Proton pump inhibitors versus H2-antagonists: a meta-analysis of their efficacy in treating bleeding...
10
Proton pump inhibitors versus H 2 -antagonists: a meta-analysis of their efficacy in treating bleeding peptic ulcer J. P. GISBERT*, L. GONZA ´ LEZ*, X. CALVET , M. ROQUE ´ à , R. GABRIEL§, & J. M. PAJARES* *Department of Gastroenterology and §Department of Clinical Epidemiology, University Hospital ‘La Princesa’, Madrid, Spain; Servei de Medicina, Corporacio´Sanita`ria Parc Taulı´, Sabadell, Spain; and àCenter d’Estudis, Programes i Serveis Sanitaris (CEPSS), Barcelona, Spain Accepted for publication 26 February 2001 SUMMARY Purpose: To evaluate whether proton pump inhibitors are more effective than H 2 -antagonists (H 2 -A) for the treatment of bleeding peptic ulcer. Data sources: PubMed database until January 2000. Study selection: Comparative randomized trials of proton pump inhibitors (omeprazole, lansoprazole, or pantop- razole) vs. H 2 -A (cimetidine, ranitidine or famotidine). Data extraction: Meta-analysis combining the odds ratios (OR) of the individual studies in a global OR (Peto method). Outcomes evaluated: Persistent or recurrent bleeding, need for surgery, or mortality. Data synthesis: Eleven studies fulfilled the inclusion criteria and contained data for at least one of the planned comparisons. Persistent or recurrent bleeding was reported in 6.7% (95% CI: 4.9–8.6%) of the patients treated with proton pump inhibitors, and in 13.4% (95% CI: 10.8–16%) of those treated with H 2 -A (OR 0.4; 95% CI: 0.27–0.59) (v 2 -homogeneity test, 18; P 1 0.09). Surgery was needed in 5.2% (95% CI: 3.4–6.9%) of the patients treated with proton pump inhibitors, and in 6.9% (95% CI: 4.9–8.9%) of the patients treated with H 2 -A (OR 0.7; 95% CI: 0.43–1.13). Respective percentages for mortality were 1.6% (95% CI: 0.9–2.9%) and 2.2% (95% CI: 1.3–3.7%) (OR 0.69; 95% CI: 0.31–1.57). Sub-analysis: Five studies evaluated the effect of both therapies given in bolus injections on persistent or recurrent bleeding rate, which was 6% (95% CI: 3.6–8.3%) and 8.1% (95% CI: 5.3–10.9%), respectively (OR, 0.57; 95% CI: 0.31–1.05). Persistent or recurrent bleeding in high risk patients (Forrest Ia, Ib and IIa) occurred in 13.2% (95% CI: 7.9–8%) of the patients treated with proton pump inhibitors and in 34.5% (27–42%) of those treated with H 2 -A (OR 0.28; 95% CI: 0.16–0.48). In patients not having endoscopic therapy, persistent or recurrent bleeding was reported, respect- ively, in 4.3% (95% CI: 2.7–6.7%) and in 12% (95% CI: 8.7–15%) (OR 0.24; 95% CI: 0.13–0.43). Less marked differences were observed in patients having adjunct endoscopic therapy: 10.3% (95% CI: 6.7–13.8%) and 15.2% (11.1–19.3%) (OR 0.59; 95% CI: 0.36–0.97). Moreover, the significance disappeared in this group when a single outlier study was excluded. Conclusions: Proton pump inhibitors are more effective than H 2 -A in preventing persistent or recurrent bleed- ing from peptic ulcer, although this advantage seems to be more evident in patients not having adjunct sclerosis therapy. This beneficial effect seems to be similar or even more marked in patients with Forrest Ia, Ib or IIa ulcers. However, proton pump inhibitors are not more effective than H 2 -A for reducing surgery or mortality rates. Nevertheless, the data are too scarce and heterogeneous to draw definitive conclusions, and further comparative trials are clearly warranted. Correspondence to: Dr J. P. Gisbert, Playa de Moja´car 29. Urb. Bonanza, 28669 Boadilla del Monte, Madrid, Spain. E-mail: [email protected] Aliment Pharmacol Ther 2001; 15: 917–926. Ó 2001 Blackwell Science Ltd 917
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Proton pump inhibitors versus H2-antagonists: a meta-analysis of their efficacy in treating bleeding...

Proton pump inhibitors versus H2-antagonists: a meta-analysisof their ef®cacy in treating bleeding peptic ulcer
J . P. GISBERT*, L. GONZAÂ LEZ*, X. CALVET , M. ROQUEÂ à , R. GABRIEL§, & J. M. PAJARES*
*Department of Gastroenterology and §Department of Clinical Epidemiology, University Hospital `La Princesa', Madrid,
Spain; Servei de Medicina, Corporacio SanitaÁria Parc TaulõÂ, Sabadell, Spain; and àCenter d'Estudis, Programes i Serveis
Sanitaris (CEPSS), Barcelona, Spain
Accepted for publication 26 February 2001
SUMMARY
Purpose: To evaluate whether proton pump inhibitors
are more effective than H2-antagonists (H2-A) for the
treatment of bleeding peptic ulcer.
Data sources: PubMed database until January 2000.
Study selection: Comparative randomized trials of proton
pump inhibitors (omeprazole, lansoprazole, or pantop-
razole) vs. H2-A (cimetidine, ranitidine or famotidine).
Data extraction: Meta-analysis combining the odds ratios
(OR) of the individual studies in a global OR (Peto
method).
Outcomes evaluated: Persistent or recurrent bleeding,
need for surgery, or mortality.
Data synthesis: Eleven studies ful®lled the inclusion
criteria and contained data for at least one of the
planned comparisons. Persistent or recurrent bleeding
was reported in 6.7% (95% CI: 4.9±8.6%) of the
patients treated with proton pump inhibitors, and in
13.4% (95% CI: 10.8±16%) of those treated with H2-A
(OR 0.4; 95% CI: 0.27±0.59) (v2-homogeneity test, 18;
P1 � 0.09). Surgery was needed in 5.2% (95% CI:
3.4±6.9%) of the patients treated with proton pump
inhibitors, and in 6.9% (95% CI: 4.9±8.9%) of the
patients treated with H2-A (OR 0.7; 95% CI:
0.43±1.13). Respective percentages for mortality were
1.6% (95% CI: 0.9±2.9%) and 2.2% (95% CI: 1.3±3.7%)
(OR 0.69; 95% CI: 0.31±1.57).
Sub-analysis: Five studies evaluated the effect of both
therapies given in bolus injections on persistent or
recurrent bleeding rate, which was 6% (95% CI:
3.6±8.3%) and 8.1% (95% CI: 5.3±10.9%), respectively
(OR, 0.57; 95% CI: 0.31±1.05). Persistent or recurrent
bleeding in high risk patients (Forrest Ia, Ib and IIa)
occurred in 13.2% (95% CI: 7.9±8%) of the patients
treated with proton pump inhibitors and in 34.5%
(27±42%) of those treated with H2-A (OR 0.28; 95% CI:
0.16±0.48). In patients not having endoscopic therapy,
persistent or recurrent bleeding was reported, respect-
ively, in 4.3% (95% CI: 2.7±6.7%) and in 12% (95% CI:
8.7±15%) (OR 0.24; 95% CI: 0.13±0.43). Less marked
differences were observed in patients having adjunct
endoscopic therapy: 10.3% (95% CI: 6.7±13.8%) and
15.2% (11.1±19.3%) (OR 0.59; 95% CI: 0.36±0.97).
