Potential influence of interleukin-1 haplotype IL1β-511*TIL1RN*1 in conferring low risk to middle...
8
Potential influence of interleukin-1 haplotype IL-1-511*T-IL-1RN*1 in conferring low risk to middle third location of esophageal cancer: A case–control study Rohit Upadhyay a , Meenu Jain a , Shaleen Kumar b , Uday C. Ghoshal c , Balraj Mittal a, * a Department of Genetics, Sanjay Gandhi Post Graduate Institute of Medical Sciences, Raibareilly Road, Lucknow 226014, India b Department of Radiotherapy, Sanjay Gandhi Post Graduate Institute of Medical Sciences, Raibareilly Road, Lucknow 226014, India c Department of Gastroenterology, Sanjay Gandhi Post Graduate Institute of Medical Sciences, Raibareilly Road, Lucknow 226014, India Received 12 October 2007; received in revised form 19 January 2008; accepted 24 January 2008 Summary Interleukin (IL)-1 gene polymorphisms affect several inflammatory diseases, includ- ing cancer. Therefore, we studied genetic association of biallelic (-511CT) polymorphism of IL-1 and 86-bp VNTR polymorphism of IL-1RN in 159 patients with esophageal cancer (EC) and 194 age- and gender-matched healthy controls. Genetic analysis for IL-1 polymorphisms was performed by polymerase chain reaction-restriction fragment length polymorphism. The fre- quencies of IL-1 (-511CT) and IL-1RN (variable number tandem repeat) genotypes, alleles, and haplotypes did not differ significantly between patients and controls. However, IL-1 -511TT genotype and T1 haplotype combination illustrated low risk for disease at the middle third location of the tumor (odds ratio [OR] 0.27; 95% confidence interval [CI] 0.11– 0.62; p 0.002; OR 0.462; 95% CI 0.253– 0.845, p 0.01). In conclusion, subjects with IL-1 -511TT genotype or IL-1*T-IL-1RN*1 (T1) haplotype had lower risk for middle third tumor location of EC in a northern Indian population. © 2008 American Society for Histocompatibility and Immunogenetics. Published by Elsevier Inc. All rights reserved. KEYWORDS Interleukin-1; Esophageal cancer; IL-1 haplotype Introduction Esophageal cancer (EC), an aggressive upper gastrointestinal malignancy, presents as locally advanced disease with poor prognosis. Inflammation plays an important role in tumor initiation, growth, metastasis, and cancer pathogenesis [1]. The interleukin (IL)-1 cytokine system is vital for the local control of tumor growth, particularly in regulating “protumori- genic” activities within the tumor microenvironment, and con- tributes to angiogenesis, tumor proliferation, and tumor inva- sion [2,3]. The most compelling evidence for the role of inflammation in gastrointestinal malignancy comes from stud- * Corresponding author. Fax: 91 - 522 - 2668017, 2668074. E-mail address: [email protected]/[email protected] (B. Mittal). Human Immunology (2008) 69, 179 –186 0198-8859/$ -see front matter © 2008 American Society for Histocompatibility and Immunogenetics. Published by Elsevier Inc. All rights reserved. doi:10.1016/j.humimm.2008.01.012
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Potential influence of interleukin-1 haplotype IL1β-511*TIL1RN*1 in conferring low risk to middle...

PIt
RB
a
b
Ic
2
R
I
Em
M
Human Immunology (2008) 69, 179–186
0d
otential influence of interleukin-1 haplotypeL-1�-511*T-IL-1RN*1 in conferring low risk to middlehird location of esophageal cancer: A case–control study
ohit Upadhyaya, Meenu Jaina, Shaleen Kumarb, Uday C. Ghoshalc,alraj Mittala,*
Department of Genetics, Sanjay Gandhi Post Graduate Institute of Medical Sciences, Raibareilly Road, Lucknow 226014, IndiaDepartment of Radiotherapy, Sanjay Gandhi Post Graduate Institute of Medical Sciences, Raibareilly Road, Lucknow 226014,
ndiaDepartment of Gastroenterology, Sanjay Gandhi Post Graduate Institute of Medical Sciences, Raibareilly Road, Lucknow26014, India
eceived 12 October 2007; received in revised form 19 January 2008; accepted 24 January 2008
Summary Interleukin (IL)-1 gene polymorphisms affect several inflammatory diseases, includ-ing cancer. Therefore, we studied genetic association of biallelic (-511C�T) polymorphism ofIL-1� and 86-bp VNTR polymorphism of IL-1RN in 159 patients with esophageal cancer (EC) and194 age- and gender-matched healthy controls. Genetic analysis for IL-1 polymorphisms wasperformed by polymerase chain reaction-restriction fragment length polymorphism. The fre-quencies of IL-1� (-511C�T) and IL-1RN (variable number tandem repeat) genotypes, alleles,and haplotypes did not differ significantly between patients and controls. However, IL-1�
-511TT genotype and T1� haplotype combination illustrated low risk for disease at the middlethird location of the tumor (odds ratio [OR] � 0.27; 95% confidence interval [CI] � 0.11–0.62;p � 0.002; OR � 0.462; 95% CI � 0.253–0.845, p � 0.01). In conclusion, subjects with IL-1�
-511TT genotype or IL-1�*T-IL-1RN*1 (T1) haplotype had lower risk for middle third tumorlocation of EC in a northern Indian population.© 2008 American Society for Histocompatibility and Immunogenetics. Published by Elsevier Inc.All rights reserved.
KEYWORDSInterleukin-1;
Esophageal cancer;
IL-1 haplotype
piTcgts
ntroduction
sophageal cancer (EC), an aggressive upper gastrointestinalalignancy, presents as locally advanced disease with poor
* Corresponding author. Fax: �91 - 522 - 2668017, 2668074.E-mail address: [email protected]/[email protected] (B.
iittal).
