
Phosphatidylcholine-Specific Phospholipase C Activation in Epithelial Ovarian Cancer Cells
Upload
independentCategory
view
1download
0
CORRESPONDENCE
Need for a Three-Focused Approach to Nonalcoholic Fatty Liver Disease
To the Editor:
We read with interest the reviews by Ghouri et al.1 and Marti-nez et al.2 Ghouri et al. analyzed the association of nonalcoholicfatty liver disease (NAFLD) with cardiovascular disease (CVD) andconcluded that although a diagnosis of NAFLD should prompt di-abetes screening, it is insufficient for considering patients to be athigh risk for CVD. Martinez et al. evaluated noninvasive methodsfor assessing liver fibrosis and recommended that those tests withthe highest diagnostic accuracy be validated against liver biopsy tofacilitate their implementation in clinical practice.
We meta-analyzed prospective data regarding the natural historyof NAFLD and studies assessing the diagnostic accuracy of nonin-vasive methods for liver disease severity against liver biopsy inNAFLD, and we reached the following conclusions3:
1. The two NAFLD histological subtypes, simple steatosis (SS)and nonalcoholic steatohepatitis (NASH), have different risks ofliver-related complications: SS progresses to cirrhosis in less than5% of cases; NASH progresses to cirrhosis in 10% to 15% of casesover 10 years and in 25% to 30% of cases in the presence ofadvanced fibrosis.3
2. NAFLD patients have a 1.44- to 2.05-fold higher rate ofCVD (depending on whether the diagnosis is based on an amino-transferase elevation or radiological/histological criteria) than thegeneral population; restricting the analysis to studies adjusting formetabolic syndrome did not change the risk. Importantly, CVDmortality did not differ among NAFLD histological subtypes.3
3. NAFLD conveys a 2-fold increased risk of developing diabe-tes in comparison with the general population3; restricting theanalysis to studies adjusting for metabolic syndrome did notchange the risk. Whether the risk of diabetes differs amongNAFLD histological subtypes remains unclear: in a community-based study, the 13-year incidence of diabetes was 2.98-fold higherin NASH patients versus SS patients.3
According to our analysis, a diagnosis of NAFLD shouldprompt a thorough three-focus assessment of cardiovascular, meta-bolic, and liver-related risks (Table 1).4
Liver-related risk assessment remains problematic because itrequires liver histology. Three noninvasive methods have been
extensively validated: enzyme-linked immunosorbent assay-detectedcytokeratin 18 fragments (9 studies enrolling 856 participants) forthe detection of NASH and the NAFLD fibrosis score (13 studiesenrolling 3064 participants) and FibroScan (6 studies enrolling563 participants) for the detection of advanced fibrosis. We believethat these methods should be promptly implemented in diagnosticalgorithms to select patients for liver biopsy in routine clinicalpractice while we continue to search for the ideal noninvasivemarker.
GIOVANNI MUSSO, M.D.1
ROBERTO GAMBINO, PH.D.2
MAURIZIO CASSADER, PH.D.21Gradenigo Hospital, Turin, Italy2Department of Internal Medicine
University of Turin, Turin, Italy
References1. Ghouri N, Preiss D, Sattar N. Liver enzymes, nonalcoholic fatty liver
disease, and incident cardiovascular disease: a narrative review and clini-cal perspective of prospective data. Hepatology 2011;52:1156-1161.
2. Martinez S, Crespo G, Navasa M, Forns X. Non-invasive assessment ofliver fibrosis. Hepatology 2011;52.
3. Musso G, Gambino R, Cassader M, Pagano G. Meta-analysis: naturalhistory of non-alcoholic fatty liver disease (NAFLD) and diagnostic ac-curacy of non-invasive tests for liver disease severity. Ann Med; doi:10.3109/07853890.2010.518623.
4. Stein JH, Korcarz CE, Hurst RT, Lonn E, Kendall CB, Mohler ER, et al.Use of carotid ultrasound to identify subclinical vascular disease and evaluatecardiovascular disease risk: a consensus statement from the American Societyof Echocardiography Carotid Intima-Media Thickness Task Force endorsedby the Society for Vascular Medicine. J Am Soc Echocardiogr 2008;21:93-111.
CopyrightVC 2011 by the American Association for the Study of Liver Diseases.View this article online at wileyonlinelibrary.com.DOI 10.1002/hep.24070Potential conflict of interest: Nothing to report.
Table 1. Suggested Evaluation of Patients With NAFLD
Disease Risk NAFLD Assessment
Diabetes Measure the body mass index, waist circumference, fasting plasma glucose and insulin level, and hemoglobin A1c level.*
Perform the 75-g oral glucose tolerance test in NAFLD patients without known diabetes according to standard guidelines
(i.e., the American Diabetes Association) to classify their glucose tolerance.
Calculate the fasting index of insulin resistance (homeostasis model assessment of insulin resistance), which is associated
with the severity of liver disease and has prognostic value in NAFLD.
CVD Assess smoking status, measure blood pressure, plasma total cholesterol, low density lipoprotein (LDL)-cholesterol,
high density lipoprotein(HDL) cholesterol and triglycerides.
Calculate the CVD risk score (i.e., Framingham risk score).
Perform B-mode carotid ultrasonography in patients without diabetes or established CVD who have intermediate CVD risk
(Framingham risk score ¼ 6%-20%) to measure carotid intima-media thickening according to recent guidelines6 (optional).
Liver-related
(end-stage liver disease)
Apply noninvasive tests (i.e., the serum cytokeratin 18 fragment assay, NAFLD fibrosis score, and FibroScan) to
screen for the presence of NASH with or without advanced fibrosis.
If noninvasive tests yield a high probability of NASH (with or without advanced fibrosis), refer to a gastroenterologist
for liver biopsy, the assessment of complications of cirrhosis (hepatic failure, portal hypertension, esophageal varices,
and hepatocellular carcinoma), experimental treatments, and tight monitoring.
Liver biopsy remains necessary for staging and monitoring the course of liver disease in patients with NASH and if
the diagnosis of NAFLD is in doubt.
*According to recent guidelines, hemoglobin A1c can be used for screening for type 2 diabetes.
1773

Reply:
We thank Musso and colleagues for their useful comments onour article. We agree that a comprehensive approach to patientswith nonalcoholic fatty liver disease, namely one which considerstheir diabetes and cardiovascular risk, as well as their long-termliver-related risk, is needed. We wish only to make some points ofclarification which will help hepatologists to efficiently assess cardi-ovascular and diabetes risk in their patients. First, there have beenrecent calls, recently verified by the World Health Organization, todiagnose diabetes by measurement of hemoglobin A1c (HbA1c),and this measure has the advantage of being measurable on non-fasting samples.1 Of interest, HbA1c is at least as good as fastingglucose at assessing microvascular risk and appears to be the bestglycemic predictor of macrovascular risk, performing even betterthan the 2-hour glucose tolerance test.2 We would therefore argueagainst routine oral glucose tolerance testing in patients with non-alcoholic fatty liver disease, because of both clinical and economicalconcerns. Second, the benefit of testing for insulin as a prognosticfactor, we believe, remains to be proven. At present, we wouldadvise against measuring insulin routinely, at least until thisapproach has been shown to be cost-effective. Third, lipid tests toenhance prediction of cardiovascular disease (as part of nationalcardiovascular risk guidelines or algorithms) also do not requirefasting, as recently shown by the Emerging Risk Factor Collabora-tion group.3 Rather, nonfasting total cholesterol (or low-densitylipoprotein cholesterol or non–high-density lipoprotein cholesterol)and high-density lipoprotein cholesterol adequately reflect lipid-associated vascular risk and perform as well as fasting lipids3 forrisk prediction. Fasting is therefore not required to test for diabe-tes, or indeed cardiovascular risk, in the majority of patients.Finally, we have recently proposed4 how combined vascular and di-abetes screening may be conducted by simply adding a nonfastingHbA1c test to nonfasting lipids as part of a cardiovascular risk
screen, a simple process which may be easily added to other rou-tine tests conducted in most hepatology and hepatology-relatedclinics.
NAZIM A. GHOURI, M.D.DAVID PREISS, M.D.NAVEED SATTAR, M.D.*Institute of Cardiovascular & Medical Sciences,
British Heart Foundation Glasgow Cardiovascular Research CentreUniversity of GlasgowGlasgow, UK
References1. International Expert Committee. International Expert Committee
report on the role of the A1C assay in the diagnosis of diabetes. Diabe-tes Care 2009;32:1327–1334.
2. Sarwar N, Aspelund T, Eiriksdottir G, Gobin R, Seshasai SR, ForouhiNG, et al. Markers of dysglycaemia and risk of coronary heart diseasein people without diabetes: Reykjavik prospective study and systematicreview. PLoS Med 2011;7:e1000278.
3. Emerging Risk Factors Collaboration;Di Angelantonio E, Sarwar N,Perry P, Kaptoge S, Ray KK, Thompson A, et al. Major lipids, apolipo-proteins, and risk of vascular disease. JAMA 2009;302:1993–2000.
4. Preiss D, Khunti K, Sattar N.Combined cardiovascular and diabetesrisk assessment in primary care. Diabet Med 2011;28:19–22.
CopyrightVC 2011 by the American Association for the Study of Liver Diseases.View this article online at wileyonlinelibrary.com.DOI 10.1002/hep.24138Potential conflict of interest: Nothing to report.
Association Between Virological Response and Decline in Hemoglobin Concentration DuringPegylated Interferon and Ribavirin Therapy in HCV Genotype 1: Another Story
To the Editor:
We read with great interest the article in HEPATOLOGY by Sievertet al.,1 which retrospectively evaluated the CHARIOT study of871 treatment-naive patients who were infected with hepatitis Cvirus (HCV) genotype 1 (HCV-1) to determine whether hemoglo-bin decline is associated with sustained virological response (SVR)achieved through pegylated interferon (PegIFN) and ribavirin treat-ment. With 16% of patients developing anemia (serum hemoglo-bin <100 g/L) and 76% of patients developing a hemoglobindecline of >30 g/L from baseline, SVR rate was higher in anemicpatients compared to those without anemia (61% versus 50%,respectively; P ¼ 0.02). The authors concluded that the develop-ment of anemia or experience of a decline in hemoglobin of >30g/L predicts better SVR in HCV-1 patients who receive PegIFN/ribavirin treatment which has also been reported in the post hocanalysis of the IDEAL study by Sulkowski et al. (74%).2
We examined the 100 Taiwanese HCV-1 patients who received48-week PegIFN/ribavirin treatment in our randomized trial thatenrolled a total of 200 patients.3 The means (6standard devia-tions) for baseline, lowest, and decline of hemoglobin levels were146 6 14 g/L, 103 6 17 g/L, and 42 6 14 g/L, respectively. Wefound 45% of patients developed anemia (serum hemoglobin<100 g/L) and 78% developed hemoglobin decline of >30 g/Lfrom baseline. With 79 patients (79%) achieving SVR, the SVR ratewas similar between patients with and without anemia (77.8% versus
80%, P ¼ 0.786). Also, the SVR rate in patients with hemoglobindecline >30 g/L was similar compared to patients without hemoglo-bin decline >30 g/L (78.2% versus 81.8%, P ¼ 1.000). The means(6standard deviations) for baseline, lowest, and decline of hemoglo-bin level were similar between patients with and without SVR (1466 13 g/L versus 143 6 15 g/L, P ¼ 0.286; 104 6 17 versus 102 619 g/L, P ¼ 0.670; 43 6 14 versus41 6 14 g/L, P ¼ 0.600). Thetreatment-related anemia seems to play a minimal role in predictingSVR in Taiwanese patients infected with HCV-1.
