
Orthopedic communication about osteoarthritis treatment: Does patient race matter?

Thrombosis Research 123 (2009) 687–696
Contents lists available at ScienceDirect
Thrombosis Research
j ourna l homepage: www.e lsev ie r.com/ locate / th romres
Review Article
Use of antifibrinolytic therapy to reduce transfusion in patients undergoingorthopedic surgery: A systematic review of randomized trials
Yoan K. Kagoma a, Mark A. Crowther b,⁎, James Douketis b, Mohit Bhandari c, John Eikelboom b, Wendy Lim b
a Applied Science and Engineering, University of Toronto, Toronto, Ontario, Canadab Departments of Medicine and Hematology, McMaster University (St. Joseph's Hospital / Hamilton General Hospital), Hamilton, Ontario, Canadac Department of Clinical Epidemiology and Biostatistics and Surgery (Division of Orthopedics), McMaster University, Hamilton, Ontario, Canada
⁎ Corresponding author. Room L208, St Joseph's HospE-mail address: [email protected] (M.A. Crow
0049-3848/$ – see front matter © 2008 Published by Edoi:10.1016/j.thromres.2008.09.015
a b s t r a c t
a r t i c l e i n f oArticle history:
Background: Minimizing bl Received 26 May 2008Received in revised form 4 September 2008Accepted 29 September 2008Available online 12 November 2008eeding and transfusion is desirable given its cost, complexity and potential foradverse events. Concerns have been heightened by recent data demonstrating that bleeding events maypredict worse outcomes and by warnings about the safety of erythropoietic stimulating agents. Prior smallstudies suggest that antifibrinolytic agents may reduce bleeding and transfusion need in patients undergoingtotal hip replacement (THR) or total knee arthroplasty (TKA). However, no single study has been large enoughto definitively determine if these agents are safe and effective. To address this issue we performed asystematic review of randomized trials describing the use of tranexamic acid, epsilon aminocaproic acid, oraprotinin administration in the perioperative setting.Methods: MEDLINE, EMBASE, CINAHL and the Cochrane databases were searched for relevant trials. Twoindependent reviewers abstracted total blood loss, transfusion requirements, and venous thromboembolism(VTE) rates. Data were combined using the Mantel-Haenszel method and dichotomous data expressed asrelative risk (RR) with 95% confidence intervals (CI).Results: Patients receiving antifibrinolytic agents had reduced transfusion need (RR 0.52; 95% CI, 0.42 to 0.64;Pb0.00001), reduced blood loss and no increase in the risk of VTE (RR 0.95% CI, 0.80 to 1.10, I2=0%, P=0.531).Conclusions: We conclude that antifibrinolytic agents may reduce bleeding and transfusion in patientsundergoing THR or TKA who receive appropriate antithrombotic prophylaxis. There is a need for a large,adequately powered prospective study to carefully examine the safety and efficacy of these agents.
© 2008 Published by Elsevier Ltd.
Contents
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 688Methods . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 688
Search Methodology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 688Study Identification and Selection . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 688Validity Assessment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 688Data Abstraction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 688Statistical Analyses . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 688Subgroup Analyses . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 689
Results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 689Study and Patient Characteristics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 689Study Quality. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 689Clinical Outcome Assessment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 692
Total Blood Loss . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 692Transfusion Requirements . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 693VTE Complications . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 694
Discussion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 695Conflict of interest statement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 695References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 695
ital, 50 Charlton Ave East, Hamilton, Ontario, Canada L8N 4A6. Tel.: +1 905 521 6024; fax: +1 905 540 6568.ther).
lsevier Ltd.

688 Y.K. Kagoma et al. / Thrombosis Research 123 (2009) 687–696
Introduction
In 2004, over 480,000 total knee arthroplasties (TKA) and over230,000 total hip replacements (THR) were performed in the UnitedStates [1]. About half of patients undergoing THR and TKA requiretransfusion with an average transfusion requirement of 2.0 units [2]and total average blood loss of 1,500 mL [3]. TKA generally has lowerintra-operative losses due to tourniquet use but is complicated byhigher hidden blood loss [4]. Despite blood-sparing techniques suchas cell salvage, normovolemic hemodilution, and surgical hemostasistechniques, bleeding requiring transfusion is still frequently encoun-tered peri- and post-operatively. This need for transfusion isconcerning as increasing data suggests that both bleeding andresultant transfusions are associated with an increased risk foradverse outcomes. Among patients with acute coronary syndromes,patients who undergo transfusion have increased rates of death andmyocardial infarction, even after adjustment for important confound-ing factors [5,6].
Furthermore, alternatives to transfusion including the use oferythropoietic stimulating agents (ESAs) may also be associatedwith an increased risk of adverse outcomes. ESAs are used to facilitatethe ability for patients to donate autologous blood units fortransfusion and to hasten the recovery of the hemoglobin level aftersurgery. Although effective in raising the hemoglobin level, theseagents are expensive and have recently been shown to increase therisk for deep vein thrombosis in patients undergoing orthopedicsurgery [7]. Routine use of these agents as a method to reducetransfusion is consequently problematic; the frequency with whichthey are actually used in patients undergoing major orthopedicsurgery is, to our knowledge, unknown.
Antifibrinolytic agents such as tranexamic acid (TXA), epsilonaminocaproic acid (EACA) and aprotinin are widely available agentswhich enhance hemostasis, thus potentially reducing blood loss andthe need for transfusion. EACA and TXA are synthetic amino acidderivatives which bind reversibly to plasminogen, inhibiting bindingto fibrin and activation to plasmin [8,9]. Aprotinin, a bovine lung tissueextract, is a naturally occurring polypeptide protease inhibitor thatbinds and inhibits plasmin [10]. However, like ESAs, these agents mayalso increase the risk of venous thromboembolism (VTE), as wasdemonstrated in cardiac surgery patients receiving aprotinin [11,12].
Currently, although extensively studied in cardiovascular andvascular surgery[5,6] there is a lack of data examining the efficacyand safety of these agents in other surgical settings. Despite theselimitations, a recent meta-analysis [13] suggests that intravenousantifibrinolytic agents are effective in reducing transfusion require-ments in patients undergoing various types of orthopaedic surgery.We performed a systematic review and meta-analysis of randomizedtrials to assess whether antifibrinolytic agents (TXA, EACA, aprotinin)reduce bleeding and transfusion requirements in patients undergoingjoint replacement, as well as their effect on the rate of VTE.
Methods
Search Methodology
We sought published randomized trials that evaluated TXA, EACA,or aprotinin in patients undergoing THR or TKA. A comprehensivesearch strategy was developed in consultation with a professionallibrarian. The search was limited to papers and abstracts written inEnglish. The electronic databases searched were: MEDLINE (1966 toMay Week 4 2007), Cumulative Index to Nursing & Allied HealthLiterature (1982 to May Week 4 2007), PubMed (May 30, 2007),EMBASE (1980 to 2007 May Week 21), Cochrane Database ofSystematic Reviews (to May 30, 2007). Manufacturers were contactedfor additional unpublished trials. Reference lists of included studiesand relevant reviews were checked for additional trials.
Study Identification and Selection
Studies were included if they: (1) enrolled adult patients under-going THR or TKA; (2) randomly assigned patients to receive TXA,EACA, or aprotinin; (3) compared the active treatment to placebo or notreatment; 4) reported one or more of the following outcomes: a)bleeding, b) transfusion, or c) VTE. Studies were excluded if they werenon-English language, if there were multiple study arms and theinformation specific for one antifibrinolytic agent could not beabstracted, or if the surgery was a revision procedure. Twoindependent reviewers selected studies with disagreements resolvedby consensus. The reviewers were masked to both the author andjournal of publication.
