
Esthetic Treatment of Peripheral Giant Cell Granuloma Using a Subepithelial Connective Tissue Graft...
7
Case Report Esthetic Treatment of Peripheral Giant Cell Granuloma Using a Subepithelial Connective Tissue Graft and a Split-Thickness Pouch Technique Ron Lev,* Ofer Moses,* Dan Holtzclaw, † and Haim Tal* Background: Peripheral giant cell granuloma (PGCG) is a reactive hyperplastic lesion involving the gingiva or alveolar mucosa consisting of proliferating endothelial cells, a rich capillary bed, chronic inflam- matory cells, fibroblasts, and giant cells. After complete clinical removal of PGCG recurrence occurs in about 10% of cases, and may result in an esthetic and func- tional soft tissue defect. This report describes a surgical procedure involving complete removal of a gingival PGCG in the maxillary esthetic zone and immediate tissue restoration achieving complete gingival aug- mentation. Methods: A 15-year-old female presented with a red, nodular, asymptomatic lesion, approximately 3.5 mm in diameter, located above the maxillary left lateral incisor. The lesion was excised down to the underlying root resulting in a 6 · 5-mm mucogingival dehiscence defect. Corrective surgery included a sub- epithelial connective tissue graft peripherally covered by the surrounding gingiva and stabilized by 5/0 resorbable sutures. Results: Healing was uneventful, resulting in healthy and esthetic gingiva. Microscopic examina- tion of the biopsy specimen was consistent with the diagnosis of PGCG. Conclusions: PGCG may follow an aggressive course, sometimes requiring preemptive surgical in- tervention. Grafting a subepithelial connective tissue graft peripherally covered by the surrounding gin- giva, without raising a gingival flap, successfully eliminated the gingival defect. The free gingival mar- gin of the neighboring teeth and the mucogingival junction remained unchanged. J Periodontol 2010; 81:1092-1098. KEY WORDS Case report; connective tissue; giant cell; giant cell reparative; gingival diseases; granuloma; hyperplasia. P eripheral giant cell granuloma (PGCG) is a non- neoplastic, reactive hyperplastic lesion (RHL) involving the gingiva or alveolar mucosa. The etiology is unknown; it has been suggested that an injury to the periodontal ligament and gingiva initi- ating a reactive hyperplastic response in the peri- osteum plays a role. 1 Among other hyperplasias, it can be considered an overexuberant local response of tissue to injury. 2 The initiating injury stimulates the formation of granulation tissue consisting of proliferating endothe- lial cells, a rich capillary bed, chronic inflammatory cells, and fibroblasts. The granulation tissue soon be- comes covered with stratified squamous epithelium. Most lesions are sessile, clinically asymptomatic, and smoothly contoured or lobulated with dark red appearance caused by rich vascularity; it is moder- ately soft and spongy and blanches under mild digital pressure. 1,3,4 RHLs include pyogenic granuloma, hormonal (pregnancy) tumor, epulis fissuratum, epulis granulo- matosa, pulp polyp, inflammatory papillary hy- perplasia, peripheral ossifying fibroma, acquired (traumatic) hemangioma, fibrous hyperplasia (fi- broma), and PGCG, the latter being less common (1.5%). 5 The differential diagnosis of RHL includes other types of lesions, such as parulis, hemangioma, Ka- posi sarcoma, metastatic tumors, primary benign or malignant mesenchymal tumors, amelanotic mela- noma, traumatic neuroma, gingival cyst of the adult, and, uncommonly, squamous cell carcinoma. Apart from parulis, which is an inflammatory reaction (sinus tract), all the aforementioned lesions are rarities and may be considered in the differential diagnosis if no ir- ritant is found or if the underlying bone shows resorp- tion or symptoms of a primary tumor elsewhere. PGCG differs from other RHLs in the presence of multinucleated giant cells of unknown origin. 1,6,7 Dark red is the predominant color, but it may be bluish or pale pink, polypoid or nodular, located on the * Department of Periodontology, School of Dental Medicine, Tel Aviv University, Ramat Aviv, Israel. † Private practice, Austin, TX. doi: 10.1902/jop.2010.090674 Volume 81 • Number 7 1092
-
Upload
bradleystrawser -
Category
Documents
-
view
0 -
download
0
Transcript of Esthetic Treatment of Peripheral Giant Cell Granuloma Using a Subepithelial Connective Tissue Graft...