We showed the percentage of hemoglobin decline >30 g/L(78%) in Taiwanese patients who received PegIFN/ribavirin treat-ment without erythropoietin was similar to reports by Sievert et al.(76%) and Sulkowski et al. (74%). Nevertheless, we reported ahigher percentage (45%) of anemia (serum hemoglobin <100 g/L)in Taiwanese patients than that reported by Sievert et al. (16%)1
and Sulkowski et al. (29%).2 In addition to the lack of erythro-poietin use in our study, another major reason for the higher rateof ribavirin-related anemia may be due to the significantly lowerbody weight (67.5 kg) of our patients than those of Sievert et al.(77.9 kg) and Sulkowski et al. (83.4 kg), leading to relativelyhigher initial ribavirin exposure (up to 15 mg/kg body weight/day).2 The high ribavirin exposure—just as the water that bears theboat is the same that swallows it up—may induce more anemiaduring treatment but leads to a higher SVR rate. In addition, therecent novel finding showed Asian patients have the highest fre-quency of the advantageous genotype in the gene region encoding
1774 CORRESPONDENCE HEPATOLOGY, May 2011

interleukin-28B (IL-28B, also called IFNk3), which is a very strongpredictor of treatment response.4 We have recently conducted alarge-scale study5 to test 552 Taiwanese HCV-1 patients; of these,469 (85.0%) have favorable rs8099917, located �8 kilobasesupstream of the IL-28B TT genotype, which enhances the treat-ment outcome in HCV-1 infection6,7 and is associated with therapid virological response in HCV genotype 2 infection in Taiwan-ese patients.8 Taken together, it is not difficult to understand whyTaiwanese HCV-1 patients have a high SVR rate with PegIFN/rib-avirin therapy. We consider that such a good response in TaiwaneseHCV-1 patients might also possibly contribute to minimizing therole of anemia on predicting the treatment outcome shown by Sie-vert et al.1 and Sulkowski et al.,2 and further studies are needed.
CHIA-YEN DAI, M.D., PH.D.1,2,3
CHUNG-FENG HUANG, M.D., M.S.1,2,5
JEE-FU HUANG, M.D.1,4,6
WAN-LONG CHUANG, M.D., PH.D.1,4
MING-LUNG YU, M.D., PH.D.1,4,51Hepatobiliary Division, Department of Internal Medicine, and
2Hepatobiliary Division, Department of Occupational Medicine,Kaohsiung Medical University Hospital, Kaohsiung, Taiwan
3Graduate Institute of Medicine and 4Faculty of Internal Medicine,College of Medicine, Kaohsiung Medical University, Kaohsiung,Taiwan
5Department of Internal Medicine, Kaohsiung Municipal Ta-TungHospital, Kaohsiung, Taiwan
6Department of Internal Medicine, Kaohsiung Municipal Hsiao-KangHospital, Kaohsiung, Taiwan
References1. Sievert W, Dore GJ, McCaughan GW, Yoshihara M, Crawford DH,
Cheng W, et al. Virological response is associated with decline in he-moglobin concentration during pegylated interferon and ribavirintherapy in HCV genotype 1. HEPATOLOGY 2011; doi:10.1002/hep.24180.
2. Sulkowski M, Shiffman M, Afdhal N, Reddy K, McCone J, Lee W,et al. Hepatitis C virus treatment-related anemia is associated withhigher sustained virologic response rate. Gastroenterology 2011;139:1602-1611.
3. Yu ML, Dai CY, Huang JF, Chiu CF, Yang YH, Hou NJ, et al. Rapidvirological response and treatment duration for chronic hepatitis C geno-type 1 patients: A randomized trial. HEPATOLOGY 2008;47:1884-1893.
4. Ge D, Fellay J, Thompson AJ, Simon JS, Shianna KV, Urban TJ, et al.Genetic variation in IL28B predicts hepatitis C treatment-induced viralclearance. Nature 2009;461:399-401.
5. Huang CF, Dai CY, Huang JF, Chuang WL, Yu ML. The linkage ofhepatitis C viral genotype and interleukin-28B genetic polymorphismsin Asian patients. HEPATOLOGY 2011;53:367-368.
6. Tanaka Y, Nishida N, Sugiyama M, Kurosaki M, Matsuura K, Saka-moto N, et al. Genome-wide association of IL28B with response topegylated interferon-alpha and ribavirin therapy for chronic hepatitisC. Nat Genet 2009;41:1105-1109.
7. Suppiah V, Moldovan M, Ahlenstiel G, Berg T, Weltman M, AbateML, et al. IL28B is associated with response to chronic hepatitis Cinterferon-alpha and ribavirin therapy. Nat Genet 2009;41:1100-1104.
8. Yu ML, Huang CF, Huang JF, Chang NC, Yang JF, Lin ZY, et al. Roleof interleukin-28B polymorphisms in the treatment of hepatitis C virusgenotype 2 infection in Asian patients. HEPATOLOGY 2011;53:7-13.
CopyrightVC 2011 by the American Association for the Study of Liver Diseases.View this article online at wileyonlinelibrary.com.DOI 10.1002/hep.24204Potential conflict of interest: Nothing to report.
Reply:
We thank Professor Yu and colleagues for their interest in ourstudy.1 In the CHARIOT (Collaborative group HepAtitis C studyusing PegasysRBV Induction dose in genOType one) study of 871patients, we showed that patients with anemia or a hemoglobindecline of >30 g/L from baseline had higher sustained virologicalresponse (SVR) rates compared to those who did not experience sim-ilar hematological changes. A similar outcome was reported from theIDEAL (Individualized Dosing Efficacy Versus Flat Dosing to AssessOptimal Pegylated Interferon Therapy) study of 3023 patients.2
Both study populations were primarily Caucasian. Yu and colleaguesexamined a subset of 100 patients from a total study population of200 Taiwanese patients treated with pegylated interferon and ribavirinfor 48 weeks and found a higher rate of anemia development (45%)and a similar rate of patients with a hemoglobin decline of >30 g/Lfrom baseline (78%). There was no significant difference in SVR ratesbetween patients with and patients without the hematological changes.We therefore further analyzed the CHARIOT study population strati-fied by ethnicity (Asian, n ¼ 118 versus non-Asian, n ¼ 778). Asianpatients were more likely to develop anemia than non-Asians (27%versus 14%, P < 0.001) but had a similar likelihood of hemoglobindecline >30 g/L from baseline (71% versus 74%, P ¼ 0.494). Withinthe Asian population, SVR rates were not significantly higher for thosewith anemia (71% versus 59%, P ¼ 0.188) or those with hemoglobindecline >30 g/L from baseline (74% versus 66%, P ¼ 0.379). Withinthe non-Asian population, SVR rates were higher for those with ane-mia (57% versus 46%, P ¼ 0.036) and those with hemoglobin decline>30 g/L from baseline (51% versus 36%, P < 0.001). These contrast-ing levels of significance may relate to sample size, because the SVRdifferential for the impact of anemia was similar in the Asian (12%)and non-Asian (11%) populations.
An alternative explanation, as proposed by Yu et al., may relateto the higher proportion of patients with a favorable interleukin-28B (IL28B) genotype,3 leading to an overall higher SVR rate.Although the SVR rate within the CHARIOT Asian populationwas not as high as in the Taiwanese study (79%) it was signifi-cantly higher than the non-Asian population (68% versus 47%,P < 0.001). Ultimately, multivariate analysis including IL28B ge-notype and on-treatment anemia in a large treatment populationwill be required to conclusively demonstrate the relative influenceof each factor on treatment outcome.4
WILLIAM SIEVERT, M.D.1
GREGORY J. DORE, B.SC., M.B., B.S., PH.D.2
STUART K. ROBERTS, M.D.3
On behalf of the CHARIOT Study Group1Gastroenterology and Hepatology Unit
Monash Medical Centre and Centre for Inflammatory DiseasesMonash University, Melbourne, Australia
2National Centre in HIV Epidemiology and Clinical ResearchUniversity of New South Wales and St Vincent’s HospitalSydney, Australia
3Alfred Hospital, Melbourne, Victoria, Australia
References1. Sievert W, Dore GJ, McCaughan GW, Yoshihara M, Crawford DH,
Cheng W, et al. Virological response is associated with decline in he-moglobin concentration during pegylated interferon and ribavirin ther-apy in HCV genotype 1. HEPATOLOGY 2011; doi:10.1002/hep.24180.
2. Sulkowski M, Shiffman M, Afdhal N, Reddy K, McCone J, Lee W, et al.Hepatitis C virus treatment-related anemia is associated with higher sus-tained virologic response rate. Gastroenterology 2011;139:1602-1611.
3. Ge D, Fellay J, Thompson AJ, Simon JS, Shianna KV, Urban TJ, et al.Genetic variation in IL28B predicts hepatitis C treatment-induced viralclearance. Nature 2009;461:399-401.
HEPATOLOGY, Vol. 53, No. 5, 2011 CORRESPONDENCE 1775

4. Thompson AJ, Muir AJ, Sulkowski M, Ge D, Fellay J, Shiana KV,et al. Interleukin-28B polymorphism improves viral kinetics and is thestrongest pretreatment predictor of sustained virologic response in ge-notype 1 hepatitis C virus. Gastroenterology 2011;139:120-129.
CopyrightVC 2011 by the American Association for the Study of Liver Diseases.View this article online at wileyonlinelibrary.com.DOI 10.1002/hep.24250Potential conflict of interest: Nothing to report.
Patatin-Like Phospholipase Domain Containing 3 Sequence Variant and Hepatocellular Carcinoma
To the Editor:
In a recent article in HEPATOLOGY, Valenti et al.1 reported anassociation of the patatin-like phospholipase domain containing 3(PNPLA3) isoleucine-to-methionine substitution at position 148(I148M; rs738409) with hepatitis C virus (HCV)-related chronicliver disease. In particular, they showed this genetic variant wasassociated with fatty liver and fibrosis progression in two independ-ent cohorts of Caucasians with chronic HCV. In one study cohort,they also reported an independent association with hepatocellularcarcinoma (HCC) in homozygous 148M carriers.1 Our goal was toexamine the latter association in a cohort of individuals withHCV-related cirrhosis, comparing those with and without HCC.
We genotyped a total of 221 (male/female ¼ 141/80) Cauca-sians at the Department of Gastroenterology, ‘‘Sapienza’’ Universityof Rome, Italy, for the PNPLA3 148M allele. Inclusion criteriawere presence of clinical cirrhosis, HCV RNA positivity, surveil-lance for HCC for at least 2 years, and alcohol consumption of<20 and <30 g/day for women and men, respectively. Mean agewas 58 6 11 years, 31% had diabetes, and 41% had radiologicaland/or histological diagnosis of HCC.
We performed a multivariate analysis that included HCC as de-pendent variable and age, sex, diabetes, and the 148M genotype(148M homozygotes versus the other genotypes) as covariates. Wefound homozygosity for the 148M allele to be independently asso-ciated with HCC (odds ratio ¼ 2.23, 95% confidence interval ¼1.60-3.50, P ¼ 0.008; Table 1).
