
Oxidative & nitrosative stress in depression: Why so much stress?
17
Please cite this article in press as: Moylan, S., et al., Oxidative & nitrosative stress in depression: Why so much stress? Neurosci. Biobehav. Rev. (2014), http://dx.doi.org/10.1016/j.neubiorev.2014.05.007 ARTICLE IN PRESS G Model NBR 1953 1–17 Neuroscience and Biobehavioral Reviews xxx (2014) xxx–xxx Contents lists available at ScienceDirect Neuroscience and Biobehavioral Reviews jou rn al h om epage: www.elsevier.com/locate/neubiorev Review Oxidative & nitrosative stress in depression: Why so much stress? Steve Moylan a,h,∗ , Michael Berk a,b,c,d,h,j , Olivia M. Dean a,b,d , Yuval Samuni a , Q1 Lana Williams a,d , Adrienne O’Neil a,c , Amie C. Hayley a , Julie A. Pasco a,e , George Anderson f , Felice Jacka a , Michael Maes a,g,i a IMPACT Strategic Research Centre, School of Medicine, Deakin University, Geelong, Victoria, Australia b Florey Institute for Neuroscience and Mental Health University of Melbourne, Parkville, Victoria, Australia c School of Public Health and Preventive Medicine, Monash University, Prahran, Victoria, Australia d University of Melbourne, Department of Psychiatry, Level 1 North, Main Block, Royal Melbourne Hospital, Parkville 3052, Australia e Northwest Academic Centre, University of Melbourne, St. Albans, Victoria, Australia f CRC Scotland & London, London, United Kingdom g Department of Psychiatry, Chulalongkorn University, Faculty of Medicine, Bangkok, Thailand h Barwon Health, Geelong, Victoria, Australia i Department of Psychiatry, State University of Londrina, Londrina, Brazil j Orygen Youth Health Research Centre, University of Melbourne, Parkville, Victoria, Australia a r t i c l e i n f o Article history: Received 3 February 2014 Received in revised form 17 April 2014 Accepted 13 May 2014 Keywords: Depression Bipolar disorder Oxidative & nitrosative stress Inflammation Antioxidants Autoimmune a b s t r a c t Many studies support a crucial role for oxidative & nitrosative stress (O&NS) in the pathophysiology of unipolar and bipolar depression. These disorders are characterized inter alia by lowered antioxidant defenses, including: lower levels of zinc, coenzyme Q10, vitamin E and glutathione; increased lipid perox- idation; damage to proteins, DNA and mitochondria; secondary autoimmune responses directed against redox modified nitrosylated proteins and oxidative specific epitopes. This review examines and details a model through which a complex series of environmental factors and biological pathways contribute to increased redox signaling and consequently increased O&NS in mood disorders. This multi-step process highlights the potential for future interventions that encompass a diverse range of environmental and molecular targets in the treatment of depression. © 2014 Published by Elsevier Ltd. Contents 1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00 2. Depression-related pathways causing O&NS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00 2.1. Activated immune-inflammatory pathways . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00 2.2. Leaking gut and the microbiome . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00 Abbreviations: 5-HT, 5-hydroxytryptophan; 5-HTTLPR, serotonin transporter linked polymorphic region; 8-iso, 8-iso-prostaglandin F2; 8-OHdG, 8-hydroxy- 2 -deoxyguanosine; ATP, adenosine triphosphate; BH4, 5,6,7,8-tetrahydrobiopterin; CMI, cell mediated immune; CRH, corticotrophin releasing hormone; DAMP, damage-associated molecular pattern; DNA, eeoxyribonucleic acid; GPX, glutathione peroxidase; GSH, glutathione; HDL, high density lipoprotein; HPA, hypothalamic–pituitary–adrenal axis; IDO, indoleamine 2,3-dioxygenase; IFN, interferon-alpha; IFN, interferon-gamma; Ig, immunoglobulin; IgG, immunoglobulin G; IgM, immunoglobulin M; IL-1, interleukin-1; IL-10, interleukin-10; IL-12, interleukin-12; IL-1, interleukin-1; IL-2, interleukin-2; IL-4, interleukin-4; IL-6, interleukin-6; iNOS, inducible nitric oxide synthase; KYNA, kynurenic acid; LDL, low-density lipoprotein; LPS, lipopolysaccharide; MAPK, mitogen-activated protein kinases; MDA, malon- dialdehyde; NAC, N-acetylcysteine; NDMA, N-methyl-d-aspartate; NF-B, nuclear factor (NF)-B; nNOS, neuronal nitric oxide synthase; NO, nitric oxide; NOS, nitric oxide synthase; NOX, NADPH oxidase complex.; Nrf2, nuclear factor erythroid 2-related factor; NSE, nitrosative specific epitopes; O&NS, oxidative & nitrosative stress; ONOO-, peroxynitrite; OSA, obstructive sleep apnoea; OSE, oxidation specific epitope; Ox-LDL, oxidized low density lipoprotein; Ox-PLP, oxidized phospholipids; PAMP, pathogen- associated molecular pattern; PIC, pro-inflammatory cytokine; PON1, paraxonase 1; PRR, pattern recognition receptor; QUIN, quinolinic acid; RNS, reactive nitrogen species; ROS, reactive oxygen species; SOD, Superoxide dismutase; SSRI, selective serotonin reuptake inhibitor; TCA, trycyclic antidepressant; TLR, Toll-like receptor; TNF-, tumor necrosis factor-alpha; TRYCAT, tryptophan catabolite. ∗ Corresponding author at: C/o IMPACT Strategic Research Centre, School of Medicine, Deakin University, Kitchener House, Geelong Hospital, Ryrie St., Geelong, Victoria 3220, Australia. Tel.: +61 342153306; fax: +61 342153491. E-mail address: [email protected] (S. Moylan). http://dx.doi.org/10.1016/j.neubiorev.2014.05.007 0149-7634/© 2014 Published by Elsevier Ltd. 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36
Transcript of Oxidative & nitrosative stress in depression: Why so much stress?

N
R
O
SQ1
LGa
b
c
d
e
f
g
h
i
j
a
ARRA
KDBOIAA
C
2dhIidspaRn
3
h0
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
ARTICLE IN PRESSG ModelBR 1953 1–17
Neuroscience and Biobehavioral Reviews xxx (2014) xxx–xxx
Contents lists available at ScienceDirect
Neuroscience and Biobehavioral Reviews
jou rn al h om epage: www.elsev ier .com/ locate /neubiorev
eview
xidative & nitrosative stress in depression: Why so much stress?
teve Moylana,h,∗, Michael Berka,b,c,d,h,j, Olivia M. Deana,b,d, Yuval Samunia,ana Williamsa,d, Adrienne O’Neil a,c, Amie C. Hayleya, Julie A. Pascoa,e,eorge Andersonf, Felice Jackaa, Michael Maesa,g,i
IMPACT Strategic Research Centre, School of Medicine, Deakin University, Geelong, Victoria, AustraliaFlorey Institute for Neuroscience and Mental Health University of Melbourne, Parkville, Victoria, AustraliaSchool of Public Health and Preventive Medicine, Monash University, Prahran, Victoria, AustraliaUniversity of Melbourne, Department of Psychiatry, Level 1 North, Main Block, Royal Melbourne Hospital, Parkville 3052, AustraliaNorthwest Academic Centre, University of Melbourne, St. Albans, Victoria, AustraliaCRC Scotland & London, London, United KingdomDepartment of Psychiatry, Chulalongkorn University, Faculty of Medicine, Bangkok, ThailandBarwon Health, Geelong, Victoria, AustraliaDepartment of Psychiatry, State University of Londrina, Londrina, BrazilOrygen Youth Health Research Centre, University of Melbourne, Parkville, Victoria, Australia
r t i c l e i n f o
rticle history:eceived 3 February 2014eceived in revised form 17 April 2014ccepted 13 May 2014
a b s t r a c t
Many studies support a crucial role for oxidative & nitrosative stress (O&NS) in the pathophysiologyof unipolar and bipolar depression. These disorders are characterized inter alia by lowered antioxidantdefenses, including: lower levels of zinc, coenzyme Q10, vitamin E and glutathione; increased lipid perox-idation; damage to proteins, DNA and mitochondria; secondary autoimmune responses directed againstredox modified nitrosylated proteins and oxidative specific epitopes. This review examines and details a
eywords:epressionipolar disorderxidative & nitrosative stress
nflammation
model through which a complex series of environmental factors and biological pathways contribute toincreased redox signaling and consequently increased O&NS in mood disorders. This multi-step processhighlights the potential for future interventions that encompass a diverse range of environmental andmolecular targets in the treatment of depression.
ntioxidantsutoimmune
© 2014 Published by Elsevier Ltd.
ontents
Please cite this article in press as: Moylan, S., et al., Oxidative & nitrosatRev. (2014), http://dx.doi.org/10.1016/j.neubiorev.2014.05.007
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2. Depression-related pathways causing O&NS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2.1. Activated immune-inflammatory pathways . . . . . . . . . . . . . . . . . . . . . . .2.2. Leaking gut and the microbiome . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Abbreviations: 5-HT, 5-hydroxytryptophan; 5-HTTLPR, serotonin transporter lin′-deoxyguanosine; ATP, adenosine triphosphate; BH4, 5,6,7,8-tetrahydrobiopterin;
amage-associated molecular pattern; DNA, eeoxyribonucleic acid; GPX, glutathypothalamic–pituitary–adrenal axis; IDO, indoleamine 2,3-dioxygenase; IFN�, interfer
gM, immunoglobulin M; IL-1, interleukin-1; IL-10, interleukin-10; IL-12, interleukin-12NOS, inducible nitric oxide synthase; KYNA, kynurenic acid; LDL, low-density lipoproteinialdehyde; NAC, N-acetylcysteine; NDMA, N-methyl-d-aspartate; NF-�B, nuclear factorynthase; NOX, NADPH oxidase complex.; Nrf2, nuclear factor erythroid 2-related factoreroxynitrite; OSA, obstructive sleep apnoea; OSE, oxidation specific epitope; Ox-LDL, oxssociated molecular pattern; PIC, pro-inflammatory cytokine; PON1, paraxonase 1; PRR,
OS, reactive oxygen species; SOD, Superoxide dismutase; SSRI, selective serotonin reupecrosis factor-alpha; TRYCAT, tryptophan catabolite.∗ Corresponding author at: C/o IMPACT Strategic Research Centre, School of Medicine,220, Australia. Tel.: +61 342153306; fax: +61 342153491.
E-mail address: [email protected] (S. Moylan).
ttp://dx.doi.org/10.1016/j.neubiorev.2014.05.007149-7634/© 2014 Published by Elsevier Ltd.
ive stress in depression: Why so much stress? Neurosci. Biobehav.
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00
ked polymorphic region; 8-iso, 8-iso-prostaglandin F2; 8-OHdG, 8-hydroxy-CMI, cell mediated immune; CRH, corticotrophin releasing hormone; DAMP,ione peroxidase; GSH, glutathione; HDL, high density lipoprotein; HPA,
on-alpha; IFN�, interferon-gamma; Ig, immunoglobulin; IgG, immunoglobulin G;; IL-1�, interleukin-1�; IL-2, interleukin-2; IL-4, interleukin-4; IL-6, interleukin-6;; LPS, lipopolysaccharide; MAPK, mitogen-activated protein kinases; MDA, malon-
(NF)-�B; nNOS, neuronal nitric oxide synthase; NO, nitric oxide; NOS, nitric oxide; NSE, nitrosative specific epitopes; O&NS, oxidative & nitrosative stress; ONOO-,idized low density lipoprotein; Ox-PLP, oxidized phospholipids; PAMP, pathogen-pattern recognition receptor; QUIN, quinolinic acid; RNS, reactive nitrogen species;take inhibitor; TCA, trycyclic antidepressant; TLR, Toll-like receptor; TNF-�, tumor
Deakin University, Kitchener House, Geelong Hospital, Ryrie St., Geelong, Victoria

ARTICLE IN PRESSG ModelNBR 1953 1–17
2 S. Moylan et al. / Neuroscience and Biobehavioral Reviews xxx (2014) xxx–xxx
2.3. Activation of the Toll-like receptor radical cycle . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 002.4. The tryptophan catabolite (TRYCAT) pathway . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 002.5. The glutamate–cystine cycle . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 002.6. Mitochondrial dysfunction. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 002.7. Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00
3. Depression-related factors causing dysregulated O&NS pathways . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 003.1. Genetic polymorphisms in O&NS genes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 003.2. Psychological stressors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 003.3. Medical comorbid disorders and conditions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 003.4. Obesity and metabolic syndrome . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 003.5. Sleep disorders . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 003.6. Cigarette smoking . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 003.7. Dietary factors. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 003.8. Vitamin D status . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 003.9. Sedentary lifestyle and exercise . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00
4. Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00Funding . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00
Acknowledgements . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00 . . . . . .
1
cmgpiaWataptooif
leaw((eed2os2
toofp2Hge2b
Q2
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60
61
62
63
64
65
66
67
68
69
70
71
72
73
74
75
76
77
78
79
80
81
82
83
84
85
86
87
88
89
90
91
92
93
94
95
96
97
98
99
100
101
102
103
104
105
106
107
108
109
110
111
112
113
114
115
116
117
118
119
120
121
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. Introduction
Many studies support dysregulated redox signaling as beingrucial in the pathophysiology and neuroprogressive nature ofajor depression (Maes et al., 2011a). Reactive oxygen and nitro-
en species (ROS and RNS), including peroxynitrite, superoxides,eroxides and nitric oxide (NO), are produced during normal phys-
ologic processes and, through interacting with proteins, fatty acidsnd DNA, perform numerous roles in regulation of cellular function.hen present in excess however, ROS/RNS can lead to structural
nd functional changes that produce cellular injury. These poten-ially toxic effects are offset under normal conditions by intrinsicntioxidant mechanisms that participate in the physiologic and/orathologic metabolism of ROS/RNS (Maes et al.). Increased oxida-ive and nitrosative stress (O&NS), which can arise as a consequencef raised production of ROS and RNS and/or decreased availabilityf antioxidant defenses, may cause damage to cellular components,nduce harmful autoimmune responses, and ultimately facilitateailure of normal cellular processes.
People with unipolar and bipolar depression display dysregu-ated redox signaling (Lee et al., 2013; Maes et al., 2011a; Moylant al., 2013c; Scapagnini et al., 2012). Studies using clinical andnimal models have demonstrated that depression is associatedith increased levels of redox products such as malondialdehyde
MDA, a marker for lipid peroxidation) and 8-iso-prostaglandin F28-iso) (a marker of arachidonic acid peroxidation) (Dimopoulost al., 2008; Forlenza and Miller, 2006; Galecki et al., 2009; Yagert al., 2010). Additionally, other studies have reported oxidativeamage to DNA, as measured by increased levels of 8-hydroxy-′-deoxyguanosine (8-OHdG) in serum (Forlenza and Miller, 2006)xidative damage to RNA in post-mortem hippocampus in depres-ion (Che et al., 2010) and telomere shortening (Shalev et al.,014).
Studies conducted in depressed populations demonstrate sus-ained increases in O&NS. These effects result in depleted levelsf n-3 fatty acid concentrations (Peet et al., 1998), a loweredxidative potential index of serum (Maes et al., 1999), reducedunctioning of antioxidant systems represented by lower levels oflasma concentrations of vitamin E (Maes et al., 2000; Owen et al.,005) and C (Khanzode et al., 2003), decreased albumin levels (Vanunsel et al., 1996), lowered levels of antioxidants including zinc,
Please cite this article in press as: Moylan, S., et al., Oxidative & nitrosatRev. (2014), http://dx.doi.org/10.1016/j.neubiorev.2014.05.007
lutathione (GSH) and coenzyme Q10 (Maes et al.), and lower lev-ls of amino acids, such as tryptophan and tyrosine (Maes et al.,000). Similarly, alterations of antioxidant-enzyme levels haveeen reported. For example, levels of superoxide dismutase (SOD)
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 00
and glutathione peroxidase (GpX) are lower in depressed patients(Maes et al., 2011a). Paraoxonase 1 (PON1), an antioxidant enzymebound to high-density lipoprotein (HDL), was significantly reducedin unipolar, but not bipolar, depression (Vargas et al., submitted for
publication). Impairment of these aforementioned antioxidant sys-tems contributes to the pathophysiology of depression via loweredprotection to ROS and RNS, which may result in increased risk ofsustained O&NS damage (Forlenza and Miller, 2006; Maes et al.,2011a).
NO is an important mediator in many neural processes. Rodentssubjected to acute and chronic immobilization stress exhibitincreased levels of inducible nitric oxide synthase (iNOS). AlthoughNO levels, iNOS and neuronal NOS (nNOS) expression are increasedin depression, recent studies have indicated that NOS participates inthe mechanisms underlying antidepressant efficacy (Galecki et al.,2012; Maes et al., 2008b). This suggests that NO may have differ-ential effects at different sites during the course and treatment ofdepression. Persistently increased levels of NO and O2
− may leadto the formation of peroxynitrite (ONOO ) and subsequent oxida-tion, nitration and nitrosylation of proteins, thereby contributingto cellular injury (Maes et al., 2008b, 2011d).
Major depression and bipolar depression are also accompaniedby increased autoimmune responses against newly formed oxida-tion specific epitopes (OSEs), following structural damage by O&NS(Maes et al., 2007, 2011d, 2013b). Immunoglobulin (Ig)G and IgM-mediated immune responses against OSEs of membrane fatty acids,like oxidized low density lipoprotein (LDL), oleic acid, MDA and aze-laic acid, and anchorage molecules, such as phosphatidyl inositol,palmitic acid, myristic acid and farnesyl-l-cysteine, can be seen indepression (Maes et al., 2007, 2011d, 2013b). This may have pro-found functional consequences as oxidative damage to membranes,especially to the major anchorage molecules, may affect the opera-tion of hundreds of functionally “anchored” proteins that regulatebasic cellular processes, including cell survival, growth, apoptosis,cell-signaling, neuroplasticity and neurotransmission (Maes et al.,2011a).
Chronically increased NO, following iNOS activation, can nitro-sylate (NSO or NO) proteins and amino acids yielding newNO-adducts (NO-neoepitopes) like NO-tyrosine, NO-tryptophan,NO-arginine, NSO-cysteine and NO-albumin. The consequenthyper-nitrosylation may cause dysfunction to intracellular signal-
ive stress in depression: Why so much stress? Neurosci. Biobehav.
ing, as well as competitively inhibit the palmitoylation of anchoredproteins to the membrane (Maes et al., 2008b, 2011d, 2012a).Moreover, some of these NO adducts can be immunogenic andtherefore contribute to further autoimmune responses directed
122
123
124
125

