Cirrhosis and muscle cramps: Evidence of a causal relationship
10
Cirrhosis and Muscle Cramps: Evidence of a Causal Relationship PAOLO ANGELI, 1 GRAZIA ALBINO, 1 PAOLO CARRARO, 2 MANUELA DALLA PRIA, 1 CARLO MERKEL, 1 LORENZA CAREGARO, 1 ERICA DE BEI, 1 ANDREA BORTOLUZZI, 1 MARIO PLEBANI, 2 AND ANGELO GATTA 1 The aim of the study was to define the features, preva- at rest, frequently at night, are asymmetric, and affect lence, and pathophysiology of therapy for muscle most of the gastrocnemius muscle and small muscles cramps in cirrhotic patients. The first protocol study of the foot. 1,2 In 1985 and later in 1988 Konikoff and included 294 cirrhotic patients and 194 age- and sex- Theodor reported a higher prevalence of true muscle matched controls. Controls were defined as inpatients cramps in 33 patients with cirrhosis as compared with or outpatients without any clinical and laboratory evi- that observed in a matched population without cirrho- dence of liver disease. Features and prevalence of mus- sis and suggested the inclusion of muscle cramps cle cramps were defined on the basis of a standard ques- among the recognized symptoms of cirrhosis. 3,4 The tionnaire. As far as the pathophysiological associations findings and conclusions were supported in larger se- of muscle cramps were concerned, the following parame- ries of patients by Chao et al 5 and by Kobayashi et al. 6 ters were evaluated: mean arterial pressure (MAP), nu- tritional status, liver function tests, plasma volume (PV), However, these studies did not demonstrate a relation- plasma renin activity (PRA), and electrolyte, mineral, ship between prevalence of muscle cramps and the and acid-base status. The prevalence of cramps was stage of cirrhosis evaluated by both clinical and labora- higher in cirrhotic patients than in controls, and it was tory features. Furthermore, even considering the related to the duration of recognized cirrhosis and to poorly understood pathophysiology of muscle cramps, 1,2 the severity of liver function impairment. At a multiple no plausible explanation for the relation between cir- regression analysis, the presence of ascites, low values rhosis and muscle cramps was presented. Even Koni- of MAP, and high values of PRA were the independent koff et al. 7 suggested, subsequently, that a vitamin E predictive factors for the occurrence of cramps in cir- deficiency may play a role in the pathogenesis of muscle rhosis. In the second protocol study, the effects of a sus- cramps in these patients, it is still uncertain whether tained expansion of the effective circulating volume in- duced by intravenous infusion of human albumin were muscle cramps can be considered a symptom of cirrho- compared with those of a placebo in 12 cirrhotic patients sis. A recent review did not report muscle cramps with more than three cramp crises a week. Compared among the musculoskeletal manifestations of liver dis- with the placebo, albumin reduced the cramp frequency ease. 8 Furthermore, muscle cramps have also been con- (P õ .01). In conclusion, an increased prevalence of true sidered as a side effect of diuretics in cirrhotic patients muscle cramps occurs in patients with cirrhosis. Our with ascites. 5,9 Even if cramps do not appear as a major data indicate that the pathophysiological link between clinical problem in patients with cirrhosis, their fre- cirrhosis and cramps may be represented by the reduc- quency and severity may sometimes seriously affect tion of the effective circulating volume. They also indi- their quality of life. Thus, efforts to better understand cate that weekly infusion of human albumin may be an the origin of this symptom appear justified. effective treatment for cramps in cirrhosis. (HEPATOL- OGY 1996; 23:264-273.) The aims of this study were to evaluate the preva- lence of cramps in cirrhosis according to cause and se- verity of the disease. In addition, studies were per- Painful involuntary skeletal muscle contractions may be separated into true cramps, contracture, tet- formed to define its pathophysiology. any, or dystonia on the basis of their signs and symp- MATERIALS AND METHODS toms. True cramps are the most common form, occur First Protocol Study Abbreviations: s, serum; CPK, creatine phosphokinase; 24-h, 24-hour; U, From October 1989 to November 1992, 224 consecutive urinary; MAP, mean arterial pressure; HR, heart rate; PV, plasma volume; cirrhotic patients admitted to our Institute were examined PRA, plasma renin activity; PA, plasma aldosterone. for the study. During same period, 194 controls, defined as From the 1 Institute of Clinical Medicine and 2 Institute of Laboratory Medi- inpatients or outpatients without any clinical and laboratory cine, University of Padua, Padua, Italy. evidence of liver disease, were evaluated. Each patient was Received May 9, 1994; accepted September 13, 1995. questioned about painful involuntary skeletal muscle con- Address reprint requests to: Paolo Angeli, M.D., Istituto di Medicina Clin- tractions through the use of a standard questionnaire admin- ica, Universita ` di Padova, Via Giustiniani 2, cap. 35100, Padova, Italy. istered by the same interviewer. A portion of the question- Copyright q 1996 by the American Association for the Study of Liver naire included 15 items concerning the clinical setting of Diseases. 0270-9139/96/2302-0010$3.00/0 painful involuntary skeletal muscle contractions (onset, pre- 264 m4730$0011 01-19-96 09:13:12 hepa WBS: Hepatology
Transcript of Cirrhosis and muscle cramps: Evidence of a causal relationship

Cirrhosis and Muscle Cramps: Evidence of aCausal Relationship
PAOLO ANGELI,1 GRAZIA ALBINO,1 PAOLO CARRARO,2 MANUELA DALLA PRIA,1 CARLO MERKEL,1
LORENZA CAREGARO,1 ERICA DE BEI,1 ANDREA BORTOLUZZI,1 MARIO PLEBANI,2 AND ANGELO GATTA1
The aim of the study was to define the features, preva- at rest, frequently at night, are asymmetric, and affectlence, and pathophysiology of therapy for muscle most of the gastrocnemius muscle and small musclescramps in cirrhotic patients. The first protocol study of the foot.1,2 In 1985 and later in 1988 Konikoff andincluded 294 cirrhotic patients and 194 age- and sex- Theodor reported a higher prevalence of true musclematched controls. Controls were defined as inpatients cramps in 33 patients with cirrhosis as compared withor outpatients without any clinical and laboratory evi- that observed in a matched population without cirrho-dence of liver disease. Features and prevalence of mus- sis and suggested the inclusion of muscle crampscle cramps were defined on the basis of a standard ques-
among the recognized symptoms of cirrhosis.3,4 Thetionnaire. As far as the pathophysiological associationsfindings and conclusions were supported in larger se-of muscle cramps were concerned, the following parame-ries of patients by Chao et al5 and by Kobayashi et al.6ters were evaluated: mean arterial pressure (MAP), nu-
tritional status, liver function tests, plasma volume (PV), However, these studies did not demonstrate a relation-plasma renin activity (PRA), and electrolyte, mineral, ship between prevalence of muscle cramps and theand acid-base status. The prevalence of cramps was stage of cirrhosis evaluated by both clinical and labora-higher in cirrhotic patients than in controls, and it was tory features. Furthermore, even considering therelated to the duration of recognized cirrhosis and to poorly understood pathophysiology of muscle cramps,1,2
the severity of liver function impairment. At a multiple no plausible explanation for the relation between cir-regression analysis, the presence of ascites, low values rhosis and muscle cramps was presented. Even Koni-of MAP, and high values of PRA were the independentkoff et al.7 suggested, subsequently, that a vitamin Epredictive factors for the occurrence of cramps in cir-deficiency may play a role in the pathogenesis of musclerhosis. In the second protocol study, the effects of a sus-cramps in these patients, it is still uncertain whethertained expansion of the effective circulating volume in-