Liver disease is a spectrum of conditions deriving from the pres-ence of chronic liver damage over many years. It ranges from sim-ple hepatocellular damage, to liver inflammation, fibrosis, cirrhosis,and ultimately HCC. The PNPLA3 I148M variant has been previ-
ously associated with nonalcoholic2 as well as alcoholic liver dis-ease.3 Valenti et al. showed for the first time an association of the148M allele with HCV-related liver steatosis and fibrosis. Theyalso found a possible link with HCC. Our results support the lat-ter association.
These data are consistent with the hypothesis of liver diseasebeing a continuum of conditions where chronic stress acts on a ge-netically susceptible background, in a ‘‘two-hit’’ pathogeneticmodel. The PNPLA3 protein function remains mostly obscure,and at this time it is difficult to generate a hypothesis that mayexplain the association that was found.
Longitudinal studies on HCV fibrosis progression and HCConset are needed to confirm the PNPLA3 association, and func-tional studies are required to understand the mechanisms underly-ing it.
STEFANO GINANNI CORRADINI, M.D., Ph.D.1
MARIA ANTONELLA BURZA, M.D.1,2
ANTONIO MOLINARO, M.D.1
STEFANO ROMEO, M.D., Ph.D.2,31Department of Clinical Medicine
Sapienza University of Rome, Italy2Institute of Metabolic Science
University of Cambridge, UK3Department of Molecular and Clinical Medicine and Center for
Cardiovascular and Metabolic ResearchUniversity of Gothenburg, Sweden
References1. Valenti L, Rumi M, Galmozzi E, Aghemo A, Del Menico B, De Nicola
S, et al. Patatin-like phospholipase domain containing 3 I148M poly-morphism, steatosis, and liver damage in chronic hepatitis C. HEPATO-
LOGY 2011;53:791-799.2. Romeo S, Kozlitina J, Xing C, Pertsemlidis A, Cox D, Pennacchio LA,
et al. Genetic variation in PNPLA3 confers susceptibility to nonalco-holic fatty liver disease. Nat Genet 2008;40:1461-1465.
3. Tian C, Stokowski RP, Kershenobich D, Ballinger DG, Hinds DA.Variant in PNPLA3 is associated with alcoholic liver disease. Nat Genet2011;42:21-23.
CopyrightVC 2011 by the American Association for the Study of Liver Diseases.View this article online at wileyonlinelibrary.com.DOI 10.1002/hep.24244Potential conflict of interest: Nothing to report.
Table 1. Risk of Developing HCC in Italian Individuals WithHCV-Related Cirrhosis (n 5 221)
Characteristic Odds Ratio
95% Confidence
Interval P Value
Age (years) 1.06 1.03-1.10 0.007
Sex (Female) 0.55 0.28-1.07 0.080
Diabetes 1.04 0.52-2.10 0.905
PNPLA3 148M
homozygotes
2.23 1.6-3.5 0.008
Genotype frequencies were in Hardy-Weinberg equilibrium.
1776 CORRESPONDENCE HEPATOLOGY, May 2011

Patatin-Like Phospholipase Domain-Containing Protein 3 Genotype and HepatocellularCarcinoma in Chronic Hepatitis C
To the Editor:
We thank Ginanni Corradini and coworkers for their interestin our work.1
We have recently reported that the Ile148Met PNPLA3 (patatin-like phospholipase domain-containing protein 3) genotype, a stronggenetic determinant of hepatic fat accumulation and progressive alco-holic as well as nonalcoholic steatohepatitis,2,3 influences steatosis de-velopment, liver fibrosis, possibly antiviral treatment response, and thedevelopment of hepatocellular carcinoma (HCC) in patients withchronic hepatitis C (CHC).1 Furthermore, almost contemporarily, Caiet al. found that, in line with our results, PNPLA3 genotype was asso-ciated with steatosis in patients with CHC who are not affected by vi-ral genotype 3,4 whereas Muller et al. very recently confirmed theassociation of PNPLA3 genotype with steatosis and cirrhosis in Ger-man patients with CHC.5 These data suggest that PNPLA3 genotype(1) is a strong determinant of metabolic steatosis in CHC, (2) plays acausal role in determining the progression of liver disease, and (3)that the evaluation of PNPLA3 genotype might help identify patientswho are at higher risk of complications, and in particular HCC, andmight possibly be useful for the stratification of patients in studiesaimed at HCC prevention. However, this latter conclusion awaits con-firmation in larger prospective studies, because it was based on a ret-rospective analysis of 325 patients (107 with cirrhosis) who were fol-lowed at a single center.1
In response to our article, Ginanni Corradini et al. now reportan association between homozygosity for the 148M PNPLA3 vari-ant and HCC in a retrospective analysis conducted in an Italianpopulation of 221 patients with CHC-related cirrhosis withoutexcessive alcohol intake, which was independent of age, sex, anddiabetes, thus providing an independent validation of our findingsin another population, albeit of similar ethnicity.6 Strikingly,the magnitude of the association (odds ratio ¼ 2.23, confidenceinterval ¼ 1.6-3.5 and odds ratio ¼ 2.16, confidence interval ¼1.3-3.6 in this and our report, respectively) adjusted for the sameconfounders was also very consistent between the two studies.
As previously discussed,1 we agree that larger prospectivestudies in ethnically different populations and different liver dis-eases are required to confirm the association between PNPLA3genotype and HCC, and functional studies on the still-mysteri-ous PNPLA3 function are urgently needed. Nevertheless, theseexciting findings may open new perspectives for the prevention
and treatment of the complications of liver diseases, includingbut not limited to CHC.
LUCA VALENTI, M.D.MASSIMO COLOMBO, M.D.SILVIA FARGION, M.D.Department of Internal Medicine
A.M. Migliavacca Center for Liver DiseaseFirst Division of GastroenterologyUniversita degli Studi, Fondazione IRCCS ‘‘Ca’ Granda’’Ospedale Maggiore PoliclinicoMilan, Italy
References1. Valenti L, Rumi MG, Galmozzi E, Aghemo A, Del Menico B, De
Nicola S, et al. PNPLA3 I148M polymorhism, steatosis, and liver dam-age in chronic hepatitis C. HEPATOLOGY 2011;53:791-799.
2. Romeo S, Kozlitina J, Xing C, Pertsemlidis A, Cox D, Pennacchio LA,et al. Genetic variation in PNPLA3 confers susceptibility to nonalco-holic fatty liver disease. Nat Genet 2008;40:1461-1465.
3. Valenti L, Al-Serri A, Daly AK, Galmozzi E, Rametta R, DongiovanniP, et al. Homozygosity for the PNPLA3 / adiponutrin I148M polymor-phism influences liver fibrosis in patients with nonalcoholic fatty liverdisease. HEPATOLOGY 2011;51:1209-1217.
4. Cai T, Dufour JF, Muellhaupt B, Gerlach T, Heim M, Moradpour D,et al. Viral Genotype-specific role of PNPLA3, PPARG, MTTP andIL28B in hepatitis C virus-associated steatosis. J Hepatol 2011; doi:10.1016/j.jhep.2010.12.020.
5. Muller T, Buch S, Berg T, Hampe J, Stickel F. Distinct, alcohol-modu-lated effects of PNPLA3 genotype on progression of chronic hepatitisC. J Hepatol 2011; doi:10.1016/j.jhep.2011.01.025.
6. Ginanni Corradini S, Burza MA, Molinaro A, Romeo S. Patatin-likephospholipase domain containing 3 sequence variant and hepatocellularcarcinoma. HEPATOLOGY 2011; doi:10.1002/hep.24244.
CopyrightVC 2011 by the American Association for the Study of Liver Diseases.View this article online at wileyonlinelibrary.com.DOI 10.1002/hep.24265Potential conflict of interest: Nothing to report.
The Impact of Human Immunodeficiency Virus Infection in Liver Transplantationfor Hepatocellular Carcinoma
To the Editor:
We read with great interest the article by Vibert et al.1 regard-ing their experience with liver transplantation (LT) for hepatocellu-lar carcinoma (HCC) in patients also infected with humanimmunodeficiency virus (HIV). It was very interesting to note thatthe authors reported the widest single-center experience in this fieldso far, focusing on an intent-to-treat analysis comparing HIV-posi-tive and HIV-negative patients listed for LT. The main messagefrom this experience is that HIV-positive patients are characterizedby a higher dropout rate while on the waiting list, thus impairingthe intent-to-treat analysis without a significant impact on the
overall survival and HCC recurrence in comparison with the con-trol group. However, in considering only the HIV-positive patientswho underwent transplantation, three (19%) of 16 patients wereoutside the Milan criteria and one (6%) of 16 patients was outsidethe University of California San Francisco (UCSF) criteria. Immu-nosuppressive therapy was based on calcineurin inhibitors (cyclo-sporine or tacrolimus) in all patients. It is not clear to us why thesepatients, with a higher tumor burden, did not receive an mTOR(mammalian target of rapamycin) inhibitor–based immunosuppres-sive regimen. In vitro2,3 as well as in vivo4,5 studies have shown thestrong antitumor effect of rapamycin. In addition, as we reportedin a previous article,6 rapamycin is able to inhibit HIV
HEPATOLOGY, Vol. 53, No. 5, 2011 CORRESPONDENCE 1777

progression, both reducing CCR5 gene expression on the surface ofboth lymphocytes and macrophages and interfering with the abilityof differentiating monocytes to become susceptible targets for HIVinfection. Furthermore, it is well-established that the HIV TATprotein, that is secreted by HIV infected cells and taken up by nor-mal cells, drives hepatocarcinogenesis in patients with cirrhosis.7,8
These are the reasons why rapamycin should be suggested as theimmunosuppressive drug of choice in HIV-infected patients whohave undergone LT for HCC, especially when pathological exami-nation shows a tumour outside Milan or UCSF criteria.
Another question that arises from reading this interesting workis the CD4 T cell count in the group of HIV-infected patientswho underwent LT. Two patients had a pre-LT CD4 count of27/lL and 70/lL, respectively, with a very minimal survival (1 and8 months, respectively). From June 2003 to January 2011, 27patients underwent deceased donor LT at our center for end-stageliver disease, which was associated with HCC in 14 cases. MedianCD4 T cell count in our experience was 295/lL (range 119-956/lL). A CD4 T cell count lower than 100/lL is an absolute contra-indication according to our National Protocol for LT in HIV-posi-tive patients; this is because of the high infection risk and the poorassociated post-LT survival.9 These concerns outline the necessityfor an absolutely strict selection of HIV-positive patients toundergo LT because of the complexity in the management of thesepatients and the shortage of organs available for transplantation.
FABRIZIO DI BENEDETTO, M.D., PH.D.1
GIUSEPPE TARANTINO, M.D.1
ROBERTO MONTALTI, M.D.1
GIUSEPPE D’AMICO, M.D.1
STEFANIA COCCHI, M.D.2
GIORGIO E. GERUNDA, M.D.11Liver and Multivisceral Transplant Center and 2Clinic
of Infectious Diseases, Department of InternalMedicine and Medical Specialties, University ofModena and Reggio Emilia Modena, Italy
References1. Vibert E, Duclos-Vallee JC, Ghigna MR, Hoti E, Salloum C, Guettier C,
et al. Liver transplantation for hepatocellular carcinoma: The impact ofhuman immunodeficiency virus infection. HEPATOLOGY 2011;53:475-482.
