
Role of MRI in Crohn's disease
12
REVIEW Role of MRI in Crohn’s disease R. Sinha a, *, P. Murphy b , P. Hawker c , S. Sanders d , A. Rajesh e , R. Verma e Departments of a Radiology, b Surgery, c Gastroenterology, d Pathology, GI Unit, South Warwickshire NHS Trust & IBD Network, Coventry & South Warwickshire, and e Department of Radiology, University Hospitals of Leicester, Leicester, UK Received 7 July 2008; received in revised form 18 August 2008; accepted 20 August 2008 The traditional imaging of Crohn’s disease has relied on barium and computed tomography (CT) examinations. In recent years magnetic resonance imaging (MRI) has emerged as an imaging method that can be used in the diagnosis and assessment of Crohn’s disease. The advantages of MRI include lack of ionizing radiation and its superior tissue contrast resolution. The clinical progression of Crohn’s disease can be variable, and MRI can be used to assess inflam- matory status, disease progression, and complications of Crohn’s disease. MRI of the small bowel is an evolving tech- nique and it has the potential to become the preferred technique for imaging of small bowel Crohn’s disease in the future. ª 2008 The Royal College of Radiologists. Published by Elsevier Ltd. All rights reserved. Introduction Crohn’s disease (CD) is a chronic inflammatory disease of the gastrointestinal tract that is char- acterized by ulceration, strictures, and fistula formation. CD commonly affects young adults and typically runs a chronic relapsing and remitting course. The indolent nature of the disease leads to frequent imaging examinations for monitoring disease activity and severity in order to guide appropriate treatment. The use of immune-modu- lating drugs has increased the need for accurate assessment of the activity and severity of disease. Cross-sectional imaging investigations, such as computed tomography (CT) and magnetic reso- nance imaging (MRI) are particularly suited to assess the macroscopic features, extramural ab- normalities, and complications. The high tissue contrast obtained using MRI, coupled with the absence of ionizing radiation, makes it ideally suited for imaging patients with CD. The purpose of this article is to review the role of MRI in CD. The advantages and disadvantages of MRI as compared with ultrasonography (US), CT, conven- tional enteroclysis (CE), and wireless capsule endoscopy (WCE) are also discussed. Aetiology and clinical features CD has a worldwide distribution but is more prevalent in Northern Europe and North America. 1 The disease most often afflicts young adults with the peak incidence between 15e25 years. A sec- ond lower peak has been reported in the 50e80 year age group. 2 Worldwide there is an equal sex distribution, although the female to male ratio is high when only colitis is considered. Extensive jejuno-ileitis is commoner in younger patients, whereas older patients tend to have localized enteritis. The precise cause is unknown, and therefore, a causal treatment is not yet available. However, there is evidence that the disease is due to an abnormal mucosal response to an unknown antigen. 3 Genetic factors may determine suscepti- bility to CD as up to 5% of patients have another affected family member. The onset of CD can be insidious and patients may present with vague abdominal symptoms or complications arising from CD such as perineal * Guarantor and correspondent: R. Sinha, Department of Clin- ical Radiology, Warwick Hospital, Lakin Road, Warwick CV34 5BW, UK. Tel.: þ01-92-649-5321; fax: þ01-92-648-2612. E-mail address: [email protected] (R. Sinha). 0009-9260/$ - see front matter ª 2008 The Royal College of Radiologists. Published by Elsevier Ltd. All rights reserved. doi:10.1016/j.crad.2008.08.006 Clinical Radiology (2009) 64, 341e352
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Role of MRI in Crohn's disease
Clinical Radiology (2009) 64, 341e352
REVIEW
Role of MRI in Crohn’s disease
R. Sinhaa,*, P. Murphyb, P. Hawkerc, S. Sandersd, A. Rajeshe, R. Vermae
Departments of aRadiology, bSurgery, cGastroenterology, dPathology, GI Unit, South Warwickshire NHSTrust & IBD Network, Coventry & South Warwickshire, and eDepartment of Radiology, UniversityHospitals of Leicester, Leicester, UK
Received 7 July 2008; received in revised form 18 August 2008; accepted 20 August 2008
The traditional imaging of Crohn’s disease has relied on barium and computed tomography (CT) examinations. In
recent years magnetic resonance imaging (MRI) has emerged as an imaging method that can be used in the diagnosisand assessment of Crohn’s disease. The advantages of MRI include lack of ionizing radiation and its superior tissuecontrast resolution. The clinical progression of Crohn’s disease can be variable, and MRI can be used to assess inflam-matory status, disease progression, and complications of Crohn’s disease. MRI of the small bowel is an evolving tech-nique and it has the potential to become the preferred technique for imaging of small bowel Crohn’s disease in thefuture.ª 2008 The Royal College of Radiologists. Published by Elsevier Ltd. All rights reserved.Introduction
Crohn’s disease (CD) is a chronic inflammatorydisease of the gastrointestinal tract that is char-acterized by ulceration, strictures, and fistulaformation. CD commonly affects young adultsand typically runs a chronic relapsing and remittingcourse. The indolent nature of the disease leads tofrequent imaging examinations for monitoringdisease activity and severity in order to guideappropriate treatment. The use of immune-modu-lating drugs has increased the need for accurateassessment of the activity and severity of disease.
Cross-sectional imaging investigations, such ascomputed tomography (CT) and magnetic reso-nance imaging (MRI) are particularly suited toassess the macroscopic features, extramural ab-normalities, and complications. The high tissuecontrast obtained using MRI, coupled with theabsence of ionizing radiation, makes it ideallysuited for imaging patients with CD. The purposeof this article is to review the role of MRI in CD.The advantages and disadvantages of MRI as
* Guarantor and correspondent: R. Sinha, Department of Clin-ical Radiology, Warwick Hospital, Lakin Road, Warwick CV345BW, UK. Tel.: þ01-92-649-5321; fax: þ01-92-648-2612.
E-mail address: [email protected] (R. Sinha).
0009-9260/$ - see front matter ª 2008 The Royal College of Radiolodoi:10.1016/j.crad.2008.08.006
compared with ultrasonography (US), CT, conven-tional enteroclysis (CE), and wireless capsuleendoscopy (WCE) are also discussed.
Aetiology and clinical features
CD has a worldwide distribution but is moreprevalent in Northern Europe and North America.1
The disease most often afflicts young adults withthe peak incidence between 15e25 years. A sec-ond lower peak has been reported in the 50e80year age group.2 Worldwide there is an equal sexdistribution, although the female to male ratio ishigh when only colitis is considered. Extensivejejuno-ileitis is commoner in younger patients,whereas older patients tend to have localizedenteritis. The precise cause is unknown, andtherefore, a causal treatment is not yet available.However, there is evidence that the disease is dueto an abnormal mucosal response to an unknownantigen.3 Genetic factors may determine suscepti-bility to CD as up to 5% of patients have anotheraffected family member.
The onset of CD can be insidious and patientsmay present with vague abdominal symptoms orcomplications arising from CD such as perineal
gists. Published by Elsevier Ltd. All rights reserved.

342 R. Sinha et al.
sinuses, anorectal fistulae, or abscesses. Chronicdiarrhoea is the most common presenting symp-tom; abdominal pain and weight loss are present in70 and 60% cases, respectively, before diagnosis,whereas perineal fistulas are present in 10% ofpatients at time of diagnosis.
