Oral Antioxidants Improve Leg Blood Flow During Exercise in Patients with Chronic Obstructive...
31
1 Oral Antioxidants Improve Leg Blood Flow During Exercise 1 in Patients with Chronic Obstructive Pulmonary Disease 2 3 4 Matthew J. Rossman 1,2 , Joel D. Trinity 1,3 , Ryan S. Garten 1,3 , Stephen J. Ives 1,4 , Jamie D. 5 Conklin 1,5 , Zachary Barrett-O’Keefe 1,2 , Melissa A. H. Witman 1,3 , Amber D. Bledsoe 6 , David E. 6 Morgan 6 , Sean Runnels 6 , Van R. Reese 1,3 , Jia Zhao 1.3 , Markus Amann 1, 3 , D. Walter Wray 1, 2, 3 , 7 and Russell S. Richardson 1,2, 3 8 9 10 1 Geriatric Research, Education, and Clinical Center 11 George E. Whalen VA Medical Center, Salt Lake City, Utah 12 13 2 Department of Exercise and Sport Science 14 University of Utah, Salt Lake City, Utah 15 16 3 Department of Internal Medicine, Division of Geriatrics 17 University of Utah, Salt Lake City, Utah 18 19 4 Department of Health and Exercise Sciences 20 Skidmore College, Saratoga Springs, New York 21 22 5 Department of Internal Medicine, Division of Respiratory, Critical Care and Occupational 23 Pulmonary Medicine 24 University of Utah, Salt Lake City, Utah 25 26 5 Department of Anesthesiology, 27 University of Utah, Salt Lake City, Utah 28 29 Corresponding Author: 30 31 Russell S. Richardson 32 VA Medical Center Bldg 2, Rm 1D25 33 500 Foothill Drive 34 Salt Lake City, UT 84148 35 801.582.1565 Ext. 4344 36 Fax 801.584.5658 37 [email protected] 38 39 40 Conflicts of Interest: None. 41 Funding: National Institutes of Health grant PO1 HL 09830, HL-103786 and HL-116579 and a 42 VA Merit grant E6910R 43 Short Title: Leg blood flow and oxidative stress in COPD 44 Keywords: Chronic bronchitis, emphysema, oxidative stress, exercise, oxygen transport 45 46 Articles in PresS. Am J Physiol Heart Circ Physiol (July 17, 2015). doi:10.1152/ajpheart.00184.2015 Copyright © 2015 by the American Physiological Society.
Transcript of Oral Antioxidants Improve Leg Blood Flow During Exercise in Patients with Chronic Obstructive...

1
Oral Antioxidants Improve Leg Blood Flow During Exercise 1 in Patients with Chronic Obstructive Pulmonary Disease 2
3 4 Matthew J. Rossman1,2, Joel D. Trinity1,3, Ryan S. Garten1,3, Stephen J. Ives1,4, Jamie D. 5 Conklin1,5, Zachary Barrett-O’Keefe1,2, Melissa A. H. Witman1,3, Amber D. Bledsoe6, David E. 6 Morgan6, Sean Runnels6, Van R. Reese1,3, Jia Zhao1.3, Markus Amann1, 3, D. Walter Wray1, 2, 3, 7 and Russell S. Richardson1,2, 3 8 9 10 1Geriatric Research, Education, and Clinical Center 11 George E. Whalen VA Medical Center, Salt Lake City, Utah 12 13 2Department of Exercise and Sport Science 14 University of Utah, Salt Lake City, Utah 15 16 3Department of Internal Medicine, Division of Geriatrics 17 University of Utah, Salt Lake City, Utah 18 19 4 Department of Health and Exercise Sciences 20 Skidmore College, Saratoga Springs, New York 21 22 5Department of Internal Medicine, Division of Respiratory, Critical Care and Occupational 23 Pulmonary Medicine 24 University of Utah, Salt Lake City, Utah 25 26 5Department of Anesthesiology, 27 University of Utah, Salt Lake City, Utah 28 29 Corresponding Author: 30 31 Russell S. Richardson 32 VA Medical Center Bldg 2, Rm 1D25 33 500 Foothill Drive 34 Salt Lake City, UT 84148 35 801.582.1565 Ext. 4344 36 Fax 801.584.5658 37 [email protected] 38 39 40 Conflicts of Interest: None. 41 Funding: National Institutes of Health grant PO1 HL 09830, HL-103786 and HL-116579 and a 42 VA Merit grant E6910R 43 Short Title: Leg blood flow and oxidative stress in COPD 44 Keywords: Chronic bronchitis, emphysema, oxidative stress, exercise, oxygen transport 45 46
Articles in PresS. Am J Physiol Heart Circ Physiol (July 17, 2015). doi:10.1152/ajpheart.00184.2015
Copyright © 2015 by the American Physiological Society.
2
ABSTRACT: 47 48
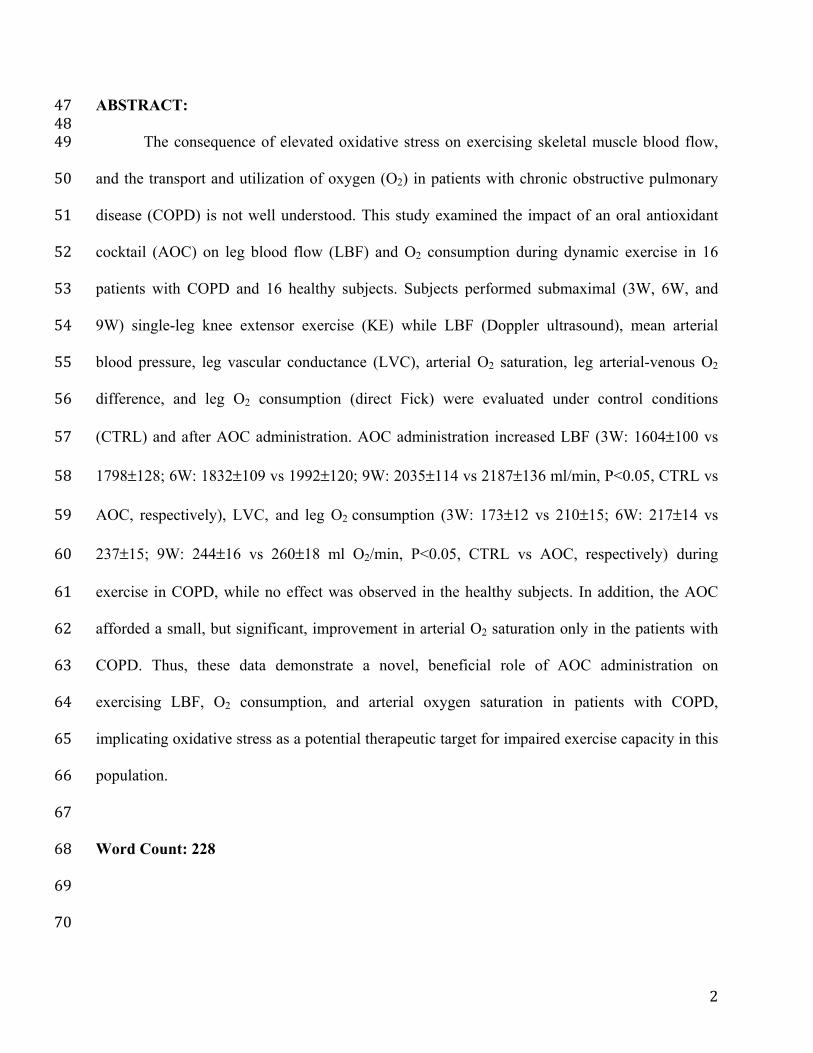
The consequence of elevated oxidative stress on exercising skeletal muscle blood flow, 49 and the transport and utilization of oxygen (O2) in patients with chronic obstructive pulmonary 50 disease (COPD) is not well understood. This study examined the impact of an oral antioxidant 51 cocktail (AOC) on leg blood flow (LBF) and O2 consumption during dynamic exercise in 16 52 patients with COPD and 16 healthy subjects. Subjects performed submaximal (3W, 6W, and 53 9W) single-leg knee extensor exercise (KE) while LBF (Doppler ultrasound), mean arterial 54 blood pressure, leg vascular conductance (LVC), arterial O2 saturation, leg arterial-venous O2 55 difference, and leg O2 consumption (direct Fick) were evaluated under control conditions 56 (CTRL) and after AOC administration. AOC administration increased LBF (3W: 1604±100 vs 57 1798±128; 6W: 1832±109 vs 1992±120; 9W: 2035±114 vs 2187±136 ml/min, P<0.05, CTRL vs 58 AOC, respectively), LVC, and leg O2 consumption (3W: 173±12 vs 210±15; 6W: 217±14 vs 59 237±15; 9W: 244±16 vs 260±18 ml O2/min, P<0.05, CTRL vs AOC, respectively) during 60 exercise in COPD, while no effect was observed in the healthy subjects. In addition, the AOC 61 afforded a small, but significant, improvement in arterial O2 saturation only in the patients with 62 COPD. Thus, these data demonstrate a novel, beneficial role of AOC administration on 63 exercising LBF, O2 consumption, and arterial oxygen saturation in patients with COPD, 64 implicating oxidative stress as a potential therapeutic target for impaired exercise capacity in this 65 population. 66 67 Word Count: 228 68 69 70

