
Polymorphisms in the genes ERCC2, XRCC3 and CD3EAP influence treatment outcome in multiple myeloma...
10
Polymorphisms in the genes ERCC2, XRCC3 and CD3EAP influence treatment outcome in multiple myeloma patients undergoing autologous bone marrow transplantation Annette Vangsted 1 * , Peter Gimsing 2 , Tobias W. Klausen 1 , Bjørn A. Nexø 3 ,H ˚ akan Wallin 4 , Pernille Andersen 5 , Peter Hokland 6 , Søren T. Lillevang 7 and Ulla Vogel 4 1 Department of Haematology, Herlev University Hospital of Copenhagen, DK-2730 Herlev, Denmark 2 Department of Haematology, Rigshospitalet, University Hospital of Copenhagen, DK-2100 Copenhagen, Denmark 3 Institute of Human Genetics, University of Aarhus, DK-8000 Aarhus C, Denmark 4 National Institute of Occupational Health, DK-2100 Copenhagen, Denmark 5 Department of Clinical Immunology, Rigshospitalet, University Hospital of Copenhagen, DK-2100 Copenhagen, Denmark 6 Department of Haematology, University Hospital of Aarhus, DK-8000 Aarhus, Denmark 7 Department of Clinical Immunology, University Hospital of Odense, DK-5270 Odense, Denmark Individual variations in the ability to cope with DNA damage by DNA repair may be essential for the response to chemotherapy, since cancer cells from patients with an effective DNA repair may survive treatment. We have studied the effect on time to treatment failure (TTF) and overall survival (OS) of polymorphism in the DNA repair genes ERCC1, ERCC2 and XRCC3, and in the apopto- tic genes PPP1R13L and CD3EAP in 348 patients with multiple myeloma undergoing autologous bone marrow transplantation. Carriers of the variant C-allele of ERCC2 K751Q, the variant T- allele of XRCC3 T241M and the variant A-allele of CD3EAP G- 21A had a 1.3-fold, 1.8-fold and 1.9-fold longer TTF, respectively, than homozygous wild type carriers (p 5 0.006, p 5 0.004, p < 0.001). The polymorphism CD3EAP G-21A also had significant effect on OS (p < 0.045). The polymorphism ERCC2 K751Q may to be related to sex, since the prolonged TTF was only seen in women (p 5 0.001). Carriers of the combination of variant alleles of ERCC2 K751Q and XRCC3 T241M had 2.8-fold longer TTF (p 5 0.0002). This indicates that suboptimal repair of both DNA mechanisms favors prolonged TTF and that polymorphism in ERCC2, XRCC3 and CD3EAP predicts the outcome for patients treated with autologous stem cell transplantation. ' 2006 Wiley-Liss, Inc. Key words: chemotherapy; DNA repair genes; polymorphism; multiple myeloma; treatment outcome It is becoming increasingly clear that interindividual variation in the response to chemotherapy in cancer is important. In this report we have attempted to elucidate whether polymorphism in DNA repair genes influences the outcome in patients with multiple myeloma (MM). Younger patients with MM are usually treated with high-dose therapy with melphalan, followed by autologous stem cell trans- plantation (ASCT), which has resulted in significantly increased overall survival (OS) and quality of life. 1 However, time to treat- ment failure (TTF) varies considerably among patients. Because DNA repair is essential for correcting damages caused by DNA damaging therapy, individual variation in DNA repair capacity may be central in resistance to chemotherapy. Cells from MM patients who relapse after treatment with melphalan exhibit increased repair capacity when compared to cells from patients without previous treatment. 2 Moreover, genetic variations that modify DNA repair capacity influence the outcome of chemotherapy. 3–5 The genes ERCC1 and ERCC2 are involved in the nucleotide excision repair (NER), which is responsible for repair of bulky DNA damages caused by chemotherapy. 6,7 ERCC1 encodes a sub- unit of the endonuclease, which makes the incision 5 0 of the DNA damage in NER. 6 ERCC2 encodes a subunit of the transcription factor TFIIH, which is essential for both transcription and NER. 6 The polymorphisms ERCC2 N312D and ERCC2 K751Q result in amino acid substitutions (Fig. 1) and the variant alleles have been associated with increased levels of DNA adducts and low DNA repair capacity. 8,9 XRCC3 (located on chromosome 14q32) is required for efficient repair of double strand breaks via homolo- gous recombination repair, correct chromosomal segregation, as well as the repair of DNA cross links. 10 PPP1R13L encodes an in- hibitor of the RelA subunit of the transcription factor NF-jB, which has a central function in apoptotic regulation in most can- cers as well as in MM. 11 Changes in the PPP1R13L level have been shown to modify cisplatin-induced apoptosis. 12 The 3 0 -end of CD3EAP, also named CAST and ASE-1, (antisense to ERCC1) is overlapping with the ERCC1 transcript. 13 CD3EAP is an ubiqui- tous nuclear protein, which may be involved in T-cell activation. 14 Homozygous carriers of the haplotype ERCC1 N118N A , CD3EAP G-21A G and PPP1R13L IVS1 A4364G A have been shown to be at a much higher risk for basal cell carcinoma, 15,16 breast cancer and lung cancer. 17,18 The haplotype was not associated with risk of testis cancer or lung cancer in males. 18,19 We hypothesized that polymorphisms, which may modify DNA repair capacity and apo- ptosis, would modify the response to chemotherapy. In a popula- tion of 348 patients with MM treated with high dose chemother- apy we have studied the effect on TTF and OS of the DNA repair gene polymorphisms ERCC2 K751Q, ERCC2 D312N, XRCC3 T241M and ERCC1 N118N, and 2 other polymorphisms, PPP1R13L IVS1 A4364G and CD3EAP A-21G, which together with ERCC1 N118N, define the previously studied haplotype. We report that 2 DNA repair gene polymorphisms, ERCC2 K751Q and XRCC3 T241M, and the polymorphism CD3EAP G-21A sig- nificantly influence the outcome of high-dose chemotherapy; for CD3EAP G-21A and ERCC2 K751Q the effect may be contained in women only. Grant sponsors: Købmand Sven Hansen and Hustru Ina Hansen Fund, Dir. Leo Nielsen’s and Hustru Margrethe Nielsen’s Medical Research Fund, Folketingsmand Jens Christensen and Hustru Korna Christensen’s Fund, The Danish Medical Association Research Fund/Mimi & Victor Larsen’s Fund. *Correspondence to: Department of Haematology, Copenhagen University of Herlev, Herlev Ringvej 75, 2730 Herlev, Denmark. Fax: 45-44532518. E-mail: [email protected] Received 20 April 2006; Accepted after revision 12 September 2006 DOI 10.1002/ijc.22411 Published online 27 November 2006 in Wiley InterScience (www.interscience. wiley.com). Abbreviations: ASCT, autologous stem cell transplantation; CD3EAP, CD3e molecule, epsilon associated protein (also named ASE-1, antisense to ERCC1); CI, confidence interval; ERCC1, excision-repair cross-comple- menting 1; ERCC2, excision-repair cross-complementing 2; MM, multiple myeloma; NER, nucleotide excision repair; OS, overall survival; PPP1R13L, protein phosphatase 1, regulatory (inhibitor) subunit 13 like (also named RAI, RelA associated inhibitor); RR, relative risk; TTF, time to treatment failure; XRCC3, X-ray repair cross-complementing group 3. Int. J. Cancer: 120, 1036–1045 (2006) ' 2006 Wiley-Liss, Inc. Publication of the International Union Against Cancer
-
Upload
southerndenmark -
Category
Documents
-
view
1 -
download
0
Transcript of Polymorphisms in the genes ERCC2, XRCC3 and CD3EAP influence treatment outcome in multiple myeloma...

Polymorphisms in the genes ERCC2, XRCC3 and CD3EAP influence treatment
outcome in multiple myeloma patients undergoing autologous
bone marrow transplantation
Annette Vangsted1*, Peter Gimsing2, Tobias W. Klausen1, Bjørn A. Nexø3, Hakan Wallin4, Pernille Andersen5,Peter Hokland
6, Søren T. Lillevang
7and Ulla Vogel
4
1Department of Haematology, Herlev University Hospital of Copenhagen, DK-2730 Herlev, Denmark2Department of Haematology, Rigshospitalet, University Hospital of Copenhagen, DK-2100 Copenhagen, Denmark3Institute of Human Genetics, University of Aarhus, DK-8000 Aarhus C, Denmark4National Institute of Occupational Health, DK-2100 Copenhagen, Denmark5Department of Clinical Immunology, Rigshospitalet, University Hospital of Copenhagen, DK-2100 Copenhagen, Denmark6Department of Haematology, University Hospital of Aarhus, DK-8000 Aarhus, Denmark7Department of Clinical Immunology, University Hospital of Odense, DK-5270 Odense, Denmark
Individual variations in the ability to cope with DNA damage byDNA repair may be essential for the response to chemotherapy,since cancer cells from patients with an effective DNA repair maysurvive treatment. We have studied the effect on time to treatmentfailure (TTF) and overall survival (OS) of polymorphism in theDNA repair genes ERCC1, ERCC2 and XRCC3, and in the apopto-tic genes PPP1R13L and CD3EAP in 348 patients with multiplemyeloma undergoing autologous bone marrow transplantation.Carriers of the variant C-allele of ERCC2 K751Q, the variant T-allele of XRCC3 T241M and the variant A-allele of CD3EAP G-21A had a 1.3-fold, 1.8-fold and 1.9-fold longer TTF, respectively,than homozygous wild type carriers (p 5 0.006, p 5 0.004, p <0.001). The polymorphism CD3EAP G-21A also had significanteffect on OS (p < 0.045). The polymorphism ERCC2 K751Q mayto be related to sex, since the prolonged TTF was only seen inwomen (p 5 0.001). Carriers of the combination of variant allelesof ERCC2 K751Q and XRCC3 T241M had 2.8-fold longer TTF(p 5 0.0002). This indicates that suboptimal repair of both DNAmechanisms favors prolonged TTF and that polymorphism inERCC2, XRCC3 and CD3EAP predicts the outcome for patientstreated with autologous stem cell transplantation.' 2006 Wiley-Liss, Inc.
