
Intraoperative graft flow assessment for myocardial surgical ...
Upload
independentCategory
view
1download
0
C
Rpdrcs2blGC
O9
F
A
Int. J. Radiation Oncology Biol. Phys., Vol. 64, No. 4, pp. 1122–1128, 2006Copyright © 2006 Elsevier Inc.
Printed in the USA. All rights reserved0360-3016/06/$–see front matter
doi:10.1016/j.ijrobp.2005.09.020
LINICAL INVESTIGATION Rectum
PROGNOSTIC FACTORS FOR DISEASE-FREE SURVIVAL IN PATIENTSWITH T3–4 OR N� RECTAL CANCER TREATED WITH PREOPERATIVE
CHEMORADIATION THERAPY, SURGERY, ANDINTRAOPERATIVE IRRADIATION
JUAN A. DÍAZ-GONZÁLEZ, M.D., PH.D.,*† FELIPE A. CALVO, M.D., PH.D.,‡
JAVIER CORTÉS, M.D., PH.D.,§ JOSÉ L. GARCÍA-SABRIDO, M.D., PH.D.,� MARINA GÓMEZ-ESPÍ, M.D.,‡
EMILIO DEL VALLE, M.D.,� FERNANDO MUÑOZ-JIMÉNEZ, M.D.,� AND EMILIO ÁLVAREZ, M.D., PH.D.¶
*Department of Oncology, Clinica Universitaria, University of Navarra, Navarra, Spain; †Sloan-Kettering Institute for Cancer Research,Memorial Sloan-Kettering Cancer Center, New York, NY; Departments of ‡Oncology, �General Surgery, and ¶Pathology, Hospital
General Universitario Gregorio Marañón, Madrid, Spain; §Department of Oncology, Hospital Vall d’Hebron, Barcelona, Spain
Purpose: Fluoropyrimidine-radiosensitizing agents in conjunction with preoperative radiotherapy have provento induce tumor and nodal downstaging effects, sphincter preservation promotion, and mid-term favorablesurvival rates. Intraoperative electron beam radiation therapy may improve pelvic control in patients with locallyadvanced rectal cancer stages. Potential predictive factors for response and disease-free survival, with intenselocal multidisciplinary approach, are analyzed.Methods and Materials: One hundred fifteen patients with rectal cancer were treated with oral 5-fluorouracil orTegafur with preoperative radiotherapy, surgery, and intraoperative electron beam radiation therapy to identifypotential pre- and on-treatment characteristics that might be of prognostic value for disease outcome. Univariateand multivariate analyses were performed.Results: Older patients and those treated with Tegafur were more likely to achieve a major histologic response,categorized as persistence of minimal residual microscopic disease foci in the surgical specimen (“mic” response).Factors unfavorably associated with disease-free survival in the multivariate model were male gender and persistenceof macroscopic disease in the rectal wall (“mac” response). Accordingly, 3-year disease-free survival rates in thegroups of patients with 0, 1, or 2 of these risk factors were 100%, 81%, and 53%, respectively (p < 0.001).Conclusions: Females with an intense pathologic response (pTmic residue) to preoperative chemoradiotherapyhave an excellent 3-year disease-free survival. This information might be of interest for stratification of patientsin the development of adjuvant treatment trials. © 2006 Elsevier Inc.
Rectal cancer, Prognostic factors, Preoperative chemoradiation, Surgery, Intraoperative radiotherapy.
ctSPoheiaimH
MEvR
INTRODUCTION
adical surgery is the cornerstone in the management ofatients with locally advanced rectal carcinoma. Inci-ences of local recurrences in contemporary reportsange from 15% to 45% and are a formidable oncologichallenge, because they are associated with disablingymptoms that lead to catastrophic medical outcomes (1,). During the past two decades, several attempts haveeen made to improve the outcome of patients withocally advanced rectal cancer. Studies conducted by theastrointestinal Tumor Study Group (3, 4) and the Northentral Cancer Treatment Group (5) concluded that the
Reprint requests to: Felipe A. Calvo, M.D., Ph.D., Department ofncology, Hospital Gregorio Marañón, Madrid, Spain. Tel: (�34)1-586-8599; E-mail: [email protected]
J. A. Díaz-González was supported by a postdoctoral grant fromundación Ramón Areces.The first two authors contributed equally to this article.
cknowledgments—The authors are indebted to Emiliano Calvo,A
1122
ombination of postoperative chemotherapy and radio-herapy improved local tumor control and survival intage II and III rectal cancer relative to surgery alone.reoperative radiotherapy has also been found to improveverall survival as compared with surgery alone (6, 7). Itas been reported to be more dose efficient than postop-rative radiotherapy (8) and to induce a tumor downstag-ng effect, which potentially improves the probability of
complete resection and sphincter-preserving surgeryndication, particularly if combined with concurrent che-otherapy, with a benefit in local control promotion (9).owever, some patients still develop local recurrences
.D., Ph.D., who reviewed this manuscript. We thank Bioscienceditors for editorial assistance. This work has the scientific super-ision of GICOR (Grupo de Investigación Clínica en Oncologíaadioterapica).Received June 10, 2005, and in revised form Aug 28, 2005.
ccepted for publication Sept 15, 2005.

