
Improving outcome in patients undergoing liver surgery
14
Improving outcome in patients undergoing liver surgery Katarzyna Furrer, Michelle Lucinda DeOliveira, Rolf Graf and Pierre-Alain Clavien Department of Visceral and Transplantation Surgery, University Hospital of Z¨ urich, 8091-Z ¨ urich, Switzerland Keywords ischemia – liver – outcome – surgery Abbreviations ATP, adenosine tri-phosphate; BSA, body surface area; CT, computed tomography; DNA, deoxyribonucleic acid; ICU, intensive care unit; MEGX, monoethylglycinexylidide; MRI, magnetic resonance imaging; TNF-a, tumor necrosis factor alpha Correspondence Pierre-Alain Clavien, MD, PhD, Department of Visceral and Transplantation Surgery, University Hospital of Z ¨ urich, R ¨ amistrasse 100, 8091 Z¨ urich, Switzerland. Tel: 141 (0) 44 255 33 00 Fax: 141 (0) 44 255 44 49 e-mail: [email protected] Received 8 May 2006 accepted 30 November 2006 DOI:10.1111/j.1478-3231.2006.01416.x Abstract Liver surgery is associated with many factors, which may affect outcome. Preoperative assessment of patient’s general condition, resectability, and liver reserve are paramount for success. The Child–Pugh score and other scoring systems only partially enables to assess the risk associated with liver surgery. The presence of portal hypertension per se is a major risk factor for hepatectomy. Intraoperatively, any attempts should be made to minimize blood loss. Low central venous pressure and inflow occlusion best prevent bleeding. Ischemic precondi- tioning and intermittent clamping are routinely applied in many centers to protect against long periods of ischemia, although the mechanisms of protection remain unclear. In this review we describe recent advances in activated pathways associated with protection against ischemia. Postoperatively, the best factor impacting on outcome probably resides in experienced medical care particularly in the intensive care setting. Currently, no drug or gene therapy approaches has reached the clinic. The future relies on new insight into mechanisms of ische- mia–reperfusion injury. Considerable progress has been made in many areas of liver surgery over the past two decades including better selection of patients for surgery, the availability of novel modalities to preoperatively manipulate tumor and liver volumes, novel operative techniques, and an optimization of the postoperative management. The development of centers of excellence with high volume of patients and formal training of liver surgeons has also significantly contributed in improving outcomes. In this review, we will successively cover preoperative, intraoperative, and postoperative strategies, which may prevent or correct complications related to major liver resection. Preoperative strategies The first step in preoperative evaluation of a candidate for liver surgery is to secure that he/she is fit for surgery, that the indication is adequate and the tumor is resectable. Evaluation of operability related to the general condition of the patient and indications for liver resection related to specific tumors are beyond the scope of this review. Here, we will focus on the evaluation of the liver reserve and available interven- tion to increase the volume of a putative remnant volume. Preoperative imaging of liver lesions Several imaging techniques are currently for the pre- operative assessment of liver tumors and to identify the best strategy for resection. These techniques and their respective sensitivities are summarized in Table 1. Evaluation of liver reserve Tumor patient A general health assessment with a careful history and physical examination for symptoms and signs of portal hypertension is the first step in the evaluation of patients with benign or malignant liver tumor. Before liver surgery the patient’s overall condition should be assessed, coexisting medical illnesses ex- cluded and the liver disease should be diagnosed and staged. Preoperative investigations should include radiology, full blood count with estimation of tumor markers (a-fetoprotein, carcinoembryonic antigen, Ca19-9), assessment of liver and renal function, and a Liver International (2007) 26 c 2007 The Authors. Journal compilation c 2007 Blackwell Munksgaard Liver International ISSN 1478-3223
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Improving outcome in patients undergoing liver surgery

Improvingoutcome in patients undergoing liver surgeryKatarzyna Furrer, Michelle Lucinda DeOliveira, Rolf Graf and Pierre-Alain Clavien
Department of Visceral and Transplantation Surgery, University Hospital of Zurich, 8091-Zurich, Switzerland
Keywords
ischemia – liver – outcome – surgery
Abbreviations
ATP, adenosine tri-phosphate; BSA, body
surface area; CT, computed tomography;
DNA, deoxyribonucleic acid; ICU, intensive
care unit; MEGX, monoethylglycinexylidide;
MRI, magnetic resonance imaging; TNF-a,
tumor necrosis factor alpha
Correspondence
Pierre-Alain Clavien, MD, PhD, Department of
Visceral and Transplantation Surgery, University
Hospital of Zurich, Ramistrasse 100, 8091
Zurich, Switzerland.
Tel: 141 (0) 44 255 33 00
Fax: 141 (0) 44 255 44 49
e-mail: [email protected]
Received 8 May 2006
accepted 30 November 2006
DOI:10.1111/j.1478-3231.2006.01416.x
AbstractLiver surgery is associated with many factors, which may affect outcome.
Preoperative assessment of patient’s general condition, resectability, and liver
reserve are paramount for success. The Child–Pugh score and other scoring
systems only partially enables to assess the risk associated with liver surgery. The
presence of portal hypertension per se is a major risk factor for hepatectomy.
Intraoperatively, any attempts should be made to minimize blood loss. Low central
venous pressure and inflow occlusion best prevent bleeding. Ischemic precondi-
tioning and intermittent clamping are routinely applied in many centers to protect
against long periods of ischemia, although the mechanisms of protection remain
unclear. In this review we describe recent advances in activated pathways
associated with protection against ischemia. Postoperatively, the best factor
impacting on outcome probably resides in experienced medical care particularly
in the intensive care setting. Currently, no drug or gene therapy approaches has
reached the clinic. The future relies on new insight into mechanisms of ische-
mia–reperfusion injury.
Considerable progress has been made in many areas ofliver surgery over the past two decades including betterselection of patients for surgery, the availability ofnovel modalities to preoperatively manipulate tumorand liver volumes, novel operative techniques, and anoptimization of the postoperative management. Thedevelopment of centers of excellence with high volumeof patients and formal training of liver surgeons hasalso significantly contributed in improving outcomes.In this review, we will successively cover preoperative,intraoperative, and postoperative strategies, whichmay prevent or correct complications related to majorliver resection.
Preoperative strategies
The first step in preoperative evaluation of a candidatefor liver surgery is to secure that he/she is fit forsurgery, that the indication is adequate and the tumoris resectable. Evaluation of operability related to thegeneral condition of the patient and indications forliver resection related to specific tumors are beyondthe scope of this review. Here, we will focus on theevaluation of the liver reserve and available interven-
tion to increase the volume of a putative remnantvolume.
Preoperative imaging of liver lesions
Several imaging techniques are currently for the pre-operative assessment of liver tumors and to identifythe best strategy for resection. These techniques andtheir respective sensitivities are summarized in Table 1.
Evaluation of liver reserve
Tumor patient
A general health assessment with a careful history andphysical examination for symptoms and signs ofportal hypertension is the first step in the evaluationof patients with benign or malignant liver tumor.Before liver surgery the patient’s overall conditionshould be assessed, coexisting medical illnesses ex-cluded and the liver disease should be diagnosed andstaged. Preoperative investigations should includeradiology, full blood count with estimation of tumormarkers (a-fetoprotein, carcinoembryonic antigen,Ca19-9), assessment of liver and renal function, and a
Liver International (2007)26 c� 2007 The Authors. Journal compilation c� 2007 Blackwell Munksgaard
Liver International ISSN 1478-3223

full clotting profile. Patients over 65 years of ageshould undergo detailed evaluation of their pulmon-ary and cardiac function.
Before embarking in a major liver resection, it isparamount to identify the presence of underlying liverdiseases and to assess the liver reserve. Postoperativemortality strongly correlates with the degree of pre-existing liver impairment; for example, a near zeromortality is reported by many expert surgeons inpatients with normal liver parenchyma, while a mor-tality of 10% or more is not uncommon in patientswith underlying liver diseases.
Cirrhotic patient
In cirrhotic patients additional factors are assessed.The detection of viral and serologic markers andmeasurement of viral serologic markers for HepatitisC and B as well as the type and extent of fibrosis arecrucial.
Unfortunately, how to assess and quantify liverfunction preoperatively remains controversial as nosingle biological value or test is able to accuratelypredict postoperative liver failure. Many teams, parti-cularly in Western countries, still use the Child andTurcotte (21) scoring system described for the firsttime in 1964 to assess the operative risk in cirrhoticpatients undergoing portosystemic shunt surgery forvariceal bleeding. The initial score included five vari-ables: ascites, encephalopathy, nutritional status, andserum levels of bilirubin and albumin. Patients wereranked according to three scores A–C in relation tobest (A), moderate (B), or worse (C) prognosis.
In 1973, Pugh et al. (22) used a modified version ofthis classification for patients undergoing surgicaltransection for esophageal varices. They replaced theevaluation of the nutritional status by prothrombintime and assigned a score ranging from 1 to 3 to eachvariable. Subsequently, this classification was used topredict the outcome of surgery in cirrhotic patients ingeneral, and more recently, to stratify patients on thewaiting list for liver transplantation. The expectedpostoperative mortality was found to be 10% inpatients with Child A cirrhosis (23), 30% with ChildB cirrhosis (24), and up to 80% in Child C patients(25). Therefore, currently Child–Pugh class C cirrhosisis considered as an absolute contra-indication forhepatic surgery, while Child–Pugh class B patientsshould undergo only minor hepatic resection (e.g.� two segments). In Child–Pugh class A patients the
decision to proceed with a major hepatic resectionshould rely on additional tests, particularly the evalua-tion of concomitant portal hypertension (26).
