Plasma C20-Sphingolipids predict cardiovascular events independently from conventional...
6
Plasma C 20 -Sphingolipids predict cardiovascular events independently from conventional cardiovascular risk factors in patients undergoing coronary angiography Alaa Othman a, b, c , Christoph H. Saely d, e, f , Axel Muendlein d, e, f , Alexander Vonbank d, e, f , Heinz Drexel d, e, f, g , Arnold von Eckardstein a, b , Thorsten Hornemann a, b, * a Institute for Clinical Chemistry, University Hospital Zurich, R€ amistrasse 100, 8091 Zurich, Switzerland b Centre for Integrative Human Physiology, University of Zurich, Zurich, Switzerland c Institute of Experimental and Clinical Pharmacology and Toxicology, University of Lübeck, Lübeck, Germany d Vorarlberg Institute for Vascular Investigation and Treatment (VIVIT), Feldkirch, Austria e Department of Medicine and Cardiology, Academic Teaching Hospital Feldkirch, Feldkirch, Austria f Private University of the Principality of Liechtenstein, Triesen, Liechtenstein g Drexel University College of Medicine, Philadelphia, PA, USA article info Article history: Received 3 November 2014 Received in revised form 9 March 2015 Accepted 9 March 2015 Available online 14 March 2015 Keywords: Predictive biomarker Risk factor Coronary artery disease Myocardial infarction Stroke Atypical sphingolipids Serine-palmitoyltransferase C 20 Sphingosine abstract Aims: Sphingolipids are emerging as novel players in the pathogenesis of atherosclerosis and cardio- vascular disease. Serine palmitoyltransferase (SPT) catalyzes the first and rate-limiting step in the de novo synthesis of sphingolipidsdthe condensation of palmitoyl-CoA and L-Serine. In addition to these canonical substrates, SPT can also metabolize other acyl-CoAs and amino acids, thus generating a variety of atypical sphingoid bases. In this study, we investigated the association of these atypical sphingoid bases with the presence of angiographically characterized coronary artery disease (CAD) as well as their ability to predict the incidence of cardiovascular events. Methods and results: 349 subjects, who underwent coronary angiography for the evaluation of estab- lished or suspected stable CAD, were enrolled in the study at baseline and followed up for cardiovascular events over a period of 8 years (median 7.7 years). The sphingoid base profile in the extracted plasma sphingolipids were determined by LC/MS after acid-base hydrolysis. Plasma levels of C 18 SAdiene were found to be significantly lower in CAD patients at baseline, while levels for C 16 SA, C 16 SO, C 17 SO, C 18 SA, C 18 SO, and C 19 SO and 1-deoxy sphingoid bases were not different. In the prospective analysis C 20 SO significantly predicted cardiovascular events (standardized adjusted HR ¼ 1.20, CI 95% [1.03e1.41]; p ¼ 0.022) after adjusting for traditional risk factors, the use of lipid-lowering drugs and angiographically-determined CAD at baseline. Conclusion: Plasma C 20 SO levels are independent predictive biomarkers for cardiovascular events, even after adjusting for cardiovascular risk factors including coronary stenosis. © 2015 Elsevier Ireland Ltd. All rights reserved. 1. Introduction Sphingolipids are essential components of plasma membranes and lipoproteins and have been shown to be involved in the development of atherosclerosis [1]. Elevated plasma sphingomyelin levels were found in patients with coronary artery disease (CAD) [2] and have been suggested to be associated with subclinical athero- sclerosis [3]. Sphingolipid formation is typically initiated by the conjugation of L-serine and palmitoyl-CoA, a reaction catalyzed by the enzyme serine palmitoyltransferase (SPT). SPT is a heteromeric protein that is composed of the three subunitsdSPTLC1, SPTLC2 and SPTLC3 (Suppl. Fig. 1). Besides palmitoyl-CoA the SPT can also metabolize other acyl-CoAs thereby generating a spectrum of atypical C 14 eC 20 sphingoid bases [4]. It is not fully understood how this shift in the acyl-CoA preference is regulated but it has been demonstrated that primarily the SPTLC3 subunit of SPT is respon- sible for the use of other acyl-CoAs [5,6]. Variants of the SPTLC3 * Corresponding author. Inst. for Clinical Chemistry, University Hospital Zürich, Raemistrasse 100, 8091 Zürich, Switzerland. E-mail address: [email protected] (T. Hornemann). Contents lists available at ScienceDirect Atherosclerosis journal homepage: www.elsevier.com/locate/atherosclerosis http://dx.doi.org/10.1016/j.atherosclerosis.2015.03.011 0021-9150/© 2015 Elsevier Ireland Ltd. All rights reserved. Atherosclerosis 240 (2015) 216e221
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Plasma C20-Sphingolipids predict cardiovascular events independently from conventional...

