
Pancreas and Diabetes Mellitus
46
Pancreas and Diabetes Mellitus Pharmacology Sharon Jobity MS
Transcript of Pancreas and Diabetes Mellitus

Pancreas and Diabetes MellitusPharmacology
Sharon Jobity MS
Pancreas Located in abdomen behind the stomachContains both exocrine and endocrine glands Bulk of gland composed of:Acinar cells– enzyme rich pancreatic juiceScattered among cells:Islets of Langerhans – Alpha cells – glucagon Beta cells – insulin Delta cells – somatostatin, pancreatic polypeptide


Pancreas Glucagon – 29 AA polypeptide hyperglycemic hormonePromotes glycogenolysis, gluconeogenesis, release of glucose to the blood by liver cells, fall in AA conc in bloodRelease stimulated by falling glucose levels and increase in AA levels from a mealInsulin is hypoglycemic hormone with independent but antagonistic action to glucagon on blood glucose levels

Diabetes mellitus• Diabetes mellitus (DM) is a disorder of metabolism of carbohydrate, fat, and protein associated with an absolute or relative deficiency of insulin and/or varying degrees of insulin resistance. DM should be regarded as a syndrome that includes a heterogeneous group of disorders whose common feature is persistent hyperglycemia

Disease Burden • Leading cause of blindness (12.5% of cases)
• Leading cause of end stage renal disease ESRD(42% of cases)
• 50% of all non-traumatic amputations• 2.5x increase risk of stroke• 2-4x increase in cardiovascular mortality
• DM responsible for 25% of cardiac surgeries
• Mortality in DM: 70% due to Cardiovascular disease like myocardial infarction.
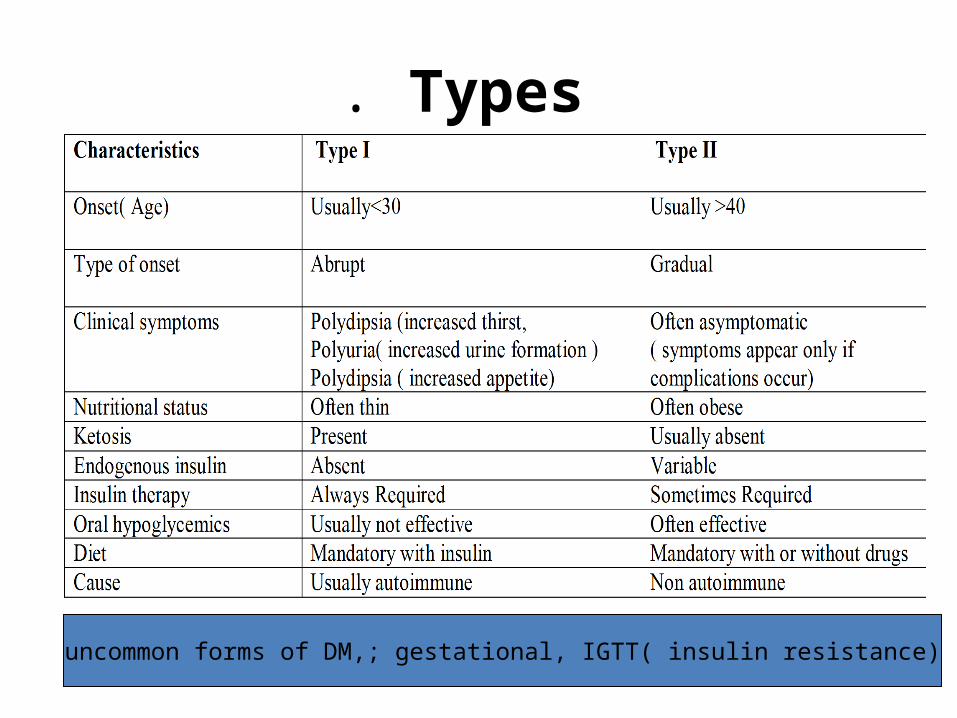
. Types
uncommon forms of DM,; gestational, IGTT( insulin resistance)