ING ModelN
iobeh
aMdi
aeaas
otaGitoifi
2
2
eDvaIwcs2acesaiitiTtoecrnMaimtaoniuiif2
126
127
128
129
130
131
132
133
134
135
136
137
138
139
140
141
142
143
144
145
146
147
148
149
150
151
152
153
154
155
156
157
158
159
160
161
162
163
164
165
166
167
168
169
170
171
172
173
174
175
176
177
178
179
180
181
182
183
184
185
186
187
188
189
190
191
192
193
194
195
196
197
198
199
200
201
202
203
204
205
206
207
208
209
210
211
212
213
214
215
216
217
218
219
220
221
222
223
224
225
226
227
228
229
230
231
232
233
234
235
236
237
238
239
240
241
242
243
244
245
246
247
248
249
ARTICLEBR 1953 1–17
S. Moylan et al. / Neuroscience and B
gainst “nitrosative specific epitopes” (NSEs) (Boullerne et al., 2002;aes et al., 2011d, 2012a). Finally, the autoimmune response
irected against some of these NSEs (e.g. NSO-cysteine) may resultn serious neurotoxic effects (Boullerne et al., 2002).
Animal studies have demonstrated that various classes ofntidepressants can reduce levels of oxidative stress markers (Erent al., 2007a,b; Maes et al., 2011a) and increase some endogenousntioxidants (Maes et al., 2011d). Further, some redox modulatorsppear to have some promise as adjunctive treatments for depres-ion (Maes et al., 2012a; Scapagnini et al., 2012).
The above observations provide greater insight into the pathol-gy of depression, but also raise a pertinent question: what arehe underlying pathways and factors that contribute to the onsetnd maintenance of the increased O&NS state in depression?reater understanding of the pathways and factors that precip-
tate a state of subchronic O&NS in depression may inform newherapeutic and preventative strategies. Here, we review numer-us pathways and factors that may contribute to increased O&NSn major depression, and discuss the potential implications of thesendings.
. Depression-related pathways causing O&NS
.1. Activated immune-inflammatory pathways
Considerable evidence supports the role of central and periph-ral immune-inflammatory processes in depression pathogenesis.epression is associated with cell-mediated immune (CMI) acti-ation, increased monocytic activation and a T helper (Th)-1-nd Th-17-like cytokine response (Leonard and Maes, 2012).n addition, recent meta-analyses demonstrate that patients
ith depression have higher serum levels of pro-inflammatoryytokines (PICs) such interleukin (IL)-1, IL-6 and tumor necro-is factor alpha (TNF�) (Dowlati et al., 2010; Howren et al.,009). Depression is also associated with increased levels ofcute phase proteins, including C-reactive protein and haptoglobin,hemokines, adhesions molecules and complement factors (Berkt al., 1997; Maes et al., 1997a; Pasco et al., 2010). An eventronger association between pro-inflammatory cytokines and LPSnd depressive-like behaviors has been reported in rodent stud-es where administration of IL-6, IL-1�, TNF� or LPS resultedn depressive-like and anxiety-like-behaviors. Similar manifesta-ions of depressive symptoms are also seen in patients undergoingmmunotherapy with IL-2 and INF-� (Dutcher et al., 2000).he reader is referred to three recent reviews demonstratinghat in depression and bipolar disorder peripheral activationf immune-inflammatory pathways coupled with elevated lev-ls of circulating LPS may contribute to neuroinflammation andonsequent neuroprogressive changes including decreased neu-oplasticity, neurogenesis, and increased neurodegeneration andeuronal apoptosis (Berk et al., 2011b; Leonard and Maes, 2012;oylan et al., 2013c). In addition, immune-inflammatory pathways
ffect the expression of key neurotransmitters thought involvedn depression pathogenesis (e.g. serotonin, noradrenaline) through
ultiple pathways. One example is through effects on 5,6,7,8-etrahydrobiopterin (Bh4). (BH4) is a critical co-factor of numerousmino acid converting enzymes responsible for the productionf neurotransmitters including NO, tryptophan, dopamine andoradrenaline (Sperner-Unterweger et al., 2014). Under acute
nflammatory conditions these BH4 related enzymes are upreg-lated, leading to increased biosynthesis of neurotransmitters
Please cite this article in press as: Moylan, S., et al., Oxidative & nitrosatRev. (2014), http://dx.doi.org/10.1016/j.neubiorev.2014.05.007
n the short term. However, chronic low-grade inflammations associated with “oxidative loss of BH4”, reducing capacityor neurotransmitter biosynthesis (Sperner-Unterweger et al.,014).
PRESSavioral Reviews xxx (2014) xxx–xxx 3
Studies assessing the effect of antidepressants on immune-inflammatory markers in depression provide further corroborationfor the role of immune-inflammatory processes in depression.Administration of tricyclic antidepressants (TCAs) and selectiveserotonin inhibitors (SSRI) has been shown to suppress CMI, whilstattenuating inflammatory biomarkers and acute phase protein lev-els in animal models (Leonard and Maes, 2012). Not surprisingly,the relationship between the immune-inflammatory response anddepression may be driven, or modulated, by underlying geneticvulnerability. A recent review of genetic variants in neurobiolog-ical pathways associated with immune activation and depressiondemonstrates that allelic variants of IL-1�, TNF-� and CRP mayincrease depression risk. SNPs in the IL-1�, IL-6 and IL-11 genes mayalso be associated with reduced responsiveness to antidepressants(Bufalino et al., 2013).
Mutual inductions between immune-inflammatory and O&NSpathways may be key in depression pathogenesis (Maes et al.,2011a, 2012a). Activation of immune-inflammatory pathways,O&NS processes and lowered antioxidant defenses are insepara-bly interrelated (Maes et al., 2012a). Activated phagocytes and M1macrophages produce large quantities of ROS and RNS. Increasedlevels of TNF� can upregulate the expression of iNOS via transloca-tion of nuclear factor kappa B (NF-�B), while interferon-gamma(IFN�) may activate the production of iNOS and thus NO bymacrophages. In different cell types, such as macrophages, neu-trophils, epithelial cells and microglia, cytokines such as IL-1, TNF�and IFN� activate ROS production (superoxide) via the NADPH oxi-dase complex (NOX). Neopterin, a surrogate marker of the Th-1-likeresponse, activates iNOS and NO production and the productionof hydrogen peroxide. On the other hand, activated O&NS path-ways may increase nuclear factor (NF)-�B, activator protein-1and mitogen-activated protein kinases (MAPK) thereby increas-ing the production of inflammatory mediators, such as PICs andchemokines.
Inflammatory and O&NS processes may also affect antioxidantdefenses. For example, the inflammatory processes in depressionare associated with lowered levels of zinc and vitamin E (Maeset al., 2011e). ROS produced in physiological conditions and duringinflammation upregulate antioxidant defense systems. In responseto O&NS, cells increase their antioxidant defenses through activa-tion of nuclear factor erythroid 2-related factor (Nrf2) (Maes et al.,2012a). Once activated, Nrf2 increases the expression of multipleendogenous antioxidants. On the other hand, severe inflamma-tion accompanied by increased ROS, as observed in inflammatorybowel disease, causes an increased consumption of tissue antioxi-dant defenses masking increased antioxidant levels due to the mildO&NS (Blau et al., 2000).
Since antioxidants, such as coenzyme Q10, zinc and glutathione,have anti-inflammatory effects, the lowered levels of those antiox-idants in depression increase the inflammatory and O&NS burden(Maes et al.). Moreover, reduced glutathione (GSH) and the regula-tion of pro-inflammatory cytokines are intimately interlinked. Forexample, the transcription of IL-1�, IL-6, and TNF� are regulatedby the redox state of the cell and depletion of GSH enhances thetranscription of these cytokines (Haddad, 2000).
Fig. 1 shows the associations between activated immune-inflammatory pathways, lowered antioxidant defenses andincreased damage by O&NS in depression. Factors that are knownto activate immune-inflammatory pathways (review: (Berk et al.,2013)) may therefore lead to downstream activation of ROS/RNSproduction and O&NS. It may be concluded that in depression, low-ered levels of antioxidants and activation of immune-inflammatory
ive stress in depression: Why so much stress? Neurosci. Biobehav.
and O&NS pathways are complex processes that exacerbate eachother via multiple feedback loops. Interactions of these seem-ingly enmeshed pathways further contribute to the complexity ofdepression pathogenesis.
250
251
252

ARTICLE ING ModelNBR 1953 1–17
4 S. Moylan et al. / Neuroscience and Biobeh
Fig. 1. Depression is characterized by multiple associations between activatedimmune-inflammatory pathways, lowered levels of key antioxidants and increasedreactive nitrogen species (RNS) and reactive oxygen species (ROS), which activatenuclear factor erythroid 2-related factor (Nrf2) increasing the expression of endoge-nous antioxidants. ROS, on the other hand, increases the consumption of antioxidantdefenses. The consequences of activated oxidative and nitrosative stress (O&NS)pathways comprise the following: (a) formation of oxidative (OSEs) and nitrosative(NSEs) specific epitopes, which may be immunogenic thereby causing autoimmuner(s
2
rrtnMrgWtcaitpbl12carm
253
254
255
256
257
258
259
260
261
262
263
264
265
266
267
268
269
270
271
272
273
274
275
276
277
278
279
280
281
282
283
284
285
286
287
288
289
290
291
292
293
294
295
296
297
298
299
300
301
302
303
304
305
306
307
308
309
310
311
312
313
314
315
316
317
318
319
320
321
322
323
324
325
326
327
328
329
330
331
332
333
334
335
336
337
esponses; (b) oxidative and nitrosative damage to various cellular components; andc) hyper-nitrosylation. These consequences of activated oxidative and nitrosativetress pathways ultimately cause a wide variety of cellular dysfunctions.
.2. Leaking gut and the microbiome
Clinically depressed patients display higher IgM and IgAesponses to lipopolysaccharides (LPS) from gram-negative bacte-ia, potentially as consequence of bacterial translocation secondaryo increased gut permeability (Maes et al., 2008a, 2012b). Gram-egative bacteria including Hafnia alvei, Pseudomonas aeruginosa,organella morganii, Proteus mirabilis, Pseudomonas putida, Cit-
obacter koseri and Klebsiella pneumoniae belong to the normalut flora and are termed commensal gut bacteria (Todar, 2006;iest, 2005). Under normal conditions the immune system is func-
ionally and geographically separated from these poorly invasiveommensal gut bacteria by an intact gut tight junction barrier (Bergnd Garlington, 1979; Wiest and Garcia-Tsao, 2005). Due to this,mmune cells are not normally primed against commensal gut bac-eria. However, when the gut wall is weakened by increased gutermeability, gram-negative bacteria can exploit the loosened gutarrier, thereby translocating from the gut into the mesenteric
ymph nodes (MLNs) or the blood stream (Berg and Garlington,979; Chavez et al., 1999; Clark et al., 2005; Wiest and Garcia-Tsao,005; Yang et al., 2003). Once bacteria are translocated, immuno-
Please cite this article in press as: Moylan, S., et al., Oxidative & nitrosatRev. (2014), http://dx.doi.org/10.1016/j.neubiorev.2014.05.007
ytes can mount an IgA or IgM-mediated immune response directedgainst the LPS of gut commensal bacteria. Measuring IgA and IgMesponses against LPS of commensal bacteria is a more sensitiveethod to detect bacterial translocation than the assay of serum
PRESSavioral Reviews xxx (2014) xxx–xxx
LPS, because it also detects bacterial LPS when bacteria have notspread into the blood circulation but when the bacteria are translo-cated into the MLNs (Maes et al., 2013a). The finding that clinicaldepression is associated with increased IgM/IgA responses to LPStherefore indicates that immune cells are activated by LPS fromgram-negative bacteria, which is translocated into the MLNs, theblood stream, or both. Because if their particular role in mucosaldefence, Th17 cells, a subset of T helper cells have a particular roleagainst gut infections and are associated with atopic, inflammatory,and autoimmune disorders. Th17 cells may disrupt the blood–brainbarrier leading to infiltration of the central nervous system, anddrive neuroprogression (Debnath and Berk, 2014).
Through binding with the Toll-like receptor (TLR)2 andTLR4 complexes, LPS activates different intracellular signalingmolecules, including NF-�� and MAPK, thereby increasing expres-sion of PIC and O&NS genes (Tsukamoto et al., 2010; Wiest andGarcia-Tsao, 2005). For example, NF-�� induces the production ofIL-1, IL-6, TNF� and iNOS (Brasier, 2006). LPS additionally activatesNOX, which in turn increases production of iNOS, NO, superox-ide and peroxides (Chan and Riches, 2001; Check et al., 2010;Peng et al., 2005). Previously, it has been shown that increasedgut permeability is accompanied by elevated plasma LPS and signsof inflammation and O&NS, with these processes being attenu-ated or reversed upon successful treatment of the leaky gut (Quanet al., 2004; Zhou et al., 2003). This is relevant to depression, asLPS administration increases nitrite, nitrate and MDA levels whilstdecreasing brain GSH levels (Tyagi et al., 2010). LPS also reduces thelevels of CC16 or uteroglobin, an endogenous anti-inflammatorysubstance, thereby increasing inflammatory potential (Franssonet al., 2007). CC16 is significantly lowered in depressed subjects; inpart explaining the immune-inflammatory responses in that illness(Rief et al., 2001).
In patients with depression there are significant and positivecorrelations between bacterial translocation (increased IgA andIgM responses to LPS) and signs of increased O&NS (Maes et al.,2012b) including increased plasma oxidized LDL antibodies, IgMresponses to NSEs, such as NO-tryptophan and NO-tyrosine, aswell as IgM responses directed against OSEs, including azelaic acid,MDA and phosphatidyl inositol (Maes et al., 2012b). These find-ings indicate that increased bacterial translocation in depressiondrives chronically activated O&NS pathways (damage to fatty acidsand proteins) and autoimmune responses directed against OSEsand NSEs (Maes et al., 2012b). Gut bacteria produce a plethora ofcompounds that influence redox signaling, with different popula-tions producing different compounds. One example is molecularhydrogen which has wide-ranging biological effects, includinganti-oxidative, anti-apoptotic and anti-inflammatory properties(Ghanizadeh and Berk, 2013).
Recently a review of the bidirectional connections between thegut and the brain summarized the evidence that gastrointestinalhomeostasis may modulate emotion, affect, neurocognitive func-tions and motivation (Mayer, 2011). Most importantly, animalsexposed to repeated restraint and acoustic stressors demonstratedincreased gut permeability, TLR4 activation and neuroinflam-mation (Garate et al., 2013). Moreover, attenuation of bacterialtranslocation through antibiotic induced intestinal decontamina-tion reduces stress-induced neuroinflammation, suggesting thatstress-induced neuroinflammation is at least partially caused byincreased bacterial translocation. For these reasons, increased bac-terial translocation may be a promising drug target in stress-relateddisorders, such as depression (Garate et al., 2013).
ive stress in depression: Why so much stress? Neurosci. Biobehav.
2.3. Activation of the Toll-like receptor radical cycle
Pattern recognition receptors (PRRs), which include TLR2 andTLR4, are an important part of the host defense system (Lucas
338
339
340

ING ModelN
iobeh
al(iTcadtc
p(siedo(t1dacs(aRw
tcoeDoi
2
dttmdlc
iIrcfuAtcaie(hap
341
342
343
344
345
346
347
348
349
350
351
352
353
354
355
356
357
358
359
360
361
362
363
364
365
366
367
368
369
370
371
372
373
374
375
376
377
378
379
380
381
382
383
384
385
386
387
388
389
390
391
392
393
394
395
396
397
398
399
400
401
402
403
404
405
406
407
408
409
410
411
412
413
414
415
416
417
418
419
420
421
422
423
424
425
426
427
428
429
430
431
432
433
434
435
436
437
438
439
440
441
442
443
444
445
446
447
448
449
450
451
452
453
454
455
456
457
458
459
460
461
ARTICLEBR 1953 1–17
S. Moylan et al. / Neuroscience and B
nd Maes, 2013). PRRs recognize pathogen-associated molecu-ar patterns (PAMPs) and damage-associated molecular patternsDAMPs), which consequently activate MAPK and/or NF-�B lead-ng to activation of immune-inflammatory and O&NS pathways.he TLRs recognize mycoplasma, fungus, viruses and LPS, a typi-al PAMP derived from gram-negative bacteria. Since depression isccompanied by increased IgM/IgA-mediated immune responsesirected against LPS of gut commensals, it may be concluded thathe TLR2/TLR4 complexes are activated by PAMP-mediated pro-esses.
Typically DAMPs, including �-defensin, high mobility grouprotein 1 (HMGB1), heat shock proteins (HSPs), extracellular matrixECM), cathelicidin (LL37), hyaluronic acid, heparin sulfate, sub-tance P and redox-derived DAMPs, appear following injury andnflammation (Carta et al., 2009; Kaczmarek et al., 2013; Lotzet al., 2007; Rubartelli and Lotze, 2007; Uchida, 2013). Redox-erived DAMPs are produced during lipid peroxidation and consistf oxidatively modified molecules, such as oxidized phospholipidsOx-PLP), oxidized LDL (Ox-LDL), 4-HNE and MDA modified pro-eins (Carta et al., 2009; Uchida, 2013). As reviewed in Section, depression is accompanied by increased levels of some redox-erived DAMPS, including oxidized LDL, oxidized phospholipidsnd MDA-derived adducts (Maes et al., 2011d). These moleculesan activate the TLR2/TLR4 complex and play a role in the down-tream activation of immune-inflammatory and O&NS pathwaysLucas and Maes, 2013). As a consequence, depression may beccompanied by a vicious cycle between TLR2/TLR4 activation andOS production causing increased levels of redox-derived DAMPs,hich further stimulate the TLRs.
Exposure to TLR agonists has been shown to sensitize and primehe TLR response to subsequent stimulation by other agonists. Psy-hosocial stressors may additionally upregulate TLR4 expressionr activation (Lucas and Maes, 2013). Thus, in depression differ-nt TLR2/TLR4 agonists, including bacterial LPS and redox-derivedAMPs, and psychosocial stressors may cause hypersensitivityf the TLR complexes, thereby activating downstream immune-nflammatory and O&NS pathways.
.4. The tryptophan catabolite (TRYCAT) pathway
Interactions between inflammation, O&NS, lowered antioxi-ant levels and bacterial translocation may occur via changes inhe tryptophan catabolite (TRYCAT) pathway. By diverting tryp-ophan metabolism away from serotonin, N-acetylserotonin and
elatonin production, increased activation of indoleamine 2,3-ioxygenase (IDO) and tryptophan 2,3-dioxygenase (TDO) have
ong been identified as being associated with depression and asso-iated conditions (Maes et al., 1993, 2011c).
IDO, a heme-centered enzyme, is upregulated in pro-nflammatory states in particular by INF�, but also IL-1, IL-6,L-18, TNF� and LPS (Maes et al., 2011a). When IDO is in its fer-ous form and in the presence of molecular oxygen, it acts toleave tryptophan to N-formylkynurenine, initiating induction ofurther TRYCATs. Alternatively, when IDO is in its ferric form ittilizes O2
− as a reducing agent to trigger the TRYCAT pathway.s such, the inflammatory state and redox status regulates how
ryptophan is utilized, with significant consequences for processeslassically associated with depression (Maes et al., 2011c; Wernernd Werner-Felmayer, 2007). In addition, lowered tryptophan andncreased levels of most TRYCATs have negative immunoregulatoryffects that suppress primary immune-inflammatory responses
Please cite this article in press as: Moylan, S., et al., Oxidative & nitrosatRev. (2014), http://dx.doi.org/10.1016/j.neubiorev.2014.05.007
Maes et al., 2011c). Thus, induction of the TRYCAT pathway mayave a protective function, but the longer-term consequence ofctivation can be crucial to alterations in neuronal activity andatterning in depression.
PRESSavioral Reviews xxx (2014) xxx–xxx 5
IDO is predominantly expressed in microglia within the CNS(Alberati-Giani and Cesura, 1998). Microglia are important reg-ulators and coordinators of central changes in depression anddepression-associated neurodegenerative disorders (Maes et al.,2011c). The activation of IDO leads to production of neuroregu-latory TRYCATs including kynurenic acid (KYNA) and quinolinicacid (QUIN). KYNA is inhibitory at the �7 nicotinic receptor, whilstQUIN is excitotoxic at N-methyl d-aspartate (NMDA) receptors byincreasing NO-mediated damage to neurons and astrocytes (Braidyet al., 2009).
Moreover, TRYCATs have anti-oxidant and pro-oxidant effects.For example, 3-hydroxykynurenine, 3-hydroxyanthranilic acid andxanthurenic acid perform antioxidant functions including scaveng-ing free radicals, reducing lipid peroxidation, and preventing thespontaneous oxidation of glutathione and damage to 2-deoxy-d-ribose (Christen et al., 1990; Goda et al., 1999; Leipnitz et al., 2007).However, 3-hydroxykynurenine, 3-hydroxyanthranilic and quino-linic acid also display pro-oxidant effects by generating ROS (e.g.superoxide and hydrogen peroxide) and causing lipid peroxidationand oxidative cell damage (Dykens et al., 1987; Goldstein et al.,2000; Guidetti and Schwarcz, 1999; Murakami et al., 2006; Okudaet al., 1998; Rios and Santamaria, 1991; Santamaria et al., 2001;Smith et al., 2009).
Genetic variants of IDO genes may influence inflammatorystatus, thereby regulating the etiology, course and outcome ofdepression (Bufalino et al., 2013). Another important regulatorof the TRYCAT pathways is TDO, which in the CNS is predom-inantly expressed in astrocytes, although also in some neurons(Funakoshi et al., 2011). The activation of TDO is primarily mediatedby cortisol (Ren and Correia, 2000). Therefore, increased immune-inflammatory pathway activation and O&NS, through drivingincreases in hypothalamic pituitary adrenal (HPA) axis activitycommonly found in depression (Carroll, 1980), will also contributeto increased TDO, further depleting serotonin, N-acetylserotoninand melatonin, whilst changing neuroregulation by the inductionof KYNA, which is the TRYCAT predominantly produced follow-ing TDO induction. Overall, immune-inflammatory processes andO&NS, including via the regulation of IDO and TDO, are intimatelylinked to processes altered in depression.
2.5. The glutamate–cystine cycle
Prolonged oxidative stress reduces the capacity of astrocytesto import glutamate facilitating an increase in extracellular gluta-mate levels (Dallas et al., 2007). Higher extrasynaptic and lowersynaptic glutamate may play a role in depression (Sanacora et al.,2003), and depression is associated with glutamate supersensi-tivity (Berk et al., 2001). A genome-wide association study indepression demonstrated involvement of glutamatergic synapticneurotransmission genes in depression (Lee et al., 2012). Oxidative-stress increased glutamate levels can inhibit cystine uptake by thexc-antiporter system thereby causing intracellular GSH depletionand consequently oxidative-stress-induced neurotoxicity throughexcitotoxic effects, a process called “oxidative glutamate toxicity”(Murphy et al., 1989; Schubert and Piasecki, 2001) that is at leastin part mediated by increased calcium signaling.
2.6. Mitochondrial dysfunction
The mitochondrial electron transport chain (ETC) is responsi-ble for cellular energy generation via adenosine-5-triphosphate(ATP) production (Adam-Vizi and Starkov, 2010). ATP is gener-
ive stress in depression: Why so much stress? Neurosci. Biobehav.
ated by transferring electrons through complexes I–V (Green andKroemer, 2004; Lenaz, 2001). During this process electrons canescape, resulting in the reduction of molecular oxygen, whichleads to the generation of the superoxide anion (O2
−) (Green and
462
463
464
465
IN PRESSG ModelN
6 iobehavioral Reviews xxx (2014) xxx–xxx
Ki
hivcttd
astdtMpmt2ttfimisgaald
D(dlp1aecm
matdIbrmchim
oto
2
c
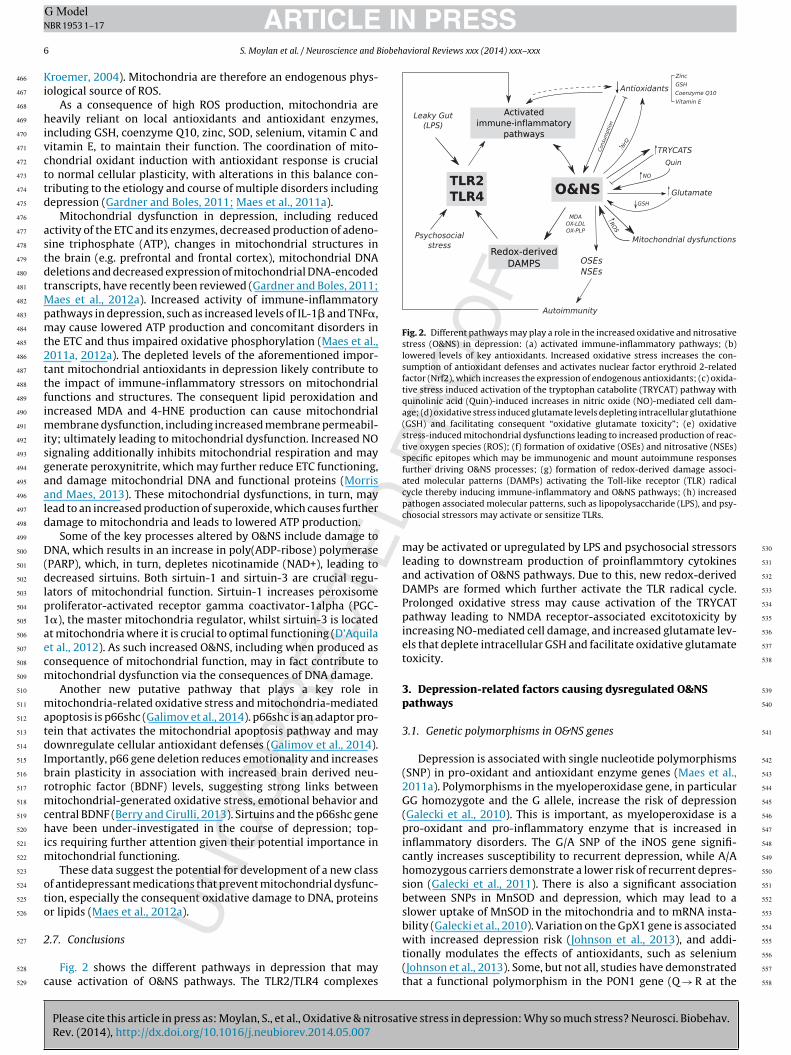
Fig. 2. Different pathways may play a role in the increased oxidative and nitrosativestress (O&NS) in depression: (a) activated immune-inflammatory pathways; (b)lowered levels of key antioxidants. Increased oxidative stress increases the con-sumption of antioxidant defenses and activates nuclear factor erythroid 2-relatedfactor (Nrf2), which increases the expression of endogenous antioxidants; (c) oxida-tive stress induced activation of the tryptophan catabolite (TRYCAT) pathway withquinolinic acid (Quin)-induced increases in nitric oxide (NO)-mediated cell dam-age; (d) oxidative stress induced glutamate levels depleting intracellular glutathione(GSH) and facilitating consequent “oxidative glutamate toxicity”; (e) oxidativestress-induced mitochondrial dysfunctions leading to increased production of reac-tive oxygen species (ROS); (f) formation of oxidative (OSEs) and nitrosative (NSEs)specific epitopes which may be immunogenic and mount autoimmune responsesfurther driving O&NS processes; (g) formation of redox-derived damage associ-ated molecular patterns (DAMPs) activating the Toll-like receptor (TLR) radical
466
467
468
469
470
471
472
473
474
475
476
477
478
479
480
481
482
483
484
485
486
487
488
489
490
491
492
493
494
495
496
497
498
499
500
501
502
503
504
505
506
507
508
509
510
511
512
513
514
515
516
517
518
519
520
521
522
523
524
525
526
527
528
529
530
531
532
533
534
535
536
537
538
539
540
541
542
543
544
545
546
547
548
549
550
551
552
553
554
ARTICLEBR 1953 1–17
S. Moylan et al. / Neuroscience and B
roemer, 2004). Mitochondria are therefore an endogenous phys-ological source of ROS.
As a consequence of high ROS production, mitochondria areeavily reliant on local antioxidants and antioxidant enzymes,
ncluding GSH, coenzyme Q10, zinc, SOD, selenium, vitamin C anditamin E, to maintain their function. The coordination of mito-hondrial oxidant induction with antioxidant response is crucialo normal cellular plasticity, with alterations in this balance con-ributing to the etiology and course of multiple disorders includingepression (Gardner and Boles, 2011; Maes et al., 2011a).
Mitochondrial dysfunction in depression, including reducedctivity of the ETC and its enzymes, decreased production of adeno-ine triphosphate (ATP), changes in mitochondrial structures inhe brain (e.g. prefrontal and frontal cortex), mitochondrial DNAeletions and decreased expression of mitochondrial DNA-encodedranscripts, have recently been reviewed (Gardner and Boles, 2011;
aes et al., 2012a). Increased activity of immune-inflammatoryathways in depression, such as increased levels of IL-1� and TNF�,ay cause lowered ATP production and concomitant disorders in
he ETC and thus impaired oxidative phosphorylation (Maes et al.,011a, 2012a). The depleted levels of the aforementioned impor-ant mitochondrial antioxidants in depression likely contribute tohe impact of immune-inflammatory stressors on mitochondrialunctions and structures. The consequent lipid peroxidation andncreased MDA and 4-HNE production can cause mitochondrial
embrane dysfunction, including increased membrane permeabil-ty; ultimately leading to mitochondrial dysfunction. Increased NOignaling additionally inhibits mitochondrial respiration and mayenerate peroxynitrite, which may further reduce ETC functioning,nd damage mitochondrial DNA and functional proteins (Morrisnd Maes, 2013). These mitochondrial dysfunctions, in turn, mayead to an increased production of superoxide, which causes furtheramage to mitochondria and leads to lowered ATP production.
Some of the key processes altered by O&NS include damage toNA, which results in an increase in poly(ADP-ribose) polymerase
PARP), which, in turn, depletes nicotinamide (NAD+), leading toecreased sirtuins. Both sirtuin-1 and sirtuin-3 are crucial regu-
ators of mitochondrial function. Sirtuin-1 increases peroxisomeroliferator-activated receptor gamma coactivator-1alpha (PGC-�), the master mitochondria regulator, whilst sirtuin-3 is locatedt mitochondria where it is crucial to optimal functioning (D’Aquilat al., 2012). As such increased O&NS, including when produced asonsequence of mitochondrial function, may in fact contribute toitochondrial dysfunction via the consequences of DNA damage.Another new putative pathway that plays a key role in
itochondria-related oxidative stress and mitochondria-mediatedpoptosis is p66shc (Galimov et al., 2014). p66shc is an adaptor pro-ein that activates the mitochondrial apoptosis pathway and mayownregulate cellular antioxidant defenses (Galimov et al., 2014).
mportantly, p66 gene deletion reduces emotionality and increasesrain plasticity in association with increased brain derived neu-otrophic factor (BDNF) levels, suggesting strong links betweenitochondrial-generated oxidative stress, emotional behavior and
entral BDNF (Berry and Cirulli, 2013). Sirtuins and the p66shc geneave been under-investigated in the course of depression; top-
cs requiring further attention given their potential importance initochondrial functioning.These data suggest the potential for development of a new class
f antidepressant medications that prevent mitochondrial dysfunc-ion, especially the consequent oxidative damage to DNA, proteinsr lipids (Maes et al., 2012a).
Please cite this article in press as: Moylan, S., et al., Oxidative & nitrosatRev. (2014), http://dx.doi.org/10.1016/j.neubiorev.2014.05.007
.7. Conclusions
Fig. 2 shows the different pathways in depression that mayause activation of O&NS pathways. The TLR2/TLR4 complexes
cycle thereby inducing immune-inflammatory and O&NS pathways; (h) increasedpathogen associated molecular patterns, such as lipopolysaccharide (LPS), and psy-chosocial stressors may activate or sensitize TLRs.
may be activated or upregulated by LPS and psychosocial stressorsleading to downstream production of proinflammtory cytokinesand activation of O&NS pathways. Due to this, new redox-derivedDAMPs are formed which further activate the TLR radical cycle.Prolonged oxidative stress may cause activation of the TRYCATpathway leading to NMDA receptor-associated excitotoxicity byincreasing NO-mediated cell damage, and increased glutamate lev-els that deplete intracellular GSH and facilitate oxidative glutamatetoxicity.
3. Depression-related factors causing dysregulated O&NSpathways
3.1. Genetic polymorphisms in O&NS genes
Depression is associated with single nucleotide polymorphisms(SNP) in pro-oxidant and antioxidant enzyme genes (Maes et al.,2011a). Polymorphisms in the myeloperoxidase gene, in particularGG homozygote and the G allele, increase the risk of depression(Galecki et al., 2010). This is important, as myeloperoxidase is apro-oxidant and pro-inflammatory enzyme that is increased ininflammatory disorders. The G/A SNP of the iNOS gene signifi-cantly increases susceptibility to recurrent depression, while A/Ahomozygous carriers demonstrate a lower risk of recurrent depres-sion (Galecki et al., 2011). There is also a significant associationbetween SNPs in MnSOD and depression, which may lead to aslower uptake of MnSOD in the mitochondria and to mRNA insta-bility (Galecki et al., 2010). Variation on the GpX1 gene is associated
ive stress in depression: Why so much stress? Neurosci. Biobehav.
with increased depression risk (Johnson et al., 2013), and addi-tionally modulates the effects of antioxidants, such as selenium(Johnson et al., 2013). Some, but not all, studies have demonstratedthat a functional polymorphism in the PON1 gene (Q → R at the
555
556
557
558

