
Current Therapeutic Approaches in Inflammatory Bowel Disease
Upload
utsouthwesternCategory
view
1download
0
Best Practice & Research Clinical Gastroenterology 27 (2013) 225–233
Contents lists available at SciVerse ScienceDirect
Best Practice & Research ClinicalGastroenterology
5
Advanced precancerous lesions in the smallbowel mucosa
Robert M. Genta, M.D. a,b,c,d,e,*, Linda A. Feagins, M.D. b,c,d,e
aMiraca Life Sciences Research Institute, Irving, TX, USAbDepartment of Pathology, Veterans Affairs North Texas Health Care System, Dallas, TX, USAcDepartment of Medicine, Veterans Affairs North Texas Health Care System, Dallas, TX, USAdDepartment of Pathology, University of Texas Southwestern Medical Center, Dallas, TX, USAeDepartment of Medicine, University of Texas Southwestern Medical Center, Dallas, TX, USA
Keywords:Duodenal adenomaSmall intestinal dysplasiaCancer risk in Crohn’s diseaseCancer risk after proctocolectomyPouchitis
* Corresponding author. Miraca Life Sciences, 66(Office); fax: þ1 (214) 596 7415.
E-mail address: [email protected]
1521-6918/$ – see front matter Published by Elsevhttp://dx.doi.org/10.1016/j.bpg.2013.03.013
a b s t r a c t
The small intestine has comparatively low rates of epithelialcancers and is, for the most part, inaccessible to ordinary endo-scopic visualization. As a result, few solid data are available on thepathological, clinical, and therapeutic aspects of epithelial dysplasiain the small intestine.In this review, we discuss the duodenal adenoma, the most readilyvisualized dysplastic lesion of the small intestine and the only onethat can be detected in an early phase and resected endoscopicallybefore it progresses to high-grade or invasive carcinoma. Particularemphasis is placed on the relationship between duodenal ade-noma and colon neoplasia. Because of their different behaviour,detection and management of ampullary adenomas is discussedseparately.Even if the absolute risk remains small, the incidence of adeno-carcinoma in the small bowel is increased 32-fold in patients withileal Crohn’s disease. Therefore, the follow up and management ofthese patients is discussed with particular emphasis on theoccurrence of dysplasia in the small bowel mucosa of the post-restorative proctocolectomy patients.
Published by Elsevier Ltd.
55 North MacArthur Blvd, Irving, TX 75039, USA. Tel.: þ1 (214) 596 7440
du (R.M. Genta).
ier Ltd.
R.M. Genta, L.A. Feagins / Best Practice & Research Clinical Gastroenterology 27 (2013) 225–233226
Introduction and definitions
Adenocarcinoma of the small intestine is a rare, orphan malignancy: a recent study from the Sur-veillance, Epidemiology and End Results (SEER) cancer registry suggests that between 2000 and 3000adenocarcinomas of the small intestine are diagnosed in the US each year, with an annual incidence of0.6–0.8 per 100,000 person-years [1]. This is in contrast to 160,000 cases of adenocarcinoma of thecolorectum (current annual incidence around 36 per 100,000 person-years) and 21,000 cancers of thestomach [2]. The ratio of colon to small intestinal cancer (w100:2) is similar around the world [3].
In light of this very low frequency and the inaccessibility of most of the jejunum and ileum to or-dinary endoscopic visualization, it is not surprising that there is a dearth of data regarding the path-ological, clinical, and therapeutic aspects of epithelial dysplasia in the small intestine. In this review‘advanced precancerous lesions’ are defined as the phenotypic alterations covering the gap betweenregenerative or metaplastic changes and invasive carcinoma; in other words, low-grade and high-grade intraepithelial neoplasia, which may eventually progress to gastric adenocarcinoma [4].
