
Ovarian mucinous cystadenocarcinoma with mural nodule of carcinomatous derivation a light and...
8
Ovarian Mucinous Cystadenocarcinoma with Mural Nodule of Carcinomatous Derivation A Light and Electron Microscopic Study BERNARD CZERNOBILSKY, MD,' RAM DGANI, MD,t AND LAWRENCE M. ROTH, MDS A case of an ovarian mucinous tumor with a mural nodule is reported. The epithelial elements consisted of benign, low malignant potential, and invasive mucinous carcinoma. The latter was present in one focus near the surface of the mural nodule as well as in some shallow depressed areas in the cyst wall. The nodule itself was made up of highly malignant, anaplastic cells which on light microscopic ex- amination showed some similarities to the cells previously described in the sarcomatous and in some of the sarcoma-like mural nodules. However, analysis of light microscopic features in our case showed continuity and histologic similarities between the malignant mucinous cells and the sarcoma-appearing elements in the mural nodule. Ultrastructural features also supported an epithelial origin of the cells within the mural nodule. This case is the first of its kind with light and electronmicroscopic docu- mentation and supports an epithelial origin for some of the mural nodules in ovarian mucinous tumors. Cancer 51:141-148, 1983. HE NEWLY RECOGNIZED entities Of SarCOmatOUS and T sarcoma-like mural nodules occumng in ovarian mucinous tumors were described by Prat and Scully in 1979.'.*In their cases these mural nodules were sharply demarcated from the overlying mucinous epithelial component. It is of considerable interest that Prat and Scully mentioned in an addendum' a case in which the mural nodules in an ovarian mucinous cystadenocar- cinoma consisted of undifferentiated carcinoma with osteoclast-like giant cells rather than sarcoma or sar- coma-like tissue. We have recently encountered a case of an ovarian mucinous cystadenocarcinoma with a mural nodule composed of histologically malignant spindle, pleomor- phic, and giant cells, which on light and electron mi- croscopic examination appeared to be of epithelial rather than sarcomatous origin. This report, which is the first documented case of an ovarian mural nodule of adenocarcinomatous origin, adds to our knowledge of the histogenesis of mural nodules in ovarian mucinous neoplasms. Case Report A 75-year-old white Jewish woman, gravida 9, para 9, whose last menstrual period occurred 18 years previously, was ad- mitted to the hospital for a lower abdominal mass discovered three weeks prior to admission by her physician. Her initial complaint at that time was generalized weakness. There was no uterine bleeding. On physical examination a large fixed, nonpainful right abdominal mass reaching the umbilicus was found. The uterus was small and the left adnexa were unremarkable. A cervical polyp was seen. The remaining physical examination and lab- oratory data were within normal levels. was identified. Peritoneal fluid was absent and washings were From the Departments of Pathology and Obstetrics 8~ Gynecology, A laparotomy was performed and a right ovarian cystic Kaplan Hospital, Rehovot, Israel and the Department of Pathology, Indiana Universitv School of Medicine. Indianaoolis. Indiana. * Professor of Pathology, Medical School of the Hebrew University and Hadassah, Jerusalem and Chief, Department of Pathology, Kaplan Hospital, Rehovot, Israel. t Senior Gynecologist, Department of Obstetrics & Gynecology, Kaplan Hospital, Rehovot, Israel. Professor of Pathology and Director of Surgical Pathology, Indiana University School of Medicine, Indianapolis, Indiana. Address for reprints: B. Czernobilsb, MD, Dept. of Patholow. Kaplan Hospital, 76- 100 Rehovot, Israel. The authors wish to thank MS. Riva Lotsova, MS. Naomi and Mr. Yair Shimron for excellent technical assistance. Accepted for publication November 9, 198 I. obtained from the cul-de-sac and lateral paracolic gutters. On exploration of the abdominal cavity and pelvis, including lap- aroscopy of liver and diaphragm, no evidence of metastatic spread was found. After a frozen section, diagnosis of mucin- ous Carcinoma with malignant mural nodule was made, total hysterectomy, bilateral salpingo-oophorectomy, total omen- tectomy and pelvic lymph node sampling were performed. The postoperative course was uneventful. It was elected to treat her with adjuvant whole-pelvic irradiation. She is living and well 12 months after surgery. 0008-543X/83/0101/0141 $1.20 0 American Cancer Society 141
Transcript of Ovarian mucinous cystadenocarcinoma with mural nodule of carcinomatous derivation a light and...

