Dhahbi IRBM 2014 Reference database of the gait cycle for young healthy Tunisian adults
Upload
independentCategory
view
0download
0
Review
Prevention and early treatment of in¯uenza in healthy adults
V. Demicheli a, T. Je�ersonb,*, D. Rivetti c, J. Deeksd
aInstitute of Medical Statistics, University of Pavia, Pavia, ItalybCochrane Centre and Cochrane Vaccines Field, Summertown Pavillion, Middle Way, Oxford OX2 7LG, UK
cEnvironmental Epidemiology Unit, ARPA, Alessandria, ItalydSystematic Reviews Unit, Institute of Health Sciences, Oxford, UK
Received 27 January 1999; received in revised form 20 June 1999; accepted 14 July 1999
Abstract
Introduction: We present three systematic reviews carried out within the Cochrane Collaboration, focusing on a di�erent
in¯uenza intervention in healthy adults: Vaccines; Ion Channel Inhibitor antivirals and Neuraminidase Inhibitor (NIs) antivirals.The objectives were to identify, retrieve and assess all studies evaluating the e�ects of these interventions in prophylaxis andearly treatments of in¯uenza and the frequency of adverse events. Additionally we present the results of the economic evaluation
of e�ective alternatives in order to de®ne the most cost-e�ective intervention. The economic evaluation is set in the context ofthe British Army.Methods: Studies were identi®ed using a standard Cochrane search strategy. Any randomised or quasi-randomised studies in
healthy individuals aged 14±60 years were considered for inclusion in the systematic review. Those which met inclusion criteria
were assessed for quality and their data meta-analysed. The economic model was constructed using Cost-e�ectiveness and Cost-utility study designs.Results: Live aerosol vaccines reduced cases of clinical in¯uenza A with virological con®rmation (by serology and/or viral
isolation) by 48% (95%CI: 24±64%), whilst recommended inactivated parenteral vaccines have an e�cacy of 68% (95%CI: 49±79%). Vaccine e�ectiveness in reducing clinical in¯uenza cases (i.e. without virological con®rmation) was lower, with e�cacies of13 and 24% respectively. Use of the vaccine signi®cantly reduced time o� work, but only by 0.4 days (95%CI: 0.1±0.8 days).
Analysis of vaccines matching the circulating strain gave higher estimates of e�cacy, whilst inclusion of all other vaccinesreduced the e�cacy. When compared to placebo for the prevention of in¯uenza, oral amantadine was 61% (95%CI: 51±69%)e�cacious (RR 0.39 Ð 95%CI: 0.31±0.49), and oral rimantadine was 64% (95%CI: 41±78%) e�cacious (RR 0.36 Ð95%CI:
0.22±0.59). When compared to placebo for the treatment of in¯uenza, oral amantadine signi®cantly shortened duration of fever(by 1.00 days Ð 95%CI: 0.73±1.29), and oral rimantadine signi®cantly shortened duration of fever (by 1.27 days Ð 95%CI:0.77±1.77). When compared to placebo, NIs were 74% (95%CIs: 50±87%) e�ective in preventing naturally occurring cases ofclinically de®ned in¯uenza. In a treatment role, NIs shortened the duration of symptoms by one day (Weighted Mean Di�erence
Ð 1.0; 95%CIs: ÿ1.3 to ÿ 0.6) when a clinical case de®nition is used. The economic results show that in healthy adults,inactivated vaccines appear the best buy.Conclusions: If assessed from the point of view of e�ectiveness and e�ciency, vaccines are undoubtedly the best preventive
means for clinical in¯uenza in healthy adults. However, when safety and quality of life considerations are included, parenteralvaccines have such low e�ectiveness and high incidence of trivial local adverse e�ects that the trade-o� is unfavourable. This isso even when the incidence of in¯uenza is high and adverse e�ect quality of life preferences are rated low. We reached similar
conclusions for antivirals and NIs even at high in¯uenza incidence levels. On current evidence we conclude in healthy adultsaged 14±60 the most cost-e�ective option is not to take any action. # 2000 Elsevier Science Ltd. All rights reserved.
Vaccine 18 (2000) 957±1030
0264-410X/00/$ - see front matter # 2000 Elsevier Science Ltd. All rights reserved.
PII: S0264-410X(00 )00332 -1
www.elsevier.com/locate/vaccine
* Corresponding author. Tel.: +44-1865-516300; fax: +44-1865-
516311.
E-mail address: [email protected] (T. Je�erson).
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 959
1.1. Prevention and early treatment of in¯uenza . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9591.1.1. In¯uenza vaccines . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9591.1.2. Ion channel inhibitor antivirals (Amantadine and Rimantadine) . . . . . . . . . . 961
1.1.3. Neuraminidase inhibitor antivirals (NIs) . . . . . . . . . . . . . . . . . . . . . . . . . . . 9621.2. Rationale for the economic evaluation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 962
2. Methods . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 963
2.1. Methods for the reviews. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9632.1.1. Objectives. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9632.1.2. Selection criteria . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 963
2.1.3. Search strategy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9632.1.4. Methods for the economic evaluation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 966
3. Results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 967
3.1. Results of the reviews . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9673.1.1. Description of studies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9673.1.2. Methodological quality of included studies . . . . . . . . . . . . . . . . . . . . . . . . . 970
3.2. E�ects of in¯uenza vaccines . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9713.2.1. E�ect of vaccination on clinical cases of in¯uenza . . . . . . . . . . . . . . . . . . . . 9713.2.2. E�ect of vaccination on serologically con®rmed cases of in¯uenza . . . . . . . . 9713.2.3. E�ect of vaccination on other outcomes . . . . . . . . . . . . . . . . . . . . . . . . . . . 971
3.2.4. Recommended vaccines . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9723.2.5. Vaccine matching the circulating strain . . . . . . . . . . . . . . . . . . . . . . . . . . . . 972
3.3. E�ects of amantadine and rimantadine . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 972
3.3.1. Comparison A Ð oral amantadine compared to placebo in in¯uenzaprevention . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 974
3.3.2. Comparison B Ð oral rimantadine compared to placebo in in¯uenza
prevention . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9743.3.3. Comparison C Ð oral amantadine compared to oral rimantadine in in¯uenza
prevention . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9753.3.4. Comparison D Ð oral amantadine compared to placebo in in¯uenza
treatment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9753.3.5. Comparison E Ð oral rimantadine compared to placebo in in¯uenza
treatment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 976
3.3.6. Comparison F Ð oral amantadine compared to oral rimantadine in in¯uenzatreatment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 976
3.3.7. Comparison G Ð oral amantadine compared to oral aspirin in in¯uenza
treatment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9773.3.8. Comparison H Ð inhaled amantadine compared to placebo in in¯uenza
treatment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 977
3.4. E�ects of NIs . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9773.5. Results of the economic evaluation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 979
4. Discussion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 979
4.1. In¯uenza vaccines . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9794.2. Amantadine and rimantadine . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9814.3. Neuraminidase inhibitors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 982
4.4. Overall comments . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9824.5. Economic evaluation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 982
Acknowledgements . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 983
Appendix A. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 984
Appendix B . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 985
Appendix C . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 986
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1030
V. Demicheli et al. / Vaccine 18 (2000) 957±1030958

1. Introduction
In¯uenza is an acute respiratory infection caused
by a virus, of which three serotypes are known (A, B
and C). In¯uenza causes an acute febrile illness with
myalgia, headache and cough. Although the median
duration of the acute illness is three days (duration
can vary between serotypes and subtypes), cough and
malaise can persist for weeks. Complications of in¯u-
enza include otitis media, pneumonia, secondary bac-
terial pneumonia, exacerbations of chronic respiratory
disease and bronchiolitis in children. Additionally,
in¯uenza can cause a range of non-respiratory com-
plications including febrile convulsions, Reye's syn-
drome and myocarditis [1].
The in¯uenza virus is composed of a lipid mem-
brane surrounding a protein shell and a core consist-
ing of several RNA complexes. On the lipid
membrane are two viral glycoproteins which act as
powerful antigens: neuraminidase (N antigen) and
hemagglutinin (H antigen). Hemagglutinin facilitates
the entry of the virus into cells of the respiratory epi-
thelium, while neuraminidase facilitates the release of
newly produced viral particles (so-called virions) from
infected cells. The in¯uenza virus has a marked pro-
pensity to mutate its external antigenic composition
to escape the hosts' immune defences. Given this
extreme mutability, the World Health Organisation
(WHO) has introduced a classi®cation of each viral
subtype based on H and N typing. Additionally,
strains are classi®ed on the basis of antigenic type of
the nucleoprotein core (A, B or C), geographical lo-
cation of ®rst isolation, strain serial number and year
of isolation. Every item is separated by a slash mark
(e.g. A/Wuhan/359/95 [H3N2]).
In this century there have been four pandemics
caused by so-called antigenic shift (a major change
in H con®guration with or without a concomitant
change in N and perhaps viral alteration of tissue
tropism) leading to the appearance of a new sub-
type against which there is little circulating natural
immunity. Pandemics are thought to originate in
Southern China where ducks (the animal reservoir
and breeding ground for new strains), pigs (which
are thought to be the biological intermediate host
or `mixing vessel') and humans live in very close
proximity [2]. Minor changes in viral antigenic
con®gurations, known as `drift', cause local or
more circumscribed epidemics. The recently isolated
Hong Kong avian in¯uenza (A/HK/156/97 [H5N1]
virus appears to be an example of a zoonotic
infection with direct spread of the avian virus to
humans [3±5]. Pandemics by de®nition cause a
very high morbidity and mortality burden [6]. The
1918±19 pandemic is estimated to have caused up
to 40 million deaths world-wide.
1.1. Prevention and early treatment of in¯uenza
E�orts to prevent or treat in¯uenza have had their
mainstay in two separate approaches: vaccines and
antivirals (ion channel inhibitors and neuraminidase
inhibitors).
1.1.1. In¯uenza vaccines
Current in¯uenza vaccines are of four types:
1. whole virion vaccines which consist of complete
viruses which have been `killed'; or inactivated, so
that they are not infectious but retain their strain-
speci®c antigenic properties.
2. subunit virion vaccines which are made of surface
antigens (H and N) only.
3. split virion vaccines in which the viral structure is
broken up by a disrupting agent.
4. live vaccines (as yet unlicensed).
The ®rst three types of vaccines contain the two sur-
face antigens; whole virion and split vaccines also con-
tain antigens which are thought to contribute to a
higher rate of vaccine reactions compared to subunit
vaccines.
Appendix A shows a list of in¯uenza vaccine produ-
cers and products world-wide, compiled by WHO in
1996 [7].
Periodic antigenic drifts and shifts pose problems
for vaccine production and procurement, as a new
vaccine closely matching circulating antigenic con-
®guration must be produced and procured for the
beginning of each new in¯uenza `season'. To achieve
this, WHO has established a world-wide surveillance
system allowing identi®cation and isolation of viral
strains circulating in the di�erent parts of the globe.
Sentinel practices recover viral particles from the
naso-pharynx of patients with in¯uenza-like symp-
toms and the samples are swiftly sent to the labora-
tories of the national in¯uenza centres (110
laboratories in 79 countries). When new strains are
detected the samples are sent to one of the four
WHO reference centres (London, Atlanta, Tokyo and
Melbourne) for antigenic analysis. Information on cir-
culating strains is then sent to WHO, who in
February of each year recommends, through a com-
mittee, the strains to be included in the vaccine for
the forthcoming `season'. Individual governments may
or may not follow WHO recommendations.
Australia, New Zealand and more recently South
Africa follow their own recommendations for vaccine
content.
Surveillance and early identi®cation thus play a cen-
V. Demicheli et al. / Vaccine 18 (2000) 957±1030 959
tral part in the composition of the vaccine.
Traditionally, in¯uenza vaccines have been targeted to
the elderly and those at serious risk of complications.
Despite clear theoretical advantages in the use of vac-
cines, their uptake has been patchy. Studies in family
practices suggest that 20% is a reasonable estimate of
in¯uenza vaccine utilisation in the Canadian popu-
lation [8±10]. The current low level of in¯uenza vac-
cine uptake in targeted populations may re¯ect
uncertainty on the part of primary care and public
health practitioners and health policy decision-makers
regarding vaccine e�ectiveness.
One possible reason may be the diversity of regu-
lations for the ®nancing and reimbursement of the
vaccines. Other reasons may include perceived low
e�cacy due to the mutable viral con®guration, the
perceived commonality of the disease, which may
breed contempt and, strangely, a misperception of the
burden imposed by the disease on society. Nowhere
is this more marked than in the case of healthy
adults in employment, a population which would
most bene®t from protection against in¯uenza.
Epidemics in settings such as schools, barracks, pris-
ons, o�ces, hospitals and industrial complexes cause
great losses, but are seldom prevented by vaccination
of sta�.
Despite the publication over a period of more than
®ve decades of a large number of reports of con-
trolled clinical trials, there remains substantial uncer-
tainty about the clinical e�ectiveness of in¯uenza
vaccine. This uncertainty is manifested in widely vary-
ing estimates of vaccine e�ectiveness in the current
health care literature. For example MMWR states:
`The e�ectiveness of in¯uenza vaccine in preventing
or attenuating illness varies, depending primarily on
the age and immunocompetence of the vaccine recipi-
ent and the degree of similarity between the virus
strains included in the vaccine and those that circu-
late during the in¯uenza season. When a good match
exists between vaccine and circulating viruses, in¯u-
enza vaccine has been shown to prevent illness in ap-
proximately 70±90% of healthy persons aged <65
years' [11].
To our knowledge there are no systematic reviews
of the e�ects of vaccination on healthy adults,
although there are several examples of reviews in the
elderly such as the studies by Gross and Strassburg
[12,13]. For example, Strassburg meta-analysed 17
controlled studies of in¯uenza vaccine e�ectiveness
among elderly subjects. However all but two of the
primary studies included in his analysis were non-ex-
perimental [13]. The only attempt at a comprehensive
review of the in¯uenza vaccine e�ectiveness literature
was conducted by Couch for the US O�ce of
Technology Assessment. Couch reviewed 68 trials
`reporting e�ectiveness against naturally occurring
in¯uenza' (56 type A in¯uenza, 12 type B) [14]. His
sources for identi®cation of primary studies were: CG
Lossli, International Bibliography of In¯uenza 1930±
59; Medlars Service of NLM; and Cumulative Index
Medicus. His ®ndings included the following:
. The range of e�ectiveness for each virus type was 0±
96%
. The majority of trials reported e�ectiveness greater
than 60% for homologous virus challenge, but pro-
tection against heterologous virus was more variable
[14]
. The commonly quoted ®gure of 70% protection
against illness (`clinical in¯uenza') in these circum-
stances (`if the epidemic virus is antigenically similar
to the vaccine virus and if vaccine is given in the im-
mediate few months preceding exposure') seems
reasonable' [14]
The wide variation in protection observed in controlled
trials may be related to features of the in¯uenza virus,
the vaccine, the target population or the study design.
The most salient of these are discussed below.
1.1.1.1. The virus. The phenomenon of antigenic drift/shift among in¯uenza viruses can result in a less thanperfect Ð and at times non-existent Ð match betweenvaccine strain(s) and prevalent strain(s). The protectivee�ect of vaccination would be expected to vary withthe closeness of the antigenic match. There are twoclinically important types of in¯uenza virus Ð A andB.
1.1.1.2. The vaccine. Vaccines may vary in antigenicpotency, composition (e.g. monovalent, bivalent, triva-lent or polyvalent) or method of preparation (e.g. liveor inactivated; whole virus, split virus or subunit vac-cines, aqueous or oil adjuvant). In¯uenza vaccines mayact to modify as well as prevent illness.
1.1.1.3. The target population. Study populations varyin age, health status and type of living arrangements(e.g. institutional, communal or independent house-hold). Some of these characteristics may a�ect immuneresponsiveness to vaccination or likelihood of contract-ing in¯uenza (which in turn a�ects statistical powerand the play of chance on observed e�ect size).
1.1.1.4. The study design. Protective e�ect in clinicaltrials might be substantially in¯uenced by the outcomemeasure used. In¯uenza cannot be satisfactorily distin-guished on clinical grounds from respiratory infectionscaused by other Ð chie¯y viral Ð organisms. As aconsequence, dilution of any e�ect of intervention can
V. Demicheli et al. / Vaccine 18 (2000) 957±1030960

be expected when purely clinical outcome measures
are used. This is particularly true when the incidence
of in¯uenza is low, when the period of observation
extends beyond the usual four to 12 week annual
period of in¯uenza activity, or when the de®nition of
illness is imprecise (e.g. respiratory illness). To the
extent that in¯uenza vaccine modi®es illness which itdoes not prevent, protection might be greater for out-
comes which re¯ect complications of in¯uenza (e.g.
hospitalisation with respiratory illness) rather than
primary infection (e.g. acute respiratory illness). Con-
ventionally, serological diagnosis is based on a four-
fold or greater increase in antibody titre to one or
more virus antigens. There is evidence that vaccinated
individuals are less likely than non-vaccinated persons
to mount an antibody rise following infection with an
in¯uenza virus antigenically related to strains con-
tained in the vaccine. This phenomenon is thought to
be based, at least in part, on higher pre-infection
antibody titres which result from vaccination. Serolo-
gical methods will therefore `miss' cases of in¯uenza
among vaccinated subjects and could be expected to
produce a spuriously high observed protective e�ect.
Hobson has suggested (without citing supportive evi-
dence) that virus isolation results may be similarly
biased. He proposes that vaccines which fail to pro-tect against clinical illness may reduce the amount
and duration of virus shedding [15].
Other study design features which might in¯uence
observed vaccine e�ectiveness include method of al-
location, extent of blinding and type of virus chal-
lenge (natural or arti®cial). Variability would be
expected to be greater in studies with small sample
sizes.
The de®ciencies of most current and past reviews of
in¯uenza vaccine e�ectiveness can be summarised as
follows:
1. lack of comprehensiveness in the identi®cation of
primary studies
2. lack of methodological assessment of primary stu-
dies
3. failure to satisfactorily account for (or in some
cases, to acknowledge) the marked variability in
vaccine e�ectiveness among controlled studies
4. failure to provide estimates of vaccine e�ectiveness
under conditions of imperfect antigenic matching
between vaccines and prevalent viruses (that is,
when vaccines contain either a di�erent strain or a
di�erent subtype of in¯uenza virus than the preva-
lent virus)
5. lack of credible estimates of vaccine e�ectiveness in
speci®c populations currently targeted for in¯uenza
vaccination (for example, institutionalised elderly,
community-dwelling elderly and persons with under-
lying medical conditions associated with a high risk
of complications [16,17].
These de®ciencies help to explain discrepancies in
reported vaccine e�ectiveness in the existing literature.
Moreover, they can be expected to give rise to uncer-
tainty among clinicians and policy-makers regarding
the expected e�ectiveness of in¯uenza vaccine in the
population groups for which annual in¯uenza vacci-
nation is currently recommended. In this scenario a
systematic review of the e�ects of vaccines against
naturally occurring in¯uenza is necessary to enable de-
cision-makers to devise strategies to deal with in¯uenza
based on evidence.
1.1.2. Ion channel inhibitor antivirals (Amantadine andRimantadine)
The main antiviral compounds used against in¯u-
enza are amantadine hydrochloride and rimantadine
hydrochloride (amantadine and rimantadine for
short). Amantadine (an anti-Parkinsonism) was intro-
duced in the 1950s and found to have antiviral ac-
tivity in 1965. In the USA, amantadine was licensed
for the treatment and prophylaxis of in¯uenza A/
H2N2 infections by the FDA in 1966 and for pro-
phylaxis and treatment of all in¯uenza A infections
in 1976. Rimantadine was licenced in 1993 [18]. In
the USA, while amantadine is licensed for treatment
and prophylaxis of adults and children over the age
of one, rimantadine is licensed only for prophylaxis
in children as well as for treatment and prophylaxis
in adults [18]. In the UK amantadine only is licensed
and is administered orally at a recommended does of
100 mg a day in healthy adults for ®ve days (treat-
ment role) or 100 mg a day as long as the risk of
infection lasts (prophylaxis role).
Both compounds interfere with the replication cycle
of type A (but not type B) viruses [19] and are thought
to be e�cacious and, given their virus-speci®c action,
relatively free of adverse e�ect. Drug resistant H3N2
subtype in¯uenza A viruses have been isolated during
treatment with amantadine and rimantadine, especially
in institutions, but their clinical signi®cance is unclear
[20].
Given both drugs' apparent e�cacy in both pro-
phylactic and therapeutic roles (if administration is
started in time), their relatively scarce use is surpris-
ing [1]. Explanations for this ®nding include lack of
awareness of the drugs and their properties by medi-
cal practitioners, lack of a rapid diagnostic capability
and concern over their adverse e�ects, which include
epilepsy. Even more surprising is the list of indi-
cations for use of both drugs. While subjects at high
risk (i.e. subjects with underlying debilitating pathol-
ogies and the elderly) are included, healthy adults, es-
V. Demicheli et al. / Vaccine 18 (2000) 957±1030 961

pecially those working in institutions (such as health-
care workers, nursing home attendants and the mili-
tary) are not. These groups are likely to greatly
bene®t from the use of the drugs, which could have a
direct impact on length of sickness absence and
diminish considerably the burden of in¯uenza epi-
demics to society. Additionally a non-systematic
review of the evidence of the e�cacy of rimantadine
identi®ed ®ve small double-blind placebo-controlled
trials of both drugs in a prophylaxis role and nine
trials in a treatment role [21]. The largest study con-
tained 378 individuals, indicating the need to attempt
pooling data to derive more precise estimates of e�ect
and safety for the compounds. This systematic review
of the e�ects of amantadine and rimantadine in
healthy adults excludes children, the elderly and indi-
viduals with pre-existing pathologies. However, given
the impact of in¯uenza in these populations, systema-
tic reviews of the e�ects of amantadine and rimanta-
dine in children, elderly and at-risk groups should
also be carried out in the future.
1.1.3. Neuraminidase inhibitor antivirals (NIs)
In recent years a new generation of antiviral com-
pounds has been developed and is currently in pre-
registration phase III trials. These compounds, known
collectively as neuraminidase inhibitors (NIs), are:
. Nebulised Zanamivir developed by GlaxoWellcome
PLC (UK).
. Oral Oseltamivir (formerly known as Ro 64-0796
or GS 4104) co-developed by Gilead Sciences Inc.
(Foster City, CA, USA) and Ho�mann-La Roche
Ltd (Basle, CH). Gilead Sciences Inc. still retains
the intellectual property rights to Oseltamivir.
Zanamivir is a so-called second-generation NI, whereas
Oseltamivir represents the third generation of such
compounds [22]. NIs act by inhibiting the entry of
viral particles into the target cell and subsequent
release of virions from the infected cell, neuraminidase
being essential for both functions. Both Oseltamivir
and Zanamivir appear to be e�ective against In¯uenza
A and B, while amantadine is e�ective only against
in¯uenza A.
NIs could be used in both a preventive role and to
diminish the severity of the illness [23], to:
. treat infected individuals
. supplement protection against infection in individ-
uals not fully protected by vaccination
. provide protection for individuals unable to receive
vaccine (e.g. individuals allergic to eggs)
. provide short term prophylaxis in family settings
. supplement vaccination during pandemics when vac-
cine stocks may be limited
. control outbreaks in institutions such as nursing
homes or prisons
. control outbreaks in settings such as factories,
o�ces or the military
. generally interrupt viral transmission.
Ho�mann-La Roche and GlaxoWellcome are target-
ing the registration and marketing of their com-
pounds to the year 2000 in¯uenza season [24]. As
NIs are likely, if proved e�ective and safe, to become
a major form of prophylaxis and treatment of in¯u-
enza, reviewing and updating the available evidence is
necessary to provide an accurate assessment of their
e�ects.
1.2. Rationale for the economic evaluation
J95, the British Army's ICD-based surveillance sys-
tem, indicated that in soldiers respiratory disease is the
second highest cause of morbidity and sixth highest
cause of productivity losses (measured in working days
lost, or WDL) both on world-wide military operations
and when in barracks [25]. Further work carried out
by the Department of Public Health of the University
of Glasgow [26] shows that within the `respiratory dis-
ease' code block approximately 40% of the morbidity
in the 1996±1997 season was caused by clinical in¯u-
enza. In some Army subpopulations (such as recruits
undergoing training) the burden of respiratory disease
is much higher (37 attendances per 1000 personnel per
month in Training Establishment compared to 13 at-
tendances per 1000 personnel per month in the rest of
the Army). In¯uenza, then, is an important recurring
public health problem for the British Army, as it
threatens the health and hence e�ciency of its work-
force, the most important resource that any organis-
ation has at its disposal.
Before embarking in a major expenditure pro-
gramme to purchase large quantities of these inter-
ventions (given that clinical in¯uenza is a disease of
such high incidence among the military) the Ministry
of Defence of the United Kingdom wanted to make
sure that resources used in the prevention programme
would be recouped by its bene®ts. This provided the
rationale for an economic evaluation comparing the
costs and e�ects of each course of action. However,
preliminary work prior to undertaking the evaluation
indicated that there were considerable uncertainties as
to the e�ectiveness and safety of vaccines, antivirals
and NIs. This provided the main reason for the com-
missioning of three Cochrane reviews [27±29] prior to
carrying out the economic evaluation. The evaluation
has been conducted and reported according to the
BMJ guidelines for economic submissions [30].
V. Demicheli et al. / Vaccine 18 (2000) 957±1030962
2. Methods
2.1. Methods for the reviews
2.1.1. Objectives
In comparisons between groups intended for the
interventions and control/placebo groups the following
hypotheses were tested:
2.1.1.1. Cases. There is no di�erence in the number ofcases of in¯uenza and their severity.
2.1.1.2. Adverse e�ects. There is no di�erence in thenumber and severity of adverse e�ects (both systemicand localised).
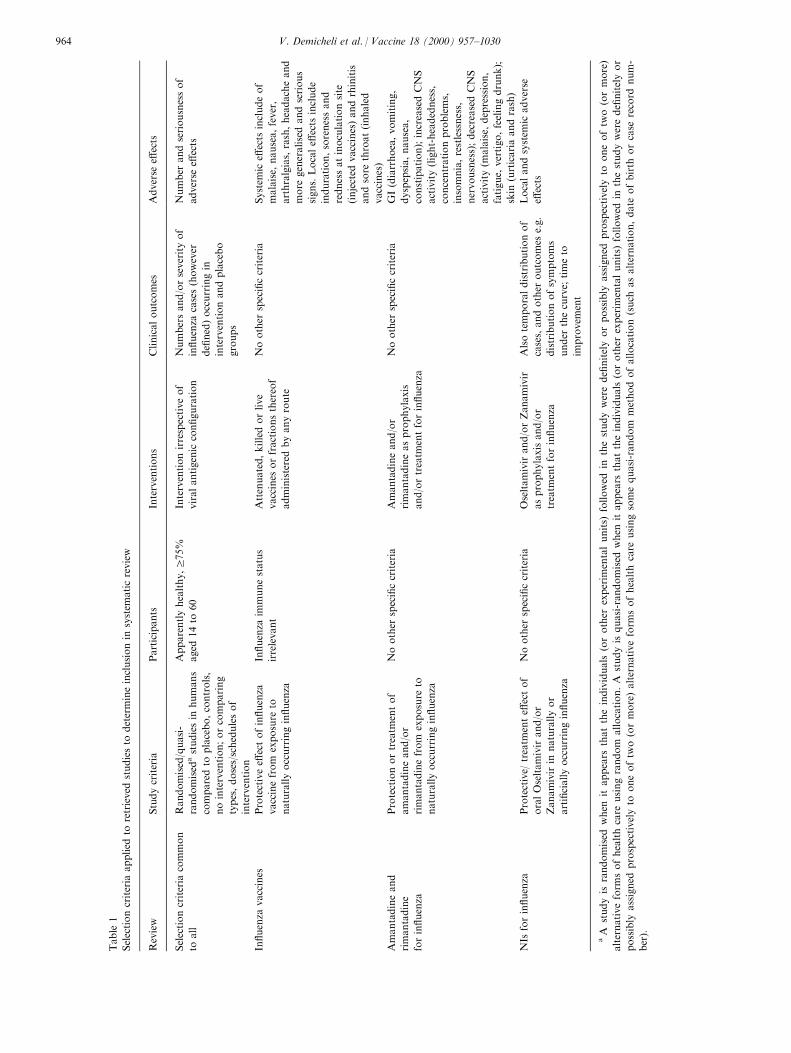
2.1.2. Selection criteria
See Table 1.
2.1.3. Search strategy
. A MEDLINE search was carried out using the
extended search strategy of the Cochrane Acute
Respiratory Infections (ARI) Group [31] with the
following search terms or combined sets from 1966
to the end of 1997 in any language: in¯uenza; route
(oral) OR route (parenteral); vaccine; amantadine;
rimantadine; neuraminidase inhibitors; Oseltamivir ;
GS 4104; Ro 64-0796; Zanamivir
. The bibliography of retrieved articles was examined
in order to identify further trials
. A search was carried out of the Cochrane
Controlled Trials Register (CCTR) and of
EMBASE (1990±97 for In¯uenza Vaccines and for
NIs; 1985 to 1997 for Amantadine and
Rimantadine)
. The journal Vaccine was handsearched from its ®rst
issue to the end of 1997 [32,33]
. The manufacturers, ®rst or corresponding authors
of evaluated studies and researchers active in the
®eld were contacted in order to locate unpublished
trials.
2.1.3.1. Trial quality assessment. Two reviewers readall trials retrieved in the search and applied inclusioncriteria. Trials ful®lling these criteria were assessed forquality and results analysed by the same authors. Dis-agreements on trial quality were arbitrated by a thirdauthor. Assessment of trial quality were made accord-ing to the following criteria:
1. generation of allocation schedule (de®ned as the
methods of generation of the sequence which
ensures random allocation).
2. measure(s) taken to conceal treatment allocation
(de®ned as methods to prevent selection bias, i.e. to
ensure that all participants have the same chance of
being assigned to one of the arms of the trial. This
protects the allocation sequence before and during
allocation)
3. number of drop-outs of allocated healthcare worker
participants from the analysis of the trial (de®ned as
the exclusion of any participants for whatever
reason Ð deviation from protocol, loss to follow-
up, withdrawal, discovery of ineligibility; while the
unbiased approach analyses all randomised partici-
pants in the originally assigned groups regardless of
compliance with protocol, known as intention to
treat analysis)
4. measures taken to implement double blinding (a
double-blind study is one in which observer(s) and/
or subjects are kept ignorant of the group to which
the subjects are assigned, as in an experiment, or of
the population from which the subjects come, as in
a non-experimental situation. Unlike allocation con-
cealment, double blinding seeks to prevent ascer-
tainment bias and protects the sequence after
allocation)
For criteria 2, 3 and 4 there is empirical evidence that
low quality in their implementation is associated with
exaggerated trial results [34] and it is reasonable to
infer a quality link between all four items. The four
criteria were assessed by answering a questionnaire; see
Appendix B.
2.1.3.2. Data collection. The following data wereextracted, checked and recorded:
. Characteristics of trials: date; location; setting; case
de®nitions used (clinical, serological, virological);
surveillance system; type and length of epidemic
(de®nition used, characteristics of circulating virus);
sponsor (speci®ed, known or unknown); publication
status
. Characteristics of participants: number of partici-
pants; age; gender; ethnic group; risk category; occu-
pation
. Characteristics of interventions: type of intervention;
type of placebo; dose; treatment or prophylaxis
schedule; length of follow-up (in days); route of ad-
ministration
. Characteristics of outcome measures:* Numbers and seriousness of in¯uenza cases (how-
ever de®ned) occurring in vaccine and placebo
groups. Other outcome measures used to assess
e�ects included cases of in¯uenza clinically
de®ned; cases of in¯uenza clinically de®ned on
the basis of a speci®c list of symptoms and/or
signs; cases of in¯uenza con®rmed by laboratory
V. Demicheli et al. / Vaccine 18 (2000) 957±1030 963
Table
1
Selectioncriteria
applied
toretrieved
studiesto
determineinclusionin
system
aticreview
Review
Studycriteria
Participants
Interventions
Clinicaloutcomes
Adverse
e�ects
Selectioncriteria
common
toall
Randomised/quasi-
randomised
astudiesin
humans
comparedto
placebo,controls,
nointervention;orcomparing
types,doses/schedulesof
intervention
Apparentlyhealthy,r
75%
aged
14to
60
Interventionirrespectiveof
viralantigenic
con®guration
Numbersand/orseverityof
in¯uenza
cases(however
de®ned)occurringin
interventionandplacebo
groups
Number
andseriousnessof
adverse
e�ects
In¯uenza
vaccines
Protectivee�
ectofin¯uenza
vaccinefrom
exposure
to
naturallyoccurringin¯uenza
In¯uenza
immunestatus
irrelevant
Attenuated,killedorlive
vaccines
orfractionsthereof
administeredbyanyroute
Noother
speci®ccriteria
System
ice�
ects
includeof
malaise,
nausea,fever,
arthralgias,rash,headacheand
more
generalisedandserious
signs.Locale�
ects
include
induration,sorenessand
rednessatinoculationsite
(injected
vaccines)andrhinitis
andsore
throat(inhaled
vaccines)
Amantadineand
rimantadine
forin¯uenza
Protectionortreatm
entof
amantadineand/or
rimantadinefrom
exposure
to
naturallyoccurringin¯uenza
Noother
speci®ccriteria
Amantadineand/or
rimantadineasprophylaxis
and/ortreatm
entforin¯uenza
Noother
speci®ccriteria
GI(diarrhoea,vomiting,
dyspepsia,nausea,
constipation);increasedCNS
activity(light-headedness,
concentrationproblems,
insomnia,restlessness,
nervousness);decreasedCNS
activity(m
alaise,
depression,
fatigue,
vertigo,feelingdrunk);
skin
(urticariaandrash)
NIs
forin¯uenza
Protective/
treatm
ente�
ectof
oralOseltamivirand/or
Zanamivirin
naturallyor
arti®ciallyoccurringin¯uenza
Noother
speci®ccriteria
Oseltamivirand/orZanamivir
asprophylaxisand/or
treatm
entforin¯uenza
Alsotemporaldistributionof
cases,andother
outcomes
e.g.
distributionofsymptoms
under
thecurve;
timeto
improvem
ent
Localandsystem
icadverse
e�ects
aA
studyis
randomised
when
itappears
thattheindividuals
(orother
experim
entalunits)
followed
inthestudywerede®nitelyorpossibly
assigned
prospectivelyto
oneoftw
o(ormore)
alternativeform
sofhealthcare
usingrandom
allocation.A
studyis
quasi-randomised
when
itappears
thattheindividuals
(orother
experim
entalunits)
followed
inthestudywerede®nitelyor
possibly
assigned
prospectivelyto
oneoftw
o(ormore)alternativeform
sofhealthcare
usingsomequasi-random
methodofallocation(such
asalternation,date
ofbirth
orcase
record
num-
ber).
V. Demicheli et al. / Vaccine 18 (2000) 957±1030964

tests; hospital admissions; complications; working
day lost in episodes of sickness absence regardless
of cause* Adverse e�ects: presence and type, with local
symptoms presented in the analysis separately
from systemic symptoms; number of withdrawals
due to adverse e�ects. Individual adverse e�ects
have been considered in the analysis, as well as
a combined endpoint (any or highest symptom).
2.1.3.3. De®nitionsEpidemic period. Four di�erent de®nitions of `epi-
demic period' were found:
. the interval between the ®rst and the last virus iso-
lation in the community
. the interval during which in¯uenza virus was recov-
ered from more than a stated percentage of ill subjects
. the period during which an increase of respiratory
illness more than a stated percentage was recorded
. the winter period taken as a proxy for epidemic
period.
The data were included regardless of the de®nition of
epidemic period used in the primary study. When data
were presented for the epidemic period and the entire
follow-up period, those occurring during the former
were considered.
Clinically de®ned case. A clinically de®ned case was
assumed as any case de®nition based on symptoms
without further speci®cation. The speci®c de®nition
was assumed as:
. `¯u-like illness' according to a prede®ned list of
symptoms (including the CDC case de®nition for
surveillance)
. `upper respiratory illness' according to a prede®ned
list of symptoms.
When more than one de®nition was given for the same
trial, data related to the more speci®c de®nition were
included.
Laboratory con®rmation of cases. The laboratory
con®rmation of cases found were:
. virus isolation from culture
. four-fold antibody increase (HI) in acute or conva-
lescent phase sera
. four-fold antibody increase (HI) in post-vaccination
or post-epidemic phase sera.
When more than one de®nition was given for the same
trial, data related to the more sensitive de®nition (sero-
conversion) were included.
Hospital admission rates. Hospital admission rateswere calculated as the proportion of cases hospitalisedfor respiratory causes.Complications. Complications were considered as the
proportion of cases complicated by bronchitis, pneu-monia or otitis.
2.1.3.4. Data synthesis. The relative risks of events(cases of in¯uenza, deaths, and adverse e�ects) com-paring treatment and placebo/control groups fromthe individual trials were combined using Mantel-Haenszel meta-analytical techniques. We did not com-bine estimates from treatment and prophylactic trialsas these were conducted to answer di�erent studyquestions. Between-trial variability in results wasexamined and incorporated into the estimates ofuncertainty of treatment e�ect using random e�ectsmodels where appropriate. In treatment trials thechoice of methods for combining the estimates ofseverity of in¯uenza depended on the format inwhich the data was presented. Where possible, com-parisons were made between the mean duration ofsymptoms in the two groups, and methods for com-bining di�erences in means were used. Speci®cally,where the data were presented as the number of sub-jects with duration of symptoms beyond a cut-o�time period these were presented as `Cases with feverat 48 h'. The bewildering array of outcomes used inthe treatment trials (see Results section) prevented usfrom using more than the `cases with fever' outcome.Included trials did not contain su�cient informationto enable us to assess the number of cases with nodocumented fever at entry into the trial.
For the vaccine trials, separate analyses were per-
formed for live aerosol vaccines, inactivated parent-
eral vaccines and inactivated aerosol vaccines.
Clinical in¯uenza outcomes were speci®ed according
to whether speci®c criteria were or were not used, for
which estimates were produced separately, and com-
bined (where trials reported both de®nitions, only the
wider de®nition was retained for analysis). Vaccine
e�cacy was estimated by calculating the common
relative risk, using the Mantel-Haenszel method (®xed
e�ect model) when the trial results were consistent, or
the DerSimonian and Laird method (random e�ects
model) when signi®cant heterogeneity was evident
between the study results. Between-study heterogen-
eity is to be expected in vaccine trials as there are
unpredictable systematic di�erences between trials in
circulating strains and levels of local immunity. Once
the relative risk (RR) had been obtained, vaccine e�-
cacy (VE) was calculated as VE=1-RR. Similar ana-
lyses were also undertaken for other events, such as
complications, hospital admissions and adverse
e�ects.
V. Demicheli et al. / Vaccine 18 (2000) 957±1030 965