Duodenal adenoma
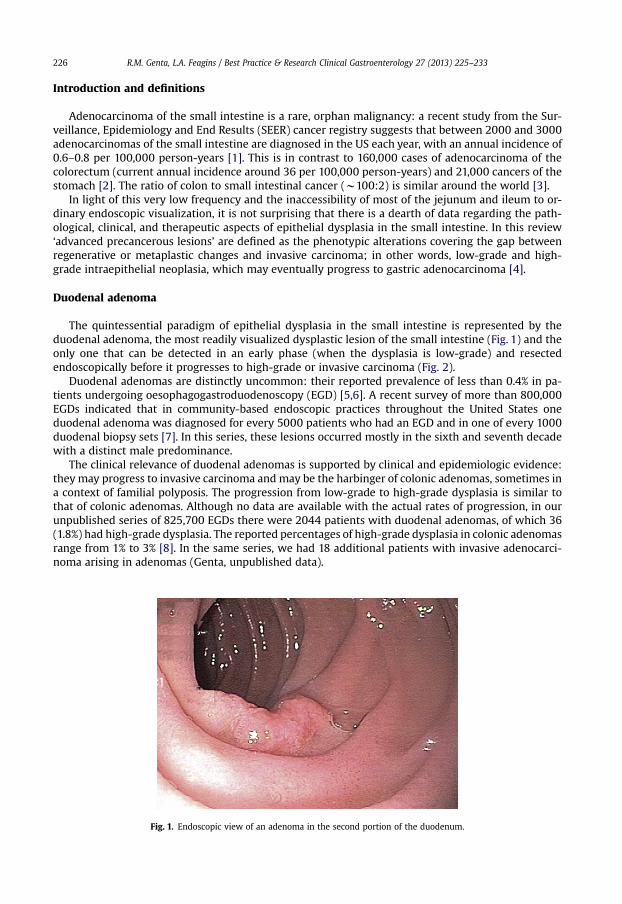
The quintessential paradigm of epithelial dysplasia in the small intestine is represented by theduodenal adenoma, the most readily visualized dysplastic lesion of the small intestine (Fig. 1) and theonly one that can be detected in an early phase (when the dysplasia is low-grade) and resectedendoscopically before it progresses to high-grade or invasive carcinoma (Fig. 2).
Duodenal adenomas are distinctly uncommon: their reported prevalence of less than 0.4% in pa-tients undergoing oesophagogastroduodenoscopy (EGD) [5,6]. A recent survey of more than 800,000EGDs indicated that in community-based endoscopic practices throughout the United States oneduodenal adenoma was diagnosed for every 5000 patients who had an EGD and in one of every 1000duodenal biopsy sets [7]. In this series, these lesions occurred mostly in the sixth and seventh decadewith a distinct male predominance.
The clinical relevance of duodenal adenomas is supported by clinical and epidemiologic evidence:they may progress to invasive carcinoma and may be the harbinger of colonic adenomas, sometimes ina context of familial polyposis. The progression from low-grade to high-grade dysplasia is similar tothat of colonic adenomas. Although no data are available with the actual rates of progression, in ourunpublished series of 825,700 EGDs there were 2044 patients with duodenal adenomas, of which 36(1.8%) had high-grade dysplasia. The reported percentages of high-grade dysplasia in colonic adenomasrange from 1% to 3% [8]. In the same series, we had 18 additional patients with invasive adenocarci-noma arising in adenomas (Genta, unpublished data).
Fig. 1. Endoscopic view of an adenoma in the second portion of the duodenum.

Fig. 2. A: Typical large polypoid duodenal adenoma. Approximately 98% of these adenomas show only low-grade dysplasia wheninitially biopsied or resected (panel B). High-grade dysplasia (panel C) is more common in ampullary adenomas and may be difficultto distinguish from invasive carcinoma, particularly when these lesions are removed piecemeal and there are no clear margins toevaluate.