ING ModelN
iobeh
1(bastaappe
mmc
3
OcfStlh(pI(saaoaeccri2suloK
lwPac(ieersabe
3
a
559
560
561
562
563
564
565
566
567
568
569
570
571
572
573
574
575
576
577
578
579
580
581
582
583
584
585
586
587
588
589
590
591
592
593
594
595
596
597
598
599
600
601
602
603
604
605
606
607
608
609
610
611
612
613
614
615
616
617
618
619
620
621
622
623
624
625
626
627
628
629
630
631
632
633
634
635
636
637
638
639
640
641
642
643
644
645
646
647
648
649
650
651
652
653
654
655
656
657
658
659
660
661
662
663
664
665
666
667
668
669
670
671
672
673
674
675
676
677
678
679
680
ARTICLEBR 1953 1–17
S. Moylan et al. / Neuroscience and B
92 position) increases the odds of unipolar and bipolar depressionVargas et al., 2013). In addition, gene by environmental effects maye involved. For example, an interaction between PON1 gene SNPnd smoking is associated with bipolar depression (Vargas et al.,ubmitted for publication). While polymorphisms of glutamate cys-eine ligase, a key synthetic enzyme in the glutathione pathwaysre associated with disorders such as schizophrenia, this does notppear to be the case in depression (Berk et al., 2011a). SNPs ofro-inflammatory cytokine genes, including IL-1 and IL-6, may alsoredict responsiveness to treatment with antidepressants (Baunet al., 2010; Uher et al., 2010).
Therefore, underlying genetic vulnerabilities produced by poly-orphisms in pro-oxidant, antioxidant and inflammatory genesay contribute to the O&NS processes in depression especially in
onditions of increased ROS/RNS production.
.2. Psychological stressors
A vast literature suggests psychosocial stressors may induce&NS pathways and reduce antioxidant defenses. Psychologi-al stress causes a pro-oxidant state and oxidative damage toatty acids (Aleksandrovskii Iu et al., 1988; Pertsov et al., 1995;osnovskii and Kozlov, 1992). Morimoto et al. (2008) reportedhat in postmenopausal women, mental stress induces increasedipid peroxidation as measured by plasma 4-HNE. In nurses withigh job stress, significantly decreased levels of alpha-tocopherolvitamin E) and a significant relationship between MDA levels anderceived stress ratings have been detected (Tsuboi et al., 2006).
n workers from a pre-hospital emergency service, Casado et al.2006) observed a significant association between occupationaltress and erythrocyte MDA levels. In females, stress variables, suchs perceived stress and workload and less coping with stress, weressociated with increased levels of 8-OHdG (Irie et al., 2001). Stress-rs such as examination stress decrease plasma antioxidant activitynd increases oxidative stress-induced damage to DNA (Sivonovat al., 2004). Conversely, lifestyle-modifying programs may signifi-antly improve antioxidant defenses. For example, in patients withoronary artery disease an intensive lifestyle modification programesulted in statistically significant increases in plasma total antiox-dant capacity, vitamin E and erythrocyte GSH (Jatuporn et al.,003). In animal models, many different types of psychophysicaltressors, including immobilization stress, restraint stress, chronicnpredictable stress and chronic mild stress, were shown to cause
owered levels of antioxidants, such as GSH, and increased lipid per-xidation, as measured with MDA and 4-HNE (Ahmad et al., 2010;ubera et al., 2011; Moretti et al., 2012; Wang et al., 2012).
As psychological stressors may cause O&NS, the role of psycho-ogical trauma has been examined in animal models and individuals
ith post-traumatic stress disorder (PTSD). An animal model ofTSD demonstrated that increased expression of oxidative stressnd pro-inflammatory cytokine mRNA in the brain and systemicirculation are associated with the onset and exacerbation of PTSDWilson et al., 2013). In patients with PTSD, however, no changesn urinary 8-OHdG could be detected, while protein carbonyl lev-ls were lower in the PTSD group (Ceprnja et al., 2011). Millert al. (2013) identified a variant in the gene retinoid-related orphaneceptor alpha (RORA) as being protective against the effects oftress on the brain, and subsequent development of PTSD. Theuthors concluded that this gene plays a crucial role in guardingrain cells from the detrimental effects of oxidative stress (Loguet al., 2013).
Please cite this article in press as: Moylan, S., et al., Oxidative & nitrosatRev. (2014), http://dx.doi.org/10.1016/j.neubiorev.2014.05.007
.3. Medical comorbid disorders and conditions
Depression is highly comorbid with many systemic immunend O&NS-related disorders (e.g. Chronic Obstructive Pulmonary
PRESSavioral Reviews xxx (2014) xxx–xxx 7
Disorder; COPD, atherosclerosis, rheumatoid arthritis, inflam-matory bowel disease, psoriasis, diabetes type 1 and type 2,HIV-infection), neuroinflammatory and O&NS-related brain disor-ders (e.g. Parkinson’s disease, Alzheimer’s disease, stroke, multiplesclerosis) and conditions accompanied by increased inflammatorypotential and O&NS (hemodialysis, IFN�-based immunotherapy)(Maes et al., 2011b). Depression may be triggered by these disor-ders or conditions, or worsen outcomes for those in whom thesedisorders are present (Maes et al., 2011b).
Increased O&NS and immune-inflammatory pathways mayunderpin the comorbidity and interaction between depression andthese related conditions (Maes et al., 2011a; Wolkowitz et al.,2011). Recently, it has been proposed that the underlying biologicalprocesses driving depression intimately overlap with neurodegen-erative processes, suggesting that depression may be more than acomorbidity but rather is intertwined with degenerative processes(Anderson and Maes, 2013b). Oxidative stress drives telomereshortening, a key mechanism underlying the aging process (Phillipset al., 2013), and therapies that reduce oxidative stress such aslithium are associated with longer telomeres (Martinsson et al.,2013). There may be additional effects of aging on O&NS pathwaysand a number of ‘age-related’ disorders such as cardiovascular dis-ease (CVD) (Maes et al., 2011e), stroke (El Kossi and Zakhary, 2000),diabetes (Maritim et al., 2003), metabolic syndrome (Hansel et al.,2004), and sleep apnea (Jelic et al., 2008); all of which are recog-nized to share common origins of increased O&NS (Forlenza andMiller, 2006).
3.4. Obesity and metabolic syndrome
Accumulating clinical and epidemiological evidence suggeststhat obesity contributes to the pathogenesis of depression (Atlantiset al., 2009). Cross-sectional studies have linked obesity withdepression (Atlantis and Baker, 2008; de Wit et al., 2010) and neg-ative affect (Pasco et al., 2013), and a series of longitudinal studieshave demonstrated this association is bi-directional (Luppino et al.,2010; Pan et al., 2012). Traditionally regarded as an energy storagedepot, adipose tissue is now recognized as having a role in bothphysical and mental health.
Excessive accumulation of adipose tissue in obesity perturbs theregulatory network of neural circuits and circulatory messengersthat has evolved to maintain energy homeostasis. As one of thecell types in adipose tissue, adipocytes (fat cells) serve as depotsfor energy storage and mobilization. Adipocytes produce biolog-ically active molecules known as adipokines (or adipocytokines)that have pro-inflammatory or anti-inflammatory activities, andthese include leptin, TNF� and adiponectin. Leptin is a pro-inflammatory cytokine that plays a key role in regulating energyintake and expenditure and signals the brain when adipocytesbecome enlarged to modify appetite and behavior (Jequier, 2002).TNF� is a pro-inflammatory cytokine that stimulates the acutephase reaction and adiponectin is an anti-inflammatory factor. Cir-culating levels of leptin (Pasco et al., 2008a; Solin et al., 1997) andTNF� (Kern et al., 1995) are elevated in obesity and raised levels ofboth factors have been reported in depression (Halaris et al., 2012;Pasco et al., 2008a). By contrast, adiponectin levels are reduced inobesity (Ryo et al., 2004) and depression (Leo et al., 2006).
In the obese state, enlarged mature adipocytes become stressedand macrophages accumulate in the expanded adipose tissue,releasing a host of pro-inflammatory cytokines and establishinga low-grade inflammatory state. Such adipose tissue dysregulationalso impairs the differentiation of pre-adipocytes and favors the
ive stress in depression: Why so much stress? Neurosci. Biobehav.
storage of excess lipid in other tissues (ectopic depots) (Gustafsonet al., 2009), which is metabolically toxic.
Adipose tissue dysregulation induces oxidative stress and adi-pose tissue itself is considered an important source of ROS
681
682
683
684

ING ModelN
8 iobeh
(tEpasics
atlyn
hnsepas
pssi
3
sab1tes(coIadtbrma
wio2dplhmoMrdas
685
686
687
688
689
690
691
692
693
694
695
696
697
698
699
700
701
702
703
704
705
706
707
708
709
710
711
712
713
714
715
716
717
718
719
720
721
722
723
724
725
726
727
728
729
730
731
732
733
734
735
736
737
738
739
740
741
742
743
744
745
746
747
748
749
750
751
752
753
754
755
756
757
758
759
760
761
762
763
764
765
766
767
768
769
770
771
772
773
774
775
776
777
778
779
780
781
782
783
784
785
786
787
788
789
790
791
792
793
794
795
796
797
798
799
800
801
802
803
804
805
806
807
808
ARTICLEBR 1953 1–17
S. Moylan et al. / Neuroscience and B
Furukawa et al., 2004; Houstis et al., 2006; Lee et al., 2009), poten-ially through the stimulation of NOX (Furukawa et al., 2004).vidence from mouse models suggests that oxidative stress in adi-ose tissue hampers adipogenesis through Wnt signaling (Funatond Miki, 2010), thereby promoting undesirable ectopic fat depo-ition and further aggravating health. It is even hypothesized thatmbalances in immune-inflammatory and O&NS pathways are theommon soil from which insulin resistance, dyslipidemia and obe-ity may develop (Bryan et al., 2013).
Metabolic syndrome, a clustering of conditions includingbdominal (central) obesity, high blood pressure, plasma glucose,riglycerides, and low HDL levels), is accompanied by increasedevels of MDA, advanced oxidation protein products, lipid hydrox-peroxides and nitric oxide metabolites (plasma concentrations ofitrite and nitrate) (Bortolasci et al., 2014; Sankhla et al., 2012).
Patients with metabolic syndrome have higher MDA levels, lipidydroxyperoxides and advanced oxidation protein products, butot NO metabolites, when compared with controls; however thetatus of serum total antioxidants in metabolic syndrome remainsquivocal (Vargas et al., submitted for publication). Interestingly,araoxonase Q192R functional genotypes or activity phenotypesre associated not only with depression, but also with the metabolicyndrome (Bortolasci et al., 2014).
These findings suggest that activation of immune-inflammatoryathways and oxidative stress balance may underpin both depres-ion and the metabolic syndrome. Therefore, the metabolicyndrome when comorbid with depression may increase themmune-inflammatory and oxidative burden.
.5. Sleep disorders
Numerous studies have indicated a bidirectional link betweenleep disturbances and depression (Tsuno et al., 2005). Prospectivend longitudinal studies have demonstrated that sleep distur-ances predict later episodes of major depression (Breslau et al.,996; Perlis et al., 1997), and symptomatic depression is recognizedo act as a proxy for the later development of insomnia (Breslaut al., 1996; LeBlanc et al., 2009). These findings have further beenustained after accounting for possible lifestyle factors such as ageChang et al., 1997), gender (Taylor et al., 2005), general medicalonditions (Taylor et al., 2005) and prior history of a depressiver sleep disorder (Buysse et al., 2008; Neckelmann et al., 2007).n addition, numerous studies have demonstrated that individu-ls with obstructive sleep apnea (OSA) often exhibit high rates ofepression (Harris et al., 2009; Schroder and O’Hara, 2005), withhe degree of depressive symptoms thought to reflect nocturnaliomarkers such as the hypoxemia nadir (McCall et al., 2006) andelative disease severity (Millman et al., 1989). Despite this, theechanisms that underlie the association between disturbed sleep
nd depression have not yet been fully elucidated.Sleep has a number of restorative functions. Sleep disruption,
hether acute or chronic, endogenously or exogenously mediated,s associated with increased risk for later development of seri-us medical illnesses to which O&NS contributes (Foster et al.,007; Ozkan et al., 2008). Individuals with primary sleep disor-ers and OSA typically exhibit activation of immune-inflammatoryathways, including increased IL-6, IL-8 and prostaglandin E2
evels and lowered plasma tryptophan (Song et al., 1998) andigher 8-isoprostane (Alonso-Fernandez et al., 2009) but lower NOetabolites (Ozkan et al., 2008). Patients with primary sleep dis-
rders also show significantly lower activity of GpX and higherDA concentrations than controls (Gulec et al., 2012), compa-
Please cite this article in press as: Moylan, S., et al., Oxidative & nitrosatRev. (2014), http://dx.doi.org/10.1016/j.neubiorev.2014.05.007
able to research investigating individuals diagnosed with majorepression (Bilici et al., 2001). Volna et al. (2011) found a strongssociation between OSA symptomology and markers of oxidativetress, and significant inverse correlations between mean blood
PRESSavioral Reviews xxx (2014) xxx–xxx
hemoglobin oxygen saturation and matrix metalloproteinase 9, C-reactive protein and fibrinogen. The oxygen desaturation indexwas additionally correlated with advanced glycation end products.Sleep fragmentation and intermittent hypoxia largely determinethe molecular signature of OSA, including oxidative stress andinflammation, although comorbid obesity may play a role due toits impact on shared molecular pathways (Arnardottir et al., 2009,2012). Mitigation of nocturnal symptoms via night-time therapyalso appears to neutralize the degree of O&NS damage in OSApatients (Alonso-Fernandez et al., 2009).
Preliminary findings derived from animal studies have high-lighted the potential of melatonin administration as an effectivetherapeutic agent in regard to its O&NS effects (Manda and Bhatia,2003). Although the possible therapeutic benefits of this hormonein the treatment of a range O&NS specific disorders has been previ-ously described (see review (Reiter et al., 2009)), and independentreports have profiteered the usefulness of melatonin in a rangeof sleep-disordered populations (Reiter et al., 2007), there is lit-tle information integrating this knowledge regarding the possibleefficacy of this hormone in targeting sleep-disorder specific O&NS.Moreover, the availability of a unified model describing the impactof O&NS damage in sleep disorders is currently lacking, and thuscurrently available treatment options are unable to effectively tar-get underlying mechanisms associated with O&NS. Future researchwill therefore benefit from both further exploring the relationshipbetween insomnia and O&NS, as well as systematically assessingthe efficacy of melatonin as a possible therapeutic option.
3.6. Cigarette smoking
The prevalence of cigarette smoking is significantly higherin individuals suffering from depressive and anxiety disorders(Moylan et al., 2012; Pasco et al., 2008b) than those without. Thismay be linked, at least in part, to the inter-relationship betweencigarette smoking and precipitated oxidative stress (Moylan et al.,2013b). Cigarette smoke contains many chemicals that increaselevels of O&NS and is a substantial source of exogenous free radi-cals (Stedman, 1968). Multiple animal models have demonstratedthat exposure to cigarette smoke can lead to increases in levelsof brain O&NS, as demonstrated by increased levels of reactiveoxygen species, including superoxide, thiobarbituric acid reactivesubstances (TBARS), carbonylated proteins and markers of lipidperoxidation (Anbarasi et al., 2005; Luchese et al., 2009; Stangherlinet al., 2009; Thome et al., 2011; Tuon et al., 2010). In additions tothese changes, exposure to cigarette smoke appears to be associ-ated with lowered levels of antioxidant enzymes, such as catalase,vitamins (A, C, E), GpX, glutathione reductase, PON1, glutathioneand SOD (Anbarasi et al., 2005; Luchese et al., 2009).
As with other factors that stimulate production of O&NS, acuteexposure to cigarette smoke appears to provoke a protectiveincrease in antioxidant enzymes. However, more chronic exposureoverwhelms these defences and leaves the system vulnerable tocellular damage. This is important, as factors which can assist theadaptive protective mechanisms, such as augmentation with vita-min E or active exercise (Thome et al., 2011; Tuon et al., 2010),appear to assist by limiting the increase in O&NS provoked byexposure to cigarette smoke. Investigations also reveal that themajor addictive component of cigarette smoke, nicotine, may beresponsible for the major proportion of increased O&NS attributedto cigarette smoke exposure. For example, studies utilizing exoge-nous administration of nicotine to isolate cell lines in culture leadto reduced production of antioxidant enzymes and increased mark-
ive stress in depression: Why so much stress? Neurosci. Biobehav.
ers of lipid peroxidation, lactate dehydrogenase activity and TBARS(Bhagwat et al., 1998; Yildiz et al., 1998). Given the interactionbetween cigarette smoking and O&NS balance, coupled with theassociative findings between O&NS and depressive and anxiety
809
810
811
812

