
Current Therapeutic Approaches in Inflammatory Bowel Disease
16
3668 Current Pharmaceutical Design, 2010, 16, 3668-3683 1381-6128/10 $55.00+.00 © 2010 Bentham Science Publishers Ltd. Current Therapeutic Approaches in Inflammatory Bowel Disease Amir Ali Sohrabpour 1 , Reza Malekzadeh 1 and Ali Keshavarzian 2, * 1 Digestive Disease research Center, Shariati Hospital, Tehran University of Medical Sciences, Tehran, Iran, 2 Division of Digestive Diseases, Department of Internal Medicine, Rush University Medical Center, Chicago, Illinois 60612, USA Abstract: Inflammatory bowel disease (IBD) is a chronic, relapsing, inflammatory disorder of the gastrointestinal tract and is broadly classified into Crohn’s disease (CD) and ulcerative colitis (UC). In the last decade, our understanding of the etiology and pathogenesis of this group of disorders has been improved. More specifically, recent development of biologics and use of immunomodulator agents in IBD have made it possible to robustly control mucosal inflammation and heal mucosal ulcerations and thus provide an opportunity to po- tentially modify disease course and prevent complications and future surgery. However, unfortunately we have not identified reliable, sensitive and specific markers to predict disease course and to identify those patients with aggressive and progressive course that would benefit from early use of biologics to prevent future complication and surgery. Thus, optimal medical management of IBD has remained multifaceted and individualized. Our primary therapeutic goals have remained unchanged and are to: [1] improve patient quality of life by treating flare ups [induction of remission], maintaining remission, and treating symptoms like diarrhea; [2] predict and prevent/treat complication; [3] prevent/treat nutritional deficiency and maintain optimal nutrition, [4] provide appropriate psychosocial support, and of course [5] attempt to modify disease course in those with aggressive disease. We can achieve these goals by appropriate use of therapeu- tic agents that include 5-aminosalicylates, corticosteroids, immunosuppressive agents, antibiotics, nutritional support, and the biologic agents. Information from well designed double blind placebo controlled trials combined with knowledge of the potential impact of patient and disease characteristics on disease course which can assist us to individualized treatment plan will be the guide for us to appropriately use these therapeutic agents. For example, age of the onset of the disease, patient gender and race, mode of the disease presentation, dis- ease location, disease-associated complications such as perianal disease/fistula, and serology and genetic markers can all help to indi- vidualize disease treatment. These factors can help to determine whether one should start with 5-ASA/antibiotic/steroid [step-up where there is no risk factors for aggressive disease course] or whether one should initiate biologic therapy at diagnosis [top-down approach], and whether it is most advisable to use monotherapy with biologic treatment [e.g. in young, Caucasian male or elderly] or use a combina- tion therapy with a biologic and an immunomodulator. Ongoing research promises, in a near future, development of more robust set of markers to be able to model disease behavior to more accurately predict disease course and thus decide on therapeutic approach with most appropriate efficacy/risk ratio for a given patient. Furthermore, current basic laboratory research has provided a large number of po- tential therapeutic targets to treat IBD with new promising highly specific and targeted agents. Keywords: Inflammatory bowel disease, Crohn’s disease, Ulcerative colitis, treatment, anti-TNF antibodies. INTRODUCTION Inflammatory bowel disease (IBD) is a chronic, relapsing, in- flammatory condition of the gastrointestinal tract affecting more than a million people worldwide. The incidence of IBD is assumed to be highest in developed countries and lowest in the developing regions of the world. A higher rate of IBD is observed in individu- als living in colder climates, as well as the urban population. West- ernization of lifestyles, including changes in dietary habits and en- vironmental changes such as improved sanitation and industrializa- tion are implicated in the rising trend in the incidence and preva- lence of IBD in previous low-incidence Asian countries [1-3]. IBD is a heterogeneous group of diseases that can be broadly classified into Crohn disease (CD) and ulcerative colitis (UC). The term IBD-unclassified (IBDU), previously referred as indeterminate colitis (IC), applies to the subset of 10% to 15% of patients with IBD in whom this sub-categorization is not possible. There is no gold standard single test that provides the diagnosis of IBD so as- signing a diagnosis of IBD is often not straightforward and involves integration of historical factors, physical examination findings, and evidence of inflammation on endoscopic, histologic, and radiologic evaluations [4]. The inflammation in CD is typically transmural. This frequently leads to complications from perforating disease or from progressive fibrosis and stricturing. CD can thus be thought of as fitting one of three phenotypes: inflammatory, stricturing, or perforating disease (the latter including abscesses and fistulae). Disease behavior is not *Address correspondence to this author at the Division of Digestive Dis- eases, Department of Internal Medicine, Rush University Medical Center, Chicago, Illinois 60612; Tel: +9821 8241 5300; Fax: +9821 8241 5400; E-mail: [email protected] necessarily constant in an individual patient. Indeed, inflammatory disease frequently progresses to penetrating disease, and then to fibrosis and stricturing. Perianal disease, including abscesses and fistulae, is commonly encountered, particularly in conjunction with terminal ileal disease [5]. Inflammation in UC is limited to the mucosal layer of the colon. The rectum is virtually always involved, with inflammation extend- ing proximally in a confluent fashion. The extent of proximal in- volvement is variable. Unlike CD, UC is frequently acute or suba- cute in onset. Like CD, the subsequent clinical course is one of recurring episodes of symptomatic disease interspersed with epi- sodes of relative (or complete) quiescence [6]. Although UC and CD have significant differences, many (but not all) of the treatments available for one are also effective for the other. Both diseases usually have waxing and waning intensity and severity. In most cases, symptoms do correspond well with the degree of inflammation present for either disease, although this is not universally true. In the last decade, our understanding of this enigmatic group of disorders has improved. Genetic, environ- mental, infectious, and immunologic factors are all thought to play a role in the etiology and pathogenesis of IBD [7]. Optimal medical management of IBD is multifaceted and indi- vidualized. Except for mild cases (primarily UC), most patients require combination therapy to achieve sustained response or re- mission. Fine-tuning of treatment is based upon clinical, biochemi- cal, endoscopic, and histologic responses that depend upon consid- erations of drug doses, routes, and timings and drug–drug syner- gies. Despite advances in our ability to predict clinical course in specific patients, the individual response to IBD therapy often is idiosyncratic [8].
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Current Therapeutic Approaches in Inflammatory Bowel Disease

3668 Current Pharmaceutical Design, 2010, 16, 3668-3683
1381-6128/10 $55.00+.00 © 2010 Bentham Science Publishers Ltd.
Current Therapeutic Approaches in Inflammatory Bowel Disease
Amir Ali Sohrabpour1, Reza Malekzadeh
1 and Ali Keshavarzian
2,*
1Digestive Disease research Center, Shariati Hospital, Tehran University of Medical Sciences, Tehran, Iran,
2Division of Digestive
Diseases, Department of Internal Medicine, Rush University Medical Center, Chicago, Illinois 60612, USA
Abstract: Inflammatory bowel disease (IBD) is a chronic, relapsing, inflammatory disorder of the gastrointestinal tract and is broadly classified into Crohn’s disease (CD) and ulcerative colitis (UC). In the last decade, our understanding of the etiology and pathogenesis of
this group of disorders has been improved. More specifically, recent development of biologics and use of immunomodulator agents in IBD have made it possible to robustly control mucosal inflammation and heal mucosal ulcerations and thus provide an opportunity to po-
tentially modify disease course and prevent complications and future surgery. However, unfortunately we have not identified reliable, sensitive and specific markers to predict disease course and to identify those patients with aggressive and progressive course that would
benefit from early use of biologics to prevent future complication and surgery. Thus, optimal medical management of IBD has remained multifaceted and individualized. Our primary therapeutic goals have remained unchanged and are to: [1] improve patient quality of life
by treating flare ups [induction of remission], maintaining remission, and treating symptoms like diarrhea; [2] predict and prevent/treat complication; [3] prevent/treat nutritional deficiency and maintain optimal nutrition, [4] provide appropriate psychosocial support, and of
course [5] attempt to modify disease course in those with aggressive disease. We can achieve these goals by appropriate use of therapeu-tic agents that include 5-aminosalicylates, corticosteroids, immunosuppressive agents, antibiotics, nutritional support, and the biologic
agents. Information from well designed double blind placebo controlled trials combined with knowledge of the potential impact of patient and disease characteristics on disease course which can assist us to individualized treatment plan will be the guide for us to appropriately
use these therapeutic agents. For example, age of the onset of the disease, patient gender and race, mode of the disease presentation, dis-ease location, disease-associated complications such as perianal disease/fistula, and serology and genetic markers can all help to indi-
vidualize disease treatment. These factors can help to determine whether one should start with 5-ASA/antibiotic/steroid [step-up where there is no risk factors for aggressive disease course] or whether one should initiate biologic therapy at diagnosis [top-down approach],
and whether it is most advisable to use monotherapy with biologic treatment [e.g. in young, Caucasian male or elderly] or use a combina-tion therapy with a biologic and an immunomodulator. Ongoing research promises, in a near future, development of more robust set of
markers to be able to model disease behavior to more accurately predict disease course and thus decide on therapeutic approach with most appropriate efficacy/risk ratio for a given patient. Furthermore, current basic laboratory research has provided a large number of po-
tential therapeutic targets to treat IBD with new promising highly specific and targeted agents.
Keywords: Inflammatory bowel disease, Crohn’s disease, Ulcerative colitis, treatment, anti-TNF antibodies.
INTRODUCTION
Inflammatory bowel disease (IBD) is a chronic, relapsing, in-flammatory condition of the gastrointestinal tract affecting more than a million people worldwide. The incidence of IBD is assumed to be highest in developed countries and lowest in the developing regions of the world. A higher rate of IBD is observed in individu-als living in colder climates, as well as the urban population. West-ernization of lifestyles, including changes in dietary habits and en-vironmental changes such as improved sanitation and industrializa-tion are implicated in the rising trend in the incidence and preva-lence of IBD in previous low-incidence Asian countries [1-3].
IBD is a heterogeneous group of diseases that can be broadly classified into Crohn disease (CD) and ulcerative colitis (UC). The term IBD-unclassified (IBDU), previously referred as indeterminate colitis (IC), applies to the subset of 10% to 15% of patients with IBD in whom this sub-categorization is not possible. There is no gold standard single test that provides the diagnosis of IBD so as-signing a diagnosis of IBD is often not straightforward and involves integration of historical factors, physical examination findings, and evidence of inflammation on endoscopic, histologic, and radiologic evaluations [4].
The inflammation in CD is typically transmural. This frequently leads to complications from perforating disease or from progressive fibrosis and stricturing. CD can thus be thought of as fitting one of three phenotypes: inflammatory, stricturing, or perforating disease (the latter including abscesses and fistulae). Disease behavior is not
*Address correspondence to this author at the Division of Digestive Dis-
eases, Department of Internal Medicine, Rush University Medical Center,
Chicago, Illinois 60612; Tel: +9821 8241 5300; Fax: +9821 8241 5400; E-mail: [email protected]
necessarily constant in an individual patient. Indeed, inflammatory disease frequently progresses to penetrating disease, and then to fibrosis and stricturing. Perianal disease, including abscesses and fistulae, is commonly encountered, particularly in conjunction with terminal ileal disease [5].
Inflammation in UC is limited to the mucosal layer of the colon. The rectum is virtually always involved, with inflammation extend-ing proximally in a confluent fashion. The extent of proximal in-volvement is variable. Unlike CD, UC is frequently acute or suba-cute in onset. Like CD, the subsequent clinical course is one of recurring episodes of symptomatic disease interspersed with epi-sodes of relative (or complete) quiescence [6].
Although UC and CD have significant differences, many (but not all) of the treatments available for one are also effective for the other. Both diseases usually have waxing and waning intensity and severity. In most cases, symptoms do correspond well with the degree of inflammation present for either disease, although this is not universally true. In the last decade, our understanding of this enigmatic group of disorders has improved. Genetic, environ-mental, infectious, and immunologic factors are all thought to play a role in the etiology and pathogenesis of IBD [7].
Optimal medical management of IBD is multifaceted and indi-vidualized. Except for mild cases (primarily UC), most patients require combination therapy to achieve sustained response or re-mission. Fine-tuning of treatment is based upon clinical, biochemi-cal, endoscopic, and histologic responses that depend upon consid-erations of drug doses, routes, and timings and drug–drug syner-gies. Despite advances in our ability to predict clinical course in specific patients, the individual response to IBD therapy often is idiosyncratic [8].
Current Therapeutic Approaches in Inflammatory Bowel Disease Current Pharmaceutical Design, 2010, Vol. 16, No. 33 3669
We reviewed the current therapeutic approaches in inflamma-tory bowel disease by searching English-language publications in PubMed and Cochrane database and references from relevant arti-cles published between 1970 and September 2010. The main search terms were inflammatory bowel disease, UC, CD, remission, treat-ment, therapy, management, and maintenance. We selected articles on the basis of quality, relevance to the illness, importance in illus-trating an effective therapy, or the level of attention that they have received in the field.
THERAPEUTIC AGENTS
Therapeutic recommendations depend on the disease location, disease severity, and disease-associated complications. Therapeutic approaches are individualized according to the symptomatic re-sponse and tolerance to medical intervention.
Present therapeutic approaches should be considered sequential to treat "acute disease" or "induce clinical remission," and then to "maintain response / remission."
5-AMINOSALICYLATES
Sulfasalazine, the parent compound of all ASAs used in IBD, was developed as a treatment for rheumatoid arthritis. It was later discovered to also benefit patients with IBD. 5-ASA agents are likely to have multiple anti-inflammatory effects, including inhibi-tion of cyclooxygenase, lipoxygenase, B-cells, and several key inflammatory cytokines, inhibition of T-cell proliferation, presenta-tion of antigen to T cells, and antibody production by B cells; inhi-bition of macrophage and neutrophil adhesion; and decreased pro-duction of IL-1 and TNF. Most recently, 5-ASA has been shown to activate selective peroxisome proliferators activated receptor ligand- (PPAR- ), a nuclear receptor that controls cell proliferation and apoptosis. The active moiety in sulfasalazine is 5-ASA and sulfapyridine moiety makes it possible for majority of sulfasalazine
to reach the colon and release 5-ASA through colonic bacteria. However, sulfasalazine also has anti-inflammatory effects through inhibiting NFkB and its anti-oxidant activity. Since therapeutic doses of sulfasalazine are tolerated poorly in up to 30% of patients, pharmaceutical companies have attempted to deliver 5-ASA to the distal small bowel and colon through the means other than sul-fapyridine moiety. This resulted in development of a variety of mesalamine derivatives; they differ in their site of active drug re-lease. These delivery systems include coating with protective mate-rials that release the drug in a pH or osmotic-dependent manner to achieve controlled (Pentasa) or delayed (Asacol, Apriso and Lialda) delivery; and diazo-bonding the drug to a second 5-ASA molecule (olsalazine) or to an inert carrier (balsalazide). The site of delivery of coated preparations depends largely on the properties of the coat-ing material used and its pH sensitivity. Some preparations (Pen-tasa) release half of the dose in the small intestine and the remain-der in the colon and other preparations release mesalamine in the distal terminal ileum and beyond. Diazo-bonded preparations have release profiles closely resembling that of sulfasalazine [9].
CD
5-ASA agents are generally safe and well tolerated and are used commonly for the treatment of mild active CD and for maintenance of remission, but their efficacy is not well established for either role and evidence suggests that this approach is minimally effective as compared with placebo and less effective than systemic corticoster-oid therapy. The most convincing evidence for a benefit has been for use of sulfasalazine in treatment of active CD involving the colon [10].