lable at ScienceDirect
Atherosclerosis 240 (2015) 216e221
Contents lists avai
Atherosclerosis
journal homepage: www.elsevier .com/locate/atherosclerosis
Plasma C20-Sphingolipids predict cardiovascular events independentlyfrom conventional cardiovascular risk factors in patients undergoingcoronary angiography
Alaa Othman a, b, c, Christoph H. Saely d, e, f, Axel Muendlein d, e, f, Alexander Vonbank d, e, f,Heinz Drexel d, e, f, g, Arnold von Eckardstein a, b, Thorsten Hornemann a, b, *
a Institute for Clinical Chemistry, University Hospital Zurich, R€amistrasse 100, 8091 Zurich, Switzerlandb Centre for Integrative Human Physiology, University of Zurich, Zurich, Switzerlandc Institute of Experimental and Clinical Pharmacology and Toxicology, University of Lübeck, Lübeck, Germanyd Vorarlberg Institute for Vascular Investigation and Treatment (VIVIT), Feldkirch, Austriae Department of Medicine and Cardiology, Academic Teaching Hospital Feldkirch, Feldkirch, Austriaf Private University of the Principality of Liechtenstein, Triesen, Liechtensteing Drexel University College of Medicine, Philadelphia, PA, USA
a r t i c l e i n f o
Article history:Received 3 November 2014Received in revised form9 March 2015Accepted 9 March 2015Available online 14 March 2015
Keywords:Predictive biomarkerRisk factorCoronary artery diseaseMyocardial infarctionStrokeAtypical sphingolipidsSerine-palmitoyltransferaseC20Sphingosine
* Corresponding author. Inst. for Clinical ChemistrRaemistrasse 100, 8091 Zürich, Switzerland.
E-mail address: [email protected] (T. H
http://dx.doi.org/10.1016/j.atherosclerosis.2015.03.0110021-9150/© 2015 Elsevier Ireland Ltd. All rights rese
a b s t r a c t
Aims: Sphingolipids are emerging as novel players in the pathogenesis of atherosclerosis and cardio-vascular disease. Serine palmitoyltransferase (SPT) catalyzes the first and rate-limiting step in the denovo synthesis of sphingolipidsdthe condensation of palmitoyl-CoA and L-Serine. In addition to thesecanonical substrates, SPT can also metabolize other acyl-CoAs and amino acids, thus generating a varietyof atypical sphingoid bases. In this study, we investigated the association of these atypical sphingoidbases with the presence of angiographically characterized coronary artery disease (CAD) as well as theirability to predict the incidence of cardiovascular events.Methods and results: 349 subjects, who underwent coronary angiography for the evaluation of estab-lished or suspected stable CAD, were enrolled in the study at baseline and followed up for cardiovascularevents over a period of 8 years (median 7.7 years). The sphingoid base profile in the extracted plasmasphingolipids were determined by LC/MS after acid-base hydrolysis. Plasma levels of C18SAdiene werefound to be significantly lower in CAD patients at baseline, while levels for C16SA, C16SO, C17SO, C18SA,C18SO, and C19SO and 1-deoxy sphingoid bases were not different. In the prospective analysis C20SOsignificantly predicted cardiovascular events (standardized adjusted HR ¼ 1.20, CI 95% [1.03e1.41];p ¼ 0.022) after adjusting for traditional risk factors, the use of lipid-lowering drugs andangiographically-determined CAD at baseline.Conclusion: Plasma C20SO levels are independent predictive biomarkers for cardiovascular events, evenafter adjusting for cardiovascular risk factors including coronary stenosis.
© 2015 Elsevier Ireland Ltd. All rights reserved.
1. Introduction
Sphingolipids are essential components of plasma membranesand lipoproteins and have been shown to be involved in thedevelopment of atherosclerosis [1]. Elevated plasma sphingomyelinlevels were found in patients with coronary artery disease (CAD) [2]
y, University Hospital Zürich,
ornemann).
rved.
and have been suggested to be associated with subclinical athero-sclerosis [3]. Sphingolipid formation is typically initiated by theconjugation of L-serine and palmitoyl-CoA, a reaction catalyzed bythe enzyme serine palmitoyltransferase (SPT). SPT is a heteromericprotein that is composed of the three subunitsdSPTLC1, SPTLC2and SPTLC3 (Suppl. Fig. 1). Besides palmitoyl-CoA the SPT can alsometabolize other acyl-CoAs thereby generating a spectrum ofatypical C14eC20 sphingoid bases [4]. It is not fully understood howthis shift in the acyl-CoA preference is regulated but it has beendemonstrated that primarily the SPTLC3 subunit of SPT is respon-sible for the use of other acyl-CoAs [5,6]. Variants of the SPTLC3

A. Othman et al. / Atherosclerosis 240 (2015) 216e221 217
gene were shown in two previous GWAS studies to be associatedwith differences in the plasma levels of several sphingomyelinspecies [7], as well as with an increased risk for myocardialinfarction [8]. Also, two small proteins (ssSPTa/b) which interactwith SPT were reported to modulate the affinity of SPT for variousacyl-CoA substrates [9,10]. Besides other acyl-CoAs the SPT can alsometabolize L-alanine and glycine under certain conditions. Thisforms a category of atypical 1-deoxysphingolipids (1-deoxySLs)which are involved in the pathogenesis of the inherited neuropathyHSAN1 [11,12]. As the metabolic precursors for serine, alanine andglycine emerge from the glycolysis, the SPT reaction provides afunctional link between fatty acid and carbohydrate metabolism.We demonstrated previously that 1-deoxySLs plasma levels aresignificantly elevated in metabolic syndrome (MetS) [13] and dia-betes type 2 (T2DM) [14], two major risk factors for cardiovasculardisease [15]. In this paper we explored the potential of atypicalsphingoid bases as biomarkers in cardiovascular disease.