Ovarian Mucinous Cystadenocarcinoma with Mural Nodule of Carcinomatous Derivation
A Light and Electron Microscopic Study
BERNARD CZERNOBILSKY, MD,' RAM DGANI, MD,t AND LAWRENCE M. ROTH, MDS
A case of an ovarian mucinous tumor with a mural nodule is reported. The epithelial elements consisted of benign, low malignant potential, and invasive mucinous carcinoma. The latter was present in one focus near the surface of the mural nodule as well as in some shallow depressed areas in the cyst wall. The nodule itself was made up of highly malignant, anaplastic cells which on light microscopic ex- amination showed some similarities to the cells previously described in the sarcomatous and in some of the sarcoma-like mural nodules. However, analysis of light microscopic features in our case showed continuity and histologic similarities between the malignant mucinous cells and the sarcoma-appearing elements in the mural nodule. Ultrastructural features also supported an epithelial origin of the cells within the mural nodule. This case is the first of its kind with light and electronmicroscopic docu- mentation and supports an epithelial origin for some of the mural nodules in ovarian mucinous tumors.
Cancer 51:141-148, 1983.
HE NEWLY RECOGNIZED entities Of SarCOmatOUS and T sarcoma-like mural nodules occumng in ovarian mucinous tumors were described by Prat and Scully in 1979.'.* In their cases these mural nodules were sharply demarcated from the overlying mucinous epithelial component. It is of considerable interest that Prat and Scully mentioned in an addendum' a case in which the mural nodules in an ovarian mucinous cystadenocar- cinoma consisted of undifferentiated carcinoma with osteoclast-like giant cells rather than sarcoma or sar- coma-like tissue.
We have recently encountered a case of an ovarian mucinous cystadenocarcinoma with a mural nodule composed of histologically malignant spindle, pleomor- phic, and giant cells, which on light and electron mi- croscopic examination appeared to be of epithelial
rather than sarcomatous origin. This report, which is the first documented case of an ovarian mural nodule of adenocarcinomatous origin, adds to our knowledge of the histogenesis of mural nodules in ovarian mucinous neoplasms.
Case Report
A 75-year-old white Jewish woman, gravida 9, para 9, whose last menstrual period occurred 18 years previously, was ad- mitted to the hospital for a lower abdominal mass discovered three weeks prior to admission by her physician. Her initial complaint at that time was generalized weakness. There was no uterine bleeding.
On physical examination a large fixed, nonpainful right abdominal mass reaching the umbilicus was found. The uterus was small and the left adnexa were unremarkable. A cervical polyp was seen. The remaining physical examination and lab- oratory data were within normal levels.
was identified. Peritoneal fluid was absent and washings were
From the Departments of Pathology and Obstetrics 8~ Gynecology, A laparotomy was performed and a right ovarian cystic Kaplan Hospital, Rehovot, Israel and the Department of Pathology, Indiana Universitv School of Medicine. Indianaoolis. Indiana.
* Professor of Pathology, Medical School of the Hebrew University and Hadassah, Jerusalem and Chief, Department of Pathology, Kaplan Hospital, Rehovot, Israel.
t Senior Gynecologist, Department of Obstetrics & Gynecology, Kaplan Hospital, Rehovot, Israel.
Professor of Pathology and Director of Surgical Pathology, Indiana University School of Medicine, Indianapolis, Indiana.
Address for reprints: B. Czernobilsb, MD, Dept. of Patholow. Kaplan Hospital, 76- 100 Rehovot, Israel.
The authors wish to thank MS. Riva Lotsova, MS. Naomi and Mr. Yair Shimron for excellent technical assistance.
Accepted for publication November 9, 198 I .
obtained from the cul-de-sac and lateral paracolic gutters. On exploration of the abdominal cavity and pelvis, including lap- aroscopy of liver and diaphragm, no evidence of metastatic spread was found. After a frozen section, diagnosis of mucin- ous Carcinoma with malignant mural nodule was made, total hysterectomy, bilateral salpingo-oophorectomy, total omen- tectomy and pelvic lymph node sampling were performed. The postoperative course was uneventful. It was elected to treat her with adjuvant whole-pelvic irradiation. She is living and well 12 months after surgery.