2. Koehl GE, Andrassy J, Guba M, Richter S, Kroemer A, Scherer MN, et al.Rapamycin protects allografts from rejection while simultaneously attackingtumors in immunosuppressed mice. Transplantation 2004;77:1319-1326.
3. Wang Z, Zhou J, Fan J, Qiu SJ, Yu Y, Huang XW, et al. Effect of rapa-mycin alone and in combination with sorafenib in an orthotopic modelof human hepatocellular carcinoma. Clin Cancer Res 2008;14:5124-5130.
4. Schnitzbauer AA, Zuelke C, Graeb C, Rochon J, Bilbao I, Burra P,et al. A prospective randomised, open-labeled, trial comparing siroli-mus-containing versus mTOR-inhibitor-free immunosuppression inpatients undergoing liver transplantation for hepatocellular carcinoma.BMC Cancer 2011;10:190.
5. Toso C, Merani S, Bigam DL, Shapiro AM, Kneteman NM. Sirolimus-basedimmunosuppression is associated with increased survival after liver transplanta-tion for hepatocellular carcinoma. HEPATOLOGY 2011;51:1237-1243.
6. Di Benedetto F, Di Sandro S, De Ruvo N, Montalti R, Ballarin R,Guerrini GP, et al. First report on a series of HIV patients undergoingrapamycin monotherapy after liver transplantation. Transplantation2011;89:733-738.
7. Di Benedetto F, De Ruvo N, Berretta M, Masetti M, Montalti R, Di
Sandro S, et al. Don’t deny liver transplantation to HIV patients with
hepatocellular carcinoma in the highly active antiretroviral therapy era.
J Clin Oncol 2006;24:e26-e27.
8. Altavilla G, Caputo A, Lanfredi M, Piola C, Barbanti-Brodano G,
Corallini A. Enhancement of chemical hepatocarcinogenesis by the
HIV-1 TAT gene. Am J Pathol 2000;157:1081-1089.
9. Di Benedetto F, De Ruvo N, Berretta M, Masetti M, Montalti R, DiSandro S, et al. Hepatocellular carcinoma in HIV patients treated byliver transplantation. Eur J Surg Oncol 2008;34:422-427.
CopyrightVC 2011 by the American Association for the Study of Liver Diseases.View this article online at wileyonlinelibrary.com.DOI 10.1002/hep.24235Potential conflict of interest: Nothing to report.
Reply:
We agree with these authors that one of the main problemsconcerning patients infected with human immunodeficiency virus(HIV)who have hepatocellular carcinoma (HCC) is the high rateof dropouts on the waiting list for liver transplantation (LT).1
Although controversial results have been published regarding theprognosis of HCC in HIV-infected patients, the kinetics of tumorprogression in HIV-infected subjects seems to be particularlyrapid.2,3 We need specific markers of poor prognosis and HCCtumor progression in these patients in order to improve patientselection and guide neoadjuvant and adjuvant therapies.
As for the CD4 cell count, we agree with the authors thatgreat caution is necessary regarding the indications of LT inpatients with a CD4 T cell count lower than 100/lL. However,because of the lack of clear data to demonstrate the influenceof the CD4 T cell count on HCC progression before LT andon survival after LT, it is difficult to exclude such patientsfrom a transplantation program. In the event of a low CD4cell count before LT, one of the main objectives during thepost-LT period is to prevent a marked drop in the CD4 cellcount; for this reason, a rapid reintroduction of highly activeantiretroviral therapy (HAART) after LT needs to be discussedin such cases.
We also agree with the authors that mTOR (mammalian tar-get of rapamycin) inhibitor-based immunosuppressive regimensmust be tried in such patients.4 We contributed to the Silverstudy on sirolimus after LT for HCC, and rapamycin and siroli-mus are currently being evaluated in our center for the treat-ment of HIV-infected patients who have undergone transplanta-tion for HCC. However, mTOR inhibitors are metabolized bycytochrome P4503A4, and interactions with HAART therapyneed to be avoided. Moreover, Raltegravir, an HIV-1 integraseinhibitor that is metabolized primarily by UGT1A1 (uridinediphosphate glucuronosyltransferase 1 family, polypeptide A1)and is not affected by cytochrome P450 inhibitors or inducers,could be suggested as the drug of choice among nucleosidereverse transcriptase inhibitors.5
In conclusion, the definition of new prognostic markers forHCC before LT, an active neoadjuvant therapy that can preventdropouts, and the specific management of immunosuppression arethe main objectives to be achieved in the very near future withrespect to these HIV-infected patients.
JEAN-CHARLES DUCLOS-VALLEE, M.D.1,2,3
RENE ADAM, M.D., PH.D.1,4,5
ERIC VIBERT, M.D.1,2,3
DIDIER SAMUEL, M.D.1,2,31Assistance Publique–Hopitaux de Paris, Hopital Paul Brousse,
Centre Hepato-Biliaire, Villejuif, France2Institut National de la Sante et de Recherche Medicale (INSERM),
Unite 785, Villejuif, France3Universite Paris-Sud, Unite Mixte de Recherche (UMR)-S785,
Villejuif, France4INSERM, Unite 776, Villejuif, France5Universite Paris-Sud, UMR-S776, Villejuif, France
1778 CORRESPONDENCE HEPATOLOGY, May 2011
References1. Vibert E, Duclos-Vallee JC, Ghigng MR, Hoti E, Salloum C, Gaettier C,
et al. Liver transplantation for hepatocellular carcinoma: The impact ofhuman immunodeficiency virus infection. HEPATOLOGY 2011;53:475-482.
2. Puoti M, Bruno R, Soriano V, Donato F, Gaeta GB, Quinzan GP, et al.Hepatocellular carcinoma in HIV-infected patients: epidemiological fea-tures, clinical presentation and outcome. AIDS 2004;18:2285-2293.
3. Brau N, Fox RK, Xiao P, Marks K, Naqvi Z, Taylor LE, et al. Presenta-tion and outcome of hepatocellular carcinoma in HIV-infected patients: aU.S. Canadian multicenter study. J Hepatol 2007;47:527-537.
4. Di Benedetto F, Di Sandro S, De Ruvo N, Montalti R, Ballarin R,Guerrini GP, et al. First report on a series of HIV patients undergoing
rapamycin monotherapy after liver transplantation. Transplantation2011;89:733-738.
5. Bickel M, Anadol E, Vogel M, Hofmann WP, von Hentig N,
Kuetscher J, et al. Daily dosing of tacrolimus in patients treated with
HIV-1 therapy containing a ritonavir-boosted protease inhibitor or ral-
tegravir. J Antimicrob Chemother 2011;65:999-1004.
CopyrightVC 2011 by the American Association for the Study of Liver Diseases.View this article online at wileyonlinelibrary.com.DOI 10.1002/hep.24264Potential conflict of interest: Nothing to report.
Noninvasive Assessment of Cystic Fibrosis–Associated Liver Disease With AcousticRadiation Force Impulse Imaging
To the Editor:
We read with great interest the article by Lewindon et al.1 Theauthors elegantly addressed the issue of hepatic disease in the natu-ral history of patients with cystic fibrosis (cystic fibrosis–associatedliver disease [CFLD]). Liver fibrosis, ranging from grade 1 to 4,was detected by dual-pass biopsy in most of the patients (77.5%).
Incident portal hypertension (PHT) occurred in up to 42% ofpatients. Notably, clinical characterization did not predict the indi-vidual’s risk of liver fibrosis or PHT, whereas dual-pass liver biopsywas informative of such risk.
The need for noninvasive, user-friendly, and quick techniques toquantify liver fibrosis in systemic disease also emerges for cystic fibro-sis. Novel tissue strain imaging techniques, i.e., transient elastography2
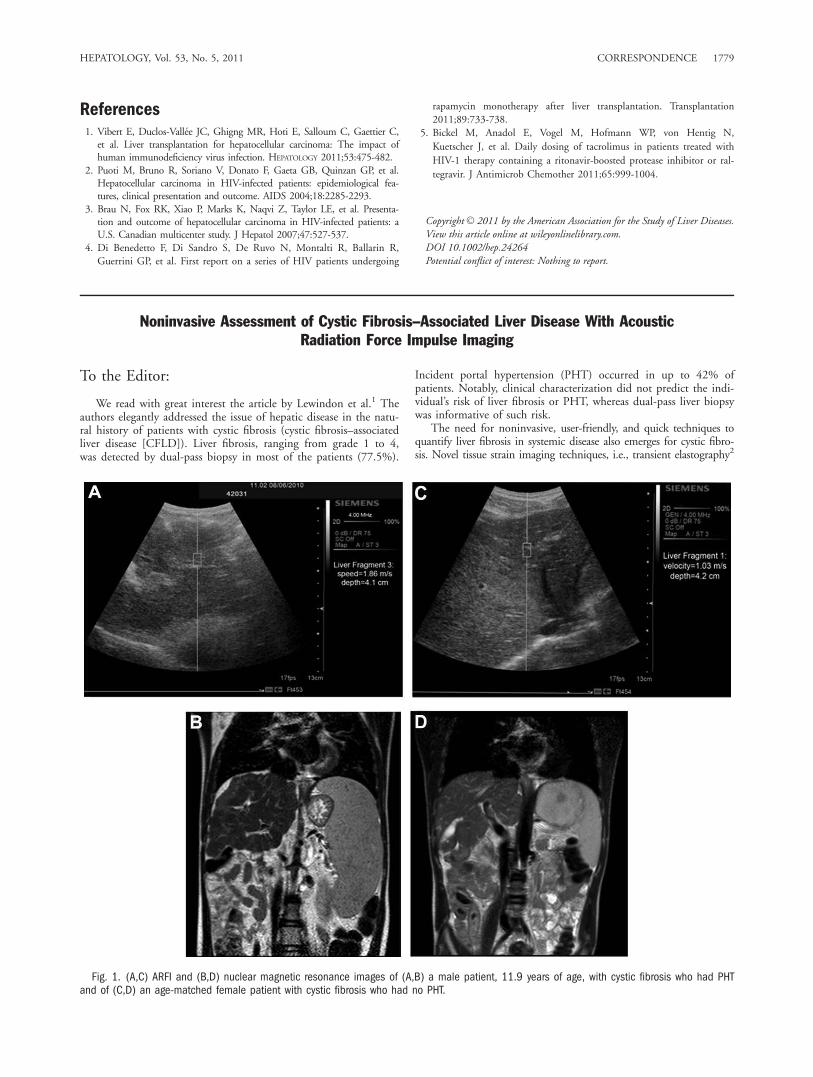
Fig. 1. (A,C) ARFI and (B,D) nuclear magnetic resonance images of (A,B) a male patient, 11.9 years of age, with cystic fibrosis who had PHTand of (C,D) an age-matched female patient with cystic fibrosis who had no PHT.