CD in the paediatric population may commonlypresent with systemic and extraintestinal ratherthan gastrointestinal symptoms. Isolated gastrodu-odenal disease is seen more commonly in paediat-ric patients and reported in 30e62% of patients onendoscopy and jejunal disease is also commoner inchildren as compared with adults.4,5
In the older age group, women are affectedmore frequently, and isolated involvement of thecolon rather than small bowel is commoner.5
Pathological findings
The earliest macroscopic feature of CD is shallowaphthoid mucosal ulceration, histologically corre-sponding to early mucosal ulceration over a muco-sal lymphoid follicle. CD most commonly involvesthe terminal ileum and ileocaecal region. Aph-thous ulcers progress to frank ulceration, and inlate stages, extensive linear and transmural ulcersmay be present. Advanced ulceration with bulgingof the oedematous residual mucosal islands leadsto the ‘‘cobblestone pattern’’. CD involves thewhole thickness of the bowel and also extends intothe mesentery and the lymph nodes draining thebowel. The classic macroscopic features of long-standing disease include fat wrapping, strictureformation, mucosal cobblestoning, linear mucosalulceration (classically on the mesenteric aspectof the bowel), deep mucosal fissuring, and fistulaformation. Another feature of CD is the presenceof clearly defined normal intestinal segmentsbetween diseased segments (termed ‘‘skip le-sions’’) and this pattern of discontinuous involve-ment is considered pathognomic of CD.
Neoplasia in CD
There is increased risk for adenocarcinoma of af-fected intestinal segments and the risk of colorectalcancer in Crohn’s colitis is four to 20 times higherthan that of the normal population, with an in-cidence of up to 1.8%.6,7 Defunctioned segments ofbowel have higher risk for developing cancer. Carci-noma may present as a stricturing lesion that can bedifficult to differentiate from benign strictures re-lated to CD. Lymphoma has been reported to presentas multifocal areas of increased nodularity and
strictures on barium examinations.8 Neoplastic le-sions should also be distinguished from stricturoplas-ties as both may appear as annular lesions withshouldered margins.9 Bowel cancer must be sus-pected when bowel obstruction in CD does not re-spond to conventional treatment and nasaldecompression.
Role of MRI in CD
Several scientific reports have reported that theinherent tissue contrast resolution obtained onMRI can provide good mural and extramuraldetail.10e19 Although as yet there is not enough ev-idence that MRI can identify early mucosal ulcers,some studies have shown that MRI has a good cor-relation with barium enteroclysis in demonstrationof mucosal lesions.10,20 MRI studies have reportedsensitivities and specificities ranging between88e98 and 78e100%, respectively, in the detectionof CD. MRI has also been used in the detection andfollow-up of CD in paediatric patients with sensi-tivity and specificity values 84e96 and 92e100%,respectively.14,21
MRI versus other diagnostic techniques
MRI versus CE. Prospective comparative trialsbetween MR enteroclysis (MRE) and CE have re-ported sensitivity and specificity ranges for MREof 82.5e89 and 100%, respectively, in the detec-tion of bowel ulceration; 100 and 88e92.9% inthe detection of stenosis; and 75e100 and97.8e100% in the detection of fistulae.13,22e25 Asignificantly higher number of abscesses, fibro-fatty proliferation, lymphadenopathy, and skip le-sions are detected on MRI than CE.13,22,26 In theirstudy, Umschaden et al.26 report that in 24% ofthe patients MRI demonstrated abnormalities notseen at CE, whereas another study detected of70% more abnormalities with MRE as comparedwith CE.27 MRE can provide identical functionalinformation regarding strictures and bowel ob-struction as compared with CE.26 A recent criti-cally appraised article has concluded that MREcompares favourably with CE in terms of diagnosticyield but is inferior in detection of early mucosalabnormalities.25
MRI versus CT. There are no robust studies di-rectly comparing CT with MRI in CD. One prospec-tive study that directly compared MRE with CTenteroclysis (CTE) showed better overall agree-ment for CTE than MRE (0.52 versus 0.42).28 How-ever, in this study the proof of disease, as basedon the findings at CTE combined with histological,

Role of MRI in Crohn’s disease 343
surgical, laboratory, and clinical data, was notavailable for each patient and, therefore, accu-rate evaluation of reported sensitivity and speci-ficity results cannot be performed. A comparisonof contrast-enhanced MRI with CT using oral con-trast media showed much higher sensitivity andspecificity for MRI.15 CT has high diagnostic sensi-tivity in suspected CD. Studies have reported sen-sitivities of 80e86.3% for CT when compared withCE, and 80e88% compared with ileocolonosco-py.24,29e31 CT enterography has also been reportedto be more sensitive than barium follow-throughexaminations in detection of active CD and extra-intestinal complications.32 Early mucosal lesions(such as aphthoid lesions) are not accurately visu-alized on CT or MRI, making them less suitable asa first-line examination for suspected early dis-ease. Extramural complications are well visualizedon CT, although the higher contrast resolution ofMRI makes it more suitable for the detection offistulae and abscesses than CT.24,33
MRI versus WCE. A prospective comparativestudy between MR enterography (MREG), CE,andWCE has shown CE to be the least sensitive andWCE to be the most sensitive technique in the de-tection of CD.34 MREG was less sensitive than WCE(83 versus 100%), although a statistically significantdifference between the performance of WCE andMREG was not detected.
Many studies have reported a higher diagnosticyield for WCE compared with radiological investi-gations. A meta-analysis comparing imaging versusWCE has shown yields of 30 versus 69%, respec-tively.35 However, the increase in use of WCE hasalso highlighted its limitations. Poor localizationof bowel abnormalities, camera retention, contra-indications in obstructive or stricture disease, andfalse-positive results are some of the significantdrawbacks of WCE. Furthermore as CD, by nature,has significant transmural, extraintestinal progres-sion, radiological investigations that provide muraland extramural detail provide complimentaryinformation to the WCE examination.36,37
MRI versus push enteroscopy. Double-balloon orpush enteroscopy have also been advocated forevaluation of the small bowel. The advantages ofthis method are the ability to directly visualizethe bowel mucosa and biopsy suspicious lesions.The disadvantages include patient discomfort andlong examination times. A pilot series has reportedcomparable findings for MRE and double-balloonenteroscopy in CD.38
MRI versus US. The advantages of US include itsnon-invasiveness and widespread availability.However, the significant disadvantages includeoperator dependence and the difficulty of viewing
the gastrointestinal tract in its entirety. US hashigh sensitivity in detection of CD, particularlydisease involving the terminal ileum. In a meta-analysis, the sensitivity and specificity ranges ofan US examination were reported to rangebetween 75e94 and 67e100%, respectively.39
MRI versus scintigraphy. Several studies havereported the use of labelled-leukocyte imagingin detecting CD and assessing its inflammatory ac-tivity.40e43 Labelled leukocytes are used becausemucosal infiltration with leukocytes is typicallypresent in active CD. Tc-99 m HMPAO is a com-monly used agent because of its greater availabil-ity, better image quality and lower radiationdose.44e46 Direct comparative studies betweenMRI and scintigraphy have not been reported, al-though the sensitivity and specificity of leuko-cyte-labelled scintigraphy has been reported torange between 76e94.7 and 77.8e93.3%, respec-tively.23 In recent years 2- [18F]-fluoro-2-deoxy-D-glucose positron-emission tomography (FDG-PET)has been used to assess inflammatory activity inCD.47e49 Neurath et al.49 reported strong correla-tion between MRI and FDG-PET findings in CD, al-though reported lower specificity values forMRI.49 The usefulness of PET in differentiating be-tween active and indolent CD is unclear and itsrole in diagnosis of CD needs evaluation in largerstudies.
Overview of imaging techniques versus MRI
Overall imaging techniques (US, MRI, scintigraphy,or CT) have high per-patient sensitivity (84.3e93%)and specificity (84.5e95.6%) for the diagnosis ofinflammatory bowel disease; although CT hada significantly lower sensitivity and specificitycompared with MRI and scintigraphy on a per-segment basis. Therefore, it may be justified touse any of these methods based on their advan-tages and disadvantages and local expertise.
Although CT is widely used in CD, it does carrya high radiation burden and the results of a recentmeta-analysis conclude that it is preferable to usea non-ionizing technique, such as US or MRI, inCD.23 A recent study has highlighted the high cu-mulative radiation dosages imparted to patientswith CD, mainly due to the increased use of CT.50
In this study CT accounted for up to 84.7% of thecumulative dose imparted to patients and 15.5%of patients had cumulative dosage in excess of75 mSv. The carcinogenic effect of radiation canbe particularly significant in patients with CDwho already have an increased risk of developinggastrointestinal, hepatobiliary cancer, and smallbowel lymphoma.