Validity Assessment
Two independent reviewers assessed each study according to theJadad Scale [14]. The Jadad Scale is a validated scoring systemwherebya study is given one point for the presence of randomization, blinding,and a description of patient attrition. A further two points are given ifthe methods of randomization and blinding are appropriate, to amaximum of five points. A score of ≤2 indicates “low” quality, while≥3 indicates “high” quality. Quality is further described by presentingthemethod of treatment concealment, themethod of blinding, the useof an intention-to-treat analysis, and the objectivity of the measuredoutcomes. We also collected information describing how the studywas funded. Reviewers weremasked to both the author and journal ofpublication. Any disagreements were resolved by consensus.
Data Abstraction
Two independent reviewers abstracted data and disagreementsresolved by consensus. Study characteristics such as patient demo-graphics and study design as well as the following 3 outcomes wererecorded: (1) transfusion requirements measured by number of unitstransfused and number of patients transfused (autologous andheterologous); (2) total bleeding, measured intraoperatively byweighing surgical sponges, postoperatively through drainage, orperioperatively through the hemoglobin balance method whichmeasures loss through comparison of pre- and postoperativehemoglobin concentrations (hematoma volumes as well as hiddenor internal blood loss were excluded); and (3) symptomatic orasymptomatic VTE confirmed using objective methods.
Statistical Analyses
Three primary analyses were performed. For the first analysisexamining total blood loss, the mean blood loss (in mL) and standarddeviations provided for each study were pooled to calculate aweighted mean difference (WMD). The strengths of conclusionsdrawn from this analysis are limited, however because we observedsignificant heterogeneity among studies. To reduce the heterogeneity,we calculated a standardized mean difference (SMD) using a fixedeffects model and further stratified the analysis by type of surgery. TheSMD is the difference between two means (treatment and controlgroups) divided by an estimate of the within-group standarddeviation. It provides a unitless comparison for studies in whichoutcomes (e.g., bleeding) have been measured in slightly differentways. A value N0.8 is considered clinically significant, although thisvalue is arbitrary [15]. The second analysis assessed the relative risk(RR) of any transfusion, where the proportion of patients whounderwent transfusion was compared in patients who received, anddid not receive, antifibrinolytic agents. The third analysis assessed theRR for VTE, where a WMD was calculated. A WMD was used toaccommodate for the fact that many studies had no VTEs reportedwhich does not allow for a RR to be calculated. The WMD was then

689Y.K. Kagoma et al. / Thrombosis Research 123 (2009) 687–696
converted to a RR by assuming an incidence rate of 29.6% in the controlgroup. This rate was based on the average of deep vein thrombosis(DVT) occurrence rates (proximal and distal DVTs detected byvenography) in THR and TKA patients with thromboprophylaxis[16]. For further comparisons, the risk difference (RD) of the VTE datawas calculated. Data were combined using the Mantel-Haenszelmethod and random effects model. All calculations were completedusing Review Manager (RevMan, Version 4.2.8 for Windows; Oxford,England: The Cochrane Collaboration, 2005). Heterogeneity wasassessed using the I2 statistic, which is interpreted as approximatelythe proportion of total variation in study estimates that is due toheterogeneity rather than sampling error [17]. A value of over 40%waschosen as significant heterogeneity. The statistical significance of theeffect was assessed using the Z-statistic with p-value [17].
Subgroup Analyses
Three a priori subgroup analyses were performed assessing the 3major outcomes by: (1) type of surgery (THR vs. TKA); (2) type ofantifibrinolytic agent used [9] (studies assessing combination anti-fibrinolytic agents were excluded from this analysis); (3) number ofdoses given (1 vs. N1, assessing dose effect [8]).
Results
Our search strategy identified a total of 283 articles (Fig. 1). Nounpublished articles were found. One [44] additional article wasretrieved through reference review. Subsequently, 226 articles wereexcluded after title and abstract screening using the predefinedinclusion and exclusion criteria. Of the remaining 57 articles, 26 wereexcluded: 1[18] was not published in English, 2[19,20] did not reportthe outcome measurements in a quantitative manner, 7[21–27] wereexcluded due to inclusion of patients undergoing other types ofsurgery, 1[28] was a comparative study with desmopressin, 8[29–36]were excluded since they did not have contemporaneous controlgroups, 3[37–39] were not randomized, 3[40–42] were duplicatestudies, 1[43] had multiple arms from which data could not beextracted, and 2[44,45] were excluded due to inadequacies in datareporting.
Fig. 1. Study selection and rationale for inclusion/exclusion.
Twenty-nine studies were included in the review, 26 studies wereincluded in the bleeding analysis, 25 studies in the transfusionanalysis, and 27 studies in the VTE analysis. Cohen's Kappa forInterrater Agreement was 0.94 (95% CI, 0.89-0.99) indicating nearperfect agreement between the two reviewers for study selection.
Study and Patient Characteristics
Of the 29 included studies, study size ranged from19 to 301 patients.Sixteen studies involved THR [46–48,51–53,55–57,59,65,67,69–72]while 13 were TKA [41,49,50,54,58,60–64,66,68,73]. TXA was studiedin 19[36,49–66] studies, aprotinin in 6[47,67–71 studies, and EACA in 1[72] study. Combination studies were as follows: aprotinin/EACA [72],EACA/TXA [73], and TXA/aprotinin [41].
Most TXA doses were weight-adjusted, ranging from 10 to 15 mg/kg (Table 2). EACA doses ranged from 12.5 to 100 mg/kg, as well asfixed (not weight adjusted) doses of 5 to 10 g. All aprotinin dosageswere a variation of the regimens recommended in the productmonograph[10] for coronary artery bypass graft surgery.
Timing of antifibrinolytic agent administration was variable. In 5[47,48,59,67,71] studies, initial administration was at or aroundinitiation of anaesthesia, in 10 studies, initial administration wasprior to the commencement of surgery [46,52,53,55–57,62,65,70,72]and in 1 study the antifibrinolytic was given at the end of surgery[51].In 9[41,49,50,54,58,60,61,66,73] studies, initial administration wasgiven prior to tourniquet release and 1[68] prior to tourniquetinflation. One study[69] did not specify the timing of administration,2[63,64] administered multiple doses at varying times. Assessment oftiming was complicated by studies with multiple study arms, multipledoses or constant infusions were given.
In 2[46,64] studies patients did not receive pharmacologic DVTprophylaxis, in 2[68,69] DVT prophylaxis was not reported, and in theremaining 25 studies a combination of mechanical and/or pharmaco-logic thromboprophylaxis was used (see Table 1). In 19 studies[41,46,48,49,51,54,55–63,65,67,72,73], clinically suspected VTE wasinvestigated with ultrasound, venography, and/or ventilation perfu-sion scans. In 8 studies[47,48,52,53,59,64,66,70], routine screening forVTE was conducted by ultrasound, venography and/or ventilationperfusion scans. In 3[68,69,71] studies the method of VTE assessmentused was unclear.
The follow-up period was variable and ranged from 3 days to3 months. Initial enrollment in all studies was 2060 patients with 79patients excluded (4.1%) from the analysis by original authors due toprotocol violations, death and other factors. Data on outcome eventsfor these patients was either limited or not available. Exclusion criteriaused in the included studies were factors which increase bleeding risk(coagulopathy, anemia, anticoagulant drugs), allergy to antifibrinoly-tic agents, thromboembolic disease, history of coagulopathy, orprevious renal or hepatic failure. No patients allocated to antifibrino-lytic therapy were lost to follow-up. One[68] study was stoppedprematurely after a patient given aprotinin underwent an above-kneeamputation; the contribution of aprotinin to this event was unknown.