Moreover, the signi®cance disappeared in this group
when a single outlier study was excluded.
Conclusions: Proton pump inhibitors are more effective
than H2-A in preventing persistent or recurrent bleed-
ing from peptic ulcer, although this advantage seems to
be more evident in patients not having adjunct sclerosis
therapy. This bene®cial effect seems to be similar or
even more marked in patients with Forrest Ia, Ib or IIa
ulcers. However, proton pump inhibitors are not more
effective than H2-A for reducing surgery or mortality
rates. Nevertheless, the data are too scarce and
heterogeneous to draw de®nitive conclusions, and
further comparative trials are clearly warranted.
Correspondence to: Dr J. P. Gisbert, Playa de MojaÂcar 29. Urb. Bonanza, 28669 Boadilla del Monte, Madrid, Spain.E-mail: [email protected]
Aliment Pharmacol Ther 2001; 15: 917±926.
Ó 2001 Blackwell Science Ltd 917

INTRODUCTION
Acute upper gastrointestinal haemorrhage is a major
cause of morbidity and mortality, with peptic ulcer being
the most frequent source of bleeding.1 It has been
estimated that approximately 2±3% of duodenal ulcer
(DU) patients who are not receiving antisecretory therapy
are likely to develop haemorrhage during each year of
follow-up study, giving a cumulative risk of haemor-
rhage after 5 years of approximately 10±14%.2 Patients
with bleeding ulcers account for an overall mortality
rate that has remained around 5±10% for the past
50 years, despite improved medical and surgical treat-
ments, the development of diagnostic and therapeutic
endoscopy, and the availability of intensive care units.3
Data from in vitro studies suggest that clotting proceeds
more ef®ciently and the dissolution of clots by proteo-
lytic enzymes occurs more slowly at high pH levels.4±7
Both acid and pepsin alter coagulation by interfering
with the intrinsic and extrinsic coagulation system,
®brinogen polymerization, and platelet aggregation.4
Therefore, pharmaco-therapy of bleeding ulcers attempts
to improve the microenvironment at the bleeding point
by keeping the gastric pH above the proteolytic range
for pepsin to stabilize the clotting process.
Traditionally, pharmacological treatment for bleeding
peptic ulcer has included H2-receptor antagonists, but
these drugs have shown only marginal bene®cial effects
or no effect at all when compared with placebo.1, 8±10
The lack of a clear bene®cial effect of H2-antagonists
could be due, at least in part, to the limited control of
gastric pH. This is because at the conventional recom-
mended doses of these drugs, intragastric pH cannot be
maintained higher than 4.0 for a long period in patients
with a bleeding peptic ulcer.11±13
On the other hand, intravenous proton pump inhib-
itors produce consistently high intragastric pH values in
patients with bleeding peptic ulcers, whereas cimetidine
or ranitidine is less effective.14±17 However, as the half-
life of omeprazole in the circulation is short, it has been
suggested that it needs to be given in continuous
infusion instead of in bolus injections. Nevertheless,
although some placebo-controlled trials have demon-
strated a bene®cial effect of proton pump inhibitors on
bleeding peptic ulcer, other studies have demonstrated
no effect in outcome of bleeding when comparing
proton pump inhibitors and placebo.18±21
The prevention of even a low effect is a worthwhile aim
for a condition that is common.9 However, in order to
reliably detect such a moderate effect on persistent or
recurrent bleeding, need for surgery, or mortality, the
randomization of a large number of patients is required.
Most of the studies comparing proton pump inhibitors
vs. H2-antagonists have a relatively small sample size,
thus lacking the power to reliably demonstrate the
differences between the two regimens. Although several
well-designed randomized clinical trials comparing the
two drugs have been published, no formal meta-analysis
has been performed to date. Therefore, our aim was to
conduct a meta-analysis of the studies comparing
proton pump inhibitors and H2-antagonists for the
treatment of bleeding peptic ulcer.
PATIENTS AND METHODS
Search strategy
Bibliographical searches were performed in the PubMed
(Internet) database, including studies available until
January 2000, looking for the following words (all ®elds):
bleeding, cimetidine, ranitidine, famotidine, omeprazole,
lansoprazole, pantoprazole, proton pump inhibitor, pep-
tic ulcer. References of reviews on the treatment of
bleeding peptic ulcer, and from the articles selected for
the study, were also examined in search of articles
meeting inclusion criteria. Articles published in any
language were included. The bibliographic searches were
performed independently by two different reviewers.
Selection criteria
The selection criteria were as follows: (i) articles had to
report comparative randomized trials; (ii) they had to
include at least one branch of treatment consisting of
a histamine H2-antagonist (cimetidine, ranitidine or fa-
motidine, which were pooled together in the present
meta-analysis) and another branch with a proton pump
inhibitor (omeprazole, lansoprazole, or pantoprazole, also
pooled together); (iii) studies had to evaluate these
therapies in patients with bleeding gastroduodenal ulcer;
(iv) the effect of therapy had to be evaluated by means of
at least one of the following variables: persistent or recur-
rent bleeding, need for surgery, or mortality; (v) only stud-
ies that clearly stated information about the number of
treated patients in each therapeutic group were included.
Publications identi®ed as duplicates were excluded.
The quality of the studies was assessed using a score
proposed by Jadad et al. based on three items:22
918 J. P. GISBERT et al.
Ó 2001 Blackwell Science Ltd, Aliment Pharmacol Ther 15, 917±926

(i) randomization (one point if yes, or two points if the
method to generate the sequence of randomization
was described and was appropriate); (ii) double-
blinding (one point if yes, or two points if the method
of double-blinding was described and was appropriate);
and (iii) description of withdrawals and dropouts (one
point).
Sub-analyses were planned a priori to compare
studies in sub-groups depending on: omeprazole dose
(40 mg/12 h and 40 mg/8 h), schemes of drug adminis-
tration (bolus injections and continuous infusion),
endoscopic (Forrest) classi®cation [active bleeding (Ia,
Ib) and non-active bleeding (IIa, IIb, IIc)],23 and the
application of concomitant endoscopic therapy. All
these factors have been reported to in¯uence, in some
studies, the risk of persistent or recurrent bleeding or the
effect of proton pump inhibitor on bleeding peptic ulcer.