344 R. Sinha et al.
Among the non-ionizing techniques, the advan-tages of MRI over US include multiplanar imagingability, comprehensive assessment of the entiregastrointestinal tract and easier follow-up ofdisease with MRI images. The ability to distinguishfibrotic from inflammatory strictures and highsensitivity for detecting abscesses and fistulaeare the other important advantages. The disad-vantages of MRI are its longer examination timeand lack of consensus regarding oral contrastagents and timing of image acquisition in theenterographic technique.
MRI technique
The cardinal principle behind obtaining diagnosticsmall bowel images is good distension and opaci-fication of the bowel lumen coupled with ultrafastMRI sequences and intravenous contrast. Collapsedloops of bowel can even hide large lesions and mayappear falsely thickened. Distension of the smallbowel can be achieved with intubation or non-intubation techniques. For the intubation tech-nique (MRE) a nasojejunal catheter is placed at theduodeno-jejunal flexure and 1.5e2 l of iso-osmoticcontrast medium is infused. Imaging of bowel isperformed once contrast reaches the ileocaecaljunction. MRE produces excellent distension of thebowel and can provide detailed luminal informa-tion that is useful in identifying early muralchanges and also highlighting sub-acute or partialstrictures. However, these advantages have to becounter-balanced by the complexity of the pro-cedure and associated patient discomfort. Naso-jejunal intubation can be uncomfortable for thepatient and sedation or anxiolytics may beneeded.51 MREG is another technique where a largevolume of oral contrast medium is ingested by thepatient prior to imaging. Although the entero-graphic technique may be less uncomfortable forthe patient, it may not produce optimal and uni-form distension of the bowel lumen. Consistentdistension of the proximal bowel may also not beachieved on the enterographic technique as com-pared with the enteroclysis examination.
There is still no consensus on the amount of oralcontrast medium needed for an enterographicexamination and timing of image acquisition.Some studies have advocated long duration ofcontrast medium ingestion.52 Other investigatorsadvocate repeated imaging immediately after in-gestion until the contrast medium reaches the ter-minal ileum before formal imaging sequences areperformed. The second approach is less practicalas it increases the amount of examination timeneeded for the investigation.53 Kuehle et al.51
studied the effect of different types and volumesof oral contrast medium on bowel distension andtiming of image acquisition and found that gooddistension of the bowel was achieved with1350 ml contrast medium (1.2e2% sorbitol solutionand 0.2% locust bean gum) and no additional dis-tension was achieved by increasing the contrastmedium volume to 1800 ml.65 Water was found toprovide inadequate distension at all volumes.Ajaj et al.54 reported no significant differences inbowel distension with either 1000, 1200, or1500 ml mannitol solution. The optimal time forimaging the duodenum and proximal jejunum hasbeen reported to range between 0e15 min,whereas the distal jejunum and ileum can beappropriately imaged between 20e35 min aftercontrast medium ingestion.51 Lohan et al.55 has re-ported a mean time of 55 min for imaging and rec-ommends initial imaging at 20 min after contrastmedium ingestion to assess progress of the con-trast medium bolus and adjusting the timing ofthe examination accordingly.
Patients prefer MREG over MRE because there isless abdominal discomfort and nausea.56,57 Fur-thermore, patients are still exposed to radiationduring placement of the naso-jejunal catheterand the logistics of using two diagnostic rooms intandem needs to be considered.
The sensitivity of MREG for diagnosing CD hasbeen reported to be lower than the sensitivity ofMRE (p¼ .046), whereas specificity values arecomparable.23 However, a prospective, random-ized study showed a similar diagnostic sensitivityfor MREG as compared with MRE (88 versus 88%),and recommended enterographic examinationsfor follow-up of established CD.56 In the paediatricpopulation, MREG has been proposed as a less inva-sive technique as opposed to MRE. Studies have re-ported excellent patient tolerance of the MREGtechnique with high sensitivity and specificities inthe paediatric subgroup of CD.58e60
Oral contrast media. Several enteral contrastagents have been described that include water,methylcellulose, or solutions containing locust-bean gum, mannitol, and polyethyl glycol. Theseagents work by retarding the resorption of waterin the intestine. Superparamagnetic agents havealso been used as oral contrast agents, and theywork by altering signal intensity within the bowellumen. Enteral contrast agents may be positive,i.e., they produce increased signal intensity withinthe bowel lumen, whereas negative agents causea signal drop out. Biphasic agents behave as posi-tive or negative agents depending on the imagingsequence applied. Studies have reported differentadvantages and disadvantages for positive and

Role of MRI in Crohn’s disease 345
negative contrast agents, although there does notseem to be any significant difference in terms ofdiagnostic accuracy.61 Combined small and largebowel MRI has also been proposed as a feasibleand useful technique by some investigators.62,63
MRI sequences (Table 1). In recent years high-resolution, ultra-fast sequences based onsteady-state precession have been emerged asthe predominant technique for imaging of thesmall and large bowel in CD. Different manufac-turers’ call these sequences true fast imagingwith steady-state with free precession (true-FISP), balanced fast field echo (FFE) or fast imag-ing employing steady state precession (FIESTA).These sequences are relatively insensitive to mo-tion artefacts and provide uniform luminal opaci-fication and high contrast between the bowelwall, lumen, and the mesentery. The disadvan-tage of these sequences is a black boundary arte-fact along the bowel wall that may mask smalllesions or abnormalities. Fat suppression mayhelp in reducing the effects of the black-bound-ary artefact. Hohl et al.60 reported high sensitiv-ity and specificity (93.3 and 100%) of true-FISPsequences in detecting inflammatory lesions ofthe small bowel, and this sequence had greaterdiagnostic accuracy than T1, T2, and half-Fourieraxial single-shot fast spin-echo (HASTE) se-quences (80, 53.3, and 13.3%, respectively).They reported that the true-FISP had a significantsuperiority in soft-tissue differentiation comparedwith other sequences.
Table 1 Overview of MR Sequences for small bowel imaging use
MRI sequences 1.HASTE with fatsaturation (similarto SSFSE)
2.True-FISP& withoutsaturationto FIESTA;
Plane Coronal Coronal an
No. of sections 1 19e25Section thickness (mm) 50 4Field of view (mm2) 512� 512 512� 400Repetition time (ms) 5000 2.5e4.0Echo time (ms) 1080 1.6e1.8Flip angle (�) 90e140 50e80
MR enterography - Patients drink 1300 ml mannitol solution dividedimaged at 55 min with sequence 1 to assess progress of contrastsequences 2e4 performed. Small field of view, thin-section, truefor further characterization of disease.MR fluoroscopy can be performed using sequence 1 imaged every 6state with free precession) sequences.[HASTE, half-Fourier axialFIESTA, fast imaging employing steady state precession; bFFE, baangle shot; 3D, three-dimensional; VIBE, volumetric interpolated
Fast MRI sequences obviate the need for longbreath-holds and thus reduce motion or respiratoryartefacts. MRI images are also acquired usingT2-weighted fast sequences based on rapid acqui-sition and relaxation (RARE). Different manufac-turers call these sequences HASTE, or single shotfast spin echo (SSFSE). These sequences producehigh contrast between the lumen and the bowelwall. These sequences also do not have theblack-boundary artefact, although they are suscep-tible to motion artefacts produced by flow void. Dueto k-space filtering effects, visualization of the mes-enteric structures is impaired on these sequences.
Two-dimension (2D) or dimension spoilt gradientecho T1-weighted sequences are used to acquirecontrast-enhanced images. Fat saturation can beused to increase contrast resolution and alsoallows better assessment of bowel enhancement.64
Three-dimensional (3D) acquisitions allow thinnercollimation and allow multiplanar reconstruction(MPR), but are more prone to artefact production.Contrast-enhanced sequences using 2D and3D-FLASH (fast low angle shot) or volumetric se-quences, such as VIBE (volumetric interpolatedbreath-hold examination) have been reported inscientific literature.