ING ModelN
iobeh
dudigdi2
etivriedtrwestei
2aairNindTi(tetadcimoafoi2cesp
3
cowefr
813
814
815
816
817
818
819
820
821
822
823
824
825
826
827
828
829
830
831
832
833
834
835
836
837
838
839
840
841
842
843
844
845
846
847
848
849
850
851
852
853
854
855
856
857
858
859
860
861
862
863
864
865
866
867
868
869
870
871
872
873
874
875
876
877
878
879
880
881
882
883
884
885
886
887
888
889
890
891
892
893
894
895
896
897
898
899
900
901
902
903
904
905
906
907
908
909
910
911
912
913
914
915
916
917
918
919
920
921
922
923
924
925
926
927
928
929
930
931
932
933
934
935
936
937
938
ARTICLEBR 1953 1–17
S. Moylan et al. / Neuroscience and B
isorders, it is possible that exposure to cigarette smoke, partic-larly in vulnerable individuals, plays a contributing role in theevelopment of depression through modulation of O&NS. Indeed,
t was recently demonstrated that interactions between PON1enotypes and smoking significantly increased the odds of bipolarepression, while decreased PON1 activity levels, but not smok-
ng, significantly predicted unipolar major depression (Vargas et al.,013).
However, it should be noted that nicotine has some anti-stressffects, with its activation of nicotinic receptors affording protec-ion in a number of neurodegenerative and psychiatric conditions,ncluding Parkinson’s disease (Anderson and Maes, 2013a), in partia improvements in arousal-associated cognition. Alpha7 nicotiniceceptor activation in murine regulatory T cells potentiates theirmmuno-suppressive capacity (Wang et al., 2010), exacerbating theffects of nicotine via immune system regulation in different CNSisorders (Quik et al., 2012). Given the role of gut permeability inhe modulation of depression, it is of note that nicotine amelio-ates ulcerative colitis, partly by increasing regulatory T cells, butorsens Crohn’s disease, where it increases Th17 cells (Galitovskiy
t al., 2011). Cigarette smokers also show a decreased incidence ofome inflammatory and allergic disorders, partly mediated by nico-ine effects on mast cells (Linneberg et al., 2001). As such, nicotineffects on O&NS in isolated cells require balance with its effects onmmune system regulation.
Some of the effects of cigarette smoke are mediated by,3,7,8-tetrachlorodibenzo-p-dioxin (TCDD), which activates theryl hydrocarbon receptor, which, as well as inducing oxidantsnd antioxidants also increases IDO, contributing to TRYCATnduction and serotonin depletion. TCDD-inducible poly (ADP-ibose) polymerase (TiPARP/ARTD14) (Opitz et al., 2011) decreasesAD+, in turn lowering sirtuins and PGC-1� and thereby inhibit-
ng mitochondrial function (Diani-Moore et al., 2010). However,icotine may have some direct protective effects at mitochon-ria, suggesting that nicotine effects will interact with those ofCDD in the regulation of mitochondrial function. Other factorsn cigarette smoke including 2,3,6-trimethyl-1,4-naphthoquinoneTMN), a MAO-A/B inhibitor, also provide protection, partly viahe decreased metabolism of serotonin and dopamine (Castagnolit al., 2003). Taking these diverse effects together, it is possiblehat the level of stimulated oxidative stress induced by nicotinend cigarette smoke may alter the balance between protective andamaging effects to cellular structures. Nicotine stimulates acetyl-holine receptors in a more sustained fashion than normally occursn acetylcholine transmission. Depending upon the conditions, this
ay lead to production of a small, but still regulated amountf oxidative stress that can potentially even augment importantspects of cell signaling that may exert protective effects to cellularunction. However, persistent exposure to increased signaling mayverwhelm intrinsic protective mechanisms, leading to chronicallyncreased oxidative stress leading to cellular damage (Moylan et al.,013b; Newman et al., 2002). As such, depending on the individualonditions present, nicotine and cigarette smoke may have diverseffects on processes driving the biological underpinnings of depres-ion, including via the regulation of O&NS, immune-inflammatoryrocesses and their interaction.
.7. Dietary factors
Levels of ROS/RNS and an individual’s endogenous antioxidantapacity are influenced by dietary factors. Fruits, vegetables, oliveil, nuts and other plant foods are all potent sources of antioxidants,
Please cite this article in press as: Moylan, S., et al., Oxidative & nitrosatRev. (2014), http://dx.doi.org/10.1016/j.neubiorev.2014.05.007
hile a range of dietary derived amino acids, found in meats, veg-tables, whole grains, eggs and yoghurt, are important precursorsor the body’s endogenous antioxidant, GpX. In contrast, high satu-ated fat diets (Morrison et al., 2010) and hyperglycaemia (Yu et al.,
PRESSavioral Reviews xxx (2014) xxx–xxx 9
2006) increase ROS. The effects of dietary factors on the incidenceof depression are exemplified in the PREDIMED randomized trial(Sanchez-Villegas et al., 2013). In patients with comorbid type 2diabetes, 3-year exposure to a Mediterranean diet (rich in olive oil,fruit, vegetables, legumes, tomato, garlic, onion and fish, but low inmeat, cream, butter, fast foods and sugar) supplemented with nutswas significantly and inversely associated with a lower incidenceof depression.
The dietary minerals selenium, copper, manganese and zinc arerequired as cofactors by oxidative enzymes (Parletta et al., 2013).Selenium is also a co-factor in the synthesis of GSH and its relatedenzymes. Selenium appears to play a role in modulating moodand has been shown to be inversely associated with an increasedlikelihood of de novo major depressive disorder (Pasco et al.,2012). In West Texas, residential selenium levels in groundwaterhave been significantly and negatively associated with depressivesymptoms, explaining up 17% of their variance (Johnson et al.,2013).
Reduced dietary intakes of zinc-rich foods have been associatedwith increased odds for depression (Jacka et al., 2012). Decreasedserum zinc is commonly described in individuals with depres-sion (Maes et al., 1994, 1997b; McLoughlin and Hodge, 1990) andis negatively correlated with illness severity (Maes et al., 1994).A meta-analysis showed that zinc supplementation has clinicalefficacy in treatment-resistant depression as an adjunct to antide-pressants as well as a stand-alone intervention (Lai et al., 2012).Zinc’s antidepressant activity can be explained by its anti-oxidativeand anti-inflammatory effects, and also by its neuroprotectiveeffects related to the modulation of neurogenesis, n-3 metabolism,NMDA receptor and glutamate levels (Szewczyk et al., 2011). Forexample, zinc administration mitigated apoptosis and behavioralchanges in rats exposed to malathion, a toxic insecticide knownto induce depressive behaviors and oxidative damage to the brain(Brocardo et al., 2007).
Vitamins A, C and E, present in fruits, vegetables and nuts,(Bolling et al., 2011), are antioxidants that scavenge free rad-icals, protect against cell damage, and upregulate antioxidantcapacity (Parletta et al., 2013). As noted previously, vitaminsE and C are significantly lowered in depressed patients. Thereare few intervention studies examining vitamins in relation todepression, although one randomized, double-blinded, placebocontrolled trial did demonstrate improvements in subjective moodin healthy middle-aged men using a high-dose B vitamin com-plex with vitamin C and minerals (Kennedy et al., 2010). In animalmodels of depression, administration of vitamin E yields a signif-icant antidepressant-like effect, while long-term treatment alsoimproves the antioxidant defenses in the prefrontal cortex andhippocampus (Lobato et al., 2010).
Another vitamin that appears important in depression patho-genesis is vitamin B6. The active form of vitamin B6, pyridoxol-5-phosphate, can influence synthesis of key neurotransmitters dueto its role in tryptophan metabolism. Deficiency in pyridoxol-5-phosphate is associated with depression expression (Hvas et al.,2004) and higher intakes of vitamin B6 appear to be protectiveagainst depression expression (Skarupski et al., 2010).
Reduced folate intake (Tolmunen et al., 2004) and folate status(Nanri et al., 2012) is associated with an increased risk for depres-sion. A Cochrane review supports the use of folate as an adjunctivetreatment in major depression, although it is still unclear as towhether supplementation will benefit both those with low and nor-mal levels of folate (Taylor et al., 2004). At this time however thereis no evidence that folate is useful as a monotherapy (Luberto et al.,
ive stress in depression: Why so much stress? Neurosci. Biobehav.
2013). Recent reviews concluded that folic acid levels should bemeasured and corrected in treatment-resistant depression and insubjects with increased risk for deficiencies in folic acid (Lazarouand Kapsou, 2010).
939
940
941
942

IN PRESSG ModelN
1 iobehavioral Reviews xxx (2014) xxx–xxx
dantm
bpodntrnrcnbei(
tmwlldmcsaoiio2aBodtat
3
a2ucC(anaDDgi
hoe
Fig. 3. This figure shows the wide array of factors that may contribute to increasedoxidative and nitrosative stress (O&NS) in depression. Increased O&NS, in turn,activates the Toll-like receptor (TLR) radical cycle through formation of redox-derived damage associated molecular patters (DAMPs), including malondialdehyde(MDA) and oxidized low density lipoprotein (ox-LDL) and phospholipids (ox-PLP),which further activate immune-inflammatory and O&NS pathways by stimulatingTLRs. The TLR radical cycle is further activated or sensitized by increased levels oflipopolysaccharide (LPS) from gram-negative bacteria, psychosocial stressors and
943
944
945
946
947
948
949
950
951
952
953
954
955
956
957
958
959
960
961
962
963
964
965
966
967
968
969
970
971
972
973
974
975
976
977
978
979
980
981
982
983
984
985
986
987
988
989
990
991
992
993
994
995
996
997
998
999
1000
1001
1002
1003
1004
1005
1006
1007
1008
1009
1010
1011
1012
1013
1014
1015
1016
1017
1018
1019
1020
1021
1022
1023
1024
1025
1026
1027
1028
1029
1030
1031
1032
1033
1034
1035
1036
1037
1038
1039
1040
ARTICLEBR 1953 1–17
0 S. Moylan et al. / Neuroscience and B
In elderly (>70 years of age) Japanese individuals, a tomato-richiet, which contains high levels of lycopene, was inversely associ-ted with depressive symptoms (Niu et al., 2013). In the same studyo significant association was detected between depressive symp-oms and the intake of other vegetables, suggesting that lycopenes
ay have the potential to prevent depressive symptoms.Polyphenols, found in particular abundance in herbs and spices,
erries, green tea, nuts, red wine and other plant foods, also haveotent antioxidant properties. In elderly subjects, the higher intakef green tea polyphenols is accompanied by a reduced incidence ofepressive symptoms, while in animal models green tea polyphe-ols show antidepressant-like effects, which are in part relatedo their antioxidant effects (Liu et al., 2013; Zhu et al., 2012). Aecent paper reviewed the antidepressant potential of polyphe-ols, such as curcumin, ferulic acid, hesperidin, rutin, quercetin andesveratrol (Pathak et al., 2013). Resveratrol, one of the phenolicompounds abundant in berries, grapes, red wine, and peanuts, isot only a strong antioxidant and anti-inflammatory compound,ut also is neuroprotectant (Joseph et al., 1999). Polyphenols maynhance brain plasticity by modulating signaling pathways tonduce the activation of key molecules and proteins, such as BDNFWilliams et al., 2008).
The brain is particularly vulnerable to oxidative damage dueo the high content of polyunsaturated fatty acids in erythrocyte
embranes. The activated immune-inflammatory and O&NS path-ays that commonly accompany depression result in increased
ipid peroxidation, which may account for the decreased levels ofong chain fatty acids regularly observed in those with depressiveisorders (Berk and Jacka, 2012). Such peroxidation decreases cellembrane fluidity and can damage membrane proteins. While long
hain n-3 fatty acids help to mitigate the impact of these processes,upplementation with nutritional antioxidants, such as vitamins And E, polyphenols, lycopenes and zinc might prevent lipid per-xidation. Pre-treatment with antioxidants can prevent cell lossn animal models of acute stress (Lee et al., 2006), while studiesn rodents demonstrate that the adverse effects of high fat dietsn BDNF expression are ameliorated by antioxidants (Wu et al.,004b). Similarly, adverse effects of induced traumatic brain injuryre ameliorated by n-3 PUFAs (Wu et al., 2004a). Moreover vitamins6, B12 and folate can reduce levels of homocysteine, increasesxidative stress in endothelial cells (Parletta et al., 2013). Theseata indicate that nutrient sufficiency is likely to play an impor-ant role in reducing the impact of O&NS on the brain via increasedntioxidant and anti-inflammatory effects and related neuropro-ection.
.8. Vitamin D status
Vitamin D is a secosteroid that has a primary role in bonend muscle health. Widespread vitamin D deficiency, particularly5-hydroxyvitamin D, has been identified among western pop-lations at higher latitudes and cultures with restrictive dressodes (Pasco et al., 2001). Many adverse health outcomes includingVD, osteoporosis and cancer are linked to vitamin D insufficiencyNowson et al., 2012). Additionally, Vitamin D has many less well-ppreciated roles in neural physiology and immune regulation thatotably overlap with the pathophysiology of depression. Vitamin Dlso impacts on sleep and circadian rhythms. Receptors for vitamin
are found in brain regions important in mood regulation. Vitamin influences cell proliferation in the developing brain and embryo-enesis as well as influencing neuronal growth. It also plays a rolen glucocorticoid physiology (Eyles et al., 2011).
Please cite this article in press as: Moylan, S., et al., Oxidative & nitrosatRev. (2014), http://dx.doi.org/10.1016/j.neubiorev.2014.05.007
Cross-sectional and prospective data suggest that serum 25-ydroxyvitamin D insufficiency is associated with an increased riskf developing depression (Kjaergaard et al., 2012). There is, how-ver, inconsistent clinical trial data of the antidepressant effects of
1041
autoimmune responses directed against oxidative (OSEs) and nitrosative (NSEs)specific epitopes.
supplementation with vitamin D, with both positive and null trialsreported (Lansdowne and Provost, 1998; Sanders et al., 2011).
Vitamin D also has roles in preventing DNA damage and regu-lating cell growth. Preclinical data suggest that vitamin D reducesoxidative stress mediated damage, particularly to DNA, evidencedby reduced 8-OHdg, reduced chromosomal aberrations, the pre-vention of telomere shortening and the inhibition of telomeraseactivity. It also regulates the cell cycle, preventing propagation ofdamaged DNA, and regulates cell death pathways and apoptosis(Nair-Shalliker et al., 2012). Vitamin D3 can reverse the inductionof diabetes by streptozotocin in animal models; a state which isassociated with reduced antioxidant defenses including superox-ide dismutase and GpX (George et al., 2012). In elderly subjects withglucose intolerance, a significant association has been observedbetween oxidative stress markers, particularly advanced glycationend products, advanced oxidation protein products, LDL suscep-tibility to oxidation and NO metabolic pathway products with25(OH)D levels. This effect was more marked in hyperglycemic sub-jects, a state known to be linked to oxidative stress (Gradinaru et al.,2012).
Early life vitamin D deficiency is associated with increasedblood pressure and vascular oxidative stress (Argacha et al., 2011).Calcitriol can reduce expression of inflammation and oxidativestress markers in patients receiving hemodialysis with secondaryhyperparathyroidism (Wu et al., 2011). Calcitriol increases brainglutathione levels, and is a catalyst for GSH production, a find-ing concordant with both the role of GSH as a principal redoxdefense, and in the modulation of depression (Garcion et al., 2002).Some of the efficacy of valproate in bipolar disorder is mediated byan increase in bcl-2 associated anthanogen-1 (BAG-1), which pre-vents the nuclear translocation of cortisol’s glucocorticoid receptor,thereby preventing many of the effects of this stress hormone,including in neuroinflammatory disorders such as multiple sclero-sis (Anderson and Rodriguez, 2011). BAG-1 also transports vitaminD3 to the nuclear vitamin D receptor, suggesting that stress and
ive stress in depression: Why so much stress? Neurosci. Biobehav.
depression associated O&NS may be intimately involved in the reg-ulation of vitamin D3 effects, partly via BAG-1 regulation. Togetherthese findings suggest that oxidative stress may play a modulatory
1042
1043
1044