duced by intravenous infusion of human albumin were muscle cramps can be considered a symptom of cirrho-compared with those of a placebo in 12 cirrhotic patients sis. A recent review did not report muscle crampswith more than three cramp crises a week. Compared among the musculoskeletal manifestations of liver dis-with the placebo, albumin reduced the cramp frequency ease.8 Furthermore, muscle cramps have also been con-(P õ .01). In conclusion, an increased prevalence of true sidered as a side effect of diuretics in cirrhotic patientsmuscle cramps occurs in patients with cirrhosis. Our with ascites.5,9 Even if cramps do not appear as a majordata indicate that the pathophysiological link between clinical problem in patients with cirrhosis, their fre-cirrhosis and cramps may be represented by the reduc-
quency and severity may sometimes seriously affecttion of the effective circulating volume. They also indi-their quality of life. Thus, efforts to better understandcate that weekly infusion of human albumin may be anthe origin of this symptom appear justified.effective treatment for cramps in cirrhosis. (HEPATOL-
OGY 1996;23:264-273.) The aims of this study were to evaluate the preva-lence of cramps in cirrhosis according to cause and se-verity of the disease. In addition, studies were per-Painful involuntary skeletal muscle contractions
may be separated into true cramps, contracture, tet- formed to define its pathophysiology.any, or dystonia on the basis of their signs and symp-
MATERIALS AND METHODStoms. True cramps are the most common form, occurFirst Protocol Study
Abbreviations: s, serum; CPK, creatine phosphokinase; 24-h, 24-hour; U, From October 1989 to November 1992, 224 consecutiveurinary; MAP, mean arterial pressure; HR, heart rate; PV, plasma volume; cirrhotic patients admitted to our Institute were examinedPRA, plasma renin activity; PA, plasma aldosterone. for the study. During same period, 194 controls, defined as
From the 1Institute of Clinical Medicine and 2Institute of Laboratory Medi- inpatients or outpatients without any clinical and laboratorycine, University of Padua, Padua, Italy. evidence of liver disease, were evaluated. Each patient was
Received May 9, 1994; accepted September 13, 1995. questioned about painful involuntary skeletal muscle con-Address reprint requests to: Paolo Angeli, M.D., Istituto di Medicina Clin-tractions through the use of a standard questionnaire admin-ica, Universita di Padova, Via Giustiniani 2, cap. 35100, Padova, Italy.istered by the same interviewer. A portion of the question-Copyright q 1996 by the American Association for the Study of Livernaire included 15 items concerning the clinical setting ofDiseases.
0270-9139/96/2302-0010$3.00/0 painful involuntary skeletal muscle contractions (onset, pre-
264
m4730$0011 01-19-96 09:13:12 hepa WBS: Hepatology

HEPATOLOGY Vol. 23, No. 2, 1996 ANGELI ET AL. 265
cipitant events, frequency, duration, relief, and associated drugs and were maintained on a normocaloric diet with so-dium, phosphorus, calcium, and magnesium content of 1.85,symptoms). Moreover, questions were asked about drug in-
take, drinking habits, and the general level of daily physical 1.15, 0.65, and 0.215 g/d, respectively. At the end of the equili-bration period, the following parameters were evaluated afteractivity. Each subject was asked to indicate the intensity
of involuntary skeletal muscle contraction–related pain by an overnight fast: hematocrit, serum and 24-hour urinarycreatinine excretion (s-Cr and 24-h UCr, respectively), serummarking a 10-cm line that was labeled ‘‘no pain’’ at one end
and the ‘‘worst pain possible’’ at the other (visual analogue and 24-hour urinary Na excretion (s-Na and 24-h UNa, re-spectively), serum and 24-hour urinary K excretion (s-K andscale).10 Cirrhotic patients were also asked to define the onset
of cramps according to both the diagnosis of cirrhosis and to 24-h UK, respectively), serum and urinary PO4 excretion (s-PO4 and 24-h UPO4, respectively), serum and 24-hour uri-the appearance of ascites.
All patients underwent a complete physical examination nary Mg excretion (s-Mg and 24-h UMg, respectively), serumand 24-hour urinary Ca excretion (s-Ca and 24-h UCa), ion-during which signs of thyroid disease, tetany (Trousseau’s
and Chvostek’s signs), peripheral neuropathy, and clinically ized s-Ca, arterial pH, arterial pCO2, and arterial bicarbon-ate plasma concentration. Moreover, brachial arterial pres-silent ischemia were sought. Inclusion criteria for cirrhotic
patients was a histologically or clinically demonstrated cir- sure (MAP), heart rate (HR), plasma volume (PV), plasmarenin activity (PRA), and plasma aldosterone (PA) were eval-rhosis along with the absence of major complications (hepatic
encephalopathy, infection, gastrointestinal bleeding) except uated in the supine position. Blood for the evaluation of labo-ratory parameters was withdrawn from a peripheral vein.for ascites. In patients with ascites at the time of inclusion,
the history of diuretic therapy was also elicited. Exclusion PV was evaluated by means of an isotope dilution techniqueusing 125I-albumin.20 After a 24-hour baseline urine collec-criteria for both cirrhotic patients and controls were
• Evidence of diseases known to be associated with muscle tion, a load of 30 mmol of Mg sulfate was administered intra-venously in 0.5% dextrose water over 12 hours.19,21,22 Urinecramps (vascular occlusive disease, peripheral neuropathy,
cancer, diabetes mellitus, and postphlebitic syndrome) or was collected for 24 hours from the beginning of the infusion.Preload and postload urine were analyzed for Mg and Cr. Forthat contraindicate procedures of the study (severe renal fail-
ure, advanced respiratory insufficiency, and disturbances of the purpose of the study an s-Mg õ0.65 mmol/L as well as aretention of more than 50% of the Mg load, despite a baselinecardiac conduction).
• Use of drugs known to induce (digitalis, cimetidine, clor- s-Mg in the normal range, were considered indicative of Mgdeficiency.21,22fibrate, lithium, opiates, nifedipine, b2-agonists, b-blockers,
penicillamine) or relieve muscle cramps (quinine, antispasticdrugs, verapamil, and vitamin E).2,6,11-14 As far as the diseases Second Protocol Studyconsidered as exclusion criteria, in addition to those reportedby Joekes in 1982,15 diabetes mellitus, postphlebitic syn- From June 1993 to October 1994, 20 cirrhotic patients with
muscle cramps seen in our outpatient liver clinic were consid-drome,16 severe renal failure, silent ischemia, and asympto-matic peripheral neuropathy were included. In the case of ered as candidates for this study. Inclusion criteria for cir-
rhotic patients were histologically or clinically demonstrateddiabetes, hypoglycemia is a well-known cause of true musclecramps2; in addition, diabetes is commonly associated with cirrhosis and absence of major complications (hepatic enceph-
alopathy, infection, gastrointestinal bleeding) except for asci-magnesium deficiency.17,18 Severe renal failure (creatinineclearance õ40 mL/min), advanced respiratory insufficiency, tes and a history at the time of inclusion of ordinary true
cramps for at least 1 year with an average of at least threeand disturbances of cardiac conduction were part of the exclu-sion criteria because the intravenous Mg load for the evalua- crises a week in the previous 2 months. In patients with
ascites or peripheral edema at the time of inclusion, a goodtion of Mg deficiency is contraindicated.19 To include onlycontrols with ordinary true cramps, diseases characterized control through diuretic therapy in the previous 6 months
was also requested. The exclusion criteria were the same asby derangement of fluid, electrolyte, mineral, and acid-basehomeostasis were considered as exclusion criteria in controls. for protocol 1. Continued alcohol intake, electrolyte or acid-
base imbalance, or a history of allergy to serum componentsAs a result of the adopted exclusion criteria, controls hadonly minor and transient medical problems. were also considered as exclusion criteria.
