proposal form - `The Global Fund to Fight AIDS, Tuberculosis ...
72
Application Form for Proposals to the Global Fund Page 1 of 72 Geneva, March 2003 For the use of the Global Fund Secretariat: Date Received: ID No: PROPOSAL FORM Before starting to fill out this proposal form, please read the Guidelines for Proposals carefully. When completing each question in the proposal form, please note the reference given to the corresponding section of the guidelines. This form is divided into 4 main parts : SECTION I is an executive summary of the proposal and should be filled out only AFTER the rest of the form has been completed. SECTION II asks for information on the applicant. SECTION III seeks summary information on the country setting. SECTIONS IV to VIII seeks details on the content of the proposal for each component. How to use this form : 1. Please read ALL questions carefully. Specific instructions for answering the questions are provided. 2. Where appropriate, indications are given as to the approximate length of the answer to be provided. Please try, as much as possible, to respect these indications. 3. All answers, unless specified otherwise, should be provided in the form. If submitting additional pages, please mark clearly on the pages which section and numbered question this relates to. 4. To avoid duplication of efforts, we urge you to make maximum use of existing information (e.g., from programme documents written for other donors/funding agencies). 5. When using tables, all cells are automatically expanded as you write in them. Should you wish to add a new row, place the cursor on the outside of the cell at the bottom right-hand corner of the table and press ENTER. To copy tables, select all cells in the table and press CTRL+C. Place cursor where you would like the new table to begin and press CTRL+V. 6. Please DO NOT fill in shaded cells.
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of proposal form - `The Global Fund to Fight AIDS, Tuberculosis ...

Application Form for Proposals to the Global Fund Page 1 of 72
Geneva, March 2003 For the use of the Global Fund Secretariat: Date Received: ID No:
PROPOSAL FORM
Before starting to fill out this proposal form, please read the Guidelines for Proposals carefully. When completing each question in the proposal form, please note the reference given to the corresponding section of the guidelines.
This form is divided into 4 main parts: SECTION I is an executive summary of the proposal and should be filled out only AFTER the rest of the form has been completed. SECTION II asks for information on the applicant. SECTION III seeks summary information on the country setting. SECTIONS IV to VIII seeks details on the content of the proposal for each component. How to use this form: 1. Please read ALL questions carefully. Specific instructions for answering the
questions are provided.
2. Where appropriate, indications are given as to the approximate length of the answer to be provided. Please try, as much as possible, to respect these indications.
3. All answers, unless specified otherwise, should be provided in the form. If submitting additional pages, please mark clearly on the pages which section and numbered question this relates to.
4. To avoid duplication of efforts, we urge you to make maximum use of existing information (e.g., from programme documents written for other donors/funding agencies).
5. When using tables, all cells are automatically expanded as you write in them. Should you wish to add a new row, place the cursor on the outside of the cell at
the bottom right-hand corner of the table and press ENTER. To copy tables, select all cells in the table and press CTRL+C. Place cursor
where you would like the new table to begin and press CTRL+V.
6. Please DO NOT fill in shaded cells.

Application Form for Proposals to the Global Fund Page 2 of 72
SECTION I: Executive summary of Proposal
Please note: The Executive Summary will be used to present an overview of the proposal to various members of the Secretariat, the Technical Review Panel and the Board of the Global Fund. The proposal once approved becomes public information. TO BE COMPLETED AFTER THE OTHER SECTIONS HAVE BEEN FILLED OUT General information: Table I.a Proposal title (Title should reflect scope of proposal):
Building a coordinated national response to tuberculosis and HIV/AIDS in Macedonia
Country or region covered:
Macedonia
Name of applicant: CCM Macedonia Constituencies represented in CCM
6 Government – Health ministry
6 UN/Multilateral agency
(write the number of members from each
14 Government – Other ministries
0 Bilateral agency
Category):
6 NGO/Community-based organisations
4 Academic/Educational Organisations
2 Private Sector 3 Religious/Faith groups
1 People living with HIV/TB/Malaria*
5 Other (please specify): Professional Associations/Chambers
If the proposal is NOT submitted through a CCM, briefly state why:
Not Applicable
Specify which component(s) this proposal is targeting and the amount requested from the Global Fund**:
Table I.b Amount requested from the GF (USD thousands) Year 1 Year 2 Year 3 Year 4 Year 5 Total Component(s) x HIV/AIDS 2442 1907 1961 N/A N/A 6310
(mark with X): x Tuberculosis 723 419 330 326 335 2133
Malaria
HIV/TB
Total 3165 2326 2291 326 335 8443
Total funds from other sources for activities related to proposal
1921 2083 2294 2348 2404 11050
Please specify how you would like your proposal to be evaluated*** (mark with X): The Proposal should be evaluated as a whole The Proposal should be evaluated as separate components x
* According to national epidemiological profile/characteristics ** If the proposal is fully integrated, whereby one component cannot be separated from another, and where splitting budgets would not be realistic or feasible, only fill the “Total” row. *** This will ensure the proposal is evaluated in the same spirit as it was written. If evaluated as a whole, all components will be considered as parts of an integrated proposal. If evaluated as separate components, each component will be considered as a stand-alone component.

Application Form for Proposals to the Global Fund Page 3 of 72
Brief proposal summary (1 page) (please include quantitative information where possible): • Describe the overall goals, objectives and main activities per component,
including expected results and timeframe for achieving these results: TB Component – The goal of this component is to achieve WHO recommended targets for TB control. This will be achieved by pursuing three objectives. The first is to strengthen the national health care system for TB patients. Activities within this objective will strengthen hospital treatment, laboratory diagnosis and drug management in the country so that all laboratories have quality assurance results available by the end of year 3 and all units are using the new drug management system by the end of year 4. The second objective is to expand coverage of the DOTS program from 50-100% of the country. Activities include refurbishing the National Education Center in TB Control, training of staff, IEC and social support for TB patients so that the number of units implementing DOTS rises from 16 to 32 by year 4 and 100% of patients receive DOTS during the initial phase by year 4. The third objective is to improve the supervision, monitoring and evaluation of the national TB program. Activities involve strengthening national data collection and monitoring and supervisions systems so that all units are implementing a package of activities by year 4 and the number of people defaulting treatment has fallen to 5% by year 5. HIV/AIDS Component – The goal of this component is to build a coordinated national response to prevent a major HIV/AIDS epidemic in Macedonia. This will be achieved by pursuing ten objectives. The first six of these are focused on preventing HIV transmission amongst vulnerable groups including young people, injecting drug users, sex workers, men who have sex with men, the Roma community and prisoners. Expected results include dramatically increasing the number of members of vulnerable groups reached with targeted HIV/AIDS interventions in three years, for example increasing IDUs reached from 2680 to 6500, sex workers from 103 to 250, men who have sex with men from 250 to 750 and reaching 21 300 Roma people and 1500 prisoners, where currently there are no HIV/AIDS interventions targeted for these groups. The seventh objective aims to improve access to and the quality of HIV counseling and testing. The expected result of this is that the number of people being tested voluntarily for HIV rises from 250 currently to 1000 in three years. The eighth objective is to improve HIV/AIDS surveillance in the country. The expected result of this is that the country will produce reports on biologic surveillance figures and figures for behavioral surveillance amongst vulnerable groups annually. The ninth objective is to provide health care and psychosocial support for PLWHAs. The expected results of this are that the numbers receiving such services will increase including at least 20 people to be receiving ARVs within 3 years. The tenth objective is to strengthen coordination and capacity of the national response to HIV/AIDS. The expected result is that within three years 90% of CCM members express the view that capacity is increasing and that the national response is well-coordinated. • Specify the beneficiaries of the proposal per component and the benefits
expected to accrue to them (including target populations and their estimated number):
TB Component – Every year 350 TB in-patients and 750 TB outpatients will benefit from improved quality of treatment as a result of rehabilitation of 2 inpatient facilities, improvement of the system for diagnosis and treatment of TB and expansion of the DOTS program. Every year 340 health staff (60 specialists in lung diseases, 200 general practitioners, 20 lab technicians, 60 nurses) will benefit from training. 10 country-level and 10 central-level statisticians will benefit from specially designed software for data collection processing. The general population and vulnerable sub-populations (prisoners, Roma, refugees, internally displaced people) will benefit from education. The country’s entire population will benefit indirectly from decreasing TB morbidity and mortality. HIV/AIDS Component – Members of vulnerable groups will benefit from carefully-targeted interventions aimed at reducing transmission of HIV. Over 500 000 young people will

Application Form for Proposals to the Global Fund Page 4 of 72
receive a brochure about HIV/AIDS and other educational materials within two years. More than 4900 IDUs will benefit from harm reduction programs in 2 years, with at least 1500 benefiting from drug treatment programs within the same time period. Sex workers will receive many benefits including improved access to medical and social services, which is expected to benefit 160 street-based women in 2 years. Men who have sex with men will benefit from improved access to condoms and a centre specific for their needs. Members of the Roma community will benefit from information about HIV/AIDS and improved access to condoms. Prisoners will benefit from being involved in HIV/AIDS prevention activities with 80 being trained as peer educators in 2 years. 900 prisoners are expected to benefit from improved prison health services. A wide range of people will benefit from improved access to counseling and testing, particularly in areas outside of Skopje. Health professionals and others working in the AIDS field will benefit from improved surveillance data and a more coordinated national response to the epidemic. • If there are several components, describe the synergies, if any, expected from the
combination of different components (By synergies, we mean the added value the different components bring to each other, or how the combination of these components may have effects beyond the effects of each component taken)
TB and HIV are inextricably linked to each other with both spreading rapidly amongst socially-marginalised and vulnerable sub-populations. In addition, HIV predisposes to TB and TB is a common opportunistic infection in PLWHAs. Therefore, these programs offer opportunity for considerable synergies between the two components. These include: o The establishment of a joint coordinating mechanism for the two diseases o Close cooperation between the two sectors in the development of this proposal,
particularly sections 1-3 o Measures to improve capacity to tackle one disease will inevitably benefit the other,
particularly where these result in increased capacity within the health sector. o Activities targeting particularly vulnerable groups with education messages for one
disease will have beneficial effects for the other • Indicate if the proposal is to scale up existing efforts or initiate new activities.
Explain how lessons learned and best practices have been reflected in this proposal and describe innovative aspects to the proposal
TB Component – The activities proposed under the TB component largely build on existing activities and the current health care system. For example, activities within the first objective will strengthen current practices relating to hospital treatment, laboratory diagnosis and drug management. In addition, activities have been designed based on international standards of best practice, e.g. relating to DOTS. HIV/AIDS Component – The activities described in this proposal constitute a significant attempt to drastically scale up activities which have been being implemented on a relatively small scale in the country, such as prevention activities amongst young people, IDUs, sex workers, and MSM, counselling and testing, care and support for PLWHAs and surveillance. The program also includes new activities, such as HIV prevention activities among prisoners and with the Roma community. There are many innovative elements in the proposal, such as the development of a partnership between an NGO and a government department to work in prisons. The activities described in this proposal build on experience gained and lessons learned from within the country and also draw on good practice from other countries, for example in the design of harm reduction and drug treatment programs.

Application Form for Proposals to the Global Fund Page 5 of 72
SECTION II: Information about the applicant
Table IIa serves to help you know which questions you should answer in this Section, reflecting the different types of application mechanisms and proposals. For further guidance on who can apply, refer to Guidelines Part II.
Table IIa
Application mechanism
Type of proposal Questions to answer
National CCM Country-wide proposal (Guidelines Para. 10–13) 1–9 Regional CCM Coordinated Regional proposal from multiple
countries reflecting national CCM composition (Guidelines Para. 27-28)
1–10
Small Island States proposal with representation from all participating countries but without need for national CCM (Guidelines Para. 29)
Sub-national CCM Sub-national proposal (Guidelines Para. 30) 1–9 and 11 Non-CCM In-country proposal (Guidelines Para. 31-35) 12 – 16 Regional Non-CCM
Regional proposal (Guidelines Para. 34) 12 – 15 and 17
Proposals from countries in complex emergencies will be dealt with on a case-by-case basis (Guidelines Para. 35) Country Coordinating Mechanism (CCM)
Table IIb
Preliminary questions (Yes/No) a). Has the CCM applied to the Fund in previous rounds? No b). Has the composition of the CCM changed since the last submission? N/A c). If composition of CCM has changed, briefly outline changes (e.g., list of new members or sector representatives):
N/A
1. Name of CCM (e.g., CCM Country name, National Committee to fight AIDS, TB and
Malaria, etc): CCM Macedonia
2. Date of constitution of the current CCM (The date the CCM was formed for the purpose of the Global Fund application. If the CCM builds on or uses existing processes – which is encouraged – please explain this in Question 3):
Macedonia’s CCM was formerly constituted on 14th April 2003 by bringing together existing national commissions on TB and HIV/AIDS (see question 3).
3. Describe the background and the process of forming the CCM (including whether the CCM is an entirely new mechanism or building on existing bodies, how the other partners were contacted and chosen, etc.), (1 paragraph):
The CCM has been established by joining two existing Committees on HIV/AIDS† and TB. Furthermore, both Committees had previously been expanded to include members from other ministries and sectors because previously, members of these bodies had largely been drawn from the Ministry of Health. The selection of which organizations to invite to be members of these two committees was guided by the desire to make them as inclusive and representative as possible, ensuring that key players from a
† Macedonia originally established an AIDS Commission within the MoH in the 1980s. A national multisectoral committee was established in 2003. It is this latter committee that has been used to form part of the CCM.

Application Form for Proposals to the Global Fund Page 6 of 72
variety of sectors were included, for example NGOs, faith-based groups and academic institutions. Each member organization has delegated a person to represent them and their interests in the CCM. CCM formation has been supported and officially recognized by the Government and its constituent ministries. In addition, representatives of the UN Theme and Technical Groups on HIV/AIDS are included within the CCM. It is acknowledged that this process has produced a committee which is larger than that recommended by the Global Fund. However, this has been necessary to ensure adequate and full representation of all interested parties in both diseases in the country. Measures to ensure that the CCM operates effectively are described in detail in section 4.
3.1. If the CCM is or includes an already existing body, briefly describe the work previously done, programmes implemented and results achieved (1 paragraph): The pre-existing committees on AIDS and TB served as advisory bodies to the Ministry of Health. In this capacity they were involved in numerous consultations and have been involved in work on country strategies for the two diseases. These committees were also involved in drafting national programs on preventive health care, TB, immunization and HIV/AIDS. All of these programs have been recognized by the government.
4. Describe the organisational processes (e.g., secretariat, sub-committee, stand-alone; describe the decision-making mechanism. Provide Terms of Reference, operating rules or other relevant documents as attachments), (1 paragraph):
The CCM has two main structures – an advisory committee and a standing committee. The advisory committee consists of all members of the two previous committees on HIV/AIDS and TB. Its main purpose is to ensure that all major stakeholders in the two diseases are included in consultations and discussions. Its functioning is described in a set of Operating Rules (see Annex 1). A smaller Standing Committee of between 10-15 people is responsible for most routine business of the CCM and for ensuring that decisions are taken in a timely manner. Operating rules have also been established for this committee (see Article 9 CCM Operating Rules). This committee took responsibility for writing this proposal and for submitting it for approval to the whole CCM. The standing committee is able to co-opt additional members for specific purposes. The Ministry of Health acts as Secretariat to the CCM through administrative staff nominated by The State Secretary of Health.
5. Describe the mode of operation of the CCM (e.g., frequency of meetings, functions and responsibilities of the CCM. Provide the minutes or records of previous meetings as attachments), (1 paragraph): The advisory/main committee of the CCM will meet at least once per year and will have overall responsibility for following up HIV/AIDS and TB activities described in this proposal. Efforts will be made to make decisions through discussion and by consensus but where this is not possible, decisions will be made by simple majority. The standing committee will meet more frequently, at least six times per year. This committee will prepare draft documents for approval by the main committee and will be responsible for ensuring that CCM decisions are implemented. Copies of sample minutes of meetings of the CCM and its standing committee are attached (Annex 7).
6. Describe plans to enhance the role and functions of the CCM in the next 12
months, including plans to promote partnerships and broader participation as well as communicating with wider stakeholders, if required (1 paragraph):
The CCM, in general, and its standing committee will carefully monitor the performance of the CCM over time and make recommendations for improvement and strengthening as appropriate. In particular, the CCM will review regularly the size of the main committee and consider whether it is possible to reduce this without adversely affecting stakeholder ownership of the process. CCM proceedings will be a matter of public record and the standing committee will endeavour to ensure that the activities of the CCM and any programs it operates are effectively communicated with

Application Form for Proposals to the Global Fund Page 7 of 72
key stakeholders, in particular, and the country’s population, in general.

Application Form for Proposals to the Global Fund Page 8 of 72
7. Members of the CCM
Please note: All representatives of organisations included in the CCM must sign this page to be included in the original, hard-copy proposal sent to the Secretariat. The signatures must reach the Secretariat before the deadline for submitting proposals. Please print additional pages if necessary, including the following statement:
“We the undersigned hereby certify that we have participated throughout the CCM process and have had sufficient opportunities to influence the process and this application. We have reviewed the final proposal and are happy to support it. We further pledge to continue our involvement in the CCM if the proposal is approved and as it moves to implementation”
Table II.7 Agency/Organisation (including type*)
Name of representative
Title Date Signature
Ministry of Health Dr Rexep Selmani
Minister of Health
Main role in CCM Chair of the CCM and contact person between CCM and senior political structures
Agency/Organisation (including type*)
Name of representative
Title Date Signature
Ministry of Health Dr Nikola Panovski
Deputy Minister of Health
Main role in CCM Deputy Chair of the CCM and Deputy Chair of the National Multisectoral Commission on HIV/AIDS Agency/Organisation (including type*)
Name of representative
Title Date Signature
Ministry of Health Dr Avzilatif Xemaili
State Secretary
Main role in CCM Current Chair of the National Multisectoral Commission on TB
Agency/Organisation (including type*)
Name of representative
Title Date Signature
Ministry of Health Dr Borislav Josifovski
Head of the Department for Preventive and Primary Health care
Main role in CCM Member of the Standing Committee of the CCM and responsible for the development of health protection programmes within the Ministry of Health
* E.g. People living with HIV/TB/malaria, NGOs/Community-based organisations, Private Sector, Religious/Faith-based groups, Academic/Educational Sector, Government Sector.

