
Oxcarbazepine (Trileptal) in the treatment of bipolar disorders: a review of efficacy and...
12
Journal of Affective Disorders 72 (2002) S23–S34 www.elsevier.com / locate / jad Review Oxcarbazepine (Trileptal) in the treatment of bipolar disorders: a review of efficacy and tolerability * Jonathan S.E. Hellewell Department of Psychiatry, Trafford General Hospital, Moorside Road, Urmston, Manchester M41 5SL, UK Abstract Oxcarbazepine, although structurally similar to carbamazepine, is metabolised very differently. As a consequence, oxcarbazepine’s pharmacokinetic profile is comparatively less complex, and a more predictable, linear relationship between oxcarbazepine and blood levels is apparent. Furthermore, hepatic enzyme induction is considerably less with oxcarbazepine. Unlike carbamazepine, oxcarbazepine does not appear to induce its own metabolism, nor is it highly protein bound. These pharmacokinetic and metabolic characteristics raise the expectation that potential for drug interactions and side effects with oxycarbazepine will be less than that reported for carbamazepine. This review compares the pharmacokinetic and metabolic profiles of the two drugs and the available efficacy and safety data of carbamazepine and oxcarbazepine, in the treatment of bipolar disorder. 2002 Published by Elsevier Science B.V. Keywords: Oxcarbazepine (trileptal); Bipolar disorders; Review; Efficacy; Tolerability 1. Introduction indicate that oxcarbazepine is effective in the acute treatment of mania, with efficacy similar to that seen Oxcarbazepine (Trileptal) has recently been made with haloperidol or lithium. available in a number of European countries and the Moreover, the agent appears to be well-tolerated. US. Despite its recent introduction, there have been a Carbamazepine, to which oxcarbazepine is structur- number of studies conducted over the past twenty to ally related, is a particularly well-researched treat- thirty years, which provide positive indications of its ment in bipolar disorders. Thus, the studies demon- utility in bipolar disorders. In addition, oxcar- strating the efficacy of carbamazepine in acute and bazepine has been widely employed as an anticon- maintenance phases of bipolar treatment may provide vulsant and, in this setting, has been found to be both a useful indication of the utility of the newer agent. effective and well-tolerated. Comparative studies Despite its undoubted efficacy, the utility of carbam- azepine is limited both by its side effects and also by its complicated pharmacokinetics and drug interac- *Tel.: 1 44-161-746-2680; fax: 1 44-870-052-6955. tions. Although oxcarbazepine may show similar E-mail address: [email protected] (J.S.E. Hellewell). efficacy to carbamazepine in affective disorders, the 0165-0327 / 02 / $ – see front matter 2002 Published by Elsevier Science B.V. PII: S0165-0327(02)00338-5
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Oxcarbazepine (Trileptal) in the treatment of bipolar disorders: a review of efficacy and...
Journal of Affective Disorders 72 (2002) S23–S34www.elsevier.com/ locate/ jad
Review
O xcarbazepine (Trileptal) in the treatment of bipolar disorders: areview of efficacy and tolerability
*Jonathan S.E. Hellewell
Department of Psychiatry, Trafford General Hospital, Moorside Road, Urmston, Manchester M41 5SL, UK
Abstract
Oxcarbazepine, although structurally similar to carbamazepine, is metabolised very differently. As a consequence,oxcarbazepine’s pharmacokinetic profile is comparatively less complex, and a more predictable, linear relationship betweenoxcarbazepine and blood levels is apparent. Furthermore, hepatic enzyme induction is considerably less with oxcarbazepine.Unlike carbamazepine, oxcarbazepine does not appear to induce its own metabolism, nor is it highly protein bound. Thesepharmacokinetic and metabolic characteristics raise the expectation that potential for drug interactions and side effects withoxycarbazepine will be less than that reported for carbamazepine. This review compares the pharmacokinetic and metabolicprofiles of the two drugs and the available efficacy and safety data of carbamazepine and oxcarbazepine, in the treatment ofbipolar disorder. 2002 Published by Elsevier Science B.V.
Keywords: Oxcarbazepine (trileptal); Bipolar disorders; Review; Efficacy; Tolerability
1 . Introduction indicate that oxcarbazepine is effective in the acutetreatment of mania, with efficacy similar to that seen
Oxcarbazepine (Trileptal) has recently been made with haloperidol or lithium.available in a number of European countries and the Moreover, the agent appears to be well-tolerated.US. Despite its recent introduction, there have been a Carbamazepine, to which oxcarbazepine is structur-number of studies conducted over the past twenty to ally related, is a particularly well-researched treat-thirty years, which provide positive indications of its ment in bipolar disorders. Thus, the studies demon-utility in bipolar disorders. In addition, oxcar- strating the efficacy of carbamazepine in acute andbazepine has been widely employed as an anticon- maintenance phases of bipolar treatment may providevulsant and, in this setting, has been found to be both a useful indication of the utility of the newer agent.effective and well-tolerated. Comparative studies Despite its undoubted efficacy, the utility of carbam-
azepine is limited both by its side effects and also byits complicated pharmacokinetics and drug interac-*Tel.: 144-161-746-2680; fax:1 44-870-052-6955.tions. Although oxcarbazepine may show similarE-mail address: [email protected](J.S.E.
Hellewell). efficacy to carbamazepine in affective disorders, the
0165-0327/02/$ – see front matter 2002 Published by Elsevier Science B.V.PI I : S0165-0327( 02 )00338-5
S24 J.S.E. Hellewell / Journal of Affective Disorders 72 (2002)S23–S34
agents are metabolised very differently; there are incongruent psychotic symptoms (Brambilla et al.,thus grounds to predict that side effects will be fewer 2001). Since a partial response to single agents inand interactions less complicated with this agent than acute mania is often the rule rather than the excep-with carbamazepine. This review will first consider tion, the clinician needs to maintain an awareness ofcarbamazepine’s role in affective disorders, in order the various combination strategies (Hellewell, 2001).to set the later findings with oxcarbazepine in their Unfortunately, research evidence guiding the use ofwider context. However, the differences between the agents in combination is generally lacking. Small ettwo agents will be explored fully, so as to highlight al. (1995), however, showed that the use of carbam-potential advantages of the newer agent. The studies azepine together with lithium was as effective as theexamining the potential contribution of oxcar- combination of haloperidol and lithium, and thatbazepine to the treatment of affective disorders will there were fewer neurological side effects withbe reviewed in detail and suggestions will be given carbamazepine than haloperidol. In a similar vein,for future areas of study. Lenzi et al. (1986) demonstrated that the combina-
tion of carbamazepine and chlorpromazine was aseffective as that of chlorpromazine and lithium.