Before the study, all patients underwent a complete physi-Definitions. The differential diagnosis of involuntary skel-etal muscle contractions was based on the approach proposed cal examination. After an overnight fast and 2 hours of re-
cumbency, serum albumin, total serum bilirubin, prothrom-by McGee.2 True muscle cramps were defined as asymmetricpainful muscle involuntary contractions that occur at rest. bin time, s-Cr, serum urea (s-urea), s-Na, s-K, MAP, HR,
PRA, and PA were evaluated. The design of the study pro-Contracture was defined as an involuntary skeletal contrac-tion or stiffness that develops during exercise and that, un- vided an 8-week ‘‘run-in’’ period and then a ‘‘drug-on’’ cross-
over (fixed order) period. The ‘‘run-in’’ period was planned tolike true muscle cramps, is not relieved by stretching theinvolved muscle. Tetany was defined as involuntary skeletal establish the baseline number of cramp crises. Patients had
to keep a diary noting the daily number of cramps. Patientsmuscle contractions with characteristic associated symptomssuch as paresthesia, hyperventilation, and with characteris- who did not keep an adequate record or who reported an
average of less then three cramp crises a week during thetic signs. Finally, dystonia was defined as an involuntaryskeletal muscle contraction that occurs with specific tasks. ‘‘run-in’’ period were excluded from the study.
Those considered eligible at the end of the ‘‘run-in’’ periodCollection of Laboratory Data. After an overnight fast, thefollowing parameters were evaluated 48 hours after admis- received a placebo (100 mL 5% dextrose solution intrave-
nously) each Friday for 4 weeks (placebo period). At the endsion: serum albumin, total serum bilirubin, prothrombintime, serum creatine phosphokinase activity (s-CPK), serum of the placebo period, they received human albumin (100 mL
25% human albumin solution intravenously) each Friday foraldolase activity (s-aldolase). Nutritional status was investi-gated by means of triceps skinfold and midarm muscle cir- 4 weeks (albumin period). Because the duration of the possi-
ble effects of albumin on cramp frequency was not predict-cumference measurements. An equilibration period of at least5 days was begun. During this period, patients received no able, the order in which ‘‘solution-on’’ periods were assigned
m4730$0011 01-19-96 09:13:12 hepa WBS: Hepatology

266 ANGELI ET AL. HEPATOLOGY February 1996
was not randomized. To avoid a possible spontaneous change (12%) controls and 53 cirrhotic patients (24%) were ex-of cramp frequency, a washout period of 2 months was pro- cluded. Twenty-one controls were excluded for diseasesvided for each patient at the end of the albumin period (wash- (10 patients for diabetes mellitus, 6 for vascular occlu-out period). Physicians were aware of which solution was sive disease, 4 for postphlebitic syndrome, 1 for cancer),infused, and patients were not. To keep the patients blinded, whereas only 2 controls were excluded for use of drugs.the bottles and the infusion systems were covered by alumi-
Thirty-two cirrhotic patients were excluded for dis-num foil. Serum albumin, total serum bilirubin, serum pro-eases (11 for diabetes mellitus, 8 for cancer, 3 for vascu-thrombin activity, s-Cr, s-urea, s-Na, s-K, MAP, HR, PRA,lar occlusive disease, 3 for postphlebitic syndrome, 1and PA were reevaluated after an overnight fast and 2 hours
of recumbency 4 days after the last placebo or albumin infu- for thyroid disease, 4 for hepatic encephalopathy, and 2sion and at the end of the washout period. for severe renal failure). Twenty-one cirrhotic patients
Informed consent was obtained from all of the patients were excluded for the use of drugs (12 for b-blockers,after a full explanation of the purpose and nature of all proce- 8 for digitalis, 1 for b-agonist). Controls and cirrhoticdures. The study conformed with the 1975 Declaration of
patients were matched as far as age (55 { 13 vs. 57Helsinki ethical guidelines.{ 11, P ÅNS), sex (73 females and 98 males in controlsAnalytical Methods. Serum albumin, total serum bilirubin, s-and 62 females and 109 males in cirrhotic patients, PCr, s-urea, s-CPK, s-aldolase, s-Na, 24-hrUNa, s-K, 24-hrUK, s-
PO4, 24-hrUPO4, s-Mg, 24-hrUMg, s-Ca, and 24-hrUCa were Å NS) and degree of physical activity (93 with reducedmeasured using a standard autoanalyzer (SRA-2000; Technicon physical activity, 68 with normal physical activity andDiagnostics, Terrytown, NY). Ionized Ca was evaluated in serum, 10 with intensive physical activity in the control groupas suggested by Burns et al,23 by means of an ion-selective elec- versus 109, 57, and 5, respectively in the cirrhotictrode (ICA2 Radiometer, Copenhagen, Denmark). Arterial pH, group, P Å NS). Diagnosis of cirrhosis was based onPaCO2, and HCO3 were evaluated by a digital acid-base analyzer
clinical and laboratory findings and in 138 patients was(ABL 300; Instrumentation Laboratory 243, Paderno Dugnano,histologically proven. The cause of cirrhosis was alcoholItaly). Brachial artery pressure was measured with a standardinduced in 91 patients, hepatitis virus B– or hepatitismercury sphygmomanometer. Diastolic pressure was recorded
at the disappearance of Korotkoff’s sounds. 125I-albumin plasma virus C–related in 62, and cryptogenetic in 18 patients.radioactivity was determined with a g-scintillation counter. PRA One hundred cirrhotic patients had ascites at the timewas determined by radioimmunoassay for angiotensin I (Renin of inclusion in the study.Maia Kit, Biodata, Rome, Italy), PA was determined by radioim- Features of Muscle Cramps in Cirrhotics and Con-munoassay (Aldosterone Maia Kit, Biodata, Rome, Italy).
