
Pyogenic granuloma – the quest for optimum treatment: Audit of treatment of 408 cases
6
Pyogenic granuloma e the quest for optimum treatment: Audit of treatment of 408 cases * A.V. Giblin*, A.J.P. Clover, A. Athanassopoulos, P.G. Budny Department of Plastic and Reconstructive Surgery, Stoke Mandeville Hospital, Mandeville Road, Aylesbury, Buckinghamshire HP21 8AL, UK Received 25 April 2006; accepted 10 October 2006 KEYWORDS Pyogenic granuloma; Lobular capillary haemangioma; Treatment; Recurrence Summary Pyogenic granuloma is a common, acquired, benign vascular lesion of skin and mucous membranes which may occasionally present intravascularly or subcutaneously. Pyogenic granuloma occur in all age groups and although they may eventually regress, removal of unsightly, bleeding or uncomfortably positioned lesions is usually sought before this takes place. This is a retrospective study of 408 cases of pyogenic granuloma that were analysed by the Stoke Mandeville Histopathology laboratory between 1994 and 2004. This study was carried out to review the sex, age and anatomic distribution of the lesions and to assess the most success- ful form of treatment on the basis of recurrence risk and other measures such as aesthetic re- sult, acceptability and appropriateness of the procedure with respect to the patient. There was a slight male preponderance especially among children. The exception to this was lesions on mucous membranes, which were more common in women. Head and neck was the most common anatomical location, in particular the cheek and intraoral locations. Fewest re- currences were noted following excision and direct closure although all techniques investi- gated showed an acceptably low recurrence rate. Whatever technique is used it must yield material for histopathological analysis to ensure the exclusion of differential diagnoses. ª 2007 British Association of Plastic, Reconstructive and Aesthetic Surgeons. Published by Elsevier Ltd. All rights reserved. Pyogenic granuloma (PG) are common, acquired, benign vascular proliferations which may occur anywhere on the skin or mucosa 1 and even intravascularly 2 at any age. While PG are thought to constitute 0.5% of all childhood skin nod- ules, 3 population data for adults are scarce but studies have determined a prevalence rate for intraoral lesions of one lesion in 25 000. 4,5 The literature offers conflicting views as to the sex ratio of PG, however, it is clear that mucosal lesions are up to twice as common in women than men. 6 * Presented in part at The British Society of Plastic Surgeons Winter Meeting, December 2004. * Corresponding author. Royal Marsden Hospital, Melanoma and sarcoma surgery, 203 Fulham Road, London SW3 6JJ, UK. Tel.: þ44 0207 352 8171x2265; fax: þ44 0207 808 2232. E-mail address: [email protected] (A.V. Giblin). 1748-6815/$ - see front matter ª 2007 British Association of Plastic, Reconstructive and Aesthetic Surgeons. Published by Elsevier Ltd. All rights reserved. doi:10.1016/j.bjps.2006.10.018 Journal of Plastic, Reconstructive & Aesthetic Surgery (2007) 60, 1030e1035
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Pyogenic granuloma – the quest for optimum treatment: Audit of treatment of 408 cases

Journal of Plastic, Reconstructive & Aesthetic Surgery (2007) 60, 1030e1035
Pyogenic granuloma e the quest for optimumtreatment: Audit of treatment of 408 cases*
A.V. Giblin*, A.J.P. Clover, A. Athanassopoulos, P.G. Budny
Department of Plastic and Reconstructive Surgery, Stoke Mandeville Hospital, Mandeville Road, Aylesbury,Buckinghamshire HP21 8AL, UK
Received 25 April 2006; accepted 10 October 2006
KEYWORDSPyogenic granuloma;Lobular capillaryhaemangioma;Treatment;Recurrence
Summary Pyogenic granuloma is a common, acquired, benign vascular lesion of skin andmucous membranes which may occasionally present intravascularly or subcutaneously.Pyogenic granuloma occur in all age groups and although they may eventually regress, removalof unsightly, bleeding or uncomfortably positioned lesions is usually sought before this takesplace.