wds(p(sbnpib1og1etm
P
fr[cCtmtdcwpcnec
apawbqw
P
G5t1oiaD
ctp
pgwdnrhwcm
aaocucorc
Ombca
S
qde
gsdpe
ttn
wtpgtvt
mthact
1123Prognostic factors in preoperative treatment of rectal cancer ● J. A. DÍAZ-GONZÁLEZ et al.
ith survival compromise. By administering tumoricidaloses to the postsurgical area at risk (generally presacralpace), intraoperative electron beam radiation therapyIOERT) does intensify irradiation and may improveelvic control without increasing normal tissue toxicity10). Moreover, to further improve local control andurvival, studies have been designed to explore the com-ination of active chemotherapeutic agents simulta-eously with preoperative radiotherapy (11–17). Fluoro-yrimidine-radiosensitizing agents, such as 24-h i.v.nfusion of 5-fluorouracil (5-FU) and oral Tegafur, haveeen shown to produce promising antitumor activity (12,8). In previous analysis, combined treatment with flu-ropyrimidine-based chemotherapy and radiation therapy, sur-ery, and IOERT reported attractive cancer control rates (12,8). To analyze potentially relevant clinico-pathologic param-ters of interest for risk stratification in future prospectiverials, a large cohort of patients homogenously treated and withature follow-up time has been studied.
METHODS AND MATERIALS
atient populationTo be entered into the study, patients had to fulfill all of the
ollowing criteria: biopsy-proven primary adenocarcinoma of theectum (Stage T3–4N0 or any T N� according to the TNM systemAmerican Joint Committee on Cancer, 5th edition]), no previoushemotherapy or radiation therapy to the pelvis, and an Easternooperative Oncology Group performance status of 0–2. Addi-
ional eligibility criteria included a serum creatinine level of �1.6g/dL and liver profile levels of no more than three times greater
han the control level, and also adequate bone marrow reserve,efined as leukocyte count �3 � 109/L (absolute granulocyteount �1.5 � 109/L) and platelet count �75 � 109/L. Patientsith severe comorbid conditions or a history of concomitant orrevious malignancy, other than basal cell carcinoma of the skin,arcinoma in situ of the cervix, or completely resected synchro-ous in situ or T1 colon cancer in the previous 5 years werexcluded. Patients were at least 18 years of age and gave informedonsent.
Tumor staging was established as the result of a combinedssessment with physical examination, digital rectal examination,roctocolonoscopy, endorectal ultrasound (95% of the patients),bdominal CT scan, chest X-ray, complete blood cell count withhite blood cell differential and platelet counts, and standardiochemical profiles. Patients with locally advanced disease re-uiring exenteration or multiorgan resection for radical surgery orith any evidence of distant metastasis were excluded.
rotocol schedulePreoperative radiotherapy consisted of the delivery of 45 to 50.4
y over 5 to 6 weeks with conventional daily fractions of 1.8 Gy,days per week as described previously (12). Concurrent chemo-
herapy consisted of two different consecutive regimens. Between995 and 1998, patients received 5-FU, 500–1,000 mg/m2 daily,n Days 1–4 and Days 21–24, administered as a 24-h continuous.v. infusion. Between 1998 and 2001, 400 mg of Tegafur wasdministered orally 3 times a day (every 8 hours) from Day 1 to
ay 28 of radiotherapy, including weekends. A complete blood lount was performed every week during preoperative chemoradia-ion. A chest and abdominal CT and an endorectal ultrasound wereerformed 4 weeks after chemoradiation.Radical surgery was programmed 4 to 6 weeks after the com-
letion of preoperative chemoradiation. A total of 19 senior sur-eons were involved in this combined modality program. Thereere no strict criteria for selection of the type of surgical proce-ure or appropriateness of safety distal margin distance. There waso written record available regarding the practice of total meso-ectal excisions. The institutional IOERT program characteristicsave been described previously (19, 20). Adjuvant chemotherapyith 4–6 courses of bolus 5-FU (425 mg/m2) together with leu-
ovorin (20 mg/m2), on Days 1–5 every 21 days, was recom-ended following intramural protocols.Pathologic examination of the surgical specimen was performed
s described previously (12). Categorization of pathologic findingsfter chemoradiation was based upon an estimation of the amountf residual cancer relative to the extent of the initial tumor. pTmic
ategory was considered for surgical specimens with minimal resid-al cancer consisting of microscopically isolated nests of neoplasticells surrounded by regenerated fibrotic repair tissue, independentlyf depth involvement in the rectal wall. Pathologically completeesponses were included in this category. All the other responses wereonsidered to pertain to the pTmac response category.
Acute toxicity was scored according to the Radiation Therapyncology Group/European Organization for Research and Treat-ent of Cancer scale. After surgery, follow-up included complete
lood cell count, carcinoembryonic antigen, general biochemistry,hest X-ray, and an abdominal CT scan every 6 months for 5 years,nd annually thereafter. A colonoscopy was performed every year.
tatisticsClinical nodal staging may present some inaccuracies; conse-
uently, the evaluation of downstaging including N stage may intro-uce some bias, so the term “downstaging” used to describe thefficacy of treatment was defined specifically as T stage downstaging.
Disease-free survival (DFS) was calculated from the date of sur-ery to the date of progression (local and/or distant), and overallurvival was calculated from the first date of treatment to the date ofeath or last follow-up. Only patients who completed the treatmentrogram (chemoradiation followed by surgery and IOERT) wereligible for this analysis.
To identify a point for dichotomizing the distance of the tumoro the anal margin for optimal preservation of the anorectal sphinc-er, and consequently to determine the optimal cutoff value, aonparametric receiver operating characteristic analysis was used.The significance of differences in proportions was calculated
ith Chi-square test and the differences in means with Student’stest. A logistic regression analysis was used to assess the inde-endent significance of factors predictive of response, defined asrade of residual tumor (mac/mic categories): Age, gender, pre-reatment clinical stage, anal–tumor distance, circumferential in-olvement, tumor grade, dose of radiotherapy, and type of chemo-herapy were studied.