trols. Painful involuntary skeletal muscle contractionsCalculations. The formula used to calculate the percent-in cirrhotic patients had the features of true crampsage of Mg load retention was (the creatinine level was ex-except for one case in which tetany was found. Datapressed in mmol/L)24:from this patient were excluded from further analysis.Few differences were found in the main characteristics
100 11 0 (postload 24-h UMg 0 preload24-h UMg)/24-h UCr 1 postload 0 24-h UCr
Total elemental Mg infused of muscle cramps between controls and cirrhotic pa-tients. Cramps were painful (6.3 { 2.2 vs. 6.7 { 2.0MAP was calculated as the diastolic pressure plus one thirdcm, P Å NS), lasted in most of the cases for less thanof the pulse pressure. Plasma volume was calculated as pre-4 minutes (70% vs. 79%, P Å NS), and had severalviously reported.20
Statistical Analysis. The data are expressed by mean localizations in each patient. Cramps involved mainly{ SD. Differences in the prevalence of muscle cramps be- the lower extremities and particularly the calves (righttween controls and cirrhotic patients as well as between cir- calf: 77% vs. 80%, P Å NS; left calf: 64% vs. 67%, Prhotic subgroups or between baseline and posttreatment Å NS), the feet (right foot: 38% vs. 48%, P Å NS; leftnumber of cramps were evaluated by Fisher’s exact test. Dif- foot: 16% vs. 22%, P ÅNS), and the thighs (right thigh:ferences in clinical and laboratory features between cirrhotic
16% vs. 28%, P Å NS; left thigh: 12% vs. 9%, P Å NS)patients with and without muscle cramps were tested by thein both groups. The involvement of the upper extremit-ANOVA and subsequently by Student’s t test for paired or
unpaired data or Bonferroni’s test, depending on the numbers ies, the abdomen, or the neck was slightly more fre-of groups or subgroups. To simultaneously assess the com- quent in cirrhotic patients than in controls (9% vs. 2%,bined value of clinical and pathophysiological data in de- P Å NS). Although cramps developed more frequentlytermining the occurrence of cramps, a multiple logistic re- at rest in both groups (64% vs. 42%, P Å NS), sleepgression analysis was performed considering presence of was recorded as a precipitating factor of cramps moreascites, MAP, prothrombin time, serum bilirubin, serum al-
frequently by controls (33% vs. 15%, P õ .005). Thebumin, s-Na, s-K, s-PO4, s-Ca, ionized s-Ca, s-pH, serum PV,prevalence of muscle cramps in controls and cirrhoticPRA, and PA as possible covariates. An interactive forward
selection procedure was used, with Põ .10 as the enter limit, patients is reported in Table 1. No difference was ob-and Pú .15 as the removed limit. All statistical computations served in the frequency of cramps between controlswere performed using the LR program of the Biomedica Data evaluated as inpatients or outpatients. Muscle crampsProgram (Statistical Software BMDP, Los Angeles, CA). A were more frequent in cirrhotic patients than in con-5% probability level was regarded as significant. trols. When cirrhotic patients were divided into preas-
RESULTS citic and ascitic patients to examine the possible patho-First Protocol Study genetic role of diuretic therapy, the prevalence of
muscle cramps in preascitic cirrhotic patients re-Sample. One hundred seventy-one controls and 171cirrhotic patients were included in the study, and 23 mained higher than in controls. Nevertheless, a higher
m4730$0011 01-19-96 09:13:12 hepa WBS: Hepatology

HEPATOLOGY Vol. 23, No. 2, 1996 ANGELI ET AL. 267
TABLE 1. Prevalence of Cramps in Controls and Cirrhotic Patients
Preascitic AsciticCirrhotic Cirrhotic Cirrhotic
Controls Patients Patients Patients P* P† P‡ P§
1 crisis during a lifetime 69/171 (40%) 123/170 (72%) 46/71 (65%) 77/99 (78%) õ.001 õ.001 õ.001 NS¢3 crises per year 57/171 (33%) 111/170 (65%) 38/71 (54%) 73/99 (74%) õ.001 õ.005 õ.001 õ.01¢3 crises per month 23/171 (13%) 83/170 (49%) 27/71 (38%) 56/99 (57%) õ.001 õ.001 õ.001 õ.025¢3 crises per week 15/171 (9%) 49/170 (29%) 16/71 (23%) 33/99 (33%) õ.001 õ.025 õ.001 NS
* P Å comparison between cirrhotic patients as a whole and controls.† P Å comparison between preascitic cirrhotic patients and controls.‡ P Å comparison between ascitic cirrhotic patients and controls.§ P Å comparison between preascitic and ascitic cirrhotic patients.
frequency of cramps were observed in ascitic cirrhotic Ca, and higher levels of PRA and PA as compared withpatients without cramps (Table 4). According to thepatients as compared with preascitic patients.
Clinical and Laboratory Features in Controls and multiple regression analysis, significant covariateslinked to the occurrence of cramps were PRA, presenceCirrhotic Patients. Laboratory parameters were eval-
uated in all cirrhotic patients and, moreover, in a sub- of ascites, and MAP. The statistical parameters of theregression are illustrated in Table 5.group of 53 controls, including all of the control subjects
with at least three crises of cramps a month. Clinical Clinical and Laboratory Features in Preascitic and As-citic Cirrhotic Patients With and Without Cramps. Asand laboratory data are shown in Table 2.
Clinical and Laboratory Features in Controls With shown in Table 6, when cirrhotic patients with and with-out cramps were divided into preascitic and ascitic sub-and Without Cramps. Considering controls with at
least three crises of cramps a month as patients with groups, lower MAP and higher levels of PRA and PA stillpersisted in patients with cramps in both cirrhotic sub-cramps, no significant difference was observed in any
of considered clinical parameters between controls with groups. In addition, lower PV and 24-h UNa patients withcramps were observed only in the ascitic subgroup. As farcramps (n Å 23) and without cramps (n Å 148). In
particular, no difference was observed in age (56 { 12 as the liver tests were concerned, a difference in total s-bilirubin was found between patients with and withoutvs. 55 { 11 years, respectively; P Å NS), sex (15 males/
8 females vs. 83 males/65 females, respectively; P cramps only in the preascitic subgroup (22.2 { 16.4 vs.35.8 { 29.2 mmol/L, P õ .025). In addition, no differenceÅ NS), level of physical activity (13 with reduced level,
8 with normal level, 2 with increased level vs. 80, 60, was found between patients with and without cramps withrespect to potassium, magnesium, and acid-base status inand 8, respectively, P Å NS), MAP (99 { 9 vs. 101
{ 9 mm Hg, respectively, P Å NS), and HR (72 { 9 vs. both subgroups. Total s-Ca was lower in ascitic cirrhoticpatients with cramps as compared with those without72 { 8 beats/min, respectively, P Å NS). Likewise, no
difference was observed in any of the considered clini- (2.07 { 0.17 vs. 2.15 { 0.14, P õ .025), but no differencewas found when the ionized s-Ca was considered (1.23cal and laboratory parameters between controls with
(n Å 23) and without (n Å 30) cramps. In particular, { 0.06 vs. 1.23 { 0.05, P Å NS).no difference was observed in PV (2,961{ 640 vs. 2,793
Second Protocol Study{ 967 mL, respectively; P Å NS), PRA (2.33 { 1.77 vs.2.37 { 1.72 ng/mL/hr, respectively, P Å NS), and PA Sample. Twelve patients completed the study. Seven
patients were excluded from the study at the end of(80.5 { 48.2 vs. 78.9 { 51.2 pg/mL, respectively, PÅ NS). the run-in period. Four subjects had an average of less
than three cramp crises a week, and the other threeClinical and Laboratory Features in Cirrhotic Pa-tients With and Without Cramps. Table 3 shows the patients had not kept an adequate record in the diary.
