
Circulating Cytokines Reflect Mucosal Inflammatory Status in Patients with Crohn’s Disease
11
ORIGINAL ARTICLE Circulating Cytokines Reflect Mucosal Inflammatory Status in Patients with Crohn’s Disease Farid Ljuca • Adnan Gegic • Nermin N. Salkic • Nada Pavlovic-Calic Received: 9 March 2009 / Accepted: 24 September 2009 Ó Springer Science+Business Media, LLC 2009 Abstract Background There is a great need for a simple activity assessment tool that can reliably predict activity in patients with Crohn’s disease (CD). Aim To investigate the relationship between serum cytokines and endoscopic activity of CD using Crohn’s Disease Endoscopic Index of Severity (CDEIS) as a gold standard. Methods We prospectively evaluated 32 firmly estab- lished CD patients using ileocolonoscopy, CDEIS score, and Crohn’s Disease Activity Index (CDAI) score. Blood samples for cytokine analysis were obtained 1 day prior to procedure. Results The correlation between CDEIS and CDAI was moderate (r = 0.43; P = 0.01); however, the correlation between CDEIS and inflammatory cytokines was excellent, with the highest coefficients for tumor necrosis factor alpha (TNFa) and interleukin-6 (IL-6) (r = 0.96 and r = 0.96, respectively; P \ 0.001). CDEIS and anti-inflammatory cytokines were correlated nonlinearly (power function). We identified two separate models for predicting CDEIS value, based on the best performing pro-inflammatory [CDEIS = 0.445 9 (IL-6) - 5,143] and anti-inflammatory [CDEIS = 27.478 9 (IL-10) -0.71 ] cytokines. Both IL-6 and IL-10 models had high adjusted R 2 values (0.916 and 0.954, respectively). IL-6 had excellent diagnostic accuracy for detecting patients with CDEIS [ 7 (active disease), with area under the receiver operating characteristic (ROC) curve of 1.0 [95% confidence interval (CI) = 0.89–1.0; P \ 0.001]. Conclusion Serum cytokine levels are excellent predic- tors of endoscopic activity in patients with CD. Keywords Crohn’s disease Cytokine Tumor necrosis factor Interleukin Crohn’s Disease Endoscopic Severity Index Crohn’s Disease Activity Index Introduction Treatment of CD is a clinically demanding process that quite often has to be individualized for each patient. For this reason clinicians have the need for constant monitoring and evaluation of disease status, usually through various clinical, biochemical, and endoscopic assessments. Various instruments for measuring disease activity have been developed over the last two decades, but few of them have been widely adopted by gastroenterology practitio- ners. Some of these instruments are based mostly on clinical features of the patient, some are based on quality-of-life parameters, some take into account biochemical markers, and some are based exclusively on the endoscopic appear- ance of intestinal mucosa [1]. However, most of them are associated with various problems; they either poorly predict the level of mucosal inflammation (e.g., CDAI score) or they are hard to use in clinical settings or in clinical trials (e.g., CDEIS score) [2, 3]. Crohn’s Disease Endoscopic Farid Ljuca, Adnan Gegic, and Nermin Salkic contributed equally to this paper. F. Ljuca Faculty of Medicine, University of Tuzla, Univerzitetska 1, Tuzla, Bosnia and Herzegovina A. Gegic N. N. Salkic (&) N. Pavlovic-Calic Department of Gastroenterology, Internal Medicine Hospital, University Clinical Center Tuzla, Trnovac bb, 75000 Tuzla, Bosnia and Herzegovina e-mail: [email protected] 123 Dig Dis Sci DOI 10.1007/s10620-009-1016-9
Transcript of Circulating Cytokines Reflect Mucosal Inflammatory Status in Patients with Crohn’s Disease

ORIGINAL ARTICLE
Circulating Cytokines Reflect Mucosal Inflammatory Statusin Patients with Crohn’s Disease
Farid Ljuca • Adnan Gegic • Nermin N. Salkic •
Nada Pavlovic-Calic
Received: 9 March 2009 / Accepted: 24 September 2009
� Springer Science+Business Media, LLC 2009
Abstract
Background There is a great need for a simple activity
assessment tool that can reliably predict activity in patients
with Crohn’s disease (CD).
Aim To investigate the relationship between serum
cytokines and endoscopic activity of CD using Crohn’s
Disease Endoscopic Index of Severity (CDEIS) as a gold
standard.
Methods We prospectively evaluated 32 firmly estab-
lished CD patients using ileocolonoscopy, CDEIS score,
and Crohn’s Disease Activity Index (CDAI) score. Blood
samples for cytokine analysis were obtained 1 day prior to
procedure.
Results The correlation between CDEIS and CDAI was
moderate (r = 0.43; P = 0.01); however, the correlation
between CDEIS and inflammatory cytokines was excellent,
with the highest coefficients for tumor necrosis factor alpha
(TNFa) and interleukin-6 (IL-6) (r = 0.96 and r = 0.96,
respectively; P \ 0.001). CDEIS and anti-inflammatory
cytokines were correlated nonlinearly (power function).
We identified two separate models for predicting CDEIS
value, based on the best performing pro-inflammatory
[CDEIS = 0.445 9 (IL-6) - 5,143] and anti-inflammatory
[CDEIS = 27.478 9 (IL-10)-0.71] cytokines. Both IL-6
and IL-10 models had high adjusted R2 values (0.916 and
0.954, respectively). IL-6 had excellent diagnostic accuracy
for detecting patients with CDEIS[7 (active disease), with
area under the receiver operating characteristic (ROC)
curve of 1.0 [95% confidence interval (CI) = 0.89–1.0;
P \ 0.001].
Conclusion Serum cytokine levels are excellent predic-
tors of endoscopic activity in patients with CD.
Keywords Crohn’s disease � Cytokine �Tumor necrosis factor � Interleukin �Crohn’s Disease Endoscopic Severity Index �Crohn’s Disease Activity Index
Introduction
Treatment of CD is a clinically demanding process that
quite often has to be individualized for each patient. For
this reason clinicians have the need for constant monitoring
and evaluation of disease status, usually through various
clinical, biochemical, and endoscopic assessments.
Various instruments for measuring disease activity have
been developed over the last two decades, but few of them
have been widely adopted by gastroenterology practitio-
ners. Some of these instruments are based mostly on clinical
features of the patient, some are based on quality-of-life
parameters, some take into account biochemical markers,
and some are based exclusively on the endoscopic appear-
ance of intestinal mucosa [1]. However, most of them are
associated with various problems; they either poorly predict
the level of mucosal inflammation (e.g., CDAI score) or
they are hard to use in clinical settings or in clinical trials
(e.g., CDEIS score) [2, 3]. Crohn’s Disease Endoscopic
Farid Ljuca, Adnan Gegic, and Nermin Salkic contributed equally to
this paper.