Case Report
Esthetic Treatment of Peripheral Giant Cell GranulomaUsing a Subepithelial Connective Tissue Graftand a Split-Thickness Pouch Technique
Ron Lev,* Ofer Moses,* Dan Holtzclaw,† and Haim Tal*
Background: Peripheral giant cell granuloma(PGCG) is a reactive hyperplastic lesion involving thegingiva or alveolar mucosa consisting of proliferatingendothelial cells, a rich capillary bed, chronic inflam-matory cells, fibroblasts, and giant cells. After completeclinical removal of PGCG recurrence occurs in about10% of cases, and may result in an esthetic and func-tional soft tissue defect. This report describes a surgicalprocedure involving complete removal of a gingivalPGCG in the maxillary esthetic zone and immediatetissue restoration achieving complete gingival aug-mentation.
Methods: A 15-year-old female presented witha red, nodular, asymptomatic lesion, approximately3.5 mm in diameter, located above the maxillary leftlateral incisor. The lesion was excised down to theunderlying root resulting in a 6 · 5-mm mucogingivaldehiscence defect. Corrective surgery included a sub-epithelial connective tissue graft peripherally coveredby the surrounding gingiva and stabilized by 5/0resorbable sutures.
Results: Healing was uneventful, resulting inhealthy and esthetic gingiva. Microscopic examina-tion of the biopsy specimen was consistent with thediagnosis of PGCG.
Conclusions: PGCG may follow an aggressivecourse, sometimes requiring preemptive surgical in-tervention. Grafting a subepithelial connective tissuegraft peripherally covered by the surrounding gin-giva, without raising a gingival flap, successfullyeliminated the gingival defect. The free gingival mar-gin of the neighboring teeth and the mucogingivaljunction remained unchanged. J Periodontol 2010;81:1092-1098.
KEY WORDS
Case report; connective tissue; giant cell; giant cellreparative; gingival diseases; granuloma;hyperplasia.
Peripheral giant cell granuloma (PGCG) is a non-neoplastic, reactive hyperplastic lesion (RHL)involving the gingiva or alveolar mucosa. The
etiology is unknown; it has been suggested that aninjury to the periodontal ligament and gingiva initi-ating a reactive hyperplastic response in the peri-osteum plays a role.1 Among other hyperplasias, itcan be considered an overexuberant local responseof tissue to injury.2
The initiating injury stimulates the formation ofgranulation tissue consisting of proliferating endothe-lial cells, a rich capillary bed, chronic inflammatorycells, and fibroblasts. The granulation tissue soon be-comes covered with stratified squamous epithelium.Most lesions are sessile, clinically asymptomatic,and smoothly contoured or lobulated with dark redappearance caused by rich vascularity; it is moder-ately soft and spongy and blanches under mild digitalpressure.1,3,4
RHLs include pyogenic granuloma, hormonal(pregnancy) tumor, epulis fissuratum, epulis granulo-matosa, pulp polyp, inflammatory papillary hy-perplasia, peripheral ossifying fibroma, acquired(traumatic) hemangioma, fibrous hyperplasia (fi-broma), and PGCG, the latter being less common(1.5%).5
The differential diagnosis of RHL includes othertypes of lesions, such as parulis, hemangioma, Ka-posi sarcoma, metastatic tumors, primary benign ormalignant mesenchymal tumors, amelanotic mela-noma, traumatic neuroma, gingival cyst of the adult,and, uncommonly, squamous cell carcinoma. Apartfrom parulis, which is an inflammatory reaction (sinustract), all the aforementioned lesions are rarities andmay be considered in the differential diagnosis if no ir-ritant is found or if the underlying bone shows resorp-tion or symptoms of a primary tumor elsewhere.
PGCG differs from other RHLs in the presence ofmultinucleated giant cells of unknown origin.1,6,7
Dark red is the predominant color, but it may be bluishor pale pink, polypoid or nodular, located on the
* Department of Periodontology, School of Dental Medicine, Tel AvivUniversity, Ramat Aviv, Israel.
