Analysis and Introduction of Effective Permeability with ...
Upload
khangminh22Category
view
0download
0
I954
On the Bromide Test of Permeability of the Barrier betweenBlood and Cerebrospinal Fluid-an Assessment
BY G. HUNTERElectro-medical Research Unit, Medical Research Council, Stoke Mandeville Hospital, Aylesbury, Bucks
HONOR V. SMITH AND L. MARGARET TAYLORDepartment of Surgery, Radcliffe Infirmary, Oxford
(Received 3 September 1953)
The publication of Walter's monograph (1929) onthe blood/cerebrospinal-fluid barrier was followedby the widespread use ofthe bromide test in diseasedconditions of the brain and spinal cord. Thebromide test consists in the administration ofbromide to the patient; after allowing 24 hr. forequilibration with the cerebrospinal fluid (c.s.f.),the content of bromide in the serum and c.s.f. isdetermined. The permeability of the barrier is thenjudged by the magnitude of the ratio (bromide/unitvol. serum)/(bromide/unit vol. c.s.f.). Walter foundnormal control ratios to lie in the range 2-90-3-30(mean 3-10). In pathological states causing thegreatest increase in permeability (syphilitic ortuberculous meningitis) the ratio was near 2-0,although a few values as low as 1-50 have beenrecorded. On the other hand, ratios over 3-50 werefound in a number of conditions.Walter emphasized certain desirable features of
the bromide test. Bromide is excreted very slowly,so the blood level remains relatively constant overlong periods (days or weeks), permitting adequatetime for the establishment of equilibrium betweenblood and c.s.f., and making possible several testswithout further bromide administration. Bromidedoes not enter metabolism and might thus beexpected to qualify as a test substance for perme-ability. It is neither bound by, nor adsorbed to,protein. It can be determined with adequate pre-cision at low levels in serum or c.s.f. It is neitherdisliked by, nor toxic to, patients, and at the levelsused is unlikely to affect barrier permeability. Itsnormal distribution between serum and c.s.f. givesa ratio well removed from unity so that decreases orincreases in permeability are readily recognized.A fairly extensive study ofneurological conditions
with the bromide test has enabled us to examine anumber of points relevant to the test which havereceived little or no attention. From the beginningwe regarded the auric chloride method of bromidedetermination (Walter, 1919; Malamud, Mullins &Brown, 1933; Katzenelbogen & Czarski, 1934) withsome scepticism. Since several workers havequestioned its reliability (e.g. Lovell & Brown,
1934; Tod, 1933; Mishkis, Ritchie & Hastings,1933; Fremont-Smith, Dailey & Sloan, 1935; Gray &Moore, 1942) a method based upon iodometrictitration (Hunter, 1953), and regarded as moreaccurate, has been used throughout. With thismethod, however, the ratios obtainedwere markedlylower than those commonly reported, our mean fornearly normal controls being 2-60 (S.D. 0.30). Thisnecessitated the examination of sera and c.s.f. byboth methods, and it was found that there iscommonly present in human serum a substance thatreacts like bromide with auric chloride solutions togive a brown colour. With c.s.f. the two methodsgive results in near agreement but with serum theresult by the auric chloride method is commonly toohigh, and an erroneously high bromide distributionratio is obtained.As bromide tests are carried out under ordinary
hospital working conditions, the technique forcollecting blood should be as simple as possible. Theuse of whole blood overcomes analytical uncer-tainties that may arise from uneven distribution ofions between cells and plasma, but it necessitates ananticoagulant, and is less suitable than plasma orserum for studies on the balance of electrolytes withother body fluids. Therefore we decided to use serumfor brormide analysis; this raised the questionwhether there was a 'shift' of bromide, like that ofchloride, with changing pH and degree of oxygena-tion of haemoglobin. This seemed probable from thelittle information available, especially on humanblood. The normal distribution of administeredbromide between plasma and corpuscles also seemedto call for further observation since false bromidedistribution ratios might arise through alteration ofthe serum bromide after taking the blood. Some ofour blood samples might be kept several days beforethe serum was separated from the clot.
In the determination of serum/c.s.f. bromideratios Walter states that blood and c.s.f. were taken24 hr. after the last oral dose of bromide. Yet thereis little information in the literature as to how longadministered bromide takes to reach equilibriumwith the c.s.f. Nor is there adequate evidence that
588

BLOOD-CEREBROSPINAL FLUID BARRIER
the ratio is consistent from day to day in the sameperson in similar conditions. This paper describesexperiments designed to assess the general re-liability of the Walter test.The convention that Br. = bromide in serum and
(Br), =bromide in serum water has been followed.Other subscripts used are p = plasma, c = cells, andc.s.f. = cerebrospinal fluid.
EXPERIMENTAL
Determination of bromide. The iodometric titrationmethod of Hunter (1953) and the colorimetric auric chloridemethod as modified by Katzenelbogen & Czarski (1934)were used.