F. Ljuca
Faculty of Medicine, University of Tuzla, Univerzitetska 1,
Tuzla, Bosnia and Herzegovina
A. Gegic � N. N. Salkic (&) � N. Pavlovic-Calic
Department of Gastroenterology, Internal Medicine Hospital,
University Clinical Center Tuzla, Trnovac bb, 75000 Tuzla,
Bosnia and Herzegovina
e-mail: [email protected]
123
Dig Dis Sci
DOI 10.1007/s10620-009-1016-9

Severity Index (CDEIS) score is currently the only tool that
can reliably evaluate the degree and extent of mucosal
inflammation [4].
The role of cytokines in inflammatory bowel disease
pathogenesis is firmly established. The activation of central
immune-cell populations in inflamed intestinal mucosa is
accompanied by the production of a wide variety of
inflammation mediators, including various cytokines, e.g.,
interleukin-1 (IL-1), IL-6, tumor necrosis factor alpha
(TNFa), interferon gamma (IFNc), and others [5]. Some of
these released cytokines have pro-inflammatory properties
(e.g., IL-1, IL-6, IL-12, TNFa, and IFNc) whereas others
have anti-inflammatory properties (e.g., IL-4, IL-10, and
IL-11).
Although cytokine concentrations are highest at the
inflammation site, they are also easily detectable in plasma
as well. Several reports have established the relationship of
mucosal or plasma levels of cytokines with disease activity
in CD and ulcerative colitis patients [6–9]. Some studies
reported increased levels of pro-inflammatory cytokines
such as IL-6 in active CD and increased levels of anti-
inflammatory cytokines such as IL-10 during recovery
phases of CD [10, 11]. However, all of those studies either
omitted to use CDEIS as a gold standard or investigated
only a limited set of cytokines.
The need for a CD activity assessment tool that is
accurate, simple, easy to use, and readily available in
routine clinical and research practice is obvious. Therefore
we aimed to investigate the relationship between inflam-
matory/anti-inflammatory serum cytokines and mucosal
activity in patients with firmly established CD, using
CDEIS as a gold standard. We hypothesized that serum
cytokines might be used as serum markers of mucosal
activity of CD.
Subjects and Methods
During a 2-year period (2004–2006) we prospectively
recruited all patients referred to our institution for clinical
reevaluation of established CD. The study protocol con-
formed to the Declaration of Helsinki and was approved by
the University Clinical Center Tuzla Ethics Committee.
Inclusion criteria were firmly established diagnosis of CD
(based on a characteristic combination of history data,
laboratory tests, radiology, endoscopy, and histology) and
referral for ileocolonoscopy by the gastroenterologist in
charge of the patient. We excluded all patients without
complete ileocolonoscopy and those with previous history
of surgical procedures related to CD, consequently evalu-
ating only patients with intact bowel and small intestine.
We also excluded all patients treated with anti-TNFamedication(s) (infliximab) during the year prior to
evaluation and patients with clinical or laboratory param-
eters indicating other concomitant disease that might have
systemic inflammatory response (respiratory and genito-
urinary infections, other autoimmune diseases, etc.).
Each patient scheduled for evaluation was given a 7-day
diary with items of relevance to CDAI score (number of
liquid stools, abdominal pain, general well-being, use of
antidiarrheal medications, fever [37.8�C). The diary was
completed with a final entry on the day before procedure,
and then returned to investigators. A blood sample for
standard laboratory tests and cytokines analysis was taken
from each patient upon admission to the diagnostic site,
1 day before ileocolonoscopy. Body weight and height
were measured after thorough physical examination, during
which any presence of extraintestinal manifestations or
abdominal mass were also recorded. A single experienced
gastroenterologist performed all of the mentioned exam-
inations and recorded findings immediately.
The following day, the same gastroenterologist per-
formed total colonoscopy with ileoscopy at least 10 cm in
length in a patient prepared for the procedure in the usual
fashion. Ileum was reached and explored in all patients.
The intestinal mucosa was carefully evaluated for presence
and length of lesions with relevance to CDEIS score and
findings were recorded immediately after the procedure.
For calculating CDEIS, as described by score authors,
the intestine was divided into five segments: ileum, right
colon, transverse colon, left and sigmoid colon, and rec-
tum [4]. The extent of disease involvement in each of the
five segments was determined by examining the presence
of mucosal lesions (pseudopolyps, healed ulcerations,
frank erythema or mucosal swelling, aphthoid ulcers,
superficial or deep ulcers, and nonulcerated or ulcerated
stenosis) and by estimating the percentage of both that
involvement and the ulcerated surface on a 10-cm linear
analog scale for the segment (score between 0 and 10,
with a score of 0 meaning no lesions or ulcerations at all,
and a score of 10 meaning 100% involvement of the
segmental surface; for partially explored segments and for
the ileum, the 10-cm linear scale represented the surface
effectively explored). In each segment the presence of a
superficial ulcer was scored as 6 and a deep ulcer was
scored as 12 (0 if absent). The sum of the score of
involved surface, the score of ulcerated surface, and the
scores of superficial and deep ulcers of each segment was
divided by the number of segments examined, and a score
of 3 was added if either ulcerated or nonulcerated stenosis
was present. The lowest possible CDEIS was 0, repre-
senting an intestine without any lesions, and higher scores
(up to a maximum of 44) indicated more severe disease
[4].
CDAI score was also calculated in a standardized
manner, as previously described [12].
Dig Dis Sci
123

Cytokines Assay
Cytokine levels were determined in the University of
Ljubljana Faculty of Medicine Laboratory (Ljubljana,
Slovenia). Enzyme-linked immunosorbent assay (ELISA)
kit for IL-1 was obtained from Biosource; IL-4, IL-6, IL-10,
IL-11, IL-12, tumor necrosis factor alpha (TNFa), and
gamma interferon (IFNc) ELISA kits were obtained from
Sanquin (Amsterdam, The Netherlands). ELISA was per-
formed by coating 96-well polystyrene microtiter plates
(Nalge Nunc International, Roskilde, Denmark) with a
specific monoclonal antibody. Standards and samples were
added after the plates were blocked, and the plates were
incubated overnight at 4�C. A specific biotinylated antibody
was added to all wells after they were washed, and they
were incubated for 1 h at room temperature. The plates
were washed and incubated for 30 min with horseradish
peroxidase-conjugated streptavidin. After removal of non-
bound horseradish peroxidase conjugate by washing,
3-30,5,50-tetramethylbenzidine substrate reagent solution
(ICN Biomedicals Inc., Aurora, OH) was added to the wells.
