Rapid mechanical squeezing with pulsed optomechanics - arXiv
Upload
khangminh22Category
view
1download
0
TECHNOLOGY REVIEW (MINI-HTA)
PULSED ELECTROMAGNETIC
FIELD THERAPY – AN UPDATE
Malaysian Health Technology Assessment Section (MaHTAS)
Medical Development Division
Ministry of Health Malaysia
017/2020

MaHTAS Technology Review
i
Malaysian Health Technology Assessment Section (MaHTAS)
Medical Development Division
Ministry of Health Malaysia
Level 4, Block E1, Precinct 1
Government Office Complex
62590, Putrajaya
Tel: 603 8883 1229
Available online via the official Ministry of Health Malaysia website: http://www.moh.gov.my
e-ISBN: 978-967-2887-08-9
DISCLAIMER
This technology review (mini-HTA) is prepared to assist health care decision-makers and health
care professionals in making well-informed decisions related to the use of health technology in
health care system, which draws on restricted review from analysis of best pertinent literature
available at the time of development. This technology review has been subjected to an external
review process. While effort has been made to do so, this document may not fully reflect all
scientific research available. Other relevant scientific findings may have been reported since the
completion of this technology review. MaHTAS is not responsible for any errors, injury, loss or
damage arising or relating to the use (or misuse) of any information, statement or content of this
document or any of the source materials.
Please contact [email protected] if further information is required.
SUGGESTED CITATION: Roza S, Syful AMF and Izzuna MMG. Pulsed electromagnetic field therapy – an update. Technology Review. Ministry of Health Malaysia: Malaysian Health Technology Assessment Section (MaHTAS); 2020.38p. Report No.: 017/2020. e-ISBN: 978-967-2887-08-9
DISCLOSURE: The author of this report has no competing interest in this subject and
the preparation of this report is entirely funded by the Ministry of Health Malaysia.

MaHTAS Technology Review
ii
AUTHORS
Dr. Roza Sarimin Public Health Physician Head of Health Technology Assessment Unit Malaysian Health Technology Assessment Section (MaHTAS) Medical Development Division, Ministry of Health Malaysia Mr. Syful Azlie Md. Fuzi Principal Assistant Director Health Technology Assessment Unit Malaysian Health Technology Assessment Section (MaHTAS) Medical Development Division, Ministry of Health Malaysia
REVIEWERS
Dr. Izzuna Mudla Mohamed Ghazali Public Health Physician Deputy Director Malaysian Health Technology Assessment Section (MaHTAS) Medical Development Division, Ministry of Health Malaysia
EXTERNAL REVIEWERS (alphabetical order)
Dato’ Dr. Fazir Mohamad Consultant Orthopaedic Head of Orthopaedic Department Hospital Kuala Lumpur Dato’ Dr. Rohan Malek Consultant Urologist, Hospital Selayang Head of Urology Services, Ministry of Health Dr. Saiful Safuan Mohd Sani Consultant Physician Head of General Internal Medicine Unit Hospital Kuala Lumpur Dr. Sharmini Diana Parampalem Consultant Obstetrics & Gynaecology Head of Obstetrics & Gynaecology Department Hospital Pulau Pinang

MaHTAS Technology Review
iii
EXECUTIVE SUMMARY
Background
Musculoskeletal diseases comprise of several conditions characterized by pain, limitation in mobility and functional ability, with substantial impact on quality of life, mental well-being, and impose considerable cost on individual, health system as well as disability insurance. Worldwide burden of musculoskeletal disorders increased from 2000 to 2015 as quantified using daily adjusted life years (DALYs), with median proportion of years lived with disability (YLDs) due to musculoskeletal disorders was 11.8% in 2000 to 13.5% in 2015. The largest contribution to the YLDs among the musculoskeletal disorders is due to back and neck pain, followed by osteoarthritis. Back pain is the most common presentation of spinal pathologies, affecting patient health and quality of life. It is expected between 60 and 80% of the world population will experience LBP during lifetime, with 65% being recurrent and longstanding episodes. Approximately one in five patients with back pain will require intervention, commonly spinal fusion, with annual estimated cost of nine billion USD. Pharmaceutical options in musculoskeletal disorders are often associated with adverse effects, whereas some interventions were invasive associated with complication such as migration (for implanted device) and infection. Though intervention such as spinal fusion following spinal pathologies can improve quality of life, outcomes may be negatively impacted by complication such as non-union and hardware failure. Hence, there is a demand for intervention free of side effects and less invasive. Pulsed electromagnetic field (PEMF) therapy provided an alternative approach to treating bone and joint diseases since 1970s, especially for elderly or those who are unable to undergo surgery or take medications. Pulsed electromagnetic fields devices are usually applied directly on the targeted body or using full body therapy system. The PEMF was reported as a non-invasive and non-thermal approach to accelerate the repair of delayed and non-union fractures and chronic wounds, and reduced pain and inflammation. There is increasing interest in the application of magnetic and electromagnetic fields for therapeutic purposes. The largest interest is in its potential in the alleviation of pain. The National Institutes of Health estimated that more than 48 million Americans suffer chronic pain that resulted in a $65 billion loss of productivity and over $100 billion spent on pain care. Despite the inconsistencies in effectiveness and safety of this procedure, it is being used as a modality of treatment for a wide range of applications including to heal damaged tissue and bone, to relieve injury related pain, to stimulate organs, to treat depression, diabetes, as well as used for skin lifting and skin rejuvenation, as advertised by one of a wellness center in Sibu, Sarawak. This technology review was conducted following a request from the Private Medical Practice Control Unit, Sarawak State Health Department to provide the current best scientific evidence on effectiveness, safety and cost-effectiveness of PEMF to heal damaged tissue and bone, to relieve pain, to stimulate organs, to treat depression, to treat diabetes, as well as for skin lifting and skin rejuvenation.

MaHTAS Technology Review
iv
Objective/ aim
The objective of this technology review is to assess the effectiveness, safety and cost-effectiveness of PEMF to heal damaged tissue and bone, to relieve pain, to stimulate organs, to treat depression, to treat diabetes, as well as for skin lifting and skin rejuvenation Results and conclusion
The review included sixteen studies which consisted of systematic reviews with or without meta-analysis (seven), RCT (eight) and cost-effectiveness analysis (one). The included articles were published between 2016 and 2020. The studies were conducted in countries such as US, Germany, Italy, Poland, Egypt and the Netherland. This review included a total of 3,529 participants enrolled from all the studies. Sample size for each of the included studies ranged from 27 to 914 participants. The longest follow-up of the included study was up to 12 months. There is wide variation in the study population of this review, in which mostly were osteoarthritis, low back pain, and post-operative spinal surgery patients as well as patients with mild to moderate metabolic disorder, benign prostatic hyperplasia and female patients with primary dysmenorrhea. The intervention, PEMF therapy, varies widely in duration of application (ranged from five days to three weeks) and frequency of application from four times a day to twice a week).
Effectiveness Based on the above review, there was sufficient good level of evidence retrieved on PEMF to be used in the treatment of patients with osteoarthritis, LBP and post-operative (spinal surgery). However, there was limited evidence retrieved on PEMF to be used in the treatment of patients with mild to moderate metabolic disorder, benign prostatic hyperplasia and patients with primary dysmenorrhoea. No evidence retrieved on PEMF use in the treatment of patients with depression, diabetes, as well as in its use for skin lifting and skin rejuvenation. The PEMF appeared beneficial in reducing pain and improving physical function in patients with knee and hand OA, but not in patients with cervical OA, compared with placebo or sham.
• Reduction in pain score was observed after treatment with PEMF in patients affected by knee OA compared to placebo or sham group (SMD -0.54, 95%CI -1.04 to -0.04) and hand OA (SMD -2.85, 95%CI -3.65 to -2.04), at short term (longest follow-up 24 weeks), but not in cervical OA.
• Significant improvement in function was observed following PEMF in patients with knee (SMD -0.34, 95%CI -0.53 to -0.14), and hand OA (SMD -1.49, 95%CI -2.12 to -0.86), compared with the sham group, but not in patients with cervical OA.
• No improvement in WOMAC stiffness score (WMD -0.50, 95%CI –1.09 to 0.09) (five studies, n=301), was observed following PEMF in patients with knee OA, compared to placebo.
Good level of evidence retrieved, demonstrating benefits of PEMF to relieve pain and improve functionality in patients with LBP until 12 weeks of follow-up, compared to sham treatment.
• In patients with LBP, reduction in pain intensity following PEMF was observed, from baseline to the endpoint, with Cohen effect size ranged from 0.21 (95%CI -0.78 to1.18) to 1.01(95%CI 0.33 to 1.64). Improvement in disability using Oswestry

MaHTAS Technology Review
v
Disability Index, has been demonstrated following PEMF, from baseline to week six however the effect size was small [ranged d= 0.10 (95%CI -0.52 to 0.72) to d=0.15 (95%CI -0.49 to 0.78)], compared to sham group. This difference is persisted at week-12 of follow-up.
Limited fair level of evidence retrieved on PEMF in the treatment of patients post spinal surgery, fracture with cast immobilisation, mild to moderate metabolic syndrome, benign prostate hyperplasia and primary dysmenorrhoea.
• For post-operative spinal fusion patients, PEMF increased the odds of a successful fusion by 2.5 times relative to control.
• In patients with fracture (distal radius) on cast immobilisation, PEMF appeared beneficial in reducing pain, improving mobility, touch (exteroceptive) sensation and reducing disability of the upper limb (the arm, shoulder, and hand).
• In patients with mild to moderate metabolic disorder, PEMF may improve blood pressure (BP) at rest and during exercise, and increase plasma circulating Nitric Oxide (NO) level
o Significant increase in NO was observed following PEMF (16.5 ± 5.6 µmol/L to 22.2 ± 12.5 µmol/L, p=0.04), compared to the sham group.
o Significant reduction in SBP (reduce by 11.3 ± 13.4mmHg), DBP (reduce by 6.4 ± 7.9 mmHg) and MAP (reduce by 8.0 ± 9.0 mmHg) in participants with underlying hypertension (at rest) (SBP≥140 mmHg) has been demonstrated following PEMF, compared to sham with hypertension.
o Evaluation of BP at peak exercise showed the PEMF reduced peak SBP by 14.4 ± 20.3 mmHg (p=0.04), compared to increase in SBP in the sham group by 6.0 ± 20.9 mmHg. No difference between groups for peak DBP and peak MAP showed.
• In patients with benign prostatic hyperplasia aged 55 to 65 years, PEMF combined with pelvic floor and aerobic exercises improved Residual Urine, Flow Rate, Prostate Specific Antigen and International Prostate Symptom Score, compared with PEMF alone or placebo
• In patients with primary dysmenorrhea aged between 18 to 24 years, PEMF is beneficial in alleviating pain and decreasing prostaglandin level in blood
Safety The PEMF therapy appeared safe and well tolerated in the study population with mild adverse events reported. The electro-magnetic field devices were approved by the USFDA (Class III) within the category of bone growth simulation/osteogenesis stimulation. Peripheral electromagnetic field was approved by USFDA (Class III) device to aid wound healing. The wearable ActiPatch PEMF Device was FDA 510k cleared as adjunctive treatment of musculoskeletal pain related to plantar fasciitis of the heel and osteoarthritis of the knee, and the wearable RecoveryRx PEMF Device was FDA cleared for adjunctive treatment of postoperative pain. The use of this device is well tolerated. However, it’s use is contraindicated in patients with implanted electrical devices like pacemakers or intrathecal pumps and should be used with caution in certain conditions such as Grave’s disease or active bleeding.

MaHTAS Technology Review
vi
Cost-effectiveness There was limited evidence retrieved on cost-effectiveness of PEMF. Based on cost utility analysis from societal perspective done in Netherland, the PEMF cannot be considered as a cost-effective treatment for acute fractures of the scaphoid bone, when comparing the effects of PEMF to standard health care in terms of QALY’s.
Methods
Studies were identified by searching electronic databases. The following databases were searched through the Ovid interface: MEDLINE(R) In-process and other Non-Indexed Citations and Ovid MEDLINE(R) 1946 to present. EBM Reviews-Cochrane Database of Systematic Reviews (2005 to March 2021), EBM Reviews-Cochrane Central Register of Controlled Trials (March 2021), EBM Reviews – Database of Abstracts of Review of Effects (1st Quarter 2021), EBM Reviews-Health Technology Assessment (1st Quarter 2021), EBM Reviews-NHS Economic Evaluation Database (1st Quarter 2021). Parallel searches were run in PubMed. Appendix 3 showed the detailed search strategies. No limits were applied to the search. The last search was run on 1 March 2021. Additional articles were identified from reviewing the references of retrieved articles. Among the tools used to assess the risk of bias and methodological quality of all the articles retrieved are the Cochrane Risk of Bias (ROB)2 and Critical Appraisal Skills Programme (CASP) checklist. All full text articles were then graded based on guidelines from the US/Canadian Preventive Services Task Force.

