
Fatty Acids, IL6, and TNFα Polymorphisms: An Example of Nutrigenetics in Crohn's Disease
Upload
independentCategory
view
1download
0
PergamonThrombosisResearch.Vol. 87, No. 6, pp. 539-546,1997
CopyrightO 1997Elsevier SciencxLtdPrimedin tie USA. AUrightsresa-ved
0049-3848/97 $17.00 + .00
PII S0049-3848(97)00183-7
PERSISTENCE OF HEMOSTATIC ALTERATIONS INPATIENTS AFFECTED BY CROHN’S DISEASE AFTER
BOWEL SURGERY
ElenaChiarantini,RosaVRIanzan01,AgatinaAlessan&lloLiottaz, AnnaPaolaCellai2,IsabellaWirP,DomenicoPrisco,ErniliaAntonucci,FrancescoTonellil,RosannaAbbate,IstitutodiClinicaMedicaGeneralee Cardiologia,IDipartimentodiFisiopatologiaclinica,
Uniti3di Chirurgia, Universitydi Firenze,zAziendaOspedalieraCareggi,Florence,Italy
(Received30June 1997byEditorM. Cattaneo;reviwd/accef.?ted24Juiy 1997)
ABSTRACTIn Crohn’sdisease (CD) a conditionof hypercoagulabilitywith increasedriskfor thrombotic events has been reported. In this study we have investigatedhemostaticparameters in thirty-onepatientsaffected by CD before, 3 and 12months after bowel operation, and in thirty healthy controls. Before surgeryplateletnumber(PLT), fibrinogen(Fbg), prothrombinfragment F1+2 (F1+2),PAI and whole blood-spontaneous platelet aggregation (WB-SPA) weresignificantlyhigher( pat leastcO.0005)in patientsthan in controls,whilefactorXIII (F XIII) was significantly lower (p at least <0.005). Three and twelvemonths after surgery PLT, FBG and WB-SPA significantly decreased incomparisonto pre-surgeryvalues(respectivelyp at [email protected] pcO.01),butPLTand Fbg were still significantlyhigherthan in controlsat 3 and 12months(p4.01). At threeand 12monthsafteroperationF XIII was significantlyhigherin comparison with pre-surgery values (p at least <0.05). The presence ofantiphospholipidantibodies(aPL) was not differentbetween CD patientsandcontrols before surgery, whereas it significantly increased 12 months aftersurgery(p&05). Our resultssuggestthat in CD hemostaticchangesare onlyin part influencedby localflogisticprocessesand thatan inflammatorysystemicconditionmayprovokeboththe boweland extraintesthudmanifestationsof CD.@1997Elsevier ScienceL/d
Key words:Crohn’sdisease,coagulation,fibrinolysis,antiphospholipidantibodiesCorresponding author: Elena Chiarantini MD, Istituto di Clinica Medica Generale eCardiologia,Universitydi Firenze,VialeMorgagni,85,50134 FIRENZE,Italy,Fax 0039-55-4378638,Phone0039-55-4277954
539
540 HEMOSTASISALTERATIONS Vol. 87, No. 6
Crohn’sdisease(CD)is a systemicdisorder,as indicated by the extraintestinalsymptomsand by the recurrenceof diseaseafter surgery,in which arterialand venousthromboticevents frequently occur (l). In CD a conditionof hypercoagulabilityhas been reported,independentlyof thepresenceof previousthromboticevents(2-12).A thrombophilicstatehas been supposedto be one of the pathogeneticfactors of disease, through multifocalintestinalmicroinfarctions(8).Also antiphospholipidantibodies(13-16)whichhavebeenfoundin CD couldplaya role in promotingtheconditionof thrombophilia.In order to investigate whether hemostatic]alterationsare dependenton the intestinalinflammationof CD, or expressthe systemicinflammatorystate, we have studiedthirty-onesubjectsaffectedby CD,beforeandafterboweloperation.