0008-543X/83/0101/0141 $1.20 0 American Cancer Society
141

142 CANCER January 1 1983 VOl. 5 1
Results
Gross and Histologic Findings
The right ovarian cyst measured 12 cm in diameter and presented a smooth external surface to which a nor- mal fallopian tube was attached. The cut surface showed a predominantly unilocular cyst with a few secondary small locules measuring up to 0.5 cm arising from the inner surface. The majority of the inner surface was smooth, but several oval-shaped shallow, slightly de- pressed, yellow-white rough areas were observed. A sin- gle firm gray-white focally hemorrhagic mural nodule measuring as its base 3.0 X 1.5 cm and projecting 2.0 cm into the cavity was present (Fig. 1). The surface of this nodule was covered by fibrinous material. On the cut section near the surface a small mucoid area was noted. The contents of the cyst consisted of a stringy mucoid fluid.
The uterus weighed 60 g, was small and showed no abnormalities except for an 0.8 cm long endocervical
On light microscopic examination, the cyst wall and loculated areas were lined by a single layer of mature mucinous epithelium which was partially denuded. In areas well formed mucous glands were present under- neath the surface lining. The cyst wall consisted mostly of nonspecific fibrous tissue. In the loculated areas the stroma was more cellular. Near the mural nodule and partly covering it, as well as in the vicinity of the shallow depressed areas, the lining showed stratification of up to three layers of mucinous cells with a filigree pattern, moderate nuclear atypia and occasional mitotic figures (Fig. 2). Most of the surface of the mural nodule was ulcerated and a thick fibrin cap covered the underlying
Polyp.
FIG. 1. Portion of cyst wall showing protruding mural nodule
Material and Methods
Tissue for light microscopy was fixed in 10% buffered formalin. Routine paraffin block sections were stained with hematoxylin and eosin (H & E), periodic acid Schiff (PAS), mucicarmine, alcian blue at pH 2.5, trichrome, and Prussian blue.
Small fragments from the mural nodule, and rough- ened oval depressions were fixed in 2% glutaraldehyde either initially or following formalin fixation. They were then postfixed in 2% osmium tetroxide for 1 hour, de- hydrated through graded alcohols, propylene oxide and embedded in Epon 8 12. Thick sections were cut for light and ultrastructural correlation and stained with tolu- idine blue. Thin sections were cut on a Sorvall MT-2B ultramicrotome, stained with uranyl acetate and lead citrate and examined with a Philips EM-201 electron microscope.
FIG. 2. Cyst wall adjacent to mural nod- ule lined by several layers of mucinous epithelium showing filigree pattern (H & E, X36).

No. 1 OVARIAN MUCINOUS C A WITH MURAL NODULE * C'zernobilsky et al.
FIG. 3. High magnification of area of invasive adenocarcinoma showing tumor cells floating in a mucous pool to the left and similar appearing cells invading fi- brous stroma to the right. A fold of benign surface epithelium is noted in the top cen- ter of the field (H & E, XlSO).
necrotic and hemorrhagic tissue. In a single focus near the surface of the mural nodule there was a pool of mucus which contained neutrophils and clusters of highly atypical epithelial cells sometimes forming glands. At the margins of this mucous pool and beneath the ulcerated surface, epithelial cells and glands with nuclear features similar to those floating in the mucus, trailed off into the surrounding fibrous stroma that also showed a moderate chronic inflammatory cell reaction consist- ing primarily of lymphocytes and plasma cells (Fig. 3). In areas a desmoplastic reaction was very prominent. In the deeper areas the tumor was composed of aggre-
143
gates of very atypical polygonal or spindle cells showing large vesicular nuclei with occasional inconspicuous nucleoli. Tumor giant cells, multinucleated tumor cells and abnormal mitoses were also present (Fig. 4). Forty high power fields were counted for mitotic rate and an average of 9 mitoses, many highly atypical, per 10 fields were found. The tumor nodule was fairly well circum- scribed and presented a pushing border which was heavily infiltrated by lymphocytes. Sections from the roughened, slightly depressed areas showed foci of in- vasive, poorly differentiated, mucinous carcinoma with abundant extracellular mucin production. Moderate
FIG. 4. Deeper portion of mural nodule showing a sarcomatous appearance with tumor giant cells and scattered inflam- matory reaction. An abnormal mitosis is present in upper portion of the field ( H & E, X225).

144 CANCER January 1 1983 VOl. 51
chronic inflammatory reaction with capillary prolifera- tion and fibroblasts was present in this area. No bizarre stromal cells were identified.