Comparison of resultsfrom iodometric andauric chloride methods
Table 1 shows bromide values obtained on seraand c.s.f. and the resulting ratios, by the twomethods. The colours obtained with auric chloridewere read in a photoelectric colorimeter at 450 m .e.,in the region of maximum absorption for auricbromide (which is the substance that gives thebrown colour), and also at 500 miu., as likely toaccord better with readings in a visual colorimeter.It will be seen that there is fair concordance withboth the titrimetric and the colorimetric method, ateither wavelength, for c.s.f. With serum, however,the values obtained colorimetrically are higher andoften much higher, especially at 500 myi., than thecorresponding titrimetric values. The first four caseslisted in Table 1 have about normal permeabilitieswith a mean ratio, by the titration method of 2-67 orby the colorimetric method at 450 m1z. of 2-79 andat 500 miu. of 3-11, a value the same as the Waltermean. The lower ratios are similarly increased in the
three cases of tuberculous meningitis. Moststriking perhaps are the values on the sera of thefive individuals not treated with bromide; theirsera contained usually less than 1 mg. Br/100 ml.according to the iodometric method but much moreaccording to the colorimetric method. It may benoted that Gray & Moore (1942), in an examinationof blood from seventy-six subjects who had re-ceived no bromide, obtained by the auric chloridemethod results indicating 16-53 mg. Br/100 ml. innine of these cases, although no bromide wasdetected by other tests.
It seems that human sera, normal and patho-logical, contain a substance (or substances) which isnot bromide but which produces, like bromide, abrown colour in auric chloride solution and that thissubstance is responsible for the high mean value ofthe ratio Br,/Brc, f obtained when auric chloride isused to determine bromide in serum. The nature ofthe interfering substance in serum is unknown;a variety of substances in dilute solution, such asiodide, sulphide, thiosulphate, guaiacol, increase thebrown colour of auric chloride solutions under theconditions of the test, whereas small amounts ofuric acid or ascorbic acid nearly completely dis-charge the colour with formation of metallic gold.On such grounds alone it is not surprising that theuse ofthis reagent leads to uncertain results in bloodserum.
Rate of equilibration of bromide betweenplasma and corpuscles
The experiments recorded in Table 2 show thatequilibration of bromide between plasma andcorpuscles is established within 5 min. of additionof bromide in vitro and within 30 min. in vivo.
Table 1. Bromide distribution ratios in serum and cerebrospinal fluidBromide was determined by iodometric titration and by the auric chloride method. In the latter the absorption was
measured at 450 and at 500 mi.Auric chloride method, measurement at
Patient
No. Diagnosis94S Palsy97S Pain98S Pain99S Disseminated sclerosis
1958X Tuberculous meningitis113X f (treated cases)
Normal120X141X Meningitis127X134X Transverse myelitis
lodometric titrationmethod
Bromide in
Br,Br,,...f.
2-612-692-652-731-431-682-07
Serum C.s.f.(mg./l00 ml.)18-8 7-218-8 7-020-7 7-818-3 6-722-8 15-926-4 15-727-6 13-30-905 --041.-10-9 -
450 mu.
Bromide in. _W~~
Serum C.s.f.(mg./100 ml.)16-2 7-018-3 6-623-8 8-422-1 6-824-6 14-228-2 15-736-0 14-11-83-8
- 4.-76-35-7
tsr,
Br.,.f.2-312-782-813-271-731-792-55
500 M.u.
Bromide in
Serum C.s.f. Br,(mg./100 ml.) Brc 8 i22-3 7-2 3-1023-0 7-3 3-1526-1 8-2 3-1825-0 8-3 3-0029-7 15-0 1-9836-0 15-3 2-3540-8 14-1 2-90
- 5.-4- 44-5- 8-1 -_- 18-0-- 17-1
Vol. 56 589
ID-

G. HUNTER, H. V. SMITH AND L. M. TAYLOR I954
Table 2. Rate of equilibration of bromide with blood in vitro and in vivo
In vitro. NaBr (as 0-6 ml. of isotonic glucose solution containing 5-38 mg. Br) was added to 20 ml. heparinized blood.Samples (3 ml.) were taken for analysis at intervals. The packed cell volume was 48-5 %.In vivo. Heparinized blood was obtained after intravenous injection of NaBr.
Bromide (mg./100 ml.)
Time afteraddition ofNaBr
(min.)In vitro
51015306017 hr.
In vivo3026 hr.
Plasma(a)
32-132-633*032-532-632*5
27*823-7
Cells(b)
193
Whole bloodt ~A
Calc. from Br0Found a and b brp
26-6
15-413-3
26-1
0550-56
Table 3. Effect of pH on equilibration of blood with bromide added in vitro and in vivo
In vitro. NaBr in isotonic glucose solution was added to fresh, heparinized human blood. The mixed blood was dividedinto four parts. One part was untreated; N-NaOH or N acetic acid in bromide-free saline was added to the others to givethe range of plasma pH shown. After 15 min. the bloods were centrifuged and bromide determined. (The top layer ofcells containing 'buffy coat' was removed and discarded.) It was assumed that plasma and cells contained 93 and 70%of water, respectively (Maizels, 1936; Harris & Maizels, 1952).In vivo. Heparinized blood was taken from two patients who had previously received bromide.
Bromide (mg./100 ml.)
Plasma42-040-236-035-118-117-715-815-211-811-710-0
Cells
24*626-428*428-27-69.59-89.95-87 07-2
Plasmawater45*243-238-737-719-419-017-016-312-712-6
Cell (Br),water (Br)p35*1 0.7737-7 0-8740-6 1-0540-2 1-0610.9 0 5613-6 0-7214-0 0*8214-1 0*868-3 0-65
10.0 0*790*9610-8 10-3
Plasma pHat 2008*07*87-57-27-987.577X157*008-007-567*18
Effect of pH on distribution of bromidebetween plasma and cells
Table 3 shows that the ratios of bromide in cell
water to bromide in plasma water, (Br)0/(Br)p,vary inversely as the pH. It may be noted that thechange in plasma water through addition of solu-tions of base and acid is less than 1% and has beenneglected in the calculation.