Study Quality
Masking of study group was variable: 20 studies were double-blinded, 1[63] study was single-blinded, 1[54] study was semi-blindedand in 7[41,46,64,68–71] studies masking was unclear. Quality wasgenerally good; 21 studies received a high Jadad rating. The randomiza-tion sequence was described in 18[46,47,49,50,54,55,56,58–66,71,73]studies. No studies indicated the use of intention-to-treat analysis. Inter-rater agreement for validity assessment (high or low quality ranking)was good; Kappa=0.93 (95% CI, 0.78-1.07)[74].
Sixteen studies declared their sources of support: 1[68] author re-ceived support from a pharmaceutical company, 7[47,55,60,62,65,70,73]received financial support for the study from external sources such as

Table 1Study Characteristics
Study, Year Patients (Tx/C) Treatment Dose Control Transfusion Criteria DVT Prophylaxis, Dosage DVT Screening Method, Timing
Janssens, 1994 40 (20/20) Aprotinin 2×106 KIU (B), 5×105/h intraop to max3.5×106 KIU
S Maintenance of Hct at 30% Fraxiparin 100 IU/kg12 h b/f surgery,150 IU starting on post-op d 4
Daily clinical exam +/-venogram
Thorpe, 1994 19 (8/9) Aprotinin 5×105 KIU×2 b/f and following TRNQT, then1×106 KIU over 2 h
Similaranestheticmanagement
Clinical Decision - -
Compostella, 1997 100 (50/50) Aprotinin 2×106 KIU followed by 5×106 KIU/h S Hctb27% - -Hayes, 1996 40 (20/20) Aprotinin 5×104 KIU IV over 10 min then 2×106 KIU
over 20 min b/f incisionS Clinical Decision Enoxaparin and TED stocking Venogram, on Post-Op
Day 7Petsatodis, 2006 50 (25/25) Aprotinin (B) 2×104 KIU/kg at anesthesia followed by
(I) of 5×104 KIU/hrS - Enoxaparin, 2 hrs pre-op and 2 hrs
post-op-
Harley, 2002 55 (26/29) EACA LD of 150 mg/kg over 20 min then 12.5 mg/kghourly for 5 h
S Hbb80 g/L post-op or Hctb0.24intra-op
Heparin, 5000 U q12h until INRN2.0,.Coumadin×6 weeks
Daily clinical exam +/-venogram or V/Q scan
Benoni, 1996 96 (43/43) TXA 10 mg/kg (max 1 g) IV at EOS repeated every3 h, +/- extra dose when heavy bleeding
S Clinical Decision/Hbb100 g/L Dalteparin 5000 IU or Enoxaparin 40 mgfor 7-10d starting evening b/f surgery
Clinical Exam +/- venogramor V/Q
Benoni, 2000 40 (20/19) TXA 10 mg/kg IV at EOS, repeated after 3 h S Clinical Decision Enoxaparin 40 mg for 10d starting eveningb/f op
Clinical Exam
Ekbäck, 2000 40 (20/20) TXA (B) of 10 mg/kg b/f incision then (I) of1.0 mg·kg-1·h-1 for 10 h then (B) of 10 mg/kg3 h later
S Hctb27% after autologous PRBCtransfusion
Dalteparin, evening b/f surgery up to 10dpost op
US, on day 3 and 21
Benoni, 2001 40 (18/20) TXA IV 10 mg/kg in 5-10 min S Clinical Decision Enoxaparin 40 mg day b/f surgery to 7-10dpost-op
Clinical Exam
Hiippala, 1995 29 (15/13) TXA (B) 15 mg/kg 2-5 mins b/f TRNQT deflation 0.9% NaCl Hbb100 g/L Enoxaparin, 40 mg evening b/f surgery untildischarge or mobility
Clinical Exam
Orpen, 2005 30 (15/14) TXA IV 15 mg/kg at cement mixing NS Hbb 9 g/dL Fragmin, evening b/f surgery until discharge Color DUSHusted, 2003 40 (20/20) TXA (B) 10 mg/kg IV then (I) 1 mg/kg/hour for 10 h S Hbb75% baseline value and clinical
symptomsLWMH, day b/f surgery until discharge Clinical Exam +/- US
Garneti, 2004 50 (25/25) TXA (B) 10 mg/kg IV at anesthesia S - Stockings and foot pumps, 48 h post-op Belfast +/- Duplex Scan +/-venogram
Good L, 2003 55 (27/24) TXA 10 mg/kg IV b/f TRNQT release S Hbb90 g/L Dalteparin 5000 IU evening after surgerythen 5000 IU for 10d
Clinical Exam +/- US
Hiippala, 1997 90 (39/38) TXA 15 mg/kg IV b/f TRNQT deflation then 10 mg/kg3-4 h and 6-7 h after initial dose
S Hbb10 g/dL Enoxaparin, 40 mg on evening b/f surgeryuntil discharge or mobility
Clinical Exam +/- Venogram
Jansen, 1999 42 (20/20) TXA 15 mg/kg 30 min b/f inflation of TRNQT thenrepeated every 8 h for 3 days
S Packed Cell Volumeb26% in anypost-op measure
Fraxiparin, starting day b/f surgery untildischarge
Clinical Exam
Zohar, 2004 80 (20,20,20/20) TXA a) IV (B) of 15 mg/kg over 30 min followed by IVof 10 mg/kgh until 12 h after deflation of TRNQT
- Maintain HctN28% Enoxaparin, 40 mg/d starting b/f surgeryand for duration of hospital admission
Daily Exam with DUS, on5th Post-op daya) long
b) same as a) except IV infusion stopped 2 h afterTRNQT deflation then 1 g oral TXA given at 6, 12 hb) shortc) 1 g given orally 60 min b/f op then 1 g every6 h post-op for 18 hc) oral
690Y.K
.Kagomaet
al./Throm
bosisResearch
123(2009)
687–696

Yamasaki, 2004 40 (20/20) TXA 1000 mg of whole body TXA 5 min b/f op by IV P - None Clinical Exam +/- ascendingphlebography
Veien, 2002 30 (15/15) TXA 10 mg/kg (to 1 g max) b/f TRNQT release andrepeated 3 h later
- Hctb28% Fragmin, 500 U (I) on evening b/f surgeryuntil discharg r mobility
Clinical Exam
Tanaka, 2001 99 (24,22,27/26) TXA a) 20 mg/kg 10 min b/f surgery b) 20 mg/kg 10 minb/f deflation of TRNQT
S - None Venography, 7-14 days post-opas well as perfusion lung scan
c) 10 mg/kg 10 min b/f surgery and 10 min b/fdeflation of TRNQT
Niskanen, 2005 40 (19/20) TXA 10 mg/kg in 100 mL saline injection by IV over5-10 min b/f surgery then repeated 8 h and16 h after first injection