2. Methods
2.1. Patients and study design
For the study, we enrolled 349 individuals who underwentcoronary angiography for the evaluation of established or sus-pected stable CAD [16] between September 1999 and October 2000.Anthropometric data, clinical chemistry laboratory parameters andcoronary angiography (Judkin's technique) was determined for allstudy participants at baseline. The Ethics Committee of the Uni-versity of Innsbruck approved the current study, and all partici-pants gavewritten informed consent. Patients with coronary arterystenoses �50% were diagnosed with significant CAD. The extent ofCAD was defined as the number of significant coronary stenoses ina given patient.
T2DM was diagnosed according to World Health Organisation(WHO) criteria [17] (Fasting glucose levels �7 mmol/l; plasmaglucose levels �11.1 mmol/l 2 h after an oral glucose challenge(75 g) or a previous diagnosis of T2DM by a physician).
Metabolic syndrome was defined according to the criteria of theNational Cholesterol Education Program-Adult Treatment Panel III[18]. Metabolic syndrome was present when three or more of thefollowing criteria were met: waist circumference >102 cm in menor >88 cm in women; triglycerides �1.7 mmol/l (150 mg/dl); HDL-cholesterol <1.0 mmol/l (40 mg/dl) in men or <1.3 mmol/l (50 mg/dl) in women; blood pressure �130/�85 mmHg; and fastingglucose �6.1 mmol/l (110 mg/dl).
Patients were followed-up over a period of 8 years forcardiovascular-related events, including non-fatal myocardialinfarction, non-fatal stroke, need for a coronary artery bypass graft,percutaneous coronary intervention, non-coronary vascular sur-gery, and mortality due to cardiac or non-cardiac vascular reasons.Out of the 349 patients, three had missing data for the date of lastcontact and were excluded from the prospective analysis. Datawere collected both from patient records and from standardizedinterviews, and were cross-checked between these sources.
2.2. Clinical chemistry
Venous blood samples were collected after overnight fastingand at least 12 h before angiography. Laboratory analysis was per-formed on fresh serum or blood samples. HbA1c was analyzed byhigh-performance liquid chromatography (HPLC) on a Menarini-Arkray KDK HA 8140 (Arkray KDK, Kyoto, Japan). Triacylglycerols,total cholesterol, HDL and other clinical chemistry variables weremeasured on Hitachi 717 or 911 systems (Roche).
2.3. Sphingolipid analysis
The sphingoid base profile was analyzed as described before[13], with some minor modifications. Briefly, 0.5 ml methanolincluding 200 pmol of the internal standards d7-sphingosine andd7-sphinganine (d7SA, d7SO; Avanti Polar Lipids, Alabaster,Alabama, USA) was added to 100 ml of plasma. Lipids wereextracted for 1 h under constant agitation at 37 �C. Precipitatedproteins were pelleted by centrifugation and the supernatanttransferred to a new tube. For lipid hydrolysis, 75 ml of meth-anolic HCl (1 N HCl and 10 M H2O in methanol) was added to thesupernatant and incubated for 16 h at 65 �C followed by theaddition of 100 ml of 10 M KOH. To this mix, 625 ml chloroformwas added followed by 100 ml 2 N ammonium hydroxide and0.5 ml alkaline water. The mixture was intensively vortexed andphases were separated by centrifugation at 16,000 g for 5 min.The upper phase was removed and the lower organic phasewashed three times with alkaline water (500 ml NH4OH (25%) in250 ml H2O). Finally, the lipids were dried under N2 and storedat �20 �C until analysis.
The sphingoid bases were separated on a C18 column (Uptispere120 Å, 5 mm, 125 � 2 mm, Interchim, Montluçon, France) andanalyzed on a TSQ Quantum Ultra mass spectrometer (Thermo,Reinach, BL, Switzerland). Each sample was measured as asingleton. Intra- and Inter-assay coefficient of variation (CV%) of themethod was between 5% and 20%.
Plasma sphingoid bases are usually N-acylated and conjugatedto different head groups, giving rise to a great variety of differentsphingolipid species. In this study, weweremostly interested in thesphingoid base composition of the plasma sphingolipidome.Therefore, the N-acyl chains and head groups were removed byhydrolysis prior LC/MS analysis. Hence, it is important to note thatthe here reported sphingoid base concentrations reflect the totalsphingoid base composition for all the individual sphingolipidsub classes (e.g. ceramides, sphingomyelins, glycosphingolipidsetc.).
