
Prognostic value of C-reactive protein levels in patients with cirrhosis
21
Prognostic value of C-reactive protein levels in patients with cirrhosis Vincent DI MARTINO (1,2), Caroline COUTRIS (1), Jean-Paul CERVONI (1), Stavros DRITSAS (1,2), Delphine WEIL (1), Carine RICHOU (1), Claire VANLEMMENS (1), Thierry THEVENOT (1,2). (1) Service d’Hépatologie et de soins intensifs digestifs, CHRU Jean Minjoz, 25030 Besançon Cedex, France. (2) Université de Franche Comté, UFR-SMP, Besançon, France. Running title: CRP and liver cirrhosis Key words: Liver cirrhosis, C-reactive protein, inflammation, MELD score, prognosis. Counts: Title: 72 characters. Summary: 260 words. Text: 2841 words. 29 references. 2 tables. 3 Figures. Abbreviations: CRP: C-reactive Protein; MELD: Model for End-stage Liver Disease; AUROC: Area Under Receiver Operating Characteristic Curve; HR: Hazard Ratio; SOFA: Sequential Organ Failure Assessment; SIRS: Systemic Inflammatory Response Syndrome; ACCI: Age-adjusted Charlson Comorbidity Index; ANOVA: Analysis of Variance; HIV: Human Immunodeficiency Virus; HCC: Hepatocellular Carcinoma; HCV: Hepatitis C Virus; HBV: Hepatitis B Virus; NO: Nitric Oxide; OR: Odds Ratio. Conflict of Interest: Nothing to disclose. Funding: This study was not supported by any pharmaceutical company or governmental agency. Author contributions: Study Conception: VDM, JPC. Data collection: CC. Statistical analyses: VDM. Manuscript Drafting: VDM, CC. Critical revision of the manuscript for important intellectual content: JPC, TT, SD, DW. Correspondence to: Prof. Vincent DI MARTINO, Service d’Hépatologie, CHRU jean Minjoz, 25030 Besançon Cedex, France. Tel: 33 3 81668421. Fax: 33 3 81668417. E-mail: vdimartino@chu- besancon.fr. This article has been accepted for publication and undergone full peer review but has not been through the copyediting, typesetting, pagination and proofreading process which may lead to differences between this version and the Version of Record. Please cite this article as an ‘Accepted Article’, doi: 10.1002/lt.24088 This article is protected by copyright. All rights reserved.
-
Upload
chu-besancon -
Category
Documents
-
view
3 -
download
0
Transcript of Prognostic value of C-reactive protein levels in patients with cirrhosis

Prognostic value of C-reactive protein levels in patients with
cirrhosis
Vincent DI MARTINO (1,2), Caroline COUTRIS (1), Jean-Paul CERVONI (1), Stavros DRITSAS (1,2),
Delphine WEIL (1), Carine RICHOU (1), Claire VANLEMMENS (1), Thierry THEVENOT (1,2).
(1) Service d’Hépatologie et de soins intensifs digestifs, CHRU Jean Minjoz, 25030 Besançon Cedex,
France. (2) Université de Franche Comté, UFR-SMP, Besançon, France.
Running title: CRP and liver cirrhosis
Key words: Liver cirrhosis, C-reactive protein, inflammation, MELD score, prognosis.
Counts: Title: 72 characters. Summary: 260 words. Text: 2841 words. 29 references. 2 tables. 3
Figures.
Abbreviations: CRP: C-reactive Protein; MELD: Model for End-stage Liver Disease; AUROC: Area
Under Receiver Operating Characteristic Curve; HR: Hazard Ratio; SOFA: Sequential Organ Failure
Assessment; SIRS: Systemic Inflammatory Response Syndrome; ACCI: Age-adjusted Charlson
Comorbidity Index; ANOVA: Analysis of Variance; HIV: Human Immunodeficiency Virus; HCC:
Hepatocellular Carcinoma; HCV: Hepatitis C Virus; HBV: Hepatitis B Virus; NO: Nitric Oxide; OR: Odds
Ratio.
Conflict of Interest: Nothing to disclose.
Funding: This study was not supported by any pharmaceutical company or governmental agency.
Author contributions: Study Conception: VDM, JPC. Data collection: CC. Statistical analyses: VDM.
Manuscript Drafting: VDM, CC. Critical revision of the manuscript for important intellectual content:
JPC, TT, SD, DW.
Correspondence to: Prof. Vincent DI MARTINO, Service d’Hépatologie, CHRU jean Minjoz, 25030
Besançon Cedex, France. Tel: 33 3 81668421. Fax: 33 3 81668417. E-mail: vdimartino@chu-
besancon.fr.
This article has been accepted for publication and undergone full peer review but has not beenthrough the copyediting, typesetting, pagination and proofreading process which may lead todifferences between this version and the Version of Record. Please cite this article as an‘Accepted Article’, doi: 10.1002/lt.24088
This article is protected by copyright. All rights reserved.