S Hct of 0.28-0.30 and clinicalsituation
Dalteparin an elastic leg dressing Clinical Exam +/- US
Ray, 2005 45 (15,15/15) a) Aprotinin, a) 1×104 KIU test dose followed by 2×106
KIU over 30 min after anesthesia followed by0.5×106 KIU/h for 3 h
S - Aspirin 150 m , foot stockings, andfoot pump
Clinical Exam and US, onDay 2 and 5
b) EACAb) 10 g in 250 mL IV S over 30 min after anesthesiathen 5 g in 250 mL IV S over 3 h
Camarasa, 2006 128 (35,32/60) a) EACA a) 100 mg/kg before TRNQT deflation then perfusionof 1 g/h during 3 h
S Hbb8 g/dl or b10 g/dl for thosewith associated conditions suchas COPD
Dalteparin, 5 0 IU night b/f surgeryand continue or 40 days
Clinical Examination +/- US
b) TXA b) 10 mg/kg IV before TRNQT deflation then 3 h laterLemay, 2004 40 (20/19) TXA Test dose of 1 mL then 10 mg/kg iv followed by
infusion of 1 mg/kghr until skin closureS Either 90 g/L or 70 g/L based on
age, history, & genderDalteparin, 5 0 Units twice dailystarted day o rgery, anti-stasisstocking, and rly mobilization
US, between post-op day5-10 or earlier
Johansson, 2005 119 (47/53) TXA 15 mg/kg in 100 mL NS S Hbb90 g/L with consideration ofwell-being
Dalteparin, 25 IU (I) twice on day ofsurgery and t 5000 IU until mobilization
Patient Record
Engel, 2001 36 (24/12) a) TXA a) 15 mg/kg then 10 mg/kg after 3 h - Hbb10 g/dL Certoparin, 30 IU evening b/f surgeryuntil discharg r mobility
Clinical Exam +/-Venographyb) Aprotinin b) 1×106 KIE b/f TRNQT deflation then infusion of
5×105 KIE/h for 4 hMurkin, 2000 301 (69,68,75/68) Aprotinin a) 5×105 KIU after anesthesia S Hctb18% or clinical decision Warfarin, 10 m orally on evening of
operation (wi n 12 h after skin closure)to patients w INRb1.3
US, 5-10 days post-opa) low b) 1×106 KIU followed by 2.5×105 KIU/hb) medium c) 2×106 KIU followed by infusion of 5.0×105 KIU/hc) high
Molloy, 2007 150 (50,50/50) TXA 500 mg IV b/f deflation of TRNQT and repeat 3 h later - Hctb25% 150 mg Aspir single dose evening b/fsurgery and d y for 6 weeks post-op
Clinical Evidence
TKR – Total Knee Replacement, THA – Total Hip Arthroplasty, ⁎ - Median Value, † - Estimated Standard Deviation, ‡ - WEIGHTED Mean Value, § - Summation of Perioperative & DrainMedi , ∥ - Calculated from 95% CI, d – day, a,b,c, etc – indicate multipletreatment arms, b/f – before, B – Bolus, s.c. – subcutaneous, Hb – hemoglobin, Hct – hematocrit, INR – international normalized ratio, Tx – treatment group, KIU –Kallikrein Inactivator Un , IU - international units, OD – once daily, TRNQT – tourniquet, I –injection,US–ultrasound,DUS–Doppler ultrasound, SD– standarddeviation,DVT–deepvein thrombosis, LD– loadingdose, op–operation,NS–normal saline, g–grams, PRBC–prepar redblood cells, ⁎⁎ - all lowmolecularweight heparins givenoncedaily and subcutaneous unless otherwise indicated, S – Saline, P – placebo, EOS – end of surgery.
691Y.K
.Kagomaet
al./Throm
bosisResearch
123(2009)
687–696
0 Ie o
d
g
00d f
00f suea00hen00e o
gthiith
inail
ansitsed

692 Y.K. Kagoma et al. / Thrombosis Research 123 (2009) 687–696
pharmaceutical or biotechnology companies, or research foundations,and 5[48,49,51,52,57] studies reported both sources of funding. Onlythree [56,59,64] studies declared no competing interests.
Clinical Outcome Assessment
Total Blood LossTotal blood losswas examined in 26 studies (see Table 2) with a total
of 1432patients. ApooledWMDfor all patientswas completedhowever,the data showed important heterogeneity (I2=89.6%) and consequently
Table 2Patient Characteristics
Study, Year Initial Number of Patients,(Patients Analyzed Tx/C)
Mean Age Tx[SD]/C[SD] MeaTx[S
Janssens, 1994 40, (20/20) 64.9[13.2] / 65.3[15.3] 144
Thorpe, 1994 19, (8/9) [n/a] / [n/a] 663
Compostella, 1997 100, (50/50) 68⁎ / 67⁎ 826Hayes, 1996 40, (20/20) 70[7.9] / 72.9[10.3] 1186
Petsatodis, 2006 50, (25/25) 58.4[12.5] / 59.6[10.9] 107
Harley, 2002 55, (26/29) 69[11] / 69[10] 867
Benoni, 1996 96, (43/43) 76[7] / 74[7] 730
Benoni, 2000 40, (20/19) 69.5[10] / 68[10] 990
Ekbäck, 2000 40, (20/20) 66.4[9] / 65.6[8.8] 1130
Benoni, 2001 40, (18/20) 66[9.5] / 68[9.4] 759
Hiippala, 1995 29, (15/13) 70[n/a] / 60[n/a] 847
Orpen, 2005 30, (15/14) 73[n/a] / 69[n/a] 660
Husted, 2003 40, (20/20) 65[n/a] / 67[n/a] 814
Garneti, 2004 50, (25/25) 69.6[11.99] / 67.6[11.4] 144
Good, 2003 55, (27/24) 72[n/a] / 72[n/a] 104
Hiippala, 1997 90, (39/38) 70[7] / 69[5] 689
Jansen, 1999 42, (20/20) 70.7[n/a] / 71.0[n/a] 678
Zohar, 2004 80, (20,20,20/20) 73[8],69[7],69 [10] / 73[7] Tota
Yamasaki, 2004 40, (20/20) 55.5[14.2] / 61.2[6.9] 135
Veien, 2002 30, (15/15) 70.5[9.5] / 69.5[9.0] 409
Tanaka, 2001 99, (24,22,27/26) 65[n/a],65[n/a],65[n/a] / 65 720
Niskanen, 2005 40, (19/20) 66[9.1] / 65[8.2] 792
Ray, 2005 45, (15,15/15) 72[n/a],72[n/a] / 69[n/a] -
Camarasa, 2006 128, (35,32/60) 73[n/a] / 73[n/a] 109
Lemay, 2004 40, (20/19) 59.7[10.3] / 53.6[12.8] 130
Johansson, 2005 119, (47/53) 69[7] / 68[8] 969
Engel, 2001 36, (24/12) 71[9],68[11] / 66[11] 837.