MaHTAS Technology Review
vii
TABLE OF CONTENTS
Disclaimer and Disclosure i Authors ii External reviewers ii Executive summary iii Abbreviations viii
1.0 BACKGROUND 1
2.0 OBJECTIVE/AIM 2
3.0 TECHNICAL FEATURES 2
4.0 METHODS 5 4.1 SEARCHING 5
4.2 SELECTION 6 5.0 RESULTS 6
5.1 RISK OF BIAS 8 5.2 EFFICACY/ EFFECTIVENESS 11
5.3 SAFETY 27 5.4 ECONOMIC IMPLICATION/COST-EFFECTIVENESS ANALYSIS 28 5.5 ORGANISATIONAL 30 5.6 SOCIAL 31
6.0 CONCLUSION 31 7.0 REFERENCES 33 8.0 APPENDICES 36
APPENDIX 1 - HIERARCHY OF EVIDENCE FOR EFFECTIVENESS 36 APPENDIX 2 - SEARCH STRATEGY 37 APPENDIX 3 - EVIDENCE TABLE 38

MaHTAS Technology Review
viii
ABBREVIATION
ADR Adverse dug reaction
ALP Alkaline Phosphatase
BPH Benign Prostate Hyperplasia
CC Capacitative coupling
CI Confidence Interval
DALY Daily adjusted life years
DASH Disability of arm, shoulder and hand
DBP Diastolic blood pressure
DC Direct current
EMF Electromagnetic field
HILT High Intensity Laser Therapy
HTO High Tibial Osteotomy
Hz Heartz
IQR Interquartile Range
IPSS International prostate symptom score
LBP Low back pain
LUTS Lower urinary tract symptom
MAP Mean arterial pressure
MOH Ministry of Health
NO Nitric Oxide
ODI Oswestry Disability Index
OR Odds Ratio
OTA Orthopedic Trauma Association
PEMF Pulsed Electromagnetic Field
PV Prostate volume
QALY Quality Adjusted Life Years
QOL Quality of Life
RCT Randomised controlled trial
ROB Risk of bias
RR Relative risk
SBP Systolic blood pressure
SE Standard Error
SMD Standardized Mean Difference
SR Systematic review
TENS Transcranial Electrical Neural Stimulation
TNFα Tumour necrosis factor alpha
VAS Visual Analogue Scale
WMD Weighted Mean Difference
WOMAC Western Ontario and McMaster Universities Osteoarthritis Index

MaHTAS Technology Review
1
1.0 BACKGROUND
Musculoskeletal diseases comprise of several conditions characterized by pain and limitation in mobility, dexterity and functional ability, with associated impact on mental well-being and quality of life.1 Worldwide burden of musculoskeletal disorders as quantified using daily adjusted life years (DALYs) increased from 2000 to 2015, with median proportion of years lived with disability (YLDs) (Interquartile range, IQR 25 to 75) due to musculoskeletal disorders was 11.8% (8.3 to 15.1) in 2000 to 13.5% (9.6 to 16.6) in 2015.The largest contribution to the YLDs among the musculoskeletal disorders is due to back and neck pain, followed by osteoarthritis.2,3 The most common and disabling musculoskeletal diseases are back and neck pain, osteoarthritis, tendinopathy, fibromyalgia and myofascial pain.1 Back pain is the most common presentation of numerous spinal pathologies, significantly affecting patient health and quality of life.4 Chronic low back pain (LBP) increases linearly from the third decade of life until 60 years.5 It is expected between 60 and 80% of the world population will experience LBP during lifetime, with 65% being recurrent and longstanding episodes.6 Approximately one in five patients with back pain will require intervention, commonly spinal fusion, with annual estimated cost of nine billion USD. 4 Osteoarthritis, one of the most common joint diseases worldwide, affects large proportion of the population especially the elderly, leading to pain and disability.7 Pharmaceutical options in musculoskeletal disorders are often associated with adverse side effects, whereas some interventions were invasive options that have been associated with complication such as migration (for implanted device) and infection.8 Though intervention such as spinal fusion following spinal pathologies can significantly improve quality of life, outcomes may be negatively impacted by complication such as non-union and hardware failure.9 Total knee arthroplasty for treating knee OA, may not be suitable for all patients and may not be a permanent solution as patients often need reoperation within 20 years.10 Many patients are turning towards non-pharmacological therapies to avoid side effects of long term use of conventional treatment.11 Hence, there is a demand for less invasive approach and free of side effects. PEMF therapy has provided an alternative approach to treating bone and joint diseases since 1970s, especially for elderly or those who are unable to undergo surgery or take medications.12 Pulsed electromagnetic field therapy (PEMF) is an emerging approach in relieving pain, that uses electric current with the aim of modifying pain signal and works to enhance cellular activity healing and repair.13,14
Pulsed electromagnetic fields devices are usually applied directly on the targeted body or using full body therapy system. Magnetotherapy provides a non-invasive, safe, and easy method to directly treat the site of injury, the source of pain and inflammation, and other types of diseases and pathologies. Pulsed electromagnetic fields are one important modality in magnetotherapy. Magnetic and electromagnetic fields are now recognised by the 21st century medicine as real physical entities that promise the healing of various health problems. There is increasing interest in the application of magnetic and electromagnetic fields for therapeutic purposes.15 Pulsed electromagnetic field therapy (PEMF) has been reported as a non-invasive and non-thermal approach to accelerate the repair of delayed and non-union fractures and chronic wounds, and the reduction of pain and inflammation.16
Magnetic field therapy was applied to promote bone healing, treat osteoarthritis and inflammatory diseases of the musculoskeletal system, alleviate pain, enhance healing of ulcers and reduce spasticity.17 The largest interest in general public is in the potential of

MaHTAS Technology Review
2
electromagnetic field therapy (EMF) to help in the alleviation of pain. The National Institutes of Health estimated that more than 48 million Americans suffer chronic pain that resulted in a $65 billion loss of productivity and over $100 billion spent on pain care.18 Despite the inconsistencies in effectiveness and safety of this procedure, it is being used as a modality of treatment for a wide range of applications including to heal damaged tissue and bone, to relieve injury related pain, to stimulate organs, to treat depression, to treat diabetes, as well as for skin lifting and skin rejuvenation, as advertised by one of a wellness center in Sibu, Sarawak. This technology review was conducted following a request from the Private Medical Practice Control Unit, Sarawak State Health Department to provide the current best scientific evidence on effectiveness, safety and cost-effectiveness of PEMF to heal damaged tissue and bone, to relieve pain, to stimulate organs, to treat depression, to treat diabetes, as well as for skin lifting and skin rejuvenation.
2.0 OBJECTIVE / AIM
The objective of this technology review is to assess the effectiveness, safety and cost-effectiveness of PEMF therapy to heal damaged tissue and bone, to relieve pain, to stimulate organs, to treat depression, to treat diabetes, as well as for skin lifting and skin rejuvenation.
3.0 TECHNICAL FEATURES
This review is focused on the modalities that utilize pulsed electromagnetic fields (PEMF), one type of low-frequency electromagnetic (EMF) signals, also known as low field magnetic stimulation (LFMS) that uses electromagnetic fields to exert its effects. Contemporary magnetotherapy began in Japan immediately after World War II by introducing both magnetic and electromagnetic fields in clinical practice. During the period of 1960 to 1985, nearly all European countries designed and manufactured their own magnetotherapeutic systems which utilized various waveshapes.15
In 2017 the wearable ActiPatch PEMF Device was FDA 510k Cleared (application K152432), for adjunctive treatment of musculoskeletal pain related to: (1) plantar fasciitis of the heel; and (2) osteoarthritis of the knee. In 2019 the wearable RecoveryRx PEMF Device was FDA Cleared (application K190251), for adjunctive treatment of postoperative pain. Recently, in January 2020 the wearable ActiPatch was granted FDA 510k Clearance, (application K192234), for over the counter marketing relating to adjunctive treatment of musculoskeletal pain. 19 (Figure 1)
The original PEMF devices consisted of a Helmholtz coil which generated a magnetic field. (Figure 2). The patient's body was placed inside the magnetic field to deliver treatment. Today, the majority of PEMF wellness devices resembles a typical yoga mat in dimensions but is slightly thicker to house several flat spiral coils to produce an even electromagnetic field. A frequency generator is then used to energize the coils to create a pulsed electromagnetic field. A variety of consumer PEMF devices are sold and marketed as FDA registered wellness devices. The majority are manufactured in Germany, Austria and Switzerland and are imported into North America as electric massagers or full body electric
MaHTAS Technology Review
3
yoga mats. They are either placed on a massage table for clinical use or directly on the floor in the home to practice simple yoga postures.19 (Figure 3) Magnetotherapy includes at least six groups of electromagnetic fields, developed and utilized in different countries of the world during the last 50 years; 18 • Static/permanent magnetic fields: can be created by various permanent magnets as
well as by passing direct current through a coil. • Low-frequency sine wave electromagnetic fields: mostly utilize 60 Hz (in the US and
Canada) and 50 Hz (in Europe and Asia) frequency in distribution lines. • PEMF is usually low-frequency fields with very specific shapes and amplitudes. The
large variety of commercially available PEMF devices makes it difficult to compare their physical and engineering characteristics, presenting a major obstacle when attempting to analyze the putative biological and clinical effects obtained when different devices are used.
• Pulsed Radiofrequency Fields (PRF): utilize the selected frequencies in the radiofrequency range: 13.56, 27.12 and 40.68MHz.
• Transcranial magnetic/electric stimulation: is a method of treatment of selected areas of the brain with short but intensive magnetic pulses.
• Millimeter waves: have a very high-frequency range of 30 to 100 GHz. In the last ten years this modality has been used for treatment of a number of diseases, especially in the countries of the former Soviet Union.
Extremely low frequency (≤300Hz) electromagnetic field are non-ionizing and athermal. 20 A subset of ELF electromagnetic field, PEMF, displays frequency at the lower end of the electromagnetic spectrum, from 6Hz to 500Hz. Another characteristic of PEMF waveform is their rate of change. High rate of change (such as tesla, second) are able to induce significant biological current in tissues, thereby enabling them to have greater biological effects than waveform of lower rates of change, if the biological effect is dependent on the magnitude of the induced current. 20 Time-varied or pulsed magnetic fields have three main components: frequency, intensity, and waveform. 21
• Electromagnetic field frequency is measured in cycles per second (Hertz, abbreviated Hz). Frequency is tied to wavelength. Most PEMF systems use low frequencies and long wavelengths, from 1 Hz up to 10,000 Hz or so, although a few systems will produce frequencies higher than this. Extremely low frequency (ELF) magnetic fields are those with a frequency at or below 3,000 Hz.
• Magnetic field intensity (flux density) is basically a measurement of the strength of a magnetic field. The intensity of a magnetic field is responsible for how much ‘charge’ is induced in the stimulated tissues. For therapeutic purposes, PEMF vary drastically in intensity, and are measured commonly in either gauss (for higher-intensity systems) or microTesla (for lower-intensity systems). There are 100 microTesla in 1 gauss.
• A huge variety of waveforms exist in nature, in the body, and in PEMF devices. The most common are sinus, sawtooth, and square, though there are trapezoidal, rectangular, impulse, triangular, and many other different options in engineering PEMF devices
The waveforms associated with PEMF can be asymmetric, biphasic and quasi-rectangular or quasi-triangular in shape. However, most ELF sources of electromagnetic stimulation

MaHTAS Technology Review
4
produce a sinusoidal form. In 1979, the USFDA approved both quasi-rectangular or quasi-triangular waveform as safe and efficacious form of treatment disorders associated with fractures. The PEMF therapy is based on low frequency signal, with a wide range of frequencies, which will produce membrane disturbances and activation of multiple intracellular pathways. Extremely low frequency magnetic fields in the pico tesla and mili tesla ranges aimed at improving neurotransmission and correcting local immune pathology. 21 Mechanism of action There are two methods in which PEMF stimulation can be non-invasively applied to biological systems; capacitative or inductive coupling. Capacitative coupling (CC) does not involve any contact with the body. In contrast, direct coupling requires the placement of opposing electrodes in direct contact with the skin surface surrounding the tissue of interest. Inductive coupling does not require the electrodes to be in direct contact with the skin. Rather, the time changing magnetic field of the PEMF induces an electric field (Faraday’s law of induction), which in turn produces a current in the body’s connective tissue. PEMF and capacitative coupling are non-invasive technique involving electrodes or a fitted coil placed over the skin. In contrast, direct current (DC) electrical stimulation involves surgical implantation of a cathode at the fusion site and an anode within the soft tissue, providing constant direct stimulation to the site.22
Pulsed Electromagnetic Fields promote the synthesis of skeletal extracellular matrix. The physiologic process of the response of skeletal cells to PEMF is the synthesis of extracellular matrix structural and signalling molecules in the wound. The result of the signalling processes is to instruct skeletal cells to synthesize structural extracellular matrix and signalling molecules and enhance the ability of skeletal tissues to respond to changing physicochemical environments and biomechanical demands, and facilitate healing.19
PEMF can alter gene and protein expression. PEMF therapy involves generating a PEMF with a coil located within an applicator pad that is placed adjacent to the area of the body to be treated. In the case of a PEMF device used in some trials, a carrier frequency (27.12MHz) is also employed. Biological effects using this approach is most likely occur via induction of electrical current within the tissue.23
Figure 1: Pulsed electromagnetic field (PEMF) therapy device (left) and PEMF in patch form (right)

MaHTAS Technology Review
5
Figure 2: Example of PEMF application on different body parts
Figure 3: Full body electric yoga mat containing pulsed electromagnetic field therapy
4.0 METHODS
4.1 SEARCHING
Electronic databases searched through the Ovid interface:
• MEDLINE(R) In-Process and Other Non-Indexed Citations and Ovid MEDLINE (R) 1946 to present
• EBM Reviews – Cochrane Central Registered of Controlled Trials – January 2021
• EBM Reviews – Database of Abstracts of Review of Effects – 1st Quarter 2021
• EBM Reviews – Cochrane Database of Systematic Reviews – 2005 to January 2021
• EBM Reviews – Health Technology Assessment – 1st Quarter 2021
• EBM Reviews - NHS Economic Evaluation Database - 1st Quarter 2021 Other databases:
• PubMed
• Horizon Scanning database (National Instutute of Health research (NIHR) Innovation Observatory, Euroscan International Network)
• Other websites: US FDA, INAHTA, MHRA General databases such as Google and Yahoo were used to search for additional web-based materials and information. Additional articles retrieved from reviewing the bibliographies of retrieved articles or contacting the authors. The search was limited to articles on human, on studies published from 2015 onwards, systematic review and randomized controlled trial in the design. There was no language limitation in the search. Appendix 1 showed the detailed search strategies. The last search was conducted on the 1 March 2021.