ARTICLE IN PRESSG ModelNBR 1953 1–17
S. Moylan et al. / Neuroscience and Biobehavioral Reviews xxx (2014) xxx–xxx 11
Fig. 4. This figure demonstrates a model depicting the interrelationship between (neuro)inflammation, oxidative and nitrosative stress (O&NS), mood disorders and theprocess of neuroprogression. Multiple medical, environmental and genetic factors predispose to (neuro)inflammation and increased O&NS. (Neuro)inflammation and O&NSproducts contribute to expression of mood disorder symptoms and to neuroprogressive processes. These products also lead to direct cell damage and dysfunction thatcontribute to disorder expression, neuroprogression, and to development of autoimmune responses that reinforce a (neuro)inflammatory and O&NS state. This reinforcingc n chac
r2
3
t(tiaiaerehdeaheiacLw
dcH
Q3
1045
1046
1047
1048
1049
1050
1051
1052
1053
1054
1055
1056
1057
1058
1059
1060
1061
1062
1063
1064
1065
1066
1067
1068
1069
1070
1071
1072
1073
1074
1075
1076
1077
1078
1079
1080
1081
1082
1083
1084
1085
1086
1087
1088
1089
1090
1091
1092
1093
1094
1095
1096
1097
1098
ycle contributes to further neuroprogression, and subsequent staging of depressiohronicity. LPS – lipopolysaccharide.
ole in the interaction between vitamin D and mood (Autier et al.,013).
.9. Sedentary lifestyle and exercise
Despite the known health benefits of exercise it is estimatedhat more than 30% of the global population are physically inactiveOrganisation, 2002). With increasing sedentary behavior comeshe risk of many diseases, including depression. Physical inactiv-ty across the lifespan has been cross-sectionally and prospectivelyssociated with depression (Teychenne et al., 2008). In a studynvestigating self-reported levels of physical activity in childhoodnd adult depression, low physical activity levels throughout thearly years was associated with up to a 35% increased risk of self-eported depression in adulthood (Jacka et al., 2010). Furthermore,pidemiological studies of younger, middle aged and older adults,ave shown habitual physical activity to reduce the likelihood ofe novo depression (Brown et al., 2005; Pasco et al., 2011; Sagatunt al., 2007; Strawbridge et al., 2002). These observational findingsre somewhat supported by intervention studies where exerciseas been demonstrated to be effective in treating depression (Rimert al., 2012). For example, older patients with depression random-zed to a twice-weekly exercise group for 10 weeks demonstrated
modest reduction in depression scores compared to non-exerciseontrols (weekly health education talks) (Mather et al., 2002).arger effect sizes are reported when comparison is made to aaiting list or placebo treatment (Rimer et al., 2012).
Please cite this article in press as: Moylan, S., et al., Oxidative & nitrosatRev. (2014), http://dx.doi.org/10.1016/j.neubiorev.2014.05.007
Exercise is likely to influence the rate of depression and relatedisorders through numerous biochemical, physiological and psy-hological pathways (Eyre and Baune, 2012; Moylan et al., 2013a).owever, O&NS is likely to act as a prominent mechanism by which
racterized by increasing sensitivity to relapse, treatment resistance and symptom
this occurs. O&NS has been shown to be increased in those whoare physically inactive as well as in individuals following acuteexercise, whereas chronic or habitual exercise has been shownto be associated with a reduction in O&NS via an up regulationof antioxidant defenses (Gomes et al., 2012). For example, in asmall group of physical inactive medical students, levels of MDAwere shown to be increased when compared with age-matchedfootball players under regular training (Metin et al., 2003). Antioxi-dant enzyme levels are increased in response to exercise, indicatingthat physical activity has the ability to diminish lipid peroxidation(Djordjevic et al., 2012; Evelson et al., 2002; Fisher-Wellman andBloomer, 2009; Metin et al., 2003). Exercise, like antidepressants,is a significant inducer of neurogenesis, with melatonin furtherpotentiating the effects of exercise on rodent neurogenesis (Liu
et al., in press). Given the role of O&NS in both depression andexercise, these data highlight the possibility of O&NS modulatingexercise-induced mood improvements. However, further researchinto the optimal type, duration and intensity of the exercise isrequired.
4. Conclusions
Fig. 3 summarizes the pathways and factors that may contributeto O&NS in depression. A vicious cycle of activated immune-inflammatory pathways, lowered antioxidant levels, redox-derivedDAMPs and activation of the TLR4 complex with downstreamproduction of immune-inflammatory mediators and ROS/RNS
ive stress in depression: Why so much stress? Neurosci. Biobehav.
characterizes depression. Psychosocial stressors, metabolic syn-drome and obesity, sleep disorders, smoking, lowered vitaminD status, a diet low in antioxidants, such as selenium, folate,zinc, lycopenes and polyphenols, and a sedentary lifestyle may
1099
1100
1101
1102

ING ModelN
1 iobeh
crOa
ecseOnadpttTrTNatbHmbtoib2
rpadcttOpOFtkinadairarairpvatpiaip
Q4
Q5
Q6
1103
1104
1105
1106
1107
1108
1109
1110
1111
1112
1113
1114
1115
1116
1117
1118
1119
1120
1121
1122
1123
1124
1125
1126
1127
1128
1129
1130
1131
1132
1133
1134
1135
1136
1137
1138
1139
1140
1141
1142
1143
1144
1145
1146
1147
1148
1149
1150
1151
1152
1153
1154
1155
1156
1157
1158
1159
1160
1161
1162
1163
1164
1165
1166
1167
1168
1169
1170
1171
1172
1173
1174
1175
1176
1177
1178
1179
1180
1181
1182
1183
1184
1185
1186
1187
1188
1189
1190
1191
1192
1193
1194
1195
1196
1197
1198
1199
1200
1201
1202
1203
1204
1205
1206
1207
1208
1209
1210
1211
1212
1213
1214
1215
1216
1217
1218
1219
1220
1221
1222
1223
1224
1225
1226
1227
1228
1229
1230
1231
1232
1233
1234
ARTICLEBR 1953 1–17
2 S. Moylan et al. / Neuroscience and B
ontribute to activated O&NS pathways in depression. Neu-oinflammatory brain disorders and systemic immune- and&NS-related disorders and conditions characterized by O&NS aredditionally associated with the onset of depression.
Activated peripheral immune-inflammatory pathways and low-red peripheral antioxidant defenses may have consequences forentral immune-inflammatory and O&NS pathways. As previouslyummarized (Leonard and Maes, 2012), peripherally increased lev-ls of LPS and pro-inflammatory cytokines, driven by activated&NS pathways and lowered antioxidant defenses, may cause braineuroinflammation. The latter involves not only inflammation butlso O&NS processes fueled by a systemic loss of antioxidantefenses and increased gut permeability. Activated central O&NSathways may cause lipid peroxidation, and result in new forma-ion of redox-derived DAMPs that in turn may further activatehe TLR radical cycle in the brain. Increased levels of peripheralRYCATs, such as kynurenine, may pass the blood brain bar-ier to exert depressogenic and neurotoxic activities in the brain.he peripheral autoimmune processes directed against OSEs andSEs may have grave consequences for CNS functions. In patientsnd animals with autoimmune conditions, including lupus ery-hematosus, associations have been detected between serum andrain autoantibodies and neuropsychiatric symptoms (Zameer andoffman, 2001). These behavioral changes accompanying autoim-une diseases are centrally mediated through increased blood
rain barrier permeability and infiltration of white blood cellshrough the choroid plexus (Zameer and Hoffman, 2001). More-ver, some of the IgM autoantibodies directed against NSEs that arencreased in depressed patients (e.g. S–NO–cysteine) are known toe highly neurotoxic and to cause demyelination (Boullerne et al.,002).
Fig. 4 depicts the wide-angle lens picture emerging from theeviewed research literature, demonstrating that activation oferipheral and central immune-inflammatory and O&NS pathwaysre linked to expression of mood disorder symptoms, staging ofepression and to neuroprogressive processes. A series of medi-al, environmental and genetic factors predispose and contributeo development of increased levels of peripheral inflammationhat can precipitate development of neuroinflammation. Activated&NS pathways and lowered antioxidant defenses also drive thisrocess. Increased neuroinflammation and central activation of&NS pathways have two broad, non-mutually exclusive, effects.irst, they can influence development of depressive symptomshrough effects on cellular functioning and through influencingey factors underpinning depression effects (e.g. through impair-ng normal neurotransmitter synthesis and metabolism). Second,euroinflammatory and O&NS products cause direct cellular dam-ge (e.g. lipid peroxidation) and dysfunction. Cellular damage andysfunction contributes to expression of depressive symptoms (asbove) and to processes underlying neuroprogression, includingncreased neuronal apoptosis and decreased neurogenesis and neu-oplasticity. The cell damage in addition can further stimulateutoimmune pathways, leading to further increases in central neu-oinflammation and O&NS and reinforcing further depressogenicnd neuroprogressive effects. These effects contribute to the stag-ng of depression, increasing the likelihood of recurrence, treatmentesistance and a chronic depressive state. The delineation of theseathways highlights multiple opportunities for therapeutic inter-ention in preventing and/or reducing levels of neuroinflammationnd O&NS in depression. Future research should delineate whetherhe pathways involved in the immune-inflammatory and O&NSathophysiology of depression are useful as state, trait or stag-
Please cite this article in press as: Moylan, S., et al., Oxidative & nitrosatRev. (2014), http://dx.doi.org/10.1016/j.neubiorev.2014.05.007
ng biomarkers for depression. Lastly, understanding of the processnd its constituents offers both molecular targets for pharmacolog-cal intervention and environmental targets for public health andreventive approaches.
PRESSavioral Reviews xxx (2014) xxx–xxx
Funding
MB has received Grant/Research Support from the NIH, Cooper-
ative Research Centre, Simons Autism Foundation, Cancer Councilof Victoria, Stanley Medical Research Foundation, MBF, NHMRC,Beyond Blue, Rotary Health, Geelong Medical Research Foundation,Bristol Myers Squibb, Eli Lilly, Glaxo SmithKline, Organon, Novar-tis, Mayne Pharma, Servier and Woolworths, has been a speakerfor Astra Zeneca, Bristol Myers Squibb, Eli Lilly, Glaxo SmithK-line, Janssen Cilag, Lundbeck, Merck, Pfizer, Sanofi Synthelabo,Servier, Solvay and Wyeth, and served as a consultant to AstraZeneca, Bristol Myers Squibb, Eli Lilly, Glaxo SmithKline, JanssenCilag, Lundbeck Merck and Servier. MB, AO, FNJ have receivedfunding from Meat and Livestock, Australia. JAP has receivedGrant/Research support from the NHMRC, Perpetual, Amgen, BUPAFoundation and Arthritis Australia and has received speaker feesfrom Amgen and Sanofi Aventis. OMD has received Grant supportfrom the Brain and Behavior Foundation, Simons Autism Founda-tion, Stanley Medical Research Institute, Lilly, NHMRC, an AlfredDeakin Postdoctoral Research Fellowship and an ASBD/Serviergrant. LW has received Grant/Research support from Eli Lilly, Pfizer,The University of Melbourne, Deakin University and the NHMRC.
Acknowledgements
MB is supported by a NHMRC Senior Principal Research Fellow-ship. AO is supported by a NHMRC ECR Fellowship (1052865).
References
Adam-Vizi, V., Starkov, A.A., 2010. Calcium and mitochondrial reactive oxygenspecies generation: how to read the facts. J. Alzheimer’s Dis. 20 (Suppl. 2),S413–S426.
Ahmad, A., Rasheed, N., Banu, N., Palit, G., 2010. Alterations in monoamine levelsand oxidative systems in frontal cortex, striatum, and hippocampus of the ratbrain during chronic unpredictable stress. Stress 13, 355–364.
Alberati-Giani, D., Cesura, A.M., 1998. Expression of the kynurenine enzymes inmacrophages and microglial cells: regulation by immune modulators. AminoAcids 14, 251–255.
Aleksandrovskii Iu, A., Poiurovskii, M.V., Neznamov, G.G., Seredeniia, S.B., Krasova,E.A., 1988. Lipid peroxidation in emotional stress and neurotic disorders. Zh.Nevropatol. Psikhiatr. Im. S.S. Korsakova 88, 95–101.
Alonso-Fernandez, A., Garcia-Rio, F., Arias, M.A., Hernanz, A., de la Pena, M., Pierola, J.,Barcelo, A., Lopez-Collazo, E., Agusti, A., 2009. Effects of CPAP on oxidative stressand nitrate efficiency in sleep apnoea: a randomised trial. Thorax 64, 581–586.
Anbarasi, K., Vani, G., Balakrishna, K., Devi, C.S., 2005. Effect of bacoside A onmembrane-bound ATPases in the brain of rats exposed to cigarette smoke. J.Biochem. Mol. Toxicol. 19, 59–65.
Anderson, G., Maes, M., 2013a. Neurodegeneration in Parkinson’s disease: inter-actions of oxidative stress, tryptophan catabolites and depression withmitochondria and sirtuins. Mol. Neurobiol..
Anderson, G., Maes, M., 2013b. Oxidative/nitrosative stress and immuno-inflammatory pathways in depression: treatment implications. Curr. Pharm.Des..
Anderson, G., Rodriguez, M., 2011. Multiple sclerosis, seizures, and antiepileptics:role of IL-18, IDO, and melatonin. Eur. J. Neurol. 18, 680–685.
Argacha, J.F., Egrise, D., Pochet, S., Fontaine, D., Lefort, A., Libert, F., Goldman, S., vande Borne, P., Berkenboom, G., Moreno-Reyes, R., 2011. Vitamin D deficiency-induced hypertension is associated with vascular oxidative stress and alteredheart gene expression. J. Cardiovasc. Pharmacol. 58, 65–71.
Arnardottir, E.S., Mackiewicz, M., Gislason, T., Teff, K.L., Pack, A.I., 2009. Molecularsignatures of obstructive sleep apnea in adults: a review and perspective. Sleep32, 447–470.
Arnardottir, E.S., Maislin, G., Schwab, R.J., Staley, B., Benediktsdottir, B., Olafsson, I.,Juliusson, S., Romer, M., Gislason, T., Pack, A.I., 2012. The interaction of obstruc-tive sleep apnea and obesity on the inflammatory markers C-reactive proteinand interleukin-6: the Icelandic Sleep Apnea Cohort. Sleep 35, 921–932.
Atlantis, E., Baker, M., 2008. Obesity effects on depression: systematic review ofepidemiological studies. Int. J. Obes. 32, 881–891.
Atlantis, E., Goldney, R.D., Wittert, G.A., 2009. Obesity and depression or anxiety.BMJ 339, b3868.
Autier, P., Boniol, M., Pizot, C., Mullie, P., 2013. Vitamin D status and ill health: a
ive stress in depression: Why so much stress? Neurosci. Biobehav.
systematic review. Lancet Diabetes Endocrinol..Baune, B.T., Dannlowski, U., Domschke, K., Janssen, D.G., Jordan, M.A., Ohrmann, P.,
Bauer, J., Biros, E., Arolt, V., Kugel, H., Baxter, A.G., Suslow, T., 2010. The inter-leukin 1 beta (IL1B) gene is associated with failure to achieve remission andimpaired emotion processing in major depression. Biol. Psychiatry 67, 543–549.
1235
1236
1237
1238
1239

ING ModelN
iobeh
B
B
B
B
B
B
B
B
B
B
B
B
B
Q7B
B
B
B
B
B
B
B
B
CC
C
C
C
C
1240
1241
1242
1243
1244
1245
1246
1247
1248
1249
1250
1251
1252
1253
1254
1255
1256
1257
1258
1259
1260
1261
1262
1263
1264
1265
1266
1267
1268
1269
1270
1271
1272
1273
1274
1275
1276
1277
1278
1279
1280
1281
1282
1283
1284
1285
1286
1287
1288
1289
1290
1291
1292
1293
1294
1295
1296
1297
1298
1299
1300
1301
1302
1303
1304
1305
1306
1307
1308
1309
1310
1311
1312
1313
1314
1315
1316
1317
1318
1319
1320
1321
1322
1323
1324
1325
1326
1327
1328
1329
1330
1331
1332
1333
1334
1335
1336
1337
1338
1339
1340
1341
1342
1343
1344
1345
1346
1347
1348
1349
1350
1351
1352
1353
1354
1355
1356
1357
1358
1359
1360
1361
1362
1363
1364
1365
1366
1367
1368
1369
1370
1371
1372
1373
1374
1375
1376
1377
1378
1379
1380
1381
1382
1383
1384
1385
1386
1387
1388
1389
1390
1391
1392
1393
1394
1395
1396
1397
1398
1399
1400
1401
1402
1403
1404
1405
1406
ARTICLEBR 1953 1–17
S. Moylan et al. / Neuroscience and B
erg, R.D., Garlington, A.W., 1979. Translocation of certain indigenous bacteria fromthe gastrointestinal tract to the mesenteric lymph nodes and other organs in agnotobiotic mouse model. Infect. Immun. 23, 403–411.
erk, M., Jacka, F., 2012. Preventive strategies in depression: gathering evidence forrisk factors and potential interventions. Br. J. Psychiatry 201, 339–341.
erk, M., Johansson, S., Wray, N.R., Williams, L., Olsson, C., Haavik, J., Bjerkeset, O.,2011a. Glutamate cysteine ligase (GCL) and self reported depression: an associ-ation study from the HUNT. J. Affect. Disord. 131, 207–213.
erk, M., Kapczinski, F., Andreazza, A.C., Dean, O.M., Giorlando, F., Maes, M., Yucel, M.,Gama, C.S., Dodd, S., Dean, B., Magalhaes, P.V., Amminger, P., McGorry, P., Malhi,G.S., 2011b. Pathways underlying neuroprogression in bipolar disorder: focuson inflammation, oxidative stress and neurotrophic factors. Neurosci. Biobehav.Rev. 35, 804–817.
erk, M., Plein, H., Ferreira, D., 2001. Platelet glutamate receptor supersensitivity inmajor depressive disorder. Clin. Neuropharmacol. 24, 129–132.
erk, M., Wadee, A.A., Kuschke, R.H., O’Neill-Kerr, A., 1997. Acute phase proteins inmajor depression. J. Psychosom. Res. 43, 529–534.
erk, M., Williams, L.J., Jacka, F.N., O’Neil, A., Pasco, J.A., Moylan, S., Allen, N.B., Stuart,A.L., Hayley, A.C., Byrne, M.L., Maes, M., 2013. So depression is an inflammatorydisease, but where does the inflammation come from? BMC Med. 11, 200.
erry, A., Cirulli, F., 2013. The p66(Shc) gene paves the way for healthspan:evolutionary and mechanistic perspectives. Neurosci. Biobehav. Rev. 37,790–802.
hagwat, S.V., Vijayasarathy, C., Raza, H., Mullick, J., Avadhani, N.G., 1998.Preferential effects of nicotine and 4-(N-methyl-N-nitrosamine)-1-(3-pyridyl)-1-butanone on mitochondrial glutathione S-transferase A4-4 induction andincreased oxidative stress in the rat brain. Biochem. Pharmacol. 56, 831–839.
ilici, M., Efe, H., Koroglu, M.A., Uydu, H.A., Bekaroglu, M., Deger, O., 2001. Antioxida-tive enzyme activities and lipid peroxidation in major depression: alterationsby antidepressant treatments. J. Affect. Disord. 64, 43–51.
lau, S., Kohen, R., Bass, P., Rubinstein, A., 2000. Relation between colonicinflammation severity and total low-molecular-weight antioxidant profiles inexperimental colitis. Dig. Dis. Sci. 45, 1180–1187.
olling, B.W., Chen, C.Y., McKay, D.L., Blumberg, J.B., 2011. Tree nut phytochemi-cals: composition, antioxidant capacity, bioactivity, impact factors. A systematicreview of almonds, Brazils, cashews, hazelnuts, macadamias, pecans, pine nuts,pistachios and walnuts. Nutr. Res. Rev. 24, 244–275.
ortolasci, C.C., Vargas, H.O., Souza-Nogueira, A., Moreira, E.G., Nunes, S.O., Berk, M.,Dodd, S., Barbosa, D.S., Maes, M., 2014. Paraoxonase (PON)1 Q192R functionalgenotypes and PON1 Q192R genotype by smoking interactions are risk factorsfor the metabolic syndrome, but not overweight or obesity. Redox Rep. (in press).
oullerne, A.I., Rodriguez, J.J., Touil, T., Brochet, B., Schmidt, S., Abrous, N.D., LeMoal, M., Pua, J.R., Jensen, M.A., Mayo, W., Arnason, B.G., Petry, K.G., 2002.Anti-S-nitrosocysteine antibodies are a predictive marker for demyelination inexperimental autoimmune encephalomyelitis: implications for multiple sclero-sis. J. Neurosci. 22, 123–132.
raidy, N., Grant, R., Adams, S., Brew, B.J., Guillemin, G.J., 2009. Mechanism forquinolinic acid cytotoxicity in human astrocytes and neurons. Neurotox. Res.16, 77–86.
rasier, A.R., 2006. The NF-kappaB regulatory network. Cardiovasc. Toxicol. 6,111–130.
reslau, N., Roth, T., Rosenthal, L., Andreski, P., 1996. Sleep disturbance and psy-chiatric disorders: a longitudinal epidemiological study of young adults. Biol.Psychiatry 39, 411–418.
rocardo, P.S., Assini, F., Franco, J.L., Pandolfo, P., Muller, Y.M., Takahashi, R.N.,Dafre, A.L., Rodrigues, A.L., 2007. Zinc attenuates malathion-induced depressant-like behavior and confers neuroprotection in the rat brain. Toxicol. Sci. 97,140–148.
rown, W.J., Ford, J.H., Burton, N.W., Marshall, A.L., Dobson, A.J., 2005. Prospectivestudy of physical activity and depressive symptoms in middle-aged women. Am.J. Prev. Med. 29, 265–272.
ryan, S., Baregzay, B., Spicer, D., Singal, P.K., Khaper, N., 2013. Redox-inflammatorysynergy in the metabolic syndrome. Can. J. Physiol. Pharmacol. 91, 22–30.
ufalino, C., Hepgul, N., Aguglia, E., Pariante, C.M., 2013. The role of immune genesin the association between depression and inflammation: a review of recentclinical studies. Brain Behav. Immun. 31, 31–47.
uysse, D.J., Angst, J., Gamma, A., Ajdacic, V., Eich, D., Rossler, W., 2008. Prevalence,course, and comorbidity of insomnia and depression in young adults. Sleep 31,473–480.
arroll, B.J., 1980. Dexamethasone suppression test in depression. Lancet 2, 1249.arta, S., Castellani, P., Delfino, L., Tassi, S., Vene, R., Rubartelli, A., 2009. DAMPs and
inflammatory processes: the role of redox in the different outcomes. J. Leukoc.Biol. 86, 549–555.
asado, A., De Lucas, N., Lopez-Fernandez, E., Sanchez, A., Jimenez, J.A., 2006. Lipidperoxidation, occupational stress and aging in workers of a prehospital emer-gency service. Eur. J. Emerg. Med. 13, 165–171.
astagnoli, K., Petzer, J.B., Steyn, S.J., van der Schyf, C.J., Castagnoli Jr., N., 2003. Inhi-bition of human MAO-A and MAO-B by a compound isolated from flue-curedtobacco leaves and its neuroprotective properties in the MPTP mouse model ofneurodegeneration. Inflammopharmacology 11, 183–188.
eprnja, M., Derek, L., Unic, A., Blazev, M., Fistonic, M., Kozaric-Kovacic, D., Franic,
Please cite this article in press as: Moylan, S., et al., Oxidative & nitrosatRev. (2014), http://dx.doi.org/10.1016/j.neubiorev.2014.05.007
M., Romic, Z., 2011. Oxidative stress markers in patients with post-traumaticstress disorder. Coll. Antropol. 35, 1155–1160.
han, E.D., Riches, D.W., 2001. IFN-gamma + LPS induction of iNOS is modulated byERK, JNK/SAPK, and p38(mapk) in a mouse macrophage cell line. Am. J. Physiol.Cell Physiol. 280, C441–C450.
PRESSavioral Reviews xxx (2014) xxx–xxx 13
Chang, P.P., Ford, D.E., Mead, L.A., Cooper-Patrick, L., Klag, M.J., 1997. Insomnia inyoung men and subsequent depression. The Johns Hopkins Precursors Study.Am. J. Epidemiol. 146, 105–114.
Chavez, A.M., Menconi, M.J., Hodin, R.A., Fink, M.P., 1999. Cytokine-induced intesti-nal epithelial hyperpermeability: role of nitric oxide. Crit. Care Med. 27,2246–2251.
Che, Y., Wang, J.F., Shao, L., Young, T., 2010. Oxidative damage to RNA but not DNA inthe hippocampus of patients with major mental illness. J. Psychiatry Neurosci.35, 296–302.
Check, J., Byrd, C.L., Menio, J., Rippe, R.A., Hines, I.N., Wheeler, M.D., 2010. Src kinaseparticipates in LPS-induced activation of NADPH oxidase. Mol. Immunol. 47,756–762.
Christen, S., Peterhans, E., Stocker, R., 1990. Antioxidant activities of some trypto-phan metabolites: possible implication for inflammatory diseases. Proc. Natl.Acad. Sci. U.S.A. 87, 2506–2510.
Clark, E., Hoare, C., Tanianis-Hughes, J., Carlson, G.L., Warhurst, G., 2005. Interferongamma induces translocation of commensal Escherichia coli across gut epithelialcells via a lipid raft-mediated process. Gastroenterology 128, 1258–1267.
D’Aquila, P., Rose, G., Panno, M.L., Passarino, G., Bellizzi, D., 2012. SIRT3 gene expres-sion: a link between inherited mitochondrial DNA variants and oxidative stress.Gene 497, 323–329.
Dallas, M., Boycott, H.E., Atkinson, L., Miller, A., Boyle, J.P., Pearson, H.A., Peers, C.,2007. Hypoxia suppresses glutamate transport in astrocytes. J. Neurosci. 27,3946–3955.
de Wit, L., Luppino, F., van Straten, A., Penninx, B., Zitman, F., Cuijpers, P., 2010.Depression and obesity: a meta-analysis of community-based studies. Psychia-try Res. 178, 230–235.
Debnath, M., Berk, M., 2014. Th17 pathway-mediated immunopathogenesis ofschizophrenia: mechanisms and implications. Schizophr. Bull..
Diani-Moore, S., Ram, P., Li, X., Mondal, P., Youn, D.Y., Sauve, A.A., Rifkind, A.B., 2010.Identification of the aryl hydrocarbon receptor target gene TiPARP as a mediatorof suppression of hepatic gluconeogenesis by 2,3,7,8-tetrachlorodibenzo-p-dioxin and of nicotinamide as a corrective agent for this effect. J. Biol. Chem.285, 38801–38810.
Dimopoulos, N., Piperi, C., Psarra, V., Lea, R.W., Kalofoutis, A., 2008. Increased plasmalevels of 8-iso-PGF2alpha and IL-6 in an elderly population with depression.Psychiatry Res. 161, 59–66.
Djordjevic, D.Z., Cubrilo, D.G., Barudzic, N.S., Vuletic, M.S., Zivkovic, V.I., Nesic,M., Radovanovic, D., Djuric, D.M., Jakovljevic, V., 2012. Comparison of bloodpro/antioxidant levels before and after acute exercise in athletes and non-athletes. Gen. Physiol. Biophys. 31, 211–219.
Dowlati, Y., Herrmann, N., Swardfager, W., Liu, H., Sham, L., Reim, E.K., Lanctot,K.L., 2010. A meta-analysis of cytokines in major depression. Biol. Psychiatry67, 446–457.
Dutcher, J.P., Logan, T., Gordon, M., Sosman, J., Weiss, G., Margolin, K., Plasse, T., Mier,J., Lotze, M., Clark, J., Atkins, M., 2000. Phase II trial of interleukin 2, interferonalpha, and 5-fluorouracil in metastatic renal cell cancer: a cytokine workinggroup study. Clin. Cancer Res. 6, 3442–3450.
Dykens, J.A., Sullivan, S.G., Stern, A., 1987. Oxidative reactivity of the tryptophanmetabolites 3-hydroxyanthranilate, cinnabarinate, quinolinate and picolinate.Biochem. Pharmacol. 36, 211–217.
El Kossi, M.M., Zakhary, M.M., 2000. Oxidative stress in the context of acute cere-brovascular stroke. Stroke 31, 1889–1892.
Eren, I., Naziroglu, M., Demirdas, A., 2007a. Protective effects of lamotrigine, arip-iprazole and escitalopram on depression-induced oxidative stress in rat brain.Neurochem. Res. 32, 1188–1195.
Eren, I., Naziroglu, M., Demirdas, A., Celik, O., Uguz, A.C., Altunbasak, A., Ozmen, I., Uz,E., 2007b. Venlafaxine modulates depression-induced oxidative stress in brainand medulla of rat. Neurochem. Res. 32, 497–505.
Evelson, P., Gambino, G., Travacio, M., Jaita, G., Verona, J., Maroncelli, C., Wikinski,R., Llesuy, S., Brites, F., 2002. Higher antioxidant defences in plasma and lowdensity lipoproteins from rugby players. Eur. J. Clin. Invest. 32, 818–825.
Eyles, D., Burne, T., McGrath, J., 2011. Vitamin D in fetal brain development. Semin.Cell Dev. Biol. 22, 629–636.
Eyre, H., Baune, B.T., 2012. Neuroimmunological effects of physical exercise indepression. Brain Behav. Immun. 26, 251–266.
Fisher-Wellman, K., Bloomer, R.J., 2009. Acute exercise and oxidative stress: a 30year history. Dynam. Med. 8, 1.
Forlenza, M.J., Miller, G.E., 2006. Increased serum levels of 8-hydroxy-2’-deoxyguanosine in clinical depression. Psychosom. Med. 68, 1–7.
Foster, G.E., Poulin, M.J., Hanly, P.J., 2007. Intermittent hypoxia and vascular func-tion: implications for obstructive sleep apnoea. Exp. Physiol. 92, 51–65.
Fransson, M., Adner, M., Uddman, R., Cardell, L.O., 2007. Lipopolysaccharide-induceddown-regulation of uteroglobin in the human nose. Acta Otolaryngol. (Stockh.)127, 285–291.
Funakoshi, H., Kanai, M., Nakamura, T., 2011. Modulation of tryptophan metabolism,pomotion of neurogenesis and alteration of anxiety-related behavior in trypto-phan 2, 3-dioxygenase-deficient mice. Int. J. Tryptophan Res. 4, 7.
Funato, Y., Miki, H., 2010. Redox regulation of Wnt signalling via nucleoredoxin. FreeRadic. Res. 44, 379–388.
Furukawa, S., Fujita, T., Shimabukuro, M., Iwaki, M., Yamada, Y., Nakajima, Y.,
ive stress in depression: Why so much stress? Neurosci. Biobehav.
Nakayama, O., Makishima, M., Matsuda, M., Shimomura, I., 2004. Increasedoxidative stress in obesity and its impact on metabolic syndrome. J. Clin. Invest.114, 1752–1761.
Galecki, P., Galecka, E., Maes, M., Chamielec, M., Orzechowska, A., Bobinska, K.,Lewinski, A., Szemraj, J., 2012. The expression of genes encoding for COX-2, MPO,
1407
1408
1409
1410
1411

