
Protection of chemolithoautotrophic bacteria exposed to simulated Mars environmental conditions
Upload
khangminh22Category
view
3download
0
PRESUMPTIVE BENEFITS FOR WAR FIGHTERS EXPOSED TO BURN PITS AND OTHER TOXINS
ACT OF 2020

2
September 15, 2020 Dear Colleague: After the Vietnam War, an entire generation of servicemembers came back from war sick from exposure to Agent Orange while they were deployed. It took decades for Congress to legislate their illnesses as service-connected and require the Department of Veterans Affairs to provide Vietnam veterans with the health and benefits they earned and deserve. And now, it is happening again. Twenty years of the Global War on Terror (GWOT) have created yet another generation of sick servicemembers returning with ailments caused by exposure to a wide array of toxic chemicals and carcinogens, from burn pits, to burning jet fuel, oil-well fires, industrial solvents, depleted uranium, and many others. Within months or years of returning from deployment, exposed servicemembers and veterans now suffer from respiratory illnesses, cancers, and other diseases. Many of these illnesses have resulted in permanent disabilities and even death. The Department of Veterans Affairs and the Department of Defense have been dismissing the serious health effects of these exposures. They keep hiding behind promises about “ongoing studies” to prove whether the illnesses are service-connected, which would grant veterans with access to VA health and disability services. Yet, it is well established that burning regular household waste releases carcinogens, neuro-disruptors, and heavy metals that can have devastating effects on the lungs, heart, brain, thyroid, and immune system. Both federal and state government agencies have compiled decades of research linking these toxins to diseases. It’s why using burn pits on American soil is against the law and exposure to other toxins is highly regulated. We have seen this movie before, and we have a solution. Please join us in cosponsoring the Presumptive Benefits for War Fighters Exposed to Burn Pits and Other Toxins Act of 2020 which would provide access to VA health and disability services for GWOT veterans, including Afghanistan, Iraq, Gulf War, K2 and every other country where our servicemembers fought and were exposed to toxins. Sick veterans should not have to spend their time collecting paperwork to access VA services they have earned and deserve. To cosponsor, please contact [email protected] in Congressman Ruiz’s office or [email protected] in Senator Gillibrand’s office.
Sincerely,
Kirsten Gillibrand Raul Ruiz, M.D. U.S. Senator Member of Congress

3
Presumptive Benefits for War Fighters Exposed to Burn Pits and Other Toxins Act of 2020
Senator Kirsten Gillibrand Congressman Raul Ruiz, M.D.
To cosponsor or questions, please contact [email protected] in Congressman Ruiz’s office or [email protected] in Senator Gillibrand’s office.
The bill would establish a list of new diseases as service-connected for which veterans can receive VA benefits as a result of toxic exposure while serving in the military. The bill would amend 38 U.S.C. (the same section that provided for Vietnam veterans exposed to Agent Orange), to add a new list of diseases where it is presumed that they got this disease as a result of their exposure. The following conditions will be added to the list:
• Asthma that was diagnosed after service in a country or territory listed
• Cancer of any type • Chronic bronchitis • Chronic obstructive pulmonary disease • Constrictive bronchiolitis or obliterative
bronchiolitis
• Emphysema • Granulomatous disease • Interstitial lung disease • Lymphoma • Pleuritis • Pulmonary fibrosis • Sarcoidosis
The bill outlines the criteria for veterans who can be considered for presumptive conditions as those having served on active duty on or after August 2, 1990 and having spent a minimum of 15 or more cumulative days in one of the countries identified in the bill, or received a campaign medal for deployment to one of the missions considered part of the Global War on Terror, including Gulf War. These countries are:
• Afghanistan • Bahrain • Burkina Faso • Cameroon • Chad • Diego Garcia • Djibouti • Egypt • Ethiopia • Gabon • Ghana • Iraq
• Jordan • Kenya • Kuwait • Kyrgyzstan • Libya • Mali • Niger • Nigeria • Oman • Pakistan • Philippines • Saudi Arabia
• Somalia • South Sudan • Sudan • Syria • Tajikistan • Tunisia • Turkey • United Arab
Emirates • Uzbekistan • Yemen
In addition, the Secretary of Veterans Affairs, in conjunction with the National Academies, are directed to evaluate petitions to determine whether there is scientific evidence of a link between human disease and exposure to one of the covered toxins, for potential addition to the list. Following the recommendation by the National Academy the Secretary must add that disease to the list or publicly state why it is not being added. Finally, the bill would create a presumption for disability or death incurred by a civilian federal employee caused by the same list of diseases, and would make it compensable under the Federal Employees’ Compensation Act (FECA) if that employee had served overseas in same list of countries or territories in support of military operations.

TABLE OF CONTENTSTABLE OF CONTENTSTABLE OF CONTENTS
DEAR COLLEAGUE .................................................................................................................................. 2
PRESUMPTIVE WAR FIGHTERS TOXINS ACT 2020 ........................................................................ 3
I. ISSUE ......................................................................................................................................................... 5
The Truth About Burn Pits...................................................................................................................... 7
II. WHY ARE BURN PITS BAD? ............................................................................................................. 8
III. SUMMARY OF BURN PITS, SANDSTORMS, IEDS, METALS, AND OTHER AIRBORNE HAZARDS .................................................................................................................................................... 9
U.S. Air Force Memo – Burn Pit Health Hazards ...................................................................................10 U.S. Air Force Memo – Air Quality Summary on Bagram Airfield (BAF) ..............................................12 U.S. Air Force Memo – Waiver of Requirements to include Occupational and Environmental Monitoring Summaries in Individual Medical Records ...........................................................................13 Balad Air Sampling Summary ..................................................................................................................14
IV. HOW MANY SERVICE MEMBERS ARE SICK? ...........................................................................15
Burn Pits 360 – Burn Pit Registry Heat Map ...........................................................................................16 Burn Pits 360 Registry Members by State and Congressional District ...................................................17 Burn Pits 360 Registry Self-Reported Symptoms and Illnesses ................................................................24 VA Airborne Hazards and Open Burn Pit Registry Enrollment Table .....................................................26 Burn Pits 360 Registry Self-Reported Cancers ........................................................................................27
V. EXAMPLES OF IMPACT ON AMERICAN SERVICE MEMBERS ..............................................28
SSG Will Thompson - U.S. Army ..............................................................................................................28 CAPT Le Roy Torres - U.S. Army ............................................................................................................29 TSgt Amie Muller - U.S. Air Force...........................................................................................................30 COL David McCracken - U.S. Army ........................................................................................................31
VI. SCIENTIFIC EVIDENCE ...................................................................................................................32
Burn Pits 360 - Toxic Exposure Table .....................................................................................................33 Congressional Letter of Support – Richard Meehan, MD .......................................................................46 Congressional Letter of Support – Allyn Harris, MD ..............................................................................49 Congressional Letter of Support – Robert Miller, MD ............................................................................50 Congressional Letter of Support – Anthony Szema, MD ..........................................................................51 Additional Scientific Literature ................................................................................................................52
VII. VA CLAIMS HISTORY .....................................................................................................................54
Media: How the VA is Failing to Track Veterans Burn Pit Claims .........................................................55
VIII. MEDIA AND NEWSPAPER COVERAGE ....................................................................................60
IX. DIGITAL MEDIA .................................................................................................................................67
X. FALLEN HEROES ................................................................................................................................70
XI. MILITARY TOXIC EXPOSURE COALITION ...............................................................................71

5
I - ISSUE
It all burned. Human waste, aerosols, Styrofoam, medical waste, biohazardous materials, body parts, trucks, and explosives. Hundreds of tons of waste produced on Coalition bases in Iraq and Afghanistan were burned in football field-sized hollows of roiling flame and unceasing smoke, propelled by jet and diesel fuels – as American soldiers lived, worked, and slept on site.
Unsurprisingly, many of our veterans are now sick and dying from lung diseases, cancers, and respiratory illnesses after inhaling this toxic smoke while serving our country overseas. Yet, the Department of Veterans Affairs and the Department of Defense continue to ignore our veterans’ suffering and death caused by their own department policies.
The VA claims it has no evidence that soldiers are facing long-term health problems due to their exposure to toxic military burn pits. The VA and the DoD refuse to investigate or acknowledge the consequences of their policies. And as a result, service members who survived the battlefield are returning home to become delayed casualties of war, suffering and dying from lung diseases, cancers, and respiratory illnesses caused by their exposure to toxic chemicals.
It is well established that burning regular household waste releases carcinogens, neuro-disruptors, and heavy metals that can have devastating effects on the lungs, heart, brain, thyroid, and immune system. Both federal and state government agencies have compiled decades of research linking these toxins to diseases and birth defects. It’s why using burn pits on American soil is against the law.
It is hard then to believe the VA and DoD don’t “know enough” about these burn pits to take action to help our service members and their families. In fact, internal memos that are now publicly available show that the VA and DoD actually are aware of this problem and continue to ignore it. In 2006, Air Force bioenvironmental engineer, Lt. Col. Darrin Curtis, observed an “operational health risk to those that have been, are now and will be deployed to [Joint Base] Balad,” due to burn pit exposure. Air Force chief of aeromedical services, Lt. Col. James Elliott agreed, stating, “the known carcinogens . . . released by the burn pit present both an acute and a chronic health hazard to our troops and the local population.”
A 2011 memo from Army environmental science engineer, Cpt. G. Michael Pratt, based on eight years of samples at Bagram Air Field, Afghanistan, assessed the air quality as “unhealthy.” Cpt. Pratt concluded, there may be an increased risk of long-term heart and lung conditions as a result of poor air quality and particulate matter, primarily contributed by the burn pit on site.
But because the VA refuses to acknowledge the connection between burn pits and toxic exposures, thousands of veterans have been refused VA care for their conditions. They are denied outside referrals to doctors who specialize in the field, and if their disease takes their lives, their dependents receive no benefits to help them in the years to come without their loved ones.
For every soldier returning with horrific health defects, there are untold numbers of service members who continue to be subjected to burn pit sites and toxic smoke to this day.
The DoD and VA must acknowledge the reality and gravity of the problems toxic chemicals from burn pits have caused and take immediate action to end the use of the 9 active burn pits once and for all.

6
In addition, Congress must make health care and compensation available to veterans and service members who are suffering exposure-related health effects. And, we must pass legislation that grants surviving families of deceased veterans the benefits they deserve.
All our efforts to obtain compensation through the judicial system have come to an end, as the courts held that the political question doctrine prevented the dispute from being heard. The big defense contractors were granted sovereign immunity. In the course of the litigation, KBR successfully argued that it was acting under military supervision and is immune from liability. The courts never took up the question of whether the burn pits caused harm.
Decades of advocacy begins with the suffering, the wounded and the dead whose families are now calling on congress demanding justice. Congress must act quickly, the question shouldn’t be scientific. The question should be, Are we fulfilling our moral obligation to protect and serve these service men and women that borne the burden of America’s defense. It’s time we recognize these injuries as an instrumentality of war.
We must take action to chip away at the complex web of barriers, erected by entrenched political and bureaucratic interests, which deprive a class of injured Veterans of healthcare and benefits.
Veterans continue to die without appropriate care. We must pass the ‘‘Presumptive Benefits for War Fighters Exposed to Burn Pits and Other Toxins Act of 2020’’.

7
8
II - WHY ARE BURN PITS BAD?
It has long been established that the burning of waste and garbage has significant negative impacts on the environment and human health. Carcinogenic toxins such as dioxin, polycyclic aromatic hydrocarbons, and small sharp particulate matter can wreak havoc on the respiratory, immune, and central nervous system as well as the heart, liver, and kidneys. Particulate matter can affect health on two-time scales. The first time scale is long-term exposure, lasting from months to years, which can influence the incidence and susceptibility to chronic disease. Sanders et al. (2005) surveyed 15,000 military personnel deployed to OEF/OIF. It was estimated that 69.1% reported respiratory illness while 17% required medical care. Chronic exposure to particulate matter can result in “increases in lower respiratory symptoms, chronic obstructive pulmonary disease (COPD), reduced lung function, and a reduced life expectancy.” The reduced life expectancy may be attributed to “cardiopulmonary mortality.”
Long term PM2.5 exposure is associated with a 6% increase in the risk of death. The relative risk for deaths from cardiovascular diseases and lung cancer are estimated to be 12% and 14%, respectively, per 10 μg/m3 increase in PM2.5 levels.
The second time scale is short-term exposure, which may display as acute health events. King et al. (2008) presented at the American Thoracic Society (ATS) “a case series of 47 soldiers with recent deployment in the Iraq War that presented with unexplained dyspnea.” All of the cases were exposed to sand storms, smoke, and dust. Many soldiers were exposed to a sulfur fire in Mishraq in 2003. After diagnosis and analysis, researchers found that 51% of the soldiers had lung pathologies consistent with bronchiolitis.
Sources:[1] Lorber, M. (2001). Indirect exposure assessment at the United States Environmental Protection Agency. Toxicology and industrial health, 17(5-10), 145-156.[2] Weese, C. B., & Abraham, J. H. (2009). Potential health implications associated with particulate matter expo sure in deployed settings in southwest Asia. Inhalation toxicology, 21(4), 291-296.
9
III - SUMMARY OF BURN PITS, SANDSTORMS, IEDS, METALS, AND OTHER AIRBORNE HAZARDS
Since the 1980’s, the Environmental Protection Agency’s (EPA) has been aware of the damaging effects burning garbage has on human health. In a 1980 health-assessment of a municipal solid waste incinerator in Ohio, the EPA found dangerous levels of toxins and particulate matter in the surrounding residential area. Further, it was discovered that the proximity to the garbage-burning incinerator spiked the predicted lifetime cancer risks of the nearby neighborhoods and, thus, triggered immediate regulatory activity.
There are several toxins and particulates that are released during the burning process: (1) carcinogenic polycyclic aromatic hydrocarbons; (2) volatile organic compounds,which can worsen existing respiratory and heart conditions causing further damage to the liver, kidneys, and central nervous system; (3) hexachlorobenze, which can cause cancer and lead to kidney and liver damage;1 and (4) other small particulate matter. Inhalation of small particulate dust (~10 μg/m3) can trigger asthma even in the absence of allergic sensitization.
Most United States soldiers deployed during Operation Iraqi Freedom and the other campaigns involved in the War on Terror served extended or multiple tours of duty. The unique climate of Iraq and the Middle East leads to frequent and severe sandstorms and exposed these soldiers to unfavorably dusty conditions. Measured air pollution levels in the ambient air of Balad, Iraq, between Jan. 2004 – Apr. 2006, were recorded several 10-fold higher than acceptable particulate limits.
Additional sundry airborne hazards include: inhalation of improvised explosive devices (roadside bombs), vehicle improvised explosive devices, blast overpressure from friendly and combatant mortar fire leading to shear stress on delicate lung tissue, as well as tank fired rounds, sandstorms, known as Shamal and Sharq, oil well and sulfur fires, and seasonal pollen counts.

10

11

12

13

14
2008
2004
2006
2007
2005
AFIO
H R
epor
t Sam
plin
g Ja
n -A
pr
Bal
ad A
ir S
ampl
ing
Sum
mar
yAs
of 1
Jan
200
8

15
IV - HOW MANY SERVICE MEMBERS ARE SICK?
According to recent estimates by the U.S. Government Accountability Office and the Department of Defense, there were at least 230 burn pits in Iraq and Afghanistan. Further, it is estimated over 3.5 million military personnel have been exposed to the burn pits.[1] The largest of these burn pits were located at Balad Air Base, Iraq, (Camp Anaconda) and comprised 10-acres of burning trash 24-hours a day, 365-days a year, from 2003-2009.
All U.S. military personnel entered Iraq by flying into this airbase. Many military personnel, private contractors, and civilian workers have all been negatively affected by burn pits and as a result, have developed several serious health issues. Under certain conditions, military personnel can go to the VA for support, however, oftentimes private contractors and civilian workers have nowhere to turn.[2]
Although there is a registry for veterans and military personnel, there needs to be a more comprehensive registry for contractors and civilian workers who developed health problems due to their burn pit exposure. Ideally, a comprehensive registry would facilitate remedial action and benefits for those who manifested illness and provide a record for those who develop related issues later in life.
Moreover, the fallout from burn pits will likely continue into future generations. This was the first campaign that saw women serving in combat and studies have shown maternal exposure to airborne hazards has been linked to preterm birth and restricted fetal growth. Meaning that, deployed women exposed to these conditions run the risk of having future childbirth issues. There has also been evidence of increased birth deformities for Iraqi children born near burn pit locations.[3]
Sources:[1] A. Bennet (2019). America’s ‘sacred obligation.’ 3.5 Million Troops Exposed to Airborne Toxins Since 9/11. ConnectingVets.com [2] D. Sagalyn (2014). Photo Essay: The Burn Pits of Iraq and Afghanistan. PBS (2014)[3] Melody, S. M., Ford, J., Wills, K., Venn, A., & Johnston, F. H. (2019). Maternal exposure to short-to medium- term outdoor air pollution and obstetric and neonatal outcomes: A systematic review. Environmental Pollution, 244, 915-925.