A number of metabolic tests (Table 2) have beenproposed to assess the hepatic functional reserve.These tests include the clearance of indocyanine green(ICG) (37) caffeine (38), lidocaine (34) and lidocainederivatives test [monoethylglycinexylidide (MEGX)](37), galactose elimination capacity (31), and thetechnetium-99m galactosyl human serum albuminscan (39). Clearance of these compounds not onlydepends on hepatic metabolism but often also onhepatic blood flow. The ICG test is probably the mostpopular test, particularly in Asia. ICG is exclusivelycleared by the liver and it has been shown thatexcretion measured at 15 min (ICG R15) is a safe
Table 1. Imaging of liver lesions
Imaging tool Detection Sensitivity (%)
Ultrasound Benign liver lesions malignant liver lesions HCC 60–70 (1)64–94 (2)20–72 (3, 4)
CT Malignant liver lesions HCC 77–95 (5–7)52–98 (8, 9)
MRI Benign liver lesions malignant liver lesions HCC 70 (10)69–86 (5, 11)97 (9)
CT angiography Malignant liver lesions HCC 93–97 (12, 13)91–98 (14, 15)
MR angiography Malignant liver lesions HCC cholangiocarcinoma 97 (12)93 (14)99 (16)
FDG-PET Malignant liver lesions cololorectal cancer-liver metastases recurrence 82 (17)97 (18)
PET-CT Cololorectal cancer-liver metastases recurrence 89–93 (19, 20)
CT, computer tomography; FDG-PET, fluor-18-deoxyglucose-positron emission tomography; HCC, hepatocellular carcinoma; MRI, magnetic resonance
imaging.
Liver International (2007)c� 2007 The Authors. Journal compilation c� 2007 Blackwell Munksgaard 27
Furrer et al. Liver surgery
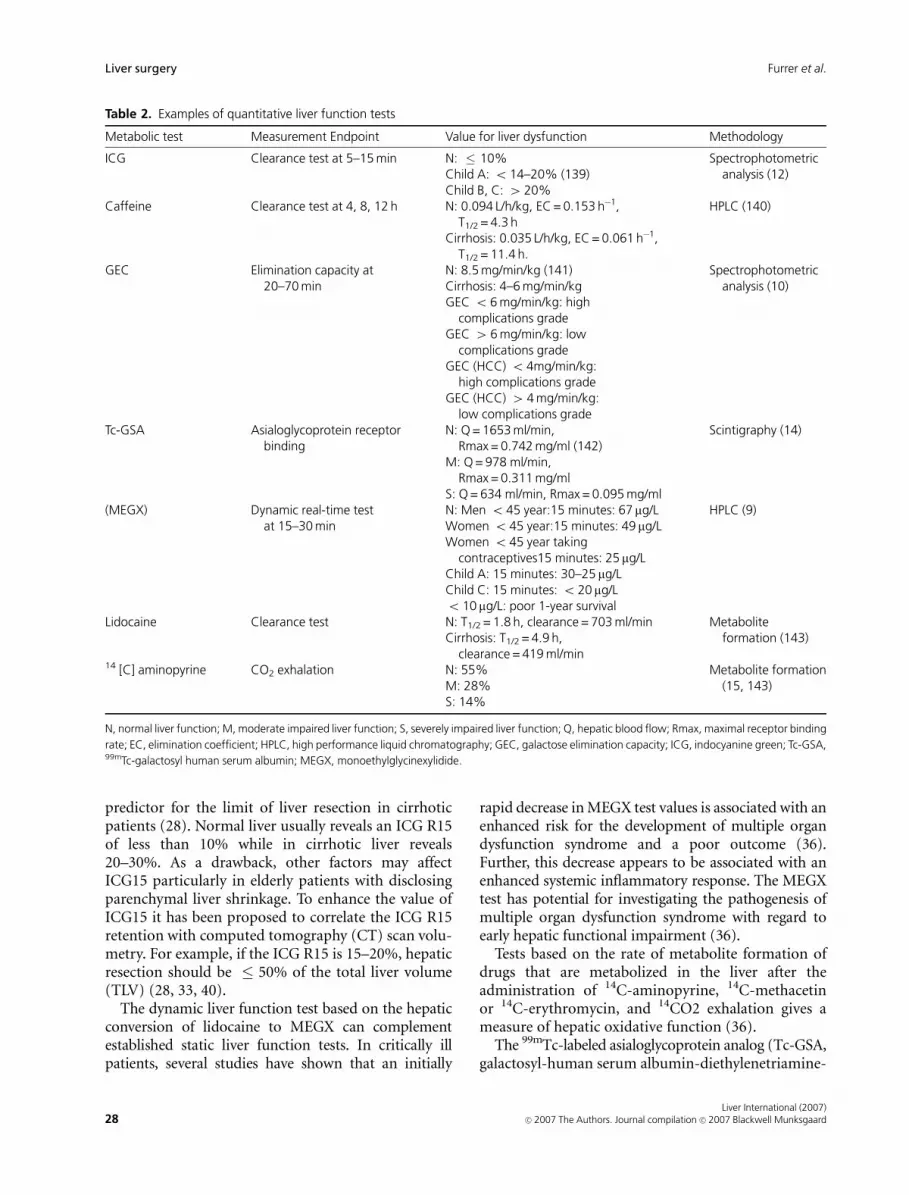
predictor for the limit of liver resection in cirrhoticpatients (28). Normal liver usually reveals an ICG R15of less than 10% while in cirrhotic liver reveals20–30%. As a drawback, other factors may affectICG15 particularly in elderly patients with disclosingparenchymal liver shrinkage. To enhance the value ofICG15 it has been proposed to correlate the ICG R15retention with computed tomography (CT) scan volu-metry. For example, if the ICG R15 is 15–20%, hepaticresection should be � 50% of the total liver volume(TLV) (28, 33, 40).
The dynamic liver function test based on the hepaticconversion of lidocaine to MEGX can complementestablished static liver function tests. In critically illpatients, several studies have shown that an initially
rapid decrease in MEGX test values is associated with anenhanced risk for the development of multiple organdysfunction syndrome and a poor outcome (36).Further, this decrease appears to be associated with anenhanced systemic inflammatory response. The MEGXtest has potential for investigating the pathogenesis ofmultiple organ dysfunction syndrome with regard toearly hepatic functional impairment (36).
Tests based on the rate of metabolite formation ofdrugs that are metabolized in the liver after theadministration of 14C-aminopyrine, 14C-methacetinor 14C-erythromycin, and 14CO2 exhalation gives ameasure of hepatic oxidative function (36).
The 99mTc-labeled asialoglycoprotein analog (Tc-GSA,galactosyl-human serum albumin-diethylenetriamine-
Table 2. Examples of quantitative liver function tests
Metabolic test Measurement Endpoint Value for liver dysfunction Methodology
ICG Clearance test at 5–15 min N: � 10%Child A: o 14–20% (139)Child B, C: 420%
Spectrophotometricanalysis (12)
Caffeine Clearance test at 4, 8, 12 h N: 0.094 L/h/kg, EC = 0.153 h�1,T1/2 = 4.3 h
Cirrhosis: 0.035 L/h/kg, EC = 0.061 h�1,T1/2 = 11.4 h.
HPLC (140)
GEC Elimination capacity at20–70 min
N: 8.5 mg/min/kg (141)Cirrhosis: 4–6 mg/min/kgGEC o 6 mg/min/kg: high
complications gradeGEC 46 mg/min/kg: low
complications gradeGEC (HCC) o 4mg/min/kg:
high complications gradeGEC (HCC) 4 4 mg/min/kg:
low complications grade
Spectrophotometricanalysis (10)
Tc-GSA Asialoglycoprotein receptorbinding
N: Q = 1653 ml/min,Rmax = 0.742 mg/ml (142)
M: Q = 978 ml/min,Rmax = 0.311 mg/ml
S: Q = 634 ml/min, Rmax = 0.095 mg/ml
Scintigraphy (14)
(MEGX) Dynamic real-time testat 15–30 min
N: Men o 45 year:15 minutes: 67 mg/LWomen o 45 year:15 minutes: 49 mg/LWomen o 45 year taking
contraceptives15 minutes: 25 mg/LChild A: 15 minutes: 30–25 mg/LChild C: 15 minutes: o 20 mg/Lo 10 mg/L: poor 1-year survival
HPLC (9)
Lidocaine Clearance test N: T1/2 = 1.8 h, clearance = 703 ml/minCirrhosis: T1/2 = 4.9 h,
clearance = 419 ml/min
Metaboliteformation (143)
14 [C] aminopyrine CO2 exhalation N: 55%M: 28%S: 14%
Metabolite formation(15, 143)
N, normal liver function; M, moderate impaired liver function; S, severely impaired liver function; Q, hepatic blood flow; Rmax, maximal receptor binding
rate; EC, elimination coefficient; HPLC, high performance liquid chromatography; GEC, galactose elimination capacity; ICG, indocyanine green; Tc-GSA,99mTc-galactosyl human serum albumin; MEGX, monoethylglycinexylidide.
Liver International (2007)28 c� 2007 The Authors. Journal compilation c� 2007 Blackwell Munksgaard
Liver surgery Furrer et al.

pentaacetic acid) has been applied to human hepaticreceptor imaging (41). Liver scintigraphy using Tc-GSA has recently been used in some centers as amethod for the quantitative measurement of func-tional hepatocyte mass unaffected by liver tumors orbiliary obstruction (42). Another proposed test is thegalactose elimination capacity test (31). It was demon-strated in a prospective study to be a strong indepen-dent and valuable predictor for long and shortoutcome in patients with primary and secondaryhepatic tumors undergoing resection.
