
Distribution of four polymorphisms in the tumour necrosis factor (TNF) genes in patients with...
6
C1in Exp Immunol 1996; 103:391-396 Distribution of four polymorphisms in the tumour necrosis factor (TNF) genes in patients with inflammatory bowel disease (IBD) G. BOUMA, B. XIA, 1. B. A. CRUSIUS, G. BIOQUE, I. KOUTROUBAKIS, B. M. E. VON BLOMBERG*, S. G. M. MEUWISSEN & A. S. PEN A Departments oj Gastroenterology and *Pathology, Free University Hospital, Amsterdam, The Netherlands ( Accepted jor publication 15 November 1995) SUMMARY In 153 patients with IBD, 64 with Crohn's disease (CD), and 89 with ulcerative colitis (UC), as well as in 54 healthy controls (HC), the frequencies of four known di-allelic polymorph isms in the genes for TNF-a and Iymphotoxin alpha (LTa) were investigated. In the Dutch population, the alleles of these four polymorphisms are present in only five combinations, called TNF haplotypes: TNF-C, -E, -H, -I, -Po Furthermore, the relation with the presence of perinuclear anti-neutrophil cytoplasmic autoantibodies (P-ANCA) was studied. A small, but statistically significant, associa- tion between the polymorphism at position -308 in the promoter region of the TNF-a gene and UC was found. The frequency of the uncommon TNF -a -308 allele 2 was found to be decreased in patients with UC compared with HC (allele frequency of allele 2 in UC patients O· 15 versus 0·25 in HC, P = 0,044). No significant differences in distribution of the TNF haplotypes were found between IBD patients and HC, although there was a tendency towards a higher frequency of the TNF-C haplotype in UC patients compared with controls (haplotype frequency 22% versus 13%; P = 0'19). No statistically significant differences in distribution of the TNF haplotypes were observed between P-ANCA-positive and P-ANCA-negative UC patients. The strength of the associations indicates that TNF genes are not markers for the predisposition to suffer from IBD. They may, however, be markers of subsets of patients with UC and CD. Keywords inflammatory bowel disease Crohn's disease ulcerative colitis HLA association tumour necrosis factor-alpha lymphotoxin a gene polymorphism haplotype INTRODUCTION groups (for reviews, see [1,2]). In spite of the fact that these observations strongly support the contribution of genetic fac- Although the etiology of the IBD, Crohn's disease (CD) and tors in the pathogenesis of IBD. the relevant genes have not ulcerative colitis (UC)' is unknown, several observations have been identified. shown that there may be a genetic predisposition underlying In recent years, there have been several studies on HLA these diseases. These include the increased familial incidence, associations in IBD. An association of HLA-DR2 with UC has the higher prevalence of disease in monozygotic versus dizygo- been shown in some studies, especially those of Japanese UC tic twins, the higher prevalence in first degree relatives versus patients [3-7], but was not found in a study by Duerr & Neigut spouses, and the differences in prevalence in diverse ethnic [8]. An association between CD and the HLA-DRI allele has been found, and was recently confirmed [4,9]. The associations B'x. present address: Department of Gastroenterology, 2nd observed are, however, weak and inconclusive. Affiliated Hospital, Hubei Medical University Wuhan, Hubei, P.R. Although striking associations exist between different China. alleles of the MHC and various autoimmulfe diseases, the l.K. present address: Department of Gastroenterology, University role of MHC class I or II molecules in many of these diseases Hospital of Heraklion, 71 J 10 Heraklion, Crete, Greece. remains largely unknown. It is even questionable whether these Correspondence: Professor A. S. Pena MD, PhD, Department of Gastroenterology, Free University Hospital, De Boelelaan 1117,1081 genes are responsible for the predisposition to the disease, HV Amsterdam, The Netherlands. rather than markers for other closely linked genes. TNF-a 1996 Blackwell Science 391
-
Upload
immunogenetics -
Category
Documents
-
view
0 -
download
0
Transcript of Distribution of four polymorphisms in the tumour necrosis factor (TNF) genes in patients with...

C1in Exp Immunol 1996; 103:391-396
Distribution of four polymorphisms in the tumour necrosis factor (TNF) genes in patients with inflammatory bowel disease (IBD)
G. BOUMA, B. XIA, 1. B. A. CRUSIUS, G. BIOQUE, I. KOUTROUBAKIS, B. M. E. VON BLOMBERG*, S. G. M. MEUWISSEN & A. S. PEN A Departments oj Gastroenterology and *Pathology,
Free University Hospital, Amsterdam, The Netherlands
( Accepted jor publication 15 November 1995)
SUMMARY
In 153 patients with IBD, 64 with Crohn's disease (CD), and 89 with ulcerative colitis (UC), as well as in 54 healthy controls (HC), the frequencies of four known di-allelic polymorph isms in the genes for TNF-a and Iymphotoxin alpha (LTa) were investigated. In the Dutch population, the alleles of these four polymorphisms are present in only five combinations, called TNF haplotypes: TNF-C, -E, -H, -I, -Po Furthermore, the relation with the presence of perinuclear anti-neutrophil cytoplasmic autoantibodies (P-ANCA) was studied. A small, but statistically significant, association between the polymorphism at position -308 in the promoter region of the TNF-a gene and UC was found. The frequency of the uncommon TNF-a -308 allele 2 was found to be decreased in patients with UC compared with HC (allele frequency of allele 2 in UC patients O· 15 versus 0·25 in HC, P = 0,044). No significant differences in distribution of the TNF haplotypes were found between IBD patients and HC, although there was a tendency towards a higher frequency of the TNF-C haplotype in UC patients compared with controls (haplotype frequency 22% versus 13%; P = 0'19). No statistically significant differences in distribution of the TNF haplotypes were observed between P-ANCA-positive and P-ANCA-negative UC patients. The strength of the associations indicates that TNF genes are not markers for the predisposition to suffer from IBD. They may, however, be markers of subsets of patients with UC and CD.