2.4. Statistical analysis
Continuous variables were log-transformed and themeanswerecompared using the two-sided t-test. Categorical variables werecompared using the Chi-square test. Prospective analysis of car-diovascular events was done using KaplaneMeier curves and Coxhazard regression models (univariate and multivariate). Contin-uous variables were standardized in standard deviation units bysubtracting each value from the average and then dividing it by thestandard deviation. Hazard ratios are reported per increase of onestandard deviation. Univariate Cox regression models were calcu-lated to evaluate the predictive potential of each variable. Multi-variate Cox regression models were performed to evaluate thepredictive role of individual variables after adjusting for other sig-nificant variables from the univariate model (with a hazard ratio(HR) lower limit of 95% CI > 1.00). The model was adjusted for age,sex, history of smoking, HDL-C, waist-to-hip ratio, HbA1c, creati-nine, GFR, CRP, systolic and diastolic blood pressure, the use oflipidelowering drugs (including statins and fibrates) and the extentof CAD determined by angiography. Schoenfeld residuals werecalculated for each of the covariates and plotted against time-to-event to visually check for the fulfillment of the proportionalityassumption and linear regression models using the Schoenfeldresiduals as dependent variables weremade. None of the covariatesshowed major violation of the proportionality assumption. Statis-tical analyses were performed in SPSS16.0 (IBM, Zurich,Switzerland).

A. Othman et al. / Atherosclerosis 240 (2015) 216e221218
3. Results
Baseline characteristics of the study cohort showed significantdifferences in cardiovascular risk factors between individuals with
Table 1Baseline and cardiovascular event rates of patients with (CADþ) and without(CAD�) coronary artery disease.
CAD� (n ¼ 134) CADþ (n ¼ 215) p
Age (years) 61.8 ± 9.9 63.5 ± 10.2 0.151Sex (Female) (%) 64 (47.77%) 48 (22.33%) <0.001Hypertension (WHO) 69 (51.5%) 112 (52.1%) 0.913T2DM (%) 35 (26.12%) 76 (35.35%) 0.072History of smoking (%) 64 (47.77%) 147 (68.38%) <0.001Extent of CAD
(no. of stenoses)0 2.4 ± 1.4
MetS ATP III Definition (%) 52 (38.81%) 102 (47.45%) 0.114BMI (kg/m2) 28.0 ± 4.5 26.8 ± 4.2 0.016Waist circumference (cm) 96.2 ± 13.8 95.7 ± 10.9 0.935Waist-to-Hip ratio 0.94 ± 0.10 0.96 ± 0.08 0.026Cholesterol (mmol/l) 5.7 ± 1.0 5.5 ± 1.2 0.080LDL-C (mmol/l) 3.4 ± 0.8 3.3 ± 1.0 0.178HDL-C (mmol/l) 1.4 ± 0.5 1.1 ± 0.3 <0.001Triglycerides (mmol/l) 1.8 ± 1.5 2.0 ± 1.2 0.001Glucose (mmol/l) 6.5 ± 2.0 7.0 ± 2.6 0.035HbA1c (%) 6.2 ± 1.1 6.5 ± 1.2 0.007Insulin (mU/ml) 11.8 ± 8.9 13.6 ± 14.7 0.439HOMA-IR 3.4 ± 2.6 4.4 ± 4.8 0.089Systolic BP (mm Hg) 137.7 ± 24.2 136.4 ± 20.9 0.739Diastolic BP (mm Hg) 80.4 ± 12.6 78.1 ± 12.5 0.088CRP (mg/dl) 0.8 ± 1.4 0.9 ± 1.3 0.282S. Potassium (mmol/l) 4.3 ± 0.4 4.4 ± 0.5 0.089S. Creatinine (mg/dl) 1.1 ± 0.5 1.2 ± 0.7 0.002GFR (Mayo) 87.7 ± 19.1 84.5 ± 21.4 0.139T2DM treatment (%) 35 (26.12%) 76 (35.35%) 0.071Diuretics (%) 54 (40.3%) 69 (32.1%) 0.118Anti-hypertensive drugs (%) 101 (75.38%) 184 (85.59%) 0.016Lipid lowering drugs (%) 41 (30.6%) 134 (62.33%) <0.001Plasma SphingolipidsC16SO (mmol/l) 15.47 ± 4.83 14.52 ± 5.68 0.050C16SA (mmol/l) 0.49 ± 0.22 0.46 ± 0.25 0.080C17SO (mmol/l) 8.09 ± 2.5 7.57 ± 2.72 0.040C18PhytoSO (mmol/l) 0.12 ± 0.04 0.12 ± 0.05 0.176C18SAdiene (mmol/l) 29.23 ± 7.80 26.35 ± 7.73 <0.001C18SO (mmol/l) 96.44 ± 17.84 90.51 ± 21.75 0.001C18SA (mmol/l) 3.64 ± 1.42 3.25 ± 1.48 0.002C19SO (mmol/l) 2.80 ± 1.16 2.80 ± 1.24 0.752C20SO (mmol/l) 0.18 ± 0.06 0.18 ± 0.06 0.922C20SA (mmol/l) 0.03 ± 0.02 0.03 ± 0.01 0.4761-deoxySO (mmol/l) 0.18 ± 0.11 0.18 ± 0.12 0.4711-deoxySA (mmol/l) 0.08 ± 0.04 0.08 ± 0.05 0.191Cardiovascular eventsTotal (cumulative)
cardiac and vascularevents (n ¼ 126)
28 (20.9%) 98 (45.58%) <0.001
Mortality due to cardiacor vascular reasons(n ¼ 69)
19 (14.18%) 50 (23.26%) 0.38
Non-fatal myocardialinfarction (n ¼ 26)
2 (1.49%) 24 (11.16%) <0.001
Non-fatal stroke (n ¼ 19) 5 (3.73%) 14 (6.51%) 0.266Coronary artery bypass
graft (n ¼ 18)1 (0.75%) 13 (6.05%) 0.014
Percutaneous coronaryintervention (n ¼ 48)
6 (4.48%) 42 (19.53%) <0.001
Peripheral vascular surgery(non-coronary) (n ¼ 24)
8 (5.97%) 16 (7.44%) 0.597