198-8859/$ -see front matter © 2008 American Society for Histocompatibioi:10.1016/j.humimm.2008.01.012
rognosis. Inflammation plays an important role in tumornitiation, growth, metastasis, and cancer pathogenesis [1].he interleukin (IL)-1 cytokine system is vital for the localontrol of tumor growth, particularly in regulating “protumori-enic” activities within the tumor microenvironment, and con-ributes to angiogenesis, tumor proliferation, and tumor inva-ion [2,3]. The most compelling evidence for the role of
nflammation in gastrointestinal malignancy comes from stud-lity and Immunogenetics. Published by Elsevier Inc. All rights reserved.

it
akpnpnpT(w[IlIaefa[s[aqt[scc
IgbpIhlt
S
S
D1
metebmBcftaohm2oici
S
Akfd
G
P5TTacu7mApnC
G
Pgml5atcspStSrbsnc
180 R. Upadhyay et al.
es indicating that IL-1 cytokine gene polymorphisms increasehe risk of gastric cancer and its precursors [4,5].
IL-1 cluster genes are located at chromosome 2q12 [6]nd are composed of three related genes within a 430-ilobase region: IL-1�, IL-1�, and IL-1RN, which encode theroinflammatory cytokines IL-1�, IL-1�, and their endoge-ous receptor antagonist IL-1RA, respectively. Numerous re-orted polymorphisms exist in the IL-1� (-511 C�T, -31 T�C,t5810 A�T, �3953 C�T) and IL-RN genes (Intron-2 [86-baseair (bp) variable number tandem repeat (VNTR)] nt8006�C, nt8061 C�T, nt9589 A�T, nt11100 T�C) [7]. In IL-1�-511C�T) gene polymorphism, the variant allele (-511T)as associated with higher susceptibility to gastric cancer
8,9]. Helicobacter pylori-infected patients carrying theL-1� -511T allele demonstrated increased gastric mucosalevels of IL-1� cytokine in gastric mucosa [7]. The activity ofL-1� is modulated by an endogenous inhibitor, the receptorntagonist (IL-1RA), which binds to IL-1 receptor withoutxerting an effector function [10]. In the IL-1RN gene codingor IL-1RA, a functional VNTR polymorphism in intron 2 playsn important role in human immune response and cancer risk11]. The IL-1RN gene exists in six allelic variants corre-ponding to one to six copies of the 86-bp sequence repeat12]. The 4-repeat (IL-1RN*1) and 2-repeat (IL-1RN*2) allelesre most common, whereas others occur at a combined fre-uency of �5%. The polymorphic IL-1RN gene results in quan-itative differences in both IL-1RA and IL-1� production13,14]. Association of IL-1� and IL-1RN polymorphisms weretudied with susceptibility to liver, lung, prostate, and ovarianancers with inconsistent results [15], but studies regardingancer of the esophagus are limited [16].
Previous studies postulated that it is not the IL-1RN orL-1� genes alone, but the haplotypes of the IL-1RN and IL-1�enes that play important roles in modulating the suscepti-ility to certain disease states [17–19]. Therefore, in theresent study, we aimed to investigate the association ofL-1� (-511C�T) and IL-1RN (VNTR) at allele, genotype, andaplotype interface with EC using case–control analysis, fol-owed by evaluation of their association with clinical pheno-ypes and environmental factors.
ubjects and methods
tudy subjects
uring a 31/ year period from August 2003 to April 2007, a total of
ABBREVIATIONS
ADC adenocarcinomabp base pairCI confidence intervalEC esophageal cancerIL interleukinOR odds ratioPCR polymerase chain reactionSCC squamous cell carcinomaVNTR variable number tandem repeats
2
59 histopathology confirmed patients (74.2% males and 25.8% fe- s
ales, mean age 56.6 years � 12 old, range 30–84 years) werenrolled from the outpatient clinics of Radiotherapy and Gastroen-erology, Sanjay Gandhi Post-Graduate Institute of Medical Sci-nces, Lucknow. Patients’ diagnosis was confirmed on endoscopiciopsy by pathologists. Patients were excluded if they had secondalignancy like corrosive esophageal injury, Achalasia injury, orarrett’s esophagus. The patient’s information was recorded ac-ording to cancer proforma, which included demography, pedigree,amily history of chronic diseases, clinical investigations (histology,umor location, and lymph nodes), tobacco, smoking, alcohol, andny work-related exposure to toxic chemicals, as described previ-usly [20]. At the same time, a total of 194 unrelated, age-matched,ealthy controls (paramedical staff and healthy volunteers) (65.5%ales and 34.5% females, mean age 53.6 years � 11.2 old, range
0–85 years) were also recruited from the same source populationf northern India. Informed consent was obtained from all recruitedndividuals and the study was approved by the institutional ethicsommittee (ethically approved at the 28th Ethics Committee Meet-ng held on 14.05.2003 at SGPGI).
ample collection
venous blood sample (5 ml) was collected form each patient andept frozen until DNA extraction. The genomic DNA was extractedrom peripheral blood leukocytes using the salting-out method, asescribed previously [20].
enotyping for IL-1� (-511 C>T) polymorphism
olymerase chain reaction (PCR) was conducted in a total volume of0 �l with 25 pmol of each primer; as reported by Rad et al. [21], 5=GG CAT TGA TCT GGT TCA TC 3= and 5= GTT TAG GAA TCT TCC CACT 3=; genomic DNA (100–150 ng); 10� Taq polymerase buffer (5 �l),nd 1.5 units of Taq DNA polymerase (Bangalore Genei, India). PCRonditions were as follows: initial denaturation of 95°C for 5 min-tes, 35 cycles of 95°C for 30 seconds, 55°C for 30 seconds, and2°C for 30 seconds, followed by a final extension of 72°C for 5inutes. PCR products were digested by restriction endonucleasevaI (MBI Fermentas) at 37°C overnight and then analyzed by 10%olyacrylamide gel electrophoresis using a 50-bp ladder. IL-1� ge-otypes were coded as follows: 304 bp for T/T; 190 and 114 bp for/C; 304 � 190 and 114 bp for C/T genotype (Figure 1a).