During the examination bowel paralysis isinduced by intravenous injection of buscopan orglucagon. Changes in bowel kinetics can also beevaluated on MR fluoroscopy to demonstrate eitheran obstructive element or abnormalities in peri-stalsis. MR fluoroscopy can provide functional
d by the authors
withfat(similarbFFE)
3.HASTE with fatsaturation (similarto SSFSE)
4. Contrast-enhanced2D FLASH or 3D VIBEwith Fat Saturation
d axial Coronal and axial Coronal and axialunenhanced andenhanced (60 s aftercontrast mediumadministration)
19e25 644 1.5512� 512 288� 3121200 2.5e5.1280 1e2.590e140 10e20
in two aliquots. Each aliquot is drunk over 25 min and patient. If ileo-caecal region is opacified, buscopan is injected and-FISP sequences are performed for abnormal bowel segments
e8 s or single-section true-FISP (true fast imaging with steady-single-shot fast spin-echo; SSFFE, single shot fast field echo;lanced fast field echo; 2D, two-dimensional; FLASH, fast lowbreath-hold examination.]
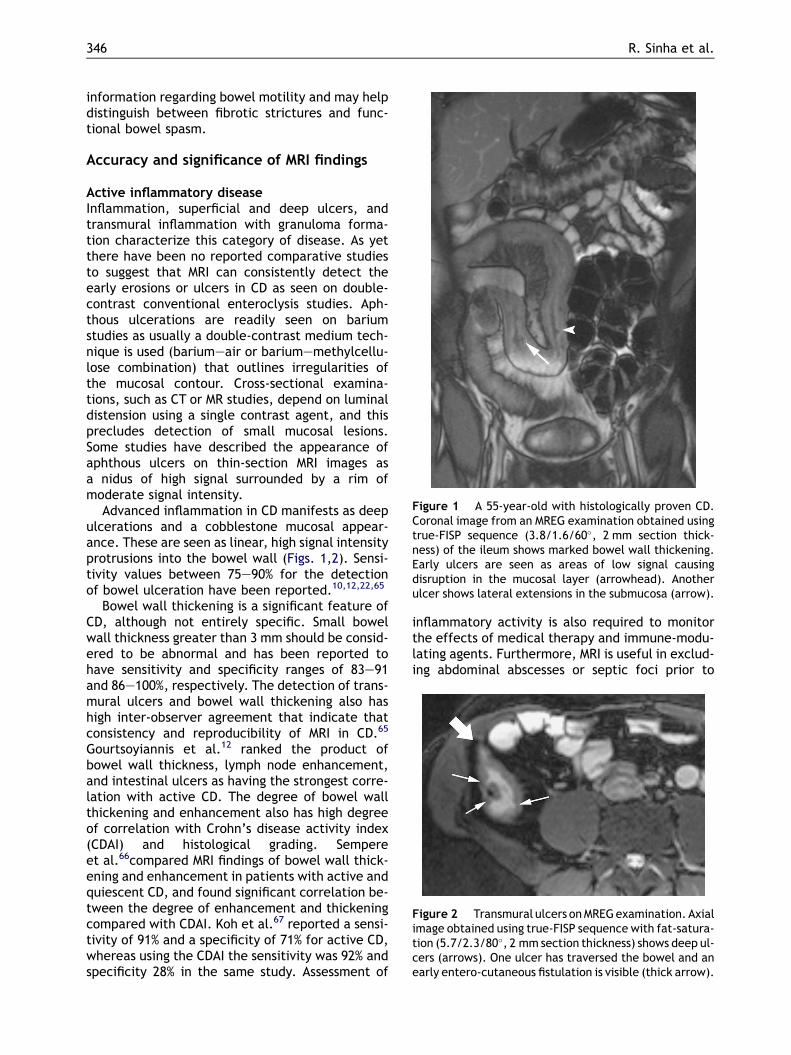
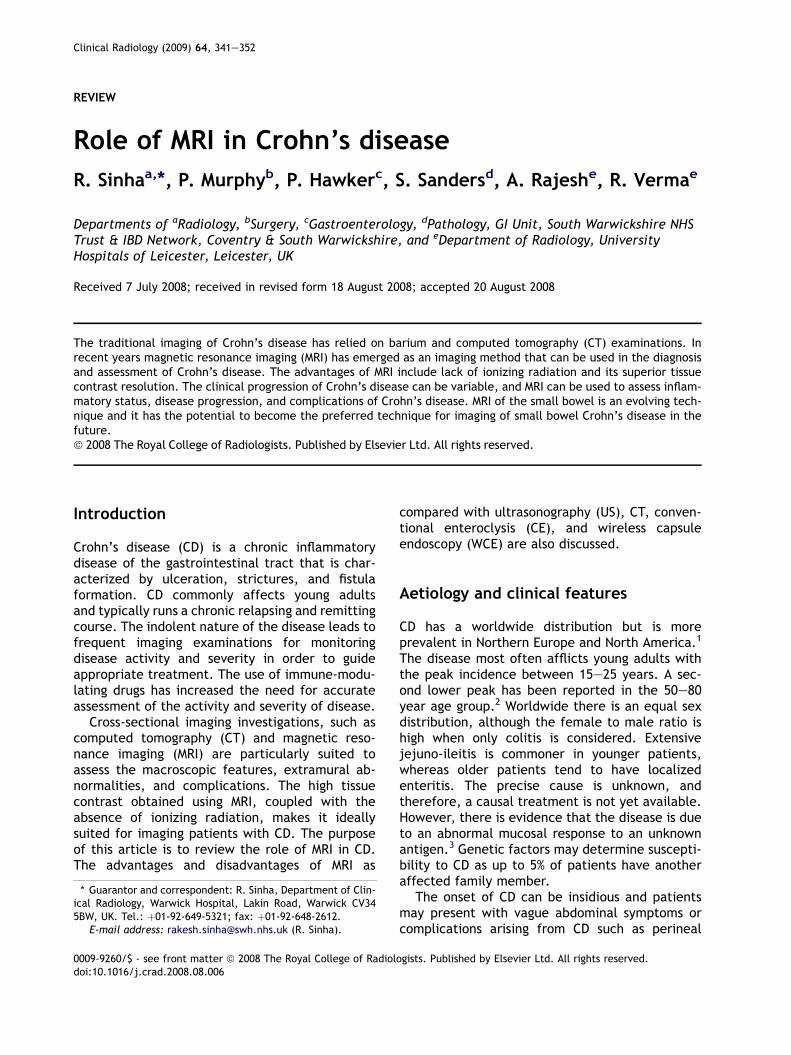
Figure 1 A 55-year-old with histologically proven CD.Coronal image from an MREG examination obtained usingtrue-FISP sequence (3.8/1.6/60�, 2 mm section thick-ness) of the ileum shows marked bowel wall thickening.Early ulcers are seen as areas of low signal causingdisruption in the mucosal layer (arrowhead). Anotherulcer shows lateral extensions in the submucosa (arrow).
Figure 2 Transmural ulcers on MREG examination. Axialimage obtained using true-FISP sequence with fat-satura-tion (5.7/2.3/80�, 2 mm section thickness) shows deep ul-cers (arrows). One ulcer has traversed the bowel and anearly entero-cutaneous fistulation is visible (thick arrow).
346 R. Sinha et al.
information regarding bowel motility and may helpdistinguish between fibrotic strictures and func-tional bowel spasm.
Accuracy and significance of MRI findings
Active inflammatory diseaseInflammation, superficial and deep ulcers, andtransmural inflammation with granuloma forma-tion characterize this category of disease. As yetthere have been no reported comparative studiesto suggest that MRI can consistently detect theearly erosions or ulcers in CD as seen on double-contrast conventional enteroclysis studies. Aph-thous ulcerations are readily seen on bariumstudies as usually a double-contrast medium tech-nique is used (bariumeair or bariumemethylcellu-lose combination) that outlines irregularities ofthe mucosal contour. Cross-sectional examina-tions, such as CT or MR studies, depend on luminaldistension using a single contrast agent, and thisprecludes detection of small mucosal lesions.Some studies have described the appearance ofaphthous ulcers on thin-section MRI images asa nidus of high signal surrounded by a rim ofmoderate signal intensity.