Key words: chemotherapy; DNA repair genes; polymorphism; multiplemyeloma; treatment outcome
It is becoming increasingly clear that interindividual variationin the response to chemotherapy in cancer is important. In thisreport we have attempted to elucidate whether polymorphism inDNA repair genes influences the outcome in patients with multiplemyeloma (MM).
Younger patients with MM are usually treated with high-dosetherapy with melphalan, followed by autologous stem cell trans-plantation (ASCT), which has resulted in significantly increasedoverall survival (OS) and quality of life.1 However, time to treat-ment failure (TTF) varies considerably among patients. BecauseDNA repair is essential for correcting damages caused by DNAdamaging therapy, individual variation in DNA repair capacity maybe central in resistance to chemotherapy. Cells from MM patientswho relapse after treatment with melphalan exhibit increased repaircapacity when compared to cells from patients without previoustreatment.2 Moreover, genetic variations that modify DNA repaircapacity influence the outcome of chemotherapy.3–5
The genes ERCC1 and ERCC2 are involved in the nucleotideexcision repair (NER), which is responsible for repair of bulkyDNA damages caused by chemotherapy.6,7 ERCC1 encodes a sub-unit of the endonuclease, which makes the incision 50 of the DNAdamage in NER.6 ERCC2 encodes a subunit of the transcriptionfactor TFIIH, which is essential for both transcription and NER.6
The polymorphisms ERCC2 N312D and ERCC2 K751Q result inamino acid substitutions (Fig. 1) and the variant alleles have been
associated with increased levels of DNA adducts and low DNArepair capacity.8,9 XRCC3 (located on chromosome 14q32) isrequired for efficient repair of double strand breaks via homolo-gous recombination repair, correct chromosomal segregation, aswell as the repair of DNA cross links.10 PPP1R13L encodes an in-hibitor of the RelA subunit of the transcription factor NF-jB,which has a central function in apoptotic regulation in most can-cers as well as in MM.11 Changes in the PPP1R13L level havebeen shown to modify cisplatin-induced apoptosis.12 The 30-endof CD3EAP, also named CAST and ASE-1, (antisense to ERCC1)is overlapping with the ERCC1 transcript.13 CD3EAP is an ubiqui-tous nuclear protein, which may be involved in T-cell activation.14
Homozygous carriers of the haplotype ERCC1 N118NA, CD3EAPG-21AG and PPP1R13L IVS1 A4364GA have been shown to be ata much higher risk for basal cell carcinoma,15,16 breast cancer andlung cancer.17,18 The haplotype was not associated with risk oftestis cancer or lung cancer in males.18,19 We hypothesized thatpolymorphisms, which may modify DNA repair capacity and apo-ptosis, would modify the response to chemotherapy. In a popula-tion of 348 patients with MM treated with high dose chemother-apy we have studied the effect on TTF and OS of the DNA repairgene polymorphisms ERCC2 K751Q, ERCC2 D312N, XRCC3T241M and ERCC1 N118N, and 2 other polymorphisms,PPP1R13L IVS1 A4364G and CD3EAP A-21G, which togetherwith ERCC1 N118N, define the previously studied haplotype. Wereport that 2 DNA repair gene polymorphisms, ERCC2 K751Qand XRCC3 T241M, and the polymorphism CD3EAP G-21A sig-nificantly influence the outcome of high-dose chemotherapy; forCD3EAP G-21A and ERCC2 K751Q the effect may be containedin women only.
Grant sponsors: Købmand Sven Hansen and Hustru Ina Hansen Fund,Dir. Leo Nielsen’s and Hustru Margrethe Nielsen’s Medical ResearchFund, Folketingsmand Jens Christensen and Hustru Korna Christensen’sFund, The Danish Medical Association Research Fund/Mimi & VictorLarsen’s Fund.*Correspondence to: Department of Haematology, Copenhagen
University of Herlev, Herlev Ringvej 75, 2730 Herlev, Denmark.Fax: 45-44532518. E-mail: [email protected] 20 April 2006; Accepted after revision 12 September 2006DOI 10.1002/ijc.22411Published online 27November 2006 inWiley InterScience (www.interscience.
wiley.com).
Abbreviations: ASCT, autologous stem cell transplantation; CD3EAP,CD3e molecule, epsilon associated protein (also named ASE-1, antisenseto ERCC1); CI, confidence interval; ERCC1, excision-repair cross-comple-menting 1; ERCC2, excision-repair cross-complementing 2; MM, multiplemyeloma; NER, nucleotide excision repair; OS, overall survival;PPP1R13L, protein phosphatase 1, regulatory (inhibitor) subunit 13 like(also named RAI, RelA associated inhibitor); RR, relative risk; TTF, timeto treatment failure; XRCC3, X-ray repair cross-complementing group 3.
Int. J. Cancer: 120, 1036–1045 (2006)' 2006 Wiley-Liss, Inc.
Publication of the International Union Against Cancer

Material and methods
Subjects
Patients were recruited from August 1994 to August 2004 from4 participating Danish centers in Denmark with a catchment popu-lation of about 5 million inhabitants. One hundred eighty-fivepatients diagnosed with MM in high-dose treatment protocolsincluding ASCT (NMSG no. 5/94, 7/98 and 11/00) administratedby the Nordic Myeloma Study Group (NMSG),20 and 163 patientstreated identically, but not registered in the NMSG protocols,were included.
The study was approved by the Danish Ethical Committee (01-158/03).
Clinical data and response criteria
The diagnosis of MM was accepted if criteria A 1 C, A 1 D orB 1 C 1 D of the following were attained. Three patients withsmoldering myeloma were included (C 1D). A: serum monoclo-nal compartment concentration of immunoglobulin IgG > 30 g/L,IgA > 20 g/L, the presence of an M-protein of IgD or IgE regard-less of concentration, or Bence-Jones proteinuria > 1 g/24 hr; B:M-protein in serum or urine at a lower concentration thandescribed under A; C: at least 10% plasma cells in bone marrowaspirate or biopsy-verified plasmacytoma of bone or soft tissue;and D: osteolytic bone lesions. Staging was according to Durieand Salmon.21
Progression was defined by a more than 25% increase in serumM-protein or 25% increase in immunoglobulin levels above uppernormal levels, confirmed by 2 separate measurements within a1-month interval. Increase of Bence-Jones proteinuria to morethan 1.0 g/24 hr or other signs of progression such as hypercalce-mia, progressive skeletal disease or soft-tissue plasmacytomawere also considered as progression. In patients for whom progres-sion could not be evaluated from the above-mentioned criteria,progression was defined as a 25% increase in infiltration of plasmacells in bone marrow. Occurrence of secondary malignancies anddeath without progression was considered as events not related toprogression. TTF and OS were calculated from date of transplan-tation to date of progression or death. Eleven patients died duringtransplantation. Two patients died from other cancer forms thanfrom MM, and 2 patients died of other causes. These patients wereincluded in the analysis of OS, but they were censored at time ofdeath in the analysis of TTF. Sixty-eight patients, including the 11patients who died during the transplantation procedure, were fol-lowed up less than 2 years.
Eligibility criteria
NMSG no. 5/94: All patients younger than 60 years could beincluded, provided they were not considered ineligible for induc-tion therapy because of severe chronic heart or lung disease, other
active malignancy or severe coincident illness, psychiatric diseaseor abuse, terminal illness or refusal. NMSG no. 7/98 and NMSGno. 11/00: As described in NMSG no. 5/94, but with inclusion ofall patients younger than 65 years. Patients not included in theabove-mentioned high-dose treatment protocols were submitted toASCT in accordance to the judgment of eligibility by the treatingphysician.
NMSG treatment protocols
NMSG no. 5/94: Induction therapy with VAD (vincristine, dox-orubicin and dexamethasone; peripheral blood stem cell harvest atregeneration after cyclophosphamide, high-dose chemotherapywith melphalan followed by ASCT, maintenance therapy withinterferon. Patients were transplanted only if they had an initialresponse to chemotherapy before harvesting.1 NMSG no. 7/98: Asdescribed for NMSG no. 5/94, but patients were included in thestudy regardless of their response to the induction treatment.22
NMSG no. 11/00: The treatment strategy was the same as forNMSG no. 7/98 except for the induction treatment. The patientswere randomized to treatment with either 3 series of VAD or 2–3series of cyclophosphamide (1 g/m2) combined with dexametha-sone (40 mg daily for 4 days). Twenty-nine patients were treatedwith VAD and 33 patients were treated with cyclophosphamide.There was no difference in TTF and OS in the 2 treatment groups.
The patients not included in the above-mentioned high-dosetreatment protocols were treated according to the judgment by thetreating physician. Standard induction chemotherapy for thisgroup of patients was VAD or cyclophosphamide (1 g/m2) anddexamethasone (40 mg daily for 4 days). Induction treatment wasfollowed by peripheral blood stem cell harvest at regeneration af-ter cyclophosphamide, high-dose chemotherapy with melphalanfollowed by ASCT, maintenance therapy with interferon.
Human tissue samples
Peripheral blood mononuclear cell was purified from 292 leuka-pheresis products by buffy coat preparation. From 56 patients 10lm sections were collected 10 times from paraffin-embeddedbone marrow samples. Material was not available for 19 patientsundergoing autologous bone marrow transplantation and thesepatients were not included in the study.