enotyping for IL-1RN (VNTR) polymorphism
CR analysis was carried out in a total volume of 50 �l containingenomic DNA (100–150 ng); 10 pmol of each primer; 10� Taq poly-erase buffer (5 �l), and 1.5 units of Taq DNA polymerase (Banga-
ore Genei). The primers for the IL-1RN (VNTR) in intron 2 were (F)= CTCAGCAACACTCCTAT 3= and (R) 5= TCCTGGTCTGCAGGTAA 3=,ccording to Tarlow et al. [22]. Amplification was performed underhe following conditions: denaturing step at 95°C for 5 minutes, 35ycles of 95°C for 30 seconds, 58°C for 30 seconds, and 72°C for 30econds and 1 cycle of extension at 72°C for 10 minutes. The PCRroducts were separated by electrophoresis on a 2% agarose gel.izing of product was performed using a 50-bp ladder. Gel documen-ation was done using an Alphaimager 1220 (Alpha Innotech Corp.,an Leandro, CA, USA). Allele 1 (4 repeats) was 410 bp, allele 2 (2epeats) 240 bp, allele 3 (3 repeats) 325 bp, allele 4 (5 repeats) 500p, and allele 5 (6 repeats) 595 bp (Figure 1b). Twenty percent ofamples from patients and controls, including samples of each ge-otype, were regenotyped by other laboratory personnel. No dis-repancy existed after sequencing of the randomly selected 10%
amples.
S
Tqwpftetr2tjumtst
R
C
Cc(mppotf
fqe
Dga
ICI3dfdd2qcc-cpi9-
e1st0
Ag
TthpppnA1
llOccag(
H(
S
FClpn1
181Influence of IL-1 haplotype in esophageal cancer
tatistical analysis
he direct gene counting method was used to determine the fre-uency of genotypes and alleles. To ensure that the controls usedere representative in the general population and to exclude theossibility of genotyping error, deviation of the observed genotyperequencies of IL-1� (-511C�T) and IL-1RN (VNTR) polymorphisms inhe controls was compared with that expected under Hardy–Weinbergquilibrium using the goodness-of-fit �2 test. Statistical analysis ofhe IL-1� and IL-1RN haplotype frequency and linkage disequilib-ium calculations were conducted using Arlequin software, ver..00, by the expectization and maximization algorithm [23]. Geno-ype and haplotype risk was expressed as an age- and gender-ad-usted OR (odds ratio) with 95% confidence interval (CI) estimatedsing binary logistic regression statistics. Bonferroni’s correction (aultiple-comparison correction) was applied to significant associa-
ions (p [pcorr]). The significance level for all statistical tests waset at p � 0.05. The collected data were analyzed using the statis-ical software SPSS, ver. 12.0 (SPSS, Inc., Chicago, IL, USA).
esults
haracteristics of study participants
linical characteristics involved 92.5% (147/159) squamousell carcinoma (SCC) and 7.5% (12/159) adenocarcinomaADC) patients. More than 50% of tumors were localized iniddle third region of the esophagus (79/147). About 80%atients used some form of tobacco. A significant number ofatients also reported alcohol usage (49/132, 37.1%) andccupational exposure (41/131, 30%). Information regardingumor location was not available in all patients. Similarly,
igure 1. (a) Gel picture of IL-1� C�T polymorphism. Lane 1,T genotype; lane 2, 50-bp DNA ladder; lane 3, TT genotype;
ane 4, CC genotype. (b) Gel picture of IL-1RN (VNTR) polymor-hism. Lane 1, 50-bp DNA ladder; lane 2, 2/4; lane 3, 1/3 ge-otype; lane 4, 2/3 genotype; lane 5, 1/1; lane 6, 2/2; lane 7,/2.
or the environmental exposure, history was not available f
or all patients. Some individuals refused to answer certainuestions if they were regarded as too private (alcohol andxposure).
istribution of IL-1� (-511C>T) and IL-1RN (VNTR)enotypes in esophageal cancer patientsnd controls
n controls, the frequency of IL-1� (-511C�T) genotypes CC,T, and TT was 12.9, 47.4, and 39.7% and the frequency of
L-1RN (VNTR) genotypes 1/1, 1/2, 2/2, and 1/4 was 52.6,9.2, 6.7, and 1.5%, respectively. The observed frequencyid not differ significantly from expected in controls andollowed Hardy–Weinberg equilibrium (p � ns). Also, theistribution of IL-1� (-511C�T) and IL-1RN (VNTR) genotypesid not differ between patients and controls (Tables 1 and). However, for IL-1� (-511C�T) polymorphism, the fre-uency of the -511TT genotype was lower in patients (34%)ompared with controls (39.7%) but did not confer signifi-ant protection (OR 0.55, 95% CI � 0.28–1.0, p � 0.07). The511T allele frequency was also lower in patients (57.5%)ompared with controls (63.4%; OR 0.80, 95% CI � 0.58–1.0,� 0.154). After study participants were stratified accord-
ng to gender, -511TT genotype forced lower risk (OR � 0.47,5% CI � 0.22–0.99, p � 0.04) to males compared with other511CT genotypes.