Advanced inflammation in CD manifests as deepulcerations and a cobblestone mucosal appear-ance. These are seen as linear, high signal intensityprotrusions into the bowel wall (Figs. 1,2). Sensi-tivity values between 75e90% for the detectionof bowel ulceration have been reported.10,12,22,65
Bowel wall thickening is a significant feature ofCD, although not entirely specific. Small bowelwall thickness greater than 3 mm should be consid-ered to be abnormal and has been reported tohave sensitivity and specificity ranges of 83e91and 86e100%, respectively. The detection of trans-mural ulcers and bowel wall thickening also hashigh inter-observer agreement that indicate thatconsistency and reproducibility of MRI in CD.65
Gourtsoyiannis et al.12 ranked the product ofbowel wall thickness, lymph node enhancement,and intestinal ulcers as having the strongest corre-lation with active CD. The degree of bowel wallthickening and enhancement also has high degreeof correlation with Crohn’s disease activity index(CDAI) and histological grading. Sempereet al.66compared MRI findings of bowel wall thick-ening and enhancement in patients with active andquiescent CD, and found significant correlation be-tween the degree of enhancement and thickeningcompared with CDAI. Koh et al.67 reported a sensi-tivity of 91% and a specificity of 71% for active CD,whereas using the CDAI the sensitivity was 92% andspecificity 28% in the same study. Assessment of
inflammatory activity is also required to monitorthe effects of medical therapy and immune-modu-lating agents. Furthermore, MRI is useful in exclud-ing abdominal abscesses or septic foci prior to
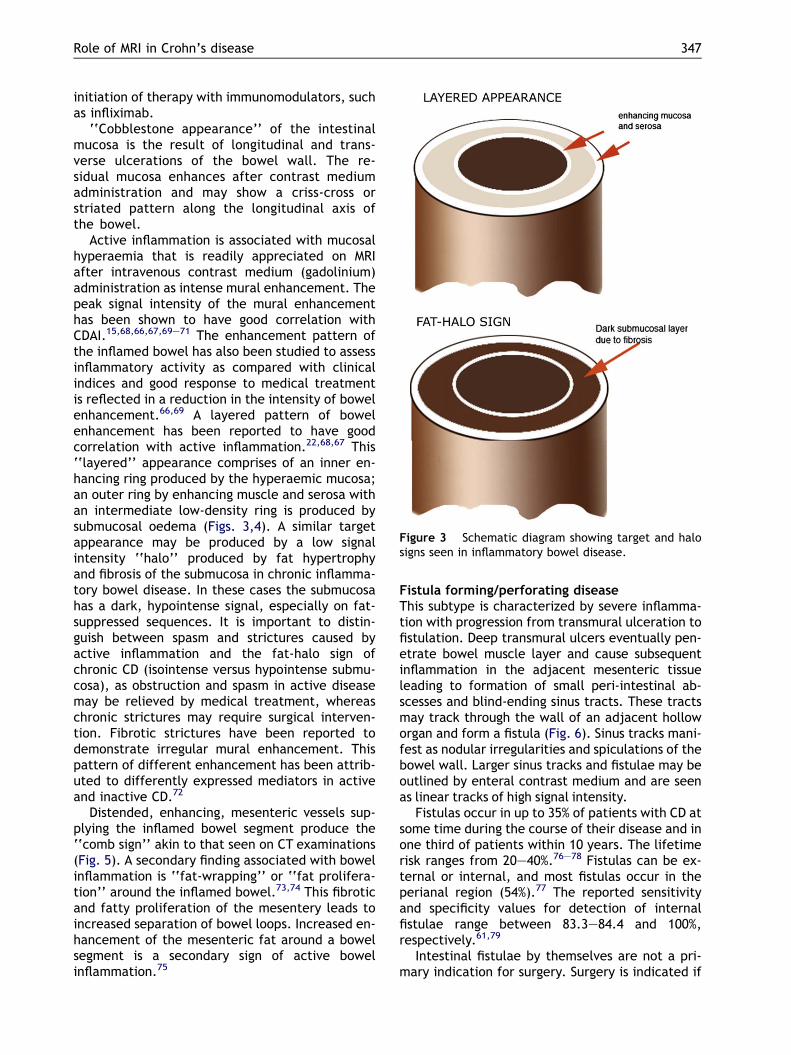
Figure 3 Schematic diagram showing target and halosigns seen in inflammatory bowel disease.
Role of MRI in Crohn’s disease 347
initiation of therapy with immunomodulators, suchas infliximab.
‘‘Cobblestone appearance’’ of the intestinalmucosa is the result of longitudinal and trans-verse ulcerations of the bowel wall. The re-sidual mucosa enhances after contrast mediumadministration and may show a criss-cross orstriated pattern along the longitudinal axis ofthe bowel.
Active inflammation is associated with mucosalhyperaemia that is readily appreciated on MRIafter intravenous contrast medium (gadolinium)administration as intense mural enhancement. Thepeak signal intensity of the mural enhancementhas been shown to have good correlation withCDAI.15,68,66,67,69e71 The enhancement pattern ofthe inflamed bowel has also been studied to assessinflammatory activity as compared with clinicalindices and good response to medical treatmentis reflected in a reduction in the intensity of bowelenhancement.66,69 A layered pattern of bowelenhancement has been reported to have goodcorrelation with active inflammation.22,68,67 This‘‘layered’’ appearance comprises of an inner en-hancing ring produced by the hyperaemic mucosa;an outer ring by enhancing muscle and serosa withan intermediate low-density ring is produced bysubmucosal oedema (Figs. 3,4). A similar targetappearance may be produced by a low signalintensity ‘‘halo’’ produced by fat hypertrophyand fibrosis of the submucosa in chronic inflamma-tory bowel disease. In these cases the submucosahas a dark, hypointense signal, especially on fat-suppressed sequences. It is important to distin-guish between spasm and strictures caused byactive inflammation and the fat-halo sign ofchronic CD (isointense versus hypointense submu-cosa), as obstruction and spasm in active diseasemay be relieved by medical treatment, whereaschronic strictures may require surgical interven-tion. Fibrotic strictures have been reported todemonstrate irregular mural enhancement. Thispattern of different enhancement has been attrib-uted to differently expressed mediators in activeand inactive CD.72
Distended, enhancing, mesenteric vessels sup-plying the inflamed bowel segment produce the‘‘comb sign’’ akin to that seen on CT examinations(Fig. 5). A secondary finding associated with bowelinflammation is ‘‘fat-wrapping’’ or ‘‘fat prolifera-tion’’ around the inflamed bowel.73,74 This fibroticand fatty proliferation of the mesentery leads toincreased separation of bowel loops. Increased en-hancement of the mesenteric fat around a bowelsegment is a secondary sign of active bowelinflammation.75
Fistula forming/perforating diseaseThis subtype is characterized by severe inflamma-tion with progression from transmural ulceration tofistulation. Deep transmural ulcers eventually pen-etrate bowel muscle layer and cause subsequentinflammation in the adjacent mesenteric tissueleading to formation of small peri-intestinal ab-scesses and blind-ending sinus tracts. These tractsmay track through the wall of an adjacent holloworgan and form a fistula (Fig. 6). Sinus tracks mani-fest as nodular irregularities and spiculations of thebowel wall. Larger sinus tracks and fistulae may beoutlined by enteral contrast medium and are seenas linear tracks of high signal intensity.
