
Enzymes in feces: Useful markers of chronic inflammatory bowel disease
Upload
khangminh22Category
view
0download
0
© 2010 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY
Abstracts S413
INFLAMMATORY BOWEL DISEASE
1140
Diff erences in Infl ammatory Bowel Disease Between Caucasian, African American, Hispanic and Caribbean Populations in an Outpatient ClinicLeon Kurtz, MD, Ronald Greenberg, MD, Maurice Cerulli, MD. Long Island Jewish Medical Center, New Hyde Park, NY.
Purpose: Infl ammatory Bowel Disease (IBD) is more prevalent in Caucasian populations. Despite this, African Americans have a more severe presentation of disease, necessitating increased surgical interventions and higher incidence of extra-intestinal manifestations. Sparse data exists in the literature on people of Caribbean and Hispanic ethnicity with IBD.Methods: We conducted a retrospective chart review analysis at a single adult gastroenterology ambulatory clinic analyzing diff erences in phenotypic pre-sentation of IBD and various utilized treatment regimens between Caucasian and Non-Caucasian populations.Results: Analysis revealed that Non-Caucasians have isolated ileal or ileo-colonic Crohn’s Disease (CD) while Caucasians have predominant isolated colonic involvement. CD related surgeries (41% vs. 7%, p=0.03) and utilization of immunomodulator therapy (63% vs. 27%, p=0.02) were more frequent in Non-Caucasian populations compared to Caucasians. Th e phenotypic presen-tation of IBD in the Caribbean and Hispanic population was similar to African Americans with IBD.Conclusion: CD related surgeries and utilization of immunomodulators are more commonly utilized in Non-Caucasian populations. Th is data supports prior observations between ethnicity and disease phenotype in IBD. Carib-bean and Hispanic populations trended to have a similar disease presenta-tion and treatment utilization to African-American populations. Further studies are still needed on a larger scale to adequately understand the disease phenotype in Non-Caucasian populations and formulate optimal treatment algorithms between ethnicities.
1141
Concomitant Use of Adalimumab and Immunomodulators or Corticoste-roids Compared with Adalimumab Alone: Pooled Safety Analysis
2010 Presidential PosterWilliam Sandborn, MD,1 Jean-Frédéric Colombel, MD,2 James Lewis, MD,3 Mark Osterman, MD,3 Anne Robinson, PharmD,4 Bidan Huang, PhD,4 Paul Pollack, MD,4 Roopal Th akkar, MD4. 1. Mayo Clinic, Rochester, MN; 2. Uiversity de Lille, Lille, France; 3. University of Pennsylvania, Philadelphia, PA; 4. Abbott, Abbott Park, IL.
Purpose: To assess the incidence of serious infections in patients with Crohn’s disease (CD) using adalimumab in combination with immunomodulators and/or corticosteroids.Methods: Th e proportion of patients with treatment-emergent serious infec-tions was determined from the cumulative adverse event data in lead-in and long-term studies of adalimumab in CD (CLASSIC I and II, CHARM, GAIN, and ADHERE) among patients who received at least 1 dose. Proportions and rates of serious infection were assessed across treatment groups according to receipt of immunomodulators (IMM, i.e., 6-MP, AZA, and methotrexate) and/or corticosteroids at lead-in study baseline. Proportions were compared using Fisher’s exact test.Results: In the pooled analysis, serious infection occurred in 10.0% (64/638) of patients using IMM in combination with adalimumab compared with 7.2% (59/821) of patients using adalimumab without IMM (p=0.058). In both groups, baseline use of corticosteroid was associated with increased serious infections (see Table). Within the subgroup receiving adalimumab without IMM, corticosteroid use was associated with a signifi cantly increased pro-portion of patients with serious infections compared with adalimumab alone (p=0.034). Serious infections were observed most commonly in patients receiving adalimumab plus both IMM and corticosteroids (p=0.005, com-pared with adalimumab alone).
Conclusion: Patients with Crohn’s disease treated with corticosteroids and IMMs in combination with adalimumab are at the highest risk of experiencing treatment-emergent serious infections.Disclosure: Dr Sandborn - Consultant, research support: Abbott Dr Colombel - Consultant: Abbott Dr Lewis - Consultant: Abbott Dr Osterman - Consultant: Abbott Dr Robinson - Employee, Abbott Dr Huang - Employee, Abbott Dr Pollack - Employee, Abbott Dr Th akkar - Employee, Abbott.
1142
Safety of Adalimumab in Global Clinical Trials of Patients with Crohn’s DiseaseJean-Frédéric Colombel, MD,1 Remo Panaccione, MD,2 William Sandborn, MD,3 Paul Rutgeerts, MD,4 Stephen Hanauer, MD,5 Walter Reinisch, MD,6 Anne Robinson, PharmD,7 Winnie Lau, PhD,7 Alexandra Cardoso, PharmD,7 Paul Pollack, MD7. 1. University of Lille, Lille, France; 2. University of Calgary, Calgary, AB, Canada; 3. Mayo Clinic, Rochester, MN; 4. University Hospital Gasthuisberg, Leuven, Belgium; 5. University of Chicago, Chicago, IL; 6. Medical University Vienna, Vienna, Austria; 7. Abbott, Abbott Park, IL.
Purpose: Adalimumab (ADA), a fully human anti-TNF monoclonal antibody, is approved in Europe for treating patients with severely active Crohn’s disease (CD) who have had an inadequate response to conventional therapy.Methods: All patients with CD participating in the pivotal randomized con-trolled clinical trials, open-label extensions, and Phase IIIb studies were evalu-ated for safety at regular intervals. Rates of adverse events (AEs) of interest to physicians prescribing anti-TNF therapy were assessed per 100-patient-years (100-PYs) of ADA exposure. Standardized mortality ratios were calculated using the World Health Organization 2003 age- and sex-matched US mortal-ity data.Results: As of 6 November, 2009, the ADA CD clinical trial safety data-base contained data for 3603 patients (4088-PYs of ADA exposure). Table 1 compares AE rates observed in all clinical trials in CD at the 6 November 2009 cutoff to those from the 15 April 2008 safety update.1 Observed cases of lymphoma (2), tuberculosis (3), congestive heart failure (2), and demy-elinating disease (6) have not increased since the previous update. The AE rates were comparable to those reported in rheumatoid arthritis trials.2 The calculated standardized mortality ratio in ADA-treated patients with CD, 0.48 (95% confidence interval [CI]: 0.15, 1.12), is lower than the rate of 1.52 (95% CI: 1.32, 1.74) reported in a recent meta-analysis of patients with CD.3
Conclusion: Th e safety profi le and AE rates for ADA in CD were similar to those reported previously for ADA and other TNF antagonists in CD popu-lations.4,5 ADA was well-tolerated, and no new safety signals were identifi ed. References: 1. Colombel DDW 2009; Poster W1089. 2. Burmester Ann Rheum Dis 2009; 68:1863 3. Canavan Aliment Pharmacol Th er 2007; 25:861 4. Colom-bel Gastroenterology 2004; 126:19 5. Lichtenstein Clin Gastroenterol Hepatol 2006; 4:621.Disclosure: Dr Colombel - Consultant: Abbott Dr Panaccione - Consultant, research support, lecture fees: Abbott Dr Sandborn - Consultant, research support: Abbott Dr Rutgeerts - Consultant, research support: Abbott Dr Hanauer - Consultant: Abbott Dr Reinisch - Consultant: Abbott Dr Robinson - Employee: Abbott Dr Lau - Employee: Abbott Dr Cardoso - Employee: Abbott Dr Pollack - Employee: Abbott.
Treatment-emergent serious infections by baseline concomitant therapy
Therapy N SI a n ( % ) SI a E / 100-PYs b P value*
ADA c alone 528 30 (5.7) 3.2
ADA + IMM (no CS d ) 370 33 (8.9) 5.3 0.064
ADA + CS (no IMM) 293 29 (9.9) 7.0 0.034
ADA + IMM + CS 268 31 (11.6) 8.6 0.005
*Comparing proportion, versus ADA alone. a serious infections; b events per 100 patient-years; c adalimumab; d corticosteroid.

The American Journal of GASTROENTEROLOGY VOLUME 105 | SUPPLEMENT 1 | OCTOBER 2010 www.amjgastro.com
AbstractsS414
1143
Current Practice and Perception of Screening for Medication Adherence in Infl ammatory Bowel Disease: Results of a Nationwide SurveyArvind Trindade, MD, Andrew Tinsley, MD, Th omas Ullman, MD. Th e Dr Henry D. Janowitz Division of Gastroenterology, Mount Sinai School of Medicine, New York, NY.
Purpose: A recent paper from President Obama’s chief healthcare advisor calls for medication adherence as a priority for healthcare reform, as adherence to medica-tion in chronic diseases improves outcomes; with the infl ammatory bowel diseases being no exception. Th e current practice of physician screening for medication adherence is unknown. Th e goal of this study was to determine current practice and perception of screening for medication adherence in the USA in IBD.Methods: A ten-question survey was mailed electronically to gastroenterolo-gists whose electronic-mail address was listed in the American College of Gas-troenterology database. Physicians who cared for IBD patients were invited to answer the survey.Results: 6,830 surveys were sent to gastroenterologists nationwide. 395 physi-cians who cared for IBD patients fully completed the survey. Th e true response rate is unknown as the number of physicians caring for IBD patients in the data-base is unknown. 77% (n=303) of physicians who responded stated they screen for adherence to medication. Of the 77% that screened for adherence, only 19% (n=58) use accepted measures of screening for adherence (pill counts, prescrip-tion refi ll rates, or adherence surveys). Th e remaining 81% used patient inter-view to screen for adherence, a measure considered least accepted to determine adherence, as it overestimates adherence. Th e average number of IBD patients seen in one week, type of practice (academic versus private), number of years post training, or age had no statistical signifi cance in predilection or prefer-ence of screening. 89% of responders thought screening was very important or important versus 11% who thought screening was somewhat important or not important. 99% of responders thought improving adherence would improve health related outcomes. 95% of responders thought determining a low adherer to medicine was important because an intervention can increase adherence. 74% of responders would use an adherence survey in practice if one were vali-dated for IBD in at least 75% of encounters. 48% would use it in every patient.Conclusion: Th e vast majority of gastroenterologists surveyed recognize that adherence to medication is important and improves outcomes. Th e majority of physicians are screening for non-adherence in IBD patients, but are not using accepted measures for adherence detection. Changing the way physcians screen for adherence may detect more low adherers to medication.
1144
Comorbid Diabetes Mellitus Increases the Risk For Surgery in Patients with Crohn’s DiseaseJason Harper, MD, Scott Lee, MD. University of Washington, Seattle, WA.
Purpose: Th e prevalence of diabetes is rapidly increasing. Given the eff ects of hyperglycemia on wound healing and tissue regeneration, comorbid
diabetes may aff ect the natural history of Crohn’s disease (CD). We examined the period prevalence of surgical intervention in a diabetic cohort with CD compared to a control population.Methods: We compared a cohort of individuals diagnosed with CD prior to January 1, 2004 with comorbid diabetes to a non-diabetic control population and compared the period prevalence of surgical intervention between 2004 to 2009. Covariates of interest included age, gender, BMI, biologic use, length of time since diagnosis of CD and corticosteroid use. Unadjusted and adjusted odds-ratios were calculated regarding need for surgical intervention.Results: A total of 239 patients were identifi ed, 25 of whom met the criteria for diagnosis with diabetes. Th e period prevalence of CD-specifi c surgery in the diabetic cases was 68.0% and in the non-diabetic controls, 30.1%. Th e unadjusted OR for surgical intervention in the diabetic cohort was 4.9 (95% CI 2.0 - 11.9). Comparison of independent variables between the case and con-trol groups revealed no signifi cant diff erence in mean age (P=0.30), sex ratio (P=0.69), mean time since diagnosis of CD (P=0.94) or corticosteroid use (P=0.29). Th ere were signifi cant diff erences in mean Harvey-Bradshaw Index (P=0.03) and mean SIBDQ scores (P=0.006) between groups. Th ere were also signifi cant diff erences in BMI distribution (P=0.01) and use of biologic therapy (P=0.01). Regression analysis failed to identify any signifi cant eff ect interaction among the covariates; stratifi cation of patients by BMI groups did reveal a mild confounding eff ect, with a fi nal adjusted OR of 4.4 (95% CI 1.8-10.8). Patients with corticosteroid-induced diabetes had a similar period prevalence of surgery as compared to patients with idiopathic type 1 or type 2 diabetes (P=1.0).Conclusion: Diabetes mellitus is a novel risk factor predicting need for surgery in patients with CD, and is associated with worse subjective disease outcomes as well. Th is knowledge compliments the already established risk factors that predict surgical intervention in patients with CD, such as smoking or earlier age at diagnosis. Th e eff ect of diabetes mellitus is independent of corticosteroid use and not simply a proxy for the same.
1145
Prognosis for Lymphoma in Patients with Infl ammatory Bowel Disease Treated with 6-mercaptopurine or AzathioprineKeith Sultan, MD,1 Burton Korelitz, MD, MACG,2 Daniel Present, MD, MACG,3 Seymour Katz, MD, MACG,1 Iuliana Shapira, MD1. 1. North Shore University Hospital, Manhasset, NY; 2. Lenox Hill Hospital, New York, NY; 3. Mount Sinai School of Medicine, New York, NY.
Purpose: An increased risk of lymphoma in patients with Crohn’s disease (CD) and ulcerative colits (UC) has never been confi rmed. However, treat-ment of CD with 6-mercaptopurine (6MP) and azathioprine (AZA) has been associated with a four fold increase in the risk of lymphoma compared to non-treated patients and the general population. Lymphoma occurs in 4 out of every 10,000 CD patients treated with 6MP/AZA. Despite this small number, lymphoma remains a feared complication of treatment. Recent reports of hep-atosplenic T cell lymphoma in patients treated with both 6MP/AZA and infl ix-imab have worsened these fears. Currently, little is known about the prognosis of lymphoma occurring in the infl ammatory bowel disease (IBD) population, specifi cally those treated with 6MP/AZA.Methods: A retrospective case series of IBD patients at three academic centers were analyzed from a database of 8,780 total records. All patients with a diag-nosis of lymphoma were identifi ed and analyzed for IBD type, medication use, lymphoma type and outcome following medical treatment. Another database of 600 lymphoma patients from an academic Hematology and Oncology cen-ter was searched for IBD patients and analyzed in the same fashion.Results: In all, 14 patients with a diagnosis of lymphoma were identifi ed, 12 with CD and 2 with UC. Th e one female case had CD. Th ere was only one Hodgkin’s lymphoma. Cases are summarized in the table below.Conclusion: While the number of IBD patients who develop lymphoma remains small, concern among patients and practitioners remains dispropor-tionately high. While hepatosplenic T cell lymphoma is rapidly progressive and uniformly fatal, there is no evidence that prior 6MP/AZA use alone and non-Hodgkin’s lymphoma follows a similar severe course. From our own series only two cases treated with 6MP/AZA exhibited a rapid clinical decline. Our data suggest that those who developed lymphoma aft er treatment with 6MP/AZA had a prognosis no more ominous than those not so treated.
[1142]
AE of interest
All CD trials as of 15 Apr 2008 ( N =3160; 3402-PYs)
E (E / 100-PYs)
All CD trials as of 6 Nov 2009 ( N =3603; 4088-PYs)
E (E / 100-PYs)
Any AE 20399 (599.6) 24875 (608.4)
Any serious AE 1170 (34.4) 1473 (36.0)
Any AE leading to discon-tinuation
556 (16.3) 695 (17.0)
Infectious AE 3917 (115.1) 4953 (121.1)
Serious infections 225 (6.6) 270 (6.6)
Malignantneoplasms 44 (1.3) 54 (1.3)
Injection-site pain 138 (4.1) 321 (7.9)
Opportunistic infections 64 (1.9) 82 (2.0)
Any fatal AE 4 (0.1) 6 (0.1)

© 2010 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY
Abstracts S415
1146
Oral Tacrolimus Th erapy is Useful for Patients with Intractable Ulcerative ColitisNagamu Inoue, MD,1 Riko Saito, MD,2 Katsuyoshi Matsuoka, MD,2 Tadakazu Hisamatsu, MD,2 Susumu Okamoto, MD,2 Haruhiko Ogata, MD,1 Yasushi Iwao, MD,1 Toshifumi Hibi, MD2. 1. Center for Diagnostic and Th erapeutic Endoscopy, Keio University School of Medicine, Tokyo, Japan; 2. Keio University School of Medicine - Division of Gastroenterology and Hepatology, Department of Internal Medicine, Tokyo, Japan.
Purpose: Immunosuppressive therapy with intravenous ciclosporin is an alternative treatment option to total colectomy for patients with severely-active ulcerative colitis (UC), while the benefi ts of oral administration of tacrolimus are not well defi ned. As it was recently approved for clinical use in Japan, we evaluate the effi cacy and safety of tacrolimus in patients with intractable UC.Methods: Twenty patients with intractable UC, including those refractory to conventional therapy (n=5), dependent to corticosteroids (n=4) and easy to recurrence (n=4), were orally administered tacrolimus to induce remission with trough whole-blood levels of 10-15 ng/mL for two week and then maintained with those of 5-10 ng/mL. Median treatment duration was 4.7 months (1-7 months) and median follow-up duration was 5.2 months (1-8 months). Evaluation of the clinical response was based on a modifi ed Truelove-Witts clinical activity index (CAI) and endoscopic response was assessed by Baron’s score before and three months aft er starting the treat-ment. Moreover, prognosis during or aft er the treatment with tacrolimus was assessed.Results: Trough levels of the drug reached to target level in 9.0 days (mean, 3-19 days). CAI scores signifi cantly decreased from 10.7 ± 4.8 to 5.3 ± 3.2 at week 2 (p < 0.0001). Remission was achieved in 35%, improvement was achieved in 35% of patients while 30% of patients did not respond to treat-ment. Endoscopic scores decreased from 2.7 ± 0.6 to 1.6 ± 1.6 by week 12. In 11 patients (55%) treated with corticosteroids at the initiation of tacroli-mus therapy, corticosteroids were successfully tapered or discontinued. Four patients underwent proctocolectomy within 6 months. Adverse events were tremor (5%), renal function impairment (10%), hyperkalaemia (5%), hypo-magnesemia (85%) and none of serious events were observed.Conclusion: Th ese fi ndings suggested that short-term oral administration of tacrolimus produced a good clinical response as well as steroid tapering eff ect in patients with intractable UC.
1147
Setting Priorities for Comparative Eff ectiveness Research in Infl ammatory Bowel Disease: Results of an International Provider Survey, Expert RAND Panel, and Patient Focus GroupsAdam Cheifetz, MD,1 Gil Melmed, MD,2 Brennan Spiegel, MD, M.S.H.S.,3 Jennifer Talley, none,4 Shane Devlin, MD,5 Laura Harrell, MD,6 Peter Irving, MD,7 Jennifer Jones, MD,8 Gil Kaplan, MD,5 Patricia Kozuch, MD,9 Miles Sparrow, MD,10 Fernando Velayos, MD,11 Leonard Baidoo, MD,12 Brian Bressler, MD,13 Corey Siegel, MD14. 1. Medicine/GI, Beth Israel Deaconess Medical Center, Boston, MA; 2. Cedars-Sinai Medical Center, Los Angeles, CA; 3. VA Greater Los Angeles Healthcare System, Los Angeles, CA; 4. CURE Digestive Disease Research Center, Los Angeles, CA; 5. University of Calgary, Calgary, AB, Canada; 6. University of Chicago, Chicago, IL; 7. Guy’s and St. Th omas’ Hospital, London, United Kingdom; 8. University of Saskatchewan, Saskatoon, SK, Canada; 9. Jeff erson University, Philadelphia, PA; 10. Th e Alfred Hospital, Melbourne, VIC, Australia; 11. University of California San Francisco, San Francisco, CA; 12. University of Pittsburgh, Pittsburgh, PA; 13. University of British Columbia, Vancouver, BC, Canada; 14. Dartmouth-Hitchcock Medical Center, Lebanon, NH.
Purpose: Comparative eff ectiveness research (CER) is an emerging fi eld that compares the relative eff ectiveness of alternative strategies to prevent, diag-nose, or treat patients that are typical of day-to-day clinical practice. To focus goals for CER in infl ammatory bowel disease (IBD) it is important to identify research questions that practitioners and patients believe are important. We sought to develop a priority list of CER studies (CERs) for IBD.Methods: Following the Institute of Medicine’s approach for developing CER priorities, we developed and administered a survey to gastroenterologists (GIs) asking them to suggest important CERs in IBD. Th e survey was electronically distributed to an international sample of GIs from North America, UK and Aus-tralia. In addition, an international panel of 13 IBD experts (BRIDGe group) independently proposed CERs. Two patient focus groups were also convened to solicit their opinions of priority IBD research topics. All CERs were compiled and divided into 21 topic categories. Th e candidate CERs were then presented to the expert panel using the validated RAND/UCLA method. Th e panel rated the proposed CERs using a standard 1-9 point scale (1=lowest priority; 9=high-est; >7=high priority). Following the initial ratings the panel met in person to discuss and re-rate priorities. Disagreement was assessed using a validated index accounting for response distributions over the 9-point scale.Results: Responses were collated into 234 unique CERs proposed by the GIs, experts and patients. Based on the initial round of rating, the RAND panel
[1145] Table 1 .
Patient / gender / IBD type Age at lymphoma
diagnosis, yrs 6MP / AZA Lymphoma type / distribution Survival at last follow- up (yrs)
1 male, CD 53 Yes CNS < 1, expired
2 male, CD 69 Yes B cell, diffuse, low grade, multiple lymph node groups 11
3 male, CD 50 Yes Large B cell, liver, marrow, retroperitoneal mass 14, expired
4 male, CD 58 No Large cleaved cell, liver, multiple lymph node groups 1
5 male, CD 30 No Ileo-cecal 5
6 male, CD 50 Yes Non-Hodgkins, lung 6
7 male, UC 52 Yes Non-Hodgkins < 1, expired
8 female, CD 53 Yes Large cell follicular, groin nodes 4.5
9 male, CD 74 No Low grade B cell, marrow, diffuse adenopathy 4.5
10 male, UC 44 No Follicular B cell, Stage IIIS 6.5
11 male, CD 50 No Diffuse large B cell Liver mass 1
12 male, CD 45 No Hodgkins Stage IVB 3, expired
13 male, CD 55 Yes Diffuse low grade B cell 3
14 male, CD 83 No Lymphoplasmacytic, Marrow, Peritoneal, lung 2, expired
HBI remission rates.

The American Journal of GASTROENTEROLOGY VOLUME 105 | SUPPLEMENT 1 | OCTOBER 2010 www.amjgastro.com
AbstractsS416
selected 87 CERs to re-rate, of which 40 were rated as high priority. Disagree-ment was observed in only 5 of 87 CERs. Th e highest priority CERs (scores >7.7) related to comparing the eff ectiveness of: withdrawal of biologic or immunomodulator agents for Crohn’s patients in remission; anti-TNF mono-therapy versus combination therapy in patients failing thiopurines; biologics vs. thiopurines for prevention of post-operative recurrence; the utility of colo-noscopy in guiding post-operative management; the use of infl iximab levels vs. standard infl iximab dosing to guide therapy; the use of biomarkers to predict outcomes and response to therapy; the use of biologics in inducing remission and mucosal healing in Crohn’s disease; and cyclosporine vs. infl iximab vs. surgery in steroid refractory UC.Conclusion: We systematically developed a list of high priority CERs for IBD based on a survey of GIs, expert review, and patient input. Th is list may guide IBD researchers and funding agencies towards the most important CERs that would impact day-to-day clinical practice.Disclosure: GYM: Consultant and/or Research Support (Centocor, Setpoint, Amgen, Celgene), Speaker’s Bureau (Abbott, P&G, Shire), Advisory Board (UCB). CAS: Advisory board (Abbott, UCB, P&G), Consultant and research support (Elan, P&G), CME activities (Abbott, UCB). BMS: Research (Takeda, Rose Pharma A/S, Prometheus, Novartis), Advisory Board (Prometheus, Takeda, Ironwood, Procter & Gamble, AstraZeneca). BB: Advisory Board (Abbott, Scher-ing-Plough Canada, Shire, Ferring,), Speaker’s Bureau (Abbott, Schering-Plough Canada, Shire, Takeda). AC: Speaker’s bureau (UCB, P&G, Shire, and Abbott), Advisory board (Abbott, UCB, Schering-Plough Canada). JJ: Consulting, speak-er’s Bureau and educational funding (Schering-Plough Canada, UCB Pharma, Shire, P&G and Abbott). MS: Research Support (Ferring Pharmaceuticals, Abbott Pharmaceuticals), Advisory Board (Schering-Plough Pharmaceuticals). FV: Research support (P&G). PI: Advisory Board (Abbott, Shire, Falk), Speaker’s Bureau ( Shire, Abbott, MSD, Merck). SD: Speaker’s Bureau (Scheringing-Plough, Abbott, Merck, Shire), Advisory Board (Abbott, UCB, Merck). GK: Advisory Board (Schering-Plough, Abbott, UCB, Shire). LH: Consultant (Abbott, Salix), Research support (Glycominds). LB: Advisory board (UCB), Speaker’s bureau (Centocor, Salix). PK: None.Funding Source: Unrestricted funding for the in-person Scottsdale RAND Appropriateness Panel meeting was generously provided by Proctor and Gamble Pharmaceuticals, Abbott, and Shire. Unrestricted funding for the BRIDGe group is provided by Abbott, Shire, UCB, and Proctor and Gamble Pharmaceuticals.
1148
Patient Response to Anti-TNF Dose Escalation in Crohn’s Disease Using Health Claims DataDavid Rubin, MD,1 Rob Sederman, BS2. 1. University of Chicago Medical Center, Chicago, IL; 2. C1 Consulting, Summit, NJ.
Purpose: Studies of claims databases have shown that dose escalation of adali-mumab (ADA) and infl iximab (IFX) occurs in 20-60% of Crohn’s disease (CD) patients taking ADA or IFX. We used claims data (PharMetrics database) to assess patients’ response to these dose changes.Methods: Claims data included were from patients diagnosed with CD, con-tinuously enrolled for 6 months before and 3 months aft er their fi rst anti-TNF claim, who had at least 1 postinduction anti-TNF claim. Dose escalation was defi ned for IFX as ≤4 weeks between maintenance doses or ≥75% increase in vials compared with induction (using cost data), and for ADA as weekly dose ≥40 mg (≥2x recommended maintenance dose). Response to dose escalation was measured by continuation/discontinuation of the drug. Kaplan-Meier and Cox regression (controlling for age, gender, comorbidities, and fi rst anti-TNF) were used to estimate mean times to escalation and discontinuation. Medica-tion use aft er anti-TNF discontinuation (steroids, immunosuppressants, new biologic) and CD-related surgeries in patients with and without dose escala-tion were compared.Results: IFX: 3866 patients were identifi ed (60% aged 30-60, 56% female); 28% had dose escalation and IFX was the fi rst anti-TNF used (IFX-1L) in 99% of cases. ADA: 935 patients were identifi ed (69% aged 30-60, 61% female); 24% of patients had dose escalation, among whom 65% used ADA-1L (35% ADA-2L aft er IFX). Mean time to dose escalation aft er induction was 10.4 months (95% CI, 8.7-12.0) for IFX, 3.0 months (2.2-3.9) for ADA-1L, and 1.8 months (1.2-2.4) for ADA-2L. Mean time to drug discontinuation aft er dose escalation
was 12.6 months (95% CI, 10.4-14.9) for IFX, 3.7 months (1.8-5.6) for ADA-1L, and 4.7 (2.4-7.1) for ADA-2L. 36% of IFX patients remained on therapy at 12 months aft er dose escalation compared with 38% and 33% of ADA-1L and ADA-2L patients remaining on therapy at 6 months. Mean time on mainte-nance therapy was extended for patients who had dose escalation compared with those who did not (IFX, 23.0 vs. 13.5 months; ADA-1L, 6.7 vs. 4.9 months; ADA-2L, 6.5 vs. 3.0 months). Overall, 47-62% of patients who had dose escala-tion and 53-60% of those who did not received prescription therapy for CD or underwent surgery within 6 months of anti-TNF discontinuation.Conclusion: Among CD patients receiving IFX and ADA, dose escalation was common (24-28%), occurred quickly (within 2-10 months), and extended duration of therapy (3-10 months). Dose escalation occurred sooner and extended therapy for less time in patients receiving ADA compared with those receiving IFX. Further investigation of anti-TNF dosing and response patterns in clinical practice are warranted.Disclosure: Dr Rubin - Consultancy for UCB Mr. Sederman - Consultancy for UCB.
1149
Compassionate Use of Certolizumab Pegol in Patients with Crohn’s Disease Who Have Failed Previous TNF Inhibitor Th erapiesSeverine Vermeire, MD, PhD,1 Stefanie Howaldt, MD,2 Daan Hommes, MD,3 Brian Bressler, MD,4 Jean-Frédéric Colombel, MD,5 Krassimir Mitchev, MD, PhD,6 Paul Rutgeerts, MD, PhD1. 1. University Hospital Gasthuisberg, Leuven, Belgium; 2. Private Practice, Hamburg, Germany; 3. University of Leiden, Leiden, Netherlands; 4. St. Paul’s Hospital, Vancouver, BC, Canada; 5. Hôpital Claude Huriez, Lille, France; 6. UCB, Braine l’Alleud, Belgium.
Purpose: Th e effi cacy and safety of certolizumab pegol (CZP), the only Fc-free, PEGylated Fab’ anti-TNF, in Crohn’s disease (CD) has been shown in 2 large Phase III trials1,2. A compassionate use program (COMPAS) allows physicians to use CZP in resistant cases. Here we report the eff ectiveness of CZP in CD in real-world clinical practice.Methods: COMPAS includes patients with CD for whom approved conser-vative therapies had failed. Th e recommended CZP dose regimen followed that of the submitted label (400 mg subcutaneous [sc] induction at Weeks 0, 2, and 4, then 400 mg sc maintenance every 4 weeks). Treatment was deemed eff ective if there was a clinical response (clinical improvement satisfactory to both patient and investigator with the patient remaining on treatment) and no adverse events (AEs) leading to withdrawal.Results: By November 6, 2009, COMPAS involved 346 gastroenterologists in 18 countries, with 823 requests received from physicians. Drug-release criteria were met by 779 patients, and 657 patients had been treated with CZP. Most patients were also receiving immunosuppressants and/or corti-costeroids at baseline. At Week 8, 76.6% (503/657) of patients responded to CZP treatment. Of these, 70.2% (461/657) were still in response after 8 weeks; 58.3% (383/657) remained on treatment at Week 20, 45.2% (297/657) at Week 32, and 38.5% (253/657) at Week 40. The vast majority of the patients had failed treatment with 1 or 2 anti-TNFs at inclusion in COMPAS. Sixty-one serious AEs occurred in 35 patients, including small intestine carcinoma (history of severe CD/successive immunosuppres-sives/5 months’ therapy), acute left cardiac insufficiency and renal failure (obesity and family history of myocardial infarction/2 weeks’ therapy), and acute urticaria (patient had similar reactions to previous anti-TNF therapies). Two deaths occurred (1 due to myocardial infarction and the other respiratory failure) and were judged unlikely to be, or not, related to treatment.Conclusion: COMPAS off ers a chance for patients with CD to receive CZP in real-life conditions. CZP is eff ective in patients with diffi cult to treat CD and those who had previously failed other TNF inhibitor therapies. Despite inclu-sion of only patients with severe and resistant disease, the clinical effi cacy and safety profi les of CZP in this study were similar to those in controlled clinical trials. References 1. Sandborn WJ, et al. N Engl J Med 2007;357:228-238. 2. Schreiber S, et al. N Engl J Med 2007;357:239-250.Disclosure: Dr Vermiere - Consultant for and research and grant support from UCB Dr Howaldt - None Dr Hommes - Consultant for UCB Dr Bressler - None Dr Colombel - Consultant for and research and grant support from UCB Dr Mitchev - Employee of UCB Dr Rutgeerts - Consultant for UCB.

© 2010 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY
Abstracts S417
1150
Certolizumab Pegol 400 mg Rapidly Reduced the Signs and Symptoms of Crohn’s Disease in Greek Patients Who Previously Failed Infl iximab Th erapyJohn Triantafi llidis, MD,1 Dimitrios Karamanolis, MD,2 Georgios Kitis, MD,3 Etienne Ernault, PhD,4 Gerasimos Mantzaris, MD, PhD2. 1. Saint Panteleimon General Hospital, Nicea, Greece; 2. Evangelismos Hospital, Athens, Greece; 3. George Papanikolaou General Hospital, Th essaloniki, Greece; 4. UCB, Brussels, Belgium.
Purpose: In the treatment of Crohn’s disease (CD), failure to receive rapid relief from disease signs and symptoms can lead to therapy switching. It is therefore important to determine effi cacy and onset of action of a new therapy aft er switching. Th is study assessed the rapidity of response to treatment with 400 mg certolizumab pegol (CZP; the only Fc-free, PEGylated Fab’ anti-TNF with effi cacy in CD1,2) in reducing the signs and symptoms of moderate to severe CD in Greek patients who failed on infl iximab (IFX) therapy.Methods: In this open-label, multicenter, single-cohort study conducted in Greece (NCT00307931), adult patients with moderate to severe CD (CD Activity Index [CDAI] score, 220-450) had previously responded to IFX ther-apy but were no longer responding or had developed intolerance. CZP 400 mg was administered subcutaneously to all patients at baseline (>8 weeks aft er last dose of IFX) and at Weeks 2, 4, 8, and 12. In this analysis, CDAI compo-nents (number of loose/liquid stools, abdominal pain, and general well-being) reported in patient diary cards were assessed in the fi rst 7 days of treatment (aft er initial CZP dose at baseline) to determine rapidity of response. p values were calculated using nonparametric tests.Results: Th e intent-to-treat population consisted of 16 patients (43.8% male; mean age, 42.5 years [SD 15.4]). Th ree patients withdrew prior to receiving study drug and are not included in this analysis. At baseline, the median number of loose/liquid stools was 4.9; rapid improvement was seen as early as Day 1 aft er receiving CZP, with a change in the median number of loose/liquid stools of -1.30 (p<0.01) and -1.00 (p=0.09) at Day 7. Abdominal pain also showed rapid improvement, with 10 (76.9%) patients reporting none/mild abdominal pain and 3 (23.1%) reporting moderate/severe abdominal pain at Day 1 compared with 8 (61.5%) having moderate/severe abdominal pain at baseline. Patients maintained improvement from baseline, with 4 (30.8%) reporting moderate/severe pain at Day 7. At baseline, 7 (53.8%) patients rated their well-being as poor/very poor; at Day 1 patients’ well-being improved, with only 2 (15.4%) scoring poor/very poor. Th is was maintained at Day 7, with 4 (30.8%) patients rating their condition poor/very poor. At Day 7, 4 (30.8%) patients reported being generally well, an improvement from 1 (7.7%) patient at baseline.Conclusion: Patients who had previously failed IFX therapy experienced rapid relief in the signs and symptoms of CD following treatment with CZP 400 mg. References 1. Sandborn WJ, et al. N Engl J Med 2007;357:228-238. 2. Schreiber S, et al. N Engl J Med 2007;357:239-250.Disclosure: Triantafi llidis - Financial support for research from UCB Karamano-lis - Financial support for research from UCB Kitis - None Ernault - Employee of UCB Mantzaris - None.
1151
Patient Self-assessed HBI Correlates Highly with Physician-Assessed HBI in the Secure RegistryBrian Feagan, MD,1 Scott Lee, MD,2 Gary Lichtenstein, MD,3 Edward Loft us, MD,4 David Binion, MD,5 Juan Pablo Guzman, MD,6 Ralph Bloomfi eld, MSc,7 Douglas Wolf, MD8. 1. Robarts Research Institute, London, ON, Canada; 2. University of Washington School of Medicine, Seattle, WA; 3. University of Pennsylvania School of Medicine, Philadelphia, PA; 4. Mayo Clinic, Rochester, MN; 5. University of Pittsburgh Department of Medicine, Pittsburgh, PA; 6. UCB, Raleigh, NC; 7. UCB, Slough, United Kingdom; 8. Atlanta Gastroenterology Associates, Atlanta, GA.
Purpose: Th e SECURE Registry compares the long-term safety of Crohn’s disease (CD) patients treated with certolizumab pegol (CZP) with a non-CZP-treated control population. Patient- and physician-derived modifi ed Harvey-Bradshaw Index (HBI) scores were compared in these patients, pro-viding an analysis that has not previously been investigated.
Methods: SECURE (NCT00844285) is a long-term observational study in the United States that will assess 2000 CZP-treated CD patients and 2000 CD patients treated with steroids, immunosuppressives, or other biologic agents for up to 10 years. Gastroenterologists and internal medicine physicians from community-based and academic practice settings will follow patients using regular clinic visits and direct patient follow-up (Web/mail surveys and tele-phone calls). Medications will be prescribed according to usual patient/physi-cian judgment. To assess the potential value of the HBI as a patient-reported outcome, we compared baseline physician-derived HBI scores and modifi ed patient HBI scores (omitting the abdominal mass item).Results: As of March 1, 2010, 819 patients had been recruited, 270 into the CZP cohort (median age, 40.0 years [range, 15-81]; 62% female) and 549 into the comparison cohort (median age, 42 years [range, 9-88]; 58% female). At baseline, 41%, 40%, and 10% of patients in the CZP cohort had mild to moder-ate, moderate to severe, and severe disease activity, respectively, and 9% were in remission. In the non-CZP cohort, 42%, 17% and 3% of patients had mild to moderate, moderate to severe, and severe disease activity, respectively, and 38% were in remission. Fift y-six percent of patients in the CZP cohort and 65% of patients in the non-CZP cohort had disease duration of ≥5 years; 61% and 65%, respectively, had previously used biologic agents as therapy. Interest-ingly, based on 781 patients with paired assessments, the baseline physician and modifi ed patient HBI scores were highly correlated (regression coeffi cient r=0.990 [95 %CI, 0.968-1.000], R2=0.908, p<0.0001).Conclusion: Patients recruited into the CZP and non-CZP arms of SECURE had similar demographics. However, patients treated with CZP had more severe dis-ease activity. Th e high correlation observed between patient and physician assess-ment on the modifi ed HBI suggests that this instrument may be highly valuable for use in clinical studies when a regular physical examination is not feasible. Vali-dation of patient self-assessed HBI for CD clinical research is warranted.Disclosure: Feagan - Consultancy and research support from UCB Lee - Con-sultant for UCB Lichtenstein - Consultant for UCB Loft us - Consultancy and research support from UCB Binion - Consultancy and research support from UCB Guzman - Employee of UCB Bloomfi eld - Employee of UCB Wolf - Con-sultant for UCB.
1152
Long-term Remission with Certolizumab Pegol in Crohn’s Disease: Effi cacy Over 4.5 Years in Patients with No Prior TNF Inhibitor Exposure (PRECiSE 3 Study)Gary Lichtenstein, MD,1 Ole Th omsen, MD,2 Stefan Schreiber, MD, PhD,3 Ian Lawrance, MD, PhD,4 Stephen Hanauer, MD,5 Ralph Bloomfi eld, MSc,6 William Sandborn, MD7. 1. University of Pennsylvania School of Medicine, Philadelphia, PA; 2. Herlev Hospital, Copenhagen, Denmark; 3. Christian Albrechts University, Kiel, Germany; 4. University of Western Australia, Fremantle, WA, Australia; 5. University of Chicago Medical Center, Chicago, IL; 6. UCB Pharma, Slough, United Kingdom; 7. Mayo Clinic, Rochester, MN.
Purpose: Th e purpose of this study was to evaluate remission rates in patients (pts) who received certolizumab pegol (CZP) for 6 months (26 weeks) in PRE-CiSE 2 (P2) and a further 4.5 years in PRECiSE 3 (P3) and to determine if remission rates are aff ected in pts without previous TNF inhibitor exposure.Methods: Pts completing P2 (NCT00152425) were eligible to enter P3 (NCT00160524) and receive CZP 400 mg every 4 weeks. Effi cacy and safety data for pts who received CZP in P2 and continued with open-label CZP treat-ment in P3 (P3-CZP population) are presented. Th e Harvey-Bradshaw index (HBI) was used to measure disease activity (remission=score of ≤4). Remission rates were analyzed from the baseline of P2 in the P3-CZP population and in a subset of this population who had never received infl iximab (IFX-naïve). Remission rates were calculated using non-responder imputation (NRI), observed case (OC), and last observation carried forward (LOCF) analyses.Results: Of the 141 pts in the P3-CZP population, 114 were IFX-naïve. At the start of P3 (Week [Wk] 0), 75% (105/141) and 78% (89/114) of the P3-CZP and IFX-naïve populations were in remission, respectively. Remission rates for the P3-CZP population aft er 1 (Wk 26 of P3), 2 (Wk 78 of P3), 3 (Wk 130 of P3), 4 (Wk 182 of P3), 4.5 (Wk 206 of P3), and 5 (Wk 226 of P3) years (LOCF) were 69%, 69%, 64%, 64%, 63%, and 62%, respectively, and 69%, 68%, 65%, 65%, 63%, and 62% for the IFX-naïve pts (Table).

The American Journal of GASTROENTEROLOGY VOLUME 105 | SUPPLEMENT 1 | OCTOBER 2010 www.amjgastro.com
AbstractsS418
Conclusion: Continuous CZP 400 mg therapy provided long-term remission for more than 4.5 years in pts who initially responded to CZP induction therapy. Sustained long-term remission rate was observed in both all P3 pts receiving CZP and in P3 pts receiving CZP with no previous exposure to infl iximab.Disclosure: Dr Lichtenstein - Consultancy and Financial Support for Research from UCB Dr Th omsen - no disclosures for UCB Dr Schreiber - Financial Support for Research from UCB Dr Lawrance - Consultancy for UCB Dr Hanauer - Consultancy and Financial Support for Research from UCB Ralph Bloomfi eld - Employee of UCB Dr Sandborn - Financial Support for Research from UCB. Consulting Fees paid to Mayo Clinic from UCB.Th is research was supported by an industry grant from UCB Pharma.
1153
Long-term Maintenance of Remission with No Dose Escalation Aft er Re-induction with Certolizumab Pegol in Patients with Crohn’s Disease Exacerbation Who Were Naïve to Anti-TNF Treatment: 4-Year Results from the PRECiSE 4 StudyWilliam Sandborn, MD,1 Stefan Schreiber, MD, PhD,2 Stephen Hanauer, MD,3 Jean-Frédéric Colombel, MD,4 Ralph Bloomfi eld, MSc,5 Gary Lichtenstein, MD6. 1. Mayo Clinic, Rochester, MN; 2. Christian Albrechts University, Kiel, Germany; 3. University Of Chicago Medical Center, Chicago, IL; 4. Hopital Claude Huriez, Lille, France; 5. UCB Pharma, Slough, United Kingdom; 6. University of Pennsylvania School of Medicine, Philadelphia, PA.
Purpose: Patients (pts) who experienced disease exacerbation on either active or placebo maintenance therapy in PRECiSE 2 (P2) were re-induced with cer-tolizumab pegol (CZP). Th e purpose of this study was to evaluate the long-term (4-year) sustainability of remission (total Harvey-Bradshaw index [HBI] score of ≤4 points) and safety of CZP in anti-TNF naïve vs. non-naïve pts who were in remission at Week (Wk) 4 of PRECiSE 4 (P4).Methods: In P2 (NCT00152425), pts (n=428) who responded to induction therapy with CZP at Wk 6 were randomized to continuous therapy with CZP or placebo (drug interruption) during Wks 6-26. Pts who had an exacerbation of symptoms before Wk 26 could enter P4 (NCT00160706), an open-label extension study. In P4, pts received CZP 400 mg at Wks 0, 2, and 4 followed by every 4-week (q4w) maintenance therapy with CZP 400 mg through Wk 208 (4 years). Th us, pts receiv-ing active treatment were given 1 single extra dose, and then continued with q4w maintenance therapy in P4. Disease activity was measured using the HBI.Results: A total of 124 pts entered P4 from P2: 49 pts who had been randomized to CZP and 75 pts who had been randomized to placebo. Among these pts, 84 were anti-TNF naïve and 40 were non-naïve. By Wk 4, 38% (47/124) achieved HBI remission (intent-to-treat [ITT]). Aft er 1, 2, 3, and 4 years of q4w CZP 400 mg maintenance therapy in naïve vs. non-naïve pts, remission was maintained in 68% vs. 47%; 71% vs. 64%; 60% vs. 70%; and 63% vs. 50% pts, respectively (observed case [OC]) (Table). In general, rates of remission were similar in the naïve vs. non-naïve pts. No new safety concerns were identifi ed.Conclusion: CZP 400 mg re-induction successfully recaptured and maintained remission in pts with disease exacerbation who were naïve to anti-TNF treat-ment. Th ese data suggest that a long-term benefi t is achieved with a re-induc-tion strategy in anti-TNF naïve pts with Crohn’s disease who lost response due to drug interruption or loss of initial response to active therapy with no dose escalation.Disclosure: Dr Lichtenstein - Consultancy and Financial Support for Research from UCB Dr Schreiber - Financial Support for Research from UCB Dr Hanauer -
Consultancy and Financial Support for Research from UCB Ralph Bloomfi eld - Employee of UCB Dr Sandborn - Financial Support for Research from UCB. Consulting Fees paid to Mayo Clinic from UCB Dr Colombel - Consultancy, Lecturer, Grant and Research Support from UCB.Th is research was supported by an industry grant from UCB Pharma.
1154
Endoscopic Improvement in Patients with Active Crohn’s Disease Treated with Certolizumab Pegol: Results of Blinded Central Reading of Recorded Endoscopies from the MUSIC Study (NCT00297648)Xavier Hebuterne, MD, PhD,1 Marc Lémann, MD,3 Jean-Louis Dupas, MD, PhD,6 Yoram Bouhnik, MD, PhD,5 Matthieu Allez, MD,3 Edouard Louis, MD, PhD,7 Krassimir Mitchev, MD, PhD,4 Etienne Ernault, MSc,4 Jean-Frédéric Colombel, MD2. 1. CHU Nice, Nice, France; 2. CHU Lille, Lille, France; 3. Hopital Saint Louis, Paris, France; 4. UCB Pharma, Braine Alleud, Belgium; 5. Hopital Beaujon, Clichy, France; 6. CHU Amiens, Amiens, France; 7. CHU Liege, Liege, Belgium.
Purpose: MUSIC, an open-label intervention study, evaluated the eff ect of certolizumab pegol on endoscopic improvement in patients with active mod-erate to severe Crohn’s disease (CD). In addition to evaluation by the local endoscopist, recorded endoscopies were evaluated by 2 central readers and are reported here.Methods: Patients (N=89) with active endoscopic disease (ulcerations in ≥2 intestinal segments with a CD Endoscopic Index of Severity [CDEIS] score ≥8 points) received subcutaneous certolizumab pegol 400 mg at Weeks 0, 2, and 4 and every 4 weeks up to 54 weeks. Th e primary end point was change from baseline in CDEIS score at Week 10. Secondary end points included evalua-tion of mucosal ulcerations, endoscopic response (>5-point improvement in CDEIS score vs. baseline), remission (CDEIS score <6), and complete remis-sion (CDEIS score <3) at Week 10. Each of 2 pairs of central readers (JLD and YB, EL and MA), blinded to the local readings, was randomly assigned half of the recorded endoscopies for CDEIS scoring. For each pair mean CDEIS was calculated; in case of discrepancies between the 2 readers regarding the pres-ence and severity of ulcers, the worse result was taken into account.Results: A total of 44 patients had evaluable recorded endoscopies at baseline and Week 10. Change from baseline to Week 10 in mean (SD) CDEIS score was signifi cant (-3.79 [4.24]; p<0.0001). At Week 10, the number of patients achieving endoscopic response was 37%, remission was 45%, and complete remission was 20% for central readings, compared with 61%, 42%, and 11%,
[1152] HBI remission rates
P3-CZP, % (95 % CI for percentage remission) IFX-na ï ve, % (95 % CI for percentage remission)
LOCF OC NRI LOCF OC NRI
Year 1 (Wk 26 of P3) 69 (61.1 – 76.4) 74 (66.5 – 81.9) 65 (57.4 – 73.1) 69 (60.9 – 77.9) 75 (66.2 – 83.3) 65 (56.2 – 73.7)
Year 2 (Wk 78 of P3) 69 (61.1 – 76.4) 84 (76.2 – 92.1) 49 (40.7 – 57.2) 68 (59.9 – 77.0) 83 (74.0 – 92.2) 47 (38.2 – 56.5)
Year 3 (Wk 130 of P3) 64 (55.9 – 71.8) 82 (71.9 – 91.5) 35 (26.9 – 42.6) 65 (56.2 – 73.7) 82 (71.9 – 92.8) 37 (28.0 – 45.7)
Year 4 (Wk 182 of P3) 64 (55.9 – 71.8) 79 (66.9 – 91.2) 23 (16.4 – 30.4) 65 (56.2 – 73.7) 81 (67.6 – 93.5) 25 (16.7 – 32.5)
Year 4.5 (Wk 206 of P3) 63 (55.2 – 71.1) 83 (70.4 – 95.3) 21 (13.9 – 27.2) 63 (54.3 – 72.0) 81 (66.7 – 94.6) 22 (14.3 – 29.5)
Year 5 (Wk 226 of P3) 62 (54.4 – 70.4) 77 (54.0 – 99.8) 7 (2.9 – 11.3) 62 (53.4 – 71.2) 73 (46.4 – 99.0) 7 (2.3 – 11.7)
HBI remission rate
Anti-TNF naive, % (n / N) Non-naive, % (n / N)
OC ITT OC ITT
Wk 4 40 (32 / 81) 38 (32 / 84) 43 (15 / 35) 38 (15 / 40)
Wk 52 (Year 1) 68 (34 / 50) 40 (34 / 84) 47 (8 / 17) 20 (8 / 40)
Wk 104 (Year 2) 71 (25 / 35) 30 (25 / 84) 64 (7 / 11) 18 (7 / 40)
Wk 156 (Year 3) 60 (12 / 20) 14 (12 / 84) 70 (7 / 10) 18 (7 / 40)
Wk 180 (Year 3.5) 71 (12 / 17) 14 (12 / 84) 60 (6 / 10) 15 (6 / 40)
Wk 208 (Year 4) 63 (10 / 16) 12 (10 / 84) 50 (5 / 10) 13 (5 / 40)

© 2010 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY
Abstracts S419
respectively, for local readings. At baseline, 77% had deep ulcerations; by Week 10, 32% had improved to superfi cial and 2% had completely healed for central readings, compared with 92%, 42%, and 5%, respectively, for local readings.Conclusion: Central reading of recorded paired endoscopies confi rmed sta-tistically signifi cant improvement in CDEIS scores at Week 10 in patients with active CD treated with certolizumab pegol. Overall, the results supported the initial fi ndings with nonblinded local readings.Disclosure: Dr Hebuterne - Consultant for UCB Lemann- Consultant for UCB Dupas - None Bouhnik - Consultant for UCB Allez - Consultant for UCB Louis - None Mitchev - Employee of UCB Ernault - Employee of UCB Colombel - Consultant, Lecturer, Grant and Research Support from UCB.Th is research was supported by an industry grant from UCB.
1155
Eff ect of the PEG Component of Certolizumab Pegol on Calcium Flux in Cellular SystemsAndrew Nesbitt, PhD, Sabrina Lamour, BSc, Gianluca Fossati, PhD. UCB, Slough, United Kingdom.
Purpose: Certolizumab pegol (CZP), the only Fc-free, PEGylated Fab’ anti-TNF, has a very low incidence of injection site pain (ISP) in all clinical studies. Th is could be due to inhibition of mast cell degranulation by the PEG compo-nent of CZP1. Mast cells may be involved in mediating ISP as they are present at high numbers in the skin and can rapidly secrete many infl ammatory media-tors. Changes in calcium (Ca2+) fl ux from intracellular stores or by infl ux from outside of the cell are primary indicators of cell activation, and when mast cells degranulate, this is preceded by Ca2+ fl ux into the cell. PEG has been shown to bind metal ions (in particular Ca2+)2, and the aim of this study was to deter-mine if PEG could inhibit Ca2+ fl ux in a cellular system.Methods: Peripheral blood monocytes, positively isolated using MACS beads, were incubated for 30 min with the fl uorophore Fluo-4, which changes its fl u-orescence emission when it chelates Ca2+. Ca2+ fl ux was measured using fl ow cytometry by detecting the Fluo-4 emission at 515-535 nm. Ionomycin (a Ca2+ ionophore) was added at 2 μg/mL and the emission measured over a 4-min period relative to background, which was assessed for 1 min prior to ionomycin addition. Th e eff ect of a range of concentrations of the 40 kDa PEG component of CZP on Ca2+ fl ux induced by ionomycin was assessed. In addition, the eff ect of PEG on ionomycin-induced Ca2+ fl ux in cultured mast cells was determined by a similar method except that the Ca2+ fl ux was measured using a fl uorimeter.Results: Ionomycin caused a dramatic fl ux of Ca2+ in the monocytes. PEG mediated a dose-dependent inhibition of Ca2+ fl ux in these cells over a range of concentrations from 40 mg/mL. Th is is a physiologic concentration of PEG as the equivalent concen-tration of PEG that is injected into patients is 88.9 mg/mL. Th e half maximal inhibi-tory concentration (IC50) for inhibition of the Ca2+ fl ux by PEG was around 10 mg/mL. Th e maximum inhibition observed was 84.2% obtained at 40 mg/mL, with the eff ect titrating out at around 1 mg/mL. In mast cells the IC50 was around 11 mg/mL.Conclusion: Th e PEG component of CZP inhibits Ca2+ fl ux in monocytes and mast cells at a concentration relevant to the site of injection. Th is could explain the eff ect of CZP observed on inhibition of mast cells and the low levels of ISP observed with CZP in the clinic. Inhibition of Ca2+ fl ux would only be expected at the site of injection as systemic concentrations of the drug are below the levels where an eff ect is seen. Th is property of PEG merits further investigation as low levels of ISP are important for compliance during treatment. References 1. Lamour S, et al. Ann Rheum Dis 2009;68(suppl 3):188. 2. Buschmann H. Z Phys Chem 1984;139:113.Disclosure: Drs Fossati and Nesbitt are both employees of UCB, the manufacturer of certolizumab pegol.
1156
Induction Th erapy with Certolizumab Pegol in Patients with Moderate to Severe Crohn’s Disease: A Placebo-Controlled TrialWilliam Sandborn, MD,1 Stefan Schreiber, MD, PhD,2 Brian Feagan, MD,3 Paul Rutgeerts, MD, PhD,4 Ziad Younes, MD,5 Ralph Bloomfi eld, MSc,6 Juan Pablo Guzman, MD, MSc,7 Geert D’Haens, MD, PhD8. 1. Mayo Clinic, Rochester, MN; 2. Christian Albrechts University, Kiel, Germany; 3. Robarts Research Institute, London, ON, Canada; 4. University Hospital Gasthuisberg, Leuven, Belgium; 5. GastroOne, Memphis, TN; 6. UCB, Slough, United Kingdom; 7. UCB, Raleigh, NC; 8. Imelda General Hospital, Bonheiden, Belgium.
Purpose: In the pivotal phase III trials PRECiSE 1 and 2, certolizumab pegol (CZP) has been shown to be effi cacious for reducing the signs and symptoms
and maintaining response in patients with moderate to severe Crohn’s disease (CD). Th e aim of the present study was to further evaluate the effi cacy and safety of CZP during induction treatment.Methods: In this double-blind trial (NCT00552058), adult patients (male or female, aged 18-75 years, N=439) with active CD (CD Activity Index [CDAI] 220-450) were randomly assigned to receive CZP 400 mg or placebo subcutane-ously at Weeks 0, 2, and 4. Th e primary end point was remission rate (CDAI score ≤150) at Week 6. Secondary end points were response rates (decrease in CDAI score ≥100 from Week 0) at Weeks 2, 4, and 6, the remission rate (CDAI score ≤150) at Week 6 in subgroups of patients stratifi ed by the baseline C-reactive pro-tein (CRP) concentration, and the proportion of patients with adverse events.Results: Data from the intent-to-treat population are shown (Table 1). At Week 6, the remission rate was 32% for CZP vs. 25% for placebo (p=0.174). Response rates at Weeks 2 and 4, but not Week 6, were signifi cantly greater with CZP treatment vs. placebo (Table 1). Among patients with baseline CRP concentrations ≥5 mg/L, the remission rates were signifi cantly greater (p<0.05) for CZP vs. placebo (Table 2). Approximately one-third of all patients with a baseline CRP ≥5 mg/L achieved remission at Week 6 with CZP induction. Th e safety profi le was consistent with that observed in previous trials with CZP and other anti-TNF agents, with no new safety signals.Conclusion: In patients with moderate to severe CD, induction treatment with CZP 400 mg at Weeks 0, 2, and 4 failed to demonstrate a statistically signifi cant increase in the pre-specifi ed clinical remission end point at Week 6. However, the remission and response rates in the CZP group were numerically greater than placebo at all time points. CZP showed statistically signifi cant and clini-cally meaningful superiority vs. placebo in patients with signs of active infl am-mation (baseline CRP ≥5 mg/L). Th is result confi rms that inclusion criteria in controlled randomized trials in infl ammatory bowel disease should comprise objective criteria for infl ammatory disease activity. CZP was well tolerated. No new safety issues were identifi ed.Disclosure: Dr Sandborn - Financial Support for Research from UCB, Lecture fees paid by UCB to Mayo Clinic Dr Schreiber - Financial Support for Research from UCB Dr Feagan - Financial Support for Research and Consultancy for UCB Dr Rutgeerts - Financial Support for Research, Lecturer and Consultancy for UCB Dr Younes - Financial Support for Research and Lecturer for UCB Ralph Bloomfi eld - Employee of UCB Juan Pablo Guzman - Employee of UCB Dr D’Haens - Lecturer for UCB.Th is research was supported by an industry grant from UCB Pharma.
Table 1 . Clinical remission and response rates
Clinical remission (CDAI score ≤ 150), n ( % )
Week Placebo (n=209) CZP 400 mg (n=215) P value
2 33 (15.8) 50 (23.3) 0.033
4 40 (19.1) 57 (26.5) 0.063
6 53 (25.4) 68 (31.6) 0.174
Clinical response (decrease in CDAI score ≥ 100 from Week 0), n ( % )
Week Placebo ( n =209) CZP 400 mg ( n =215) P value
2 42 (20.1) 71 (33.0) 0.001
4 55 (26.3) 76 (35.3) 0.024
6 71 (34.0) 87 (40.5) 0.179
Table 2 . Patients achieving clinical remission (CDAI score ≤ 150)
CRP concentration Placebo, % ( n = 209) CZP 400 mg, % ( n = 215)
< 4 mg / L 27.1 28.8
≥ 4 mg / L 24.5 33.1
≥ 5 mg / L 22.5 33.8*
≥ 6 mg / L 20.0 33.3*
≥ 7 mg / L 20.2 33.3*
≥ 8 mg / L 20.6 34.3*
≥ 9 mg / L 20.8 34.7*
≥ 10 mg / L 19.8 33.3*
* P < 0.05.

The American Journal of GASTROENTEROLOGY VOLUME 105 | SUPPLEMENT 1 | OCTOBER 2010 www.amjgastro.com
AbstractsS420
1157
Health-Related Quality of Life Improvements in Patients with Active Crohn’s Disease Following Treatment with Certolizumab Pegol in the MUSIC Study (NCT00297648)Xavier Hebuterne, MD, PhD,1 Marc Lémann, MD,2 Geoff roy Coteur, PhD,3 Etienne Ernault, MSc,3 Jean-Frédéric Colombel, MD4. 1. CHU Nice, Nice, France; 2. Saint-Louis Hospital, Paris, France; 3. UCB, Braine l’Alleud, Belgium; 4. Hopital Huriez, Lille, France.
Purpose: To assess change in health-related quality of life (HRQoL) in patients with Crohn’s disease (CD) treated with certolizumab pegol (CZP) in the MUSIC study.Methods: Patients in the MUSIC study had active CD (CD Activity Index score >225 to <450) and were treated with open-label CZP (400 mg subcutaneously [sc] every 2 weeks for 3 doses, then 400 mg sc every 4 weeks) for up to 54 weeks. Patients completed the Infl ammatory Bowel Disease Questionnaire (IBDQ) at baseline, Week 10, and Week 54 to assess HRQoL. Th e IBDQ includes 32 ques-tions that examine 4 aspects of patients’ lives: bowel symptoms, systemic symp-toms, emotional function, and social function (range of total score, 32-224). Least squares (LS) mean change (SD) in IBDQ total scores from baseline to Week 10 and Week 54 were evaluated; categorical rates of response (increase in IBDQ total score of ≥16 points) and remission (IBDQ total score ≥170 points) at each time point were also assessed. An exploratory analysis of the correlation between HRQoL remission as measured by the IBDQ and endoscopic remission as measured by the CD Endoscopic Index of Severity (remission, <6 points) was also performed.Results: A total of 89 patients entered the study; the IBDQ was completed by 78 patients at Week 10 and by 50 patients at Week 54. At baseline, mean (SD) IBDQ total score was 120.2 (29.8). At Week 10, LS mean (SD) change in IBDQ total score was 43.8 (33.8), the response rate was 66.3% (95% CI for percent-age response, 55.5-76.0%), and the remission rate was 43.8% (95% CI, 33.3-54.7%). At Week 54, LS mean (SD) change in IBDQ total score was 44.1 (32.8), the response rate was 43.8% (95% CI, 33.3-54.7%), and the remission rate was 29.2% (95% CI, 20.1-39.8%). In the intent-to-treat population with an available endoscopic assessment at Week 10, the overall IBDQ remission rate was 69.7% in patients with endoscopic remission compared with 33.3% in patients not reaching endoscopic remission. Similar results were observed at Week 54.Conclusion: In patients with active CD, treatment with CZP at recommended dosages resulted in substantial improvement in HRQoL at both 10 and 54 weeks of therapy as measured by the IBDQ. Higher rates of IBDQ remission were asso-ciated with endoscopic remission compared with nonremission. Further evalu-ation of the impact of CZP therapy on improvement in HRQoL is warranted.Disclosure: Ernault - Employee UCB Coteur - Employee of UCB Colombel - Consultant, Lecturer, Grant and Research Support from UCB Lemann - Consul-tant for UCB Hebuterne - Consultant for UCB.Th is research was supported by an industry grant from UCB.
1158
Colectomy and Mortality Rates in Infl ammatory Bowel Disease: A Nationwide AnalysisJohn Wysocki, MD,1 N. Teddy Winstead, MD, MSPH2. 1. Tulane School of Medicine, New Orleans, LA; 2. Ochsner Clinic Foundation, New Orleans, LA.
Purpose: To analyze nationwide adult (>=18 years) inpatient data from 2002-2007 to determine statistical signifi cant factors in colectomy and mortality rates for patients presenting with fulminant infl ammatory bowel disease.Methods: Th is is a cross-sectional retrospective study using hospital discharge data from the US Nationwide Inpatient Sample from 2002-2007. Patient admis-sion characteristics were analyzed. Th ere were a total of 161,903 and 95,201 discharged patients with Crohns Disease (CD) and Ulcerative Colitis (UC), respectively, as identifi ed by ICD-9 code. Th e primary outcomes were inpatient colectomy (total or partial) and mortality rate. Risk factors specifi c to UC (C. diffi cile infection and proximity of colitis) were also analyzed.Results: Discharges of patients with CD and UC increased from 2002-2007 by 24.3% and 25.4%, respectively. Overall inpatient mortality of patients with CD and UC has remained relatively constant from 2002-2007 at 0.89% and 1.79%, respectively. Mortality rate for UC patients with inpatient colectomy was nearly four times greater than patients who did not have a colectomy. Procedure rates (either partial or total colectomy) associated with CD and UC decreased by 13.7% and 22.8%, respectively, from 2002-2007. Patients with concomitant
C. diffi cile infection were more likely to have a colectomy. Patients with panco-litis UC were four times more likely to have colectomy compared to other types of UC (ileocolitis, proctitis), while patients with left sided UC were two times more likely to have colectomy compared to other types of UC.Conclusion: Colectomy rates for UC and CD have decreased with time, how-ever inpatient mortality has remained relatively constant over the past decade. Patients with pancolitis were more likely to have a colectomy performed com-pared to patients with less extensive presentations of disease.
1159
Spontaneous Splenic Rupture: A Rare Complication of Acute Pancreatitis in a Patient with Crohn’s DiseaseGhulam Mujtaba, MD,1 Amir Butt, MD,1 Josmi Joseph, MD,1 Mukul Arya, MD,2 Sury Anand, MD1. 1. Th e Brooklyn Hospital Center, Brooklyn, NY; 2. Wyckoff Heights Medical Center, Brooklyn, NY.
Purpose: Spontaneous rupture of the spleen is a rare disorder and has been reported to occur in hematological, neoplastic, and infectious process involv-ing the spleen or as a complication of pancreatitis. We report a case of splenic rupture in a patient with poorly controlled Crohn’s disease (CD) presenting with acute pancreatitis. A case report: A 37 years old male with known history of Crohn’s colitis was admitted with a complaint of upper abdominal pain for 2 weeks. Examination revealed left upper quadrant tenderness without guard-ing, mass or rebound. Initial laboratory investigations revealed a WBC of 17.9 and Hgb of 7.9. Serum amylase was 202 IU/L (reference range: 45-200 IU/L) and lipase was 177 IU/L (reference range: 35-95 IU/L). Ultrasound of abdomen was normal. Contrast-enhanced CT scan of abdomen showed hemoperitoneum from spontaneous splenic rupture, splenic vein thrombosis, markedly edema-tous pancreas and peripancreatic infl ammatory changes. Patient was treated conservatively for the ruptured spleen as it was well localized. Discussion:Spon-taneous splenic rupture has been reported with acute pancreatitis, splenic vein thrombosis, perisplenic adhesions, and acute infl ammation of ectopic intras-plenic pancreatic tissue. Pancreatitis has been described in the setting of poorly controlled Crohn’s disease. In this case, the combination of poorly controlled CD, acute pancreatitis and splenic rupture are probably interconnected.
Figure 1: Splenic hemorrhage identifi ed by arrow.
Figure 2: Splenic vein thrombosis identifi ed by arrow.