Mucicarmine, PAS and alcian blue stains revealed the presence of intracellular mucin in the single and mul- tilayered epithelial cell lining of the cyst. Some of it was within goblet cells. The mucinous nature of the extra- cellular material near the surface of the nodule was con- firmed by mucicarmine, PAS and alcian blue stains. Occasional tumor cells and glands in the nodule also stained positively with these stains. The trichrome stain
FIG. 5. Electron micrograph of superficial area of mural nodule showing tumor cells forming a glandular lumen containing secretory substance. The luminal border is lined by stubby microvilli. Nuclei show evenly distributed chromatin and one has a markedly irregular contour (X5600).
showed a variable pattern with extensive collagenization in areas where the tumor cells were dispersed in the fibrous portion of the mural nodule to virtual absence of collagen in the areas where polygonal and spindle type tumor cells were heavily aggregated. In the areas near the ulcerated surface of the mural nodule much hemosiderin pigment was present.
The opposite ovary was atrophic and showed scat- tered surface epithelial inclusion cysts. The fallopian tubes were not remarkable. The endometrium showed mild cystic hyperplasia with an occasional mitotic figure.
FIG. 6. An intracytoplasmic lumen lined by stubby microvilli is present in neoplastic epithe- lial cells of superficial portion of mural nodule. Adjacent cell membranes show some immature desmosomes (X8300).

No. 1 OVARIAN MUCINOUS CA WITH MURAL NODULE - Czernobilsky et ul. 145
FIG. 7. Electron micrograph of a tumor cell from the deep area of the mural nodule showing extremely irregular nuclear contour, prominent nucleolus and lysosome-like dense bodies. The cell is sharply demarcated from the collagenous stroma in the lower right-hand portion of the field. Small accumulations of electron dense ma- terial are present between collagen bundles (X12000).
The myometrium was unremarkable. In the cervix a benign endocervical polyp was identified. The omentum and pelvic lymph nodes were free of tumor. Peritoneal washings were negative on cytologic examination.
Electronmicroscopic findings
Cells from the superficial area of the mural nodule showing cords and irregular neoplastic glands invading fibrous stroma in the 1 pm sections, showed at the ul- trastructural level glandular differentiation as evidenced by luminal surfaces with a stubby microvillous lining. Luminal secretory substance containing mucous gran- ules was abundant (Fig. 5). The borders of adjacent ep- ithelial cells showed well-developed tripartate junctions. Several epithelial cells showed intracytoplasmic lumina lined by similar microvilli (Fig. 6). In some areas ad- jacent cell membranes demonstrated prominent infold- ings. Tumor cells were demarcated from the stroma by an indistinct basal lamina. Cytoplasm contained abun- dant free ribosomes, occasional strands of smooth and rough endoplasmic reticulum, mucous granules and small numbers of mitochondria. Nuclei showed even distribution of chromatin with occasional nucleoli. Nu- clear membranes sometimes exhibited prominent in- foldings producing a lobulated appearance of the nuclear contour (Fig. 7).
In 1 pm sections of the deeper areas, cords of tumor cells were evident but no glandular formations were seen. Ultrastructurally clusters of tumor cells that dif- fered from those described above by the absence of glan- dular or intracytoplasmic lumina were evident in this
area. Immature desmosomes were present but were not as numerous as in the more superficial areas of the tumor.
Neoplastic cells from the deepest portion of the mural nodule were more irregular, varying from spindle to polygonal in shape. Nuclear-cytoplasmic ratios were often high. Nuclear contours were sometimes extremely irregular and nucleoli were occasionally more promi- nent. However, the chromatin remained evenly distrib- uted. Contents of cytoplasmic organelles were similar to that previously described, except that an occasional cell had more developed endoplasmic reticulum, which was sometimes dilated and rarely contained amorphous material of variable electron density. No mucin granules were present. Where tumor cells were closely apposed, they were attached by occasional tight junctions or rarely by desmosomes of the macula adherens type (Fig. 8). No basal lamina separated the clusters of tumor cells from the collagenous stroma, but occasionally an amor- phous electron dense material was present along the epithelial cell membrane or between adjacent collagen bundles (Fig. 9). This material was similar in density to the more dense portion of the material observed in tu- mor cells within the dilated cisternal granular endo- plasmic reticulum.