Application Form for Proposals to the Global Fund Page 9 of 72
“We the undersigned hereby certify that we have participated throughout the CCM process and have had sufficient opportunities to influence the process and this application. We have reviewed the final proposal and are happy to support it. We further pledge to continue our involvement in the CCM if the proposal is approved and as it moves to implementation”
Agency/Organisation (including type*)
Name of representative
Title Date Signature
Ministry of Health Ms Snezana Cicevalieva
Head of the Department for European Integration and International Coordination
Main role in CCM Member of the Standing Committee of the CCM
Agency/Organisation (including type*)
Name of representative
Title Date Signature
Institute for Epidemiology, Faculty of Medicine
Dr Vesna Velik Stefanovska
National AIDS Coordinator
Main role in CCM Member of the Standing Committee of the CCM and current national AIDS Coordinator
Agency/Organisation (including type*)
Name of representative
Title Date Signature
Institute for Lung Diseases and TB
Dr Liljana Simonovska
National TB Coordinator
Main role in CCM Member of the Standing Committee of the CCM and current National TB Coordinator
Agency/Organisation (including type*)
Name of representative
Title Date Signature
Institute for Lung Diseases and TB
Dr Stefan Talevski
TB Specialist
Main role in CCM Member of the Standing Committee of the CCM
“We the undersigned hereby certify that we have participated throughout the CCM process and have had sufficient opportunities to influence the process and this application. We have reviewed the final proposal and are

Application Form for Proposals to the Global Fund Page 10 of 72
happy to support it. We further pledge to continue our involvement in the CCM if the proposal is approved and as it moves to implementation”
Agency/Organisation (including type*)
Name of representative
Title Date Signature
Institute for Lung Diseases and TB
Dr Cveta Vragoterova
TB Specialist
Main role in CCM Member of the National Multisectoral Commission on TB
Agency/Organisation (including type*)
Name of representative
Title Date Signature
Private Sector Dr Teuta Damjaha
Representative
Main role in CCM Member
Agency/Organisation (including type*)
Name of representative
Title Date Signature
Associations of Private Doctors
Dr Stoe Stojmanovski
Representative
Main role in CCM Member
Agency/Organisation (including type*)
Name of representative
Title Date Signature
Ministry of Education and Science
Ms Emilija Stavridis
Adviser
Main role in CCM Representative of the Ministry of Education and science and has key role within the CCM in giving advice on inclusion of HIV/AIDS/STIs related topics in the school curricula
Agency/Organisation (including type*)
Name of representative
Title Date Signature
Ministry of Education and Science
Ms Naziktere Sulejmani
Adviser
Main role in CCM Representative of the Ministry of Education and science and has key role within the CCM in giving advice on inclusion of HIV/AIDS/STIs related topics in the school curricula

Application Form for Proposals to the Global Fund Page 11 of 72
“We the undersigned hereby certify that we have participated throughout the CCM process and have had sufficient opportunities to influence the process and this application. We have reviewed the final proposal and are happy to support it. We further pledge to continue our involvement in the CCM if the proposal is approved and as it moves to implementation”
Agency/Organisation (including type*)
Name of representative
Title Date Signature
Ministry of Foreign Affairs
Ms Donka Gligorova
Head of Unit
Main role in CCM Member
Agency/Organisation (including type*)
Name of representative
Title Date Signature
Ministry of Justice Dr Zivko Ristevski
Doctor in the Military Hospital
Main role in CCM Representative of the Ministry of Justice and has key role within the CCM in giving advice on promoting safe behavior among young people doing military service Agency/Organisation (including type*)
Name of representative
Title Date Signature
Ministry of Interior Dr Vladimir Nikolovski
Medical Adviser
Main role in CCM Member of the Standing Committee of the CCM
Agency/Organisation (including type*)
Name of representative
Title Date Signature
Ministry of Finance Ms Ljubica Jovcevska
Adviser in the Budget Department
Main role in CCM Member of the Standing Committee of the CCM and has key role within the CCM in giving advice on financial issues Agency/Organisation (including type*)
Name of representative
Title Date Signature
Ministry of Justice Mr Ljupco Shapcevski
Head of the prisons
Main role in CCM Representative of the Ministry of Justice and has key role within the CCM in giving advice on preventing HIV transmission among prisoners
* E.g. People living with HIV/TB/malaria, NGOs/Community-based organisations, Private Sector, Religious/Faith-based groups, Academic/Educational Sector, Government Sector.

Application Form for Proposals to the Global Fund Page 12 of 72
“We the undersigned hereby certify that we have participated throughout the CCM process and have had sufficient opportunities to influence the process and this application. We have reviewed the final proposal and are happy to support it. We further pledge to continue our involvement in the CCM if the proposal is approved and as it moves to implementation”
Agency/Organisation (including type*)
Name of representative
Title Date Signature
Cabinet of the President of the Country
Ms Florija Ljatifi
Advisor
Main role in CCM Representative of the cabinet of the President of the country
Agency/Organisation (including type*)
Name of representative
Title Date Signature
General Assembly of Macedonia
Dr Natasha Bikova
Member of the Health Commission
Main role in CCM Member
Agency/Organisation (including type*)
Name of representative
Title Date Signature
General Assembly of Macedonia
Dr Risto Pejoski
Member of the Health Commission
Main role in CCM Member
Agency/Organisation (including type*)
Name of representative
Title Date Signature
Macedonian Medical Association
Dr Violeta Jovanovska
Senior Doctor
Main role in CCM Member
Agency/Organisation (including type*)
Name of representative
Title Date Signature
Macedonian Medical Association
Dr Slobodan Dimitrov
Chief of Laboratory
Main role in CCM Member

Application Form for Proposals to the Global Fund Page 13 of 72
“We the undersigned hereby certify that we have participated throughout the CCM process and have had sufficient opportunities to influence the process and this application. We have reviewed the final proposal and are happy to support it. We further pledge to continue our involvement in the CCM if the proposal is approved and as it moves to implementation”
Agency/Organisation (including type*)
Name of representative
Title Date Signature
Medical Chamber Dr Hristo Pop Hristov
Infectologist
Main role in CCM Member
Agency/Organisation (including type*)
Name of representative
Title Date Signature
Trade Chamber Ms Danica Zimbakova
Pharmacist
Main role in CCM Member
Agency/Organisation (including type*)
Name of representative
Title Date Signature
Health Insurance Fund Dr Jasmina Zafirovska
Representative
Main role in CCM Member of the Standing Committee of the CCM
Agency/Organisation (including type*)
Name of representative
Title Date Signature
NGO HERA Mr Stefan Stojanovik
Executive Director
Main role in CCM Member of the Standing Committee of the CCM and has key role within the CCM in giving advice on promoting safe behavior among vulnerable groups
Agency/Organisation (including type*)
Name of representative
Title Date Signature
NGO HOPS Mr Branko Dokuzovski
Executive Director
Main role in CCM Member of the Standing Committee of the CCM and has key role within the CCM in giving advice on promoting safe behavior among vulnerable groups

Application Form for Proposals to the Global Fund Page 14 of 72
“We the undersigned hereby certify that we have participated throughout the CCM process and have had sufficient opportunities to influence the process and this application. We have reviewed the final proposal and are happy to support it. We further pledge to continue our involvement in the CCM if the proposal is approved and as it moves to implementation”
Agency/Organisation (including type*)
Name of representative
Title Date Signature
NGO MIA Mr Aleksandar Kisman
Representative
Main role in CCM Member of the Standing Committee of the CCM and has key role within the CCM in giving advice on promoting safe behavior among vulnerable groups
Agency/Organisation (including type*)
Name of representative
Title Date Signature
NGO Trust Ms Suzana Peseva
Psychologist
Main role in CCM Representative of the NGO Trust and has key role within the CCM in giving advice on promoting safe behavior among vulnerable groups
Agency/Organisation (including type*)
Name of representative
Title Date Signature
People living with TB Mr Sokrati Zumbulov
Representative
Main role in CCM Member
Agency/Organisation (including type*)
Name of representative
Title Date Signature
Macedonian Information Agency
Ms Elizabeta Veljanovska
Journalist
Main role in CCM Member
Agency/Organisation (including type*)
Name of representative
Title Date Signature
Macedonian Orthodox Church
Mr Zarko Georgievski
Representative
Main role in CCM Member
Agency/Organisation (including type*)
Name of representative
Title Date Signature
Ministry of Health Dr Isljaim Besimi
Representative
Main role in CCM Member

Application Form for Proposals to the Global Fund Page 15 of 72
“We the undersigned hereby certify that we have participated throughout the CCM process and have had sufficient opportunities to influence the process and this application. We have reviewed the final proposal and are happy to support it. We further pledge to continue our involvement in the CCM if the proposal is approved and as it moves to implementation”
Agency/Organisation (including type*)
Name of representative
Title Date Signature
WHO DPR Office Dr Yukka Pukkila
Head of Office
Main role in CCM Member
Agency/Organisation (including type*)
Name of representative
Title Date Signature
WHO Liaison Office Dr Marija Kisman
Liaison Officer
Main role in CCM Member
Agency/Organisation (including type*)
Name of representative
Title Date Signature
UNICEF Ms Debora Comini
Head of Office
Main role in CCM Member
Agency/Organisation (including type*)
Name of representative
Title Date Signature
UNDP Ms Consuelo Vidal
Deputy Resident Representative
Main role in CCM Member
Agency/Organisation (including type*)
Name of representative
Title Date Signature
IOM Pasquale Lupoli
Head of Office
Main role in CCM Member
Agency/Organisation (including type*)
Name of representative
Title Date Signature
World Bank Marie-Hélène Bricknell
Head of Office
Main role in CCM Member
Application Form for Proposals to the Global Fund Page 16 of 72
“We the undersigned hereby certify that we have participated throughout the CCM process and have had sufficient opportunities to influence the process and this application. We have reviewed the final proposal and are happy to support it. We further pledge to continue our involvement in the CCM if the proposal is approved and as it moves to implementation”
Agency/Organisation (including type*)
Name of representative
Title Date Signature
Islamic Community Mr Sherif Deari Representative
Main role in CCM Member
Agency/Organisation (including type*)
Name of representative
Title Date Signature
Agency for Youth and Sport
Ms Vesna Cupik
Representative
Main role in CCM Member
Agency/Organisation (including type*)
Name of representative
Title Date Signature
Ministry of Local Self Government
Mr Miralem Asani
Advisor
Main role in CCM Member
Agency/Organisation (including type*)
Name of representative
Title Date Signature
Macedonian Red Cross Dr Vasil Tunev Representative
Main role in CCM Member
Agency/Organisation (including type*)
Name of representative
Title Date Signature
NGO El Hilal Dr Mair Iseini Representative
Main role in CCM Member

Application Form for Proposals to the Global Fund Page 17 of 72
“We the undersigned hereby certify that we have participated throughout the CCM process and have had sufficient opportunities to influence the process and this application. We have reviewed the final proposal and are happy to support it. We further pledge to continue our involvement in the CCM if the proposal is approved and as it moves to implementation”
Agency/Organisation (including type*)
Name of representative
Title Date Signature
Macedonian Journalist Association
Mr Viktorio Jakovlevski
Journalist
Main role in CCM Member
Agency/Organisation (including type*)
Name of representative
Title Date Signature
Catholic Church Mr Zoran Stojanov
Representative See attached letter
Main role in CCM Member

Application Form for Proposals to the Global Fund Page 18 of 72
7.1 Provide as attachment the following documentation for private sector and civil society CCM members:
• Statutes of organisation (official registration papers) • A presentation of the organisation, including background and history,
scope of work, past and current activities • Reference letter(s), if available • Main sources of funding
These are provided as Annex 15 and labelled with the name of each organization.
7.2 If a CCM member is representing a broader constituency, please provide a list of other groups represented.
8. Chair of the CCM and alternate Chair or Vice-Chair
Table II.8 Chair of CCM Alternate Chair/Vice-Chair Name Redzep Selmani MD Nikola Panovski MD Title
Minister of Health Republic of Macedonia
Deputy Minister of Health Republic of Macedonia
Address Ministry of Health 50 Divizija bb 1000 Skopje
Ministry of Health 50 Divizija bb 1000 Skopje
Telephone +389 2 126 206 + 389 2 126 206 Fax +389 2 113 014 + 389 2 113 014 E-mail N/A N/A Signature
9. Contact persons for questions regarding this proposal (please provide full
contact details for two persons – this is necessary to ensure expedient and responsive communications):
Please note: The persons below need to be readily accessible for technical or administrative clarification purposes by the Secretariat or the TRP members.
HIV/AIDS Component
Table II.9 Primary contact Second contact Name Vesna Velik Stefanovska, MD, PhD Čičevalieva Snežana Title
National Co-ordinator for HIV/AIDS Lawyer, Head of Sector for European Integration and International Cooperation
Address Ministry of Health 50 Divizija bb 1000 Skopje
Ministry of Health 50 Divizija bb 1000 Skopje
Telephone +389 2 119 375 +389 2 119 375 Fax +389 2 119 375 +389 2 119 375 E-mail [email protected] [email protected]

Application Form for Proposals to the Global Fund Page 19 of 72
SECTION III: General information about the country setting
Please note: For regional proposals, the information requested in this section should reflect the situation in all countries involved, either in an aggregated form or by individual country. For sub-national proposals, the information requested should reflect the situation in the particular sub-national area within the overall country context. For further guidance, refer to Guidelines Part III
18. Describe the burden or potential burden of HIV/AIDS, TB and /or Malaria: (Describe current epidemiological data on prevalence, incidence or magnitude of the diseases; its current status or stage of the diseases; major trends of the diseases disaggregated by geographical locations and population groups, where this data is available and/or relevant) (1 – 2 paragraphs per disease covered in proposal): TB Component In the last ten years, the number of people registered with tuberculosis in Macedonia has fluctuated (see figure 1). The highest rate of registered cases is in the northwestern part of country, which has the greatest concentration of refugees and internally displaced people. The case notification rate in 1999 (29.7 per 100 000) was higher than in some neighboring countries (Greece 9.0/100 000, Albania 24.6/100 000 and Yugoslavia 28.4/100 000). In addition, other epidemiological data gives further information about the nature of TB in the country. Extra pulmonary forms of tuberculosis rose from 9.6% of all cases in 1996 to 23,7% in 2002 and the percentage of TB cases among children rose from 5.4% in 1996 to 17.1% in 2002. The number of patients suffering relapse in the last five years is estimated at 7 to 11,5%. Reasons for the increasing number of TB patients in the country are numerous and include the relatively low standard of living. Certain groups are particularly vulnerable to the disease, including patients in psychiatric hospitals, prisoners, refugees and internally displaced people. Notification rates for these groups in 2002 were 165,87/100,000 in neuropsychiatry hospitals, 143.4/100,000 in prisons and 108.6/100,000 among internally displaced people and refugees. The most commonly affected age group is 25-45 years.
HIV/AIDS Component the first person with HIV in Macedonia was officially registered in 1987 and the first person with AIDS in 1989. To date, only 64 people have been found to be HIV positive in the country. However, this is almost certainly an underestimate as most people found to be positive were only tested after they became sick. The true epidemiological picture for HIV/AIDS in the country is not clear due to a relatively weak national surveillance system and the lack of specific data for the most vulnerable groups in society. Most people with AIDS in the country are male (72%) and within the age range 30-39 years. The dominant mode of transmission is reported to be heterosexual. However, stigmatization of homosexual behavior makes it possible that some of the cases declared as heterosexual could be due to homosexual/bisexual encounters. Registered cases are found in all regions of the country and among all ethnic groups. Official data also shows declining levels of sexually transmitted infections. However, there are suggestions that STI data may be underreported by a factor of three to four because of self-treatment and failure of medical staff to report all cases.
Figure 1: Numbers of registered TB cases per 100 000 population: FYROM: 1995-2002
05
1015202530354045
1995 1996 1997 1998 1999 2000 2001 2002

Application Form for Proposals to the Global Fund Page 20 of 72
There is a great deal of evidence that conditions in Macedonia are conducive to the spread of HIV/AIDS. These conditions include displacement and migration of people, the country’s location on drug trafficking routes, increasing availability of drugs, increasing number of IDUs, growth of sex work including trafficked women and rising HIV prevalence in neighboring countries. A serious HIV/AIDS epidemic could have an extremely devastating effect on the country’s vulnerable economic position. A Rapid Assessment and Response (RAR) conducted by UNICEF/CIDA in 2002 (Annex 2) concluded that first sex usually occurs without a condom, that 64.5% of sexually active girls and 43% of boys do not use condoms regularly, that sexually active girls are embarrassed to consult doctors and that 2% of young people in school were injecting drugs. The exact number of injecting drug users in the country is unknown but there are an estimated 12-15 000, mostly heroin users. It is clear that this group is particularly vulnerable to HIV. A situation analysis conducted by the UN theme group (annex 3) estimated that 70% of IDUs were Hepatitis C positive. The UNICEF RAR study on young IDUs found that HIV knowledge was low and risk behavior high within this group. Almost 70% had used injection equipment belonging to someone else and 31% had used equipment found in garbage containers in front of medical facilities or places frequented by injecting drug users. They stated that they had more than one sexual partner during the year, had had sex under the influence of drugs and that in such a state they ‘did not pay much attention to using condoms’. Macedonia also recognizes problems related to sex work. Many street-based sex workers also inject drugs (>50%) and report low usage of condoms. Macedonia has a significant Roma population and a number of inter-related factors, including poverty, make this group vulnerable to HIV/AIDS.
19. Describe the current economic and poverty situation (Referring to official indicators
such as GNP per capita, Human Development Index (HDI), poverty indices, or other information on resource availability; highlight major trends and implications of the economic situation in the context of the targeted diseases) (1–2 paragraphs): The estimated population of Macedonia is 2.1m, of these 58% live in towns, with 640 000 living in the capital, Skopje. In the 1994 census, the ethnic composition of the population was recorded as Macedonian (66%), Albanian (23%), Turks (4%), Roma (2.3%) and Serbs (2%) (see Annex 8). The country gained independence in 1991 following the collapse of Yugoslavia. This change has been extremely difficult and many factors, including border closures and internal/external armed conflict have contributed to very difficult economic circumstances. The current government was elected in September 2002. Although some progress has been made since 1996, the country is, under IMF direction, having to institute stern measures to control public expenditure including within the health sector, in order to further stabilise the macroeconomic situation. In 2002, the average per capita income was $1 876, unemployment rates were over 50% and more than 20% of the population were considered to be living in poverty (Annex 4).
Two groups of issues need to be understood to appreciate the socioeconomic situation in the country, namely those inherent to Macedonian society and those related to the state of political and economic transition. Issues within the first group include the multi-ethnic nature of Macedonian society and rural-urban migration. Particular issues relating to political and economic transition include:
• Declining levels of income and growing unemployment, particularly amongst young people
• Increase in number of people in absolute poverty • Particularly severe economic consequences for ethnic minorities • Increasing access to illegal drugs • The crisis in neighbouring Kosovo which led to the influx of many refugees
20. Describe the current political commitment in responding to the diseases (indicators of political commitment include the existence of inter-sectoral committees, recent public pronouncements, appropriate legislations, etc.) (1–2 paragraphs):

Application Form for Proposals to the Global Fund Page 21 of 72
TB Component - The Macedonian Ministry of Health (MoH) recognized the urgency of TB in the country and welcomed the World Health Organization to support the National TB Program (NTP) in 1994 (annex 5). The first support included drugs and necessary materials for bacteriological diagnosis. In addition, the MoH, one year later, sent a request for help to the Royal Netherlands Tuberculosis Associations (KNCV) for an independent assessment of TB in the country. The assessment study was conducted in 1995 and, based on those observations a proposal for a new NTP was written. By the end of 2002, the new policy of TB control, named DOTS, based on the recommendation of WHO was accepted by the MoH. According to this five year plan of TB control, a national TB Policy Committee and Central Unit, responsible for all activities of the NTP, were set up. A technical guide for the NTP has been written and already accepted by the MoH. As a result of MoH willingness to support NTP, World Bank credit was received (1996-2000) for the TB program and used for investment in the diagnosis of TB disease and laboratory equipment, especially for the National Reference Laboratory. In continuation of MoH efforts for TB control activities, the country took part in a TB surveillance pilot project in accordance with WHO DOTS strategy for TB control in the region. All activities were fully support by the MoH. The government has also pledged to increase domestic financial resources committed to TB (see section 21.3 and Annex 6).
HIV/AIDS Component – The country introduced its first AIDS program in 1985, two years prior to the first person with HIV being identified in the country. Since 1987, the National HIV/AIDS Program, oriented to addressing the health aspects of HIV/AIDS, has been implemented through the Ministry of Health and the AIDS Commission, which it established. Macedonia has not yet adopted a national strategy on HIV/AIDS but is in the process of doing so and has developed a framework for this (Annex 16). In addition, in 1996 an Inter-Ministerial State Commission for the Fight against Illicit Production and Trafficking in Drugs and the Prevention of Drug Abuse was established. The National Drug Control Strategy is supportive of the development of harm reduction approaches as one of the legitimate measures to decrease vulnerability of drug users to HIV/AIDS. In June 2001 the country signed The Declaration of Commitment on HIV/AIDS adopted in New York at the UN General Assembly Special Session on HIV/AIDS (UNGASS). Despite the severe economic hardships and health sector reforms geared towards rationalizing and reducing expenditures in the health system, the country has remained committed to tackling problems created by the collapse of the public health system and the cross border threat of HIV/AIDS. Since 2001 the Government and the President of the country have shown very strong political commitment to HIV/AIDS which resulted in the establishment of the National Multisectoral Committee on HIV/AIDS (NMC) in April 2003. It is this committee which has been used to form part of the country’s CCM (see section 3). Although most of the commitment to HIV/AIDS has been demonstrated by the MoH and NGOs, other ministries have increasingly demonstrated willingness to be actively involved in the issues. The President’s own personal commitment to the issue has been demonstrated by his involvement in World AIDS Day activities and efforts to promote tolerance and non-discrimination of PLWHAs. The government’s commitment to HIV/AIDS is illustrated by the appointment of a Cabinet Minister to head the CCM. Although the known prevalence of HIV/AIDS is low, the Government recognizes both the existence of factors that could facilitate a rapid growth of the epidemic, and the value of the existing window of opportunity to stop the spread of HIV/AIDS. It has also responded to this by pledging to increase domestic financial resources committed to AIDS (see section 21.3 and Annex 6). Local government in most urban centers provides direct logistical support to HIV/AIDS-related programs implemented by NGOs. The government has plans to make antiretroviral drugs available soon through its health systems. Although this has not yet been done, eligible PLWHAs can access other treatment and care through the Health Insurance Fund.
21. Countries classified as “Lower-Middle Income” or “Upper-Middle Income” by
the World Bank are eligible to apply only if they meet additional requirement (Guidelines Para 8). The sections below are required for proposals from these countries.