Statistics
The outcomes considered in this meta-analysis were
persistent or recurrent bleeding, need for surgery, and
mortality. The homogeneity of effects throughout
studies was appraised using a homogeneity test based
on the v2-test. Due to the low power of this test, a
minimum cut-off P-value of 0.20 was established as a
threshold of homogeneity: lower values indicated het-
erogeneity, and prevented us from relying on the
combination of the study results. Meta-analysis was
performed combining the Peto odds ratios (OR) of the
individual studies in a global OR, under the assumption-
free model (or ®xed effects model). We chose to use the
®xed effects model to obtain more precision on the
estimates, because the con®dence intervals are nar-
rower than with the random effects model. Signi®cance
and 95% con®dence intervals (95% CI) are provided for
the combined OR. All calculations were performed with
the freeware program Review Manager 4.1. The statis-
tical methods and formulae are described in the
Handbook of the Cochrane Collaboration and the
RevMan User Guide.24
RESULTS
Description of studies
Eleven studies ful®lled the inclusion criteria and con-
tained data for at least one of the planned compar-
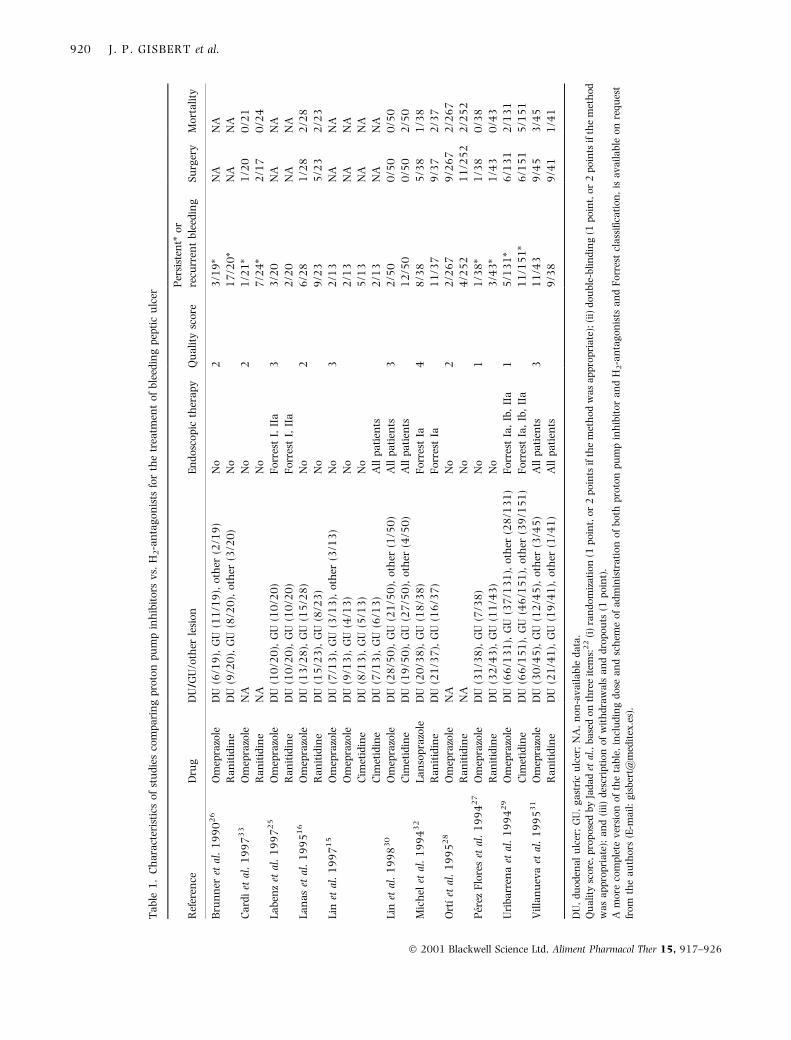
isons.15, 16, 25±33 Detailed characteristics of the studies
are shown in Table 1, where it can be seen that
omeprazole was the proton pump inhibitor used in all
but in one study (in which lansoprazole was prescribed),
whilst both cimetidine and ranitidine were given in
different studies.
Effect of therapy on persistent or recurrent bleeding
Ten out of the 11 studies gave information about the
effect of therapy on persistent or recurrent bleeding, and
in the remaining study we contacted and obtained the
data from the authors.29 Persistent bleeding was
de®ned, depending on the study, as: (a) more than
2.5 L of blood or more than 4 units blood/day
necessary to maintain haemoglobin level above
10 g/L;26, 27, 33 or (b) persistence of bleeding during
the ®rst 48 h or 72 h by clinical and endoscopic
criteria.27±29 Recurrent bleeding was de®ned,
depending on the study, as: (a) blood in the stomach
or a fresh blood clot or bleeding in the ulcer
base at endoscopy;15, 25, 26, 30±32 (b) haematemesis/
melena;16, 27, 31, 32 (c) haemodynamic and clinical
evidence of hypovolemia;16, 31, 32 or (d) decrease in
haemoglobin requiring transfusion, in all cases during
the same hospitalization and after bleeding was initially
stopped by both clinical and analytical criteria.16, 31
In total, 681 patients were treated with proton pump
inhibitors, and 671 with H2-antagonists. The results of
these studies are graphically summarized in Figure 1.
Thus, persistent or recurrent bleeding was reported in
6.7% (95% CI: 4.9±8.6%) of the patients treated with
proton pump inhibitors, and in 13.4% (95% CI:
10.8±16%) of those treated with H2-antagonists.
The OR for the effect of proton pump inhibitors vs.
H2-antagonists on persistent or recurrent bleeding was
0.4 (95% CI: 0.27±0.59). The v2 homogeneity test was
18 (P2 � 0.09), thus indicating mild heterogeneity and
suggesting the need to perform sub-analyses depending
on different factors.
Effect of therapy on the need for surgery
The results of the eight studies comparing the effects of
proton pump inhibitors (618 patients) vs. H2-antag-
onists (621 patients) on the need for surgery are
summarized in Figure 2. Surgery was needed in 5.2%
(95% CI: 3.4±6.9%) of the patients treated with proton
pump inhibitors, and in 6.9% (95% CI: 4.9±8.9%) of the
patients treated with H2-antagonists. The OR for the
PROTON PUMP INHIBITORS VS. H 2 -ANTAGONISTS IN BLEEDING PEPTIC ULCER 919
Ó 2001 Blackwell Science Ltd, Aliment Pharmacol Ther 15, 917±926
Ta
ble
1.
Ch
ara
cter
isti
cso
fst
ud
ies
com
pa
rin
gp
roto
np
um
pin
hib
ito
rsv
s.H
2-a
nta
go
nis
tsfo
rth
etr
eatm
ent
of
ble
edin
gp
epti
cu
lcer
Ref
eren
ceD
rug
DU
/GU
/oth
erle
sio
nE
nd
osc
op
icth
era
py
Qu
ali
tysc
ore
Per
sist
ent*
or
recu
rren
tb
leed
ing
Su
rger
yM
ort
ali
ty
Bru
nn
eret
al.
19
90
26
Om
epra
zole
DU
(6/1
9),
GU
(11
/19
),o
ther
(2/1
9)
No
23
/19
*N
AN
A
Ra
nit
idin
eD
U(9
/20
),G
U(8
/20
),o
ther
(3/2
0)
No
17
/20
*N
AN
A
Ca
rdi
etal
.1
99
73
3O
mep
razo
leN
AN
o2
1/2
1*
1/2
00
/21
Ra
nit
idin
eN
AN
o7
/24
*2
/17
0/2
4
La
ben
zet
al.