Distribution of IL-1RN (VNTR) genotypes in patients withsophageal cancer demonstrated a decreased frequency of/1 genotypes (44.6% in patients vs. 52.6% in controls) andlightly increased frequency of 1/4 genotypes (4.5% in pa-ients vs. 1.5% in controls; OR � 3.4; 95% CI � 0.85–14.0; p �.08).
ssociation of IL-1� (-511C>T) and IL-1RN (VNTR)enotypes with clinical characteristics in risk of EC
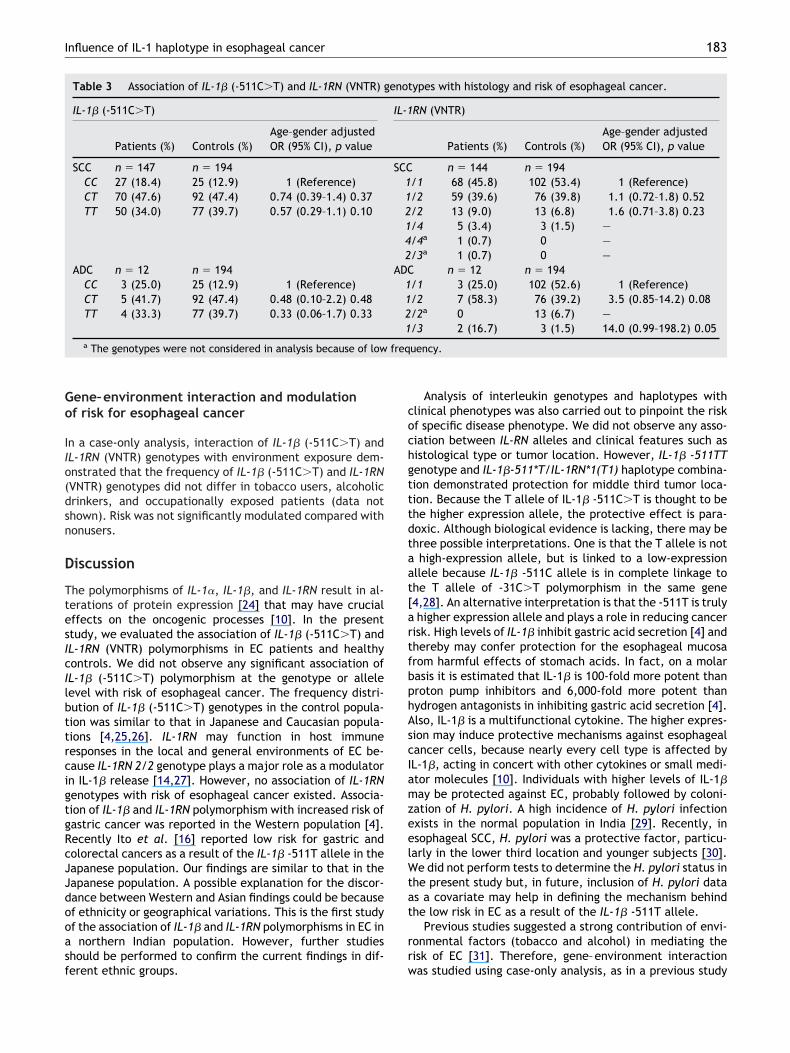
he frequency of IL-1� (-511C�T) and IL-1RN (VNTR) geno-ypes was compared in two histologies and -511TT genotypead a slightly lower frequency in both SCC (34.0%) and ADCatients (33%) compared with controls (39.7%; p � 0.10 and� 0.33, respectively; Table 3). For IL-1RN (VNTR) gene
olymorphism, genotype frequency in patients with SCC didot demonstrate any significant change but patients withDC were at threefold higher risk (OR � 3.5; 95% CI � 0.85–4.2, p � 0.08; Table 3).
When esophageal tumor location (upper, middle, orower third) was analyzed, IL-1� -511TT genotype conferredower risk in patients for middle third location (p � 0.002;R � 0.27; 95% CI � 0.12–0.62; Table 4). After Bonferroniorrection, the association remained statistically signifi-ant (pcorr � 0.009). In the other two locations (uppernd lower third), IL-1� (-511C/T) and IL-1RN (VNTR)enotypes did not appear to influence susceptibilityTable 4).
aplotype analysis of IL-1 � (-511C>T) and IL-1RNVNTR) polymorphism
ix haplotypes, C1, C2, C3, T1, T2, and T3, were observed
rom the genotype combination of IL-1� (-511C�T) and
Iip2na
cTtr0(
182 R. Upadhyay et al.
L1-RN (VNTR) polymorphisms. No linkage disequilibrium ex-sted between IL-1� (-511C�T) and IL-1RN (VNTR) polymor-hisms in patient (�2 � 5.29, p � 0.06) and control (�2 �.25, p � 0.52) populations. None of the haplotype combi-ations demonstrated significant risk of esophageal cancerfter adjusting for age and gender (Table 5). Further, asso-
Table 1 IL-1� (-511C�T) genotype frequency distribution by th
Patients (%)
IL-1� genotype n � 159CC 30 (18.9)CT 75 (47.2)TT 54 (34.0)
IL-1� allele n � 318a
C 135 (42.5)T 183 (57.5)
Males n �118CC 26 (22.0)CT 54 (45.8)TT 38 (32.2)
Females n � 41CC 4 (9.8)CT 21 (51.2)TT 16 (39.0)a Number of chromosomes.