R.M. Genta, L.A. Feagins / Best Practice & Research Clinical Gastroenterology 27 (2013) 225–233 227

R.M. Genta, L.A. Feagins / Best Practice & Research Clinical Gastroenterology 27 (2013) 225–233228
The endoscopic resection of duodenal adenomas has traditionally been considered a high-riskprocedure as the duodenal anatomy presents several challenges to the endoscopist (Fig. 3). The thinmuscle layer of the duodenum and the abundant supply of blood vessels in the submucosa increase therisk of perforation and bleeding [9]. Moreover, the duodenum receives high exposure to pancreatic andbile juices which has been postulated by some to contribute to a higher risk of delayed perforation[10,11]. Nevertheless, small studies have shown that an en bloc approach with endoscopic mucosalresection (EMR) has been successful in patients with adenomas up to 20mm in sizewhile larger lesionscan be safely removedwith a piecemeal EMR approach [12,13]. Rates of residual adenomatous tissue onfollow-up was 12–25% (particularly with a piecemeal approach), but all were able to be treated withfurther endoscopic therapy [12–14]. In one study of 21 patients, there were no complications ofperforation and only one patient experienced delayed bleeding (5%). Other centres (predominately inJapan) have found that endoscopic submucosal dissection (ESD) has lower rates of residual adeno-matous tissue on follow-up exams, but they were associated with higher rates of perforation (two ofnine or 22%) and delayed bleeding (two of nine) [11]. In a follow-up study of 988 patients (identified viaa pathology database) with duodenal adenomas, 170 (17%) had a second resection (most within oneyear), and 34 (3%) had two or more subsequent resections. However, due to study design, we do notknow how many were the result of incomplete resections and how many could be imputed to re-currences [15].
Another reason for concern in patients with a new diagnosis of duodenal adenoma is the docu-mented association with colonic adenomas. Patients with hereditary conditions causing germ line
Fig. 3. (A) Submucosal injection with a mixture of saline, epinephrine, and indigo carmine was performed prior to polypectomy.(B) Several hemoclips were placed to close the defect in the mucosa after polypectomy – [courtesy of Dr. Zeeshan Ramzan.]

R.M. Genta, L.A. Feagins / Best Practice & Research Clinical Gastroenterology 27 (2013) 225–233 229
mutations in the APC gene as well as patients with MYH-associated polyposis (MAP) have an increasedrisk for duodenal adenomas [16–20]; therefore, the unexpected finding of a duodenal adenoma,particularly in a young subject, should raise the suspicion of a polyposis syndrome. Furthermore,several studies have suggested an association between sporadic duodenal adenomas (that is, notarising in the context of a polyposis syndrome) and colonic adenomas (Table 1) [21–31]. Unfortunately,the small size of most series, the different methodologies, and the diverse origin of patients andcontrols have prevented reaching a clear consensus on the strength of this association. The overallpercentage of patients with duodenal adenomas reported to have had colonic adenomas varied from aminimum of 21% (Schneider et al, in a series of 19 patients) to a maximum of 73% (Apel et al, in 22patients) [29]; in the two largest controlled series to date (Dariusz and Jochen, 48 patients and 144controls; and Ramsoekh et al, 49 patients and 147 controls) [23,28] the combined OR (calculated fromthese authors’ reported raw data) was 4.84 (95% CI 2.93–8.00). In a series we recently presented,duodenal adenomas were strong predictors of the number, size, and degree of dysplasia of colonicadenomas [7]. According to the American Society of Gastrointestinal Endoscopy (ASGE), the recom-mendation to offer a colonoscopy to patients without known polyposis syndrome inwhom a duodenaladenoma is detected is supported by a low level of evidence (2C) [32]. Consequently gastroenterolo-gists, lacking solid evidence-based management guidelines for patients with a new diagnosis ofduodenal adenoma, are often forced to rely on the results of small studies or on the pathologist’sadvice. Was the lesion completely excised? Is there a need to follow up for recurrence? How longshould the surveillance interval be? Few of these questions can be answered with the present state ofknowledge.
Ampullary adenomas: a special case
Adenomas located around the ampulla of Vater are present in approximately 10% of all duodenaladenomas, with a reported autopsy prevalence of 0.04–0.12% [33]. Ampullary adenomas along withampullary carcinomas account for less than 10% of periampullary neoplasms, but carry a better prognosisthan the othermalignant periampullary neoplasms (namely cholangiocarcinoma and adenocarcinoma ofthe pancreas) [33]. Ampullary adenomasmay be sporadic, typically solitary, or occur in associationwith ahereditary polyposis syndrome (familial adenomatous polyposis or one of its variants), where they cancoexist with large numbers of polyps. While in a majority of cases these polyps are asymptomatic whenfound, some may also present with biliary obstruction or even recurrent pancreatitis. These adenomasare clearly precancerous lesions, and appear to follow the adenoma–carcinoma sequence similar to thatin the colon [34]. Moreover, because of the high risk of ampullary carcinoma in FAP patients, routineendoscopic surveillance is recommended [35]. Because of the high risk for malignant transformationthese polyps, whether sporadic or associated with a polyposis syndrome, have historically been treatedwith pancreatoduodenectomy, a highly invasive surgical procedure that carries high morbidity and
Table 1Studies involving patients with sporadic duodenal adenoma (DA) and evaluation of the colon.
