ON HIV/AIDS - Health and Education Resource Centre
192
Third Medium Term Plan (MTP III) 2004 - 2009 REPUBLIC OF NAMIBIA THE NATIONAL STRATEGIC PLAN HIV/AIDS
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of ON HIV/AIDS - Health and Education Resource Centre

Third Medium Term Plan(MTP III)
2004 - 2009
REPUBLIC OF NAMIBIA
THE NATIONAL
STRATEGIC PLAN
ON HIV/AIDS

ISBN NO: 99916-798—5-5 All rights reserved. Brief quotations may be reproduced without written permission provided the source is cited. Any part of this publication may be copied for planning purposes in Namibia only with clear indication of the source. This edition printed and published by: Capital Press, P.O. Box 6248, Ausspannplatz, Windhoek Tel: 061-221012, Fax 061-221015, E-mail: [email protected]
Copyright: Directorate: Special Programmes
Ministry of Health and Social Services P.O. Box 22331 Windhoek
Tel: 061-203-2822 Fax: 061 224155
Email: [email protected]

_____________________________________________________________________________________________Medium Term Plan III for HIV/AIDS
Foreword
HIV/AIDS poses the single most serious development challenge for Namibia during the next 10 to 20 years. The impact of the AIDS epidemic on all sectors of the Namibian economy is already being felt, and is expected to increase considerably over the next decade. All levels and sections of the Namibian population are being negatively affected by the spread of this virus. Adverse effects on social cohesion, human development and economic advancement are the result of the epidemic.
It was for this reason that the Government of the Republic of Namibia established the first National AIDS Control Programme in 1990. Under this programme, awareness and prevention campaigns were advocated. Subsequently, the Second Medium Term Plan was launched in March 1999 in order to intensify awareness and prevention campaigns through an expanded multi-sectoral national response. MTP II also placed increasing focus on alleviating the burden of HIV/AIDS on the infected and affected citizens of our country.
The plan focused on mobilising all partners to reduce the number of HIV infections among adults and children by strengthening the support to HIV/AIDS prevention and control efforts. It further aimed at support and strengthening the national as well as regional programme management structures to ensure effective coordination and monitoring of the National response to HIV/AIDS. It further addressed the issue of stigmatisation and discrimination, while it also strives to ensure access to quality health services for people living with HIV/AIDS.
Notwithstanding strenuous efforts, the HIV/AIDS epidemic however, continues to spread and to rob us of our loved ones, friends and neighbours. As dedicated citizens of the land of the brave, we must be undaunted and continue to put up the fight against HIV/AIDS in Namibia. Therefore, the Third Medium Term Plan goes a step further than its predecessors, since it extends and consolidates access to treatment with anti-retroviral medicines to those infected with HIV/AIDS and ensures mainstreaming of HIV/AIDS in all sectors. It further pulls together efforts from all Government Offices/Ministries/Agencies, Regions, non-governmental organisations (NGOs), Faith Based Organisations (FBOs), and Community Based Organisations (CBOs), the private sector and various development partners in order to play a distinct role in reducing the burden caused by the scourge of HIV/AIDS.
Hence, I urge all Government Offices/Ministries/Agencies Governors, the members of business fraternity, church and traditional leaders and the entire Namibian public to actively take part in all efforts which are aimed at reducing the HIV/AIDS epidemic through the framework of this important plan. It is high time to redouble our efforts in the fight against this deadly virus.
…………………………………….
Dr. Sam Nujoma
PRESIDENT OF THE REPUBLIC OF NAMIBIA
March 2004

________________________________________________________________________________________Medium Term Plan III for HIV/AIDS
Preface
The major determinants for HIV transmission lie outside the health sector. Effective management and control of the HIV/AIDS epidemic call for a multi-sectoral approach. The Third Medium-Term Plan on HIV/AIDS for the years 2004-2009 serves as a guide for sector response to the epidemic, as well as a management and coordination tool for all those involved in the fight against the epidemic. Gaps, which were identified, and recommendations from the review of the Second Medium-Term Plan were taken into account in compilation of this Third Medium-Term Plan.
The goal of the Third Medium-Term Plan has been defined. Sectoral obligations are well articulated. The Ministry of Health and Social Services together with a broad movement of partners shall continue to provide its technical support services to all sectors which are undertaking HIV/AIDS related activities. In line with its constitutional mandate to plan and manage public health, my Ministry coordinated, guided and directed the entire process of MTP III development.
In its introduction, the Plan describes the magnitude of the HIV/AIDS epidemic globally and in Namibia. It further gives a summary of the national response since 1990 as well as the principles underlying it. The Plan further describes the implementation mechanism, detailing each management structure with well-defined membership and responsibilities. The different components of the expanded national response as well as criteria for monitoring are described. Activities to achieve specified outcomes, are identified and costed. Finally, sectoral obligations and regional commitments are well articulated.
The development of the Third Medium-Term Plan on HIV/AIDS for the years 2004-2009 was a broad and participatory process. As a consequence, the plan reflects the multi-sectoral dimension very well. I acknowledge with appreciation, the contribution made by the Ministries, Offices and Agencies for the Government of the Republic of Namibia, as well as the regions, the private sector, the community-based and non governmental organisations. I commend the commitment and efficiency of the technical working group assisted by Namibia Resource Consultants for producing this Plan within good time. The financial and technical assistance provided by the European Union, GTZ, CDC, UNAIDS and USAID is highly commended. Finally, I thank the staff of the Directorate of Primary Health Care Services under the guidance of NAEC and the office of the Permanent Secretary of my Ministry, for coordinating and managing the entire process.
MTP III went through an intensive consultative process with the public and private sectors, regional committees, development partners and People Living with HIV/AIDS amongst others, and certain versions of it were presented and discussed in all thirteen administrative regions. The First Final Draft was reviewed by a joint session of the Policy Management Development and Review Committee (PMDRC) and the Ministry Management Committee. This draft was presented to the National Multi-sectoral AIDS Coordination Committee (NAMACOC), which recommended it to the National AIDS Committee. The latter endorsed it after which it was approved by Cabinet.
MTP III is a strategic plan, not an implementation plan. All partners are urged to review their existing plans and ensure that the principles and emphasis that are embodied in MTP III are brought into their plans. In addition, while the epidemic generates its own dynamic, we must be prepared to amend our response in such a way that the goal and the strategic results of this plan remain within target. The guiding principles contained in this document provide us all with the lasting values that will ensure that we do what is right when we implement this plan.
I strongly believe that the Third Medium-Term Plan on HIV/AIDS provides a comprehensive strategy for effective management and control of the HIV/AIDS epidemic and its direct consequences. I want to encourage all the stakeholders to use it as a tool and a road map for our expanded national fight against HIV/AIDS. Let us all actively work together to ensure that we reach the important targets we set ourselves!
Dr. Libertina Amathila, MP Minister of Health and Social Services Chairperson: National AIDS Committee

Foreword i
Preface ii
Abbreviations and Acronyms iv
Executive Summary viii
Chapter I Introduction 1
1.1 Background to Namibia’s Medium Term Plans
1.2 The consultative process to develop MTP III
1.3 The global HIV/AIDS epidemic
1.4 HIV/AIDS in the context of The Republic of Namibia
1.4.1 Current status and future trends of the HIV/AIDS
epidemic in Namibia
1.4.2 A summary of the national response to the epidemic
1.5 The Republic of Namibia and its international commitments in the context of HIV/AIDS
1.6 The guiding and underlying principles of the expanded national HIV/AIDS response
Chapter II Implementation Mechanisms 11 2.1 Introduction
2.2 How partners can use this strategic plan
2.3 Management and Coordination
Terms of Reference for Committees in the National Response
� National AIDS Committee (NAC) � National Multi-sectoral AIDS Co-ordination Committee (NAMACOC) � National AIDS Executive Committee (NAEC) � Sectoral Steering Committees � Technical Advisory Committee (TAC)) � Regional AIDS Co-ordination Committees (RACOC) � Constituency AIDS Co-ordination Committees (CACOC)
2.4 Technical Support
The MoHSS Directorate: Special Programmes Technical Working Groups
2.5 Human Resource Management
2.6 Resourcing the response
Resource Mobilisation Financial mechanisms
2.7 Assumptions, Risks and Risk Management
Table of Contents

Chapter III The Expanded National HIV/AIDS Programme
Response: MTP III – Plan of Action 31
3.0 Overview of the national programme response Goal, components, sub-components and strategic results
Component 1: Enabling Environment 33 Sub Component 1.1: Sustained Leadership Commitment Sub-Component 1.2 Greater Involvement of PLWHA Sub Component 1.3: Policy and Law Reform Sub Component 1.4: Interventions to reduce stigma and discrimination
Component 2: Prevention 39 Sub Component 2.1: Strengthen capacity to deliver HIV/AIDS prevention
programmes Sub-component 2.2: Target Vulnerable Populations Sub-component 2.3: Target Young People Sub-component 2.4: Target the General Population Sub-component 2.5: Interventions which reduce vulnerability
Component 3: Access To Treatment, Care And Support Services 55 Sub Component 3.1: Capacity development for the expanded treatment, care
and support response Sub Component 3.2: Treatment and care services
Component 4: Impact Mitigation Services 67 Sub-Component 4.1 Developing the capacity for local responses Sub-Component 4.2 Services for OVC and PLWHA Sub-Component 4.3 Addressing poverty
Component 5: Integrated and Co-ordinated Programme Management 73 at all Levels
Sub-component 5.1 Developing HIV/AIDS Management Capacity Sub component 5.2: Management and Co-ordination Sub component 5.3: Programme monitoring and evaluation Sub component 5.4: Surveillance and Operational Research
Chapter IV: Monitoring and Evaluation 85
4.1 Monitoring and evaluation at national, regional and sub-regional level
4.2 Outcome Indicators and targets for MTP III
Chapter V: Costing for the national HIV/AIDS response 97
Chapter VI: Sectoral obligations and commitments 99 6.1 List of sectoral clusters, lead agencies and key actors 6.2 Commitments by each Sector
Appendices 143
1 The Republic of Namibia and its international commitments in the context of HIV/AIDS
2. Regional Commitments
3. Research Topics for prioritisation
4. Index

Medium Term Plan III for HIV/AIDS
ABC Abstinence, Behaviour change, Condoms ACT AIDS Care Trust AIDS Acquired Immuno-deficiency Syndrome ALAN Association of Local Authorities in Namibia ALU AIDS Law Unit AMICAALL Alliance of Mayors and municipal leaders on HIV/AIDS in Africa ANC Ante natal clinic ARC Association of Regional Councils ART Anti-retroviral therapy ARV Anti-retroviral medicine BCC Behaviour change communication BCI Behaviour change intervention BoN Bank of Namibia CAA Catholic Aids Action CACOC Constituency AIDS Co-ordinating Committee CAFO Church Alliance For Orphans CBNRM Community-based natural resource management CBO Community-based Organisation CCN Council of Churches in Namibia CDC Centre for Disease Control and Prevention, Atlanta, USA CHS Catholic Health Services CMO Chief Medical Officer CMS Central Medical Stores COSDEC Community Skills Development Centre COTA College of the Arts CoW City of Windhoek CRIAA Centre for Research Information Africa Action CRIS Country Response Information System DACOC District AIDS Coordinating Committee DAPP Development Aid People to People in Namibia DHS Demographic Health Survey DOTs Directly observed treatment short course EIA ELISA Immuno Assay (testing) ELCAP Evangelical Lutheran Churches AIDS Programme ELCIN Evangelical Lutheran Churches in Namibia ELCRIN Evangelical Lutheran Church in the Republic of Namibia EMU Emergency Management Unit FBO Faith-based organisation FENATA Federation of Namibian Tourism Associations FHI Family Health International GDP Gross Domestic Product GF Global Fund GIPF Government Institutions Pension Fund GIPA Greater Involvement of People Living with HIV/AIDS GRN Government of the Republic of Namibia GTZ Gellschaft für Technishe Zusammenarbeit (German Technical Co-operation) HAART Highly active anti-retroviral treatment HIS Health Information System HIV Human Immuno-deficiency Virus HR Human Resources IEC Information, education, communication IPPF International Planned Parenthood Federation IPPR Institute for Public Policy Planning and Research IRDNC Integrated Rural Development and Nature Conservation
Abbreviations and Acronyms

Medium Term Plan III for HIV/AIDS
JCC Joint Co-ordinating Committee [for SME] JHU Johns Hopkins University KAP Knowledge, attitudes, practices KAYEC Katutura Youth Enterprise Centre LA Local Authority LAC Legal Assistance Centre M&E Monitoring and evaluation MAWRD Ministry of Agriculture, Water and Rural Development MDR Multi-drug resistant MET Ministry of Environment and Tourism MYFC My Future My Choice MFMR Ministry of Fisheries and Marine Resources MHETEC Ministry of Higher Education, Technology and Employment Creation MIB Ministry of Information and Broadcasting MISA Media Institute of Southern Africa MLRR Ministry of Lands, Resettlement and Rehabilitation MME on VAWC Multi-media Campaign on Violence Against Women and Children MOF Ministry of Finance MoHSS Ministry of Health and Social Services MOJ Ministry of Justice MoL Ministry of Labour MPCS Ministry of Prisons and Correctional Services MRLGH Ministry of Regional and Local Government and Housing MTI Ministry of Trade and Industry MTP II Second Medium Term Plan [1999-2004] MWACW Ministry of Women’s Affairs and Child Welfare MWTC Ministry of Works Transport and Communication NABCOA National Business Coalition on HIV/AIDS NAC National Aids Committee NaCCATuM Namibia Co-ordinating Committee for HIV/AIDS, Tuberculosis and Malaria NACOBTA Namibia Community-based Tourism Association NACOP National Aids Co-ordination Programme NACSO Namibian Association of CBNRM Support Organisations NAFWU Namibian Farm Workers Union NAG National Art Gallery NALAO Namibian Association of Local Authority Offices NAMACOC The National Multi-sectoral AIDS Coordination Committee NAMDEB NAMDEB Diamond Corporation NAMFISA Namibia Financial Institutions Supervisory Authority NAMPOL Namibian Police NAMTA Namibia Tuberculosis Association NAMBTS Namibian Blood Transfusion Service NANASO Namibia Network of AIDS Service Organisations NANAWO Namibia National Womens Organisation NANGOF Namibia Non-governmental Organisation Forum NANTU Namibia National Teachers Union NANSO Namibia National Students Union NAPPA Namibia Planned Parenthood Association NASOMA Namibia Social Marketing Association NAU Namibia Agricultural Union NBC Namibia Broadcasting Corporation NCCI Namibia Chamber of Commerce and Industry NDC Namibia Development Corporation NDF Namibia Defence Force NDP II National Development Plan II [2001-2006] NEM Namibian Essential Medicines list NEPAD New Partnership for Africa’s Development NEF Namibia Employers’ Federation

Medium Term Plan III for HIV/AIDS
NEPAD New Partnership for Africa’s Development NEPRU Namibia Economic Policy Research Unit NGO Non-governmental organization NHAG Namibia Housing Action Group NHTC National Health Training Centre NIED Namibia Institute for Education Development NIP Namibia Institute for Pathology NNFU Namibia National Farmers Union NPC National Planning Commission NPCS National Planning Commission Secretariat NQA National Qualifications Authority NRCS Namibia Red Cross Society NTN National Theatre of Namibia NWR Namibia Wildlife Resorts NYC National Youth Council OI Opportunistic infection OPM Office of the Prime Minister ORID Other Related Infectious Diseases OVC Orphans and vulnerable children OY Ombetja Yehinga PEP Post-exposure Prophylaxis PEMP Performance and Efficiency Management Programme PLWHA People living with HIV/AIDS PMTCT+ Prevention of mother to child transmission (plus on-going treatment) PON Polytechnic of Namibia PRA Participatory Rural Appraisal PSC Public Service Commission PSS Psycho-social support RAC Regional AIDS co-ordinators RACOC Regional AIDS Co-ordinating committee RCC Roads Construction Company RDCC Regional Development Coordinating Committee REMU Regional Emergency Management Unit RISE Rural Institute for Social Empowerment RMT Regional Medical Team SADC Southern African Development Community SHPA Senior Health Programme Administrator SIAPAC Social Impact Assessment and Policy Analysis Corporation SMA Social Marketing Association SME Small or Medium enterprise SSC Social Security Commission SSC Sector Steering Committee STI Sexually transmitted infection TAC Technical Advisory Committee TB Tuberculosis TBA Traditional Birth Attendants TC Take Control [Task Force] ToT Training of trainers TSC Training and Support Co-ordination Unit (MoHSS) TUCSIN The University Centre for Studies in Namibia TWG Technical Working Group UN United Nations UNAM University of Namibia UNDP United Nations Development Programme UNGASS United Nations General Assembly Special Session on HIV/AIDS UNV United Nations Volunteers USD United States dollar VCT Voluntary counselling and testing

Medium Term Plan III for HIV/AIDS
WAD Women Action for Development WBCG Walvis Bay Corridor Group WCPU Women and Child Protection Unit WHO World Health Organisation YHDP Youth Health Development Programme YWCA Young Women Christian Association

Medium Term Plan III for HIV/AIDS
viii
The Third Medium Term Plan (MTP III) process forms a unique opportunity to address the challenges that Namibia faces in combating the HIV/AIDS epidemic over the period 2004-2009. This document provides the framework for all the actors to collaborate and guide the implementation processes needed for an effective multisectoral HIV/AIDS response.
Since the first HIV/AIDS cases were reported in Namibia in 1986, the Ministry of Health and Social Services estimates that 230,000 adults and children were living with HIV/AIDS by the end of 2001. The impacts on families and communities are diverse and widespread; the effect on the national economy has correspondingly worsened as the epidemic has escalated. The Government of Namibia responded by developing strategies, priorities and mechanisms deemed necessary for each stage of the epidemic. This next plan builds on the successes and lessons learned from the MTP II (1999-2004). It adopts goals and strategies which are enshrined in key national documents such as Vision 2030 and the National Development Plan II as well as Namibia’s international commitments.
The underlying principles treat HIV/AIDS as a complex development issue that requires full and active participation of all Namibians – its leaders, government departments and civil society at large. The adverse impacts of stigma and discrimination are being increasingly recognised as key barriers to combating the epidemic. Prevention of HIV infection continues to be the mainstay of the national and international response to the epidemic but it is now recognised that voluntary counselling and testing, care, support, and treatment are mutually reinforcing mechanisms in contributing to effective prevention.
The Expanded National HIV/AIDS Programme Response for 2004-2009
The strategic results of MTP III are the following: 1. People infected and affected with HIV/AIDS enjoy equal rights in a culture of
acceptance ad openness and compassion 2. Reduced new infections of HIV and other STIs 3. All people living with or affected by HIV/AIDS have access to cost-effective and high
quality treatment, care and support services 4. Strengthened and expanded capacity of local responses to mitigate socio-
economic impacts of HIV/AIDS 5. Effective management structures and systems, optimal capacity and skills, and high
quality programme implementation at national, sectoral and regional levels. In line with the above strategic results, MTP III has five components that address the broad
strategies which need to be adopted to achieve the national goal: COMPONENT 1: ENABLING ENVIRONMENT
� Sustained leadership commitment � Greater involvement of people living with HIV/AIDS in the national response � Policy and law reform � Interventions which reduce discrimination against those affected by HIV/AIDS
MTP III National Programme Goal
The reduction in incidence of HIV infection to below epidemic threshold
Executive Summary

Medium Term Plan III for HIV/AIDS
ix
COMPONENT 2: PREVENTION
� Capacity development of service providers � Prevention interventions that target vulnerable populations � Prevention interventions which target young people � Prevention interventions which target the general population
COMPONENT 3: ACCESS TO TREATMENT, CARE AND SUPPORT SERVICES
� Capacity development, for the expanded treatment care and support response � Treatment and care services
COMPONENT 4: IMPACT MITIGATION SERVICES � Developing the capacity for local community responses � Services and support for orphans and vulnerable children � Addressing poverty, food security and nutrition
COMPONENT 5: INTEGRATED AND CO-ORDINATED PROGRAMME MANAGEMENT AT ALL LEVELS
� Developing HIV/AIDS management capacity � Management and Coordination � Programme monitoring and evaluation � Surveillance and operational research
The MTP III takes a “Results based” management approach to achieving nationally and
internationally agreed targets. These targets are listed in Chapter 4 and will provide the basis for the monitoring and evaluation system which will be put in place during 2004. These are MINIMUM results expected and they prioritise nationwide coverage and access to high quality prevention, VCT, treatment, care and mitigation services.
To achieve the minimum required results to turn the epidemic around, management and coordination will be strengthened by all partners in the multi-sectoral response. The membership and terms of reference of the decision-making and coordinating bodies at national and regional levels are provided in this plan. Implementing partners and coordinating bodies will be accountable to deliver results agreed upon results. Several mechanisms to improve technical support will be put in place.
The Directorate: Special Programmes, in the MoHSS, shall be reinforced with expanded capacity to provide support to all implementing partners. Specialist Technical Advisory Committees all key performance areas of the MPT3 will actively give leadership in their field of expertise.
Planning to build adequate human resource capacity to manage and implement the national response must be well coordinated and resourced. A National Human Resource Planning Task Force, under the responsibility of MHETEC, and the Ministry of Health and Social Services will ensure that there is training capacity across the country to overcome the spread and impact of HIV/AIDS.
Every line ministry and private sector/civil society partner is committed by this plan to budget and allocate resources to ensure their obligations related to this plan are effectively implemented.

Appendix 4
Medium Plan III for HIV/AIDS 182
Agriculture water & rural development 67-72, 103 Alcohol abuse 2, 3, 53-54 Assumptions 28-30 Awareness 46-48 Behaviour change 39-47 Blood safety 52 Capacity development 34, 40-41, 56-58, 68-69, 75-77 Caprivi Region 149 Care services 55-66 Child Welfare Sector 104-105 Condom provision 41-42, 44-45, 49, 61 Constituency AIDS Co-ordination Committees
(CACOC) 14, 24, 78 Counselling 41, 50-51, 58, 63, 65 Costing 97-98 Cultural practices 53-54 Defence 106 Directorate: Special programmes 14, 25 Discrimination 36-37 Drugs & supplies systems 60-61 Education, Sport and Culture 40, 44-46, 108 Enabling environment 33-38 Environment & Tourism Sector 110 Erongo Region 152 Faith-based organisations 34, 37, 68-71, 138 Finance, Treasury & Resources 27, 78, 112 Financial mechanisms 28, 78 Fisheries & Marine Resources Sector 113 Food security 70-72 Foreign Affairs Sector 114 Gender 2, 3, 42, 53-54, 116 General population 46-52 Global HIV/AIDS epidemic 2 HAART 57, 59, 61, 64 Hardap Region 153 Health care settings 43, 56-58 Health Services Sector 117 Home based care 48, 58, 61, 63, 65 Human resource management 26, 73, 75-77
IEC programmes 36-48, 52-53, 59 Impact mitigation services 67-72 Implementation mechanisms 11-30 Indicators 85-95 Infection prevention and management 43 Information and Media Sector 120-121 Information flows 79 Infrastructure Sector 122 International commitments 8, 143-148 Karas Region 156 Kavango Region 159 Khomas Region 162 Kunene Region 164 Laboratory services 60 Labour, trade and industry Sector 123 Lands, Resettlement and Rehabilitation Sector 124 Law reform 35 Leadership 9, 33, 34, 73, 77, 78, 80, 81 Legal Sector 125 Legislative Sector 127 Local authorities 37, 45, 46, 48, 52-53, 68, 135 Local community-based responses 67-72 Monitoring and Evaluation 73, 81, 85-95 Mainstreaming 80 Management and co-ordination 12, 73-83 Management structures 14, 78 Mining and Energy Sector 129 Mobile workers 41-42 National AIDS Committee (NAC) 14, 15, 17, 78, 86 National AIDS Executive Committee (NAEC) 14, 18 National Multi-sectoral AIDS Co-ordination Committee (NAMACOC) 14, 16 NGOs 9-10, 77, 139-140 Nutrition 57-58, 61, 62, 64, 67-72 Ohangwena Region 167 Omaheke Region 170 Omusati Region 173 Opportunistic infections 57, 62 Organogram 14 Orphans & vulnerable children 5, 41-46, 66,
67-72, 104-105
Index

Appendix 4
Medium Plan III for HIV/AIDS 183
Oshana Region 174 Oshikoto Region 177 Otjozondjupa Region 179 People with disabilities 41-42 PEP 43, 54 PLWHA 35, 67-71 PMTCT+ services 40, 61-62 Policy 6-7, 35-36 Poverty 2, 3, 67-72 Prevention 39-53 Principles guiding MTP III 9 Prisons & correctional services 41-42, 59, 54, 130 Private sector 9-10, 141 Programme management 73-83 Programme monitoring 81-83 Public services co-ordination Sector 101 Quality Assurance 77 RACOC 14, 22, 35, 40-43, 46-49, 54, 65, 67-71,
73-82 RACE 40, 44-45 Regional and local governance Sector 133 Reproductive health 57, 59 Research 59, 66, 82-83, 181 Resource mobilisation 27, 78 Risk management 28-30
Schools 44-45, 68 Sectoral policies 36 Sectoral steering committees 14, 19, 99-100 Social mobilisation 36-45, 46-47, 48, 52-53, 59 Social welfare and housing 69-72 STI management 50 Stigma 10, 33, 36 Supplies procurement 60-61 Support services 55-66 Surveillance 74, 83 Targets 85-95 TB 48, 59, 63, 72 Technical support 25-26, 75-76 Technical Advisory Committees 14, 21, 26 Terms of reference 15-24 Traditional authorities 33-34, 46, 53, 71, 100, 133 Treatment 55-66 Uniformed services 41-42, 53-54, 106, 130 Violence 53-54 Voluntary counselling and testing 41, 51, 62, 63, 69 Vulnerability 41-46, 53-54, 59, 66 Women 2, 3, 41-42, 52-53, 116 Workplace programmes 47-48, 80 Young people 44-46 Youth 44-46, 54, 136

Introduction
Medium Term Plan III for HIV/AIDS 1
This Chapter gives the background to the development of MTP III. It describes the global HIV/AIDS epidemic, and the current status and future trends in Namibia. It summarises what has been achieved under MTPII and highlights the main findings of its Mid Term Review. It gives the main international commitments to which Namibia is committed, which this plan will aim to meet. Also this chapter describes the process for developing this plan and how the plan will reach all organisations assisting in the response.
1.1 Background to Namibia’s Medium Term Plans In 1986 the first four cases of HIV/AIDS were reported in Namibia. By the 31st December 2003, a
cumulative number of 136,068 cumulative HIV/AIDS cases had been recorded by the Ministry of Health and Social Services. In an effort to control the unfolding epidemic, since 1990 a number of consecutive plans were developed which stipulate the strategies and priorities deemed to be required for that stage of the epidemic.
In March 1999, His Excellency the President of the Republic of Namibia, Dr Sam Nujoma launched the Second National Strategic Plan on HIV/AIDS covering the period from 1999 until 2004. The Second Medium Term Plan (MTP II) is a five year strategic plan that guides the health and multisectoral responses to HIV/AIDS. The Second Medium Term Plan stipulates goals and broad objectives, strategies and responsibilities of sectors in strengthening the multi-sectoral responses to HIV/AIDS. The document also defines the management structure for the National Aids Co-ordination Programme at national and regional levels.
The Second Medium Term Plan on HIV/AIDS will expire in March 2004. However, the challenges posed by the epidemic have not dissipated. It is therefore necessary to provide another framework for the continuation of the fight against HIV/AIDS through the Third Medium Term Plan on HIV/AIDS. As part of the preparations, a midterm review of MTP II was conducted in February 2003. The recommendations from this review have fed into the development of MTP III. The MTP III is consistent with the United Nations General Assembly Special Session (UNGASS) Declaration of Commitment, Namibia’s Second National Development Plan and Namibia’s Vision 2030.
1.2 The Consultative Process to Develop MTP III The goal of rapid and significant expansion of the prevention, treatment, care and support,
and impact mitigation responses to the STI/HIV and AIDS epidemics in Namibia cannot be achieved by Government alone. It requires all organisations and individuals, from communities, ministries, parastatals, the private sector, non government organisations, faith based organisations, trade unions organisations of people living with HIV/AIDS and development partners to become more actively involved in the planning and implementation of the response. Specific population groups like, women, people living with disabilities, and other vulnerable population groups at national and regional levels are included. The consultative process for the development of MTP III aimed to build on the ideas and experiences of people who are infected by HIV/AIDS, of those who are working tirelessly in the response and those who are being affected by this deepening epidemic in their work, their families and communities. Consultations were therefore held in all sectors and in all regions of Namibia in the process of developing the MTP III.
The process for developing MTP III was undertaken under the overall responsibility of the Permanent Secretary of MoHSS, Dr. K. Shangula. A Core Group to oversee the development of MTP III was established in the MoHSS, representing all Directorates of the Ministry, UNAIDS and some of the Technical Advisors in the MoHSS. The core group reported to the National AIDS Executive
Chapter I Introduction

Introduction
Medium Term Plan III for HIV/AIDS 2
Committee (NAEC) chaired by the Under Secretary, Dr. N. Forster in the drafting stages and finally to the Permanent Secretary.
Every Ministry, through its Permanent Secretary and its HIV Focal Persons, was tasked with calling a sector-wide meeting, involving all key organisations (Key Actors) which work in that sector. In MTP III each sector has its own page of objectives to which all Key Actors in the sector are encouraged to commit themselves. These can be found in Chapter 6. Similarly, each region through its Regional AIDS Coordinating Committee (RACOC) was consulted in the preparation of a regional commitment page of activities reflected in Appendix 2. Each organisation and sector is tasked to commit itself to carrying out some of these planned activities during the next five years.
A working document for MTP 3 was circulated in December 2003 to all sectors and all regions through sector focal people and through Regional AIDS Coordinators. Comments on this document were fed into the first draft which was made available in February 2004. The National Multi-Sectoral AIDS Co-ordination Committee (NAMACOC) followed by the National AIDS Committee (NAC) endorsed the last version of MTP III, prior to its final approval by Cabinet. The launch of the Third Medium Term Plan was officiated by His Excellency President Sam Nujoma in April 2004.
1.3 The global HIV/AIDS epidemic
In 2003 the global HIV/AIDS epidemic killed more than 3 million people, 2.3 million of whom were in sub-Saharan Africa. An estimated 5 million acquired the human immunodeficiency virus (HIV) in 2003 bringing to 40 million the number of people living with the virus around the world. Of these 40 million, 26.6 million people are in sub-Saharan Africa. In other sub-Saharan African countries, the epidemic has gained a firm foothold and shows little sign of weakening with some notable exceptions. In Southern Africa, HIV prevalence is maintaining alarmingly high levels in the general population.
Figure 1: Summary of HIV/AIDS data for Global and Sub-Saharan Africa
Deaths in 2003 New Infections in 2003
People living with HIV/AIDS
Global 3 million 5 million 40 million Sub-Saharan Africa 2.3 million 3.2 million 26,6 million
HIV prevalence varies considerably across the continent, ranging from less than 1% in Mauritania to almost 40% in Botswana and Swaziland. More than one in five pregnant women are HIV-infected in most countries in Southern Africa, while elsewhere in sub-Saharan Africa median HIV prevalence1 in antenatal clinics exceeded 10% in a few countries. Encouragingly however, sustained prevention efforts in a few countries in West and East Africa (principally Senegal and Uganda) demonstrate that a national HIV/AIDS epidemic can be checked through concerted human efforts.
The driving factors, along with the circumstances and interventions that might inhibit the spread of HIV, must still be better understood. Nevertheless, in Southern Africa, poverty, mobility, high levels of inequality in income, alcohol abuse, inequality in status and access to resources between urban and rural populations and between men and women, high percentage of female headed households, and high percentage of households with members living long distances from each other all contribute to very high vulnerability of our citizens to HIV/AIDS infection.

Introduction
Medium Term Plan III for HIV/AIDS 3
1.4 HIV/AIDS in the context of the Republic of Namibia
1.4.1 Current status and future trends of the HIV/AIDS epidemic in Namibia All the factors mentioned above contribute considerably to the spread of HIV infection in
Namibia. Of particular importance in our country are the following: a) the high mobility of individuals between different places in the country b) cross-border travel, c) high prevalence of STIs, d) widespread alcohol and substance abuse, e) gender inequalities, f) poverty, g) certain cultural practices, h) the disintegration of traditional family structures, i) intergenerational sex between older men and young women, and j) ignorance.
Heterosexual intercourse and mother to child transmission are the most common modes of transmission in Namibia.
Figure 2:
C ru d e H IV p re v a le n c e ra tio in p re g n a n t w o m e n , b ia n n u a l s u rv e y s 1 9 9 2 -2 0 0 2 , N a m ib ia
2 2 .01 9 .3
1 7 .41 5 .4
8 .4
4 .2
0
5
1 0
1 5
2 0
2 5
3 0
1 9 9 2 1 9 9 4 1 9 9 6 1 9 9 8 2 0 0 0 2 0 0 2
% H
IV p
reva
lenc
e
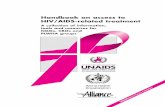
It is encouraging to note that several recent research findings provide evidence that the HIV
epidemic in Namibia may be beginning to stabilise, though the prevalence ratio is still alarmingly high. The most recent sentinel sero-survey of pregnant women done in 2002 revealed that 931 of 4227 pregnant women were infected with HIV giving a crude HIV prevalence ratio of 22.0% (Figure 2). The HIV prevalence among pregnant women ranged from a high of 43% in Katima Mulilo to a low of 9% in Opuwo. The four sites with the highest prevalence were Katima Mulilo (43%), Oshakati (30%), Grootfontein (30%) and Walvis Bay (28%). HIV prevalence exceeded 20% in 13 (62%) of the 21 sites. Only one site, Opuwo (9%), was found to have HIV prevalence remaining below 10%. The highest prevalence was in urban locations (27% to 43%) and in rural sites close to major movement corridors (see Figure 3).

Introduction
Medium Term Plan III for HIV/AIDS 4
Figure 3. Map of HIV prevalence among pregnant women in different sentinel
sites, Namibia 2002
Compared to the 2000 sero-survey, an increase in the prevalence ratio was observed in 12
(67%) of the 18 sites, for which data is available, and a decrease in the remaining 6 sites. A decline in HIV prevalence was observed in Windhoek, Walvis Bay, Swakopmund, Engela, Nankudu, and Keetmanshoop.
HIV/AIDS has been the leading cause of death since 1996. In 1999, AIDS was responsible for 26%
of all reported deaths, and for 46% of deaths in the 15 - 49 year age group.. According to the 2001 Population and Housing Census, the number of deaths has increased 80% in the three preceding years. The MoHSS estimates that in some parts of the country between 50 – 70% of hospital admissions are HIV/AIDS-related. Figure 4 shows relevant MoHSS hospital in-patient data since 1995.
<10%
10-14 %
15-19 %
20-24 %
25-29 %
30-39 %
>40 %

Introduction
Medium Term Plan III for HIV/AIDS 5
Figure 4: In-patient statistics related to HIV/AIDS in state health facilities
Year Total admission
from all causes
HIV
related admissions
Total deaths
from all causes
AIDS
Related deaths
1995 150 017 1 826 (1.2%) 6 405 628 (9.8%)
1996 163 279 2 620 (1.6%) 7 473 1 125 (15.1%)
1997 169 311 3 908 (2.3%) 8 283 1 539 (18.6%)
1998 157 045 5 155 (3.3%) 9 810 2 179 (22.2%)
1999 153 645 6 878 (4.4%) 10 670 2 823 (26.0%)
2000 164 295 7 376 (4.0%) 12 370 3 304 (26.7%)
2001 186 985 6 881 (3.6%) 13 482 3 020 (22.4%)
2002 170 168 9 248 (5.4%) 12 625 2 788 (22.1%)
2003 166 746 9 654 (5.8%) 13 508 2 804 (20.8%)
Information on orphanhood, particularly for children, provides an indirect indicator for adult mortality. It also reflects on the degree of dependency at household level and demonstrates the social impact of the epidemic. Close to 14% of the children under fifteen in Namibia have lost one or both parents. The regions of Caprivi, Kavango, Ohangwena, Omusati and Oshana are the most hit by the orphan situation.
Figure 5: Numbers of orphans aged below 15 years by area, Namibia (Census 2001)
Children Under 15 Orphaned
By one Parent By both parents
Area # of children under 15
# % # %
Namibia 717 850 87587 12.2 9 590 1.3
Urban 181 480 17 008 9.4 1 846 1.0
Rural 536 370 70 579 13.2 7 744 1.4
Caprivi 31 030 5 444 17.5 842 2.7
Erongo 30 392 2 134 7.0 191 0.6
Hardap 24 299 2 184 9.0 231 1.0
Karas 21 093 1 855 8.8 202 1.0
Kavango 88 978 11 962 13.4 1 556 1.7
Khomas 71 063 5 622 7.9 569 0.8
Kunene 28 095 1 979 7.0 157 0.6
Ohangwena 110 264 16 212 14.7 1 679 1.5
Omaheke 27 596 2 061 7.5 224 0.8
Omusati 100 428 14 682 14.6 1 445 1.4
Oshana 63 705 9 854 15.5 1 065 1.7
Oshikoto 69 839 9 288 13.3 940 1.3
Otjozondjupa 51 068 4 310 8.4 489 1.0

Introduction
Medium Term Plan III for HIV/AIDS 6
1.4.2 A summary overview of the national response to the epidemic to date The National AIDS Control Programme (NACP) was launched in 1990 soon after Independence.
The Short Term Plan followed closely behind. This in turn was followed by the First Medium Term Plan launched in 1992 to cover the period 1992-1998. The NACP was to co-ordinate and manage HIV/AIDS patient care and preventative activities. The NACP was based within the Ministry of Health and Social Services, but it supported activities implemented by other ministries and NGOs.
The review of the First Medium Term Plan conducted in 1997 found that extensive awareness campaigns had been undertaken to good effect, that political commitment had been clearly articulated and that management structures were in place. The recommendations focused on the further development of programme management, initiating more targeted IEC campaigns and strengthening multi-sectoral involvement.
The Second Medium Term Plan (MTP II) was launched in 1999 for the period 1999-2004. MTP II established the National AIDS Co-ordination Programnme (NACOP), replacing the National AIDS Control Programme. MTP II set out six broad objectives for the NACOP. These were to i) reduce the number of HIV infections in both adults and children through the strengthening of support to preventive efforts; ii) ensure that all Namibians living with HIV and their families have access to services that are affordable, of high quality and responsive to their needs; iii) empower individuals, families and community members with knowledge and skills related to prevention, home-based care and self-protection against HIV/AIDS infection; iv) ensure that all Namibians living with HIV and their families are not subjected to any form of discrimination; v) establish national and regional programme management structures for the co-ordination and monitoring of the implementation of the national response; and vi) ensure continuous support by both national and international communities in order to address the socio-economic impact of HIV/AIDS.
MTP II provided a comprehensive framework for the national multi-sectoral and sub-regional response to HIV/AIDS. It aimed to:
Involve all sectors to expand the national response to HIV and AIDS Link prevention to care and support for persons or families affected by HIV and
AIDS to reduce stigmatisation Strengthen the capacities of regional councils and local authorities to co-
ordinate, manage and monitor HIV and AIDS activities Establish partnerships with private sector and civil society organisations to
implement programmes. The Second National Development Plan (NDP II) complements the strategies and targets laid
out in MTP II. During a Round Table meeting with donors in February 2003, MTP II and NDP II targets were brought into line with the indicators developed for the Namibian application to the Global Fund to Fight HIV/AIDS, Tuberculosis (TB) and Malaria (GFATM).
As part of the MTP II and NDP II, a “Menu of Partnership Options” was compiled in 2002, canvassing for support amongst and enhancing the partnership by private sector organisations in the fight against AIDS. The process of applying for the Global Fund was also instrumental in bringing all sectors together in a co-ordinated effort to prioritise and plan.
In Vision 2030, HIV/AIDS is addressed as a cross-cutting issue in each sector, and more specifically under the theme of Population, Health and Development. The strategies highlight the need for leadership at all levels, a multi-sectoral approach, the promotion of policies to combat stigma and discrimination, the inclusion of HIV/AIDS in all development plans, a greater understanding of the impact of HIV/AIDS on all the different sectors, and an enhanced ability to monitor impact.

Introduction
Medium Term Plan III for HIV/AIDS 7
Namibia is in the process of finalising a stand-alone National HIV/AIDS policy. However, many of the individual policy and strategy elements are in place, for example:
The Namibian Constitution provides a Bill of Rights that addresses issues of HIV/AIDS and human rights. In addition, various guidelines and procedure manuals have been developed
The Namibian HIV Charter of Rights and a Code on HIV/AIDS in Employment have been compiled, defining the legal and human rights of PLWHAs and making education for AIDS awareness and prevention available at all workplaces. There is also an active non-governmental AIDS Law Unit in the Legal Assistance Centre, which assists PLWHA to claim their rights
Policies or guidelines on reporting, notification, confidentiality and surveillance have been published
A sectoral impact assessment and subsequent formulation of a sector policy on HIV/AIDS has been completed by the two Education ministries
Policies and/or strategies and guidelines have been developed (or are being finalised), for a wide range of health interventions such as Prevention of Mother to Child Transmission, Post Exposure Prophylaxis, access to Anti-retroviral therapy (ART) and Voluntary Counselling and Testing
Cabinet also approved the establishment of a Permanent Task Force on Orphans and Vulnerable Children (OVC) to oversee finalisation of a policy on orphans and other children in need of care and protection.
In February 2002 the MTP II was reviewed in February 2003. The recommendations from the Review have guided the formulation of the third Medium Term Plan (MTP III). The Mid-term Review of the MTP II highlighted the considerable progress that has been made in terms of:
• Political commitment • Establishing the structures for policy development and management of the
response • HIV/AIDS policy development in a wide range of areas • Foundations to reduce discrimination and adoption of a human rights
approach to the epidemic • Raised awareness through social mobilisation • Introduction of workplace policies and establishment of some model private
sector workplace programmes • Increased level of community lead initiatives supported by faith-based
organisations and NGOs • Foundations laid for a strengthened and expanded health sector response
including services for PMTCT, VCT, home-based care and improved access to essential medical laboratory service
• Significant progress in the development of training curricula and modules in a wide range of health interventions, and general and multi-sectoral modules
• Widening range of partners involved in the response and strong partnerships being forged between stakeholders
• High HIV/AIDS awareness among the general population (at 89%) but generally inadequate translation into intentions to act
• Development of regional structures and additional regional capacity to manage and co-ordinate the response.
The Mid Term Review of MTP II concluded that although much progress has been made and
good ground work done, several areas of the national response needed strengthening. Many of

Introduction
Medium Term Plan III for HIV/AIDS 8
these centre on the capacity to plan, co-ordinate, and monitor the national and local responses, in particular the multi-sectoral response. The specific problems include:
• Relatively weak structures, systems and processes for inclusive policy development, co-ordination and monitoring of the response at central and at regional levels
• The absence in the programming of specific links between various HIV/AIDS related issues (such as sexual and reproductive health and rights, STIs, HIV/AIDS and TB infection), and inadequate consideration of the contributions to the epidemic of the effects of important socio-economic conditions such as gender inequality, violence, substance abuse and general poverty.
• Slow formulation of policies and laws e.g. the Child Care and Protection Bill leave significant gaps in the coherence of the expanded response.
• Limited capacity (people and skills) for HIV/AIDS/TB programme planning and management at all levels, within and outside the MOHSS and most other stakeholders
• The relatively under-developed multi-sectoral response, particularly in the public sector, where HIV/AIDS is not yet systematically mainstreamed
• Uncertain financial flows and pipeline blockages, and lack of mechanisms to channel public funds to sub-regional level and non-state actors
• Untapped potential for a more expanded, efficient and co-ordinated response, especially at local levels
• Need for more research to inform targeted strategies taking into account regional differences
• Lack of a clearly defined, co-ordinated and balanced HIV/AIDS-related research programme linked to a long-term research agenda
• Lack of targeted behaviour change communication and interventions especially for vulnerable groups and specific cultural and age groups
• Unsystematic and unstructured support to regional and sub-regional level to enhance local responses
• Weak mechanisms for monitoring and evaluation (M and E), networking, sharing of experiences and replication of best practices.
The current Third Medium Term Plan (MTP III) builds on the strengths of the previous programme and addresses the areas identified for renewed attention and commitment, as well as for human resource capacity building, improved financing and enhanced coordination and cooperation.
1.5 The Republic of Namibia and its international commitments in the context of HIV/AIDS
Namibia Is signatory to a wide range of international and regional agreements, treaties, conventions, declarations and commitments. A more detailed description of those relevant to this plan can be found in Appendix 1. Two international commitments of particular relevance to the national HIV/AIDS response are the UN Millennium Development Goals [2000) and the UNGASS Declaration of Commitment on HIV/AIDS [2001]. The targets for these commitments have been taken into consideration in the development of this document as have the other conventions and agreements.
Namibia was amongst the 147 heads of State and Government and 189 member states which adopted the Millennium Declaration issued by the United Nations during the Millennium Summit, New York, 6-8 September 2000. Namibia, along with other member states, resolved –
• by the year 2015, to have halted and begun to reverse the spread of HIV/AIDS

Introduction
Medium Term Plan III for HIV/AIDS 9
• to provide special assistance to children orphaned by HIV/AIDS • to encourage the pharmaceutical industry to make essential drugs more widely
available and affordable by all who need them in developing countries [United Nations General Assembly Resolution 55/2], and
• to give greater opportunities to the private sector, non-governmental organisations and civil society to contribute to the realisation of the above and other Millennium Development Goals and programmes.
Namibia is required to monitor its progress towards the achievement of HIV/AIDS-related Millennium Development Goals.
The UNGASS Declaration of Commitment on HIV/AIDS [2001), which comprises more than 100 paragraphs, and includes the establishment of a Global AIDS and Health Fund, was adopted during the United Nations General Assembly 26th Special Session on HIV/AIDS held in New York, from 25-27 June 2001. Broadly, by becoming a signatory to the Declaration, Namibia agreed to the following priorities in the fight against HIV/AIDS:
• To ensure that all people, but particularly the youth, know what to do to avoid infection
• To stop the transmission of HIV from mother to child • To provide treatment to all those infected • To intensify the search for a vaccine as well as a cure, and • To care for all whose lives have been devastated by AIDS, particularly AIDS orphans
According to UNGASS, Namibia monitors its progress towards these goals. The indicators are included in the MTP III target and indicator table in Chapter 4.
The Medium Term Plan III takes cognisance of these guiding documents, the commitments
agreed upon, and the various indicators required. The MTP III provides a concrete national expression to these commitments and integrates them with the previously planned interventions, thus providing critical components in scaling up Namibia’s response to HIV/AIDS, TB and STIs in the country.
1.6 The guiding and underlying principles of the expanded national HIV/AIDS response
This section described the most important guiding principles for the implementation of MTP III. The guiding principles are the main values that most be taken into account during all aspects of operationalisation of a plan. They bring together all stakeholders through a Charter of Values that must inform everything that is done for the implementation of a plan. Given the fact that a dynamic epidemic such as HIV/AIDS required continuous responsiveness for which it is very difficult to plan over a five year time horizon, the guiding principles and values play a particularly important role, namely that of providing overriding and long lasting guidance for decision making and action at all levels of implementation of MTP III. The following principles therefore must underpin all strategies contained in MTP III:
HIV/AIDS is a development issue. HIV/AIDS is more than a public health priority. It is a complex, multi-faceted problem affecting all aspects of society and impacting on development goals. Underdevelopment, in turn, provides the context for the spread of HIV infection and the disempowerment of PLWHA and those affected to take effective steps to mitigate impacts.
Multi-sectoral engagement. As the epidemic is complex, affects all parts of society, involves individual, institutional and social behaviour, and far transcends the health sector, an effective national response must be multi-sectoral in spirit and structure.