DNA purification
DNA for analysis was purified from PMBC by the salting outmethod23 or from paraffin-embedded tissue by phenol extractionas described in Ref. 24.
Detection of single nucleotide polymorphisms
The polymorphisms are presented in Figure 1. The dbSNP webaddress is www.ncbi.nlm.nih.gov/entrez/query.fcgi?db5snp
Genotypes were determined on an ABI 7500 using endpointreadings. Ten microliter reactions contained about 50 ng DNA,5 lL mastermix (Applied Biosystems, Birkerød, Denmark), 100 nMof each probe and 900 nM primers. Controls were included ineach run, and 10–50% of the samples was retyped for reproduci-bility and gave 99–100% identical results. Moreover, for 10 per-sons, both DNA from bone marrow and from leukapheresis prod-ucts were typed with identical results. ERCC2 K751Q (rs1052559)(XPD exon23, AfiC) and ERCC2 D312N (rs1799793) (XPDexon10, GfiA) were determined as previously described.25
PPP1R13L VS1 A4364G (rs1970764) (RAI intron1, AfiG) wasdetermined as previously described in Ref. 19. CD3EAP G-21A(rs967591) (ASE-1, exon1 GfiA) was determined using the pri-mers 50-TCTGCAACCTGGTGCGAG-30, 50-CCTTTCTCCTTCC-ACCAACG-30 and the probes G-allele: 50-FAM-AGGGTTGCCT-GAGGTGTGGGTCC-BHQ, A-allele: Yakima Yellow-AGGGTTACCTGAGGTGTGGGTCC-BHQ-30. The reactions were runfor 40 cycles for 15 sec at 94�C, 60 sec at 62�C. ERCC1 N118N(rs3177700) (ERCC1 exon4, AfiG) was determined using the pri-mers 50-GATGGCTTCTGCCCTTCG T-30 and 50-GGGAAT-
FIGURE 1 – Graphical presentation of the studied SNPs on chromo-some 19. The ERCC1 polymorphism is silent and does not result in anamino acid substitution. The CD3EAP polymorphism is G to A trans-version in the 50 untranslated region of the mRNA. The PPP1R13Lpolymorphism is in intron 1 of the PPP1R13L gene. The ERCC2D312N polymorphism gives rise to the Asp to Asn amino acid substi-tution in position 312 of ERCC2. ERCC2 K751Q gives rise to the Lysto Gln substitution in position 751 in ERCC2.
1037GENE POLYMORPHISMS IN MULTIPLE MYELOMA TREATMENT
TACGTCGCCAAATTC-30 and the probes G-allele: 5-Fam-CGTGCGCAACGTGCCC-BHQ-30, A-allele: 50-Yakima Yellow-CGTGCGCAATGTGCCCTG-BHQ-30 (TAGCopenhagen, Copen-hagen, Denmark). The reactions were run for 40 cycles for 15 sec at94�C, 60 sec at 63�C. XRCC3 T241 M (rs861535) (XRCC3 18067,CfiT) was determined as previously described.26
A varying number of PCR reactions failed for each genotype.These PCR reactions were repeated using 1/10 the amount ofDNA and 3 times the amount of DNA. If 3 independent attemptsfailed, the genotype was left undetermined. Nearly 40% of thePCR reactions for XRCC3 T241M failed, probably because theassay is very sensitive to iron-containing impurities of hemoglobinfrom the DNA purification step.
Statistical methods
SPSS statistical software was used for all calculations (SPSS forWindows, Rel. 14.0.0. 2005, SPSS, Chicago). All tests were 2-sided and p values < 0.05 were regarded as significant.
Fisher’s exact test was used for comparing categorical variablesand Mann–Whitney test was used for comparing continuous withcategorical variables. Kaplan–Meier method and the log rank testwere used to compare TTF and OS between groups. The Cox pro-
portional hazards model, log-likelihood statistics, was applied forunivariate analyses of covariates and for multivariate analysis.Significant variables with a p value < 0.05 by univariate analysiswere included in the multivariate Cox analyses to identify varia-bles of independent significance. In accordance to the Bonferronicorrection for multiple comparisons the p value was lowered from0.05 to 0.004.
Results
Study population
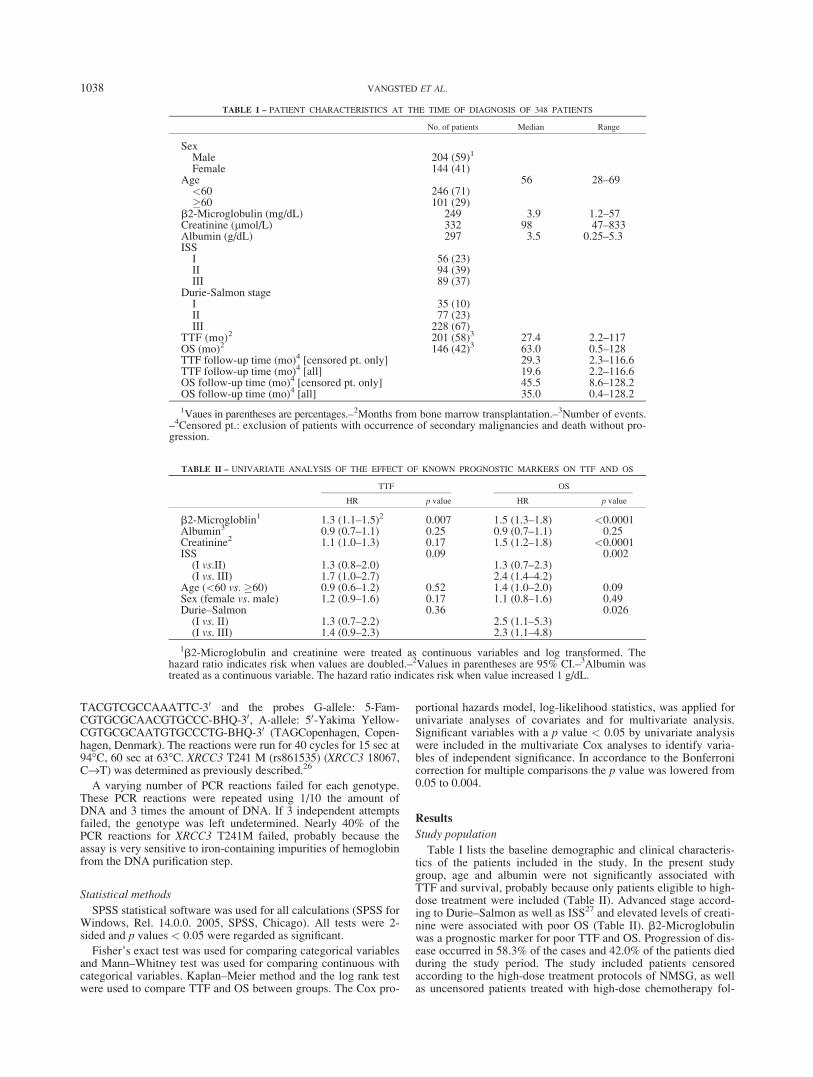
Table I lists the baseline demographic and clinical characteris-tics of the patients included in the study. In the present studygroup, age and albumin were not significantly associated withTTF and survival, probably because only patients eligible to high-dose treatment were included (Table II). Advanced stage accord-ing to Durie–Salmon as well as ISS27 and elevated levels of creati-nine were associated with poor OS (Table II). b2-Microglobulinwas a prognostic marker for poor TTF and OS. Progression of dis-ease occurred in 58.3% of the cases and 42.0% of the patients diedduring the study period. The study included patients censoredaccording to the high-dose treatment protocols of NMSG, as wellas uncensored patients treated with high-dose chemotherapy fol-
TABLE I – PATIENT CHARACTERISTICS AT THE TIME OF DIAGNOSIS OF 348 PATIENTS
No. of patients Median Range
SexMale 204 (59)1
Female 144 (41)Age 56 28–69<60 246 (71)�60 101 (29)
b2-Microglobulin (mg/dL) 249 3.9 1.2–57Creatinine (lmol/L) 332 98 47–833Albumin (g/dL) 297 3.5 0.25–5.3ISSI 56 (23)II 94 (39)III 89 (37)
Durie-Salmon stageI 35 (10)II 77 (23)III 228 (67)
TTF (mo)2 201 (58)3 27.4 2.2–117OS (mo)2 146 (42)3 63.0 0.5–128TTF follow-up time (mo)4 [censored pt. only] 29.3 2.3–116.6TTF follow-up time (mo)4 [all] 19.6 2.2–116.6OS follow-up time (mo)4 [censored pt. only] 45.5 8.6–128.2OS follow-up time (mo)4 [all] 35.0 0.4–128.2
1Vaues in parentheses are percentages.–2Months from bone marrow transplantation.–3Number of events.–4Censored pt.: exclusion of patients with occurrence of secondary malignancies and death without pro-gression.
TABLE II – UNIVARIATE ANALYSIS OF THE EFFECT OF KNOWN PROGNOSTIC MARKERS ON TTF AND OS
TTF OS
HR p value HR p value
b2-Microgloblin1 1.3 (1.1–1.5)2 0.007 1.5 (1.3–1.8) <0.0001Albumin3 0.9 (0.7–1.1) 0.25 0.9 (0.7–1.1) 0.25Creatinine2 1.1 (1.0–1.3) 0.17 1.5 (1.2–1.8) <0.0001ISS 0.09 0.002(I vs.II) 1.3 (0.8–2.0) 1.3 (0.7–2.3)(I vs. III) 1.7 (1.0–2.7) 2.4 (1.4–4.2)
Age (<60 vs. �60) 0.9 (0.6–1.2) 0.52 1.4 (1.0–2.0) 0.09Sex (female vs. male) 1.2 (0.9–1.6) 0.17 1.1 (0.8–1.6) 0.49Durie–Salmon 0.36 0.026(I vs. II) 1.3 (0.7–2.2) 2.5 (1.1–5.3)(I vs. III) 1.4 (0.9–2.3) 2.3 (1.1–4.8)
1b2-Microglobulin and creatinine were treated as continuous variables and log transformed. Thehazard ratio indicates risk when values are doubled.–2Values in parentheses are 95% CI.–3Albumin wastreated as a continuous variable. The hazard ratio indicates risk when value increased 1 g/dL.