A meta-analysis of three double-blind randomized controlled trials of mesalamine (Pentasa 4 g daily) in active CD found a mod-est overall clinical benefit reflected as a 25 points reduction in CD Activity Index (CDAI) compared with placebo [11]. However, the
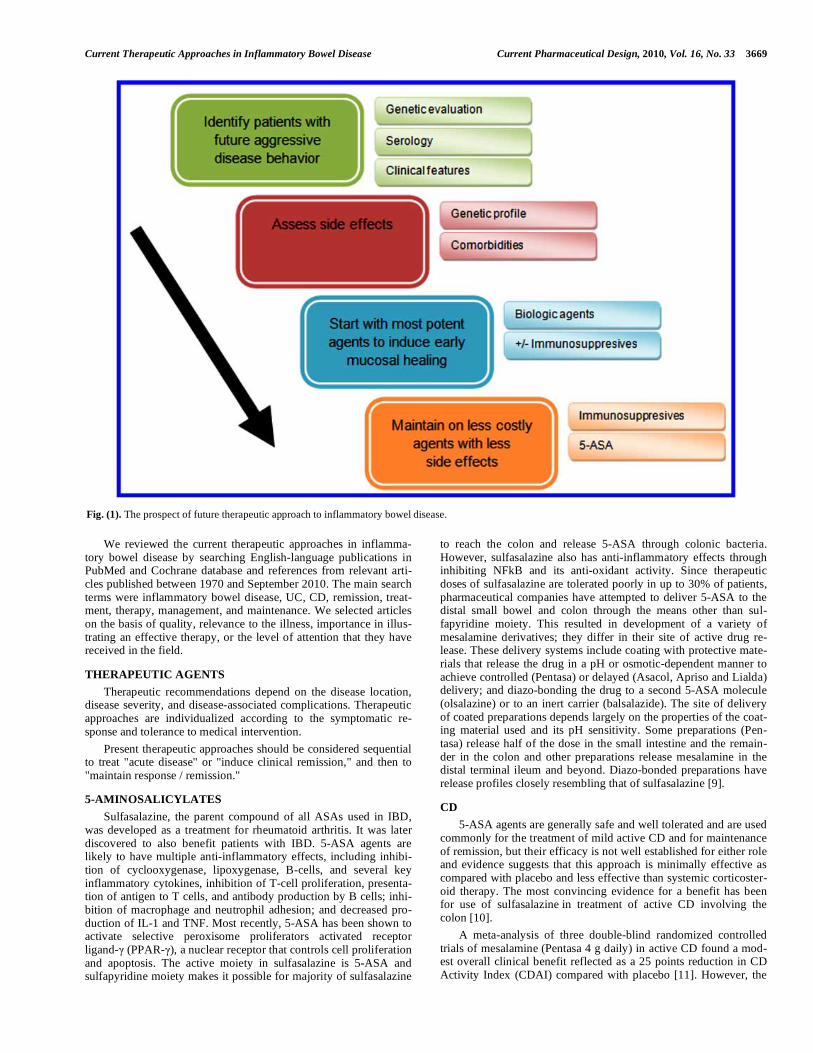
Fig. (1). The prospect of future therapeutic approach to inflammatory bowel disease.

3670 Current Pharmaceutical Design, 2010, Vol. 16, No. 33 Sohrabpour et al.
largest RCT of Pentasa in active CD, that appeared not to show effectiveness of Pentasa, was never published in full manuscript and thus was not included in the meta-analysis. A similar CDAI remission rate of 45% was seen with Asacol, 3.2 g/d for 16 weeks, in ileocolonic CD [12]. Thus, one can conclude that there is no evidence for use of mesalamine for treatment of active CD.
When initiated within three months of a medically-induced remission, mesalamine (2 g bid), in contrast to placebo, prevented more relapses over a two year period [13]. A Cochrane review of seven randomized placebo-controlled trials concluded that treat-ment with 5-ASA agents for at least six months did not confer an advantage over placebo in patients with medically-induced remis-sion [14].
Rectal applications of mesalamine have never been evaluated in controlled trials in patients with distal colonic CD, but are generally believed to be effective in mild-to-moderate distal CD.
Three randomized controlled trials have failed to verify a defi-nite role for sulfasalazine in the long term prevention of postopera-tive CD [15-17]. Data for mesalamine has been equivocal in this setting and there is little support for the routine use of mesalamine for prevention of postoperative recurrence [18].
In summary, the role of 5-ASA products to treat active CD or as a maintenance medication is equivocal at best and ineffective for postoperative maintenance. Nonetheless, it may be a reasonable choice as first-line therapy for the treatment of mild CD in selected groups of patients. If so, sulfasalazine should be reserved for pa-tients with predominantly colonic disease, while time or pH-dependent release mesalamine are appropriate for patients with small bowel disease.
UC
Aminosalicylates (5-ASA) continue to be the first-line agent for the induction and maintenance of remission in mild to moderately active UC. There is firm evidence in support of sulfasalazine, but drug intolerance in up to a third of patients limits its use [19]. Therefore, non-sulfa-containing 5-ASA agents have been studied as well. One of the biggest challenges in 5-ASA therapy is poor ad-herence, which is reported to occur in up to 60% of patients on long-term treatment with 5-ASA[20] and is associated with an in-creased risk of disease flares [21].
Recent Cochrane reviews have analyzed the effectiveness of the newer 5-ASA medications for the induction and maintenance of remission in UC. No significant differences were found between 5-ASA and sulfasalazine in induction of remission or response, al-though a trend towards 5-ASA superiority was observed [22]. The newer preparations had a statistically significant therapeutic inferi-ority relative to sulfasalazine in maintenance therapy [23]. A recent meta-analysis of six randomized trials suggested balsalazide as more effective than mesalazine in induction of remission, while no benefit was found for balsalazide compared with mesalazine in preventing relapse [24]. Another meta-analysis of twenty random-ized controlled trials found no significant difference between sul-fasalazine and mesalamine or olsalazine in terms of efficacy and tolerability in UC [25]. Choice of 5-ASA agent should be based upon tolerability, ability to titrate dose to effect and cost.
CORTICOSTEROIDS
Corticosteroids bind to a cytoplasmic receptor and then enter the nucleus to interact with glucocorticoid-response elements on the chromosomal DNA, with a variety of antiinflammatory effects in-cluding inhibition of the recruitment and proliferation of lympho-cytes, monocytes and macrophages, migration of neutrophils to sites of inflammation, and decreased production of soluble inflam-matory mediators including cytokines, leukotrienes, and prosta-glandins [26]. Despite well-known adverse effects of steroids, when
used appropriately, they are generally safe and result in rapid symp-tomatic improvement.
CD
Corticosteroids are highly effective in induction of remission in patients with active CD [27]. It should be noted that some experts, including one of the authors [AK] do not use corticosteroids in patients with fistulizing CD because corticosteroids do not appear to be effective in this subset of CD and also could increase the risk of infectious complications like abscess. However, there has been no RCT in this subset of patients to objectively substantiate this view.
If there is a controversy for use of corticosteroids in treatment of active fistulizing CD, there is no disagreement that corticoster-oids must not be used as a maintenance medication for CD. Indeed, overwhelming evidence indicate that corticosteroids play no sig-nificant role in long term therapy in CD and its long term use is associated with unacceptable and harmful side effects [28].
The systemic effects of standard glucocorticoid formulations have led to the development of more potent formulations that are less well-absorbed and have increased first-pass metabolism. Con-trolled ileal-release budesonide has been nearly equal to prednisone for ileocolonic CD and more effective than mesalamine for induc-tion of remission in CD, with fewer glucocorticoid side effects [29, 30].
Studies examining the effectiveness of budesonide in maintain-ing remission have produced disparate results. A recent Cochrane meta-analysis which focused on 11 studies, concluded that budesonide was not more effective than placebo for maintaining remission [31].
The use of conventional systemic corticosteroids in patients with clinically quiescent CD does not appear to reduce the risk of relapse over a 24 month period of follow-up [32].
UC
The majority of patients with moderate to severe active UC benefit from oral or parenteral glucocorticoids. Although no study has directly compared the efficacy of oral and parenteral glucocor-ticoids, the latter commonly are used in severe disease. No ade-quately designed controlled study has been performed to confirm the clinical impression that continuous infusion of parenteral gluco-corticoids is superior to pulse therapy.
Topically applied glucocorticoids in liquid and foam formula-tions are also beneficial for distal colitis and may serve as an ad-junct in those who have rectal involvement plus more proximal disease. Hydrocortisone enemas or foam may control active dis-ease, although they have no proven role as maintenance therapy [33]. Randomized studies have demonstrated that topical 5-ASA is more effective than topical glucocorticoids [34,35]. The combina-tion of topical steroids and topical mesalamine may be more effica-cious than either alone in the short-term treatment of distal UC [36].
Oral systemic steroids should not be used as continuous therapy due to their side effects. In chronically active distal colitis, how-ever, the long term rectal administration of steroid enemas or foams may be acceptable due to their low systemic bioavailability [37].
IMMUNOSUPPRESSIVE AGENTS
CD
Immunosuppressive agents such as azathioprine (AZA), 6-mercaptopurine (6MP) and methotrexate (MTX) have been studied for induction of active moderate-to-severe corticosteroid-dependent CD. The therapeutic role of these agents for treatment of active disease remains controversial due to their perceived relatively slow-acting effect and adverse effects. However, there is no controversy in regards to their steroid sparing effects in patients with prednisone dependent disease.

Current Therapeutic Approaches in Inflammatory Bowel Disease Current Pharmaceutical Design, 2010, Vol. 16, No. 33 3671
A meta-analysis of AZA and 6MP for the induction of remis-sion included eight randomized placebo controlled trials (n= 425). The odds ratio (OR) of a response to azathioprine or 6-mercap-topurine therapy compared with placebo in active CD was 2.43. A steroid sparing effect was seen. Adverse events requiring with-drawal from a trial, principally allergy, leukopenia, pancreatitis, and nausea were increased with active therapy [38].
However, a response to these medications will usually be seen within three to six months and they generally require concomitant corticosteroids for induction of remission, with a gradual reduction in the steroid dose after one to two months of treatment with azathioprine or 6MP.
Seven trials of azathioprine therapy and one of 6-mercap-topurine were included in a recent Cochrane review. Azathioprine used among patients with non-active CD is effective for reducing the risk of disease recurrence over a 6 month to 2 year period. Higher doses of azathioprine (2.5 mg/day) were more effective than lower doses (1.0 or 2.0 mg/day) for preventing disease recurrence. 6MP may be effective for reducing the risk of disease recurrence over a 2 year period [39].
Azathioprine and 6MP are required to be metabolized to their therapeutically active product 6-thioguanine (6TG) [40]. 6TG is not only the therapeutically active metabolite of the Azathioprine/6MP; it is also the primary cause of leucopenia, the most serious side effect of these drugs. One of The rate limiting enzymes involved in Azathioprine/6MP metabolism is thiopurine methyltransferase (TPMT). TPMT enzyme activity dictates the 6TG levels and thus low enzyme activity that occur in up to 11% of subjects and lack of the enzyme that occur in 0.3% of population will result in high 6TG levels and profound and dangerous leucopenia [41,42]. It is there-fore most advisable to check the enzyme levels prior to starting the medication and either avoid its use in those with no enzyme activity or adjust the dose in those with low enzyme levels. Alternatively, one should start with low dose [e.g. 50 mg of Azathioprine and 25 mg of 6MP] and check CBC in 5-7 days and increase the dose every 1-2 weeks if assessing enzyme activity is not available. Re-gardless, CBC and LFT should be checked regularly while the pa-tients are taking these medications. We suggest checking CBC every 3 months and LFT every 6 months. We also suggest monitor-ing the compliance and effective dosing of the medications by measuring blood 6TG levels. Indeed, one should not consider therapeutic failure unless the patient is taking adequate dose of Azathioprine/ 6MP that achieve 6TG levels of 260 [43] for at least 3-6 months. Alternative means of monitoring adequate dosing is to aim for WBC of 4000-500 and elevated MCV [44] in those patients with normal serum B12 and folate.
Methotrexate is a folate analog and reversible competitive in-hibitor of dihydrofolate reductase (DHFR). Methotrexate interferes with DNA synthesis and also has multiple anti-inflammatory effects including decreased pro-inflammatory cytokine production and lymphocyte apoptosis [45]. There is evidence from a single large randomized trial to recommend the use of methotrexate 25 mg in-tramuscularly weekly for induction of remission and complete withdrawal from steroids in patients with refractory CD [46,47]. Concomitant therapy with folic acid 1 mg/day may diminish ad-verse effects to methotrexate. Optimal strategies for surveillance liver biopsies in these patients have not been established. Mounting experience suggests that the incidence of hepatotoxicity is low and that surveillance liver biopsies based upon the cumulative metho-trexate dose may not be warranted [48].
Intramuscular methotrexate maintains remission in CD. At a dose of 15 mg/week, it is safe and effective for maintenance of remission in CD [49]. Oral methotrexate (12.5 to 15 mg/week) does not appear to be effective for maintenance of remission in CD [50].
Use of methotrexate should be reconsidered in those patients with high risk of hepatic side effects. In fact one of the authors [AK] does not recommend using methotrexate in patients with high risk of nonalcoholic steatohepatitis (NASH) [obesity, Type 2 diabe-tes and metabolic syndrome] or those with excessive use of alcohol. We also suggest careful monitoring of liver function [initially every 3-4 months and then every 2 months if the cumulative dose is more than 2 grams] and regular lung auscultation.
The use of mycophenolate mofetil has been proposed as an alternative immunosuppressive therapy for patients either refractory or intolerant to AZA/6MP. It is an anti-metabolite with pharma-codynamic properties similar to AZA and 6-MP but a more rapid onset of action. A randomized controlled trial comparing mycophe-nolate mofetil to AZA in 70 steroid-dependent CD patients with moderately active disease showed similar response rates [51].
Uncontrolled case series suggested that tacrolimus may be use-ful in the treatment of perianal disease [52,53]. In a small controlled clinical trial, patients treated with oral tacrolimus (0.2 mg/kg per day) had a higher response rate (defined as closure of at least 50% of fistulas) at week 4 compared to placebo (43% vs. 8%), but no differences were observed in terms of complete fistula closure [54]. The drug also may be effective as a topical agent for oral and peri-anal ulcerating disease [55-56].
UC
Cyclosporine A (CSA) is a safe and effective therapy for se-vere, steroid-refractory UC [57]. Intravenous cyclosporine mono-therapy may be as effective as intravenous glucocorticoids in pa-tients with severely active UC [58]. The relatively quick response makes the short-term [59] of cyclosporine potentially attractive, but the long-term benefit is unclear, when adverse events such as cy-closporine-induced nephrotoxicity may become more obvious. Side effects and drug interactions with CSA are common, some of which may be life-threatening. Thus, patients receiving therapy must be carefully monitored [60]. Careful monitoring the blood level during IV infusion for treatment of acute UC and during oral treatment will not only decrease the frequency of side effects, it will also enhance its effectiveness.
The evidence for the effectiveness of azathioprine and 6-mercaptopurine for the maintenance of remission in UC is still con-troversial. However, its steroid sparing effects in patients with prednisone dependent UC is well established. Azathioprine may be an effective treatment for patients who have failed or cannot toler-ate standard maintenance therapy with 5-ASA or sulfasalazine or for patients who require repeated courses of corticosteroids to in-duce remission. There is insufficient evidence to assess superiority of azathioprine alone, or azathioprine in addition to standard main-tenance, as compared to standard maintenance with 5-ASA or sul-fasalazine only [61].