16
BURN
PIT
S 36
0 - B
URN
PIT
REG
ISTR
Y M
AP
The
regi
stry
is a
com
preh
ensi
ve a
nd c
onfid
entia
l vol
unta
ry h
ealth
sur
vey
that
w
ill a
llow
us
to b
ette
r und
erst
and
the
heal
th o
utco
mes
of o
ur s
ervi
ce m
en a
nd
wom
en e
xpos
ed to
Airb
orne
haz
ards
and
bur
n pi
ts. T
he d
ata
colle
cted
th
roug
h th
e re
gist
ry w
ill a
llow
us
to c
olla
bora
te w
ith in
depe
nden
t res
earc
hers
an
d m
edic
al in
stitu
tions
to tr
ack
and
inve
stig
ate
illne
ss, r
ecov
ery,
and
deat
hs.
5,90
8Ve
tera
ns

17
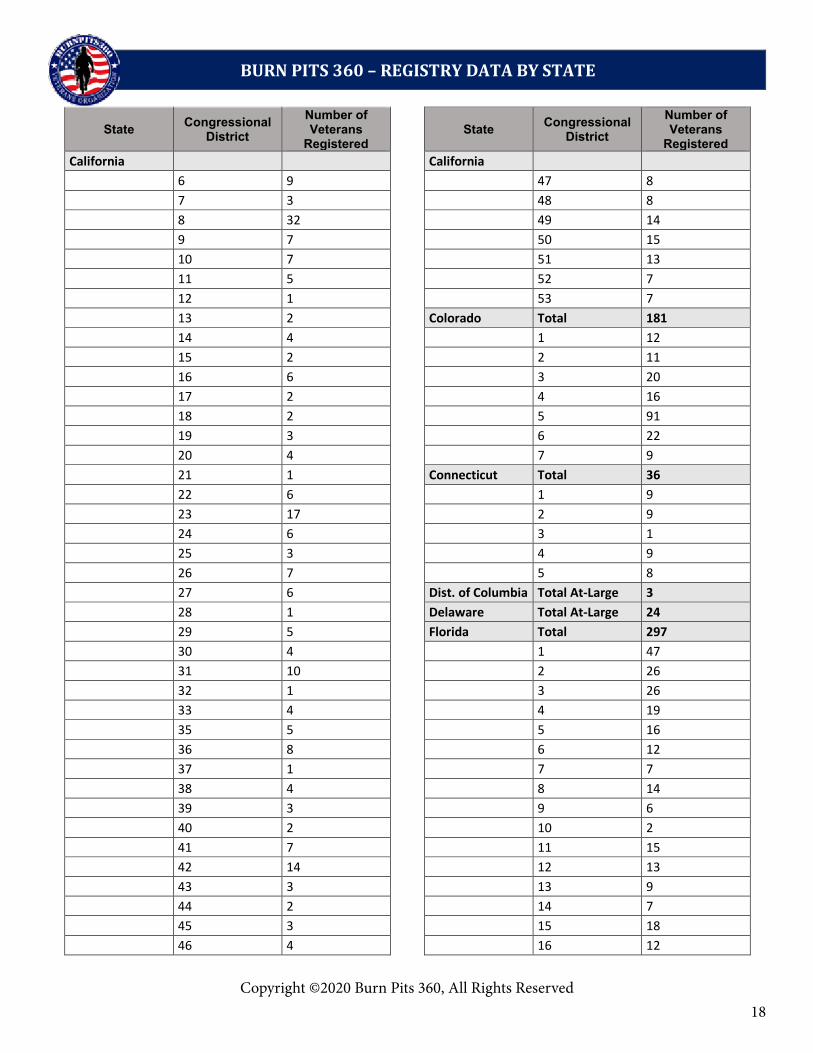
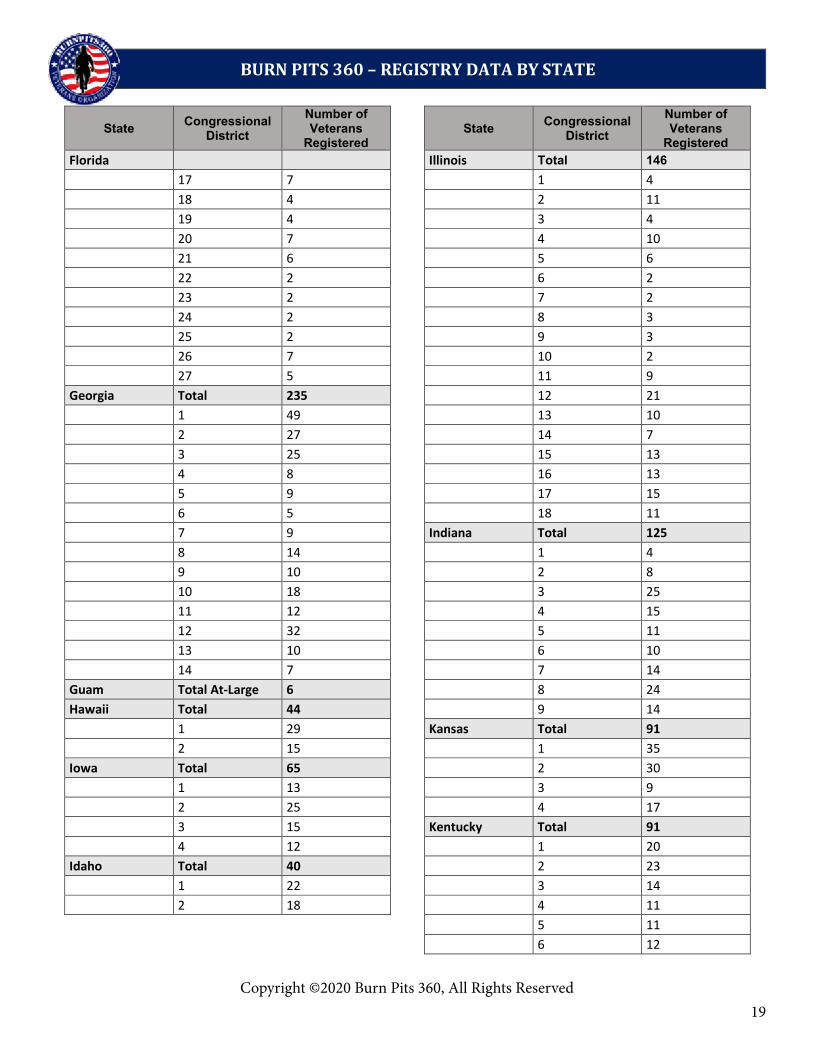
SNAPSHOT OF BURN PITS 360 REGISTRY MEMBERS BY STATE AND CONGRESSIONAL DISTRICT
BURN PITS 360 – REGISTRY DATA BY STATE
Copyright ©2020 Burn Pits 360, All Rights Reserved.
Why Register?
In 2013 Congress enacted Public Law 112-260, directing The Department of Veterans Affairs to establish and maintain the Airborne Hazards and Open Burn Pit Registry for service members who may have been exposed to toxic airborne chemicals and fumes generated by open air burn pits.
According to the VA, research does not show evidence of long-term health problems from exposure to burn pits. The VA registry does not permit service members to submit updated health information or for a dependent to submit a death entry by proxy. Burn Pits 360 established the registry in 2010 to monitor the health of service members and Veterans exposed to open air burn pits. The Burn Pit 360 registry allows eligible Veterans and service members to document their exposures, report health concerns, submit updated health and death entries through an online questionnaire that allows us to track changes in physical and mental health over time, gaps in care and denial of VA benefits. What will the data be used for?
The registry is a comprehensive and confidential voluntary health survey that will allow us to better understand the health outcomes of our service men and women exposed to Airborne hazards and burn pits. The data collected through the registry will allow us to collaborate with independent researchers and medical institutions to track and investigate illness, recovery, and deaths.
State Congressional District
Number of Veterans
Registered State Congressional
District Number of Veterans
Registered Alaska At-Large 60 Arizona Total 132
Alabama Total 121 1 10
1 10 2 34
2 36 3 15
3 17 4 11
4 20 5 16
5 20 6 10
6 15 7 5
7 3 8 20
Arkansas Total 57 9 11
1 25 California Total 339
2 13 1 12
3 11 2 8
4 8 3 14
American Samoa At-Large 2 4 14
5 3
Copyright ©2020 Burn Pits 360, All Rights Reserved
18
BURN PITS 360 – REGISTRY DATA BY STATE
Copyright ©2020 Burn Pits 360, All Rights Reserved.
State Congressional District
Number of Veterans
Registered State Congressional
District Number of Veterans
Registered California California 6 9 47 8 7 3 48 8 8 32 49 14 9 7 50 15 10 7 51 13 11 5 52 7 12 1 53 7 13 2 Colorado Total 181 14 4 1 12 15 2 2 11 16 6 3 20 17 2 4 16 18 2 5 91 19 3 6 22 20 4 7 9 21 1 Connecticut Total 36 22 6 1 9 23 17 2 9 24 6 3 1 25 3 4 9 26 7 5 8 27 6 Dist. of Columbia Total At-Large 3 28 1 Delaware Total At-Large 24 29 5 Florida Total 297 30 4 1 47 31 10 2 26 32 1 3 26 33 4 4 19 35 5 5 16 36 8 6 12 37 1 7 7 38 4 8 14 39 3 9 6 40 2 10 2 41 7 11 15 42 14 12 13 43 3 13 9 44 2 14 7 45 3 15 18 46 4 16 12
Copyright ©2020 Burn Pits 360, All Rights Reserved
19
BURN PITS 360 – REGISTRY DATA BY STATE
Copyright ©2020 Burn Pits 360, All Rights Reserved.
State Congressional District
Number of Veterans
Registered State Congressional
District Number of Veterans
Registered Florida Illinois Total 146 17 7 1 4 18 4 2 11 19 4 3 4 20 7 4 10 21 6 5 6 22 2 6 2 23 2 7 2 24 2 8 3 25 2 9 3 26 7 10 2 27 5 11 9 Georgia Total 235 12 21 1 49 13 10 2 27 14 7 3 25 15 13 4 8 16 13 5 9 17 15 6 5 18 11 7 9 Indiana Total 125 8 14 1 4 9 10 2 8 10 18 3 25 11 12 4 15 12 32 5 11 13 10 6 10 14 7 7 14 Guam Total At-Large 6 8 24 Hawaii Total 44 9 14 1 29 Kansas Total 91 2 15 1 35 Iowa Total 65 2 30 1 13 3 9 2 25 4 17 3 15 Kentucky Total 91 4 12 1 20 Idaho Total 40 2 23 1 22 3 14 2 18 4 11 5 11 6 12
Copyright ©2020 Burn Pits 360, All Rights Reserved

20
BURN PITS 360 – REGISTRY DATA BY STATE
Copyright ©2020 Burn Pits 360, All Rights Reserved.
State Congressional District
Number of Veterans
Registered State Congressional
District Number of Veterans
Registered Louisiana Total 93 Michigan 1 17 12 7 2 8 13 5 3 9 14 1 4 38 Minnesota Total 93 5 9 1 10 6 12 2 15 Massachusetts Total 91 3 9 1 18 4 11 2 15 5 4 3 10 6 13 4 8 7 13 5 6 8 18 6 3 Missouri Total 174 7 4 1 8 8 9 2 19 9 18 3 34 Maryland Total 92 4 52 1 10 5 9 2 23 6 15 3 8 7 18 4 9 8 19 5 13 Mississippi Total 83 6 9 1 13 7 8 2 19 8 12 3 14 Maine Total 25 4 37 1 11 Montana Total At-Large 26 2 14 North Carolina Total 211 Michigan Total 146 1 10 1 20 2 39 2 16 3 30 3 11 4 11 4 21 5 10 5 7 6 11 6 7 7 14 7 16 8 48 8 12 9 19 9 9 10 4 10 9 11 4 11 5 12 5
Copyright ©2020 Burn Pits 360, All Rights Reserved

21
BURN PITS 360 – REGISTRY DATA BY STATE
Copyright ©2020 Burn Pits 360, All Rights Reserved.
State Congressional District
Number of Veterans
Registered State Congressional
District Number of Veterans
Registered North Carolina New York 13 6 9 3 North Dakota Total At-Large 22 10 2 Nebraska Total 35 11 5 1 17 12 1 2 12 13 4 3 6 15 1 New Hampshire Total 30 17 3 1 14 18 14 2 16 19 8 New Jersey Total 69 20 9 1 11 21 30 2 9 22 8 3 16 23 3 4 10 24 11 5 2 25 3 6 2 26 1 7 3 27 7 8 3 Ohio Total 177 9 2 1 13 10 3 2 8 11 3 3 4 12 5 4 11 New Mexico Total 65 5 8 1 26 6 13 2 22 7 16 3 17 8 7 Nevada Total 59 9 11 1 3 10 15 2 18 11 6 3 15 12 15 4 23 13 4 New York Total 150 14 12 1 13 15 21 2 7 16 13 3 5 Oklahoma Total 127 4 3 1 21 5 1 2 15 6 1 3 20 7 4 4 57 8 3 5 14
Copyright ©2020 Burn Pits 360, All Rights Reserved

22
BURN PITS 360 – REGISTRY DATA BY STATE
Copyright ©2020 Burn Pits 360, All Rights Reserved.
State Congressional District
Number of Veterans
Registered State Congressional
District Number of Veterans
Registered Oregon Total 51 Tennessee Total 168 1 8 1 21 2 17 2 13 3 5 3 14 4 15 4 17 5 6 5 9 Pennsylvania Total 153 6 19 1 7 7 60 2 13 8 6 3 1 9 9 4 9 Texas Total 865 5 3 1 24 6 5 2 20 7 5 3 22 8 5 4 24 9 17 5 16 10 12 6 20 11 6 7 13 12 17 8 18 13 12 9 6 14 4 10 16 15 10 11 16 16 9 12 24 17 10 13 16 18 8 14 5 Puerto Rico Total At-Large 18 15 22 Rhode Island Total 20 16 38 1 9 17 15 2 11 18 7 South Carolina Total 94 19 11 1 22 20 33 2 22 21 30 3 11 22 9 4 8 23 24 5 13 24 10 6 10 25 72 7 8 26 20 South Dakota Total At-Large 16 27 103 28 37 29 2 30 11
Copyright ©2020 Burn Pits 360, All Rights Reserved

23
BURN PITS 360 – REGISTRY DATA BY STATE
Copyright ©2020 Burn Pits 360, All Rights Reserved.
State Congressional District
Number of Veterans
Registered State Congressional
District Number of Veterans
Registered Texas Wisconsin 31 99 5 5 32 5 6 17 34 38 7 10 35 29 8 9 36 10 West Virginia Total 45 Utah Total 61 1 16 1 34 2 15 2 5 3 14 3 7 Wyoming Total At-Large 16 4 15 Virginia Total 269 1 40 2 34 3 34 4 28 5 13 6 12 7 20 8 29 9 17 10 20 11 22 Vermont Total At-Large 15 Washington Total 178 1 6 2 23 3 22 4 17 5 13 6 12 7 7 8 23 9 2 10 53 Wisconsin Total 84 1 8 2 9 3 21 4 5
Copyright ©2020 Burn Pits 360, All Rights Reserved

24Copyright ©2020 Burn Pits 360, All Rights Reserved
1 Copyright ©2020 Burn Pits 360, All Rights Reserved.
BURN PITS 360 REGISTRY SELF-REPORTED SYMPTOMS & ILLNESSES
The following symptoms and illnesses listed here are self-reported from the Burn Pits 360 Registry.
SYMPTOMS
Abdominal pain Autoimmune Behavior changes (e.g., restlessness) Blood in stool Blurred vision Blurred vision Body aches Chest pain Confusion and disorientation Congestion Constipation Cough - General Cough - Passing (comes and goes) Cough - Persistent Diarrhea Diarrhea - Severe Difficult or painful urination Difficulty breathing Difficulty swallowing Dizziness Drooling Drowsiness Edema Excessive tearing Eye discomfort and redness Eye problems Facial paralysis Fatigue Fever Foot pain or ankle pain Foot swelling or leg swelling Headache Heart palpitations High Blood Pressure Hip pain Infertility Joint pain
Knee pain Loss of appetite Loss of muscle control and muscle twitching Low back pain Low blood pressure (hypotension) Low Vitamin D Memory Loss Minor skin or eye irritation Nasal congestion Nausea or vomiting Neck pain Numbness or tingling in hands Paleness (pallor) or flushed or yellowish skin Pelvic pain: Female Pelvic pain: Male Rapid heart rate Rectal bleeding Runny nose Seizures Shortness of breath Shoulder pain Skin changes Skin lesions/rashes Sleep Apnea Sore throat Soreness or stiffness in the joints Stomach cramps Stomach Distention Sweating Thirst Thyroid problems Toxic brain injury/hypoxic Encephalopathy Trembling Urinary problems Weakness Wheezing