1038 VANGSTED ET AL.
lowed by ASCT. Statistical analysis showed no difference in TTFand OS between the 3 different treatment protocols, betweenpatients treated with VAD or cyclophosphamide and dexametha-zone and the uncensored patients not included in the protocols.
Single nucleotide polymorphism
Genotypes of ERCC2 K751Q, ERCC2 D312N, PPP1R13L IVSA4364G, CD3EAP G-21A, ERCC1 N118N and XRCC3 T241Mwere determined. There was no difference in the allele frequenciesamong patients dependent on the participating centers, and the al-lele frequencies of the patients with MM were similar to those pre-viously observed for controls in the Danish Diet, Cancer and Healthcohort,17,18,25,26 indicating that the polymorphisms in this subgroupof patients were not associated with risk of MM (results not shown).The 5 polymorphisms which are located on chromosome 19q13.2-3were in linkage disequilibrium. The linkage patterns were exactlythe same as previously reported for Danish study populations.17
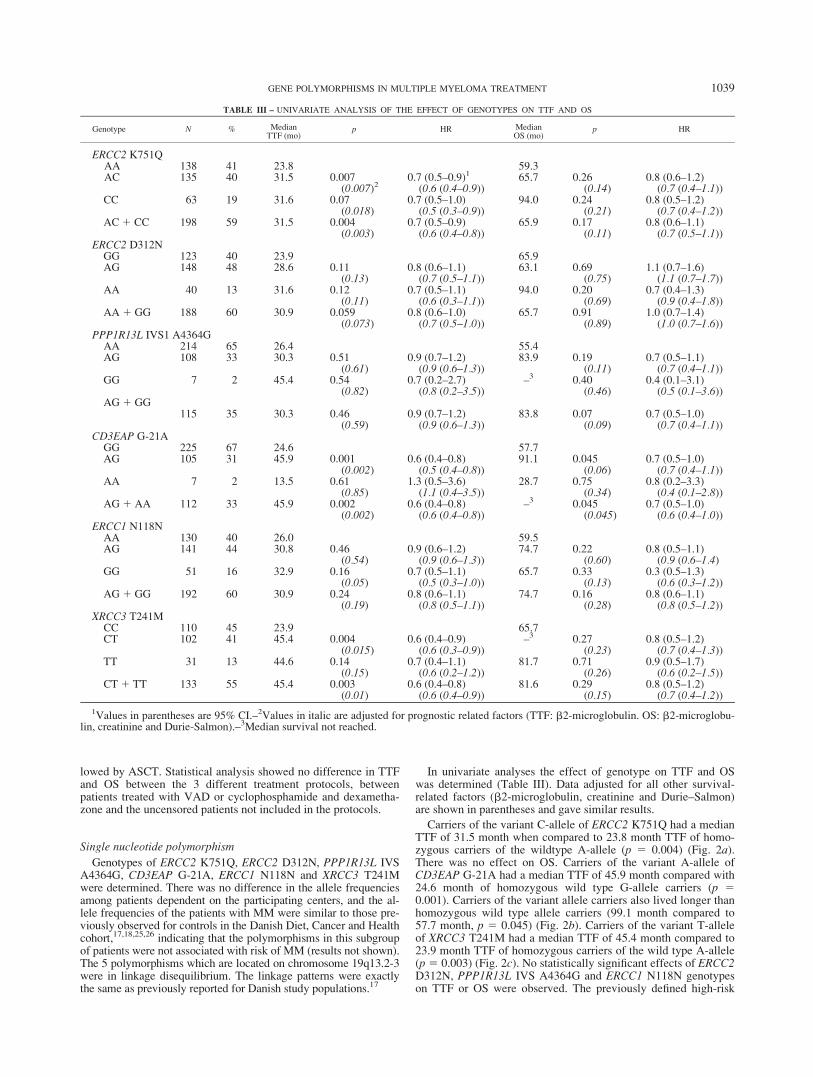
In univariate analyses the effect of genotype on TTF and OSwas determined (Table III). Data adjusted for all other survival-related factors (b2-microglobulin, creatinine and Durie–Salmon)are shown in parentheses and gave similar results.
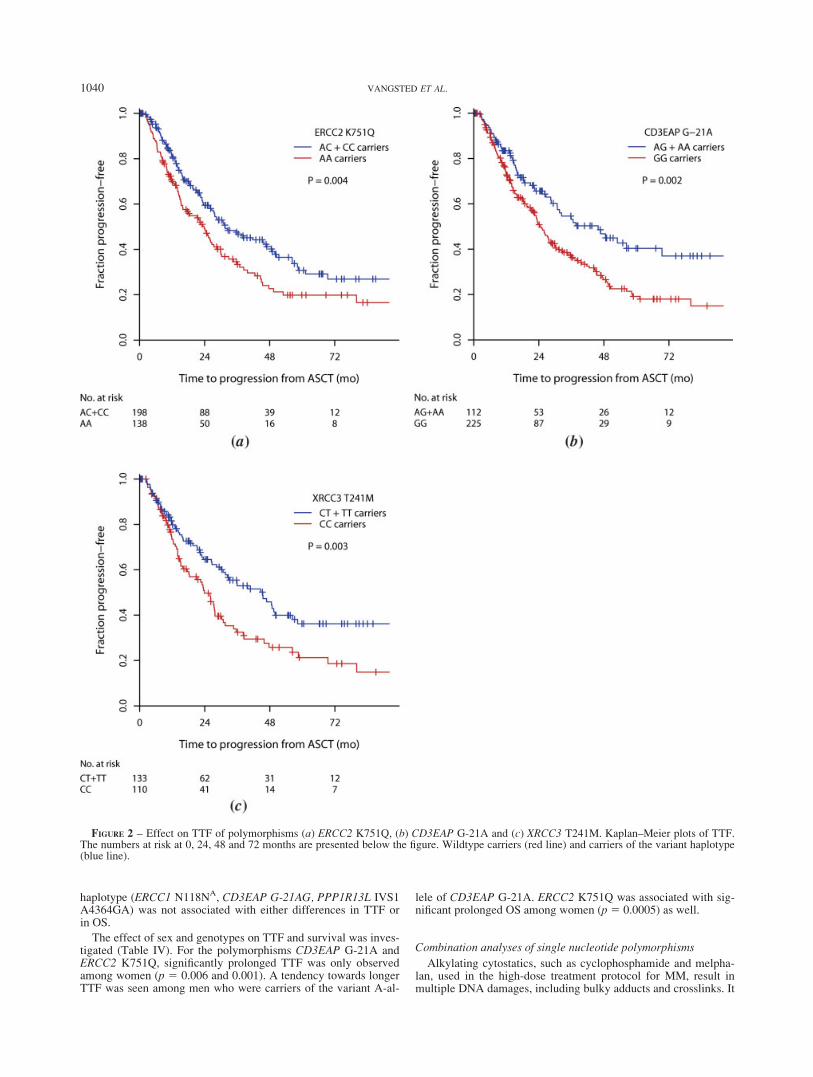
Carriers of the variant C-allele of ERCC2 K751Q had a medianTTF of 31.5 month when compared to 23.8 month TTF of homo-zygous carriers of the wildtype A-allele (p 5 0.004) (Fig. 2a).There was no effect on OS. Carriers of the variant A-allele ofCD3EAP G-21A had a median TTF of 45.9 month compared with24.6 month of homozygous wild type G-allele carriers (p 50.001). Carriers of the variant allele carriers also lived longer thanhomozygous wild type allele carriers (99.1 month compared to57.7 month, p 5 0.045) (Fig. 2b). Carriers of the variant T-alleleof XRCC3 T241M had a median TTF of 45.4 month compared to23.9 month TTF of homozygous carriers of the wild type A-allele(p 5 0.003) (Fig. 2c). No statistically significant effects of ERCC2D312N, PPP1R13L IVS A4364G and ERCC1 N118N genotypeson TTF or OS were observed. The previously defined high-risk
TABLE III – UNIVARIATE ANALYSIS OF THE EFFECT OF GENOTYPES ON TTF AND OS
Genotype N % MedianTTF (mo)
p HR MedianOS (mo)
p HR
ERCC2 K751QAA 138 41 23.8 59.3AC 135 40 31.5 0.007 0.7 (0.5–0.9)1 65.7 0.26 0.8 (0.6–1.2)
(0.007)2 (0.6 (0.4–0.9)) (0.14) (0.7 (0.4–1.1))CC 63 19 31.6 0.07 0.7 (0.5–1.0) 94.0 0.24 0.8 (0.5–1.2)
(0.018) (0.5 (0.3–0.9)) (0.21) (0.7 (0.4–1.2))AC1 CC 198 59 31.5 0.004 0.7 (0.5–0.9) 65.9 0.17 0.8 (0.6–1.1)
(0.003) (0.6 (0.4–0.8)) (0.11) (0.7 (0.5–1.1))ERCC2 D312N
GG 123 40 23.9 65.9AG 148 48 28.6 0.11 0.8 (0.6–1.1) 63.1 0.69 1.1 (0.7–1.6)
(0.13) (0.7 (0.5–1.1)) (0.75) (1.1 (0.7–1.7))AA 40 13 31.6 0.12 0.7 (0.5–1.1) 94.0 0.20 0.7 (0.4–1.3)
(0.11) (0.6 (0.3–1.1)) (0.69) (0.9 (0.4–1.8))AA 1 GG 188 60 30.9 0.059 0.8 (0.6–1.0) 65.7 0.91 1.0 (0.7–1.4)
(0.073) (0.7 (0.5–1.0)) (0.89) (1.0 (0.7–1.6))PPP1R13L IVS1 A4364G
AA 214 65 26.4 55.4AG 108 33 30.3 0.51 0.9 (0.7–1.2) 83.9 0.19 0.7 (0.5–1.1)
(0.61) (0.9 (0.6–1.3)) (0.11) (0.7 (0.4–1.1))GG 7 2 45.4 0.54 0.7 (0.2–2.7) –3 0.40 0.4 (0.1–3.1)
(0.82) (0.8 (0.2–3.5)) (0.46) (0.5 (0.1–3.6))AG 1 GG
115 35 30.3 0.46 0.9 (0.7–1.2) 83.8 0.07 0.7 (0.5–1.0)(0.59) (0.9 (0.6–1.3)) (0.09) (0.7 (0.4–1.1))
CD3EAP G-21AGG 225 67 24.6 57.7AG 105 31 45.9 0.001 0.6 (0.4–0.8) 91.1 0.045 0.7 (0.5–1.0)
(0.002) (0.5 (0.4–0.8)) (0.06) (0.7 (0.4–1.1))AA 7 2 13.5 0.61 1.3 (0.5–3.6) 28.7 0.75 0.8 (0.2–3.3)
(0.85) (1.1 (0.4–3.5)) (0.34) (0.4 (0.1–2.8))AG 1 AA 112 33 45.9 0.002 0.6 (0.4–0.8) –3 0.045 0.7 (0.5–1.0)
(0.002) (0.6 (0.4–0.8)) (0.045) (0.6 (0.4–1.0))ERCC1 N118N
AA 130 40 26.0 59.5AG 141 44 30.8 0.46 0.9 (0.6–1.2) 74.7 0.22 0.8 (0.5–1.1)
(0.54) (0.9 (0.6–1.3)) (0.60) (0.9 (0.6–1.4)GG 51 16 32.9 0.16 0.7 (0.5–1.1) 65.7 0.33 0.3 (0.5–1.3)
(0.05) (0.5 (0.3–1.0)) (0.13) (0.6 (0.3–1.2))AG 1 GG 192 60 30.9 0.24 0.8 (0.6–1.1) 74.7 0.16 0.8 (0.6–1.1)
(0.19) (0.8 (0.5–1.1)) (0.28) (0.8 (0.5–1.2))XRCC3 T241M