Keywords inflammatory bowel disease Crohn's disease ulcerative colitis HLA association tumour necrosis factor-alpha lymphotoxin a gene polymorphism haplotype
INTRODUCTION groups (for reviews, see [1,2]). In spite of the fact that these observations strongly support the contribution of genetic fac
Although the etiology of the IBD, Crohn's disease (CD) and tors in the pathogenesis of IBD. the relevant genes have not
ulcerative colitis (UC)' is unknown, several observations have been identified.
shown that there may be a genetic predisposition underlying In recent years, there have been several studies on HLA
these diseases. These include the increased familial incidence, associations in IBD. An association of HLA-DR2 with UC has
the higher prevalence of disease in monozygotic versus dizygobeen shown in some studies, especially those of Japanese UC
tic twins, the higher prevalence in first degree relatives versus patients [3-7], but was not found in a study by Duerr & Neigut
spouses, and the differences in prevalence in diverse ethnic [8]. An association between CD and the HLA-DRI allele has been found, and was recently confirmed [4,9]. The associations
B'x. present address: Department of Gastroenterology, 2nd observed are, however, weak and inconclusive. Affiliated Hospital, Hubei Medical University Wuhan, Hubei, P.R. Although striking associations exist between differentChina.
alleles of the MHC and various autoimmulfe diseases, thel.K. present address: Department of Gastroenterology, University role of MHC class I or II molecules in many of these diseases Hospital of Heraklion, 71 J 10 Heraklion, Crete, Greece. remains largely unknown. It is even questionable whether theseCorrespondence: Professor A. S. Pena MD, PhD, Department of
Gastroenterology, Free University Hospital, De Boelelaan 1117,1081 genes are responsible for the predisposition to the disease, HV Amsterdam, The Netherlands. rather than markers for other closely linked genes. TNF-a
~-' 1996 Blackwell Science 391

G. Bouma et at. 392
and lymphotoxin alpha (LTQ or TNF-,B) are potent prointlamrna tory and immunomodulatory cytokint:s that playa central role in the initiation and regulation of the immune rcsponse. The genes for these cytokines are tandemly arranged in the central rcgion of the MHC between the iLA-B and HLA-D locus, at the short arm of chromosome 6. This location has pr:ompted much speculation about the role ofT F-a and LTI'\' in the etiology of MHC-associatcd disease'. especially thosc with an inflammatory or autoimmune component [10]. In support of this, Jacob et al. showed that HLA-DR2-positive individuals produce less TNF-a than individuals that ar H ADRJ-positive [11]. J-1LA-linked polymorphic variations within the TNF genes have been claimed to be responsible for differences in secretion. Messer et al. found that a Ncol restriction fragment length polymorphism (RFLP) in the first intron of the LTo- gene influences LTa secretion, whereas an association betwt:en this polymorphism and production of T F-it was described by Pociot et al. [12-14J. An AspHI RFLP, also in the fir t intron of the LTo gene, was described by erencik el al. [15]. Wilson el al. showed that a polymorphi"m at position -308 in the promoter region or the F-o' gene is strongly linked to the HLA-AI, -B8, -DR3 ancestral haplotype, and suggested that variations at this position might be important in the regulation of TNF-Q production [16,17]. A second polymorphism, at position -238 in the promoter region of the TNF-a gene, has been described by D'Alfonso & Momiglian Richiardi [18]. We have recently shown lhat in the Dutch p pulation, the allcles of these Cour polymorphisl11s are present in only Ii combinations, that have been called T F haplotypes: TNF-C, -E, -H, -I, -P (Fig. I) [19].
Since 1990, several authors have reported the presence of perinuclear anti-neutrophil cytoplasmic antibodies (P-A CA) in the serum or the majority of patients suffering from UC [20]. in most of these studies, the presence of P-A CA in UC patients does not correlate with disease activity or extent or the disease, and is detectable even years after colectomy [21]. This, together with the observation that this autoantibody has been found in asymptomatic relatives of patients with UC, suggests that its presence is not secondary to inflammation. Therefore, it has been suggested that P-ANCA may serve as a marker for a genetically controlled immunoregulatory disturbance [21,22]. The finding that P-A CA positivity was mainly
TNF-a LTa
-IJ tt ~ .I
Haplotype -238 -308 A5pHl Ncol
TNF-C G G(1) 2 1(aa26=a5n)
TNF·E G A(2) 2 1(aa26=a5n)
TNF-H A G(1) 2 2(aa26=th r)
TNF·I G G(l) 2 2(aa26=thr)
TNF·P G G(l) 2(aa26=thr)
Fig. I. Schematic representation of the tandemly arranged T F-a and Iympholoxin alpha (LTa or TNF-{i) genes. 0, Untranslated parts of the exons; _, translated parts. The arrow indicates the direction of transcrip· tion. Positions of the four di-allelic polymorphisms are marked.
found in a group of HLA-DR2-positive patients strengthened this hypothesis [23].
We have previously studied the T F-Q -308 polymorphism in lBD patients [24]. In the present study we report on the distribution of all four polymorphisrns and the TNF haplotypes in IBD patients and healthy control:. We have also investigated whether the pre ence of P-ANCA is correlated with these polymorphisms or the T F haplotypes.