25Copyright ©2020 Burn Pits 360, All Rights Reserved
2 Copyright ©2020 Burn Pits 360, All Rights Reserved.
BURN PITS 360 REGISTRY SELF-REPORTED SYMPTOMS & ILLNESSES
TOP 10 REPORTED CANCERS
SKIN BRAIN
ESOPHAGEAL LEUKEMIA
LYMPHOMA LUNG
SOFT TISSUE SARCOMA TESTICULAR PROSTATE
BLOOD
OTHER CANCERS (2011-2018)
Acoustic neuroma blastoma Acute Lymphoblastic Lymphoma Acute myeloid leukemia Adenoid Cystic Carcinoma Anaplastic Astrocytoma Anaplastic Astrocytoma Aplastic Anemia Bladder Breast Cancer Chordoma - Skull base Chronic Lymphatic Leukemia Chronic Lymphocytic Leukemia b-cell Stage 0 Chronic Myelogenous Leukemia Dermatofibrosarcoma Protuberans Diffuse Large B-Cell Lymphoma Dysgerminoma (Ovarian Cancer Epithelial Mucinous Cancer (ovarian cancer) Esophageal Leukoplasia Ewings Sarcoma Gastroesophageal adenocarcinoma
Glioblastoma Hemochromatosis Hepatoid adenocarcinoma Hodgkins lymphoma Large Cell Lymphoma Liver Lymphatic Cancer Medulloblastoma meningioma brain tumor Neuroendocrine carcinoma Non Hodgkins Diffuse Large Cell Lymphoma Pancreatic Polycythemia Vera Renal Cell Carcinoma Round Blue Cell Soft tissue sarcoma Soft Tissue, Leiomyosarcoma Squamous cell mouth Synovial sarcoma Testicular Thyroid

26
19 BURN PIT 360 - PREPARED BY SZEMA RESEARCH TEAM, HOFSTRA-NORTHWELL SCHOOL OF MEDICINE
The Airborne Hazards and Open Burn Pit Registry Number of Participants
The Airborne Hazards and Open Burn Pit Registry allows eligible Veterans and service members to document their exposure to airborne hazards such as burn pit smoke through an online questionnaire. In total, 186,051 Veterans and service members completed the questionnaire since the start of the registry in June 2014 through the 1st Quarter of Fiscal Year 2020 (December 31, 2019).
Number of Participants* by Location June 2014 through 1st Quarter Fiscal Year 2020
U.S. State /Territory
Number of Participants
U.S. State /Territory (continued)
Number of Participants
U.S. State /Territory (continued)
Number of Participants
Alabama 4,393 Alaska 1,432 Kansas 2,651 North Dakota 594 American Samoa
3 Kentucky 3,153 Ohio 3,967 Louisiana 2,548 Oklahoma 4,152
Arizona 4,576 Maine 706 Oregon 1,266 Arkansas 1,756 Maryland 4,406 Pennsylvania 4,527 California 12,162 Massachusetts 1,962 Puerto Rico 73 Colorado 5,642 Michigan 2,915 Rhode Island 503 Connecticut 902 Minnesota 2,325 South Carolina 3,905 Delaware 739 Mississippi 1,708 South Dakota 919 District of Columbia
333 Missouri 3,241 Tennessee 5,170 Montana 762 Texas 22,039
Florida 11,252 Nebraska 1,454 Utah 1452 Georgia 8,312 Nevada 2,284 Vermont 616 Guam 10 New
Hampshire 692 Virginia 10,762
Hawaii 2,356 Washington 5,435 Idaho 950 New Jersey 2,260 West Virginia 1,036 Illinois 3,712 New Mexico 1,805 Wisconsin 2,393 Indiana 2,486 New York 4,995 Wyoming 476 Iowa 1,367 North Carolina 10,535 Unknown 7,184 Other Armed Forces locations outside the U.S.
Americas 94 Europe 2,815 Pacific 1,072
*Participants are Veterans and service members who have submitted a complete questionnaire.

27
28
V - EXAMPLES OF IMPACT ON AMERICAN SERVICE MEMBERS
U.S. ARMY- SSG WILL THOMPSON
My name is retired SSG William Joseph Thompson. I served 23 years, 3 months and 11 days in United States Army and WVARNG. I deployed twice with the WVARNG to Iraq. I was stationed at camp Stryker on the Victory Complex. My symptoms of frequent coughing started in September 2009 while in Iraq. I was treated for allergies by my doctors and PA’s. I returned to Fort Stewart, Ga and after I mentioned to the doctors I had been having a frequent cough, they did a CXR that revealed bilateral pneumonia. They treated me with antibiotics and sent me home to WV to follow up with my PCP in one week. I followed up with my doctor, Dr. Remines and after a CT scan, he discovered that I had pulmonary fibrosis with pulmonary nodules. He stated my lungs looked like an 80 year old coal miners lungs. He referred me to Walter Reed Army Medical Center where I was treated by Dr. Jacob Collins for 6 months. He admitted me to the warrior transition unit at Walter Reed and after 6 months of testing, which included an open lung biopsy, I was informed I had titanium, magnesium, iron and silica in my lungs. They diagnosed me with Hypersensitivity Pneumonitis with Pulmonary fibrosis.
I am a warrior of the United States of America. I gave my lungs for my country. The toxins in the air from burn pits and toxic dust in Iraq has changed my life forever. I will never be the way that I used to be. I am glad to be alive and home when others did not get that chance. I have heard so many times from the VA “we don’t know how to treat you” or “you don’t qualify or fit into the parameters for benefits”. I have been denied TSGLI because the Army does not think having a lung transplant is a “traumatic event”. I have been denied housing adaptation 3 times from the VA because I was not dismembered or don’t meet their qualifications Although I was 100% service connected through the Army and the VA, I do not qualify to receive my retirement until age 60 because my injuries were not “combat related”.
I may not live to be 60. Every day for me is a battle I continue to fight. I still have to battle infections and try to keep my body healthy from lung rejection. Hopefully, after hearing my story, it will bring awareness, not only for me but other veterans who are battling the same VA system that still doesn’t recognize injuries related to burn pit exposures and toxic dust from Iraq and Afghanistan.

29
U.S. ARMY - CAPTAIN LE ROY TORRES
My name is Retired Captain Le Roy Torres. I served a dual role as a Texas State Trooper (14 years) and a United States Army Soldier (23 years). I was deployed to Balad, Iraq from 2007 to 2008 where I was exposed to toxic chemicals from one of the largest open-air burn pits which was 10 acres in size.
As a man, a husband and a father I have felt stripped of my dignity, honor and health. Imagine returning home from war only to face a system of delay and deny, an employer unwilling to accommodate a war injury resulting in the involuntary end of my police career, foreclosure letters, repossession notices and denial of compensation claims.
As a military combat Veteran and First responder my mission to serve is etched in my soul and heart and I will do so until that flag is draped over my coffin. Since returning from Iraq I have had over 250 medical visits and was hospitalized immediately upon returning from Iraq.
The lack of specialized health care services from the VA and DOD forced me to exhaust my life savings to access specialized health care. I was diagnosed with war lung disease (constrictive bronchiolitis), a toxic brain injury that has the same effects of CTE brain injury found in NFL football players and many other illnesses that debilitate my body’s ability to function.
The mental and emotional trauma is from being shamed and treated like a defendant having to prove that I should have the right to keep my job after being injured in war. My employer The Department of Public Safety came to my house and stripped me of my credentials and my patrol car in front of my family like a criminal. I was punished for serving my country.
I graduated with my master’s degree while on my military leave and returned to war two weeks later. Why is this important? We go to war to serve our country knowing the uncertainty of death or injury. What we don’t plan on is returning home to fight a whole new war of having to prove our illnesses and injuries. None of us return from War with the hopes of losing our careers, homes and families.
Our employers and our government continue to hide behind the curtain of sovereign immunity.
Decades of advocacy begins with the suffering, the wounded and the dead whose families are now calling on congress demanding justice. The 9/11 World Trade Center first responders were told by our government that the air was safe, they too are sick and dying. After a decade of building systemic momentum we have joined efforts with our 9/11 first responders, the Feal Good Foundation and Jon Stewart to apply their blue print of grassroots advocacy. It’s time to deliver hope to the service men and women that borne the burden of America’s defense. It’s time we recognize these injuries as an instrumentality of war.

30
U.S. AIR FORCE - TECHNICAL SERGEANT AMIE MULLER
Technical Sergeant Amie M. Muller served in the Active Duty Air Force in Security Forces, and in the Minnesota Air National Guard as a military photojournalist. She created a program to honor fallen service members by providing the surviving family with collected videos and photographs. Muller would document the transfer of the remains, military funerals, and honor guard. Some of the noted services she covered were for a Tuskegee airman and a soldier killed in the Fort Hood mass shooting. As a skilled graphic artist, Muller designed Minnesota’s Gold Star License plate for the families of military members killed-in-action.
She was deployed twice to Balad, embedded with a military intelligence squadron. At Balad, the burn pits were more than 10 acres in size. Every day the pit burned at all hours and consumed an estimated 100 to 200 tons of waste per day. Amie’s barracks were near the burn pits.
When she returned home in 2007, she began experiencing health problems that were unusual for a woman in her 30s. She felt fatigued and suffered from constant migraines. She then started to suffer from abdominal pain and gastrointestinal problems. When she was hospitalized for the pain, the doctors found a tumor on her pancreas. Amie was diagnosed with Stage III pancreatic cancer, and nine months later she passed away. She was only 36. She is survived by her husband and three children.

31
U.S. ARMY - COLONEL DAVID MCCRACKEN
David McCracken grew up in New Castle, Pennsylvania. He was the son of a Korean War veteran and a homemaker. As a child, David loved school and was highly intelligent. He went on to be an industrial hygienist and his love for the military drove him to enlist in the Army.
David and Tammy were married for 16 years and met while working at the United States Military Academy in West Point, NY. According to his wife Tammy, David was always fit and lean. He was an avid weightlifter and runner before he left for his tour in Iraq. When David returned from Baghdad in 2009, he developed a dry cough. The cough persisted and soon headaches began plaguing him. His situation worsened as he started to develop cognitive issues, disorientation, and confusion. In 2011, doctors discovered an aggressive brain tumor. He was only 46.
David passed within a few months of the tumor’s discovery. He is survived by his wife and three young children. Tammy suspects that David’s exposure to burn pits caused his tumor. David was stationed at the same base and time frame as Former Vice President Joe Biden’s son, Beau Biden. Both men developed glioblastoma multiforme, a lethal form of brain cancer.

32
VI - SCIENTIFIC EVIDENCE
The foundational burn pit study was a retrospective review of veterans from the Northport Veterans Affairs Medical Center in New York. In that review, researchers analyzed and compared the medical records of 6,233 soldiers who served between 2004 and 2007 (920 of which were deployed, the remaining 5,313 remained stateside). The results showed a 53% increase in the rate of new-onset asthma among the Iraq-deployed soldiers. This data comports with the dangerously elevated levels of small particulate matter (10μg/m3) routinely recorded in Balad, Iraq, between 2004-2006. Next, researchers analyzed data from 7,151 veterans who served between 2004 and 2010. Of that sample, 1,816 were deployed to Iraq/Afghanistan. After controlling for all variables, including smoking, new-onset asthma rates were found to be six times higher in the deployed group (6.2% vs 0.7%). Moreover, the deployed group was significantly more likely to show symptoms and require spirometry over the non-deployed veterans (14.5%vs 1.8%). Air pollution and the burning of waste in open-air burn pits were considered as likely causes. Furthermore, researchers noted that the latency period for the development of lung diseases, like chronic obstructive pulmonary disease, is decades, and these findings may become more skewed over time. In a descriptive case series, 80 soldiers with inhalation exposure from their deployment to Iraq/Afghanistan were evaluated for dyspnea using pulmonary-function testing and CT scans. Additionally, 49 of those soldiers underwent lung biopsies. All of the biopsy samples were abnormal and 38 of those samples were likely due to constrictive bronchiolitis. The results of the non-invasive CT tests found air trappings or centrilobular nodules in a quarter of the soldiers. Last, the pulmonary-function test results were inferior compared to military control subjects. The studies above paired with the fact that 14% of U.S. Army medic visits in Iraq were for acute respiratory illness, opens the door for the connection between post-deployment diseases and cancers and the exposure to hazardous environmental conditions and open-air burn pits.
Sources:[1] Szema, A. M., Peters, M. C., Weissinger, K. M., Gagliano, C. A., & Chen, J. J. (2010, September). New-onset asthma among soldiers serving in Iraq and Afghanistan. In Allergy and Asthma Proceedings (Vol. 31, No. 5, p. 67).[2] Szema, A. M., Salihi, W., Savary, K., & Chen, J. J. (2011). Respiratory symptoms necessitating spirometry among soldiers with Iraq/Afghanistan war lung injury. Journal of occupational and environmental medicine, 53(9), 961-965.[3] King, M. S., Eisenberg, R., Newman, J. H., Tolle, J. J., Harrell Jr, F. E., Nian, H., ... & Miller, R. F. (2011). Constrictive bronchiolitis in soldiers returning from Iraq and Afghanistan. New England Journal of Medicine, 365(3), 222-230.

33Copyright ©2020 Burn Pits 360, All Rights Reserved
1 Copyright ©2020 Burn Pits 360, All Rights Reserved.
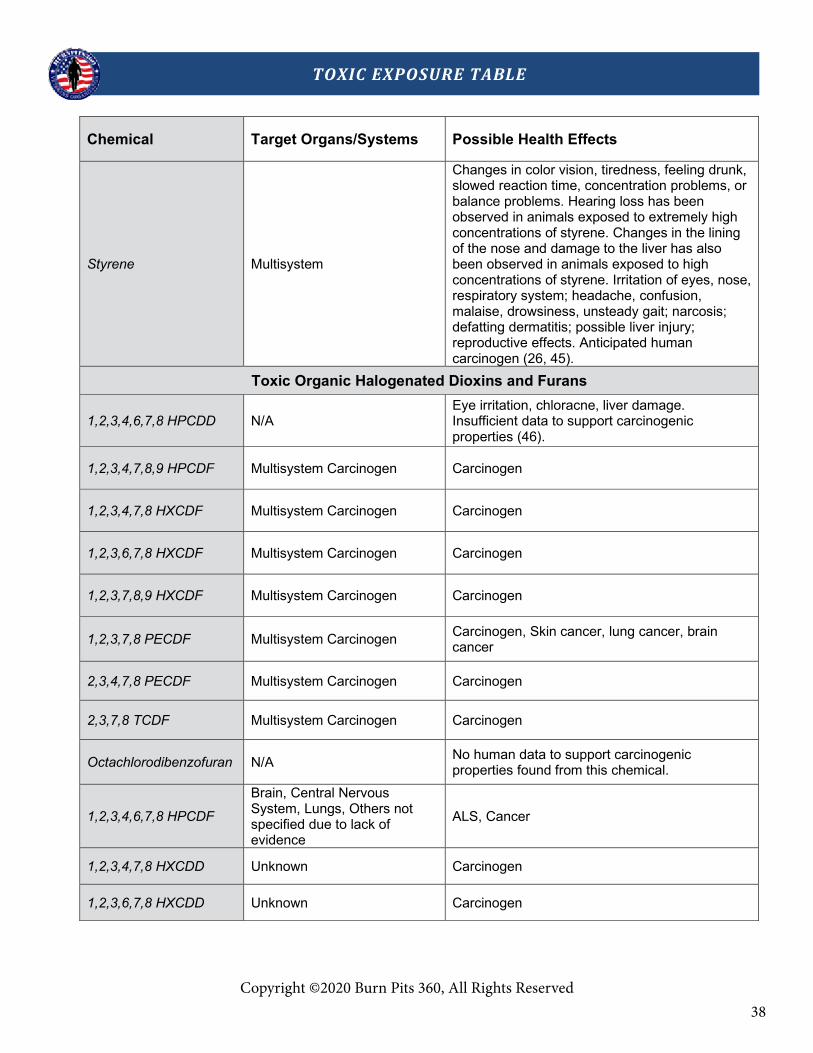
TOXIC EXPOSURE TABLE
This Toxic Exposure Table is based on the VA Training Letter 10-03 which was created in 2010 in order to educate regional office employees about specific environmental hazards that presented potential health risks to service members and Veterans. It also provided guidance to VA employees on handling claims for disabilities that may have resulted from environmental hazards while on Active Duty. Finally, the VA Training Letter 10-03 also provided “fact sheets” that could be used as a resource for VA examiners when they conduct Compensation and Pension (C&P) examinations. These “fact sheets” listed the identified toxic substances that service members were exposed to. We have compiled these toxic substances and included them the exposure table below. Our scientific committee reviewed the listed toxic substances and outlined the possible health effects that are currently supported by peer reviewed literature.
Chemical Target Organs/Systems Possible Health Effects
POLYCYCLIC AROMATIC HYDROCARBONS (PAHS)
Acenaphthene Liver and Kidneys Irritation of nose, throat and lungs upon inhalation. May affect liver and kidneys (1).
Anthracene Multisystem: Skin, blood, stomach, liver, intestines, lymph
Burning, itching and edema, a buildup of fluid in tissues, headaches, nausea, loss of appetite, inflammation or swelling of the stomach and intestines (2).
Benzo(a)pyrene Hematological, Immunological, Neurological
Mucous membrane irritation, dermatitis, bronchitis, cough, dyspnea, conjunctivitis, photosensitization, aplastic anemia, allergic reactions, keratoses, discoloration of the cornea and epithelioma lid margin in chronic exposure, pulmonary edema, reproductive effects and leukemia (9).
Genotoxic effects.
Benzo(b)fluoroanthene Hematological, Immunological, Neurological
Probable human carcinogen. Has shown lung, skin, and liver cancers in animal models. Skin and eye irritation (10).
Breathing benzene can cause drowsiness, dizziness, and unconsciousness; long-term benzene exposure causes effects on the bone marrow and can cause anemia and leukemia. Benzene has been found in at least 1,000 of the 1,684 National Priority List sites identified by the Environmental Protection Agency (EPA).

