
Incidence and Phenotype of Inflammatory Bowel Disease, Based on Results from the Asia-Pacific...
10
Incidence and Phenotype of Inflammatory Bowel Disease Based on Results From the Asia-Pacific Crohn’s and Colitis Epidemiology Study SIEW C. NG, 1 WHITNEY TANG, 1 JESSICA Y. CHING, 1 MAY WONG, 1 CHUNG MO CHOW, 2 A. J. HUI, 3 T. C. WONG, 4 VINCENT K. LEUNG, 5 STEVE W. TSANG, 6 HON HO YU, 7 MO FONG LI, 7 KA KEI NG, 8 MICHAEL A. KAMM, 9 CORRIE STUDD, 9 SALLY BELL, 9 RUPERT LEONG, 10 H. JANAKA DE SILVA, 11 ANURADHANI KASTURIRATNE, 11 M. N. F. MUFEENA, 11 KHOON LIN LING, 12 CHOON JIN OOI, 12 POH SENG TAN, 13 DAVID ONG, 13 KHEAN L. GOH, 14 IDA HILMI, 14 PISES PISESPONGSA, 15 SATHAPORN MANATSATHIT, 16 RUNGSUN RERKNIMITR, 17 SATIMAI ANIWAN, 17 YU FANG WANG, 18 QIN OUYANG, 18 ZHIRONG ZENG, 19 ZHENHUA ZHU, 19 MIN HU CHEN, 19 PIN JIN HU, 19 KAICHUN WU, 20 XIN WANG, 20 MARCELLUS SIMADIBRATA, 21 MURDANI ABDULLAH, 21 JUSTIN CY WU, 1 JOSEPH J. Y. SUNG, 1 and FRANCIS K. L. CHAN, 1 on behalf of THE ASIA–PACIFIC CROHN’S AND COLITIS EPIDEMIOLOGIC STUDY (ACCESS) STUDY GROUP 1 Institute of Digestive Disease, Department of Medicine and Therapeutics, Li Ka Shing Institute of Health Sciences, The Chinese University of Hong Kong, Hong Kong, China; 2 Department of Pediatrics, Chinese University of Hong Kong, Hong Kong, China; 3 Alice Ho Miu Ling Nethersole Hospital, Hong Kong, China; 4 North District Hospital, Hong Kong, China; 5 United Christian Hospital, Hong Kong, China; 6 Tseung Kwan O Hospital, Hong Kong, China; 7 Kiangwu Hospital, Macau, China; 8 Hospital Conde S Januario, Macau, China; 9 St Vincent’s Hospital and University of Melbourne, Melbourne, Australia; 10 Bankstown and Concord Hospitals, Sydney, Australia; 11 Faculty of Medicine, University of Kelaniya, Ragama, Sri Lanka; 12 Singapore General Hospital, Singapore; 13 National University Hospital of Singapore, Singapore; 14 University of Malaya Medical Centre, Kuala Lumpur, Malaysia; 15 Maharaj Nakorn Chiangmai Hospital, Chiangmai, Thailand; 16 Siriraj Hosptial, Bangkok, Thailand; 17 King Chulalongkorn Memorial Hospital, Bangkok, Thailand; 18 West China Hospital, Sichuan University, Chengdu, China; 19 The First Affiliated Hospital of San Yat Sen University, Guangzhou, China; 20 Department of Gastroenterology, Xijing Hospital, Fourth Military Medical University, Shaanxi, China; and 21 University of Indonesia, Depok, Indonesia BACKGROUND & AIMS: Inflammatory bowel diseases (IBD) are becoming more common in Asia, but epidemi- ologic data are lacking. The Asia-Pacific Crohn’s and Colitis Epidemiology Study aimed to determine the inci- dence and phenotype of IBD in 8 countries across Asia and in Australia. METHODS: We performed a prospec- tive, population-based study of IBD incidence in pre- defined catchment areas, collecting data for 1 year, starting on April 1, 2011. New cases were ascertained from multiple overlapping sources and entered into a Web-based database. Cases were confirmed using standard criteria. Local endoscopy, pathology, and pharmacy records were searched to ensure completeness of case capture. RESULTS: We identified 419 new cases of IBD (232 of ul- cerative colitis [UC], 166 of Crohn’s disease [CD], and 21 IBD-undetermined). The crude annual overall incidence values per 100,000 individuals were 1.37 for IBD in Asia (95% confidence interval: 1.251.51; 0.76 for UC, 0.54 for CD, and 0.07 for IBD-undetermined) and 23.67 in Australia (95% confidence interval: 18.4629.85; 7.33 for UC, 14.00 for CD, and 2.33 for IBD-undetermined). China had the highest incidence of IBD in Asia (3.44 per 100,000 indi- viduals). The ratios of UC to CD were 2.0 in Asia and 0.5 in Australia. Median time from symptom onset to diag- nosis was 5.5 months (interquartile range, 1.415 months). Complicated CD (stricturing, penetrating, or perianal dis- ease) was more common in Asia than Australia (52% vs 24%; P ¼ .001), and a family history of IBD was less common in Asia (3% vs 17%; P < .001). CONCLUSIONS: We per- formed a large-scale population-based study and found that although the incidence of IBD varies throughout Asia, it is still lower than in the West. IBD can be as severe or more severe in Asia than in the West. The emergence of IBD in Asia will result in the need for specific health care resources, and offers a unique op- portunity to study etiologic factors in developing nations. Keywords: ACCESS; Intestine; Inflammation; Rate. Watch this article’s video abstract and others at http://tiny.cc/j026c. Scan the quick response (QR) code to the left with your mobile device to watch this article’s video abstract and others. Don’t have a QR code reader? Get one by searching ‘QR Scanner’ in your mobile device’s app store. C rohn’s disease (CD) and ulcerative colitis (UC) are chronic inflammatory bowel diseases (IBD) of unknown etiology. It is estimated that up to 1.4 million people in the United States and 250,000 people in the United Kingdom suffer from IBD. This chronic condition is without a medical cure and commonly requires a life- time of care and medication. The burden of IBD varies in different countries and populations. In recent decades, the IBD incidence in tradi- tionally high-incidence areas, such as the United States and Europe, has been relatively stable 1,2 and the disease has become more prevalent in previously low incidence areas, including Asia. 3,4 Hospital-based studies in Asia have shown an increasing number of treated patients. 5–7 Improved physician awareness and better diagnostic mo- dalities are unlikely to account fully for this rise. This in- crease most likely relates to environmental and lifestyle factors, as countries in Asia undergo socioeconomic change and rapid industrialization. 8 Variations in disease incidence Abbreviations used in this paper: CD, Crohn’s disease; CI, confidence interval; IBD, inflammatory bowel disease; IBD-U, inflammatory bowel diseaseundetermined; UC, ulcerative colitis. © 2013 by the AGA Institute 0016-5085/$36.00 http://dx.doi.org/10.1053/j.gastro.2013.04.007 GASTROENTEROLOGY 2013;145:158–165 CLINICAL AT
Transcript of Incidence and Phenotype of Inflammatory Bowel Disease, Based on Results from the Asia-Pacific...