Bromide distribution in blood collectedfrom hospital patients
Venous blood was collected in a syringe and mixeddirectly with heparin in a cork-ed test tube. The tube,with cork in place to prevent loss of carbon dioxide,was centrifuged. From twenty-four observations on
nineteen patients suffering from a variety ofneurological conditions and including only one
febrile case, the ratio (Br),/(Br)p was found to be0-84 (S.D. 0.08). The observations are not givenseparately as there seemed to be no relationshipbetween (Br)./(Br)P and sex, age, pathologicalcondition, or plasma pH.
Shift of bromide in stored blood
It seemed possible that on storage of blood a
change in the ratio (Br)0/(Br)p might occur even ifthere wasno change inpH. Accordingly the bromidelevel was followed in heparinized blood kept atroom temperature and in clotted blood stored ina refrigerator for several days. The packed cell
Blood no.
1 (868S)2341 (76S)2341 (75S)23
BromideaddedIn vitro
In vivo
In vivo
590

BLOOD-CEREBROSPINAL FLUID BARRIER.
Table 4. Effect of storaqe on pkssma or serum bromide
Heparinized blood was stored at 200 and clotted blood at 4°. Plasma and cell water were assumed to be 93 and 70%,respectively.
Time of storage pH of plasmaof blood or serum
No. (days hr.) at 200
Packedcell
volume
Bromide
Plasmaor serum
Heparinized blood37 24-0- 21-8- 21-442 20-3
20-1- 19-141 20-4- 19-944 17-1
16-5
Clotted blood- 29-4
29-328-313-813-613-320-3
- 19-820-319-7
- 18-918-9
- 18-1
(mg./100 ml.) Maximum fallA in plasma or
Plasma when serum bromideCells (Br)e,/(Br)p= 1 (%)
13-3
12-5
13-7
12-0
22-0
18-8
19-6
16-7
10-8
6
2-5
3-5
3-7
3-6
3-0
4-2
volume of the former was determined and thebromide level expected in the plasma when theanion becomes evenly distributed in cell and plasmawater was calculated. The results from severalexperiments are given in Table 4 which shows thatall plasma or serum values tend to fall towards thecalculated level.
DISCUSSION
Equilibration of bromide with bloodIt is apparent from Table 2 that bromide added
in vitro or in vivo to human blood rapidly reachesequilbrium with the cells. This finding is in accordwith the observations of Hastings & Van Dyke(1931) on dog blood. Table 3 shows that whetherbromide is added in vitro or in vivo to blood itsdistribution between the cells and plasma varies,like chloride, with pH. This finding is also in accordwith those of Hastings & Van Dyke (1931) and ofHastings, Harkins & Liu (1932), when very largeamounts ofbromide were given to dogs. Ifthe ratiosin Table 3 are plotted against pH they have aboutthe same slope, with a shift of 0 3 pH unit causinga change of about 10% in the ratio. The chlorideshift with pH as found by Harris & Maizels (1952)has a similar magnitude. At normal blood pH the
magnitude of the chloride ratio, (Cl)0/(Cl)P is bygeneral consent (see Owen & Power, 1953) close to0 70 for man. In nine female epileptic patients,Notkin, Garcia & Killian (1933) found a mean
bromide ratio of 0-80 from bloods collected withoutprecautions to exclude air. Their correspondingchloride ratio was 0-82. In four patients withbromide intoxication, Mason (1936) found a mean
chloride ratio of 0-73 and a corresponding bromideratio of 0-80. In dogs, Weir & Hastings (1939) founda chloride ratio of 0-72 and a bromide ratio of 0-76(ten observations). Our bromide ratio, fromtwenty-four observations on nineteen persons, is0-84 (S.D. 0.08). This is significantly higher than thefew values previously reported for human blood andserves to emphasize that bromide displaces more
than its chloride equivalent from erythrocytes.Hastings and his associates used venous blood
collected under anaerobic conditions. Our bloodsamples were collected with minimum exposure toair, but not with strict anaerobic technique, withsome consequent oxidation of haemoglobin and loss
of carbon dioxide both of which actions would tendto lower the ratio. From the observed pH's therecould not have been serious carbon dioxide loss, butat any rate the ratio of 0 84 found should be
72 0O548
74
277
0-54
812
17
1
7-587*567-567-567-404
8324
4
1
2
87
690
3612
7-727-807-607-637-617-647-507-547-717-247-577-577-52
91 24t0
VoI. 56 591

G. HUNTER, H. V. SMITH AND L. M. TAYLORslightly below the physiological. Or, had the bloodbeen collected under anaerobic conditions, weshould expect the mean distribution of bromidebetween cells and plasma to be close to 0-85.