3
New and Noteworthy: This research has identified the ability of antioxidants to increase 71 skeletal muscle blood flow and oxygen consumption during exercise in patients with Chronic 72 Obstructive Pulmonary Disease (COPD). Thus, targeting oxidative stress may have important 73 therapeutic implications for improving oxygen transport and utilization, and therefore exercise 74 tolerance, in patients with COPD. 75 76 77

4
INTRODUCTION: 78 COPD is a pro-inflammatory condition that primarily impacts the lungs, resulting in 79 diminished pulmonary function (29). Other detrimental sequelae of this condition include 80 mitochondrial (35) and skeletal muscle (31) dysfunction, and, consequently, exercise intolerance 81 and decreased fatigue resistance are recognized hallmarks of patients with COPD (3). 82 Interestingly, peripheral vascular function is also impaired in these patients (24). Through the 83 release of autocrine and paracrine factors which modulate vascular tone, the vasculature plays a 84 critical role in regulating skeletal muscle blood flow (37), and therefore the delivery of O2 and 85 nutrients. As such, poor vascular function also has the potential to influence exercise capacity 86 and fatigability in patients with COPD (39). However, the mechanistic link between COPD, 87 vascular dysfunction, and exercising skeletal muscle blood flow remains to be elucidated. 88 Peripheral vascular dysfunction in COPD has been attributed to numerous factors, 89 including systemic inflammation and oxidative stress (20, 24). Indeed, relative to age-matched 90 healthy subjects, both elevated systemic inflammation and oxidative stress have been well 91 documented in patients with COPD (6, 24, 32). Specific to oxidative stress, our group has 92 recently demonstrated the beneficial effects of an acutely administered, oral antioxidant cocktail 93 (AOC) on vascular function, as assessed by flow-mediated dilation, in patients with COPD (24). 94 The AOC, and the dosing strategy employed, has previously been documented to reduce O2 and 95 carbon centered free radicals in patients with COPD (40). Thus, the improvement in vascular 96 function following AOC administration in the prior work was attributed to the free radical 97 scavenging ability of the AOC, restoration of the redox balance in the patients, and potentially, a 98 subsequent improvement in nitric oxide (NO) bioavailability (24). Based on these findings, 99

5
targeting oxidative stress with an acute AOC appears to represent a viable mechanism for 100 improving peripheral vascular function in patients with COPD. 101 Oxidative stress may impair vascular function, and potentially adversely impact vascular 102 control during exercise, by enhancing endothlin-1 activity (19, 43), potentiating angiotensin-II 103 mediated vasoconstriction (17), augmenting sympathetically-mediated vascular tone (42), and 104 suppressing cyclooxygenase-2 mediated dilation (21), in addition to, among these and other 105 mechanisms, directly reducing the bioavailability of the vasodilator NO. With regard to NO, 106 Crecelius et al. (16) documented an improvement in forearm blood flow in older individuals 107 during rhythmic handgrip exercise with an intra-arterial infusion of ascorbate, and this effect was 108 abrogated when ascorbate was co-infused with a NO synthase inhibitor. In addition, Wray et al. 109 (46) documented elevated end plantar flexion exercise muscle perfusion, assessed by nuclear 110 magnetic resonance spectroscopy, following administration of the AOC in older individuals. 111 Collectively, these studies suggest that there are numerous mechanisms by which oxidative stress 112 may adversely impact vascular control during exercise, and implicate antioxidant administration 113 and free radical scavenging as strategies to improve exercise hyperemia, potentially through an 114 improvement in NO bioavailability. 115 Therefore, the purpose of this study was to examine the impact of an acutely 116 administered oral AOC on LBF and O2 transport in the exercising skeletal muscle of patients 117 with COPD and healthy subjects. We tested two hypotheses: First, administration of the AOC 118 would improve exercising LBF in patients with COPD, with less of an effect in healthy subjects. 119 Second, the increase in LBF following AOC administration would be accompanied by an 120 improvement in redox balance, assessed by blood markers of antioxidant status relative to 121 markers of oxidative stress. 122

6
METHODS: 123 Subjects: A total of 32 subjects, 16 patients with COPD, and 16 age and sex matched healthy 124 subjects, completed this study. Subjects were included in the study based on spirometric 125 evidence of either COPD (patients with COPD) or normal lung function (healthy subjects) and 126 sedentary to low physical activity levels (assessment described below). Exclusion criteria for the 127 study included: Hypertension or other overt cardiovascular disease, diabetes, neuromuscular 128 disease, known cancer, and obesity. All subjects performed standard pulmonary function tests 129 during an initial visit to the laboratory. General morphometric characteristics, and peak KE work 130 rate, were also determined during this visit. The Institutional Review Boards of the University of 131 Utah and the Salt Lake City VA Medical Center approved all protocol and written, informed 132 consent was obtained from all participants prior to their inclusion in the study. 133 134 Physical Activity Level: Prior to participation in the study, physical activity was assessed by a 135 subjective modified physical activity level recall questionnaire (41) in all subjects, with the goal 136 of matching physical activity levels between patients with COPD and healthy subjects. After this 137 initial data collection, physical activity was further evaluated, to confirm similar physical activity 138 levels between groups, by objective accelerometry in a representative subset of 20 subjects (10 139 subjects per group). The physical activity questionnaire included items regarding the average 140 type, frequency, intensity, and duration of physical activity in any given week (23). For the 141 accelerometry, 10 patients with COPD and 10 healthy subjects wore accelerometers (GT1M; 142 Actigraph, Pensacola, FL) for seven consecutive days after receiving standardized operating 143 instructions. Average total daily physical activity was expressed as both the average steps per 144 day and, to better characterize the intensity of physical activity, the average total accelerometer 145