† Private practice, Austin, TX. doi: 10.1902/jop.2010.090674
Volume 81 • Number 7
1092
gingival or edentulous ridge, more commonly in themandible, rubbery to soft on palpation, and predom-inantly found in whites, with a relative predilection forfemales aged 30 to 70 years.1,8-12 There may also bea cupping resorption of the underlying bone. Micro-scopically, varying degrees of inflammation and vas-cularity with scattering of multinucleated giant cells,extravasated erythrocytes, and varying amounts ofhemosiderin may be observed.
PGCG should be completely removed and exam-ined microscopically. Chronic irritants should beeliminated. Because the recurrence rate of PGCG afterexcision is approximately 10%, cases involving theselesions should be closely followed.1,13 Full excision ofPGCG lesions containing a border of normal tissuemay result in a severe mucogingival defect and es-thetic impairment. Prevention of these post-surgicaldefects may be accomplished with preemptive peri-odontal plastic surgical techniques at the time of ex-cisional biopsy.14,15 The present report describesa case in which a PGCG in the maxillary esthetic zonewas excisionally biopsied and a resultant mucogingi-val defect was prevented by simultaneous treatmentwith a subepithelial connective tissue graft.
CASE DESCRIPTION AND RESULTS
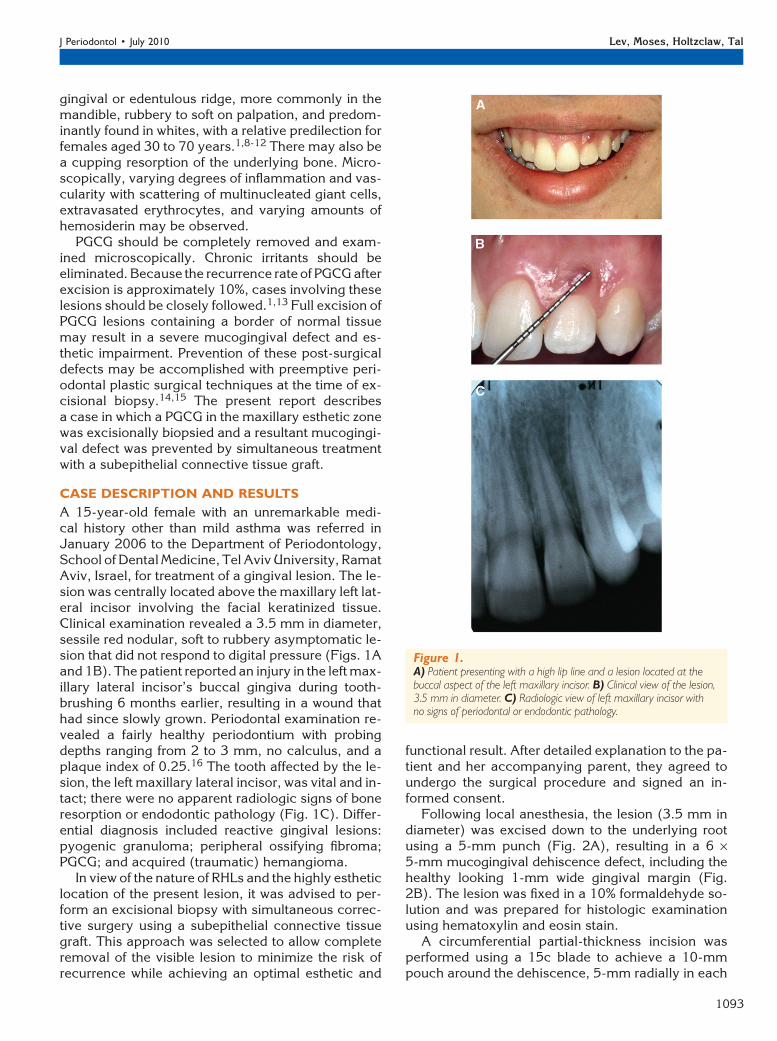
A 15-year-old female with an unremarkable medi-cal history other than mild asthma was referred inJanuary 2006 to the Department of Periodontology,School of Dental Medicine, Tel Aviv University, RamatAviv, Israel, for treatment of a gingival lesion. The le-sion was centrally located above the maxillary left lat-eral incisor involving the facial keratinized tissue.Clinical examination revealed a 3.5 mm in diameter,sessile red nodular, soft to rubbery asymptomatic le-sion that did not respond to digital pressure (Figs. 1Aand 1B). The patient reported an injury in the left max-illary lateral incisor’s buccal gingiva during tooth-brushing 6 months earlier, resulting in a wound thathad since slowly grown. Periodontal examination re-vealed a fairly healthy periodontium with probingdepths ranging from 2 to 3 mm, no calculus, and aplaque index of 0.25.16 The tooth affected by the le-sion, the left maxillary lateral incisor, was vital and in-tact; there were no apparent radiologic signs of boneresorption or endodontic pathology (Fig. 1C). Differ-ential diagnosis included reactive gingival lesions:pyogenic granuloma; peripheral ossifying fibroma;PGCG; and acquired (traumatic) hemangioma.