The reaction was stopped by addition of 1.8 M H2SO4. The
absorbance of all ELISAs was read at 450 nm with a
Milenia microtiter plate reader (Diagnostic Products Cor-
poration Nederland BV, Breda, The Netherlands). Standard
curves for the various cytokines ranging from 0.25 to 5 pg/
ml and up to 300–1,000 pg/ml were constructed by a four-
parameter regression formula and plotted as a linear curve
(log–log). Cytokine concentrations of experimental samples
were calculated with Elisa plus software version 3.01
(Meddata Inc., New York, NY) [13, 14].
Statistical Analysis
All statistical analysis procedures were performed using
SPSS version 12.0 (SPSS, Chicago, IL). Standard parameters
of descriptive statistics were used for determination of
baseline characteristics. All variables satisfied criteria for
accepting a normal distribution on testing with the
Kolmogorov–Smirnov test. Student’s T-test with correction
for unequal variances, where appropriate, or analysis of
variance (ANOVA) test for more than two variables, was
used to compare quantitative variables. Post hoc analysis
after performing ANOVA was made by using Tukey test.
Chi-square test was used to compare categorical variables.
Pearson’s correlation with two-tailed significance was used
to investigate the strength of links between analyzed
variables.
Curve estimation regression analysis was used to
investigate nonlinear relationships between anti-inflam-
matory cytokines and CDEIS score. Simple linear regres-
sion analysis was used to evaluate the best performing
pro-inflammatory cytokine for the prediction of CDEIS
value. A similar approach was used for anti-inflammatory
cytokines, only we used nonlinear regression analysis
based on a power model.
In order to validate the regression models in the setting
of a limited sample size, we used the ‘‘bootstrap’’ method
[15]. We randomly split the sample 300 times into test and
validation groups. Each time, after splitting the sample, a
regression analysis (linear or nonlinear) was performed
with CDEIS as a dependent and IL-6 or IL-10 as an
independent variable. Cross-validation between test and
validation groups was performed each time after splitting.
Coefficients for each particular regression analysis and
cross-validation were recorded. In this way we were able to
analyze the distribution of the obtained regression and
correlation coefficients with a final aim of improving
robustness and validity of analysis. The entire procedure
was performed automatically by using a custom-made
script created in SPSS Syntax Editor.
A 95% level of significance was accepted for all tests.
Results
We initially recruited 37 patients, but 5 of them were
excluded due to various exclusion criteria. Finally, a
sample of 32 patients was analyzed. Median age of the
study sample was 40 years (25–75 percentile: 26–49 years)
with a range of 18–71 years. There were 21/32 (65.6%)
males and 11/32 (34.4%) females (ratio 1.91:1). Summary
statistics for CDAI, CDEIS, and cytokine levels are pre-
sented in Table 1.
Median time since diagnosis was 22 months (25–75
percentile: 16–32 months), ranging from 9 to 53 months.
All of the patients were receiving therapy with mesalazine at
the time of evaluation. There were also 22/32 (68.75%)
patients on concomitant therapy with systemic corticoste-
roids and 6/32 (18.8%) patients on concomitant azathio-
prine, but there were no patients on methotrexate or
anti-TNFa drugs. Patients treated with concomitant corti-
costeroids were on a mean (±standard deviation, SD) daily
dose of 15 mg (±10 mg) of prednisone equivalent. We did
not find any significant difference in values of cytokines,
CDEIS or CDAI score between patients on versus off
corticosteroids (P [ 0.05).
Half of our patients (16/32) had ileal localization of the
disease. An additional 12/32 patients (37.5%) had ileoco-
lonic localization, while the remaining 4/32 patients
(12.5%) had colonic localization. We compared average
values of measured cytokines according to disease locali-
zation. As seen from Table 2, there was a significant
between-group difference in cytokine levels, with a clear
tendency for lower levels of pro-inflammatory cytokines
and higher levels of anti-inflammatory cytokines in patients
Dig Dis Sci
123

with ileal localization when compared with those with
ileocolonic/colonic localization. Post hoc group-by-group
analysis with Tukey test also confirmed this (Table 3).
There were 18 (56.3%) patients with CDAI B150 and 14
(43.8%) patients with CDAI [150. Patients with CDAI
[150 (mean ± SD: 17.54 ± 11.46) had significantly
higher (corr. t = 19.11; df = 14; P = 0.01) CDEIS than did
patients with CDAI B150 (8.26 ± 2.58), with a mean dif-
ference of 9.27 (95% CI = 2.58–15.97). There were 13/18
(72.2%) patients with CDEIS [7 (endoscopically active
disease) within the group of those with CDAI B150 (clinical
remission), in comparison with 13/14 (92.9%) patients
within the group of those with CDAI [150 (v2 = 1.06;
df = 1; P = 0.30).