7
counts per minute for each subject was parsed into sedentary, low-, moderate-, and high-intensity 146 activity using device-specific software (Actilife, Actigraph, Pensacola, FL). Previous research 147 has documented the validity and reliability of the Actigraph GT1M in the estimation of daily 148 physical activity (1, 44). 149 150 Exercise Protocols and General Procedures: Prior to data collection, all subjects were 151 familiarized with KE exercise during 1 to 3 laboratory visits, during which subjects practiced 152 performing the KE workloads and durations required for the study. On the experimental day, 153 subjects reported to the laboratory following a 12 hour fast and rested for ~30 minutes prior to all 154 procedures. Subsequently, catheters were placed in the femoral artery and vein using sterile 155 technique, as previously described (4). After catheter placement, subjects rested for an additional 156 30 minutes before beginning KE exercise as presented in Figure 1. KE exercise was performed at 157 60 rpm on a cycle erogmeter (Monark, Sweden) modified to allow KE exercise (38). Briefly, this 158 exercise modality recruits the quadriceps muscle group for active leg extension from 90 to ~170 159 degrees before a lever arm attached to a flywheel passively returns the leg to 90 degrees. Due to 160 the potentially long-lasting effects of the AOC, the AOC trial was always performed after the 161 CTRL condition. In addition, the invasive nature of the study and subject risk associated with 162 catheter placement, precluded separation of the study into two separate days. However, of note, 163 our group has previously documented the reproducibility of hemodynamic measurements 164 achieved with this serial exercise testing experimental design, without an intervention, across a 165 range of exercise intensities (8). Each workload (3, 6, and 9 Watts) was sustained for three 166 minutes. One-minute of rest was allowed between each stage. LBF, mean arterial pressure 167 (MAP), leg O2 consumption, and heart rate (HR) were assessed during the last minute of baseline 168

8
and each exercise stage. Blood samples were taken anaerobically during the last minute of both 169 baseline and each exercise stage. 170 171 Antioxidant Supplementation: All subjects were instructed to refrain from vitamin 172 supplementation for at least five days prior to data collection. On the experimental day, the AOC 173 was administered in a split dose, consumed 2 and 1.5 hours prior to the second exercise bout, to 174 improve absorption and maximize the time of antioxidant efficacy. The first dose consisted of 175 300 mg α-lipoic acid, 500 mg vitamin C and 200 IU of vitamin E, and the second dose consisted 176 of the same amounts of α-lipoic acid and vitamin C and 400 IU of vitamin E. This AOC, and the 177 dosing strategy employed, has been previously documented to lower carbon and O2-centered free 178 radical levels, as measured by EPR spectroscopy, and improve vascular function in patients with 179 COPD (24, 40). 180 181 Central Cardiovascular Responses: Arterial blood pressure measurements were collected 182 continuously from an indwelling catheter placed in the common femoral artery, with the pressure 183 transducer at the level of the catheter (Transpac IV, Abbott Laboratories). MAP (in mmHg) was 184 calculated as follows: MAP = diastolic arterial pressure + (arterial pulse pressure × 0.33). Heart 185 rate was monitored from a standard three-lead ECG, a component of the data-acquisition device 186 (Biopac, Goleta, CA). 187 188 Leg Blood Flow and Vascular Conductance: Measurements of femoral artery blood velocity 189 and vessel diameter in the leg being studied were performed at rest and during the last minute of 190 each exercise stage, using a Logic 7 ultrasound system (General Electric Medical Systems, WI, 191

9
USA) as previously described (9). The Logic 7 was equipped with a linear array transducer, 192 operating at an imaging frequency of 9 MHz. The blood velocity profile was obtained with the 193 same transducer with a Doppler frequency of 5 MHz operated in the high-pulsed repetition 194 frequency mode. LBF was calculated as: LBF = (mean femoral artery blood velocity)π(femoral 195 artery vessel diameter/2)2 × 60. LVC was calculated as LBF/arterial catheter-derived MAP. 196 197 Blood Analysis: A standard lipid panel was obtained for all subjects. At rest, and in the last 15 s 198 of each exercise stage, femoral arterial and venous blood samples (1-2 ml) were collected and 199 one ml of each sample was presented to a GEM 4000 combined blood gas analyzer and co-200 oximeter (Instrumentation Laboratories, Bedford, MA). Arterial and venous blood hemoglobin 201 (Hb) concentration, and hemoglobin O2 saturation, was measured by co-oximetry. The GEM 202 4000 also contains different polymer film electrochemical sensors specific for relevant 203 substrates, which were used to measure the partial pressure of O2 and carbon dioxide, as well as 204 lactate and pH. Arterial (CaO2) and venous (CvO2) blood O2 content (in ml/dl) were calculated 205 as: blood O2 content = 1.39 (Hb) x O2 saturation/100) + 0.003 x PO2. Leg O2 consumption (VO2; 206 in ml/min) was calculated as: VO2 = (CaO2 – CvO2) x LBF. 207 208 Oxidative Stress and Inflammation: Venous blood samples taken at rest were centrifuged to 209 collect plasma, and the plasma samples were stored at -80°C until analysis. Lipid peroxidation, a 210 marker of oxidant damage, was assessed by plasma malondialdehyde (MDA) levels (Bioxytech 211 LPO-586, Foster City, CA). Total antioxidant capacity was evaluated by determining the ferric 212 reducing ability of plasma (FRAP), using the method described by Benzie and Strain (10). The 213 efficacy of the AOC specific to plasma ascorbate levels was assayed as previously described (11) 214

10
(CosmoBio, Carlsbad, CA). Endogenous antioxidant activity was assessed by catalase activity in 215 the plasma (45) (Cayman Chemical Company, Ann Arbor, MI). Plasma C-reactive protein levels, 216 an index of systemic inflammation, were determined by a high sensitivity ELISA assay (R & D 217 Systems, Minneapolis, MN). 218 219 Statistical Analysis: Independent samples t-tests were used to determine differences in subject 220 characteristics, including physical activity-related variables. A 2 x 2 mixed-design analysis of 221 variance (ANOVA) was used to evaluate the effect of the AOC on indices of antioxidant status, 222 inflammation, and oxidative stress. When a significant effect was detected, differences were 223 identified using paired t-tests for the within-subject factor (AOC), and independent t-tests for the 224 between-subject factor (COPD vs healthy subjects). A 2 x 3 (subject x workload) ANOVA was 225 used to determine differences between patents with COPD and healthy controls (subject factor) 226 on physiological variables measured during exercise (workload: 3, 6, and 9 Watts) and a 2 X 3 227 (AOC x workload) repeated-measures ANOVA was used to identify significant changes in 228 measured variables due to AOC administration within healthy subjects and the patient group. A 229 Tukey post-hoc analysis was used if a significant main effect is found. Statistical significance 230 was set at α = 0.05 for all tests. All data are expressed as mean ± standard error of the mean. 231 232 233 234 235 236 237