MaHTAS Technology Review
6
4.2 SELECTION A reviewer screened the titles and abstracts against the inclusion and exclusion criteria and then evaluated the selected full-text articles for final article selection. The inclusion and exclusion criteria were: Inclusion criteria
Population Patients with osteoarthritis, low back pain, musculoskeletal pain, post-operation, fractures, other patients metabolic syndrome, benign prostatic hyperplasia, primary dysmenorrhoea
Interventions Pulsed electromagnetic field therapy
Comparators conventional therapy, sham, placebo
Outcomes Pain control, pain intensity, analgesic consumption, stiffness, function/disability, fusion success rate, osseous classification, blood pressure, prostate volume, residual urine, adverse events, complications
Study design Systematic reviews (SR), randomised control trials (RCTs)
Type of publication
English, full text articles
Exclusion criteria
Study design Case report, survey, anecdotal, animal studies
Type of publication
Non-English
Intervention Other magnetic field including static magnetic fields and high-frequency EMF as well as electroporation and electrical stimulation
Relevant articles were critically appraised using Cochrane Risk of Bias (ROB)2 and Critical Appraisal Skills Programme (CASP) checklist and evidence graded according to the US/Canadian Preventive Services Task Force (See Appendix 2). Data were extracted from included studies using a pre-designed data extraction form (evidence table as shown in Appendix 6) and presented qualitatively in narrative summaries. No meta-analysis was conducted for this review.
5.0 RESULTS
This review was conducted as per the guidelines outlined by the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) statement. A total of 156 titles were identified through the Ovid interface: MEDLINE(R) In-process and other Non-Indexed Citations and Ovid MEDLINE(R) 1946 to present, EBM Reviews-Cochrane Database of Systematic Reviews (2005 to February 2021), EBM
MaHTAS Technology Review
7
Reviews-Cochrane Central Register of Controlled Trials (March 2021), EBM Reviews-Database of Abstracts of Review of Effects (1st Quarter 2021), EBM Reviews-Health Technology Assessment (1st Quarter 2021), EBM Reviews-NHS Economic Evaluation Database (1st Quarter 2021) and PubMed. Search was limited to English language, studies conducted in human and studies published 2015 onwards. Thirty-eight articles were identified from references of retrieved articles. After removal of 54 duplicates, 140 titles were screened. A total of 140 titles were found to be potentially relevant and abstracts were screened using the inclusion and exclusion criteria. Of these, 118 abstracts were found to be irrelevant. Twenty-two potentially relevant abstracts were retrieved in full text. After applying the inclusion and exclusion criteria and critical appraisal to the 22 full text articles, 16 full text articles were included and six full text articles were excluded. (Figure 4). The review included sixteen studies, consisted of systematic reviews with or without meta-analysis (seven), RCT (eight) and cost-effectiveness analysis (one). Of the 16 included articles in this review, fifteen studies were included in the effectiveness and the safety section, and one study was in the cost-effectiveness section. The included articles were published between 2016 and 2020. The studies were conducted in countries such as US, Germany, Italy, Poland, Egypt and the Netherland. This review included a total of 3,529 participants enrolled from all the studies. Sample size for each of the included studies ranged from 27 to 914 participants. The longest follow-up of the included study was up to 12 months. There is wide variation in the study population of this review, in which mostly were osteoarthritis, low back pain, and post-operative patients as well as patients with metabolic disorder, benign prostatic hyperplasia and female patients with primary dysmenorrhoea. The intervention, PEMF therapy, in the included studies varies in duration of application for each session from five to 30 minutes, total duration of application (from four weeks to eight weeks), frequency of each application (from one to three times a day), intensity and frequency of the device, with most frequent frequency was between 25 to 30Hz. There were no articles retrieved from the scientific databases on PEMF therapy to stimulate organs, to treat depression, to treat diabetes, as well as for skin lifting and skin rejuvenation.

MaHTAS Technology Review
8
Figure 4: Flow chart of study selection in the review according to the PRISMA guidelines 5.1 RISK OF BIAS / QUALITY ASSESSMENT OF INCLUDED STUDIES
Risk of bias of the studies included in this review was evaluated independently by two reviewers, RS and SAMF on specified domain based on CASP checklist, except for RCT where Cochrane Risk of Bias 2 (RoB2) was used. Any disagreements were resolved through discussion until consensus was reached. For RCT, the risk of bias was evaluated in accordance with the method recommended by the Cochrane Handbook for Systematic Review of Interventions. The content of the assessment consisted mainly of the following items; random sequence generation, allocation concealment, blinding of participants and
Number of additional records identified from other sources
(n=38)
Number of records after duplicates removed (n=140)
Number of records identified through electronic databases
searching (n=156)
Number of records
screened (n=140)
Number of records
excluded (n=118)
Number of full-text articles assessed for eligibility
(n=22)
Number of full-text
articles excluded (n=6)
with reasons: - Study was already included in
systematic review and meta-analysis (n=2)
- Irrelevant study design (n=4)
Number of full-text articles included in qualitative synthesis
(n=16)

MaHTAS Technology Review
9
researcher, blinding of outcome assessment, incomplete outcome data, selective reporting and overall risk of bias. Trials having three or more high risk of bias were considered as having poor methodological quality. The plot of the domain-level judgements for each individual result was generated using robvis, a web app designed for visualizing risk-of-bias assessments. 24 The results were illustrated in the figure as below.(Figure 5).
Figure 5a: Assessment of risk of bias of systematic review (CASP)

MaHTAS Technology Review
10
Figure 5b: Assessment of risk of bias of included RCTs (RoB2)
Criteria/domain assessed
Hann
em
ann e
t
al. 2
01
5
A well-define question posed? +
Comprehensive description of competing alternative given? +
Effectiveness established? +
Effects of intervention identified, measured and valued
appropriately? +
All important and relevant resources required and health
outcome costs for each alternative identified, measured in
appropriate units and valued credibly?
+
Costs and consequences adjusted for different times at which
they occurred (discounting)? -
Results of the evaluation? +
Incremental analysis of the consequences and costs of
alternatives performed? +
Sensitivity analysis performed? -
Figure 5c: Assessment of risk of bias of economic evaluation (CASP)
MaHTAS Technology Review
11
5.2 EFFECTIVENESS
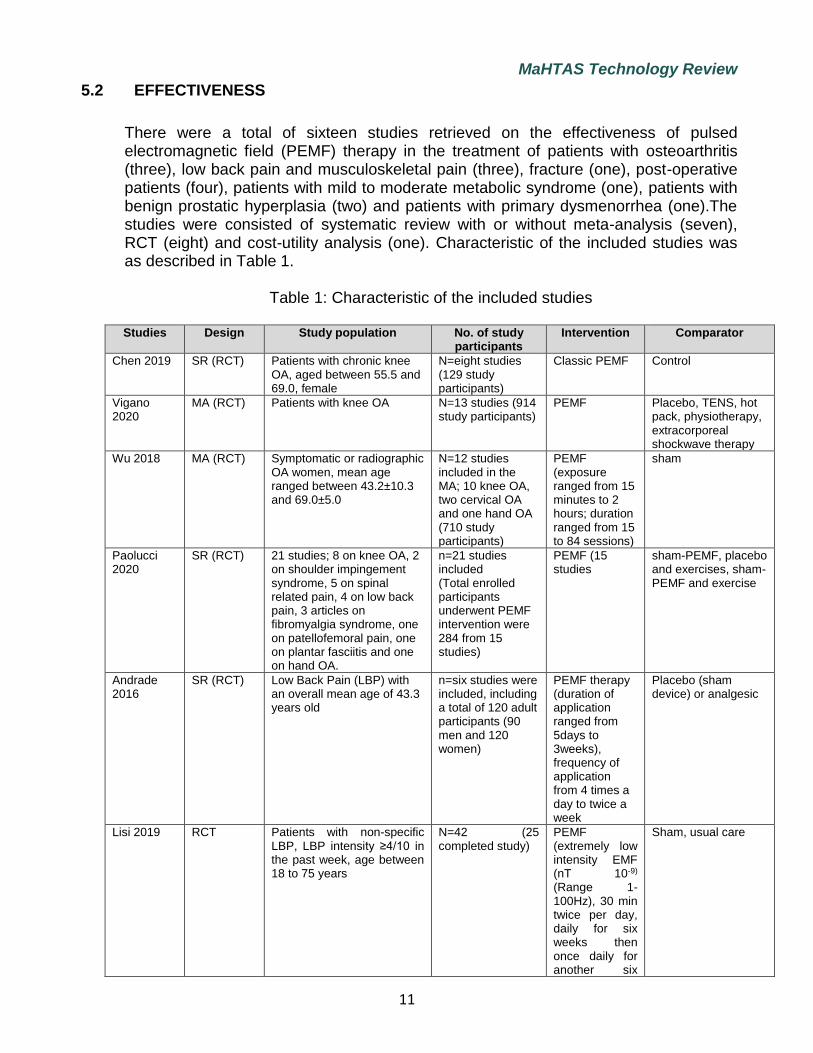
There were a total of sixteen studies retrieved on the effectiveness of pulsed electromagnetic field (PEMF) therapy in the treatment of patients with osteoarthritis (three), low back pain and musculoskeletal pain (three), fracture (one), post-operative patients (four), patients with mild to moderate metabolic syndrome (one), patients with benign prostatic hyperplasia (two) and patients with primary dysmenorrhea (one).The studies were consisted of systematic review with or without meta-analysis (seven), RCT (eight) and cost-utility analysis (one). Characteristic of the included studies was as described in Table 1.
Table 1: Characteristic of the included studies Studies Design Study population No. of study
participants Intervention Comparator
Chen 2019 SR (RCT) Patients with chronic knee OA, aged between 55.5 and 69.0, female
N=eight studies (129 study participants)
Classic PEMF Control
Vigano 2020
MA (RCT) Patients with knee OA N=13 studies (914 study participants)
PEMF Placebo, TENS, hot pack, physiotherapy, extracorporeal shockwave therapy
Wu 2018 MA (RCT) Symptomatic or radiographic OA women, mean age ranged between 43.2±10.3 and 69.0±5.0
N=12 studies included in the MA; 10 knee OA, two cervical OA and one hand OA (710 study participants)
PEMF (exposure ranged from 15 minutes to 2 hours; duration ranged from 15 to 84 sessions)
sham
Paolucci 2020
SR (RCT) 21 studies; 8 on knee OA, 2 on shoulder impingement syndrome, 5 on spinal related pain, 4 on low back pain, 3 articles on fibromyalgia syndrome, one on patellofemoral pain, one on plantar fasciitis and one on hand OA.
n=21 studies included (Total enrolled participants underwent PEMF intervention were 284 from 15 studies)
PEMF (15 studies
sham-PEMF, placebo and exercises, sham-PEMF and exercise
Andrade 2016
SR (RCT) Low Back Pain (LBP) with an overall mean age of 43.3 years old
n=six studies were included, including a total of 120 adult participants (90 men and 120 women)
PEMF therapy (duration of application ranged from 5days to 3weeks), frequency of application from 4 times a day to twice a week
Placebo (sham device) or analgesic
Lisi 2019 RCT Patients with non-specific LBP, LBP intensity ≥4/10 in the past week, age between 18 to 75 years
N=42 (25 completed study)
PEMF (extremely low intensity EMF (nT 10-9)
(Range 1-100Hz), 30 min twice per day, daily for six weeks then once daily for another six
Sham, usual care

MaHTAS Technology Review
12
Studies Design Study population No. of study participants
Intervention Comparator
weeks
Sorrell 2018 RCT Patients with persistent LBP after lumbar surgery
N=41 (36 completed)
PEMF (38µs and 42 µs)
Sham
Akhter 2020 MA (RCT) Patients aged 18 and older undergoing spinal fusion surgery at any level (cervical, lumbar, thoracic) for any degenerative spinal pathology (mean age: 51.2 years (intervention))
n=seven studies included, (n=941 participants)
postoperative electrical stimulation (n=487)
placebo or sham stimulation (n=454)
Ziegler 2019
RCT Patients underwent high tibial osteotomy (mean age 54.1 years: intervention)
N=74 ELF-PEMF Placebo
Zhang 2020 MA (RCT) Patients underwent mammaplasty
N=four studies (164 women)
PEMF Placebo
Krzyzanska 2020
RCT Patients with distal radius fracture during cast immobilization
N= 52 (27 PEMF, 25 control)
PEMF Control
Kim 2020 RCT Patient with mild to moderate metabolic syndrome
N=48 (44 completed study 23 PEMF, 21 sham)
PEMF Sham
Elgohany 2017
RCT Patients with benign prostatic hyperplasia (BPH)
N=60 (A: PEMF & Pelvic floor exercise, B: PEMF, C: placebo)
PEMF, PEMF & PFE
Placebo
Tenuta 2019
RCT Naïve patients with BPH and lower urinary tract symptom
N=27 PEMF (frequency 4-12 Hz, intensity 1000 Gauss)
-
Thabet 2017
RCT Patients with primary dysmenorrhea, aged between 18 to 24 years
N=52 PEMF HILT
Hannemann 2015
CUA (societal perspective)
Patients with acute scaphoid fractures (aged more than 18 years)
N=102 PEMF Standard care, placebo
An earlier Technology Review on Pulsed Radiofrequency Electromagnetic Field for pain and wound therapy has been conducted (2012) by MaHTAS. This review included six studies which were published up to 2014. They found the pulsed radiofrequency electromagnetic field seemed to have the potential as an adjunct therapy to accelerate and improve wound healing and reduce pain. However, the quality of the evidence was not satisfactory due to insufficient sample size and short study period. 25
Another review (Information Brief) then was conducted in 2016 on Pulsed Electromagnetic Mattress (Parmed Ultra 3D Mat). The review found effectiveness of the Pulsed Electromagnetic Mattress (Parmed Ultra 3D mat) for the various health benefits claim could not be determined. With regards to safety, the use of this device is contraindicated in patients with implanted electrical devices like pacemakers or intrathecal pumps and should be used with caution in certain conditions such as Grave’s disease or active bleeding.26