Table 2 Comparison of mean cytokine levels according to disease localization: analyzed by ANOVA
Cytokine Disease localization Mean SD Minimum Maximum P-value (ANOVA)
IL-1 Ileal 27.46 13.97 9.80 49.70 0.004
Ileocolonic 46.11 16.16 29.80 80.90
Colonic 55.40 29.16 35.10 98.70
IL-4 Ileal 7.45 4.78 1.80 20.40 0.011
Ileocolonic 3.33 1.87 0.90 5.80
Colonic 2.88 1.94 0.80 5.50
IL-6 Ileal 29.11 12.62 10.80 51.80 0.006
Ileocolonic 47.38 17.33 30.40 82.60
Colonic 55.05 28.31 33.80 96.80
IL-10 Ileal 7.47 5.12 2.00 22.80 0.014
Ileocolonic 3.31 1.80 0.70 5.80
Colonic 2.68 1.97 0.70 5.40
IL-11 Ileal 7.74 5.93 1.90 26.60 0.026
Ileocolonic 3.33 1.86 0.90 5.70
Colonic 2.80 1.83 0.90 5.30
IL-12 Ileal 29.30 14.08 11.50 50.90 0.006
Ileocolonic 47.94 17.31 31.10 89.00
Colonic 56.78 28.97 34.20 99.30
TNFa Ileal 33.05 12.47 10.50 54.60 0.007
Ileocolonic 51.04 19.39 31.30 97.90
Colonic 60.58 27.86 35.90 100.60
INFc Ileal 32.37 13.25 7.40 56.90 0.005
Ileocolonic 51.39 17.77 34.80 92.30
Colonic 60.40 28.95 37.40 102.80
Cytokine levels are expressed as picograms per milliliter (pg/ml)
IL interleukin, IFNc interferon gamma, TNFa tumor necrosis factor alpha, SD standard deviation, ANOVA analysis of variance
Table 1 Summary statistics for
values of CDAI, CDEIS, and
cytokines
Cytokine levels are expressed as
picograms per milliliter (pg/ml)
CDAI Crohn’s Disease Activity
Index, CDEIS Crohn’s Disease
Endoscopic Index of Severity,
IL interleukin, IFNc interferon
gamma, TNFa tumor necrosis
factor alpha
Mean SD Median Minimum Maximum 25–75 Percentile
CDAI 151.81 82.24 124.50 56.00 370.00 91.00–205.00
CDEIS 12.32 8.98 9.20 4.20 40.40 7.45–14.10
IL-1 37.95 19.79 37.35 9.80 98.70 30.30–43.90
IL-10 5.31 4.36 4.50 0.70 22.80 2.30–5.60
IL-11 5.47 4.89 4.65 0.90 26.60 2.50–5.65
IL-12 39.73 20.08 39.10 11.50 99.30 31.25–46.80
IL-4 5.33 4.16 4.75 0.80 20.40 2.60–5.65
IL-6 39.20 19.29 36.65 10.80 96.80 30.80–44.80
IFNc 43.01 20.07 39.65 7.40 102.80 35.35–50.70
TNFa 43.24 19.99 38.35 10.50 100.60 32.10–52.90
Dig Dis Sci
123
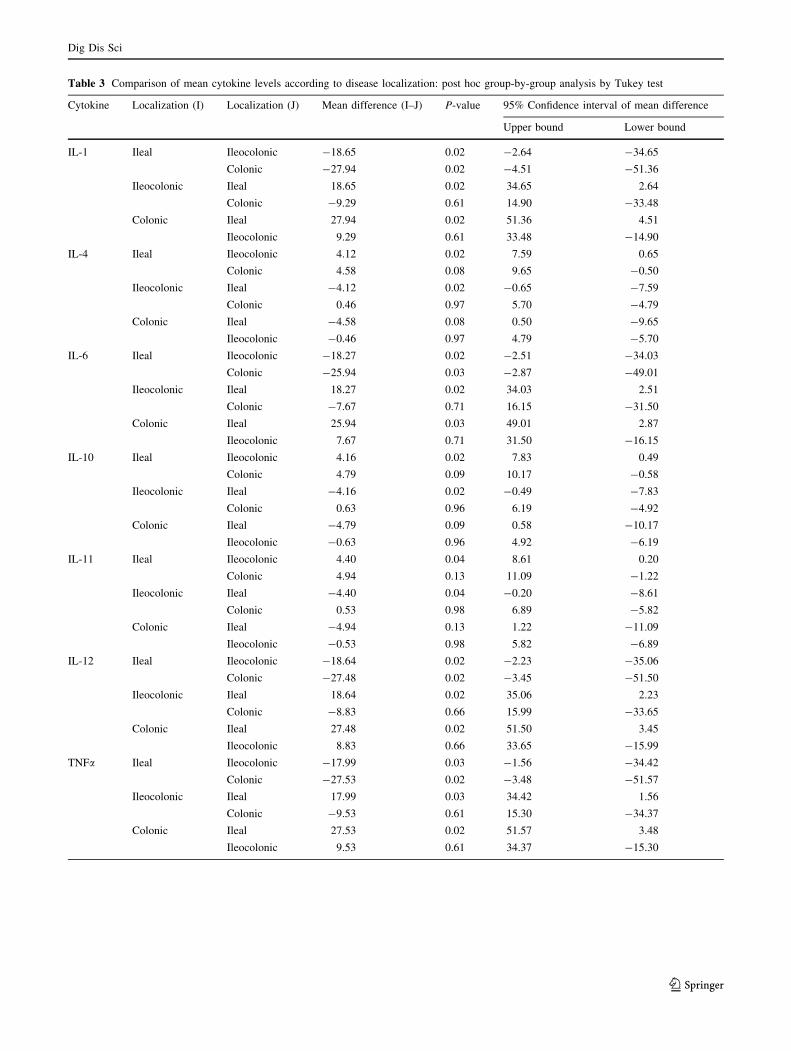
Table 3 Comparison of mean cytokine levels according to disease localization: post hoc group-by-group analysis by Tukey test
Cytokine Localization (I) Localization (J) Mean difference (I–J) P-value 95% Confidence interval of mean difference
Upper bound Lower bound
IL-1 Ileal Ileocolonic -18.65 0.02 -2.64 -34.65
Colonic -27.94 0.02 -4.51 -51.36
Ileocolonic Ileal 18.65 0.02 34.65 2.64
Colonic -9.29 0.61 14.90 -33.48
Colonic Ileal 27.94 0.02 51.36 4.51
Ileocolonic 9.29 0.61 33.48 -14.90
IL-4 Ileal Ileocolonic 4.12 0.02 7.59 0.65
Colonic 4.58 0.08 9.65 -0.50
Ileocolonic Ileal -4.12 0.02 -0.65 -7.59
Colonic 0.46 0.97 5.70 -4.79
Colonic Ileal -4.58 0.08 0.50 -9.65
Ileocolonic -0.46 0.97 4.79 -5.70
IL-6 Ileal Ileocolonic -18.27 0.02 -2.51 -34.03
Colonic -25.94 0.03 -2.87 -49.01
Ileocolonic Ileal 18.27 0.02 34.03 2.51
Colonic -7.67 0.71 16.15 -31.50
Colonic Ileal 25.94 0.03 49.01 2.87
Ileocolonic 7.67 0.71 31.50 -16.15
IL-10 Ileal Ileocolonic 4.16 0.02 7.83 0.49
Colonic 4.79 0.09 10.17 -0.58
Ileocolonic Ileal -4.16 0.02 -0.49 -7.83
Colonic 0.63 0.96 6.19 -4.92
Colonic Ileal -4.79 0.09 0.58 -10.17
Ileocolonic -0.63 0.96 4.92 -6.19
IL-11 Ileal Ileocolonic 4.40 0.04 8.61 0.20
Colonic 4.94 0.13 11.09 -1.22
Ileocolonic Ileal -4.40 0.04 -0.20 -8.61
Colonic 0.53 0.98 6.89 -5.82
Colonic Ileal -4.94 0.13 1.22 -11.09
Ileocolonic -0.53 0.98 5.82 -6.89
IL-12 Ileal Ileocolonic -18.64 0.02 -2.23 -35.06
Colonic -27.48 0.02 -3.45 -51.50
Ileocolonic Ileal 18.64 0.02 35.06 2.23
Colonic -8.83 0.66 15.99 -33.65
Colonic Ileal 27.48 0.02 51.50 3.45
Ileocolonic 8.83 0.66 33.65 -15.99
TNFa Ileal Ileocolonic -17.99 0.03 -1.56 -34.42
Colonic -27.53 0.02 -3.48 -51.57
Ileocolonic Ileal 17.99 0.03 34.42 1.56
Colonic -9.53 0.61 15.30 -34.37
Colonic Ileal 27.53 0.02 51.57 3.48
Ileocolonic 9.53 0.61 34.37 -15.30
Dig Dis Sci
123

A correlation matrix of CDAI, CDEIS, and cytokines is
presented in Table 4, showing that all correlations were
significant. The correlation between CDAI and CDEIS
appeared to be positive and low to moderate in strength.