Table 2 IL-1RN (VNTR) genotype frequency distribution by the
Patients (%)
IL1-RN genotype (n � 159)1/1 71 (44.6)1/2 66 (41.5)2/2 13 (8.3)1/4 7 (4.5)2/3a 1 (0.06)4/4 1 (0.06)
IL1-RN allele n � 318b
1 215 (67.6)2 94 (29.3)3a 1 (0.3)4 8 (2.8)
Males n � 1181/1 49 (41.5)1/2 53 (44.9)2/2 9 (7.6)1/4 5 (4.2)
Females n � 411/1 22 (53.7)1/2 13 (31.7)2/2 4 (9.8)1/4 2 (4.9)a The genotypes and alleles were not considered in analysis becb
Number of chromosomes.iation of all the variant haplotype combinations (T1�,2�, T1T2�) was analyzed with histology and location ofumor. Individuals with the T1� combination were at lowerisk for middle third tumor location (OR 0.462, 95% CI �.253–0.845, P � 0.01) after adjusting for age and genderTable 6).
e–control status and association with risk of esophageal cancer.
Controls (%)Age–gender adjustedOR (95% CI), p value
n � 19425 (12.9) 1 (Reference)92 (47.4) 0.72 (0.38–1.2) 0.25177 (39.7) 0.55 (0.28–1.0) 0.07
n � 388a
142 (36.6) 1 (Reference)246 (63.4) 0.80 (0.58–1.08) 0.154n � 12818 (14.1) 1 (Reference)58 (45.3) 0.66 (0.32–1.3) 0.2652 (40.6) 0.47 (0.22–0.99) 0.04
n � 667 (10.6) 1 (Reference)
34 (51.5) 1.0 (0.27–4.2) 0.9125 (37.9) 0.92 (0.22–3.8) 0.91
control status and association with risk of esophageal cancer.
Controls (%)Age–gender adjusted OR(95% CI), p value
(n � 194)102 (52.6) 1 (Reference)76 (39.2) 1.23 (0.77–1.9) 0.3713 (6.7) 1.56 (0.67–3.6) 0.293 (1.5) 3.45 (0.85–14.0) 0.080 —0 —
n � 388b
283 (73.0) 1 (Reference)102 (26.2) 1.187 (0.854–1.651) 0.306
03 (0.8) 4.269 (1.129–16.144) 0.032
n � 12870 (54.7) 1 (Reference)48 (37.5) 1.5 (0.89–2.7) 0.118 (6.3) 1.5 (0.56–4.4) 0.382 (1.6) 3.6 (0.66–19.7) 0.13
n � 6632 (48.5) 1 (Reference)28 (42.4) 0.70 (0.29–1.6) 0.435 (7.6) 1.6 (0.37–7.2) 0.501 (1.5) 3.1 (0.26–37.0) 0.36
of low frequency in patients and controls.
e cas
case–
ause
Go
IIo(dsn
D
TtesIcIlbttrcigtgRcJJdooasf
cochgtttdtaat[artfbphAscIamzeelWtat
rr
freq
183Influence of IL-1 haplotype in esophageal cancer
ene–environment interaction and modulationf risk for esophageal cancer
n a case-only analysis, interaction of IL-1� (-511C�T) andL-1RN (VNTR) genotypes with environment exposure dem-nstrated that the frequency of IL-1� (-511C�T) and IL-1RNVNTR) genotypes did not differ in tobacco users, alcoholicrinkers, and occupationally exposed patients (data nothown). Risk was not significantly modulated compared withonusers.
iscussion
he polymorphisms of IL-1�, IL-1�, and IL-1RN result in al-erations of protein expression [24] that may have crucialffects on the oncogenic processes [10]. In the presenttudy, we evaluated the association of IL-1� (-511C�T) andL-1RN (VNTR) polymorphisms in EC patients and healthyontrols. We did not observe any significant association ofL-1� (-511C�T) polymorphism at the genotype or alleleevel with risk of esophageal cancer. The frequency distri-ution of IL-1� (-511C�T) genotypes in the control popula-ion was similar to that in Japanese and Caucasian popula-ions [4,25,26]. IL-1RN may function in host immuneesponses in the local and general environments of EC be-ause IL-1RN 2/2 genotype plays a major role as a modulatorn IL-1� release [14,27]. However, no association of IL-1RNenotypes with risk of esophageal cancer existed. Associa-ion of IL-1� and IL-1RN polymorphism with increased risk ofastric cancer was reported in the Western population [4].ecently Ito et al. [16] reported low risk for gastric andolorectal cancers as a result of the IL-1� -511T allele in theapanese population. Our findings are similar to that in theapanese population. A possible explanation for the discor-ance between Western and Asian findings could be becausef ethnicity or geographical variations. This is the first studyf the association of IL-1� and IL-1RN polymorphisms in EC in
northern Indian population. However, further studieshould be performed to confirm the current findings in dif-
Table 3 Association of IL-1� (-511C�T) and IL-1RN (VNTR) g
IL-1� (-511C�T)
Patients (%) Controls (%)Age–gender adjustedOR (95% CI), p value
SCC n � 147 n � 194CC 27 (18.4) 25 (12.9) 1 (Reference)CT 70 (47.6) 92 (47.4) 0.74 (0.39–1.4) 0.37TT 50 (34.0) 77 (39.7) 0.57 (0.29–1.1) 0.10
ADC n � 12 n � 194CC 3 (25.0) 25 (12.9) 1 (Reference)CT 5 (41.7) 92 (47.4) 0.48 (0.10–2.2) 0.48TT 4 (33.3) 77 (39.7) 0.33 (0.06–1.7) 0.33
a The genotypes were not considered in analysis because of low
erent ethnic groups. w
Analysis of interleukin genotypes and haplotypes withlinical phenotypes was also carried out to pinpoint the riskf specific disease phenotype. We did not observe any asso-iation between IL-RN alleles and clinical features such asistological type or tumor location. However, IL-1� -511TTenotype and IL-1�-511*T/IL-1RN*1(T1) haplotype combina-ion demonstrated protection for middle third tumor loca-ion. Because the T allele of IL-1� -511C�T is thought to behe higher expression allele, the protective effect is para-oxic. Although biological evidence is lacking, there may behree possible interpretations. One is that the T allele is nothigh-expression allele, but is linked to a low-expression
llele because IL-1� -511C allele is in complete linkage tohe T allele of -31C�T polymorphism in the same gene4,28]. An alternative interpretation is that the -511T is trulyhigher expression allele and plays a role in reducing cancer
isk. High levels of IL-1� inhibit gastric acid secretion [4] andhereby may confer protection for the esophageal mucosarom harmful effects of stomach acids. In fact, on a molarasis it is estimated that IL-1� is 100-fold more potent thanroton pump inhibitors and 6,000-fold more potent thanydrogen antagonists in inhibiting gastric acid secretion [4].lso, IL-1� is a multifunctional cytokine. The higher expres-ion may induce protective mechanisms against esophagealancer cells, because nearly every cell type is affected byL-1�, acting in concert with other cytokines or small medi-tor molecules [10]. Individuals with higher levels of IL-1�ay be protected against EC, probably followed by coloni-
ation of H. pylori. A high incidence of H. pylori infectionxists in the normal population in India [29]. Recently, insophageal SCC, H. pylori was a protective factor, particu-arly in the lower third location and younger subjects [30].e did not perform tests to determine the H. pylori status in
he present study but, in future, inclusion of H. pylori datas a covariate may help in defining the mechanism behindhe low risk in EC as a result of the IL-1� -511T allele.