Gastrointestinal bleeding occurred in one patient dur-prevalence of muscle cramps in cirrhotic subgroups ac-cording to sex, etiology and history of liver disease, ing the placebo period, and this patient was dropped
from the study. The diagnosis of cirrhosis was histo-drinking habits in the alcoholic cirrhotic patients,Child-Pugh score, presence of ascites, type of diuretic logically proven in 10 of the 12 patients. Their cause
of cirrhosis was hepatitis virus C–related in 8, alco-therapy, and level of physical activity. As in the controlgroup, patients with at least three crises of cramps a holic in 2, and cryptogenic in 2 patients. Clinical,
hemodynamic, and biochemical features of the 12 pa-month were considered as patients with cramps. Theprevalence of muscle cramps appears to be related to tients are reported in Table 7. As far as the Child-
Pugh score is concerned, 2 patients were in class A,the duration and severity of the liver disease and inparticular to the presence of ascites. As in controls, no 7 in class B, and 3 in class C. Nine of the 12 patients
had ascites or peripheral edema at the time of inclu-differences in s-CPK and s-aldolase were found be-tween patients with and without cramps. Patients with sion. The same types and dosage of diuretics were
used in these patients throughout the study. Five ofcramps showed a more severe impairment of liver func-tion tests, lower levels of MAP, PV, 24-h UNa, total s- 12 patients had functional renal failure (s-urea ¢30
m4730$0011 01-19-96 09:13:12 hepa WBS: Hepatology

268 ANGELI ET AL. HEPATOLOGY February 1996
TABLE 2. Data on Mean Arterial Pressure, Heart Rate, Plasma Volume, Plasma Renin Activity, and Electrolyte, Mineral,and Acid-Base Status in Controls and in Preascitic and Ascitic Cirrhotic Patients
Preascitic Cirrhotic Ascitic CirrhoticControls Patients Patients P* P† P‡
MAP (mm Hg)§ 100 { 9 99 { 12 94 { 11 NS õ.001 õ.025HR (beats/min)§ 72 { 9 72 { 12 77 { 12 NS NS NSTSK (cm)\ 1.79 { 1.13 1.46 { 0.78 1.34 { 0.82 NS NS NSAMC (cm)\ 30.97 { 3.78 29.51 { 3.65 27.44 { 4.41 NS õ.05 õ.05MAMC (cm)\ 25.34 { 2.39 24.92 { 2.83 23.20 { 2.85 NS õ.05 õ.005Ht (%)\ 39.9 { 4.3 38.7 { 5.3 33.9 { 6.0 NS õ.001 õ.001s-osmolality (mOsm/k)\ 277 { 5 277 { 8 271 { 11 NS õ.025 õ.025s-Na (mmol/L)\ 141 { 2 139 { 3 136 { 5 NS õ.001 õ.00124-h UNa (mmol)\ 100 { 45 97 { 46 38 { 21 NS õ.001 õ.001s-K (mmol/L)\ 4.3 { 0.3 4.1 { 0.4 4.2 { 0.5 NS NS NS24-h UK (mmol)\ 36 { 16 31 { 13 30 { 16 NS NS NSPRA (ng/mL/hr)\ 2.35 { 1.71 1.66 { 2.15 9.28 { 8.28 NS õ.001 õ.001PA (pg/mL)\ 79.8 { 48.4 80.3 { 109.1 499.7 { 216.9 NS õ.001 õ.025Total s-Ca (mmol/L)\ 2.34 { 0.16 2.22 { 0.16 2.11 { 0.16 õ.005 õ.001 õ.001Ionized s-Ca (mmol/L)\ 1.24 { 0.02 1.23 { 0.02 1.23 { 0.05 NS NS NS24-h UCa (mmol)\ 3.76 { 1.75 2.66 { 1.47 1.92 { 1.65 õ.05 õ.001 NSs-PO4 (mmol/L)\ 1.11 { 0.26 1.10 { 0.28 1.09 { 0.28 NS NS NS24-h UPO4 (mmol)\ 13.4 { 8.4 12.5 { 8.7 12.5 { 8.4 NS NS NSs-Mg (mmol/L)\ 0.85 { 0.09 0.73 { 0.09 0.76 { 0.12 õ.001 õ.001 õ.00124-h UMg (mmol)\ 2.33 { 1.29 2.65 { 1.45 2.52 { 1.76 NS NS NS% patients with reduced s-Mg\ 0/53 7/71 (10%) 11/99 (11%) õ.05 õ.05 NS% patients with normal s-Mg but with
Mg deficiency evidenced by IV Mgload\ 5/53 (9%) 49/64 (77%) 63/88 (72%) õ.001 õ.001 NS
Arterial pH\ 7.41 { 0.02 7.42 { 0.02 7.45 { 0.04 NS õ.025 õ.005PaCO2 (mm Hg)\ 38.96 { 3.60 36.97 { 5.44 33.31 { 4.14 NS õ.001 õ.0025HCO3 (mmol/L)\ 24.79 { 2.28 23.67 { 2.64 23.04 { 3.15 NS NS NS
Abbreviations: MAP, mean arterial pressure; HR, heart rate; TSK, triceps skinfold; AMC, midarm circumference; MAMC, midarm musclecircumference; Ht, hematocrit; s, serum; 24-h U, 24-hour urinary excretion; PRA plasma renin activity; PA, plasma aldosterone; HCO3,arterial bicarbonate plasma concentration.
* Comparison between preascitic cirrhotic patients and controls.† Comparison between cirrhotic patients and controls.‡ Comparison between preascitic and ascitic cirrhotic patients.§ Parameter evaluated in 171 controls.\ Parameters evaluated in 53 controls.
mg/dL, urinary Na concentration õ10 mmol/L, urine { 6 days. Compared with the ‘‘run-in’’ values, no changeswere observed in hemodynamic and biochemical featuresto plasma osmolality ratio ú1, normal fresh urine
sediment and no proteinuria) at the inclusion time. during the placebo period. As expected, a significant in-crease in serum albumin occurred after human albuminEffects of Placebo or Human Albumin Administra-
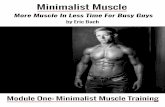
tion on Cramps. As compared with the run-in and wash- infusion, whereas no change was observed in MAP, HR,and PRA (Table 7). Nevertheless, if only the nine patientsout frequencies of cramps, no change was observed dur-
ing the placebo period (5.9 { 2.6 vs. 6.4 { 2.8, vs. 5.3 who responded to human albumin infusion were consid-ered, a significant increase of MAP (98 { 9 mm Hg) was{ 2.1 episode/week, PÅNS), whereas a significant reduc-
tion was evident during the albumin period (2.5 { 2.9 observed compared with the placebo (93 { 6 mm Hg, Põ .01) and washout (91 { 9 mm Hg, P õ .05) values. Inepisode/week, P õ .001, P õ .001, and P õ .001, respec-
tively). Individual changes in the frequency of muscle addition, a significant reduction of PRA (5.01 { 5.59 ng/mL/hr) was found compared with the ‘‘run-in’’ (11.16cramps after placebo or human albumin administration
are reported in Fig. 1. In 9 of the 12 treated patients, a { 10.04 ng/mL/hr, P õ .01), placebo (13.25 { 12.11 ng/mL/hr, P õ .01), and washout (13.36 { 13.19) values.reduction of the frequency of cramps was observed during
the albumin period. In particular, two of these nine pa-DISCUSSIONtients did not suffer with cramps during treatment with
human albumin, whereas the other seven subjects experi- Epidemiological Studyenced aú65% reduction in the number of cramps. Duringthe washout period, the frequency of cramps gradually Our study confirms that the muscle cramps that oc-
cur in cirrhosis are true muscle cramps that presentreturned toward baseline values. The mean duration ofthe effect of human albumin infusion on cramps was 15 only slight differences in their clinical setting when
m4730$0011 01-19-96 09:13:12 hepa WBS: Hepatology

HEPATOLOGY Vol. 23, No. 2, 1996 ANGELI ET AL. 269
TABLE 3. Clinical and Laboratory Features in Cirrhotic Patients With and Without Cramps
Cirrhotic Patients Cirrhotic PatientsWithout Cramps With Cramps
(n Å 87) (n Å 83) P
Age (yr) 56 { 10 58 { 12 NSSex (M/F) 55/32 54/29 NSOnset of cramps according to diagnosis of cirrhosis
Before — 15/83 (18%)After — 59/83 (71%) õ.001Undetermined — 9/83 (11%)
History of cirrhosis (mo) 43 { 56 62 { 44 õ.025Cause of cirrhosis
Alcoholic 45/87 (52%) 46/83 (55%)Posthepatitic 32/87 (37%) 26/83 (31%) NSOther 10/87 (11%) 11/83 (13%)
Continuing alcohol abuse in alcoholic cirrhotic patients (yes/no) 26/28 20/17 NSChild-Pugh score
A 31/87 (36%) 13/83 (16%)B 38/87 (44%) 38/83 (46%) õ.05C 18/87 (21%) 32/83 (39%)
AscitesNever occurred 44/87 (51%) 27/83 (32%)Present at the time of inclusion 43/87 (49%) 56/83 (67%) õ.025
Onset of cramps according to the appearance of ascitesBefore — 21/56 (37%)After — 24/56 (43%) NSUndetermined — 11/56 (20%)
Types of diuretics in ascitic cirrhotic patientsAntialdosteronic drugs 13/43 (30%) 9/56 (16%)High ceiling diuretics 4/43 (9%) 4/56 (7%) NSCombined diuretic therapy 26/43 (60%) 43/56 (77%)
Level of physical activity:Reduced 48/87 (55%) 57/83 (69%)Normal 36/87 (41%) 24/83 (29%) NSIncreased 3/87 (3%) 2/83 (2%)
MAP (mm Hg) 100 { 11 93 { 11 õ.001HR (beats/min) 74 { 11 75 { 10 NSTSK (cm) 1.52 { 0.89 1.27 { 0.71 NSAMC (cm) 29.08 { 4.61 27.49 { 3.75 NSMAMC (cm) 24.29 { 3.23 23.49 { 2.64 NSs-Albumin (g/dL) 3.6 { 0.8 3.2 { 0.7 õ.0025s-Total bilirubin (mg/dL) 2.1 { 3.0 2.9 { 2.4 NSProthrombin activity (%) 55 { 14 50 { 14 õ.025s-CPK (U/L) 69.1 { 55.0 68.7 { 71.2 NSs-Aldolase (U/L) 5.9 { 3.3 6.2 { 3.3 NS
NOTE. Patients with ¢3 crises of cramps per month were considered patients with cramps.Abbreviations: MAP, mean arterial pressure; HR, heart rate; TSK, triceps skinfold; AMC, mid-arm circumference; MAMC, mid-arm
muscle circumference; s, serum; CPK, creatine phosphokinase activity.