Application Form for Proposals to the Global Fund Page 22 of 72
21.1 Co-financing: describe in both narrative and quantitative terms how
domestic or external resources will be used to co-finance the activities described in this proposal, indicating the source and the extent of co-financing (i.e., what percentage of the budget for the proposal is covered by other resources and what percentage is being requested from the Global Fund) (2–3 paragraphs)
As the purpose of this program is to strengthen and significantly expand the country’s response to both TB and HIV/AIDS, the financial resources currently committed to those initiatives can be considered as co-financing. The most easily defined contribution to this co-financing is direct government funding to the TB and HIV/AIDS programs. In 2003, budgets for these stood at 10m and 5.5m denars respectively (approximately $200k and $110k). However, the true amount of co-financing is considerably more than this as this does not include government funding to other parts of the health sector, e.g. through the Health Insurance Fund, which support these direct programs and also does not include other domestic and external resources flowing to other sectors, e.g. through NGOs. All these amounts have been estimated and included in the figures posted in the budget table in the Executive Summary of this proposal. This amount is estimated to be $1.92m in 2004 and rising to $2.40m by 2008. However, these figures are estimations as no reliable system for collecting this information is currently in place. This issue is to be addressed as part of this program. Based on this, co-financing will account for 38% of the program’s financing in year 1, rising to 88% in year 5. It is proposed that a system be established as part of this program to readily calculate this figure at least on an annual basis.
21.2. Focus on poor or vulnerable populations: describe how underserved
populations of poor and vulnerable groups will be targeted by the proposal (2–3 paragraphs)
One of the distinctive features of the program proposed in this document is its strong emphasis on poor and vulnerable sub-populations within the country. TB Component - It is well-recognised that tuberculosis disproportionately affects poor and vulnerable people. Consequently, this component has an intrinsic focus on these groups. In particular: • NTP will advocate for sustained political will in support of disease
surveillance and continued health monitoring of the poor population • Training of health professionals within the TB program will focus on
increasing national capacity to provide services to poor and vulnerable groups
• Trained community health nurses will make sure that TB patients from different vulnerable groups complete the full course of treatment
• Mutual cooperation will be established with other ministries, NGOs, private sector, faith-based organisations and associations of former TB patients
• DOTS will be provided free of charge to all Macedonian citizens and uninsured persons
• The program will work through NGOs to provide social support of TB patients and their families
HIV/AIDS Component - The HIV/AIDS component of this proposal is targeted to those sub-populations who are particularly vulnerable to HIV. Because of the multisectoral approach of the proposed program, the CCM is able to draw on the rich and varied experience of a number of organizations from different sectors which have a proven track record of working with these groups, which include:

Application Form for Proposals to the Global Fund Page 23 of 72
• Young people – many of the activities with young people will be carried out by NGOs, drawing on their experience and that from governmental and international agencies
• IDUs – NGOs will play a leading role in expanding harm reduction services with the government spearheading a decentralization of the drug treatment program
• Sex workers – This will be led by NGOs and will focus on the most marginalized group, i.e. street-based sex workers
• MSM – This activity will be NGO-led and will focus on identifying and supporting men who have sex with men
• Roma community – According to official statistics, the Roma community constitutes 2% of the country’s population and is widely recognized as the most marginalized ethnic group. The program will conduct activities with them through NGOs already working with them on other issues.
• Prisoners – Activities in prisons will focus on both HIV prevention and drug treatment through a unique partnership between Ministry of Justice and an NGO
• PLWHAs – The program will seek to provide medical treatment and social support to PLWHAs through both governmental and NGO provision.
21.3 Greater reliance on domestic resources: describe in both narrative and
quantitative terms how over the duration of the proposal the activities described will be increasingly financed using domestic resources, including the changes in the percentage of the budget covered by domestic vs. Global Fund resources (2–3 paragraphs)
Despite the harsh macroeconomic environment and the measures which are in place to control public expenditure, the government has budgeted for significant increases in expenditure on both TB and HIV/AIDS over the next three years (see Annex 6). TB expenditure is planned to increase from current levels of 10m denars to 24.6m denars by 2006. This is equivalent to US$492k at current rates of exchange and would represent almost a 150% increase in direct TB expenditure in three years. Similarly, HIV expenditure is budgeted to increase from current levels of 5.5m denars to 13.6m denars in 2006. This is equivalent to US$272k at current rates of exchange and would also represent almost a 150% increase in direct HIV/AIDS expenditure within three years. Naturally, these budgeted increases are ambitious, given current economic uncertainties in the country. However, the government at the highest level is committed to these increases.
22. National context
22.1. Indicate the percentage of the total government budget allocated to health (optional for NGO applicants):
Health is financed in the country in two main ways. First, most health care is paid for through the National Health Insurance Fund. Secondly, funds from the central budget are used for financing specific health programs including TB and HIV/AIDS, paying for some health care for those ineligible for the Health Insurance Fund (see Annex 6) and for health insurance of those made redundant as a result of structural reform. In 2002, funds amounting to around US$6m, available from the privatization of “Telecom”, were spent on construction of health facilities. Expenditure on health care over the past 4 years has ranged from 5.4% to 6.1% of the GDP. This has been a per capita expenditure of from around US$85 to US$110 dollars.
22.2. Indicate national health spending for 2001, or latest year available, in the Table III.22.2 (optional for NGO applicants):
Table III.22.2 Total national health
spending Specify year: Spending per capita (USD)

Application Form for Proposals to the Global Fund Page 24 of 72
(USD) 2001 Public * 181.1m 86 Private ** 5.9m 2.8 Total 187.0m 89 From total, how much is from external donors?
N/A N/A
*) Including the expenditures of the National Health Insurance Fund and government central budget. **) This amount is an estimation provided by the Health Insurance Fund of money spent by individuals as part of cost sharing. No figures are available for money spent in private health facilities.
22.3. Specify in Table III.22.3, if possible, earmarked expenditures for HIV/AIDS, TB and/or Malaria *(expenditures from the health, education, social services and other relevant sectors):
Table III.22.3 Total earmarked expenditures from government, external donors, etc. Specify Year:2003
In US dollars:
HIV/AIDS 111 000 Tuberculosis 200 000 Malaria Total 311 000
*) The funds are only those from the central budget for vertical health programs
(Annex 6).
22.4. Does the country benefit from external budget support, Highly Indebted Poor Countries (HIPC) initiatives, Sector-Wide Approaches? If yes, how are these processes contributing to efforts against HIV/AIDS, TB and/or malaria? (1–2 paragraphs) (optional for NGO applicants):
No
22.5. Describe the current national capacity (state of systems and services) that
exist in response to HIV/AIDS, TB and/or Malaria (e.g., level of human resources available, health and other relevant infrastructure, types of interventions provided, mechanisms to channel funds, existence of social funds, etc.) (2–3 paragraphs):
Macedonia has relatively well-developed health and social infrastructure, which is available to meet the needs of TB patients, PLWHAs and members of vulnerable sub-populations. The health system is highly centralized and functions at three levels: primary, secondary and tertiary (see Annex 8). The primary level includes the services of primary health care centers which engage in curative, preventive and promotional health care activities. The services provided by these centers are generally of good quality except in some rural areas. The secondary level includes small to medium sized hospitals and the tertiary level includes the big hospitals. There are 18 primary health care centers, 16 medical centers, 7 specialized hospitals, 18 university medical clinics, 16 specialized institutions and two specialized polyclinics. Among governmental health institutions there are two gynecological clinics. Staffing levels are adequate although there are shortages of equipment in some places. The national health system has 23,451 employees with 4,449 medical doctors, of whom 2,801 are specialists. The overall doctor-population ratio is 1:455. Private medical services exist at each of the three levels. There are 516 private medical and 377 private dental centers.

Application Form for Proposals to the Global Fund Page 25 of 72
The Health Care Law of 1991 set the basis for the current healthcare system. It established three types of health insurance: mandatory, supplemental mandatory and voluntary insurance. Mandatory health insurance covers those employed in the public and private sectors, the retired, students, the disabled, and their dependants. Certain citizens who are not covered (stateless and social care recipients) are subsidized by the State budget, as is child and maternal care for the uninsured. The availability of social funds within the country is limited meaning that people without health insurance often have limited access to health care. Particular concern has been expressed about the potential number of HIV positive people who do not have medical insurance. Extending services to include these people is a key feature of this program. TB Component - The Macedonian National Tuberculosis Program was created according to WHO recommendations at the end of 2000. It is based upon the DOTS strategy. Its aim is to provide an effective system of tuberculosis control in the country. The NTP (Annex 5), as a part of the Macedonian health system, is a five year development plan for TB control in the country, outlining a new policy, a comprehensive strategy regarding structure and organization, detailed plans for implementation and training, and budget for investment and recurrent costs. The Ministry of Health, through a TB Policy Committee, has a clear description of their responsibilities and duties. Within the Institute for Lung Diseases and Tuberculosis, a Central Unit headed by the National TB Program Manager is in charge of coordinating all activities of the program. The National TB Laboratory is a part of the Central Unit and provides a tertiary level of bacteriological examination. It is responsible for all activities concerning microbiological examinations of TB disease, including sensitivities testing, quality control, scientific work etc. During the intensive phase of treatment, TB patients are treated in three hospitals for lung disease and tuberculosis or in one hospital for children. Two hospitals have secondary level of laboratories. 15 dispensaries provide a network, which coordinates the TB control regionally. Ten of them have possibility to perform sputum smear examination and present first level of bacteriological diagnosis.
Diagnosis and treatment, especially during the continuation phase, remain the task of dispensaries, which should protect and coordinate the preventive measures in the system for public health care. With gradual reduction of the number of TB dispensaries, their role in TB control will be increasingly performed by primary health care professionals. The role of the GP in TB control will be more important than in the past. Other health care institutions (Clinics within the Medical School, Medical Services in the Army, Prison Health Services and Psychiatric Institutions) are also involved in NTP. The health sector in general is undergoing organizational reform, which could have some influence on the NTP. All activities of the program are presented in this proposal, including diagnosis, especially bacteriological confirmation of the disease, notification of TB cases, cohort analysis, monitoring and evaluation of the program, quality control, education and training of medical staff. Every year, the Central Unit is obliged to propose an annual plan for TB control for the next year to the Ministry of Health.
HIV/AIDS Component – A key feature of the response to HIV/AIDS in Macedonia has been the emergence of a number of NGOs who are working closely with a number of vulnerable groups. These NGOs not only operate from fixed bases but also carry out a wide range of outreach activities. Consequently, many people from vulnerable sub-populations find services offered by NGOs to be readily accessible to them. This is particularly important in the current environment where many people from these vulnerable groups find themselves subject to considerable stigma and discrimination. However, there is need for these NGOs to develop further institutional capacity, to work more cooperatively with each other, to facilitate the development of other NGOs (particularly outside the capital) and to establish sustainable sources of funding.
22.6. Name the main national and international agencies involved in national responses to HIV/AIDS, TB and/or Malaria and their main programmes (NGO applicants should specify partner organisations): TB Component

Application Form for Proposals to the Global Fund Page 26 of 72
Table III. 22.6 Name of Agency Type of Agency (e.g.,
Government, NGO, private, bilateral, multilateral, etc.)
Main programs (for example, comprehensive HIV/AIDS prevention; DOTS expansion over 3 years, etc.)
Budget (Specify time period)
Ministry of Health Government Prevention
2003 $200k
Health Insurance Fund Public All activities of TB control N/A
WHO humanitarian assistance office
UN Organization Drug supply 2000-2003 No financial details available
WHO/ ECHO TB Pilot project 2000-2002 $1 000 000
KNCV NGO Technical advice to NTP 1995-1999 World Bank X-ray and laboratory equipment 1996-2000
$750 000 Project HOPE NGO TB pilot project-technical advise 1990-2000
No financial details available
Macedonian Red Cross
NGO Organization of TB week celebration
N/A
HIV/AIDS Component
Name of Agency Type of Agency (e.g., Government, NGO, private, bilateral, multilateral, etc.)
Main programs (for example, comprehensive HIV/AIDS prevention; DOTS expansion over 3 years, etc.)
Budget (Specify time period)‡
Ministry of Health Government Prevention 2003 US$ 111 000
National Health Insurance Fund
Public Treatment 2002 US$ 84 418
UNICEF UN Agency Prevention 2002 US$ 135 000
USAID Bilateral Prevention 2002 US$ 200 000
Norwegian Government
Bilateral Prevention 2002 US$ 25 000
SIDA Bilateral Prevention 2002 US$ 455 000
HOPS NGO Prevention among drug users and commercial sex workers
2002 US$116 100
HERA NGO Prevention among young people and general population
2002 US$ 109 776
TRUST NGO Prevention among drug users 2002 US$ 32 800
MIA NGO Prevention among young people 2002 US$ 36 531
Izbor NGO Prevention among drug users 2002 US$ 39 000
Via Vita NGO Prevention among drug users 2002 US$ 30 000
‡ Some of the amounts reported here may overlap, for example if a local NGO receives funds from an international donor.
Application Form for Proposals to the Global Fund Page 27 of 72
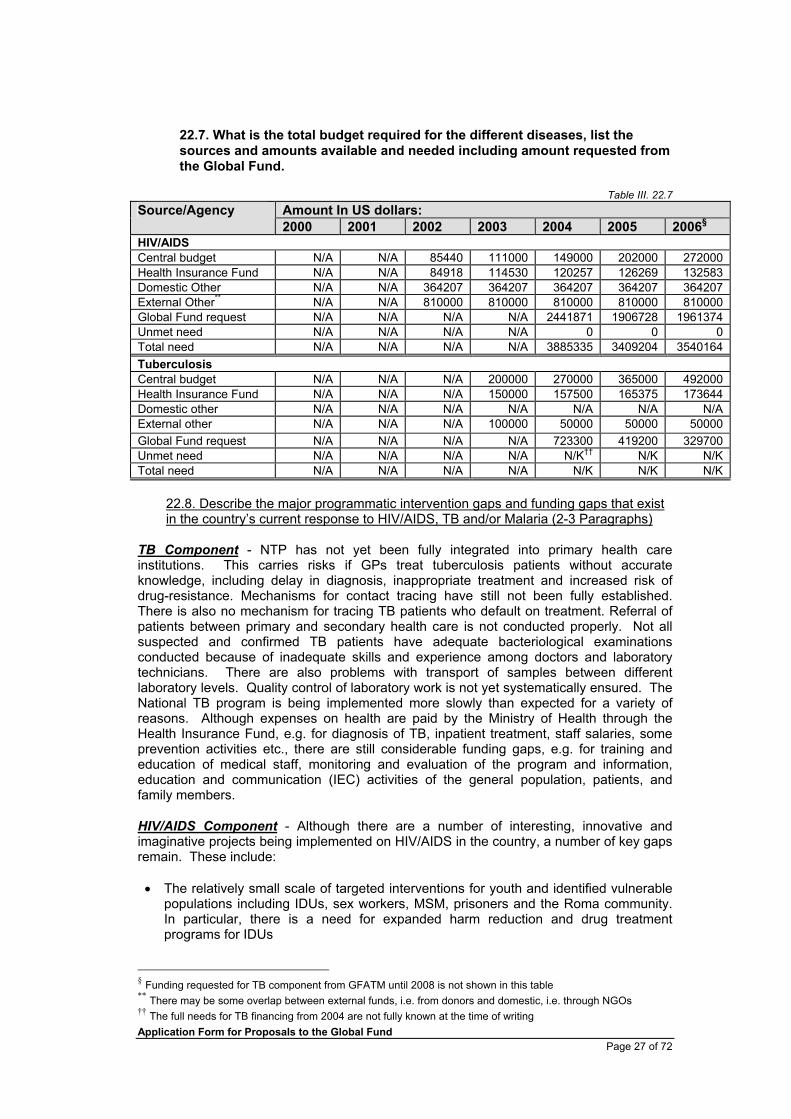
22.7. What is the total budget required for the different diseases, list the sources and amounts available and needed including amount requested from the Global Fund.
Table III. 22.7
Amount In US dollars: Source/Agency 2000 2001 2002 2003 2004 2005 2006§
HIV/AIDS Central budget N/A N/A 85440 111000 149000 202000 272000 Health Insurance Fund N/A N/A 84918 114530 120257 126269 132583 Domestic Other N/A N/A 364207 364207 364207 364207 364207 External Other** N/A N/A 810000 810000 810000 810000 810000 Global Fund request N/A N/A N/A N/A 2441871 1906728 1961374 Unmet need N/A N/A N/A N/A 0 0 0 Total need N/A N/A N/A N/A 3885335 3409204 3540164 Tuberculosis Central budget N/A N/A N/A 200000 270000 365000 492000 Health Insurance Fund N/A N/A N/A 150000 157500 165375 173644 Domestic other N/A N/A N/A N/A N/A N/A N/A External other N/A N/A N/A 100000 50000 50000 50000 Global Fund request N/A N/A N/A N/A 723300 419200 329700 Unmet need N/A N/A N/A N/A N/K†† N/K N/K Total need N/A N/A N/A N/A N/K N/K N/K
22.8. Describe the major programmatic intervention gaps and funding gaps that exist in the country’s current response to HIV/AIDS, TB and/or Malaria (2-3 Paragraphs)
TB Component - NTP has not yet been fully integrated into primary health care institutions. This carries risks if GPs treat tuberculosis patients without accurate knowledge, including delay in diagnosis, inappropriate treatment and increased risk of drug-resistance. Mechanisms for contact tracing have still not been fully established. There is also no mechanism for tracing TB patients who default on treatment. Referral of patients between primary and secondary health care is not conducted properly. Not all suspected and confirmed TB patients have adequate bacteriological examinations conducted because of inadequate skills and experience among doctors and laboratory technicians. There are also problems with transport of samples between different laboratory levels. Quality control of laboratory work is not yet systematically ensured. The National TB program is being implemented more slowly than expected for a variety of reasons. Although expenses on health are paid by the Ministry of Health through the Health Insurance Fund, e.g. for diagnosis of TB, inpatient treatment, staff salaries, some prevention activities etc., there are still considerable funding gaps, e.g. for training and education of medical staff, monitoring and evaluation of the program and information, education and communication (IEC) activities of the general population, patients, and family members. HIV/AIDS Component - Although there are a number of interesting, innovative and imaginative projects being implemented on HIV/AIDS in the country, a number of key gaps remain. These include: • The relatively small scale of targeted interventions for youth and identified vulnerable
populations including IDUs, sex workers, MSM, prisoners and the Roma community. In particular, there is a need for expanded harm reduction and drug treatment programs for IDUs
§ Funding requested for TB component from GFATM until 2008 is not shown in this table ** There may be some overlap between external funds, i.e. from donors and domestic, i.e. through NGOs †† The full needs for TB financing from 2004 are not fully known at the time of writing