A single trial of oral methotrexate 12.5 mg weekly showed no benefit over placebo in remission induction in patients with active UC [62].
Only one trial has studied the effect of methotrexate on mainte-nance therapy in patients with UC. It randomized 30 patients to oral methotrexate (12.5 mg/week) and 37 to placebo. No significant effect was observed, and the authors concluded that the available evidence is not sufficient to recommend the use of methotrexate to maintain remission in patients with UC [63].
Few trials have examined the efficacy of mycophenolate mofetil (MMF) in UC. A pilot randomized study of patients with chronic active UC receiving concomitant prednisolone failed to show superiority of MMF over AZA throughout the one-year study period in terms of efficacy and side effect profile [64].
Tacrolimus may be effective for short-term clinical improve-ment in patients with refractory UC [65].

3672 Current Pharmaceutical Design, 2010, Vol. 16, No. 33 Sohrabpour et al.
ANTIBIOTICS, PROBIOTICS, AND PREBIOTICS
Interactions between intestinal microbes and the host are the subject of intensive ongoing research since they may influence a variety of diseases. Part of this research involves the deliberate manipulation of the intestinal microflora with a therapeutic inten-tion. The greatest experience has been in the inflammatory bowel diseases. There are three general methods by which the intestinal microflora can be altered: administration of antibiotics, prebiotics (i.e. dietary components that promote the growth and metabolic activity of beneficial bacteria), or probiotics (i.e. beneficial bacte-ria). Combination of these methods is also possible (synbiotics) [66].
Antibiotics have a well-established role in the treatment of pyo-genic complications of the inflammatory bowel diseases (IBD), such as abscesses and wound infections. In contrast, their benefit in the treatment of the primary disease processes of CD, UC, and pouchitis has not been well-established in carefully-designed clini-cal trials, although they are used commonly [67-69].
Probiotics are living organisms in foods and dietary supple-ments that might beneficially affect the host in a number of ways, including improving its intestinal microbial balance, blocking adhe-sion sites on colonocytes (which might improve mucosal barrier function), and enhancing local immune response [70]. They exert their effects on numerous cell types involved in the innate and adaptive immune responses, such as epithelial cells, dendritic cells, monocytes/macrophages, B cells, T cells, including T cells with regulatory properties, and NK cells [71].
CD
Luminal bacterial microbiota have been hypothesized to be a putative etiological factor in CD and this has led to the use of anti-biotics for treating patients with mild-to-moderate luminal and peri-anal diseases [72].
Metronidazole, 10 or 20 mg/kg, has been compared with pla-cebo for mild to moderate disease and was not more effective than placebo for inducing remission. Patients with colonic involvement fared better than those with isolated ileal involvement, which has been a consistent finding in several studies [73]. Two small pla-cebo-controlled trials with metronidazole 1 g daily and metronida-zole 800 mg daily in combination with cotrimoxazole did not dem-onstrate efficacy in the treatment of active CD [74,75].
Although antibiotic therapy is frequently used in the treatment of perianal fistulae, there are no randomized controlled trials to support this practice. Most of the studies of perianal fistulizing disease treated with antibiotics are uncontrolled and the sample sizes are small. Non-suppurative perianal complications of CD typically respond to metronidazole alone [76,77] or in combination with ciprofloxacin [78]. Ciprofloxacin is increasingly used to treat CD. For perianal fistulas, ciprofloxacin may be similar in efficacy to metronidazole and with fewer side effects [79], and its addition might improve the response to infliximab [80].
Rifaximin is a non-systemic antibiotic, since it is essentially non-absorbable from the gut. It has particular indications for trav-eler's diarrhea. There has been interest in recent years in the poten-tial roles of rifaximin in CD. An uncontrolled trial of rifaximin, 200 mg tid, reported benefits over 16 weeks in patients with active dis-ease [81], but a small, multi-center placebo-controlled trial of 12-weeks duration failed to demonstrate superiority of rifaximin 800 mg daily or bid compared with placebo [82].
One important question concerning antibiotics and CD is their ineffectiveness in about 40–50% of patients. An interesting light on this problem has been shed by a study on the relationship between antibiotic response and NOD2/CARD15 gene variants in CD pa-tients with perianal disease. A complete fistula response was re-corded in 33.3% of patients with NOD2/CARD15 wild type com-pared with none of those with NOD2/CARD15 variants [83].
Clinical trials of probiotics in CD have shown mixed results. The available data do not support clinical effectiveness of probiotic therapy for either induction or maintenance of remission in patients with CD [69, 84].
UC
Antibiotics have a limited role in the management of UC, and controlled trials assessing the addition of intravenous metronidazole [85] or metronidazole and tobramycin [86] to parenteral steroids in severe colitis did not show benefit compared to steroids alone. A controlled trial included 28 patients with moderate to severe, steroid refractory disease who were randomly assigned to either rifaxi-min 400 mg twice daily or placebo for 10 days, while intravenous corticosteroids were continued [87]. Although overall clinical out-comes were not different, stool frequency, rectal bleeding, and sig-moidoscopy scores were significantly improved in the rifaximin-treated group.
The primary role of antibiotics in the treatment of UC is in the management of its suppurative complications. A course of broad-spectrum antibiotics is often prescribed in patients with severe ster-oid-refractory colitis before they are considered refractory to medi-cal therapy [88]. One should not hesitate to start broad-spectrum antibiotics for all patients who present with fulminant disease with high fever, leukocytosis with bandemia and peritoneal signs or megacolon. However, there is no direct evidence for this commonly used strategy.
There is limited evidence that probiotics added to standard ther-apy may provide modest benefits in terms of reduction of disease activity in patients with mild to moderately severe UC. Whether probiotics are as effective in patients with severe and more exten-sive disease and whether they can be used as an alternative to exist-ing therapies is unknown [89].
Studies evaluating probiotics for maintaining remission of UC are limited by trial design and use of different probiotics with vari-able bacterial contents. Thus, questions remain regarding optimal probiotic, dosing, specific patient populations, and placement in therapy [90,91].
Probiotic use, although generally considered a safe intervention, may have some potential negative effects. Bacteremia and endo-carditis have been described with lactic acid bacteria [92]. Other theoretic risks include antibiotic resistance transfer from the probi-otics bacteria to other bacteria in the gastrointestinal tract and im-munologic effects [93]. These issues need to be considered when contemplating the use of probiotics in the severely ill UC patient who is likely at a greater risk of bacterial translocation across the diseased colonic mucosa.
NUTRITION
CD
A combination of factors contributes to the pathogenesis of malnutrition in IBD including reduced nutrient intake, malabsorp-tion, increased energy expenditure, and enteral protein loss.
Diverting the fecal stream in patients with CD can treat and even prevent disease, whereas reinfusion of ileostomy contents leads to new inflammatory changes within only one week [94]. The putative mechanisms are bowel rest, provision of nutrients, altera-tion of bowel flora or alteration of antigenic stimuli.
The role of enteral nutrition in CD is controversial. No placebo-controlled trials of nutritional therapy for active CD have been per-formed. A recent Cochrane systematic review demonstrated that corticosteroids were more effective than enteral nutrition for induc-ing remission of active CD (odds ratio 0.33, 95% CI 0.21–0.53). Protein composition did not influence the effectiveness of EN in the treatment of active CD. A non-significant trend favoring very low fat and/or very low long chain triglyceride content was show [95].

Current Therapeutic Approaches in Inflammatory Bowel Disease Current Pharmaceutical Design, 2010, Vol. 16, No. 33 3673
A Cochrane review looking into 2 small studies came to no firm conclusion regarding the effectiveness of enteral nutrition for main-tenance of remission in CD [96].
At present time, the only appropriate use of enteral diets is as an adjunctive therapy to support a patient's nutrition.
In severe disease, there is no specific role for total parenteral nutri-tion in addition to steroids. Nutritional support through enteral (elemental or partially digested products) feeding or parenteral hy-peralimentation (if enteral feeding is not feasible) is indicated, after 5–7 days, for patients who are unable to maintain adequate nutri-tional requirements [10]. However, it should be emphasized that balanced food and enteral route are the safest and best means of nutritional support.
Increasingly, specific nutrients are being considered for their therapeutic properties. An example includes the use of omega-3 free fatty acids. A recent meta-analysis and a systematic review have concluded that omega-3 fatty acids are safe but probably inef-fective for maintenance of remission in CD [97,98].
UC
In contrast to CD, where enteral nutrition or bowel rest with total parenteral nutrition can at least temporarily improve disease, multiple studies have not found elemental and parenteral nutrition with or without bowel rest to have any therapeutic advantage in patients with UC, although they can occasionally be used as ad-juncts to drug therapy in more severely ill patients.[99,100]. Thus the role of nutrition in UC is only for nutritional support in patients with severe disease who are not able to maintain their normal nutri-tional state.
Short-chain fatty acids (SCFA), especially butyrate, a by-product of anaerobic fermentation of undigested carbohydrates within the colon, are an important energy source for colonic epithe-lial cells [101]. It has been proposed that UC may result from a metabolic defect in SCFA oxidation in the colon and that this defect may be corrected by supraphysiologic luminal levels of SCFA in the colon. Clinical trials published suggest that topical SCFA pro-vide an effective primary and/or adjunctive treatment in patients with mild to moderate distal UC at substantial cost savings and without significant side effects [102].
Omega 3 fatty acids (fish oil) have no place in induction or maintenance of remission in UC [103,104].
BIOLOGIC AGENTS
CD
Tumor necrosis factor alpha (TNF ) has several biologic activi-ties and there is increasing evidence suggesting a central role for TNF in CD [105] (Table 1).
Infliximab was the first biological response modifier shown to be effective in CD. It is a chimeric (25% mouse / 75% human) anti-body against TNF . It has provided a powerful new tool for the treatment of moderately to severely active CD that is refractory to conventional therapy. It was initially shown to be effective in the treatment of moderate to severe medically refractory disease when given as single infusion. Overall, 33% of all infliximab patients compared to 4% of placebo achieved remission at wk 4 (P = 0.005). Statistical analyses demonstrated no effect of concomitant medica-tion or disease location on the response rates or remission rates. There was no statistically significant difference between the three doses of infliximab used in the trial, although the 5 mg/kg body weight dose consistently yielded the highest response and remission rates. While significantly more infliximab patients maintained a response at 12 wk, 37% relapsed, suggesting that a single dose was insufficient [106].
ACCENT I was a large multicenter randomized double-blind international trial studying remission maintenance in non-fistulizing
CD patients treated with infliximab. At week 0, all patients received a single 5 mg/kg intravenous infusion of infliximab. They were then stratified according to their response and then randomly assigned to one of three groups: Group 1 — Placebo infusions at weeks 2, 6, and every 8 weeks thereafter until week 46; Group 2 — 5 mg/kg of infliximab at weeks 2 and 6 followed by 5 mg/kg every 8 weeks; and Group 3 — 5 mg/kg of infliximab at weeks 2 and 6 followed by 10 mg/kg every 8 weeks thereafter. Patients who had responded at anytime to infliximab therapy but then worsened clinically were eligible to crossover to active, episodic treatment with infliximab (5, 10, 15 mg/kg for patients originally assigned to group 1, 2, and 3, respectively). After 10 weeks, there was a statistically significant improvement in the response and remission rates in the two groups that received scheduled maintenance therapy. Also, the initial clini-cal response was maintained significantly more often in the two groups that received scheduled maintenance therapy [107]. The ACCENT I trial clearly demonstrated that scheduled treatment was more effective than episodic treatment in maintaining remission, and that antibodies to infliximab were minimized by this approach [108]. Significantly more patients in the maintenance therapy groups had discontinued steroids at wk 54, and fewer hospitaliza-tions and surgeries related to CD had occurred in them. There were no differences in serious adverse events between the three groups.
Infliximab is also effective in the treatment of fistulizing CD. In the ACCENT II study, 306 patients with one or more draining ab-dominal or perianal fistulas (at least 3 month's duration) received an induction regimen of three infliximab infusions (5 mg/kg). One hundred ninety five patients with a response at week 10 and 14 as well as 87 with no response were randomized to placebo or inflixi-mab (5 mg/kg) every 8 week until week 54. Time to loss of re-sponse was significantly longer for patients in the infliximab group than placebo (>40 vs. 14 weeks, P < 0.001). Furthermore, at week 54, 36% in the infliximab group compared to 19% in the placebo group had no draining fistulas (P = 0.009) [109]. In a follow-up report of 192 patients who were classified as responders and ran-domized to maintenance infliximab (5 mg/kg every eight weeks) or placebo, those receiving infliximab had significantly fewer hospi-talizations, surgeries, and procedures compared with placebo [110].
Adalimumab is a recombinant fully human IgG1 monoclonal antibody directed against TNF that also induces T-cell and mono-cytes apoptosis [111]. Unlike infliximab, which requires an intrave-nous infusion, adalimumab is administered by a subcutaneous self injection pen.
Its efficacy in CD was initially evaluated in the CLASSIC I trial. It demonstrated that adalimumab can be used for the induction of remission in patients with moderate to severe CD patients naive to anti-TNF therapy and is effective with respect to placebo to in-duce clinical remission (CDAI<150 points) and clinical response (CDAI decrease of 100 points) in treated patients. From this trial, the authors concluded that a 160-mg induction dose followed by 80 mg at week 2 was effective in inducing remission [112].
The CLASSIC II study followed patients who achieved remis-sion in the first trial and randomized them to either placebo, or adalimumab 40 mg weekly or every other week. Clinical remission at week 56 was seen in 44%, 83%, and 79% of patients, and clinical response at week 56 was seen in 56%, 79%, and 89%, respectively. Most patients treated with adalimumab in this trial were able to discontinue steroids by the end of the study. These data suggest that the maintenance of remission can be achieved in the majority of patients who achieved remission with induction therapy [113].