MATERIAL AND METHODS
StudypopulationThirty-one patients (17 males and 14 females, age: mean*SD = 33.8+11, range=14-64years)affectedby CD andsubmittedto boweloperationwereprospectivelystudied.Diagnosis of CD was documented by clinical, endoscopic, radiologic and histologicstudies.Disease activity of CD was assessed according to the Crohn’sDiseaseActivityIndex (CDAI) score (17). No patienthad physicalsignsor laboratorydata suggestingthepresence of liver or biliary tract disease. Five patients had suffered from thromboticepisodesaftertheCD hadbeendiagnosed;the last thromboticepisodehadoccurredat leastfour monthsbeforetheadmissionof the patientto the study.All patientswere assuming5-aminosalycilicacid (5-ASA) (1,600-2,000mtiday) and 11 of them also metronidazole(1,500 mg/day).
- . .
The hemostatic systemwas studied7-10 days before surgery.All but one patientsweresubmittedto resection of the affected bowel segment.The margins of resection did notshow microscopic signs of inflammation. Stricturoplastywas performed in only onepatient.In 8 patientsclosureof fistulawas alsoperformed. All patientswere controlled3months after surgery and 23 also 12 months after bowel operation. Whole blood-spontaneousplatelet aggregationwas carried out in 16 patients at 3 months and in 12patientsat 12months.Nopatienthad beenaffectedby thromboticeventsafter surgery.Allpatients were still assuming 5-ASA (1,600-2,000 mg/day). All patients gave theirinformedconsentto usepartof theirbloodsamplesfor an experimentalstudy.Thirtyapparentlyhealthycontrolsofequivalentsexandagewerealsoinvestigated.
ExperimentalprocedureAll venipunctureswere performedbetween8 and 10a.m., with 19Gneedles,usinga two-syringe technique. Blood samples were centrifuged for 15 min at 2,000 g at 4°C andplasmasampleswere storedat -SO°Candassayedwithinonemonth.Platelet number (PLT), prothrombin time (IT), activated partial thromboplastin time(aPTT) and fibrinogen(Fbg)were evaluatedby routinemethods.ProthrombinfragmentF1+2 (F1+2) was measuredby ELISA (EnzygnostF1+2, BehringwerkeAG, Germany);antithrombin(AT)andproteinC (PC)activitieswereevaluatedby automatedchromogenicmethods ( DADE, Switzerland) and protein S (PS) activity by clotting method(InstrumentationLaboratory,Italy); factor XIII (F XIII) was evaluatedby immunologicalmethod ( BehringwerkeAG). Plasminogen(PLG) and plasminogenactivator inhibitoractivity(PAI)were evaluatedby chromogenicmethods(Plasminogen,BehringwerkeAG,and PM-Activity,Biopool, Sweden).Whole blood-spontaneousplatelet aggregation (wB-SPA) was evaluated by countingplatelets in WB before and after stirring the samples in aggregometer for 20’ andcalculatingtheaggregationpercentage(18).LupusAnticoagulant(LA)wasevaluatedby dilutedaP_IT(Pathromtin,BehringwerkeAG,diluted 1:50)(19), Kaolin ClottingTime (20) (KCT), diluted RussellViperVenomtest(DRVVT),( DW TEST,Ortho,Itrdy)(21),TissueThromboplastinInhibitionTime(TITT,

Vol. 87, No. 6 HEMOSTASISALTERATIONS 541
CalciplastinaBaldacci,Italy, 1:1000)(22).As confirmationtest, the plateletneutralizationprocedurewas used (StaclotPNP,Stage, France).Anticardiolipinantibodies(aCL) were evaluatedby ELISA (First CardiolipinIgG-IgM,Eurospital,Italy); the cut-offlevel of positivitywas 20 GPL/mlfor IgG and 20 MPL/mlfor IgMantibodies.
StatisticalanalysisThe analyseswere performedby an IBMPS2/70computerandBMDPstatisticalsoftware.Demographic data and parametric results were analyzed by analysis of variance, thedifferencesbetween3 monthsand beforesurgery,between 12 monthsand before surgeryand between 3 monthsand 12monthsby t-test for paired data, the differencesbetweenhealthysubjectsand CD patientsbeforesurgery,3 monthsand 12 monthsvaluesby t-testfor independentdata;thefrequencyof aPLby Fisher’sexacttest.Unless otherwise indicated, results are given as mean and standard deviation. Allprobability values reported are two-tailed, with values less than 0.05 consideredstatisticallysignificant.