Introduction
Medium Term Plan III for HIV/AIDS 10
Broad political commitment. As the UNGASS Declaration states, “Leadership by governments in combating HIV/AIDS is essential and their efforts should be complemented by the full and active participation of civil society, the business community, and the private sector. Leadership involves personal commitment and concrete actions.”
Civil society involvement. As sub-components of a multi-sectoral approach and political commitment, the involvement of civil society is nevertheless worthy of highlighting as a central principle in the response. Without meaningful involvement of those groups representing all segments of society, the response will be inadequate. In particular, groups representing PLWHA need to be involved not only as meaningful participants in policy and programme discussions, but also in the organisations and agencies that implement programmes. The Greater Involvement of People with AIDS (GIPA) principle is therefore regarded as a critical element of MTP III.
Reduction of stigma and discrimination. The adverse impacts of stigma and discrimination are being increasingly recognised as key barriers to combating the epidemic. Commitment to reducing stigma and discrimination is therefore a central guideline and principle in all strategies contained in MTP III.
Prevention to care continuum. A cornerstone to our expanded national response is recognition and adoption of programmes that address the epidemic at all stages from prevention to care, support and treatment. UNGASS emphasises “…that care, support, and treatment can contribute to effective prevention through increased acceptance of voluntary and confidential counselling and testing and by keeping PLWHA and vulnerable groups in close contact with health-care systems and facilitating their access to information, counselling, care and preventive supplies.”
Human rights based approaches. All international declarations on HIV/AIDS acceded to by Namibia reference the absolute need to utilise strong human rights approaches for combating the HIV/AIDS epidemic. The reasons for this are well documented and related to fundamental rights such as access to health care, information, reproductive and sexual rights, and gender equity. In addition, human rights approaches have powerful programmatic effects as they reduce vulnerability to HIV/AIDS and also help prevent stigma and discrimination against people living with or at risk of HIV/AIDS.
Prioritisation. Resource allocation must take into consideration defined priorities based on the vulnerability of various affected groups and communities and the potential impact of the interventions.
Good governance, transparency and accountability. An effective national response requires government to provide leadership in mobilising resources, included but not limited to financial resources. Prudent management of resources at all levels and in all sectors must be ensured at all times.
Access to care. Equal access to basic care and services must be guaranteed for all persons infected and affected by HIV/AIDS.
Confidentiality and privacy. In line with our national policy, HIV testing must be voluntary with guaranteed confidentiality and adequate pre- and post-test counselling both in the public and private sectors. PLWHA and those affected consulting care and support services must be assured of privacy.
Responsiveness and flexibility. The national response must continuously be able to respond to the changing nature of the epidemic, its impacts, and the latest research, information and developments concerning HIV/AIDS.

Implementation mechanisms
Medium Term Plan III for HIV/AIDS
11
2.1 Introduction
This chapter describes how this strategic plan can be used by implementing partners as a guide to develop their own implementation plans. It describes how this complex, multisectoral response, with all its different partners and activities, will be co-ordinated and managed at national, regional and local levels. This expanded response will also require more intensive technical support and an introduction is given to the new Directorate of Special Programmes within the Ministry of Health and Social Services.
Mechanisms to disburse the financial resources needed by those implementing MTP III activities are described.
2.2 How partners can use this strategic plan
This MTP III has been developed to assist planners, implementers, and monitoring and evaluation agencies to focus their efforts in expanding the response to the HIV/AIDS epidemic in Namibia and to reach the targets set in Chapter 4. As such, it is a tool and this section gives some guidelines on how best to use it.
The MTP III is a description of the minimum elements and commitments of the national HIV/AIDS response, but it is not an implementation plan in itself. The MTP III is based on key strategies and underlying principles (see Chapter 1). It sets implementation targets for key indicators which will measure how far we have achieved the desired outcomes (see Chapter 4). It proposes the activities which need to be carried out as steps in reaching the strategic outcomes - a reduced growth in HIV infections and an improved survival and quality of life of those infected and affected. MTP III details the target populations for the activities and the responsible agencies that will execute them (see Chapter 3). These details allow the National Programme to be costed so that resource mobilisation can proceed to finance the expanded response (Chapter 5).
Implementing partners now need to take the MTP III a step further by developing their own implementation plans for the many activities listed. These implementation plans will contain the specific details on how the various activities in the MTP III will be executed. These implementation plans need to be budgeted so that precise funding can be provided for implementation.
There are many activities currently being implemented in areas of prevention, treatment care and support, and impact mitigation. It is important that these activities continue and are expanded. However, it is equally important that implementing partners review their activities to ensure that they are in alignment with the national programme thinking in the MTP III. A number of key issues need to be appreciated before implementing partners develop or review their implementation plans.
Implementing partners should appreciate the underlying principles of the national response and ensure that their projects and programmes embody these principles. They should also appreciate their specific commitments to the expanded response. For example, partners involved in providing VCT should appreciate that confidentiality and privacy is a key principle.
Implementing partners should find their specific activities reflected in the MTP III and understand how these fit into the context of a holistic response. The MTP III provides Outcome tables that are made up of specific activities. For example, one of the Prevention Component outcomes is
Chapter II: Implementation Mechanisms

Implementation mechanisms
Medium Term Plan III for HIV/AIDS
12
to provide VCT to the general population. One activity to do this will be to establish mobile VCT services.
Implementing partners should attempt to network with other partners involved in similar and related activities in order to explore collaborative projects and to co-ordinate their activities. The MTP III stipulates many instances where MoHSS Directorate: Special Programmes will facilitate this networking.
There should be an appreciation of the project output indicators for each of the activities that an implementing partner is involved with. This is the first step in ensuring that activities are being successfully carried out. Continuing the example above of mobile VCT services, the MTP III states that the output indicator for this will be the cumulative number of mobile VCT services provided and the percentage of regions covered. Each implementing partner will be obliged to report to MoHSS Directorate: Special Programmes according to MTP III established outcome indicators.
There should also be an understanding of the overall outcome that any specific activity is helping to reach and the indicators that will be used to measure achievements to reach these outcomes. Achieving the output suggested above will help implementing partners developing mobile VCT services to reach their outcome of increased access by vulnerable groups, young people and the general population to quality VCT services. One indicator to measure this will be the percentage of VCT clients tested for HIV at VCT sites that have received their sero-status results by region, gender and age group. Key outcome indicators, with their targets for 2007 and 2009, are described in Chapter 4 and implementing partners will be required to provide this data to monitoring and evaluation partners.
The primary responsible implementing partner for each activity is highlighted in the activity tables and they will be held accountable for ensuring that that activity meets the required targets agreed upon in Chapter 4. The other implementing partners listed below the responsible partner, are partnering with the primary responsible partner. The list may not be complete and indeed, as we are requiring an expanded response, we encourage partners to expand their range of activities, their coverage and assist new partners in joining the response.
2.3 Management and Co-ordination
An expanded, multi-sectoral response in these five main strategic areas requires improved management and co-ordination. Implementing partners and co-ordinating bodies will need to be made responsible and accountable for achieving the desired results to which they commit themselves, at national, regional and local levels. Co-ordinating bodies will strengthen mechanisms for continuous learning through performance monitoring and reporting. The key outcome indicators will be used by all implementing partners and co-ordinating bodies to monitor performance, the coverage in all regions and in each sector, and gaps which need to be filled. Performance will need to be reviewed every year and plans adjusted to ensure that we meet these minimum targets.
The process of developing MTP III has encouraged co-ordinating bodies to re-examine their terms of reference, their membership and their responsibilities to provide the required leadership and authority and to strengthen the management of the response. Technical Advisory Committees and Sectoral Steering Committees are now formalised to provide greater focus.
The National AIDS Committee (NAC) is the highest policy decision making body on matters related to HIV/AIDS. It is attended by Cabinet ministers and Regional Governors to ensure that policy and resource mobilisation is adequate.
The National Multi-sectoral AIDS Co-ordination Committee (NAMACOC) will provide the leadership for multi-sectoral and regional implementation. It will be attended at Permanent Secretary level and will include equivalent regional and civil society participants. It will review progress and adopt annual work plans and budgets. It will meet at such a time that fits in well with the GRN

Implementation mechanisms
Medium Term Plan III for HIV/AIDS
13
budget planning cycle. Another NAMACOC meeting will focus on key issues and best practice. NAMACOC will give recommendations to the NAC. NAMACOC will call a national stakeholders conference every two years to ensure full stakeholder participation in the national response.
The National AIDS Executive Committee (NAEC) provides the technical leadership and it will be responsible for co-ordinating the detailed implementation of the multi-sectoral response. Its membership reflects the hands-on experience required to deal with implementation issues. It will be attended by key sectors and key technical people to cover the five components of the MTP III.
The Sectoral Steering Committee will involve all key actors working in that sector and will thus be wider than most current Ministry HIV/AIDS committees. The Sectoral Steering Committee will be responsible for the implementation of sector-specific HIV/AIDS interventions and for mainstreaming HIV/AIDS into all aspects of their organisations’ core functions. Through impact assessments and establishing appropriate policies, the committee will ensure that the sector’s core functions minimise the spread of HIV/AIDS and supports programmes which address the impact of the epidemic on their target groups. It will actively work towards establishing workplace programmes across the sector.
The Regional AIDS Co-ordinating Committee (RACOC) in each region will co-ordinate between civil society and government at regional level and between the national and regional institutions. RACOCs will take responsibility to co-ordinate and supervise HIV/AIDS developments in each region and will support local committees to take community actions. Some regions have decentralised their RACOC to district level and have formed DACOCs.
The Constituency AIDS Co-ordinating Committee (CACOC) will take responsibility to co-ordinate and manage the multi-sectoral response at local level. Some regions have established District-level AIDS Committees or other structures which have essentially the same function and same terms of reference as the CACOCs.
These co-ordinating committees are supported, where appropriate, by the Directorate: Special Programmes within the MoHSS and by regional technical officers from a number of different ministries.
The organogram on the next page shows the lines of reporting between these bodies and the implementing partners. The terms of reference for the co-ordination committees follow the organogram.

Implementation mechanisms
Medium Term Plan III for HIV/AIDS
14
Figure 6: Organogram of the National AIDS Co-ordination Programme National Level - - - - - Leadership; Policy, Resource mobilisation Multi-sectoral Leadership & co-ordination
Technical Input Mainstreams, co-ordinates
Co-ordinates implementation monitors HIV/AIDS to local Level
Regional level - - - - - -
Co-ordinates multi—sectoral response Technical support at regional and local levels
Local Level - - - - - - Related Steering Committees
Co-ordinates local response
Implementation Reporting line Technical support
RACOCs
NAC
NAEC
NAMACOC
Sub-regional AIDS Committees (DACOC or CACOC)
GRN, Local Authorities, NGOs, FBOs, CBOs, private sector, Parastatals
Technical Advisory
Committees
RAC / SHPA / + Technical Team
MoHSS Directorate
Special Programmes
Sector Steering
Committees
Regional Working Groups

Implementation mechanisms
Medium Term Plan III for HIV/AIDS
15
The National AIDS Committee, NAC, provides the national leadership. Below Cabinet, it is the highest policy decision making body on matters related to HIV/AIDS. One of the key strategies in MTP III is to sustain leadership commitment to take action.
Responsibility
� NAC is responsible for initiating and approving policy for an expanded response to the HIV/AIDS epidemic, referring key policy issues to Cabinet
� It will provide leadership commitment for the regional and sectoral response � It will ensure sustained political commitment and broad support for the programme
throughout the country � Each Minister is responsible for her/his own sector’s HIV/AIDS resource mobilisation,
ensuring that the budget is sufficient for the implementation of the sector’s commitments in the plan and national, regional and local levels.
Membership
Minister for Health and Social Services (Chairperson) Minister of Regional and Local Government and Housing (Deputy Chair) Regional Governors: (13) Minister of Basic Education, Sport and Culture Minister of Defence Minister of Finance Minister of Higher Education Technology and Employment Creation Minister of Information and Broadcasting Minister of Justice Minister of Labour The Director General: National Planning Commission Secretariat Minister of Prisons and Correctional Services Minister of Women Affairs and Child Welfare Permanent Secretary: MoHSS (Secretary).
Secretariat to NAC: NAEC with support of Expanded National AIDS Response Support Division, Directorate: Special Programmes, Department Health and Social Welfare Policy, MoHSS.
Frequency of meetings
Every six months. Provision is made for extra-ordinary meetings.
The National AIDS Committee, NAC

Implementation mechanisms
Medium Term Plan III for HIV/AIDS
16
Responsibility
� NAMACOC is responsible for the co-ordination and overall implementation of the national and multi-sectoral response.
� To advise NAC on policy issues � To provide the leadership for sectoral and regional implementation � Resource management
Membership
Permanent Secretary from each of the following Ministry – (Alternate: Deputy Permanent Secretary or Under-Secretary)
Ministry of Health and Social Services (Chairperson) Ministry of Regional and Local Government and Housing (Deputy Chair) National Planning Commission Secretariat Office of the Prime Minister (Head of Department Level) Ministry of Finance Ministry of Basic Education, Sport and Culture Ministry of Defence Ministry of Home Affairs Ministry of Higher Education Technology and Employment Creation Ministry of Information and Broadcasting Ministry of Justice Ministry of Labour Ministry of Prisons and Correctional Services Ministry of Women Affairs and Child Welfare Ministry of Works, Transport and Communication
Undersecretary of all 13 regions Representatives, of equivalent standing, of
Association of Local Authorities (ALAN) Association of Regional Councils (ARC) Church Alliance for Orphans (CAFO) Council of Churches of Namibia (CCN) Lironga Eparu Medical Association of Namibia Namibia Business Coalition on AIDS (NABCOA) Namibia National Teachers Union (NANTU) Namibia National Womens Organisation (NANAWO) Namibia Non-Governmental Organisation Forum (NANGOF) Namibia Youth Council Namibian Network of AIDS Service Organisations (NANASO) National Chamber of Commerce and Industry (NCCI) National Union of Namibian Workers (NUNW) Partnership Forum (two delegates) UN Theme group on HIV/AIDS (two delegates)
The National Multi-sectoral AIDS Co-ordination Committee NAMACOC

Implementation mechanisms
Medium Term Plan III for HIV/AIDS
17
Secretariat to NAMACOC: NAEC with support of Expanded National AIDS Response Support Division, Directorate: Special Programmes; Department Health & Social Welfare Policy.
Specific Tasks 1. To review overall progress towards outcomes 2. To report on each sector’s progress towards outputs and outcomes 3. To review strategies in view of the epidemic’s changing impact 4. To review sectoral plans and budgets for the next year prior to submission to
the NAC 5. Representatives have specific responsibility to report to and from their Sectoral
Steering Committees, their regions and/or their membership 6. To call a National Conference of all Key Actors at least every two years, to
review progress, share experiences and disemminate best practice.
Frequency of meetings Every six months. Provision is made for extra-ordinary meetings.

Implementation mechanisms
Medium Term Plan III for HIV/AIDS
18
Responsibility � NAEC is responsible for the implementation of the decisions of NAC and NAMACOC, covering all
components and all sectors. � It will meet to co-ordinate the detailed implementation of the multi-sectoral response. � It will monitor the detailed progress towards outcomes and outputs of each MTP III component. � It will resolve implementation issues, referring decisions to NAMACOC when appropriate.
Membership
Its membership should reflect the hands-on experience required to deal with implementation issues for the multi-sectoral response - that of at least Director level. Membership will include one representative from each of the following:
Ministry of Health and Social Services (Chairperson: Under-secretary) Ministries responsible for Education (HAMU)(one representative) Ministry of Finance Ministry of Information and Broadcasting Office of the Prime Minister National Planning Commission Secretariat Ministry for Regional and Local Government and Housing Lironga Eparu NANASO NABCOA UNAIDS Country Coordinator Chair: Partnership Forum Director and Deputy Director: Special Programmes, MoHSS. MoHSS Directorate: Special Programmes Technical Advisors (co-opted) Secretariat to NAEC: Directorate of Special Programmes, MoHSS.
Specific Tasks
1. To review quarterly reports on braod activities, indicators and progress towards outcomes from the Sectoral Steering Committees, RACOCs, and other relevant committees, programme officers, development projects and other stakeholders;
2. To organise meetings of NAC and NAMACOC; 3. To co-ordinate activities, identify gaps and address weaknesses; 4. To communicate with all stakeholders and co-opt them as and when required.
Frequency of meetings: Monthly.
National AIDS Executive Committee (NAEC)

Implementation mechanisms
Medium Term Plan III for HIV/AIDS
19
This expanded and accelerated national response requires a greater involvement by ministries, parastatals, the private sector, NGOs and faith-based organisations, in fact from all of society. Grouping organisations by sector builds partnerships with common interests and provides opportunities to share resources and common experience. Some sectors are already having regular meetings with partners to discuss issues of sector interest. On such committees’ agendas, HIV/AIDS will be included as a regular agenda section to cover the following responsibilities and tasks. In other sectors, the ministerial HIV/AIDS Committee will be expanded to include Key Actors from the sector. The obligations and commitments of each sector can be found in Chapter 6.
Responsibility
The Sectoral Steering Committee will be responsible for:
� Engaging the sector’s leadership and spear-heading the response throughout the sector � Implementation of sector specific HIV/AIDS related interventions, involving all its Key Actors � Mainstreaming the entire process within the Sector from sectoral policies to implementation,
technical support supervision, M&E, public information and accountability; � Ensuring that HIV/AIDS interventions support local and community responses � Its own sector’s resource mobilisation and budgets.
Sectoral Clusters
Key Actors within the sector, which are currently involved or should be involved in the national HIV/AIDS response, will be invited to attend Sector Steering Committees by the Lead Agency. Sectoral Steering Committees should be dynamic and responsive to the changes within the sector and to the changing impact of the epidemic.
The Lead Agency of the Sector
The Lead Agency will be responsible for the following:
1 To establish a Sectoral Steering Committee which will be responsible for co-ordinating the Key Actors and the sector’s implementation plan
2 To provide the Secretariat for that Sector Steering Committee 3 To appoint a senior person within the sector to co-ordinate and supervise the
implementation of the HIV/AIDS activity plan for that specific sector 4 To appoint at least one full-time post of HIV/AIDS focal person for the sector 5 To allocate resources for the implementation of its sector specific activity plan on
HIV/AIDS. Supplementary resources will be mobilised through the donor communities.
The Lead Agency can be replaced by another Key Actor from within the sector, by majority vote at a Sectoral Steering Committee meeting.
Membership
Experienced Key Actors from within the GRN and private, NGO and faith-based sectors and development partners working in that sector, and PLWHAs
Chairperson: A senior official within the Lead Agency
Secretariat to Sector Steering Committee: The Lead Agency.
Sectoral Steering Committees

Implementation mechanisms
Medium Term Plan III for HIV/AIDS
20
Specific Tasks
The Sectoral Steering Committee will be responsible for the following:
1. To assess the impact of the epidemic on the sector and amend policies guidelines and work plans accordingly
2. To develop sector specific annual costed work plans on HIV/AIDS for implementation at national and regional/constituency levels
3. To assess resource requirements, including HRD, by identifying resource gaps and development needs
4. To co-ordinate implementation plans and activities through all partners 5. To educate everybody within the sector on HIV/AIDS, from top management to
the lowest rank 6. To facilitate Key Actors in the sector to implement and monitor comprehensive,
holistic workplace programmes which cover prevention, care and support to all its employees and sector beneficiaries and which eliminate any form of discrimination against PLWHA or their families
7. To submit progress reports on HIV/AIDS activity plans to the National AIDS Executive Committee on a quarterly basis
8. Assist the Training Support Co-ordination Unit, MoHSS with the identification of training and capacity-building needs within the sector
9. Provide technical backstopping to implementers in the sector 10. Provide progress reports 11. Identify research needs, co-ordinate studies and communicate additional
research needs to the relevant Technical Advisory Committee.
Frequency of meetings
The Sectoral Steering Committee will meet at least every three months, or more often, as required by its work plan.
Reporting
Sectoral Steering Committees report to NAMACOC and NAEC will review their quarterly reports/minutes.
Method of Work
The Sectoral Steering Committee may appoint working groups to work on specific aspects/areas related to the overall strategy.

Implementation mechanisms
Medium Term Plan III for HIV/AIDS
21
Responsibility
� For each area of special focus, the Technical Advisory Committees (TACs) will provide technical expertise as required by their terms of reference. These will be developed on appointment.
Areas of Special focus
The Chairperson of NAMACOC shall establish TACs as and when the need arises.
Membership
Experienced Key Actors from within the GRN and private, NGO and faith-based sectors, development partners and support groups for PLWHAs.
Secretariat to TACs: Directorate of Special Programmes, MoHSS.
Frequency of meetings
Monthly or as required.
Technical Advisory Committees

Implementation mechanisms
Medium Term Plan III for HIV/AIDS
22
The Regional AIDS Co-ordinating Committee (RACOC) in each region co-ordinates between civil society and government at regional level and between the national and regional institutions.
Responsibility
� To co-ordinate and manage the multi-sectoral response at regional and local levels.
Membership
The most senior representative at regional level from each of the following:
Regional Governor (Chairperson) Ministry of Health and Social Services (Co-Chairperson) Local Authorities Chairpersons of CACOCs Traditional Authorities Local NGOs and CBOs implementing programme interventions NCCI representative Chairperson: Regional Youth Committee Chairperson: Lironga Eparu or largest membership PLWHA support group in the region Ministry of Agriculture Water and Rural Development Ministry of Basic Education, Sport and Culture Ministry of Defence Ministry of Environment and Tourism Ministry of Higher Education Training and Employment Creation Ministry of Information and Broadcasting Ministry of Justice Ministry of Lands Resettlement and Rehabilitation Ministry of Women Affairs and Child Welfare NAMPOL Under Secretary, Regional Council Director: Regional Development (RC)
Secretariat: The Regional AIDS Coordinator (RAC) Senior Health Programme Administrator (SHPA) (MoHSS) Regional Development Planner (RP)
Specific Tasks
The RACOC will be responsible to:
1. Co-ordinate the development of all HIV/AIDS action plans in the region for the expanded multi sectoral response
2. Co-ordinate sub-regional structures (CACOCs etc) to ensure implementation of regional HIV/AIDS action plan and avoid duplication
3. Develop and co-ordinate transparent mechanisms for resource mobilisation, allocation and utilisation
Regional AIDS Co-ordinating Committees

Implementation mechanisms
Medium Term Plan III for HIV/AIDS
23
4. Develop effective evaluation tools to monitor the process of the regional and sub-regional HIV/AIDS plan
5. Co-ordinate the development of regional IEC materials and ensure dissemination
6. Ensure support to the infected and affected persons in the region 7. Improve access to good quality and affordable condoms in the region 8. Ensure availability of care services for HIV/AIDS infected persons and those
suffering from AIDS 9. Collaborate with all sectors to ensure that they mobilise resources for sectoral
activities for the multi-sectoral response to the HIV epidemic at regional and local level
10. Facilitate capacity building for CBOs and support groups in HIV/AIDS programme development, including proposal writing, implementation and monitoring and evaluation
11. Preparing and presenting an annual budget for RACOC general (non-sector specific) HIV/AIDS activities to the Regional Council who in turn submit it to MRLGH for funding
12. Overseeing all donor funds donated to RACOC for HIV/AIDS activities 13. Report to NAEC and to the Regional Council on a quarterly basis.
Frequency of meetings
Four times a year
Reporting
To NAMACOC twice per a year To Regional Council four times a year

Implementation mechanisms
Medium Term Plan III for HIV/AIDS
24
Responsibility
� To co-ordinate and manage the multi-sectoral response at local level
Membership
The most senior representative at Constituency level from each of the following:
Constituency Councillor or Mayor (Chairperson) Primary Health Care Supervisor (Co-chairperson) Local NGOs Local CBOs Chairperson: Constituency Youth Committee Private sector representatives from the constituency Public sector officials in the constituency: extension officers, liaison officers, clinic sisters, school principals, police, etc. Traditional authorities Local Authorities
Specific Tasks
The CACOC will be responsible to:
1. Identification of problems relating to HIV/AIDS in the constituency 2. Prepare local level HIV/AIDS/TB annual action plans 3. Mobilise local groups to monitor the number of and support to orphans, vulnerable
children and people living with HIV/AIDS….. 4. Ensure the implementation of the plan 5. Mobilise and distribute resources from RACOC and other sources 6. Monitor and evaluate the activities of the plan 7. Compile monitoring reports on key indicators to present to RACOC 8. Report back on RACOC meetings to community.
Frequency of meetings
Four times a year, before the RACOC meeting.
Reporting
To RACOC 4 times a year.
Constituency AIDS Co-ordinating Committee – CACOC

Implementation mechanisms
Medium Term Plan III for HIV/AIDS
25
2.4 Technical Support
The breadth of activities required to overcome this epidemic means that no one person can be an expert in all aspects of the response. At national and regional levels, technical expertise for each activity will be co-ordinated through specific posts within the new Directorate for Special Programmes. In addition, Technical Advisory Committees (TACs) will be established to pool the expertise from implementing partners and other experts.
The MoHSS Directorate: Special Programmes
In 2002, Cabinet approved the new structure of the MoHSS which makes provision for a new Directorate to design, manage and direct policy development, strategic planning, resource mobilisation, co-ordination, facilitation, monitoring and evaluation of the national response across all sectors to reduce the impact of HIV/AIDS, TB and Malaria on the Namibian population.
The Directorate has two divisions, one focusing on the health sector requirements and the other on the multi-sectoral response. A summary of the Directorate’s sub-divisions is as follows:
Directorate: Special Programmes
Health Sector Expanded National AIDS Response Co-ordination
(Multi-sectoral)
Resource Management
Response Monitoring & Evaluation
Resource Mobilisation & Development Cooperation
Training Support Co-ordination
Expanded National AIDS
Response Support
TB Control
Malaria Control
HIV/AIDS Control

Implementation mechanisms
Medium Term Plan III for HIV/AIDS
26
This expanded staffing will strengthen the MoHSS’s capacity to co-ordinate and manage the breadth of programmes within MTP III and its support to other partners. For example, there will be one staff member responsible for working with the national level line ministries. However, to establish the required level of response within each ministry and each region, the OPM and MoHSS will plan, develop and strengthen additional human resource capacity throughout the public sector.
Technical Advisory Committees
Technical Advisory Committees will provide technical expertise to the national response. The following existing committees already serve as TACs
• the Committee on Higher Education and Training (MHETEC), • the Take Control Task Force (MIB), • the Standing Committee on Condoms/Commodities Supply and Distribution (MoHSS), • the Technical Advisory Committee on Patient Care and Disease Control (MoHSS) • the Management Committee on the same (MoHSS), • the Steering Committee and the Working Group on OVC (MWACW).
The chairperson of NAMACOC will establish TACs as and when the need arises, for example
policy and legal committee to deal with legal issues pertaining to HIV/AIDS.
2.5 Human Resource Management
A major emphasis of MTP III will be to sensitise senior management in all organisations to invest in workplace programmes. They also need to ensure that the human resources required to carry out core functions and their contribution to combating HIV/AIDS and its impacts are well planned for and in place.
A senior manager needs to provide the leadership to mainstream HIV/AIDS in all aspects of the organisation. Human resource departments must be adequately staffed to professionally manage the required response. For the public sector, the Office of the Prime Minister will guide the Human Resource Division within each ministry to address human resource planning.
The following responsibilities will be formalised:
• Senior manager (usually the CEO, PS or deputy), with specific responsibility to oversee mainstreaming of HIV/AIDS (see outcome 5.2.4) and to co-ordinate with other organisations in the sector (See outcome 5.2.1)
• Human Resource manager with specific responsibility to reassess HR planning and staffing needs, implement capacity development and establish and implement extended workplace programmes (see outcomes 5.1.1, 5.1.2 and 2.4.2)
• Sector Focal Persons with specific responsibilities to a) refer department managers to the correct technical assistance within MoHSS Directorate: Special Programmes and its partners and b) refer staff to the point of treatment, care and support such as the nearest voluntary counselling and testing centre (VCT). At regional level, they may take on greater responsibilities in assisting the HR manager to implement workplace programmes.
• Peer Educators assist with the implementation of workplace programmes. These are usually voluntary posts and are therefore not formalised within job descriptions.
Building the human resource capacity to strengthen the delivery required for each of the components of MTP III, at national, regional and local levels, requires considerable planning, co-ordination and investment. The National Human Resource Planning Task Force, under the responsibility of Ministry of Higher Education, Technology and Employment Creation (MHETEC) will

Implementation mechanisms
Medium Term Plan III for HIV/AIDS
27
spear-head the planning process. It will assess the national training capacity of all existing training institutions and specialised NGOs service providers. The Training Support Co--ordination Unit (TSC Unit), within MoHSS, will assess training requirements, develop and cost a master implementation plan and mobilise resources.
2.6 Resourcing the response
Resource Mobilisation
Responsibility for financing the response must be shared by government and all sectors of society. In addition, many international partners have given support to Namibia’s efforts and have continued to pledge financial resources to achieve specific results. The MoHSS Directorate: Special Programmes sub-division: Resource Mobilisation & Development Cooperation will be responsible for co-ordinating the resources required for each of the outcomes and for identifying gaps.
The table below gives an overview of the responsibilities of Namibian partners to finance the national response.
Figure 7: Areas of responsibilities of major partners in resourcing the national response
Partner Area of major financial responsibility Reference in Ch 3
Each line Ministry Delivering core functions related to response Mainstreaming HIV/AIDS Fulfilling Sector Commitments Implementing a workplace programme Providing adequate human resources to managing HIV/AIDS
All activity tables 5.2.4 Chapter 6 2.4.2 5.1.1
Office of the Prime Minister
Guidance on Human Resource Development for HIV/AIDS posts in Public Sector Development of HIV/AIDS policies in the public sector HIV/AIDS programme resourcing and monitoring as part of PEMP Accountable for workplace programmes in public sector
5.1.1 1.3.2 5.2.2 & 5.3 2.4.2
National Planning Commission Secretariat
Development planning, co-ordination and monitoring at macro-level Co-ordination and resourcing of public sector development budgets Policy formulation on the resourcing of NGOs International resource co-ordination Planning and mainstreaming HIV/AIDS
5.2.1 5.2.2 5.2.2 5.2.2 5.2.4
Ministry of Finance Compilation and resourcing of public sector operational budgets (workplace programmes and other relevant interventions)
5.2.2
Ministry of Health and Social Services
Micro-level planning, co-ordination and monitoring Acquiring and maintaining international contributions
5..2.1 5.2.2

Implementation mechanisms
Medium Term Plan III for HIV/AIDS
28
Partner Area of major financial responsibility Reference in Ch 3
MRLGH In addition to the above: Financing RACOC and CACOC plans of action
Regional Commitment pages, Appendix 2
MIB In addition to the above: Social mobilisation, campaigns and BCI
Component 2
MHETEC Planning for human resources capacity development and developing national training mechanisms for HIV/AIDS expanded response
5.1.1 & 5.1.2
Regional Councils Supporting the establishment of CACOCs Supporting and funding core RACOC activities
4.1.1 5.2.1 & 5.2.2
Local Authorities Supporting prevention, care and mitigation responses Workplace programmes
2.4.1 & component 4 2.4.2
Private Sector Workplace programmes Supporting prevention, treatment, care and mitigation responses
2.4.2 2.4.1 & component 4
NGOs & FBOs Delivering core functions related to the response Supporting prevention and mitigation responses
All activity tables 2.4.1 & component 4
Local communities Supporting prevention and mitigation responses 2.4.1 & component 4
Financial Mechanisms
The highest priority will be given by each Ministry to adequately plan and budget for their contribution to the National response. Each Permanent Secretary, as the accounting officer, will be responsible for ensuring that their ministry’s workplan and budget adequately finances HIV/AIDS local responses in every constituency, appropriate to that ministry’s core function. Some examples are: NPCS will support community level, participatory poverty and HIV/AIDS impact assessments and action plans; MAWRD will train water point committee members and farmers associations and will seed the development of rural development income generating opportunities which target people affected by HIV/AIDS.
2.6 Assumptions, Risks and Risk Management
With the passage of time and the influence of external factors, programme control decreases and risk increases. It is important that the assumptions the plan makes, and the risks it takes are identified with key stakeholders and steps are proposed to manage these risks. This will require the development of a risk management strategy and is a priority task for the partners in the governance structure.
Assumption 1: The programme will receive timely and sufficient funding to effectively undertake HIV/AIDS programming.
Risk Analysis: Medium
Risk Assessment and Mitigation Strategy: The MTP III will require considerable funds, beyond the amount the government is able to provide. Line ministries will have to review their plans and budgets for the coming years and re-prioritise some activities. Combating HIV/AIDS is an NDP2 strategic goal for which considerable commitment is required.

Implementation mechanisms
Medium Term Plan III for HIV/AIDS
29
External development partners have already committed themselves to various aspects of the plan and may be reluctant to fund other activities. Committed leadership and real progress on some of the outcomes may persuade them to invest further.
Assumption 2: Highly competent staff in the MoHSS Directorate: Special Programmes will be recruited and retained.
Risk Analysis: Medium
Risk Assessment and Mitigation Strategy: There is a general shortage of trained Namibian professionals in the skill areas identified as critical to the functioning of the new Directorate. The competency and leadership required to co-ordinate the multi-sectoral response will require three candidates of the highest calibre. The director and two deputies will be responsible for one of the largest and most complex programmes operating within government. Further, delivery on the targets will have a “live or die” impact on the lives of thousands of people throughout Namibia. Their staff will also be able to provide the required technical support to implementing partners. Staff recruitment will be based on proven competencies.
Assumption 3: All organisations involved in HIV/AIDS co-operate in co-ordination efforts.
Risk Analysis: Low
Risk Assessment and Mitigation Strategy: There is some risk that the National HIV/AIDS Co-ordination Programme will not be able to marshal the wide array of institutions, agencies and organisations to co-ordinate a national effort. Some organisations have been working independently for years and may be reluctant to take direction from the various co-ordinating bodies. They may not co-operate in the collection of and reporting on data. There is some risk that different parts of Government may not co-operate fully, due to protection of bureaucratic imperatives, inefficiency, or conflicting policy interpretation (e.g. condoms available to prison inmates). Participation of multi-sectoral stakeholders, line ministries, and leadership in the NAC and NAMACOC should serve to mitigate this risk. NAMACOC should be able to engage these organisations in national-level strategy and planning in their areas of expertise, particularly if the organisations can participate as full partners.
Assumption 4: Implementing partners have sufficient financial and management capacity to undertake expanded HIV/AIDS programming.
Risk Analysis: Medium
Risk Assessment and Mitigation Strategy: The implementing partners possess a range of capacities, and particularly at local level, they will require intensive initial support from the programme. Such capacity development will not only be in technical areas of the response but in basic project management functions such as planning, financial management and monitoring and reporting. Risk mitigation will require a comprehensive capacity development strategy at the national, regional and community levels and the involvement of the larger more established national implementing partners, as builders of capacity. This strategy, as detailed in section 5.1.4, is a high priority.
Assumption 5: Decision- and opinion-maker leadership is vocal, forthright and strong.
Risk Analysis: Medium
Risk Assessment and Mitigation Strategy: Leadership is a key success factor and an important mitigation strategy that will be promoted through the NAC and NAMACOC, and a broad spectrum of decision and opinion makers.

Implementation mechanisms
Medium Term Plan III for HIV/AIDS
30
Assumption 6: Social, cultural and economic conditions will support behavioural change.
Risk Analysis: High
Risk Assessment and Mitigation Strategy: The conditions that have shaped the growing HIV/AIDS epidemic in Namibia are also those that have shaped a number of other social ills. Large economic and social disparities, a large mobile male population, traditional values which discourage an open and informed discussion of human sexuality, and the low status of women all contribute to risk behaviours. Well known risk mitigation strategies, i.e. targeted IEC, life skills training, youth mobilisation, etc., are not considered sufficient to foster broadly based behavioural change under these conditions. Creating closer links between HIV/AIDS and more traditional development programmes may offer a promising avenue of hope if the full influence of the NAC and NAMACOC can be brought to bear on the issue. Increased advocacy at the community level with the custodians of culture, i.e. traditional leaders, faith leaders, etc., is another strategy that could influence the underlying sexual values and beliefs that can spawn an HIV/AIDS epidemic. Mitigating strategies are planned to reduce this risk throughout the components.

Medium Plan III for HIV/AIDS 31
Overview of the national programme response
The increasing rate of infection, the rapidly increasing numbers of people developing AIDS, the numbers of people, young and old who are dying and leaving families without breadwinners or carers requires every organisation and individual to act. We all need to look at ways of rapidly and significantly expanding a multi sectoral response to the HIV/AIDS epidemic. The national programme goal with its five strategic results, is therefore as follows:
NATIONAL PROGRAMME GOAL
COMPONENT 1: ENABLING ENVIRONMENT People infected and affected with HIV/AIDS enjoy equal rights in a culture of acceptance, openness and compassion COMPONENT 2: PREVENTION Reduced new infections of HIV and other STIs COMPONENT 3: ACCESS TO TREATMENT, CARE AND SUPPORT SERVICES Access to cost effective and high quality treatment, care and support services for all people living with, or affected by HIV/AIDS COMPONENT 4: IMPACT MITIGATION SERVICES Strengthened and expanded capacity for local responses to mitigate socio-economic impacts of HIV/AIDS COMPONENT 5: INTEGRATED AND CO-ORDINATED PROGRAMME MANAGEMENT AT ALL LEVELS Effective management structures and systems, optimal capacity and skills, and high quality programme implementation at national, sectoral, regional and local levels
Chapter III The expanded National HIV/AIDS Programme Response: MTP III – Plan of action
MTP III National Programme Goal
The reduction in incidence of HIV infection to below epidemic threshold

32
32
MTP3 III National Programme Goal The reduction in incidence of HIV infection to below epidemic threshold
Figure 11: HIV/AIDS THIRD MEDIUM TERM PLAN: PROGRAMME OVERVIEW
2 Prevention
1 Enabling Environment
5 Programme Management
3 Treatment, Care, & Support
1.1 Capacity development:
Leadership
1.1.1 Sustained leadership commitment
1.3 Policy & law reform
1.3 1 National policy devt. & law reform
1.3.2 Sectoral & Instit- utional policies
1.4 Interventions to reduce stigma discrimination
1.4.1 Social mobilisation to combat discrimination
1.4.2 Actions to prevent & address discrimination
2.1 Capacity development:
prevention
2.2 Target vulnerable populations
2.1.1 Capacity development
2.3 Target young people
2.2.1 Target BCI for vulnerable populations
2.2.2 Prevention of transmission in health care settings
2.4 Target the general population
2.4.1 Social mobilisation & awareness
2.4.2 Workplace programmes
2.4.3 Expand condom provision
2.4.4 Strengthen STI management
2.4.5 Voluntary counselling & testing
3.1 Capacity development: Treatment,
care and support
3.1.1 Capacity development 3.1.2 IEC to support
expanded treatment, care & support programmes
3.2.1 Laboratory services for HIV/AIDS management
3.2.2 Drugs & supplies systems 3.2.3 PMTCT+ services 3.2.4 Management of
opportunistic infections 3.2.5 Collaborative TB/HIV/AIDS
services 3.2.6 Provision of HAART 3.2.7 Home-based care 3.2.8 Access to care for
vulnerable populations 4.3.1Addressing poverty, food security, nutrition & housing
5.1 Developing of HIV/AIDS management capacity
5.1.1 Human resource planning
5.1.2 Human resource development
5.1.3 Quality assurance 5.1.4 Capacity development
5.2.1 Management structures 5.2.2 Resource mobilisation &
flow mechanisms 5.2.3 Information flows 5.2.4 Mainstreaming 5.2.5 Management processes
5.3 Programme monitoring &
evaluation
5.4.1 Multi-sectoral HIV/AIDS
research coordination 5.4.2 Surveillance &
Research
5.1 Management & co-ordination
5.3.1 Monitoring & evaluation
3.2 Treatment and Care services
5.4 Surveillance and operational
research
2.3.1 BCI in schools 2.3.2 BCI for youth
1.2 PLWHA involvement
1.2.1 Increase participation
2.5 Interventions to reduce
vulnerability
2.5.1 Addressing vulnerability
4.1.1. Establish, strengthen & support communities to take action to respond to HIV/AIDS/STIs and TB.
4.1.2 Develop the capacity of local support groups of PLWHA and their families
4.2.1Comprehensive services for OVC, their carers and PLWHA
4.2 Services for OVC &
PLWHA
4.3 Addressing poverty
4 Impact Mitigation
4.1 Capacity development:
Local responses

Component 1: Enabling Environment
Medium Plan III for HIV/AIDS 33
An enabling environment, including the necessary leadership, policies, and anti-discriminatory practices in all sectors is critical to the success of the entire expanded response to HIV/AIDS/STI/TB epidemics. Having clear policies in place is a necessary condition to enable and facilitate the contributions of all stakeholders. Stigma and discrimination against people living with HIV/AIDS affects the spread and impact of the disease in several ways. Fear of being identified with HIV/AIDS stops people from seeking voluntary counselling and testing, which is vital to prevention, care and treatment efforts. An enabling environment, free of discrimination and stigma for HIV positive people, will contribute to greater up-take in testing, increased disclosure of status to others, particularly to partners and family, and adoption of positive living habits. The four sub-components for the Enabling Environment are
1.1 Capacity development for Leadership Commitment 1.2 Greater Involvement of People Living with HIV/AIDS 1.3 Policy and Law Reform 1.4 Interventions to Reduce Stigma and Discrimination.
Sustained leadership commitment builds the capacity and willingness of leaders to engage in the national response to HIV/AIDS. Leadership is required in all sectors and at all levels so political, religious, traditional, private sector and NGO leaders will be provided with relevant information. They will inform their constituencies about HIV/AIDS, STIs and TB prevention, treatment, care and support and advocate to address stigma and discrimination. Leadership will be critical in mainstreaming HIV/AIDS in all workplaces, programmes, communities, and institutions.
Greater Involvement of People Living with HIV/AIDS (PLWHA) is a cornerstone for creating an enabling environment. The effective involvement of PLWHA indecision making, planning and implementing the response has been shown to have a significant impact both on how the epidemic is perceived and on expanding the response. As stigma and discrimination are reduced, PLWHA will be in a better position to participate, while the activism, advocacy and involvement of PLWHA can itself be a significant force in breaking down discrimination.
Policy development and law reform will facilitate the establishment of a legal and social environment which encourages openness about HIV/AIDS and in which PLWHA receive fair and equitable treatment. To create an enabling environment that effectively addresses stigma and discrimination, existing laws and policies must be reviewed and reformed where necessary.
Interventions to reduce stigma and discrimination recognise that these are major obstacles to effective HIV prevention, care, treatment and support. Namibia’s policies concerning human rights for people living with HIV/AIDS must still be translated into acceptance by all communities, employers and families.
A results-based approach means that achieving results in these four sub-components will
produce the following:
COMPONENT 1 Enabling Environment
Strategic resultPeople infected and affected with HIV/AIDS enjoy equal rights in a culture of
acceptance, openness and compassion.