Previous studies suggested a strong contribution of envi-onmental factors (tobacco and alcohol) in mediating theisk of EC [31]. Therefore, gene–environment interaction
ypes with histology and risk of esophageal cancer.
RN (VNTR)
Patients (%) Controls (%)Age–gender adjustedOR (95% CI), p value
n � 144 n � 194/1 68 (45.8) 102 (53.4) 1 (Reference)/2 59 (39.6) 76 (39.8) 1.1 (0.72–1.8) 0.52/2 13 (9.0) 13 (6.8) 1.6 (0.71–3.8) 0.23/4 5 (3.4) 3 (1.5) —/4a 1 (0.7) 0 —/3a 1 (0.7) 0 —
n � 12 n � 194/1 3 (25.0) 102 (52.6) 1 (Reference)/2 7 (58.3) 76 (39.2) 3.5 (0.85–14.2) 0.08/2a 0 13 (6.7) —/3 2 (16.7) 3 (1.5) 14.0 (0.99–198.2) 0.05
uency.
enot
IL-1
SCC112142
ADC1121
as studied using case-only analysis, as in a previous study

[eociM
be
smd
quen
184 R. Upadhyay et al.
32]. In the present study, no interaction of environmentalxposures with interleukin genotypes indicated modulationf risk for EC. Recently, a study with high-thoroughput mi-roarray assay demonstrated differentially expressed genesn response to cigarette smoke, e.g., SOD2, CYP1B1, ATF,APK14, and SERPINB2 [33]. In future, these genes may
Table 4 Association of IL-1� (-511C�T) and IL-1RN (VNTR) g
Patients (%) (n � 159)
IL-1�
Upper (n � 22)CC 3 (13.6)CT 8 (36.4)TT 11 (50.0)
Middle (n � 79)CC 44 (55.7)CT 17 (21.5)TT 44 (55.7)
Lower (n � 46)CC 6 (13.0)CT 19 (41.3)TT 21 (45.7)
IL-1RNUpper (n � 22)
1/1 6 (27.3)1/2 11 (50.0)2/2 1 (4.5)1/4 4 (18.2)2/3b 0
Middle (n � 79)1/1 40 (50.6)1/2 28 (35.4)2/2 9 (11.4)1/4 1 (1.3)2/3b 1 (1.3)
Lower (n � 46)1/1 23 (50.0)1/2 17 (37.0)2/2 3 (6.6)1/3 2 (4.3)4/4b 1 (2.1)
a Age- and gender-adjusted.b Genotypes were not considered in analysis because of low fre* After Bonferroni correction, p value � 0.009.
Table 5 Distribution of IL-1� (-511C�T) and IL-1RN (VNTR)
HaplotypePatients(Na � 314) (%)
Contro(Na �
C1 101 (32.2) 107 (2C2 30 (9.4) 33 (8C3 1 (0.3) 1 (0T1 113 (36) 173 (4T2 63 (20.1) 69 (1T3 6 (1.9) 2 (0
a Total number of chromosomes (patients or controls having geb
Age- and gender-adjusted odds ratio.e promising candidate genes for studying the gene–nvironmental interactions in EC.
The study had limitations of low sample size. These re-ults do, however, provide interesting new clues for furtherulticentric association studies in larger patient cohorts inifferent populations, as well as for further research aimed
ypes with tumor location and risk of esophageal cancer.
Controls (%) (n � 194) ORa (95% CI), p value
25 (12.9) 1 (Reference)92 (47.4) 0.85 (0.20–3.5) 0.8277 (39.7) 1.23 (0.30–4.9) 0.76
25 (12.9) 1 (Reference)92 (47.4) 0.66 (0.32–1.3) 0.2677 (39.7) 0.27 (0.11–0.62) 0.002*
25 (12.9) 1 (Reference)92 (47.4) 1.0 (0.35–2.8) 0.9777 (39.7) 1.0 (0.44–3.4) 0.68
102 (52.6) 1 (Reference)76 (39.2) 2.4 (0.85–7.0) 0.0913 (6.7) 1.2 (0.14–11.6) 0.823 (1.5) —0 —
102 (52.6) 1 (Reference)76 (39.2) 0.92 (0.51–1.6) 0.7713 (6.7) 1.8 (0.72–4.7) 0.203 (1.5) —0 —
102 (52.6) 1 (Reference)76 (39.2) 0.97 (0.48–1.8) 0.8613 (6.7) 0.98 (0.25–3.8) 0.983 (1.5) —0 —
cy.
otypes and risk of esophageal cancer.