ING ModelN
1 iobeh
G
G
G
G
G
G
G
G
G
G
G
G
G
G
G
G
G
G
H
H
H
H
H
H
H
I
J
J
1412
1413
1414
1415
1416
1417
1418
1419
1420
1421
1422
1423
1424
1425
1426
1427
1428
1429
1430
1431
1432
1433
1434
1435
1436
1437
1438
1439
1440
1441
1442
1443
1444
1445
1446
1447
1448
1449
1450
1451
1452
1453
1454
1455
1456
1457
1458
1459
1460
1461
1462
1463
1464
1465
1466
1467
1468
1469
1470
1471
1472
1473
1474
1475
1476
1477
1478
1479
1480
1481
1482
1483
1484
1485
1486
1487
1488
1489
1490
1491
1492
1493
1494
1495
1496
1497
1498
1499
1500
1501
1502
1503
1504
1505
1506
1507
1508
1509
1510
1511
1512
1513
1514
1515
1516
1517
1518
1519
1520
1521
1522
1523
1524
1525
1526
1527
1528
1529
1530
1531
1532
1533
1534
1535
1536
1537
1538
1539
1540
1541
1542
1543
1544
1545
1546
1547
1548
1549
1550
1551
1552
1553
1554
1555
1556
1557
1558
1559
1560
1561
1562
1563
1564
1565
1566
1567
1568
1569
1570
1571
1572
1573
1574
1575
1576
1577
1578
ARTICLEBR 1953 1–17
4 S. Moylan et al. / Neuroscience and B
iNOS, and sPLA2-IIA in patients with recurrent depressive disorder. J. Affect.Disord. 138, 360–366.
alecki, P., Maes, M., Florkowski, A., Lewinski, A., Galecka, E., Bienkiewicz, M.,Szemraj, J., 2011. Association between inducible and neuronal nitric oxide syn-thase polymorphisms and recurrent depressive disorder. J. Affect. Disord. 129,175–182.
alecki, P., Smigielski, J., Florkowski, A., Bobinska, K., Pietras, T., Szemraj, J., 2010.Analysis of two polymorphisms of the manganese superoxide dismutase gene(Ile-58Thr and Ala-9Val) in patients with recurrent depressive disorder. Psychi-atry Res. 179, 43–46.
alecki, P., Szemraj, J., Bienkiewicz, M., Florkowski, A., Galecka, E., 2009. Lipid perox-idation and antioxidant protection in patients during acute depressive episodesand in remission after fluoxetine treatment. Pharmacol. Rep. 61, 436–447.
alimov, E.R., Chernyak, B.V., Sidorenko, A.S., Tereshkova, A.V., Chumakov, P.M.,2014. Prooxidant properties of p66shc are mediated by mitochondria in humancells. PLoS ONE 9, e86521.
alitovskiy, V., Qian, J., Chernyavsky, A.I., Marchenko, S., Gindi, V., Edwards, R.A.,Grando, S.A., 2011. Cytokine-induced alterations of alpha7 nicotinic receptor incolonic CD4 T cells mediate dichotomous response to nicotine in murine modelsof Th1/Th17- versus Th2-mediated colitis. J. Immunol. 187, 2677–2687.
arate, I., Garcia-Bueno, B., Madrigal, J.L., Caso, J.R., Alou, L., Gomez-Lus, M.L., Mico,J.A., Leza, J.C., 2013. Stress-induced neuroinflammation: role of the Toll-likereceptor-4 pathway. Biol. Psychiatry 73, 32–43.
arcion, E., Wion-Barbot, N., Montero-Menei, C.N., Berger, F., Wion, D., 2002. Newclues about vitamin D functions in the nervous system. Trends Endocrinol.Metab. 13, 100–105.
ardner, A., Boles, R.G., 2011. Beyond the serotonin hypothesis: mitochondria,inflammation and neurodegeneration in major depression and affective spec-trum disorders. Prog. Neuropsychopharmacol. Biol. Psychiatry 35, 730–743.
eorge, N., Kumar, T.P., Antony, S., Jayanarayanan, S., Paulose, C.S., 2012. Effectof vitamin D3 in reducing metabolic and oxidative stress in the liver ofstreptozotocin-induced diabetic rats. Br. J. Nutr. 108, 1410–1418.
hanizadeh, A., Berk, M., 2013. Molecular hydrogen: an overview of its neurobio-logical effects and therapeutic potential for bipolar disorder and schizophrenia.Med. Gas Res. 3, 11.
oda, K., Hamane, Y., Kishimoto, R., Ogishi, Y., 1999. Radical scavenging propertiesof tryptophan metabolites. Estimation of their radical reactivity. Adv. Exp. Med.Biol. 467, 397–402.
oldstein, L.E., Leopold, M.C., Huang, X., Atwood, C.S., Saunders, A.J., Hartshorn, M.,Lim, J.T., Faget, K.Y., Muffat, J.A., Scarpa, R.C., Chylack Jr., L.T., Bowden, E.F., Tanzi,R.E., Bush, A.I., 2000. 3-Hydroxykynurenine and 3-hydroxyanthranilic acid gen-erate hydrogen peroxide and promote alpha-crystallin cross-linking by metalion reduction. Biochemistry 39, 7266–7275.
omes, E.C., Silva, A.N., de Oliveira, M.R., 2012. Oxidants, antioxidants, and the ben-eficial roles of exercise-induced production of reactive species. Oxid. Med. Cell.Longevity 2012, 756132.
radinaru, D., Borsa, C., Ionescu, C., Margina, D., Prada, G.I., Jansen, E., 2012. Vitamin Dstatus and oxidative stress markers in the elderly with impaired fasting glucoseand type 2 diabetes mellitus. Aging Clin. Exp. Res. 24, 595–602.
reen, D.R., Kroemer, G., 2004. The pathophysiology of mitochondrial cell death.Science 305, 626–629.
uidetti, P., Schwarcz, R., 1999. 3-Hydroxykynurenine potentiates quinolinate butnot NMDA toxicity in the rat striatum. Eur. J. Neurosci. 11, 3857–3863.
ulec, M., Ozkol, H., Selvi, Y., Tuluce, Y., Aydin, A., Besiroglu, L., Ozdemir, P.G., 2012.Oxidative stress in patients with primary insomnia. Prog. Neuropsychopharma-col. Biol. Psychiatry 37, 247–251.
ustafson, B., Gogg, S., Hedjazifar, S., Jenndahl, L., Hammarstedt, A., Smith, U., 2009.Inflammation and impaired adipogenesis in hypertrophic obesity in man. Am. J.Physiol. Endocrinol. Metab. 297, E999–E1003.
addad, J.J., 2000. Glutathione depletion is associated with augmenting aproinflammatory signal: evidence for an antioxidant/pro-oxidant mechanismregulating cytokines in the alveolar epithelium. Cytokines Cell. Mol. Ther. 6,177–187.
alaris, A., Meresh, E., Fareed, J., Hoppensteadt, D., Kimmons, S., Sinacore, J., 2012. 2.Tumor necrosis factor alpha as a biomarker in major depressive disorder. BrainBehav. Immun. 26 (Suppl. 1), S1.
ansel, B., Giral, P., Nobecourt, E., Chantepie, S., Bruckert, E., Chapman, M.J., Kon-tush, A., 2004. Metabolic syndrome is associated with elevated oxidative stressand dysfunctional dense high-density lipoprotein particles displaying impairedantioxidative activity. J. Clin. Endocrinol. Metab. 89, 4963–4971.
arris, M., Glozier, N., Ratnavadivel, R., Grunstein, R.R., 2009. Obstructive sleep apneaand depression. Sleep Med. Rev. 13, 437–444.
oustis, N., Rosen, E.D., Lander, E.S., 2006. Reactive oxygen species have a causal rolein multiple forms of insulin resistance. Nature 440, 944–948.
owren, M.B., Lamkin, D.M., Suls, J., 2009. Associations of depression with C-reactiveprotein, IL-1, and IL-6: a meta-analysis. Psychosom. Med. 71, 171–186.
vas, A.M., Juul, S., Bech, P., Nexo, E., 2004. Vitamin B6 level is associated withsymptoms of depression. Psychother. Psychosom. 73, 340–343.
rie, M., Asami, S., Nagata, S., Miyata, M., Kasai, H., 2001. Relationships betweenperceived workload, stress and oxidative DNA damage. Int. Arch. Occup. Environ.Health 74, 153–157.
Please cite this article in press as: Moylan, S., et al., Oxidative & nitrosatRev. (2014), http://dx.doi.org/10.1016/j.neubiorev.2014.05.007
acka, F.N., Maes, M., Pasco, J.A., Williams, L.J., Berk, M., 2012. Nutrient intakes andthe common mental disorders in women. J. Affect. Disord. 141, 79–85.
acka, F.N., Pasco, J.A., Williams, L.J., Leslie, E.R., Dodd, S., Nicholson, G.C., Kotowicz,M.A., Berk, M., 2010. Lower levels of physical activity in childhood associatedwith adult depression. J. Sci. Med. Sport 14, 222–226.
PRESSavioral Reviews xxx (2014) xxx–xxx
Jatuporn, S., Sangwatanaroj, S., Saengsiri, A.O., Rattanapruks, S., Srimahachota,S., Uthayachalerm, W., Kuanoon, W., Panpakdee, O., Tangkijvanich, P.,Tosukhowong, P., 2003. Short-term effects of an intensive lifestyle modifica-tion program on lipid peroxidation and antioxidant systems in patients withcoronary artery disease. Clin. Hemorheol. Microcirc. 29, 429–436.
Jelic, S., Padeletti, M., Kawut, S.M., Higgins, C., Canfield, S.M., Onat, D., Colombo,P.C., Basner, R.C., Factor, P., LeJemtel, T.H., 2008. Inflammation, oxidative stress,and repair capacity of the vascular endothelium in obstructive sleep apnea.Circulation 117, 2270–2278.
Jequier, E., 2002. Leptin signaling, adiposity, and energy balance. Ann. N.Y. Acad. Sci.967, 379–388.
Johnson, L.A., Phillips, J.A., Mauer, C., Edwards, M., Balldin, V.H., Hall, J.R., Barber, R.,Conger, T.L., Ho, E.J., O’Bryant, S.E., 2013. The impact of GPX1 on the associa-tion of groundwater selenium and depression: a Project FRONTIER study. BMCPsychiatry 13, 7.
Joseph, J.A., Shukitt-Hale, B., Denisova, N.A., Bielinski, D., Martin, A., McEwen, J.J.,Bickford, P.C., 1999. Reversals of age-related declines in neuronal signal trans-duction, cognitive, and motor behavioral deficits with blueberry, spinach, orstrawberry dietary supplementation. J. Neurosci. 19, 8114–8121.
Kaczmarek, A., Vandenabeele, P., Krysko, D.V., 2013. Necroptosis: the release ofdamage-associated molecular patterns and its physiological relevance. Immu-nity 38, 209–223.
Kennedy, D.O., Veasey, R., Watson, A., Dodd, F., Jones, E., Maggini, S., Haskell, C.F.,2010. Effects of high-dose B vitamin complex with vitamin C and minerals onsubjective mood and performance in healthy males. Psychopharmacology (Berl.)211, 55–68.
Kern, P.A., Saghizadeh, M., Ong, J.M., Bosch, R.J., Deem, R., Simsolo, R.B., 1995. Theexpression of tumor necrosis factor in human adipose tissue. Regulation byobesity, weight loss, and relationship to lipoprotein lipase. J. Clin. Invest. 95,2111–2119.
Khanzode, S.D., Dakhale, G.N., Khanzode, S.S., Saoji, A., Palasodkar, R., 2003. Oxida-tive damage and major depression: the potential antioxidant action of selectiveserotonin re-uptake inhibitors. Redox Rep. 8, 365–370.
Kjaergaard, M., Waterloo, K., Wang, C.E., Almas, B., Figenschau, Y., Hutchinson, M.S.,Svartberg, J., Jorde, R., 2012. Effect of vitamin D supplement on depression scoresin people with low levels of serum 25-hydroxyvitamin D: nested case-controlstudy and randomised clinical trial. Br. J. Psychiatry 201, 360–368.
Kubera, M., Obuchowicz, E., Goehler, L., Brzeszcz, J., Maes, M., 2011. In animal mod-els, psychosocial stress-induced (neuro)inflammation, apoptosis and reducedneurogenesis are associated to the onset of depression. Prog. Neuropsychophar-macol. Biol. Psychiatry 35, 744–759.
Lai, J., Moxey, A., Nowak, G., Vashum, K., Bailey, K., McEvoy, M., 2012. The effi-cacy of zinc supplementation in depression: systematic review of randomisedcontrolled trials. J. Affect. Disord. 136, e31–e39.
Lansdowne, A.T., Provost, S.C., 1998. Vitamin D3 enhances mood in healthy subjectsduring winter. Psychopharmacology (Berl.) 135, 319–323.
Lazarou, C., Kapsou, M., 2010. The role of folic acid in prevention and treatmentof depression: an overview of existing evidence and implications for practice.Complement. Ther. Clin. Pract. 16, 161–166.
LeBlanc, M., Merette, C., Savard, J., Ivers, H., Baillargeon, L., Morin, C.M., 2009. Inci-dence and risk factors of insomnia in a population-based sample. Sleep 32,1027–1037.
Lee, H., Lee, Y.J., Choi, H., Ko, E.H., Kim, J.W., 2009. Reactive oxygen species facilitateadipocyte differentiation by accelerating mitotic clonal expansion. J. Biol. Chem.284, 10601–10609.
Lee, P.H., Perlis, R.H., Jung, J.Y., Byrne, E.M., Rueckert, E., Siburian, R., Haddad, S.,Mayerfeld, C.E., Heath, A.C., Pergadia, M.L., Madden, P.A., Boomsma, D.I., Pen-ninx, B.W., Sklar, P., Martin, N.G., Wray, N.R., Purcell, S.M., Smoller, J.W., 2012.Multi-locus genome-wide association analysis supports the role of glutamater-gic synaptic transmission in the etiology of major depressive disorder. Transl.Psychiatry 2, e184.
Lee, S.Y., Lee, S.J., Han, C., Patkar, A.A., Masand, P.S., Pae, C.U., 2013. Oxida-tive/nitrosative stress and antidepressants: targets for novel antidepressants.Prog. Neuropsychopharmacol. Biol. Psychiatry 46, 224–235.
Lee, Y.J., Choi, B., Lee, E.H., Choi, K.S., Sohn, S., 2006. Immobilization stress inducescell death through production of reactive oxygen species in the mouse cerebralcortex. Neurosci. Lett. 392, 27–31.
Leipnitz, G., Schumacher, C., Dalcin, K.B., Scussiato, K., Solano, A., Funchal, C.,Dutra-Filho, C.S., Wyse, A.T., Wannmacher, C.M., Latini, A., Wajner, M., 2007.In vitro evidence for an antioxidant role of 3-hydroxykynurenine and 3-hydroxyanthranilic acid in the brain. Neurochem. Int. 50, 83–94.
Lenaz, G., 2001. The mitochondrial production of reactive oxygen species: mecha-nisms and implications in human pathology. IUBMB Life 52, 159–164.
Leo, R., Di Lorenzo, G., Tesauro, M., Cola, C., Fortuna, E., Zanasi, M., Troisi, A., Siracu-sano, A., Lauro, R., Romeo, F., 2006. Decreased plasma adiponectin concentrationin major depression. Neurosci. Lett. 407, 211–213.
Leonard, B., Maes, M., 2012. Mechanistic explanations how cell-mediated immuneactivation, inflammation and oxidative and nitrosative stress pathways and theirsequels and concomitants play a role in the pathophysiology of unipolar depres-sion. Neurosci. Biobehav. Rev. 36, 764–785.
Linneberg, A., Nielsen, N.H., Madsen, F., Frolund, L., Dirksen, A., Jorgensen, T., 2001.
ive stress in depression: Why so much stress? Neurosci. Biobehav.
Factors related to allergic sensitization to aeroallergens in a cross-sectionalstudy in adults: The Copenhagen Allergy Study. Clin. Exp. Allergy 31, 1409–1417.
Liu, J., Somera-Molina, K.C., Hudson, R.L., Dubocovich, M.L., 2013. Melatonin potenti-ates running wheel-induced neurogenesis in the dentate gyrus of adult C3H/HeNmice hippocampus. J. Pineal Res. 54, 222–231.
1579
1580
1581
1582
1583