Besides these tests or scoring systems, the presenceof underlying liver diseases per se may affect outcomeof liver surgery. Hepatic steatosis is common and mayresult from a variety of conditions such as alcohol,chemo-therapeutics, certain industrial and biologicaltoxins, and obesity (31, 43–47). Steatosis increases therisk of liver resections and may enhance the suscept-ibility of the liver parenchyma to ischemic injury (48).Fatty liver disease may also interfere with liver regen-eration.
Liver resection in patients with steatosis is asso-ciated with an increased risk of postoperative mortal-ity when compared with patients disclosing lean livers(14% vs 2%) (49). Thus, major hepatectomy should beperformed with caution in patients with moderate tosevere (Z30%) steatosis. Although hepatic steatosis isnow an established risk factor for surgery, little isknown about the mechanisms of injury. In animalexperiments, steatosis is associated with decreasedATP production and a disturbance of sinusoidal flow(50, 51). Further contributing factors may includeKupffer cell dysfunction (52) and leukocyte adhesion(53). Steatosis plays a role when the liver is subjectedto oxidative stress (54) and may make the liverparenchyma vulnerable to ischemic injury (48). Fattyhepatocytes have reduced tolerance against ischemiawith a predominant necrotic form of cell death. Inaddition, the ability of hepatocytes to regenerate aftermajor tissue loss is impaired in the steatotic liver (55).
Hepatocellular and obstructive cholestasis are alsoimportant risk factors for liver surgery. The presenceof obstructive jaundice increases the risk of resection,even in noncirrhotic patients such as those withcholangiocarcinoma (56, 57). Chemotherapy is in-creasingly used in patients with liver cancer causingmorphologic changes including microsteatosis, fibro-sis, and inflammation. Severe steato-hepatitis can beassociated with preoperative administration of irino-tecan or oxaliplatin, especially in the obese and canaffect the ability to perform large liver resections (58).The sinusoidal obstruction, complicated by peri-sinu-soidal fibrosis and veno-occlusive lesions of the non-
tumoral liver, should be included in the list of theadverse side effects of colorectal systemic chemother-apy, in particular related to the use of oxaliplatin (59).Here also caution is advised, although no data isavailable that enables to accurately assess the riskassociated with surgery in these patients.
Preoperative estimation of future remnantliver volume
The liver has a unique regenerative ability, whichallows patients to rapidly recover from major tissueloss. Imaging techniques has been used to estimateliver regeneration after hepatectomy using differentmethods: scintigraphy (60, 61), ultrasound (62, 63),CT (64, 65) and MRI (66).
Urata et al. (67) proposed a formula tailored to theAsian population. Each formula may be prone toinherent errors. Thus the right formula has to beapplied, otherwise there will be a miscalculation ofthe future remnant liver.
In view of different body surface between Asianpopulation and people living in Western countries,actual liver volume is determined from a formulacorrelating TLV and body surface area (BSA) (68).Today radiological imaging enables us to accuratelyassess parenchyma hepatic resection rate (PHPR) aswell to predict the extent of outflow impairmentbefore certain types of liver resections (69, 70).
The PHPR has been applied for livers with anintrahepatic mass and can be calculated as follows:PHPR (%) = (resected liver volume� tumor volume)divided by (TLV� tumor volume)� 100 (28).
Resection up to 70% (or 0.6% of a ratio betweenremnant liver and patient weight) are well tolerated inpatients with normal liver.
In a clinical study of Yigitler et al. (71) the incidenceof complications after major hepatectomy includingliver failure was found similar in patients with aremnant liver volume of � 30% compared with pa-tients with a remnant liver volume of Z60%, althoughthe former group had a longer hospital and ICU stay.
Often large tumors cannot be resected because ofthe inability to preserve enough remnant liver. Animportant focus has been the development of inter-ventions to enable an increase in size of a putativeremnant liver including portal vein embolization andligation.
Preoperative portal vein embolization andportal vein ligation
Takayasu et al. (72) observed hypertrophy after portalocclusion resulting from hilar cholangiocarcinoma
Liver International (2007)c� 2007 The Authors. Journal compilation c� 2007 Blackwell Munksgaard 29
Furrer et al. Liver surgery

and Honjo et al. (73) first reported portal ligation inpatients with hepatocellular carcinoma.
Preoperative portal vein embolisation (PVE) of ahemi-liver containing a tumor induces compensatoryhypertrophy of the contra-lateral hemi-liver. Emboli-zation is performed percutaneously by an expertinterventional radiologist usually using cyanoacrylateglue mixed with lipiodol, polyvinyl alcohol or particlesadministration (74). In 1986, Kinoshita et al. (75) firstreported on the use of PVE to limit extension of portaltumor thrombi from hepatocellular carcinoma andstrengthened the effect of transarterial embolization.In 1990, Makuuchi et al. (76) reported the first use ofpreoperative PVE performed solely to induce left liverhypertrophy before major hepatic resection in patientswith hilar cholangiocarcinoma (77).
Liver hypertrophy occurs usually within a 2–4 weeksperiod. The indication for such a procedure remains amatter of debate. Most would agree that a predictedremnant liver volume � 25–30% might justify pre-operative embolization. In cirrhotic patients, thisfigure may reach 35–40%, and the inability to inducehypertrophy may represent a contra-indication forsurgery. The implementation of preoperative contralateral portal occlusion by embolization or sutureligation effectively prevents posthepatectomy liver fail-ure (78, 79). In prospective data from Broering et al.(80) portal vein embolization resulted in a signifi-cantly more efficient increase in liver volume and ashorter hospital stay than portal vein ligation althoughportal vein ligation was found to be safe and effective.
We designed a clinical study (81) to evaluate theeffects of concomitant unilateral portal vein ligationcombined with selective intraarterial chemotherapy onsafety, ability to induce contra-lateral hypertrophy,tumor growth, and resectability. The combination ofportal vein ligation with intraarterial chemotherapywas safe and demonstrated a concomitant atrophy ofthe hemi-liver ipsi lateral to the ligated portal vein aswell as contra lateral hypertrophy and no negativeimpact on tumor growth in the regenerating hemi-liver.
Nutritional status
The purpose of nutritional support in patients under-going hepatobliliary surgery is to decrease postopera-tive morbidity and mortality. However, perioperativenutrition in patients with limited liver function afterpartial hepatic resection is still controversial. Nutri-tional intervention should restore immunity, supportsanabolism, and attenuate the catabolic response toinjury.
The use of indirect calorimetry enables the calcula-tion of the nonprotein respiratory quotient, defined asthe ratio of energy produced by carbohydrate metabo-lism to energy generated by fat oxidation, whichconfirms whether a patient has an altered pattern offuel consumption (82). In patients with an alteredpattern a nutritional regime is implemented to correctthe imbalance e.g. by enteral nutrition.
The nutritional risk factors for postoperative com-plications in hepatobliliary surgery have been estab-lished 20 years ago and include: weight loss above 14%of lean body mass weight over the previous 6 months,serum and albumin under 3 g/dl, a hematocrit of lessthan 30% and total body potassium under 85% ofnormal (83–85).
The usefulness of branched-chain amino acid(BCAA) supplementation remains controversial, butthe most recent data promote their therapeutic poten-tial in improved survival, serum albumin concentra-tion, and quality of life in patients with decompensatecirrhosis (82).
In our institution, we begin a per oral diet as soon aspossible without a nasogastric tube to prevent gastro-intestinal atrophy and preserve the normal gut flora. Ifthe patient is unable to consume a diet orally in 3–4days after liver resection, a jejunal feeding tube can beplaced for early enteral nutrition. Early enteral nutri-tion after liver resection compared with parenteralnutrition it is associated with a decreased incidenceof postoperative complications (86). The benefit ofparenteral nutrition were predominately seen in ahigh-risk group with underlying cirrhosis undergoingmajor hepatectomy (86) and in patients whereenteral feeding cannot be achieved (82). The nutri-tional support in cirrhotic patients should focus onmaintaining adequate protein and caloric intake. Stra-tegies include the consumption of frequent smallmeals and a late evening snack to reduce proteinbreakdown (82).
The potential modulation of inflammatory andcytokine reaction with immunonutrition may reducefurther infection rates and shorten ICU and hospitallength of stay (87).
Intraoperative strategies
Many factors have contributed to improved outcomein patients undergoing hepatic surgery including abetter understanding of the liver anatomy, new tools toaccurately assess the liver volume, the routine use ofintraoperative ultrasound (IOUS), anesthetic supportunder fluid restriction guidelines, hepatic vascularcontrol, and novel hepatic parenchymal transection
Liver International (2007)30 c� 2007 The Authors. Journal compilation c� 2007 Blackwell Munksgaard
Liver surgery Furrer et al.

devices. Which of these factors best contributed toimproved outcome remains speculative.
Delineation of segmental liver anatomy allows ahepatic resection with maximum preservation of liverparenchyma, but extended hepatectomy is required inmany patients with liver tumors. Liver resection inpatients with cirrhosis, which is commonly, associatedwith hepatocellular carcinoma, needs a careful ap-proach. In our center, Child–Pugh class C is a contra-indication for hepatic resection, while Child–Pughclass B cirrhotic patient may be candidate for minorresection. For those patients Child–Pugh class A, thesurgical strategy depends on more refined evaluationof liver function reserve. Major hepatectomy is contra-indicated in patients with clinically portal hyperten-sion, whereas for those patients Child–Pugh classwithout portal hypertension, preoperative PVE maybe necessary for a minimum future remnant liver of40% after extended resection.