Complications of Diabetes Mellitus.:
i. Acute complications-diabetic keto acidosis( diabetic coma)
- Hyperosmolar Hyperglycemic State /Hyperosmolar Dehydration Syndrome
ii. Late complications- Microvascular • a. Retinopathy - Cataracts and glaucoma more common in DM , small pupils that respond poorly to light
• b. Nephropathy - end stage renal disease• c. Neuropathy - Includes various peripheral sensorimotor and autonomic neuropathies, poor wound healing, ulcer formation, amputations
TreatmentInsulin• rapid acting (0–5 hours),• short acting (0–8 hours),• intermediate acting (2 to 16 hours), and
• long acting (4 to 36 hours).
Oral antidiabetic medication

Insulin• Simple protein(poly peptide) consisting of 51amino acids
Biosynthèsis and secretion• Translated in pancreatic-cells as a large single-
chain polypeptide called preproinsulin, then further processed to proinsulin by specific endopeptidases and packaged into storage granules prior to release.
• Proinsulin has little inherent biological activity and must be converted to insulin by the action of specific proteases in the Golgi apparatus; this enzyme action results in the formation of insulin and C (connecting) peptide.
• Both insulin and C-peptide are stored in the pancreatic -cell granules, and both are liberated during insulin secretion.
• Though it is unclear whether C-peptide has any function after it enters the circulation

Insulin Secretion Insulin is continuously secreted at a low basal level during fasting, but a postprandial rise in serum glucose or amino acid levels can augment blood levels of insulin several fold. • Glucose-induced stimulation of insulin release from cells is biphasic.
• The initial rapid rise in insulin that follows a rise in glucose is termed the first phase of insulin release and is thought to reflect the release of the presynthesized insulin in the storage granules;
• delayed and prolonged rise in insulin secretion follows.
Regulation• Other nutrients ( arginine, leucine) and several hormones ( glucagon, growth hormone, secretin, gastrin cholecystokinin, pancreozymin, adreno-corticotropin) modulate insulin release.
• The autonomic nervous system also participates in the regulation of the rate of insulin secretion.
• Islets of Langerhans receives both cholinergic and adrenergic innervation. Insulin secretion is enhanced by vagal (cholinergic) and diminished by sympathetic (adrenergic) stimulation

Biochemical and Pharmacological Actions
IN ADDITION TO stimulating glucose uptake by tissues
insulin has five major physiological effects on fuel homeostasis.
• (1) Diminish hepatic glycogenolysis by inhibiting glycogen phosphorylase;
• (2) promote hepatic glucose storage into glycogen by stimulating glycogen synthetase;
• (3) inhibit hepatic gluconeogenesis (i.e., convert noncarbohydrate substrates like amino acids into glucose);
• (4) Inhibit lipolysis by inhibiting hormone-sensitive
lipase activity, thereby decreasing plasma free fatty acid and glycerol levels;
• (5) promote the active transport of amino acids into cells
for incorporation into protein,
Molecular mechanisms of insulin action.
• Insulin binds reversibly with high affinity-specific insulin receptor on the cell membrane surface
• The insulin receptor is a hetero-tetrameric tyrosine kinase receptor composed of two α-and two β-subunits.
• Insulin binds to the α-subunit on the extracellular surface of the cell and activates tyrosine kinase activity in the intracellular portion of the β -subunit.
• This results in the autophosphorylation of insulin β -receptor subunit and the phosphorylation of tyrosine residues on cytoplasmic proteins, termed the insulin receptor substrate (IRS) 1 &2.

Molecular mechanisms of insulin action.
• This network of phosphorylations within the cell represents insulin's second messanger and results in multiple effects, including translocation of glucose transporters ( GLUT ) to the cell membrane with resultant increase in glucose uptake; increased glycogen synthase activity and increased glycogen formation;
• Multiple effects on protein synthesis, lipolysis, and lipogenesis through activation of transcription factors that enhance DNA synthesis and cell growth and division also occur.


Insulin Preparations• Human insulin (e.g. Humulin,
Novolin) produced by rDNA technology is now widely available
• Some insulins have been modified through genetic engineering to produce insulin analogues, derivatives that possess novel pharmacokinetic properties (lispro, insulin aspart, and insulin glargine).