11
RESULTS: 238 Subject Characteristics: Subject characteristics are documented in Table 1. Patients with 239 COPD exhibited reduced pulmonary function relative to the healthy subjects, and blood gas 240 characteristics consistent with COPD (Table 1). Apart from pulmonary function, arterial blood 241 gases, and pulmonary disease medications, the healthy subjects were well matched with the 242 patients with COPD (Table 1). By experimental design, in general, physical activity levels were 243 relatively similar between the healthy subjects and the patient group, resulting in similar peak 244 KE work rates between groups (Table 1). Two of the patients with COPD were current smokers, 245 who refrained from the use of tobacco products for 12 hours prior to all data collection. Four 246 patients qualified for supplemental O2; only one of these patients, however, required the use of 247 supplemental O2 during exercise (the blood gas data for the individual utilizing supplemental O2 248 was excluded from the analyses). 249 250 Antioxidants, Oxidative Stress and Inflammation: Baseline plasma ascorbate was not 251 different between patients with COPD and the healthy subjects (Figure 2C). Relative to the 252 healthy subjects, patients with COPD exhibited a reduced antioxidant capacity, as assessed by 253 FRAP (Figure 2B). In addition, C-reactive protein, a marker of systemic inflammation, was 254 elevated in patients with COPD compared to the healthy subjects (Figure 2A). Plasma catalase 255 activity and malondialdehyde levels were not different between patients with COPD and the 256 healthy subjects (Figure 2D and E). Administration of the AOC increased plasma ascorbate 257 levels similarly in both groups (Figure 2A). Interestingly, however, both FRAP (Figure 2B) and 258 catalase activity (Figure 2D) were only increased in the patients with COPD as a consequence of 259 ingesting the AOC. 260

12
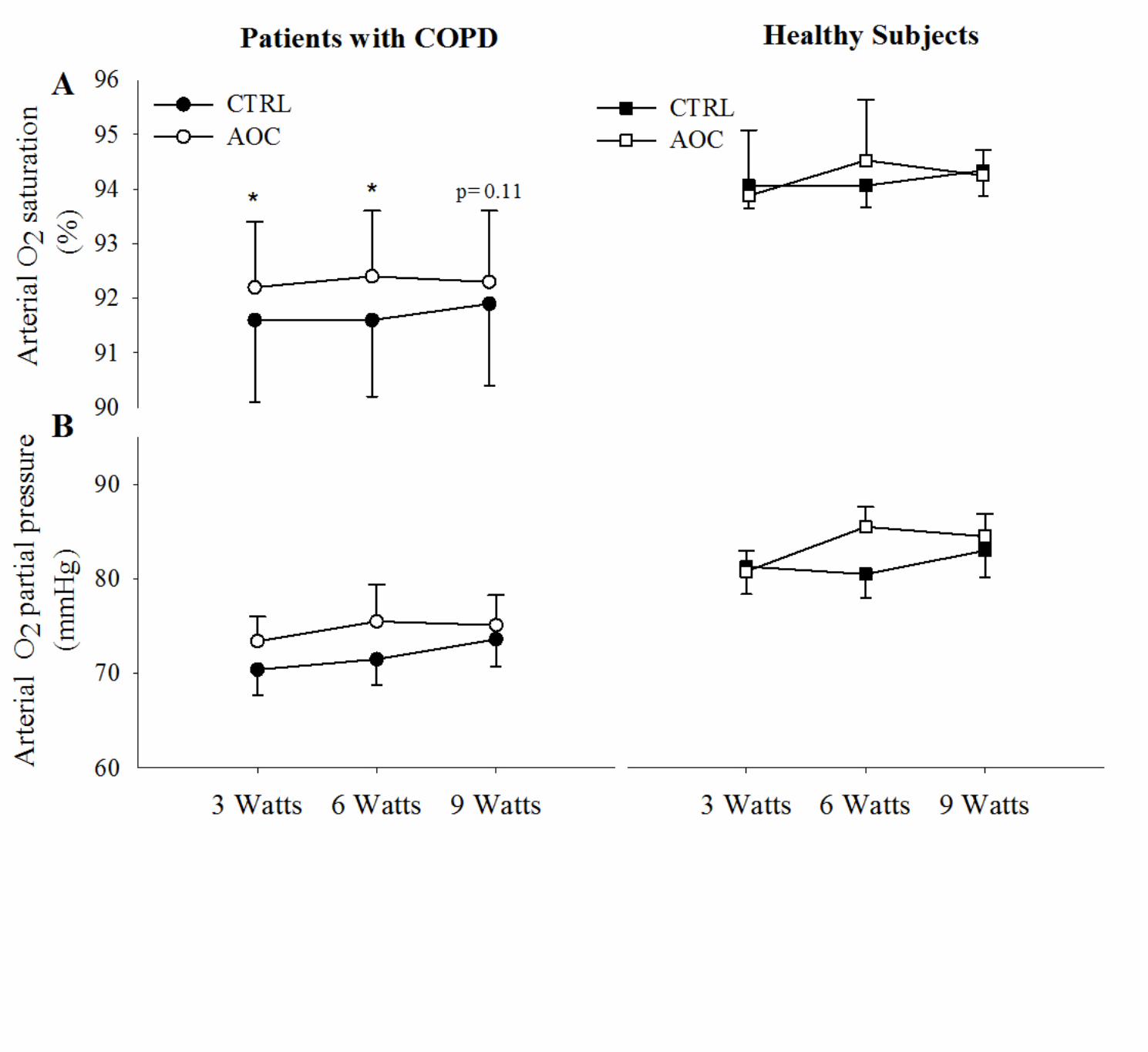
Resting Responses: In patients with COPD at rest, administration of the AOC did not impact 261 MAP, LBF, LVC, HR, CaO2, leg arterial-venous O2 difference, net lactate release or venous pH 262 (Table 2), however, arterial O2 saturation was elevated slightly (91.7 ± 1.3 vs 92.2 ± 1.1%, 263 CTRL vs AOC, respectively), but significantly. In contrast, in the healthy subjects, LBF and 264 LVC were elevated following the AOC consumption; while the other measured variables were 265 unchanged (Table 2). 266 267 Exercise Responses: During exercise at 3, 6, and 9 Watts, LBF was elevated relative to the 268 CTRL condition following AOC consumption in patients with COPD (Figure 3A, Table 2). The 269 elevated LBF, in combination with an unaltered arterial-venous O2 difference, resulted in an 270 increase in leg O2 consumption in the AOC condition in the patients with COPD (Figure 3). In 271 the healthy subjects, LBF, arterial-venous O2 difference, and leg O2 consumption were unaltered 272 by AOC administration (Figure 3A, B, and C, Table 2). In addition, LVC was elevated with the 273 AOC over the CTRL condition in the patients with COPD (Figure 4), but not in the healthy 274 subjects. SaO2 was also elevated in the AOC trial compared to CTRL conditions only in the 275 patents with COPD (Figure 5A), while PaO2 was unchanged (Figure 5B). Neither SaO2 nor PaO2 276 were impacted by the AOC in healthy subjects (Figures 5A and B). CaO2 was not different 277 between conditions in either group, because in the patient group the elevated SaO2 was offset by 278 a small, but significant, decrease in hemoglobin concentration during exercise in the AOC 279 condition (Table 2). 280 281 282 283

13
DISCUSSION: 284 This study examined the impact of an acutely administered, oral AOC with previously 285
documented efficacy, on exercise-induced skeletal muscle blood flow, vasodilation, O2 transport 286 and utilization during small muscle mass exercise in patients with COPD and age and sex 287 matched healthy subjects. Patients with COPD exhibited basal evidence of elevated 288 inflammation and reduced antioxidant capacity. AOC consumption improved antioxidant status 289 in the patients with COPD, and these alterations led to favorable changes in the central and 290 peripheral cardiorespiratory responses to exercise. Specifically, LBF and LVC during single-leg 291 KE were augmented in patients with COPD following AOC consumption, while no changes 292 were observed in the healthy subjects. The elevation in LBF, in combination with an unaltered 293 arterial-venous O2 difference from CTRL conditions, led to increased O2 consumption during 294 exercise in the patients with COPD. In addition, arterial O2 saturation was improved, at rest and 295 during exercise, in patients with COPD with the AOC, whereas there was no apparent effect in 296 the healthy subjects. These data demonstrate beneficial effects of antioxidant administration on 297 exercise-induced hemodynamics and skeletal muscle metabolism in patients with COPD, and 298 indicate that impaired O2 transport, as a consequence of elevated oxidative stress, may represent 299 a novel mechanistic link between oxidative stress and exercise intolerance in this population. 300 301 Oxidative Stress and Exercise: Oxidative stress has previously been documented to be elevated 302 in patients with COPD relative to age-matched, healthy subjects at rest (6, 24, 32). In addition, 303 indices of oxidative stress, such as protein carbonyls, have been inversely correlated with disease 304 severity (6). Exercise appears to especially augment oxidative stress in patients with COPD, and 305 as such, markers of oxidative damage are typically elevated in patients with COPD in 306