Values are shown as mean ± SD for the continuous variables and numbers andpercentage of total for the categorical variables. p values were calculated usingunpaired two sided t-tests on the log transformed continuous variables. For thecategorical variables, the p valuewas calculated using the Chi square test. Bonferronicorrection for multiple comparisons was applied (level of statistical significance isp < 0.001). Variables in bold are significant after the Bonferroni correction. CAD,coronary artery disease, MetS, metabolic syndrome HOMA-IR, Homeostatic modelassessment-insulin resistance, K, serum potassium, CRP, C-reaction protein, GFR(Mayo) Glomerular filtration rate (Mayo equation).
significant coronary artery disease (CADþ) and subjects who didnot have significant CAD (CAD�) (Table 1). In the CAD þ group thenumber of males (p < 0.001) and smokers (p < 0.001) was signifi-cantly higher whereas HDL-C was significantly lower in theCAD þ group (p < 0.001). Plasma LDL-C was not significantlydifferent among the CADþ and CAD� groups as a result of thetreatment with lipid-lowering drugs and the use of lipid-loweringdrugs was significantly higher in the CADþ group (p < 0.001).
The concentrations of the individual sphingoid bases at baselineare shown in Table 1. In CADþ patients, plasma levels of C18SAdienewas significantly lower than in controls (p < 0.001). Plasma levels ofC17SO, C18SA and C18SO were by trend different among the groupsbut did not reach the significance limit after the correction formultiple comparisons. In contrast, plasma concentrations of C16,C19, and C20- sphingoid bases, as well as 1-deoxy sphingoid bases,were not significantly different between the groups at baseline.
During follow-up, 126 individuals (36%) suffered from vascularevents (Table 1). This included mortality due to cardiac or vascularreasons, non-fatal MI, non-fatal stroke, coronary artery bypassgraft, percutaneous coronary intervention and peripheral vascularsurgery. As expected, MI (p < 0.01), coronary artery bypass graft(p< 0.05), percutaneous coronary intervention (p < 0.001) and totalcardiovascular events (p < 0.001) were significantly increased inthe CADþ group. Interestingly, stroke, peripheral vascular surgeryand mortality were not significantly different between CADþ andCAD� groups. This is mainly due the fact that CAD diagnosis wasdone by coronary angiography which does not necessarily reflectthe atherosclerotic state of the carotids or peripheral vessels.
We then compared the plasma sphingoid base backbones inpatients with and without cardiovascular events (Table 2). C20SOplasma levels were significantly elevated in patients with cardio-vascular events (p < 0.05) while C18SAdiene levels were signifi-cantly lower in the same group (p < 0.05). All other sphingoid basedwere not significantly different.
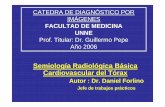
To evaluate the predictive potential of plasma sphingoid baseswe used both univariate and multivariate approaches. In the uni-variate approach, plasma levels of C20SO were significantly asso-ciated with total cardiovascular event risk (Fig. 1A). In contrast,plasma levels of C18SAdine were inversely associated with totalcardiovascular events (Fig. 1B), (log rank p < 0.05 comparing pa-tients with higher and lower than median plasma levels). Univar-iate Cox regression models (Table 3) showed similar results with asignificant standardized HR for C20SO (1.18, CI 95% [1.02e1.37];p < 0.05) and C18SAdiene (0.79 CI 95% [0.66e0.95]; p < 0.05). Othersphingoid bases did not show any significant association with totalcardiovascular events. Traditional risk factor such as male sex,
Table 2Plasma sphingoid bases in patient with and without cardiovascular events.
No cumulative events(n ¼ 223)
Cumulative events(n ¼ 126)
p
C16SO 15.03 ± 5.55 14.63 ± 5.07 0.634C16SA 0.48 ± 0.25 0.45 ± 0.23 0.119C17SO 7.92 ± 2.82 7.5 ± 2.29 0.291C18PhytoSO 0.12 ± 0.05 0.11 ± 0.04 0.104C18SAdiene 28.25 ± 8.4 26.04 ± 6.65 <0.05C18SO 93.03 ± 21.32 92.33 ± 19.09 0.810C18SA 3.43 ± 1.46 3.35 ± 1.43 0.384C19SO 2.77 ± 1.24 2.84 ± 1.14 0.372C20SO 0.17 ± 0.06 0.18 ± 0.05 <0.05C20SA 0.03 ± 0.01 0.03 ± 0.01 0.481doxSO 0.18 ± 0.12 0.18 ± 0.1 0.933doxSA 0.08 ± 0.05 0.08 ± 0.04 0.464
Values are shown as mean ± SD. p values were calculated using the unpaired twosided t-test on the log transformed variables. Variables in bold were significant(p < 0.05).