Correlation of CDEIS with anti-inflammatory cytokines
(IL-4, IL-10, and IL-11) was negative and also low to
moderate in strength. However, correlation between
CDEIS and pro-inflammatory cytokines (IL-1, IL-6,
IL-12, IFNc, and TNFa) appeared to be excellent. Nota-
bly, the correlation between CDAI and all cytokines was
similar in strength to the correlation between CDAI and
CDEIS, with negative coefficients for anti-inflammatory
cytokines.
Additional analysis showed that, in contrast to pro-
inflammatory cytokines that exhibited linear correlation
with CDEIS score, anti-inflammatory cytokines exhibited
nonlinear correlation with CDEIS, corresponding to the
power function (y = a 9 xb). Relationships between each
of the evaluated cytokines and CDEIS are depicted in
Figs. 1, 2, 3, and 4.
We used regression analysis to construct a prediction
model for CDEIS based on cytokine values. Since there
were significant correlations between cytokine variables,
which would produce undesirable multicollinearity in a
final model if entered together, we tested each cytokine
separately in order to choose the parameter with best pre-
dictive power.
On testing pro-inflammatory cytokines using linear
regression analysis, each was a significant predictor of
CDEIS value, but IL-6 showed the best performance. The
model that included IL-6 (b = 0.957; P \ 0.001) as an
independent variable was highly significant (F = 325.69;
df = 1; P \ 0.001). The equation identified for this model
was CDEIS = 0.445 9 (IL-6) - 5.143. The adjusted R2
value was 0.916, which indicates that 91.6% of the vari-
ance in CDEIS was explained by TNFa value (a very large
effect). The standard error of the estimate by this model
was 2.65. A graphical representation of this regression line
in relation to observed data is depicted in Fig. 1.
Nonlinear regression analysis was conducted to inves-
tigate how well anti-inflammatory cytokines predicted
CDEIS value. Each of the anti-inflammatory cytokines
exhibited excellent performance for prediction of CDEIS
value, but the model that included IL-10 (b = -0.977;
P \ 0.001) performed the best (F = 617.18; df = 1;
P \ 0.001). The equation identified for this model was
CDEIS = 27.478 9 (IL-10)-0.71 with adjusted R2 value of
0.954 and standard error of the estimate of 0.126. A
graphical representation of this regression line in relation to
observed data is depicted in Fig. 2.
A model that included IFNc was also evaluated
[CDEIS = 0.424 9 (IFNc) - 5.926]; however, the adjus-
ted R2 value, although rather high, was somewhat lower
(0.89) than that of the other two models and it was not
further explored.
Receiver operating characteristics analysis was per-
formed in order to test the diagnostic performance of IL-6
for detecting patients with CDEIS [7, which was sug-
gested as a threshold to distinguish between patients with
active disease and those in remission [16]. The area under
the ROC curve (AUROC) was 1.0 (95% CI = 0.89–1.0;
P \ 0.001) for a cutoff value of 15.9 pg/ml. This threshold
had 100% sensitivity (95% CI = 86.7–100), specificity
(95% CI = 54.1–100), and positive and negative predictive
values. A dot diagram depicting the observed cases in
regard to the proposed cutoff value is presented in Fig. 5.
In order to test the validity of the IL-6-based predictive
model for CDEIS and to increase the robustness of the
results in the setting of a limited sample size, we used the
bootstrap method, as described in the ‘‘Methods’’ section.
After splitting the sample 300 times (into test and valida-
tion groups) and performing linear regression and internal
cross-validation each time, we analyzed the distribution of
all of the obtained coefficients.
The mean (±SD) R2 value was 0.91 ± 0.03 and each of
the 300 regression models was statistically significant
(P \ 0.001). The average correlation coefficient obtained
for the validation groups was 0.95 ± 0.037.
Table 3 continued
Cytokine Localization (I) Localization (J) Mean difference (I–J) P-value 95% Confidence interval of mean difference
Upper bound Lower bound
INFc Ileal Ileocolonic -19.02 0.02 -2.76 -35.28
Colonic -28.03 0.02 -4.23 -51.84
Ileocolonic Ileal 19.02 0.02 35.28 2.76
Colonic -9.01 0.64 15.58 -33.59
Colonic Ileal 28.03 0.02 51.84 4.23
Ileocolonic 9.01 0.64 33.59 -15.58
Cytokine levels are expressed as picograms per milliliter (pg/ml)
IL interleukin, IFNc interferon gamma, TNFa tumor necrosis factor alpha
Dig Dis Sci
123

Similar analysis was performed in order to test the
validity of IL-10 as a predictor of CDEIS. The only dif-
ference was that, instead of linear regression, we performed
nonlinear, power model regression after each split of the
sample. The mean (±SD) R2 value was 0.95 ± 0.02 and
each of the 300 regression models was statistically signif-
icant (P \ 0.001). The average correlation coefficient
obtained for the validation groups was 0.98 ± 0.014.
Discussion
Mucosal healing is considered the ultimate aim of treat-
ment in CD. It has been demonstrated that achieving this
specific goal reduces the number of hospitalizations and
surgical procedures, which additionally emphasizes its
clinical relevance [17, 18]. Consequently, clinicians need a
reliable yet easy to use disease activity index that is cheap
and simple, preferably consisting of widely available and
easy-to-collect parameters [3].
The Crohn’s Disease Activity Index (CDAI), being one
of the first developed clinical monitoring tools, is to date
the most widely accepted index for clinical monitoring and
the instrument most frequently used in clinical trials [12].