Bleeding during hepatic surgery correlates withshort and long-term survival rates in most studies.Therefore, strategies to prevent intraoperative hemor-rhage have become very popular, and are best achievedby inflow occlusion (Pringle maneuver (88) – Fig. 1).Additionally, the use of a low central vein pressure(CVP) by the anesthesia team is paramount to preventback flow bleeding during hepatic transection. LowCVP is optimal at the levels ranging between 1 and5 mm Hg, which does not put the patient at risk for airembolism or systemic tissue hypo-perfusion withresulting renal failure. Thus, management of fluids
and the appropriate use of catecholamine are crucial tosecure bloodless transection and optimal hemostasis(69, 89, 90).
While inflow occlusion effectively prevents bloodloss during parenchyma transection, it causes ischemicinjury to the liver. The normal liver well tolerates up to45–60 min of ischemia, but significant and irreversibleinjury may occur thereafter, particularly followingmajor hepatectomy. Livers with underlying diseases(e.g. steatosis and fibrosis) poorly tolerate ischemia,and significant injury may occur already after a 30 minperiod of ischemia. Therefore, strategies have beendeveloped to improve tolerance of the liver againstischemic injury. Currently only two strategies effec-tively confer protection in both experimental modelsand clinical studies, namely intermittent clamping,and ischemic preconditioning (Fig. 2).
Intermittent clamping of the portal triad, consistingin repeated ischemic periods (10–30 min) interruptedby short intervals of reperfusion (5–15 min), wasintroduced in clinical practice by Makuuchi in 1987(91) and is currently routinely used in many centers.The protective effects of intermittent clamping againstischemic injury have been established in clinical andexperimental studies (92, 93). For example, Belghiti etal. (92) found that intermittent clamping was superiorto continuous inflow occlusion in a series of 86patients undergoing major liver resection. A similarobservation was made by Vajdova et al. (94) whereperiods of prolonged ischemia were used.
Ischemic preconditioning involves a short periodof inflow occlusion (usually 10 min) followed usuallyby 10 min of reperfusion before the prolongedcontinuous ischemic insult, during which theparenchyma transection is performed. Ischemic
Fig. 1. Schematic drawing of the Pringle maneuver beforeresection of a tumor bearing liver segment. Anatomical positionof the clamp around the porta hepatis. The Pringle maneuverincludes occlusion of blood flow by tightening the clamp usuallyup to 45–60 min in normal liver and not more than 30 min inlivers with underlying diseases.
A
C
B
Fig. 2. Surgical protective strategies (A) continuous ischemia,(B) ischemic preconditioning, and (C) intermittent inflowocclusion. Ischemia periods are drawn in black and reperfusionperiods in white.
Liver International (2007)c� 2007 The Authors. Journal compilation c� 2007 Blackwell Munksgaard 31
Furrer et al. Liver surgery

preconditioning was shown to be superior to contin-uous inflow occlusion in two clinical studies (95, 96).Whether ischemic preconditioning is superior to in-termittent clamping remains unknown. In a mousemodel, we could show that both strategies confer ahigh degree of protection up to 75 min of ischemia,but intermittent clamping was superior for longerperiods. We concluded that that ischemic precondi-tioning might be preferable for most liver resection asit is not associated with bleeding during the successivereperfusion periods included in intermittent clampingprotocols. However, if a long resection time is antici-pated intermittent clamping should be preferred (93).We also found in another study that longer ischemicintervals (up to 30 min) followed by 5 min of reperfu-sion are also highly protective (97). However, there areno clinical data available at this point.
How both strategies confer protection remains un-clear. Our current understanding of the underlyingbiological principle is that cells are primed by variouskinds of sub injurious stress, which trigger defensemechanisms against subsequent injury of the same ordifferent types (98–100). Although the benefit ofischemic preconditioning in the liver has already beensuggested in a clinical pilot study (95) and a largerandomized study (96), knowledge of the molecularmechanisms remains vague. We showed in a mousemodel that a short period of ischemic preconditioningcauses a sublethal oxidative stress, which subsequentlytriggers strong antioxidant and antiapoptotic effects atthe time of prolonged ischemia (101). Several media-tors have been proposed to play a critical role in theprotective pathways including adenosine, nitric oxide(102), oxidative stress (101), some heat shock proteins(Hsps) (103) and tumor necrosis factor a (TNF-a)(104–106).
In addition to the extracellular mediators, studies inheart and liver indicate that the ischemic precondi-tioning process involves activation of intracellularmessengers such as protein kinase C, adenosine mono-phosphate-activated protein kinase, p38 mitogen-acti-
vated protein kinase, Ik kinase, and signal transducersand activators of transcription-1. The downstreamconsequences of these pathways could be cytoprotec-tive by abrogation of cell death pathways (such asactivation of vacuolar adenosine triphosphatases, in-hibition of intracellular Na accumulation, and cellswelling), stimulating antioxidant and other cellularprotective mechanisms, and by initiating entry intothe cell cycle (107–109). Whether intermittent clamp-ing acts through similar mechanisms is unclear as thismodality has not been explored in depth in animalmodels. We observed similar antiapoptotic and anti-necrotic effects in both modalities suggesting that atleast in part similar pathways may be activated (68).The identification of the underlying mechanisms isparamount to enable more selective protective strate-gies and the discovery of effective drugs.
Assuming that any type of ischemia should beavoided, novel transection devices are continuouslyput on the market with the claim that they enablebloodless hepatic resection obviating the need forinflow occlusion. Although some devices or strategiesmay reach such a goal, none has gained unanimousacceptance (110). The most popular devices are shownin Table 3. They include the cavitron ultrasonicsurgical aspirator (CUSAs; Tyco Helthcare, Mans-field, MA), the water jet (Helix Hydrojets; Erbe,Tubingen, Germany), the bipolar vessel sealing(Ligasures; Valleylab, Bouler, CO), and the Tissue-Link Monopolar Floating Ball (TissueLinks; Dover,NH). CUSAs is an aspirator, which provides tissuefragmentation using ultrasonic energy (114, 111). TheHydrojets is a water jet device connected to a pencil-like hand piece, which is used to separate intrahepaticvessels and bile ducts from the surrounding parench-yma (110). LigaSures is an ultrasonic dissector thatuses bipolar electrothermal energy resulting in sealingof vessels into coagulated cords, which are then simplydivided with scissors under direct vision (112).TissueLinks is a unipolar cooled radiofrequency abla-tion device that promotes a much greater depth of
Table 3. Most common devices used in liver resection
Device Manufacturer Effect Advantages/disadvantages
CUSAs Tyco Helthcare Tissue fragmentation byultrasonic energy
Selective dissection (it leaves blood vessels, urethers,and connective tissue skeletonized and intact)
Helix Hydro-jets Erbe Tissue fragmentation by waterdissection and suction
High tissue selectivity, organ-saving resection,no trauma to surrounding tissue (110)
Ligasures Valleylab Sealing of vessels into coagulatedcords
Ineffective for thin-walled veins (little collagen in theirwalls) and on intrahepatic portal hypertension (112)
TissueLinks Tissuelink Medical Depth coagulation Ablation of the dissected surface may promote anoncological extension of surgical margins (113)
Liver International (2007)32 c� 2007 The Authors. Journal compilation c� 2007 Blackwell Munksgaard
Liver surgery Furrer et al.

coagulation than with standard cautery. Topp et al.(113) showed that this device, accompanied by inflowocclusion, allows a depth of ablation greater than20 mm. It may be used for ablation of the dissectionsurface promoting an oncological extension of theresection margins. Very few data is currently availablevalidating or comparing these techniques, which havebeen often used without evidence of their superiorityover other available devices. Our group recently re-ported a randomized study in 100 noncirrhotic, non-cholestatic patients comparing the standard crushingtechnique performed under inflow occlusion, withthree devices marketed for bloodless transection:CUSAs, Hydrojets, and TissueLinks. The resultsshow superiority of the standard crushing techniquein terms of blood loss, speed of resection, and cost.This study however, did not investigate whether thesedevices may be beneficial for specific types of resectionor in the presence of cirrhosis (114). At this pointwe would like to speculate that the availability ofseveral of these techniques in high volume centers iscrucial to tailor the surgical approach to specificsituations. For example, while we use the simplecrushing technique in most liver resections, we usethe hydrojet for our living donor hepatectomy, andtissue link in situations where we have concerns aboutpositive margins.
Outcome of a liver resection strongly relies on theexperience of the surgeon and the team as a whole.While such a parameter is difficult to quantify, there isa clear correlation between case volume and clinicaloutcome. For example, it was observed that thehospital mortality was 1.5%, 5.3%, and 9.3% incenters performing, respectively, Z15, 7–15, and o 7liver resections per year (115). Fong at al. (116)confirmed this relationship of perioperative outcomewith surgical volume (high-volume center was definedas 4 25 cases) for hepatectomies, suggesting that thesurvival advantage remains valid even beyond theperioperative period. Thus, it is tempting to incrimi-nate the surgical skill of the team as a major factor-influencing outcome. In addition, we would like tosubmit that formal training of the surgeon in terms ofhepato-biliary fellowships including exposure to livertransplantation might become the single most impor-tant factor-affecting outcome in complex liver surgery.
Postoperative strategies
Outcome of complex surgery must also rely onoptimal postoperative care. ICU management withphysicians familiar with this population of patients isparamount for rapid recovery and early discharge. A
review on ICU management is beyond the scope of thisreview, but below we present potential promisingpharmacological approaches, which may prevent orminimize reperfusion injury.