GASTROENTEROLOGY 2013;145:158–165
CLIN
ICALAT
Incidence and Phenotype of Inflammatory Bowel Disease Based onResults From the Asia-Pacific Crohn’s and Colitis Epidemiology StudySIEW C. NG,1 WHITNEY TANG,1 JESSICA Y. CHING,1 MAY WONG,1 CHUNG MO CHOW,2 A. J. HUI,3 T. C. WONG,4
VINCENT K. LEUNG,5 STEVE W. TSANG,6 HON HO YU,7 MO FONG LI,7 KA KEI NG,8 MICHAEL A. KAMM,9 CORRIE STUDD,9
SALLY BELL,9 RUPERT LEONG,10 H. JANAKA DE SILVA,11 ANURADHANI KASTURIRATNE,11 M. N. F. MUFEENA,11
KHOON LIN LING,12 CHOON JIN OOI,12 POH SENG TAN,13 DAVID ONG,13 KHEAN L. GOH,14 IDA HILMI,14
PISES PISESPONGSA,15 SATHAPORN MANATSATHIT,16 RUNGSUN RERKNIMITR,17 SATIMAI ANIWAN,17 YU FANG WANG,18
QIN OUYANG,18 ZHIRONG ZENG,19 ZHENHUA ZHU,19 MIN HU CHEN,19 PIN JIN HU,19 KAICHUN WU,20 XIN WANG,20
MARCELLUS SIMADIBRATA,21 MURDANI ABDULLAH,21 JUSTIN CY WU,1 JOSEPH J. Y. SUNG,1 and FRANCIS K. L. CHAN,1
on behalf of THE ASIA–PACIFIC CROHN’S AND COLITIS EPIDEMIOLOGIC STUDY (ACCESS) STUDY GROUP1Institute of Digestive Disease, Department of Medicine and Therapeutics, Li Ka Shing Institute of Health Sciences, The Chinese University of Hong Kong, Hong Kong,China; 2Department of Pediatrics, Chinese University of Hong Kong, Hong Kong, China; 3Alice Ho Miu Ling Nethersole Hospital, Hong Kong, China; 4North DistrictHospital, Hong Kong, China; 5United Christian Hospital, Hong Kong, China; 6Tseung Kwan O Hospital, Hong Kong, China; 7Kiangwu Hospital, Macau, China; 8HospitalConde S Januario, Macau, China; 9St Vincent’s Hospital and University of Melbourne, Melbourne, Australia; 10Bankstown and Concord Hospitals, Sydney, Australia;11Faculty of Medicine, University of Kelaniya, Ragama, Sri Lanka; 12Singapore General Hospital, Singapore; 13National University Hospital of Singapore, Singapore;14University of Malaya Medical Centre, Kuala Lumpur, Malaysia; 15Maharaj Nakorn Chiangmai Hospital, Chiangmai, Thailand; 16Siriraj Hosptial, Bangkok, Thailand; 17KingChulalongkornMemorial Hospital, Bangkok, Thailand; 18West China Hospital, SichuanUniversity, Chengdu, China; 19The First Affiliated Hospital of San Yat SenUniversity,Guangzhou, China; 20Department of Gastroenterology, Xijing Hospital, Fourth Military Medical University, Shaanxi, China; and 21University of Indonesia, Depok, Indonesia
Abbreviations used in this paper: CD, Crohn’s disease; CI, confidenceinterval; IBD, inflammatory bowel disease; IBD-U, inflammatory boweldisease�undetermined; UC, ulcerative colitis.
© 2013 by the AGA Institute0016-5085/$36.00
http://dx.doi.org/10.1053/j.gastro.2013.04.007
BACKGROUND & AIMS: Inflammatory bowel diseases(IBD) are becoming more common in Asia, but epidemi-ologic data are lacking. The Asia-Pacific Crohn’s andColitis Epidemiology Study aimed to determine the inci-dence and phenotype of IBD in 8 countries across Asiaand in Australia. METHODS: We performed a prospec-tive, population-based study of IBD incidence in pre-defined catchment areas, collecting data for 1 year,starting on April 1, 2011. New cases were ascertained frommultiple overlapping sources and entered into aWeb-baseddatabase. Cases were confirmed using standard criteria.Local endoscopy, pathology, and pharmacy records weresearched to ensure completeness of case capture.RESULTS: We identified 419 new cases of IBD (232 of ul-cerative colitis [UC], 166 of Crohn’s disease [CD], and 21IBD-undetermined). The crude annual overall incidencevalues per 100,000 individuals were 1.37 for IBD in Asia(95% confidence interval: 1.25�1.51; 0.76 for UC, 0.54 forCD, and 0.07 for IBD-undetermined) and 23.67 in Australia(95% confidence interval: 18.46�29.85; 7.33 for UC, 14.00for CD, and 2.33 for IBD-undetermined). China had thehighest incidence of IBD in Asia (3.44 per 100,000 indi-viduals). The ratios of UC to CD were 2.0 in Asia and 0.5in Australia. Median time from symptom onset to diag-nosis was 5.5months (interquartile range, 1.4�15months).Complicated CD (stricturing, penetrating, or perianal dis-ease) wasmore common in Asia than Australia (52% vs 24%;P ¼ .001), and a family history of IBD was less common inAsia (3% vs 17%; P < .001). CONCLUSIONS: We per-formed a large-scale population-based study and foundthat although the incidence of IBD varies throughoutAsia, it is still lower than in the West. IBD can be assevere or more severe in Asia than in the West. Theemergence of IBD in Asia will result in the need forspecific health care resources, and offers a unique op-portunity to study etiologic factors in developingnations.
Keywords: ACCESS; Intestine; Inflammation; Rate.
Watch this article’s video abstract and others athttp://tiny.cc/j026c.
Scan the quick response (QR) code to the left withyour mobile device to watch this article’s videoabstract and others. Don’t have a QR code reader?Get one by searching ‘QR Scanner’ in your mobiledevice’s app store.
rohn’s disease (CD) and ulcerative colitis (UC) are
Cchronic inflammatory bowel diseases (IBD) ofunknown etiology. It is estimated that up to 1.4 millionpeople in the United States and 250,000 people in theUnited Kingdom suffer from IBD. This chronic conditionis without a medical cure and commonly requires a life-time of care and medication.The burden of IBD varies in different countries andpopulations. In recent decades, the IBD incidence in tradi-tionally high-incidence areas, such as the United States andEurope, has been relatively stable1,2 and the disease hasbecome more prevalent in previously low incidence areas,including Asia.3,4 Hospital-based studies in Asia haveshown an increasing number of treated patients.5–7
Improved physician awareness and better diagnostic mo-dalities are unlikely to account fully for this rise. This in-crease most likely relates to environmental and lifestylefactors, as countries in Asia undergo socioeconomic changeand rapid industrialization.8 Variations in disease incidence

July 2013 IBD INCIDENCE IN ASIA 159
CLINICALAT
might reflect differences in the distribution ormagnitude ofthe impact of environmental etiologic factors.3,9
Incidence data can provide valuable information aboutthemagnitude of the problem, aswell as ameans to estimatethe burden of disease and anticipate health care needs.9 Thisis particularly important in IBD, a chronic incurable diseasethat affects mostly young people at an age when they aremost active in their private and professional life. In addi-tion, careful descriptive epidemiological studies can offerclues to the etiology of these diseases.
A number of population-based studies in IBD have beenpublished from Europe, North America, and Australia.10–13
However, there are no published studies comparing inci-dence or prevalence rates between different regions of Asia-Pacific. Little is also known about the regional differences inthe severity of disease at presentation. Challenges in Asia-Pacific include difficulty in defining catchment areas andthe lack of uniform criteria for case ascertainment. Much ofthese data are hospital-based, and so there is a bias in termsof assessing only those populations that access the hospi-tals under study. Even within Asia incidence and prevalencerates of IBD vary according to geography and ethnicgroups.3 The highest rates have been reported in India(particularly of UC), Japan, and the Middle East, and overallrising trends of IBD are seen in East Asia. A recent sys-tematic review has shown that the incidence of IBD isincreasing globally; however, this review points to a gap inthe literature with regard to the epidemiology of IBD indeveloping countries, including Asia.1
In the current study, we report the incidence and diseasecharacteristics of CD and UC at presentation for a 1-yearperiod across nine countries in the Asia-Pacific region.
MethodsStudy Setting and Study Population
The Asia-Pacific Crohn’s and Colitis Epidemiology(ACCESS) study was conducted in 21 centers in 12 cities in 9countries (considering Hong Kong and Macau separately frommainland China) across Asia-Pacific. The countries involved wereAustralia, mainland China, Hong Kong, Indonesia, Macau,Malaysia, Singapore, Sri Lanka, and Thailand. Study populationand centers were selected based on the following predefinedcriteria: well-defined boundaries and relatively geographicallyisolated; stable population that is demographically similar interms of age, socioeconomic status, and ethnic makeup to therest of the population within the region or country; populationsunder study have equivalent access to health care; and in-vestigators within the region have the ability to recruit patients,enter patient data, and follow-up patients.
Incident IBD cases diagnosed between April 1, 2011 andMarch 31, 2012 were enrolled and entered into a Web-baseddatabase (http://www.access-apibd.com/access/). Details of thebackground population and demographics of each region areshown in the Appendix.
Case Identification and Ascertainment
Unlike some countries with universal health systems thathave accurate coding for diagnostic and therapeutic registry
data,14,15 countries in Asia and Australia have no such system.Although most of the residents in Asia and in Australia usepublic health system, a small minority has comprehensive privatehealth insurance and, therefore, patients attending both publicand private clinics and hospitals needed to be identified. In mostcountries in Asia, suspected IBD cases diagnosed by generalpractitioners or in private clinics are almost exclusively referredinitially to the central public hospitals for investigations anddisease confirmation and follow-up.
To ensure maximum case capture, a multifaceted approach tocase identification was used. Patients were recruited fromoutpatient clinics and inpatient wards from all hospitals within apredefined catchment area. Before study initiation, all gastroen-terologists, pediatricians, surgeons, and pathologists within eachregion were informed of the study and its aims by letters andmeetings. They were requested to report or refer all patients withsuspected IBD to the gastroenterologists within each hospital.These patients were classified as “medically referred.” Eachmonth, all doctors were contacted by e-mail and reminded of thestudy. Every 3 months, main investigators from each region metwithin Asia-Pacific to discuss patient recruitment.