MaHTAS Technology Review
13
5.2.1 a) Patients with osteoarthritis (knee)
• pain control, stiffness, physical function
Chen L, et al. (2019) evaluated effect of PEMF therapy on pain, stiffness and physical function in patients with knee osteoarthritis in a systematic review (SR) and meta-analysis (MA) of RCT. These databases (PubMed, EMBASE, Web of Science and Cochrane Library) were searched up to April 2018. In this SR, RCT comparing PEFT with placebo for patients with knee osteoarthritis were included. Data for primary outcomes including pain, stiffness and physical function were extracted. Patients baseline and primary outcome both presented the severity of joint pain, assessed by Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) questionnaire containing 24 items divided into three subscales; pain (5 items), stiffness (2 items) and physical function (17 items) or a-10cm Visual Analogue Scale (VAS) score for pain. Data from eight RCT involving 421 patients were pooled. Overall quality assessment indicated all included studies had a low or moderate risk of bias according to the Cochrane Handbook for SR of Intervention Method. Sensitivity analysis was performed to estimate the effect of single study on overall pooled effects and heterogeneity. Publication bias was not performed due to limited number of studies included. All statistical analysis was performed using RevMan version 5.3. The study population were patients with chronic knee OA, based on radiological or clinical criteria of the American College of Rheumatology, with mean age ranged was between 55.5 and 69.0, female, body mass index (BMI) ranged between 27.0 and 33.5. A total of eight studies were included in the MA, with length of follow-up ranged from nine to 12 months. They found PEFT had an effect in improving physical function (WMD=-5.28, 95%CI-9.45 to -1.11), but have no advantage in reducing WOMAC total score (four studies, n=218)(WMD=-7.80, 95%CI -16.08 to 0.47), WOMAC pain score (WMD=-1.06, 95%CI -2.30 to 0.17) (five studies, n=301);VAS pain score (WMD=-0.88, 95%CI -2.06 to 0.31) (five studies, n=233), or WOMAC stiffness score (WMD=-0.50, 95%CI –1.09 to 0.09) (five studies, n=301), compared to placebo. The authors concluded the PEFT is beneficial for improving physical function despite having no advantage in treating pain and stiffness. The PEFT may be useful as adjuvant for non-surgical management of knee OA. Further RCT are needed to confirm these findings and determine the optimal parameters and treatment regimen for PEFT.27 level I
Vigano M, et al. (2020) in another meta-analysis of RCT evaluated pain and functional scores in patients affected by knee OA after treatment with PEMF. The purpose of this systematic review and meta-analysis was to evaluate the effect of electromagnetic field treatment on the symptoms of knee OA. In addition, the influence of the type of control group and other covariates have been investigated to identify the sources of heterogeneity in the results of the available clinical trials. This meta-analysis was prepared in accordance with the Cochrane Collaboration methodology and PRISMA guidelines. Only RCTs on human patients affected by knee OA evaluating pain and activity/disability score using VAS and/or WOMAC were included. Four electronic databases (MEDLINE, EMBASE, Web of Science, Cochrane) were searched up to February 29, 2020. Risk of bias were independently evaluated at study level by two authors according to the Cochrane Handbook guidelines, a ‘high’, ‘unclear’, or ‘low’ risk of bias was associated with each of the categories: generation of the random

MaHTAS Technology Review
14
sequence, allocation concealment, blinding of caregivers, patients and outcome assessors, incomplete outcome data collection, and selective reporting. Main outcomes were self-reported pain and activity scores collected by VAS and/or WOMAC at short term after treatment. Short-terms outcomes (0 to 6 weeks) after the end of the treatment were considered for the meta-analysis. Statistical analysis was performed using R Studio supported by R v3.6.1, using meta, 34 metafor, and dmetar packages. Nine studies out of 13 adopted a placebo control group with inactive device for electromagnetic fields generation, while four compared these treatments with different combination of alternative therapies: physiotherapy, TENS, hyperthermia, and shock waves. The OA severity according to Kellgren-Lawrence (KL) classification was available in only six studies, four studies KL grade two to three, one (KL >2), and one reporting no restrictions (0-4). In this review, 13 RCTs comprising 914 unique patients were included in the analysis. Overall reduction in pain score was observed at short term after treatment (standardized mean difference, SMD=−0.4059, 95%CI -0.69,-0.12, I2 74%)(Figure 5a) while improvement in the activity score (disability) was in favor of PEMFs however was not significant (SMD=−0.4452, 95%CI -0., I2 = 62.4%) (Figure 5b). Type of control (i.e., placebo or alternative therapies) and time of follow-up resulted as the two major elements influencing the outcomes. Subgroup analysis based on the type of control revealed that placebo-controlled trials (n=9) demonstrated a significant reduction of pain indexes after treatment (SMD −0.6285, 95%CI -0.91 to -0.35) with reduction of heterogeneity (I2=58.7%) (Figure 5c). The length of follow-up resulted to be another factor influencing the results. Longer follow-ups significantly reduce the differences observed between control and treatment groups, favoring control (p=0.0083). The restriction of the analysis to placebo-controlled trials demonstrated higher SMD between treatment and control groups, with lower p value for pain, while statistical significance became evident also for the activity score. On the contrary, no differences were observed pooling only studies comparing pulsed electromagnetic or magnetic fields to alternative treatments. In addition, longer follow-up correlated with lower differences between treated and control patients. They concluded PEMF therapy are safe and effectively relieves knee OA symptoms at short term, but it is not superior to other conservative therapies such as physiotherapy. 28 level I
Figure 5a: Forest plots comparing pain score in knee OA patients treated
with PEMF (or PMF) therapy and controls in all studies

MaHTAS Technology Review
15
Figure 5b: Forest plots comparing disability score (WOMAC) in knee OA patients treated
with PEMF (or PMF) therapy and controls in all studies
Figure 5c: Forest plots comparing pain score in knee OA patients treated
with PEMF (or PMF) therapy and controls in placebo-controlled studies only
b) Osteoarthritis (knee, cervical, hand)
• Pain control, function
Wu Z, et al. (2018) in another meta-analysis of RCT evaluated efficacy and safety of the pulsed electromagnetic field in osteoarthritis. PubMed, Embase, Cochrane library and web of science databases were searched through 13 October 2017. In this review, RCT comparing the efficacy of PEMF therapy with sham control in patients with OA were included. Pain, function, adverse effects and characteristic of patients were extracted. Excluded studies were experimental studies, studies for postoperative rehabilitation, subjects treated with short wave or PES or any other physical therapies. Methodological quality was evaluated based on Cochrane Handbook, consisted of seven domains. Trials involving three or more high risk of bias were considered as poor methodological quality. RevMan v5.2 was used to perform the statistical analysis. They included 12 studies in the MA; ten on knee OA, two involving cervical OA and another one involving hand OA. Study population involved patients who had symptomatic or radiographic OA (n=710 participants, women, mean age ranged between 43.2±10.3 and 69.0±5.0), mean BMI ranged between 27.0 ± 4.0 and 33.5±1.9). The intervention was PEMF (exposure ranged from 15 minutes to 2 hours; duration ranged from 15 to 84 sessions), compared to sham, with the longest follow-up was up to 42 days (six weeks). They found, the PEMF group showed more significant

MaHTAS Technology Review
16
pain alleviation than the sham group in knee OA (SMD=-0.54, 95%CI -1.04 to -0.04), and hand OA (SMD=-2.85, 95%CI -3.65 to -2.04), but not in cervical OA. Similarly, comparing with the sham control treatment, significant function improvement was observed in the PEMF group in both knee and hand OA patients (SMD=-0.34, 95%CI -0.53 to -0.14, and SMD=-1.49, 95%CI -2.12 to -0.86, respectively), but not in patients with cervical OA. Sensitivity analysis suggested that the exposure duration ≤30 minutes per session exhibited better effects compared with exposure duration >30minutes per session. The author’s concluded that PEMF could alleviate pain and improve physical function for patients with knee and hand OA, but not for patients with cervical OA. 29 level I
5.2.2 Musculoskeletal pain
• Pain control, function
Paolucci T et al.(2020) in Italy also conducted SR of RCT on electromagnetic field therapy, from a rehabilitative perspective in the management of musculoskeletal pain. The review aimed to describe the use of electromagnetic therapy in the rehabilitation field by investigating its efficacy in acute and chronic pain in the musculoskeletal disorders. Database search was conducted from these sources; PubMed, Cochrane, PEDro, SCOPUS, and Web Of Science (WoS). Randomised controlled trials including cross over design published between January 2009 and December 2018, assessing musculoskeletal pain condition in adult more than 18 years were included. The quality of each study was assessed using PEDro (Physiotherapy Evidence Database) scale, consisting of 11 items. Trials scoring ≥6 were considered high quality, and ≤5 of low quality. Risk of bias was assessed using Cochrane domain-based evaluation framework. Overall, a total of 21 studies were included (eight on knee OA, two on shoulder impingement syndrome, five on spinal related pain, four on low back pain, three articles on fibromyalgia syndrome, one on patellofemoral pain, one on plantar fasciitis and one on hand OA). Of these, 15 studies evaluated PEMF as intervention involving 284 total enrolled participants. The intervention, PEMF (evaluated in 15 studies), varies in type; extremely low-frequency magnetic field (one), pulsed radiofrequency electromagnetic field (two), electromagnetic transduction therapy (one), pulsed electromagnetic energy (one), magnetic resonance treatment (one). The PEMF treatment also varies in frequency, intensity and number/duration of session, compared to sham-PEMF, placebo and exercises or sham-PEMF and exercise, with longest follow-up reached 16 weeks. Results showed PEMF at low intensity and frequency (from 1Hz up to 100Hz) are commonly used with efficacy in resolving musculoskeletal pain. Electromagnetic field therapy relieves pain and improves function in patients with various musculoskeletal pain. Among non-pharmacological treatments, PEMF have beneficial therapeutic effects on knee joint tissue. The authors concluded, the EMF therapy is well tolerated, effective with no negative side effects, which can be integrated with rehabilitation for the treatment of chronic and acute pain in musculoskeletal diseases, but further studies are needed to examine the use of more standardized protocols.30 level I

MaHTAS Technology Review
17
5.2.3 Low back pain
• Pain, function Andrade R et al. (2016) in another SR of RCT evaluated pulsed electromagnetic field therapy to assess the effectiveness of PEMF therapy in reducing pain and clinical symptomatology in patients with low back pathological condition. Database search using PubMed, Scopus, Cochrane library and PEDro database was conducted from January 2005 to August 2015. Methodological quality assessed using PEDro scale and level of evidence was set according to the Oxford Center for Evidence-based Medicine scale. The SR included RCT and prospective studies, and was reported according to the PRISMA statement. Main outcome was quantification of pain intensity over time. A total of six studies were included, including a total of 120 adult participants (90 men and 120 women), with LBP with an overall mean age of 43.3 years old. The intervention, PEMF therapy, varies in duration of application (ranged from five days to three weeks) and frequency of application from four times a day to twice a week, compared to placebo (sham device) or analgesic, with follow-up ranged from three to seven weeks. In terms of pain, all studies reported reduction in pain intensity following intervention in the experimental group, from baseline to the endpoint, with reduction in pain intensity from 2.1 to 6.4 points out of 10 on the VAS or numerical pain rating scale. Cohen effect size ranged from 0.21 (95%CI -0.78,1.18) to 1.01(95%CI 0.33, 1.64). Effect size indicate a tendency to reduction of the pain intensity favoring the PEMF groups. In terms of functionality, several scales and indexes were used to quantify participants’ function, Oswestry Disability Index, Patient Specific Functional Scale, Korean version of Roland-Morris Disability Questionnaire, Modified version of Functional Activity Scale and Quebec Pain and Disability Index. The most commonly reported scale, Oswestry Disability Index, found large mean differences from baseline to endpoints, however the effect size was small [ranged d= 0.10 (95%CI -0.52 to 0.72) to d=0.15 (95%CI -0.49 to 0.78) (two studies)]. One study showed large effect size following PEMF (d=1.54, 95%CI 0.81,2.21) using the modified Oswestry Low Back Pain Disability Questionnaire. When used alone, PEMF seem to have greater effect in reducing pain intensity in LBP patients (effect size ranged from, d=0.94 (95%CI 0.25, 1.59) to d=1.01(95%CI 0.33, 1.64). The authors concluded that PEMF seems able to relieve pain intensity and improve functionality in individuals with LBP. It can be a potential alternative to the conventional pharmacological therapy due to low risk associated with its use. However, they suggested further research to evaluate PEMF effects on the different condition of LBP, with standardized protocol, larger sample and adjustment for LBP confounders. 31 level I
Lisi AJ, et al. (2019) evaluated effectiveness of PEMF therapy device for non-specific LBP in a pilot RCT in Bridgeport, US. The objective was to compare effectiveness of a portable PEMF device with a sham device for participants with mixed-duration non-specific LBP. This is a double blind, randomised, sham-controlled, parallel group study assessing the effect of a PEMF treatment device on pain and disability in patients with non-specific LBP. Inclusion criteria were LBP intensity ≥4/10 in the past week on the numerical rating scale (NRS); diagnosis of non-specific LBP condition, age 18 to 75 years, fluent in written and spoken English; post-menopausal and abstinent or having effective birth control during the study period if the women are sexually active. The