Pharmacological approach
The use of protective drugs against ischemia–reperfu-sion injury and major hepatic tissue loss is best basedon the knowledge of pathways involved in ischemicinjury and liver regeneration. Many drugs have beenproposed, and we would refer to previous reviews formore insight into the pharmacologic approach of liverinjury (117). Here we will limit the discussion to someantioxidant drugs, pentoxiphyline, and prostaglan-dins.
Antioxidants
Liver surgery causes activation of Kupffer cells, whichare the main source of vascular reactive oxygenspecies (118). The importance of superoxide anionsin ischemic injury has been demonstrated in variousanimal models for example through the protectiveeffects of superoxide dismutase (SOD), and morerecently through the availability of transgenic animalsoverexpressing human SOD. However, evidence for abeneficial effect of antioxidant strategies in the clinicalpractice is still lacking.
Pentoxifylline
Pentoxifylline, a methylxanthine theobromine deri-vate, is a hemorrheologic drug that has been used inthe treatment of occlusive arterial disease and hemor-rhagic shock. Pentoxifylline may act through severalmechanisms. It has been shown that hepatic bloodflow and hepatocellular function were improved bypentoxifylline treatment (119, 120). A possible me-chanism of action include, intracellular elevation ofadenosine monophosphate phosphodiesterase levelswith consecutive increase of intracellular levels ofcyclic adenosine monophosphate (121). Pentoxifyllinereduces the synthesis of TNF-a synthesis, release fromKupffer cells and prevents upregulation of TNF-aexpression in a model of warm ischemic liver injuryin the mouse (106). It furthermore potentiates nitricoxide production (122). This pharmacologic agentpossesses certainly the primary function owing toimproved microcirculation and tissue oxygenationthrough reduction of blood viscosity and decreasedplatelet aggregation (123). Pentoxifylline blocks
Liver International (2007)c� 2007 The Authors. Journal compilation c� 2007 Blackwell Munksgaard 33
Furrer et al. Liver surgery

platelet-derived growth factor (PDGF) fibroprolifera-tion (124), vascular endothelial growth factor andtissue factor (125). Yet, to this day no clinical studieshave been presented that would show a beneficialeffect of pentoxifylline on liver ischemia injury andhepatic regenerative activity (126). The beneficialeffects need to be confirmed in phase I or II studiesbefore routine use (127).
Prostaglandins
Prostaglandins are biologically active polyunsaturatedfatty acids arising from arachidonic acid. They arelocal regulatory factors and mediators of inflamma-tion in conjunction with cytoprotection. In the last 20years the cytoprotective role of prostaglandins wasinvestigated in the liver under healthy and pathologicconditions (128, 129). The liver synthesizes all pro-ducts of this cascade, and is a target of their biologicalaction. It acts in the biodegradation of prostanoidsand elimination of most of their final metabolites(130). This results in the perturbation of microcircula-tion. Prostaglandins are released mainly by activatedKupffer cells during the reperfusion phase (131). Theprotective action of prostaglandin I2 (PGI2) andprostaglandin E1 (PGE1) include their ability to reducethe release of proteases and the generation of oxygenfree radicals from activated leukocytes (129, 132).Both can improve hepatic microcirculation and stabi-lity of hepatocellular membranes (133).
PGE1 has several potential therapeutic effects, in-cluding cytoprotection, vasodilatation and inhibitionof platelet aggregation (133). The pretreatment withPGE1 reduces intracellular concentration of calciumand decreases the production of superoxide anion(134) and protects the liver against ischemia–reperfu-sion injury by reducing leukocyte-endothelial celladhesion via downregulation of adhesions molecule(ICAM-1) in the endothelium (135). Cytoprotectiveeffects of PGE1 also include the suppression of throm-boxane A2 production and a concurrent increase inPGI2 production. The clinical use of pharmacologicdoses of natural prostaglandins is limited because ofdrug-related side effects and currently there is noevidence of a benefit (136).
Gene targeting
Historically, gene therapy has been proposed for treat-ing diseases caused by inherited or spontaneous genet-ic mutations in somatic cells e.g. single gene disorders.Gene targets, such as antiapoptotic proteins (B-celllymphocytic-leukemia protooncogene-2 binding atha-nogene, Bcl-2 Bag 1) have been successfully used in
animal models. Bcl-2 and Bcl-xl can protect cells fromapoptosis induced by hypoxia and the mechanismappears to be independent of the detoxification ofreactive oxygen species (137, 138).
Hepatocyte growth factor (HGF) is a pluripotentgrowth factor displaying a remarkable ability to pro-mote tissue repair and organ regeneration after injury,possibly through inhibition of DNA fragmentationand apoptosis (139).
Ogura et al. (140) reported that recombinant HGFaccelerates serum albumin recovery quickly after re-section of cirrhotic liver. HGF gene delivery by elec-troporation (a method used in transformation and tointroduce DNA into living cells) in vivo is a potentialtherapeutic approach for hepatic resection in livercirrhosis (141).
Targeting the liver by gene therapy is a promisingnew tool that requires ethical discussion before reach-ing the clinical level.
Liver rescue system
Postoperative liver failure may result from manyfactors including a too small remnant liver, ischemicinjury, preexisting liver disease, and sepsis. The clinicalmanifestation is a septic like syndrome associated withmultiorgan failure, where the underlying mechanismsremain poorly understood. The ‘toxin hypothesis’implicates a variety of toxins that accumulate as aresult of impaired hepatic metabolism and detoxifica-tion (142). A few dialysis devices have been proposedas detoxification strategies e.g. albumin dialysis, whichutilizes the scavenging functions of albumin for theremoval of toxins. The molecular adsorbents regulat-ing system (MARS) is one such extracorporeal livesupport device where blood crosses an albumin-im-pregnated membrane. In clinical trials, the MARSsystem was found to improve hyperbilirubinemia andhepatic encephalopathy in patients with chronic andacute liver failure, but a recent meta-analysis reportedthat MARS treatment had no significant survivalbenefit, when compared with standard medical ther-apy (143). No data is currently available to indicatethat MARS has any impact in patients with liver failureafter hepatectomy.
Future perspectives
The improvement of outcome in patients undergoingliver surgery must still rely on optimal pre-, intra-, andpostoperative evaluation and management. Currentlyonly surgical strategies i.e. ischemic preconditioningand intermittent clamping have proven protective
Liver International (2007)34 c� 2007 The Authors. Journal compilation c� 2007 Blackwell Munksgaard
Liver surgery Furrer et al.

effects against ischemic reperfusion injury and areroutinely used in clinical practice.
All other modalities need to be better evaluated inphase I or II studies before routine use. The pharma-cologic agents, e.g. antioxidants, pentoxifylline, andprostaglandins could be potentially beneficial in thefuture. Finally, gene therapy is a promising elegantalternative strategy that requires an ethical debatebefore introduction into clinical trial.
References
1. Harvey CJ, Albrecht T. Ultrasound of focal liver lesions. Eur
Radiol 2001; 11: 1578–93.
2. Lim JH, Kim SH, Lee WJ, Choi D, Lim HK. Ultrasono-
graphic detection of hepatocellular carcinoma: correlation
of preoperative ultrasonography and resected liver pathol-
ogy. Clin Radiol 2006; 61: 191–7.
3. Bennett GL, Krinsky GA, Abitbol RJ, Kim SY, Theise ND,
Teperman LW. Sonographic detection of hepatocellular
carcinoma and dysplastic nodules in cirrhosis: correlation
of pretransplantation sonography and liver explant pathol-
ogy in 200 patients. Am J Roentgenol 2002; 179: 75–80.
4. Teefey SA, Hildeboldt CC, Dehdashti F, et al. Detection of
primary hepatic malignancy in liver transplant candidates:
prospective comparison of CT, MR imaging, US, and PET.
Radiology 2003; 226: 533–42.
5. Braga HJ, Choti MA, Lee VS, Paulson EK, Siegelman ES,
Bluemke DA. Liver lesions: manganese-enhanced MR and
dual-phase helical CT for preoperative detection and char-
acterization comparison with receiver operating character-
istic analysis. Radiology 2002; 223: 525–31.
6. Kamel IR, Bluemke DA. Magnetic resonance imaging of the
liver: assessing response to treatment. Top Magn Reson
Imaging 2002; 13: 191–200.
7. Soyer P, Poccard M, Boudiaf M, et al. Detection of hypo-
vascular hepatic metastases at triple-phase helical CT:
sensitivity of phases and comparison with surgical and
histopathologic findings. Radiology 2004; 231: 413–20.
8. de Ledinghen V, Laharie D, Lecesne R, et al. Detection of
nodules in liver cirrhosis: spiral computed tomography or
magnetic resonance imaging? A prospective study of 88
nodules in 34 patients. Eur J Gastroenterol Hepatol 2002; 14:
159–65.
9. Kang BK, Lim JH, Kim SH, et al. Preoperative depiction of
hepatocellular carcinoma: ferumoxides-enhanced MR ima-
ging versus triple-phase helical CT. Radiology 2003; 226:
79–85.
10. Hussain SM, Terkivatan T, Zondervan PE, et al. Focal
nodular hyperplasia: findings at state-of-the-art MR ima-
ging, US, CT, and pathologic analysis. Radiographics 2004;
24: 3–17; discussion 18–9.
11. Kondo H, Kanematsu M, Hoshi H, et al. Preoperative
detection of malignant hepatic tumors: comparison of
combined methods of MR imaging with combined methods
of CT. Am J Roentgenol 2000; 174: 947–54.
12. Hosch WP, Schmidt SM, Plaza S, et al. Comparison of CT
during arterial portography and MR during arterial porto-
graphy in the detection of liver metastases. Am J Roentgenol
2006; 186: 1502–11.