In addition to the traditional estimate of vaccine e�-
cacy, the e�ect of vaccination on the number of clini-
cal cases was estimated by averaging the risk
di�erences (in¯uenza rate in vaccinated group minus
in¯uenza rate in control group). Where the total num-
ber of clinical in¯uenza cases depends more on the
number of other in¯uenza-like illnesses than true in¯u-
enza A illnesses, it is more likely that an intervention
will appear to reduce the total number of cases by an
absolute amount (i.e. a constant risk di�erence) than
by a relative amount (i.e. a constant relative e�ect).
As the data on average time o� work was reported
as a continuous measurement, these results were
expressed as di�erences in means, and combined using
the weighted mean di�erence method. Caution should
be exercised in interpreting these results as the data are
very skewed.
Several trials included more than one active vaccine
arm. Where several active arms from the same trial
were included in the same analysis, the placebo group
was split equally between the di�erent arms, so that
the total number of subjects in any one analysis did
not exceed the actual number in the trials.
2.1.4. Methods for the economic evaluation
2.1.4.1. Evidence-based alternative interventions to mini-mise the burden of in¯uenza. While the three Cochranereviews were underway, we assumed a hypotheticalscenario in which all available means had a preventiveand treatment impact on in¯uenza. We also consideredit likely that such means would produce adverse e�ectsand have clinical outcomes not homogeneous for qual-ity of life. In this case, the alternatives to be exploredwould be:
. which is the best single alternative
. which is the best combination of alternatives
. which is the best combination of alternatives
depending on the outcome measure considered
(avoided cases, quality weighted avoided cases,
severity of avoided cases, hospital admissions
avoided and working days lost (WDL)).
We aimed to compare these alternatives with the cur-
rent Army policy on in¯uenza prevention (do-noth-
ing).
Once the reviews had been completed, the results led
us to introduce considerable changes to our compara-
tors. The changes (with the reasons in brackets) are
summarised in Table 2.
For our evaluation we chose the viewpoint of the
funder, the MOD (UK). We thus focused on the
e�ects of preventing in¯uenza in MOD/Army person-
nel although we believe that our methods are equally
applicable to populations of employed healthy adults,
especially in an epidemic situation. These would
include emergency services and employees of compa-
nies producing essential goods and services.
We were able to test the e�ect of this assumption by
setting our results in the context of a distribution of
similar variables derived from our widely known and
recently updated systematic review of the economics of
in¯uenza [6,35,36].
We attempted to incorporate into our evaluation
individual soldier preferences for the possible preven-
tive means. One of the e�ects of adopting the view-
point and decision-making perspective of the MOD/
Army was the possibility of incorporating the in¯u-
enza preventive campaign into existing immunisation
and routine procedures at no incremental administra-
tive cost. However, in the sensitivity analysis we have
used administration costs derived from the ratio `vac-
cine cost/total administration cost' calculated from
our systematic review of the economics of in¯uenza
[6,35,36].Final selection of alternatives. Our ®nal criteria for
the choice of alternatives were:
. evidence of e�cacy;
. evidence of safety;
. practicality of organisational implementation in the
setting of the British Army.
On the basis of the ®rst criterion all remaining
alternatives in the third column of Table 2 are prac-
ticable and acceptable. However applying the other
two criteria and assuming an average in¯uenza epi-
demic period of 46 days (as in the trials included in
the reviews) the alternatives of oral amantadine, oral
rimantadine and oral Oseltamivir are no longer prac-
ticable. It is very unlikely that whole bodies of sol-
diers would comply with the requirement of
protracted daily oral drug schedules. This assumption
was further con®rmed by the ®nding of our prefer-
ence time trade-o� exercise (Table 4) in which sol-
diers preferred the risk of contracting in¯uenza to
that of experiencing adverse e�ects such as nausea or
gastrointestinal disturbances.
Two other factors contribute to making the preven-
tion of in¯uenza with antimicrobials and NIs proble-
matic. Firstly it is doubtful whether the protracted
logistical e�ort involved in maintaining the chemopro-
phylaxis campaign for 46 days is feasible. Secondly the
level and timeliness of the information required to
determine with any certainty the `beginning' and the
`end' of the in¯uenza epidemic is unlikely to be avail-
able, especially when the Army is deployed in di�erent
areas of the UK and abroad.Description of alternatives. Whereas before the
Cochrane review results our provisional decision treewas very complicated, comprising preventive and treat-
V. Demicheli et al. / Vaccine 18 (2000) 957±1030966
ment alternatives, the ®nal tree consists only of thethree preventive arms each with in¯uenza cases with orwithout adverse e�ects.Form of the economic model. On the basis of the
above considerations we de®ned an economic modelbased on the cost per avoided case to de®ne the bestpreventive strategy, and the cost per avoided caseweighted by individual preference to de®ne the choiceof the best combination of interventions. The costper avoided case was calculated by dividing the totalcosts of the interventions by the number of casesavoided.Data collection and assumptions made. We based our
model on a set of assumptions, which are summarisedin Table 3.
The variables and the ranges across which we car-
ried out our sensitivity analysis together with the
rationale are summarised in Table 4.
3. Results
3.1. Results of the reviews
3.1.1. Description of studies
Identi®ed trials are listed and described in the table
of included studies using the name of the ®rst author
and the publication year; see Appendix C. A list and
description of excluded studies (with reason for exclu-
sion) is available from the authors.
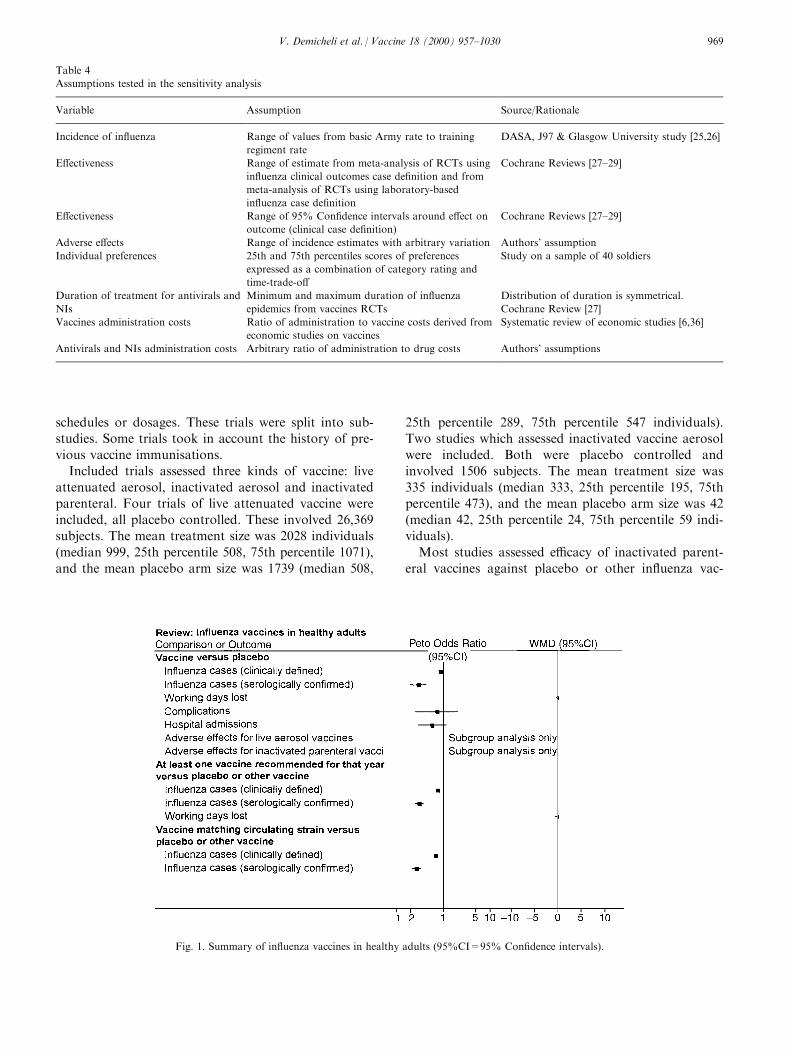
3.1.1.1. In¯uenza vaccines. The tables of comparisonswere constructed according to the following criteria(Fig. 1):
1. In¯uenza vaccine versus placebo* All studies comparing any in¯uenza vaccine
against a placebo (inert substances or non
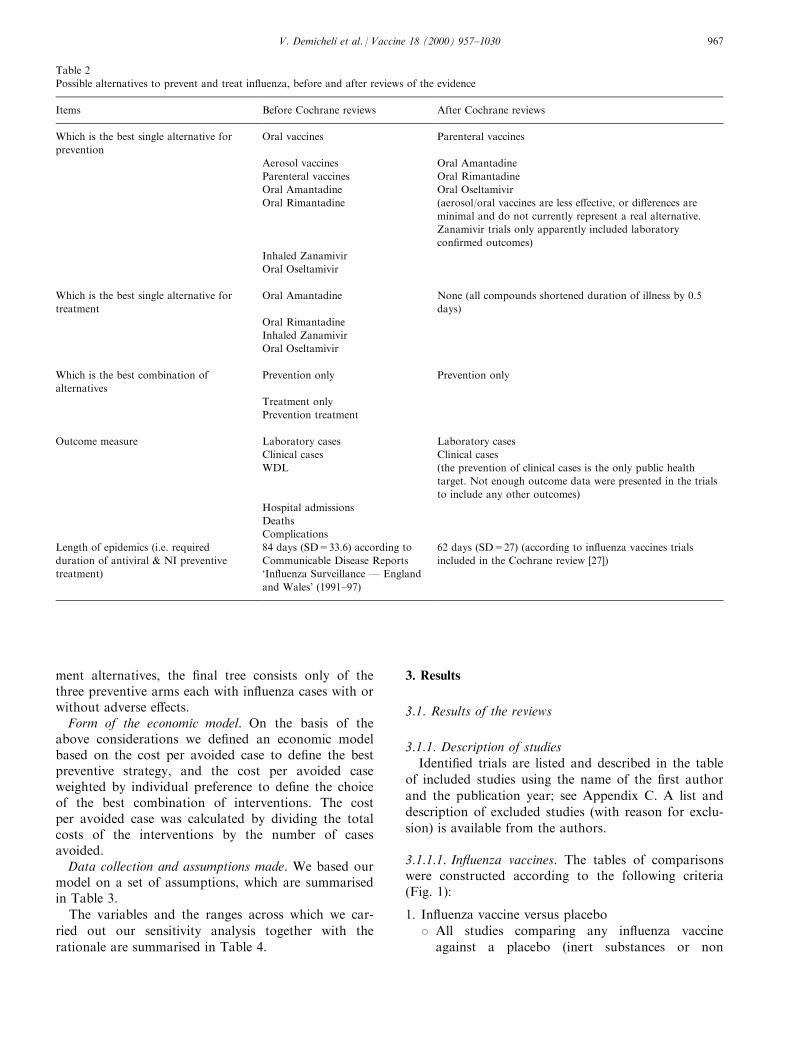
Table 2
Possible alternatives to prevent and treat in¯uenza, before and after reviews of the evidence
Items Before Cochrane reviews After Cochrane reviews
Which is the best single alternative for
prevention
Oral vaccines Parenteral vaccines
Aerosol vaccines Oral Amantadine
Parenteral vaccines Oral Rimantadine
Oral Amantadine Oral Oseltamivir
Oral Rimantadine (aerosol/oral vaccines are less e�ective, or di�erences are
minimal and do not currently represent a real alternative.
Zanamivir trials only apparently included laboratory
con®rmed outcomes)
Inhaled Zanamivir
Oral Oseltamivir
Which is the best single alternative for
treatment
Oral Amantadine None (all compounds shortened duration of illness by 0.5
days)
Oral Rimantadine
Inhaled Zanamivir
Oral Oseltamivir
Which is the best combination of
alternatives
Prevention only Prevention only
Treatment only
Prevention treatment
Outcome measure Laboratory cases Laboratory cases
Clinical cases Clinical cases
WDL (the prevention of clinical cases is the only public health
target. Not enough outcome data were presented in the trials
to include any other outcomes)
Hospital admissions
Deaths
Complications
Length of epidemics (i.e. required
duration of antiviral & NI preventive
treatment)
84 days (SD=33.6) according to
Communicable Disease Reports
`In¯uenza Surveillance Ð England
and Wales' (1991±97)
62 days (SD=27) (according to in¯uenza vaccines trials
included in the Cochrane review [27])
V. Demicheli et al. / Vaccine 18 (2000) 957±1030 967

in¯uenza vaccines) were included in this
group* Subgroup analysis were carried out for live aero-
sol vaccine, inactivated parenteral vaccine, and
inactivated aerosol vaccine* The parenteral route comprised both intramuscu-
lar and subcutaneous route* Di�erent dosages and schedules of the vaccine
and the presence of di�erent adjuvants were not
compared; and data from arms of trials compar-
ing only vaccine composition or dosage were
pooled in the analysis.
2. At least one vaccine strain recommended for that
year (as an indicator of goodness of serological ®t)
versus placebo or other vaccines:* All trials in which the studied vaccine contained
at least one of the A strains recommended for
that year by WHO or single governments (WHO
recommendations were published since 1973 only)
were included, independently from substances
used in the control arm* Subgroup analysis was carried out according to
control group for the recommended vaccine
against placebo, against in¯uenza B vaccine, and
against other non recommended A strains* Vaccines containing only a B recommended strain
were excluded from this comparison since a num-
ber of authors used monovalent B vaccine as pla-
cebo in the control arm which may generate
confusion* The compliance of the study vaccine with the o�-
cial recommendations was checked by reviewing
WHO records when possible. In case of ambigu-
ity (in the oldest trials), the opinion stated by
authors was taken into account* The compliance of a live attenuated vaccine with
the recommendation has been decided according
to the antigenic comparability to the wild strains
3. Vaccine matching circulating strain versus placebo
or other vaccines:* All trials in which the studied vaccine contained
the strain matching the circulating virus (or at
least one of several circulating viruses) were
included in this group of comparison, indepen-
dently from substances used in the control arm* Subgroup analysis was carried out according to
the control group; matching vaccine against pla-
cebo, against in¯uenza B vaccine, and against
other non recommended A strains* In cases of an incomplete match or ambiguity of
wording, the opinion stated by authors was also
taken into account. Minor viral drift clearly sta-
ted was assumed as non-matching.
Twenty papers describing 39 trials of sub-trials were
identi®ed. Some of them had more than two arms,
comparing di�erent vaccines, routes of administration,
Table 3
Basic assumptions of the model
Variable Assumption Source/Rationale
Population Army e�ectives as at 1 August 1998 Defense Analytical Services Agency (DASA)
Gender and age di�erences Only incidence di�erences will be tested in
sensitivity analysis
DASA
Incidence of in¯uenza Sickness rates for in¯uenza in 1997 DASA
E�ectiveness Meta-analysis estimate of RCTs using in¯uenza
clinical outcomes
Cochrane Reviews [27±29]
Adverse e�ects Frequent symptom reported in RCTs included
in Cochrane reviews comparable across range of
preventive interventions
Cochrane Reviews [27±29]
Individual preferences Mean score of preferences expressed as
combination of category rating and time-trade-
o�
Study on a sample of 40 soldiers
Preventive intervention costs Acquisition costs Defense Medical Supply Agency and authors'
assumption (NI)
Duration of treatment for antivirals and NIs Mean duration of in¯uenza epidemics from
vaccines RCTs
Cochrane Review [27]
Preventive intervention administration costs Nil Interviews with medical commanders
Productivity losses due to in¯uenza Nil Preventive interventions do not have di�erent
e�ects under this perspective
Productivity loss from adverse intervention
events
Nil Di�culties in valuation
V. Demicheli et al. / Vaccine 18 (2000) 957±1030968
schedules or dosages. These trials were split into sub-
studies. Some trials took in account the history of pre-
vious vaccine immunisations.
Included trials assessed three kinds of vaccine: live
attenuated aerosol, inactivated aerosol and inactivated
parenteral. Four trials of live attenuated vaccine were
included, all placebo controlled. These involved 26,369
subjects. The mean treatment size was 2028 individuals
(median 999, 25th percentile 508, 75th percentile 1071),
and the mean placebo arm size was 1739 (median 508,
25th percentile 289, 75th percentile 547 individuals).
Two studies which assessed inactivated vaccine aerosol
were included. Both were placebo controlled and
involved 1506 subjects. The mean treatment size was
335 individuals (median 333, 25th percentile 195, 75th
percentile 473), and the mean placebo arm size was 42
(median 42, 25th percentile 24, 75th percentile 59 indi-
viduals).
Most studies assessed e�cacy of inactivated parent-
eral vaccines against placebo or other in¯uenza vac-
Table 4
Assumptions tested in the sensitivity analysis
Variable Assumption Source/Rationale
Incidence of in¯uenza Range of values from basic Army rate to training
regiment rate
DASA, J97 & Glasgow University study [25,26]
E�ectiveness Range of estimate from meta-analysis of RCTs using
in¯uenza clinical outcomes case de®nition and from
meta-analysis of RCTs using laboratory-based
in¯uenza case de®nition
Cochrane Reviews [27±29]
E�ectiveness Range of 95% Con®dence intervals around e�ect on
outcome (clinical case de®nition)
Cochrane Reviews [27±29]
Adverse e�ects Range of incidence estimates with arbitrary variation Authors' assumption
Individual preferences 25th and 75th percentiles scores of preferences
expressed as a combination of category rating and
time-trade-o�
Study on a sample of 40 soldiers
Duration of treatment for antivirals and
NIs
Minimum and maximum duration of in¯uenza
epidemics from vaccines RCTs
Distribution of duration is symmetrical.
Cochrane Review [27]
Vaccines administration costs Ratio of administration to vaccine costs derived from
economic studies on vaccines
Systematic review of economic studies [6,36]
Antivirals and NIs administration costs Arbitrary ratio of administration to drug costs Authors' assumptions
Fig. 1. Summary of in¯uenza vaccines in healthy adults (95%CI=95% Con®dence intervals).
V. Demicheli et al. / Vaccine 18 (2000) 957±1030 969

cines (some of them used a monovalent in¯uenza B
vaccine as placebo). They involved 23,628 subjects.
The mean treatment size was 550 individuals (median
432, 25th percentile 161, 75th percentile 920), and the
mean placebo arm size was 358 (median 311, 25th per-
centile 66, 75th percentile 518 individuals).
Surveillance methods were prospective or retrospec-
tive, active (by phone interview or questionnaire com-
pilation) or passive (ill subjects spontaneously
presenting). Mean length of follow up was 87 days
(median 79 days, 25th percentile 61 days, 75th percen-
tile 119 days).
The duration of the epidemic was speci®ed by 17
trials. Mean length of the epidemic period was 62 days
(median 63 days, 25th percentile 42 days, 75th percen-
tile 77 days).
3.1.1.2. Amantadine and RimantadinePreventive trials. Seventeen preventive trials met the
inclusion criteria. No unpublished trials were ident-i®ed, despite receiving nine letters and three electroniccommunications from manufacturers, authors andresearchers.
The mean amantadine arm size was 494 individuals
(median 151, 25th percentile 97, 75th percentile 348),
the mean rimantadine arm size was 107 (median 108,
25th percentile 92, 75th percentile 122 individuals) and
the mean placebo arm size was 373 individuals (me-
dian 140, 25th percentile 99, 75th percentile 269). The
mean total population was 596 individuals (median
308, 25th percentile 225, 75th percentile 536). The
mean length of follow up was 28 days (median 30
days, 25th percentile 18 days, 75th percentile 42 days).Treatment trials. Ten published treatment trials were
identi®ed. No unpublished trials were identi®ed. Themean amantadine arm size was 91 individuals (median72, 25th percentile 15, 75th percentile 110), the meanrimantadine arm size was 61 (median 56, 25th percen-tile 15, 75th percentile 104 individuals) and the meanplacebo arm size was 77 individuals (median 76, 25thpercentile 14, 75th percentile 99). The mean totalpopulation was 161 individuals (median 153, 25th per-centile 30, 75th percentile 225). Mean length of followup was 25 days (median 25.5 days, 25th percentile 16days, 75th percentile 33 days).
3.1.1.3. Neuraminidase inhibitorsPreventive trials. As at 1 January 1999 four accessi-
ble preventive trials met our inclusion criteria. Afurther two preventive trials of Zanamivir in abstractformat were identi®ed (Calfee H68 and Monto ).Further data was requested from the manufacturers,GlaxoWellcome, to allow the inclusion of data fromthe trials in the review. GlaxoWellcome provided thedata as requested. The mean Zanamivir arm size was
136 individuals (median 34, 25th percentile 25, 75thpercentile 61), the mean Oseltamivir arm size was 1040(median, 25th percentile and 75th percentile 1040 indi-viduals) and the mean placebo arm size was 189 indi-viduals (median 21, 25th percentile 9, 75th percentile397). The mean total population was 475 individuals(median 68, 25th percentile 36, 75th percentile 853).Mean length of follow up was 11 days.Treatment trials. As at 1 January 1999 three accessi-
ble treatment trials were identi®ed which ful®lled theinclusion criteria. A further two treatment trials ofZanamivir in abstract format were also identi®ed.Despite a request to the manufacturers, GlaxoWell-come did not release more detailed data in time for in-clusion in the review.
The mean Zanamivir arm size was 80 individuals
(median 43, 25th percentile 25, 75th percentile 43), the
mean Oseltamivir arm size was 920 (median 1040, 25th
percentile 920, 75th percentile 1040 individuals) and
the mean placebo arm size was 107 individuals (me-
dian 85, 25th percentile 22, 75th percentile 151). The
mean total population was 315 individuals (median
243, 25th percentile 65, 75th percentile 449). Mean
length of follow up was ®ve days.Preventive and treatment trials. Only one trial was
identi®ed containing both preventive and treatmentinterventions.
3.1.2. Methodological quality of included studies
Two reviewers assessed allocation method, allo-
cation concealment, blinding and completeness of fol-
low-up.
3.1.2.1. In¯uenza vaccines. There were 20 trials in all,13 of which were placebo controlled. Three trials usedan in¯uenza B vaccine in the control arm, consideringit as a placebo. Four trials compared two or morein¯uenza vaccines but did not use a control arm.Thirteen trials reported data on adverse e�ects, butonly seven were included in the analysis: one did nothave su�cient reporting and ®ve trials did not have aplacebo arm. The overall quality of the trials wasgood.
Assessed allocation concealment was adequate in 12
of the trials, inadequate in six and unclear in two.
Fifteen trials were properly randomised, four stated
that the allocation method was quasi-random, and one
trial did not report information about randomisation.
Assessment was double blinded in 14 trials. Two trials
were single blinded and four did not mention blinding.
Two studies were ®eld trials.
3.1.2.2. Amantadine and Rimantadine. There were 27trials in all, 26 of which considered either amantadineand/or rimantadine e�cacy and one which considered
V. Demicheli et al. / Vaccine 18 (2000) 957±1030970
adverse e�ects only. Eleven preventive trials and seven
treatment trials reported su�cient data on adverse
e�ects. The quality of preventive and treatment trials
is discussed separately.Preventive trials. The quality of the preventive trials
was relatively good, considering the age of the trials.
Among the 17 preventive trials, 15 stated that the al-
location method was randomisation, although only
four mentioned a particular method and two did not
mention random allocation at all. These two trials
have therefore been classi®ed as controlled clinical
trials (CCTs) rather than RCTs. All preventive trials
were stated to be double blind with the exception of
Payler which was open and had no placebo group
(the comparison group was no intervention other
than in¯uenza vaccine at the beginning of the sea-
son).Treatment trials. Among the 10 treatment trials, nine
stated that the allocation method was randomisation;
no trials mentioned a particular method; and one
(Hornick) did not mention random allocation at all.
Major ¯aws in the reporting of trials lay in the follow-
ing:
. Lack of information on the completeness of follow-
up. In many trials there was a large di�erence
between the number randomised and the number
who actually participated
. Lack of detailed description of methods to conceal
allocation, with many trials just describing a `double
blind' procedure
. Frequent inconsistencies in the reporting of numer-
ators and denominators in various arms of trials
. In the treatment trials, the use of a bewildering
variety of outcomes, such as severity scores, of
which none are alike. This makes the task of
meta-analysis impossible and leads to a great loss of
information.
3.1.2.3. Neuraminidase inhibitors. Overall methodologi-
cal quality appeared good, in keeping with the mainly
early report nature of the results of the clinical trials
of such potentially important compounds. However,
detailed descriptions of methods and steps taken to
ensure allocation concealment were not speci®c, lead-
ing us to grade this aspect of the trials `unclear'. This
is potentially a very important point when dealing
with cases of self-limiting upper respiratory tract infec-
tions with or without systemic symptoms, in which the
potential for a placebo e�ect is great. Additionally as
some trials (the WV series for instance) relied on clini-
cal case de®nitions the potential for bias (and overesti-
mation of e�ect) is even greater.
3.2. E�ects of in¯uenza vaccines
3.2.1. E�ect of vaccination on clinical cases of in¯uenza
Trial data for the two de®nitions of in¯uenza (no
case de®nition and speci®c case de®nition) are pre-
sented separately for each of the three types of vaccine:
live aerosol, inactivated parenteral and inactivated
aerosol. Signi®cant heterogeneity was detected between
trial results for most comparisons, and the ®gures
quoted are estimated from random e�ects models.
The live aerosol vaccines were not e�ective for cases
of either de®nition. A combined analysis of data from
the two trials estimated the vaccine e�cacy to be 2%
(95%CI: ÿ5±8%).
The inactivated vaccines did o�er signi®cant protec-
tion. Taking the data from the 10 trials together,
regardless of case de®nition, the parenteral vaccine
reduced the number of cases by 29% (95%CI: 12±
42%). The e�cacy of the inactivated aerosol vaccine
was higher for the unspeci®ed case de®nition
(VE=31%, 95%CI: 5±51%) but not the speci®c in¯u-
enza case de®nition (VE=26%, 95%CI: 1±45%).
The estimates of e�cacy were more consistent when
the treatment e�ect was expressed as a risk di�erence
rather than a relative e�ect. Estimation as risk di�er-
ences suggest that 5% (95%CI: 2±8%) and 9%
(95%CI: 3±16%) fewer participants experienced in¯u-
enza like illnesses who received inactivated parenteral
vaccine and inactivated aerosol vaccine respectively.
3.2.2. E�ect of vaccination on serologically con®rmedcases of in¯uenza
Data from two studies showed that aerosol live vac-
cines reduced the number of serologically con®rmed
cases of in¯uenza by 79% (95%CI: 44±92%). Six stu-
dies provided data for inactivated parenteral vaccines,
showing a similar e�cacy of 65% (95%CI: 44±79%).
No studies of inactivated aerosol vaccine reported
numbers of serological con®rmed cases.
3.2.3. E�ect of vaccination on other outcomes
Three trials of parenteral inactivated vaccine evalu-
ated time o� work, estimating that vaccination saved
on average around 0.4 working days. This result was
nearly statistically signi®cant. Hospital admissions
were also lower, but not statistically signi®cant. There
was little di�erence in complication rates between vac-
cinated and unvaccinated groups.
3.2.3.1. Adverse e�ects Ð aerosol live vaccines. Whilstsigni®cantly more recipients experienced sore throatsafter vaccine administration than placebo adminis-tration (relative rate=2.5, 95%CI: 1.5±4.2), the overallnumber of local adverse e�ects was not signi®cantlydi�erent between vaccine and placebo groups. There
V. Demicheli et al. / Vaccine 18 (2000) 957±1030 971