MaHTAS Technology Review
18
study was conducted at University of Bridgeport’s Chiropractic Clinic, USA. Participants were randomised into active device or sham group using computer-generated tables to sequentially assigned devices at the time of enrolment. Participants were instructed to self-treat using the device for 30 minutes, two times per day daily for the first six weeks (initial treatment dose). Then, 30 minutes, once daily two to three days per week for the next six weeks (maintenance dose). Patients in each group continue to receive usual care throughout the study. Primary study end points were functional capacity assessed via the Oswestry Disability index (ODI) and pain intensity via the NRS, assessed at baseline, six and twelve weeks. The intervention group received usual care and PEMF device (MDCure and Aerotel Inc.), a class I listed therapeutic device that delivers an extremely low-intensity electromagnetic field (nT 10-9) at a set of low frequency (range one to 100Hz), and the control group received usual care and sham device. The sham devices were identical to active device, except that they were deactivated, hence no electromagnetic field energy generated when the device was turned on. They enrolled 42 participants, and 25 completed the study, however, no information given on number of participants in intervention and control group. Significant improvement in ODI scores from baseline to week six were reported in the experimental group (p<0.001), compared to the sham group (p=0.135). This difference persisted at week-12 of follow-up. Adverse events were rare and mild. They concluded the device was safe and provides preliminary evidence of effectiveness in improving function in patients with non-specific LBP. 32 level
I
Sorrell RG, et al (2018) in another RCT evaluated PEMF therapy for the treatment of chronic postoperative pain following lumbar surgery, compared to sham treatment, in the US. This study involved 41 participants with persistent LBP and/or radiating leg pain after lumbar surgery randomised (1:1:1) in a double blind, sham controlled, parallel group, multicenter trial (13 sites) in the US. The total study population (ITT) were 41 participants; sham (14), PEMF 38µs (14) and PEMF 42µs(13), of which 36 participants completed 60 days treatment protocol (per protocol). These patients were having persistent low-back and/or radiating leg pain for greater/equal to three months and less or equal to three years after lumbar surgery, on stable analgesic dosing for greater or equal to 30 days, and mean pain intensity of greater than three, less than nine on a 11-point NPRS. Eligible subjects were randomised (1:1:1) to receive one of two doses of PEMF therapy (42µs or 38µs pulse width) or treatment with a sham device. The participants underwent self-treatment twice daily for 60 days using PEMF device (Provant Therapy System, at frequency of 27.12MHz). Two pulse durations evaluated in this study (42 and 38µs pulses) are repeated every 1000µs resulting in output duty cycle of 4.2% and 3.8% and requiring an average power of <5W. Interim visits were conducted on day 15, day 30, and day 61.
The primary end point was change in pain intensity (PI) using the Numerical Pain Rating Scale (NPRS) between average baseline (days -5 to -1) and end of treatment (day 56 to 60) for lumbar and radiating leg pain. Secondary outcome measures included the Oswestry Disability Index, Beck-Depression Inventory II, Patient Global Impression of Change and consumption of analgesics. Subjects were provided with ePRO Diary login for collection of patients reported outcomes. The mean age of participants was 51.2 (12.3), 56.0 (14.3) and 50.6(12.2) for 38µs, 42µs and sham group.

MaHTAS Technology Review
19
They found in terms of pain intensity (PI), the mean-end-of-treatment PI was lower for the 42µs group, than for the other study groups, for both lumbar and radiating leg pain. The LBP scores for the 42µs pulse width group decreased by 40.2% from baseline, measured at day 60 (p=0.028), compared to 18.6% for the 38µs pulse width group (p=0.037), 25.6% for the sham group (p=0.013 per protocol population). Average radiating pain leg scores decreased by 45.0% from baseline, measured at day 60 (42µs, p=0.009), 17.0% (38µs, p=0.293) and 24.5% (sham, p=0.065). The proportion of subjects responding to therapy, time to 30% reduction in pain scores, and Patient Global Impression of Change were improved with the PEMF 42µs device over the sham control, though the results were not significant.
In terms of level of inflammatory marker, mean hsCRP was lower at day 61 compared to baseline (42µS), MD=-0.5 (95%CI-1.8,0.8) in contrast to mean hsCRP for the sham (MD=2.2, 95%CI-1.3,5.7) and 38µs group (MD=0.7,95%CI -0.4,1.8) which were higher in day 61 compared to baseline. In this study, hsCRP was assessed at baseline and day 61 following end treatment. In terms of analgesic use, all groups showed minor decrease in analgesic use. For the 38µs and 42µs pulse groups, the mean decrease in pill counts at day 56 to 60 was -0.34±0.80, and 1.06 ±1.13, and -0.67±1.38 (sham group). The authors concluded that PEMF therapy (42µs pulse width) was associated with trends for reduction in pain, compared to sham treatment in the study population.33 level I
5.2.4 Post-operative patients
a) Spinal fusion surgery (fusion success rate)
Akhter S et al. (2020) evaluated efficacy of electrical stimulation for spinal fusion, in a systematic review and meta-analysis of RCT. This review aimed to determine the efficacy of post-operative electrical stimulation on radiographic fusion rates in adult patients following spinal fusion. Systematic search was done from the date of inception to January 2018 from Cochrane Central register of Controlled Trials (CENTRAL), EMBASE, CINAHL and MEDLINE. Population of interest was individuals aged 18 and older undergoing spinal fusion surgery at any level (cervical, lumbar, thoracic) for any degenerative spinal pathology at a minimum one-year of follow-up. Trials involving tumour and fracture, with minimum follow-up of less than one year was excluded. RCT comparing either direct current (DC) electrical stimulation, capacitive coupling (CC) or PEMF stimulation to sham, placebo controlled or no stimulation as an adjunct to spinal fusion surgery were included. Fusion success rate was defined radiographically in all included trials. Risk of bias was assessed following Cochrane Handbook for SR of Intervention on domains (random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting). Data was pooled using the Mantel-Haenszel method. Subgroup analysis of type of stimulation was pre-specified to explain potential heterogeneity. Sensitivity analysis was conducted to explore impact of incomplete outcome data. The GRADE approach was used to assess the certainty (quality) of evidence. A total of eight studies included involving n=941 participants; 487 received postoperative electrical stimulation and 454 received placebo or sham stimulation. Mean age of participants were 51.2 years (intervention) and 49.9 years (control).

MaHTAS Technology Review
20
Range of (intervention treatment postoperative electrical stimulation (direct current electrical stimulation, capacitive coupling or PEMF stimulation) duration usage was minimum three months to maximum nine months. Mean hours per day was ten hours.
The overall fusion success rate demonstrated electrical stimulation (PEMF, DC or CC) increased the odds of a successful fusion by 2.5 times relative to control (OR 2.53,95%CI 1.86 to 3.43)(I2=0.00%, p=0.83). In terms of fusion rates relative to number of levels used, the odds of a successful single level fusion were three times greater in patients who received electrical stimulation compared to patients receiving no electrical stimulation (OR=3.07, 95%CI 1.75 to 5.40, p<0.001). The odds of successful multi-level fusion were 2.6 times greater in patients who received electrical stimulation compared to patients receiving no electrical stimulation (OR 2.58, 95%CI 1.56 to 4.26). In terms of fusion rates relative to stimulation type; CC has the greatest odds for successful fusion relative to control (OR 3.00,95%CI 1.45 to 4.62) followed by DC (OR 2.88, 95%CI 1.18 to 7.14) and PEMF (OR 2.59, 95%CI 1.76 to 3.80). A test for subgroup interactions by stimulation type, smoking status and number of levels fused was not significant. Sensitivity analysis conducted to explore impact of incomplete outcome data, whereby study by Goodwin et al. and Linovitz et al. were excluded. The odds of successful fusion with PEMF relative to no stimulation increased by 10% (OR 2.89,95%CI 1.50 to 5.56). The GRADE assessment of quality of evidence on outcome of fusion success rate was rated as moderate quality evidence due to indirectness.
The authors concluded that this SR found moderate quality evidence supporting the use of postoperative electrical stimulation as an adjunct to spinal fusion surgery. When compared to sham, placebo-controlled or no stimulation, patients treated with postoperative stimulation have significantly greater rates of successful radiographically defined fusion. 34 level I
b) Tibial osteotomy (osseous classification, bone alkaline phosphatese (ALP))
Ziegler P, et al. (2019) in another double blind RCT evaluated PEMF after high tibial osteotomy procedure in elderly patients in Germany. This study aimed at investigating the effect of a specific extremely low-frequency pulsed electromagnetic field (ELF-PEMF), recently identified to support osteoblast function in vitro, on bone healing after high tibial osteotomy (HTO). Patients at minimum 40 years of age, whom underwent HTO, with an HTO with opening gap of five to ten mm were included. They were randomised to ELF-PEMF or placebo treatment using MS Excel at Sachtleben GmbH, both applied by optically identical external devices seven minutes per day for 30 days following surgery. The ELF-PEMF device used, Somagen® has frequency of 16Hz and intensity of 6-282µT.Osseous consolidation was evaluated by post-surgical X-rays (7 and 14 weeks). Osseous classification, both the distance of osteotomy from medial to lateral (distance A), and the part of osteotomy gap already filled with bone (distance B), was measured. The percentage of osteotomy gap filled with new bone is obtained by dividing distance B by distance A. Serum markers (bone specific alkaline phosphatase, tartrate resistant acidic phosphatase and tumour necrosis factor alpha (TNFα, interleukin 6 (IL6), IL13) were quantified by ELISA. Data were compared by a two-sided t-test (α = 0.05). Device readouts showed excellent therapy compliance. A
MaHTAS Technology Review
21
total of 74 patients included in this study, 37 patients received ELF-PEMF and another 37 treated with placebo. Baseline parameters, including age, sex, body mass index, wedge height and blood cell count, were comparable between both groups. They found X-rays revealed faster osseous consolidation for ELF-PEMF compared to placebo treatment, which was significant in patients ≥50 years (∆mean = 0.68%/week; p=0.003). Findings were supported by post-surgically increased bone-specific alkaline phosphatase serum levels following ELF-PEMF, compared to placebo (∆mean = 2.2 µg/L; p=0.029) treatment. Adverse effects following the device were not reported. They concluded the ELF-PEMF treatment showed a tendency to accelerate osseous consolidation after HTO. This effect was stronger and more significant for patients ≥50 years. This ELF-PEMF treatment might represent a promising adjunct to conventional therapy supporting osseous consolidation in elderly patient.35 level I
c) Mammaplasty (pain control, analgesic consumption)
Zhang Li, et al. (2020) evaluated analgesic effect of pulsed electromagnetic fields for mammaplasty in a meta-analysis of RCT. The review aimed to investigate the analgesic efficacy of PEMF for pain control after mammaplasty. Databases including PubMed, EMBASE, Web of Science, EBSCO, and Cochrane library databases were systematically searched for RCT on the impact of PEMF for pain control after mammaplasty from inception to February 2020. Inclusion criteria were RCT and patients undergoing mammaplasty as study population. Primary outcome was pain score on one and three days, secondary outcome was analgesic consumption. Quality assessment of the included studies was done using Jadad score, assessing elements of randomisation, blinding, dropouts and withdrawals. RevMan version 5.3 was used for the statistical analysis. They included four RCT, total participants of 164 whom underwent surgical procedures such as breast augmentation, breast reconstruction and breast reduction. The included studies were high quality studies, with Jadad score vary from three to four. In terms of pain control, PEMF resulted in remarkably reduce pain score on one day (MD 1.34; 95%CI: -2.23 to -0.45) with significant heterogeneity, I2=96%) and three days (MD -1.86; 95%CI: -3.23 to -0.49), compared to placebo. In terms of analgesic consumption, compared to control intervention after mammaplasty, PEMF result in significantly reduced analgesic consumption (SMD-5.64, 95%CI -7.26,-4.02,with significant heterogeneity, I2=98%). Funnel plot developed was asymmetry indicating significant heterogeneity. The authors concluded that PEMF was associated with substantially reduced pain intensity after mammaplasty.36 level I
5.2.3 Fractured long bones (distal radius)
• Pain, limb function
Krzyzanska L et al. (2020) evaluated beneficial effect of PEMF during cast immobilization in patients with distal radius fracture or Colles’ fracture. This non-randomized trial was conducted in Poznan, Poland with objective to assess whether PEMF therapy during cast immobilization of distal radius fractures has beneficial effects on pain and limb function. The study included 52 patients admitted to the casualty department after a distal radius fracture based on the AO classification, type A and B according to the OTA (Orthopaedic Trauma Association), underwent cast immobilization treatment, no limitation of wrist and hand function before injury and had no contraindication to PEMF. Patients were allocated to a PEMF group (n=27) or a control group (n=25). The PEMF therapy device was produced by ASTAR ABR