CC 110 45 23.9 65.7CT 102 41 45.4 0.004 0.6 (0.4–0.9) –3 0.27 0.8 (0.5–1.2)
(0.015) (0.6 (0.3–0.9)) (0.23) (0.7 (0.4–1.3))TT 31 13 44.6 0.14 0.7 (0.4–1.1) 81.7 0.71 0.9 (0.5–1.7)
(0.15) (0.6 (0.2–1.2)) (0.26) (0.6 (0.2–1.5))CT1 TT 133 55 45.4 0.003 0.6 (0.4–0.8) 81.6 0.29 0.8 (0.5–1.2)
(0.01) (0.6 (0.4–0.9)) (0.15) (0.7 (0.4–1.2))
1Values in parentheses are 95% CI.–2Values in italic are adjusted for prognostic related factors (TTF: b2-microglobulin. OS: b2-microglobu-lin, creatinine and Durie-Salmon).–3Median survival not reached.
1039GENE POLYMORPHISMS IN MULTIPLE MYELOMA TREATMENT
haplotype (ERCC1 N118NA, CD3EAP G-21AG, PPP1R13L IVS1A4364GA) was not associated with either differences in TTF orin OS.
The effect of sex and genotypes on TTF and survival was inves-tigated (Table IV). For the polymorphisms CD3EAP G-21A andERCC2 K751Q, significantly prolonged TTF was only observedamong women (p 5 0.006 and 0.001). A tendency towards longerTTF was seen among men who were carriers of the variant A-al-
lele of CD3EAP G-21A. ERCC2 K751Q was associated with sig-nificant prolonged OS among women (p5 0.0005) as well.
Combination analyses of single nucleotide polymorphisms
Alkylating cytostatics, such as cyclophosphamide and melpha-lan, used in the high-dose treatment protocol for MM, result inmultiple DNA damages, including bulky adducts and crosslinks. It
FIGURE 2 – Effect on TTF of polymorphisms (a) ERCC2 K751Q, (b) CD3EAP G-21A and (c) XRCC3 T241M. Kaplan–Meier plots of TTF.The numbers at risk at 0, 24, 48 and 72 months are presented below the figure. Wildtype carriers (red line) and carriers of the variant haplotype(blue line).
1040 VANGSTED ET AL.
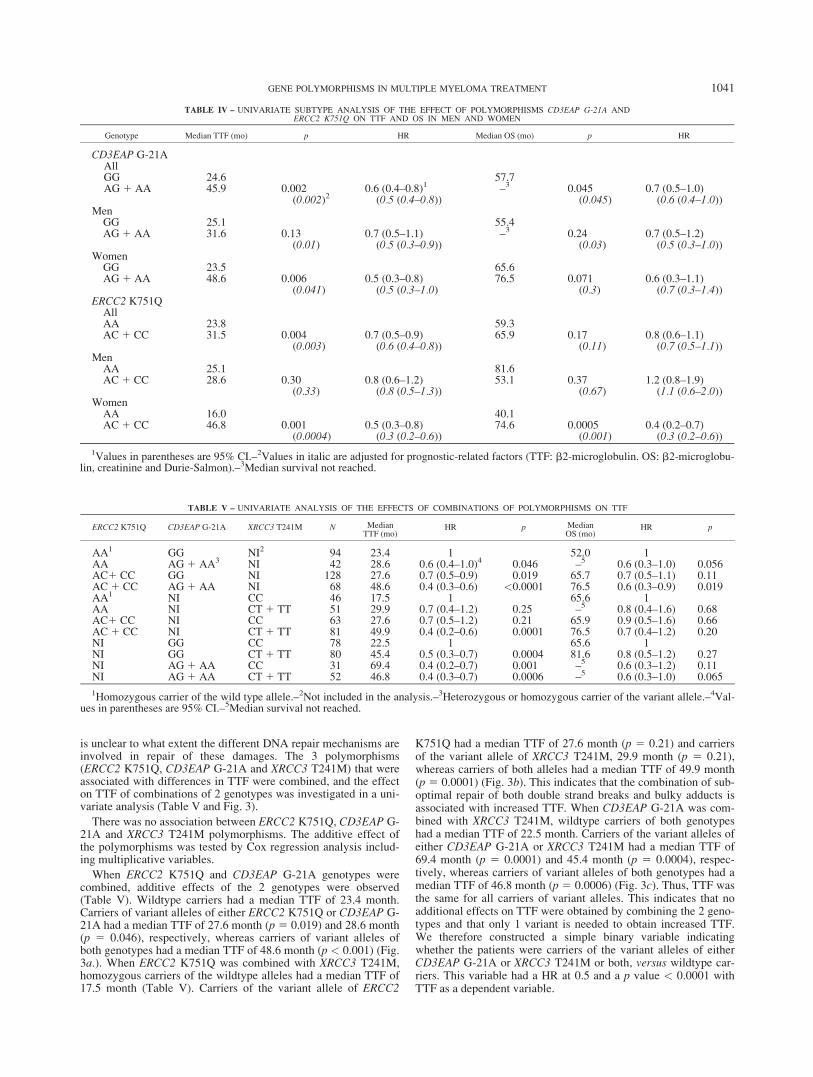
is unclear to what extent the different DNA repair mechanisms areinvolved in repair of these damages. The 3 polymorphisms(ERCC2 K751Q, CD3EAP G-21A and XRCC3 T241M) that wereassociated with differences in TTF were combined, and the effecton TTF of combinations of 2 genotypes was investigated in a uni-variate analysis (Table V and Fig. 3).
There was no association between ERCC2 K751Q, CD3EAP G-21A and XRCC3 T241M polymorphisms. The additive effect ofthe polymorphisms was tested by Cox regression analysis includ-ing multiplicative variables.
When ERCC2 K751Q and CD3EAP G-21A genotypes werecombined, additive effects of the 2 genotypes were observed(Table V). Wildtype carriers had a median TTF of 23.4 month.Carriers of variant alleles of either ERCC2 K751Q or CD3EAP G-21A had a median TTF of 27.6 month (p 5 0.019) and 28.6 month(p 5 0.046), respectively, whereas carriers of variant alleles ofboth genotypes had a median TTF of 48.6 month (p < 0.001) (Fig.3a.). When ERCC2 K751Q was combined with XRCC3 T241M,homozygous carriers of the wildtype alleles had a median TTF of17.5 month (Table V). Carriers of the variant allele of ERCC2
K751Q had a median TTF of 27.6 month (p 5 0.21) and carriersof the variant allele of XRCC3 T241M, 29.9 month (p 5 0.21),whereas carriers of both alleles had a median TTF of 49.9 month(p 5 0.0001) (Fig. 3b). This indicates that the combination of sub-optimal repair of both double strand breaks and bulky adducts isassociated with increased TTF. When CD3EAP G-21A was com-bined with XRCC3 T241M, wildtype carriers of both genotypeshad a median TTF of 22.5 month. Carriers of the variant alleles ofeither CD3EAP G-21A or XRCC3 T241M had a median TTF of69.4 month (p 5 0.0001) and 45.4 month (p 5 0.0004), respec-tively, whereas carriers of variant alleles of both genotypes had amedian TTF of 46.8 month (p 5 0.0006) (Fig. 3c). Thus, TTF wasthe same for all carriers of variant alleles. This indicates that noadditional effects on TTF were obtained by combining the 2 geno-types and that only 1 variant is needed to obtain increased TTF.We therefore constructed a simple binary variable indicatingwhether the patients were carriers of the variant alleles of eitherCD3EAP G-21A or XRCC3 T241M or both, versus wildtype car-riers. This variable had a HR at 0.5 and a p value < 0.0001 withTTF as a dependent variable.