was also no signi®cant increase in systemic side e�ects,although rates of fever and myalgia were higher in vac-cine than placebo groups. Overall 26% of vaccine reci-pients reported the combined endpoint for localreactions, whilst only 8% reported the combined end-point for systemic e�ects.
3.2.3.2. Adverse e�ects Ð inactivated vaccines. Localtenderness and soreness was more than twice as com-mon among parenteral vaccine recipients than those inthe placebo group (relative rate=2.1, 95%CI: 1.4±3.4).There were also increases in erythema (non-signi®cant),but not in duration of or arm sti�ness. The combinedlocal e�ects endpoint was signi®cantly higher for thosereceiving the vaccine (relative rate=2.6, 95%CI: 1.6±4.2), with 69% reporting some e�ect.
None of the systemic e�ects were individually more
common in parenteral vaccine recipients than placebo
recipients. However the combined endpoint was
increased, and nearly statistically signi®cant, with 26%
vaccine recipients reporting some side e�ect than pla-
cebo recipients (95%CI: 0±59%). Overall 30% of
those receiving the vaccine reported possible systemic
e�ects, although many of these equally could be attrib-
uted to in¯uenza-like illnesses.
None of the trials on inactivated aerosol vaccines
reported side-e�ects that could be included in the
analysis. The two studies which evaluated these vac-
cines included parenteral components using an in¯u-
enza B control group so that the side-e�ects of the
oral vaccine could not be estimated separately.
3.2.4. Recommended vaccines
Sixteen trials evaluated the e�ect of the vaccines rec-
ommended (by WHO or single governments) on clini-
cal cases of in¯uenza. Nine of these trials were placebo
controlled, ®ve made comparisons with in¯uenza B
vaccine, and two compared recommended in¯uenza A
vaccines with non-recommended in¯uenza A and B
vaccines. An additional trial (Tannock) only reported
serologically con®rmed cases.
Live aerosol, inactivated parenteral and inactivated
aerosol all had similar vaccine e�cacies, although the
estimate for inactivated aerosol vaccines was only
based on the results of one trial. Live aerosols had a
vaccine e�cacy of 13% (95%CI: 5±20%), inactivated
parenterals an e�cacy of 24% (95%CI: 15±32%), and
inactivated aerosols an e�cacy of 40% (95%CI: 13±
59%). Combining the data from all three vaccine types
from the placebo controlled trials, the overall estimate
of vaccine e�cacy was 24% (95%CI: 14±33%). The
estimate decreased to 22% when the non-placebo con-
trolled trials were included (Fig. 2).
Again, the individual study results were more con-
sistent when expressed as risk di�erences than relative
e�ects. Overall the percentage of participants experien-
cing clinical in¯uenza decreased by 5% (95%CI: 3±
7%) using data from the placebo controlled trials. The
reductions were 3%, 5% and 9% for the live aerosol,
inactivated parenteral and inactivated aerosol vaccines
respectively, the ®rst ®gure not being statistically sig-
ni®cant.
There were signi®cant reductions in serologically
con®rmed cases of in¯uenza for live aerosol and inacti-
vated parenteral preparations. There was no data for
inactivated aerosol vaccines. Vaccine e�cacy was esti-
mated as 48% (95%CI: 24±64%) for live aerosol vac-
cines, and 68% (95%CI: 49±79%) for inactivated
parenteral vaccines.
3.2.5. Vaccine matching the circulating strain
The highest estimates of vaccine e�cacy come from
the analyses of vaccines which were shown to match
the circulating vaccine strain. Twelve trials were
included in these analyses, and seven were placebo
controlled. Since several studies had more than two
arms, the e�cacy of the vaccines containing the match-
ing strain was compared against non-matching A or B
in¯uenza vaccines. None of the live aerosol vaccines
used in the trials matched circulating strains.
Estimates of the e�cacy of both parenteral and
aerosol inactivated vaccines in reducing cases of clini-
cal in¯uenza were similar. Overall the vaccine e�cacy
based on results of the placebo controlled trials was
37% (95%CI: 18±52%). The estimate declined to 31%
when the non-placebo controlled trials were included.
Expressing the e�cacy as a risk di�erence, on average
7% (95%CI: 4±10%) fewer participants who received
matched vaccine su�ered in¯uenza like illnesses com-
pared to placebo recipients.
The e�ect of the matched vaccine on serologically
con®rmed cases was also larger than in any other
analysis. Overall the results of seven trials reporting
serologically con®rmed cases estimated the vaccine e�-
cacy to be 72% (95%CI: 54±83%).
3.3. E�ects of amantadine and rimantadine
All trials tested the e�ects of amantadine and riman-
tadine on a wide variety of in¯uenza A viruses. None
tested the e�ects on in¯uenza B, on which the mol-
ecules are known to be ine�ective. Also, no trial tested
the role of the compounds on workplace outbreak con-
trol, which is a pity considering the trial settings (pris-
ons, factories, schools, barracks).
Some trials are likely to have included individuals
who took aspirin to relive symptoms (especially in the
V. Demicheli et al. / Vaccine 18 (2000) 957±1030972
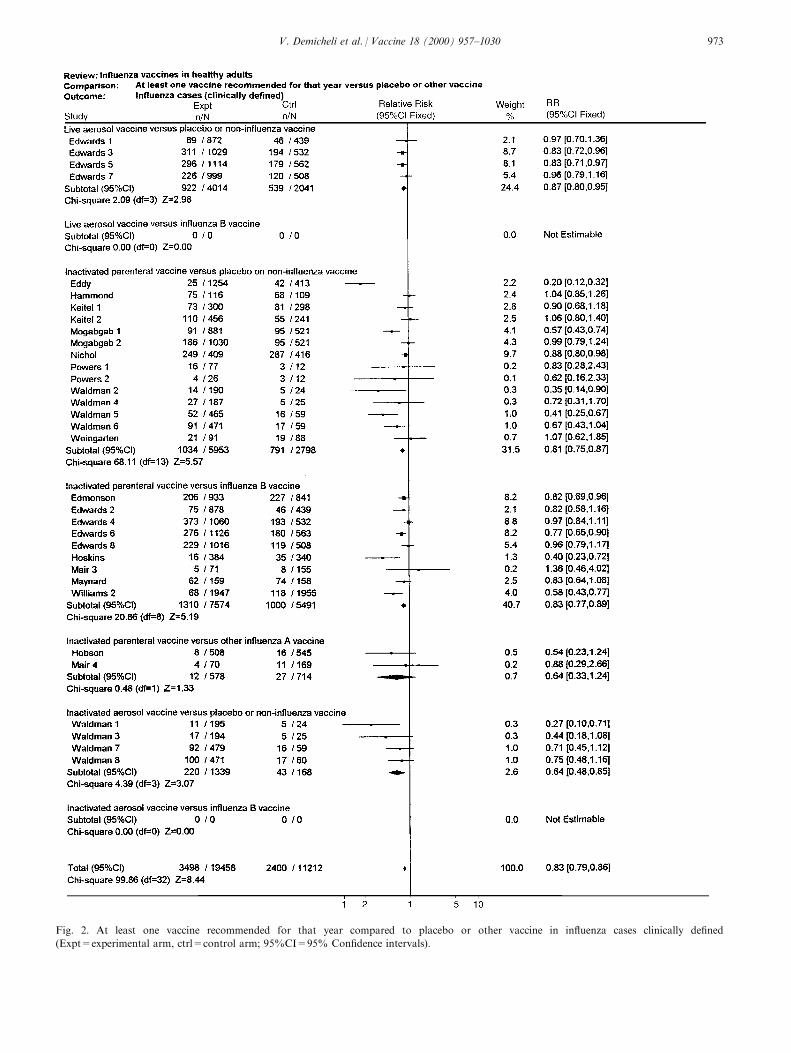
Fig. 2. At least one vaccine recommended for that year compared to placebo or other vaccine in in¯uenza cases clinically de®ned
(Expt=experimental arm, ctrl=control arm; 95%CI=95% Con®dence intervals).
V. Demicheli et al. / Vaccine 18 (2000) 957±1030 973

treatment trials). However the e�ects of this potential
confounder should have been eliminated by the process
of randomisation.
All trials commenced administration of the com-
pounds within a reasonable time lapse. When the
results of surveillance made it reasonable to do so,
treatment started at the latest 48 h after positive identi-
®cation of the ®rst case in the population and preven-
tion.
Six main comparisons were carried out:
1. Comparison A Ð oral amantadine compared to
placebo in in¯uenza prevention
2. Comparison B Ð oral rimantadine compared to
placebo in in¯uenza prevention
3. Comparison C Ð oral amantadine compared to
oral rimantadine in in¯uenza prevention
4. Comparison D Ð oral amantadine compared to
placebo in in¯uenza treatment
5. Comparison E Ð oral rimantadine compared to
placebo in in¯uenza treatment
6. Comparison F Ð oral amantadine compared to
oral rimantadine in in¯uenza treatment
Two minor comparisons, G and H, were also carried
out, each based on the results of a single trial.
For comparisons A, B and C the e�ects on `cases'
were analysed, strati®ed either on the basis of clinical-
laboratory criteria (a de®ned set of signs and symp-
toms backed up by serological con®rmation and/or
isolation of in¯uenza virus from nasal ¯uids) or clini-
cal criteria alone. The e�ects of amantadine/rimanta-
dine administration on asymptomatic cases (de®ned
only by serology or viral isolation) were not assessed,
as these are of little public health interest.
Comparisons were strati®ed on the basis of whether
participants had received vaccination or not.
Finally, the adverse e�ects in the comparisons were
assessed. The `all adverse e�ects' category includes all
types and was derived from those trials which either
did not report su�cient information to allow a more
detailed classi®cation or that presented aggregate data.
Adverse e�ects incidence is reported in the meta-analy-
sis as event per person, thus the incidence should not
be added as more than one adverse event is likely to
have taken place in the same individual during the
trial. The di�erence in incidence of adverse e�ects is of
importance, rather than the estimated incidence itself,
as the adverse e�ects reported with these drugs are
very similar to the clinical manifestations of in¯uenza
infection.
Apart from these caveats the analysis shows that all
types of adverse events were signi®cantly more likely
to happen when individuals were given amantadine
rather than placebo (with the exception of the `other'
category) but none were signi®cantly more likely to
take place in the rimantadine or placebo arms. Overall
both drugs appear to be e�ective and well tolerated,
although the evaluation of the e�ects of rimantadine
was carried out on a very small study population.
In all comparisons duration of action and protection
appeared directly related to duration of prophylaxis or
treatment with amantadine and rimantadine. This ®nd-
ing is in keeping both with the half-life of the com-
pounds which are excreted by the kidneys (at the rate
of 6.4 ml/min/kg for amantadine and 1.2 ml/min/kg
for rimantadine [37]) and the self-limiting duration of
the illness. No trials assessed onset of resistance to the
drugs although this is known to be of relatively short
induction time (10±27% of patients secrete drug-resist-
ant virus within 4±5 days of commencing treatment
[37]).
3.3.1. Comparison A Ð oral amantadine compared toplacebo in in¯uenza prevention
3.3.1.1. E�cacy. Amantadine: 61% (95%CI: 51±69%)e�cacious (RR 0.39 Ð 95%CI: 0.31±0.49) in prevent-ing clinically and laboratory de®ned in¯uenza cases;23% (95%CI: 11±34%) e�cacious (RR 0.77 95%CI:0.66±0.89) in preventing clinically de®ned in¯uenzacases (Fig. 3). There was a signi®cant variation in thetrial results for the second outcome.
3.3.1.2. Adverse events. All categories of adverse e�ectswere signi®cantly more common in participants whoreceived amantadine than placebo, except for dermato-logical changes. Nearly twice as many amantadine reci-pients experienced both increased or decreased CNSe�ects, and more than twice as many withdrew fromthe trials due to adverse e�ects (Table 5).
3.3.2. Comparison B Ð oral rimantadine compared toplacebo in in¯uenza prevention
3.3.2.1. E�cacy. Rimantadine: 72% (95%CI: ÿ8±92%) e�cacious (RR 0.28 Ð 95%CI: 0.08±1.08) inpreventing clinically and laboratory de®ned in¯uenzacases; 35% (95%CI: ÿ20±65%) e�cacious (RR 0.65Ð 95%CI: 0.35±1.20) in preventing clinically in¯uenzacases (Fig. 4). The signi®cance of these ®ndingsdepends on whether a ®xed or random e�ect model isused.
3.3.2.2. Adverse events. Rimantadine recipients werealso more likely to experience adverse e�ects than pla-cebo recipients. However, there was no evidence of anincrease in CNS-related e�ects with rimantadine andwithdrawal rates were similar in both groups (Table6).
V. Demicheli et al. / Vaccine 18 (2000) 957±1030974
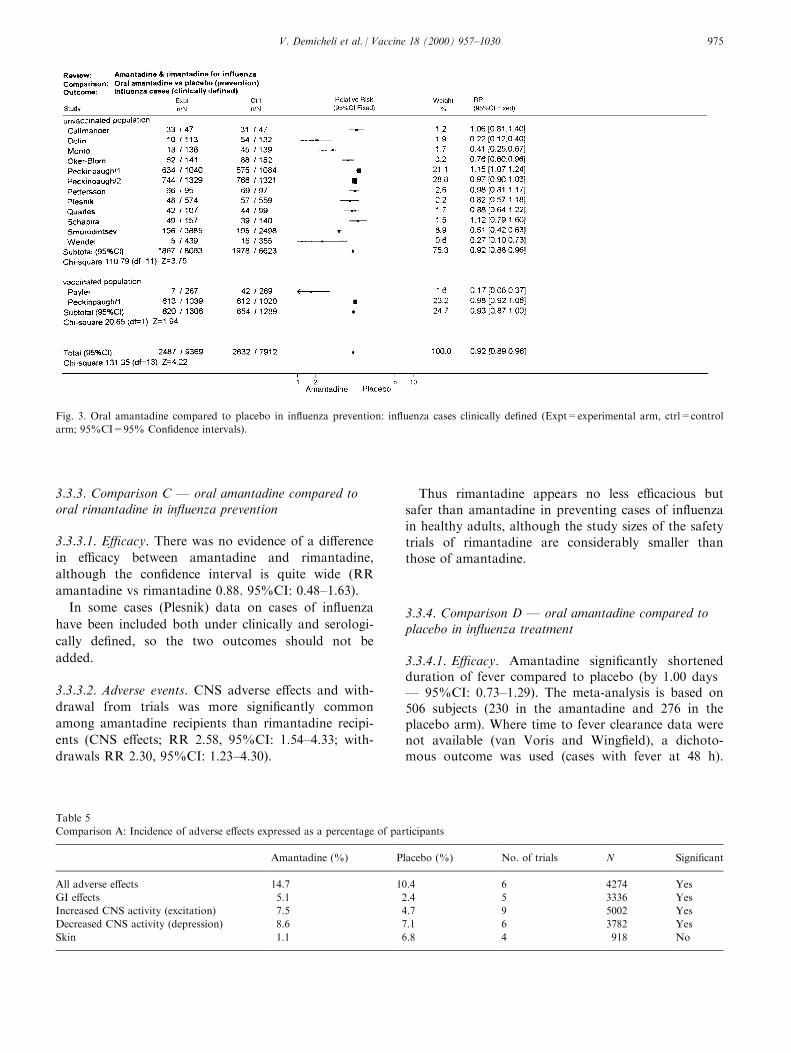
3.3.3. Comparison C Ð oral amantadine compared tooral rimantadine in in¯uenza prevention
3.3.3.1. E�cacy. There was no evidence of a di�erence
in e�cacy between amantadine and rimantadine,
although the con®dence interval is quite wide (RR
amantadine vs rimantadine 0.88. 95%CI: 0.48±1.63).
In some cases (Plesnik) data on cases of in¯uenza
have been included both under clinically and serologi-
cally de®ned, so the two outcomes should not be
added.
3.3.3.2. Adverse events. CNS adverse e�ects and with-
drawal from trials was more signi®cantly common
among amantadine recipients than rimantadine recipi-
ents (CNS e�ects; RR 2.58, 95%CI: 1.54±4.33; with-
drawals RR 2.30, 95%CI: 1.23±4.30).
Thus rimantadine appears no less e�cacious but
safer than amantadine in preventing cases of in¯uenza
in healthy adults, although the study sizes of the safety
trials of rimantadine are considerably smaller than
those of amantadine.
3.3.4. Comparison D Ð oral amantadine compared toplacebo in in¯uenza treatment
3.3.4.1. E�cacy. Amantadine signi®cantly shortenedduration of fever compared to placebo (by 1.00 daysÐ 95%CI: 0.73±1.29). The meta-analysis is based on506 subjects (230 in the amantadine and 276 in theplacebo arm). Where time to fever clearance data werenot available (van Voris and Wing®eld), a dichoto-mous outcome was used (cases with fever at 48 h).
Fig. 3. Oral amantadine compared to placebo in in¯uenza prevention: in¯uenza cases clinically de®ned (Expt=experimental arm, ctrl=control
arm; 95%CI=95% Con®dence intervals).
Table 5
Comparison A: Incidence of adverse e�ects expressed as a percentage of participants
Amantadine (%) Placebo (%) No. of trials N Signi®cant
All adverse e�ects 14.7 10.4 6 4274 Yes
GI e�ects 5.1 2.4 5 3336 Yes
Increased CNS activity (excitation) 7.5 4.7 9 5002 Yes
Decreased CNS activity (depression) 8.6 7.1 6 3782 Yes
Skin 1.1 6.8 4 918 No
V. Demicheli et al. / Vaccine 18 (2000) 957±1030 975

Amantadine was shown to be signi®cantly better thanplacebo (Peto relative risk 0.21 Ð 95%CI: 0.07±0.66).
3.3.4.2. Adverse events. In contrast to the increasedadverse e�ect rates for prevention, there was no evi-dence that amantadine recipients had increased adversee�ect rates to placebo recipients. The incidence ofadverse e�ects by comparison expressed as a percen-tage of participants is shown in Table 7.
3.3.5. Comparison E Ð oral rimantadine compared toplacebo in in¯uenza treatment
3.3.5.1. E�cacy. Rimantadine also signi®cantly shor-tened duration of fever compared to placebo (by 1.27days Ð 95%CI: 0.77±1.77). There was a signi®cantlyhigher number of afebrile cases 48 h after commencingrimantadine treatment (RR=0.17; 95%CI: 0.04±0.74).
3.3.5.2. Adverse events. There were very little dataavailable for the assessment of adverse e�ects ofrimantadine for treatment (45 participants) (Table 8).
3.3.6. Comparison F Ð oral amantadine compared tooral rimantadine in in¯uenza treatment
3.3.6.1. E�cacy. The little data available directlycomparing amantadine and rimantadine for treat-ment showed that the e�cacy of the two drugs wascomparable, although con®dence intervals are verywide.
3.3.6.2. Adverse events. There were very little dataavailable for the assessment of adverse e�ects of thedirect comparison between amantadine and rimanta-dine (33 participants).
A meta-analysis of the symptoms outcome data was
considered to further inform the assessment of the
e�ects of amantadine and rimantadine in a treatment
Fig. 4. Oral rimantadine compared to placebo in in¯uenza prevention: in¯uenza cases clinically de®ned (Expt=experimental arm, ctrl=control
arm; 95%CI=95% Con®dence intervals)
Table 6
Comparison B: Incidence of adverse e�ects expressed as a percentage of participants
Rimantadine (%) Placebo (%) No of trials N Signi®cant
All adverse e�ects 18.6 10.8 3 558 No
GI e�ects 9.0 2.2 2 357 Yes
Increased CNS activity (excitation) 6.5 4.3 3 652 No
Decreased CNS activity (depression) 9.6 1.0 1 228 No
Skin 0 0
V. Demicheli et al. / Vaccine 18 (2000) 957±1030976

role. When the outcome typology was tabulated it was
discovered that such a meta-analysis would be imposs-
ible (Table 9).
We resorted to using duration of fever (de®ned as a
temperature greater than 378C) as the only common
outcome. One drawback of this approach is the poss-
ible confounding e�ect of the presence of fever for a
variable length of time prior to and after entry to the
study (and hence at the moment of commencement of
treatment). However if random allocation had been
properly carried out, this e�ect should disappear.
3.3.7. Comparison G Ð oral amantadine compared tooral aspirin in in¯uenza treatment
In Comparison G, based on Younkin, aspirin was
signi®cantly more e�ective than amantadine in redu-
cing the length of fever (by 0.47 days Ð 95%CI: 0.17±
0.76). This observation is based on 29 individuals.
Aspirin is well known for being a very e�ective anti-
pyretic and anti-in¯ammatory drug, however it does
not inhibit viral replication and as such remains a
symptomatic remedy.
3.3.8. Comparison H Ð inhaled amantadine comparedto placebo in in¯uenza treatment
In comparison H (based on Hayden's 1980 trial)
inhaled amantadine was no more e�cacious than pla-
cebo in bringing down the respiratory or constitutional
symptom score (Weighted Mean Di�erence Ð 1.0 Ð
95%CI: 3.64±1.64 and ÿ2.0 Ð 95%CI: 16.9±12.9 re-
spectively). This comparison also is based on small
numbers of participants (20). Not surprisingly, aman-
tadine caused signi®cantly more nasal irritation (RR
6.11 Ð 95%CI: 0.86±43.3). Inhaled amantadine does
not appear to be particularly e�ective but has a high
incidence of local adverse e�ects which would make
compliance di�cult.
The interpretation of Comparisons G and H is
made di�cult by the small numbers involved and the
presence of single trials.
3.4. E�ects of NIs
When compared to placebo, NIs are 55% (95%CIs:
29±71%) e�ective in preventing naturally occurring
cases of laboratory con®rmed in¯uenza and 67% e�ec-
tive (95%CIs: 90±8%) in experimental in¯uenza when
given intravenously. Overall NIs are 60% e�ective
(95%CIs: 76±33%) (Fig. 5).
When the outcome is de®ned as cases of serologi-
cally con®rmed in¯uenza, NIs are 74% e�ective
(95%CIs: 50±87%) in preventing naturally occurring
in¯uenza and 86% e�ective (95%CIs: 12±98%) in pre-
venting experimentally induced in¯uenza. Overall they
are 76% e�ective (95%CIs: 55±87%) in preventing
cases of laboratory con®rmed in¯uenza. Both com-
pounds appear safe, but as yet no direct comparisons
have been carried out, so there can be no comment
upon their relative e�ects.
The adverse event pro®le (local nasal irritation) of
Zanamivir appears little di�erent to placebo (OR 1.19
Ð 95%CIs: 0.39±3.62). However this may be due to
the relatively small denominator (112 individuals).
Oseltamivir appears to have a signi®cantly higher inci-
dence of systemic adverse e�ects than placebo (OR
1.68 Ð 95%CIs: 1.14±2.49).
Table 7
Comparison D: Incidence of adverse e�ects expressed as a percentage of participants
Amantadine (%) Placebo (%) No. of trials N Signi®cant
GI e�ects 13.8 13.4 3 494 No
Increased CNS activity (excitation) 3.5 5.0 2 475 No
Decreased CNS activity (depression) 56.4 65.2 3 491 Yes
Skin 0.9 0.4 2 465 No
Table 8
Comparison E: Incidence of adverse e�ects expressed as a percentage of participants
Rimantadine (%) Placebo (%) No of trials N Signi®cant
GI e�ects Ð Ð 0 0 Ð
Increased CNS activity (excitation) 28.6 28.6 1 14 No
Decreased CNS activity (depression) 0 8.3 1 31 No
Skin Ð Ð 0 0 Ð
V. Demicheli et al. / Vaccine 18 (2000) 957±1030 977
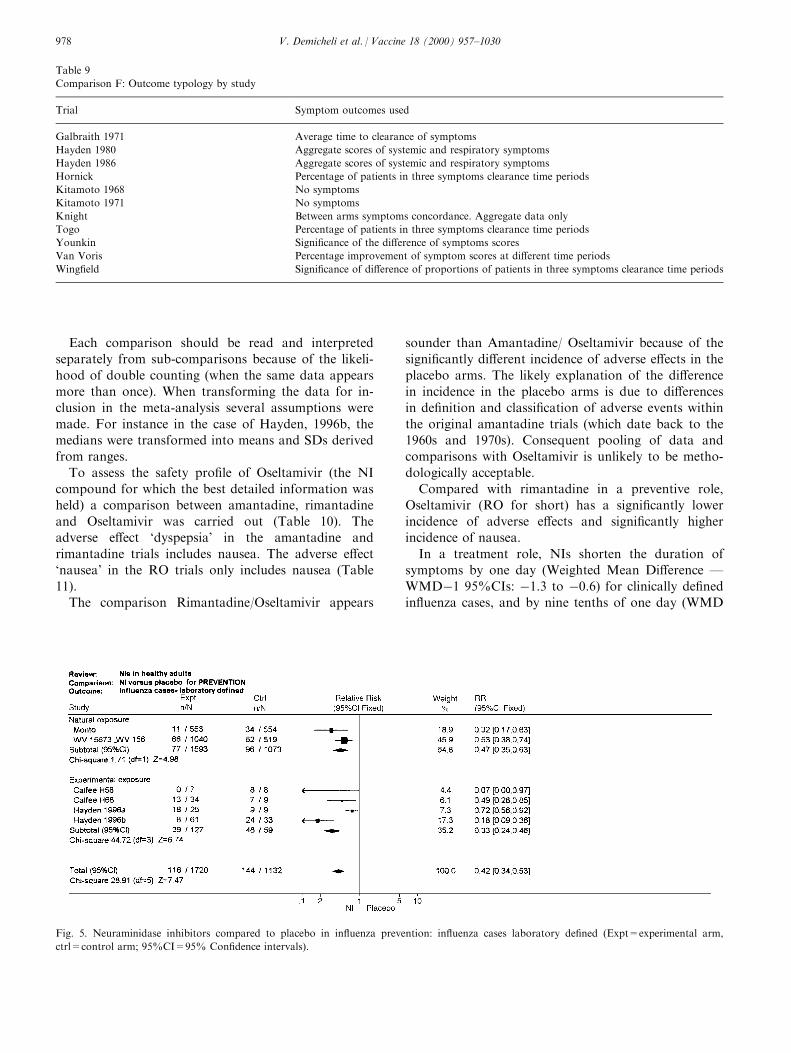
Each comparison should be read and interpreted
separately from sub-comparisons because of the likeli-
hood of double counting (when the same data appears
more than once). When transforming the data for in-
clusion in the meta-analysis several assumptions were
made. For instance in the case of Hayden, 1996b, the
medians were transformed into means and SDs derived
from ranges.
To assess the safety pro®le of Oseltamivir (the NI
compound for which the best detailed information was
held) a comparison between amantadine, rimantadine
and Oseltamivir was carried out (Table 10). The
adverse e�ect `dyspepsia' in the amantadine and
rimantadine trials includes nausea. The adverse e�ect
`nausea' in the RO trials only includes nausea (Table
11).
The comparison Rimantadine/Oseltamivir appears
sounder than Amantadine/ Oseltamivir because of the
signi®cantly di�erent incidence of adverse e�ects in the
placebo arms. The likely explanation of the di�erence
in incidence in the placebo arms is due to di�erences
in de®nition and classi®cation of adverse events within
the original amantadine trials (which date back to the
1960s and 1970s). Consequent pooling of data and
comparisons with Oseltamivir is unlikely to be metho-
dologically acceptable.
Compared with rimantadine in a preventive role,
Oseltamivir (RO for short) has a signi®cantly lower
incidence of adverse e�ects and signi®cantly higher
incidence of nausea.
In a treatment role, NIs shorten the duration of
symptoms by one day (Weighted Mean Di�erence Ð
WMDÿ1 95%CIs: ÿ1.3 to ÿ0.6) for clinically de®ned
in¯uenza cases, and by nine tenths of one day (WMD
Table 9
Comparison F: Outcome typology by study
Trial Symptom outcomes used
Galbraith 1971 Average time to clearance of symptoms
Hayden 1980 Aggregate scores of systemic and respiratory symptoms
Hayden 1986 Aggregate scores of systemic and respiratory symptoms
Hornick Percentage of patients in three symptoms clearance time periods
Kitamoto 1968 No symptoms
Kitamoto 1971 No symptoms
Knight Between arms symptoms concordance. Aggregate data only
Togo Percentage of patients in three symptoms clearance time periods
Younkin Signi®cance of the di�erence of symptoms scores
Van Voris Percentage improvement of symptom scores at di�erent time periods
Wing®eld Signi®cance of di�erence of proportions of patients in three symptoms clearance time periods
Fig. 5. Neuraminidase inhibitors compared to placebo in in¯uenza prevention: in¯uenza cases laboratory de®ned (Expt=experimental arm,
ctrl=control arm; 95%CI=95% Con®dence intervals).
V. Demicheli et al. / Vaccine 18 (2000) 957±1030978
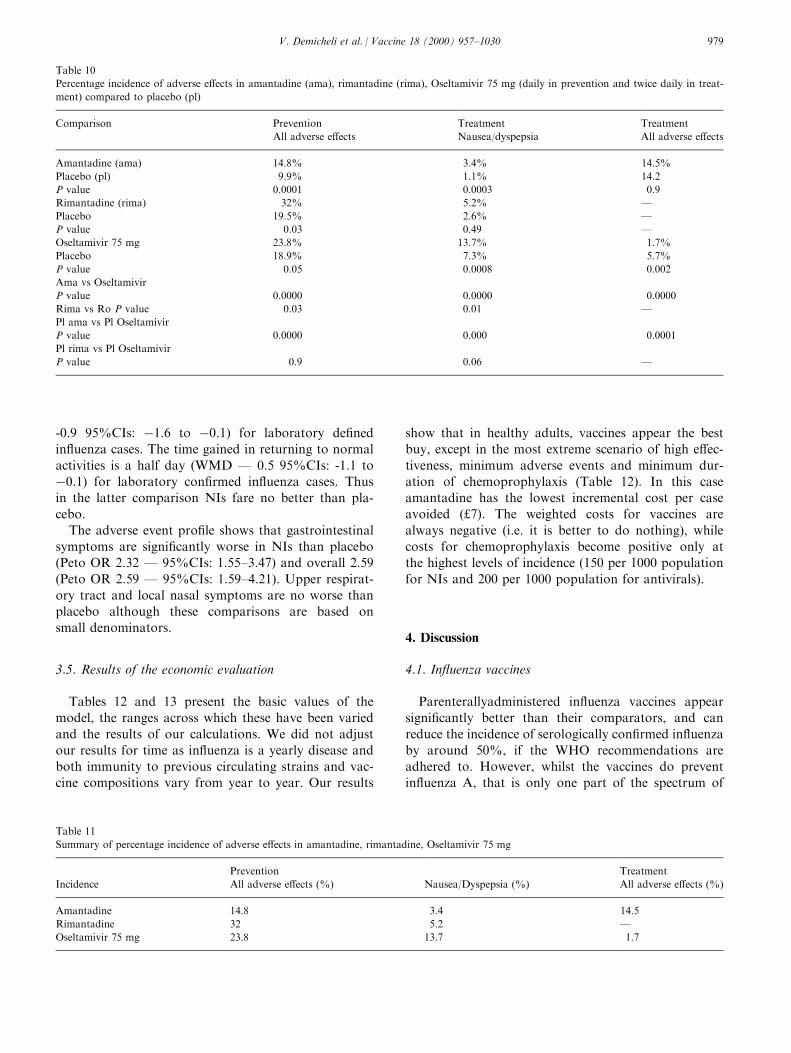
-0.9 95%CIs: ÿ1.6 to ÿ0.1) for laboratory de®ned
in¯uenza cases. The time gained in returning to normal
activities is a half day (WMD Ð 0.5 95%CIs: -1.1 to
ÿ0.1) for laboratory con®rmed in¯uenza cases. Thus
in the latter comparison NIs fare no better than pla-
cebo.
The adverse event pro®le shows that gastrointestinal
symptoms are signi®cantly worse in NIs than placebo
(Peto OR 2.32 Ð 95%CIs: 1.55±3.47) and overall 2.59
(Peto OR 2.59 Ð 95%CIs: 1.59±4.21). Upper respirat-
ory tract and local nasal symptoms are no worse than
placebo although these comparisons are based on
small denominators.
3.5. Results of the economic evaluation
Tables 12 and 13 present the basic values of the
model, the ranges across which these have been varied
and the results of our calculations. We did not adjust
our results for time as in¯uenza is a yearly disease and
both immunity to previous circulating strains and vac-
cine compositions vary from year to year. Our results
show that in healthy adults, vaccines appear the best
buy, except in the most extreme scenario of high e�ec-
tiveness, minimum adverse events and minimum dur-
ation of chemoprophylaxis (Table 12). In this case
amantadine has the lowest incremental cost per case
avoided (£7). The weighted costs for vaccines are
always negative (i.e. it is better to do nothing), while
costs for chemoprophylaxis become positive only at
the highest levels of incidence (150 per 1000 population
for NIs and 200 per 1000 population for antivirals).
4. Discussion
4.1. In¯uenza vaccines
Parenterallyadministered in¯uenza vaccines appear
signi®cantly better than their comparators, and can
reduce the incidence of serologically con®rmed in¯uenza
by around 50%, if the WHO recommendations are
adhered to. However, whilst the vaccines do prevent
in¯uenza A, that is only one part of the spectrum of
Table 10
Percentage incidence of adverse e�ects in amantadine (ama), rimantadine (rima), Oseltamivir 75 mg (daily in prevention and twice daily in treat-
ment) compared to placebo (pl)
Comparison Prevention Treatment Treatment
All adverse e�ects Nausea/dyspepsia All adverse e�ects
Amantadine (ama) 14.8% 3.4% 14.5%
Placebo (pl) 9.9% 1.1% 14.2
P value 0.0001 0.0003 0.9
Rimantadine (rima) 32% 5.2% Ð
Placebo 19.5% 2.6% Ð
P value 0.03 0.49 Ð
Oseltamivir 75 mg 23.8% 13.7% 1.7%
Placebo 18.9% 7.3% 5.7%
P value 0.05 0.0008 0.002
Ama vs Oseltamivir
P value 0.0000 0.0000 0.0000
Rima vs Ro P value 0.03 0.01 Ð
Pl ama vs Pl Oseltamivir
P value 0.0000 0.000 0.0001
Pl rima vs Pl Oseltamivir
P value 0.9 0.06 Ð
Table 11
Summary of percentage incidence of adverse e�ects in amantadine, rimantadine, Oseltamivir 75 mg
Prevention Treatment
Incidence All adverse e�ects (%) Nausea/Dyspepsia (%) All adverse e�ects (%)
Amantadine 14.8 3.4 14.5
Rimantadine 32 5.2 Ð
Oseltamivir 75 mg 23.8 13.7 1.7
V. Demicheli et al. / Vaccine 18 (2000) 957±1030 979
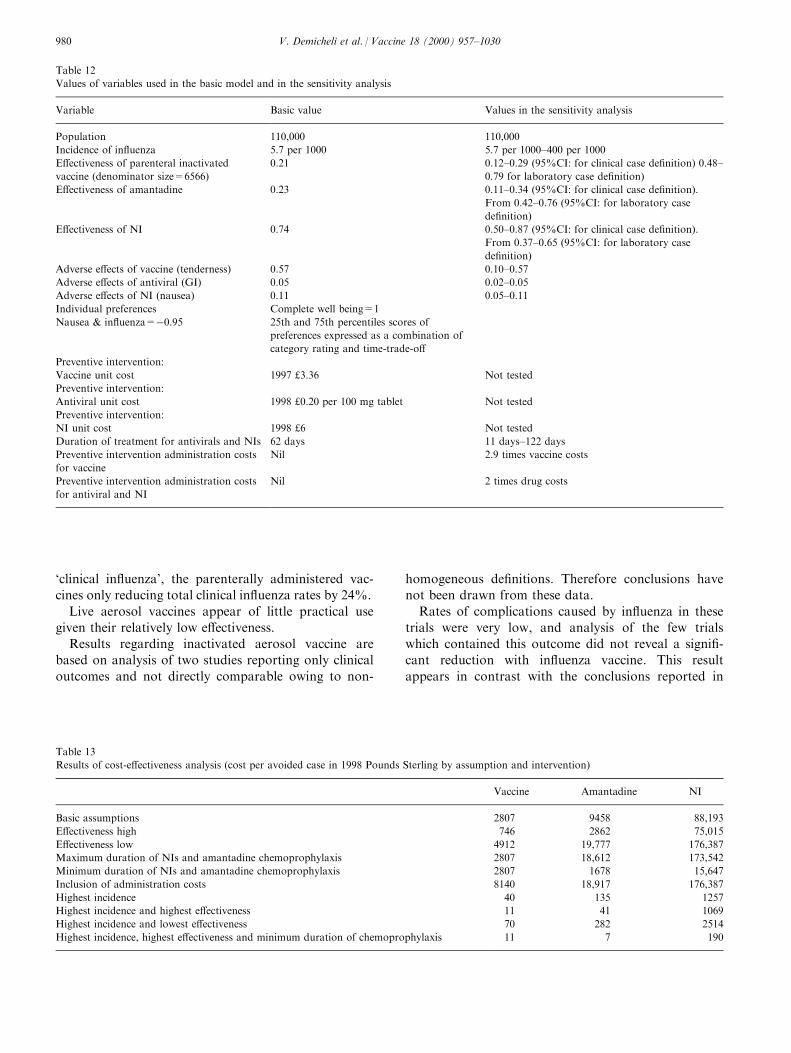
`clinical in¯uenza', the parenterally administered vac-
cines only reducing total clinical in¯uenza rates by 24%.
Live aerosol vaccines appear of little practical use
given their relatively low e�ectiveness.
Results regarding inactivated aerosol vaccine are
based on analysis of two studies reporting only clinical
outcomes and not directly comparable owing to non-
homogeneous de®nitions. Therefore conclusions have
not been drawn from these data.
Rates of complications caused by in¯uenza in these
trials were very low, and analysis of the few trials
which contained this outcome did not reveal a signi®-
cant reduction with in¯uenza vaccine. This result
appears in contrast with the conclusions reported in
Table 12
Values of variables used in the basic model and in the sensitivity analysis
Variable Basic value Values in the sensitivity analysis
Population 110,000 110,000
Incidence of in¯uenza 5.7 per 1000 5.7 per 1000±400 per 1000
E�ectiveness of parenteral inactivated
vaccine (denominator size=6566)
0.21 0.12±0.29 (95%CI: for clinical case de®nition) 0.48±
0.79 for laboratory case de®nition)
E�ectiveness of amantadine 0.23 0.11±0.34 (95%CI: for clinical case de®nition).
From 0.42±0.76 (95%CI: for laboratory case
de®nition)
E�ectiveness of NI 0.74 0.50±0.87 (95%CI: for clinical case de®nition).
From 0.37±0.65 (95%CI: for laboratory case
de®nition)
Adverse e�ects of vaccine (tenderness) 0.57 0.10±0.57
Adverse e�ects of antiviral (GI) 0.05 0.02±0.05
Adverse e�ects of NI (nausea) 0.11 0.05±0.11
Individual preferences Complete well being=1
Nausea & in¯uenza=ÿ0.95 25th and 75th percentiles scores of
preferences expressed as a combination of
category rating and time-trade-o�
Preventive intervention:
Vaccine unit cost 1997 £3.36 Not tested
Preventive intervention:
Antiviral unit cost 1998 £0.20 per 100 mg tablet Not tested
Preventive intervention:
NI unit cost 1998 £6 Not tested
Duration of treatment for antivirals and NIs 62 days 11 days±122 days
Preventive intervention administration costs
for vaccine
Nil 2.9 times vaccine costs
Preventive intervention administration costs
for antiviral and NI
Nil 2 times drug costs
Table 13
Results of cost-e�ectiveness analysis (cost per avoided case in 1998 Pounds Sterling by assumption and intervention)
Vaccine Amantadine NI
Basic assumptions 2807 9458 88,193
E�ectiveness high 746 2862 75,015
E�ectiveness low 4912 19,777 176,387
Maximum duration of NIs and amantadine chemoprophylaxis 2807 18,612 173,542
Minimum duration of NIs and amantadine chemoprophylaxis 2807 1678 15,647
Inclusion of administration costs 8140 18,917 176,387
Highest incidence 40 135 1257
Highest incidence and highest e�ectiveness 11 41 1069
Highest incidence and lowest e�ectiveness 70 282 2514
Highest incidence, highest e�ectiveness and minimum duration of chemoprophylaxis 11 7 190
V. Demicheli et al. / Vaccine 18 (2000) 957±1030980
the literature regarding elderly people, probably due to
the general rarity of complications caused by respirat-
ory infection in healthy adults. Hospitalisation was
assessed only in one trial, and showed a signi®cant
bene®t from vaccination.
Working days lost in placebo recipients and vaccine
recipients were signi®cantly reduced in the vaccinated
group, but by less than half a day on average.
Safety does not appear to be a particular problem
with any of the vaccines, either for incidence or sever-
ity, although given the low e�ectiveness of the aerosol
vaccines, the e�ects classi®ed as adverse may be caused
by in¯uenza. Either way, the public health safety pro-
®le of the vaccines is acceptable.
The results of this review seem to discourage the utilis-
ation of vaccination against in¯uenza in healthy adults
as public health measure. Having healthy adults at low
risk of complications due to respiratory disease, the use
of the vaccine may be only advised as individual protec-
tion measure in very speci®c cases.
The major di�erences in e�ect size between out-
comes highlight the need for careful consideration of
the best study design to assess the e�ects of public
health measures such as vaccines. Additionally more
work needs to be carried out on the combined use of
vaccines, antivirals and NIs when licensed.
4.2. Amantadine and rimantadine
The results of the review show that both amantadine
and rimantadine are e�cacious and relatively safe in
prevention and treatment of cases of in¯uenza A. The
role of amantadine in prophylaxis (61% e�ective) and
treatment (shortens duration of illness by one day) is
beyond question and does not need to be investigated
further compared to placebo. Rimantadine appears
equally e�cacious in prevention (72%), but in direct
comparison with placebo, when a random e�ects
model is applied the lower bound of the 95%, con®-
dence does not achieve statistical signi®cance.
Two connected explanations for this ®nding may be
given: the ®rst is that of insu�cient numbers (there are
clinical data for approximately 700 rimantadine and
2500 amantadine recipients in the review). The second
explanation is centred on the methods of statistical
analysis used: the di�erence between rimantadine and
placebo for the prevention of clinically and serologi-
cally de®ned in¯uenza cases is highly signi®cant if a
®xed e�ect model is used (RR 0.36, 95%CI: 0.22±0.59).
It is likely that with more clinical data available the
e�ectiveness of rimantadine would be beyond doubt.
Rimantadine is equally therapeutically e�cacious,
shortening duration of fever by just over one day.
However, again, this observation is based on 54 patients
only. There do not appear to be signi®cant di�erences in
e�ectiveness in either roles between the two compounds,
although again the comparisons are based on small
numbers with large con®dence intervals.
The safety pro®le of the two drugs appears however
signi®cantly di�erent; with rimantadine causing signi®-
cantly fewer CNS adverse e�ects than amantadine
(being no di�erent than placebo) and causing fewer
withdrawals from the trials. Although these obser-
vations are based on smaller numbers of rimantadine
recipients, amantadine de®nitely causes signs of signi®-
cantly increased and decreased CNS activity, an e�ect
which is not easily acceptable by healthy adults, es-
pecially in employment which require concentration
and mental ®tness. The conclusion may be drawn that
from available evidence, rimantadine appears the bet-
ter choice for prevention.
Signi®cantly decreased CNS activity is caused by
amantadine in a treatment role, but this appears to be
the only signi®cant adverse e�ect of both compounds
in a treatment role, although numbers of patients are
again very low. Low numbers make the interpretation
of the other two comparisons equally di�cult.
In future more attention should be paid to the
assessment of adverse events of the two compounds,
particularly those of rimantadine which at present are
based on relatively small numbers.
The quality of the trials was not good, with signi®-
cant numbers of studies failing to give adequate
descriptions of methods and of results. This may be in
part due to the number of older trials in the review.
Both quality of trial conducting and reporting should
be improved and adverse e�ects and case outcome
de®nitions should be standardised.
No trials assessed onset of resistance, but data from
a review citing two studies demonstrated that 10 to
27% of patients treated with rimantadine secreted
drug-resistant virus within four to ®ve days of com-
mencing treatment [37]. Finally, carrying out sub-
analysis by dose was considered (100, 200, 300 mg
daily), but decided against this given the small size of
the resulting meta-analysis. This policy will be re-con-
sidered if any further data become available.
Both drugs can be used e�ectively for the prevention
and treatment of in¯uenza, both in vaccinated and
unvaccinated populations. However, the higher inci-
dence of CNS adverse e�ects of amantadine makes
rimantadine the current antiviral of choice against in¯u-
enza.
There is a requirement for better reported trials, par-
ticularly those assessing amantadine and rimantadine
directly in both prevention and treatment roles.
Attention should be paid to the assessment of adverse
events of the two compounds, particularly those of
V. Demicheli et al. / Vaccine 18 (2000) 957±1030 981
rimantadine which at present are based on relatively
small numbers. Quality of trial conducting and report-
ing should be improved and adverse e�ects and case
outcome de®nitions should be standardised.
4.3. Neuraminidase inhibitors
As far as is known by the authors, this review pro-
vides the most comprehensive current evidence of the
e�ects of NIs on humans exposed to in¯uenza either
naturally or experimentally. The results of the meta-
analysis show that NIs are e�ective in preventing in¯u-
enza A and B and shortening duration of illness. The
safety pro®le of the compounds is good overall,
although there is concern about the acceptability of
Oseltamivir given the high incidence of nausea it
causes. Further assessment of the safety of this com-
pound is necessary.
As increasing amounts of data become available (as
can be seen by the number of studies awaiting assess-
ment following publication) the review will be updated
and further comparisons added. These are likely to
include direct comparisons between compounds, and
comparisons of di�erent doses and schedules.
Overall the quality of trials was di�cult to assess as
a proportion of trials were either in an unpublished or
an abstract format. The quality of the two published
studies was reasonable. As NIs have a clear e�ect, it is
now time to concentrate on more pragmatic trials in
individuals exposed to naturally acquired in¯uenza.
4.4. Overall comments
Overall the evidence that we assembled in our
Cochrane reviews was based on relatively small denomi-
nators. For instance, the parenteral inactivated vaccine
trials meta-analysis is based on 16 studies with a total of
23,000 individuals. The trials were carried out world-
wide over a 30-year time span during which, assuming a
low incidence of ®ve per 1000, there would have been
over eight million cases of in¯uenza in the UK alone.
We do not know whether such trial size is su�cient
to properly evaluate an intervention (vaccines) which
could be given yearly to large cohorts world-wide for a
very common infectious disease, especially since the
vaccine is e�ectively a new product each year.
Many of the 17 antiviral trials did not report adverse
events, thus our evaluation of the crucial safety pro®le
of these was based on ®ve studies with a total of ap-
proximately 3000 individuals. Again the overall knowl-
edge base may be insu�cient to reach ®rm conclusions
in this most important aspect of quality.
There is a notable di�erence between e�ect size on
clinically-de®ned outcomes and those based on a lab-
oratory-con®rmed case de®nition. This is likely to be
caused by a high intervention e�cacy against the in¯u-
enza virus, which is equivalent to a low e�ectiveness in
the context of an in¯uenza epidemic. This in turn
raises the problem of whether RCTs are the best de-
sign to assess the e�ectiveness of public health
measures such as vaccination. We are aware that the
alternatives (context-speci®c non-randomised studies)
are prone to confounders and hence problems of in-
terpretation of results.
4.5. Economic evaluation
By taking the perspectives of e�ectiveness, safety
and e�ciency into account in the evaluation of the
e�ects of prevention and treatment of in¯uenza, we
were able to assess the relative importance of each per-
spective in answering the study question. By basing
our economic model on systematically assembled and
evaluated evidence we reached relatively ®rm con-
clusions. The ®rst e�ect of such a methodological
approach was to prune our decision tree considerably;
thus the treatment arms were deleted because of the
small e�ect size. Our tree went from a `before' state of
a prevention/treatment combination leading to 11 de-
cision nodes and 165 terminal nodes to an `after' state
of preventive alternatives only with one decision node
and 12 terminal nodes. Although antivirals and NIs
signi®cantly shortened the duration of illness when
compared to placebo (0.5 to one day), this e�ect had
little practical signi®cance. However, the use of sys-
tematic review methods to de®ne comparators had the
drawbacks of discarding data because of inappropriate
format and of reliance on what data were available.
One of the consequences of the latter drawback is the
impossibility of evaluating the use of NIs in local out-
break control situations. A consequence of the former
was the exclusion from the decision-making process of
all trials with inappropriate outcome measures.
We were able to exclude inhaled or live attenuated
vaccines from our evaluation because of little e�ect or
little di�erence in e�ect with parenteral vaccines. Of
the remaining contenders, rimantadine is not licensed
in the UK but has a better safety pro®le than amanta-
dine (which is available in UK). As physicians we
would not recommend the use of amantadine in
healthy adults, given the high incidence of major CNS
excitant and depressant adverse e�ects seen in our
Cochrane meta-analysis [8].
Such adverse e�ects are likely to prove very danger-
ous in healthy adults, especially those undertaking
emergency service duty during an in¯uenza outbreak.
Despite this ®nding that ruled out the use of amanta-
dine, we decided to keep amantadine in our model and
V. Demicheli et al. / Vaccine 18 (2000) 957±1030982