The score is based on eight independent variables (number
of liquid stools, severity of abdominal pain, general well-
being, presence of extraintestinal manifestations, need for
antidiarrheal drugs, presence of abdominal mass, hemato-
crit value, and body weight) monitored via 7-day diary.
Nevertheless, CDAI score is prone to interobserver vari-
ability [19]. It also correlates poorly with inflammatory
status of the intestinal mucosa, which is one of its greatest
Table 4 Correlation matrix for CDAI, CDEIS, and cytokines
CDEIS CDAI IL-4 IL-10 IL-11 IL-1 IL-6 IL-12 IFNc TNFa
CDEIS
r N/A 0.434 -0.627 -0.601 -0.559 0.939 0.957 0.943 0.948 0.957
P 0.0130 0.0001 0.0003 0.0009 \0.0001 \0.0001 \0.0001 \0.0001 \0.0001
CDAI
r 0.434 N/A -0.442 -0.419 -0.412 0.453 0.445 0.466 0.466 0.467
P 0.0130 0.0114 0.0170 0.0192 0.0093 0.0108 0.0072 0.0071 0.0071
IL-4
r -0.627 -0.442 N/A 0.992 0.981 -0.801 -0.793 -0.798 -0.809 -0.788
P 0.0001 0.0114 \0.0001 \0.0001 \0.0001 \0.0001 \0.0001 \0.0001 \0.0001
IL-10
r -0.601 -0.419 0.992 N/A 0.994 -0.769 -0.762 -0.765 -0.786 -0.764
P 0.0003 0.0170 \0.0001 \0.0001 \0.0001 \0.0001 \0.0001 \0.0001 \0.0001
IL-11
r -0.559 -0.412 0.981 0.994 N/A -0.723 -0.719 -0.718 -0.745 -0.723
P 0.0009 0.0192 \0.0001 \0.0001 \0.0001 \0.0001 \0.0001 \0.0001 \0.0001
IL-1
r 0.939 0.453 -0.801 -0.769 -0.723 N/A 0.996 0.996 0.989 0.978
P \0.0001 0.0093 \0.0001 \0.0001 \0.0001 \0.0001 \0.0001 \0.0001 \0.0001
IL-6
r 0.957 0.445 -0.793 -0.762 -0.719 0.996 N/A 0.993 0.991 0.985
P \0.0001 0.0108 \0.0001 \0.0001 \0.0001 \0.0001 \0.0001 \0.0001 \0.0001
IL-12
r 0.943 0.466 -0.798 -0.765 -0.718 0.996 0.993 N/A 0.989 0.987
P \0.0001 0.0072 \0.0001 \0.0001 \0.0001 \0.0001 \0.0001 \0.0001 \0.0001
IFNc
r 0.948 0.466 -0.809 -0.786 -0.745 0.989 0.991 0.989 N/A 0.990
P \0.0001 0.0071 \0.0001 \0.0001 \0.0001 \0.0001 \0.0001 \0.0001 \0.0001
TNFa
r 0.957 0.467 -0.788 -0.764 -0.723 0.978 0.985 0.987 0.990 N/A
P \0.0001 0.0071 \0.0001 \0.0001 \0.0001 \0.0001 \0.0001 \0.0001 \0.0001
CDAI Crohn’s Disease Activity Index, CDEIS Crohn’s Disease Endoscopic Index of Severity, IL interleukin, IFNc interferon gamma,
TNFa tumor necrosis factor alpha, r Pearson correlation coefficient, P significance level
Dig Dis Sci
123

limitations [20, 21]. Given the fact that mucosal healing is
presently considered a main treatment goal in CD, recent
reviews suggest that CDAI cannot remain as primary
endpoint in clinical trials [3].
Our results also suggest that CDAI correlates poorly
with mucosal status (Table 2). The development of CDAI
was based on laboratory markers that later failed to be
proved reliable predictors of mucosal inflammation, and a
considerable part of the score is based on purely subjective
symptoms, thus leading to its limitations and failure to
predict inflammation [3]. In our sample we also found over
70% of patients with CDEIS[7 (those with endoscopically
active disease) within those defined to be in remission
according to CDAI (CDAI B150), which further under-
lines the imperfection of CDAI.
At present, severity of mucosal inflammation assessed by
endoscopy is considered the gold standard for disease activity
in CD. Crohn’s Disease Endoscopic Index of Severity
(CDEIS) proposed by a group of French investigators
(GETAID group) in 1989 emerged in the following years as a
gold standard for evaluation of endoscopic activity [4]. This
index is based on endoscopic findings in five segments of the
gut (ileum, right colon, transverse colon, left and sigmoid
colon, and rectum). The elaboration of the score requires
analog scale transformation. Based on data from five pro-
spective GETAID studies that included 562 colonoscopies
performed in 231 patients, it has been suggested that endo-
scopic remission might be defined as CDEIS score lower than
6 or 7 [16]. The CDEIS, although reliable and reproducible, is
rather time consuming and technically demanding.
However, CDEIS is currently the only tool that can
reliably evaluate activity of mucosal inflammation. The
score is based on ileocolonoscopy findings, which can lead
to numerous practical problems that are a serious obstacle
for routine application, and its use can be complex in
clinical trials. Ileocolonoscopy is invasive, expensive, and
time consuming; the major part of the small bowel is not
within the reach of endoscopy, therefore remaining outside
of this particular scoring system, which might lead to
potential underestimation. Although there are proposed
threshold values for remission or response following
medical therapy, their validity is still under evaluation [16].
In the recent literature there have been several attempts
to identify serum indices of mucosal inflammation. To date,
several serum markers of CD activity, alone or in various
combinations, have been evaluated. Most of the published
studies reported significant but rather weak correlations
with severity of mucosal inflammation [20–24]. Some of the
evaluated parameters include hemoglobin, hematocrit,
erythrocyte sedimentation rate (ESR), albumin, C-reactive
protein (CRP), platelets, a1-antitrypsin, orosomucoid, and
sialic acid. One study reported a high correlation rate of
serum albumin (r = 0.8) with mucosal inflammation, but
the study sample was not uniform and included 28 patients
with CD colitis and ulcerative colitis [25].
