
Psychotherapy with chronic inflammatory bowel disease patients: A Review
10
Psychotherapy with Chronic Inflammatory Bowel Disease Patients: A Review Jo ¨rn von Wietersheim, PhD and Henrik Kessler, MD Abstract: Two distinct factors have lead in the past to the develop- ment of several psychotherapeutic treatments for patients with inflammatory bowel diseases (IBD). First, clinicians and researchers believe that psychologic and somatic factors in chronic IBD, Crohn’s disease, and ulcerative colitis) are connected. In addition, IBD reduces the health-related quality of life for these patients. The purpose of the psychotherapies is to influence the somatic course of the disease, the psychological state of the patients, or the patients’ health related quality of life. This report evaluates the existing studies with regard to the effectiveness of psychotherapy IBD patients received in addition to medical treatment. We have identified 10 psychotherapy studies and 4 additional studies on self management and patient education on this topic. The studies significantly differ from each other in regard to psychotherapeutic methods, inclusion criteria, and outcome assess- ments. The results so far lead to the conclusion that psychotherapy does not have an impact on the course of the disease but, in some cases, positively influences the patient’s psychologic state (such as depres- sion, anxiety, and health related quality of life or coping with the disease). Thus, psychotherapy cannot, in general, be recommended for all patients with chronic IBD. Patients, however, that display a tendency toward psychologic problems, especially as it pertains to their illness, might profit from it. Key Words: Crohn’s disease, ulcerative colitis, psychotherapy, psychology, quality of life, review (Inflamm Bowel Dis 2006;12:1175–1184) A few years after Crohn’s disease had first been described by Crohn et al, 1 some publications speculated whether psychosomatic factors caused this disease or influenced its course. 2,3 Researchers also suspected that ulcerative colitis was caused by psychologic factors. 3Y5 As a result, researchers tried to identify typical personality traits, specific conflict constellations, or psychiatric abnormalities in patients with inflammatory bowel disease (IBD). These attempts failed. 6 First, the findings regarding personality traits and psychiatric symptoms were inconsistent. In addition, it was found that higher scores of neuroticism, depression, inhibition, and emotional instability, which were sometimes found, are typical for many patients with chronic diseases and not specific for IBD patients. In addition, researchers found that there was a correlation between the actual disease activity and the psychologic data that was being studied. Patients undergoing an acute relapse showed more signs of depression and anxiety while testing mostly normal when in remission. 7 Also, it is possible that the manner in which patients were recruited was biased. Patients with IBD who were recruited from a gastroenterological outpatient center or an internal medicine unit had significantly fewer mental problems than IBD patients from psychosomatic clinics. 8 Physical complaints as well as mental problems can adversely affect a patient’s quality of life. This has been shown by several studies of patients with ulcerative colitis and Crohn’s disease. 9,10 Both diseases are mostly chronic, with recurring relapses. Psychosomatic research hypothesized that there might be some psychosocial factors that help trigger relapses. There are several studies and summaries on this particular subject. 11Y20 It appears that increased stress could help reactivate the disease. Clinical studies have shown that elevated stress levels or life events can increase the relapse probability in patients with ulcerative colitis. 16,18 IBD patients with higher depression scores also were more likely to have a relapse. 19 It is assumed that increased stress and life events influence the endocrine and the immune system, which are mediators of the inflammatory process. Maunder 21 showed which stress-related factors might affect the disease activity in IBD patients (such as substance P, vasoactive intestinal protein, tumor necrosis factor alpha). The suspected connection between psychologic factors and relapses led to the question of whether psychotherapy is helpful for patients with IBD. This review summarizes and evaluates the results of the published psychotherapy studies. Studies were identified by searching the databases Medline, Psychlit, and Psyndex. The search strategy combined the keywords (MESH) ulcerative colitis or Crohn disease with psych* (as in psychotherapy, psychology, etc.). Another search included this combination and the additional keyword CLINICAL REVIEW Inflamm Bowel Dis & Volume 12, Number 12, December 2006 1175 Received for publication January 26, 2006; accepted July 26, 2006. University Hospital for Psychosomatic Medicine and Psychotherapy, University of Ulm, Ulm, Germany. Reprints: Jo ¨rn von Wietersheim, PhD, University Hospital for Psychosomatic Medicine and Psychotherapy, Am Hochstraess 8, 89081 Ulm, Germany (e-mail: [email protected]) Copyright * 2006 by Lippincott Williams & Wilkins Copyr ight © Lippincott Williams & Wilkins. Unauthor iz ed reproduction of this article is prohibited.
-
Upload
ruhr-uni-bochum -
Category
Documents
-
view
4 -
download
0
Transcript of Psychotherapy with chronic inflammatory bowel disease patients: A Review
Psychotherapy with Chronic Inflammatory BowelDisease Patients: A Review
Jorn von Wietersheim, PhD and Henrik Kessler, MD
Abstract: Two distinct factors have lead in the past to the develop-ment of several psychotherapeutic treatments for patients withinflammatory bowel diseases (IBD). First, clinicians and researchersbelieve that psychologic and somatic factors in chronic IBD, Crohn’sdisease, and ulcerative colitis) are connected. In addition, IBD reducesthe health-related quality of life for these patients. The purpose of thepsychotherapies is to influence the somatic course of the disease, thepsychological state of the patients, or the patients’ health related qualityof life. This report evaluates the existing studies with regard to theeffectiveness of psychotherapy IBD patients received in addition tomedical treatment. We have identified 10 psychotherapy studies and 4additional studies on self management and patient education on thistopic. The studies significantly differ from each other in regard topsychotherapeutic methods, inclusion criteria, and outcome assess-ments. The results so far lead to the conclusion that psychotherapy doesnot have an impact on the course of the disease but, in some cases,positively influences the patient’s psychologic state (such as depres-sion, anxiety, and health related quality of life or coping with thedisease). Thus, psychotherapy cannot, in general, be recommended forall patients with chronic IBD. Patients, however, that display atendency toward psychologic problems, especially as it pertains totheir illness, might profit from it.