recognized cirrhosis and to the severity of liver functioncompared with controls. Moreover, it confirms thatimpairment as judged by both clinical and laboratorymuscle cramps were more frequently observed in cir-findings. These observations, evidencing a close conti-rhotic patients than in those without liver disease, de-guity in time and space between the two clinical vari-spite the criteria adopted to define the presence ofables, represent a step of critical value for consideringcramps, as observed by other authors previously.4,5,8
muscle cramps as a symptom of cirrhosis. Our studyTo analyze the frequency of cramps in relation to thealso clarifies to what extent muscle cramps are depen-duration and the severity of the liver disease, a fre-dent on the presence of ascites and thus on diureticquency of at least three cramp crises a month was con-therapy. It was observed that a causal relationship be-sidered to define a patient with cramps, insofar as thistween the liver disease and muscle cramps already ex-frequency has been considered a compliant of clinicalists in preascitic cirrhotic patients. In addition, al-relevance.6,12-14 Muscle cramps occurred in more thanthough the presence of ascites and the consequent70% of cirrhotic patients after recognition of cirrhosis,
and their prevalence was related to the duration of diuretic therapy seem to increase the prevalence of
m4730$0011 01-19-96 09:13:12 hepa WBS: Hepatology

270 ANGELI ET AL. HEPATOLOGY February 1996
TABLE 4. Data on Plasma Volume, Plasma Renin Activity, and Electrolyte, Mineral, and Acid-Base Statusin Cirrhotic Patients With and Without Cramps
Cirrhotic Patients Cirrhotic PatientsWithout Cramps With Cramps
(n Å 87) (n Å 83) P
Plasma volume (mL) 4072 { 939 3565 { 846 õ.05Ht (%) 36.9 { 6.3 34.9 { 5.9 NSs-Osmolality (mOsm/kg) 274 { 9 272 { 11 NSs-Na (mmol/L) 138 { 4 136 { 6 õ.002524-hr UNa (mmol) 79 { 43 52 { 43 õ.025s-K (mmol/L) 4.2 { 0.5 4.1 { 0.4 NS24-hr Uk (mmol) 31 { 16 30 { 14 NSPRA (ng/mL/hr) 2.97 { 4.45 9.32 { 8.50 õ.001PA (pg/mL) 156.8 { 286.2 529.3 { 716.6 õ.001s-Ca (mmol/L) 2.19 { 0.14 2.12 { 0.18 õ.005s-Ionized Ca (mmol/L) 1.23 { 0.04 1.23 { 0.05 NS24-h UCa (mmol) 2.50 { 1.86 1.92 { 1.35 NSs-PO4 (mmol/L) 1.10 { 0.26 1.10 { 0.29 NS24-h UPO4 (mmol) 11.9 { 8.5 12.9 { 8.5 NSs-Mg (mmol/L) 0.73 { 0.10 0.76 { 0.12 NS24-h UMg (mmol) 2.59 { 1.58 2.54 { 1.72 NS% Patients with reduced s-Mg 11/87 (13%) 7/83 (8%) NS% Patients with normal s-Mg but with Mg deficiency evidenced
by IV Mg load 57/76 (75%) 55/76 (72%) NSArterial pH 7.44 { 0.04 7.43 { 0.04 NSPaCO2 (mm Hg) 35.43 { 5.19 34.02 { 4.73 NSHCO3 (mmol/L) 23.53 { 3.02 23.04 { 2.93 NS
NOTE. Patients with ¢3 crises of cramps per month were considered patients with cramps.Abbreviations: Ht, hematocrit; s, serum; 24-h U, 24-hour urinary excretion; PRA, plasma renin activity; PA, plasma aldosterone; HCO3,
arterial bicarbonate plasma concentration.
cramps and are predictive with respect to their occur- cirrhosis and muscle cramps. Particular attention wasgiven to fluid, electrolyte, mineral, and acid-base disor-rence, it was observed that more than half of ascitic
cirrhotic patients began to suffer from cramps before ders on the basis of their role in the pathogenesis ofcramps in other clinical situations2,25-27 and their highthe onset of ascites and the initiation of diuretic ther-
apy. Diuretics, in fact, seem to stress the increase of prevalence in cirrhosis and in associated conditionssuch as chronic alcoholism.28-31 The main finding of theprevalence of cramps related to the progression of the
liver disease. Our epidemiological data represent the study concerns the possible role of volume homeostaticdisturbances in the pathogenesis of cramps in cirrhoticfirst clear evidence of previous suggestions that a
causal relationship rather than a simple association patients. The lower levels of MAP in our patients, thereduced levels of urinary sodium excretion, and themay exist between cirrhosis and muscle cramps.increased levels of PV and PRA in those with ascites
Pathophysiological and Therapeutical Study are well in keeping with previous observations.19,32-34
These findings have been recently reorganized in theSeveral hypotheses were tested in an attempt to es-so-called arterial vasodilatation hypothesis.35 Briefly,tablish the nature of the causal relationship betweenthe activation of renin-aldosterone system and othervasoactive and sodium retentive influences related to
TABLE 5. Multiple Logistic Regression Analysis an initial peripheral arterial vasodilatation contributefor the Prediction of the Occurrence through renal sodium retention to increase the plasmaof Cramps in Cirrhotic Patients
volume, which represents the final step of homeostaticSE Improvement adjustment, to maintain proper arterial blood pressure.
Covariate Coefficient (Coefficient) (x0sq) P When compared with patients devoid of cramps, thehigher values of PRA, along with lower levels of MAPPRA (ng/mL/
min) 00.18 0.056 15.99 õ.001 and similar levels of plasma volume found in preasciticAscites* 01.58 0.704 3.79 õ.025 cirrhotics with cramps, suggest that the homeostaticMAP (mm Hg) 0.064 0.029 5.37 õ.025 mechanism responsible for the maintenance of blood
pressure may have been partially ineffective or it hadNOTE. Index Å 04.59 0 (0.18 1 PRA) 0 (1.58 1 ascites) / (0.064not fully completed its compensatory increase in1 MAP). Probability of being free of cramps Å eIndex/(1 / eIndex).plasma volume. The more relevant differences in MAPAbbreviations: PRA, plasma renin activity; MAP, mean arterialand PRA found between ascitic cirrhotic patients withpressure.