In countries with an IBD patient support group, memberswere informed of the study and invited to participate. In addi-tion, advertisements were placed in local newspapers and healthknowledge lectures were arranged to prompt patients with sus-pected IBD symptoms to consult a doctor. These patients wereclassified as “self-referred” cases. Finally, a search of endoscopyand histology reports at each hospital was performed for thestudy period using diagnostic keywords, including “inflamma-tory bowel disease,” “Crohn’s disease,” “ulcerative colitis,” “in-testinal/colonic ulcer,” “proctitis,” and “proctosigmoiditis.” Casenotes of additional incident patients were reviewed by a specialistdoctor. Pharmacy records in hospitals were also searched fortrade and generic names of sulfasalazine and mesalamine drugsprescribed during the study period. Case notes of patientsidentified through pharmacies were reviewed to confirm thediagnosis of IBD and letters were mailed to patients from theirphysician inviting them to participate in the study. These pa-tients were referred to as “invited.”
In Australia, >300 general practitioners across the study areawere contacted before and during study to capture primary carecases. When a case was identified, demographics, clinical, endo-scopic, and histological results were retrieved from the treatingphysician after patient consent was obtained.
A central coordinator within each region cross checked in-formation from general practitioners, gastroenterologists, pedi-atricians, surgeons, endoscopy centers, pathology laboratories,and pharmacy records to ensure completeness of case captureand case verification. Follow-up review of case notes was per-formed 3 months after diagnosis and every 3 months subse-quently to ensure diagnosis remained accurate.
Case Definition
All patients were required to meet IBD diagnostic criteriaon the basis of clinical symptoms, endoscopy, histology, andradiology.16 In each incident case, variables collected includeddisease location and behavior using the Montreal classification,17
family history of IBD, smoking status, extraintestinal manifes-tations, and drug therapy at diagnosis.
Other diagnoses, including infections, intestinal tuberculosis,amoebiasis, and nonsteroidal anti-inflammatory drug�inducedulceration, were rigorously excluded. Stools were sent for Clos-tridium difficile toxins, microscopy, culture and sensitivity, ova,
160 NG ET AL GASTROENTEROLOGY Vol. 145, No. 1
CLIN
ICALAT
cysts, and parasites. Intestinal tissue biopsies were obtained fortuberculosis polymerase chain reaction and culture. In suspectedcases, interferon gamma�releasing assay and computed tomog-raphy scans were also performed to exclude tuberculosis. Caseswere only included if the diagnosis remained certain at 6-monthfollow-up. Cases were excluded if screening for infectious enter-itis was positive, the diagnosis was doubtful after fullinvestigations or if the patient lived outside the capture area. Atstudy completion, an audit was performed by external in-vestigators in 3 randomly selected sites to review case notes andconfirm case ascertainment and diagnosis.
The study was approved by local ethics committees of each siteand patients consented to having their data collected. Australiancases were included through an opt-out consent process.
Table 1
AustraliaMainlandMainlandMainlandHong KoIndonesiMacauMalaysiaSingaporSri LankThailandThailandTotal
Data and Statistical Analysis
Crude incidence rates were calculated for IBD, CD, andUC for 2011�2012 based on the number of patients diagnosedcompared with the total population at risk. Projected populationdata by age and sex were obtained from the National Census orDepartment of Statistics of individual countries. Incidence rateswere reported with 95% confidence intervals (CI), assuming aPoisson distribution. Incidence rates were age standardized usingthe World Health Organization’s Standard Population.18 A c2
test was used to compare demographics and disease classificationbetween groups. Significance was defined as P < .05.
ResultsIncidence of IBD
During the 1-year period, 419 new IBD cases wereidentified, including 232 (55.4%) ulcerative colitis (UC),166 (39.6%) Crohn’s disease (CD), and 21 (5.0%) IBD-undetermined (IBD-U).
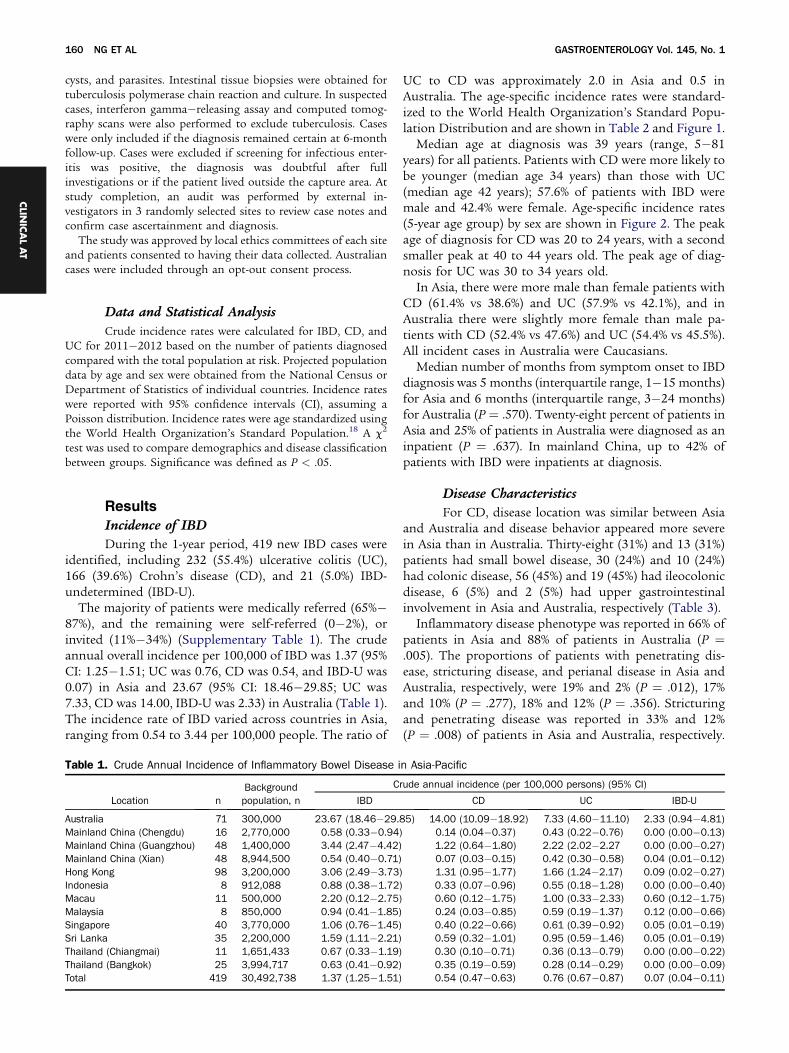
The majority of patients were medically referred (65%�87%), and the remaining were self-referred (0�2%), orinvited (11%�34%) (Supplementary Table 1). The crudeannual overall incidence per 100,000 of IBD was 1.37 (95%CI: 1.25�1.51; UC was 0.76, CD was 0.54, and IBD-U was0.07) in Asia and 23.67 (95% CI: 18.46�29.85; UC was7.33, CD was 14.00, IBD-U was 2.33) in Australia (Table 1).The incidence rate of IBD varied across countries in Asia,ranging from 0.54 to 3.44 per 100,000 people. The ratio of
. Crude Annual Incidence of Inflammatory Bowel Disease i
Location nBackgroundpopulation, n
C
IBD
71 300,000 23.67 (18.46�29.China (Chengdu) 16 2,770,000 0.58 (0.33�0.94China (Guangzhou) 48 1,400,000 3.44 (2.47�4.42)China (Xian) 48 8,944,500 0.54 (0.40�0.71)
ng 98 3,200,000 3.06 (2.49�3.73a 8 912,088 0.88 (0.38�1.72
11 500,000 2.20 (0.12�2.75)8 850,000 0.94 (0.41�1.85)
e 40 3,770,000 1.06 (0.76�1.45)a 35 2,200,000 1.59 (1.11�2.21)(Chiangmai) 11 1,651,433 0.67 (0.33�1.19)(Bangkok) 25 3,994,717 0.63 (0.41�0.92)
419 30,492,738 1.37 (1.25�1.51)
UC to CD was approximately 2.0 in Asia and 0.5 inAustralia. The age-specific incidence rates were standard-ized to the World Health Organization’s Standard Popu-lation Distribution and are shown in Table 2 and Figure 1.
Median age at diagnosis was 39 years (range, 5�81years) for all patients. Patients with CD were more likely tobe younger (median age 34 years) than those with UC(median age 42 years); 57.6% of patients with IBD weremale and 42.4% were female. Age-specific incidence rates(5-year age group) by sex are shown in Figure 2. The peakage of diagnosis for CD was 20 to 24 years, with a secondsmaller peak at 40 to 44 years old. The peak age of diag-nosis for UC was 30 to 34 years old.