HEPATOLOGY, Vol. 53, No. 5, 2011 CORRESPONDENCE 1779

or acoustic radiation force impulse imaging (ARFI),3 may representvaluable options in the evaluation and follow-up of CFLD. ARFI isan imaging technique that involves targeting an anatomic region tobe interrogated for elastic properties with use of a region-of-interestcursor while performing real-time B-mode imaging.3
Here, we report results of ARFI evaluation (ACUSON S2000;Siemens, Erlanger, Germany) in 40 patients affected by cysticfibrosis (age 12 6 5.1 years). Ten successful measurements ofshear-wave speed were obtained in each patient in the deep rightlobe, taking care not to capture any vascular or biliary structure.Diagnosis of PHT was based on presence of splenomegaly andesophageal varices. Patients with PHT (n ¼ 12, Fig. 1A,B) had sig-nificantly greater median velocities (1.56 6 0.47 versus 1.1 60.19 m/second; P ¼ 0.001) and velocities at each measurement(P from 0.046 to 0.001) than patients who were free of PHT (n ¼28, Fig. 1C,D). The receiving operating characteristic (ROC)analysis was applied to evaluate ability of speed measurement todetect PHT (area under the ROC curve ¼ 0.82, 95% confi-dence interval 0.65-0.98; P ¼ 0.002). On ROC analysis, thecutoff value of 1.3 m/second, previously reported as diagnosticin adults with fibrosis from viral hepatitis,3 had sensitivity of0.75 and specificity of 0.79. Thus, ARFI seems to be an accu-rate methodology to investigate CFLD. Nevertheless, accuracyto assess grade of fibrosis, reproducibility, and diagnostic cutoffvalues for shear-wave speed should be carefully evaluated inlarger and controlled studies.
We congratulate the authors on the emphasis they put on theimportance of liver fibrosis staging in patients with cystic fibrosis,1
and we certainly agree that liver biopsy must be considered inmanagement of such patients unless noninvasive techniques arevalidated.
MELANIA MANCO, M.D., PH.D.CRISTINA LO ZUPONE, M.D.ALESSANDRO LATINI, M.D.VINCENZINA LUCIDI, M.D.LIDIA MONTI, M.D.Bambino Gesu Hospital and Research Institute, Rome, Italy
References1. Lewindon PJ, Shepherd RW, Walsh MJ, Greer RM, Williamson R,
Pereira TN, et al. Importance of hepatic fibrosis in cystic fibrosisand the predictive value of liver biopsy. HEPATOLOGY 2011;53:193-201.
2. Menten R, Leonard A, Clapuyt P, Vincke P, Nicolae AC, Lebecque P.Transient elastography in patients with cystic fibrosis. Pediatr Radiol2011;40:1231-1235.
3. Friedrich-Rust M, Wunder K, Kriener S, Sotoudeh F, Richter S,Bojunga J, et al. Liver fibrosis in viral hepatitis: noninvasive assessmentwith acoustic radiation force impulse imaging versus transient elastogra-phy. Radiology 2009;252:595-604.
CopyrightVC 2011 by the American Association for the Study of Liver Diseases.View this article online at wileyonlinelibrary.com.DOI 10.1002/hep.24245Potential conflict of interest: Nothing to report.
Reply: The Utility of Noninvasive Imaging inCystic Fibrosis Liver Disease
We welcome the report by Manco et al. highlighting the impor-tance of detecting and monitoring the severity of fibrosis and theneed for reliable, noninvasive assessments of hepatic fibrosis inpatients with cystic fibrosis liver disease (CFLD). In a study of an
uncharacterized cohort of 40 children with cystic fibrosis (CF),they compared acoustic radiation force impulse (ARFI) imagingvalues from 12 children with evidence of portal hypertension tovalues from 28 children without portal hypertension. The sensitiv-ity and specificity of an ARFI cutoff value of 1.3 m/s, which hadbeen validated in adults with viral hepatitis, were 0.75 and 0.79,respectively, for the detection of portal hypertension in patientswith CF; however, the relative importance of each value for a childwith CF remains to be determined.
Noninvasive assessments such as serum marker measurements,transient elastography, and ARFI imaging have been validated forthe detection of liver fibrosis in adults with liver diseases (particu-larly chronic viral hepatitis). Studies in pediatric populations arecomplicated by the physicochemical influences of children’s smallersize and growth. Children also have a different spectrum of etiolo-gies for severe liver disease, with the majority of liver diseases thatlead to transplantation being cholestatic in nature (including CF);extrahepatic cholestasis has been shown to increase liver stiffness(as measured by transient elastography), which may confound val-ues ascribed to fibrosis severity.1 Hence, there is a need to validatenormal and abnormal ranges and cutoff values for age and sex, foreach modality, for each etiology of hepatic fibrosis, and in pediatricand adult cohorts.
We previously demonstrated the value of serum markers of ma-trix remodeling in differentiating patients with CFLD (particularlywith early fibrosis) from both CF children without liver diseaseand age-matched controls.2 Others have compared transient elas-tography with standard clinical assessments, including ultrasoundexaminations, in children and adults with CF.3 However, as wedemonstrated in our recent article,4 standard clinical assessmentsare not reliable for the detection of liver fibrosis in an individual,especially before the evolution of established cirrhosis and/or portalhypertension. The utility of these modalities can be determinedonly through the comparison of noninvasive assessments of fibrosiswith liver biopsy and, more importantly, with long-term hard end-points such as portal hypertension and transplantation.
We congratulate Manco et al. on establishing a potential rolefor ARFI imaging in children with CF. The next step for eachnoninvasive modality will be the validation of the obtained val-ues for the early detection and monitoring of liver fibrosis inpatients with CFLD (particularly children) to permit improvedclinical surveillance and provide a platform for monitoring ther-apeutic intervention.
PETER J. LEWINDON, M.D.1,2,3
GRANT A. RAMM, PH.D.1,31Hepatic Fibrosis Group
Queensland Institute of Medical ResearchBrisbane, Australia
2Department of GastroenterologyRoyal Children’s HospitalBrisbane, Australia
3Faculty of MedicineUniversity of QueenslandBrisbane, Australia
References1. Millonig G, Reimann FM, Friedrich S, Fonouni H, Mehrabi A, Buch-
ler MW, et al. Extrahepatic cholestasis increases liver stiffness (Fibro-Scan) irrespective of fibrosis. HEPATOLOGY 2008;48:1718-1723.
2. Pereira TN, Lewindon PJ, Smith JL, Murphy TL, Lincoln DJ, Shep-herd RW, et al. Serum markers of hepatic fibrogenesis in cystic fibrosisliver disease. J Hepatol 2004;41:576-583.
3. Witters P, De Boeck K, Dupont L, Proesmans M, Vermeulen F, ServaesR, et al. Non-invasive liver elastography (FibroScan) for detection ofcystic fibrosis-associated liver disease. J Cyst Fibros 2009;8:392-399.
1780 CORRESPONDENCE HEPATOLOGY, May 2011

4. Lewindon PJ, Shepherd RW, Walsh MJ, Greer RM, Williamson R,Pereira TN, et al. Importance of hepatic fibrosis in cystic fibrosisand the predictive value of liver biopsy. HEPATOLOGY 2011;53:193-201.
CopyrightVC 2011 by the American Association for the Study of Liver Diseases.View this article online at wileyonlinelibrary.com.DOI 10.1002/hep.24288Potential conflict of interest: Nothing to report.
Methods and Interest of Noninvasive Assessment of Liver Fibrosis Are Still in Debate
To the Editor:
In their interesting review of noninvasive assessment of liverfibrosis,1 Martınez et al. note that ‘‘the introduction of noninvasivemethods in clinical practice is making such slow headway in thefield of hepatology’’. However, their statement that ‘‘an exception tothis rule is France, where three well-validated methods (FibroTest,Fibrometer, and FibroScan) have been approved by the public healthsystem and are routinely used in clinical practice’’ has to be discussed.
Certainly, there is no doubt about wide use of these methods inclinical practice, despite the restrictions stated by the FrenchNational Authority for Health (Haute Autorite de Sante [HAS]).2
In February 2011, the Social Health Insurance finalized thedecisional process of listing those techniques for eligibility forreimbursement, subject to very strict rules according to this advice.Transient elastography, for example, will be reimbursed only whenperformed by specialists, for the follow-up of untreated patientswith chronic hepatitis C and no evidence of cirrhosis, once a yearonly (with the exception of patients presenting a risk of rapid evo-lution to cirrhosis).
One should also be careful when qualifying noninvasive meth-ods of liver fibrosis assessment as ‘‘well-validated’’ in ‘‘largecohorts’’ of patients. First, numerous accuracy studies of thesemethods were carried out and published by their manufacturers orinventors. The largest independent one, to date, is the Fibrosticstudy comparing the diagnostic accuracy of biomarkers to that oftransient elastography (FibroScan) in one and the same populationof 1307 patients with chronic hepatitis,3,4 but it was unfortunatelypublished too recently for Martınez et al. to take it into account intheir review. Second, performance of noninvasive methods is cer-tainly good for diagnosing cirrhosis but poor for significant fibro-sis; the Fibrostic study did not even reach the minimum values of85% sensitivity and specificity deemed high enough by Martınezet al. Moreover, the Fibrostic study results showed the ability ofnoninvasive tests to confirm or rule out significant fibrosis was sat-isfactory in limited ranges of high or low values only.3 Third, accu-racy is only a step toward a possible usefulness of a test.5 As rightlystressed by Martınez et al. at the end of their article, the improve-ment of patient outcomes is more relevant. However, the predic-tion of clinical endpoints by noninvasive methods was onlyrecently investigated by very few studies, and to our knowledge, nostudy assessed their ability to predict response to therapy.
We all wish that noninvasive methods could allow us to avoidliver biopsy while ensuring that patients will be managed as well or
better than with old techniques. Therefore, studies are needed inorder to specify their contribution to the choice of patient manage-ment for improving clinical endpoints or treatment response.
FRANCOISE DEGOS, M.D., PH.D.1
LOUIS LEBRUN, M.D., PH.D.2
PAUL PEREZ, M.D., PH.D.3
ISABELLE DURAND-ZALESKI, M.D., PH.D.21Assistance Publique–Hopitaux de Paris (AP-HP), Hopital Beaujon,
Hepatology Department, Institut National de la Sante et de laRecherche Medicale Unite 773, Clichy, France
2AP-HP, Departement de la recherche clinique et du developpement -Unite de recherche clinique en economie de la sante, Paris, France
3Centre Hospitalier Universitaire de Bordeaux, Clinical EpidemiologyUnit and Centre d’investigation clinique et d’epidemiologie clinique7, Bordeaux, France
References1. Martınez SM, Crespo G, Navasa M, Forns X. Noninvasive assessment
of liver fibrosis. HEPATOLOGY 2011;53:325-335.2. French Haute Autorite de Sante. Noninvasive methods for measuring
hepatic fibrosis/cirrhosis—opinion on the acts [Methodes non invasives demesure de la fibrose/cirrhose hepatique—avis sur les actes]. December2008. Available at http://www.has-sante.fr/portail/jcms/c_783807/avis-has-tests-non-invasifs-mesure-fibrose-cirrhose-decembre-2008.Accessed March 2011.
3. Degos F, Perez P, Roche B, Mahmoudi A, Asselineau J, Voitot H, et al.Diagnostic accuracy of FibroScan and comparison to liver fibrosis bio-markers in chronic viral hepatitis: a multicenter prospective study (theFIBROSTIC study). J Hepatol 2011;53:1013-1021.