INSULIN PREPARATIONS

INSULIN GLARGINEInsulin glargine is a soluble, "peakless" (ie, having a broad plasma concentration plateau), long-acting insulin analog. This product was designed to provide reproducible, convenient, background insulin replacement. SUBSTITUTION• The attachment of two arginine molecules to the B-chain carboxyl .
• The terminal substitution of a glycine for asparagine at the A21 position
Analog created that is soluble in an acidic solution but precipitates in the more neutral body pH Individual insulin molecules slowly dissolve away from the crystalline depot and provide a low, continuous level of circulating insulin.• Insulin glargine has a slow onset of action (1–1.5 hours) and achieves a maximum effect after 4–6 hours. This maximum activity is maintained for 11–24hours or longer.
• Glargine is usually given once daily

Adverse effects of insulin
• The most common side effect is -hypoglycemia, CNS symptoms : tremors, lethargy, hunger, confusion, motor and sensory deficits, seizures, and unconsciousness.
• Adrenergic manifestations : anxiety, palpitations, tachycardia, and diaphoresis.
In many cases, diabetics are aware that hypoglycemia is developing, and prompt administration of oral carbohydrates (e.g., fruit juice or glucose tablets) can restore normoglycemia.

Adverse Reactions to Insulin:
• Coma, Unconscious: In more severe cases , intravenous glucose or intramuscular glucagon is required to reverse the hypoglycemia.
• Weight Gain: Frequent side effect of insulin therapy due to increased caloric storage of glucose by insulin, and also due to renal sodium retention resulting in fluid retention and edema.
• Allergic reactions: Due to the use of animal-derived insulins, but less frequently, since the use of recombinant DNA-derived human insulin became widespread.
local lipodystrophy (lipohypertrophy or lipoatrophy): Due to repeated subcutaneous injections of insulin in fatty areas over time.• Hypokalemia : can follow acute insulin
administration, an effect that is due to the stimulation of Na–K–ATPase.

Oral hypoglycemic agents
1.Sulfonylureas-1st generation-Chloropropamide,Tolbutamide-2nd generation- Gliclazide
Glibenclamide (gluburide) Glipizide
-3rd generation-Glimepiride.2. Meglitinides- ripaglinide ,nataglinide3. Biguanides- metformin4. α- glucosidase inhibitors- acarbose 5. Thiazolidinediones- rosiglitazon,
piogltazone

SulfonylureasMechanism of action
The primary mechanism of action of the sulfonylureas is direct stimulation of insulin release from the pancreatic β-cells.
In the presence of viable pancreatic -cells, sulfonylureas enhance the release of endogenous insulin, thereby reducing blood glucose levels.
At higher doses, these drugs also decrease hepatic glucose production
Dosage 250mg -500mg/day The sulfonylureas are ineffective for the management of type I and severe type II diabetes mellitus, since the number of viable -cells is small.


Sulfonylureas -Mechanism of action
The sulfonylurea receptor was identified as an adenosine triphosphate (ATP) sensitive potassium (KATP) channel that is present on the β-cell membrane surface.
Closure of these KATP channels causes -cell membrane depolarization and triggers the opening of voltage-dependent calcium channels. The influx of calcium into the -cell triggers insulin granule fusion to the β-cellmembrane and insulin release.
Sulfonylurea binding to its receptor directly promotes the closure of these KATP channels, lowering the threshold for glucose-dependent insulin release

Pharmacokinetics of the sulfonylureas
1st generation members have short half lives.
2nd generation is administered once, twice or several times daily.
3rd generation is administered once daily. All sulfonylurea are metabolized by liver and their metabolites are excreted in urine with about 20 % excreted unchanged.
Sulfonylurea should be administered with caution to patients with either renal or hepatic insufficiency.

Adverse Reactions : Sulfonylureas may induce hypoglycemia especially in elderly patients with impaired hepatic or renal functions- These cases of hypoglycemia are treated by I/V glucose infusion Other side effects: hypersensitivity, weight gain, headache, GI upset.
The hypoglycemic effect of sulphonylureas may be enhanced if metabolism or excretion is affected by other drugs or they are displaced from plasma proteins.
These side effects are fewer in the 2nd generation and rare in the 3rd generation.

Drug InteractionsThe drugs that enhance the effect of sulfonylureas. NSAIDs Salicylates Sulfonamide ß-blockers Chloramphenicol Diazepam MAOIDrugs that reduce /suppress the effect of sulphonylureas Barbiturates Thiazide and loop diuretics Sympathomimetics Corticosteroids Oestrogen / Progesterone combinations

Contraindications:
Type 1 DM Pregnancy and Lactation.(Cat –C)
Prolonged hypoglycemia (4 to 10 days)has been reported in children borne to mothers taking sulfonylureas at the time of delivery. Significant hepatic or renal failure increase the risk of hypoglycemia.