19
97
25
Om
epra
zole
DU
(10
/20
),G
U(1
0/2
0)
Fo
rres
tI,
IIa
33
/20
NA
NA
Ra
nit
idin
eD
U(1
0/2
0),
GU
(10
/20
)F
orr
est
I,II
a2
/20
NA
NA
La
na
set
al.
19
95
16
Om
epra
zole
DU
(13
/28
),G
U(1
5/2
8)
No
26
/28
1/2
82
/28
Ra
nit
idin
eD
U(1
5/2
3),
GU
(8/2
3)
No
9/2
35
/23
2/2
3
Lin
etal
.1
99
71
5O
mep
razo
leD
U(7
/13
),G
U(3
/13
),o
ther
(3/1
3)
No
32
/13
NA
NA
Om
epra
zole
DU
(9/1
3),
GU
(4/1
3)
No
2/1
3N
AN
A
Cim
etid
ine
DU
(8/1
3),
GU
(5/1
3)
No
5/1
3N
AN
A
Cim
etid
ine
DU
(7/1
3),
GU
(6/1
3)
All
pa
tien
ts2
/13
NA
NA
Lin
etal
.1
99
83
0O
mep
razo
leD
U(2
8/5
0),
GU
(21
/50
),o
ther
(1/5
0)
All
pa
tien
ts3
2/5
00
/50
0/5
0
Cim
etid
ine
DU
(19
/50
),G
U(2
7/5
0),
oth
er(4
/50
)A
llp
ati
ents
12
/50
0/5
02
/50
Mic
hel
etal
.1
99
43
2L
an
sop
razo
leD
U(2
0/3
8),
GU
(18
/38
)F
orr
est
Ia4
8/3
85
/38
1/3
8
Ra
nit
idin
eD
U(2
1/3
7),
GU
(16
/37
)F
orr
est
Ia1
1/3
79
/37
2/3
7
Ort
õÂet
al.
19
95
28
Om
epra
zole
NA
No
22
/26
79
/26
72
/26
7
Ra
nit
idin
eN
AN
o4
/25
21
1/2
52
2/2
52
Pe r
ezF
lore
set
al.
19
94
27
Om
epra
zole
DU
(31
/38
),G
U(7
/38
)N
o1
1/3
8*
1/3
80
/38
Ra
nit
idin
eD
U(3
2/4
3),
GU
(11
/43
)N
o3
/43
*1
/43
0/4
3
Uri
ba
rren
aet
al.
19
94
29
Om
epra
zole
DU
(66
/13
1),
GU
(37
/13
1),
oth
er(2
8/1
31
)F
orr
est
Ia,
Ib,
IIa
15
/13
1*
6/1
31
2/1
31
Cim
etid
ine
DU
(66
/15
1),
GU
(46
/15
1),
oth
er(3
9/1
51
)F
orr
est
Ia,
Ib,
IIa
11
/15
1*
6/1
51
5/1
51
Vil
lan
uev
aet
al.
19
95
31
Om
epra
zole
DU
(30
/45
),G
U(1
2/4
5),
oth
er(3
/45
)A
llp
ati
ents
31
1/4
39
/45
3/4
5
Ra
nit
idin
eD
U(2
1/4
1),
GU
(19
/41
),o
ther
(1/4
1)
All
pa
tien
ts9
/38
9/4
11
/41
DU
,d
uo
den
al
ulc
er;
GU
,g
ast
ric
ulc
er;
NA
,n
on
-av
ail
ab
led
ata
.Q
ua
lity
sco
re,
pro
po
sed
by
Jad
ad
etal
.,b
ase
do
nth
ree
item
s:2
2(i
)ra
nd
om
iza
tio
n(1
po
int,
or
2p
oin
tsif
the
met
ho
dw
as
ap
pro
pri
ate
);(i
i)d
ou
ble
-bli
nd
ing
(1p
oin
t,o
r2
po
ints
ifth
em
eth
od
wa
sa
pp
rop
ria
te);
an
d(i
ii)
des
crip
tio
no
fw
ith
dra
wa
lsa
nd
dro
po
uts
(1p
oin
t).
Am
ore
com
ple
tev
ersi
on
of
the
tab
le,
incl
ud
ing
do
sea
nd
sch
eme
of
ad
min
istr
ati
on
of
bo
thp
roto
np
um
pin
hib
ito
ra
nd
H2
-an
tag
on
ists
an
dF
orr
est
cla
ssi®
cati
on
,is
av
ail
ab
leo
nre
qu
est
fro
mth
ea
uth
ors
(E-m
ail
:g
isb
ert@
med
itex
.es)
.
920 J. P. GISBERT et al.
Ó 2001 Blackwell Science Ltd, Aliment Pharmacol Ther 15, 917±926

effect of proton pump inhibitors vs. H2-antagonists on
the need for surgery was 0.7 (CI 95%: 0.43±1.13).
Results of the meta-analysis were homogeneous
(P3 � 0.78).
Effect of therapy on mortality
The effect on mortality of the two therapies evaluated in
this meta-analysis can be seen in Figure 3, where the
eight studies selected are represented graphically, inclu-
ding 618 patients treated with proton pump inhibitors
and 621 treated with H2-antagonists. Mortality was
1.6% (95% CI: 0.9±2.9%) in patients treated with proton
pump inhibitors and 2.2% (1.3±3.7%) in those receiving
H2-antagonists. The OR for the effect on the mortality
was 0.69 (95% CI: 0.31±1.57). Results obtained with
different studies were homogeneous (P4 � 0.63).
Sub-analysis on the ef®cacy of therapy
on bleeding peptic ulcer
Dose of proton pump inhibitors. The initial intention was
to perform separate comparisons for the different doses
of omeprazole; however, in only three studies were the
omeprazole doses of 40 mg/8 h used (vs. H2-antago-
nists in bolus injections), so the number of studies was
considered too small to combine and compare the
results. When we again attempted to perform separate
comparisons with omeprazole, doses of 40 mg/12 h, we
found only three studies, and in each fewer than 30
patients were treated with those doses, thus precluding
adequate comparison of the study results.
Scheme of administration of the drugs. Five studies
evaluated the effect of both therapies given in bolus
injections on persistent or recurrent bleeding rate (402
patients received proton pump inhibitors, and 369
received H2-antagonists). Re-bleeding was detected in
6% (95% CI: 3.6±8.3%) and 8.1% (95% CI: 5.3±10.9%),
respectively, with an OR for this comparison of 0.57
(95% CI: 0.31±1.05%). When evaluating the need for
surgery, also with bolus injections of both drugs, it was
necessary in 5.3% (95% CI: 3±7.5%) of the patients
treated with proton pump inhibitors, and in 7.2%
(95% CI: 4.6±9.9%) of those receiving H2-antagonists,
with an OR for this comparison of 0.68 (95% CI:
Figure 1. Proton pump inhibitors vs. H2-antagonists. Effect on persistent or recurrent bleeding of peptic ulcer.