Component 1: Enabling Environment
Medium Plan III for HIV/AIDS 34
1. Leaders and opinion setters consistently speak out about HIV/AIDS to combat discrimination, aid prevention programmes, and improve access to treatment, care and support
2. Relevant policies implemented 3. All necessary legal frameworks in place 4. People express accepting attitudes towards PLWHAs.
Indicators for these outcomes can be found in Chapter 4. If these results are achieved, we will reach a long term strategic outcome that people infected and affected with HIV/AIDS enjoy equal rights in a culture of acceptance, openness and compassion.
Sub-component 1.1 Capacity Development of Leadership 1.1.1 Sustained leadership commitment
Activities to achieve the outcome
Suggested project output Indicators
Implementing Partners
1. Raise awareness and understanding of the human rights based response to HIV/AIDS among political, traditional and religious leaders and decision makers through social mobilisation campaigns and targeted IEC
# of sessions held with target groups.
NAMACOC, MIB, MoHSS ALU, CCN
2. Facilitate the National Assembly and the National Council each to hold annual special sessions on HIV/AIDS, the first of which will be familiarisation with MTP III, starting in 2004
Minutes of session available
NAC, OPM, NAMACOC, MoHSS
3. Ensure that HIV/AIDS and TB are a normal agenda item on all public management structures e.g. Cabinet, PS management meetings, Regional Council meetings, traditional authority meetings etc. (see 5.2.1) starting in 2004 and on going
HIV/AID on agendas NAC, NAMACOC
4. Provide religious leaders with the necessary skills and attitudes to integrate reduction of stigma, discrimination, prevention, treatment and other HIV/AIDS/TB issues into their existing programmes starting with familiarisation of MTP 3 in 2004 (see 1.4.1)
# of religious personnel trained
CCN Church leaders CAFO
5. Provide all mayors, local councillors and local authority officials with relevant IEC material on HIV/AIDS and training on the management implications, governance, advocacy and co-ordination required of HIV/AIDS programmes
# of individuals receiving materials and training
MRLGH, AMICAALL, ALAN, ALU
6. Leaders in all sectors monitor a) the implementation of their bodies’ policies and programmes in keeping with national policies and international obligations, and ensure b) sufficient budget allocations for the implementation from 2004 (see 5.2)
Budget allocations in place
All
7. Ensure that the designated representatives from religious, sectoral, support groups of PLWHA and civil organisations attend and report back on the national and regional co-ordinating bodies of which they are members
Level of attendance of designated leaders at meetings of co-ordinating committees (NAC, NAMACOC, NAEC, RACOC, CACOC etc)
NAMACOC CCN, AMICAALL, ALAN, NANASO, Lironga Eparu
8. Encourage leaders to speak out on how they are personally affected by HIV/AIDS, their losses and success stories
# of leaders making personal statements
NAMACOC
Outcome: 80% of political, religious and traditional leaders and other opinion-setters, advocate for behaviour change, for reduced discrimination and stigma and for access to services and

Component 1: Enabling Environment
Medium Plan III for HIV/AIDS 35
Sub-component 1.2: Greater Involvement of PLWHA
1.2.1 Greater involvement of PLWHA
Activities to achieve the outcome Suggested project
output Indicators Implementing Partners
1. Build capacity and sustainability of national and regional organisations of PLWHA through training in advocacy skills, decision making processes, project management, and resource management
# of PLWHA groups per region trained
NANASO, NGOs RACOCs
2. Undertake awareness workshops for PLWHA on the MTP III, and training workshops on advocacy, communication skills and self esteem
# of PLWHA trained by gender and location
NANASO, NGOs, Lironga Eparu LAC, IBIS, RACOCs
3. Actively involve PLWHA as peer educators, trainers, counsellors and advisors to workplace and other HIV programmes in all sectors including the link between TB and HIV/AIDS and on importance of the National TB Programme as part of the HIV/AIDS strategy
# of PLWHA serving in these positions
All, NANASO, Lironga Eparu, NGOS, Private Sector, Ministries
4. Involve PLWHA in all appropriate national and regional decision making bodies pertaining to HIV and TB programmes
# decision-making bodies with PLWHA representation
NAC, NAMACOC RACOC, Sectors
Sub-component 1.3: Policy and Law Reform
1.3.1 National policy development and law reform
Activities to achieve the outcome
Suggested project Output Indicators
Implementing Partners
1. Develop a comprehensive national policy on HIV/AIDS by end of 2004
Policy launched MoHSS, OPM NANASO
2. Dissemination of national policy and training of implementers starting in 2005
# of copies disseminated and training sessions held
NAMACOC, MoJ, MoHSS MIB
3. Review existing legislation and propose new laws and policy reform on anti-discrimination, labour law, insurances and medical aid starting 2004
# of new laws proposed and promulgated
MoJ, Law Reform Commission, MoL, ALU
4. Review existing legislation and enact new laws and policy on family law – with specific reference to inheritance, customary marriage, co-habitation, marital property and divorce
Legislation enacted MoJ, Law Reform Commission, LAC
Outcome: National HIV/AIDS policy is developed by 2004 and all relevant law reform is undertaken to create a framework to a) reduce vulnerability to HIV b) improve access to prevention, care, support and treatment services and c) mitigate the impact by 2009
Outcome: 100% participation of PLWHA in planning, decision making and implementation for the expanded human rights response to HIV/AIDS

Component 1: Enabling Environment
Medium Plan III for HIV/AIDS 36
Activities to achieve the outcome
Suggested project Output Indicators
Implementing Partners
5. Review existing and enact new legislation, policies and procedures to provide for the protection of vulnerable children, to facilitate their access to services, and to eliminate any discrimination against vulnerable children
Legislation enacted MoJ, Law Reform Commission, LAC, MoHSS Parliament
6. Undertake law, policies and procedures reform to amend and /or set aside laws that a) increase vulnerability to HIV/AIDS b) hinder access to care, support and treatment c) impede mitigation of impact beginning in 2004
# of amended or repealed legislation compared to # of laws in need of amendment
MoJ, Law Reform Commission, ALU, Parliament
1.3.2 Sectoral and institutional policy development and reform
Activities to achieve the outcome
Suggested project Output Indicators
Implementing Partners
1. Rationalise existing sectoral and institutional HIV/AIDS policies with national policy by 2005
# of policies revised Ministries, Private Sector, NGOs
2. Review other national and sectoral policies and laws with a view to mainstreaming HIV/AIDS and addressing vulnerability, poverty, substance abuse, violence and impact by 2005
Policies and legislation in place
MoJ, Law Reform Commission, LAC,
3. Ensure that every sector has an HIV/AIDS policy in line with the national policy by 2005 and that all include issues dealing with socio-economic influences/factors
# of sector policies Each Ministry
4. Undertake a detailed assessment of the social assistance policy and procedures to make them more responsive to the needs of OVC and PLWHA. (see also 4.2.1)
Revised policy and procedures
MoHSS, CAA NRCS, Lironga Eparu Other NGOs
Sub-component 1.4: Interventions to Reduce Stigma and Discrimination
1.4.1 Social Mobilisation to Combat Discrimination
Activities to achieve the outcome
Suggested project Output Indicators
Implementing Partners
1. Provision of simple and accurate information in accessible formats and in local languages to the general population on HIV/AIDS, STIs and TB, including information on treatment, stigma and discrimination
# and quality of information available
MoHSS, MIB TC, ACT. CAA, ALU, NANASO,
Outcome: All sectoral and institutional HIV/AIDS related policies are developed or reviewed in conjunction with the National Policy to ensure an expanded multi-sectoral and human rights approach by 2009
Outcome: Appropriate and accessible social mobilisation aimed at reducing discrimination against, and stigmatisation of, those living with and affected by HIV/AIDS, STIs or TB

Component 1: Enabling Environment
Medium Plan III for HIV/AIDS 37
Activities to achieve the outcome
Suggested project Output Indicators
Implementing Partners
2. Increase multi-media efforts to reduce stigma and discrimination of HIV/AIDS, STIs & TB
Time and space given to such campaigns
MIB, Take Control NBC, MISA, NABCOA, ALU
3. Run regional information and awareness workshops to increase understanding of impact of stigma and discrimination on HIV and on social cohesion generally starting in 2004 and on-going
# of constituencies reached
Local authorities ALU ACT
4. Train and sensitise media practitioners to ensure sensitive media coverage pf HIV and AIDS
# of media practitioners trained
MIB, TC,NBC MISA, ALU
5. Provide information to schools, churches, health facilities and extension workers in all sectors, in local languages on the negative impact of stigma and discrimination. (see also 1.1.1) and on appropriate strategies to address stigma and discrimination
# of institutions reached
Take Control MBESC CCN FBOs
6. Develop a targeted campaign at insurance companies and financial institutions to adopt non-discriminatory practices with regard to people infected and affected by HIV/AIDS
# of insurance companies reached
MoF, Motorite, Bank of Namibia, NAMFISA, ALU
1.4.2 Actions to Reduce Stigma and Discrimination
Activities to achieve the outcome
Suggested project output indicators
Implementing Partners
1. Ensure the enactment, implementation and enforcement of laws and policies that address stigma and discrimination in all sectors and institutions (see 1.3.1 and 1.3.2)
Policies in place All Ministries NGOs, LAs Regional Councils
2. Provision of legal advice and assistance to access remedies for discrimination
# of people receiving legal advice
Office of the Ombudsman, Legal Aid, ALU, Law Society
3. Conduct training of community paralegals to render advice on the rights of PLWHA starting in 2004 and continuing
# of paralegals trained # of people who accessed the service
ALU Other NGOs
4. Conduct training of justice officials, social workers and educators concerning the rights of PLWHA and TB, starting in 2004
# of officials receiving training
MoJ, UNAM, Colleges, ALU
5. Establish or identify a body to investigate cases of discrimination and institute corrective measures
# of cases investigated and successfully concluded
Office of the Ombudsman OPM
Outcome: Counselling and legal assistance is provided to all persons living with or affected by HIV/AIDS/STIs or TB who have suffered discrimination and stigmatisation and request such assistance

Component 2: Prevention
Medium Plan III for HIV/AIDS 39
Prevention of the transmission of HIV remains the cornerstone of the strategy to overcome the epidemic. MTP II was successful in focusing on mass media campaigns and almost all sectors of the population are aware of how HIV/AIDS is transmitted and how they can protect themselves.
In this Third Medium Term Plan, the prevention strategy is based on the theory that behaviour change is a process of awareness that influences attitudes to create intentions to change behaviour. MTP III will therefore sustain the awareness programmes and encourage individuals to change behaviour to reduce risks of infection. Behaviour change requires specific, well targeted communication and interventions targeting those who are vulnerable to HIV because of their social status, lifestyles, work and living patterns. Individuals need to understand why they are at risk and how they can reduce that risk. The strategy recognises the need to empower people so that they want to and are able to protect themselves from HIV infection.
MTP III emphasises interventions which are known to have a strong influence in promoting behaviour change. Workplace programmes, with peer educators, have proven to be effective vehicles for promoting awareness, good attitudes, intentions and behaviour change. All partners in the fight against AIDS can assist in ensuring that condoms are available everywhere and at all times. Sexually transmitted infections are known to increase ones risk to HIV infection considerably, so speedy treatment and good management of STIs must be promoted. Strong communication and social mobilisation strategies are required to help people understand sexuality, sexual and reproductive health and rights, and to promote rapid identification and treatment of TB in the community and the workplace. Good TB care is the first life-saving treatment for PLWHA and it prevents this communicable disease from spreading to family members and close working colleagues.
Knowing your HIV status is an important step in changing your behaviour so that you remain HIV negative or in adopting safe sex practices so that you do not infect others. The expansion of voluntary counselling and testing will also enable those infected to enrol for treatment, care and support programmes.
The health sector will ensure that medical practices and infection control are strengthened and that their workers are protected from both HIV and TB infection. Safe blood transfusion products must continue to be guaranteed.
Finally, MTP III will encourage partners to focus on addressing difficult social and cultural factors which influence vulnerability such as poverty, gender inequality, traditional practices, alcohol abuse and violence.
All these strategies have been placed within five sub-components:
2.1 Strengthening capacity to deliver HIV /AIDS prevention programmes 2.2 Target vulnerable populations 2.3 Target behaviour change interventions at young people 2.4 Target the general population 2.5 Interventions to reduce vulnerability
COMPONENT 2 Prevention
Strategic resultReduced new infections of HIV and other STIs

Component 2: Prevention
Medium Plan III for HIV/AIDS 40
The results of all these strategies should lead to the following outcomes by the end of MTP III:
• A range of service providers with the capacity to provide high quality prevention services
• Reduced infection rates among vulnerable population groups. These include migrant and mobile workers, people with disabilities, pregnant women and their partners, mobile communities, farm workers and their families, minorities and other vulnerable groups
• The reduction of new infections of HIV and other STIs among children and young people in and out of educational institutions
• Reduced rate of new infections of HIV and other STIs in the general population
This component will not be able to reduce transmission of HIV and other STIs without the results of the other components. Prevention needs strong leadership and advocacy, appropriate policies and legal reform issues (see component 1: the enabling environment). The availability of treatment, care and support (See Component 3) can contribute to people wanting to know their HIV status. Improved programme management and coordination, strengthened monitoring, and behavioural change surveillance and research (component 5) are also pre-requisites for achieving the strategic result of reducing transmission of HIV, TB and STIs.
Although Prevention of Mother to Child Transmission (PMTCT) is a prevention programme, it needs considerable medical supervision and health service management. For these reasons it has been placed under Component 3: Treatment Care and Support services.
Sub-component 2.1: Strengthen capacity to deliver HIV/AIDS prevention programmes 2.1.1 Strengthen the capacity of those promoting behaviour change
Activities to achieve the outcome
Suggested project Output Indicators
Implementing Partners
1. Regularly improve knowledge and skills on sexual and reproductive health and rights, HIV/AIDS prevention issues, behaviour change communications and social mobilisation interventions among peer educators, technical staff, leaders, ministry focal persons and all other agents of behaviour change
# number of trained people # and types of interventions
MoHSS / MIB Regional AIDS Coordinators
2. Strengthen the capacity of Regional AIDS Coordinating Committees for Education (RACE), cluster schools, school focal points and school board members
# of school participating and regularity of activities N$ spent on HIV/AIDS capacity development, per region
MBESC
3. Build capacity among teachers, tutors, instructors and lecturers on HIV/AIDS issues, life-skills, sexuality and sexual health
% of teachers/trainers/lecturers trained in HIV/AIDS issues Increase of teachers discussing issues with youth
MBESC, MHETEC, MoHSS
Outcome: 100% of organisations and individuals delivering prevention interventions have improved knowledge and skills on HIV/AIDS and behaviour change

Component 2: Prevention
Medium Plan III for HIV/AIDS 41
Activities to achieve the outcome
Suggested project Output Indicators
Implementing Partners
4. Train all staff in basic social mobilisation to ensure more community-based approaches and involvement of communities in interventions for increased behaviour change
# of trainings in regions and/or constituencies # people trained in IEC material development # of community activities
MIB
5. Train service providers to develop outreach programmes to serve the communities and vulnerable populations such as mobile workers and people living in remote areas
# number of service providers trained in outreach programmes # of regions and constituencies reached
MoHSS MIB NGOs
6. Establish forum for the exchange of ideas and experiences and sharing of resources and facilities
# number of regular meetings and targeted interventions by partners # & types of information exchanges
MIB NANASO
7. Train people among vulnerable groups in counselling skills, to work in mainstream counselling services, including people who can communicate in Namibian sign language
# of people trained and working Awareness and behaviour change among vulnerable groups
MoHSS NGOs
8. Train youth peer educators in gender, sexual reproductive health and alcohol and drug abuse
Reduction of new HIV infections among youth Reduction in teenage pregnancies
MHETEC, MWACW
9. Train peer educators in all sectors in condom promotion and promotion of partner reduction
# of people trained in condom promotion Increase in condom use
MoHSS, Private & NGO sectors All Ministries,
10. Train media practitioners on HIV/AIDS issues, including sensitivity of language
#of media practitioners trained by media type (mass, community and regional media) # Type and coverage in media
MIB. JHU, UNAM, Polytechnic
11. Train RACOCs, CACOCs, NGOs, FBOs to use media for HIV/AIDS prevention
#of organisations trained Use of media by organisations
MIB. JHU, UNAM, Polytechnic
12. Train VCT staff and health workers in STI and VCT management (refer to 3.1.1)
# heath care workers trained in STI management, by year, cadre
MoHSS, and many others
13. Train professional & community counsellors for VCT
# of professional and community counsellors trained
NGOs, UNAM

Component 2: Prevention
Medium Plan III for HIV/AIDS 42
Sub-component 2.2: Target vulnerable populations
2.2.1: Target behaviour change interventions for vulnerable populations1
Activities to achieve the outcome
Suggested project Output Indicators
Implementing Partners
1. Develop and implement a comprehensive HIV/AIDS policy, including a condom distribution policy, to create a supportive and human rights based environment for prisoners and to reduce stigma and discrimination among prisoners and staff of the MPCS
Policy in place Rate and rapidness of implementation
Min. of Prisons & Correctional Services (MPCS)
2. Include PLWHAs in prisons in planning and implementation of all interventions and establish support groups for PLWHA
# of PLWHAs included in programmes
MPCS
3. Develop and implement behaviour change intervention targeting prisoners, such as access to IEC materials, referrals to STI, VCT, PMTCT, care, treatment and support services and PEP services for rape victims
# of behaviour change interventions in place Reduction in risk behaviour and HIV infections among prisoners
MPCS
4. Ensure provision of HAART, and PMTCT+, to prison inmates and uniformed services
# of prisoners accessing treatment Reduction of deaths due to AIDS in prisons
MPCS / MoHSS
5. Research the socio-economic conditions of mobile workers and their families which may make them vulnerable to HIV/AIDS infection in order to develop appropriate BCI
# of research papers available
MoHSS MTWC, NGOs
6. Develop targeted behaviour change communication and interventions (BCI) for mobile workers, including IEC materials and male and female condom provision
# of IEC interventions targeting mobile workers # of people who use condoms Reduced new infections among mobile communities
MoHSS MTWC, NGOs
7. Develop targeted behaviour change communication and interventions (BCI) for sex workers, including IEC materials, male and female condom provision, VCT, PEP
# of IEC interventions targeting sex workers
MoHSS
8. Establish baseline data on HIV/AIDS and disability through assessment visits to all regions
Data on HIV and disability available
NFPDN2, MLRR NGOs
1 Many vulnerable groups have been identified in Namibia. Interventions will target the following groups: Mobile populations and people who spend long periods away from home and their families; these include migrant workers, long-distance truck drivers, uniformed services and extension staff. Women and girls are particularly at risk due to their previously disadvantaged status and some cultural practises. People with disabilities, farm workers, minority and other vulnerable groups require special attention. The work, lifestyles and situation of transactional sex workers, street children, substance abusers, prison inmates and, on their release, their families are all at risk. Lastly, the growing group of people living with HIV/AIDS requires specially targeted prevention programmes.
2 National Federation of People with Disabilities in Namibia
Outcome: Targeted behaviour change communication and interventions (BCI) in place for vulnerable populations, such as IEC materials, male and female condom provision, STI, VCT, PMTCT prevention services, and post exposure prophylaxis for rape survivors to reduce new infections

Component 2: Prevention
Medium Plan III for HIV/AIDS 43
Activities to achieve the outcome
Suggested project Output Indicators
Implementing Partners
9. Develop and make widely accessible specific IEC materials for people with disabilities (PWDS) e.g. Braille, cassettes, videos with sign language
# of leaflets capacity and language appropriate material
MIB, MLRR NFPDN NGOs
10. Organise workshops targeting vulnerable youth and adult, including people with disabilities, providing information on HIV/AIDS and services available
# of workshops held NFPDN NGOs of PWDs
11. Develop and implement training for HIV/AIDS service providers on how to include vulnerable groups in their mainstream programmes
# of NGO service providers attending
NFPDN, MLRR
12.Ensure “Mainstream” HIV/AIDS organisations network and include PWDs in their HIV/AIDS activities
# interventions including PWDs
RACs, NANASO, MoHSS
13. Strengthen the implementation of mainstreaming gender into HIV/AIDS programmes
# of HIV/AIDS programmes which mainstream gender
MWACW All organisations
14. Develop, translate and distribute IEC materials for behaviour change targeting women, (including pregnant women, grandmothers and traditional birth attendants)
# of IEC materials produced
MWACW MIB, MoHSS
15. Support sport, art, culture, theatre, fashion and interactive programmes to increase awareness and self-esteem among all target groups, especially youth.
# and type of activities Participation and response of general public
MIB, TC MBESC, MHETEC, NAG, COTA, RACOC, CACOC, NGOs, FBOs, Community groups, NTN,
16. Develop activities which target marginalised or self-excluded groups
# involvement of marginalised or self-excluded groups
MRLGH, NRCS, UNICEF, FBOs
2.2.2 Prevention of transmission in health care settings
Activities to achieve the outcome Suggested Project Output
Indicators Implementing Partners
1. Finalise and distribute the revised Infection Control Guidelines to reduce occupational exposure to blood, body fluids and other potentially infectious materials that contain blood pathogens, particularly HIV, Hepatitis B and C
# of finalised Infection Control Guidelines printed and distributed
MoHSS
2. Finalise and distribute the post-exposure prophylaxis (P.E.P.) Guidelines aimed to protect health workers at risk of infection
# of finalised P.E.P. Guidelines printed and distributed
MoHSS
3. Conduct ongoing education and training among workplace management and health workers on universal precautions with regard to infection control and P.E.P, in public and private sectors
# of trained health workers at all levels with regard to infection control and P.E.P.
MoHSS, Private & Church Health sector, NGOs
4. Raise awareness and strengthen the legal responsibilities and accountability of employers to health workers, in terms of provision of
# of well-informed, responsible employers aware of their legal responsibilities, in terms of provision
MoHSS, MoL, Private & Church Health sectors,
Outcome: All health facilities adhere to national infection control and Post-exposure Prophylaxis (PEP) policies

Component 2: Prevention
Medium Plan III for HIV/AIDS 44
Activities to achieve the outcome Suggested Project Output Indicators
Implementing Partners
universal precautions & P.E.P. (with reference to Labour Act)
of universal precautions & P.E.P. at the workplace
NGOs, unions
5. Develop strategies for affordable access to counselling for all health workers and their families
# of public and private sector workplaces implementing national strategies for counselling # of health workers and their families counselled
MoHSS, Private & Church Health sector, NGOs
6. Establish HIV/AIDS counsellors’ support groups in the private and public health care settings
# of HIV/AIDS counsellors’ support groups available in each facility
MoHSS, Private health sector, NGOs
7. Establish infection control committees and occupational health structures at all workplaces to facilitate the implementation and provision of universal precautions & P.E.P
# of infection control committees and occupational health structures at workplaces
MoHSS, MOL, Private health sector, NGOs, unions
8. Educate health care workers on how to protect themselves from contracting TB in the workplace
# of health workers diagnosed with TB
MoHSS
9. Enforce TB infection control policy
# of reported infringements, per district MoHSS

Component 2: Prevention
Medium Plan III for HIV/AIDS 44
Sub-component 2.3: Target Behaviour change interventions1 at young people 2.3.1 Behaviour change interventions in schools
Activities to achieve the outcome
Suggested project Output Indicators
Implementing Partners
1. Promote and enforce the Education Policy on HIV/AIDS in all schools
% of school adhering to all aspects of the policy
MBESC
2. Revise curricula & resource materials to include appropriate life skills, sexuality, sexual health and HIV/AIDS education for learners/ students as part of the curriculum, also to include issues of teenage pregnancy, violence and substance abuse
% of curricula revised, by Grade, subject
NIED (MBESC)
3. Develop and distribute to all school libraries IEC materials regarding life skills, self-esteem, sexuality, sexual health, HIV/AIDS, TB, discrimination, children's rights, gender equality and other relevant social and equity issues
# of HIV/AIDS and TB brochures/booklets/posters produced by theme and # of copies distributed (by district)
MBESC, NGOs, FBOs, NRCS, MIB
4. Increase behavioural change communication (BCC) approaches and materials with learners for learners, adapted to the situation in each region to seek actual behaviour change
# of learners in AIDS Awareness Clubs and # and types of activities Involvement of learners in planning of TC material
TC, Schools, OY, NGOs
5. Design and implement a mandatory course for all teacher trainers, teachers-in-training, principals and teachers to make them HIV competent in the classroom
# of teachers trained to be HIV competent
MBESC MHETEC
6. Provide additional advanced courses for school staff in speciality areas such as care, counselling, prevention techniques, planning and management
# of teachers with advanced course certificates
MBESC MHETEC
7. Implement continuing life skills, sexual health, TB, HIV and AIDS education prevention programmes in all primary & secondary schools for all learners/students & staff
% of schools teaching HIV/AIDS prevention during the last curriculum year (rural/Urban)*
MBESC, NGOs
8. Develop partnerships between MBESC and other key actors to conduct life skills, sexuality, HIV/AIDS programmes in schools
# of memoranda of understanding signed # of joint programmes running
MBESC, NGOs, MHETEC
9. Strengthen and expand the Health Promoting Schools programme in primary and secondary schools in all regions
# of schools participating MoHSS MBESC
10. Expand the life skills, sexuality, HIV/AIDS and TB information campaigns targeting parents
# of schools disseminating information to parents # churches reaching out to parents # materials available to parents
Take Control MHETEC, FBOs
1 Behaviour change interventions (BCIs) include life skills promoting abstinence, delay in first sexual encounter, be faithful to a partner of known HIV status; male and female condom provision; counselling; STI and VCT services; post exposure prophylaxis for rape victims; expanded adolescent friendly health services and social services
Outcome: 100% of children receive behaviour change communication in primary schools and behaviour change interventions in secondary schools

Component 2: Prevention
Medium Plan III for HIV/AIDS 45
Activities to achieve the outcome
Suggested project Output Indicators
Implementing Partners
11. Continue to ensure a supply of potable water and latrines in all schools to create an orderly and hygienic environment where nutrition is guaranteed and health messages can prevail
% of schools with potable water and latrines
MTWC, MBESC
2.3.2 Behaviour change interventions for youth2
Activities to achieve the outcome
Suggested project Output Indicators
Implementing Partners
1. Develop and implement life skills, sexuality, sexual and reproductive health & rights, TB, STIs, HIV and AIDS programmes and curricula, including violence and substance abuse, in all tertiary institutions for all learners/students & staff
# of tertiary institutions with such an HIV/AIDS programme # and types of regular activities
MHETEC All tertiary institutions
2. Increase behavioural change communication (BCC) approaches and materials with students for students, adapted to the situation in each region to seek actual behaviour change
# and quality of materials available regular and monitored distribution of material
Take Control, Tertiary institutions, OY,
3. Expand the implementation of adolescent friendly health services (including information on sexual and reproductive rights) at all health centres, clinics, hospitals. and tertiary institutions
# of adolescent friendly health facilities, per region
MOHSS
4. Implement strategies to reach out-of-school youth # of strategies implemented MHETEC, TC, Lifeline/Childline, CAA,
5. Expand the range of behaviour change interventions easily accessible to young people to include the peer education training approach on related sexual and reproductive health services and HIV/AIDS prevention projects, condoms, STI and VCT services, post exposure prophylaxis (PEP) for rape victims, violence and substance abuse
# of tertiary institutions offering BCI # and types of material available
MHETEC, MoHSS All tertiary institutions NAPPA, NGOs, FBOs
6. Expand provision of youth-friendly multi-purpose centres in all major centres (see 2.5.1 below)
# of multi-purpose centres accommodating youth
MHETEC, LAs, MRLGH, MoHSS
7. Provide training opportunities for youth in computers, drama, peer education, and other skills through multi-purpose centres (see 2.5.1 below)
# of multi-purpose centres offering such training # of youth trained
MHETEC NGOs
8. Develop facilities and programmes to provide opportunities aimed at reducing risk in youth by improving self-esteem and pride through sports, culture, community service and skills development (see 2.5.1 below)
# of youth enrolled in sport or skills development programmes # of sports facilities available
MHETEC COSDECs, NAMCOL, KAYEC, LAs FBOs, NGOs
2 Behaviour change interventions (BCIs) include life skills promoting abstinence, delay in first sexual encounter, be faithful to a partner of known HIV status; male and female condom provision; counselling; STI and VCT services; post exposure prophylaxis for rape victims; expanded adolescent friendly health services and social services
Outcome: 100% of youth in tertiary education and out-of-school youth have access to behaviour change interventions (BCIs)

Component 2: Prevention
Medium Plan III for HIV/AIDS 46
Activities to achieve the outcome
Suggested project Output Indicators
Implementing Partners
9. Support skills training centres in their provision of vocational and employable skills training programmes to vulnerable groups, particularly young women (see 2.5.1 below)
# of youth (by region and gender) enrolled in such programmes
MHETEC COSDECs, NAMCOL, KAYEC, LAs, NGOs
Sub-component 2.4: Target the general population 2.4.1: Social mobilisation and awareness
Activities to achieve the outcome
Suggested project Output Indicators
Implementing Partners
1. Strengthen co-ordination of national, regional and local social mobilisation programmes and increase outreach for HIV prevention, care and support through regular contact meetings and visits with TC task force, RIO3, RACOC
Monthly TC meetings # of joint meetings, workshops, training courses and M&E visits with MRLGH, MIB, RAC, RIO, MHSS IEC, NYC Monthly activity reports
MIB, Take Control (TC) Task Force members4 RACOC, CACOC Regional and local authorities AAMICAAL
2. Provide I.E.C. tools, material and equipment to national, regional and community programme communication structures with e.g. support for international and national commemorations such as World AIDS Day, cultural and interactive activities
No. of regular video shows and dissemination of material in all 13 regions Regular publication of material from and in the regions Use of audio visual vans # of constituencies and people reached
MIB, Regional and local Authorities, RACOC, CAC Take Control partners, especially GRN and development partners, NGOs, FBOs
3. Develop a national IEC strategy for TB and TB/HIV to improve health seeking behaviour, enhance early reporting and detection, increase successful treatment completion
Long term IEC strategy formulated IEC strategy implemented Biannual survey of TB awareness in community conducted
MoHSS: Special Programmes NGOs Relevant sectors
4. Develop information material, community and interpersonal activities, use of role models, culture and self-esteem programmes for behaviour change
# of and types of material developed # of HIV/AIDS radio programmes & TV programmes produced and # hours aired # of HIV/AIDS brochures/booklets /posters produced & distributed # of and types of activities carried out in regions # of communities reached # of role models
MIB, NYC, Ombetja Yehinga, UNAM, NamCol, JHU, Take Control Task Force members RACOC, CAC, MFMC FBOs
3 RIO: Regional information officers, in employ of MIB, combined training and activities 4 Take Control (TC) Task Force: Co-ordinator Ministry of Information and Broadcasting (MIB) • AIDS Care Trust • ALU (LAC) • AMICAAL• CAA • CCN • Channel 7 • Christ’s Hope • CLASH • CRIS • German Development Service •FHI • FAWENA • Gospel Outreach • Lifeline/Childline• Lironga Eparu • MBESC • MHA (NamPol) • MHETEC • MIB • MLRR • MISA Namibia • MOD • MOHSS • MPCS •Mubasen • MWACW • NABTA • NABCOA • MoHSS: Special programmes, • NamCol • NAPPA • NaSoMa• NBC • NNAD • NRCS • NYC • Ombetja Yehinga • Open Talk (NYC) • Radio Energy • SMA•Telecom • The Namibian • UNAIDS • UNESCO • UNFPA • UNICEF• USAID • Voluntary Service Overseas, • Walvis Bay MPC • White Ribbon • Windhoek City Council • WHO • Youth for Christ • YouthNet (FHI) • All RACOCs
Outcome: 100% of the general population are targeted with social mobilisation and awareness interventions for the prevention of HIV, TB and STIs

Component 2: Prevention
Medium Plan III for HIV/AIDS 47
Activities to achieve the outcome
Suggested project Output Indicators
Implementing Partners
5. Include the use of indigenous languages in media as a means of communication
# of materials developed in local languages
MIB
6. Involve leaders at national, regional, constituency, local and tribal level in prevention activities through awareness creation, social mobilisation and personal speeches e.g. publicise testimonies through activities, material development, art and cultural programmes
# of leaders involved in advocacy and social mobilisation meetings, pamphlets, videos and other forums # of politicians who testify to personal losses
Take Control Task Force members and development partners MHSS, MRLGH Traditional Leaders Council NA and NC
7. Promote materials and activities to increase awareness of rights of HIV positive people and their families to care, support and services that are affordable, of high quality and responsive to their needs, and elimination of discrimination development
# and type of activities (art, theatre and culture, interpersonal communication); Rate of involvement of PLWHA # of material developed Videos, printed materials and events for testimonies of those infected and affected
MIB, Lironga Eparu CAA, NRCS, ALU LAC, TC, FBOs, NGOs
8. Support art, culture, theatre, fashion, sport and interactive programmes to increase awareness and self-esteem in all communities
# and type of activities Participation and response of general public
MIB, MBESC, NAG, NTN, COTA, RACOC, CAC, Community groups, NGOs, FBOs, TC
9. Disseminate regular publications and updates on HIV/AIDS, STIs and TB and related issues through websites, electronic and printed media, including development of special supplements and programmes for specific commemorations (see 5.2.2)
# and type of material on developments in Namibia in the mass media Regularity of media coverage Updating of websites and # of hits Regional reports and participation
MIB, UNAM, Polytechnic, JHU, MHSS, MWACW, MRLGH, Media, TC
2.4.2: Workplace programmes
Activities to achieve the outcome
Suggested project Output Indicators
Implementing Partners
1. Establish management and co-ordination mechanisms to support workplace programming in the public and private sector
Management and co-ordinating mechanism in place
OPM, MoHSS, umbrella bodies5
2. Expand guidelines for workplace programmes in the public and private sector
Implementation for workplace programmes developed
OPM MoHSS,, LAC6
3. Develop standardised training modules, toolkits, and mechanisms for workplace interventions
# of standardised modules and mechanisms developed
OPM MoHSS
5 such as NABCOA, NANASO, JCC, ACT, LAC, WBCG, Walvis Bay Multi-Purpose Centre 6 The AIDS Law Unit in the Legal Assistance Centre in 2003 brought out a guideline document on workplace programmes
Outcome: 90% of enterprises and all line ministries have expanded behaviour change interventions (BCI) in the workplace linking prevention, treatment, care and support in place

Component 2: Prevention
Medium Plan III for HIV/AIDS 48
Activities to achieve the outcome
Suggested project Output Indicators
Implementing Partners
4. Involve PLWHAs at appropriate levels of programme design and implementation
# PLWHAs involved in programme design, training & implementation # of advertisements encouraging PLWHA to apply
Lironga Eparu All organisations
5. Create supportive and human rights based environment for HIV/AIDS responses in the public and private sector
# of workplaces in public and private sector with human rights based policies and programmes in place
OPM, NABCOA, All sectors
6. Create awareness in workplace management to mainstream HIV/AIDS, STIs and TB into programming and budgeting cycles
# of workplaces understanding concept of mainstreaming of HIV/AIDS
NPCS, MoF, umbrella bodies
7. Ensure that TB receives high prominence in workplace programmes as both diseases occur at the same time, or in succession in the same individual
# of workplaces promoting awareness of TB signs & symptoms, early diagnosis & DOTS programmes
MoHSS All organisations
8. Develop and design targeted implementation strategies for different stakeholders eg, SME, informal sector, NGOs & CBOs
# of different stakeholders having implementation strategies in place % of enterprises registered with NCCI with workplace programmes # of workers accessing services
NANASO JCC
9. Establish and formalise Public-Private Partnerships for workplace programme interventions
# of Public-Private Partnerships established
OPM, NPCS
10. Design and implement community outreach workplace programmes – including prevention, care, support and treatment and support for OVCs
# of workplace programmes with community outreach components # of OVCs receiving support from workplaces as part of social responsibility
OPM, NABCOA, Local Authorities
11. Ensure that insurance companies and medical aid schemes have non-discriminatory policies in place that cover all HIV/AIDS related aspects
% of insurance companies with non-discriminatory policies in place
OPM, MoF MoL, ALU
12. Develop, design and implement behaviour change interventions for different target groups
# number of behaviour change interventions in place
MIB MoHSS
13. Establish support groups in workplaces in public and private sector
# number of support groups established in workplaces
HRD in all organisations
14. Develop strategies for access to treatment and care programmes for all workers in the public and private sectors
# number of workplaces having strategies and providing treatment, care and support programmes # of workers on treatment Reduction of AIDS related deaths
MoL, OPM
15. Develop comprehensive M & E system for workplace programmes
# of workplaces having comprehensive M & E systems in place National reporting system
OPM MoHSS NPCS

Component 2: Prevention
Medium Plan III for HIV/AIDS 49
2.4.3: Expand condom provision
Activities to achieve the outcome
Suggested project Output Indicators
Implementing Partners
1. Develop and implement a national policy on condom forecasting, supply, promotion and distribution by 2004
Policy in place and being implemented
MoHSS
2. Develop, implement and closely monitor condom (male & female) procurement / logistics management system and plan of action
# of reports of condom stock-outs MoHSS
3. Coordinate condom procurement and testing with quality assurance
% increase per year of procured condoms passing quality assurance testing
MoHSS
4. All sectors to procure and distribute condoms to meet annually agreed targets
# of male and female condoms distributed free through public sector
MoHSS All Lead Agencies
5. Ensure and support effective male and female condom social marketing services by marketing different brands to different segmented groups
# of male and female condoms distributed through social marketing
NaSoMa SMA
6. Strengthen community outlets to provide all sexually active people in Namibia with condoms through free provision and through social marketing
# of community outlets supplied, by supplier, per region, # of outlets trained on correct storage of condoms
RACOC
7. Provide adolescent friendly reproductive health information and services
% of health facilities with adolescent friendly services Use of facilities by youth
MoHSS
8. Train peer educators in all sectors in condom promotion (ref 2.1.1 above)
# of people trained in condom promotion # activities and outreach of peer educators
MoHSS, All Ministries, Private & NGO sector
9. Promote correct and consistent use of male and female condoms
MoHSS, MWACW All Ministries, Private & NGO sector
10. Conduct knowledge, attitudes, behaviour and practice studies (refer to section 5.4.3)
% of people reporting the consistent use of a condom during sexual intercourse with a non-regular sexual partner by gender, residence & age (15-19, 20-24, 25-49) * MoHSS
11. Monitor and evaluate condom logistics and usage
M&E reports MoHSS
12. Conduct operational research on clients’ preferences for condom brands
Research conducted MoHSS
Outcome: The proportion of sexually active women aged 15-49 consistently using condoms (male or female) during sexual intercourse increased from 8.9% in 2000 to 60% by 2009

Component 2: Prevention
Medium Plan III for HIV/AIDS 50
2.4.4: Strengthen STI Management
Activities to achieve the outcome
Suggested project Output Indicators
Implementing Partners
1. Conduct STI research and maintain STI database to improve STI service delivery
Aetiological study completed Resistance study completed STI health seeking behaviour research completed STI patient satisfaction survey completed
MoHSS: Special programmes, UNAM, NAPPA
2. Review STI treatment guidelines to reflect drug resistance to some of the drugs that might have occurred since the initial guidelines were developed
STI guidelines disseminated MoHSS: Special programmes, STI Technical Committee
3. Conduct regular sensitivity test to medicines (antibiotics)used for STI treatment
# of Tests conducted MoHSS: Special programmes,, NIP
4. Conduct a feasibility study into the establishment of a STI Reference Centre at Katutura Hospital, as a national centre for clinical and laboratory excellence
Feasibility study conducted Findings acted upon
MoHSS: Special programmes, UNAM, WHO
5. Clarify partners’ roles and strengthen STI IEC material production and dissemination, to include behaviour change in local contexts & languages
STI IEC materials disseminated to PHC clinics, hospitals, VCT sites
MoHSS: Special programmes,, MIB, SHPA, IEC Unit
6. Re-orientate and train various cadres of health providers (ref 3.1.1 below)
MoHSS: Special programmes,
7. Strengthen supportive supervision in all health facilities
# & length of supervisory visits MoHSS: Special programmes,
8. Pilot social marketing of STI drugs for urethral discharge with traditional healers, and the involvement of pharmaceutical companies in the social marketing of STI syndromic ‘over the counter’ drugs
Pilot programmes assessed MoHSS: Special programmes,, SMA
9. Strengthen STI surveillance, monitoring and evaluation, including annual planning and monitoring workshop with RACs and SHPAs and annual supervisory visits to regions
STI data base established STI regional surveillance training workshops held Biannual STD/HIV sero survey report completed
MoHSS: Special programmes,
Outcome: 80% reduction of STI cases by 2009 per syndrome through strengthened STI management and research at all levels of health care delivery

Component 2: Prevention
Medium Plan III for HIV/AIDS 51
2.4.5: Voluntary Counselling and Testing (VCT)
Activities to achieve the outcome
Suggested project Output Indicators
Implementing Partners
1. Conduct a needs assessment for mobile site planning
Assessment report SMA
2. Establish static VCT centres Cumulative number of static VCT centres to be established (% of regions covered)
MoHSS, SMA, CCN, CAA, Philippi Trust, NALAO
3. Establish VCT services in public hospitals # of public hospitals offering VCT services # of uptake of VCT
MoHSS
4. Establish mobile VCT services to also reach mobile and vulnerable communities
Cumulative number of mobile VCT services (% of regions covered) # of people reached
SMA
5. Conduct social marketing events and disseminate educational materials on VCT, e.g. media (posters, stickers, etc), ceremonies; hold information sessions with local stakeholders
# launch ceremonies # materials distributed # increase in uptake of services
SMA, TC
6. Train field officers & community volunteers to do door to door mobilisation for HIV testing
# of field officers trained # of households reached Increased uptake of VCT
Development Aid from People to People in Namibia (DAPP)
7. Increase peer educators in the workplace who promote VCT services
# peer educators trained per year # of households reached Increased uptake of VCT
MoHSS AIDS Care Trust
8. Encourage TB patients to go for VCT % of TB patients taking up VCT MoHSS 9. Map available support services for VCT clients
for both static and mobile services including: home based care; ongoing counselling / peer counselling; medical support inc. PMTCT; Legal services; spiritual support
% of VCT clients taking up referral to other services
SMA
10. Train volunteer pastors and other counsellors for service at CCN VCT centres
# pastors trained # of people reached by trained pastors
Council of Churches in Namibia
11. Rollout VCT services and rapid HIV testing
Cumulative # of clients receiving VCT services per annum # of clients at fixed centres # of clients at mobile centres
MoHSS, SMA, CCN, CAA, Philippi Trust, Khomas
12. Evaluate the VCT programme every 2 years Evaluation conducted and acted upon
MoHSS
13. Expand a national information system for VCT to all VCT centres
# centres with information system
MOHSS VCT Technical Working Group, SMA, CCN, CAA
14 Refer VCT clients to other services (e.g. clinics, social services)
% of clients who have been referred to other services
VCT centres
Outcome: Increased access and use by vulnerable groups, young people and the general population to quality VCT services at 45 centres in Namibia