Fistulas occur in up to 35% of patients with CD atsome time during the course of their disease and inone third of patients within 10 years. The lifetimerisk ranges from 20e40%.76e78 Fistulas can be ex-ternal or internal, and most fistulas occur in theperianal region (54%).77 The reported sensitivityand specificity values for detection of internalfistulae range between 83.3e84.4 and 100%,respectively.61,79
Intestinal fistulae by themselves are not a pri-mary indication for surgery. Surgery is indicated if

Figure 4 Contrast-enhanced, axial, T1-weighted, 3Dsource image obtained on an MREG examination with vol-umetric interpolated breath-hold examination (5.3/2.4/10�, 2.5 mm section thickness) shows the inflamed termi-nal ileum with layered enhancement (arrows) comprisingof enhancing mucosa and serosa with the isointense,oedematous, submucosal layer in between (b) Axial,T1-weighted, 3D source image obtained with volumetricinterpolated breath-hold examination (5.3/2.4/10�,2.5 mm section thickness) shows the fat halo sign ofchronic Crohn’s disease manifesting as enhancing mucosaand serosa with a dark, hypointense submucosal layer.
Figure 5 MREG examination in a 55-year-old womanwith CD. Coronal image obtained using true-FISP se-quence (5.7/2.3/80�, 4 mm section thickness) showsthe thickened, inflamed segments of the ileum withassociated engorged mesenteric vessels producing the‘‘comb sign’’. Note separation of bowel loops due tofat proliferation of the mesentery.
348 R. Sinha et al.
fistulae connect to the renal tract causing renalimpairment or infection; if their drainage is causefor personal embarrassment and hygiene; or ifthey create a significant bypass resulting in in-testinal malabsorption. The global assessment ofthe bowel along with MPR images can also be ofhelp in planning surgical treatment.
Abdominal abscesses and inflammatory massesare less frequent than fistulae but are more oftenan indication to operative intervention. Smallerabscesses may be treated with antibiotics ordrained percutaneously under CT or ultrasoundguidance. Percutaneous, image-guided drainagemay obviate the need for surgery in a significantproportion of patients.80
Fibrostenotic diseaseThis pattern of disease is typically characterizedby bowel obstruction. On MRI a fixed narrowing ofthe affected segment without any significantbowel wall thickening or inflammation is seen.Chronic fibrotic strictures are typically hypoin-tense on both T1 and T2-weighted sequences(Fig. 7). Fibrotic strictures may show minor, inho-mogeneous contrast enhancement without anyevidence of oedema or surrounding mesentericinflammation or hyperaemia. MRE combined withMR fluoroscopy can provide functional assessmentof bowel obstruction and strictures similar to thoseobtained on CE with less patient discomfort.26
Commonly the obstruction is caused by a singlestricture and treatment is carried out by resectionand primary anastomosis.81 The terminal ileum isthe commonest affected location requiring surgeryand accounts for up to 40e50% of cases referred tosurgeons. Furthermore, one third of patients haverecurrent disease after ileocolic resection within10 years.82 MRI can provide useful information inthis setting by differentiating between fibroticand inflammatory strictures.64

Figure 6 MREG examination showing sinuses and fistu-lae. Coronal image obtained using true-FISP sequencewith fat-saturation (5.4/2.3/80�, 2 mm section thick-ness) shows multiple linear inflammatory sinuses(arrows) arising from the terminal ileum and a sinusthat has progressed to fistulation by communicationwith the adjacent bowel (ileo-ileal fistula) (arrowhead).
Figure 7 A 33-year-old man with CD and obstructivesymptoms. Contrast-enhanced, axial, T1-weighted, 3Dsource image obtained with volumetric interpolatedbreath-hold examination (5.3/2.4/10�, 2.5 mm sectionthickness) shows multiple strictures in the distal ileum(arrows). The strictures show minor, inhomogeneouscontrast enhancement and hypointense signal is seen inthe submucosal layer indicative of fibrosis. Note lack of oe-dema or inflammation in the surrounding mesenteric fat.
Role of MRI in Crohn’s disease 349
Perineal CDIt is estimated that perineal fistulas occur in30e50% of patients with CD and patients withrectal CD have almost a 100% incidence of perinealfistulas.83 The role of MRI in the diagnosis and indelineating the anatomy of perineal fistulae andinflammation has been extensively covered inscientific literature.84,85
Future potential
Higher field strength magnets and emerging tech-niques, such as parallel imaging, may help inimproving spatial and temporal resolution on MRI.It is possible that with parallel imaging high-resolu-tion 3D datasets comprising isotropic voxels of theentire abdomen could be produced within a singlebreath-hold.86 Hohl et al.87 reported the value ofparallel-imaging sequences that enable acquisitionof whole-body images within one breath-hold. 3Ddatasets would enable high-resolution MPR
reconstructions. Parallel imaging techniques alsohave the potential for improving dynamic imaging(such as MR fluoroscopy) due to their greater tempo-ral resolution combined with high spatialresolution.
Conclusion
The advantages of MRI in CD include its highsensitivity in diagnosis of disease and importantrole in assessment of inflammatory activity. Theability to distinguish fibrotic from inflammatorystrictures and high sensitivity for detectingabscesses and fistulae are the other importantadvantages that can help in guiding medical orsurgical treatment of patients.
Its non-ionizing nature is a particularly signifi-cant advantage. In the authors’ opinion, MRIexaminations should be the preferred cross-sec-tional technique in CD in view of the high radiationdosage imparted during CT examinations.88 Work-force limitations and expertise permitting, MREGwith its higher patient acceptability can providea valid alterative to barium or CT examinations inthe imaging of patients with CD.
References
1. Maglinte D, Gourtsoyiannis N, Rex D, et al. Classification ofsmall bowel Crohn’s subtypes based on multimodality imag-ing. Radiol Clin North Am 2003;41:285e303.

350 R. Sinha et al.
2. Fleischer DE, Grimm IS, Friedman LS. Inflammatory boweldisease in older patients. Med Clin North Am 1994;78:1303e19.
3. Przemioslo RT, Ciclitira PJ. Pathogenesis of Crohn’s disease.QJM 1995;88:525e7.
4. Halligan S, Nicholls S, Bartram CI, et al. The distribution ofsmall bowel Crohn’s disease in children compared to adults.Clin Radiol 1994;49:314e6.
5. Wills JS, Lobis IF, Denstman FJ. Crohn disease: state of theart. Radiology 1997;202:597e610.
6. Richards ME, Rickert RR, Nance FC. Crohn’s disease-associ-ated carcinoma. A poorly recognized complication of in-flammatory bowel disease. Ann Surg 1989;209:764e73.
7. Ribeiro MB, Greenstein AJ, Sachar DB, et al. Colorectal ade-nocarcinoma in Crohn’s disease. Ann Surg 1996;223:186e93.
8. Glick SN, Teplick SK, Goodman LR, et al. Development oflymphoma in patients with Crohn disease. Radiology 1984;153:337e9.
9. Kelly IM, Bartram CI. Pseudotumoral appearance of smallbowel strictureplasty for Crohn’s disease. Abdom Imaging1993;18:366e8.
10. Masselli G, Brizi G, Parrella A, et al. Crohn disease: magneticresonance enteroclysis. Abdom Imaging 2004;29:326e34.
11. ChouCK, ChenLT, SheuRS, etal.MRImanifestationsof gastro-intestinal wall thickening. Abdom Imaging 1994;19:389e94.
12. Gourtsoyiannis N, Papanikolaou N, Grammatikakis J, et al.Assessment of Crohn’s disease activity in the small bowelwith MR and conventional enteroclysis: preliminary results.Eur Radiol 2004;14:1017e24.
13. Gourtsoyiannis N, Grammatikakis J, Papamastorakis G,et al. Imaging of small intestinal Crohn’s disease: compari-son between MR enteroclysis and conventional enteroclysis.Eur Radiol 2006;16:1915e25.
14. Darbari A, Sena L, Argani P, et al. Gadolinium-enhancedmagnetic resonance imaging: a useful radiological tool in di-agnosing pediatric IBD. Inflamm Bowel Dis 2004;10:67e72.
15. Low RN, Francis IR. MR imaging of the gastrointestinal tractwith i.v., gadolinium and diluted barium oral contrastmedia compared with unenhanced MR imaging and CT.AJR Am J Roentgenol 1997;169:1051e9.