Figure 2. Proton pump inhibitors vs. H2-antagonists. Effect on the need for surgery of bleeding peptic ulcer.
PROTON PUMP INHIBITORS VS. H 2 -ANTAGONISTS IN BLEEDING PEPTIC ULCER 921
Ó 2001 Blackwell Science Ltd, Aliment Pharmacol Ther 15, 917±926

0.37±1.26%). Finally, the mortality rate was 1.8%
(95% CI: 0.9±3.8%) and 1.4% (95% CI: 0.6±3.2%),
respectively, with bolus injections of proton pump
inhibitors and H2-antagonists, with an OR of 1.25
(95% CI: 0.40±3.97%). Results obtained in different
studies with bolus injections were homogeneous for all
comparisons. Other comparisons, evaluating other
schemes of administration, were precluded due to the
low number of studies in each group.
Endoscopic (Forrest) classi®cation. Although the initial (a
priori) intention was to perform sub-analyses (plural)
comparing the effect of the therapy on active ulcer
bleeding (Forrest Ia, Ib) and non-active ulcer bleeding
(Forrest IIa, IIb, IIc), the number of studies was
considered too small to combine and compare the
results. Therefore, we classi®ed (a posteriori, ad hoc
analysis) the studies into those with high or low risk of
persistent or recurrent bleeding. Thus, persistent or
recurrent bleeding in high risk patients (Forrest Ia, Ib
and IIa, that is, with active bleeding or non-bleeding
visible vessel) occurred in 13.2% (95% CI: 7.9±18%) of
the patients treated with proton pump inhibitors and in
34.5% (95% CI: 27±42%) of those treated with H2-
antagonists (OR 0.28; 95% CI: 0.16±0.48). The het-
erogeneity of the results (P5 � 0.02) disappeared when
we excluded the study of Villanueva et al., in which
adjunct endoscopic therapy was performed (OR 0.15;
95% CI: 0.08±0.3; P6 � 0.64).31
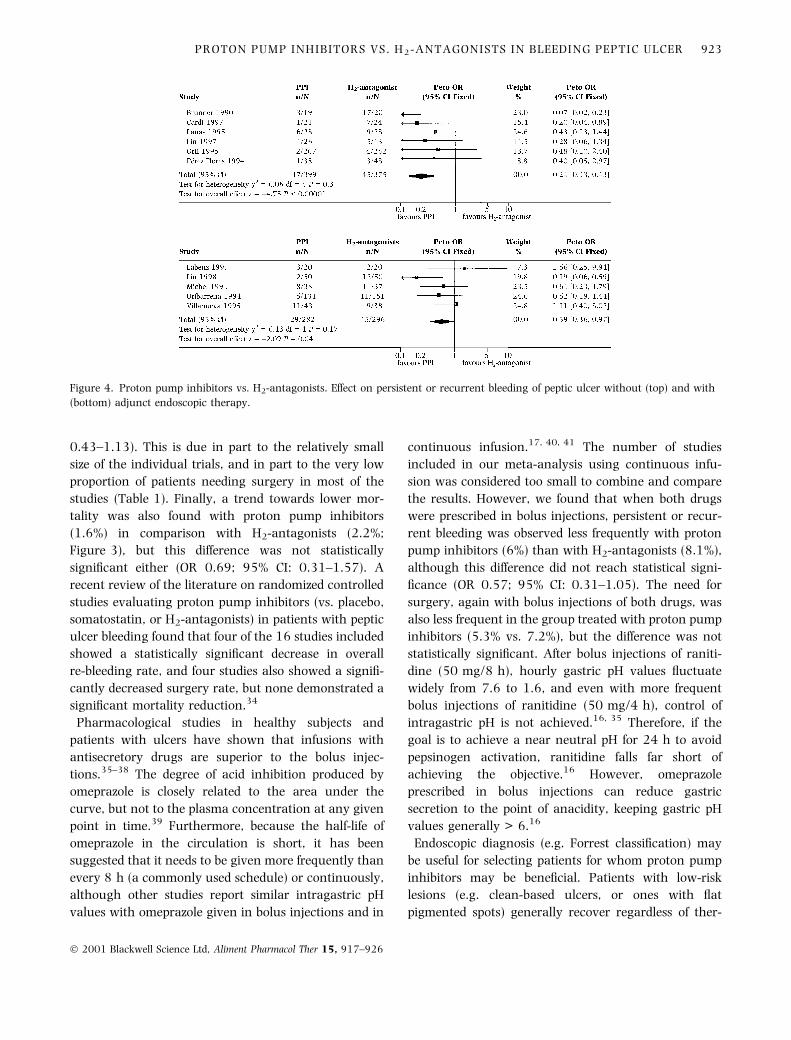
Endoscopic therapy. In patients who did not have
endoscopic therapy, persistent or recurrent bleeding
was reported in 4.3% (95% CI: 2.7±6.7%) of those
treated with proton pump inhibitors and in 12%
(95% CI: 8.7±15%) of those treated with H2-antagonists
(OR 0.24; 95% CI: 0.13±0.43). The corresponding
®gures for patients having endoscopic therapy (during
the treatment) were 10.3% (95% CI: 6.7±13.8%) and
15.2% (95% CI: 11.1±19.3%) (OR 0.59; 95% CI:
0.36±0.97%; Figure 4). The homogeneity of the results
(P7 � 0.27) was higher when we excluded the study of
Lin et al., in which heater probe thermocoagulation or
multipolar electrocoagulation instead of sclerosis was
performed (OR 0.77; 95% CI: 0.04±1.35%; P8 � 0.78).30
DISCUSSION
Pharmacological treatment for bleeding peptic ulcer has
traditionally included H2-antagonists drugs, with con-
troversial results. It remains unknown whether more
recent and powerful antisecretory drugs, namely proton
pump inhibitors, are superior to H2-antagonists in the
treatment of bleeding peptic ulcer. Several well-designed
randomized clinical trials comparing the two drugs have
been published, but the results have been contradictory,
and to date no formal meta-analysis has been per-
formed.
In the present meta-analysis, 11 studies ful®lled the
inclusion criteria and compared the effect of proton
pump inhibitors vs. H2-antagonists on bleeding peptic
ulcer (Table 1).15, 16, 25±33 When combining the results
of the studies (Figure 1) it was observed that persistent
or recurrent bleeding was less frequent with proton
pump inhibitors (6.7%) than with H2-antagonists
(13.4%) (OR 0.4; 95% CI: 0.27±0.59%). Surgery was
needed in 5.2% of the patients treated with proton
pump inhibitors, and in 6.9% of those receiving
H2-antagonists (Figure 2), which indicates a trend
towards better results with the proton pump inhibitors,
though this difference was not statistically signi®cant.
Nevertheless, the available data on the need for surgery
may lack the power to reliably demonstrate a number of
moderate but clinically important effects (the OR was
0.7, but con®dence interval limits ranged from to
Figure 3. Proton pump inhibitors vs. H2-antagonists. Effect on the mortality for bleeding peptic ulcer.