These data have been confirmed by another study (CHARM) which showed that adalimumab administered weekly or every other week was superior to placebo for maintaining remission at 56 weeks (36% every other week, 41% weekly and 12% placebo). The adalimumab groups also had significantly more steroid discontinua-tion and complete fistula closure. In this study, weekly administra-

3674 Current Pharmaceutical Design, 2010, Vol. 16, No. 33 Sohrabpour et al.
Table 1. Landmark Trials for Anti-TNF Agents in CD
Main Findings Design N Subjects
Infliximab
• Multiple infusions were more effective than single
infusion
• The efficacy of the scheduled therapy was better
compared with the efficacy of the episodic strategy
• Higher number of infliximab treated individuals were
able to discontinue corticosteroids while remaining in
remission
• Placebo
• Infliximab (5 mg/kg) q8w
• Infliximab (10 mg/kg) q8w
573 Nonfistulizing CD re-
sponding to a single infu-
sion (5 g/kg)
ACCENT I
[178]
• Higher response rate and complete fistula closure in
infliximab recipients
• Less hospitalizations and fewer surgical procedures in
infliximab recipients than placebo group
• Placebo
• Infliximab (5 mg/kg) q8w
306 Fistulizing CD responding
to a three-dose induction
regimen
ACCENT II
[109]
Adalimumab
• Adalimumab is effective to induce clinical remission
and clinical response in moderate to severe CD pa-
tients naive to anti-TNF therapy
• A 160-mg induction dose followed by 80 mg at week
2 was effective in inducing remission
• Placebo
• Adalimumab (40/20 mg)
2wks apart
• Adalimumab (80/40 mg)
2wks apart
• Adalimumab (160/80 mg)
2wks apart
299 Moderate to severe CD
patients naive to anti-TNF
therapy
CLASSIC I
[112]
• Placebo
• Adalimumab 40 mg q2w
• Adalimumab 40 mg weekly
55 Patients in remission at
wk 4 of CLASSIC I trial
CLASSIC II
[113]
• Higher rates of remission in the adalimumab groups
• More steroid discontinuation and complete fistula
closure in adalimumab groups
• Sustained improvements in health-related quality of
life measures in adalimumab groups
• Adalimumab (80/40 mg)
2wks apart, then:
• Placebo
• Adalimumab 40 mg q2w
• Adalimumab 40 mg) weekly
778 Patients with moderately
to severely active CD
CHARM
[115,116]
• Adalimumab was effective to induce clinical remis-
sion and clinical response
• Placebo
• Adalimumab (160/80 mg)
2wks apart
325 Patients not responding or
intolerant to infliximab
GAIN [209]
Certolizumab
• Certolizumab modestly improves response rate in
moderate to severe CD patients
• No significant improvement in remission rates ob-
served compared to placebo
• Placebo
• Certolizumab (400 mg) at
wks 0, 2, and 4 and then
q4w
662 Moderate to severe CD
patients refractory to
standard therapy
PRECiSE 1
[119]
• Significantly higher maintenance of response in cer-
tolizumab group compared with placebo
• Placebo
• Certolizumab (400 mg) q4w
668 Patients with moderate to
severe CD who responded
to treatment with certoli-
zumab pegol (400 mg)
PRECiSE 2
[120]
• By the end of the 3-year study period, only one third
of patients remained in remission
• Placebo
• Certolizumab (400 mg) q4w
428 Patients who completed
PRECiSE 1 or PRECiSE
2 trials
PRECiSE 3
[121]
• Reinduction with certolizumab pegol is effective for
treating patients who have relapsed after successful
induction therapy
• Placebo
• Certolizumab (400 mg) at
wks 2, and 4 and then q4w
124 Patients who relapsed in
PRECiSE 1 or PRECiSE
2 trials
PRECiSE 4
[122]

Current Therapeutic Approaches in Inflammatory Bowel Disease Current Pharmaceutical Design, 2010, Vol. 16, No. 33 3675
tion of adalimumab at 40 mg per week resulted in a response that was as efficacious as adalimumab dosing every other week [114]. Subsequent analyses showed that patients treated with adalimumab had a significantly lower 1-year risk of both all-cause and CD-related hospitalization and surgery [115] and sustained improve-ments in health-related quality of life measures through week 56 than placebo patients [116].
The GAIN study evaluated the use of adalimumab in patients who had persistent symptoms on infliximab therapy or were intol-erant to this latter agent. It showed that 21% of patients achieved remission compared with 7% of the placebo group. Thus, adalimu-mab provided a viable alternative to infliximab therapy, especially in those patients who experienced infusion reactions, despite the fact that these antibodies are fully human and are not necessarily less immunogenic. However, in the GAIN study both the adalimu-mab and placebo responses were numerically lower than those in the CLASSIC I trial. This lower efficacy could be related to the longer duration of disease with increased fibrostenosis, the presence of more refractory disease and the loss of response to TNF inhibi-tion [117].
Certolizumab pegol is a pegylated humanized Fab fragment of an anti-TNF monoclonal antibody with a high affinity for TNF . Unlike other monoclonal antibodies such as infliximab and adali-mumab, certolizumab pegol does not contain an Fc portion and consistently it does not induce in-vitro complement activation, anti-body-dependent cellular cytotoxicity or apoptosis [118]. This drug is injected subcutaneously.
The PRECiSE 1 study, a multicenter, randomized, double-blind, placebo-controlled trial, compared subcutaneous certolizu-mab to placebo in patients with moderate-severe CD. The primary endpoints were induction of a response at week 6 and a response at both weeks 6 and 26. Response rates at week 6 and 26 were signifi-cantly higher in the certolizumab group (35% vs. 27% and 23% vs. 16%, respectively). Response rates were increased in a subset of patients with a baseline serum C-reactive protein (CRP) level of at least 10 mg/L. However, rates of remission did not differ signifi-cantly between the groups or in the subset with higher CRP levels [119].
The subsequent PRECiSE 2 trial randomized CD patient re-sponders to the open induction regimen, to maintenance therapy with certolizumab at a dose of 400 mg or placebo every 4 weeks through week 24. At week 26, 48% of certolizumab patients com-pared with 29% of placebo patients showed clinical remission, and 63% compared with 36% showed clinical response based on CDAI. Safety and tolerability were similar to other anti-TNF agents, al-though patients treated with certolizumab had lower rates of autoan-tibody formation [120].
PRECiSE 3 reported results of the long-term use of certolizu-mab. For those patients without any drug interruption, 66.1% of patients had a response at week 80 and 62.1% of patients were in remission based on the Harvey–Bradshaw Scale [121].
Patients who experienced a significant worsening of symptoms necessitating study withdrawal at week 2 in PRECiSE 1 and at week 6 in PRECiSE 2 were eligible to enter the extension study PRECiSE 4, in which they received reinduction with certolizumab pegol and then continued dosing every 4 weeks. At week 4 of PRECiSE 4, response rates were 65%. Response was maintained in 55% of these responders, through week 52 [122].
The FACTS survey documented a 50% rate of response in pa-tients with fistulizing CD treated with certolizumab [123].
Studies evaluating the efficacy of infliximab, adalimumab, and certolizumab have generally shown similar results but no studies have directly compared them. The decision whether to use adalimumab, infliximab, or certolizumab in patients with CD re-quiring anti-TNF therapy will mostly be influenced by the conven-ience (and availability in individual countries) of subcutaneous
administration of adalimumab and certolizumab pegol at home contrasted against office based infusion, cost and patient and/or third party payer choice. It is advisable not to switch between TNF antibodies if the patient is responding. The dose and/or schedule of TNF antibody might be adjusted if the patient begins to lose the response.
Natalizumab is a monoclonal antibody against the integrin- 4 (95% humanized and 5% murine-derived) that is administered by intravenous infusion. By binding to the 4 chain, it disrupts leuko-cyte adhesion to the endothelium and subsequent migration into the gut mucosa. Tissue studies show that endothelial cells from IBD patients demonstrate increased 4-mediated leukocyte adhesion [124]. By blocking this pathway, the concept is that there would be a decrease in inflammation and CD severity due to reduced cell traffic into inflamed tissues [125].
Four large studies have examined the use of natalizumab for the treatment of CD [126-129]. A Cochrane meta-analysis including these trials showed that natalizumab (300 mg or 3 to 4 mg/kg) is effective for induction of clinical response and remission in patients with moderately to severely active CD. Natalizumab appears to provide greater benefit in patients with elevated C-reactive protein levels, active disease despite the use of immunosuppressants, or prior anti-TNF therapy [130].
A meta-analysis of 24 trials in CD using TNF antagonists evaluated three major safety concerns: death, malignancy and seri-ous infection. There was no difference in death between anti-TNF and control groups for all trials (0.21 vs 0.05%). Malignancy was found in five patients receiving open-label treatment in studies prior to those that included placebo randomization; however, the overall frequency was not different (0.24 vs 0.39%). Serious infections were also similar between groups (2.09 vs 2.13%) [131].
UC
The role of anti-TNF therapy in active UC, steroid-dependent UC, refractory pouchitis, and in maintenance of disease remission is evolving. TNF is expressed at high levels in the colonic mucosa of patients with UC [132]. There is also an increased production of TNF by colonic lamina propria mononuclear cells and high con-centrations of TNF in stool of patients with UC [133,134].
While several small studies of infliximab collectively showed equivocal efficacy in UC, the ACT (Active Ulcerative Colitis Tri-als) 1 and 2 provided definitive evidence supporting its efficacy in this population. In both the studies, a significantly higher proportion of patients in the infliximab groups (5 or 10 mg/kg at weeks 0, 2, 6 and then every 8 weeks) than in the placebo groups achieved clini-cal response and remission at week 8, and these outcomes were generally maintained through the end of the studies. There was no major difference in efficacy between the two doses of infliximab (5 and 10 mg/kg). Furthermore, infliximab treatment also correlated with significant differences in the proportion of patients who expe-rienced mucosal healing [135], an important finding in light of re-cent evidence suggesting that mucosal healing is significantly asso-ciated with a low risk of future colectomy [136] and is a strong predictor of a reduced risk of cancer in UC patients [137]. In both studies, infliximab patients successfully discontinued corticoster-oids in a significantly higher percentage with respect to the placebo group.
Infliximab seems to be effective as a rescue therapy to avoid colectomy in severe UC unresponsive to intravenous steroids in the short-term [138] and long-term [139] follow-up. Infliximab might be used in severe colitis instead of steroids if they are contraindi-cated [140].
Adalimumab appears to be of clinical benefit for patients with UC, including those who have previously lost their response to or cannot tolerate infliximab. In an open-label study of adalimumab in 20 patients with UC including 13 patients with prior loss of re-

3676 Current Pharmaceutical Design, 2010, Vol. 16, No. 33 Sohrabpour et al.
sponse or intolerance to infliximab, at weeks 8 and 24, the rates of clinical response were 25 and 50 percent, respectively, and the rates of clinical remission were 5 and 20 percent, respectively. The rate of mucosal healing was 30 percent at week 8 [141].
In another small open-label study, adalimumab was well toler-ated and effective in maintaining clinical remission in a subgroup of UC patients who had lost response or intolerance to infliximab [142].
The main possible adverse events related to the use of anti-TNF therapy include the increased risk of infections [143,144], neuro-logical events [145,146], worsening congestive heart failure [147] and the risk of lymphoma [148] and other malignancies. Issues surrounding the development of antibodies and autoimmunity are also of concern. In addition, interest has been directed toward the risk of vaccine preventable disease in the setting of anti-TNF ther-apy.
A history of TB exposure should be taken and a purified protein derivative (PPD) or Quantiferon assay or chest x-ray be performed in patients who are going to receive any anti-TNF agent [149]. Hepatitis B reactivation is a smaller concern; however, reactivation has been reported, and therefore hepatitis B surface and core anti-bodies should be checked [150].
Lymphoma risk has been discussed as a possible side effect, but it is unclear if increased risk is due to treatment or the underlying disease [151]. A series of patients with hepatosplenic T-cell lym-phoma has been reported in infliximab-treated patients [152]. Longer-term data across all agents is still needed to better under-stand the malignancy risk of these medications.
Antibodies against interleukin (IL)-12, IL-23, and IL-17, impli-cated in the pathogenesis or Crohn disease, are currently being stud-ied as potential therapeutic agents.
OTHER POTENTIAL ANTI-INFLAMMATORY AGENTS
Endogenous opioids and opioid antagonists have been shown to play a role in healing and repair of tissues. In an open-labeled pro-spective trial, low-dose naltrexone (4.5 mg/d), an opioid antagonist, was tested in 17 patients with active CD. The patients had a CDAI score of 220–450 and were treated for 3 months. At 1 month after treatment, 76% had achieved a response to therapy (a decrease in the CDAI score by 70 points), and at 8 and 12 weeks, 88% showed a response. Four weeks after discontinuation of therapy, 73% con-tinued to show a response. At 1 month after starting therapy, 29% of the patients had achieved a remission (a CDAI score of 150 points or less), and at weeks 8 and 12 of therapy, 53 and 47%, re-spectively, had achieved remission. Four weeks after discontinua-tion of therapy, 33% of the subjects were in clinical remission. Therefore, at some point during the 16-wk trial, 89% of patients exhibited a response (P < 0.001), and 67% achieved a remission (P = 0.07). ESR and CRP levels were significantly decreased at 3 months. Improvement in quality of life was recorded with low-dose naltrexone compared with baseline [153].
The peroxisome proliferator activated receptor (PPAR ) is a nuclear receptor highly expressed in the colon and playing a key role in bacterial induced inflammation. Animal studies have dem-onstrated impaired PPAR expression in colonic epithelial cells of mice with experimental inflammatory colitis [154]. The functional significance of impaired PPAR expression at the cellular level in inflamed human colonic epithelium is not well described [155]. Few studies have examined the effect of thiazolidinediones in pa-tients with UC. A controlled trial from China compared rosiglita-zone 4 mg/d plus 5-ASA 2 g/d daily with 5-ASA 2 g/d alone, given for 4 weeks in patients with mild or moderately active UC and showed significant decrease in disease activity assessed by Mayo score [156]. Another multicenter randomized, double blind, pla-cebo-controlled clinical trial compared the efficacy of rosiglitazone 4 mg orally twice daily versus placebo twice daily for 12 weeks in
105 patients with mild to moderately active UC. After 12 weeks of therapy, 23 patients (44%) treated with rosiglitazone and 12 pa-tients (23%) treated with placebo achieved clinical response (p=0.04). Remission was achieved in 9 patients (17%) treated with rosiglitazone and 1 patient (2%) treated with placebo (p=0.01). Quality of life was significantly improved at week 8 but not thereaf-ter [157]. There is growing concerns about the increased risk of myocardial infarction in diabetic patients treated with oral rosiglita-zone (and perhaps other synthetic PPAR ligands) [158]. In an out-standing study, 14 patients with active distal UC were randomized to either topical rosiglitazone (4 mg) or mesalazine (1 g) enema treatment once daily for 14 days. Rosiglitazone enema treatment was well tolerated and significantly reduced the Mayo UC score from, similar to the effect of mesalazine [159].
SYMPTOMATIC TREATMENT
IBD is a chronic debilitating disease affecting many aspects of human physiology and diminishing the patient's quality of life. Many patients are rather young and the psychosocial as well as economic burden of the disease is also significant [160]. The short-term and long-term complications imposed by therapeutic modali-ties are another area needing concern. In addressing the symptoma-tology of patients, one should consider the many associated organic and functional problems and help the patient put up with them. It should also be noted that GI symptoms in patients with IBD can be due to non-inflammatory causes and thus use of additional anti-inflammatory medication adds no benefit and could be associated with unnecessary side effects. For example, diarrhea in patients with CD and ileal resection could be due to bile acid-induced colo-nic secretion and should be treated with bile acid binding agents. Bloating, abdominal cramp and diarrhea in patients with IBD could be due to bacteria overgrowth or dietary factors [e.g. lactose or fructose intolerance] which are best treated with dietary modifica-tion. Abdominal pain in Crohn’s patients could be due to stricture requiring balloon dilatation or surgery. Of course, irritable bowel syndrome is common in IBD patients. Also, several IBD drugs can cause GI symptoms and should be considered as a possibility in those symptomatic patients with no evidence of active inflamma-tion. Examples are mesalamine induced-diarrhea and even bloody diarrhea, abdominal pain with diarrhea, fever and joint pain from azathioprine-induced vasculitis. Thus, comprehensive assessment of patients using careful history and physical with appropriated and targeted laboratory and radiological/endoscopic tests is essential for optimal management of patients with IBD.
Functional bowel disorders should be in mind in symptomatic patients. A substantial number of patients with UC in remission reported bowel symptoms highly suggestive of IBS despite no signs of active inflammation [161]. A study on IBD patients in long-standing remission, as assessed by laboratory, clinical, and endo-scopic parameters, demonstrated that 57% of patients with CD and 33% of patients with UC, experience IBS-like symptoms during remission [162]. Sleep parameters also greatly influence quality of life even when the disease is in remission [163], and sleep concerns need to be addressed as part of IBD management [164].
Supportive or resuscitative therapy with fluid and electrolytes is indicated for dehydrated patients. Transfusions are necessary in the setting of anemia and active hemorrhage.
Bone loss should be anticipated as a potentially serious compli-cation in all patients. Bone density should be checked at regular intervals, with appropriate medical management of bone loss. Se-rum 25-OH vitamin D should be checked regularly and corrected accordingly. Low serum vitamin not only negatively impacts bone, it also promotes inflammatory processes. Strategies to preserve bone density include smoking cessation, calcium and vitamin D supplementation, and bisphosphonates in patients at the highest risk and without contraindications [165].