The survival function was estimated using the Kaplan–Meierethod (21). The difference in survival rates between groups was
ested for significance using the log–rank test. A Cox proportionalazard regression was performed to estimate prognostic factorsssociated with disease-free survival: age, gender, pretreatmentlinical stage, anal–tumor distance, circumferential involvement,umor grade, dose of radiotherapy, type of chemotherapy, patho-
ogic stage, downstaging, mac/mic category response, and the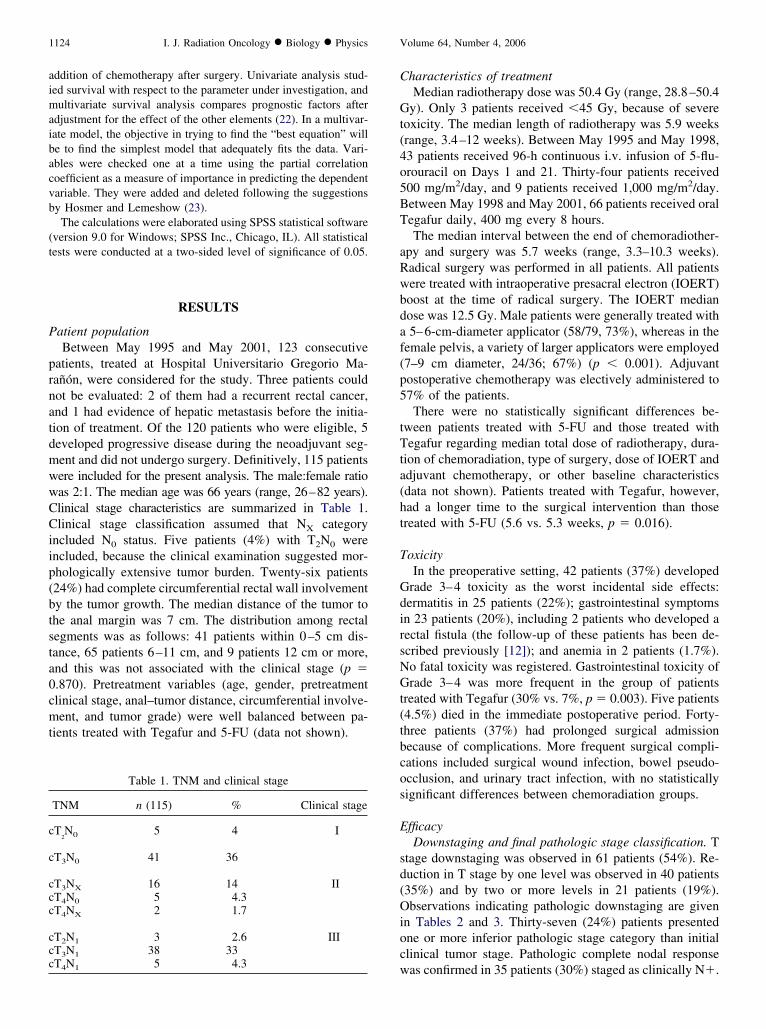
aimaibacvb
(t
P
prnatdmwwCCiip(btsta0cmt
C
Gt(4o5BT
aRwbdaf(p5
tTta(ht
T
GdirsNGt(tbcos
E
sd(Oioc
c
c
ccc
ccc
1124 I. J. Radiation Oncology ● Biology ● Physics Volume 64, Number 4, 2006
ddition of chemotherapy after surgery. Univariate analysis stud-ed survival with respect to the parameter under investigation, andultivariate survival analysis compares prognostic factors after
djustment for the effect of the other elements (22). In a multivar-ate model, the objective in trying to find the “best equation” wille to find the simplest model that adequately fits the data. Vari-bles were checked one at a time using the partial correlationoefficient as a measure of importance in predicting the dependentariable. They were added and deleted following the suggestionsy Hosmer and Lemeshow (23).
The calculations were elaborated using SPSS statistical softwareversion 9.0 for Windows; SPSS Inc., Chicago, IL). All statisticalests were conducted at a two-sided level of significance of 0.05.
RESULTS
atient populationBetween May 1995 and May 2001, 123 consecutive
atients, treated at Hospital Universitario Gregorio Ma-añón, were considered for the study. Three patients couldot be evaluated: 2 of them had a recurrent rectal cancer,nd 1 had evidence of hepatic metastasis before the initia-ion of treatment. Of the 120 patients who were eligible, 5eveloped progressive disease during the neoadjuvant seg-ent and did not undergo surgery. Definitively, 115 patientsere included for the present analysis. The male:female ratioas 2:1. The median age was 66 years (range, 26–82 years).linical stage characteristics are summarized in Table 1.linical stage classification assumed that NX category
ncluded N0 status. Five patients (4%) with T2N0 werencluded, because the clinical examination suggested mor-hologically extensive tumor burden. Twenty-six patients24%) had complete circumferential rectal wall involvementy the tumor growth. The median distance of the tumor tohe anal margin was 7 cm. The distribution among rectalegments was as follows: 41 patients within 0–5 cm dis-ance, 65 patients 6–11 cm, and 9 patients 12 cm or more,nd this was not associated with the clinical stage (p �.870). Pretreatment variables (age, gender, pretreatmentlinical stage, anal–tumor distance, circumferential involve-ent, and tumor grade) were well balanced between pa-
ients treated with Tegafur and 5-FU (data not shown).