In Asia, there were more male than female patients withCD (61.4% vs 38.6%) and UC (57.9% vs 42.1%), and inAustralia there were slightly more female than male pa-tients with CD (52.4% vs 47.6%) and UC (54.4% vs 45.5%).All incident cases in Australia were Caucasians.
Median number of months from symptom onset to IBDdiagnosis was 5 months (interquartile range, 1�15 months)for Asia and 6 months (interquartile range, 3�24 months)for Australia (P ¼ .570). Twenty-eight percent of patients inAsia and 25% of patients in Australia were diagnosed as aninpatient (P ¼ .637). In mainland China, up to 42% ofpatients with IBD were inpatients at diagnosis.
n Asia-P
rude ann
85) 14) 0
10
) 1) 0
0000000
Disease Characteristics
For CD, disease location was similar between Asiaand Australia and disease behavior appeared more severein Asia than in Australia. Thirty-eight (31%) and 13 (31%)patients had small bowel disease, 30 (24%) and 10 (24%)had colonic disease, 56 (45%) and 19 (45%) had ileocolonicdisease, 6 (5%) and 2 (5%) had upper gastrointestinalinvolvement in Asia and Australia, respectively (Table 3).
Inflammatory disease phenotype was reported in 66% ofpatients in Asia and 88% of patients in Australia (P ¼.005). The proportions of patients with penetrating dis-ease, stricturing disease, and perianal disease in Asia andAustralia, respectively, were 19% and 2% (P ¼ .012), 17%and 10% (P ¼ .277), 18% and 12% (P ¼ .356). Stricturingand penetrating disease was reported in 33% and 12%(P ¼ .008) of patients in Asia and Australia, respectively.
acific
ual incidence (per 100,000 persons) (95% CI)
CD UC IBD-U
.00 (10.09�18.92) 7.33 (4.60�11.10) 2.33 (0.94�4.81).14 (0.04�0.37) 0.43 (0.22�0.76) 0.00 (0.00�0.13).22 (0.64�1.80) 2.22 (2.02�2.27 0.00 (0.00�0.27).07 (0.03�0.15) 0.42 (0.30�0.58) 0.04 (0.01�0.12).31 (0.95�1.77) 1.66 (1.24�2.17) 0.09 (0.02�0.27).33 (0.07�0.96) 0.55 (0.18�1.28) 0.00 (0.00�0.40).60 (0.12�1.75) 1.00 (0.33�2.33) 0.60 (0.12�1.75).24 (0.03�0.85) 0.59 (0.19�1.37) 0.12 (0.00�0.66).40 (0.22�0.66) 0.61 (0.39�0.92) 0.05 (0.01�0.19).59 (0.32�1.01) 0.95 (0.59�1.46) 0.05 (0.01�0.19).30 (0.10�0.71) 0.36 (0.13�0.79) 0.00 (0.00�0.22).35 (0.19�0.59) 0.28 (0.14�0.29) 0.00 (0.00�0.09).54 (0.47�0.63) 0.76 (0.67�0.87) 0.07 (0.04�0.11)
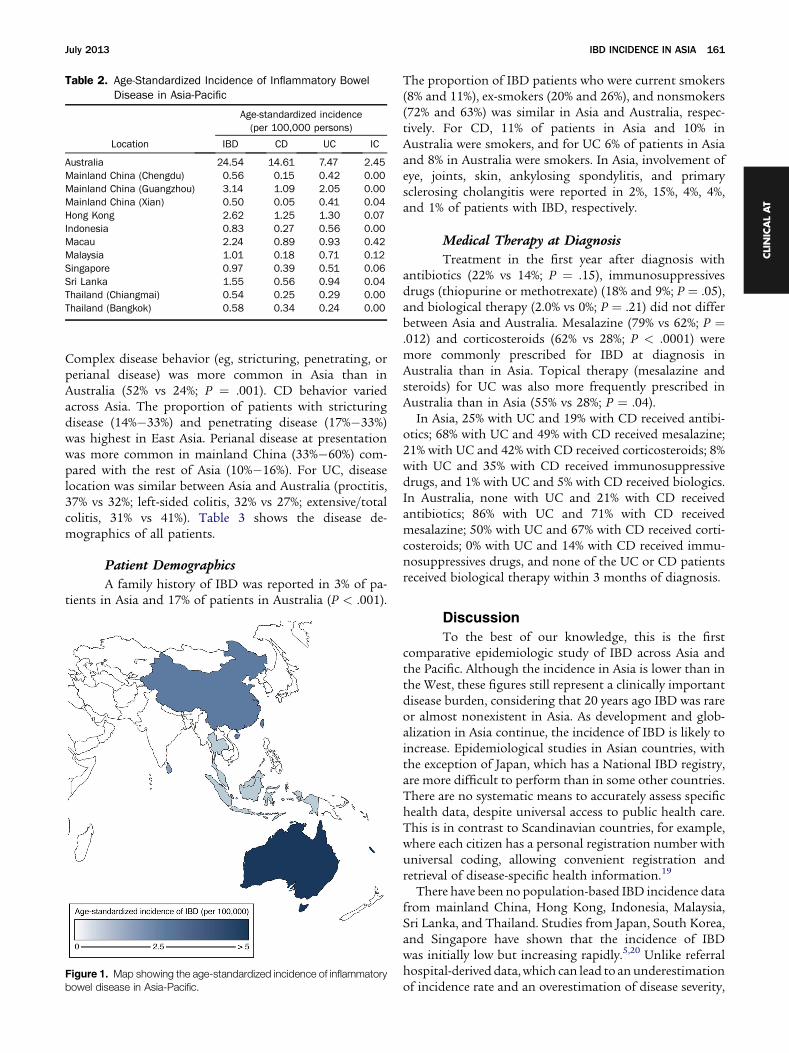
Table 2. Age-Standardized Incidence of Inflammatory BowelDisease in Asia-Pacific
Location
Age-standardized incidence(per 100,000 persons)
IBD CD UC IC
Australia 24.54 14.61 7.47 2.45Mainland China (Chengdu) 0.56 0.15 0.42 0.00Mainland China (Guangzhou) 3.14 1.09 2.05 0.00Mainland China (Xian) 0.50 0.05 0.41 0.04Hong Kong 2.62 1.25 1.30 0.07Indonesia 0.83 0.27 0.56 0.00Macau 2.24 0.89 0.93 0.42Malaysia 1.01 0.18 0.71 0.12Singapore 0.97 0.39 0.51 0.06Sri Lanka 1.55 0.56 0.94 0.04Thailand (Chiangmai) 0.54 0.25 0.29 0.00Thailand (Bangkok) 0.58 0.34 0.24 0.00
July 2013 IBD INCIDENCE IN ASIA 161
CLINICALAT
Complex disease behavior (eg, stricturing, penetrating, orperianal disease) was more common in Asia than inAustralia (52% vs 24%; P ¼ .001). CD behavior variedacross Asia. The proportion of patients with stricturingdisease (14%�33%) and penetrating disease (17%�33%)was highest in East Asia. Perianal disease at presentationwas more common in mainland China (33%�60%) com-pared with the rest of Asia (10%�16%). For UC, diseaselocation was similar between Asia and Australia (proctitis,37% vs 32%; left-sided colitis, 32% vs 27%; extensive/totalcolitis, 31% vs 41%). Table 3 shows the disease de-mographics of all patients.
Figure 1bowel d
Patient Demographics
A family history of IBD was reported in 3% of pa-tients in Asia and 17% of patients in Australia (P < .001).
. Map showing the age-standardized incidence of inflammatoryisease in Asia-Pacific.
The proportion of IBD patients who were current smokers(8% and 11%), ex-smokers (20% and 26%), and nonsmokers(72% and 63%) was similar in Asia and Australia, respec-tively. For CD, 11% of patients in Asia and 10% inAustralia were smokers, and for UC 6% of patients in Asiaand 8% in Australia were smokers. In Asia, involvement ofeye, joints, skin, ankylosing spondylitis, and primarysclerosing cholangitis were reported in 2%, 15%, 4%, 4%,and 1% of patients with IBD, respectively.
Medical Therapy at Diagnosis
Treatment in the first year after diagnosis withantibiotics (22% vs 14%; P ¼ .15), immunosuppressivesdrugs (thiopurine or methotrexate) (18% and 9%; P ¼ .05),and biological therapy (2.0% vs 0%; P ¼ .21) did not differbetween Asia and Australia. Mesalazine (79% vs 62%; P ¼.012) and corticosteroids (62% vs 28%; P < .0001) weremore commonly prescribed for IBD at diagnosis inAustralia than in Asia. Topical therapy (mesalazine andsteroids) for UC was also more frequently prescribed inAustralia than in Asia (55% vs 28%; P ¼ .04).