RESULTS
DegreeofactivityBeforeboweloperationthe diseasewas quiescentin 6 patients,activein 17and severein8. Threemonthsafter surgery,allbutonepatienthad inactivediseaseandnormalvaluesoferythrocytesedimentationrate, serumC reactiveproteinandwhitebloodcell count.In one patient, affected by severe CD before surgery,three monthsafter bowel resectionCDAIindicatedactivedisease;erythrocytesedimentationrate was 67 mndh and serumCreactiveproteinwas35 mg/1.Twelvemonthsafter surgery, only two patientswere affectedby active disease(the onementionedbeforeand anotherone,affectedby quiescentCD beforesurgeryand 3 monthsafter). They showed laboratory findings of inflammation (increase in erythrocytesedimentationrate and in serumC reactiveprotein).Increasederythrocytesedimentationrate, but a normal value of serumC reactiveprotein,was found in only one patient withquiescentdisease.
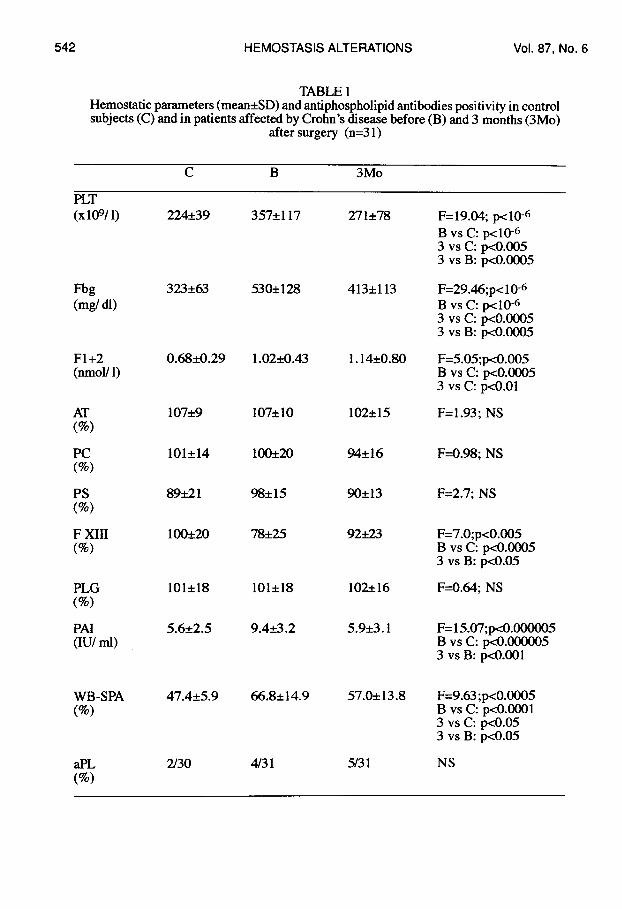
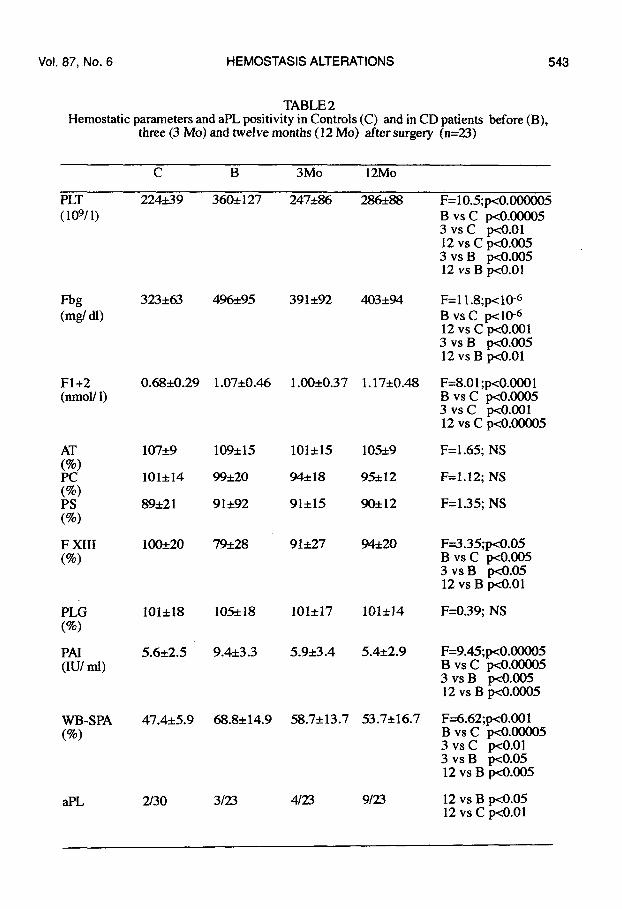
HemostaticparametersBeforesurgery,PT and aPTT werenot signit3cantlydifferentbetweenpatientsand controlsubjects;PLT, Fbg, F1+2, PAIactivityandWB-SPAwere significantlyhigherin patientsthan in controlsubjects,whileFXIIIwas significantlylower(table 1).The presence of antiphospholipidantibodies(aPL) was higher in CD patients than inhealthysubjects:2/31patientswere LA-positiveand 1bothLA-andaCL-positive,but thedifferencewasnot significant(table 1).No significantdifferencewasfound in PLT,Fbg, F1+2 and PAIvalueswithrespectto thedifferentdegreesofactivity.On the contrary, FXH1 was significantly higher in patients with inactive disease(107%*27) than in patients with active (72%*18) and severe (70%+22) disease. Nodifferenceeitherin hemostaticparametersor in thefrequencyof aPL betweenpatientswhohad or had notpreviouslysufferedfromthromboticeventswasobserved.Three and 12 months after surgery, PLT, Fbg and WB-SPAsignificantlydecreasedincomparisonwith the preoperativestatus,but PLT and Fbg were still significantlyhigherthan in control subjectsboth at 3 monthsand at 12 months,whereasWB-SPA only at 3months(tables 1and 2).F1+2 did not change after 3 and 12 months, and was still significantlyhigher than incontrols(tables 1and 2).At both 3 and 12 monthsF XIII significantlyincreased in comparisonwith pre-surgeryvalues,withno statisticaldifferencewithhealthysubjects(tables1and2).The number of aPL-positivepatients was higher 3 months (5/31) and 12 months (9/23)
542 HEMOSTASISALTERATIONS Vol. 87, No. 6