13. Sahani D, Saini S, Pena C, et al. Using multidetector CT for
preoperative vascular evaluation of liver neoplasms: techni-
que and results. Am J Roentgenol 2002; 179: 53–9.
14. Choi D, Kim S, Lim J, et al. Preoperative detection of
hepatocellular carcinoma: ferumoxides-enhanced MR ima-
ging versus combined helical CT during arterial portogra-
phy and CT hepatic arteriography. Am J Roentgenol 2001;
176: 475–82.
15. Kim HC, Kim TK, Sung KB, et al. Preoperative evaluation of
hepatocellular carcinoma: combined use of CT with arterial
portography and hepatic arteriography. Am J Roentgenol
2003; 180: 1593–9.
16. Lee MG, Park KB, Shin YM, et al. Preoperative evaluation of
hilar cholangiocarcinoma with contrast-enhanced three-di-
mensional fast imaging with steady-state precession magnetic
resonance angiography: comparison with intraarterial digital
subtraction angiography. World J Surg 2003; 27: 278–83.
17. Bohm B, Voth M, Geoghegan J, et al. Impact of positron
emission tomography on strategy in liver resection for
primary and secondary liver tumors. J Cancer Res Clin
Oncol 2004; 130: 266–72.
18. Huebner RH, Park KC, Shepherd JE, et al. A meta-analysis
of the literature for whole-body FDG PET detection of
recurrent colorectal cancer. J Nucl Med 2000; 41: 1177–89.
19. Cohade C, Osman M, Leal J, Wahl RL. Direct comparison of
(18)F-FDG PET and PET/CT in patients with colorectal
carcinoma. J Nucl Med 2003; 44: 1797–803.
20. Selzner M, Hany TF, Wildbrett P, McCormack L, Kadry Z,
Clavien PA. Does the novel PET/CT imaging modality
impact on the treatment of patients with metastatic color-
ectal cancer of the liver? Ann Surg 2004; 240: 1027–34
discussion 1035–6.
21. Child CG, Turcotte JG. Surgery and portal hypertension.
Major Probl Clin Surg 1964; 1: 1–85.
22. Pugh RN, Murray-Lyon IM, Dawson JL, Pietroni MC,
Williams R. Transection of the oesophagus for bleeding
oesophageal varices. Br J Surg 1973; 60: 646–9.
23. Mansour A, Watson W, Shayani V, Pickleman J. Abdominal
operations in patients with cirrhosis: still a major surgical
challenge. Surgery 1997; 122: 730–5; discussion 735–6.
24. Propst A, Propst T, Zangerl G, Ofner D, Judmaier G, Vogel
W. Prognosis and life expectancy in chronic liver disease.
Dig Dis Sci 1995; 40: 1805–15.
25. Riley TR III, Bhatti AM. Preventive strategies in chronic
liver disease: part II. Cirrhosis. Am Fam Physician 2001; 64:
1735–40.
26. Bruix J, Castells A, Bosch J, et al. Surgical resection of
hepatocellular carcinoma in cirrhotic patients: prognostic
value of preoperative portal pressure. Gastroenterology 1996;
111: 1018–22.
Liver International (2007)c� 2007 The Authors. Journal compilation c� 2007 Blackwell Munksgaard 35
Furrer et al. Liver surgery

27. Poon RT, Fan ST. Assessment of hepatic reserve for indica-
tion of hepatic resection: how I do it. J Hepatobiliary
Pancreat Surg 2005; 12: 31–7.
28. Lee SG, Hwang S. How I do it: assessment of hepatic
functional reserve for indication of hepatic resection. J
Hepatobiliary Pancreat Surg 2005; 12: 38–43.
29. Jodynis-Liebert J, Flieger J, Matuszewska A, Juszczyk J.
Serum metabolite/caffeine ratios as a test for liver function.
J Clin Pharmacol 2004; 44: 338–47.
30. Herold C, Regn S, Ganslmayer M, Ocker M, Hahn EG,
Schuppan D. Can quantitative tests of liver function dis-
criminate between different etiologies of liver cirrhosis? Dig
Dis Sci 2002; 47: 2669–73.
31. Redaelli CA, Dufour JF, Wagner M, et al. Preoperative
galactose elimination capacity predicts complications and
survival after hepatic resection. Ann Surg 2002; 235: 77–85.
32. Ha-Kawa SK, Tanaka Y, Hasebe S, et al. Compartmental
analysis of asialoglycoprotein receptor scintigraphy for
quantitative measurement of liver function: a multicentre
study. Eur J Nucl Med 1997; 24: 130–7.
33. Schneider PD. Preoperative assessment of liver function.
Surg Clin North Am 2004; 84: 355–73.
34. Oellerich M, Burdelski M, Lautz HU, Schulz M, Schmidt
FW, Herrmann H. Lidocaine metabolite formation as a
measure of liver function in patients with cirrhosis. Ther
Drug Monit 1990; 12: 219–26.
35. Goldberg DM, Brown D. Advances in the application of
biochemical tests to diseases of the liver and biliary tract:
their role in diagnosis, prognosis, and the elucidation of
pathogenetic mechanisms. Clin Biochem 1987; 20: 127–48.
36. Oellerich M, Armstrong VW. The MEGX test: a tool for the
real-time assessment of hepatic function. Ther Drug Monit
2001; 23: 81–92.
37. Clavien PA, Emond J, Vauthey JN, Belghiti J, Chari RS,
Strasberg SM. Protection of the liver during hepatic surgery.
J Gastrointest Surg 2004; 8: 313–27.
38. McDonagh JE, Nathan VV, Bonavia IC, Moyle GR, Tanner
AR. Caffeine clearance by enzyme multiplied immunoassay
technique: a simple, inexpensive, and useful indicator of
liver function. Gut 1991; 32: 681–4.
39. Mitsumori A, Nagaya I, Kimoto S, et al. Preoperative
evaluation of hepatic functional reserve following hepatect-
omy by technetium-99m galactosyl human serum albumin
liver scintigraphy and computed tomography. Eur J Nucl
Med 1998; 25: 1377–82.
40. Wu CC, Cheng SB, Ho WM, Chen JT, Liu TJ, P’Eng FK.
Liver resection for hepatocellular carcinoma in patients
with cirrhosis. Br J Surg 2005; 92: 348–55.
41. Kokudo N, Vera DR, Makuuchi M. Clinical application of
TcGSA. Nucl Med Biol 2003; 30: 845–9.
42. Wakabayashi H, Nishiyama Y, Ushiyama T, Maeba T, Maeta
H. Evaluation of the effect of age on functioning hepatocyte
mass and liver blood flow using liver scintigraphy in
preoperative estimations for surgical patients: comparison
with CT volumetry. J Surg Res 2002; 106: 246–53.
43. Neuschwander-Tetri BA, Caldwell SH. Nonalcoholic steato-
hepatitis: summary of an AASLD single topic conference.
Hepatology 2003; 37: 1202–19.
44. McClain CJ, Mokshagundam SP, Barve SS, et al. Mechan-
isms of non-alcoholic steatohepatitis. Alcohol 2004; 34:
67–79.
45. Yu MC, Yuan JM. Environmental factors and risk for
hepatocellular carcinoma. Gastroenterology 2004; 127: S72–8.
46. Markiewski MM, DeAngelis RA, Lambris JD. Liver inflam-
mation and regeneration: two distinct biological phenom-
ena or parallel pathophysiologic processes? Mol Immunol
10th Meeting Complement Hum Dis 2006; 43: 45–56.
47. Yang SQ, Lin HZ, Lane MD, Clemens M, Diehl AM. Obesity
increases sensitivity to endotoxin liver injury: implications
for the pathogenesis of steatohepatitis. Proc Natl Acad Sci
USA 1997; 94: 2557–62.
48. Selzner M, Rudiger HA, Sindram D, Madden J, Clavien PA.
Mechanisms of ischemic injury are different in the steatotic
and normal rat liver. Hepatology 2000; 32: 1280–8.
49. Selzner M, Clavien PA. Fatty liver in liver transplantation
and surgery. Semin Liver Dis 2001; 21: 105–13.
50. Fukumori T, Ohkohchi N, Tsukamoto S, Satomi S. Why is
fatty liver unsuitable for transplantation? Deterioration of
mitochondrial ATP synthesis and sinusoidal structure dur-
ing cold preservation of a liver with steatosis. Transplant
Proc 1997; 29: 412–5.
51. Seifalian AM, Piasecki C, Agarwal A, Davidson BR. The
effect of graded steatosis on flow in the hepatic parenchymal
microcirculation. Transplantation 1999; 68: 780–4.
52. Zhong Z, Connor H, Stachlewitz RF, et al. Role of free
radicals in primary nonfunction of marginal fatty grafts
from rats treated acutely with ethanol. Mol Pharmacol 1997;
52: 912–9.
53. Nakano H, Nagasaki H, Barama A, et al. The effects of N-
acetyl–cysteine and anti-intercellular adhesion molecule-1
monoclonal antibody against ischemia–reperfusion injury
of the rat steatotic liver produced by a choline–methionine-
deficient diet. Hepatology 1997; 26: 670–8.
54. Powell EE, Jonsson JR, Clouston AD. Steatosis: co-factor in
other liver diseases. Hepatology 2005; 42: 5–13.
55. Selzner M, Clavien PA. Failure of regeneration of the
steatotic rat liver: disruption at two different levels in the
regeneration pathway. Hepatology 2000; 31: 35–42.
56. Belghiti J, Hiramatsu K, Benoist S, Massault P, Sauvanet A,
Farges O. Seven hundred forty-seven hepatectomies in the
1990s: an update to evaluate the actual risk of liver resec-
tion. J Am Coll Surg 2000; 191: 38–46.