In Asia, 25% with UC and 19% with CD received antibi-otics; 68% with UC and 49% with CD received mesalazine;21% with UC and 42% with CD received corticosteroids; 8%with UC and 35% with CD received immunosuppressivedrugs, and 1% with UC and 5% with CD received biologics.In Australia, none with UC and 21% with CD receivedantibiotics; 86% with UC and 71% with CD receivedmesalazine; 50% with UC and 67% with CD received corti-costeroids; 0% with UC and 14% with CD received immu-nosuppressives drugs, and none of the UC or CD patientsreceived biological therapy within 3 months of diagnosis.
Discussion
To the best of our knowledge, this is the firstcomparative epidemiologic study of IBD across Asia andthe Pacific. Although the incidence in Asia is lower than inthe West, these figures still represent a clinically importantdisease burden, considering that 20 years ago IBD was rareor almost nonexistent in Asia. As development and glob-alization in Asia continue, the incidence of IBD is likely toincrease. Epidemiological studies in Asian countries, withthe exception of Japan, which has a National IBD registry,are more difficult to perform than in some other countries.There are no systematic means to accurately assess specifichealth data, despite universal access to public health care.This is in contrast to Scandinavian countries, for example,where each citizen has a personal registration number withuniversal coding, allowing convenient registration andretrieval of disease-specific health information.19
There have been no population-based IBD incidence datafrom mainland China, Hong Kong, Indonesia, Malaysia,Sri Lanka, and Thailand. Studies from Japan, South Korea,and Singapore have shown that the incidence of IBDwas initially low but increasing rapidly.5,20 Unlike referralhospital-derived data,which can lead to anunderestimationof incidence rate and an overestimation of disease severity,
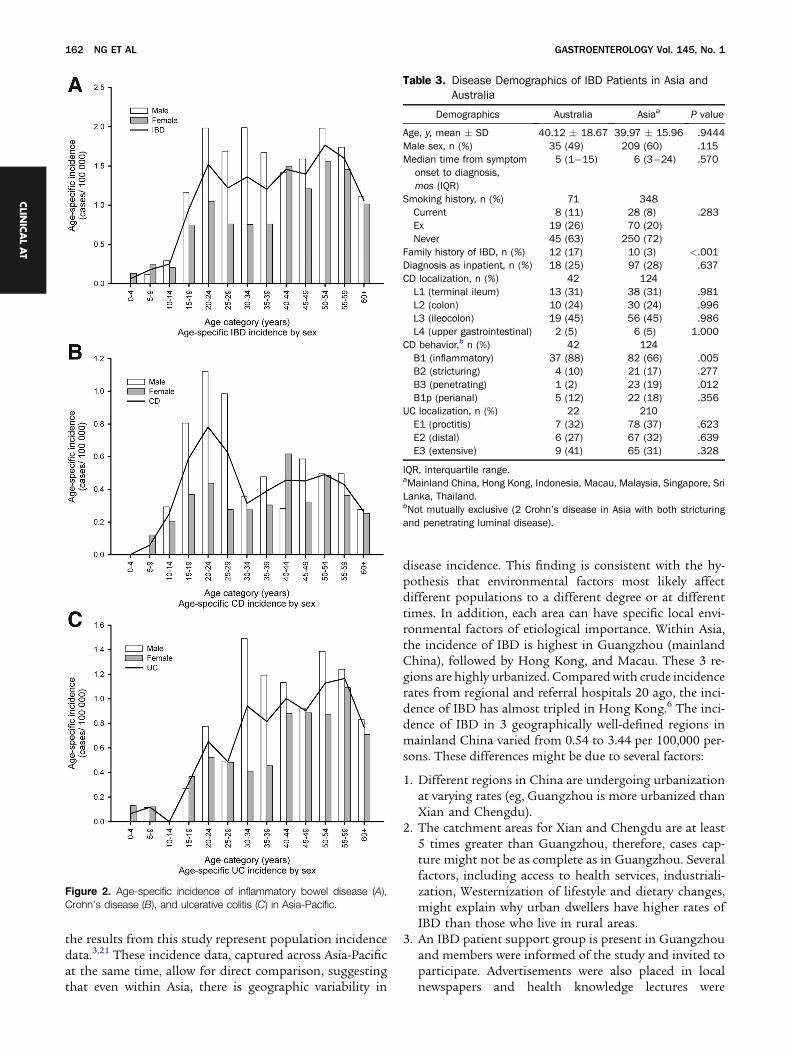
Figure 2. Age-specific incidence of inflammatory bowel disease (A),Crohn’s disease (B), and ulcerative colitis (C) in Asia-Pacific.
Table 3. Disease Demographics of IBD Patients in Asia andAustralia
Demographics Australia Asiaa P value
Age, y, mean � SD 40.12 � 18.67 39.97 � 15.96 .9444Male sex, n (%) 35 (49) 209 (60) .115Median time from symptom
onset to diagnosis,mos (IQR)
5 (1�15) 6 (3�24) .570
Smoking history, n (%) 71 348Current 8 (11) 28 (8) .283Ex 19 (26) 70 (20)Never 45 (63) 250 (72)
Family history of IBD, n (%) 12 (17) 10 (3) <.001Diagnosis as inpatient, n (%) 18 (25) 97 (28) .637CD localization, n (%) 42 124
L1 (terminal ileum) 13 (31) 38 (31) .981L2 (colon) 10 (24) 30 (24) .996L3 (ileocolon) 19 (45) 56 (45) .986L4 (upper gastrointestinal) 2 (5) 6 (5) 1.000
CD behavior,b n (%) 42 124B1 (inflammatory) 37 (88) 82 (66) .005B2 (stricturing) 4 (10) 21 (17) .277B3 (penetrating) 1 (2) 23 (19) .012B1p (perianal) 5 (12) 22 (18) .356
UC localization, n (%) 22 210E1 (proctitis) 7 (32) 78 (37) .623E2 (distal) 6 (27) 67 (32) .639E3 (extensive) 9 (41) 65 (31) .328
IQR, interquartile range.aMainland China, Hong Kong, Indonesia, Macau, Malaysia, Singapore, SriLanka, Thailand.bNot mutually exclusive (2 Crohn’s disease in Asia with both stricturingand penetrating luminal disease).
162 NG ET AL GASTROENTEROLOGY Vol. 145, No. 1
CLIN
ICALAT
the results from this study represent population incidencedata.3,21 These incidence data, captured across Asia-Pacificat the same time, allow for direct comparison, suggestingthat even within Asia, there is geographic variability in
disease incidence. This finding is consistent with the hy-pothesis that environmental factors most likely affectdifferent populations to a different degree or at differenttimes. In addition, each area can have specific local envi-ronmental factors of etiological importance. Within Asia,the incidence of IBD is highest in Guangzhou (mainlandChina), followed by Hong Kong, and Macau. These 3 re-gions are highly urbanized. Compared with crude incidencerates from regional and referral hospitals 20 ago, the inci-dence of IBD has almost tripled in Hong Kong.6 The inci-dence of IBD in 3 geographically well-defined regions inmainland China varied from 0.54 to 3.44 per 100,000 per-sons. These differences might be due to several factors:
1. Different regions in China are undergoing urbanizationat varying rates (eg, Guangzhou is more urbanized thanXian and Chengdu).
2. The catchment areas for Xian and Chengdu are at least5 times greater than Guangzhou, therefore, cases cap-ture might not be as complete as in Guangzhou. Severalfactors, including access to health services, industriali-zation, Westernization of lifestyle and dietary changes,might explain why urban dwellers have higher rates ofIBD than those who live in rural areas.
3. An IBD patient support group is present in Guangzhouand members were informed of the study and invited toparticipate. Advertisements were also placed in localnewspapers and health knowledge lectures were

July 2013 IBD INCIDENCE IN ASIA 163
CLINICALAT
arranged to prompt patients with suspected IBDsymptoms to consult a doctor.
The incidence of IBD in Australia is consistent withresults of a previous study from the same region, and ishigher than the rest of Asia. This is likely becauseAustralia shares many possible environmental risk factorsand similar genetic background as northwest Europe andthe United States, where disease incidence is high.12 Inaddition, all general practitioners in the Geelong region inAustralia received regular written information about thestudy, which might have increased awareness of IBD,reducing the threshold for investigation and referral andresulting in earlier diagnosis. This might have artificiallyraised the incidence rate in the study year.