Component 2: Prevention
Medium Plan III for HIV/AIDS 52
2.4.6: Safety of blood transfusion products
Activities to achieve the outcome Suggested project
output indicators Implementing Partners
1. Train counsellors to counsel blood donors before and after donations
# of trained counsellors MoHSS: Special programmes
2. Advocate blood safety in High schools and centres of Higher Education by training school principals and educators on the importance, purpose and function of NAMBTS, thus developing an interest on donation of safe blood
# of schools that donate blood # of educators and principals targeted
Namibian Blood Transfusion (NAMBTS), MBESC and MHETEC
3. Strengthen the capacity of current and new personnel to render a quality and efficient service
# of trained personnel NAMBTS
4. Mobilise resources and apply for funds from development partners
Funds available Programmes implemented
NAMBTS Development Partners
5. Continuous upgrading of equipment to ensure blood safety, such as equipment to test for the transfusion transmissible infections
N$ spent on equipment procurement
NAMBTS Development Partners
6. Generate and establish working policies for NAMBTS Operational policies in place
NAMBTS
Outcome: Continued safety of blood transfusion products and the rational use of these products

Component 2: Prevention
Medium Plan III for HIV/AIDS 53
2.5 Interventions to reduce vulnerability
2.5.1 Addressing vulnerability based on gender inequality, violence and alcohol abuse
Activities to achieve the outcome
Suggested project Output Indicators
Implementing Partners
1. Conduct and disseminate research on the role of traditional and cultural practices, values and beliefs in the transmission of HIV, sexual violence and abuse
Research available # of forums and people reached
MWACW, Traditional authorities, Local authorities
2. Train service providers (magistrates, police, social workers, prosecutors) on the Combating of Rape Act, Combating of Domestic Violence Act, Vulnerable Witness Act
# of service providers trained and better services to survivors Reduction in time between rape and court outcome
MOJ, MoHSS, LAC, MWACW, MHA,
3. Expand the social mobilisation campaign that addresses the connection between sexual and domestic violence and the spread of HIV/AIDS, STIs, including issues which contribute to risk behaviour
# & types of material # of people with access to material on sexual violence
MWACW, TC, MMC on VAWC
4. Target young women for income generating opportunities, further education, and skills training to develop their economic independence
# of young women involved in skills training programmes
MHETEC, MWACW, Namibia Girl Child Organisation WAD, NWN, Sister Namibia, Big Issue
5. Develop and enforce appropriate systems and safe guards to prevent sexual harassment, exploitation or assault of imprisoned offenders, and to support and protect those coming forward with complaints and needs
# of victims reporting offences # and types of prevention strategies preventative policing # fast tracking of cases
MWACW, MHA Namibian Police and WCPU, MOJ, MMC on VAWC7, NALAO
6. Develop and support prevention strategies and services for men and women who abuse alcohol, and their partners
# of organisations offering appropriate counselling
MoHSS, MWACW, NGOs
7. Expand access for men and women to counselling on domestic violence
# of people receiving counselling
MWACW, NGOs, MOHSS, Women and Child Protection Units
8. Increase production and dissemination of IEC material in all the local languages related to the dangers of alcohol abuse, especially as it relates to unsafe sexual practices and violence
# of booklets, leaflets, pamphlets available % of regions and constituencies with appropriate material
MWACW, MOHSS, MMC on VAWC, NGOs, WCPU
9. Identify and assist NGOs involved in alcohol abuse counselling to expand their services
# of NGOs assisted to expand services # people reached & rehabilitated
MoHSS
7 Multimedia Campaign on Violence against Women and Children
Outcome: Every region has programmes in place which address gender inequality, cultural practices, violence and alcohol abuse as a means of reducing vulnerability to HIV infection

Component 2: Prevention
Medium Plan III for HIV/AIDS 54
Activities to achieve the outcome
Suggested project Output Indicators
Implementing Partners
10. Regional and local authorities to mainstream prevention of violence and address alcohol abuse in all programmes and community mobilisation
# of regional and local authorities addressing this # and types of interventions
RACOC, DACs, NALAO, AMMICAAL, MWACW, WCPU, MoHSS
11. Regional and local authorities to provide appropriate and safe recreational opportunities for youth as alternatives to drinking and violence
# and types of recreational facilities Reduction in cases of violence, teenage pregnancy, alcohol abuse and HIV infections among youth
MRLGH, MWACW, MBESC, MHETEC
12. Provide comprehensive HIV post exposure prophylaxis after occupational exposure and rape (see 3.2.6)
# of PEP regimen provided MoHSS

Component 3: Treatment, Care and Support Services
Medium Plan III for HIV/AIDS 55
Treatment, care and support are indispensable and integral components to the response to the
HIV/AIDS epidemic and the Ministry of Health and Social Services considers them priority areas of investment and intervention for the welfare of the people of Namibia. Investing in the care and support of people living with HIV/AIDS can among others: i) complement and enhance prevention activities; ii) improve the quality of life; iii) maintain the working capacity of people infected and affected by AIDS; iv) decrease the social impact of AIDS; and v) prevent the secondary spread of infectious diseases like tuberculosis.
MTP III places more priority on care and support than had been the case previously. This is in keeping with the growing burden of disease. However, this Plan also reinforces the prevention to care continuum as well as the need to integrate prevention into this continuum wherever possible.
Priority will be placed on developing quality services. Various activities to reduce discrimination against and misconceptions about PLWHAs will be implemented, as these inhibit access to services that are available. See Component 1 for more details.
The care and support needs of PLWHA, and those most affected, will be addressed through the provision of a continuum of integrated quality services that can respond to the varying demands of PLWHAs. This extends from the time an individual may seek HIV testing, or be required to undergo testing; through the needs for primary health care support for minor HIV complications and interventions, including the provision of preventive therapy; to the management of more serious opportunistic infections and the provision of highly active antiretroviral therapy (HAART); and to the time when palliative interventions may be required in terminal stages. Alongside these medical interventions in the care continuum, will be the provision of psychosocial and community and home-based care and support.
Figure 12 below shows the implementation continuum of the different interventions required
COMPONENT 3Access to Treatment, Care and Support Services
Strategic Result: Access to cost effective and high quality treatment, care and support services for all people
living with, or affected by HIV/AIDS

Component 3: Treatment, Care and Support Services
Medium Plan III for HIV/AIDS 56
The strategy to respond to the continuum of care and support needs of PLWHA and those most affected is fourfold.
Firstly, accelerated HIV/AIDS care will be aimed at strengthening the provision of essential care countrywide, while ensuring increased access to comprehensive care in selected settings.
Secondly, the capacity to provide quality and integrated responses throughout the health care delivery system is in short supply. This will be addressed through scaled up training programmes and appropriate referral of more complicated cases to more sophisticated services for the management of these difficult to manage consequences of HIV infection. For this reason, integrated primary health continuum of care services need to include and be linked to tertiary institutions.
Thirdly, the responsibility to extend care and support services to the general population will fall to those care and support centres with established experience. These centres will need to achieve a level of excellence and best practice in order to maintain quality of care and support in this expansion phase. The aim, therefore, will be to build critical sites of best practice that are able to offer quality continuum of care services and provide capacity development and backup to more peripheral services.
Fourthly, it will be important to ensure that the care and support responses to HIV/AIDS are not “verticalised”. Every effort will be made to integrate minimum HIV/AIDS care and support initiatives into the existing health care and social support delivery systems. This will be especially important for TB management, as this condition is the major HIV/AIDS complication in Namibia. Efforts to mainstream HIV/AIDS care and support will also target traditional health care systems.
Progress towards the outcomes planned within this component is expected to lead to the following strategic outcomes:
• Continued increase in access to treatment information for all infected and affected by HIV and AIDS, and access to quality treatment, care and support services for PLWHAs
• Increased quality of life of PLWHAs, (including parents enrolled through PMTCT programmes)
• Reduced maternal transmission of HIV infection to newborns
Sub-component 3.1 Capacity development for the expanded treatment, care and support response
3.1.1: Capacity Development
Activities to achieve the outcome
Suggested project Output Indicators
Implementing Partners
1. Regular programme monitoring by the Programme Management and Technical Advisory Committees on Patient Care and Disease Management
# of meetings of Committees on Patient Care and Disease Management held and outcomes followed-up
MoHSS
Outcome: 100% of health care personnel have improved capacity to implement, monitor and supervise comprehensive case management, using updated guidelines and protocols
Formatted: Bullets and Numbering
Formatted: Bullets and Numbering
Formatted: Bullets and Numbering

Component 3: Treatment, Care and Support Services
Medium Plan III for HIV/AIDS 57
Activities to achieve the outcome
Suggested project Output Indicators
Implementing Partners
2. Review and produce clinical, laboratory and psychosocial support guidelines
Clinical, laboratory and psycho-social support guidelines produced & used
MoHSS, TAC: Patient Care and Disease Management
3. Distribute clinical, laboratory and psychosocial support guidelines to health and social services
Guidelines received by providers and other interested parties
MoHSS
4. Establish a Training Co-ordination Committee to determine and monitor training needs, guide training selection, standardise training curricula, and assess training efficiency and quality
Meetings of Training Co-ordination Committee held Training needs determined and monitored Training curricula standardised Quality assurance of training carried out
MoHSS
5. Produce standardised training materials to train trainers and care givers working with PLWHA and those most affected
TOT, trainer and trainee training materials produced # of people trained
MoHSS
6. Integrate STI, HIV/AIDS, TB and reproductive health into existing health and psychosocial training curricula
Integrated curricula produced and used
MoHSS, UoM
7. Assess and strengthen the capacity of the National Health Training Centre to train care givers working with PLWHA and those most affected
Strengthened National Health Training Centre # of caregivers trained
MoHSS
8. Train national ToTs for integrated STI/HIV/TB & reproductive health training
# of STI/HIV/TB ToTs trained # of people trained by TOTs
NHTC, MoHSS Directorate: Special Programmes, NGOs
9. Update existing treatment manuals for clinics and pocket manuals for all health workers to include revised aspects on HIV/AIDS, TB, STI, OIs, Reproductive Health, nutrition
Updated manuals distributed
Primary Health Care, MoHSS
10. Target health workers with campaigns to adopt a caring attitude to PLWHA and those affected
Health workers campaign conducted
MoHSS
11. Make treatment, care and support services ‘friendly’ towards PLWHA and those affected
Criteria established for ‘friendly’ services # of services accredited as ‘friendly’ services
MoHSS
12. Train professional and non professional health and social support personnel to provide care and support to PLWHA and those affected
# of professional health care workers trained in: • VCT • Integrated HIV/AIDS and TB
• Reproductive health
# (%) of licensed doctors trained in comprehensive case management # (%) of nurses trained in: • comprehensive case
management • HAART dispensing
MoHSS Directorate: Special Programmes, MoHSS, NHTC, FHI, CDC, SMA, UNAM, Namibian Red Cross, Catholic AIDS Action, TAKMOAS, AIDS Care Trust, Philippi Namibia, ELCAP and LAC, Lironga Eparu
Formatted: Bullets and Numbering
Formatted: Bullets and Numbering

Component 3: Treatment, Care and Support Services
Medium Plan III for HIV/AIDS 58
Activities to achieve the outcome
Suggested project Output Indicators
Implementing Partners
13. Train professional and non professional health and social support personnel to provide care and support to PLWHA and those affected
(continued)
# of community volunteers & care givers trained in providing community home based care by district # community counsellors trained per year # of professional counsellors trained per year (full-time & short course) # of lay counsellors trained # PLWHA trained as VCT counsellors # PLWHA trained as DOTS supervisors # trained nutritional management in HIV and infant & young child feeding # technologists trained in viral, PCR and Flow-cytometry techniques # health workers trained to perform rapid HIV testing
Mohss Directorate: Special Programmes, MoHSS, NHTC, FHI, CDC, SMA, UNAM, Namibian Red Cross, Catholic AIDS Action, TAKMOAS, AIDS Care Trust, Philippi Namibia, ELCAP and LAC, Lironga Eparu
14. Strengthen training of health workers in STI syndromic management
STI training manuals printed # of SHPAs sent on advanced training # of health workers trained in STI syndromic management # of doctors trained in syndromic management
MoHSS Directorate: Special Programmes
15. Develop standardised reporting systems for care and support providers (VCT, PMTCT, OI Management, HAART, HBC)
Standardised reporting systems developed
MoHSS
16. Develop and use accreditation criteria and approaches for community counsellors and HBC workers
Accreditation systems developed for counsellors and HBC workers % personnel working with PLWHAs and those affected accredited
MoHSS, NHTC, UNAM
Formatted: Bullets and Numbering
Formatted: Bullets and Numbering

Component 3: Treatment, Care and Support Services
Medium Plan III for HIV/AIDS 59
3.1.2: IEC to support expanded treatment, care and support programmes
Activities to achieve the outcome
Suggested project Output Indicators
Implementing Partners
1. Conduct research into the general population’s understanding and experience of treatment, care and support for HIV/AIDS and barriers to accessing services
Research conducted Sharing, dissemination & implementation of research recommendations
UNAM
2. Develop a communication strategy to improve understanding of the continuum of treatment, care and support for HIV/AIDS and how to overcome barriers to accessing services (incl messaging, nature of communication materials required and dissemination)
Communication strategy developed
MIB, MoHSS, JHU, CCP, Care and support providers, PLWHAs
3. Conduct a comprehensive treatment literacy campaign for the general public and PLWHA to improve understanding of the continuum of treatment, care and support for HIV/AIDS and how to overcome barriers to accessing services
# & type of material # of people with access to the information
MIB, TC, MoHSS, JHU
Conduct social mobilisation and produce materials on PMTCT, targeting young women, traditional birth attendants, traditional healers, mothers & grandmothers
# & type of material # of people with access to the information
MIB, TC, MoHSS, JHU
4. Include TB in Communication and Social Mobilisation programmes, as an inseparable part of HIV/AIDS control to improve health seeking behaviour, enhance early reporting and detection and increase successful treatment completion
Integrated Communication and Social Mobilisation programmes in place
MIB, TC, MoHSS, JHU, NAMTA, NBC
5. Promote coverage by national and local media of treatment, care and support services
Increased coverage by national and local media of services # of people accessing treatment
MIB, TC, MoHSS, JHU
6. Provide IEC to vulnerable groups such as the prison inmate population and sex workers about HIV/AIDS & STI treatment, care and support programmes, especially TB as an opportunistic infection, and increase ‘treatment literacy’ for people infected and those affected by HIV/AIDS
# of sex workers receiving IEC on treatment literacy # of sex workers accessing treatment
MoHSS
7. Develop & disseminate IEC materials in reproductive health
# & type produced MIB, TC, MoHSS, JHU
8. Develop small media (videos, tapes) to improve understanding of the continuum of treatment, care and support for HIV/AIDS and how to overcome barriers to accessing services
Small media developed Small media disseminated
MoHSS
9. Develop a small media communication campaign for health workers to improve their understanding of HAART
Small media developed & disseminated
MoHSS
Outcome: 50% of the general population have a satisfactory level of knowledge on treatment, care and support for HIV/AIDS
Formatted: Bullets and Numbering
Formatted: Bullets and Numbering

Component 3: Treatment, Care and Support Services
Medium Plan III for HIV/AIDS 60
Sub-component 3.2 Treatment and Care Services
3.2.1: Laboratory Services
Activities to achieve the outcome
Suggested project Output Indicators
Implementing Partners
1. Develop a policy and protocols for, and quality control system for monitoring of, rapid HIV testing
Policy disseminated Quality control system developed
National Institute of Pathology (NIP)
2. Accredit training of nurses/ counsellors by NIP in the use of rapid testing and quality control
# of certified nurses / counsellors NIP
3. Conduct Phase II validation of rapid test Phase II underway NIP
4. Roll out rapid testing within VCT centres # of VCT sites with rapid testing NIP
5. Implement quality control/assurance and continuing monitoring & evaluation of rapid testing
Quality control and monitoring implemented # of quality tests & % success rate
NIP
6. Expand CD4, viral load and HIV EIA testing sites where needed or appropriate and train laboratory workers to carry out these tests
# of CD4 sites # of viral load sites # of HIV EIA sites
NIP
7. Obtain accreditation for NIP laboratories NIP accredited # laboratories accredited
NIP
8. Assess the feasibility of ARV drug resistance monitoring
Feasibility study completed NIP
3.2.2: Drugs and Supplies Systems
Activities to achieve the outcome
Suggested project Output Indicators
Implementing Partners
1. Assess and strengthen the current capacity in the MoHSS to monitor and track the drug distribution pipeline at the various important points in the supply chain
Assessment completed # of monitoring assessments & regularity of supplies Capacity strengthened
Central Medical Stores (CMS)
2. Improve supply chain tracking through the computerisation of the central and regional medical stores to link them electronically
Computerised inventory control system replaced
CMS
3. Develop a routine tracking and reporting system to ensure that information is collated and available for regular checking against actual physical stock levels and for bulk procurement planning
Tracking and reporting system developed # of drug shortages
CMS
4. CMS to develop a social marketing plan to notify outlets of additional stock
Social marketing plan Rate & distribution of drugs
CMS
Outcome: Satisfactory laboratory capacity for monitoring HIV/AIDS disease management and VCT quality assurance
Outcome: Management systems for forecasting, procurement and supply of essential drugs and commodities are able to meet an expanded HIV/AIDS response

Component 3: Treatment, Care and Support Services
Medium Plan III for HIV/AIDS 61
5. Develop Ministry guidelines for drug procurement (such as PMTCT-PLUS and related activities)
Guidelines obtained & implemented % adherence & orders by CMS
CMS, MoHSS
6. Ensure co-ordination between the Procurement Task Group, under the NaCCATuM secretariat, and the MoHSS
Joint meetings held Procurement & supplies rate
Procurement Task Group, MoHSS
7. Investigate possible joint procurement mechanisms with other countries, which could further reduce costs of generic ARVs
Proposal developed CMS
8. Obtain consensus on the minimum contents of the HBC kit so that this combination can be ordered through the state procurement mechanisms
Consensus obtained # of HBC kits ordered # HBC kits distributed & used, by region
CMS, HBC organisations
9. Increase procurement of additional Public Sector condoms for free distribution and Procurement of Social Marketing Condoms through the multi-sectoral Standing Committee on Condom Procurement and Distribution (see 2.4.3)
# of Public Sector condoms procured & distributed, by region Female Male # of Social marketing condoms procured
CMS
3.2.3: PMTCT-Plus Services
Activities to achieve the outcome
Suggested project Output Indicators
Implementing Partners
1. Strengthen PMTCT-PLUS Technical Working Group with a co-ordinating and technical role
# of recommendations adopted
MoHSS
2. Develop, launch and distribute national guidelines for PMTCT-PLUS, Safe Obstetric Practices and Infant and Young Child Feeding guidelines
# of guidelines developed and distributed
MoHSS and its main partners for PMTCT-PLUS programmes
3. Strengthen capacity for national co-ordination of HIV/AIDS training & supply chain management for PMTCT–PLUS
% of PMTCT+ trained staff in each PMTCT+ service
MoHSS
4. Ensure that PMTCT-PLUS centres have enough rooms for comprehensive VCT/PMTCT-PLUS activities;
# Hospitals with VCT/PMTCT-PLUS centre
MoHSS
5. Develop pool of ToTs and supervisors for each Health Region
# of ToTs /supervisors (re)trained MoHSS
6. Rollout programme in phased coverage # of hospitals with PMTCT-PLUS services in place % of eligible women enrolled in PMTCT-PLUS programme % of HIV+ pregnant women who choose at birth to exclusively breastfeed for 4 months or choose replacement feeding
MoHSS
Outcome: 90% of HIV+ pregnant women, their children and partners, have access to PMTCT+ services and receive a complete course of ARV prophylaxis to prevent mother to child transmission

Component 3: Treatment, Care and Support Services
Medium Plan III for HIV/AIDS 62
Activities to achieve the outcome
Suggested project Output Indicators
Implementing Partners
7. Conduct operational research Reasons for low uptake of PMTCT Clinical nutritional management of HIV and AIDS, infant and young child feeding
MoHSS
8. Monitor integrated implementation of PMTCT-PLUS (including VCT and medical treatment with HAART and for OIs) guidelines and programmes in hospitals
% Namibian pregnant women received VCT % of eligible babies receiving Nevirapine % of children HIV negative at 18 months
MoHSS
3.2.4: Management of Opportunistic Infections
Activities to achieve the outcome
Suggested Project Output Indicators
Implementing Partners
1. Develop policies, guidelines and protocols to guide the three main levels1 of care for PLWHA, including clinical nutritional care
Policies, guidelines and protocols developed and disseminated # of people living positively with HIV without drugs # of PLWHA being treated at primary care level, secondary & tertiary care level
MoHSS
2. Finalise a policy on chemoprophylaxis of commonly occurring OIs and develop guidelines and protocols
Policies, guidelines and protocols developed and disseminated
MoHSS
3. Regularly distribute protocols, guidelines and standards for HIV/AIDS management
# of hospitals & medical practitioners who have and use the guidelines
MoHSS
4. Take stock of essential HIV/AIDS drugs at all levels of care and ensure their availability
# of stock outs MoHSS
5. Conduct regular clinic supervision to assess quality of OI management by both PHCS and SHPA and sometimes with MoHSS Directorate: Special Programmes staff
# of supervision visits, by clinic, by region # of integrated supervision visits carried out according to schedule with evidence of feedback to regions
CMO, MoHSS, MoHSS Directorate: Special Programmes
6. Conduct regular assessments of training needs of health care workers to manage HIV/AIDS during supervisory visits & organise training
# of clinic staff trained SHPA, MoHSS
7. Conduct operational research to profile the spectrum of AIDS related illnesses and presentation of HIV in Namibia
# of PLWHA & types of illnesses MoHSS
1 . The Primary level corresponds to clinics and Health Centres; the Secondary level to the district hospitals while the Tertiary level should correspond to the Regional Referral and National Referral hospitals.
Outcome: Increased access by PLWHAs to opportunistic infections prevention, comprehensive case management services and palliative care
Formatted: Bullets and Numbering

Component 3: Treatment, Care and Support Services
Medium Plan III for HIV/AIDS 63
3.2.5: Collaborative TB/HIV/AIDS Services
Activities to achieve the outcome
Suggested project Output Indicators Implementing Partners
1. Create effective co-ordination within MoHSS Directorate: Special Programmes and sectors on TB/HIV technical policy and implementation, at all levels
TB and HIV/AIDS guidelines formulated and disseminated Representation of TB and HIV/AIDS experts in meetings and committees where TB and HIV/AIDS interests overlap
MoHSS Special Programmes, Church Health Services, NGOs Relevant sectors
2. Strengthen intensified case finding for active TB in all PLWHA in VCT and clinic settings
Counsellors in VCT centres trained in TB screening Awareness of health workers increased about TB in PLWHA # of clients referred by VCT sites for TB examination and diagnosis
MoHSS Special Programmes NGOs Relevant sectors
3. Provide access to VCT for TB patients
# of TB patients tested for HIV and counselled each year
Nat. TB Control Programme
4. Provide TB patients with knowledge and care to prevent HIV infection
BCI provided to all TB patients (such as STI referral, condoms, IEC materials)
Nat. TB Control Programme
5. Promote and provide Cotrimoxazole Preventative Therapy (CPT) to eligible HIV+ TB patients during their treatment
# of HIV+ TB patients on Cotrimoxazole Preventative Therapy (CPT) Educate and support HIV+ TB patients to adhere to Cotrimoxazole Preventative Therapy
Nat. TB Control Programme
6. Strengthen TB control in the HBC environment
# of patients with TB receiving directly observed treatment (DOT) and support from home based care workers # of patients referred for TB diagnosis by home based care workers
Nat. TB Control Programme NGOs
7. Establish referral systems between different services for PLWHA and PLWTB
Referral systems established Referral systems introduced
MOHSS Special Programmes NGOs Relevant sectors
Outcome: PLWHA and PLWTB have access to a continuum of care and support services for TB and HIV/AIDS diagnosis, in all health care facilities and home based care services in public and private sector

Component 3: Treatment, Care and Support Services
Medium Plan III for HIV/AIDS 64
3.2.6: Provision of HAART
Activities to achieve the outcome
Suggested project Output Indicators
Implementing Partners
1. Increase national capacity to supervise and support HAART and comprehensive care programme
Hire 5 national coordinators for MOHSS (1 doctor, 1 nurse, 1 counsellor, 1 pharmacist, 1 dietitian, 1 M&E officer)
MoHSS
2. Distribute and regular update Namibian guidelines on comprehensive HIV disease management
# of regions received guidelines and updates
MoHSS TAC: Patient Care and Disease Control
3. Build collaboration between the public and private sector in the provision of HAART
Regular interactive fora held between public and private sector
MoHSS, medical aid administrators, Medical Association
4. Review existing HAART provision to determine patient flow plans, and job definitions of key staff
Patient flow plans and key job definitions determined
MoHSS
5. Expand the number of facilities providing HAART
Cumulative number of facilities providing HAART
MoHSS
6. Expand access of AIDS patients to HAART Cumulative number of patients on HAART
MoHSS
7. Expand the number of health care facilities with capacity to provide PEP
Cumulative number of health care facilities with capacity to provide PEP
MoHSS
8. Provide comprehensive HIV post exposure prophylaxis after occupational exposure and rape
# of PEP regimen provided MoHSS
9. Educate family members to serve as the treatment supervisor for patients on HAART, supported by trained providers
# home-based care providers trained to train and support family members as HAART supervisors
NGOs providing HBC, CCN, MoHSS Case Management Unit
10. Implement PMTCT-PLUS and HAART component in all hospitals for PMTCT-PLUS
# hospitals where HAART component implemented
MoHSS
11. Ensure hospitals /districts have capacity to support home visits to PMTCT-PLUS programme families
# health districts/hospitals with home visit support capacity
MoHSS
12. Monitor integrated implementation of PMTCT-PLUS (including VCT and medical treatment with HAART, for OIs and clinical nutrition management) guidelines and programme in hospitals
%of partners reached % of eligible pregnant women and partners on HAART
MoHSS
13. Provide eligible HIV positive pregnant women with HAART and clinical nutrition care
# of (pregnant and post delivery) women treated with HAART in target population (cumulative)
MoHSS
14. Provide eligible HIV positive pregnant women’s partners with HAART and clinical nutrition care
# of partners treated with HAART in target population (cumulative)
MoHSS
15. Provide eligible HIV positive children with HAART and clinical nutrition care
# of children treated with HAART in target population (cumulative)
MoHSS
Outcome: 30,000 PLWHA are receiving Highly Active Anti-retroviral Treatment (HAART) in public and private settings

Component 3: Treatment, Care and Support Services
Medium Plan III for HIV/AIDS 65
3.2.7: Home Based Care
Activities to achieve the outcome
Suggested project Output Indicators
Implementing Partners
1. Establish additional NGO/CBO/ FBO/PLWHA home based care groups
# of NGO/CBO/FBO PLWHA Support Groups by district
MoHSS, Health Districts Church Health Services, RACOCs, sub contracted NGOs
2. Train Field Officers (incl. PLWHAs) to run Positive Living Courses; establish support groups around VCT centres; produce tool kit for Positive Living Course & for Support Groups
# people trained # support groups established around VCT centres # positive Living tool kits produced # Support Groups toolkits produced
Development Aid from People to People in Namibia (DAPP)
3. Establish referral systems between NGO/CBO/FBO PLWHA HBC groups and the formal health care systems
Referral systems developed and functional
MoHSS, Health districts, HBC organisations
4. Train and support HBC volunteers to identify TB cases promptly and supervise DOTS
# of TB referrals from HBC groups MoHSS
5. Improve networking among NGO/CBO/FBO PLWHA HBC groups to promote horizontal learning
Network meetings between NGO/CBO/FBO PLWHA Support Groups
MoHSS, District Hospitals, RACOCs, HBC organisations
6. Provide technical support to NGO/CBO/FBO PLWHA HBC groups from central level
# of technical support contacts with NGO/CBO/FBO PLWHA Support Groups
MoHSS, NGOs
7. Investigate mechanisms to support and recognise HBC providers
Incentives developed Recognition provided
8. Distribute and replenish home based care kits to NGO/CBO/FBO PLWHA HBC groups
# of HBC kits distributed by region # of HBC kits replenished by region
MoHSS, NGOs
Outcome: Quality home based care services, including community based care and psycho-social support are available in all 96 constituencies

Component 3: Treatment, Care and Support Services
Medium Plan III for HIV/AIDS 66
3.2.8: Access to Care for Vulnerable Populations
Activities to achieve the outcome
Suggested project Output Indicators
Implementing Partners
1. Conduct an assessment of the barriers that exist in accessing treatment, care and support services by vulnerable populations, OVCs and students
Assessment recommendations considered and acted upon
MoHSS, PLWHA from special populations, OVCs and students
2. Establish consultative forums with representatives from vulnerable populations, OVCs and students to promote improved access to services
Consultative forums established Forums meet annually
MoHSS
3. Increase public awareness of the importance of HIV/AIDS care and support and the need to support PLWHA and those affected to access these services
Public campaign conducted MoHSS
4. Establish appropriate co-ordination mechanisms with public health services for offenders arriving at and leaving the MPCS institutions, including prisoners on remand, imprisoned pregnant women living with HIV/AIDS delivering in external facilities, in order to ensure a continuum of care (HAART, PMTCT+, other)
# of prisoners receiving continuous treatment & care Reduction of deaths due to AIDS in prisons
MPCS / MoHSS MHA
5. Ensure mobile and migrant workers have access to treatment, care and support including access to HAART, PMTCT
# Mobile workers accessing treatment Reduction in deaths
MoHSS
Outcome: 100% of vulnerable populations have access to comprehensive medical, psychosocial and palliative care

Component 4: Impact mitigation services
Medium Plan III for HIV/AIDS 67
Strategies are required that focus on building local responses to the impact of the epidemic. Local responses are a combination of i) building the knowledge and skills of key actors in the community ii) facilitating support from different sectors especially local authorities, education, health, agriculture and iii) building the capacity of service providers such as local NGOs. The Local Response approach has proven effective in developing capacities of local communities to tackle HIV/AIDS issues within their own environment. The success of this approach will depend in some measure on the management and co-ordination mechanisms proposed in Component 5, in particular the availability and accessibility of financial resources for community-based interventions and capacity building of local NGOs providing training and services.
To address adequately the needs of orphans and vulnerable children a number of policies and legislation must be enacted (see Component 1). A system of social assistance grants is in place including foster grants, maintenance grants and disability grants. The criteria and procedures for accessing these grants and other available services to mitigate the impact of HIV/AIDS will be streamlined. The provision of various other mitigating services available to workers and their families are discussed under Workplace Programmes in 2.4.2. and under Home-Based Care in 3.2.7.
This strategic result is divided into three sub-components:
4.1 Developing the capacity of local responses 4.2 Services for OVC and PLWHA 4.3 Addressing poverty
Achieving results in these three sub-components will contribute to the following overall desired results:
1. Continued increase in access to community-led quality programme interventions for PLWHAs, OVCs and those affected by HIV/AIDS and TB.
2. PLWHAs and TB and affected people provided with skills training and support by type e.g. advocacy & income generation and by region.
3. Social assistance is accessed by OVC, their caregivers and PLWHA in all thirteen regions. 4. School age OVC attend school.
Indicators for these outcomes can be found in Chapter 4 on Monitoring. If the results are
achieved we will reach our long term strategic outcome of an increase in quality of life of PLWHAs, OVCs and those affected by HIV/AIDS and TB.
Strategic Result:Strengthened and expanded capacity of local responses to mitigate socio-economic impacts of
HIV/AIDS
COMPONENT 4Impact mitigation services

Component 4: Impact mitigation services
Medium Plan III for HIV/AIDS 68
Sub-component 4.1: Developing the Capacity of Local Responses 4.1.1 Establish, strengthen and support communities to take action to respond to HIV/AIDS/STIs and TB
Activities to achieve the outcome
Suggested project Output Indicators
Implementing Partners
1. Extend service delivery capacity in all relevant sectors by developing mechanisms to sustain community volunteers (see also 5.1.1 and 5.1.2)
Options in place for remunerating, recognising and assisting community volunteers
OPM, All sectors NGOs NANASO
2. Expand and establish Constituency and Village HIV/AIDS committees and train their members in HIV/AIDS advocacy, local response development, and programme management (see 5.2.1) by 2006
# of constituencies with active HIV/AIDS Committees
Regional Councils MoHSS Directorate: Special Programmes, Trad. Authorities
3. Enable community HIV committees to conduct participatory risk and impact assessments, develop action plans, implement them and monitor the outcomes
# of community groups implementing their own HIV/AIDS action plans based on local assessment
MAWRD, MWACW LAs, RACOCs NGOs, NALAO
4. Ensure that existing community committees, such as water point committees, ECD committees, development committees etc. have an HIV/AIDS component in their training and plans
# of community based committees trained in HIV/AIDS issues including prevention, treatment, care and support.
Regional Councils MAWRD MWACW All sectors
5. Conduct community based nutrition surveillance and monitoring
# of communities trained in nutrition surveillance & monitoring
MoHSS, NGOs
6. Build the capacity of mayors, municipal leaders and local authority institutions to initiate, expand, co-ordinate and manage local responses to HIV/AIDS, including the provision of relevant and up-to date information in support of HIV/AIDS advocacy, sensitisation and programme development (see 1.1.1)
# of projects initiated by local authorities
Local Authorities, ALAN, AMICAALL, LAC
7. Train community counsellors (including home-based care givers) in psycho-social support for OVC with an approved curriculum (see also HBC 3.2.4)
# of community volunteers trained in providing care and support including psycho-social support for OVC
MOHSS CAA, Red Cross, CCN, RACOCs, CACOCs
8. Establish HIV/AIDS Committees at every school that develop partnerships with CBOs and other service agencies to develop the schools as centres of support for OVC and HIV/AIDS prevention activities
% of schools with functioning HIV/AIDS committees
MBESC, MHETEC IBIS
9. Provide training, technical assistance and financing of community organisations and local NGOs to assist with OVC and affected families
# of CBOs and NGOs which receive technical and financial assistance
RACOCs, NANASO, NGOs, local authorities MAWRD, MWACW
10. Develop, maintain and support foster parent pools in all regions
# of carers registered and trained with the pool
MoHSS MWACW, FBOs, NGOs
Outcome: 80% of targeted communities have a local response to HIV/AIDS

Component 4: Impact mitigation services
Medium Plan III for HIV/AIDS 69
Activities to achieve the outcome
Suggested project Output Indicators
Implementing Partners
11. Integrate HIV/AIDS, STIs and TB interventions into all existing church programmes e.g. youth services, confirmation classes, marriage preparation, men’s clubs, camps, retreats and choirs and build the capacity of congregations to expand and deliver strong prevention programmes focusing on delay and faithfulness and providing appropriate and accurate information on condoms (see 1.1.1)
# of congregations using HIV/AIDS information and materials.
CCN, FBOs, Lironga Eparu
4.1.2 Develop the capacity of local support groups of PLWHA and their families
Activities to achieve the outcome
Suggested project output indicators
Implementing Partners
1. All RACOCs to monitor the number of support groups and the support they receive in their region
Data on number of support groups receiving support
RACOCs
2. Strengthen the development of PLWHA organisations, such as Lironga Eparu, particularly at regional and local levels and provide technical assistance and material resources where needed
# of member groups annual plans and budgets in place
NANASO, NGOs Lironga Eparu RACOCs, MAWRD, MoHSS
3. Establish support groups around the country with emphasis on linking with VCT centres
# of constituencies with support groups
SMA, Lifeline Support Groups, MoHSS, NGOs
4. Train extension officers and field workers in every sector in positive living and provide IEC material on positive living
# of extension workers trained and in possession of relevant material
MAWRD, MWACW All relevant ministries, NGOs
5. Build and support emerging coping mechanisms and initiatives of PLWHA and affected families especially by IGA
# of groups identified and supported
NGOs, IBIS Extension workers
Sub-component 4.2: Services for OVC and PLWHA 4.2.1 Comprehensive services for OVC, their carers and PLWHA
Activities to achieve the outcome
Suggested project Output Indicators
Implementing Partners
1. OVC Policy adopted and implemented by 2005 (see 1.3.2) Published Policy MWACW
2. Management plan for the OVC Trust Fund developed and implemented 2005
Management Plan operational
MWACW
Outcome: Increased number of well functioning support groups for PLWHA and their families
Outcome: Guaranteed access to comprehensive services for 85% of OVC, their caregivers, especially older people, and PLWHA in all 13 regions

Component 4: Impact mitigation services
Medium Plan III for HIV/AIDS 70
Activities to achieve the outcome
Suggested project Output Indicators
Implementing Partners
3. Finalisation and adoption of procedures to simplify access to grants (see 1.3 .2) in 2004
Legislation in place MOJ, MOHSS, MWACW NGOs, LAC
4. Improve access to all relevant social assistance grants by streamlining the process, reducing the complexity and reducing inter-regional disparities according to the Poverty Alleviation Strategy of 2002 (see also 1.3.2) starting in 2004
# of recipients of grants MoHSS, MWACW, MOJ
5. Orient the distribution of social workers and establish the use of para-professional to ensure better coverage by social grant programmes starting in 2005
MWACW MoHSS NGOs
6. Compile and disseminate information to caregivers and the public on how to access social grants, benefits and other statutory services for OVC and PLWHA, including exemption from school fund, examination fees and health services by 2005
# of OVC accessing services through the exemption policies and # of grants provided
MoHSS, MWACW MBESC, MIB, ALU, CAA
7. Develop alternative methods for covering school development fund through both community initiatives and government and private sector contributions in 2004
# of schools receiving external support to cover OVC costs.
MBESC, MWACW, NGOs
8. Establish and strengthen counselling and care services in all educational institutions starting in 2004 and on-going
# of voluntary school counsellors trained
MBESC, MHETEC, NGOS
9. Target preventative child health care services for young children in the care of the elderly (particularly 0-3 year olds) and strengthen growth monitoring to identify children who are not thriving
# of elderly carers reached
MoHSS Church health services, NGOs
10. Expand support to community early childhood education centres catering for OVC and raise the awareness in communities on the importance of early childhood education for all infected and affected children
# of centres catering for OVC and receiving material support
MWACW Nat. ECD Association, NGOs
11. Conduct training of peer educators and paralegals to render advice on the rights of OVC and their caregivers
(see 1.4.2)
# of educators trained/year
LAC, NGOs
12. Training of justice officials, social workers and educators concerning processing of grants and inheritance (see 1.4.2)
# of officials trained MWACW, MoJ, LAC, MBESC, Colleges of Education
13. Develop, up-date, maintain and share national database on OVC
Data base in place MWACW NGOs, NPCS
14. Ensure OVC have priority access to OVC-friendly hostels, food, prevention, care and health services
% of OVCs in hostels MBESC MOHSS
15. Ensure all school-going age OVC attend school and are not deterred from participation in formal education through school development fund or other material contributions requested by schools.
% of OVC of school going age attending school
MBESC, NGOs
16. Registration and adherence with guidelines of all institutional care facilities for OVC
% of institutions registered MoHSS, MWACW
17. Ensure that OVC obtain birth certificates and national identification documents and that all necessary documents (e.g. death certificates) are available to assist families affected by HIV/AIDS accessing assistance.
% of OVC obtaining necessary documents
MHA

Component 4: Impact mitigation services
Medium Plan III for HIV/AIDS 71
Sub-Component 4.3 Addressing poverty
4.3.1 Addressing poverty, food security, nutrition and housing
Activities to achieve the outcome
Suggested project output indicators
Implementing Partners
1. Identify OVC and households affected by HIV/AIDS in need of support (food aid and other specific services) by 2005 and update annually
Data base available OPM MoHSS MWACW
2. Establish and strengthen community-based self-help and income generating projects and skills training especially for child headed households, families with large numbers of OVC, particularly those headed by the elderly and other made vulnerable by HIV/AIDS
# of groups trained MWACW MAWRD, Red Cross, CCN, ELCAP, CAFO
3. Ensure that HIV/AIDS, STI and TB, and other contributing social problems such as violence and alcohol abuse are an integral component in all development projects (see 5. 2.4)
% of development projects with an HIV/AIDS component
NPCS, NANASO NANGOF MAWRD
4. Expand cash based labour intensive public works programmes to target members of families caring for OVC, especially youth headed households, and PLWHA
# of affected people receiving
MWTC MAWRD
5. Provide a feeding programme for OVC identified through the school counselling programme around school clusters
Cumulative # of children in feeding programme
MBESC, MWACW, NGOs
6. Provide material support such as shoes and school uniforms for OVC most in need and provide extremely needy households with OVC temporary food baskets
# of OVC receiving assistance
MWACW CAA, Red Cross, CCN, ELCAP, CAFO
7. Agricultural extension workers to ensure that families affected by HIV/AIDS (especially child headed households, families with large numbers of OVC, particularly those headed by the elderly) benefit from all relevant programmes such as improved seed dissemination and plant varieties, nutrition training, appropriate agricultural technology, intensifying labour saving activities in the production and processing of food, adequate and fertile land provision and irrigation structures
# of target families reached
MAWRD. EMU NGOs
8. Expand programmes in the small and micro enterprise sectors, which enable child headed households and families with large numbers of OVC to generate income
# of target families reached
MTI, JCC, MAWRD
9. Traditional authorities assist to eradicate inheritance and other cultural practices which increase the vulnerability of women and OVC, especially concerning wife inheritance, land rights and homes. (see 1.3.2)
# of women and children who lose the right to live in their homes
MRLGH AMICAALL ALAN
10. Realign national drought relief programme, emergency food assistance and food for work programmes so that PLWHA and families affected by HIV/AIDS (especially child headed households, families with large numbers of OVC, particularly those headed by the elderly) are prioritised
# of targeted families receiving such assistance
EMU MAWRD Regional Council
Outcome: 85% of those HIV/AIDS affected families in need receive support to address the depressed socio-economic conditions and the need for income, food security, nutrition and housing of OVC, PLWHA receive support

Component 4: Impact mitigation services
Medium Plan III for HIV/AIDS 72
Activities to achieve the outcome
Suggested project output indicators
Implementing Partners
11. Provide and/or mobilise social support to eligible TB patients • Food parcels for TB patients on medication especially
during DOTS; • Social assessment • Referral to organisations that work in the area of income
generating projects
Food parcels available at TB treatment sites # of TB patients referred for social assessments # of TB patients referred to income generating projects
Nat. TB Control Programme, NAMTA, NGOs
12. Expand social welfare services and the capacity of social workers to address poverty and other social issues by providing training in different dimensions of poverty reduction and addressing violence and substance abuse
# of social workers trained
MoHSS UNAM NGOs
13. Increase provision of vocational training, business training and other income generating services to HIV/AIDS affected families
# HIV/AIDS affected families trained
MHETEC/MTI, Private sector, UNAM, KAYEC

Component 5: Integrated and Coordinated Management
Medium Plan III for HIV/AIDS
73
The success of the rapidly expanded multi-sectoral response to fight HIV/AIDS, STIs and TB will depend on the effective and co-ordinated management of activities implemented by all levels of government and civil society. Every person in Namibia has a role and responsibility. The aim of this component is therefore to ensure that effective management structures and systems are put in place and supported, that optimal capacity and skills are built so that implementing partners can deliver high quality programmes at national, sectoral, regional and local levels.
The four sub-components reflect the focus for the next five years:
5.1: Developing HIV/AIDS Management Capacity 5.2: Management and Co-ordination 5.3: Programme monitoring and evaluation 5.4: Surveillance and research.
This chapter includes developing HIV/AIDS management capacity at all levels and within all sectors to respond to the rapidly growing impact of the epidemic. (Developing the technical capacity to expand prevention, treatment, care and support programmes is dealt with under components 2 and 3 respectively.) All institutions will have to plan for and implement an expansion of the number of skilled people delivering interventions, improved technical support and adequate supervision. The personnel compliment required for the expanded response must be well-planned and managed to also account for attrition from HIV/AIDS and TB mortality and reduced productivity from AIDS and TB absenteeism in every workforce. Minimum standards need to be set for quality training, service delivery and management practices. Best practices need to be identified, appraised, rewarded, monitored and replicated.
Strengthening Management and Co-ordination will ensure that the structures, systems, processes, tools and skills are in place for planning, managing and co-ordinating the response at all levels. The capacity of co-ordinating committees, such as sectoral steering committees and RACOCs, will be built so that they can identify gaps or duplication in provision, and respond appropriately.
MTP III will address the constraints of inadequate funding for community responses. Appropriate financing mechanisms will be strengthened for sectors and regions so that programme implementation takes place at the local level. Appropriate bodies will be trained in financial and contractual management. All organisations will be encouraged to mainstream HIV/AIDS, STIs and TB into the management of their core functions. It is critical that STIs and TB are included in mainstreaming, at all levels, as TB is a communicable disease and it is the first life-saving treatment for PLWHA; STIs are often the first gap for HIV infection. Institutional capacity will be built so that good management practices incorporate research, participatory planning, supervision, regular monitoring and reviews as normal practice.
Monitoring and Evaluation will be an essential element in managing the programme. Every organisation – from CBO, NGO, business enterprise and each government unit – needs to monitor its activities and know that they are achieving the desired results (outcomes) and having a positive impact in reducing the epidemic. Every organisation will need to take responsibility for monitoring the core indicators which are given in Chapter 4.
COMPONENT 5Integrated and co-ordinated Programme Management at all levels
Strategic result:Effective management structures and systems, optimal capacity and skills, and high qualityprogramme implementation at national, sectoral and regional levels

Component 5: Integrated and Coordinated Management
Medium Plan III for HIV/AIDS
74
An overarching framework will be established for surveillance and research which will strengthen the co-ordination of research on HIV/AIDS and related issues. The MoHSS will ensure that the HIV/AIDS sero-sentinel surveys will continue and be expanded as the need arises. The monitoring of behavioural change will be strengthened through behavioural sentinel surveys in the form of second generation surveillance and rapid knowledge, attitudes and practices (KAP) studies. Contextual research including impact studies, law and policies, and issues of human rights will be conducted. A database will be developed whereby all research activities and their coverage will be captured. This will be added to the main HIV/AIDS database and website.
The Health Information System will be strengthened so that the prevalence of HIV/AIDS, STIs, TB and other opportunistic diseases can be closely monitored. Epidemiology reporting will be annual. As treatment is rolled out, greater understanding will be gained through bio-medical and operational research.
Within the next 5 years, we plan to achieve the following outcomes and strategic result:
• A national human resource plan in place by 2005, detailing the adequate number of posts required for HIV/AIDS and TB management and response implementation in all sectors
• Programme implementing staff, volunteers and management in all organisations are trained and supported to effectively handle their role
• Effective, efficient and accountable institutional structures and processes in place at national, regional & local levels by 2004 with increased capacity to effectively plan, co-ordinate and manage the implementation of quality interventions of the multi-sectoral response for HIV/AIDS from 2005 onwards
• Systematic mainstreaming of HIV/AIDS, STIs and TB in all sectors and all organisations, with dedicated staff, and budgeted plans for the incorporation of HIV/AIDS, STIs and TB in the workplace and its core functions by 2005
• Effective monitoring, surveillance and research which enables programme implementers and managers to measure their progress towards targets in place by 2004
These, together, will achieve the strategic result that effective management structures and systems, optimal capacity and skills, and high quality programme implementation at national, sectoral, regional and local levels are in place. Parts may take more than 5 years to achieve at all levels but that is the long term aim of this component.
As improved management contributes to the outcomes of all other components, it will contribute to the national goals of:
Reduced vulnerability of people to and reduced transmission of HIV and other STIs;
Decreased STI, HIV/AIDS and TB morbidity and AIDS and TB mortality;
Mitigation against the social and economic impacts of HIV and AIDS on infected individuals and affected families and communities and
• Increased quality of life of PLWHAs and those affected by HIV/AIDS.