This is a retrospective study of 408 cases of pyogenic granuloma that were analysed by theStoke Mandeville Histopathology laboratory between 1994 and 2004. This study was carried outto review the sex, age and anatomic distribution of the lesions and to assess the most success-ful form of treatment on the basis of recurrence risk and other measures such as aesthetic re-sult, acceptability and appropriateness of the procedure with respect to the patient.
There was a slight male preponderance especially among children. The exception to this waslesions on mucous membranes, which were more common in women. Head and neck was themost common anatomical location, in particular the cheek and intraoral locations. Fewest re-currences were noted following excision and direct closure although all techniques investi-gated showed an acceptably low recurrence rate. Whatever technique is used it must yieldmaterial for histopathological analysis to ensure the exclusion of differential diagnoses.ª 2007 British Association of Plastic, Reconstructive and Aesthetic Surgeons. Publishedby Elsevier Ltd. All rights reserved.
* Presented in part at The British Society of Plastic SurgeonsWinter Meeting, December 2004.
* Corresponding author. Royal Marsden Hospital, Melanoma andsarcoma surgery, 203 Fulham Road, London SW3 6JJ, UK. Tel.:þ44 0207 352 8171x2265; fax: þ44 0207 808 2232.
E-mail address: [email protected] (A.V. Giblin).
1748-6815/$-seefrontmatterª2007BritishAssociationofPlastic,Reconstdoi:10.1016/j.bjps.2006.10.018
Pyogenic granuloma (PG) are common, acquired, benignvascular proliferations which may occur anywhere on theskin or mucosa1 and even intravascularly2 at any age. WhilePG are thought to constitute 0.5% of all childhood skin nod-ules,3 population data for adults are scarce but studies havedetermined a prevalence rate for intraoral lesions of onelesion in 25 000.4,5 The literature offers conflicting viewsas to the sex ratio of PG, however, it is clear that mucosallesions are up to twice as common in women than men.6
ructiveandAestheticSurgeons.PublishedbyElsevierLtd.All rightsreserved.

Pyogenic granuloma the quest for optimum treatment 1031
Mucosal lesions are especially common in pregnancy, possi-bly due to hormonal influences.7
These, usually solitary, smooth, bright red, rapidlygrowing papules often ulcerate and bleed and this, to-gether with cosmetic factors, brings many patients to seektreatment. A number of treatments are recognised for PGof which the standard is thought to be complete excisionand surgical closure. This may, of course, leave a scar andalthough other treatments such as shave and cautery,curettage and laser ablation or photocoagulation appearless efficient in clearing these notoriously recurring lesions,they may leave less of a cosmetic defect for lesions thatmight have resolved without intervention.
Spontaneous involution of less mature lesions has beenreported, especially post partum in cases which appearedduring pregnancy,8 or where a stimulus such as a foreign bodyis removed,9 whereas older lesions tend to become increas-ingly fibrotic and therefore to persist.10 It was this regressionon stimulus removal that prompted Requena et al.9 to sug-gest PG should be considered a form of vascular hyperplasia.
Some methods of treatment fail to provide samples forhistopathological analysis. This must be considered be-cause, despite the fact that clinical characteristics com-bined with a history of a fast growing, easily bleeding lesionare often enough to distinguish a PG, up to 18% of lesionsmay be misdiagnosed.11 The differential diagnosis includes:spitz naevus, common warts, true haemangiomas, amela-notic melanoma, squamous cell carcinoma and spindlecell tumours, amongst others.
This retrospective analysis was undertaken to examinethe distribution of PG and to assess the efficacy oftreatment modalities.
Method
This was a retrospective study of 408 cases of PG in adultsand children registered in the Stoke Mandeville Hospitalhistopathology database. Inclusion criteria required a histo-logical diagnosis of PG within the decade 1 January 1994 to31 December 2003.