4. Degos F, Perez P, Asselineau J, Bedossa P. Diagnostic accuracy of Fibro-Scan and comparison to liver fibrosis biomarkers in chronic viral hepa-titis: a multicenter prospective study (the FIBROSTIC study). JHepatol 2011; doi:10.1016/j.jhep.2011.01.015
5. Knottnerus JA, ed. The Evidence Base of Clinical Diagnosis. London:BMJ Books; 2002.
CopyrightVC 2011 by the American Association for the Study of Liver Diseases.View this article online at wileyonlinelibrary.com.DOI 10.1002/hep.24276Potential conflict of interest: Nothing to report.
Noninvasive Assessment of Liver Fibrosis: The Need for Better Validation
To the Editor:
We read with interest the review by Martınez et al. on noninva-sive assessment of liver fibrosis,1 but some important points werenot discussed.
First, the authors mention that the relatively high misclassifica-tion of the ‘‘gold standard’’ (liver biopsy) makes it impossible fornoninvasive tests to achieve high concordances. This is indeed truefor noninvasive tests whose development was independent fromliver histology (e.g., elastography). However, serum markers have
HEPATOLOGY, Vol. 53, No. 5, 2011 CORRESPONDENCE 1781

been calibrated with direct reference to sets of liver biopsies. There-fore, the perfect serum marker would replicate even the misclassifi-cations of the ‘‘golden’’ histological standard and could theoreticallyreach an AUROC (area under the receiver operating characteristiccurve) of 1.
Second, the explosive development and overenthusiastic accep-tance of noninvasive markers is not always supported by sufficientevidence and validation. In our meta-analysis on elastography, weexposed issues such as invalidated stiffness cutoffs for specific liverdisease stages and low methodological quality in the vast majorityof published studies.2 In numerous studies, the maximum intervalbetween elastography and liver biopsy was >3-6 months; in suchcases, there is an erroneous assumption that fibrosis remains stableover these periods of time. Furthermore, from all publications,only six studies had both optimal histological and elastographymeasurements.2
Third, the authors correctly state that liver biopsy is more of areference standard than a gold standard for assessing fibrosis. As wehave pointed out before, histological ‘‘scores’’ of fibrosis are ordinalcategories that incorporate both architectural changes and fibrosis,and have no quantitative relationship between them.3 Therefore,using them as continuous variables is inappropriate.3 Validation ofnoninvasive markers of ‘‘fibrosis’’ should ideally use quantitative histo-logical measures. We have described such a measure, namely, collagenproportionate area, and correlated it with hepatic venous pressure gra-dient.4 More importantly, we evaluated its prognostic value withrespect to patient outcome.5 Notably, collagen proportionate area per-formed better than Ishak staging and hepatic venous pressure gradientfor predicting decompensation (AUROC ¼ 0.97).5
In conclusion, the way forward involves carefully designed stud-ies that validate noninvasive fibrosis markers against quantitativehistological measures and/or clinical outcomes. Because we are ulti-mately treating patients, the clinical consequences of false positiveand false negative classifications should be incorporated in the vali-dation processes.
EMMANUEL A. TSOCHATZIS, M.D.1
GIACOMO GERMANI, M.D.1
ANDREW HALL, M.D.2
PINELOPI M ANOUSOU, M.D.1
AMAR P. DHILLON, M.D.2
ANDREW K. BURROUGHS, M.D., F.MED.SCI.11The Royal Free Sheila Sherlock Liver Centre
and University Department of SurgeryRoyal Free Hospital and University College LondonLondon, UK
2Department of Cellular Pathology, UCL Medical SchoolRoyal Free Campus, Rowland Hill Street, London, UK
References1. Martınez SM, Crespo G, Navasa M, Forns X. Noninvasive assessment
of liver fibrosis. Hepatology 2011;53:325–335.2. Tsochatzis EA, Gurusamy KS, Ntaoula S, Cholongitas E, Davidson
BR, Burroughs AK. Elastography for the diagnosis of severity of fibrosisin chronic liver disease: a meta-analysis of diagnostic accuracy. J Hepa-tol 2011; doi:10.1016/j.jhep.2010.07.033
3. Germani G, Burroughs AK, Dhillon AP. The relationship between liverdisease stage and liver fibrosis: a tangled web. Histopathology 2011;57:773–784.
4. Calvaruso V, Burroughs AK, Standish R, Manousou P, Grillo F, LeandroG, et al. Computer-assisted image analysis of liver collagen: relationship toIshak scoring and hepatic venous pressure gradient. Hepatology 2009;49:1236–1244.
5. Manousou P, Dhillon AP, Isgro G, Calvaruso V, Luong TV, TsochatzisE, et al. Digital image analysis of liver collagen predicts clinical out-
come of recurrent hepatitis C virus 1 year after liver transplantation.Liver Transpl 2011;17:178–188.
CopyrightVC 2011 by the American Association for the Study of Liver Diseases.View this article online at wileyonlinelibrary.com.DOI 10.1002/hep.24271Potential conflict of interest: Nothing to report.
Reply:
We appreciate the letters of Tsochatzis et al. and Degos et al.regarding our recent review. We essentially agree with their com-ments but would like to stress a few points.
It is obviously very relevant to maximize the diagnostic accuracyof any diagnostic test. In the case of noninvasive markers of liverfibrosis, the latter applies particularly to confirm or exclude thepresence of cirrhosis, because there are important clinical implica-tions derived from this finding (i.e., screening for hepatocellularcarcinoma and gastroesophageal varices). We all would agree thatin this setting most of the noninvasive methods widely used inclinical practice perform well. Regarding the identification of sig-nificant fibrosis, the diagnostic accuracy is certainly lower. How-ever, their performance in the area of viral hepatitis C is probablyacceptable. As an example in our own field, we are using theModel for End-Stage Liver Disease (MELD) score to predict the3-month survival in patients awaiting liver transplantation (withthe obvious consequences in a patient’s life—or death) with diag-nostic accuracies not far from those used to exclude significantfibrosis. The MELD score has been widely validated in differentcohorts of patients with a prediction in 3-month survival rangingfrom 0.76-0.87.1,2 Identifying or excluding significant fibrosis haslimited practical implications in real life and, in the field of viralhepatitis, it may become less relevant once antiviral treatment effi-cacy increases.
Regarding the comment by Tsochatzis et al. on the use of thecollagen proportionate area as a histological standard (based on itsquantitative nature) we believe this is a good approach.3 The prog-nostic value regarding patient outcome was excellent in their study,although the results need validation in other cohorts. Using suchmethodology, however, will not preclude one of the main problemsof liver biopsy, which is sampling error.
Finally, as we stressed in our review and as was noticed byDegos et al., using noninvasive methods to predict clinical out-comes is probably the most important goal. It is in this particulararea where we need more and well-designed studies.
STELLA M. MARTINEZ, M.D.GONZALO CRESPO, M.D.MIQUEL NAVASA, M.D., PH.D.XAVIER FORNS, M.D., PH.D.Liver Unit, Hospital Clınic
Institut d’Investigacions Biomediques August Pi i Sunyer (IDIBAPS)Centro de Investigacion Biomedica en Red de EnfermedadesHepaticas y Digestivas (Ciberehd) Barcelona, Spain
References1. Cholongitas E, Marelli L, Shusang V, Senzolo M, Rolles K, Patch D,
Burroughs AK. A systematic review of the performance of the modelfor end-stage liver disease (MELD) in the setting of liver transplanta-tion. Liver Transpl 2006;12:1049-1061.
2. Kamath PS, Kim WR; Advanced Liver Disease Study Group. Themodel for end-stage liver disease (MELD). HEPATOLOGY 2007;45:797-805.
1782 CORRESPONDENCE HEPATOLOGY, May 2011

3. Manousou P, Dhillon AP, Isgro G, Calvaruso V, Luong TV, TsochatzisE, Xirouchakis E, et al. Digital image analysis of liver collagen predictsclinical outcome of recurrent hepatitis C virus 1 year after liver trans-plantation. Liver Transpl 2011;17:178-188.
CopyrightVC 2011 by the American Association for the Study of Liver Diseases.View this article online at wileyonlinelibrary.com.DOI 10.1002/hep.24300Potential conflict of interest: Nothing to report.
Beta-Blockers in Patients with Cirrhosis and Refractory Ascites
To the Editor:
The provocative article by Serste et al.1 about the negativeimpact of propranolol on the survival of patients with cirrhosisand refractory ascites ends with the recommendation that beta-blockers should not be used in patients with refractory ascites.Some of the methodological concerns of the study are addressed inthe accompanying editorial: the lack of causality between the maincause of death (hepatocellular carcinoma) and beta-blocker therapy,the lack of consecutive patient enrolment, and the misbalancebetween groups with sicker patients in the beta-blocker group.2
The editorial also points out that a randomized controlled trialwould have been the most appropriate tool for evaluating theeffects of beta-blockers. Although we agree, we think that carefullyanalyzed observational data may provide us with firm clues aboutcausality even without balanced randomization.
Serste et al.1 linked beta-blocker therapy to increased mortalitywith a proportional hazards model. Through automatic backwardmodeling, the criterion for selecting the final model strategy wasstatistical significance. We think that an explanatory strategy forbuilding the Cox model, using time-dependent covariates and apropensity score to adjust for the potential confounding factors,would have enriched the study.3–5 In this way, instead of beingdriven by significance tests, covariates would have entered andremained in the explanatory model as a result of their modificationeffect on the association of therapy and mortality.3 Moreover, theycould have checked for confounding and likely interactions toexplore whether the observed effect was the same in different sub-sets of patients, as the editorialists claimed. Besides, the use oftime-dependent covariates would have allowed fine-tuning of thebeta-blocker therapy duration and would have better addressed itsinfluence on outcomes.4 Finally, a propensity score, which definesthe probability that an individual will receive a specific treatmentbased on his or her pretreatment characteristics, is useful for over-coming the imbalance between groups when treatment assignmentis not random.5 Specifically, in Serste et al.’s study, the propensityscore would have corrected the effect of beta-blockers for patientcharacteristics such as the presence of varices, which heavily condi-tions their prescription. With such an analysis, the focus of themodel would have been the influence of beta-blockers on survival
rather than the identification of factors influencing survival; hence,it would have offered more clues to the causal effect. The proposedapproach would add robustness to the interesting results providedby Serste et al.
AGUSTIN ALBILLOS, M.D., PH.D.1,3
JAVIER ZAMORA, M.D., PH.D.2,41Departments of 1Gastroenterology and Hepatology and2Clinical Biostatistics
Ramon y Cajal University HospitalRamon y Cajal Institute of Health Research (IRYCIS)University of AlcalaMadrid, Spain
Network Centers for Biomedical Research in3Hepatic and Digestive Diseases (Ciberhd) and
4Epidemiology (Ciberesp), Public HealthCarlos III Institute of HealthMadrid, Spain
References1. Serste T, Melot C, Francoz C, Durand F, Rautou PE, Valla D, et al.
Deleterious effects of beta-blockers on survival in patients with cirrhosisand refractory ascites. HEPATOLOGY 2010;52:1017-1022.
2. Wong F, Salerno F. Beta-blockers in cirrhosis: friend and foe? HEPATOLOGY
2010;52:811-813.3. Clark TG, Bradburn MJ, Love SB, Altman DG. Survival analysis part
IV: further concepts and methods in survival analysis. Br J Cancer2003;89:781-786.