ING ModelN
iobeh
L
L
L
L
L
L
L
M
M
M
M
M
M
M
M
M
M
M
M
M
M
M
M
Q8
1584
1585
1586
1587
1588
1589
1590
1591
1592
1593
1594
1595
1596
1597
1598
1599
1600
1601
1602
1603
1604
1605
1606
1607
1608
1609
1610
1611
1612
1613
1614
1615
1616
1617
1618
1619
1620
1621
1622
1623
1624
1625
1626
1627
1628
1629
1630
1631
1632
1633
1634
1635
1636
1637
1638
1639
1640
1641
1642
1643
1644
1645
1646
1647
1648
1649
1650
1651
1652
1653
1654
1655
1656
1657
1658
1659
1660
1661
1662
1663
1664
1665
1666
1667
1668
1669
1670
1671
1672
1673
1674
1675
1676
1677
1678
1679
1680
1681
1682
1683
1684
1685
1686
1687
1688
1689
1690
1691
1692
1693
1694
1695
1696
1697
1698
1699
1700
1701
1702
1703
1704
1705
1706
1707
1708
1709
1710
1711
1712
1713
1714
1715
1716
1717
1718
1719
1720
1721
1722
1723
1724
1725
1726
1727
1728
1729
1730
1731
1732
1733
1734
1735
1736
1737
1738
1739
1740
1741
1742
1743
1744
1745
1746
1747
1748
1749
1750
ARTICLEBR 1953 1–17
S. Moylan et al. / Neuroscience and B
obato, K.R., Cardoso, C.C., Binfare, R.W., Budni, J., Wagner, C.L., Brocardo, P.S., deSouza, L.F., Brocardo, C., Flesch, S., Freitas, A.E., Dafre, A.L., Rodrigues, A.L., 2010.Alpha-tocopherol administration produces an antidepressant-like effect in pre-dictive animal models of depression. Behav. Brain Res. 209, 249–259.
ogue, M.W., Baldwin, C., Guffanti, G., Melista, E., Wolf, E.J., Reardon, A.F., Uddin, M.,Wildman, D., Galea, S., Koenen, K.C., Miller, M.W., 2013. A genome-wide asso-ciation study of post-traumatic stress disorder identifies the retinoid-relatedorphan receptor alpha (RORA) gene as a significant risk locus. Mol. Psychiatry18, 937–942.
otze, M.T., Zeh, H.J., Rubartelli, A., Sparvero, L.J., Amoscato, A.A., Washburn,N.R., Devera, M.E., Liang, X., Tor, M., Billiar, T., 2007. The grateful dead:damage-associated molecular pattern molecules and reduction/oxidation reg-ulate immunity. Immunol. Rev. 220, 60–81.
uberto, C.M., White, C., Sears, R.W., Cotton, S., 2013. Integrative medicine for treat-ing depression: an update on the latest evidence. Curr. Psychiatry Rep. 15, 391.
ucas, K., Maes, M., 2013. Role of the Toll like receptor (TLR) radical cycle in chronicinflammation: possible treatments targeting the TLR4 pathway. Mol. Neurobiol.48, 190–204.
uchese, C., Pinton, S., Nogueira, C.W., 2009. Brain and lungs of rats are differentlyaffected by cigarette smoke exposure: antioxidant effect of an organoseleniumcompound. Pharmacol. Res. 59, 194–201.
uppino, F.S., de Wit, L.M., Bouvy, P.F., Stijnen, T., Cuijpers, P., Penninx, B.W., Zitman,F.G., 2010. Overweight, obesity, and depression: a systematic review and meta-analysis of longitudinal studies. Arch. Gen. Psychiatry 67, 220–229.
aes, M., Christophe, A., Delanghe, J., Altamura, C., Neels, H., Meltzer, H.Y., 1999.Lowered omega3 polyunsaturated fatty acids in serum phospholipids andcholesteryl esters of depressed patients. Psychiatry Res. 85, 275–291.
aes, M., D’Haese, P.C., Scharpe, S., D’Hondt, P., Cosyns, P., De Broe, M.E., 1994.Hypozincemia in depression. J. Affect. Disord. 31, 135–140.
aes, M., De Vos, N., Pioli, R., Demedts, P., Wauters, A., Neels, H., Christophe, A., 2000.Lower serum vitamin E concentrations in major depression. Another marker oflowered antioxidant defenses in that illness. J. Affect. Disord. 58, 241–246.
aes, M., Delange, J., Ranjan, R., Meltzer, H.Y., Desnyder, R., Cooremans, W., Scharpe,S., 1997a. Acute phase proteins in schizophrenia, mania and major depression:modulation by psychotropic drugs. Psychiatry Res. 66, 1–11.
aes, M., Fisar, Z., Medina, M., Scapagnini, G., Nowak, G., Berk, M., 2012a. Newdrug targets in depression: inflammatory, cell-mediated immune, oxidative andnitrosative stress, mitochondrial, antioxidant, and neuroprogressive pathways.And new drug candidates–Nrf2 activators and GSK-3 inhibitors. Inflammophar-macology 20, 127–150.
aes, M., Galecki, P., Chang, Y.S., Berk, M., 2011a. A review on the oxidative andnitrosative stress (O&NS) pathways in major depression and their possiblecontribution to the (neuro)degenerative processes in that illness. Prog. Neu-ropsychopharmacol. Biol. Psychiatry 35, 676–692.
aes, M., Kubera, M., Leunis, J.C., 2008a. The gut-brain barrier in major depression:intestinal mucosal dysfunction with an increased translocation of LPS from gramnegative enterobacteria (leaky gut) plays a role in the inflammatory pathophys-iology of depression. Neuroendocrinol. Lett. 29, 117–124.
aes, M., Kubera, M., Leunis, J.C., Berk, M., 2012b. Increased IgA and IgM responsesagainst gut commensals in chronic depression: further evidence for increasedbacterial translocation or leaky gut. J. Affect. Disord. 141, 55–62.
aes, M., Kubera, M., Leunis, J.C., Berk, M., Geffard, M., Bosmans, E., 2013a. In depres-sion, bacterial translocation may drive inflammatory responses, oxidative andnitrosative stress (O&NS), and autoimmune responses directed against O&NS-damaged neoepitopes. Acta Psychiatr. Scand. 127, 344–354.
aes, M., Kubera, M., Mihaylova, I., Geffard, M., Galecki, P., Leunis, J.C., Berk, M.,2013b. Increased autoimmune responses against auto-epitopes modified byoxidative and nitrosative damage in depression: implications for the pathwaysto chronic depression and neuroprogression. J. Affect. Disord. 149, 23–29.
aes, M., Kubera, M., Obuchowiczwa, E., Goehler, L., Brzeszcz, J., 2011b. Depres-sion’s multiple comorbidities explained by (neuro)inflammatory and oxidative& nitrosative stress pathways. Neuroendocrinol. Lett. 32, 7–24.
aes, M., Leonard, B.E., Myint, A.M., Kubera, M., Verkerk, R., 2011c. The new‘5-HT’ hypothesis of depression: cell-mediated immune activation inducesindoleamine 2,3-dioxygenase, which leads to lower plasma tryptophan and anincreased synthesis of detrimental tryptophan catabolites (TRYCATs), both ofwhich contribute to the onset of depression. Prog. Neuropsychopharmacol. Biol.Psychiatry 35, 702–721.
aes, M., Meltzer, H.Y., Scharpe, S., Bosmans, E., Suy, E., De Meester, I., Cal-abrese, J., Cosyns, P., 1993. Relationships between lower plasma l-tryptophanlevels and immune-inflammatory variables in depression. Psychiatry Res. 49,151–165.
aes, M., Mihaylova, I., Kubera, M., Leunis, J.C., 2008b. An IgM-mediated immuneresponse directed against nitro-bovine serum albumin (nitro-BSA) in chronicfatigue syndrome (CFS) and major depression: evidence that nitrosative stressis another factor underpinning the comorbidity between major depression andCFS. Neuroendocrinol. Lett. 29, 313–319.
aes, M., Mihaylova, I., Kubera, M., Leunis, J.C., Geffard, M., 2011d. IgM-mediatedautoimmune responses directed against multiple neoepitopes in depression:new pathways that underpin the inflammatory and neuroprogressive patho-physiology. J. Affect. Disord. 135, 414–418.
Please cite this article in press as: Moylan, S., et al., Oxidative & nitrosatRev. (2014), http://dx.doi.org/10.1016/j.neubiorev.2014.05.007
aes, M., Mihaylova, I., Leunis, J.C., 2007. Increased serum IgM antibodies directedagainst phosphatidyl inositol (Pi) in chronic fatigue syndrome (CFS) and majordepression: evidence that an IgM-mediated immune response against Pi is onefactor underpinning the comorbidity between both CFS and depression. Neu-roendocrinol. Lett. 28, 861–867.
PRESSavioral Reviews xxx (2014) xxx–xxx 15
Maes, M., Ruckoanich, P., Chang, Y.S., Mahanonda, N., Berk, M., 2011e. Multipleaberrations in shared inflammatory and oxidative & nitrosative stress (IO&NS)pathways explain the co-association of depression and cardiovascular disorder(CVD), and the increased risk for CVD and due mortality in depressed patients.Prog. Neuropsychopharmacol. Biol. Psychiatry 35, 769–783.
Maes, M., Vandoolaeghe, E., Neels, H., Demedts, P., Wauters, A., Meltzer, H.Y., Alta-mura, C., Desnyder, R., 1997b. Lower serum zinc in major depression is a sensitivemarker of treatment resistance and of the immune/inflammatory response inthat illness. Biol. Psychiatry 42, 349–358.
Manda, K., Bhatia, A.L., 2003. Prophylactic action of melatonin againstcyclophosphamide-induced oxidative stress in mice. Cell Biol. Toxicol.19, 367–372.
Maritim, A.C., Sanders, R.A., Watkins 3rd., J.B., 2003. Diabetes, oxidative stress, andantioxidants: a review. J. Biochem. Mol. Toxicol. 17, 24–38.
Martinsson, L., Wei, Y., Xu, D., Melas, P.A., Mathe, A.A., Schalling, M., Lavebratt, C.,Backlund, L., 2013. Long-term lithium treatment in bipolar disorder is associatedwith longer leukocyte telomeres. Transl. Psychiatry 3, e261.
Mather, A.S., Rodriguez, C., Guthrie, M.F., McHarg, A.M., Reid, I.C., McMurdo, M.E.,2002. Effects of exercise on depressive symptoms in older adults with poorlyresponsive depressive disorder: randomised controlled trial. Br. J. Psychiatry180, 411–415.
Mayer, E.A., 2011. Gut feelings: the emerging biology of gut-brain communication.Nat. Rev. Neurosci. 12, 453–466.
McCall, W.V., Harding, D., O’Donovan, C., 2006. Correlates of depressive symptomsin patients with obstructive sleep apnea. J. Clin. Sleep Med. 2, 424–426.
McLoughlin, I.J., Hodge, J.S., 1990. Zinc in depressive disorder. Acta Psychiatr. Scand.82, 451–453.
Metin, G., Atukeren, P., Alturfan, A.A., Gulyasar, T., Kaya, M., Gumustas, M.K., 2003.Lipid peroxidation, erythrocyte superoxide-dismutase activity and trace metalsin young male footballers. Yonsei Med. J. 44, 979–986.
Miller, M.W., Wolf, E.J., Logue, M.W., Baldwin, C.T., 2013. The retinoid-related orphanreceptor alpha (RORA) gene and fear-related psychopathology. J. Affect. Disord.151, 702–708.
Millman, R.P., Fogel, B.S., McNamara, M.E., Carlisle, C.C., 1989. Depression as a man-ifestation of obstructive sleep apnea: reversal with nasal continuous positiveairway pressure. J. Clin. Psychiatry 50, 348–351.
Moretti, M., Colla, A., de Oliveira Balen, G., dos Santos, D.B., Budni, J., de Freitas, A.E.,Farina, M., Severo Rodrigues, A.L., 2012. Ascorbic acid treatment, similarly to flu-oxetine, reverses depressive-like behavior and brain oxidative damage inducedby chronic unpredictable stress. J. Psychiatr. Res. 46, 331–340.
Morimoto, K., Morikawa, M., Kimura, H., Ishii, N., Takamata, A., Hara, Y., Uji, M.,Yoshida, K., 2008. Mental stress induces sustained elevation of blood pressureand lipid peroxidation in postmenopausal women. Life Sci. 82, 99–107.
Morris, G., Maes, M., 2013. Mitochondrial dysfunctions in myalgic encephalomyeli-tis/chronic fatigue syndrome explained by activated immuno-inflammatory,oxidative and nitrosative stress pathways. Metab. Brain Dis., 1–18.
Morrison, C.D., Pistell, P.J., Ingram, D.K., Johnson, W.D., Liu, Y., Fernandez-Kim, S.O.,White, C.L., Purpera, M.N., Uranga, R.M., Bruce-Keller, A.J., Keller, J.N., 2010.High fat diet increases hippocampal oxidative stress and cognitive impairmentin aged mice: implications for decreased Nrf2 signaling. J. Neurochem. 114,1581–1589.
Moylan, S., Eyre, H.A., Maes, M., Baune, B.T., Jacka, F.N., Berk, M., 2013a. Exercising theworry away: how inflammation, oxidative and nitrogen stress mediates the ben-eficial effect of physical activity on anxiety disorder symptoms and behaviours.Neurosci. Biobehav. Rev. 37, 573–584.
Moylan, S., Jacka, F.N., Pasco, J.A., Berk, M., 2012. Cigarette smoking, nicotinedependence and anxiety disorders: a systematic review of population-based,epidemiological studies. BMC Med. 10, 123.
Moylan, S., Jacka, F.N., Pasco, J.A., Berk, M., 2013b. How cigarette smoking mayincrease the risk of anxiety symptoms and anxiety disorders: a critical reviewof biological pathways. Brain Behav. 3, 302–326.
Moylan, S., Maes, M., Wray, N.R., Berk, M., 2013c. The neuroprogressive nature ofmajor depressive disorder: pathways to disease evolution and resistance, andtherapeutic implications. Mol. Psychiatry 18, 595–606.
Murakami, K., Haneda, M., Yoshino, M., 2006. Prooxidant action of xanthurenic acidand quinoline compounds: role of transition metals in the generation of reac-tive oxygen species and enhanced formation of 8-hydroxy-2’-deoxyguanosinein DNA. Biometals 19, 429–435.
Murphy, T.H., Miyamoto, M., Sastre, A., Schnaar, R.L., Coyle, J.T., 1989. Glutamatetoxicity in a neuronal cell line involves inhibition of cystine transport leading tooxidative stress. Neuron 2, 1547–1558.
Nair-Shalliker, V., Armstrong, B.K., Fenech, M., 2012. Does vitamin D protect againstDNA damage? Mutat. Res. 733, 50–57.
Nanri, A., Hayabuchi, H., Ohta, M., Sato, M., Mishima, N., Mizoue, T., 2012. Serumfolate and depressive symptoms among Japanese men and women: a cross-sectional and prospective study. Psychiatry Res. 200, 349–353.
Neckelmann, D., Mykletun, A., Dahl, A.A., 2007. Chronic insomnia as a risk factor fordeveloping anxiety and depression. Sleep 30, 873–880.
Newman, M.B., Arendash, G.W., Shytle, R.D., Bickford, P.C., Tighe, T., Sanberg, P.R.,2002. Nicotine’s oxidative and antioxidant properties in CNS. Life Sci. 71,2807–2820.
ive stress in depression: Why so much stress? Neurosci. Biobehav.
Niu, K., Guo, H., Kakizaki, M., Cui, Y., Ohmori-Matsuda, K., Guan, L., Hozawa, A.,Kuriyama, S., Tsuboya, T., Ohrui, T., Furukawa, K., Arai, H., Tsuji, I., Nagatomi, R.,2013. A tomato-rich diet is related to depressive symptoms among an elderlypopulation aged 70 years and over: a population-based, cross-sectional analysis.J. Affect. Disord. 144, 165–170.
1751
1752
1753
1754
1755