The sex, age and pregnancy status (of women) werenoted. Those aged 17 years or less were classified aschildren. The distribution of lesions was categorised ac-cording to anatomic location: head and neck, trunk (in-cluding back), upper limb and lower limb.
Distribution was further subdivided according to epider-mis type involved: skin or mucous membranes (intraoral,conjunctival, intranasal).
The method of treatment was recorded: excision andlinear closure, curettage or shave excision with or withoutcautery, or cautery alone (chemical and thermal). Re-current granuloma were grouped according to the unsuc-cessful primary treatment modality and reportedcompleteness of removal of the original lesion was noted.
Patient case notes were reviewed to ensure that allrecurrences were recorded, as subsequent treatmentsmight not have yielded histopathological specimens andwould therefore not have been picked up by the primarysearch. It was not possible to comment on those lesionsthat were treated during the audit period with destructivetechniques where material was not made available for
histopatholgical analysis as these cases would not havebeen entered in the searched database.
Results
Histopathology
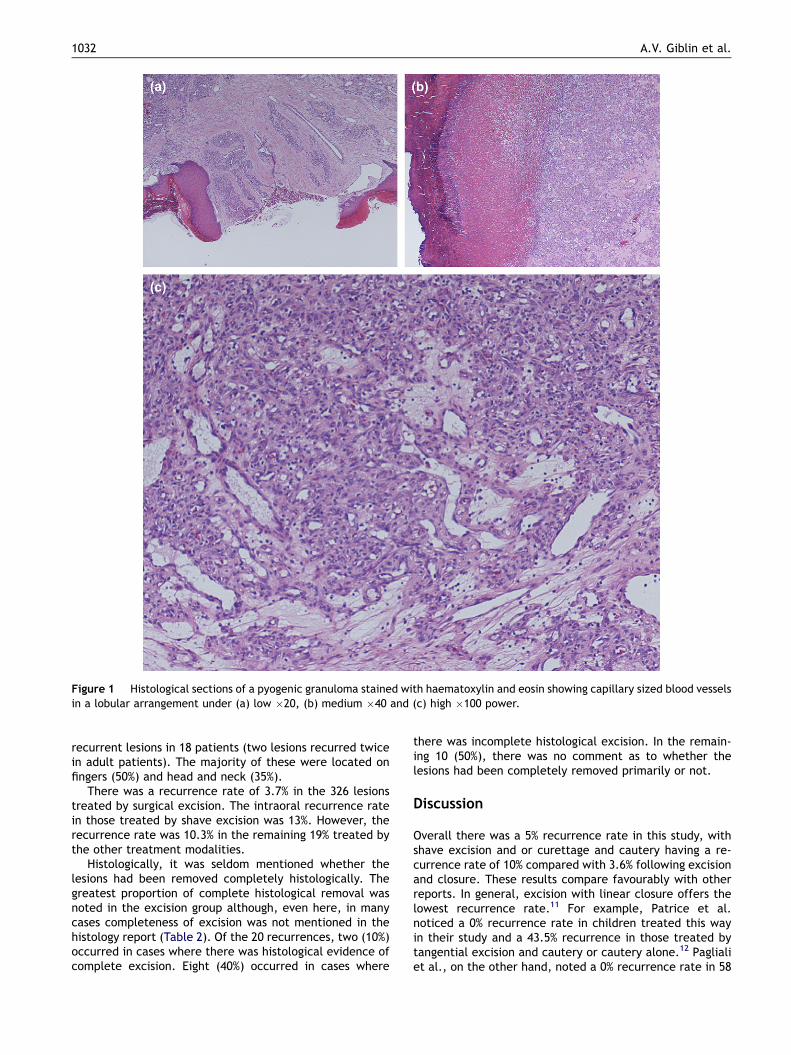
Overall 408 PG were recorded in the histopathology reportsof 388 patients whose specimens were analysed in theStoke Mandeville Hospital laboratory. PG was diagnosed onthe basis of a polypoid or raised skin or mucosal lesionshowing a proliferation of capillary-sized blood vessels ina lobular arrangement. An epidermal collarette was oftenpresent at the periphery of the lesion and ulceration andinflammation frequently superimposed (Fig. 1). There wereno histological features of malignancy.