Component 5: Integrated and Coordinated Management
Medium Plan III for HIV/AIDS
75
Sub-component 5.1 Developing HIV/AIDS Management Capacity
5.1.1 Human Resource Planning
Activities to achieve the outcome
Suggested project Output Indicators
Implementing Partners
1. Compile periodic reports on a) staff losses through deaths, resignation, promotion, studies; b) absenteeism, sick leave c) Requests for transfers due to disability;
# of desk top analyses of workforce # of institutions conducting voluntary prevalence testing
Personnel Officers in all sectors OPM
2. Assess the human resource requirements to carry out MTP III implementation plans and detail prioritised training needs of all sectors, MoHSS, from 2004 onwards
# of training assessments of Key Actors received by the MoHSS, annually
MoHSS All Key Actors
3. The impact of HIV/AIDS on human resources to be factored into the long, medium and short-term human resource plans by 2005 (see 2.4.2 and 5.1.2)
# of sectors with strategic human resource plans
All Ministries Private, NGO, FBO sectors
4. Establish strategies for the public sector to address the loss of productivity, (such as relief teachers, ensuring access to ARV treatment for critical service providers and exploring ways to extend service delivery capacity to volunteers)
Strategies in place OPM, MoJ, Attorney General’s Office, MBESC
5. Strengthen capacity for HIV/AIDS and TB programme support within each ministry and establish a career path structure by 2005
# of HIV/AIDS/TB/STI posts established, by ministry, by region
OPM All ministries
6. Quantify resources required and budget accordingly to implement human resource plans
# of sectors with financing plans for HR planning
All Ministries Private, NGO, FBO sectors
5.1.2 Human Resource Development
Activities to achieve the outcome
Suggested project Output
Indicators Implementing Partners
1. Mobilise the National Human Resource Planning Task Force, under the responsibility of NPCS, to revise the National HR Plan to include HIV/AIDS, to implement and monitor the planning process, from 2004 on-going
Quarterly monitoring reports produced
NPCS, MHETEC, OPM and MoHSS
2. Establish the Training Support Co--ordination Unit (TSC Unit), within MoHSS, to co-ordinate HIV/AIDS, STI, TB and Malaria training of all stakeholders nationally
# & types of training co-ordinated
MoHSS
3. Map existing training infrastructure, capacity & potential nationwide in 2004
Up-to-date inventory of trainers and training institutions available
MHETEC / MoHSS Training Providers
Outcome: To have created a training capacity for the multi-sectoral HIV/AIDS, TB and STI responses by 2007 and ensured that the technical support required is built by 2009
Outcome: Ensure that the personnel required for an expanded response is well planned and managed to also account for attrition and absenteeism by 2007

Component 5: Integrated and Coordinated Management
Medium Plan III for HIV/AIDS
76
Activities to achieve the outcome
Suggested project Output Indicators
Implementing Partners
4. Assess and monitor training gaps in the national provision from 2004
# of new HIV/AIDS/TB related courses available
TACs, TSC Unit, MoHSS
5. Provide a range of choice of training opportunities in the level, type and length of courses to provide the required MTP III implementation skills as well as skills to perform core functions
# of training places available, by institution, type of course # of people trained, by skill type, level
MHETEC Training Providers, All sectors
6. Promote the provision of mentorship & on-the-job training by training providers, from 2004 onwards
# of trainees receiving practical follow-up after training
Training Providers All sectors
7. Conduct TOT training to promote the mainstreaming of TB and STIs in HIV/AIDS human resource development in all organisations
% of organisations with HRD departments mainstreaming TB, STIs and HIV/AIDS
MoHSS, All sectors All organisations
8. Award performance-based contracts to NGOs, private sector & parastatals to provide agreed numbers of qualified graduates to meet MTP III implementation needs, from 2004 onwards
# of people trained using performance-based contracts
MoHSS MHETEC
9. Support integration of HIV/AIDS, TB and STIs in pre- & in-service training curricula in all tertiary education courses in 2004
% of all tertiary courses with HIV/AIDS/TB in the curriculum
MHETEC, MoHSS, All training institutions
10. Co-ordinate and regularly disseminate all training opportunities required by the national response, available in Namibia and regionally1 from 2004
# of brochures disseminated # of people applying for training
TSC Unit, MoHSS All Training Providers
11. Design mechanisms to financially contribute to the provision of HIV/AIDS related training and bursaries for trainees, in 2004
# of N$ spent on HRD training subsidies # of graduates assisted
MHETEC / MoHSS
12. Strengthen Technical Advisory Committees (TACs) and Standing Committees to co-ordinate technical input to sectors and partners and monitor performance, from 2004 onwards
# of meetings of each TAC annually
MoHSS All sectors
13. Provide technical support for programme development and national training in all components of MTP III, from 2004 onwards
# days of technical assistance provided # of technical specialist support visits provided by the MoHSS Directorate: Special Programmes annually, by type, by region
MoHSS, Training & Development Partners, All sectors
14. Address challenge of incentives for volunteers e.g. peer educators and HBC volunteers
# of volunteers receiving incentives (by type e.g. material, skills training, cash)
MoHSS, NGOs
1 The Training Co-ordination subcommittee will assist with the identification of training and capacity-building needs until such time as the Training Support Co-ordination Unit is operationalised.

Component 5: Integrated and Coordinated Management
Medium Plan III for HIV/AIDS
77
5.1.3: Quality Assurance
Activities to achieve the outcome
Suggested project Output
Indicators Implementing Partners
1. Accredit courses on HIV/AIDS related issues e.g. home based care, Psycho-social support, HIV/AIDS programme management
# of new courses accredited TSC Unit, MoHSS NQA, UNAM, PON, NIED
2. Establish basic course competencies and outcomes (minimum standards) for all courses on HIV/AIDS and TB issues and award performance-related certificates, from 2005 onwards
# of training providers issuing performance-related certificates
Training Support Co-ordination Unit, MoHSS, All Training Providers
3. Establish & monitor the implementation of minimum standard guidelines for VCT, PMTCT+, TB control, HBC, social mobilisation and communication, HAART, workplace & OVC etc
# of minimum standard guidelines (e.g. VCT, PMTCT+, TB Control, HBC, social mobilisation and communication, HAART, workplace & OVC) developed # partners using guidelines
TSC Unit, MoHSS, All partners, UNAM, Polytechnic
4. Establish nation-wide system for identifying best practices and give rewards to their implementers (certificates, incentives, rewards, promotion and publicity)
# of rewards established and awarded
TSC Unit, MoHSS Key Actors, RACOCs, NGOs
5.1.4 Institutional Capacity Development of NGO Service Providers
Activities to achieve the outcome
Suggested project Output
Indicators Implementing Partners
1. Train managers and senior staff in programme management
# of managers trained MoHSS, Training providers
2. Train managers and senior staff to effectively utilise and manage funds and to foster co-operation with national and international development partners
# of managers trained in financial management
Training providers
3. Build institutional capacity of service providers’ umbrella bodies to assist and support members
# of training sessions carried out by umbrella bodies
Training providers
4. Organise seminars involving both sectoral steering committees, established service providers and small organisations, at regional level, for support through technical and skills transfer
# of small organisations receiving support
Training providers
5. Train decision-makers, staff and volunteers on their roles of responsibilities
# number of people trained on their roles and responsibilities
Training providers
6. Expand the provision of Internet Computer Training, such as training modules available on CD ROM & the MoHSS Directorate: Special Programmes website, to expand coverage and access to quality training in technical and managerial skills
# of computer-based training courses available
MHETEC / MoHSS / Training providers
Outcome: Quality assurance systems in place and monitored to ensure that minimum standards are adhered to by 2007
Outcome: Financial and management capacity of 85% of institutions delivering HIV.AIDS, STI & TB programmes is strengthened by 2009

Component 5: Integrated and Coordinated Management
Medium Plan III for HIV/AIDS
78
Sub-component 5.2 Management and co-ordination
5.2.1: Management Structures
Activities to achieve the outcome
Suggested project Output
Indicators Implementing Partners
1. Strengthen existing multisectoral HIV/AIDS management / co-ordination committees to lead the response, at national level
# of regular minuted national, regional and sectoral management meetings with evidence of follow up
MoHSS, All Ministries Regional Councils, NGOs, FBOs, Private Sector
2. Expand existing and establish new Sectoral Steering Committees to strengthen the response within each sector
Sectoral Steering Committees, involving Key Actors in civil society in place
Lead Agencies in all Sectors
3. Strengthen RACOCs to fulfil their terms of reference (see Chapter 2)
# RACOCs co-ordinating & monitoring implementation
MoHSS, MRLGH
4. Establish sub-regional committees at district and/or constituency levels to lead the local response
# of functioning district & constituency AIDS co-ordinating committees (DACOCs & CACOCs) in place
RACOCs Local communities
5. Establish an HIV/AIDS committee within every institution to manage its response
% of Key Actors per sector, with HIV/AIDS committees in place
All organisations
6. Provide effective secretariat support and resources to enable structures to function
# of committees with effective secretariat
All organisations
5.2.2: Resource mobilisation and flow mechanisms
Activities to achieve the outcome
Suggested project Output
Indicators Implementing Partners
1. Mobilise resources through adequate GRN budgeting, successful proposals to development partners and from civil society
# of N$ available for HIV/AIDS programmes in Namibia
% of spending used per outcomes
MoF, NPCS, OPM, MRLGH, MoHSS, All Ministries, Regional Councils; LAs, NGOs, FBOs, Private Sector
2. Strengthen mechanisms and build capacity of GRN for donor co-ordination and feedback to the different sectors and partners
# of discussions between GRN and donor partners
NPCS, MoF, MoHSS
3. Build capacity of RACOCs, NGOs, FBOs and CBOs to plan and cost annual workplans to incorporate into funding proposals for small and medium sized projects
# of successful funding applications
MRLGH, MoHSS
Outcome: The budgeted comprehensive HIV/AIDS plans of the 3 national, 13 regional, 26 sectoral and 96 constituency management structures are resourced by 2005 onwards
Outcome: 100% of 3 national, 13 regional, 26 sectoral and 96 constituency management structures have a budgeted comprehensive HIV/AIDS plan which they monitor and review annually

Component 5: Integrated and Coordinated Management
Medium Plan III for HIV/AIDS
79
4. Build capacity of RACOCs & local authorities to scrutinise proposals, disburse funds and monitor progress
# of local funding agents in place (Reg. Councils & LAs)
MRLGH, MoHSS
5. Establish effective mechanisms for financial disbursement to support regional/local responses, its management, reporting and evaluation
# of constituencies, local authorities & communities that have accessed outside financial resources, delivered local responses and successfully completed reports
MRLGH, MoHSS
5.2.3 Information Flows
Activities to achieve the outcome
Suggested project Output Indicators
Implementing Partners
1. Supply community and school libraries under the MBSEC with HIV/AIDS materials from a central HIV/AIDS resource centre
# of resources loaned out per year
MBESC, MIB,
2. Create and update annually, website and database of national & local activities, service providers, and monitoring data on progress of MTP III
Database of national and local activities developed and updated annually
MoHSS
3. Develop methods to share best practice, e.g. organise information-sharing sessions, workshops at regional and national levels, and electronic networks
Evidence of best practice dissemination and uptake
MIB, Key Actors
4. Organise national conferences for all Key Actors to review progress and make recommendations
# of national conferences MoHSS/ NAMACOC, MIB
5. Organise study tours for peer review # of study tours MoHSS
6. Facilitate development of horizontal & vertical communication and networking systems
Evidence of widespread knowledge of policies, strategies, structures, guidelines and plans.
MoHSS Lead Agencies
Outcome: Readily accessible, up-to-date information is available, regularly disseminated to all stakeholders and used for policy development and planning.

Component 5: Integrated and Coordinated Management
Medium Plan III for HIV/AIDS
80
5.2.4 Mainstreaming2
Activities to achieve the outcome
Suggested project Output Indicators
Implementing Partners
1. Lead the process of mainstreaming in the public sector from 2004 onwards
# of ministries & parastatals with workplace programmes
OPM, NPCS
2. Develop practical, sector/programme-specific guidelines for planning and budgeting HIV/AIDS related issues and activities.
# of sectoral implementation guidelines disseminated
MoHSS Directorate: Special Services, MoF, NPCS
3. Sensitise top & middle management # of PS regularly attending MoHSS Directorate: Special Services committees # management staff trained
OPM, MoHSS, NPCS
4. Develop capacity of sectoral HIV/AIDS focal points to strengthen response at national and regional levels, involving PLWHA
Evidence of increased capacity MoHSS: Special Programmes
5. Facilitate lead agencies and key actors to conduct rapid risk and impact assessments to understand how AIDS is affecting their core functions and their target groups
# of impact assessments conducted and disseminated # of workplace plans with impact mitigation strategies
NPCS Sectoral Lead Agencies Key Actors
6. Systematically include HIV/AIDS, STI &TB in all sectoral and programme analyses, strategies and plans in all organisations – ministries, parastatals, private, NGO, FBO and SME sector
# of organisations implementing mainstreaming
All organisations
7. Develop supportive human resource management policies (see 5.1.1)
# of Key Actors with human resource plans in place, by sector
All organisations
8. Facilitate establishment of supportive workplace programmes and treatment regimes (see 2.4.2)
% of large enterprises/ companies/ministries that have workplace policies & programmes # of workers on treatment
All organisations
2 Incorporating the implications of HIV/AIDS into normal everyday considerations and actions of an organisation is
called mainstreaming. Mainstreaming of HIV/AIDS has two aspects to consider – how HIV/AIDS is affecting the core functions of an organisation and how HIV/AIDS is affecting the organisation itself. Every organisation needs to understand how, in its ordinary work, it can reduce the risk of infection and the impact of AIDS. It needs to incorporate its response into core function plans and internally through adequate HRD and workplace programmes.
Outcome: Systematic mainstreaming of HIV/AIDS, STIs and TB in all sectors and all organisations, with dedicated staff, and budgeted plans for the incorporation of HIV/AIDS and TB into core functions by 2005

Component 5: Integrated and Coordinated Management
Medium Plan III for HIV/AIDS
81
5.2.5 Management Processes
Activities to achieve the outcome
Suggested project Output
Indicators Implementing Partners
1. Inform senior management on the impact of HIV/AIDS on core functions and within the organisation (see 5.2.4)
% of Management knowledgeable about the impact of HIV/AIDS
HR and development planners within all partners
2. Develop action plans and budget for HIV/AIDS, STI and TB activities on annual basis
# of budgeted action plans in place
NAMACOC, All Partners
3. Hold regular, inclusive meetings to review progress towards the organisation’s outputs, using appropriate indicators. (see 5.3.1)
# of review meetings held,(by key actor, by sector)
All Implementing partners
4. Adjust work plans and resource allocation to build on successes and to address constraints
Evidence of rolling plans All Implementing partners
5. Hold annual reviews, involving PLWHA to assess change towards short-term outcomes and to revise plans and budgets for long-term plans.
# of annual reviews held to revise work plans
NAMACOC All Implementing partners
Sub-component 5.3: Programme monitoring and evaluation 5.3.1 Monitoring and Evaluation
Activities to achieve the outcome
Suggested project Output Indicators
Implementing Partners
1. Develop an overall M & E co-ordination plan for all sectors
M&E plan in place by 2004 MoHSS
2. Disseminate monitoring handbook to all implementing partners in 2004
% of implementers with M&E handbook accessible
MoHSS
3. Train and mentor implementing partners in the collection, verification and validation of data by 2005
% of organisations that have submitted MoHSS Directorate: Special Services Activity Reports on time/yr
MoHSS
4. Train and mentor implementing partners in results based monitoring with regular reviews and adjustments to implementation plans
# of partners trained and mentored in RBM monitoring # of reviews
MoHSS
5. Improve quality of reporting between key actors, lead agencies & co-ordinating bodies
Level of satisfaction with written reports received and feedback given
All Key Actors
6. Strengthen a standardised reporting system to HIS, MoHSS from public, private and NGO health facilities
% of public, private, NGO & FBO health facilities using the standardised reporting system
MOHSS, private health care institutions, NGOs
Outcome: 100% of implementing partners report on all the required indicators to their co-ordinating body and MoHSS Directorate: Special Programmes
Outcome: 95% of all implementing partners use the project management cycle

Component 5: Integrated and Coordinated Management
Medium Plan III for HIV/AIDS
82
7. Disseminate annual publication, the National HIV/AIDS M&E Report by MoHSS Directorate: Special Programmes from 2005 onwards
M&E report available MoHSS
8. Hold regular review meetings to monitor progress reports from staff and all implementing partners, 2004 onwards
# of performance review & planning meetings held
NAEC, All implementing partners
9. Conduct a participatory mid term review of MTP III during 2007
MTR report produced # & types of outcomes
MoHSS All implementing partners
Sub- component 5.4 Surveillance and operational research
5.4.1 Multi-sectoral HIV/AIDS research co-ordination
Activities to achieve the outcome Suggested project Output Indicators
Implementing Partners
1. Strengthen the existing national research co-ordination body to co-ordinate multi-sectoral HIV/AIDS, STI & TB research
# of meetings per year
# of participating institutions/departments
NPCS, MHETEC, MoHSS, UNAM, Polytechnic, NEPRU, IPPR, Institute for Public Health Research, UNAM, SIAPAC, NGOs, private sector
2. Establish an overarching framework and policy to co-ordinate research activities, with a prioritised national research agenda, including socio-economic issues that contribute to the spread of HIV/AIDS, STI and TB
Framework, policy & agenda disseminated
NPCS, OPM, MoHSS, UNAM, NEPRU, SIAPAC All sectors & main implementing partners
3. Incorporate HIV/AIDS research into existing research policies
HIV/AIDS Research policy in place
MHETEC, MoHSS
4. Identify contextual, operational and bio-medical research priority areas3
List of research priority areas available in each sector
MHETEC, NPCS, MoHSS, other sectors
5. Create and update a national database of HIV/AIDS, STIs & TB research (see 5.4.1)
# of hits on MoHSS Directorate: Special Services website accessible to stakeholders
UNAM, MOHSS, NEPRU, SIAPAC HIV focal person from each sector
6. Strengthen the research unit within MoHSS, and other key organisations, including the capacity to write research proposals for funding (see also 5.1.1)
Available budget for research
Staff competencies within Unit
MoHSS, UNAM, Polytechnic
3 Research identified during the MTP III process is listed in Appendix 3
Outcome: HIV/AIDS surveillance and research is co-ordinated and implemented, based on national priorities

Component 5: Integrated and Coordinated Management
Medium Plan III for HIV/AIDS
83
5.4.2 Surveillance and research
Activity to achieve the outcomes
Suggested project output indicators
Implementing Partners
1. Conduct and expand national sero-surveillance on a biennial basis
# of surveys # of sentinel sites
MoHSS
2. Continue conducting Demographic Health Survey (DHS) every five years and add questions for new indicators
DHS reports MoHSS, private health care institutions, NGO institutions
3. Conduct national behavioural surveys and second generation (behavioural surveillance) survey bi-annually
# of population-based surveillance studies # of studies on risk behaviour, types of risk behaviour and risks associated with such behaviours, particularly among the youth.
MoHSS, NPCS, private health care institutions, NGO institutions, academics
4. Continue compiling HIV/AIDS/STI/TB epidemiological report bi-annually
# of epidemiological studies on the rate and extent of HIV infection and monitoring the course of the epidemic
MoHSS, private health care institutions, NGO institutions
5. Conduct research in priority areas Number of research reports per sector as per priority areas
NPCs, MoHSS
Outcome: Surveillance and research on STI, TB and HIV/AIDS issues are conducted according to scheduled monitoring and research plans

Chapter IV: Monitoring and Evaluation
Medium Plan III for HIV/AIDS
85
4.1 Monitoring and evaluation at national, regional and local level
The MTP III presents an expanded national response to the HIV/AIDS epidemic in Namibia. Its implementation will involve many implementing agencies. The GRN and several development partners will commit an increased amount of resources to its operationalisation. It is important that such resources bring about positive returns through achievement of the strategic results and outcomes outlined in this plan. In a critical area of public health and national development such as HIV/AIDS, it is even more imperative to demonstrate the effectiveness of programmes not only at the national level, but also at regional and local levels since the well-being of Namibia is at stake.
The complexity of the institutional arrangements outlined in the plan requires multi-level approaches to the monitoring and evaluation of programmes and activities. At the same time, the approaches will facilitate inter- and intra-level monitoring and evaluation particularly for cross-cutting issues such as policy, resource mobilisation and utilisation, programme design and implementation.
The GRN through the National AIDS Committee (NAC) will monitor the overall effectiveness of MTP III’s strategies. It will monitor processes of resource mobilisation, allocation and utilisation in the public sector. It will further monitor the extent to which its decentralised management and administrative structures facilitate HIV/AIDS prevention and mitigation efforts and the integration of HIV/AIDS within the public sector machinery at national and regional council levels.
NACOP will monitor stakeholder programme design and implementation at all levels through active participation and on-going co-ordination of stakeholder activities. It will collaborate with the stakeholders and implementing partners to develop an overall M & E co-ordination plan. This national M & E co-ordination plan will define each M & E data source for the core indicators of MTP III and specify how and how often data will flow from each component, level and source to a central repository at MoHSS Directorate: Special Programmes. It will include a flow chart depicting data flows. The Directorate will include a flow chart depicting data flows. NACOP will develop a number of information products based on data received and disseminate these information products to all relevant stakeholders to keep them appraised of progress with regard to the implementation of the Medium Term Plan 3. A monitoring handbook for MTP III implementing partners and the Global Fund recipients will be produced separately from this plan.
As part of the management process, annual reviews will be scheduled and adjustments to plans and targets will have to be justified. A mid term review of MTP III will take place in 2007 so targets have been set for 2007 and 2009 for each of the core indicators to assist the evaluation process.
Chapter IV Monitoring and evaluation

Chapter IV Monitoring and Evaluation
Medium Plan III for HIV/AIDS 86
4.2 Core Impact and Outcome Indicators with targets for MTP III
Impact Assessment
GOAL Ref No.
Impact Indicator Baseline
2004
Short Term Targets
Early 2007
Medium term Targets
20091
Responsible Agency
Reduced incidence of HIV infection to below epidemic threshold (1%)
1 HIV prevalence among pregnant women [by age group 13-19, 20-24, and 25-29), and residence] *2
13-19 age group 20-24 age group 25-29 age group 30-34 age group 35-39 age group 40-44 age group 45+ age group
11%3 22% 28% 27% 21% 16% 12%
9% 15% 21% 20% 16% 14% 10%
7% 12% 18% 17% 14% 12% 9%
NAC, GRN, NGOs, FBOs, Private Sector, Development partners
Outcomes Assessment
Component 1: Enabling Environment
Programme Sub Components, and
Outcomes
Ref. no.
Outcome Indicators Baseline
2004
Short Term Targets
Early 2007
Medium term Targets
2009
Responsible Agency
Sub Component 1.1 Capacity development of Leadership
Outcome 1.1.1 Sustained Leadership Commitment
2 3
The amount of national funds spent by the GRN on HIV/AIDS annually * 4 GRN Development Budget (N$’000): Operational expenditure ceiling MoHSS, (N$’000) % of attendance of designated leaders at national and regional HIV/AIDS coordination meetings
73,814 1,575,131
71%
50,000 1,680,956 (2005-06)
80%
- -
90%
NAC, GRN, NGOs, FBOs, Private Sector, Development partners
1 Targets are cumulative figures, unless stipulated 2 * UNGASS Indicator 3 MoHSS 2002 HIV Sentinel Survey 4 Medium Term Expenditure Framework (2003/04 - 2005/06)

Chapter IV Monitoring and Evaluation
Medium Plan III for HIV/AIDS 87
Programme Sub Components, and
Outcomes
Ref. no.
Outcome Indicators Baseline
2004
Short Term Targets
Early 2007
Medium term Targets
2009
Responsible Agency
Sub-Component 1.2 Greater Involvement of PLWHA
Outcome 1.2.1 Greater involvement of PLWHA and vulnerable populations
4 5
# of PLWHAs provided with advocacy and communication skills training % of coordination meetings (all levels) which include PLWHA
- -
50
60%
50
100%
Lironga Eparu, PLWHA networks, MoHSS, NGOs
Sub-Component 1.3 Policy and Law Reform
Outcome 1.3.1 National policy development and law reform
6
National Composite Policy Index
12/20
16/20
20/20
MoHSS Directorate: Special Programmes, MoJ, ALU
Outcome 1.3.2 Sectoral and Institutional Policies
7 % of large enterprises/ companies (including line ministries) that have HIV/AIDS workplace policies *5
Less than 10%
80% 26 sectors
with policies
100% 26 sectors implement
policies
All Ministries, Private sector, Civil society
Sub-Component 1.4 Intervention to reduce Stigma and Discrimination Outcome 1.4.1 Social mobilisation to combat discrimination
8 % of population expressing accepting attitudes towards PLWHAs by gender, residence and level of education
- 75% 100% MoHSS, MIB, Lironga Eparu
Outcome 1.4.2 Actions to address stigma & discrimination
9 % of people knowing where to go for legal assistance or counselling regarding stigma and discrimination (DHS)
- 30% 80% All Ministries, MoJ, ALU
5 * UNGASS indicator

Chapter IV Monitoring and Evaluation
Medium Plan III for HIV/AIDS 88
Component 2: Prevention
Programme Sub Components, and
Outcomes
Ref. no.
Outcome Indicators Baseline
2004
Short Term Targets
Early 2007
Medium term Targets
2009
Responsible Agency
Sub Component 2.1: Strengthen capacity to deliver HIV/AIDS prevention programmes
Outcome 2.1.1 Capacity Development: Prevention
10
% of schools with teachers who have been trained in life-skills-based HIV/AIDS education and taught it during the last curriculum year by type of school (primary/secondary) * 6
N.B. The outcome of good other capacity building will be reflected in improved prevention services below
-
50%
75%
MoHSS MIB
MBESC
Sub-component 2.2: Target Vulnerable Populations
Outcome 2.2.1 Targeted BCI for vulnerable populations
11 % of people reporting the consistent use of a condom during sexual intercourse with a non-regular sexual partner by gender, residence & age (15-19, 20-24, 25-29)* women 25-29 age group 7
women 30-39 age group women 40-49 age group
34%8 19% 9%
45% 25% 15%
55% 32% 20%
MIB, MoHSS, MPCS, MWACW,
All Key Actors
Outcome 2.2.2 Prevention of transmission in health care settings
12
% of health care facilities that apply national standards for infection prevention
-
80%
100%
MoHSS Tertiary Care
Sub-component 2.3: Target BCI at Young People
Outcome 2.3.1 Target BCI in schools
13 # of young people taught life-skill-based HIV/AIDS education in past 12 months by type of school and gender
100,000 400,000 500,000 MBESC NGOs
6 * UNGASS Indicator 7 Under 24s are monitored in section 2.2.3 above 8 DHS 2000, p177 % of women who have had sexual intercourse in the past year who used a condom during last sexual intercourse with any partner.

Chapter IV Monitoring and Evaluation
Medium Plan III for HIV/AIDS 89
Programme Sub Components, and
Outcomes
Ref. no.
Outcome Indicators Baseline
2004
Short Term Targets
Early 2007
Medium term Targets
2009
Responsible Agency
Outcome 2.3.2 BCI for Youth
14 15 16
% of young people aged 15-24 who both correctly identify ways of preventing the sexual transmission of HIV and who reject major misconceptions about HIV transmission by gender & residence *9 % of people reporting the consistent use of a condom during sexual intercourse with a non-regular sexual partner by gender, residence & age 5-24 *
women 15-19 age group women 20-24 age group
Median age at first sex among 20-24 year-olds by gender & residence
men 20-24 age group: women 20-24 age group:
+-86% (2000)
48.5%10 38%
16.7 18.2
95%
60% 50%
17.5 19
99%
80% 60%
19 20
MHETEC Dir. Adult
Education, Further Education Institutions, NGOs
Sub-component 2.4: Target the General Population Outcome 2.4.1 Social Mobilisation and Awareness
17
% of sexually active respondents who had sex with a non-regular partner within the previous 12 months by gender11
19%
17%
15%
MIB All Key Actors
Outcome 2.4.2 Workplace programmes
18 19
% of large enterprises/companies (incl line ministries) that have HIV/AIDS workplace programmes * # of employees in all sectors that have been reached by work place programmes
# 36 -
80%
60,000 public 20,000private
90%
90,000 public 35,000 private
OPM MoHSS, NABCOA
9 * UNGASS Indicator 10 DHS 2000, p177 % of women who have had sexual intercourse in the past year who used a condom during last sexual intercourse with any partner. 11 DHS 2000 p174

Chapter IV Monitoring and Evaluation
Medium Plan III for HIV/AIDS 90
Programme Sub Components, and
Outcomes
Ref. no.
Outcome Indicators Baseline
2004
Short Term Targets
Early 2007
Medium term Targets
2009
Responsible Agency
Outcome 2.4.3 Expand condom provision
20 21 22
# of male and female condoms distributed through social marketing annually # of male and female condoms distributed free through public sector (annually) % of people reporting the consistent use of a condom during sexual intercourse with a non-regular sexual partner by gender, residence & age (15-19, 20-24, 25-29)* women 25-29 age group 12
women 30-39 age group women 40-49 age group
3,780,000
15,000,000 (2001)
34%13 19% 9%
4,500,000
40,500,000
45% 25% 15%
5,105,800 -
55% 32% 20%
MoHSS NaSoMa, SMA, All Key Actors:
NGOs, All Ministries,
Private Sector
Outcome 2.4.4 Strengthen STI management
23
% of patients with STIs at health care facilities who have been diagnosed, treated, and counselled according to national management guidelines * 14
-
75%
95%
MoHSS
Directorate: Special
Programmes, SHPA
Outcome 2.4.5 VCT
24 25
# of health facilities that apply national standards for voluntary counselling & testing * # of clients tested for HIV and receiving their sero-status results by region, gender and age group per annum
6
9900
13 28,000
45 30,800
MoHSS Church-based
Health Services, NGOs, Private
Sector Outcome 2.4.6 Safety of blood transfusion products
26 # and % of health facilities (hospitals & private clinics) that apply national guidelines for storage, distribution, & transfusions
39/3915
100%
100%
MoHSS Blood Transfusion
Service
Sub-component 2.5: Interventions to reduce vulnerability Outcome 2.5.1 Addressing vulnerability
27 # and types of interventions by region
13
26
52
MWACW, NGOs, Traditional and
Local Authorities,
12
Under 24s are monitored in section 2.2.3 above 13 DHS 2000, p177 % of women who have had sexual intercourse in the past year who used a condom during last sexual intercourse with any partner. 14 * UNGASS Indicator 15 20 NIP laboratories, BTS in Oshakati, 9 private clinics, 5 hospitals in Windhoek, 4 other hospitals nationwide.

Chapter IV Monitoring and Evaluation
Medium Plan III for HIV/AIDS 91
Component 3: Equal Access to Treatment, Care and Support Services
Programme Sub Components, and
Outcomes
Ref. No.
Outcome Indicators Baseline
2004
Short Term Targets
Early 2007
Medium term Targets
2009
Responsible Agency
Sub Component 3.1: Capacity Development for the expanded treatment, care and support response
Outcome 3.1.1 Capacity development of treatment, care and support service providers
28 29 30
# of service providers trained per district to implement, monitor & supervise comprehensive case management including HAART (includes clinicians, nurses, pharmacists, technologists & counsellors) # of home based care providers trained to provide training & support to family members on HAART # of community volunteers/members/ caregivers trained in providing care and support to orphans and other vulnerable children by region N.B A considerable range of training is planned the outcomes of which will be reflected in improved treatment, care and services below
150
2500
1,500
325
6,600
4,600
900
8,000
6,000
MoHSS Church- based Health Services, NGOs, Private
Sector
Outcome 3.1.2 Promoting treatment literacy
31 % of 15-49 year age group have correct knowledge of the principal services and key therapies available for treatment, care and support
- 40% 60% MoHSS Church- based Health Services, NGOs, Private
Sector Sub Component 3.2: Treatment and Care Services Outcome 3.2.1 Laboratory Services
32
# of testing sites by region rapid tests HIV Elisa tests CD4 laboratories Viral load Hepatitis B
0 7 2 1 2
13 10 4 2 3
45 12 4 2 3
NIP MoHSS

Chapter IV Monitoring and Evaluation
Medium Plan III for HIV/AIDS 92
Programme Sub Components, and
Outcomes
Ref. No.
Outcome Indicators Baseline
2004
Short Term Targets
Early 2007
Medium term Targets
2009
Responsible Agency
Outcome 3.2.2 Drugs and Supplies
33 34
# and % of health facilities with drugs for OIs in stock and no stock outs of >1 week in last 12 months by district % of health facilities where ARV services are being offered with no ARV drug stock outs of >1 week in last 12 months
- -
98%
98%
100%
100%
MoHSS, Church- based Health Services,
Outcome : 3.2.3 PMTCT + Services
35 36
% of HIV-infected infants born to HIV-infected mothers *16 % of HIV+ pregnant women receiving a complete course of ARV prophylaxis to prevent vertical transmission *
30%
6/45
20%
13/45
15%
100%
MoHSS Church- based Health Services,
Outcome 3.2.4 Management of Opportunistic Infections
37
% of health facilities that provide treatment for opportunistic infections according to guidelines
-
70%
90%
MoHSS Church- based Health Services,
Outcome 3.2.5 Collaborative TB/HIV/AIDS services
38 39 40
% of TB patients tested for HIV and counselled each year TB treatment success rate # of TB patients on HAART
< 5%
69%
100
50%
75%
1,500
90%
85%
3,500
MoHSS Church- based
Health Services,, NGOs
Outcome 3.2.6 HAART Provision
41 42
# of people receiving HAART by gender (adult, child) * # of facilities providing HAART
800 7
18,000 13
25,000 35
MoHSS Church- based Health Services,
Outcome 3.2.7 Home Based Care
43 44
# of community volunteers & caregivers providing home based care by district & constituency % of chronically ill clients receiving home based care, by gender & district
2,500
35%
6,600
70%
8,000
95%
MoHSS
NGOs
Outcome 3.2.8 Access to care for vulnerable populations
No core indicators
16 * UNGASS Indicator

Chapter IV Monitoring and Evaluation
Medium Plan III for HIV/AIDS 93
Component 4: Impact Mitigating Services
Programme Sub Components, and
Outcomes
Ref. No.
Outcome Indicators Baseline
2004
Short Term Targets
Early 2007
Medium term Targets
2009
Responsible Agency
Sub-component 4.1: Developing the Capacity of Local Responses Outcome 4.1.1 Developing capacity for community-based responses
45
% of constituencies implementing HIV/AIDS community action plans,
- 60/96
80%
Councillors, MWACW, MBESC,
CAFO, CAA, NGOs
Outcome 4.1.2 Developing the capacity of support groups for PLWHA
46 47
# of PLWHAs provided with skills training to manage support groups % of constituencies with support groups
- -
100
50%
150
90% NGOs
Sub-Component 4.2: Services for OVC and PLWHA
Outcome 4.2.1 Services for OVC and PLWHA
48 49 50 51
# and % of households with OVC that have received support through grants (maintenance & foster parent grants) from the government Ratio of current school attendance among orphans to that of non-orphans *
# of OVC and PLWHA enrolled in community based care and support projects Number of PLWA receiving disability/social grants
10,813 -
<20
X17
30% increase
1 ( 0 difference)
1000 -
80% increase
1 (0 difference)
1610 -
MWACW NGOs, MBESC
CAFO, CAA
Sub Component 4.3: Addressing poverty
Outcome 4.3.1 Addressing poverty, food security, nutrition and housing
52 53
# of local groups of HIV affected people trained in income generating skills training by region # of orphans and vulnerable children receiving material & psychosocial support, food, by gender & region
2 -
260
50,000
500
100,000
MAWRD, MBESC, MoHSS, CAFO, KAYEC, CAA OPM, Governors
17 14,730 people claim the disability grant nationwide for many kinds of disability but this is not disaggregated at national level.