SUBJECTS AND M °nIODS
Blood samples were obtained from 153 unselected IBD patients, 64 with CD (44 females, 20 males; mean age 39 years, range 19- 67 years) and 89 with C (43 females, 46 males; mean age 45 years, range 20 84 years), attending the Department oT Gastroenterology over a 2-year period. Blood samples from 54 healthy controls (HC) (24 females, 30 males; mean age 36 years, range 24-60 years) served as controls. All subjects were recruited from The Netherlands and were caucasian. Diagnosis or CD or was based on the conventional clinical, radiological, endoscopic, and patholo ical criteria, as described by Lennard-Jones et al. [25].
TNF-a. alld LTa polymorphisms Genomic DNA was extracted from anti-coagulated blood by a conventional proteinase K digestion/phenol-chloroform extraction method. Typing of the di-allelic R LP at position -308 in the T F-Q promotcr (TNF-a: -308) was performed by polymerase chain reaction (PCR) amplification (using a 5' primer 5'-AGGCAATAGGTTTT GGG C T-3' and 5'-TCCTCC TG TCCGATT G-3' as the 3' primer) and col digestion as described by Wilson et (71. [16]. A single-strand conformation polymorphism mcthod was optimized for the detection of di-allelic polymorphisms at both positions 308 and -238 in the T F-a gene.
PCR fragments spanning sequences from position -396 to -69 were generated using a 5' primer 5'-TICCTGCATC TGTCTGGAA-3' and a 3' primer 5'- A GG AAA TCCTT GT-3' as de cribed by O'Alfonso & Momigliano Richiardi [18]. The 328 base pair (bp) fragments were denatured and run on pre-cast non-denaturing 12·5% polyacrylamide PhastGels. Horizontal electrophoresis and silver staining were performed scmi-automatically with the PhastSystem (Pharmacia LKB Biotechnology AB, ppsala, Sweden).
P R amplification with primers located in the 5' untranslated region and third intron of the LTOo gene (5' primer 5'CCGT CGTGCTlTGGACT -3' and 3' primer 5'AGAG TGGTGGGGACATGTCTG-3') resulted in 740 bp fragments that wcre either cut (allele LTa col·l) or remained intact (allele LT 0' Ncol*2) following incubation with the restriction enzyme col [12] (Fig. 2). For typing the AspHT RFLP described by F rencik et al., the 740-bp P R fragmcnts were digested with the isoschizomer BsiHKAI ( ew England Biolabs, Beverly, MA) [15]. This re.ulted in 425-bp and 315-bp fragments (allele LTa AspHl'" I) or the undigested 740-bp fragment (allele L 0' AspHI *2). Fragments from individual digests were analysed by electrophorcsLs in O' I% ethidium bromide-stained [. 5% agarose gels.
Indirect immunofluorescence technique The standard ANCA indirect immunofluorescence technique
(f'J [996 Blackwell Science Ltd, Clinical and Experimental Immlll1.ology, 103:391-396
393 TNF polymorphisms in /BD
LTa Ncol RLFP
allele bp
*2 740
*1 555
*1 185
2 3 4
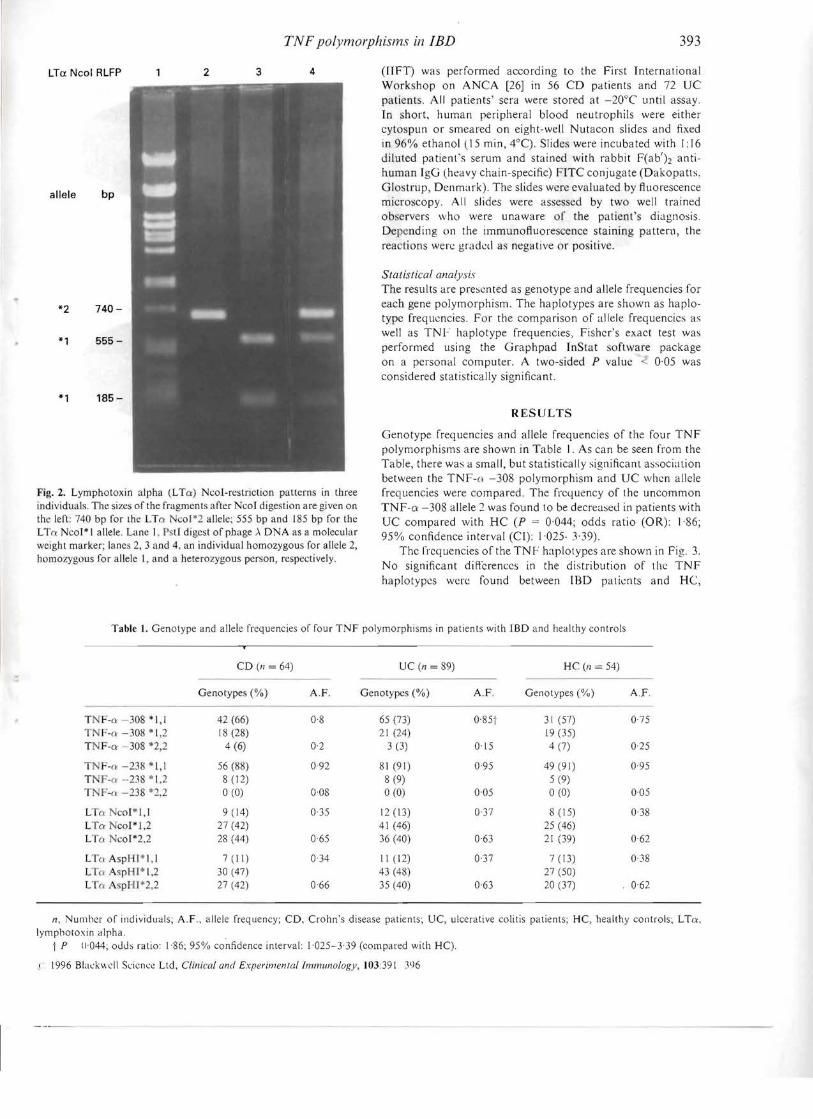
Fig. 2. Lymphotoxin alpha (LTCI:) Ncal-restriction pallerns in three individuals. The sizes of the fragments after Nco! digestion are given on the left: 740 bp for the LTn co'·2 allele: 555 bp and 185 bp for the LTo: Nco!* I allele. Lane I. PstI digest of phage II DNA as a molecular weight marker; lanes 2, 3 and 4. an individual homozygous for allele 2, homozygous for allele l, and a heterozygous person, respectively.