Current Therapeutic Approaches in Inflammatory Bowel Disease Current Pharmaceutical Design, 2010, Vol. 16, No. 33 3677
A daily multivitamin should be added if there are any dietary restrictions. It is reasonable to suggest supplementation with folic acid based upon data suggesting that it might protect against the development of dysplasia [166].
In patients with abdominal cramping and diarrhea, it is advis-able to restrict fresh fruit and fresh vegetables, caffeine, carbonated beverages, and sorbitol-containing products. Anti-diarrheal and anti-cholinergic agents can help to alleviate symptoms.
Patients with ileal disease or resection can require parenteral vitamin B12 supplementation or the addition of resins to control bile salt diarrhea. Iron supplementation also may be needed. Serum vitamin B12 should be checked regularly in patients with ileal CD who are not on monthly subcutaneous injection [167].
Lactose intolerance is frequently noted in patients with UC. Patients with suggestive symptoms should undergo a lactose breath hydrogen test to confirm the diagnosis. Calcium supplementation should be maintained in patients on a limited lactose intake to minimize the risk of bone loss [168].
Because sulfasalazine inhibits absorption of folic acid, the latter usually is co-administered at dosages of 1 to 2 mg/d [169].
Patients who are especially troubled by psychosocial stresses may benefit from minor tranquilizers. Limited data suggest that stress can worsen the disease [170]. These medications should be used as adjuncts to behavior modification and involvement in a social support group.
All patients with IBD and in particular those on immune modu-lators [Azathioprine/6MP, methotrexate, biologics] should be vac-cinated. Patients with CD should be advised against smoking since smoking worsens the course of CD [171].
THERAPEUTIC APPROACH AND GOALS
The traditional clinical practice and recommended treatment for CD arranges the therapeutic agents in a step-up manner according to disease severity with an ultimate goal to maintain clinical remis-sion [10]. The term 'step-up' refers to a sequential treatment strategy that often begins with a less effective, potentially less toxic treat-ment strategy, with escalation to the highly effective but potentially more toxic treatment strategies in patients who failed each line of therapy.
Clinical trials in patients with rheumatoid arthritis evolved from studies of conventional therapies to studies of earlier interventions in patients at high risk of disease progression. The Best study showed that early aggressive treatment with infliximab in patients with rheumatoid arthritis may slow disease progression and prevent disease sequels like joint deformity [172]. In this multicenter, ran-domized trial, initial combination therapy including either predniso-lone or infliximab resulted in less radiographic damage after 1 year than monotherapy or step-up combination therapy. Radiologic damage is a surrogate marker for disease progression in RA, and its attenuation is considered an important endpoint. Endoscopic mu-cosal healing seems to be its equivalent in CD. The assessment of disease activity in UC and CD has traditionally been accomplished by assessing clinical indices that are highly symptom based, such as the CDAI or Harvey-Bradshaw Index (HBI) in CD, and the Mayo score, among others, for UC [173,174]. Patients with IBD often have symptoms that are not related to inflammatory lesions of the GI tract. Moreover, CDAI has been shown to lack correlation to the presence and degree of endoscopic lesions in CD [175]. The dis-connect between mucosal lesions and symptoms is illustrated by studies of postoperative recurrence of CD. Within a year after intes-tinal resection, at least 70% of patients have recurrent disease endo-scopically, yet clinical recurrence occurs in only one-third by 3 years, implying that endoscopic lesions and symptoms may not correlate [176].
The value of mucosal healing on outcomes in CD was demon-strated in several studies. In a prospective randomized controlled trial, patients with newly diagnosed treatment-naïve CD received either early combined immunosuppression therapy with infliximab and azathioprine, or conventional treatment with corticosteroids. Follow-up of the patient cohort for up to 4 years showed that endo-scopic remission, regardless of treatment, was associated with fewer relapses and a reduced need for repeated infliximab treatment [177]. During ACCENT I trial which evaluated infliximab for maintenance therapy of CD, mucosal healing was associated with a significantly lower need for hospitalizations [178]. Data from a large cohort of CD patients demonstrated that the presence of mu-cosal healing during therapy with infliximab was strongly associ-ated with a lower risk of major abdominal surgery [179]. In a Nor-wegian population-based study, mucosal healing after 1 year of medical treatment was reported to be predictive of reduced subse-quent disease activity and need for anti-inflammatory therapies. This study was performed before the introduction of biologic agents and suggests that the achievement of mucosal healing by any means is valuable and is not reflective only of the effect of biologic agents [136].
The available therapeutic agents differ in terms of their ability to induce mucosal healing. Corticosteroids are highly effective in induction of clinical remission, but are not associated with signifi-cant mucosal healing in CD and UC patients. In a multicenter pro-spective study, patients with CD who were treated with predniso-lone (1 mg/kg/day) for up to 7 weeks, 92% of patients underwent clinical remissions within 7 weeks of treatment. However, only 29% of patients in clinical remissions were also in endoscopic re-mission [180]. Although earlier postoperative prevention studies had demonstrated a lower endoscopic recurrence rate with 6MP compared with placebo (43% vs. 64%) [181], the SONIC study that evaluated AZA versus infliximab versus infliximab in combination with AZA in patients with active CD demonstrated a rate of mu-cosal healing of only 16.5% with AZA at 26 weeks [182]. There is little data regarding mucosal healing ability of methotrexate [183]. Infliximab induces endoscopic mucosal healing in CD patients [184,185]. In the open-label EXTEND trial, Rutgeerts and col-leagues found that induction plus maintenance therapy with adalimumab was better than induction therapy alone in maintaining remission in patients with moderate-to-severe ileocolonic CD. After 52 weeks, 24% of adalimumab patients had maintained mucosal healing, compared with none of the placebo patients [186]. Endo-scopic healing has been demonstrated in an open-label trial of cer-tolizumab pegol in 89 patients. Preliminary data indicated that after 1 year of treatment with certolizumab pegol (400 mg every 4 weeks), 55% of patients experienced endoscopic remission [187].
If a therapeutic agent induces significant and durable mucosal healing, which in turn reduces complications and the need for sur-gical intervention; it could potentially slow down or even stop the progression and change the natural course of the disease. D'Haens and colleagues investigated the early biological treatment effect on treatment naïve CD patients with active disease, all of whom had a CD diagnosis of less than 4 years. Top-down and step-up therapy were compared in this randomized controlled trial. Patients received either early combination immunosuppression (top-down) or con-ventional (step-up) treatment. The conventional therapy consisted of an initial treatment with steroids, followed by AZA if patients became steroid-dependant or steroid-refractory, followed by in-fliximab if immunosuppression failed to control the symptoms. The early combination immunosuppression therapy consists of initial treatment of infliximab and AZA, with repeat infliximab infusion as needed (episodic) for patients with disease relapse and failure to respond to corticosteroids or infliximab. Patients in the early com-bination (top-down) therapy group had a significantly higher pro-portion in early induction of remission, a lower relapse rate, a lower mean number of days of corticosteroid use and complete mucosal

3678 Current Pharmaceutical Design, 2010, Vol. 16, No. 33 Sohrabpour et al.
healing in 75% of the early combination immunosuppression (top-down) group, compared with 21% in the conventional (step-up) treatment group at 2 years [188].
There is growing evidence that a strategy of earlier use of more potent therapies (biologic agents) may be the optimal approach to therapy in selected patients. In CHARM trial, the rate of mainte-nance of remission with adalimumab was higher in patients with less disease duration. Fifty five percent of patients with disease duration less than 2 years, 35% of those with a disease duration of 2 to 5 years, and 37% of those with disease longer than 5 years were in remission after 26 weeks [189]. In the PRECiSE 2 study evaluat-ing maintenance of response and remission with certolizumab pegol in CD, 62% of patients maintained response at week 26. However, in those with an elevated CRP and a disease duration of less than 2 years, the maintenance of response was 90% (P = .02), suggesting that early use of an anti-TNF agent was more successful [120].
SONIC (Study of Biologic and Immunomodulator Naive Pa-tients in Crohn’s Disease) researchers recruited 508 patients with moderate to severe CD who were naive to Immunomodulators and biologic agents. The patients were randomized to infliximab mono-therapy, azathioprine (AZA) monotherapy, or infliximab plus azathioprine combination therapy. The proportion of patients achieving steroid-free clinical remission at week 26 was signifi-cantly greater with infliximab monotherapy (44%) and infliximab plus AZA combination therapy (57%) than with AZA monotherapy (31%, p = 0.009 vs. infliximab monotherapy; p < 0.001 vs. combi-nation therapy). Similar numerical trends were found at week 50. At week 26, the proportion of patients with mucosal healing was significantly greater in those receiving infliximab monotherapy (30%) and infliximab plus AZA combination therapy (44%) than in those given AZA monotherapy (17%). Serious infections developed in 3.9% of patients in the combination therapy group, 4.9% of those in the infliximab group, and 5.6% of those in the azathioprine group. The SONIC trial demonstrates that earlier treatment with infliximab may provide better control of CD. The efficacy of an infliximab-based treatment strategy, either as monotherapy or as combination therapy, is superior to that of azathioprine monother-apy in azathioprine naive patients, with the benefit sustained over 50 weeks. In addition, a high C-reactive protein level and/or mu-cosal lesions at baseline may be identifiers for patients who can experience a significant benefit from earlier infliximab therapy. Steroid-free remission at week 26 was significantly improved in patients with a high CRP level and/or extensive endoscopic lesions at baseline. In patients with a normal baseline CRP level (<0.8 mg/dl), the rate of steroid-free clinical remission among the treat-ment groups was not statistically different. However, in patients with a high baseline CRP level (>0.8 mg/dl), the proportion of those achieving steroid-free remission was greater with infliximab plus AZA combination therapy (63.5%) and infliximab monotherapy (47.5%) than with AZA monotherapy (27.6%) [182].
Advocates of top-down strategy should take into account the potential risks of novel agents discussed above; moreover, a par-ticular effort should be made to identify patients with spontaneous disabling course of the disease, who should be properly considered for enrollment in early intensive therapy trials.
Patients with CD exhibiting deep and extensive ulcerations at colonoscopy have a more aggressive clinical course with an in-creased rate of penetrating complications and surgery [190]. Peri-anal lesions, the need for steroids to treat the first flare, and ileo-colonic location of the disease have also been suggested as predic-tive markers [191]. Disease onset before the age of 40 has been found by some [192], but not others [191] to predict subsequent aggressive course. Predictors of CD recurrence after surgery in-clude cigarette smoking [193], and penetrating rather than strictur-ing disease [194]. Studies evaluating a relationship between NOD2/CARD15 status and risk for postoperative recurrence have been negative so far [195].
An array of serologic markers is being evaluated for predicting disease behavior. Several studies have shown that Anti-Saccharo-myces cerevisiae mannan antibodies (ASCA) correlates with dis-tinct clinical phenotypes in Crohn disease. Presence of ASCA is associated with ileal disease, young age at onset, fibrostenotic and penetrating behavior, and multiple bowel surgeries [196-199]. The presence of anti-OmpC antibodies in Crohn disease is associated with internal perforating disease and requirement for surgery in adults [198]. Patients with Crohn disease with anti-I2 are more likely to have stenosing ileal disease and to require surgical resec-tion [198]. An increasing number of positive serologic markers portend a more aggressive disease behavior with a higher frequency of complications and surgery [200]. Presence of anti-CBir1 expres-sion is associated with internal penetrating, and fibrostenotic and fistulizing complications [201]. These and other predictive meas-ures are crucial because they could help us save on resources and potential toxicity by limiting use of these agents to those destined to have favorable response.
Unlike CD the main concern in long-standing ulcerative colitis UC is the development of dysplasia rather than structural derange-ments. The best evidence for prevention of dysplasia currently ex-ists for 5-aminosalicylates, and similar evidence is lacking for in-fliximab [202]. Therefore, at present, there is little rationale for a top-down approach to managing UC. There will be patients who will have an accelerating disease course and would likely benefit from earlier intervention, but the current tools do not allow reliable advance identification of these patients.
POSTSURGICAL MANAGEMENT OF IBD
Recurrence of CD is frequent after surgery and its prevention remains a problem in the medical management of these patients. Postoperative recurrence can be defined by endoscopic findings, symptoms, or the need for a subsequent resection. Endoscopic re-currence precedes clinical recurrence. A meta-analysis of random-ized trials evaluating postoperative maintenance therapies estimated that among patients treated with placebo, pooled relapse rates were 24 percent (95% CI 13 to 35 percent) [203].
Scheduled postoperative assessment for recurrence, to allow for early detection and intervention, is important. There are a range of clinical, laboratory-based, radiological, and endoscopic evaluation parameters that have been assessed.
As of today, none of the medications traditionally used to treat the spontaneous disease (i.e. mesalamine, steroids, immunosuppres-sive drugs and antibiotics) has shown a clear benefit.
In the largest study, conducted as part of the European Coop-erative Crohn’s Disease Study to examine 5-ASA for postoperative Crohn’s prophylaxis, 318 patients were randomized to receive pla-cebo or 5-ASA (Pentasa) 4 g daily over 18 months. Clinical recur-rence rates were not significantly different between the 5-ASA group (24.5%) and placebo group (31.4%), but post-hoc analysis revealed a significant effect in the subgroup of patients with iso-lated small bowel disease [204].
In a randomized, placebo-controlled trial, metronidazole (20 mg/kg/day), started within 7 days postoperatively and continued for 12 weeks, was associated with significant reductions in severe en-doscopic CD recurrence [205]. Despite their promising efficacy, the long-term use of these antibiotics is limited by their side effects, including peripheral neuropathy [206].
In a prospective, randomized, open-label study, AZA (2 mg/kg/day) was compared to mesalamine (3 g/d) and clinical re-lapse risk was equal between the groups at 24 months [207]. In another trial 6MP (50 mg/day) was more effective compared to placebo in prevention of clinical as well as endoscopic recurrence after 2 years [181].
Most postoperative studies define recurrence by endoscopic and clinical recurrence, but the time to recurrence and duration of trials

Current Therapeutic Approaches in Inflammatory Bowel Disease Current Pharmaceutical Design, 2010, Vol. 16, No. 33 3679
vary widely. This fact is reflected in the wide range of efficacy response demonstrated between different therapeutic agents.
The combination of metronidazole and azathioprine was com-pared to metronidazole alone in a controlled trial, in which patients receiving combination therapy suffered recurrence rates of 43.7% after 1 year compared with 69% in the group not receiving azathio-prine [208].
Recent data indicate that infliximab is highly effective in pre-venting relapse in the majority of patients. In a double-blind pla-cebo-controlled trial to assess efficacy of infliximab in the postop-erative setting, patients who underwent surgery for Crohn disease were randomized to either infliximab (5 mg/kg administered as a standard 3-dose induction, with a maintenance dose every 8 weeks) or placebo for 1 year. Infliximab or placebo was started within 4 weeks of surgery. Corticosteroids and antibiotics were discontinued within 12 weeks of surgery. AZA, 6MP, or 5-ASA products were continued as long as the patients were maintained on stable doses for at least 12 weeks before starting the study. The study found that 9.1% in the infliximab group developed endoscopic recurrence, compared with 84.6% in the placebo group (P = .0006). Further-more, the infliximab patients had a lower risk of endoscopic, his-tologic, and clinical recurrence at 1 year [185]. An implication of these studies is that infliximab appears extremely effective when given very early to prevent disease recurrence after surgery.