One micron-thick sections of a slightly depressed rough area in the inner lining of the cyst, showed ultra- structurally clusters of neoplastic epithelial cells within loose strands of mucus. Nuclei were often peripherally located and showed evenly distributed chromatin, some irregularity of the nuclear contour and an occasional prominent nucleolus. Cytoplasm was abundant, con-

146 CANCER January 1 1983 Vol. 5 1
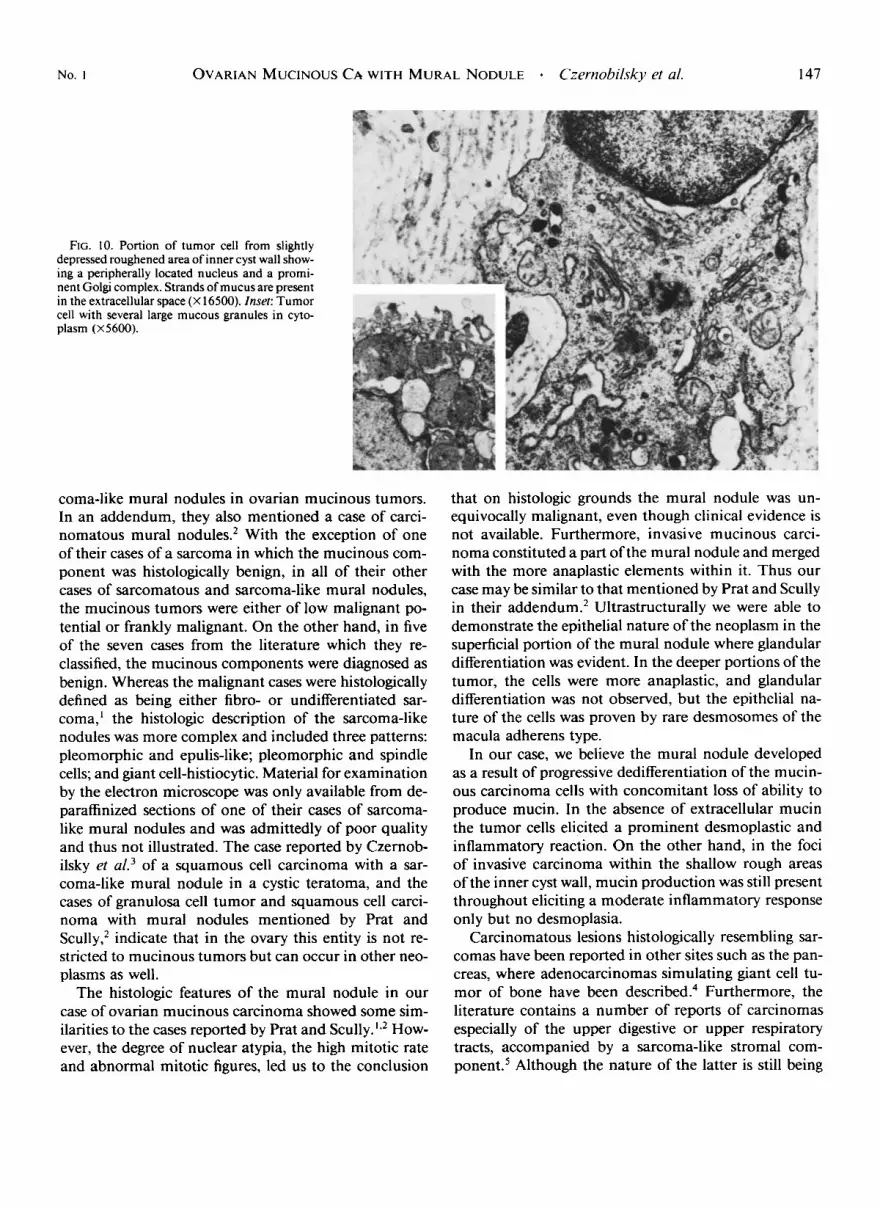
taining strands of granular and smooth endoplasmic re- ticulum. Some cells had a prominent Golgi complex and large mucous granules. Occasional mitochondria and scattered lysosome-like dense bodies were also observed. Individual cells showed irregular processes but no sur- face specializations were identified (Fig. 10).
Sections from the stroma of the smooth surfaced cyst wall showed spindle-shaped fibroblasts and abundant collagen.
FIG. 8. Desmosomes of the macula adherens type are present between tumor cells in deep por- tion of mural nodule (X52000).