(lIFT) was performed according to the First International Workshop on ANCA [26] in 56 CD patients and 72 UC patients. All patients' sera were stored at -20°C until assay. In short, human peripheral blood neutrophils were either cytospun or smeared on eight-well Nutacon slides and fixed in 96% ethanol (15 min, 4°C). Slides were incubated with 1:16 diluted patient's serum and stained with rabbit F(ab'h antihuman IgG (heavy chain-specific) FITC conjugate (Dakopatts, Glostrup, Denmark). The slides were evaluated by fluorescence microscopy. All slides were assessed by two well trained observers who were unaware of the patient's diagnosis. Depending on the immunofluorescence staining pattern, the reactions were graded as negative or positive.
Statistical analysis The results are presented as genotype and allele frequencies for each gene polymorphism. The haplotypes are shown as haplotype frequencies. For the comparison of allele frequencies as well as TNF haplotype frequencies, Fisher's exaet test was performed using the Graphpad InStat software package on a personal computer. A two-sided P value < 0·05 was considered statistically significant.
RESULTS
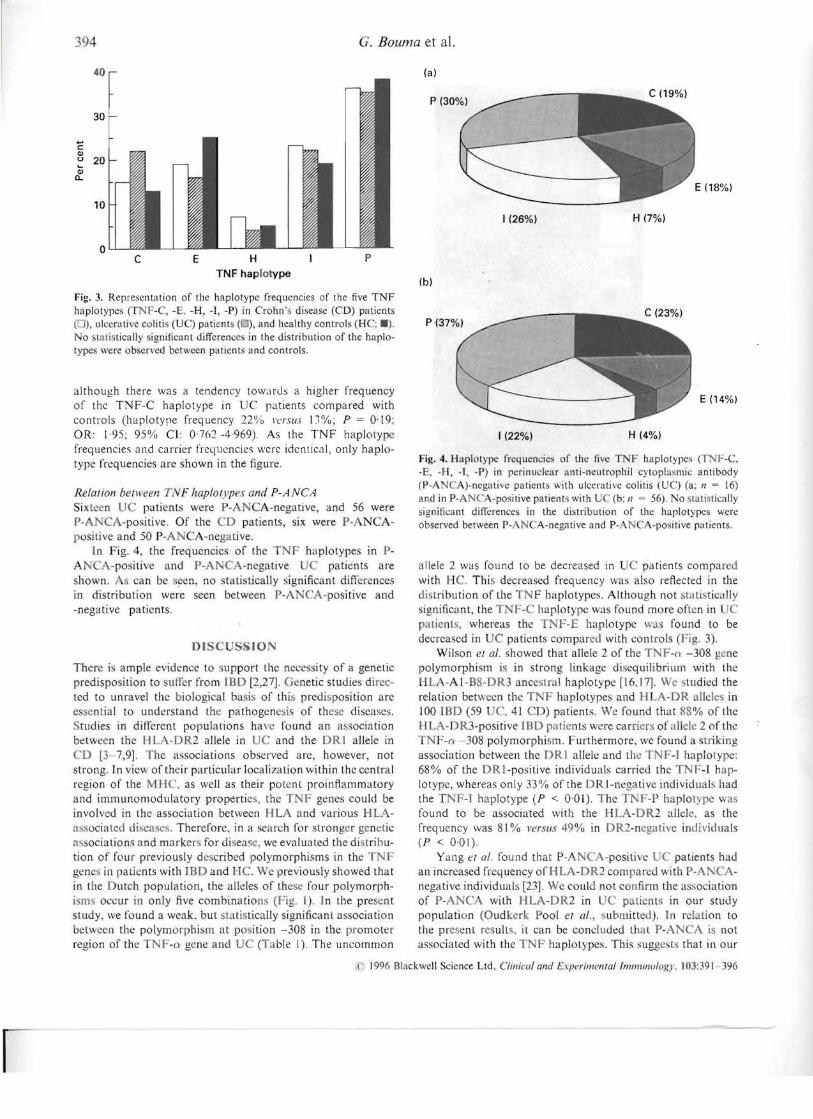
Genotype frequencies and allele frequencies of tile four TNF polymorphisms are shown in Table I. As can be seen from the Table, there was a small, but statistically significant association between the TNF-o -308 polymorphism and UC when allele frequencies were compared. The frequency of the uncommon TNF-o: -308 allele 2 was found to be decreased in patients with UC compared with HC (P == 0'044; odds ratio (OR): 1'86; 95% confidence interval (CI): 1,025- 3· 39).