In view of the nature of RHLs and the highly estheticlocation of the present lesion, it was advised to per-form an excisional biopsy with simultaneous correc-tive surgery using a subepithelial connective tissuegraft. This approach was selected to allow completeremoval of the visible lesion to minimize the risk ofrecurrence while achieving an optimal esthetic and
functional result. After detailed explanation to the pa-tient and her accompanying parent, they agreed toundergo the surgical procedure and signed an in-formed consent.
Following local anesthesia, the lesion (3.5 mm indiameter) was excised down to the underlying rootusing a 5-mm punch (Fig. 2A), resulting in a 6 ·5-mm mucogingival dehiscence defect, including thehealthy looking 1-mm wide gingival margin (Fig.2B). The lesion was fixed in a 10% formaldehyde so-lution and was prepared for histologic examinationusing hematoxylin and eosin stain.
A circumferential partial-thickness incision wasperformed using a 15c blade to achieve a 10-mmpouch around the dehiscence, 5-mm radially in each
Figure 1.A) Patient presenting with a high lip line and a lesion located at thebuccal aspect of the left maxillary incisor. B) Clinical view of the lesion,3.5 mm in diameter. C) Radiologic view of left maxillary incisor withno signs of periodontal or endodontic pathology.
J Periodontol • July 2010 Lev, Moses, Holtzclaw, Tal
1093

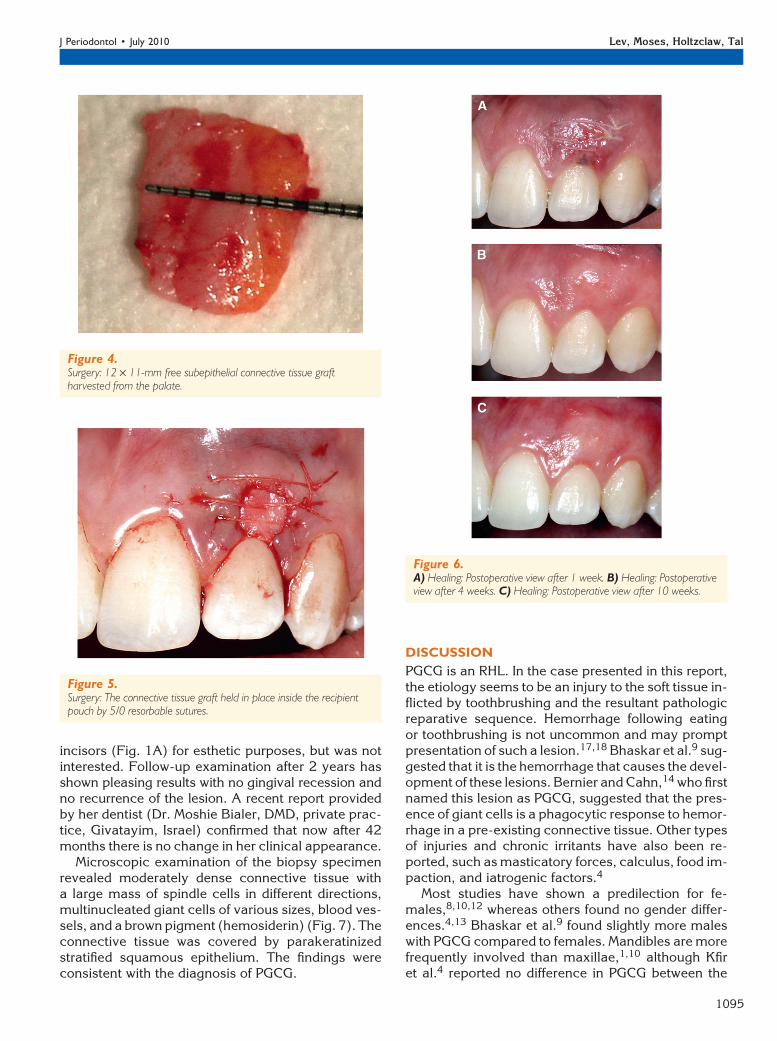
direction (Fig. 3), and the exposed root surface wasthoroughly planed with hand instruments aiming atboth root coverage outcomes and avoiding recur-rence of the lesion. The interdental papillae were leftintact to minimize the possibility of recession duringhealing and to avoid further esthetic impairment inthe esthetic zone. A subepithelial connective tissuegraft measuring 11 · 12 · 2 mm was harvested fromthe palate opposing the first and second right maxil-lary molars. The graft (Fig. 4) was contoured to fitthe formerly prepared recipient bed. The donor sitewas sutured with five 4/0 silk sutures.