Discussion
In 1979 Prat and S~u l ly l .~ reported nine cases of sar- comatous and sarcoma-like mural nodules in ovarian mucinous tumors, reviewed the literature on this subject and, in addition, reclassified seven previously reported cases collected from the literature. Based on light mi- croscopic findings and clinical information, Prat and Scullyl,2 presented a total of two sarcomas and 14 sar-
FIG. 9. Tumor cell from deep portion of mural nodule showing profiles of granular endoplasmic reticulum as well as free ribosomes. Amorphous electron dense material is present at the junction of the cell membrane and the collagenous stroma (X34000).
No. I OVARIAN MUCINOUS CA WITH MURAL NODULE Czernobifsky et al. 147
FIG. 10. Portion of tumor cell from slightly depressed roughened area of inner cyst wall show- ing a peripherally located nucleus and a promi- nent Golgi complex. Strands of mucus are present in the extracellular space (X 16500). Insef: Tumor cell with several large mucous granules in cyto- plasm (X5600).
coma-like mural nodules in ovarian mucinous tumors. In an addendum, they also mentioned a case of carci- nomatous mural nodules.2 With the exception of one of their cases of a sarcoma in which the mucinous com- ponent was histologically benign, in all of their other cases of sarcomatous and sarcoma-like mural nodules, the mucinous tumors were either of low malignant po- tential or frankly malignant. On the other hand, in five of the seven cases from the literature which they re- classified, the mucinous components were diagnosed as benign. Whereas the malignant cases were histologically defined as being either fibro- or undifferentiated sar- coma,' the histologic description of the sarcoma-like nodules was more complex and included three patterns: pleomorphic and epulis-like; pleomorphic and spindle cells; and giant cell-histiocytic. Material for examination by the electron microscope was only available from de- paraffinized sections of one of their cases of sarcoma- like mural nodules and was admittedly of poor quality and thus not illustrated. The case reported by Czernob- ilsky et ~ 1 . ~ of a squamous cell carcinoma with a sar- coma-like mural nodule in a cystic teratoma, and the cases of granulosa cell tumor and squamous cell carci- noma with mural nodules mentioned by Prat and S c ~ l l y , ~ indicate that in the ovary this entity is not re- stricted to rnucinous tumors but can occur in other neo- plasms as well.
The histologic features of the mural nodule in our case of ovarian mucinous carcinoma showed some sim- ilarities to the cases reported by Prat and Scully.'*2 How- ever, the degree of nuclear atypia, the high mitotic rate and abnormal mitotic figures, led us to the conclusion
that on histologic grounds the mural nodule was un- equivocally malignant, even though clinical evidence is not available. Furthermore, invasive mucinous carci- noma constituted a part of the mural nodule and merged with the more anaplastic elements within it. Thus our case may be similar to that mentioned by Prat and Scully in their addendum.2 Ultrastructurally we were able to demonstrate the epithelial nature of the neoplasm in the superficial portion of the mural nodule where glandular differentiation was evident. In the deeper portions of the tumor, the cells were more anaplastic, and glandular differentiation was not observed, but the epithelial na- ture of the cells was proven by rare desmosomes of the macula adherens type.
In our case, we believe the mural nodule developed as a result of progressive dedifferentiation of the mucin- ous carcinoma cells with concomitant loss of ability to produce mucin. In the absence of extracellular mucin the tumor cells elicited a prominent desmoplastic and inflammatory reaction. On the other hand, in the foci of invasive carcinoma within the shallow rough areas of the inner cyst wall, much production was still present throughout eliciting a moderate inflammatory response only but no desmoplasia.
Carcinomatous lesions histologically resembling sar- comas have been reported in other sites such as the pan- creas, where adenocarcinomas simulating giant cell tu- mor of bone have been de~cribed.~ Furthermore, the literature contains a number of reports of carcinomas especially of the upper digestive or upper respiratory tracts, accompanied by a sarcoma-like stromal com- p ~ n e n t . ~ Although the nature of the latter is still being

148 CANCER January 1 1983 VOl. 5 1
debated, there is evidence that in at least some instances the spindle cell component is of epithelial deri~ation.~.'