MaHTAS Technology Review
22
(Bielsko-Biała, Poland). The patient’s hand, wrist and distal forearm were placed inside a concentric coil applicator 345 mm in diameter and 440mm in height generating a magnetic field intensity of six to ten mT and a frequency of 25 to 30Hz, and each treatment lasted approximately 30 minutes. Altogether, the patients received 22 treatments over six weeks. Outcomes including pain; forearm and arm circumference; range of motion; disabilities of the arm, shoulder, and hand score; and touch sensation were evaluated on the day of the plaster cast dressing, three and six weeks after. Range of joint motion was measured using a goniometric method according to the rules of the International Standard Orthopaedic Measurement. Grip strength was measured using a Jamar dynamometer (Poland), and the results are expressed in kilograms (kg). Touch sensation (two-point discrimination) sense perception was measured using a standardized Dellon’s discriminator (two-point discrimination test). The DASH (disabilities of the arm, shoulder, and hand) questionnaire was used to assess the disability of the upper limb. Both the PEMF and control groups started rehabilitation that consisted of active shoulder, elbow, and finger mobilization exercises three times a day on the day following the injury and cast immobilization. The mean age of participants was 60.8 ± 15.0 years. Majority of participants were female (n=22 in PEMF group and n=23 in control group). They found in comparison to the control group, the PEMF group reported significant changes after three and six weeks of treatment: lower pain levels, greater mobility of upper-limb joints, improvement in exteroceptive (touch) sensation and reduction in disability of the upper limb (disabilities of the arm, shoulder and hand). They suggested early addition of PEMF treatment, during cast immobilization of distal radius fractures, has beneficial effects on the pain, exteroceptive sensation, range of motion, and daily functioning of patients with distal radius fracture with cast immobilization.37 level I
5.2.4 Patients with metabolic syndrome
• Blood pressure and circulating nitric oxide (NO)
Kim C et al. (2020) in a double blind RCT in the US evaluated effect of PEMF on blood pressure (BP) and Nitric Oxide (NO) in 48 participants with mild to moderate metabolic syndrome. Metabolic syndrome was defined as individuals who had two or more of following five criteria: hypertension (systolic blood pressure 130 mmHg), dyslipidemia (i)(triglyceride 150 mg/dl), hyperglycaemia (fasting glucose 100 mg/dl), obesity (body mass index >30 kg/m2) and dyslipidemia (ii) (high density lipoprotein <40 mg/dl (male) and <50 mg/dl (female). Effect of PEMF on free calcium and calmodulin dependent nitric oxide signaling pathway, which is one of the components for controlling vascular tone and BP has been suggested. Finally out of 48 study participants, 44 completed the study of which 23 participants underwent PEMF therapy and 21 participants underwent sham therapy for 12 weeks. At the initial assessment, subjects underwent a series of tests to include resting BP measured in triplicate using sphygmomanometer (767 series, Welch Allyn, Germany), blood for NO level, followed by an incremental exercise test on a cycle ergometer. The BP was measured at rest and near the end of submaximal exercise pre- and 12-week post-therapy. Additionally, plasma NO was measured at similar time points. A portable PEMF device (Bioboosti, Biomobie, Shanghai, China) was utilized with adjustable magnetic field strength range (X-axis: 0.22 ± 0.05mT, Y-axis: 0.20 ± 0.05 mT and Z-axis: 0.06 ± 0.02mT) and working

MaHTAS Technology Review
23
frequency (30 ± 3Hz). For the sham group, the sham PEMF devices were modified to deliver no micromagnetic field when turned on. The participants were instructed to use their device three times per day (16 minutes each session, or 48 minutes per day), on both hands in morning and afternoon, and both feet at night. The mean age was 58.0±11.5 and 58.6±10.2 (PEMF and sham group, respectively). The baseline systolic BP (SBP) and diastolic BP (DBP) was 135.8±8.1 mmHg, 82.3±3.9 mmHg (PEMF) and 130.5±7.7, 79.3±4.1 (sham). They found significant increase in NO after PEMF therapy (16.5±5.6 µmol/L to 22.2±12.5 µmol/L p=0.04), however there was no increase reported in the sham group (20.8±12.9 µmol/L to 17.7±5.8 µmol/L, p=0.37). Following PEMF therapy, for resting BP, although the PEMF group demonstrated a fall in SBP, DBP and MAP when compared to the sham group, these differences were not significant (p=0.16, p=0.20 and p=0.14), respectively. For resting BP, there were no differences in SBP, DBP or mean arterial pressure (MAP) between groups (p>0.05). During exercise, following PEMF, reduction in peak SBP has been demonstrated, from 191.9±11.5 mmHg to 182.9±10.5 mmHg (p=0.04), however it was not significant in the sham group, from 189.1±12.4 mmHg to 189.1±14.3 mmHg (p=0.57). Following PEMF therapy, significant inverse association were demonstrated between baseline SBP and change in SBP (r= -0.71, p<0.01); and between MAP and change in MAP following therapy (r= -0.60, p <0.01), however there was no association found in sham group.38 level I (Figure 6)
Figure 6: Relationship between SPB and MAP, and the changes in SBP and MAP
after 12 weeks therapy in PEMF and sham group. Participants with underlying hypertension (at rest) (SBP≥140 mmHg) in PEMF (n=11) had significant reduction in SBP (reduce by 11.3 ± 13.4mmHg), DBP (reduce by 6.4 ± 7.9 mmHg) and MAP (reduce by 8.0 ± 9.0 mmHg) when compared to sham with hypertension (n=9) (p<0.05). Evaluation of BP at peak exercise demonstrated that the PEMF subgroup showed a significant reduction in peak SBP by 14.4 ± 20.3 mmHg (p=0.04), compared to increase in SBP observed in the sham subgroup by 6.0 ± 20.9 mmHg, but not significant (p=0.41). However, peak DBP and peak MAP remained no difference between subgroups (p=0.67 and p=0.24, respectively). They concluded PEMF may increase plasma NO level and improve BP at rest and during exercise. However, this beneficial effect appears to be more pronounced in
MaHTAS Technology Review
24
subjects with existing hypertension. This result may suggest that PEMF has the potential to be utilized as one of a non-pharmacological technique to control BP. 38 level I
5.2.5 Benign prostatic hyperplasia
• Residual urine, flow rate, prostate volume, International Prostate Symptom Score (IPSS) Elgohary HM, et al. (2017) in another RCT conducted in Egypt, evaluated PEMF with or without exercise therapy in the treatment of benign prostatic hyperplasia (BPH). The study aimed to investigate the effect of PEMF with or without exercise therapy in the treatment of BPH. They involved 60 male patients aged 55 to 65 years with BPH, prostate specific antigen (PSA)<4 ng/ml with no clear abnormalities on urological examination. Patients with symptoms for less than six months, acute or chronic urethritis, urinary stones, bacterial or inflammatory chronic prostatitis or chronic pelvic pain syndrome, bladder cancer, urethral strictures, neurogenic bladder dysfunction, restricted mobility, and antimicrobial or anti-inflammatory medication up to four weeks before study enrollment were excluded. Patients were randomly assigned to Group A (n=20; patients who received PEMF in addition to pelvic floor and aerobic exercises), Group B (n=20; patients who received PEMF), and Group C (n=20; patients who received placebo electromagnetic field) in this double-blind controlled trial.
Each subject underwent these assessments, including post-void residual urine, urine flow rate, prostate specific antigen, white blood cells count, and International Prostate Symptom Score were weighed, before and after a four-week intervention by the same therapist. Urodynamic investigation and measurement of post-void residual urine and urine flow rate for each patient pre- and post-treatment by DANTIC UD 5000/5500 urodynamic examination system. Prostate specific antigen (PSA), white blood cell (WBCs) count, and International Prostate Symptom Score (IPSS) were assessed before and after a four-week intervention. An EMF device (PMT-120 Desktop, ElectroMeds, USA) with a period of 20 to 1,100 nanoseconds and an intensity of 0.12 to 18 microtesla and a decreased damping of at least 0.05 and a repetition rate between the trains in the range of 25 to 30Hz, was applied to the perineum, conducted 30 minutes for each day, five times each for four progressive weeks. After four weeks of treatment, patients were re-assessed using total PSA, complete blood count values, post-void residual urine, estimated urine flow rate, and IPSS. The final sample consisted of 60 patients, 20 in each group and demographically homogenous. The results showed no significant differences in the baseline values of post-void residual urine (F=1.12, p=0.33), urine flow rate (F=1.69, p=0.19), total PSA (F=0.36, p=0.70), WBCs (F=1.19, p=0.31), and IPSS (F=2.64, p=0.08) among the three groups. They found significant differences post-intervention in intragroup comparison, Group A and B in all parameters. (Table 2a). Group C showed non-significant differences in all measured variables except for IPSS. All parameters showed highly significant differences in favor of Group A, in the comparison among groups post-intervention, as revealed by ANOVA: Residual Urine (F=11.91, p=0.0001), Flow Rate (F=24.11, p=0.0001), PSA (F=51.04, p=0.001), WBC (F=7.93, p=0.001), and IPSS (F=31.77, p=0.0001).

MaHTAS Technology Review
25
There was significant difference between Groups A and C; and between Groups B and C. (Table 2b) They concluded the present study demonstrated that electromagnetic field had a significant impact on the treatment of BPH. Accordingly, electromagnetic field can be utilized alone or in combination with other physiotherapy modalities. Moreover, clinicians should have the capacity to perceive the advantages accomplished using extra treatment alternatives. Electromagnetic field is a safe, non-invasive method and can be used for the treatment of benign prostatic hyperplasia.38
level I
Table 2a: Values assessed before and after intervention
Table 2b: Symptom scores and free uroflowmetry for all groups
before and after treatment
Tenuta M, et al. (2019) in another RCT in Rome, Italy evaluated the effects of PEMF on prostate volume (PV) in BPH. This interventional trial involved 27 naive patients with BPH and lower urinary tract symptoms (LUTS). At baseline(V0), all patients had blood tests, transrectal ultrasound, and questionnaires [(IPSS, International Index of Erectile Function-15 (IIEF-15)] and received a perineal PEMF device (Magcell®Microcirc, Physiomed Elektromedizin). PEMF was delivered on perineal area five minutes twice daily for 28 days, then (V1) all baseline evaluations were repeated. Afterward, nine patients continued therapy for three more months (PT group) and 15 discontinued (FU group). A four-month evaluation(V2) was performed in both groups. Median age of patients was 67 years.
The result showed a reduction was observed both at V1 and at V2 in Prostate Volume: [PVV0 44.5 mL (38.0;61.6) vs PVV1 42.1 mL (33.7;61.5, p=0.039) vs PVV2 41.7mL (32.7;62.8, p=0.045)].

MaHTAS Technology Review
26
The IPSS was reduced both at V1 and at V2: IPSSV0 11 (5.7;23.2) vs IPSSV1 10 (6;16, p=0.045) vs IPSSV2 9 (6;14, p= 0.015). The IPSS was significantly reduced at V1: IPSSV0 11 (5.7;23.2) vs IPSSV1 10 (6;16), p= 0.045. The IPSS-QoL also significantly improved at V1: IPSS-QoLV0 3 (1;3.25) vs IPSSV1 1 (1;3), p=0.018. No correlation was found for change in PV, whereas a moderate and strong correlation was found between baseline IPSS and ΔIPSSV1 (rs =0.540, p=0.004) or between baseline IPSS and ΔIPSS V2 (rs =0.800, p<0.001) respectively.
The PV reduction in patients without metabolic syndrome (ΔPVV1nMetS −4.7 mL, 95%CI −7.3 to -2.0) was greater than in affected patients (ΔPVV1MetS 1.7 mL, 95%CI −2.69 to 6.1)(p=0.017, Relative RiskMetS = 6). No changes were found in gonadal hormones, sexual function, PSA level, inflammatory markers compared to baseline assessment. They concluded PEMF reduces PV and improves LUTS in a relative short time (after 28 days of therapy), in BPH patients. Symptoms improved in a short time, with high compliance and no effects on hormonal and sexual function or any side effects. Patients with moderate-severe LUTS and without MetS seem to benefit more from this treatment. 39 level II-I
5.2.7 Primary dysmenorrhoea (pain intensity, serum prostaglandin)
Thabet AAE, et al. (2017) in another RCT evaluated effectiveness of high-intensity laser therapy (HILT) versus pulsed electromagnetic field in the treatment of primary dysmenorrhea in a total of 52 girls aged between 18 to 24 years diagnosed with primary dysmenorrhea in Egypt. They were randomly assigned into two groups of equal numbers using a GraphPad program (San Diego, USA). The treatment was three sessions every cycle for three consecutive cycles where group (A) included those participants treated with HILT 15 min/session and group (B) those who were treated with PEMF 30 min/session.
All patients were evaluated before starting the treatment as well as after the end of treatment by present pain intensity (PPi) scale and the prostaglandin level (serum PGF2α) in blood; and pain relief (PR) scale at the end of treatment for both groups. The PR is similar to PPi scale in which zero equal no relief, one equal slight relief, two equal good relief, three equal excellent relief and four equal complete relief.
The results showed a significant decrease in the severity of pain, statistically significant decrease in prostaglandin level in blood, and a statistically significant pain alleviation in both groups.
The PPi score mean fell considerably following the application of treatment for both groups compared to the baseline values (p<0.0001). Post intervention mean value of pain relief showed that the mean value was 3.2 ± 0.85 for HILT group and 2.65 ± 1.02 for PEMF, (p<0.05).
Following HILT, in group (A), the mean concentration for serum PGF2α was 32.85 ± 3.92 pg/ml prior to treatment, reduced to 13.50 ± 2.80 pg/ml following treatment (mean difference (MD)= 19.35). Following PEMF, in group (B), the mean concentration of PGF2α was 32.77 ± 3.89 pg/ml, reduce to 15.19 ± 2.38 pg/ml.