Chapter IV Monitoring and Evaluation
Medium Plan III for HIV/AIDS 94
Component 5: Integrated and Co-ordinated Programme Management at all levels
Programme Sub Components, and
Outcomes
Ref. No.
Outcome Indicators Baseline
2004
Short Term Targets
Early 2007
Medium term
Targets 2009
Responsible Agency
Sub-component 5.1 Developing HIV/AIDS Management Capacity
Outcome 5.1.1 Human resource planning
54 # of national and sectoral long, medium and short-term human resource plans in place that take account of the current skills gaps, the required expanded national response, attrition, absenteeism & the roll-out of AIDS treatment.
1 25 26 All Ministries
Outcome 5.1.2 Human resource development18
55 # of planners & managers of implementing partners trained in HIV/AIDS programme management and M&E, by sector, by region
10%
80%
95%
MoHSS, All Key Actors
Outcome 5.1.3 Quality Assurance
See:12, 23, 24, 26, 33 and 37
See quality assurance indicators embedded in components
MoHSS
Outcome 5.1.4 Institutional Capacity development of NGO service providers
56 # of planners & managers of implementing partners trained in HIV/AIDS programme management and M&E, by sector, by region
10%
80%
95%
MoHSS, All Key Actors
Sub-component 5.2 Management and Coordination
Outcome 5.2.1 Management structures
57 % of 3 national, 13 regional and 26 sectoral management structures with a budgeted comprehensive HIV/AIDS plan which is financed annually
10%
85%
100%
MoHSS All Ministries
Regional Councils
Outcome 5.2.2 Resource mobilisation and flow mechanisms
58 # of regions with multisectoral HIV/AIDS plans integrated into Regional Development plans / poverty reduction plans, budgeted, financed and implemented
0 13 13 Regional Councils
Outcome 5.2.3 Information flows
59 # of hits on MoHSS Directorate: Special Programmes website accessible to stakeholders
0 50/month 100/month MoHSS All Key Actors
18 Indicators which reflect capacity developed under the other components are not reflected here again

Chapter IV Monitoring and Evaluation
Medium Plan III for HIV/AIDS 95
Programme Sub Components, and
Outcomes
Ref. No.
Outcome Indicators Baseline
2004
Short Term Targets
Early 2007
Medium term
Targets 2009
Responsible Agency
Outcome 5.2.4 Mainstreaming
60 # of line ministries reaching 80% of criteria measuring mainstreaming (e.g. policy, annual plans, guidelines, budget, management committees with HIV/AIDS on agenda)
2 12 23 OPM, NPCS, MoHSS
All Ministries
Outcome 5.2.5 Management Processes
61 # of implementing partners using the management planning cycle
10 50 95% Implementing partners
Sub component 5.3: Programme monitoring and evaluation Outcome 5.3.1 Monitoring and Evaluation
62 % of organisations that have submitted the required number of completed MoHSS Directorate: Special Programmes Activity Reports on time in the past 12 months
- 95% 100% All implementing Partners
Sub component 5.4 Surveillance and operational research Outcome 5.4.1 Multi-sectoral HIV/AIDS research coordination
63 64
# of surveillance studies conducted # of research studies conducted
-
0
60%
50%
100%
85%
NPCS MoHSS
Outcome 5.4.2 Surveillance & Research
65 % of surveillance and research conducted according to the scheduled monitoring and research plan
- 50% 85% MoHSS & NPCS

Costing the National HIV/AIDS response
Medium Term Plan III for HIV/AIDS 97
The costing of MTP III was calculated by small groups of implementing partners and technical assistants who costed each individual activity within each broad activity. The data was approximately 95% complete. These were totalled by sub-component and a blanket 20% was added as a contribution towards overheads, which would include staff time, administration etc. The estimated costs for each sub-component are given below and should be viewed as indicative. Summary of Estimated Costs by Component and Sub-components
COST PER ANNUM [N$] COMPONENT AND SUBCOMPONENT Year 1 Year 2 Year 3 Year 4 Year 5 Total
COMPONENT 1: ENABLING ENVIRONMENT
SUBCOMPONENT 1.1: Leadership 2,565,750.00 2,618,250.00 2,880,750.00 570,750.00 570,750.00 9,206,250.00
SUBCOMPONENT 1.2: Greater Involvement of PLWHA 1,610,000.00 1,610,000.00 1,610,000.00 2,292,500.00 2,292,500.00 9,415,000.00
SUBCOMPONENT 1.3: Policy and Law Reform 1,535,750.00 1,362,250.00 131,250.00 0.00 0.00 3,029,250.00 SUBCOMPONENT 1.4: Interventions to Reduce Stigma and Discrimination 3,652,500.00 3,652,500.00 3,652,500.00 3,652,500.00 3,652,500.00 18,262,500.00
COMPONENT TOTAL 9,364,000.00 9,243,000.00 8,274,500.00 6,515,750.00 6,515,750.00 39,913,000.00
ADD 20% OVERHEADS 1,872,800.00 1,848,600.00 1,654,900.00 1,303,150.00 1,303,150.00 7,982,600.00
OVERALL COMPONENT TOTAL 11,236,800.00 11,091,600.00 9,929,400.00 7,818,900.00 7,818,900.00 47,895,600.00
COMPONENT 2: PREVENTION SUBCOMPONENT 2.1: Strengthen Capacity to Deliver HIV/AIDS Prevention Programmes 21,397,070.00 21,306,070.00 27,124,570.00 27,033,570.00 27,177,070.00 124,038,350.00
SUBCOMPONENT 2.2: Target Special Populations 9,421,032.00 9,812,200.00 6,062,200.00 5,756,200.00 5,756,200.00 36,807,832.00 SUBCOMPONENT 2.3: Target Behaviour Change Intervention at Young People 67,660,000.00 57,580,000.00 55,010,000.00 19,160,000.00 19,160,000.00 218,570,000.00
SUBCOMPONENT 2.4: Target the General Population 113,957,628.00 107,059,400.00 109,208,900.00 108,727,400.00 110,976,900.00 549,930,228.00
SUBCOMPONENT 2.5: Interventions to Reduce Vulnerability 300,000.00 1,200,000.00 700,000.00 600,000.00 600,000.00 3,400,000.00
COMPONENT TOTAL 212,735,730.00 196,957,670.00 198,105,670.00 161,277,170.00 163,670,170.00 932,746,410.00
ADD 20% OVERHEADS 42,547,146.00 39,391,534.00 39,621,134.00 32,255,434.00 32,734,034.00 186,549,282.00
OVERALL COMPONENT TOTAL 255,282,876.00 236,349,204.00 237,726,804.00 193,532,604.00 196,404,204.00 1,119,295,692.00
Chapter V Costing the National HIV/AIDS response

Costing the National HIV/AIDS response
Medium Term Plan III for HIV/AIDS 98
COST PER ANNUM [N$] COMPONENT AND SUBCOMPONENT Year 1 Year 2 Year 3 Year 4 Year 5 Total
COMPONENT 3: EQUAL ACCESS TO TREATMENT, CARE AND SUPPORT SERVICES SUBCOMPONENT 3.1: Capacity Development For The Expanded Treatment, Care And Support Response 10,590,931.00 10,121,811.00 7,967,971.00 7,278,291.00 7,518,971.00 43,477,975.00
SUBCOMPONENT 3.2: Treatment and Care Services 242,250,670.00 293,057,790.00 358,940,600.00 369,463,650.00 398,013,600.00 1,661,726,310.00
COMPONENT TOTAL 252,841,601.00 303,179,601.00 366,908,571.00 376,741,941.00 405,532,571.00 1,705,204,285.00
ADD 20% OVERHEADS 50,568,320.20 60,635,920.20 73,381,714.20 75,348,388.20 81,106,514.20 341,040,857.00
OVERALL COMPONENT TOTAL 303,409,921.20 363,815,521.20 440,290,285.20 452,090,329.20 486,639,085.20 2,046,245,142.00
COMPONENT 4: IMPACT MITIGATION SERVICES
SUBCOMPONENT 4.1: Developing the Capacity of Local Responses 6,836,000.00 11,401,000.00 11,152,500.00 13,670,000.00 13,628,000.00 56,687,500.00
SUBCOMPONENT 4.2: Services for OVC and PLWHA 19,517,250.00 26,147,250.00 4,091,250.00 9,191,000.00 41,191,000.00 100,137,750.00
SUBCOMPONENT 4.3: Addressing Poverty 13,615,000.00 15,615,000.00 16,932,500.00 16,932,500.00 18,932,500.00 82,027,500.00
COMPONENT TOTAL 39,968,250.00 53,163,250.00 32,176,250.00 39,793,500.00 73,751,500.00 238,852,750.00
ADD 20% OVERHEADS 7,993,650.00 10,632,650.00 6,435,250.00 7,958,700.00 14,750,300.00 47,770,550.00
OVERALL COMPONENT TOTAL 47,961,900.00 63,795,900.00 38,611,500.00 47,752,200.00 88,501,800.00 286,623,300.00
COMPONENT 5: INTEGRATED AND CO-ORDINATED PROGRAMME MANAGEMENT AT ALL LEVELS
SUBCOMPONENT 5.1: Developing HIV/AIDS Management Capacity 17,813,250.00 29,285,500.00 26,111,000.00 26,160,000.00 26,197,000.00 125,566,750.00
SUBCOMPONENT 5.2: Management and Co-ordination 2,011,000.00 1,656,000.00 1,956,000.00 756,000.00 1,956,000.00 8,335,000.00
SUBCOMPONENT 5.3: Programme Monitoring and Evaluation 1,500,000.00 1,500,000.00 1,500,000.00 1,500,000.00 1,500,000.00 7,500,000.00
SUBCOMPONENT 5.4: Surveillance and Research 2,065,980.00 2,421,715.00 3,000,000.00 1,775,060.00 3,000,000.00 12,262,755.00
COMPONENT TOTAL 23,390,230.00 34,863,215.00 32,567,000.00 30,191,060.00 32,653,000.00 153,664,505.00
Add 20% Overheads 4,678,046.00 6,972,643.00 6,513,400.00 6,038,212.00 6,530,600.00 30,732,901.00
Overall Component Total 28,068,276.00 41,835,858.00 39,080,400.00 36,229,272.00 39,183,600.00 184,397,406.00
OVERALL MTP III TOTAL COST 645,959,773.20 716,888,083.20 765,638,389.20 737,423,305.20 818,547,589.20 3,684,457,140.00

Chapter VI: Sectoral obligations and commitments
Medium Plan III for HIV/AIDS
99
This expanded and accelerated national response requires a greater involvement by ministries, parastatals, the private sector, NGOs and faith-based organisations, in fact from all of society. Grouping organisations by sector builds partnerships with common interests and provides opportunities to share resources and common experience.
A list of sectors can be found below. It recommends the Lead Agency for the sector and lists Key Actors which are currently involved, or should be involved, in the national response. The Sectoral Steering Committee will be established and supported by the Lead Agency. The Sector Steering Committee should be dynamic and responsive to the changes within the sector and to the changing impact of the epidemic. The terms of reference for Sector Steering Committees are presented in Chapter 2.
The following pages contain the obligations and commitments which individual Lead Agencies or Sectoral Steering Committees have agreed upon. These should correspond to the activity tables in Chapter 3 where appropriate implementing partners have been identified for specific activities; those implementing partners indicated in bold in Chapter 3 will be held responsible for ensuring that that activity takes place. It is therefore important to not only rely on your own sector pages as your guide but also to consult the main activity tables in Chapter 3.
6.1 List of Sectoral Clusters, Lead Agencies and Key Actors Sector Cluster Lead
Agency Other Key Actors Representatives to include among others:
Public Services Co-ordination
OPM Office of the President, public service unions, GIPF, PSC, Employers Federation
Agriculture Water and Rural Development
MAWRD Lands and Resettlement, Dir: Forestry MET; Community Development in MWACW, NNFU, NAU, NAFWU, AgriBank, NDC, NGOs e.g. RISE, CRIAA; NAMWATER, NAB, NDC
Child Welfare MWACW OVC Standing Committee, MoHSS Dir: Social Services, NGOs: e.g. Namibia Red Cross Society, Catholic AIDS Action, CCN, ELCAP, SSC, Lironga Eparu, CAFO
Defence MoD NDF Education and Culture
Joint HIV/AIDS Unit, MBESC / MHETEC
MHETEC, NIED, Adult Education: COSDECs, NAMCOL, NANTU, NANSO, TUCSIN, Sports Codes, Clubs, UNAM, Polytechnic, Voc. Training Colleges, Colleges of Education, NYC, NGOs e.g. Ombetja Yehinga, Total Child Project, Childline/Lifeline
Environment and Tourism
Directorate Tourism (MET)
MET, NWR, Namibia Tourism Board, FENATA, Namibian Association of CBNRM Support Organisations (NACSO), NACOBTA, NNF
Finance, Treasury and Resources
NPC MoF, Treasury, NPC, Office of the Auditor General, Banking & Insurance sectors, GIPF, NEPRU, IPPR
Fisheries MFMR MFMR, fishing companies, unions Foreign Affairs MFA UN Agencies, Foreign Missions and Diplomatic
Communities, Development Volunteers eg. VSO, UNV Gender MWACW Line ministries, NANAWO, Girl Child Project, Sister Namibia,
WAD, Khomas Women in Development, Nnawib, UNAM, WCPU, LAC
Chapter VI Sectoral obligations and commitments

Chapter VI: Sectoral obligations and commitments
Medium Plan III for HIV/AIDS
100
Sector Cluster Lead Agency
Other Key Actors Representatives to include among others:
Health and Social Services
MoHSS Directorate: Special Programmes
MoHSS, Lironga Eparu, Nurses Association, other medical agencies, NaSoMa, SMA, Church and private health services, NAMBTS, NIP, NGOs delivering prevention, treatment, care & support, medical insurance companies, Medical and para-medical boards, traditional healers, TBA, health sector & HIV/AIDS training institutions, development partners
Information and Media
MIB NBC, Take Control Task Force, MISA, print media, radio stations, advertising agencies, MoHSS: IEC, MBESC, John Hopkins University, media training institutions, MWACW, MBESC, MHETEC
Infrastructure MWTC NAMPOST, TELECOM, NAMWATER, LAs, ALAN, TransNamib, RCC, Air Namibia, WBCG, RCC, Air Namibia
Labour, Trade and Industry
MoL MTI, NABCOA, unions, NCCI, Retail industry, Namibian Business Coalition, Retail industry, JCC, Okatumbatumba Hawkers Association, NEF, Labour Advisory Council,
Lands, Resettlement and Rehabilitation
MLRR MLRR, National Federation of People with Disabilities in Namibia; MBESC Directorate: Special Education, MoHSS: Rehab, MoHSS Directorate: Social Services, Ehafo
Legal MoJ MoJ, Offices of Attorney General and Ombudsman, Law Society, LAC, Legal Dept in UNAM, Assoc. of Para-Legals, NAMFISA
Legislative Parliamentary Speakers
National Assembly, National Council, Cabinet
Mining and Energy MME Chamber of Mines, NAMDEB, Oil companies, unions, NAMCOR, Small Miners Federation. NAMPOWER, ECB
Prisons and Correctional Services
MPCS MPCS, ALU, Lironga Eparu, organisations supporting rehabilitation (CRIS, BRIDGE, PFB & others)
Regional and local government and housing
MRLGH ALAN, ARC, NELAO, AMICAALL , Regional Councils, Traditional Leaders, Land Boards, Directorate of Housing, City of Windhoek, National Housing Action Group (NHAG)
Local Authorities Coordinated by: ALAN and AMICAALL and NALAO to target Local Authorities throughout Namibia
Youth MHETEC National Youth Council, MHETEC: YHDP, Ombetja Yehinga, NANSO, Girl Child Project; City of Windhoek Junior Councillors; NYS, YouthNet, YWCA, CCN Youth Desk, Catholic Youth League, ELCIN Youth Desk, Lirongo Eparu ambassadors, NAPPA, KAYEC
Faith-based Organisations
CCN CAFO, CAA, ELCIN, ELCRIN, CHS, Church AIDS Network, HIV/AIDS Church Forum
NGOs NANASO AIDS Service Organisations and other NGOs, NANGOF, Lironga Eparu
Private Sector NABCOA Representatives of members of NABCOA, NCCI, Chamber of Mines, Okatumbatumba Hawkers Association, Namibia Shebeen Association, Professional associations, ALU, ACT

Chapter VI: Sectoral obligations and commitments
Medium Term Plan III for HIV/AIDS 101
Lead Agency: Office of the Prime Minister Key Actors: Office of the President, Office of the Prime Minister: Operations;
Public Service Union, Government Institution Pension Fund, Public Service Commission, Employers’ Federation
Target Groups: All managers and staff in the Public sector
Sector Objectives 1. Engage the sector’s leadership and spear-head the response throughout the
sector
2. Mainstream HIV/AIDS within the Sector from sectoral policies to implementation, technical support supervision, M&E, public information and accountability
This Sector’s Commitments in MTP III Chapter 3 Reference Public Service Coordination’s Commitments Ref Enabling Environment Secretary to Cabinet will champion advocacy and sensitisation and be up-to-date on programmes in O/M/As regarding HIV/AIDS
1.1.1
HIV/AIDS to be on the Agenda during the Permanent SecretariesMeeting urging them to support the workplace programmes, attend NAMACOC meetings and lead the response in their sector
1.1.1
Presentations on impact of HIV/AIDS can be made to the top management so that they become involved from the start of all programmes
1.1.1
Top managers will provide moral and financial support to the HIV/AIDS programmes and activities in O/M/As and will include HIV/AIDS in all their speeches
1.1.1
Increase involvement of Medical Aid companies and GIPF in the fight against HIV/AIDS
1.1.1
All budgets will reflect HIV/AIDS activities 1.1.1 PLWHAs will be supported to speak up and join in the campaigns 1.2.1 PLWHA will be involved in decision making and development of policies 1.2.1 Ensure wellness programmes that will support PLWHAs 1.2.1 Policy And Legal Reforms Ensure the development and implementation of National Policy on HIV/AIDS. 1.3.1 Ensure that the National Policy on HIV/AIDS is in line with the ILO code on employment, SADDEC and other existing legal framework
1.3.1
Review all existing legal framework of the Public Service of Namibia to be in line with the HIV/AIDS pandemic
1.3.2
Ensure the development and implementation of Public Service Charter on non-discrimination and stigmatisation (translated in all local languages)
1.3.1
Sector: Public Service Coordination

Chapter VI: Sectoral obligations and commitments
Medium Term Plan III for HIV/AIDS 102
Public Service Coordination’s Commitments Ref Review EMU criteria for food assistance to include people in need infected and affected by HIV/AIDS
1.3.1
Ensure information and education to combat discrimination through workshops, seminars and training
1.4.1
Ensure counselling and legal assistance is available in the workplace. Make counselling rooms available
1.4.2
Prevention 2 Train peer counsellors and have peer counselling services in place 2.4.2 Advocate and lobby for Management to invest in workplace programmes (resources, finances, personnel)
2.4.2
Streamline gender throughout the activities and programmes of O/M/As and in the Public Service Training courses
2.5.1
Ensure the implementation of Gender Policy 2.5.1 Mitigating the impact 4 Make the information available to OVCs on where to get assistance 4.2.1 Protect the rights of OVCs by a policy on the rights of OVCs 4.2.1 Programme Management and Coordination Permanent Secretaries to give brief report of HIV/AIDS activities intheir O/M/As during the PS's meetings to the Secretary of Cabinet
5.2.1
Ensure the creation of full time post in O/M/As for HIV/AIDS coordination. Such coordinator could report to PS
5.2.1
Create a position in the OPM Private Office for a person to work as HIV/AIDS coordinator to liaise with the Directorate of Special Programmes in the MoHSS
5.2.1
Provide clear terms of reference for HIV/AIDS focal people and empower them to fulfil their responsibilities
5.2.1
Mainstream HIV/AIDS in the existing Public service training modules 5.2.4 Top managers should mainstream HIV/AIDS in all programmes and projects 5.2.4

Chapter VI: Sectoral obligations and commitments
Medium Term Plan III for HIV/AIDS 103
Lead Agency Ministry of Agriculture Water and Rural Development Key Actors to be involved: MLRR, MET Forestry, Community Development in
MWACW, NNFU, NGOs, NAU, NAFWU, Agribank, NDC, RISE, CRIAA, IRDNC, NAB, NAMWATER,
Target Groups: All staff, extension officers, farmers, women, youth, and farm workers
Sector Objectives:
1. Disseminate information to key actors in the sector 2. Include HIV/AIDS information with all extension work target groups 3. Co-ordinate and plan activities, resource mobilisation and research
This Sector’s Commitments in MTP III Chapter 3 Reference Review and revise the national Agricultural policy in order to guide all stakeholders with regard to the pandemic
1.3.2
Finalise and launch HIV/AIDS policy for MAWRD 1.2.2 Develop activities which address the Sector’s vulnerable groups including: farmers associations, farm workers, cooperatives, women groups, extension officers/technicians
2.2.1
Develop support and counselling groups within the Ministry 2.4.2 Purchase condoms and distribute every Friday in all male and female Toilets at national and regional level offices
2.4.3
Training and awareness on HIV/AIDS for all extension officers/technicians 2.1.1 Train HIV/AIDS focal people in MAWRD and regional HIV/AIDS committees 2.1.1 Include HIV/AIDS information in all extension work in particular with the water point committees
2.4.1
Develop IEC material for behaviour change to distribute to all employees and to target group
2.4.1
Encourage all employees to be tested and to access their Medical Aid Fund for treatment if necessary
2.4.2
Through our extension staff to encourage and facilitate discussions during farmers’ information sessions, so that communities can develop their own coping strategies
4.1.1
Assist Farmers associations, women groups, and youth groups to identify and establish income generating projects
4..3.1
Consider and implement ways of enhancing nutrition and food security for the identified vulnerable groups
4.3.1
Appoint full time HIV/AIDS focal point and national and regional level within the Ministry
5.1.1
Ensure an annual budget line for HIV/AIDS activities 5.2.2 Human Resource Division to provide training to enhance skills and knowledge on HIV/AIDS pandemic
5.1.2 & 5.1.3
Develop guidelines and plans of action 5.2.2
Sector: Agriculture Water and Rural Development

Chapter VI: Sectoral obligations and commitments
Medium Term Plan III for HIV/AIDS 104
Lead Agency: OVC Permanent Task Force, Ministry of Women’s Affairs and Child Welfare
Key Actors: MoHSS Directorate: Social Services, NGOs: e.g. Namibia Red Cross Society, Catholic AIDS Action, Council of Churches, ELCAP, Social Security Commission, Lironga Eparu, CAFO, Local Authorities, NECD Association, Permanent Task Force
Target Groups: Persons living with HIV/AIDS, their families, caregivers, orphans and other Vulnerable Children, community based organisations, youth groups, women’s groups, churches
Sector Objectives
1. To improve the quality of life of all children 2. To empower families and communities to take part in children’s issues 3. To strengthen capacity of staff in the division
This Sector’s Commitments in MTP III Chapter 3 Reference Child Welfare’s Commitments Ref Enabling Environment Strengthen existing and establish new regional and constituency OVC forums. 1.1.1 Train home based care volunteers on HIV/AIDS and psycho social support for OVC 1.1.1 Involve OVC in decision making 1.2.1 Prevention Establish lists of potential foster carers in the regions 2.2.1 Education and awareness raising on OVC and care givers rights and responsibilities based on OVC policy
2.2.1
Develop and distribute IEC materials on OVC and caregivers rights and responsibilities
2.2.1
Develop and distribute a comprehensive guide on grants and OVC Trust Fund 2.2.1 Treatment, Care and Support Develop and Implement guidelines and procedures for institutions in line with the Child Care and Protection Act
3.1.1
Mobilise resources for funding of regional OVC workplans 3.1.1 Train social workers and TOTs on psycho social support to PLWHA and OVC 3.1.1 Provision of grants and subsidies to families, caregivers and institutions taking care of OVC in need
3.1.2
Provision of services to facilitate access to support and protection for OVC and caregivers
3.2.7
Provision of food baskets to needy OVC Impact Mitigation Ensure adoption and implementation of OVC policy 4.2.1 Support implementation of the National OVC strategic plan 4.2.1 Establish, update and maintain the data system on OVC 4.2.1 Develop innovative systems for channelling resources to household and 4.3.1
Sector: Child Welfare

Chapter VI: Sectoral obligations and commitments
Medium Term Plan III for HIV/AIDS 105
Child Welfare’s Commitments Ref communities caring for OVC Lobby for promulgation of outstanding bills: Child Care and Protection and Child Status
4.2.1
Managing the HIV/AIDS response Organise study tours for best practices for OVC stakeholders 5.2.3 Develop and adopt monitoring and evaluation strategy framework/tool 5.3.1 Develop a comprehensive and costed strategic action plan for OVC 5.2.5 Review and update situation analysis information to include child headed household and gender breakdown
5.4.2
Conduct research on OVC issues as per priority area 5.4.2

Chapter VI: Sectoral obligations and commitments
Medium Term Plan III for HIV/AIDS 106
Lead Agency: Ministry of Defence / Namibia Defence Force Key Actors: MOD Staff and NDF Members, Public and Communities where
appropriate Target Groups: Active duty service members, eligible family members, military
health care providers, personnel and staff members of MOD/NDF, the population in the surrounding as appropriate.
Sector Goal: To ensure and secure effective, physically and mentally healthy MOD/NDF members, by significantly reducing and efficiently managing HIV/AIDS/STI/TB and Malaria.
Sector Objectives 1. Prevent HIV and sexually transmitted infections (STI) among service members
according to the Military Action Prevention Programme (MAPP) through proper female and male condom use, and intensive Information, Education and Communication (IEC) provision
2. Reduce the number of new HIV/AIDS/STI/TB infections among active members by a measurable percentage during MTP 3
3. Strengthen already established Voluntary Counselling and Testing (VCT), treatment of Opportunistic Infections (OI), new Anti-Retroviral (ARV) therapy, care and support services (home based care), for the infected and affected members
4. Carry out regular monitoring, assessment, surveillance and research studies within the force, in order to determine the magnitude and impact of the epidemic, and effectiveness of programme activities, aimed at proper planning, managing and budgeting
This Sector’s Commitments in MTP III Chapter 3 Reference Defence Sector’s Commitments Ref Enabling Environment Intensify sensitisation and advocacy with sectoral leadership (political & military) and management to improve sectoral response to HIV/AIDS/STI/TB and other related infectious diseases
1.1.1
Establish policy, guidelines and management structure for effective response to the epidemic
1.3.2
Address stigma and discrimination of PLWA (uniformed individuals) 1.4.1 Prevention Scale up IEC provision, condom distribution as well as other necessary materials 2.2.1 Develop BCI programmes aimed at MOD/NDF members 2.2.1 Support trainer of trainers (TOT) courses to develop multi-disciplinary teams for promoting HIV/AIDS/STI/TB/Malaria education, counselling, care and support
2.1.1 & 3.1.2
Conduct training of personnel, instructors, and peer educators 2.1.1 & 3.1.2
Implement an HIV/AIDS awareness campaign at all military bases using drama, 2.2.1
Sector: Defence

Chapter VI: Sectoral obligations and commitments
Medium Term Plan III for HIV/AIDS 107
Defence Sector’s Commitments Ref edutainment, videos and talks according to the Military Action Prevention Programme Prevent HIV and hepatitis transmission among uniformed members and the provision of PEP to military health workers at risk
2.2.2
Support the creation of additional VCT facilities and uniformed population friendly multi-purpose centres
2.4.1
Distribution of male and female condoms 2.4.3 Campaign vigorously to raise awareness on STI and syndromic treatment approach application for NDF members
2.4.4
Provide other hobbies and alternatives to alcohol and risky sexual behaviour for uniformed personnel and members (sport, drama, etc.)
2.5.1
Treatment, Care an Support Train more HBC counsellors and strengthen the community in their role in HBC support
3.1.1
Provide treatment literacy for all MOD/NDF members, including Unit Commanders and health workers on treatment for OI, VCT, PMTCT and HAART, and make sure there are no confusion or myths
3.2
Ensure and secure treatment, care and support to infected and affected members of the Army, Maritime Wing and the Air Wing as well as the general personnel, and develop activities for addressing stigma and discrimination among the force and members
3.2
Collaborate with MoHSS and other stakeholders in the provision of HAART 3.2.6 Establish a home-based care centre in MOD/NDF for the infected military members 3.2.7 Impact Mitigation Develop and support local activities based on community response to HIV/AIDS (positive living with HIV/AIDS etc.) support groups, poverty alleviation programmes, food security, nutrition and housing
4.1.1
HIV/AIDS/STI/TB Management Response Strengthen MOD/NDF programme planning and management structure in order to improve coordination and monitoring of HIV/AIDS/STI response, with emphasis on resource mobilisation, human resource development and information management
5.2
Develop action plans and budget for HIV/AIDS/STI/TB/Malaria and other related infectious diseases activities on annual basis
5.2.5
Monitor and evaluate in order to ensure and secure data collection, which would facilitate effective planning and improve our understanding of the magnitude of the HIV/AIDS/STI problems at hand
5.3
Conduct impact assessment studies to have first hand knowledge supported by variables, and act on the findings
5.4.2
HIV/STI surveillance system must be in place 5.4.2 Design and undertake HIV vulnerability, risk behaviour and coping strategies research study among MOD/NDF members during MTP III
5.4.2

Chapter VI: Sectoral obligations and commitments
Medium Term Plan III for HIV/AIDS 108
Lead Agency: Ministry of Basic Education Sport and Culture, (MBESC) and the Ministry of Higher Education Technology and Employment Creation (MHETEC): HIV/AIDS Management Unit (HAMU)
Key Actors: MHETEC, Namibian Institute for Educational Development (NIED), National Namibian Teachers Union (NANTU), National Namibian Students Organisation (NANSO), TUCSIN, Childline/Lifeline, Sports Codes, Clubs, University of Namibia (UNAM), Polytechnic, Vocational Training Colleges, Teacher Training Colleges, FAWENA, Ombetja Yehinga, Total Child Project, KAYEC, other NGOS
Target Groups: All learners, teachers, students, lecturers, tutors, instructors, institution workers, school boards, parents
Sector Objective: To reduce the transmission of HIV, mitigating its social and economic impact of AIDS on the Namibian Education system at all levels
This Sector’s Commitments in MTP III Chapter 3 Reference
Education Sector’s Commitments Ref Enabling Environment To protect all learners/students from any form of discrimination in particular orphans and other vulnerable children and learners/students infected or affected by HIV and AIDS
1.3.3
To develop and enforce appropriate systems and safe guards to prevent sexual harassment abuse, exploitation or assault of learners/students and education institution and education sector employees
1.3.4
To create and promote awareness and action for the rights of all learners/students in particular orphans and other vulnerable children/students infected or affected by HIV and AIDS.
1.4.1
To ensure that all employees infected are treated fairly and are not discriminated against in terms of recruitment, appointment, transfer and development and to create a culture of acceptance, openness and compassion in the workplace
1.4.2
Prevention To include HIV and AIDS education programmes as part of the pre and in-services programmes of teachers that provide knowledge on continuing life-skills, sexual health and HIV/AIDS and skills to deal with the impact of HIV and AIDS
2.1.1
To implement continuing life skills, sexual health, HIV and AIDS education prevention programmes in all educational institutions for all learners/students, education sector employees and stakeholders
2.3.1
To ensure that age and ability-appropriate, accurate, and scientific defensible life skills, sexual health and HIV and AIDS education and resource materials are made available to learners/students as part of the curriculum in language and terms that are
2.3.1
Sector: Education

Chapter VI: Sectoral obligations and commitments
Medium Term Plan III for HIV/AIDS 109
Education Sector’s Commitments Ref understandable To ensure that all education institutions and education sector employees are aware of and apply the universal First Aid precautions to prevent them to contract the HIV/AIDS virus
2.4.2
To ensure that all employers in the education sector provide accurate information on HIV and AIDS including advocacy, counselling and testing and prevention methods to all employees
2.4.2
To review the package of benefits in the sector that is available to employees, with a view to ensuring that infected employees are not disadvantaged or discriminated against
2.4.2
Treatment, Care an Support and Impact mitigation To ensure that OVC are not deterred from participation in formal education through school development fund or other material contributions requested by schools.
4.2.1
To provide holistic care, counselling and support services to orphans other vulnerable children and learners/students infected or affected by HIV and AIDS
3.2.8 and 4.2.1
To expand the provision of vocational training and other income earning opportunities to vulnerable young people especially child headed households, families with large numbers of OVC, particularly those headed by the elderly
4.3.1
HIV/AIDS/STI/TB Management Response To develop and implement clear and consistent guidelines and regulations to manage absenteeism and productivity to reduce its impact in the classroom and the workplace
5.1.1
To ensure that management structures and support systems are in place at all levels of the education sector to effectively implement HIV/AIDS policy and monitor and evaluate associated programmes
5.1.1
To ensure systems and structures are in place to provide the data/information necessary to support the HIV and AIDS management unit’s role in coordinating effective planning, budgeting, implementation and review of the HIV/AIDS management response
5.2.1
To ensure that advisory committees function in every institution that coordinate efforts/activities in the sector through development of partnerships with service and community
5.2.1

Chapter VI: Sectoral obligations and commitments
Medium Term Plan III for HIV/AIDS 110
Lead Agency: Directorate: Tourism, MET Key Actors: MET, Namibia Wildlife Resorts, Namibia Tourism Board,
Federation of Namibian Tourism Associations (FENATA), Namibian Association of CBNRM Support Organisations (NACSO), Namibia Nature Foundation
Target Groups: Conservancy members, parastatal and private sector, MET staff and their families, Namibian and international tourists
Sector Objectives 1. To create awareness among staff and family members and all stakeholders of the tourism
sector about HIV/AIDS, modes of transmission, prevention, etc 2. To facilitate a process in order to ensure the achievement of desired goals (strategic plan) 3. To promote social mobilisation 4. To access and provide timely information relating to the epidemic in order to stimulate action 5. To have a supportive attitude and to promote appropriate sexual and social behavioural
change amongst employees 6. To strengthen coordination with stakeholders to effectively embark upon HIV/AIDS
preventative programmes 7. To sensitise partner organisations about the disease 8. To establish employee committees and involve their families 9. To educate employees and their families about prevention, symptoms, and the use of safety
mechanisms such as condoms
This Sector’s Commitments in MTP III Chapter 3 Reference Environment and Tourism Sector’s Commitments Ref Component 1. Enabling Environment Build capacity between all levels within in MET and stakeholders, namely the top and middle management and employees at the shop level to be able to execute activities.
1.1.1
Design HIV/AIDS policies and programmes for the sector 1.3.2 Raise awareness through provision of information on discriminating and stigma 1.4.1 Component 2. Prevention Link with other organisations such as churches, youth groups, women groups, men groups and schools and build capacity on behavioural change.
2.1.1
Build capacity of vulnerable people: Women, men, children and community at large
2.2.1
Promote prevention of HIV/AIDS through IEC materials, messages and dissemination of information on HIV/AIDS throughout the tourism sector.
2.4.1
Arrange activities to celebrate World AIDS Day 2.4.1 Design I.E.C. materials collaboratively with other partners working in the field 2.4.1 Link with schools and programmes on HIV/AIDS within communities attached to conservancies and field work
2.4.1
Sector: Environment and Tourism

Chapter VI: Sectoral obligations and commitments
Medium Term Plan III for HIV/AIDS 111
Environment and Tourism Sector’s Commitments Ref Make provision for care and support to staff and families affected through counselling, home-based care and general care
2.4.2
Design workplace programmes (action plans) 2.4.2 Facilitate weekly discussions or meetings on a variety of HIV/AIDS related topics amongst staff in departments
2.4.2
Strengthen condom supplies and distribution channels within the sector 2.4.3 Promote the use of voluntary counselling and testing (VCT) 2.4.5 Component 4. Impact Mitigation Sensitise the sector’s organisations and employees to identify contributing factors towards the spread of the disease and assist tourism-based communities and staff members to identify pillars to be put in place to mitigate this impact
4.1.1
Build capacity on safe livelihood programmes 4.3.1 Assist organisations, conservancies and communities to come up with activities to address identified problems and develop action plans to overcome the problems.
4.3.1
Link needy communities with the Emergency Management Unit for drought relief food
4.3.1
5. Managing the HIV/AIDS response Appoint a Social Welfare Office to steer the HIV/AIDS activities in the MET 5.1.1 Establish HIV/AIDS committees in all the directorates of MET 5.2.1 Establish relevant committees/forums to steer the programme at all levels within the tourism sector
5.2.1
Share information and experience through workshops and educational tours to all regions
5.2.3
Ensure that HIV/AIDS reporting is mainstreamed into routine reports 5.2.4 Integrate quarterly HIV/AIDS activities into routine workplans 5.2.4 Provide logistics and technical support to all levels 5.2.4 Ensure that a sound monitoring system is in place at all levels within the sector - Indicators in action plans.
5.3.1
Feedback on monthly management and staff meetings through formal reporting. 5.3.1 Data collection and research in require areas 5.4.2 Integrate HIV/AIDS activities into the lead agency (MET) action plan 5.4.2

Chapter VI: Sectoral obligations and commitments
Medium Term Plan III for HIV/AIDS 112
Lead Agency: National Planning Commission Key Actors: Ministry of Finance, Treasury, Office of the Auditor General,
Banking sector and Insurance sector representatives, Government Institutions Pension Fund, NEPRU, Institute for Public Policy Research
Target Groups: Ministry staff, NPC staff, Parastatals staff, Auditor General staff and the general public
Sector Objectives: 1. To investigate the impact of HIV/AIDS on the national economy 2. To ensure that all sectors allocate funds from their budgets for HIV/AIDS related activities 3. To plan and ensure integration of HIV/AIDS related activities into the sector annual plans 4. To distribute information on HIV/AIDS to its staff members and public 5. To procure condoms and distribute amongst the Ministry staff
This Sector’s Commitments in MTP III Chapter 3 Reference
Finance Treasury and Resource’s Commitments Ref Enabling Environment To protect all employees from any form of discrimination and in particular those infected or affected by HIV and AIDS to create a culture of acceptance, openness, and compassion in the workplace
1.4.2
Prevention Sensitise and encourage other institutions and sectors to carry out workers’ AIDS risk analysis in the workplace
2.4.2
Establish a workplace programme which distributes information on the prevention of HIV infection and raises workers’ awareness of risk behaviours
2.4.2
Procure and distribute condoms to its staff 2.4.2 Impact mitigation Mainstream HIV/AIDS into poverty reduction and development programmes 4.3.1 Management and Coordination Strengthen the National Human Resource Planning Task Force to revise the National HR Plan to include HIV/AIDS, to implement and monitor the planning process, from 2004 on-going
Build capacity of sector members on HIV/AIDS programmes and budgeting. 5.1.2 Strengthen mechanisms and build capacity of GRN for donor coordination and feedback to the different sectors and partners
5.2.2
Coordinate consultative meetings on HIV/AIDS resources mobilisation with relevant sectors and partners.
5.2.2
Review budgets and proposals to ensure the implementation of HIV/AIDS related action plans by all sectors.
5.2.2
Facilitate line ministries and sectors to conduct impact assessments to understand how AIDS is impacting on their sector, affecting their core functions and their target groups
5.2.4
Strengthen the existing national research coordination body to coordinate multi-sectoral HIV/AIDS, STI & TB research
5.4.1`
Sector: Faith-based Organisations Sector: Finance, Treasury and Resources

Chapter VI: Sectoral obligations and commitments
Medium Term Plan III for HIV/AIDS 113
Co-ordinating Bodies Ministry of Fisheries and Marine Resources Key Actors to be involved: MFMR, fishing and processing companies, unions
Target Groups: Internal staff members, (permanent & casual) families of staff, friends of staff.
Fisheries Sector Objectives: 1. Develop and implement a conducive policy framework for HIV/AIDS and other life
threatening diseases 2. Provide appropriate moral and socio–economic support to infected and affected
target groups 3. Provide awareness, understanding and openness about HIV/AIDS, its causes and
effects 4. Provide and improve access to appropriate preventative measures, devices and
services 5. Ensure appropriate and sufficient funds on a continuous basis for HIV/AIDS related
activities
Fisheries Sector Commitments in MTP III Chapter 3 Reference Component 2 Prevention
Create continuous awareness by establishing dialogue 2.4.1
Support and promote the use of comprehensive appropriate IEC material 2.4.1
Develop and implement workplace policies to prevent discriminatory practices against PLWA
2.4.2
Render moral support to affected and infected people 2.4.2
Support, strengthen and expand counselling and other psychological support services
2.4.2
Component 4 Impact Mitigation
Establish and manage and HIV/AIDS benefit fund to assist affected and infected employees
4.3.1
Component 5 Integrated Management
Identify and train human resources for HIV/AIDS internal and external 5.1.2
Establish and strengthen regional programme management structures 5.2.1
Conduct mid-term review of HIV/AIDS programmes 5.3.1
Establish planning and management programme 5.2.4
Support research and surveys conducted by respective sectors 5.4.2
Sector: Fisheries

Chapter VI: Sectoral obligations and commitments
Medium Term Plan III for HIV/AIDS 114
Lead Agency: Ministry of Foreign Affairs Key Actors: Ministry of Foreign Affairs, Foreign Missions and Diplomatic
Communities, (both inside and outside the country), UN Agencies, Development Volunteer Agencies
Target Groups: Staff in the Ministry of Foreign Affairs at the Namibia Missions abroad, studying/travelling Namibians abroad, foreign missions, embassies and all diplomatic communities in Namibia, and other foreigners
Specific Sector Objectives 1. To advocate and facilitate dialogue for support for the National Response on HIV/AIDS 2. To disseminate information on HIV/AIDS to the Namibians outside the country through
our Missions abroad 3. To provide care and support to those infected within the sector and outside the
country 4. To budget for the procurement and distribution of the HIV/AIDS Workplace Programme 5. To co-ordinate and plan activities, resource mobilisation and research for the country
from foreign countries and Agencies 6. To ensure maintenance of information flow between Namibia and International
Communities 7. To organise quarterly debriefing sessions on HIV/AIDS with all Embassies/High
Commissions in Namibia 8. To distribute condoms to Head office and Namibian missions abroad 9. To participate in dialogue and discussions in foreign countries to solicit information flow
and support 10. To gather information related to HIV/AIDS through the respective foreign missions, UN
Agencies, etc
This Sector’s Commitments in MTP III Chapter 3 Reference
Foreign Affairs Sector’s Commitments Ref Enabling Environment Development of the National Foreign Affairs HIV/AIDS Policy in order to guide all stakeholders with regard to the implementation of the Ministry’s Plan of Action
1.3.1
Review insurance and pension schemes 1.3.2 Prevention Implementation of the Foreign Affairs Workplace Programme
2.4.2
Distribution of condoms and HIV/AIDS information material 2.4.1 & 2.4.3
Engage expertise and knowledge of AIDS Care Trust on Namibia (ACT) and other HIV/AIDS experts on the best means and methods of informing the employees about all aspects of HIV/AIDS and in implementing the prevention programme (training, counselling and home based care)
2.4.2
Sector: Foreign Affairs

Chapter VI: Sectoral obligations and commitments
Medium Term Plan III for HIV/AIDS 115
Foreign Affairs Sector’s Commitments Ref Provide IEC material and peer education to promote behaviour change, STI treatment, VCT,HAART, use of condoms and reduction of stigma and discrimination
2.4.2
Train employees to be peer educators as an effective tool to convey behaviour change messages.
2.4.2
Promotion of Voluntary Counselling and Home Based Care 2.4.2 Provide advise as how to access treatment of STI, management of TB, provision of VCT, and HAART
2.4.2
HIV/AIDS/STI/TB Management Response Undertake an impact assessment (internal and external), 5.1.1 Appoint HIV/AIDS Focal Person/Coordinator and HIV/AIDS Committee. These are responsible for the running, implementing and monitoring of the HIV/AIDS Programme
5.1.1
Presentation to the Management/Heads of Mission: Equip Management/Heads of Mission with necessary skills on how to manage HIV/AIDS in the workplace. This includes information on financial implications, management guidelines, legal issues and condom distribution.
5.1.2
Train middle management/supervisors: Support from management is crucial for the success of the HIV/AIDS Programme. As a result of a specific training they will understand the implications of HIV/AIDS on the workforce as well as the importance of the programme and their role in its implementation
5.1.2
Form a Planning Committee: Establish a task team to lay the groundwork for the training programme. The team will design the programme, co-ordinate and supervise the implementation.
5.2.1
Report on changes of key indicators of impact of HIV/AIDS on the Foreign Ministry (such as absenteeism, medical retirements, funeral attendances and production delays); obtain feedback from peer educators; and obtain supervisors’ views and experiences
5.3

Chapter VI: Sectoral obligations and commitments
Medium Term Plan III for HIV/AIDS 116
Lead Agency: Ministry of Womens Affairs and Child Welfare Key Actors: Line Ministries, NANAWO, Girl Child Organisation, Sister
Namibia, WAD, Khomas Women in Development, Nnawib, UNAM, WCPU, LAC
Target Groups: Ministry staff, women, men, youth, traditional leaders and communities. Sector Objectives: 1. Ensure that gender is mainstreamed into HIV/AIDS programming 2. To educate women, men and children about their legal rights. 3. To empower women economically in order to reduce their dependence on their male counterparts. 4. To reduce incidences of gender based violence.
This Sector’s Commitments in MTP III Chapter 3 Reference Gender Sector’s Commitments Ref Component 1. Enabling Environment Ministerial committee to be well trained on HIV/AIDS pandemic to enable them to train and implement HIV/AIDS related programmes
1.1.1
Conduct legal literacy programmes in the communities 1.4.2 Component 2. Prevention Provide training to staff and target group to enhance skill and knowledge on the HIV/AIDS pandemic
2.1.1 & 2.4.1
Training of youth peer educators in gender and sexual reproductive health 2.1.1 Develop and Translate IEC materials for behaviour change to distribute to all employee and the target group
2.2.1
Conduct meetings for discussions and information dissemination on gender issues that relate to HIV/AIDS
2.4.1
Encourage employees to be tested and to utilise their medical aid scheme 2.4.5 Component 4. Impact mitigation Mobilisation of women to take part in income generating activities 4.1.1 Capacity building for women in business 4.1.1 Component 5: Integrated Management Develop strategy and guideline for gender mainstreaming into HIV/AIDS programmes
5.2.4
Develop HIV/AIDS Plan of Action for HIV/AIDS intervention within the Ministry 5.2.4 Ensure adequate annual budget line for HIV/AIDS and it’s proper utilisation 5.4.2 Conduct research on socio-economic issues with in order to determine the influence that they have on HIV/AIDS infections
5.4.2
Sector: Gender

Chapter VI: Sectoral obligations and commitments
Medium Term Plan III for HIV/AIDS 117
Lead Agency: Ministry of Health and Social Services (MoHSS) Directorate: Special Programmes
Key Actors: MoHSS, church and private health services, Medical and para-medical boards, Nurses Association and other medical agencies, Blood Transfusion Service (BTS), National Institute of Pathology, medical insurance companies, health sector & HIV/AIDS training institutions, traditional healers, traditional birth attendants, NGOs delivering treatment, care and support services, development partners
Target Groups: The general public, implementing partners, health sector staff
Sector Objectives 1. To create an enabling environment for the national and health sector response 2. To reduce new infections of HIV, STI and TB by providing HIV/AIDS prevention services, I.E.C
materials, TB & STI treatment, condoms and other supplies 3. To integrate HIV/AIDS into STI care, reproductive health and all relevant health care services 4. To provide cost effective and high quality treatment, care and support to those infected
and affected by HIV/AIDS, STI and TB 5. To mitigate the impact of HIV/AIDS at local level 6. (The MoHSS) to coordinate the overall, multisectoral national response 7. To provide technical support to partners in all sectors engaged in the HIV/AIDS response at
all levels 8. To implement expanded workplace programmes in the health sector
This Sector’s Commitments in MTP III Chapter 3 Reference Health Sector’s Commitments Responsibility Ref Activities to achieve Objective 1:Create an enabling environment Promote leadership and adequate mobilisation to respond to the epidemic across all sectors
All Key Actors 1.1.1
Increase participation of people living with HIV/AIDS (PLWHA) in decision-making bodies of the Response
All Key Actors 1.2.1
Develop a national and a health sectoral HIV/AIDS policy MoHSS 1.3.1 & 1.3.2
Develop a policy on nutrition supplementation for people living with HIV/AIDS.
MoHSS 1.3.2
Activities to achieve Objective 2 & 3: Reduce new infections Coordinate prevention programmes which target marginalised populations
MoHSS 2.2.1
Develop and disseminate well targeted IEC materials MoHSS 2.2.2 Integrate HIV/AIDS/STI services into adolescent friendly health services and actively expand the Health Promoting Schools programme
MoHSS 2.2.2 & 8.1
Promote establishment of workplace programmes in all sectors. MoHSS, NGOs 2.4.2
Sector: Health

Chapter VI: Sectoral obligations and commitments
Medium Term Plan III for HIV/AIDS 118
Health Sector’s Commitments Responsibility Ref Ensure the countrywide forecasting, supply, distribution and availability of condoms and promote the consistent use of female and male condoms through public, private and social marketing systems
MoHSS and All key actors
2.4.3
Promote the importance of speedy STI and TB detection among the public and strengthen the management and treatment of both diseases
All Key Actors and MoHSS/NACOP
2.4.4 & 3.2.5
Provide and sustain high quality voluntary counselling and testing services in all regions
MoHSS and partners
2.4.5
Ensure safe blood transfusion products NAMBTS & Ministries of basic and higher education
2.4.6
Mobilise sectoral and societal action on alcohol and substance abuse and promote responsible drinking
Social Services, All Key Actors, NGOs Shebeens Association
2.5.1
Provide Post-exposure Prophylaxis (PEP) for rape survivors as well as Health professionals exposed during duty through occupational health risks in all regions and strengthen psychosocial support of all affected persons
MoHSS & MHA (Women and Child protection Unit)
2.5.1
Activities to achieve Objective 4: Provide treatment, care and support Develop and coordinate a communication strategy to improve understanding of the continuum of treatment, care and support for HIV/AIDS, STI and TB and how to overcome barriers to accessing services
NACOP and all Key Actors
3.1.1
Develop & disseminate sector relevant policies, guidelines and minimum standards on prevention, treatment, care and support
MoHSS & Key Actors
3.2 & 1.3.2
Strengthen the capacity of laboratory and pharmaceutical services to support treatment and care
NIP, CMS 3.2.1 &
Strengthen the clinical management of HIV/AIDS related diseases MoHSS, church health services
3.2.4 & 3.2.5
Strengthen HAART PMTCT, STI and TB programmes in all facilities offering the services
NACOP, Dev Partners & All health service providers
Promote provision of psychosocial support and home based care to all people in all regions by all Key actors
MoHSS, NACOP & all Key actors
3.2.7 & 4.2.1
Ensure NGOs and CBOs are equipped to provide and support relevant treatment, care and support
MoHSS, church health services
3.2.7
Promote the Patient’s Charter to ensure that health workers adopt a caring attitude to all, including marginalised people
All Key Actors 3.2.8
Activities to achieve Objective 5: To mitigate impact Improve access to all relevant social assistance grants by streamlining the process
Social Services 4.2.1
Compile and disseminate information to caregivers and the public on how to access social grants, benefits and other statutory services for OVC and PLWHA
Social Services 4.2.1
Build the capacity of social workers and community workers to identify and register people eligible for social grants in order to address poverty related issues by providing training.
MoHSS, NGOs UNAM,
4.3.1