Table 1. TNM and clinical stage
TNM n (115) % Clinical stage
T2N0 5 4 I
T3N0 41 36
T3NX 16 14 IIT4N0 5 4.3T4NX 2 1.7
T2N1 3 2.6 IIIT3N1 38 33
wT4N1 5 4.3
haracteristics of treatmentMedian radiotherapy dose was 50.4 Gy (range, 28.8–50.4
y). Only 3 patients received �45 Gy, because of severeoxicity. The median length of radiotherapy was 5.9 weeksrange, 3.4–12 weeks). Between May 1995 and May 1998,3 patients received 96-h continuous i.v. infusion of 5-flu-rouracil on Days 1 and 21. Thirty-four patients received00 mg/m2/day, and 9 patients received 1,000 mg/m2/day.etween May 1998 and May 2001, 66 patients received oralegafur daily, 400 mg every 8 hours.The median interval between the end of chemoradiother-
py and surgery was 5.7 weeks (range, 3.3–10.3 weeks).adical surgery was performed in all patients. All patientsere treated with intraoperative presacral electron (IOERT)oost at the time of radical surgery. The IOERT medianose was 12.5 Gy. Male patients were generally treated with5–6-cm-diameter applicator (58/79, 73%), whereas in the
emale pelvis, a variety of larger applicators were employed7–9 cm diameter, 24/36; 67%) (p � 0.001). Adjuvantostoperative chemotherapy was electively administered to7% of the patients.There were no statistically significant differences be-
ween patients treated with 5-FU and those treated withegafur regarding median total dose of radiotherapy, dura-
ion of chemoradiation, type of surgery, dose of IOERT anddjuvant chemotherapy, or other baseline characteristicsdata not shown). Patients treated with Tegafur, however,ad a longer time to the surgical intervention than thosereated with 5-FU (5.6 vs. 5.3 weeks, p � 0.016).
oxicityIn the preoperative setting, 42 patients (37%) developed
rade 3–4 toxicity as the worst incidental side effects:ermatitis in 25 patients (22%); gastrointestinal symptomsn 23 patients (20%), including 2 patients who developed aectal fistula (the follow-up of these patients has been de-cribed previously [12]); and anemia in 2 patients (1.7%).o fatal toxicity was registered. Gastrointestinal toxicity ofrade 3–4 was more frequent in the group of patients
reated with Tegafur (30% vs. 7%, p � 0.003). Five patients4.5%) died in the immediate postoperative period. Forty-hree patients (37%) had prolonged surgical admissionecause of complications. More frequent surgical compli-ations included surgical wound infection, bowel pseudo-cclusion, and urinary tract infection, with no statisticallyignificant differences between chemoradiation groups.
fficacyDownstaging and final pathologic stage classification. T
tage downstaging was observed in 61 patients (54%). Re-uction in T stage by one level was observed in 40 patients35%) and by two or more levels in 21 patients (19%).bservations indicating pathologic downstaging are given
n Tables 2 and 3. Thirty-seven (24%) patients presentedne or more inferior pathologic stage category than initiallinical tumor stage. Pathologic complete nodal response
as confirmed in 35 patients (30%) staged as clinically N�.
Pp
apmit3r0ewss1O
tactw(p
ofT7dna(2sMi8
fc
sT
ttdgficot3
tttatu
tmlOmtatsasp
hoatcdpstids
C
C
1125Prognostic factors in preoperative treatment of rectal cancer ● J. A. DÍAZ-GONZÁLEZ et al.
athologic Tmic response category was established in 50atients (43.5%).Factors predictive of response. A logistic regression