Fig. 1. Univariate Kaplan Meier plots (A and B) for plasma C20SO and C18SAdiene. The cohort was sorted into two groups; higher (red) and lower (blue) than the median values ofC20SO and C18SAdiene, respectively. The table below shows the number of patients at risk at 0, 2, 4, 6 and 8 years for each group. P values were calculated using log rank test. (Forinterpretation of the references to color in this figure legend, the reader is referred to the web version of this article.)
A. Othman et al. / Atherosclerosis 240 (2015) 216e221 219
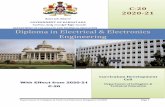
smoking, waist to hip ratio, HDL-C, HbA1c, CRP and GFR weresignificantly associated with total cardiovascular events(Supplementary Table 1). Multivariate Cox hazard regressionmodels were used to adjust for those cardiovascular risk factorsthat were significant in the univariate models as well as othertraditional risk factors and lipid lowering drugs. After adjusting themodels to these predictors, C20SO remained significantly associatedwith the risk to develop cumulative cardiovascular events (adjustedstandardized HR (1.20, CI 95% [1.03e1.41]; p < 0.05), whereasC18SAdiene did not (Fig. 2). It is noteworthy that all the variables inthis model fulfilled the proportionality assumption of Cox propor-tional hazard regression including those factors that are known toaffect plasma lipids such as sex and the use of lipid-lowering drugs.Therefore a further stratification based on sex or the use of lipidlowering drugs is not necessary and would yield to similar results.Interestingly, while C20SO was a significant predictor of for car-diovascular events, its baseline levels were not significantlydifferent between the CADþ and CAD� groups.
Table 3Univariate Cox hazard regression models for total cardiovascular events.Continuous variables were log-transformed and standardized into units of standarddeviation (SD). Hazard ratios are expressed as increases of SD units.
HR (95% CI) per 1 SD p
C16SO 0.9(0.75e1.08) 0.247C16SA 0.87(0.72e1.07) 0.168C17SO 0.85(0.71e1.02) 0.072C18PhytoSO 0.87(0.72e1.06) 0.143C18SAdiene 0.79(0.66e0.95) <0.05C18SO 0.96(0.81e1.15) 0.642C18SA 0.95(0.79e1.15) 0.593C19SO 1.02(0.86e1.21) 0.857C20SO 1.18(1.02e1.37) <0.05C20SA 0.98(0.82e1.18) 0.8101-deoxySO 1(0.84e1.18) 0.9321-deoxySA 0.95(0.79e1.14) 0.553
4. Discussion
Here we investigated the association of plasma sphingoid baseswith coronary atherosclerosis and their ability to predict cardio-vascular events. At baseline, we found plasma levels of C18SAdiene
Fig. 2. Adjusted Cox hazard regression models for the plasma sphingoid bases aspredictors for total cardiovascular events. The Forest plot shows the hazard ratio (filledcircle) and the 95% CI as horizontal error bar for the individual plasma sphingoid bases.Models were built using the standardized variables. Each bar represents a different Coxregression model for the individual sphingoid base and was adjusted for age, sex,smoking, HDL, waist-to-hip ratio, HbA1c, creatinine, GFR, CRP, systolic and diastolicblood pressure, the use of lipid lowering drugs and the extent of coronary arterystenosis as graded by angiography. **p < 0.05.

A. Othman et al. / Atherosclerosis 240 (2015) 216e221220
to be significantly lower in CAD patients while the levels of othersphingoid bases were not different compared to the control group.This seems to contradict earlier reports which showed increasedplasma sphingomyelin (SM) levels in patients with CAD [2,3] or nosignificant association of plasma SM with incident CAD events[19,20]. However, in contrast to these earlier reports, our study didnot focus on SM levels but on the sphingoid base composition oftotal plasma sphingolipids. Although ~95% of the sphingolipids inplasma are sphingomyelins [21], only 60% of the total plasmasphingomyelins contain a C18SO backbone [21]. In the previousstudies, total SM levels were determined enzymatically by therelease of phosphocholine after treatment with sphingomyelinase[22]. Such assay cannot detect alterations in the sphingoid basecomposition. A recent lipidomic analysis of plasma from patientswith stable and unstable CAD showed that certain sphingomyelinsubspecies were decreased while others were increased in CADcompared to controls [23]. In contrast, our study focused on thesphingoid base composition of all plasma sphingolipids, includingceramides and glycosphingolipids. This highlights the importanceof considering both the sphingoid base backbone and the N-acylchain of plasma sphingolipids, as these are of different metabolicorigin and may play different roles in CAD.