14
comparison to healthy subjects following exercise (32). Interestingly, this amplified oxidant 307 production during exercise in COPD occurs following exercise which minimally taxes the 308 pulmonary system, such as isolated quadriceps exercise (14, 15), implying that organs beyond 309 the lung may be contributing to the free radical production. Increased oxidative stress in patients 310 with COPD has been attributed to mitochondrial electron transport chain dysfunction (35) and 311 the systemic inflammation (29) accompanying COPD, among other factors (36). 312
The current data supports the concept of elevated oxidative stress and inflammation in 313 patients with COPD. Specifically, decreased plasma antioxidant capacity and increased C-314 reactive protein levels were documented in the patients with COPD relative to the healthy 315 subjects (Figure 2). Administration of the AOC partially corrected the pro/antioxidant imbalance 316 only in the patient group, increasing both FRAP and catalase activity, with minimal effects in 317 healthy subjects (Figure 2). Although not examined in the current study, these data are in 318 accordance with the previously observed free-radical diminishing effects of the AOC in patients 319 with COPD using ex-vivo spin-trapping and electron paramagnetic resonance spectroscopy (24, 320 40). In the current study, the absence of a change in antioxidant or oxidant status in the healthy 321 subjects, despite an equal increase in plasma ascorbate (Figure 2A), is likely due to the absence 322 of a substantial redox imbalance in these healthy individuals. Thus, these data further document 323 elevated oxidative stress in patients with COPD, as well as beneficial effects of antioxidant 324 administration on redox balance in patients with COPD, that may be useful in the face of the 325 elevated free radical production during exercise in this population. 326 327 Exercise Hyperemia and Oxidative Stress: Independent of COPD, aging itself is characterized 328 by a pro-inflammatory, pro-oxidant phenotype, which has been implicated as a causative factor 329

15
in the age-associated decline in vascular function (18). As such, previous research has suggested 330 that the increase in oxidative stress with age may impair resting limb blood flow and exercise 331 hyperemia (12, 13, 16, 46). There are numerous mechanisms by which oxidative stress may 332 impair vascular control and limb blood flow, including the amplification of vasoconstrictor 333 activity (17, 19, 42, 43) or by diminishing the bioactivity of vasodilating agents, such as 334 cyclooxygenase 2 (21) and NO (16). Accordingly, antioxidant administration has been 335 documented to augment resting blood flow and exercise-induced hyperemia in older individuals 336 (16, 25, 46), although this is not a universal observation (34). Likewise, an abnormal 337 pro/antioxidant balance has repeatedly been documented in patients with COPD (6, 24, 30), as 338 observed in the current study (Figure 2). In addition, our group has previously observed 339 beneficial effects of AOC administration on vascular function in patients with COPD (24). 340 Collectively, these observations support the possibility that oxidative stress may negatively 341 impact skeletal muscle blood flow in this population. 342
Similar to previous research in older individuals, the current data, for the first time, 343 demonstrate an augmented exercise hyperemia following AOC administration in patients with 344 COPD (Figure 3A). The increase in LBF in the patients with COPD was observed across all 345 submaximal workloads (Figure 3), and can be attributed to an increase in LVC (Figure 4), as 346 MAP was unaffected by AOC administration. These data imply an increase in leg vasodilation 347 during exercise in the patients with COPD, providing a novel mechanism to target with the goal 348 of improving O2 transport in this population. 349 Oxygen Transport and Utilization: In the presence of increased LBF following AOC 350 administration, and no change in arterial-venous O2 difference, exercising skeletal muscle O2 351 consumption was elevated in the patients with COPD (Figure 3). Although the typical response 352

16
to augmented O2 delivery is to decrease O2 extraction, and thereby maintain O2 consumption, 353 according to the Fick principle (22), there is growing evidence that skeletal muscle can increase 354 or decrease VO2 at a given workload when O2 availability is altered (4, 5, 7, 28, 33) and these 355 changes in VO2 do not always result in compensatory changes in glycolytic metabolism. 356 Accordingly, our group (4) and others (33), have previously observed lower levels of VO2 during 357 exercise, and unchanged lactate production, with interventions that result in decreased skeletal 358 muscle blood flow. Similarly, enhanced blood flow has led to augmented skeletal muscle VO2 359 without a corresponding decrease in lactate production (5, 8). Collectively, these data suggest 360 that the total energy consumed by the muscle at a given workload may vary with changes in 361 blood flow and O2 delivery. The potential functional consequences of these changes in VO2 have 362 been examined by Amann et al. (2, 5), who demonstrated that augmented LBF during 363 submaximal KE in heart failure patients resulted in an increase in skeletal muscle VO2, which 364 attenuated exercise-induced skeletal muscle fatigue. 365
The data from the current study support the notion that augmented exercise hyperemia 366 may enhance skeletal muscle VO2 during exercise, as observed following AOC administration in 367 the patients with COPD (Figure 3). In line with previous research (4, 8, 33), the changes in VO2 368 in the patients with COPD were not accompanied by changes in glycolytic metabolism, as 369 evidenced by a lack of an effect of the AOC on lactate release (Table 2). As enhanced muscle 370 VO2 has been suggested to lead to greater fatigue resistance during exercise (2, 5), it is tempting 371 to speculate that increased VO2 during exercise may enhance fatigue resistance in COPD. 372 Central Responses: Secondary to a significant ventilation-perfusion mismatch in their diseased 373 lungs (26), patients with COPD are typically characterized by depressed arterial O2 saturation 374 and reduced PaO2. In addition, the degree of hypoxemia is inversely related to exercise capacity, 375

17
and hypoxemia exacerbates oxidative stress in patients with COPD (27). As expected, the 376 patients with COPD in the current study exhibited reduced PaO2 and SaO2 relative to healthy 377 subjects at rest (Table 1) and during exercise (Figure 5). Interestingly, following AOC 378 administration, a small, but significant, increase in SaO2, but no change in PaO2, was observed in 379 patients with COPD, both at rest and during exercise, whereas no impact of the AOC was 380 observed in healthy subjects (Figures 5A and B). These data indicate that at a similar PaO2 as 381 CTRL conditions, SaO2 was elevated following AOC administration in the patients with COPD. 382 Therefore, although it is difficult to elucidate the precise mechanism responsible for the increase 383 in SaO2, it may have been due to a direct effect of AOC administration at the lung or an increase 384 in Hb affinity for O2. The increased Hb-O2 affinity may have been related to a decrease in 385 metabolic perturbation during exercise as a consequence of the increase in aerobic metabolism 386 afforded by the AOC (Figure 3C), although no measurable changes in lactate or pH were 387 observed (Table 2). Although the practical significance of the ~1% increase in saturation is 388 questionable, as this increase was accomplished with a relatively small antioxidant dose, the 389 impact on saturation of further decreases in oxidative stress with a more potent antioxidant 390 intervention potentially deserves further examination. In addition, an increase in SaO2 has the 391 potential to improve CaO2 and O2 delivery, which would likely have beneficial effects for 392 exercising skeletal muscle (2). CaO2, however, was not altered in the patients in the current study 393 because of the small, but significant, decrease in hemoglobin concentration that offset the 394 increased SaO2, and maintained CaO2 (Table 2). These data do, however, suggest that reducing 395 oxidative stress in patients with COPD has the potential to attenuate arterial hypoxemia, which 396 may improve exercise tolerance in this population. 397