Murkin, 2000 301, (69,68,75/68) 63.7[n/a],65.5[n/a],63.4[n/a] /63.2 [n/a]
Tota
Molloy, 2007 150, (50,50/50) n/a 1215
⁎ - Median Value, † - Estimated Standard Deviation, ‡ - Weighted Mean Value, § - Summatdeviation , SD – Standard Deviation, Tx – treatment group, C – control group, n/a – not ava
the datawas stratified by TKA and THR and a SMDwas calculated.Whenanalyzed by surgery type, antifibrinolytic agents were associated withsignificant decreases in total blood loss for patients undergoing eitherTKA and THR. The SMD for TKA and THR were -1.12 (95% CI, -1.31 to-0.93) and -0.89 (95% CI, -1.05 to –0.72), respectively (see Fig. 2).Whenanalyzed by antifibrinolytic type, theWMD for TXA, EACA and aprotininwere -393mL (95% CI, -442 to -345), -331mL (95%CI, -544 to -118) and-639 mL (95% CI, -725 to -536), respectively. All comparisons werestatistically significant. Analysis by the number of doses showed similarresults to the analysis by surgery type.
n Total Blood Loss, mLD]/C[SD]
Allogeneic Transfusions,units Tx/C
Incidence of DVT
6[514]/1943[700] - Tx: 0Control: 4 DVT
⁎[286.7†]/960⁎ [431.7†] 1/6 Tx: 1Control: 0
[340]/1832[410] - -[414]/1274[347] - Tx: 0
Control: 1 DVT (below knee)3.2[388]/1496.2[545] 17/25 Tx: 0
Control: 0[207]/1198[544] 4/7 Tx: 0
Control: 0[280]/1410[480] 8/24 Tx: 4 DVT
Control: 3 DVT, 1 PE§ [210†]/950§ [162.5†] 9/15 Tx: 3 DVT
Control: 3 DVT[400]/1770[523] 1/1 Tx: 1 DVT
Control: 1 DVT[275.8∥]/996[398∥] 4/8 Tx: 1 PE
Control: 1 PE[356]/1549[574] 10/12 Tx: 0
Control: 2 DVT, 1 PE[317.6∥]/726[333.0∥] 1/3 Tx: 0
Control: 0[1323.8∥]/1231[1692.7∥] 2/7 Tx: 0
Control: 03[809]/1340[665] 16/14 Tx: 1 PE
Control: 05⁎[368.7†]/1426⁎[620.9†] 3/14 Tx: 2 DVT
Control: 2 DVT[289]/1509[643] 17/34 Tx: 2 DVT
Control: 2 DVT, 1 PE[352]/1419[607] 2/13 Tx: 0 DVT
Control: 2 DVTl Blood Loss Not Given 9/20 Tx: 0
Control: 00[477]/1667[401] 0/0 Tx: 0
Control : 0.7[174.9]/761.7[313.1] 0/2 Tx: 0
Control: 0.4‡[187.2⁎⁎]/1470[264.8] 47/26 Tx: 0
Control: 0[390.1∥]/1102[485.2∥] 5/8 Tx: 0
Control: 06/3 Tx: 0
Control: 09[535]/1784[660] 5/23 Tx: 0
Control: 08[462]/1469[405] 0/8 Tx: 0
Control: 0[434]/1324[577] 8/23 Tx: 0
Control: 05‡[287.9⁎⁎]/865[375] 5/3 Tx: 3
Control: 0l Blood Loss Not Given 66/32 Tx: 13
Control: 7[499]/1415[416] 5/11 Tx: 0
Control: 0
ion of Perioperative & Drain Medians, ∥ - Calculated from 95% CI, ⁎⁎ - pooled standardilable.
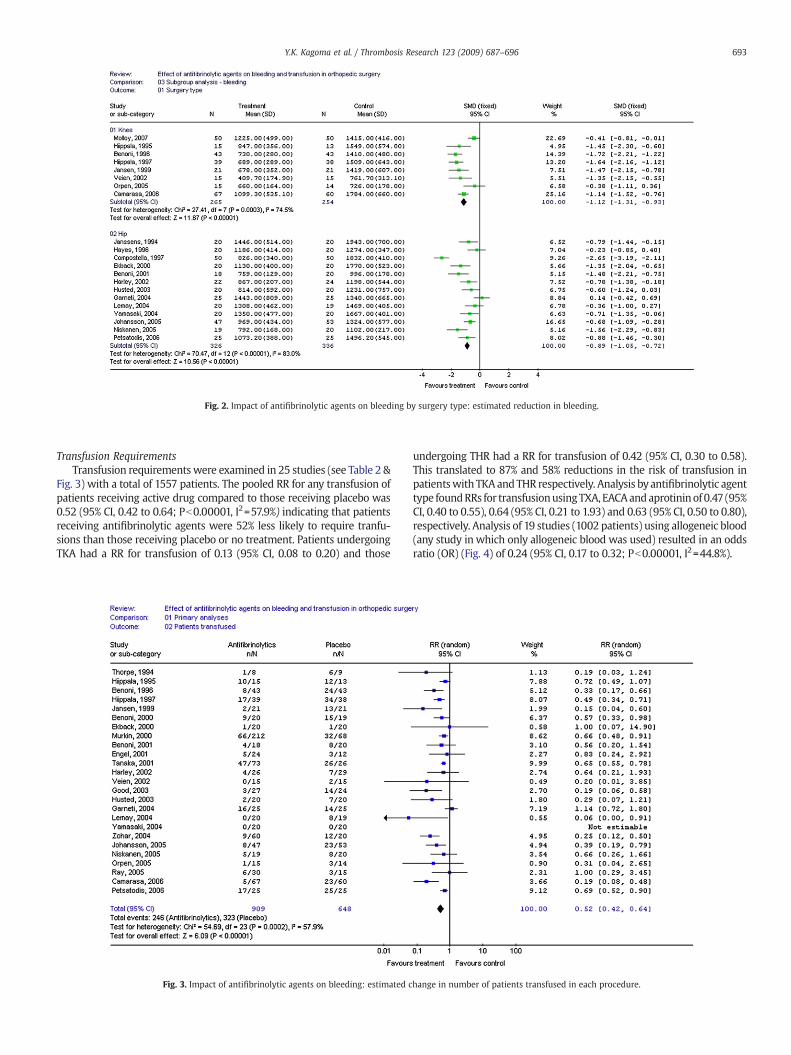
Fig. 2. Impact of antifibrinolytic agents on bleeding by surgery type: estimated reduction in bleeding.
693Y.K. Kagoma et al. / Thrombosis Research 123 (2009) 687–696
Transfusion RequirementsTransfusion requirementswere examined in 25 studies (see Table 2 &
Fig. 3) with a total of 1557 patients. The pooled RR for any transfusion ofpatients receiving active drug compared to those receiving placebo was0.52 (95% CI, 0.42 to 0.64; Pb0.00001, I2=57.9%) indicating that patientsreceiving antifibrinolytic agents were 52% less likely to require tranfu-sions than those receiving placebo or no treatment. Patients undergoingTKA had a RR for transfusion of 0.13 (95% CI, 0.08 to 0.20) and those
Fig. 3. Impact of antifibrinolytic agents on bleeding: estimated c
undergoing THR had a RR for transfusion of 0.42 (95% CI, 0.30 to 0.58).This translated to 87% and 58% reductions in the risk of transfusion inpatientswith TKAandTHR respectively. Analysis byantifibrinolytic agenttype foundRRs for transfusionusingTXA, EACAandaprotininof 0.47 (95%CI, 0.40 to 0.55), 0.64 (95% CI, 0.21 to 1.93) and 0.63 (95% CI, 0.50 to 0.80),respectively. Analysis of 19 studies (1002 patients) using allogeneic blood(any study in which only allogeneic blood was used) resulted in an oddsratio (OR) (Fig. 4) of 0.24 (95% CI, 0.17 to 0.32; Pb0.00001, I2=44.8%).
hange in number of patients transfused in each procedure.

Fig. 4. Impact of antifibrinolytic agents on bleeding: estimated change in number of patients transfused in each procedure (excluding autologous transfusions).
694 Y.K. Kagoma et al. / Thrombosis Research 123 (2009) 687–696
VTE ComplicationsTwenty-seven studies (1637 patients) reported VTE complications.