Cross sectional at baseline, we did not see a difference in theC20SO levels between CAD patients and controls. However, theprospective analysis of the follow-up data showed that low levels ofC18SAdiene and increased levels of C20SO at baseline were predic-tive for the risk to develop cardiovascular events. Even afteradjusting for cardiovascular risk factors, including the extent ofCAD as determined by angiography C20SO levels remained signifi-cant predictors for CAD. From a statistical point, this indicates thatplasma C20SO levels are reflecting the risk for cardiovascular eventsindependent of the atherosclerotic burden which is typicallyassessed by angiography as a gold standard.
C20SO is a minor component of plasma sphingolipids and re-flects less than 1% of the total sphingoid bases in plasma [21]. Thepresence of a C20SO backbone was reported in gangliosides of ratand human brains [24], in gangliosides of human stomach mucosa[25] and in SM of rat liver [26]. The concentration of C20SO wasshown to increase with age in human and rat brains [24,27] andusing imaging mass spectrometry, C20-based sphingolipids wereshown to exist in distinct areas of the rat hippocampus dependingon age [28]. Little is known about the source of C20SO in plasma andits regulation and metabolism. It was shown that SPT can also usestearoly-CoA as a substrate to form C20-based sphingolipids [29].This reaction is likely mediated by the SPTLC3 subunit of SPT whichwas shown previous to be associated with increased risk formyocardial infarction [8].
A major strength of the here presented study is the combinationof an angiography-based CAD diagnosis with a prospective follow-up investigation. However, with respect to the limitations, it isimportant to consider that the analyzed cohort might not faithfullyrepresent the risk in the general population. Therefore, the pre-dictive potential of C20SO for the general population needs to beverified in a larger and lower risk cohort. Also the possible contri-bution of diet and physical activity on plasma C20SO levels needs tobe evaluated in follow up studies. However, the extrapolations ofthe risk predictions might nevertheless be relevant to clinical set-tings where the prevalence of cardiovascular disease is high. Theobservation that, by trend C18SAdiene was inversely associatedwith total cardiovascular events argues for a protective effect of thismetabolite and warrants further investigations on the use ofC18SAdiene as a neutraceutical in functional food compositions[30].
In summary, we demonstrated that increased levels of C20SO areindependent and predictive biomarkers for the risk to develop
cardiovascular events. Elucidating the underlying metabolicmechanisms which link changes in sphingolipid metabolism withthe increased risk for cardiovascular events is therefore of scientificand clinical importance.
Conflict of interest
There are no conflicts of interest to disclose.
Acknowledgments
We specially thank Irina Alecu for proofreading the manuscript.This work was supported by grants from the Zurich Center of
Integrated Human Physiology, University of Zurich (ZIHP); the 7thFramework Program of the European Commission (“RESOLVE”,Project number 305707) and “radiz”dRare Disease Initiative Zur-ich, University of Zurich.
Appendix A. Supplementary data
Supplementary data related to this article can be found at http://dx.doi.org/10.1016/j.atherosclerosis.2015.03.011.
References
[1] T. Hornemann, T.S. Worgall, Sphingolipids and atherosclerosis, Atherosclerosis226 (2013) 16e28.
[2] X.C. Jiang, F. Paultre, T.A. Pearson, et al., Plasma sphingomyelin level as a riskfactor for coronary artery disease, Arterioscler. Thromb. Vasc. Biol. 20 (2000)2614e2618.
[3] J.C. Nelson, X.C. Jiang, I. Tabas, et al., Plasma sphingomyelin and subclinicalatherosclerosis: findings from the multi-ethnic study of atherosclerosis, Am. J.Epidemiol. 163 (2006) 903e912.
[4] Y.A. Hannun, L.M. Obeid, Many ceramides, J. Biol. Chem. 286 (2011)27855e27862.
[5] T. Hornemann, S. Richard, M.F. Rütti, et al., Cloning and initial characterizationof a new subunit for mammalian serine-palmitoyltransferase, J. Biol. Chem.281 (2006) 37275e37281.
[6] T. Hornemann, A. Penno, M.F. Rütti, et al., The SPTLC3 subunit of serine pal-mitoyltransferase generates short chain sphingoid bases, J. Biol. Chem. 284(2009) 26322e26330.
[7] T. Illig, C. Gieger, G. Zhai, et al., A genome-wide perspective of genetic varia-tion in human metabolism, Nat. Genet. 42 (2010) 137e141.
[8] A.A. Hicks, P.P. Pramstaller, A. Johansson, et al., Genetic determinants ofcirculating sphingolipid concentrations in European populations, PLoS Genet.5 (2009) e1000672.
[9] G. Han, S.D. Gupta, K. Gable, et al., Identification of small subunits ofmammalian serine palmitoyltransferase that confer distinct acyl-CoA sub-strate specificities, Proc. Natl. Acad. Sci. U. S. A. 106 (2009) 8186e8191.
[10] J.M. Harmon, D. Bacikova, K. Gable, et al., Topological and functional charac-terization of the ssSPTs, small activating subunits of serine palmitoyl-transferase, J. Biol. Chem. 288 (2013) 10144e10153.