Authors and year DA andcolonoscopy
Any colonicadenoma (%)
Advanced colonicadenomaa (%)
Colonic adeno-carcinoma (%)
Control patients withcolonic adenomab (%)
Seifert et al (1992) [30] 7 4 (57) n.a n.a. n.a.Apel et al (2004) [22] 22 16 (73) n.a 1 (5) n.a.Murray et al (2004) [26] 34 12 (35) 6 (18) 7 (21) 26/102 (25)Ford et al (2004) [24] 11 4 (36) 3 (27) 0 n.aSchneider et al (2005) [29] 19 4 (21) 1 (5) 1 (5) 27/104 (26)Pequin et al (2007) [27] 35 11 (31) 8 (23) 2 (6) 17/70 (24)Ramsoekh et al (2008) [28] 49 17 (35) 9 (18) 4 (8) 21/147 (14)Lagarde et al (2009) [25] 29 15 (52) 4 (14) 3 (10) 11/58 (19)Dariusz et al (2009) [23] 48 31 (65) n.a. 5 (10) 35/144 (24)Abbass et al (2010) [21] 17 9 (53) n.a. n.a. n.aGonzalez-Ortiz
et al (2010) [31]21 9 (43) 4 (19) n.a. 38/84 (45)
a Advanced adenoma defined in previous studies as size �10 mm, villous component, and/or high-grade dysplasia.b Age and sex matched controls.
R.M. Genta, L.A. Feagins / Best Practice & Research Clinical Gastroenterology 27 (2013) 225–233230
mortality. Today, with the advances in therapeutic endoscopy, an attempt is typically made beforeconsidering surgery [36]. Similar to sporadic non-ampullary adenomas, attempts to remove these en blocshould be the goal for polyps up to 2 cm in size, but will often require a piecemeal technique for largerlesions [36]. One study observed a linear relationship between size and presence of invasive cancer andfound that lesions less than 25 mm in size did not demonstrate any invasion [37]. Complications asso-ciated with endoscopic ampullectomy have been reported to occur in 9%–20% of patients [36], andinclude bleeding, acute pancreatitis, papillary stenosis, cholangitis and, more rarely, perforation.
Sporadic adenomas in the distal small intestine
Adenomas located distal to the papilla are rare. Although they rarely produce obstructive symptomsor occult blood loss, most remain clinically silent until complicated by the development of carcinoma.Thus, in this location, the discovery of lesions at the precancerous stage is highly unusual [1].
Although both macroscopic and histologic features of small intestinal adenomas are virtuallyidentical to those of the colon, and the criteria for grading epithelial dysplasia are the same, there is animportant difference in staging these neoplasms when they invade the lamina propria [38,39]. Colonicadenomas with high-grade dysplasia and foci of adenocarcinoma that invade only the lamina propria(‘intramucosal carcinoma’) are staged as in situ lesions (pTis). In contrast, similar lesions invading thelamina propria of the small intestine are staged as invasive carcinomas (pT1) because the lamina propriain this location (as opposed to the colon) contains an extensive network of lymphatic vessels [40].
Small intestinal adenomas in familial polyposis
Until the recent introduction of new imaging techniques (such as the capsule endoscopy) the extentto which hereditary polyposis syndromes affected the small intestine beyond the duodenum remainedunclear. The little information regarding numbers and the distribution of polyps in these patients wasderived from relatively rare surgical and autopsy specimens. Recent studies using video capsuleendoscopy and double balloon enteroscopy have revealed that up to 90% of patients with familialpolyposis have polyps in the jejunum and ileum [41,42]. Interestingly, the degree of duodenal polyposisappears to correlate with the presence of adenomas in the jejunum and ileum [41,43,44]. However, theclinical significance andmalignant potential of these polyps is uncertain. Some experts have advocatedsurveillance of the small bowel in FAP patients with severe duodenal polyposis (given their higher riskfor jejunal and ileal polyps) using video capsule endoscopy; if large (>1 cm) polyps are seen in thesmall bowel, this should be followed by double balloon enteroscopy. Since only limited data areavailable, the outcomes of such surveillance programs are still largely unknown [45].