Key Words: Crohn’s disease, ulcerative colitis, psychotherapy,psychology, quality of life, review
(Inflamm Bowel Dis 2006;12:1175–1184)
A few years after Crohn’s disease had first been describedby Crohn et al,1 some publications speculated whether
psychosomatic factors caused this disease or influenced itscourse.2,3 Researchers also suspected that ulcerative colitiswas caused by psychologic factors.3Y5 As a result, researcherstried to identify typical personality traits, specific conflictconstellations, or psychiatric abnormalities in patients withinflammatory bowel disease (IBD). These attempts failed.6
First, the findings regarding personality traits and psychiatricsymptoms were inconsistent. In addition, it was found thathigher scores of neuroticism, depression, inhibition, andemotional instability, which were sometimes found, aretypical for many patients with chronic diseases and notspecific for IBD patients. In addition, researchers found thatthere was a correlation between the actual disease activityand the psychologic data that was being studied. Patientsundergoing an acute relapse showed more signs of depressionand anxiety while testing mostly normal when in remission.7
Also, it is possible that the manner in which patients wererecruited was biased. Patients with IBD who were recruitedfrom a gastroenterological outpatient center or an internalmedicine unit had significantly fewer mental problems thanIBD patients from psychosomatic clinics.8
Physical complaints as well as mental problems canadversely affect a patient’s quality of life. This has been shownby several studies of patients with ulcerative colitis andCrohn’s disease.9,10 Both diseases are mostly chronic, withrecurring relapses. Psychosomatic research hypothesized thatthere might be some psychosocial factors that help triggerrelapses. There are several studies and summaries on thisparticular subject.11Y20 It appears that increased stress couldhelp reactivate the disease. Clinical studies have shown thatelevated stress levels or life events can increase the relapseprobability in patients with ulcerative colitis.16,18 IBDpatients with higher depression scores also were more likelyto have a relapse.19 It is assumed that increased stress and lifeevents influence the endocrine and the immune system,which are mediators of the inflammatory process. Maunder21
showed which stress-related factors might affect the diseaseactivity in IBD patients (such as substance P, vasoactiveintestinal protein, tumor necrosis factor alpha). The suspectedconnection between psychologic factors and relapses led tothe question of whether psychotherapy is helpful for patientswith IBD. This review summarizes and evaluates the resultsof the published psychotherapy studies.
Studies were identified by searching the databasesMedline, Psychlit, and Psyndex. The search strategy combinedthe keywords (MESH) ulcerative colitis or Crohn disease withpsych* (as in psychotherapy, psychology, etc.). Anothersearch included this combination and the additional keyword
CLINICAL REVIEW
Inflamm Bowel Dis & Volume 12, Number 12, December 2006 1175
Received for publication January 26, 2006; accepted July 26, 2006.University Hospital for Psychosomatic Medicine and Psychotherapy, University
of Ulm, Ulm, Germany.Reprints: Jorn von Wietersheim, PhD, University Hospital for Psychosomatic
Medicine andPsychotherapy,AmHochstraess 8, 89081Ulm,Germany (e-mail:[email protected])
Copyright * 2006 by Lippincott Williams & Wilkins
Copyr ight © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

stress management. The search included material from 1980 tothe end of 2005. In addition, the references list of each studywas screened for additional studies. In addition to studiesrelated to psychotherapeutic techniques, we found somestudies that are more related to patient education. Some ofthese were also included here, but we did not conduct a formalliterature search for that segment.
A meta-analysis did not appear appropriate because thereare only a few studies, and these differ from each other in manyrespects such as inclusion criteria (active disease, remission),sample selection (consecutive or self-selected), treatmentvariables (type of psychotherapy, duration of therapy, grouptherapy, individual therapy, or self help context, inpatient oroutpatient treatment), and outcome variables (disease course,IBD symptoms, health-related quality of life, psychopathology).
STUDIES REGARDING THE EFFECTIVENESSOF PSYCHOTHERAPEUTIC TREATMENTFOR PATIENTS WITH INFLAMMATORY
BOWEL DISEASESThe goal of psychotherapy with IBD patients could be to
improve the course of the disease, to change psychologicfactors such as depression and dysfunctional coping, or toimprove the patient’s quality of life. Our literature researchproduced 10 studies dealing with psychotherapeutic treat-ments of patients with IBD. We also found four additionalstudies that are more related to patient education and selfmanagement. It is important to point out that in all studies,psychotherapy was used as a supplementary treatment. Allpatients simultaneously received conservative therapy. Table 1shows an overview of the psychotherapy studies. These studiescan be divided into two subgroups: those using psychodynamictherapy (including psychoanalysis and supportive-expressivetherapy) and those using behavior therapy, predominantlystress management training. Psychodynamic therapy addressesmore underlying problems and conflicts, and the behaviortherapy addresses more specific problematic cognitions anddysfunctional behavior (e.g., problems in stress management).
Studies Involving PsychodynamicPsychotherapy
The earliest studies regarding the effectiveness ofpsychotherapy for ulcerative colitis were conducted 50 yearsago (1956), as published by O’Connor et al.22 They examinedthe impact psychoanalytic therapy had on somatic data(symptoms, proctoscopy) and the psychologic state of thepatients compared with a control group only receivingmedication. The researchers did not, however, use a random-ized design. There were 57 patients each in the therapy and thecontrol groups. Researchers concluded that the patients in thepsychotherapy group did better. Because of the specificmanner by which the patients had been referred (referral for
psychiatric consultation or directly to a psychoanalytic depart-ment), many of the patients in the therapy group weresuffering from severe psychiatric problems (19 patients withschizophrenia, 34 with personality disorders). As a result, thepatients included in this study did not constitute a representa-tive sample for ulcerative colitis patients. The researchers alsodid not conduct statistical significance testing.
Kunsebeck et al23 investigated the effects of supportivepsychotherapy on patients with Crohn’s disease with regard toits effect on the course of the disease and coping skills. At thebeginning of the study, all patients were experiencing an acuteepisode; in addition to medical treatment, they receivedpsychotherapy during their stay at the hospital. Twenty-ninepatients participated in this study. Patients were assigned to thetwo groups in the order they were admitted to the hospital. Theearlier patients were assigned to the intervention group (n = 15),and patients admitted to the hospital at a later point wereassigned to the control group (n = 14). The interventionconsisted of supportive psychotherapy. The data collected atadmission, discharge, and 4 months and 13 months afterdischarge consisted of disease activity, amount and duration ofhospitalizations and operations, depression, anxiety, and per-sonality traits. The data for both groups was comparable at thepoint of admission. The average disease activity indexes of 235(intervention group) and 214 patients (control group) were quitehigh. The scores for depression and anxiety were above normal.In the therapy group, the scores for depression and anxietydecreased significantly during the 13 months the study wasbeing conducted. The scores of the control group declined alsobut remained at a higher level with regard to depression andanxiety. There were no differences in regard to most of thesomatic data. The patients in the therapy group, however,required significantly less inpatient or outpatient treatments oroperations during the observation period. Half of the patients inthe therapy group continued with outpatient psychotherapyafter their discharge.