used its less frequent GI adverse e�ects, broadly
comparable to those of NIs. From a GI point of
view however, amantadine has a better safety pro®le
that rimantadine. As rimantadine's e�ects on the
CNS are no di�erent than those of placebo, rimanta-
dine would be considered a better candidate as a com-
parator were it registered in the UK. However when the
likely duration of treatment is taken into consideration
(62 days), the probable logistic burden and compliance
problems of compounds to be administered daily (such
as antivirals and NIs) make them an unpractical choice.
The only remaining intervention, vaccines, should then
become the solution to our study problem. Thus the
economic evaluation was a posteriori made redundant
by evidence of e�ects which ruled out all the alterna-
tives. Had we built our economic model using an a
priori conceptual framework and had we fed it esti-
mates derived from single studies of the relevant inter-
ventions, it is likely that we would have retained a very
complicated decision tree with many di�erent alterna-
tives and reached a di�erent conclusion.
If assessed from an e�ectiveness and e�ciency
point of view, vaccines are undoubtedly the best pre-
ventive means for in¯uenza in healthy adults.
However when safety and quality of life consider-
ations are included, parenteral vaccines have such low
e�ectiveness and high incidence of trivial local
adverse e�ects that the trades-o� are unfavourable.
This is so even when the incidence of in¯uenza is
high and adverse e�ect quality of life preferences are
lowly rated. We reached similar conclusions for anti-
virals and NIs even at high in¯uenza incidence levels.
We conclude that the most cost-e�ective option is
not to take any action.
We believe that our methods are applicable to other
healthy adult population groups with several caveats.
The costs of administration of a preventive pro-
gramme and indirect costs of interventions (time spent
being vaccinated or taking medication) would need to
be carefully valued in a non-military population.
Individual preferences would have to be assessed in
the reference population.
The impact of in¯uenza di�ers on the basis of sick-
ness certi®cation patterns that are speci®c to employ-
ment groups.
However problematical the economics of in¯uenza
prevention are, these pale into insigni®cance when
compared to the uncertainty still surrounding epide-
miological knowledge of the disease and of its conse-
quences and remedies.
Acknowledgements
This study was funded by the Ministry of Defence
of the United Kingdom (MOD(UK)).
In¯uenza vaccines in healthy adults Ð The authors
gratefully acknowledge the help received by Drs Brian
Hutchison, Alan Hampson, Andy Oxman and
Donatella Tiberti for data extraction and Mrs Carol
Hobbs for assistance with trial retrieval.
Amantadine and Rimantadine for in¯uenza in healthy
adults Ð The authors would like to thank Drs Aoki,
Couch, Hayden, and Monto for helpful comments on
the draft protocol and Mrs Carol Hobbs for assistance
with trial retrieval.
Neuraminidase inhibitors for in¯uenza in healthy
adults Ð The authors would like to thank Professor
Arnold Monto, Drs Penelope Ward, Bina Rawal for
the help received and Mrs Carol Hobbs for assistance
with trial retrieval.
Economic evaluation Ð The authors gratefully
acknowledge the assistance given by the editorial base
of the Cochrane Acute Respiratory Infections Group
to the Cochrane reviews and by Stephen Morris. The
authors also gratefully acknowledge the extensive edi-
torial assistance given by Ms Elizabeth Hayden and
Dr Abraham Palache.
Potential con¯ict of interest Ð Dr Je�erson is an ad
hoc consultant for Ho�mann-La Roche Ltd.
V. Demicheli et al. / Vaccine 18 (2000) 957±1030 983

Appendix A. Producers of in¯uenza vaccines and their products [7]
Country Producer Product type
Australia CSL Ltd Split virionBulgaria MA Research Institute of Infectious and Parasitic Diseases Live vaccineCanada IAF BIO Va. Inc. Trivalent whole virion, split virionFrance Pasteur-Merieux Serums & Vaccines Whole virion, split virionGermany Behringwerke Aktiengesellischaft Split virion liquidGermany Veb Sachsisches Serumwerk Dresen Split virionHungary Omnivest Institute InactivatedItaly BIOCINE spa Whole virion, subunit virionItaly Istituto Sieroterapico Italiano spa Whole, split and subunit virionItaly Istituto Vaccinogeno Pozzi spa Whole, split and subunit virionJapan Denka Seiken Co. Whole virionJapan The Chemo-Sero-Therapeutic Research Institute Whole virionJapan The Kitasato Institute Whole virionJapan The Research Foundation for Microbial Diseases of Osaka
UniversityWhole virion
Korea Boryung Biopharma Co. Whole virionKorea Cheil Foods and Chemicals Inc. Whole virionKorea Dong Shin Pharmaceutical Co Ltd Whole virionKorea DongÐA Pharmaceutical Co Ltd Whole virionKorea Korea Green Cross Corporation Whole virionKorea Korea Vaccine Co Ltd Whole virionKorea LG Chemical Ltd Whole virionNetherlands Solvay Pharmaceuticals bv Whole virion, subunit virionRomania Cantacuzino Institute Whole virion, split virionRomania Stefan S Nicolau Institute of Virology Whole virionRussianFederation
Bacteriological preparations division of the St PetersburgInstitute for Vaccine and Serum Research
Live intranasal, whole virion
RussianFederation
Immunopreparat Whole virion
RussianFederation
Irkutsk Bilogical Preparation Company Intranasal
RussianFederation
Pasteur Institute St Petersburg Whole virion
Slovakia Imuna sp. Subunit virionSwitzerland Swiss Serum and Vaccine Institute Berne Whole virionUK Evans Medical Subunit virionUSA Connaught Laboratories Inc. Subunit virion, whole virionUSA Parke Davis Subunit virion, whole virionUSA Wyeth Laboratories Inc. Subunit virionYugoslavia Institute of Immunology and Virology Torlak Whole virion
V. Demicheli et al. / Vaccine 18 (2000) 957±1030984
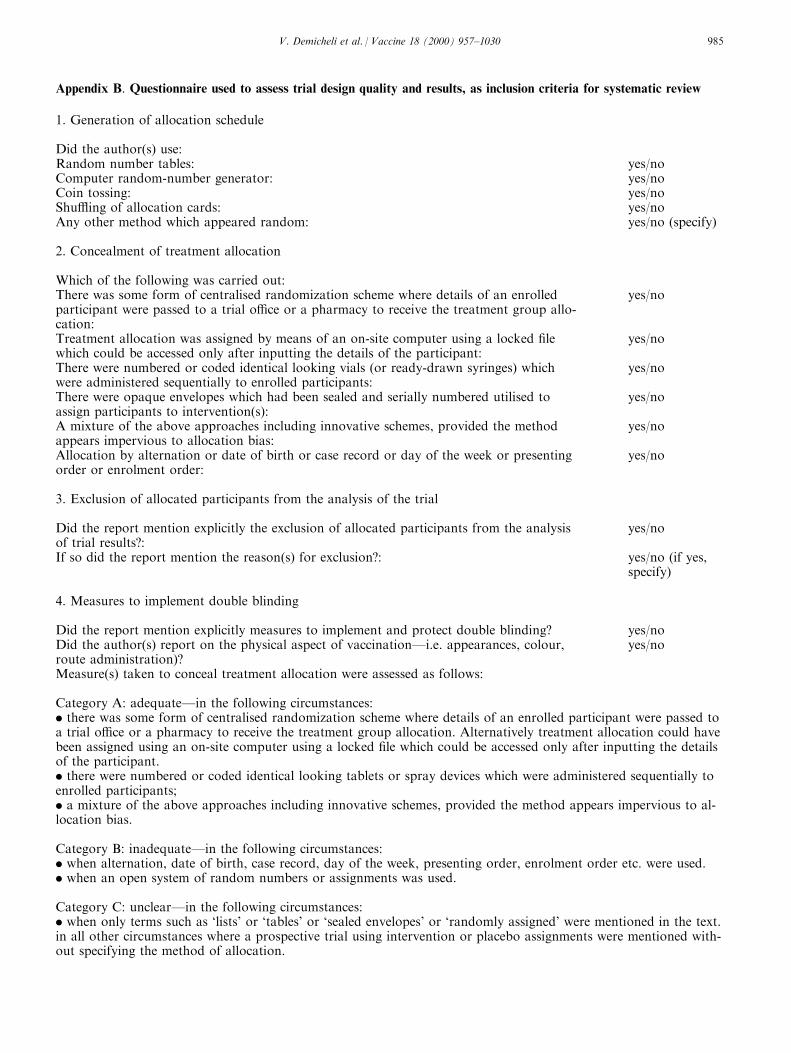
Appendix B. Questionnaire used to assess trial design quality and results, as inclusion criteria for systematic review
1. Generation of allocation schedule
Did the author(s) use:Random number tables: yes/noComputer random-number generator: yes/noCoin tossing: yes/noShu�ing of allocation cards: yes/noAny other method which appeared random: yes/no (specify)
2. Concealment of treatment allocation
Which of the following was carried out:There was some form of centralised randomization scheme where details of an enrolledparticipant were passed to a trial o�ce or a pharmacy to receive the treatment group allo-cation:
yes/no
Treatment allocation was assigned by means of an on-site computer using a locked ®lewhich could be accessed only after inputting the details of the participant:
yes/no
There were numbered or coded identical looking vials (or ready-drawn syringes) whichwere administered sequentially to enrolled participants:
yes/no
There were opaque envelopes which had been sealed and serially numbered utilised toassign participants to intervention(s):
yes/no
A mixture of the above approaches including innovative schemes, provided the methodappears impervious to allocation bias:
yes/no
Allocation by alternation or date of birth or case record or day of the week or presentingorder or enrolment order:
yes/no
3. Exclusion of allocated participants from the analysis of the trial
Did the report mention explicitly the exclusion of allocated participants from the analysisof trial results?:
yes/no
If so did the report mention the reason(s) for exclusion?: yes/no (if yes,specify)
4. Measures to implement double blinding
Did the report mention explicitly measures to implement and protect double blinding? yes/noDid the author(s) report on the physical aspect of vaccinationÐi.e. appearances, colour,route administration)?
yes/no
Measure(s) taken to conceal treatment allocation were assessed as follows:
Category A: adequateÐin the following circumstances:. there was some form of centralised randomization scheme where details of an enrolled participant were passed toa trial o�ce or a pharmacy to receive the treatment group allocation. Alternatively treatment allocation could havebeen assigned using an on-site computer using a locked ®le which could be accessed only after inputting the detailsof the participant.. there were numbered or coded identical looking tablets or spray devices which were administered sequentially toenrolled participants;. a mixture of the above approaches including innovative schemes, provided the method appears impervious to al-location bias.
Category B: inadequateÐin the following circumstances:. when alternation, date of birth, case record, day of the week, presenting order, enrolment order etc. were used.. when an open system of random numbers or assignments was used.
Category C: unclearÐin the following circumstances:. when only terms such as `lists' or `tables' or `sealed envelopes' or `randomly assigned' were mentioned in the text.in all other circumstances where a prospective trial using intervention or placebo assignments were mentioned with-out specifying the method of allocation.
V. Demicheli et al. / Vaccine 18 (2000) 957±1030 985
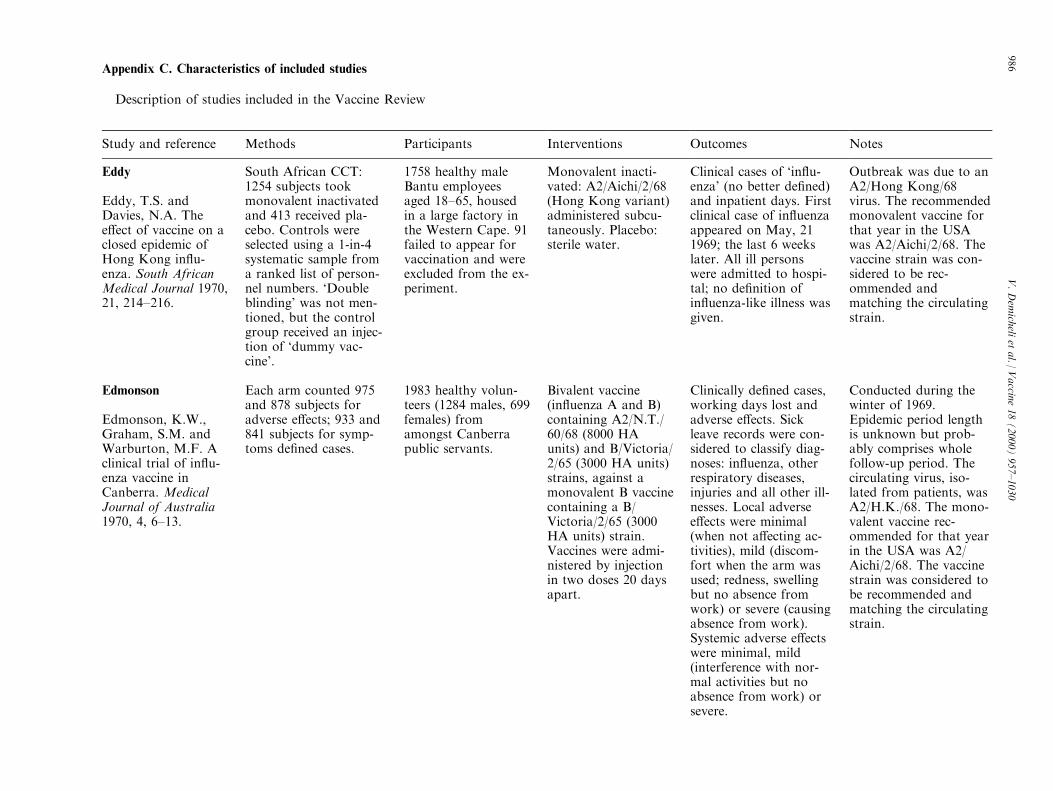
Appendix C. Characteristics of included studies
Description of studies included in the Vaccine Review
Study and reference Methods Participants Interventions Outcomes Notes
Eddy
Eddy, T.S. andDavies, N.A. Thee�ect of vaccine on aclosed epidemic ofHong Kong in¯u-enza. South AfricanMedical Journal 1970,21, 214±216.
South African CCT:1254 subjects tookmonovalent inactivatedand 413 received pla-cebo. Controls wereselected using a 1-in-4systematic sample froma ranked list of person-nel numbers. `Doubleblinding' was not men-tioned, but the controlgroup received an injec-tion of `dummy vac-cine'.
1758 healthy maleBantu employeesaged 18±65, housedin a large factory inthe Western Cape. 91failed to appear forvaccination and wereexcluded from the ex-periment.
Monovalent inacti-vated: A2/Aichi/2/68(Hong Kong variant)administered subcu-taneously. Placebo:sterile water.
Clinical cases of `in¯u-enza' (no better de®ned)and inpatient days. Firstclinical case of in¯uenzaappeared on May, 211969; the last 6 weekslater. All ill personswere admitted to hospi-tal; no de®nition ofin¯uenza-like illness wasgiven.
Outbreak was due to anA2/Hong Kong/68virus. The recommendedmonovalent vaccine forthat year in the USAwas A2/Aichi/2/68. Thevaccine strain was con-sidered to be rec-ommended andmatching the circulatingstrain.
Edmonson
Edmonson, K.W.,Graham, S.M. andWarburton, M.F. Aclinical trial of in¯u-enza vaccine inCanberra. MedicalJournal of Australia1970, 4, 6±13.
Each arm counted 975and 878 subjects foradverse e�ects; 933 and841 subjects for symp-toms de®ned cases.
1983 healthy volun-teers (1284 males, 699females) fromamongst Canberrapublic servants.
Bivalent vaccine(in¯uenza A and B)containing A2/N.T./60/68 (8000 HAunits) and B/Victoria/2/65 (3000 HA units)strains, against amonovalent B vaccinecontaining a B/Victoria/2/65 (3000HA units) strain.Vaccines were admi-nistered by injectionin two doses 20 daysapart.
Clinically de®ned cases,working days lost andadverse e�ects. Sickleave records were con-sidered to classify diag-noses: in¯uenza, otherrespiratory diseases,injuries and all other ill-nesses. Local adversee�ects were minimal(when not a�ecting ac-tivities), mild (discom-fort when the arm wasused; redness, swellingbut no absence fromwork) or severe (causingabsence from work).Systemic adverse e�ectswere minimal, mild(interference with nor-mal activities but noabsence from work) orsevere.
Conducted during thewinter of 1969.Epidemic period lengthis unknown but prob-ably comprises wholefollow-up period. Thecirculating virus, iso-lated from patients, wasA2/H.K./68. The mono-valent vaccine rec-ommended for that yearin the USA was A2/Aichi/2/68. The vaccinestrain was considered tobe recommended andmatching the circulatingstrain.
V.Dem
icheli
etal./
Vaccin
e18(2000)957±1030
986
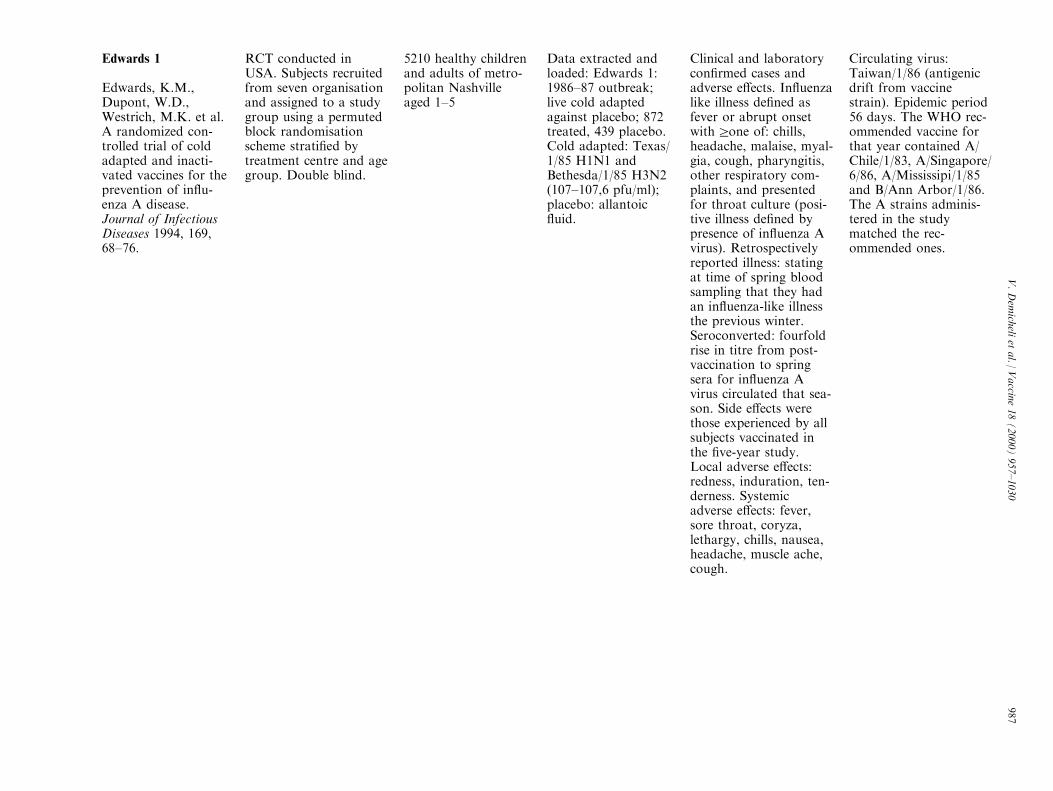
Edwards 1
Edwards, K.M.,Dupont, W.D.,Westrich, M.K. et al.A randomized con-trolled trial of coldadapted and inacti-vated vaccines for theprevention of in¯u-enza A disease.Journal of InfectiousDiseases 1994, 169,68±76.
RCT conducted inUSA. Subjects recruitedfrom seven organisationand assigned to a studygroup using a permutedblock randomisationscheme strati®ed bytreatment centre and agegroup. Double blind.
5210 healthy childrenand adults of metro-politan Nashvilleaged 1±5
Data extracted andloaded: Edwards 1:1986±87 outbreak;live cold adaptedagainst placebo; 872treated, 439 placebo.Cold adapted: Texas/1/85 H1N1 andBethesda/1/85 H3N2(107±107,6 pfu/ml);placebo: allantoic¯uid.
Clinical and laboratorycon®rmed cases andadverse e�ects. In¯uenzalike illness de®ned asfever or abrupt onsetwithrone of: chills,headache, malaise, myal-gia, cough, pharyngitis,other respiratory com-plaints, and presentedfor throat culture (posi-tive illness de®ned bypresence of in¯uenza Avirus). Retrospectivelyreported illness: statingat time of spring bloodsampling that they hadan in¯uenza-like illnessthe previous winter.Seroconverted: fourfoldrise in titre from post-vaccination to springsera for in¯uenza Avirus circulated that sea-son. Side e�ects werethose experienced by allsubjects vaccinated inthe ®ve-year study.Local adverse e�ects:redness, induration, ten-derness. Systemicadverse e�ects: fever,sore throat, coryza,lethargy, chills, nausea,headache, muscle ache,cough.
Circulating virus:Taiwan/1/86 (antigenicdrift from vaccinestrain). Epidemic period56 days. The WHO rec-ommended vaccine forthat year contained A/Chile/1/83, A/Singapore/6/86, A/Mississipi/1/85and B/Ann Arbor/1/86.The A strains adminis-tered in the studymatched the rec-ommended ones.
V.Dem
icheli
etal./
Vaccin
e18(2000)957±1030
987
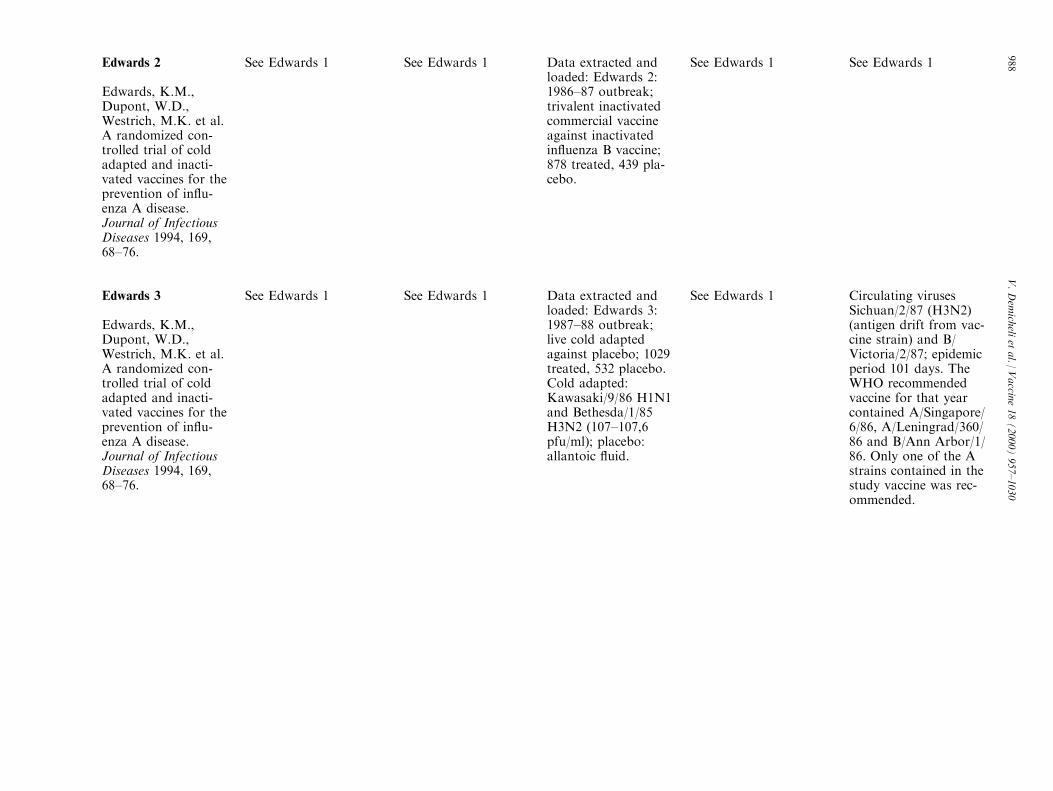
Edwards 2
Edwards, K.M.,Dupont, W.D.,Westrich, M.K. et al.A randomized con-trolled trial of coldadapted and inacti-vated vaccines for theprevention of in¯u-enza A disease.Journal of InfectiousDiseases 1994, 169,68±76.
See Edwards 1 See Edwards 1 Data extracted andloaded: Edwards 2:1986±87 outbreak;trivalent inactivatedcommercial vaccineagainst inactivatedin¯uenza B vaccine;878 treated, 439 pla-cebo.
See Edwards 1 See Edwards 1
Edwards 3
Edwards, K.M.,Dupont, W.D.,Westrich, M.K. et al.A randomized con-trolled trial of coldadapted and inacti-vated vaccines for theprevention of in¯u-enza A disease.Journal of InfectiousDiseases 1994, 169,68±76.
See Edwards 1 See Edwards 1 Data extracted andloaded: Edwards 3:1987±88 outbreak;live cold adaptedagainst placebo; 1029treated, 532 placebo.Cold adapted:Kawasaki/9/86 H1N1and Bethesda/1/85H3N2 (107±107,6pfu/ml); placebo:allantoic ¯uid.
See Edwards 1 Circulating virusesSichuan/2/87 (H3N2)(antigen drift from vac-cine strain) and B/Victoria/2/87; epidemicperiod 101 days. TheWHO recommendedvaccine for that yearcontained A/Singapore/6/86, A/Leningrad/360/86 and B/Ann Arbor/1/86. Only one of the Astrains contained in thestudy vaccine was rec-ommended.
V.Dem
icheli
etal./
Vaccin
e18(2000)957±1030
988
Edwards 4
Edwards, K.M.,Dupont, W.D.,Westrich, M.K. et al.A randomized con-trolled trial of coldadapted and inacti-vated vaccines for theprevention of in¯u-enza A disease.Journal of InfectiousDiseases 1994, 169,68±76.
See Edwards 1 See Edwards 1 Data extracted andloaded: Edwards 4:1987±88 outbreak;trivalent inactivatedcommercial vaccineagainst inactivatedin¯uenza B vaccine;1060 treated, 532 pla-cebo. Inactivated vac-cine formula:Taiwan/1/86 H1N1and Leningrad/360/86H3N2 (15 mg eachstrain). B strain con-tained in the vaccineswas not described.
See Edwards 1 See Edwards 1
Edwards 5
Edwards, K.M.,Dupont, W.D.,Westrich, M.K. et al.A randomized con-trolled trial of coldadapted and inacti-vated vaccines for theprevention of in¯u-enza A disease.Journal of InfectiousDiseases 1994, 169,68±76.
See Edwards 1 See Edwards 1 Data extracted andloaded: Edwards 5:1988±89 outbreak;live cold adaptedagainst placebo; 1114treated, 562 placebo.Cold adapted:Kawasaki/9/86 H1N1and Los Angeles/2/87H3N2 (107±107,6pfu/ml); placebo:allantoic ¯uid.
See Edwards 1 Circulating virusesTaiwan/1/86 (H1N1)and B/Yamagata/16/88;epidemic period 78 days.WHO recommendedvaccine contained A/Singapore/6/86, A/Sichuan/2/87 and B/Beijing/1/87. Only oneof the A strains con-tained in the study vac-cine was recommended.The vaccine was con-sidered to be rec-ommended andmatching the circulatingstrain.
V.Dem
icheli
etal./
Vaccin
e18(2000)957±1030
989
Edwards 6
Edwards, K.M.,Dupont, W.D.,Westrich, M.K. et al.A randomized con-trolled trial of coldadapted and inacti-vated vaccines for theprevention of in¯u-enza A disease.Journal of InfectiousDiseases 1994, 169,68±76.
See Edwards 1 See Edwards 1 Data extracted andloaded: Edwards 6:1988±89 outbreak;trivalent inactivatedcommercial vaccineagainst inactivatedin¯uenza B vaccine;1126 treated, 562 pla-cebo; Inactivated vac-cine formula:Taiwan/1/86 H1N1and Sichuan/2/87H3N2 (15 mg eachstrain). B strain con-tained in vaccines notdescribed.
See Edwards 1 See Edwards 1
Edwards 7
Edwards, K.M.,Dupont, W.D.,Westrich, M.K. et al.A randomized con-trolled trial of coldadapted and inacti-vated vaccines for theprevention of in¯u-enza A disease.Journal of InfectiousDiseases 1994, 169,68±76.
See Edwards 1 See Edwards 1 Data extracted andloaded: Edwards 7:1989±90 outbreak;live cold adaptedagainst placebo; 999treated, 508 placebo.Cold adapted:Kawasaki/9/86 H1N1and Los Angeles/2/87H3N2 (107±107,6pfu/ml); placebo:allantoic ¯uid.
See Edwards 1 Circulating virusShangai/11/87 (H3N2);epidemic period 80 days.WHO recommendedvaccine contained A/Singapore/6/86, A/Shanghai/11/87 and B/Yamagata/16/88. Onlyone A strain containedin study vaccine was rec-ommended. The vaccinewas considered to berecommended andmatching the circulatingstrain
V.Dem
icheli
etal./
Vaccin
e18(2000)957±1030
990