Di Martino V et al.- 2
ABSTRACT
Identifying cirrhosis with poor short-term prognosis remains crucial to improve the allocation of
liver grafts. The purpose of this study was to assess the prognostic value of a model combining the
variation of CRP levels within 15 days, the MELD score and the presence of comorbidities in
decompensated cirrhotic patients with Child-Pugh>B7 and to test the relevance of this model in
compensated cirrhotic patients. Data of cirrhotic patients without hepatocellular carcinoma,
extrahepatic malignancy, HIV infection, organ transplantation, seen between January 2010 and
December 2011 were collected. Multivariate analyses of predictors of 3-months mortality used Cox
models adjusted on the Age-ajusted Charlson Comorbidity Index (ACCI). The prognostic
performance (AUROCs) of the 3-variables model was compared to that of the MELD score. 241
patients met the inclusion criteria, including 109 patients with Child-Pugh>B7 hospitalized for
decompensation. In these severe patients, the 3-month mortality was independently predicted by
the MELD (HR=1.10, 95%CI:1.05-1.14, p<0.001), and CRP>32mg/L at baseline and day-15 (HR=2.21,
95%CI:1.03-4.76, p=0.042). This model was better than the MELD alone (AUROC, 0.789 vs.0.734,
p<0.05). In the whole cirrhotic population, the 3 month mortality was also predicted by high MELD
scores (HR=1.11, 95%CI:1.07-1.16,p<10-4) and CRP>10mg/L at baseline and day 15 (HR=2.89,
95%CI:1.29-6.48, p<0.001), but the AUROCs of the 3 variables model and of the MELD score alone
were no longer significantly different (0.89 vs. 0.88, NS). In conclusion, prognostic models
incorporating variations in CRP predict 3-month mortality in cirrhotic patients. Such models are
particularly relevant in patients with decompensated cirrhosis but provide limited increase of
prediction when compared to the MELD in the whole cirrhotic population.
Page 2 of 21
John Wiley & Sons, Inc.
Liver Transplantation
This article is protected by copyright. All rights reserved.

Di Martino V et al.- 3
The prognosis of cirrhotic patients remains difficult to assess despite its substantial improvement
over the last decades1,2, particularly due to the development of liver transplantation. The context of
organ shortage makes crucial to optimize organ allocation by giving priority to the sickest patients,
thus emphasizing the need for accurate short-term prognosis assessment. Currently, patients eligible
for liver transplantation are sorted according to their MELD score3, an indicator of liver function.
However, it has been shown that the short-term prognosis of patients with end-stage liver failure
largely depends on events that worsen temporarily or are superimposed to liver failure. These events
are better taken into account by general prognostic scores numbering organ failures (such as the
Acute Physiology and Chronic Health Evaluation (APACHE) and the Sequential Organ Failure
Assessment (SOFA) scores) than scores specifically dedicated to liver failure, such as the Child-Pugh
or MELD scores. A key event for prognosis seems to be the existence of a systemic inflammatory
response syndrome (SIRS)4,5
, which has been shown to increase mortality6,7
, complications of portal
hypertension, and encephalopathy8,9 in cirrhotic patients with or without renal failure. It therefore
seems appropriate to test prognostic models incorporating together parameters of liver function and
parameters reflecting SIRS. In a previous prospective study we suggested that CRP was an accurate
marker of SIRS and was able to predict 6-month mortality in patients with cirrhosis1. This study
included hospitalized cirrhotic patients with Child-Pugh score greater than B7 and suggested the
good prognostic value of a 3-variables model incorporating MELD score, assessment of extrahepatic
comorbidities, and variation of CRP levels within 15 days.
The aims of this study were therefore: 1) to provide a validation of this model in a new cohort of
patients; 2) to investigate whether CRP is still useful for predicting mortality in the general
population of cirrhotic patients, i.e., without clinical decompensation and with Child-Pugh A score; 3)
to investigate whether this model is able to predict 3-month mortality to make it more appropriate
for the context of liver transplantation.
Page 3 of 21
John Wiley & Sons, Inc.
Liver Transplantation
This article is protected by copyright. All rights reserved.

Di Martino V et al.- 4
PATIENTS AND METHODS
Study design
We conducted a prospective observational cohort study. The protocol for this study was approved by
the Besançon University Hospital Institutional Review Board (CPP Est-2).
Patients
All consecutive cirrhotic patients admitted between January 2010 and December 2011 in our
University Hospital were prospectively included if they fulfilled the following criteria: 1) cirrhosis
either histologically-proven or considered obvious by clinical, biochemical and morphological criteria;
2) no hepatocellular carcinoma, 3) no progressive extrahepatic malignancy, organ transplant or HIV
infection, 4) obtained consent. There were no exclusion criteria regarding age or Child-Pugh score.
Patients enrolled in our previous study were not eligible for the present study.
Data collection
Ninety-four variables were recorded at admission and during follow-up at day 15, and month six.
They concerned demographics (sex, age), cause and history of liver disease, relevant comorbidities as
assessed by the Age-adjusted Charlson comorbidity index (ACCI10), reason for admission (with a
specific distinction between planned hospitalizations (for routine paracentesis, endoscopy or other
diagnostic procedures) and unplanned hospitalization (in the event of decompensation) , clinical
status on admission including the SIRS criteria5, liver biochemistry, assessment of renal function,
culture of blood, urine, and ascitis (if any), and measurement of serum routine CRP and Procalcitonin.
Statistical analyses
Quantitative variables were expressed by their mean ± SE or median (with the 95% CI) in the event of
abnormal distribution. Comparisons of subgroups of patients regarding variations of CRP levels were
Page 4 of 21
John Wiley & Sons, Inc.
Liver Transplantation
This article is protected by copyright. All rights reserved.