16. Maccioni F. Current status of gastrointestinal MRI. AbdomImaging 2002;27:358e60.
17. Maglinte D, Chernish S, Kelvin F, et al. Crohn disease of thesmall intestine: accuracy and relevance of enteroclysis.Radiology 1992;184:541e5.
18. Marcos HB, Semelka RC. Evaluation of Crohn’s disease usinghalf-fourier RARE and gadolinium-enhanced SGE sequences:initial results. Magn Reson Imaging 2000;18:263e8.
19. Semelka RC, Shoenut JP, Silverman R, et al. Bowel disease:prospective comparison of CT and 1.5-T pre- and postcon-trast MR imaging with T1-weighted fat-suppressed andbreath-hold FLASH sequences. J Magn Reson Imaging1991;1:625e32.
20. Prassopoulos P, Papanikolaou N, Grammatikakis J, et al. MRenteroclysis imaging of Crohn disease. RadioGraphics 2001;21:S161e172.
21. Laghi A, Borrelli O, Paolantonio P, et al. Contrast enhancedmagnetic resonance imaging of the terminal ileum in chil-dren with Crohn’s disease. Gut 2003;52:393e7.
22. Masselli G, Casciani E, Polettini E, et al. Assessment ofCrohn’s disease in the small bowel: prospective comparisonof magnetic resonance enteroclysis with conventional en-teroclysis. Eur Radiol 2006;16:2817e27.
23. Horsthuis K, Bipat S, Bennink RJ, et al. Inflammatory boweldisease diagnosed with US, MR, scintigraphy, and CT:meta-analysis of prospective studies. Radiology 2008;247:64e79.
24. Horsthuis K, Stokkers P, Stoker J. Detection of inflammatorybowel disease: diagnostic performance of cross-sectionalimaging modalities. Abdom Imaging 2008;33:417e24.
25. Ryan ER, Heaslip ISE. Magnetic resonance enteroclysis com-pared with conventional enteroclysis and computed tomog-raphy enteroclysis: a critically appraised topic. AbdomImaging 2008;33:34e7.
26. Umschaden HW, Szolar D, Gasser J, et al. Small-bowel dis-ease: comparison of MR enteroclysis images with conven-tional enteroclysis and surgical findings. Radiology 2000;215:717e25.
27. Frøkjaer JB, Larsen E, Steffensen E, et al. Magnetic reso-nance imaging of the small bowel in Crohn’s disease. ScandJ Gastroenterol 2005;40:832e42.
28. Schmidt S, Lepori D, Meuwly J, et al. Prospective compar-ison of MR enteroclysis with multidetector spiral-CT enter-oclysis: interobserver agreement and sensitivity by meansof ‘‘sign-by-sign’’ correlation. Eur Radiol 2003;13:1303e11.
29. Hassan C, Cerro P, Zullo A, et al. Computed tomography en-teroclysis in comparison with ileoscopy in patients withCrohn’s disease. Int J Colorectal Dis 2003;18:121e5.
30. Minordi LM, Vecchioli A, Guidi L, et al. Multidetector CT en-teroclysis versus barium enteroclysis with methylcellulosein patients with suspected small bowel disease. Eur Radiol2006;16:1527e36.
31. Wold PB, Fletcher JG, Johnson CD, et al. Assessment ofsmall bowel Crohn disease: noninvasive peroral CT enterog-raphy compared with other imaging methods and endoscopydfeasibility study. Radiology 2003;229:275e81.
32. Hara AK, Leighton AJ, Heigh RI, et al. Crohn’s disease of thesmall bowel: preliminary comparison between CT enterog-raphy, capsule endoscopy, small bowel follow-through,and ileoscopy. Radiology 2006;238:128e34.
33. Koelbel G, Schmiedl U, Majer MC, et al. Diagnosis of fistulaeand sinus tracts in patients with Crohn disease: value of MRimaging. AJR Am J Roentgenol 1989;152:999e1003.
34. Albert JG, Martiny F, Krummenerl A, et al. Diagnosis ofsmall bowel Crohn’s disease: a prospective comparison ofcapsule endoscopy with magnetic resonance imaging andfluoroscopic enteroclysis. Gut 2005;54:1721e7.
35. Triester SL, Leighton JA, Leontiadis GI, et al. A meta-analysis ofthe yield of capsule endoscopy compared to other diagnosticmodalities in patients with non-stricturing small bowel Crohn’sdisease. Am J Gastroenterol 2006;101:954e64.
36. Maglinte D, Sandrasegaran K, Chiorean M, et al. Radiologicinvestigations complement and add diagnostic informationto capsule endoscopy of small-bowel diseases. AJR AmJ Roentgenol 2007;189:306e12.
37. Sandrasegaran K, Maglinte DDT, Jennings SG, et al. Capsuleendoscopy and imaging tests in the elective investigation ofsmall bowel disease. Clin Radiol 2008;63:712e23.
38. Seiderer J, Herrmann K, Diepolder H, et al. Double-balloonenteroscopy versus magnetic resonance enteroclysis in di-agnosing suspected small-bowel Crohn’s disease: results ofa pilot study. Scand J Gastroenterol 2007;42:1376e85.
39. FraquelliM,Colli A,Casazza G,et al.Role ofUS indetectionofCrohn disease: meta-analysis. Radiology 2005;236:95e101.
40. Cucchiara S, Celentano L, de Magistris TM, et al. Colono-scopy and technetium-99m white cell scan in childrenwith suspected inflammatory bowel disease. J Pediatr1999;135:727e32.
41. Dhote R, Beades E, Le Dinh T, et al. Scintigraphy using leu-kocytes marked with 99m-Tc-HMPAO in Crohn’s disease.Acta Gastroenterol Belg 1995;58:353e63.
42. Almer S, Granerus G, Strom M, et al. Leukocyte scintigraphycompared to intraoperative small bowel enteroscopy and
Role of MRI in Crohn’s disease 351
laparotomy findings in Crohn’s disease. Inflamm Bowel Dis2007;13:164e74.
43. Rispo A, Imbriaco M, Celentano L, et al. Small bowel Crohn’sdisease: comparison of enteroclysis, bowel sonography andTc-99m-HMPAO leukocyte scintigraphy. Eur Rev Med Phar-macol Sci 2004;8:219e24.
44. Giaffer MH. Labelled leucocyte scintigraphy in inflamma-tory bowel disease: clinical applications. Gut 1996;38:1e5.
45. Mansfield JC, Giaffer MH, Tindale WB, et al. Quantitativeassessment of overall inflammatory bowel disease activityusing labelled leucocytes: a direct comparison between in-dium-111 and technetium-99m HMPAO methods. Gut 1995;37:679e83.
46. Sciarretta G, Furno A, Mazzoni M, et al. Technetium-99mhexamethyl propylene amine oxime granulocyte scintigra-phy in Crohn’s disease: diagnostic and clinical relevance.Gut 1993;34:1364e9.
47. Louis E, Ancion G, Colard A, et al. Noninvasive assessmentof Crohn’s disease intestinal lesions with (18)F-FDG PET/CT. J Nucl Med 2007;48:1053e9.
48. Madsen SM, Thomsen HS, Munkholm P, et al. Inflammatorybowel disease evaluated by low-field magnetic resonanceimaging. Comparison with endoscopy, 99mTc-HMPAO leuco-cyte scintigraphy, conventional radiography and surgery.Scand J Gastroenterol 2002;37:307e16.
49. Neurath MF, Vehling D, Schunk K, et al. Noninvasive assess-ment of Crohn’s disease activity: a comparison of 18F-fluoro-deoxyglucose positron emission tomography, hydromagneticresonance imaging, and granulocyte scintigraphy with la-beled antibodies. Am J Gastroenterol 2002;97:1978e85.
50. Desmond AN, O’Regan K, Curran C, et al. Crohn’s disease:factors associated with exposure to high levels of diagnosticradiation. Gut 2008;. doi:10.1136/gut.2008.151415.