(%) p value OR (95% CI)b
— Reference0.890 1.06 (0.459–2.45)0.834 0.740 (0.044–12.3)0.410 0.79 (0.462–1.37)0.775 1.10 (0.564–2.1)0.226 4.59 (0.39–54.1)
e count n � 0 were not included in the haplotype construction).
enot
hapl
ls385)
8).5).2)4.7)8).6)
notyp

al
pasd-lgssbEaoas
A
TCWBc
R
[
[
[
[
[
[
T2 n
185Influence of IL-1 haplotype in esophageal cancer
t elucidating the causal relationship of genotype and hap-otype with tumor location of EC.
To conclude, the present study illustated that IL-1 geneolymorphisms IL-1RN (VNTR) and IL-1� (-511C�T), at thellele or genotype level, had little or no influence on overallusceptibility of esophageal malignancy. However, a geneticifference in the IL-1� -511TT genotype and haplotype IL-1B511*T-IL-1RN*1 appeared to be associated with significantower risk for middle third anatomical location of esopha-eal tumor. This may represent a potential tool to assess theusceptibility and outcome of esophageal cancer. In future,ite-specific treatment protocols can be designed on theasis of IL-1 genotype or haplotype for better prognosis ofC. However, the role of other linked polymorphisms in IL-1�nd TNF� cannot be excluded. Thus, genetic analysis ofther cytokines and their interactions among themselvesnd environmental factors will be required to better under-tand this complex interplay in the development of EC.
cknowledgments
he study was sponsored by research grants from the Indianouncil of Medical Research (ICMR), Government of India.e gratefully acknowledge the assistance of Dr. Sandeephattacharya from King George Medical University in sampleollection.
eferences
[1] Smyth MJ, Cretney E, Kershaw MH, Hayakawa Y. Cytokines incancer immunity and immunotherapy. Immunol Rev 2004;202:275.
[2] Apte R, Voronov E. Interleukin 1: a major pleotropic cytokine intumor–host interactions. Semin Cancer Biol 2002;12:277.
[3] Pantschenko AG, Pushkar I, Anderson KH, Wang Y, Miller LJ,Kurtzman SH, et al. The interleukin-1 family of cytokines andreceptors in human breast cancer: implications for tumor pro-
Table 6 Association of IL-1� (-511C�T) and IL-1RN (VNTR) hesophageal cancer.
Haplotype
Histology (%)
Controls (n � 194) SCCa (n � 147) ADCb (n
T1� 37 (19.1) 40 (27.2) 3 (25)T1� 157 (80.9) 107 (72.8) 9 (75)T2� 115 (59.3) 84 (57.1) 7 (58.3)T2� 79 (40.7) 63 (42.9) 5 (41.7)T1T2� 67 (34.5) 96 (65.3) 7 (58.3)T1T2� 127 (65.5) 51 (34.7) 5 (41.7)
a Controls vs. SCC.b Controls vs. ADC.c Controls vs. upper third location.d Controls vs. middle third location.e Controls vs. lower third location.* Significant difference is shown in boldface (p � 0.01, OR � 0
T1� � patients who were T1 negative; T2� � patients who werewho were T1 and T2 positive; T1T2� � patients who were T1 and
gression. Int J Oncol 2003;23:269.
[4] El-Omar EM, Carrington M, Chow WH, McColl KE, Bream JH,Young HA, et al. Interleukin-1 polymorphisms associatedwith increased risk of gastric cancer. Nature 2000;404:398.
[5] Macarthur M, Hold GL, El-Omar EM. Inflammation and cancer II.Role of chronic inflammation and cytokine gene polymorphismsin the pathogenesis of gastrointestinal malignancy. Am JPhysiol Gastrointest Liver Physiol 2004;286:G515.
[6] Steinkasserer A, Spurr NK, Cox S, Jeggo P, Sim RB. The humanIL-1 receptor antagonist gene (IL1RN) maps to chromosome2q14-q21, in the region of the IL-1 alpha and IL-1 beta loci.Genomics 1992;13:654.
[7] Bidwell J, Keen L, Gallagher G, Kimberly R, Huizinga T,McDermott MF, et al. Cytokine gene polymorphism in humandisease: on-line databases. Genes Immun 1999;1:3.
[8] Figueiredo C, Machado JC, Pharoah P, Seruca R, Sousa S, Car-valho R, et al. Helicobacter pylori and interleukin 1 genotyp-ing: an opportunity to identify high-risk individuals for gastriccarcinoma. J Natl Cancer Inst 2002;94:1680.
[9] Machado JC, Figueiredo C, Canedo P, Pharoah P, Carvalho R,Nabais S, et al. A proinflammatory genetic profile increases therisk for chronic atrophic gastritis and gastric carcinoma. Gas-troenterology 2003;125:364.
10] Dinarello CA. Biologic basis for interleukin-1 in disease. Blood1996;87:2095.
11] Hu Z, Shao M, Chen Y, Zhou J, Qian J, Xu L, et al. Allele 2 of theinterleukin-1 receptor antagonist gene (IL1RN*2) is associatedwith a decreased risk of primary lung cancer. Cancer Lett 2006;236:269.
12] Vamvakopoulos JE, Taylor CJ, Morris-Stiff GJ, Green C, Met-calfe S. The interleukin-1 receptor antagonist gene: a single-copy variant of the intron 2 variable number tandem repeat(VNTR) polymorphism. Eur J Immunogenet 2002;29:337.
13] Arend WP, Gabay C. Physiologic role of interleukin-1 receptorantagonist. Arthritis Res 2000;2:245.