Patients receiving antifibrinolytic agents (949 patients) had 35 episodesofVTEwhile 688patientswhodidnot receive antifibrinolytic agents hada total of 31 episodes. TheRR forVTEwas0.95 (95%CI, 0.80 to 1.10, I2=0%,P=0.531). The risk difference (RD, see Fig. 5), a measure of the absolutechange in risk thatmaybe attributed to theuse of antifibrinolytic agents,
Fig. 5. Impact of antifibrinolytic agents o
was 0.00 (95% CI, -0.02 to 0.01), again suggesting no difference in VTErates between groups.When analyzed by antifibrinolytic agent type, theRDs for TXA, EACA and aprotininwere -0.01 (95% CI, -0.04 to 0.02), 0.00(95% CI, -0.07 to 0.07) and -0.04 (95% CI, -0.09 to 0.02), respectively.However, the strength of these conclusions are limited by the lack ofsystematic investigation and reporting of VTE complications, as well asthe small numbers of events.
n risk of venous thromboembolism.

695Y.K. Kagoma et al. / Thrombosis Research 123 (2009) 687–696
Discussion
Among patients undergoing elective THR or TKA, antifibrinolyticagents reduce bleeding, reduce the risk of transfusion by almost 50%and do not appear to increase the risk of VTE. These observations areconsistent with those found in the cardiovascular surgery literature[5,6] and are of particular clinical importance given the observationthat from 1995 to 2004 the rates of inpatient hip and kneereplacements increased by 38% and 70% respectively in patients overage 65 in the United States[1]. Such increases will be associated withincreasing bleeding complications andwill place additional burden onthe blood transfusion system, unless methods to reduce bleeding arefound. Minimizing bleeding and the need for transfusion is not onlycost-saving, but associated with decreased patient risk and complica-tions including volume overload, transfusion reactions and exposureto infectious agents [5,75]. Techniques such as autologous donation,intraoperative hemodilution and/or controlled hypotension increasecosts, pose additional logistical problems and may be immunomodu-latory [55,76]. Antifibrinolytic agents avoid many of these complica-tions, are widely available and inexpensive.
Our analysis does have several limitations. There was significantheterogeneity in the doses and type of antifibrinolytic agent, timing ofadministration, and a lack of standardized dose regimens for THR andTKA. Differences in surgical techniques and transfusion thresholds arelikely to have contributed to the differences observed betweenstudies. Lastly, estimating blood loss was variable, since blood dueto hematomas [57] or tissue extravasation [77] were rarely measuredand only 5[51,55,57,60,70] studies used a method to account for thissource of blood loss. Few studies reported the type of surgicalhemostasis (i.e., electrical cauterization, tissue adhesives) utilized;these techniques are known to reduce blood loss during surgery [70].It is likely that these inconsistencies across all studies contributed tothe high I2 values seen in statistical analyses. Nonetheless, theselimitations are mitigated in large part by the fact that differencesshould be balanced between groups within the individual studiescontributing to this analysis. Furthermore, across all studies the sameeffect was seen: antifibrinolytic agents reduced bleeding irrespectiveof dose, type, route or timing of its use.
This meta-analysis raises several important questions. Firstly, theshort half-life of these drugs raise the possibility that bleeding couldbe further reduced if multiple doses of these agents were adminis-tered. Biologic plausibility suggests that antifibrinolytic agents shouldbe administered after surgical hemostasis has been achieved butbefore significant fibrinolysis has occurred; thus the first dose of theseagents is perhaps optimally administered at the end of, or immedi-ately after the procedure. The potential for these drugs to causepostoperative thrombosis needs to be more carefully explored anddiligent reporting of all adverse events (including others such asmyocardial infarction and mortality) must be adopted. Aprotinin hasrecently been linked to higher mortality rates when compared to TXAand EACA in cardiovascular surgery[78,79] and these findings willlikely prevent further use of aprotinin to reduce blood loss in a clinicalsetting[80] regardless of patient population.
To date, use of antifibrinolytic agents in patients undergoingelective THR and TKA has been limited. Our results indicate that theymay reduce bleeding by at least 300 mL and reduce (by about 50%) oreliminate the need for transfusion inmany patients. TXA and EACA areboth inexpensive and widely available, making them a promisingtherapy for the prevention of surgical blood loss. The potentialbenefits of such therapy include lower total procedure costs,[47,65,72]due to reduced transfusion requirements, reduced exposure to thecomplications of bleeding and transfusion as well as a reducedperioperative need for ESAs. However given the heterogeneity of thepooled estimates, low number of studies, variance in dosing, andunclear toxicity profile of these agents, a large randomized placebo-controlled trial is warranted to examine blood loss, transfusion and
thromboembolic complications using antifibrinolytic agents in ortho-pedic procedures. Such a studymust be powered to assess the effect ofantifibrinolytic agents on blood loss and transfusion as primaryefficacy outcomes and the effect on thromboembolic complications asthe primary safety outcome.
Conflict of interest statement
Dr Crowther holds a career investigator award from the Heart andStroke Foundation of Ontario. Dr Crowther has received researchfunds, been on advisory boards, spoken on behalf and/or providedconsultation services to: Pfizer, Sanofi Aventis, Leo Laboratories, Bayer,Boehringher Ingelheim, Artisan Pharma and Octapharma.
References
[1] National Hospital Discharge Survey 2004. National Center for Health Statistics;2004.
[2] Bierbaum BE, Callaghan JJ, Galante JO, Rubash HE, Tooms RE,Welch RB. An Analysisof BloodManagement in Patients Having a Total Hip or Knee Arthroplasty. J Bone JtSurg 1999;81:2–10.
[3] R. Carver, R. Cooper: Anaesthesia for joint replacement surgery. AnaesthesiaUK.2005.
[4] Sehat KR, Evans RL, Newman JH. Hidden blood loss following hip and kneearthroplasty. J Bone Jt Surg (Br) 2004;86B:561–5.
[5] Rao SV, Eikelboom JA, Granger CB, Harrington RA, Califf RM, Bassand JP. Bleedingand blood transfusion issues in patients with non-ST-segment elevation acutecoronary syndromes. Eur Heart J 2007;28:1193–204.
[6] Yang X, Alexander KP, Chen AY, Roe MT, Brindis RG, Rao SV, et al. The Implicationsof Blood Transfusions for Patients With Non-ST – Segment Elevation AcuteCoronary Syndromes. J Am Coll Cardiol 2004;46(8):1490–5.
[7] A Study to Confirm the Safety and Efficacy of Epoetin Alfa (PROCRIT®)Administered Perioperatively vs. the Standard of Care in Blood Conservation inPatients Undergoing Major Elective Spinal Surgery (SPINE Study). Johnson andJohnson Pharmaceutical Research and Development; 2007.
[8] Mannucci PM. Hemostatic Drugs. N Engl J Med 1998;339(4):245–53.[9] Prentice CRM. Basis of Antifibrinolytic Therapy. J Clin Pathol Suppl 1980;14:35–40.[10] Trasylol Product Monograph, Bayer Pharmaceuticals; 2006[11] Mangano DT, Tudor IC, Dietzel C. The Risk Associated with Aprotinin in Cardiac
Surgery. N Engl J Med 2006;354:353–65.[12] FDA Statement Regarding New Trasylol Data. U.S. Food and Drug Administration;
2006.[13] Zufferey P, Merquiol F, Laporte S, Decousus H, Mismetti P, Auboyer C, et al. Do
Antifibrinolytics Reduce Allogeneic Blood Transfusion in Orthopedic Surgery?Anesthesiology 2006;2105:1034–6.
[14] Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJM, Gavaghan DJ, et al.Assessing the Quality of Reports of Randomized Clinical Trials: Is BlindingNecessary? Control Clin Trials 1996;17:1–12.