Application Form for Proposals to the Global Fund Page 28 of 72
• Limited access to counselling and testing services. In addition, the quality of these services is variable
• Limited access to medical care and support for PLWHAs. In particular, there is still a strong sense of stigma and discrimination within Macedonian society as a whole
• Limited availability of important biologic and behavioural surveillance data relating to the spread and development of the epidemic
• Relatively limited capacity within the HIV/AIDS response and a degree of fragmentation of services and approaches
22.9. If a SWAp or a similar fund pooling mechanism exists in your country, briefly describe how it is functioning and if you anticipate using it to administer the Global Fund grant
Not Applicable

Application Form for Proposals to the Global Fund Page 29 of 72
SECTIONS IV – VIII: Detailed information on each component of the proposal
PLEASE COMPLETE THE FOLLOWING SECTIONS FOR EACH COMPONENT Please copy sections IV – VIII as many times as there are components Please note: a component refers to a disease, so the proposal will have more than one component only if it covers more than one disease. There should only be 1 component per disease. If there are any objectives or broad activities within a particular component that are of a system-wide/cross-cutting nature such as capacity building or infrastructure development that may go beyond the scope of that particular component, please indicate those aspects clearly and specify how they would relate to other components of the proposal when detailing them in Question 26. If this is a fully integrated proposal, where two or more components are linked in such a way which would not make it realistic or feasible to separate, mark the boxes in Table IV.23 to identify all diseases which would be directly affected by this integrated component.
SECTION IV – Scope of proposal 23. Identify the component that is detailed in this section (mark with X):
Table IV.23 Component x HIV/AIDS
(mark with X): Tuberculosis
Malaria
HIV/TB
24. Provide a brief summary of the component (Specify the rationale, goal, objectives, activities, expected results, how these activities will be implemented and partners involved) (2–3 paragraphs): Although Macedonia has relatively few people who are known to be HIV positive, concerns have been expressed that the country is vulnerable to the disease and that the true situation regarding HIV/AIDS in the country is not fully known because of poorly-developed national surveillance systems. The goal of this program is to build a co-ordinated national response to prevent a major HIV/AIDS epidemic in the country.
This program has a total of five main areas of emphasis grouped around ten objectives. The five areas are • Preventing the spread of HIV/AIDS amongst vulnerable sub-populations
including young people, IDUs, sex workers, prisoners, MSM and the Roma community
• Improving access to and the quality of counselling and testing services • Improving the provision of care and support for PLWHAs • Improving national biologic and behavioural surveillance systems • Strengthening capacity and coordination within the national response to
HIV/AIDS
This proposal is being submitted along with a proposal for a TB program in the country. Both programs will be overseen by the Macedonian Country Coordinating Mechanism which has been formed by bringing together two existing committees working on HIV/AIDS and TB respectively. The CCM is led by the

Application Form for Proposals to the Global Fund Page 30 of 72
Minister of Health and brings together representatives from a wide variety of different organizations concerned about the two diseases. The Ministry of Health will act as secretariat to the CCM and is also proposed as the principal recipient for GFATM funds. Activities specified within particular objectives will be delivered and managed by a range of organizations, including NGOs and government with a strong track record of work in this field.
25. Indicate the estimated duration of the component:
Table IV.25 From (month/year): January 2004 To (month/year): December 2006 26. Detailed description of the component for its FULL LIFE-CYCLE: Please note: Each component should have ONE overall goal, which should translate into a series of specific objectives. In turn each specific objective should be broken-down into a set of broad activities necessary to achieve the specific objectives. While the activities should not be too detailed they should be sufficiently descriptive to understand how you aim to achieve your stated objectives. Indicators: In addition to a brief narrative, for each level of expected result tied to the goal, objectives and activities, you will need to identify a set of indicators to measure expected result. Where applicable this set of indicators should include the core indicators as listed in Annex A. Baseline data: Baseline data should be given in absolute numbers and percentage. If baseline data is not available, please refer to Guidelines. Baseline data should be from the latest year available, and the source must be specified. Targets: Clear targets should be provided in absolute numbers and percentage.
26.1. Goal and expected impact (Describe overall goal of component and what impact, if applicable, is expected on the targeted populations, the burden of disease, etc.) (1–2 paragraphs):
Please note: the impact may be linked to broader national-level programmes within which this component falls. If that is the case, please ensure the impact indicators reflect the overall national programme and not just this component. Please specify in Table IV.26.1 the baseline data. Targets to measure impact are only required for the end of the full award period.
The overall goal of the program is to build a coordinated national response to prevent a major HIV/AIDS epidemic in Macedonia. Currently, it appears that there are relatively few people with HIV/AIDS in the country. However, surveillance systems are not well-developed and the country is vulnerable to the epidemic for a number of reasons. Various responses have started in the country but they are relatively small in scale and uncoordinated in nature. This program builds on recent initiatives to extend HIV/AIDS activities beyond the health sector. It will seek to scale-up existing successful activities, introduce a range of new activities and strengthen overall coordination and cooperation. It will link to activities proposed to strengthen TB management and treatment in the country, which forms an additional component to this proposal.

Application Form for Proposals to the Global Fund Page 31 of 72
Table IV.26.1
Goal: To build a co-ordinated national response to prevent a major HIV/AIDS epidemic in Macedonia
Impact indicators Baseline‡‡ Target (last year of proposal)
Year: Year:
Percent of IDUs who are HIV infected Percent of MSM who are HIV infected Percent of sex workers who are HIV infected Percent of prisoners who are HIV infected
No information is available for these as no systematic studies have been conducted. A key element of this proposal is establishing a system of biologic surveillance. Targets will be set based on baselines established in first year of the program
26.2. Objectives and expected outcomes (Describe the specific objectives and
expected outcomes that will contribute to realizing the stated goal) (1 paragraph per specific objective):
Question 26.2 must be answered for each objective separately. Please copy Question 26.2 as many times as there are objectives. Please note: the outcomes may be linked to broader programmes within which this component falls. If that is the case, please ensure the outcome/coverage indicators reflect the overall national programme and not just this component. Specify in Table IV.26.2 the baseline data to measure outcome/coverage indicators. Targets are only required for Year 2 onwards.
This program is focused on achieving ten specific objectives. These have been selected based on the need to focus efforts on vulnerable groups identified as most at risk of HIV/AIDS in Macedonia. This has been done by means of a broad consultative process which has included not only all key players within the country, but has also drawn on external technical inputs, e.g. from UNAIDS, UNDP, UNICEF, WHO and USAID. The program’s ten objectives are:
1. To prevent HIV transmission among young people. Currently, several NGOs are working on this objective. In this program, these activities will be scaled up and linked together. Coverage will be monitored by measuring and aggregating the number of young people aged 15-24 educated in HIV prevention. Although some baseline information is available from different NGOs, there is currently no system for aggregating this information. Such a system will be developed within the first six months of operation of this program.
Table IV.26.2
Objective: 1 To prevent HIV transmission among young people Outcome/coverage indicators Baseline Targets Year: Year 2: Year 3: Year 4: Year 5: Number of young people aged 15-24 educated in HIV prevention
No reliable baseline data. This will be gathered in first 6 months of program and targets set
2. To prevent transmission of HIV and blood-borne diseases among IDUs.
There are currently some programs in the country providing harm reduction
‡‡ All baselines are for 2002 unless stated otherwise

Application Form for Proposals to the Global Fund Page 32 of 72
measures for IDUs and drug treatment and rehabilitation. Both these approaches will be supported and significantly expanded through this program and they will be linked more closely together. Currently, rates of HIV infection among IDUs in the country appear low. However, there is a significant problem with other blood-borne diseases, such as hepatitis C. Consequently, activities will have a broad focus on prevention of all blood-borne infections and not HIV/AIDS only. Coverage under this objective will be measured by the number of IDUs receiving targeted HIV/AIDS interventions which will include needle exchange services, drug treatment programs etc.
Objective: 2 To prevent transmission of HIV and blood-borne diseases among
IDUs Outcome/coverage indicators Baseline Targets Year:
2002 Year 2: Year 3: Year 4: Year 5:
Number of injecting drug users receiving targeted HIV/AIDS interventions
2680 5900 6500
3. To prevent HIV transmission among sex workers and their clients. Currently,
NGOs are providing some services to sex workers on a small scale in the country. These will be significantly expanded through this program. Coverage will be measured by recording the number of sex workers and their clients reached through such programs. It is expected that the number of sex workers reached through such programs will rise from just over 100 currently to 250 in three years. Currently, no data is available for the number of clients reached. Systems for recording this data will be established within the first six months of the program’s establishment.
Objective: 3 To prevent HIV transmission among sex workers and their clients Outcome/coverage indicators Baseline Targets Year:
2002 Year 2: Year 3: Year 4: Year 5:
Number of sex workers reached with targeted HIV/AIDS interventions
103 200 250
Number of clients of sex workers reached with targeted HIV/AIDS interventions
No reliable baseline data. This will be gathered in first 6 months of program and targets set
4. To prevent HIV transmission among men who have sex with men (MSM).
Currently, NGOs are conducting some limited work with this group but it is hampered by limited openness about this issue in this country. Activities will be significantly expanded through this program. Coverage will be measured by recording the number of MSM reached with targeted HIV/AIDS interventions. It is expected that the numbers reached will rise from 250 currently to 750 in three years.
Objective: 4 To prevent HIV transmission among MSM Outcome/coverage indicators Baseline Targets Year: Year 2: Year 3: Year 4: Year 5: Number of men who have sex with men reached with targeted HIV/AIDS interventions
250 500 750
5. To prevent HIV transmission among the Roma community. Although some
Roma people have access to general HIV/AIDS activities, there are currently no programs specifically-focused on HIV/AIDS within the Roma community. Under this program, such activities will be introduced. Coverage will be measured by the

Application Form for Proposals to the Global Fund Page 33 of 72
number of Roma people educated in HIV prevention. It is expected that this will rise from the current level of zero to 21 300 in three years.
Objective: 5 To prevent HIV transmission among the Roma community Outcome/coverage indicators Baseline Targets Year: Year 2: Year 3: Year 4: Year 5: Number of Roma people educated in HIV prevention
0 10.200
21.300
6. To prevent HIV transmission among prisoners. Currently, there is no specific
program of HIV prevention in the country’s prisons. It is proposed that one be established under this program through a partnership between the Ministry of Justice and an NGO. Coverage will be measured by recording the number of prisoners reached with targeted HIV/AIDS intervention. It is expected that this number will rise from the current level of zero to 1500 within three years.
Objective: 6 To prevent of HIV transmission among prisoners Outcome/coverage indicators Baseline Targets Year: Year 2: Year 3: Year 4: Year 5: Number of prisoners reached with targeted HIV/AIDS interventions
0 800 1500
7. To improve access to and quality of HIV counselling and testing. Currently,
there are a number of programs offering HIV counselling and testing in the country. In general, NGOs offer counselling and government health institutions offer testing. Under this program, it is proposed to increase access to these services and to improve and standardise their quality. Coverage will be measured by recording the number of people receiving HIV testing through this part of the program (i.e. it will be recorded separately from surveillance activities). It is expected that the number of people receiving HIV tests will rise from current levels of 250 per year to 1000 per year within three years.
Objective: 7 To improve access to and quality of HIV counselling and testing Outcome/coverage indicators Baseline Targets Year: Year 2: Year 3: Year 4: Year 5: Number of people receiving HIV testing (not including testing for routine surveillance)
250 700
1000
8. To improve HIV/AIDS/STI surveillance and forecasting to strengthen
planning of the national response. A key gap identified in the country’s situation and response analysis was the limited availability of accurate biologic and behavioral surveillance data concerning the extent of HIV/AIDS/STI in the country. The activities within this objective are largely based on recommendations made rapid assessment of the system conducted in November 2002 (see annex 9A§§). Achievement of this objective will be demonstrated by the production and distribution of national report on biologic and behavioral surveillance amongst vulnerable sub-populations annually.
§§ Annexes denoted by a number only relate to both components within this proposal, i.e. TB and HIV/AIDS. Those marked with a T relate to Tuberculosis only, whereas those marked with an A related to HIV/AIDS only.

Application Form for Proposals to the Global Fund Page 34 of 72
Objective: 8 To improve HIV/AIDS/STI surveillance and forecasting to
strengthen planning of the national response Outcome/coverage indicators Baseline Targets Year: Year 2: Year 3: Year 4: Year 5: National reports of HIV/AIDS and STI biologic surveillance annually
0 1 1 2 2
Yearly reports on risk behavior of vulnerable sub-populations
0 1 1 1 1
9. To provide health care and psychosocial support to PLWHAs. Currently,
PLWHAs receive medical treatment at the Clinic for Infectious Diseases in Skopje and limited psychosocial support from a variety of places. Under this program, services will be expanded and improved in quality. Coverage will be measured by recording the number of people living with HIV/AIDS receiving such services. Currently, no baseline figures for this are available. These will be collected within six months of the start of the program and targets set on the basis of those and forecasts based on surveillance data.
Objective: 9 To provide health care and psychosocial support to PLWHAs Outcome/coverage indicators Baseline Targets Year: Year 2: Year 3: Year 4: Year 5: The number of PLWHA having access to health care and psychosocial support
No reliable baseline data. This will be gathered in first 6 months of program and targets set
10. To strengthen coordination and capacity of the national response to
HIV/AIDS. A key focus of this program is to build the capacity of institutions working on HIV/AIDS individually and the capacity of the national response as a whole. In this regard, the program will have a strong focus on building coordination and cooperation among key players. The outcome will be monitored by measuring the percentage of CCM members who believe that capacity is increasing and that the response is well-coordinated. Currently, no figures for this exist. Baselines will be established during the first six months of the program. It is expected that satisfaction levels will reach 90% within three years.
Objective: 10 To strengthen coordination and capacity of the national response to
HIV/AIDS. Outcome/coverage indicators Baseline Targets Year: Year 2: Year 3: Year 4: Year 5: Percentage of CCM members who believe that capacity is increasing and the response to HIV/AIDS is well-coordinated in the country
N/A 80% 90%
26.3. Broad activities related to each specific objective and expected output
(Describe the main activities to be undertaken, such as specific interventions, to achieve the stated objectives) (1 short paragraph per broad activity):
Please note: Process/output indicators for the broad activities should directly reflect the specified broad activities of THIS component. Specify in Table IV.26.3 below the baseline data to measure process/output indicators. Targets need to be specified for the first two years of the component. For each broad activity, specify in Table IV.26.3 who the implementing agency or agencies will be.

Application Form for Proposals to the Global Fund Page 35 of 72
It is proposed to reach objective 1 through thirteen broad activities carried out mainly by a number of NGOs who work directly with children and young people using a range of methods which are innovative and creative in nature and include young people as active participants in the activities and associated processes. These prevention activities will be inclusive of young people from all ethnic groups living in Macedonia. Specific activities for young people from the Roma community are included under objective 5.
The first activity focuses on trying to learn from current peer education activities and to increase the quality of those activities. Four workshops will be held each year in which NGO staff will be able to identify best practice for peer education and upgrade their own skills in this area.
The second activity involves establishing a pilot educational center for young people on HIV/AIDS/STI and reproductive health: Ultimately, it would be good to have such facilities in every community, either located within existing community facilities, or in dedicated facilities where such services do not exist. This pilot project will explore possible approaches and make suggestions for ways in which this approach can be developed in the future. The third activity consists of training of youth peer educators. It is planned to increase the numbers of training workshops from the current level of 2 per year, to 15 per year by the end of year 2. Each training course will train approximately 10 peer educators. The fourth activity involves promoting and distributing condoms among young people. This will involve identifying places in each community where good quality condoms can be obtained and providing free distribution of condoms in poor neighborhoods. Participating agencies will include NGOs and the Agency for Youth and Sport. These activities will include all ethnic groups in the country and will be combined with advocacy efforts to lower condom prices making them more accessible for young people. The fifth activity will involve targeted information dissemination for young people. Educational materials will be developed in order that issues relating to HIV/AIDS/STIs can be easily understood. This material will be distributed through public campaigns, educational events and will be continuously accessible in certain public places. This will contribute to the spread of key information about these diseases and the promotion of safe sexual behavior. The brochures will be focused on HIV/STI, reproductive health, open conversation between children and parents, young people’s rights as patients, drug use etc. The sixth activity involves a national media campaign using TV and radio to spread information, skills and awareness of HIV/AIDS/STI through a combination of educational and entertainment methods. A media campaign will be developed using TV, radio and print. For TV, a 30 minute youth-oriented entertainment program will be developed that includes a drama component based on real life situations. For radio a social marketing format will be used to promote messages on HIV/AIDS prevention. Information will be printed in all major newspapers in the Macedonian, Albanian and Turkish languages. These activities will involve national TV and radio (MRTV), 2 TV stations with national broadcasting, 6 local TV stations, 8 local radio stations and 4 major newspapers The seventh activity involves developing an interactive web-page on HIV/AIDS/STIs, designed to be easily accessible to young people. Web chat rooms will be used as a link for this site, which will be named CHATTING GUIDE. It will be primary designed as a site for improving web-chatting skills, but it will also offer information about HIV/AIDS/STI. It is based on a model that has been used in other countries, e.g. the Netherlands. Young people will be guided through the site, step by step in an interactive and interesting manner. Through these steps they will receive information on HIV/AIDS/STI. This site will offer the possibility of conducting research surveys,

Application Form for Proposals to the Global Fund Page 36 of 72
particularly about socially sensitive issues, such as same sex sexual experiences. The web site will feature links to other important resources. The eighth activity involves the development of a publication that promotes open, inter-generational conversations on HIV/AIDS/STI, i.e. between young people and their parents. This approach will build on the family as a key social institution and will seek to increase such conversations which are currently often limited, particularly on issues relating to sex. This publication will seek to initiate open conversation and positive attitudes and behaviors on sexual issues within families and will be linked to a series of workshops on these issues. The ninth activity involves training of health and social service providers in the skills required to provide Youth Friendly Services. This approach will use existing re-training schemes focused on GPs, nurses, and school health workers. In addition, it will also involve work to include such training in pre-service training for nurses, doctors, social workers and psychologists. The tenth activity involves developing and integrating life skills health-based education within the school curricula. As 75% of young people are enrolled in secondary school education, schools are an important forum for receiving information on HIV/AIDS and reproductive health. This activity will promote health education in the school curriculum, providing baseline knowledge on health, including reproductive. A team of professionals will review the health education law. A special program for teaching on sex and HIV/AIDS/STI issues will be developed followed by a guide for health education in schools. The eleventh activity involves training of teachers in primary and secondary schools on HIV/AIDS/STI and sexual issues and is linked to a process of revising the school curricula to include these issues (activity 12). They will be trained to teach pupils according to their age, level of education and knowledge on these topics. This activity will allow children to access relevant information on this issue and will also contribute more open discussion about sex and sexual issues. In the first year, one teacher per school will be trained and in the second year two more teachers per school will be trained. The twelfth activity is production of a training manual for teachers: This activity is aimed at helping the teachers adapt to the changes made within the school curriculum. The manual will be distributed to each trained teacher in each primary and secondary school in the country. It will consist of the developed and integrated life skills health based education which has been incorporated into the school curriculum
The final activity focuses on promoting safe behavior among a particular group of young people, those doing national service. Currently, all males aged 18-30 are required to do nine months military service. This activity would include HIV/AIDS education into their basic training program. Activities would also extend to the estimated 7 000 military professionals in the armed forces. Initial activities will focus on ten of the country’s twelve military recruiting centers. As part of this activity, four military medical/social staff representatives already working in each of the ten health centers will be trained in information, education and communication (IEC) related to HIV/AIDS/STIs topics through five-day seminars. Approximately 40 military medical/social staff representatives will be trained during the first year and they will be responsible for promoting safe behavior among the recruits as well as professional soldiers. In subsequent years, there will be one three-day seminar for previously-trained staff to allow them to update their knowledge. Also as part of this activity, printed materials developed as part of other activities within this objective will be distributed amongst young people doing national service.