The subepithelial connective tissue graft was in-serted into the recipient pouch and was furtherstabilized by three 5/0 polylactic-polyglycolic acid re-sorbable interrupted sutures crossing over or throughthe graft and the surrounding gingiva. The graft wasadhered to the exposed root surface for 3 minutesand was left uncovered opposing the mucogingival
dehiscence defect (Fig. 5). Postoperative instructionsincluded analgesics as needed, and a 0.2% chlorhex-idine mouthwash was prescribed twice a day for a 3-week period of time, followed by a 3-week gentlebrushing using an extrasoft toothbrush.
Palatal sutures were removed 1 week after the sur-gery, and the resorbable sutures at the recipient sitewere removed after 2 weeks. Healing was uneventfulat both donor and recipient sites. At 1 week, the ex-posed portion of the graft was partially covered witha fibrin clot and was reddish in appearance; marginalnecrosis was observed at the most coronal border(Fig. 6A).
At 2 and 4 weeks after surgery, the recipient sitewas fully covered by epithelium, matching in colorto the surrounding gingiva (Fig. 6B). After 10 weeks,the gingiva presented with normal appearance, andwas esthetically pleasing (Fig. 6C). The patient wasadvised to correct surgically the discrepancy on thegingival margin between the right and left central
Figure 2.A) Surgery: 5-mm punch incision circumscribing the lesion. B) Surgery:dehiscence-type defect created following full excision of the lesion.
Figure 3.A) Surgery: Circumferential split-thickness incision creating a recipientpouch. B) Surgery: Clinical view of the 10-mm deep recipient pouch site.
Esthetic Treatment of Peripheral Giant Cell Granuloma Volume 81 • Number 7
1094
incisors (Fig. 1A) for esthetic purposes, but was notinterested. Follow-up examination after 2 years hasshown pleasing results with no gingival recession andno recurrence of the lesion. A recent report providedby her dentist (Dr. Moshie Bialer, DMD, private prac-tice, Givatayim, Israel) confirmed that now after 42months there is no change in her clinical appearance.
Microscopic examination of the biopsy specimenrevealed moderately dense connective tissue witha large mass of spindle cells in different directions,multinucleated giant cells of various sizes, blood ves-sels, and a brown pigment (hemosiderin) (Fig. 7). Theconnective tissue was covered by parakeratinizedstratified squamous epithelium. The findings wereconsistent with the diagnosis of PGCG.
DISCUSSION
PGCG is an RHL. In the case presented in this report,the etiology seems to be an injury to the soft tissue in-flicted by toothbrushing and the resultant pathologicreparative sequence. Hemorrhage following eatingor toothbrushing is not uncommon and may promptpresentation of such a lesion.17,18 Bhaskar et al.9 sug-gested that it is the hemorrhage that causes the devel-opment of these lesions. Bernier and Cahn,14 who firstnamed this lesion as PGCG, suggested that the pres-ence of giant cells is a phagocytic response to hemor-rhage in a pre-existing connective tissue. Other typesof injuries and chronic irritants have also been re-ported, such as masticatory forces, calculus, food im-paction, and iatrogenic factors.4
Most studies have shown a predilection for fe-males,8,10,12 whereas others found no gender differ-ences.4,13 Bhaskar et al.9 found slightly more maleswith PGCG compared to females. Mandibles are morefrequently involved than maxillae,1,10 although Kfiret al.4 reported no difference in PGCG between the
Figure 4.Surgery: 12 · 11-mm free subepithelial connective tissue graftharvested from the palate.