34Copyright ©2020 Burn Pits 360, All Rights Reserved
2 Copyright ©2020 Burn Pits 360, All Rights Reserved.
TOXIC EXPOSURE TABLE
Chemical Target Organs/Systems Possible Health Effects
Benzo(k)fluoroanthene Hematological, Immunological, Neurological
Probable carcinogen. Eye and skin irritant (11).
Breathing benzene can cause drowsiness, dizziness, and unconsciousness; long-term benzene exposure causes effects on the bone marrow and can cause anemia and leukemia. Benzene has been found in at least 1,000 of the 1,684 National Priority List sites identified by the Environmental Protection Agency (EPA).
Dibenz (a,h) anthracene Hematological, Immunological, Neurological
Dizziness, vomiting, unconsciousness, cancers, and other health effects from prolonged exposures. Genotoxic in mammalian cells (3).
Fluorene Hematological Decreased red blood cells, packed cell volume and hemoglobin (4).
Naphthalene Hematological, Liver, Neurological, Lungs, Eyes
Headache, nausea, vomiting, diarrhea, malaise, confusion, anemia, jaundice, convulsions coma, cataracts, retinal hemorrhage, hemolytic anemia (EPA, 5).
Pyrene Lungs, Neurological, Renal, Liver, Bone/Marrow
Probable human carcinogen. Depending on type of exposure (IE Tar, coal, smoke, etc.) cancer of the kidneys, lungs, skin, brain, and bone (12, 13).
Acenaphthylene Multisystem Cancer
The CDC warns to treat all these material as carcinogens. Samples and unused standard (extremely small doses) are considered Toxic Waste. Health effect is cancerous (13).
Benzo(a)anthracene Hematological, Immunological, Neurological
Probable carcinogen. Aplastic anemia and reproductive effects seen in animal models (14).
Breathing benzene can cause drowsiness, dizziness, and unconsciousness; long-term benzene exposure causes effects on the bone marrow and can cause anemia and leukemia. Benzene has been found in at least 1,000 of the 1,684 National Priority List sites identified by the Environmental Protection Agency (EPA).

35Copyright ©2020 Burn Pits 360, All Rights Reserved
3 Copyright ©2020 Burn Pits 360, All Rights Reserved.
TOXIC EXPOSURE TABLE
Chemical Target Organs/Systems Possible Health Effects
Benzo(g,h,i)perylene Unknown
Unknown carcinogenicity (15). Similar PAH have demonstrated carcinogenic and reproductive effects in animal models (16).
Breathing benzene can cause drowsiness, dizziness, and unconsciousness; long-term benzene exposure causes effects on the bone marrow and can cause anemia and leukemia. Benzene has been found in at least 1,000 of the 1,684 National Priority List sites identified by the Environmental Protection Agency (EPA).
Chrysene Immune System Increased risk for tumor and cancer exposure (17).
Fluoranthene Skin, Bone, Lung, Brain, Neurological, Hematological
Irritant. Contact burns, nausea, tachycardia, cardiac arrhythmias, liver injury, pulmonary edema, and respiratory arrest (18). Potential endocrine disruptor. Limited evidence of carcinogenicity (19).
Indeno(1,2,3-cd)pyrene Multisystem Carcinogen Increased allergic inflammation and airway eosinophilia (20). Carcinogen (21).
Phenanthrene Unknown
Inadequate studies to determine carcinogenic properties. Currently considered a non-carcinogenic PAH, but structurally similar to carcinogenic PAHs (22). Irritant (23).
VOLATILE ORGANIC COMPOUNDS (VOC)
Acetone Neurological
CNS depression, dermatitis , dizziness , headache, eye irritation, nose irritation, irritation of the throat, delayed reaction times, nephropathy through oral exposure (EPA, 6).

36Copyright ©2020 Burn Pits 360, All Rights Reserved
4 Copyright ©2020 Burn Pits 360, All Rights Reserved.
TOXIC EXPOSURE TABLE
Chemical Target Organs/Systems Possible Health Effects
Benzene Immune System, Blood
Drowsiness, dizziness, rapid heart rate, headaches, tremors, confusion, and unconsciousness. Eating or drinking foods containing high levels of benzene can cause vomiting, irritation of the stomach, dizziness, sleepiness, convulsions, rapid heart rate, and death. Long-term exposure to high levels of benzene in the air can cause leukemia, particularly acute myelogenous leukemia, often referred to as AML (24). Breathing benzene can cause drowsiness, dizziness, and unconsciousness; long-term benzene exposure causes effects on the bone marrow and can cause anemia and leukemia. Benzene has been found in at least 1,000 of the 1,684 National Priority List sites identified by the Environmental Protection Agency (EPA, 25).
Chlorodifluoromethane
Respiratory system, Cardiovascular system, Central Nervous System, Liver, Kidneys, Spleen
Irritation respiratory system; confusion, drowsiness, ringing in ears; heart palpitations, cardiac arrhythmias; asphyxia; liver, kidney, spleen injury; liquid: frostbite (26).
Acrolein Cardiovascular, hematological, ocular, respiratory
Irritation of upper respiratory tract and eyes, respiratory congestion, dyspnea, cyanosis, fever (27). Suppression of immune responses, may play a role in lung cancer (28, 29).
Carbon Disulfide
Central nervous system, peripheral nervous system, cardiovascular system, eyes, kidneys, liver, skin, reproductive system
Chest pain, respiratory problems, vomiting and nausea, polyneuropathy, nerve conduction abnormalities, increased risk of toxic encephalopathy, blisters with contact, cardiovascular disease, gastritis, retinopathy, Parkinson’s-like symptoms (26, 31, 32).
Chloromethane Liver, Neurological, Renal, reproductive system
Dizziness, nausea, vomiting; visual disturbance, stagger, slurred speech, convulsions, coma; liver, kidney damage; potential reproductive, teratogenic effects, potential occupational carcinogen (26, 33)
Ethylbenzene Developmental (effects during periods when organs are developing) , Neurological
Carcinogen. Neurological changes or defects with birth. Potential increase for cancers related to exposures. Irritation of eyes, skin, mucous membrane; headache; dermatitis; narcosis, coma (26, 34, 35).

37Copyright ©2020 Burn Pits 360, All Rights Reserved
5 Copyright ©2020 Burn Pits 360, All Rights Reserved.
TOXIC EXPOSURE TABLE
Chemical Target Organs/Systems Possible Health Effects
Hexachlorobutadiene Eyes, skin, respiratory system, kidneys
In animals: Kidney failure, blood issues, fluid retention. Potential human carcinogen (26, 36).
Methylene Chloride Eyes, skin, cardiovascular system, central nervous system
irritation eyes, skin; lassitude (weakness, exhaustion), drowsiness, dizziness; numb, tingling sensations in limbs; nausea; potential carcinogen (26, 37).
Propylene Unknown CNS toxicity, hyperosmolarity, hemolysis, cardiac arrhythmia, and lactic acidosis (38, 39, 40, 41).
Toluene Immunological, Neurological, Eyes, Skin, Respiratory
Irritation to eyes, skin, nose, throat; choke, paroxysmal cough; chest pain, retrosternal soreness; nausea, vomiting, abdominal pain; bronchitis, bronchospasm, pulmonary edema; dyspnea, asthma; conjunctivitis, lacrimation; dermatitis, skin sensitization; ataxia, tremors, seizure, potential carcinogen; fetotoxic in animal studies (26, 42). Toluene may be contaminated with benzene (42, 43).
Hexane Central Nervous System, Eyes, Skin, Respiratory systems
Brain and neurological changes and effects, neuropathy (44).
n-Hexane: irritation eyes, nose; nausea, headache; peripheral neuropathy: numb extremities, muscle weak; dermatitis; dizziness; chemical pneumonitis (aspiration liquid) (26).
Hexane isomers: irritation eyes, skin, respiratory system; headache, dizziness; nausea; chemical pneumonitis (aspiration liquid); dermatitis (26).
m/p-Xylene Eyes, Nose, Throat, Lungs, Skin, Brain
High levels of xylene in air can cause eye and mucous membrane irritation, dyspnea, and central nervous system effects, such as headaches, dizziness, forgetfulness, delayed reaction times, and poor coordination (ATSDR, 2007).
Pentane Eyes, skin, respiratory system, central nervous system
Irritation eyes, skin, nose; dermatitis; chemical pneumonitis (aspiration liquid); drowsiness; In Animals: narcosis (26).
38Copyright ©2020 Burn Pits 360, All Rights Reserved
6 Copyright ©2020 Burn Pits 360, All Rights Reserved.
TOXIC EXPOSURE TABLE
Chemical Target Organs/Systems Possible Health Effects
Styrene Multisystem
Changes in color vision, tiredness, feeling drunk, slowed reaction time, concentration problems, or balance problems. Hearing loss has been observed in animals exposed to extremely high concentrations of styrene. Changes in the lining of the nose and damage to the liver has also been observed in animals exposed to high concentrations of styrene. Irritation of eyes, nose, respiratory system; headache, confusion, malaise, drowsiness, unsteady gait; narcosis; defatting dermatitis; possible liver injury; reproductive effects. Anticipated human carcinogen (26, 45).
Toxic Organic Halogenated Dioxins and Furans
1,2,3,4,6,7,8 HPCDD N/A Eye irritation, chloracne, liver damage. Insufficient data to support carcinogenic properties (46).
1,2,3,4,7,8,9 HPCDF Multisystem Carcinogen Carcinogen
1,2,3,4,7,8 HXCDF Multisystem Carcinogen Carcinogen
1,2,3,6,7,8 HXCDF Multisystem Carcinogen Carcinogen
1,2,3,7,8,9 HXCDF Multisystem Carcinogen Carcinogen
1,2,3,7,8 PECDF Multisystem Carcinogen Carcinogen, Skin cancer, lung cancer, brain cancer
2,3,4,7,8 PECDF Multisystem Carcinogen Carcinogen
2,3,7,8 TCDF Multisystem Carcinogen Carcinogen
Octachlorodibenzofuran N/A No human data to support carcinogenic properties found from this chemical.
1,2,3,4,6,7,8 HPCDF
Brain, Central Nervous System, Lungs, Others not specified due to lack of evidence
ALS, Cancer
1,2,3,4,7,8 HXCDD Unknown Carcinogen
1,2,3,6,7,8 HXCDD Unknown Carcinogen

39Copyright ©2020 Burn Pits 360, All Rights Reserved
7 Copyright ©2020 Burn Pits 360, All Rights Reserved.
TOXIC EXPOSURE TABLE
Chemical Target Organs/Systems Possible Health Effects
1,2,3,7,8,9 HXCDD Unknown Carcinogen
1,2,3,7,8 PECDD Unknown Acute toxicity, long term exposure toxic
2,3,4,6,7,8 HXCDF Eyes, Mucus Membranes, other soft tissue and moist organs
Eye irritation, serious eye damage, long lasting harmful effects to aquatic life are noted, acute toxicity.
2,3,7,8 TCDD Developmental (teratogen), immune, hepatic, lymphatic, respiratory systems
allergic dermatitis, chloracne, lung cancer, soft tissue sarcomas, lymphoma, stomach carcinoma; GI distress in animals: carcinogen , in animals: hemorrhage, in animals: kidney damage, in animals: liver damage, eye irritant, porphyria, possible reproductive effects , possible teratogenic effects (7,8).
40Copyright ©2020 Burn Pits 360, All Rights Reserved
8 Copyright ©2020 Burn Pits 360, All Rights Reserved.
TOXIC EXPOSURE TABLE
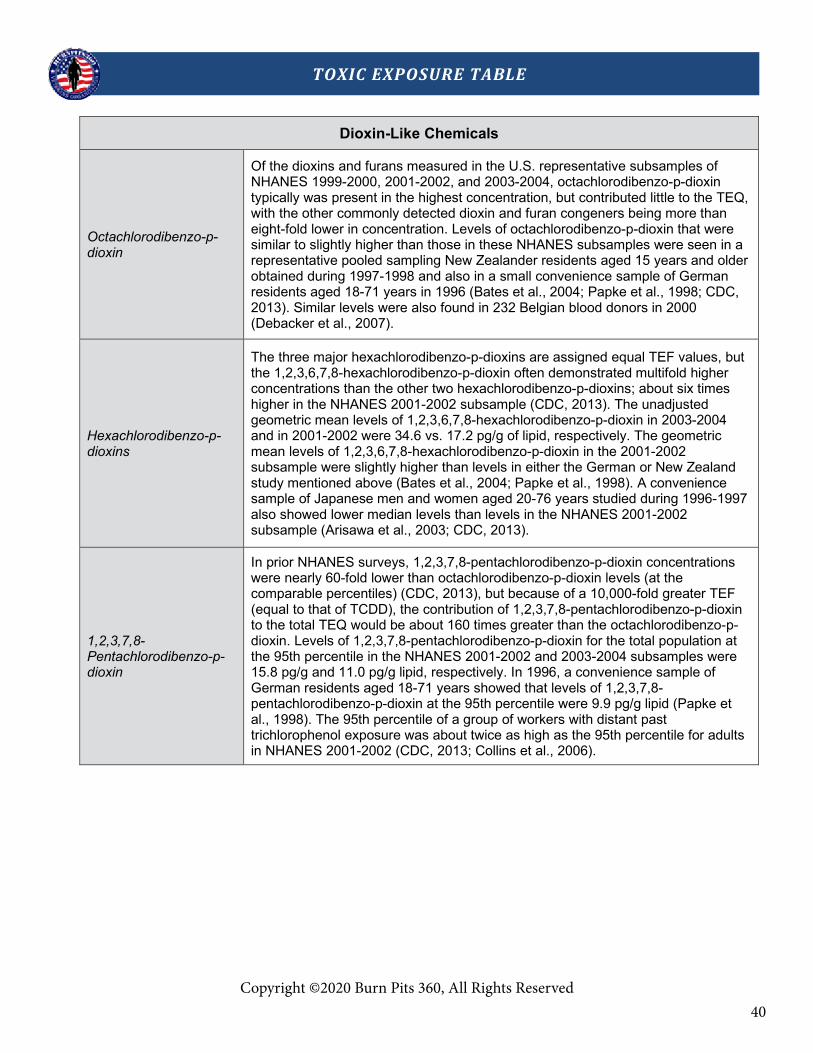
Dioxin-Like Chemicals
Octachlorodibenzo-p-dioxin
Of the dioxins and furans measured in the U.S. representative subsamples of NHANES 1999-2000, 2001-2002, and 2003-2004, octachlorodibenzo-p-dioxin typically was present in the highest concentration, but contributed little to the TEQ, with the other commonly detected dioxin and furan congeners being more than eight-fold lower in concentration. Levels of octachlorodibenzo-p-dioxin that were similar to slightly higher than those in these NHANES subsamples were seen in a representative pooled sampling New Zealander residents aged 15 years and older obtained during 1997-1998 and also in a small convenience sample of German residents aged 18-71 years in 1996 (Bates et al., 2004; Papke et al., 1998; CDC, 2013). Similar levels were also found in 232 Belgian blood donors in 2000 (Debacker et al., 2007).
Hexachlorodibenzo-p-dioxins
The three major hexachlorodibenzo-p-dioxins are assigned equal TEF values, but the 1,2,3,6,7,8-hexachlorodibenzo-p-dioxin often demonstrated multifold higher concentrations than the other two hexachlorodibenzo-p-dioxins; about six times higher in the NHANES 2001-2002 subsample (CDC, 2013). The unadjusted geometric mean levels of 1,2,3,6,7,8-hexachlorodibenzo-p-dioxin in 2003-2004 and in 2001-2002 were 34.6 vs. 17.2 pg/g of lipid, respectively. The geometric mean levels of 1,2,3,6,7,8-hexachlorodibenzo-p-dioxin in the 2001-2002 subsample were slightly higher than levels in either the German or New Zealand study mentioned above (Bates et al., 2004; Papke et al., 1998). A convenience sample of Japanese men and women aged 20-76 years studied during 1996-1997 also showed lower median levels than levels in the NHANES 2001-2002 subsample (Arisawa et al., 2003; CDC, 2013).
1,2,3,7,8-Pentachlorodibenzo-p-dioxin
In prior NHANES surveys, 1,2,3,7,8-pentachlorodibenzo-p-dioxin concentrations were nearly 60-fold lower than octachlorodibenzo-p-dioxin levels (at the comparable percentiles) (CDC, 2013), but because of a 10,000-fold greater TEF (equal to that of TCDD), the contribution of 1,2,3,7,8-pentachlorodibenzo-p-dioxin to the total TEQ would be about 160 times greater than the octachlorodibenzo-p-dioxin. Levels of 1,2,3,7,8-pentachlorodibenzo-p-dioxin for the total population at the 95th percentile in the NHANES 2001-2002 and 2003-2004 subsamples were 15.8 pg/g and 11.0 pg/g lipid, respectively. In 1996, a convenience sample of German residents aged 18-71 years showed that levels of 1,2,3,7,8-pentachlorodibenzo-p-dioxin at the 95th percentile were 9.9 pg/g lipid (Papke et al., 1998). The 95th percentile of a group of workers with distant past trichlorophenol exposure was about twice as high as the 95th percentile for adults in NHANES 2001-2002 (CDC, 2013; Collins et al., 2006).