Di Martino V et al.- 5
performed using the chi-square, Student t test and ANOVA. Correlations between CRP level and
MELD score were evaluated by the Spearman rank test.
Statistical analyses were performed separately in the whole study population and in the subset of
patients with Child-Pugh >B7 hospitalized for clinical decompensation. This latter population
constituted a validation cohort of results previously published.
For these two analyses, the primary outcome measure for prognosis was the 3-month mortality rate.
Patients were separated in three groups defined by the variation of CRP levels between baseline and
day 15 as defined previously, with relevant thresholds of CRP assessed by the Youden index. Group A
(validation cohort) or group A’ (whole population) were defined by persistently high CRP levels (at
baseline and day-15); Group B (validation cohort) or B’ (whole population) were defined by high CRP
levels at baseline with subsequent decrease below threshold at day-15; Group C (validation cohort)
or C’ (whole population) were defined by CRP levels below threshold at baseline. Patients’ group
according to CRP variation and other factors affecting prognosis were evaluated using the Kaplan-
Meier model and log-rank test for univariate analyses, and the proportional Hazard Regression (Cox)
Model for multivariate analysis. To include in the model the variation of CRP level within the first 15
days as a predictive factor of mortality, day 15 was considered as the starting point and patients who
died within the first 15 days were not included in the survival analysis. Patients transplanted during
follow-up were included and considered as alive with the liver transplant date marking the end of
follow-up. The performances of MELD, baseline CRP, and multivariate model for predicting short-
term mortality were compared using the comparison of the AUROCs. All statistical analyses were
performed using the NCSS package for Windows.
Page 5 of 21
John Wiley & Sons, Inc.
Liver Transplantation
This article is protected by copyright. All rights reserved.

Di Martino V et al.- 6
RESULTS
Study population
Five hundred and five cirrhotic patients were admitted during the study period. Seventy-four patients
were excluded because they participated to the previous study; 138 patients had HCC, 7 patients
were HIV-infected, 7 patients were organ recipients and 16 patients had solid cancer or hematologic
malignancies. Twenty-two additional patients were excluded because of missing data. A total of 241
cirrhotic patients were thus finally included (Figure 1). Their characteristics are summarized in table
1. Briefly, there were 160 men (66.4%); the median age was 60 yrs (95%CI: 59-62 yrs); the cirrhosis
was related to alcohol for 140 patients (58.1%), to a metabolic syndrome for 40 patients (16.6%),
HCV or HBV for 28 patients (11.6%) and other disease (Wilson, hemochromatosis, autoimmune,
cryptogenic) for 33 patients (13.7%). Eighty-eight patients (36.5%) were Child-Pugh A, 64 patients
(26.5%) Child-Pugh B, and 89 patients (36.9%). Child-Pugh C Ninety-two patients (38.2%) were
hospitalized for endoscopic procedure or paracentesis (planned hospitalization) and 149 patients
(61.8%) for decompensation (unplanned hospitalization). The median MELD was 14.06 (95%CI:
11.42–15.72). The CRP value ranged from 1 to 372 mg/L (median 10 mg/l, 95%CI: 8-12). We
identified 69 overt bacterial infections (28.6%) including 20 spontaneous peritonitis (8.3%) and 18
bacteremia (7.5%). Among the 33 alcoholic patients with a Maddrey discriminant function>32 who
underwent transjugular liver biopsy, 23 patients had histologically-proven alcoholic hepatitis. It
represented 9.5% of the whole cohort and 21.1% of decompensated patients. Seventy-three patients
(30.3%) had SIRS as defined by the ACCP/SCCM consensus conference5. One hundred thirteen
patients (46.9%) had extrahepatic comorbidities, including 30 cardiac failures (12.4%), 18 respiratory
failures (7.4%), 15 renal failures unrelated to hepatorenal syndrome (6.2%). The median Age-ajusted
Charlson Comorbidity Index (ACCI)10
was 5 and ranged from 3 to 12. The subgroup of patients Child-
Pugh>B7 hospitalized for decompensation included 109 patients (45.27%).
Page 6 of 21
John Wiley & Sons, Inc.
Liver Transplantation
This article is protected by copyright. All rights reserved.

Di Martino V et al.- 7
During a 14 months median follow-up (range: 15 days to 38 months), 76 patients (31.3%) died
including 38 deaths at month 3 and 51 deaths at month 6. Fifteen patients (6.2%) underwent liver
transplantation.
Determination of optimal cut-offs of CRP levels for predicting 3 month mortality
High baseline CRP levels were significantly associated with 3 month mortality (CRP=40.9±6.7 in
patients who died vs. 17.5±2.4 in others, p=0.0002). The AUROC was 0.783 (95%CI: 0.701-0.844).
Using the Youden index, the best discriminant value of CRP was 10mg/L (the upper normal range).
With this cut-off, the prediction of 3 month mortality was true for 62% of patients, the sensitivity was
89% and the negative predictive value was 97%. When considering the changes in CRP levels
between baseline and day 15 using this cut-off, 72 patients belonged to group A’, 21 to group B’ and
120 to Group C’.
In similar ROC curve analysis restricted to patients with decompensated cirrhosis and a Child-Pugh
score >B7 (validation cohort), the AUROC was 0.635 (95%CI: 0.509-0.734), and the best discriminant
value of CRP given by the Youden index was 32mg/L, which gave the following performance
indicators for predicting 3 month mortality: Sensitivity: 51%, specificity: 70%, NPV: 75%, well-
classified: 64%. When considering the changes in CRP levels between baseline and day 15 using this
cut-off, 19 patients belonged to group A, 20 to group B and 69 to Group C.
Predictors of 3 month mortality in decompensated cirrhotic patients
In univariate analyses restricted to Child-Pugh>B7 cirrhotic patients hospitalized for decompensation,
the 3-month mortality was significantly associated with the Child-Pugh C stage, a high MELD score,
the presence of SIRS, bacteriemia, overt bacterial infection and particularly spontaneous peritonitis.
Page 7 of 21
John Wiley & Sons, Inc.
Liver Transplantation
This article is protected by copyright. All rights reserved.