Meglitinides:Similar to sulphonylureas
Designed to minimize mealtime blood glucose peaks
Fast acting, short duration non-sulfonylurea
Stimulation of pancreatic insulin release by closing ß-cells KATP channels
Very rapid onset of action and short duration (TMAX = 1 hour, metabolized by liver )
No hypoglycemic metabolites

Clinical efficacy:
– Improves postprandial glycemia – Less effective in decreasing fasting blood glucose levels and HbA1C
• drawbacks:– Fails to provides a stable 24 hours blood glucose control
– Complicated dosage style (3-8 tablets/daily)

Biguanides :• Biguanides are derivatives of the antimalarial agent Chloroguanide. Which is found to have hypoglycemic action.
• The most commonly used member of biguanides is Metformin.

Biguanides – Mechanism of Action
• Biguanides- Antihyperglycemic and not Hypoglycemic
• It does not stimulate pancreas to secrete insulin and does not cause hypoglycemia even in large doses.
• Also it has no effect on secretion of Glucagon or Somatostatin
• Decreases the intestinal absorption of CHO• Increases glucose uptake (GLUT 4)• Increases glucose utilization (glycogensynthase)• Increases glycolysis via anaerobic pathway (lactic acidosis)

Metformin
Indications: Metformin works best in patients with significant hyperglycemia and is often considered first-line therapy
in the treatment of mild to moderate type II overweight diabetics who demonstrate insulin resistance
Type 2 diabetes failed on diet Metformin can be given alone or in combination with sulfonylureas or Insulin

MetforminCLINICAL EFFICACY
• Study demonstrated a marked reduction in cardiovascular comorbidities and diabetic complications in metformin treated individuals.
• Metformin has also been used to treat hirsutism in individuals with polycystic ovarian syndrome and may enhance fertility in these women, perhaps by decreasing androgen levels and enhancing insulin sensitivity.
PK/PD
Metformin is well absorbed from small intestine, stable, does not bind to plasma proteins, excreted unchanged in urine.
Not metabolized by the liver Half life of Metformin is 1.5 - 4.5 hours, taken in three doses with meals
Pregnancy (Cat – B) Dosage -500mg bid-max 2000mg

Adverse EffectsOccur in 20-25 % of patients. Diarrhea, abdominal discomfort, nausea, metallic taste, decreased absorption of vitamin B12.More serious: Lactic acidosis

Contraindications
• Patients with renal or hepatic impairment.
• Past history of lactic acidosis.
• Heart failure, Chronic lung disease.
These conditions predispose to increased lactate production which causes lactic acidosis can be potentially fatal

α Glucosidase Inhibititor (Acarbose )
Indicated for Type 2 diabetes, in conjunction with diet and with other anti-diabetic therapies
Mode of action: Poorly absorbed 1% (act locally in G.I.T.) competitively inhibits intestinal alpha-glucosidases and modulating the postprandial digestion and absorption of carbohydrates like starch and disaccharides

• Dose:– 50mg to 100mg 3 times daily before meals
• Side effects:– Flatulence (77%) – Diarrhea– Abdominal pain (21%)– Decreased iron absorption
5. Thiazolidenediones(sometimes termed glitazones)
Rosiglitazone and Pioglitazone• Have insulin-sensitizing properties. They all act to decrease insulin resistance and enhance insulin action in target tissues.

Mode of action:• Insulin sensitizer (increase insulin sensitivity in muscle, adipose tissue & liver)
• They are not insulin secretagogues (Not insulin releasers)
• Thiazolidinediones activate the nuclear peroxisome proliferator–activated receptor- γ (PPAR- γ) , a nuclear orphan receptor that is predominantly expressed in adipose tissue and to a lesser extent in muscle, liver, and other tissues.
• The endogenous ligand for the PPAR- γ receptor is postulated to be prostaglandinJ2, and it appears to work by heterodimerizing with other nuclear receptors to modulate the expression of insulin-sensitive genes.

• Indication:–They are used in combination therapy-not alone. In case of severe insulin deficiency should be combined with sulfonylurea or metformin or both
• Side effects Edema
Hepatotoxicity weight gain Dyslipidaemia (increases LDL, cholesterol)

PD/PKPregnancy (Cat- C)Dose 4mg daily in combination with 2nd or 3rd generation sulphonylureaMechanism requires presence of insulin therefore not recommended in Type 1 diabetes.





