Given the often incomplete response to lithium in2 . Carbamazepine in acute mania acute mania, it is useful to note that carbamazepine
has been found to be effective in patients with aThe effectiveness of carbamazepine in acute mania proven history of lithium resistance (Lerer et al.,
has been examined in a number of studies, using a 1987; Okuma et al., 1990; Post et al., 1987). Thevariety of experimental designs (reviewed by Post drug has also shown proven effectiveness inet al., 1996). Comparisons have been made with schizoaffective patients (Emrich et al., 1985; Gon-both conventional antipsychotics and with lithium. calves and Stoll, 1985). There is also evidence toDouble-blind comparisons with the conventional support a particular role in the many patients inantipsychotics chlorpromazine (Okuma et al., 1979) whom affective disorders are complicated by organicor haloperidol (Stoll et al., 1986) have shown factors (Porter et al., 1999; Joffe, 1991).equivalent efficacy with perhaps a slightly sloweronset of response (Brown et al., 1989), althoughantipsychotics appear to be associated with a greaterburden of side effects. 3 . Carbamazepine in depressive disorders
Studies comparing carbamazepine and lithium inacute mania have tended to indicate no pattern of There have been a number of comparative studiesconsistent difference between the two agents of carbamazepine in depression (reviewed by Bram-(Okuma et al., 1990; Small et al., 1996), although billa et al., 2001). Carbamazepine has been studiedLerer et al. (1987) reported superior efficacy with both as an augmentation therapy, with lithiumcarbamazepine. Mixed states, moreover, tend to (Kramlinger and Post, 1989; Rybakowski et al.,respond better to carbamazepine than to lithium 1999) or MAOIs (Ketter et al., 1995) and as(Walden and Grunze, 2000); similarly, rapid cycling monotherapy (e.g. Ballenger and Post, 1980; Post ethas been shown to respond better to carbamazepine al., 1986). In many of these studies, enrolled patientsthan to lithium (Okuma, 1993; Denicoff et al., 1994). were refractory to either lithium or antidepressants.Moreover, carbamazepine appears also to be of Although there is still a need for large-scale, ran-equivalent efficacy in acute mania to valproate domised placebo-controlled studies, the available(Emrich et al., 1985; Vasudev et al., 2000). data, as reviewed by Brambilla et al. (2001), suggest
Generally, only 60–90% of patients suffering from that carbamazepine, either alone or in combinationa typical manic state respond to lithium (Him- with antidepressant drugs, may be useful in themelhoch et al., 1976; Secunda et al., 1985; Swann et treatment of both unipolar and bipolar depression.al., 1986); response rates tend to be still lower for Both the severity of illness and a history of rapidpatients with atypical features, depressive or mood- cycling have been found to be predictors of acute

J.S.E. Hellewell / Journal of Affective Disorders 72 (2002)S23–S34 S25
antidepressant response to carbamazepine (Kram- Similarly, Kishimoto (1992), in a retrospectivelinger and Post, 1989; Post et al., 1986). study, found evidence for greater effectiveness of
lithium and carbamazepine in combination, com-pared with their use in monotherapy. In reviewing
4 . Effectiveness in the prophylaxis of affective these studies, Porter et al. (1999) concluded that thedisorder combination of lithium and carbamazepine appeared
well-tolerated, especially if the additional drug isThere is good evidence that carbamazepine is introduced gradually and recommended that the
effective in the prophylaxis of bipolar disorders (see addition of carbamazepine be an early consideration,Post et al., 1996 and Brambilla et al., 2001 for should response to lithium prove inadequate.reviews). Carbamazepine appears to be equally effec- Rapid cycling, or the occurrence of four or moretive in reducing the frequency of both manic and episodes of major affective disorder within a onedepressive episodes. There are a number of studies year period, poses particular challenges to the clini-indicating that carbamazepine has broadly similar cian (Walden and Grunze, 2000). Patients with thiseffectiveness to lithium in the prophylaxis of major pattern of illness often do not respond well to lithiumaffective disorders (Placidi et al., 1986; Watkins et (Swann et al., 1986). The response to carbamazepineal., 1987; Lusznat et al., 1988, Coxhead et al., 1992). in rapid cycling appears to be superior to that withGreil et al. (1997), for example, using the substantial lithium (Okuma, 1993; Denicoff et al., 1994). Portercohort of 144 bipolar patients, compared the effec- et al. (1999) have argued that this superior responsetiveness of carbamazepine and lithium over two and suggests that the clinician should be prepared toa half years’ treatment. While lithium appeared to be move immediately to the combination of carbamaz-superior in terms of recurrence rate, discontinuation epine and lithium, when dealing with the patient withdue to adverse effects and the need for additional a rapid cycling pattern of illness.medication, patients on carbamazepine reportedfewer side effects. These data suggest that carbamaz-epine may be best suited, when used in monotherapy,for those patients in whom lithium proves ineffective 5 . Carbamazepine in the treatment of affectiveor poorly tolerated. disorder—summary
Irrespective of the drug used, a substantial propor-tion of bipolar patients fail to derive benefit from There is good evidence to support the use ofmonotherapy (Hellewell, 2001). This suggests that carbamazepine in the acute treatment of bipolarclinicians need to become familiar with the use of affective disorders. Efficacy in acute mania appearsmood stabilising drugs in combination, although to be broadly comparable with that for anti-there is a lack of studies that might be used to guide psychotics, valproate and lithium; in addition theredecisions as to the switching and sequencing of is evidence for additional effectiveness in patientsmedications. Fortunately, there are a number of with atypical or mixed presentations. On reviewingstudies that support the addition of carbamazepine to this data, Brambilla et al. (2001) concluded thatlithium as prophylactic treatment in patients with a carbamazepine should be regarded as a treatment ofhistory of poor response to mood stabilisers used in choice for lithium-resistant or intolerant patients.monotherapy. Denicoff et al. (1994) for example, There is also good evidence to support the use ofcarried out a study in which patients were treated for carbamazepine in the prophylaxis of bipolar dis-the first year with either lithium or carbamazepine in orders. Carbamazepine appears to have similarmonotherapy, after which there was a year during efficacy to that of lithium and may have fewer sidewhich patients were switched to the other treatment, effects. There appears to be a particular role foralso in monotherapy. This was followed by one year carbamazepine in the maintenance treatment ofon combination therapy. Response to the combina- atypical or rapid-cycling disorders and for the manytion therapy appeared to be superior to the individual patients who cannot tolerate or prove resistant totreatments in monotherapy. lithium treatment.
S26 J.S.E. Hellewell / Journal of Affective Disorders 72 (2002)S23–S34
6 . The tolerability of carbamazepine—side handling of other drugs is also affected, an importanteffects clinical consequence of this being that plasma levels
of oral contraceptives are reduced by carbamazepineAlthough reasonably well-tolerated, for some and that either higher doses of contraceptives or
patients, carbamazepine can be associated with un- alternative methods should be used. Other drugs ofacceptable side effects. These can include CNS which plasma levels can be significantly loweredeffects such as blurred vision, ataxia and dizziness, include the antipsychotics, antidepressants andall of which are reversible and often dose-dependent. macrolide antibiotics.Thus, it is important that, where the clinical situation Plasma levels of carbamazepine are also affectedallows, dosing should be started at a low level and by those drugs metabolised by the P450 3A4 iso-titrated gradually, as side effects and clinical re- enzyme. In particular, a number of the antidepres-sponse permit. In addition to the CNS effects, rashes sants, such as some of the selective serotonin reup-occur commonly; these should be monitored closely take inhibitors and nefazodone, may inhibit thesince severe reactions can occasionally develop. It is metabolism of carbamazepine, leading to both in-prudent to discontinue carbamazepine if the rash creased plasma levels and also side effects. Plasmaworsens or if this is accompanied by other symp- levels can also be elevated by calcium antagoniststoms. such as diltiazem and verapamil.