57. Emond JC, Samstein B, Renz JF. A critical evaluation of
hepatic resection in cirrhosis: optimizing patient selection
and outcomes. World J Surg 2005; 29: 124–30.
58. Fernandez FG, Ritter J, Goodwin JW, Linehan DC, Hawkins
WG, Strasberg SM. Effect of steatohepatitis associated with
irinotecan or oxaliplatin pretreatment on resectability of
hepatic colorectal metastases. J Am Coll Surg 2005; 200:
845–53.
Liver International (2007)36 c� 2007 The Authors. Journal compilation c� 2007 Blackwell Munksgaard
Liver surgery Furrer et al.
59. Rubbia-Brandt L, Audard V, Sartoretti P, et al. Severe
hepatic sinusoidal obstruction associated with oxaliplatin-
based chemotherapy in patients with metastatic colorectal
cancer. Ann Oncol 2004; 15: 460–6.
60. Rollo FD, DeLand FH. The determination of liver mass
from radionuclide images. Radiology 1968; 91: 1191–4.
61. Lin TY, Lee CS, Chen CC, Liau KY, Lin WS. Regeneration of
human liver after hepatic lobectomy studied by repeated
liver scanning and repeated needle biopsy. Ann Surg 1979;
190: 48–53.
62. Carr D, Duncan JG. Liver volume determination by
ultrasound: a feasibility study. Br J Radiol 1976; 49:
776–8.
63. Van Thiel DH, Hagler NG, Schade RR, et al. In vivo hepatic
volume determination using sonography and computed
tomography. Validation and a comparison of the two
techniques. Gastroenterology 1985; 88: 1812–7.
64. Nagasue N, Yukaya H, Ogawa Y, Kohno H, Nakamura T.
Human liver regeneration after major hepatic resection. A
study of normal liver and livers with chronic hepatitis and
cirrhosis. Ann Surg 1987; 206: 30–9.
65. Chen MF, Hwang TL, Hung CF. Human liver regeneration
after major hepatectomy. A study of liver volume by
computed tomography. Ann Surg 1991; 213: 227–9.
66. Ogasawara K, Une Y, Nakajima Y, Uchino J. The significance
of measuring liver volume using computed tomographic
images before and after hepatectomy. Surg Today 1995; 25:
43–8.
67. Urata K, Hashikura Y, Ikegami T, Terada M, Kawasaki S.
Standard liver volume in adults. Transpl Proc 2000; 32:
2093–4.
68. Vauthey JN, Abdalla EK, Doherty DA, et al. Body surface
area and body weight predict total liver volume in Western
adults. Liver Transpl 2002; 8: 233–40.
69. Jarnagin WR, Gonen M, Fong Y, et al. Improvement in
perioperative outcome after hepatic resection: analysis of
1,803 consecutive cases over the past decade. Ann Surg 2002;
236: 397–406; discussion 406–7.
70. Imamura H, Seyama Y, Kokudo N, et al. One thousand fifty-
six hepatectomies without mortality in 8 years. Arch Surg
2003; 138: 1198–206; discussion 1206.
71. Yigitler C, Farges O, Kianmanesh R, Regimbeau JM, Abdalla
EK, Belghiti J. The small remnant liver after major liver
resectio: how common and how relevant? Liver Transpl
2003; 9: S18–25.
72. Takayasu K, Muramatsu Y, Shima Y, Moriyama N, Yamada
T, Makuuchi M. Hepatic lobar atrophy following obstruc-
tion of the ipsilateral portal vein from hilar cholangiocarci-
noma. Radiology 1986; 160: 389–93.
73. Honjo I, Suzuki T, Ozawa K, Takasan H, Kitamura O.
Ligation of a branch of the portal vein for carcinoma of the
liver. Am J Surg 1975; 130: 296–302.
74. Abdalla EK, Hicks ME, Vauthey JN. Portal vein emboliza-
tion: rationale, technique and future prospects. Br J Surg
2001; 88: 165–75.
75. Kinoshita H, Sakai K, Hirohashi K, Igawa S, Yamasaki O,
Kubo S. Preoperative portal vein embolization for hepato-
cellular carcinoma. World J Surg 1986; 10: 803–8.
76. Makuuchi M, Thai BL, Takayasu K, et al. Preoperative
portal embolization to increase safety of major hepatectomy
for hilar bile duct carcinoma: a preliminary report. Surgery
1990; 107: 521–7.
77. Madoff DC, Abdalla EK, Vauthey JN. Portal vein emboliza-
tion in preparation for major hepatic resection: evolution of
a new standard of care. J Vasc Interv Radiol 2005; 16:
779–90.
78. Uesaka K, Nimura Y, Nagino M. Changes in hepatic lobar
function after right portal vein embolization. An appraisal
by biliary indocyanine green excretion. Ann Surg 1996; 223:
77–83.
79. Tanaka H, Kinoshita H, Hirohashi K, Kubo S, Lee KC.
Increased safety by two-stage hepatectomy with preopera-
tive portal vein embolization in rats. J Surg Res 1994; 57:
687–92.
80. Broering DC, Hillert C, Krupski G, et al. Portal vein
embolization vs. Portal vein ligtion for induction of hyper-
trophy of the future liver remnant. J Gastrointest Surg 2002;
6: 905–13; discussion 913.
81. Selzner N, Pestalozzi BC, Kadry Z, Selzner M, Wildermuth
S, Clavien PA. Downstaging colorectal liver metastases by
concomitant unilateral portal vein ligation and selective
intra-arterial chemotherapy. Br J Surg 2006; 93: 587–92.
82. Henkel AS, Buchman AL. Nutritional support in patients
with chronic liver disease. Nat Clin Pract Gastroenterol
Hepatol 2006; 3: 202–9.
83. Pitt HA, Cameron JL, Postier RG, Gadacz TR. Factors
affecting mortality in biliary tract surgery. Am J Surg 1981;
141: 66–72.
84. Halliday AW, Benjamin IS, Blumgart LH. Nutritional risk
factors in major hepatobiliary surgery. J Parenter Enteral
Nutr 1988; 12: 43–8.
85. Harrison J, McKiernan J, Neuberger JM. A prospective
study on the effect of recipient nutritional status on out-
come in liver transplantation. Transpl Int 1997; 10: 369–74.
86. Richter B, Schmandra TC, Golling M, Bechstein WO.
Nutritional support after open liver resection: a systematic
review. Dig Surg 2006; 23: 139–45.
87. Grimble RF. Immunonutrition. Curr Opin Gastroenterol
2005; 21: 216–22.
88. Pringle J. Notes on the arrest of hepatic haemorrhage due to
trauma. Ann Surg 1908; 48: 541–9.
89. Smyrniotis V, Kostopanagiotou G, Theodoraki K, Tsantou-
las D, Contis JC. The role of central venous pressure and
type of vascular control in blood loss during major liver
resections. Am J Surg 2004; 187: 398–402.
90. Melendez JA, Arslan V, Fischer ME, et al. Perioperative
outcomes of major hepatic resections under low central
venous pressure anesthesia: blood loss, blood transfusion,
and the risk of postoperative renal dysfunction. J Am Coll
Surg 1998; 187: 620–5.
Liver International (2007)c� 2007 The Authors. Journal compilation c� 2007 Blackwell Munksgaard 37
Furrer et al. Liver surgery
91. Makuuchi M, Mori T, Gunven P, Yamazaki S, Hasegawa H.
Safety of hemihepatic vascular occlusion during resection of
the liver. Surg Gynecol Obstet 1987; 164: 155–8.
92. Belghiti J, Noun R, Malafosse R, et al. Continuous versus
intermittent portal triad clamping for liver resection: a
controlled study. Ann Surg 1999; 229: 369–75.
93. Rudiger HA, Kang KJ, Sindram D, Riehle HM, Clavien PA.
Comparison of ischemic preconditioning and intermittent
and continuous inflow occlusion in the murine liver. Ann
Surg 2002; 235: 400–7.
94. Vajdova K, Heinrich S, Tian Y, Graf R, Clavien PA. Ischemic
preconditioning and intermittent clamping improve mur-
ine hepatic microcirculation and Kupffer cell function after
ischemic injury. Liver Transpl 2004; 10: 520–8.
95. Clavien PA, Yadav S, Sindram D, Bentley RC. Protective
effects of ischemic preconditioning for liver resection per-
formed under inflow occlusion in humans. Ann Surg 2000;
232: 155–62.
96. Clavien PA, Selzner M, Rudiger HA, et al. A prospective
randomized study in 100 consecutive patients undergoing
major liver resection with versus without ischemic precon-
ditioning. Ann Surg 2003; 238: 843–50; discussion 851–2.
97. Kang KJ, Jang JH, Lim TJ, et al. Optimal cycle of inter-
mittent portal triad clamping during liver resection in the
murine liver. Liver Transpl 2004; 10: 794–801.
98. Jaeschke H. Molecular mechanisms of hepatic ischemia–r-
eperfusion injury and preconditioning. Am J Physiol Gastro-
intest Liver Physiol 2003; 284: G15–26.
99. Cavalieri B, Perrelli MG, Aragno M, et al. Ischemic pre-
conditioning attenuates the oxidant-dependent mechan-
isms of reperfusion cell damage and death in rat liver. Liver
Transpl 2002; 8: 990–9.
100. Schauer RJ, Gerbes AL, Vonier D, op den Winkel M,
Fraunberger P, Bilzer M. Induction of cellular resistance
against Kupffer cell-derived oxidant stress: a novel concept
of hepatoprotection by ischemic preconditioning. Hepatol-
ogy 2003; 37: 286–95.