922 J. P. GISBERT et al.
Ó 2001 Blackwell Science Ltd, Aliment Pharmacol Ther 15, 917±926
0.43±1.13). This is due in part to the relatively small
size of the individual trials, and in part to the very low
proportion of patients needing surgery in most of the
studies (Table 1). Finally, a trend towards lower mor-
tality was also found with proton pump inhibitors
(1.6%) in comparison with H2-antagonists (2.2%;
Figure 3), but this difference was not statistically
signi®cant either (OR 0.69; 95% CI: 0.31±1.57). A
recent review of the literature on randomized controlled
studies evaluating proton pump inhibitors (vs. placebo,
somatostatin, or H2-antagonists) in patients with peptic
ulcer bleeding found that four of the 16 studies included
showed a statistically signi®cant decrease in overall
re-bleeding rate, and four studies also showed a signi®-
cantly decreased surgery rate, but none demonstrated a
signi®cant mortality reduction.34
Pharmacological studies in healthy subjects and
patients with ulcers have shown that infusions with
antisecretory drugs are superior to the bolus injec-
tions.35±38 The degree of acid inhibition produced by
omeprazole is closely related to the area under the
curve, but not to the plasma concentration at any given
point in time.39 Furthermore, because the half-life of
omeprazole in the circulation is short, it has been
suggested that it needs to be given more frequently than
every 8 h (a commonly used schedule) or continuously,
although other studies report similar intragastric pH
values with omeprazole given in bolus injections and in
continuous infusion.17, 40, 41 The number of studies
included in our meta-analysis using continuous infu-
sion was considered too small to combine and compare
the results. However, we found that when both drugs
were prescribed in bolus injections, persistent or recur-
rent bleeding was observed less frequently with proton
pump inhibitors (6%) than with H2-antagonists (8.1%),
although this difference did not reach statistical signi-
®cance (OR 0.57; 95% CI: 0.31±1.05). The need for
surgery, again with bolus injections of both drugs, was
also less frequent in the group treated with proton pump
inhibitors (5.3% vs. 7.2%), but the difference was not
statistically signi®cant. After bolus injections of raniti-
dine (50 mg/8 h), hourly gastric pH values ¯uctuate
widely from 7.6 to 1.6, and even with more frequent
bolus injections of ranitidine (50 mg/4 h), control of
intragastric pH is not achieved.16, 35 Therefore, if the
goal is to achieve a near neutral pH for 24 h to avoid
pepsinogen activation, ranitidine falls far short of
achieving the objective.16 However, omeprazole
prescribed in bolus injections can reduce gastric
secretion to the point of anacidity, keeping gastric pH
values generally > 6.16
Endoscopic diagnosis (e.g. Forrest classi®cation) may
be useful for selecting patients for whom proton pump
inhibitors may be bene®cial. Patients with low-risk
lesions (e.g. clean-based ulcers, or ones with ¯at
pigmented spots) generally recover regardless of ther-
Figure 4. Proton pump inhibitors vs. H2-antagonists. Effect on persistent or recurrent bleeding of peptic ulcer without (top) and with
(bottom) adjunct endoscopic therapy.
PROTON PUMP INHIBITORS VS. H 2 -ANTAGONISTS IN BLEEDING PEPTIC ULCER 923
Ó 2001 Blackwell Science Ltd, Aliment Pharmacol Ther 15, 917±926

apy. Our results show that persistent or recurrent
bleeding in high risk patients (Forrest Ia, Ib and IIa, e.g.
with active bleeding or non-bleeding visible vessel) was
less frequent with proton pump inhibitors than with
H2-antagonists (13.2% vs. 34.5%; OR 0.28; 95%
CI: 0.16±0.48). This difference was higher than that
previously calculated with all studies (OR for all Forrest
stages: 0.4), suggesting that the bene®cial effect of
proton pump inhibitors (against H2-antagonists) is
similar or even more marked in patients with Forrest I
or IIa ulcers.
Nevertheless, we should bear in mind the possible
confounding role of adjunct endoscopic therapy, which
has been proven effective in the treatment of bleeding
ulcers.42 The study of Villanueva et al., in which
endoscopic therapy was performed and showed no
bene®t of omeprazole over H2-antagonists in Forrest Ia,
Ib and IIa patients, contrasts markedly with the other
studies (in which, excepting the study of Lin et al.,
endoscopy therapy was not performed).15, 31 The results
were no longer heterogeneous when the study of
Villanueva et al. was excluded from the analysis.31 In
this respect, our meta-analysis shows that in patients
who do not have endoscopic therapy, persistent or
recurrent bleeding is less frequent with proton pump
inhibitors than with H2-antagonists (4.3% vs. 12%; OR
0.24) (Figure 4). However, the difference with these two
drugs on patients who underwent endoscopic therapy
was less clear (10.3% vs. 15.2%; OR 0.59; Figure 4).
Furthermore, the differences were no longer statistically
signi®cant (and homogeneity increased) when we
excluded the study of Lin et al., in which heater probe
thermocoagulation or multipolar electrocoagulation
instead of sclerosis was performed.30 These results
suggest that the bene®cial effect of proton pump
inhibitors on bleeding peptic ulcer, when compared
with H2-antagonists, may be mainly or exclusively
observed in those patients not having adjunct endo-
scopic therapy, and that when sclerosis is performed the
advantage of proton pump inhibitors could be limited or
even lost altogether. In other words, injection therapy
may be so effective that the additional effect of the
antisecretory drugs may be minimal. Because endo-
scopic therapy for bleeding peptic ulcers is routinely
performed (when indicated) in most centres, the role of
proton pump inhibitors may be considered less import-
ant in the future if these data are con®rmed. Most of
the patients with an actively bleeding ulcer or a visible
vessel have a very low risk of re-bleeding after
endoscopic therapy and will not therefore bene®t from
any adjunct therapy. Nonetheless, recurrence of bleed-
ing, even with endoscopic therapy, is a signi®cant
problem in selected patients with bleeding peptic ulcer.1
The risk factors for re-bleeding after endoscopic therapy
have been previously described: ulcer greater than
2 cm; haemodynamic instability; advanced age; active
haemorrhage during endoscopy; and location high in
the lesser curvature.43, 44 Measures leading to a reduc-
tion in bleeding rate in this group of patients could
result in a better outcome, although this point has not
been speci®cally investigated. Further prospective stud-
ies are needed to compare endoscopic therapy vs.
combined therapy in this sub-group of patients with
high risk of re-bleeding.