18
Experimental considerations: It is important to acknowledge potential limitations of the current 398 study. Specifically, the AOC trial was always performed after the CTRL trial, which does not 399 exclude the possibility of an order effect. However, due to the invasive nature of catheter 400 placement, the t CTRL and AOC trials had to be performed on the same day. In addition, 401 because of the potential long-lasting effects of the AOC, the AOC trial always had to be 402 performed last. Importantly, our group has previously documented the reproducibility of 403 hemodynamic measurements achieved with sequential exercise bouts, and no intervention, across 404 a range of exercise intensities (8). Thus, we are confident that the observed changes are most 405 likely due to the intervention, and the favorable impact of decreasing oxidative stress in patients 406 with COPD. Additionally, and somewhat surprisingly, despite minimalistic blood sampling to 407 avoid a change in hemoglobin, hemoglobin levels were lower in the patients with COPD in the 408 second, AOC, trial. As there was no evidence of greater bleeding in the patients with COPD, this 409 could simply have been the effect of random variation in the measurement (i.e. a type 1 error). 410 Importantly, arterial oxygen content, which actually has the ability to affect blood flow, was not 411 different between trials (Table 2). 412 Summary and Conclusions: The purpose this study was to examine the impact of an AOC on 413 oxidative stress and antioxidant capacity, and subsequently exercise hemodynamics during small 414 muscle mass exercise in patients with COPD and healthy subjects. Patients with COPD exhibited 415 evidence of reduced antioxidant capacity relative to healthy subjects. Administration of the AOC 416 improved the redox balance in the patients with COPD, with little effect in the healthy subjects. 417 These favorable changes in redox balance were accompanied by improved LBF and LVC as well 418 as increased skeletal muscle O2 consumption during submaximal KE exercise in patients with 419 COPD, while minimal effects were observed in healthy subjects. In addition, arterial O2 420

19
saturation was improved at rest and during exercise in patients with COPD following AOC 421 administration. Collectively, these data illustrate the role of oxidative stress in the integration of 422 O2 transport and utilization during exercise in this population, and further implicate oxidative 423 stress in the systemic pathophysiological consequences of COPD. 424 425

20
References: 426 1. Abel MG, Hannon JC, Sell K, Lillie T, Conlin G, and Anderson D. Validation of the 427 Kenz Lifecorder EX and ActiGraph GT1M accelerometers for walking and running in adults. 428 Applied physiology, nutrition, and metabolism = Physiologie appliquee, nutrition et metabolisme 429 33: 1155-1164, 2008. 430 2. Amann M, and Calbet JA. Convective oxygen transport and fatigue. J Appl Physiol 431 104: 861-870, 2008. 432 3. Amann M, Regan MS, Kobitary M, Eldridge MW, Boutellier U, Pegelow DF, and 433 Dempsey JA. Impact of pulmonary system limitations on locomotor muscle fatigue in patients 434 with COPD. Am J Physiol Regul Integr Comp Physiol 299: R314-324, 2010. 435 4. Amann M, Runnels S, Morgan DE, Trinity J, Fjeldstad A, Wray DW, Reese VR, 436 and Richardson RS. On the Contribution of Group Iii and Iv Muscle Afferents to the 437 Circulatory Response to Rhythmic Exercise in Humans. J Physiol 589: 3855-3866, 2011. 438 5. Amann M, Venturelli M, Ives SJ, Morgan DE, Gmelch B, Witman MA, Jonathan 439 Groot H, Walter Wray D, Stehlik J, and Richardson RS. Group III/IV muscle afferents 440 impair limb blood in patients with chronic heart failure. International journal of cardiology 174: 441 368-375, 2014. 442 6. Barreiro E, de la Puente B, Minguella J, Corominas JM, Serrano S, Hussain SN, 443 and Gea J. Oxidative stress and respiratory muscle dysfunction in severe chronic obstructive 444 pulmonary disease. Am J Respir Crit Care Med 171: 1116-1124, 2005. 445 7. Barrett-O'Keefe Z, Helgerud J, Wagner PD, and Richardson RS. Maximal strength 446 training and increased work efficiency: contribution from the trained muscle bed. Journal of 447 applied physiology 113: 1846-1851, 2012. 448 8. Barrett-O'Keefe Z, Ives SJ, Trinity JD, Morgan G, Rossman MJ, Donato AJ, 449 Runnels S, Morgan DE, Gmelch BS, Bledsoe AD, Richardson RS, and Wray DW. 450 Endothelin-A-Mediated Vasoconstriction During Exercise With Advancing Age. The journals of 451 gerontology Series A, Biological sciences and medical sciences 2014. 452 9. Barrett-O'Keefe Z, Ives SJ, Trinity JD, Morgan G, Rossman MJ, Donato AJ, 453 Runnels S, Morgan DE, Gmelch BS, Bledsoe AD, Richardson RS, and Wray DW. Taming 454 the "sleeping giant": the role of endothelin-1 in the regulation of skeletal muscle blood flow and 455 arterial blood pressure during exercise. Am J Physiol Heart Circ Physiol 304: H162-169, 2013. 456 10. Benzie IF, and Strain JJ. The ferric reducing ability of plasma (FRAP) as a measure of 457 "antioxidant power": the FRAP assay. Anal Biochem 239: 70-76, 1996. 458 11. Bradley DW, Emery G, and Maynard JE. Vitamin C in plasma: a comparative study 459 of the vitamin stabilized with trichloroacetic acid or metaphosphoric acid and the effects of 460 storage at -70 degrees, -20 degrees, 4 degrees, and 25 degrees on the stabilized vitamin. Clin 461 Chim Acta 44: 47-52, 1973. 462 12. Casey DP, Madery BD, Curry TB, Eisenach JH, Wilkins BW, and Joyner MJ. Nitric 463 oxide contributes to the augmented vasodilatation during hypoxic exercise. J Physiol 588: 373-464 385, 2010. 465 13. Casey DP, Walker BG, Curry TB, and Joyner MJ. Ageing reduces the compensatory 466 vasodilatation during hypoxic exercise: the role of nitric oxide. J Physiol 589: 1477-1488, 2011. 467 14. Couillard A, Koechlin C, Cristol JP, Varray A, and Prefaut C. Evidence of local 468 exercise-induced systemic oxidative stress in chronic obstructive pulmonary disease patients. 469 Eur Respir J 20: 1123-1129, 2002. 470