[15] Cohen J. Statistical power analysis for the behavioral sciences (2nd ed.). Hillsdale,NJ: Lawrence Earlbaum Associates; 1988.
[16] Xing KH, Morrison G, Lim W, Douketis J, Odueyungbo A, Crowther M. Has theIncidence of deep vein thrombosis inpatients undergoing total hip/knee arthroplastychanged over time? A systematic review of randomized controlled trials. Thromb Res2008.
[17] ReviewManager (RevMan)Version 4.2.8 forWindows;Oxford, England: The CochraneCollaboration, 2005.
[18] Cvachovec K, Sechovska H, Berousek J, Popelka S, HladikovaM. Aprotinin (antilysinspofa) - its effect on the reduction of haemorrhage in post-operative period inpatients with THA. Acta Chir Orthop Traumatol Cechoslov 2001;68(5):311–4.
[19] Ketterl R, Haas S, Wendt P, Stemberger A, Fritsche HM, Kienzle H, et al. The Effect ofAprotinin on the Blood Lactate Level, The Platelet Function and on Parameters ofCoagulation Following Total Hip Replacement. Haemostasis 1982;12(Suppl2):68.
[20] Haas S, Ketterl R, Stemberger A, Wendt P, Fritsche HM, Kienzle H, et al. The Effect ofAprotinin on Platelet Function, Blood Coagulation and Blood Lactate Level in TotalHip Replacement – A Double Blind Clinical Trial. Thromb Haemost 1983;50(1).
[21] Ozay K, Doğu H, Erkal H, Aydm F, Azali G, Arikan Z. Aprotinin infusion during majororthopaedic surgery. Br J Anaesth 1995;74(suppl):A.201.
[22] Capdevila X, Calvet Y, Biboulet P, Biron C, Rubenovitch J, d'Athis F. AprotininDecreases Blood Loss and Homologous Transfusions in Patients Undergoing MajorOrthopedic Surgery. Anesthesiology 1998;88(1):50–7.
[23] Samama CM, Langeron O, Rosencher N, Capdevila X, Rouche P, Pegoix M, et al.Aprotinin Versus Placebo in Major Orthopedic Surgery: A Randomized, Double-Blinded, Dose-Ranging Study. Anesth Analg 2002;95:287–93.
[24] Amar D, Grant FM, Zhang H, Boland PJ, Leung DH, Healey JA. AntifibrinolyticTherapy and Perioperative Blood Loss in Cancer Patients Undergoing MajorOrthopedic Surgery. Anesthesiology 2003;98(2):337–42.
[25] Murkin JM, Shannon NA, Bourne RB, Rorabeck CH, Cruickshank M, Wyile G.Aprotinin Decreases Blood Loss in Patients Undergoing Revision or Bilateral TotalHip Arthroplasty. Anesth Analg 1995;80:343–8.
[26] Shiga T, Wajima Z, Inoue T, Sakamoto A. Aprotinin in Major Orthopedic Surgery: ASystematic Review of Randomized Controlled Trials. Anesth Analg 2005;101:1602–7.

696 Y.K. Kagoma et al. / Thrombosis Research 123 (2009) 687–696
[27] Jeserschek R, Clar H, Aigner C, Rehak P, Primus B, Windhager R. Reduction of bloodloss using high-dose aprotinin in major orthopaedic surgery. J Bone Jt Surg [Br]2003;85B:174–7.
[28] Zohar E, Fredman B, Ellis MH, Ifrach N, Stern A, Jedeikin R. A comparative study ofthe postoperative allogeneic blood-sparing effects of tranexamic acid and ofdesmopressin after total knee replacement. Transfusion 2001;41:1285–9.
[29] K. Ido:Reductionofblood lossusing tranexamicacid in total kneeandhiparthroplasties.[30] Kasper SM, Elsner F, Hilgerst D, Ground S, Rütt J. A Retrospective study of the
effects of small-dose aprotinin on blood loss and transfusion needs during totalhip arthroplasty. Eur J Anaesthesiol 1998;15:669–75.
[31] Benoni G, Carlsson A, Petersson C, Fredin H. Does Tranexamic Acid Reduce BloodLoss in Knee Arthroplasty? Am J Knee Surg 1995;8(3):88–92.
[32] Singbartl G, Kantak S, Munkel H. Adjunct aprotinin administration is at least acost-neutral blood saving measure in infective knee revision surgery. Curr OpinClin Exp Res 2001;3(3):146–55.
[33] Hynes M, Calder P, Scott G. The use of tranexamic acid to reduce blood loss duringtotal knee arthroplasty. The Knee 2003;10:375–7.
[34] Kinzel V, Shakespeare D, Derbyshire D. The effect of aprotinin on blood loss inbilateral total knee arthroplasty. The Knee 2005;12:107–11.
[35] Singbartl G, Kantak S, Munkel H. Transfusion-Related Cost of Adjunct AprotininApplication in One-Step Infected Hip Revision Arthroplasty – Cost-MinimizingAnalysis. Infus Ther Transfus Med 2001;28:74–9.
[36] Yamasaki S, Masuhara K, Fuji T. Tranexamic Acid Reduces Postoperative Blood Lossin Cementless Total Hip Arthroplasty. J Bone Jt Surg Am 2005;87:766–70.
[37] McCarthy MW, Coley KC. Aprotinin for Prophylaxis of Blood Loss. Ann Pharmac-other 1994;28(11):1246–8.
[38] Coats T, Hunt B, Roberts I, Shakur H. Antifibrinolytic agents in traumatichaemorrhage. Indian J Pharmacol 2005;37(1):3–4.
[39] Hynes MC, Calder P, Rosenfeld P, Scott G. The use of tranexamic acid to reduceblood loss during total hip arthroplasty: an observational study. Ann R Coll SurgEngl 2005;87(2):99–101.
[40] C. Little: Effect of tranexamic acid in total knee arthroplasty – pilot study. Unpublished.[41] Engel JM, Hohaus T, Ruwoldt R, Menges T, Jürgensen I, Hempelmann G. Regional
Hemostatic Status and Blood Requirements After Total Knee Arthroplasty Withand Without Tranexamic Acid or Aprotinin. Anesth Analg 2001;92:775–80.
[42] Ellis M, Zohar E, Ifrach N, Stern A, Sapir O, Fredman B. Oral tranexamic acid in totalknee replacement: results of a randomized study. Vox Sanguinis 2004;87(Suppl3):S50.
[43] D'AmbrosioA,Borghi B,D'AmatoG,AntonacciG,Valeri F. Reducingperioperativebloodloss in patients undergoing total hip arthroplasty. Int J Artfi Organs 1999;22(1):47–51.
[44] Duquenne P, Lhoest L, Henkes W, De Sart F. Tranexamic Acid Reduces Post-operative Blood Losses Associated with Elective Total Hip Replacement. J Bone JtSurg (Br) 1999;81B(Suppl 2):233–4.
[45] Langdown A, Field J, Grote J, Himayat H. Aprotinin (Trasylol) Does Not ReduceBleeding in Primary Total Hip Arthroplasty. J Arthroplast 2000;15(8):1009–12.
[46] Yamasaki S, Masuhara K, Fuji T. Tranexamic acid reduces blood loss aftercementless total hip arthroplasty – prospective randomized study in 40 cases.Int Orthop 2004;28:69–73.
[47] Murkin JM, Haig GM, Beer KJ, McCutchen J, Communale ME, Hall R, et al. AprotininDecreases Exposure to Allogeneic Blood During Primary Unilateral Total HipReplacement. J Bone Joint Surg Am 2000;82:675–84.