In a randomized, controlled, multicenter study, Jantscheket al7,24 investigated the effect of psychodynamic psycho-therapy on patients with Crohn’s disease in regard to the courseof the disease and to psychologic symptoms. The study lasted2 years. Patients were recruited from four German universityclinics. Overall, 108 (of 488 screened) patients fulfilled thestrict and precisely documented inclusion criteria and wererandomized into the control group (standardized medication)and the intervention group (standardized medication andadditional psychotherapy during the first of the 2 years ofthe study) at a 1:2 ratio. The intervention consisted of psycho-dynamic psychotherapy (e.g., approximately 26 therapysessions) and also autogenic training (approximately 17sessions) during the first year of the study. At the beginningof the study, there were no differences between the two groupswith respect to somatic, sociodemographic, and psychologiccriteria. After 2 years, 23% of the control group and 30% of the
von Wietersheim and Kessler Inflamm Bowel Dis & Volume 12, Number 12, December 2006
1176 * 2006 Lippincott Williams & Wilkins
Copyr ight © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

therapy group had not experienced a relapse. Twenty-ninepercent of the control group and 17% of the therapy group hadto undergo surgery. In regard to the somatic course of thedisease, the therapy group did better than the control group butnot significantly (P G 0.125). After 1 year, the scores fordepression, anxiety, quality of life, and psychologic symptomsdid not differ significantly. It is important to mention that mostpsychologic data, particularly for patients in remission, werewithin the normal range.
The study conducted by Maunder and Esplen25 testedthe effect of supportive-expressive group psychotherapy forpatients with IBD. In this uncontrolled study, 30 subjectswith IBD (21 with Crohn’s disease, 9 with ulcerative colitis)underwent 20 weekly sessions of supportive-expressivegroup psychotherapy in a small group setting. The groupdiscussions were related to emotion-evoking issues anddiscussions about disease related topics such as self-image,stigma, and conflict with health care professionals. Psycho-logic variables were measured at the beginning and the end ofthe therapy. Scores regarding quality of life, anxiety, ordepression did not change significantly over the course oftreatment. Only the scores for maladaptive coping decreased.The authors did not provide any information about somaticchanges in the patients.
Studies Involving Behavior TherapyThe study by Milne et al26 examined the impact a stress
management program has on the course of the disease and onthe patient’s psychosocial level of functioning. The studyincluded 80 patients with IBD. The patients were randomizedinto an intervention and a control group. The interventiongroup received stress management training in a group setting(6 sessions, each lasting 3 hours). The training emphasizedplanning techniques (time management, problem solving),communication skills, and relaxation (autogenic training).Medical treatment was determined by the patient’s physicianand was not standardized. Patients from both groups wereinterviewed by Bblinded[ investigators after 4, 8, and12 months (course of disease, medication) and also filled outquestionnaires to provide additional psychologic data. Despitethe randomization of the two groups, they differed signifi-cantly. At the beginning of the study, the patients in theintervention group tested higher with regard to disease activity(Crohn’s Disease Activity Index, 143 vs. 90) and had a higherstress index (34 vs. 23). Over the course of the study, theintervention group improved significantly regarding diseaseactivity and stress index, whereas there was no change in thecontrol group.
Schwarz et al27 studied the effects of outpatient behaviortherapy in patients with Crohn’s disease and ulcerative colitis incomparison with a control group (waitlist control group). Thetwo groups with 11 and 10 patients, respectively, were verysmall. The therapy, consisting of 12 1 hour sessions, included
information about IBD, progressive muscle relaxation, thermalbiofeedback, and cognitive coping strategies. The patients kepta diary, in which they noted symptoms, nutrition, andmedication on a daily basis. They also completed a numberof psychologic questionnaires regarding depression, anxiety,and life stress at the beginning and the end of the study. Theresearchers found that psychotherapy had no significant effecton either the somatic symptoms or the psychologic variables.Most patients in the therapy group, however, believed that thetherapy had had a positive effect and indicated that they werebetter able to cope with the disease now.
Mussell et al28 studied 28 patients (14 with Crohn’sdisease, 14 with ulcerative colitis, no control group) toresearch whether 12 sessions of cognitive behavior therapyin a group setting would reduce illness-related anxiety andconcerns, help the patient cope more effectively, or would helpreduce the stress level. The treatment consisted of psycho-education about IBD provided by a gastroenterologist,information about how cognition and emotions generate stress,training regarding adaptive cognitive coping strategies fordisease-related and routine stress, and progressive musclerelaxation training. This treatment was followed by threeadditional sessions every 3 months. The researchers collecteddata at the beginning and the end of treatment and during thefollow-up sessions. Nine months after the conclusion of thetherapy, the patients had lower depression scores and werebetter able to cope, but the latter was only significant forwomen. Scores for illness-related anxiety had decreased in allpatients. The overall results for psychopathology and activecoping had not changed during this time period.
Larsson et al29 researched the impact of a group trainingprogram that had specifically been tailored toward IBDpatients with high anxiety scores. Forty-nine patients withIBD and high anxiety levels were randomized into the therapygroup. Seventeen patients were on a waiting list and served asthe control group. The training was conducted in a groupsetting and consisted of eight sessions dealing with somaticand psychosocial factors of IBD and stress management. Inaddition to anxiety and depression, the researchers alsoassessed the general and health-related quality of life and thepatient’s opinion about the training. Six months after thetraining, none of the psychologic instruments indicated asignificant change in the scores. The patients, however, weresatisfied with the training, which had provided them with moreinformation about their illness. The authors highlight howimportant it is that the patient is adequately informed about thedisease. However, they cannot claim that the training had asignificant impact on the psychologic state of the patients.They believe that there was no impact because the high levelof anxiety has become an integral part of the patients’personality because they had been sick for a long time(average 20 yr). This severe anxiety cannot perhaps not bechanged by 8 hours of training.