The worldwide incidence rate of UC varies greatly, be-tween 0.5 and 24.5 per 100,000 persons, and that of CDvaries between 0.1 and 16 per 100,000 persons world-wide.1,2 Longitudinal studies from the West during thepast 50 years have shown an increasing incidence of UCfirst, followed by a rise in the incidence of CD.15,19,22
Consistent with studies from developing countries,3 wehave shown that UC is the predominant disease in Asiaand is twice as common as CD. In countries that havebecome Westernized, including Hong Kong, the ratio ofUC to CD appeared to be narrowing.
In Australia, the incidence of IBD-U was 2.33, and inAsian countries the incidence was nearly zero. The samedisease definitions were used in Asian and Australia cen-ters. However, we cannot exclude that these definitionswere applied slightly differently.
In high-incidence areas, UC occurs more frequently inmen and CD occurs 20%�30% more frequently in females,although in low-incidence areas CD has been reportedmore frequently in men, as in our study.2,4 We have alsoshown that Asian patients with IBD have less familialclustering (only 3%). Low rates of family history in Asiansare likely to relate to the short time that these diseaseshave been present in the population; this is likely to in-crease as the incidence and prevalence of disease rise.
The disease location for CD and UC described in thisstudy were broadly similar to those reported in otherAsian and Western studies.4,23–25 We have also reportedIBD phenotypic data across different Asian countries atdiagnosis in the population-based setting. Previousstudies reporting disease characteristics in secondary ortertiary centers can be associated with referral bias andconfounded by delayed presentation and more compli-cated disease behavior.4,21,26,27 Contrary to common belief,complicated disease behavior for CD was as common inAsia as in Australia. Such finding is unlikely to be due todelayed presentation or late case identification as themedian time from symptom onset to disease diagnosiswas similar and relatively short. It is also unlikely to bedue to referral bias, whereby the most severe cases werereferred to tertiary care. However, we cannot exclude thatIBD patients with the mildest symptoms might have beenmissed. In addition, these mildly affected IBD subjects
might choose to seek complementary or alternative ther-apy initially. We believe that taking these factors into ac-count, the phenotype of CD in Asia does appear to be assevere as in the West. A large proportion of patients inAsia were inpatients at the time of disease diagnosis, eitherdue to complicated severe disease or differences in clinicalpractice. These data are consistent with studies in Asia andon Asian patients in the West that have demonstratedhigher hospitalization rates of Asian than Western IBDpatients.28,29 This severity of disease has health care im-plications in terms of the need for immunosuppressivedrugs, biologic therapy, recurrent hospitalizations, andsurgery.2
Rates of smoking did not differ between IBD patients inAsia and Australia. Although smoking has been shown to astrong risk factor for CD and protective for UC, it is un-likely to account for the geographic variability of IBD. Ourdata are consistent with a recent cross-sectional observa-tional study that showed that there were fewer smokersamong Chinese with CD in Hong Kong than Caucasianswith CD in Australia.30 Medical therapy at presentationwas similar between Asia and Australia, except the use ofcorticosteroids, which was more common in Australia. It isunclear whether disease was more severe than in Asia, asdata on disease activity were not captured.
Although >4.2 billion people live in the Asia-Pacific re-gion, there are no widely based population-based incidencedata related to IBD in Asia. Until recently, IBD was notconsidered a public health problem in Asia.31 The collec-tion of accurate epidemiological data in Asia has beenhampered by limited access of IBD patients to health carefacilities, poor physician and patient awareness of disease,and diagnostic challenges due to symptom overlap withinfective enteritis. This study provides information on theincidence of IBD in a very wide geographical area, where fewincidence studies have been conducted previously. It alsoprovides a valuable basis to study disease prevalence, assessincidence trends over time, and to start planning healthcare resource provision. We have selected well-definedgeographic areas within Asia with relatively stable pop-ulations serviced by identifiable groups of hospitals. NewIBD cases were likely to be captured within these hospitals,ensuring near-complete case ascertainment. Although onequarter of UC patients in Asia had received antibiotics atdiagnosis, this is a common clinical practice in Asiawhereby antibiotic use has become more liberal and notbecause of misdiagnosis with infectious causes. Infectiousenteritis were rigorously excluded and every case wasfollowed-up for 6 to 12months to ensure that the diagnosisof IBD remained certain. Index cases were identified frommultiple overlapping sources and cross checked, and thediagnosis was confirmed by a large panel of experiencedgastroenterologists treating IBD patients.
This study has several limitations. The populationstudied was much bigger than those studied recently inpopulation-based studies inAustralia12 andNewZealand.11
Because of the relatively low disease incidence in Asia, alarge at-risk population was required to determine

164 NG ET AL GASTROENTEROLOGY Vol. 145, No. 1
CLIN
ICALAT
incidence with reasonable accuracy. It is possible that pa-tients who had mild disease in the community or whowere seen in private centers and not subsequently referredto hospitals would have been missed, although it isbelieved that most people with a significant chronicmedical condition (such as IBD) are referred from privateto public sectors. Patients who have sought alternativeforms of treatment, including complementary and alter-native medicine might not have been captured. In addi-tion, patients in primary care can be captured in Australia,although it could not be registered accurately in otherareas. This would have in any case led to an underesti-mation of the true incidence of IBD in Asia. Although wehave used a multifaceted approach for capturing the cases,it is difficult to establish the exact capture rate in thisepidemiologic study. The proportion of medically referredsubjects in this study (65%�87%) was relatively consistentwith figures from population-based studies in New Zea-land and Australia (65%�80%).11,12 The remaining 20%�30% of incident cases were invited or self-referred. Toaddress whether the magnitude of incomplete capturemight influence the regional variation in incidence, weperformed sensitivity analysis and found that even whenwe assumed a 30% missing rate within each country, it didnot negate the regional variation observed in this study(Supplementary Table 2). In addition, when we assumed a50% incidence missed rate in the region with the lowestreported incidence (0.5 per 100,000 in Xian, MainlandChina), the sensitivity analysis showed an incidence of 1.0per 100,000, which is still much lower than Guangzhou inMainland China, which has one of the highest diseaseincidence. Secondly, differing access to health care acrossthe different centers can play a role in both the differencesin incidence of IBD across regions and the severity ofdisease at diagnosis. Sood et al reported previously thatUC incidence rates in India were higher compared withprevious incidence studies in India, when a householdsurvey was conducted and individuals screened positive forUC were sent for diagnostic sigmoidoscopy or colonos-copy.32 Variations in accuracy, efficiency, and quality ofregistration between areas cannot be ruled out as acontributing factor to differing incidences. Thirdly, theincidence estimates from each center might not reflectaccurate extrapolations to the national level. For instance,although we have studied the incidences in 5 cities inChina, these cities do not necessarily represent Chinabecause we have not included the incidence in Shanghaiand Beijing. Not all centers invited were able to participatein the study. Our data support the observation that inci-dence of IBD can vary not only between but also withincountry, as has been reported in studies from France.33,34
For this study, we have selected mostly centers withinurban areas in Asia that have equivalent and easy access tohealth care. Therefore, these results might not representincidence data outside of urban cities in Asia. Lastly, a1-year time frame might be too short to document vari-ability of incidence. Apart from Japan, there is no IBDregistry system in the rest of Asia, therefore, the data
reported here probably represent the closest estimate tothe true incidence of IBD. However, a longer time periodwill be necessary to average out the variability.
In conclusion, the population incidence of IBD acrossAsia-Pacific is lower than in the West. The emergence ofIBD in Asia indicates an important role for environmentalfactors in pathogenesis. The emerging incidence in Asiaoffers a unique opportunity to study etiologic factors,particularly factors associated with Western lifestyle,including improved home amenities, refrigeration, con-sumption of protein and carbohydrate-rich diets, wide-spread use of antibiotics, vaccination, and industrialpollution. The complex disease behavior for CD in Asiahas major implications for local health care planning andresource allocation.
Supplementary Material
Note: To access the supplementary materialaccompanying this article, visit the online version ofGastroenterology at www.gastrojournal.org, and at http://dx.doi.org/10.1053/j.gastro.2013.04.007.
References
1. Molodecky NA, Soon IS, Rabi DM, et al. Increasing incidence andprevalence of the inflammatory bowel diseases with time, based onsystematic review. Gastroenterology 2012;142:46–54.
2. Cosnes J, Gower-Rousseau C, Seksik P, et al. Epidemiology andnatural history of inflammatory bowel diseases. Gastroenterology2011;140:1785–1794.
3. Thia KT, Loftus EV Jr, Sandborn WJ, et al. An update on the epide-miology of inflammatory bowel disease in Asia. Am J Gastroenterol2008;103:3167–3182.
4. Hou JK, El-Serag H, Thirumurthi S. Distribution and manifestations ofinflammatory bowel disease in Asians, Hispanics, and AfricanAmericans: a systematic review. Am J Gastroenterol 2009;104:2100–2109.