41Copyright ©2020 Burn Pits 360, All Rights Reserved
9 Copyright ©2020 Burn Pits 360, All Rights Reserved.
TOXIC EXPOSURE TABLE
2,3,7,8-Tetrachlorodibenzo-p-dioxin
TCDD is considered the most potent of the dioxin-like chemicals and environmental exposure usually results in very low serum concentrations. In the NHANES 2003-2004 subsample, the 95th percentile for the total population (12 years and older) was 5.2 picograms/gram (pg/g) of lipid. In 1996, the 95th percentile for lipid-adjusted serum TCDD levels in 139 Germans aged 18-71 years was 4.3 pg/g of lipid, with that percentile comprising mainly older individuals (Papke, 1998). In contrast, the most highly exposed females following the Seveso, Italy, factory explosion had median lipid adjusted levels of 272 pg/g lipid in 1976 (Eskenazi et al., 2004). TCDD levels in chemical plant workers with higher exposures have ranged as high as 2,000 pg/g lipid (IARC, 1997). Median serum TCDD levels measured in chemical production workers 15 years after workplace exposure ended were 68 pg/g of lipid (Calvert et al., 1996; Calvert et al., 1999). TCDD levels in the U.S. general population were also lower than workers with past trichlorophenol exposure (Collins et al., 2006) and lower than Vietnam veterans 20 years after duty-related exposure to Agent Orange (median serum TCDD concentration was 12.2 pg/g of lipid) (Henriksen et al., 1997).
Polychlorinated dibenzofurans
Of the polychlorinated dibenzofurans, the following could be characterized at the 95th percentiles (or lower) in the NHANES 1999-2000, 2001-2002 and 2003-2004 subsamples:1,2,3,4,6,7,8-heptachlorodibenzofuran, 1,2,3,4,7,8-hexachlorodibenzofuran, 1,2,3,6,7,8-hexachlorodibenzofuran, and 2,3,4,7,8-pentachlorodibenzofuran. Generally, these levels are similar to other large population studies. In 237 workers with past exposure to trichlorophenol, where little polychlorinated dibenzofuran exposure would be expected, higher percentiles values were similar to a referent population and to the NHANES 1999-2000 and 2001-2002 subsamples (Collins et al., 2007; CDC, 2013). In 232 Belgian blood donors from the year 2000, the geometric mean level of 1,2,3,4,6,7,8-heptachlorodibenzofuran was several times lower than the geometric mean value in the NHANES 2001-2002 subsample of adults and the other dibenzofurans examined in the Belgian donors were lower than the limits of detection in NHANES 2000-2001 (CDC, 2013; Debacker et al., 2007). In Yucheng rice oil contamination victims when examined 15 years after their exposure, levels of the polychlorinated dibenzofurans were still hundreds of times higher than in levels for the U.S. population observed in the NHANES subsamples (Hsu et al., 2005).
Coplanar PCBs
The coplanar PCBs typically contribute less than about 15% to the total TEQ in the U.S. population (Ferriby et al., 2007). In the NHANES 2001-2002 subsample, the geometric mean levels of PCBs 126 and 169 for adults aged 20 years and older were similar or slightly lower than those reported from a representative pooled sample of New Zealanders in 1996-1997 (Bates et al., 2004; CDC, 2013) and from a smaller sample of non-occupationally exposed men and women aged 20-76 years in Japan in 1999 (Arisawa et al., 2003). Higher levels of these PCBs have been reported for persons consuming sport fish caught in the Great Lakes region (Turyk et al., 2006).In 311 residents of northern Italy, serum PCB 126 and 169 were not detectable, though other PCBs tended to be higher than in the recent NHANES subsamples (Apostoli et al., 2005; CDC, 2013).

42Copyright ©2020 Burn Pits 360, All Rights Reserved
10 Copyright ©2020 Burn Pits 360, All Rights Reserved.
TOXIC EXPOSURE TABLE
Mono-ortho-substituted PCBs
Of the mono-ortho-substituted PCB congeners, the most frequently detected in general population studies are PCBs 118 and 156. Of these, PCB 118 levels were higher than levels of PCB 156 in the NHANES 1999-2000, 2001-2002, and 2003-2004 subsamples, although PCB 156 contributes more to the TEQ because its TEF is five-fold greater than the TEF of PCB 118. Although these PCBs are relatively less potent (i.e., lower TEFs), their contribution to the total TEQ in the U.S. population is about 25% (Ferriby et al., 2007) since they are present in much higher concentrations than are the coplanar PCBs, dioxins, and furans. In a convenience sample of the U.S. population in 1988 (Patterson et al., 1994), levels of PCB 118 were five-fold higher than in the NHANES 1999-2002 subsamples (CDC, 2013). Comparable levels of PCB 156 levels in NHANES 1999-2000 were slightly lower than those reported for a Canadian population study in 1994 (Longnecker et al., 2000). In a referent population of 311 residents in northern Italy during 2001-2003, the 95th percentile levels of PCB 156 and PCB 118 were two to three times higher than for the NHANES 1999-2002 subsamples (Apostoli et al., 2005; CDC, 2013). Levels of PCB 156 and PCB 118 were slightly higher in a Swedish study of 150 men than in the NHANES 1999-2000 subsample, possibly due to higher fish intake in the Swedish population (Glynn et al., 2000; CDC, 2013). However, in fish-consuming Japanese men and women studied during 1996-1997, PCB 118 levels at the 75th percentile were similar to levels in the NHANES 2001-2002 subsample (Arisawa et al., 2003). Finding a measurable amount of one or more of the polychlorinated dibenzo-p-dioxins, dibenzofurans, coplanar or mono-ortho-substituted biphenyls in serum does not mean that the level of one or more of these chemicals causes an adverse health effect. Biomonitoring studies of serum polychlorinated dibenzo-p-dioxins, dibenzofurans, coplanar or mono-ortho-substituted biphenyls provide physicians and public health officials with reference values so that they can determine whether or not people have been exposed to higher levels of polychlorinated dibenzo-p-dioxins, dibenzofurans, coplanar or mono-ortho-substituted biphenyls than levels found in the general population. Biomonitoring data can also help scientists plan and conduct research on exposure and health effects.
Notes
1. Toxic Organic Halogenated Dioxins and Furans: Specific information regarding many of the individual compounds is difficult to locate. Most have not been well studied and may simply be lumped together with other dioxins and furans. Chlorinated dibenzo-p-dioxins (CDDs) are regarded as human carcinogens based on sufficient animal data. Other health effects include chloracne; a severe dermatological condition characterized by acne-like lesions. Rashes, skin discoloration, and liver damage are also possible complications from exposure. CDDs have varying harmful effects and have been divided into eight groups based on the position of chlorine molecules. Exposure may occur through inhalation, orally, or with direct skin contact. How CDDs are broken down by the body is not well understood though CDDs may be found in higher concentrations in liver and adipose tissue after exposure (47). Chlorodibenzofurans (CDFs) have not been characterized for their ability to cause cancers and have not been shown to cause cancer in animal studies. Health effects in humans include dermatological conditions, eye irritation with discharge, vomiting, diarrhea, anemia, lung infections, numbness, nervous system effects, and liver changes. Children born to exposed mothers had skin irritation and more difficulty learning (48).

43Copyright ©2020 Burn Pits 360, All Rights Reserved
11 Copyright ©2020 Burn Pits 360, All Rights Reserved.
TOXIC EXPOSURE TABLE
Citation List
1. National Center for Biotechnology Information. PubChem Database. Acenaphthene, CID=6734, https://pubchem.ncbi.nlm.nih.gov/compound/Acenaphthene (accessed on Mar. 19, 2020)
2. NM, Issa & NM, El-Sherif. (2018). Histological and Immunohistochemical Study on the Toxic Effects of Anthracene on the lung and liver of Adult Male Albino Rats and the Possible Protective Role of Ocimum gratissimum Extract. Journal of Cell Biology and Histology. 1. 10.15744/2638-082X.1.103.
3. National Center for Biotechnology Information. PubChem Database. Dibenz[a,h]anthracene, CID=5889, https://pubchem.ncbi.nlm.nih.gov/compound/Dibenz_a_h_anthracene (accessed on Mar. 20, 2020)
4. U.S. Environmental Protection Agency. 1989. Mouse oral subchronic toxicity study. Prepared by Toxicity Research Laboratories, LTD., Muskegon, MI for the Office of Solid Waste, Washington, DC.
5. U.S. Environmental Protection Agency. Toxicological Review of Naphthalene (CAS No. 91-20-3) in Support of Summary Information on the Integrated Risk Information System (IRIS). National Center for Environmental Assessment, Cincinnati, OH. 1998.
6. U.S. Environmental Protection Agency. Toxicological Review of Acetone (CAS No. 67-64-1) in Support of the Summary Information on the Integrated Risk Information System (IRIS). U.S. Environmental Protection Agency, Washington, D.C. 2003.
7. National Center for Biotechnology Information. PubChem Database. CID=15625, https://pubchem.ncbi.nlm.nih.gov/compound/2_3_7_8-Tetrachlorodibenzo-P-dioxin (accessed on Mar. 20, 2020)
8. Agency for Toxic Substances and Disease Registry (ATSDR). Toxicological Profile for Chlorinated Dibenzop-Dioxins. Public Health Service, U.S. Department of Health and Human Services, Atlanta, GA. 1998.
9. National Center for Biotechnology Information. PubChem Database. Benzo[a]pyrene, CID=2336, https://pubchem.ncbi.nlm.nih.gov/compound/Benzo_a_pyrene (accessed on Apr. 1, 2020)
10. New Jersey Department of Health and Senior Services. Hazardous Substance Fact Sheet: Benzo(b)fluoranthene (CAS No. 205-99-2). New Jersey Department of Health and Senior Services, Trenton, N.J. 1995 [Revised 2001]. (accessed Apr. 1, 2020)
11. National Center for Biotechnology Information. PubChem Database. Benzo[k]fluoranthene, CID=9158, https://pubchem.ncbi.nlm.nih.gov/compound/Benzo_k_fluoranthene (accessed on Apr. 1, 2020)
12. Faust, Rosmarie A., Oak Ridge National Laboratory, Chemical Hazard Evaluation Group. Toxicity Summary for Pyrene. Oak Ridge, T.N. 1993.
13. “CDC - NIOSH Pocket Guide to Chemical Hazards - Coal Tar Pitch Volatiles.” Centers for Disease Control and Prevention, Centers for Disease Control and Prevention, 4 Oct. 2019, www.cdc.gov/niosh/npg/npgd0145.html.
14. United States Environmental Protection Agency. Integrated Risk Information System (IRIS) Chemical Assessment Summary of Benz[a]anthracene (CASRN 56- 55-3). Office of Research and Development, National Center for Environmental Assessment, Washington, DC. 1990.
15. Faust, Rosmarie A., Oak Ridge National Laboratory, Chemical Hazard Evaluation Group. Toxicity Summary for Benzo(g,h,i) perylene. Oak Ridge, TN:1994.
16. Agency for Toxic Substances and Disease Registry (ATSDR). Public Health Statement, Polycyclic Aromatic Hydrocarbons. Atlanta, GA: U.S. Department of Health and Human Services, 1990.
17. National Center for Biotechnology Information. PubChem Database. Chrysene, CID=9171, https://pubchem.ncbi.nlm.nih.gov/compound/Chrysene (accessed on Apr. 1, 2020)
18. National Center for Biotechnology Information. PubChem Database. Fluoranthene, CID=9154, https://pubchem.ncbi.nlm.nih.gov/compound/Fluoranthene (accessed on Apr. 1, 2020)

44Copyright ©2020 Burn Pits 360, All Rights Reserved
12 Copyright ©2020 Burn Pits 360, All Rights Reserved.
TOXIC EXPOSURE TABLE
19. Ndiya Ogba, Chongmin Wang & Samir Raychoudhury (2005) Differential Effects of Fluoranthene and Benzo[a]pyrene in MCF–7 Cells, Journal of Environmental Science and Health, Part A, 40:5, 927-936, DOI: 10.1081/ESE-200056110
20. Wong, T., Lee, C., Su, H. et al. A prominent air pollutant, Indeno[1,2,3-cd]pyrene, enhances allergic lung inflammation via aryl hydrocarbon receptor. Sci Rep 8, 5198 (2018). https://doi.org/10.1038/s41598-018-23542-9
21. National Center for Biotechnology Information. PubChem Database. Indeno[1,2,3-cd]pyrene, CID=9131, https://pubchem.ncbi.nlm.nih.gov/compound/Indeno_1_2_3-cd_pyrene (accessed on Apr. 1, 2020)
22. Zhong, Y. et al. Metabolism of [D10]Phenanthrene to Tetraols in Smokers for Potential Lung Cancer Susceptibility Assessment: Comparison of Oral and Inhalation Routes of Administration. Journal of Pharmacology and Experimental Therapeutics July 1, 2011, 338 (1) 353-361; DOI: https://doi.org/10.1124/jpet.111.18171
23. National Center for Biotechnology Information. PubChem Database. Phenanthrene, CID=995, https://pubchem.ncbi.nlm.nih.gov/compound/Phenanthrene (accessed on Apr. 1, 2020)
24. Khalade, A., Jaakkola, M.S., Pukkala, E. et al. Exposure to benzene at work and the risk of leukemia: a systematic review and meta-analysis. Environ Health 9, 31 (2010). https://doi.org/10.1186/1476-069X-9-31
25. Agency for Toxic Substances and Disease Registry (ATSDR). 2007. Toxicological profile for Benzene. Atlanta, GA: U.S. Department of Health and Human Services, Public Health Service.
26. NIOSH pocket guide to chemical hazards. Department of Health and Human Services, Center for Disease Control and Prevention, DHHS (NIOSH). Online. NIOSH Publications, US.
27. Agency for Toxic Substances and Disease Registry (ATSDR). Toxicological Profile for Acrolein. 28. Public Health Service, U.S. Department of Health and Human Services, Atlanta, GA. 2007. 29. Stevens JF, Maier CS. Acrolein: sources, metabolism, and biomolecular interactions relevant to human
health and disease. Mol Nutr Food Res. 2008;52(1):7–25. doi:10.1002/mnfr.200700412 30. Lambert C, Li J, Jonscher K, Yang TC, et al. Acrolein inhibits cytokine gene expression by alkylating
cysteine and arginine residues in the NF-kappaB1 DNA binding domain. J. Biol. Chem. 2007;282:19666–19675.
31. Agency for Toxic Substances and Disease Registry (ATSDR). 1996. Toxicological profile for Carbon Disulfide. Atlanta, GA: U.S. Department of Health and Human Services, Public Health Service.
32. Swaen, G.M.H., Braun, C. & Slangen, J.J.M. Mortality of Dutch workers exposed to carbon disulfide. Int Arch Occup Environ Health 66, 103–110 (1994). https://doi.org/10.1007/BF00383365
33. Agency for Toxic Substances and Disease Registry (ATSDR). 1998. Toxicological profile for Chloromethane. Atlanta, GA: U.S. Department of Health and Human Services, Public Health Service.
34. Agency for Toxic Substances and Disease Registry (ATSDR). 2010. Toxicological profile for Ethylbenzene. Atlanta, GA: U.S. Department of Health and Human Services, Public Health Service.
35. Huff J, Chan P, Melnick R. Clarifying carcinogenicity of ethylbenzene. Regul Toxicol Pharmacol. 2010;58(2):167–172. doi:10.1016/j.yrtph.2010.08.011
36. Agency for Toxic Substances and Disease Registry (ATSDR). 2019. Toxicological profile for hexachlorobutadiene (Draft for Public Comment). Atlanta, GA: U.S. Department of Health and Human Services, Public Health Service.
37. Agency for Toxic Substances and Disease Registry (ATSDR). 2000. Toxicological profile for Methylene Chloride. Atlanta, GA: U.S. Department of Health and Human Services, Public Health Service.
38. Tuohy KA, Nicholson WJ, Schiffman F. Agitation by sedation. Lancet. 2003;361(9354):308.