TABLE1Hemostaticparameters(mean&SD)andantiphospholipidantibodiespositivityin controlsubjects(C) andin patientsaffectedby Crohn’sdiseasebefore(B) and3 months(3Mo)
after surgery (n=31)
c B 3M0
(Xlo%l)
Fbg(mgldl)
F1+2(nmol/1)
AT(%)
Pc(%)
Ps(%)
F XIII(%)
PLG(%)
PAI(IUlml)
WB-SPA(%)
aPL(%)
z~~s$)
s~~(js
0.68*0.29
107*9
101*14
89*21
1O(E2O
101+18
5.6*2.5
47.4*5.9
230
357*117
530*128
1.02+0.43
107*1O
10&t20
98*15
78*25
101+18
9.4*3.2
66.8&14.9
4/31
271*78
413*113
1.14*0.80
102*15
94*16
90*13
!ZM23
102*16
5.9*3. 1
57.0*13.8
5/31
F=19.04;pc10-bB VS C: pdO-G3 Vsc: pco.oo53 vs B: pdNO05
F=29.46;p<10-bB VS C: p-dO-b3 Vsc: ~o.00053 vs B: pcO.0005
F=5.05;p<0.005B VS C: pcO.00053 Vsc: ~o.ol
F=l.93; NS
F=O.98;NS
F=2.7; NS
F=7.O;p<O.005B VS C: @.00053 vs B: wO.05
F=O.64;NS
F=15.07;pco.m5B Vsc: p.dm53 vs B: pcO.001
F=9.63;x0.0005B VS C: wO.00013 Vsc: yo.053 vs B: ~0.05
NS
vol. 87, No.6 HEMOSTASISALTERATIONS 543
TABLE2HemostaticparametersandaPLpositivityin Controls(C) and in CDpatients before(B),
three(3 Mo)and twelvemonths(12 Mo) after surge~ (n=23)
c B 3M0 12M0
PLT 224&39 36&127 247*86 286A8 F=1O.5;WO.OOOOO5(109/1)
Fbg(mg/dl)
F1+2(nmol/1)
AT(%)Pc(%)Ps(%)
F XIII(%)
PLG(%)
PAI(IU/ml)
WB-SPA(%)
aPL
323*63
0.68*0.29
107*9
101*14
89*21
10&20
101+18
5.6*2.5
47.4*5.9
2/30
496*95
1.07~0.46
109*15
99*2O
91*92
79*28
10S18
9.4*3.3
68.8*14.9
3123
391*92
1.00*0.37
101*15
94*18
91*15
91*27
101*17
5.9*3.4
58.7*13.7
4/23
403*94
1.17+0.48
105*9
95*12
90*12
94*2O
101*14
5.4*2.9
53.7*16.7
9/23
B VS C ‘~0.000053 Vsc ~o.ol12 Vsc ~o.oo53 vs B [email protected] vs B ~0.01
F=l 1.8;p-dO-GB VS C wICG12Vsc po.ool3 vs B @M10512vs B p4.01
F=8.ol;p<o.0001B VS C @.00053 Vsc p-dMIOl12 Vsc ~o.0ooo5
F=l.65; NS
F=l.12; NS
F=l.35; NS
F=3.35;~0.05B VS C @l.0053 vs B pcO.0512 vs B p4.01
F=O.39;NS
F=9.45;P0.00005B VS C [email protected] vs B @M10512vs B ~0.0005
F=6.62;Ix0.001B VS C @.000053 Vsc ~o.ol3 vs B pcO.0512 vs B PO.005
12 vs B txO.0512 Vsc &o.ol

544 HEMOSTASISALTERATIONS Vol. 87, No. 6
afteroperation,witha significantdifferencebetween12monthsandbeforesurgery.Sevenpatients,who were aPL negativebefore surgery, became aPL-positiveafter 12 months.OneaPL-positivepatientbecamenegativeat3 monthsaftersurgery.Forno parametera significantdifferencewasfoundbetween3 and 12months.
DISCUSSION