Application Form for Proposals to the Global Fund Page 37 of 72
TableIV.26.3
Objective:1 To prevent HIV transmission among young people Main activities Process/Output Baseline Targets Responsible/Implementing Indicators (indicate
one per activity; refer to Annex A)
(Specify year)
Year 1 Year 2 agency or agencies
Workshop discussions among NGO's to upgrade and identify best practice for peer education
Number of annual workshops
0 4 4 MIA, HERA, HOPS, TRUST
Establishing pilot educational center for HIV/AIDS/STI and reproductive health.
Pilot educational center established
0 1 N/A MoE, Agency for youth and sport, MIA, HERA, HOPS Local Government
Peer education activities
Number of peer education training workshops annually
2 12 15 MIA, HERA, Agency for youth and sport, youth NGO's
Condom promotion activities
Number of condoms distributed annually
100 000 120 000 150 000 MIA, HERA, HOPS, Agency for youth and sport, MoE, municipalities
Targeted information dissemination for young people
Number of printed and distributed brochures annually
0 300 000 350 000 MIA, HERA, HOPS
National media campaign using TV and radio to spread information, skills and awareness of HIV/AIDS/STI through educational and entertainment methods.
Number of HIV/AIDS-related shows broadcast on national and local media annually
7 150 150 MRTV, national and local TV and radio stations,
Developing an interactive web-page on HIV/AIDS/STI
Annual number of users of the information of the web-page
0 10 000 15 000 MIA,
Development of publication that promotes inter-generational conversations on HIV/AIDS/ STI
Number of publications disseminated to parents annually
0 1 000 1 000 MIA, HERA, HOPS,
Training health and social service providers on Youth Friendly Services skills
Number of health and social service providers who are trained to be youth friendly annually
0 75 75 MOH, Agency for Youth and Sports, Medical Faculty and NGOs, Ministry of Labor and Social Welfare
Develop and integrate life-skills health based education within the school curricula
Program defined for teaching on HIV/AIDS/STI and reproductive health issues
0 1 N/A MoE, NGO's Bureau of Education of MoE.

Application Form for Proposals to the Global Fund Page 38 of 72
Objective:1 To prevent HIV transmission among young people Main activities Process/Output Baseline Targets Responsible/Implementing Indicators (indicate
one per activity; refer to Annex A)
(Specify year)
Year 1 Year 2 agency or agencies
Training of teachers in primary and secondary schools on HIV/AIDS/STI and reproductive health issues
Number of teachers trained per year
0 393 786 MoE, Institute of Epidemiology, Medical Chamber, Macedonian Medical Association, NGO's
Production of training manual for teachers
Number of manuals distributed per year
0 393 786 MoE, NGO's Bureau of Education of MoE.
Promoting safe behavior among young people doing military service
Number of recruits receiving HIV/AIDS education annually
N/A 13 000 16 000 MoD, Institute of Epidemiology, Medical Chamber, Macedonian Medical Association
The second objective is particularly important because injecting drug users are the most vulnerable group to rising HIV/AIDS infection rates in the region. IDU numbers have increased substantially over the past decade across Macedonia. Apart from unsafe injecting practices, many drug users may engage in unsafe sexual behavior including a cross over between injecting drug users and sex work. According to official state statistics, 80% of intravenous drug users are infected with hepatitis C. Consequently, this objective includes a focus on preventing other blood-borne infections in addition to HIV/AIDS. The ten main activities are broadly focused on both harm reduction activities and drug treatment programs. The first activity focuses on providing additional resources to three existing programs in the country (Skopje, Strumica and Bitola), resulting in increasing numbers of injecting drug users receiving harm reduction services. Additional resources will be used to expand both services within stationary and mobile units. Services include exchange and proper disposal of injecting equipment, peer education on HIV/AIDS, safe injecting, safe sex, treatment of consequences of long term and improper injecting, other medical and social services and counseling, counseling and referral for drug treatment. The second activity will involve the introduction of seven new HR programs, 2 in the capital Skopje and 5 in other cities in the country. Centers will offer both stationary and mobile services. This activity will include services specifically targeting sex workers who inject drugs. As part of this activity, training and technical support will be provided to new centers from existing ones. The third activity will focus on trying to improve IDUs experience of accessing health and social care by trying to break down stigma and discrimination experienced by IDUs from health and social service personnel. This will be done primarily through training. Emphasis will also be placed on trying to improve access to medical treatment by lobbying for IDUs to be included in the provision of social insurance, as many are currently excluded because of not having completed primary school. IDUs themselves would be actively involved in all lobbying and advocacy activities. The fourth activity focuses on the police and aims to generate a more understanding environment for IDUs. Currently use of drugs is illegal and IDUs are treated as criminals and face various legal, social, health and administrative problems. These may include repressive police measures, arrest, interrogation and physical harassment. This environment is particularly severe in some parts of the country and makes it difficult for NGOs and others to reach IDUs with harm reduction programs and other interventions. This activity will focus on training of police professionals in harm reduction principles and creating an enabling environment for such interventions.

Application Form for Proposals to the Global Fund Page 39 of 72
The fifth activity involves campaigning to try to promote a more positive attitude towards people who use drugs and towards harm reduction programs, in particular. In addition to specific problems faced by IDUs in relation to attitudes of health professionals and the police, they experience widespread stigma and discrimination within society as a whole. This activity will use a mixture of information strategies to seek to promote more positive attitudes towards IDUs The sixth activity focuses on establishing a national strategy for decentralization of drug treatment programs and building support for these. There is strong commitment from both government and NGOs to establishing these much-needed services. The key input required for these are dedicated and motivated human resources who will be committed to the decentralization process. The seventh activity involves decentralizing drug treatment services to an additional six centers throughout the country. This initiative would be a bold and significant input to a much-needed process by making funds available, particularly for the human resources for this activity. This would allow new and motivated staff to be recruited specifically for these centers. The eighth and ninth activities are linked to the decentralization of drug treatment and involve the provision of counseling/early interventions and establishment of self help groups respectively. The final activity involves provision of training for three different groups. One day training seminars will be held for key local leaders and national decision makers to brief them on the national strategy and the implementation plans. Continuous education will be offered to staff of the units, consisting of three three-day workshops in the first year and one in subsequent years.
TableIV.26.3
Objective:2 To prevent transmission of HIV and blood-borne diseases among IDUs Main activities Process/Output Baseline Targets Responsible/Implementing indicators (indicate one
per activity; refer to Annex A)
(Specify year)
Year 1 Year 2 agency or agencies
Scaling up three existing harm reduction programs
Number of injecting drug users receiving harm reduction interventions annually
2000
2900
3300
HOPS, Izbor, Via Vita
Establishing 7 new harm reduction programs including development of special services for sex workers who are IDUs and female IDUs
Number of injecting drug users receiving harm reduction interventions annually
N/A 1000 1600 HOPS, Izbor, Via Vita, Opcija Ohrid, HELP Gostivar and other NGOs
Training of health and social workers from primary health care and social welfare services in harm reduction principles and work with IDUs
Number of health and social workers who received training annually
N/A 50 30 HOPS, Izbor, Via Vita, Opcija Ohrid, HELP Gostivar and other NGOs Ministry of Labor and Social Welfare

Application Form for Proposals to the Global Fund Page 40 of 72
Objective:2 To prevent transmission of HIV and blood-borne diseases among IDUs Main activities Process/Output Baseline Targets Responsible/Implementing indicators (indicate one
per activity; refer to Annex A)
(Specify year)
Year 1 Year 2 agency or agencies
Training of police professionals in the basic principles of harm reduction and work with IDU
Number of police professionals who receive training annually
N/A 25 25 HOPS, Izbor, Via Vita, Opcija Ohrid, HELP Gostivar and other NGOs
Campaign to create more positive public opinion towards harm reduction programs, in particular, and IDUs, in general.
Number of people receiving information annually
N/A 1000 1500 HOPS, PASSAGE, Izbor, Via Vita, Opcija Ohrid, HELP Gostivar and other NGOs
Developing a national strategy to decentralize drug treatment activities
Strategy developed 0 1 1 Ministry of Health, NGOs
Improving access to drug treatment – decentralization of treatment services for drug users through six new centers
Number of injecting drug users receiving treatment annually
680 800 1000 Ministry of Health, NGOs
Providing pre treatment-counseling and referring to decentralized treatment facilities
Number of people receiving counseling and early intervention annually
c150 300 500 Ministry of Health, NGOs
Development of self-help support networks for drug users on treatment
Number of injecting drug users involved in self help/support groups annually
80-100 300 400 Ministry of Health, NGOs
Training seminars for community leaders, staff working in decentralized centers and decision makers
Number of seminars held annually
0 5 1 Ministry of Health, NGOs
The third objective consists of four broad activities focused on sex workers and their clients. The first activity is promotion of safer sexual practices among sex workers and their clients. This activity will focus on the poorest and most vulnerable group of sex workers, i.e. street-based sex workers. A key part of this activity is implementation of outreach activities and distribution of free condoms, lubricants and informational materials on safer sexual practices to street-based sex workers. Specially designed materials for safer sexual behavior combined with oral information will be provided also to the clients on outreach by trained outreach workers.

Application Form for Proposals to the Global Fund Page 41 of 72
The second activity is about providing a range of professional services for commercial sex workers through outreach. This includes social assistance and counseling, legal consultations and medical assistance and counseling including gynecological checks, STI tests and treatment etc. In order to inform and prepare future stuff for field work with vulnerable groups, this activity will include education of students in the Institute for Social Work and Policy. The third activity is focused on providing services through a ‘drop-in’ facility. These drop-in services will include practical facilities, such as laundry, showers, free meals, in addition to psycho-social support from a team of professionals (including social worker, psychologist, legal adviser etc.). The final activity is focused on developing activities designed to prevent young women beginning sex work. These activities will target youth under 18. These activities will be based on peer educational sessions among high school population in schools and other informal places.
Objective:3 To prevent HIV transmission among sex workers and their clients Main activities Process/Output Baseline Targets Responsible/Implementing indicators (indicate one
per activity; refer to Annex A)
(Specify year)
Year 1 Year 2 agency or agencies
Number of sex workers reached with targeted HIV/AIDS interventions annually
103 135 200 Promotion of safer sex, condom use and distribution of free condoms among sex workers and their clients
Number of clients reached with targeted HIV/AIDS interventions annually
0 1 200 2 500
HOPS
Providing medical and social support for sex workers including STI treatment
Number of sex workers using medical, social and legal services annually
103 125 160 HOPS
Provision of drop-in center for sex workers
Number of sex workers using drop-in facilities annually
0 50 100 HOPS
Prevention of entry into sex work among young women
Number of young people reached with prevention interventions annually
0 1000 2500
HOPS
Objective 4 includes four broad activities focused on men who have sex with men. This group is felt to be vulnerable in the country because of experience in other countries and because this group is highly stigmatized and discriminated against meaning that men in this group are highly secretive about their sexual activities. Consequently, it is difficult to identify these people and to reach them with targeted activities. The first activity will focus on the production of appropriate literature for MSM in the Macedonian and Albanian languages. To date, there has only been one booklet (produced in 1999) on this issue. Under this program, a range of relevant printed materials will be produced including HIV educational and prevention materials that directly address the needs and situation of this group. Other media options will also be considered. The materials will be distributed nationwide. The distribution will be by ethnic Macedonian and Albanian peers. The second activity will seek to address a current problem, namely that condoms/lubricants are not readily available in the country and are not generally used in the MSM community. One NGO, HERA, conducted a survey among 200 MSM who reported that they either never or rarely use condoms in their sexual intercourse. Initially,

Application Form for Proposals to the Global Fund Page 42 of 72
condoms and lubricants will be made available free of charge to promote their use. This provision will be phased out over the life of the program and replaced with more sustainable approaches such as social marketing, improved availability etc. The third activity will seek to establish a national gay and lesbian center that includes a website, helpline, counseling and other services related to HIV/AIDS/STIs and gay and lesbian issues. Personnel will be trained to perform these tasks as well as needed outreach activities. The center will be established within existing NGO premises. The helpline will be based on the existing helpline which will operate with extended hours and will act as a central point for gay and lesbian information related to HIV/AIDS in Skopje. The center will serve as a base for training and outreach activities for MSM.
The final activity recognizes that currently very few organizations currently target HIV/AIDS information and counseling at MSM. Activities will aim at increasing the number of organizations doing this, particularly in cities other than Skopje, to create a network of support for the MSM community.
Objective:4 Prevention of HIV transmission among vulnerable groups/reducing vulnerability MSM Main activities Process/Output Baseline Targets Responsible/Implementing indicators (indicate one
per activity; refer to Annex A)
(Specify year)
Year 1 Year 2 agency or agencies
Production and distribution of targeted HIV prevention literature.
Number of distributed brochures annually
200 (1999)
2 000 3 000 HERA-Skopje
Free distribution of condoms and lubricants through clubs and other locals frequented by MSM
Number of distributed condoms annually
2000 (2001)
10 000 15 000 HERA-Skopje
Establishment of national gay and lesbian centre focusing on HIV/AIDS
Working hours of the Hotline (per month) Number of pre and post testing sessions in the Counselling service (hours per month)
60
40
150
100
240
200
HERA-Skopje, CHCR-Skopje
Expand the number of organizations working with MSM on HIV/AIDS
Number of organizations with HIV/AIDS activities focused on MSM
2 3 5 HERA-Skopje, CHCR-Skopje
The fifth objective includes seven broad activities targeted on the Roma community, who constitute 2% of the country’s population (approx 44 000 people) and are its most economically and socially marginalized ethnic group. A UNICEF/World Bank study of Roma youth in 1999 showed that 27% live in temporary makeshift housing with minimal facilities, 48% are without indoor plumbing, 55% of Roma mothers had not completed primary school and 31% of Roma children did not attend school. The first activity will involve training peer educators. Representatives selected from all Roma communities will be trained as peer educators through workshops, held by professional peer trainers and representatives from NGOs. Two five-day workshops will be held in the first year and one in subsequent years. The selection criteria for participants will include holding an informal leadership position in the target group, reliability, communication skills, previous experience and readiness to devote sufficient time and efforts to the implementation of the project activities. Peer educators will be trained in

Application Form for Proposals to the Global Fund Page 43 of 72
HIV/STI and reproductive health issues and how to promote open conversation between children and parents. The second activity will involve expanding peer education activities in Roma communities using peer educators trained in activity 2. It is envisaged that these activities will take place throughout the country. It is estimated that during a year each of the peers would contact approximately 130-150 Roma. The third activity will focus on training of social and health professionals to engage more constructively with members of the Roma community. Through a three-day seminar social and health care professionals will be trained to improve their IEC skills related to Roma people to make their communications more culturally sensitive and adapted to target groups. This activity will cover the specifics of Roma culture, behavior and beliefs in order to improve the work of the professionals with this vulnerable group. The fourth activity involves seeking to detect STIs early among Roma women. Currently, many members of the Roma community often lack health insurance and are reluctant to attend for medical examinations unless they are very sick. Consequently, the campaign "FOR MY HEALTH" will be launched offering counseling and free examinations through the already existing primary care medical network. The fifth activity involves promoting and distributing condoms. Because of widespread poverty among Roma people and the relatively high price of good quality condoms, this activity will seek to distribute condoms among the Roma community for both contraception and HIV prevention. A strong focus will be placed on addressing existing social norms, such as male dominance in sex decision making. A combined strategy will be used whereby condoms are provided free and ensuring that in each community there is at least one place where good quality condoms can be purchased continuously. The sixth activity will focus on developing, printing and distributing information materials tailored to the needs of the Roma people. Brochures will be developed which will cater for literate populations and those with extremely limited literacy. The brochures will focus on HIV/STI, reproductive health, open conversations between children and parents, patient's rights, drug use etc. All materials will be based on the languages spoken in local Roma communities. The final activity will consist of a local media campaign focused on HIV/AIDS/STI awareness for the Roma community. The first audio and video spot related to safe behavior in the context of HIV/STI prevention and prevention of drug use will be produced. It will be specially tailored to the needs of Roma people. The local radio and TV stations will contribute by broadcasting them on a regular basis. The local Roma media have a significant influence which can be used positively in HIV/AIDS prevention activities.
Objective:5 To prevent HIV transmission among the Roma community Main activities Process/Output Baseline Targets Responsible/Implementing indicators
(indicate one per activity; refer to Annex A)
(Specify year)
Year 1 Year 2 agency or agencies
Training of Roma peer educators
Number of peer educators trained per year
3 24 18 MIA, Roma NGOs
Expanded peer outreach activities in Roma communities
Number of Roma people educated per year
Not known
2 300 3 700 MIA, Roma NGOs
Training of social and health care professionals for better IEC with Roma people
Number of social and health care professionals trained per year
0 26 13 Institute of Epidemiology, Medical Chamber Ministry of Labor and Social Welfare

Application Form for Proposals to the Global Fund Page 44 of 72
Objective:5 To prevent HIV transmission among the Roma community Main activities Process/Output Baseline Targets Responsible/Implementing indicators
(indicate one per activity; refer to Annex A)
(Specify year)
Year 1 Year 2 agency or agencies
Early detection of STIs among Roma women of reproductive age
Number of STIs examinations performed among Roma population in reproductive age (annually)
Not known
3 700 7 300 MoH, Primary Health Care Centers, Medical Centers,
Condom promotion and free distribution
Number of condoms distributed annually
10 000 65 000 100 000 MIA, Local Roma NGOs
Tailored information distribution for Roma people, including people with very limited literacy
Number of brochures distributed annually
Not known
34 000 25 000 MIA, local Roma NGOs
Roma local media campaign for HIV/AIDS/STI awareness
Number of special educative shows broadcasted on local Roma TV and radio annually
1 48 96 BTR, SUTEL, MRTV , production media house
The sixth objective is focused on preventing HIV transmission among prisoners. There are a total of eight prisons in Macedonia. They house 1 573 prisoners, of whom 98% are male. There are also special facilities for juveniles. A report in 2000 (produced by the Clinic for Infectious Diseases, WHO, MoH and MoJ) highlighted that a high percentage of prisoners are drug users involved in high risk sexual behavior. Access to health services is poor, with a lack of medical staff and available drug treatment. The five broad activities proposed here will be implemented jointly between the government and an NGO. The first activity will focus on training of prison social and medical staff in IEC activities. Four three-day workshops will be held in the first year and three in the second year. It is planned that staff representatives dealing with adults and juveniles will be trained separately because of the different challenges presented by these different groups. During the first year it is planned that 200 people will be trained and 150 in the second year. The government has developed a training centre which could be used for this purpose. The second activity will focus on training peer educators among prisoners. This activity will be developed in partnership with an NGO with a strong track record in running peer education programs. This is a new and very innovative way of working for the country. It is expected to increase access to HIV/AIDS/STI information and to promote safe behavior among the prisoners. During the first year from each of the eight prisons, 6 selected prisoners will be trained. During the second year it is expected that 80 of them will be acting as peer educators. The third activity will focus on improving access to health services and will concentrate on strengthening these facilities which are very poorly equipped. Particular focus will be placed on improving the services needed by IDUs. Under this activity it is planned to renovate the main prison hospital/clinic in Skopje which is responsible for any major medical treatment required by prisoners. The fourth activity will involve developing, printing and distributing printed materials for prisoners. These materials will be designed taking into consideration the information collected through the behavioural survey described in activity 1. It will be tailored to the

Application Form for Proposals to the Global Fund Page 45 of 72
needs of the prisoners and will be adapted for both literate prisoners and those with limited literacy. There will be three different types of brochures focusing on HIV/AIDS prevention, STI information and prevention and condom promotion. It is also planned that separate brochures be developed for social and medical staff working within the prisons. The final activity involves a limited and targeted condom distribution in prisons on the basis that that they have visits from partners and are at times released for weekends. Whilst recognizing the limited nature of this move, it is an important and innovative approach to seeking to control the spread of HIV in the country’s prisons.