Mural nodules in ovarian mucinous tumors may rep- resent anaplastic carcinoma, a true sarcoma,' or a re- active process either to extracellular mucin' or to re- peated hemorrhage.8 In order to establish the true nature of the mural nodules in ovarian mucinous and possibly other epithelial neoplasms, the material must be care- fully studied ultrastructurally in addition to light mi- croscopic examination. This does not mean to imply that sarcomatous or sarcoma-like mural nodules do not exist, but a carcinomatous origin must first be consid- ered. The absence of an overlying low malignant poten- tial or frankly malignant epithelial neoplasm does not entirely eliminate a carcinomatous origin of the mural nodule since focal areas of epithelial malignancy might not be detected when, as in our case, most of the surface of the mural nodule becomes ulcerated and necrotic.
Other ovarian neoplasms, composed of both epithelial and malignant stromal components such as adenosar- coma' and mesodermal (Mullenan) mixed tumors" can easily be differentiated from the mucinous tumors with mural nodules since in the former the epithelial and stromal elements are intimately mixed throughout, whereas the previously described mural nodules were sharply demarcated from the epithelial lining of the cyst wall.',' In our case, the blending of epithelial and stromal elements was limited to one area only. Otherwise, the two elements were completely separated as in the cases reported by Prat and Scully.'.*
It is difficult to evaluate the biologic behavior of ovar- ian mucinous tumors with mural nodules since the for- mer ranges from benign, low malignant potential, to invasive carcinoma; whereas the latter encompasses a spectrum of reactive lesions, sarcomas, and carcinomas. As might be expected, histologically malignant mural nodules often have behaved aggressively since two pa- tients with apparent sarcoma died of tumor' and a third with carcinoma' had a recurrence following rupture of the tumor. In our case, the tumor was confined to the ovary but follow-up at this time is still limited.
In conclusion, the case reported here stresses the im- portance of a careful histologic analysis of mural nodules in ovarian mucinous tumors, in which ultrastructural examination is of paramount importance. With the help of the latter, the histogenesis of the mural nodule can usually be established. Classification of a mural nodule as reactive, sarcomatous or carcinomatous may deter- mine the proper treatment and prognosis in these pa- tients.
ADDENDUM
Since the acceptance of this article, Prat e/ ul. (Prat J, Young RH. Scully RE. Ovarian mucinous tumors with foci of anaplastic carci- noma, Cancer 1982; 50:300-304) published a series of four ovarian mucinous tumors with foci of anaplastic carcinoma that also appeared in the form of mural nodules.
REFERENCES
I . Prat J , Scully RE. Sarcomas in ovarian mucinous tumors: A report of two cases. Cancer 1979; 44:1327-1331.
2. Prat J, Scully RE. Ovarian mucinous tumors with sarcoma-like mural nodules: A report of seven cases. Cancer 1979; 44: 1332-1344.
3. Czernobilsky B, Rotenstreich L, Lancet M. Ovarian dermoid with squamous carcinoma-pseudosarcoma. Arch Puthol 1972: 93: 14 I - 144.
4. Rosai J. Carcinoma of pancreas simulating giant cell tumor of bone: Electron microscopic evidence of its acinar cell origin. Cancer 1968; 22:333-344.
5. Lane N. Pseudosarcoma (polypoid sarcoma-like masses) asso- ciated with squamous-cell carcinoma of the mouth, fauces and larynx: Report of 10 cases. Cuncer 1957: 10:19-41.
6. Lichtiger B, Mackay MB, Tessmer CF. Spindle cell variant of squamous carcinoma: A light and electron microscopic study of 13 cases. Cancer 1970; 26: I3 I I - 1320.
7 . Battifora H. Spindle cell carcinoma: Ultrastructural evidence of squamous origin and collagen production by the tumor cells. Cancer 1976; 31:2215-2282.
8. Leschke H. Estraossare Riesenzellengeschwulste und die Deu- tung Ihrer Entstehung in Cystadenomen des Ovar aus jungem Gran- ulationsgewebe. Virchows Arch Pa/hol Anal 195 1; 320: 164-1 73 .
9. Clement PB, Scully RE. Extra-uterine mesodermal (Mullenan) adenosarcoma: A clinicopathological analysis of five cases. Am J CIin
10. Czernobilsky B, La Barre GC. Carcinosarcoma and mixed me- sodermal tumor of the ovary: A clinicopathologic analysis of 9 cases. Ohtet Gynecol 1968; 31:21-32.
Puthd 1918; 69~276-283.




