[48] Ray M, Hatcher S, Whitehouse SL, Crawford S, Crawford R. Aprotinin and epsilonaminocaproic acid are effective in reducing blood loss after primary total hiparthroplasty – a prospective randomized double-blind placebo-controlled study. JThromb Haemost 2005;3:1421–7.
[49] Benoni G, Fredin H. Fibrinolytic Inhibitionwith Tranexamic Acid Reduces Blood Lossand Blood Transfusion After Knee Arthroplasty. J Bone Jt Surg [Br] 1996;78B:434–40.
[50] Molloy DG, Archbold HAP, Ogonda L, McConway J, Wilson RK, Beverland DE.Comparison of topical fibrin spray and tranexamic acid on blood loss after totalknee replacement – A Prospective, Randomised Controlled Trial. J Bone Jt Surg (Br)2007;89-B:306–9.
[51] Benoni G, Lethagen S, Nilsson P, Fredin H. Tranexamic acid, given at the end of theoperation, does not reduce postoperative blood loss in hip arthroplasty. ActaOrthop Scand 2000;71(3):250–4.
[52] Ekbäck G, Axelsson K, Ryttberg L, Edlund B, Kjellberg J, Weckström J, et al.Tranexamic Acid Reduces Blood Loss in Total Hip Replacement Surgery. AnesthAnalg 2000;91:1124–30.
[53] Lemay E, Guay J, Côté C, Roy A. Tranexamic acid reduces the need for allogenic redblood cell transfusions in patients undergoing total hip replacement. Can J Anesth2004;51(1):31–7.
[54] Veien M, Sørensen JV, Madsen F, Juelsgaard P. Tranexamic acid given intraopera-tively reduces blood loss after total knee replacement: a randomized, controlledstudy. Acta Anaesthesiol Scand 2002;46:1206–11.
[55] Johansson T, Pettersson LG, Lisander B. Tranexamic acid in total hip arthroplastysaves blood and money. Acta Orthop 2005;76(3):314–9.
[56] Husted H, Blønd L, Sonne-Holm S, Holm G, Jacobsen TW, Gebuhr. Tranexamic acidreduces blood loss and blood transfusions in primary total hip arthroplasty. ActaOrthop Scand 2003;74(6):665–9.
[57] Benoni G, Fredin H, Knebel R, Nilsson P. Blood conservation with tranexamic acidin total hip arthroplasty. Acta Orthop Scand 2001;72(5):442–8.
[58] Hiippala S, Strid L, Wennestrand M, Arvela V, Mäntylä S, Ylinen J, et al. Tranexamicacid (Cyklokapron) reduces perioperative blood loss associated with total kneearthroplasty. Br J Anaesth 1995;74:534–7.
[59] Garneti N, Field J. Bone Bleeding During Total Hip Arthroplasty After Administra-tion of Tranexamic Acid. J Arthroplast 2004;19(4):488–93.
[60] Good L, Peterson E, Lisander B. Tranexamic acid decreases external blood loss butnot hidden blood loss in total knee replacement. Br J Anaesth 2003;90(5):596–9.
[61] Hiippala ST, Strid LJ, Wennerstrand MI, Arvela JVV, Niemelä HM, Mäntylä SK, et al.Tranexamic Acid Radically Decreases Blood Loss and Transfusions Associated withTotal Knee Arthroplasty. Anesth Analg 1997;84:839–44.
[62] Jansen AJ, Andreica S, Claeys M, D'Haese, Camu F, Jochmans K. Use of tranexamicacid for an effective blood conservation strategy after total knee arthroplasty. Br JAnaesth 1999;83(4):596–601.
[63] Zohar E, Ellis M, Ifrach N, Stern A, Sapir O, Fredman B. The Postoperative Blood-Sparing Efficacy of Oral Versus Intravenous Tranexamic Acid After Total KneeReplacement. Anesth Analg 2004;99:1670–83.
[64] Tanaka N, Sakahashi H, Sato E, Hirose K, Ishima T, Ishii S. Timing of theadministration of tranexamic acid for maximum reduction in blood loss inarthroplasty of the knee. J Bone Joint Surg [Br] 2001;83B:702–5.
[65] Niskanen RO, Korkala OL. Tranexamic acid reduces blood loss in cemented hiparthroplasty. Acta Orthop 2005;26(6):829–32.
[66] Orpen NM, Little C, Walker G, Crawford EJP. Tranexamic acid reduces early post-operative blood loss after total knee arthroplasty: A prospective randomizedcontrolled trial of 29 patients. The Knee 2006;13:106–10.
[67] Janssens M, Joris J, David JL, Lemaire R, Lamy M. High Dose Aprotinin ReducesBlood Loss in Patients Undergoing Total Hip Replacement Surgery. Anesthesiology1994;80:23–9.
[68] Thorpe CM, Murphy WG, Logan M. Use of aprotinin in knee replacement surgery.Br J Anaesth 1994;73:408–10.
[69] Compostella FA, Marcante P, Marcate S, Dosso P. High dose aprotinin in electivetotal HIP replacement surgery: Effects on bleeding and renal function. Br J Anaesth1997;78(Suppl1):66.
[70] Hayes A, Murphy DB, McCarroll M. The Efficacy of Single-Dose Aprotinin 2 MillionKIU in Reducing Blood Loss and Its Impact on the Incidence of Deep VenousThrombosis in Patients Undergoing Total Hip Replacement Surgery. J Clin Anesth1996;8:357–60.
[71] Petsatodis G, Samoladas E, Christodoulou A, Hatzokos I, Pournaras I. Does AprotininReduce Blood Loss in Total Hip Arthroplasty? Proquest Nurs J 2006;29(1):75–7.
[72] Harley BJ, Beaupré LA, Jones A, Cinats JG, Guenther CR. The effect of epsilonaminocaproic acid on blood loss in patients who undergo primary total hipreplacement: a pilot study. Can J Surg 2002;45(3):185–90.
[73] Camarasa MA, Ollé G, Serra-Prat M, Martín A, Sánchez, Ricós P, et al. Efficacy ofaminocaproic, tranexamic acids in the control of bleeding during total kneereplacement: a randomized clinical trial. Br J Anaesth 2006;96:576–82.
[74] Mackinnon A. A spreadsheet for the calculation of comprehensive statistics forthe assessment of diagnostic tests and inter-rater agreement. Comput Biol Med2000;30(3):127–34.
[75] Mercuriali F, Inghilleri G. Transfusion risks and limitations. Minerva Anestesiol1999;65(5):286–92.
[76] Nielsen HJ. Detrimental effects of perioperative blood transfusion. Br J Surg1995;82(5):582–7.
[77] Sehat KR, Evans R, Newman JH. How much blood is really lost in total kneearthroplasty? Correct blood management should take hidden loss into account.The Knee 2005;7(3):151–5.
[78] Schneeweiss S, Seeger JD, Landon J, Walker AM. Aprotinin during Coronary-ArteryBypass Grafting and Risk of Death. N Engl J Med 2008;358(8):771–83.
[79] Fergusson DA, et al. A Comparison of Aprotinin and Lysine Analogues in High-RiskCardiac Surgery. N Engl J Med 2008;358(22):2319–31.
[80] Ray WA, Stein CM. The Aprotinin Story – Is BART the Final Chapter? N Engl J Med2008;358(22):2398–9.
Copyright © 2022 FDOKUMEN




