Inflamm Bowel Dis & Volume 12, Number 12, December 2006 Psychotherapy with Chronic Inflammatory Bowel Disease Patients
* 2006 Lippincott Williams & Wilkins 1177
Copyr ight © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

TABLE1.Overview
ofPsych
otherapyStudieswithPatients
withChronic
Inflammatory
BowelDisease
Study
Recruitmentof
StudyParticipan
tsDesignan
dAssessm
ents
Intervention
MeasuredFactors
MainFindings
O’Con
ner
etal,19
64UC
Partlymatched
controlgrou
pPsychoanalytically
oriented
PT
Ratings
ofsymptom
sandproctoscop
ySligh
tlybetter
diseasecourse
inthePTgrou
p,go
odrespon
seof
patientsto
PT
n=57
,therapy
Follow-upob
servations
to8years
Psycholog
icrespon
seto
psycho
therapy
n=57
,control
outpatientsin
psycho
analytic
unit
Kun
sebeck
etal,19
87CD
Con
trolled,
admission
,discharge,4and13
mo
postho
spitalization
Sup
portivePT
Disease
activity,course
ofdisease,
depression
,anxiety,
person
ality
PTim
proved
depression
and
anxiety;
noinfluenceon
somatic
data
butless
use
n=15
,therapy
n=14
,controlinpatient
internal
med.
Jantschek
etal,19
98CD
Multicenter
RCT
before
therapy
Psychod
ynam
icshort
therapy,
autogenic
training
Cou
rseof
disease,
depression
,anxiety,
qualityof
life,
mentalstatus
PTdidno
tinfluencepsycho
logic
orsomatic
factors;somew
hat
less
surgery,
positive
selfevaluation
n=72
,intervention
Follow-upevery3mo
for2yr
n=36,control
outpatientsof
internal
medicineunit
Maund
erand
Esplen,
2001
n=21
,CD
Prospective,no
control
Sup
portive-expressive
grou
ptherapy
IBD
concerns,
symptom
s,qu
alityof
life,depression
,anxiety,
maladaptive
coping
Onlyredu
ctions
inmaladaptive
coping
,no
tin
otherpsycho
logic
data
orin
qualityof
life
n=9,
UCou
tpatients
Pre-post
Milne etal,19
86CD/UC
RCTfollow
-upafter4,
8,and12
mo
Stressmanagem
ent
(problem
solving,
commun
ication,
autogenictraining
)
Disease
activity
stress
index
Stressmanagem
entim
prov
edCDAIandstress
index,
but
controlgrou
pvery
different
n=40
,therapy
n=40,control
outpatientsof
internal
medicineunit
von Wietersheim and Kessler Inflamm Bowel Dis & Volume 12, Number 12, December 2006
1178 * 2006 Lippincott Williams & Wilkins
Copyr ight © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

Schwarz
etal,19
91IBD
RCTpre-po
st,follow
-up
after3mo
12sessions
PMR,
biofeedb
ack,
cogn
itive
coping
strategies
Disease
activity,
depression
,anxiety,
stress
index
Betterdevelopm
entin
waiting
list
grou
p,subjectively
better
coping
withIBD
intherapygrou
p
n=11,Therapy
n=10
,waiting
list
outpatients
Mussel
etal,20
03n=14
,CD
Prospective,no
control
Behaviortherapyin
grou
psetting(training,
coping
techniqu
es,PMR)
Psychop
atho
logy,coping
,disease-relatedconcerns
Reduced
illness-relatedconcerns,
inwom
en.additional
improv
ementof
depression
n=14
,UC
outpatientsin
clinical
remission
3mo,
pre,
post,3/6/9mo
follow
-up
Larsson
etal,20
03CD/UC
Prospective,rand
omized,sm
all
controlgrou
p(w
aiting
list)
before
training
and6months
follow
-up
Patient
training
,stress
managem
ent
Anx
iety,depression
,disease-specificqu
ality
oflife,ov
erallqu
ality
oflife
Traininghadno
impact
onmentalstate,
butpatients
enjoyedtraining
n=49
,intervention
n=17,controlinternal
medicineoutpatients
with
high
degree
ofanxiety
Garcia-Vega
and
Rodriguez,
2004
CD
RCTwith3grou
ps,pre,
post,
follow
-upafter6and12
mo
Stressmanagem
ent
treatm
ent,self-directed
stress
managem
ent
prog
ram
CD
symptom
ssuch
asdiscom
fort,tiredn
ess,
diarrhea
Inbo
thtreatm
entgrou
ps,
redu
ctionof
tiredn
ess,
constipation
,abdo
minal
pain;
nodifference
betweenthe
treatm
entgrou
ps
n=30
,intervention
n=15
,control
Eisenbruch
etal,20
05n=30
,UC
Prospective,rand
omized,
controlled
Bod
y-mind-therapy
(stressmanagem
ent,
exercise,diet,selfcare,
60ho
urs)
Quality
oflife,perceived
stress,diseaseactivity,
endo
crine,
and
labo
ratory
data
Improv
ementin
somequ
alityof
life
scales
andbo
welsymptom
s;no
grou
pdifferencesin
disease
activity,endo
crine,
and
immun
eparameters
n=15
,intervention
Pre,po
stn=15
,control
Firstfour
studiesaremorerelatedto
psychodynamic
therapies,thelatter
tobehavioral
therapies.
CD,Crohn
’sdisease;
UC,ulcerative
colitis;IBD,inflam
matorybo
wel
disease;
CDAI,Crohn
’sDisease
ActivityIndex;
RCT,rand
omized
controlled
trail;PT,psychotherapy;
PMR,progressive
musclerelaxation
.
Inflamm Bowel Dis & Volume 12, Number 12, December 2006 Psychotherapy with Chronic Inflammatory Bowel Disease Patients
* 2006 Lippincott Williams & Wilkins 1179
Copyr ight © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

Garcia-Vega and Fernandez-Rodriguez30 studied theeffectiveness of two stress management programs for patientswith Crohn’s disease. They compared three groups. The firstgroup received 6 individual sessions of manualized stressmanagement. The second group received a self-directed stressmanagement program, in which the patients followed a writtenguidebook on stress management techniques and worked withan audiotape for home practice relaxation (6 sessions). Thethird group was the control group and received conventionalmedical treatment. The groups were randomized and consistedof 15 patients each. None of the patients was experiencing anacute episode. They were asked to use a diary to documentsymptoms such as general discomfort, fatigue, diarrhea,constipation, abdominal pain, and distended abdomen on adaily basis. The study did not include any additionalpsychologic data. After the treatment, the patients who hadreceived stress management training were less fatigued, lessconstipated, and had less abdominal pain and a less distendedabdomen. The patients in the self-directed group had verysimilar results, whereas no significant changes were observedin the control group.