Application Form for Proposals to the Global Fund Page 46 of 72
Objective:6 To prevent HIV transmission among prisoners Main activities Process/Output Baseline Targets Responsible/Implementing indicators
(indicate one per activity; refer to Annex A)
(Specify year) 2003
Year 1
Year 2
agency or agencies
Training of prison social and medical staff in conducting IEC
Number of prison social and medical staff trained per year
5 200 150 MoJ, Institute of Epidemiology, Medical Chamber, MIA,
Training of peer educators among prisoners
Number of prisoners acting as peer educators (cumulative)
0 48 80 MoJ, Institute of Epidemiology, MIA
Improving access to health services
Number of prisoners receiving good health services including a drug treatment annually
N/A 500
900 MoJ, MoH
Tailored information distribution for prisoners
Number of printed and distributed brochures annually
N/A 4 800 6 300 MoJ, MIA
Condom promotion and distribution
Number of condoms distributed annually
N/A 7 000 10 000 MoJ
Objective 7 is focused on improving access to and quality of HIV counselling and testing services. Although much of this objective focuses on testing and the counselling associated with it, the emphasis on counselling goes beyond simply that which is related to testing. It is proposed to achieve this objective through seven main activities. The first activity involves increasing the number of testing centers offering HIV testing in the country with a particular focus on public health institutes, which currently have responsibility for this. There are ten centres for public health in the country, though only four of them currently perform HIV tests. The others do not currently perform HIV tests due to lack of enzymes, testing machines or other needs. In addition, two other facilities, the Clinic for Infectious Diseases and the Republican Institute for Health Protection also perform HIV testing. The Clinic for Infectious Diseases acts as a referral laboratory and is able to perform Western Blot confirmatory tests. A total of six institutions need capacity and infrastructure biulding in order to start performing both HIV testing and counseling.
The second activity will be a new and innovative approach which will seek to take counseling and testing services to vulnerable populations where they are located through the use of outreach teams in non-hospital settings. This work will be possible through NGOs with existing contacts with vulnerable sub-populations. Outreach teams will include members of NGOs and peers from among the population being offered counselling and testing. Outreach activities will include the distribution of condoms and lubricants. These NGOs and peers will act as facilitators between these sub-populations and medical institutions, in order to facilitate outreach testing and counselling with mobile teams. As this is a new and exciting innovation, it is proposed to start this in the second year, having spent the first year developing a national strategy for this through a broad consultative process led by a working group established for this purpose.
The third activity will focus on the development of a training manual and protocols for counseling and testing. To date, there are no protocols on counseling in the country, although some protocols on HIV testing do exist. No consistent training

Application Form for Proposals to the Global Fund Page 47 of 72
for counseling is also available. The proposed activity would be to organize a working group to develop a manual and protocols for testing and counseling. A series of pilot seminars will then be organized on HIV counseling and testing using these materials. Following these, further seminars will then be held to train members of sub-populations on HIV testing and counseling.
The fourth activity involves training of competent counselors from within the NGO sector. This will enhance the quality of HIV/AIDS counseling and will promote HIV testing. This broad activity includes an internationally-facilitated workshop on counselling best practice.
The fifth activity will involve training of medical personnel in issues relating to HIV testing. A series of pilot seminars will be organized on this issue. There is some experience in this area, although to date a very limited (50) number of health personnel have been trained in HIV testing and counseling.
The sixth activity involves integration of counseling/testing into the medical/social service system through inclusion of HIV counseling and testing issues in the curicula of medical and social educational institutions. This will be establlished through legislation The final activity involves development and dissemmination of leaflets promoting HIV testing and counseling. NGOs have experience of producing this type of brochures.
Objective:7 Development of HIV counseling and expanded access to HIV testing. Main activities Process/Output Baseline Targets Responsible/Implementing indicators
(indicate one per activity; refer to Annex A)
(Specify year)
Year 1 Year 2 agency or agencies
Increasing number of testing centers
Number of testing centers and facilities
6 10 12 MoH
Outreach teams for counseling on HIV/AIDS
Number of outreach activities for HIV/AIDS counseling
0 0 30 HERA, MIA, HOPS, TRUST, MoH
Development of training manual with protocols for counseling/ testing
Number of printed manuals distributed annually
0 1 000 1 000 HERA, MIA, HOPS, TRUST, MoH, RIHP, CID
Training of competent counselors
Number of counselors trained (cumulative)
10 20 50 HERA
Training of health providers on counseling and testing
Number of medical personnel trained (cumulative)
100 300 500 MoH
Integration of counseling/ testing into the medical/social service system
Material developed for integration into curricula
N/A 1 N/A MoH
Production of brochures on HIV/AIDS counseling and testing
Number of printed brochures
120 000 200 000 400 000 HERA, MIA, TRUST, HOPS

Application Form for Proposals to the Global Fund Page 48 of 72
Objective 8 focuses on increasing national capacity to conduct biologic and behavioral surveillance relating to HIV/AIDS and STIs. This data is vital in assessing the actual position of the country in relation to the epidemic currently and for forecasting the likelihood of disease spread in the future. Seven broad activities are proposed under this objective. The first activity is to increase the capacity of the Ministry of Health to use currently available HIV/AIDS/STI case report data for public health action. In order to increase the capacity of Ministry of Health staff to analyze and use existing HIV/AIDS/STI data, a workshop will be held in the first year to address aspects of data analysis, interpretation, report writing and dissemination, and the use of the resulting data for programming and policy making. This will involve all national providers and users of these data, as well as the involvement of external technical support to help guide the process and provide experience from a national setting that has faced similar issues. In addition, planning and review workshops will be held annually. The second activity will involve training in second generation surveillance. In order to build capacity in second generation surveillance in the country, training workshops will be held for health professionals working within the surveillance system in Macedonia. This activity will also play a role in drawing more institutions and their staff into the system. It is proposed to hold 4 four-day workshops per year with an estimated number of 30 people attending each workshop. The number of workshops will be highest in the first year in order to establish initial levels of training which will be updated and upgraded in workshops in subsequent years. The third activity will be to develop a written protocol for the HIV/AIDS/STI surveillance system. A formal written protocol is essential so that all stakeholders are clear on their respective roles and understand the various surveillance procedures. A formal protocol will also serve as a template against which to evaluate the existing surveillance system. This type of evaluation could be done fairly easily and would offer suggestions to strengthen data quality and completeness within the HIV/AIDS/STI case reporting system. It is proposed to develop this written protocol by the end of the first year through an approach which involves participation of all major stakeholders. The fourth activity will involve conducting serological surveys and prevalence studies among vulnerable sub-populations including IDUs, sex workers, prisoners, MSM and STI patients. Serological surveys will be carried out to assess HIV prevalence rates among vulnerable groups. These groups will include those identified in this proposal but others may be added based on the outcome of the workshops described earlier in this section and the way the HIV/STIs spread in the country over time. These surveys would be carried out through collaboration between technical experts and NGOs/government institutions working with these vulnerable sub-populations. A report showing the results of these surveys will be produced annually. The fifth activity involves behavior surveys and studies among vulnerable sub-populations including IDUs, sex workers, prisoners, MSM, Roma population and young people. Based on the recommendations of an external review, behavioral surveillance of vulnerable sub-populations is identified as the next priority for the country’s surveillance system. Access to these groups had been identified as a challenge which will be overcome by working closely with NGOs already working with these groups. This activity will be carried out for each recognized sub-population. A report showing the results of these surveys will be produced annually. The sixth activity involves improving reporting and feedback within the national HIV/AIDS/STI surveillance system. In order to strengthen the national HIV/AIDS/STI surveillance system an improved and updated reporting form is required as the current form has been in use for more than 20 years. In addition, current STI report forms only cover syphilis and gonorrhoea and this needs to be extended. Current usage of these forms is sub-optimal and efforts will be made to increase this, particularly by providing regular feedback of data and its interpretation to health professionals. This feedback will

Application Form for Proposals to the Global Fund Page 49 of 72
seek to include both public and private health sectors. Meetings will be held in 20 different municipalities with private and public sector health professionals to explain the new forms. The final activity involves developing a laboratory quality assurance program for HIV testing. To ensure accurate diagnosis of HIV for clinical purposes and also for surveillance purposes, the Clinic for Infectious Diseases [CID] laboratory should develop and coordinate a quality assurance and training program for all laboratories performing HIV tests in the country. The central CID laboratory will also seek to participate in an international quality assurance program to maintain its own capacity and to build capacity to conduct the national quality assurance program by developing linkages with a national laboratory that has developed proficiency in both national quality assurance programs.
Objective:8 To improve HIV/AIDS/STI surveillance and forecasting to strengthen planning of the national response
Main activities Process/Output
Baseline Targets Responsible/Implementing
indicators (indicate one per activity; refer to Annex A)
(Specify year)
Year 1 Year 2 agency or agencies
Increase capacity of the Ministry of Health to use currently available HIV/AIDS/STI case report data for public health action
Workshops conducted annually
0 1 1 Ministry of Health, National Public Health Institute, Institute of Epidemiology
Training in second generation surveliance
Number of training workshops annually
0 4 2 Ministry of Health, National Public Health Institute, Institute of Epidemiology
Develop a written protocol for the HIV/AIDS/STI surveillance system.
Written protocol for HIV/AIDS/STI surveillance system developed
0 1 N/A Ministry of Health, National Public Health Institute, Institute of Epidemiology, Clinic of Dermatology, Clinic of Infectious Diseases
Serological surveys and prevalence studies among vulnerable sub-populations including IDUs, sex workers, prisoners, MSM and STI patients
Survey reports and results published
0 1 1 Ministry of Health, National Public Health Institute, Institute of Epidemiology, NGOs
Behavior surveys and studies among vulnerable sub-populations including IDUs, sex workers, prisoners, MSM, Roma population and young people
Survey reports and reports published
0 1 1 Ministry of Health, National Public Health Institute, Institute of Epidemiology, Institute of Sociology, NGOs

Application Form for Proposals to the Global Fund Page 50 of 72
Objective:8 To improve HIV/AIDS/STI surveillance and forecasting to strengthen planning of the national response
Main activities Process/Output
Baseline Targets Responsible/Implementing
indicators (indicate one per activity; refer to Annex A)
(Specify year)
Year 1 Year 2 agency or agencies
Improving reporting and feedback within the national HIV/AIDS/STI surveillance system
Reporting forms for HIV/AIDS/STIs updated and improved
0 1 N/A Ministry of Health, National and Private Health Sector, Institute of Epidemiology, Institute of Public Health
Develop a laboratory quality assurance program for HIV testing
Written protocol developed and reference laboratory nominated
0 1 N/A Ministry of Health, Public Health Institutes, Clinic for Infectious Diseases, Central Biochemical Laboratory, Institute for Transfusiology
Objective 9 focuses on providing health care and psychosocial support to PLWHAs. Currently, there are relatively few known people living with HIV/AIDS in Macedonia. However, this situation may not reflect the true number of people living with HIV/AIDS. This reported number may increase with improved surveillance and increased access to testing. Currently, access to antiretroviral drugs is very limited. Support is requested from GFATM to assist with this process and for funding for antiretroviral therapy for those people who are unable to access this treatment in other ways. There are six broad activities that will contribute to reaching this objective. The first activity focuses on inclusion of ARVs on the drug list reimbursed by the Health Insurance Fund. This is referred to as the ‘positive list’. Currently 3 ARVs drugs are included on the list, but there is strong commitment by the Ministry of Health and Health Insurance Fund to add additional ARVs on this list. In addition, these drugs need to be registered in the country and activities to support this process will be included within this broad activity. The second activity recognises the need for establishment of national guidelines for treatment and care of PLWHAs as one of the main prerequisites for delivery of good health care. Currently WHO and CDC guidelines for treatment and care are being used but under this activity, guidelines specific for Macedonia will be produced. Once the national guidelines have been developed they will be printed as a booklet and disseminated through the health care network. The third activity involves training for health professionals on the clinical management of PLWHAs, with a particular focus on treatment with ARVs. This will involve bringing foreign experts for training purposes and taking national health providers to other countries to see how treatment and care are organised. The fourth activity is focused on providing improved treatment and care infrastructure. To achieve this, part of the Clinic for Infectious Diseases will be refurbished involving the provision of additional patient rooms and offices for counselling. This will allow daily follow up of patients. In order to assure good quality monitoring of the therapy, the Immunological Laboratory within the Clinic, which serves as a national reference laboratory, will be equipped with PCR, CD4 cell counter, test kits, and microscope. The key output expected of this is that PLWHAs benefit from improved standards of care including access to ARVs. The fifth and sixth activity are linked as they are both focused on the provision of psychosocial support for PLWHAs. The former is focused on training of health and social workers, NGO volunteers and faith based organisations’ members on how to provide

Application Form for Proposals to the Global Fund Page 51 of 72
psychosocial support, while the latter is focused on provision of such services. Currently some NGOs provide support for PLWHAs and their families. These activities are intended to improve the quality and reach of these services.

Application Form for Proposals to the Global Fund Page 52 of 72
Objective:9 To provide health care and psychosocial support to PLWHAs
Main activities Process/Outpu
t Baseline Targets Responsible/Implementing
Indicators (indicate one per activity; refer to Annex A)
(Specify year)
Year 1 Year 2 agency or agencies
Inclusion of ARV on the drug list reimbursed by the Health Insurance Fund
Number of ARVs included on the drug list reimbursed by the Health Insurance Fund
3 6 12 Ministry of Health, Health Insurance Fund, Clinic for Infectious diseases
National Guidelines for treatment and care of PLWHAs
Developed National Guidelines for treatment and care of PLWHAs
0 1 n/a Clinic for Infectious diseases
Provision of training to health professionals on the clinical management of PLWHAs , with particular focus on ARVs
Number of health professionals trained
0 5 10 Clinic for Infectious diseases
Building up the treatment and care infrastructure
Number of PLWHAs receiving ARVs
N/A 10 15 Clinic for Infectious diseases
Provision of training for psychosocial support for PLWHAs including development of written training
Number of health and social workers, NGO volunteers and faith-based organisations’ members trained (cumulative)
0 10 30 Clinic for Infectious Diseases , Ministry of Labour and Social Welfare, NGO HERA, NGO MIA, Faith-based organisations
Provision of psychosocial support for PLWHAs
Number of PLWHAs receiving psychosocial support
Currently, no baseline figures for this are available. These will be collected within six months of the start of the program and targets set on the basis of those and forecasts based on surveillance data.
Clinic for Infectious Diseases, Ministry of Labour and Social Welfare, NGO HERA, NGO MIA, Faith-based organisations
Objective 10 underpins all the other objectives because the capacity and coordination which are developed here will contribute significantly to the successful implementation of the other objectives. It is proposed to implement this objective through 12 broad activities. The first activity focuses on building the institutional capacity of the various agencies that will implement this program. Building of technical capacity has been covered under specific objectives. However, this activity will focus on building capacity in more general areas such as management, financial management, reporting, personnel management etc. This is particularly important in the NGO sector as more organizations are formed to work in this area.