A transient leucopaenia occurs in about 10% ofpatients and a persistent leucopaenia in about 2%.These usually appear early in the course of treat- 8 . Oxcarbazepine and carbamazepine—ment. Thrombocytopenia occurs in about 2% of similarities and differencespatients and may become clinically manifest aspetechia (Jefferson and Greist, 1987). The risk of Both carbamazepine and oxcarbazepine have tri-aplastic anemia and agranulocytosis with carbamaz- cyclic structures. These appear quite similar, al-epine is approximately five to eight times greater though there is the important difference of an oxygenthan in the general population. However, since these atom at the 10 position in the centre ring. For thisabnormalities occur extremely uncommonly in the reason, oxcarbazepine is sometimes referred to as thegeneral population, the risk with carbamazepine is 10-keto analog of carbamazepine.actually quite low. Nonetheless, carbamazepine This apparently subtle variation in chemical struc-should not be used in combination with clozapine. ture results in marked differences in routes of
Carbamazepine is often associated with elevated metabolism and pharmacology. The major metaboliteplasma levels of hepatic enzymes; although rare in of carbamazepine is carbamazepine-10,11-epoxide. Itoccurrence, hepatocellular damage caused by car- is likely that this metabolite is responsible for manybamazepine may be fatal. A further, potentially of the side effects associated with carbamazepine.serious, although uncommon side effect of carbam- CYP 3A4 is the main enzyme involved in formationazepine is that of hyponatraemia (plasma sodium of the epoxide metabolite. The epoxide metabolite, in,125 mmol / l). turn, is converted to carbamazepine-10,11-dihydro-
10-hydroxide by the enzyme epoxide hydrolase.Since valproate inhibits this enzyme, blood levels of
7 . Drug interactions with carbamazepine the epoxide metabolite can be increased when car-bamazepine is administered with valproate, leading
Carbamazepine is metabolised in the liver by the to a greater burden of side effects (Ketter and Post,cytochrome P450 3A4 isoenzyme. However, carbam- 1994).azepine also induces the activity of this enzyme, In contrast to carbamazepine, which undergoessuch that, after 3–4 weeks’ treatment, metabolism of oxidation, primarily by CYP 3A4 to the 10,11-carbamazepine tends to be greater, and plasma levels epoxide, oxcarbazepine is reduced by a cytosoliccorrespondingly lower, than when treatment was arylketone reductase to the 10-monohydroxy deriva-begun. The induction of cytochromes means that the tive (MHD). Unlike CYP 3A4, arylketone reductase

J.S.E. Hellewell / Journal of Affective Disorders 72 (2002)S23–S34 S27
is not an inducible enzyme. Thus, whereas carbamaz- doses of between 15 and 20 mg. Mania scores, asepine induces its own metabolism, this does not rated by the Bech–Rafaelson Mania Rating Scaleoccur with oxcarbazepine (Wellington and Goa, (BRMRS, 1979), improved in both groups over the 22001). As oxcarbazepine does not induce its own weeks’ treatment, although early improvementsmetabolism, there is therefore a linear relationship appeared greatest in the oxcarbazepine treatedbetween dose and blood level of the drug. Moreover, patients.as oxcarbazepine is not metabolised to the epoxide, A further open study was conducted by Velikonjaone might reasonably expect fewer side effects in and Heinrich (1984), using patients with manicclinical use. syndromes or schizoaffective psychosis. Ten patients
In contrast to carbamazepine, oxcarbazepine is a were treated with both oxcarbazepine (900 mg permuch weaker inducer of cytochrome P450 3A4/5, day) and antipsychotics. Antipsychotic doses wereand it inhibits only the 2C19 enzyme. For this lower in patients receiving oxcarbazepine than in areason, there are few clinically significant drug matched group not receiving oxcarbazepine, sug-interactions, although the plasma levels of the oes- gesting that the oxcarbazepine allowed the use oftrogen and progesterone components of oral contra- lower antipsychotic doses than would otherwise haveceptives tend to be reduced. High-dose contracep- been needed.tives, or alternative means of contraception, should A recent open-label study, reported in a prelimin-be used to counteract this effect. Oxcarbazepine is ary publication (Munoz, 2002), investigated thenot highly bound to plasma proteins; there are thus mood stabilizing effects of oxcarbazepine (titrated tofew significant interactions with the other drugs that 300–2400 mg/day) as adjunctive therapy, over 12compete for protein-binding sites, such as phenytoin weeks, in 28 patients with bipolar disorder. Of these,and warfarin. 21 were manic and seven were depressed at enroll-
ment.At the final visit, the mean dose of oxcarbazepine
was 1063 mg/day for patients initially manic and9 . Studies of oxcarbazepine in bipolar disorders 959 mg/day for patients initially depressed. Of the
28 patients who completed the study, concomitantControlled studies of oxcarbazepine in bipolar medications included antipsychotics, mood stabi-
disorder are few in number but are strongly sug- lizers and antidepressants (Table 1). At baseline, thegestive of a role for the drug in affective disorders. average number of concomitant mediations per pa-
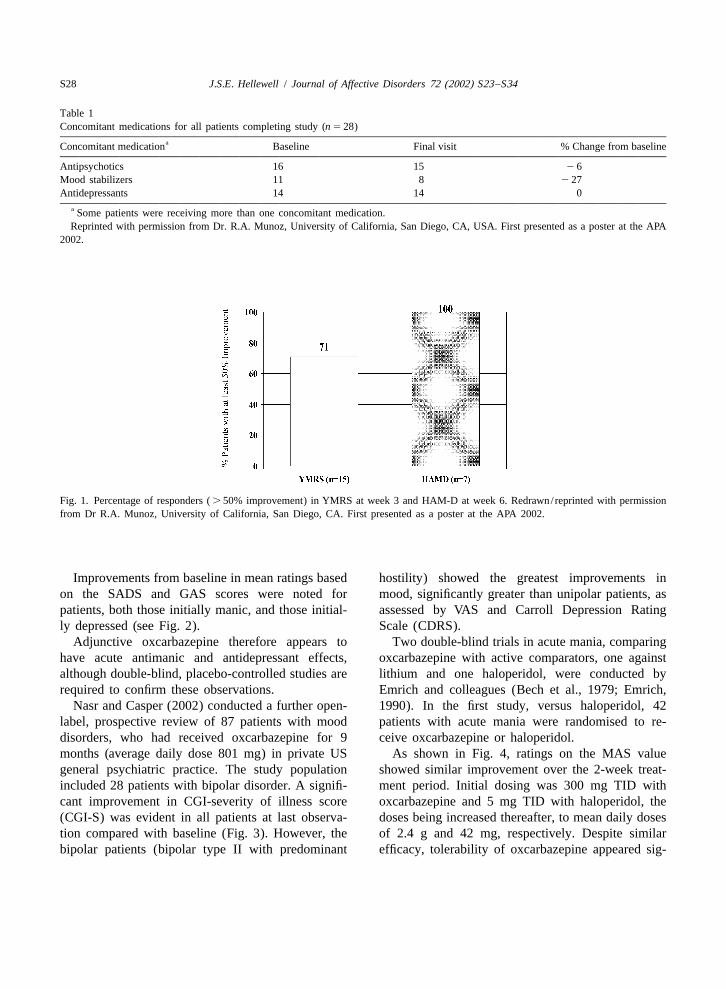
One of the first evaluations of oxcarbazepine in tient was 3.761.2. A reduction of 27% in concomi-affective disorders was reported by Emrich et al. tant medications (to 3.261.1) was seen over the 12(1983), who treated six patients in a double-blind, weeks of the study.placebo-controlled study, using crossover ABA de- Fifteen patients (71%) with mania showed$ 50%sign. Patients were suffering from ‘maniform psy- improvement as defined by the Young Mania Ratingchoses’ and had ICD-9 diagnoses of either manic- Scale (YMRS) within 3 weeks of starting treatment.depressive or schizoaffective psychosis. The authors Notably, all depressed patients showed$ 50% im-report substantial changes in mania ratings, made provement in depressive symptoms, as assessed byusing the Inpatient Multidimensional Psychiatric the Hamilton Rating Scale for Depression (HAM-D),Scale (1962). by week 6 (Fig. 1). A mean weight loss of2 2%
¨Muller and Stoll (1984) reported an open, multi- was reported at endpoint and although low sodiumcentre study, in which oxcarbazepine was adminis- levels (, 125 mEq/ l) were reported in four patients,tered to 48 patients with mania. Good results were no discontinuations were necessary.observed in over 80% of subjects, while over 90% Nine (60%) of the 15 responders in the manicwere rated as showing good tolerability. The same group remained euthymic throughout the remaining 9authors also conducted a comparative trial, in which weeks of the study, and all seven (100%) of thepatients were randomised to receive oxcarbazepine, responders in the depressed group remainedat doses of 0.9–1.2 g per day, or haloperidol, at daily euthymic for the remainder of the study.