Several studies have established a connection between
disease activity and levels of circulating cytokines (both
pro-inflammatory and anti-inflammatory), implying their
potential use as monitoring tools [6, 10, 11]. Mitsuyama
et al. reported that serum concentrations of IL-10 increased
Fig. 1 Scattergram depicting the linear relationship between IL-6
and CDEIS. Solid line represents the equation identified by linear
regression: CDEIS = 0.445 9 (IL-6) - 5,143
Fig. 2 Scattergram depicting the nonlinear (power) relation-
ship between IL-10 and CDEIS. Solid line represents the equa-
tion identified by nonlinear (power function) regression:
CDEIS = 27.478 9 (IL-10)-0.71
Dig Dis Sci
123

during phases of disease resolution, while serum levels of
IL-6 and CRP increased during the active phase of CD
[11]. However, disease activity of CD in this particular
study was assessed according to scores established by the
International Organization for the Study of Inflammatory
Bowel Disease (IOIBD), which is also a clinical and not an
endoscopic activity index [26]. Our study is the first
attempt to correlate CDEIS (as the most reliable mucosal
activity index) with serum cytokine levels.
Our results suggest that circulating cytokines could be
used as reliable and noninvasive markers of endoscopic
activity in CD. According to our findings, levels of pro-
Fig. 3 Scattergrams depicting
the nonlinear (power)
relationships between anti-
inflammatory cytokines (IL-4
and IL-11) and CDEIS. Solidline in each diagram represents
the nonlinear (power) regression
line
Fig. 4 Scattergrams depicting
the linear relationship between
pro-inflammatory cytokines
(IL-1, IL-6, IL-12, and INF-c)
and CDEIS. Solid line in each
diagram represents the linear
regression line
Dig Dis Sci
123

inflammatory and anti-inflammatory cytokines predict the
degree of endoscopic activity with more than adequate
accuracy. Pro-inflammatory cytokines, due to their positive
linear relationship with mucosal inflammation, are perhaps
easier to use in routine clinical practice, especially after
CDEIS thresholds for remission and therapy response are
validated. ROC analysis of the diagnostic accuracy of IL-6
for predicting patients with endoscopically active disease
(CDEIS [7) demonstrated excellent diagnostic perfor-
mance, thus proposing another possible clinical application.
Apparently, anti-inflammatory cytokines provide even
better prediction of CDEIS score, with standard error of
estimate of 0.126 for IL-10 and very high R2 values.
However, due to their nonlinear and negative correlation
with CDEIS, they are less straightforward markers,
although they could be used in clinical trials or in any other
situation where accurate prediction of mucosal status is of
value.
In our paper we are proposing the utilization of two
cytokines: IL-6 and IL-10. However, the scattergrams for
the relationships between CDEIS and other anti-inflam-
matory and pro-inflammatory cytokines evaluated in this
study (Figs. 3, 4) look almost identical to those in Figs. 1
and 2. Our choice of IL-6 and IL-10 was based on the fact
that their regression models had the best R2 values and also
on the fact that their relationships with disease activity
were already established in previous studies, although
without validation against CDEIS [11]. However, in any
future research with a larger sample, this choice can be
reevaluated and perhaps any of the cytokines evaluated in
our research might prove to be better.
There is reasonable consensus that mucosa of patients
with established Crohn’s disease is dominated by CD4?
lymphocytes with type 1 helper-T cell (Th1) phenotype,
characterized by production of IFNc and IL-2 [5]. There-
fore, one may assume that IL-2 and/or IFNc levels could
have a significant predictive potential for prediction of
mucosal status. Although we have not measured IL-2, we
did evaluate the prognostic performance of IFNc and found
it to be excellent, although slightly inferior to that of IL-6
and IL-10, which led us to prefer the IL-6 and IL-10
models.
In a recent paper, Italian authors reported significantly
higher levels of serum IL-6 and TNFa in patients with
perianal CD when separately compared with groups of
patients with small bowel CD and healthy controls [27].
We have also observed a clear difference in serum cytokine
levels in three different CD localization groups (Tables 2,
3) with higher levels of anti-inflammatory cytokines and
lower levels of pro-inflammatory cytokines in patients with
ileal localization of the disease. Whether this is a result of
the extent of intestinal surface involved or perhaps a result
of different disease behavior and different immunological
response in ileojejunal phenotype of the disease (which is
already recognized as a separate and distinct form of CD)
remains to be answered [28–30].
There are several important limitations of this study that
need to be addressed. Sample size is the obvious issue, but
CD is a relatively rare disease in our region, with 140 new
cases detected in the 12-year period of 1995–2006 [31].
Therefore, obtaining a reasonably large sample would
significantly prolong this research. One could also raise
questions about validation of the proposed score(s).
Although we used the bootstrap method in order to increase
the robustness of our internal validation, we agree that
external validation would provide more reliable results.
Another important issue is the value of cytokines as
markers of mucosal inflammation in patients receiving
different types of treatment, particularly anti-TNFa ther-
apy. In order to test this, one would need a significantly
larger sample and a substantial number of patients on anti-
TNFa drugs. Bearing in mind the relative prevalence of the
CD in our region and the fact that anti-TNFa treatment is
very expensive and not affordable for most of our patients,
achieving these conditions was not possible in our setting.
However, in this context, it is very important to note that
our sample included patients receiving different types of
treatment (except anti-TNFa), with a variable time since
initiating treatment and since diagnosis. In a diverse sam-
ple such as this, cytokines predicted the degree of mucosal
inflammation with more than good accuracy. Nonetheless,
the true value of cytokines in noninvasive monitoring of
therapy response is the question of great clinical signifi-
cance that needs to be answered in future studies.
Despite limitations, we believe that this study brings
very important information about the relationship between
circulating cytokines and endoscopic activity of CD. This
Fig. 5 Dot diagram depicting the observed cases in regard to the
proposed cutoff value of 15.9 pg/ml for IL-6
Dig Dis Sci
123

fact, on its own, might be the first step in the direction of
creating the simple and reliable CD activity index that we
all need so much.
To conclude, serum cytokines are excellent predictors of
mucosal inflammation in patients with CD. The best per-
forming predictor for mucosal inflammation among the
pro-inflammatory cytokines was IL-6, while the best per-
forming anti-inflammatory cytokine appeared to be IL-10,
although others were almost as good as those two. We
propose predictive models based on IL-6 and/or IL-10 that
might be used as accurate and simple mucosal activity
monitoring tools in CD.
References
1. Sostegni R, Daperno M, Scaglione N, et al. Review article:
Crohn’s disease: Monitoring disease activity. Aliment PharmacolTher. 2003;17(Suppl 2):11–17.
2. Biancone L, De Nigris F, Del Vecchio Blanco G, et al. Review
article: Monitoring the activity of Crohn’s disease. AlimentPharmacol Ther. 2002;16(Suppl 4):29–33.
3. Minderhoud IM, Samsom M, Oldenburg B. What predicts
mucosal inflammation in Crohn’s disease patients? InflammBowel Dis. 2007;13:1567–1572.