© 2010 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY
Abstracts S421
1160
Th erapeutic Single-balloon Enteroscopy for Small Intestinal Stenosis May Modify Outcome of Patients with Crohn’s Disease Receiving Infl iximabAtsushi Yoshida, MD, Kentaroh Takatsuka, MD, Fumiaki Ueno, MD, Kenji Kobayashi, MD, Shogo Iwabuchi, MD. Ofuna Chuo Hospital, Kamakura, Japan.
Purpose: Progression of stenosis aft er administration of infl iximab is occa-sionally encountered in patients with Crohn’s disease, and surgical opera-tion is required. We evaluated effi cacy of single-balloon enteroscopy in these patients.Methods: Ten patients with Crohn’s disease with small intestinal stenosis, which was detected either by enteroscopy or barium meal, were placed on scheduled administration of infl iximab, and followed for the mean period of 33.3 month (4 to 96 month). During the follow up period, balloon dilatation was attempted using single-balloon enteroscopy (Olympus Medical Systems, Tokyo, Japan) for symptomatic small intestinal stenosis. Only when endo-scopic therapy was unsuccessful, the patients underwent surgical operation.Results: Seven patients developed stenotic symptoms during the follow up period, and totally 9 procedures of enteroscopy were performed. In 2 patients, endoscopic dilatation was unsuccessful because of failure to approach to the ste-notic lesions, and surgical operation was performed. Endoscopic dilatation was successful in remaining 5 patients. No complication was encountered in associa-tion with the endoscopic dilatation. Th e other 3 patients remained asymptomatic and received only pharmacological intervention. In all 10 patients, corticosteroid was withdrawn, and endoscopic remission was confi rmed.Conclusion: In signifi cant portion of Crohn’s disease patients with small intes-tinal stenosis who are on scheduled administration of infl iximab, endoscopic dilatation using single-balloon enteroscopy is benefi cial to avoid surgical inter-vention, and improved clinical outcome is expected.
1161
Prevalence of Bone Demineralization in AfroCaribbeans with Infl amma-tory Bowel DiseaseCharles Koczka, MD, Adam Goodman, MD. SUNY Downstate Medical Center, Brooklyn, NY.
Purpose: Osteoporosis/osteopenia has been increasingly recognized as a dis-ease process concurrent with infl ammatory bowel disease (IBD). Several incit-ing factors include malabsorption of Vitamin D and calcium, corticosteroid therapy, infl ammatory cytokines, and smoking. Racial variation of osteopo-rosis in IBD patients has been poorly described. We sought to identify risk factors for bone demineralization in AfroCaribbean (AC) with IBD.Methods: A retrospective chart review was performed from a 10-year-old pro-spectively collected database of IBD patients (age >18 years) seen at a large urban university medical center. Data on dual energy X-ray absorptiometry (DXA) scanning, use of steroids, bisphosphonates, calcium, and vitamin D, as well as blood chemistries were collected and analyzed using the student’s t-test and chi-square test as appropriate.Results: 115 charts of AC IBD patients [37 Crohn’s disease (CD), 2 indeter-minate colitis, 76 ulcerative colitis (UC)] were reviewed of which 24 patients (14 UC, 10 CD) had DXA scanning performed.10 patients had T-scores > -1, 14 patients had scores of < -1 of which 6 patients had scores <-2.5. 14 patients with a T-score of < -1 (mean age of 51 years, SD +/–20.4) were compared to ten patients with DXA scores > -1 (mean age 50.1 years, SD +/–14.9).Two patients with T-scores <-1 had fractures while none were observed in the comparison group (p=0.5). Mean body mass index (BMI) for those with T-scores <-1 was 23.9 kg/m2 compared to 31.5 kg/m2 in those with T-scores >-1 (p=0.0034). Two thirds of the patients with lower T-scores were prescribed treatment. See Table 1 for results.Conclusion: Screening for bone demineralization in ethnic populations with IBD is lacking as only 21% of AC IBD patients seen in our institution had a DXA scan. Of those who were scanned, more than half of the patients had T-scores suggestive of bone demineralization. Although elevated BMI was pro-tective against demineralization in AC patients with IBD, these results should prompt further studies to determine the prevalence and signifi cance of bone demineralization in minority populations with IBD.
1162
Are Infl ammatory Markers Predictive of Length of Hospital Stay in Patients with Infl ammatory Bowel Disease?Charles Koczka, MD, Adam Goodman, MD, Meira Abramowitz, MD, Pragati Jain, MS. SUNY Downstate Medical Center, Brooklyn, NY.
Purpose: Formulas such as the Crohn’s Disease Activity Index and Harvey Bradshaw Index rely on subjective criteria and have had poorly documented relationships to infl ammation in the gut and extraintestinal tissues. C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) levels, however, have served as objective measures of IBD activity. If CRP and ESR forecast severity of disease, then a prolonged hospital stay might be expected. We sought to determine if CRP and ESR were correlated with length of hospital stay (LOS) in IBD patients and if there was a diff erence in those with Crohn’s disease (CD) compared to ulcerative colitis (UC).Methods: IRB-approved retrospective study of 35 IBD patients admitted for an IBD fl are in the past 10 years. Inclusion criteria were age >18, diagnosis of UC or CD,ESR and/or CRP taken within the fi rst 2 days of admission, and an admission for an IBD fl are. Statistical analysis done using SAS version 9.2.Results: All patients were of AfroCaribbean descent. Seventeen patients had CD and 18 patients had UC. Fourteen patients had IBD for more than 5 years. Mean age was 38 years. Fift een patients had extraintestinal manifestations (EIM). For all IBD patients, mean CRP level was 62.0 mg/L (normal value <0.4) and mean ESR was 58.7 mm/hr (normal value 0-20). Average LOS was 8.1 days. Correlation of CRP with LOS was r=0.21 (p=0.29) and ESR with LOS r=0.271 (p=0.13). Stronger correlations were found with males (CRP r=0.40 and ESR r=0.48 in males; CRP r=0.22 and ESR r=0.23 in females). No diff erence was found in those with >5 years of IBD compared to <5 years (p=0.43). No diff erence was found in those with EIM compared to those without (p=0.79).In UC patients, mean CRP was 56.7 mg/L and ESR was 58 mm/hr, with a mean LOS of 8.9 days. Correlation of CRP with LOS was r=0.36 (p=0.18) and ESR with LOS being r=0.30 (p=0.22). In CD patients, mean CRP was 69 mg/L and ESR was 59 mm/hr, with the mean LOS being 7.2 days. Correlation of CRP with LOS was r=0.02 (p=0.94) and with ESR and LOS r= 0.26(p=0.38).Conclusion: We found no correlation between infl ammatory markers and LOS. Diff erences may not have been seen due to our small sample size. In addi-tion, our results come solely from AfroCaribbeans, an oft en under-reported group of IBD patients. Whether our fi ndings can be applied to other ethnic IBD populations remain to be seen. No data have been available correlating infl ammatory markers and LOS in ethnic populations. We question if stronger correlations could found among other ethnicities given that racial diff erences in phenotypic expression of IBD have been previously reported. In the mean-time, though CRP and ESR have been correlated with disease activity, we do not encourage the use of these markers in forecasting LOS.
Characteristics Tscore < -1 N =14
Tscore > -1 N =10
P value
BMI (kg / m2) 23.9 31.5 0.0034
Females ( % ) 71 90 0.35
Years of IBD at time of DXA 8.7 10.7 0.56
Ulcerative Colitis ( % ) 57 60 1.0
Fractures 2 0 0.5
Smokers ( % ) 21 10 0.6
Taking steroids at time of DXA ( % ) 64 60 1.0
Taking calcium or Vitamin D prior to DXA ( % )
14 30 0.62
Prescribed calcium, Vitamin D, or Bisphos-phonate ( % )
64 40 0.43
Alkaline Phosphatase (U / L) 103.6 83.8 0.24
Serum Calcium (mg / dL) 9.7 9.4 0.1
Serum Creatinine (mg / dL) 0.9 0.7 0.36

The American Journal of GASTROENTEROLOGY VOLUME 105 | SUPPLEMENT 1 | OCTOBER 2010 www.amjgastro.com
AbstractsS422
1163
Prospective Evaluation of the Clinical Utility of Spiral Deep Small Bowel Enteroscopy (SBE) in Patients with Known or Suspected Crohn’s Disease (CD)Jill Gaidos, MD, Joel Judah, MD, Dennis Collins, MD, Peter Draganov, MD.Medicine, Univ. of Florida, Gainesville, FL.
Purpose: Spiral enteroscopy (SE) is a new modality for examination of the deep small bowel. Its role in the management of Crohn’s disease (CD) has not been well defi ned. Th erefore, we evaluated the clinical utility of spiral enteros-copy in patients with known or suspected CD.Methods: Th is is a prospective cohort study. All patients referred to our insti-tution for SE with known or suspected CD were considered. All patients signed IRB approved research informed consent.Results: From April 2008 to April 2010, 11 patients (5 male, 6 female) mean age 49.5 years (21-77 years) with known or suspected CD presented to our hospi-tal to undergo SE. Indications included abnormalities noted on capsule endos-copy (n=3), CT enterography (n=4, 1 of whom also had an abnormal capsule endoscopy), CT (n=2), small bowel follow through (n=1), and in 1 patient the SBE was performed to retrieve a retained wireless capsule. Th ree patients had a confi rmed diagnosis of CD and 1 of ulcerative colitis. All procedures were per-formed antegrade. Th e procedure was successfully completed in 9/11 patients (82%). It failed in 2 (18%), one due to overtube malfunction and the other was due to an inability to engage the small bowel with the spiral overtube, precluding advancement of the enteroscope. Th e median procedure time was 44.5 minutes (range 25 - 59 minutes). Th e median depth of insertion in the 9 completed ante-grade cases was 214 cm (range 120 - 300 cm) beyond the ligament of Treitz. One patient was found to have infl ammation in the mid and proximal jejunum and a stricture in the mid jejunum; the biopsies showed an ulcer, consistent with the patient’s history of Crohn’s disease, and the stricture was treated with balloon dilation. One patient was found to have a jejunal diverticulum as an incidental fi nding. Th e remaining 8 enteroscopies were normal. Random biopsies were obtained in 2 patients and revealed normal small intestinal mucosa in both. Th e retained capsule was successfully retrieved. Th ere were no complications.Conclusion: Th is is the fi rst report of the use of spiral enterscopy in patients with known or suspected CD. Th e procedure can be safely and successfully completed in the majority of patients. Th erapy was successfully performed in the two patients with positive fi ndings. A majority of patients had normal enteroscopy, and the correlation between prior small bowel evaluation and spiral enteroscopy was poor. Further studies with long term follow-up are war-ranted to better defi ne the negative predictive value of a normal deep small bowel enteroscopy in patients with suspected CD.
1164
Activity of STS-1 in Patients with Infl ammatory Bowel DiseaseGuo Jun Huang, MD, Ramona Rajapakse, MD, Nicholas Carpino, PhD. Medicine, Stony Brook University, Stony Brook, NY.
Purpose: Suppressor of TCR Signaling-1 & -2 (STS-1 & STS-2) are phospha-tases that have been shown to negatively regulate T cell signaling pathways. Cells isolated from STS-1/2-/- mice display a striking hyper-sensitivity to in vitro TCR cell stimulation. Mutant mice also have increased susceptibility to auto-immunity, in a mouse model of multiple sclerosis. To determine if the STS proteins were involved in the etiology of IBD (Crohn’s colitis and ulcer-ative colitis), STS protein and enzyme activity levels were examined in diseased patients.Methods: STS-1 was obtained from peripheral lymphocytes by cell lysis, followed by immunoprecipitation. STS-1 phosphatase activity toward the artifi cial sub-strate pNPP was measured, and protein levels were assessed by Western analysis.Results: Ninety-one patients were enrolled and 63 patients [32 controls, 9 males; 31 IBD patients, 13 males] completed the study. Th e ratio of phosphotase activity over STS-1 activity/concentration (STS-1 activity ratio) was compared between 1) controls and IBD group, 2) controls compared to IBD with & without infl ammation on colonoscopy, and 3) IBD patients on anti-TNF agents, steroids plus mesalamine, mesalamine, and 6-mercaptopurine (6MP). Using the
Mann-Whitney test, the STS-1 activity ratio between the control group (median=0.190) & the IBD group (median=0.124) was not signifi cant (p=0.280). Using the Krukal-Wallis test, the STS-1 activity ratio between the control group (median=0.190), IBD with infl ammation group (median=0.199), and IBD without infl ammation group (0.0688) were not signifi cant (p=0.195). Using the Krukal-Wallis test, the STS-1 activity ratio between groups using the anti-TNF (median=0.151), steroids plus mesalamine (median=0.470), mesalamine (median=0.101), and 6MP (median=0.0636) were not signifi cant (p=0.621).Conclusion: While the above data is preliminary, it suggests that levels of STS-1 protein and phosphatase activity do not correlate with the occurrence of IBD. We are currently examining the possible correlation of STS-2 activity and expression level with the development of IBD.
1165
Preoperative Magnetic Resonance Enterography (MRE) Accurately Iden-tifi es Pathologic and Surgically Confi rmed Penetrating and Obstructive Complications of Crohn’s DiseaseSean Lynch, MD, Richard Bloomfeld, MD, MS, Ryan Mott, MD, Gregory Waters, MD, David Childs, MD, John Leyendecker, MD. Gastroenterology, Wake Forest University Baptist Medical Center, Winston Salem, NC.
Purpose: Crohn’s disease is a chronic infl ammatory disorder oft en marked by penetrating or obstructive complications. Frequently, these complications lead to surgical therapy for Crohn’s disease patients. Successful preoperative identifi cation of a penetrating or obstructive phenotype is crucial for proper surgical planning. Magnetic resonance enterography (MRE) is oft en used to identify complications of Crohn’s disease. Th e aim of this retrospective study is to describe the accuracy of MRE in identifying pathologically and surgically proven complications of Crohn’s disease.Methods: All MRE exams performed at our tertiary care medical center over the past 30 months were retrospectively identifi ed by chart review and those patients who had undergone surgery for Crohn’s disease following a MRE examination were selected. Th e radiographic images, surgical reports, and pathologic slides/reports were independently re-examined for evidence of penetrating (abscesses and fi stulae) or obstructive (strictures) disease. Th e radiographic fi ndings were compared to the composite gold standard of the surgical/pathologic fi ndings. Complications were recorded and analyzed on a per patient basis.Results: 20 patients who had received a MRE exam followed by surgical ther-apy for Crohn’s disease were identifi ed. Th e mean time between the MRE exam and surgery was 80 days. MRE accurately predicted the surgical/pathologic presence or absence of strictures in 17/20 patients (accuracy 85%, sensitivity 89%, specifi city 50%), abscesses in 19/20 patients (accuracy 95%, sensitivity 100%, specifi city 94%), and fi stulae in 15/20 patients (accuracy 75%, sensitiv-ity 100%, specifi city 66%). Of the 9 patients incorrectly identifi ed, the majority were false positive results (7 of 9 patients).Conclusion: MRE accurately identifi es penetrating and obstructive compli-cations in patients with Crohn’s disease and aff ords a means of identifying patients who may benefi t from surgical intervention.
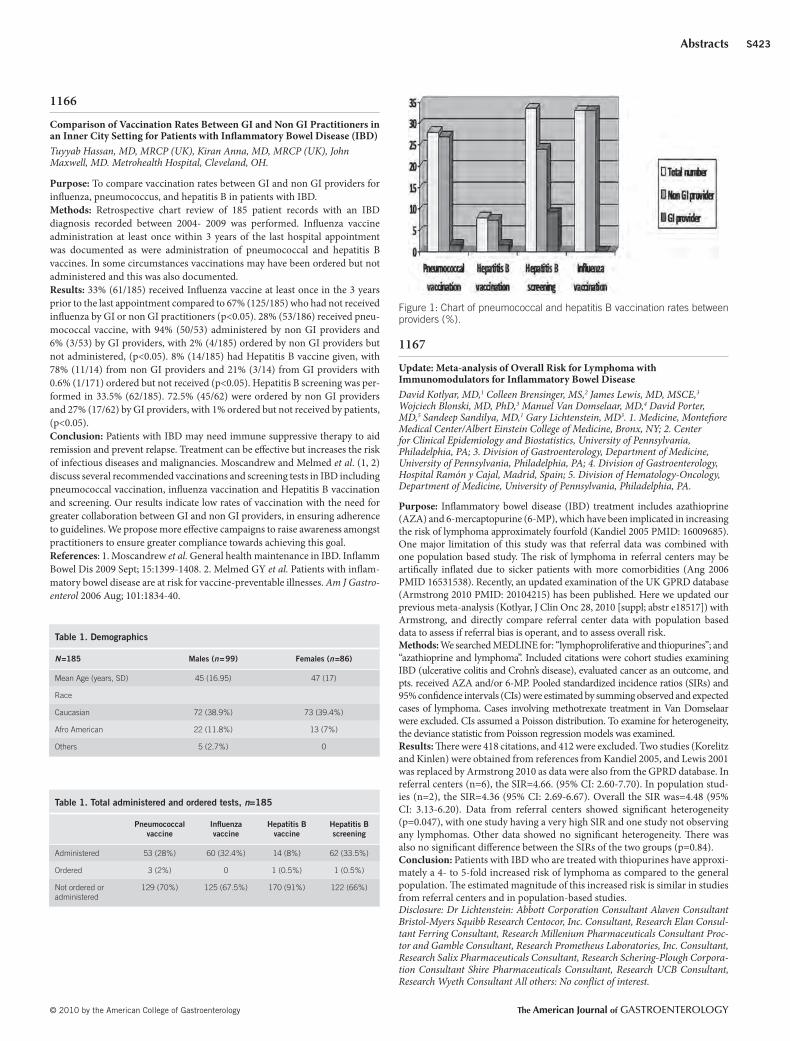
© 2010 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY
Abstracts S423
1166
Comparison of Vaccination Rates Between GI and Non GI Practitioners in an Inner City Setting for Patients with Infl ammatory Bowel Disease (IBD)Tuyyab Hassan, MD, MRCP (UK), Kiran Anna, MD, MRCP (UK), John Maxwell, MD. Metrohealth Hospital, Cleveland, OH.
Purpose: To compare vaccination rates between GI and non GI providers for infl uenza, pneumococcus, and hepatitis B in patients with IBD.Methods: Retrospective chart review of 185 patient records with an IBD diagnosis recorded between 2004- 2009 was performed. Infl uenza vaccine administration at least once within 3 years of the last hospital appointment was documented as were administration of pneumococcal and hepatitis B vaccines. In some circumstances vaccinations may have been ordered but not administered and this was also documented.Results: 33% (61/185) received Infl uenza vaccine at least once in the 3 years prior to the last appointment compared to 67% (125/185) who had not received infl uenza by GI or non GI practitioners (p<0.05). 28% (53/186) received pneu-mococcal vaccine, with 94% (50/53) administered by non GI providers and 6% (3/53) by GI providers, with 2% (4/185) ordered by non GI providers but not administered, (p<0.05). 8% (14/185) had Hepatitis B vaccine given, with 78% (11/14) from non GI providers and 21% (3/14) from GI providers with 0.6% (1/171) ordered but not received (p<0.05). Hepatitis B screening was per-formed in 33.5% (62/185). 72.5% (45/62) were ordered by non GI providers and 27% (17/62) by GI providers, with 1% ordered but not received by patients, (p<0.05).Conclusion: Patients with IBD may need immune suppressive therapy to aid remission and prevent relapse. Treatment can be eff ective but increases the risk of infectious diseases and malignancies. Moscandrew and Melmed et al. (1, 2) discuss several recommended vaccinations and screening tests in IBD including pneumococcal vaccination, infl uenza vaccination and Hepatitis B vaccination and screening. Our results indicate low rates of vaccination with the need for greater collaboration between GI and non GI providers, in ensuring adherence to guidelines. We propose more eff ective campaigns to raise awareness amongst practitioners to ensure greater compliance towards achieving this goal. References: 1. Moscandrew et al. General health maintenance in IBD. Infl amm Bowel Dis 2009 Sept; 15:1399-1408. 2. Melmed GY et al. Patients with infl am-matory bowel disease are at risk for vaccine-preventable illnesses. Am J Gastro-enterol 2006 Aug; 101:1834-40.
1167
Update: Meta-analysis of Overall Risk for Lymphoma with Immunomodulators for Infl ammatory Bowel DiseaseDavid Kotlyar, MD,1 Colleen Brensinger, MS,2 James Lewis, MD, MSCE,3 Wojciech Blonski, MD, PhD,3 Manuel Van Domselaar, MD,4 David Porter, MD,5 Sandeep Sandilya, MD,1 Gary Lichtenstein, MD3. 1. Medicine, Montefi ore Medical Center/Albert Einstein College of Medicine, Bronx, NY; 2. Center for Clinical Epidemiology and Biostatistics, University of Pennsylvania, Philadelphia, PA; 3. Division of Gastroenterology, Department of Medicine, University of Pennsylvania, Philadelphia, PA; 4. Division of Gastroenterology, Hospital Ramón y Cajal, Madrid, Spain; 5. Division of Hematology-Oncology, Department of Medicine, University of Pennsylvania, Philadelphia, PA.
Purpose: Infl ammatory bowel disease (IBD) treatment includes azathioprine (AZA) and 6-mercaptopurine (6-MP), which have been implicated in increasing the risk of lymphoma approximately fourfold (Kandiel 2005 PMID: 16009685). One major limitation of this study was that referral data was combined with one population based study. Th e risk of lymphoma in referral centers may be artifi cally infl ated due to sicker patients with more comorbidities (Ang 2006 PMID 16531538). Recently, an updated examination of the UK GPRD database (Armstrong 2010 PMID: 20104215) has been published. Here we updated our previous meta-analysis (Kotlyar, J Clin Onc 28, 2010 [suppl; abstr e18517]) with Armstrong, and directly compare referral center data with population based data to assess if referral bias is operant, and to assess overall risk.Methods: We searched MEDLINE for: “lymphoproliferative and thiopurines”; and “azathioprine and lymphoma”. Included citations were cohort studies examining IBD (ulcerative colitis and Crohn’s disease), evaluated cancer as an outcome, and pts. received AZA and/or 6-MP. Pooled standardized incidence ratios (SIRs) and 95% confi dence intervals (CIs) were estimated by summing observed and expected cases of lymphoma. Cases involving methotrexate treatment in Van Domselaar were excluded. CIs assumed a Poisson distribution. To examine for heterogeneity, the deviance statistic from Poisson regression models was examined.Results: Th ere were 418 citations, and 412 were excluded. Two studies (Korelitz and Kinlen) were obtained from references from Kandiel 2005, and Lewis 2001 was replaced by Armstrong 2010 as data were also from the GPRD database. In referral centers (n=6), the SIR=4.66. (95% CI: 2.60-7.70). In population stud-ies (n=2), the SIR=4.36 (95% CI: 2.69-6.67). Overall the SIR was=4.48 (95% CI: 3.13-6.20). Data from referral centers showed signifi cant heterogeneity (p=0.047), with one study having a very high SIR and one study not observing any lymphomas. Other data showed no signifi cant heterogeneity. Th ere was also no signifi cant diff erence between the SIRs of the two groups (p=0.84).Conclusion: Patients with IBD who are treated with thiopurines have approxi-mately a 4- to 5-fold increased risk of lymphoma as compared to the general population. Th e estimated magnitude of this increased risk is similar in studies from referral centers and in population-based studies.Disclosure: Dr Lichtenstein: Abbott Corporation Consultant Alaven Consultant Bristol-Myers Squibb Research Centocor, Inc. Consultant, Research Elan Consul-tant Ferring Consultant, Research Millenium Pharmaceuticals Consultant Proc-tor and Gamble Consultant, Research Prometheus Laboratories, Inc. Consultant, Research Salix Pharmaceuticals Consultant, Research Schering-Plough Corpora-tion Consultant Shire Pharmaceuticals Consultant, Research UCB Consultant, Research Wyeth Consultant All others: No confl ict of interest.
Table 1 . Demographics
N =185 Males ( n = 99) Females ( n =86)
Mean Age (years, SD) 45 (16.95) 47 (17)
Race
Caucasian 72 (38.9 % ) 73 (39.4 % )
Afro American 22 (11.8 % ) 13 (7 % )
Others 5 (2.7 % ) 0
Table 1 . Total administered and ordered tests, n =185
Pneumococcal
vaccine Infl uenza vaccine
Hepatitis B vaccine
Hepatitis B screening
Administered 53 (28 % ) 60 (32.4 % ) 14 (8 % ) 62 (33.5 % )
Ordered 3 (2 % ) 0 1 (0.5 % ) 1 (0.5 % )
Not ordered or administered
129 (70 % ) 125 (67.5 % ) 170 (91 % ) 122 (66 % )
Figure 1: Chart of pneumococcal and hepatitis B vaccination rates between providers (%).

The American Journal of GASTROENTEROLOGY VOLUME 105 | SUPPLEMENT 1 | OCTOBER 2010 www.amjgastro.com
AbstractsS424
1168
Serology Correlation with Findings on Capsule Endoscopy (CE) in Chil-dren with Infl ammatory Bowel Disease (IBD)Bisher Abdullah, MD, Alan Paschall, MD. Mary Bridge Children‘s Hospital and Health Center, Tacoma, WA.
Purpose: To evaluate the diagnostic yield of IBD serology in the absence of histology for fi ndings on CE.Methods: Retrospectively reviewed the records of children who all underwent CE, IBD serology testing, small bowel radiographic studies, EGD and colonos-copy with biopsies at our institution between March 2007 and May 2010.Results: Total 50 patient. Twenty-fi ve females (50%) were part of the study. Age ranging from 8 to 18 years with a mean age of 16 years. Th e indications were unexplained abdominal pain, diarrhea, hematochezia and/or weight loss. In the selected patients, fi ndings were suggestive of small bowel Crohn’s disease (CD) on CE in 15/50 (30%). From the patients with positive small bowel CD on CE only 4/15 (26.6%) had positive serology for CD. Furthermore IBD serologies were positive for CD in 7/35 (20%) of patients with normal small bowel on CE.Conclusion: In the diagnosis of small bowel CD in children, Serologic testing for IBD did not add a signifi cant diagnostic value to CE.
1169
Th e Impact of Capsule Endoscopy on Management of Infl ammatory Bowel Disease: A Single Tertiary Care Center ExperienceMillie Long, MD, MPH, Edward Barnes, MD, Kim Isaacs, MD, PhD, Douglas Morgan, MD, MPH, Hans Herfarth, MD, PhD. University of North Carolina at Chapel Hill, Chapel Hill, NC.
Purpose: Capsule endoscopy (CE) is performed with frequency to assess activity of symptomatic infl ammatory bowel disease (IBD). It is unknown whether CE fi nd-ings directly impact the management of IBD. We aimed to defi ne results of CE in symptomatic Crohn’s disease (CD), indeterminate colitis (IC) and pouchitis and to determine whether CE is associated with management changes in each subtype.Methods: We conducted a retrospective cohort study of all CEs performed at the University of North Carolina Hospitals (UNCH) from 2003-2009. Th e study was then limited to those CEs performed for an indication of previ-ously diagnosed IBD. Th e capsules also had to leave the stomach. Descriptive statistics were used to compare IBD specifi c medications, surgeries and imag-ing studies in the 3 months prior and 3 months aft er CE.Results: Of 907 CEs performed from 2003-2009 at UNCH, 128 were for an indication of symptomatic IBD and 124 capsules left the stomach (86 for CD, 15 for IC, 23 for pouchitis). Findings in CD consisted of erythema (12.8%), few apthae/ulcers (17.4%), multiple apthae/ulcers (22.1%), stenosis (8.1%) and ste-
nosis with retention (17.4%). Only 22.1% of CEs performed for symptomatic CD were normal. Findings in IC were most oft en normal (53.3%) or consisted of erythema (26.7%). Findings in pouchitis were most oft en normal (34.8%) or had few aphthae (43.8%). In CD, 61.6% had a change in medication in the 3 months aft er the CE, with 39.5% initiating a new IBD medication; most com-monly budesonide. In the 3 months following CE, 12.8 % of patients with CD underwent surgery. Severe fi ndings on CE in patients with CD, as compared to no/minimal fi ndings, resulted in signifi cant diff erences in medication changes (73.2% vs. 51.1%, p=0.04), addition of medications (58.5% vs. 22.2%, p<0.01), and surgeries (21.9% vs. 4.4%, p=0.01) in the ensuing 3 months.Conclusion: CE was performed frequently in patients with symptomatic IBD at a tertiary care center. Th ose with CD were most likely to have positive fi nd-ings, followed by those with pouchitis and those with IC. CE resulted in man-agement changes in the majority of cases, regardless of the specifi c CE fi ndings or the subtype of IBD. Overall, CE impacts the management of IBD.
1170
Characterization of Patients of Diff erent Ethnicities with Infl ammatory Bowel Disease and Primary Sclerosing CholangitisOriana Damas, MD,1 Darius Jahann, MD,1 Cynthia Levy, MD2. 1. Dept of Medicine, Division of Internal Medicine. Univ. of Miami Miller School of Medicine/Jackson Memorial Hospital, Miami, FL; 2. Dept of Medicine, Division of Hepatology. University of Miami Miller School of Medicine/Jackson Memorial Hospital, Miami, FL.
Purpose: Primary Sclerosing Cholangitis (PSC) is a well known extra-intes-tinal manifestation of Infl ammatory Bowel Disease (IBD); yet little is known about the epidemiology of PSC in IBD. Our aim was to determine the phe-notypic characteristics of PSC-IBD in patients of diff erent race and ethnic-ity. Th ose examined include Hispanics, Afro-Caribbeans, African-Americans (AA) and Caucasian-Americans (CA).Methods: Th is retrospective cohort study was performed at a university-affi li-ated hospital and a tertiary-care referral center in Miami, FL. We identifi ed adult patients with ICD-9 codes 555.X or 556.X and 576.1 for whom outpatient IBD follow-up took place between 1999-2010. Ethnicity was self-reported. Outcomes measured were IBD subtype, colectomy rate, PSC presentation, PSC involvement (intrahepatic, extrahepatic or both), orthotopic liver transplant, comorbidities and malignancies.Results: Twenty-three patients were identifi ed with PSC-IBD: 6 Hispanics, 5 Afro-Caribbeans, 6 CA, and 6 AA. Among Whites, 6 were Hispanic and 6 CA. In Blacks, 5 were Afro-Caribbean and 6 AA. Median age of diagnosis was 27 yrs for Whites and 34 yrs for Blacks (p=0.49). Th ere were 9 males and 14 females. Median follow up time was 1.7 yrs and 4.2 yrs for Whites and Blacks, respectively (p=0.55). Whites had 25% Crohn’s disease and 75% ulcerative
[1167] Meta-analysis of Standardized Incidence Ratios (SIR)
Referral center study Observed Expected SIR 95 % CI No. of pts.
Connell (PMID: 7910274) 0 0.52 0 NA 755
Farrell (PMID: 10986211) 2 0.05 37.5 (3.53-138) 238*(as calculated by Kandiel 2005)
Fraser (PMID:12144571) 3 0.65 4.64 (0.87-13.7) 626
Kinlen (Am J Med 1985;78:44-9) 2 0.16 12.5 (1.18-46.0) 321
Korelitz (PMID: 10566724) 3 0.61 4.91 (0.93-14.5) 486
Van Domselaar (PMID: 19889478) 5 1.23 4.07 (1.28-9.56) 345
Combined 15 3.22 4.66 (2.60-7.70) 2,771
Population Based Study Observed Expected SIR 95 % CI No. of pts.
Armstrong (PMID: 20104215) 4 1.24 3.23 (0.84-8.34) 1,955
Beaugerie (PMID: 19837455) 17 3.58 4.75 (2.76-7.62) 8,676
Combined 21 4.82 4.36 (2.69-6.67) 10,631
Overall Data Observed Expected SIR 95 % CI No. of pts.
All studies 36 8.04 4.48 (3.13-6.20) 13,402
NA=Not applicable CI=Confi dence Interval SIR=Standardized Incidence Ratio.

© 2010 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY
Abstracts S425
colitis; Blacks comprised of 10% Crohn’s disease and 90% ulcerative colitis. A total of 4 patients underwent colectomy: 3 CA and 1 AA. PSC presentation, includ-ing total bilirubin, AST, ALT, albumin, PT, and development of fatigue, pruritus, gastrointestinal bleeding, encephalopathy or ascites, did not vary by ethnicity or race. However, jaundice was present in 45% of Blacks at presentation compared to 8% of Whites despite only 1 patient with sickle cell disease (p=0.07). For patients with imaging results available, 1 had extrahepatic disease, 1 intrahepatic and 10 involvement of both. Six patients underwent liver transplantation: 67% Black and 33% White (p=0.37). Diabetes was the predominant comorbidity among patients (13%). Malignancies were identifi ed in 22% of patients: 40% of these in Afro-Caribbeans (1 hepatocellular carcinoma, 1 colorectal carcinoma) and 60% in CA (1 cholangiocarcinoma, 2 colorectal carcinomas) (p=0.07); suggesting a trend towards more malignancies between these two groups.Conclusion: In our study, the phenotypic presentation of PSC-IBD did not diff er signifi cantly among patients of the aforementioned ethnicities or races, although larger studies are needed to further characterize such diff erences. Additionally, understanding the association cultural identity has with the phe-notypic presentation of PSC can help individualize management and therapy.
1171
Prevalence and Risk of Avascular Osteonecrosis in Infl ammatory Bowel DiseaseChristian Stone, MD, MPH,1 Jiajing Chen, MPH,2 Paula Buchanan, PhD,2 Michael Williams, MD,2 Glenn Gordon, MD,2 Mahendran Jayaraj, MD,1 Th omas Burroughs, PhD2. 1. University of Nevada School of Medicine, Las Vegas, NV; 2. St. Louis University School of Medicine, St. Louis, MO.
Purpose: Avascular necrosis (AVN) of bone is a dreaded complication of pro-longed steroid use. Case series in patients with infl ammatory bowel disease (IBD) have reported an association between steroids and AVN of the hip/neck of femur and other sites. However, the prevalence of AVN has not been studied in depth in a large IBD population. Given that IBD patients oft en develop ste-roid-dependent disease, we sought to investigate the prevalence of AVN in IBD and to determine whether risk is related to length of steroid exposure.Methods: Using a large administrative health claims database, we conducted a retro-spective cohort analysis to determine the prevalence AVN in IBD and identify factors associated with AVN occurrence. ICD-9 codes were used to identify subjects with IBD and diagnosis of AVN. We excluded subjects who also had diagnoses of lupus and other disorders for which steroids are used frequently. Treatment with steroids was docu-mented and categorized into four exposure groups based on duration of use. All sub-jects were followed forward in time until the occurrence of AVN, end of capture period (Dec 2006) or end of enrollment. Th e prevalence of AVN in IBD was compared to that in a non-IBD population (1:5 ratio). Logistic regression was used to calculate indepen-dent risk (expressed as odds ratio [OR]) for AVN stratifi ed by steroid exposure.Results: 53,434 IBD subjects were included and mean follow-up time was 2.4 years. Th e overall prevalence of AVN was 0.3% in IBD and 0.2% in non-IBD subjects. Th e rates were similar for Crohn’s disease (CD) and ulcerative colitis (UC) but the steroid exposure overall was greater in CD. Th e risk of AVN with any steroid exposure compared to none was greater in CD (OR=2.1, P=0.0019) than in UC (OR=1.1, P=0.74). In a multivariate analysis, risk of AVN increased with longer steroid exposure, aft er adjustment for age and gender (Table).Conclusion: Among IBD patients, risk of AVN increases signifi cantly with greater duration of steroid use. Th e prevalence is higher in CD than in UC but this diff erence may be due to lower steroid exposure in UC. Th ere does not appear to be an increased risk for AVN due to IBD alone.
1172
Ocean State Crohn’s and Colitis Area Registry (OSCCAR): Incidence of Crohn’s Disease and Ulcerative Colitis in a Prospective, Population-Based Inception Cohort in Rhode IslandSamir Shah, MD,1 Neal Leleiko, MD, PhD,1 Sheldon Lidofsky, MD,1 Renee Bright, MS,1 Stacey Grabert, PharMD, MS,2 Meaghan Law, BS,1 Heather Moniz, BS,1 Barbara Bancroft , RN,1 Kristina Suorsa, BS,1 Mitul Patel, MD,1 Jennifer Vancura, BS,1 Adam Harris, MD,1 Bharati Kalasapudi, BA,1 Elisabeth Cole, MS,2 Bruce Sands, MD, MS3. 1. Lifespan and Brown University, Providence, RI; 2. Massachusetts General Hospital, Boston, MA; 3. Mount Sinai School of Medicine, New York, NY.
Purpose: OSCCAR, a novel, prospective, population-based inception cohort of patients with infl ammatory bowel disease (IBD), was conceived to deter-mine incidence, better understand the natural history and factors that infl u-ence disease outcomes.Methods: Residents of Rhode Island with newly diagnosed Crohn’s disease (CD), ulcerative colitis (UC), or indeterminate colitis (IC) were eligible for enrollment beginning January 1, 2008. Diagnosis of IBD was confi rmed using criteria from the NIDDK IBD Genetics Consortium. Individuals diagnosed before January 2008, unwilling to provide consent, and those imprisoned or pregnant at diagnosis were excluded. Research assistants collected demographic data, medical history and disease related information, quality of life and disease activity questionnaires, blood, urine and stool samples, with quarterly follow-up in the fi rst year, then every 6 months. 97 of 98 gastroenterologists/colorectal surgeons in RI and 11 in MA agreed to refer patients. Practice billing data were queried and chart reviews were conducted to capture missed referrals. Billing data has been reviewed for all but 11 physicians. IRB approval was obtained.Results: 237 newly diagnosed CD patients and 274 newly diagnosed UC/IC patients were identifi ed between January 1, 2008 and December 31, 2009. Th e age distribution for CD was bimodal (graph 1) in contrast to that of UC (graph 2). Unadjusted incidence rates for 2008 and 2009 were calculated: IBD 21-27, CD 10.4-11.6, UC 9.3-14.3 and IC 0.8-1.1 per 100,000 cases. 103 of the 237 CD patients and 77 of the 274 UC/IC patients enrolled in OSCCAR. Demographic information (sex, race, ethnicity, smoking status and NSAID use) is presented in table 1.Conclusion: Preliminary data from RI suggests an incidence rate of IBD higher than previously reported in the US. Funding:CCFA/CDC 5U01DP000340-03 and NIH 1R21DK078555-02.Disclosures: Dr Samir A. Shah (Th e Rhode Island Hospital/Lifespan Principal Investigator and co-PI with Dr Sands in this study: OSCCAR) is on the speaker’s bureau for the following companies involved in making medicines used for the treatment of IBD: Abbott, Prometheus, Warner-Chilcott (formerly Proctor & Gamble for the drug Asacol), and UCB. He and his group are/have been involved in registries and/or clinical studies with Centocor and Elan Pharmaceuticals. Dr. Bruce Sands (the MSSM Principal Investigator in this study) receives fi nan-cial compensation as a consultant and lecturer to several companies which either develop or assess medicines used for the treatment of infl ammatory bowel disease (IBD). Th ese companies include BiogenIDEC, Millennium Pharma-ceuticals, Proctor & Gamble Pharmaceuticals, Abbott Immunology, Amgen, CommonHealth, Prometheus Laboratories, Axcan Pharma, VMS, Centocor,
Steroid duration (days) Odds ratio for AVN
CD UC All IBD
≤ 60 1.6 0.9 1.3
61 – 180 2.3* 1.5 2.3*
> 180 4.8* 1.8 3.4*
* P < 0.001.

The American Journal of GASTROENTEROLOGY VOLUME 105 | SUPPLEMENT 1 | OCTOBER 2010 www.amjgastro.com
AbstractsS426
Elan Pharmaceuticals, Astellas, Chandler Chico Agency, Strategic Consultants Inc., and Cequent Pharmaceuticals (of which he owns stock options).Dr. Neal LeLeiko receives research support as a consultant to several companies which either develop or assess medicines used for the treatment of infl ammatory bowel disease (IBD). Th ese companies include Centocor and Astra Zeneca.
1173
Global Reduction of Crohn’s Disease Risk, with Increasing Lactase Non Persistence is Associated with Inverse Relationship to NOD2 Mutations in Healthy PopulationsBarry Burstein, Bsc,2 Andrew Szilagyi, MD FRCPC,1 Brian Smith, PhD2. 1. Medicine, Division of Gastroenterology, Jewish General Hospital, Montreal, YT, Canada; 2. Jeff erson Medical College, Philadelphia, PA.
Purpose: Increasing national prevalence of lactase non persistence(LNP) is associated with global risk reduction of IBD incidence (Shrier I et al. Nutr
Cancer 2008). Th e mechanism isn’t clear. We assess a possible relationship between national NOD2 mutations frequency (%) and LNP%. Although, mul-tiple genes are involved with IBD, NOD2 is the best polymorphism investi-gated to date.Methods: Th e literature was searched for any NOD2% mutation (R702W, G908R and 1007fsinsC) in healthy controls (HC), patients with Crohn’s disease (CD) or ulcerative colitis (UC). Multiple reports from same countries were combined with a weighted average where necessary (8 countries). Frequencies of national LNP%, based on biopsies or physiological studies, were obtained from previ-ously published lists and individual reports. Comparisons and analysis used linear regression and statistical signifi cance was accepted at p<0.05.Results: On NOD2%, 9018 healthy controls (33 populations,[Ps]), 7898 with CD (34Ps) and 3042 multi-ethnic patients with UC (15Ps) were included. Compari-sons were possible between LNP% and NOD2% in HC, CD(31Ps) or UC(15Ps). Th ere was a positive correlation between NOD2 mutations in HC and CD (r2=0.4, p=0.0001). Correlations between LNP% and NOD2% in HC was inverse (r2=0.35, p=0.00037). Comparison of LNP% with NOD2% in CD was also inverse but weak (r2=0.13, p=0.04). Similar analysis for UC revealed a weak inverse rela-tionship with LNP% (r2=0.014, p=0.3). However, NOD2% in CD vs. UC showed positive relationship as with controls (r2=0.67, p=0.0002). Sub analysis of Euro-pean countries however, eliminates negative relationships with HC, r2=0.6%, and converts LNP% with CD to a weak positive one. r2 =29.3% p=0.03.Conclusion: Incidence of CD decreases from north(west) to south(east). Reports reveal marked heterogeneity in NOD2% mutations in diff erent coun-tries and ethnic groups residing in same countries in HC or CD. Globally, increasing LNP% appears to reduce risk of CD and is echoed by a moderate inverse relationship with NOD2 mutations. However, the apparent opposite outcome in Europe suggests there is unlikely to be a direct link between poly-morphisms of NOD2 and lactase. Because CD depends on interactions of com-plex factors, other variables and polymorphisms are needed to explain apparent association of reduction of IBD risk with increasing LNP% of populations.
1174
Presenting Symptoms at Diagnosis of Crohn’s Disease and Ulcerative Colitis: Results from the Ocean State Crohn’s and Colitis Area Registry (OSCCAR)
Mitul Patel, MD,1 Samir Shah, MD,1 Neal Leleiko, MD, Ph.D.,1 Sheldon Lidofsky, MD,1 Renee Bright, MS,1 Stacey Grabert, PharMD, MS,2 Meaghan Law, BS,1 Heather Moniz, BS,1 Barbara Bancroft , RN,1 Kristina Suorsa, BS,1 Adam Harris, MD,1 Jennifer Vancura, BS,1 Bharati Kalasapudi, BA,1 Elisabeth Cole, MS,2 Bruce Sands, MD, MS3. 1. Lifespan and Brown University, Providence, RI; 2. Massachusetts General Hospital, Boston, MA; 3. Mount Sinai School of Medicine, New York, NY.
Purpose: Th e Ocean State Crohn’s and Colitis Area Registry (OSCCAR) is a novel population-based, prospective inception cohort of patients with infl am-matory bowel disease in Rhode Island. Presenting symptoms of enrolled patients were recorded and analyzed to assess the current presentation of IBD.Methods: Residents of Rhode Island with newly diagnosed Crohn’s disease (CD), ulcerative colitis (UC), or indeterminate colitis (IC) were eligible for enrollment beginning January 1, 2008. Diagnosis of IBD was confi rmed using criteria from the NIDDK IBD Genetics Consortium. Individuals diagnosed before January 2008, unwilling to provide consent, and those imprisoned or pregnant at diagnosis were excluded. Research assistants collected demo-graphic data, medical history and disease related information, quality of life and disease activity questionnaires, blood, urine and stool samples, with quar-terly follow-up in the fi rst year, then every 6 months. 97 of 98 gastroenterolo-gists/colorectal surgeons in RI and 11 in MA agreed to refer patients. Practice billing data were queried and chart reviews were conducted to capture missed referrals. IRB approval was obtained.Results: Th e mean time from diagnosis to enrollment was approximately 66 days in 2008 and 64 days in 2009. Abdominal pain and fatigue were the most common symptoms reported by both adult and pediatric patients with
Baseline demographics of enrolled patients
Charateristics Crohn’s Disease ( N =103) % ( n )
Ulcerative Colitis and Indeterminant Colitis ( N =77) % ( n )
Female 53.4 (55) 46.8 (36)
Male 46.6 (48) 53.2 (41)
Pediatric 33.0 (34) 20.8 (16)
Adult 67.0 (69) 79.2 (61)
Race
Caucasian 86.4 (89) 93.5 (72)
African American 4.9 (5) 2.6 (2)
More than 1 1.9 (2) 0.0 (0)
Other 4.9 (5) 2.6 (2)
Refused / Unknown 1.9 (2) 1.3 (1)
Ethnicity
Hispanic 9.7 (10) 5.2 (4)
Not Hispanic 89.3 (92) 93.5 (72)
Refused / Unknown 1.0 (1) 1.3 (1)
Tobacco Use
Current smoker 12.6 (13) 7.8 (6)
Former smoker 17.5 (18) 27.3 (21)
Never smoked 68.9 (71) 63.6 (49)
Refused / Unknown 1.0 (1) 1.3 (1)
NSAID Use
Yes 12.6 (13) 20.7 (16)
No 87.3 (90) 79.2 (61)

© 2010 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY
Abstracts S427
CD at presentation and year 1 (table 1). Weight loss and decreased appetite were common presenting symptoms in the pediatric population (#3, and #4 respectively), whereas they were not common in the adult CD population. As one would expect, loose/watery stools, urgency, increased frequency of bowel movements and bleeding were the most common symptoms reported by patients with UC at enrollment (Table 2).Conclusion: Th is prospective description of presenting symptoms in IBD may facilitate earlier evaluation and diagnosis. Fatigue was a common symptom at presentation for both CD and UC/IC but more frequently reported with CD. A large proportion of patients report persistent symptoms at 1 year from diagno-sis. Funding: CCFA/CDC 5U01DP000340-03 and NIH 1R21DK078555-02.
1175
Medical Th erapy of IBD in the First Year Aft er Diagnosis: Prelimi-nary Results from the Ocean State Crohn’s and Colitis Area Registry (OSCCAR)Adam Harris, MD,1 Samir Shah, MD,1 Neal Leleiko, MD, Ph.D.,1 Sheldon Lidofsky, MD,1 Renee Bright, MS,1 Stacey Grabert, PharMD, MS,2 Meaghan Law, BS,1 Heather Moniz, BS,1 Barbara Bancroft , RN,1 Kristina Suorsa, BS,1 Mitul Patel, MD,1 Jennifer Vancura, MS,1 Bharati Kalasapudi, BA,1 Elisabeth Cole, MS,2 Bruce Sands, MD, MS3. 1. Lifespan and Brown University, Providence, RI; 2. Massachusetts General Hospital, Boston, MA; 3. Mount Sinai School of Medicine, New York, NY.
Purpose: Th e Ocean State Crohn’s and Colitis Area Registry (OSCCAR) is a novel population-based, prospective inception cohort of patients with infl am-
matory bowel disease (IBD) in Rhode Island. Th e frequency of medications used to treat IBD during the fi rst year aft er diagnosis was analyzed with a focus on steroids, immunomodulators and biologics.Methods: Residents of Rhode Island with newly diagnosed Crohn’s disease (CD), ulcerative colitis (UC), or indeterminate colitis (IC) were eligible for enrollment beginning January 1, 2008. Diagnosis of IBD was confirmed using criteria from the NIDDK IBD Genetics Consortium. Individuals diagnosed before January 2008, unwilling to provide consent, and those imprisoned or pregnant at diagnosis were excluded. Research assistants collected demographic data, medical history and disease related infor-mation, quality of life and disease activity questionnaires, blood, urine and stool samples, with quarterly follow-up in the first year, then every 6 months. 97 of 98 gastroenterologists/colorectal surgeons in RI and 11 in MA agreed to refer patients. Practice billing data were queried and chart reviews were conducted to capture missed referrals. IRB approval was obtained.Results: For enrolled patients, medical therapy during the fi rst year is sum-marized in tables 1 & 2. 5-ASA was the mainstay of therapy for UC, and a high rate of 5-ASA use was observed in CD. Th e rate of immunomodulator use was much higher in pediatric compared to adult patients (both CD and UC). CD patients were more likely to be on an immunomodulator or anti-TNF agent compared with UC patients. A substantial percentage of patients were started on anti-TNF therapy early aft er diagnosis.Conclusion: Among patients captured in this prospective, inception cohort from RI, different patterns of medication usage are seen in adult and pediatric patients, as well as in UC and CD. More than half of patients were exposed to steroids in the first year after diagnosis. A large por-tion of CD patients were on 5-ASA despite the lack of evidence sup-porting its use for this indication. Long term follow-up of these patients will yield insight into prescribing patterns and clinical effectiveness of various IBD therapies. Funding:CCFA/CDC 5U01DP000340-03 and NIH 1R21DK078555-02.
[1174] OSCCAR: Top 10 Symptoms in Patients with Crohn’s Disease.
Symptom Baseline % ( n ) Year 1 % ( n )
Abdominal pain 83.5 (81) 61.5 (24)
Tiredness or fatigue 81.4 (79) 61.5 (24)
Incontinence or leakage of stool 71.9 (18) 10.5 (4)
Abdominal tenderness 65.6 (63) 51.3 (20)
Cramping with a bowel movement 62.5 (60) 53.9 (21)
Loose stools or watery bowel movements 62.5 (60) 53.9 (21)
Abdominal bloating or distention 61.7 (58) 53.9 (21)
Sense of incomplete emptying after a bowel movement
59.3 (54) 51.3 (20)
Increased number or frequency of bowel movements
58.3 (56) 39.5 (15)
Weight loss 57.7 (56) 30.6 (11)
[1174] OSCCAR: Top 10 symptoms in patients with ulcerative colitis and indeterminant colitis
Symptom Baseline % ( n ) Year 1 % ( n )
Loose stools or watery bowel movements
93.0 (66) 69.6 (16)
Urgent bowel movements 90.1 (64) 52.2 (12)
Increased number or frequency of bowel move-ments
88.6 (62) 39.1 (9)
Passage of blood with bowel movement 87.0 (60) 45.5 (10)
Cramping with a bowel movement 75.0 (51) 47.8 (11)
Foul smelling gas 72.5 (50) 47.8 (11)
Increased passage of gas 72.1 (49) 50.0 (11)
Tiredness or fatigue 70.0 (49) 69.9 (16)
Abdominal pain 68.6 (48) 69.9 (16)
Uncertain whether gas / bowel movement is about to be passed
68.1 (47) 52.2 (12)
OSCCAR: medication use in patients with Crohn’s disease
Class Baseline
( N =103) % ( n ) 3 Months
( N =93) % ( n ) 6 Months
( N =75) % ( n ) 9 Months
( N =62) % ( n ) Year 1
( N =49) % ( n )
Anti-diarrheals 2.9 (3) 0.0 (0) 0.0 (0)
5-ASA 69.9 (72) 66.7 (50) 63.3 (31)
Antibiotics 30.1 (31) 29.3 (22) 20.4 (10)
Entocort 12.6 (13) 11.8 (11) 12.0 (9) 3.2 (2) 4.1 (2)
Any Steroid 42.7 (44) 41.9 (39) 33.3 (25) 21.0 (13) 24.5 (12)
Immunomod-ulators
6.8 (7) 21.3 (16) 28.6 (14)
Biologics 4.9 (5) 16.0 (12) 20.4 (10)
OSCCAR: medication use in patients with ulcerative colitis and indeterminant colitis
Class Baseline
( N =77) % ( n ) 3 Months
( N =63) % ( n ) 6 Months
( N =49) % ( n ) 9 Months
( N =37) % ( n ) Year 1
( N =30) % ( n )
Anti-diarrheals 10.4 (8) 2.0 (1) 0.0 (0)
5-ASA 92.2 (71) 79.6 (39) 76.7 (23)
Antibiotics 10.4 (8) 2.0 (1) 3.3 (1)
Any Steriod 50.6 (39) 39.7 (25) 20.4 (10) 13.5 (5) 16.7 (5)
Immunomodu-lators
5.2 (4) 6.1 (3) 10.0 (3)
Biologics 0.0 (0) 6.1 (3) 10.0 (3)

The American Journal of GASTROENTEROLOGY VOLUME 105 | SUPPLEMENT 1 | OCTOBER 2010 www.amjgastro.com
AbstractsS428
1176
Eff ect of Disease Duration on “Deep Remission”: Results from the EXTEND TrialJean-Frédéric Colombel, MD,1 Stefan Schreiber, MD,2 Paul Rutgeerts, MD,3 William Sandborn, MD,4 Mei Yang, PhD,5 Kathleen Lomax, MD,5 Paul Pollack, MD,5 Roopal Th akkar, MD,5 Anne Camez, MD,6 Bidan Huang, PhD,5 Qian Zhou, PhD,5 Parvez Mulani, PhD,5 Jingdong Chao, PhD5. 1. Centre Hospitalier Universitaire de Lille, Lille, France; 2. Christian Albrechts University, Kiel, Germany; 3. University Hospital Gasthuisberg, Leuven, Belgium; 4. Mayo Clinic, Rochester, MN; 5. Abbott, Abbott Park, IL; 6. Abbott GmbH & Co. KG, Ludwigshafen, Germany.
Purpose: Adalimumab (ADA) therapy in patients with shorter Crohn’s disease (CD) duration appears to be associated with improved clinical outcomes and less side eff ects in the CHARM trial.1 We investigated the rela-tionship between CD duration and response to ADA in the EXTEND trial.Methods: EXTEND was a placebo (PBO)-controlled study of moderate to severe CD patients with baseline mucosal ulceration. Patients received open-label ADA 160/80 mg induction therapy at Weeks 0/2 and were randomized at Week 4 to blinded maintenance therapy with ADA 40 mg every other week or PBO through Week 52. Eff ects of CD duration (≤2, >2-≤5, >5 years) on deep remission (defi ned as complete mucosal healing and clinical remission [CDAI <150]) was compared at Week 52 for ADA and PBO-treated patients from the intention-to-treat population.Results: Of 129 patients randomized at Week 4 (64, ADA; 65, PBO), CD duration was ≤2 years for 18 patients (14%), >2-≤5 years for 26 patients (20%), and >5 years for 85 patients (66%). An overall signifi cant eff ect of ADA therapy vs. PBO was shown on deep remission aft er stratifying by CD duration (Table, CMH test). Because of small sample size for patients with shorter CD duration, patients from the <2 and >2-≤5 groups were pooled. Th e rate of deep remission with ADA was signifi cantly higher than PBO in patients within each CD duration ≤5 and >5 years (p=0.009 and 0.008, respectively, Chi-square test). Th ere was a numerical trend for a relationship between rates of deep remission and CD duration with ADA therapy (Table), but no statistical signifi cance.Conclusion: ADA maintenance therapy led to higher rates of deep remission compared to PBO in patients regardless of CD duration. Th ere was a trend for higher rates of deep remission with shorter CD duration with ADA therapy, which was not statistically signifi cant, likely because of small sample size.Reference: 1. Schreiber S et al. Early Crohn’s Disease Shows High Levels of Remission to Th erapy With Adalimumab: Sub-analysis of CHARM. Abstract: Presented at Digestive Diseases Week, 2007.Disclosure: Dr Colombel - Advisory Committees or Review Panels: Abbott, AstraZeneca Pharmaceuticals LP, Centocor, Inc, Danone Research, Elan Phar-maceuticals, Inc, Millennium Research Group, Schering-Plough Corp, UCB, Inc; Consulting: Abbott, ActoGeniX, Albireo Pharma: Consulting, AstraZen-eca Pharmaceuticals LP, Bayer AG, Biogen Idec, Boehringer Ingelheim GmbH, Bristol-Myers Squibb Co., Cellerix SL, Centocor, Inc., Chemocentryx, Cosmo Technologies Ltd, Danone Research, Elan Pharmaceuticals, Inc., Genentech Inc., Giuliani SpA, Given Imaging, GlaxoSmithKline, Hutchison MediPharma Limited, Milan, Millennium Research Group, Ocera Therapeutics, Inc., Pfizer Inc,, Schering-Plough Corp., UCB, Inc.; Speaking and Teaching: Abbott, Cen-tocor, Inc, Elan Pharmaceuticals, Inc, Given Imaging Dr Schreiber - Financial support for research: UCB; Lecture fee(s): Abbott, Essex; Consultancy: Abbott, Schering-Plough Dr Rutgeerts - Consulting: Abbott, Actogenics, Bris-tol-Myers Squibb Co., Centocor, Inc., Genentech Inc., Italfarmako, Millen-nium Research Group, NovImmune, Schering-Plough Corp., UCB Pharma; Grant/Research Support: Abbott, Centocor, Inc, Schering-Plough, UCB Pharma Dr Sandborn - Financial Support for Research: Abbott Laboratories, Bristol Meyers Squibb, CentocorOrthoBiotech, Genentech, Millennium Phar-maceuticals, Novartis, Pfizer, Shire Pharmaceuticals, UCB Pharma, Warner Chilcott (previously Procter & Gamble); Consultancy: ActoGenix, Abbott Laboratories (fees paid to Mayo), AGI Therapeutics, Albireo, Alfa Wasser-mann, AM-Pharma, Amgen, Anaphore, Astellas Pharma, Athersys, Atlantic Healthcare Limited, Axcan Pharma, BioBalance Corporation, Celegene, Bris-tol Meyers Squibb (fees paid to Mayo), Celek Pharmaceuticals, Cellerix, Cen-tocorOrthoBiotech (fees paid to Mayo), Chemocentryix, CoMentis, Cosmo Technologies, Cytokine Pharmasciences, Eagle Pharmaceuticals, Eisai Medi-cal Research, Elan Pharmceuticls (fees paid to Mayo), Eli Lilly, Enteromed-ics, Ferring Pharmaceuticals, Flexion Therapeutics, Funxional Therapeutics
Limited, Genentech (fees paid to Mayo), Given Imaging, GlaxoSmithKline, KaloBios Pharmaceuticals, Merck Research Laboratories, Merck Serono, Novo Nordisk, Pfizer (fees paid to Mayo), Procter & Gamble (fees paid to Mayo), Purgenesis Technologies, Regeneron Pharmaceuticals, Salient Phar-maceuticals, Salix Pharmaceuticals, Santarus, Schering Plough Corporation, Shire Pharmaceuticals (fees paid to Mayo), Sigmoid Pharma, Sitrtis Pharma-ceuticals, SLA Pharma, Takeda (fees paid to Mayo), Tillotts Pharma, UCB Pharma (fees paid to Mayo), Vascular Biogenics, Viamet Pharmaceuticals, Wyeth Drs Yang, Lomax, Pollack, Thakkar, Camez, Huang, Zhou, Mulani, Chao - Employment: Abbott; Shareholder: Abbott.Th is research was supported by an industry grant from Abbott.
1177
Eff ect of Adalimumab Induction Th erapy on Clinical Laboratory Parameters Suggesting Improved Nutrition and Infl ammation Status in Patients with Moderately to Severely Active Ulcerative ColitisWalter Reinisch, MD,1 William Sandborn, MD,2 Daan Hommes, MD,3 Roopal Th akkar, MD,4 Paul Pollack, MD,4 Ashish Kumar, PhD,4 Wendy Kampman, MD,5 Andreas Lazar, MD6. 1. Medical University Vienna, Vienna, Austria; 2. Mayo Clinic, Rochester, MN; 3. Leiden University Medical Center, Leiden, Netherlands; 4. Abbott, Abbott Park, IL; 5. Abbott, Rungis, France; 6. Abbott, Ludwigshafen, Germany.
Purpose: To describe the evolution of clinical laboratory indicators of nutri-tional status and infl ammation in patients with moderately to severely active ulcerative colitis (UC) enrolled in a large randomized, placebo-controlled study of adalimumab for induction of remission.Methods: Adult patients with moderately to severely active UC, failing treat-ment with corticosteroids and/or immunosuppressants, were enrolled and randomized to receive subcutaneous ADA160/80 (160 mg at Week 0, 80 mg at Week 2, 40 mg at Weeks 4 and 6), ADA80/40 (80 mg at Week 0, 40 mg at Weeks 2, 4, and 6) or placebo. Dosing of concomitant corticosteroids and/or immunosuppressants were maintained stable during the 8-week study. Mean changes from baseline in hemoglobin, hematocrit, red cell count, total protein, albumin, and median changes from baseline in C-reactive protein (CRP), were assessed at intervals in the safety population (all patients who received at least 1 dose of study drug). Analyses were performed on observed cases; comparisons between the ADA groups and the placebo group were made using 1-way analysis of variance (mean changes) or the Kruskal-Wallis test (median changes).Results: In the safety population, 521 of 576 patients completed 8 weeks (placebo, n=204/223; ADA80/40, n=118/130; ADA160/80, n=199/223). Changes from baseline at Week 8 are shown in the table. ADA160/80 treatment was associated with statistically significant changes from base-line in the clinical laboratory parameters shown, compared with placebo treatment.Conclusion: In this study, adalimumab therapy for 8 weeks was associated with statistically and clinically signifi cant improvements in several nutritional indicators and direct and indirect markers of infl ammation, compared with placebo treatment.Disclosure: Dr Reinisch - Consultant: Abbott Dr Sandborn - Consultant, research funding: Abbott Dr Hommes - Consultant, research funding: Abbott Dr Th akkar - Employee: Abbott Dr Pollack - Employee: Abbott Dr Kumar - Employee: Abbott Dr Kampman - Employee: Abbott Dr Lazar - Employee: Abbott.
Week 52 deep remission rate 2
CD duration (years) Placebo Adalimumab P value CMH 1
≤ 2 0 / 9 (0.0) 3 / 9 (33.3) < 0.001*
< 2- ≤ 5 0 / 15 (0.0) 2 / 11 (18.2)
> 5 0 / 41 (0.0) 7 / 44 (15.9)
Data: n / N ( % ) *Statistically signifi cant 1 vs. placebo, adjusted for baseline disease duration (Cochran-Mantel-Haenszel test) 2 Complete mucosal healing (judged by the endoscopist) AND clinical remission (CDAI < 150).