Probable errorfrom bromide shtftOur immediate purpose in determining the
distribution ratio of bromide between corpusclesand plasma was to assess the extent ofthe error thatmight arise from the bromide shift. As the bromideratio is much nearer unity than the chloride ratio,the bromide shift is likely to be the source of asmaller error in serum bromide determination thanis the chloride shift in serum chloride determination.Also, the pH change in venous blood with loss of alittle carbon dioxide would not be expected to belarge, as it tends to be compensated by the con-current formation of more oxyhaemoglobin. If wetake an instance when (Br)e/(Br)= 0-84, thepacked cell volume is 45 %, the cells contain 70%and the plasma 93% ofwater, and the cell water andplasma water contain 16-8 and 20 mg. Br/100 ml.,respectively, it can readily be calculated that, if thebromide becomes equally distributed between celland plasma water, the fall in level ofplasma bromidewould be 1-1 mg. Br or 5.9 %, and a physiologicalBrp/Br_.. of 2-50 would be decreased to 2-35. Inbloods where the (Br)c/(Br)p is appreciably less than0-84, especially when the packed cell volume ishigh, the error could be perhaps over 10 %, but withthe procedure used in the present research it seemsimprobable that any error arising from bromideshift is likely to exceed 2-3%. This estimate ofpossible error from bromide shifts may be comparedwith the observed values shown in Table 4. Herethe heparinized bloods were kept at room temper-ature to hasten equilibrium. After 4 days' storagethe plasma bromide values were close to the expectedequilibrium values, and only one sample had a valuegreater than 10% below the initial value. Withclotted blood at 40, as might be expected, thebromide shift to the corpuscles is slower. Evenwith prolonged storage ofup to 1-2 days, the greatestfall was 4-2 %.We may thus conclude, on the evidence of rapid
equilibration of administered bromide with cor-puscles and plasma, and from the magnitude of theratio of the distribution of bromide betweencorpuscles and plasma, that, under the conditions ofcollection and storage of the blood at 40, no seriouserrors in the ratio Br5/Br01,.f. are likely to arise frombromide shift after the blood has been drawn.
Equilibration of bromide with extracellular fluidThere is evidence in the literature that bromide
equilibrates within a few hours with extracellularfluid. For example, Brodie, Friedman & Ferraro(1941) have suggested its use as a measure of extra-
cellular fluid some 3 hr. after oral administration inman. Greenberg et al. (1943), from experiments ondogs with 82Br, found it to be completely distributedin the body within 1 or 2 hr. We have followed in afew subjects the blood level at short intervals afterintravenous administration of sodium bromide, anda typical case (Table 5) shows that the serum-bromide level falls rather rapidly for about 2 hr.following intravenous administration. After about2 hr. the rate of fall rapidly decreases. During thefirst 2-3 hr., presumably, equilibrium is takingplace with the body's extracellular fluids.
Table 5. Rate offall of blood bromide followingintravenous administration
Time afterinjection
(hr.)0-251-02-08-0
24-0
Bromide(mg./100 ml.)
r
Serum24-822-820-419-218-2
Fall/hr.
2-72-40-60-06
Persistence in blood of administered bromide
Some 24 hr. after giving the bromide we havefound the rate of fall to be commonly less than1-0 mg. Br/100 ml. serum/day. Thus if the initialblood level is over 30 mg./100 ml. serum, determin-able amounts ofbromide will remain for some weeks.We shall later consider the matter of further ad-ministration of bromide in prolonged studies onpatients, with the related question of a possiblevariation of the ratio Br./Br,., with different bloodbromide levels, but the persistence of administeredbromide in the body fluid is an important aspect ofthe barrier test, and a matter of some physiologicalinterest. Palmer & Clarke (1933) demonstrated inthe dog that the percentage of bromide in urinehalides is less than the percentage of bromide inblood halides. They found, however, that the ratioofthose urine andbloodpercentages was constant ona constant chloride intake. On a salt-poor diet itwas 0-40 and on a high salt diet it was about 0-70.Similar ratios were found in a few patients withbromide dermatitis. It therefore appeared that thekidney preferentially excretes chloride. A similarconclusion is reached by Smith & Walker (1938) andby Bodansky & Modell (1941). Bromide is notremoved from the plasma by increased excretion ofurine but only by replacement by dietary chloride.Palmer & Clarke (1933> recorded about 120 mg.Br/100 ml. blood 30 min. after intravenous ad-ministration to a dog on a salt-poor diet, and4-5 months later the blood still contained about16 mg./100 ml. We have determined serum/c.s.f.ratios on patients who had about 7 mg. Br/100 ml.
592 I954

BLOOD-CEREBROSPINAL FLUID BARRIERserum more than 50 days after they had receivedbromide to the extent of about 35 mg./100 ml. ofserum, and who had had the ordinary hospital saltintake. We commonly find that the relationshipbetween serum bromide and time after bromideadministration is of a linear rather than an ex-ponential type, indicating that the rate of bromideloss is largely independent of its level in the serum.Whether or not the kidney excretes bromide
in preference to chloride has long been a vexedquestion. Mason (1936) supports the findings ofPalmer & Clarke (1933) but Frey (1932) andMoller (1932) believe that the kidney does notdistinguish between chloride and bromide. Thequestion should, perhaps, be re-examined withmodem methods for bromide determination.