nalysis was used to assess the independent significance ofre- and on-treatment variables as predictive factors oficroscopic residual disease (mic category). In the univar-
ate analysis, the use of Tegafur as concomitant chemo-herapy with radiation therapy showed an odds ratio (OR) of.97 (p � 0.001). Similarly, a tendency to achieve more micesponses with older age was observed (OR 1.03, p �.056). In the multivariate analysis, after adjustment for theffects of the other variables, older patients and those treatedith Tegafur were more likely to achieve a relevant re-
ponse—with only residual microscopic disease in the surgicalpecimen (mic category)—than those treated with 5-FU (OR,.04; 95% confidence interval [CI], 1.01–1.08; p � 0.038, andR, 4.25; 95% CI, 1.79–9.98; p � 0.001, respectively).A sphincter-saving procedure was performed in 69 pa-
ients (60%), i.e., in 28% of patients with tumors between 3nd 6 cm from anal verge, and in 89% with tumors over 6m from the anal verge. The multivariate analysis showedhat there was a greater probability of sphincter preservationith tumors located 6 cm superiorly from the anal verge
OR, 26.49; 95% CI, 8.97–78.21; p � 0.001) and in femaleatients (OR, 3.22; 95% CI, 1.09–9.55; p � 0.028).Relapse of disease and survival. With a median follow-up
f 36.9 months (range, 6–83.4 months), median disease-ree and overall survival had not yet been reached (Fig. 1).hree-year disease-free and overall survivals were both4%, and pelvic control was 94%. Seven patients (6.1%)eveloped pelvic recurrence (3 isolated and 4 with synchro-ous metastatic disease) and 24 (21%) distant metastaseslone. Only two recurrences were localized in presacral areaIOERT boosted area). The median time to local relapse was3 months (range, 10–55 months). Patients with mic re-ponse had fewer local relapses (2% vs. 9%, p � 0.136).etastasis and overall relapse rate was significantly lower
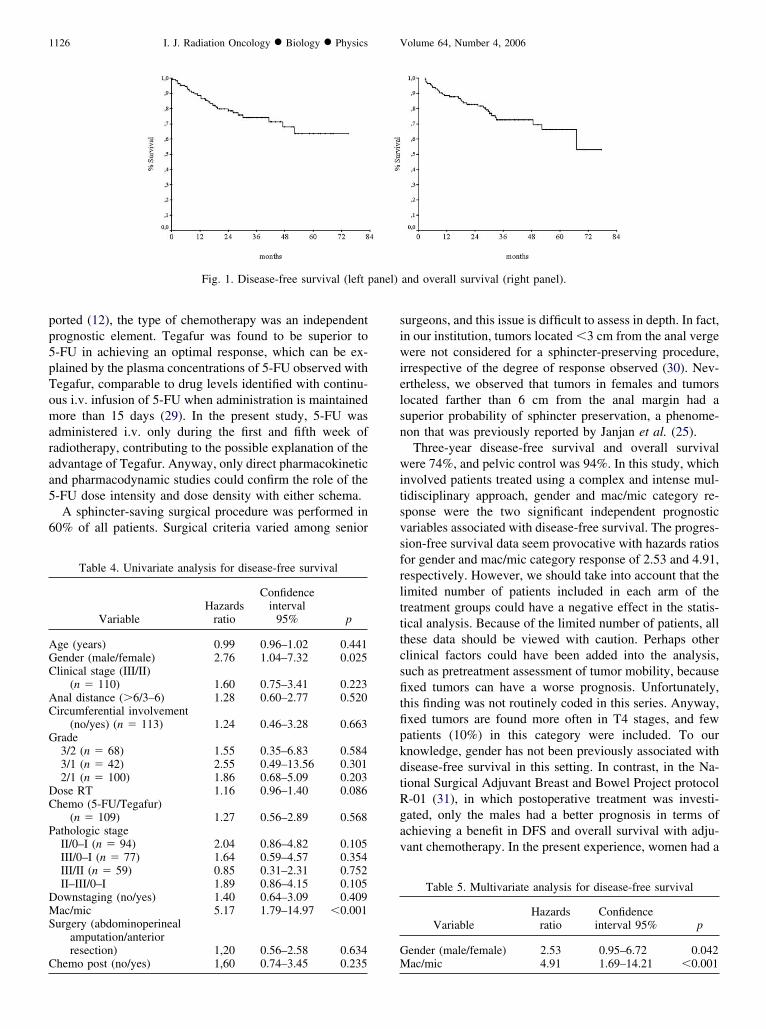
n the mic response subgroup (6% vs. 32%, p � 0.001, and% vs. 37%, p � 0.001, respectively).Thirteen variables were subjected to univariate analysis
or prognostic significance (Table 4): Male gender and macategory were associated with adverse prognosis.
The variables were entered into the multivariate regres-ion analysis using the Cox proportional hazards model.
Table 2. Observations on pathologic downstaging accordingto T status
Pathologic stage
pT0 pT1 pT2 pT3 pT4
linical stagecT2 2 2 4 0 0 8cT3 5 12 31 42 5 95cT4 0 1 2 7 2 12
7 15 37 49 7 115
he selection was based upon their statistical significance in
he univariate analysis and their potential clinical interac-ion. Two of these factors were identified to have indepen-ent significance for disease-free survival in the Cox model:ender and mac/mic category (Table 5). Based on thesendings, patients with no risk factors (female and micategory response) had a 3-year DFS of 100%, patients withne risk factor had a 3-year DFS of 81.3%, and those withwo risk factors (male and mac category response) had a-year DFS of 53% (p � 0.001) (Fig. 2).
DISCUSSION
Pretreatment or treatment-related prognostic factors for pa-ients with locally advanced rectal carcinoma can be charac-erized. The current analysis indicates that among the 13 po-ential prognostic variables analyzed, two of them, male gendernd pTmac category, are independent adverse prognostic fea-ures for prediction of relapse in patients who have been treatedsing an intensive multidisciplinary approach.