Elsenbruch et al31 researched the effect a BMind-Body-Therapy[ has on patients with ulcerative collitis in remission.The intervention group consisted of 15 patients, whereas 15patients on a waiting list served as the control group. Thetherapy consisted of a 60 hour training program, whichincluded stress management training, some exercise, Mediter-ranean diet, behavioral techniques, and self-care strategies.Quality of life, perceived stress, and disease symptoms wereassessed with standardized questionnaires. In addition, re-searchers also measured disease activity (Clinical ActivityIndex), endocrine laboratory parameters, leukocytes and lympho-cyte subsets in peripheral blood, and the b-adrenergic modu-lation of tumor necrosis factor-a production in vivo. The scoresfrom patients in the intervention group improved in regard tosome of the eight Short Form-36 quality of life scales, but onlythe changes regarding the mental health scale were statisticallysignificant. Researchers also noted significant changes in theinflammatory bowel disease quality of life index. In contrastwith these psychologic changes, however, there were nosignificant group differences regarding somatic data such asdisease activity, endocrine, and immune parameters.
As previously mentioned, our database research yieldednot only studies regarding psychotherapy of patient with IBD,but also some studies focusing on patient education and selfmanagement. Table 2 summarizes the details of those studies.
Kennedy et al32 conducted a multicenter, randomized,controlled study to assess the effectiveness and costs of apatient-orientated self management program for patients withIBD. Seven hundred patients were recruited and assigned toeither a control group or an intervention group. Cliniciansworking with the intervention group received a 2 hour trainingin patient-centered consultations. In collaboration with the
individual patient, they developed a self-management plan forthis patient, which was documented in a guidebook. Thisguidebook also contained information about research on,treatment of, and self management of IBD and indicated areaswhere the patient’s choices might influence treatment deci-sions. During the 1 year follow-up, self managing patients hadsignificantly fewer hospital visits without this leading to anincrease in the number of visits to their regular doctor. Thescores for quality of life, anxiety, and depression did not differbetween the intervention and control group. The authorsconclude that their new self management program is efficientin reducing health care costs for IBD patients.
In a randomized, controlled study, Waters et al33 assessedthe effects of a formal educational program for patients withIBD. Sixty-nine patients received a special IBD educationalprogram and standard care or just standard care alone. The12 hour educational program was divided into sessions lasting3 hours each and was administered over the course of 4 weeks.It included general information about anatomy, pathophysi-ology of IBD, therapy, and discussions about disease manage-ment. During the 8 week follow-up testing, the group that hadundergone the training scored significantly higher regardingknowledge about the disease and patient satisfaction. Thescores regarding quality of life and medication adherence weresimilar in both groups. In both groups, however, increasedhealth care use was associated with poorer medicationadherence and lower perceived health. Scores regarding thequality of life remained the same. There was no informationon somatic outcome variables.
In a prospective study by Bregenzer et al,34 73 patientswith IBD (40 Crohn’s disease, 33 ulcerative colitis) whoattended a training program were compared with 72 controlpatients. The training program, which was conducted in agroup setting, consisted of four 2 hour sessions. The maintopics of these sessions were information about the somaticaspects of IBD, nutrition, social problems, stress management,and training in coping techniques. Data was assessed at thebeginning of the study and after 3, 6, and 10 months. Thedisease activity remained unchanged in both groups. Through-out the study, the patients’ illness-related knowledge increased.Depression and quality of life parameter improved only inpatients with initially high results, but this was true for bothgroups. The patients of the intervention group reported,however, that they were satisfied with the training and thatthey would be able to accept more responsibility forthemselves and their illness.
Shepanski et al35 researched the effect of an IBDsummer camp on the health-related quality of life in childrenand adolescents with IBD. This was sponsored by the Crohn’sand Colitis Foundation of America, with all the families of thecampers being members of the foundation. Throughout theweek, the children participated in group activities such astubing, swimming, kayaking, miniature golf, basketball,
von Wietersheim and Kessler Inflamm Bowel Dis & Volume 12, Number 12, December 2006
1180 * 2006 Lippincott Williams & Wilkins