Small intestinal dysplasia and cancer in Crohn’s disease
The risk of adenocarcinoma in the small bowel is increased 32-fold in patients with ileal Crohn’sdisease; however, because of the rarity of small bowel adenocarcinoma in the general population, evenwith this dramatic increase the absolute risk remains small [46]. The mechanism of carcinogenesis inpatients with Crohn’s disease is likely to be analogous to the mechanisms that lead to colorectal cancerin patients with ulcerative colitis. The underlying chronic active inflammatory process, similar in thetwo conditions [47], may lead to dysplasia and promote the progression to adenocarcinoma [48,49].Data in this regard are largely anecdotal: one study of eight cases of small intestinal adenocarcinomasassociated with Crohn’s disease found dysplasia, in most cases adjacent to the carcinoma, but in onecase also distant from the tumour [48]. A single case report details the progression of flat low-gradedysplasia to adenocarcinoma in the small intestinal mucosa over the course of 18 months of follow-up of a patient with Crohn’s disease [49].
Concerns for the occurrence of dysplasia in the small bowel mucosa of the post-restorative proc-tocolectomy (i.e., with a pouch) have also been raised, particularly in patients who underwent proc-tocolectomy for colon cancer. After the creation of an ileal pouch, the mucosa of the pouch adapts to itsnew role as a reservoir; three distinct mucosal patterns have been described: (1) normal or mildatrophic mucosa (type A); (2) transient atrophic response, with temporary moderate to severe villous

R.M. Genta, L.A. Feagins / Best Practice & Research Clinical Gastroenterology 27 (2013) 225–233 231
atrophy (type B); and (3) permanent atrophy with total or subtotal villous atrophy accompanied bysevere pouchitis (type C) [50,51]. The type C pattern has been associated with dysplasia in severalstudies. Another study found that patients with long-standing pouches who also have concurrentprimary sclerosing cholangitis had an increased incidence of dysplasia in the pouch as compared topatients with a pouch but no cholangitis [52]. The overall incidence of dysplasia in the pouch, however,remains distinctly uncommon: in one prospective study only one of 138 patients (0.7%) followed up foralmost six years developed epithelial dysplasia while undergoing pouch surveillance [53].
Summary
Duodenal adenoma, the most readily visualized dysplastic lesion of the small intestine and the onlyone that can be detected in an early phase and resected endoscopically before it progresses to high-grade or invasive carcinoma, is a rare tumour, occurring in approximately one in every thousandsubjects who have an EGD. Its importance is threefold: (1) unless removed, it may progress to invasiveadenocarcinoma; (2) it may be associated with a familial polyposis syndrome; and (3) it has a sig-nificant associationwith colonic neoplasia. Therefore, the first detection of a duodenal adenoma shouldtrigger a colonoscopy and, particularly in young patients, a search for familial polyposis.
Ampullary adenomas (sporadic or associated with a polyposis syndrome) have a higher risk formalignant transformation; therefore, these polyps have historically been treated with pan-creatoduodenectomy, a highly invasive surgical procedure that carries high morbidity and mortality.Today, with the advances in therapeutic endoscopy, an attempt at endoscopic therapy is typically madebefore considering surgery.
Crohn’s disease with small intestinal involvement is a risk factor for adenocarcinoma. Even if theabsolute risk remains small, the incidence of adenocarcinoma in the small bowel is increased 32-fold inpatients with ileal Crohn’s disease; patients with restorative proctocolectomy are also at increased risk.Therefore, surveillance is indicated in patients with Crohn’s disease, whether or not intestinalresections have been performed.
Practice points
� Small intestinal dysplastic lesions are rare and difficult to detect before they progress tocancer.
� Duodenal adenoma represents the most accessible small intestinal dysplastic/neoplasticlesion and the only one that can be detected, removed, and followed up using traditionalendoscopic methods.
� Because of their frequent association with colon polyps, the detection of unexpectedduodenal adenomas should prompt a colonoscopy.
� Young patients with duodenal adenomas should be worked up for familial polyposis.