45
13 Copyright ©2020 Burn Pits 360, All Rights Reserved.
TOXIC EXPOSURE TABLE
39. Kelner MJ, Bailey DN. Propylene glycol as a cause of lactic acidosis. J Anal Toxicol. 1985;9(1):40–42. 40. O'Donnell J, Mertl SL, Kelly WN. Propylene glycol toxicity in a pediatric patient: the dangers of diluents.
J Pharm Pract. 2000;13(3):214–224. 41. Lim TY, Poole RL, Pageler NM. Propylene glycol toxicity in children. J Pediatr Pharmacol Ther.
2014;19(4):277–282. doi:10.5863/1551-6776-19.4.277 42. Agency for Toxic Substances and Disease Registry (ATSDR). 2017. Toxicological profile for Toluene.
Atlanta, GA: U.S. Department of Health and Human Services, Public Health Service. 43. Dawn Tharr Column Editor & Irena Kudla (1997) Case Studies Exposure to Benzene-Contaminated
Toluene and Bone Marrow Disorders—A Retrospective Exposure Assessment, Applied Occupational and Environmental Hygiene, 12:1, 11-14, DOI: 10.1080/1047322X.1997.10389448
44. Agency for Toxic Substances and Disease Registry (ATSDR). 1999. Toxicological profile for n-Hexane. Atlanta, GA: U.S. Department of Health and Human Services, Public Health Service.
45. Agency for Toxic Substances and Disease Registry (ATSDR). 2010. Toxicological profile for Styrene. Atlanta, GA: U.S. Department of Health and Human Services, Public Health Service.
46. National Center for Biotechnology Information. PubChem Database. CID=37270, https://pubchem.ncbi.nlm.nih.gov/compound/Heptachlorodibenzo-p-dioxin (accessed on Apr. 1, 2020)
47. Agency for Toxic Substances and Disease Registry (ATSDR). 1998. Toxicological profile for Chlorinated Dibenzo-p-dioxins (CDDs). Atlanta, GA: U.S. Department of Health and Human Services, Public Health Service.
48. Agency for Toxic Substances and Disease Registry (ATSDR). 1994. Toxicological Profile for chlorodibenzofurans (CDFs). Atlanta, GA: U.S. Department of Health and Human Services, Public Health Service.
Copyright ©2020 Burn Pits 360, All Rights Reserved

46
The leading respiratory hospital in the nation.
Main Health Campus 1400 Jackson St. Denver, CO 80206 303-388.4461 800.423.8891 njhealth.org
To Congressional Staff 06.01.2018 Regarding: Small Airway Injury Due to Deployment Related Lung Disease (DRLD), Airborne Hazard exposures and VA Disability Evaluation Criteria Background Over 2.5 million US service men and woman have honorably served in Iraq and Afghanistan in support of OIF and OEF since 2001. Forty percent of those returning from service rely on VA providers and a significant number of those seeking care have experienced respiratory symptoms and diseases associated with deployment. While the specific cause(s) for deployment related lung disease (DRLD) have not been proven, there are many significant exposures which have been implicated. The air quality in those regions is poor due to; high levels of ambient air particulates, industrial air pollution, combat operations and open air burn pits used for disposing of medical waste, metals, plastics, electronics and other combustible products (1). The first incinerators were not placed in Iraq until 2009. These activities contribute to high levels of air particulate matter (PM2.5), an exposure which is linked to several cardiovascular and pulmonary disorders (2). The Department of Defense has consistently documented airborne PM2.5 concentrations throughout Iraq and Afghanistan that exceed US Military Exposure Guidelines (3). These high levels of particulate matter carry toxins, noxious agents and microbes that can lodge in the small airways of the lung and result in diseases such as asthma, constrictive bronchiolitis, emphysema and other disorders (4). Both DOD and civilian academic medical centers have described respiratory diseases associated with military deployment. The Millennium Cohort Study, which surveyed 46,000 deployers, reported a higher incidence of respiratory symptoms in deployers compared to non-deployers. Other studies have shown an increased incidence of asthma, eosinophilic pneumonia, constrictive bronchiolitis, granulomatous lung disease and emphysema in deployers, many of whom were never smokers (5-10). Unfortunately, the magnitude of the problem is not quantified as there are no longitudinal studies to adequately determine the long-term health consequences of veterans exposed to inhalation hazards due to OIF and OEF deployments. There are a number of unique challenges in diagnosing lung diseases following deployment to Southwest Asia, particularly for those diseases affecting the small airways of the lungs. Non-invasive studies such as pulmonary function testing (PFTs), high resolution computed tomography (HRCT) and cardiopulmonary exercise testing (CPET) are normal in some patients. For many, the only definitive diagnostic test has been surgical lung biopsy. This disparity between non-invasive testing and more invasive lung biopsy is well-recognized in patients

47
The leading respiratory hospital in the nation.
suffering from small airways disease such as constrictive bronchiolitis and was acknowledged by the United States Defense Health Board in its 2014 study on (DRLD) (11-12). One large DOD facility, which did not pursue video-assisted thorascopic surgical lung biopsies (VATS), was unable to identify the cause of respiratory symptoms in 40% of their deployers (13). Symptomatic deployers may face discharge from military service because they are unable to pass mandatory fitness testing (8). In summary, a substantial number of service members have returned from OIF and OEF with respiratory diseases that are both unique to deployment and difficult to diagnose. This group of veterans requires specialty care which is not consistently found throughout the VA system. Moreover, the current VA disability guidelines do not adequately address some of the respiratory disability issues affecting service men and women returning from OIF and OEF. Recommendations
1. The diagnosis of deployment-related lung disease (DRLD) requires specialized pulmonary evaluation and testing, which may include metabolic exercise testing, complete pulmonary function testing, high resolution chest CT scans that are interpreted by thoracic radiologists and sometimes surgical lung biopsy. Since these capabilities are not available at most VA medical centers, the VA should encourage providers to refer veterans suffering from these complex exposure related pulmonary disorders using the “VA Choice” option to academic or tertiary referral centers with expertise in DRLD.
2. The current VA disability criteria for DRLD and, specifically, small airways disease should be revised (14). Current clinical disability guidelines requiring resting PFTS and oxygen saturation testing for bronchitis, asthma and COPD are not sufficient for assessing small airway injury due to Southwest Asia inhalation exposures.
Richard Meehan, MD CAPT, MC, USN (ret) Co-Director, NJH Center for Deployment Related lung Disease Professor of Medicine Rheumatology Division National Jewish Health 1400 Jackson St Denver, CO 80206

48
The leading respiratory hospital in the nation.
References
1. National Research Council. Long-Term Health consequences of exposure to Burn Pits in Iraq and Afghanistan. Washington DC the National Academies Press; 2011:
2. World Health Organization. Burden of Disease from the joint effects of household and ambient air pollution for 2012. Geneva Switzerland: Public Health, Social and Environmental Determinations of Health Department. World Health Organization. 2014
3. Engelbrecht JP, McDonald EV, Gillies JA, Jayanty RK, Casuccio G, Gertler AW. Characterizing mineral dusts and other aerosols from the middle- East Part 1: ambient sampling. Inhal Toxicol. 2009; 21: 297-326.
4. Leski TA, Malanoski AP, Gregory MJ, Lin B, Stenger DA. Application of a broad-range resequencing array for detection of pathogens in desert dust samples from Kuwait and Iraq. Applied Environ Microbiology 2011; 77: 4285-4292.
5. Smith B, Wong CA, Smith TC, Boyko EJ, et al. Newly reported respiratory symptoms and conditions among military personnel deployed to Iraq and Afghanistan A prospective population based study. Am J Epidemiol 2009; 170: 1433-1442.
6. Szema AM, Peters MC Weissinger KM et al. New onset asthma among soldiers serving in Iraq and Afghanistan. Allergy Asthma Proc. 2010l31:L67-71.
7. Shorr AF, Scoville SL, Cersovsky, Shankd GD et al Acute Eosinophilic pneumonia among US military personnel Deployed in or near Iraq. JAMA 2004; 292:2997-3005
8. King MS Eisenberg R, Newman JH et al Constrictive bronchiolitis in soldiers returning from Iraq and Afghanistan N Engl J Med 2011l 365:222-230.
9. Rose C, Abraham J Harkins D Miller R et al. Overview and recommendations for Medical Screening and Diagnostic Evaluation for post-Deployment Lung Disease in Returning US Warfighters. J Occ Env Med. 2012; 54:746-658.
10. Dhoma S, Gottschall B, Robinson M, Williams A, Meehan R, Groshong S. Lung disease in deployers returning from Afghanistan and Iraq. Am J Respir Crit Care Med. 2013; 187: A3669.
11. Madar CS, Lewin-Smith MR, Franks TJ, Harley RA, Klaric JS, Morris MJ. Histological diagnosis of military personnel undergoing lung biopsy after deployment to southwest Asia. Lung; 2017; DOI 10.1007/s00408-017-0009-2
12. Rose C, Abraham J Harkins D Miller R et al. Overview and recommendations for Medical Screening and Diagnostic Evaluation for post-Deployment Lung Disease in Returning US Warfighters. J Occ Env Med. 2012; 54:746-658.
13. Morris MJ, Dodson DW, Lucero PF et al. Study of active duty military for pulmonary disease related to environmental dust exposure (STAMPEDE). Am J Respir Crit Care Med 2014; 190: 77-84.
14. www.benefits.va.gov/warms/docs/regs/38CFR/BOOKC/PART4/S4_97.doc
§4.97—Schedule of ratings–respiratory system 4.97-1

49
DEPARTMENT OF VETERANS AFFAIRS G. V. “Sonny” Montgomery Veterans Affairs Medical Center Jackson, MS 39216
January 27, 2016 Dear Senator,
Many veterans of the wars in Iraq and Afghanistan are returning home disabled from a respiratory condition known as constrictive bronchiolitis. This disease affects young, non-smoking men and women and presents as slowly progressive shortness of breath. In its mildest form it limits exercise capacity, and in its more severe form affects daily life sometimes requiring supplemental oxygen 24 hours a day.
I serve veterans as a pulmonologist at the VA Medical Center in Jackson, Mississippi where I am confronting this disease daily. Currently, there are over 100 patients seen at our hospital with this condition confirmed or suspected. The medical community needs your support for research dollars to learn more about this disease and possible treatments. We also need constrictive bronchiolitis listed as a presumptive service connected disease as it is clearly related to airborne exposures suffered in the theater of OEF/OIF. Thank you for your support in this matter and I would be happy to answer any questions you may have. Sincerely, Allyn Harris, M.D. Assistant Professor Division of Pulmonary/Critical Care G.V. Sonny Montgomery VA Medical Center Jackson, MS [email protected]

50

51

52
ADDITIONAL SCIENTIFIC LITERATURE
1. Aguilar, P. R., Michelson, A. P., & Isakow, W. (2016). Obliterative Bronchiolitis. Transplantation, 100(2), 272–283. https://doi.org/10.1097/TP.0000000000000892
2. Coughlin, S. S., & Szema, A. (2019). Burn Pits Exposure and Chronic Respiratory Illnesses among Iraq and Afghanistan Veterans. Journal of environment and health sciences, 5(1), 13–14. https://doi.org/10.15436/2378-6841.19.2429
3. Falvo, M. J., Sotolongo, A. M., Osinubi, O. Y., Helmer, D. A., Galvin, J. R., & Franks, T. J. (2020). Diagnostic Workup of Constrictive Bronchiolitis in the Military Veteran. Military medicine, usaa192. Advance online publication. https://doi.org/10.1093/milmed/usaa192
4. Harrington, A. D., Schmidt, M. P., Szema, A. M., Galdanes, K., Tsirka, S. E., Gordon, T., & Schoonen, M. (2017). The Role of Iraqi Dust in Inducing Lung Injury in United States Soldiers-An Interdisciplinary Study. GeoHealth, 1(5), 237–246. https://doi.org/10.1002/2017GH000071
5. King, M. S., Eisenberg, R., Newman, J. H., Tolle, J. J., Harrell, F. E., Jr, Nian, H., Ninan, M., Lambright, E. S., Sheller, J. R., Johnson, J. E., & Miller, R. F. (2011). Constrictive bronchiolitis in soldiers returning from Iraq and Afghanistan. The New England journal of medicine, 365(3), 222–230. https://doi.org/10.1056/NEJMoa1101388
6. Lentz, R. J., Fessel, J. P., Johnson, J. E., Maldonado, F., Miller, R. F., & Rickman, O. B. (2016). Transbronchial Cryobiopsy Can Diagnose Constrictive Bronchiolitis in Veterans of Recent Conflicts in the Middle East. American journal of respiratory and critical care medicine, 193(7), 806–808. https://doi.org/10.1164/rccm.201509-1724LE
7. Lin, D., Li, J., Razi, R., Qamar, N., Levine, L., Zimmerman, T., Hamidi, S. A., Schmidt, M., Golightly, M. G., Rueb, T., Harrington, A., Garnett, M., Antonawich, F., McClain, S., Miller, E., Cox, C., Huang, P. H., & Szema, A. M. (2018). Rux largely restores lungs in Iraq PM-exposed mice, Up-regulating regulatory T-cells (Tregs). Experimental lung research, 44(3), 153–166. https://doi.org/10.1080/01902148.2018.1459957
8. Mammarappallil, J. G., Shofer, S., Carraway, M. S., Tucker, J., Womack, S., Ainslie, M., & Charles, H. C. (2020). Utilization of 19F MRI for Identification of Iraq-Afghanistan War Lung Injury. Military medicine, 185(Suppl 1), 50–56. https://doi.org/10.1093/milmed/usz284
9. Rose C, Abraham J, Harkins D, et al. Overview and recommendations for medical screening and diagnostic evaluation for postdeployment lung disease in returning US warfighters. J Occup Environ Med. 2012;54(6):746-751. doi:10.1097/JOM.0b013e31825297ba
10. Savabieasfahani, M., Basher Ahamadani, F., & Mahdavi Damghani, A. (2020). Living near an active U.S. military base in Iraq is associated with significantly higher hair thorium and increased likelihood of congenital anomalies in infants and children. Environmental pollution (Barking, Essex : 1987), 256, 113070. https://doi.org/10.1016/j.envpol.2019.113070
11. Sotolongo, A., Falvo, M., Santos, S., Johnson, I., Arjomandi, M., Hines, S., Krefft, S., & Osterholzer, J. (2020). Military Burn Pits. American journal of respiratory and critical care medicine, 201(7), P13–P14. https://doi.org/10.1164/rccm.2017P13
12. Szema A. M. (2013). Occupational Lung Diseases among Soldiers Deployed to Iraq and Afghanistan. Occupational medicine & health affairs, 1, 10.4172/2329-6879.1000117. https://doi.org/10.4172/2329-6879.1000117
13. Szema, A., Mirsaidi, N., Patel, B., Viens, L., Forsyth, E., Li, J., Dang, S., Dukes, B., Giraldo, J., Kim, P., & Burns, M. (2017). Proposed Iraq/Afghanistan War-Lung Injury (IAW-LI) Clinical Practice Recommendations: National Academy of Sciences’ Institute of Medicine Burn Pits Workshop. American journal of men’s health, 11(6), 1653–1663. https://doi.org/10.1177/1557988315619005
14. Szema, A. M., Peters, M. C., Weissinger, K. M., Gagliano, C. A., & Chen, J. J. (2010). New-onset asthma among soldiers serving in Iraq and Afghanistan. Allergy and asthma proceedings, 31(5), 67–71. https://doi.org/10.2500/aap.2010.31.3383