In this study relevant changes in hemostaticsystem were observedfor 12 monthsaftersurgery,despitea decreasein thedegreeofactivity.F XIII, whose decrease in CD is attributedto its depositionon the affected bowelareas(24) and isnot linkedto the inflammato~ state,returnedtonormalvaluesafter surgery.Differently,two hemostaticparameterswhichbehave as “acutephasereactant”- PLT andFbg-,remainedsignificantlyhigherthanin healthysubjects,althoughsignificantlylower3and 12 monthsafter surgery than before. A specificmarker of blood clottingactivation(F1+2) showed that a conditionof hypercoagulabilitywas still present in these patientsafter bowel operation.WB-SPAsignificantlydecreasedafter3 and 12monthsand at 12monthsit wasnothigherthan in controlgroup.In our study the prevalence of aPL positivitybefore surgery has been 12.9Yo;in otherstudiespercentagesup to 2570have been reported(14); aPL have not been found strictlyrelated to the activityof the disease,even if a lower prevalencehas been observedin thequiescent phase (16,25). Interestingly,in this study the prevalence of aPL antibodypositivityincreased after bowel operation.At the best of our knowledgethis is the firstreport of this phenomenon.The resultsof our studydo not allowto rule out a causativeroleof the surgicalprocedurein triggeringaPLpresence.No studiesare availablein whicha follow-upof aPL behaviorhasbeen carriedout in CDpatients,independentlyof surgicalprocedure, neither aPL appearance after surgery has been investigated. The higherfrequency of aPL in quiescent phase after surgery suggests that in these patients aPLpresencemaypredicttheevolutionof diseaseevenbeforetheappearanceofclinicalsigns.In fact, someauthorsreportedan early recurrence(after a few months)of microscopicaland, morefrequently, microscopicallesionsafter bowelresection,and most importantly,theselesionswere not associatedto clinicalsignsof the disease(26-28).Furtherfollow-upof thepatientswho had becomeaPL-positiveafter surgerymightdemonstratethe possibleprognosticmeaningof aPL.The behaviorof PLTand Fbg, whosedecreaseis, likely,secondaryto the reductionin theamountof inflammatorytissuefollowingthe operation,doesnotruleout the persistenceofa systemicinflammatorystate, and, on the other hand, they tend to increaseagain at 12monthswhilebloodclottingactivationis persistent,as observedthroughoutthe study.In our opinion,these results1)indicatethat in CD changesof hemostaticsystemare onlyin part influenced by local flogistic intestinal processes; and 2) suggest that theinflammatorysystemic condition, which provokes both the bowel and extraintestinalmanifestationsof CD,maybe stillactive,and evenin progress,alsoin the quiescentphaseofactivityof intestinalalterationsaftersurgery,at leastin thefirstpost-operativeperiod.