Di Martino V et al.- 8
The survival rate was significantly lower in group A patients compared with others (p=0.020). At 3
months, it was 57.0% in group A vs. 70.0% in group B and 76.7% in group C; at 6 months, it was
50.7%, 65.0% and 66.0% in group A, B and C, respectively (Figure 2A). The 3 variables prognostic
model (including ACCI, MELD and group A as defined by CRP variations) was able to predict 3 month
mortality (AUROC=0.789; 95%CI: 0.679-0.875). Group A (HR=2.21; 95%CI: 1.03-4.76, p=0.042) and
MELD score (HR=1.10; 95%CI: 1.05-1.14, p<0.001) had independent influence on 3 month mortality.
There was no correlation between the CRP levels and MELD score (R² <0.001, p=NS).
Predictors of 3-month mortality in the general population
In univariate analysis, the 3 month mortality was significantly associated with group A' (OR=7.33;
95% CI: 3.18-16.89, p<10-4). The 3 month survival was 69.2% (95%CI: 58.3-80.2%) in group A’, 75.4%
(95%CI:56.6-94.2) in group B’, and 96.6% (95%CI: 93.4-99.9%) in group C’, (p<0.001; Figure 2B). Other
significant predictors were Child-Pugh >B7 (OR=23.26; 95%CI: 5.45-99.20, p<10-4), MELD>18
(OR=10.38; 95%CI: 4.47-24.10, p<10-4
), histologically proven alcoholic hepatitis (OR=2.67; 95%CI:
1.01-7.01, p=0.040), overt bacterial infection (OR=11.20; 95% CI: 5.04-24.90, p<10-4), positive blood
culture (OR=15.31; 95%CI: 5.29-44.26, p<10-4), pneumonia (OR=6.57; 95%CI:2.29-18.81; p< 0.001),
spontaneous peritonitis (OR=8.87; 95%CI: 3.37-23.36, p<10-4
), SIRS (OR=14.53; 95%CI: 5.36-39.36,
p<10-4) (and all SIRS criteria considered separately), cardiac failure (OR=3.30; 95%CI: 1.40-7.78,
p=0.004), and unplanned hospitalization (OR=30.12; 95%CI: 4.05-223.76, p<10-4
). The use of beta-
blockers had no significant impact on 3-month mortality.
Group A' patients were more often younger than 60yrs (42.7 vs. 26.7% p=0.012), had more often a
Child-Pugh score B or C (50.7 vs. 3.9% p<10-4), a MELD>18 (56.0 vs. 21.2%, p<10-4), a SIRS (72.7 vs.
16.5%, p<10-4), a bacterial infection (62.1 vs. 21.1%, p<10-4), positive blood cultures (88.2 vs. 29.1%,
p<10-4
), spontaneous peritonitis (85.0 vs. 28.5%, p<10-4
), alcoholic hepatitis (68.2 vs. 29.8%,
p=0.0003) and have been more often hospitalized for decompensation (49.6 vs. 6.4% p<10-4) than
Page 8 of 21
John Wiley & Sons, Inc.
Liver Transplantation
This article is protected by copyright. All rights reserved.

Di Martino V et al.- 9
others. There was no significant relationship between group A’ and sex, extrahepatic morbidities,
and etiology of cirrhosis. CRP and MELD were positively correlated (R²=0.056, p<0.001), conversely to
that observed in the subset of more severe patients.
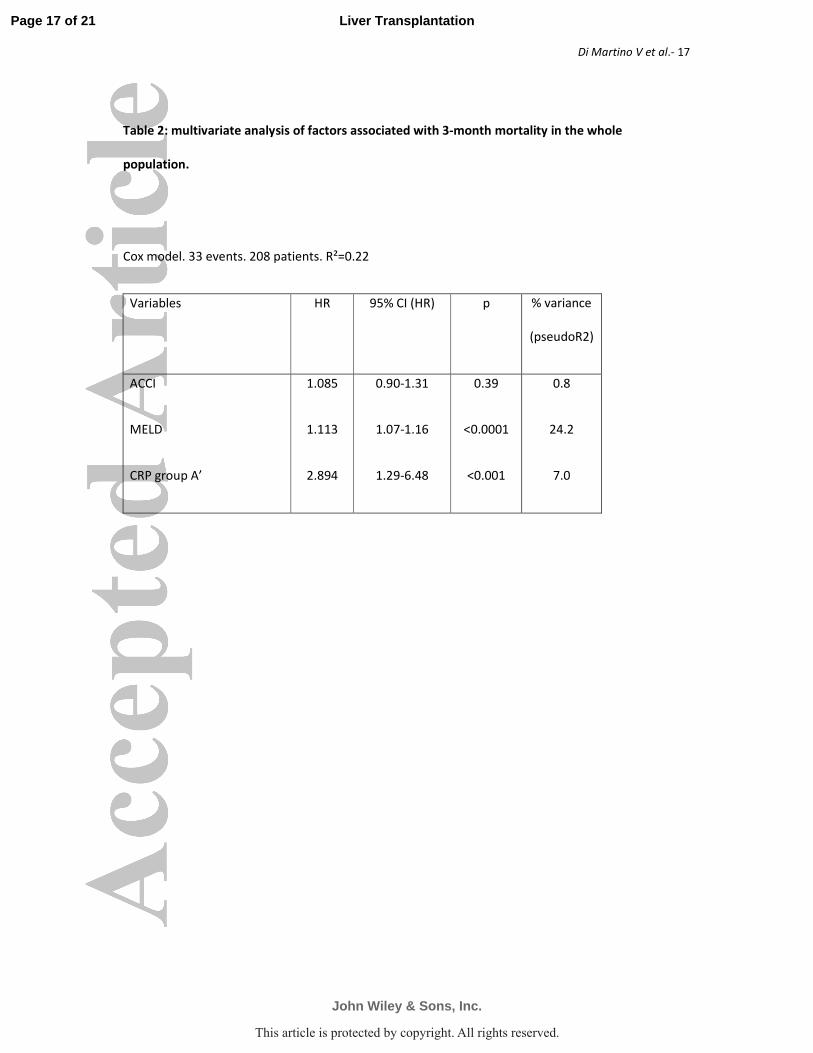
Through Cox regression multivariate analysis adjusted on ACCI, the MELD score (HR=1.113, 95%CIHR:
1.07-1.16, p<10-4
), and the group A' according to the CRP variations (HR=2.894, 95% CIHR: 1.29-6.48,
p<0.001) were significant predictors of 3 month mortality (Table 2). The AUROC of the 3 variable
model was 0.895 (95%CI: 0.843-0.930).
Sensitivity analyses
Sensitivity analyses were performed to investigate whether group A’ was able to predict 6 month
mortality when excluding patients with histologically proven alcoholic hepatitis, or considering
separately patients with or without bacterial infection. When restricting survival analysis on patients
without alcoholic hepatitis and without infection, the 3 month survival was 85.2% in group A’ vs.
96.4% in other patients (p=0.003). Similar results were obtained when removing from analysis only
patients with alcoholic hepatitis or only patients with bacterial infection. In a sensitivity analysis
restricted to infected patients, the difference in 3 month survival was still significant between group
A’ patients vs. others (50.1% vs. 79.8%, p=0.028).
Performance of the 3 variables prognostic model vs. MELD score alone
In the general population, the prognostic performance of the 3 variables Cox model (incorporating
MELD, ACCI, and group A’ as performed in the previous study) was 0.895 (AUROC; 95%CI: 0.843-
0.930). When compared to the performance of the MELD score alone (AUROC: 0.876; 95% CI: 0.817-
0.916), the difference was not significant (p=0.18; Figure 3). In contrast, in the restricted population
Page 9 of 21
John Wiley & Sons, Inc.
Liver Transplantation
This article is protected by copyright. All rights reserved.