53
15. Szema, A. M., Reeder, R. J., Harrington, A. D., Schmidt, M., Liu, J., Golightly, M., Rueb, T., & Hamidi, S. A. (2014). Iraq dust is respirable, sharp, and metal-laden and induces lung inflammation with fibrosis in mice via IL-2 upregulation and depletion of regulatory T cells. Journal of occupational and environmental medicine, 56(3), 243–251. https://doi.org/10.1097/JOM.0000000000000119
16. Szema, A. M., Salihi, W., Savary, K., & Chen, J. J. (2011). Respiratory symptoms necessitating spirometry among soldiers with Iraq/Afghanistan war lung injury. Journal of occupational and environmental medicine, 53(9), 961–965. https://doi.org/10.1097/JOM.0b013e31822c9f05
17. Szema, A. M., Schmidt, M. P., Lanzirotti, A., Harrington, A. D., Lyubsky, S., Reeder, R. J., & Schoonen, M. A. (2012). Titanium and iron in lung of a soldier with nonspecific interstitial pneumonitis and bronchiolitis after returning from Iraq. Journal of occupational and environmental medicine, 54(1), 1–2. https://doi.org/10.1097/JOM.0b013e31824327ca
18. Thatcher, T. H., Woeller, C. F., Thakar, J., Khan, A., Hopke, P. K., Smith, M. R., Uppal, K., Walker, D. I., Go, Y. M., Jones, D. P., Krahl, P. L., Mallon, T. M., Sime, P. J., Phipps, R. P., & Utell, M. J. (2019). Analysis of Postdeployment Serum Samples Identifies Potential Biomarkers of Exposure to Burn Pits and Other Environmental Hazards. Journal of occupational and environmental medicine, 61 Suppl 12(Suppl 12), S45–S54. https://doi.org/10.1097/JOM.0000000000001715

54
VII - VA CLAIMS HISTORY
The VA recently (February 2019) reported its total burn pit related disability claims as approximately 10,500 since 2007. The VA arrived at this number by merely conducting a word search for “burn pits” in its database of rating decisions. This results in the number of “reported” burn-pit related claims being not only disingenuous, but deceptive.
More often than not, the phrase “burn pits” never appears in rating decisions, even when a Veteran actually uses the phrase in his or her claim. Also, in most claims, Veterans either don’t know to use that phrase, or they use other terms, such as smoke, environmental toxins, exposures, or none of the above.
To put the VA’s “reported” number in better context, there have been approximately 250,000 claims filed by Veterans (or their survivors) who served in Iraq and/or Afghanistan since 9/11 just for some form of respiratory disability, and this number does not include the numerous claims for immune related disorders, neurological disorders, cancers, etc., that could be related to burn pits.
Nearly 100,000 claims from Veterans with post 9/11 service in Iraq and/or Afghanistan just since 2010 have been coded with the special identifier of “Environmental hazard in Gulf War.” So, while it is likely that the VA has no method to determine a truly accurate number of burn-pit related claims, the method they chose and the number they reported is one of the least accurate methods of all.
This is neither incompetence nor an oversight, which leaves one question, “Why is VA so drastically downplaying these numbers?”

55
Just 10,588 burn-pit claims have been filed since Sept. 11, 2001, Veterans Affairs said in response to a Freedom of Information Act request from a veterans advocacy group. But that’s only a fraction of what veterans advocates say they expected to see. Veterans have filed 98,017 claims for “environmental claims” since 9/11, and at least 200,000 people have signed up for VA’s burn-pit registry, according to VA. That means burn-pit claims make up slightly less than 10% of VA’s total number of environmental exposure claims for veterans returning from Iraq and Afghanistan. That makes it difficult for experts and researchers to track veterans to look for trends, for legislators to watch so they can properly fund VA and provide legislation for benefits, and for veterans service organizations to learn from as they determine how best to help veterans file claims. Kerry Baker, who helps veterans appeal VA disability claims and who previously worked for VA’s Veterans Benefits Administration, said he has been personally involved to some extent with more than 1,000 burn-pit claims. “There’s no way I’ve been involved with 10% of the nation’s burn pit claims,” he said. “So I want to know how they are getting these numbers.” The military burned as much as 250 tons of trash a day at Joint Base Balad alone, as well as tons more in open pits in Iraq and Afghanistan—as close as one mile away from service members’ living quarters. (Juneau, Alaska, produces about 83 tons of trash a day.) In 2006, an Air Force bioenvironmental engineer called the pit at Joint Base Balad an “acute health hazard” and worried people on base would face chronic health problems. Most large bases in Iraq and Afghanistan had burn pits, and the military burned everything from Styrofoam from the dining facilities to petroleum products to paints and solvents, releasing contaminants, including benzene, an aircraft fuel known to cause leukemia; arsenic; Freon; ethylbenzene; formaldehyde; hydrogen cyanide; nitrogen dioxide; sulfuric acid; and xylene. The biggest issue? Dioxin, which is the same chemical that was used to make Agent Orange during the Vietnam War. It has been linked to cancers, diabetes, and birth defects. It also can interfere with the immune system. The Environmental Protection Agency explains that dioxin is a byproduct of burning materials—including wood, which is why burning trash in the backyard is banned in most cities. “What surprised me were the unbelievably low numbers they’re reporting,” said Baker, who has been tracking veterans with health issues they believe are associated with burn pits since 2008. “It’s so inaccurate.” And Rosie Torres, who, along with her husband, retired Army Capt. Le Roy Torres, filed the FOIA request on behalf of Burn Pits 360, said veterans shouldn’t have had to ask for the numbers.

56
“It should be coming from them,” she said. “They should be willingly delivering this information to the public, but we have to force them to do this.” VA responded to questions from The War Horse by processing them as a FOIA request. But in their written response to Burn Pits 360, VA officials said they included only cases that specifically state “burn pit” or “BPE” “within the text of the decision”—which doesn’t include if the veteran used the term when filing an initial claim—for the FOIA request. And, they said, the 98,017 figure could include veterans exposed to other environmental hazards in Iraq or Afghanistan. “They just did a word search in their corporate database for ‘burn pits’ or ‘bp’—that I’ve rarely seen people use in a burn pit claim,” Baker said. “The vast majority of these cases don’t mention burn pits, even when a veteran says ‘burn pit’ when he raises his claim. So a veteran might say, ‘burn pits,’ but the adjudicators might say ‘environmental hazards in Iraq and Afghanistan.’” If VA searched the corporate database, they looked at rating decisions, not the veteran’s initial claim or record, Baker said—but the rating decision probably won’t say “burn pit.” And veterans themselves may not have used the term “burn pit.” “The training letter even told adjudicators, ‘Don’t refuse development under this policy if they don’t use “burn pits’’ as a basis for their claims because [veterans] might not know about it or might not associate their disability with burn pits,’” Baker said. “There’s no way you’re going to catch even a majority if all you’re doing is a corporate word search. There’s just no way.” Baker said “Gulf War Environmental Special Issue,” the term used in VA’s burn pit training letter, would have turned up many more cases than “burn pit.” “Ten thousand cases is just not remotely close to accurate,” Baker said. But the VA figures also show an astonishingly low rate of approval of burn pit claims: Of the 10,588 claims, only 2,360 veterans had their benefits granted, and 8,228 veterans had their claims denied. The numbers are low for approved claims for all environmental-exposure claims, as well. VA’s numbers show that veterans who served in Southwest Asia claimed 248,610 respiratory conditions since Sept. 11, 2001. Of those, VA said 61,734 conditions were granted benefits and 93,957 were not. Baker also found it curious that the burn pit cases go back as far as 2007, because prior to a 2010 training letter that laid out how to adjudicate a burn pit claim, there had been no VA policy on burn pit claims, he said. “So my first questions was, ‘How did you get a number from 2007?’” Baker said. “The numbers they are using aren’t using the tracking mechanism from the training letter.” And he still sees problems with adjudication: If a person gets sick while still in the military, their illness is typically awarded service-connection. But if a person gets out of the military, even with documented exposure to burn pits, and later develops bronchiolitis, their case is not being approved. “Those ones, I don’t see any improvement whatsoever,” he said. In its FOIA request, Burn Pits 360 also asked about a specific disorder: constrictive bronchiolitis. In 2008, Robert Miller, a pulmonologist at Vanderbilt University Medical Center, began performing biopsies on the lungs of Fort Campbell soldiers no longer able to run fast enough to pass their physical fitness tests after deploying to Iraq. The soldiers also quickly became tired with normal activity and generally had difficulty breathing. Many of those 101st Airborne soldiers had been exposed to a sulfur-

57
emitting factory—but many had not. After the biopsies, Miller found that more than 100 soldiers had constrictive bronchiolitis, a rare condition typically seen in lung-transplant patients or as a result of toxic fumes. It affects the smallest airways of the lungs and isn’t detectable through typical respiratory tests. But VA doesn’t have rating criteria for constrictive bronchiolitis. In the past, it has simply used “constrictive bronchitis,” and then rated veterans based on whether they had normal pulmonary function tests, Baker said. And they do—because constrictive bronchiolitis doesn’t normally show up on pulmonary function tests. The FOIA request asked if progress had been made on creating rating criteria for constrictive bronchiolitis. “That’s why Rosie [Torres] wants presumption for at least bronchiolitis,” Baker said. “We are working with Senator [Kirsten] Gillibrand on a toxic exposure burn pit presumptive coverage bill that will be ready in September,” Torres said. Gillibrand’s office did not respond to a request for comment. On Aug. 28, Burn Pits 360, along with Grunt Style, will host a conference in preparation of the bill featuring Miller, Jon Stewart, former VA Secretary David Shulkin, and Baker, among others, Torres said. “Veterans and service members are sick and dying,” Torres said. “According to the Burn Pits 360 registry, we know there are veterans struggling with illnesses that live in every state and congressional district nationwide. This conference is a form of hope for so many left fighting a system of delay and deny.” In response to the FOIA request, VA said the Veterans Benefits Administration is revising its respiratory condition regulation. “Since VBA is still engaged in the deliberative process, VBA is unable to share details concerning possible revisions,” the FOIA response states, and did not confirm whether constrictive bronchiolitis will be included in the proposed changes. Torres said she’s thinking in terms of what will help veterans now. For now, there are no clinical guidelines for veterans exposed to burn pit smoke, and there are problems within the benefits adjudication system for veterans who say they’re sick because of the burn pits. Many conditions connected to environmental hazard exposure don’t appear until years after a person has been exposed—as has been demonstrated with first responders to the World Trade Center who encountered smoke similar to what service members breathed in Iraq and Afghanistan—and veterans who claim exposure have a hard time claiming benefits. “I don’t think more studies are the answer,” Torres said. “The reality is people are dying.” Torres had physicians investigate science-based, peer-reviewed material and identify which exposures could cause health problems for veterans, and then gave the information to Congress members and Veterans Affairs. Torres and Baker also asked VA for information about people filing for benefits after a death, but didn’t receive it. “They may still be working through some of the data,” Torres said. The pair also asked for cancer numbers since 9/11. Instead, they received cancer numbers from within the 10,000 burn pit claims, Baker said.

58
“Ten thousand five hundred burn-pit claims and 200 cancers?” Torres said. “I don’t think they’re capturing things correctly.” As Baker and Torres have pushed the issue since 2008, a coalition of veterans service organizations has also formed to insist that the issue be addressed.
Research shows respiratory symptoms and asthma rates are higher in service members and veterans who deployed to Iraq and Afghanistan versus those who did not. And veterans who have joined Veterans Affairs’ burn pit registry also report high instances of hypertension and lung disease. More than 1.9 million people have deployed to Iraq and Afghanistan since the wars began. But since the burn-pit story first broke in 2008, there has been little progress in ensuring veterans receive disability benefits associated with the burn pits, including for respiratory disorders. To that end, Burn Pits 360 has brought on Jon Stewart and Ted Koppel to promote the cause, and Rosie Torres is working with Congress members on legislation that would cause veterans’ claims to be approved automatically for respiratory illnesses if they can show they were exposed to a burn pit. The House passed legislation in July that includes $840 million for medical research that must include toxic exposures, including for burn pits. It also would expand the burn pit registry and improve training for medical personnel about the effects of burn pits. The Senate will now decide if it will pass similar legislation. VA does not acknowledge a connection between poor long-term respiratory health and the burn pits. “At this time, research does not show evidence of long-term health problems from exposure to burn pits. VA continues to study the health of deployed Veterans,” VA’s website states. But a new study published in Military Medicine conducted by the VA’s Airborne Hazards and Burn Pits Center of Excellence at the War Related Illness and Injury Study Center found that respiratory issues in service members who deployed to Iraq and Afghanistan may be, in part, connected to physical training in polluted areas. Service members at Balad and other bases ran outside and worked out in gyms near the burn pits. Researchers found that while veterans’ pulmonary function tests came up normal, many of those same veterans say they wheeze or feel short of breath after they exercise. The researchers wrote this is known to happen in people with asthma—as well as with athletes. It tends to be worse in athletes exposed to particulate matter or “gaseous irritants,” they wrote. “Although the exact mechanism for increased prevalence of [exercise-induced bronchoconstriction] in athletic populations remains to be fully established, repeated bouts of exercise hyperpnoea in polluted environments has been identified as an important risk factor,” they wrote. The researchers asked 24 veterans—19 of whom were deployed on a base with a burn pit—who had never been diagnosed with an illness or sought care for burn pit exposure to take a spirometry test to check their lung function, and then to exercise on a treadmill. After exercising, the veterans took another spirometry test. Spirometry tests check how much people inhale, as well as how much and how quickly they exhale. They found that the veterans the researchers found had exercise-induced bronchoconstriction were less likely to have smoked and had shorter cumulative deployment lengths, but respiratory symptoms were similar among all of the veterans: One in two reported coughing, and one in three reported wheezing, shortness of breath and sputum production. However, the researchers found that the

59
deployed veterans not diagnosed with asthma did not have a higher rate of EIB than would be expected in a civilian population of people who have not been diagnosed with asthma. (Recruits are screened for respiratory issues before joining the military.) But, using “less conservative criteria,” the researchers found that 42% of the veterans “demonstrated evidence of acute airway narrowing” after exercising. “This finding is particularly concerning in that our sample was non-treatment seeking yet reported frequent lower respiratory symptoms,” they wrote. Only 38% of the veterans met recommended levels of exercise, and prior research found that people with exercise-induced respiratory issues stop or avoid exercise, they wrote, and expressed the need for more research. In May, the Defense Department released a “clinical tool box” for providers. The military advises service members to sign up for VA’s burn pit registry. Then, the service member may request a physical exam through the registry site. However, it is notoriously difficult to enroll in the registry. (After multiple attempts, this reporter, an Army veteran, tried again in July, logged in, learned she needed to update a phone number to enter the system, and then learned she needed to wait 23 minutes to speak to an agent on the phone to update her phone number.) Of those who have registered, 72% report neurological problems, 40% report allergies, 37% report hypertension, 19% report immune-system issues, 14% report asthma and 13% report chronic bronchitis, VA documents show. Last October, Eric Shuping, VA’s director of Post-911 Era Environmental Health Program, spoke to veterans service organizations about environmental hazards in Iraq and Afghanistan to explain how VA had addressed problems identified in a 2017 Institute of Medicine report about the burn pits. Only 10% of people who request a physical examination after completing the registry complete one. By August 2019, only 2,942 had completed an exam. Shuping’s slide deck shows VA is trying to get the word out about exams to VA employees, as well as train them about how to conduct them. The registry takes about 40 minutes to complete, according to Shuping’s PowerPoint slide deck. From June 2014 to March 2019, 90,125 did not complete the registry, while 170,693 did. VA should eliminate the section requiring veterans to report previous addresses, their nonmilitary work history, their home environment, community and hobbies, and instead focus on information “that may only be useful in epidemiologic studies of the population,” the Institute of Medicine said, Shuping’s slides showed. But VA found that 38% of veterans never started the questionnaire, and 37% didn’t make it through the deployment section. A contract has been put out to bid and will be completed in 2021 to bring in external experts to revamp the registry questionnaire, Shuping’s slides state. But Torres said veterans and their families shouldn’t have to wait for the government to prove what she says has already been proven. “It’s already there,” she said. “That’s what bothers me so much. I don’t understand why we still need to prove it.”