MaHTAS Technology Review
27
With comparison between both groups there was a statistically significant decrease in the severity of pain, significant decrease in the blood levels of PGF2α, in group (A) than group (B). They concluded both HILT and PEMF were effective in the treatment of primary dysmenorrhoea with HILT being superior to PEMF.40 level I
5.3 SAFETY
There were five studies retrieved on the safety of PEMF in the treatment of osteoarthritis, postoperative pain following lumbar surgery, spinal fusion, musculoskeletal pain and non-specific LBP; consisted of three systematic reviews and two RCTs.
Wu Z, et al. in the meta-analysis of RCT (12 studies) evaluated efficacy and safety of the PEMF therapy compared with sham control, in patients with osteoarthritis. They found three trials reported adverse events, of each treatment group, mainly increase knee pain, hip pain, spine pain, vomiting, warm sensation, increase blood pressure, numbness of feet, paraesthesia of feet, cardiomyopathy, with no AE-related dropouts in each trial. The combined results showed no significant difference in AE between sham and PEMF group (RR=0.83, 95%CI 0.26 to 2.64, p=0.75).29 level I
Sorrell RG, et al. (2018) in the RCT conducted in the US, evaluated PEMF therapy for the treatment of chronic postoperative pain following lumbar surgery, compared to sham treatment, whereby 41 participants were involved. In this study, adverse events were reported in all groups, those underwent 42µs PEMF (46.2%), 38µs PEMF (21.4%) and sham group (35.7%). Musculoskeletal disorders were the most common adverse event reported including back pain, disc protrusion and extremity pain.33 level I
Akhter S, et al. (2020) in another systematic review and meta-analysis of RCT evaluated efficacy of electrical stimulation for spinal fusion. In this review, out of seven included studies, adverse event was only reported in one trial.34 level I
Paolucci et al. (2020) in the SR of RCT conducted on electromagnetic field therapy in the management of musculoskeletal pain found the EMF therapy was well tolerated.17level I
Lisi AJ, et al. (2019) in the RCT conducted to evaluate effectiveness of PEMF therapy device for non-specific LBP in Bridgeport, US involving 42 participants of which 25 completed the study found that adverse events were rare and mild. 32 level I Electro-magnetic field devices were approved by the US Food & Drug Administration (FDA) (Class III) within the category of bone growth simulation/osteogenesis stimulation.42 In 2004, a pulsed electromagnetic field system was approved by the FDA as an adjunct to cervical fusion surgery in patients at high risk for non-fusion.43
Peripheral electromagnetic field was approved by USFDA as class III device to aid wound healing.44
The wearable ActiPatch PEMF Device was FDA 510k Cleared, application # K152432, for adjunctive treatment of musculoskeletal pain related to: (1) plantar fasciitis of the
MaHTAS Technology Review
28
heel; and (2) osteoarthritis of the knee, in 2017. This Clearance was for Over-the-Counter use. In 2019, the wearable RecoveryRx PEMF Device was FDA Cleared, Application K190251, for ‘adjunctive treatment of postoperative pain’.44 Recently, in January 2020 the wearable ActiPatch was granted FDA 510k Clearance, application # K192234, for Over-the-Counter Marketing relating to ‘adjunctive treatment of musculoskeletal pain’.45
The US Food and Drug Administration (FDA) has approved a certain number of electromagnetic field generators for the following three applications: 1) the stimulation of osteogenesis in cases of non-healing fractures; 2) congenital pseudoarthrosis; and 3) spinal fusion. Three of these devices generate low-frequency pulsed electromagnetic fields. Two devices on the list above were approved by Health Canada.48 The only absolute contraindication for use of a PEMF device is placing an active applicator over implanted electrical devices like pacemakers, cochlear implants, intrathecal pumps, as the magnetic field can shut the device off or otherwise interfere with its function. The PEMFs are contraindicated in organ transplant patients, as there is a chance that PEMFs may stimulate or activate a more aggressive rejection process by stimulating the immune system. Safety of PEMFs has not been established in pregnancy, although there is no evidence of harm. PEMFs should be used with caution in Grave’s disease or in the case of active bleeding. Extremely high intensity PEMFs should be used with caution or with professional guidance in people with implanted metals, such as joint replacements, dental implants, mechanical heart valves, metal stents, or metal staples in blood vessel, because extremely high intensity PEMFs may stimulate the nerves in the area of the metal, causing sharp pain.21
5.4 ECONOMIC EVALUATION / COST-EFFECTIVENESS ANALYSIS
Only one study (cost-utility analysis) retrieved on the cost-effectiveness of PEMF for the treatment of patients with scaphoid fracture.
Hannemann PFW et al. (2015) conducted a cost-utility analysis in the Netherlands on PEMF compared to standard health care in the treatment of acute scaphoid fractures. The scaphoid has an essential role in proper functionality of the wrist, mainly affecting the young and working population and prolonged cast immobilization leads to more working days lost with socio-economic consequences. Hence, an economic evaluation was carried out from a societal perspective, alongside a double-blind, randomized, placebo-controlled, multicenter trial involving five centres in the Netherlands. The time horizon was similar to the clinical study from the moment of inclusion until 12 months follow-up. One hundred and two (n=102) patients with a clinically and radiographically proven fracture of the scaphoid were included in the study and randomly allocated to either active bone growth stimulation or standard health care, using a placebo. All fractures were treated conservatively with immobilization in a below elbow cast with the first metacarpal and proximal phalanx immobilized. Electromagnetic stimulation was administered continuously for 24 hours a day using a PEMF bone growth stimulator incorporated into the cast. The PEMF device was removed six weeks after the start of treatment.
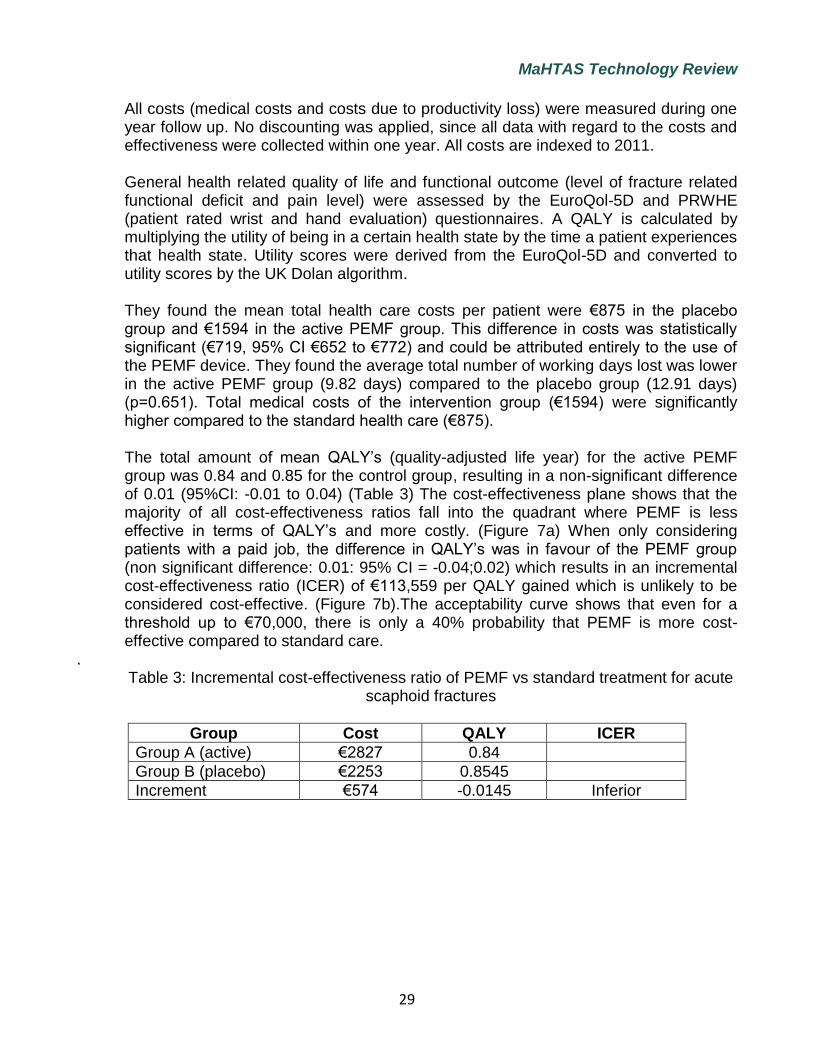
MaHTAS Technology Review
29
All costs (medical costs and costs due to productivity loss) were measured during one year follow up. No discounting was applied, since all data with regard to the costs and effectiveness were collected within one year. All costs are indexed to 2011. General health related quality of life and functional outcome (level of fracture related functional deficit and pain level) were assessed by the EuroQol-5D and PRWHE (patient rated wrist and hand evaluation) questionnaires. A QALY is calculated by multiplying the utility of being in a certain health state by the time a patient experiences that health state. Utility scores were derived from the EuroQol-5D and converted to utility scores by the UK Dolan algorithm. They found the mean total health care costs per patient were €875 in the placebo group and €1594 in the active PEMF group. This difference in costs was statistically significant (€719, 95% CI €652 to €772) and could be attributed entirely to the use of the PEMF device. They found the average total number of working days lost was lower in the active PEMF group (9.82 days) compared to the placebo group (12.91 days) (p=0.651). Total medical costs of the intervention group (€1594) were significantly higher compared to the standard health care (€875). The total amount of mean QALY’s (quality-adjusted life year) for the active PEMF group was 0.84 and 0.85 for the control group, resulting in a non-significant difference of 0.01 (95%CI: -0.01 to 0.04) (Table 3) The cost-effectiveness plane shows that the majority of all cost-effectiveness ratios fall into the quadrant where PEMF is less effective in terms of QALY’s and more costly. (Figure 7a) When only considering patients with a paid job, the difference in QALY’s was in favour of the PEMF group (non significant difference: 0.01: 95% CI = -0.04;0.02) which results in an incremental cost-effectiveness ratio (ICER) of €113,559 per QALY gained which is unlikely to be considered cost-effective. (Figure 7b).The acceptability curve shows that even for a threshold up to €70,000, there is only a 40% probability that PEMF is more cost-effective compared to standard care.
. Table 3: Incremental cost-effectiveness ratio of PEMF vs standard treatment for acute
scaphoid fractures
Group Cost QALY ICER
Group A (active) €2827 0.84
Group B (placebo) €2253 0.8545
Increment €574 -0.0145 Inferior

MaHTAS Technology Review
30
Figure 7a: Cost-effectiveness plane for the incremental cost per QALY
Figure 7b: Cost-effectiveness plane for the incremental cost per QALY (for working patients only)
They concluded from societal perspective, this study showed that the desired effects in terms of cost-effectiveness were not met. When comparing the effects of PEMF to standard health care in terms of QALY’s, PEMF cannot be considered a cost-effective treatment for acute fractures of the scaphoid bone.47
The cost of the electromagnetic field generator devices is estimated at about $5,000 CDN.48
5.5 ORGANISATIONAL
Electrotherapy modalities, which also known as electrophysical agents aimed to reduce pain and improve function via an increase in energy (electrical, sound, light, or thermal) into the body are delivered by various clinicians, including physiotherapists, chiropractors and osteopaths. Examples include pulsed electromagnetic field therapy