Figure 5.Surgery: The connective tissue graft held in place inside the recipientpouch by 5/0 resorbable sutures.
Figure 6.A) Healing: Postoperative view after 1 week. B) Healing: Postoperativeview after 4 weeks. C) Healing: Postoperative view after 10 weeks.
J Periodontol • July 2010 Lev, Moses, Holtzclaw, Tal
1095

jaws. Most studies have reported that PGCG lesionsvary in size between 5 and 15 mm in diameter: Kfiret al.4 reported a mean size of 12 mm, with most le-sions ranging between 6 and 10 mm in diameter;82% of lesions were smaller than 15 mm. Similar find-ings were published by Mighell et al.13 and Zhanget al.19 At only 3.5 mm in diameter, the PGCG ofthe present case was relatively small. However, its lo-cation in the maxillary anterior esthetic zone resultedin high patient awareness and may have been the rea-son for the relatively early diagnosis at such a smallsize. All age groups seemed to be affected by PGCGlesions, with a range of 2 to 86 years (mean, 31 to49.6 years) and a peak frequency in the fourth to sixthdecades of life.19,20 Appearance of such a lesion in anadolescent patient required special socioestheticconsiderations; however, the nature of the lesion de-manded complete removal in view of the tendencyto recur.1,13
Treatment of PGCG lesions is comprised of surgicalexcision of the lesion and elimination of possible irri-tating factors. The extent of surgical excision differs inthe literature. Kfir et al.4 suggested a simple conser-vative excision, as did Mighell et al.,13 although thelatter found a 22% recurrence rate, which he related
to incomplete removal of the lesion. Recurrences inthe study by Mighell et al.13 were re-excised to thelevel of the periosteum and experienced no furtherrecurrences. Mighell et al.13 also reported that spec-imens that were histopathologically incompletely ex-cised did not always recur, indicating that partialexcision may be sufficient in some cases wherechronic irritation factors were removed. However,Flaitz21 suggested that growth may recur with super-ficial resection. Recurrences may be related to lack ofinclusion of periosteum or periodontal ligament in theexcised specimen.22 Chaparro-Avendano et al.23 de-scribed resection by either a scalpel or a carbon diox-ide laser, the latter being of limited applicability inlesions with adjacent bone involvement where carefulsurgical curettage is required. A more aggressive re-section was suggested by Eronat et al.24 describingcomplete excision including the base of the lesion,with resection of the affected bone and removal ofbordering teeth and tooth germs.
The esthetic location of the lesion in the presentcase dictated a treatment that included a periodontalplastic surgery procedure. A variety of procedures toachieve this goal have been documented includingautogenous or allogeneic tissue grafting, guided tissue
Figure 7.A) Histologic view revealed moderately dense connective tissue with a large mass of spindle cells in different directions, multinucleated giant cell bloodvessels and hemosiderin (hematoxylin and eosin; original magnification ·10). B) Higher magnification histologic view revealed findings consistent withthe diagnosis of peripheral giant cell granuloma (hematoxylin and eosin; original magnification ·20). Arrows = giant cells; asterisks = blood vessels.
Esthetic Treatment of Peripheral Giant Cell Granuloma Volume 81 • Number 7
1096

regeneration, coronally positioned flaps, and pedicleflaps. A subepithelial connective tissue graft was con-sidered to be advantageous for root coverage witha concurrent gain of lost keratinized tissue in view ofthe authors’ experience and review of recent re-ports.25-27 Furthermore, in the present case, espe-cially in view of the high lip line, we chose to avoida coronally positioned flap, leaving the mucogingivaljunction (MGJ) undistorted and the neighboring papil-lae untouched. Avoiding coronal positioning of theMGJ resulted in optimal esthetic appearance with nogingival deformation or scarring. Treating a similar le-sion by a coronally positioned flap and a subepithelialconnective tissue graft, Sahingur et al.15 observed re-cession associated with a neighboring tooth during thehealing period.