Di Martino V et al.- 10
(Child> B7 and unplanned hospitalization) the same model predicted significantly better than the
MELD score alone the 3-month mortality (AUROC: 0.789 vs. 0.734, p<0.05) (Figure 3).
Predictors of 6 month mortality
All the previous analyses have been performed for discriminating survivors vs. non-survivors at 6
months. The same predictors were identified, with similar cutoffs of CRP levels. The impact of
extrahepatic comorbidities was slightly stronger. (data not shown).
DISCUSSION
This study provided two relevant results. First, it confirmed that the variation of CRP level is a useful
tool for predicting short-term mortality in hospitalized cirrhotic patients with a Child-Pugh stage
greater than B7. In this population, the relevant cut-off of CRP was 32mg/L, close to that found in the
first set of patients1. We thus provided a convincing internal validation of the results previously
published. Second, we demonstrated that our prognostic model still works in patients with less
severe cirrhosis, as reflected by lower Child-Pugh scores and planned hospitalizations. In that
population, the relevant cut-off of CRP was 10mg/L, i.e., the upper normal value. However, the
increase in predicting 3 month mortality provided by our model appears to be marginal compared to
that already given by the MELD score alone.
Our study had the advantage of collecting prospectively numerous data in an unselected population,
thus avoiding selection bias. The sample size was adequate to allow multivariate analyses and to
compare the performance of different prognostic models. In addition, the assessment of
comorbidities was performed by the ACCI (quantitative index) rather than a qualitative indicator
(presence or absence of extrahepatic comorbidities), which enabled us to analyze more accurately
Page 10 of 21
John Wiley & Sons, Inc.
Liver Transplantation
This article is protected by copyright. All rights reserved.