Application Form for Proposals to the Global Fund Page 53 of 72
The second activity focuses on meeting the reporting requirements of the program, both internal and external and both financial and narrative. This will involve strengthening the human resources capacity of the Principal Recipient and other groups involved in reporting, e.g. implementing agencies. The third activity focuses on enabling people working within the program to develop useful links by networking with others working in similar fields in other countries through making trips to those countries. The fourth activity focuses on ensuring that the program is adequately monitored and evaluated at three different levels – goal, objective and activity. This involves strengthening of the capacity of the Principal Recipient and implementing agencies. The fifth activity involves having a series of meetings to discuss progress of the program, including any problems that might be encountered. This activity includes provision for holding an annual HIV/AIDS conference. The sixth activity involves sharing lessons learned from the program through their publication. This activity provides for one such publication in each of years 2 & 3. The seventh activity provides for development and review of a National HIV/AIDS Strategy. This is currently in an advanced state of preparation. It is proposed to be finalized and publicized in year 1 and reviewed in year 3. The eighth activity provides for audits to be carried out at all levels of the program. The ninth activity involves activities which will contribute to development of additional policies and strategies, particularly at national level. It is envisaged that these would expand on and strengthen the National HIV/AIDS Strategy and may in some cases require supporting legislation. The tenth activity explicitly focuses on the CCM and its standing committee with the intention of supporting these structures and making sure they function effectively. The eleventh activity involves establishing a system for calculating the amount of money being spent nationally on HIV/AIDS annually. It is proposed that a firm of accountants be hired to do this on an annual basis. The final activity involves liaison with politicians to keep them informed of program progress and to continue to build political support for HIV/AIDS activities in the country.
Objective:10 To strengthen coordination and capacity of the national response to HIV/AIDS Main activities Process/Output Baseline Targets Responsible/Implementing indicators
(indicate one per activity; refer to Annex A)
(Specify year)
Year 1 Year 2 agency or agencies
Building institutional capacity of participating organisations
Number of workshops held
0 4 4 Principal Recipient, CCM Standing Committee
Reporting Quarterly reports submitted to GFATM on time and to required standard
N/A 4 4 Principal Recipient

Application Form for Proposals to the Global Fund Page 54 of 72
Objective:10 To strengthen coordination and capacity of the national response to HIV/AIDS Main activities Process/Output Baseline Targets Responsible/Implementing indicators
(indicate one per activity; refer to Annex A)
(Specify year)
Year 1 Year 2 agency or agencies
Establishing linkages
Number of people making international visits
0 2 2 CCM Standing Committee
Ensuring effective M&E
Reports on progress of program produced on time and to required standard
0 4 4 Principal Recipient
Meetings Number of meetings held
0 10 10 CCM Standing Committee
Sharing lessons learned
Number of publications
0 0 1 CCM Standing Committee
Development and Review of National Strategy
National Strategy introduced (Y1) and reviewed (Y3)
0 1 N/A CCM
Audits Program and individual projects conducted as required
0 100% 100% Principal Recipient
Policy development
Number of policies introduced
0 2 2 CCM Standing Committee
CCM and standing committee
Number of meetings of CCM Standing Committee
N/A 5 5 CCM
Systems for tracking national expenditure on HIV/AIDS
Annual report on national expenditure on HIV/AIDS
0 1 1 Principal Recipient
Liaison with politicians
Number of politicians reached
0 20 20 CCM Standing Committee
27. Describe how the component adds to or complements activities already
undertaken by the government, external donors, the private sector or other relevant partner: (e.g., does the component build on or scale-up existing programs; does the component aim to fill existing gaps in national programs; does the proposal fit within the National Plan; is there a clear link between the component and broader development policies and programmes such as Poverty Reduction Strategies or Sector-Wide Approaches, etc.) (2–3 paragraphs):
To date, HIV/AIDS activities have been implemented on a project basis that target only a small percentage of the people in need. Further these projects have generally not been co-ordinated and have been sporadic in duration. The program detailed in this application represents an integrated approach at the national level. Further, it increases the scope activities to include vulnerable sub-populations that have not previously been included, e.g. Roma and prisoners. The program proposed in this document builds on the

Application Form for Proposals to the Global Fund Page 55 of 72
foundation of previous activities but is far more comprehensive than anything that has been implemented previously. Within the application, programs can be divided between those that build on existing activities and those in which no significant programs are now active. Objectives 1 (Youth), 2 (IDUs), 3 (Sex workers), 4 (MSM) currently have significant levels of activities, largely developed and implemented by the NGOs. Objectives 7 (Counselling and testing), 8 (Surveillance), 9 (Care for PLWHA) and 10 (Strengthening of national response to HIV/AIDS) are currently being addressed in a relatively minimal way and will be significantly expanded through this program. Objectives 5 (Roma) and 6 (Prisons) represent completely new activities. 28. Describe innovative aspects to the component: (1–2 paragraphs) The program blends well established activities with those that bring an innovative approach to reaching vulnerable sub-populations. In particular the objectives targeting the Roma community and prisons are particularly innovative. The Roma community is a vulnerable sub-population for a number of reasons including the fact that it is by far the lowest socio-economic group in Macedonia and outreach is made particularly difficult by widespread illiteracy and social exclusion. The program addresses this by using peer-counsellors and personal outreach within the community. Prisons are particularly vulnerable to HIV/AIDS infection and the prison authorities in Macedonia are very receptive to addressing this issue including training of personnel, peer counselling and improved health services so that an integrated approach can be implemented in the prison system. 29. Briefly describe how the component addresses the following issues (1 paragraph per item):
29.1. The involvement of beneficiaries such as people living with HIV/AIDS: Given the limited number of PLWHA in Macedonia, they have not yet become actively involved in policy and implementation. This absence is recognised as a problem. Objective 9 has several broad activities focused on PLWHA that will raise awareness and will support the establishment of self-help groups and active communities of PLWHA. This goes beyond the focus of delivering peer support, but will also start lobbying for treatment, monitoring treatment information and actively shaping the information delivered by peers. Other beneficiaries will also be involved in design, implementation and M&E of specific activities. This is already the case in certain areas of work, e.g. with IDUs and sex workers and will be expanded in these and other areas. 29.2. Community participation: Community participation in the application is highlighted by the strong involvement of NGOs. NGOs form a vital link in civil society to assure the involvement of citizens within the community in these activities. The decentralisation of medical services to the local government level also strengthens community involvement and this is reflected in the facilities and provision of services to IDUs and to youth. On a more targeted basis, the use of peer counsellors in the Roma, youth and prison communities provides direct participation of these groups. 29.3. Gender equality issues Gender issues are covered both by general population interventions, as well as targeted at marginalized groups. All the models for interventions in the general population and youth are well disbursed with activities by gender. The gender implications of HIV/AIDS and other STIs will be addressed in outreach materials and trainings. Many of the activities of the program will focus on women that lack equal opportunities within their life and community, including women involved in sex work and women from the Roma community.

Application Form for Proposals to the Global Fund Page 56 of 72
29.4. Social equality issues Social equality and the increased risk and lack of access to socio-economically disadvantaged groups is directly addressed. This is shown in the targeting of vulnerable populations of which four of the six target groups are economically disadvantaged and five of the six groups suffer from discrimination. The provision of VCT and care and support are designed to be inclusive across social and economic distinctions.
29.5. Human Resources development: The lack of human resources to address HIV/AIDS is a fundamental barrier. The training of medical and support personnel, peer counsellors and educational personnel is a fundamental and crucial element of this proposed program across objectives. Steps have been built into program design which will institutionalise the building of human resources, e.g. by the adapting of appropriate curricula and developing of protocols and manuals.

A
SECTION V – Budget information 30. Indicate the summary of the financial resources requested from the Global
Fund by year and budget category:
Table V.30
Resources needed (USD)
Year 1 Year 2 Year 3 (Estimate)
Year 4 (Estimate)
Year 5 (Estimate)
Total
Human Resources
613162 650579 755620 N/A N/A 2019361
Infrastructure/ Equipment
786135 252303 194180 N/A N/A 1232618
Training/ Planning
304548 280729 257992 N/A N/A 843269
Commodities/ Products
502072 445734 459830 N/A N/A 1407636
Drugs 52010 97002 106641 N/A N/A 255653
Monitoring and Evaluation
51740 45023 45923 N/A N/A 142686
Administrative 121168 124101 129705 N/A N/A 374974
Other 11036 11257 11482 N/A N/A 33775
Total 2441871 1906728 1961374 N/A N/A 6309973
3c
Pb Pfu Ulsm
*
C
The budget categories may include the following items: Human Resources: Consultants, recruitment, salaries, etc. Infrastructure/Equipment: Building infrastructure, cars, microscopes, etc. Training/Planning: Training, workshops, meetings, etc. Commodities/Products: Bednets, condoms, syringes, educational material, etc. Drugs: ARVs, drugs for opportunistic infections, TB drugs, anti-malaria drugs, etc. Monitoring & Evaluation: Data collection, analysis, reporting, etc. Administrative: Overhead, costs for Principal Recipients associated with managing the project, audit costs, etc Other (please specify):
pplication Form for Proposals to the Global Fund Page 57 of 72
1. For drugs and commodities/products, specify in the table below the use of the ommodity, unit costs, volumes and total costs, for the FIRST YEAR ONLY:
lease indicate the International Non-proprietary Name of the medicines, rather than the rand names.
lease indicate what the commodity/drug will be used for (e.g., whether antiretrovirals are or prevention of mother-to-child transmission or adult treatment; whether insecticides are sed for net treatment, retreatment or indoor residual spraying).
nit prices for pharmaceutical products should be the lowest of: prices currently available ocally; public offers from manufacturers; or price information for public information ources.*** If prices from sources other than those specified above are used, a rationale ust be included.
** Sources and Prices of Selected Drugs and Diagnostics for People Living With HIV/AIDS. openhagen/Geneva, UNAIDS/UNICEF/WHO-HTP/MSF, 3rd edition, May 2002

Application Form for Proposals to the Global Fund Page 58 of 72
Volumes indicated in the table below should be consistent with activity targets specified in section 26 when these activities involve procurement. The Total Cost of Drugs and Commodities/Products should equal the sum of the Commodities/Products and Drugs lines for Year 1 in the table above.
Table V.31 Item/unit (using International Non-proprietary Names for pharmaceuticals)
Purpose Unit cost (USD)
Volume (specify measure)
Total cost (USD)
Educational Materials Brochures for young people x 5 types
0.16 300000 48000
Intergenerational conversation publication
3.00 1000 3000
Life skills manual for teachers 20.00 400 8000Peer Education manual
Educational materials for objective 1 with young people
3.00 1000 3000Doverba harm reduction brochures
0.25 20000 5000
HOPS harm reduction brochures
0.25 40000 10000
Via Vitola harm reduction brochures
0.30 30000 9000
Izbor harm reduction brochures
Educational materials for objective 2 with IDUs
0.30 8000 2400
Booklets for sex workers Educational materials for objective 3 with sex workers
0.20 8000 1600
Booklets for MSM Educational materials for objective 4 with MSM
0.50 5000 2500
Brochures for Roma community
0.16 34000 5440
Training booklet
Educational materials for objective 5 with Roma community
1.60 50 80
Brochures for prisoners - 3 types
0.30 15000 4500
Brochures for prison staff
Educational materials for objective 6 with prisoners
1.00 1000 1000
Counseling manual 3.00 2000 6000Counseling brochure
Materials to support objective 7 on counselling and testing
0.16 400000 64000
Biologic surveillance reports 2.00 1000 2000Questionnaires for behavior studies
0.10 14400 1440
Report of behavior surveys
Reports and materials for objective 8 on surveillance 2.00 1000 2000
National protocol on ARV Printed 5.00 300 1500
(http://www.who.int/medicines/library/par/hivrelateddocs/prices-eng.pdf); Market News Service, Pharmaceutical starting materials and essential drugs, WTO/UNCTAD/International Trade Centre and WHO (http://www.intracen.org/mns/pharma.html); International Drug Price Indicator Guide on finished products of essential drugs, Management Sciences for Health in collaboration with WHO (published annually) (http://www.msh.org); First-line tuberculosis drugs, formulations and prices currently supplied/to be supplied by Global Drug Facility (http://www.stoptb.org/GDF/drugsupply/drugs.available.html)

Application Form for Proposals to the Global Fund Page 59 of 72
Item/unit (using International Non-proprietary Names for pharmaceuticals)
Purpose Unit cost (USD)
Volume (specify measure)
Total cost (USD)
treatment Manual on psychosocial care 5.00 100 500Guidelines on working with PLWHAs
materials for objective 9 on care for PLWHAs
5.00 300 1500
Posters 0.30 25000 7500Production of TV programs for media campaign
8000.00 6 48000
Production of radio programs 2400.00 1 2400HIV/AIDS messages in newspapers
Additional educational material for objective 1 with young people 80.00 48 3840
Posters for Roma community 0.30 10000 3000Production and broadcast of videos
3750.00 4 15000
Production and broadcast of audios
Additional educational material for objective 5 with Roma community
400.00 5 2000
Condoms For young people 0.30 120000 36000For IDUs – HOPS 0.30 50000 15000For IDUs - Via Vita 0.30 26000 7800For IDUs - new centers 0.30 40000 12000For IDUs – Izbor 0.30 20000 6000For sex workers and clients 0.30 25000 7500Lubricants 0.30 25000 7500For MSM 0.30 8000 2400Lubricants 0.30 8000 2400For Roma community 0.30 65000 19500For prisons 0.30 7500 2250For counseling teams
Condoms and lubricants for use in each objective
0.30 7000 2100 Other commodities Medical materials to treat consequences of injecting per person per year
1.07 3900 4180
Injecting equipment per person per year
13.26 3900 51700
Disposal of injecting equipment per person per year
For use with IDUs in objective 2
0.69 3900 2700
Hygiene materials per person per year
For use with sex workers in objective 3
7.41 135 1000
Laboratory consumables per center
For centers providing HIV testing
10000.00 4 40000
Medical supplies for Roma community per person per year
For use with Roma community for early diagnosis of STIs
0.66 3700 2442
Gloves 0.06 7500 450Plastic protection for face and eyes
3.00 75 225
Masks 0.12 750 90Metal garbage bins
For use in prisons – objective 6
20.00 13 260

Application Form for Proposals to the Global Fund Page 60 of 72
Item/unit (using International Non-proprietary Names for pharmaceuticals)
Purpose Unit cost (USD)
Volume (specify measure)
Total cost (USD)
White coats 2.50 30 75Disinfectant (liters) 10.00 150 1500Swabs 100Syringes and needles
0.05 1000 50Rapid HIV tests for surveillances
1.00 450 450
HIV tests for surveillance
To be used in surveillance program 5.00 750 3750
HIV tests 5.00 200 1000Other medical tests
For medical treatment of PLWHAs
5.00 1490 7450
Drugs Methadone per person per year
150.00 250 37500
Transportation of Methadone to decentralized centers
100.00 12 1200
Methadone per person per year – prisons
For treatment of IDUs
150.00 10 1500
ARVs per person per year For treatment of PLWHAs
1181.00 10 11810
Total Cost of Drugs and Commodities/Products 554082
31.1. Budget justification: Please indicate assumptions or formulas used to calculate volume of drug/commodity necessary to achieve coverage targets specified in section 26. Detailed explanations for all assumptions and formulae used to calculate costs are given in the detailed budget which is included with this application. In relation to drugs and some other products, costs have been calculated based on an annual price per person treated. Detailed justification of these annual prices per person treated are either supplied in the budget document, e.g. for ARV treatment or can be made available on request. 31.2. In cases where Human Resources (HR) is an important share of the budget, explain to what extent HR spending will strengthen health systems capacity at the patient/target population level, and how these salaries will be sustained after the proposal period is over (1 paragraph):
Human resources are an important share of the budget for this program, comprising 32% over three years. This investment will be focused on health and other systems which deliver services to the most vulnerable sub-populations in Macedonia. Ensuring there are adequate levels of well-trained and highly motivated staff to deliver the results envisaged by this program will be a key factor in determining the success of this program. For example, the provision of additional staff for drug treatment programs is considered essential if these are to be effectively decentralized. The cost of these human resources will be met from a combination of domestic and external resources after completion of the program. It is envisaged that the cost of these salaries will eventually be covered from domestic resources. However, it is unlikely to be possible to fully achieve this within a three year period. It is envisaged that progress towards this will be made during the life of the program but that some external resources will still be needed from other sources, e.g. for support to NGOs for longer than this period.
32. If you are receiving funding from other sources than the Global Fund for activities related to this component, indicate in the Table below overall funding

Application Form for Proposals to the Global Fund Page 61 of 72
received over the past three years as well as expected funding until 2005 in US dollars†††:
Table V.32
1999 2000 2001 2002 2003 2004 2005 Domestic (public and private)
N/A N/A N/A 170358 589737 633464 692476
External N/A N/A N/A 810000 810000 810000 810000Total N/A N/A N/A 980358 1399737 1443464 1502476 Please note: The sum of yearly totals of Table V.32 from each component should correspond to the yearly total in Table 1.b of the Executive Summary. For example, if Year 1 in the proposal is 2003, the column in Table 1.b labelled Year 1 should have in the last row the total of funding from other sources for 2003 for all components of the proposal.
33.Provide a full and detailed budget as attachment, which should reflect the broad budget categories mentioned above as well as the component’s activities. It should include unit costs and volumes, where appropriate. See Annex 14A 34. Indicate in the Table below how the requested resources will be allocated to the
implementing partners, in percentage: Table V.34
Resource allocation to implementing partners* (%)
Year 1 Year 2 Year 3 (Estimate)
Year 4 (Estimate)
Year 5 (Estimate)
Total
Government
41 39 43 N/A N/A 41
NGOs/ Community-Based Org.
59 61 57 N/A N/A 59
Private Sector 0 0 0 N/A N/A 0
People living with HIV/TB/ malaria
0 0 0 N/A N/A 0
Academic/ Educational Organisations
0.4 0.3 0.1 N/A N/A 0.3
Faith-based Organisations
0 0 0 N/A N/A 0
Others (please specify)
0 0 0 N/A N/A 0
Total 100% 100% 100% 100% 100% 100%Total in USD 2441871 1906851 1961374 N/A N/A 6310095
• If there is only one partner, please explain why.
††† Systems for collecting this information are relatively underdeveloped in Macedonia and will be strengthened as part of this program. Figures prior to 2001 are not available. Figures from 2002 are estimates only. There are some resources which are not captured within this analysis such as private sector expenditure on HIV/AIDS and indirect public spending on it. In addition, there may be some overlap in funds reported as domestic and external, e.g. if an external donor provides funding to a domestic NGO.

Application Form for Proposals to the Global Fund Page 62 of 72
Please note that a detailed one year work plan and an indicative work plan for the second year need to be provided with detailed budget. See template in Annex B to this form. This is attached as Annex 10A. Please note: The following three sections (VI, VII and VII) are all related to proposal/component implementation arrangements. If these arrangements are the same for all components, you do not need to answer these questions for each component. If this is the case, please indicate clearly in which component the required information can be found. All relevant information for the proposed HIV/AIDS component is found in this document. The budget for the functioning of the Principal Recipient for both TB and HIV/AIDS components has been included in the budget for the HIV/AIDS component. SECTION VI – Programmatic and Financial management information
Please note: Detailed description of programmatic and financial management and arrangements are outlined in Guidelines Para. VI. 67 – 74, including the main responsibilities and roles of the Principal Recipient (PR).
35. Identify your Principal Recipient(s) (PR)
Table VI.35 Name of PR Ministry of Health N/A Name of contact
Dr Rexep Selamni Minister of Health
Address 50 Divizija bb 1000 Skopje Macedonia
Telephone +389 2 126 206 Fax +389 2 113 014 E-mail N/A
Please note: If you are suggesting having several Principal Recipients, please copy Table VI.35 below.
35.1. Briefly describe why you think this/these organisation(s) is/are best suited to undertake the role of a Principal Recipient for your proposal/component (e.g. previous experience in similar functions, capacity and systems in place, existing contacts with sub recipients etc) (1–2 paragraphs)
The Ministry of Health is the lead ministry in responding to HIV/AIDS in the country and is considered by the CCM well-placed to act both as Principal Recipient for funds received from the Global Fund and secretary to the CCM itself. The MoH has previous experience of managing large amounts of World Bank funds through the establishment of a Program Implementation Unit (PIU). The Ministry has effective working relationships with all organizations included in this proposal. It is proposed to establish a unit within the MoH specifically to fulfill this role. Staff will be deployed from within the MoH to do this. These staff will bring experience of financial management, procurement and monitoring and evaluation which will be accommodated within the well-established institutional framework provided by the Ministry. Additional monitoring and evaluation skills will be drawn in from other institutions, governmental, academic and civil society. Strengthening the biologic and