© 2010 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY
Abstracts S429
1178
Improved Adherence and Persistence With Once-Daily Lialda® Th erapy for Ulcerative Colitis in the United States: Retrospective Analysis of a Multi-plan Claims DatabaseLinnette Yen, MS,1 David Klingman, PhD,2 Paul Hodgkins, PhD1 . 1. Shire Pharmaceuticals, Wayne, PA; 2. IMS Health Incorporated, Falls Church, VA.
Purpose: To assess persistence and adherence with once-daily Lialda® versus other 5-aminosalicylate (5-ASA) medications among patients with ulcerative colitis (UC) using real-world data.Methods: Retrospective analysis using IMS LifeLink Health Plan Claims data from Jan 1, 2007 to Mar 31, 2009 in the US. Adults (age ≥18 y) diagnosed with UC receiving ≥1 5-ASA prescription between Jul 1, 2007 and Jun 30, 2008 were included and categorized by index therapy (fi rst 5-ASA pharmacy claim): Lialda®, Asacol®, Pentasa®, Colazol®, Dipentum®, or sulfasalazine. Patients had ≥1 diagnosis of UC (ICD-9 556.xx) and no 5-ASA use ≤180 days pre-index and continuous enrollment in a health plan for ≥180 days pre- and 360 days post-index. Follow-up continued until disenrollment/end of study period. Patients with diagnosed Crohn’s disease (555.x) or irritable bowel disease (564.1) in their claims history were excluded. Persistence was defi ned as days until discontinuation of index 5-ASA therapy (gap in cover-age of up to twice the days’ supply from last fi ll of that drug), or switch from that drug. Adherence was defi ned as percentage of days covered (PDC) by index 5-ASA, analyzed during successive 90-day intervals and cumulative 180-day intervals post-index. Patients with a PDC ≥80% were considered adherent.Results: A total of 4245 patients (median age 47 y; 53% female) were included in the analysis. Of these, the index drug for 58.5% of patients was Asacol®, 15.6% Lialda®, 11% Colazol®, 11% sulfasalazine, 2.5% Pentasa®, and 0.7% Dipentum®. Persistence with treatment was highest among patients initiated on Lialda® (25.3%; P<0.0001 vs. other 5-ASAs combined). Median duration of persistence was 99 days for patients initiated on Lialda® compared with 79 days for other 5-ASAs combined (P=0.0011). Adherence during the fi rst 18 months aft er initiation of therapy was signifi cantly greater for Lialda® (21.8%) than for all other 5-ASAs combined (10.9%; P=0.0001) and numeri-cally greater than the individual comparators, eg, Dipentum® (14.3%) and Asacol® (10.9%) (not statistically analyzed). Across successive 90-day inter-vals, Lialda® patients remained the most adherent, but in each treatment group, levels of adherence declined over time, to 21.1% for Lialda® during the fi nal 90-day interval (vs. 46.6% for days 1-90) and 13.9% (vs. 41.5% for days 1-90) for all other 5-ASAs combined (P=0.0189).Conclusion: Using real-world data, patients initiating Lialda® were signifi -cantly more persistent and adherent with index therapy than patients pre-scribed other 5-ASA formulations. Increased persistence and adherence may reduce UC relapse rates, and hence resource utilization and cost. Supported by funding from Shire Development Inc.Disclosure: Linnette Yen, MS - Employee and stockholder: Shire Pharmaceuticals David Klingman, PhD - Paid Consultant through his employer: IMS Health Paul Hodgkins, PhD - Employee and stockholder: Shire Pharmaceuticals.Th is research was supported by an industry grant from Shire Pharmaceutical, Inc.
1179
Compliance and Adherence with 5-ASA Th erapy for Ulcerative Colitis in Canada: A Retrospective Analysis of a Large Claims DatabaseLinnette Yen, MS,1 Richard Lavoie, MS,2 Jordan Rudner, MS,3 Brihad Abhyankar, FRCS,4 Subrata Ghosh, MD5. 1. Shire Pharmaceuticals, Wayne, PA; 2. Shire Canada, Montréal, QC, Canada; 3. Brogan Inc., Montréal, QC, Canada; 4. Shire UK, Basingstoke, United Kingdom; 5. University of Calgary, Calgary, AB, Canada.
Purpose: To assess compliance (both adherence and persistence) with 5-ASA therapies among patients with ulcerative colitis (UC) in a real-world setting.Methods: A 6-month observational follow-up retrospective cohort analysis was conducted using Brogan Inc. Private Drug Plan claims data. Participants (any age) newly initiated on one of the available 5-ASA products (either treat-ment-naïve or switching from another 5-ASA product with no claim for that 5-ASA in the preceding 6 months) between June 2008 and June 2009 with at least 6 months claims history prior to and aft er their index 5-ASA claim were included. Six-month persistence, adherence rates, and adherence ratios were calculated for: Mezavant® (known as Lialda®, US), Asacol® 400 mg and 800 mg, Pentasa®, and Salofalk®. Participants were classifi ed as either persistent (a sub-sequent claim for a specifi ed 5-ASA product within a predefi ned grace period following the fi rst claim for that product) or non-persistent. Adherence rate was calculated as the total days’ supply while the patient was persistent divided by the number of calendar days expanded while the patient was persistent. Partici-pants who scored >80% were considered adherent. Chi-square testing was used to compare persistence and adherence (>80% and >90%) between products.Results: A total of 15,545 patients (average age, 43.55 y) were analyzed. Of these, 13.2% initiated on Mezavant®, 25.7% Asacol® 400 mg, 11.9% Asacol® 800 mg, 23.2% Pentasa®, and 25.8% Salofalk®. Aft er 6 months, persistence was signifi cantly higher among patients initiated on Mezavant® (44%) compared with Asacol® 400 mg (21%), Asacol® 800 mg (27%), Pentasa® (26%), and Salo-falk® (28%) (P<0.0001 for all comparisons). Signifi cantly more patients on Mezavant® continued therapy beyond their initial prescription claim (70%) and achieved adherence >80% (88%) and >90% (70%) compared with Asacol® 400 mg (45%, 81%, and 62%, respectively), Asacol® 800 mg (53%, 82%, and 63%, respectively), Pentasa® (49%, 79%, and 60%, respectively), and Salofalk® (52%, 81%, and 60%, respectively) (P<0.0001 and P<0.001, respectively, for all comparisons).Conclusion: In this Canadian private drug claims database, adherence and persistence rates diff ered between the diff erent 5-ASA products. Over 6 months, patients initiating on Mezavant® were signifi cantly more persistent, more likely to continue treatment aft er the initial claim, and signifi cantly more likely to achieve adherence >80% and >90% than other 5-ASA products cur-rently approved for use in this Canadian cohort. Mezavant®, with less frequent dosing and lower pill burden, may increase compliance, which could lead to reduced UC relapse and thus help reduce the economic burden of this chronic disease. Supported by funding from Shire Development Inc.Disclosure: Linnette Yen, MS: Employee; owns company stock Richard Lavoie: Shire Pharmaceuticals: Employee Jordan Rudner: Shire Pharmaceuticals: Paid consultant through his employer Brogan, Inc. Brihad Abhyankar, FRCS: Shire Pharmaceuticals: Paid employee; stock options Subrata Ghosh, MD: Shire Phar-maceuticals: Advisory Committee; Ferring: Speaker honorarium.Th is research was supported by an industry grant from Shire Pharmaceuticals, Inc.
1180
Randomized, Double-blind, Placebo-Controlled Trial of Andrographis Paniculata Extract (HMPL-004) in Patients with Moderately Active Crohn’s DiseaseWilliam Sandborn, MD,3 Stephan Targan, MD,2 Vera Byers, MD, PhD,1 Tom Tang, MD4 . 1. Immunology Inc., Incline Village, NV; 2. Cedars-Sinai Medical Center, Los Angeles, CA; 3. Mayo Clinic, Rochester, MN; 4. Hutchison MediPharma, Shanghai, China.
Purpose: HMPL-004 is an extract of the herb Andrographis Paniculata, which inhibits pro-infl ammatory cytokines including TNF-α, IL-1β, and NF-κB. We evaluated HMPL-004 for Crohn’s Disease (CD).
[1177]
Change from baseline a Placebo ADA80 / 40 ADA160 / 80
Hemoglobin (g / L) − 0.1 4.4* 4.9*
Hematocrit (fraction) − 0.001 0.014* 0.014*
Red blood cells ( × 10 12 / L) 0.05 0.16 † 0.19*
Total protein (g / L) 0.4 1.5 ‡ 1.7 †
Albumin (g / L) 0.7 1.3 1.7 †
CRP (mg / L) b − 0.10 − 0.47 − 0.87*
a Mean changes, except median change for CRP. b Excludes 1 patient without confi rmed UC at baseline. * P < 0.001; † P < 0.01; ‡ P < 0.05.

The American Journal of GASTROENTEROLOGY VOLUME 105 | SUPPLEMENT 1 | OCTOBER 2010 www.amjgastro.com
AbstractsS430
Methods: Patients with moderate CD (CDAI 220-400 + CRP > upper limit of normal) despite stable doses of concomitant medications were randomized to oral HMPL-004, 1200 mg/day or placebo for 8 weeks. Th e primary endpoint was clinical response-100 (CDAI reduction of 100 points) at 8 weeks. Second-ary endpoints included response- 70 and remission (CDAI <150 points). Miss-ing data were handled by worst observation carried forward.Results: One hundred and one patients were enrolled at 26 sites in the US and Ukraine (HMPL-004 n=51 and placebo n=50). At week 8 the clinical response-100 rates in the HMPL-004 and placebo groups were 37.3% and 22% (p=0.087), respectively. Th e corresponding response-70 and remission rates were 49% and 32% (p=0.061) and 29.4% and 14% (p=0.069), respectively. Th e mean baseline CRP was 23.5 mg/L in the HMPL-004 group and decreased 11.8 mg/L at week 8 (p=0.004). Th e mean baseline CRP was 14.2 mg/L in the placebo group and decreased to 10.0 mg/L at week 8 (p=0.008). Th e mean change in CRP from baseline to week 8 was 11.7 mg/L in the HMPL-004 group and 4.2 mg/L in the placebo group (p=0.068). Th irty-three of 51 (64%) patients in the HMPL-004 group and 28 of 50 (56%) patients in the placebo group reported adverse events (AEs), of which none were considered probably or defi nitely related to study medication. Th ere was an increase in skin rash and slight increase in bronchitis and urinary tract infections in the HMPL-004 group. Two of 51 (4%) patients in the HMPL-004 group developed serious AEs (SAEs), both were related to CD exacerbation. Four of 50 (8%) patients in the placebo group developed SAEs, 3 were related to CD exacerbation and 1 patient developed lung cancer.Conclusion: Patients with moderately active CD treated with Andrographis Paniculata extract (HMPL-004) 1200 mg/day had numerically greater rates of clinical response -100, response-70 and remission and a numerically greater reduction from baseline in mean CRP concentration as compared with pla-cebo, but these numeric trends did not reach statistical signifi cance. A dose ranging study of HMPL-004 for active ulcerative colitis demonstrated signifi -cant effi cacy for induction of response, remission, and mucosal healing for an 1800 mg/day dose but not a 1200 mg/day dose. An additional trial to investi-gate the safety and effi cacy of higher doses of HMPL-004 in CD is planned.Disclosure: Dr Sandborn - Consultant: Hutchison MediPharma, Ltd. Dr Targan - Consultant: Hutchison MediPharma, Ltd. Dr Byers - Consultant: Hutchison MediPharma Ltd. Dr Tang - Employee: Hutchison MediPharma Ltd.Th is research was supported by an industry grant from Hutchison MediPharma Ltd.
1181
Adalimumab is Eff ective for Inducing Clinical Remission at Week 4 Regard-less of Baseline Corticosteroid Use: Pooled Analysis of Four Clinical TrialsJean-Frédéric Colombel, MD,1 Paul Rutgeerts, MD,2 Walter Reinisch, MD,3 William Sandborn, MD,4 Julian Panés, MD,5 Anne Camez, MD,6 Paul Pollack, MD,7 Roopal Th akkar, MD,7 Bidan Huang, PhD,7 Mei Yang, PhD,7 Jingdong Chao, PhD,7 Parvez Mulani, PhD7. 1. Centre Hospitalier Universitaire de Lille, Lille, France; 2. University Hospital Gasthuisberg, Leuven, Belgium; 3. Medical University Vienna, Vienna, Austria; 4. Mayo Clinic, Rochester, MN; 5. Hospital Clinic, Barcelona, Spain; 6. Abbott GmbH & Co. KG, Ludwigshafen, Germany; 7. Abbott, Abbott Park, IL.
Purpose: We investigated the impact of baseline corticosteroid use on Week 4 clinical remission rates using data from four clinical trials of patients with moderate to severe Crohn’s disease.
Methods: Data from EXTEND, CLASSIC I, GAIN, and CHARM were pooled for this post-hoc analysis; data were summarized for the adalimumab 160/80 mg and 80/40 mg induction regimens. Corticosteroid dosing remained sta-ble throughout the 4 week induction period. Clinical remission (CDAI <150) rates for patients with and without baseline corticosteroid use were compared at Week 4. Nonresponder imputation was used for missing data. Th e mean change in CDAI score from baseline was also investigated. A t-test was per-formed to compare the mean change diff erence and a chi-square test was per-formed to compare the diff erences in proportion between the subgroups.Results: Th ere were no signifi cant diff erences in the rate of clinical remission at Week 4 following induction therapy nor in mean change from baseline in CDAI between patients receiving baseline corticosteroids vs. those who were not; one exception was observed at Week 4 which had a higher remission rate for the pooled 80/40 mg group in patients who were not receiving corticoster-oids, p < 0.05 (Table).Conclusion: Baseline corticosteroids do not appear to infl uence the pattern of clinical remission nor changes in CDAI score from baseline aft er induction therapy with adalimumab.Disclosure: Dr Colombel - Advisory Committees or Review Panels: Abbott, AstraZeneca Pharmaceuticals LP, Centocor, Inc, Danone Research, Elan Phar-maceuticals, Inc, Millennium Research Group, Schering-Plough Corp, UCB, Inc.; Consulting: Abbott, ActoGeniX, Albireo Pharma: Consulting, AstraZen-eca Pharmaceuticals LP, Bayer AG, Biogen Idec, Boehringer Ingelheim GmbH, Bristol-Myers Squibb Co., Cellerix SL, Centocor, Inc., Chemocentryx, Cosmo Technologies Ltd, Danone Research, Elan Pharmaceuticals, Inc., Genentech Inc., Giuliani SpA, Given Imaging, GlaxoSmithKline, Hutchison MediPharma Limited, Milan, Millennium Research Group, Ocera Th erapeutics, Inc., Pfi zer Inc,, Schering-Plough Corp., UCB, Inc.; Speaking and Teaching: Abbott, Cen-tocor, Inc, Elan Pharmaceuticals, Inc, Given Imaging Dr Rutgeerts - Consult-ing: Abbott, Actogenics, Bristol-Myers Squibb Co., Centocor, Inc., Genentech Inc., Italfarmako, Millennium Research Group, NovImmune, Schering-Plough Corp., UCB Pharma; Grant/Research Support: Abbott, Centocor, Inc, Scher-ing-Plough, UCB Pharma Dr Reinisch - Consultancy: Abbott Dr Sandborn - Financial Support for Research: Abbott Laboratories, Bristol Meyers Squibb, CentocorOrthoBiotech, Genentech, Millennium Pharmaceuticals, Novartis, Pfi zer, Shire Pharmaceuticals, UCB Pharma, Warner Chilcott (previously Procter & Gamble); Consultancy: ActoGenix, Abbott Laboratories (fees paid to Mayo), AGI Th erapeutics, Albireo, Alfa Wassermann, AM-Pharma, Amgen, Anaphore, Astellas Pharma, Athersys, Atlantic Healthcare Limited, Axcan Pharma, BioBalance Corporation, Celegene, Bristol Meyers Squibb (fees paid to Mayo), Celek Pharmaceuticals, Cellerix, CentocorOrthoBiotech (fees paid to Mayo), Chemocentryix, CoMentis, Cosmo Technologies, Cytokine Pharma-sciences, Eagle Pharmaceuticals, Eisai Medical Research, Elan Pharmceuticls (fees paid to Mayo), Eli Lilly, Enteromedics, Ferring Pharmaceuticals, Flexion Th erapeutics, Funxional Th erapeutics Limited, Genentech (fees paid to Mayo), Given Imaging, GlaxoSmithKline, KaloBios Pharmaceuticals, Merck Research Laboratories, Merck Serono, Novo Nordisk, Pfi zer (fees paid to Mayo), Procter & Gamble (fees paid to Mayo), Purgenesis Technologies, Regeneron Pharma-ceuticals, Salient Pharmaceuticals, Salix Pharmaceuticals, Santarus, Scher-ing Plough Corporation, Shire Pharmaceuticals (fees paid to Mayo), Sigmoid Pharma, Sitrtis Pharmaceuticals, SLA Pharma, Takeda (fees paid to Mayo), Tillotts Pharma, UCB Pharma (fees paid to Mayo), Vascular Biogenics, Viamet Pharmaceuticals, Wyeth Dr Panes - Consultant: Abbott, Schering-Plough; Research grants: Abbott, Schering-Plough; Speakers bureau: Abbott, Scher-ing-Plough Drs. Camez, Pollack, Th akkar, Huang, Yang, Chao, and Mulani - Employement: Abbott; Shareholder: Abbott.Th is research was supported by an industry grant from Abbott.
[1181] Clinical remission rates at week 4: patients with and without baseline corticosteroid use
No Baseline Corticosteroids Baseline Corticosteroids
Analysis group Remission rate n / N ( % ) Baseline CDAI
Mean ± SD CDAI Mean change from
Baseline ± SD Remission rate n / N ( % ) Baseline CDAI
Mean ± SD CDAI Mean change from
Baseline ± SD
Pooled 160 / 80 mg Induction 1,2
68 / 258 (26) 313.2 ± 59.1 − 136.9 ± 85.8 40 / 112 (36) 306.2 ± 68.4 − 105.9 ± 91.8
Pooled 80 / 40 mg Induction 1,2
151 / 548 (28)* 313.2 ± 61.0 − 105.2 ± 89.5 83 / 381 (22) 310.7 ± 63.3 − 97.2 ± 87.9
1 Includes moderate + severe CD patients 2 Includes EXTEND, CLASSIC I, GAIN studies 3 Includes CLASSIC I and CHARM studies * P =0.046 vs. patients with baseline corticosteroid use (chi-square test); all other results were non-signifi cant.

© 2010 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY
Abstracts S431
1182
Resource Utilization and Health Care Costs Associated with Diverticulitis: Results from A Retrospective Claims Database AnalysisLinnette Yen, MS,1 Keith Davis, MA,2 George Longstreth, MD,3 Paul Streck, MD,1 Paul Hodgkins, PhD1. 1. Shire Pharmaceuticals, Wayne, PA; 2. RTI Health Solutions, Triangle Park, NC; 3. Kaiser Permanente, San Diego, CA.
Purpose: Th e purpose of this study was to assess the all-cause resource uti-lization and health care costs of patients diagnosed with diverticulitis and to compare them to a matched control population.Methods: Medical claims data from the Ingenix IMPACT Managed Care database between 2005 and 2008 were analyzed. Th e database included medical, hospital discharge, and pharmacy claims. Patients with a primary diagnosis of diverticulitis followed by acute antibiotic treatment were identi-fi ed (n=36,636). A control group (2:1) without a diagnosis of diverticulitis and matching age (+/- 3 years), gender, and dates of health plan enrollment was identifi ed from the same database (n=73,272). Patients’ fi rst observed diverticulitis diagnosis defi ned their index date. Th e index date for controls was assigned as the index date of their respective match from the diverticu-litis group. Minimum follow-up was 12 months for both groups (defi ned by continuous health plan enrollment) and all outcomes were evaluated over 12 months post-index. Generalized linear models with a log-link function and gamma distribution were used to estimate health care costs. Nega-tive binomial regression models were used to estimate resource utilization (eg, count data on number of hospitalizations, medical visits, etc.). Nonpara-metric t-tests were used to assess diff erences in cost and resource utilization data between the diverticulitis and control groups. Cost data were adjusted to 2009 dollars.Results: Rates of resource utilization and health care costs were signifi cantly higher for patients with diverticulitis compared to the control group. Specifi -cally, for diverticulitis patients the rates of hospitalization, ER visit, and offi ce visits were 8-fold (Incidence Rate Ratio (IRR)= 8.1), 4 fold (IRR=3.7), and 2 fold (IRR=2.3) higher than the control group, respectively; all P<0.001. Due to higher resource utilization, adjusted mean total annual health care costs were substantially higher in diverticulitis cases ($16,933 vs. $7,028; P<0.0001). Th e major drivers for the cost diff erence were hospitalizations ($6,554 vs. $1,374; P<0.0001), ER ($1,022 vs. $120; P<0.0001), outpatient/ancillary costs ($4,289 vs. $2,168; P<0.0001), and offi ce visits ($2,280 vs. $1,420; P<0.0001).Conclusion: Patients with a diagnosis of diverticulitis are costly. Th e economic burden is therefore signifi cant to payers, with 12-month all-cause costs 2.6 times higher than patients without diverticulitis. Th ere is a need for newer therapies that improve health outcomes and lower the burden of this disease by preventing recurrences of the disorder. Supported by funding from Shire Development Inc.Disclosure: Linnette Yen, MS: Shire Pharmaceuticals: Employee; stockholder Keith Davis, MA: Shire Pharmaceuticals: Consultant George Longstreth, MD: Shire Pharmaceuticals: Scientifi c Advisory Board Paul Streck, MD: Shire Phar-maceuticals: Employee Paul Hodgkins, PhD: Shire Pharmaceuticals: Employee; stockholder.Th is research was supported by an industry grant from Shire Pharmaceutical, Inc.
1183
PYRAMID Registry: Observational Study of Adalimumab in Crohn’s Disease at Year 2Geert D’Haens, MD, PhD,1 Walter Reinisch, MD,2 Jack Satsangi, MD,3 Edward Loft us, MD,4 Remo Panaccione, MD,5 Debbie Tokimoto, MD,6 Lawrence McNamee, BS,6 Kathleen Lomax, MD6. 1. Imelda GI Clinical Research Center, Bonheiden, Belgium; 2. Medical University of Vienna, Vienna, Austria; 3. Western General Hospital, Edinburgh, United Kingdom; 4. Mayo Clinic, Rochester, MN; 5. University of Calgary, Calgary, AB, Canada; 6. Abbott, Abbott Park, IL.
Purpose: Adalimumab, a fully human anti-tumor necrosis factor (TNF) monoclonal antibody, is approved for the treatment of Crohn’s disease (CD) and has been shown to induce and maintain remission in patients with CD. Our objective was to assess the long-term safety of adalimumab as prescribed
according to local product labels in PYRAMID, an ongoing observational registry initiated in September 2007 in 24 countries (421 sites), now at year 2.Methods: Patients enrolled in PYRAMID during a 2-year enrollment period, with a 6-year study duration for each patient. Study visits are recommended every 3 months through Year 1, then every 6 months. Th e primary endpoint is safety, including all serious adverse events (SAEs) and adverse events of special interest (AEIs) in an anti-TNF-exposed population.Results: As of Dec 1, 2009, the fully enrolled study included 5,043 patients (mean age, 38 years; 57% female; 96% white). Th e majority of patients were enrolled outside of North America (34% from US and Canada). Approximately half (49%) had been previously treated with biologics, 35% were treated with concomitant immunosuppressants, and 29.5% with concomitant corticoster-oids. Most patients (88%) were new adalimumab users at enrollment, with the remainder continuing from prior adalimumab studies. As of Dec 1, 2009, total adalimumab exposure was 5362.8 patient years. Th e discontinuation rate was 10.1%; 4.8% discontinued for lack of effi cacy. At least 1 treatment-emer-gent SAE occurred in 11.5% of patients, the most frequent being CD (3.2%), intestinal obstruction (1.3%), and abdominal pain (0.6%); 1.1% of SAEs were uncoded (inquiries pending). Th ere were 7 deaths: 1 motor vehicle accident, 2 suicides, 3 cases of sepsis, and 1 lymphoma; one of the sepsis cases was consid-ered possibly related to the study drug. AEIs are listed in the table.Conclusion: At the 2 year timepoint, there were no new clinical concerns regarding incidence of deaths, SAEs, or AEIs, and no new safety signals were observed.Disclosure: Dr D’Haens - Consultant: Abbott Dr Reinisch - Consultant: Abbott Dr Satsangi - Consultant: Abbott Dr Loft us - Consultant: Abbott Dr Panaccione - Consultant, research support: Abbott Dr Tokimoto - Employee: Abbott Dr McNa-mee - Employee: Abbott Dr Lomax - Employee: Abbott.
1184
Natalizumab Use in Patients with Crohn’s Disease and Relapsing Multi-ple Sclerosis: Updated Utilization and Safety Results from the TOUCH,™ Prescribing Program, the Pregnancy Registry, and the INFORM and TYGRIS StudiesAnthony Pepio, PhD,1 Lori Taylor, PhD,1 Mariska Kooijmans, MD, PhD,2 Lynda Cristiano, MD,2 Carmen Bozic, MD,2 Grainne Quinn, MD3. 1. Elan Pharmaceuticals, Inc., South San Francisco, CA; 2. Biogen Idec, Inc., Cambridge, MA; 3. Elan Pharma International Ltd., Dublin, Ireland.
Purpose: To report the most recent data on natalizumab utilization and safety in patients with Crohn’s disease (CD) and relapsing multiple sclerosis (MS).Methods: Natalizumab was approved by the FDA for use in CD in 2008. Th e TYSABRI Outreach: Unifi ed Commitment to Health (TOUCH™) Prescribing Program, CD INFORM: Investigating Natalizumab through Further Obser-vational Research and Monitoring, TYSABRI Global ObseRvation Program In Safety (TYGRIS), and pregnancy registry are ongoing risk management programs or studies designed to further evaluate the safety of natalizumab. TOUCH™ is a mandatory prescribing program for all patients, physicians, and infusion centers in the United States that ensures appropriate and informed use of natalizumab. Th e purpose of TOUCH™ is to monitor patients for serious opportunistic infections (OIs), including progressive multifocal leu-koencephalopathy (PML). CD INFORM is a voluntary study in the United
Adverse event of special interest Any adalimumab ( N =5043) n ( % )
Any opportunistic infectionincluding TB 13 (0.3) a
Any intestinal obstruction / stricture 118 (2.3)
Any malignancies 17 (0.3)
Any lupus / lupus-like syndrome 2 ( < 0.1)
Any demyelinating disorders 0
Any congestive heart failure 2 ( < 0.1)
AE leading to permanent discontinuation of adalimumab 114 (2.3)
a Disseminated TB, 1 patient; TB, 2 patients; Opportunistic infections excluding TB, 10 patients.

The American Journal of GASTROENTEROLOGY VOLUME 105 | SUPPLEMENT 1 | OCTOBER 2010 www.amjgastro.com
AbstractsS432
States collecting patient history, effi cacy as assessed by the Harvey Bradshaw Index (HBI), Health Related Quality of Life outcomes, and serious adverse events (SAE) in CD patients. TYGRIS is a voluntary global observational study evaluating the long-term safety of natalizumab in MS. Post-marketing surveil-lance data from countries that do not participate in TOUCH™ or TYGRIS are also collected. Th is abstract provides updates on natalizumab utilization and safety data from these programs in both indications.Results: As of the end of March 2010, ~67,700 patients have been exposed to natalizumab in the post-marketing setting, predominately for MS. As of 6 May 2010, 49 confi rmed cases of PML had been reported in the post-marketing setting (all in MS patients). Th ere were 11 deaths; 38 of the 49 (78%) natalizu-mab-treated patients who developed PML have survived and exhibit varying levels of disability. CD INFORM has enrolled 84 patients with an average HBI at time of entry of 8.3 as of 23 May 2010. Of the 51 CD patients with an HBI assessment following 6 months of natalizumab therapy, the average score was 4.7, a mean decrease of 2.8 points from baseline. Th e overall SAE incidence in CD INFORM was 16.7% (n=14), though only 2.4% (n=2) was considered treatment related. As of 23 February 2010, there were 198 women (including 1 woman with CD) enrolled prospectively in the pregnancy registry where the outcome of the pregnancy was unknown at time of enrollment. Follow-up was ongoing in 51 cases and 151 outcomes have been reported (4 patients with twins resulted in 2 outcomes for each pregnancy). Th e most current exposure and safety data from patients receiving natalizumab worldwide will be pre-sented.Conclusion: Cumulative data from both indications suggest a safety profi le consistent with the product labeling of natalizumab.Disclosure: Drs Anthony Pepio and Lori Taylor are employees of Elan Pharma-ceuticals, Inc. Drs Mariska Kooijmans, Lynda M. Cristiano, and Carmen Bozic are employees of Biogen Idec, Inc. Dr Grainne Quinn is an employee of Elan Pharma International Ltd.
1185
Evaluation of the Incidence of Anti-JC Virus Antibodies in a Cohort of Natalizumab-Treated PatientsAnthony Pepio, PhD,1 Lori Taylor, PhD,1 Mark Jaros, PhD,1 Simonetta Mocci, MD, PhD,1 Julie Taylor, PhD,1 Ted Yednock, PhD,1 Tatiana Plavina, PhD,2 Leonid Gorelik, PhD,2 Susan Goelz, PhD,2 Meena Subramanyam, PhD2. 1. Elan Pharmaceuticals, Inc., South San Francisco, CA; 2. Biogen Idec, Inc., Cambridge, MA.
Purpose: To evaluate an assay to detect antibodies (Abs) to the JC virus (JCV) in Crohn’s disease (CD) and multiple sclerosis (MS) patients and to evaluate JCV antibody status in patients who later developed progressive multifocal leukoen-cephalopathy (PML). JC virus infection underlies the development of PML, a lytic infection of oligodendrocytes that occurs rarely in natalizumab-treated patients. Currently available techniques utilized to identify the presence of JCV DNA in blood have not proven predictive of the risk of developing PML.Methods: An ELISA for detecting anti-JCV Abs in human serum and plasma was evaluated. Th e method was shown to be sensitive, specifi c and to have acceptable precision. An assay cut point was established using sera from a broad panel of CD and MS patients.Results: Evaluation of over 800 sera samples collected from natalizumab-treated MS patients demonstrated the presence of distinct sero-positive (JCV Ab+) and sero-negative (JCV Ab-) populations. Consistent with 2 recently published large studies in healthy volunteers, 46% of these MS patients were classifi ed as negative and 54% as positive for anti-JCV antibodies. Antibody status of individual MS patients was generally stable over time (~5 years) with ~2% seroconversion per year. Serum samples from 316 CD patients participat-ing in the pivotal studies were also analyzed. All patients had a baseline sample and at least 3 additional time points (median: 9 time points). Of these patients, 56% were JCV Ab+ (177/316). Concurrent use of immunosuppressants or ster-oids did not appear to signifi cantly alter this rate. Th e rate of seroconversion was similar to results in MS patients. Serum samples from 15 patients who developed PML were also analyzed. Samples were collected 16-180 months prior to the clinical diagnosis of PML, in some cases prior to commencing
natalizumab. In all 15 patients with PML, serum samples were JCV Ab+ prior to the onset of PML, suggesting pre-existing JCV infection in these patients.Conclusion: Th e novel 2-step assay provides a preliminary classifi cation of patients as sero-negative or sero-positive with respect to anti-JCV Abs. Addi-tional analyses are ongoing to determine whether the presence or absence of anti-JCV Abs may be a potential tool for PML risk stratifi cation.Disclosure: Anthony Pepio, Lori K. Taylor, Mark Jaros, Simonetta Mocci, and Ted Yednock are employees of Elan Pharmaceuticals, Inc. Tatiana Plavina, Leonid Gorelik, Susan Goelz, and Meena Subramanyam are employees of Biogen Idec, Inc. Julie Taylor was previously an employee of Elan Pharmaceuticals and is now employed by Janssen Alzheimer Immunotherapy.
1186
Safety and Outcome of Endoscopic Th erapy for Ileal Pouch StricturesBo Shen, MD, Elaine Queener, LPN, Lei Lian, MD, Feza Remzi, MD, Ravi Kiran, MD. Cleveland Clinic, Cleveland, OH.
Purpose: Endoscopic management of ileal pouch strictures has not been sys-temically studied. Th e aim of the study was to evaluate endoscopic balloon dilation and needle knife therapy of pouch strictures with pouch patients with or without Crohn’s disease (CD).Methods: Consecutive pouch pts from our Pouchitis Clinic who underwent non-fl uoroscopy-guided outpatient endoscopic therapy were studied. Pouch pts with underlying familial adenomatous polyposis were excluded. Th e loca-tion, number, degree (range 0-3), and length of strictures and balloon size were documented. All procedures were performed by a single endoscopist. Safety and outcome were evaluated.Univariable and multivariable analyses were per-formed.Results: A total of 150 pts were studied consisting of those with acute pouchitis (N=10), chronic pouchitis (N=26), CD of the pouch (N=62), cuffi tis (N=12), and surgery-associated strictures(N=40). Th e mean age was 44.1 +/- 13.4 yrs, with 66 being female (44%) and 12 being chronic NSAID users (8%). Concur-rent use of immumodulators and biologics for underlying pouch disorders was in 25 (16.7%) and 4 (2.7%) pts, respectively. Th e median duration of ulcerative colitis before colectomy was 5.1 (1.75-9.6) yrs. Stricture locations: inlet (96), outlet (73), aff erent limb (33), & pouch body (2). 42 pts (28%) had multiple strictures. A cumulative of 646 strictures were endoscopically dilated, with a total of 406 pouchoscopies using the gastroscope. Th e median degree of stric-ture score was 1 (1-2); and the median stricture length was 1 (0.5-1.25) cm. Th e median balloon size was 20 (18-20) mm. Technical success measured by the passage of gastroscope aft er the dilation was 100%. 10 pts with refractory stric-tures had endoscopic needle knife therapy. Of 406 therapeutic endoscopies per-formed, there were 2 perforations (0.46%) and 4 tranfusion-required bleeding (0.98%). With a median follow-up of 9.6 (6-17) yrs, 19 pts (12.7%) developed pouch failure (Fig), with risk factors showed in the Cox model (Table).Conclusion: Endoscopic treatment of pouch stricture is safe and effi cacious, by improving pouch survival. Underlying diagnosis of CD of the pouch and surgery-related strictures, multiple strictures are the risk factors for pouch failure.
Cox model for risk factors of pouch failure in patients with strictures
Variable Hazard ratio (95 % CI) P value
Number of stricture 1.69 (1.07 – 2.68) 0.02
Cumulative frequency of stricture dilatation
0.95 (0.87 – 1.04) 0.25
Number of pouchoscopy 1.08 (0.9 – 1.3) 0.41
Degree of stricture 1.22 (0.59 – 2.5) 0.59
Balloon size 0.82 (0.64 – 1.05) 0.12
Final pouch diagnosis (Crohn ′ s or surgical complications)
1.61 (0.99 – 2.61) 0.05

© 2010 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY
Abstracts S433
1187
Ganciclovir is Ineff ective at Reducing Colectomy Rate in Infl ammatory Bowel Disease in Patients with Superimposed Cytomegalovirus InfectionRaed Alzafi ri, MD,1 Adrian Gologan, MD,2 Esther Lamoureux, MD,2 Ghaith Habboub, Bsc,1 Polymnia Galiatsatos, MD,1 Andrew Szilagyi, MD1. 1. Jewish General Hospital, Medicine, Montreal, QC, Canada; 2. Jewish General Hospital, Pathology, Montreal, QC, Canada.
Purpose: Role of cytomegalovirus(CMV) infection in infl ammatory bowel disease (IBD) is debated. Its discovery in refractory IBD leads to use of anti-virals despite lack of proof of effi cacy. Th is retrospective study evaluates IBD patients to determine eff ect of CMV antiviral therapy on outcome.Methods: Pathological reports of patients with CMV complicating IBD over 9 years (Jan 2000 - Nov 2009) were scrutinized.CMV diagnosis was his-topathological and immunostain (started in 2005;16 cases 2005-9, and 19 cases 2000-4). Admitted patient’s charts (ulcerative colitis [UC] or Crohn’s disease [CD]) were reviewed. Colectomies and death were compared for those on or off antiviral treatment. Demographics: age, sex, IBD subtype, site, duration, treatment (especially immunomodulators or biologics) prior to and during hospitalization, white count (x 10e9), hemoglobin (g/L) and albumin (g/L) were abstracted and tabulated. Histological intensity of CMV based on reports, was graded 1=1viral inclusion body, 2 >1-<4 inclusion bodies and 3=multi-ple ≥4. Colectomy and deaths were also compared in IBD patients admitted emergently during the same period. Chi squared with Fisher Exact test and unpaired student t-tests were used. All p-values were 2 tailed and signifi cance was accepted at p ≤0.05 level.Results: 35 CMV cases were found; 13 female, 20 UC, (9/20 left sided only, 11/20 pancolitis); 15 CD[6/15 ileocolonic and 9/15 colonic ), 10/35 previ-ously on 5ASA only. 12 were treated with ganciclovir (5 mg/kg) and 23 were not. 3 colectomies (25%) and 2 deaths (5.7%) occurred in the treated group. Th ere were 8 colectomies (CMV found post surgery, 34.8%) and no deaths in the untreated group (colectomy rates, p=0.71). No parameter reached signifi cance. Same parameters evaluated between colectomized and non colectomized patients showed low albumin was signifi cant (colectomized; mean ±SD, 25.9±7.8 vs. non colectomized 32.2±8.9 g/L, p=0.050). Frequency of intensity score 3 (7/10), was higher in the colectomized group ( p=0.004, Fisher test). During the same period 579 other patients (369 CD and 210 UC) were admitted. Th ere were 64 (40 CD and 24 UC) partial or total colectomies (64/579 [11.1%] vs. 11/35 CMV+ [31.4%], p<0.001). Death rates were similar (14/557, 2.5% p=0.24, Fisher exact).Conclusion: In UC and colonic CD patients, histologically confi rmed CMV, especially high intensity was associated with increased severity of disease and colectomy rates. Use of ganciclovir did not reduce rate of colectomy or death. Any true benefi t to antiviral agents will likely require prospective trials. Th e
fi ndings support that CMV co-infection should be thoroughly ruled out in severe cases of IBD. Prognostic value of histopathology needs to be verifi ed.
1188
Effi cacy of Certolizumab Pegol in Preoperative Management of Ileal Crohn’s StricturesCharles Randall, MD,1 Raul Ramos, MD,1 Carlo Taboada, MD,1 Christopher Fincke, MD,2 Russell Havranek, MD,2 Franz Zurita, MD,2 David Stump, MD,2 Gary Gossen, MD,1 Armando Martinez, MD3. 1. Research, Gastroenterology Research of San Antonio, San Antonio, TX; 2. Gastroenterology Clinic of San Antonio, San Antonio, TX; 3. University of Texas Health Science Center at San Antonio, San Antonio, TX.
Purpose: Since the advent of biologics we have made great strides in manag-ing Ileal Crohn’s Disease. Medications however cannot reverse fi brostenosis and subsequent ileal strictures, thus surgery remains an important treatment tool. Because surgical therapy is easier to accomplish in the absence of acute infl ammation we are investigating the role of Certolizumab Pegol (CZP) pre-operatively. Th is paper represents data on the fi rst 3 patients of an ongoing long-term study.Methods: Th is is a prospective study that follows patients with ileal Crohn’s stric-tures through their operations. Patients referred to our IBD clinic are enrolled in this study if they demonstrate active Ileal Crohn’s Disease in addition to an ileal stricture that requires surgical intervention. All patients underwent an MR Enterography (MRE) during screening and again prior to surgery. Each received CZP from selection until surgery. Th e primary endpoint of the study was reduc-tion in active disease by the time of operation. Th e secondary endpoint was a decrease in the amount of small intestine resected during surgery.Results: 3 patients have completed the study. Th ey received 6 months of CZP prior to surgery. Preoperative MRE showed resolution of the acute disease. At laparoscopy the resolution of active Crohn’s was confi rmed. All patients had resections limited to the strictured areas. Th e surgeon also felt that intraopera-tive time was less due to lack of active infl ammation.Conclusion: 1. Th e primary endpoint of the study was observed. No infl am-mation was seen at preoperative MRE or at laparoscopy. 2. All patients had ileal resections limited to the strictured areas thus preserving non-stenotic healthy bowel. Th is satisfi ed our secondary endpoint. 3. Th e early results of our ongoing study are encouraging. Additional cases will be required to fully assess the benefi t of CZP before surgery.Disclosure: Dr Randall - Consultant: UCB, Speakers Bureau.
1189
Safety Analysis from a Phase IIa Multicenter Study with Interferon-β-1a in Active Moderate to Severe Ulcerative ColitisPhilip Miner, MD,1 Salam Zakko, MD,2 Arthur McAllister, MS,3 Fabio Cataldi, MD3. 1. Oklahoma Foundation for Digestive Research, Oklahoma City, OK; 2. Connecticut Gastroenterology Institute, Bristol, CT; 3. Biogen IDec, Cambridge, MA.
Purpose: Ulcerative colitis (UC) is a chronic and recurring infl ammatory dis-order of the colon is associated with an increased risk of colon cancer and com-plications requiring medical and surgical intervention. Th e effi cacy of currently marketed UC-modifying therapies is limited by their safety and tolerability.Methods: 123 subjects with moderate to severe active UC were randomized in a double blind pilot study to receive Interferon-β-1a (IFN) 30 μg IM or placebo (P) twice at WK, 62 IFN and 61 P, for 12 weeks and a safety follow-up at week 16 (for Czech Rep at week 20). Th e dose tested in this study was twice the dose approved for the treatment of multiple sclerosis (MS). Subjects were required to receive 1 or more of the following treatments in any combination: steroids, AZA/6-MP, oral 5-ASA. Subjects were required to maintain stable doses of these treatments aft er randomization to week 8 (week 12 for 5-ASA). Th e pri-mary endpoint was clinical response at Week 8, defi ned as a decrease from baseline in the Total Mayo Score. Th e secondary endpoints were the safety and tolerability of IFN and the % of subjects, with a decrease in the SCCAI score of ≥3 points at Week 8.
[1186]

The American Journal of GASTROENTEROLOGY VOLUME 105 | SUPPLEMENT 1 | OCTOBER 2010 www.amjgastro.com
AbstractsS434
Results: IFN has an established safety and tolerability profi le with over 15 years of experience and over a million patient-years of exposure in MS. Overall the study drug was very well tolerated and the adverse events with an incidence of 5% or more are showed in table 1. In the P group all reports were of mild severity, 5 subjects symptoms started on Day 1 and ceased on Day 9 at the lat-est and for 1 subject, symptoms started aft er dosing completed. In IFN, all the reports were mild to moderate in severity, oft en reported on days of dosing and the 8 cases of pyrexia were independent of cases of infl uenza-like illness. 3 SAEs were reported in the P group, 2 worsening of UC (1 subject became anemic) and 1 tibia fracture; 1 worsening of UC in IFN. Th ere were only 8 AEs leading to discontinuation of the study drug, 2 in P and 6 in IFN; 4 of these events were previously described as SAEs. Of the other 5 reports in IFN, 3 were worsening of UC, of moderate to severe nature; 1 mild allergic dermatitis and 1 fl u-like illness/injection site pain on the fi rst day of dosing of moderate sever-ity. As known with this drug, no serious infections were seen in this study.Conclusion: Overall Interferon-β-1a showed a very positive safety and toler-ability profi le in subjects with moderate to severe active UC dosed at twice of the approved MS dose. Interferon-β-1a in this study showed a lower incidence of AEs compared to the known safety and tolerability profi le of this class of drugs. In addition the low incidence of AEs and SAEs led to a small number of discontinuations from study drug.Disclosure: Phil B. Miner Consultant Biogen Idec Salam Zakko Consultant Biogen Idec Arthur McAllister Employee Biogen Idec Fabio CataldiEmployee Biogen Idec.Th is research was supported by an industry grant from Biogen Idec.
1190
Achievement of Early Deep Remission Predicts Better Long-Term Outcomes for Adalimumab-Treated Patients with Crohn’s Disease: Data from EXTENDJean-Frédéric Colombel, MD,1 Paul Rutgeerts, MD,2 William Sandborn, MD,3 Mei Yang, PhD,4 Kathleen Lomax, MD,4 Paul Pollack, MD,4 Roopal Th akkar, MD,4 Anne Camez, MD,5 Naijun Chen, MS,4 Jingdong Chao, PhD,4 Parvez Mulani, PhD4. 1. Centre Hospitalier Universitaire de Lille, Lille, France; 2. University Hospital of Gasthuisberg, Leuven, Belgium; 3. Mayo Clinic, Rochester, MN; 4. Abbott Laboratories, Abbott Park, IL; 5. Abbott GmbH & Co. KG, Ludwigshafen, Germany.
Purpose: To explore the impact of early deep remission on long-term out-comes in the 52-week EXTEND trial.Methods: Patients in EXTEND, a study of mucosal healing in patients with moderate to severe ileocolonic CD (CDAI 220-450), received open-label adalimumab 160-/80-mg induction therapy at Weeks 0/2 and were rand-omized at Week 4 to maintenance therapy with adalimumab (ADA) 40 mg every other week (eow) or placebo through Week 52. From Week 8, patients with fl ares/nonresponse could receive open-label (OL) ADA 40 mg eow (weekly if fl ares/nonresponse continued). Endoscopic assessment was per-formed at baseline, Week 12 (or unscheduled visits at Weeks 8-12 prior to switch to OL or dropout), time of switch to OL (if aft er Week 12), and Week
52 (or early termination). Early deep remission was defi ned as observed mucosal healing+clinical remission (CDAI <150) at Week 12. Relation-ships of early deep remission with Infl ammatory Bowel Disease Question-naire (IBDQ) remission status (IBDQ ≥170), Short-Form 36 Health Survey (SF-36) normal status (Physical Component Summary [PCS]/Mental Com-ponent Summary [MCS] ≥50), and Work Productivity and Activity Impair-ment Questionnaire (WPAI) improvements at Week 52 and hospitalization from Week 12 through Week 52 were assessed. Data were analyzed using multiple linear regressions and logistic regressions, with control for baseline QOL/WPAI scores.Results: ADA-treated patients achieving early deep remission tended to have fewer hospitalizations, better Week-52 QOL, and less productivity impairment compared with patients not achieving deep remission (table). Patients with early deep remission were ~5 times more likely to achieve both IBDQ remission and a normal SF-36 PCS score (both p<0.05) at Week 52. No patients achieving early deep remission were hospitalized. Th ere were 3 CD-related surgeries in the non-deep remission group and 0 in the deep remission group.Conclusion: Achievement of early deep remission predicted better long-term outcomes in ADA-treated patients with moderate to severe ileocolonic CD.Disclosure: J-F Colombel: Advisory Boards and/or Consulting: Abbott, Acto-GeniX, Albireo Pharma, Astra Zeneca, Bayer Schering Pharma, Biogen Idec, Boehringer-Ingelheim, Bristol-Myers Squibb, Cellerix SL, Centocor, Chemo-centryx Inc, Cosmo Technologies Ltd, Danone France, Elan Pharmaceuticals Inc, Genentech, Giuliani SPA, Given Imaging, GlaxoSmithKline, Merck and Co Inc, Millenium Pharmaceuticals Inc, NeoVacs SA, Ocerra Th erapeutics Inc (previously named Renovia Inc), Otsuka American Pharmaceuticals Inc, PDL Biopharma (previously named Protein Design Labs), Pfi zer Inc, Ribo Vacs Biotech, Schering-Plough Corporation, Shire Pharmaceuticals, Synta Phar-maceutical Corporation, Teva Pharmaceuticals and Petah Tikva, Th erakos, UCB Pharma (previously named Celltech Th erapeutics Ltd) and Wyeth Phar-maceuticals. Grant Support: Astra-Zeneca, Danisco, Danone, Dysphar, Fer-ring, Giuliani SPA, Lesaff re, Mapi Naxis, Ocerra Th erapeutics Inc (previously named Renovia Inc), Roquette, Schering-Plough Corporation, UCB Pharma. Lecture Fees from speaking at continuing medical education events indirectly sponsored by a commercial sponsor: Abbott, Astra Zeneca, Centocor, Elan Pharmaceuticals Inc, Falk Pharma, Ferring, Given Imaging, Otsuka Ameri-can Pharmaceuticals Inc, PDL Biopharma, Schering-Plough Corporation, Shire Pharmaceuticals, UCB Pharma. Stock: Intestinal Biotech Development. P Rutgeerts: Advisor: Elan Pharmaceuticals; Ferring Pharmaceuticals; Procter and Gamble; Schering-Plough; UCB. Consultant: Abbott; Astra Zeneca; Bris-tol-Myers Squibb; Centocor; Elan Pharmaceuticals; Ferring Pharmaceuti-cals; GlaxoSmithKline; Procter and Gamble; Schering-Plough; Shire; UCB. Grant/Research Support: Abbott; Bristol-Myers Squibb; Centocor; Elan Phar-maceuticals; Ferring Pharmaceuticals; Millenium Pharmaceuticals; Procter and Gamble; Schering-Plough. Speaker’s Fees: Abbott; Astra Zeneca; Axcan Pharma; Byk Solvay; Centocor; Elan Pharmaceuticals; Jansen; Procter and Gamble; Prometheus; Schering-Plough; Shire. WJ Sandborn: Financial Support for Research: Abbott Laboratories, Bristol Meyers Squibb, CentocorOrthoBio-tech, Genentech, Millennium Pharmaceuticals, Novartis, Pfi zer, Shire Phar-maceuticals, UCB Pharma, Warner Chilcott (previously Procter & Gamble).Lecture Fees: None. Consultancy: ActoGenix, Abbott Laboratories (fees paid to Mayo), AGI Th erapeutics, Albireo, Alfa Wassermann, AM-Pharma, Amgen, Anaphore, Astellas Pharma, Athersys, Atlantic Healthcare Limited, Axcan Pharma, BioBalance Corporation, Celegene, Bristol Meyers Squibb (fees paid to Mayo), Celek Pharmaceuticals, Cellerix, CentocorOrthoBiotech (fees paid to Mayo), Chemocentryix, CoMentis, Cosmo Technologies, Cytokine Pharmasci-ences, Eagle Pharmaceuticals, Eisai Medical Research, Elan Pharmaceuticals (fees paid to Mayo), Eli Lilly, Enteromedics, Ferring Pharmaceuticals, Flexion Th erapeutics, Funxional Th erapeutics Limited, Genentech (fees paid to Mayo), Given Imaging, GlaxoSmithKline, KaloBios Pharmaceuticals, Merck Research Laboratories, Merck Serono, Novo Nordisk, Pfi zer (fees paid to Mayo), Procter & Gamble (fees paid to Mayo), Purgenesis Technologies, Regeneron Pharma-ceuticals, Salient Pharmaceuticals, Salix Pharmaceuticals, Santarus, Scher-ing Plough Corporation, Shire Pharmaceuticals (fees paid to Mayo), Sigmoid Pharma, Sitrtis Pharmaceuticals, SLA Pharma, Takeda (fees paid to Mayo), Tillotts Pharma, UCB Pharma (fees paid to Mayo), Vascular Biogenics, Viamet Pharmaceuticals, Wyeth. Shareholder: None. Directorships: None. Other: None. M Yang: Employee/Stock: Abbott. KG Lomax: Employee/Stock: Abbott. PF Pol-lack: Employee/Stock: Abbott. R Th akkar: Employee/Stock: Abbott. A Camez: Employee/Stock: Abbott. N Chen: Employee/Stock: Abbott. J Chao: Employee/Stock: Abbott. PM Mulani: Employee/Stock: Abbott.
Table 1 .
P n =61 ( % ) IFN n =62 ( % )
Number with an event 35 (57) 52 (84)
Infl uenza-like illness 6 (10) 25 (40)
Headache 3 (5) 11 (18)
Pyrexia 2 (3) 8 (13)
Ulcerative colitis 5 (8) 6 (10)
Myalgia 0 4 ( 6)
Hypertension 0 3 ( 5)
Upper respiratory tract infection 0 3 ( 5)
Anemia 6 (10) 1 ( 2)

© 2010 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY
Abstracts S435
1191
Relative Accuracy of Diff erent Modalities for the Diagnosis of Pouch- vaginal Fistula in Infl ammatory Bowel Disease Patients Aft er Restorative ProctocolectomyHillary Rockey, BA, Udayakumar Navaneethan, MD, Ravi Kiran, MD, Bo Shen, MD. Cleveland Clinic, Cleveland, OH.
Purpose: Th e current gold standard for diagnosing pouch-vaginal fi stula (PVF) is symptomatology. Pouchoscopy (PES), gastrografi n enema (GGE), magnetic resonance imaging (MRI), exam under anesthesia (EUA), gynecological pelvic exam, vaginoscopy, vaginogram, and computerized tomography (CT) may be used to support diagnosis, but the accuracy of these diagnostic modalities has not been evaluated. Th e aim of this study was to determine the accuracy of these diagnostic modalities to optimize the diagnosis of PVF.Methods: Data of all infl ammatory bowel disease (IBD) patients with PVF pre-senting to a subspecialty Pouchitis Clinic were reviewed. Patients with symp-toms of PVF who had 1 or more of the following diagnostic modalities used for diagnosis of PVF: PES, GGE, MRI, EUA, gynecological pelvic exam, vagi-noscopy, vaginogram, and CT were included. Pouch patients with underlying familial adenomatous polyposis were excluded.Results: A total of 52 eligible female patients were identifi ed. Th e mean age was 40.7±10.4 years. Forty-six patients (88.5%) had a preoperative diagnosis of ulcera-tive colitis (UC), 2 (3.8%) Crohn’s disease, and 4 (7.7%) indeterminate colitis. Th e mean duration of UC before surgery was 5.3±5.6 years, and mean duration of the pouch aft er construction was 11.5±5.8 years. Of the 9 available tests, PES, EUA, MRI, and GGE were most commonly used. Th e mean number of diagnostic tests per patient was 3.7±1.5. Overall, EUA appeared to have the most reasonable accuracy (85.0%). Of the patients with negative EUA, 1 patient was diagnosed by PES, and 1 patient was diagnosed by both MRI and PES. CT pelvis (5.0%) and CT enterography (15.4%) had the lowest accuracy; all other modalities were between 33.3%-57.1% accurate. Representative PVF features are shown in Figure.
Conclusion: While being the most commonly performed modality, EUA is also the most diagnostically accurate modality for PVF, but a combined assessment of diff erent diagnostic modalities may be needed.
1192
Quality-of-Life and Work Productivity Outcomes with Adalimumab for Patients Previously Treated with High-Dose Infl iximab for Crohn’s DiseaseRemo Panaccione, MD,1 Edouard Louis, MD, PhD,2 David Binion, MD,3 Mei Yang, PhD,4 Naijun Chen, MS,4 Kathleen Lomax, MD,4 Parvez Mulani, PhD,4 Jingdong Chao, PhD4. 1. University of Calgary, Calgary, AB, Canada; 2. University of Liège, Liège, Belgium; 3. University of Pittsburgh, Pittsburgh, PA; 4. Abbott Laboratories, Abbott Park, IL.
Purpose: To assess quality-of-life and work productivity outcomes for patients with Crohn’s disease (CD) who received high-dose infl iximab (IFX) prior to entering an adalimumab (ADA) clinical trial for CD.Methods: Data from 3 open-label clinical trials of ADA for CD were reviewed: ACCESS, CARE, and CHOICE. High-dose IFX was defi ned as a maintenance dosage greater than the recommended initial dosage for CD (ie, ≥7 mg/kg) or a shorter dosing interval (ie, ≤every 6 weeks). Paired Wilcoxon signed-rank tests were used to compare Short Infl ammatory Bowel Disease Questionnaire (SIBDQ) and Work Productivity and Activity Impairment Questionnaire (WPAI) scores between baseline and each follow-up visit for all patients with prior high-dose IFX maintenance therapy who received ADA 160-/80-mg induction therapy followed by ADA 40-mg every-other-week (eow) main-tenance therapy during the trial. For patients who switched from ADA eow to ADA weekly, the last observations at the time patients changed to weekly therapy were carried forward to impute the outcome values. Subgroup analyses for patients who responded well but discontinued IFX owing to intolerance were conducted for CHOICE. Because of the small sample size, the subgroup analysis was not conducted for ACCESS or CARE.Results: SIBDQ and WPAI scores at study endpoint for high-dose IFX users who received ADA 40 mg eow as maintenance therapy improved signifi cantly from baseline (table). Results were similar for the subgroup of patients who responded initially but developed intolerance to IFX in CHOICE.Conclusion: Aft er receiving treatment with ADA 160/80 induction followed by ADA eow maintenance therapy, patients with prior high-dose IFX therapy experienced signifi cant improvements in patient-reported outcomes.Disclosure: R Panaccione: Consultant: Abbott, AstraZeneca, Ferring, Schering-Plough, Shire, Centocor, Elan, Glaxo-Smith Kline, UCB, Proctor and Gamble,
Table . Comparison of diagnostic accuracy for pouch-vaginal fi stula
Number of cases Cases with PVF detected with the test
%
Pouchoscopy 48 23 47.9 %
MRI 23 8 34.9 %
CT pelvis 20 1 5.0 %
CT enterography 13 2 15.4 %
EUA 40 34 85.0 % *
GYN exam 3 1 33.3 %
Vaginoscopy 4 2 50.0 %
Vaginogram 7 4 57.1 %
Gastrografi n Enema 34 9 26.3 %
* P < 0.05 vs. other groups with sample sizes > 10.
Figure: Pouch-vaginal fi stula on imaging and endoscopic modalities used in the diagnosis of pouch-vaginal fi stula.
[1190]
Deep remission (Week 12)
Yes, % ( N =11) No, % ( N =53)
All-cause hospitalization 0 17
CD-related hospitalization 0 9
Week-52 IBDQ remission 64 a 26
Week-52 SF-36 MCS normal 36 25
Week-52 SF-36 PCS normal 55 a 19
Week-52 WPAI impairment, LS mean
Total work productivity impairment 23 44
Total activity impairment 18 a 43
a P < 0.05.

The American Journal of GASTROENTEROLOGY VOLUME 105 | SUPPLEMENT 1 | OCTOBER 2010 www.amjgastro.com
AbstractsS436
Bristol Myers Squibb. Speaker’s Fees: Abbott, AstraZeneca, Byk Solvay, Axcan, Jansen, Schering-Plough, Shire, Centocor, Elan, Prometheus, Proctor and Gam-ble. Advisory Boards: Abbott, Ferring, Schering-Plough, Shire, Elan, Proctor and Gamble. Research/Educational Support: Abbott, Ferring, Axcan, Jansen, Schering-Plough, Centocor, Millennium, Elan, Proctor and Gamble, Bristol Myers Squibb. E Louis: Grant/Research Support: AstraZeneca, Schering-Plough. Speaker’s Fees: AstraZeneca, UCB, Abbott, Schering-Plough, Ferring. Advisory Boards: Abbott, UCB, Ferring. DG Binion: Speaker’s Fees: Abbott Laboratories, Centocor, Elan, Procter & Gamble, Prometheus, Salix, Shire, UCB. Grant/Research Support: National Institute of Health, Centocor, Elan, Biogen, Procter & Gamble. M Yang: Employee/Stock: Abbott N Chen: Employee/Stock: Abbott KG Lomax: Employee/Stock: Abbott PM Mulani: Employee/Stock: Abbott J Chao: Employee/Stock: Abbott.
1193
Comparison of Medical Costs Among Patients Using Adalimumab and Infl iximab: A Retrospective Study (COMPAIRS)Daniel Sussman, MD,1 Nisa Kubiliun, MD,1 Jingdong Chao, PhD,2 Parvez Mulani, PhD,2 Carol Gillis, PharMD,2 Mei Yang, PhD,2 Mei Lu, -,3 Maria Abreu, MD1. 1. University of Miami, Miami, FL; 2. Abbott Laboratories, Abbott Park, IL; 3. Analysis Group, Inc., Boston, MA.
Purpose: Anti-tumor necrosis factor (anti-TNF) medications have never been compared in a direct fashion under real-world circumstances. Th e purpose of this study was to compare health care utilization and costs using insurance data for patients with Crohn’s disease (CD) who newly initiated anti-TNF therapy with adalimumab (ADA) or infl iximab (IFX).Methods: Patients with ≥2 diagnoses of CD (ICD-9-CM: 555.XX) who initi-ated ADA or IFX therapy between January 2000 and March 2009 were identi-fi ed from the Medstat MarketScan® database. Patients had to be continuously enrolled at least 6 months before and aft er anti-TNF initiation. Patients with prior biologic therapy (ie, anti-TNF or natalizumab) or colitis (ICD-9-CM: 556.x) were excluded. ADA and IFX groups were matched 1:1 using a propensity
score stratifi ed by age, residence, inpatient visit utilization, and steroid use at baseline. Th e primary endpoint was 6-month direct cost of health care. Th e secondary endpoints compared health care utilization between groups.Results: Aft er propensity matching, demographic, clinical, and health care uti-lization characteristics were similar between the ADA (n=623) and IFX (n=623) groups at baseline. During the 6-month interval following anti-TNF initiation, health care costs were signifi cantly lower for ADA compared with IFX therapy (table). Both all-cause and CD-related hospitalization decreased for both ADA and IFX groups (not shown). Emergency department (ED) use and hospitaliza-tion in the 6-month follow-up period were similar between groups.Conclusion: In this real-world analysis of patients with CD who newly initi-ated with ADA or IFX, ADA-treated patients had signifi cantly lower health care costs. Hospitalization and ED utilization were similar between groups.Disclosure: DA Sussman: No disclosures. N Kubiliun: No disclosures. J Chao: Employee/Stock: Abbott. PM Mulani: Employee/Stock: Abbott. CA Gillis: Employee/Stock: Abbott. M Yang: Employee/Stock: Abbott. M Lu: Employee: Analysis Group; under contract with Abbott. M Abreu: Consultant: Abbott, Amgen, Elan, Opson, Prometheus, Salix, UCB.
1194
Mucosal Healing in Patients Receiving Certolizumab Pegol for Crohn’s Disease (CHARTER Study)Charles Randall, MD,1 Christian Herrera, MD,3 Carlo Taboada, MD,1 Christopher Fincke, MD,2 Russell Havranek, MD,2 Franz Zurita, MD,2 David Stump, MD,2 Gary Gossen, MD,1 Daniela Vidaurri, MD3. 1. Research, Gastroenterology Research of San Antonio, San Antonio, TX; 2. Gastroenterology Clinic of San Antonio, San Antonio, TX; 3. University of Texas Health Science Center at San Antonio, San Antonio, TX.
Purpose: Th e introduction of biological agents has been popularized by research showing statistically signifi cant responses and remission rates. Only a few studies have commented on mucosal healing. Th is paper presents the preliminary results of an ongoing study.
[1192] Mean changes in SIBDQ and WPAI from baseline to study endpoint a
Access Care Choice
All All All Intolerant to IFX
High-dose IFX followed by ADA, N 48 138 349 84
SIBDQ 9.1 ( P < 0.001) 11.7 ( P < 0.001) 8.8 ( P < 0.001) 9.7 ( P < 0.001)
WPAI
Absenteeism − 4.2 ( P =0.28) − 13.0 ( P < 0.001) − 7.3 ( P < 0.001) − 7.0 ( P =0.017)
Presenteeism − 18.8 ( P =0.0022) − 16.8 ( P < 0.001) − 16.4 ( P < 0.001) − 19.4 ( P < 0.001)
TWPI − 20.3 ( P =0.0012) − 19.0 ( P < 0.001) − 19.3 ( P < 0.001) − 21.0 ( P < 0.001)
TAI − 18.1 ( P < 0.001) − 22.7 ( P < 0.001) − 19.1 ( P < 0.001) − 22.5 ( P < 0.001)
TWPI, total work productivity impairment; TAI, total activity impairment. a Study endpoint was Week 24 for ACCESS and CHOICE and Week 20 for CARE.
[1193] Mean health care costs (Per Person) during the 6 months after initiating anti-TNF Therapy (US $ )
All-cause CD-related a
ADA ( N =623) IFX ( N =623) ADA ( N =623) IFX ( N =623)
Anti-TNF drug costs — — 10,709 12,401
Other prescription drug costs 1,334 b 1,639 546 857
Medical service-related costs c
Hospitalization 3,357 5,166 3,257 4,961
Outpatient visit 2,482 b 4,565 1,579 b 3,659
Total medical service-related costs 6,842 b 10,316 5,199 b 9,059
Total health care costs 18,885 b 24,355 16,454 b 22,316
Total health care costs, excluding anti-TNF agents
8,176 b 11,955 5,745 b 9,916
a Based on diagnosis of CD or related comorbidities (eg, malnutrition, anemia, abdominal symptoms, etc). b P < 0.0005 vs. IFX. c Medical costs other than hospitalization and outpatients visits are not shown.