Copyr ight © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
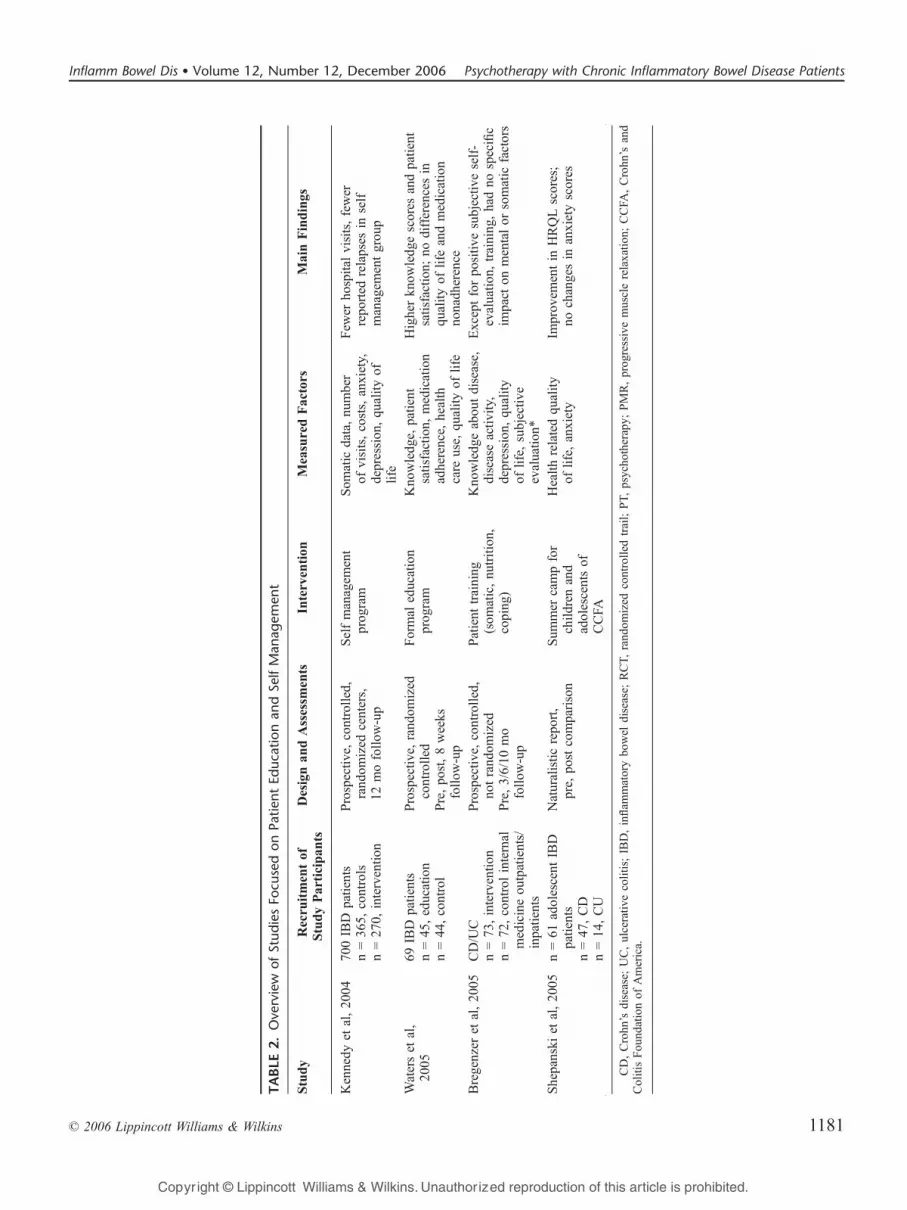
TABLE2.Overview
ofStudiesFo
cusedonPatientEducationandSelfManagement
Study
Recruitmentof
StudyParticipan
tsDesignan
dAssessm
ents
Intervention
MeasuredFactors
MainFindings
Kennedy
etal,20
0470
0IBD
patients
n=36
5,controls
n=27
0,intervention
Prospective,controlled,
rand
omized
centers,
12mofollow
-up
Selfmanagem
ent
prog
ram
Som
atic
data,nu
mber
ofvisits,costs,anxiety,
depression
,qu
alityof
life
Few
erho
spital
visits,fewer
repo
rted
relapses
inself
managem
entgrou
p
Waterset
al,
2005
69IBD
patients
n=45
,education
n=44
,control
Prospective,rand
omized
controlled
Pre,po
st,8weeks
follow
-up
Formal
education
prog
ram
Kno
wledg
e,patient
satisfaction
,medication
adherence,
health
care
use,
qualityof
life
Higherkn
owledg
escores
andpatient
satisfaction
;no
differencesin
qualityof
life
andmedication
nonadh
erence
Bregenzer
etal,20
05CD/UC
n=73
,intervention
n=72
,controlinternal
medicineoutpatients/
inpatients
Prospective,controlled,
notrand
omized
Pre,3/6/10
mo
follow
-up
Patient
training
(som
atic,nu
trition,
coping
)
Kno
wledg
eabou
tdisease,
diseaseactivity,
depression
,qu
ality
oflife,subjective
evaluation
*
Exceptforpo
sitive
subjective
self-
evaluation
,training
,hadno
specific
impact
onmentalor
somatic
factors
Shepanski
etal,20
05n=61
adolescent
IBD
patients
n=47
,CD
n=14
,CU
Naturalisticreport,
pre,
postcomparison
Sum
mer
campfor
children
and
adolescentsof
CCFA
Healthrelatedqu
ality
oflife,anxiety
Improv
ementin
HRQLscores;
nochangesin
anxietyscores
CD,Crohn
’sdisease;
UC,ulcerative
colitis;
IBD,inflam
matorybo
wel
disease;
RCT,rand
omized
controlled
trail;PT,psycho
therapy;
PMR,progressivemusclerelaxation
;CCFA
,Crohn
’sand
ColitisFou
ndationof
America.
Inflamm Bowel Dis & Volume 12, Number 12, December 2006 Psychotherapy with Chronic Inflammatory Bowel Disease Patients
* 2006 Lippincott Williams & Wilkins 1181
Copyr ight © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

adventure course, arts and crafts, dance, and cooking. Medicalsupervision was provided by experienced physicians andnurses. The campers had no formal IBD educational classes,but there were many informal conversations among thecampers and between campers and counselors about theirillness. The study evaluates questionnaires from 61 patients (of125 individuals who had consented to participate). Forty-sevenhad Crohn’s disease, and 14 had ulcerative colitis, ranging inage from 9 to 16 years. There were small, but statisticallysignificant, improvements regarding the total scores for healthrelated quality of life, bowel symptoms scores, socialfunctioning scores, and treatment interventions scores. Thescores for anxiety, however, did not change.
SUMMARY AND CONCLUSIONSThe results of the psychotherapy studies can be summar-
ized as follows: only one study23 showed an (indirect) influenceof psychotherapy on the somatic course of the illness (lessreadmissions to the hospital and fewer operations). However,this study had very small samples and was not randomized.Most other studies failed to show such an influence. Theresults of the largest psychotherapy study24 showed tendenciesin that direction, but this were not statistically significant.Another study30 illustrated the impact of a stress managementprogram on disease related symptoms such as fatigue, diarrhea,constipation, and abdominal pain. Some studies showed thatpsychotherapy influences psychologic factors such as depres-sion, anxiety, coping, and stress index,23,26,28 but this could notbe repeated in others.24,25,27,29,33 In some studies,24,26,27,29,33,34
the patients themselves believed that they had subjectivelyprofited from the study.
The studies used very different psychotherapeutic methods(individual and group therapy, psychodynamic methods,behavior therapy, relaxation therapy, and special stress manage-ment training). Because of the lack of studies, it is not possibleto decide whether one therapy is superior to another. Psycho-dynamic therapies and behavior therapy appear to have hadsimilar results, but it appears that stress management trainingwas used more often than the other methods.
We therefore feel confident in making the followingassumptions:Psychotherapy mainly affects the psyche. There were only
very few and inconsistent somatic effects, such as amore favorable course of the disease. Psychotherapyappears to have a positive impact on the patients’depression and anxiety and helps patients cope withtheir illness. In most of the studies, patients indicatedhaving subjectively profited from the intervention andthat it had become easier for them to cope with theillness. From a methodologic viewpoint, these findingsdeal with the general problems of satisfaction studiesbecause the patients often give positive feed-back given
that this is socially desired. A possible conclusionwould be, however, that psychotherapy does not affectthe course of disease itself but influences the psyche ofthe patients and how they deal with their illness.