51. Kuehle C, Ajaj W, Ladd S, et al. Hydro-MRI of the smallbowel: effect of contrast volume, timing of contrast admin-istration, and data acquisition on bowel distention. AJR AmJ Roentgenol 2006;187:375e85.
52. Lomas DJ, Graves MJ. Small bowel MRI using water as a con-trast medium. Br J Radiol 1999;72:994e7.
53. Patak MA, Froehlich JM, von Weymarn C, et al. Non-invasivedistension of the small bowel for magnetic-resonance imag-ing. Lancet 2001;358:987e8.
54. Ajaj W, Goehde SC, Schneemann H, et al. Dose optimizationof mannitol solution for small bowel distension in MRI.J Magn Reson Imaging 2004;20:648e53.
55. Lohan D, Cronin C, Meehan C, et al. MR small bowel enter-ography: optimization of imaging timing. Clin Radiol 2007;62:804e7.
56. Negaard A, Paulsen V, Sandvik L, et al. A prospective ran-domized comparison between two MRI studies of the smallbowel in Crohn’s disease, the oral contrast method andMR enteroclysis. Eur Radiol 2007;17:2294e301.
57. Negaard A, Sandvik L, Berstad AE, et al. MRI of the smallbowel with oral contrast or nasojejunal intubation inCrohn’s disease: randomized comparison of patient accep-tance. Scand J Gastroenterol 2008;43:44e51.
58. Godefroy C, Pilleul F, Dugougeat F, et al. Value of contrast-enhanced MR enterography in pediatric Crohn’s disease:preliminary study. J Radiol 2005;86:1685e92.
59. Pilleul F, Godefroy C, Yzebe-Beziat D, et al. Magnetic reso-nance imaging in Crohn’s disease. Gastroenterol Clin Biol2005;29:803e8.
60. Hohl C, Haage P, Krombach GA, et al. Diagnostic evaluationof chronic inflammatory intestinal diseases in children andadolescents: MRI with true-FISP as new gold standard?Rofo 2005;177:856e63.
61. Rieber A, Aschoff A, Nussle K, et al. MRI in the diagnosis ofsmall bowel disease: use of positive and negative oral con-trast media in combination with enteroclysis. Eur Radiol2000;10:1377e82.
62. Narin B, Ajaj W, Gohde S, et al. Combined small and largebowel MR imaging in patients with Crohn’s disease: a feasi-bility study. Eur Radiol 2004;14:1535e42.
63. Rottgen R, Herzog H, Lopez-Hanninen E, et al. Combinationof dynamic MR enteroclysis (Sellink) and MR colonography todiagnose Crohn’s disease. Rofo 2005;177:1131e8.
64. Shoenut JP, Semelka RC, Silverman R, et al. Magnetic reso-nance imaging in inflammatory bowel disease. J Clin Gas-troenterol 1993;17:73e8.
65. Negaard A, Sandvik L, Mulahasanovic A, et al. Magnetic res-onance enteroclysis in the diagnosis of small-intestinalCrohn’s disease: diagnostic accuracy and inter- andintra-observer agreement. Acta Radiol 2006;47:1008e16.
66. Sempere G, Martinez Sanjuan V, Medina Chulia E, et al. MRIevaluation of inflammatory activity in Crohn’s disease. AJRAm J Roentgenol 2005;184:1829e35.
67. Koh D, Miao Y, Chinn R, et al. MR imaging evaluation of theactivity of Crohn’s disease. AJR Am J Roentgenol 2001;177:1325e32.
68. Del Vescovo R, Sansoni I, Caviglia R, et al. Dynamic contrastenhanced magnetic resonance imaging of the terminalileum: differentiation of activity of Crohn’s disease. AbdomImaging 2007;33:417e24.
69. Florie J, Wasser M, Arts-Cieslik K, et al. Dynamic contrast-enhanced MRI of the bowel wall for assessment of diseaseactivity in Crohn’s disease. AJR Am J Roentgenol 2006;186:1384e92.
70. Low R, Sebrechts C, Politoske D, et al. Crohn disease withendoscopic correlation: single-shot fast spin-echo and gado-linium-enhanced fat-suppressed spoiled gradient-echo MRimaging. Radiology 2002;222:652e60.
71. Pauls S, Gabelmann A, Schmidt SA, et al. Evaluating bowelwall vascularity in Crohn’s disease: a comparison of dy-namic MRI and wideband harmonic imaging contrast-enhanced low MI ultrasound. Eur Radiol 2006;16:2410e7.
72. Koutroubakis IE, Tsiolakidou G, Karmiris K, et al. Role of an-giogenesis in inflammatory bowel disease. Inflamm BowelDis 2006;12:515e23.
73. Maccioni F, Bruni A, Viscido A, et al. MR imaging in patientswith Crohn disease: value of T2- versus T1-weighted gadoli-nium-enhanced MR sequences with use of an oral superpar-amagnetic contrast agent. Radiology 2006;238:517e30.
74. Desreumaux P, Ernst O, Geboes K, et al. Inflammatory alter-ations in mesenteric adipose tissue in Crohn’s disease. Gas-troenterology 1999;117:73e81.
75. Peyrin-Biroulet L, Chamaillard M, Gonzalez F, et al. Mesen-teric fat in Crohn’s disease: a pathogenetic hallmark or aninnocent bystander? Gut 2007;56:577e83.
76. Bell SJ, Williams AB, Wiesel P, et al. The clinical course offistulating Crohn’s disease. Aliment Pharmacol Ther 2003;17:1145e51.
77. Herrmann K, Michaely H, Zech C, et al. Internal fistulas inCrohn disease: magnetic resonance enteroclysis. AbdomImaging 2006;31:675e87.
78. Schwartz DA, Loftus EV, Tremaine WJ, et al. The naturalhistory of fistulizing Crohn’s disease in Olmsted County, Min-nesota. Gastroenterology 2002;122:875e80.
79. Schreyer AG, Geissler A, Albrich H, et al. Abdominal MRIafter enteroclysis or with oral contrast in patients withsuspected or proven Crohn’s disease. Clin GastroenterolHepatol 2004;2:491e7.
80. Gervais DA, Hahn PF, O’Neill MJ, et al. Percutaneousabscess drainage in Crohn disease: technical success and

352 R. Sinha et al.
short- and long-term outcomes during 14 years. Radiology2002;222:645e51.
81. Michelassi F, Balestracci T, Chappell R, et al. Primary andrecurrent Crohn’s disease. Experience with 1379 patients.Ann Surg 1991;214:230e8.
82. Bernell O, Lapidus A, Hellers G. Risk factors for surgery andrecurrence in 907 patients with primary ileocaecal Crohn’sdisease. Br J Surg 2000;87:1697e701.
83. Szurowska E, Wypych J, Izycka-Swieszewska E. Perianalfistulas in Crohn’s disease: MRI diagnosis and surgical plan-ning: MRI in fistulazing perianal Crohn’s disease. AbdomImaging 2007;32:705e18.
84. Rasul I, Wilson SR, MacRae H, et al. Clinical and radiolog-ical responses after infliximab treatment for perianal
fistulizing Crohn’s disease. Am J Gastroenterol 2004;99:82e8.
85. Van Assche G, Vanbeckevoort D, Bielen D, et al. Magneticresonance imaging of the effects of infliximab on perianalfistulizing Crohn’s disease. Am J Gastroenterol 2003;98:332e9.
86. Patak MA, von Weymarn C, Froehlich JM. Small bowel MRimaging: 1.5T versus 3T. Magn Reson Imaging Clin N Am2007;15:383e93.
87. Hohl C, Honnef D, Krombach G, et al. Pediatric bowel MRI d
accelerated parallel imaging in a single breathhold. Rofo2008;180:402e9.
88. Sinha R, Nwokolo C, Murphy PD. Magnetic resonance imag-ing in Crohn’s disease. BMJ 2008;336:273e6.




