© 2010 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY
Abstracts S437
Methods: Prospective analyses of patients beginning certolizumab pegol within the last 12 months were eligible to participate in the study. 24 patients with known mucosal lesions received certolizumab pegol per standard pro-tocol that included induction followed by maintenance of 400mg every 4 weeks. All patients had active erosions or ulcerations prior to treatment. A Harvey-Bradshaw Index (HBI) was used to correlate symptoms with endo-scopic appearance.Results: Of the 24 patients, 10 had follow-up colonoscopies following initiation of therapy. Th e average time to colonoscopy was 6 months post-induction. Th e range was 4-9 months. 7 patients had complete colonic mucosal healing; 2 had resolution of their ulcers or erosions but had friability and erythema; and the tenth patient, though improved endoscopically, had persistent erosions. 6 of these patients also had Ileal disease. 2 had no change in their endoscopic appear-ance; 2 showed moderate improvement; and 2 had complete mucosal healing. 8 patients were in clinical remission by the HBI and 2 showed response.Conclusion: 1. Colonic healing can be expected early in the course of therapy. 2. Ileal healing occurs, but at a slower rate than does the colon. 3. Mucosal healing lags behind clinical remission and response. 4. Continuing investiga-tion will allow a better understanding of time required to see healing and what percent of patients we expect to have mucosal healing.Disclosure: Dr Randall - Consultant: UCB, Speakers Bureau.
1195
How Patients View Probiotics: Findings from a Multicenter Focus Group Study of Patients with Chronic Digestive DiseasesMaryBeth Mercer, MPH,1 Margaret Brinich, BA,1 Gail Geller, ScD,2 Krista Harrison, BA,2 Janelle Highland, MA,1 Katherine James, MPH,3 Patricia Marshall, PhD,4 Jennifer McCormick, PhD,3 Jon Tilburt, MD, MPH,3 Ruth Farrell, MD,1 Richard Sharp, PhD1. 1. Cleveland Clinic, Cleveland, OH; 2. Johns Hopkins, Baltimore, MD; 3. Mayo Clinic, Rochester, MN; 4. Case Western Reserve University, Cleveland, OH.
Purpose: Patients with chronic digestive diseases have access to a large and growing number of probiotic products marketed to improve digestive health. It is unclear what role patients expect their gastroenterologists to play as they consider adding probiotics to their treatment plan. Understanding patients’ knowledge, attitudes and expectations of probiotics may assist gastroenterolo-gists in engaging their patients in productive discussions about this emerging therapeutic option.Methods: Patients with IBD, IBS and pouchitis were recruited from outpatient GI clinics at Cleveland Clinic, Mayo Clinic and Johns Hopkins. Qualitative data was collected using focus group discussions that were audio-recorded and transcribed. Data analysts used QSR NVivo 8 soft ware to code the transcripts. Inductive analytic methods were utilized to identify themes and draw interpre-tations from the narratives.Results: Twenty-two focus groups (N=136) were held between March and August 2009. Patients had variable familiarity with probiotics and had learned about them primarily from advertisements and the internet. Th ey viewed probi-otics as an appealing alternative to pharmaceutical drugs and understood them as a more natural, low risk, though possibly less eff ective, therapeutic option. Although patients expressed interest in using probiotics, many were hesitant to use them without consulting their gastroenterologists. Patients were skeptical about information available from popular media and expressed a desire for more detailed scientifi c information, particularly about safety and effi cacy, from their physicians. Th ey also voiced concerns about how probiotics would impact their current treatments and wanted guidance from their gastroenterologists on how probiotics may fi t into their treatment regimen. Despite concerns about their use, patients were reluctant to abandon pharmaceutical drugs due to modest expectations of benefi ts from probiotics. Patients weighed the risks and benefi ts of probiotics as they would for any therapy they would consider using to treat their digestive disease. Disease severity and satisfaction with current treatments were key factors patients considered when thinking about using probiotics.Conclusion: Patients with chronic digestive diseases are interested in using probiotics but have many unanswered questions about them. Our findings suggest that patients will likely turn to their gastroenterologists for comprehensive information about probiotics and for guidance on how they may fit within their treatment plan. Gastroenterologists should
be prepared to educate their patients on probiotics and ensure that they understand the potential benefits and risks in order to facilitate informed decision-making.
1196
Th e Social and Economic Impact on Crohn’s Patients Receiving Certolizumab (SAVE Trial)Charles Randall, MD,1 Christian Herrera, MD,3 Carlo Taboada, MD,1 Christopher Fincke, MD,2 Russell Havranek, MD,2 Franz Zurita, MD,2 David Stump, MD,2 Gary Gossen, MD,1 Daniela Vidaurri, MD,3 Nicholas Martinez, MD3. 1. Research, Gastroenterology Research of San Antonio, San Antonio, TX; 2. Gastroenterology Clinic of San Antonio, San Antonio, TX; 3. University of Texas Health Science Center at San Antonio, San Antonio, TX.
Purpose: Most research in Crohn’s Disease focuses on clinical response and remission. As scrutiny of health-care costs rises it becomes important to evaluate social and economic benefi ts of a given treatment. Certolizumab has been commercially available for 24 months at the time of this writing. In our registry of Crohn’s patients we have begun to analyze outcome data for psychosocial issues. Th is paper presents preliminary results of an ongoing study.Methods: 30 patients receiving Certolizumab within the last 24 months were followed both prospectively and retrospectively. Data was recorded on hospi-talizations, surgeries, insurance acceptance, absence from work or school and sense of well being. Quality of life (QOL) was determined using the simple 5 point scale which evaluates fatigue, energy, physical limitations, stress and social situations. Th e maximum score is 25 (worst) and 0 (best). Comparisons were made before and during therapy. Th e primary objectives were positive economic benefi t of treatment and improved QOL.Results: 26 patients were available for follow-up. Th ere were no admissions for disease exacerbation or any surgeries. No insurance denials were encountered. 2 patients missed work but these absences occurred during induction. Th e mean pretreatment QOL score was 16.10 while the score during the mainte-nance phase declined to a mean of 8.3. Mean follow-up time was 12 months.Conclusion: 1. Th e primary objective of a positive economic impact was made with no hospitalizations, surgeries and limited absenteeism. 2. Th e other pri-mary objective of improved QOL was also seen with a drop in the QOL score from 16.10 to 8.3 during the course of treatments. 3. Both objectives were observed over a mean follow-up time of 12 months.Disclosure: Dr Randall - Consultant: UCB, Speakers Bureau.
1197
Effi cacy of MR Enterography for Evaluation of Known or Suspected Crohn’s DiseaseAdam Harris, MD, David Grand, MD, Vinay Kampalath, BA, Michael Beland, MD, William Chen, MD, Samir Shah, MD. Lifespan and Brown University, Providence, RI.
Purpose: To study the effi cacy of MR enterography (MRE) in evaluating Crohn’s disease using endoscopic/histologic evaluation within 90 days of the MRE as the gold standard.Methods: 850 consecutive patients with known or suspected Crohn’s disease underwent routine MRE without pharmacologic bowel paralysis. Of these, 310 patients also underwent endoscopy with biopsy(s) within 90 days. Th e sensitivity and specifi city of the MRE compared to endoscopy and pathology were retrospectively evaluated.Results: In 310 consecutive patients, the overall sensitivity and specifi city of MRE (using endoscopy as a gold standard) were 84% and 76% respectively (kappa=0.58). Th e results improved as the time between the MRE and endos-copy decreased. In 162 patients who underwent endoscopy within 30 days of MRE, the sensitivity remained 84% but the specifi city increased to 82% (kappa= 0.65). Th e specifi city further improved if the MRE was compared to a positive result in either the endoscopy or pathology increasing to 89% with a positive predictive value of 88% and a negative predictive value of 84% (kappa=0.71).Conclusion: MRE highly correlates with endoscopic and histologic asses-ment for evaluation of known or suspected Crohn’s disease noninvasively and

The American Journal of GASTROENTEROLOGY VOLUME 105 | SUPPLEMENT 1 | OCTOBER 2010 www.amjgastro.com
AbstractsS438
without the exposure to ionizing radiation of CT enterography. Pharmacologic bowel paralysis is not necessary for reliable diagnosis.
1198
MR Detection of Colonic Crohn’s Disease Without Use of Colon Prepara-tion or Anti-Peristaltic AgentsVinay Kampalath, BA, Adam Harris, MD, David Grand, MD, Michael Beland, MD, Samir Shah, MD. Lifespan and Brown University, Providence, RI.
Purpose: Published studies of MR enterography (MRE) have focused on the detection of small bowel disease. We report the effi cacy of MRE for the detec-tion of colonic Crohn’s disease without colon preparation or anti-peristaltic agent.Methods: 850 consecutive patients with known or suspected Crohn’s disease underwent routine MRE without the use of pharmacologic bowel paraly-sis or colonic preparation. Of these, 310 patients also underwent endoscopy with biopsy(s). Th e sensitivity and specifi city of the MRE for the detection of colonic Crohn’s disease was retrospectively evaluated.Results: Of the 310 patients in our cohort, 143 patients underwent endoscopy and biopsy(s) within 30 days of the MRE. Th e sensitivity and specifi city of MRE for the detection of colonic Crohn’s disease (using pathology as a gold standard) was 67% and 97% respectively (kappa=0.69). Th e positive predictive value was 88% and the negative predictive value was 91%.Conclusion: MRE detects colonic involvement of Crohn’s disease with a high specifi city and negative predictive value. Colonic preparation and anti-peri-staltic agents are not required for accurate diagnosis. MRE is currently not as sensitive in detecting colonic as it is in detecting small bowel Crohn’s disease.
1199
Impact of Age at Diagnosis and Crohn’s Disease PhenotypeSandra Quezada, MD, MS, Raymond Cross, MD, MS. Gastroenterology, University of Maryland Medical Center, Baltimore, MD.
Purpose: Crohn’s disease (CD) primarily aff ects young adults; however 15% of patients are diagnosed at an advanced age. Previous studies report that older patients are less likely to have penetrating phenotypes and more likely to have colonic disease location. However, no studies have classifi ed patients using the Montreal classifi cation system. Our objective was to compare CD phenotype by age of diagnosis in a tertiary referral cohort.Methods: Demographics, disease behavior, disease location, and extraintes-tinal manifestations were compared by the following age of diagnosis groups: <17 years, 17-40 years, 41-59 years, and ≥60 years.Results: 467 patients evaluated between July 1, 2004 and April 19, 2010 were included. Mean age of diagnosis was 27.8±14.9 years. 17% (n=78) were diag-nosed under age 17, 67% (n=312) were diagnosed between 17 and 40 years of age, 11% (n=55) were diagnosed between age 41 and 59, and 5% (n=22) were diagnosed at age ≥ 60. Gender, race, smoking history, and EIM did not diff er by age at diagnosis. 33%, 30%, 13%, and 14% of patients diagnosed at <17, 17-40, 41-59, and ≥60 years of age had a family history of IBD respectively (p<0.015). Mean disease duration from time of diagnosis was 22.4, 13.0, 8.5, and 5.5 years in patients diagnosed at <17, 17-40, 41-59, and ≥60 years respec-tively (p<0.001). As age of diagnosis increased, the proportion of patients with isolated colonic disease increased (see Table). Further, as age of diagnosis increased the proportion of patients with nonstricturing/nonpenetrating phe-notype increased (see Table). Aft er adjustment for disease duration (<10 years
vs. ≥10 years), patients diagnosed at 60 or older were 64% less likely to develop complicated disease (stricturing or penetrating disease) compared to younger cohorts (OR 0.39, 95% CI 0.25, 0.60).Conclusion: Patients diagnosed with CD over age 60 are more likely to have isolated colonic disease and less likely to have complicated disease behavior than patients diagnosed at a younger age. Our results suggest that older patients have distinct clinical phenotypes. If our results are confi rmed, providers will be able to individualize treatments according to age at diagnosis.
1200
Mucosal Healing in Patients with Ulcerative Colitis Associates with a Reduced Colectomy Risk, High Incidence of Symptomatic Remission, and Corticosteroid-Free StateWilliam Sandborn, MD,1 Paul Rutgeerts, MD, PhD,2 Walter Reinisch, MD,3 Dirk Esser, PhD,4 Y. Wang, PhD,5 Yinghua Lang, PhD,6 Colleen Marano, PhD,6 Richard Strauss, MD,6 Bjorn Oddens, MD,5 Brian Feagan, MD,7 Stephen Hanauer, MD,8 Gary Lichtenstein, MD,9 Daniel Present, MD,10 Bruce Sands, MD,11 Jean-Frédéric Colombel, MD12. 1. Mayo Clinic, Rochester, MN; 2. U Hospital Gasthuisberg, Leuven, Belgium; 3. U Hosp Vienna, Wien, Austria; 4. Centocor BV, Leiden, Netherlands; 5. Schering Corp, Kenilworth, NJ; 6. Centocor R&D, Malvern, PA; 7. Robarts Research Institute, London, ON, Canada; 8. U of Chicago, Chicago, IL; 9. U of Pennsylvania, Philadelphia, PA; 10. Mount Sinai Medical Center, New York, NY; 11. Mass General Hosp/Harvard Med School, Boston, MA; 12. CHRU Lille, Lille, France.
Purpose: To assess whether there is an association between degree of mucosal healing (MH) at wk 8 and clinical outcomes in patients with moderate-to-severe ulcerative colitis (UC) in ACT1 and ACT2.Methods: MH at wk 8 was assessed using the Mayo endoscopic subscore clas-sifi cation (0-normal, 1-mild, 2-moderate, 3-severe disease). A post-hoc log-rank test was used to examine the distribution of time to colectomy through wk 54 across the 4 endoscopy subgroups for IFX and PBO-treated patients, respectively (ACT 1 and ACT 2 combined). Th e proportion of patients with symptomatic remission (stool frequency score of 0/1 and a rectal bleeding score of 0) and corticosteroid-free status were assessed at wk 30 (ACT 1 and ACT 2 combined) and at wk 54 (ACT 1).Results: IFX patients who had endoscopy subscores of 0 or 1 at wk 8 were less likely to progress to colectomy through wk 54 (Table; p=0.0004). Small event numbers in PBO patients precluded a clear conclusion for PBO. IFX patients with lower endoscopy scores at wk 8 were more likely to be in symptomatic remission at wk 30 (71% (0); 51% (1); 23% (2); 10% (3), p<0.0001). Among those receiving corticosteroids prior to starting IFX-treatment, patients were more likely to be corticosteroid-free at wk 30 as their degree of MH improved at wk 8 (62% (0); 46% (1); 20% (2); 10% (3), p<0.0001). Similar trends in symptomatic remission and the attainment of a corticosteroid-free status were observed at wk 54 for IFX patients in ACT 1. Although a lower proportion of PBO patients achieved symptomatic remission or became corticosteroid-free vs. IFX patients, similar trends of improved outcomes at wks 30 and 54 were associated with the degree of MH attained by PBO patients at wk 8.Conclusion: Patients with moderate-to-severe UC, who achieve early mucosal healing, are less likely to go on to colectomy through 1 year of follow-up. Improved endoscopic outcomes were associated with a greater likelihood of achieving symptomatic remission and eliminating corticosteroids.Disclosure: Dr Sandborn-Investigator, Centocor R&D, Inc Dr Rutgeerts-Investi-gator, Centocor R&D, Inc Dr Reinisch-Investigator, Centocor R&D, Inc Dr Esser-Employee-Centocor BV Drs Wang and Oddens-Employees-Schering Corp Drs Lang, Marano, Strauss-Employees-Centocor R&D, Inc Dr Feagan-Investigator, Centocor
[1199] Crohn’s disease phenotype by age of diagnosis
Variable < 17 years 17 – 40 years 41 – 59 years > =60 years P value*
Location L1 L2 L3 L4 15 (20) 15 (20) 44 (59) 1 (1) 111 (38) 53 (18) 116 (40) 9 (3) 19 (37) 20 (38) 13 (25) 0 (0) 4 (20) 11 (55) 4 (20) 1 (5) < 0.0001
Behavior B1 B2 B3 20 (26) 24 (31) 34 (43) 105 (34) 96 (31) 111 (35) 31 (56) 18 (33) 6 (11) 14 (64) 3 (14) 5 (23) 0.0001
Perianal disease (Yes) 35 (45) 101 (32) 7 (13) 6 (22) 0.0014
*Pearson chi-square test.

© 2010 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY
Abstracts S439
R&D, Inc Dr Hanauer-Investigator, Centocor R&D, Inc Dr Lichtenstein-Investigator, Centocor R&D, Inc Dr Present-Investigator, Centocor R&D, Inc Dr Sands-Investiga-tor, Centocor R&D, Inc Dr Colombel-Investigator, Centocor R&D, Inc.Th is research was supported by an industry grant from Centocor R&D, Inc.
1201
Top-Down versus Step-Up Th erapy in Pediatric Patients with New Onset Crohn’s DiseaseAli Minhas, MBBS, Orooj Khan, MBBS, Maya Srivastava, MD, PhD. Medicine, State University of New York at Buff alo, Williamsville, NY.
Purpose: Top-down (TD) therapy with tumor necrosis factor inhibitors early in disease course of adult Crohn’s disease (CD) has been shown to result in decreased steroid dependence, hospitalization, complications, and disease activity compared to conventional step-up (SU) therapy. However, data regard-ing the effi cacy of the TD approach in children are limited, due to concerns regarding potential side eff ects including lymphoma, and diffi culty with insur-ance approval. Th e goal of this study was to begin to compare the outcome of TD versus SU therapy in our pediatric patients with new onset CD.Methods: We conducted a retrospective analysis of patients with CD seen in our practice using diagnostic codes 555.0,555.1, 555.2. Sixteen pediatric patients with new diagnosis CD identifi ed as diagnosed within the last 1 year and with Crohn’s
disease activity index (CDAI) greater than 200 were included for study. Eleven had been treated with TD, 5 with SU therapy. Mean ages (SU 14.6years+/-2.4 and TD 14.27years+/-3.2, p=0.8435); gender (SU 63% male; TD 61% male), and CDAI were similar (SU 271+/-86 and TD 273+/-71, p=0.9743) in the two groups. Pri-mary endpoints were remission at 4 and 52 weeks (CDAI less than 150), secondary endpoints were disease complication rate, hospitalization, and surgery. Two-tailed Fisher’s exact test and unpaired t test were used to compare the two groups.Results: In the TD group 72% of patients achieved remission in 4 weeks as did 60% of the SU group (p=1.000). Mean CDAI was 116+/-42 for the TD patients, 173+/-68 for the SU patients at 4 weeks (p=0.0585). 100% of patients in the SU group versus 45% in the TD group developed complications of CD (p=0.0934). Also, 80% of patients in the SU group were hospitalized, only 45% in the TD group (p=0.3077). Surgical rates were 60% in the SU group, and 9% in the TD patients (p=0.0632). At 52 weeks CDAI was 82.9+/-29.3 for TD group, and 95.6+/-41.8 for the SU group (p=0.5274). One patient in the SU group was excluded from 52 week CDAI as he had undergone permanent colectomy/ileostomy and thus CDAI could not be calculated.Conclusion: Although not statistically signifi cant, most likely due to small sample size, there is a clear trend suggesting the use of biologic agents early in disease course may reduce the risk of hospitalization, surgery and disease complications in children within the fi rst year of their diagnosis of CD. Larger studies comparing safety and effi cacy of TD versus SU treatment should be conducted in the pediatric age group.Disclosure: Dr Srivastava - Consultant Centocor Speaker’s bureau.
1202
Th e Infl uence of Anti-TNF Th erapy on the Course of Chronic Hepatitis C Virus (HCV) Infection in Patients with Infl ammatory Bowel Disease (IBD)Ming Lin, MD,1 Wojciech Blonski, MD, PhD,2 Colleen Brensinger, MS,2 Anna Buchner, MD, PhD,2 K.Rajender Reddy, MD,2 Gary Lichtenstein, MD2. 1. Department of Medicine, Pennsylvania Hospital, Philadelphia, PA; 2. Division of Gastroenterology, University of Pennsylvania, Philadelphia, PA.
Purpose: Anti-TNF therapy has been widely used for IBD management. Th e potential for immunosuppressive therapy to exacerbate a pt with underlying
[1200] Table. Kaplan-Meier estimates of time to colectomy
Wk 8 endoscopy score Number of colectomies
Colectomy-free prob at wk 54 ( % )
P -value*(log rank)
Pts randomized to IFX ( n =466**)
0 ( n =120) 6 95 0.0004
1 ( n =175) 8 95
2 ( n =114) 14 87
3 ( n =57) 10 80
* P -value indicates the difference in distributions of time to colectomy among the 4 endoscopy score subgroups **patients who had a colectomy or discontinued before wk 8 were not included.
[1202] Patients ’ demographics and disease characteristics
Patient #
Gender
(M / F)
Age
(yrs)
IBD subtype
(CD or UC) Duration of IBD (yrs) Duration of HCV (yrs)
Duration of infl ixi-
mab therapy (yrs) HCV genotype Liver histology (stage)
1 F 64 CD 46 1 4 Unable to genotype
(low viral load)
1
2 M 56 UC 5 10 3 N / A 2
3 F 72 UC 7 1 1 1 Fibrosure score 0.2
(minimal fi brosis)
4 M 50 UC 9 8 3 1a 4
5 F 85 UC 64 50 0.5 N / A N / A
[1202] Hepatic biochemical tests, viral load and IBD disease activity score before (1) and after (2) anti-TNF therapy
Patient # AST 1(u / L) AST 2 (u / L) ALT 1 (u / L) ALT 2 (u / L) ALP 1 (u / L) ALP 2 (u / L)
Viral Load 1
(IU / ml)
Viral Load 2
(IU / ml)
IBD Disease activity
score 1 (points)
IBD disease activity
score 2 (points)
1 24 24 23 14 56 61 891 N / A 8 5
2 28 18 39 16 129 145 2,172,660 2,400,000 9 2
3 35 33 34 22 86 73 2,786,118 2,128,414 5 1
4 49 109 35 51 43 72 11,000,000 6,838,000 7 4
5 100 46 145 41 125 114 10,900,000 N / A 9 8

The American Journal of GASTROENTEROLOGY VOLUME 105 | SUPPLEMENT 1 | OCTOBER 2010 www.amjgastro.com
AbstractsS440
chronic HCV has been a major concern. Th e literature on the outcome of anti-TNF Rx in pts with IBD and chronic HCV infection is limited to 3 case reports (4 total pts). Th e aim was to critically analyze the impact of anti-TNF Rx on the course of chronic HCV infection in pts with both IBD and HCV infection.Methods: A retrospective review of the electronic database in our health sys-tem was done to identify pts with a diagnosis of both IBD and HCV infection. Data was assessed on demographics, duration of IBD and HCV infection, HCV RNA levels, HCV genotype, liver histology, hepatic biochemical tests (HBT) and IBD disease activity index pre and post anti-TNF Rx (Harvey-Bradshaw Index for CD and partial Mayo Score for UC).Results: 4274 IBD pts and 3523 HCV pts were identifi ed from 10/1998-05/2010. 37 pts had concurrent HCV infection, of which, 14 pts were excluded due to incomplete records. 23 pts with HCV were eligible (61% CD; 39% UC), but only 5 pts (22%) received anti-TNF Rx (infl iximab). 80% of HCV infec-tions were blood transfusion related, and 2 of 5 pts received peginterferon and ribavirin (both non-responders to HCV therapy). Th e mean age was 65(±14) yrs, and the mean duration of IBD and HCV were 26(±27) and 14(±21) yrs, respectively. Th e mean duration of anti-TNF Rx was 27(±18) mos. Th e mean AST, ALT and ALP pre anti-TNF Rx were 47(±31)u/L, 55(±51)u/L, 88(±39)u/L compared to post Rx of 46(±36)u/L, 29(± 16)u/L, 93(± 35)u/L (p=0.95; p=0.26; p=0.55). Th e mean viral load was 5,320,000(± 4,929,000) IU/mL pre anti-TNF Rx and 3,789,000(± 2,644,000) IU/mL post Rx (p=0.37). Th e mean partial Mayo Score was 7.5(± 1.9) vs. 3.8(± 3.1) points pre and post anti-TNF Rx, respectively (p=0.06). Overall, 3 of 5 pts had a clinical remission, 1 had a clinical response and the other had no response to infl iximab. When compared to baseline, 1 pt had HBT improvement, 3 pts remained stable and 1 pt had HBT elevation, which is likely due to progressive liver disease in view of HIV co-infection.Conclusion: Th is represents the fi rst critical analysis assessing the impact of anti-TNF Rx on the course of chronic HCV in IBD pts. Concurrent HCV infec-tion in IBD pts is uncommon. Treatment of IBD with infl iximab in HCV pts did not result in hepatic biochemical tests fl ares while there was an improve-ment in the IBD disease activity score. However, our results should be inter-preted with caution due to the small number of pts studied. Future prospective studies on large number of pts are warranted to further evaluate the impact of anti-TNF Rx on the hepatic biochemical tests in pts with IBD and concomitant chronic HCV infection.Disclosure: Gary R. Lichtenstein, Md Potential Confl ict of Interest Declara-tion Abbott Corporation Consultant Alaven Consultant Bristol-Myers Squibb Research Centocor Orthobiotech Consultant, Research Elan Consultant Ferring Consultant, Research Millenium Pharmaceuticals Consultant Proctor and Gam-ble Consultant, Research Prometheus Laboratories, Inc. Consultant, Research Salix Pharmaceuticals Consultant, Research Schering-Plough Corporation Con-sultant Shire Pharmaceuticals Consultant, Research UCB Consultant, Research Warner Chilcotte Consultant, Research Wyeth Consultant.
1203
A Multicenter, Randomized Study to Evaluate the Effi cacy and Safety of Mesalamine Suppositories 1 g at Bedtime and 500 mg Twice Daily in Patients with Active Mild-to-Moderate Ulcerative ProctitisMark Lamet, MD, FACG. Th e Center for Gastrointestinal Disorders, Hollywood, FL.
Purpose: To evaluate the eff ects of a mesalamine 1-g suppository administered QHS compared with a 500 mg suppository administered BID on measures of UP disease activity (eg, disease extension, mucosal appearance), remission, onset of therapeutic response, safety and compliance in 97 patients with UP.Methods: 6-week, multicenter, parallel-group study was conducted and previ-ously effi cacy variable and individual published (Lamet et al 2005) with Disease Activity Index (DAI) at week 6 as the primary components of DAI at week 6 (ie, stool frequency, rectal bleeding, mucosal appearance, global assessment) as sec-ondary variables. Other outcome measures, not initially reported, were remission rates (DAI<3 units at weeks 3 and 6), disease extension and complete response to treatment (DAI=0; evaluated by post-hoc, exploratory analyses) and safety.Results: DAI values aft er 6 weeks of treatment with mesalamine suppositories were reduced (± standard deviation) from 6.6 ± 1.5 to 1.6 ± 2.3 in the 500 mg BID group, and from 6.1 ± 1.5 to 1.3 ± 2.2 in the 1-g QHS group. Mucosal appear-ance signifi cantly improved from 1.8 ± 0.5 to 0.8 ± 0.7 aft er 3 weeks and to 0.5 ± 0.7 aft er 6 weeks of treatment in the 500 mg BID group (P≤0.0062 for both) and
from 1.7 ± 0.5 to 0.9 ± 0.5 aft er 3 weeks and to 0.4 ± 0.6 aft er 6 weeks of treatment in the 1-g QHS group (P≤0.0001 for both). Remission rates were comparable (78.3% [500 mg BID] vs. 86.1% [1 g QHS]), onset of response generally occurred within 3 weeks of treatment initiation, and a decrease in disease extension length was reported (>70%) aft er 6 weeks of treatment in both groups. Aft er 6 weeks of 500 mg BID therapy, 22 patients (41.5%) and 29 patients (54.7%) reported complete response and resolved disease extension, respectively, compared with 15 patients (34%) and 25 patients (56.8%), respectively, in the 1-g QHS group. Mesalamine was well tolerated, and compliance in both groups was >96%.Conclusion: Mesalamine 500 mg BID and 1 g QHS suppositories are safe and eff ective treatments for patients with UP. Most patients reported onset of response within 3 weeks and UP remission and reduced disease extension aft er 6 weeks of treatment. Th ese additional fi ndings attest to the healing eff ect of mesalamine sup-positories on the mucosa, corroborating symptom relief. Th e validity of a more convenient timing of suppository administration (ie, QHS) was also confi rmed. Disclosure: Research was funded in part by Axcan Pharma Inc, QC, Canada.Th is research was supported by an industry grant from Axcan Pharma.
1204
Predictors of Early and Sustained Response to Infl iximab in Patients with Ulcerative ColitisEmily Rostholder, MD, Awais Ahmed, MBBS, Alan Moss, MD. Beth Israel Deaconess Medical Center, Boston, MA.
Purpose: Infl iximab (IFX) is effi cacious in treating ulcerative colitis (UC), but also has a number of serious side eff ects. Whether IFX should be used alone, or in combination with other immunomodulators in UC is unknown. Our aim was to determine clinical variables associated with response to IFX in patients with UC.Methods: Retrospective analysis of demographic, clinical and biochemical variables associated with response to IFX in patients with UC over 12 months. Chi-square test or Fisher’s exact test was used to analyze dichotomous vari-ables, and Wilcoxon test for continuous variables. A multivariate model was constructed where appropriate.Results: 62 patients had complete data for inclusion in the analysis. In total, 77% of patients treated with IFX had a primary response, 40% were in remis-sion at 12 months, and 35% of patients required a colectomy during follow-up. In a univariate analysis, age, duration of disease, and prior azathioprine/6-MP use, were signifi cantly associated with primary response. Concomitant aza-thioprine/6-MP use was not associated with a higher rate of remission, or ster-oid-free remission, at 12 months. Patients with UC for >2 years had a reduced risk of progression to colectomy (OR 0.2, 95% CI 0.1, 0.6). In those patients who were steroid-refractory (N=31), 65% had a primary response, 32% were in remission at 12 months, and 42% had a subsequent colectomy. Both age and disease duration, but not concomitant azathioprine/6MP use, were signifi -cantly associated with primary response to IFX in this group.Conclusion: Th e response and remission rates seen in clinical practice are sim-ilar to published rates from clinical trials. Patients with UC for >2 years had better clinical outcomes than recently-diagnosed patients with this condition. Th e use of concomitant immunomodulators was not associated with improved long-term clinical outcomes in this cohort.
1205
Prevalence and Characteristics of Patients with IBD Who Develop Serrated AdenomasWojciech Blonski, MD, PhD,1 Kimberly Dumoff , MD,1 Irene Sonu, MD,1 Ming Valerie Lin, MD,2 Gary Lichtenstein, MD1. 1. University of Pennsylvania, Philadelphia, PA; 2. Pennsylvania Hospital, Philadelphia, PA.
Purpose: Recent evidence suggests that serrated adenomas occur in pts with infl ammatory bowel disease (IBD). Th us far there has only been evaluation of colectomy specimens. One study demonstrated that serrated adenomas juxtapose colorectal carcinoma in 29% of IBD pts and 3% of controls (Rubio CA. Anticancer Res. 2000). Another study identifi ed a characteristic molecu-lar profi le of serrated polyps detected in 36 IBD pts and suggested that these

© 2010 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY
Abstracts S441
lesions might be involved in the development of colorectal cancer in pts with IBD (Bossard C. Oncol Rep. 2007). Since data on serrated adenomas in pts with IBD are evolving it is important to characterize the cohort of patients who develop these lesions. Th e aim of this study was to assess the characteris-tics and the prevalence of serrated adenomas in a cohort of pts with IBD in a surveillance program at our institution.Methods: A retrospective review of our electronic patient pathology database was performed to identify pts with serrated adenomas. Th e records of pts with IBD in our inpatient and outpatient electronic medical record system were cross referenced to identify which pts had both IBD and serrated adenomas. Our electronic pathology database was searched to identify the number of pts with IBD whose colonic histological specimens were obtained during surveil-lance colonoscopy in our institution.Results: Overall there were 213 pts with serrated adenomas and 258 IBD pts with colon biopsies and colectomies identifi ed in our pathology database from May 2008 to November 2009. Th ere were 4 (1.55%) IBD pts identifi ed who had detected serrated adenomas. Th e results are presented in the Table. Th ere were 3 pts with Crohn’s disease (CD) presenting with sessile serrated adenomas and 1 patient with ulcerative colitis (UC) presenting with polypoid serrated lesions (one DALM lesion with low grade dysplasia in the cecum and a nondysplastic polypoid lesion in the rectum).Conclusion: Th is study establishes that serrated adenomas occur in pts with IBD who undergo surveillance colonoscopy. Th ese lesions have occurred in pts with longstanding disease. Given the precancerous potential of these lesions it is important to recognize that these lesions do occur in IBD pts. Future studies are needed to defi ne the true neoplastic potential of these lesions and the clini-cal course of IBD in pts with these lesions.
1206
Treatment Adjustment Indicators in Patients with Crohn’s Disease on Inf-liximab Maintenance Th erapy: Analysis of Long-Term Claims DataEdward Loft us Jr, MD,1 Mei Yang, PhD,2 David Laitinen, MPH,2 Shivaji Manthena, -,2 Jingdong Chao, PhD,2 Parvez Mulani, PhD2. 1. Mayo Clinic, Rochester, MN; 2. Abbott Laboratories, Abbott Park, IL.
Purpose: Long-term data on infl iximab persistency are limited for patients with Crohn’s disease (CD) on infl iximab maintenance therapy, and there are few studies on predictors for treatment adjustment. We examined occurrence of events that potentially indicate treatment adjustment using data from a large health care claims database and explored the predictors of treatment adjust-ment.Methods: Th e I3 database (United Health) contains patient-level information from April 1, 2000 to March 31, 2009. Patients included in the analysis met the selection criteria of ≥2 diagnostic codes for CD; 6 months of continuous eligibility prior to and 12 months following the date of fi rst infl iximab infusion; and an initial response to infl iximab, defi ned as no occurrence of any of the following events during the fi rst 4 infusions: dose escalation, CD-related emer-gency department (ED) visit or hospitalization, CD-related surgery, new fi s-tula, or initiation of a new biologic therapy. Patients were also required to have received infl iximab maintenance therapy, defi ned as a minimum of 8 infusions. A potential treatment adjustment event (PTAE) was defi ned as the occurrence
of dose escalation, CD-related ED visit or hospitalization, CD-related surgery, new fi stula, or initiation of a new biologic therapy. Th e cumulative probabilities of PTAEs were estimated using Kaplan-Meier methods. Predictors for PTAEs were analyzed with proportional-hazard models.Results: Th e sample included 388 patients with CD who met the criteria for an initial response to infl iximab maintenance therapy. Kaplan-Meier estimates for both 2-year and 3-year PTAE rates are provided in the table. Overall, 78% of patients experienced a PTAE to infl iximab by 3 years. CD-related hospital or ED visits and dose escalation were the most common types of PTAE. Corti-costeroid use was a predictor for overall PTAE, CD-related surgery, CD-related ED or inpatient visit and new biologic use; Charlson comorbidity index score was a predictor for CD-related ED or inpatient visits.Conclusion: Using long-term observational data from a large health care claims database, we found that most patients with CD in the real-world setting who initially responded to infl iximab required subsequent treatment adjust-ment, and patients with prior corticosteroid use were more likely to require this adjustment.Disclosure: EV Loft us Jr: Consulting Fees: Abbott, Elan, PDL BioPharma, Procter & Gamble, Salix, UCB. Grant/Research Support: Abbott, ActoGeniX, Otsuka America, PDL BioPharma, Procter & Gamble, Schering-Plough, UCB. M Yang: Employee/Stock: Abbott. D Laitinen: Employee/Stock: Abbott. S Manthena: Employee: Abbott. J Chao: Employee/Stock: Abbott. PM Mulani: Employee/Stock: Abbott.
1207
Adalimumab Induction Th erapy Improves Health-Related Quality of Life in Patients with Moderately to Severely Active Ulcerative ColitisWalter Reinisch, MD,1 William Sandborn, MD,2 Roopal Th akkar, MD,3 Andreas Lazar, MD,3 Bidan Huang, PhD,3 Parvez Mulani, PhD,3 Jingdong Chao, PhD3. 1. Medical University of Vienna, Vienna, Austria; 2. Mayo Clinic, Rochester, MN; 3. Abbott Laboratories, Abbott Park, IL.
Purpose: To investigate the eff ects of adalimumab induction therapy on health-related quality of life (HRQOL) in patients with ulcerative colitis (UC).Methods: Anti-tumor necrosis factor (anti-TNF)-naïve patients with mod-erately to severely active UC (Mayo score ≥6 points and endoscopic subscore ≥2 points) despite treatment with corticosteroids and/or immunosuppressants
[1205]
Case number Age [yrs] Gender IBD Type Duration of IBD [yrs]
Duration of IBD at the time of detection of
serrated adenoma [yrs] Disease Extent Location and Size of Serrated Adenoma Follow-up
1 34 F CD 9 8 Rectosigmoid Hepatic fl exure (1.5 cm)
Ileocecectomy at 18 months, no serrated adenomas
2 48 M CD 11 10 Left Sided Rectum (0.7 cm) 24 months
3 50 F CD 20 20 Pancolitis and terminal ileum
Ascending colon (2.0 cm)
Right colectomy after 15 months-ser-rated adenoma in ascending colon (1.5 cm)
4 36 M UC 21 21 Left Sided -Rectum (2.0 cm) -Cecum (1.0 cm)
Proctocolectomy at 6 months
[1206]
Year 2 ( % ) Year 3 ( % )
Overall PTAE 70 78
Dose escalation 41 48
CD-related ED or inpatient visit 33 43
CD-related surgery 19 26
New fi stula 6 9
Initiation of new biologic therapy 8 14

The American Journal of GASTROENTEROLOGY VOLUME 105 | SUPPLEMENT 1 | OCTOBER 2010 www.amjgastro.com
AbstractsS442
were enrolled in an 8-week, randomized, placebo-controlled induction trial. Patients (N=186) were randomized 1:1 to subcutaneous adalimumab (160 mg at Week 0, 80 mg at Week 2, and 40 mg at Weeks 4 and 6) or placebo. Patients being treated with corticosteroids and/or immunosuppressants remained on stable dosages. Subsequent to approval of the Crohn’s disease indication in Europe, in which the recommended induction dose was 80/40 mg (or 160/80 mg if a more rapid response was needed), the protocol was amended to prespecify enrollment of 390 additional patients who were ran-domized 1:1:1 to the original adalimumab 160-/80-mg regimen; adalimu-mab 80 mg at Week 0 and 40 mg at Weeks 2, 4, and 6; or placebo. HRQOL was measured by the Infl ammatory Bowel Disease Questionnaire (IBDQ) and Mental and Physical Component Summary (MCS and PCS) scores of the Short Form 36 Health Survey (SF-36). Th e intention-to-treat population enrolled aft er the protocol amendment was analyzed. Changes from baseline were compared using 1-way ANCOVA with treatment as a factor and base-line value as a covariate.Results: Patients treated with the 160-/80-mg induction regimen had signifi -cant improvements in IBDQ and SF-36 PCS scores vs. placebo at Week 4 that were maintained at Week 8 (table). With the 80-/40-mg induction regimen, only SF-36 scores at Week 4 were signifi cantly better than placebo. SF-36 MCS scores were not signifi cantly improved in either adalimumab group.Conclusion: Anti-TNF-naive patients with moderate to severe UC who failed conventional therapy experienced signifi cant improvements in IBDQ and SF-36 PCS scores through Week 8 with adalimumab 160-/80-mg induction ther-apy vs. placebo. HRQOL improvements with the 80-/40-mg induction were inconsistent.Disclosure: W Reinisch: Consultant/Advisory Committee: Abbott, Aesca, Centocor, Genentech, Novartis, Schering-Plough, UCB. Consultant/Speaker: Ferring. WJ Sandborn: Financial Support for Research: Abbott Laborato-ries, Bristol Meyers Squibb, CentocorOrthoBiotech, Genentech, Millennium Pharmaceuticals, Novartis, Pfi zer, Shire Pharmaceuticals, UCB Pharma, Warner Chilcott (previously Procter & Gamble).Lecture Fees: None. Consul-tancy: ActoGenix, Abbott Laboratories (fees paid to Mayo), AGI Th erapeutics, Albireo, Alfa Wassermann, AM-Pharma, Amgen, Anaphore, Astellas Pharma, Athersys, Atlantic Healthcare Limited, Axcan Pharma, BioBalance Corpora-tion, Celegene, Bristol Meyers Squibb (fees paid to Mayo), Celek Pharmaceu-ticals, Cellerix, CentocorOrthoBiotech (fees paid to Mayo), Chemocentryix, CoMentis, Cosmo Technologies, Cytokine Pharmasciences, Eagle Pharmaceu-ticals, Eisai Medical Research, Elan Pharmaceuticals (fees paid to Mayo), Eli Lilly, Enteromedics, Ferring Pharmaceuticals, Flexion Th erapeutics, Funx-ional Th erapeutics Limited, Genentech (fees paid to Mayo), Given Imaging, GlaxoSmithKline, KaloBios Pharmaceuticals, Merck Research Laboratories, Merck Serono, Novo Nordisk, Pfi zer (fees paid to Mayo), Procter & Gamble (fees paid to Mayo), Purgenesis Technologies, Regeneron Pharmaceuticals, Salient Pharmaceuticals, Salix Pharmaceuticals, Santarus, Schering Plough Corporation, Shire Pharmaceuticals (fees paid to Mayo), Sigmoid Pharma, Sitrtis Pharmaceuticals, SLA Pharma, Takeda (fees paid to Mayo), Tillotts Pharma, UCB Pharma (fees paid to Mayo), Vascular Biogenics, Viamet Pharmaceuticals, Wyeth. Shareholder: None. Directorships: None. Other: None. R Th akkar: Employee/Stock: Abbott. A Lazar: Employee/Stock: Abbott. B Huang: Employee/Stock: Abbott. PM Mulani: Employee/Stock: Abbott. J Chao: Employee/Stock: Abbott.
1208
Achievement of Early Deep Remission Is Associated with Lower Rates of Weekly Dosing for Adalimumab-Treated Patients with Crohn’s Disease: Data from EXTENDWilliam Sandborn, MD,1 Jean-Frédéric Colombel, MD,2 Kathleen Lomax, MD,3 Paul Pollack, MD,3 Roopal Th akkar, MD,3 Anne Camez, MD,4 Naijun Chen, MS,3 Mei Yang, PhD,3 Jingdong Chao, PhD,3 Parvez Mulani, PhD3. 1. Mayo Clinic, Rochester, MN; 2. Centre Hospitalier Universitaire de Lille, Lille, France; 3. Abbott Laboratories, Abbott Park, IL; 4. Abbott GmbH & Co. KG, Ludwigshafen, Germany.
Purpose: To explore the relationship between early deep remission and rates of dosage adjustment for patients with Crohn’s disease (CD).Methods: EXTEND was a study of the eff ects of adalimumab on mucosal healing in patients with moderate to severe ileocolonic CD (Crohn’s Disease Activity Index [CDAI] 220-450). Patients received open-label adalimumab 160-/80-mg induction therapy at Weeks 0/2 and were randomized at Week 4 to maintenance therapy with adalimumab 40 mg every other week (eow) or placebo through Week 52. From Week 8, patients with fl ares or nonresponse could receive open-label adalimumab 40 mg eow. Th e maintenance regimen could be adjusted to weekly open-label adalimumab for continued fl ares/non-response. Endoscopic assessments of mucosal disease activity were performed at baseline, Week 12 (or unscheduled visits Weeks 8-12 prior to switch to open-label), time of switch to open-label adalimumab (if aft er Week 12), and Week 52 (or early termination). Early deep remission was defi ned as mucosal healing (visually determined) plus clinical remission (CDAI <150) at Week 12. Rates of moving to open-label eow and weekly therapy through Week 52 were compared between patients randomized to blinded adalimumab maintenance therapy who achieved Week-12 deep remission and those who did not.Results: Sixty-four patients were randomized to adalimumab maintenance therapy at Week 4. Adalimumab-treated patients who achieved deep remission by Week 12 had signifi cantly lower rates of dosage adjustment compared with patients not achieving early deep remission (table). No patients achieving early deep remission moved to weekly therapy.Conclusion: Deep remission, defi ned as complete mucosal healing plus clini-cal remission, may be an important treatment goal in CD. Patients in EXTEND who achieved deep remission by Week 12 were less likely than those who did not achieve deep remission to move to open-label eow dosing and subse-quently receive weekly therapy.Disclosure: WJ Sandborn: Consultant and/or Advisory Board: Abbott (fees paid to employer, Mayo Clinic), ActoGeniX, AGI Th erapeutics, Alba Th erapeutics, Albireo, AM-Pharma, Amgen, Ardea Biosciences, Aspreva, Astellas, Athersys, Atlantic Healthcare, Axcan, BioBalance, Bristol-Myers Squibb, Celegene, Celek, Cellerix, Centocor Ortho Biotech (fees paid to employer, Mayo Clinic), Cerimon, Chemocentryx, CombinatoRx, CoMentis, Cosmo Technologies, Cytokine Phar-masciences, Eagle, Eisai Medical Research, Elan, Enteromedics, Enzo Th erapeu-tics, Ferring, Flexion Th erapeutics, Funxional Th erapeutics, Genentech, Genzyme, Given Imaging, GlaxoSmithKline, Human Genome Sciences, Hutchison Medi-pharma, Ironwood, KaloBios, Merck Research Laboratories, MerckSerono, Mil-lennium Pharmaceuticals, Nisshin Kyorin, Novo Nordisk, Ocera Th erapeutics, Pfi zer, Procter & Gamble (fees paid to employer, Mayo Clinic), Prometheus, Pur-genesis Technologies, Salient, Salix, Santarus, Schering-Plough, Shire (fees paid to employer, Mayo Clinic), Sigmoid, Sirtris, SLA (UK), Teva, Tillotts, Tioga, UCB (fees paid to employer, Mayo Clinic), VBL, Ventech, Viamet, Wyeth. Research Support: Abbott, Bristol-Myers Squibb, Celltech, Centocor Ortho Biotech, Genen-tech, Millennium Pharmaceuticals, Novartis, Otsuka American, PDL Biopharma, Pfi zer, Procter & Gamble, Robarts Research Institute, Shire, UCB. J-F Colombel: Advisory Boards and/or Consulting: Abbott, ActoGeniX, Albireo Pharma, Astra Zeneca, Bayer Schering Pharma, Biogen Idec, Boehringer-Ingelheim, Bristol-Myers Squibb, Cellerix SL, Centocor, Chemocentryx Inc, Cosmo Technologies Ltd, Danone France, Elan Pharmaceuticals Inc, Genentech, Giuliani SPA, Given Imaging, GlaxoSmithKline, Merck and Co Inc, Millenium Pharmaceuticals Inc, NeoVacs SA, Ocerra Th erapeutics Inc (previously named Renovia Inc), Otsuka American Pharmaceuticals Inc, PDL Biopharma (previously named Protein Design Labs), Pfi zer Inc, Ribo Vacs Biotech, Schering-Plough Corporation, Shire Pharmaceuticals, Synta Pharmaceutical Corporation, Teva Pharmaceuticals and Petah Tikva, Th erakos, UCB Pharma (previously named Celltech Th erapeutics Ltd) and Wyeth Pharmaceuticals. Grant Support: Astra-Zeneca, Danisco, Dan-one, Dysphar, Ferring, Giuliani SPA, Lesaff re, Mapi Naxis, Ocerra Th erapeutics Inc (previously named Renovia Inc), Roquette, Schering-Plough Corporation,
[1207] Mean HRQOL scores over time (last observation carried forward)
Placebo Adalimumab
80 / 40 mg Adalimumab 160 / 80 mg
IBDQ
Baseline 125 126 132
Week 4 146 149 163 a
Week 8 152 153 168 b
SF-36 PCS
Baseline 40 41 42
Week 4 43 45 c 47 a
Week 8 44 46 49 a
a P < 0.001 vs. placebo. b P < 0.01 vs. placebo. c P < 0.05 vs. placebo.

© 2010 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY
Abstracts S443
UCB Pharma. Lecture Fees from speaking at continuing medical education events indirectly sponsored by a commercial sponsor: Abbott, Astra Zeneca, Cen-tocor, Elan Pharmaceuticals Inc, Falk Pharma, Ferring, Given Imaging, Otsuka American Pharmaceuticals Inc, PDL Biopharma, Schering-Plough Corporation, Shire Pharmaceuticals, UCB Pharma. Stock: Intestinal Biotech Development. PM Mulani: Employee/Stock: Abbott. KG Lomax: Employee/Stock: Abbott. PF Pollack: Employee/Stock: Abbott. R Th akkar: Employee/Stock: Abbott. A Camez: Employee/Stock: Abbott. N Chen: Employee/Stock: Abbott. M Yang: Employee/Stock: Abbott. J Chao: Employee/Stock: Abbott.
1209
Markov Model Projection of Remission Status for Early Vs. Delayed Step-Up Adalimumab Use in Moderate to Severe Crohn’s DiseaseEdward Loft us Jr, MD,1 Jingdong Chao, PhD,2 Mei Yang, PhD,2 Paul Pollack, MD,2 Zhiyi Li, -,3 Roopal Th akkar, MD,2 Parvez Mulani, PhD2. 1. Mayo Clinic, Rochester, MN; 2. Abbott Laboratories, Abbott Park, IL; 3. Analysis Group, Inc., Boston, MA.
Purpose: No randomized clinical trials have compared early treatment with anti-TNF agents and conventional delayed step-up treatment for patients with moderate to severe Crohn’s disease (CD). Th e goal of this study was to project remission rates in patients with moderate to severe CD with early vs. delayed step-up use of adalimumab (ADA) using a Markov model.Methods: Th e Markov model considered 4 states: remission, no remission but response, no remission and no response, and discontinuation. Each treatment cycle was 4 weeks. In the early treatment arm, patients with shorter disease duration (onset ≤2 years) would start ADA without prior use of immunomod-ulators (IMMs). In the step-up treatment arm, patients with longer disease duration (onset >2 years) would be treated with IMMs before switching to ADA owing to lack of response for 2 consecutive months. Transitional proba-bilities for patients on ADA were estimated using a multinomial logistic model using data from the CHARM trial,1 specifi cally the treatment arm of ADA 40 mg every other week. Transitional probabilities for patients on IMM treatment in the step-up treatment arm were derived from literature.2 One-year remis-sion rates with early and step-up use of ADA were projected with the estimated transitional probabilities.Results: Th e multinomial logistic model estimated that patients in the early ADA treatment arm had a higher probability of transitioning from moder-ate/severe disease to remission during the induction cycle (Weeks 0-4) than did patients in the step-up arm (64.6% vs. 34.0%, p=0.0018). Aft er achieving remission, early use patients had a higher probability of staying in remission than did step-up patients (91.8% vs. 78.2%, p<0.0001). Using the estimated transitional probabilities, the Markov model projected early use patients to have a remission rate of 58.3% at the end of 1 year, with cumulative time in remission of 0.69 years. For step-up patients, the model projected a remission rate of 40.7% at the end of 1 year, with cumulative time in remission of 0.39 years.Conclusion: Early initiation with ADA was projected in a 1-year Markov model to result in higher remission rates and longer time in remission than delayed step-up therapy. References: 1 Colombel JF, et al. Gastroenterology. 2007;132:52-65. 2 Silver-stein MD, et al. Gastroenterology. 1999;117:49-57.Disclosure: EV Loft us Jr: Consulting Fees: Abbott, Elan, PDL BioPharma, Procter & Gamble, Salix, UCB. Grant/Research Support: Abbott, ActoGeniX, Otsuka
America, PDL BioPharma, Procter & Gamble, Schering-Plough, UCB. J Chao: Employee/Stock: Abbott. M Yang: Employee/Stock: Abbott. PF Pollack: Employee: Abbott. Stock: Abbott, Human Genome Sciences, Johnson & Johnson (Janssen). Z Li: Employee: Analysis Group; under contract with Abbott. R Th akkar: Employee/Stock: Abbott. PM Mulani: Employee/Stock: Abbott.
1210
Racial Diff erences in Use of Biologics for Crohn’s Disease in a Medicaid PopulationMark Flasar, MD,1 Parvez Mulani, PhD,2 Mei Yang, PhD,2 Jingdong Chao, PhD,2 Mei Lu, -,3 Raymond Cross, MD, MS1. 1. University of Maryland School of Medicine, Baltimore, MD; 2. Abbott Laboratories, Abbott Park, IL; 3. Analysis Group, Inc., Boston, MA.
Purpose: Immunomodulator (IMM) and biologic (anti-TNF) use in African Americans (AA) with Crohn’s disease (CD) has been reported to be lower than in white patients (W); few data exist for Hispanic patients (H). We assessed racial diff erences in initiation of anti-TNF agents for patients with CD using Medicaid data.Methods: Medicaid databases from Florida, Kansas, and New Jersey were exam-ined to identify all patients with CD (≥2 encounters with ICD-9 for CD) from August 1998 to March 2009. CD-related treatment (antibiotics, steroids, aminosal-icylates, IMMs, and anti-TNF agents), CD-related medical comorbidities, CD location, CD behavior, surgery, and health care utilization were assessed from CD diagnosis until the fi rst anti-TNF claim or end of claims. Cox proportional-hazards model was used to assess the eff ect of race on odds of anti-TNF agent initiation.Results: We identifi ed 8,105 patients with CD; 7,284 had race data (4,602 W; 1,219 AA; 663 H; 800 other). Of these, 22% W, 24% AA, 25% H, and 29% of other patients were excluded owing to an ICD-9 code for ulcerative coli-tis, yielding a total of 5,575 patients with CD (3,590 W; 924 AA; 494 H; 567 other) for analysis. 18%, 17%, and 17% of W, AA, and H patients started IMMs aft er a CD diagnosis (p=not signifi cant). 7%, 9%, and 5% of W, AA, and H patients initiated anti-TNF agents aft er a CD diagnosis (p=not signifi cant). Aft er adjusting for CD-related medications, comorbidities, and demography, the Cox model did not reveal an association between AA patients and odds of biologic use compared with W patients (HR 1.20, 95% CI 0.93-1.54), nor between H and W patients (HR 0.68, 95% CI 0.46-1.02). To further adjust for CD severity, we analyzed patients hospitalized aft er CD diagnosis (n=3,428). Anti-TNF treatment was initiated less oft en in H than W or AA patients (4% vs. 8% and 7%, p=0.027 for H vs. W). Th e Cox model showed that H patients were signifi cantly less likely to use anti-TNF agents than W patients (HR 0.39, 95% CI 0.22-0.71). No diff erences between W and AA patients were found in mean doses of or time to fi rst dose of anti-TNF agents.Conclusion: Initiation of anti-TNF agents was similar in W and AA patients but lower in H patients. Further research is needed to confi rm these fi ndings in a commercially insured population because it is possible that anti-TNF agents may be underused among all racial groups in the Medicaid population.Disclosure: M Flasar: Consultant: UCB Pharma. Research Funding: Abbott, Cen-tocor. PM Mulani: Employee/Stock: Abbott. M Yang: Employee/Stock: Abbott. J Chao: Employee/Stock: Abbott. M Lu: Employee: Analysis Group; under con-tract with Abbott. R Cross: Advisory Board: Abbott, UCB. Consultant: Abbott. Research Funding: Abbott, Centocor. Speaker’s fees: Abbott.
1211
Higher Th erapeutic Tacrolimus Trough Levels Are Associated with Fewer Surgical Resections in Crohn’s Disease Patients Refractory to Anti-TNFα Th erapyMark Gerich, MD,1 Darrell Pardi, MD,2 David Bruining, MD,2 Patricia Kammer,2 Brenda Becker,2 William Tremaine, MD2. 1. University of Colorado Denver, Aurora, CO; 2. Mayo Clinic Rochester, Rochester, MN.
Purpose: Several small retrospective studies have reported encouraging response rates of Crohn’s disease (CD) patients treated with tacrolimus. We sought to determine the relationship of tacrolimus blood levels to the response rate in Crohn’s disease refractory to standard therapies.Methods: Th is was a single center, retrospective, observational study. Potential cases were identifi ed by searching electronic medical records from January 1,
[1208] Rates of adalimumab dosage adjustment with and without early deep remission
Deep Remission Outcome Yes ( N =11) No ( N =53) P Value a
Open-label eow, b % (n / N) 9 (1 / 11) 49 (26 / 53) 0.02
Weekly therapyc, % (n/N) 0 (1 / 11) 28 (15 / 53) 0.05
a P Values from Fisher’s exact test. b Dosage adjustment to open-label adalimumab eow for fl are / nonresponse. c Dosage adjustment to open-label adalimumab weekly therapy for continued fl are / nonresponse.

The American Journal of GASTROENTEROLOGY VOLUME 105 | SUPPLEMENT 1 | OCTOBER 2010 www.amjgastro.com
AbstractsS444
2000 to April 1, 2010, that included the words “Crohn” and either “tacrolimus” or “Prograf.” Inclusion criteria were symptomatic Crohn’s disease refractory to one or more anti-TNFα agent subsequently treated with tacrolimus. Exclusion criteria were: indeterminate colitis; perianal fi stulas without other evidence of Crohn’s disease; less than one month of follow-up without adverse eff ects that required termination of therapy; and tacrolimus therapy primarily for post-transplant immunosuppression or treatment of pyoderma gangrenosum. Demo-graphic and clinical data were collected. Response was defi ned as a clinician’s assessment of improvement aft er at least 7 days treatment of one or more of the following: bowel movement frequency, fi stula output, rectal bleeding, abdomi-nal pain, extraintestinal manifestations (EM), or overall well-being. Remission required all of the following: <3 stools/day (excluding subjects with a previous resection), no bleeding, abdominal pain or EM, and increased well-being.Results: Th ere were 26 treatment courses among 24 eligible patients, with one patient treated with three separate courses of tacrolimus aft er long intervals. 96% had failed infl iximab; 23% had failed two biologics; 8% had failed three biologics. 31% were steroid-dependent. Overall response and remission rates were 65% and 19%, respectively, at a median follow up of 56 months. Data for surgery (resection or diversion) and adverse events (AE) is presented in the table below. Supra-therapeutic trough levels of >15 ng/ml were associated with a less favorable outcome than therapeutic levels. Serious adverse events included one Port-a-Cath infection and 9 (35%) episodes of acute kidney injury. Th ere were no deaths attributable to tacrolimus.Conclusion: In patients with Crohn’s disease refractory to anti-TNFα therapy, tacrolimus treatment at a higher therapeutic trough level appears to reduce the need for surgery, but adverse events are frequent.
1212
Effi cacy of Adalimumab Th erapy in Patients with Crohn’s Disease Who Were Unresponsive to or Intolerant of Infl iximab: Six Years of Experience in a Single Gastroenterology CenterIra Shafran, MD, David Cangemi, MS, Patricia Burgunder, ARNP. Shafran Gastroenterology Center, Winter Park, FL.
Purpose: Th is retrospective chart review assessed the effi cacy of adalimumab for the improvement of Crohn’s disease symptoms in patients who were unre-sponsive to or intolerant of infl iximab and evaluated potential predictors of nonresponse to infl iximab therapy.Methods: Medical records from patients with Crohn’s disease who were unre-sponsive to or intolerant of infl iximab and had Crohn’s disease activity index (CDAI) score of ≥225 were identifi ed from a single gastroenterology center from 2004 to 2010. Infl ammatory bowel disease questionnaire (IBDQ) score and CDAI score were assessed at baseline and approximately every 3 months during therapy. Patients were classifi ed as responders (defi ned as reduction in CDAI score >100, elimination of steroids [if steroid dependent at baseline], and improvement in IBDQ score >30) and nonresponders. Endoscopic heal-ing, disease phenotype (infl ammatory, fi brostenotic, fi stulizing), prior surgery, concomitant therapy, smoking, and narcotic use were compared between responders and nonresponders.Results: Of 71 charts examined, 44 (62%) fulfi lled inclusion criteria (18 males, 26 females; mean age, 39 years; mean disease duration, 18 years). All patients received induction therapy with adalimumab 160 mg at week 0 and adalimumab 80 mg at week 2. Patients who responded to initial therapy were maintained on adalimumab 40 mg every other week, and patients who did not were maintained on adalimumab 40 mg weekly. Th irty-four percent of patients were responders (15 of 44 patients; mean duration of therapy, 39 months), and 66% were nonresponders
(29 of 44 patients; mean duration of therapy, 16 months). Disease phenotype and mean disease duration did not diff er between responders and nonresponders. Th ree of the 15 responders (20%) required weekly administration of adalimumab. All responders who were receiving steroids at baseline (n=6) had elimination of steroids during adalimumab therapy, and endoscopic healing was evident in 5 of 7 responders (71%) who underwent endoscopic evaluations. A greater per-centage of nonresponders reported smoking (45%) and narcotic use (55%) versus responders (7% and 13%, respectively). Seventeen of 29 nonresponders (59%) required surgery within 6 months aft er discontinuation of adalimumab therapy. Patients with fi brostenotic disease, prior surgery, smoking, and steroid depend-ence had an increased risk of complications that resulted in surgery.Conclusion: Adalimumab induced and maintained clinical response in 34% of patients with Crohn’s disease who were intolerant of or unresponsive to inf-liximab. Cessation of smoking and narcotic use may increase the probability of response to adalimumab in these patients.Disclosure: Dr Shafran - Consultant: Salix Pharmaceuticals, Inc.; Patty Burgunder - None.
1213
Analysis of Anti-drug Antibodies (ADA) to Adalimumab in Patient Serum Using a Novel Homogeneous Mobility Shift AssayShui Long Wang, MD, Linda Ohrmund, BS, Nicholas Ling, PhD, Sharat Singh, PhD. Prometheus Laboratories, Inc., San Diego, CA.
Purpose: Anti-TNF-α drugs such as infl iximab (IFX) and adalimumab have been shown to be eff ective in treating infl ammatory bowel disease (IBD). However, induction of ADA in the treated patients may reduce the drug’s effi -cacy and/or induce adverse eff ects. Indeed, ADAs have been found not only in patients treated with IFX, but also in patients treated with adalimumab. Moni-toring of ADA and drug levels in individual patients may help optimize treat-ment and dosing of the patient. We have developed a proprietary mobility shift assay to accurately measure in the serum both HACA (Human Anti-Chimeric Antibody) and IFX from IFX-treated patients. Th is assay overcame the major limitation of the current solid-phase assays for detecting HACA, namely the inability to accurately detect HACA in the presence of IFX in circulation. In the present study, we have evaluated this new assay to measure serum ADA and drug levels in patients treated with the humanized antibody drug, adalimumab.Methods: Th e mobility shift assay was based on the shift in retention time of a free antigen versus the antigen-antibody immunocomplex on size-exclusion chromatography. Fluorophore-labeled adalimumab or TNF-α and internal control were mixed with serum samples to measure the mobility shift of free adalimumab and TNF-α in the presence of ADA or drug. Th e changes in the ratio of free adalimumab or TNF-α to internal control are the indicators of the immunocomplex formation. Serum concentrations of ADA or adalimumab were determined with standard curves generated by incubating with diff er-ent concentrations of anti-human IgG antibody or purifi ed adalimumab. Using this assay, we measured adalimumab and ADA levels in sera collected from IBD patients treated with adalimumab.Results: Dose-response curves were generated with anti-human IgG antibody for the measurement of mobility shift of labeled adalimumab. Th e detection limit of the assay was 1 ng of anti-human IgG. Detection of ADA was also demonstrated in the presence of exogenously added adalimumab. Sera from fi ft y healthy controls were tested for the ADA and all of the samples had the ADA levels below the detection limit. To measure the drug concentration in patients treated with adalimumab, we generated a standard curve with
[1211]
Tacrolimus trough Surgical rate Time to surgery (mos.) Surgery within 1 yr. AE rate Dose reduction due to AE Discontinuation due to AE
< 5 ng / ml 60 % 9.3 67 % 60 % 20 % 60 %
5 – 10 ng / ml 50 % 7.3 80 % 90 % 30 % 38 %
10 – 15 ng / ml 38 % 33.3 0 % 75 % 40 % 13 %
> 15 ng / ml 67 % 10.0 50 % 67 % 33 % 33 %

© 2010 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY
Abstracts S445
diff erent amount of adalimumab on the mobility shift of labeled TNF-α and the detection limit of adalimumab is 10 ng.Conclusion: We have applied our proprietary mobility shift assay to measure the ADA and adalimumab levels in serum samples from patients treated with adalimumab. Th e assay was found to be reproducible with high sensitivity and accuracy, and can be used to evaluate ADA and drug levels in serum samples from patient treated with adalimumab.Disclosure: Dr Wang - Employee: Prometheus Laboratories, Inc. Mrs. Ohrmund - Employee: Prometheus Laboratories, Inc. Dr Ling - Consultant: Prometheus Lab-oratories, Inc. Dr Singh - Employee: Prometheus Laboratories, Inc.
1214
Ulcerative Proctitis Patients’ Preferences for Topical Formulations of MesalamineSteven Sanderson, MD,1 Jeannette Barrett, PhD,2 Herbert Swanson,2. 1. Steven J Sanderson, MD, Plymouth, MN; 2. Axcan Pharma, Bridgewater, NJ.
Purpose: Ulcerative proctitis (UP) is a common infl ammatory bowel disease associated with signifi cant morbidity. Topical mesalamine (5-aminosalicylic acid; 5-ASA) reduces symptoms, disease fl ares, improves outcomes, and is considered fi rst-line therapy. Dosing oral 5-ASA encumbers a large pill burden and carries increased risk of adverse events, but 5-ASA suppositories have low systemic absorption and fast onset of action (within days). Social factors have prevented patients from using rectal formulations. Th is study assessed patient perceptions and preferences for 5-ASA suppositories vs. enemas in the man-agement of UP and potential eff ects of their use on compliance.Methods: Two phases of research were utilized. Phase 1, a qualitative study, used semi-structured, individual-depth methodology to explore UP treatment issues and validated questions asked in phase 2, an online survey of patients with UP on maintenance therapy.Results: Fourteen patients with UP and 21 gastroenterologists were interviewed in phase 1; 250 patients completed phase 2. Of these patients, 60% were female, 74% were Caucasian, 83% were 25-54 years old, and 57% perceived their UP as at least moderate severity. Symptoms (Table) were completely controlled in only 4% of patients despite oral 5-ASA maintenance therapy. Medication convenience was important; 84% of patients reported traveling during the past year, with 33% traveling >3 weeks/year. Patients experienced ~6 UP fl ares over the past year. Forty percent of patients perceived their UP had not improved and 12% reported their UP had worsened since diagnosis. Of patients prescribed topical mesalamine, 62% would use a suppository without hesitation, while 38% would use an enema. Among patients who perceived their UP was worsening, >90% were willing to take a sup-pository compared with ~50% willing to take an enema. Suppositories were rated by 90% of patients as clean or cleaner than enemas and 87% rated suppositories as being as discrete as or more discrete than enemas. Most patients (82%) reported that suppositories take the same or less time to administer than enemas and 86% rated suppositories as equal or superior to enemas in terms of portability.Conclusion: Mesalamine suppositories are a safe and well-accepted thera-peutic option for patients with UP and may improve compliance compared with oral and enema formulations. Th is research was funded in part by Axcan Pharma Inc, QC, Canada.Disclosure: Dr Barrett and Herbert Swanson are employees of Axcan Pharma Inc. Dr Sanderson does not have a relevant fi nancial relationship.Th is research was supported by an industry grant from Axcan Pharma.
1215
Th e Comparison of the Eff ectiveness of Hyperbaric Oxygen and Medical Ozone Th erapy Against Acute Distal Colitis in a Rat ModelAhmet Guven, Asc Prof, Bulent Uysal, Asc Prof, Emin Oztas, Prof, Mehmet Yasar, Prof, Tuncer Cayci, Asc Prof, Ahmet Korkmaz, Prof. Pediatric Surgery, Gulhane Military Medical Academy, Ankara, Turkey.
Purpose: Previous studies have shown that hiperbaric oxygen (HBO) is eff ec-tive in reducing severity of acute distal colitis (ADC). On the other hand, ozone therapy (OT) is shown to reduce infl ammation in several pathological entities. Th us, we designed a study to evaluate the effi cacy of OT in an experimental rat model of ADC and to compare eff ects of both HBO and OT in this entity.Methods: Forty Sprague-Dawley rats were divided into four groups: sham, ADC, ADC+HBO, ADC+OT groups. All groups except sham group were sub-jected to ADC procedure, which was induced by intracolonic installation of %4 acetic acid to investigate acute phase of infl amation. ADC+HBO group underwent to hyperbaric oxygen chamber at 2.8 atmosphere absolute pressure with 100 % O2 inhalation for 90 minutes twice in a day and ADC+OT group received 0.7 mg/kg/day ozone/oxygen mixture intraperitoneally for a total of 4 days aft er induction of colitis. Th e surviving animals were killed at the 5th day and their distal colons were harvested for biochemical and histopathologic analysis.Results: Th e Malondialdehyde (MDA) levels in the ADC group were sig-nifi cantly higher when comparing with the other groups indicating increased damage in tissue with colitis (p<0.05, ADC vs. the other groups). Althougt the MDA levels were decreased in the ADC+HBO and the ADC+OT groups, only that of ADC+OT group was statistically signifi cant (p<0.005, ADC+OT vs. AP). Th e tissue Superoxydedismutase (SOD) activity in ADC group were sig-nifi cantly lower than the sham-operated group (p<0.05, ADC vs. sham-oper-ated). Th ere is no signifi cantly diff erence for the tissue SOD activities between the treatment groups and the sham-operated group. Th e diff erence between all groups in terms of the values of the Gluthatione dismutase (GSH-Px) activity were not statistically signifi cant. At the histopathological evaluation, there is a signifi cant improvement in the ADC+OT group.Conclusion: Our data showed that OT reduced severity in the experimental ADC compared with HBO in term of oxidative stress, histopathologic damage score. Th ese fi ndings suggest that it is possible to improve the outcome of ADC by using ozone therapy as an adjuvant therapy.
Symptom Ever experiencing
( %)
Experiencing “ almost continually ” over past 12 Months
( % )
Symptom ranks in Top 3 “ most
troublesome symp-toms, ” (% )
Diarrhea 75 27 41
Bleeding 56 12 27
Bloating / gas 66 40 29
Frequent use of toilet 58 34 22
Urgency 52 26 25