S28 J.S.E. Hellewell / Journal of Affective Disorders 72 (2002)S23–S34
Table 1Concomitant medications for all patients completing study (n 5 28)
aConcomitant medication Baseline Final visit % Change from baseline
Antipsychotics 16 15 2 6Mood stabilizers 11 8 2 27Antidepressants 14 14 0
a Some patients were receiving more than one concomitant medication.Reprinted with permission from Dr. R.A. Munoz, University of California, San Diego, CA, USA. First presented as a poster at the APA
2002.
Fig. 1. Percentage of responders (. 50% improvement) in YMRS at week 3 and HAM-D at week 6. Redrawn/reprinted with permissionfrom Dr R.A. Munoz, University of California, San Diego, CA. First presented as a poster at the APA 2002.
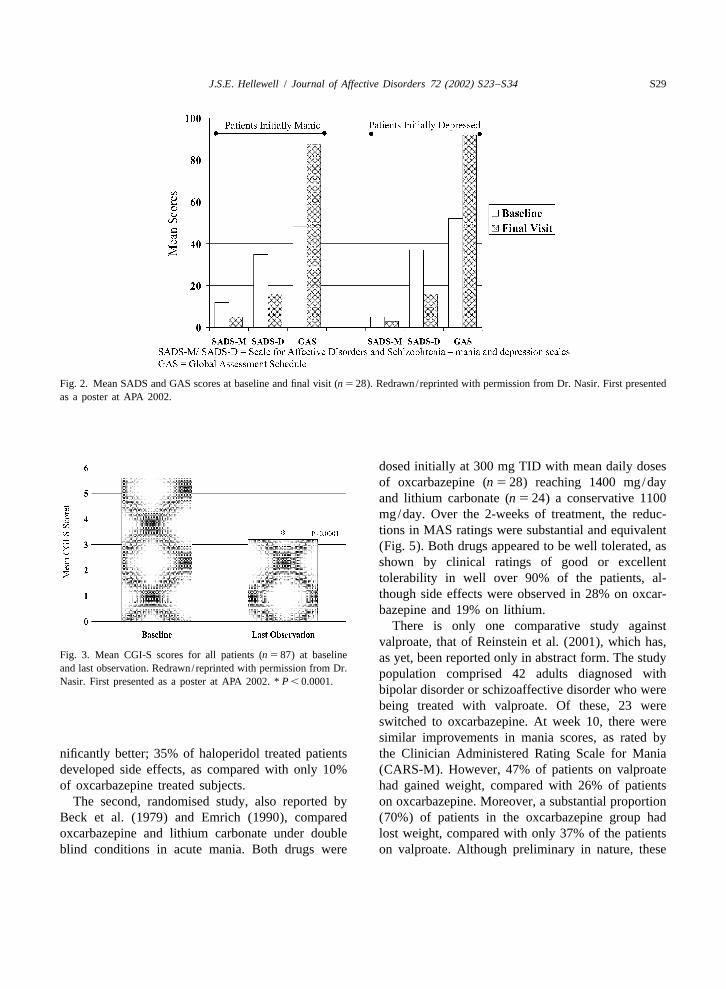
Improvements from baseline in mean ratings based hostility) showed the greatest improvements inon the SADS and GAS scores were noted for mood, significantly greater than unipolar patients, aspatients, both those initially manic, and those initial- assessed by VAS and Carroll Depression Ratingly depressed (see Fig. 2). Scale (CDRS).