MaHTAS Technology Review
31
(PEMF) and other modalities such as therapeutic ultrasound, low-level laser therapy (LLLT), and transcutaneous electrical nerve stimulation (TENS). 49
5.6 SOCIAL Sorrell RG, et al (2018) in the RCT evaluating pulsed electromagnetic field therapy for the treatment of chronic postoperative pain following lumbar surgery, compared to sham treatment, in the US involving 41 participants with persistent LBP found good compliance of the device in the treatment group, with mean total duration of device usage per subject during the study was 57.2±4.4, 49.7±14.5 and 46.7±17 hours, respectively for the 42µs, 38µs and sham group, based on the device usage meter data.33
5.7 LIMITATION Our review has several limitations. The selection of the studies was done by one reviewer, however appraisal was done by two reviewers. Although there was no restriction in language during the search, only English full text articles were included in the report. This review is limited to studies published in 2015 onwards, as this is an update of our previous assessment. Study population of this intervention is diverse and volume of available evidence varies with the study population. Few head-to-head comparisons or trials of PEMF against current practice were made in the included studies. There is lack of longer-term data on the measure of effectiveness. No indirect treatment comparison through network meta-analysis done in the included studies. While majority of the included studies had low risk of bias, one of them had high risk of bias. In the included SR or MA in this review, those included studies which had a high risk of bias may affect its methodological quality. Lack of local data on cost and utility of the interventions and comparator prohibit the generation of local cost-utility analysis.
6.0 CONCLUSION
Effectiveness Based on the above review, there was good level of evidence retrieved on PEMF to be used in the treatment of patients with osteoarthritis and LBP. However, there was limited fair level of evidence retrieved on PEMF to be used in the treatment of patients post spinal surgery, fracture with cast immobilisation, patients with mild to moderate metabolic disorder, benign prostatic hyperplasia and patients with primary dysmenorrhoea. No evidence retrieved on PEMF use in the treatment of patients with depression, diabetes, as well as in its use for skin lifting and skin rejuvenation, hence its effectiveness and safety for these indications could not be determined.
The PEMF appeared beneficial in reducing pain and improving physical function in patients with knee and hand OA, but not in patients with cervical OA, compared with placebo or sham.
MaHTAS Technology Review
32
Good level of evidence retrieved demonstrating benefits of PEMF to relieve pain and improve functionality in patients with LBP until 12 weeks of follow-up, compared to the sham group.
Limited fair level of evidence retrieved on PEMF in the treatment of patients post spinal surgery, fracture with cast immobilisation, mild to moderate metabolic syndrome, benign prostate hyperplasia and primary dysmenorrhea.
• For post-operative spinal fusion patients, PEMF increased the odds of a successful fusion by 2.5 times relative to control.
• In patients with fracture (distal radius) on cast immobilisation, PEMF appeared beneficial in reducing pain, improving mobility, touch (exteroceptive) sensation and reducing disability of the upper limb (the arm, shoulder, and hand).
• In patients with mild to moderate metabolic disorder, PEMF may improve blood pressure at rest and during exercise, and increase plasma circulating Nitric Oxide level, compared with sham group.
• In patients with benign prostatic hyperplasia aged 55 to 65 years, PEMF combined with pelvic floor and aerobic exercises improved Residual Urine, Flow Rate, Prostate Specific Antigen and International Prostate Symptom Score, compared with PEMF alone or placebo.
• In patients with primary dysmenorrhea aged between 18 to 24 years, PEMF is beneficial in alleviating pain and decreasing prostaglandin level in blood.
Safety The PEMF therapy appeared safe and well tolerated in the study population with mild adverse events reported. The devices were approved by the USFDA (Class III) within the category of bone growth simulation/osteogenesis stimulation. Peripheral electromagnetic field was approved by USFDA (Class III) device to aid wound healing. The wearable ActiPatch PEMF Device was FDA 510k cleared as adjunctive treatment of musculoskeletal pain related to plantar fasciitis of the heel and osteoarthritis of the knee, and the wearable RecoveryRx PEMF Device was FDA cleared for adjunctive treatment of postoperative pain. The use of this device is well tolerated. However, it’s use is contraindicated in patients with implanted electrical devices like pacemakers or intrathecal pumps and should be used with caution in certain conditions such as Grave’s disease or active bleeding. Cost-effectiveness There was limited evidence retrieved on cost-effectiveness of PEMF. Based on cost utility analysis from societal perspective done in Netherland, PEMF cannot be considered as a cost-effective treatment for acute fractures of the scaphoid bone, when comparing the effects of PEMF to standard health care in terms of QALY’s.
MaHTAS Technology Review
33
7.0 REFERENCE
1. Hawker GA, Mian S, Kendzerska T, et al. Measures of adult pain: visual analog scale for pain (VAS pain), numeric rating scale for pain (NRS pain), McGill pain questionnaire (MOQ), short-term McGill pain questionnaire (SF-MPQ), chronic pain grade scale (CPGS), short form 36 bodily pain scale (SF36-BPS) and measure of intermittent and constant osteoarthritis pain (ICOAP),Arthritis Care Res (Hoboken) 2011;63(suppl 11):S240-252.
2. Disease GBD, Injury I, Prevalence C. Global, regional and national incidence, prevalence and years lived with disability for 354 disease and injuries for 195 countries and territories.1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018;392(10159):1789-858.
3. Sebbag E, Felten R, Sagez F, et al. The worldwide burden of musculoskeletal diseases: a systematic analysis of musculoskeletal diseases: a systematic analysis of the World Health Organisation Burden of Diseases Dtabase. Ann Rheum Dis 2019;78(6):844-848.
4. Elfering A and Mannion AF. Chapter 6. Epidemiology and risk factors of spinal disorders.In Boos N, Aebi M (eds).Spinal disorders. Springer, Berlin, Heidelberg 2008;153-173.
5. Meucci RD, Fassa AG, Faria NM.Prevalence of chronic low back pain: systematic review. Rev Saude Publica 2015; 49:S0034-89102015000100408.
6. Airaksinen O, Brox J, Cedraschi C, et al. Chapter 4: European guidelines for the management of chronic non-specific low back pain.Eur Spine J 2006;15:s192-300.
7. Bijlsma JW, Berenbaum F, Lafeber FP. Osteoarthritis: an update with relevance for clinical practice.Lancet 2011;377:2115-26.
8. Chou R, Huffman LH. Guideline for the evaluation and management of low back pain: Evidence review.Glenview IL. American Pain Society 2007.
9. Rajaee SS, Bae HW, Kanim LEA, et al. Spinal fusion in the US Analysis of trends from 1998 to 2008.Spine 2021; 37(1);67-76.
10. Richmond JC. Surgery for osteoarthritis of the knee. Rheum Dis Clin North Am 2013;39:203-211.
11. Lee YC, Shmerling RH. The benefit of nonpharmacologic therapy to treat symptomatic osteoarthritis.Curr Rheumatol Rep 2008; 10:5-10.
12. Kalemaj Z, Dbernard IC, Buti J. Efficacy of surgical and non-surgical intervention on accelerating orthodontic movement: a systematic review. Eur J Oral Implantol 2015;8:9-24.
13. Guo L, Kubat NJ, Isenberg RA. Pulsed radio frequency anergy use in human medical application. Electromegn Biol Med 2011;30(1):21-45.
14. Krammer A, Horton S,Tumity S. Pulsed electromagnetic energy as an adjunct to physiotherapy for the treatment of acute low back pain: a randomized controlled trial. NZ J Physiother 2015;43:16-22.
15. Markov MS. Expanding Use of Pulsed Electromagnetic Field Therapies, Electromagnetic Biology and Medicine, 2007;26:3, 257-274, DOI:10.1080/15368370701580806
16. Pilla AA. Mechanisms and therapeutic application of time-varying and static magnetic field.Biological and medical aspectsof electromagnetic field 2007;3
17. Quittan M, Schuhfried O, Wiesinger GF, et al. Clinical effectiveness of magnetic field therapy - a review of the literature. Acta Med Austriaca 2000;27(3):61-68.
18. Markov, MS. Magnetic and electromagnetic field therapy: basic principles of application for pain relief. In: Rosch, P. J., Markov, M. S., eds. Bioelectromag. Med. New York: Marcel Dekker, 2004: pp. 251-264.
19. Pulsed electromagnetic field therapy. Wikipedia. https://en.wikipedia.org/wiki/Pulsed_electromagnetic_field_therapy
20. Shupak NM. The Radio Science Bulletin 2003;307. 21. Dr Pawluk.com. Medical authority for magnetic field therapy. Available at
https://www.drpawluk.com/education/pemf-information/frequency-intensity-and-waveform/ (accessed online on 25 February 2021)

MaHTAS Technology Review
34
22. Gan JC, Fredericks DC & Glazer PA. Direct Current and Capacitive Coupling Electrical Stimulation Upregulates Osteopromotive Factors for Spinal Fusions. Spine 2005; 15, 57-59.
23. Guo L, Kubat NJ, Isenberg RA. Pulsed radio frequency energy (PRFE) use in human medical applications. Electromagn Biol Med 2011;30(1):21-45
24. McGuinness, LA, Higgins, JPT. Risk-of-bias VISualization (robvis): An R package and Shiny web app for visualizing risk-of-bias assessments. Res Syn Meth. 2020; 1- 7. https://doi.org/10.1002/jrsm.1411
25. Maharita AR, Rugayah B, Izzuna MMG. Pulsed radiofrequency electromagnetic field for pain and wound therapy. Malaysian Health Technology Assessment Section. Ministry of Health. Technology Review 2012.
26. Nur Farhana M, Junainah S. Pulsed Electromagnetic Mattress (Parmed Ultra 3D Mat). Malaysian Health Technology Assessment Section. Ministry of Health. Information Brief 2016.
27. Chen L, Duan X, Xing F, et al. Effects of pulsed electromagnetic field therapy on pain, stiffness and physical function in patients with knee osteoarthritis: a systematic review and meta-analysis of randomized controlled trials. J Rehabil Med 2019; 51:821-827.
28. Vigano M, Orfei CP, Ragni E, et al. Pain and functional scores in patients affected by knee osteoarthritis after treatment with pulsed electromagnetic and magnetic field: a meta analysis. Cartilage 2020;1-12
29. Wu Z, Ding X, Lei G, et al. Efficacy and safety of the pulsed electromagnetic field in osteoarthritis: a meta-analysisBMJ Open 2018;8:e022879.doi:10.1136/bmjopen-2018-022879
30. Paolucci T, Pezzi L, Centra AM, et al. Electromagnetic field therapy: a rehabilitative perspective in the management of musculoskeletal pain-a systematic review. Journal of Pain Research 2020;13:1385-1400.
31. Andrade R, Duarte H, Pereira R, et al. Pulsed electromagnetic field therapy effectiveness in low back pain: a systematic review of randomized controlled trials. Porto Biomed J 2016;1(5):156-163.
32. Lisi AJ, Scheinowitz M, Saporito R, et al. A pulsed electromagnetic field therapy device for non-specific low back pain: a pilot randomized controlled trial. Pain Ther 2019;8:133-140.
33. Sorrell RG, Muhlenfeld J, Moffett J, et al. Evaluation of pulsed electromagnetic field therapy for the treatment of chronic postoperative pain following lumbar surgery: a pilot, double blind, randomized, sham controlled clinical trial. Journal of Pain Research 2018;11:1209-1222.
34. Akhter s, Qureshi AR, Aleem I, et al. Efficacy of electrical stimulation for spinal fusion: a systematic review and meta-analysis of randomized controlled trial. Nature Scientific Reports 2020;10:4568.https://doi.org/10.1038/s41598-020-61266-x
35. Ziegler P, Nussler AK, Wilbrand B, et al. Pulsed electromagnetic field therapy improves osseous classification after high tibial osteotomy in elderly patients- a randomized, placebo-controlled, double blind trial. Journal of Clinical Medicine 2019;8:2008. doi:10.3390/jcm8112008
36. Zhang Li, Ding W, Ji Y.Analgesic effect of pulsed electromagnetiv fields for mammaplasty. A meta-analysis of randomized controlled studies.
37. Krzyzanska L, Straburzynska-Lupa A, Raglewska P, et al. Beneficial effects of pulsed electromagnetic field during cast immobilisation in patients with distal radius fracture. BioMed Research International 2020;6849352.https://doi.org/10.1155/2020/6849352
38. Kim CH, Weatley-Guy CM, Stewart GM, et al. The impact of pulsed electromagnetic field therapy on blood pressure and circulating nitric oxide levels: a double blind, randomized study in subjects with metabolic syndrome. Blood pressure 2020;29(1):47-54.
39. Elgohary HM, Tantawy SA. Pulsed electromagnetic field therapy with or without exercise therapy in the treatment of benign prostatic hyperplasia. J Phys Ther Sci 2017;29:1305-1310.
MaHTAS Technology Review
35
40. Tenuta M, Tarsitano MG, Mazzotta P, et al. Therapeutic use of pulsed electromagnetic field therapy reduces prostate volume and lower urinary tract symptoms in benign prostatic hyperplasia. Andrology 2020;8:1076-1085.
41. Thabet AAE, Elsodany AM, Battecha KH, et al. High intensity laser therapy versus pulsed electromagnetic field in the treatment of primary dysmenorrhea. J Phys Ther Sc 2017;29:1742-1748.
42. Waldorff EI, Zhang N, Ryaby JT. Pulsed electromagnetic field applications: A corporate perspective. Journal of Orthopaedic Translation 2017; 9:60-68.
43. USFDA. Nonthermal Shortwave Therapy Device Indicated for Over the Counter Use for The Treatment of Pain. Available at https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfpmn/pmn.cfm?ID=K152432
44. USFDA. K190251.RecoveryRx® Regulation Number: 21 CFR 890.5290. Shortwave Diathermy Regulatory Class: Class II. https://www.accessdata.fda.gov/cdrh_docs/pdf19/K190251.pdf
45. USFDA.K192234. ActiPatch® Regulation Number: 21 CFR 890.5290. Shortwave Diathermy Regulatory Class: Class II. https://www.accessdata.fda.gov/cdrh_docs/pdf19/K192234.pdf
46. Health Canada. Listing of Medical Devices Licenses. February 2, 2000 update. Available at: http://www.hcsc.gc.ca/hpb-dgps/therapeut/htmlfrn/ md_lic.html.2000
47. Hannemann PFW, Essers BAB, Schots JPM te al. Functional outcome and cost-effectiveness of pulsed electromagnetic fields in the treatment of acute scaphoid fractures: a cost utility analysis. BMC Muscululoskeletal Disorders 2015;16:84.DOI 10.1186/s12891-015-0541-2
48. Health Canada. Electromagnetic Devices. It's Your Health. September 29,1998. Ottawa. 49. Page MJ, Green S, Mrocki MA, et al. Electrotherapy modalities for rotator cuff disease.
Cochrane Database of Systematic Reviews 2016, Issue 6. Art. No.: CD012225. DOI: 10.1002/14651858.CD012225.
MaHTAS Technology Review
36
APPENDIX 1: HIERARCHY OF EVIDENCE FOR EFFECTIVENESS
DESIGNATION OF LEVELS OF EVIDENCE
I Evidence obtained from at least one properly designed randomized controlled trial.
II-I Evidence obtained from well-designed controlled trials without randomization.
II-2 Evidence obtained from well-designed cohort or case-control analytic studies,
preferably from more than one centre or research group.
II-3 Evidence obtained from multiple time series with or without the intervention. Dramatic
results in uncontrolled experiments (such as the results of the introduction of penicillin
treatment in the 1940s) could also be regarded as this type of evidence.
III Opinions or respected authorities, based on clinical experience; descriptive studies
and case reports; or reports of expert committees.
SOURCE: US/CANADIAN PREVENTIVE SERVICES TASK FORCE (Harris 2001)

MaHTAS Technology Review
37
APPENDIX 2: SEARCH STRATEGY
Ovid MEDLINE® In-Process & Other Non-indexed Citations and Ovid MEDLINE® 1946
to present
1 pulsed electromagnetic field therapy.tw. (101)
2 electromagnetic field therapy.tw. (140)
3 osteoarthritis.tw. (67048)
4 low back pain.tw. (28213)
5 metabolic syndrome.tw. (52262)
6 benign prostate hyperplasia.tw. (1728)
7 depression.tw. (346238)
8 facial rejuvenation.tw. (1188)
9 1 or 2 (140)
10 3 and 9 (18)
11 4 and 9 (8)
12 5 and 9 (2)
13 6 and 9 (0)
14 7 and 9 (6)
15 8 and 9 (0)
17 limit 9,10,11,12,14 to (english language and humans)(156)
OTHER DATABASES
EBM Reviews – Cochrane Central
Registered of Controlled Trials
Similar MeSH, keywords, limits used as per
MEDLINE search
EBM Reviews – Database of Abstracts
of Review of Effects
EBM Reviews – Cochrane database of
systematic reviews
EBM Reviews – Health Technology
Assessment
NHS economic evaluation database
PubMed Similar MeSH, keywords, limits used as per
MEDLINE search INAHTA
US FDA

MaHTAS Technology Review
38
APPENDIX 3: EVIDENCE TABLE
Only available upon request.
Copyright © 2022 FDOKUMEN