AcknowledgementThis work was supportedin part by a grantfrom Ministerodell’Universitile dellaRicercaScientificaeTecnologica(n.12.02.212).

Vol.87, No. 6 HEMOSTASISALTERATIONS 545
REFERENCES1.GLIKMANR.M.Inflammatov boweldisease:ulcerativecolitisand Crohn’sdisease.In“Harrison’s.Principlesof internalmedicine”. K J Isselbacher,E Braunwald,JD Wilson,JR Martin, AS Fauci, DL Fauci. pp 1403-1417,Mc GRAW-HILLInc.(eds),NewYork1994.2. LAM A, BORDA IT, INWOOD MJ, and THOMSON S. Coagulation studies inulcerativecolitisandCrohn’sdisease.Gastroenterology68, 245-25,1975.3. TALBOTRW, HEI?PELJ, DOZOIS RR and BEART RW.Vascularcomplicationsofinflammatoryboweldisease.MayoClinProc61, 140-145,1986.4. EDWARDSRL, LEVINE JB, GREEN R, DUFFY M, MATHEWSE, BRANDEW,and RICKLESFR. Activationof bloodcoagulationin Crohn’sdisease.Increasedplasmafibrinopeptide A levels and enhanced generation of monocyte tissue factor activity.Gastroenterology92,329-337, 1987.5. KOENIGS KP, Mc PHEDRANP and SPIROHM.Thrombosisin inflammatoryboweldisease.J ClinGastroenterol9, 617-621, 1987.6. CONLAN MJ, HAIRE WD and BURNETT DA. Prothrombotic abnormalities ininflammatoryboweldisease.DigDis Sci 34, 1089-1093,1989.7. DE JONG E, PORTE RJ, KNOT EAR, VERHEIJEN JH and DEES J. Disturbedfibrinolysisin patientswith inflammatoryboweldisease.A studyin bloodplasma,colonmucosa,and feces. Gut 30, 1S8-194,1989.8. WAKEFIELD A, COHENZ and LEVY G. Procoagulantactivityin gastroenterology.‘Gut31, 239-241, 1990.9. VECCHI M, CA’ITANEOM, DE FRANCHIS R and MANNUCCI PM. Risk ofthromboemboliccomplicationsin patients with inflammatorybowel disease. Study ofhemostatic measurements.Int JClin Lab Res 21,165-170,1991.10. HUDSON M, HUTTON RA, WAKEFIELDAJ, SAWYERRAM, and POUNDERRE. Evidencefor activationof coagulationin Crohn’sdisease.BloodCoag Fibrinolysis3,7773-778, 1992.11. WEBBERLEY MJ, HART MD and MELIKIAN V. Thromboembolism ininflammatoryboweldisease:roleofplatelets.Gut34, 247-251, 1993.12. SIMI M, LEARDI S, TEBANO MT, CASTELLI M, COSTANTINI FM andSPERANZAW. Raised plasma concentrations of platelet factor 4 (PF 4) in Crohn’sdisease.Gut 28,333-338,1987.13.VIANNAJL, D’CRUZDP,KHAMASTAMA, ASHERSONRA and HUGHES GR.Anticardiolipinantibodiesin a patient with Crohn’s disease and thrombosis. Clin ExpRheumatol10, 165-168,1992.14. REICHT G , PETRITSCH W, WENZL H, EHERER A, HINTERLEITNER TA,AUER-GRUMBACHP and KREJS GJ. Increased anticardiolipinantibodiesin patientswithinflammatoryboweldisease.Gastroenterolgy104,A768, 1993.15.CHAMOUARDP, GRUNEBAUML, WIESEL ML, FREYSSINETJM, DUCLOSB, CAZENAVEJP and BAUMANNR. Prevalence