Edwards 8
Edwards, K.M.,Dupont, W.D.,Westrich, M.K. et al.A randomized con-trolled trial of coldadapted and inacti-vated vaccines for theprevention of in¯u-enza A disease.Journal of InfectiousDiseases 1994, 169,68±76.
See Edwards 1 See Edwards 1 Data extracted andloaded: Edwards 8:1989±90 outbreak;trivalent inactivatedcommercial vaccineagainst inactivatedin¯uenza B vaccine;1016 treated, 508 pla-cebo Inactivated vac-cine formula:Taiwan/1/86 H1N1and Shanghai/11/87H3N2 (15 mg eachstrain). B strain con-tained in the vaccineswas not described.
See Edwards 1 See Edwards 1
Hammond
Hammond, M.L.,Ferris, A.A., Faine,S. et al. E�ective pro-tection against in¯u-enza after vaccinationwith subunit vaccine.Medical Journal ofAustralia 1978, 1,301±303.
Australian CCT, doubleblind. Coded identicallooking vials weresequentially adminis-tered to enrolled partici-pants.
225 volunteers, medi-cal students or sta�members of theMonash University.116 subjects in thevaccine group and109 subjects in theplacebo group.
A trivalent, subunitvaccine containing200 IU of A/Victoria/3/75, 250 IU of A/Scotland/840/74 and300 IU of B/HongKong/8/73 (as issuedfor general use), wascompared against pla-cebo (diphtheria andtetanus toxoids).Vaccines were admi-nistered subcu-taneously.
Clinical and laboratorycon®rmed cases.In¯uenza de®ned as: suf-fering a respiratory ill-ness associated with theisolation of in¯uenzavirus, a four-fold orgreater rise in antibodytitre occurred betweenpostvaccination andpostepidemic sera, orboth. Adverse e�ects arenot considered.
Epidemic in¯uenza wasde®ned by virus iso-lation and serology testsand lasted from middleApril to middle August1976. Outcomes weredetected during thewhole epidemic period.A/Vic/3/75 was isolatedfrom patients. The rec-ommended formula forthat year was: A/Victoria/3/75, A/Scotland/840/74 and ofB/Hong Kong/8/73.
V.Dem
icheli
etal./
Vaccin
e18(2000)957±1030
991
Hobson
Hobson, D., Baker,F.A., Chivers, C.P. etal. A comparison ofmonovalent HongKong in¯uenza virusvaccine with vaccinescontaining only pre-1968 Asian strains inadult volunteers.Journal of Hygiene1970, 68, 369±378.
UK RCT comparingmonovalent inactivatedvaccine of Hong Kongstrain of in¯uenza Avirus against polyvalentvaccine containing onlypre-1968 Asian viruses.Volunteers allocated toone of three groups byrandom numbers.Double-blinding main-tained throughout trialby coded preparation.Vaccines administeredintramuscularly in twogroups and placebo(saline) administerednasally. The third groupreceived both vaccines:monovalent nasally;polyvalent intramuscu-larly.
1601 volunteers,industrial workersaged 16±64.
Data extracted andloaded: Polyvalentintramuscular(N= 545) againstmonovalent intramus-cular in¯uenza A(N= 508) polyvalentformula was: A2/Eng/12/64 3000 HAunits, A2/Eng/76/666000 HA units, B/Eng/5/66 3000 HAunits, B/Swiss/265/673000 HA units mono-valent was a HongKong virus: A2/Eng/344/68 7000 HA units
Clinical cases andWDLS. Clinical caseswere de®ned as `respirat-ory illness' or `clinicalin¯uenza' according tothe clinical syndromescharacterised by Stuart-Harris (1965).
Epidemic period lasted10 weeks. Vaccine e�-cacy was evaluatedduring the whole 1968±69 in¯uenza season (23weeks). The viral strainisolated from patientswas antigenically identi-cal to A2/Eng/344/68.The monovalent vaccinerecommended for thatyear in the USA wasA2/Aichi/2/68 (a HongKong virus). The mono-valent A vaccine wasconsidered to be rec-ommended and match-ing the circulatingstrain.
V.Dem
icheli
etal./
Vaccin
e18(2000)957±1030
992

Hoskins
Hoskins, T.W.,Davies, J.R., Allchin,A. et al. Controlledtrial of inactivatedin¯uenza vaccine con-taining the A/HongKong strain duringan outbreak of in¯u-enza due to the A/England/42/72 strain.Lancet 1973, 21, 116±120.
Quasi-randomised,double blind, not pla-cebo controlled trial,conducted in a UKboarding school. Boyswere allocated to thetwo arms of the studyaccording to date ofbirth. The vaccines werelabelled according to acode.
800 boys 11±19 year-old. 384 subjectsreceived in¯uenza Avaccine; 340 boysreceived in¯uenza Bvaccine.
Monovalent inacti-vated in¯uenza Avaccine containingthe A/Hong Kong/68strain vs monovalentinactivated in¯uenzaB vaccine. Studylasted three years(1970±72): boys werere-vaccinated stayingin the same vaccinegroup, and newentrants were allo-cated as before. Viralstrain used in vac-cines were:Ðwinter1970±71: A2/HongKong/X31/68 (H3N2)200 IU and B/England/5/66 200IUÐwinter 1971±72:A2/Hong Kong/X31/68 (H3N2) 200 IUand B/England/5/66200 IUÐwinter1972±73: A2/HongKong/1/68X (H3N2)200 IU and B/Victoria/98926/70 200IU. Each vaccine wasgiven subcutaneously.
Clinical and laboratorycon®rmed cases andadverse e�ects. Clinicalcases de®ned as `febrilerespiratory infection'.Laboratory casesde®ned by isolation ofan in¯uenza virus fromthroat swabs or a four-fold or greater rise inantibody titre occurredbetween acute and con-valescent sera. Reactionsto vaccination hadinsu�cient de®nition tobe extracted.
The protective e�cacyof the vaccines was eval-uated during an out-break of in¯uenza dueto A/England/42/72, astrain which had under-gone to a recent anti-genic shift. The epidemicperiod lasted fromDecember 5 toDecember 15, 1972. Therecommended formulafor those years in theUSA was A2/Aichi/2/68,B/Massachusetts/1/72.The vaccine was con-sidered to match one ofthe recommendedstrains.
V.Dem
icheli
etal./
Vaccin
e18(2000)957±1030
993
Keitel 1
Keitel, W.A., Cate,T.R. and Couch,R.B. E�cacy ofsequential annualvaccination with inac-tivated in¯uenza virusvaccine. AmericanJournal ofEpidemiology 1988,127, 353±364.
RCT Volunteers ran-domly allocated toreceive vaccine or pla-cebo using a table ofrandom numbersaccording to prior vacci-nation experience. Threegroups were formed:®rst vaccinated, multi-vaccinated and placebo.Each arm counted, re-spectively, 162, 138 and298 subjects. Doubleblind.
598 healthy volun-teers, 30±60 yearsold, working in theTexas Medical Centerin Huston, Texas, orin surrounding indus-trial companies.
Data extracted andloaded: Keitel 1:1983±84 outbreak;trivalent inactivated,killed whole, intra-muscularly adminis-tered, commercialvaccine against pla-cebo; 300 treated, 298placebo Each dose ofthe commercial vac-cine contained 15 mgof hemagglutinin ofeach of the followingin¯uenza strains: A/Philippines/2/82(H3N2), A/Brazil/11/78 (H1N1) and B/Singapore/222/79.Placebo was sterilesaline for injection.
Clinical and laboratorycon®rmed cases.Illnesses classi®ed as`any', `¯u-like' (lowerrespiratory and/or sys-temic illness) or `febrile'(oral temperature ofr37.8) from ®ndings atinitial examination.Symptoms and signs ofdisease of trachea,bronchi and/or lungwere designated lowerrespiratory illness.Systemic illness de®nedby: myalgia, malaise,fatigue, lethargy, chills,sweats and anorexia.Laboratory con®rmationwas based on cultureand/orrfour-fold rise inantibody titre betweenpostvaccination (pre-epi-demic), acute, convales-cent and/or spring(postepidemic) sera, andis reported separatelyfor in¯uenza A or in¯u-enza B and for cultureor serological positivity.Authors don't specifywhen culture and serolo-gical con®rmation areobtained on same sub-ject. Adverse e�ects arenot considered.Outcomes were detectedduring the whole epi-demic period ('intervalduring which commu-nity surveillance recov-ered in¯uenza virusesfromr10% of personwith febrile respiratoryillness per calendarweek').
The epidemic periodwas from January 8 toMarch 17, 1984. Viralstrains isolated fromcases were A/Victoria/7/83 (H1N1) and B/USSR/100/83. TheWHO recommendedformula for that yearwas: A/Brazil/11/78, A/Philippines/2/82 and ofB/Singapore/222/79.
V.Dem
icheli
etal./
Vaccin
e18(2000)957±1030
994

Keitel 2
Keitel, W.A., Cate,T.R. and Couch,R.B. E�cacy ofsequential annualvaccination with inac-tivated in¯uenza virusvaccine. AmericanJournal ofEpidemiology 1988,127, 353±364.
See Keitel 1 See Keitel 1 Data extracted andloaded: Keitel 2:1984±85 outbreak;trivalent inactivated,killed whole, intra-muscularly adminis-tered, commercialvaccine against pla-cebo; 456 treated, 241placebo Commercialvaccine for fall of1984 contained 15 mgof hemagglutinin ofeach of followingin¯uenza strains: A/Philippines/2/82(H3N2), A/Chile/1/83(H1N1) and B/USSR/100/83.Placebo was sterilesaline for injection.
See Keitel 1 Epidemic period wasfrom January 6 toMarch 9, 1985. Theviral strain isolated fromcases was an A/Philippines/2/82(H3N2)-like. The WHOrecommended formulafor that year was: A/Philippines/2/82(H3N2), A/Chile/1/83(H1N1) and B/USSR/100/83. The vaccine wasconsidered to be rec-ommended and match-ing the circulatingstrain.
Mair 1
Mair, H.J., Sansome,D.A.W. and Tillett,H.E. A controlledtrial of inactivatedmonovalent in¯uenzaA vaccines in generalpractice. Journal ofHygiene 1974, 73,317±327.
UK CCT, with allo-cation by day of birth.Double blind. Comparestwo monovalent, inacti-vated, intramuscularlyadministered in¯uenzaA vaccines against amonovalent inactivatedin¯uenza B vaccine usedas placebo.
507 volunteers,patients from generalpractices. Completefollow up wasobtained for 465 ofthem. Three armswhich counted, re-spectively, 141,169and 155 subjects.
Data extracted andloaded: Mair 1:monovalent in¯uenzaA matching circulat-ing strain (N = 85)against monovalent B(N= 155). Vaccinestrains were respect-ively: A/England/42/72 (H3N2) (recombi-nant XPR8, 600 IU),B/Victoria/98926/70(400 IU).
Clinical and laboratorycon®rmed cases andadverse e�ects. Illnessde®ned as `any symp-toms of in¯uenza'.Laboratory con®rmationby in¯uenza virus iso-lation from throat swabsor four-fold rise in anti-body titre between acuteand convalescent sera.Local adverse e�ectswere mild (slight swel-ling, aching) or severe(painful, red and swollenarm). Systemic adversee�ects were mild (slightpyrexia, mild aching ofback and limbs) orsevere (in¯uenza-likesymptoms).
Trial was conductedduring the 1972±73in¯uenza season. Thefollow up period lasted13 weeks. Authors don'tspecify the length of theepidemic period. Viralstrains isolated fromcases was A/England.The recommended for-mula for that year in theUSA was A2/Aichi/2/68,B/Massachusetts/1/72.
V.Dem
icheli
etal./
Vaccin
e18(2000)957±1030
995

Mair 2
Mair, H.J., Sansome,D.A.W. and Tillett,H.E. A controlledtrial of inactivatedmonovalent in¯uenzaA vaccines in generalpractice. Journal ofHygiene 1974, 73,317±327.
See Mair 1 See Mair 1 Data extracted andloaded: Mair 2:monovalent in¯uenzaA matching circulat-ing strain (N = 84)against monovalent A(N= 141). Vaccinestrains were respect-ively: A/England/42/72 (H3N2) (recombi-nant XPR8, 600 IU),A/Hong Kong/1/68(H3N2) (recombinantX31, 600 IU).
See Mair 1 See Mair 1
Mair 3
Mair, H.J., Sansome,D.A.W. and Tillett,H.E. A controlledtrial of inactivatedmonovalent in¯uenzaA vaccines in generalpractice. Journal ofHygiene 1974, 73,317±327.
See Mair 1 See Mair 1 Data extracted andloaded: Mair 3:monovalent rec-ommended in¯uenzaA strain (N= 71)against monovalent B(N= 155). Vaccinestrains were respect-ively: A/Hong Kong/1/68 (H3N2) (recom-binant X31, 600 IU),B/Victoria/98926/70(400 IU).
See Mair 1 See Mair 1
Mair 4
Mair, H.J., Sansome,D.A.W. and Tillett,H.E. A controlledtrial of inactivatedmonovalent in¯uenzaA vaccines in generalpractice. Journal ofHygiene 1974, 73,317±327.
See Mair 1 See Mair 1 Data extracted andloaded: Mair 4:monovalent rec-ommended in¯uenzaA strain (N= 70)against monovalent A(N= 169). Vaccinestrains were respect-ively: A/Hong Kong/1/68 (H3N2) (recom-binant X31, 600 IU),A/England/42/72(H3N2) (recombinantXPR8, 600 IU).
See Mair 1 See Mair 1
V.Dem
icheli
etal./
Vaccin
e18(2000)957±1030
996

Maynard
Maynard, J.E., Dull,H.B., Hanson, M.L.,et al. Evaluation ofmonovalent and poly-valent in¯uenza vac-cines during anepidemic of type A2and B in¯uenza.American Journal ofEpidemiology 1968,87, 148±157.
Randomised, not pla-cebo controlled Alaskantrial with no of blinding,comparing a monovalentinactivated in¯uenza Aand a monovalent inac-tivated in¯uenza B vac-cine against thestandard commercialpolyvalent AB formu-lation. All vaccinesadministered subcu-taneously.
502 volunteer stu-dents 14±18 year-old,not previously immu-nised. 488 completedthe study.
Data extracted andloaded: Standardcommercial poly-valent AB formu-lation (N = 159)against monovalent B(N= 158) polyvalentformula: A/PR8 100CCA, A1/AnnArbor/1/57 100 CCA,A2/Jap/170/62 100CCA, A2/Taiwan/1/64 100 CCA, B/Maryland/1/59 200CCA. monovalent B:B/Maryland/1/59 400CCA
Clinical and laboratorycon®rmed cases.Adverse e�ects not con-sidered. A case wasde®ned `in¯uenza-like'with three of: fever,cough, headache, myal-gia, sore throat.Serological studies weredone on one-third ran-dom sample from eachof the three groups.Laboratory con®rmationseen by four-fold rise inantibody titre betweenpost-vaccination andpost-epidemic sera.Throat swabs and acuteconvalescent sera werecollected from a few illindividuals to con®rmcirculating in¯uenzavirus. Attack rates byvaccine groups werereported for clinical ill-ness during the wholeepidemic period.
Protective e�cacy ofvaccines was evaluatedduring a simultaneousoutbreak of in¯uenza Aand B virus strains,peaking in February andMarch 1966 respectively.Epidemic period fromFebruary 17 to March18 de®ned by increase inabsenteeism. Circulatingstrains were B/Alaska/1/66 and an A2 virus;both had only minorantigenic variation fromB/Maryland and A2/Taiwan contained in thevaccines. Recommendedformula that year in theUSA: A/PR8, A1/AnnArbor/1/57, A2/Jap/170/62, A2/Taiwan/1/64, B/Maryland/1/59 andcompletely matched thepolyvalent vaccine.
V.Dem
icheli
etal./
Vaccin
e18(2000)957±1030
997
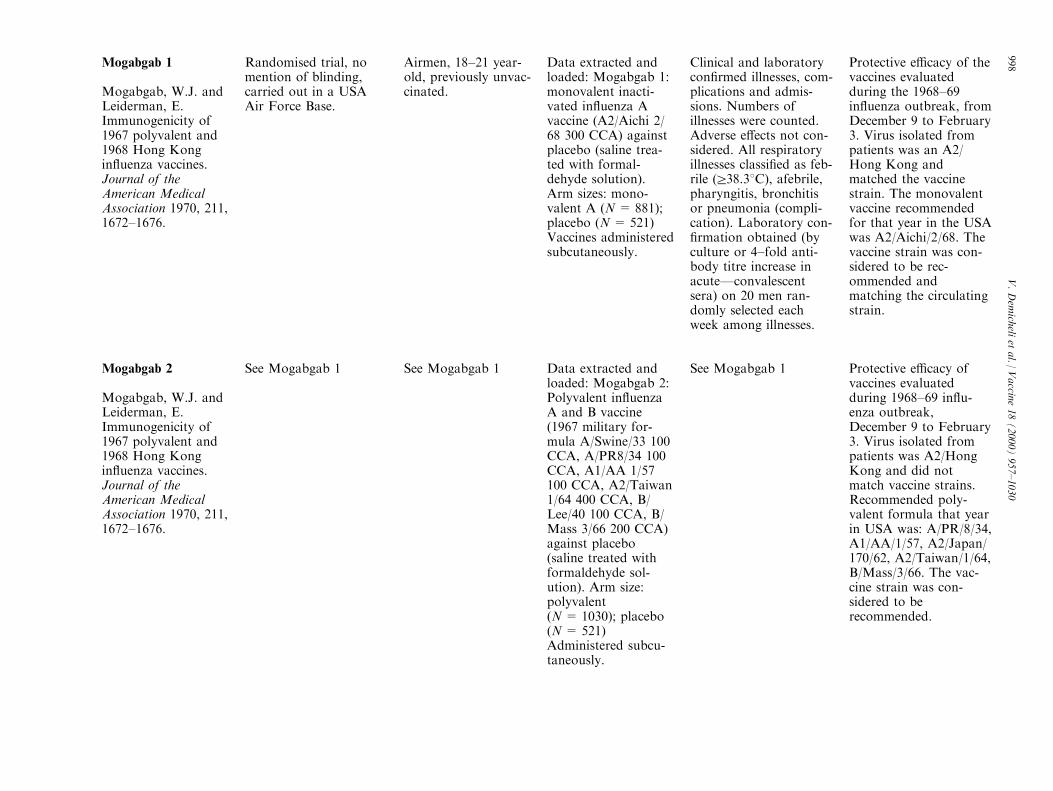
Mogabgab 1
Mogabgab, W.J. andLeiderman, E.Immunogenicity of1967 polyvalent and1968 Hong Kongin¯uenza vaccines.Journal of theAmerican MedicalAssociation 1970, 211,1672±1676.
Randomised trial, nomention of blinding,carried out in a USAAir Force Base.
Airmen, 18±21 year-old, previously unvac-cinated.
Data extracted andloaded: Mogabgab 1:monovalent inacti-vated in¯uenza Avaccine (A2/Aichi 2/68 300 CCA) againstplacebo (saline trea-ted with formal-dehyde solution).Arm sizes: mono-valent A (N = 881);placebo (N = 521)Vaccines administeredsubcutaneously.
Clinical and laboratorycon®rmed illnesses, com-plications and admis-sions. Numbers ofillnesses were counted.Adverse e�ects not con-sidered. All respiratoryillnesses classi®ed as feb-rile (r38.38C), afebrile,pharyngitis, bronchitisor pneumonia (compli-cation). Laboratory con-®rmation obtained (byculture or 4±fold anti-body titre increase inacuteÐconvalescentsera) on 20 men ran-domly selected eachweek among illnesses.
Protective e�cacy of thevaccines evaluatedduring the 1968±69in¯uenza outbreak, fromDecember 9 to February3. Virus isolated frompatients was an A2/Hong Kong andmatched the vaccinestrain. The monovalentvaccine recommendedfor that year in the USAwas A2/Aichi/2/68. Thevaccine strain was con-sidered to be rec-ommended andmatching the circulatingstrain.
Mogabgab 2
Mogabgab, W.J. andLeiderman, E.Immunogenicity of1967 polyvalent and1968 Hong Kongin¯uenza vaccines.Journal of theAmerican MedicalAssociation 1970, 211,1672±1676.
See Mogabgab 1 See Mogabgab 1 Data extracted andloaded: Mogabgab 2:Polyvalent in¯uenzaA and B vaccine(1967 military for-mula A/Swine/33 100CCA, A/PR8/34 100CCA, A1/AA 1/57100 CCA, A2/Taiwan1/64 400 CCA, B/Lee/40 100 CCA, B/Mass 3/66 200 CCA)against placebo(saline treated withformaldehyde sol-ution). Arm size:polyvalent(N= 1030); placebo(N= 521)Administered subcu-taneously.
See Mogabgab 1 Protective e�cacy ofvaccines evaluatedduring 1968±69 in¯u-enza outbreak,December 9 to February3. Virus isolated frompatients was A2/HongKong and did notmatch vaccine strains.Recommended poly-valent formula that yearin USA was: A/PR/8/34,A1/AA/1/57, A2/Japan/170/62, A2/Taiwan/1/64,B/Mass/3/66. The vac-cine strain was con-sidered to berecommended.
V.Dem
icheli
etal./
Vaccin
e18(2000)957±1030
998

Monto
Monto, A.S.,DeWolfe Miller, F.and Maassab, H.F.Evaluation of an atte-nuated, cold recombi-nant in¯uenza B virusvaccine. Journal ofInfectious Diseases1982, 145, 57±64.
Randomised, singleblind, placebo controlledUSA trial. Subjects weregiven a serial numberpreviously assigned ran-domly by a code to thevaccine or placebogroup.
306 volunteer univer-sity students. 154 par-ticipants in vaccinearm, placebo arm152. 144 and 140 stu-dents respectivelycompleted study.
Monovalent, live atte-nuated, intranasalin¯uenza B vaccineagainst placebo (vac-cine diluent). Thevaccine virus, coldrecombinant, wasproduced by recom-bining the attenuatedB/Ann Arbor/1/66with a wild strain B/Hong Kong/8/73.
Clinical and laboratorycon®rmed cases andadverse e�ects. Patientssu�ered a respiratory ill-ness if they hadr2 res-piratory symptoms.Cases were laboratorycon®rmed by an increasein antibody titre against3 in¯uenza B virus anti-gens, i.e. if there was afour-fold increase froman initial sample.Adverse e�ects werede®ned as sore throat,coryza, hoarseness,cough, muscle aches,temperature >100 Foccurred during the ®rstthree days after vacci-nation.
Protective e�cacy ofvaccine evaluated during1979±80 outbreak; epi-demic period de®ned by®rst and last isolation(February 11±March18). Circulating virusstrains were B/Singapore/79±like andB/Buenos Aires/79±like,antigenically di�erentfrom vaccine. WHO rec-ommended formula thatyear: A/USSR/90/77 orA/Brazil/11/78, A/Texas/1/77, B/Hongkong/5/72, and did notmatch the strains usedto produce the recombi-nant virus.
Nichol
Nichol, K.L., Lind,A., Margolis, K.L. etal. The e�ectivenessof vaccination againstin¯uenza in healthy,working adults. NewEngland Journal ofMedicine 1995, 333,889±893.
USA RCT on full-timeemployed volunteers.Randomisation per-formed according to acomputer-generated ran-domisation schedule.Double blinding wasensured by preloaded,coded identical lookingsyringes.
849 healthy volun-teers, 18±64 years;841 had follow upinterviews to ascer-tain side e�ects.Complete follow updata were obtainedfor 416 of 422 pla-cebo recipients and409 of 419 vaccinerecipients.
A subvirion, trivalent,parenteral in¯uenzaA and B vaccine wascompared against pla-cebo (vaccine dilu-ent). Vaccine strainswere A/Texas/36/91,A/Shangdong/9/93,B/Panama/45/90.
Clinical cases symptomsde®ned, WDL, andadverse e�ects. Patientswere de®ned as cases ifthey hadrone upperrespiratory illness (asore throat associatedwith fever or cough last-ingr24 h). Localadverse e�ects werede®ned as arm soreness.Systemic adverse e�ectswere de®ned as fever,tiredness, feeling underthe weather, muscleache, headache.
Trial was conductedduring the 1994±95in¯uenza season. Thefollow up period wasde®ned as 1 December,1994 to 31 March, 1995(the in¯uenza season).The USA recommendedformula for that yearwas: A/Texas/36/91, A/Shangdong/9/93, B/Panama/45/90.
V.Dem
icheli
etal./
Vaccin
e18(2000)957±1030
999
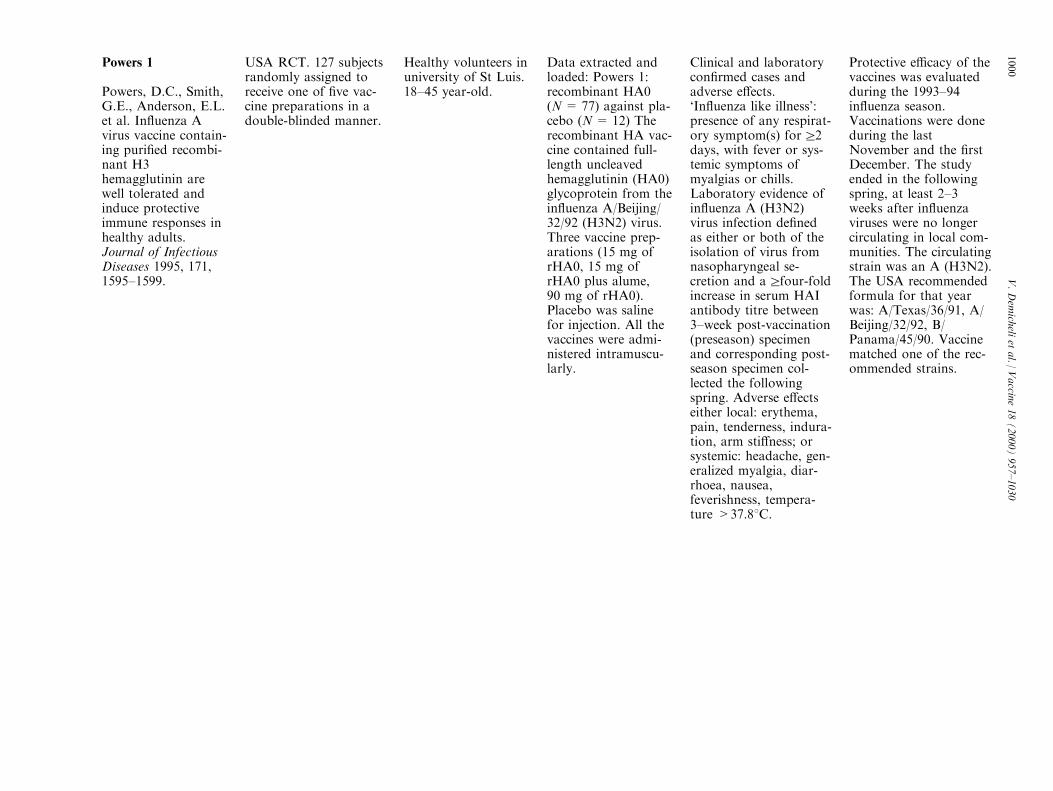
Powers 1
Powers, D.C., Smith,G.E., Anderson, E.L.et al. In¯uenza Avirus vaccine contain-ing puri®ed recombi-nant H3hemagglutinin arewell tolerated andinduce protectiveimmune responses inhealthy adults.Journal of InfectiousDiseases 1995, 171,1595±1599.
USA RCT. 127 subjectsrandomly assigned toreceive one of ®ve vac-cine preparations in adouble-blinded manner.
Healthy volunteers inuniversity of St Luis.18±45 year-old.
Data extracted andloaded: Powers 1:recombinant HA0(N= 77) against pla-cebo (N = 12) Therecombinant HA vac-cine contained full-length uncleavedhemagglutinin (HA0)glycoprotein from thein¯uenza A/Beijing/32/92 (H3N2) virus.Three vaccine prep-arations (15 mg ofrHA0, 15 mg ofrHA0 plus alume,90 mg of rHA0).Placebo was salinefor injection. All thevaccines were admi-nistered intramuscu-larly.
Clinical and laboratorycon®rmed cases andadverse e�ects.`In¯uenza like illness':presence of any respirat-ory symptom(s) forr2days, with fever or sys-temic symptoms ofmyalgias or chills.Laboratory evidence ofin¯uenza A (H3N2)virus infection de®nedas either or both of theisolation of virus fromnasopharyngeal se-cretion and arfour-foldincrease in serum HAIantibody titre between3±week post-vaccination(preseason) specimenand corresponding post-season specimen col-lected the followingspring. Adverse e�ectseither local: erythema,pain, tenderness, indura-tion, arm sti�ness; orsystemic: headache, gen-eralized myalgia, diar-rhoea, nausea,feverishness, tempera-ture >37.88C.
Protective e�cacy of thevaccines was evaluatedduring the 1993±94in¯uenza season.Vaccinations were doneduring the lastNovember and the ®rstDecember. The studyended in the followingspring, at least 2±3weeks after in¯uenzaviruses were no longercirculating in local com-munities. The circulatingstrain was an A (H3N2).The USA recommendedformula for that yearwas: A/Texas/36/91, A/Beijing/32/92, B/Panama/45/90. Vaccinematched one of the rec-ommended strains.
V.Dem
icheli
etal./
Vaccin
e18(2000)957±1030
1000