21
15. Couillard A, Maltais F, Saey D, Debigare R, Michaud A, Koechlin C, LeBlanc P, 471 and Prefaut C. Exercise-induced quadriceps oxidative stress and peripheral muscle dysfunction 472 in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med 167: 1664-473 1669, 2003. 474 16. Crecelius AR, Kirby BS, Voyles WF, and Dinenno FA. Nitric oxide, but not 475 vasodilating prostaglandins, contributes to the improvement of exercise hyperemia via ascorbic 476 acid in healthy older adults. Am J Physiol Heart Circ Physiol 299: H1633-1641, 2010. 477 17. de Groot AA, van Zwieten PA, and Peters SL. Involvement of reactive oxygen species 478 in angiotensin II-induced vasoconstriction. Journal of cardiovascular pharmacology 43: 154-479 159, 2004. 480 18. Donato AJ, Eskurza I, Silver AE, Levy AS, Pierce GL, Gates PE, and Seals DR. 481 Direct evidence of endothelial oxidative stress with aging in humans: relation to impaired 482 endothelium-dependent dilation and upregulation of nuclear factor-kappaB. Circ Res 100: 1659-483 1666, 2007. 484 19. Donato AJ, Gano LB, Eskurza I, Silver AE, Gates PE, Jablonski K, and Seals DR. 485 Vascular endothelial dysfunction with aging: endothelin-1 and endothelial nitric oxide synthase. 486 Am J Physiol Heart Circ Physiol 297: H425-432, 2009. 487 20. Eickhoff P, Valipour A, Kiss D, Schreder M, Cekici L, Geyer K, Kohansal R, and 488 Burghuber OC. Determinants of systemic vascular function in patients with stable chronic 489 obstructive pulmonary disease. Am J Respir Crit Care Med 178: 1211-1218, 2008. 490 21. Gano LB, Donato AJ, Pasha HM, Hearon CM, Jr., Sindler AL, and Seals DR. The 491 SIRT1 activator SRT1720 reverses vascular endothelial dysfunction, excessive superoxide 492 production, and inflammation with aging in mice. Am J Physiol Heart Circ Physiol 307: H1754-493 1763, 2014. 494 22. Gonzalez-Alonso J, Richardson RS, and Saltin B. Exercising skeletal muscle blood 495 flow in humans responds to reduction in arterial oxyhaemoglobin, but not to altered free oxygen. 496 J Physiol 530: 331-341, 2001. 497 23. Groot HJ, Trinity JD, Layec G, Rossman MJ, Ives SJ, and Richardson RS. Perfusion 498 pressure and movement-induced hyperemia: evidence of limited vascular function and 499 vasodilatory reserve with age. Am J Physiol Heart Circ Physiol 304: H610-619, 2013. 500 24. Ives SJ, Harris RA, Witman MA, Fjeldstad AS, Garten RS, McDaniel J, Wray DW, 501 and Richardson RS. Vascular dysfunction and chronic obstructive pulmonary disease: the role 502 of redox balance. Hypertension 63: 459-467, 2014. 503 25. Jablonski KL, Seals DR, Eskurza I, Monahan KD, and Donato AJ. High-dose 504 ascorbic acid infusion abolishes chronic vasoconstriction and restores resting leg blood flow in 505 healthy older men. Journal of applied physiology 103: 1715-1721, 2007. 506 26. Kent BD, Mitchell PD, and McNicholas WT. Hypoxemia in patients with COPD: 507 cause, effects, and disease progression. International journal of chronic obstructive pulmonary 508 disease 6: 199-208, 2011. 509 27. Koechlin C, Maltais F, Saey D, Michaud A, LeBlanc P, Hayot M, and Prefaut C. 510 Hypoxaemia enhances peripheral muscle oxidative stress in chronic obstructive pulmonary 511 disease. Thorax 60: 834-841, 2005. 512 28. Larsen FJ, Schiffer TA, Borniquel S, Sahlin K, Ekblom B, Lundberg JO, and 513 Weitzberg E. Dietary inorganic nitrate improves mitochondrial efficiency in humans. Cell 514 metabolism 13: 149-159, 2011. 515

22
29. Maclay JD, and MacNee W. Cardiovascular disease in COPD: mechanisms. Chest 143: 516 798-807, 2013. 517 30. MacNee W. Pulmonary and systemic oxidant/antioxidant imbalance in chronic 518 obstructive pulmonary disease. Proceedings of the American Thoracic Society 2: 50-60, 2005. 519 31. Maltais F, Decramer M, Casaburi R, Barreiro E, Burelle Y, Debigare R, Dekhuijzen 520 PN, Franssen F, Gayan-Ramirez G, Gea J, Gosker HR, Gosselink R, Hayot M, Hussain SN, 521 Janssens W, Polkey MI, Roca J, Saey D, Schols AM, Spruit MA, Steiner M, Taivassalo T, 522 Troosters T, Vogiatzis I, Wagner PD, and COPD AEAHCoLMDi. An official american 523 thoracic society/european respiratory society statement: update on limb muscle dysfunction in 524 chronic obstructive pulmonary disease. Am J Respir Crit Care Med 189: e15-62, 2014. 525 32. Mercken EM, Hageman GJ, Schols AM, Akkermans MA, Bast A, and Wouters EF. 526 Rehabilitation decreases exercise-induced oxidative stress in chronic obstructive pulmonary 527 disease. Am J Respir Crit Care Med 172: 994-1001, 2005. 528 33. Mortensen SP, Gonzalez-Alonso J, Damsgaard R, Saltin B, and Hellsten Y. 529 Inhibition of nitric oxide and prostaglandins, but not endothelial-derived hyperpolarizing factors, 530 reduces blood flow and aerobic energy turnover in the exercising human leg. J Physiol 581: 853-531 861, 2007. 532 34. Nyberg M, Blackwell JR, Damsgaard R, Jones AM, Hellsten Y, and Mortensen SP. 533 Lifelong physical activity prevents an age-related reduction in arterial and skeletal muscle nitric 534 oxide bioavailability in humans. J Physiol 590: 5361-5370, 2012. 535 35. Puente-Maestu L, Tejedor A, Lazaro A, de Miguel J, Alvarez-Sala L, Gonzalez-536 Aragoneses F, Simon C, and Agusti A. Site of mitochondrial reactive oxygen species 537 production in skeletal muscle of chronic obstructive pulmonary disease and its relationship with 538 exercise oxidative stress. American journal of respiratory cell and molecular biology 47: 358-539 362, 2012. 540 36. Rahman I. The role of oxidative stress in the pathogenesis of COPD: implications for 541 therapy. Treatments in respiratory medicine 4: 175-200, 2005. 542 37. Richardson RS. Oxygen transport and utilization: an integration of the muscle systems. 543 Advances in physiology education 27: 183-191, 2003. 544 38. Richardson RS, Frank LR, and Haseler LJ. Dynamic knee-extensor and cycle 545 exercise: functional MRI of muscular activity. Int J Sports Med 19: 182-187, 1998. 546 39. Rossman MJ, Garten RS, Groot HJ, Reese V, Zhao J, Amann M, and Richardson 547 RS. Ascorbate infusion increases skeletal muscle fatigue resistance in patients with chronic 548 obstructive pulmonary disease. Am J Physiol Regul Integr Comp Physiol 305: R1163-1170, 549 2013. 550 40. Rossman MJ, Groot HJ, Reese V, Zhao J, Amann M, and Richardson RS. Oxidative 551 stress and COPD: the effect of oral antioxidants on skeletal muscle fatigue. Med Sci Sports Exerc 552 45: 1235-1243, 2013. 553 41. Taylor HL, Jacobs DR, Jr., Schucker B, Knudsen J, Leon AS, and Debacker G. A 554 questionnaire for the assessment of leisure time physical activities. Journal of chronic diseases 555 31: 741-755, 1978. 556 42. Thomas GD, Zhang W, and Victor RG. Impaired modulation of sympathetic 557 vasoconstriction in contracting skeletal muscle of rats with chronic myocardial infarctions: role 558 of oxidative stress. Circ Res 88: 816-823, 2001. 559