TABLE IV – UNIVARIATE SUBTYPE ANALYSIS OF THE EFFECT OF POLYMORPHISMS CD3EAP G-21A ANDERCC2 K751Q ON TTF AND OS IN MEN AND WOMEN
Genotype Median TTF (mo) p HR Median OS (mo) p HR
CD3EAP G-21AAllGG 24.6 57.7AG 1 AA 45.9 0.002 0.6 (0.4–0.8)1 –3 0.045 0.7 (0.5–1.0)
(0.002)2 (0.5 (0.4–0.8)) (0.045) (0.6 (0.4–1.0))Men
GG 25.1 55.4AG 1 AA 31.6 0.13 0.7 (0.5–1.1) –3 0.24 0.7 (0.5–1.2)
(0.01) (0.5 (0.3–0.9)) (0.03) (0.5 (0.3–1.0))Women
GG 23.5 65.6AG 1 AA 48.6 0.006 0.5 (0.3–0.8) 76.5 0.071 0.6 (0.3–1.1)
(0.041) (0.5 (0.3–1.0) (0.3) (0.7 (0.3–1.4))ERCC2 K751Q
AllAA 23.8 59.3AC1 CC 31.5 0.004 0.7 (0.5–0.9) 65.9 0.17 0.8 (0.6–1.1)
(0.003) (0.6 (0.4–0.8)) (0.11) (0.7 (0.5–1.1))Men
AA 25.1 81.6AC1 CC 28.6 0.30 0.8 (0.6–1.2) 53.1 0.37 1.2 (0.8–1.9)
(0.33) (0.8 (0.5–1.3)) (0.67) (1.1 (0.6–2.0))Women
AA 16.0 40.1AC1 CC 46.8 0.001 0.5 (0.3–0.8) 74.6 0.0005 0.4 (0.2–0.7)
(0.0004) (0.3 (0.2–0.6)) (0.001) (0.3 (0.2–0.6))
1Values in parentheses are 95% CI.–2Values in italic are adjusted for prognostic-related factors (TTF: b2-microglobulin. OS: b2-microglobu-lin, creatinine and Durie-Salmon).–3Median survival not reached.
TABLE V – UNIVARIATE ANALYSIS OF THE EFFECTS OF COMBINATIONS OF POLYMORPHISMS ON TTF
ERCC2 K751Q CD3EAP G-21A XRCC3 T241M N MedianTTF (mo)
HR p MedianOS (mo)
HR p
AA1 GG NI2 94 23.4 1 52.0 1AA AG 1 AA3 NI 42 28.6 0.6 (0.4–1.0)4 0.046 –5 0.6 (0.3–1.0) 0.056AC1 CC GG NI 128 27.6 0.7 (0.5–0.9) 0.019 65.7 0.7 (0.5–1.1) 0.11AC1 CC AG 1 AA NI 68 48.6 0.4 (0.3–0.6) <0.0001 76.5 0.6 (0.3–0.9) 0.019AA1 NI CC 46 17.5 1 65.6 1AA NI CT 1 TT 51 29.9 0.7 (0.4–1.2) 0.25 –5 0.8 (0.4–1.6) 0.68AC1 CC NI CC 63 27.6 0.7 (0.5–1.2) 0.21 65.9 0.9 (0.5–1.6) 0.66AC1 CC NI CT 1 TT 81 49.9 0.4 (0.2–0.6) 0.0001 76.5 0.7 (0.4–1.2) 0.20NI GG CC 78 22.5 1 65.6 1NI GG CT 1 TT 80 45.4 0.5 (0.3–0.7) 0.0004 81.6 0.8 (0.5–1.2) 0.27NI AG 1 AA CC 31 69.4 0.4 (0.2–0.7) 0.001 –5 0.6 (0.3–1.2) 0.11NI AG 1 AA CT 1 TT 52 46.8 0.4 (0.3–0.7) 0.0006 –5 0.6 (0.3–1.0) 0.065
1Homozygous carrier of the wild type allele.–2Not included in the analysis.–3Heterozygous or homozygous carrier of the variant allele.–4Val-ues in parentheses are 95% CI.–5Median survival not reached.
1041GENE POLYMORPHISMS IN MULTIPLE MYELOMA TREATMENT
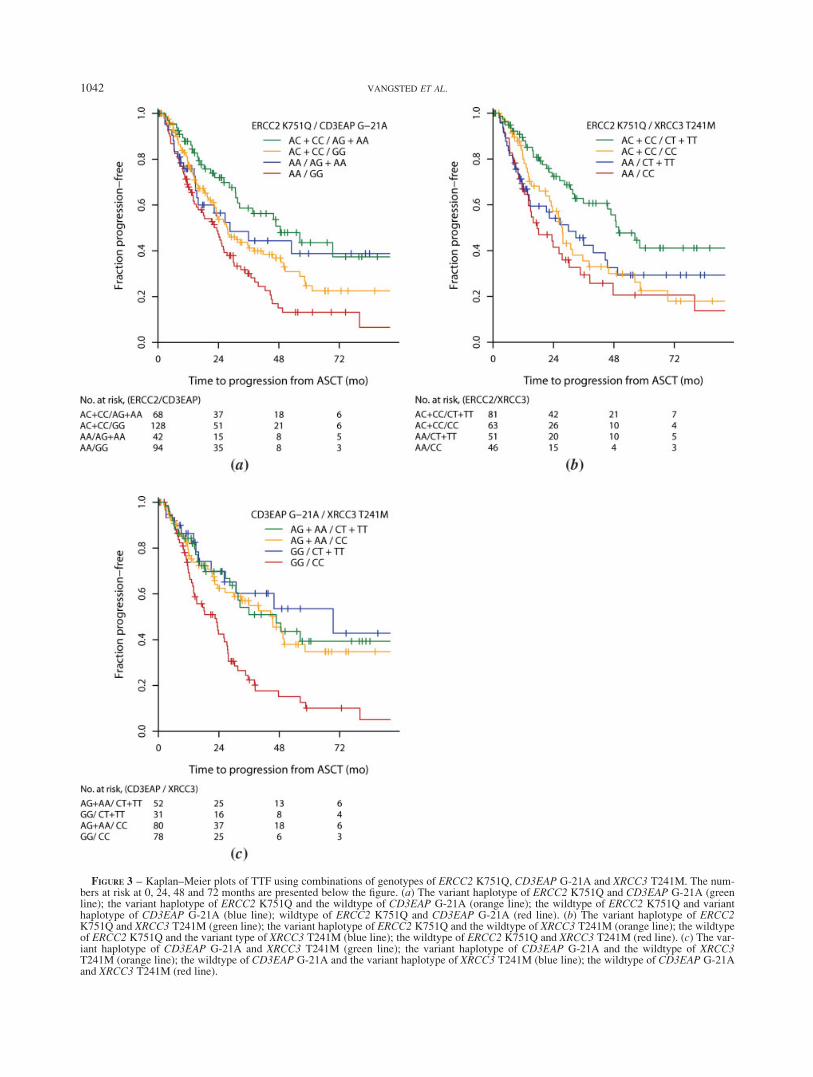
FIGURE 3 – Kaplan–Meier plots of TTF using combinations of genotypes of ERCC2 K751Q, CD3EAP G-21A and XRCC3 T241M. The num-bers at risk at 0, 24, 48 and 72 months are presented below the figure. (a) The variant haplotype of ERCC2 K751Q and CD3EAP G-21A (greenline); the variant haplotype of ERCC2 K751Q and the wildtype of CD3EAP G-21A (orange line); the wildtype of ERCC2 K751Q and varianthaplotype of CD3EAP G-21A (blue line); wildtype of ERCC2 K751Q and CD3EAP G-21A (red line). (b) The variant haplotype of ERCC2K751Q and XRCC3 T241M (green line); the variant haplotype of ERCC2 K751Q and the wildtype of XRCC3 T241M (orange line); the wildtypeof ERCC2 K751Q and the variant type of XRCC3 T241M (blue line); the wildtype of ERCC2 K751Q and XRCC3 T241M (red line). (c) The var-iant haplotype of CD3EAP G-21A and XRCC3 T241M (green line); the variant haplotype of CD3EAP G-21A and the wildtype of XRCC3T241M (orange line); the wildtype of CD3EAP G-21A and the variant haplotype of XRCC3 T241M (blue line); the wildtype of CD3EAP G-21Aand XRCC3 T241M (red line).
1042 VANGSTED ET AL.

Multivariate analysis of prognostic markers
The polymorphisms were compared to known prognostic fac-tors (b2-microglobulin, creatinine, albumin, sex, age and Durie–Salmon stage). No significant correlations were found (data notshown) except for the XRCC3 T241M polymorphism and age(high age associated to wild type XRCC3 T241M, p5 0.02).