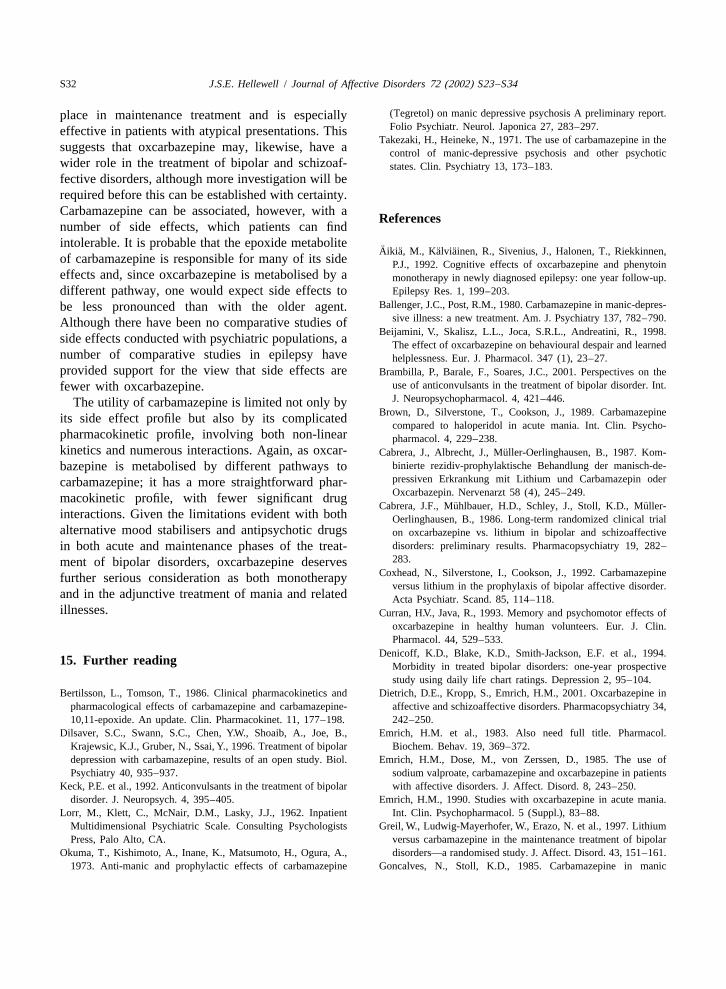
Adjunctive oxcarbazepine therefore appears to Two double-blind trials in acute mania, comparinghave acute antimanic and antidepressant effects, oxcarbazepine with active comparators, one againstalthough double-blind, placebo-controlled studies are lithium and one haloperidol, were conducted byrequired to confirm these observations. Emrich and colleagues (Bech et al., 1979; Emrich,
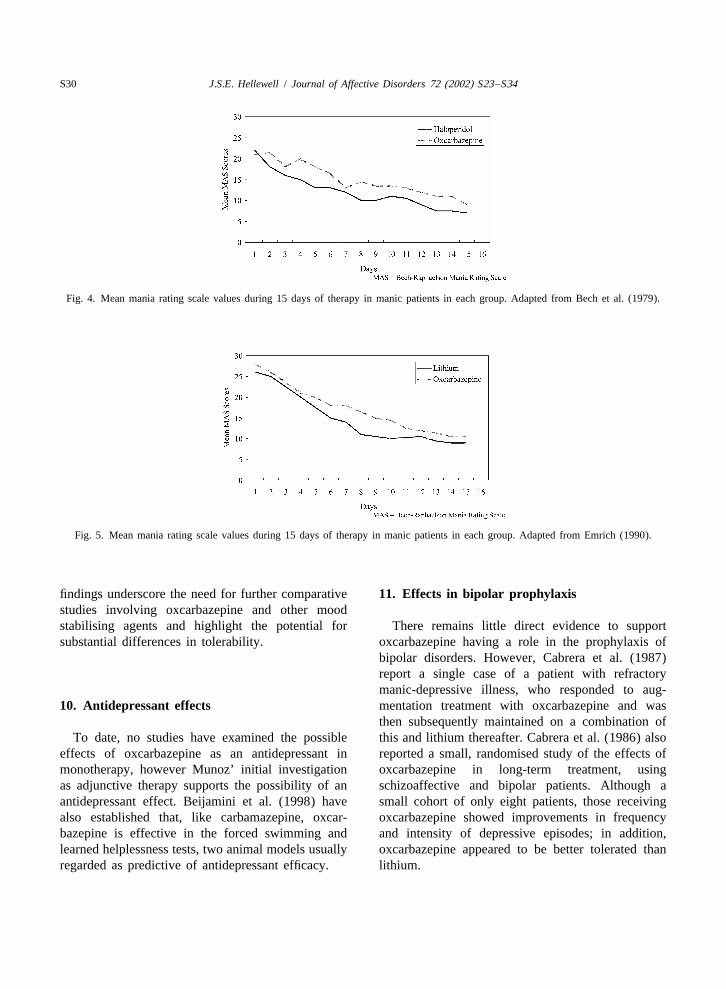
Nasr and Casper (2002) conducted a further open- 1990). In the first study, versus haloperidol, 42label, prospective review of 87 patients with mood patients with acute mania were randomised to re-disorders, who had received oxcarbazepine for 9 ceive oxcarbazepine or haloperidol.months (average daily dose 801 mg) in private US As shown in Fig. 4, ratings on the MAS valuegeneral psychiatric practice. The study population showed similar improvement over the 2-week treat-included 28 patients with bipolar disorder. A signifi- ment period. Initial dosing was 300 mg TID withcant improvement in CGI-severity of illness score oxcarbazepine and 5 mg TID with haloperidol, the(CGI-S) was evident in all patients at last observa- doses being increased thereafter, to mean daily dosestion compared with baseline (Fig. 3). However, the of 2.4 g and 42 mg, respectively. Despite similarbipolar patients (bipolar type II with predominant efficacy, tolerability of oxcarbazepine appeared sig-
J.S.E. Hellewell / Journal of Affective Disorders 72 (2002)S23–S34 S29
Fig. 2. Mean SADS and GAS scores at baseline and final visit (n 5 28). Redrawn/reprinted with permission from Dr. Nasir. First presentedas a poster at APA 2002.
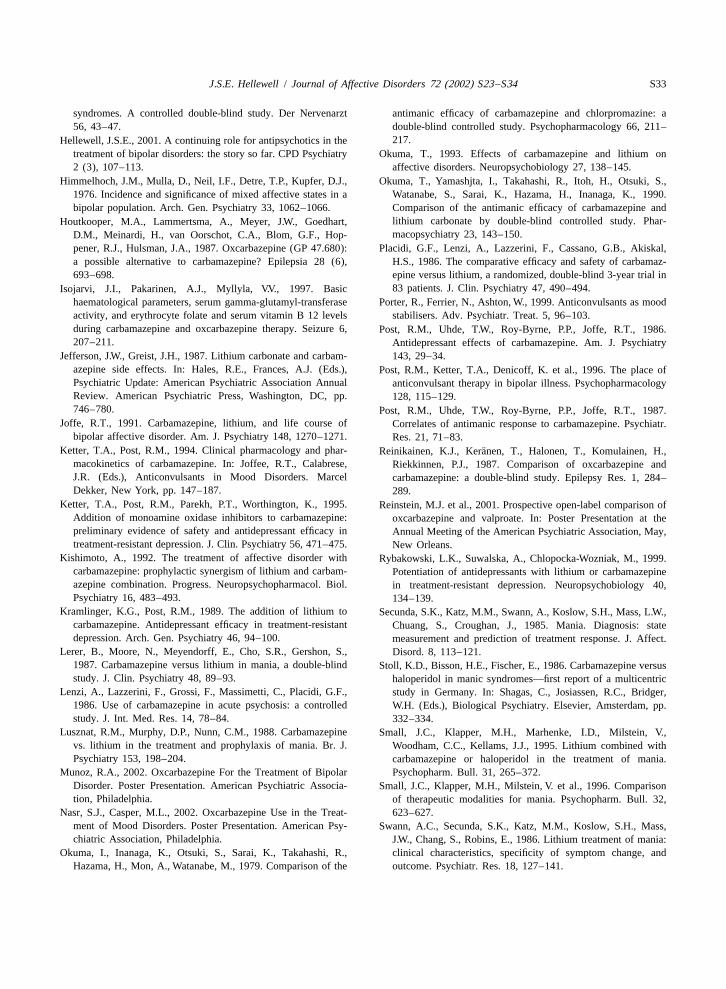
dosed initially at 300 mg TID with mean daily dosesof oxcarbazepine (n 5 28) reaching 1400 mg/dayand lithium carbonate (n 5 24) a conservative 1100mg/day. Over the 2-weeks of treatment, the reduc-tions in MAS ratings were substantial and equivalent(Fig. 5). Both drugs appeared to be well tolerated, asshown by clinical ratings of good or excellenttolerability in well over 90% of the patients, al-though side effects were observed in 28% on oxcar-bazepine and 19% on lithium.