The freq uencies of the TN F haplotypes are shown in Fig. 3. No significant differences in the distribution of tl1e TNF haplotypes were found between IBD patients and He,
Table 1. Genotype and allele frequencies of four TNF polymorphisms in patients with lED and healthy controls
CD (n == 64) UC (n == 89) HC (n == 54)
Genotypes (%) A.F. Genotypes (%) A.F. Genotypes (Ofu) AT
T F-CI: -308 *1,1 TNF-n -308 *1,2 T F-CI: --308 *2,2
42 (66) 18 (28)
4 (6)
08
0·2
65 (73) 2l (24)
3 (3)
0'85t
0·l5
31 (57) 19 (35) 4 (7)
075
025
T T T
F-o: -238 *1,1 'F-a ·-138 *1,2 F-u -138 *2,2
56 (88) 8 (12) 0(0)
092
0·08
81 (91) 8 (9) 0(0)
0·95
0·05
49 (91) 5 (9) 0(0)
0·95
005
L (~ co!'I,1 LTo: Ncol*I,2 LT" NcoI*2.2
9 (14) 27 (42) 28 (44)
0·35
0·65
12 ([3) 41 (46) 36 (40)
0·37
0·63
8 (15) 25 (46) 21 (39)
0·38
062
LT"AspHI·I,1 LTnAspHJ*I,2 L (> AspHI*2,2
7 (11) 30 (47) 27 (42)
034
0·66
II (12) 43 (48) 35 (40)
0·37
063
7 (13) 27 (50) 20 (37)
038
0·62
n, Numhcr of individuals; A.F., allele frequency; CD, Crohn's disease patients; UC, ulcerative colitis patients; HC, healthy controls; LTo:, Iymphotoxin alpha.
1 P 11'044; ouus ratio: 1·86: 95% confidence interval: 1,025-3'39 (compared with HC).
)' 1996 Blackwell Science Ltd, Clinical and Experimenlallmmlll1ology, 103:391 396
40
394 · Bouma et al.
30
.... c: Ql U 20 .... Ql a.
10
0 C E H
TNF haplotype
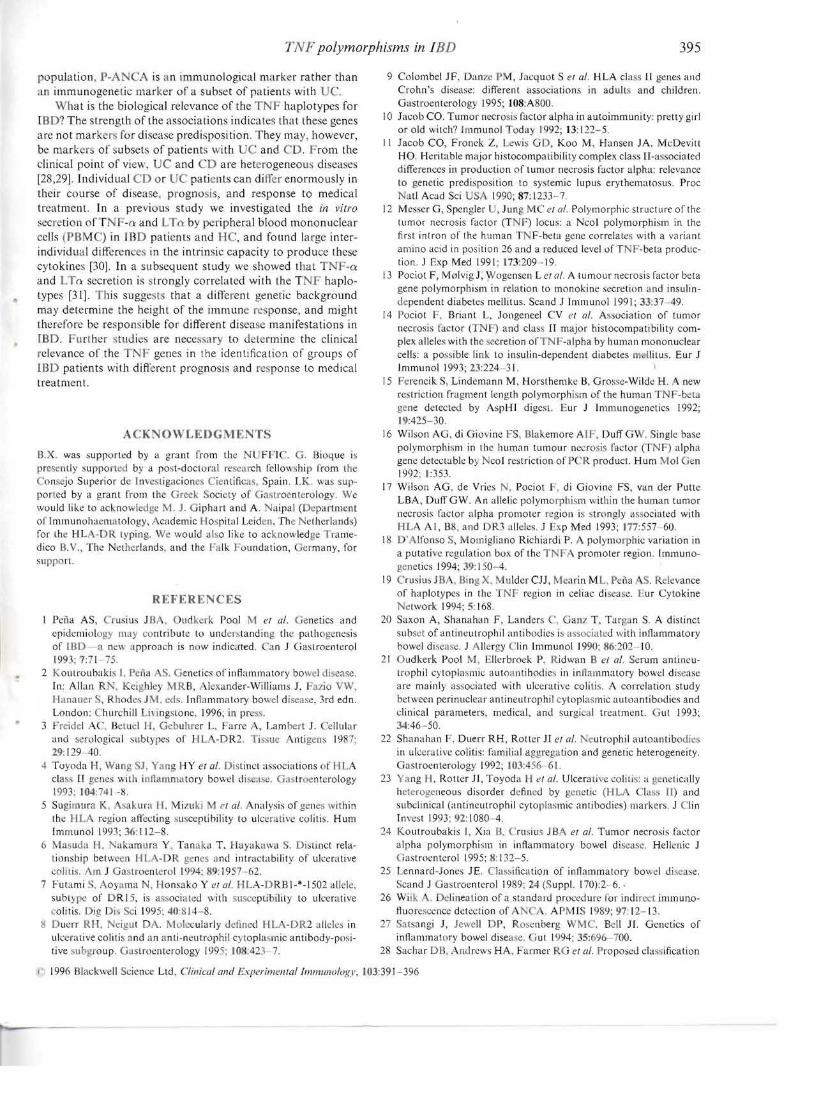
Fig. 3. Representation of the haplotype frequencies of the five TNF haplotypes CfNF-C, -E. -H, -T, -P) in Crohn's disease (CD) patients (0), ulcerative colitis (UC) patients (119), and healthy controls (HC; 11). No statistically significant differences in the distribution of the haplotypes were observed bctwcen patients and controls.
although there was a tendency towards a higher frequency of the TNF-C haplotype in UC patients compared with controls (haplotype frequency 22% versus DOlo; P = 0·\9; OR: 1·95; 95% CI: 0762 -4,969). As the TNF haplotype frequencies and carrier frequencies were identical, only haplotype frequencies are shown in the figure.