Gastric secretion of bromideSince the observations of Nencki & Schoumov-
Simanowsky (1894) on the presenoe of bromide inthe gastric juice of dogs given bromide, there hasbeen repeated mention of gastric secretion as apossible factor in lowering serum bromide. Daven-port & Fisher (1940) have clearly shown that inPavlov pouches in dogs the rate of secretion ofbromide is of the same order as the rate of secretionof chloride, and the concentration of bromide in thegastric juice is of the order of 50% higher than thatin plasma. The recent observation of Gabrieli (1950)that this bromide is not secreted with the hydro-chloric acid of the juice does not affect this point inour argument, but is suggestive in the study of thephysiology of bromide. It seems unlikely that thevolume of gastric juice in any short period could bemore than 3-4% of the volume of the extracellularfluid and only the 50% excess over the plasma levelcould be regarded as likely to change the plasmalevel. Thus we should not expect a fall in plasmabromide level of more than 1-2% following a veryactive period of gastric secretion and such analteration is within the usual analytical variation.Fleischacker & Scheiderer (1928) maintain thatblood for the bromide barrier test should be taken inthe post-absorptive state, but their values (by theauric chloride method) of less than 5% dropfollowing food can hardly be regarded as significant.
Equilibrium between plasma and cerebrospinal fluidWalter (1929) recommended an interval of 24 hr.
between the last oral dose of bromide and lumbarpuncture. This interval seems to have been generallyaccepted, though there is a paucity of evidence asto the length of time really necessary. Stem &Gautier (1921) demonstrated the presence ofbromide in the c.s.f. of animals 1-25, 3 and 16 hr.after intravenous administration of relatively largedoses. Wallace & Brodie (1940), after intravenousinjection of 22 g. of sodium bromide to a dog
Biochem. 1954, 56
Table 6. Equilibrium with cerebrospinal fluid afterintravenous injection of sodium bromide
Values in parentheses are for ventricular fluid.
No.
56S
Diagnosis
Head injury
598 Subacute combineddegeneration ofspinal cord
Br.Br...8,
24-3-=4-805-123-1-f--=3-00
22-8-6 =4-0722-09- ==2-29
79X Tuberculous 24-0meningitis 16-9
22-6 1-45
34X Pneumococcal 19-7 1-23meningitis 16-0
=1.27
90X Schizophrenia 23-8
22-4- =2-80
28X Pulmonary 240-76tuberculosis 8-7
21-48-0 =2-68
l05X Lymphocytic 18-2=28meningitis 8-0
11-1-l=2-18
98X Tuberculous 27-7meningitis with 3 .8201hydrocephalus (11-10)
25-7 145
(3-72)24-518-1 135
(2-85)11-18-3 =1-34(2-31)
Time afterinjectionof NaBr
(days hr.)
5
28
5
24
12
28
20
44
21
48
25
48
24
10
5
24
48
7
weighing 22 kg., found Br./Br,..,.. to be nearlyconstant after 7 hr. and constant from 24 hr. to13 days. The c.s.f. was drawn from the cisternanmagna. With 82Br, Greenberg et al. (1943) founda plateau level in about 2 hr. in the dog. Table 6shows some ofour results with human subjects. It is
38
VoI. 56 593
I

G. HUNTER, H. V. SMITH AND L. M. TAYLOR
clear that an interval of about 5 hr., at which wehave made many other observations with similarresults, is insufficient. In the meningitis cases,79X, 34X, equilibrium was attained in 12 and20 hr., respectively, but in this condition, as will beshown elsewhere, the barrier permeability is greatlyincreased and such cases may give a false impressionof the time interval necessary with the barriernormal. In the case of schizophrenia, 90X, 21 hr.was insufficient, and in cases 28X and 105X, 25 and24 hr. were barely sufficient. In the case of hydro-cephalus, 98X, in which we got a more continuousrecord for both lumbar and ventricular fluids,24 hr. was insufficient; in 48 hr. equilibrium wasreached with the lumbar fluid but not with theventricular. We have followed another case ofhydrocephalus at shorter time intervals up to 24 hr.with similar results.
Although the evidence from Table 6 is not asextensive as might be desired for the more normalcases, it suggests that 24 hr. should be the minimalinterval between intravenous bromide dosage andlumbar puncture for the purposes of the bromidetest. With oral dosage, a considerably longer intervalshould be set.
Concentration of bromide in cerebrospinal fluidat different levels in the neural axis
Masserman (1934), in many observations onparetic and schizophrenic patients, found that thelumbar fluid contained slightly more bromide thanthe cisternal and in seven cases Bau-Prussak &Prussak (1927) reported higher bromide values inthe lumbar than in the cisternal fluids. Our ownobservations are mostly from rather extreme neuro-pathological conditions which will be discussedelsewhere. However, for Table 7 we have selectedsix cases where the fluids, as judged from thediagnosis, condition of the patient and concentra-tion of protein in the fluids, are likely to be suffi-ciently near normal for a comparison of them to bevalid. It may be seen that the bromide concentra-tion of the ventricular fluid is about half that of thelumbar, with a resultant distribution ratio between4 0 and 5 0. In two cases the bromide level ofcisternal fluid was about midway between that oflumbar and ventricular fluid. It is clear thatvalues obtained from either ventricular or cisternalfluid should not be compared with those obtainedfrom lumbar fluid.
Table 7. Bromide and protein concentrations of cerebrospinal fluid at different levels in the neural axis
Bromide and protein values are expressed as mg./100 ml.