Psychotherapy is especially beneficial for those who need it.In studies that showed no effect of psychotherapy onpsychologic variables, patients usually were already inthe subclinical range before the intervention. Thiscould be interpreted as a Bground effect[ (no furtherimprovement possible). Because of this fact, somestudies concentrated on patients with initially clinicallyrelevant values for depression or anxiety.
The need for psychotherapy varies significantly. Miehsleret al36 developed a questionnaire regarding the need forpsychologic care for patients with IBD. The scales onthe questionnaire address the need for various types ofpsychosocial interventions: disease-oriented counseling,Bintegrated psychosomatic care[, which focuses on theinteraction of biological, psychologic, and social sub-systems as they pertain to the current situation thepatient finds him or herself in, and patients requiringintensive (professional) psychotherapy because of emo-tional stress or behavioral problems.
There is no proof that one therapy is superior to another.Different forms of treatment have been used (psycho-dynamic therapy, behavior therapy, relaxation, etc.). Sofar, there has not been a systematic comparisonbetween the various therapies.
Patients with Crohn’s disease or ulcerative colitis could responddifferently to psychotherapy. Post hoc analyses indi-cated different effects of psychotherapy on patientswith Crohn’s disease or ulcerative colitis. Overall,Crohn’s disease patients have more psychologic com-plaints,37 which indicates a different starting positionor a mentally and physically more challenging illness.Future studies should take this into consideration.Overall, the existing results give no general indication
that patients with IBD should undergo psychotherapeutictreatment. We suspect that there are Brisk patients[ in whompsychosocial components have a bigger influence on thecourse of disease than in other patients. That group wouldprobably benefit from psychotherapeutic treatment. Thefollowing risk factors, which can also appear in combination,can be drawn from the existing literature and cited research:obvious psychopathology, especially depressive symptoms,(chronic) mental stress, indication for an interaction of stressand symptoms, as well as dysfunctional coping techniques.
A gastroenterologist who is considering recommendingpsychotherapy or psychologic consultation to a patient withIBD should consider the following questions (and also askthe patient):Is the patient under a lot of stress that could possibly
trigger relapses?
von Wietersheim and Kessler Inflamm Bowel Dis & Volume 12, Number 12, December 2006
1182 * 2006 Lippincott Williams & Wilkins
Copyr ight © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

How is the patient coping with the disease?Does he or she show signs of depression?Does the patient have a social support system?
The physician then can decide, together with the patientand possibly a psychotherapist, which type of intervention(disease-oriented counseling, Bintegrated psychosomaticcare[, Bspecialized psychotherapy[) would be most appro-priate for this patient.
These recommendations are in concordance with theEuropean evidence based guideline on the management ofCrohn’s disease, which indicates that psychotherapy is usefulif IBD patients have an addition psychologic disorder, suchas depression, anxiety, or a reduced quality of life withpsychological distress, as well as maladaptive coping withthe illness.38
From a methodologic perspective, it is important to notethat IBD varies significantly throughout its course. This hasbeenwell documented and is influenced by somatic factors suchas localization, course of disease, immune parameter, andmedication. Therefore, the claim that psychotherapy has a(verifiable) influence on the course of the disease is veryambitious. This is especially true for the most common studydesign, a comparison between treatment with an effectivemedication and this medication with additional psychotherapy.For methodologic reasons alone, it is clear that the possibleadditive effects cannot be very strong. It would be more realisticto find out whether psychotherapy influences the patient’spsyche, health related quality of life, or disease coping.Although it could theoretically be expected that a betterpsychologic state would positively influence the course of thedisease, it would be very difficult to prove this scientifically.
Psychotherapeutic methods such as those presented inthis study have also been used with similar results inconnection with many other somatic illnesses such as coronaryheart disease, bronchial asthma, cancer, and skin diseases.39 Inthat context, chronic IBDs are probably no more or lessBpsychosomatic[ than other illnesses.
Further studies on psychotherapy with IBD patientsshould focus on the risk patients mentioned above. It would behelpful to recognize these (possible with an effective screeningprocedure) and to investigate the impact of a (manualized)psychotherapy in a controlled study. The main outcomevariables should be psychopathology, quality of life, or howthe patient deals with daily stress.
A large percentage of the patients would probablybenefit from detailed information about the illness and aconsultation regarding self-management of the illness. Onestudy illustrated that patient education programs reduceddoctor visits, and two studies indicated that it produced betterinformed patients. One study was able to show that the scoresregarding health related quality of life slightly improved.Therefore, these therapies could be recommended for manypatients (as opposed to more intensive psychotherapy).
REFERENCES1. Crohn BB, Ginzburg L, Oppenheimer GD. Regional ileitis. JAMA.
1932;99:1323Y1329.2. Bockus HL. Present status of chronic regional or cicatrizing enteritis.
JAMA. 1945;127:449Y456.3. Alexander F. Psychosomatic Medicine. New York: Norton; 1950.4. Engel GL. Studies of ulcerative colitis III. The nature of the psychologic
process. Am J Med. 1955;19:231.5. Engel GL. Biologic and psychologic features of the ulcerative colitis
patient. Gastroenterology. 1961;40:313.6. Drossman DA, Ringel Y. Psychosocial factors in ulcerative colitis and
Crohn’s disease. In: Balfour Sartor R, Kirsner JB, eds. Kirsner’sInflammatory Bowel Diseases, ed 6. Edinburg: Saunders; 2004:342Y356.
7. Keller W, Pritsch M, von Wietersheim J, et al. Effect of psychotherapyand relaxation on the psychosocial and somatic course of Crohn’sdisease: main results of the German prospective multicenter psycho-therapy treatment study on Crohn’s disease. J Psychosom Res.2004;56:687Y696.
8. Deter HC, Manz R, Becker M, et al. Soziale Unterstutzung in ihrerBeziehung zu korperlichen und seelischen Befunden bei Morbus CrohnPatienten. Z Psychosom Med Psychother. 1991;37:45Y59.
9. Guthrie E, Jackson J, Shaffer J, et al. Psychological disorder and severityof inflammatory bowel disease predict health-related quality of life inulcerative colitis and Crohn’s disease. Am J Gastroenterol. 2002;97:1994Y1999.
10. Bernklev T, Jahnsen J, Aadland E, et al, and the IBSEN Study Group.Health-related quality of life in patients with inflammatory bowel diseasefive years after the initial diagnosis. Scand J Gastroenterol. 2004;39:365Y373.
11. North CS, Clouse RE, Spitznagel EL, et al. The relation of ulcerativecolitis to psychiatric factors: a review of findings and methods. Am JPsychiatry. 1990;147:974Y981.