Relation beNcell TNF haplotypes and P-ANCA Sixteen UC patients were P-AN A-negative, and 56 were P-A CA-positive. Of the CD patients, six were P-ANCApositive and 50 P-ANCA-negative.
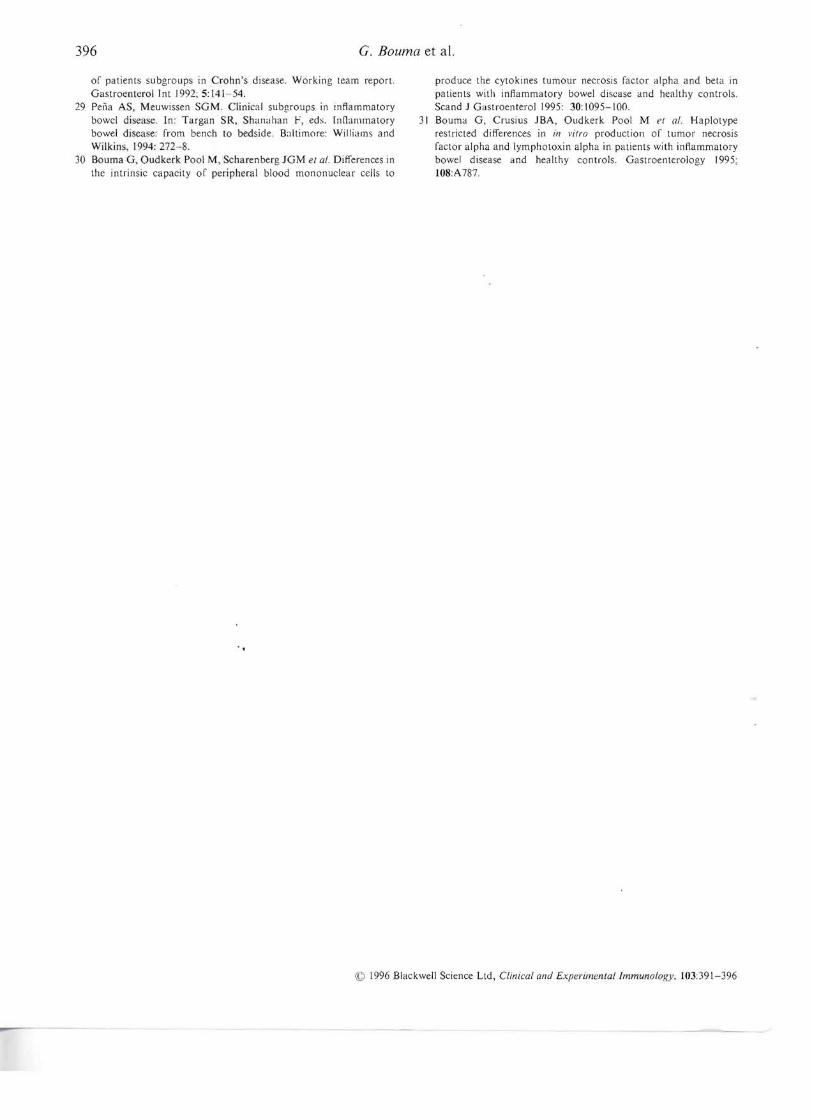
]n Fig. 4, the frequencies of the NF haplotypes in pAN A-positive and P-A CA-negative patients are shown. scan been, no statistically ignifieant differences in distribution were seen between P-ANCA-positive and -negative patients.
Of CUS ION
There is ample evidence to 'upport the nee ssity of a genetic predisposition to suffer from IBD [2,27]. G netic studies directed to unravel the biological basis of this predi. position arc essential to understand the pathogenesis of these disea. cs.
tudies in different populations have found an association belw en the HL - R2 allele in UC and the DRI allele in CD [3-7,9]. The associations observed are, however, not strong. In vie, of their particular localization within the central region of the MHC, as well as their pot nt proinftammatory and immunomodulatory properties, the TNF genes could be involved in the association between HLA and various HLAa 'sociated disease. Therefore, in a search for stronger genetic associations and marke for disea e, we evaluated the distribution of four previously described polymorphisms in the gen s in patients with IBD and He. We previously showed that in tile Dutch population, the alleles of these four polymorphism occur in only five combinations (Fig. I). In the present study. we found a weak. but statistically significanl association betwe n the polymorphism at po ition -308 in the promoter region of the TN -n gene and DC (Table I). The uncommon
p
(a)
1(26%) H (7%)
(b)
1(22%) H (4%)
E (14%)
Fig. 4. Haplotype frequencies of the five TNF haplotypes (TNF-C, -E, -H, -I, -P) in perinuclear anti-neutrophil eytoplasmic antibody (P-A CA)-negative patients with ulcerative colitis ( C) (a; 17 = (6)
and in P-A CA-positive patients with U (b; 1/ = 56). No stati ·tically significant differences in the distribution of the haplotypes were observed between P-ANCA-negative and P-ANCA-positive patients.
allele 2 was found to be decreased in C patients compar d with He. This decreased frequency was also reflected in the distribution of the T F haplotypes. Although not statistically significant, the TNF-C haplot pe was found more often in C patients whereas the TNF-E haplotype was found to be decreased in UC patients compared with controls (Fig. 3).