60
VIII - MEDIA AND NEWSPAPER COVERAGE
19 BURN PIT 360 - PREPARED BY SZEMA RESEARCH TEAM, HOFSTRA-NORTHWELL SCHOOL OF MEDICINE
VIII - MEDIA AND NEWSPAPER COVERAGE
Toxic Inferno: How Burning Military Trash is Poisoning Our Troops (2019) https://connectingvets.radio.com/articles/13-platoon-dead-or-sick-toxic-exposures-iraq
America’s ‘sacred obligation.’ 3.5 million troops exposed to airborne toxins since 9/11 (2019) https://connectingvets.radio.com/articles/35-million-us-troops-exposed-airborne-toxins-911
More Veterans Are Getting Cancer, and Some Suspect It’s Due to Burn Pits in Iraq and Afghanistan (2019) https://taskandpurpose.com/burn-pit-cancer
Photo Essay: The Burn Pits of Iraq and Afghanistan (2014) https://www.pbs.org/newshour/world/photo-essay-burn-pits-iraq-afghanistan

6119
BURN PIT 360 - PREPARED BY SZEMA RESEARCH TEAM, HOFSTRA-NORTHWELL SCHOOL OF MEDICINE
Thousands of Veterans Fear "Burn Pits" Exposed Them to Lethal Disease (2019) https://www.cbsnews.com/news/burn-pit-military-lung-disease-thousands-of-veterans-fear-burn-pits-exposed-them-to-lethal-disease-2019-08-17/
Contractors Sickened by Military Burn Pits Left to Fend for Themselves (2016) https://www.military.com/daily-news/2016/10/19/contractors-sickened-military-burn-pits-left-fend-themselves.html
A New Coalition is Fighting for Vets Sickened by Environmental Hazards (2019) https://www.military.com/daily-news/2019/06/12/new-coalition-fighting-vets-sickened-environmental-hazards.html
Risk for Exposure-Related Respiratory Diseases Varies Among US Military Personnel (2019) https://www.healio.com/pulmonology/practice-management/news/online/%7B8bb26e30-a277-442a-b018-4975e9a6c6fd%7D/risk-for-exposure-related-respiratory-diseases-varies-among-us-military-personnel?page=2
Veterans Urged to Learn More About Hazardous Environments and Burn Pit Exposure (2019) https://clarksvillenow.com/local/veterans-urged-to-learn-more-about-hazardous-environments-and-burn-pit-exposure/
Home Fires: In Balad, Smoke and Fire (2010) https://opinionator.blogs.nytimes.com/2010/01/20/home-fires-in-balad-smoke-and-fire/?searchResultPosition=14
Decorated Vermont Veteran Dealing With Terminal Cancer After Burn Pit Exposure (2018) https://www.foxnews.com/us/decorated-vermont-veteran-dealing-with-terminal-cancer-after-burn-pit-exposure
Former Burn Pit Inspector Says Warnings Were Largely Ignored by Pentagon Officials During Iraqi War (2018)

6219 BURN PIT 360 - PREPARED BY SZEMA RESEARCH TEAM, HOFSTRA-NORTHWELL SCHOOL OF MEDICINE
https://www.foxnews.com/us/former-burn-pit-inspector-says-warnings-were-largely-ignored-by-pentagon-officials-during-iraq-war
Local Producers Team Up With Jon Stewart to Help Vets (2019) https://local21news.com/news/local/local-company-teams-up-with-jon-stewart-to-help-vets
New 'Heat Maps' of Burn Pit Exposures Could Help Show Risks, But DoD Data is Unreliable (2019) https://connectingvets.radio.com/articles/burn-pit-heat-maps-show-exposures-risk-of-illness
Under Toxic Fire: Veterans Believe Exposure to Burn Pits Made Them Sick (2019) https://www.firstcoastnews.com/article/news/under-toxic-fire-veterans-believe-exposure-to-burn-pits-made-them-sick/77-99327cda-ae76-417b-b850-7d702927bbba
Burn Pits: The New Agent Orange (2017) https://www.huffpost.com/entry/military-burn-pits-the-new-agent-orange_b_9322334
Veterans Claiming Illness From Burn Pits Lose Court Fight (2019) https://radio.wosu.org/post/veterans-claiming-illness-burn-pits-lose-court-fight#stream/0
This Generation's Agent Orange? Congressman Ruiz's Bill Aims to Aid Vets Exposed to ‘Burn Pits’ (2019) https://www.desertsun.com/story/news/politics/2019/08/14/ruiz-bill-classify-burn-pit-exposure-alongside-agent-orange/1999313001/
Sec Def Says He'll Work with VA on Vets' Environmental Health Concerns (2016) https://www.military.com/daily-news/2019/08/28/secdef-says-hell-work-va-vets-environmental-health-concerns.html
Veterans Health Guide (2019) https://www.drugwatch.com/health/veterans/

6319 BURN PIT 360 - PREPARED BY SZEMA RESEARCH TEAM, HOFSTRA-NORTHWELL SCHOOL OF MEDICINE
DoD and VA to Host Closed-Door Conference on Burn Pits (2019) https://www.military.com/daily-news/2019/03/13/dod-and-va-host-closed-door-conference-burn-pits.html
National Guard Head Backs Burn Pit Exposure Awareness Bill (2019) https://vtdigger.org/2019/03/28/national-guard-head-backs-burn-pit-exposure-awareness-bill/
Veterans Fighting for Benefits after Exposure to Burn Pits in Iraq and Afghanistan (2018) https://www.nbcchicago.com/news/local/veterans-fighting-for-benefits-after-exposure-to-burn-pits-in-iraq-and-afghanistan/169021/
Sens. Klobuchar and Tillis: We Can’t Let Burn Pits Become the New Agent Orange (2019) https://www.klobuchar.senate.gov/public/index.cfm/2016/5/sens-klobuchar-and-tillis-we-can-t-let-burn-pits-become-the-new-agent-orange
Fighting the Agent Orange Battle of the 9/11 Generation (2019) https://www.ozy.com/the-new-and-the-next/shes-making-sure-vets-who-inhaled-toxic-fumes-get-their-due/232136/
Wounded Warrior Project Announced Formation of Toxic Exposures Coalition (2019) https://newsroom.woundedwarriorproject.org/2019-06-06-Wounded-Warrior-Project-Announce-Formation-of-Toxic-Exposures-Coalition
Lawmakers Call for Action on Burn Pit Exposure (2019) https://www.military.com/daily-news/2019/05/03/lawmakers-call-action-burn-pit-exposure.html

6419
BURN PIT 360 - PREPARED BY SZEMA RESEARCH TEAM, HOFSTRA-NORTHWELL SCHOOL OF MEDICINE
Supreme Court Upholds Appellate Decision on Burn Pits Lawsuits (2015) https://www.foxnews.com/us/supreme-court-upholds-appellate-decision-on-burn-pit-lawsuits
ATS: Military Deployment to Southwest Asia May Lead to Respiratory AE’s (2019) https://www.pulmonologyadvisor.com/author/virginia-schad/
Petraeus: US has ‘Sacred Obligation’ to Help Burn-Pit Veterans (2018) https://www.foxnews.com/us/petraeus-us-has-sacred-obligation-to-help-burn-pit-veterans
Jon Stewart Lends His 9/11 Advocacy to Help GIs Exposed to Burn Pits in Iraq, Afghanistan (2019) https://www.caller.com/story/news/local/texas/state-bureau/2019/09/16/jon-stewart-calls-action-help-burn-pit-victims/2340088001/
Committee will Study Respiratory Diseases Related to Military Burn Pits, Dust (2019) https://www.military.com/daily-news/2019/04/12/committee-will-study-respiratory-diseases-related-military-burn-pits-dust.html
Bipartisan Support Grows on the Hill for Reform of Burn Pit Vet Support System (2018) https://www.foxnews.com/us/bipartisan-support-grows-on-the-hill-for-reform-of-support-system-for-burn-pit-vets
VFW-Supported Burn-Pit Bill Introduced to House (2019) https://www.vfw.org/media-and-events/latest-releases/archives/2019/11/vfw-supported-burn-pit-bill-introduced-to-house
Gillibrand Voices Support for Veterans Exposed to Burn Pits (2019) https://www.wcax.com/content/news/Gillibrand-voices-support-for-veterans-exposed-to-burn-pits-565492822.html
WFAA Original: Stop Collecting Burn Pit Data and Start Treating Troops, Is the Toxic Legacy of the Iraq War Deforming Children Near US Bases? (2018) https://www.ehn.org/is-the-toxic-legacy-of-the-iraq-war-deforming-children-near-us-bases-2640288680.html

6519
BURN PIT 360 - PREPARED BY SZEMA RESEARCH TEAM, HOFSTRA-NORTHWELL SCHOOL OF MEDICINE
The Things They Burned (2016) https://newrepublic.com/article/138058/things-burned
New Study Documents Depleted Uranium Impacts on Children in Iraq (2019) https://www.foreignpolicyjournal.com/2019/09/21/new-study-documents-depleted-uranium-impacts-on-children-in-iraq/
Environmental Poisoning’ of Iraq Is Claimed (2014) https://www.nytimes.com/2014/03/27/world/middleeast/environmental-poisoning-of-iraq-is-claimed.html?searchResultPosition=31
‘Indefensible’: Report Reveals Extent of ‘Burn Pit’ Pollution Inhaled by US Troops in Afghanistan (2015) https://www.foxnews.com/politics/indefensible-report-reveals-extent-of-burn-pit-pollution-inhaled-by-us-troops-in-afghanistan
Court Determines Military Burn Pits Caused Lung Disease in Service Members (2018) https://www.foxnews.com/world/court-determines-military-burn-pits-caused-lung-disease-in-service-members
U.S. Military Is Scrutinized Over Trash Burning in Afghanistan (2014) https://www.nytimes.com/2014/07/23/us/us-military-is-scrutinized-over-trash-burning-in-afghanistan.html?searchResultPosition=16
Military Contractor KBR Turned Away by SCOTUS (2015) https://www.militarytimes.com/news/your-military/2015/01/20/military-contractor-kbr-turned-away-by-scotus/

6619
BURN PIT 360 - PREPARED BY SZEMA RESEARCH TEAM, HOFSTRA-NORTHWELL SCHOOL OF MEDICINE
Burn-Pit Exposure Likely Leads to Higher Cancer Mortality Rate Among Army Vets: New Study (2018) https://www.foxnews.com/us/burn-pit-exposure-likely-leads-to-higher-cancer-mortality-rate-among-army-vets-new-study
Should Service in Iraq and Afghanistan be a Recognized Health Hazard for Vets Applying for Benefits? (2019) https://www.militarytimes.com/news/pentagon-congress/2019/11/22/proposed-legislation-would-name-service-in-iraq-afghanistan-a-health-hazard-to-us-troops/
Open Burn Pits Made Tens of Thousands of Vets Sick, and the VA Isn’t Working (2019) https://www.nationalreview.com/2019/08/open-burn-pits-illness-veterans-administration-overhaul-needed/
Congress Poised to Help Veterans Exposed to ‘Burn Pits’ Over Decades of War (2019) https://www.nytimes.com/2019/02/12/us/politics/veterans-burn-pits-congress.html?searchResultPosition=4
Veterans Go Back to Court Over Burn Pits. Do They Have a Chance? (2018) https://www.nytimes.com/2018/05/17/magazine/burn-pits-veterans.html?searchResultPosition=3
The Burn Pits: The Poisoning of America’s SoldiersBy Joseph Hickman

67
IX - DIGITAL MEDIA
19 BURN PIT 360 - PREPARED BY SZEMA RESEARCH TEAM, HOFSTRA-NORTHWELL SCHOOL OF MEDICINE
IX - DIGITAL MEDIA
Veterans Say Burn Pit Exposure Made Them Sick (2019) https://www.youtube.com/watch?v=axdXA2bFRXk
The Deadly Legacy of Burn Pits (2013) https://www.youtube.com/watch?v=ydcifH0SQmI
Did Military Burn Pits Make Soldiers Sick? (2014) https://www.youtube.com/watch?v=1VppHqKQyqk
VA Airborne Hazards and Open Burn Pit Registry For Veterans and Service Members (2016) https://www.youtube.com/watch?v=Hg9_TCFl-7o
What is Burn Pit Legislation About? (2019) https://www.youtube.com/watch?v=w357IEBXYmc
Iraqi Burn Pit (2009) https://www.youtube.com/watch?v=jbqa_wm23Cw
Burn Pit Exposure Causes Lung Disease in Veterans (2013) https://www.youtube.com/watch?v=ndurf-mLvMo

6819
BURN PIT 360 - PREPARED BY SZEMA RESEARCH TEAM, HOFSTRA-NORTHWELL SCHOOL OF MEDICINE
Susan Burke is Leading a Lawsuit on Behalf of Veterans Sickened by Burn Pits in Iraq and Afghanistan (2014) https://www.youtube.com/watch?v=uY9TCbgu9ns
Burn Pits Haunt Veterans From Afghanistan and Iraq (2014) https://www.youtube.com/watch?v=IWD4IQw2Ga4
Iraq War Burn Pit Toxic Effects Revealed (2016) https://www.youtube.com/watch?v=tPtVDw3iDQI
Veterans Concerned About “Burn Pit” Exposure After Deployments (2017) https://www.youtube.com/watch?v=Nmy5x7KjbQE
Burn Pits Are Killing Our Veterans (2019) https://www.youtube.com/watch?v=KtH8yXNMs9w
Iraq and Afghan War Vets Exposed to Toxic Air Struggle for Breath and a Diagnosis (2018) https://www.youtube.com/watch?v=zW86Qip-KzA
Thousands of Veterans Suffering After Toxic Smoke Exposure (2019) https://www.youtube.com/watch?v=hhs8WYS1SFM
Military’s Burn Pits Blamed for Lasting Health Problems (2018) https://www.youtube.com/watch?v=ajhsKD029TI
Burn Pits: with Military Medical Expert and Retired Navy Captain, Dr. Cassano (2018) https://www.youtube.com/watch?v=2RGA2RlMl8g
Burn Pits, the New Agent Orange (2019) https://www.youtube.com/watch?v=BFEOKxLYn5A

6919
BURN PIT 360 - PREPARED BY SZEMA RESEARCH TEAM, HOFSTRA-NORTHWELL SCHOOL OF MEDICINE
Burn Pits and Betrayal: How the U.S. Poisoned its Veterans (2017) https://www.youtube.com/watch?v=_PyfiP3h2Qw
Sensible Solutions - The Open Burn Pits Registry Act (2019) https://www.youtube.com/watch?v=lrSJJBIMnTI
Under Toxic Fire: Veterans Believe Exposure to Burn Pits Made Them Sick https://www.youtube.com/watch?v=5LXyrMjASiA
Local Veteran Pleads for Congressional Action on 'Burn Pits' https://www.youtube.com/watch?v=d8y2WGpN_M0
Rep. Mast Discusses Burn Pit Exposure at Veterans Affairs Hearing https://www.youtube.com/watch?v=HJZpH_Xz8sA
Senate Passes Bill To Help Veterans Affected by Toxic Burn Pits https://www.youtube.com/watch?v=Vc1mgMPngIU
Klobuchar Bill Aims to Help Vets Exposed to Burn Pits https://www.youtube.com/watch?v=AHMofl1XaCU
Veterans Demand of the VA https://www.youtube.com/watch?v=2CiDNo9WEGc
Veterans Hope Burn Pit Bill Will Provide VA Health Care and Disability Benefits https://www.youtube.com/watch?v=UIZQTdME-o4

70

71
MILITARY TOXIC EXPOSURE COALITION 2020

72
Copyright © 2022 FDOKUMEN




