A detailed differential diagnosis was set beforetreatment plan and the patient was notified that it isdifficult clinically to distinguish PGCG from pyogenicgranuloma and other reactive lesions, and that the dif-ference is seen only histologically. Furthermore, thepatient was informed of a need for a second surgicalprocedure in case of lesion recurrence or an unlikelyhistopathologic diagnosis of a rarity, such as a malig-nant tumor. It is noteworthy that it is difficult to distin-guish PGCG clinically from other reactive lesions,especially from pyogenic granuloma, and that in rarecases, giant cell granulomas may represent an oralmanifestation of hyperparathyroidism.28,29 Lesionsof hyperparathyroidism, known as ‘‘brown tumors,’’appear centrally and may perforate the bone mimick-ing PGCG.30 Histologically, brown tumors cannot bedistinguished from giant cell granulomas and shouldbe suspected when multiple lesions appear or whenlesions recur despite adequate treatment.31 In suchcases, serum biochemistry at time of lesion presenta-tionshouldbeperformed toexcludeor proveadiagno-sis of hyperparathyroidism.
The prognosis of surgical removal of PGCG is good;approximately 10% of the lesions excised were re-ported to recur, and re-excision must be performed.1
A thorough search of the relevant literature providedno information about the course of time during whichpost-surgical recurrence occurs, but in most cases ithappened after a few weeks. Our 2-year follow-upwas, therefore, a period of time long enough to ensurethe patient that she was safe from recurrence.
CONCLUSIONS
PGCG may follow an aggressive course, sometimes re-quiring preemptive surgical intervention, resulting ina significant defect in the gingiva. The present caseshows that grafting a subepithelial connective tissuegraft peripherally covered by the surrounding gingiva,without raising a gingival flap, successfully eliminatesthe gingival defect, with excellent results after 6 weeks.
Over a 3.5-year period of time the free gingival marginand the MGJ of the treated site and neighboring teethremained unchanged.
ACKNOWLEDGMENTS
This study was supported by the Gerald A. NiznickChair of Implant Dentistry, Tel Aviv University. Theauthors report no conflicts of interest related to thiscase report.
REFERENCES1. KatsikerisN,Kakarantza-AngelopoulouE,Angelopoulos
AP. Peripheral giant cell granuloma. Clinicopatho-logic study of 224 new cases and review of 956 re-ported cases. Int J Oral Maxillofac Surg 1988;17:94-99.
2. Priddy RW. Inflammatory hyperplasias of the oralmucosa. J Can Dent Assoc 1992;58:311-315;319-321.
3. Neville BW, Damm DD, Allen CM, Bouquot JE. Softtissue tumors. In: Neville BW, Damm DD, Allen CM,Bouquot JE, eds. Oral & Maxillofacial Pathology, 2nded. Philadelphia: WB Saunders Company; 2002:12:437-495.
4. Kfir Y, Buchner A, Hartsen LS. Reactive lesions of thegingiva. A clinicopathological study of 741 cases. JPeriodontol 1980;51:655-661.
5. Wood NK, Goaz PW. Peripheral oral exophytic lesions.In: Wood NK, Goaz PW, eds. Differential Diagnosis ofOral and Maxillofacial Lesions, 5th ed. St. Louis: Mosby-Year Book; 1997:10:130-161.
6. Sapp JP. Ultrastructure and histogenesis of peripheralgiant cell reparative granuloma of the jaws. Cancer1972;30:1119-1129.
7. Jaffe HL. Giant-cell reparative granuloma, traumaticbone cyst, and fibrous (fibro-osseous) dysplasia of thejawbones. Oral Surg Oral Med Oral Pathol 1953;6:159-175.
8. Eversole LR, Rovin S. Reactive lesions of the gingiva.J Oral Pathol 1972;1:30-38.
9. Bhaskar SN, Cutright DE, Beasley JD 3rd, Perez B.Giant cell reparative granuloma (peripheral): Report of50 cases. J Oral Surg 1971;29:110-115.
10. Buchner A, Calderon S, Ramon Y. Localized hyper-plastic lesions of the gingiva: A clinicopathologicalstudy of 302 lesions. J Periodontol 1977;48:101-104.
11. Carvalho YR, Loyola AM, Gomez RS, Araujo VC.Peripheral giant cell granuloma. An immunohisto-chemical and ultrastructural study. Oral Dis 1995;1:20-25.
12. Giansanti JS, Waldron CA. Peripheral giant cell gran-uloma: Review of 720 cases. J Oral Surg 1969;27:787-791.
13. Mighell AJ, Robinson PA, Hume WJ. Peripheral giantcell granuloma: A clinical study of 77 cases from 62patients, and literature review. Oral Dis 1995;1:12-19.