* Ascites absent Å 0; ascites present Å 1. cramps and those without cramps, along with the ob-
m4730$0011 01-19-96 09:13:12 hepa WBS: Hepatology

HEPATOLOGY Vol. 23, No. 2, 1996 ANGELI ET AL. 271
TABLE 6. Data on Mean Arterial Pressure, Heart Rate, Plasma Volume, Plasma Renin Activity, and Sodium Metabolism inPreascitic and Ascitic Cirrhotic Patients With and Without Cramps
Preascitic Cirrhotic Preascitic Cirrhotic Ascitic Cirrhotic Ascitic CirrhoticPatients Without Patients With Patients Patients With
Cramps Cramps Without Cramps Cramps(n Å 44) (n Å 27) P (n Å 43) (n Å 56) P
MAP (mm Hg) 102 { 11 94 { 12 õ.0025 97 { 9 92 { 11 õ.025HR (beats/min) 72 { 8 72 { 10 NS 77 { 13 77 { 10 NSPlasma volume (mL) 3,475 { 887 3,471 { 1036 NS 4,278 { 879 3,596 { 796 õ.005s-NA (mmol/L) 140 { 4 139 { 3 NS 137 { 4 135 { 6 NS24-h UNa (mmol) 101 { 45 93 { 49 NS 49 { 23 30 { 14 õ.001PRA (ng/mL/h) 1.10 { 0.85 2.41 { 3.02 õ.05 4.62 { 5.60 12.28 { 8.38 õ.001PA (pg/mL) 52.0 { 51.9 121.8 { 153.2 õ.05 239.1 { 361.3 682.1 { 784.0 õ.001
NOTE. Patients with ¢3 crises of cramps per month were considered patients with cramps.Abbreviations: MAP, mean arterial pressure; HR, heart rate; s, serum; 24-h U, 24-hour urinary excretion; PRA, plasma renin activity;
PA, plasma aldosterone.
served lower levels of plasma volume and urinary Na the effective circulating volume. The magnitude of thereduction of cramps obtained by means of albumin ad-excretion in patients with cramps, suggest two possible
explanations. The first involves the possibility of a ministration was comparable to that obtained by otherauthors,12,38 in particular, by Lee et al, with quinidinemore advanced stage on the continuum in the process
of vasodilation-mediated arterial underfilling, and the in a placebo-controlled study.12 Although comparativestudies are needed, weekly human albumin infusionsecond revolves around a potential detrimental effect
of the diuretic therapy on the circulatory homeostasis may represent an alternative to quinidine in the treat-ment of cramps in cirrhotic patients, particularly con-in patients with cramps. Our data thus suggest that a
reduced effective plasma volume per se may be involved sidering that the use of quinidine requires the monitor-ing of both the serum levels of the drug and thein the pathophysiology of cramps in cirrhosis. This hy-
pothesis, which is well in keeping with the clinical ob- electrocardiogram in these patients.Proposing a mechanism by which an effective plasmaservation that muscle cramps are one of the earliest
symptoms of the hypovolemic state,36,37 is further sup- volume contraction results in muscle cramps can onlybe speculative, because the pathogenesis of cramps isported by the results of the multiple regression analysis
and overall by the results of the therapeutical study, unknown.39-41 Accepting the neurogenic origin ofcramps and considering that symptoms induced by hy-which showed that the infusion of human albumin was
more effective than a placebo in reducing the cramp povolemia are primarily related to decreased tissueperfusion,36 an alteration of the neural cell membranefrequency. Even if the dosage of albumin was totally
empirical, it resulted in a reduction in PRA and an excitability may be suggested as a consequence of hypo-perfusion. In light of this comment, it appears interest-increase in MAP in patients who responded to it. Albu-
min seems to reduce cramp frequency by improving ing to discover that blood flow to nerves does not auto-
TABLE 7. Hemodynamic and Biochemical Data Before, During, and After Treatmentfor Muscle Cramps in Cirrhotic Patients (n Å 12)
Parameters Run-in Period Placebo Period Albumin Period Washout Period
MAP (mm Hg) 93.3 { 9.3 90.9 { 10.1 95.2 { 11.8 90.0 { 9.2HR (beats/min) 84.7 { 10.0 83.2 { 12.3 81.0 { 11.0 84.5 { 8.7s-Total bilirubin (mg/dL) 2.0 { 1.8 1.8 { 1.5 1.8 { 2.0 1.8 { 1.6Prothrombin activity (%) 59.9 { 14.0 61.5 { 13.9 61.1 { 12.3 59.0 { 12.6s-Albumin (g/dL) 3.1 { 0.5 3.1 { 0.5 3.5 { 0.4†‡* 3.1 { 0.4s-Na (mmol/L) 136 { 5 136 { 4 137 { 4 136 { 4s-K (mmol/L) 4.2 { 0.6 4.5 { 0.6 4.2 { 0.4 4.4 { 0.4s-Urea (mg/dL) 48.0 { 34.1 51.7 { 35.64 47.8 { 33.6 50.9 { 35.1s-Creatinine (mg/dL) 0.9 { 0.5 1.0 { 0.4 0.9 { 0.4 1.0 { 0.4PRA (ng/mL/h) 11.60 { 10.80 13.34 { 12.83 6.84 { 8.65 12.84 { 12.55PA (pg/mL) 528.7 { 609.4 615.9 { 716.5 417.2 { 568.8 583.1 { 672.6No. of episodes of cramps/wk 6.4 { 2.8 6.2 { 2.5 2.5 { 2.9*†‡ 5.3 { 2.1
Abbreviations: s, serum; PRA, plasma renin activity; PA, plasma aldosterone.* P õ .001 when compared with run-in value.† P õ .001 when compared with placebo value.‡ P õ .001 when compared with washout value.
m4730$0011 01-19-96 09:13:12 hepa WBS: Hepatology

272 ANGELI ET AL. HEPATOLOGY February 1996
et al. Muscle cramps in liver cirrhosis. Chinese J Gastroenterol1989;6:163-169.
6. Kobayashi Y, Kawasaki T, Yoshimi T. Muscle cramps in chronicliver disease and treatment with antispastic agent (eperisonehydrochloride). Dig Dis Sci 1992;37:1145-1149.
7. Konikoff F, Ben-Amitay G, Halpern Z, Weisman Y, Fishel B,Theodor E, Rattan J, et al. Vitamin E and cirrhotic musclecramps. Isr J Med Sci 1991;27:221-223.
8. Asherson RA, Hughes GRV. Musculoskeletal problems in liverdisease. In: McIntyre N, Benhamou JP, Bircher J, et al., eds.Oxford textbook of hepatology. Oxford: Oxford Medical Publica-tions, 1991:1260-1263.
9. Salerno F. Large volume paracentesis and volume re-expansion:can synthetic plasma expanders safely replace albumin? J Hepa-tol 1992;14:143-145.
10. Chapman CR, Casey KL, Dubner R, Foley KM, Gracely RH,Reading AE. Pain measurement: an overview. Pain 1985;22:1-31.
11. Davies DM. Drug-induced disorders of muscles, joints, bones andconnective tissues. Adverse Drug Reaction Bulletin 1985;112:416-419.
12. Lee FY, Lee SD, Tsai YT, Lai KH, Chao Y, Lin HC, Wang SS,et al. A randomized controlled clinical trial of quinidine in the
FIG. 1. Individual changes in the frequency of muscle cramps treatment of cirrhotic patients with muscle cramps. J Hepatolafter intravenous administration of placebo and human albumin. 1991;12:236-240.
13. Baltodano N, Gallo BV, Weidler DJ. Verapamil vs quinine inrecumbent nocturnal leg cramps in the elderly. Arch Intern Med1988;148:1969-1970.