The univariate significant polymorphisms were tested in a mul-tivariate analysis to see whether they had independent prognosticvalue. They were tested separately against the statistically signifi-cant parameters from the univariate analyses to calculate adjustedhazard ratios and p values. b2-Microglobulin was not analyzedroutinely in 1 center. Therefore, only 240 patients were availablein the multivariate analysis with the CD3EAP G-21A and ERCC2K751Q polymorphisms, and 160 patients were available with theXRCC3 T241M polymorphism.
The adjusted hazard ratios and p values were similar to theunadjusted hazard ratios (Table VI).
Using a wider range of commonly used prognostic variables (allshown in Table II except for ISS) and a backward stepwisemethod, all polymorphisms stayed in the model as statistically sig-nificant prognostic factors (data not shown).
We constructed a multivariate analysis including all the valuesfrom the univariate analysis.
The multivariate analysis showed that known prognosticmarkers such as stage according to Durie–Salmon and ISS werenot prognostic markers for TTF. Elevated b2-microglobulin levelwas a prognostic marker for adverse TTF and OS. Creatinine lev-els correlated to poor OS. The polymorphisms ERCC2 K751Q,CD3EAP G-21A and XRCC3 T241M were significant prognosticmarkers for prolonged TTF, but only CD3EAP G-21A was a prog-nostic marker for prolonged OS.
Discussion
In this study we have explored the importance of genetic consti-tution for prognosis in a cohort of 348 patients treated with high-dose chemotherapy and ASCT. We report 3 new parametersrelated to genetic variations that influences TTF. In univariateanalysis as well as Cox multivariate analysis, which included 146patients (and 223 when b2-microglobulin and ISS were excluded),we found a statistically significant effect on TTF of ERCC2K751Q, CD3EAP G-21A and XRCC3 T241M and on OS ofCD3EAP G-21A. We have found that carriers of variant alleles ofthe polymorphisms ERCC2 K751Q and XRCC3 T241M had anincreased TTF when compared to homozygous carriers of thewildtype allele. The 2 polymorphisms results in amino acid substi-tutions that probably modify the catalytic capacity of the DNArepair enzymes.28
Our interpretation of the results is that in treatment with high-dose alkylating chemotherapy it is an advantage to have low DNArepair capacity. With a low DNA repair capacity it is more likelythat tumor cells are killed by the high-dose therapy, because unre-paired DNA damage will make the cells go into apoptosis. With a
high DNA repair capacity, efficient DNA repair may allow tumorcells to escape apoptosis, eventually leading to relapse for thepatient. Melphalan, which was used for bone marrow ablation, isan alkylating agent giving rise to bulky DNA adducts and DNAcrosslinks.29 XRCC3 and certain NER genes are known to be cru-cial for the repair of crosslinks and NER in general takes care ofbulky adducts. Thus, it is a reasonable assumption that NER aswell as double-strand–breakage repair plays a role in the cellularresponse to the drug.
This assumption is supported by our findings of the longest TTFof 49.9 month in the subgroup of patients with the alleles associ-ated with suboptimal repair in both NER and double strand repair.No effect was however seen on survival. This may be explainedby the use of new drugs such as IMiDs and proteasome inhibitorsat progression of disease after ASTC or because less events of OSwas registered. In contrast, patients with ineffective DNA repairmay be at risk for secondary malignancies.
Few studies have focused on polymorphisms and the outcomeof chemotherapy. Different chemotherapeutic agents vary in theamount and type of DNA damage induced and to which extent ap-optosis is induced. Furthermore, the interplay between geneticallydetermined factors, such as DNA repair efficiency and apoptosisthreshold, on the one hand, and treatment regimen on the other,require large study groups of homogeneous populations and treat-ment strategies for evaluation of the relationship between poly-morphisms and treatment outcome. In a large study of 341 elderlypatients with acute leukemia, it was found that carriers of the vari-ant homozygote of ERCC2 K751Q had the poorest prognosis andthis genotype was associated with the highest risk of developingAML after chemotherapy.5 We selected a large group of patientsthat included the majority of the patients in Denmark who weretreated in accordance to the treatment protocols of NMSG. In oursetting, patients carrying the variant allele of ERCC2 K751Q hadthe best prognosis. Which DNA repair status is favorable maythus vary depending on the type of cancer and chemotherapeutictreatment strategies.
The polymorphism CD3EAP G-21A was associated with largedifferences in both TTF and OS, and 31% were carriers of thefavorable variant allele. No previously published work has showneffect on treatment outcome in relation to polymorphisms inCD3EAP. The function of CD3EAP protein is unknown, but itcolocalizes with the RNA polymerase I transcription initiation fac-tor UBF/NOR-90 throughout all stages of the cell cycle.13 Itslocalization could suggest that the protein impinges on ribosomesynthesis, one of the central features of cell proliferation. Involve-ment in the immune function of this gene product has been sug-gested.14 However, the studied polymorphism in CD3EAP doesnot result in amino acid substitutions and it is located close to thegenes ERCC1 and PPP1R13L. The effect on TTF and OS wasonly observed for heterozygous carriers of CD3EAP G-21A. Thisindicates that it may not be the polymorphism itself that has bio-logical impact but rather a polymorphism that cosegregates withit. It is therefore possible that the variant allele of CD3EAP G-21A is a marker for another genetic variation that modifies thefunction of ERCC1 or PPP1R13L and the polymorphism maytherefore not be involved in the causal explanation of the pro-longed TTF and OS. Our combination analysis suggests an inde-pendent function of CD3EAP G-21A and ERCC2 K751Q.
Our results indicate that polymorphism in CD3EAP G-21A andERCC2 K751Q may have effects on TTF, and for ERCC2 K751Qalso on OS, in women only. Data from the Danish Cancer Registrycollected from 1989 to 2001, including all 3,500 patients with MM,indicate that women have a small but statistically significant longersurvival when compared to men. Thus, women had a median OS of26 months when compared to 22 months for men (p5 0.02).
There are several examples of interaction between gender andpolymorphisms in this specific chromosomal region. Amongwomen in the Danish Diet, Cancer and Health cohort consistingof 57,000 Danes, homozygous carriers of the haplotype ERCC1
TABLE VI – MULTIVARIATE ANALYSIS OF CHARACTERISTICAFFECTING TTF
ParameterTTF
p value Relative risk
B2-Microglobulin1 0.001 1.4 (1.2–1.8)2
ERCC2 K751Q 0.009 0.5 (0.3–0.8)CD3EAP G-21A
or XRCC3 T241M30.0001 0.4 (0.2–0.6)
1b2-Microglobulin and creatinine were treated as continuous varia-bles and log transformed. The hazard ratio indicates risk when valuesare doubled.–2Values in parentheses are 95% CI.–3The hazard ratiosof progression for the variants were calculated with respect to havingwildtype in CD3EAP G21A and XRCC3-T241M. The p value is forall combinations used as a categorical variable.
1043GENE POLYMORPHISMS IN MULTIPLE MYELOMA TREATMENT
N118NA, CD3EAP G-21AG and PPP1R13L IVS1 A4364GA wereat increased risk of breast cancer,17 an effect that is not foundamong males with cancer of the testis.19 In a large study of 1,092lung cancer cases and 1,240 controls, a borderline statistically sig-nificant interaction was found between ERCC2 Asp312Asn andgender in relation to risk of lung cancer,30 and in a recent study of428 lung cancer cases and 800 controls, the relation between risk oflung cancer and the haplotype ERCC1 N118NA, CD3EAP G-21AG
and PPP1R13L IVS1 A4364GA was statistically significantly dif-ferent between the 2 genders and only female carriers were atincreased risk. Furthermore, gene-smoking interaction with the hap-lotype was detected among women, but not among men.31
Abnormalities of chromosome 13 and translocations involvingthe IgH gene locus (14q32) have been associated with survivaland response to high-dose treatment.32,33 These analyses arerelated to the biology of the tumor cell and require purification ofmyeloma cells from bone marrow sample. In this study we presentdata that individuals with polymorphisms in ERCC2 K751Q,CD3EAP G-21A and XRCC3 T241M have prolonged TTF. Theseresults may explain part of the differences in TTF noted amongpatients. Our results indicate that high-dose therapy may be bene-ficial for MM patients with defective DNA repair, while treatment
improvements, such as dose escalation or inclusion of drugsknown to inhibit DNA repair, may be relevant for carriers of thewildtype alleles.
Acknowledgements
Participants of NMSG. H. Knudsen, E. Gaarsdal, B. Ingemann,C. Lønskov and H. Larsen, all from KAS Herlev; S.T. Clausenand T. Nørgaard, both from Hillerød Sygehus; L. Drivsholm andP.P. Clausen, both from Næstved Sygehus; K. Bendix, A. Lønskov,A.Z. Kudsk and J.L. Nielsen, all from Arhus Amtssygehus; M.Frederiksen, Haderslev Sygehus; B. Bengtsson and N. Korsgaard,both from Esbjerg Sygehus; E. Ludvigsen, Sønderborg Sygehus;C. Rygaard, H.S. Hvidovre Hospital; H.K. Thomsen and A. Kjøge,both from Bispebjerg Hospital; F. Egede, Sygehus Syd Svendborg;E. Worthington, Tønder Sygehus; O.V. Gadeberg, Vejle Sygehus;N. Abildsgard and N. Tinggaard, both from Odense Sygehus; H.Gregersen, Aalborg Sygehus; H. Kiær, Sygehus Fyn Svendborg;J.C. Andreassen and H.lK. Nielsen, both from Sygehus Vestsjæl-land; H. Sciolla, Rigshospitalet; A. Juhl, Nykøbing Falster Syge-hus; B. �a Steig, Landssjukrahusid, Faroe Islands; B. Bach, ViborgSygehus. All these persons are from Denmark.