Wilson el at. showed that allele 2 of the TNF-a -308 gene polymorphism is in strong linkage di -equilibrium with the IlLA-AI-B8-DRJ anc . tral haplotype [16.17]. We studied the relation between the TNF haplotypes and H A-DR alleles in 100 IBD (59 UC, 41 CD) patients. We found that 88% of the HLA- R3-positive IBD patients w re carriers of allele 2 of the TNF-()' -308 polymorphism. Furthermore. we found a striking association between the RI allele and the TNF-I haplotype: 68% of the DRI-positive individuals carried the TNF-I haplotyp , whereas only 33% of the DR I-negativ individuab had the T F-I haplotype (P < 001). Th TNF-P haplotype ~ a found to be associated with the HLA-DR2 allel , as the frequency was 81 % versus 49% in DR2-ncgative individuals (P < 0'01).
Yang el af. found that P-A A-positive patients had an increased fr quency of HLA-DR2 compared ith P-ANCAnegative individual [23]. WI;;; could not eenfirm the association of P-A CA with HLA-DR2 in C patients in our study population (Oudkerk Pool et al., ubmitlcd). In relation to the present results. it can be concluded that P-ANCA is not associated with the TNF haplotype~. This ,;uggest that in our
() 1996 Blackwell Science Ltd, Clin;ml and Exper;mel1tallmlJlllllUlogy. 103:391-396
395 TNF polymorphisms in lED
population. P-A CA is an immunological marker rather than an immunogenetic marker of a subset of patients with C.
What is the biological relevance of the TNF haplotypes for 180') The strength of the associations indicates that these genes are not marker for disease predisposition. They may however, be markers of subsets of patient~ with UC and CO. From the clinical point of view, UC and CD are heterogeneoLls diseases [28,29]. Individual CD or C patients can differ enormously in their course of dIsease. prognosis, and response to medical treatment. In a previous study we investigated the in vitro
secretion ofT -0: and LTo: by peripheral blood mononuclear cells (PBM ) in IBO patients and He, and found large interindividuuJ difference. in the intrinsic capacity to produce these cytokines [30J. In a subsequent study we showed that TNF-o: and LTrl' sccretion is strongly correlated with the TNF haplotypes [31]. This suggests that a ditlerent genetic background may determine the height of the immune response, and might therefore be responsible for different disease manifestations in IBD. Further studies are nece. sary to determine the clinical relevance of the TNF genes in the identification of groups of IBO patients with differcnt prognosis and re ponse to medical treatment.
ACKNOWLEDGME 1'5
ll.X was supported by a grant from the N FII G. BiQljue i~
prc"ently :;upported by a post-doctoral re e!lrch fello ship from the onsejo Superior de Inve tigacione. Cientiftcas. Spain. I.K. \\IUS sup
poned by a grant from thc Greek Society of ;(slroenterology. We wuuld like to acknowledge M. J. Giphart aDd A. Naipal (Depat·tment oflmmunohael1l11tology, Academic Hospital Leiden, [he Netherlands) fOt' the H LA-DR lyping. We would abo Ii e to acknowledge Tramedieo B. V., The Netherlands. and the Falk Foundation, ermany, for support.
REFERENCES
Peiia AS, Crtlsius JBA. Oudkcrk 1'001 M cl al. Genetics and epidemiology may contribut~ to understanding the pathogene.sis of lHD a new llpproach is now indicated. ~an J Gastroenterol 1993; 771 75.
2 KOUll'Oubakis 1, Pena S. enetie, 01' inflammatory bowel disease In Allan RN, Keighley MRB, lexander-Williams J, Fazio VW. !-Ian::llIer S, Rhodes JM. ed' Inflammatory bowel disease. 3rd edn. London: hurchill Livingstone. 1996; in preS,',.
3 Freidel AC. Betucl H. Gebuhrer L, ['aITe A, Lamhert J. ellular and serological subtypes of HLA-DR2 Ti 'sue ntigen 1987; 29:129-40.
4 Toyoda 1-1, Wang J. Yang!-lY ct al. Distinct associations of l-ILA clas~ [J genes with il1namm'ttory bowel di ea e. astroenterology 1993; 104:741-~
5 SuginllIr::I K, i\sakuta H. Mi 4 uki el al. Analysis of genes within the HLA region affecting su.,ceptihility to ulcerative colitis. Hum Immunol 1993; 36:112-8.
6 Masuda fl. akumura Y. Tanaka 1', Hayakawa S. Di tinct relalionship between HI. -DR genes and intractability of ulcerative eoliti:; Am J Gastroentcrol 1994: 89: 1957 -62.
7 FutHmi • Aoyama N. Honsako Y eJ al. IILA-DRBI-*-1502 allele. subtype of DR 15, is associated with susceptibility to ulcerative colitis. Dig Di:. ci 1995; 40:814-8.
1I Ducrr RH. eigut DA. Molecularly defined H LA-DR2 alleles in ulcerative coliti, and an anti-neutrophil c. toplasmic antibody-pOSItive subgroup. Gastroenterology 1995; 108:423- 7.