Cerebrospinal fluid
Patient no.and diagnosis
36X. Rhinorrhoea39X. Fits34X. Intracranialtumour65X. Psychosis50X. Cystic glioma88X. Tuberculousmeningitis, partlyhealed
Serum(S)
Bromide12*028-711-7
Lumbar(L)
Bromide Protein5*4 48
12*1 224-5 16
Cisternal(C)
r-Bri
33-8 12*1 3525*6 11 0 6035-5 23-5 69
Ventricular(V)
omide Protein Bromide Protein
- - 7*1 222*8 11
6*9 178*7 60 7-8 92
14-6 45 10-5 23
SIL S/C S/V2-22 - 4-442-37 4*042-60 - 4-18
2*71 4'902-33 2-94 3-281.51 2.43 3-38
Table 8. Effect of repeated tappings on bromide level of lumbar cerebrospinal fluid
Patient no.and diagnosis
36X. Cerebrospinal fluidrhinorrhoea
39X. Infantile hemiplegia
1015. Disseminated sclerosis
* Not used for bromide determination.
Sampleno.123123412*3
Approx. vol.tapped(ml.)101051510105374
Intervalbetweensamples(min.)
1020
201010
22
Bromide(mg./100 ml.) s
6-05-34-78-98*78-78*710-8
9-7
594 I954

BLOOD-CEREBROSPINAL FLUID BARRIER
Table 9. The distribution of bromide between blood and cerebrospinal fluid in control patients
ConditionDisseminated sclerosisPsychosis
No. ofcases2010
Br.
Mean2*602-60
Effect of repeated lumbar punctures on thebromide level of cerebrospinal fluid
Fleischacker & Scheiderer (1930) found a fall offrom 4-5 to 9 0% in withdrawing successively three5 ml. samples of lumbar fluid, and Walter (1929) hasa warning on this point. On two of three patientsour observations (Table 8) were made in the courseof lumbar air encephalograms (cases 39X, 1OIS).In ohie of these and in case 36X there was a markedfall in bromide, while in case 39X the fall was lessthan might have been expected with the removalof relatively large amounts of fluid. It is clear,however, that a considerable error may arise,where large amounts of fluid are removed, ifthe first drawn fluid is not used for the bromideanalysis.
The normal distribution of bromide betweenserum and cerebrospinal fluid
With the precautions implied above, the ratioBr./Brc.,f has been determined in over 200 cases,and in a number of these many times. All the cases,however, were hospital patients and like mostworkers in this field we have no control values fromhealthy subjects. From a variety of apparentlybenign neurological conditions like headache,neuralgia, anxiety neurosis, epilepsy, motor neuronedisease, we found rather a high standard deviationand chose as controls a less heterogeneous groupconsistingoften psychotic patientswithnormal c.s.f.protein and twenty cases of disseminated sclerosis,in which the c.s.f. protein did not exceed 50 mg./100 ml. (Table 9). It is no doubt fortuitous that thetwo groups gave precisely the same ratios andstandard deviations. In choosing such patients ascontrols it may be remarked that, according toWalter (1929), there is a tendency towards highratios or decreased permeability in schizophrenicpatients and the ratio is in the normal range incases of multiple sclerosis provided the c.s.f. proteinis normal. In using cases of psychosis and dissemi-nated sclerosis as controls we are not suggestingthat in such conditions the barrier permeability isnormal. It would seem in fact that our controlswere comparable with those chosen by mostworkers, in that they gave a mean serum/c.s.f.bromide ratio of about 3-10 by the auric chloridemethod (2.60 by the iodometric method).
No. of cases with ratioI~~~~~~~r
S.D. < 2*15 2-15-2*44 2*45-2*74 2-75-3-04 > 3*040*30 1 5 7 7 0030 0 3 3 3 1
c E0 3C
U E0c 1C*
co
6co._
2-5
2-0
1-5
1.0
10 20 30 40 50 60 70 80 90 100Time (days)
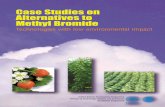
Fig. 1. Case of a psychotic patient who received orally1-0 g. NaBr thrice daily for 3 days. About 60 hr. after thelast dose bromide values in serum and c.s.f. were 35'2and 13-3 mg. Br/100 ml., respectively (ratio 2.65). Thepatient was then given tuberculin intrathecally, andthe bromide levels in serum and c.s.f. were followedover a period of 102 days. Between 50 and 60 days thepatient was given another similar oral course of NaBr.x- x, serum; ®-®3, c.s.f.
Repeated tests on the same patientFew repeated Walter bromide tests on the same
patient have been recorded. Walter (1925) reportedrepeat values on four patients at times varyingfrom 9 to 37 days after the initial observations, andconcluded that the ratio was very constant and un-influenced by time and amount of bromide present.Further observations of this kind are desirable.Fig. 1 illustrates our findings in a case where a rapidand profound change in barrier permeabilityoccurred following intrathecal administration oftuberculin; the medical aspects of which will bediscussed elsewhere. The main features of this casehave been repeatedly observed in other patients.The following points may be observed:
(a) The consistently diminishing values obtainedon the serum, except at about a week from the startwhen the blood values remained constant overseveral days and indeed on one day showed a slightrise. Such changes could well have been due tochanges in the water balance as a result of thetreatment. As remarked earlier the fall in bloodbromide tends to be linear with time. Walter (1929)records a similar curve obtained from his own bloodover about 50 days.