The American Journal of GASTROENTEROLOGY VOLUME 105 | SUPPLEMENT 1 | OCTOBER 2010 www.amjgastro.com
AbstractsS446
1216
Interferon-b-1a in Active Moderate to Severe Ulcerative Colitis: Effi cacy and Safety from a Phase IIa Multicenter StudyPeter Mannon, MD,1 Remo Panaccione, MD,2 Philip Miner, MD,3 Arthur McAllister, MS,4 John O’Gorman, PhD,4 Fabio Cataldi, MD4. 1. University of Alabama at Birmingham, Birmingham, AL; 2. University of Calgary, Calgary, AB, Canada; 3. Oklahoma Foundation for Digestive Research, Oklahoma City, OK; 4. Biogen Idec, Cambridge, MA.
Purpose: IL-13, the cytokine active in the mouse oxazalone model of ulcera-tive colitis (UC), is elevated in human disease and directly damaging to gut epithelium. IL-13 represents a novel target for new drug development in UC. Type 1 interferons can block IL-13 production and receptor signaling in human CD4 cells. In an open label pilot study, 16 patients with moderately active UC treated with interferon-b-1a (IFNb), 30 μg IM/wk for 12 doses, reported 81% clinical response and 44% remission rates. Responders also showed signifi cant decreases in CD4 production of IL-13. Given these very promising results, a phase IIa study was conducted.Methods: Patients (age 18-65) with moderate to severe UC-modifi ed Mayo Score 6-13 were enrolled into a multicenter, randomized, double-blind, pla-cebo-controlled study. Patients must have had an established diagnosis of UC for at least 6 months; >20 cm of active disease at screening endoscopy. Sta-ble doses of the following concomitant medications in any combination were required: corticosteroids, AZA/6-MP, and 5-ASA. Patients were randomized 1:1 to receive IFNb 30 μg IM or placebo (P) twice at WK, for 12 weeks and with a safety follow-up at week 16. Th e primary endpoint was clinical response at Week 8, defi ned as a decrease from baseline in the Total Mayo Score of at least 3 points and at least 30%, accompanied by a decrease in the subscore for rectal bleeding of at least 1 point or absolute subscore of 0 or 1. Th e secondary endpoints were the safety and tolerability of IFNb and the % of subjects with a decrease in the Short Clinical Colitis Activity Index (SCCAI) score of ≥3 points at Week 8.Results: Th e intent to treat (ITT) population included 123 patients, 61 in P and 62 in IFNb. At week 8, 53% of patients on IFNb vs. 44% on P were in clinical response (P= 0.35). 122 patients were evaluable for the analysis of the second-ary endpoint at week 8. 64% of patients on IFNb vs. 46% on P showed clinical response based on the SCCAI at week 8 (P= 0.05). In this study the safety and tolerability was overall very positive, consistent with the established safety profi le of IFNb. No serious infections were seen and 4 SAEs were reported, 3 on P and 1 on IFNb; 2 worsening of UC and 1 tibia fracture in P; worsening of UC in IFNb.Conclusion: IFNb did not meet the primary endpoint of clinical response based on the Mayo score but all week 8 endpoints showed a trend towards effi -cacy. IFNb met the key secondary endpoint with statistically signifi cant SCCAI clinical response. IFNb showed a very good safety and tolerability profi le in the UC population mirroring the safety profi le with this drug in MS. Th ese interesting results suggest blocking IL-13 production with IFNb may be useful in treatment of ulcerative colitis.Disclosure: Peter Mannon consultant for Biogen Idec Remo Panaccione consul-tant for Biogen Idec Philip B. Miner consultant for Biogen Idec Arthur McAllister employee of Biogen Idec John O’Gorman employee of Biogen Idec Fabio Cataldi employee of Biogen Idec.Th is research was supported by an industry grant from Biogen Idec.
1217
Th e Mechanisms of Sai-rei-to, a Herbal Drug, in the Treatment of Experimental ColitisNoriko Nakajima, MD, PhD, AGAF, Yuichi Akai, MD, PhD, Taichi Nakagawa, MD, Naoto Kunoki, MD, Shun Kobayashi, MD, Ryu Nishiyama, MD, PhD, Mitsuhiko Moriyama, MD, PhD. Nihon University School of Medicine, Tokyo, Japan.
Purpose: Current medical management of IBD consists of aminosalicylats (ASAs), steroids, and immunosuppressant therapies including azathioprine, and recently TNF-α antibody therapy has also been used. But treatment with these drugs reduces immunity which may be a trigger for adverse events including infection. Sai-rei-to (SRT), a type of kampo medicine (Japanese herbal medicine), is a compound drug made from the crude extracts of various medicinal plants. Th ese plants and extracts have been reported to have an anti-infl ammatory action. Recently in Japan, the administration of SRT was shown to reduce the amount of steroid administration required for IBD patients. But the mechanisms of the eff ect of this drug for IBD are unknown. In this study, we demonstrated the eff ect of SRT on colonic epithelial cell proliferation and apoptosis in rats with TNBS-induced experimental colitis.Methods: SRT, prednisolone (PSL) and 5-ASA (ASA) were administered in various combinations to TNBS rats for 4 weeks. Aft er the rats were sacrifi ced, any infl ammatory change of the colonic mucosa was studied using Matt’s classifi cation. Th e cell proliferation of colonic mucosa was studied the BrdU uptake, and apoptosis cells were stained by Tunel method.Results: Th e treatment of SRT, PSL and ASA alone signifi cantly reduced colonic infl ammation (TNBS control:39.75±1.26, vs. SRT:34.33±1.09, PSL:31.11±1.89, ASA:33.57±1.26) and there was no signifi cant diff erence on the infl ammation between these drugs. PSL administration signifi cantly decreased the number of BrdU-labeled cells (TNBS control:4.66±1.1, vs. PSL:3.44±2.1), but SRT and ASA did not infl uence the number of BrdU-labeled cells (SRT:4.63±1.1, ASA:4.64±3.2). Both ASA and SRT administration increased the number of total cells in colonic pits (TNBS control:42.61±21.8, ASA:57.11±13.7, SRT:74.34±19.9). In the SRT+ASA group, administration of SRT further increased the number of total cells which had already been increased by ASA treatment (SRT+ASA:72.64±22.7). SRT and ASA treatment alone increased the number of cells above the prolif-erative zone (TNBS control:24.8±17.3, vs. SRT:56.63±26.3, ASA:39.19±17.8). ASA, PSL and SRT alone signifi cantly decreased the number of apoptosis cells (TNBS control:9.53±2.17, vs. ASA:1.52±0.29, PSL:1.62±0.6, SRT:0.4±0.18). In the SRT+ASA group (ASA:1.52±0.29, vs. SRT+ASA:0.36±0.05) administration of SRT further decreased apoptosis cells which had been decreased by ASA.Conclusion: Th e treatment of SRT alone decreased colonic infl ammation similar to PSL and ASA. SRT reduced both the colonic cells above the PZ zone and the apop-tosis cells. From these data, the eff ect of SRT treatment for IBD is not an inducer of proliferation, and reduces and protects the desquamated colonic epithelial cells.
1218
Th e Role of Preoperative Internal Medicine Consultations for Ulcerative Colitis Patients Undergoing ColectomiesSonia Cerquozzi, MD, Marie-Claude Proulx, BSc, MSc, Christopher MA, BSc, James Hubbard, BSc, MSc, William Ghali, MD, MPH, FRCPC, Gil Kaplan, MD, MPH, FRCPC. Medicine, University of Calgary, Calgary, AB, Canada.
Purpose: Despite advances in medical therapy, a colectomy is performed in approximately 30-40% of patients with ulcerative colitis (UC). Internists are
[1215] Histopathological score of the each group
Groups Infl ammation Edema Ulceration Necrosis Total Score
Sham − − − − 0
Control + + + + + + + + + + + + + + 14
ADC + OT + + + + + + + + 8
ADC + HBO + + + + + + + + + + 10

© 2010 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY
Abstracts S447
oft en asked to evaluate a patient prior to surgery in order to determine the patient’s risks in the proposed procedure. UC is associated with numerous extra-intestinal manifestations such as arthritis, primary sclerosing cholangitis, thromboembolic disease, and asthma. Furthermore, postoperative complica-tions occur commonly (~30%) following colectomy for UC. Th us, preopera-tive internal medicine consults may infl uence postoperative outcomes. Th e purpose of this study was to determine the prevalence of preoperative inter-nal medicine consults for UC patients undergoing colectomy and evaluate the patient characteristics that predict referral for preoperative internal medicine consultation.Methods: Population-based surveillance was conducted in the Calgary Health Region between January 1, 1996 and December 31, 2007 using administra-tive databases to identify all adults (≥18 years) with ICD-9/10 coding for UC and a colectomy (n=582). All medical charts were reviewed. Th e primary out-come was the presence of a preoperative internal medicine consult prior to the operation. Logistic regression analysis was used to determine independent predictors of patients receiving a preoperative internal medicine consult. Point estimates were presented as adjusted odds ratios (OR) with 95% confi dence intervals (CI).Results: Among the 582 UC patients who underwent a colectomy, 23% received a preoperative internal medicine consult. Th e median age at operation was 40 years (interquartile range: 30-53 years), 60% were males, 40% were current or ex-smokers, and 44% had no preoperative comorbidities. Independent pre-dictors of preoperative internal medicine consults included age (64 years ver-sus 18-34 years: OR 4.51, 95% CI: 2.16-9.4), comorbidities (>2 comorbidities vs. none: OR 6.76, 95% CI: 3.39-13.49), and indication of surgery was cancer (OR 2.01, 95% CI: 1.01-3.99).Conclusion: Th e majority of UC patients who undergo colectomy did not receive a preoperative internal medicine consult. Preoperative consults were predominantly requested for elderly patients with underlying comorbidities and UC patients who were operated for colorectal cancer. Future studies are necessary to determine whether wider spread use of preoperative internal medicine consults would improve postoperative outcomes.
1219
Does the Dye-based Chromoendoscopy Improve Dysplasia Detection in Patients Undergoing Surveillance Colonoscopy for Long term Ulcerative Colitis (UC)? Meta-analysis
2010 ACG/Centocor IBD Abstract AwardAnna Buchner, MD, PhD, Wojciech Blonski, MD, PhD, Colleen Brensinger, MS, Ming Lin, MD, Gary Lichtenstein, MD. Gastroenterology, University of Pennsylvania, Philadelphia, PA.
Purpose: Colorectal cancer (CRC) risk is elevated in pts with long-term ulcerative colitis (UC). Endoscopic surveillance with biopsies is performed to identify dysplasia, a precursor lesion of CRC. Use of dye-based chromoendos-copy (CE) in UC surveillance is supported by European GI societies and the CCFA, however, recently published guidelines by ACG and AGA recommend random and targeted biopsies of raised lesions and do not yet suggest the rou-tine use of CE. In the US, few physicians use CE in colonoscopic evaluation of IBD pts. Our study aim is to compare the diagnostic yield of CE vs. white light colonoscopy (WLE) for dysplasia during surveillance colonoscopy in the published literature.Methods: Databases examined in this meta-analysis include MEDLINE, EMBASE, Cochrane Collaboration, Journals@OVID, Cochrane, CAB, and OVID Healthstar. Full-length, English, prospective studies were included for analysis. Th e pooled estimate of odds ratio (OR) for the association between CE/WLE and dysplasia (IN) detection was calculated with random eff ects models and the heterogeneity in ORs across studies was examined.Results: We identifi ed 2525 articles; 2494 were rejected, 31 were included in full review and 6 met inclusions criteria. Th ere were 1584 pts with UC under-going surveillance colonoscopy including 878 pts with CE exam and 868 with WLE exam. CE had a signifi cant benefi t in detecting dysplasia. Th e diff erence in the number of pts with CE detected dysplasia (IN) was statistically signifi -cant [pooled OR=2.79 (95% CI 1.91-4.08), but not with signifi cant heterogene-ity (p=0.5)]. CE had a signifi cant benefi t in detecting IN in fl at mucosa [pooled
OR=2.47(0.67-8.67) with signifi cant heterogeneity (p=0.036)]. CE had no ben-efi t in detecting IN in raised mucosa (“polypoid” mucosa): [pooled OR=0.74 (0.33-1.65) with no signifi cant heterogeneity (p=0.3)].CE had a signifi cant benefi t in detecting IN in targeted biopsies [pooled OR=2.15 (1.38-3.33) with-out signifi cant heterogeneity (p=0.67)].Conclusion: Th is study represents the fi rst meta-analysis of the role of CE in detecting dysplasia during surveillance colonoscopy in pts with long term UC. Th is confi rms an overall signifi cant benefi t of the CE for the detection of dys-plasia in fl at mucosa and in targeted biopsies but it does not demonstrate a benefi t in detecting dysplasia in visible, raised (“polypoid”) mucosal lesions.
1220
Th e Impact of Health Insurance Coverage and Socioeconomic Status in Access to Care in Patients with Infl ammatory Bowel DiseaseVeroushka Ballester, MD, Roberto Vendrell, MD, Yelitza Sanchez, PhD, Juan Zevallos, MD, Esther Torres, MD, MACG. Department of Medicine, University of Puerto Rico-School of Medicine, San Juan, Puerto Rico.
Purpose: A study of prevalence of IBD in Puerto Rico showed a signifi cant dif-ference between patients with commercial insurance (CI) versus those insured through a government sponsored (GS) capitated managed care system (61.5 vs. 14.6 per 100,000).To determine if the type of health insurance, CI or GS, infl uenced the time to referral to a specialist, and overall patient satisfaction in patients attending the clinics of the UPR Center for IBD.Methods: 155 patients with a diagnosis of IBD from the UPR Center for IBD participated in the study. Th ree patients with Medicare insurance were excluded from the analysis. Th e data was collected through a questionnaire distributed at the clinics. Demographic, socioeconomic and health care uti-lization data was collected. STATA v10 was used for descriptive statistics and Pearson chi-square was used to calculate diff erences between proportions. A logistic regression analysis was conducted to assess several dependent vari-ables simultaneously. Th e study was approved by the MSC IRB.Results: 97/152 (64.0%) were covered by commercial insurance and 55 (36.0%) were covered by the government sponsored health plan. CI patients reported higher levels of education (p=0.0003) and income (p=0.0001) as compared to GS patients. Both groups reported similar satisfaction with their medical insurance (91.8% and 89.1% respectively, p=0.58). Of the 113 patients referred to a gastroenterologist by their primary physician, 68 (60.0%) were CI and 45 (40.0%) were GS (p=0.05). Median delay before referral to a gastroenterolo-gist was 1 month for CI and 6 months for GS. Ten patients were never referred to a gastroenterologist, 1 (10%) was CI and 9 (90%) were GS (p=0.0004). All 29 patients who directly visited a gastroenterologist were CI. Of the 36 patients referred to a gastroenterologist within one month of diagnosis, 30 (83.3%) were CI and only 6 (16.7%) were GS (p=0.0006). Th is diff erence was sustained aft er adjusting by gender, education and income.Conclusion: Our study shows that commercially insured patients with IBD attending the UPR IBD clinic are more timely referred to a gastroenterologist

The American Journal of GASTROENTEROLOGY VOLUME 105 | SUPPLEMENT 1 | OCTOBER 2010 www.amjgastro.com
AbstractsS448
as compared to patients with a government sponsored plan. Delay in referral to subspecialty care could be a factor in the diff erence in prevalence between the CI and the GS individuals with IBD in Puerto Rico. A study of all patients participating in GS coverage is necessary to validate this fi nding, as we studied only patients who were receiving subspecialty care. If confi rmed, this high-lights the importance of appropriate educational intervention at the primary care level. Supported by the UPR SoM Endowed Health Services Research Center, Grants 5S21MD000242 and 5S21MD000138, NCMHD-NIH.
1221
Vitamin D Defi ciency and Abnormal DEXA Scans in Infl ammatory Bowel Disease PatientsBincy Abraham, MD, MS, Hoda Malaty, MD. Baylor College of Medicine, Houston, TX.
Purpose: Infl ammatory bowel diseases (IBD), mainly ulcerative colitis and Crohn’s disease are chronic, heterogenic, lifelong illnesses with a great poten-tial for disability. Studies using dual-energy X-ray absorptiometry (DEXA) scans have suggested a high prevalence of osteoporosis in IBD. Interference with bone repair and remodeling in IBD patients can occur not only through the use of corticosteroid use and excess of infl ammatory cytokines, but also from calcium and vitamin D malabsorption, both of which are important to bone health. Vitamin D defi ciencies have been reported in IBD patients but prior studies have been confl icting in its association with bone density. We aimed to determine the association between vitamin D defi ciency and abnor-mal bone density in IBD patients.Methods: A prospective study was conducted on a cohort of patients diag-nosed with IBD based on clinical, radiologic, endoscopic and histological data. Children and adults between the ages 10 and 70 of whom were diagnosed with IBD participated in the study between 2008 and 2010. Demographic data, dis-ease sub-type, vitamin D levels and DEXA scan results were recorded. Th e data were analyzed using the Chi-square, Fisher exact and Student t-tests. We defi ned Vitamin D defi ciency as Vitamin D 25-hydroxy levels less than 30 ng/mL. DEXA scan results were considered abnormal if osteopenia and osteoporosis were found.Results: Th ere were 161 IBD patients in the studied cohort. Reduction in bone density with a diagnosis of either osteopenia or osteoporosis was found among 22% of the studied patients of whom 50% were below the age of 40. Th e patients with an abnormal bone density exam had signifi cantly higher rate of vitamin D defi ciency than those who had normal DEXA scans (40%. vs. 1%, respectively, OR=8.7; 95% CI=2.4-19.8, p=0.001). Th is association remained aft er controlling for corticosteroid intake and age, and it was consistent among females and males, independently. Of interest, CD patients were found to have
a higher rate of abnormal bone density exams compared to UC patients (34% vs. 13%, respectively, OR=4.2; 95% CI=1.8-11.7, P=0.02). Both CD and UC patients diagnosed with osteoporosis had signifi cantly higher rate of Vitamin D defi ciency irrespective of prednisone intake.Conclusion: Abnormal bone density was relatively high among our IBD patients with Vitamin D defi ciency irrespective to age, gender, or corticoster-oid use that would place them at signifi cantly higher risk of having an abnor-mal DEXA result. It remains important for those caring for IBD patients to evaluate for Vitamin D nutritional defi ciency and for its potential consequence of osteopenia or osteoporosis.
1222
Ethnicity is a Predictor of Pouchitis in Asian Ulcerative Colitis Patients Undergoing Ileal Pouch Anal Anastomosis SurgeryBoon Bee George Goh, MBBS, MRCP,1 Khoon-Lin Ling, MBBS, PHD,1 San-Choon Kong, MBBS, MRCP, MD,1 Choong-Leong Tang, MBBS, MMED (Surg), FRCS (Ed), FAMS,2 Choon Jin Ooi, MBBS, FRCP,1 Kelvin Th ia, MBBS, MRCP1. 1. Gastroenterology & Hepatology, Singapore General Hospital, Singapore; 2. Colorectal Surgery, Singapore General Hospital, Singapore.
Purpose: Little is known about the burden of pouchitis and the associated risk factors in Asian UC patients aft er IPAA. Th e aims of this study were to assess the cumulative risk of pouchitis and its predictive factors.Methods: Th is was a retrospective study involving UC patients of Asian ethnic-ity identifi ed through our institution Infl ammatory Bowel Disease (IBD) and IPAA registry. Clinical information relating to UC phenotypes, indications for surgery, endoscopic, pathologic and clinical outcomes relating to post-opera-tive complications and pouchitis were abstracted from the electronic medi-cal records and clinical charts. Patients who underwent IPAA for FAP were excluded. Pouchitis was diagnosed based on typical symptoms in the exclusion of other causes. Th e Kaplan-meier method was used to estimate cumulative incidence of pouchitis, and Cox proportional hazards regression models used to assess univariate association between putative factors and time to development of pouchitis. Results were expressed as median (IQR) unless otherwise stated.Results: A total of 52 UC patients with IPAA performed between 1990 and 2009 were included. Th e age at IPAA surgery was 44 (37-56) years, with a fol-low-up duration 61 months (17-115) post surgery. Th irty patients (57.7%) were male and the racial distributions were Chinese 67.3%, Indians 19.2% and Malays 13.5%. Th e extents of disease were proctitis 9.6%, left -sided 28.8% and extensive 61.6%. Th e indications for IPAA were medically refractory 71.2%, malignancy 7.7%, toxic megacolon 5.8% and refractory bleeding 5.8%. A total of 14 complications (anastomotic leak/abscess 10, ileal fi stula 4) were seen within 3 months of ileostomy closure post-IPAA. A total of 18 patients experienced at least 1 pouchitis event. Th e cumulative incidence of pouchitis
[1222] Table 1 . Univariate association between putative risk factors and time to development of fi rst pouchitis
Factors Patients, n (Total, 52) Events, n (Total, 18) Hazard ratio (95 % CI) Signifi cance level ( ρ )
Chinese Ethnicity 35 11 1.0 ref. 0.038
Indian / Malay Ethnicity 17 7 3.48 (1.07 – 11.35)
No complications 40 12 1.0 ref. 0.548
Complications 12 6 1.54 (0.38 – 6.30)
Limited disease 20 3 1.0 ref. 0.408
Extensive disease 32 15 1.89 (0.42 – 8.53)
platelet count ≤ 440 # 34 13 1.0 ref. 0.251
Platelet count > 440 14 4 0.51 (0.16 – 1.62)
Age at surgery < 40 years 17 8 1.0 ref. 0.966
Age at surgery ≥ 40 years 35 10 1.02 (0.39 – 2.70)
Male 30 11 1.0 ref. 0.455
Female 22 7 0.83 (0.50 – 1.36)
# Platelet count pre-operative, normal range: 140 – 440 × 10(9) / L; missing, n =4.

© 2010 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY
Abstracts S449
at 1, 5 and 10 years post-IPAA were 0.14 (95% CI, 0.03-0.24), 0.23 (95% CI, 0.09-0.36) and 0.53 (95% CI, 0.33-0.73) respectively. In our univariate analysis (Table 1), Malay and Indian ethnicity were signifi cantly associated with the development of pouchitis.Conclusion: Th e risk of pouchitis appears to be lower among Asian UC patients aft er IPAA compared to Caucasian patients. Malay and Indian UC patients were 3.5 times more likely than Chinese UC patients to develop pouchitis.
1223
Anti-Tumor Necrosis Factor Th erapy for Infl ammatory Bowel Disease Management in Liver Transplant Recipients
Arya Mohabbat, MD, William Sandborn, MD, Edward Loft us, MD, Russell Wiesner, MD, David Bruining, MD. Mayo Clinic, Rochester, MN.
Purpose: Ulcerative colitis (UC) or Crohn’s disease can be diffi cult to manage following orthotopic liver transplantation (OLT) despite conventional immu-nosuppressive therapy. We sought to evaluate the effi cacy and safety of anti-tumor necrosis factor (anti-TNF) agents for the management of infl ammatory bowel disease (IBD) following OLT.Methods: All patients with an established diagnosis of UC or Crohn’s dis-ease who underwent OLT at the Mayo Clinic between January 1, 1985 and December 30, 2009 were identifi ed. Patients were included if they had received anti-TNF therapy post-OLT. Medical records were reviewed to obtain patient demographic, clinical, and outcomes data. Response was defi ned as a clini-cian’s assessment of improvement aft er 12 weeks of usage and mucosal healing was defi ned as the absence of ulcerations on follow-up endoscopy.Results: Of the 8 patients identifi ed, median age was 42 years and 38% were females. All patients had an IBD diagnosis prior to OLT, 3 with UC and 5 with Crohn’s disease. Median IBD disease duration was 17 years (range, 5-48 years). All patients underwent OLT for primary sclerosing cholangitis (PSC), 3 also had cholangiocarcinoma. Th ree patients had received anti-TNF therapy before OLT, but no anti-TNF agents were continued at the time of OLT. Median time from OLT to anti-TNF usage was 3.5 years (range, 1-14 years). Agents admin-istered included infl iximab (n=4), infl iximab followed by adalimumab (n=2), and adalimumab (n=2). Reasons for changing from infl iximab to adalimu-mab included infusion reaction (n=1) and loss of response (n=1). Th e most common indications for anti-TNF agents were diarrhea (n=6), diarrhea with penetrating disease (n=1), and diarrhea with extra-intestinal disease manifes-tations (n=1). Clinical response was demonstrated in 7 of 8 patients with initial therapy. Of the two patients changed to adalimumab, only one demonstrated a clinical response (patient with infl iximab allergy). Mucosal healing was dem-onstrated in 3 of 7 patients. Five patients were tapered off prednisone. Four infections in 3 patients were reported while on anti-TNF therapy, including oral candidiasis, Clostridium diffi cile colitis, pneumonia, and cryptosporidi-osis. One individual developed an Epstein-Barr virus-positive polymorphic post-transplant lympho-proliferative disorder in the absence of depleting antilymphocyte therapy. No organ rejection was reported while on anti-TNF therapy. One death occurred due to complications from recurrent PSC.Conclusion: Initiation of anti-TNF therapy post-OLT appears to be an eff ec-tive option for IBD management. Further studies are needed to adequately assess potential risks.Disclosure: Dr Bruining: Centocor-past research support.
1224
Clinical Utility of Infl ammatory Bowel Disease Serology Testing in Patients with Indeterminate ColitisSiddharth Sura, MD, MPH, Awais Ahmed, MBBS, Adam Cheifetz, MD, Alan Moss, MD. Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, MA.
Purpose: Among patients with infl ammatory bowel disease (IBD), approxi-mately 15% have features of overlap between Crohn’s disease (CD) and
ulcerative colitis (UC), and have historically been described as having “inde-terminate colitis” (IC). IBD serology testing is oft en used in clinical practice to help distinguish UC or CD from patients with IC. Th ere is little data on the characteristics of serology testing in this setting. Th e purpose of this study is to determine the test characteristics of IBD serology in predicting UC or CD disease behavior in a cohort of patients with IC.Methods: Individuals meeting criteria for IC were identifi ed from a cohort of patients who underwent IBD serology testing between 2001 and 2007. Serolo-gies tested included pANCA, ASCA, anti-OmpC, and anti-CBir1. One year aft er serology testing, individual diagnoses were re-evaluated and categorized as IC, UC, or CD. Data analysis was conducted with JMP, Version 8 (SAS Insti-tute Inc., Cary, NC).Results: 117 subjects met criteria for IC and had at least one year follow-up data. Th e initial diagnosis of IC was signifi cantly associated with positive pANCA (p<0.0001) and elevated anti-OmpC (p=0.02). At one year aft er serol-ogy testing, 58 (50%) of the patients with IC were re-classifi ed as UC, 49 (42%) as CD, and 10 (9%) remained IC. Th e sensitivity/specifi city of serology for a subsequent diagnosis of UC or CD was; pANCA for UC 78%/44%; ASCA for CD 18%/84%; and anti-OmpC for CD 27%/75%. Th e likelihood ratio of a sub-sequent diagnosis of UC with a positive ANCA was 1.4 (95% CI: 1.1-1.8), CD with a positive ASCA was 1.1 (95% CI: 0.5-2.5), and CD with a positive anti-OmpC was 1.1 (95% CI: 0.6-2.0).Conclusion: Th e majority of patients initially diagnosed as IC evolved clini-cal characteristics of UC or CD within 12 months of diagnosis in this cohort. pANCA was associated with a high sensitivity and low specifi city for UC in this setting, whereas ASCA and anti-OmpC were associated with high specifi -city and low sensitivity for CD.
1225
Knowledge and Attitudes About Cervical Cancer Risk Factors and Human Papilloma Virus Infection in Female Patients with Infl ammatory Bowel DiseaseJosé Rivera-Acosta, MD,1 Maysabel Aponte, MD,1 Irene Villamil, MD,1 Josefi na Romaguera, MD,3 Ana Ortiz, PhD,2 Esther Torres, MD, MACG1. 1. University of Puerto Rico Center for Infl ammatory Bowel Disease, San Juan; 2. University of Puerto Rico Comprehensive Cancer Center, San Juan; 3. University of Puerto Rico, Department of Obstetrics and Gynecology, San Juan.
Purpose: Women with infl ammatory bowel disease (IBD) may be at increased risk of human papilloma virus (HPV) infection and HPV related malignancies. Most studies show poor knowledge about cervical cancer risk factors, includ-ing the role of HPV. Despite being a high-risk population, there is no study about knowledge and attitudes about HPV infection and other cervical cancer risk factors in the IBD population. Th e purpose of this study is to describe the knowledge and attitudes of IBD female patients about HPV infection and the HPV vaccine.Methods: We performed a cross-sectional study in 147 consecutive patients attending the Clinics of the University of Puerto Rico Center for IBD. An interviewer-administered questionnaire was used to collect information on demographics, lifestyles and HPV related knowledge of participants. Bivari-ate analysis using the chi-square statistic was used to examine the association between HPV knowledge and risk factors.Results: Mean age of participants was 36.6 years (SD=13.91 years); 53% had Crohn’s disease, 43% ulcerative colitis and 4% indeterminate colitis. One-third (33%) of women had never heard of HPV and 42% did not know about the exist-ence of HPV vaccines. Among those who had ever heard about HPV, 80% knew that HPV can cause cervical cancer, 58% knew that the virus is sexually transmit-ted, and only 31% knew that genital warts are caused by HPV. A considerable percentage of the participants knew about risk factors for HPV infection. Among those who knew of about the vaccine, 75% learned about its existence through the media, while only 17% through their doctor/health care professional. Younger women (15-29 years) and those with higher educational attainment (college grad-uates) had increased awareness of HPV and the HPV vaccine (p<0.05). Only 3 women (2%) had been vaccinated against HPV, although 50% indicated that they would defi nitely/probably vaccinate against HPV in the future.Conclusion: Our study documents low knowledge of HPV and HPV vac-cine in this population of IBD patients in Puerto Rico. Although vaccination

The American Journal of GASTROENTEROLOGY VOLUME 105 | SUPPLEMENT 1 | OCTOBER 2010 www.amjgastro.com
AbstractsS450
coverage is low in this population, women are receptive to the possibility of vaccination in the future. Given that this population may be at an increased risk of HPV infection and related morbidities, education and vaccination programs should be promoted among them.
1226
Clinical Utility of Infl ammatory Bowel Disease Serology Testing in Patients with Suspected Infl ammatory Bowel DiseaseSiddharth Sura, MD, MPH, Awais Ahmed, MBBS, Adam Cheifetz, MD, Alan Moss, MD. Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, MA.
Purpose: Patients with a clinical suspicion of infl ammatory bowel disease (IBD) oft en undergo IBD serology testing in clinical practice to distinguish IBD from other conditions. Th e performance of serology testing in this popula-tion is unclear. Th e purpose of this study is to determine the utility of serology testing in identifying IBD among a cohort of individuals with suspected IBD.Methods: Individuals with disease suspicious for IBD but without diagnos-tic criteria for CD, UC, or indeterminate colitis (IC) were identifi ed from a cohort of patients who underwent IBD serology testing between 2001 and 2007. Serologies tested included perinuclear anti-neutrophil cytoplasmic antibody (pANCA), anti-Saccharomyces cerevisiae antibody (ASCA), anti-outer membrane porin C antibody (anti-OmpC), and anti-CBir1 fl agellin antibody (anti-CBir1). One year aft er serology testing, each individual’s diagnosis was re-evaluated and categorized as IBD or non-IBD based on pre-determined criteria. Data analysis was conducted with JMP, Version 8 (SAS Institute Inc., Cary, NC).Results: 77 subjects were determined by their gastroenterologists to have disease characteristics suspicious for IBD, and did not meet diagnostic crite-ria for IBD. At time of serology testing, 55% had abnormality on colonoscopy and 21% had abnormality on small bowel follow through. One year aft er serology testing, 34/77 (44%) had developed diagnostic features consist-ent with IBD, with the majority diagnosed as CD (31%). Positive pANCA (p=0.0002) was signifi cantly associated with a diagnosis of IBD at twelve months. Based on standard antibody cutoff s, the likelihood ratio of evolving into IBD was 8.2 (95% CI: 2.0-34.0) for pANCA positive patients, 2.5 (95% CI: 0.7-9.4) for ant-OmpC positive patients, and 1.7 (95% CI: 0.6-4.4) for ASCA positive patients.Conclusion: pANCA may be useful in identifying individuals at risk of devel-oping diagnostic features of IBD among a cohort of individuals suspicious for having IBD.
1227
Utilization of Wound Ostomy Continence Nurses at a Tertiary Care Medical CenterMarcum Gillis, MD, Donna Craven, RN, BSN, CWON, Tim Chilson, RN, BSN, CWON, Jill Fowler, RN, BSN, CWON, Jill Smith, RN, BSN, CWON, Richard Bloomfeld, MD. Wake Forest University, Winston-Salem, NC.
Purpose: Wound Ostomy Continence Nurses (WOCN) off er a wide variety of services and are specifi cally trained to counsel, mark, and care for stomas and enteric tubes such as feeding tubes. Th is study was performed to describe the clinical utilization of WOCN at a tertiary care medical center and to assess the eff ect of pre-operative ostomy counseling and marking by WOCN on post-operative ostomy related complication rates.Methods: A retrospective chart review for all consults placed to WOCN was performed for the year 2009. Consults concerning colostomies, ileostomies, and enteric feeding tubes were included. Patient demographics, the reason for obtaining a WOCN consult, whether pre-operative counseling and skin mark-ing (C&M) were performed, and the presence of post-operative stoma related complications (e.g. skin breakdown, appliance leakage, and inability to care for appliance) were recorded. For patients with new stomas, the data were ana-lyzed to determine if complication rates were related to whether or not patients received pre-operative C&M.
Results: During the study period, 1784 WOCN consults were placed; 705 consults (40% of total consults) involving 390 patients were related to stoma or enteric tube management and were included. Th e mean age of the patients was 54 years with 50% female and 50% male. Th e majority of con-sults were placed by surgical specialties (74%), followed by medicine and its subspecialties (17%), pediatrics (5%), OB/Gyn (4%), and ED (1%). Only 3% of the consults were originated by gastroenterologists. For the 390 patients, 208 (53%) consults were placed for new stoma management; 131 (34%) were for issues related to established stomas (e.g. skin problems, appliance problems, or counseling); 26 (7%) were for enteric tube management (i.e. leakage around the tube); 22 (6%) were for counseling in patients that did not have a stoma placed during the study period; and 3 (1%) were for other reasons. Stoma related complication rates for new stomas were similar for patients who received pre-operative C&M compared to those who did not (27% vs. 24%).Conclusion: WOCN provide a valuable service to patients with gastroen-terological disorders that require stomas or enteric tubes. Short-term stoma related complications were similar whether or not pre-operative C&M was provided. Although most WOCN consultations are placed by surgeons, gas-troenterologists should be aware of the services that these nurses can provide our patients.
1228
Health Maintenance Strategies for the IBD Patient in Private PracticeIra Shafran, MD, Patricia Burgunder, MSN, ARNP. Shafran Gastroenterology Center, Winter Park, FL.
Purpose: Our community based IBD practice acknowledges the importance of developing consistent health maintenance strategies specifi c to the needs of the IBD population. Immunization status, B12 and vitamin D testing, osteoporosis screening and cancer surveillance are essential components of a comprehensive plan. We have strived to understand the real risk and preva-lence of non-immunity among our IBD population (both biologic exposed and naive patients), in order to implement an appropriate and cost eff ective program for screening and immunizing both before and during treatment decisions.Methods: Forty two IBD patients (38 Crohn’s, 4 UC) were evaluated between 1/1/2010 and 4/30/2010. Fift y seven percent (24 of 42 patients) were on biologic or immunosuppressive therapies at the time of evaluation. Serum titers were drawn to identify active immunity to measles, mumps, rubella, varicella, hepatitis A & B. Both vitamin B12 and vitamin D levels were also obtained. All 48 patients were advised to obtain DEXA scan and all female patients (16) were advised to obtain yearly PAP testing and HPV screening.Results: Ninety three percent of patients demonstrated active immunity to measles, 86% to mumps, 90% to rubella, 100% to varicella with only 8% immune to hepatitis A and 21% to hepatitis B. B12 levels were low in 19% of patients with 36% found to be vitamin D deficient. Of the 42 patients advised to obtain DEXA scanning, 9 patients (21%) completed the exam; 4 having normal bone density, 4 with osteopenia, and 1 with osteoporo-sis. One of 16 female patients scheduled PAP testing. All 18 patients not on immunosuppressants were advised to update all immunizations, with those immunocompromised advised to avoid all live virus vaccines. All patients who were vitamin B12 and D deficient were started on appropriate replacement.Conclusion: Th e role of the gastroenterologist as primary decision maker in the health care of IBD patients is essential to assure that patients are educated, and that a general preventative health maintenance plan is implemented. We are continuing to provide guidance to our patients on a broad range of issues such as vaccinations, osteoporosis screening and cancer/dysplasia surveillance. Our analysis clearly uncovered issues with non-adherence to recommendations in regards to DEXA scanning and PAP testing specifi cally, warranting dynamic follow up strategies to encourage improved adherence to health maintenance recommendations.

© 2010 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY
Abstracts S451
1229
Racial Diff erences in the Prevalence of Infl ammatory Bowel Disease in the United States: A Population-Based Analysis of the Medical Expenditure Panel Survey, 1996-2007Y. Richard Wang, MD, PhD, John Cangemi, MD, Michael Picco, MD, PhD. Division of Gastroenterology, Mayo Clinic, Jacksonville, FL.
Purpose: We aimed to compare racial diff erences in the prevalence of infl am-matory bowel disease in the United States (U.S.). Previous estimates on the prevalence of infl ammatory bowel disease in the U.S. were limited to local or insured populations, therefore lacking geographical or racial representations.Methods: Th e Medical Expenditure Panel Survey (http://www.meps.ahrq.gov) is a nationally representative survey of individuals, their medical conditions, and associated use of medical care in the U.S. since 1996. It was used to esti-mate the prevalence of infl ammatory bowel disease in the U.S. and its diff er-ences by racial groups. Th e multivariate logistic model was used to test the association between the prevalence of infl ammatory bowel disease and race.Results: Of the universe of 202,468 individuals surveyed between 1996 and 2007, 204 were diagnosed with Crohn’s disease and 109 were diagnosed with ulcerative colitis, with an adjusted U.S. prevalence of 114 per 100,000 persons for Crohn’s disease (95% confi dence interval [CI]: 95-133) and 65 per 100,000 persons for ulcerative colitis (95% CI: 48-86). Th e prevalence of infl ammatory bowel disease was signifi cantly higher in White individuals (Crohn’s disease and ulcerative colitis: 148 and 82 per 100,000) than in Hispanic (15 and 32 per 100,000), Black (65 and 26 per 100,000), and Asian (40 and 36 per 100,000) individuals (all p<0.05, Figure 1). Racial groups diff ered in education and fam-ily income levels (Percentage with college education: White 43% vs. Hispanic 21% vs. Black 29% vs. Asian 53%; Percentage with low family income: White 24% vs. Hispanic 53% vs. Black 49% vs. Asian 25%). Racial diff erences in the prevalence of infl ammatory bowel disease (vs. White) remained signifi cant in multivariate logistic regressions controlling for age, sex, region, education, and family income (all p<0.05).Conclusion: In this recent, large and nationally representative sample of the U.S. population, the prevalence of infl ammatory bowel disease was lower than previous estimates. Th ere were signifi cant racial diff erences in the prevalence of infl ammatory bowel disease. Whether some diff erences refl ect unmeasured factors such as lack of access to medical care and under-diagnosis is an impor-tant question for future research.
1230
Effi cacy of Certolizumab Pegol Th erapy in Patients With Crohn’s DiseaseIra Shafran, MD, Sayel Al-Maani, BS, Patricia Burgunder, MSN, ARNP. Shafran Gastroenterology Center, Winter Park, FL.
Purpose: Prior literature has suggested a marked decrease in the effi cacy of biologic therapy in TNF exposed Crohn’s disease patients. Our aim of this analysis is to evaluate the eff ectiveness of certolizumab pegol in Crohn’s dis-ease, comparing TNF naïve and TNF exposed patients in a private practice setting.
Methods: We performed a retrospective chart review of 17 patients with Crohn’s disease on certolizumab pegol from June 2008 to May 2010. Certoli-zumab pegol 400 mg was administered in each patient with CDAI (Crohn’s Disease Activity Index) scores obtained at baseline and each injection visit routinely. Clinical response was defi ned as reduction of at least 100 points from the baseline CDAI, with remission defi ned as a score of 150 or less. Prior therapy, surgery, disease phenotype, smoking, and narcotic use were compared between responders and non-responders.Results: Seventeen charts were reviewed (7 males, 10 females; mean age, 40 years; mean disease duration, 7.8 years). All patients received standard induction therapy with 400 mg SQ at 0, 2 and 4 weeks. Patients who responded to induction dosing (76%, 13 of 17 patients) were continued on maintenance therapy of 400 mg monthly. Twenty-nine percent (5 of 17) achieved remis-sion with a mean duration of therapy of 10.6 months, with 47% (8 of 17) of patients meeting the defi nition of clinical response. At 11 months, 41 % of the intent to treat population maintained remission/response. Prior TNF use was reported in 76% of evaluated patients (TNF naïve 24%, 4 of 17). Past surgeries were documented in 53% of patients. All 4 TNF naïve patients (100%) had no prior surgical history and achieved clinical remission or response (mean disease duration, 4.5 years).Conclusion: Certolizumab pegol induced clinical remission or response in 76% of patients with Crohn’s disease, and maintained remission in 41% of patients at 11 months of therapy. All 4 TNF naïve patients achieved remis-sion or response and maintained durability of certolizumab pegol. All primary and secondary non-responders had prior TNF exposure. While TNF naive patients in this analysis demonstrated evident effi cacy, we believe there is also clear benefi t for the use of certolizumab pegol despite prior TNF exposure. Th e analysis of larger numbers of patients and longer durations of therapy, in the community setting, are necessary.
1231
Vitamin D Defi ciency and Its Potential Link to Ulcerative Colitis Disease ActivityStacey Blanck, MD, Colleen Brensinger, MS, Gary Lichtenstein, MD, Faten Aberra, MD, MSCE. Hospital of the University of Pennsylvania, Philadelphia, PA.
Purpose: Previous studies on experimental mouse models have suggested a role of Vitamin D in immune system regulation and IBD disease severity. In this study, we examine the relationship between Vitamin D levels and clinical disease activity in human subjects with ulcerative colitis (UC). We hypothe-sized that patients with Vitamin D defi ciency will display increased UC disease activity as compared to patients with normal Vitamin D levels.Methods: A cross-sectional study was performed by querying the outpatient electronic medical record of our health system for patients seen in the gas-troenterology clinic from January 2007 to October 2009 who carried both a diagnosis of UC and a documented 25-OH Vitamin D level within 30 days of their clinic visit. Demographic and clinical variables were collected including patient age, gender, years with UC diagnosis, current medications (immune-modulators, steroids, biologics, antibiotics, 5-ASA and Vitamin D supplemen-tation), NSAID exposure and smoking history. Clinical disease activity was calculated using the 6-point partial Mayo index based on symptoms recorded in the patient’s gastroenterology clinic notes. Active disease was defi ned as a 6-point index score of ≥1. Vitamin D defi ciency was defi ned as a 25-OH D level below 30 ng/mL. Data were analyzed using the chi-square distribution test.Results: 34 patients met inclusion criteria (53% female, mean age 45.7 ± 24.7 years). 15 patients had normal Vitamin D levels and 19 patients were Vitamin D defi cient. 12 patients had vitamin D levels <20 ng/mL. Vitamin D defi cient patients were statistically more likely to have increased disease activity than patients with normal Vitamin D levels (p=0.04), with 68% of defi cient patients displaying active disease compared with 33% in the suffi cient group. Th ere was also a statistically signifi cant association between Vitamin D status and need for treatment with steroids, with a higher percentage of Vitamin D defi cient patients (47%) requiring such treatment compared with 7% in the suffi cient
Figure 1: Prevalence of Crohn’s disease and ulcerative colitis by race in the United States (U.S.), 1996-2007.

The American Journal of GASTROENTEROLOGY VOLUME 105 | SUPPLEMENT 1 | OCTOBER 2010 www.amjgastro.com
AbstractsS452
group (p=0.02). Th ere was no association between season of visit and disease activity.Conclusion: Vitamin D defi ciency is common among patients with active UC, particularly those requiring corticosteroids. Further investigation is needed to determine the clinical utility of Vitamin D monitoring in patients with UC and whether there is a role for Vitamin D as a treatment for UC.
1232
Anti-Saccharomyces cerevisiae Antibodies as a Prognostic Indicator in Crohn’s DiseaseCatarina Rodrigues, MD, Sara Alberto, MD, Leonel Ricardo, MD, Julieta Félix, MD, Alexandra Martins, MD, Eduardo Pires, MD, Joao Deus, MD. Gastroenterology, Professor Fernando Fonseca’s Hospital, Amadora, Portugal.
Purpose: Anti-Saccharomyces cerevisiae antibodies (ASCA) are relatively spe-cifi c serological markers of Crohn’s Disease (CD) and have been suggested as useful tools in diagnosis and prognostic stratifi cation of patients. Th e purpose was to determine the association of ASCA with the phenotypic characteristics and prognosis of CD.Methods: We included 206 patients with CD, 95 men and 111 women for whom we evaluated the location and behavior of the disease and the need for corticosteroid therapy, immunosuppression, biological therapy, hospitaliza-tion and surgery. ASCA serology was determined by ELISA (IBDX® ELISA kits; GlyCochip®), considering seropositivity for values> 1/100. Th e statistical analysis was performed with SPSS 17.0 soft ware (Chi2 test).Results: According to the Montreal classifi cation, we identifi ed seven patients A1 (3.4%), 127 A2 (61.7%) and 72 A3 (35.0%); 98 patients L1 (47.6%), 31 L2 (15.0%), 75 L3 (36.4%) and 23 L4 (11.2%); 22 patients B1 (59.2%), 43 B2 (20.9%) and 41 B3 (19.9%). Perianal disease was present in 58 patients (28.2%). One hundred and twelve patients (54.4%) required at least one cycle of ster-oids, 64 (31.1%) were treated with azathioprine and 28 (13.6%) with biological therapy. Eighty-one patients (39.3%) required hospitalization and 69 (33.5%) underwent surgery. ASCA were positive in 104 patients (50.5%). Th e seroposi-tivity was associated statistically signifi cantly with ileal disease (46% vs. 26%, p=0.01), fi brostenosing or penetrating behavior (28% vs. 13%, p <0.0001) and with the need for immunosuppression (19% vs. 12%, p=0.044), hospitalization (24% vs. 16%, p=0.021) and surgery (22% vs. 11%, p=0.001).Conclusion: According to our series ASCA positive patients have a more frequent ileal involvement, a greater need for immunosuppression and a worse course of disease. Th ese could be considered when making treatment decisions.
1233
Treatment of Infl ammatory Bowel Disease with Anti-TNF Agents in Patients with Chronic Hepatitis C Virus (HCV) Infection - A Systematic Review of LiteratureWojciech Blonski, MD, PhD,1 Ming Valerie Lin, MD,2 Anna Buchner, MD, PhD,1 K.Rajender Reddy, MD,1 Gary Lichtenstein, MD1. 1. University of Pennsylvania, Philadelphia, PA; 2. Pennsylvania Hospital, Philadelphia, PA.
Purpose: Anti-tumor necrosis factor (TNF) therapy has been shown to be highly effi cacious in the treatment of infl ammatory bowel disease (IBD). However, there is a concern that inhibition of TNF may have immunosup-pressive eff ects leading to HCV replication and worsening of liver disease. Th e aim of this study was to perform a systematic review of the literature regarding the treatment of IBD with anti-TNF agents in patients with chronic HCV infection.Methods: A systematic search of the literature was performed. Databases of literature examined included MEDLINE, EMBASE and PUBMED using key words: hepatitis C, ulcerative colitis, Crohn’s disease, infl ammatory bowel dis-ease, anti-TNF, infl iximab, certolizumab and adalimumab. Articles searched were from 1910 to May 2010. Only full-length, English-written original studies and case-reports that described the eff ects of anti-TNF treatment on the course of IBD and the liver function in patients with IBD and concomitant chronic HCV infection were included in the analysis. [1
23
3]
Cas
e no
A
utho
rs
Patie
nt’s
age
at
pres
enta
tion
and
gend
er
HC
V ch
arac
teri
stic
s
IBD
ch
arac
teri
stic
s
Hep
atic
bio
chem
i-ca
l tes
ts
Ant
i-TN
F th
erap
y
Con
com
itan
t an
ti-
HC
V th
erap
y
Out
com
e IB
D
Out
com
e H
CV
1 C
ampb
ell a
nd
Gho
sh 2
001
39 y
rs M
ale
Not
ava
ilabl
e C
D
Stab
le
Sing
le d
ose
5 m
g / kg
N
o C
D r
emis
sion
for
3 m
onth
s H
CV
PC
R n
egat
ive
at 1
6 w
k of
fol-
low
-up
( < 4
x 10
3 co
pies
/ ml).
2 H
oltm
ann,
Gal
le
and
Neu
rath
200
3 26
yrs
Fem
ale
geno
type
1b,
vira
l lo
ad 7
.4 ×
10 7 c
opie
s / m
l
CD
U
ncha
nged
Si
ngle
dos
e 5
mg /
kg
No
Clin
ical
res
pons
e af
ter
2 w
k Vi
ral l
oad
- 3.
7 x
107
copi
es / m
l at
12
wk
- 3.
3 x1
06 c
opie
s / m
l at
9 m
onth
s
3 H
oltm
ann,
Gal
le
and
Neu
rath
200
3 32
yrs
Mal
e ge
noty
pe 1
vira
l lo
ad 3
.6 ×
10 5 c
opie
s / m
l
CD
N
orm
al
Sing
le d
ose
5 m
g / kg
N
o D
isap
pear
ance
of l
eft i
schi
orec
tal
cuta
neou
s fi s
tula
afte
r 2
wk,
no
rela
pse
with
in 1
8 m
onth
s fo
llow
up
Vira
l loa
d 2.
5 × 10
5 co
pies
/ ml a
t 6
wk
and
12 m
onth
s
4 A
bdem
alek
, Liu
and
Va
lent
ine
2007
54
yrs
Mal
e ge
noty
pe 1
C
D
Stab
le
5 m
g / kg
q6
wk
pegy
late
d in
terf
eron
an
d rib
aviri
n fo
r 48
wk
Clin
ical
rem
issi
on
HC
V ne
gativ
e 4
yrs
afte
r th
e an
tivi-
ral t
hera
py

© 2010 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY
Abstracts S453
Results: Th e search yielded a total of 1312 articles, of which 10 were included in full review and only 3 met inclusion criteria. Th ese 3 studies were case reports, describing a total of 4 cases of treatment with anti-TNF agent, inf-liximab, in patients with IBD (namely Crohn’s disease [CD]) and concomitant chronic HCV infection. Th e excluded 7 articles were either review articles, original articles not evaluating anti-TNF treatment in patients with IBD or case report describing the disseminated aspergillosis in patient with chronic HCV infection and CD who was treated with infl iximab but not providing any details on the course of CD or the hepatic biochemical tests. Th e fi ndings of these studies are presented in the Table. Th ere were no original studies identi-fi ed that assessed the treatment of IBD with anti-TNF agent in patients with chronic HCV infection.Conclusion: Th ere are limited data on the use of anti-TNF agents in patients with IBD and chronic HCV infection. Th e results of our systematic review indicate that therapy with anti-TNF agents does not exacerbate the course of chronic HCV infection. Further, in the limited data available, interferon based therapy has been successfully used to clear HCV infection, while not inducing a fl are of liver disease. Large scale studies are needed to fully evaluate the eff ects of anti-TNF treatment on the course of chronic HCV infection in patients who have a background of IBD. Th e course of IBD while on interferon based therapy also needs to be assessed in larger studies.Disclosure: Gary R. Lichtenstein, Md Potential Confl ict of Interest Declara-tion Abbott Corporation Consultant Alaven Consultant Bristol-Myers Squibb Research Centocor Orthobiotech Consultant, Research Elan Consultant Ferring Consultant, Research Millenium Pharmaceuticals Consultant Proctor and Gam-ble Consultant, Research Prometheus Laboratories, Inc. Consultant, Research Salix Pharmaceuticals Consultant, Research Schering-Plough Corporation Con-sultant Shire Pharmaceuticals Consultant, Research UCB Consultant, Research Warner Chilcotte Consultant, Research Wyeth Consultant.
1234
Eff ect of Age, Gender, and Ethnicity on Radiation Exposure Among a Multi-Ethnic Infl ammatory Bowel Disease Population of Low Socioeconomic StatusJason Hou, MD, Selvi Th irumurthi, MD, MS, Hoda Malaty, MD, PhD. Gastroenterology and Hepatology, Baylor College of Medicine, Houston, TX.
Purpose: Radiographic imaging is an important tool for diagnosis and man-agement of infl ammatory bowel disease (IBD). However, there is a paucity of data quantifying ionizing radiation exposure in patients with IBD. Th e eff ect of age, gender and ethnicity on ionizing radiation exposure in patients with IBD of low socioeconomic status (SES) has not been reported. Our aim was to quantify and compare the eff ect of age, gender and ethnicity on ionizing radia-tion exposure among adult patients with IBD in a county hospital system.Methods: A retrospective study was conducted on patients with IBD in the Harris County Hospital District (HCHD). Adult patients with IBD were iden-tifi ed using ICD-9 CM diagnostic codes (555.x [Crohn’s disease, CD] and 556.x [ulcerative colitis, UC]). Primary chart review was performed on all patients identifi ed with at least one inpatient or outpatient IBD diagnostic code between 2000-2006. Patients with clinical, radiologic, endoscopic or histologic data consistent with IBD were included in the analysis. Demographic data, disease characteristics and radiographic imaging data were collected. Radiation expo-sure was calculated using total number of imaging studies performed during the study period and reference estimates of radiation dose per study. Th e data were analyzed using the Chi-square, Fisher exact and Student t-tests.Results: Among 549 patients identifi ed, 278 patients qualifi ed for this study. Fift y-four percent of the patients were female, 54% with CD, 30% Caucasian, 44% African American and 26% Hispanic. Th e mean length of follow up was 5.5 years. Th e mean total radiation exposure was 35.7 millisieverts (mSv) per patient. Patients with CD received over 1.5 times the radiation dose as patients with UC (43.7+/- 51 vs. 26.6+/-45 mSv, p=0.05). Overall, there was no diff er-ence in radiation exposure between men and women (33.4+/-49 vs. 37.5+/-49 mSv, p=0.49). However, in male patients < age 35, there was a trend towards increased radiation exposure compared to females (39.8+/-64 vs. 23.8+/-32 mSv, p=0.18). Twenty-one percent of patients < age 35 received greater than 75 mSv of radiation. Th ere were no diff erences in radiation exposure between ethnic groups.
Conclusion: HCHD patients with IBD are exposed to significant amounts of ionizing radiation. There was a trend in male patients < age 35 being exposed to more radiation than females. Our results are clinically relevant in the context of established gender trends for cancer risk in patients with IBD. High levels of radiation exposure among our patients with low SES may be due to lack of routine care or inadequate medical therapy and bears further study.
1235
Higher Weight Based Doses of Adalimumab Reduces Risk of Surgery at 6 MonthsRaja Taunk, MD,1 Ellen Scherl, MD,1 Harrison Lakehomer, BA,1 Heejung Bang, PhD,2 Nicole Green, BA,1 Brian Bosworth, MD1. 1. Gastroenterology and Hepatology, Weill Medical College of Cornell University, New York, NY; 2. Department of Biostatistics, Weill Cornell Medical College, New York, NY.
Purpose: Anti-TNFα therapy has demonstrated effi cacy in the treatment of moderate-severe Crohn’s disease (CD). Both infl iximab (IFX) and adalimu-mab (ADA) have similar rates of remission and response, however both their mode of administration and dosing strategy are diff erent. Whereas IFX is pre-scribed as a weight based regimen of 5mg/kg or 10 mg/kg infusion, ADA is given subcutaneously in fi xed dosing fashion, independent of patient’s weight. No study has controlled for weight and its possible eff ect on remission rates or need for surgical intervention aft er induction with ADA. Hypothesis: Weight is an important factor in inducing remission in Crohn’s disease, and induc-tion regimens with a higher mg/kg dose of ADA are more likely to result in decreased need for surgery.Methods: Th e Consortium on Outcomes of Biologic Th erapy in IBD (COBI) is a prospectively compiled database of patients treated for CD between July 2002 and September 2009 with anti-TNF therapy. A retrospective analysis was performed to determine the eff ect of induction dosing mg/kg on our primary endpoint, the need for surgical intervention at 6 months time. Both Univariate and Multivariate Analysis were performed. Secondary outcomes were remis-sion and response rates as measured by Harvey Bradshaw Index (HBI).Results: Th ere were 78 patients who received ADA therapy for CD. Of those, only 58 had suffi cient data regarding weight, HBI, and surgery to be included in analysis. Th e mean age for initiation of ADA was 34 years (range 12-73, 56% female). Th e induction dose was calculated as the mg of ADA received over the 4 week induction period. Th e range of ADA dosing was 1.73-7.8 mg/kg. Th ere was an association between lower ADA concentration during induction and need for surgical intervention at 6 months (OR 0.49, 95% CI: 0.28-0.84). Th is held signifi cance in both univariate and multivariate analysis (p=0.009). Initial HBI scores were correlated with need surgical intervention but the study was not powered to detect impact of weight based dosing on remission rates.Conclusion: ADA at higher mg/kg dosing during the induction period of 4 weeks was correlated with a decreased need for surgical intervention at 6 months. Th e optimal dosing regimen for ADA has been previously described at 160 mg/80 mg, however heavier patients may warrant even higher induc-tion dosing given a likely lower serum concentration in these heavier patients. Trough levels are not commercially available, and existing data has not been stratifi ed by weight. Th is study demonstrates that a weight based regimen may lead to optimization of ADA. A prospective study where mg/kg dosing is cor-related with serum concentration is warranted.Disclosure: Dr Scherl - Speaker’s Bureau: Abbott.
1236
Risk Factors for the Development of Alopecia in Infl ammatory Bowel DiseaseRajesh Shah, MD, Bincy Abraham, MD, MS, Joseph Sellin, MD. Baylor College of Medicine, Houston, TX.
Purpose: Alopecia is a common complaint from infl ammatory bowel disease (IBD) patients in clinical practice. Th e aim of our study is to evaluate the prev-alence of alopecia in IBD patients and correlate alopecia with medication use, disease activity, and vitamin or mineral defi ciency.

The American Journal of GASTROENTEROLOGY VOLUME 105 | SUPPLEMENT 1 | OCTOBER 2010 www.amjgastro.com
AbstractsS454
Methods: In this survey, 58 IBD patients were recruited from the Baylor Col-lege of Medicine associated institutions. Prior to their clinic appointment, IBD patients were given a questionnaire to fi ll out. Th e data was then analyzed for signifi cant diff erences between the alopecia and non-alopecia cohorts.Results: Th e prevalence of alopecia in our population was 34%, which is signifi -cantly diff erent from the previously reported 0.8% seen in ulcerative colitis patients (P=0.0003). None of the epidemiological data showed any statistically signifi cant diff erences. Th ere were trends for mild disease (odds ratio 0.19 with 95% CI of 0.02-1.59) and severe disease (odds ratio 3.80 with 95% CI of 0.64-22.57), but these again did not reach statistical signifi cance. Th ere were no signifi cant diff erences in vitamin defi ciencies between alopecia and non-alopecia cohorts. Th ere was a trend towards vitamin D defi ciency (odds ratio 0.32 with 95% CI of 0.06-1.56), but this did not reach statistical signifi cance. No medications commonly used to treat IBD were correlated with the development of alopecia. Th e prevalence of patients stat-ing they experienced an episode of alopecia with fl are was 17%.Conclusion: Th e prevalence of alopecia in the study population is much higher than the previously reported fi gures. Th is study showed that no epidemiologi-cal factors can reliably be used to predict an IBD patient will develop alopecia. Severe disease may be associated with alopecia development, but further study will be needed to explore this. None of the common vitamin and mineral defi -ciencies seen in IBD patients were associated with alopecia. Prior studies have been linked to alopecia via the vitamin D-dependent rickets syndrome, how-ever our study showed only a trend toward vitamin D defi ciency. Th is trend and prior association to alopecia suggests further studies are needed. Finally, the medications used to treat IBD were not signifi cantly correlated with alo-pecia. Th e prevalence of alopecia is more common than previously reported, but the risk factors associated with this will need further study.
1237
A Meta-analysis of Age-specifi c Risk for Lymphoma with Immunomodula-tors for Infl ammatory Bowel DiseaseDavid Kotlyar, MD,1 Laurent Beaugerie, MD,2 James Lewis, MD, MSCE,3 Colleen Brensinger, MS,4 Wojciech Blonski, MD, PhD,3 Manuel Van Domselaar, MD,5 Gary Lichtenstein, MD3. 1. Medicine, Montefi ore Medical Center/Albert Einstein College of Medicine, Bronx, NY; 2. Department of Gastroenterology, Assistance Publique-Hôpitaux de Paris (AP-HP), Hôpital Saint- Antoine, Université Pierre et Marie Curie Paris-VI, Paris, France; 3. Division of Gastroenterology, Department of Medicine, University of Pennsylvania Health System, Philadelphia, PA; 4. Center for Clinical Epidemiology and Biostatistics, Philadelphia, PA; 5. Division of Gastroenterology, Hospital Ramón y Cajal, Madrid, Spain., Madrid, Spain.
Purpose: Th e overall risk of lymphoma with immunomodulators, azathioprine (AZA) and 6-mercaptopurine(6-MP)has been reported in several population based cohorts and in referral based studies but none have examined the risk per age group.A prior Markov analysis (Gastro 118(6):1018) suggested that if the overall relative risk (RR) was ∼3, then pts >50 on immunomodulators would have a negative eff ect on their remaining quality adjusted life-yrs(QALY) while those <50 would have benefi t. We aimed to discern RRs per age decile using raw data from previously published studies.Methods: Primary raw data was obtained from all studies evaluated for analy-sis. Four studies were included for analysis: 2 population-based -- CESAME (Lancet 2009) and Lewis (Gastro. 2001) and 2 referral center based trials Kore-litz (AJG 1999), Fraser (APT2002). Th ere are 9,975 patients in the CESAME
trial (Beaugerie) included here because only patients which were confi rmed never to have taken thiopurines at the end of follow up were excluded from the original data set. Th e standardized incidence ratio (SIR) was calculated for each age decile (e.g. 0-10, 10-20 yr olds). Pooled standardized incidence ratios (SIRs) and 95% confi dence intervals (CIs) were estimated by summing the observed and expected numbers of lymphomas across studies, stratifi ed by each age decile. CIs were estimated assuming that the incidence of lymphoma followed a Poisson distribution. To test the heterogeneity, the deviance statistic from Poisson regression models for each of the studies was examined.Results: No signifi cantly elevated risk was seen in the age ranges of 0-20, 30-50 or 60-70. Between ages 20-30 the SIR was noted to be 6.4 with 95% CI (1.67-16.6), in 50-60 yr olds 5.5 with 95% CI (2.20-11.5), and 70-80 yr olds 5.3 with 95% CI(1.68-12.5). Data on those older than 80 was not included due to low numbers of pts analyzed. For the CESAME study only, absolute risk was 0 in 0-19 yr olds, 0.504 cases per 1,000 pt yrs in 20-30 yr olds, 0.019 cases per 1,000 pt yrs in 30-40 yr olds, 0.017 cases per 1,000 pt yrs in 40-50 yr olds, 0.881 cases per 1,000 pt yrs in 50-60 yr olds, 0.813 cases per 1,000 pt yrs in 60-70 yr olds, and 5.68 cases per 1,000 pt yrs in 70-80 yr olds.Conclusion: Th is represents the fi rst report of age based risk stratifi cation of lymphoma with antimetabolite use in IBD pts. Th ese data suggest that the rela-tive risk of lymphoma with thiopurines is not disproportionately elevated in young pts. As has been previously suggested by the Markov model this data suggests that the risk to benefi t ratio of thiopurine use in elderly IBD pts may be less favorable given the baseline and the absolute risk of lymphoma is higher.Heterogeneity was nonsignifi cant for any decile. Referral centers and Popula-tion center results were not statisically signifi cantly diff erent.Disclosure: Gary R. Lichtenstein, MD Potential Confl ict of Interest Declara-tion Abbott Corporation Consultant Alaven Consultant Bristol-Myers Squibb Research Centocor Orthobiotech Consultant, Research Elan Consultant Ferring Consultant, Research Millenium Pharmaceuticals Consultant Proctor and Gamble Consultant, Research Prometheus Laboratories, Inc. Consultant, Research Salix Pharmaceuticals Consultant, Research Schering-Plough Corporation Consultant Shire Pharmaceuticals Consultant, Research UCB Consultant, Research Warner Chilcotte Consultant, Research Wyeth Consultant.
1238
Granulocyte/ Monocyte Absorption for Infl iximab Refractory Crohn’s DiseaseKoji Kamikozuru, PHD, MD, Ken Fukunaga, PHD, MD, Hiroto Miwa, Professor, Takayuki Matsumoto, Professor. Hyogo college of Medicine, Nishinomiya, Hyogo, Japan.
Purpose: Peripheral immune-disorder has been focused to play an important role in ignition and development of Crohn’s disease (CD) and anti-cytokine therapy with biologics has been recognized as the main therapeutic strategy for refractory CD patients. In Japan, infl iximab (IFX), a chimeric monoclonal IgG1 antibody against tumor necrosis factor (TNF)-α, has been an only one available among the biologics. IFX has been associated with a signifi cant improvement of patients’ quality of life. However, it has been recognized that many patients who revealed resistance to IFX or initially respond well to IFX worsen during repeated administration. Hence, we have hypothesized that the granulocyte/ monocytes absorption (GMA), an extracorporeal hemoabsorp-tion therapy removing patient’s peripheral granulocytes and monocytes semi-selectively, could be eff ective for such IFX refractory CD patients. In Japan, the
[1237] Combined meta-analysis of risk of lymphoma in IBD pts on thiopurines per age decile
Age decile Observed cases Expected cases SIR 95 % Confi dence interval
0 – 19 (combined) 1 0.09123 10.961 (0.004385 – 62.83)
20 – 29 4 0.62351 6.4153 (1.66862 – 16.5885)
30 – 39 1 1.09195 0.91579 (0.000366 – 5.24956)
40 – 49 3 1.22727 2.44445 (0.46084 – 7.2359)
50 – 59 7 1.26388 5.5385 (2.19540 – 11.4759)
60 – 69 to 70 – 79 3 – 5 1.13966 – 0.93973 2.63236 – 5.32068 (0.49627 – 7.7921) – (1.67889- 12.5157)
Heterogeneity was nonsignifi cant for any decile. Referral centers and Population center results were not statisically signifi cantly different.