Chapter VI: Sectoral obligations and commitments
Medium Term Plan III for HIV/AIDS 119
Health Sector’s Commitments Responsibility Ref Activities to achieve Objective 6: (MoHSS) To coordinate the national response
Plan for adequate human resource capacity in the health sector MoHSS, Dev Partners & All Key Actors
5.1.1 & 5.1.2
Provide the secretariat for NAC, NAMACOC and NAEC and technical support to all other coordinating bodies in the national response
NACOP & NPC 5.2.1
Promote commitment by MOF, NPC, MRLGH and OPM to ensure adequate financial resources are in place to respond at all levels
MoHSS 5.2.2
Ensure that readily available, up-to-date information is available and regularly disseminated to all stakeholders and support the stakeholders in the development as well as dissemination of a user-friendly M&E system
MoHSS and Key actors
5.2.3
Develop and disseminate a user-friendly M&E system for the whole national response
MoHSS 5.3.1
Coordinate and implement surveillance, HIS and research MoHSS 5.4 Activities to achieve Objective 7: To provide technical support to partners
Strengthen the technical capacity of partners promoting behaviour change, particularly relating to health factors and interventions affecting transmission of HIV/AIDS, STI and TB
All Key Actors 2.1.1, 2.4.2
NACOP to coordinate quality training in treatment, care and support services, of professional and non-professional staff, delivered by Key Actors in the health sector
MoHSS NHTC, NACOP and Key Actors
3.1.1
Provide technical support to community initiatives All Key Actors 4.1 Activities to achieve Objective 7: To implement workplace programmes in the health sector
Assess the impact of HIV/AIDS in the health sector’s workplaces and its effect on delivering its core functions
All Key Actorsand Dev Partners
5.4.2
Establish workplace programmes in all health sector institutions All Key Actors 2.4.2 Strive for the prevention of HIV transmission in all health care settings Key Actors 2.2.2 Provide Post-exposure Prophylaxis (PEP) to health workers at risk of infection
All health service providers
2.2.2

Chapter VI: Sectoral obligations and commitments
Medium Term Plan III for HIV/AIDS 120
Lead Agency: Ministry of Information and Broadcasting Key Actors: NBC, MISA, media training institutions (UNAM and Polytechnic),
print, broadcast, electronic, community and corporate media, advertising agencies, MoHSS: IEC, MBESC, MHETEC, MWACW, NYC, John Hopkins Institute, Take Control Task Force1
Target Groups: The general public, the information and media communities
Sector Objectives Coordination of and support to social mobilisation at all levels, including advocacy, community involvement and behaviour change communication
This Sector’s Commitments in MTP III Chapter 3 Reference
Information and Media Sector’s Commitments Ref Enabling Environment Mobilisation of institutional, community, spiritual, traditional, political and private sector leadership to advocate for support, behaviour change, reduced discrimination and stigma for equal access to services and care
1.1.1
Support and publicise testimonies of PLWHA and vulnerable groups to eradicate stigma and discrimination
1.2.1
Coordinate information and communication on policy and law reform issues to ensure all people know their rights and access to justice and services
1.3.1
Coordination of IEC to combat HIV-related discrimination 1.4.1 Prevention Develop and make widely accessible specific IEC materials for vulnerable people, including with disabilities, e.g. Braille, cassettes, videos with sign language, in San and other minority languages
2.2.1
Develop, design and translate and distribute behaviour change interventions for different target groups, including women
2.2.1
Support sport, art, culture, theatre, fashion and interactive programmes to increase awareness and self-esteem
2.2.1
Strengthen co-ordination of national, regional and local information, education and communication (IEC) programmes and increase outreach for HIV prevention, care and support through regular contact meetings and visits with TC task force, RIO2, RACOC
2.4.1
1 Take Control (TC) Task Force: Co-ordinator Ministry of Information and Broadcasting (MIB) • AIDS Care Trust • ALU (LAC) • AMICAAL• CAA • CCN • Channel 7 • Christ’s Hope • CLASH • CRIS • ded •FHI • FAWENA • Gospel Outreach • Lifeline/Childline• Lironga Eparu • MBESC • MHA (NamPol) • MHETEC • MIB • MLRR • MISA Namibia • MOD • MOHSS • MPCS •Mubasen • MWACW • NABTA • NABCOA • NACOP • NamCol • NAPPA • NaSoMa• NBC • NNAD • NRCS • NYC • Ombetja Yehinga • Open Talk (NYC) • Radio Energy • SMA•Telecom • The Namibian • UNAIDS • UNESCO • UNFPA • UNICEF• USAID • VSO RAISA • Walvis Bay MPC • White Ribbon • Windhoek CC • WHO • Youth for Christ • YouthNet (FHI) • All RACOCs 2 RIO: Regional information officers, in employ of MIB, combined training and activities
Sector: Home AffairsSector: Information and Media

Chapter VI: Sectoral obligations and commitments
Medium Term Plan III for HIV/AIDS 121
Information and Media Sector’s Commitments Ref Provide I.E.C. tools, material and equipment to national, regional and community programme communication structures with e.g. support for international and national commemorations such as World AIDS Day, cultural and interactive activities
2.4.1
Develop information material, community and interpersonal activities, use of role models, culture and self-esteem programmes for behaviour change
2.4.1
Involve leaders at national, regional, constituency, local and tribal level in prevention activities through awareness creation, social mobilisation and personal speeches e.g. publicise testimonies through activities, material development, art and cultural programmes
2.4.1
Promote materials and activities to increase awareness of rights of HIV positive people and their families to care, support and services that are affordable, of high quality and responsive to their needs, and elimination of discrimination development
2.4.1
Support art, culture, theatre, fashion, sport and interactive programmes to increase awareness and self-esteem in all communities
2.4.1
Disseminate regular publications and updates on HIV/AIDS and related issues through websites, electronic and printed media, including development of special supplements and programmes for specific commemorations
2.4.1
Develop, design and implement targeted workplace programmes for different stakeholders in the information and media sectors linking rights, prevention, treatment, care and support, including issues of substance abuse and violence
2.4.2
Develop and enforce appropriate systems and safe guards to prevent sexual harassment, exploitation or assault of imprisoned offenders, and to support and protect those coming forward with complaints and needs
2.5.1
Increase production and dissemination of IEC material in all the local languages related to the dangers of alcohol abuse, especially as it relates to unsafe sexual practices
2.5.1
IEC programmes to support expanded treatment, care and support programmes, including PMTCT, STIs, TB and other opportunistic diseases, HBC and support
3.1.2
Impact Mitigation IEC for impact mitigation, including on OVC, poverty, food security and community-based interventions
4.1.1
Managing the HIV/AIDS response Train personnel at all levels, particularly personnel officers and media managers 5.1.2 Strengthen coordination, management, dissemination, monitoring and evaluation capacity of social mobilisation programmes and training of key actors in information and media sector
5.2.1 5.44.1
Strengthen networking platforms and reporting systems for increased information flow of national social mobilisation programmes through the Take Control Task Force, regional and constituency AIDS committees, mobile communication and information sharing mechanisms
5.2.2
Conduct sectoral impact assessment and develop strategies to mitigate impact 5.5.4 Mainstream HIV/AIDS, TB and other related issues into ministerial programmes and budgets, monitoring, evaluation systems and research
5.3.1 5.4.2

Chapter VI: Sectoral obligations and commitments
Medium Term Plan III for HIV/AIDS 122
Lead Agency: Ministry of Works, Transport and Communication Key Actors: NAMPOST, TELECOM, NAMWATER, Local Authorities, Association
of Local Authorities in Namibia (ALAN), TransNamib, Roads Construction Corporation (RCC), Air Namibia, Walvis Bay Corridor Group (WBCG)
Target Groups: Employees, local communities neighbouring infrastructural projects
This Sector’s Commitments in MTP III Chapter 3 Reference
Infrastructure Sector’s Commitment Ref Enabling Environment The Ministry of Works, Transport and Communication will approach all role players in the Transport Sector to expand the number of role players that positively contribute to the prevention of HIV/AIDS infection and to the reduction of its impact
1.1.1
Train MWTC management in HIV/AIDS related issues in order to give the required assistance to the respective committees within the Ministry and the sector at large
1.1.1
Continue to include all Regional and District Offices of the Ministry as well as the identification of HIV/AIDS focal persons in the respective regions and district and their training.
1.1.1
Prevention Strengthen existing workplace programmes and encourage other organisations to establish their own programmes
2.4.2
Distribute condoms on a regular basis and continue to train peer educators, al all levels, in condom promotion and the promotion of partner reduction
2.4.3
Treatment and Care Services Create an environment where staff members can be counselled and obtain general information regarding HIV/AIDS, STIs and TB
3.1
Continue to train all MWTC HIV/AIDS Committee members more advanced HIV/AIDS related matters, including home base care and counselling so that they will serve their respective workforces more effectively
3.1.1
Integrated and Coordinated Programme Management Establish a Sectoral Steering Committee to coordinate Key Actors in the Infrastructure sector
5.2.1
Establish and strengthen Ministerial HIV/AIDS Committees at all regional and district MWTC offices
5.2.1
Continue to increase MTWC budget allocations for HIV/AIDS activities 5.2.2
Sector: Infrastructure

Chapter VI: Sectoral obligations and commitments
Medium Term Plan III for HIV/AIDS 123
Lead Agency: Directorate: Labour Services, Ministry of Labour (MoL) Key Actors: MoL, MTI, unions, Namibia Chambers of Commerce and
Industry, Namibian Business Coalition on AIDS (NABCOA), Retail industry, Joint Consultative Conference, Hawkers Association, Namibia Employers Federation, Labour Advisory Council, Namibia Shebeen Association
Target Groups: The workforce, employers,
Introduction:
HIV/AIDS severely threatens both productivity and demand for goods and services. AIDS results in increased health care costs, medical insurance, death benefits, disabilities and pension payments. The Ministry of Labour, which is directly monitoring the workforce of Namibia, has realised the importance of addressing the HIV/AIDS pandemic. The Directorate of Labour Services, which deals with HIV/AIDS at the workplace, is aware of the tremendous tasks lying ahead to be more effective in addressing the pandemic and all other related concerns with in the working environment.
This Sector’s Commitments in MTP III Chapter 3 Reference
Labour, Trade and Industry Sector’s Commitments Ref Prevention through education Implementation of the National Code on HIV/AIDS at all workplaces 1.3.2 Ensure that infected workers are not discriminated against at the workplace 1.4.2 Prevention by social mobilisation 2.4.1 Through all possible media, TV, radio, and newspapers awareness campaigns must be strengthened
2.4.1
Dissemination of pamphlets, booklets and any other sources of information in order to raise awareness
2.4.1
Place adverts, e.g. sign boards, in workplaces and in workplaces 2.4.1 The Directorate of Labour Services will enhance education at work through tripartite workshops, workplace meetings, counselling and safety talks
2.4.2
Ensure through inspections that the safety structures (committees) at workplaces are in place as stipulated by the Labour Act
2.4.2
Ensure that employers and employees implement the provisions of the National Code on HIV/AIDS
2.4.2
All stakeholders are well informed on the content of the National Code 2.4.2 Prevention by changing attitudes In Labour too, we should educate the workers and the employers that protected sex bears a responsibility which goes beyond their privacy, personal choice or taste
2.4.2
Educate workforce and public at large to behave responsibly 2.4.2 Encourage voluntary test in order to ensure that workers know their HIV/AIDS status, thus to prevent further infections
2.4.2
Counselling for those infected and affected to refrain from stigmatisation 2.4.2 Labour inspectors to distribute condoms at workplaces during inspections 2.4.3
Sector: Labour, Trade and Industry

Chapter VI: Sectoral obligations and commitments
Medium Term Plan III for HIV/AIDS 124
Lead Agency: Ministry of Lands Resettlement and Rehabilitation
Key Actors: MLRR, National Federation of People with Disabilities in Namibia, Directorate. Special Education, MoHSS (Rehab), Directorate of Social Services, Ehafo.
Target Groups: Staff members, resettled people, people with disabilities and the public at large.
Sector Objectives 1. To ensure that staff, people with disabilities and resettled people are fully informed and
sensitised on HIV/AIDS. 2. To ensure availability and easy access to HIV/AIDS information and condoms/femidoms for staff,
resettled people as well as people with disabilities. 3. To provide care and support to HIV infected individuals and those suffering from AIDS. 4. To develop policies that facilitates the protection of people with disabilities to enjoy their right to
safe sex and practice family planning without being discriminated against. 5. To make information available on HIV/AIDS awareness in an accessible format for people with
disabilities e.g. Braille or large print.
This Sector’s Commitments in MTP III Chapter 3 Reference Lands Resettlement and Rehabilitation Sector’s Commitments Ref Enabling Environment Create continuous awareness through sector committees 1.1.1 Render moral support to infected and affected people 1.2.1 Involve those who are affected in the planning of the activities 1.2.1 Develop and implement HIV/AIDS policy for the sector 1.3.2 Prevention Develop activities which address the Sector’s vulnerable groups such as resettled people, people with disabilities and public at large
2.2.1
Develop and implement workplace policy to prevent discriminatory practice against people living with HIV/AIDS (PLWHA)
2.4.2
Treatment, Care and Support 3 To facilitate care and support for the sector’s vulnerable groups who are infected and affected by HIV/AIDS
3.2.8
Impact Mitigation Establish coordination with other organisations representing PLWHA 4.1.2 HIV/AIDS/STI/TB Management Response Appoint full time HIV/AIDS focal person 5.1.1 Provide training to enhance skills and knowledge on HIV/AIDS pandemic 5.1.2 Ensure an annual budget line for HIV/AIDS activities 5.2.2 Develop guidelines and plans of action 5.2.5
Sector: Lands Resettlement and Rehabilitation

Chapter VI: Sectoral obligations and commitments
Medium Term Plan III for HIV/AIDS 125
Lead Agency: Ministry of Justice Key Actors: Offices of Attorney General and Ombudsman, Law Society,
Legal Assistance Centre, University of Namibia: Justice Department and other relevant partners, NAMFISA
Target Groups: The general public and Sectors
This Sector’s Commitments in MTP III Chapter 3 Reference
Legal Sector’s Commitments Ref Enabling Environment Consider adopting a broad anti-discrimination law that includes discrimination on the basis of HIV
1.3.1
Review all existing legislation to identify that which impedes access to services for PLWHAs and OVC and to reform same
1.3.1
Undertake law reform to amend or set aside laws that a) increase vulnerability to HIV/AIDS b) hinder access to treatment, care and support or c) impede mitigation of impact
1.3.1
Put in place laws that facilitate a) reduction of vulnerability b) access to treatment, care and support and c) mitigation of impact
1.3.1
Conduct systematic review of laws and policies to ensure no arbitrary discrimination is present
1.3.2
Policy guidelines tailor made for particular Sector Review legislation to ensure that all legislation adhere to international standards
1.3.2
Sensitise lawyers, magistrates, judges and other legal personnel on nature of HIV generally as well as on the need for a human rights based approach to the epidemic and what that means and on national HIV/AIDS policy when it becomes available
1.4.1
Donors to be approached for funds for provision of information material and other educational programs by the Sector
1.4.1
Statute required to modify common law on contract and to enable NAMFISA to regulate the insurance sector so as to ensure equal access to insurance for PLWHA
1.4.2
Prevention Educate staff members in the sector on the nature of the disease as well as preventative measures
2.4.2
Ensure that people’s rights are adequately protected in the workplace and in the community and that they can come out freely and become actively involved in all activities
2.4.2
Review existing customary law to identify customary law practices that increase vulnerability to HIV or increase the impact of HIV and enact appropriate law reform
2.5.1
Capacity development for Treatment and Care Services Train paralegals to act as resource persons in communities and to assist and train healthcare workers on legal issues
3.1.1
Mitigating the impact Legal Sector to make legal practitioners available to address communities and render legal advice to PLWHAs on a pro bono basis
4.1.1
Sector: Legal

Chapter VI: Sectoral obligations and commitments
Medium Term Plan III for HIV/AIDS 126
Legal Sector’s Commitments Ref Lawyers/Legal Aid directorate (MOJ) to assist in the writing of wills and to advise on insurance contracts and other legal problems associated with HIV/AIDS
4.2.1
Inform people on procedures to access social assistance grants and other services 4.2.1 Integrated and Coordinated Programme Management 5 Assess the impact of HIV/AIDS on the sector 5.1.1 Training of personnel at all levels, particularly personnel officers 5.1.2 Establish a centralised information centre and an HIV coordinator in every region who will provide information and give direction
5.2.1
Sectoral structures to be established. Composition of structure to be worked out by Steering Committee
5.2.1
Circulate information in the sector via e-mail and the creation of a website for use by this Sector and other Sectors
5.2.3
Share the information at meetings through the discussion of minutes 5.2.3 Sector to identify and appoint a full-time career public servants as the HIV/AIDS/STI/TB program officers to enable the Sectors to carry out their mandate effectively
5.2.4
The Steering Committee in liaison with the focal persons will monitor indicators 5.3.1

Chapter VI: Sectoral obligations and commitments
Medium Term Plan III for HIV/AIDS 127
Lead Agency: Parliamentary Presiding Officers
Key Actors: National Assembly, National Council, Cabinet
Target Groups: The Nation
Sector Objectives: It is important for Parliamentarians to be knowledgeable about HIV and AIDS and to be key
partners in developing policies, programmes and legislation that advance effective prevention, treatment, support and care for PLWHA. Hence they are to strive for the achievement of the desired goals by creating an environment conducive for preventing new infections, eliminating discrimination and stigmatisation associated with the epidemic. Parliamentarians will do everything within their sphere of influence to:-
influence public opinion and lead their constituents towards attitudes supportive of an effective national response to the epidemic by increasing public knowledge and understanding of relevant issues
ensure that legislations that they vote on to become acts of parliament protects human rights, advances effective prevention, treatment, support and care programmes
ensure political commitment and better governance essential for a rights-based response to HIV and AIDS
mobilise the involvement of government, private sector and civil society to discharge their societal responsibilities in responding appropriately to the epidemic and
ensure that adequate and consistent financial resources are allocated to support and enhance effective HIV and AIDS national programmes that are consistent with human rights principles.
This Sector’s Commitments in MTP III Chapter 3 Reference Legislative Sector’s Commitments Ref Enabling Environment Legislative Committees on HIV and AIDS can provide on-going forum for parliamentarians to deepen their understanding of the epidemic through regular briefings, policy discussions and can serve as a vehicle for the law reform
1.1.1
Acting as bridge between Parliament, the statutory and voluntary sectors, providing a forum for the exchange of information
1.1.1
Ensuring that HIV and AIDS is kept on the political agenda through Parliamentary debates , questions and meetings with Ministers
1.1.1
The Parliamentarians need to combine intellect, tolerance, compassion and resolve to address the most important issues that cause suffering among communities and PLWHA
1.1.1
Strong personal commitments from political and civil society leaders are vital to promote national and local understanding and cooperation, avoid denial and stigma, and secure the full commitment and accountability of all sectors. These contributions will significantly lead to increased openness and some of the strides necessary in curbing HIV infection
1.1.1
Prevent forced testing 1.3.1 Raising awareness of HIV and AIDS issues in Parliament and encouraging balanced policies based on accurate information;
1.3.1
Sector: Legislative

Chapter VI: Sectoral obligations and commitments
Medium Term Plan III for HIV/AIDS 128
Legislative Sector’s Commitments Ref Prevent discrimination and stigma 1.4.1 Prevention Implement the workplace programme through a work place HIV/AIDS committee, including peer education, management and staff training, and community outreach to staff and family members
2.4.2
Treatment Promote antiretroviral treatment 3.2.6 Impact Mitigation Prevent malnutrition 4.3.1 Advocate reduction of poverty and vulnerability and building of community capacity and that of individuals to enable them to respond to the epidemic. Such attention should ensure access to basic education, health, and social services
4.1.1
Special attention should be given to the growing number of orphans and children made vulnerable through death or incapacity of one or both parents
4.2.1
Managing the HIV/AIDS response Parliamentary Committees 5.2.1 Sectoral Committee and Parliamentary Staff 5.2.1 Constituency Committees 5.2.1 Improved information and knowledge management is an essential enabling element in the fight against this pandemic.
5.2.3
Consistent Budget Allocation 5.2.4 Regularly monitoring the Programme implementations from national to local levels
5.3.1

Chapter VI: Sectoral obligations and commitments
Medium Term Plan III for HIV/AIDS 129
Lead Agency Ministry of Mines and Energy Key Actors to be involved: Ministry of Mines and Energy, Unions,
NAMPOWER, Chamber of Mines and Oil Companies
Target Groups Mineworkers, workers, families, employees and relevant communities
Sector Objectives 1. To prevent HIV/AIDS within the Mining and the energy providing communities 2. To ensure compliance to the National Code on HIV/AIDS in employment.
This Sector Commitments in MTP III Chapter 3 Reference Mining and Energy Sector’s Commitments Ref To ensure the development of educational programmes on HIV/AIDS for all the relevant communities
2.4.1
To ensure development and dissemination of HIV/AIDS information to all the communities
2.4.1
To acquire and distribute condoms through social marketing strategies 2.4.3 To ensure review of company policies inline with the National Code on HIV/AIDS in employment
1.3.2
To ensure existence of care and support services within Key Actors for the infected and affected workers and management staff
2.4.2
Sector: Mining and energy

Chapter VI: Sectoral obligations and commitments
Medium Term Plan III for HIV/AIDS 130
Lead Agency: Ministry of Prisons and Correctional Services Key Actors: MPCS, Aids Law Unit, Lironga Eparu, organisations supporting
rehabilitation (CRIS, BRIDGE, PFB, others) Target Groups: All imprisoned offenders, all MPCS staff, relevant community
members (relatives of offenders and others)
Sector Objectives 1. To have established an enabling legal and policy framework for the sectoral response to STIs
and the HIV/AIDS epidemic and their impacts 2. To have developed and implemented prevention, care and support programmes for staff
(workplace) and for imprisoned offenders 3. To have involved AIDS service organisations in the sectoral response in general and in
promotion of positive living in particular 4. To have conducted research and surveillance in order to have evidence-based policies
This Sector’s Commitments in MTP III Chapter 3 Reference
Prisons and Correctional Service’s Commitments Ref. Enabling Environment To sensitise and advocate with sector leadership and management, as well as relevant community members, for improved sectoral response to HIV/AIDS (using research results)
1.1.1
To review legal issues hindering the sector’s adequate response to HIV/AIDS, concerning prevention, care and support, and pursue legal changes through appropriate channels
1.2.1
To develop and implement a comprehensive sectoral policy for HIV/AIDS response in prisons and correctional institutions (for staff as well as imprisoned offenders), aiming to offer the imprisoned offenders the same scope and quality of prevention, care and support services as those in the general community
1.2.2
To develop activities to address and reduce stigma and discrimination among both the imprisoned offenders as well as in the MPCS workplace
1.3
Prevention among imprisoned offenders To strengthen the capacity of MPCS to design and deliver appropriate prevention programmes, through improved knowledge and skills and strengthened management capacity
2.1
To develop and implement a behaviour change programme targeting imprisoned offenders, including the development of relevant and effective IEC materials
2.2.1
To establish a male condom procurement and distribution policy, within the (changed) legal framework
2.2.1
To develop and enforce appropriate systems and safe guards to prevent sexual harassment, exploitation or assault of imprisoned offenders, and to support and protect those coming forward with complaints and needs
2.2.1
To maintain current STI treatment services 2.2.1 To develop and implement adequate VCT services as well as PEP services for rape victims, in accordance with current guidelines, policies and protocols
2.2.1
Sector: Prisons and Correctional Services

Chapter VI: Sectoral obligations and commitments
Medium Term Plan III for HIV/AIDS 131
Prisons and Correctional Service’s Commitments Ref. To maintain and strengthen existing coordination with public health services on PMTCT in order to ensure appropriate services for female imprisoned offenders involved
2.2.1
Employees Assistance Programme
To strengthen the capacity of MPCS to design and deliver appropriate comprehensive workplace programmes linking prevention, treatment, care and support, through improved knowledge and skills and strengthened management capacity
2.4.2
To develop and implement a workplace behaviour change and support programme with appropriate referral to existing STI, VCT, PMTCT, care, treatment and support services
2.4.2
To design and implement a condom provision policy, including its financial implications, to ensure access to male and female condoms by all staff in all institutions country-wide
2.4.2
To maintain the current policy on prevention of transmission in healthcare settings (for staff as well as imprisoned offenders), including existing PEP services for health workers at risk of infection with HIV
2.2.2 2.4.2
Treatment Care and Support for imprisoned offenders
Ensure that the prison health system has the knowledge and capacity to implement, monitor and supervise comprehensive HIV/AIDS treatment, care and support programmes, including the provision of HAART and treatment of opportunistic infections, using updated guidelines and protocols
3.1.1
Ensure adequate support for HIV/AIDS care providers, as part of a comprehensive support programme for health care providers
3.1.1
Provide information and education to the general imprisoned offenders’ population about HIV/AIDS treatment, care and support programmes, especially TB as an opportunistic infection, and increase ‘treatment literacy’ for people infected and those affected by HIV/AIDS
3.1.2
Improve existing opportunistic infection and comprehensive case management services, including palliative care and attention for HIV/TB dual infection, with special attention for drug provision coordination
3.2.2
Establish provision of HAART, including PMTCT+, in prison health services for persons meeting the existing inclusion criteria
3.2.3
Establish appropriate coordination mechanisms with public health services for offenders arriving at and leaving the MPCS institutions, including imprisoned pregnant women living with HIV/AIDS delivering in external facilities, in order to ensure a continuum of care (HAART, PMTCT+, other)
3.2.3
Review the early release policy in order to ensure taking into account the situation of people living with HIV/AIDS
?
Expand existing (informal) prisoner-to-prisoner care and support activities to include care for people living with HIV/AIDS, and ensure coordination with external services for home-based care for arriving and leaving offenders
3.2.4
Establish an appropriate management plan to plan and monitor access to and coverage of treatment, care and support
3.2.6
Impact Mitigation among imprisoned offenders and related affected persons Establish coordination with aids service organisations and those representing people living with HIV/AIDS, in order to ensure the provision of additional services (such as to promote positive living)
4.1.1
Maintain current support for people living with HIV/AIDS concerning special diets, adequate shelter and clothing and other
4.1.4

Chapter VI: Sectoral obligations and commitments
Medium Term Plan III for HIV/AIDS 132
Prisons and Correctional Service’s Commitments Ref.
Managing the HIV/AIDS response
Review and strengthen the sector’s programme planning and management structures for enhanced coordination, accountability and monitoring of the HIV/AIDS response, addressing resource mobilisation, human resource development and information flows issues
5.1
Ensure to obtain the identified necessary external technical support for programme development and training
5.2.1
Ensure quality assurance of the MPCS HIV/AIDS response programme through the development of minimum standards and best practices and their monitoring
5.2.2
In the framework of the overall prison health service M&E system, develop and implement a monitoring and evaluation system to ensure data collection, assessment of resource use and results achievement against performance data, facilitation of planning and improved understanding of the epidemic
5.3.1
Put in place a n HIV and STI surveillance system 5.4.1 Improve the current health information system with respect to HIV/AIDS, STIs and TB 5.4.2 Design and undertake research into HIV vulnerability, HIV/AIDS risk behaviour and coping strategies of people living with or affected by HIV/AIDS, in the context of the prison community and human rights policies and obligations
5.4.2

Chapter VI: Sectoral obligations and commitments
Medium Term Plan III for HIV/AIDS 133
Lead Agency: Ministry of Regional and Local Government and Housing Key Actors: ALAN, NELAO, AMICAALL, local authorities including town
councils, Regional Councils, RACs, RACOCs, DACOCs, CACOCs, ARC, CoW, Traditional Leaders, Land Boards, Governors, relevant NGOs.
Target Groups: Regional and constituency planning, coordination and implementation bodies relevant for the HIV/AIDS response, both governmental and non-governmental; as well as the populations of each constituency and region
Sector Objectives 1. Ensure protection of residents within corresponding regions, constituencies and town
council areas against HIV/AIDS infection 2. To coordinate HIV/AIDS prevention, care, support and impact mitigation activities in
respective regions, including those of the government, NGOs and the private sector 3. To ensure resource mobilisation for regional and constituency HIV/AIDS responses,
through the Regional Council budgeting procedures for multi-sectoral activities as well as through adequate budgeting on regional level by each governmental sector, NGO and private sector business
4. To plan, manage and implement HIV/AIDS prevention, care, support and impact mitigation activities at regional and local authority level.
This Sector’s Commitments in MTP III Chapter 3 Reference Regional and Local Governance Sector’s Commitments Ref Enabling Environment Provide traditional leaders with IEC on HIV/AIDS so that hey can advocate for reduction in discrimination, access to treatment care and support, and behaviour change
1.1.1
Sensitise and mobilise all the governors to champion a non-discriminatory, human rights approach to the HIV/AIDS epidemic, and to use every opportunity to address HIV/AIDS with their constituencies
1.1.1
Ensure that Regions and local authorities have HIV/AIDS policies for their workplaces 1.3.1 Prevention Assist each region to undertake an assessment of particularly vulnerable groups and the reasons for vulnerability
2.2.1
Strengthen and expand IEC and behaviour change programmers in regions, especially outside urban centres
2.41
Establish additional HIV-testing facilities in the regions 2.4.5 Ensure that traditional authorities take steps to see that traditional inheritance practices which might be harmful to OVC, especially concerning inheritance, are abolished
2.5.1
Treatment Care and Support Use the regional IEC and Advocacy Committees to produce IEC material for treatment literacy, dealing especially with the particular regional context with regard to VCT, PMTCT, and HAART
3.1.2
Sector: Regional & Local Governance

Chapter VI: Sectoral obligations and commitments
Medium Term Plan III for HIV/AIDS 134
Regional and Local Governance Sector’s Commitments Ref Through the RACOCs, coordinate home-based care provision at regional level, ensuring sufficient volunteers are trained, adequately equipped and supported
3.2.4
Use World AIDS Day to acknowledge the contribution of volunteers in the expanded response to HIV/AIDS
3.2.4
Impact Mitigation Expand the establishment of multi-purpose centres that can accommodate youth and mitigate risk behaviour
4.1.1
Improve care for orphans and vulnerable children through community care 4.1.2 Managing the HIV/AIDS response Ensure direct representation of local authorities in national as well as regional level coordinating bodies such as RACOCs for the HIV/AIDS response (other than through ALAN, NELAO or AMICAALL)
5.1.1
Assist local authorities to design and implement HIV/AIDS local responses, including workplace activities, and to obtain the necessary resources to this end
5.1.1
Ensure that regions have sufficient information based on participatory research into the impact of HIV/AIDS to plan and monitor their programmes
5.4.2

Chapter VI: Sectoral obligations and commitments
Medium Term Plan III for HIV/AIDS 135
Coordinating Bodies: ALAN and AMICAALL and NALAO
Key Actors to be involved: Local Authorities throughout Namibia Target Groups: Those HIV/AIDS infected and affected populations in
cities, towns and villages Sector Objectives: 1. Empower local authorities to respond more effectively to the HIV/AIDS epidemic in their
constituencies and to work together with these communities
2. Build the capacity of mayors, and municipal leaders and local authority institutions to initiate or expand local responses to HIV/AIDS
3. Increase access by local authorities to relevant and up-to date information in support of
HIV/AIDS advocacy, sensitisation and programme development
4. Apply the comparative advantage of local authorities in coordination and implementation of local responses.
This Sector’s Commitments in MTP III Chapter 3 Reference Enabling Environment 1 All mayors, local councillors and local authority officials receive relevant IEC material on HIV/AIDS
1.1.1
Conduct training and sensitisation activities for local authorities on the HIV/AIDS epidemic, management implications, governance, advocacy and Co-ordination
1.1.1
Local authorities contribute to national policy dialogue through articulation of local realities
1.3.1
Prevention 2 Mobilise local capacity to protect and support young people in staying free of HIV/AIDS infection, and in appropriate care and support for those infected and affected
2.3.2
Develop workplace programmes for all municipalities 2.4.2 Mitigating the Impact 4 Capacity building for local authorities on project management of community-based responses to HIV/AIDS and use of limited resources
4.1.1
The Local Authority will act as a local funding agent for community responses 4.1.1 Identify through a needs assessment process, community based HIV/AIDS response projects
4.1.1
Work together with private sector and civil society people living with HIV/AIDS and other partners in the community
4.1.2
Ensure that all Local Authorities have a Plan of Action for combating the impact of HIV/AIDS on communities, and an HIV/AIDS coordinating committee
4.3.1
Programme Management and Coordination 5 All local authorities undertake a rapid impact assessment to inform planning 5.1.1 All local authorities undertake a strategic planning process to mainstream HIV/AIDS into the municipal service agenda
5.1.5
Develop monitoring system, including client feedback, for programmes 5.3.1
Sector: Local Authorities

Chapter VI: Sectoral obligations and commitments
Medium Term Plan III for HIV/AIDS 136
Lead Agency: MHETEC with National Youth Council Key Actors: MHETEC, NYC and its 13 Regional Forums, Ombetja Yehinga,
NANSO, YouthNet, Young Women Christian Association (YWCA), Disabled National Youth Council, Girl Child Project, Open Talk, CoW Junior Councillors, NYS, Youth Health Development Programme (YHDP), CCN Youth Desk, Catholic Youth League, SWAPO Youth League, ELCIN Youth Desk, Lironga Eparu Ambassadors of Hope, NAPPA, KAYEC
Target Groups: All in-school and out-of-school Namibian youth
Sector Objectives 1. To prevent spread of HIV/AIDS among in-school and out-of-school youth 2. To ensure active participation and action of young people in the national response to the
HIV/AIDS epidemic 3. To ensure availability of HIV/AIDS and sexuality and reproductive rights information and life
skills education as well as condoms for young people 4. To ensure provision of treatment, care and support to young people living with HIV/AIDS 5. To develop policies which allow young people to enjoy sexuality without fear of infection or
unwanted pregnancy and without sexual violence, with attention for the empowerment of young women and the differential needs of young women and men
6. To support relevant programmes of youth organisations and assist these in capacity building
This Sector’s Commitments in MTP III Chapter 3 Reference Youth Sector’s Commitments Ref Enabling Environment Ensure that youth leaders engage in HIV/AIDS advocacy and creating an enabling environment for visible actions
1.1.1
Prevention Strengthen the capacity of youth organisations for delivering prevention programmes through improved knowledge and skills development as well as management capacity building
2.1
Strengthen the capacity of existing youth-friendly services for BCC, male and female condom provision, STI education and VCT, and add STI treatment as new component
2.3 2.4
Raise the issue of lacking confidentiality for youth visiting health services (for family planning, condoms testing and other) with appropriate authorities
2.2.1
Ensure expansion of IEC and behaviour change interventions concerning sexuality, reproductive health and HIV/AIDS, for youth to rural areas, including through the regional and constituency youth forums
2.3
Ensure greater involvement of youth organisations in developing and implementing peer education programmes in schools, including the setting up and continued support to aids awareness clubs
2.3.1
Reinforce existing programmes for older youth and facilitate youth organisations to reach youth in the regions at constituency level, through churches and other channels as a way to reach whole families including youth and their parents
2.3.2
Sector: Youth

Chapter VI: Sectoral obligations and commitments
Medium Term Plan III for HIV/AIDS 137
Youth Sector’s Commitments Ref Implement the NYC 2004-2005 action plan ‘kicking aids out of sports’ 2.3.3 Treatment Care and Support Ensure youth organisations and BCI programmes targeting youth to have the right information for referral for treatment, care and support and increasing treatment literacy of youth
3.1
Ensure that HAART services and HIV/AIDS care and management in general are accessible for young people living with HIV/AIDS
3.2
Increase involvement of young people in HBC activities 3.2.4 Impact Mitigation Ensure that youth leaders and youth organisations pursue increased support for OVC
4.1.1
Managing the HIV/AIDS response Co-ordinate the Youth Sector activities and ensure involvement of all relevant stakeholders
5.2.1
Improve co-ordination on regional levels, including between youth organisations and Regional Aids Co-ordinators
5.2.1
Ensure greater involvement of youth organisations in other relevant sectors as well as in major national forums dealing with coordinated management of the HIV/AIDS response (including monitoring & evaluation and research issues)
5.2.1 5.3 5.4
Strengthen resource mobilisation for youth organisations and programmes targeting young people
5.1.2
Mobilise resources for implementation of HIV/AIDS related programmes through youth organisations
5.2.2

Chapter VI: Sectoral obligations and commitments
Medium Term Plan III for HIV/AIDS 138
Co-ordinating Bodies: Council of Churches in Namibia (CCN), Church Alliance
for Orphans (CAFO), and Church AIDS Network (CAN).
Key Actors: Members of all organisations Target Groups: Religious leaders, youth, vulnerable groups, community
volunteers, all congregation members
Sector Objectives 1. Religious leaders and identified laity have the necessary attitudes and skills to address
HIV/AIDS in their communities and to be in the forefront of HIV/AIDS program activities, especially in reducing stigma and discrimination
2. Integrate HIV/AIDS interventions into all existing church programs e.g. youth services, confirmation classes, marriage preparation, men’s clubs, camps, retreats and choirs.
3. PLWHA, children and families affected by HIV/AIDS receive holistic care and support from congregational-community initiatives.
This Sector’s Commitments in MTP III Chapter 3 Reference Be a righteous and Biblical voice concerning issues of gender, justice and bias as it affects HIV/AIDS reducing stigma and discrimination.
1.1.1
Call on clergy and laity to model abstinence before marriage and fidelity and tolerance and compassion to al those infected and affected by HIV/AIDS.
1.1.1
Empower PLWHA in local congregations as resource people for changing attitudes and developing appropriate congregational responses
1.3.2
Build the capacity of congregations to expand and deliver strong prevention programmes focusing on abstinence and faithfulness and providing appropriate and accurate information on condoms
2.1.1 and 2.1.2
Train religious leaders in HIV/AIDS information, behaviour change communication, counselling and referrals, and the importance of reducing stigma and discrimination
2.1.1
Develop and disseminate locally responsive material related to HIV/AIDS prevention, care and support incorporating a religious perspective
2.3.1
Develop programmes emphasizing parenting and healthy family life creating an environment for open discussion on sexuality
2.3.1 & 2.3.2
Promote youth-appropriate interventions including peer education, youth based IEC materials, and youth centres, including an emphasis on abstinence, delay, and faithfulness
2.3.2
Mainstream gender equity in every structure and programme 2.5.1 Facilitate home-based care training for those interested volunteer groups in congregations or at ecumenical level and provide material and moral support to home-based care providers
3.2.4
Establish and promote ideal models of OVC care, optimally in a family setting ensuring a safety net for all children.
4.1.1
Develop and expand programmes in the community that address the poverty and suffering caused by HIV/AIDS at household level
4.3.1
Advocate for consistent and frequent FBO representation and participation in policy formation and programme co-ordination, development and implementation
5.1.1
Sector: Faith-Based Organisations

Chapter VI: Sectoral obligations and commitments
Medium Term Plan III for HIV/AIDS 139
Coordinating Bodies NANASO and NANGOF and Lironga Eparu Key Actors to be involved: Members of both organisations, other NGOs
Target Groups: HIV/AIDS infected and affected people throughout Namibia, especially vulnerable communities, CBOs, support groups, NGO staff
NGO Sector Objectives: 1. Develop the capacity of all members, especially smaller, rural organisations through access to
technical support and small grants 2. Support local responses to HIV/AIDS by training in HIV/AIDS project management and
providing up-to-date information 3. Consistent and frequent participation in all relevant coordinating mechanisms to ensure that
NGO/CBO needs and contributions are understood at national and regional level 4. Improve capacity of sector for monitoring and evaluation
This Sector’s Commitments in MTP III Chapter 3 Reference NGO Sector’s Commitments Ref Enabling Environment Provide information, materials and training in local languages to traditional healers, religious, political and traditional leaders and other community leaders concerning the necessary change in attitudes and in behaviour and reduction of discrimination of those living with and affected by HIV/AIDS, STIs and TB
1.1.1
To organise and participate in AIDS awareness campaigns to influence the general public and opinion leaders
1.1.1
Deal with HIV/AIDS as a human rights issue and provide basic client services in terms of legal advice, litigation, policy formation and education and advocacy.
1.2.2 1.3.3
Prevention To develop or use existing behaviour change communication material and interventions for targeted groups based on research within communities, and ensure consistent expression of basic ABCD messages in the sector
2.2 and 2.3
Targeted behaviour change communication and interventions (BCI) for children and young people in primary and secondary educations/institutions including comprehensive life skills intervention efforts with a sexual and reproductive health component and counselling services
2.3.1
Expand social mobilization and awareness interventions that target the general population for the prevention of HIV and STI infections
2.4.1
Develop and implement workplace programmes and policies 2.4.2 Scale up the country wide supply and distribution of male and female condoms for the general through public, private and social marketing mechanisms
2.4.3
Provide Adolescent Friendly Reproductive Health information and services 2.4.3 Expand Voluntary Counselling and Testing provision and support the training of community counsellors
2.4.5
Treatment, Care and Support 3 Facilitate and train community home-based care groups
3.2.4
Sector: Non-Governmental Organisations

Chapter VI: Sectoral obligations and commitments
Medium Term Plan III for HIV/AIDS 140
NGO Sector’s Commitments Ref Provide the general public with IEC on treatment and care for PLWHA. 3.1.2 Mitigating the Impact Mobilise and support through training and resource mobilisation CBOs to actively and constructively participate in HIV/AIDS programmes
4.1.1
Capacity building for the Network of People Living With HIV/AIDS as well as promoting and providing support groups for people living with HIV/AIDS
4.1.2
Expand and improve the care and support available for orphans and vulnerable children
4.2.1
Develop a national community educational campaign to ensure non-discriminatory access to the available social assistance grants, allowances and other services for OVC and people living with and affected by HIV/AIDS.
4.2.1
Programme Management and Coordination Ensure NGOs/CBOs are represented at all levels in programme coordination and management structures
5.2.1
Strengthen and coordinate national and regional resource mobilization and flow mechanisms to support the HIV/AIDS STI and TB programmes at all levels
5.2.2
To ensure horizontal learning through sharing best practices with members through newsletters, workshops, and other effective communication systems
5.2.3
To develop, annually update and maintain the Directory of NGOs/CBOs 5.2.4 Develop monitoring and evaluation systems and procedures 5.3.1

Chapter VI: Sectoral obligations and commitments
Medium Term Plan III for HIV/AIDS 141
Lead Agency: Namibian Business Coalition on AIDS (NABCOA)
Key Actors: Representatives of members of NABCOA, NCCI, Chamber of Mines, Joint Consultative Committee (JCC), Okatumbatumba Hawkers Association (OHA), Namibia Shebeen Association (NSA), Namibia Employers Federation (NEF), Professional Associations, AIDS Law Unit, AIDS Care Trust
Target Groups: Leadership, Employers, Self-employed, SMEs & Informal Sector
Sector Objectives 1. To mobilise the private sector to implement HIV/AIDS prevention, care treatment, support and
impact mitigation policies and programmes in the workplace in line with MTP III 2. Prevent and minimise HIV infections through workplace and community education programmes 3. Share and implement best practices addressing HIV/AIDS 4. Raise awareness on the impact of the HIV/AIDS epidemic, its impact on the national economy
and the need for an expanded national response 5. To ensure national private sector development and implementation of workplace programmes
and policies for addressing HIV/AIDS at every workplace in a non-discriminatory manner 6. To ensure acceptance and compliance to the National Code(s) on HIV/AIDS in employment
and ALL other/subsequent codes/guidelines and/or Acts of Parliament 7. To facilitate a process to provide guidelines for the effective implementation of a policy
framework for affordable treatment (antiretroviral) for PLWHA 8. To develop innovative approaches to assist smaller and informal employers to implement
appropriate HIV/AIDS prevention, care, treatment, support and impact mitigation programmes in the workplace
9. Establish ongoing M&E strategies of workplace programmes as well continuous analysis of the Private Sector National Alignment Strategies Successfully Managing HIV/AIDS appropriate response Workplace Programmes
This Sector’s Commitments in MTP III Chapter 3 Reference Private sector’s Commitment Ref Enabling Environment Mobilise the private sector nationally through business membership organisations about HIV/AIDS Epidemic with relevant IEC materials with innovative approaches e.g. local languages; one-on-one meetings and involving PLWHA (GIPA Principles)
1.1.1 1.2.1
Develop comprehensive/continuous training programmes at major companies & centres with increased human resource training budgets
2.1.1
Encompass smaller businesses into the fold of larger ones in a true smart partnership and/or public-private partnership arrangement where applicable (e.g. local authorities). Branches of business membership organisations will assist with the outreach programmes to smaller towns
2.1.1
To ensure the development and implementation of workplace programmes and policies with emphatic non-discriminatory clauses
1.4.1 2.4.2
To widely implement increased condom distribution and management thereof as an up-scaling of the preventative measures
2.4.3
Sector: Private Sector