Funding
Dr. Feagins is supported by the Office of Medical Research, Department of Veterans Affairs,Washington, D.C., and the Harris Methodist Health Foundation, Dr. Clark R. Gregg Fund, Dallas, Texas.
Conflict of interest statement
Drs. Genta and Feagins have no conflicts of interest related to the preparation or contents of thismanuscript.
References
*[1] Overman MJ, Hu CY, Kopetz S, Abbruzzese JL, Wolff RA, Chang GJ. A population-based comparison of adenocarcinoma ofthe large and small intestine: insights into a rare disease. Ann Surg Oncol 2012;19:1439–45.

R.M. Genta, L.A. Feagins / Best Practice & Research Clinical Gastroenterology 27 (2013) 225–233232
[2] American Cancer Society. Cancer facts and figures. Atlanta: American Cancer Society; 20122012.[3] American Cancer Society. Global cancer facts and figures. 2nd ed. Atlanta: American Cancer Society; 2011.[4] Rugge M, Correa P, Dixon MF, Hattori T, Leandro G, Lewin K, et al. Gastric dysplasia: the Padova international classifi-
cation. Am J Surg Pathol 2000;24:167–76.[5] Jepsen JM, Persson M, Jakobsen NO, Christiansen T, Skoubo-Kristensen E, Funch-Jensen P, et al. Prospective study of
prevalence and endoscopic and histopathologic characteristics of duodenal polyps in patients submitted to upperendoscopy. Scand J Gastroenterol 1994;29:483–7.
*[6] Schottenfeld D, Beebe-Dimmer JL, Vigneau FD. The epidemiology and pathogenesis of neoplasia in the small intestine.Ann Epidemiol 2009;19:58–69.
[7] Genta RM, Sonnenberg A. Duodenal adenomas are strongly associated with an increased risk for colonic neoplasia. Am JGastroenterol 2012;107(S1):S128.
[8] Gupta S, Balasubramanian BA, Fu T, Genta RM, Rockey DC, Lash R. Polyps with advanced neoplasia are smaller in the rightthan in the left colon: implications for colorectal cancer screening. Clin Gastroenterol Hepatol 2012;10:1395–401.
[9] Ponchon T. Endoscopic mucosal resection. J Clin Gastroenterol 2001;32:6–10.*[10] Matsumoto S, Miyatani H, Yoshida Y. Endoscopic submucosal dissection for duodenal tumors: a single-center experience.
Endoscopy 2013;45:136–7.*[11] Honda T, Yamamoto H, Osawa H, Yoshizawa M, Nakano H, Sunada K, et al. Endoscopic submucosal dissection for su-
perficial duodenal neoplasms. Dig Endosc 2009;21:270–4.[12] Alexander S, Bourke MJ, Williams SJ, Bailey A, Co J. EMR of large, sessile, sporadic nonampullary duodenal adenomas:
technical aspects and long-term outcome (with videos). Gastrointest Endosc 2009;69:66–73.[13] Sohn JW, Jeon SW, Cho CM, Jung MK, Kim SK, Lee DS, et al. Endoscopic resection of duodenal neoplasms: a single-center
study. Surg Endosc 2010;24:3195–200.[14] Apel D, Jakobs R, Spiethoff A, Riemann JF. Follow-up after endoscopic snare resection of duodenal adenomas. Endoscopy
2005;37:444–8.[15] Hurrell JM, Genta RM. Duodenal adenomas: clinical, endoscopic, and histopathologic characteristics in 1,132 patients.