Powers 2
Powers, D.C., Smith,G.E., Anderson, E.L.et al. In¯uenza Avirus vaccine contain-ing puri®ed recombi-nant H3hemagglutinin arewell tolerated andinduce protectiveimmune responses inhealthy adults.Journal of InfectiousDiseases 1995, 171,1595±1599.
See Powers 1 See Powers 1 Data extracted andloaded: Licensed tri-valent (N = 26)against placebo(N= 12) Licensedsubvirion trivalentAB vaccine contained15 mg/dose of eachthe HAs from in¯u-enza A/Texas/36/91(H1N1), A/Beijing/32/92 (H3N2) and B/Panama/45/90 virusesPlacebo was salinefor injection. All thevaccines were admi-nistered intramuscu-larly.
See Powers 1 See Powers I. Vaccinematched the rec-ommended formula.
Rytel
Rytel, M.W., Jakson,L.J., Niebojewski,R.A. et al. Field trialof live attenuatedin¯uenza A/B(`Alice'/R-75) vaccine.American Journal ofEpidemiology 1977,105, 49±55.
USA RCT, single blind.Subjects randomlyassigned to three sub-groups.
Three subgroupsreceived either twodoses of the vaccine(N = 47), one dose ofvaccine and one doseof placebo (N = 48)or two doses of pla-cebo (N = 48) 14days apart.
E�cacy of a single ordouble doses a liveattenuated, bivalent,intranasal in¯uenza A(containing 10 exp7,2EID50) and B (con-taining 10 exp7,8EID50 ) vaccine wastested against placebo(5% sucrose).Vaccine virus strainswere A/England/42/72 (H3N2) and B/Hong Kong/5/72.
Laboratory con®rmedcases (presence of a ¯u-like illness:rthree symp-toms of acute respirat-ory disease andtemperature greater then37.2; and virus isolationand/or four fold rise inantibody titre in seraobtained at 30 days and6 months following im-munisation) and adversee�ects (URI symptomsand cough; subdividedinto moderate andsevere). No generaladverse e�ects de®nitiongiven (again distin-guished among moder-ate and severe).
Conducted during the1974±75 in¯uenza sea-son in which a twomonths epidemic periodis described by theauthors with no refer-ence to a de®nition. Thefollow-up period of thestudy was genericallyde®ned as `winter andspring', lasted sixmonths and comprisedthe epidemic period. Thecirculating strain was A/PortChalmers/1/73(H3N2) and presented aslight antigenic driftwhen compared withvaccine strain.
V.Dem
icheli
etal./
Vaccin
e18(2000)957±1030
1001

Sumarokow
Sumarokow, A.A.,Popov, V.F.,Nefedova, L.A. et al.A study of live in¯u-enza vaccines in acontrolled trial.Zhumal MikrobiologiiEpidemiologiiImmunobiologii 1971,48, 46±52.
Russian ®eld trial.Vaccinations were car-ried out using codedpreparation.
76150 persons. A ®rststudy group of 36665children 3±12 yearsold. A second studygroup counted 39485subjects aged 13±25.Only data regardingthe latter wereextracted and loaded.
Compared two livevaccines against pla-cebo. Strains used inthe vaccines were notreported. Study armswere the following:Ðallantoic intranasalvaccine; N= 9945Ðplacebo; N = 9942Ðtissue vaccine for oraladministration;N = 9817Ðplacebo;N = 9781 Only datafrom the ®rst twogroups were includedin the meta-analysis.
Clinical and laboratorycon®rmed cases, deaths,severity. Clinical out-comes were all acute res-piratory infections.Laboratory con®rmationof illness was obtainedby virus isolation ordemonstration of sero-conversion. Bronchitis,opti and pneumoniawere considered as com-plications.
Outcomes were detectedduring the entire periodof in¯uenza outbreak.Epidemic period de®nedas the period of highestin¯uenza morbidity,lasting 11 weeks fromthe 22January to the 10April. Virus circulatingwas A2/Hong Kong/68,and did not matched thevaccine strains.
Tannock
Tannock, G.A.,Bryce, D.A., Hensley,M.J. et al. Responsesto one or two dosesof a deoxycholatesubunit in¯uenza vac-cine in a primedpopulation. Vaccine1984, 2, 100±105.
Australian CCT doubleblind, placebo con-trolled,. Volunteers allo-cated by alternation toreceive one or two dosesof a trivalent subunitvaccine or placebo.
88 volunteers, aged16±64, sta� from aNewcastle Hospitaland CommonwealthSteel Corporation. 46volunteers assigned toeach treatment; onlyindividuals receivingexpected doses ofvaccine consideredpart of study (29, 27and 32 for eachgroup). Complete fol-low up data wereobtained for 18, 19,and 20 subjects re-spectively.
Trivalent vaccine (A/Brazil/11/78, A/Bangkok/1/79, B/Singapore/222/797 mg each) againstplacebo (sterilesaline). Vaccine orplacebo was adminis-tered by the subcu-taneous route.
Laboratory con®rmedcases (respiratory illness,retrospectively reported,was associated with a 4±fold antibody titreincrease between post-vaccination and postepi-demic sera) and adversee�ects. Reactions to vac-cination were local reac-tion: redness, swelling,warmth or irritation;local pain: pain on con-tact, pain with pressure,continuous pain, orrestriction of arm move-ment; systemic reaction:fever, chills, sweating,drowsiness or insomnia.
Follow up period of 20weeks and comprisedthe epidemic period(year 1981) Viral strainisolated from patientswas A/Bangkok/1/79.The recommended for-mula for that year was:A/Brazil/11/78, A/Bangkok/1/79, B/Singapore/222/79
V.Dem
icheli
etal./
Vaccin
e18(2000)957±1030
1002
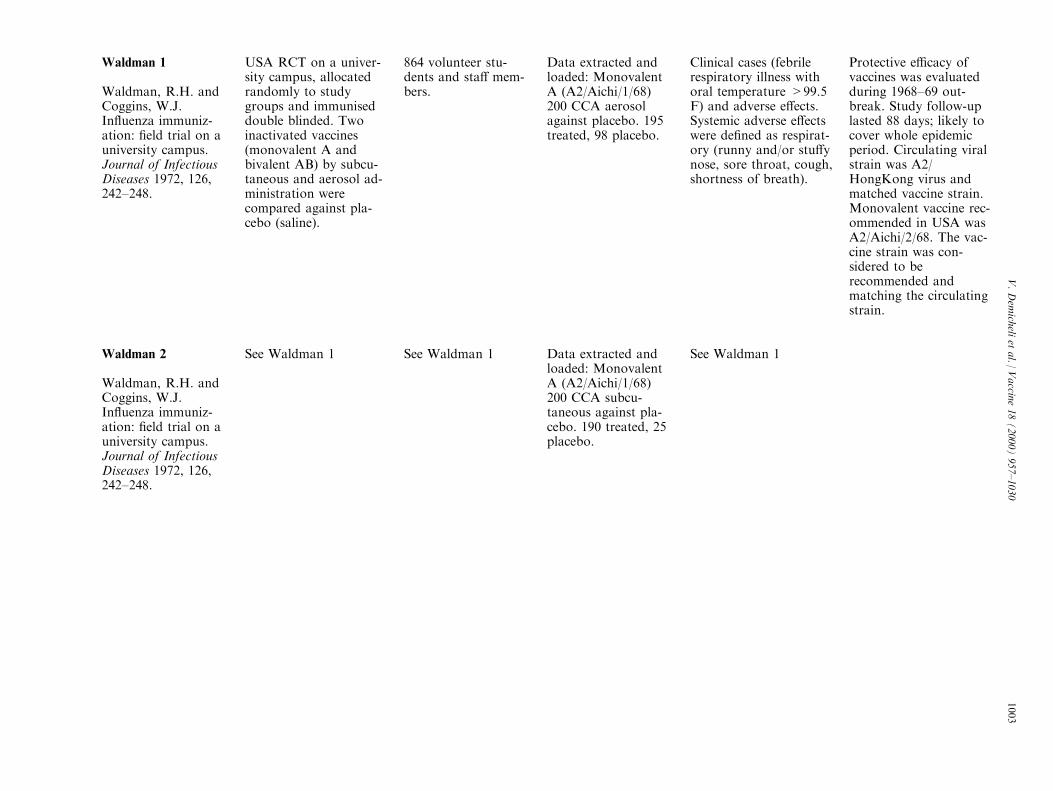
Waldman 1
Waldman, R.H. andCoggins, W.J.In¯uenza immuniz-ation: ®eld trial on auniversity campus.Journal of InfectiousDiseases 1972, 126,242±248.
USA RCT on a univer-sity campus, allocatedrandomly to studygroups and immuniseddouble blinded. Twoinactivated vaccines(monovalent A andbivalent AB) by subcu-taneous and aerosol ad-ministration werecompared against pla-cebo (saline).
864 volunteer stu-dents and sta� mem-bers.
Data extracted andloaded: MonovalentA (A2/Aichi/1/68)200 CCA aerosolagainst placebo. 195treated, 98 placebo.
Clinical cases (febrilerespiratory illness withoral temperature >99.5F) and adverse e�ects.Systemic adverse e�ectswere de®ned as respirat-ory (runny and/or stu�ynose, sore throat, cough,shortness of breath).
Protective e�cacy ofvaccines was evaluatedduring 1968±69 out-break. Study follow-uplasted 88 days; likely tocover whole epidemicperiod. Circulating viralstrain was A2/HongKong virus andmatched vaccine strain.Monovalent vaccine rec-ommended in USA wasA2/Aichi/2/68. The vac-cine strain was con-sidered to berecommended andmatching the circulatingstrain.
Waldman 2
Waldman, R.H. andCoggins, W.J.In¯uenza immuniz-ation: ®eld trial on auniversity campus.Journal of InfectiousDiseases 1972, 126,242±248.
See Waldman 1 See Waldman 1 Data extracted andloaded: MonovalentA (A2/Aichi/1/68)200 CCA subcu-taneous against pla-cebo. 190 treated, 25placebo.
See Waldman 1
V.Dem
icheli
etal./
Vaccin
e18(2000)957±1030
1003

Waldman 3
Waldman, R.H. andCoggins, W.J.In¯uenza immuniz-ation: ®eld trial on auniversity campus.Journal of InfectiousDiseases 1972, 126,242±248.
See Waldman 1 See Waldman 1 Data extracted andloaded: Bivalent AB(A2/Japan/170/62 150CCA, A2/Taiwan/1/64 150 CCA and B/Massachusttes/3/66200 CCA) aerosolagainst placebo. 194treated, 25 placebo.
See Waldman 1 Protective e�cacy ofvaccines evaluatedduring 1968±69 out-break. Follow-up lasted88 days and is likely tohave covered the wholeepidemic period.Circulating viral strainwas A2/HongKongvirus. Recommendedpolyvalent formula inUSA was: A/PR/8/34,A1/AA/1/57, A2/Japan/170/62, A2/Taiwan/1/64,B/Mass/3/66 The vac-cine strain was con-sidered to berecommended.
Waldman 4
Waldman, R.H. andCoggins, W.J.In¯uenza immuniz-ation: ®eld trial on auniversity campus.Journal of InfectiousDiseases 1972, 126,242±248.
See Waldman 1 See Waldman 1 Data extracted andloaded: Bivalent AB(A2/Japan/170/62 150CCA, A2/Taiwan/1/64 150 CCA and B/Massachusttes/3/66200 CCA) subcu-taneous against pla-cebo. 187 treated and23 placebo.
See Waldman 1 See Waldman 3
V.Dem
icheli
etal./
Vaccin
e18(2000)957±1030
1004
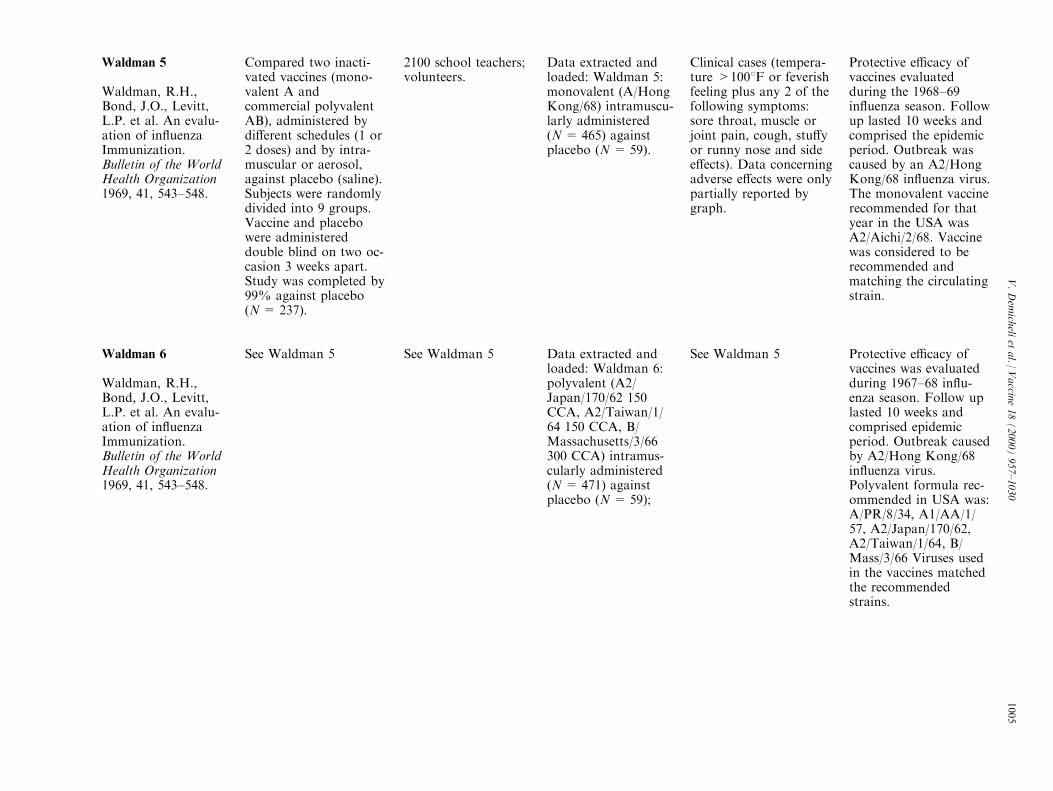
Waldman 5
Waldman, R.H.,Bond, J.O., Levitt,L.P. et al. An evalu-ation of in¯uenzaImmunization.Bulletin of the WorldHealth Organization1969, 41, 543±548.
Compared two inacti-vated vaccines (mono-valent A andcommercial polyvalentAB), administered bydi�erent schedules (1 or2 doses) and by intra-muscular or aerosol,against placebo (saline).Subjects were randomlydivided into 9 groups.Vaccine and placebowere administereddouble blind on two oc-casion 3 weeks apart.Study was completed by99% against placebo(N = 237).
2100 school teachers;volunteers.
Data extracted andloaded: Waldman 5:monovalent (A/HongKong/68) intramuscu-larly administered(N= 465) againstplacebo (N = 59).
Clinical cases (tempera-ture >1008F or feverishfeeling plus any 2 of thefollowing symptoms:sore throat, muscle orjoint pain, cough, stu�yor runny nose and sidee�ects). Data concerningadverse e�ects were onlypartially reported bygraph.
Protective e�cacy ofvaccines evaluatedduring the 1968±69in¯uenza season. Followup lasted 10 weeks andcomprised the epidemicperiod. Outbreak wascaused by an A2/HongKong/68 in¯uenza virus.The monovalent vaccinerecommended for thatyear in the USA wasA2/Aichi/2/68. Vaccinewas considered to berecommended andmatching the circulatingstrain.
Waldman 6
Waldman, R.H.,Bond, J.O., Levitt,L.P. et al. An evalu-ation of in¯uenzaImmunization.Bulletin of the WorldHealth Organization1969, 41, 543±548.
See Waldman 5 See Waldman 5 Data extracted andloaded: Waldman 6:polyvalent (A2/Japan/170/62 150CCA, A2/Taiwan/1/64 150 CCA, B/Massachusetts/3/66300 CCA) intramus-cularly administered(N= 471) againstplacebo (N = 59);
See Waldman 5 Protective e�cacy ofvaccines was evaluatedduring 1967±68 in¯u-enza season. Follow uplasted 10 weeks andcomprised epidemicperiod. Outbreak causedby A2/Hong Kong/68in¯uenza virus.Polyvalent formula rec-ommended in USA was:A/PR/8/34, A1/AA/1/57, A2/Japan/170/62,A2/Taiwan/1/64, B/Mass/3/66 Viruses usedin the vaccines matchedthe recommendedstrains.
V.Dem
icheli
etal./
Vaccin
e18(2000)957±1030
1005