References
1. Lenhoff S, Hjorth M, Holmberg E, Turesson I, Westin J, Nielsen JL,Wisloff F, Brinch L, Carlson K, Carlsson M, Dahl IM, Gimsing P,et al., for the Nordic Myeloma Study Group. Impact on survival ofhigh-dose therapy with autologous stem cell support in patientsyounger than 60 years with newly diagnosed multiple myeloma: apopulation-based study. Blood 2000;95:7–11.
2. Spanswick VJ, Craddock C, Sekhar M, Mahendra P, Shankaranar-ayana P, Hughes RG, Hochhauser D, Hartley JA. Repair of DNAinterstrand crosslinks as a mechanism of clinical resistance to melpha-lan in multiple myeloma. Blood 2002;100:224–9.
3. Isla D, Sarries C, Rosell R, Alonso G, Domine M, Taron M, Lopez-Vivanco G, Camps C, Botia M, Nunez L, Sanchez-Ronco M, SanchezJJ, et al. Single nucleotide polymorphisms and outcome in docetaxel–cisplatin-treated advanced non-small-cell lung cancer. Ann Oncol2004;15:1194–203.
4. Stoehlmacher J, Park DJ, Zhang W, Yang D, Groshen S, Zahedy S,Lenz HJ. A multivariate analysis of genomic polymorphisms: predic-tion of clinical outcome to 5-FU/oxaliplatin combination chemother-apy in refractory colorectal cancer. Br J Cancer 2004;91:344–54.
5. Allan JM, Smith AG, Wheatley K, Hills RK, Travis LB, Hill DA,Swirsky DM, Morgan GJ, Wild CP. Genetic variation in XPD predictstreatment outcome and risk of acute myeloid leukemia followingchemotherapy. Blood 2004;104:3872–7.
6. Wood RD. Nucleotide excision repair in mammalian cells. J BiolChem 1997;272:23465–8.
7. de Boer J, Hoeijmakers JH. Nucleotide excision repair and humansyndromes. Carcinogenesis 2000;21:453–60.
8. Matullo G, Palli D, Peluso M, Guarrera S, Carturan S, Celentano E,Krogh V, Munnia A, Tumino R, Polidoro S, Piazza A, Vineis P.XRCC1, XRCC3, XPD gene polymorphisms, smoking and 32P-DNAadducts in a sample of healthy subjects. Carcinogenesis 2001;22:1437–45.
9. Qiao Y, Spitz MR, Shen H, Guo Z, Shete S, Hedayati M, GrossmanL, Mohrenweiser H, Wei Q. Modulation of repair of ultraviolet dam-age in the host-cell reactivation assay by polymorphic XPC and XPD/ERCC2 genotypes. Carcinogenesis 2002;23:295–9.
10. Liu N, Lamerdin JE, Tebbs RS, Schild D, Tucker JD, Shen MR,Brookman KW, Siciliano MJ, Walter CA, Fan W, Narayana LS, ZhouZQ, et al. XRCC2 and XRCC3, new human Rad51-family members,promote chromosome stability and protect against DNA cross-linksand other damages. Mol Cell 1998;1:783–93.
11. Yang JP, Hori M, Sanda T, Okamoto T. Identification of a novel in-hibitor of nuclear factor-jB, RelA-associated inhibitor. J Biol Chem1999;274:15662–70.
12. Bergamaschi D, Samuels Y, O’Neil NJ, Trigiante G, Crook T, HsiehJK, O’Connor DJ, Zhong S, Campargue I, Tomlinson ML, KuwabaraPE, Lu X. iASPP oncoprotein is a key inhibitor of p53 conservedfrom worm to human. Nat Genet 2003;33:162–7.
13. Whitehead CM, Winkfein RJ, Fritzler MJ, Rattner JB. ASE-1: a novelprotein of the fibrillar centres of the nucleolus and nucleolus organizerregion of mitotic chromosomes. Chromosoma 1997;106:493–502.
14. Yamazaki T, Hamano Y, Tashiro H, Itoh K, Nakano H, Miyatake S,Saito T. CAST, a novel CD3e-binding protein transducing activationsignal for interleukin-2 production in T cells. J Biol Chem 1999;274:18173–80.
15. Yin J, Rockenbauer E, Hedayati M, Jacobsen NR, Vogel U, GrossmanL, Bolund L, Nexo BA. Multiple single nucleotide polymorphisms onhuman chromosome 19q13.2–3 associate with risk of basal cell carci-noma. Cancer Epidemiol Biomarkers Prev 2002;11:1449–53.
16. Vogel U, Hedayati M, Dybdahl M, Grossman L, Nexo BA. Polymor-phisms of the DNA repair gene XPD: correlations with risk of basalcell carcinoma revisited. Carcinogenesis 2001;22:899–904.
17. Nexo BA, Vogel U, Olsen A, Ketelsen T, Bukowy Z, Thomsen BL,Wallin H, Overvad K, Tjonneland A. A specific haplotype of singlenucleotide polymorphisms on chromosome 19q13.2–3 encompassingthe gene RAI is indicative of post-menopausal breast cancer beforeage 55. Carcinogenesis 2003;24:899–904.
18. Vogel U, Laros I, Jacobsen NR, Thomsen BL, Bak H, Olsen A, Buk-owy Z, Wallin H, Overvad K, Tjonneland A, Nexo BA, Raaschou-Nielsen O. Two regions in chromosome 19q13.2–3 are associatedwith risk of lung cancer. Mutat Res 2004;546:65–74.
19. Laska MJ, Nexo BA, Vistisen K, Poulsen HE, Loft S, Vogel U. Poly-morphisms in RAI and in genes of nucleotide and base excision repairare not associated with risk of testicular cancer. Cancer Lett 2005;225:245–51.
20. Hippe E, Westin J, Wisloff F. Nordic Myeloma Study Group, the first15 years: scientific collaboration and improvement of patient care.Eur J Haematol 2005;74:185–93.
21. Durie BG, Salmon SE. A clinical staging system for multiple my-eloma. Correlation of measured myeloma cell mass with presentingclinical features, response to treatment, and survival. Cancer 1975;36:842–54.
22. Lenhoff S, Hjorth M, Westin J, Brinch L, Backstrom B, Carlson K,Christiansen I, Dahl IM, Gimsing P, Hammerstrom J, Johnsen HE,Juliusson G, et al. Impact of age on survival after intensive therapyfor multiple myeloma: a population-based study by the Nordic My-eloma Study Group. Br J Haematol 2006;133:389–96.
23. Miller SA, Dykes DD, Polesky HF. A simple salting out procedure forextracting DNA from human nucleated cells. Nucleic Acids Res1988;16:1215.
24. Saber AT, Nielsen LR, Dictor M, Hagmar L, Mikoczy Z, Wallin H.K-ras mutations in sinonasal adenocarcinomas in patients occupation-ally exposed to wood or leather dust. Cancer Lett 1998;126:59–65.
25. Vogel U, Olsen A, Wallin H, Overvad K, Tjonneland A, Nexo BA.Effect of polymorphisms in XPD, RAI, ASE-1 and ERCC1 on therisk of basal cell carcinoma among Caucasians after age 50. CancerDetect Prev 2005;29:209–14.
26. Jacobsen NR, Nexo BA, Olsen A, Overvad K, Wallin H, TjonnelandA, Vogel U. No association between the DNA repair gene XRCC3T241M polymorphism and risk of skin cancer and breast cancer. Can-cer Epidemiol Biomarkers Prev 2003;12:584–5.
27. Greipp PR, San Miguel J, Durie BG, Crowley JJ, Barlogie B, Blade J,Boccadoro M, Child JA, Harousseau JL, Kyle RA, Lahuerta JJ,
1044 VANGSTED ET AL.
Ludwig H, et al. International staging system for multiple myeloma.J Clin Oncol 2005;23:3412–20.
28. Hou SM, Falt S, Angelini S, Yang K, Nyberg F, Lambert B, Hem-minki K. The XPD variant alleles are associated with increased aro-matic DNA adduct level and lung cancer risk. Carcinogenesis 2002;23:599–603.
29. Sunters A, Springer CJ, Bagshawe KD, Souhami RL, Hartley JA. Thecytotoxicity, DNA crosslinking ability and DNA sequence selectivityof the aniline mustards melphalan, chlorambucil and 4-[bis(2-chloroe-thyl)amino] benzoic acid. Biochem Pharmacol 1992;44:59–64.
30. Zhou W, Liu G, Miller DP, Thurston SW, Xu LL, Wain JC, LynchTJ, Su L, Christiani DC. Gene–environment interaction for theERCC2 polymorphisms and cumulative cigarette smoking exposurein lung cancer. Cancer Res 2002;62:1377–81.
31. Vogel U, Sørensen M, Hansen RD, Tjønneland A, Overvad K, NexøBA, Raaschou-Nielsen O. Gene–environment interactions betweensmoking and a haplotype of RAI, ASE-1 and ERCC1 polymorphismsamong women in relation to risk of lung cancer in a population-basedstudy. Cancer Lett, in press.
32. Moreau P, Facon T, Leleu X, Morineau N, Huyghe P, Harousseau JL,Bataille R, Avet-Loiseau H. Recurrent 14q32 translocations determinethe prognosis of multiple myeloma, especially in patients receiving in-tensive chemotherapy. Blood 2002;100:1579–83.
33. Desikan R, Barlogie B, Sawyer J, Ayers D, Tricot G, Badros A, Zan-gari M, Munshi NC, Anaissie E, Spoon D, Siegel D, Jagannath S,et al. Results of high-dose therapy for 1000 patients with multiple my-eloma: durable complete remissions and superior survival in the ab-sence of chromosome 13 abnormalities. Blood 2000;95:4008–10.
1045GENE POLYMORPHISMS IN MULTIPLE MYELOMA TREATMENT




