38-2
Vol. 56 595

596 G. HUNTER, H. V. SMITH AND L. M. TAYLOR I954(b) The c.s.f. values are likewise on a continuous
curve with only two points slightly erratic. The peakc.s.f. value of 35 9 mg. Br/100 ml. was the meanof close triplicate determinations. It is not onlymuch higher than the corresponding serum value(30.5) but higher than the serum peak at the start.This surprising bromide distribution will be dis-cussed elsewhere.
(c) The values of the ratio Br,/Br,,,.ff. also lie ona smooth curve, despite a large change in the bloodlevel between the 50th and 60th day.
(d) When the observations were stopped, theratio, 2-40, was still somewhat lower than its initialvalue, indicating that the barrier had not yet quiterecovered from its treatment more than 3 monthsearlier.From such considerations Fig. 1 is taken as
evidence of the general reliability of the bromidetest. It also proves, and we have further similarevidence on the same point, that the ratio is inde-pendent of the level of bromide in the blood-atleast within the limits recommended for the test.
SUMMARY1. The bromide test of meningeal permeability
(Walter, 1929) has been critically examined.2. The auric chloride method for estimation of
bromide in serum is unreliable, and values for theserum/cerebrospinal fluid bromide ratio determinedby this method are too high.
3. When bromide is added to human blood anequilibrium between plasma and erythrocytes isestablished in a few minutes. At this equilibriumthe ratio (Br- in cell water)/(Br- in plasma water) is0-84 (S.D. 0.08) and from the magnitude of this ratioit is inferred that administered bromide replacesmore than its equivalent of chloride in the humanerythrocyte. The ratio also varies inversely with thepH of the blood.
4. Onstorage ofbloodtheserumbromide tends tofall to a level corresponding to an even distributionthroughout the blood water. With clotted bloodstored in a refrigerator this process is probably notcomplete for 1 or 2 weeks. When the serum isseparated within 1-2 days the bromide level is notlikely to have dropped more than 2-3%.
5. Intravenously injected bromide takes severalhours to equilibrate with the extracellular fluid ofthe body.
6. Administered bromide persists in the bloodfor several weeks. Our evidence favours the viewthat the kidney excretes chloride in preference tobromide.
7. Intravenously injected bromide, except wherethere is increased barrier permeability, normallytakes about 24 hr. to equilibrate with the lumbarcerebrospinal fluid -and longer with ventricularfluid.
8. The bromide concentration of cerebrospinalfluid decreases on ascending the neural axis. Innearly normal cases the bromide concentration inventricular cerebrospinal fluid is about half that oflumbar.
9. A significant error in the bromide distributionratio between serum and cerebrospinal fluid canarise if much lumbar fluid is removed before thespecimen is taken.
10. In thirty cases with nearly normal meningesthe bromide distribution ratio between serum andcerebrospinal fluid was 2-60 (S.D. 0.30). This ratio isindependent of the level of bromide in the serum.
This paper is part of a study on the circulation of thecerebrospinal fluid initiated by Dr R. B. Bourdillon. We areindebted to Dr Ritchie Russell for some of the samplesexamined and to MrA. A. Goldspink for technical assistance.One of us (L.M.T.) is the recipient of a grant from theMedical Research Council.
REFERENCES
Bau-Prussak, S. & Prussak, L. (1927). Enciphale. 22, 176.Bodansky, 0. & Modell, W. (1941). Amer. J. Phy8iol. 133,216P.
Brodie, B. B., Friedman, M. M. & Ferraro, L. R. (1941).J. biol. Chem. 140, xxi.
Davenport, H. W. & Fisher, R. B. (1940). Amer. J. Phy8iol.131, 165.
Fleischacker, H. & Scheiderer, G. (1928). Z. ge8. Neurol.P8ychiat. 116, 692.
Fleischacker, H. & Scheiderer, G. (1930). Dt8ch. med.Wschr. 56, 1657.
Fremont-Smith, F., Dailey, M. E. & Sloan, D. H. (1935).Arch. Neurol. Paychiat., Chicago, 33, 764.
Frey, E. (1932). Arch. exp. Path. Pharmak. 163, 393.Gabrieli, E. (1950). Nature, Lond., 165, 247.Gray, M. G. & Moore, M. (1942). J. Lab. din. Med. 27,
680.Greenberg, D. M., Aird, R. B., Boelter, M. D., Campbell,W. W., Cohn, W. E. & Murayama, M. M. (1943). Amer. J.Physiol. 140, 47.
Harris, E. J. & Maizels, M. (1952). J. Phy8iol. 118, 40.Hastings, A. B. &Van Dyke, H. B. (1931). J. biol. Chem. 92,
13.Hastings, A. B., Harkins, H. N. & Liu, S. K. (1932). J. biol.
Chem. 94, 681.Hunter, G. (1953). Biochem. J. 54, 42.Katzenelbogen, S. & Czarski, T. (1934). Proc. Soc. exp. Biol.,
N.Y., 32, 136.Lovell, H. W. & Brown, J. R. (1934). Proc. Soc. exp. Biol.,
N.Y., 32, 516.Maizels, M. (1936). Biochem. J. 30, 821.Malamud, W., Mullins, B. M. & Brown, J. R. (1933). Proc.