Age
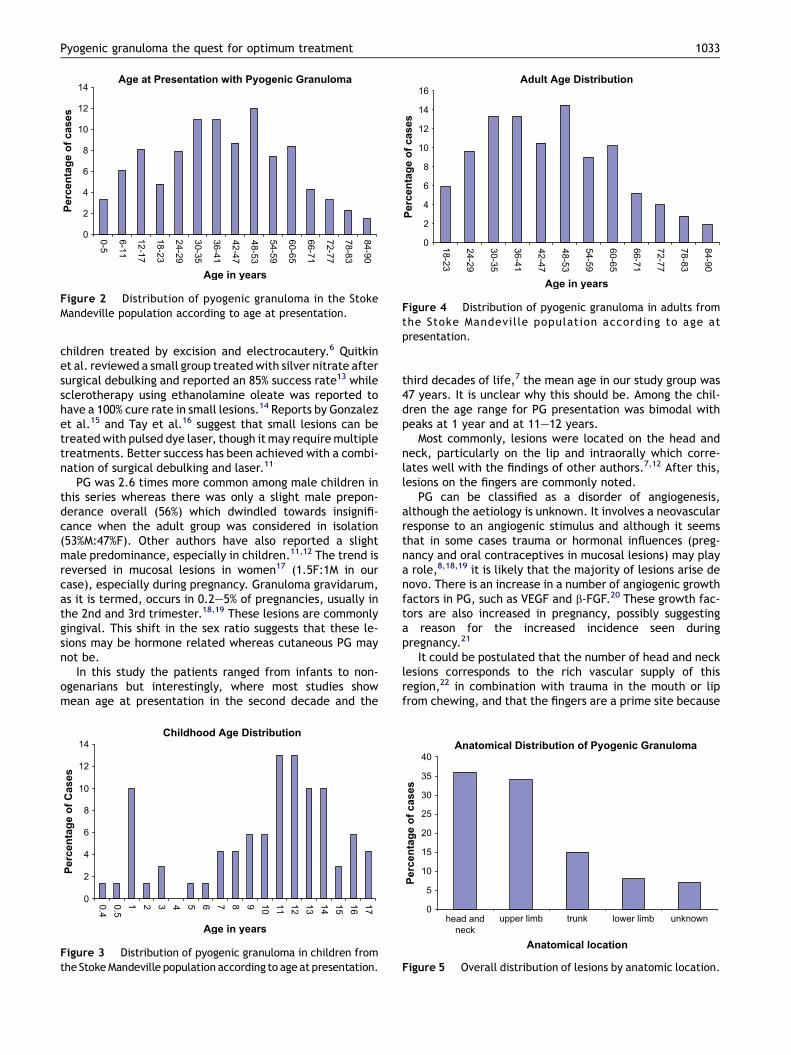
The mean age of the patients was 40.5 years (age range 5monthse90 years) (Fig. 2). Eighteen per cent (69) of the pa-tients were children (17 years and under) with a mean ageat the time of treatment of 10 years and a median of 11years (Fig. 3). The mean age at treatment for the adultgroup was 47 years (Fig. 4).
Sex
Of the 388 patients, 56% were male and 46% were female.Of the female patients, 16 (9.5%) were pregnant. Seventy-two per cent of the children in the studied group weremale.