5. Yang SK, Yun S, Kim JH, et al. Epidemiology of inflammatory boweldisease in the Songpa-Kangdong district, Seoul, Korea, 1986-2005:a KASID study. Inflamm Bowel Dis 2008;14:542–549.
6. Leong RW, Lau JY, Sung JJ. The epidemiology and phenotype ofCrohn’s disease in the Chinese population. Inflamm Bowel Dis 2004;10:646–651.
7. Prideaux L, Kamm MA, De Cruz PP, et al. Inflammatory bowel diseasein Asia: a systematic review. J Gastroenterol Hepatol 2012;27:1266–1280.
8. de Silva HJ, de Silva NR, De Silva AP, et al. Emergence of inflam-matory bowel disease ‘beyond the West’: do prosperity and improvedhygiene have a role? Trans R Soc Trop Med Hyg 2008;102:857–860.
9. Bernstein CN, Shanahan F. Disorders of a modern lifestyle: recon-ciling the epidemiology of inflammatory bowel diseases. Gut 2008;57:1185–1191.
10. Bernstein CN, Wajda A, Svenson LW, et al. The epidemiology of in-flammatory bowel disease in Canada: a population-based study. AmJ Gastroenterol 2006;101:1559–1568.
11. Gearry RB, Richardson A, Frampton CM, et al. High incidence ofCrohn’s disease in Canterbury, New Zealand: results of an epide-miologic study. Inflamm Bowel Dis 2006;12:936–943.
12. Wilson J, Hair C, Knight R, et al. High incidence of inflammatorybowel disease in Australia: a prospective population-based Austra-lian incidence study. Inflamm Bowel Dis 2010;16:1550–1556.
13. Vind I, Riis L, Jess T, et al. Increasing incidences of inflammatorybowel disease and decreasing surgery rates in Copenhagen City andCounty, 2003�2005: a population-based study from the DanishCrohn colitis database. Am J Gastroenterol 2006;101:1274–1282.

July 2013 IBD INCIDENCE IN ASIA 165
CLINICALAT
14. Bernstein CN, Blanchard JF, Rawsthorne P, et al. Epidemiology ofCrohn’s disease and ulcerative colitis in a central Canadian province:a population-based study. Am J Epidemiol 1999;149:916–924.
15. Ekbom A, Helmick C, Zack M, et al. The epidemiology of inflamma-tory bowel disease: a large, population-based study in Sweden.Gastroenterology 1991;100:350–358.
16. Lennard-Jones JE. Classification of inflammatory bowel disease.Scand J Gastroenterol Suppl 1989;170:2–6.
17. Satsangi J, Silverberg MS, Vermeire S, et al. The Montreal classifi-cation of inflammatory bowel disease: controversies, consensus, andimplications. Gut 2006;55:749–753.
18. Ahmad OB, Boschi-Pinto C, Lopez AD. Age standardization of rates: anew WHO standard. Global Programme on Evidence for Health PolicyDiscussion Paper Series: No. 31. Geneva: World Health Organization;2001.
19. Munkholm P, Langholz E, Nielsen OH, et al. Incidence and prevalenceof Crohn’s disease in the county of Copenhagen, 1962-87: a sixfoldincrease in incidence. Scand J Gastroenterol 1992;27:609–614.
20. Morita N, Toki S, Hirohashi T, et al. Incidence and prevalence ofinflammatory bowel disease in Japan: nationwide epidemiologicalsurvey during the year 1991. J Gastroenterol 1995;30(Suppl8):1–4.
21. Jiang L, Xia B, Li J, et al. Retrospective survey of 452 patients withinflammatory bowel disease in Wuhan city, central China. InflammBowel Dis 2006;12:212–217.
22. Loftus EV Jr, Silverstein MD, Sandborn WJ, et al. Ulcerative colitis inOlmsted County, Minnesota, 1940-1993: incidence, prevalence, andsurvival. Gut 2000;46:336–343.
23. Wang YF, Zhang H, Ouyang Q. Clinical manifestations of inflammatorybowel disease: East andWest differences. J Dig Dis 2007;8:121–127.
24. Jess T, Riis L, Vind I, et al. Changes in clinical characteristics, course,and prognosis of inflammatory bowel disease during the last 5decades: a population-based study from Copenhagen, Denmark.Inflamm Bowel Dis 2007;13:481–489.
25. Henriksen M, Jahnsen J, Lygren I, et al. Ulcerative colitis and clinicalcourse: results of a 5-year population-based follow-up study (theIBSEN study). Inflamm Bowel Dis 2006;12:543–550.
26. Song XM, Gao X, Li MZ, et al. Clinical features and risk factors forprimary surgery in 205 patients with Crohn’s disease: analysis of aSouth China cohort. Dis Colon Rectum 2011;54:1147–1154.
27. Oriuchi T, Hiwatashi N, Kinouchi Y, et al. Clinical course and longtermprognosis of Japanese patients with Crohn’s disease: predictive factors,rates of operation, and mortality. J Gastroenterol 2003;38:942–953.
28. Wang YF, Ouyang Q, Hu RW. Progression of inflammatory boweldisease in China. J Dig Dis 2010;11:76–82.
29. Sewell JL, Yee HF Jr, Inadomi JM. Hospitalizations are increasingamong minority patients with Crohn’s disease and ulcerative colitis.Inflamm Bowel Dis 2010;16:204–207.
30. Prideaux L, Kamm MA, De CP, et al. Comparison of clinical charac-teristics and management of inflammatory bowel disease in HongKong versus Melbourne. J Gastroenterol Hepatol 2012;27:919–927.
31. Ouyang Q, Xue LY. Inflammatory bowel disease in the 21(st) centuryin China: turning challenges into opportunities. J Dig Dis 2012;13:195–199.
32. Sood A, Midha V, Sood N, et al. Incidence and prevalence of ulcer-ative colitis in Punjab, North India. Gut 2003;52:1587–1590.
33. Nerich V, Monnet E, Etienne A, et al. Geographical variations ofinflammatory bowel disease in France: a study based on nationalhealth insurance data. Inflamm Bowel Dis 2006;12:218–226.
34. Ng SC, Bernstein CN, Vatn MH, et al. Geographical variability andenvironmental risk factors in inflammatory bowel disease. Gut 2013;62:630–649.
Received January 5, 2013. Accepted April 2, 2013.
Reprint requestsAddress requests for reprints to: Siew C. Ng, MD, PhD, Institute of
Digestive Disease, Department of Medicine and Therapeutics, ChineseUniversity of Hong Kong, Hong Kong. e-mail: [email protected];fax: þ 852 2637 3852.
AcknowledgmentsThe authors are grateful to Y. K. Tse for statistical input, Sunny Wong
for illustration, and Honson Lam for input on database amendmentand updates. The authors are thankful to Drs. K. C. D. Mettananda,Nilesh Fernandopulle, Shaman Rajindrajith, P. R. Waraketiya,S. K. Weerasinghe, A. Ranaweera, Prof. S. JdeS Hewavisenthi,Prof. A. P. de Silva (Sri Lanka), Nazri Mustaffa (Sydney), Fan Siok Chiang(Singapore), Jessica Leung and Rosita Chan (Hong Kong), Zhang JunWen (Macau), and all other gastroenterologists and staff at everyhospital who have assisted in identification and recruitment of patients.
Conflicts of interestThe authors disclose no conflicts.
FundingUnrestricted educational grants from Ferring pharmaceuticals, Hong
Kong, and Direct Grant Faculty of Medicine Chinese University of HongKong were used to support the database setup and maintenance of thisstudy. The study sponsors have no contribution in the study design,analysis, interpretation of data, and publication.

Appendix.
Country Background population and demographic
Australia The study was conducted in the geographically defined region of Geelong, located 75 km to the southwest of Melbourne.Geelong is the second largest city in the southern state of Victoria. According to the 2010 Australian census, the populationof Geelong and surrounding regions was 300,000 compared to the overall Australian population of 20.4 million. TheGeelong area has well-defined boundaries and is relatively geographically isolated. There is one central pathology andendoscopy center in Geelong.
Mainland China The incidence study in mainland China was conducted in 3 geographically defined regions.Zhongshan, located 70 km to the south of Guangzhou in Guangdong province. According to the 2010 Chinese census, the
population of Zhongshan and surrounding regions was 1.46 million. This compares with the overall China population of1370 million. The Zhongshan area has well-defined boundaries and is relatively geographically isolated. There are 4 publichospitals and migration rates are low.