12. North CS, Alpers DH, Helzer JE, et al. Do life events or depressionexacerbate inflammatory bowel disease? Ann Intern Med. 1991;114:381Y386.
13. Gerbert B. Psychosocial aspects of Crohn’s disease. J Beh Med.1980;3:41Y58.
14. Duffy LC, Zielezny MA, Marshall JR, et al. Relevance of major stressevents as an indicator of disease activity prevalence in inflammatorybowel disease. J Behav Med. 1991;17:101Y110.
15. von Wietersheim J, Overbeck A, Kiel K, et al. Die Bedeutungrezidivauslosender Ereignisse bei Patienten mit chronisch-entzundlichenDarmerkrankungen. Ergebnisse einer prospektiven Langsschnittstudieuber drei Jahre. Psychother Psychosom Med Psychol. 1994;44:58Y64.
16. Levenstein SC, Pantera C, Varvo V, et al. Stress and exacerbation inulcerative colitis: a prospective study of patients enrolled in remission.Am J Gastroenterol. 2000;95:1213Y1220.
17. Traue HC, Kosarz P. Everyday stress and Crohn’s disease activity: anxtime series analysis of 20 single cases. Int J Behav Med. 1999;6:101Y119.
18. Bitton A, Sewitch MJ, Peppercorn MA, et al. Psychosocial determinantsof relapse in ulcerative colitis: a longitudinal study. Am J Gastroenterol.2003;98:2203Y2208.
19. Mittermaier CC, Dejaco C, Waldhoer T, et al. Impact of depressive moodon relapse in patients with inflammatory bowel disease: a prospective18-month follow-up study. Psychosom Med. 2004;66:79Y84.
20. Mardini HE, Kip KE, Wilson JW. Crohn’s disease: a two-yearprospective study of the association between psychological distress anddisease activity. Dig Dis Sci. 2004;49:492Y497.
21. Maunder R. Mediators of stress effects in inflammatory bowel disease:not the usual suspects. J Psychosom Res. 2000;48:569Y577.
22. O’Conner JF, Daniels G, Flood C, et al. An evaluation of theeffectiveness of psychotherapy in the treatment of ulcerative colitis.Ann Int Med. 1964;60:587Y602.
23. Kunsebeck HW, Lempa W, Freyberger H. Kurz- und Langzeiteffekteerganzender Psychotherapie bei Morbus Crohn. In: Lamprecht F, ed.Spezialisierung und Integration in Psychosomatik und Psychotherapie.Berlin: Springer; 1987:253Y262.
24. Jantschek G, Zeitz M, Pritsch M, et al. Effect of psychotherapy on thecourse of Crohn’s disease. Results of the German prospective multicenter
Inflamm Bowel Dis & Volume 12, Number 12, December 2006 Psychotherapy with Chronic Inflammatory Bowel Disease Patients
* 2006 Lippincott Williams & Wilkins 1183
Copyr ight © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

psychotherapy treatment study on Crohn’s disease. Scand J Gastroenterol.1998;33:1289Y1296.
25. Maunder RG, Esplen MJ. Supportive-expressive group psychotherapyfor persons with inflammatory bowel disease. Can J Psychiatry. 2001;46:622Y626.
26. Milne B, Joachim G, Niedhardt J. A stress management program forinflammatory bowel disease patients. J Adv Nurs. 1986;11:561Y567.
27. Schwarz SP, Blanchard EB. Evaluation of a psychological treatment forinflammatory bowel disease. Behav Res Ther. 1991;29:167Y177.
28. Mussell M, Bocker U, Nagel N. Reducing psychological distress inpatients with inflammatory bowel disease by cognitive-behaviouraltreatment: exploratory study of effectiveness. Scand J Gastroenterol.2003;38:755Y762.
29. Larsson KM, Sundberg Hjelm M, Karlbom U, et al. A group-basedpatient education programme for high-anxiety patients with Crohndisease or ulcerative colitis. Scand J Gastroenterol. 2003;38:763Y769.
30. Garcia-Vega E, Fernandez-Rodriguez C. A stress management pro-gramme for Crohn’s disease. Behav Res Ther. 2004;42:367Y383.
31. Elsenbruch S, Langhorst J, Popkirowa K, et al. Effects of mind-bodytherapy on quality of life and neuroendocrine and cellular immunefunctions in patients with ulcerative colitis. Psychother Psychosom.2005;74:277Y287.
32. Kennedy AP, Nelsen E, Reeves D, et al, and the North-West RegionalGastrointestinal Research Group. A randomized controlled trial to assessthe effectiveness and cost of a patient orienteated self management
approach to chronic inflammatory bowel disease. Gut. 2004;53:1639Y1645.
33. Waters BM, Jensen L, Fedorak RN. Effects of formal education forpatients with inflammatory bowel disease: a randomized controlled trial.Can J Gastroenterol. 2005;19:235Y244.
34. Bregenzer N, Lange A, Furst A, et al. Patient education ininflammatory bowel disease increases patients’ knowledge but does notinfluence long-term psychological well-being. Z Gastroenterol. 2005;43:367Y371.
35. Shepanski MA, Hurd LB, Culton K, et al. Health-related quality of lifeimproves in children and adolescents with inflammatory bowel diseaseafter attending a camp sponsored by the Crohn’s and Colitis Foundationof America. Inflamm Bowel Dis. 2005;11:164Y170.
36. Miehsler W, Weichselberger M, Offerlbauer E, et al. Assessing thedemand for psychological care in chronic diseases: development andvalidation of a questionnaire based on the example of inflammatorybowel disease. Inflamm Bowel Dis. 2004;10:637Y645.
37. Simren M, Axelsson J, Gillberg R, et al. Quality of life in inflammatorybowel disease in remission: the impact of IBS-like symptoms andassociated psychological factors. Am J Gastroenterol. 2002;97:389Y396.
38. Caprilli R, Gassuli MA, Escher JC, et al. European evidence basedconsensus on the diagnosis and management of Crohn’s disease: specialsituations. Gut. 2006;55:36Y58.
39. Fava GA, Sonino N. Psychosomatic medicine: emerging trends andperspectives. Psychother Psychosom. 2000;69:184Y197.
von Wietersheim and Kessler Inflamm Bowel Dis & Volume 12, Number 12, December 2006
1184 * 2006 Lippincott Williams & Wilkins
Copyr ight © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.




