14. Bernier JL, Cahn LR. Peripheral giant cell reparativegranuloma. J Am Dent Assoc 1954;49:141-148.
15. Sahingur SE, Cohen RE, Aguirre A. Esthetic manage-ment of peripheral giant cell granuloma. J Periodontol2004;75:487-492.
16. Turesky S, Gilmore ND, Glickman I. Reduced plaqueformation by the chloromethyl analogue of victamineC. J Periodontol 1970;41:41-43.
17. Andersen L, Fejerskov P, Philipsen HP. Oral giant cellgranulomas: A clinical and histological study of 129
J Periodontol • July 2010 Lev, Moses, Holtzclaw, Tal
1097

new cases. Acta Pathol Microbiol Scand A 1973;81:606-616.
18. Anneroth G, Sigurdson A. Hyperplastic lesions of thegingiva and alveolar mucosa. A study of 175 cases.Acta Odontol Scand 1983;41:75-86.
19. Zhang W, Chen Y, An Z, Geng N, Bao D. Reactivegingival lesions: A retrospective study of 2,439 cases.Quintessence Int 2007;38:103-110.
20. Motamedi MH, Eshghyar N, Jafari SM, et al. Peripheraland central giant cell granulomas of the jaws: Ademographic study. Oral Surg Oral Med Oral PatholOral Radiol Endod 2007;103:e39-e43.
21. Flaitz CM. Peripheral giant cell granuloma: A poten-tially aggressive lesion in children. Pediatr Dent 2000;22:232-233.
22. Regezi JA, Sciubba JJ. Red-blue lesions. In: RegeziJA, Sciubba JJ, Fletcher J, eds. Oral Pathology:Clinical Pathological Correlations, 4th ed. Philadel-phia: WB Saunders Company; 1999:4:114-117.
23. Chapparo-Avendano AV, Berini-Aytes L, Gay-EscodaC. Peripheral giant cell granuloma. A report of fivecases and review of the literature. Med Oral Patol OralCir Bucal 2005;10:53-57;48-52.
24. Eronat N, Aktug M, Giinbay T, Unal T. Peripheral giantcell granuloma: Three case reports. J Clin Pediatr Dent2000;24:245-248.
25. Oates TW, Robinson M, Gunsolley JC. Surgical ther-apies for the treatment of gingival recession. Asystematic review. Ann Periodontol 2003;8:303-320.
26. Chambrone L, Chambrone D, Pustiglioni FE, ChambroneLA, Lima LA. Can subepithelial connective tissue
grafts be considered the gold standard procedure inthe treatment of Miller Class I and II recession-typedefects? J Dent 2008;36:659-671.
27. Chambrone L, Sukekava F, Araujo MG, Pustiglioni FE,Chambrone LA, Lima LA. Root coverage proceduresfor the treatment of localized recession-type defects.Cochrane Database Syst Rev 2009;15:CD007161.
28. Parbatani R, Tinsley GF, Danford MH. Primary hyper-parathyroidism presenting as a giant-cell epulis. OralSurg Oral Med Oral Pathol Oral Radiol Endod 1998;85:282-284.
29. Burkes EJ Jr., White RP Jr. A peripheral giant-cellgranuloma manifestation of primary hyperparathy-roidism: Report of case. J Am Dent Assoc 1989;118:62-64.
30. Smith BR, Fowler CB. Primary hyperparathyroidismpresenting as a ‘‘peripheral’’ giant cell granuloma. JOral Maxillofac Surg 1988;46:65-69.
31. Okada H, Davies JE, Yamamoto H. Brown tumor of themaxilla in a patient with secondary hyperparathyroid-ism: A case study involving immunohistochemistry andelectron microscopy. J Oral Maxillofac Surg 2000;58:233-238.
Correspondence: Professor Haim Tal, Department of Peri-odontology, School of Dental Medicine, Tel Aviv University,Ramat Aviv 69978, Israel. Fax: 972-3-5230362; e-mail:[email protected].
Submitted December 2, 2009; accepted for publicationFebruary 24, 2010.
Esthetic Treatment of Peripheral Giant Cell Granuloma Volume 81 • Number 7
1098




