14] Vamvakopoulos J, Green C, Metcalfe S. Genetic control of IL-1beta bioactivity through differential regulation of the IL-1receptor antagonist. Eur J Immunol 2002;32:2988.
15] Balasubramanian SP, Azmy IA, Higham SE, Wilson AG, Cross SS,Cox A, et al. Interleukin gene polymorphisms and breast can-cer: a case control study and systematic literature review. BMC
types with clinical characteristics and risk of
Location (%)
) Upperc (n � 22) Middled (n � 79) Lowere (n � 46)
4 (18.2) 26 (32.9) 10 (21.7)18 (81.8) 53* (67.1) 36 (78.3)12 (54.5) 48 (60.8) 19 (41.3)10 (45.5) 31 (39.2) 27 (58.7)13 (59.1) 56 (70.9) 30 (65.2)9 (40.9) 23 (29.1) 16 (34.8)
, 95% CI � 0.253–0.845). T1� � patients who were T1 positive;sitive; T2� � patients who were T2 negative; T1T2� � patientsegative.
aplo
� 12
.462T2 po
Cancer 2006;6:188.

[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
186 R. Upadhyay et al.
16] Ito H, Kaneko K, Makino R, Konishi K, Kurahashi T, Yamamoto T,et al. Interleukin-1beta gene in esophageal, gastric and colo-rectal carcinomas. Oncol Rep 2007;18:473.
17] Hurme M, Santtila S. IL-1 receptor antagonist (IL-1Ra) plasmalevels are co-ordinately regulated by both IL-1Ra and IL-1betagenes. Eur J Immunol 1998;28:2598.
18] Wilkinson RJ, Patel P, Llewelyn M, Hirch CS, Pasvol G, SnounouG, et al. Influence of polymorphism in the genes for theinterleukin (IL)-1 receptor antagonist and IL-1beta on tubercu-losis. J Exp Med 1999;189:1863.
19] Joos L, McIntyre L, Ruan J, Connett JE, Anthonisen NR, WeirTD, et al. Association of IL-1beta and IL-1 receptor antagonisthaplotypes with rate of decline in lung function in smokers.Thorax 2001;56:863.
20] Jain M, Kumar S, Rastogi N, Lal P, Ghoshal UC, Tiwari A, et al.GSTT1, GSTM1 and GSTP1 genetic polymorphisms and interac-tion with tobacco, alcohol and occupational exposure inesophageal cancer patients from North India. Cancer Lett2006;242:60.
21] Rad R, Prinz C, Neu B, Neuhofer M, Zeitner M, Voland P, et al.Synergistic effect of Helicobacter pylori virulence factors andinterleukin-1 polymorphisms for the development of severehistological changes in the gastric mucosa. J Infect Dis 2003;188:272.
22] Tarlow JK, Blakemore AI, Lennard A, Solari R, Hughes HN,Steinkasserer A, et al. Polymorphism in human IL-1 receptorantagonist gene intron 2 is caused by variable numbers of an86-bp tandem repeat. Hum Genet 1993;91:403.
23] Schneider S, Roessli D, Excoffier L. Arlequin ver. 2.00. Softwarefor population genetics data analysis. Switzerland: Geneticsand Biometry Laboratory, University of Geneva, 2000.
24] Hulkkonen J, Vilpo J, Vilpo L, Koski T, Hurme M. Interleukin-1beta, interleukin-1 receptor antagonist and interleukin-6
plasma levels and cytokine gene polymorphisms in chronic lym-phocytic leukemia: correlation with prognostic parameters.Haematologica 2000;85:600.
25] Kato S, Onda M, Yamada S, Matsuda N, Tokunaga A, MatsukuraN. Association of the interleukin-1 beta genetic polymorphismand gastric cancer risk in Japanese. J Gastroenterol 2001;36:696.
26] Furuta T, El-Omar EM, Xiao F, Shirai N, Takashima M, SugimuraH. Interleukin 1beta polymorphisms increase risk of hypochlo-rhydria and atrophic gastritis and reduce risk of duodenal ulcerrecurrence in Japan. Gastroenterology 2002;123:92.
27] Santtila S, Savinainen K, Hurme M. Presence of the IL-1RA allele2 (IL1RN*2) is associated with enhanced IL-1beta production invitro. Scand J Immunol 1998;47:195.
28] Hamajima N, Matsuo K, Saito T, Tajima K, Okuma K, Yamao K,et al. Interleukin 1 polymorphisms, lifestyle factors, and Heli-cobacter pylori infection. Jpn J Cancer Res 2001;92:383.
29] Ghoshal UC, Tiwari S, Dhingra S, Pandey R, Ghoshal U, Singh H.Frequency of Helicobacter pylori and CagA antibody in patientswith gastric neoplasms and controls: The Indian enigma. Dig DisSci (In press).
30] Wu DC, Wu IC, Lee JM, Hsu HK, Kao EL, Chou SH, et al. Helico-bacter pylori infection: a protective factor for esophagealsquamous cell carcinoma in a Taiwanese population. Am J Gas-troenetrology 2005;100:588.
31] Straif K, Weiland SK, Bungers M, Holthenrich D, Taeger D, Yi S,et al. Exposure to high concentrations of nitrosamines and can-cer mortality among a cohort of rubber workers: Occup EnvironMed 2000;57:180.
32] Jain M, Kumar S, Ghoshal UC, Tiwari A, Mittal B. Role of GSTM3polymorphism in the risk of developing esophageal cancer.Cancer Epidemiol Biomark Prev 2007;16:178.
33] van Leeuwen DM, van Agen E, Gottschalk RW, Vlietinck R,Gielen M, van Herwijnen MH, et al. Cigarette smoke-induceddifferential gene expression in blood cells from monozygotic
twin pairs. Carcinogenesis 2007;28:691.