Chengdu, the capital of Sichuan Province, lies in the hinterland of the Chengdu Plain, in central Sichuan. The study populationof 7.68 million was drawn from the 10 districts of Chengdu, which have well-defined boundaries and are relativelygeographically isolated. There are 24 hospitals involved in these districts.
Xi’an, In Shaanxi Province the geographically defined region of Xi’an is 1 of the 8 largest cities in China. Incident cases werecaptured from 7 districts with a population of 5.13 million. Xi’an has well-defined boundaries and is relatively geographicallyisolated. The study population for all 3 areas was demographically similar in terms of age, socioeconomic status, and ethnicmakeup to the rest of China.
Hong Kong The study was conducted in the North East and Kowloon East territory. According to the 2011 Hong Kong population censusthese 2 territories have a population of 3.7 million people served by 5 public hospitals. The population is ethnicallyhomogenous Chinese with a very low migratory rate.
Indonesia The study was conducted in the geographically defined region of Central Jakarta, with a population of 912,088 based on the2011 Jakarta City Bureau for Demographics and Civil-Related Administration Census. This population accounts for 10.7% ofJakarta’s total population of 8.52 million. Central Jakarta area has well-defined boundaries and high population density, and5 public and 7 private hospitals. The study population is demographically similar in terms of age, socioeconomic status, andethnic makeup to the rest of the Indonesian population. Ethnic groups in Jakarta mostly consists of Betawinese, Sundanese,Javanese, Minang, Chinese, and Arabs.
Macau Macau has a stable population of approximately 500,000 people served by 2 hospitals. Macau is situated southwest of HongKong and next to Guangzhou; 95% of Macau’s population is of Chinese descent from the Guangdong Province and the restare of Portugese or mixed Chinese-Portuguese ancestry. It is geographically well defined and has a stable population. Allsubjects with IBD will be diagnosed in these 2 hospitals.
Malaysia The study was conducted in the geographically defined region of Kinta Valley, approximately 205 km north of Kuala Lumpur.The region consists of the city of Ipoh, the capital of the state of Perak, and its surrounding towns and villages. According tothe 2010 census from Department of Statistics Malaysia, the population of Kinta Valley was 852,200. Ipoh is served by 3public and 2 private hospitals. The population of Malaysia is 28.5 million. There are 3 main ethnic groups in Malaysia;Malays, Chinese and Indians. The ethnic mix in Kinta Valley is representative of urban populations in Malaysia but not ruralareas where the residents are predominantly Malays. It is a stable population with low migration.
Singapore The background population of 3.8 million, based on the 2011 national census, constitutes the permanent citizens ofSingapore. It is a highly urbanized city. There are 6 public and 12 private hospitals or medical centers within the catchmentarea; 74% of the residents are of Chinese, 13% of Malay, and 9% of Indian descent.
Sri Lanka The study was conducted in the Gampaha district, which is adjoining the Colombo district. According to the 2009 census it hada population of 2.2 million, of which 91% are Sinhalese, 3.6% Tamil, 3.8% Muslim, and 1.7% others. The district has goodhealth care facilities and one main referral center for diagnosis and management of IBD. There are 5 other hospitals withspecialist services (3 public and 2 private). Most specialists in the district cover both public and private sectors and majorityof subjects diagnosed in the private sector are also captured.
Thailand The incidence study in Thailand was conducted in 2 cities.Chiangmai, Chiangmai metropolitan and Chiangrai metropolitan are 2 regions in Northern Thailand with well-defined
boundaries and stable population. Chiangmai is served by 1 university hospital and 4 private hospitals and Chiangrai isserved by 1 regional hospital. The total population of Chiangmai and Chiangrai is approximately 1.6 million people, and thetotal population of Thailand is 66 million people.
Bangkok, the participating hospitals in Bangkok cover approximately 70% of the population in a catchment area with apopulation of 3.9 million. Nearby provinces in close proximity to Bangkok are Nonthaburi and Patumthani. Thesocioeconomic status of population in Bangkok and its boundary area is higherthan the rest of the country. The ethnicity ofthe population in and around Bangkok is mainly Thai and Chinese.
165.e1 NG ET AL GASTROENTEROLOGY Vol. 145, No. 1
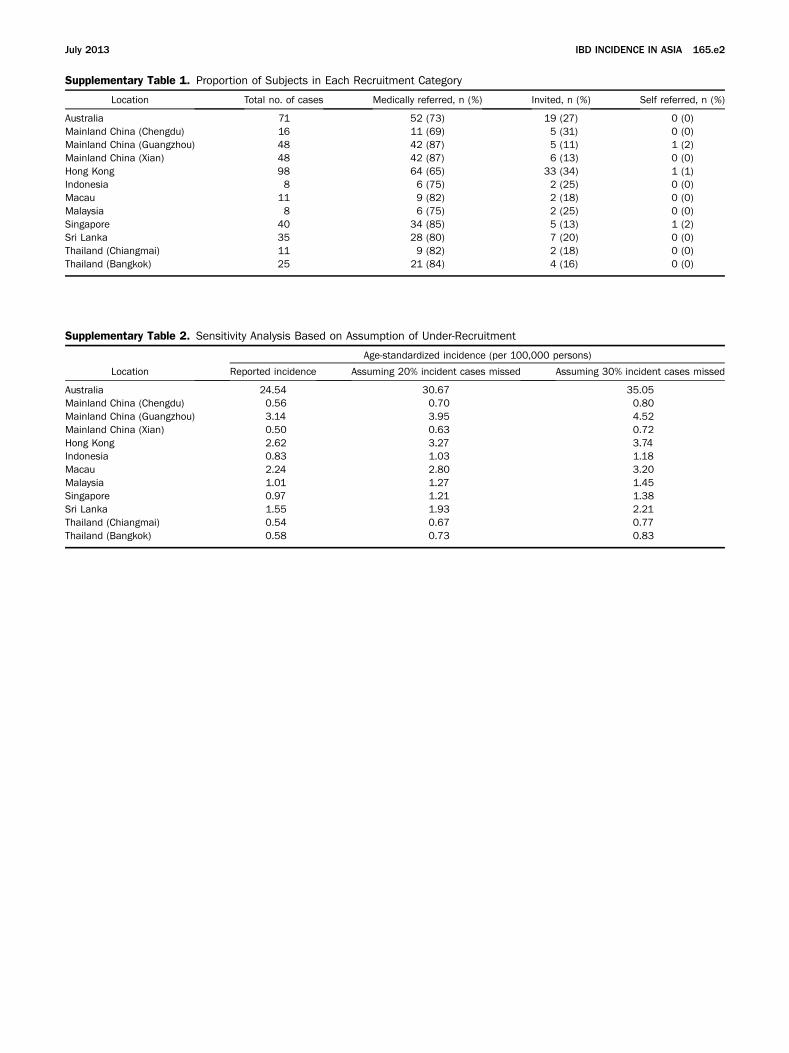
Supplementary Table 2. Sensitivity Analysis Based on Assumption of Under-Recruitment
Age-standardized incidence (per 100,000 persons)
Location Reported incidence Assuming 20% incident cases missed Assuming 30% incident cases missed
Australia 24.54 30.67 35.05Mainland China (Chengdu) 0.56 0.70 0.80Mainland China (Guangzhou) 3.14 3.95 4.52Mainland China (Xian) 0.50 0.63 0.72Hong Kong 2.62 3.27 3.74Indonesia 0.83 1.03 1.18Macau 2.24 2.80 3.20Malaysia 1.01 1.27 1.45Singapore 0.97 1.21 1.38Sri Lanka 1.55 1.93 2.21Thailand (Chiangmai) 0.54 0.67 0.77Thailand (Bangkok) 0.58 0.73 0.83
Supplementary Table 1. Proportion of Subjects in Each Recruitment Category
Location Total no. of cases Medically referred, n (%) Invited, n (%) Self referred, n (%)
Australia 71 52 (73) 19 (27) 0 (0)Mainland China (Chengdu) 16 11 (69) 5 (31) 0 (0)Mainland China (Guangzhou) 48 42 (87) 5 (11) 1 (2)Mainland China (Xian) 48 42 (87) 6 (13) 0 (0)Hong Kong 98 64 (65) 33 (34) 1 (1)Indonesia 8 6 (75) 2 (25) 0 (0)Macau 11 9 (82) 2 (18) 0 (0)Malaysia 8 6 (75) 2 (25) 0 (0)Singapore 40 34 (85) 5 (13) 1 (2)Sri Lanka 35 28 (80) 7 (20) 0 (0)Thailand (Chiangmai) 11 9 (82) 2 (18) 0 (0)Thailand (Bangkok) 25 21 (84) 4 (16) 0 (0)
July 2013 IBD INCIDENCE IN ASIA 165.e2




