Di Martino V et al.- 11
the prognostic consequences of comorbidities in cirrhotic patients. Such information is often missing
in the literature. Another advantage of this study is to have expanded the analysis of the prognostic
value of CRP to less severe cirrhotic patients, thus allowing us to generalize our findings to the
general cirrhotic population. We confirmed the deleterious impact of alcoholic hepatitis, bacterial
infection, and SIRS, as already described in the literature11–13
. Interestingly, the prognostic relevance
of CRP variations, although still significant, was much lower in the whole population than in the
population of severe cirrhotic patients. This was clearly illustrated when comparing the performance
of our 3 variables model and that of the MELD (figure 3). This finding was probably the consequence
of a higher variability of MELD in the whole population, thus increasing its power. We also found that
CRP and MELD were correlated in the whole population and were not in the subset of severe
cirrhotic patients. This makes our prognostic model particularly useful in the setting of end-stage
liver disease. In this context, systemic inflammation, a condition able to compromise survival, may be
frequent but poorly predicted by the variations of MELD. The measure of a simple and reproducible
marker of SIRS such as CRP seems thus interesting. Conversely, in patients with compensated
cirrhosis, the prognostic value of CRP variations is statistically significant but its clinical significance
probably remains limited.
SIRS is common in severe cirrhotic patients. It is the consequence of overt or occult bacterial
infections14 favored by an increased permeability of the gastrointestinal tract, a decrease in serum
concentrations of fibronectin, complement and opsonins and an impairment of phagocytic function
and chemotaxis of neutrophils15. The activation of the inflammatory response is promoted by the
bacterial translocation of gram-negative bacilli and gram-positive cocci from the gastrointestinal tract
to the mesenteric lymph nodes and/or other extra-intestinal sites16. Bacterial translocation is the
consequence of bacterial growth17,18, structural19 and functional changes (exsudative enteropathy)20
of the mucosa and a deficiency of mucosal T lymphocytes21
and immunoglobulin A22
. Bacterial
translocation may increase the production of NO in the splanchnic circulation aggravating portal
hypertension and abnormal liver flow23,24
. It also activates peritoneal macrophages which produce
Page 11 of 21
John Wiley & Sons, Inc.
Liver Transplantation
This article is protected by copyright. All rights reserved.
Di Martino V et al.- 12
pro-inflammatory cytokines (IL2, IL12, TNF alpha). Such pro-inflammatory response is exacerbated by
interleukin-625. In cirrhotics with ascites, Albillos et al. found that high concentrations of
lipopolysaccaride binding protein stimulate the secretion of Tumor Necrosis Factor-alpha and
interleukin-626. The clinical diagnosis of SIRS may be difficult in the event of cirrhosis: hypersplenism
can hide hyperleucocytosis or worsen leukopenia, subclinical encephalopathy may lead to an
increase in respiratory rate and induce hypocapnia, tachycardia is frequently associated with
hyperkinetic syndrome but can conversely be hidden by beta-blockers. CRP is synthesized in the
acute phase of inflammation in response to IL6 and its concentration is not modified by liver
impairment27. It seems to be a good marker of SIRS, which is easily available, inexpensive, and more
accurate than clinical parameters of SIRS for identifying systemic inflammation in cirrhotic patients.
We have shown that a simple measurement of CRP at baseline and at day 15 provided a powerful
tool for predicting short-term mortality in hospitalised cirrhotic patients. Interestingly, high baseline
CRP levels could remain elevated over time despite the resolution of bacterial infection in some
patients. This suggests that systemic inflammation may become persistent and acts as an
autonomous disease. In the event of bacterial infection, the value of serial CRP measures for
predicting mortality of cirrhotic patients was underlined by other authors: prognosis was significantly
better in patients who quickly recovered from bacterial infection and experienced reduction in the
CRP levels28, as also observed in our series. Our findings are also in keeping with those of a
multicenter study recently published29
, which found that high CRP levels, as well as
hyperleukocytosis, were strong predictors of death in cirrhotic patients. However, this study did not
investigate the relevance of serial measures of CRP, and its strong prognostic value out of the context
of sepsis.
The applicability of our findings to the context of liver transplantation seems good. It may allow to
better sort patients with intermediate MELD scores in the waiting list. Although it requires a 15-days
follow-up to become available, our model helps avoiding the prioritization of infected patients to
liver transplantation, contrary to what a single measure of CRP would produce.
Page 12 of 21
John Wiley & Sons, Inc.
Liver Transplantation
This article is protected by copyright. All rights reserved.
Di Martino V et al.- 13
In conclusion, CRP level, and particularly its variation, is a true prognostic marker in cirrhotic patients,
particularly powerful in the event of advanced liver failure. It allows identifying cirrhotic patients with
poor short-term prognosis. A model combining MELD and CRP variations may sort the candidates for
liver transplantation better than the MELD score alone. Such model warrants external validations.
REFERENCES
1. Cervoni JP, Thévenot T, Weil D, Muel E, Barbot O, Sheppard F, et al. C-reactive protein predicts
short-term mortality in patients with cirrhosis. J Hepatol 2012;56:1299–304.
2. D’Amico G, Garcia-Tsao G, Pagliaro L. Natural history and prognostic indicators of survival in
cirrhosis: a systematic review of 118 studies. J Hepatol 2006;44:217–31.
3. Wiesner R, Edwards E, Freeman R, Harper A, Kim R, Kamath P, et al. Model for end-stage liver
disease (MELD) and allocation of donor livers. Gastroenterology 2003;124:91–6.
4. Malik R, Mookerjee RP, Jalan R. Infection and inflammation in liver failure: two sides of the same
coin. J Hepatol 2009;51:426–9.
5. American College of Chest Physicians/Society of Critical Care Medicine Consensus Conference:
definitions for sepsis and organ failure and guidelines for the use of innovative therapies in
sepsis. Crit Care Med 1992;20:864–74.
6. Navasa M, Follo A, Filella X, Jiménez W, Francitorra A, Planas R, et al. Tumor necrosis factor and
interleukin-6 in spontaneous bacterial peritonitis in cirrhosis: relationship with the development
of renal impairment and mortality. Hepatology 1998;27:1227–32.
7. Thabut D, Massard J, Gangloff A, Carbonell N, Francoz C, Nguyen-Khac E, et al. Model for end-
stage liver disease score and systemic inflammatory response are major prognostic factors in
patients with cirrhosis and acute functional renal failure. Hepatology 2007;46:1872–82.
8. Rolando N, Wade J, Davalos M, Wendon J, Philpott-Howard J, Williams R. The systemic
inflammatory response syndrome in acute liver failure. Hepatology 2000;32:734–9.
9. Shawcross DL, Sharifi Y, Canavan JB, Yeoman AD, Abeles RD, Taylor NJ, et al. Infection and
systemic inflammation, not ammonia, are associated with Grade 3/4 hepatic encephalopathy,
but not mortality in cirrhosis. J Hepatol 2011;54:640–9.
10. Charlson M, Szatrowski TP, Peterson J, Gold J. Validation of a combined comorbidity index. J Clin
Epidemiol 1994;47:1245–51.
11. Arvaniti V, D’Amico G, Fede G, Manousou P, Tsochatzis E, Pleguezuelo M, et al. Infections in
patients with cirrhosis increase mortality four-fold and should be used in determining prognosis.
Gastroenterology 2010;139:1246–1256, 1256.
Page 13 of 21
John Wiley & Sons, Inc.
Liver Transplantation
This article is protected by copyright. All rights reserved.