There is only one comparative study againstvalproate, that of Reinstein et al. (2001), which has,
Fig. 3. Mean CGI-S scores for all patients (n 5 87) at baseline as yet, been reported only in abstract form. The studyand last observation. Redrawn/reprinted with permission from Dr. population comprised 42 adults diagnosed withNasir. First presented as a poster at APA 2002. *P , 0.0001.
bipolar disorder or schizoaffective disorder who werebeing treated with valproate. Of these, 23 wereswitched to oxcarbazepine. At week 10, there weresimilar improvements in mania scores, as rated by
nificantly better; 35% of haloperidol treated patients the Clinician Administered Rating Scale for Maniadeveloped side effects, as compared with only 10% (CARS-M). However, 47% of patients on valproateof oxcarbazepine treated subjects. had gained weight, compared with 26% of patients
The second, randomised study, also reported by on oxcarbazepine. Moreover, a substantial proportionBeck et al. (1979) and Emrich (1990), compared (70%) of patients in the oxcarbazepine group hadoxcarbazepine and lithium carbonate under double lost weight, compared with only 37% of the patientsblind conditions in acute mania. Both drugs were on valproate. Although preliminary in nature, these
S30 J.S.E. Hellewell / Journal of Affective Disorders 72 (2002)S23–S34
Fig. 4. Mean mania rating scale values during 15 days of therapy in manic patients in each group. Adapted from Bech et al. (1979).
Fig. 5. Mean mania rating scale values during 15 days of therapy in manic patients in each group. Adapted from Emrich (1990).
findings underscore the need for further comparative 1 1. Effects in bipolar prophylaxisstudies involving oxcarbazepine and other moodstabilising agents and highlight the potential for There remains little direct evidence to supportsubstantial differences in tolerability. oxcarbazepine having a role in the prophylaxis of
bipolar disorders. However, Cabrera et al. (1987)report a single case of a patient with refractorymanic-depressive illness, who responded to aug-
1 0. Antidepressant effects mentation treatment with oxcarbazepine and wasthen subsequently maintained on a combination of
To date, no studies have examined the possible this and lithium thereafter. Cabrera et al. (1986) alsoeffects of oxcarbazepine as an antidepressant in reported a small, randomised study of the effects ofmonotherapy, however Munoz’ initial investigation oxcarbazepine in long-term treatment, usingas adjunctive therapy supports the possibility of an schizoaffective and bipolar patients. Although aantidepressant effect. Beijamini et al. (1998) have small cohort of only eight patients, those receivingalso established that, like carbamazepine, oxcar- oxcarbazepine showed improvements in frequencybazepine is effective in the forced swimming and and intensity of depressive episodes; in addition,learned helplessness tests, two animal models usually oxcarbazepine appeared to be better tolerated thanregarded as predictive of antidepressant efficacy. lithium.

J.S.E. Hellewell / Journal of Affective Disorders 72 (2002)S23–S34 S31
1 2. Oxcarbazepine is well tolerated Although a double-blind study would be needed toconfirm this, it is likely that a correspondingly lower
In general, oxcarbazepine is well tolerated when prevalence of side effects would be seen in psychiat-used in a psychiatric population (Dietrich et al., ric populations. Moreover, the greatly reduced bur-2001). The most frequent side effects associated with den of clinical monitoring with oxcarbazepine isoxcarbazepine treatment include dizziness, sedation, likely to further simplify treatment, may enhanceand blurred vision. For most patients, however, the patient satisfaction and thereby outcome.drug is not sedative (Dietrich et al., 2001). Gastroin-testinal distress may also occur. Rash is another sideeffect and, although this occurs less frequently than 1 3. Dosingwith carbamazepine, 25–30% of patients with hyper-sensitivity to carbamazepine are also hypersensitive The dosages required with both carbamazepineto oxcarbazepine. As with carbamazepine, clinically and oxcarbazepine vary widely from patient tosignificant hyponatraemia has occasionally been patient; the daily oral dose of carbamazepine isreported. usually in the region of 600–1800 mg, whereas with
Oxcarbazepine does not show any significant oxcarbazepine, optimal doses are usually within thehepatic effects and, as such, does not require liver range of 900–2400 mg/day (Walden and Grunze,monitoring. The potentially serious complications 2000). Oxcarbazepine is given twice daily; thisthat can occur, albeit rarely, with carbamazepine of regimen is often regarded by clinicians as optimal inaplastic anemia and agranulocytosis, have not been acute manic states. There are, as yet, no studiesobserved with oxcarbazepine (Dietrich et al., 2001). examining the relationship between plasma levelsFurthermore, there have been reports of abnormal and clinical efficacy in bipolar disorder. Thus, deci-haematological indices on carbamazepine returning sions about dosing should usually be based upon theto normal following a switch to oxcarbazepine patient’s clinical condition.(Isojarvi et al., 1997). Two studies have indicated In acute mania, a reasonable dosing schedulethat, in clinical use, oxcarbazepine does not cause might be to commence treatment with doses in thesignificant impairments in cognitive function (Curran region of 150 mg twice daily for inpatients with
¨ ¨and Java, 1993; Aikia et al., 1992). manic syndromes, with consideration being given toAlthough generally free of significant phar- increasing of dose every few days, assuming side
macokinetic interactions, oxcarbazepine does reduce effects are tolerated.plasma concentrations of the oestrogen and proges-terone components of oral contraceptives. Thismeans that high-dose contraceptives, or alternative 1 4. Conclusionsmeans of contraception, should be used in women ofchildbearing age. Oxcarbazepine has shown similar efficacy to both
As the epoxide metabolite of carbamazepine, haloperidol and lithium, when studied in acutewhich is believed to contribute to many of the side mania. Clinical studies have indicated that the agenteffects, does not occur with oxcarbazepine treatment, not only brings about substantial improvements inthere are grounds for predicting a relative freedom symptoms, as measured by rating scales, but also thatfrom side effects with the newer agent. There have, the use of oxcarbazepine allows the use of lowerto date, been no comparative studies of tolerability doses of other medications. There are, as yet, in-carried out using psychiatric populations. However, sufficient data with which to judge whether the drugtwo studies examining the comparative tolerability of is also effective in maintenance treatment. Carbam-carbamazepine and oxcarbazepine in patients with azepine, to which oxcarbazepine is structurally re-epilepsy have indicated that the side effect advan- lated, is however, one of the better characterisedtages of the newer agent may be more than theoret- anticonvulsants, with proven efficacy in both acuteical, and may be evident in clinical practice and maintenance treatment of bipolar disorders.(Reinikainen et al., 1987; Houtkooper et al., 1987). Furthermore, carbamazepine has a well-established
S32 J.S.E. Hellewell / Journal of Affective Disorders 72 (2002)S23–S34
(Tegretol) on manic depressive psychosis A preliminary report.place in maintenance treatment and is especiallyFolio Psychiatr. Neurol. Japonica 27, 283–297.effective in patients with atypical presentations. This
Takezaki, H., Heineke, N., 1971. The use of carbamazepine in thesuggests that oxcarbazepine may, likewise, have a control of manic-depressive psychosis and other psychoticwider role in the treatment of bipolar and schizoaf- states. Clin. Psychiatry 13, 173–183.fective disorders, although more investigation will berequired before this can be established with certainty.Carbamazepine can be associated, however, with aR eferencesnumber of side effects, which patients can findintolerable. It is probable that the epoxide metabolite ¨ ¨ ¨ ¨Aikia, M., Kalviainen, R., Sivenius, J., Halonen, T., Riekkinnen,of carbamazepine is responsible for many of its side P.J., 1992. Cognitive effects of oxcarbazepine and phenytoineffects and, since oxcarbazepine is metabolised by a monotherapy in newly diagnosed epilepsy: one year follow-up.