Anatomic location
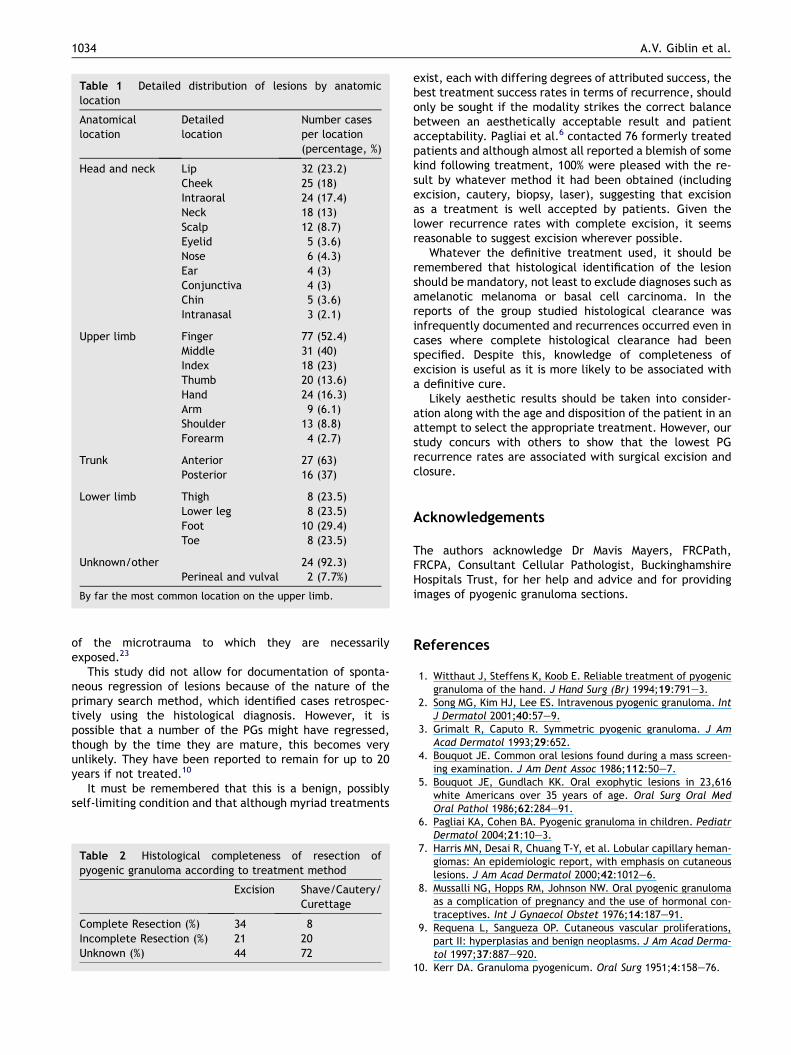
A little over a third (36%) of PGs were located in the headand neck area, followed by a third on the upper limb, 15%on the trunk and 8% on the lower limb (7% had no record ofposition of the lesion) (Fig. 5). The male to female ratio formucosal lesions was 1:1.5. Table 1 shows the breakdown oflocations within the regions described. The most commonhead and neck locations were cheek and intraoral lesions,followed by lip lesions.
By far the most common location on the upper limbwas the fingers, especially the middle finger (40%). Theanterior trunk was a more frequent site than the posteriorand in the lower limb the distribution was fairly uniformthroughout.
Mucosal cases comprised 29% (five) of lesions in pregnantwomen, which contrasted notably with the smaller per-centage (8%) these lesions represented in the female groupoverall.
Treatment and recurrence
Eighty per cent of the lesions were treated by surgicalexcision, while 19% were treated by curettage, shaveexcision or cautery or a combination of these. Overall,this resulted in a recurrence rate of 5%. There were 20
1032 A.V. Giblin et al.
Figure 1 Histological sections of a pyogenic granuloma stained with haematoxylin and eosin showing capillary sized blood vesselsin a lobular arrangement under (a) low �20, (b) medium �40 and (c) high �100 power.
recurrent lesions in 18 patients (two lesions recurred twicein adult patients). The majority of these were located onfingers (50%) and head and neck (35%).
There was a recurrence rate of 3.7% in the 326 lesionstreated by surgical excision. The intraoral recurrence ratein those treated by shave excision was 13%. However, therecurrence rate was 10.3% in the remaining 19% treated bythe other treatment modalities.