and significanceof anticardiolipinantibodiesin Crohn’sdisease.Dig Dis Sci 39, 1501-1504,1994.16. CHIARANTINIE, VALANZANOR,ALESSANDRELLOLIOTTAA, CELLAIAP,FEDI S, ILARI I, PRISCOD, TONELLIF and ABBATER.Hemostatic abnormalitiesininflammatoryboweldisease.ThrombRes82, 137-146,19%.17. BEST WR, BECKTEL JM, SINGELTONJW and KERN F Jr. Developmentof aCrohn’sdiseaseactivityindex.Gastroenterology70,439-444, 1976.18. GRAY RP, HENDRA TJ, PATTERSONDLH, and YUDKIN JS. “Spontaneous”plateletaggregationin wholebloodin diabeticssurvivorsof acute myocardialinfarction.ThrombHaemost 70,932-936, 1993.19. ALVING BN, BALDWIN PE, RICHARDS RL and JAKSON BJ. The dilutephospholipidaPTT: a sensitive assay for verification of lupus anticoagulant. ThrombHaemost54, 709-712, 1985.20. EXNER TE, RICKARD KA and KRONBERG H. A sensitive test demonstratingLupusAnticoagulantanditsbehavioral patterns.BrJHaematol 40, 143-151, 1978.21. THIAGARAJANP, PENGO V and SHAPIRO SS. The use of dilute Russell vipervenomtimefor the diagnosisof LupusAnticoagulant.Blood 68,869-874, 1986.22. SCHLEIDERMA, NACHMANRL, JAFFEEA and COLEMANM. A clinicalstudy
546 HEMOSTASISALTERATIONS Vol. 87, No.6
of theLupusAnticoagulant.Blood 48, 499-509, 1976.23.TRIPLEI”TDA, BRANIYI’JT, KALZORD, and SCHAFFERJ. Laboratorydiagnosisof Lupus Inhibitors:a comparisonof the neutralizationprocedure.Am J Clin Pathol 79,678-672,1983.24. HUDSON M, WAKEFIELD AJ, HUTTON RA, SANKEY EA, DHILLON AP,MORE L, SIM R, and POUNDERRE. FactorXIII subunitand Crohn’sdisease.Gut 34,75-79, 1993.25. SCHAUFELBERGER HD, UHR MR, SMITH AC, LOGAN RPH, GORDAN-SMITHEC and MISIEWICZJJ; Platelet activationin inflammatorybowel disease.Gut34, s50 (abstract), 1993.26. COLLINS CE and RAMPTON DS. Platelet dysfunction: a new dimension in
atoryboweldisease.Gut 36, 5-8, 1995.inflamm27. CHAMOUARDP, DUCLOS B, BAUMANN R, GRUNEBAUML, WIESEL ML,FREYSSINET JM and CAZENAVEJP; Antiphospholipidantibodies in inflammatoryboweldisease;(letter).Dig Dis Sci 7, 1524-15251995.28. RUTGEEKIX P, GEBOES K, VANTRAPPENG, BEILS J, KARREMANS R andHIELE M. Predictabilityof the postoperativecourseof Crohn’sdisease.Gastroenterology99,956-9631990.29. OLAISON G, SMEDH K and SJODAHLR. Natural course of Crohn’sdiseaseafterileocolicresection:endoscopicalyvisualizedileal ulcerspreceding symptoms.Gut 33,331-335, 1992.30. RUTGEERTSP, HIELE M, GEBOES K, PEETERS M, PENNICKX F, AERTS Rand KARREMANS R. Controlled trials of metronidazole treatment for prevention ofCrohn’srecurrenceafterilealresection.Gastroenterology108, 1617-1622,1995.
Copyright © 2022 FDOKUMEN




