ING ModelN
1 iobeh
N
O
O
O
O
O
P
P
P
P
P
P
P
P
P
P
P
P
P
P
P
Q
Q
R
R
R
R
R
R
1756
1757
1758
1759
1760
1761
1762
1763
1764
1765
1766
1767
1768
1769
1770
1771
1772
1773
1774
1775
1776
1777
1778
1779
1780
1781
1782
1783
1784
1785
1786
1787
1788
1789
1790
1791
1792
1793
1794
1795
1796
1797
1798
1799
1800
1801
1802
1803
1804
1805
1806
1807
1808
1809
1810
1811
1812
1813
1814
1815
1816
1817
1818
1819
1820
1821
1822
1823
1824
1825
1826
1827
1828
1829
1830
1831
1832
1833
1834
1835
1836
1837
1838
1839
1840
1841
1842
1843
1844
1845
1846
1847
1848
1849
1850
1851
1852
1853
1854
1855
1856
1857
1858
1859
1860
1861
1862
1863
1864
1865
1866
1867
1868
1869
1870
1871
1872
1873
1874
1875
1876
1877
1878
1879
1880
1881
1882
1883
1884
1885
1886
1887
1888
1889
1890
1891
1892
1893
1894
1895
1896
1897
1898
1899
1900
1901
1902
1903
1904
1905
1906
1907
1908
1909
1910
1911
1912
1913
1914
1915
1916
1917
1918
1919
1920
1921
1922
ARTICLEBR 1953 1–17
6 S. Moylan et al. / Neuroscience and B
owson, C.A., McGrath, J.J., Ebeling, P.R., Haikerwal, A., Daly, R.M., Sanders, K.M.,Seibel, M.J., Mason, R.S., Working Group of: A., New Zealand, B., Mineral Society,E.S.o.A., Osteoporosis, A., 2012. Vitamin D and health in adults in Australia andNew Zealand: a position statement. Med. J. Aust. 196, 686–687.
kuda, S., Nishiyama, N., Saito, H., Katsuki, H., 1998. 3-Hydroxykynurenine, anendogenous oxidative stress generator, causes neuronal cell death with apop-totic features and region selectivity. J. Neurochem. 70, 299–307.
pitz, C.A., Litzenburger, U.M., Sahm, F., Ott, M., Tritschler, I., Trump, S., Schumacher,T., Jestaedt, L., Schrenk, D., Weller, M., Jugold, M., Guillemin, G.J., Miller, C.L., Lutz,C., Radlwimmer, B., Lehmann, I., von Deimling, A., Wick, W., Platten, M., 2011. Anendogenous tumour-promoting ligand of the human aryl hydrocarbon receptor.Nature 478, 197–203.
rganisation, W.H., 2002. World Health Report. World Health Organistion Press,Switzerland.
wen, A.J., Batterham, M.J., Probst, Y.C., Grenyer, B.F., Tapsell, L.C., 2005. Low plasmavitamin E levels in major depression: diet or disease? Eur. J. Clin. Nutr. 59,304–306.
zkan, Y., Firat, H., Simsek, B., Torun, M., Yardim-Akaydin, S., 2008. Circulating nitricoxide (NO), asymmetric dimethylarginine (ADMA), homocysteine, and oxidativestatus in obstructive sleep apnea-hypopnea syndrome (OSAHS). Sleep Breath.12, 149–154.
an, A., Sun, Q., Czernichow, S., Kivimaki, M., Okereke, O.I., Lucas, M., Manson, J.E.,Ascherio, A., Hu, F.B., 2012. Bidirectional association between depression andobesity in middle-aged and older women. Int. J. Obes. 36, 595–602.
arletta, N., Milte, C.M., Meyer, B.J., 2013. Nutritional modulation of cognitive func-tion and mental health. J. Nutr. Biochem. 24, 725–743.
asco, J.A., Henry, M.J., Nicholson, G.C., Sanders, K.M., Kotowicz, M.A., 2001. VitaminD status of women in the Geelong Osteoporosis Study: association with diet andcasual exposure to sunlight. Med. J. Aust. 175, 401–405.
asco, J.A., Jacka, F.N., Williams, L.J., Evans-Cleverdon, M., Brennan, S.L., Kotowicz,M.A., Nicholson, G.C., Ball, M.J., Berk, M., 2012. Dietary selenium and majordepression: a nested case–control study. Complement. Ther. Med. 20, 119–123.
asco, J.A., Jacka, F.N., Williams, L.J., Henry, M.J., Nicholson, G.C., Kotowicz, M.A.,Berk, M., 2008a. Leptin in depressed women: cross-sectional and longitudinaldata from an epidemiologic study. J. Affect. Disord. 107, 221–225.
asco, J.A., Nicholson, G.C., Williams, L.J., Jacka, F.N., Henry, M.J., Kotowicz, M.A.,Schneider, H.G., Leonard, B.E., Berk, M., 2010. Association of high-sensitivity C-reactive protein with de novo major depression. Br. J. Psychiatry 197, 372–377.
asco, J.A., Williams, L.J., Jacka, F.N., Brennan, S.L., Berk, M., 2013. Obesity andthe relationship with positive and negative affect. Aust. N.Z. J. Psychiatry 47,477–482.
asco, J.A., Williams, L.J., Jacka, F.N., Henry, M.J., Coulson, C.E., Brennan, S.L., Leslie,E., Nicholson, G.C., Kotowicz, M.A., Berk, M., 2011. Habitual physical activity andthe risk for depressive and anxiety disorders among older men and women. Int.Psychogeriatr. 23, 292–298.
asco, J.A., Williams, L.J., Jacka, F.N., Ng, F., Henry, M.J., Nicholson, G.C., Kotowicz,M.A., Berk, M., 2008b. Tobacco smoking as a risk factor for major depressivedisorder: population-based study. Br. J. Psychiatry 193, 322–326.
athak, L., Agrawal, Y., Dhir, A., 2013. Natural polyphenols in the management ofmajor depression. Expert Opin. Invest. Drugs 22, 863–880.
eet, M., Murphy, B., Shay, J., Horrobin, D., 1998. Depletion of omega-3 fatty acidlevels in red blood cell membranes of depressive patients. Biol. Psychiatry 43,315–319.
eng, T., Lu, X., Feng, Q., 2005. NADH oxidase signaling induces cyclooxygenase-2expression during lipopolysaccharide stimulation in cardiomyocytes. FASEB J.19, 293–295.
erlis, M.L., Giles, D.E., Buysse, D.J., Tu, X., Kupfer, D.J., 1997. Self-reported sleepdisturbance as a prodromal symptom in recurrent depression. J. Affect. Disord.42, 209–212.
ertsov, S.S., Balashova, T.S., Kubatieva, A.A., Sosnovskii, A.S., Pirogova, G.V.,Abramov, V.M., 1995. Lipid peroxidation and antioxidant enzymes in rat brain inacute emotional stress: effect of interleukin-1beta. Biulleten’ eksperimental’noibiologii i meditsiny 120, 244–247.
hillips, A.C., Robertson, T., Carroll, D., Der, G., Shiels, P.G., McGlynn, L., Benzeval, M.,2013. Do symptoms of depression predict telomere length? Evidence from thewest of Scotland twenty-07 study. Psychosom. Med. 75, 288–296.
uan, Z.F., Yang, C., Li, N., Li, J.S., 2004. Effect of glutamine on change in earlypostoperative intestinal permeability and its relation to systemic inflammatoryresponse. World J. Gastroenterol. 10, 1992–1994.
uik, M., Perez, X.A., Bordia, T., 2012. Nicotine as a potential neuroprotective agentfor Parkinson’s disease. Mov. Disord. 27, 947–957.
eiter, R.J., Paredes, S.D., Manchester, L.C., Tan, D.X., 2009. Reducing oxida-tive/nitrosative stress: a newly-discovered genre for melatonin. Crit. Rev.Biochem. Mol. Biol. 44, 175–200.
eiter, R.J., Tan, D.X., Manchester, L.C., Pilar Terron, M., Flores, L.J., Koppisepi, S.,2007. Medical implications of melatonin: receptor-mediated and receptor-independent actions. Adv. Med. Sci. 52, 11–28.
en, S., Correia, M.A., 2000. Heme: a regulator of rat hepatic tryptophan 2,3-dioxygenase? Arch. Biochem. Biophys. 377, 195–203.
ief, W., Pilger, F., Ihle, D., Bosmans, E., Egyed, B., Maes, M., 2001. Immunological dif-ferences between patients with major depression and somatization syndrome.
Please cite this article in press as: Moylan, S., et al., Oxidative & nitrosatRev. (2014), http://dx.doi.org/10.1016/j.neubiorev.2014.05.007
Psychiatry Res. 105, 165–174.imer, J., Dwan, K., Lawlor, D.A., Greig, C.A., McMurdo, M., Morley, W., Mead, G.E.,
2012. Exercise for depression. Cochrane Database Syst. Rev. 7, CD004366.ios, C., Santamaria, A., 1991. Quinolinic acid is a potent lipid peroxidant in rat brain
homogenates. Neurochem. Res. 16, 1139–1143.
PRESSavioral Reviews xxx (2014) xxx–xxx
Rubartelli, A., Lotze, M.T., 2007. Inside, outside, upside down: damage-associatedmolecular-pattern molecules (DAMPs) and redox. Trends Immunol. 28,429–436.
Ryo, M., Nakamura, T., Kihara, S., Kumada, M., Shibazaki, S., Takahashi, M., Nagai, M.,Matsuzawa, Y., Funahashi, T., 2004. Adiponectin as a biomarker of the metabolicsyndrome. Circ. J. 68, 975–981.
Sagatun, A., Sogaard, A.J., Bjertness, E., Selmer, R., Heyerdahl, S., 2007. The associa-tion between weekly hours of physical activity and mental health: a three-yearfollow-up study of 15–16-year-old students in the city of Oslo, Norway. BMCPublic Health 7, 155.
Sanacora, G., Rothman, D.L., Mason, G., Krystal, J.H., 2003. Clinical studies imple-menting glutamate neurotransmission in mood disorders. Ann. N.Y. Acad. Sci.1003, 292–308.
Sanchez-Villegas, A., Martinez-Gonzalez, M.A., Estruch, R., Salas-Salvado, J., Corella,D., Covas, M.I., Aros, F., Romaguera, D., Gomez-Gracia, E., Lapetra, J., Pinto, X.,Martinez, J.A., Lamuela-Raventos, R.M., Ros, E., Gea, A., Warnberg, J., Serra-Majem, L., 2013. Mediterranean dietary pattern and depression: the PREDIMEDrandomized trial. BMC Med. 11, 208.
Sanders, K.M., Stuart, A.L., Williamson, E.J., Jacka, F.N., Dodd, S., Nicholson, G., Berk,M., 2011. Annual high-dose vitamin D3 and mental well-being: randomisedcontrolled trial. Br. J. Psychiatry 198, 357–364.
Sankhla, M., Sharma, T.K., Mathur, K., Rathor, J.S., Butolia, V., Gadhok, A.K., Vardey,S.K., Sinha, M., Kaushik, G.G., 2012. Relationship of oxidative stress withobesity and its role in obesity induced metabolic syndrome. Clin. Lab. 58,385–392.
Santamaria, A., Galvan-Arzate, S., Lisy, V., Ali, S.F., Duhart, H.M., Osorio-Rico, L.,Rios, C., St’astny, F., 2001. Quinolinic acid induces oxidative stress in rat brainsynaptosomes. Neuroreport 12, 871–874.
Scapagnini, G., Davinelli, S., Drago, F., De Lorenzo, A., Oriani, G., 2012. Antioxidantsas antidepressants: fact or fiction? CNS Drugs 26, 477–490.
Schroder, C.M., O’Hara, R., 2005. Depression and obstructive sleep apnea (OSA). Ann.Gen. Psychiatry 4, 13.
Schubert, D., Piasecki, D., 2001. Oxidative glutamate toxicity can be a component ofthe excitotoxicity cascade. J. Neurosci. 21, 7455–7462.
Shalev, I., Moffitt, T.E., Braithwaite, A.W., Danese, A., Fleming, N.I., Goldman-Mellor,S., Harrington, H.L., Houts, R.M., Israel, S., Poulton, R., Robertson, S.P., Sugden,K., Williams, B., Caspi, A., 2014. Internalizing disorders and leukocyte telomereerosion: a prospective study of depression, generalized anxiety disorder andpost-traumatic stress disorder. Mol. Psychiatry.
Sivonova, M., Zitnanova, I., Hlincikova, L., Skodacek, I., Trebaticka, J., Durackova,Z., 2004. Oxidative stress in university students during examinations. Stress 7,183–188.
Skarupski, K.A., Tangney, C., Li, H., Ouyang, B., Evans, D.A., Morris, M.C., 2010. Lon-gitudinal association of vitamin B-6, folate, and vitamin B-12 with depressivesymptoms among older adults over time. Am. J. Clin. Nutr. 92, 330–335.
Smith, A.J., Smith, R.A., Stone, T.W., 2009. 5-Hydroxyanthranilic acid, a tryptophanmetabolite, generates oxidative stress and neuronal death via p38 activation incultured cerebellar granule neurones. Neurotox. Res. 15, 303–310.
Solin, M.S., Ball, M.J., Robertson, I., de Silva, A., Pasco, J.A., Kotowicz, M.A., Nicholson,G.C., Collier, G.R., 1997. Relationship of serum leptin to total and truncal bodyfat. Clin. Sci. 93, 581–584.
Song, C., Lin, A., Bonaccorso, S., Heide, C., Verkerk, R., Kenis, G., Bosmans, E., Scharpe,S., Whelan, A., Cosyns, P., de Jongh, R., Maes, M., 1998. The inflammatory responsesystem and the availability of plasma tryptophan in patients with primary sleepdisorders and major depression. J. Affect. Disord. 49, 211–219.
Sosnovskii, A.S., Kozlov, A.V., 1992. Increased lipid peroxidation in the rat hypotha-lamus after short-term emotional stress. Biulleten’ eksperimental’noi biologii imeditsiny 113, 486–488.
Sperner-Unterweger, B., Kohl, C., Fuchs, D., 2014. Immune changes and neurotrans-mitters: possible interactions in depression? Prog. Neuropsychopharmacol. Biol.Psychiatry 48, 268–276.
Stangherlin, E.C., Luchese, C., Ardais, A.P., Nogueira, C.W., 2009. Passive smoke expo-sure induces oxidative damage in brains of rat pups: protective role of diphenyldiselenide. Inhal. Toxicol. 21, 868–874.
Stedman, R.L., 1968. The chemical composition of tobacco and tobacco smoke. Chem.Rev. 68, 153–207.
Strawbridge, W.J., Deleger, S., Roberts, R.E., Kaplan, G.A., 2002. Physical activityreduces the risk of subsequent depression for older adults. Am. J. Epidemiol.156, 328–334.
Szewczyk, B., Kubera, M., Nowak, G., 2011. The role of zinc in neurodegenerativeinflammatory pathways in depression. Prog. Neuropsychopharmacol. Biol. Psy-chiatry 35, 693–701.
Taylor, D.J., Lichstein, K.L., Durrence, H.H., Reidel, B.W., Bush, A.J., 2005. Epidemiologyof insomnia, depression, and anxiety. Sleep 28, 1457–1464.
Taylor, M.J., Carney, S.M., Goodwin, G.M., Geddes, J.R., 2004. Folate for depressivedisorders: systematic review and meta-analysis of randomized controlled trials.J. Psychopharmacol. (Oxf.) 18, 251–256.
Teychenne, M., Ball, K., Salmon, J., 2008. Physical activity and likelihood of depressionin adults: a review. Prev. Med. 46, 397–411.
Thome, G.R., Spanevello, R.M., Mazzanti, A., Fiorenza, A.M., Duarte, M.M., da Luz,S.C., Pereira, M.E., Morsch, V.M., Schetinger, M.R., Mazzanti, C.M., 2011. Vitamin
ive stress in depression: Why so much stress? Neurosci. Biobehav.
E decreased the activity of acetylcholinesterase and level of lipid peroxidationin brain of rats exposed to aged and diluted sidestream smoke. Nicotine TobaccoRes. 13, 1210–1219.
Todar, K., 2006. Todar’s Online Textbook of Bacteriology. University of Wisconsin-Madison Department of Bacteriology.
1923
1924
1925
1926
1927

ING ModelN
iobeh
T
T
T
T
T
T
U
U
V
V
V
W
W
W
severe burns: a randomized, double-blind, controlled clinical trial. J. ParenteralEnteral Nutr. 27, 241–245.
Zhu, W.L., Shi, H.S., Wei, Y.M., Wang, S.J., Sun, C.Y., Ding, Z.B., Lu, L., 2012. Green tea
1928
1929
1930
1931
1932
1933
1934
1935
1936
1937
1938
1939
1940
1941
1942
1943
1944
1945
1946
1947
1948
1949
1950
1951
1952
1953
1954
1955
1956
1957
1958
1959
1960
1961
1962
1963
1964
1965
1966
1967
1968
1969
1970
1971
1972
1973
1974
1975
1976
1977
1978
1979
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
2017
2018
2019
ARTICLEBR 1953 1–17
S. Moylan et al. / Neuroscience and B
olmunen, T., Hintikka, J., Ruusunen, A., Voutilainen, S., Tanskanen, A., Valkonen,V.P., Viinamaki, H., Kaplan, G.A., Salonen, J.T., 2004. Dietary folate and the riskof depression in Finnish middle-aged men. A prospective follow-up study. Psy-chother. Psychosom. 73, 334–339.
suboi, H., Tatsumi, A., Yamamoto, K., Kobayashi, F., Shimoi, K., Kinae, N., 2006. Pos-sible connections among job stress, depressive symptoms, lipid modulation andantioxidants. J. Affect. Disord. 91, 63–70.
sukamoto, H., Fukudome, K., Takao, S., Tsuneyoshi, N., Kimoto, M., 2010.Lipopolysaccharide-binding protein-mediated Toll-like receptor 4 dimerizationenables rapid signal transduction against lipopolysaccharide stimulation onmembrane-associated CD14-expressing cells. Int. Immunol. 22, 271–280.
suno, N., Besset, A., Ritchie, K., 2005. Sleep and depression. J. Clin. psychiatry 66,1254–1269.
uon, T., Valvassori, S.S., Lopes-Borges, J., Fries, G.R., Silva, L.A., Kapczinski, F.,Quevedo, J., Pinho, R.A., 2010. Effects of moderate exercise on cigarette smokeexposure-induced hippocampal oxidative stress values and neurological behav-iors in mice. Neurosci. Lett. 475, 16–19.
yagi, E., Agrawal, R., Nath, C., Shukla, R., 2010. Effect of melatonin on neuroin-flammation and acetylcholinesterase activity induced by LPS in rat brain. Eur. J.Pharmacol. 640, 206–210.
chida, K., 2013. Redox-derived damage-associated molecular patterns: ligandfunction of lipid peroxidation adducts. Redox Biol. 1, 94–96.
her, R., Perroud, N., Ng, M.Y., Hauser, J., Henigsberg, N., Maier, W., Mors, O., Pla-centino, A., Rietschel, M., Souery, D., Zagar, T., Czerski, P.M., Jerman, B., Larsen,E.R., Schulze, T.G., Zobel, A., Cohen-Woods, S., Pirlo, K., Butler, A.W., Muglia, P.,Barnes, M.R., Lathrop, M., Farmer, A., Breen, G., Aitchison, K.J., Craig, I., Lewis,C.M., McGuffin, P., 2010. Genome-wide pharmacogenetics of antidepressantresponse in the GENDEP project. Am. J. Psychiatry 167, 555–564.
an Hunsel, F., Wauters, A., Vandoolaeghe, E., Neels, H., Demedts, P., Maes, M., 1996.Lower total serum protein, albumin, and beta- and gamma-globulin in majorand treatment-resistant depression: effects of antidepressant treatments. Psy-chiatry Res. 65, 159–169.
argas, H.O., Nunes, S.O., Pizzo de Castro, M., Cristina Bortolasci, C., Sabbatini Bar-bosa, D., Kaminami Morimoto, H., Venugopal, K., Dodd, S., Maes, M., Berk, M.,2013. Oxidative stress and lowered total antioxidant status are associated witha history of suicide attempts. J. Affect. Disord. 150, 923–930.
olna, J., Kemlink, D., Kalousova, M., Vavrova, J., Majerova, V., Mestek, O., Svar-cova, J., Sonka, K., Zima, T., 2011. Biochemical oxidative stress-related markersin patients with obstructive sleep apnea. Med. Sci. Monitor 17, CR491–CR497.
ang, C., Wu, H.M., Jing, X.R., Meng, Q., Liu, B., Zhang, H., Gao, G.D., 2012. Oxidativeparameters in the rat brain of chronic mild stress model for depression: relationto anhedonia-like responses. J. Membr. Biol. 245, 675–681.
ang, D.W., Zhou, R.B., Yao, Y.M., Zhu, X.M., Yin, Y.M., Zhao, G.J., Dong, N., Sheng,Z.Y., 2010. Stimulation of alpha7 nicotinic acetylcholine receptor by nicotine
Please cite this article in press as: Moylan, S., et al., Oxidative & nitrosatRev. (2014), http://dx.doi.org/10.1016/j.neubiorev.2014.05.007
increases suppressive capacity of naturally occurring CD4+CD25+ regulatory Tcells in mice in vitro. J. Pharmacol. Exp. Therapeut. 335, 553–561.
erner, E.R., Werner-Felmayer, G., 2007. Substrate and cofactor requirements ofindoleamine 2,3-dioxygenase in interferon-gamma-treated cells: utilization ofoxygen rather than superoxide. Curr. Drug Metab. 8, 201–203.
PRESSavioral Reviews xxx (2014) xxx–xxx 17
Wiest, R., 2005. Bacterial translocation. Biosci. Microflora 24, 61–90.Wiest, R., Garcia-Tsao, G., 2005. Bacterial translocation (BT) in cirrhosis. Hepatology
41, 422–433.Williams, C.M., El Mohsen, M.A., Vauzour, D., Rendeiro, C., Butler, L.T., Ellis, J.A.,
Whiteman, M., Spencer, J.P., 2008. Blueberry-induced changes in spatial work-ing memory correlate with changes in hippocampal CREB phosphorylationand brain-derived neurotrophic factor (BDNF) levels. Free Radic. Biol. Med. 45,295–305.
Wilson, C.B., McLaughlin, L.D., Nair, A., Ebenezer, P.J., Dange, R., Francis, J., 2013.Inflammation and oxidative stress are elevated in the brain, blood, and adrenalglands during the progression of post-traumatic stress disorder in a predatorexposure animal model. PLoS ONE 8, e76146.
Wolkowitz, O.M., Mellon, S.H., Epel, E.S., Lin, J., Dhabhar, F.S., Su, Y., Reus, V.I.,Rosser, R., Burke, H.M., Kupferman, E., Compagnone, M., Nelson, J.C., Blackburn,E.H., 2011. Leukocyte telomere length in major depression: correlations withchronicity, inflammation and oxidative stress – preliminary findings. PLoS ONE6, e17837.
Wu, A., Ying, Z., Gomez-Pinilla, F., 2004a. Dietary omega-3 fatty acids normalizeBDNF levels, reduce oxidative damage, and counteract learning disability aftertraumatic brain injury in rats. J. Neurotrauma 21, 1457–1467.
Wu, A., Ying, Z., Gomez-Pinilla, F., 2004b. The interplay between oxidative stress andbrain-derived neurotrophic factor modulates the outcome of a saturated fat dieton synaptic plasticity and cognition. Eur. J. Neurosci. 19, 1699–1707.
Wu, C.C., Chang, J.H., Chen, C.C., Su, S.B., Yang, L.K., Ma, W.Y., Zheng, C.M., Diang, L.K.,Lu, K.C., 2011. Calcitriol treatment attenuates inflammation and oxidative stressin hemodialysis patients with secondary hyperparathyroidism. Tohoku J. Exp.Med. 223, 153–159.
Yager, S., Forlenza, M.J., Miller, G.E., 2010. Depression and oxidative damage to lipids.Psychoneuroendocrinology 35, 1356–1362.
Yang, R., Han, X., Uchiyama, T., Watkins, S.K., Yaguchi, A., Delude, R.L., Fink, M.P.,2003. IL-6 is essential for development of gut barrier dysfunction after hemor-rhagic shock and resuscitation in mice. Am. J. Physiol. 285, G621–G629.
Yildiz, D., Ercal, N., Armstrong, D.W., 1998. Nicotine enantiomers and oxidativestress. Toxicology 130, 155–165.
Yu, T., Robotham, J.L., Yoon, Y., 2006. Increased production of reactive oxygen speciesin hyperglycemic conditions requires dynamic change of mitochondrial mor-phology. Proc. Natl. Acad. Sci. U.S.A. 103, 2653–2658.
Zameer, A., Hoffman, S.A., 2001. Immunoglobulin binding to brain in autoimmunemice. J. Neuroimmunol. 120, 10–18.
Zhou, Y.P., Jiang, Z.M., Sun, Y.H., Wang, X.R., Ma, E.L., Wilmore, D., 2003. The effect ofsupplemental enteral glutamine on plasma levels, gut function, and outcome in
ive stress in depression: Why so much stress? Neurosci. Biobehav.
polyphenols produce antidepressant-like effects in adult mice. Pharmacol. Res.65, 74–80.
2020
2021




