Histologically, it was seldom mentioned whether thelesions had been removed completely histologically. Thegreatest proportion of complete histological removal wasnoted in the excision group although, even here, in manycases completeness of excision was not mentioned in thehistology report (Table 2). Of the 20 recurrences, two (10%)occurred in cases where there was histological evidence ofcomplete excision. Eight (40%) occurred in cases where
there was incomplete histological excision. In the remain-ing 10 (50%), there was no comment as to whether thelesions had been completely removed primarily or not.
Discussion
Overall there was a 5% recurrence rate in this study, withshave excision and or curettage and cautery having a re-currence rate of 10% compared with 3.6% following excisionand closure. These results compare favourably with otherreports. In general, excision with linear closure offers thelowest recurrence rate.11 For example, Patrice et al.noticed a 0% recurrence rate in children treated this wayin their study and a 43.5% recurrence in those treated bytangential excision and cautery or cautery alone.12 Paglialiet al., on the other hand, noted a 0% recurrence rate in 58
Pyogenic granuloma the quest for optimum treatment 1033
children treated by excision and electrocautery.6 Quitkinet al. reviewed a small group treated with silver nitrate aftersurgical debulking and reported an 85% success rate13 whilesclerotherapy using ethanolamine oleate was reported tohave a 100% cure rate in small lesions.14 Reports by Gonzalezet al.15 and Tay et al.16 suggest that small lesions can betreated with pulsed dye laser, though it may require multipletreatments. Better success has been achieved with a combi-nation of surgical debulking and laser.11
PG was 2.6 times more common among male children inthis series whereas there was only a slight male prepon-derance overall (56%) which dwindled towards insignifi-cance when the adult group was considered in isolation(53%M:47%F). Other authors have also reported a slightmale predominance, especially in children.11,12 The trend isreversed in mucosal lesions in women17 (1.5F:1M in ourcase), especially during pregnancy. Granuloma gravidarum,as it is termed, occurs in 0.2e5% of pregnancies, usually inthe 2nd and 3rd trimester.18,19 These lesions are commonlygingival. This shift in the sex ratio suggests that these le-sions may be hormone related whereas cutaneous PG maynot be.
In this study the patients ranged from infants to non-ogenarians but interestingly, where most studies showmean age at presentation in the second decade and the
Childhood Age Distribution
0
2
4
6
8
10
12
14
0.40.51 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17
Age in years
Percen
tag
e o
f C
ases
Figure 3 Distribution of pyogenic granuloma in children fromthe Stoke Mandeville population according to age at presentation.
Age at Presentation with Pyogenic Granuloma
0
2
4
6
8
10
12
14
0-5
6-11
12-17
18-23
24-29
30-35
36-41
42-47
48-53
54-59
60-65
66-71
72-77
78-83
84-90
Age in years
Percen
tag
e o
f cases
Figure 2 Distribution of pyogenic granuloma in the StokeMandeville population according to age at presentation.
third decades of life,7 the mean age in our study group was47 years. It is unclear why this should be. Among the chil-dren the age range for PG presentation was bimodal withpeaks at 1 year and at 11e12 years.
Most commonly, lesions were located on the head andneck, particularly on the lip and intraorally which corre-lates well with the findings of other authors.7,12 After this,lesions on the fingers are commonly noted.
PG can be classified as a disorder of angiogenesis,although the aetiology is unknown. It involves a neovascularresponse to an angiogenic stimulus and although it seemsthat in some cases trauma or hormonal influences (preg-nancy and oral contraceptives in mucosal lesions) may playa role,8,18,19 it is likely that the majority of lesions arise denovo. There is an increase in a number of angiogenic growthfactors in PG, such as VEGF and b-FGF.20 These growth fac-tors are also increased in pregnancy, possibly suggestinga reason for the increased incidence seen duringpregnancy.21
It could be postulated that the number of head and necklesions corresponds to the rich vascular supply of thisregion,22 in combination with trauma in the mouth or lipfrom chewing, and that the fingers are a prime site because
Adult Age Distribution
0
2
4
6
8
10
12
14
16
18-23
24-29
30-35
36-41
42-47
48-53
54-59
60-65
66-71
72-77
78-83
84-90
Age in years
Percen
tag
e o
f cases
Figure 4 Distribution of pyogenic granuloma in adults fromthe Stoke Mandeville population according to age atpresentation.