4. Hosmer DW, Lemeshow S. Applied Survival Analysis: Regression Mod-eling of Time to Event Data. New York, NY: John Wiley & Sons;1999:248-253.
5. D’Agostino RB. Propensity score methods for bias reduction in thecomparison of a treatment to a non-randomized control group. Stat Med1998;17:2265-2281.
CopyrightVC 2011 by the American Association for the Study of Liver Diseases.View this article online at wileyonlinelibrary.com.DOI 10.1002/hep.24032Potential conflict of interest: Nothing to report.
Pathogen DNA Also Contributes to Interferon Regulatory Factor 3 Activation in Hepatic Cells:Implications for Alcoholic Liver Diseases
To the Editor:
We read with great interest the recent article by Petrasek andcolleagues,1 who reported that interferon regulatory factor 3(IRF3) activation and type I interferon (IFN) production inparenchymal cells have protective effects in patients with alcoholicliver disease (ALD). The authors also suggested that IRF3 activa-
tion is a result of hepatic exposure to bacterial lipopolysaccharide(LPS). However, the authors failed to discuss gut bacterial and he-patic virus DNA, which is another immune-stimulating agent inaddition to LPS that may also contribute to IRF3 activation in liverparenchymal cells and should be involved in the process of ALD.
Besides LPS, excessive drinking of alcohol also results in anelevation of bacterial DNA in the portal blood.2 Recent studies
HEPATOLOGY, Vol. 53, No. 5, 2011 CORRESPONDENCE 1783

have indicated that intracellular bacterial DNA can strongly acti-vate IRF3 in liver parenchymal cells3 and thus induce the pro-duction of type I IFNs. In this respect, we suggest that gut-derived bacterial DNA also contributes to IRF3 activation andmay play a key role in the prevention of alcoholic liver injury.
We also believe that DNA-mediated hepatic IRF3 activation hasgreat significance in China because of the high rate of hepatitis B vi-rus (HBV) infection. Intracellular virus DNA4 has been proved tostrongly activate IRF3 and induce type I IFN production. However,recent studies have found that components of HBV3 inhibit IRF3activation via cleavage of the mitochondrial antiviral signaling protein,which is an essential component that activates IRF3 and thus inducesthe production of type I IFNs.5 Considering the current findings byPetrasek et al.,1 we hypothesize that HBV may also hinder the preven-tion functions of IRF3 and type I IFNs via the inhibition of the mi-tochondrial antiviral signaling protein and that HBV infection mayincrease the risk of ALD. This requires further investigation.
YUE WANG, M.D.YINGJUN GUO, M.D.FANG WANG, M.D.SHUHAN SUN, M.D.Department of Medical Genetics
Second Military Medical UniversityShanghai, People’s Republic of China
References1. Petrasek J, Dolganiuc A, Csak T, Nath B, Hritz I, Kodys K, et al.
Interferon regulatory factor 3 and type I interferons are protective inalcoholic liver injury in mice via cross-talk of parenchymal and myeloidcells. HEPATOLOGY 2011; DOI: 10.1002/hep.24059.
2. Miura K, Kodama Y, Inokuchi S, Schnabl B, Aoyama T, OhnishiH, et al. Toll-like receptor 9 promotes steatohepatitis by induc-tion of interleukin-1beta in mice. Gastroenterology 2011;139:323-334.
3. Wei C, Ni C, Song T, Liu Y, Yang X, Zheng Z, et al. The hepatitis Bvirus X protein disrupts innate immunity by downregulating mitochon-drial antiviral signaling protein. J Immunol 2011;185:1158-1168.
4. Chiu YH, Macmillan JB, Chen ZJ.RNA polymerase III detects cyto-solic DNA and induces type I interferons through the RIG-I pathway.Cell 2009;138:576-591.
5. Sun Q, Sun L, Liu HH, Chen X, Seth RB, Forman J, et al. The spe-cific and essential role of MAVS in antiviral innate immune responses.Immunity 2006;24:633-642.
CopyrightVC 2011 by the American Association for the Study of Liver Diseases.View this article online at wileyonlinelibrary.com.DOI 10.1002/hep.24089Potential conflict of interest: Nothing to report.
Bile Acid Sequestrants Improve Glycemic Control in Type 2 Diabetes: A ProposedMechanism Implicating Glucagon-Like Peptide 1 Release
To the Editor:
In HEPATOLOGY, Brufau et al.1 recently reported their examina-tion of the effect of colesevelam, a potent bile acid sequestrant, onglycemic control and bile acid kinetics in patients with type 2 dia-betes. Colesevelam improved glycemic parameters and caused theexpected increase in cholic acid synthesis. However, the authors‘‘found no correlation between markers of insulin resistance/glucosemetabolism and bile acid metabolism,’’ and they concluded thata firm link between bile acid and glucose metabolism in type 2diabetes mellitus remained elusive.
The purpose of this note is to propose a mechanism by whichcolesevelam improves glycemic control in patients with type 2diabetes. The mechanism is increased release of glucagon-like pep-tide 1 (GLP-1) from the L cells of the ileum. This GLP-1 releaseis induced by fatty acids that reach the ileum because of defectivemicellar solubilization in the jejunum.
In a healthy person, fatty acids are generated by pancreaticlipases acting at the triglyceride/water interface. Fatty acids are solu-bilized in mixed micelles with conjugated bile acids. Normally, fattyacid absorption is remarkably efficient and complete by the proximaljejunum. When a bile acid sequestrant is administered, it binds bileacids, removes them from solution, and decreases the fatty acid con-centration in the aqueous phase.2 Fatty acids that are not solubilizedin micelles can be absorbed by the diffusion of individual moleculesthrough the aqueous boundary layer, but this is a slow process. Fattyacids will remain in an emulsified form; experimentally, absorptionfrom an emulsion is slower than absorption from a micellar solu-tion.3 As a result, fatty acids will pass into the ileum, where theywill enter L cells and stimulate GLP-1 release. In rats, biliary diver-sion changes the site of fatty acid absorption from predominantlythe jejunum to both the jejunum and the ileum.4
This proposed mechanism can also explain why intestinal trans-position or anti-obesity operations that cause fatty acids to reachthe ileum improve type 2 diabetes.
This proposed mechanism does not exclude substances inplasma such as cholecystokinin5 or bile acid derivatives6 acting onL cells from the basolateral side and evoking GLP-1 release.
ALAN F. HOFMANN, M.D.Department of Medicine
University of California, San DiegoLa Jolla, CA 92093-063Email: [email protected]
References1. Brufau G, Stellaard F, Prado K, Bloks VW, Jonkers E, Boverhof R,
et al. Improved glycemic control with colesevelam treatment in patientswith type 2 diabetes is not directly associated with changes in bile acidmetabolism. HEPATOLOGY 2011;52:1455-1464.
2. Poley JR, Hofmann AF.Role of fat maldigestion in pathogenesis of stea-torrhea in ileal resection. Fat digestion after two sequential test mealswith and without cholestyramine. Gastroenterology 1976;71:38-44.
3. Hoffman NE, Hofmann AF.A comparison of the rate of absorption ofmicellar and nonmicellar oleic acid: a jejuna perfusion study in man.Am J Dig Dis 1973;18:489-492.
4. Knoebel LK.Intestinal absorption of micellar and nonmicellar lipid.Am J Physiol 1972;223:255-261.
5. Beglinger S, Drewe J, Schirra J, Goke B, D’Amato M, BeglingerC.Role of fat hydrolysis in regulating glucagon-like peptide-1 secretion.J Clin Endocrinol Metab 2011;95:879-886.
6. Thomas C, Gioiello A, Noriega L, Strehle A, Oury J, Rizzo G, et al.TGR5-mediated bile acid sensing controls glucose homeostasis. CellMetab 2009;10:167-177.
CopyrightVC 2011 by the American Association for the Study of Liver Diseases.View this article online at wileyonlinelibrary.com.DOI 10.1002/hep.24100Potential conflict of interest: Nothing to report.
1784 CORRESPONDENCE HEPATOLOGY, May 2011

Is Endotoxemia a Therapeutic Target in Liver Injury?
To the Editor:
Dr. Nolan states1 that alcoholic liver disease is the target forearlier interventions with antiendotoxin therapy, although it is stilldifficult to prevent or suppress the progression of endotoxin-medi-ated liver injury by antiendotoxin therapy in clinical settings de-spite solid evidence of its effectiveness in the experimental models.Nolan refers to a study that showed a progressive rise of meanplasma endotoxin levels from 10 pg/mL in mild fatty liver to 60pg/mL in severe cirrhosis with alcoholic hepatitis.2 However, posi-tive correlations of endotoxin levels with the severity of liver injurydo not necessarily mean the harmful effects of modest endotoxemiaon the liver. A high plasma concentration of endotoxin exceeding1,000 pg/mL is the predictor of death in hepatic failure, while theclinical implications of modest endotoxemia is unclear. Endotoxinactivates tumor necrosis factor alpha (TNF-a) and nuclear factorkappa-B (NF-jB) signaling pathways, which are involved in themaintenance of the ordered balance between cell proliferation andapoptosis in the liver. Modest endotoxemia in chronic liver injurymight be a response to an increased demand for TNF-a and NF-jB signaling. In such conditions, antiendotoxin therapy should beperformed with caution. The gut is a reservoir of endotoxinbecause a single Escherichia coli contains about 2 million lipopoly-saccharide (LPS) molecules per cell and 1 g of human feces contain1.0-10 mg endotoxin.3 As mentioned in the present article, chang-ing the gut flora with the use of prebiotics, probiotics, or both(symbiotics) seems a safe and promising approach in chronic liverdisease. However, to confirm the effectiveness of probiotic or sym-biotic therapy, larger randomized controlled trials would berequired, because each sample size in previous trials is too small toyield level 1 evidence.4 In a small clinical trial, symbiotic-relatedimprovement in ICGR15 was not related to endotoxin levels.5 Ihope that such treatment strategies using probiotics or symbiotics
for patients with chronic liver disease will be performed regardlessof plasma endotoxin levels, because endotoxin activity in vitro doesnot actually reflect its biological toxicity in vivo.6
TETSUJI FUJITA, M.D.Department of Surgery
Jikei University School of MedicineTokyo, Japan
References1. Nolan JP. The role of intestinal endotoxin in liver injury: a long and
evolving history. Hepatology 2011;52:1829-1835.2. Fukui K. Relation of endotoxin, endotoxin binding proteins and mac-
rophages to severe alcoholic liver injury and multiple organ failure.Alcohol Clin Exp Res 2005;29:172S-179S
3. Magalhaes PO, Lopes AM, Mazzola PG, Rangel-Yagui C, Penna TCV,Pessoa A Jr. Methods of endotoxin removal from biological prepara-tions: a review. J Pharm Pharmaceut Sci 2007;10:388-404.
4. Bengmark S. Bio-ecological control of chronic liver disease and ence-phalopathy. Metab Brain Dis 2009;24:223-236.
5. Riordan SM, Skinner NA, Mclver CJ, Liu Q, Bengmark S, Bihari D,et al. Synbiotic-associated improvement in liver function in cirrhoticpatients: relation to changes in circulating cytokine messenger RNAand protein levels. Microb Ecol Health Dis 2007;19:7-16.