14. Ayres S, Mihan R. Nocturnal leg cramps (systremma): a progressregulate and that it is greatly dependent on bloodreport on response to vitamin E. South Med J 1974;67:1308-volume.42 Accepting the muscular origin of the cramps,1312.according to what has been recently observed in pa-
15. Joekes AM. Cramp: a review. J R Soc Med 1982;75:546-549.tients with hemodialysis-associated cramps, a greater 16. Jorgensen PW, Jorgensen T, Andersen M, Kirchhoff M. Postphle-reduction of effective circulating volume with a conse- bitic syndrome and general surgery: an epidemiologic investiga-
tion. Angiology 1991;42:397-403.quent more pronounced activation of the sympathetic17. Nadler JL, Malayan S, Luong H, Shaw S, Natarajan R, Rudenervous system would result in a larger derecruitment
RK. Intracellular free magnesium deficiency plays a key role inof skeletal muscle capillaries and thus would reduce to increased platelet reactivity in type II diabetes mellitus. Diabe-a larger extent skeletal muscle blood flow in cirrhotic tes Care 1992;15:833-841.
18. Grafton G, Baxter MA. The role of magnesium in diabetes melli-patients with cramps.43
tus: a possible mechanism for the development of diabetic com-Conversely, our data apparently exclude a patho-plications. J Diabetic Complications 1992;6:143-149.genic role for electrolyte and mineral disorders even if
19. Dyckner T, Wester PO. Magnesium deficiency: guidelines forthe serum levels of Na, K, PO4, and Ca do not necessar- diagnosis and substitution therapy. Acta Med Scand 1982;ily reflect their intracellular levels in patients with cir- 661(Suppl):37-41.
20. Angeli P, Caregaro L, Menon F, Sacerdoti D, De Toni R, Merkelrhosis.44 The possible role of Mg deficiency was ex-C, Gatta A. Variability of atrial natriuretic peptide plasma levelscluded with greater accuracy because its prevalencein ascitic cirrhotics: pathophysiological and clinical implications.was investigated by Mg intravenous load, which corre- HEPATOLOGY 1992;16:1389-1394.
lates well with intracellular Mg.1921. Berkelhammer C, Bear RA. A clinical approach to common elec-
In conclusion, our data suggest that a causal rela- trolyte problems: hypomagnesemia. Can Assoc J 1985;132:360-368.tionship rather than a simple association may exist
22. Kobrin SM, Goldfarb S. Magnesium deficiency. Semin Nephrolbetween cirrhosis and muscle cramps. The cirrhosis-1990;10:525-535.induced arterial underfilling may play a role in the 23. Burns J, Law RWG, Paterson CR. Measurement of plasma ion-
pathogenesis of cramps. Weekly infusion of human al- ized calcium: comparison of calcium-titrated sodium heparin andbumin solution is effective in the treatment of cramps lithium heparin as anticoagulants. Med Lab Sci 1987;44:187-
189.in cirrhosis by improving effective circulating volume.24. Ryzen E, Elbaum N, Singer FR, Rude RK. Parenteral magne-
sium tolerance testing in the evaluation of magnesium defi-Acknowledgments: We thank Sticca Antonietta andciency. Magnesium 1985;4:1137-1147.Paul Marcucci for their technical assistance in the
25. Neal CR, Resnikoff E, Unger AM. Treatment of dialysis-relatedpreparation of this paper. muscle cramps with hypertonic dextrose. Arch Intern Med1981;141:171-173.REFERENCES 26. Stwewart WK, Fleming LW, Manuel MA. Muscle cramps duringmaintenance hemodialysis. Lancet 1972;i:1049-1051.1. Layzer RB, Rowland LP. Cramps. N Engl J Med 1971;285:31-
27. Knochel JP. Neuromuscular manifestations of electrolyte disor-40.ders. Am J Med 1982;72:521-535.2. McGee SR. Muscle cramps. Arch Intern Med 1990;150:511-518.
28. Hecker R, Sherlock S. Electrolyte and circulatory changes in3. Konikoff F, Theodor E. Painful muscle cramps in liver cirrhosis.terminal liver failure. Lancet 1956;2:1121-1125.Br Med J 1985;290:286.
29. Knochel JP. Derangements of univalent and divalent ions in4. Konikoff F, Theodor E. Painful muscle cramps: a symptom ofchronic alcoholism. In: Epstein M, ed. The kidney in liver dis-liver cirrhosis? J Clin Gastroenterol 1986;8:669-672.
5. Chao Y, Lee FY, Tsai YT, Lin HC, Chang TT, Wang SS, Wu JC, ease. Baltimore: Williams & Wilkins, 1988:132-153.
m4730$0011 01-19-96 09:13:12 hepa WBS: Hepatology

HEPATOLOGY Vol. 23, No. 2, 1996 ANGELI ET AL. 273
30. Angeli P, Gatta A, Caregaro L, Luisetto G, Menon F, Merkel C, 37. Schrier RW. Pathogenesis of sodium and water retention in high-output and low-output cardiac failure, nephrotic syndrome, cir-Bolognesi M, et al. Hypophosphatemia and renal tubular dys-
function in alcoholics: are they related to liver function impair- rhosis, and pregnancy. N Engl J Med 1988;319:1127-1134.38. Matsuzaki Y, Tanaka N, Osuga T. Is taurine effective for treat-ment? Gastroenterology 1991;100:502-512.
31. Oster JR, Perez GO. Acid-base homeostasis and pathophysiology ment of painful muscle cramps in liver cirrhosis? Am J Gas-troenterol 1993;88:1466-1467.in liver disease. In: Epstein M, ed. The kidney in liver disease.
Baltimore: Williams & Wilkins, 1988:119-131. 39. Rowland LP. Cramps, spasms and muscle stiffness. Rev Neurol1985;141:261-273.32. Schrier RW, Carmelo C. Hemodynamics and hormonal alter-
ations in hepatic cirrhosis. In: Epstein M, ed. The kidney in liver 40. Norris FH, Gasteiger EL, Chatfield PO. An electromyographicstudy of induced and spontaneous muscle cramps. EEG Clindisease. Baltimore: Williams & Wilkins, 1988:265-285.
33. Rector WG Jr, Ibarra F. Intravascular volume in cirrhosis: reas- Neurophysiol 1957;9:139-147.41. Tahmoush AJ, Alonso RJ, Tahmoush GP, Heiman-Patterson TD.sessment using improved methodology. Dig Dis Sci 1988;33:460-
466. Cramp-fasciculation syndrome: a treatable hyperexcitable pe-ripheral nerve disorder. Neurology 1991;41:1021-1024.34. Arroyo V, Gines P, Jimenenez W, Rodes J. Ascites, renal failure,
and electrolyte disorders in cirrhosis: pathogenesis, diagnosis, 42. Takeuchi M, Low PA. Dynamic peripheral nerve metabolic andvascular responses to exsanguination. Am J Physiol 1987;and treatment. In: McIntyre N, Benhamou JP, Bircher J, et al,
eds. Oxford textbook of hepatology. Oxford: Oxford Medical Pub- 253:E349-E353.43. Kaplan B, Wang T, Rammohan M, Del Greco F, Molteni A, Atkin-blications, 1991:429-470.
35. Schrier RW, Arroyo V, Bernardi M, Epstein M, Henriksen JH, son AJ. Response to head-up tilt in cramping and noncrampinghemodialysis patients. Int J Clin Pharmacol Ther ToxicolRodes J. Peripheral arterial vasodilating hypothesis: a proposal
for the initiation of renal sodium and water retention in cirrho- 1992;30:173-180.44. Moller P, Bergstrom J, Furst P, Hellstrom K. Muscle biopsysis. HEPATOLOGY 1988;8:1151-1157.
36. Rose BD. Hypovolemic states. In: Rose BD, ed. Clinical physiol- studies in patients with moderate liver cirrhosis with specialreference to energy-rich phosphagens and electrolytes. Scand Jogy of acid-base and electrolyte disorders. Singapore: McGraw
Hill International Editions, 1989:361-388. Gastroenterol 1984;19:267-272.
m4730$0011 01-19-96 09:13:12 hepa WBS: Hepatology