Several studies have emphasized the importance of iden-ifying clinical prognostic factors to individualize the treat-ent approach in locally advanced rectal cancer. Thymidy-
ate synthase polymorphisms (24), Eastern Cooperativencology Group performance status, clinical stage, tumorobility, circumference of the rectal wall involved in the
umor (25), and time lapsed before surgery (26) have beenssociated with downstaging. No definitive prognostic fac-ors for prediction of response to treatment have been con-istently identified, and more importantly, few data arevailable associated with disease-free survival. The presenttudy was aimed at analyzing specific factors potentiallyredictive of response and disease-free survival.Downstaging effects of locally advanced rectal cancers
ave been well studied and are a frequent feature in pre-perative chemoradiation trials (27, 28). In the presentnalysis, only the clinical stage before treatment was statis-ically associated with downstaging; in fact, patients withlinical Stage III were three times more likely to showownstaging than patients with Stage II. However, olderatients and those treated with Tegafur were more likely tohow an intense pathologic response (mic category) thanhose treated with 5-FU. There were no statistically signif-cant differences associated with the other variables, butata should be interpreted with caution given the limitedtatistical power of the patients’ cohort. As previously re-
Table 3. Observations on pathologic downstaging accordingto N status
Pathologic stage
pN0 pN1 pN2 pNX
linical stagecN0 41 8 1 0 50cN4 35 9 1 2 47cNX 15 2 0 1 18
91 19 2 3 115
pp5pTomaraa5
6
siwielsn
witsvsfrltttcsfitfipkdtRgav
anel)
AGC
AC
G
DC
P
DMS
CG
1126 I. J. Radiation Oncology ● Biology ● Physics Volume 64, Number 4, 2006
orted (12), the type of chemotherapy was an independentrognostic element. Tegafur was found to be superior to-FU in achieving an optimal response, which can be ex-lained by the plasma concentrations of 5-FU observed withegafur, comparable to drug levels identified with continu-us i.v. infusion of 5-FU when administration is maintainedore than 15 days (29). In the present study, 5-FU was
dministered i.v. only during the first and fifth week ofadiotherapy, contributing to the possible explanation of thedvantage of Tegafur. Anyway, only direct pharmacokineticnd pharmacodynamic studies could confirm the role of the-FU dose intensity and dose density with either schema.A sphincter-saving surgical procedure was performed in
0% of all patients. Surgical criteria varied among senior
Fig. 1. Disease-free survival (left p
Table 4. Univariate analysis for disease-free survival
VariableHazards
ratio
Confidenceinterval
95% p
ge (years) 0.99 0.96–1.02 0.441ender (male/female) 2.76 1.04–7.32 0.025linical stage (III/II)
(n � 110) 1.60 0.75–3.41 0.223nal distance (�6/3–6) 1.28 0.60–2.77 0.520ircumferential involvement
(no/yes) (n � 113) 1.24 0.46–3.28 0.663rade3/2 (n � 68) 1.55 0.35–6.83 0.5843/1 (n � 42) 2.55 0.49–13.56 0.3012/1 (n � 100) 1.86 0.68–5.09 0.203
ose RT 1.16 0.96–1.40 0.086hemo (5-FU/Tegafur)
(n � 109) 1.27 0.56–2.89 0.568athologic stageII/0–I (n � 94) 2.04 0.86–4.82 0.105III/0–I (n � 77) 1.64 0.59–4.57 0.354III/II (n � 59) 0.85 0.31–2.31 0.752II–III/0–I 1.89 0.86–4.15 0.105
ownstaging (no/yes) 1.40 0.64–3.09 0.409ac/mic 5.17 1.79–14.97 �0.001
urgery (abdominoperinealamputation/anteriorresection) 1,20 0.56–2.58 0.634
hemo post (no/yes) 1,60 0.74–3.45 0.235 M
urgeons, and this issue is difficult to assess in depth. In fact,n our institution, tumors located �3 cm from the anal vergeere not considered for a sphincter-preserving procedure,
rrespective of the degree of response observed (30). Nev-rtheless, we observed that tumors in females and tumorsocated farther than 6 cm from the anal margin had auperior probability of sphincter preservation, a phenome-on that was previously reported by Janjan et al. (25).
Three-year disease-free survival and overall survivalere 74%, and pelvic control was 94%. In this study, which
nvolved patients treated using a complex and intense mul-idisciplinary approach, gender and mac/mic category re-ponse were the two significant independent prognosticariables associated with disease-free survival. The progres-ion-free survival data seem provocative with hazards ratiosor gender and mac/mic category response of 2.53 and 4.91,espectively. However, we should take into account that theimited number of patients included in each arm of thereatment groups could have a negative effect in the statis-ical analysis. Because of the limited number of patients, allhese data should be viewed with caution. Perhaps otherlinical factors could have been added into the analysis,uch as pretreatment assessment of tumor mobility, becausexed tumors can have a worse prognosis. Unfortunately,
his finding was not routinely coded in this series. Anyway,xed tumors are found more often in T4 stages, and fewatients (10%) in this category were included. To ournowledge, gender has not been previously associated withisease-free survival in this setting. In contrast, in the Na-ional Surgical Adjuvant Breast and Bowel Project protocol-01 (31), in which postoperative treatment was investi-ated, only the males had a better prognosis in terms ofchieving a benefit in DFS and overall survival with adju-ant chemotherapy. In the present experience, women had a
and overall survival (right panel).
Table 5. Multivariate analysis for disease-free survival
VariableHazards
ratioConfidence
interval 95% p
ender (male/female) 2.53 0.95–6.72 0.042
ac/mic 4.91 1.69–14.21 �0.001
strbiocmpprlraadcddrssimOdrtsp
acrHswirMptfyprt(alrstd
wae(co
iwrrc3ci
caafpmpt
Fm
1127Prognostic factors in preoperative treatment of rectal cancer ● J. A. DÍAZ-GONZÁLEZ et al.
ignificantly longer time to disease progression, a findinghat is not easy to interpret. No presacral relapses wereegistered, perhaps as a result of the improved use of IOERTecause of the anatomic characteristics of the female pelvisn which larger applicators can be adapted: in the majorityf women, 7–9 cm diameter applicators were used vs. 5–6m diameter applicators in men (p � 0.001). However, theain prognostic factor for disease-free survival in the
resent analysis was the mac/mic response category. Thoseatients with occasional cancer foci in the rectal wall (micesponse) had an appreciably, statistically significantlyonger disease-free survival. Few studies have analyzed theelationship between tumor degree of response to preoper-tive chemoradiation therapy and outcome, using appropri-te statistical methodology. Janjan et al. (25) observed thatisease-free survival was worse when nonresponders wereompared to downstaged patients, but interestingly, evi-ence of any type of response was more significant than theegree of response. Valentini et al. found similar results,eporting a positive impact in local control, disease-freeurvival, and overall survival in patients achieving down-taging (32). It has also been reported that patients achiev-ng a complete pathologic response after preoperative che-oradiation did not have a better disease-free survival (33).n the other hand, Berger et al. (34) described no statisticalifference among patients achieving a complete pathologicesponse, but some suggestion of an improved outcome inhis subgroup of patients was advocated. However, themall number of patients with completely sterilized tumors
ig. 2. Three-year disease-free survival based on gender andac/mic response.