How do we explain the fact that results are better with
proton pump inhibitors than with H2-antagonists in
bleeding peptic ulcer? Some authors have demonstrated
that intravenous omeprazole produces consistently
high intragastric pH values in patients with bleeding
peptic ulcers, whereas H2-antagonists are less
effective.14±16, 41 This loss of effectiveness of ranitidine
may be due to tolerance (tachyphylaxis), which is
known to occur in response to repetitive doses of
H2-antagonists, but has never been found with proton
pump inhibitors.45, 46 As stated above, both acid and
pepsin alter coagulation by interfering with the coagu-
lation system, ®brinogen polymerization, and platelet
aggregation.4 Therefore, parenteral proton pump inhib-
itors seem to be more effective than H2-antagonists in
keeping the gastric pH above the proteolytic range for
pepsin in bleeders. Furthermore, omeprazole can heal
96% of ranitidine-resistant peptic ulcerations, and
several case reports have been published where intra-
venous omeprazole was able to stop the bleeding from
peptic lesions that did not respond to ranitidine
treatment.10 26, 46±51 Finally, because intravenous proton
pump inhibitors are more expensive than intravenous
H2-antagonists, further studies are needed to evaluate
the cost±effectiveness relationship of these two drugs.
The present meta-analysis has several limitations.
First, the signi®cant variability between studies makes
combination of the results dif®cult. For example, there
was a marked variability between studies with respect
to location of peptic ulcer, dose of proton pump
inhibitors and H2-antagonists, scheme of administration
of the drugs, Forrest classi®cation of the bleeding ulcer,
and concomitant endoscopic therapy. Second, the
relatively low number of studies (and patients in each
924 J. P. GISBERT et al.
Ó 2001 Blackwell Science Ltd, Aliment Pharmacol Ther 15, 917±926

study) included in the meta-analysis sometimes preclu-
ded adequate comparisons of outcomes, depending on
the status of important variables such as dose and
scheme of administration of proton pump inhibitors, or
Forrest classi®cation. Furthermore, comparisons
depending on Forrest classi®cation were performed
a posteriori (ad hoc analysis) and were not planned
a priori. Finally, overall analysis must be quali®ed
because of the poor data that are available (see quality
scores of the studies in Table 1).
In summary, the results of the present meta-analysis
indicate that proton pump inhibitors are more effective
than H2-antagonists in preventing persistent or recur-
rent bleeding from peptic ulcer, although this advantage
seems to be restricted to those patients who do not have
adjunct sclerosis therapy. Nevertheless, the data are too
scarce and heterogeneous to draw de®nitive conclusions
and further randomized clinical trials comparing proton
pump inhibitors and H2-antagonists are clearly
warranted.
ACKNOWLEDGEMENTS
We are indebted to Brenda Ashley and Michael
Maudsley for assistance with the English.
This study was not funded by any pharmaceutical
company.
REFERENCES
1 Laine L, Peterson WL. Bleeding peptic ulcer. N Engl J Med
1994; 331: 717±27.
2 Mignon M, Penston JG, Deltenre M, Ruszniewski P, Dobrill G.
Natural history of duodenal ulcer disease: are we at a turning
point? Gastroenterol Int 1994; 7: 95±113.
3 Gilbert DA. Epidemiology of upper gastrointestinal bleeding.
Gastrointest Endosc 1990; 36: S8±13.
4 Green FW Jr, Kaplan MM, Curtis LE, Levine PH. Effect of acid
and pepsin on blood coagulation and platelet aggregation. A
possible contributor to prolonged gastroduodenal mucosal
hemorrhage. Gastroenterology 1978; 74: 38±43.
5 Patchett SE, O'Donoghue DP. Pharmacological manipulation
of gastric juice: thrombelastographic assessment and impli-
cations for treatment of gastrointestinal haemorrhage. Gut
1995; 36: 358±62.
6 Patchett SE, Enright H, Afdhal N, O'Connell W, O'Donoghue
DP. Clot lysis by gastric juice: an in vitro study. Gut 1989; 30:
1704±7.
7 Chaimoff C, Creter D, Djaldetti M. The effect of pH on platelet
and coagulation factor activities. Am J Surg 1978; 136:
257±9.
8 RollhauSeries C, Fleischer DE. Nonvariceal upper gastroin-
testinal bleeding: an update. Endoscopy 1997; 29: 91±105.
9 Collins R, Langman M. Treatment with histamine H2 antag-
onists in acute upper gastrointestinal hemorrhage. Implica-
tions of randomized trials. N Engl J Med 1985; 313: 660±6.
10 Falk A, Darle N, Haglund U, Tornqvist A. Histamine2-receptor
antagonists in gastroduodenal ulcer haemorrhage. Scand J
Gastroenterol 1985; 110(Suppl.): 95±100.
11 Reynolds JR, Walt RP, Clark AG, Hardcastle JD, Langman MJ.
Intragastric pH monitoring in acute upper gastrointestinal
bleeding and the effect of intravenous cimetidine and raniti-
dine. Aliment Pharmacol Ther 1987; 1: 23±30.
12 Peterson WL, Barnett C, Feldman M, Richardson CT. Reduc-
tion of twenty-four-hour gastric acidity with combination
drug therapy in patients with duodenal ulcer. Gastroenterol-
ogy 1979; 77: 1015±20.
13 Merki HS, Witzel L, Kaufman D, et al. Continuous intravenous
infusions of famotidine maintain high intragastric pH in
duodenal ulcer. Gut 1988; 29: 453±7.
14 Labenz J, Borsch G. Role of Helicobacter pylori eradication in
the prevention of peptic ulcer bleeding relapse. Digestion
1994; 55: 19±23.
15 Lin HJ, Lo WC, Perng CL, Wang K, Lee FY. Can optimal acid
suppression prevent rebleeding in peptic ulcer patients with a
non-bleeding visible vessel: a preliminary report of a ran-
domized comparative study. Hepatogastroenterology 1997;
44: 1495±9.
16 Lanas A, Artal A, Blas JM, Arroyo MT, Lopez-Zaborras J, Sainz
R. Effect of parenteral omeprazole and ranitidine on gastric pH
and the outcome of bleeding peptic ulcer. J Clin Gastroenterol
1995; 21: 103±6.
17 Kiilerich S, Rannem T, Elsborg L. Effect of intravenous infu-
sion of omeprazole and ranitidine on twenty-four-hour
intragastric pH in patients with a history of duodenal ulcer.
Digestion 1995; 56: 25±30.
18 Khuroo MS, Yattoo GN, Javid G, et al. A comparison of
omeprazole and placebo for bleeding peptic ulcer. N Engl J Med
1997; 336: 1054±8.
19 Hasselgren G, Lind T, Lundell L, et al. Continuous intravenous
infusion of omeprazole in elderly patients with peptic ulcer
bleeding. Results of a placebo-controlled multicenter study.
Scand J Gastroenterol 1997; 32: 328±33.
20 Schaffalitzky de Muckadell OB, Havelund T, Harling H, et al.
Effect of omeprazole on the outcome of endoscopically treated
bleeding peptic ulcers. Randomized double-blind placebo-
controlled multicentre study. Scand J Gastroenterol 1997; 32:
320±7.
21 Daneshmend TK, Hawkey CJ, Langman MJ, Logan RF, Long
RG, Walt RP. Omeprazole versus placebo for acute upper
gastrointestinal bleeding: randomised double blind controlled
trial. Br Med J 1992; 304: 143±7.
22 Jadad AR, Moore RA, Carroll D, et al. Assessing the quality of
reports of randomized clinical trials: Is blinding necessary?
Controlled Clin Trials 1996; 17: 1±12.