4. Mary JY, Modigliani R. Development and validation of an
endoscopic index of the severity for Crohn’s disease: A pro-
spective multicentre study. Groupe d’Etudes Therapeutiques des
Affections Inflammatoires du Tube Digestif (GETAID). Gut.1989;30:983–989.
5. Podolsky DK. Inflammatory bowel disease. N Engl J Med.
2002;347:417–429.
6. Nancey S, Hamzaoui N, Moussata D, et al. Serum interleukin-6,
soluble interleukin-6 receptor and Crohn’s disease activity. DigDis Sci. 2008;53:242–247.
7. Yamamoto T, Nakahigashi M, Saniabadi AR, et al. Impacts of
long-term enteral nutrition on clinical and endoscopic disease
activities and mucosal cytokines during remission in patients with
Crohn’s disease: A prospective study. Inflamm Bowel Dis.
2007;13:1493–1501.
8. Yamamoto T, Umegae S, Kitagawa T, Matsumoto K. Systemic
and local cytokine production in quiescent ulcerative colitis and
its relationship to future relapse: A prospective pilot study. In-flamm Bowel Dis. 2005;11:589–596.
9. Spoettl T, Hausmann M, Klebl F, et al. Serum soluble TNF
receptor I and II levels correlate with disease activity in IBD
patients. Inflamm Bowel Dis. 2007;13:727–732.
10. Mahida YR, Kurlac L, Gallagher A, Hawkey CJ. High circulating
concentrations of interleukin-6 in active Crohn’s disease but not
ulcerative colitis. Gut. 1991;32:1531–1534.
11. Mitsuyama K, Tomiyasu N, Takaki K, et al. Interleukin-10 in the
pathophysiology of inflammatory bowel disease: increased serum
concentrations during the recovery phase. Mediators Inflamm.
2006;2006:26875.
12. Best WR, Becktel JM, Singleton JW, Kern F Jr. Development of
a Crohn’s disease activity index. National cooperative Crohn’s
disease study. Gastroenterology. 1976;70:439–444.
13. de Jager W, Prakken BJ, Bijlsma JW, Kuis W, Rijkers GT.
Improved multiplex immunoassay performance in human plasma
and synovial fluid following removal of interfering heterophilic
antibodies. J Immunol Methods. 2005;300:124–135.
14. de Jager W, te Velthuis H, Prakken BJ, Kuis W, Rijkers GT.
Simultaneous detection of 15 human cytokines in a single sample
of stimulated peripheral blood mononuclear cells. Clin Diagn LabImmunol. 2003;10:133–139.
15. Fox J. Bootstrapping, In: Fox J, ed. Applied Regression Analysis,Linear Models, and Related Methods Thousand Oaks, CA: Sage;
1997.
16. Mary JY, Lemann M, Colombel JF, Lerebours E, Soule JC,
Gendre JP, Modigliani R, The GETAID. Endoscopic remission
and response in Crohn’s disease: An objective definition using the
CDEIS, In: 13th United European Gastroenterology Week.
Copenhagen: Denmark; 2005.
17. Hanauer SB, Feagan BG, Lichtenstein GR, et al. Maintenance
infliximab for Crohn’s disease: The ACCENT I randomised trial.
Lancet. 2002;359:1541–1549.
18. Rutgeerts P, Feagan BG, Lichtenstein GR, et al. Comparison of
scheduled and episodic treatment strategies of infliximab in
Crohn’s disease. Gastroenterology. 2004;126:402–413.
19. de Dombal FT, Softley A. IOIBD report no 1: Observer variation
in calculating indices of severity and activity in Crohn’s disease.
International organisation for the study of inflammatory bowel
disease. Gut. 1987;28:474–481.
20. Cellier C, Sahmoud T, Froguel E, et al. Correlations between
clinical activity, endoscopic severity, and biological parameters
in colonic or ileocolonic Crohn’s disease. A prospective multi-
centre study of 121 cases. The Groupe d’Etudes Therapeutiques
des Affections Inflammatoires Digestives. Gut. 1994;35:231–235.
21. Modigliani R, Mary JY, Simon JF, et al. Clinical, biological,
and endoscopic picture of attacks of Crohn’s disease. Evolution
on prednisolone. Groupe d’Etude Therapeutique des Affections
Inflammatoires Digestives. Gastroenterology. 1990;98:811–818.
22. Tromm A, Tromm CD, Huppe D, et al. Evaluation of different lab-
oratory tests and activity indices reflecting the inflammatory activity
of Crohn’s disease. Scand J Gastroenterol. 1992;27:774–778.
23. Simonis B, Heine M, Heene DL, Gladisch R. Evaluation and
validation of a Crohn’s disease inflammatory activity index
reflecting pattern of endoscopic severity. Scand J Gastroenterol.1998;33:283–288.
24. Solem CA, Loftus EV Jr, Tremaine WJ, et al. Correlation of C-
reactive protein with clinical, endoscopic, histologic, and radio-
graphic activity in inflammatory bowel disease. Inflamm BowelDis. 2005;11:707–712.
25. Moran A, Jones A, Asquith P. Laboratory markers of colono-
scopic activity in ulcerative colitis and Crohn’s colitis. Scand JGastroenterol. 1995;30:356–360.
26. Myren J, Bouchier IA, Watkinson G, et al. The O.M.G.E. Mul-
tinational Inflammatory Bowel Disease Survey 1976–1982. A
further report on 2, 657 cases. Scand J Gastroenterol Suppl.1984;95:1–27.
27. Ruffolo C, Scarpa M, Faggian D, et al. Cytokine network in
rectal mucosa in perianal Crohn’s disease: Relations with
inflammatory parameters and need for surgery. Inflamm BowelDis. 2008;14:1406–1412.
28. Freeman HJ. Long-term clinical behavior of jejunoileal
involvement in Crohn’s disease. Can J Gastroenterol. 2005;19:
575–578.
29. Freeman HJ. Long-term natural history of Crohn’s disease. WorldJ Gastroenterol. 2009;15:1315–1318.
30. Touze I, Gower-Rousseau C, Grandbastien B, et al. Diffuse je-
juno-ileitis of Crohn’s disease: a separate form of the disease?
Gastroenterol Clin Biol. 1999;23:307–311.
31. Pavlovic-Calic N, Salkic NN, Gegic A, Smajic M, Alibegovic E.
Crohn’s disease in Tuzla region of Bosnia and Herzegovina: A
12-year study (1995–2006). Int J Colorectal Dis. 2008;23:
957–964.
Dig Dis Sci
123




