Epilepsy Res. 1, 199–203.different pathway, one would expect side effects toBallenger, J.C., Post, R.M., 1980. Carbamazepine in manic-depres-be less pronounced than with the older agent.
sive illness: a new treatment. Am. J. Psychiatry 137, 782–790.Although there have been no comparative studies ofBeijamini, V., Skalisz, L.L., Joca, S.R.L., Andreatini, R., 1998.
side effects conducted with psychiatric populations, a The effect of oxcarbazepine on behavioural despair and learnednumber of comparative studies in epilepsy have helplessness. Eur. J. Pharmacol. 347 (1), 23–27.provided support for the view that side effects are Brambilla, P., Barale, F., Soares, J.C., 2001. Perspectives on the
use of anticonvulsants in the treatment of bipolar disorder. Int.fewer with oxcarbazepine.J. Neuropsychopharmacol. 4, 421–446.The utility of carbamazepine is limited not only by
Brown, D., Silverstone, T., Cookson, J., 1989. Carbamazepineits side effect profile but also by its complicatedcompared to haloperidol in acute mania. Int. Clin. Psycho-
pharmacokinetic profile, involving both non-linear pharmacol. 4, 229–238.kinetics and numerous interactions. Again, as oxcar- ¨Cabrera, J., Albrecht, J., Muller-Oerlinghausen, B., 1987. Kom-
binierte rezidiv-prophylaktische Behandlung der manisch-de-bazepine is metabolised by different pathways topressiven Erkrankung mit Lithium und Carbamazepin odercarbamazepine; it has a more straightforward phar-Oxcarbazepin. Nervenarzt 58 (4), 245–249.macokinetic profile, with fewer significant drug
¨ ¨Cabrera, J.F., Muhlbauer, H.D., Schley, J., Stoll, K.D., Muller-interactions. Given the limitations evident with both Oerlinghausen, B., 1986. Long-term randomized clinical trialalternative mood stabilisers and antipsychotic drugs on oxcarbazepine vs. lithium in bipolar and schizoaffective
disorders: preliminary results. Pharmacopsychiatry 19, 282–in both acute and maintenance phases of the treat-283.ment of bipolar disorders, oxcarbazepine deserves
Coxhead, N., Silverstone, I., Cookson, J., 1992. Carbamazepinefurther serious consideration as both monotherapyversus lithium in the prophylaxis of bipolar affective disorder.
and in the adjunctive treatment of mania and related Acta Psychiatr. Scand. 85, 114–118.illnesses. Curran, H.V., Java, R., 1993. Memory and psychomotor effects of
oxcarbazepine in healthy human volunteers. Eur. J. Clin.Pharmacol. 44, 529–533.
Denicoff, K.D., Blake, K.D., Smith-Jackson, E.F. et al., 1994.1 5. Further reading Morbidity in treated bipolar disorders: one-year prospective
study using daily life chart ratings. Depression 2, 95–104.Bertilsson, L., Tomson, T., 1986. Clinical pharmacokinetics and Dietrich, D.E., Kropp, S., Emrich, H.M., 2001. Oxcarbazepine in
pharmacological effects of carbamazepine and carbamazepine- affective and schizoaffective disorders. Pharmacopsychiatry 34,10,11-epoxide. An update. Clin. Pharmacokinet. 11, 177–198. 242–250.
Dilsaver, S.C., Swann, S.C., Chen, Y.W., Shoaib, A., Joe, B., Emrich, H.M. et al., 1983. Also need full title. Pharmacol.Krajewsic, K.J., Gruber, N., Ssai, Y., 1996. Treatment of bipolar Biochem. Behav. 19, 369–372.depression with carbamazepine, results of an open study. Biol. Emrich, H.M., Dose, M., von Zerssen, D., 1985. The use ofPsychiatry 40, 935–937. sodium valproate, carbamazepine and oxcarbazepine in patients
Keck, P.E. et al., 1992. Anticonvulsants in the treatment of bipolar with affective disorders. J. Affect. Disord. 8, 243–250.disorder. J. Neuropsych. 4, 395–405. Emrich, H.M., 1990. Studies with oxcarbazepine in acute mania.
Lorr, M., Klett, C., McNair, D.M., Lasky, J.J., 1962. Inpatient Int. Clin. Psychopharmacol. 5 (Suppl.), 83–88.Multidimensional Psychiatric Scale. Consulting Psychologists Greil, W., Ludwig-Mayerhofer, W., Erazo, N. et al., 1997. LithiumPress, Palo Alto, CA. versus carbamazepine in the maintenance treatment of bipolar
Okuma, T., Kishimoto, A., Inane, K., Matsumoto, H., Ogura, A., disorders—a randomised study. J. Affect. Disord. 43, 151–161.1973. Anti-manic and prophylactic effects of carbamazepine Goncalves, N., Stoll, K.D., 1985. Carbamazepine in manic
J.S.E. Hellewell / Journal of Affective Disorders 72 (2002)S23–S34 S33
syndromes. A controlled double-blind study. Der Nervenarzt antimanic efficacy of carbamazepine and chlorpromazine: a56, 43–47. double-blind controlled study. Psychopharmacology 66, 211–
217.Hellewell, J.S.E., 2001. A continuing role for antipsychotics in thetreatment of bipolar disorders: the story so far. CPD Psychiatry Okuma, T., 1993. Effects of carbamazepine and lithium on2 (3), 107–113. affective disorders. Neuropsychobiology 27, 138–145.