23
43. Van Guilder GP, Westby CM, Greiner JJ, Stauffer BL, and DeSouza CA. 560 Endothelin-1 vasoconstrictor tone increases with age in healthy men but can be reduced by 561 regular aerobic exercise. Hypertension 50: 403-409, 2007. 562 44. Welk GJ, Blair SN, Wood K, Jones S, and Thompson RW. A comparative evaluation 563 of three accelerometry-based physical activity monitors. Med Sci Sports Exerc 32: S489-497, 564 2000. 565 45. Wheeler CR, Salzman JA, Elsayed NM, Omaye ST, and Korte DW, Jr. Automated 566 assays for superoxide dismutase, catalase, glutathione peroxidase, and glutathione reductase 567 activity. Anal Biochem 184: 193-199, 1990. 568 46. Wray DW, Nishiyama SK, Monnet A, Wary C, Duteil SS, Carlier PG, and 569 Richardson RS. Antioxidants and aging: NMR-based evidence of improved skeletal muscle 570 perfusion and energetics. Am J Physiol Heart Circ Physiol 297: H1870-1875, 2009. 571 572 573

24
Table 1. Subject characteristics
Healthy Subjects COPD
Age, yr 68 ± 2 62 ± 3
Male/Female 13/3 13/3
Height, m 1.73 ± 0.02 1.74 ± 0.02
Weight, kg 75 ± 4 85 ± 4
BMI, kg/m2 25 ± 1 28 ± 1
Peak knee-extensor work rate, W 31 ± 3 26 ± 3
Glucose, mg/dl 84 ± 4 84 ± 3
Cholesterol, mg/dl 201 ± 14 202 ± 16
HDL, mg/dl 52 ± 3 61 ± 5
LDL, mg/dl 132 ± 10 120 ± 13
Triglycerides, mg/dl 94 ± 16 117 ± 14
Pulmonary function Forced vital capacity, l (% predicted) 4.7 ± 0.3 (113 ± 5) 4.1 ± 0.3* (94 ± 5*)
Forced expiratory volume in one s, l/s (% predicted) 3.4 ± 0.2 (115 ± 4) 1.8 ± 0.2* (54 ± 6*)
FEV1/FVC (%) 75 ± 1 48 ± 4*
Resting arterial blood gases Oxyhemoglobin, % 94.4 ± 0.5 91.7 ± 1.2*
Partial pressure of oxygen, mmHg 87 ± 4 71 ± 3*
Partial pressure of carbon dioxide, mmHg 30 ± 1 35 ± 1*
Bicarbonate, mmol/l 19.7 ± 0.5 23.4 ± 0.8*
pH 7.43 ± 0.01 7.43 ± 0.01
Medications (% of Group) Long Acting Beta Agonists 0% 26%
Short Acting Beta Agonists 0% 80%
Acetylcholine Antagonists 0% 53%
Inhaled Corticosteroids 15% 33%
Physical Activity, n = 10/group Sedentary, min/day 1215 ± 17 1156 ± 75
Light, min/day 153 ± 9 127 ± 20
Moderate, min/day 26 ± 5 15 ± 6
High, min/day 0.4 ± 0.2 0.1 ± 0.01*
Steps, counts/day 5101 ± 671 3798 ± 728 COPD, chronic obstructive Pulmonary Disease; FEV1/FVC, forced expiratory volume in one s relative to forced vital capacity; BMI, body mass index; Values expressed as mean ± S.E.M. *Significantly different from healthy subjects.
574 575 576 577 578 579 580

25
Table 2. Impact of antioxidant cocktail administration on selected physiological variables at rest and during exercise Work Rate Rest 3 Watts 6 Watts 9 Watts
Healthy Subjects Mean arterial pressure, mmHg CTRL 119±2 127±3 125±2 127±3
AO 117±2 124±2 125±3 127±2 HR, beats/min CTRL 64±2 76±4 78±4 81±5
AO 64±2 77±4 79±4 83±5 Leg O2 Delivery (l/min) CTRL 0.06±.01 0.31±0.03 0.36±0.02 0.41±0.02
AO 0.06±0.01 0.32±0.02 0.38±0.02 0.41±0.02 Hemoglobin (g/dl) CTRL 15±0.3 14.8±0.2 14.8±0.2 14.8±0.2
AO 14.8±0.4 15.0±0.3 14.8±0.2 14.8±0.2 Arterial O2 Content (ml/dl) CTRL 19.9±0.3 19.6±0.2 19.6±0.2 19.7±0.3
AO 19.6±0.3 19.8±0.3 19.8±0.3 19.7±0.3 Net lactate release, mmol/min CTRL 8±18 338±82 417±113 975±179
AO 34±10 343±99 571±184 799±212 Venous pH CTRL 7.41±0.01 7.31±0.01 7.30±0.01 7.29±0.01
AO 7.38±0.01 7.29±0.02 7.28±0.02 7.27±0.02 COPD
Mean arterial pressure, mmHg CTRL 129±4# 137±4# 137±4# 138±4# AO 131±4# 138±4# 136±4# 140±4#
HR, beats/min CTRL 72±4 87±4 90±4 92±4 AO 72±4 85±4 87±4 90±4
Leg O2 Delivery (l/min) CTRL 0.05±0.01 0.3±0.02 0.34±0.02 0.38±0.02 AO 0.06±0.01 0.32±0.02 0.36±0.02 0.39±0.03
Hemoglobin (g/dl) CTRL 14.0±0.4 14.3±0.4 14.1±0.4 14.3±0.4 AO 13.9±0.4 13.8±0.4* 14.0±0.4* 13.8±0.4*
Arterial O2 Content (ml/dl) CTRL 18.1±0.4# 18.5±0.4# 18.2±0.4# 18.5±0.5# AO 18.0±0.4# 17.9±0.4# 18.3±0.4# 18.0±0.4#
Net lactate release, mmol/min CTRL 48±7 1777±373# 1968±369# 2083±442# AO 70±11 1606±346# 1596±298# 2258±461#
Femoral Venous pH CTRL 7.38±0.01 7.29±0.02 7.28±0.02 7.27±0.02 AO 7.38±0.01 7.31±0.02 7.29±0.02 7.28±0.02
Values expressed as mean ± S.E.M. *Significantly different from control (CTRL) conditions. #Significantly different from 581 healthy subjects. 582 583 584 585 586 587 588 589 590 591 592 593

26
Figure 1. Experimental Protocol. Arrows indicate points at which leg blood flow was recorded 594 and arterial and venous blood samples were obtained. 595 596 Figure 2. Impact of an antioxidant cocktail (AOC) on indices of oxidative stress, antioxidant 597 capacity and inflammation in patients with chronic obstructive pulmonary disease (COPD) and 598 healthy subjects. Values are presented as mean ± S.E.M *Significantly different from the control 599 (CTRL) condition, p < 0.05. #Significantly different from healthy subjects, p < 0.05. 600 601 Figure 3. Impact of an antioxidant cocktail (AOC) on exercising leg blood flow (A), oxygen 602 extraction (B) and oxygen consumption (C) in patients with chronic obstructive pulmonary 603 disease (COPD) and healthy subjects. Values are presented as mean ± S.E.M. *Main effect of 604 AOC, p < 0.05. 605 606 Figure 4. Impact of an antioxidant cocktail (AOC) on leg vascular conductance during exercise 607 in patients with chronic obstructive pulmonary disease (COPD) and healthy subjects. Values are 608 presented as mean ± S.E.M. *Significantly different from the control (CTRL) condition within 609 patients with COPD. 610 611 Figure 5. Impact of an antioxidant cocktail (AOC) on arterial oxygen saturation (A) and partial 612 pressure (B) during exercise in patients with chronic obstructive pulmonary disease (COPD) and 613 healthy subjects. Values are presented as mean ± S.E.M. *Main effect of AOC, p < 0.05. 614 615