© 2010 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY
Abstracts S455
weekly GMA therapy has been approved by national health-insurance policy since Feb. 2009. In this study, we aimed to evaluate the clinical effi ciency of GMA for IFX refractory CD patients who have treated with or without IFX since then.Methods: Subjects were 12 CD patients. Th eir mean clinical disease activity index (CDAI) and CD duration were 222.68 points and 10.8 years, respectively. Th eir type of CD were 4 colonic type and 8 ileocolonic type. Th ree had past episode(s) of intestinal resection. Th ree had been stopped IFX, because of infu-sion-reaction and/or ineff ectiveness, and 6 did not accept to be given IFX. We have applied 5-10 times of the weekly GMA sessions for them instead of IFX for remission induction. Also, 3 were repeated 3-4 times of weekly GMA prior to their IFX infusion every 8 weeks because of loose of its response.Results: Th e remission induction therapy with 5-10 GMA has been demon-strated signifi cant decrease of CDAI without IFX (P=0.05). And, IFX and GMA combination therapy has indicated to maintain the patients in stable clinical remission without experiencing shorten and increase IFX administration.Conclusion: IFX appears to induce and maintain remission of CD, but it may lose its effi cacy aft er repeated administration. GMA is safe and by selectively depleting elevated/activated leukocytes may be a useful adjunct for IFX effi cacy.
1239
Childhood Environmental Exposures as Risk Factors for Pouchitis in Patients with Ulcerative ColitisRafael Cordero-Arill, MD,1 Yadira Correa, MD,1 Yahaira Moreno, MD,1 Lilliana Morales, MD,1 Manuel Betancourt, BS,1 Roberto Vendrell, MD,1 Carmen Gonzalez-Keelan, MD,1 Kent Taylor, Ph.D,2 Esther Torres, MD, MACG1. 1. University of Puerto Rico School of Medicine, San Juan; 2. Medical Genetics Institute, Cedars Sinai Medical Center, Los Angeles, CA.Purpose: Pouchitis is the most common long-term complication of ileal pouch-anal anastomosis(IPAA). Although a signifi cant association between childhood environmental factors and UC has been documented, there are no studies evaluating a possible relationship between these factors and pou-chitis. Th e aim of this study is to assess whether childhood environmental exposures are risk factors for developing pouchitis in patients with UC aft er IPAA.Methods: 141 patients with UC were identifi ed from a database of patients recruited for the IBD Genetics Consortium between 1995 and 2008. Patients were from the community or the University of Puerto Rico Center for Infl am-matory Bowel Diseases clinics. 88 were followed in our clinics and had a record with documented disease evolution and treatment. Patients had consented previously for the release of information for research purposes. Demographic characteristics and treatment data was gathered retrospectively; subjects were assigned to Group A: no surgery (n=35), B: surgery other than IPAA (n=6),and C: IPAA (n=47). We focused on patients with IPAA who also participated in a dysplasia surveillance protocol, where interval pouchoscop-ies with biopsies were performed. Recorded childhood environmental factors were urban vs. rural living, running water, toilet inside home, public sewer, breast feeding history, socioeconomic status and education. Presence of pou-chitis using histological criteria was determined by an expert pathologist. An individual pouchitis rate was determined dividing number of pouchitis by number of pouchoscopies.Results: No correlation of statistical signifi cance was found between individ-ual exposures (not having running water p=0.66, not having a toilet at home p=0.90, not having public sewer service p=0.79) and recurrent pouchitis (rate >0.5). All three variables combined had no statistical signifi cance (p=0.79). Breast feeding, education, and socioeconomic status did not signifi cantly change this outcome either. However, 21/29 (72%) patients with pouchitis were not exposed to environmental risk factors.Conclusion: Although no signifi cance was found between exposure to risk fac-tors during childhood and recurrent pouchitis, lack of exposure to risks was prevalent in pouchitis. Th is fi nding is compatible with the hygiene hypothesis suggested in previous studies. Supported by the UPR SoM Endowed Health Services Research Center Grants 5S21MD000242 and 5S21MD000138, NCMHD-NIH;Grant 5P20RR011126(NCRR,NIH);and NIDDK U01 DK62413 (IBDGRC).
1240
Th e Rate of Development of Complicated Crohn’s Disease (Penetrating or Stricturing) Increases with Calendar Decade of Diagnosis: Reality or Bias?Michael Picco, MD, PhD, John Cangemi, MD, Y. Richard Wang, MD, PhD. Gastroenterology, Mayo Clinic, Jacksonville, FL.
Purpose: Th e rate of development of complicated (penetrating or stricturing) Crohn’s disease (CD) may be infl uenced by patient characteristics but also bias of patient selection or inaccurate classifi cation in historical cohort studies. We determined if calendar decade of diagnosis infl uenced rate of development of complicated disease.Methods: 207 patients with non-stricturing non-penetrating CD were fol-lowed from diagnosis to development of complications or last clinic follow-up. Th e infl uences of decade of diagnosis and patient specifi c characteristics including Montreal classifi cation and medication use on the rate of develop-ment of complicated disease in a historical cohort were determined.Results: Duration of disease was far longer in patients diagnosed before 1990 compared to aft er 1990 (24.6 vs. 6.8 years; p<0.001). Th e proportion diagnosed before age 40 was lower (30 vs. 48%, p=0.02) and surgery rates higher (68 vs. 30%; p<0.001) in the earlier diagnosis group. Immunomodulator use was equal in both groups (34%) yet time to fi rst immunomodulator prescription was signifi cantly longer in the earlier group (17.6 vs. 3.5 yrs; p<0.001). Kaplan Meier analysis was performed to study the rate of development of complica-tions by decade of diagnosis (Figure). Rates of development of complicated disease were unusually low among patients diagnosed before 1990. In a Cox proportional hazards model, only calendar decade of diagnosis (HR 6.9; p<0.001) and age at diagnosis aft er age 40 (HR 0.29; p=0.006) infl uenced the hazard of development of complications.Conclusion: Earlier calendar decade of diagnosis of CD is associated with a lower rate of progression to complicated disease. While this might refl ect changes in disease course with calendar time, it likely represents a bias in patient selection (survival bias) or inaccurate behavior classifi cation because of diff erences in technology to detect and defi ne disease complications. Such biases must be taken into account in historical cohort studies.
1241
Infectious Exacerbations of IBD in an Outpatient IBD Center Are Associ-ated with a High Rate of Clostridium diffi cile with Good Clinical OutcomeChristopher Fain, DO, Inge Hanschu, PA, Ann Silverman, MD. Henry Ford Hospital, Detroit, MI.
Purpose: Little is known about the frequency, management and outcomes of outpatients with infectious complications of infl ammatory bowel disease. We sought to characterize the organisms causing infectious exacerbations at our IBD center.

The American Journal of GASTROENTEROLOGY VOLUME 105 | SUPPLEMENT 1 | OCTOBER 2010 www.amjgastro.com
AbstractsS456
Methods: We performed a retrospective analysis of exacerbations in IBD patients under the care of a single gastroenterologist from January 2008 to 2010. Patient exacerbations had clinical signs and symptoms and required modifi cation of therapy. All had stool for culture, O and P, and C. diff toxin except for 8 patients. We identifi ed patient demographics, disease course and therapy. We documented outcomes including mortality, ICU admissions, sur-gical interventions, and hospitalizations.Results: We identifi ed 180 IBD patients with 112 exacerbations. 37 (33%) had C. diff infection (19 male, 18 female, mean age 34). Of the patients with C. diff , 2 patients had coinfection with giardia, 1 with shigella, 1 with CMV. No other organisms were detected. In patients with C. diff , 19 had ulcerative colitis and 18 had Crohn’s disease (all with colon involvement). 65% of patients had identifi able risk factors for C. diff infection. Baseline therapy in these patients included: 8% anti-TNF, 16% combination immunosuppressives; 19% steroids; 3% 6MP; 5% topical steroids. 80% were on mesalamine. C. diff was treated with vancomycin in 49%, vancomycin and metronidazole in 35%, and metro-nidazole in 16%. Besides antibiotics, 3 patients were started on 6MP, and 2 had their dose of 6MP increased. Mesalamine was started or the dose increased in 51%. 81% of patients required the addition of corticosteroids, half needing IV steroids. No patient died, needed surgical intervention, or ICU admission dur-ing the study period. 57% required hospital admission, usually for IV steroid treatment. 24% had recurrent C. diff infection.Conclusion: In our cohort of IBD patients, infectious exacerbations were asso-ciated primarily with C. diff . infection. Aggressive medical management with steroids, antibiotics, and additional combination therapy resulted in a good out-come as defi ned by no mortality, surgical intervention or ICU admission.
1242
Treatment of Newly Diagnosed Ulcerative Proctitis in Community-Based PracticeJames Richter, MD,1 Sophie Kushkuley, BS,2 Gerry Oster, PhD2. 1. Massachusetts General Hospital; Harvard Medical School, Boston, MA; 2. Policy Analysis Inc., Brookline, MA.
Purpose: Treatment of ulcerative proctitis (UP) is aimed at controlling infl am-mation and reducing symptoms. While orally administered 5-aminosalicylates (“5-ASAs”) traditionally have been the mainstay of acute and maintenance therapy for UP, 5-ASA suppositories or enemas are generally considered to be fi rst-line therapy, due to evidence that they are more eff ective at inducing and maintaining remission. Little is known, however, about how UP is typically treated in community-based practice.Methods: Using a large US healthcare claims database, we identifi ed all per-sons with evidence of newly diagnosed UP (ICD-9-CM 556.2, 556.3) between 1/1/2005 and 12/31/2007, based on: (1) ≥2 encounters for UP ≤90 days apart; (2) evidence of sigmoidoscopy/colonoscopy within 60 days of fi rst visit for UP (“index date”); and (3) no evidence of receipt of any medication used to treat UP (eg, 5-ASA, glucocorticoid, etc.) in the year preceding index date. All patients were followed for 365 days from their index date. We examined pharmacotherapy for UP over post-index periods of 30 days and 365 days alternatively.Results: We identifi ed a total of 518 patients with newly diagnosed UP. Mean (SD) age was 48 (16) years, and there were equal numbers of men and women. Forty-fi ve percent of patients were seen by a gastroenterologist at initial visit. In the 30-day post-index period, 37% of patients had evidence of receipt of mesalamine suppository; 23%, an oral 5-ASA; 12%, mesalamine enema; 12%, rectal hydrocortisone; and 6%, oral prednisone. Antidiarrheals, antimetabo-lites, and TNF inhibitors were rarely used. Over the entire 365-day post-index period, the number of patients ever-prescribed 5-ASA suppositories increased to 45%; oral 5-ASAs, 38%; 5-ASA enemas, 18%; and systemic glucocorticoids, 20%. Combination and sequential treatment was frequent. Over 365 days, 24% of patients had evidence of receipt of both oral and rectal 5-ASAs; 11%, rectal 5-ASAs and rectal steroids; 2%, rectal 5-ASAs and budesonide; and 11%, rectal 5-ASAs and systemic steroids.Conclusion: While local therapy is commonly prescribed in patients with newly diagnosed UP, approximately one in four patients receive an oral 5-ASA preparation. In the year following diagnosis, one in fi ve patients receive
systemic steroids—a marker of failure of conservative therapy and/or disease progression. Our fi ndings suggest that treatment of newly diagnosed UP by community-based physicians largely conforms to guidelines and recommen-dations. Support: Th is research was funded by Axcan Pharma Inc., which manufactures and markets a 5-ASA suppository (Canasa®).Disclosure: Th is research was funded by Axcan Pharma Inc., which manufactures and markets a 5-ASA suppository (Canasa®).
1243
Use of Anti-TNF Th erapy is Associated with Decreased Utilization of Diagnostic Imaging and Radiation Dose in Crohn’s Disease
2010 ACG/Centocor IBD Abstract AwardSeema Patil, MD, Ankur Rustgi, MBBS, MPH, Fauzia Vandermeer, MD, Raymond Cross, MD, MS. University of Maryland, Baltimore, MD.
Purpose: Diagnostic imaging is used frequently in patients with Crohn’s dis-ease (CD); therefore CD patients may be exposed to high amounts of radia-tion from diagnostic imaging in their lifetime. Frequent exposure to radiation increases the risk of malignancy. Tumor necrosis factor (TNF) antagonists are eff ective for treatment of CD and decrease health care utilization. Th e impact of anti-TNF therapy on radiation exposure has not been determined.Methods: 60 patients initiated on anti-TNF therapy with at least one year of fol-low up at a tertiary care referral center between 2004 and 2008 were included. All radiologic studies done 1 year before and 1 year aft er initiation of anti-TNF therapy were recorded. Th e annual cumulative eff ective dose of radiation was calculated using standardized eff ective doses. Demographics, disease pheno-type, and extraintestinal manifestations of disease (EIM) were collected. Dif-ferences in the number of diagnostic tests and cumulative radiation dose used the year prior and year aft er anti-TNF were compared.Results: Th e mean age was 34.3+/-11.0 years. 62% were female. 79% were Caucasian and 20% were African-American. 22%, 14%, and 64% were current, former and never smokers respectively. 25%, 48%, 13%, and 12% had ileal, ileocolonic, colonic, and upper tract disease respectively. 24%, 36%, and 40% had infl ammatory, stricturing, and penetrating disease respectively. 30% had perianal disease. 70% had EIM. 52% and 48% were treated with infl iximab and adalimumab or certolizumab respectively. In the year prior to anti-TNF treat-ment, patients underwent 5.6+/-4.8 imaging tests compared to 4.0+/-7.9 the year aft er anti-TNF (p=0.0002). CT exams decreased from 3.2+/-2.8 the year prior to anti-TNF compared to 1.3+/-2.6 the year aft er (p<0.0001). Fluoro-scopic exams decreased from 0.48+/-0.8 to 0.17+/-0.5 (p=0.01). Radiation dose decreased 17.6+/-25.4 mSv the year aft er anti-TNF therapy was initiated (p<0.0001). Radiation dose from CT decreased 16.5+/-22.1 mSv (p<0.0001). Patients with ileal and ileocolonic disease location had greater reductions in radiation exposure aft er anti-TNF therapy (data not shown).Conclusion: Th e number of diagnostic imaging tests and radiation dose is decreased the year aft er anti-TNF therapy is initiated. Th is is largely explained by decreased use of CT. It is likely that these diff erences are the result of improved disease activity and less complications of disease aft er anti-TNF use; however, it is possible that the results are biased as patients about to initiate anti-TNF therapy are more likely to undergo an extensive diagnostic evalua-tion. Further research is needed to confi rm our results and to determine if the use of diagnostic imaging is decreased with prolonged follow up.Disclosure: Dr Cross-Consultant: Abbott Laboratories, Grant Support: Abbott Laboratories and Centocor, Inc.
1244
Signifi cant Diff erences in the Prescribing Patterns of Community and Expert IBD PhysiciansArun Swaminath, MD,1 Benjamin Lebwohl, MD, MS,1 Kristina Capiak, BFA, Certifi cate Pre-Medical Sciences,1 Daniel Present, MD2. 1. Columbia University Medical Center, New York, NY; 2. Mount Sinai Medical Center, New York, NY.
Purpose: Background: Th ere are currently three available anti-TNF therapies, inf-liximab (IFX), adalizumab (ADA), and certolizumab (CZA), for the treatment of

© 2010 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY
Abstracts S457
moderate-to-severe Crohn’s disease. Th ere are no guidelines that clarify which of these drugs may be better suited to individual clinical scenarios. Th ere is little under-standing of what criteria physicians use to choose among these medications. AIMS: To gather national data on the prescribing pattern, comfort levels, and algorithms gastroenterologists use in the management of their biologic requiring patients.Methods: An internet survey was emailed to members of the American Gastroen-terology Association. Responses were collected and separated into “community” and “expert” physician based on the criteria of >50% patient panel consisting of patients with infl ammatory bowel disease (IBD). Chi square and Fischer Exact test were used to determine diff erences in the responses between groups.Results: Of 3990 eligible surveys distributed, 473 replied in full (11.9%). 64 (12.6%) of these respondents met the criteria of IBD expert physician. Demo-graphic criteria of expert and community physicians are presented in the Table. Experts were comfortable using both immunomodulators (methotrexate (MTX), 6MP, AZA) and Anti-TNF therapies, with no diff erence among the specifi c Anti-TNF’s. Community physicians were equally comfortable prescribing 6MP, AZA, IFX, ADA, but less comfortable with MTX (56% vs. 86%; p < 0.0001) and CZA (68 vs. 89%; p=0.0007) than experts. When asked whether their choice of initial anti-TNF therapy has changed since the introduction of subcutaneously adminis-tered drugs, 41% of experts now off er all three as equal options, compared to 24% of community physicians (p=0.0078). While there was no diff erence in the pro-portion of experts and community physicians that still prefer infl iximab (38% in both groups, p=0.92), a greater proportion of community physicians now prefer SQ adalimumab (32%) compared to experts (14%, p=0.0055).Conclusion: Our data suggest that experts are more comfortable using a broader array of medical therapies than community physicians.
1245
Briakinumab (Anti-interleukin 12/23p40, ABT874) for Treatment of Crohn’s Disease (CD)Remo Panaccione, MD,1 William Sandborn, MD,2 Glenn Gordon, MD,3 Scott Lee, MD,4 Alan Safdi, MD,5 Shahriar Sedghi, MD,6 Brian Feagan, MD,7 Stephen Hanauer, MD,8 Ashish Kumar, PhD,9 Roberto Carcereri, MD10. 1. University of Calgary, Calgary, AB, Canada; 2. Mayo Clinic, Rochester, MN; 3. Center for Digestive and Liver Diseases, Inc, Mexico, MO; 4. University of Washington Medical Center, Seattle, WA; 5. Consultants for Clinical Research, Cincinnati, OH; 6. Georgia Heart and Vascular Center, Macon, GA; 7. London Health, London, ON, Canada; 8. University of Chicago, Chicago, IL; 9. Abbott Laboratories, Abbott Park, IL; 10. Abbott Laboratories, Ludwigshafen, Germany.
Purpose: To evaluate effi cacy of briakinumab, an antibody against interleukin 12/23p40, for the induction and maintenance treatment of CD.
Methods: 230 patients (pts) with moderately to severely active CD (CDAI 220-400) were randomized 3:1:1 to briakinumab 700 mg (n=139) or 400 mg (n=45), or placebo (pbo; n=46) infusions at Weeks (Wk) 0, 4, and 8. Primary endpoint was clinical remission (CDAI<150) at Wk 6. Pts who responded (decrease from Wk 0 CDAI ≥ 70 points) to induction therapy at Wk 12 were eligible for maintenance therapy. Pts treated with induction briakinumab 400 mg (n=21) or pbo (n=14) who responded at Wk 12 received maintenance treatment with the same therapy at Wk 12, 16, and 20. Pts treated with induction briakinumab 700 mg who responded at Wk 12 were re-randomized to maintenance briaki-numab 700 mg (n=21) or 200 mg (n=21), or pbo (n=22) at Wk 12, 16, and 20 and assessed at Wk 24. Secondary end-points included clinical remission at Wk 12 and 24 (among pts responding at Wk 12).Results: Proportion of pts in remission at Wk 6 was 8.7% with pbo, 13.3% with briakinumab 400 mg (p=0.455, CI for diff erence in proportions = -8.1%, 18.1%) and 17.3% with briakinumab 700 mg (p=0.157, CI=-3.3%, 20.6%). Th e proportion of pts in remission at Wk 12 was 10.9% with pbo, 28.9% with bri-akinumab 400 mg (p=0.030, CI=1.8%, 34.9%) and 22.3% with briakinumab 700 mg (p=0.087, CI=-1.7%, 25.0%). Among pts continuing maintenance treatment, the proportion of pts in remission at Wk 24 was 28.6% in pts contin-uing pbo, 52.4% of pts continuing briakinumab 400 mg (p=0.219), and 57.1% of pts continuing briakinumab 700 mg (p=0.109). Among pts who received induction briakinumab 700 mg and were re-randomized, the proportion of pts in remission at Wk 24 was 47.6% in pts re-randomized to pbo, 42.9% of pts re-randomized to briakinumab 200 mg, and 57.1% of pts re-randomized to briakinumab 700 mg (same pts in preceding sentence who continued briakinu-mab 700 mg). 173 pts (75.2%) previously received anti-TNF therapy. Subgroup analyses suggested trends towards worse outcome for induction treatment of pts with primary non-response to anti-TNF therapy. During the induction portion of the study, serious adverse events (SAEs) occurred in 4.5% of pts on briakinumab and 8.7% on pbo, including 0.5% with a serious infection on briakinumab and 2.2% with a non-melanoma skin cancer on pbo. During the maintenance portion of the study, SAEs occurred in 2.2% of pts on briakinu-mab and 7.1% on pbo, including 1.1% with a serious infection on briakinumab. One pt died of respiratory distress failure due to pancreatitis 2 months aft er last dose of briakinumab.Conclusion: Among pts with moderate to severe CD, briakinumab was not eff ective for induction or maintenance of remission.Disclosure: Dr Remo Panaccione: Financial Support for Research from: Abbott, Osiris Th erapeutics Inc, UCB Inc, Lecture Fee(s) from: Abbott, Centecor Inc, Elan Pharmaceuticals, Inc, Medscape, Consultancy for: Abbott, Axcan Pharma Inc, Bio-gen/IDEC, Bristol-Myers Squibb, Centocor, Inc, Chemocentryx, Elan Pharmaceuti-cals, Inc, Ferring Pharmaceuticals Inc, Genetech Inc, UCB Inc Other: Abbott, Axcan Pharma, Centocor Inc, Chemocentryx, Elan Pharmaceuticals, Inc, Genetech Inc, Lippincott Williams & Wilkins, Novartis, PDL BioPharma DrWilliam Sandborn: Financial Support for Research: Abbott Laboratories, Bristol Meyers Squibb, Cento-corOrthoBiotech, Genentech, Millennium Pharmaceuticals, Novartis, Pfi zer, Shire Pharmaceuticals, UCB Pharma, Warner Chilcott (previously Procter & Gamble) Consultancy: ActoGenix, Abbott Laboratories (fees paid to Mayo), AGI Th erapeu-tics, Albireo, Alfa Wassermann, AM-Pharma, Amgen, Anaphore, Astellas Pharma, Athersys, Atlantic Healthcare Limited, Axcan Pharma, BioBalance Corporation, Celegene, Bristol Meyers Squibb (fees paid to Mayo), Celek Pharmaceuticals, Cellerix, CentocorOrthoBiotech (fees paid to Mayo), Chemocentryix, CoMentis, Cosmo Tech-nologies, Cytokine Pharmasciences, Eagle Pharmaceuticals, Eisai Medical Research, Elan Pharmceuticls (fees paid to Mayo), Eli Lilly, Enteromedics, Ferring Pharma-ceuticals, Flexion Th erapeutics, Funxional Th erapeutics Limited, Genentech (fees paid to Mayo), Given Imaging, GlaxoSmithKline, KaloBios Pharmaceuticals, Merck Research Laboratories, Merck Serono, Novo Nordisk, Pfi zer (fees paid to Mayo), Procter & Gamble (fees paid to Mayo), Purgenesis Technologies, Regeneron Pharma-ceuticals, Salient Pharmaceuticals, Salix Pharmaceuticals, Santarus, Schering Plough Corporation, Shire Pharmaceuticals (fees paid to Mayo), Sigmoid Pharma, Sitrtis Pharmaceuticals, SLA Pharma, Takeda (fees paid to Mayo), Tillotts Pharma, UCB Pharma (fees paid to Mayo), Vascular Biogenics, Viamet Pharmaceuticals, Wyeth Dr Glenn Gordon: Abbott, Other fi nancial benefi t, Speaking and Grant/Research Support Axcan Pharma Inc., Other fi nancial benefi t, Grant/Research Support Bris-tol-Myers Squibb, Other fi nancial benefi t, Grant/Research Support Centocor, Other fi nancial benefi t, Grant/Research Support Eisai Co.Ltd, Other fi nancial benefi t, Grant/Research Support Elan Pharmaceuticals, Inc., Other fi nancial benefi t, Speak-ing Evoke Pharma, Other fi nancial benefi t, Grant/Research Support Fleming, Self: Consulting fee, Consulting Luitpold Pharmaceuticals, Other fi nancial benefi t, Grant/Research Support Merck and Company, Other fi nancial benefi t, Grant/Research
[1244] Demographic and practice-pattern information of respondents
Demographic Expert Community N =64 N =409
Years in practice ( % ) 1 – 10 years 21 (36) 130 (34)
> 10 years 37 (64) 248 (66)
Practice setting ( % ) : Private practice 18 (28) 250 (61)
Health maintenance
organization
0 17 (4)
University-based
practice
41 (64) 110 (27)
Fellow / Trainee 4 (6.25) 25 (6)
Other 1 (2) 6 (1)
Time devoted to patient care ( % ): < 50 % 13 (20) 26 (7)
> 51 % 51(80) 378 (94)
Annual number of distinct IBD
patients
363.84 ± 40.1 76 .71 ± 4.95

The American Journal of GASTROENTEROLOGY VOLUME 105 | SUPPLEMENT 1 | OCTOBER 2010 www.amjgastro.com
AbstractsS458
Support Procter & Gamble Pharmaceuticals, Other fi nancial benefi t, Speaking and Grant/Research Support Prometheus Laboratories, Other fi nancial benefi t, Speak-ing, Consulting and Grant/Research Support Revogenex, Other fi nancial benefi t, Grant/Research Support Salix Pharmaceuticals, Other fi nancial benefi t, Speaking, Consulting and Grant/Research Support Shire Pharmaceuticals Group, Other fi nan-cial benefi t, Grant/Research Support Takeda Pharmaceutical Company Ltd, Other fi nancial benefi t, Speaking and Teaching and Grant/Research Support UCB Pharma, Other fi nancial benefi t, Speaking, Consulting and Grant/Research Support Dr Scott Lee:Abbott, Self: Consulting fee, Advisory Committees or Review Panels Abbott, Self: Consulting fee, Grant/Research Support; Abbott, Self: Consulting fee, Speaking and Teaching; Centocor, Inc.,Self: Consulting fee, Advisory Committees or Review Panels; Centocor, Inc., Self: Consulting fee, Grant/Research Support Centocor, Inc., Self: Con-sulting fee, Speaking and Teaching;Elan Pharmaceuticals, Inc., Self: Grant/Research Support; Millennium Research Group, Self: Salary, Grant/Research Support; Salix Pharmaceuticals, Inc., Self: Salary, Grant/Research Support; UCB, Inc., Self: Con-sulting fee, Advisory Committees or Review Panels; UCB, Inc., Self: Consulting fee, Grant/Research Support; UCB, Inc., Self: Consulting fee, Speaking and Teaching Dr Alan Safdi: Dr Shahriar Sedghi: Salix Pharmaceuticals, Inc., Other fi nancial benefi t, Speaking and Teaching Dr Brian Feagan: Abbott, Self: Consulting fee, Consulting Abbott, Self: Consulting fee, Grant/Research Support Albireo Pharmaceuticals, Self: Consulting fee, Consulting Bristol-Myers Squibb Co., Self: Consulting fee, Grant/Research Support Celgene Corporation, Self: Consulting fee, Advisory Committees or Review Panels Centocor, Inc., Self: Consulting fee, Consulting Centocor, Inc.,Self: Consulting fee, Grant/Research Support Elan Pharmaceuticals, Inc., Self: Consult-ing fee, Advisory Committees or Review Panels Elan Pharmaceuticals, Inc., Self: Consulting fee, Consulting Funxtional Th erapeutics, Self: Consulting fee, Consult-ing GlaxoSmithKline, Self: Consulting fee, Consulting Merck - consulting fee/speak-ing Millennium Pharmaceuticals, Self: Consulting fee, Consulting NovoNordisk,Self: Consulting fee, Consulting Ore Pharmaceuticals, Inc., Self: Consulting fee, Consulting Otsuka America Pharmaceutical Inc., Self: Consulting fee, Grant/Research Support Procter & Gamble Pharmaceuticals, Self: Consulting fee, Consulting Prometheus Laboratories Inc., Self: Consulting fee, Consulting Salix Pharmaceuticals, Inc., Self: Consulting fee, Consulting Schering Canada, Self: Consulting fee, Grant/Research Support Schering-Plough Canada Inc, Self:Consulting fee, Consulting Shire Phar-maceuticals Inc., Self: Consulting fee, Consulting Tillotts Pharma, Self: Consulting fee, Advisory Committees or Review Panels UCB Pharma Inc, Self: Consulting fee, Advisory Committees or Review Panels; UCB, Inc., Self: Consulting fee, Consulting UCB, Inc., Self: Consulting fee, Speaking and Teaching Dr Stephen Hanauer: Lecture Fee(s) from: Elan Pharmaceuticals, Consultancy for: Abbott, Millenium Pharma, Novartis Pharmaceuticals, Proctor & Gamble Pharmaceuticals, Prometheus Labo-ratories Inc Other: Abbott, Amgen, Bristol-Myers Squibb, Caremark, Centocor, CVS/Caremark, Elan Pharmaceuticals, Eli Lilly, Genetech, McNeal Pharma, Millenium Pharma, Proctor & Gamble Pharmaceuticals, Salix Pharmaceuticals Inc, Shire U.S. Inc, Takeda, Warner Chilcotte, Wyeth Pharmaceuticals Ashish Kumar: Employee, Abbott Dr Roberto Carcereri: Employee, Abbott.
1246
Changing Spectrum of IBD Admissions 1998-2008: Increasing Rates of Chronic Pain, Depression and Repeat AdmissionsMarwa El Mourabet, MD, Marc Schwartz, MD, MPH, Melissa Saul, MS, Michael Dunn, MD, Miguel Regueiro, MD, Eva Szigethy, MD, PhD, David Binion, MD. University of Pittsburgh School of Medicine, Pittsburgh, PA.
Purpose: Despite treatment advances over the past decade, the number of infl ammatory bowel disease (IBD; Crohn’s disease (CD) and ulcerative colitis (UC)) patients requiring inpatient management has signifi cantly risen. Clini-cal factors underlying these admissions have not been defi ned. We sought to characterize the factors contributing to IBD admissions in a referral popula-tion comparing hospitalizations in 1998 and 2008 respectively.Methods: Retrospective search of a comprehensive electronic medical record database was performed to identify IBD patients admitted to a tertiary referral hospital during 1998 and 2008. ICD9-CM diagnosis codes for CD or UC were used to identify admission records. Analysis was performed fi rst with IBD as primary or secondary ICD9 diagnosis (Primary IBD) and then with IBD as any of 25 possible diagnostic codes (Total IBD). Statistical analysis was performed using SPSS soft ware.Results: Th ere were 262 Total IBD admissions in 1998 and 735 in 2008 (p<0.0001). Primary IBD admissions were 119 in 1998 and 447 in 2008 (p<0.0001). Overall hospital admissions increased from 1998 (28,926) to 2008 (35,505) and the rate of IBD admissions increased signifi cantly during
this time period (p<0.0001). Th e rate of Primary IBD admissions compared with Total IBD admissions increased between 1998 and 2008 (p<0.0001). CD admissions increased during the decade, which was opposite of UC, where admissions decreased (p=0.0001). Th e rate of CD surgical admissions remained unchanged, but decreased for UC (p=0.0001). C. diffi cile associated IBD admissions increased signifi cantly from 1998 to 2008 (p=0.01). Overall IBD inpatient mortality decreased from 1998 to 2008 (p=0.03). IBD patients were signifi cantly younger in 2008 compared with 1998, and had shorter lengths of stay (p=0.001). Repeat admissions for unique IBD patients increased from 18% in 1998 to 24% in 2008. Repeat admissions in 2008 were twice more common with CD patients than UC. Chronic pain admissions accounted for 5% of IBD admissions in 2008, which was not seen in 1998. IBD admissions with concomitant anxiety/depression increased signifi cantly between 1998 (5%) and 2008 (15%).Conclusion: Despite advances in medical therapy, IBD patients are admitted at increasing rates between 1998 and 2008. Factors contributing to admission have changed, with chronic pain and depression rising signifi cantly. CD patients are readmitted more frequently in 2008 compared with prior years. UC patients have fewer admissions and less surgery during this time period. Rising CD admissions and repeat admissions appear related to associated depression and chronic pain, which is an unrecognized unmet need in IBD patient care.
1247
Long-term Compliance with Mesalamine Th erapy in Patients with Quiescent Ulcerative Colitis: Results from a Long-term Phase IV Study of MMX® MesalamineSunanda Kane, MD,1 Dory Solomon, MD,2 Mary Palmen, PhD,3 Karen Barrett, MSc3. 1. Mayo Clinic College of Medicine, Rochester, MN; 2. Shire Pharmaceuticals Inc., Wayne, PA; 3. Shire Pharmaceuticals Inc., Basingstoke, United Kingdom.
Purpose: Patients with quiescent ulcerative colitis (UC) are oft en required to remain on long-term maintenance therapy to prevent recurrence of active disease. However, patients frequently report forgetting to take their medica-tion, particularly in the absence of symptoms. Th is may be made worse by the requirement for multiple tablets, with multiple times daily administration. MMX® mesalamine (Shire Pharmaceuticals Inc., USA; MMX, Cosmo Tech-nologies Ltd., Ireland) features a low pill burden and once-daily (QD) dos-ing. In this analysis of a long-term phase IV maintenance study using MMX mesalamine, we examine compliance over time with a once-daily mesalamine formulation.Methods: Th e Strategies in Maintenance for Patients Receiving Long-term Th er-apy (SIMPLE) study was a phase IV, multicenter, open-label trial conducted in 51 centers across the USA. Patients with quiescent UC (defi ned as no rectal bleed-ing and 0-1 more bowel movements than normal per day, either at enrollment or following 8 weeks’ treatment with MMX mesalamine [2.4-4.8g/day; acute phase]) received MMX mesalamine 2.4g/day QD for 12 months (maintenance phase). We examined compliance at 6 months, and 12 months aft er entry to the maintenance phase. Compliance was assessed via prescription refi ll data using the formula: [sum of days’ supply dispensed]/[sum of days in all refi ll intervals] x 100. Patients who took ≥80% of study medication were considered to be compliant.Results: In total, 208 patients were enrolled to the 12-month maintenance phase, and 207 were included in the maintenance phase effi cacy population. During the maintenance phase, 79.2 and 77.3% of patients remained compliant with their prescribed treatment at 6 and 12 months, respectively. Consider-ing all patients, average compliance with MMX mesalamine in was 86.7% by month 12. Compliance was similar in patients who entered the maintenance phase directly (87.3%) and those who fi rst required acute treatment with MMX mesalamine to achieve disease quiescence (84.8%). Examination of patient outcomes according to some predefi ned patient and disease characteristics did not identify any signifi cant diff erences.Conclusion: In this study, the majority of patients were compliant with MMX mesalamine aft er 6 months treatment, and a similar proportion were also complaint aft er 12 months. Additionally, compliance was maintained regard-less of previous treatment and was equally high in patients who entered the maintenance phase directly, and those who required additional acute phase

© 2010 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY
Abstracts S459
treatment with MMX mesalamine to achieve disease quiescence. Th is research was funded by Shire Pharmaceuticals Inc.Disclosure: Sunanda Kane - Research Funding from Shire Pharmaceuticals Inc. Dory Solomon - Employee, Shire Pharmaceuticals Inc. Mary Palmen - Employee, Shire Pharmaceuticals Inc. Karen Barrett - - Employee, Shire Pharmaceuticals Inc.Th is study was funded by Shire Pharmaceuticals Inc.
1248
Impact of Severe Colitis and Colectomy on Marital Status and Divorce in Infl ammatory Bowel DiseaseMarmy Shah, MD, Marwa El Mourabet, MD, Eva Szigethy, MD, PhD, Miguel Regueiro, MD, Michael Dunn, MD, Melissa Saul, MS, Leonard Baidoo, MD, Arthur Barrie, MD, Jason Swoger, MD, Marc Schwartz, MD, MPH, David Binion, MD. University of Pittsburgh School of Medicine, Pittsburgh, PA.
Purpose: Infl ammatory bowel disease (IBD; Crohn’s disease (CD), ulcerative colitis (UC)) signifi cantly impacts patients’ quality of life and stresses psycho-social function. Of particular concern is how illness will aff ect interpersonal relationships. A major fear of IBD patients is the need for colectomy/ostomy and how this may aff ect their relationship with signifi cant others and marital status. Currently, there is limited data regarding the impact of severe colitis and colectomy on marital status. We evaluated marriage durability in a cohort of IBD colitis patients following medical and surgical management for severe disease requiring hospitalization.Methods: We conducted a retrospective, observational study of IBD patients at a tertiary referral center. IBD patients were identifi ed with ICD 9 codes and indexed terms from hospital admissions from 2002-2008. De-identifi ed records were reviewed, including hospital course, demographic data, treat-ment, surgical procedures, out patient follow-up and marital status.Results: Among 184 patients who required hospitalization (UC 86.7%, CD 2.7%, and IC 10.6%) for IBD colitis, 59.2% were married, 3.2% were divorced, and 37.5% were single at the time of hospitalization. Mean age of the married patients was 47.1 years (range 24-79 years) and they were 40.4% female and 59.6% male. Among these married individuals 23.9% required colectomy (69.2% male, 30.8% female). Patients were followed for a mean period of 485.7 days (range 1-1860 days). Among married IBD colitis patients, 10.1% required permanent end-ileostomy and 13.8% had ileoanal reconstruction. Among 109 IBD patients who were married at the time of hospitalization for severe colitis (including individuals who required colectomy/end-ilesot-omy), none underwent divorce during the follow-up time period (1-5 years, mean 3.5 years).Conclusion: We report no increase in divorce among a large cohort of married IBD patients who required inpatient management for severe colitis (including a subset with colectomy/ileostomy). Patients with IBD have signifi cant con-cern that severe colitis and its treatments, especially colectomy/ileostomy, may damage relationships with their spouse. Our data suggests that marriage dura-bility is not adversely aff ected in IBD patients requiring hospitalization for the management of severe colitis. Th e impact of IBD colitis and its treatments on patients’ psychosocial function, interpersonal relationships and quality of life is an area of clinical investigation which warrants further study.
1249
IBD Cause-Specifi c Mortality in Monroe County, NY 1995-2006: A Popula-tion-Based Cohort StudyJames Stormont, MD, Ashok Shah, MD, MACG, Anil Sharma, MD, Tarun Kothari, MD, Lawrence Saubermann, MD, Richard Farmer, MD, MS MACP, MACG. University of Rochester Medical Center, Rochester, NY.
Purpose: Th is study was designed to examine the cause of death in infl amma-tory bowel disease (IBD) in a cohort of patients from an ongoing population-based registry in Monroe County, NY (including Rochester).Methods: During the years 1995-2000, community-derived patients with a diagnosis of IBD were sent a questionnaire and a consent form. Prior to
12/31/2000, 1121 Monroe County subjects had returned the questionnaire. Aft er exclusions, 727 subjects who had signed consent forms were used to form a cohort. Cause of death information on this cohort was obtained from the Monroe County IBD Registry and the NY State Department of Health in 2008 using data from 1995-2006. We adjusted the mortality rates for age and gender.Results: Th e overall mortality for the cohort was only slightly greater than that expected in Monroe County NY with overall Standardized Mortality Ratio (SMR) of 1.11 (95% CI: 0.86, 1.36). Th e overall male SMR was 1.16 (95% CI: 0.76, 1.56), and the overall female SMR was 1.07 (95% CI: 0.74, 1.39). Th e over-all SMR for CD was 1.27 (95% CI: 0.91, 1.64) while the SMR was 1.20 for CD males and 1.34 for CD females. Th e overall SMR for CUC was 1.01 (95% CI: 0.61, 1.40) while it was 1.26 for CUC Males and 0.87 for CUC females. Th us, statistically, our groups are no diff erent than the general population of Monroe County. Among the cohort, there were 74 deaths (10.2%). Death was from a cause primarily, secondarily, or possibly related to IBD in 28.4%. Death was primarily related to IBD in 8/74 cases, or 10.8% (7 CD & 1 CUC) and median age at death in these eight was 76.5 yrs. In addition, 27.0% of deaths were from non-related malignancy and 31.1 % were due to cardiovascular disease. Seven of the deaths secondarily related to IBD were from colo-rectal cancer, with SMR of 3.77; four of these cancers (2 CD patients & 2 CUC patients) occurred in post-surgical retained rectum or colon. Th ese cancers occurred in spite of close follow-up.Conclusion: A population-based cohort of 727 patients from Monroe County in western NY, initially diagnosed as IBD, was followed for a median of 9 years and analyzed for cause of death using the Monroe County IBD registry and NY State certifi cates. Mortality of the cohort was not signifi cantly diff erent than the general population with SMR of 1.11 (95% CI: 0.86, 1.36). Four subjects died of colo-rectal cancer occurring in post surgical retained colon in spite of close follow-up. Th is emphasizes the increased cancer risk both in chronic ulcerative colitis and Crohn’s disease colitis.Disclosure: Th is research was supported by an industry grant from P&G.
1250
rVEGF164b, a Novel Anti-angiogenic VEGF-A Isoform: A Potential Th era-peutic Option for Ulcerative ColitisWalter Cromer, BS, Chaitanya Ganta, PhD, Mihir Patel, MD, Paul Jordan, MD, Ankur Sheth, MD, James Mathis, PhD, Jonathan Alexander, PhD. Mol Cell Physiology, LSU Health Sciences Center, Shreveport, LA.
Purpose: We hypothesize that VEGF-A mediated aggravation of experimental colitis can be attenuated by treatment with an endogenous inhibitory isoform of VEGF, VEGF164b. Th e protective effi cacy of VEGF164b was investigated in the TNBS induced model of murine colitis with the purpose of determining if this endogenous antiangiogenic VEGF may be therapeutic.Methods: Mice were treated with or without an adenovirus encoding rVEGF164b prior to the induction of TNBS colitis. All experimental groups were monitored for 3d (acute) or 21d (chronic) and disease activity index score was measured daily from animal weight, stool form and fecal blood. Mice were sacrifi ced at 3d or 21d and serum and organs were harvested. Colon lengths, weights, wet/dry ratio, myeloperoxidase assay (MPO), cross sectional area of colons, histopathological analysis (including severity of infl ammation, extent of infl ammation, and cryptdamage score), protein content of serum (protein losing enteropathy) and immunostaining for Meca32 (blood vessel) and VEGFR3 (lymphatic) were performed.Results: Our results show that Ad-CMV-rVEGF164b treated animals were sig-nifi cantly protected from diarrhea and occult blood over controls. Colon lengths (decreased infl ammation), wet/dry weight ratios (vasogenic edema) and MPO (neutrophil content, both acute and chronic) were signifi cantly improved in rVEGF164b treated mice over controls. Crossectional area of the colon and his-topathology were improved in animals treated with rVEGF164b in acute TNBS colitis as was protein content of the serum. Immunostaining confi rmed a sig-nifi cant reduction in the numbers of blood vessels in the colons of rVEGF164 treated animals corresonding to inhibition of VEGF-A induced endothelial cell

The American Journal of GASTROENTEROLOGY VOLUME 105 | SUPPLEMENT 1 | OCTOBER 2010 www.amjgastro.com
AbstractsS460
proliferation by rVEGF164b in vitro. Interestingly, lymphatic proliferation was also proportionately decreased in rVEGF164b treated animals.Conclusion: Our results show that VEGF-A activity in TNBS colitis induces infl ammatory angiogenesis and aggravates disease pathology and rVEGF164b treatment can attenuate several detrimental eff ects of VEGF-A induced infl am-mation and improve the colitis disease pathology. Th is is the fi rst report on the use of an endogenous inhibitory rVEGF164b as a potential therapeutic approach for attenuating the colitis disease pathology.
1251
Increased Risk of IBD Among Military Personnel with IBSChad Porter, MPH,1 Mark Pimentel, MD, FRCP(C),2 Brooks Cash, MD,3 Tunde Akinseye, BS,4 Mark Riddle, MD, DrPH1. 1. Naval Medical Research Center, Silver Spring, MD; 2. Cedars-Sinai Medical Center, Los Angeles, CA; 3. National Naval Medical Center, Bethesda, MD; 4. George Washington University, Washington, DC.
Purpose: Irritable bowel syndrome (IBS) and infl ammatory bowel disease (IBD) oft en share overlapping symptoms, and it is oft en noted that individuals with newly diagnosed IBD have had IBS symptoms for several years preceding their IBD diagnosis. Furthermore, recent data have emerged suggesting that in some cases of IBS there are subtle infl ammatory and immune markers which share common features with the immune-mediated pathophysiology associ-ated with IBD, and both have been identifi ed to occur at higher rates aft er an episode of infectious gastroenteritis (IGE). To evaluate the risk of IBS on IBD and evaluate the eff ect of intercurrent IGE, we designed a retrospective cohort study utilizing data from the US Department of Defense medical encounter data repository.Methods: Active duty military members with IBS were identifi ed and matched with 2 subjects (one each with an unrelated acute or chronic disease). Th e medical encounter history was analyzed for the duration of service time (or disease onset) to assess for incident IBD. Episodes of IGE were assessed from documented medical encounters and by self-report using a post-deployment health assessment tool completed by each service member following deploy-ment. Relative risks were calculated using Poisson regression models to deter-mine the relationship between IBS and IBD and to control for important covariates.Results: In our dataset of 28,173 subjects, we found that IBS increased IBD risk by 8-fold with an IBD incidence of 238.1 per 100,000 person-years (95% Confi dence Interval (CI: 184.2, 291.9) compared to 27.6 per 100,000 person-years (95% CI: 15.2, 40.0) in our referent population (p<0.0001). In a subset (N=2205) of subjects that only included IBS confi rmed by negative endoscopy, the risk of IBD was 15 times that of those subjects with no antecedent IBS. Th e mean time to IBD onset following initial IBS diagnosis was 2.9 years (stand-ard deviation: 1.8). We also found an approximate 2-fold increase in IBD risk following an episode IGE (p<0.05), although our study was underpowered to observe that eff ect aft er controlling for IBS.Conclusion: Th ese data refl ect a complex interaction in the pathophysiology of IBS and IBD and suggest that intercurrent IGE may increase one’s subse-quent IBD risk. Additional studies are needed to determine whether IBS lies on the causal pathway for IBD or whether the two lie on the same pathophysi-ological spectrum of the same clinical illness.
1252
Long-term Maintenance Treatment with MMX® Mesalamine in Patients with Quiescent Ulcerative Colitis: Time to Clinical RecurrenceSunanda Kane, MD,1 Dory Solomon, MD,2 Mary Palmen, PhD,3 Karen Barrett, MSc3. 1. Mayo Clinic College of Medicine, Rochester, MN; 2. Shire Pharmaceuticals Inc., Wayne, PA; 3. Shire Pharmaceuticals Inc., Basingstoke, United Kingdom.
Purpose: Patients with ulcerative colitis (UC) oft en require life-long treatment to maintain disease quiescence. When starting a new course of maintenance treatment for quiescent UC, the length of time that patients are likely to remain
recurrence free is an important consideration for both patients and physicians. In this analysis of a phase IV study, we evaluated the time to clinical recurrence in patients receiving maintenance treatment with MMX® mesalamine (Shire Pharmaceuticals Inc., USA; MMX, Cosmo Technologies Ltd., Ireland).Methods: Th e Strategies in Maintenance for Patients Receiving Long-term Th erapy (SIMPLE) study was a phase IV, multicenter, open-label trial con-ducted in 51 centers across the USA. Patients with quiescent UC (defi ned as no rectal bleeding and 0-1 more bowel movements than normal per day, either at enrollment or following 8 weeks’ treatment with MMX mesalamine [2.4-4.8 g/day; acute phase]) received MMX mesalamine 2.4 g/day once daily (QD) for 12 months (maintenance phase). We examined clinical recurrence at 6 and 12 months. Clinical recurrence was defi ned as four or more bowel movements per day above the patient’s normal frequency and associated with urgency, abdominal pain or rectal bleeding.Results: In total, 208 patients were enrolled to the 12-month maintenance phase, and 207 were included in the maintenance phase effi cacy population. Overall, 64% of patients remained recurrence free by 12 months. Examination of patient outcomes according to some predefi ned patient and disease charac-teristics did not identify any signifi cant diff erences.Conclusion: A low proportion of patients experienced disease recurrence dur-ing the study and the time to recurrence was similar regardless of whether patients had achieved disease quiescence prior to receiving MMX mesalamine therapy, or if they fi rst required acute induction therapy with MMX mesala-mine.Disclosure: Sunanda Kane - Research funding received from Shire Pharmaceuti-cals Inc. Dory Solomon - Employee, Shire Pharmaceuticals Inc. Mary Palmen - Employee, Shire Pharmaceuticals Inc. Karen Barrett - Employee, Shire Pharma-ceuticals Inc.Th is study was funded by Shire Pharmaceuticals Inc.
1253
Th e Clinical Phenotype of Obese and Overweight Crohn’s Disease PatientsShrinivas Bishu, MD,2 Saba Hamiduzzaman, MD,1 Edgar Salas, MD,1 Adrian Dawkins, MD,4 Viral Patel, BS,1 Violetta Arsenescu, MD, PhD,3 Willem de Villiers, MD, PhD,3 Razvan Arsenescu, MD, PhD3. 1. University of Kentucky Medical Center, Lexington, KY; 2. Department of Internal Medicine, University of Kentucky Medical Center, Lexington, KY; 3. Division of Digestive Diseases and Nutrition, University of Kentucky Medical Center, Lexington, KY; 4. Department of Radiology, University of Kentucky, Lexington, KY.
Purpose: Investigate the impact of overwight and obese body habitus on the phenotype and clinical course of patients with Crohn’s disease (CD).Methods: We retrospectively reviewed the medical records of 117 consecu-tive patients with CD who presented to the gastroenterology service at the University of Kentucky Medical Center. Patients were seperated based on body mass index (BMI) into three groups: normal weight (BMI: 18.5-24.9), over-weight (BMI: 25-29.9) and obese (BMI: >30). Clinical paramaters, including the montreal classifi cation, were compared between groups. Th e unpaired stu-dents t-test was used compare groups.Results: Patients with BMI > 25 were more likely to require surgery for CD (Figure 1), were less likely to have isolated infl ammatory (B1) disease and were more likely to have lower serum levels of vitamin D. Th ere was a progressive

© 2010 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY
Abstracts S461
increase in the proportion of patients with stricturing ileocolonic (L2B2) dis-ease (Figures 2 & 3), and in the proportion needing surgery with increasing BMI. Mean values of serum Vitamin D were lower in patietns with BMI >25 (20 ng/ml) compared to those with BMI < 24.9 (25 ng/ml) (p-value: 0.36). Suprisingly, mean values of C-reactive protein were lower in overweight patients (4 mg/l) compared with normal weight patients (8 mg/l) (p-value:0.20).Conclusion: Compared to normal weight patients with CD, overweight and obese patients (BMI > 25) are more likely to have more severe disease charac-erized by a higher likelyhood of Vitamin D defi ciency, stricturing ileocolonic phenotype, and are more likely to require surgery.
1254
Medical Malpractice Litigation and Infl ammatory Bowel DiseaseTimothy Pfanner, MD,2 Marwa El Mourabet, MD,1 Marc Schwartz, MD, MPH,1 Miguel Regueiro, MD,1 Kwon Miller, BA,3 David Binion, MD1. 1. University of Pittsburgh School of Medicine, Pittsburgh, PA; 2. Texas A&M Health Science Center College of Medicine, Temple, TX; 3. Physicians Insurers’ Association of America, Rockville, MD.
Purpose: Gastroenterologists are concerned about potential litigation result-ing from care of patients with infl ammatory bowel disease (IBD). IBD patients are believed to be high-risk for malpractice litigation due to rapidly changing treatment paradigms, signifi cant side eff ects of immunosuppressive therapy, frequent requirement for surgery, relatively young age and the overall com-plexity of their illness. Th ere is limited information regarding medical mal-practice litigation in IBD at the present time. We sought to characterize the patterns of medical malpractice litigation in IBD, and to determine changes in claims during the past decade which represents the era of increased immuno-suppressive therapy.
Methods: We queried a database of malpractice closed claims maintained by the Physician’s Insurance Association of America (PIAA) between January 1, 1985 and December 31, 2008. Th e PIAA provides malpractice insurance for approximately 60% of private practice U.S. physicians.Results: Over the 24 year period there were a total of 559 claims brought against all physicians involving IBD patients. Surgeons were most com-monly named with 185 closed cases (63 resulted in payments i.e., settled in or out of court). Internists were second, with 169 closed claims (52 resulted in payment). Gastroenterologists ranked third with 81 claims involving IBD patients, of which 19 were paid. Family Practitioners were fourth with 40 closed claims (14 resulted in payment). Th e rates of IBD litigation per specialty were as follows: 6.5 cases/1000 gastroenterologists; 3.2 cases/1000 general surgeons; 0.92 cases/ 1000 general internists. Further analysis of the medical defendants in IBD litigation revealed that 40% of gastroenterolo-gists who were the target of a lawsuit had previous claim experience. Th e mean annual number of IBD related claims against gastroenterologists was 3.4 and the number decreased during the most recent decade compared with prior years. Th e most common reasons for litigation were: error in diagnosis (23%), improper performance (16%), failure to supervise a case (8%), and medication errors (7%).Conclusion: Medical malpractice litigation targeting gastroenterologists in the care of IBD patients occurs rarely and has decreased over the past decade. Gas-troenterologists who are targeted in IBD litigation have a high rate of repeat claims. Concern regarding increased use of immunosuppression and biologic therapy in IBD does not correlate with litigation patterns.
1255
Accurate Diff erentiation Between Crohn’s Disease and Ulcerative Colitis Using Novel Biomarkers from Peripheral Blood SpecimensCole Harris, MS,1 Th omas Ma, MD, PhD,2 Jonathan Leighton, MD,3 Th omas Williams, MD,4 Allison Treloar, MS,1 Lisa Davis, PhD,1 John Alsobrook II, PhD1.1. Exagen Diagnostics, Inc., Albuquerque, NM; 2. Internal Medicine, Division of Gastroenterology and Hepatology, University of New Mexico, Albuquerque, NM; 3. Division of Gastroenterology and Hepatology, Mayo Clinic, Scottsdale, AZ; 4. Department of Pathology, University of New Mexico, Albuquerque, NM.
Purpose: Accurate laboratory diff erentiation of Crohn’s disease (CD) from ulcerative colitis (UC) in infl ammatory bowel disease patients would have great clinical utility. We describe here a gene expression blood biomarker set that distinguishes patients with CD from patients with UC.Methods: In an eff ort to discover a molecular profi le diagnostic for diff erentia-tion of CD from UC we investigated 10 genes that were previously identifi ed by application of Exagen’s proprietary in silico data analysis engine1 Coperna® to publicly available full-genome expression microarray data from 85 IBD patients and 42 normal controls2. Th e expression levels of those 10 discovery phase genes were assayed in a clinical study of independently ascertained, consecutively prospectively enrolled cohorts of 192 patients with IBD: 95 with ulcerative colitis, and 97 with Crohn’s disease. Each patient’s diagnosis was confi rmed by a board-certifi ed gastroenterologist using endoscopy, radiology, biopsy and pathology. All protocols were IRB approved; informed consent was obtained and peripheral blood samples and clinical data were collected from all patients. Expression data was obtained from peripheral whole blood sam-ples (with no mononuclear enrichment) by isolating total mRNAs, synthesiz-ing cDNAs, and performing real-time quantitative PCR. Expression levels of the 10 candidate biomarker genes were assayed on each patient specimen and quantitated with a standard curve.Results: An optimal scoring algorithm for classifi cation of patients as CD or UC was derived based on 3 of the 10 tested genes (MMD, CD4, DNAJA1). Th e classifi cation of patients by clinical diagnosis and test result is given in Table 1. Th e diagnostic performance of the classifi cation is summarized in Table 2.Conclusion: Th e genes identifi ed as diff erentiating between UC and CD in this study have potential as a clinical laboratory diagnostic test.Disclosure: Cole Harris - Employee: Exagen Th omas Ma - none Jonathan Leighton - none Th omas Williams - Stockholder interest: Exagen Allison Treloar - Employee: Exagen Lisa Davis - Employee: Exagen John Alsoborok - Employee: Exagen.