Soc. exp. Biol., N.Y., 30, 1084.Mason, M. F. (1936). J. biol. Chem. 113, 61.Masserman, J. (1934). Amer. J. Physiol. 109, 193.Mishkis, M., Ritchie, E. B. & Hastings, A. B. (1933). Proc.
Soc. exp. Biol., N. Y., 30, 473.Moller, K. 0. (1932). Arch. exp. Path. Pharmak. 165,
244.

Vol. 56 BLOOD-CEREBROSPINAL FLUID BARRIER 597Nencki, M. & Schoumov-Simanowsky, E. 0. (1894).
Arch. exp. Path. Pharmak. 34,313.Notkin, J., Garcia, T. & Killian, J. A. (1933). Arch. Neurol.
P8ychiat., Chicago, 30, 114.Owen, C. A. & Power, M. H. (1953). J. biol. Chem. 200,
111.Palmer, J. W. & Clarke, H. T. (1933). J. biol. Chem.
99,435.Smith, P. K. & Walker, D. W. (1938). J. Pharmacol.
63,35.
Stern, L. & Gautier, R. (1921). Arch. int. Phy8iol. 17,138.
Tod, H. (1933). J. ment. Sci. 79, 373.Wallace, G. B. & Brodie, B. B. (1940). J. Pharmaol. 68,50.Walter, F. K. (1919). Z. ge8. Neurol. P8ychiat. 47, 380.Walter, F. K. (1925). Z. ge8. Neurol. P8ychiat. 97, 192.Walter, F. K. (1929). Die BlutsILiquor8chranke, p. 99.
Leipzig: Thieme.Weir, E. G. & Hastings, A. B. (1939). J. biol. Chem. 129,
547.
The Source of Antibody Globulin in Rabbit Milk and Goat ColostrumBY B. A. ASKONAS, P. N. CAMPBELL,* J. H. HUMPHREY AND T. S. WORK
The National In8titute for Medical Re8earch, MiU Hill, London, N.W. 7
(Received 15 September 1953)
After the intravenous injection ofradioactive aminoacids into lactating rabbits, there is an extremelyrapid and efficient incorporation of radioactivecarbon into milk proteins. The blood plasma-proteinradioactivity reached its maximum value 6 or 7 hr.after the injection, but it is only about one-tenth theactivity of a milk protein sample collected at thesame time (Campbell & Work, 1951, 1952). It hasbeen concluded that blood plasma protein is nota major and direct precursor of milk protein andthat most of the milk protein is synthesized in themammary gland from amino acids or small peptides.Amino acids isolated from radioactive rabbit caseinwere, however, of slightly higher specific activitythan the corresponding amino acids from wheyprotein, and it seemed possible that this differencemight be due to the direct transfer from blood tomilk ofa fraction ofthe plasma protein. Campbell &Work (1952) calculated that up to 25% of the totalwhey protein would have to be so transferred toaccount for the lowered radioactivity of the whey.Experiments have, therefore, been directed towardsidentification of the protein transferred from bloodto milk in the lactating rabbit. More recently wehave been interested in the biosynthesis of milkproteins in the goat, and it was hoped to extend thework to this animal.
Extensive studies on the transmission of im-munity from parent to offspring have suggested thatantibody may pass across the placental barrier un-changed; high concentrations of antibody beingfound in colostrum and traces in milk (Ehrlich,1892; Ratner, Jackson & Gruehl, 1927; Marrack,1947; McMeekin & Polis, 1949, McCarthy &McDougall, 1953). According to Smith (1948) theimmune-globulin fraction of cow colostrum isidentical with the immune-globulin of cow milk and
closely similar to, but not quite identical with, theT-globulin of cow plasma. The immune-globulinsare, however, proteins of high molecular weight,rabbit y-globulin having a molecular weight of160000 (Kabat, 1939; Nichol & Deutsch, 1948) andthere has been considerable doubt as to whether thiswhole protein passed across cell barriers or whetherit was partially degraded and resynthesized(Cohen, 1950; Calman & Murray, 1951; Brambell,Henmings & Henderson, 1951).From the work on immune-globulin, it was clear
that in so far as proteins could be transferreddirectly from rabbit blood to milk, they wouldprobably be found in the immune-globulin fraction.Moreover, any protein transferred directly to themilk during the hours immediately followingintravenous injection of a radioactive amino acidshould have the radioactivity characteristic of theplasma proteins and, 6 hr. after injection, shouldhave not more than about one-tenth the activityof protein synthesized in the mammary gland.Accordingly, a lactating rabbit was immunized withpneumococcus (type III) and was then given aninjection of [36S]methionine. Blood and milksamples were withdrawn at intervals and pneumo-coccus capsular polysaccharide (SSS III) was used toprecipitate the specific antibody from blood andmilk. The antibodies thus obtained were comparedwith one another and with the other milk and bloodproteins. A preliminary account of this investiga-tion has been published (Campbell, Humphrey &Work, 1953).An attempt was then made to reproduce in a goat
the experimental conditions already used withrabbits. However, even after a prolonged course ofintravenous injections of formalin-treated pneumo-coccus (type III) the serum antibody level did notrise above 0-4 mg./ml. The level in the milk wasmuch lower, and was too low to permit accurate
* Present address: Courtauld Institute of Biochemistry,The Middlesex Hospital, London, W.1.
Copyright © 2022 FDOKUMEN