revented any firm conclusion from being drawn. In an a
REFEREN
3. Gastrointestinal Tumor Study Group. Prolongation of the dis-
dditional study, patients with downstaging had signifi-antly superior cancer-specific and recurrence-free survivalates compared with the group without downstaging (35).owever, the degree of response and final downstaging
tatus were not analyzed. Moreover, a multivariate analysisas not reported. Perhaps the most recent and complete
nformation in regard to the influence of the degree ofesponse on outcome parameters is reported by experts at
emorial Sloan-Kettering Cancer Center. Pathologic com-lete response and �95% pathologic response were some ofhe independent variables associated with both recurrence-ree survival and overall survival in their multivariate anal-sis (17). The same group previously communicated therognostic relevance of morphologic features in treatedectal cancer (36). Interestingly, the present study differen-iates between downstaging and the degree of responsemac/mic category), and only the latter was associated withn improved outcome. Vecchio et al. (37) contribute to thisine of research, demonstrating that the tumor regressionate is an independent prognostic factor for disease-freeurvival in their series. These data support the hypothesishat it is necessary to use complementary criteria other thanownstaging to better predict the outcome of these patients.Adjuvant chemotherapy was not statistically associated
ith disease-free survival. However, it was administeredccording to the institutional protocols and was generallylected for patients with potentially the worst prognosisresistant disease to neoadjuvant chemoradiation). This factontaminates data interpretation regarding the contributionf systemic treatment.When the patients were categorized on the basis of hav-
ng 0, 1, or 2 risk factors, the 3-year disease-free survivalas remarkably discriminated. In the group of favorable
ectal cancers (women with major responses), no patientelapsed. In contrast, in the group of unfavorable rectalancer features (males with poor or no responses), the-year disease-free survival was only 53%. If these data areonfirmed, relevant implications may be established regard-ng adjuvant treatment.
In conclusion, patients with locally advanced rectal can-er who have been treated with fluoropyrimidine-based neo-djuvant chemoradiation, surgery, and IOERT have remark-ble outcome data. The cohort analysis suggests implicationsor stratification of patients based on gender and pathologicostchemoradiation findings in future adjuvant trials. Further-ore, the current findings provide useful information for
hysicians and patients when considering the potential ofhis multidisciplinary scheme in the treatment of locally
dvanced rectal cancer.CES
1. Madoff RD. Chemoradiotherapy for rectal cancer–when, why,and how? N Engl J Med 2004;351:1790–1792.
2. Wiggers T, de Vries MR, Veeze-Kuypers B. Surgery for local re-currence of rectal carcinoma. Dis Colon Rectum 1996;39:323–328.
ease-free interval in surgically treated rectal carcinoma. N EnglJ Med 1985;312:1465–1472.
4. Douglass HO, Jr, Moertel CG, Mayer RJ, et al. Survival afterpostoperative combination treatment of rectal cancer. N Engl
J Med 1986;315:1294–1295.
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
1128 I. J. Radiation Oncology ● Biology ● Physics Volume 64, Number 4, 2006
5. Krook JE, Moertel CG, Gunderson LL, et al. Effective surgi-cal adjuvant therapy for high-risk rectal carcinoma. N EnglJ Med 1991;324:709–715.
6. Improved survival with preoperative radiotherapy in resect-able rectal cancer. Swedish Rectal Cancer Trial. N Engl J Med1997;336:980–987.
7. Camma C, Giunta M, Fiorica F, Pagliaro L, Craxi A, CottoneM. Preoperative radiotherapy for resectable rectal cancer: Ameta-analysis. JAMA 2000;284:1008–1015.
8. Glimelius B, Isacsson U, Jung B, Pahlman L. Radiotherapy inaddition to radical surgery in rectal cancer: Evidence for adose-response effect favoring preoperative treatment. Int JRadiat Oncol Biol Phys 1997;37:281–287.
9. Sauer R, Becker H, Hohenberger W, et al. Preoperative versuspostoperative chemoradiotherapy for rectal cancer. N EnglJ Med 2004;351:1731–1740.
0. Mannaerts GH, Martijn H, Crommelin MA, Dries W, Repel-aer van Driel OJ, Rutten HJ. Feasibility and first results ofmultimodality treatment, combining EBRT, extensive surgery,and IOERT in locally advanced primary rectal cancer. Int JRadiat Oncol Biol Phys 2000;47:425–433.
1. Bosset JF, Magnin V, Maingon P, et al. Preoperative radio-chemotherapy in rectal cancer: Long-term results of a phase IItrial. Int J Radiat Oncol Biol Phys 2000;46:323–327.
2. Calvo FA, Gomez-Espi M, Diaz-Gonzalez JA, et al. Patho-logic downstaging of T3–4Nx rectal cancer after chemoradia-tion: 5-fluorouracil vs. Tegafur. Int J Radiat Oncol Biol Phys2001;51:1264–1270.
3. Chari RS, Tyler DS, Anscher MS, et al. Preoperative radiationand chemotherapy in the treatment of adenocarcinoma of therectum. Ann Surg 1995;221:778–786.
4. Grann A, Feng C, Wong D, et al. Preoperative combinedmodality therapy for clinically resectable uT3 rectal adeno-carcinoma. Int J Radiat Oncol Biol Phys 2001;49:987–995.