The American Journal of GASTROENTEROLOGY VOLUME 105 | SUPPLEMENT 1 | OCTOBER 2010 www.amjgastro.com
AbstractsS462
1256
MMX® Mesalamine for the Treatment of Quiescent Ulcerative Colitis: Assessment of Symptoms Over 12 Months’ TreatmentSunanda Kane, MD,1 Dory Solomon, MD,2 Mary Palmen, PhD,3 Karen Barrett, MSc3. 1. Mayo Clinic College of Medicine, Rochester, MN; 2. Shire Pharmaceuticals Inc., Wayne, PA; 3. Shire Pharmaceuticals Inc., Basingstoke, United Kingdom.
Purpose: Ulcerative colitis (UC) is associated with a number of unpleasant and frequently debilitating symptoms that can have a substantial negative impact on patients’ lives. Once a patient has achieved disease quiescence, one of the physician’s long term goals is to maintain a patient symptom free; many patients judge treatment success as continued relief from the symptoms of active disease. Here, we examine the effi cacy of MMX® mesalamine (Shire Pharmaceuticals Inc, USA; MMX; Cosmo Technologies Ltd, Ireland) in main-taining disease quiescence in patients receiving long-term treatment.Methods: Data were analysed from the Strategies in Maintenance for Patients Receiving Long-term Th erapy (SIMPLE) study, a phase IV, multicenter, open-label trial conducted in 51 centers across the USA. Patients with quiescent UC (defi ned as no rectal bleeding and 0-1 more bowel movements than nor-mal per day, either at enrollment or following 8 weeks’ treatment with MMX mesalamine [2.4-4.8g/day; acute phase]) received MMX mesalamine 2.4g/day once daily for 12 months (maintenance phase). Symptom severities were recorded and scored daily using IVRS and extracted from IVRS at every visit and included information on: frequency of bowel movements (scored: 0=0-1 more than normal per day; 1=2-3 more than normal per day; 2=≥4 more than normal per day), rectal bleeding (scored: 0=no bleeding; 1=streaks of blood; 2= obvious blood; 3=mostly blood), fecal urgency (scored: 0=no sense of urgency; 1=sense of urgency) and pain (scored: 0=no abdominal pain; 1=abdominal pain).Results: In total, 208 patients were enrolled to the 12-month maintenance phase, and 207 were included in the maintenance phase effi cacy population. Th e majority of patients had symptom scores of 0 aft er 6 and 12 months’ MMX mesalamine treatment (table).Conclusion: Aft er 6 and 12 months’ treatment with MMX mesalamine, the majority of patients had a symptom score of 0 for most of the major symptoms of UC.Disclosure: Sunanda Kane - Research Funding received from Shire Pharma-ceuticals Inc. Dory Solomon - Employee, Shire Pharmaceuticals Inc. Mary
Palmen - Employee, Shire Pharmaceuticals Inc. Karen Barrett - Employee, Shire Pharmaceuticals Inc.Th is Study was funded by Shire Pharmaceuticals Inc.
1257
Marital Status, Gender and Geriatric Crohn’s DiseaseManie Juneja, MD,2 Marwa El Mourabet, MD,1 Miguel Regueiro, MD,1 Michael Dunn, MD,1 Leonard Baidoo, MD,1 Marc Schwartz, MD, MPH,1 Jason Swoger, MD,1 Arthur Barrie, MD,1 David Binion, MD1. 1. University of Pittsburgh School of Medicine, Pittsburgh, PA; 2. West Virginia University Hospital, Morgantown, WV.
Purpose: Gender and relationship status are important psychosocial factors which infl uence prognosis in geriatric medicine, with male and widowed patients at risk for worse outcomes. Th ere is limited data regarding geriatric Crohn’s disease (CD) including the eff ect of gender and spousal status on dis-ease outcomes. We examined the geriatric CD population in a tertiary referral center to address these issues.Methods: Comprehensive analysis of geriatric CD patients ≥ 65 years who had a defi ned marital status followed in a tertiary hospital over a 2 year time period. Disease activity was determined by retrospective chart review, as deter-mined by physician global assessment, symptoms of diarrhea, abdominal pain, and endoscopic and/or radiographic evidence of activity. Active disease could include ≥ 1 clinical relapse during the follow up period while inactive patients remained in remission during the entire time. “Relationship” was defi ned as being married or having a partner while single patients were denoted “not in relationship.” Co-morbidity was estimated using the Charlson Co-morbidity index.Results: Th ere were 51 geriatric CD patients identifi ed (female 52.9%; male 47.1%; 96.1% Caucasian). Mean age of the patients was 72.5 ± 5.9 years and duration of CD was 17.4±14.2 years. 76.5% of the geriatric CD patients were in a relationship, 23.5% were not in a relationship (5.0% single,17.5% wid-owed,1.0% divorced). Disease activity was identifi ed in 29.4% of the geriat-ric CD patients over the 2 years. Th ere was no diff erence in the mean age for patients with evidence of active CD (70.5±5.8 years) and inactive CD (73.4 ± 5.8). Among geriatric CD patients with evidence of disease activity, 53.3% were in a relationship while 46.7% were not. We measured the association of marital status with clinical remission. 86.1% of geriatric CD patients in a relationship were in remission while only 13.9% of geriatric CD not in a relationship were able to achieve remission (OR: 5.43 (1.36-21.69) p=0.017). Gender did not infl uence the rate of remission vs. active disease in the geriatric CD population followed at our center over a 2 year time period. Co-morbidity was similar between male and female geriatric CD patients (males 2.0 ± 2.2 vs. females 2.7 ± 2.5; p= 0.29).Conclusion: Geriatric CD patients not in a relationship had a lower chance of maintaining remission over a two year time period compared with elderly patients with signifi cant others/partners. In our geriatric study population, gender did not correlate with CD activity and did not infl uence co-morbid-ity. Psychosocial factors infl uencing clinical course in geriatric CD warrant further, prospective investigation.
[1255] Table 1 . Classifi cation by 3-gene CD / UC differential biomarker
Clinical diagnosis CD UC
Biomarker classifi cation CD 89 12
Biomarker classifi cation CD 8 83
Fisher’s exact Odds Ratio (2-sided)=73.7, P < 2 x 10 − 16
[1255] Table 2 . Diagnostic performance of 3-gene CD / UC differential biom
CD UC
Accuracy* 90 % 90 %
Sensitivity 92 % 87 %
Specifi city 87 % 92 %
Positive predictive value* 88 % 91 %
Negative predictive value* 91 % 88 %
AUC-ROC 0.94
*Result based on study prevalences.
Proportion of patients with symptom score of 0 at 6 and 12 months
n ( % )
Symptom 6 months ( n =207) 12 months ( n =207)
Frequency of bowel movement 127 (61.4) 105 (50.7)
Rectal bleeding 137 (66.2) 117 (56.5)
Urgency 121 (58.5) 99 (47.8)
Pain 128 (61.8) 110 (53.1)

© 2010 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY
Abstracts S463
1258
Anti-platelet and Anticoagulant Th erapy in Geriatric Crohn’s DiseaseManie Juneja, MD,2 Marwa El Mourabet, MD,1 Arthur Barrie, MD,1 Jason Swoger, MD,1 Marc Schwartz, MD, MPH,1 Miguel Regueiro, MD,1 Leonard Baidoo, MD,1 Michael Dunn, MD,1 David Binion, MD1. 1. University of Pittsburgh School of Medicine, Pittsburgh, PA; 2. West Virginia University Hospital, Morgantown, WV.
Purpose: Chronic infl ammation, including Crohn’s disease (CD), is associ-ated with hypercoagulability and increased rates of vascular disease and this is especially true in elderly patients. Anti-platelet and anticoagulant ther-apy has been recommended as a preventive strategy for geriatric patients at risk for complications of atherosclerosis and thrombosis. However, there is concern that aspirin use may cause a worsening of IBD clinical status with disease fl are, and anticoagulation may be associated with a worsening of gas-trointestinal blood loss. Systematic data describing the relationship of anti-platelet agents and anti-coagulant use with CD activity among elderly CD is limited.Methods: We performed a comprehensive analysis of CD patients age ≥ 65 fol-lowed in a tertiary care hospital to determine relationship of CD activity and patients of anti-platelet and anticoagulant therapy. Data was extracted from a comprehensive electronic medical record based on ICD9 coding and indexed terms. CD activity was determined by retrospective chart reviews, with active disease defi ned by physician global assessment, clinical impression, symptoms of diarrhea and abdominal pain, and endoscopic and/or radiographic evi-dence of activity. Study duration was 24 months. Patients were labeled as active disease if they had ≥1 relapse during the study period and inactive patients remained in remission the entire time.Results: Th ere were 90 geriatric CD patients identifi ed of whom 32.2% were receiving anti-platelet/anticoagulant therapy. Among these individuals rates of antiplatelet/anticoagulant treatment included: Aspirin - 17.8%; warfarin - 11.1%; cilostazol - 1.1%; clopidogrel - 1.1%; low molecular weight heparin - 1.1%. During the study period 35.6% of the geriatric patients had active CD. Th e mean age for active CD was 71.4 ± 6.4 (years ± S.D.) and for inactive CD was 72.8 ± 6.8 (years ± S.D), p = NS. Among geriatric CD patients with active CD during the study period, 15.6% were using aspirin, while 19% of inactive geriatric CD were using aspirin. Among active geriatric CD patients, warfarin use was identifi ed in 9.4%, while 12.1% of inactive CD were using warfarin.Conclusion: Aspirin and warfarin use was not associated with a higher likeli-hood of active CD in geriatric patients. Th ese agents may be underutilized in geriatric patients with CD, who are at high risk of cardio-vascular events due to their chronic infl ammation. Prospective studies are warranted in this respect.
1259
NSAIDs and Hormone Replacement Th erapy in Geriatric Crohn’s DiseaseManie Juneja, MD,2 Marwa El Mourabet, MD,1 Jason Swoger, MD,1 Marc Schwartz, MD, MPH,1 Leonard Baidoo, MD,1 Arthur Barrie, MD,1 Michael Dunn, MD,1 Miguel Regueiro, MD,1 David Binion, MD1. 1. University of Pittsburgh School of Medicine, Pittsburgh, PA; 2. West Virginia University Hospital, Morgantown, WV.
Purpose: Th e US population is aging and the burden of patients with geriatric Crohn’s disease (CD) is increasing. Studies have suggested that infl ammatory bowel disease (IBD) including CD in elderly patients is diff erent from the dis-ease in young patients, arguing for two variant disease phenotypes. Treatment patterns may diff er between geriatric and young IBD, with elderly patients receiving medications for concomitant illness and prophylaxis of cardiac, vas-cular and bone health. Nonsteroidal antiinfl ammatory drugs (NSAIDs) and hormone replacement therapy (HRT) have been associated with initial onset of IBD and reactivation of quiescent disease in IBD. Data describing NSAIDs and HRT treatment in elderly CD is limited.Methods: We performed a comprehensive analysis of CD patients age ≥ 65 fol-lowed in a tertiary care center. We determined patterns of CD activity over an
18 month time period and its relationship with treatment patterns of NSAIDs and HRT therapy. CD activity was categorized by retrospective chart review, with active disease defi ned by physician global assessment, clinical impression, symptoms of diarrhea and abdominal pain, and endoscopic and/or radio-graphic evidence of activity. Patients were labeled as active disease if they had ≥ 1 relapse during the study period and inactive patients remained in remis-sion the entire time.Results: Th ere were 90 geriatric CD patients, with 35.6% (n = 32) showing evidence of active CD during the study time period. Th e mean age for active CD was 71.4 ± 6.4 (years ± S.D.) and for inactive CD was 72.8 ± 6.8 (years ± SD). Among geriatric patients with active CD, 9.4% were on NSAIDs while the inactive CD cohort had 15.5% receiving NSAIDs. Female constituted 54% of the geriatric CD patients (n=49) and HRT was identifi ed in only 7 patients (8% of the total and 14% of the female geriatric cohort). Among female CD patients with active disease 19% were on HRT, while 11% of inactive CD geri-atric females were on HRT (p=NS).Conclusion: Our study of geriatric CD patients suggests that use of NSAIDs and HRT did not correlate with increased rates of disease activity during an 18 month time period. Further prospective studies evaluating the use of NSAIDs and HRT in geriatric CD are warranted.
1260
Aspirin Use in Geriatric Crohn’s DiseaseManie Juneja, MD,2 Marwa El Mourabet, MD,1 Leonard Baidoo, MD,1 Marc Schwartz, MD, MPH,1 Arthur Barrie, MD,1 Miguel Regueiro, MD,1 Jason Swoger, MD,1 Michael Dunn, MD,1 David Binion, MD1. 1. University of Pittsburgh School of Medicine, Pittsburgh, PA; 2. West Virginia University Hospital, Morgantown, WV.
Purpose: Th ere is an increase in arterial thrombotic events in the elderly. Co-morbid illness associated with chronic infl ammation may further increase the risk of an arterial ischemic event, with data suggesting 5 fold increased cardio-vascular risk for those over age 70 compared with those under age 55. Anti-platelet therapy with aspirin has been recommended as a preventive strategy for geriatric patients at risk for complications of atherosclerosis and thrombo-sis. Crohn’s disease (CD) is a chronic infl ammatory illness of the gastrointesti-nal tract which can aff ect any age and increased risk of vascular disease in CD has been identifi ed. Aspirin use has been associated with CD exacerbation and it is unknown if it should be routinely used in CD patients at risk for vascular disease. Systematic data describing the use of aspirin in patients with geriatric CD is limited.Methods: Retrospective descriptive study of all CD patients followed in a 20 hospital system born prior to the year 1944. Data was extracted from a comprehensive electronic medical record (EMR) based on ICD9 coding and indexed terms and we examined all records (inpatient and outpatient) which were available in the study population. Co-morbidity was determined using Charlson’s index.Results: Th ere were 150 geriatric CD patients identifi ed in the EMR data analysis. 20% of these individuals were on aspirin therapy. In the geriatric CD cohort, rates of vascular disease were: Coronary artery disease (CAD) - 30.7%; Cerebrovascular disease (CVD) - 13.3%; peripheral vascular disease (PVD) - 8.7%. Patterns of aspirin usage in the CD patients with specifi c vascular disorders were as follows: CAD - 23.1%; CVD - 35%; PVD - 23.1 %. Next, we compared the rates of co-morbidity using Charlson’s index between patients receiving and not receiving aspirin (on aspirin 3.8±3.8, not on aspirin 2.4 ± 2.2; p=0.06). Th ere was no diff erence in the hospitaliza-tion rates for patients on aspirin (3.8±2.3) and those not on aspirin (3.4± 2.6); p= 0.625.Conclusion: In our IBD cohort, geriatric CD patients demonstrated an over-all low use of aspirin, which was identifi ed in one fi ft h of these individuals. Co-morbidity, number of concomitant illnesses and number of hospitaliza-tions, was similar between geriatric CD patients receiving and not receiving aspirin. Th ese data suggests that aspirin may be tolerated and underutilized in the elderly CD population, but prospective studies are warranted.

The American Journal of GASTROENTEROLOGY VOLUME 105 | SUPPLEMENT 1 | OCTOBER 2010 www.amjgastro.com
AbstractsS464
1261
Is Infl ammatory Bowel Disease a Risk Factor for Coronary Artery Disease?Tarun Rustagi, MD,1 Mridula Rai, MD,1 Luis Diez, MD2. 1. Department of Internal Medicine, University of Connecticut, Farmington, CT; 2. Saint Francis Hospital and Medical Center, Hartford, CT.
Purpose: Chronic infl ammation may act independently or synergistically with traditional atherosclerotic risk factors in the pathogenesis of atherosclerosis. Th e association between infl ammatory bowel disease (IBD) and coronary artery disease (CAD) has not been clearly studied. Th e purpose of this study is to assess whether IBD is a risk factor for CAD.Methods: Th is is a cross-sectional, single-center study aimed at evaluating the presence of traditional atherosclerotic risk factors in patients with IBD and CAD compared with the control (CAD alone) population. Th e medical records of 112 consecutive patients with documented IBD and CAD discharged from our hospital between October 2007 and September 2009 were reviewed for the Framingham risk factors. Th e Framingham risk score (FRS) was calculated based on age, sex, hypertension, diabetes, tobacco use, total cholesterol and HDL values. FRS of patients with IBD and CAD was compared with the FRS of 100 randomly selected age- and sex-matched patients with CAD alone. Values were expressed as mean±standard deviation. Th e eff ects of age and gender on FRS were controlled using analysis of covariance (ANCOVA). Student’s t-test was used to analyze continuous variables and χ2 test or Fisher’s exact test for categorical variables. A p value of ≤0.05 was considered signifi cant.Results: 79 patients with complete laboratory data and confi rmed IBD and CAD diagnosis were enrolled into the study group. 46 (58.2%) patients had ulcerative colitis, and 52% were males in the study group, compared to 40% males in control group (p=0.13). Mean age in IBD+CAD group was 61.39±10.1 years compared to mean age of 63.71±11.4 years in CAD alone group (p=0.16). Th ere was no signifi cant diff erence in the treat-ment for CAD between the two groups (p=0.81). Mean (unadjusted) FRS in IBD+CAD group was 7.51±3.48 compared to 8.56±3.93 in CAD alone group (p=0.06). Aft er adjusting FRS for group with age and gender as a covariate, the adjusted total FRS score was signifi cantly lower in patients with IBD and CAD as compared to those with CAD alone (7.88±3.29 vs. 9.34±3.85; p=0.008).Conclusion: FRS is lower in patients with IBD and CAD compared with the control, implying that IBD is an independent risk factor for CAD. Recurrent flares of intestinal mucosal inflammation leads to presence of excess pro-inflammatory cytokines and serum soluble adhesion molecules in IBD that could promote atherosclerosis-related inflammation, alter lipid metabolism, and contribute to plaque instability and rupture. Our results are in accordance with those published by smaller studies. Further pro-spective cohort studies are needed to accurately study the incidence of CAD in patients with IBD.
1262
HNF4 alpha: A New Susceptibility Gene for Crohn’s Disease?2010 Presidential Poster
Valerie Marcil, PhD,1 Emile Levy, MD, PhD,2 Devendra Amre, PhD,2 Alain Bitton, MD,1 Vytautas Bucionis, MD, MSc,1 Francois Boudreau, PhD,3 Fernand-Pierre Gendron, PhD,3 Claude Asselin, PhD,3 Jean-Francois Beaulieu, PhD,3 Daniel Sinnett, PhD,2 Ernest Seidman, MD1. 1. Gastroenterology, McGill University Health Center, Montreal, QC, Canada; 2. CHU Sainte-Justine Research Center, Montreal, QC, Canada; 3. CIHR Group on the Digestive Epithelium, Universite de Sherbrooke, Sherbrooke, QC, Canada.
Purpose: Hepatocyte nuclear factor 4 alpha (HNF4α) is a transcription factor mainly expressed in liver, intestine, kidney and pancreas involved in regulating many metabolic functions. Our recent studies in an experimental knock out model supports its potential implication in the physiopathology underlying IBD. However, little is known regarding its potential involvement in humans with Crohn’s disease (CD). Th e aim of this study was to evaluate the associa-tion between HNF4α genetic variants and CD.
Methods: Th e sequencing of the promoter, coding and strategic regions of the HNF4α gene was fi rst carried out in a sample population of 40 French Canadian patients, in order to identify the genetic variants prevalent in our population. Th ereaft er, the identifi ed polymorphisms were genotyped in an extensive French Canadian cohort including 350 CD patients and 650 controls.Results: Sequencing the HNF4α gene led to the identifi cation of 28 polymor-phisms. Genotyping these variants in our cohort revealed that 8 polymor-phisms demonstrated signifi cant allelic association with CD. Among these variants, one polymorphism leading to a change in the amino acid sequence of the protein, appears to be highly protective against the risk of developing CD (OR: 0.2546, P<0.00001). Moreover, haplotype analyses revealed that one spe-cifi c haplotype composed of 8 polymorphisms in high linkage disequilibrium and located in the promoter region is also protective against CD (OR: 0.5097, P<0.0027).Conclusion: In a French Canadian population, several HNF4α genetic vari-ants are associated with CD. Our genetic results further support the hypothesis of a relation between HNF4α and physiopathology underlying CD. Th is study is the fi rst to demonstrate a relationship between HNF4α genetic variants and CD susceptibility.
1263
ABSTRACT WITHDRAWN
1264
Th e Incidence of Infl ammatory Bowel Disease Across Time and Geogra-phy: A Systematic ReviewNatalie Molodecky, BSc,1 Ing Shian Soon, MD,1 Doreen Rabi, MD, MSc, FRCPC,1 William Ghali, MD, MPH, FRCPC,1 Eric Benchimol, MD, PhD, FRCPC,2 Remo Panaccione, MD, FRCPC,3 Subrata Ghosh, MD, FRCPC, FRCP(E),3 Gil Kaplan, MD, MPH, FRCPC1. 1. Departments of Medicine and Community Health Sciences, University of Calgary, Calgary, AB, Canada; 2. Division of Gastroenterology, Hepatology & Nutrition, Children’s Hospital of Eastern Ontario, Ottawa, ON, Canada; 3. Department of Medicine, University of Calgary, Calgary, AB, Canada.
Purpose: Th e incidence of infl ammatory bowel disease (IBD) varies greatly around the world with a wide range of estimates both within and between geo-graphic regions. Currently there is no comprehensive review of international incidence of IBD. Th e objectives of our study were to conduct a systematic review of the incidence of adult ulcerative colitis (UC) and Crohn’s disease (CD) worldwide and to evaluate the change in incidence across diff erent geo-graphic regions.Methods: A systematic literature search of MEDLINE (1950 to Oct. 2009) and EMBASE (1980 to Oct. 2009) databases was conducted to identify stud-ies investigating the incidence of IBD. Th e search was not limited by lan-guage to ensure capture of all appropriate papers. Two reviewers identifi ed eligible articles based on the following pre-determined criteria: (1) reported the methods used to obtain the diagnosis of IBD; (2) identifi ed a population-based cohort of IBD cases; (3) reported or provided enough information to calculate population-based incidence rates (IRs); (4) UC and/or CD were reported separately; and (5) published in full manuscript form. Studies not based on original data (e.g. review papers) were excluded. Geographic maps were created to evaluate worldwide diff erences in incidence of IBD. Time trend analyses were conducted to explore diff erences in incidence across time periods.Results: Th e search strategy retrieved 6940 unique citations and 180 studies were selected for inclusion. Of these, 120 described the incidence of UC and

© 2010 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY
Abstracts S465
137 described the incidence of CD. Th e studies were conducted in diff erent geographic regions with 76% of studies from Europe, 11% from Asia, and 8.5% from North America. Th e remainder of the countries made up less than 5% of the included studies. Th e annual IRs varied by geographic region with UC estimates ranging from 0.4 to 20.3 per 100,000 in Europe; 0.27 to 5.8 in Asia; and 0.6 to 19.2 in North America, and CD estimates ranging from 0.17 to 9.8 per 100,000 in Europe; 0.13 to 4.2 in Asia; and 0.8 to 20.2 in North America. Th ese included IRs ranged from 1950 to 2006 for Europeans studies, 1974 to 2004 for Asian studies, and 1940 to 2001 for North American studies. Time trend analyses were conducted in 61% of CD and 56% of UC studies, of which 70% of CD studies and 64% of UC studies showed increased incidence trends over time.Conclusion: Th e incidence of both UC and CD varies across geographic regions and time period. Overall, there has been an increased trend in the incidence of IBD over time. Th e incidence is greatest in European and North American countries.
1265
Th e Relationship Between Urban Environment and Infl ammatory Bowel Disease: A Systematic Review and Meta-analysisIng Shian Soon, MD,1 Natalie Molodecky, BSc,2 Doreen Rabi, MD, MSc, FRCPC,2 William Ghali, MD, MPH, FRCPC,2 Gil Kaplan, MD, MPH, FRCPC2. Department of Pediatrics and Community Health Sciences, University of Calgary, Calgary, AB, Canada; 2. Department of Medicine and Community Health Sciences, University of Calgary, Calgary, AB, Canada.
Purpose: Residing in an urban environment has been associated with the infl ammatory bowel diseases (IBD). Th e objectives of our study were to conduct a systematic review with meta-analysis of studies assessing the associ-ation between urban environment and both ulcerative colitis (UC) and Crohn’s disease (CD).Methods: A systematic literature search of MEDLINE (1950 to Oct. 2009) and EMBASE (1980 to Oct. 2009) databases was conducted to identify studies investigating the relationship between urban environment and IBD. The search was not limited by language to ensure capture of all appropri-ate papers. Two reviewers identified eligible articles based on the follow-ing pre-determined criteria: (1) investigated environmental risk factors for IBD in a case-control design or investigated the epidemiology of IBD using incident cases; (2) reported or provided enough information to calculate a measure of association between urban environment and IBD; and (3) UC and/or CD were reported separately. Studies not based on original data were excluded. Cohort and case-control studies were analyzed using inci-dence rate ratio (IRR) and odds ratio (OR) with 95% CIs, respectively. Ran-dom effects analyses were used given the potential heterogeneity between studies. Stratified and sensitivity analyses were performed to explore fac-tors that may explain heterogeneity between studies (e.g. publication year, geographic region, timing of exposure) and to assess the effects of selected study quality.Results: Th e search strategy retrieved 6940 unique citations and 30 stud-ies were selected for inclusion. Of these, 20 investigated the relationship between urban environment and UC and 22 investigated this relationship with CD. Th erefore, included in our analysis were 5 case-control UC studies, 7 case-control CD studies, 15 cohort UC studies and 15 cohort CD studies. Based on a random eff ects model, the pooled IRRs for UC and CD cohort studies were 1.20 (1.02, 1.41) and 1.37 (1.20, 1.58), respectively. For case-control studies the pooled ORs for UC and CD were 1.28 (0.99, 1.65) and 1.35 (1.23, 1.62), respectively. Th ese associations persisted across multiple stratifi ed and sensitivity analyses exploring clinical and study quality fac-tors. Heterogeneity was observed in the cohort studies for both UC and CD, whereas statistically signifi cant heterogeneity was not observed for the case-control studies.Conclusion: A positive association between urban environment and both CD and UC was found. Heterogeneity may be explained by diff erences in study design and quality factors.
1266
Infl uenza and Pneumococcal Vaccination in Immunosuppressed Infl am-matory Bowel Disease (IBD) PatientsPatricia Kozuch, MD,1 Aarati Malliah, MD,1 Jennifer Au, MD,1 Bettina Berman, RN,2 Valerie Pracilio, MPH,2 Neil Goldfarb, BA,2 Albert Crawford, PhD, MBA, MSIS2. 1. Th omas Jeff erson University Hospital, Division of Gastroenterology and Hepatology/Department of Medicine, Philadelphia, PA; 2. Jeff erson School of Population Health, Philadelphia, PA.
Purpose: Despite guidelines recommending that immunosuppressed IBD patients are vaccinated against Infl uenza (fl u) and S. pneumoniae (pneumo-coccus), low rates of vaccination in this population have been reported. Th e primary purpose of this study was to determine baseline and post-intervention rates of fl u and pneumococcal vaccination in immunosuppressed IBD patients at our institution. Th e intervention consisted of health-care provider educa-tion, reminder emails to physicians and a new vaccine documentation form for the chart. Th e “pre-intervention” or baseline rates of vaccination are reported; post-intervention data collection has not been yet completed.Methods: 100 consecutively seen IBD outpatients on ≥1 immunosuppressant including glucocorticosteroids, immunomodulators, and biologic agents were asked to complete a survey regarding prior-year fl u and past pneumococcal vaccination; they could mark one or more reasons for vaccination or non- vaccination. Outpatient chart review was conducted to assess documentation of these vaccinations.Results: 99 patients participated (56% females). 66% and 38% reported pre-vious-year fl u and past pneumococcal vaccination respectively. Chi-square analysis for age, sex, race, marital status, education level, attending physician and number of outpatient visits the previous year was signifi cant for females being more likely to have received a fl u vaccine (p=.012) and for age groups 15-26 y.o. and 43-73 y.o. being more predictive of pneumococcal vaccina-tion (p=.007). Flu and pneumococcal vaccination were documented in 22% and 30% of patients’ charts respectively. Th e most-oft cited reasons for fl u and pneumococcal vaccination were 1) GI doctor recommendation (55% and 71%), 2) belief that it was a good idea because of IBD medications (45% and 29%). Th e two most commonly given reasons for non-fl u vaccination were 1) “didn’t get around to it” (35%) and 2) “thought it might make me sick” (24%), and for non-pneumococcal vaccination were 1) lack of recommendation (71%) and 2) not believing it was necessary (27%).Conclusion: While baseline fl u and pneumococcal vaccination rates among immunosuppressed IBD patients exceeded previously reported data, approxi-mately one-third and two-thirds of patients respectively had not received these vaccinations. Patients’ reasons for not getting vaccinated were oft en errone-ous or showed lack of awareness. Documentation of vaccination was poor and lagged behind patient-reported vaccination as well as GI doctor recommenda-tion, the latter of which was encouragingly the most commonly cited reason for vaccination. Gender and age may be important variables in infl uencing vaccination rates.
1267
Demographic Diff erences Among Patients with Infl ammatory Bowel Disease in the U.S Military Health System
2010 ACG/Centocor IBD Abstract AwardJohn Betteridge, MD, Corinne Maydonovitch, BS, Ganesh Veerappan, MD. Walter Reed Army Medical Center, Washington, DC.
Purpose: Determine the demographic diff erences among patients seen for infl ammatory bowel diseases (IBD) in the U.S Military Health System.Methods: Th ere are a number of demographic and putative factors associated with IBD. Th e military population off ers a relatively consistent and unique but ethnically and geographically diverse population. We analyzed a military wide clinical database of an electronic medical record (EMR) with more than 45 million patient encounters in 2008, using ICD-9 codes to search then com-pare demographic diff erences among our military (active or retired) and civil-ian (non-military) benefi ciaries with IBD.

The American Journal of GASTROENTEROLOGY VOLUME 105 | SUPPLEMENT 1 | OCTOBER 2010 www.amjgastro.com
AbstractsS466
Results: A total of 8,194 patients were seen at direct access military hospi-tals during 2008 for ulcerative colitis or Crohn’s disease. 41.4 % were white, 8.2% were black and 50.4% were non-white, non-black. Men comprised the majority of service members (active or retired) while women comprised the majority of our civilian cohort. Th ere were slightly more civilian benefi ci-aries (53.3%) with IBD, than active or retired service member benefi ciar-ies. Th e age distribution between these two groups was similar(mean age in years: 39 +/-16 civ, 41 +/-15 mil). Th e percentage of patients with IBD peaked in the 3rd decade (24.7%) of life and declined in each subsequent decade. More people were seen with a diagnosis of UC than Crohn’s (51.9% vs. 48.1%). However, there was a gender diff erence with IBD phenotype; with male predominance for UC (54.7%) and female predominance for Crohn’s (53.7%).Conclusion: Many putative risk factors have been implicated in the develop-ment of infl ammatory bowel diseases. Our fi ndings are consistent with recent studies suggesting a male predominance in ulcerative colitis, and a female pre-dominance in Crohn’s disease. Although not a true incidence assessment, the uni-modal peak in age during the 3rd to 4th decades is supportive of recent studies. More data is needed to determine if particular service experiences in the military aff ect these diseases.
1268
Characteristics Predictive of Progression to Malignancy of Raised Colonic Lesions in Patients with Ulcerative Colitis (UC): A Systematic Review of the LiteratureWojciech Blonski, MD, PhD,1 Faten Aberra, MD,1 Anna Buchner, MD, PhD,1 Mark Osterman, MD,1 Ming Lin, MD,2 Gary Lichtenstein, MD1. 1. Division of Gastroenterology, University of Pennsylvania, Philadelphia, PA; 2. Pennsylvania Hospital, Philadelphia, PA.
Purpose: Pts with UC have an increased risk of colon cancer. Surveillance colonoscopy is currently recommended in pts with longstanding UC to identify precursor lesions that may develop into malignancy. However, it is
unknown whether certain characteristics of raised colonic lesions identifi ed during colonoscopy including endoscopic appearance, location, size and cer-tain pit patterns can predict the development of colonic malignancy. Th e aim of this study was to perform a systematic review of the literature focusing on characteristics of macroscopically visible raised colonic lesions in pts with longstanding UC that predict progression to malignancy.Methods: A systematic search of the literature was performed. Databases of literature examined included MEDLINE, EMBASE and PUBMED using key words: ulcerative colitis, dysplasia and colorectal cancer.Only full-length, Eng-lish-written prospective cohort studies of pts with UC who underwent con-ventional surveillance colonoscopy and that provided detailed characteristics of each raised lesion within the colon.Results: Th e search yielded a total of 3778 articles, of which 50 were included in full review and only 2 met inclusion criteria. Th e 48 studies were excluded as they were either retrospective studies, studies using chromoendoscopy, nar-row-band imaging, or magnifying colonoscopy or studies that did not provide detailed description of each raised lesion. Th ere were a total of 458 patients with extensive or total UC with at least of 7 year duration of whom 39 (8.3%) had detected macroscopically visible raised dysplastic lesions within colonic mucosa during surveillance colonoscopy. No standardized descriptions of identifi ed raised lesions including their pit pattern appearance and endoscopic appearance were provided in these studies. However the fi rst study clearly demonstrated that larger lesions (above 1 cm), of polypoid appearance and located in the right colon tended to progress to adenocarcinoma at the time of colectomy or repeated colonoscopy. Th e second study showed that the larger lesions (above 1 cm) had progression to adenocarcinoma at the time of colec-tomy or follow up colonoscopy. In total among these 39 patients, 17 (43.6%) had detected colon cancer during follow-up colectomy or surveillance colon-oscopy (Table).Conclusion: Overall, there is a relative lack of data regarding endoscopic characteristics of raised lesions within the colon in patients with long standing UC that would allow for systematic evaluation of factors predicting benignity or malignancy. Th e results of a very limited numbers of studies suggest that certain characteristics such as larger size, polypoid appearance and location in the right colon predict further progression of dysplasia to malignancy.
[1268]
Study Description
Blackstone et al. 1981 Single polypoid masses ( n =5 pts)
Results of biopsy at colonoscopy: Results at follow-up (6-12 months):
“ Mild ” dysplasia ( n =2 pts) -2x3 cm- transverse colon ( n =1 pt) − 3 × 4 cm- as-cending colon ( n =1 pt)
- cancer B2-transverse colon (colectomy) -cancer C2-ascending colon (colec-tomy)
“ Moderate ” dysplasia ( n =1pt) -2x2 cm-transverse colon -cancer B2-transverse colon (colectomy)
“ Severe ” dysplasia ( n =2 pts) -5x 20 cm-ascending & transverse colon ( n =1pt) -2x2 cm -sigmoid colon ( n =1pt)
- cancer B1-transverse colon (colectomy) - cancer invading stalk-sigmoid colon (colonoscopy)
Plaque-like lesions ( n =2pts)
Results of biopsy at colonoscopy: Results at follow up (6-12 months):
“ moderate ” dysplasia ( n =2) - size not reported- descending-sigmoid junction area ( n =1pt) - 2 x3 cm- ascending colon ( n =1pt)
- “ moderate ” dysplasia- descending / sigmoid colon (colectomy) - “ mild ” dyspla-sia-ascending-transverse colon (colonoscopy)
Multiple sessile polyps within 5-15 cm of colon ( n =5pts)
Results of biopsy at colonoscopy: Results at follow up (6-12 months):
“ Mild ” dysplasia ( n =3pts) - 0.5 cm-rectosigmoid junction ( n =1 pt) - 0.5-3 cm-sigmoid colon ( n =1pt) -0.6-1.5 cm-transverse colon ( n =1pt)
- “ mild ” dysplasia-rectum and sigmoid colon (colectomy) -cancer C2 (sigmoid, cecum), B2(descending colon) (colectomy) - “ mild ” dysplasia (transverse colon) (colonoscopy)
“ Moderate ” dysplasia ( n =2pts) - 1-1.5 cm-rectosigmoid junction ( n =1pt) -0.5-3 cm-sigmoid colon ( n =1pt)
- cancer B1(rectum), B2 (sigmoid) (colectomy) - moderate dysplasia-sigmoid (colectomy at 15 months)
Suzuki et al. 1998 DALM diagnosed by biopsy at colonoscopy ( n =13 pts) A) colectomy: invasive cancer: B1 ( n =4 pts), B2 ( n =2pts), C2 ( n =3pts) (size of DALM: 1-7 cm) high grade dysplasia ( n =1pt) (size of DALM: 0.7-4 cm) B) surveillance colonoscopy: low grade dysplasia ( n =3 pts) (size of DALM: 0.3-1 cm)
Adenoma diagnosed by biopsy at colonoscopy ( n =2pts)= > upon colectomy: DALM with high grade dysplasia ( n =2 pts) (size: 0.5-1.8 cm)
DALM diagnosed by polypectomy specimens ( n =1 pt) (size: 1.3 cm)= > Cancer B1 invading the stalk of polyp
Adenoma diagnosed by polypectomy specimens (n=11 pts) - low grade dysplasia (n=10 pts) (size: 0.3-0.9 cm) -high grade dysplasia (n=1 pt) (size: 0.4-0.8 cm)
Gross appearance: - DALM (2 pedunculated, 13 sessile, 13 plaque-like) -adenoma (9 pedunculated, 6 sessile, 1 plaque-like) (p<0.001 DALM vs. adenoma appearance)

© 2010 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY
Abstracts S467
1269
Microscopic Colitis-like Histologic Changes in Idiopathic Infl ammmatory Bowel Disease Patients: A Clinicopathologic Study Utilizing a National Pathology DatabaseJonathan Glickman, MD, PhD,1 Anuradha Singhal, MD2. 1. Caris Diagnostics, Newton, MA; 2. Caris Diagnostics, Irving, TX.
Purpose: Collagenous colitis (CC) and lymphocytic colitis (LC), collectively termed microscopic colitis (MC), are chronic watery diarrheal disorders that most commonly aff ect middle aged to elderly adults. Th e diagnosis rests upon characteristic histologic fi ndings in endoscopic mucosal biopsies, which also distinguish MC from idiopathic infl ammatory bowel disease (IBD) [ulcerative colitis (UC) and Crohn’s disease (CD)]. MC and IBD have diff erent treatments, natural histories, and need for endoscopic surveillance. However, the distinc-tion between MC and IBD can be diffi cult at times since they can share some histologic features. It has also been speculated that these disorders may bear some relationship, at least in some individuals. Th e objective of this study was to characterize patients in whom these disorders present either synchronously or metachronously.Methods: Th e case database of a large national pathology laboratory was searched for examples of MC or MC-like changes, and IBD (UC,CD or inde-terminate type) during the period January 2008 to May 2010. Patients with colonic mucosal biopsies showing MC who also had a biopsy-confi rmed or reported history of IBD, or with biopsies showing MC-like and IBD-like changes in the same endoscopic procedure, were identifi ed. Clinical and endo-scopic data such as demographic data (gender age), clinical symptoms, and endoscopic fi ndings were compared among the groups.Results: A total of 135 patients (mean age 61 yrs, M:F ratio 0.26:1) had both IBD and MC, out of a total of 5849 patients with MC or MC-like changes, and 11,965 patients with IBD (515,724 patients total). Th irty-seven of the patients were classifi ed as having CD, 76 as UC, and 22 with IBD of inde-terminate type. Among MC types, 43 had defi nite or probable CC, 46 had LC, 44 had mild colonic intraepithelial lymphocytosis and 2 had ileal lym-phocytosis. Of the 135 patients, 31 showed MC and IBD in the same biopsy set; 27 with chronic changes in the colon, and 3 cases with ileal involvement. Th e remaining 104 cases had a reported history of IBD and biopsies show-ing MC, without histologic evidence of involvement by IBD in the current biopsy set.Conclusion: A small subset of IBD patients develop MC-like histologic changes in their endoscopic biopsies, either concurrent with or following the diagnosis of IBD. Although this concurrence may in some cases be due to coin-cidence or prior misdiagnosis of IBD, our results suggest that MC-like histo-logic changes could also be an unusual manifestation of treatment or healing colitis, or an unusual pattern of incipient IBD. Th ese fi ndings emphasize the need for thorough biopsy sampling and review of clinical history in patients with suspected IBD and MC.
1270
Accuracy of Administrative Data in Identifying Ulcerative Colitis Patients Presenting with Acute Flare and Undergoing Colectomy
2010 Presidential PosterChristopher Ma, MD, Marcelo Crespin, BHSc, MD, Marie-Claude Proulx, BSc, MSc, Shani DeSilva, MD, James Hubbard, MSc, Martin Prusinkiewicz, BSc, Remo Panaccione, MD, FRCPC, Subrata Ghosh, MD, FRCPC, FRCP (E), Robert Myers, MD, MSc, FRCPC, Gil Kaplan, MD, MPH, FRCPC. Division of Gastroenterology. Department of Medicine and Community Health Sciences, University of Calgary, Calgary, AB, Canada.
Purpose: Administrative databases have been widely used to evaluate in-hos-pital outcomes among ulcerative colitis (UC) patients admitted for a fl are. However, the validity of administrative data defi ning admission diagnoses in UC has not been adequately validated. Th is study evaluates the accuracy of International Classifi cation of Diseases coding in identifying patients who are admitted for UC fl are or undergo colectomy.
Methods: Population-based surveillance was conducted in the Calgary Health Region between January 1, 1996 and December 31, 2007 using the Discharge Abstract Database to identify adults (≥18 years) admitted for UC. Two cohorts were identifi ed: patients admitted for UC (ICD-9:556.X, ICD-10:K51.X) and patients admitted with UC who underwent colectomy (ICD-9:45.7, 45.8; ICD-10/CCI:1.NM.87, 1.NM.89, 1.NM.91, 1.NQ.89, 1.NQ.90). UC patients who did not undergo colectomy were stratifi ed by diagnostic position (i.e. UC coded as the primary diagnosis vs. UC in diagnostic position 2 or 3). All medical charts were comprehensively reviewed and 100 charts were randomly audited to con-fi rm agreement. Th e accuracy of the administrative data in correctly identify-ing patients presenting with UC fl are and patients admitted for colectomy was assessed.Results: Th e administrative database identifi ed 697 admissions of UC that underwent colectomy; 665 charts were available for review. Th e adminis-trative data correctly identifi ed both UC and colectomy in 85.9% [95% CI: 83.2-88.5%] of cases. Reasons for misclassifi cation included: repeat admis-sions (3.8%); patients did not have UC (5.4%); and patients did not undergo colectomy (5.0%). Chart review was performed for 569 patients admit-ted for UC fl are but without colectomy. UC was the primary diagnosis in 66.1%. Overall, the administrative data was 57.1% [53.1-61.2%] accurate in identifying patients presenting with a fl are. 10 patients (1.8%) underwent colectomy, which was not recorded in the administrative data. Other reasons for misclassifi cation included: prior colectomy (12.3%); patients without UC (10.4%), or UC was a comorbidity for an unrelated admission (18.5%). Th e accuracy of administrative data identifying a UC fl are varied by diagnostic position: 79.3% [75.2-83.4%] in the primary diagnostic position; 18.7% [11.3-26.1%] in the second diagnostic position; and 8.1% [2.4-13.9%] in the third diagnostic position.Conclusion: Administrative data accurately identifi es UC patients who under-went a colectomy, but inappropriately included a subset of patients without UC or colectomy and missed a small proportion of colectomy patients. Adminis-trative data is less reliable in identifying UC patients presenting to hospital with a fl are, particularly if UC is not coded in the primary diagnostic position.
1271
Is the Natural History of Crohn’s Disease Altered by Immune Suppressant or Biologic Drug Use?
2010 ACG/Centocor IBD Abstract AwardLeyla Ghazi, MD, Seema Patil, MD, Mark Flasar, MD, MS, Raymond Cross, MD, MS Medicine, University of Maryland School of Medicine, Baltimore, MD.
Purpose: Recent studies have demonstrated superior outcomes of early biologic therapy with or without concomitant immune-suppressants (IS) compared to standard step up therapy. Th e purpose of this study is to evaluate diff erences in disease course among patients in clinical practice who are treated with early biologic therapy in comparison to those treated with initial IS with or without escalation to biologic therapy.Methods: All patients with Crohn’s disease (CD) evaluated from July 2004 to January 2010 at a tertiary referral center were included. Demographic data was obtained from a prospectively maintained clinical database. Each patient was categorized into one of two groups. Patients treated with early biologic therapy (with or without concomitant IS) were denoted as Early Bio group; patients treated with initial IS with or without escalation to biologics were denoted as Step Up group. Th e Short Form Infl ammatory Bowel Disease Questionnaire (SIBDQ) and the Harvey Bradshaw Index (HBI) were used to assess disease-specifi c quality of life and disease activity, respectively. Further, we collected information on physician global assessment of disease activity (PGA), use of steroids, and number of hospitalizations and surgeries aft er initiation of above therapy.Results: 136 CD patients met inclusion criteria; 73 (54%) in the Step Up group and 62 (46%) in the Early Bio group. Th ere was no signifi cant diff erence in gender, race, smoking status, presence of extraintestinal manifestations, dis-ease location, disease phenotype, perianal involvement or age at diagnosis

The American Journal of GASTROENTEROLOGY VOLUME 105 | SUPPLEMENT 1 | OCTOBER 2010 www.amjgastro.com
AbstractsS468
between groups. Mean HBI and SIBDQ scores at 3, 6, and 12 months were not diff erent between groups. Response rates as defi ned by the PGA were similar between groups at 3, 6, and 12 months. Th e proportion of patients on ster-oids was not signifi cantly diff erent at each time point. Early Bio patients had a greater number of surgeries at 1 year in comparison to Step Up patients (0.4 vs. 0.2, p=0.01). Th e number of hospitalizations did not diff er between groups (0.5 vs. 0.4, p=0.63).Conclusion: In clinical practice, early biologic therapy did not improve disease activity or quality of life and did not decrease the need for steroids or hospitalizations one year after initiation of therapy. However, the need for surgical intervention was higher in the early biologic group. The lat-ter is likely explained by the aggressive use of exam under anesthesia in our practice for patients with perianal disease. Our results suggest that clinical outcomes are not worsened in patients who undergo Step Up ther-apy. Therefore, an accelerated Step up approach for most patients seems reasonable. Further research is needed to evaluate outcomes at later time points.Disclosure: Dr Raymond Cross - Consultation for Abbott Pharmaceuticals; grant support from Centocor and Abbott Pharmaceuticals. Dr Mark Flasar - grant support from Procter and Gamble.
1272
Impact of Age at Diagnosis and Ulcerative Colitis Disease ExtentSandra Quezada, MD, MS, Raymond Cross, MD, MS. Gastroenterology, University of Maryland Medical Center, Baltimore, MD.
Purpose: Ulcerative colitis (UC) primarily aff ects young adults; however 12% of patients are diagnosed at an advanced age. Previous studies report that older patients are less likely to have pancolitis and more likely to have distal disease location. However, no studies have classifi ed patients using the Montreal clas-sifi cation system. Our objective was to compare UC phenotype by age of diag-nosis in a tertiary referral cohort.Methods: Th e Infl ammatory Bowel Disease Program’s Clinical Database pro-spectively documents demographic, extraintestinal manifestations of disease (EIM), and Montreal classifi cation of disease for all UC patients at each clinic visits. Demographics, disease extent, and EIM were compared by the following age of diagnosis groups: <17 years, 17-40 years, 41-59 years, ≥60 years.Results: 270 patients evaluated at a tertiary referral center between July 1, 2004 and April 19, 2010 were included. Mean age of diagnosis was 29.8 years. 8% (n=22) were diagnosed under age 17, 62% (n=167) were diagnosed between 17 and 40 years of age, 24% (n=64) were diagnosed between age 41 and 59, and 6% (n=17) were diagnosed at age ≥ 60. Gender, race, and family history of infl ammatory bowel disease did not diff er by age at diagnosis. 82%, 71%, 47%, and 18% of patients diagnosed at <17, 17-40, 41-59, and ≥60 years of age were never smokers (p<0.001). Mean disease duration from time of diagnosis was 16.7, 11.1, 8.2, and 5.5 years in patients diagnosed at <17, 17-40, 41-59, and ≥60 years respectively (p<0.001). As age of diagnosis increased, there was a trend for an increased proportion of patients with proctitis and a decreased proportion of patients with pancolitis (see Table).Conclusion: Aft er adjustment for smoking history, patients diagnosed at 60 or older were less likely to develop pancolitis compared to younger cohorts (OR 0.78, 95% CI 0.49, 1.23); however the fi nding was not statistically signifi cant. Adjusting for disease duration, did not aff ect the odds of developing pancolitis (data not shown).
1273
Rare Presentations of T cell and Natural Killer (NK) Cell Lymphomas Asso-ciated with Tumor Necrosis Factor Alpha (TNF-α) InhibitionDeepak Parakkal, MD, Eli Ehrenpreis, MD, Rumi Semer, MS, Matthew Adess, MD. Internal Medicine, NorthShore University Health System, Evanston, IL.
Purpose: Both T cells and NK cells provide surveillance for malignancies. Because TNF-α inhibition leads to impaired NK cell function, cells undergo-ing malignant transformation may escape detection and proliferate. Cases of T cell lymphomas developing in patients on TNF-α blockers are rarely described. Th e purpose of this study is to review and describe the clinical features of T cell lymphomas reported to the Food and Drug Administration (FDA) in patients receiving TNF-α blockers.Methods: Th e FDA AERS database is available for public access. Individual reports were downloaded as ASCII fi les and analyzed using a database created with the Access program (Microsoft Corp., Redmond, WA). Th e database was queried for lymphomas reported with infl iximab (Remicade, Revellex), adali-mumab (Humira, Trudexa), certolizumab (Cimzia), natalizumab (Tysabri) and etanercept (Enbrel). Full reports for all T-cell lymphomas were obtained from the FDA using the Freedom of Information Act.Results: A total of 2,097,223 fi les were downloaded from the FDA AERS system for the years 2004- September 2009. Seventy two cases of T cell lymphomas were identifi ed. Twenty four of these were previously reported in literature. Twenty three (32%) were in females. Twenty nine patients were treated for Crohn’s dis-ease (40%), 23 had rheumatoid arthritis (32%), 7 had psoriasis (10%), 5 had ulcerative colitis (7%), 4 had other autoimmune disease and the indication was unknown in 4 subjects. Twenty six (36%) of these were hepatosplenic T cell lymphomas (HSTCL), 26 cases (36%) were T cell non-Hodgkin’s lymphomas (NHL) and 4 were cutaneous T cell lymphomas. Th ere were 2 cases each of T cell lymphoblastic type lymphoma, intestinal T-cell lymphoma and NK cell lymphoma/leukemia. Th ere was 1 case each of γδ T cell lymphoma/anaplas-tic large cell lymphoma, hepatosplenic peripheral T cell lymphoma and eight other cases of undefi ned T cell lymphomas. Average patient age for HSTCl was 35.56(range 12 to 79), for other systemic lymphomas was 53.88 (range 17 to 86) and for cutaneous lymphomas was 52.75 (range 43 to 69), comparable to the age description in literature. Th e most common TNF-α inhibitors associated with lymphomas were infl iximab (30 patients) and etanercept (18 patients). Com-bined immunomodulator therapy and TNF-α inhibitors were given in 23(89%) of patients with HSTCL and 28(61%) of all others. Mean duration of therapy with anti-TNFα in non-HSTCL was 26.55 months (range 1-81 months).Conclusion: Th ese cases highlight the association between the use of anti-TNFα blockers and T/NK cell lymphomas. Improved epidemiologic analysis should advance our understanding of the relationship of TNF-α inhibition and T cell lymphoma development.
1274
Secondary Effi cacy Analysis from a Phase IIa Multicenter Study with Inter-feron-β-1a for Induction of Clinical Response in Active Moderate to Severe Ulcerative ColitisPeter Mannon, MD,1 Philip Miner, MD,2 Milan Lukas, MD,3 Arthur McAllister, MS,4 Fabio Cataldi, MD4. 1. University of Alabama at Birmingham, Birmingham, AL; 2. Oklahoma Foundation for Digestive Research, Oklahoma City, OK; 3. ISCARE, Prague, Czech Republic; 4. Biogen Idec, Cambridge, MA.
Purpose: IL-13 has emerged as a cytokine target for novel therapeutics in ulcerative colitis (UC). IL-13 is elevated in human UC and directly toxic to
[1272] Ulcerative colitis disease extent by age at diagnosis
Location < 17 years n ( % ) 17 – 40 years n ( % ) 41 – 59 years n ( % ) ≥ 60 years n ( % ) P value*
Proctitis (E1) Left sided colitis (E2) Pancolitis(E3)
0 (0) 4 (20) 16 (80) 13 (8) 42 (27) 103 (65) 4 (6) 26 (42) 32 (52) 3 (18) 5 (29) 9 (53) 0.10
*Pearson chi-square test.

© 2010 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY
Abstracts S469
epithelial cells. Given Type I interferons block IL-13 production and signaling in human CD4 cells, interferon-β-1a (IFNβ) was tested in an open label pilot study: 18 patients with moderately active UC treated with IFNβ, 30 μg IM/wk for 12 doses. Th e endpoint used was the Simple Clinical Colitis Activity Index (SCCAI). 67% of the patients showed response at Wk 12 durable to 18 weeks aft er treatment and 10 patients experienced remission at any one time. Th ese data lad to a Phase IIa multicenter, randomized, double-blind, placebo-con-trolled trial of IFNβ in UC.Methods: Patients (age 18-65) had moderate to severe UC (modifi ed Mayo Score 6-13), diagnosis of UC of at least 6 months, >20 cm of active disease, and were on stable doses of concomitant medications including corticoster-oids, AZA/6-MP, and 5-ASA. Patients were randomized 1:1 to receive IFNb 30 μg IM or placebo (P) twice at WK, for 12 weeks. Th e primary endpoint was clinical response at Week 8, defi ned as a decrease from baseline in the Total Mayo Score of ≥3 points and ≥30%, and a decrease in the subscore for rectal bleeding of ≥1 point or absolute subscore ≤1. Th e secondary endpoints were the clinical response at Weeks 8 and 12 defi ned as a decrease in the SCCAI score of ≥3 points.Results: Of 122 evaluable patients (61 IFNβ and 61 placebo), 64% of IFNβ vs. 46% placebo patients reported response at week 8 (P= 0.05). 75% of IFNβ vs. 52% placebo patients reported response at week 12 (P= 0.01) (Figure 1). Posi-tive safety and tolerability consistent with the established profi le of this drug. No serious infections were seen. 4 SAEs were reported (2 worsening of UC) and 1 tibia fracture in P; 1 worsening of UC in IFNb.Conclusion: Interferon-β-1a showed effi cacy on the secondary endpoints measured by the SCCAI in the induction of clinical response at both week 8 and 12. In this study IFNβ showed good safety and tolerability similarly to the known profi le of the drug. Th ese very encouraging results need to be further explored in larger studies to assess the potential of IFNβ as treatment of UC .Disclosure: Peter Mannon Consultant Biogen Idec Philip Mner Consultant Bio-gen Idec Milan Lukas Consultant Biogen Idec Arthur McAllister Employee Bio-gen Idec Fabio Cataldi Employee Biogen Idec.Th is research was supported by an industry grant from Biogen Idec.
1275
Assessment of the Effi cacy of Certolizumab Pegol for the Treatment of Crohn’s Disease at a Single North American CenterScott Lee, MD,1 Cynthia Ko, MD,1 Ghassan Wahbeh, MD,2 Jason Harper, MD,1 Cory Cullinan, RN,1 Scott Etter, RN,1 Mika Sinanan, MD,1 Christopher Naumann, MD,1 Chelle Wheat, BS; MPH candidate1. 1. Gastroenterology, University of Washington, Seattle, WA; 2. Seattle Children’s Hospital Research Foundation, Seattle, WA.
Purpose: While there have been multiple prospective clinical trials evaluating the effi cacy of certolizumab pegol (CZP) for the treatment of Crohn’s Disease (CD), the most recently approved anti-TNF biologic, there is limited published
data evaluating the effi cacy of CZP in clinical practice. We evaluated the effi -cacy of CZP in a single site practice. In addition, we evaluated the effi cacy of split dose modifi cation (200 mg every 2 weeks) in those patients who were having a fl are of symptoms despite remaining on a standard maintenance dose of CZP (400mg once monthly).Methods: Study Design: Th is study was a retrospective chart review of CZP treated CD patients seen at the University of Washington’s Infl ammatory Bowel Diseases Clinic (IBD) between April 1, 2008 and August 1, 2009. Effi -cacy Evaluation: Patients seen in the IBD clinic are uniformly evaluated with the Harvey-Bradshaw Index (HBI) and the Short Infl ammatory Bowel Dis-ease Questionnaire (SIBDQ). We defi ned response as any decrease in the HBI within 12 weeks of the fi rst induction dose. Remission was defi ned as an HBI of ≤ 5. Th e same outcome measures were evaluated for both standard dosing as well as for split dosing.Results: Sixty nine patients (36 women, 33 men) were included in the stand-ard dosing analysis; 43.5% met the defi nition of response and 34.8% either achieved or maintained a clinical remission. Among responders the mean change in HBI was -4.8 (p<0.001). Th irty one patients who lost response to the 400 mg once monthly dose (14 women, 17 men) were included in the split dosing analysis; 55.8% met the defi nition of response and 35.6% either achieved or maintained a clinical remission. Among responders the mean change in HBI was -3.11 (p<0.001).Conclusion: At a single North American site, certolizumab pegol induced a clinical response, as measured by the HBI, in 43.5% of Crohn’s Disease patients with standard dosing of 400 mg administered subcutaneously once per month. In addition, 34.8% of patients either achieved clinical remission or maintained a clinical remission with the traditional dosing strategy. Further, CZP induced a clinical response in 55.8% of patients who lost response to the 400 mg once monthly dose and were transitioned to split dosing of 200 mg every 2 weeks. Remission was achieved or maintained in 35.6% of CD patients following dose modifi cation. Although the sample size was limited in this analysis, these results support the eff ectiveness of CZP in clinical practice and warrant fur-ther investigation into dosing options for CZP for the treatment of Crohn’s Disease.Disclosure: Scott D. Lee, MD Consultant: UCB Pharma; Speakers Bureau: UCB Pharma; Grant/Research Support: UCB Pharma Ghassan Wahbeh, MD-Consul-tant: UCB Pharma; Speakers Bureau: UCB Pharma.
1276
Clinical Utility of Infl iximab in Treating Acute Exacerbation of Crohn’s Disease in the Treatment Naïve PatientsShachi Tyagi, MD, Michael Cannon, MD. Internal Medicine, William Beaumont Hospital, Royal Oak, MI.
Purpose: Anti-tumour necrosis factor-alpha (TNF-a) agents have revolution-ized the clinical management of infl ammatory bowel diseases (IBD) refractory to conventional medications (corticosteroids, immunomodulators). Anti- TNF-a agents such as infl iximab, adalimumab, and certolizumab have been found are more eff ective than placebo for the induction and maintenance of remission in luminal Crohn’s disease. Among the three agents, infl iximab is the only one approved by Food and Drug Administration (FDA) for the outpatient management of ulcerative colitis and both infl iximab and adalimumab have been found eff ective in maintenance of fi stula closure in Crohn’s disease. How-ever, the available level of evidence is D for the use of infl iximab in severely ill patients hospitalized for an acute exacerbation of Crohn’s disease and its role remains unknown for inpatient management of ulcerative colitis. Th erefore, we investigated the clinical response of infl iximab in IBD patients hospitalized for acute fl are-up.Methods: We conducted a retrospective review of the electronic medical records (EMR) of all patients at our institution admitted with diagnosis of acute fl are-up of ulcerative or crohn’s disease and who then underwent inpa-tient management with infl iximab between January 2007-September 2009. Factors reviewed included: age, race, sex, duration of symptom onset, extent/

The American Journal of GASTROENTEROLOGY VOLUME 105 | SUPPLEMENT 1 | OCTOBER 2010 www.amjgastro.com
AbstractsS470
location of disease, presence of co-morbid conditions, use of tobacco/alco-hol, and concomitant/past use of immunosuppressants. Clinical response was defi ned as relief/resolution of symptoms resulting in early discharge and outpatient follow-up 6-8 weeks later for next treatment dose. Non-respond-ers were identifi ed by prolonged length of hospital stay and/or if patient required surgery.Results: EMR review of over 2000 patient found that 47 patients met the inclu-sion criteria of which 24 had Crohn’s disease and 23 had ulcerative colitis. Inf-liximab treatment found 22 responders in the Crohn’s disease of which 32% had fi stulizing disease, 44% had ileal involvement and 24% had segmental dis-ease. Analysis of data from ulcerative colitis patients revealed 17 responders with smoking (OR 7.14) and prior use of immunosuppressants (OR 3.25) as positive predictors of infl iximab failure.Conclusion: Our study supports the use of infl iximab as a preferred treat-ment over steroids in patients hospitalized with an acute fl are-up of crohn’s disease without any previous exposure to anti-TNF-a agents. Th ese results demonstrate morbidity benefi t in patients with Crohn’s disease with shortened duration of stay in hospital and better treatment response for whom few thera-peutic options are available.
1277
Infl ammatory Bowel Disease Has a Benefi cial Eff ect on Glucose Metabo-lism in DiabetesAndres Yarur, MD,1 Juan Brito, MD,1 Daniel Sussman, MD,2 Amar Deshpande, MD,2 David Pechman, Medical student,1 Anup Sabharwal, MD,3 Maria Abreu, MD2. 1. Department of Medicine, University of Miami, Miami, FL; 2. Division of Gastroenterology, University of Miami, Miami, FL; 3. Division of Endocrinology, University of Miami, Miami, FL.
Purpose: Infl ammatory bowel disease (IBD) results in chronic infl ammation of the gastrointestinal tract, but it can also involve other organs. Th e endocrine function of the pancreas in patients with IBD and the association with diabetes mellitus (DM) has not been well-studied. We sought to compare the preva-lence of DM and level of glycemic control in patients with IBD and matched controls.Methods: We designed a retrospective cohort study of patients with a con-fi rmed diagnosis of either Crohn’s disease (CD) or ulcerative colitis (UC) matched by age and gender with controls in a 1:2 fashion. Th e primary out-come was the prevalence of DM (Type 1 or 2). Secondary outcomes were the degree of DM control (using glycohemoglobin level as a surrogate) and treat-ment required. As obesity and steroid use play a key role in the pathogenesis of Type 2 DM, we stratifi ed results by body mass index (BMI) and we accounted for prednisone exposure.Results: A total of 356 IBD subjects and 712 matched controls were identi-fi ed. Th e mean age was 44 years and 51% of the subjects were male. Th e prevalence of DM was 7.3% in the IBD group and 15.5% in the control group (p<0.05). Among patients with DM, the prevalence of Type 1 DM was sig-nifi cantly higher among patients with IBD compared with controls (p<0.05). 74.7% of subjects in the IBD group were corticosteroid-exposed, while no one in the control group used corticosteroids. Glycohemoglobin levels were statistically similar in IBD subjects with DM (IBD-DM) and controls with DM (c-DM) (p=0.88). In the IBD-DM cohort, fewer patients were on dia-betic medications (95 versus 83%; p<0.05), fewer patients used insulin (41 versus 35%; p<0.05), and among those on insulin, their scheduled insulin dose was lower (18 versus 30 units, p<0.05); these results maintained signifi -cance aft er stratifying by BMI.Conclusion: Th e prevalence of DM is lower in IBD patients when compared to matched controls, despite the fact they were more prednisone-exposed. Type 1 DM is more frequent in patients with IBD, which may be due to a common autoimmune mechanism. Th e IBD-DM group was less likely to receive insulin and had a lower daily insulin dose. Th ese results warrant fur-ther investigation into the relationship between IBD, glucose homeostasis, and DM management.
1278
Th e Predictive Utility of Capsule Endoscopy in Patients with Crohn’s Disease Starting Treatment with a Tumor Necrosis Factor Antagonist: A Prospective, Blinded StudyKevin Cronley, MD,2 Beth Bednarchik, RN,2 Laurie Logan, RN,2 Gregory Cooper, MD,1 Jeff ry Katz, MD,1 Gerard Isenberg, MD1. 1. Case Western Reserve University School of Medicine, Cleveland, OH; 2. Internal Medicine, University Hospital Case Medical Center, Cleveland, OH.
Purpose: Th e use of capsule endoscopy (CE) for the evaluation of Crohn’s disease (CD) has become increasingly common. However, how well CE fi nd-ings predict CD clinical activity remains uncertain. Th is pilot study aims to correlate CE fi ndings, using the Lewis score, with the Crohn’s disease activity index (CDAI) in patients starting therapy with an anti-tumor necrosis factor (anti-TNF) antibody.Methods: Patients with active CD starting anti-TNF therapy underwent CE at initiation of treatment, at 10 wks, and at 26 wks. Th e Lewis score, based on CE evaluation of small bowel villous edema, ulceration, and stenosis, was calcu-lated by an expert capsule endoscopist blinded to the patient’s clinical status. At each study visit, a CDAI was calculated, H&P performed, and lab studies obtained. Results were analyzed with students paired t-test.Results: Five patients have completed the study to date. Average CDAI before treatment was 308, at 10 wks 203, and at 26 wks 287. Th e decrease in CDAI score aft er 10 wks and 26 wks were not statistically signifi cant (p=0.10 and 0.12, respectively). Average Lewis scores before treatment was 1,157, at 10 wks 1,854, and at 26 wks 1490. Changes in the Lewis score were also not statistically signifi cant (p=0.11 and 0.49, respectively). No correlation between Lewis score and CDAI was found. (Figures 1 and 2)Conclusion: In our study, Lewis scores did not correlate with the CDAI in subjects managed with anti-TNF therapy. In fact, Lewis scores were worse at 10 wks even though CDAI scores improved. Th ese results suggest that the Lewis score may not correlate with clinical disease activity in CD patients receiving anti-TNF therapy. More patients need to be studied to confi rm these prelimi-nary results. Acknowledgements: Th is study is supported by the ASGE Given Capsule Endoscopy Research Award.