Application Form for Proposals to the Global Fund Page 63 of 72
behavioral surveillance for HIV/AIDS is a key element of that component of the proposal. Some additional capacity will be required for the MoH to fulfill the role of PR and plans to develop this are included in the proposal, e.g. through an ongoing process of staff development.
35.2. Briefly describe how your suggested Principal Recipient(s) will relate to the CCM and to other implementing partners (e.g., reporting back to the CCM, disbursing funds to sub-recipients, etc.) (1 paragraph)
The Principal Recipient will serve as secretary to the CCM so will provide all administrative and management support required by that body. In particular, the PR will prepare reports for meetings of the main CCM, which will be held at least annually, will be responsible for minute-taking and for ensuring that decisions taken are implemented. In addition, the PR will provide the same services for the CCM Standing Committee which will meet at least 5 times per year. In practice, the Team Leader of the unit within the MoH acting as PR will be an ex officio member of the Standing Committee. A particular responsibility of the Principal Recipient will be to compile quarterly and annual reports of program progress. These will be used to keep the CCM Standing Committee, the main CCM committee, GFATM and other stakeholders informed as to program progress. These reports will include narrative and financial elements, with a strong focus on monitoring of results achieved at three levels – goal, objective and activity. The Principal Recipient will be responsible for all elements of financial management of funds received from GFATM including reporting, contract negotiation, fund disbursement etc. The PR will develop all forms and documents required to perform these duties. The PR will develop contracts with all sub-recipients and will seek to provide them with support needed to ensure that activities are carried out as envisaged within this proposal. This will include exercising responsibility for objective 10 within the HIV/AIDS component of this proposal. The PR will ensure that there is regular communication with sub-recipients both individually and as a whole and this will include opportunity for sub-recipients to reflect critically on the performance of the PR. Sub-recipients will be required to submit narrative and financial reports for the areas they are working on to the PR on a quarterly basis. The PR will ensure that sub-recipients receive copies of all narrative and financial reports for the program as a whole.
36. Describe the proposed management arrangements (outline proposal
implementation arrangements, roles and responsibilities of different partners and their relations) (1–2 paragraphs)
A diagram illustrating the proposed management arrangements for the program is included as Annex 11A. The main CCM committee will have overall responsibility for coordinating the implementation of the program. As it is composed of current TB and HIV/AIDS Commissions, it will be responsible for both components of the program. It will also be responsible for liaison with the UN theme group on HIV/AIDS, whose members will be part of the CCM, and through its Chairperson, the Minister of Health for reporting on program progress to senior politicians and for seeking to ensure that both TB and HIV/AIDS remain high political priorities in the country. The CCM’s Standing Committee will be responsible for overseeing the implementation of the program. This will particularly involve reviewing reports from implementing agencies and the Principal Recipient, analyzing these and taking action to ensure achievement of results and to both prevent and address problems. The Principal Recipient will report to the CCM and will be responsible for the overall management of the program, with particular responsibilities for financial management and M&E. The PR will liaise closely with the National Coordinators for TB and HIV who have had overall responsibility for the technical aspects of this program and will remain responsible for those areas during implementation. Day to day

Application Form for Proposals to the Global Fund Page 64 of 72
implementation of specific elements of the program will be handled by implementing agencies/sub-recipients. Representatives of these groups are mostly included in both the main CCM and the Standing Committee. Where this is not the case, e.g. the Clinic for Infectious Diseases, they will be co-opted into the Standing Committee.
36.1. Explain the rationale behind the proposed arrangements (e.g., explain why you have opted for that particular management arrangement) (1 paragraph)
Four key principles underpin the selection of the proposed management arrangements:
• Utilization of existing structures – where possible, existing structures have been used. Every effort has been made to avoid duplicating such structures
• Inclusiveness and representation – every effort has been made to ensure that everyone working on TB and HIV/AIDS in the country feels involved in the process. This has not always been easy and has resulted in the combined CCM for TB and HIV/AIDS being slightly larger than optimal.
• Efficient management and decision-making systems – the formation of a standing committee and the selection of an established organization as PR means that decisions will be made in a timely manner.
• Simplicity and clarity – where possible, clear and simple structures and systems are proposed.
37. Briefly indicate links between the overall implementation arrangements
described above and other existing arrangements (including, for example, details on annual auditing and other related deadlines). If required, indicate areas where you require additional resources from the Global Fund to strengthen managerial and implementation capacity (1–2 paragraphs)
Assuming that disbursement of funds can start from January 2004, it is proposed to use the calendar year as the fiscal year. This is currently the system used by the Ministry of Health. Auditors will be selected in line with the fiduciary arrangements for grant recipients and International Standards of Audit. The evaluation of the auditor will include specific references on whether grant funds provided were used in accordance with relevant financial agreements. It will also indicate whether all necessary supporting documents, records and accounts have been kept for all expenditures. In order for the Ministry of Health to act as PR, some capacity will need to be developed. Details of this are described in this proposal and have been budgeted for.

Application Form for Proposals to the Global Fund Page 65 of 72
SECTION VII – Monitoring and evaluation information
38. Outline the plan for conducting monitoring and evaluation including the following information (1 paragraph per sub-question).
38.1. Explain the overall approach to M&E
It is proposed that the program be monitored and evaluated at three levels – goal, objective and activity. The CCM will assume overall responsibility for M&E at the goal level delegated through its Standing Committee. In practice, the main instrument to be used to monitor the goal of the HIV/AIDS component of this proposal will be the reports of the strengthened biologic surveillance work, which forms an integral part of this proposal. Secondly, responsibility for monitoring HIV/AIDS objectives will be taken up by a specially-constituted team located within the structures of the Principal Recipient. This unit will not do all the work but will be responsible for coordinating all inputs, including from implementing agencies, commissioned academics and reports of the strengthened behavioral surveillance work being carried out as part of this program. Thirdly, the responsibility for monitoring at activity level will be that of the implementing agency. In order to aid coordination with the PR and others, the Standing Committee of the CCM will designate one organization to take responsibility for coordinating M&E for each objective. Overall, the budget for Monitoring and Evaluation appears to represent 2% of total budget. However, this is a significant underestimate, because objective 8 on surveillance is almost all focused on monitoring and evaluation and some of the human resources which will be developed within the Principal Recipient will be focused specifically on M&E. Consequently, it would be more realistic to estimate that approximately 7-8% of the total budget is focused on M&E.
38.2. Describe how the beneficiaries will be involved in M&E
Beneficiaries will be involved in M&E in at least two specific ways. First, they will be actively involved in M&E at activity level through involvement with specific implementing agencies. This involvement will not be limited to M&E only but will also include other areas, such as planning and implementation. Secondly, specific care will be taken to ensure that feedback from M&E of the program at all three levels is fed back to beneficiaries through relevant implementing agencies.
38.3. Describe how the CCM or other partners will be involved in M&E (e.g.,
oversight, data review, capacity building, quality control and validation of data).
The table below shows who will be involved in each of the five specified functions at each of the three program levels:
Level Oversight Data
Review Capacity Building
Quality Control
Data Validation
Goal
The main CCM committee will oversee M&E at goal level
Objective The CCM standing committee will oversee M&E at objective level
The CCM standing committee will conduct detailed review of all M&E data generated at goal and objective level
The capacity that will be developed at these levels is for enhanced behavioural and biologic surveillance as catered for in objective 8 which falls under MoH responsibility
Quality control measures will be built into the enhanced biologic and behavioural surveillance systems and reports will be subject to external international expert scrutiny.
Data collected from biologic and behavioural surveillance studies will be validated by the internal design of the studies and by triangulating with other data

Application Form for Proposals to the Global Fund Page 66 of 72
Level Oversight Data Review
Capacity Building
Quality Control
Data Validation
The Ministry of Health will be responsible for this.
sources. The Ministry of Health will be responsible for this.
Activity The PR M&E staff will oversee M&E data at activity level
The PR M&E staff will review data at activity level
The PR M&E staff will manage the capacity building activities at this level
PR M&E staff will carry out periodic checks to verify the quality of reports received from implementing agencies
PR M&E staff will be responsible for validating data by critical analysis of data presented and by comparison with other data sources.
38.4. Describe what already exists. How does the existing health information system work and how it will be used to manage and/or report proposal data (e.g., Demographic Health Surveys, Living Standards Measurement Surveys)
Macedonia conducts an annual health survey and a report is produced each year by the State Statistical Office in both printed and electronic form. A CD version of the report for 2002 is included with this proposal (Annex 12A). The Ministry of Health also has a health information management system which collects disease statistics from public health facilities.
38.5. Prepare a table showing the following for each impact, coverage and
process indicator listed in section 26: i) the source of data, ii) periodicity of data collection, iii) how the quality of data will be determined/ensured, iv) who (the entity) will be primarily responsible for each indicator, v) and what indicators will be reported through partner organisations.
This form is attached as Annex 13A.
38.6. Describe how data will be analyzed and used by the PR, CCM, and others
Data will be used in five main ways. First data will be feedback to beneficiaries of the program through implementing agencies, to ensure that the program remains accountable to the people it is seeking to benefit. Secondly, data will be used by implementing agencies at activity level to improve activity management. This will include setting priorities and problem solving. Thirdly, data will be used by the CCM and its Standing Committee for management of the program as a whole, for policy formulation and for advocating with other groups. Fourthly, data will be stored in a variety of databases so that it is accessible to a variety of users. Finally, lessons learned from M&E data will be compiled into lessons learned publications, which will be shared within and beyond the program.
39. Recognizing that M & E plans will make use of existing monitoring systems
especially for impact and coverage indicators, national information systems may require strengthening. Please specify activities, partners and resource requirements for strengthening M&E capacities.

Application Form for Proposals to the Global Fund Page 67 of 72
Please note: Total requested from Global Fund should be consistent with the resources needed for Monitoring and Evaluation as indicated in Table V.30. Examples of activities include collecting data, improving computer systems, analyzing data, preparing reports, etc.
Table VII.39 Activities (aimed at strengthening
Partner(s) (which may
Resources Required (USD)
Monitoring and Evaluation
help in strengthening
Year 1 Year 2 Year 3 Total
Systems) M&E capacities)
Drug treatment database and networks
To be identified 5000 0 0 5000
HOPS and Izbor Databases
To be identified 1000 0 0 1000
MSM Database To be identified 1000 204 208 1412
Counseling and testing database
To be identified 1000 204 208 1412
Technical support to M&E
To be identified 2500 2550 2601 7651
System to assess national HIV/AIDS expenditure
To be identified 25000 25500 26010 76510
M&E at activity level
To be identified 16240 16565 16896 49701
Global Fund M&E request
51740 45023 45923 142686
Unmet need 0 0 0 0
Total resources needed
51740 45023 45923 142686
In addition to the activities listed in the table, additional activities will also contribute to developing national M&E capacity. These include the improved surveillance system (Y1 $123880, Y2 $94636, Y3 $87165) and the additional M&E staff within the Principal Recipient (Y1 $48040, Y2 $24235, Y3 $24270) (see explanation in 38.1).

Application Form for Proposals to the Global Fund Page 68 of 72
SECTION VIII – Procurement and supply-chain management information 40. Describe your plans for procurement and supply chain management of health
products (including pharmaceutical products, diagnostic technologies and other supplies related to the use of medicines, bednets, insecticides, aerial sprays against mosquitoes, other products for prevention [e.g., condoms], and laboratory equipment and support products [e.g., microscopes and reagents]) integral to this component’s proposed disease interventions. The plan should include.
i. Procurement responsibilities: A description of whether existing national
systems, international or other outsourced procurement agencies, or a mix of both will be used for procurement;
The program will predominantly use existing public procurement procedures. Funds have been provided within the budget for international TA to assist and advise the development of these to accommodate any additional requirements which might be needed because of the implementation of this program. Macedonia has legislation which determines how public procurement should be done. Most procurement is done centrally by the Health Insurance Fund, although individual health institutions can procure materials under certain circumstances. Pharmaceuticals can be procured in one of four ways:
o By restricted tender for amounts over 260 000 Euros o By open tender for amounts over 52 000 Euros o By supply with collection of offers for amounts over 2 600 Euros o By direct negotiation with suppliers for amounts under 2 600 Euros
In addition, all pharmaceutical products have to be registered in Macedonia (see Annex 17A). A commission within the Ministry of Health is responsible for this. This process has been streamlined and now takes an average of 30 days. A shortened procedure is available for drugs already registered in the EU, US or Japan. Fees are payable for this. Prices vary depending on whether or not the drug is supplied by an international or domestic company. There is provision for exemptions to registration. These include supply of an unregistered drug on a named patient basis, provision of drugs for urgent public health matters and for provision of certain drugs in a health facility. To date, no antiretroviral drugs have been registered in Macedonia. Similarly, methadone powder, as commonly used in drug substitution programs has not been registered. There is strong commitment within Ministry of Health to address these issues as part of this program.
ii. Procurement practices: A description of how the Interagency Operational
Principles for Good Pharmaceutical Procurement will be adhered to, including competitive purchasing from qualified manufacturers and suppliers to obtain the lowest prices for products of acceptable quality; and a description of how performance of suppliers with respect to the quality of goods and services they supply will be monitored;
The proposed procurement practices would adhere to the operational principles of the Interagency Operational Principles for Good Pharmaceutical Procurement in the following ways:
o Procurement responsibilities are clearly divided between different bodies. For example, the Ministry of Health determines which drugs may be registered in the country while other aspects of procurement are dealt with by the Health Insurance Fund
o Written procurement procedures are in place and recognised in law o Procurement is conducted and reviewed annually. The Ministry of
Finance ensures that specified procedures have been followed.

Application Form for Proposals to the Global Fund Page 69 of 72
o Macedonia does not have an Essential Drugs List but limits drugs to those which have been registered by the Ministry of Health. The Health Insurance Fund has a ‘positive’ list of drugs whose costs it will cover for insured persons
o Macedonia has been procuring drugs using generic names since 2000 o Amounts of drugs to be ordered are determined monthly by health
facilities on the basis of projected need and previous usage o Financing of drug procurement is handled through the Health
Insurance Fund who have established systems for financial management
o Most drug procurement is done annually to ensure that the largest quantities possible can be procured at once. Most drug procurement uses restricted tendering procedures, i.e. for purchases over 260 000 Euros. Macedonia spends approximately 100 -150 million Euros on drug procurement annually.
o Macedonia has four mechanisms through which drugs can be procured. These have been explained above
o Centralized purchasing through the Health Insurance Fund ensures that members of the purchasing group buy products from selected suppliers
o Criteria exist for pre-selection of suppliers, including assessment of financial status and proof of drug quality
o Macedonia has a Bureau of Drugs within the MoH which employs Inspectors of Drugs. There are two facilities for testing drug quality, at the Public Health Institute and the Faculty of Pharmacy
All imported drugs are subjected to batch sampling and require quality certification specific to that batch.
iii. Supply chain management: A description of how reliability, efficiency, and
security will be assured throughout the supply chain;
Drugs are supplied to health facilities through a system of licensed wholesalers. These are subjected to regular checks by drugs inspectors.
iv. Avoidance of diversion: A description of inventory management, stock control systems, audit systems, and other means to ensure the avoidance of diversion of products;
Drugs are supplied directly to health facilities where they are managed by pharmacists within pharmacies. The Health Insurance Fund conducts periodic checks that the people treated tallies with the drugs used.
v. Forecasting and inventory management: A description of how forecasts of the quantities of health products needed for the programme will be systematically and regularly updated, and how these forecasts will be monitored and regularly compared with actual consumption of these products;
Orders are made based on historic and projected consumption. Actual performance is monitored by individual health facilities and the Health Insurance Fund.
vi. Product selection: A list of health products to be procured, including reference to the relevant standard treatment guidelines and essential medicines lists of the World Health Organization, host country government or applicant;
All drugs and health products to be procured for the HIV/AIDS component of this proposal are itemised in table V.31. The only drugs to be procured are Methadone and ARVs. Treatment protocols for ARVs have been supplied by the Clinic for Infectious Diseases in Skopje. However, there are plans to review and revise these as part of the program as more people gain access to treatment with ARVs through the program.

Application Form for Proposals to the Global Fund Page 70 of 72
vii. Donation programmes: A description of any donation programmes that are
currently supplying health products (or which have been applied for), including the Global TB Drug Facility and drug donation programmes by pharmaceutical companies, multilateral agencies, and NGOs;
Macedonia has established guidelines for drug donations, which were used during the Kosovo crisis. However, there are not expected to be any drug donations relevant to the HIV/AIDS component of this proposal.
viii. Compliance with quality standards: A description of how compliance with quality standards for both multisource and single- or limited-source pharmaceutical products will be assured, including a description of how random samples of pharmaceutical products will be tested for compliance with applicable quality standards;
Macedonia has seven drug inspectors working within the Bureau of Drugs, MoH who carry out random sampling of pharmaceutical products.
ix. Adherence to treatment protocols, drug resistance, and adverse drug reactions: A description of how patients will be encouraged to adhere to prescribed treatment (e.g., use of fixed-dose combinations, once-a-day formulations, blister packs, and peer education and support), how drug resistance will be monitored and contained, and how adverse drug reactions will monitored;
Macedonia does not yet have an established national treatment protocol for ARVs. This will be developed as part of this program and will include measures to monitor and respond to emergence of drug resistance. There is an established procedure for dealing with adverse drug reactions, including the presence of a Center for Adverse Reactions within the Institute of Pharmacology in the medical faculty. This unit is connected to a similar unit in Sweden.
x. National and international laws: A description of how national laws and
applicable international obligations in the field of intellectual property rights will be complied with, including a description of how the flexibilities provided in the World Trade Organization’s Agreement on Trade-Related Aspects of Intellectual Property Rights (TRIPS) and referred to in the Doha Declaration on the TRIPS Agreement and Public Health will be used in a manner that achieves the lowest possible prices for products of assured quality;
Macedonia is a signatory to TRIPS and modified its laws on intellectual property rights to allow this to be signed. There are currently no plans to produce generic ARVs domestically but there is interest in accessing these, if a way can be found to do this which is compatible with Macedonia’s aspirations to join the EU. It is currently planned to focus on negotiating best price from commercial suppliers of these medicines.
xi. Procurement and supply management indicators: A description of indicators to
be used to monitor procurement and supply management (e.g., average lead time between product orders and receipt of goods, average percentage of time out of stock of products at principle warehouses and sentinel treatment facilities, price of products in the latest procurement in comparison with prices from the previous procurement of the same products and with median prices reported in international drug price indicators), with baselines if available.
These are not currently well-defined or systematically monitored. Advice on how to do this for commodities provided through this component will be provided by an international drug procurement advisor/consultant.

Application Form for Proposals to the Global Fund Page 71 of 72
41. All procurement of medicines to treat multi-drug resistant tuberculosis financed by the Global Fund must be conducted through the Green Light Committee of the Stop TB Partnership. Please for a Green Light Committee application form in Annex C.

Application Form for Proposals to the Global Fund Page 72 of 72
LIST OF ATTACHMENTS
Please note: The list of attachments is divided into two parts: the first part lists the attachments requested by the Global Fund as support for Sections III and IV. The second part is for applicants to list attachments related to other Sections such as the Information on applicants (Section II), Detailed Budget (Section IV), or other relevant information. Please note which documents are being included with your proposal by indicating a document number. General documentation: Attachment
‡‡‡ #National Poverty Reduction Strategy 4
HIV/AIDS specific documentation: Attachment #
General documentation: Attachment
#CCM Operating Rules 1National Tuberculosis Plan (NTP) 5§§§
Fiscal projection on TB and HIV/AIDS expenditure for 2004-2006 6Minutes of the Standing Committee of the CCM 7.1 & 7.2CCM Minutes 7.3Speech of Minister of Health at CCM meeting 26 May 2003 7.4Health care Systems in Transition- Macedonia Report 2000 European Observatory on Health care Systems
8
Diagram illustrating proposed management structures 11ACD-ROM containing health survey data 12ASupporting documents for civil society and private organizations 15
HIV/AIDS specific documentation: Attachment
#Rapid Assessment and Response (RAR) report 2Situation Analysis 3.1Response Analysis 3.2Rapid Assessment of HIV/AIDS/STI Surveillance 9AProposed Workplan for HIV/AIDS Component (requested in section V.34) 10AM&E Table (as requested in section VII 38.5) 13ADetailed Budget for HIV/AIDS Component 14AFramework for National HIV/AIDS Strategy 16Law on Medicaments, Remedial Medicaments and Medical Devices 17A
‡‡‡ Numbers alone have been used for annexes relating to sections of the proposal which are common, i.e. sections I-III. Where an annex relates to separate sections of the proposal, i.e. IV-VIII, it is designated as T for TB and A for HIV/AIDS §§§ This is referred to here because, although it is TB-specific, it is referred to in the common parts of the proposal