Clinicians in conjunction with patients must balance the risks of recurrence against the potential risks associated with treatment. For those at very low risk of recurrence, no therapy may be needed; however, for patients at moderate risk immunomodulators should be considered. For those at highest risk of recurrence, biologic ther-apy has emerged as appropriate treatment.
CONCLUSION
Although considerable progress has been made in recent years, a major gap in knowledge of the pathogenesis of IBD still remains. Accumulating evidence on effectiveness of biologic agents in terms of durable clinical and endoscopic improvement makes "top-down" therapy a noteworthy approach (Fig. 1). It would be based on phe-notypic risk assessment of new IBD cases by means of clinical, serologic, and genetic markers. Those with the highest risk of rapid disease progression or developing complications should be treated with the most effective therapy as early as possible. Future research also aims at developing a more individualized approach to treating patients. As of today, nearly 100 different genetic regions indicating a predisposition to IBD have been identified. These genetic ad-vances should now be used to understand the underlying immune and functional defects that lead to the increased risk of IBD. Novel therapies continue to be explored as the immunopathophysiologic underpinnings of IBD continue to be elucidated and an ultimate etiopathogenesis remains undetermined. Ongoing research will probably introduce more robust set of markers to accurately predict disease behavior and help us decide on a therapeutic approach with highest efficacy/risk ratio for every patient.
DISCLOSURE
The authors have no potential conflicts of interest relevant to this article.
REFERENCES
[1] Mir-Madjlessi SH, Forouzandeh B, Ghadimi R. Ulcerative colitis in Iran: a review of 112 cases. Am J Gastroenterol 1985; 80: 862-6.
[2] Malekzadeh R, Varshosaz R, Mir-Madjlessi SH, Tavakoli H. Rising incidence of Crohn's disease in Iran over 1989-1999.
Gastroenterology 2000; 118: A6172. [3] Vahedi H, Merat S, Momtahen S, et al. Epidemiologic
characteristics of 500 patients with inflammatory bowel disease in Iran studied from 2004 through 2007. Arch Iran Med 2009; 12:
454-60.
[4] Vucelic B. Inflammatory bowel diseases: controversies in the use
of diagnostic procedures. Dig Dis 2009; 27: 269-77. [5] Louis E, Collard A, Oger AF, et al. Behaviour of Crohn's disease
according to the Vienna classification: changing pattern over the course of the disease. Gut 2001; 49: 777-82.
[6] Kornbluth A, Sachar DB. Ulcerative colitis practice guidelines in adults: American College Of Gastroenterology, Practice Parameters
Committee. Am J Gastroenterol 2010; 105: 501-23; quiz 24. [7] Malekzadeh F, Alberti C, Nouraei M, et al. Crohn's disease and
early exposure to domestic refrigeration. PLoS One 2009; 4: e4288. [8] Tamboli CP. Current medical therapy for chronic inflammatory
bowel diseases. Surg Clin North Am 2007; 87: 697-725. [9] Desreumaux P, Ghosh S. Review article: mode of action and
delivery of 5-aminosalicylic acid - new evidence. Alim Pharmacol Ther 2006; 24 Suppl 1: 2-9.
[10] Lichtenstein GR, Hanauer SB, Sandborn WJ. Management of Crohn's disease in adults. Am J Gastroenterol 2009; 104: 465-83;
quiz 4, 84. [11] Hanauer SB, Stromberg U. Oral Pentasa in the treatment of active
Crohn's disease: A meta-analysis of double-blind, placebo-controlled trials. Clin Gastroenterol Hepatol 2004; 2: 379-88.
[12] Tremaine WJ, Schroeder KW, Harrison JM, Zinsmeister AR. A randomized, double-blind, placebo-controlled trial of the oral
mesalamine (5-ASA) preparation, Asacol, in the treatment of symptomatic Crohn's colitis and ileocolitis. J Clin Gastroenterol
1994; 19: 278-82. [13] Gendre JP, Mary JY, Florent C, et al. Oral mesalamine (Pentasa) as
maintenance treatment in Crohn's disease: a multicenter placebo-controlled study. The Groupe d'Etudes Therapeutiques des
Affections Inflammatoires Digestives (GETAID). Gastroenterology 1993; 104: 435-9.
[14] Akobeng AK, Gardener E. Oral 5-aminosalicylic acid for maintenance of medically-induced remission in Crohn's Disease.
Cochrane Database Syst Rev 2005: CD003715. [15] Summers RW, Switz DM, Sessions JT, Jr., et al. National
Cooperative Crohn's Disease Study: results of drug treatment. Gastroenterology 1979; 77: 847-69.
[16] Wenckert A, Kristensen M, Eklund AE, et al. The long-term prophylactic effect of salazosulphapyridine (Salazopyrin) in
primarily resected patients with Crohn's disease. A controlled double-blind trial. Scand J Gastroenterol 1978; 13: 161-7.
[17] Ewe K, Herfarth C, Malchow H, Jesdinsky HJ. Postoperative recurrence of Crohn's disease in relation to radicality of operation
and sulfasalazine prophylaxis: a multicenter trial. Digestion 1989; 42: 224-32.
[18] Sutherland LR. Mesalamine for the prevention of postoperative recurrence: is nearly there the same as being there?
Gastroenterology 2000; 118: 436-8. [19] Nielsen OH. Sulfasalazine intolerance. A retrospective survey of
the reasons for discontinuing treatment with sulfasalazine in patients with chronic inflammatory bowel disease. Scand J
Gastroenterol 1982; 17: 389-93. [20] Kane SV, Cohen RD, Aikens JE, Hanauer SB. Prevalence of
nonadherence with maintenance mesalamine in quiescent ulcerative colitis. Am J Gastroenterol 2001; 96: 2929-33.
[21] Higgins PD, Rubin DT, Kaulback K, Schoenfield PS, Kane SV. Systematic review: impact of non-adherence to 5-aminosalicylic
acid products on the frequency and cost of ulcerative colitis flares. Alim Pharmacol Ther 2009; 29: 247-57.
[22] Sutherland L, Macdonald JK. Oral 5-aminosalicylic acid for induction of remission in ulcerative colitis. Cochrane Database Syst
Rev 2006: CD000543. [23] Sutherland L, Macdonald JK. Oral 5-aminosalicylic acid for
maintenance of remission in ulcerative colitis. Cochrane Database Syst Rev 2006: CD000544.
[24] Rahimi R, Nikfar S, Rezaie A, Abdollahi M. Comparison of mesalazine and balsalazide in induction and maintenance of
remission in patients with ulcerative colitis: a meta-analysis. Dig Dis Sci 2009; 54: 712-21.
[25] Nikfar S, Rahimi R, Rezaie A, Abdollahi M. A meta-analysis of the efficacy of sulfasalazine in comparison with 5-aminosalicylates in
the induction of improvement and maintenance of remission in patients with ulcerative colitis. Dig Dis Sci 2009; 54: 1157-70.
[26] Katz JA. Treatment of inflammatory bowel disease with corticosteroids. Gastroenterol Clin North Am 2004; 33: 171-89, vii.

3680 Current Pharmaceutical Design, 2010, Vol. 16, No. 33 Sohrabpour et al.
[27] Benchimol EI, Seow CH, Steinhart AH, Griffiths AM. Traditional
corticosteroids for induction of remission in Crohn's disease. Cochrane Database Syst Rev 2008: CD006792.
[28] Rutgeerts P, Lofberg R, Malchow H, et al. A comparison of budesonide with prednisolone for active Crohn's disease. N Engl J
Med 1994; 331: 842-5. [29] Seow CH, Benchimol EI, Griffiths AM, Otley AR, Steinhart AH.
Budesonide for induction of remission in Crohn's disease. Cochrane Database Syst Rev 2008: CD000296.
[30] Otley A, Steinhart AH. Budesonide for induction of remission in Crohn's disease. Cochrane Database Syst Rev 2005: CD000296.
[31] Benchimol EI, Seow CH, Otley AR, Steinhart AH. Budesonide for maintenance of remission in Crohn's disease. Cochrane Database
Syst Rev 2009: CD002913. [32] Steinhart AH, Ewe K, Griffiths AM, Modigliani R, Thomsen OO.
Corticosteroids for maintenance of remission in Crohn's disease. Cochrane Database Syst Rev 2003: CD000301.
[33] Campieri M, Gionchetti P, Belluzzi A, et al. Efficacy of 5-aminosalicylic acid enemas versus hydrocortisone enemas in
ulcerative colitis. Dig Dis Sci 1987; 32: 67S-70S. [34] Marshall JK, Irvine EJ. Rectal corticosteroids versus alternative
treatments in ulcerative colitis: a meta-analysis. Gut 1997; 40: 775-81.
[35] Cohen RD, Woseth DM, Thisted RA, Hanauer SB. A meta-analysis and overview of the literature on treatment options for left-sided
ulcerative colitis and ulcerative proctitis. Am J Gastroenterol 2000; 95: 1263-76.
[36] Mulder CJ, Fockens P, Meijer JW, van der Heide H, Wiltink EH, Tytgat GN. Beclomethasone dipropionate (3 mg) versus 5-
aminosalicylic acid (2 g) versus the combination of both (3 mg/2 g) as retention enemas in active ulcerative proctitis. Eur J
Gastroenterol Hepatol 1996; 8: 549-53. [37] Rogler G. Medical management of ulcerative colitis. Dig Dis 2009;
27: 542-9. [38] Prefontaine E, Macdonald JK, Sutherland LR. Azathioprine or 6-
mercaptopurine for induction of remission in Crohn's disease. Cochrane Database Syst Rev 2010; 6: CD000545.
[39] Prefontaine E, Sutherland LR, Macdonald JK, Cepoiu M. Azathioprine or 6-mercaptopurine for maintenance of remission in
Crohn's disease. Cochrane Database Syst Rev 2009: CD000067. [40] Sahasranaman S, Howard D, Roy S. Clinical pharmacology and
pharmacogenetics of thiopurines. Eur J Clin Pharmacol 2008; 64: 753-67.
[41] Weinshilboum RM, Sladek SL. Mercaptopurine pharmacogenetics: monogenic inheritance of erythrocyte thiopurine methyltransferase
activity. Am J Hum Genet 1980; 32: 651-62. [42] Collie-Duguid ES, Pritchard SC, Powrie RH, et al. The frequency
and distribution of thiopurine methyltransferase alleles in Caucasian and Asian populations. Pharmacogenetics 1999; 9: 37-
42. [43] Osterman MT, Kundu R, Lichtenstein GR, Lewis JD. Association
of 6-thioguanine nucleotide levels and inflammatory bowel disease activity: a meta-analysis. Gastroenterology 2006; 130: 1047-53.
[44] D'Halluin PN, Tribut O, Branger B, et al. RBC 6-TGN and hematological parameters in patients with Crohn's disease treated
by azathioprine. Gastroenterol Clin Biol 2005; 29: 1264-9. [45] Pierik M, Rutgeerts P, Vlietinck R, Vermeire S. Pharmacogenetics
in inflammatory bowel disease. World J Gastroenterol 2006; 12: 3657-67.
[46] Feagan BG, Rochon J, Fedorak RN, et al. Methotrexate for the treatment of Crohn's disease. The North American Crohn's Study
Group Investigators. N Engl J Med 1995; 332: 292-7. [47] Alfadhli AA, McDonald JW, Feagan BG. Methotrexate for
induction of remission in refractory Crohn's disease. Cochrane Database Syst Rev 2005: CD003459.
[48] Te HS, Schiano TD, Kuan SF, Hanauer SB, Conjeevaram HS, Baker AL. Hepatic effects of long-term methotrexate use in the
treatment of inflammatory bowel disease. Am J Gastroenterol 2000; 95: 3150-6.
[49] Feagan BG, Fedorak RN, Irvine EJ, et al. A comparison of methotrexate with placebo for the maintenance of remission in
Crohn's disease. North American Crohn's Study Group Investigators. N Engl J Med 2000; 342: 1627-32.
[50] Patel V, Macdonald JK, McDonald JW, Chande N. Methotrexate for maintenance of remission in Crohn's disease. Cochrane
Database Syst Rev 2009: CD006884.
[51] Neurath MF, Wanitschke R, Peters M, Krummenauer F, Meyer
zum Buschenfelde KH, Schlaak JF. Randomised trial of mycophenolate mofetil versus azathioprine for treatment of chronic
active Crohn's disease. Gut 1999; 44: 625-8. [52] Lowry PW, Weaver AL, Tremaine WJ, Sandborn WJ. Combination
therapy with oral tacrolimus (FK506) and azathioprine or 6-mercaptopurine for treatment-refractory Crohn's disease perianal
fistulae. Inflamm Bowel Dis 1999; 5: 239-45. [53] Ierardi E, Principi M, Rendina M, et al. Oral tacrolimus (FK 506)
in Crohn's disease complicated by fistulae of the perineum. J Clin Gastroenterol 2000; 30: 200-2.
[54] Sandborn WJ, Present DH, Isaacs KL, et al. Tacrolimus for the treatment of fistulas in patients with Crohn's disease: a randomized,
placebo-controlled trial. Gastroenterology 2003; 125: 380-8. [55] Casson DH, Eltumi M, Tomlin S, Walker-Smith JA, Murch SH.
Topical tacrolimus may be effective in the treatment of oral and perineal Crohn's disease. Gut 2000; 47: 436-40.
[56] Hart AL, Plamondon S, Kamm MA. Topical tacrolimus in the treatment of perianal Crohn's disease: exploratory randomized
controlled trial. Inflamm Bowel Dis 2007; 13: 245-53. [57] Cheifetz AS, Stern J, Garud S, et al. Cyclosporine is safe and
effective in patients with severe ulcerative colitis. J Clin Gastroenterol 2010; [Epub ahead of print].
[58] D'Haens G, Lemmens L, Geboes K, et al. Intravenous cyclosporine versus intravenous corticosteroids as single therapy for severe
attacks of ulcerative colitis. Gastroenterology 2001; 120: 1323-9. [59] Hansen R, Thomson JM, El-Omar EM, Hold GL. The role of
infection in the aetiology of inflammatory bowel disease. J Gastroenterol 2010; 45: 266-76.
[60] Shibolet O, Regushevskaya E, Brezis M, Soares-Weiser K. Cyclosporine A for induction of remission in severe ulcerative
colitis. Cochrane Database Syst Rev 2005: CD004277. [61] Timmer A, McDonald JW, Macdonald JK. Azathioprine and 6-
mercaptopurine for maintenance of remission in ulcerative colitis. Cochrane Database Syst Rev 2007: CD000478.
[62] Oren R, Arber N, Odes S, et al. Methotrexate in chronic active ulcerative colitis: a double-blind, randomized, Israeli multicenter
trial. Gastroenterology 1996; 110: 1416-21. [63] El-Matary W, Vandermeer B, Griffiths AM. Methotrexate for
maintenance of remission in ulcerative colitis. Cochrane Database Syst Rev 2009: CD007560.
[64] Orth T, Peters M, Schlaak JF, et al. Mycophenolate mofetil versus azathioprine in patients with chronic active ulcerative colitis: a 12-
month pilot study. Am J Gastroenterol 2000; 95: 1201-7. [65] Baumgart DC, Macdonald JK, Feagan B. Tacrolimus (FK506) for
induction of remission in refractory ulcerative colitis. Cochrane Database Syst Rev 2008: CD007216.
[66] Schrezenmeir J, de Vrese M. Probiotics, prebiotics, and synbiotics--approaching a definition. Am J Clin Nutr 2001; 73: 361S-4S.