Di Martino V et al.- 14
12. Cazzaniga M, Dionigi E, Gobbo G, Fioretti A, Monti V, Salerno F. The systemic inflammatory
response syndrome in cirrhotic patients: relationship with their in-hospital outcome. J Hepatol
2009;51:475–82.
13. Mathurin P, Duchatelle V, Ramond MJ, Degott C, Bedossa P, Erlinger S, et al. Survival and
prognostic factors in patients with severe alcoholic hepatitis treated with prednisolone.
Gastroenterology 1996;110:1847–53.
14. Navasa M, Rimola A, Rodés J. Bacterial infections in liver disease. Semin Liver Dis. 1997;17:323–
33.
15. Mookerjee RP, Malaki M, Davies NA, Hodges SJ, Dalton RN, Turner C, et al. Increasing
dimethylarginine levels are associated with adverse clinical outcome in severe alcoholic
hepatitis. Hepatology 2007;45:62–71.
16. Cirera I, Bauer TM, Navasa M, Vila J, Grande L, Taurá P, et al. Bacterial translocation of enteric
organisms in patients with cirrhosis. J Hepatol. 2001;34:32–7.
17. Shindo K, Machida M, Miyakawa K, Fukumura M. A syndrome of cirrhosis, achlorhydria, small
intestinal bacterial overgrowth, and fat malabsorption. Am J Gastroenterol. 1993;88:2084–91.
18. Garcia-Tsao G, Wiest R. Gut microflora in the pathogenesis of the complications of cirrhosis. Best
Pract Res Clin Gastroenterol. 2004;18:353–72.
19. Viggiano TR, Gostout CJ. Portal hypertensive intestinal vasculopathy: a review of the clinical,
endoscopic, and histopathologic features. Am J Gastroenterol. 1992;87:944–54.
20. Stanley AJ, Gilmour HM, Ghosh S, Ferguson A, McGilchrist AJ. Transjugular intrahepatic
portosystemic shunt as a treatment for protein-losing enteropathy caused by portal
hypertension. Gastroenterology. 1996;111:1679–82.
21. Albillos A, de la Hera A, Reyes E, Monserrat J, Muñoz L, Nieto M, et al. Tumour necrosis factor-
alpha expression by activated monocytes and altered T-cell homeostasis in ascitic alcoholic
cirrhosis: amelioration with norfloxacin. J Hepatol. 2004;40:624–31.
22. Saitoh O, Sugi K, Lojima K, Matsumoto H, Nakagawa K, Kayazawa M, et al. Increased prevalence
of intestinal inflammation in patients with liver cirrhosis. World J Gastroenterol WJG.
1999;5:391–6.
23. Bellot P, García-Pagán JC, Francés R, Abraldes JG, Navasa M, Pérez-Mateo M, et al. Bacterial DNA
translocation is associated with systemic circulatory abnormalities and intrahepatic endothelial
dysfunction in patients with cirrhosis. Hepatology 2010;52:2044–52.
24. Francés R, Muñoz C, Zapater P, Uceda F, Gascón I, Pascual S, et al. Bacterial DNA activates cell
mediated immune response and nitric oxide overproduction in peritoneal macrophages from
patients with cirrhosis and ascites. Gut. 2004;53:860–4.
25. Rosenbloom AJ, Pinsky MR, Bryant JL, Shin A, Tran T, Whiteside T. Leukocyte activation in the
peripheral blood of patients with cirrhosis of the liver and SIRS. Correlation with serum
interleukin-6 levels and organ dysfunction. JAMA 1995;274:58–65.
Page 14 of 21
John Wiley & Sons, Inc.
Liver Transplantation
This article is protected by copyright. All rights reserved.

Di Martino V et al.- 15
26. Albillos A, de la Hera A, González M, Moya J-L, Calleja J-L, Monserrat J, et al. Increased
lipopolysaccharide binding protein in cirrhotic patients with marked immune and hemodynamic
derangement. Hepatology 2003;37:208–17.
27. Bota DP, Van Nuffelen M, Zakariah AN, Vincent J-L. Serum levels of C-reactive protein and
procalcitonin in critically ill patients with cirrhosis of the liver. J Lab Clin Med 2005;146:347–51.
28. Ha YE, Kang C-I, Joo E-J, Joung M-K, Chung DR, Peck KR, et al. Usefulness of C-reactive protein for
evaluating clinical outcomes in cirrhotic patients with bacteremia. Korean J Intern Med
2011;26:195–200.
29. Moreau R, Jalan R, Gines P, Pavesi M, Angeli P, Cordoba J, et al. Acute-on-chronic liver failure is a
distinct syndrome that develops in patients with acute decompensation of cirrhosis.
Gastroenterology 2013;144:1426–1437, 1437.
Page 15 of 21
John Wiley & Sons, Inc.
Liver Transplantation
This article is protected by copyright. All rights reserved.