23 Foster DN, Miloszewski KJ, Losowsky MS. Stigmata of recent
haemorrhage in diagnosis and prognosis of upper gastroin-
testinal bleeding. Br Med J 1978; 1: 1173±7.
PROTON PUMP INHIBITORS VS. H 2 -ANTAGONISTS IN BLEEDING PEPTIC ULCER 925
Ó 2001 Blackwell Science Ltd, Aliment Pharmacol Ther 15, 917±926
24 Clarke M, Oxman AD, eds. Cochrane Reviewers's Handbook
4.0. In: Review Manager (RevMan) 4.0. Oxford: The Cochrane
Collaboration, 1999.
25 Labenz J, Peitz U, Leusing C, Tillenburg B, Blum AL, Borsch G.
Ef®cacy of primed infusions with high dose ranitidine and
omeprazole to maintain high intragastric pH in patients with
peptic ulcer bleeding: a prospective randomised controlled
study. Gut 1997; 40: 36±41.
26 Brunner G, Chang J. Intravenous therapy with high doses of
ranitidine and omeprazole in critically ill patients with bleeding
peptic ulcerations of the upper intestinal tract: an open
randomized controlled trial. Digestion 1990; 45: 217±25.
27 Perez Flores R, Garcia Molinero MJ, Herrero Quiros C, et al.
The treatment of upper digestive hemorrhage of peptic origin:
intravenous ranitidine versus intravenous omeprazole. Rev
Esp Enferm Dig 1994; 86: 637±41.
28 Orti E, Canelles P, Quiles F, et al. Does the antisecretory agent
used affect the evolution of upper digestive hemorrhage? Rev
Esp Enferm Dig 1995; 87: 427±30 (in Spanish).
29 Uribarrena R, Bajador E, Simon MA, Sebastian JJ, Gomollon F.
Omeprazole and cimetidine in the treatment of upper digestive
hemorrhage. Rev Esp Enferm Dig 1994; 86: 878±83 (in
Spanish).
30 Lin HJ, Lo WC, Lee FY, Perng CL, Tseng GY. A prospective
randomized comparative trial showing that omeprazole pre-
vents rebleeding in patients with bleeding peptic ulcer after
successful endoscopic therapy. Arch Intern Med 1998; 158:
54±8.
31 Villanueva C, Balanzo J, Torras X, et al. Omeprazole versus
ranitidine as adjunct therapy to endoscopic injection in act-
ively bleeding ulcers: a prospective and randomized study.
Endoscopy 1995; 27: 308±12.
32 Michel P, Duhamel C, Bazin B, et al. Lansoprazole versus
ranitidine in the prevention of early recurrences of digestive
hemorrhages from gastroduodenal ulcers. Randomized dou-
ble-blind multicenter study. Gastroenterol Clin Biol 1994; 18:
1102±5 (in French).
33 Cardi M, Muttillo IA, Amadori L, et al. Intravenous omepraz-
ole versus ranitidine in the treatment of hemorrhagic duode-
nal ulcer: a prospective randomized study. Ann Chir 1997;
51: 136±9 (in French).
34 Bustamante M, Stollman N. The ef®cacy of proton-pump
inhibitors in acute ulcer bleeding: a qualitative review. J Clin
Gastroenterol 2000; 30: 7±13.
35 Ballesteros MA, Hogan DL, Koss MA, Isenberg JI. Bolus or
intravenous infusion of ranitidine: effects on gastric pH and
acid secretion. A comparison of relative ef®cacy and cost. Ann
Intern Med 1990; 112: 334±9.
36 Heiselman DE, Hulisz DT, Fricker R, Bredle DL, Black LD.
Randomized comparison of gastric pH control with intermittent
and continuous intravenous infusion of famotidine in ICU
patients. Am J Gastroenterol 1995; 90: 277±9.
37 Ostro MJ, Russell JA, Soldin SJ, Mahon WA, Jeejeebhoy KN.
Control of gastric pH with cimetidine: boluses versus primed
infusions. Gastroenterology 1985; 89: 532±7.
38 Peterson WL, Richardson CT. Sustained fasting achlorhydria:
a comparison of medical regimens. Gastroenterology 1985;
88: 666±9.
39 Cederberg C, Andersson T, Skanberg J. Omeprazole phar-
macokinetics and metabolism in man. Scand J Gastroenterol
1989; 24(Suppl. 166): 33±40.
40 Brunner G, Luna P, Thiesemann C. Drugs for pH control in
upper gastrointestinal bleeding. Aliment Pharmacol Ther
1995; 9: 47±50.
41 Artal A, Lanas A, Barrao ME, Moliner FJ, Blas JM, Lopez J.
Evaluation of intravenous ranitidine and omeprazole effect on
the 24-hour gastric ph-metry in duodenal ulcer hemorrhage.
Rev Esp Enferm Dig 1996; 88: 191±6 (in Spanish).
42 Cook DJ, Guyatt GH, Salena BJ, Laine LA. Endoscopic therapy
for acute nonvariceal upper gastrointestinal hemorrhage: a
meta-analysis. Gastroenterology 1992; 102: 139±48.
43 Brullet E, Calvet X, Campo R, Rue M, Catot LI, Donoso LI.
Factors predicting failure of endoscopic injection therapy
in bleeding duodenal ulcer. Gastrointest Endosc 1996; 43:
111±6.
44 Brullet E, Campo R, Calvet X, Coroleu D, Rivero E, Simo Deu J.
Factors related to the failure of endoscopic therapy for bleed-
ing gastric ulcer. Gut 1996; 39: 155±8.
45 Wilder-Smith CH, Merki HS. Tolerance during dosing with
H2-receptor antagonists. An overview. Scand J Gastroenterol
1992; 193(Suppl.): 14±9.
46 Merki HS, Wilder-Smith CH. Do continuous infusions of
omeprazole and ranitidine retain their effect with prolonged
dosing? Gastroenterology 1994; 106: 60±4.
47 Brunner G, Creutzfeldt W. Omeprazole in the long-term
management of patients with acid-related diseases resistant
to ranitidine. Scand J Gastroenterol 1989; 166(Suppl.):
101±5.
48 Collier DS, Crampton J, Everett WG. Acute haemorrhagic
gastritis controlled by omeprazole. Lancet 1989; 1: 776
(Letter).
49 Hetzel DJ, Bonnin M. Long term management of hemorrhagic
esophagitis with cimetidine and omeprazole. Aust N Z J Med
1986; 16: 226±8.
50 Vezzadini P, Tomassetti P, Marrano D, Labo G. Life-threaten-
ing gastrointestinal hemorrhage with omeprazole. Dig Dis Sci
1988; 33: 766±7 (Letter).
51 Gabbrielli M, Pennati P, Trallori G, Vannozzi G. Use of intra-
venous omeprazole in emergency cases of gastroduodenal
hemorrhage. Am J Gastroenterol 1992; 87: 1229 (Letter).
926 J. P. GISBERT et al.
Ó 2001 Blackwell Science Ltd, Aliment Pharmacol Ther 15, 917±926