9 Colombcl JF. Danle PM, Jacquot S el al. HLA class II gene:; and Crohn's di,ea,e: different assoeiations in adult, and children. Gastroenterology 1995; 108:A800
10 Jacob CO. Tumor necro i' factor alpha in autoimmunity: pretty girl or old witch'! Irnmunol Today I 92; 13: 122-5.
II Jacob CO, Fronek Z, Lewis GO, Koo M. Hansen JA. McDevitt HO. Heritable major histocompatibiLity complex class II-associated differences in production of tumor necrosis factor alpha: relevance to genetic predisposition to systemic lupus erytheIj1ato:;us. Proc Nat! Acad Sci USA 1990; 87: 1233-7
12 Messer G, Spengler U, Jung M . et al. Polymorphic structure of the tumor necrosis factor (1' F) locus: a Ncol polymorphism in the first intron of the human TNF-bcla gene correlate;; with a variant amino acid in position 26 and a reduced level of l' F-beta production. J Exp Med 1991; 173:209 ·19
13 Pociot F, Molvig J, Wogensen Lei al. A tumour necrosis factor beta gene polymorphism in relation to monokine secretion and insulindependent diabetes mellitus. Scand J Immunol 19 I; 33:37 49.
14 Pociot F, Brrant L, Jongeneel CV el al. Association of tumor necrosis factor (TNF) and class" major histocompatibility complex alleles with thesccretion ofTNF-alpha by human mononuclear cells: a possible link to insulin-dependent diabetes me litus. Eur J Immunol 1993; 23:224-31
15 Ferencik S. Lindemann 1'.1, Horsthemke B. Grosse-Wilde H. A new restriction fragment length polymorphi~rn of the human TNF-bet::l gene detected by AspHI digest. Eur J Immunogenetics 1992; 19:425-30.
16 Wilson A , di Giovine FS, Blakemore A1F. Duff GW Single base polymorphism in the human tumour necrosis factor (TNF) alpha genc detectable b~ Ncol restriction ofP R product. Hum Mol Gen 1992; 1:]53.
17 Wilson AG. de Vries N, Pociot F, di Giovine FS, van del' Pulle LBA, Dull GW. An allelic polymorphism within the 11llman tumor necrosis factor alpha promoter rt:gion i, strongly associated with HLA AI, B8, and R3 alleles. J "xp Med 1993; 177:557-60.
18 D'Alfonso $, Momigliano Richiardi P. A polymorphic variation in a putative regulation box of the T promoter region. Immunogenetics 1994; 39: 150-4.
19 Crusius J B ,Bing X. ulder cn, Mearin M L. Pena S. Relevance of haplotypes in the TNF region in celiac disease. Eur Cytokine
etwork 1994; 5: 168 20 Saxon A, Shanahan F, Landers C, Ganz 1', Targan S. A distinct
subset of anti neutrophil antibodies is associated with inflammatory bov,el disease. J llergy Ciin Immunol 1990; 86:202-10
21 udkerk Pool M. Ellerbrock P~ Ridwan B eI al. Serum antineulnJphii cytopla~mie autoanlibodies in inflammatory bowel disease are mainly asociated with ulcerative colitis. A correlation study between perinuclear anti neutrophil cytoplasmic autoantibodies and clinical parameters, medical, and surgical treatment. ut 1993; 34:46 -50
22 Shanahan F, Duerr RH, Rotter JI cl al. Neutrophil autoantibodies in ulcerative colitis: familial aggregation and genetic heterogeneity. Gastroenterology 1992; 103:456 6l
23 Y.lDg II. Rotter JI, Toyoda lei al. Ulcerative eoliti~: a genetically heterogeneous disorder defined by genetic (IJLA lass II) and subclinical (anti neutrophil cytoplasmic antibodies) markers. J Clin Invest 1993; 92: 1080-4.
24 Koutroubakis I, Xia B, Crusius J BA ('I al. Tumor necrosis factor alpha polymorphism in inflammatory bowel disease Hellenic J Gastroen terol 1995: 8: 132-5.
25 Lennard-Jones JE. Classification of inflammatory bowel diease. Scand J Gastroente.rol 1989; 24 (Suppl. (70)2-6 .
26 Wiik . Delineation of a standard procedure for indirect immunofluorescence detection of A A. APMIS 198\l; 97:12-13.
27 Satsangi J, Jewell DP, Rosenberg WM , Bell JI. Genetics of inl1ammatC'ry bowel disea 'e. Gut 1994: 35:696-700.
28 SachaI' DB. mlrews HA, Farmer RG cl al. Proposed classification
It 1996 Blackwell Science Ltd. Clillicul and E.\pcril)(clllallll7lilllllOlogl', 103:39 J~396
396 G. Bouma et al.
or patients subgroups in Crohn's disease. Working team report. Gastroenterol Int 1992; 5:141-54.
29 Peila AS, Meuwissen SGM. Clinical subgroups in inflammatory bowcl disease. In: Targan SR, Shanahan F, eds. [nfiall1l11atory bowel disease: rrom bench to bedside. Baltimore: Williams and Wilkins, 1994: 272-8.
30 Bouma G, Oudkerk Pool M, Scharenberg JGM e/ 01. Differences in the intrinsic capacity or peripheral blood mononuclear cells to
produce the cytokines tumour necrosis ractor alpha and beta in patients with inflammatory bowel disease and healthy controls. Scand J Gastroenterol 1995: 30:1095-100.
31 Bouma G, Crusius JBA, Oudkerk Pool M eI af. Haplotype restricted differences in in vilro production or tumor necrosis ractor alpha and Iymphotoxin alpha in patients with inflammatory bowel disease and healthy controls. Gastroenterology 1995; l08:A787.
© 1996 Blackwell Science Ltd, Clinical and Experimen/allmmunology, 103:391-396




