Di Martino V et al.- 16
Table 1: Patients characteristics
Whole population
(n = 241)
Pugh>B7, unplanned
hospitalization
(n = 109)
Age (years)
Sex (Males)
Etiology of cirrhosis
- Alcohol
- Virus
- Metabolic
- Other
Histologically-proven alcoholic hepatitis
Extrahepatic comorbidities
ACCI
MELD
Bacterial Infection
Spontaneous peritonitis
Pneumonia
Bacteremia
SIRS
- SIRS according to heart rate
- SIRS according to breath rate or pCO2
- SIRS according to leukocytes count
- SIRS according to body temperature
-
Baseline CRP (mg/L)
PCT (ng/ml)
Planned hospitalization
Beta-blockers
Child-Pugh A
Child-Pugh B
Child-Pugh C
60 (59-62)
160 (66.4%)
140 (58.1%)
28 (11.6%)
40 (16.6%)
33 (13.7%)
23 (9.5%)
113 (46.9%)
5.4 (5.2-5.7)
15.4 (14.3-16.5)
69 (28.6%)
20 (8.3%)
16 (6.6%)
18 (7.5%)
73 (30.3%)
69 (28.6%)
206 (85.5%)
76 (31.5%)
18 (7.5%)
21.2 (16.6-25.8)
0.69 (0.29-1.09)
92 (38.2%)
135 (56.0%)
88 (36.5%)
64 (26.5%)
89 (36.9%)
59 (57-61)
83 (76.1%)
79 (72.5%)
9 (8.2%)
9 (8.2%)
12 (11.0%)
23 (21.1%)
49 (44.9%)
5.3 (5-5.6)
21.5 (20-23.1)
57 (52.3%)
20 (18.3%)
16 (14.7%)
15 (13.8%)
55 (50.4%)
41 (37.6%)
100 (91.7%)
41 (37.6%)
14 (12.8%)
35.2 (26.2-44.2)
0.72 (0.27-1.17)
-
70 (64.2%)
-
26 (23.8%)
83 (76.1%)
ACCI: Age-Adjusted Charlson Comorbidity Index. MELD: Model for End-Stage Liver Disease. SIRS:
Systemic Inflamatory Response Syndrome. CRP: C-Reactive Protein. PCT: Procalcitonin.
Page 16 of 21
John Wiley & Sons, Inc.
Liver Transplantation
This article is protected by copyright. All rights reserved.
Di Martino V et al.- 17
Table 2: multivariate analysis of factors associated with 3-month mortality in the whole
population.
Cox model. 33 events. 208 patients. R²=0.22
Variables HR 95% CI (HR) p % variance
(pseudoR2)
ACCI
MELD
CRP group A’
1.085
1.113
2.894
0.90-1.31
1.07-1.16
1.29-6.48
0.39
<0.0001
<0.001
0.8
24.2
7.0
Page 17 of 21
John Wiley & Sons, Inc.
Liver Transplantation
This article is protected by copyright. All rights reserved.

Di Martino V et al.- 18
FIGURES LEGEND
Figure 1: Flowchart of cirrhotic patients included in our study
Figure 2: Survival according to variation of CRP levels between baseline and day 15. 2A in the
validation cohort (Child-Pugh>B7 and unplanned hospitalization, N = 109). 2B In the general
population (N=217), survival was significantly lower in groups A and A' as defined by a persistently
elevated CRP level.
Figure 3: Prediction of the 3-month mortality: comparison of MELD score and 3 variables model.
In the whole population of inpatients with cirrhosis, the MELD score accurately predicts 3 month
mortality (AUROC=0.876) whereas a Cox model (1) including MELD, Age-adjusted Charlson
comorbidity index (ACCI) and the variation of CRP levels between baseline and day 15 provided
marginal and non-significant improvement for the same prediction (AUROC=0.895). In severe
patients (as defined by Pugh >B7 and unplanned hospitalization for clinical decompensation), the
MELD score has lower variability and its power for predicting 3 month mortality decreases
(AUROC=0.734). In that population, a 3 variables Cox model (MELD, ACCI, CRP variation within 15
days, (2)) provides significant improvement for predicting 3-month mortality (AUROC=0.789, p<0.05).
(1) Index= Exp(0.08207*(ACCI) + 1.06274*(groupA', i.e., CRP>10mg/L at baseline and day-15) +
0.10699*(MELD)
(2) Index=Exp(0.49429*ACCI + 0.79383*(groupA, i.e., CRP≥32mg/L at baseline and day-15)+
0.09322*MELD)
Page 18 of 21
John Wiley & Sons, Inc.
Liver Transplantation
This article is protected by copyright. All rights reserved.

Figure 1
Inpatients with cirrhosis 1/1/2010-31/12/2011
N=505
N=263
242 Excluded First cohort N=74
HCC N=138 Transplanted N=7 HIV positive N=7
Extrahepatic malignancies N=16
22 Excluded for missing data
Whole Study population N=241
Pugh>B7 and clinical
decompensation N=109
Pugh≤ B7 or compensated
cirrhosis N=132
Validation cohort of the
3-variable model
Assessment of the prognostic value of CRP changes in
cirrhotic patients
Page 19 of 21
John Wiley & Sons, Inc.
Liver Transplantation
5960
This article is protected by copyright. All rights reserved.

0
10
20
30
40
50
60
70
80
90
100
0 3 6
months
Group A
Group B
Group C
P=0.020
Figure 2A
0
10
20
30
40
50
60
70
80
90
100
0 3 6
months
Group C’
Group B’
Group A’
P<0.0001
Figure 2B
% surviving
% surviving
Page 20 of 21
John Wiley & Sons, Inc.
Liver Transplantation
5960
This article is protected by copyright. All rights reserved.

0.00
0.25
0.50
0.75
1.00
0.00 0.25 0.50 0.75 1.00
1-Specificity
Sens
itivi
ty
3 variables model. AUROC=0.789 (0.679-0.875)
MELD. AUROC=0.734 (0.618-0.820)
Validation cohort (Pugh>B7; clinical decompensation)
Whole population
Figure 3
0.00
0.25
0.50
0.75
1.00
0.00 0.25 0.50 0.75 1.00
1-Specificity
Sens
itivi
ty
3 variables model. AUROC=0.895 (0.843-0.930)
MELD. AUROC=0.876 (0.817-0.916)
Page 21 of 21
John Wiley & Sons, Inc.
Liver Transplantation
5960
This article is protected by copyright. All rights reserved.




