5. Janjan NA, Khoo VS, Abbruzzese J, et al. Tumor downstagingand sphincter preservation with preoperative chemoradiationin locally advanced rectal cancer: The M. D. Anderson CancerCenter experience. Int J Radiat Oncol Biol Phys 1999;44:1027–1038.
6. Stryker SJ, Kiel KD, Rademaker A, Shaw JM, Ujiki GT,Poticha SM. Preoperative “chemoradiation” for stages II andIII rectal carcinoma. Arch Surg 1996;131:514–518.
7. Guillem JG, Chessin DB, Cohen AM, et al. Long-term onco-logic outcome following preoperative combined modalitytherapy and total mesorectal excision of locally advancedrectal cancer. Ann Surg 2005;241:829–838.
8. Diaz-Gonzalez JA, Calvo FA, Cortes J, et al. Preoperativechemoradiation with oral tegafur within a multidisciplinarytherapeutic approach in patients with T3–4 rectal cancer. Int JRadiat Oncol Biol Phys 2005;61:1378–1384.
9. Calvo FA, Santos A, Lozano MA, et al. Early IORT experi-ence in a public university hospital in Spain: Hospital GeneralUniversitario Gregorio Maranon (Madrid). Front Radiat TherOncol 1997;31:76–79.
0. Calvo FA, Gomez-Espi M, Diaz-Gonzalez JA, et al. Intraop-erative presacral electron boost following preoperative chemora-diation in T3–4Nx rectal cancer: Initial local effects and clinicaloutcome analysis. Radiother Oncol 2002;62:201–206.
1. Kaplan E, Meier P. Non-parametric estimation from incom-plete observations. J Am Stat Assoc 1959;53:457–481.
2. Clark TG, Bradburn MJ, Love SB, Altman DG. Survival
analysis part I: Basic concepts and first analyses. Br J Cancer2003;89:232–238.
3. Hosmer DW, Lemeshow S. Applied logistic regression. 2nded. New York: Wiley; 2000.
4. Villafranca E, Okruzhnov Y, Dominguez MA, et al. Polymor-phisms of the repeated sequences in the enhancer region of thethymidylate synthase gene promoter may predict downstagingafter preoperative chemoradiation in rectal cancer. J ClinOncol 2001;19:1779–1786.
5. Janjan NA, Abbruzzese J, Pazdur R, et al. Prognostic impli-cations of response to preoperative infusional chemoradiationin locally advanced rectal cancer. Radiother Oncol 1999;51:153–160.
6. Francois Y, Nemoz CJ, Baulieux J, et al. Influence of theinterval between preoperative radiation therapy and surgery ondownstaging and on the rate of sphincter-sparing surgery forrectal cancer: The Lyon R90–01 randomized trial. J ClinOncol 1999;17:2396.
7. Marsh RD, Chu NM, Vauthey JN, et al. Preoperative treatmentof patients with locally advanced unresectable rectal adenocarci-noma utilizing continuous chronobiologically shaped 5-fluoro-uracil infusion and radiation therapy. Cancer 1996;78:217–225.
8. Morgan MJ, Koorey DJ, Painter D, et al. Histological tumourresponse to pre-operative combined modality therapy in lo-cally advanced rectal cancer. Colorectal Dis 2002;4:177–183.
9. Ansfield FJ, Kallas GJ, Singson JP. Phase I-II studies of oraltegafur (ftorafur). J Clin Oncol 1983;1:107–110.
0. Calvo FA, Cantalapiedra R, Gomez-Espi M, et al. Ano-rectalsphincter preservation following preoperative chemoradiationin cT3–4Nx rectal cancer: Influence of tumor distance anddownstaging. Rev Oncologia 2002;4:146–153.
1. Fisher B, Wolmark N, Rockette H, et al. Postoperative adju-vant chemotherapy or radiation therapy for rectal cancer:Results from NSABP protocol R-01. J Natl Cancer Inst 1988;80:21–29.
2. Valentini V, Coco C, Picciocchi A, et al. Does downstagingpredict improved outcome after preoperative chemoradiationfor extraperitoneal locally advanced rectal cancer? A long-term analysis of 165 patients. Int J Radiat Oncol Biol Phys2002;53:664–674.
3. Pucciarelli S, Toppan P, Friso ML, et al. Complete pathologicresponse following preoperative chemoradiation therapy formiddle to lower rectal cancer is not a prognostic factor for abetter outcome. Dis Colon Rectum 2004;47:1798–1807.
4. Berger C, de MA, Garaud P, et al. Preoperative radiotherapy(RT) for rectal cancer: Predictive factors of tumor downstag-ing and residual tumor cell density (RTCD): Prognostic im-plications. Int J Radiat Oncol Biol Phys 1997;37:619–627.
5. Kaminsky-Forrett MC, Conroy T, Luporsi E, et al. Prognosticimplications of downstaging following preoperative radiationtherapy for operable T3-T4 rectal cancer. Int J Radiat OncolBiol Phys 1998;42:935–941.
6. Shia J, Guillem JG, Moore HG, et al. Patterns of morphologicalteration in residual rectal carcinoma following preoperativechemoradiation and their association with long-term outcome.Am J Surg Pathol 2004;28:215–223.
7. Vecchio FM, Valentini V, Minsky BD, et al. The relationshipof pathologic tumor regression grade (TRG) and outcomesafter preoperative therapy in rectal cancer. Int J Radiat Oncol
Biol Phys 2005;62:752–760.Copyright © 2022 FDOKUMEN




