[67] Rahimi R, Nikfar S, Rezaie A, Abdollahi M. A meta-analysis of broad-spectrum antibiotic therapy in patients with active Crohn's
disease. Clin Ther 2006; 28: 1983-8. [68] Prantera C, Scribano ML. Antibiotics and probiotics in
inflammatory bowel disease: why, when, and how. Curr Opin Gastroenterol 2009; 25: 329-33.
[69] Rahimi R, Nikfar S, Rahimi F, et al. A meta-analysis on the efficacy of probiotics for maintenance of remission and prevention
of clinical and endoscopic relapse in Crohn's disease. Dig Dis Sci 2008; 53: 2524-31.
[70] Sartor RB. Therapeutic manipulation of the enteric microflora in inflammatory bowel diseases: antibiotics, probiotics, and
prebiotics. Gastroenterology 2004; 126: 1620-33. [71] Ng SC, Hart AL, Kamm MA, Stagg AJ, Knight SC. Mechanisms of
action of probiotics: recent advances. Inflamm Bowel Dis 2009; 15: 300-10.
[72] Macfarlane S, Steed H, Macfarlane GT. Intestinal bacteria and inflammatory bowel disease. Crit Rev Clin Lab Sci 2009; 46: 25-
54. [73] Sutherland L, Singleton J, Sessions J, et al. Double blind, placebo
controlled trial of metronidazole in Crohn's disease. Gut 1991; 32: 1071-5.
[74] Blichfeldt P, Blomhoff JP, Myhre E, Gjone E. Metronidazole in Crohn's disease. A double blind cross-over clinical trial. Scand J
Gastroenterol 1978; 13: 123-7.

Current Therapeutic Approaches in Inflammatory Bowel Disease Current Pharmaceutical Design, 2010, Vol. 16, No. 33 3681
[75] Ambrose NS, Allan RN, Keighley MR, et al. Antibiotic therapy for
treatment in relapse of intestinal Crohn's disease. A prospective randomized study. Dis Colon Rectum 1985; 28: 81-5.
[76] Bernstein LH, Frank MS, Brandt LJ, Boley SJ. Healing of perineal Crohn's disease with metronidazole. Gastroenterology 1980; 79:
599. [77] Jakobovits J, Schuster MM. Metronidazole therapy for Crohn's
disease and associated fistulae. Am J Gastroenterol 1984; 79: 533-40.
[78] Arnold GL, Beaves MR, Pryjdun VO, Mook WJ. Preliminary study of ciprofloxacin in active Crohn's disease. Inflamm Bowel Dis
2002; 8: 10-5. [79] Thia KT, Mahadevan U, Feagan BG, et al. Ciprofloxacin or
metronidazole for the treatment of perianal fistulas in patients with Crohn's disease: a randomized, double-blind, placebo-controlled
pilot study. Inflamm Bowel Dis 2009; 15: 17-24. [80] West RL, van der Woude CJ, Hansen BE, et al. Clinical and
endosonographic effect of ciprofloxacin on the treatment of perianal fistulae in Crohn's disease with infliximab: a double-blind
placebo-controlled study. Alim Pharmacol Ther 2004; 20: 1329-36. [81] Shafran I, Johnson LK. An open-label evaluation of rifaximin in
the treatment of active Crohn's disease. Curr Med Res Opin 2005; 21: 1165-9.
[82] Prantera C, Lochs H, Campieri M, et al. Antibiotic treatment of Crohn's disease: results of a multicentre, double blind, randomized,
placebo-controlled trial with rifaximin. Alim Pharmacol Ther 2006; 23: 1117-25.
[83] Angelberger S, Reinisch W, Dejaco C, et al. NOD2/CARD15 gene variants are linked to failure of antibiotic treatment in perianal
fistulating Crohn's disease. Am J Gastroenterol 2008; 103: 1197-202.
[84] Butterworth AD, Thomas AG, Akobeng AK. Probiotics for induction of remission in Crohn's disease. Cochrane Database Syst
Rev 2008: CD006634. [85] Chapman RW, Selby WS, Jewell DP. Controlled trial of
intravenous metronidazole as an adjunct to corticosteroids in severe ulcerative colitis. Gut 1986; 27: 1210-2.
[86] Mantzaris GJ, Hatzis A, Kontogiannis P, Triadaphyllou G. Intravenous tobramycin and metronidazole as an adjunct to
corticosteroids in acute, severe ulcerative colitis. Am J Gastroenterol 1994; 89: 43-6.
[87] Navaneethan U, Shen B. Pros and cons of antibiotic therapy for pouchitis. Expert Rev Gastroenterol Hepatol 2009; 3: 547-59.
[88] Thukral C, Travassos WJ, Peppercorn MA. The role of antibiotics in inflammatory bowel disease. Curr Treat Options Gastroenterol
2005; 8: 223-8. [89] Mallon P, McKay D, Kirk S, Gardiner K. Probiotics for induction
of remission in ulcerative colitis. Cochrane Database Syst Rev 2007: CD005573.
[90] Do VT, Baird BG, Kockler DR. Probiotics for maintaining remission of ulcerative colitis in adults. Ann Pharmacother 2010;
44: 565-71. [91] Sang LX, Chang B, Zhang WL, Wu XM, Li XH, Jiang M.
Remission induction and maintenance effect of probiotics on ulcerative colitis: a meta-analysis. World J Gastroenterol 2010; 16:
1908-15. [92] Cannon JP, Lee TA, Bolanos JT, Danziger LH. Pathogenic
relevance of Lactobacillus: a retrospective review of over 200 cases. Eur J Clin Microbiol Infect Dis 2005; 24: 31-40.
[93] Snydman DR. The safety of probiotics. Clin Infect Dis 2008; 46 Suppl 2: S104-11; discussion S44-51.
[94] D'Haens GR, Geboes K, Peeters M, Baert F, Penninckx F, Rutgeerts P. Early lesions of recurrent Crohn's disease caused by
infusion of intestinal contents in excluded ileum. Gastroenterology 1998; 114: 262-7.
[95] Zachos M, Tondeur M, Griffiths AM. Enteral nutritional therapy for induction of remission in Crohn's disease. Cochrane Database
Syst Rev 2007: CD000542. [96] Akobeng AK, Thomas AG. Enteral nutrition for maintenance of
remission in Crohn's disease. Cochrane Database Syst Rev 2007: CD005984.
[97] Turner D, Zlotkin SH, Shah PS, Griffiths AM. Omega 3 fatty acids (fish oil) for maintenance of remission in Crohn's disease.
Cochrane Database Syst Rev 2009: CD006320. [98] Turner D, Shah PS, Steinhart AH, Zlotkin S, Griffiths AM.
Maintenance of remission in inflammatory bowel disease using
omega-3 fatty acids (fish oil): A systematic review and meta-
analyses. Inflamm Bowel Dis 2010; [Epub ahead of print]. [99] McIntyre PB, Powell-Tuck J, Wood SR, et al. Controlled trial of
bowel rest in the treatment of severe acute colitis. Gut 1986; 27: 481-5.
[100] Dickinson RJ, Ashton MG, Axon AT, Smith RC, Yeung CK, Hill GL. Controlled trial of intravenous hyperalimentation and total
bowel rest as an adjunct to the routine therapy of acute colitis. Gastroenterology 1980; 79: 1199-204.
[101] Rose DJ, DeMeo MT, Keshavarzian A, Hamaker BR. Influence of dietary fiber on inflammatory bowel disease and colon cancer:
importance of fermentation pattern. Nutr Rev 2007; 65: 51-62. [102] Kim YI. Short-chain fatty acids in ulcerative colitis. Nutr Rev
1998; 56: 17-24. [103] De Ley M, de Vos R, Hommes DW, Stokkers P. Fish oil for
induction of remission in ulcerative colitis. Cochrane Database Syst Rev 2007: CD005986.
[104] Turner D, Steinhart AH, Griffiths AM. Omega 3 fatty acids (fish oil) for maintenance of remission in ulcerative colitis. Cochrane
Database Syst Rev 2007: CD006443. [105] Plevy SE, Landers CJ, Prehn J, et al. A role for TNF-alpha and
mucosal T helper-1 cytokines in the pathogenesis of Crohn's disease. J Immunol 1997; 159: 6276-82.
[106] Targan SR, Hanauer SB, van Deventer SJ, et al. A short-term study of chimeric monoclonal antibody cA2 to tumor necrosis factor
alpha for Crohn's disease. Crohn's Disease cA2 Study Group. N Engl J Med 1997; 337: 1029-35.
[107] Hanauer SB, Feagan BG, Lichtenstein GR, et al. Maintenance infliximab for Crohn's disease: the ACCENT I randomised trial.
Lancet 2002; 359: 1541-9. [108] Hanauer SB, Wagner CL, Bala M, et al. Incidence and importance
of antibody responses to infliximab after maintenance or episodic treatment in Crohn's disease. Clin Gastroenterol Hepatol 2004; 2:
542-53. [109] Sands BE, Anderson FH, Bernstein CN, et al. Infliximab
maintenance therapy for fistulizing Crohn's disease. N Engl J Med 2004; 350: 876-85.
[110] Lichtenstein GR, Yan S, Bala M, Blank M, Sands BE. Infliximab maintenance treatment reduces hospitalizations, surgeries, and
procedures in fistulizing Crohn's disease. Gastroenterology 2005; 128: 862-9.
[111] Plosker GL, Lyseng-Williamson KA. Adalimumab: in Crohn's disease. BioDrugs 2007; 21: 125-32; discussion 33-4.
[112] Hanauer SB, Sandborn WJ, Rutgeerts P, et al. Human anti-tumor necrosis factor monoclonal antibody (adalimumab) in Crohn's
disease: the CLASSIC-I trial. Gastroenterology 2006; 130: 323-33; quiz 591.
[113] Sandborn WJ, Hanauer SB, Rutgeerts P, et al. Adalimumab for maintenance treatment of Crohn's disease: results of the CLASSIC
II trial. Gut 2007; 56: 1232-9. [114] Colombel JF, Sandborn WJ, Rutgeerts P, et al. Adalimumab for
maintenance of clinical response and remission in patients with Crohn's disease: the CHARM trial. Gastroenterology 2007; 132:
52-65. [115] Feagan BG, Panaccione R, Sandborn WJ, et al. Effects of
adalimumab therapy on incidence of hospitalization and surgery in Crohn's disease: results from the CHARM study. Gastroenterology
2008; 135: 1493-9. [116] Loftus EV, Feagan BG, Colombel JF, et al. Effects of adalimumab
maintenance therapy on health-related quality of life of patients with Crohn's disease: patient-reported outcomes of the CHARM
trial. Am J Gastroenterol 2008; 103: 3132-41. [117] Hanauer SB. Biologic therapy for inflammatory bowel disease
comes of age. Curr Gastroenterol Rep 2007; 9: 485-7. [118] Blick SK, Curran MP. Certolizumab pegol: in Crohn's disease.
BioDrugs 2007; 21: 195-201; discussion 2-3. [119] Sandborn WJ, Feagan BG, Stoinov S, et al. Certolizumab pegol for
the treatment of Crohn's disease. N Engl J Med 2007; 357: 228-38. [120] Schreiber S, Khaliq-Kareemi M, Lawrance IC, et al. Maintenance
therapy with certolizumab pegol for Crohn's disease. N Engl J Med 2007; 357: 239-50.
[121] Lichtenstein GR, Thomsen OO, Schreiber S, et al. Continuous therapy with certolizumab pegol maintains remission of patients
with Crohn's disease for up to 18 months. Clin Gastroenterol Hepatol 2010; 8: 600-9.
3682 Current Pharmaceutical Design, 2010, Vol. 16, No. 33 Sohrabpour et al.
[122] Sandborn WJ, Schreiber S, Hanauer SB, Colombel JF, Bloomfield
R, Lichtenstein GR. Reinduction with certolizumab pegol in patients with relapsed Crohn's disease: results from the PRECiSE 4
Study. Clin Gastroenterol Hepatol 2010; 8: 696-702 e1. [123] Schoepfer AM, Vavricka SR, Binek J, et al. Efficacy and safety of
certolizumab pegol induction therapy in an unselected Crohn's disease population: results of the FACTS survey. Inflamm Bowel
Dis 2010; 16: 933-8. [124] Binion DG, West GA, Volk EE, et al. Acquired increase in
leucocyte binding by intestinal microvascular endothelium in inflammatory bowel disease. Lancet 1998; 352: 1742-6.
[125] Siegmund B. Targeted therapies in inflammatory bowel disease. Dig Dis 2009; 27: 465-9.
[126] Gordon FH, Lai CW, Hamilton MI, et al. A randomized placebo-controlled trial of a humanized monoclonal antibody to alpha4
integrin in active Crohn's disease. Gastroenterology 2001; 121: 268-74.
[127] Ghosh S, Goldin E, Gordon FH, et al. Natalizumab for active Crohn's disease. N Engl J Med 2003; 348: 24-32.
[128] Sandborn WJ, Colombel JF, Enns R, et al. Natalizumab induction and maintenance therapy for Crohn's disease. N Engl J Med 2005;
353: 1912-25. [129] Targan SR, Feagan BG, Fedorak RN, et al. Natalizumab for the
treatment of active Crohn's disease: results of the ENCORE Trial. Gastroenterology 2007; 132: 1672-83.
[130] MacDonald JK, McDonald JW. Natalizumab for induction of remission in Crohn's disease. Cochrane Database Syst Rev 2007:
CD006097. [131] Peyrin-Biroulet L, Deltenre P, de Suray N, Branche J, Sandborn
WJ, Colombel JF. Efficacy and safety of tumor necrosis factor antagonists in Crohn's disease: meta-analysis of placebo-controlled
trials. Clin Gastroenterol Hepatol 2008; 6: 644-53. [132] Masuda H, Iwai S, Tanaka T, Hayakawa S. Expression of IL-8,
TNF-alpha and IFN-gamma m-RNA in ulcerative colitis, particularly in patients with inactive phase. J Clin Lab Immunol
1995; 46: 111-23. [133] Saiki T, Mitsuyama K, Toyonaga A, Ishida H, Tanikawa K.
Detection of pro- and anti-inflammatory cytokines in stools of patients with inflammatory bowel disease. Scand J Gastroenterol
1998; 33: 616-22. [134] Reinecker HC, Steffen M, Witthoeft T, et al. Enhanced secretion of
tumour necrosis factor-alpha, IL-6, and IL-1 beta by isolated lamina propria mononuclear cells from patients with ulcerative
colitis and Crohn's disease. Clin Exp Immunol 1993; 94: 174-81. [135] Rutgeerts P, Van Assche G, Vermeire S. Review article: Infliximab
therapy for inflammatory bowel disease--seven years on. Alim Pharmacol Ther 2006; 23: 451-63.
[136] Froslie KF, Jahnsen J, Moum BA, Vatn MH. Mucosal healing in inflammatory bowel disease: results from a Norwegian population-
based cohort. Gastroenterology 2007; 133: 412-22. [137] Rutter MD, Saunders BP, Wilkinson KH, et al. Cancer surveillance
in longstanding ulcerative colitis: endoscopic appearances help predict cancer risk. Gut 2004; 53: 1813-6.
[138] Jarnerot G, Hertervig E, Friis-Liby I, et al. Infliximab as rescue therapy in severe to moderately severe ulcerative colitis: a
randomized, placebo-controlled study. Gastroenterology 2005; 128: 1805-11.
[139] Kohn A, Daperno M, Armuzzi A, et al. Infliximab in severe ulcerative colitis: short-term results of different infusion regimens
and long-term follow-up. Alim Pharmacol Ther 2007; 26: 747-56. [140] Ochsenkuhn T, Sackmann M, Goke B. Infliximab for acute, not
steroid-refractory ulcerative colitis: a randomized pilot study. Eur J Gastroenterol Hepatol 2004; 16: 1167-71.