6. Fujita T. Endotoxemia in alcoholic liver disease. Hepatology 2009;50:1319.
CopyrightVC 2011 by the American Association for the Study of Liver Diseases.View this article online at wileyonlinelibrary.com.DOI 10.1002/hep.24146Potential conflict of interest: Nothing to report.
Insulin Resistance Links Nonalcoholic Fatty Liver to Cardiovascular Diseases
To the Editor:
We read with interest the article by Ghouri et al.,1 whoreviewed the evidence regarding the link between nonalcoholicfatty liver disease (NAFLD) and cardiovascular disease (CVD). Theauthors concluded that the connection between NAFLD and CVDis not well supported by existing data because of the presence ofconfounders such as age and established cardiovascular risk factors.
We agree that the main limitation of these studies is that theirresults make it difficult to distinguish the contribution of liver fatper se to the risk of CVD. However, we should consider that theliver is the main regulator of insulin sensitivity and finely tunes in-sulin-regulated metabolic pathways such as glucose and lipid home-ostasis that are involved in endothelial dysfunction and atherogene-sis. Studies in null mice have clearly substantiated this issue. Inparticular, the disruption of insulin signaling in the liver is morerelevant to whole body glucose homeostasis than its disruption inadipose tissue and muscle.2 In addition, hepatic insulin signalingregulates the secretion of very low density lipoprotein and thus lip-otoxicity and atherogenesis.3 Therefore, it is impossible to identifythe intrahepatic triglyceride level, which precisely reflects liver insu-lin resistance, as an isolated variable in the generation of CVDrisk.
Furthermore, when we consider cardiovascular mortality, weshould refer not only to coronary heart disease but also to chronicheart failure due to nonischemic cardiomyopathy, which is associ-ated with alterations in substrate utilization (cardiac work/myocar-dial oxygen consumption) occurring early in the cascade of eventsleading to impaired ventricular contractility. In this respect, Perse-ghin et al.4 demonstrated that young individuals without obesity,diabetes, or hypertension who had a fatty liver showed echocardio-graphic features of early left ventricular dysfunction and impairedenergy metabolism (measured by cardiac 31P magnetic resonancespectroscopy). The phosphocreatine/adenosine triphosphate ratio, arecognized in vivo marker of myocardial energy metabolism, wasinversely related to both plasma glucose and insulin levels in thatstudy and was also tightly related to liver fat. These findings sug-gest that NAFLD is not merely a marker of metabolic dysfunctionbut may be actively involved in the initiation and progression ofCVD.
Finally, we agree with the authors’ conclusion that methodologi-cally rigorous prospective studies evaluating not only surrogatemarkers but also liver histology are warranted in order to dissectthe precise contribution of a fatty liver to the risk of CVD. In theinterim, we suggest that there is consistent pathophysiological evi-dence indicating that the evaluation and management of a fatty
HEPATOLOGY, Vol. 53, No. 5, 2011 CORRESPONDENCE 1785

liver should be considered a mainstay for the prevention of meta-bolic CVD.
FEDERICO SALAMONE, M.D.1
FABIO GALVANO, PH.D.2
GIOVANNI LI VOLTI, M.D., PH.D.21Department of Internal Medicine, University of Catania, Catania,
Italy2Department of Biological Chemistry, University of Catania, Catania,
Italy
References1. Ghouri N, Preiss D, Sattar N. Liver enzymes, nonalcoholic fatty liver
disease, and incident cardiovascular disease: a narrative review and clini-cal perspective of prospective data. HEPATOLOGY 2011;52:1156-1161.
2. Perseghin G. Viewpoints on the way to a consensus session: where doesinsulin resistance start? The liver. Diabetes Care 2009;32(Suppl 2):S164-S167.
3. Han S, Liang CP, Westerterp M, Senokuchi T, Welch CL, Wang Q,et al. Hepatic insulin signaling regulates VLDL secretion and athero-genesis in mice. J Clin Invest 2009;119:1029-1041.
4. Perseghin G, Lattuada G, De Cobelli F, Esposito A, Belloni E, NataliG, et al. Increased mediastinal fat and impaired left ventricular energymetabolism in young men with newly found fatty liver. HEPATOLOGY
2008;47:51-58.
CopyrightVC 2011 by the American Association for the Study of Liver Diseases.View this article online at wileyonlinelibrary.com.DOI 10.1002/hep.24115Potential conflict of interest: Nothing to report.
Does the Donor Mannose-Binding Lectin Genotype Really Predict the Risk of Bacterial InfectionsAfter Liver Transplantation?
To the Editor:
With great interest, we read the recent article by De Rooijet al.1 and the accompanying editorial.2 The authors showed thatfunctional single-nucleotide polymorphisms within donor genesinvolved in the lectin complement pathway [mannose-bindinglectin 2 (MBL2), ficolin 2, and mannan-binding lectin-associatedserine protease 2 (MASP2)] determine the risk of bacterial infec-tions after liver transplantation (LT). Although this is the firststudy associating single-nucleotide polymorphisms in ficolin 2and MASP2 with the risk of infection after LT, the value of thedonor MBL2 genotype as a risk factor for infection after LT issupported by two other studies.3,4 However, a fourth study5
found no difference in the overall rate of infections betweenpatients who received liver transplants from donors with insuffi-cient MBL genotypes and those who received liver transplantsfrom donors with sufficient MBL genotypes; although there was ahigher incidence of septic shock after transplantation with MBL-insufficient livers. Moreover, the published studies used differentways to stratify MBL genotypes into groups with MBL serum lev-els predicted to be sufficient or insufficient. Donor YA/YA andYA/XA genotypes result in high serum MBL2 levels, O/O andXA/O genotypes are almost MBL2-deficient, and YA/O and XA/XA genotypes are associated with intermediate MBL2 serum lev-
els after LT.4 Although De Rooij et al. used a strict definition ofMBL insufficiency and considered only O/O and XA/O geno-types to be MBL-insufficient, Worthley et al.4 also considered theintermediate XA/XA genotype to be MBL-insufficient, and thetwo other studies3,5 also included the second intermediate geno-type (YA/O) in the MBL-insufficient group. Therefore, the valueof the donor MBL genotype and the method of its interpretationfor the early identification of LT patients at risk of infectiouscomplications are not established yet.
We studied the predictive value of donor MBL genotyping forbacterial infections in our own center. The MBL genotypes of 290donor livers used for orthotopic transplantation between 1987 and2010 were determined. Notably, this cohort represents the largestsingle-center cohort of LT patients in which associations betweenthe donor MBL2 genotype and bacterial infections have been ana-lyzed. In three different ways, we categorized donor livers as MBL-sufficient or MBL-insufficient according to the stratification sys-tems used in the cited studies, and we analyzed associations withclinically significant and laboratory-confirmed bacterial infectionsoccurring during the first 3 months after LT by chi-square analysiswith Fisher’s exact test (Table 1). Thirty-eight percent of LT recipi-ents experienced one or more infectious episodes, and this is com-parable to the numbers reported by the previous studies.1,4,5
Importantly, none of the three stratifications resulted in a
Table 1. Associations Between Donor MBL2 Genotypes and Clinically Significant Bacterial Infections After LT
MBL Genotype Stratification Clinically Significant Infection Intra-Abdominal Infection Bacteremia Pneumonia
I*
Insufficient: O/O, XA/O 22/47 (47%) 18/47 (38%) 12/47 (26%) 6/47 (13%)
Sufficient: YA/YA, YA/XA, XA/XA, YA/O 88/243 (36%) 59/243 (24%) 47/243 (19%) 12/243 (5%)
P value 0.190 0.070 0.328 0.090
II†
Insufficient: O/O, XA/O, XA/XA 31/66 (47%) 20/66 (30%) 18/66 (27%) 9/66 (14%)
Sufficient: YA/YA, YA/XA, YA/O 79/224 (35%) 57/224 (25%) 41/224 (18%) 9/224 (4%)
P value 0.112 0.432 0.120 0.008
III‡
Insufficient: O/O, XA/O, XA/XA, YA/O 51/131 (39%) 32/131 (24%) 30/131 (23%) 13/131 (10%)
Sufficient: YA/YA, YA/XA 59/159 (37%) 45/159 (28%) 29/159 (18%) 5/159 (3%)
P value 0.808 0.505 0.380 0.026
*The MBL genotypes are stratified according to the combinations of promoter �221 and exon 1 single-nucleotide polymorphisms used by De Rooij et al.1
†The MBL genotypes are stratified according to Worthley et al.4
‡The MBL genotypes are stratified according to Bouwman et al.3 and Cervera et al.5
1786 CORRESPONDENCE HEPATOLOGY, May 2011

statistically significant association between the donor MBL geno-type and clinically significant infections. In addition, when we ana-lyzed associations with site-specific infections, independently ofMBL genotype stratification, we observed no significant increasesin the risk of intra-abdominal infections or bacteremia in patientswho underwent transplantation with MBL-insufficient livers. How-ever, in two of the three types of MBL genotype stratification, sig-nificantly more pneumonia was diagnosed in patients who under-went transplantation with MBL-deficient livers.
In conclusion, this retrospective study indicates that in our cen-ter, the donor MBL2 genotype is not helpful in predicting the riskof bacterial infection after LT.
LILIAN A. CURVELO, M.D., PH.D.1
EMMELOES DE MARE-BREDEMEIJER, M.D.1
ILSE DE CANCK, M.SC.3
MARTINE VAN THIELEN, M.SC.3
GEERT KAZEMIER, M.D., PH.D.2
HEROLD METSELAAR, M.D., PH.D.1
JAAP KWEKKEBOOM, PH.D.1
Departments of 1Gastroenterology and Hepatology and 2SurgeryErasmus MC: University Medical Center RotterdamRotterdam, the Netherlands
3R&D Discovery, Innogenetics NV, Zwijnaarde, Belgium
References1. de Rooij BJ, van Hoek B, ten Hove WR, Roos A, Bouwman LH,
Schaapherder AF, et al. Lectin complement pathway gene profile of do-nor and recipient determine the risk of bacterial infections after ortho-topic liver transplantation. HEPATOLOGY 2011;52:1100-1110.
2. Razonable RR. Innate immune genetic profile to predict infection riskand outcome after liver transplant. HEPATOLOGY 2011;52:814-817.
3. Bouwman LH, Roos A, Terpstra OT, de Knijff P, van Hoek B, Verspa-
get HW, et al. Mannose binding lectin gene polymorphisms confer a
major risk for severe infections after liver transplantation. Gastroenter-
ology 2005;129:408-414.4. Worthley DL, Johnson DF, Eisen DP, Dean MM, Heatley SL, Tung JP,
et al. Donor mannose-binding lectin deficiency increases the likelihood
of clinically significant infection after liver transplantation. Clin Infect
Dis 2009;48:410-417.5. Cervera C, Balderramo D, Suarez B, Prieto J, Fuster F, Linares L, et al.
Donor mannose-binding lectin gene polymorphisms influence the out-come of liver transplantation. Liver Transpl 2009;15:1217-1224.
CopyrightVC 2011 by the American Association for the Study of Liver Diseases.View this article online at wileyonlinelibrary.com.DOI 10.1002/hep.24114Potential conflict of interest: Nothing to report.
HEPATOLOGY, Vol. 53, No. 5, 2011 CORRESPONDENCE 1787
Copyright © 2022 FDOKUMEN




