Himmelhoch, J.M., Mulla, D., Neil, I.F., Detre, T.P., Kupfer, D.J., Okuma, T., Yamashjta, I., Takahashi, R., Itoh, H., Otsuki, S.,1976. Incidence and significance of mixed affective states in a Watanabe, S., Sarai, K., Hazama, H., Inanaga, K., 1990.bipolar population. Arch. Gen. Psychiatry 33, 1062–1066. Comparison of the antimanic efficacy of carbamazepine and
lithium carbonate by double-blind controlled study. Phar-Houtkooper, M.A., Lammertsma, A., Meyer, J.W., Goedhart,macopsychiatry 23, 143–150.D.M., Meinardi, H., van Oorschot, C.A., Blom, G.F., Hop-
pener, R.J., Hulsman, J.A., 1987. Oxcarbazepine (GP 47.680): Placidi, G.F., Lenzi, A., Lazzerini, F., Cassano, G.B., Akiskal,a possible alternative to carbamazepine? Epilepsia 28 (6), H.S., 1986. The comparative efficacy and safety of carbamaz-693–698. epine versus lithium, a randomized, double-blind 3-year trial in
83 patients. J. Clin. Psychiatry 47, 490–494.Isojarvi, J.I., Pakarinen, A.J., Myllyla, V.V., 1997. Basichaematological parameters, serum gamma-glutamyl-transferase Porter, R., Ferrier, N., Ashton, W., 1999. Anticonvulsants as moodactivity, and erythrocyte folate and serum vitamin B 12 levels stabilisers. Adv. Psychiatr. Treat. 5, 96–103.during carbamazepine and oxcarbazepine therapy. Seizure 6, Post, R.M., Uhde, T.W., Roy-Byrne, P.P., Joffe, R.T., 1986.207–211. Antidepressant effects of carbamazepine. Am. J. Psychiatry
Jefferson, J.W., Greist, J.H., 1987. Lithium carbonate and carbam- 143, 29–34.azepine side effects. In: Hales, R.E., Frances, A.J. (Eds.), Post, R.M., Ketter, T.A., Denicoff, K. et al., 1996. The place ofPsychiatric Update: American Psychiatric Association Annual anticonvulsant therapy in bipolar illness. PsychopharmacologyReview. American Psychiatric Press, Washington, DC, pp. 128, 115–129.746–780. Post, R.M., Uhde, T.W., Roy-Byrne, P.P., Joffe, R.T., 1987.
Joffe, R.T., 1991. Carbamazepine, lithium, and life course of Correlates of antimanic response to carbamazepine. Psychiatr.bipolar affective disorder. Am. J. Psychiatry 148, 1270–1271. Res. 21, 71–83.
Ketter, T.A., Post, R.M., 1994. Clinical pharmacology and phar- ¨Reinikainen, K.J., Keranen, T., Halonen, T., Komulainen, H.,macokinetics of carbamazepine. In: Joffee, R.T., Calabrese, Riekkinnen, P.J., 1987. Comparison of oxcarbazepine andJ.R. (Eds.), Anticonvulsants in Mood Disorders. Marcel carbamazepine: a double-blind study. Epilepsy Res. 1, 284–Dekker, New York, pp. 147–187. 289.
Ketter, T.A., Post, R.M., Parekh, P.T., Worthington, K., 1995. Reinstein, M.J. et al., 2001. Prospective open-label comparison ofAddition of monoamine oxidase inhibitors to carbamazepine: oxcarbazepine and valproate. In: Poster Presentation at thepreliminary evidence of safety and antidepressant efficacy in Annual Meeting of the American Psychiatric Association, May,treatment-resistant depression. J. Clin. Psychiatry 56, 471–475. New Orleans.
Kishimoto, A., 1992. The treatment of affective disorder with Rybakowski, L.K., Suwalska, A., Chlopocka-Wozniak, M., 1999.carbamazepine: prophylactic synergism of lithium and carbam- Potentiation of antidepressants with lithium or carbamazepineazepine combination. Progress. Neuropsychopharmacol. Biol. in treatment-resistant depression. Neuropsychobiology 40,Psychiatry 16, 483–493. 134–139.
Kramlinger, K.G., Post, R.M., 1989. The addition of lithium to Secunda, S.K., Katz, M.M., Swann, A., Koslow, S.H., Mass, L.W.,carbamazepine. Antidepressant efficacy in treatment-resistant Chuang, S., Croughan, J., 1985. Mania. Diagnosis: statedepression. Arch. Gen. Psychiatry 46, 94–100. measurement and prediction of treatment response. J. Affect.
Lerer, B., Moore, N., Meyendorff, E., Cho, S.R., Gershon, S., Disord. 8, 113–121.1987. Carbamazepine versus lithium in mania, a double-blind Stoll, K.D., Bisson, H.E., Fischer, E., 1986. Carbamazepine versusstudy. J. Clin. Psychiatry 48, 89–93. haloperidol in manic syndromes—first report of a multicentric
Lenzi, A., Lazzerini, F., Grossi, F., Massimetti, C., Placidi, G.F., study in Germany. In: Shagas, C., Josiassen, R.C., Bridger,1986. Use of carbamazepine in acute psychosis: a controlled W.H. (Eds.), Biological Psychiatry. Elsevier, Amsterdam, pp.study. J. Int. Med. Res. 14, 78–84. 332–334.
Lusznat, R.M., Murphy, D.P., Nunn, C.M., 1988. Carbamazepine Small, J.C., Klapper, M.H., Marhenke, I.D., Milstein, V.,vs. lithium in the treatment and prophylaxis of mania. Br. J. Woodham, C.C., Kellams, J.J., 1995. Lithium combined withPsychiatry 153, 198–204. carbamazepine or haloperidol in the treatment of mania.
Munoz, R.A., 2002. Oxcarbazepine For the Treatment of Bipolar Psychopharm. Bull. 31, 265–372.Disorder. Poster Presentation. American Psychiatric Associa- Small, J.C., Klapper, M.H., Milstein, V. et al., 1996. Comparisontion, Philadelphia. of therapeutic modalities for mania. Psychopharm. Bull. 32,
Nasr, S.J., Casper, M.L., 2002. Oxcarbazepine Use in the Treat- 623–627.ment of Mood Disorders. Poster Presentation. American Psy- Swann, A.C., Secunda, S.K., Katz, M.M., Koslow, S.H., Mass,chiatric Association, Philadelphia. J.W., Chang, S., Robins, E., 1986. Lithium treatment of mania:
Okuma, I., Inanaga, K., Otsuki, S., Sarai, K., Takahashi, R., clinical characteristics, specificity of symptom change, andHazama, H., Mon, A., Watanabe, M., 1979. Comparison of the outcome. Psychiatr. Res. 18, 127–141.
S34 J.S.E. Hellewell / Journal of Affective Disorders 72 (2002)S23–S34
Vasudev, K., Goswami, U., Kohli, K., 2000. Carbamazepine and Watkins, S.F., Callender, K., Thomas, D.R., Tidmarsh, S.F., Shaw,valproate monotherapy: feasibility, relative safety and efficacy, D.M., 1987. The effect of carbamazepine and lithium onand therapeutic drug monitoring in manic disorder. Psycho- remission from affective illness. Br. J. Psychiatry 150, 180–pharmacology (Berl.) 150, 15–23. 182.
Velikonja, M., Heinrich, K., 1984. Effect of Oxcarbazepine (GP Wellington, K., Goa, K.L., 2001. Oxcarbazepine: An update on its47.680) On Affective and Schizoaffective Symptoms: A Pre- efficacy in the management of epilepsy. CNS Drugs 15, 137–liminary Report. Elsevier, Amsterdam, pp. 208–210. 163.
Walden, J., Grunze, H., 2000. Bipolar Affective Disorder—Etiolo-gy and Treatment. Georg Thieme, Stuttgart.









![[CONFERENCE PAPER] Bipolar Bozuklukta BDT](https://static.fdokumen.com/doc/165x107/63328d1f4e0143040300b9b3/conference-paper-bipolar-bozuklukta-bdt.jpg)