Waldman 7
Waldman, R.H.,Bond, J.O., Levitt,L.P. et al. An evalu-ation of in¯uenzaImmunization.Bulletin of the WorldHealth Organization1969, 41, 543±548.
See Waldman 5 See Waldman 5 Data extracted andloaded: Waldman 7:monovalent A/HongKong/68 aerosoladministered(N= 479) againstplacebo (N = 59);
See Waldman 5 See Waldman 5
Waldman 8
Waldman, R.H.,Bond, J.O., Levitt,L.P. et al. An evalu-ation of in¯uenzaImmunization.Bulletin of the WorldHealth Organization1969, 41, 543±548.
See Waldman 5 See Waldman 5 Data extracted andloaded: Waldman 8:polyvalent (A2/Japan/170/62 150CCA, A2/Taiwan/1/64 150 CCA, B/Massachusetts/3/66300 CCA) aerosoladministered(N= 471) againstplacebo (N = 59);
See Waldman 5 See Waldman 7
V.Dem
icheli
etal./
Vaccin
e18(2000)957±1030
1006
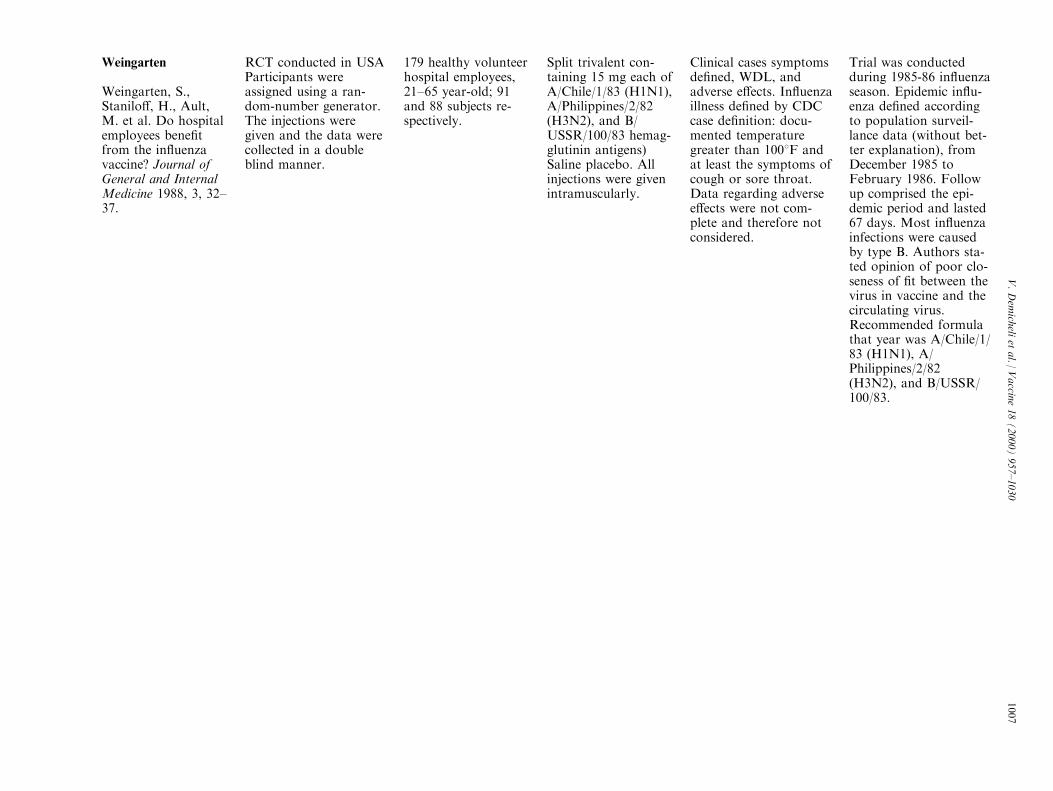
Weingarten
Weingarten, S.,Stanilo�, H., Ault,M. et al. Do hospitalemployees bene®tfrom the in¯uenzavaccine? Journal ofGeneral and InternalMedicine 1988, 3, 32±37.
RCT conducted in USAParticipants wereassigned using a ran-dom-number generator.The injections weregiven and the data werecollected in a doubleblind manner.
179 healthy volunteerhospital employees,21±65 year-old; 91and 88 subjects re-spectively.
Split trivalent con-taining 15 mg each ofA/Chile/1/83 (H1N1),A/Philippines/2/82(H3N2), and B/USSR/100/83 hemag-glutinin antigens)Saline placebo. Allinjections were givenintramuscularly.
Clinical cases symptomsde®ned, WDL, andadverse e�ects. In¯uenzaillness de®ned by CDCcase de®nition: docu-mented temperaturegreater than 1008F andat least the symptoms ofcough or sore throat.Data regarding adversee�ects were not com-plete and therefore notconsidered.
Trial was conductedduring 1985-86 in¯uenzaseason. Epidemic in¯u-enza de®ned accordingto population surveil-lance data (without bet-ter explanation), fromDecember 1985 toFebruary 1986. Followup comprised the epi-demic period and lasted67 days. Most in¯uenzainfections were causedby type B. Authors sta-ted opinion of poor clo-seness of ®t between thevirus in vaccine and thecirculating virus.Recommended formulathat year was A/Chile/1/83 (H1N1), A/Philippines/2/82(H3N2), and B/USSR/100/83.
V.Dem
icheli
etal./
Vaccin
e18(2000)957±1030
1007
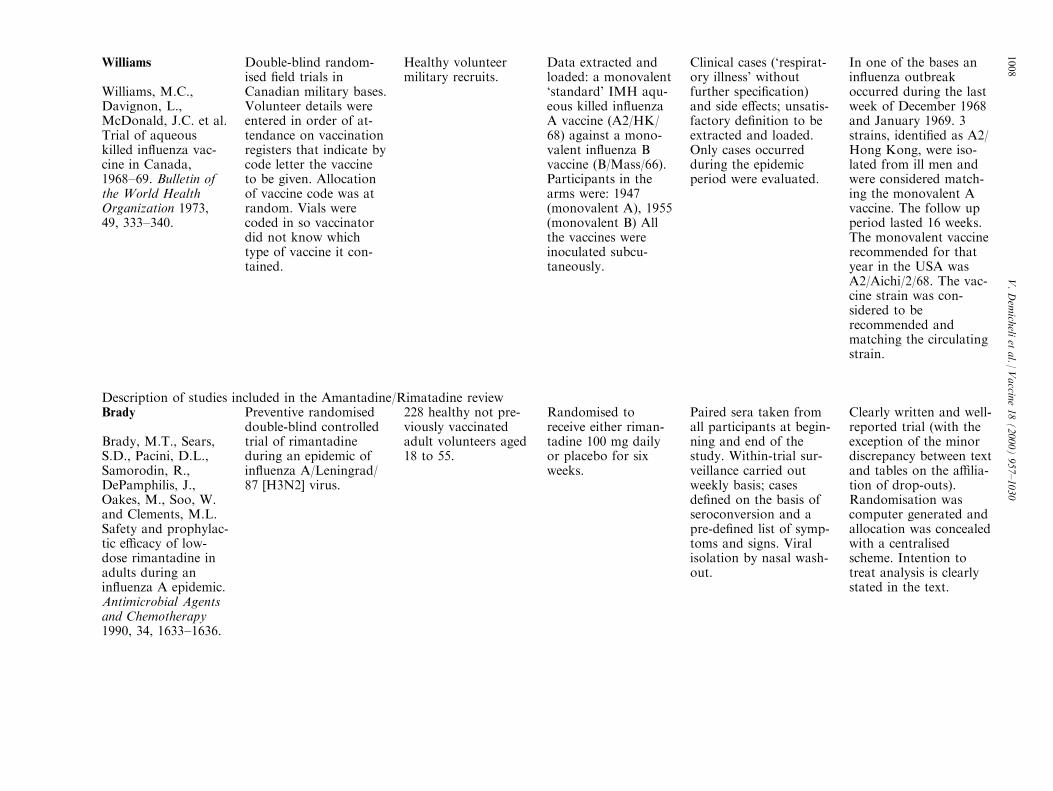
Williams
Williams, M.C.,Davignon, L.,McDonald, J.C. et al.Trial of aqueouskilled in¯uenza vac-cine in Canada,1968±69. Bulletin ofthe World HealthOrganization 1973,49, 333±340.
Double-blind random-ised ®eld trials inCanadian military bases.Volunteer details wereentered in order of at-tendance on vaccinationregisters that indicate bycode letter the vaccineto be given. Allocationof vaccine code was atrandom. Vials werecoded in so vaccinatordid not know whichtype of vaccine it con-tained.
Healthy volunteermilitary recruits.
Data extracted andloaded: a monovalent`standard' IMH aqu-eous killed in¯uenzaA vaccine (A2/HK/68) against a mono-valent in¯uenza Bvaccine (B/Mass/66).Participants in thearms were: 1947(monovalent A), 1955(monovalent B) Allthe vaccines wereinoculated subcu-taneously.
Clinical cases (`respirat-ory illness' withoutfurther speci®cation)and side e�ects; unsatis-factory de®nition to beextracted and loaded.Only cases occurredduring the epidemicperiod were evaluated.
In one of the bases anin¯uenza outbreakoccurred during the lastweek of December 1968and January 1969. 3strains, identi®ed as A2/Hong Kong, were iso-lated from ill men andwere considered match-ing the monovalent Avaccine. The follow upperiod lasted 16 weeks.The monovalent vaccinerecommended for thatyear in the USA wasA2/Aichi/2/68. The vac-cine strain was con-sidered to berecommended andmatching the circulatingstrain.
Description of studies included in the Amantadine/Rimatadine reviewBrady
Brady, M.T., Sears,S.D., Pacini, D.L.,Samorodin, R.,DePamphilis, J.,Oakes, M., Soo, W.and Clements, M.L.Safety and prophylac-tic e�cacy of low-dose rimantadine inadults during anin¯uenza A epidemic.Antimicrobial Agentsand Chemotherapy1990, 34, 1633±1636.
Preventive randomiseddouble-blind controlledtrial of rimantadineduring an epidemic ofin¯uenza A/Leningrad/87 [H3N2] virus.
228 healthy not pre-viously vaccinatedadult volunteers aged18 to 55.
Randomised toreceive either riman-tadine 100 mg dailyor placebo for sixweeks.
Paired sera taken fromall participants at begin-ning and end of thestudy. Within-trial sur-veillance carried outweekly basis; casesde®ned on the basis ofseroconversion and apre-de®ned list of symp-toms and signs. Viralisolation by nasal wash-out.
Clearly written and well-reported trial (with theexception of the minordiscrepancy between textand tables on the a�lia-tion of drop-outs).Randomisation wascomputer generated andallocation was concealedwith a centralisedscheme. Intention totreat analysis is clearlystated in the text.
V.Dem
icheli
etal./
Vaccin
e18(2000)957±1030
1008
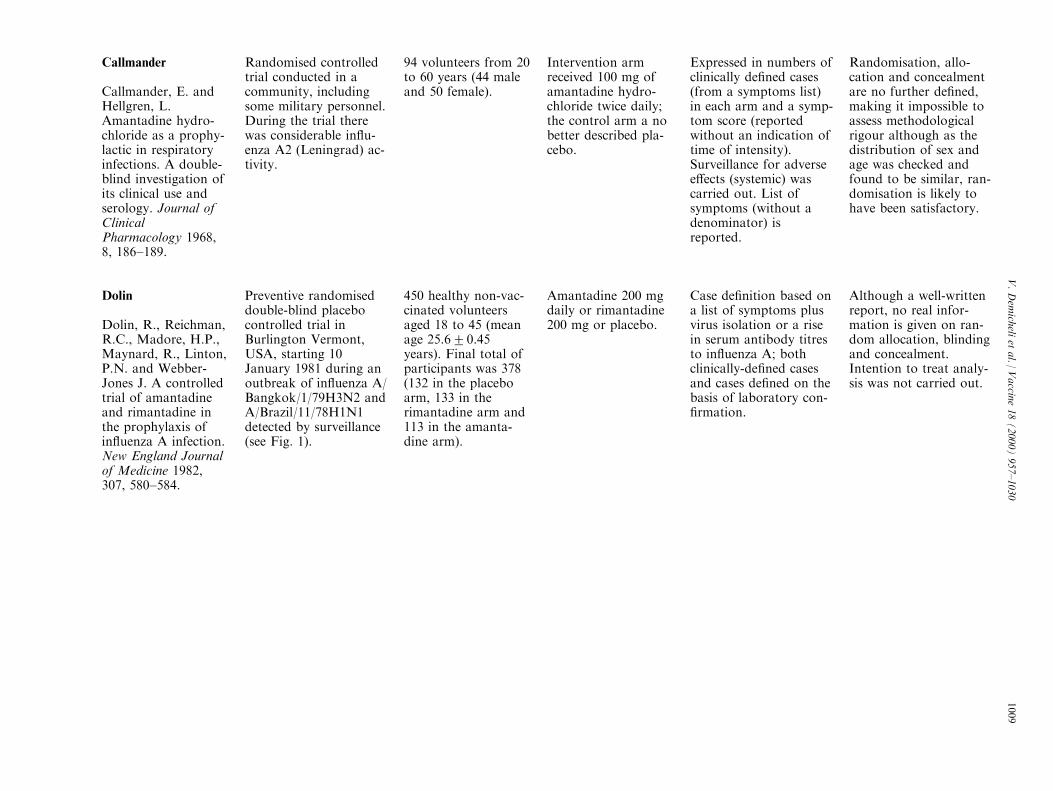
Callmander
Callmander, E. andHellgren, L.Amantadine hydro-chloride as a prophy-lactic in respiratoryinfections. A double-blind investigation ofits clinical use andserology. Journal ofClinicalPharmacology 1968,8, 186±189.
Randomised controlledtrial conducted in acommunity, includingsome military personnel.During the trial therewas considerable in¯u-enza A2 (Leningrad) ac-tivity.
94 volunteers from 20to 60 years (44 maleand 50 female).
Intervention armreceived 100 mg ofamantadine hydro-chloride twice daily;the control arm a nobetter described pla-cebo.
Expressed in numbers ofclinically de®ned cases(from a symptoms list)in each arm and a symp-tom score (reportedwithout an indication oftime of intensity).Surveillance for adversee�ects (systemic) wascarried out. List ofsymptoms (without adenominator) isreported.
Randomisation, allo-cation and concealmentare no further de®ned,making it impossible toassess methodologicalrigour although as thedistribution of sex andage was checked andfound to be similar, ran-domisation is likely tohave been satisfactory.
Dolin
Dolin, R., Reichman,R.C., Madore, H.P.,Maynard, R., Linton,P.N. and Webber-Jones J. A controlledtrial of amantadineand rimantadine inthe prophylaxis ofin¯uenza A infection.New England Journalof Medicine 1982,307, 580±584.
Preventive randomiseddouble-blind placebocontrolled trial inBurlington Vermont,USA, starting 10January 1981 during anoutbreak of in¯uenza A/Bangkok/1/79H3N2 andA/Brazil/11/78H1N1detected by surveillance(see Fig. 1).
450 healthy non-vac-cinated volunteersaged 18 to 45 (meanage 25.620.45years). Final total ofparticipants was 378(132 in the placeboarm, 133 in therimantadine arm and113 in the amanta-dine arm).
Amantadine 200 mgdaily or rimantadine200 mg or placebo.
Case de®nition based ona list of symptoms plusvirus isolation or a risein serum antibody titresto in¯uenza A; bothclinically-de®ned casesand cases de®ned on thebasis of laboratory con-®rmation.
Although a well-writtenreport, no real infor-mation is given on ran-dom allocation, blindingand concealment.Intention to treat analy-sis was not carried out.
V.Dem
icheli
etal./
Vaccin
e18(2000)957±1030
1009
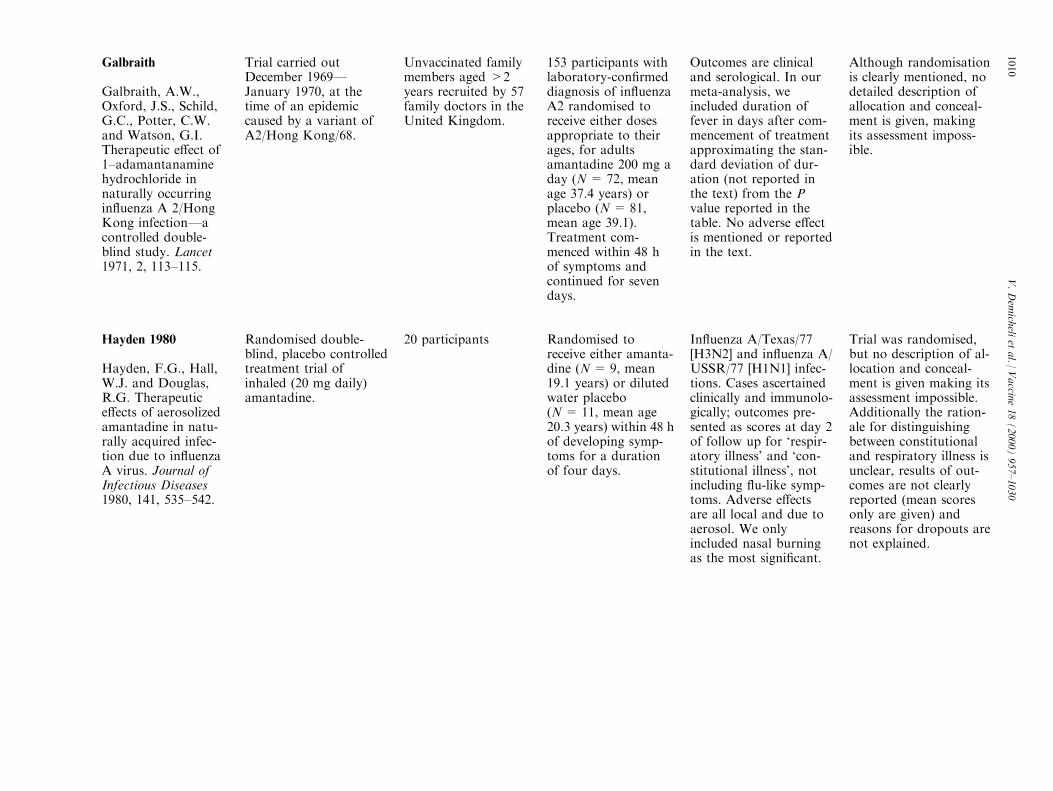
Galbraith
Galbraith, A.W.,Oxford, J.S., Schild,G.C., Potter, C.W.and Watson, G.I.Therapeutic e�ect of1±adamantanaminehydrochloride innaturally occurringin¯uenza A 2/HongKong infectionÐacontrolled double-blind study. Lancet1971, 2, 113±115.
Trial carried outDecember 1969ÐJanuary 1970, at thetime of an epidemiccaused by a variant ofA2/Hong Kong/68.
Unvaccinated familymembers aged >2years recruited by 57family doctors in theUnited Kingdom.
153 participants withlaboratory-con®rmeddiagnosis of in¯uenzaA2 randomised toreceive either dosesappropriate to theirages, for adultsamantadine 200 mg aday (N = 72, meanage 37.4 years) orplacebo (N = 81,mean age 39.1).Treatment com-menced within 48 hof symptoms andcontinued for sevendays.
Outcomes are clinicaland serological. In ourmeta-analysis, weincluded duration offever in days after com-mencement of treatmentapproximating the stan-dard deviation of dur-ation (not reported inthe text) from the Pvalue reported in thetable. No adverse e�ectis mentioned or reportedin the text.
Although randomisationis clearly mentioned, nodetailed description ofallocation and conceal-ment is given, makingits assessment imposs-ible.
Hayden 1980
Hayden, F.G., Hall,W.J. and Douglas,R.G. Therapeutice�ects of aerosolizedamantadine in natu-rally acquired infec-tion due to in¯uenzaA virus. Journal ofInfectious Diseases1980, 141, 535±542.
Randomised double-blind, placebo controlledtreatment trial ofinhaled (20 mg daily)amantadine.
20 participants Randomised toreceive either amanta-dine (N = 9, mean19.1 years) or dilutedwater placebo(N= 11, mean age20.3 years) within 48 hof developing symp-toms for a durationof four days.
In¯uenza A/Texas/77[H3N2] and in¯uenza A/USSR/77 [H1N1] infec-tions. Cases ascertainedclinically and immunolo-gically; outcomes pre-sented as scores at day 2of follow up for `respir-atory illness' and `con-stitutional illness', notincluding ¯u-like symp-toms. Adverse e�ectsare all local and due toaerosol. We onlyincluded nasal burningas the most signi®cant.
Trial was randomised,but no description of al-location and conceal-ment is given making itsassessment impossible.Additionally the ration-ale for distinguishingbetween constitutionaland respiratory illness isunclear, results of out-comes are not clearlyreported (mean scoresonly are given) andreasons for dropouts arenot explained.
V.Dem
icheli
etal./
Vaccin
e18(2000)957±1030
1010
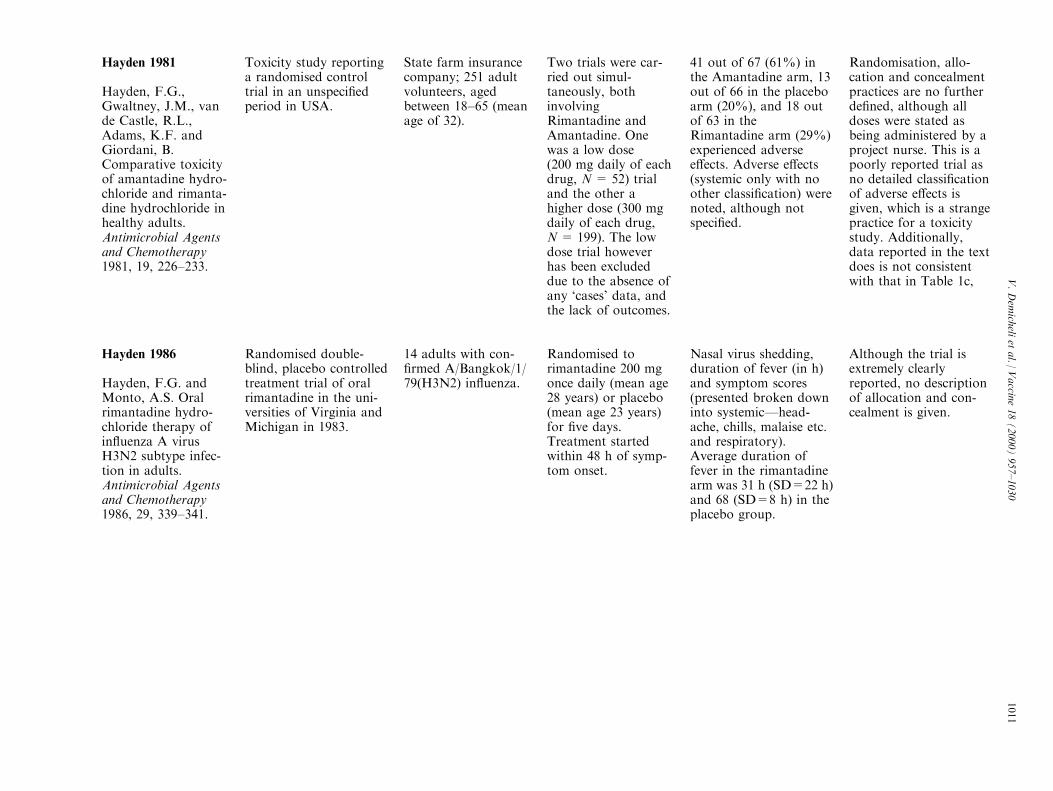
Hayden 1981
Hayden, F.G.,Gwaltney, J.M., vande Castle, R.L.,Adams, K.F. andGiordani, B.Comparative toxicityof amantadine hydro-chloride and rimanta-dine hydrochloride inhealthy adults.Antimicrobial Agentsand Chemotherapy1981, 19, 226±233.
Toxicity study reportinga randomised controltrial in an unspeci®edperiod in USA.
State farm insurancecompany; 251 adultvolunteers, agedbetween 18±65 (meanage of 32).
Two trials were car-ried out simul-taneously, bothinvolvingRimantadine andAmantadine. Onewas a low dose(200 mg daily of eachdrug, N = 52) trialand the other ahigher dose (300 mgdaily of each drug,N = 199). The lowdose trial howeverhas been excludeddue to the absence ofany `cases' data, andthe lack of outcomes.
41 out of 67 (61%) inthe Amantadine arm, 13out of 66 in the placeboarm (20%), and 18 outof 63 in theRimantadine arm (29%)experienced adversee�ects. Adverse e�ects(systemic only with noother classi®cation) werenoted, although notspeci®ed.
Randomisation, allo-cation and concealmentpractices are no furtherde®ned, although alldoses were stated asbeing administered by aproject nurse. This is apoorly reported trial asno detailed classi®cationof adverse e�ects isgiven, which is a strangepractice for a toxicitystudy. Additionally,data reported in the textdoes is not consistentwith that in Table 1c,
Hayden 1986
Hayden, F.G. andMonto, A.S. Oralrimantadine hydro-chloride therapy ofin¯uenza A virusH3N2 subtype infec-tion in adults.Antimicrobial Agentsand Chemotherapy1986, 29, 339±341.
Randomised double-blind, placebo controlledtreatment trial of oralrimantadine in the uni-versities of Virginia andMichigan in 1983.
14 adults with con-®rmed A/Bangkok/1/79(H3N2) in¯uenza.
Randomised torimantadine 200 mgonce daily (mean age28 years) or placebo(mean age 23 years)for ®ve days.Treatment startedwithin 48 h of symp-tom onset.
Nasal virus shedding,duration of fever (in h)and symptom scores(presented broken downinto systemicÐhead-ache, chills, malaise etc.and respiratory).Average duration offever in the rimantadinearm was 31 h (SD=22 h)and 68 (SD=8 h) in theplacebo group.
Although the trial isextremely clearlyreported, no descriptionof allocation and con-cealment is given.
V.Dem
icheli
etal./
Vaccin
e18(2000)957±1030
1011
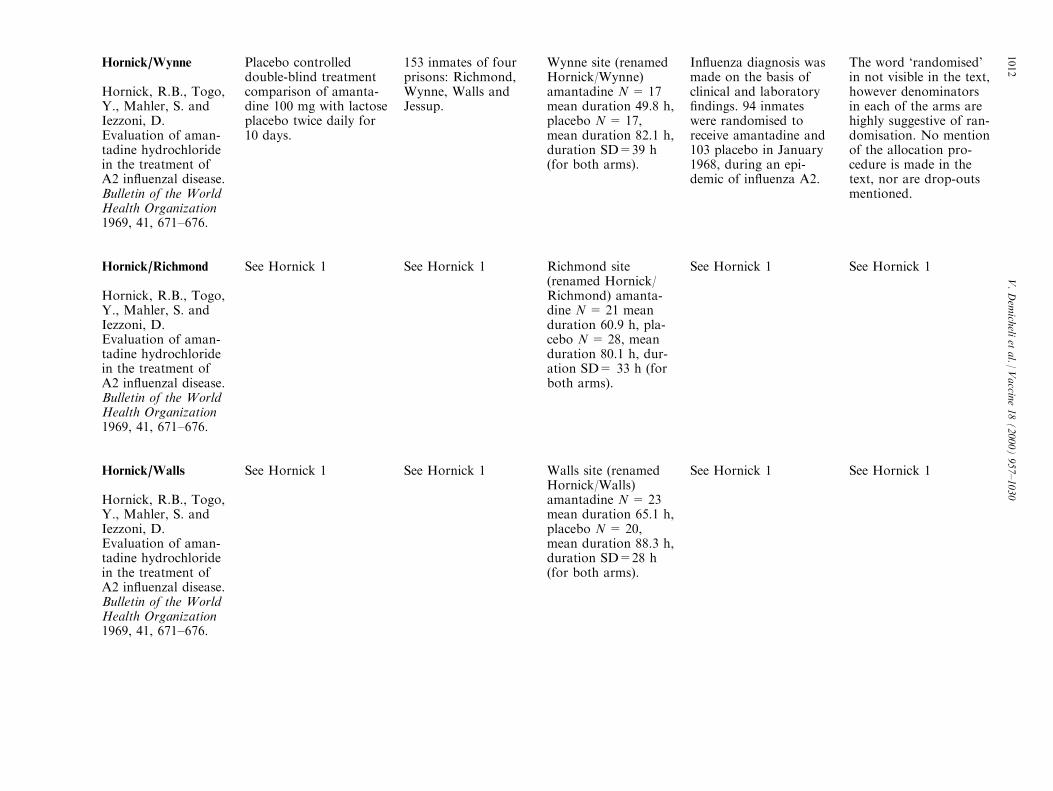
Hornick/Wynne
Hornick, R.B., Togo,Y., Mahler, S. andIezzoni, D.Evaluation of aman-tadine hydrochloridein the treatment ofA2 in¯uenzal disease.Bulletin of the WorldHealth Organization1969, 41, 671±676.
Placebo controlleddouble-blind treatmentcomparison of amanta-dine 100 mg with lactoseplacebo twice daily for10 days.
153 inmates of fourprisons: Richmond,Wynne, Walls andJessup.
Wynne site (renamedHornick/Wynne)amantadine N = 17mean duration 49.8 h,placebo N = 17,mean duration 82.1 h,duration SD=39 h(for both arms).
In¯uenza diagnosis wasmade on the basis ofclinical and laboratory®ndings. 94 inmateswere randomised toreceive amantadine and103 placebo in January1968, during an epi-demic of in¯uenza A2.
The word `randomised'in not visible in the text,however denominatorsin each of the arms arehighly suggestive of ran-domisation. No mentionof the allocation pro-cedure is made in thetext, nor are drop-outsmentioned.
Hornick/Richmond
Hornick, R.B., Togo,Y., Mahler, S. andIezzoni, D.Evaluation of aman-tadine hydrochloridein the treatment ofA2 in¯uenzal disease.Bulletin of the WorldHealth Organization1969, 41, 671±676.
See Hornick 1 See Hornick 1 Richmond site(renamed Hornick/Richmond) amanta-dine N = 21 meanduration 60.9 h, pla-cebo N= 28, meanduration 80.1 h, dur-ation SD= 33 h (forboth arms).
See Hornick 1 See Hornick 1
Hornick/Walls
Hornick, R.B., Togo,Y., Mahler, S. andIezzoni, D.Evaluation of aman-tadine hydrochloridein the treatment ofA2 in¯uenzal disease.Bulletin of the WorldHealth Organization1969, 41, 671±676.
See Hornick 1 See Hornick 1 Walls site (renamedHornick/Walls)amantadine N = 23mean duration 65.1 h,placebo N = 20,mean duration 88.3 h,duration SD=28 h(for both arms).
See Hornick 1 See Hornick 1
V.Dem
icheli
etal./
Vaccin
e18(2000)957±1030
1012

Hornick/Wynne
Hornick, R.B., Togo,Y., Mahler, S. andIezzoni, D.Evaluation of aman-tadine hydrochloridein the treatment ofA2 in¯uenzal disease.Bulletin of the WorldHealth Organization1969, 41, 671±676.
See Hornick 1 See Hornick 1 Wynne site (renamedHornick/Wynne)amantadine N = 17mean duration 49.8 h,placebo N = 17,mean duration 82.1 h,duration SD=39 h(for both arms).
See Hornick 1 See Hornick 1
Kantor
Kantor, R.J., Potts,D.W., Stevens, D.and Noble, G.R.Prevention of in¯u-enza A/USSR/77(H1N1): an evalu-ation of the sidee�ects and e�cacy ofamantadine inrecruits at Fort SamHouston. MilitaryMedicine 1980, 145,312±315.
Preventive double-blindrandomised controlledtrial of e�cacy andsafety of oral amanta-dine compared to a (notfurther de®ned) placebo,from 20 FebruaryÐ7March 1978. The targetserotype was A/USSR/77.
139 healthy parame-dic recruits (mean age22 years) in the mili-tary barracks at FortSam Houston (FSH),Texas.
Randomised toreceive either amanta-dine 100 mg tabletstwice daily (N = 64)or placebo (N = 62).
Case de®nition by a listof recognised symptomsand serological con®r-mation and adversee�ects were recorded inthe questionnaires.Paired sera wereobtained at the begin-ning of the study and®ve weeks later. Caseswere also presented byseverity.
Although the trial wasrandomised and allo-cation concealment wasprotected through a sys-tem of sealed envelopes,the di�culty in reconcil-ing ®gures and under-standing what actuallyhappened during thetrial makes this a verypoorly reported study.No reason for the lossof 20 participants to fol-low up is given.
Kitamoto 1968
Kitamoto, O.Therapeutic e�ective-ness of amantadinehydrochloride inin¯uenza A2Ðdoubleblind studies.Japanese Journal ofTuberculosis andChest Diseases 1968,15, 17±26.
Randomised double-blind, placebo controlledtreatment trial of oralamantadine, during the1967±68 in¯uenza sea-son throughout Japan.
Not speci®ed 355 participants ran-domised to amanta-dine (N = 182)(200 mg/day foradults) or placebo(N= 173) within 48 hof developing symp-toms.
Case de®nition based onsymptoms and serologi-cal con®rmation. Duringthe trial A2/Kumamoto/1/65 virus and its driftedvariants were circulatingin the community.
Although the trial isadequately reported andclearly randomised, nodescription of allocationand concealment isgiven making its assess-ment impossible.
V.Dem
icheli
etal./
Vaccin
e18(2000)957±1030
1013
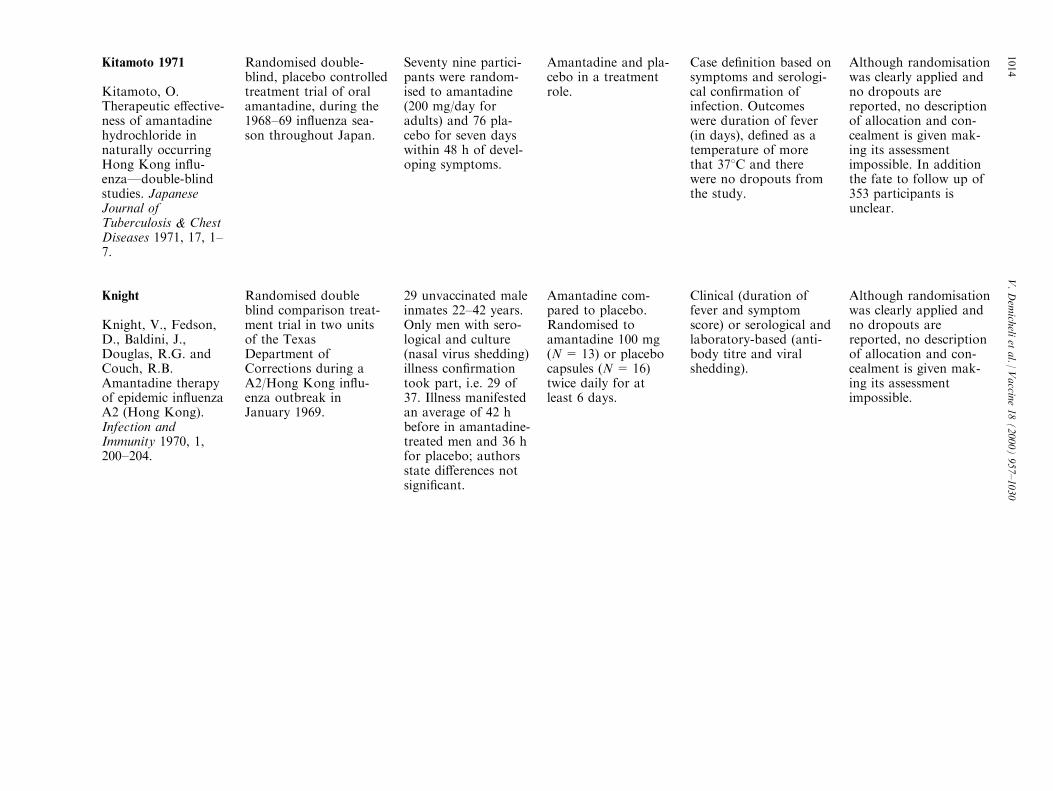
Kitamoto 1971
Kitamoto, O.Therapeutic e�ective-ness of amantadinehydrochloride innaturally occurringHong Kong in¯u-enzaÐdouble-blindstudies. JapaneseJournal ofTuberculosis & ChestDiseases 1971, 17, 1±7.
Randomised double-blind, placebo controlledtreatment trial of oralamantadine, during the1968±69 in¯uenza sea-son throughout Japan.
Seventy nine partici-pants were random-ised to amantadine(200 mg/day foradults) and 76 pla-cebo for seven dayswithin 48 h of devel-oping symptoms.
Amantadine and pla-cebo in a treatmentrole.
Case de®nition based onsymptoms and serologi-cal con®rmation ofinfection. Outcomeswere duration of fever(in days), de®ned as atemperature of morethat 378C and therewere no dropouts fromthe study.
Although randomisationwas clearly applied andno dropouts arereported, no descriptionof allocation and con-cealment is given mak-ing its assessmentimpossible. In additionthe fate to follow up of353 participants isunclear.
Knight
Knight, V., Fedson,D., Baldini, J.,Douglas, R.G. andCouch, R.B.Amantadine therapyof epidemic in¯uenzaA2 (Hong Kong).Infection andImmunity 1970, 1,200±204.
Randomised doubleblind comparison treat-ment trial in two unitsof the TexasDepartment ofCorrections during aA2/Hong Kong in¯u-enza outbreak inJanuary 1969.
29 unvaccinated maleinmates 22±42 years.Only men with sero-logical and culture(nasal virus shedding)illness con®rmationtook part, i.e. 29 of37. Illness manifestedan average of 42 hbefore in amantadine-treated men and 36 hfor placebo; authorsstate di�erences notsigni®cant.
Amantadine com-pared to placebo.Randomised toamantadine 100 mg(N= 13) or placebocapsules (N= 16)twice daily for atleast 6 days.
Clinical (duration offever and symptomscore) or serological andlaboratory-based (anti-body titre and viralshedding).
Although randomisationwas clearly applied andno dropouts arereported, no descriptionof allocation and con-cealment is given mak-ing its assessmentimpossible.
V.Dem
icheli
etal./
Vaccin
e18(2000)957±1030
1014
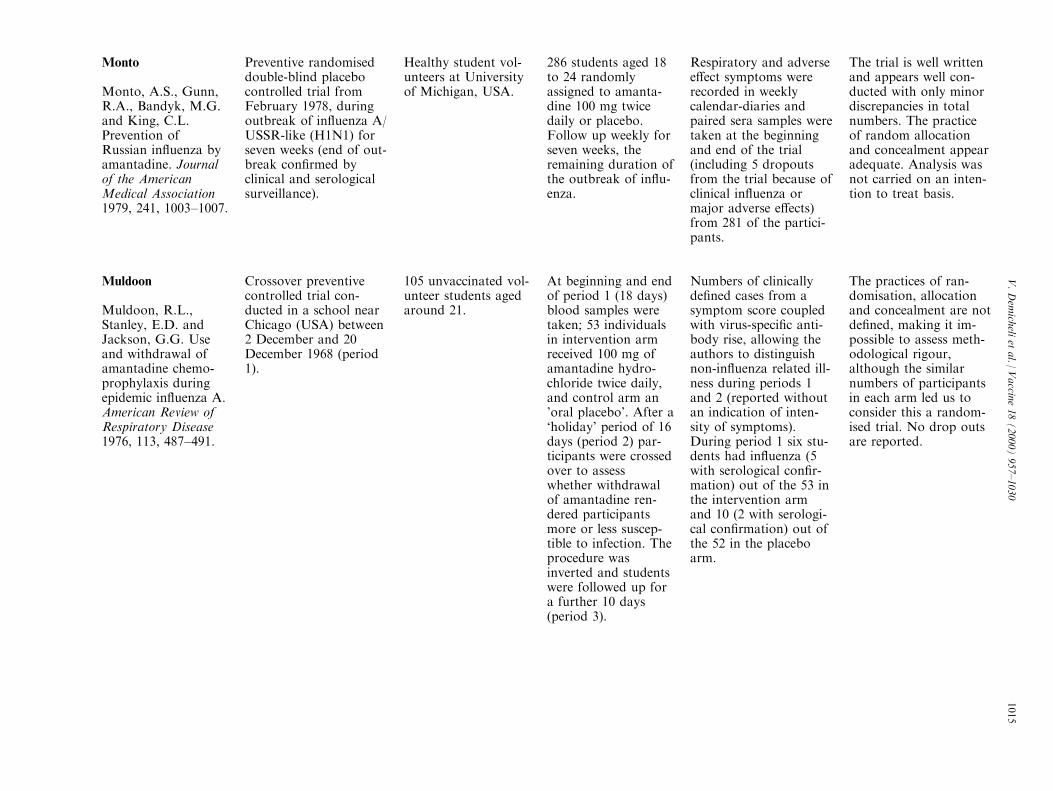
Monto
Monto, A.S., Gunn,R.A., Bandyk, M.G.and King, C.L.Prevention ofRussian in¯uenza byamantadine. Journalof the AmericanMedical Association1979, 241, 1003±1007.
Preventive randomiseddouble-blind placebocontrolled trial fromFebruary 1978, duringoutbreak of in¯uenza A/USSR-like (H1N1) forseven weeks (end of out-break con®rmed byclinical and serologicalsurveillance).
Healthy student vol-unteers at Universityof Michigan, USA.
286 students aged 18to 24 randomlyassigned to amanta-dine 100 mg twicedaily or placebo.Follow up weekly forseven weeks, theremaining duration ofthe outbreak of in¯u-enza.
Respiratory and adversee�ect symptoms wererecorded in weeklycalendar-diaries andpaired sera samples weretaken at the beginningand end of the trial(including 5 dropoutsfrom the trial because ofclinical in¯uenza ormajor adverse e�ects)from 281 of the partici-pants.
The trial is well writtenand appears well con-ducted with only minordiscrepancies in totalnumbers. The practiceof random allocationand concealment appearadequate. Analysis wasnot carried on an inten-tion to treat basis.
Muldoon
Muldoon, R.L.,Stanley, E.D. andJackson, G.G. Useand withdrawal ofamantadine chemo-prophylaxis duringepidemic in¯uenza A.American Review ofRespiratory Disease1976, 113, 487±491.
Crossover preventivecontrolled trial con-ducted in a school nearChicago (USA) between2 December and 20December 1968 (period1).
105 unvaccinated vol-unteer students agedaround 21.
At beginning and endof period 1 (18 days)blood samples weretaken; 53 individualsin intervention armreceived 100 mg ofamantadine hydro-chloride twice daily,and control arm an'oral placebo'. After a`holiday' period of 16days (period 2) par-ticipants were crossedover to assesswhether withdrawalof amantadine ren-dered participantsmore or less suscep-tible to infection. Theprocedure wasinverted and studentswere followed up fora further 10 days(period 3).
Numbers of clinicallyde®ned cases from asymptom score coupledwith virus-speci®c anti-body rise, allowing theauthors to distinguishnon-in¯uenza related ill-ness during periods 1and 2 (reported withoutan indication of inten-sity of symptoms).During period 1 six stu-dents had in¯uenza (5with serological con®r-mation) out of the 53 inthe intervention armand 10 (2 with serologi-cal con®rmation) out ofthe 52 in the placeboarm.
The practices of ran-domisation, allocationand concealment are notde®ned, making it im-possible to assess meth-odological rigour,although the similarnumbers of participantsin each arm led us toconsider this a random-ised trial. No drop outsare reported.
V.Dem
icheli
etal./
Vaccin
e18(2000)957±1030
1015

Oker-Blom
Oker-Blom, N., Hovi,T., Leinikki, P.,Palosuo, T.,Pettersson, R. andSuni, J. Protection ofman from naturalinfection with in¯u-enza A2 Hong Kongvirus by amantadine:a controlled ®eldtrial. British MedicalJournal 1970, 3, 676±678.
Preventive randomiseddouble-blind placebocontrolled trial from 20January 1969 inHelsinki, Finland for 30days.
391 healthy medicalstudents (132 femalesand 259 males) agedon average 22 years.In¯uenza A2 HongKong was the maincirculating strain atthe time.
Randomised toamantadine 100 mgor placebo (tabletscontaining calciumlactate) twice daily.Additionally theauthors analysed age-strati®ed results foreach arm (althoughthe results are notincluded in the text).
Self-reported (by ques-tionnaire) clinical symp-toms and serologicaltitres. Adverse e�ectswere recorded too.
Randomisation and allo-cation are not su�-ciently describedwhereas the placebotablets are described as`identical'. No reason isgiven for the two drop-outs from the study.
Payler
Payler, D.K. andPurdham, P.A.In¯uenza A prophy-laxis with amantadinein a boarding school.Lancet 1984, 1, 502±504.
Preventive randomisedopen trial of 536 mem-bers of Malvern BoysSchool in the UK.
Boys, 13 to 19 hadbeen previouslyimmunised in theautumn of 1982 (viralstrain not reported).
Randomised toamantadine 100 mgdaily (N = 267 or notreatment N = 269)for 14 days from 18February 1983, assoon as the cases oflaboratory-con®rmedin¯uenza weredescribed.
Case de®nition isunclear but from theresults it would appearthat clinical de®nitionsand laboratory isolateswere used. A/H1N1 wasthe prevalent viralstrain.
Although the trial wasrandomised, the designis open and the analysiswas not carried out onintention to treat.Additionally, length offollow up is notreported.
V.Dem
icheli
etal./
Vaccin
e18(2000)957±1030
1016
Peckinpaugh 1
Peckinpaugh, R.O.,Askin, F.B., Pierce,W.E., Edwards, E.A.,Johnson, D.P. andJackson, G.G. Fieldstudies with amanta-dine: acceptabilityand protection.
A randomised factorialdouble-blind controlledtrial conducted from 5December 1967 to 1June 1968.
US Naval trainees;2079 oral amantadineand 2104 placebo.
Comparison of oralamantadine (200 mgdaily) on 2079 indi-viduals and oral pla-cebo on 2104individuals, with andwithout vaccine.Administration con-tinued for 28 days.Individuals in eacharm, three days aftercommencing treat-ment were assignedto receive either vac-cine (2059 individ-uals) or subcutaneoussaline placebo (2124individuals).
Presented by interven-tion arm: amantadineand vaccineÐ1039 indi-viduals, vaccine and oralplaceboÐ1020 individ-uals, amantadine andsubcutaneous placeboÐ1040 and subcutaneousand oral placeboÐ1084individuals. Outcomesare % of participantsnot seeking treatment,sought treatment as out-patients, or admitted tolocal hospital.
The study was de®nitelyrandomised andarrangements to concealallocation appear ade-quate. The standard ofreporting is poor withoutcomes reported inhistogram form, makingestimation of their inci-dence necessary.
Peckinpaugh 2
Peckinpaugh, R.O.,Askin, F.B., Pierce,W.E., Edwards, E.A.,Johnson, D.P. andJackson, G.G. Fieldstudies with amanta-dine: acceptabilityand protection.
Study conducted fromDecember 1968 to May1969.
US Naval recruits Randomised toreceive either amanta-dine 200 mg daily(N= 1329) or pla-cebo (N = 1321)orally for 20 days.
As in Peckinpaugh 1,serological assessmentwas carried out on onefourth of participants(416 sera pairs).Outcome de®nition andpresentation were simi-lar to those inPeckinpaugh 1, as is ourtransformation of them.
The study was random-ised and arrangementsto conceal allocationappear adequate.Reporting standard ispoor with outcomesreported in histogramform, making estimationof their incidence necess-ary. Contradictory state-ments in the textconcerning de®nition ofcases and serologicaloutcomes make in-terpretation di�cult.
V.Dem
icheli
etal./
Vaccin
e18(2000)957±1030
1017