Anatomical Distribution of Pyogenic Granuloma
0
5
10
15
20
25
30
35
40
head andneck
upper limb trunk lower limb unknown
Anatomical location
Percen
tag
e o
f cases
Figure 5 Overall distribution of lesions by anatomic location.
1034 A.V. Giblin et al.
of the microtrauma to which they are necessarilyexposed.23
This study did not allow for documentation of sponta-neous regression of lesions because of the nature of theprimary search method, which identified cases retrospec-tively using the histological diagnosis. However, it ispossible that a number of the PGs might have regressed,though by the time they are mature, this becomes veryunlikely. They have been reported to remain for up to 20years if not treated.10
It must be remembered that this is a benign, possiblyself-limiting condition and that although myriad treatments
Table 1 Detailed distribution of lesions by anatomiclocation
Anatomicallocation
Detailedlocation
Number casesper location(percentage, %)
Head and neck Lip 32 (23.2)Cheek 25 (18)Intraoral 24 (17.4)Neck 18 (13)Scalp 12 (8.7)Eyelid 5 (3.6)Nose 6 (4.3)Ear 4 (3)Conjunctiva 4 (3)Chin 5 (3.6)Intranasal 3 (2.1)
Upper limb Finger 77 (52.4)Middle 31 (40)Index 18 (23)Thumb 20 (13.6)Hand 24 (16.3)Arm 9 (6.1)Shoulder 13 (8.8)Forearm 4 (2.7)
Trunk Anterior 27 (63)Posterior 16 (37)
Lower limb Thigh 8 (23.5)Lower leg 8 (23.5)Foot 10 (29.4)Toe 8 (23.5)
Unknown/other 24 (92.3)Perineal and vulval 2 (7.7%)
By far the most common location on the upper limb.
Table 2 Histological completeness of resection ofpyogenic granuloma according to treatment method
Excision Shave/Cautery/Curettage
Complete Resection (%) 34 8Incomplete Resection (%) 21 20Unknown (%) 44 72
exist, each with differing degrees of attributed success, thebest treatment success rates in terms of recurrence, shouldonly be sought if the modality strikes the correct balancebetween an aesthetically acceptable result and patientacceptability. Pagliai et al.6 contacted 76 formerly treatedpatients and although almost all reported a blemish of somekind following treatment, 100% were pleased with the re-sult by whatever method it had been obtained (includingexcision, cautery, biopsy, laser), suggesting that excisionas a treatment is well accepted by patients. Given thelower recurrence rates with complete excision, it seemsreasonable to suggest excision wherever possible.
Whatever the definitive treatment used, it should beremembered that histological identification of the lesionshould be mandatory, not least to exclude diagnoses such asamelanotic melanoma or basal cell carcinoma. In thereports of the group studied histological clearance wasinfrequently documented and recurrences occurred even incases where complete histological clearance had beenspecified. Despite this, knowledge of completeness ofexcision is useful as it is more likely to be associated witha definitive cure.
Likely aesthetic results should be taken into consider-ation along with the age and disposition of the patient in anattempt to select the appropriate treatment. However, ourstudy concurs with others to show that the lowest PGrecurrence rates are associated with surgical excision andclosure.
Acknowledgements
The authors acknowledge Dr Mavis Mayers, FRCPath,FRCPA, Consultant Cellular Pathologist, BuckinghamshireHospitals Trust, for her help and advice and for providingimages of pyogenic granuloma sections.