101. Rudiger HA, Graf R, Clavien PA. Sub-lethal oxidative stress
triggers the protective effects of ischemic preconditioning in
the mouse liver. J Hepatol 2003; 39: 972–7.
102. Peralta C, Hotter G, Closa D, Gelpi E, Bulbena O, Rosello-
Catafau J. Protective effect of preconditioning on the injury
associated to hepatic ischemia–reperfusion in the rat: role of
nitric oxide and adenosine. Hepatology 1997; 25: 934–7.
103. Redaelli CA, Tien YH, Kubulus D, Mazzucchelli L, Schilling
MK, Wagner AC. Hyperthermia preconditioning induces
renal heat shock protein expression, improves cold ischemia
tolerance, kidney graft function and survival in rats. Ne-
phron 2002; 90: 489–97.
104. Colletti LM, Kunkel SL, Walz A, et al. The role of cytokine
networks in the local liver injury following hepatic ische-
mia/reperfusion in the rat. Hepatology 1996; 23: 506–14.
105. Peralta C, Fernandez L, Panes J, et al. Preconditioning
protects against systemic disorders associated with hepatic
ischemia–reperfusion through blockade of tumor necrosis
factor-induced P-selectin up-regulation in the rat. Hepatol-
ogy 2001; 33: 100–13.
106. Rudiger HA, Clavien PA. Tumor necrosis factor alpha, but
not Fas, mediates hepatocellular apoptosis in the murine
ischemic liver. Gastroenterology 2002; 122: 202–10.
107. Carini R, De Cesaris MG, Splendore R, Bagnati M, Albano
E. Ischemic preconditioning reduces Na(1) accumulation
and cell killing in isolated rat hepatocytes exposed to
hypoxia. Hepatology 2000; 31: 166–72.
108. Carini R, De Cesaris MG, Splendore R, et al. Signal pathway
involved in the development of hypoxic preconditioning in
rat hepatocytes. Hepatology 2001; 33: 131–9.
109. Teoh N, Dela Pena A, Farrell G. Hepatic ischemic precondi-
tioning in mice is associated with activation of NF-kappaB,
p38 kinase, and cell cycle entry. Hepatology 2002; 36:
94–102.
110. McCormack L, Selzner M, Clavien PA. Radical pericystic
resection of hydatid cysts of the liver using the water jet
device: a novel approach. J Am Coll Surg 2005; 200: 976–8.
111. Yamamoto Y, Ikai I, Kume M, et al. New simple technique
for hepatic parenchymal resection using a Cavitron
Ultrasonic Surgical Aspirator and bipolar cautery equipped
with a channel for water dripping. World J Surg 1999; 23:
1032–7.
112. Strasberg SM, Drebin JA, Linehan D. Use of a bipolar vessel-
sealing device for parenchymal transection during liver
surgery. J Gastrointest Surg 2002; 6: 569–74.
113. Topp SA, McClurken M, Lipson D, et al. Saline-linked
surface radiofrequency ablation: factors affecting steam
popping and depth of injury in the pig liver. Ann Surg
2004; 239: 518–27.
114. Lesurtel M, Selzner M, Petrowsky H, McCormack L, Clavien
PA. How should transection of the liver be performed?: a
prospective randomized study in 100 consecutive patients
comparing four different transection strategies. Ann Surg
2005; 242: 814–22; discussion 822–3.
115. Choti MA, Bowman HM, Pitt HA, et al. Should hepatic
resections be performed at high-volume referral centers? J
Gastrointest Surg 1998; 2: 11–20.
116. Fong Y, Gonen M, Rubin D, Radzyner M, Brennan MF.
Long-term survival is superior after resection for cancer in
high-volume centers. Ann Surg 2005; 242: 540–4; discussion
544–7.
117. Selzner N, Rudiger H, Graf R, Clavien PA. Protective
strategies against ischemic injury of the liver. Gastroenterol-
ogy 2003; 125: 917–36.
118. Jaeschke H. Mechanisms of reperfusion injury after warm
ischemia of the liver. J Hepatobiliary Pancreat Surg 1998; 5:
402–8.
119. Peng XX, Currin RT, Thurman RG, Lemasters JJ. Protection
by pentoxifylline against normothermic liver ischemia/
reperfusion in rats. Transplantation 1995; 59: 1537–41.
120. Fabia R, Travis DL, Levy MF, Husberg BS, Goldstein RM,
Klintmalm GB. Effect of pentoxifylline on hepatic ischemia
and reperfusion injury. Surgery 1997; 121: 520–5.
Liver International (2007)38 c� 2007 The Authors. Journal compilation c� 2007 Blackwell Munksgaard
Liver surgery Furrer et al.

121. Semmler J, Gebert U, Eisenhut T, et al. Xanthine derivatives:
comparison between suppression of tumour necrosis factor-
alpha production and inhibition of cAMP phosphodiester-
ase activity. Immunology 1993; 78: 520–5.
122. Hoebe KH, Gonzalez-Ramon N, Nijmeijer SM, et al.
Differential effects of pentoxifylline on the hepatic inflam-
matory response in porcine liver cell cultures. Increase in
inducible nitric oxide synthase expression. Biochem Phar-
macol 2001; 61: 1137–44.
123. Sherer JT, Glover PH. Pentoxifylline for sickle-cell disease.
Ann Pharmacother 2000; 34: 1070–4.
124. Peterson TC. Inhibition of fibroproliferation by pentoxifyl-
line. Activity of metabolite-1 and lack of role of adenosine
receptors. Biochem Pharmacol 1996; 52: 97–602.
125. Akriviadis E, Botla R, Briggs W, Han S, Reynolds T, Shakil
O. Pentoxifylline improves short-term survival in severe
acute alcoholic hepatitis: a double-blind, placebo-controlled
trial. Gastroenterology 2000; 119: 1637–48.
126. Moser M, Zhang M, Gong Y, Johnson J, Kneteman N,
Minuk GY. Effect of preoperative interventions on outcome
following liver resection in a rat model of cirrhosis. J
Hepatol 2000; 32: 287–92.
127. Gines P, Guevara M, Arroyo V, Rodes J. Hepatorenal
syndrome. Lancet 2003; 362: 1819–27.
128. Araki H, Lefer AM. Cytoprotective actions of prostacyclin
during hypoxia in the isolated perfused cat liver. Am J
Physiol 1980; 238: H176–81.
129. Quiroga J, Prieto J. Liver cytoprotection by prostaglandins.
Pharmacol Ther 1993; 58: 67–91.
130. Huber M, Keppler D. Eicosanoids and the liver. Prog Liver
Dis 1990; 9: 117–41.
131. Decker K. Biologically active products of stimulated liver
macrophages (Kupffer cells). Eur J Biochem 1990; 192: 245–61.
132. Fantone JC, Kinnes DA. Prostaglandin E1 and prostaglan-
din I2 modulation of superoxide production by human
neutrophils. Biochem Biophys Res Commun 1983; 113:
506–12.
133. Hanazaki K, Kuroda T, Kajikawa S, Amano J. Prostaglandin
E1 reduces thromboxane A2 in hepatic ischemia–reperfu-
sion. Hepatogastroenterology 2000; 47: 807–11.
134. Matsuo KI, Togo S, Sekido H, et al. Pharmacologic pre-
conditioning effects: prostaglandin E(1) induces heat-shock
proteins immediately after ischemia/reperfusion of the
mouse liver. J Gastrointest Surg 2005; 9: 758–68.
135. Natori S, Fujii Y, Kurosawa H, Nakano A, Shimada H.
Prostaglandin E1 protects against ischemia–reperfusion
injury of the liver by inhibition of neutrophil adherence to
endothelial cells. Transplantation 1997; 64: 1514–20.
136. Totsuka E, Todo S, Zhu Y, et al. Attenuation of ischemic liver
injury by prostaglandin E1 analogue, misoprostol, and
prostaglandin I2 analogue, OP-41483. J Am Coll Surg 1998;
187: 276–86.
137. Jacobson MD, Raff MC. Programmed cell death and
Bcl-2 protection in very low oxygen. Nature 1995; 374:
814–6.
138. Shimizu S, Eguchi Y, Kosaka H, Kamiike W, Matsuda H,
Tsujimoto Y. Prevention of hypoxia-induced cell death by
Bcl-2 and Bcl-xl. Nature 1995; 374: 811–3.
139. Xue F, Takahara T, Yata Y, et al. Attenuated acute liver injury
in mice by naked hepatocyte growth factor gene transfer
into skeletal muscle with electroporation. Gut 2002; 50:
558–62.
140. Ogura Y, Hamanoue M, Tanabe G, et al. Hepatocyte growth
factor promotes liver regeneration and protein synthesis
after hepatectomy in cirrhotic rats. Hepatogastroenterology
2001; 48: 545–9.
141. Xue F, Takahara T, Yata Y, et al. Hepatocyte growth factor
gene therapy accelerates regeneration in cirrhotic mouse
livers after hepatectomy. Gut 2003; 52: 694–700.
142. Sen S, Williams R, Jalan R. Emerging indications for
albumin dialysis. Am J Gastroenterol 2005; 100: 468–75.
143. Khuroo MS, Farahat KL. Molecular adsorbent recirculating
system for acute and acute-on-chronic liver failure: a meta-
analysis. Liver Transpl 2004; 10: 1099–106.
Liver International (2007)c� 2007 The Authors. Journal compilation c� 2007 Blackwell Munksgaard 39
Furrer et al. Liver surgery




