Mod Pathol 2011;24(1s):153A.[16] Bapat B, Odze R, Mitri A, Berk T, Ward M, Gallinger S. Identification of somatic APC gene mutations in periampullary
adenomas in a patient with familial adenomatous polyposis (FAP). Hum Mol Genet 1993;2:1957–9.[17] Björk J, Akerbrant H, Iselius L, Bergman A, Engwall Y, Wahlstrom J, et al. Periampullary adenomas and adenocarcinomas in
familial adenomatous polyposis: cumulative risks and APC gene mutations. Gastroenterology 2001;121:1127–35.[18] Gallinger S, Vivona AA, Odze RD, Mitri A, O’Beirne CP, Berk TC, et al. Somatic APC and K-ras codon 12 mutations in
periampullary adenomas and carcinomas from familial adenomatous polyposis patients. Oncogene 1995;10:1875–8.[19] Kadmon M, Tandara A, Herfarth C. Duodenal adenomatosis in familial adenomatous polyposis coli. A review of the
literature and results from the Heidelberg Polyposis Register. Int J Colorectal Dis 2001;16:63–75.[20] Sarre RG, Frost AG, Jagelman DG, Petras RE, Sivak MV, McGannon E. Gastric and duodenal polyps in familial adenomatous
polyposis: a prospective study of the nature and prevalence of upper gastrointestinal polyps. Gut 1987;28:306–14.[21] Abbass R, Rigaux J, Al-Kawas FH. Nonampullary duodenal polyps: characteristics and endoscopic management.
Gastrointest Endosc 2010;71:754–9.[22] Apel D, Jakobs R, Weickert U, Riemann JF. High frequency of colorectal adenoma in patients with duodenal adenoma but
without familial adenomatous polyposis. Gastrointest Endosc 2004;60:397–9.[23] Dariusz A, Jochen R. Increased prevalance of colorectal adenoma in patients with sporadic duodenal adenoma. Eur J
Gastroenterol Hepatol 2009;21:816–8.[24] Ford AC, Rotimi O, Everett SM. Sporadic duodenal adenoma and colorectal neoplasia. Gut 2004;53:1056–7.[25] Lagarde S, Dauphin M, Delmas C, Vitry F, Bouche O, Thiefin G, et al. Increased risk of colonic neoplasia in patients with
sporadic duodenal adenoma. Gastroenterol Clin Biol 2009;33:441–5.[26] MurrayMA, ZimmermanMJ,EeHC. Sporadicduodenal adenomais associatedwithcolorectalneoplasia.Gut2004;53:261–5.[27] Pequin P, Manfredi S, Quentin V, Heresbach D, Boyer J, Siproudhis L, et al. Patients with sporadic duodenal adenoma are a
high-risk group for advanced colorectal neoplasia: results of a case-control study.Aliment Pharmacol Ther 2007;26:277–82.[28] Ramsoekh D, van Leerdam ME, Dekker E, Ouwendijk RT, van DH, Kuipers EJ. Sporadic duodenal adenoma and the as-
sociation with colorectal neoplasia: a case-control study. Am J Gastroenterol 2008;103:1505–9.[29] Schneider AR, Seifert H, Trojan J, Stein J, Hoepffner NM. Frequency of colorectal polyps in patients with sporadic ade-
nomas or adenocarcinomas of the papilla of vater–an age-matched, controlled study. Z Gastroenterol 2005;43:1123–7.[30] Seifert E, Schulte F, Stolte M. Adenoma and carcinoma of the duodenum and papilla of Vater: a clinicopathologic study.
Am J Gastroenterol 1992;87:37–42.[31] Gonzalez-Ortiz DI, Torres-Cotto C, Toro DH, Cruz-Correa M, Bigio J. Duodenal adenomas in nonpolyposis syndrome pa-
tients are not associated to colorectal neoplasia. Bol Asoc Med P R 2010;102:5–8.[32] Adler DG, Qureshi W, Davila R, Gan SI, Lichtenstein D, Rajan E, et al. The role of endoscopy in ampullary and duodenal
adenomas. Gastrointest Endosc 2006;64:849–54.[33] Martin JA, Haber GB. Ampullary adenoma: clinical manifestations, diagnosis, and treatment. Gastrointest Endosc Clin N
Am 2003;13:649–69.[34] Yamaguchi K, Enjoji M. Adenoma of the ampulla of Vater: putative precancerous lesion. Gut 1991;32:1558–61.*[35] Vasen HF, Moslein G, Alonso A, Aretz S, Bernstein I, Bertario L, et al. Guidelines for the clinical management of familial
adenomatous polyposis (FAP). Gut 2008;57:704–13.*[36] Patel R, Varadarajulu S, Wilcox CM. Endoscopic ampullectomy: techniques and outcomes. J Clin Gastroenterol 2012;46:8–15.[37] Patel R, Davitte J, Varadarajulu S, Wilcox CM. Endoscopic resection of ampullary adenomas: complications and outcomes.