© 2010 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY
Abstracts S471
1279
Combining Genetic Variants with Serological Markers Improve the Accuracy in the Diagnosis of Ulcerative ColitisFred Princen, PhD, Derren Barken, PhD, Shelly Brown, BSc, Jordan Stachelski, BSc, Cherryl Triggs, BSc, Sharat Singh, PhD. Prometheus Laboratories, San Diego, CA.
Purpose: Crohn’s disease (CD) and ulcerative colitis (UC) are two common forms of infl ammatory bowel disease (IBD). Serological markers can be used to help distinguish these diseases, although their accuracy is generally greater for CD. Th is is due to the fact that most of the diverse serologic markers are associated with CD whereas there is only one predominant UC marker, namely, anti-neutrophil cytoplasmic antibodies (ANCA). UC associated ANCA yields a perinuclear staining pattern (pANCA) on alcohol fi xed neutrophils. How-ever despite its high specifi city, only 48% of the UC cases are pANCA positive. Th e search for new IBD markers using GWAS analysis confi rmed that genetic mutations are playing an important role in the disease etiology. Numerous genetic markers have been identifi ed and associated with CD, UC or both. Th e aim of this exploratory study was to identify genetic markers that can contrib-ute, in combination with ANCA/pANCA, to better identify patients with UCMethods: DNA from well characterized UC patients (n=81) and healthy con-trol (HC, n=153) were genotyped for variants in three genes: GlI1 (rs2228224) and MDR1 (rs2032582). Diff erences in risk allele frequencies between UC and HC were analyzed using Fisher’s exact test, and odds ratio (OR) were calcu-lated with 95% confi dences intervals (CIs). Patient and control serum were tested for ANCA by ELISA and pANCA by immunofl uorescence followed by DNAse treatment on fi xed neutrophils. Predictive models were generated using random forests and validated using leave-one-out cross validation.Results: Signifi cant diff erences in risk allele frequency were found for the GlI1 (G933D) mutation in UC compared to HC (p<0.001, OR=2.64, 95% CI=1.73-4.07). For the triallelic MDR1 variants, the most common MDR1 mutation (A893S) was signifi cantly associated with UC (p=0.010, OR=1.67, 95% CI=1.11-2.51). Receiver operator characteristic (ROC) analysis was used to compare the diagnostic accuracy of ANCA/pANCA alone to the three gene variants combined with ANCA/pANCA. Th e addition of the three gene vari-ants increased the area under the ROC curve from 0.793 (CI=0.726-0.861) to 0.853 (CI=0.801-0.905).Conclusion: We have characterized a new genetic variation, GlI1 (G933D), associated with UC and confi rmed the association of MDR1 (A893S) variants with UC. In this population subset, these genetic variants, in combination with ANCA/pANCA, provided greater diagnostic accuracy for UC than ANCA/pANCA alone.Disclosure: Fred Princen, Derren Barken Shelly Brown, Jordan Stachelski, Cheryl Triggs and Sharat Singh are all employees of Prometheus Laboratories.Th is research was supported by an industry grant from Prometheus laboratory.
1280
Response to Biologic Th erapy in Crohn’s Disease Does Not Diff er By RaceSeema Patil, MD, Leyla Ghazi, MD, Ankur Rustgi, MPH, Raymond Cross, MD, Mark Flasar, MD. University of Maryland School of Medicine, Baltimore, MD.
Purpose: While tumor necrosis factor antagonists (anti-TNF) are eff ective for treatment of Crohn’s disease (CD), data suggests possible diff erences in use across racial groups. One possible reason could be diff erential response to and tolerance of anti-TNF agents by race. Th e purpose of this study was to assess for diff erences in response to and tolerance of anti-TNF therapy by race.Methods: All CD patients who were initiated on anti-TNF therapy and had ≥ 1 year of follow up at a tertiary care referral center between 2004 and 2008 were indentifi ed. Demography, Montreal classifi cation, and extraintestinal manifes-tations (EIM) were collected. Physician global assessment of response, adverse drug reactions, steroid use, hospitalizations and surgeries were recorded at 3, 6, and 12 months aft er anti-TNF initiation and compared between Caucasian (W) and non-Caucasian (NW) patients.
Results: 97 patients were analyzed; 77% (77) were Caucasian (W), 20% (19) African-American and 1% (1) Hispanic (combined as NW). 63% (61) were treated with infl iximab, 30% (29) with adalimumab, and 7% (7) with certoli-zumab. Th ere was no diff erence in age, gender, smoking status, presence of EIM, or disease location between W and NW. W had more B2 and B3 behavior (47% vs. 32% and 47% vs. 37%, respectively; p=0.08), but less perianal disease (30% vs. 60%, p=0.004) than NW. W had a higher complete response rate at 3 months; however there was no diff erence at other time points (see table). Overall prevalence of steroid use at 3, 6, and 12 months was 29%, 16% and 16% respectively without signifi cant diff erences between W and NW. Th e overall rate of severe adverse drug reactions at 3, 6, and 12 months was 1%, 1%, and 0% without diff erence by race. Th e mean number and prevalence of hospitalizations in each group was not diff erent at any time point. Th ere was a trend toward a higher prevalence of surgery in W at 12 months (17% vs. 0%, p=0.08).Conclusion: Overall response to and tolerance of anti-TNF therapy over the fi rst 12 months appeared similar between W and NW patients when therapy was started under the care of a tertiary referral CD practice. A trend to lower response at 3 months in NW compared to W did not persist at later months, while hospitalizations and surgeries were similar between W and NW. Th is suggests that diff erences in use of anti-TNF therapy should not be justifi ed by possible diff erential response by race.Disclosure: Dr Patil - none Dr Ghazi - none Mr. Rustgi - none Dr Flasar - none Dr Cross - Consultant: Abbott, Grant Funding: Centocor, Abbott.
1281
Assessment of the Safety of Certolizumab Pegol for the Treatment of Crohn’s Disease at a Single North American CenterScott Lee, MD,1 Cynthia Ko, MD,1 Chelle Wheat, BS; MPH candidate,1 Jason Harper, MD,1 Cory Cullinan, RN,1 Scott Etter, RN,1 Michele Pulling, MD,1 Mika Sinanan, MD,1 Ghassan Wahbeh, MD2. 1. Gastroenterology, University of Washington, Seattle, WA; 2. Seattle Children’s Hospital Research Foundation, Seattle, WA.
Purpose: Although the data from clinical trials in regards to the safety of CZP for the treatment of Crohn’s Disease (CD) is widely available, there is limited published data specifi cally evaluating the safety of CZP in clinical practice. As such, we evaluated the safety of CZP in a single site practice, including both standard dosing (400mg once monthly) as well as split dosing (200mg every 2 weeks).Methods: Study Design: Th is study was a retrospective chart review of CZP treated CD patients seen at the University of Washington’s Infl ammatory Bowel Diseases Clinic (IBD) between April 1, 2008 and August 1, 2009. Safety Evalu-ation: Patients seen in the University of Washington’s IBD clinic are evaluated for adverse eff ects (AE) to current clinical treatment at each visit. For this safety evaluation, the number of AEs associated with CZP while on treatment as well as 90 days post treatment discontinuation were captured and assessed in relation to both standard dosing as well as split dosing.Results: Sixty nine patients (36 women, 33 men) were included in the stand-ard dosing analysis; 12 patients reported adverse events (17%) and the total number of distinct events was 18. 9 (50%) of the AEs reported were infec-tious; 5 (28%) were considered complications secondary to CD; 3 (17%) were
Table 1
PGA response W ( % ) NW ( % ) P value
3 months: none 7.9 10 0.08
3 months: complete 52.6 25 0.08
6 months: none 6.2 5.6 0.90
6 months: complete 55.4 50 0.90
12 months: none 6.4 12.5 0.30
12 months: complete 59.6 37.5 0.30

The American Journal of GASTROENTEROLOGY VOLUME 105 | SUPPLEMENT 1 | OCTOBER 2010 www.amjgastro.com
AbstractsS472
classifi ed as drug reactions to CZP; and 1 (5.5%) patient was diagnosed with Hodgkins Lymphoma. Th irty one patients (14 women, 17 men) were included in the split dosing analysis; 5 patients reported adverse events (16%) and the total number of distinct events was 6. 4 (67%) of the AEs reported were infec-tious; 1 (17%) was considered a complication secondary to CD; and 1 (3%) was an unrelated skin disorder. A majority of patients included in this analysis and reporting infectious adverse events were on concomitant immunosuppression (78% and 100% respectively) and 6 (67%) patients reporting infections in the standard dosing group had indwelling lines.Conclusion: At a single North American site, treatment with certolizumab pegol was found to be generally safe and well tolerated. In both the stand-ard dosing group (400 mg once monthly) and the dose modifi cation group (200 mg ever 2 weeks) the most common adverse events reported were infec-tions. Only 1 AE, an injection site reaction in the standard dosing group, was assessed by the treating gastroenterologist as probably related. Although the sample size in this analysis was limited, the number of adverse events reported at this single site is comparable to the frequency in previously published clini-cal trial data.Disclosure: Scott D. Lee, MD-Consultant: UCB Pharma; Speakers Bureau: UCB Pharma; Grant/Research Support: UCB Pharma Ghassan T. Wahbeh, MD-Con-sultant: UCB Pharma; Speakers Bureau: UCB Pharma.
1282
Assessment of the Safety of Certolizumab Pegol Associated with the Time of Previous Biologic Treatment of Crohn’s Disease at a Single North Ameri-can SiteChelle Wheat, BS, MPH candidate,1 Cynthia Ko, MD,1 Ghassan Wahbeh, MD,2 Cory Cullinan, RN,1 Scott Etter, RN,1 Mika Sinanan, MD,1 Scott Lee, MD1. 1. Gastroenterology, University of Washington, Seattle, WA; 2. Seattle Children’s Hospital Research Foundation, Seattle, WA.
Purpose: During prior clinical trials, adalimumab (ADA) and infl iximab (IFX) were discontinued at a minimum of eight weeks prior to patients initiating therapy with certolizumab pegol (CZP). In clinical practice, the interval from discontinuation of ADA or IFX to initiating CZP is not standardized and oft en is shorter than 8 weeks. As there is little data available regarding the safety of this practice, we evaluated whether there are any adverse events (AEs) associ-ated with the practice of initiating CZP within a variable interval relative to the time since discontinuation of another similar therapy.Methods: Study Design: Th is study was a retrospective chart review of CZP treated CD patients seen at the University of Washington’s Infl ammatory Bowel Diseases Clinic (IBD) between April 1, 2008 and August 1, 2009. Safety Evaluation: Patients seen in the University of Washington’s IBD clinic are evaluated for AEs to current clinical treatment at each visit. For this safety evaluation, the number of AEs associated with CZP within 90 days of initiation were captured and assessed in relation to the time since discontinuation of prior biologic therapy.Results: Sixty six patients (34 women, 32 men) were included in the overall analysis. Th e average time from the discontinuation of the prior biologic to the start of certolizumab pegol was 43.2 weeks. Twenty two patients (9 women, 13 men) had a washout period of less than 8 weeks (average 3.14 weeks). Of these patients, 23% reported an adverse event, including infectious events (66%), 1 suspected drug reaction to CZP (17%), and 1 case of Hodgkins Lym-phoma (17%). Forty four patients (25 women, 19 men) had a washout period of at least 8 weeks (average 63.2 weeks). Of these patients, 20% reported an adverse event, including infectious events (46%), 4 suspected drug reactions to CZP (31%), and 3 complications due to CD (23%). Th is diff erence in the proportion of patients with AEs was not statistically signifi cant (p=0.42).Conclusion: At a single North American site, the initiation of certolizumab pegol for the treatment of Crohn’s Disease (CD) within less than 8 weeks from the discontinuation of prior biologic therapy was not associated with a signifi -cant increase in the proportion of adverse events reported by patients. As the interval prior to beginning therapy with CZP in clinical practice is not standard-ized, these results are encouraging for patients who are having active symptoms on a similar biologic and require initiation of CZP therapy prior to 8 weeks.Disclosure: Scott D. Lee, MD-Consultant: UCB Pharma; Speakers Bureau: UCB Pharma; Grant/Research Support: UCB Pharma Ghassan T. Wahbeh, MD- Consultant: UCB Pharma; Speakers Bureau: UCB Pharma.
1283
Do Quality of Life, Disease Activity, and Flares Diff er by Race in Ulcerative Colitis Over Time?Leyla Ghazi, MD,1 Raymond Cross, MD, MS,1 Alison Lydecker, MPH,2 Mark Flasar, MD, MS1. 1. Medicine, University of Maryland School of Medicine, Baltimore, MD; 2. Department of Epidemiology and Preventive Medicine, Baltimore, MD.
Purpose: Research suggests that racial disparities may exist in the treatment of ulcerative colitis (UC) patients; however this may be due to racial diff er-ences in disease activity. Our aim was to assess for racial diff erences in disease activity, quality of life, and disease fl ares over time among patients in a tertiary referral practice.Methods: Th e Infl ammatory Bowel Disease Program’s Clinical Database pro-spectively documents demography, Montreal classifi cation, disease-specifi c quality of life and disease activity for all UC patients at all clinic visits. We iden-tifi ed Caucasian (W) and African American (AA) UC patients seen between 7/1/2004-12/31/2009 with ≥2 scores for the Short Form Infl ammatory Bowel Disease Questionnaire (SIBDQ) and the Simple Clinical Colitis Activity Index (SCCAI). Regression analysis assessed for racial diff erences in SCCAI, SIBDQ scores and fl ares over time.Results: 145 UC patients met inclusion criteria; 117 (81%) were Caucasian (W) and 28 (19%) were African American (AA).Th ere were no signifi cant racial diff erences in demographics, smoking status, overall extraintestinal manifesta-tions (EIM), disease location, baseline SCCAI and SIBDQ scores and fl ares; 14% of AA patients exhibited biliary EIM compared to 2% of W (p=0.01). In year 1, SCCAI scores decrease diff erentially in W and AA (p=0.06); W SCCAI scores decrease a mean 0.6 pts with each successive visit window (p<0.01 for trend) compared to a mean 0.2 pts in AA (p=0.48 for trend). In year 1, the odds of fl are at each successive visit window decreased 23% in W (p=0.003 for trend) but was static in AA; this diff erence between W and AA trended to statistical signifi cance (p=0.08). Aft er year 1, SCCAI scores increase in W by a mean 0.8 pts at each visit window (p<0.01 for trend) while scores in AA remained static; these trends were not diff erent by race (p=0.19). Aft er year 1, the odds of fl are at each successive visit window rose 21% in W (p=0.55 for trend) and 26% in AA (p=0.60 for trend); this was not signifi cantly diff erent by race (p=0.73). SIBDQ scores increase similarly in the fi rst year for W and AA at each successive visit window (mean 2.3 and 1.9 pts, p< 0.01 for both trends), decreasing in subsequent years by a mean 2.8 pts for W (p <0.01 for trend) and 3.4 pts for AA (p=0.14 for trend). Th ere were no racial diff erences in SIBDQ trends.Conclusion: Signifi cant temporal diff erences in disease activity scores and fl are rates were not found between W and AA in a tertiary referral UC cohort; how-ever a trend to a more vigorous decrease in SCCAI was seen in W compared to AA in the fi rst year. Further investigation is needed to determine whether this represents racial diff erences in the course of UC.Disclosure: Dr Raymond Cross - Consultation for Abbott Pharmaceuticals, and grants from Centocor and Abbott Pharmaceuticals; Dr Mark Flasar - grant from Procter and Gamble.
1284
Infl ammatory Bowel Disease Exacerbations Aft er the Initiation of Aspirin and Clopidogrel (Plavix®) - A Retrospective Case Control StudyDeepak Vadada, MD, Jeevan Vinod, MD, Niket Sonpal, MD, Peter Baiocco, MD, Burton Korelitz, MD. Lenox Hill Hospital, New York, NY.
Purpose: It has recently been demonstrated that cells and molecules classi-cally implicated in the physiological process of coagulation behave abnor-mally in IBD and possibly also play an active role in disease pathogenesis and progression. Th e coagulation system represents an important component of IBD pathogenesis and may be a possible target for therapeutic interven-tion. It is now well established that clopidogrel is a crucial adjunct to aspirin therapy before and aft er percutaneous coronary intervention (PCI). Anti-platelet therapy has signifi cantly improved outcomes in patients undergoing

© 2010 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY
Abstracts S473
percutaneous interventions for coronary artery disease. Th e aim of our study is to assess the eff ect of anti-platelet therapy on patients with pre-existing infl ammatory bowel disease, aft er the initiation of the antiplatelet agents aspirin and clopidogrel.Methods: A retrospective chart review was conducted to assess disease pro-gression of patients with IBD who were started on ASA and clopidogrel (Plavix®) between January 1, 2002 and January 31, 2007. We have identifi ed approximately 41 patients with IBD who had been started on the medications aft er having a PCI for Coronary Artery Disease. Th e patients fi t the criteria of the population we wish to study and a control group of patients not on aspirin or clopidogrel with IBD was matched with the study group.Results: Th e 41 patients once analyzed revealed 20 females and 21 males. Th e median age of the sample was 68 years of age. Of the 41 patients, 15% (6) patients reported worsening of IBD symptoms. Two of those patients presented with new onset of GI bleeding. Th e remaining patients reported no change in the frequency of their IBD fl are-ups aft er the initiation of anti-platelet therapy. Th ese results were not statistically signifi cant when compared to the control group. Th is group consisted of 85 patients, 33 females and 35 males with an average age of 66 years old. 26% (22/85) (6 males;16 females) who were not on ASA or clopidogrel and were found to have fl ares in the last fi ve years. 5 of these patients had intermittent rectal bleeding and one patient required resec-tion secondary to obstruction. However an 11% lower rate of fl ares were seen to occur in patients with concomitant therapy thus implying a possible amelio-rating eff ect of ASA and clopidogrel.Conclusion: Th e fi ndings currently from this ongoing study show that no statisiti-cally signifi cant link between concomitant anti-platelet therapy and IBD exacer-bations can be commented upon. However, a lower rate of fl ares was seen in the anti-platelet group and thus a possible anti-infl ammatory eff ect of these agents may be possible in patients with a history of IBD. However further analysis with larger cohorts are required to make a more defi nitive conclusion.
1285
A Serogenetic Test Accurately Predicts the Probability of Complicated Crohn’s DiseaseDouglas Wolf, MD,1 Derren Barken, PhD,2 Susan Carroll, PhD,2 Th eresa Luna, BA,2 Fred Princen, PhD,2 Sharat Singh, PhD,2 Emil Chuang, MD2. 1. Atlanta Gastroenterology Associates, Atlanta, GA; 2. Prometheus Laboratories, San Diego, CA.
Purpose: Studies have shown that biologics are eff ective in inducing remission and altering the natural history in patients with active Crohn’s disease (CD). To appropriately use these powerful but expensive treatments, which also have potential side eff ects; it would be useful to know which patients are at risk for rapid progression to severe disease. Serologic and genetic markers have been shown to be associated with a severe disease phenotype. Recently, a serogenetic model incorporating diverse immune response markers and NOD2 variants has been developed and shown to predict the probability of complications. Th e aim of this study is to evaluate the serogenetic model’s ability to predict the probability of complications in CD patients derived from community gastro-enterology clinics.Methods: Adult CD patients (n=137, 45% male) were enrolled from 13 US sites in a cross sectional study. Patients had confi rmed CD for > 2 years. Patients were classifi ed as complicated, meaning at least one instance of stricturing or penetrating (internal or perianal) disease, or non-complicated. Blood was sent to Prometheus Laboratories for genotyping (NOD2: SNPs 8, 12, 13) and serol-ogy testing (ASCA IgA and IgG, anti-CBir1, anti-OmpC, anti-I2 and pANCA). Th e dates of both CD diagnosis and of the manifestation of the complications were known. A prediction of the complication rate was derived for each patient using the serogenetic model and the prediction was compared to the known clinical status of the patient.Results: Th ere were 79 complicated and 58 non-complicated patients. All anal-yses were performed with blinded clinical data. Th e performance of the model was assessed by construction of receiver operator characteristic (ROC) curves and comparison of the area under the curve (AUC) to the null hypothesis,
specifi cally a random predictor with an AUC=0.5. At year 5, the AUC was 0.705 (95% CI 0.610-0.799, p < 0.001) and at year 10, the AUC was 0.630 (95% CI 0.513-0.747, p =0.037). Th e model was also assessed by calculating the correla-tion between predicted and observed complications with patients divided into fi ve groups based on predicted probabilities (groups=0-20%, 20-40%, etc). Th e correlation between predicted and observed rates was 0.96 at year 5 (p=0.01) and 0.87 at year 10 (p=0.05).Conclusion: Th ese results show that this new serogenetic model is able to accurately predict the probability of complications for CD in patients derived from community gastroenterology clinics. Th is test may help physicians iden-tify patients who are at risk for rapid progression to a complicated CD phe-notype and who are thus appropriate candidates for early intervention with eff ective therapy.Disclosure: Dr Wolf - consultant and speaker for Prometheus Labs. Drs. Barken, Carroll, Chuang, Luna, Princen, Singh are employees of Prometheus Labs.Th is research was supported by an industry grant from study was funded by Prometheus.
1286
Azathioprine in Luminal Crohn’s Disease: Diff erent Strategies, Diff erent OutcomesSusana Rodrigues, MD,1 Fernando Magro, MD, PhD,1 Orquidea Ribeiro, BA,2 Susana Lopes, MD,1 Altamiro Costa Pereira, MD, PhD,2 Guilherme Macedo, MD, PhD1. 1. Hospital Sao Joao, Department of Gastroenterology, Porto, Portugal; 2. Department of Biostatistics and Medical Information, Faculty of Medicine, University of Porto, Porto, Portugal.
Purpose: Th e current goal of medical treatment in Crohn’s disease (CD) aims to alter its natural history. Th e emergence of biologicals in the clinical practice of CD challenged the existing relevance of immunosuppressants. Th e aim of the study was to evaluate the effi cacy of azathioprine (AZA) in luminal Crohn’s disease based upon the development of a major event such as hospitalisation and the need for additional medical or surgical treatment over time.Methods: Retrospective study assessed a large population of luminal CD patients treated with AZA. Th e patients were stratifi ed according to the Mon-treal Classifi cation and medical treatment: AZA monotherapy, combined therapy with AZA and infl iximab (IFX), and infl iximab monotherapy. Survival analysis starting from AZA until a major event such as hospitalisation, need for surgery or biological, namely infl iximab (IFX) was performed.Results: A population of 281 patients with luminal CD was divided into three groups: AZA (67%), IFX (8%), IFX+AZA (27%). Median age at diagno-sis was 25 years (20-33). From the 21% of patients on AZA that experienced adverse reactions, 21 patients were started on monotherapy with IFX and 39 remained without immunomodulation. 157 patients continued solely with AZA, in 41 cases following surgery and the remaining were immunosup-pressed due to steriod dependency with an average dose of 2.08 mg/kg. Ster-oid-free remission was obtained in 36% of patients treated with AZA due to steroid-dependency, and in 75% of post-operative patients (p=0.009). All of the 64 patients in the AZA+IFX group were immunosuppressed due to ster-oid-dependency. Following the introduction of IFX, 67% patients of these patients maintained steroid-free remission, having 63% of these patients eventually persisted without AZA. In the IFX monotherapy group, ster-oid-free remission was attained in 62% patients. Time from diagnosis until introduction of AZA was analyzed: ≤ 1 year, 1-3 years, or >3 years and no signifi cant diff erences were found in hospitalisations (p=0.508) or surgical events (p=0.203). 29% of all patients on AZA required IFX. Time to surgery was clearly less in the AZA monotherapy compared to IFX and AZA+IFX groups (p=0.05). Surgical rates were signifi cantly diff erent between groups (p=0.033) AZA monotherapy: 17,2%, IFX monotherapy: 0%, and combined treatment: 9%.Conclusion: Azathioprine was associated with remarkably elevated cases of adverse reactions and the majority of those treated required further medi-cal/surgical interventions. It seems particularly eff ective in the postoperative setting, and its combined use with infl iximab reduced the rate of surgical events.

The American Journal of GASTROENTEROLOGY VOLUME 105 | SUPPLEMENT 1 | OCTOBER 2010 www.amjgastro.com
AbstractsS474
1287
Does Immunosuppressive Th erapy Increase Operative Morbidity in Patients with Crohn’s Disease?Andrea Baff ord, MD, Sarah Powers, BA, Daniel Greenwald, BS, Christina Ha, MD, Stephen Gorfi ne, MD, David Chessin, MD, Joel Bauer, MD. Colon and Rectal Surgery, Mount Sinai Medical Center, New York, NY.
Purpose: An increasing number of immunomodulating agents are being used in the treatment of Crohn’s disease. Th e impact of these medications on surgical morbidity is controversial. While some published reports have demonstrated a higher rate of postoperative complications with perioperative steroid, thiopu-rine, and anti-TNF biologic therapy, others have shown no eff ect. Th erefore, the aim of this study was to examine the impact of immunosuppressive therapy on the morbidity of intestinal surgery in patients with Crohn’s disease.Methods: We performed a retrospective review of our prospectively maintained database of patients with Crohn’s disease who underwent intestinal surgery between June 1999 and May 2010. Th e eff ect of perioperative immunomodula-tion on postoperative outcomes, specifi cally anastomotic complications, was evaluated. Only those procedures in which at least one intestinal anastomosis was performed were analyzed. Predictors of postoperative morbidity among demographic and surgical variables were identifi ed. Length of hospitalization and rate of hospital readmission were compared between groups. Compari-sons were made using student’s t-test and Fisher’s exact test.Results: 237 intestinal procedures were performed in 214 patients. Of these, 41 were excluded because intestinal resection was not accompanied by anas-tomosis. 127 of the remaining 196 (64.8%) procedures were performed in patients who received immunomodulating medications within 90 days of surgery. 48 (24.5%) procedures were in patients who received more than one immunomodulating medication perioperatively. Th ere were 35 complications (17.9%). Th ere were 20 (10.2%) anastomotic complications, including 8 (4.1%) intra-abdominal abscesses, 8 (4.1%) anastomotic leaks, and 4 (2%) enterocuta-neous fi stulas. Steroids (p=0.6), 6-MP (p=0.2), and anti-TNF biologics (p=0.6) were not associated with increased postoperative anastomotic complications. Combination therapy with immunosuppressants also did not increase morbid-ity (p=0.8). Whether surgery was performed for infl ammatory (0.83), stric-turing (0.35), or penetrating (0.3) Crohn’s disease behavior, or for dysplasia or cancer (1.0) did not aff ect morbidity. Similarly, there was no association between postoperative complications and patient age (1.0), gender (0.7), ASA score (0.8), urgency of surgery (0.37), or type of surgery (0.18). Th e 30-day readmission rate and length of hospitalization were signifi cantly increased in patients who had a postoperative complication (p=0.0001 and p=0.0006, respectively).Conclusion: In our series, single agent and combination immunosuppressive therapy given within 90 days of intestinal surgery did not increase the inci-dence of surgical complications in patients with Crohn’s disease.
1288
Th e Use of Appropriate Medical Th erapy in an Underserved Population with Infl ammatory Bowel Disease (IBD)Neal Joseph, MD, Daniel Sussman, MD, John Clark, PhD, Amar Deshpande, MD. University of Miami-Jackson Memorial Hospital, Miami, FL.
Purpose: Immunomodulators and biologics are eff ective in both ulcerative colitis (UC) and Crohn’s disease (CD) for induction and maintenance of remis-sion in patients with moderate-to-severe disease activity. However, several barriers may prevent patients from getting these medications. Our aim was to examine the appropriate utilization of medical therapy in an underserved patient population in Miami, Florida.Methods: A retrospective chart review of all patients with ICD9-CM diag-noses of UC or CD was conducted in the outpatient gastroenterology clinic of Miami-Dade County’s public hospital (Jackson Memorial Hospital) from January 1, 2004 to December 31, 2009. Information concerning demograph-ics, medication history, and criteria for immunomodulator and/or biologic therapy were obtained. Patients were included if any of the following criteria were met: 1) ≥2 courses of steroids; 2) steroid-dependency; 3) steroid-refracto-
riness; 4) IBD-related surgery; 5) perianal disease; 6) active disease on 5-ASA therapy. Patients meeting these criteria and on either an immunomodulator or biologic were considered on appropriate therapy. Th e percentage of patients on appropriate medical therapy was then calculated and cohorts on appropriate and suboptimal therapy were compared.Results: 152 charts were reviewed, of which 97 (51 male, 46 female) met inclu-sion criteria. Th e mean age was 43 years, consisting of 54% Hispanics, 31% African Americans, and 15% Caucasians. Of those who met inclusion criteria, 63 (65%) were on appropriate therapy. Patients meeting only one criteria were signifi cantly less likely to be on appropriate therapy compared to those with greater than one indication (38% vs. 62%; p=0.026). Patients fi rst seen before 2008 were less likely to be on appropriate therapy compared to those fi rst seen aft er 2008 (76% vs. 52%; p=0.02). No diff erence between those on appropriate and suboptimal therapy was observed with respect to age, gender, ethnicity, IBD subtype, smoking history, or insurance status.Conclusion: In the underserved IBD population of Miami-Dade County (85% non-Caucasian), approximately two-thirds of patients met criteria for immunomodulator or biologic therapy; only 65% of these subjects were given appropriate therapy. Th is underutilization of therapy was observed in subjects meeting only one inclusion criterion and those initially seen prior to 2008. Studies examining reasons for underutilization of these resources in our patient population are currently underway.
1289
Quality of Life, Disease Activity, and Flares in Crohn’s Disease Diff er by Race Over Time?Leyla Ghazi, MD,1 Raymond Cross, MD, MS,1 Alison Lydecker, MPH,2 Mark Flasar, MD, MS1. 1. University of Maryland Medical Center, Division of Gastroenterology and Hepatology, Baltimore, MD; 2. University of Maryland School of Medicine, Department of Epidemiology and Preventive Medicine, Baltimore, MD.
Purpose: Research suggests that racial disparities may exist in the treatment of Crohn’s disease (CD) patients; however this may be due to racial diff erences in disease activity. Our aim was to assess for racial diff erences in disease activ-ity, quality of life, and disease fl ares over time among CD patients in a tertiary referral practice.Methods: Th e Infl ammatory Bowel Disease Program’s Clinical Database prospectively documents demography, Montreal classifi cation, disease-spe-cifi c quality of life and disease activity for all CD patients at all clinic visits. We identifi ed Caucasian (W) and African American (AA) CD patients seen between 7/1/2004-12/31/2009 with ≥2 scores for the Short Form Infl amma-tory Bowel Disease Questionnaire (SIBDQ) and the Harvey Bradshaw Index (HBI). Regression analysis assessed for racial diff erences in HBI, SIBDQ scores and fl ares over time.Results: 296 CD patients met criteria; 240 (81%) W, 56 (19%) AA. At base-line, no signifi cant racial diff erences in demography, extraintestinal mani-festations, smoking, disease location or behavior, HBI or SIBDQ score or fl are rates were seen. In year 1, HBI scores decreased more in W (mean 0.6 pts at each successive visit window, p<0.01 for trend) than AA (mean decrease 0.2 pts, p=0.39 for trend); trends were diff erent by race (p=0.01). W also had a 24% decrease in odds of fl are at each successive visit window (p<0.01 for trend) while AA odds of fl are remained stable (p<0.01 for W vs. AA) during year 1. Aft er year 1, HBI scores increased by a mean 0.6 pts at each successive visit window in W (p<0.01 for trend) while scores in AA continued to decrease by a mean of 0.8 pts at each visit window (p=0.23 for trend); these trends were not diff erent by race (p=0.25). Aft er year 1, the odds of fl are at each successive visit window rose 21% in W (p=0.01 for trend) but fell 25% in AA (p=0.34 for trend; p=0.07 W vs. AA). SIBDQ scores rose similarly in W and AA during (1.72 vs. 1.60 pts at each window) and subsequent to year 1 (0.94 vs. 1.27 pts).Conclusion: While quality of life remained stable, temporal diff erences in disease activity and fl ares between W and AA were found in a referral CD cohort. Disease activity and fl ares improved in W during year 1, while AA had improved disease activity and fl ares aft er year 1. Further investigation is needed

© 2010 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY
Abstracts S475
to determine whether this represents racial variation in the course of CD.Disclosure: Dr Cross: Grant support from Abbott Laboratories and Centocor, Inc. Consultant for Abbott Laboratories, UCB Pharma and Centocor, Inc. Dr Flasar: grant support from Procter and Gamble.Th is research was supported by an industry grant from Procter and Gamble.
1290
A Comparison of Dynamic Systems Models of Gastrointestinal Kinetics of Controlled Release Multimatrix System 5-Aminosalicylic Acid (5-ASA), Lialda™ with pH-dependent, Delayed Release 5-ASA (Asacol™)Deepak Parakkal, MD,1 Matthew Th orpe, BS,2 Sarah Paver, MS,2 Eli Ehrenpreis, MD,1 Bruce Hannon, PhD2. 1. Internal Medicine, NorthShore University Health System, Evanston, IL; 2. University of Illinois, Urbana-Champaign, IL.
Purpose: Our group has previously published a dynamic computer simulation of the gastrointestinal kinetics of Asacol™, a pH-dependent tablet formulation of 5-ASA in quiescent and acute ulcerative colitis (UC). Th e model predicts an asymmetric distribution of 5-ASA with Asacol™, with relatively minor reach to the distal colon. Th e model also predicted that in acute exacerbations of UC, there is a decrease total colonic 5-ASA concentrations to less than 50% of those modeled in quiescent UC. Th is model is now applied to study the colonic distribution of 5-ASA with MMX™ mesalazine (Lialda™), a controlled release tablet formulation of 5-ASA.Methods: Using published data on gastrointestinal motility, 5-ASA absorp-tion, clearance of colonic contents with defecation and release rate of 5-ASA from the slow release MMX™ mesalazine tablet(Lialda™), levels of 5-ASA in the four major segments of the colon were simulated via a dynamic model using STELLA soft ware (Isee Systems, Inc., Lebanon NH, USA). 5-ASA levels were predicted in the healthy colon as well as during variations in motility and the frequency of defecation, designed to simulate active UC. We simulated 100 days of treatment with Asacol™ tablet (release starting in the terminal ileum) compared to Lialda™ tablet (delivering drug gradually throughout the colon), and of quiescent compared to acute UC.Results: While Asacol™ demonstrated an asymmetric distribution of 5-ASA with 37, 34, 14 and 15% of drug residing on an average in the right, transverse, descending and sigmoid colon respectively, Lialda™ was shown to distribute at 20, 28, 18 and 34% to these areas respectively in quiescent UC. Simulations of acute UC with frequent bowel movements (6 times a day) reduced total colon drug levels to 45% of quiescent UC levels with Asacol™ with a distribution of 64, 28, 6 and 2% of this amount respectively in the above 4 segments of the colon. With Lialda™, total colonic levels of 5-ASA were reduced to 33% of those in quiescent UC with a distribution of 46, 31, 17 and 5% respectively in the above 4 segments of the colon.Conclusion: Our model predicts that the Lialda™ eff ectively inverts the distribu-tion of 5-ASA delivery along the colon in comparison with Asacol™, such that greater amounts reach the distal colon. Total delivery of 5-ASA from Lialda™ is more aff ected by frequent bowel movements characterizing acute UC than is Asacol™. However, the model predicts higher 5-ASA levels in the descending and sigmoid colon with Lialda™. Th is suggests that Lialda™ will have greater effi cacy in comparison to Asacol™ for distal quiescent and active UC.
1291
Hepatosplenic T-cell Lymphoma (HSTCL) in Patients Receiving Tumor Necrosis Factor Alpha (TNF-α) Inhibitors: A Review of Cases Reported to the Food and Drug Administration (FDA)Eli Ehrenpreis, MD, Deepak Parakkal, MD, Rumi Semer, MS, Matthew Adess, MD. Gastroenterology, NorthShore University HealthSystem, Highland Park, IL.
Purpose: Hepatosplenic T cell lymphoma (HSTCL) is a rare but lethal lym-phoma. Th e Study of Biologic and Immunomodulator Naive Patients in Crohn’s Disease (SONIC) trial has demonstrated the benefi t of combining infl iximab with an immunomodulator in moderate-to-severe Crohn’s disease. Unfortunately, combined immunosuppresion is also a reported risk factor for the development of HSTCL, generally in pediatric male patients with infl am-matory bowel disease (IBD). Th e purpose of the study is to review all cases of HSTCL reported to the FDA in patients receiving TNF-α blockers.
Methods: Th e FDA adverse event reporting system (AERS) database is avail-able for public access. Individual reports were downloaded as ASCII fi les and analyzed using a database created with the Access program (Microsoft Corp., Redmond, WA). Th e database was queried for lymphomas reported with the following biological agents: infl iximab, (Remicade, Revellex), adalimu-mab, (Humira, Trudexa), certolizumab, (Cimzia), natalizumab (Tysabri) and etanercept (Enbrel). Full reports for all T-cell lymphomas including HSTCL were obtained from the FDA using the Freedom of Information Act.Results: A total of 2,097,223 fi les were downloaded from the FDA AERS sys-tem for the years 2004-2009. Twenty six cases of HSTCL (8 not previously described) were identifi ed. Twenty three (89%) were in patients with IBD (3 in Ulcerative colitis) and three cases occurred in rheumatoid arthritis patients. Five cases (19%) were females. Seven cases (27%) occurred in patients > 50 yrs of age and 4 cases (15%) were seen in patients >65 yrs of age. Twenty three cases (89%) occurred in patients receiving a TNFα blocker and a second immu-nomodulator, including azathioprine (12 cases), 6-Mercaptopurine (9 cases) and methotrexate (1 case) and azathioprine with past use of methotrexate and lefl unomide in 1 case. Twenty patients received infl iximab, 3 received infl ixi-mab followed by adalimumab, 1 received infl iximab followed by adalimumab then natalizumab and 2 received adalimumab. Seventeen cases were gamma-delta tumor subtype, 5 were alpha-beta and 3 were unknown. One case showed trisomy 13 on chromosomal analysis, not typical of HSTCL. Twenty one (81%) patients were reported to have expired despite treatment.Conclusion: HSTCL is most common in pediatric males with IBD. However, adults, senior citizens, women and patients with rheumatoid arthritis receiving TNF-α blocking agents and immunomodulators are also at risk. Improved dis-ease outcomes using combination therapy described in the SONIC trial should be tempered by reports of additional patient groups developing HCTCL.
1292
Gastroenterologist-Patient Communication About Crohn’s Disease and Treatment with Biologic Th erapy: Results of an In-offi ce Linguistic StudyKimberly Persley, MD,2 Corey Eagan, MPH,1 Heidi Waters, MS, MBA,3 Meaghan Onofrey, MS1. 1. MBS/Vox, a CommonHealth Co., Parsippany, NJ; 2. University of Texas Southwestern Medical Center Presbyterian Hospital, Dallas, TX; 3. Centocor OrthoBiotech, Horsham, PA.
Purpose: To evaluate current discussions of Crohn’s disease and its treatment, an observational study was conducted using accepted sociolinguistic method-ologies.Methods: 1161 community-based gastroenterologists were invited to partici-pate; the fi rst 18 who responded and met screening criteria were enrolled in the sample. Regularly scheduled offi ce visits were recorded with patients with Crohn’s disease who were candidates for and likely to discuss biologic therapy. Separate post-visit interviews were recorded with physicians and patients, and demographic questionnaires were completed. Recordings were transcribed and analyzed using sociolinguistic techniques, including quantifi cation of top-ics discussed and time spent on each, quantifi cation and qualifi cation of ques-tions asked and answered, and identifi cation of requests for information and making of recommendations.Results: Interactions between 14 physicians and 23 patients were analyzed. Physicians were 77% male; patients were 48% female, had a mean age 38 and a mean duration of Crohn’s disease of 13 years. Mean duration of visits was 10.46 minutes (range 2.42 -26.33 minutes). Discussions of Crohn’s disease, including side eff ects, medication effi cacy, and all other medication conversation (e.g., confi rming current regimen, dosing, refi lls), made up 45% of visits. Conver-sations about symptoms and complications of the disease comprised 18% of visits. Quality of life dialogues made up less than 3% of visits. Visits were physi-cian-driven and characterized by rapid-fi re, closed-ended symptom questions. Patients’ quality of life (QOL) was rarely addressed; however, 96% of patients revealed information post-visit about how their QOL was negatively impacted by Crohn’s disease. Additionally, 39% of patients reported deliberately with-holding information about their QOL from their physician. Biologic therapy was discussed but not initiated in 11 of 23 visits. Both risks and benefi ts of biologics were mentioned, but risks were typically serious (e.g., lymphoma) while benefi ts were typically general (e.g., a biologic “might help you”). All 11

The American Journal of GASTROENTEROLOGY VOLUME 105 | SUPPLEMENT 1 | OCTOBER 2010 www.amjgastro.com
AbstractsS476
patients stated post-visit that they would be interested in learning more about new forms of treatment for Crohn’s disease.Conclusion: In-offi ce dialogue is marked by rapid-fi re, closed-ended symp-tom questions, a lack of attention to QOL, and an unbalanced presentation of biologic therapy. Th is may account for 11 of 23 visits in which biologic therapy was discussed as an option but not prescribed. Further research is needed to evaluate strategies to improve in-offi ce communication, such as incorporat-ing a validated tool into offi ce visits focused on the management of Crohn’s disease.Disclosure: Dr Persley - Consultant: Centocor Ortho Biotech.
1293
Th e Safety of Continuing Th iopurines in Patients with Infl ammatory Bowel Disease (IBD) During Hospitalization for InfectionJennifer Rockfeld, MD, Christina Ha, MD, Emily Schonfeld, MD, Mekhala Chandra, BS, Elana Maser, MD. Internal Medicine, Mount Sinai Hospital, New York, NY.
Purpose: Th is study aims to determine if IBD patients hospitalized for severe infections have a more complicated hospital course with continued thiopurine therapy.Methods: A retrospective single-center observational study of all patients with a pre-existing diagnosis of IBD hospitalized for serious infections from 2003 to 2009 was performed. Infections were identifi ed using ICD-9 coding from a hospital discharge registry listing the following infections as the primary admitting or discharge diagnoses: Clostridium diffi cile, pyelonephritis, abdom-inal abscess, pneumonia, cellulitis, osteomyelitis, cholecystitis and bacteremia. Data collected included concurrent medications, length of hospitalization, and 30-day readmission rates. Patients were excluded if they were HIV positive, had a previous organ transplant or were on chemotherapy.Results: A total of 1,993 charts were reviewed and 342 admissions met the above criteria, of which 60 were for patients treated with thiopurines. Of these hospital visits, 29 were continued on thiopurines throughout their hospitaliza-tion and 31 were discontinued. Th ere were more patients concurrently taking biologics in the group that continued on thiopurines (48.3% vs. 29.0%) and fewer patients taking steroids (10.3% vs. 25.8%). Th e median length of stay for patients who remained on thiopurines was shorter than the length of stay for patients in whom thiopurines were discontinued (6 days vs. 9 days). Th e lengths of stay for patients continuing thiopurines were similar to those pub-lished by the Centers for Disease Control for non-IBD patients excluding sepsis and cellulitis, for which our patients had longer than average hospitalizations. Th e patients who were continued on thiopurines had higher rates of readmis-sion to the hospital within 30 days for complication of the original infection or unremitting symptoms (24.1% vs. 6.5%). 42.8% of the readmissions in the group that continued thiopurines were for complications of bacteremia.Conclusion: Th e fi ndings from this small study suggest that although patients with IBD and infections continued on thiopurine therapy did not have longer lengths of stay, they did have higher rates of readmission, specifi cally during hospitalizations for bacteremia. Further data is needed to guide clinical man-agement.
1294
Osteoporosis Screening in a Tertiary Referral - Infl ammatory Bowel DiseaseLia Kaufman, MD, Edward Loft us, MD, William Sandborn, MD, Patricia Kammer, Darrell Pardi, MD. Internal Medicine, Mayo Clinic Rochester, Rochester, MN.
Purpose: Background: Many will argue that IBD patients are a unique popula-tion at high risk for developing osteoporosis. Considered the most signifi cant risk factor would be the common use of corticosteroids. Th e AGA com-mented in their 2006 Medical Position Statement, “Periodic bone mineral density assessment is recommended for patients on long-term corticosteroid
therapy (>3 months) (Grade A). Aims: To estimate the percent of patients with appropriate osteoporosis screening among infl ammatory bowel disease (IBD) patients at highest risk: those with current chronic steroid use. To describe the characteristics of IBD clinic patients needing osteoporosis screening, and to determine whether these characteristics are associated with whether or not screening was performed.Methods: A retrospective chart review was performed on 80 new referral patients seen at our IBD clinic from August 31, 2009 through January 5, 2010. Patients were excluded if they were under 18 years old, if they had a diagnosis of osteoporosis, or if they lacked a defi nitive diagnosis of IBD.Results: Th e patient population was 57.5% female and 42.5% male. Th e major-ity of patients, 86%, were Caucasian. 38.8% reported current steroid use at the time of their visit, and 37.5% had a history of steroid use greater than three months in duration; 23% had both current and chronic steroid usage. Of those with current chronic steroid use, only 28% were asked about bone density scanning during their visit; 2 patients were referred for testing, and 1 was diag-nosed with osteoporosis. Additional osteoporosis risk factors were identifi ed during the review including elevated infl ammatory markers (52.5%), low body weight (45%), signifi cant smoking history (27.5%), positive family history (21.3%) and age>65 (11.3%).Conclusion: In our tertiary referral IBD practice, the rate of appropriate oste-oporosis screening was low. Early recognition and treatment of osteoporosis has been shown to decrease the risk of fracture, decreasing morbidity and increasing the quality of patient care. Th erefore, a practice improvement pro-tocol to improve screening for osteoporosis in these patients is appropriate.
1295
Th e Use of Serum, Urine, and Fecal Neopterin to Determine Disease Activ-ity in Ulcerative ColitisNisreen Husain, MD,1 Stanley Naides, MD, PhD,2 Ken Tokoro, PhD,2 Mary Kwasny, PhD,1 Alan Buchman, MD, MSPH1. 1. Feinberg School of Medicine, Northwestern University, Chicago, IL; 2. Quest Laboratories, San Juan Capistrano, CA.
Purpose: Th ere are few noninvasive biomarkers which correlate with disease activity in ulcerative colitis (UC). Th e aim of this study was to determine if serum, urine, or fecal neopterin concentrations were associated with disease activity as determined by the Simple Clinical Colitis Activity (SCCAI) and Dis-ease Activity Indices (DAI), erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), serum albumin and, fecal lactoferrin.Methods: We prospectively enrolled a total of 52 outpatients with UC (29 clin-ically in remission, 23 active). Disease was considered active if the SCCAI was ≥3. Fecal (n=50), urine (n=115) and serum (n=120) samples were collected from healthy controls for neopterin measurement. Due to non-normality of data, medians and ranges are present. Mann-Whitney or Kruskal-Wallis tests, and Spearman’s correlation coeffi cients were employed.Results: Fecal neopterin was signifi cantly higher in UC patients compared to controls (95.2 (7, 248) vs. 12.0 (3, 379) ng/g; p<0.001); median serum neopterin levels were higher in controls, although the range was wider in UC patients (4.5 (2.3, 14.6) v 2.9 (1.5, 1.5, 57.3), p<0.001); additionally, fecal neopterin and serum neopterin were higher among those with active disease (active v. inactive fecal neopterin 135 (56, 248) and 63 (7, 182), and serum neopterin 3.8 (1.5, 21.3) v. 2.3 (1.5, 57.3), both p < 0.05). No signifi cant dif-ference in urine neopterin values was detected in controls vs. UC patients (p=0.4138). Urine neopterin was weakly but signifi cantly correlated with Hb (-0.37), Hct (-0.43), albumin (-0.38) but not with SCCAI, DAI, CRP, or ESR. Serum neopterin correlated with SCCAI (0.30), Hct (-0.30), Albumin (-0.43), CRP (0.37), and ESR (0.35) but not with Hb or DAI. Fecal neopterin correlated with SCCAI (0.48), and ESR (0.40) but not with DAI, Hb, Hct, Albumin, or CRP.Conclusion: Fecal neopterin was signifi cantly greater in patients with UC vs. controls, and was signifi cantly higher among those with active disease. For patients in remission, that suggests the likelihood of ongoing subclinical intes-tinal infl ammation. Urine neopterin did not distinguish UC patients (active or

© 2010 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY
Abstracts S477
remission) from healthy controls. Although diff erences were seen in distribu-tions of serum neopterin between UC groups and controls, it is unclear if there is a single mechanism to explain this.
1296
Biosynthesis Characteristic of TTP and TNF Can Be Regulated Th rough a Posttranscriptional Molecular LoopNaveed Aslam, PhD,2 Irum Zaheer, MBBS1. 1. Th e Methodist Hospital, Houston, TX; 2. Department of Neurobiology and Anatomy, UT Medical School, Houston, TX.
Purpose: Th e abundant expression of tumor necrosis factor (TNF) is a hall-mark of chronic infl ammation of gastrointestinal tract. Prolonged infl amma-tion can lead to infl ammatory bowel disease (IBD).Understanding of the TTP TNF loop would allow in better understanding of disease pathophysiology and treatment options at various steps of the loop.Methods: Th is involves a computaional model based on the biochemical interaction of proteins. Th is study proposes a molecular model for regulat-ing the biosynthesis characteristics of a cytokine through a posttranscriptional molecular loop. We test a hypothesis that the biosynthesis characteristics of an infl ammatory cytokine might be regulated at posttranscriptional level through a regulatory loop.Results: Th e abundant expression of tumor necrosis factor (TNF) is a hall-mark of chronic infl ammation of gastrointestinal tract. Prolonged infl amma-tion can lead to infl ammatory bowel disease (IBD). Th e TNF biosynthesis is regulated both at transcription and translation levels. However, the stimula-tion induced increase in translation rate is much higher. Th is might indicate the possibility of a posttranscriptional regulatory mechanism. How during basal conditions the TNF concentration is tightly regulated at low levels? Th e stability and translational effi ciency of TNF transcript is regulated by an AU-rich (ARE) element in 3’UTR of messenger RNA. A transacting protein TTP binds to ARE and enhances the mRNA turnover. Here, we examine a proposal that TNF homeostasis is maintained by a TTP-TNF interaction loop at posttranscriptional level. We propose a computational framework of this regulatory loop by modeling the role of AREs in mediating the mes-senger RNA stability and translation. Th e proposed posttranscriptional regulatory loop between TTP and TNF is composed of two feedback loops i.e., positive and negative. Th e mutual interaction of these feedback loops regulates the biosynthesis response of TNF during basal and infl ammatory conditions.Conclusion: Th e proposed posttranscriptional regulatory loop between TTP and TNF is composed of two feedback loops i.e., positive and negative. Th e mutual interaction of these feedback loops regulates the biosynthesis response of TNF during basal and infl ammatory conditions.Knowledge about this feed-back would help in knowing and applying treatment to these specifi c loops for a targeted treatment approach.
1297
Infl uence of Body Mass Index on Quality of Life and Disease Activity in Crohn’s Patients
2010 ACG/Centocor IBD Abstract AwardMazen Issa, MD, Ashwin Ananthakrishnan, MD, Yelena Zadvornova, MD, Amar Naik, MD, Daniel Stein, MD, Lilani Perera, MD. Medical College of Wisconsin, Milwaukee, WI.
Purpose: Over the past 2 decades there has been a dramatic increase in preva-lence of obesity in the United States. Adipocytes are recently recognized as endocrine cells that secrete a variety of bioactive substances including tumor necrosis factor a, IL-6, and IL-8. Th is would suggest an increase in the infl am-mation burden in patients with infl ammatory bowel disease and potentially result in a negative impact on health related quality of life (HRQoL). We sought to evaluate disease activity and quality of life in our Crohn’s disease (CD) patient population based on body mass index.Methods: Th is was a retrospective study evaluating all CD pts being followed in a single referral center. Demographic information and disease characteris-tics were obtained from our database. Disease activity and quality of life were measured using the Harvey Bradshaw index (HBI) and Short Infl ammatory Bowel Disease Questionnaire (SIBDQ) respectively. Mean body mass index (BMI) was obtained from patients who had at least 3 measurements of BMI, HBI and SIBDQ and was stratifi ed into three categories - Normal (< 25kg/m2), Overweight (25-29.9kg/m2), and obese (> 30kg/m2).Results: Th ere were 576 CD pts (226 men, 350 women) included with a mean age of 43 years. Approximately 33% of patients had infl ammatory disease, 40% stricturing and 27% with fi stulizing disease. Half the patients (50%) had involvement of both the small and large bowel. Ninety-one patients (15%) were current smokers. Fift y-six patients were non-white (10%). A majority of the patients were on combined immunomodulator and biologic therapy (57%) (27% on biologics alone and 10% on immunomodulators alone). Th e mean SIBDQ was 51 points with a mean HBI in our cohort of 3. Mean BMI was 26.8kg/m2 with 40%, 33%, and 27% in the normal, overweight and obese cat-egories respectively. On multivariate analysis, the obese (-2.8, 95% CI -4.4 to -1.2) and the overweight cohorts (-1.7, 95% CI -3.2 to -0.24) had modestly reduced SIBDQ compared to those with normal weight. Th ere was no diff er-ence in mean HBI by BMI. Obese patients had slightly lower number of sur-geries on adjusted analysis (-0.4, 95% CI -7 to -0.1) but were no diff erent in number of hospitalizations.Conclusion: Elevated BMI is associated with slight decrease in HRQoL in patients with Crohn’s disease but has no impact on Crohn’s disease activity represented by HBI.
1298
Clinical Effi cacy of MR Enterography in the Diagnosis and Management of Crohn’s DiseaseSiobhan Byrne, MD, Helen Fasanya-Uptagraft , MD, Sumona Saha, MD, Jessica Robbins, MD, Scott Reeder, MD, PhD, Mark Reichelderfer, MD. Internal Medicine, University of Wisconsin Hospital, Madison, WI.
Purpose: Background: Assessing small bowel Crohn’s disease (CD) activity is challenging as direct visualization is diffi cult and traditional radiographic stud-ies can result in large cumulative radiation doses. MR enterography (MRE) is a rapidly evolving diagnostic technique performed without ionizing radiation. While prior studies evaluate the technical aspects of MRE, few address its clini-cal utility. Aim: To evaluate the clinical utility of MRE in patients with known or suspected CD at a single institution.Methods: Consecutive MRE performed between 1/1/09 and 9/30/09 were reviewed. All imaging was performed on a 1.5T clinical scanner with an 8-channel phased array body coil. Patients were scanned aft er ingestion of hyperosmolar oral contrast. High resolution T2 and T1 weighted pre- and post-contrast images were obtained. Studies performed for reasons other than known or suspected CD were excluded. Patient data including clini-cal course prior to MRE and subsequent management was abstracted from the medical record and a clinical disease activity score was derived. Each

The American Journal of GASTROENTEROLOGY VOLUME 105 | SUPPLEMENT 1 | OCTOBER 2010 www.amjgastro.com
AbstractsS478
MRE was scored on a 4-point scale (1: active small bowel infl ammation defi -nitely absent, 2: probably absent, 3: probably present, 4: defi nitely present). A clinical effi cacy score (CES) was also assigned to each MRE (range 0-3, from 0: not helpful, 1: confi rmatory only, 2: contributory, led to change in management/diagnosis, 3: determined diagnosis/directly led to manage-ment change). Comparisons were made between groups to the correlation between MRE fi ndings and clinical activity and impact of the MRE on man-agement.Results: 50 of 57 MREs met inclusion criteria. MRE was ordered in 1 patient in clinical remission and showed no activity. 57% of clinically severe cases had MRE scores of 3 or 4 and 75% had defi nite activity. In mild to moderate cases by symptoms, MRE was unlikely to show active disease with 68% having MRE scores of 1 or 2. With regard to clinical effi cacy, CES >2 in 74% while MRE was considered not helpful once. MRE had the greatest impact when it was employed to diff erentiate active CD from other non-functional diagnoses. In this group, CES =3 in 60%. In the group with established CD where MRE was used to assess activity, CES = 3 in 29%.Conclusion: MRE fi ndings correlate well with clinical activity in patients with severe CD and those in remission. Most patients with clinically mild to moder-ate disease activity did not have active disease by MRE. In these patients, MRE prevented escalation of therapy and led to the work-up of alternate diagnoses. Overall, MRE was a useful tool in this clinical setting, leading to management change in 66% of cases without use of ionizing radiation.
1299
Clinical Presentation, Treatment and Outcome of Ulcerative Colitis in African American vs. Caucasian American PatientsTalha Malik, MD,1 Seidu Inusah, MS,1 Alexandra Gutierrez, MD, MPH2. 1. Medicine, University of Alabama at Birmingham, Birmingham, AL; 2. Washington University in Saint Louis, Saint Louis, MO.
Purpose: Minority patients can experience health care disparities that aff ect the natural history of their disease. We examined the presentation, treatment and outcome of ulcerative colitis (UC) in African American (AA) vs. Cauca-sian American (CA) patients seen at a university IBD clinic.Methods: Th e records of 29 AA and 52 CA UC patients seen between 2003 and 2009 were reviewed. Unadjusted analysis utilizing the chi-square test, Fisher’s exact test or Wilcoxan rank sum test as appropriate was performed to compare disease characteristics, treatment, and outcome in the two groups. Adjusted logistic regression models tested independent diff erences.Results: Th ere was no signifi cant diff erence between AA and CA patients in regard to age at diagnosis, 37 years(range 14-69) vs. 32 years(range 9-56) respectively (P=0.478). Forty eight percent of the AA patients were female compared to 38% of CA patients (P=0.392). Th e median body mass index in AA (26 kg/m2,range 20-45) and CA patients (27 kg/m2, range 18-42) was similar (P=0.371). Similarly, no signifi cant diff erences were detected between the two groups based on extra-intestinal manifestations, smoking, extent of UC, steroid utilization, 5-ASA use or family history of infl ammatory bowel disease, other autoimmune diseases, color-ectal cancer or other cancers. However, diff erences in medical treatment between the two ethnic groups were observed. Th irty one percent of AA patients received thiopurine analogues (AZA/6-MP) vs. 55% of CA patients (P=0.031). Moreover, 21% of AA patients received biologics versus 50% of CA patients (P=0.008). In terms of surgical treatment, the rate of colectomy was similar in the two groups; 13% for AA and 10% for CA patients (P=0.679). On comparing the two ethnic groups based on clinical outcome, it was noted that AA patients were not more likely to have increase disease activity at end of observation, 21% vs. 24% (P=0.758). Adjusted analysis, done to asses if ethnicity aff ected the use of immune modulators independent of age, gender, duration of disease and observation revealed that AA patients with UC were less likely to receive biologics (P=0.021 OR=0.27 95%CI 0.09-0.82). Th e eff ect of ethnicity on the use of AZA/6-MP however remained only marginally signifi cant (P=0.045 OR=0.33 95%CI 0.11-0.98).Conclusion: While these data show that there might be signifi cantly lower rates of biological agent use in AA patients with UC, they at the same time also suggest that AA patients do not seem to have worse clinical disease. Whether socioeconomic status, access to care and health beliefs also contribute to the disparity in biological agent use needs further study.
1300
Th e Use of Serum, Urine, and Fecal Neopterin to Determine Disease Activ-ity in Crohn’s DiseaseNisreen Husain, MD,1 Alan Buchman, MD, MSPH,1 Stanley Naides, MD, PhD,2 Ken Tokoro, PhD,2 Mary Kwasny, PhD1. 1. Feinberg School of Medicine, Northwestern University, Chicago, IL; 2. Quest Laboratories, San Juan Capistrano, CA.
Purpose: Th ere are few noninvasive biomarkers which correlate with disease activity in Crohn’s Disease (CD). Th e aim of this study was to determine if serum, urine, or fecal neopterin concentrations were associated with clinical activity as defi ned by the Harvey Bradshaw (HBI) or Capetown Indices, eryth-rocyte sedimentation rate (ESR), C-reactive protein (CRP), serum albumin, hemoglobin (Hb), hematocrit (Hct) and fecal lactoferrin.Methods: We prospectively enrolled 70 outpatients with CD (33 clinically in remission, 37 active). Disease was considered active if the HBI was ≥ 5. Fecal (n=50), urine (n=115) and serum (n=120) samples were collected from healthy controls for neopterin measurement. Due to non-normality of data, medians and ranges are present. Mann-Whitney or Kruskal-Wallis tests, and Spearman’s correlation coeffi cients were employed.Results: Fecal neopterin was signifi cantly higher in CD patients compared to controls (-91 (20, 322) vs. 12.0 (3, 379) ng/g; p <0.001); median serum neopterin levels were higher in controls, although the range was wider in CD patients (4.5 (2.3, 14.6) v. 3.0 (1.5, 19.0), p < 0.001); neither fecal neopterin or serum neopterin were able to diff erentiate disease activity. We failed to detect any diff erence in urine neopterin values between groups (p=0.255). Urinary neopterin was weakly, but signifi cantly correlated with HBI (0.27), Capetown index (0.27), Hb (-0.37), Hct (-0.34), Albumin (-0.36), CRP (0.38), and ESR (0.31). Serum neopterin was also correlated with HBI (0.27), Albumin (-0.38), CRP (0.43), and ESR (0.32), but not with Capetown index, Hb, Hct, or fecal lactoferrin. Fecal neopterin was not associated with any of the serum or clini-cal indices.Conclusion: Fecal neopterin was signifi cantly greater in patients with CD vs. controls. For patients in remission, that suggests the likelihood of ongo-ing subclinical intestinal infl ammation and may be a promising independent biomarker for disease. However, it was unable to distinguish between active and inactive CD. Urine neopterin did not distinguish clinically active or inac-tive patients from healthy controls. Although diff erences were seen in distribu-tions of serum neopterin between CD groups and controls, it is unclear if there is a single mechanism that might explain this.
1301
Evaluation of IBD Serology in Infl ammatory and Non-infl ammatory Dis-orders of the Ileal PouchBo Shen, MD, Emmanuel Obusez, BA, Elaine Queener, LPN. Cleveland Clinic, Cleveland, OH.
Purpose: : Infl ammatory (pouchitis, cuffi tis, Crohn’s disease of the pouch, and surgery-related stricture/fi stula/sinus) and non-infl ammatory (irrita-ble pouch syndrome) complications of the ileal pouch are common in IBD patients with restorative proctocolectomy. Th e etiopathogenesis of these disorders are largely unclear. pANCA and anti-CBir1 expression has been reported to be associated with pouchitis aft er IPAA. We postulated that alteration of commensal bacteria to the etiopathogenesis of each of these pouch disorders at diff erent degree. Th e aim of the study was to evaluate bacteria-antigen-based IBD serology for diagnosis and possible pathoge-netic role.Methods: Consecutive eligible pouch patients were recruited from the Pou-chitis Clinic. Pouch patients with underlying familial adenomatous polyposis were excluded. Diagnosis of pouch disorders were based on a combined clini-cal, endoscopic, histologic, and radiographic examinations. Serum specimens from 196 patients were analyzed for 8-marker antibody panel by Prometheus Laboratories, San Diego, CA. Demographic and clinical data were prospec-tively documented. Descriptive statistics were performed.

© 2010 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY
Abstracts S479
Results: Th e 196 patients consisted of normal pouch (N=10), irritable pouch syndrome (N=26), acute pouchitis (antibiotic-responsive or antibiotic-depend-ent forms, N=35, chronic antibiotic-refractory pouchitis (N=34), Crohn’s disease of the pouch (N=55), cuffi tis (N=15), surgery-related complications (strictures, sinuses, fi stula, prolapse N=28). In general, there were no signifi -cant diff erences in the serology markers among the 7 pouch categories, except the maker of C-Bir1 (Table). Th ere was signifi cant diff erence in ANCA level between CD of the pouch (42.6±32.8 EU/ml) and remaining pouch groups (22.5±20.5 EU/ml). Th ere was no diff erence in each of 8 serology markers between 3 phenotypes of CD of the pouch (infl ammatory, N=12; fi brostenotic N=13; and fi stulizing N=32).Conclusion: Th ere is evidence that host immune response to certain bacterial antigens in patients with various categories of pouch disorders may be diff er-ent, particularly to C-Bir fl agellin antigen.Disclosure: Bo Shen, MD, consulting for Prometheus Lab.
FUNCTIONAL BOWEL DISORDERS
1302
Irritable Bowel Syndrome and HIV: A Cross Sectional Study of the Severity of Gastrointestinal Symptoms and HIV-infected SubjectsKeri Herzog, MD, Renee Williams, MD, Ilseung Cho, MD, MSc, Craig Tenner, MD, Michael Poles, MD, PhD. NYU School of Medicine, New York City, NY.
Purpose: Irritable bowel syndrome (IBS) is a common functional bowel disorder in which bowel habits are altered in association with abdominal pain or discom-fort. Altered bowel habits, abdominal pain, and abdominal discomfort are also common complaints in the HIV+ population. To date, no studies have assessed the prevalence of IBS in the HIV+ population. Furthermore, while gastrointestinal (GI) symptoms had been found to signifi cantly impair the health-related quality of life (HRQOL) of HIV+ outpatients, it remains to be determined if IBS aff ects the HRQOL of HIV+ outpatients. Th e aims of this study were to determine the preva-lence of IBS in HIV+ outpatients and to examine the impact of IBS on the HRQOL of HIV+ subjects. We hypothesized that the prevalence of IBS is signifi cantly higher in the HIV+ outpatient population compared to the HIV- outpatient population and that these symptoms signifi cantly impair HRQOL in HIV+ outpatients.Methods: Consecutive patients seen in the VA New York Harbor Healthcare System Primary Care Clinic and Infectious Disease were invited to partici-pate in the study. GI symptoms were evaluated in 146 HIV+ subjects and 274 HIV- controls using an integrated Rome III diagnostic questionnaire for IBS. Th e HRQOL of these patients was assessed using the Medical Outcomes Study Short Form 36 (MOS SF-36) survey. Patient demographic data and HIV medi-cal history information were also collected.Results: We surveyed 416 patients (96.2% male) with a mean age of 60.5 years. Of these subjects, 38.5% were white/non-hispanic, 37.0% were black, and 19.0% were Hispanic. Th e prevalence of IBS was signifi cantly increased among HIV+ vs. HIV- outpatients (10.2% vs. 2.2%, p < 0.002 using Fisher’s exact test), according to strict ROME III criteria. All of the HIV+ subjects with IBS in our cohort were male and 53.8% were black. Th ere were no signifi cant diff erences
in the categorized distribution of CD4 counts and viral loads between IBS+ and IBS- patients. Among our HIV+ subjects, the presence of IBS was signifi -cantly associated with a decrease in the SF-36 Physical Component Summary score (HIV+ /IBS - (64.12), HIV+/IBS + (34.62), (p<0.018)).Conclusion: Our study demonstrates that in a predominantly male veteran outpatient population, there is a greater prevalence of IBS in HIV + subjects compared with HIV- subjects. Th e presence of IBS symptoms signifi cantly impairs HRQOL in HIV+ patients. IBS oft en remains unrecognized and untreated, especially in the HIV+ population, and there it is essential that healthcare providers evaluate their HIV+ patients for this syndrome so that they may be optimally treated.
1303
Week 1 Changes in Bowel and Abdominal Symptoms Following Linaclotide Treatment: Results from Two Phase 3 Trials in Chronic Constipation PatientsAnthony Lembo, MD,1 Bernard Lavins, MD,2 Steven Shiff , MD,3 James MacDougall, PhD,2 Caroline Kurtz, PhD,2 Chris O’Dea, MS,2 Harvey Schneier, MD,3 Mark Currie, PhD,2 Jeff rey Johnston, MD2. 1. Beth Israel Deaconess Medical Center, Boston, MA; 2. Ironwood Pharmaceuticals, Cambridge, MA; 3. Forest Research Institute, Jersey City, NJ.
Purpose: Linaclotide, a fi rst-in-class, minimally-absorbed, guanylate cyclase type-C receptor agonist, statistically signifi cantly improved bowel and abdominal symptoms, and patient global assessments in chronic constipation (CC) and irritable bowel syndrome with constipation patients in Phase 2b trials. Two recent, randomized, double-blind, Phase 3 trials (MD-01 and 103-303) in patients with CC demonstrated statistically signifi cant improvements in bowel and abdominal symptoms. Th e aim of this analysis is to determine the time to onset of symptom changes following treatment initiation in both Phase 3 trials.Methods: 1272 patients who met modifi ed Rome II criteria for CC, and had <3 complete spontaneous bowel movements (CSBM) per week and ≤6 SBMs per week during a 2-week baseline period were randomized to oral once-daily 133 or 266μg linaclotide or placebo for 12 weeks.Results: In pooled analyses, 67% and 57% of linaclotide 133 and 266 μg patients had an SBM within 24 hours following initial study drug dosing, vs. 39% for placebo (both P<0.0001); for CSBM results, 31% and 28% of Linaclotide 133 and 266μg patients had a CSBM vs. 12% for placebo (both p<0.0001). Results by study for bowel symptoms and weekly constipation severity were also sta-tistically signifi cantly improved for linaclotide vs. placebo (p<0.0001) aft er 1 week of treatment (Table). Statistically signifi cant improvements in bloat-ing and abdominal discomfort were obtained at Week 1 and Week 2 of treat-ment, respectively. Bowel and abdominal symptom improvements were seen throughout the 12-week treatment period. Th e week 1 incidence of diarrhea across both studies was 8%, 8%, and 1% for the 133μg, 266μg, and placebo groups, respectively.Conclusion: Once daily doses of linaclotide resulted in early and sustained statistically signifi cant improvements in bowel and abdominal symptoms during treatment of patients with CC. Diarrhea was the most common adverse event.
[1301] Comparison of serology markers in categories of ileal pouch disorders
Normal pouch
N =10 Irritable Pouch
Syndrome N =26 Acute pouchitis
N =35 Refractory pouchi-
tis N =34 Crohn’s pouch
N =55 Cuffi tis N =15 Surgery complica-
tion N =28 P
ANCA EU / ml 41.1 ± 37.6 31.9 ± 29.0 35.3 ± 32.7 38.8 ± 31.4 42.6 ± 32.8 37.5 ± 28.5 22.5 ± 20.5 0.351
ASCA-A EU / ml 21.0 ± 20.2 18.6 ± 22.8 16.9 ± 23.3 16.6 ± 19.3 16.5 ± 18.9 14.4 ± 14.8 24.1 ± 26.4 0.741
ASCA-G EU / ml 26.5 ± 11.9 19.7 ± 16.8 17.6 ± 17.9 18.6 ± 23.1 23.8 ± 24.8 20.8 ± 25.8 26.4 ± 25.6 0.758
CBir1 EU / ml 41.3 ± 31.5 25 ± 20.1 33 ± 24.8 31.0 ± 21.5 47.3 ± 27.6 31.9 ± 25.7 48.4 ± 33.6 0.002
OmpC EU / ml 32.2 ± 29.0 16.9 ± 15.0 21.1 ± 16.9 33.5 ± 2.4 29.7 ± 23.4 19.6 ± 14.6 36.2 ± 27.9 0.097
I2 EU / ml 471.2 ± 294.7 433.9 ± 454.2 371.7 ± 197.5 670.7 ± 153.5 479.4 ± 587.5 318.6 ± 197.7 446.1 ± 365.2 0.797
pANCA EU / ml 0.38 ± 0.52 0.24 ± 0.44 0.27 ± 0.46 0.33 ± 0.48 0.56 ± 0.50 0.25 ± 0.45 446.1 ± 365.2 0.127

Copyright of American Journal of Gastroenterology is the property of Nature Publishing Group and its content
may not be copied or emailed to multiple sites or posted to a listserv without the copyright holder's express
written permission. However, users may print, download, or email articles for individual use.
Copyright © 2022 FDOKUMEN




