Pettersson
Pettersson, R.F.,Hellstrom, P.E.,Penttinen, K., Pyhala,R., Tokola, O.,Vartio, T. andVisakorpi, R.Evaluation of aman-tadine in the prophy-laxis of in¯uenza A(H1N1) virus infec-tion: a controlled®eld trial amongyoung adults andhigh-risk patients.Journal of InfectiousDiseases 1980, 142,377±383.
Preventive randomisedplacebo- controlleddouble-blind trial in amilitary training centrein Finland commencingon 17 January 1978. Atthe time an epidemic ofA H1N1 was underwayin the surrounding com-munity.
192 participants (mili-tary recruits aged 21average).
Randomly assignedto receive eitheramantadine 200 mgdaily of calcium lac-tate placebo tablets.
Follow up for threeweeks and cases werede®ned on the basis ofretrospective analysis ofquestionnaires and anti-body titre rise in pairedsera. Infection within¯uenza A H3N2 virusalso was veri®ed serolo-gically.
Although the studyreport is well writtenand random allocationwas carried out on thebasis of random numbertables, allocation con-cealment was unspeci®edand intention to treatanalysis did not takeplace.
Plesnik
Plesnik, V., Heinz,F., Bindas, B. et al.Controlled study ofin¯uenza prophylaxisusing amantadineVUFB. CsEpidemiologie mikro-biologie, immunologie1977, 4. (translatedfrom Czeck).
Preventive randomiseddouble-blind controlledtrial of amantadineduring an epidemic ofin¯uenza A/Victoria/42/75 [H3N2] virus frommid March 1976 in theformer Czechoslovakiaand lasted 20 days.
1133 healthy students,industrial workersand elderly aged 10to 69.
Randomised toreceive either amanta-dine 100 mg once ortwice daily (N = 574)or placebo(N= 559), one ortwo tablets daily.
Case de®nition wasbased on in¯uenzasymptoms and antibodytitre rise from pairedsera and viral isolation(although from thetranslated text it is notclear whether this prac-tice covered the wholestudy population).Adverse e�ects arereported in detail in thetrial.
Although randomis-ation, allocation andanalysis on an intentionto treat are notdescribed, concealmentis described as a centra-lised scheme with codedtablets and is thereforeassessed as adequate.
V.Dem
icheli
etal./
Vaccin
e18(2000)957±1030
1018
Quarles
Quarles, J.M., Couch,R.B., Cate, T.R. andGoswick, C.B.Comparison of aman-tadine and rimanta-dine for prevention oftype A (Russian)in¯uenza. AntiviralResearch 1981, 1,149±155.
Preventive randomiseddouble blind placebo-controlled trial at theUniversity of Texas.Trial commenced onweek 7 (? mid February)1978 during an epidemicof in¯uenza A/USSR/90/77 virus.
444 healthy studentsaged 18 to 24 fol-lowed up for sixweeks on the basisweekly of self-report-ing.
Randomised toamantadine (100 mg),or rimantadine(100 mg), or placebo(not speci®ed) tabletstwice daily.
Cases were de®ned onthe basis of paired seraand clinical symptoms.Viral isolation fromthroat swabs was ad-ditionally carried out.
The practices of ran-domisation, allocationand concealment are notde®ned, making it im-possible to assess meth-odological rigour.Analysis on the basis ofintention to treat wasnot carried out and theoverall quality of report-ing is poor (with nocomplete details ofreasons for dropout).
Reuman
Reuman, P.D.,Bernstein, D.I.,Keefer, M.C., Young,E.C., Sherwood, J.R.and Schi�, G.M.E�cacy and safety oflow dosage amanta-dine hydrochloride asprophylaxis for in¯u-enza A. AntiviralResearch, 1989, 11,27±40.
Double-blind preventiverandomised controlledtrial. Follow up weeklyfor six weeks throughsymptom diaries andvisits; those reportingwith in¯uenza- like ill-ness had examinationand nasal washouts ontwo consecutive days.Adverse e�ects wererecorded. Randomblood tests on 48 sub-jects gave results consist-ent with compliance.Paired sera from begin-ning and end of trialwere tested for anti-bodies against A/Chile/1/83(H1N1), A/Philippines/1/82(H3N2)and B/USSR/100/83, theprevalent viruses duringthe study period. Viralassays were performedfrom nasal washouts.
476 healthy hospitalpersonnel aged 18 to55 at CincinnatiChrist Hospital,Ohio, USA duringthe 1985±86 in¯uenzaseason.
Three arms to thetrial: (a) 159 subjectsrandomly allocated toreceive amantadine100 mg/day (b) 159subjects randomly al-located to receiveamantadine 200 mg/day (c) 158 subjectsrandomly allocated toreceive identical look-ing placebo capsuleseach day.
Five participants wereinfected in the placebogroup, two subjects inthe 100 mg group andone in the 200 mggroup. The number ofparticipants with at leastone (systemic) adversee�ect was 49 in the pla-cebo arm, 47 in the100 mg arm and 71 inthe 200 mg arm, indicat-ing a clear dose-adversee�ect relationship.In¯uenza-like illness pre-de®ned from a list ofsigns and symptoms.
The study is of goodquality with computer-generated randomis-ation, checks on allo-cation concealment andgood blinding pro-cedures. No dropoutsare reported.
V.Dem
icheli
etal./
Vaccin
e18(2000)957±1030
1019
Schapira
Schapira, M., Oxford,J.S. and Galbraith,A.W. A study of 1±adamantamine hydro-chloride during the1970 Hong Kongin¯uenza epidemic.Journal of the RoyalCollege of GeneralPractitioners 1971,21, 695±697.
Placebo-controlled trialof amantadine con-ducted in the NorthernEnglish village ofKeighly by a generalpractitioner during thewinter of 1968±69.
297 healthy volun-teers from ®rms,schools, a newspaper,a bank and families.Mean age was evenlymatched at 38 years(active arm) and 38.5years (placebo arm).
Amantadine 100 mgevery 12 h (157 par-ticipants) or oil-basedplacebo capsule (140participants), ident-i®ed by a code.Follow up was 10days. Sera werescreened prior tocommencement; thosementioning symptomsof in¯uenza under-went a second anti-body titre estimationagainst A2/HongKong/1/68, the preva-lent strain. Some par-ticipants may havebeen infected prior tocommencement;authors point outthat trial is preventiveand curative.
49 of 157 volunteers intreatment arm su�eredin¯uenza symptomscompared to 39 out 140in placebo arm.However only 8 and 15cases respectively wereserologically con®rmedas in¯uenza. Twelvepaired sera were una-vailable for the 49 symp-tomatic volunteers inthe treatment arm; threepaired sera were una-vailable although theauthors do not explainthe reason for the dropouts. Adverse e�ects arenot reported.
The authors concludethat the trial provides`marginal' evidence ofpreventive e�ect ofamantadine. The prac-tices of randomisation,and allocation are notdescribed, making it im-possible to assess meth-odological rigour,although the similarnumbers of participantsin each arm led us toconsider this a random-ised trial. Allocationconcealment appearedadequate.
V.Dem
icheli
etal./
Vaccin
e18(2000)957±1030
1020

Smorodintsev
Smorodintsev, A.A.,Karpuhin, G.I.,Zlydnikov, D.M.,Malyseva, A.M.,Svecova, E.G.,Burov, S.A.,Hramcova, L.M.,Romanov, J.A.,Taros, L.J.,Ivannikov, J.G. andNovoselov, S.D. Theprophylactic e�ective-ness of amantadinehydrochloride in anepidemic of HongKong in¯uenza inLeningrad in 1969.Bulletin of the WorldHealth Organization1970, 42, 865±872.
Preventive randomiseddouble-blind placebocontrolled trial carriedout in eight engineeringschools aroundLeningrad, in the formerUSSR. The design com-prised an `internal' (daystudents) and `external'(i.e. boarders) do-noth-ing control groupswhich will not be furthertaken into considerationas they took no medi-cation.
Males, aged 18±30. Randomised toreceive amantadine100 mg daily(N= 5092) or pla-cebo tablets(N= 3175).Commenced aroundJanuary 1969 withstaggered starts,according to theresults of schoolspeci®c surveillanceagainst A2/HongKong/68 virus.Di�erential follow-upis also recordedbetween placebo andamantadine arms (30days) and controls(12 days).
Case de®nition wasbased on a list of symp-toms plus a four-foldrise in serum antibodytitres to in¯uenza A.
Although randomisationoccurred and conceal-ment is described in anadequate manner, anunknown number ofparticipants were givenamantadine syrup. Asno reference to syrupplacebo is made in thetext (only to tabletform), robustness ofblinding and conceal-ment is questionable.Additionally the numer-ous discrepancies in thetext make this a poorlyreported trial.
van Voris
van Voris, L.P.,Betts, R.F., Hayden,F.G., Christmas,W.A. and Douglas,R.G. Successful treat-ment of naturallyoccurring in¯uenzaA/USSR/77 H1N1.Journal of theAmerican MedicalAssociation 1981, 245,1128±1131.
Randomised in adouble-blind designtreatment trial.
45 students with lab-oratory con®rmedin¯uenza A/USSR/77[H1N1] in February1978 in University ofRochester, USA .
Amantadine 200 mgdaily (N = 14) orrimantadine 200 mgdaily (N = 14) orinert placebo capsules(N= 12) and fol-lowed up for ®vedays.
Symptom scores, dur-ation of temperature.We used the outcome`number of participantswith temperatures>37.58C", 48 hafter commencing medi-cation (a dichotomousoutcome). Data onmean duration of feverwere not given.
The trial is well reportedand de®nitely random-ised. Allocation conceal-ment is described andappears to be adequate.
V.Dem
icheli
etal./
Vaccin
e18(2000)957±1030
1021

Wendel
Wendel, H.A.,Snyder, M.T. andPell, S. Trial ofamantadine in epi-demic in¯uenza.ClinicalPharmacology andTherapeutics 1966, 7,38±43.
Preventive and treat-ment randomised doubleblind placebo-controlledtrial in a prison commu-nity in Philadelphia,USA in January 1963.
Prison inmates aged17±54 exposed tonaturally occurringin¯uenzaA2Japan305/57 virus.
Placebo was a lactosetablet. In the preven-tive trial 794 inmateswere randomised toreceive amantadine200 mg daily(N= 439) or placebo(N= 355). Follow-uplength was 10 days.
Cases were de®ned bothclinically and serologi-cally.
The trials are wellreported although ran-domisation was notgood (as con®rmed byuneven numbers in thearmsÐ20% excess inthe amantadine arm)and allocation conceal-ment is adequate
Wing®eld
Wing®eld, W.L.,Pollack, D. andGrunert, R.R.Therapeutic e�cacyof amantadine HC1and rimantadine HC1in naturally occurringin¯uenza A2 respirat-ory illness in man.New England Journalof Medicine 1969,281, 579±584.
Randomised doubleblind placebo-controlledtreatment trial in theVirginia StatePenitentiary, USA,during an outbreak ofin¯uenza A2/Rockville/1/65 in January-February 1968.
95 inmates whosesymptoms developedin the previous 24 h.
Randomised toamantadine 100 mg(N= 23), or rimanta-dine 150 mg (N = 24)or placebo lactosecapsules (N= 48)twice daily.Medication com-menced within 24 hof developing symp-toms and continuedfor 10 days. The ®naldenominators forwhich data are pro-vided in the report:Placebo N= 39Amantadine N= 20Rimantadine=20.
Only data relating toparticipants with tem-peratures ofr37.58C onthe ®rst day of the studywere analysed of theduration of fever out-come and one partici-pant was later found notto have a rise at the sec-ond antibody titre esti-mation. We haveincluded duration offever as the clinical out-come in our meta-analy-sis.
Randomisation and allo-cation concealment aredetailed in the text withindividual coded `vials'(which we assume tomean containers) sys-tem. Intention to treatanalysis appears to havetaken place on individ-uals who ful®lled clinicaland serological criteria.
V.Dem
icheli
etal./
Vaccin
e18(2000)957±1030
1022

Younkin
Younkin, S.W., Betts,R.F., Roth, F.K. andDouglas, R.G.Reduction in feverand symptoms inyoung adults within¯uenza A/Brazil/78H1N1 infection aftertreatment with aspirinor amantadine.Antimicrobial Agentsand Chemotherapy1983, 23, 577±582.
Randomised doubleblind comparison ofamantadine with aspirin,during an outbreak ofin¯uenza A/Brazil/78[H1N1] in the winter of1981.
48 otherwise healthycollege students aged17 to 20 from theUniversity ofRochester, NewYork, USA.Participants all hadclinical and (later)laboratory con®rmeddiagnosis of in¯u-enza.
Randomised toamantadine 100 mg aday (N = 16), 200 mga day (N = 14) oraspirin 3.25 grams aday (N = 17).
Outcomes are presentedas both symptoms scoresand duration of fever (inthe text).
Randomisation and allo-cation concealment arewell detailed in the textand concealment in par-ticular appears veryrobust with an elaboratesystem of envelopes. Touniformly make up thetablets number, theaspirin arm had two pla-cebo tablets included.Compliance was equallytested by daily question-ing.
Description of studies included in the neuraminidase inhibitor review
Calfee 1
Calfee, D.P., Peng,A.W., Cass, L.M.R.,Lob, M. and Hayden,F.G. Protective e�-cacy of intravenousZanamivir in exper-imental human in¯u-enza. Abstract H58 atthe 38th InterscienceConference ofAntimicrobial Agentsand Chemotherapyon 24±27 September1998.
Randomised placebocontrolled preventivetrial of IV Zanamivir inexperimental in¯uenza.
16 healthy adultsmale volunteers.
Saline placebo orZanamivir 600 mgtwice daily for 5 daysbeginning four hbefore inoculationwith A/Texas/91[H1N1].
A mixture of serological,clinical and laboratory-con®rmed. The authorsconclude that this studyis the ®rst to show theIV Zanamivir is protec-tive against in¯uenza(for example being100% e�ective in pre-venting viral nasal shed-ding).
The methodologicalquality of the study isdi�cult to assess as nodescription is given.Randomisation is expli-citly mentioned in thetext of the abstract.
V.Dem
icheli
etal./
Vaccin
e18(2000)957±1030
1023

Calfee 2
Calfee, D.P., Peng,A.W., Hussey, E.K.,Lobo, M. andHayden, F.G.Protective e�cacy ofreduced frequencydosing of intranasalZanamivir in exper-imental human in¯u-enza. Abstract H68 atthe 38th InterscienceConference ofAntimicrobial Agentsand Chemotherapyon 24±27 September1998.
Preventive placebo con-trolled double-blind ran-domised trial ofZanamivir nasal sprayin 43 individuals exper-imentally exposed to A/Texas/91 [H1N1] virus.
Arms 3 and 4 of thetrial were carried outon 19 subjects (10 inthe active arm and 9in the placebo arm).
Administration of asingle dose ofZanamivir beganeither 48 h, or 4 h(N= 12). These sub-jects were given intra-nasal Zanamivir dailyfor 3 days from theday of experimentalexposure).
A mixture of laboratoryand clinical but in ourreview we include dataon laboratory con®rmedindividuals with symp-toms. The authors con-clude that their trialprovides the ®rst evi-dence on humans that asingle daily dose ofZanamivir is e�caciousin the prevention ofin¯uenza.
The methodologicalquality of the studies isdi�cult to assess as nodetailed description isgiven in the abstract.Randomisation is expli-citly mentioned and wascon®rmed to thereviewers by the manu-facturers.
Hayden 1996a
Hayden, F.G., Lobo,M., Hussey, E.K. andEason, C.U. E�cacyof intranasal GG167in experimentalhuman in¯uenza Aand B virus infection.In: Options for thecontrol of in¯uenzaIII (Eds Brown, L.E.,Hampson, A.W. andWebster, R.G.).Elsevier Science,Amsterdam, 1996,pp. 718±724.
Preventive placebo con-trolled double-blind ran-domised trial ofZanamivir.
Nasal spray in 34 in-dividuals experimen-tally exposed to B/Yamagata/88 virus.
Administration ofGG167 began four hprior to inoculationwith the virus andcontinued for ®vedays. Susceptible in-dividuals wereassigned to receiveeither GG167 3.2 mgtwice daily (N = 9),or 6.4 mg twice daily(N= 8), or 6.4 mgonce daily (N = 8) oraqueous placebospray (N= 9).
Infection (viral nasalshedding and HI anti-body rise) or upper res-piratory illness de®nedas the presence ofrtworespiratory symptoms onr2 days.
The authors remark thatthe proportion of sub-jects developing illnesswas signi®cantly lowerin the two twice-dailyarms. The methodologi-cal quality of the studyis di�cult to assess asno detailed descriptionof methods is given,although a note underTable 1 describes thenecessity to randomiseeach placebo group in a3:1 ratio to preservedouble-blinding.Randomisation is expli-citly mentioned.
V.Dem
icheli
etal./
Vaccin
e18(2000)957±1030
1024
Hayden 1996b
Hayden, F.G.,Treanor, J.J., Betts,R.F., Lobo, M.,Esinhart, J.D. andHussey, E.K. Safetyand e�cacy of theneuraminidase inhibi-tor GG167 in exper-imental humanin¯uenza. Journal ofthe American MedicalAssociation 1996, 275,295±299.
As Hayden 1996a As Hayden 1996a As Hayden 1996a Outcomes were infection(viral nasal sheddingand HI antibody rise) orupper respiratory illnessde®ned as the presenceofrtwo respiratorysymptoms onr2 days.
As Hayden 1996a
V.Dem
icheli
etal./
Vaccin
e18(2000)957±1030
1025

Hayden 1997
Hayden, F.G.,Osterhaus, A.D.,Treanor, J.J.,Fleming, D.M., Aoki,F.Y., Nicholson,K.G., Bohnen, A.M.,Hirst, H.M., Keene,O. and Wightman, K.E�cacy and safety ofthe neuraminidase in-hibitor Zanamivir inthe treatment of in¯u-enza virus infections.New England Journalof Medicine 1997,337, 874±880.
Two multicentre trials inNorth America (38centres, 220 individuals)and Europe (32 centres,197 individuals) con-ducted during the 1994±95 in¯uenza season toassess the treatmente�ects of Zanamivirusing a randomised,double-blind, placebocontrolled design.
Otherwise healthy in-dividuals with symp-toms suggestive ofin¯uenza persistinglonger than 48 h.Mean ages of subjectsin the three armswere 31±33 years.
Randomised to 10 mgof inhaled Zanamivirby mouth plus 6.4 mgby intranasal spray or10 mg of inhaledZanamivir and intra-nasal placebo sprayor aqueous placeboby both routes twicedaily for ®ve days.During convalescenceHAI titres wereassessed and 262 indi-viduals had labora-tory con®rmedin¯uenza. Of these,56% were due to A/H3N2 and 44±Bvirus.
Nine placebo patientsand 10 from each of theother arms withdrew orwere lost to follow-up(explained in the text asfailure to at tend for thefollow-up visits). Themajor outcome assessedin the trial was `time toalleviation of majorsymptoms' (de®ned asabsence of fever andheadache, muscle ache,sore throat and cough).Additionally, time toresumption of usual ac-tivities are also reported.
Individuals commencingtreatment R30 h fromillness onset fared sig-ni®cantly better thanthose commencing later.Both interventions sig-ni®cantly shortened dur-ation of illnesscompared to placebo(5.3 and 5.4 days com-pared to 6.3 days).Inhaled and intranasalZanamivir signi®cantlyshortened non-e�ectivetime compared to pla-cebo. No e�ect seen onnon-in¯uenza infectedpatients (although datanot presented in text).Adverse e�ects are gen-eralised (respiratorytract and gastrointesti-nal) or local (perinasal).Authors conclude thatZanamivir is safe ande�ective treatmentagainst in¯uenza A andB if given early in ill-ness. Although clearlyrandomised, no detailsof allocation or doubleblinding are given.Intention to treat analy-sis has clearly takenplace
V.Dem
icheli
etal./
Vaccin
e18(2000)957±1030
1026
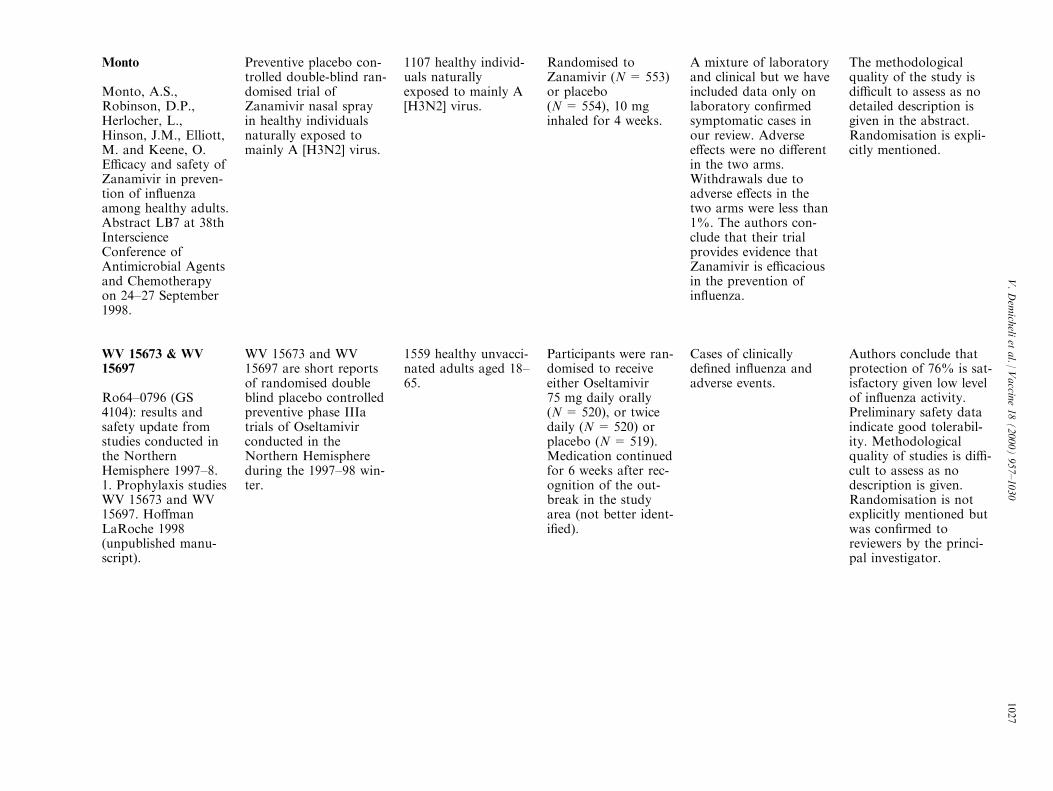
Monto
Monto, A.S.,Robinson, D.P.,Herlocher, L.,Hinson, J.M., Elliott,M. and Keene, O.E�cacy and safety ofZanamivir in preven-tion of in¯uenzaamong healthy adults.Abstract LB7 at 38thInterscienceConference ofAntimicrobial Agentsand Chemotherapyon 24±27 September1998.
Preventive placebo con-trolled double-blind ran-domised trial ofZanamivir nasal sprayin healthy individualsnaturally exposed tomainly A [H3N2] virus.
1107 healthy individ-uals naturallyexposed to mainly A[H3N2] virus.
Randomised toZanamivir (N= 553)or placebo(N= 554), 10 mginhaled for 4 weeks.
A mixture of laboratoryand clinical but we haveincluded data only onlaboratory con®rmedsymptomatic cases inour review. Adversee�ects were no di�erentin the two arms.Withdrawals due toadverse e�ects in thetwo arms were less than1%. The authors con-clude that their trialprovides evidence thatZanamivir is e�caciousin the prevention ofin¯uenza.
The methodologicalquality of the study isdi�cult to assess as nodetailed description isgiven in the abstract.Randomisation is expli-citly mentioned.
WV 15673 & WV15697
Ro64±0796 (GS4104): results andsafety update fromstudies conducted inthe NorthernHemisphere 1997±8.1. Prophylaxis studiesWV 15673 and WV15697. Ho�manLaRoche 1998(unpublished manu-script).
WV 15673 and WV15697 are short reportsof randomised doubleblind placebo controlledpreventive phase IIIatrials of Oseltamivirconducted in theNorthern Hemisphereduring the 1997±98 win-ter.
1559 healthy unvacci-nated adults aged 18±65.
Participants were ran-domised to receiveeither Oseltamivir75 mg daily orally(N= 520), or twicedaily (N = 520) orplacebo (N = 519).Medication continuedfor 6 weeks after rec-ognition of the out-break in the studyarea (not better ident-i®ed).
Cases of clinicallyde®ned in¯uenza andadverse events.
Authors conclude thatprotection of 76% is sat-isfactory given low levelof in¯uenza activity.Preliminary safety dataindicate good tolerabil-ity. Methodologicalquality of studies is di�-cult to assess as nodescription is given.Randomisation is notexplicitly mentioned butwas con®rmed toreviewers by the princi-pal investigator.
V.Dem
icheli
etal./
Vaccin
e18(2000)957±1030
1027

WV 15670
Ro64±0796 (GS4104): results andsafety update fromstudies conducted inthe NorthernHemisphere 1997±8.2. Treatment studiesWV 15670 and WV15671. Ho�manLaRoche 1998(unpublished manu-script).
WV 15670 is a shortreport of randomiseddouble blind placebocontrolled preventivephase IIIa trials ofOseltamivir. WV 15670was conducted inEurope, Canada andChina during the 1997±98 winter.
473 otherwise healthyindividuals who pre-sented with at leaston respiratory andone constitutionalsymptom were ran-domised within 36 hof onset.
Oseltamivir 75 mgdaily orally(N= 155), or twicedaily (N = 157), orplacebo (N = 161)for ®ve days.
Time to alleviation ofsymptoms expressed indays and type and inci-dence of adverse events.Additionally severity ofillness was also assessedby means of a symptomscore.
Time to alleviation ofsymptoms was signi®-cantly reduced in activearms, and 30% re-duction in symptomsscores of active arms ofboth trials. As in pro-phylaxis/ preventiontrials, nausea was mostreported systemicadverse event, especiallyat higher dose (see WV15671). Methodologicalquality of study di�cultto assess as no descrip-tion is given, in keepingwith preliminary reportnature. Randomisationis explicitly mentionedin text.
V.Dem
icheli
etal./
Vaccin
e18(2000)957±1030
1028

WV 15671
Ro64±0796 (GS4104): results andsafety update fromstudies conducted inthe NorthernHemisphere 1997±8.2. Treatment studiesWV 15670 and WV15671. Ho�manLaRoche 1998(unpublished manu-script).
WV 15671 is a shortreport of a randomiseddouble blind placebocontrolled preventivephase IIIa trials ofOseltamivir. WV 15671was conducted in theUSA during the 1997±98 winter.
368 otherwise healthyindividuals who pre-sented with at leaston respiratory andone constitutionalsymptom were ran-domised within 36 hof onset.
Participants receivedeither Oseltamivir75 mg twice dailyorally (N = 128), or150 mg twice daily(N= 122), or placebo(N= 128) for ®vedays.
As in WV 15670. Time to alleviation ofsymptoms was signi®-cantly reduced in activearms, and 30% re-duction in symptomsscores of active arms ofboth trials. As in pro-phylaxis/ preventiontrials of Oseltamivir,nausea was mostreported systemicadverse event, especiallyat the higher dose. Inview of this and lack ofsigni®cant di�erencebetween doses, trialistsrecommend that futuretrials adopt lower (75 mgtwice daily) dose.Methodological qualityof study is di�cult toassess as no descriptionis given, in keeping withnature of report.Randomisation is expli-citly mentioned in thetext.
V.Dem
icheli
etal./
Vaccin
e18(2000)957±1030
1029

References
[1] Wiselka M. In¯uenza: diagnosis, management and prophylaxis.
BMJ 1994;308:1341±5.
[2] Bonn D. Spared an in¯uenza pandemic for another year?
Lancet 1997;349:36.
[3] Belshe RB. In¯uenza as a zoonosis: how likely is a pandemic?
Lancet 1998;351:460±1.
[4] Yuen KY, Chan PKS, Peiris M, et al. Clinical features and
rapid viral diagnosis of human disease associated with avian
in¯uenza A H5N1 virus. Lancet 1998;351:467±71.
[5] Claas EC, Osterhaus ADM, van Beek R, et al. Human in¯uenza
A H5N1 virus related to a highly pathogenic avian in¯uenza
virus. Lancet 1998;351:472±7.
[6] Je�erson TO, Demicheli V. The socioeconomics of in¯uenza. In:
Nicholson, Hay, Webster, editors. Textbook of In¯uenza.
London: Blackwell, 1998. p. 541±7.
[7] World Health Organisation (WHO). International list of avail-
ability of vaccines and sera. Fourth edition. Geneva 1996
(updated February).
[8] McDowell I, Newell C, Rosser W. Comparison of three
methods of recalling patients for in¯uenza vaccination. Can
Med Assoc J 1986;135:991±7.
[9] Lukasik MH, Pratt G. The telephone: an overlooked technology
for prevention in family medicine. Can Fam Physician
1987;33:1997±2021.
[10] Gerace TM, Sangster JF. In¯uenza vaccination: a comparison
of two outreach strategies. Fam Med 1988;20:43±5.
[11] Advisory Committee on Immunisation Practices. Prevention
and control of in¯uenza. MMWR 1998;47(3 no RR-6).
[12] Gross PA, Hermogenes AW, Sacks HS, et al. The e�cacy of
in¯uenza vaccines in elderly people: A meta-analysis and review
of the literature. Annals of Internal Medicine 1995;123:518±27.
[13] Strassburg MA, Greenland S, Sorvillo FJ, et al. In¯uenza in the
elderly: report of an outbreak and a review of vaccine e�ective-
ness reports. Vaccine 1986;4:38±44.
[14] Couch R. Summary of medical literature review of e�ectiveness
of inactivated in¯uenza virus vaccines. In: Cost E�ectiveness of
In¯uenza Vaccination. Washington: O�ce of Technology
Assessment, 1981. p. 43±5.
[15] Hobson D. Assessment of the e�cacy of in¯uenza vaccines
against natural challenge. Develop Biol Standard 1975;28:285±
94.
[16] Advisory Committee on Immunisation Practices. Prevention
and control of in¯uenza. MMWR 1988;37:361±73.
[17] Advisory Committee on Immunisation Practices. Prevention
and control of in¯uenza. MMWR 1998;47(3 no RR-6.).
[18] Advisory Committee on Immunisation Practices (ACIP).
Prevention and control of in¯uenza: Part II, antiviral agents.
MMWR 1994;43:1±9.
[19] Loughlin CA. The discovery and development of therapies for
in¯uenza infections. In: Hannoun C, et al., editors. Options for
the control of in¯uenza. Amsterdam: Elsevier, 1993. p. 327±31.
[20] Hayden FG, Couch RB. Clinical and epidemiological import-
ance of in¯uenza A viruses resistant to amantadine and riman-
tadine. In: Hannoun C, et al., editors. Options for the control
of in¯uenza. Amsterdam: Elsevier, 1993. p. 333±42.
[21] Wintermeyer SM, Nahata MC. Rimantadine: a clinical perspec-
tive. The Annals of Pharmacotherapy 1995;29:299±310.
[22] Penn CR. Inhibitors of in¯uenza virus neuraminidase. In:
Nicholson KG, Hay RG, Webster AJ, editors. Textbook of
In¯uenza. London: Blackwell, 1998. p. 477±87 (Chapter 36).
[23] Couch RB. A new antiviral agent for in¯uenza: Is there a clini-
cal niche? New England Journal of Medicine 1997;337:927±8
(editorial).
[24] Pfei�er N. Firms racing to develop drugs for in¯uenza virus.
Genetic Engineering News 1997;17(1 November):1±16.
[25] Wright LA, Demicheli V, Gillespie W, Je�erson TO. Morbidity
surveillance in the British Army Ð the ®rst 12 months. J R
Army Med Corps 1998;144:11±7.
[26] McMenamin J, Morton R, McEwen J. Report of a pilot pro-
gramme of enhanced surveillance of respiratory illness in the
British Army (UK). University of Glasgow, Department of
Public Health, 1998.
[27] Demicheli V, Rivetti D, Deeks JJ, Je�erson TO. In¯uenza vac-
cines in healthy adults. Cochrane Database of Systematic
Reviews (Acute Respiratory Infections Module). Update
Software 1999 (forthcoming).
[28] Je�erson TO, Demicheli V, Deeks JJ, Rivetti D. Amantadine &
rimantadine for in¯uenza. Cochrane Database of Systematic
Reviews (Acute Respiratory Infections Module). Update
Software 1999, issue 2.
[29] Je�erson TO, Demicheli V, Deeks JJ, Rivetti D. Neuraminidase
inhibitors for in¯uenza. Cochrane Database of Systematic
Reviews (Acute Respiratory Infections Module). Update
Software 1999, issue 2.
[30] Drummond MF, Je�erson TO (for the BMJ Working Party on
guidelines for authors peer-reviewers of economic submissions
to the British Medical Journal) Buxton M Demicheli V,
Donaldson C, JoÈ nsson B, Mugford M, Rennie D, Rovira J,
Rutten F, Schulman K, Smith R, Tonks A, Torrance G, Towse
A. Guidelines for authors and peer-reviewers of economic sub-
missions to the British Medical Journal. BMJ 1996;313(3
August):275±83.
[31] Cochrane Acute Respiratory Infections Group. Search strategy
for specialised register. Cochrane Library 1998 Issue 1. Oxford:
Update Software (updated quarterly).
[32] Je�erson TO, Je�erson VM. The quest for trials on the e�cacy
of human vaccines. Results of the handsearch of `Vaccine'.
Vaccine 1996;14:461±4.
[33] Je�erson TO. Vaccine trial data systematically assembled,
pooled and disseminated by the Cochrane Collaboration.
Vaccine 1998;16:1487±95.
[34] Schulz KF, Chalmers I, Hayes RJ, Altman DG. Empirical evi-
dence of bias. Dimensions of methodological quality associated
with estimates of treatment e�ects in controlled trials. JAMA
1995;273:408±12.
[35] Je�erson TO Demicheli V. Economic evaluation of In¯uenza
vaccination and economic modelling. Can results be pooled?
Pharmacoeconomics 1996;9(Suppl 3):67±72.
[36] Je�erson TO, Demicheli V. A systematic review of world litera-
ture on the economics of in¯uenza. Information and News on
In¯uenza. European Scienti®c Working Group on In¯uenza
(Newsletter) 1997;7:6.
[37] Aoki FY. Amantadine and rimantadine. In: Nicholson KG,
Hay AJ, Webster RG, editors. Textbook of In¯uenza. London:
Blackwell, 1998. p. 457±76.
V. Demicheli et al. / Vaccine 18 (2000) 957±10301030
Copyright © 2022 FDOKUMEN