References
1. Witthaut J, Steffens K, Koob E. Reliable treatment of pyogenicgranuloma of the hand. J Hand Surg (Br) 1994;19:791e3.
2. Song MG, Kim HJ, Lee ES. Intravenous pyogenic granuloma. IntJ Dermatol 2001;40:57e9.
3. Grimalt R, Caputo R. Symmetric pyogenic granuloma. J AmAcad Dermatol 1993;29:652.
4. Bouquot JE. Common oral lesions found during a mass screen-ing examination. J Am Dent Assoc 1986;112:50e7.
5. Bouquot JE, Gundlach KK. Oral exophytic lesions in 23,616white Americans over 35 years of age. Oral Surg Oral MedOral Pathol 1986;62:284e91.
6. Pagliai KA, Cohen BA. Pyogenic granuloma in children. PediatrDermatol 2004;21:10e3.
7. Harris MN, Desai R, Chuang T-Y, et al. Lobular capillary heman-giomas: An epidemiologic report, with emphasis on cutaneouslesions. J Am Acad Dermatol 2000;42:1012e6.
8. Mussalli NG, Hopps RM, Johnson NW. Oral pyogenic granulomaas a complication of pregnancy and the use of hormonal con-traceptives. Int J Gynaecol Obstet 1976;14:187e91.
9. Requena L, Sangueza OP. Cutaneous vascular proliferations,part II: hyperplasias and benign neoplasms. J Am Acad Derma-tol 1997;37:887e920.
10. Kerr DA. Granuloma pyogenicum. Oral Surg 1951;4:158e76.

Pyogenic granuloma the quest for optimum treatment 1035
11. Kirschner RE, Low DW. Treatment of pyogenic granuloma byshave excision and laser photocoagulation. Plast ReconstrSurg 1999;104:1346e9.
12. Patrice SJ, Wiss K, Mulliken JB. Pyogenic granuloma (lobularcapillary hemangioma): a clinicopathological study of 178cases. Pediatr Dermatol 1991;8:267e76.
13. Quitkin HM, Rosenwasser MP, Strauch RJ. The efficacy of silvernitrate cauterization for pyogenic granuloma of the hand. JHand Surg 2003;28A:425e38.
14. Matsumoto K, Nakanishi H, Seike T, et al. Treatment of pyo-genic granuloma with a sclerosing agent. Dermatolog Surg2001;27:521e3.
15. Gonzalez S, Vibhagool C, Falo LD, et al. Treatment of pyogenicgranulomas with the 585nm pulsed dye laser. J Am Acad Der-matol 1996;35:428e31.
16. Tay Y-K, Weston WL, Morelli JG. Treatment of pyogenic granu-loma in children with flashlamp-pumped pulsed dye laser.Pediatrics 1997;99:368e70.
17. Angelopoulos AP. Pyogenic granuloma of the oral cavity: statis-tical analysis of its clinical features. J Oral Surg 1971;29:840e7.
18. Kroumpouzos G, Cohen LM. Dermatoses of pregnancy. J AmAcad Dermatol 2001;45:1e19.
19. Daley TD, Nartey NO, Wysocki GP. Pregnancy tumor: an analy-sis. Oral Surg Oral Med Pathol 1991;72:196e9.
20. Yuan K, Jin YT, Lin MT. The detection and comparison of angio-genesis-associated factors in pyogenic granuloma by immuno-histochemistry. J Periodontol 2000;71:701e9.
21. Yuan K, Wing LY, Lin MT. Pathogenetic roles of angiogenicfactors in pyogenic granulomas in pregnancy are modulatedby female sex hormones. J Periodontol 2002;73:701e8.
22. Pasyk VA, Thomas SV, Hassett CA. Regional differences incapillary density of the normal human dermis. Plast ReconstrSurg 1989;83:939e45.
23. Nkanza NK, Hutt MSR. Pyogenic granuloma: a study of 181cases from Malawi. East Afr Med J 1981;58:318e23.




