[11] A. Penno, M.M. Reilly, H. Houlden, et al., Hereditary sensory neuropathy type 1is caused by the accumulation of two neurotoxic sphingolipids, J. Biol. Chem.285 (2010) 11178e11187.
[12] N.C. Zitomer, T. Mitchell, K.A. Voss, et al., Ceramide synthase inhibition byfumonisin B1 causes accumulation of 1-deoxysphinganine: a novel categoryof bioactive 1-deoxysphingoid bases and 1-deoxydihydroceramides bio-synthesized by mammalian cell lines and animals, J. Biol. Chem. 284 (2009)4786e4795.
[13] A. Othman, M.F. Rutti, D. Ernst, et al., Plasma deoxysphingolipids: a novel classof biomarkers for the metabolic syndrome? Diabetologia 55 (2012) 421e431.
[14] M. Bertea, M.F. Rutti, A. Othman, et al., Deoxysphingoid bases as plasmamarkers in diabetes mellitus, Lipids Health Dis. 9 (2010) 84.
[15] Diabetes mellitus: a major risk factor for cardiovascular disease, A jointeditorial statement by the American Diabetes Association; The National Heart,Lung, and Blood Institute; The Juvenile Diabetes Foundation International;The National Institute of Diabetes and Digestive and Kidney Diseases; and TheAmerican Heart Association, Circulation 100 (1999) 1132e1133.
[16] H. Drexel, S. Aczel, T. Marte, et al., Is atherosclerosis in diabetes and impairedfasting glucose driven by elevated LDL cholesterol or by decreased HDLcholesterol? Diabetes Care 28 (2005) 101e107.
[17] M.M. Gabir, R.L. Hanson, D. Dabelea, et al., The 1997 American Diabetes As-sociation and 1999 World Health Organization criteria for hyperglycemia inthe diagnosis and prediction of diabetes, Diabetes Care 23 (2000) 1108e1112.
[18] National Cholesterol Education Program Expert Panel on Detection, E andTreatment of High Blood Cholesterol in, A, third report of the national

A. Othman et al. / Atherosclerosis 240 (2015) 216e221 221
cholesterol education program (NCEP) expert panel on detection, evaluation,and treatment of high blood cholesterol in adults (Adult treatment panel III)final report, Circulation 106 (2002), 3143e3421.
[19] A. Schlitt, S. Blankenberg, D. Yan, et al., Further evaluation of plasma sphin-gomyelin levels as a risk factor for coronary artery disease, Nutr. Metab.(Lond) 3 (2006) 5.
[20] J. Yeboah, C. McNamara, X.C. Jiang, et al., Association of plasma sphingomyelinlevels and incident coronary heart disease events in an adult population:multi-ethnic study of atherosclerosis, Arterioscler. Thromb. Vasc. Biol. 30(2010) 628e633.
[21] O. Quehenberger, A.M. Armando, A.H. Brown, et al., Lipidomics reveals aremarkable diversity of lipids in human plasma, J. Lipid Res. 51 (2010)3299e3305.
[22] M.R. Hojjati, X.C. Jiang, Rapid, specific, and sensitive measurements of plasmasphingomyelin and phosphatidylcholine, J. Lipid Res. 47 (2006) 673e676.
[23] P.J. Meikle, G. Wong, D. Tsorotes, et al., Plasma lipidomic analysis of stable andunstable coronary artery disease, Arterioscler. Thromb. Vasc. Biol. 31 (2011)2723e2732.
[24] A. Rosenber, N. Stern, Changes in sphingosine and fatty acid components of
gangliosides in developing rat and human brain, J. lipid Res. 7 (1966), 122-&.[25] A. Keranen, Fatty-acids and long-chain bases of gangliosides of human
gastrointestinal mucosa, Chem. Phys. lipids 17 (1976) 14e21.[26] A.H. Merrill, E. Wang, P.W. Wertz, Differences in the long-chain (Sphingoid)
base composition of sphingomyelin from rats Bearing Morris Hepatoma-7777,Lipids 21 (1986) 529e530.
[27] P. Palestini, M. Masserini, S. Sonnino, et al., Changes in the ceramidecomposition of rat Forebrain gangliosides with age, J. Neurochem. 54 (1990)230e235.
[28] Y. Sugiura, S. Shimma, Y. Konishi, et al., Imaging mass spectrometry tech-nology and application on ganglioside study; visualization of age-dependentaccumulation of C20-Ganglioside molecular species in the mouse Hippo-campus, PLoS One 3 (2008).
[29] V. Chigorno, M. Valsecchi, S. Sonnino, Biosynthesis of gangliosides containingC18:1 and C20:1 [3-14C]sphingosine after administrating [1-14C]palmiticacid and [1-14C]stearic acid to rat cerebellar granule cells in culture, Eur. J.Biochem. 221 (1994) 1095e1101.
[30] P. Scicchitano, M. Cameli, M. Maiello, et al., Nutraceuticals and dyslipidaemia:beyond the common therapeutics, J. Funct. Foods 6 (2014) 11e32.