[141] Afif W, Leighton JA, Hanauer SB, et al. Open-label study of adalimumab in patients with ulcerative colitis including those with
prior loss of response or intolerance to infliximab. Inflamm Bowel Dis 2009; 15: 1302-7.
[142] Oussalah A, Laclotte C, Chevaux JB, et al. Long-term outcome of adalimumab therapy for ulcerative colitis with intolerance or lost
response to infliximab: a single-centre experience. Alim Pharmacol Ther 2008; 28: 966-72.
[143] Viget N, Vernier-Massouille G, Salmon-Ceron D, Yazdanpanah Y, Colombel JF. Opportunistic infections in patients with
inflammatory bowel disease: prevention and diagnosis. Gut 2008; 57: 549-58.
[144] Colbert C, Chavarria A, Berkelhammer C. Fulminant hepatic
failure in chronic hepatitis B on withdrawal of corticosteroids, azathioprine and infliximab for Crohn's disease. Inflamm Bowel
Dis 2007; 13: 1453-4. [145] Colombel JF, Loftus EV, Jr., Tremaine WJ, et al. The safety profile
of infliximab in patients with Crohn's disease: the Mayo clinic experience in 500 patients. Gastroenterology 2004; 126: 19-31.
[146] Caspersen S, Elkjaer M, Riis L, et al. Infliximab for inflammatory bowel disease in Denmark 1999-2005: clinical outcome and
follow-up evaluation of malignancy and mortality. Clin Gastroenterol Hepatol 2008; 6: 1212-7; quiz 176.
[147] Chung ES, Packer M, Lo KH, Fasanmade AA, Willerson JT. Randomized, double-blind, placebo-controlled, pilot trial of
infliximab, a chimeric monoclonal antibody to tumor necrosis factor-alpha, in patients with moderate-to-severe heart failure:
results of the anti-TNF Therapy Against Congestive Heart Failure (ATTACH) trial. Circulation 2003; 107: 3133-40.
[148] Siegel CA, Marden SM, Persing SM, Larson RJ, Sands BE. Risk of lymphoma associated with combination anti-tumor necrosis factor
and immunomodulator therapy for the treatment of Crohn's disease: a meta-analysis. Clin Gastroenterol Hepatol 2009; 7: 874-81.
[149] Carmona L, Gomez-Reino JJ, Rodriguez-Valverde V, et al. Effectiveness of recommendations to prevent reactivation of latent
tuberculosis infection in patients treated with tumor necrosis factor antagonists. Arthritis Rheum 2005; 52: 1766-72.
[150] Millonig G, Kern M, Ludwiczek O, Nachbaur K, Vogel W. Subfulminant hepatitis B after infliximab in Crohn's disease: need
for HBV-screening? World J Gastroenterol 2006; 12: 974-6. [151] Jones JL, Loftus EV, Jr. Lymphoma risk in inflammatory bowel
disease: is it the disease or its treatment? Inflamm Bowel Dis 2007; 13: 1299-307.
[152] Ochenrider MG, Patterson DJ, Aboulafia DM. Hepatosplenic T-cell lymphoma in a young man with Crohn's disease: case report and
literature review. Clin Lymphoma Myeloma Leuk 2010; 10: 144-8. [153] Smith JP, Stock H, Bingaman S, Mauger D, Rogosnitzky M, Zagon
IS. Low-dose naltrexone therapy improves active Crohn's disease. Am J Gastroenterol 2007; 102: 820-8.
[154] Dubuquoy L, Jansson EA, Deeb S, et al. Impaired expression of peroxisome proliferator-activated receptor gamma in ulcerative
colitis. Gastroenterology 2003; 124: 1265-76. [155] Wu GD. Is there a role for PPAR gamma in IBD? Yes, no, maybe.
Gastroenterology 2003; 124: 1538-42. [156] Liang HL, Ouyang Q. A clinical trial of combined use of
rosiglitazone and 5-aminosalicylate for ulcerative colitis. World J Gastroenterol 2008; 14: 114-9.
[157] Lewis JD, Lichtenstein GR, Deren JJ, et al. Rosiglitazone for active ulcerative colitis: a randomized placebo-controlled trial.
Gastroenterology 2008; 134: 688-95. [158] Nissen SE, Wolski K. Effect of rosiglitazone on the risk of
myocardial infarction and death from cardiovascular causes. N Engl J Med 2007; 356: 2457-71.
[159] Pedersen G, Brynskov J. Topical rosiglitazone treatment improves ulcerative colitis by restoring peroxisome proliferator-activated
receptor-gamma activity. Am J Gastroenterol 2010; 105: 1595-603. [160] Sainsbury A, Heatley RV. Review article: psychosocial factors in
the quality of life of patients with inflammatory bowel disease. Aliment Pharmacol Ther 2005; 21: 499-508.
[161] Isgar B, Harman M, Kaye MD, Whorwell PJ. Symptoms of irritable bowel syndrome in ulcerative colitis in remission. Gut
1983; 24: 190-2. [162] Simren M, Axelsson J, Gillberg R, Abrahamsson H, Svedlund J,
Bjornsson ES. Quality of life in inflammatory bowel disease in remission: the impact of IBS-like symptoms and associated
psychological factors. Am J Gastroenterol 2002; 97: 389-96. [163] Ranjbaran Z, Keefer L, Farhadi A, Stepanski E, Sedghi S,
Keshavarzian A. Impact of sleep disturbances in inflammatory bowel disease. J Gastroenterol Hepatol 2007; 22: 1748-53.
[164] Keefer L, Stepanski EJ, Ranjbaran Z, Benson LM, Keshavarzian A. An initial report of sleep disturbance in inactive inflammatory
bowel disease. J Clin Sleep Med 2006; 2: 409-16. [165] Lichtenstein GR, Sands BE, Pazianas M. Prevention and treatment
of osteoporosis in inflammatory bowel disease. Inflamm Bowel Dis 2006; 12: 797-813.
[166] Lashner BA, Provencher KS, Seidner DL, Knesebeck A, Brzezinski A. The effect of folic acid supplementation on the risk
Current Therapeutic Approaches in Inflammatory Bowel Disease Current Pharmaceutical Design, 2010, Vol. 16, No. 33 3683
for cancer or dysplasia in ulcerative colitis. Gastroenterology 1997;
112: 29-32. [167] Kulnigg S, Gasche C. Systematic review: managing anaemia in
Crohn's disease. Alim Pharmacol Ther 2006; 24: 1507-23. [168] von Tirpitz C, Kohn C, Steinkamp M, et al. Lactose intolerance in
active Crohn's disease: clinical value of duodenal lactase analysis. J Clin Gastroenterol 2002; 34: 49-53.
[169] Pironi L, Cornia GL, Ursitti MA, et al. Evaluation of oral administration of folic and folinic acid to prevent folate deficiency
in patients with inflammatory bowel disease treated with salicylazosulfapyridine. Int J Clin Pharmacol Res 1988; 8: 143-8.
[170] Bitton A, Sewitch MJ, Peppercorn MA, et al. Psychosocial determinants of relapse in ulcerative colitis: a longitudinal study.
Am J Gastroenterol 2003; 98: 2203-8. [171] van der Heide F, Dijkstra A, Weersma RK, et al. Effects of active
and passive smoking on disease course of Crohn's disease and ulcerative colitis. Inflamm Bowel Dis 2009; 15: 1199-207.
[172] Goekoop-Ruiterman YP, de Vries-Bouwstra JK, Allaart CF, et al. Clinical and radiographic outcomes of four different treatment
strategies in patients with early rheumatoid arthritis (the BeSt study): a randomized, controlled trial. Arthritis Rheum 2005; 52:
3381-90. [173] Best WR, Becktel JM, Singleton JW, Kern F, Jr. Development of a
Crohn's disease activity index. National Cooperative Crohn's Disease Study. Gastroenterology 1976; 70: 439-44.
[174] Harvey RF, Bradshaw JM. A simple index of Crohn's-disease activity. Lancet 1980; 1: 514.
[175] Jones J, Loftus EV, Jr., Panaccione R, et al. Relationships between disease activity and serum and fecal biomarkers in patients with
Crohn's disease. Clin Gastroenterol Hepatol 2008; 6: 1218-24. [176] Olaison G, Smedh K, Sjodahl R. Natural course of Crohn's disease
after ileocolic resection: endoscopically visualised ileal ulcers preceding symptoms. Gut 1992; 33: 331-5.
[177] Baert F, Moortgat L, Van Assche G, et al. Mucosal healing predicts sustained clinical remission in patients with early-stage Crohn's
disease. Gastroenterology 2010; 138: 463-8; quiz e10-1. [178] Rutgeerts P, Feagan BG, Lichtenstein GR, et al. Comparison of
scheduled and episodic treatment strategies of infliximab in Crohn's disease. Gastroenterology 2004; 126: 402-13.
[179] Schnitzler F, Fidder H, Ferrante M, et al. Mucosal healing predicts long-term outcome of maintenance therapy with infliximab in
Crohn's disease. Inflamm Bowel Dis 2009; 15: 1295-301. [180] Modigliani R, Mary JY, Simon JF, et al. Clinical, biological, and
endoscopic picture of attacks of Crohn's disease. Evolution on prednisolone. Groupe d'Etude Therapeutique des Affections
Inflammatoires Digestives. Gastroenterology 1990; 98: 811-8. [181] Hanauer SB, Korelitz BI, Rutgeerts P, et al. Postoperative
maintenance of Crohn's disease remission with 6-mercaptopurine, mesalamine, or placebo: a 2-year trial. Gastroenterology 2004; 127:
723-9. [182] Colombel JF, Sandborn WJ, Reinisch W, et al. Infliximab,
azathioprine, or combination therapy for Crohn's disease. N Engl J Med 2010; 362: 1383-95.
[183] Van Assche G, Vermeire S, Rutgeerts P. The potential for disease modification in Crohn's disease. Nat Rev Gastroenterol Hepatol
2010; 7: 79-85. [184] D'Haens G, Van Deventer S, Van Hogezand R, et al. Endoscopic
and histological healing with infliximab anti-tumor necrosis factor antibodies in Crohn's disease: A European multicenter trial.
Gastroenterology 1999; 116: 1029-34. [185] Regueiro M, Schraut W, Baidoo L, et al. Infliximab prevents
Crohn's disease recurrence after ileal resection. Gastroenterology 2009; 136: 441-50 e1; quiz 716.
[186] Rutgeerts P. Adalimumab induces and maintains mucosal healing in patients with moderate to severe ileocolonic Crohn’s disease:
first results of the EXTEND trial. Digestive Disease Week: Abstract 751e; 2009; 2009.
[187] Colombel JF. Endoscopic mucosal improvement in patients with active Crohn’s disease treated with certolizumab pegol: first results
of the music clinical trial. Am J Gastroenterol 2008; 103: A1107. [188] D'Haens G, Baert F, van Assche G, et al. Early combined
immunosuppression or conventional management in patients with
newly diagnosed Crohn's disease: an open randomised trial. Lancet
2008; 371: 660-7. [189] Devlin SM, Panaccione R. Evolving inflammatory bowel disease
treatment paradigms: top-down versus step-up. Med Clin North Am 2010; 94: 1-18.
[190] Allez M, Lemann M, Bonnet J, Cattan P, Jian R, Modigliani R. Long term outcome of patients with active Crohn's disease
exhibiting extensive and deep ulcerations at colonoscopy. Am J Gastroenterol 2002; 97: 947-53.
[191] Loly C, Belaiche J, Louis E. Predictors of severe Crohn's disease. Scand J Gastroenterol 2008; 43: 948-54.
[192] Dorn SD. Predictors of Crohn's disease. Gastroenterology 2006; 131: 334-5; author reply 5.
[193] Reese GE, Nanidis T, Borysiewicz C, Yamamoto T, Orchard T, Tekkis PP. The effect of smoking after surgery for Crohn's disease:
a meta-analysis of observational studies. Int J Colorectal Dis 2008; 23: 1213-21.
[194] Sachar DB, Lemmer E, Ibrahim C, et al. Recurrence patterns after first resection for stricturing or penetrating Crohn's disease.
Inflamm Bowel Dis 2009; 15: 1071-5. [195] Maconi G, Colombo E, Sampietro GM, et al. CARD15 gene
variants and risk of reoperation in Crohn's disease patients. Am J Gastroenterol 2009; 104: 2483-91.
[196] Quinton JF, Sendid B, Reumaux D, et al. Anti-Saccharomyces cerevisiae mannan antibodies combined with antineutrophil
cytoplasmic autoantibodies in inflammatory bowel disease: prevalence and diagnostic role. Gut 1998; 42: 788-91.
[197] Vasiliauskas EA, Kam LY, Karp LC, Gaiennie J, Yang H, Targan SR. Marker antibody expression stratifies Crohn's disease into
immunologically homogeneous subgroups with distinct clinical characteristics. Gut 2000; 47: 487-96.
[198] Mow WS, Vasiliauskas EA, Lin YC, et al. Association of antibody responses to microbial antigens and complications of small bowel
Crohn's disease. Gastroenterology 2004; 126: 414-24. [199] Walker LJ, Aldhous MC, Drummond HE, et al. Anti-
Saccharomyces cerevisiae antibodies (ASCA) in Crohn's disease are associated with disease severity but not NOD2/CARD15
mutations. Clin Exp Immunol 2004; 135: 490-6. [200] Dubinsky MC, Lin YC, Dutridge D, et al. Serum immune
responses predict rapid disease progression among children with Crohn's disease: immune responses predict disease progression.
Am J Gastroenterol 2006; 101: 360-7. [201] Targan SR, Landers CJ, Yang H, et al. Antibodies to CBir1
flagellin define a unique response that is associated independently with complicated Crohn's disease. Gastroenterology 2005; 128:
2020-8. [202] Velayos FS, Terdiman JP, Walsh JM. Effect of 5-aminosalicylate
use on colorectal cancer and dysplasia risk: a systematic review and metaanalysis of observational studies. Am J Gastroenterol 2005;
100: 1345-53. [203] Renna S, Camma C, Modesto I, et al. Meta-analysis of the placebo
rates of clinical relapse and severe endoscopic recurrence in postoperative Crohn's disease. Gastroenterology 2008; 135: 1500-9.
[204] Lochs H, Mayer M, Fleig WE, et al. Prophylaxis of postoperative relapse in Crohn's disease with mesalamine: European Cooperative
Crohn's Disease Study VI. Gastroenterology 2000; 118: 264-73. [205] Rutgeerts P, Hiele M, Geboes K, et al. Controlled trial of
metronidazole treatment for prevention of Crohn's recurrence after ileal resection. Gastroenterology 1995; 108: 1617-21.
[206] Ng SC, Kamm MA. Management of postoperative Crohn's disease. Am J Gastroenterol 2008; 103: 1029-35.
[207] Ardizzone S, Maconi G, Sampietro GM, et al. Azathioprine and mesalamine for prevention of relapse after conservative surgery for
Crohn's disease. Gastroenterology 2004; 127: 730-40. [208] D'Haens GR, Vermeire S, Van Assche G, et al. Therapy of
metronidazole with azathioprine to prevent postoperative recurrence of Crohn's disease: a controlled randomized trial.
Gastroenterology 2008; 135: 1123-9. [209] Sandborn WJ, Rutgeerts P, Enns R, et al. Adalimumab induction
therapy for Crohn disease previously treated with infliximab: a randomized trial. Ann Intern Med 2007; 146: 829-38.
Received: October 16, 2010 Accepted: November 10, 2010




