Dig Dis Sci 2011;56:3235–40.[38] Buckley JA, Siegelman SS, Jones B, Fishman EK. The accuracy of CT staging of small bowel adenocarcinoma: CT/pathologic
correlation. J Comput Assist Tomogr 1997;21:986–91.[39] Pinocy J, Klotz M, Weinzierl B, Schunck R, Weber P. [Primary adenocarcinoma of the jejunum. Diagnostic challenge by a
rare tumour]. Dtsch Med Wochenschr 2008;133:1064–7.

R.M. Genta, L.A. Feagins / Best Practice & Research Clinical Gastroenterology 27 (2013) 225–233 233
*[40] Hamilton SR, Bosman FT, Boffetta P, Ilyas M, Morreau H, Nakamura S, et al. Tumors of the colon and rectum: carcinoma ofthe colon and rectum. In: Bosman FT, Carneiro F, Hruban RH, Theise ND, editors. WHO classification of tumours of thedigestive system. 2nd ed. Lyon: IARC; 2010. p. 134–46.
[41] Burke CA, Santisi J, Church J, Levinthal G. The utility of capsule endoscopy small bowel surveillance in patients withpolyposis. Am J Gastroenterol 2005;100:1498–502.
[42] Gunther U, Bojarski C, Buhr HJ, Zeitz M, Heller F. Capsule endoscopy in small-bowel surveillance of patients with he-reditary polyposis syndromes. Int J Colorectal Dis 2010;25:1377–82.
[43] Schulmann K, Hollerbach S, Kraus K, Willert J, Vogel T, Moslein G, et al. Feasibility and diagnostic utility of video capsuleendoscopy for the detection of small bowel polyps in patients with hereditary polyposis syndromes. Am J Gastroenterol2005;100:27–37.
[44] Plum N, May A, Manner H, Ell C. Small-bowel diagnosis in patients with familial adenomatous polyposis: comparison ofpush enteroscopy, capsule endoscopy, ileoscopy, and enteroclysis. Z Gastroenterol 2009;47:339–46.
[45] Koornstra JJ. Small bowel endoscopy in familial adenomatous polyposis and Lynch syndrome. Best Pract Res Clin Gas-troenterol 2012;26:359–68.
*[46] Canavan C, Abrams KR, Mayberry J. Meta-analysis: colorectal and small bowel cancer risk in patients with Crohn’s dis-ease. Aliment Pharmacol Ther 2006;23:1097–104.
*[47] Feagins LA, Souza RF, Spechler SJ. Carcinogenesis in IBD: potential targets for the prevention of colorectal cancer. Nat RevGastroenterol Hepatol 2009;6:297–305.
[48] Sigel JE, Petras RE, Lashner BA, Fazio VW, Goldblum JR. Intestinal adenocarcinoma in Crohn’s disease: a report of 30 caseswith a focus on coexisting dysplasia. Am J Surg Pathol 1999;23:651–5.
[49] Watermeyer G, Locketz M, Govender D, Mall A. Crohn’s disease-associated small bowel adenocarcinoma with pre-existing low-grade dysplasia: a case report. Am J Gastroenterol 2007;102:1545–6.
[50] Veress B, Reinholt FP, Lindquist K, Lofberg R, Liljeqvist L. Long-term histomorphological surveillance of the pelvic ilealpouch: dysplasia develops in a subgroup of patients. Gastroenterology 1995;109:1090–7.
[51] Veress B, Reinholt FP, Lindquist K, Liljeqvist L. Prospective studies of the mucosa of the ileoanal pouch. Gastroenterology1995;108:953–4.
[52] Stahlberg D, Veress B, Tribukait B, Broome U. Atrophy and neoplastic transformation of the ileal pouch mucosa in patientswith ulcerative colitis and primary sclerosing cholangitis: a case control study. Dis Colon Rectum 2003;46:770–8.
[53] Nilubol N, Scherl E, Bub DS, Gorfine SR, Marion J, Harris MT, et al. Mucosal dysplasia in ileal pelvic pouches afterrestorative proctocolectomy. Dis Colon Rectum 2007;50:825–31.
Copyright © 2022 FDOKUMEN




