Chapter VI: Sectoral obligations and commitments
Medium Term Plan III for HIV/AIDS 142
Private sector’s Commitment Ref Call for the appointment of HIV/AIDS focal persons at all workplaces (regardless of size)
2.4.2
Encourage VCT programmes within workplaces. This procedure to be accompanied by an effective stakeholder buy-in exercise
2.4.5
To undertake quarterly “HIV/AIDS Climate Surveys” and Annual Assessment Studies of the private Sector to emphasise to economic impact on business. With special reference to sub-sectors e.g. Fishing; Agriculture; Tourism; Mining etc
5.1.4 5.4.1
To plan, develop and implement appropriate programme activities with all relevant stakeholders for the SMME & Informal Sector
2.1.1 2.4.2
To widely consult with Business Namibia and its major stakeholders e.g. government; medical and insurance industries; pharmaceutical companies and international donor community on the establishment of a Policy Framework for affordable treatment (anti-retrovirals) for those living with HIV & AIDS in Namibia
3.2.1 3.2.2 3.2.7
Develop M&E strategies for adoption by businesses in order for them to adapt and adopt new ideas for effectiveness of planned activities. This to be in the format of management training programmes. Additionally, the National private sector initiatives driven by the above mentioned agencies (amongst others) to assess the national private sector response continuously and adopt M&E strategies for cascading down to the appropriate sub-sector; individual company and membership representative body hence the proposed National Private Sector Alignment Strategies
5.1.6 5.3.1
Implement training programmes for Senior and line managers on “Effective AIDS Management – in the Place of Work”. These courses to be similar to other management disciplines e.g. ‘Conflict Management’ or ‘Change Management’. It should serve as a catalyst for action by Corporate Namibia to have the HIV/AIDS Programme become a strategic intervention at their businesses. Such courses to be presented in cooperation with either UNAM or Polytechnic or others
5.1.1 5.2.1
Resource Pooling; Resource Gap Funding to be explored; investigated for implementation of certain National initiatives e.g. (a) treatment (drugs) programmes (b) cross border initiatives (trucking; migration; Refugees and (c) regional programmes (SADC)
5.1.2
Increased (a) Advocacy activities to enhance buy-in by bigger Companies into the new revised menu of partnership options (Namibia specific) to provide financial support to NGO’s at the local level (increased corporate social responsibility initiatives) and (b) Lobbying the Parliamentarians and specifically the Parliamentarian Sub-committee on Economics; Trade and Investment for increased debate and educating of the constituents on HIV/AIDS
1.1.1 1.3.1 1.3.2

Appendix 2
Medium Plan III for HIV/AIDS 149
Profile:
Caprivi Region has a population of 79,826 (2001 Census) of which 72% live in rural areas. Caprivi Region occupies a critical transportation and potential tourism niche in Namibia, linking Namibia to Botswana, Zimbabwe and Zambia. Thirty eight percent of the population are under 15 years of age. Four percent of the population have a disability, blindness predominating. Caprivi Region has the highest HIV/AIDS prevalence rate in the country at 43% of pregnant women testing positive for HIV/AIDS in 2002. Caprivi Region has experienced the fourth largest percentage increase in the number of deaths at 108% from 1999-2001. Caprivi Region has the second highest less than five mortality rate in the country. Fourteen percent of the children under fifteen have lost a mother, a father or both parents.
Caprivi Region’s Commitments in MTP III Reference
Caprivi Region’s Commitment Responsible Agency
Ref
Component 1 Enabling Environment 1 Conduct consultative meetings and hold workshops for leaders in all sectors
MoHSS, CAFO, CYDA, CAA
1.1.1
Hold workshops for local leaders at constituency level to identify problems and plan for HIV/AIDS activities
Regional Councillors
1.1.1
Lobby for mainstreaming of HIV/AIDS and budgetary from each ministry Regional Councillors
1.1.1
Sensitise traditional leaders RACOC 1.1.1 Promote participation of PLWHA in developing IEC material and advocacy work
RACOC 1.2.1
Educate employers on rights of PLWHA at the workplace. MWTC, Lironga Eparu, MBESC
1.4.2
Educate communities through mass media and open discussion on rights of PLWHA and the fight against discrimination
RACOC 1.4.1
Component 2: Prevention 2.
Train youth life-skills facilitators CAA and MBESC
2.1.1
Establish more multi-purpose youth centres for life-skills programme sites and greater media and community mobilisation. Target: 10,000 children and youth
CAA, MFMY, CBIAS, CYDA,
MHE
2.3.1 2.3.2
Run outreach workshops for parents on HIV/AIDS and communication with children. Target: 15,000
MBESC/NGOS 2.3.2
Order condoms, distribute and provide condom use training – male and female
NGOs, all ministries
2.4.3
Consider mobile and standard VCT to expand services. 5 MoHSS/NGOs 2.4.5 Improve referrals to VCT counsellors MOHSS 2.4.5 Run training workshops and establish clubs in sports, music and drama. Provide materials for the clubs: Target 10,000 youth
MBESC/MHETEC/NGOs
2.5.1
Sub-Component 3.1: Capacity development for the expanded treatment, care and support response
3.1
Train health care workers and traditional healers in PMTCT, HAART and HBC: refresher courses, workshops, in-service: Target: 10 groups per constituency: 75% of health workers, 50% of traditional healers
MoHSS, BMS, NGOs
3.1.1
Caprivi Region

Appendix 2
Medium Plan III for HIV/AIDS 150
Caprivi Region’s Commitment Responsible Agency
Ref
Train and sensitise traditional healers – establish association of Traditional Healers Target: 50% of traditional healers
MoHSS, Red Cross, CAA BMS
3.1.1
Expand home-based care groups to 10 per constituency and give refresher courses to HBC especially on dealing with the terminally ill, psycho-social support and food provision
MoHSS/CAA 3.1.1
Establish I – C – S forum for traditional healers and medical staff MoHSS 3.1.1 Standardise training curriculum MoHSS 3.1.1 Recruit two HBC giver per village MoHSS, CAA 3.1.1 Strengthen understanding of access to HAART to recruit more patients on HAART
MoHSS 3.1.2
Sub- Component 3.2: Treatment and care services 3.2 Expand PMTCT and then HAART to 3 health centres and 24 clinics MoHSS/NGOs – 3.2.3 Integrate counselling for PMTCT- 3 centres MoHSS 3.2.3 Facilitate self referrals for HAART and PMTCT via VCT MoHSS 3.2.3 Expand access to HAART by ensuring quality NIP services, adequate drug supply, and recruiting sufficient counsellors.
MoHSS 3.2.6
Standardise HBC kits, training curriculum and referral using reporting forms by holding meetings with health care workers and HBC to discuss flow and ensuring referrals from counsellors to hospitals
MoHSS 3.2.7
Consider ways to give and to standardise incentives for volunteers in the region – counsellors, HBC etc
NGOs, MoHSS, 3.2.7
Increase mobility for caretakers NGOs/MoHSS 3.2.7 Sub-component 4.1 : Developing the Capacity of Local Responses 4.1 Facilitate participatory planning with community HIV/AIDS groups (2 per constituency)
Regional Councillors
4.1.1
Decentralise funds from Regional Council to community groups
Regional Council
4.1.1
Facilitate participatory planning with community HIV/AIDS groups: 2 groups per constituency.
RAC/CAA/ NGOs
4.1.1
Train community leaders in facilitating and participatory planning techniques
RAC/CAA/ NGOs
4.1.1
Sub-Component 4.2 Comprehensive services for OVC and PLWHA 4.2 Urgent need for Ministries (MOHSS and MWACW) to identify most vulnerable beginning with up-dating data on OVC and terminally ill
MoHSS, MBESC, MWACW
4.2.1
Train counsellors in psycho-social support NGOs/MoHSS 4.2.1 Resource mobilisation for community projects RAC/RC 4.2.1 Register OVC for material support (school fees, hostels, uniforms etc) Target: 2500
MWACW 4.2.1
Include a focus in governmental projects on those made vulnerable by HIV/AIDS
All 4.3.1
Establish and expand feeding schemes such as soup kitchens for OVC through HBC groups
4.2.1
Establish and expand after school support to OVC Target: all hostels % of schools
Red Cross, CAA, MoHSS, CAFO, CYDA,
4.2.1
Sub-Component 4.3 Addressing poverty 4.3 Facilitate appropriate housing grants for PLWHA and OVC and lobby for increased material support for vulnerable families including IGA and food security
LAs MoHSS
MWACW
4.3.1
Facilitate IGA and agricultural projects – 2 groups per const. Introduce Facilitate IGA among clients and support groups: 25% of clients involved in IGAs
MWACW 4.3.1
Encourage appropriate agricultural technology especially intensifying labour saving activities
MAWRD 4.3.1

Appendix 2
Medium Plan III for HIV/AIDS 151
Caprivi Region’s Commitment Responsible Agency
Ref
Include a focus in government and non-governmental projects on those made vulnerable by HIV/AIDS
Ministries/ NGOS
4.3.1
Component 5 : Integrated and Coordinated Programme Management 5 Quarterly working meetings – monitoring and performance evaluation – at RACOC
RACOC 5.2.1
Community health to be a directorate under RC to deal with HIV/AIDS under a director with staff. (reporting to Office of Governor)
Regional Council
5.2.1
The appointment of officers in the sectors to represent on RACOC (CACOCs etc) must be at the right level and have commitment. The permanent secretaries of various Ministries to be asked to inform regions of importance of RACOC and give guidelines on appropriate person.
Governor 5.2.1
Chief Control Officer to be head of Constituency admin. to strengthen const. level committees like Constituency Development Committees. Sector extension workers will be incorporated
Regional Council/ Governor
5.2.1
Monthly reports produced by various sectors and compiled and distributed and shared by RAC
Focal people 5.2.3
Establish operating and coordinating procedures between RACOC, CACOC and VDC
RAC/NACOP 5.2.3
HIV/AIDS to be addressed at RDCC and REMU Governor 5.2.3 Improve data collection on vulnerable groups. Explore ways of using students for data collection to have reliable information
Regional Council
5.2.3
Regional and constituency HIV/AIDS annual evaluation workshop RACOC 5.3.1 Develop M and E tools for RACOC activities RAC 5.3.1 Undertake regional needs assessment. Regional
Council 5.4.3

Appendix 2
Medium Plan III for HIV/AIDS 152
Profile:
According to the 2001 Census 107,663 people reside in Erongo Region. The region is divided into seven constituencies with 80% of the population residing in an urban centre. The region has an average unemployment rate of 34%, but 42.3 % for women. 7.6 % of the children under 15 in Erongo Region have lost one or both parents. Erongo has a well developed health delivery system with 87% of its population within 10 kilometres of a health facility. Erongo also has the lowest level of malnutrition among children in the nation, nine percent. The HIV/AIDS prevalence in Erongo is high with the 2002 sero-sentinel survey revealing an infection rate in pregnant women of 25% in the port town of Walvis Bay and 16% in neighbouring Swakopmund, a key tourist destination.
Erongo Region’s Commitments in MTP III Reference Erongo Region’s Commitments Component 1: Enabling Environment Provide political, religious and traditional leaders with up-dated information and statistics on HIV/AIDS/STIs in the region in the appropriate languages
1.1.1
Community awareness raising on rights of PLWHA and OVC Training workshops for 72 politicians, 28 traditional leaders, and 48 religious leaders
1.1.1
Component 2: Prevention Work with the traditional healers association and include them in CACOCs and RACOCs 2.1.1 Develop and strengthen BCC and BCI for specific groups in Erongo Region, including youth, sex workers, truck drivers, those in the fishing industry
2.2.1
Provide alternatives to alcohol and unsafe sex for the youth by providing opportunities for training and life-skills, drama, and sport, in multi-purpose centres schools, hostels and other venues
2.3.3
Establish more condom distribution points 2..4.3 Run a regional campaign on the importance of VCT and motivate for expansion of this service
2.4.5
Equip women with skills for economic empowerment 2.5.1 Component 3: Treatment, Care and Support Improve utilisation of existing IEC materials on treatment and care especially on VCT, PMTCT and HAART, for example at ANC clinics and in maternity wards
3.1.2
Provide training and resources to volunteer home based care givers 3.2.4 Component 4: Mitigating the Impact Establish soup kitchens and feeding schemes for PLWHA and OVC 4.1.1 Expand support groups of PLWHA 4.1.1 Create a directory of CBOs in the region to facilitate harnessing local resources for local activities
4.1.1
Develop and distribute a comprehensive guide on grants available for OVC and people infected and affected by HIV/AIDS with detailed information
4.1.2
Explore how MAWRD could help with food security projects for PLWHA 4.1.4 MWACW to speed up register of OVC and grant applications 4.1.2 Component 5 : Integrated and Coordinated Programme Management Establish clear objectives and terms of reference for all co-ordinating committees 5.2.1 Co-ordinate transport requirements to ensure full participation in co-ordinating mechanisms
5.2.2
Train local focal people for all sectors 5.2.4
ERONGO REGION

Appendix 2
Medium Plan III for HIV/AIDS 153
Profile:
Hardap has a total population of 68, 249 (2001 Census) of which 72% reside in rural areas. Hardap is a sparsely populated region, consisting of deserts on both the eastern and western borders. The main source of household income is wages and salaries, although the unemployment rate is high at 34%. 15% of the population rely on pensions as their main source of income. The HIV/AIDS prevalence rate is 11% and 11% of children under fifteen have lost one or both parents.
Hardap Region’s Commitments in MTP III Reference
Hardap Region’s Commitment Responsible Agency
Ref
Sub Component 1.1: Sustained leadership commitment 1.1 Educate and train political, religious, traditional leaders, employers and senior management as trainer of trainers on HIV/AIDS issues
RAC 1.1.1
Leaders will give feedback on their actions to RACOC and to their stakeholders (constituencies, membership etc)
Leaders 1.1.1
Leaders will become involved in support groups for OVC & PLWHA to increase their understanding of their situation
Leaders 1.1.1
Sub-Component 1.2 : Greater involvement of PLWHA in the response Improve the coordination and quality of counselling and support services for PLWHA by clarifying roles and geographic areas of responsibility, and by holding regular meetings.
RACOC 1.2.1
Strengthen PLWHA’s support groups and educate PLWHA on their rights RAC, HIV/AIDS counsellors
1.2.1
Sub Component 1.4 : Reduced discrimination and stigma Educate employers, communities and scholars on human rights to reduce discrimination and stigma
RACOC 1.4.1
Train peer educators in all sectors – NGOs, Faith-based organisations, parastatals, ministries - to have a good understanding of discrimination
RACOC, TOTs, RAC
1.4.1
Organise awareness campaigns using dramas, discussions, videos Peer educators 1.4.1 Sub-Component 2.1 Outcome: Improved quality of behaviour change interventions
2
Strengthen RACOC as the umbrella coordinating body in 2004, ensuring that all service providers are represented
Regional Council
2.1.1
Establish RACOC sub-committee by 2004 to coordinate training for capacity building and the development of I.E.C. materials
RACOC, MIB 2.1.1
Conduct training needs assessments for all personnel involved in delivering behaviour change messages – such as focal persons, leaders and peer educators; set annual training plans and publicise training sessions, involving PLWHA
RACOC Training Sub-committee
2.1.1
Sub-component 2.2: Behaviour change programmes targeting mobile and migrant workers, sex workers and prisoners, young people including OVC and street children, as well as the general population
2.2
Conduct behaviour change HIV prevention campaign targeting truck drivers and other mobile workers, sex workers and migrant workers.
Mariental Municipality
2.2.1
Strengthen existing HIV/AIDS activities/programmes for prison inmates, and make condoms available to all
MPCS RACOC
2.2.1
Strengthen and expand the MHSS peer counselling programme MoHSS 2.3.1 Establish a multi-purpose youth centre in Mariental as a focal point for behaviour change interventions and other activities
MHETEC, Municipality
2.3.2
Hardap Region

Appendix 2
Medium Plan III for HIV/AIDS 154
Hardap Region’s Commitment Responsible Agency
Ref
Develop & implement workplace policies on HIV/AIDS, including training on labour rights, promoting prevention of discrimination in businesses and penalties for discrimination.
Mariental Municipality; MoL, RACOC
2.4.2
Ensure the availability of free condoms at all times in all towns, villages and in rural areas with the assistance of GRN extension staff & NAMPOL.
MoHSS, RACOC members
2.4.3
Establish 2 VCT centres with outreach services within 5 years MoHSS 2.4.5 Expand prevention services, particularly the number of counsellors throughout the region, and develop regionally-orientated IEC materials
MoHSS 2.4.5
Enforce laws on alcohol availability to youth NAMPOL 2.5.1 Sub-Component 3.1: Capacity development for the expanded treatment, care and support response
Assess training needs and conduct training for Home-based care & counselling (HBC), Highly active anti-retroviral treatment (HAART) & Prevention of mother to child transmission (PMTCT) programmes.
MoHSS, NGOs
3.1.1
Strengthen training of HBC volunteers, peer educators and focal persons & leaders to provide information to households and individuals on the progression and treatment of HIV/AIDS, sexually transmitted diseases (STI), TB and other opportunistic diseases
MoHSS, RACOC,
NACOP, line ministries
3.1.1
Sub- Component 3.2: Treatment, care and support services Make treatment available for people with AIDS by 2005 MoHSS 3.2.6 Develop an adequate, confidential referral system between care and support services, health centres and counsellors for people living with HIV/AIDS, TB or STI
MoHSS, NGOs
3.2.7
Strengthen and expand the home-based care programmes to reach all communities and households;
3.2.7
Establish a RACOC technical committee on HBC to improve supervision, coordination, monitoring and evaluation of HBC activities and to ensure regular supplies for the HBC kits;
RACOC, MoHSS
3.2.7
Sub-component 4.1 : Developing the Capacity of Local Responses 4.1 Strengthen existing/ establish constituency (CACOCs) and local authority level multi-sectoral committees to coordinate and support local responses
RACOC 4.1.1 5.1.1
Establish support systems for these local committees – funding, training of members, on-going supervision (master trainer) information sharing, networking between groups, technical assistance, monitoring and evaluation on a regular basis
MWACW 4.1.1
Sub-Component 4.2 : Comprehensive services for OVC and PLWHA 4.2 The Regional OVC Committee will report quarterly to RACOC, as a RACOC sub-committee, and coordinate / monitor OVC needs & services in the region
MWACW RACOC
4.2.1
Assign specific activities/programmes to local multi-sectoral committee members to streamline assistance to OVC
CACOC, local authorities
4.2.1
Establish and maintain a referral system of OVC between RACOC members (including MWACW) and one regional database which is available to RACOC members in all localities
MWACW RACOC
4.2.1
Develop regional criteria for OVC assistance and provide food parcels and other material assistance to those in need
RACOC OVC committee
4.2.1
Establish a regional AIDS Trust Fund by 2004 HRC 4.2.1 Sensitise schools to not discriminate against OVC RACE: MBESC 4.2.1 Ensure pensions and maintenance grants reach care-givers MoHSS 4.2.1 Provide psychological & spiritual support and counselling to families in need Churches,NGOs 4.2.1 Monitor the situation of OVC on a regular basis and conduct participatory impact studies and other research
RACOC 4.2.1
Develop clear criteria for assistance to PLWHA and their support groups, monitor process and delivery of services; regular reports
RACOC 4.2.1

Appendix 2
Medium Plan III for HIV/AIDS 155
Hardap Region’s Commitment Responsible Agency
Ref
Sub-component 4.3: Addressing poverty 4.3 Strengthen school feeding programme by sensitising schools MBESC 4.3.1 Strengthen and streamline the Regional Food Security and Nutrition Programme; The Regional Emergency Management Unit will support both rural and urban communities
MAWRD REMU
4.3.1
Provide orientation and training on backyard gardening; MAWRD 4.3.1 Negotiate with local authorities on water pricing for vulnerable people / support groups
RACOC 4.3.1
Provide health education on healthy eating habits to communities and PLWHAs
MoHSS, RACOC 4.3.1
Assess the appropriateness of the Social Housing Programme and explore how PLWHA and homeless OVC can be accommodated within low cost housing schemes
MRLGH 4.3.1
Identify programme for local economic development – identify income generating projects and develop business plans for support groups; establish a regional economic development revolving fund.
RDCC, MWACW
MTI,
4.3.1
Develop an employment creation programme for the region MHETEC 4.3.1 Component 5 : Integrated and Coordinated Programme Management Strengthen RACOC as the umbrella coordinating body in 2004, ensuring that all service providers are represented; members should have decision-making mandates
Hardap Regional
Council (HRC)
5.2.1

Appendix 2
Medium Plan III for HIV/AIDS 156
Profile:
Karas Region has a total population of 60,329 (2001 Census), fairly equally distributed between rural and urban areas. Karas Region has the lowest population density in the country at 0.4 persons per square kilometre. Wages and salaries account for the majority (69%) of household incomes, with farming accounting for only 7 percent. Although the region has three hospitals and two health centres, about 43% of the residents must still walk over an hour to a health facility. The HIV/AIDS prevalence rate in the region is 16% and 11% of the children under fifteen are orphans. Agriculture, tourism, fishing and mining are important economic sectors which attract many migrant workers, usually separating them from their families. Karas Region has two of the main cross border points with South Africa and the port of Luderitz.
Karas Region’s Commitments in MTP III Karas Region’s Commitments Responsible
Agency Reference
Sub-Component 1.1: Sustained leadership commitment 1.1 Regional Councillors to meet with traditional and church leaders on a regular basis to emphasise a stronger involvement in the fight against HIV/AIDS and to advocate for behaviour change
Governor, RACOC,
All Leaders
1.1.1
Include HIV/AIDS as a regular agenda item at every regional, sectoral and constituency meeting
All 1.1.1
Train leaders on HIV/AIDS issues and involve people living with AIDS RAC 1.1.1 Sub-Component 1.2: Greater involvement of PLWHA in the response Leaders use existing structures to mobilise community leaders and encourage people living with AIDS to be open to their families, friends and community
RACOC 1.2.1
Sub-Component 1.3: Policy and law reform Lobby to amend national policy to enable people younger than 18 years to be tested for HIV/AIDS without their parents consent
RACE 1.3.1
Sub-Component 1.4: Reduced discrimination and stigma Review the para-legal programme in Karas Region and train 25 additional volunteers as para-legals who will serve their communities and PLWHA on human rights
RACOC 1.4.1
Publicise HIV/AIDS human rights issues using NBC and community radio, newspapers, etc
RACOC, Assoc of Para-
legals
1.4.1
All leaders to address discrimination and stigma among their stakeholders Governor, All leaders
1.4.1
Sub-Component 2.1: Capacity to deliver prevention programmes 2.1 Train 160 additional volunteers and health workers in counselling and home based care, including the supervision of TB treatment (DOTS)
CAA, SHPA - MoHSS
2.1.1 2.1.1
Train all health workers in the ARV programme CMO 2.1.1
Train all clinic and outpatient health workers in STI management and treatment
SHPA - MoHSS 2.1.1
Sub-Components 2.2 Target vulnerable populations Raise awareness among truck drivers; provide condom demonstrations and increase condom outlets
RACOC, NATAU
2.2.1
Lobby NAMPOL, NDF and other ministries to station married couples RACOC, 2.2.1
Karas Region

Appendix 2
Medium Plan III for HIV/AIDS 157
Karas Region’s Commitments Responsible Agency
Reference
together NAMPOL Strengthen health education to farm workers and rural communities MAWRD, NAU,
MWACW 2.2.1
Strengthen health education for large workforces such as at Aussenkehr and Rosh Pinah clinic
MoHSS, private sector
2.2.1
Expand health care services to rural communities (e.g. VCT and anti-natal care)
MoHSS 2.2.1
Educate women (16yrs-40yrs) on the use of femidoms MWACW 2.2.1 Advocate for the amendment of policies to enable prison inmates to have access to condoms
RACOC, Councillors
2.2.1
Sub-Components 2.3: Target young people Sensitise conservative school principals and expand comprehensive life skills programmes and other interventions to all schools to facilitate behaviour change
MBESC, NGOs
2.3.2
Train out-of-school youth as trainers of trainers on prevention of HIV/AIDS and STIs and support drama groups, puppet shows and other activities
MHETEC MBESC
2.3.2
Sub-Components 2.4: Target the general population Strengthen involvement of regional and local councillors and church leaders in HIV/AIDS prevention
RACOC 2.4.1
Mainstream workplace programmes; involve top managers RACOC 2.4.2 Expand condom outlets and ensure continuous supply of male and female condoms
MoHSS 2.4.3
Expand coverage of VCT services to all districts MoHSS, CAA 2.4.5 Sub-Components 2.5: Interventions to reduce poverty Empower women to work in income generating projects to become more financially independent
MWACW 2.5.1
Advocate for a change to customary law whereby a brother-in-law inherits a widow
MWACW 2.5.1
Sub-Component 3.1: Capacity development for the expanded treatment, care and support response
3.1
Provide information to the general population on HIV/AIDS treatment, through the media, health talks, meetings etc, recognising that culture plays a big role in treatment and care
GRN, NGOs, churches, peer educators, trad.
leaders
3.1.1
Expand training of home based caregivers MoHSS, CAA 3.1.1 Train health workers for an expanded provision of HAART treatment MoHSS 3.1.1 Run awareness programmes for youth to expand access to testing, counselling and treatment
MBESC, health sector, NGOs
3.1.1
Sub-Component 3.2: Treatment, care and support services 3.2 Ensure continuous supply of drugs and other commodities MoHSS 3.2.2 Increased access to special care e.g. counselling offices at clinics MoHSS, NGOs,
CBOs 3.2.3
Increase access of people living with AIDS to HAART MoHSS 3.2.7 Increase access to treatment, care and support services in the rural areas through outreach clinics and health centres
MoHSS 3.2
Sub-component 4.1 : Developing the Capacity of Local Responses 4.1 Establish a technical working group (TWG) of RACOC to coordinate support to local responses
RACOC 4.1.1 5.1.1
Identify existing organisations and resources; perform community needs assessment and develop plans accordingly, including new programmes where needed; share best practices and involve people living with AIDS
TWG - RACOC, MRLGH
4.1.1
Sub-Component 4.2 : Comprehensive services for OVC and PLWHA 4.2 Identify organisations working with OVC and PLWHA and the services TWG-RACOC 4.2.1

Appendix 2
Medium Plan III for HIV/AIDS 158
Karas Region’s Commitments Responsible Agency
Reference
rendered; identify these organisations’ needs; Develop a plan according to needs assessment; consider “Circles of support” within communities and fight against stigma and discrimination; RACOC to budget to provide support; lobby for political and government commitment to support programmes for OVC and PLWHA. Sub-Component 4.3: Addressing poverty 4.3 Improve networking/communication, coordination and the dissemination of information
RACOC 4.3.1
Make provision of land for gardens and livestock to those infected and affected by HIV/AIDS
MLRR, MAWRD, Local Authorities
4.3.1
Continue with the school feeding programme; Provide vitamin supplements to PLWHA
MBESC MoHSS, NGOs
4.3.1
Involve local caregivers and PLWHA in local council meetings – in decision-making
Councillors 4.3.1 5.1.1
Component 5 : Integrated and Coordinated Programme Management 5 Create two additional posts within the regional council to support the RAC and RACOC
MRLGH 5.1.1
Decentralise RACOC to maintain 3 district coordinating committees which meet monthly
RACOC 5.2.1
Revitalise the Regional Emergency Management Unit (REMU) to focus on impact mitigation of HIV/AIDS
Regional Council
5.2.1
Contract partners to implement parts of the programme, distributing responsibilities to cover all components
RACOC 5.2.1
Establish and maintain a regional database of the region’s organisations
RACOC 5.2.3
All implementing partners need to report to RACOC, using a standardised reporting system
All Key Actors RACOC
5.2.3
Improved communication between RACOC, NACOP, focal persons within ministries and other implementing organisations
All 5.2.3
Develop a unified plan, with goals and objectives agreed by all participants and schedule regular meetings to keep track of short-term outcomes
RACOC 5.2.4
Establish and maintain programme monitoring tools and reporting formats
NACOP 5.3.1

Appendix 2
Medium Plan III for HIV/AIDS 159
Profile:
The Kavango Region has a total population of 202,604, of which seventy-two percent live in rural areas. Fifty-two percent of the population indicate that farming is their main source of household income. Although Kavango Region has four hospitals and numerous health centres and clinics, it must contend with the highest infant mortality rate in the country and close to fifty percent of the children may be mal- or under- nourished. Seventeen percent of the children under fifteen have lost either one or both parents. The HIV/AIDS prevalence rate is 22% (2002). AIDS is the top killer disease, followed by malaria.
Kavango Region’s Commitments in MTP III Reference
Kavango Region’s Commitment Responsible Agency
Ref
Component 1: Enabling Environment 1 Provide leaders with knowledge and information in local languages about how many people are infected, how they get infected, what should be done to address the impact of HIV/AIDS , national HIV/AIDS policies, and treatment of HIV/AIDS to share with their communities to address behaviour change and stigma and discrimination.
MoHSS/RAC/ MIB/NGOs
1.1.1
Traditional leaders to advocate against discrimination Traditional authorities
1.1.1
Spiritual leaders to address the problem of stigma and discrimination in their sermons and other public speaking occasions, and in any counselling environment.
CCN 1.1.1
Leaders to mobilise funds for local communities and to ensure the correct use of funds.
Regional Council
1.1.1
Governor to launch the ARV and PMTCT programme for Kavango Region.
Governor/ MoHSS
1.1.1
Community leaders to establish more support groups for PLWHA and to involve PLWHA in planning and implementation
Trad. Leaders, NGOs
1.2.1
Laws needed to address discrimination and to promote equal access to services.
Parliament 1.3.1
Component 2: Prevention 2
Use drama to train communities on the impact of HIV/AIDS and possible action plans (including impact of stigmatisation)
MAWRD/ NGOs
2.1.1
Identify who in the region still required awareness raising and target those very rural communities through drama and community meetings
MAWRD (DEES project)
2.2.1
Train more counsellors for VCT, including 20 nurses providing ANC. MoHSS/NGOS 2.1.1 Training in use of female condom NASOMA,
MWACW 2.1.1
Meeting with contract and mobile workers (construction workers, defence, police etc.)
MoD, MHA
2.2.1
Establish HIV/AIDS clubs at schools Target: (331 schools + 2 tertiary institutes) will target schools with 11 + age groups
MBESC, Red Cross
2.3.1
Public library to be supplied with educative materials in all media formats on HIV/AIDS –
MBESC 2.3.1 2.3.2
Existing Multi-purpose centres to undertake recreational activities to attract the youth
MHETEC, MBESC
2.3.2
Kavango Region

Appendix 2
Medium Plan III for HIV/AIDS 160
Kavango Region’s Commitment Responsible Agency
Ref
Organise sport, drama and cultural competitions for youth –
MFMC, MBESC, NGOs
2.3.1
Review workplace policies which may put people at risk – e.g. mobility – structural changes and establish proper policies in the workplace to fight stigma
Private Sector/ Ministries
2.4.2
Supply RACOC with condoms (male and female) in order for members to distribute to their groups and simplify an ordering system for condoms from the regions with medical store.
MoHSS 2.4.3
Hold meetings with teachers, church leaders, community leaders, NGOS to provide information and to look at attitudes around condoms
RAC 2.4.3
All condom distributors should give correct information about condom use and improve distribution of female condoms
MoHSS MWACW
2.4.3
Improve partner tracing for STIs management MoHSS 2.4.4 Raise awareness about VCT services and establish VCT centres at each district hospital; at all centres with ANC and some outside the hospital, including the possibility of mobile services. 1 in each constituency
MoHSS, NGOS 2.4.5
Sub-Component 3.1: Capacity development for the expanded treatment, care and support response
3.1
Conduct refresher courses for 200 HBC givers on ARV/PMTCT training of more HBC groups and refresher training
MoHSS/NGOS 3.1.1
Conduct refresher courses for 60 TBAs in PMTCT MoHSS 3.1.1 Train 80 health workers on PMTCT/ARV in order to expand provision MoHSS 3.1.1 Train lay counsellors and hold refresher training MoHSS/
Lifeline 3.1.1
Train MIS officers on PMTCT/ARV record forms Print 400 T-shirts on VCT; develop 7 bill boards; provide translated IEC materials and drama and other outreach services to uniform services and youth clubs; intensify awareness raising campaign.
RMT 3.1.2
Sub-Component 3.2 : Treatment, care and support services 3.2 PMTCT programme to strengthen partner notification MoHSS 3.2.3 Obtain a CD4 count machine for Rundu Hospital lab. And obtain Elisa test at district level by 2008
MoHSS 3.2.6
Increase the number of patients on ARV from 10 to 200 by 2004 and to 900 by 2009
MoHSS 3.2.6
Develop and monitor a referral system for HBC. to report monthly to ? MoHSS 3.2.7 HBC kits to be available at nearest centre MoHSS 3.2.7 Establish support groups for ARV clients MoHSS/NGOs 3.2.7 Sub-component 4.1 : Developing the Capacity of Local Responses 4.1 Organise community programs to support orphans – at constituency levels (crops, income generating, feeding programmes at school etc.)
community leaders and all
4.1.1
Training of constituency HIV committees in HIV/AIDS so they can facilitate community responses
RAC/RCs 4.1.1
Hold workshops in the community on HIV/AIDS awareness and its impact on agriculture
MAWRD 4.1.1
Train more peer educators and trainers in the community to assist with HIV/AIDS information, access to services and planning and implementing programmes.
NGOs/ MWACW MAWRD
4.1.1
Sub-Component 4.2: Comprehensive services for OVC and PLWHA 4.2 Traditional leaders and RC to inform OVC and caregivers about procedures and documents required to access fee exemptions for health care and education
Traditional leaders/ Reg. Councillors
4.2.1
Register OVC so they can have access to grants MWACW and 4.2.1 Develop system to streamline the application procedures and to ensure speedy provision of correct documentation to OVC and their caregivers (e.g. birth and death certificates)
MoHSS and MBESC, Red Cross, RC,
4.2.1

Appendix 2
Medium Plan III for HIV/AIDS 161
Kavango Region’s Commitment Responsible Agency
Ref
Ensure the provision of identity documents needed for OVC to access support.
MHA 4.2.1
Sub-Component 4.3 : Addressing poverty 4.3 Encourage HBC programmes or CBOs to be incorporated into food-for-work programmes so that needy volunteers may obtain food
MWACW/ MAWRD
4.3.1
Facilitate income generating projects for PLWHA MAWRD 4.3.1 Facilitate HBC givers to start IGA and supply start up funds MAWRD 4.3.1 REMU criteria for vulnerability to include people infected and affected and caregivers and inform affected communities about access to drought relief food when available and food for work programmes.
REMU 4.3.1
Raise awareness in the communities through drama and IEC about services and funds available for OVC and caregivers.
MBESC/NGOs/others
4.3.1
AETs provide technical back-up to communities that have been trained (see 4.1) on their projects (e.g. garden, nutrition, etc).
MAWRD 4.3.1
Component 5: Integrated and Coordinated Programme Management 5 Train RACOC members in HIV/AIDS programme management NACOP 5.1.1 Hold consultative meetings and extensive mobilisation of all head of departments to ensure all members attend all the RACOC meetings.
RAC Regional
Councillors
5.2.1
Regional Councillors and Traditional Leaders to speed up establishment of (and involvement in) constituency and village AIDS committees from 2 – 8
RC 5.2.1
Councillors to designate just one deputy or focal person who has the authority to act as deputy chair on CACOCs. CACOCs to meet twice per quarter
Councillors 5.2.1
Regional Council to allocate financial resources and transport to communities for constituency committees plans
Regional Council
5.2.2
Mobilise funds from donor agencies, private sectors, and others. RACOC 5.2.2 Regional Development Planner to assist in preparation of proper plan and budget for RACOC activities.
Dev. Planner 5.2.2
Improve networking with existing line ministries and NGOs RACOC 5.2.3 RAC to report regularly to the Regional Development Committee on RACOC activities.
RAC 5.2.3
Undertake operational research into awareness, determinants of behaviour and ways to support behaviour change
RACOC 5.4.2

Appendix 2
Medium Plan III for HIV/AIDS 162
Profile:
According to the 2001 Census 250,262 people reside in the Khomas Region. The region has nine constituencies, eight of which make up the main urban centre of the country, Windhoek. Migration to the capital city has caused a 5.4% population growth resulting in, among others, unemployment (29%), inadequate housing, and over-burdened support services. The region has the best health and educational facilities in the country, including two public and 2 private hospitals and 64 schools. Unlike much of the country, the vast majority of people have wages and salaries as their main source of income. Sixteen percent of the children under 15 have lost a mother, a father, or both parents. In the most recent sero-sentinel survey 27% of the pregnant women were HIV/AIDS positive, down from 31 percent in 2000. The Khomas Region has the fifth highest prevalence rate in the country.
Khomas Region’s Commitments in MTP III Reference
Khomas Region’s Commitment Ref Component 1: Enabling Environment RACOC will organise on-going HIV/AIDS sensitisation and education sessions for all leaders in Khomas Region (political, community, religious, employers) on HIV/AIDS issues such as its impact on households, workplace & the region, treatment of AIDS & opportunistic infections and nutritional requirements of PLWHA, and to include aspects in every speech
1.1.1
Regional Councillors will ensure that every Constituency Development Committee has HIV/AIDS on every meeting’s agenda
1.1.1
Leaders will mobilise communities and large employers, such as Ramatex, to plan HIV/AIDS programmes
Leaders will share public speaking platforms with people living with HIV/AIDS 1.2.1 Strengthen support groups for PLWHAs to cover all parts of the region and support their action plans
1.2.1
RACOC will encourage employers and sectors to put appropriate HIV/AIDS policies in place
1.3.2
Reduce discrimination and stigma by being good role models and using the media to promote positive living and telling the truth about HIV/AIDS
1.4.1
Component 2: Prevention Hold specific target campaigns focusing on youth, young women, street children, orphans and vulnerable children (OVC)
2.2
Establish consortiums of NGOs working with similar target groups to coordinate coverage 2.1.1 Organise a strong education campaign “Enough is Enough” on the effects of alcohol in increasing poverty, on HIV infection rates, weakening the resistance of HIV infected people to opportunistic infections, reducing their body’s ability to accept medication,
Establish and enforce a Council policy on shebeens’ opening hours and other actions which promote owners’ social responsibility towards HIV prevention, through negotiations with the Shebeen Association and its members, in all constituencies
2.2.3
Create a platform for young people to share information & debate on HIV/AIDS and to encourage them to integrate HIV/AIDS activities with other youth activities such as dramas, sport, functions
2.3.2
Actively involve political and religious leaders in prevention campaigns by training them in HIV/AIDS
2.4.1
Support NGOs & volunteers to hold HIV/AIDS prevention sessions & condom demonstrations, in bars / shebeens
2.4.1
KHOMAS REGION

Appendix 2
Medium Plan III for HIV/AIDS 163
Khomas Region’s Commitment Ref Strengthen condom availability, especially of free condoms, after hours 2.4.3 Expand VCT services in Khomas in easily accessible places such as shopping centres 2.4.5 Strengthen referral systems between VCT centres and faith-based organisations 2.4.5 Component 3: Treatment Care and Support Services
Foster partnerships of service providers at constituency level 3.1 Expand the number of information points in different constituencies, by training existing personnel and PLWHAs, to provide information on the progression of HIV to AIDS, treatment, medication, side effects, its links with alcohol and other issues
3.1.2
Assess the capacity of existing HBC organisations to meet the growing need, and encourage existing or new NGOs to meet that need
3.2.7
Strengthen and expand the Health Promoters Programme to other constituencies to promote health education, HIV prevention, community mobilisation and to provide TB and AIDS treatment supervision
3.1.1
Component 4: Impact Mitigation Services Organise training of CBOs wanting to provide support services and provide small start-up funds
4.1.1
Network with other regions with experience of supporting CBOs, & income generating activities
4.3.1
Support a Khomas fund which supports OVC to further their education 4.2.1 Component 5: Integrated and Coordinated Programme Management Chairpersons of all national & regional HIV/AIDS committees will encourage members to send mandated delegates and they will publicly report on members’ attendance.
5.1.1
RACOC will establish criteria to support community action plans; each Constituency Development Committee will develop a community HIV/AIDS plan of action, which will be supported by RACOC, and will submit a quarterly report of their activities to RACOC
5.1.1 &
5.1.2 RACOC to develop a monitoring tool for HIV/AIDS and standardise a reporting format for all members to use
5.3.1

Appendix 2
Medium Plan III for HIV/AIDS 164
Profile:
The Kunene Region has a population of 68, 735 (2001 Census) of which 75% live in rural areas. The population density is very low at .6 persons per square kilometre. Kunene Region has the lowest literacy rate in the country at 57 percent, though it is interesting to note for information and communication purposes 72% of the population have access to a radio. Kunene Region has the lowest HIV/AIDS prevalence rate with 9% of pregnant women testing positive for HIV/AIDS in 2002. Kunene Region also has the lowest rate of orphanhood with 8% of children under fifteen classified as orphans
Kunene Region’s Commitments in MTP III Reference
Kunene Region’s Commitment Responsible Agency
Ref
Component 1: Sustained leadership commitment; greater involvement of PLWHA, relevant policies developed and discrimination and stigma reduced.
1
All leaders (traditional, church, political, private sector) to be part of local AIDS committees and linked with RACOC.
RAC and RCs 1.1.1
Conduct consultative meetings and workshops with all leaders CYDA, Church, CAFO, Youth
1.1.1
Church, traditional, and civil society leaders to address their communities on HIV/AIDS and discrimination at all possible venues and opportunities and to encourage openness and support local organisations for PLWHA.
All 1.1.1
Leaders to be provided with statistics on HIV/AIDS and up-date on latest treatment and the necessary training
CMO/RAC 1.1.1
Ensure all constituencies have HIV/AIDS committees supported through new constituency offices.
Regional Councillors
1.1.1
Parliament to consider if policies about discrimination need to be translated into law.
Regional Councillor
1.1.1
Initiate a vigorous campaign through workshops, radio, TV, print media on combating discrimination.
MIB/IEC Advocacy
1.4.1
Health services to ensure that facilities promote confidentiality – for example through the use of multi-purpose centres.
MoHSS 1.4.1
Component 2: Behaviour change programmes targeting mobile and migrant workers, sex workers and prisoners, young people including OVC and street children, as well as the general population, to reduce new infections
2.
Training in condom use for sex workers and distribution of condoms and family planning by agricultural ext. workers and mobile clinics especially to farm workers and rural populations.
MoHSS MAWRD
2.2.1
Issue of CSW and men having sex with men needs to be addressed in MTP III, including access to condoms by prisoners
Parliament 2.2.1
Traditional health workers and birth attendants to be provided with essential materials and training to deliver in hygienic conditions (gloves etc). Target: 200 already identified
MoHSS 2.2.2
Kunene Region

Appendix 2
Medium Plan III for HIV/AIDS 165
Kunene Region’s Commitment Responsible Agency
Ref
Messages for the below groups need to be developed and improved with testing and reviews:
women, learners, elderly, commercial sex workers, the disabled, farm workers, prisoners, traditional health workers, road construction or extension workers, army, police, sexually active youth, the unemployed in rural areas, school leavers.
IEC - Advocacy
Committee/ MoHSS
2.2 & 2.3
Build capacity of women to be empowered to report cases of rape and negotiate safer sex and establish two women and child protection centres in Khorixas and Kamanjab
Home Affairs 2.2.3
Encourage women to go to clinics and hospitals for ante-natal and delivery MoHSS 2.2.3 Expand peer education in schools with MFMC, mass media campaigns, outreach programmes.
MBESC 2.3.1
Provision of condoms and condom use training by all Ministries which have outreach programmes including greater distribution of female condoms
MoHSS
2.4.3
Establish 3 new VCT centres with outreach capacity at Opuwo, Outjo and Khorixas including training more counsellors
MoHSS/SMA 2.4.5
Communities to be made aware of new laws protecting women. LAs, NGOs, RCs 2.5.1 Use youth in community development projects. NGOs/Church 2.5.1 Develop activities to address alcohol abuse and drug abuse and encourage delay of sexual debut.
Churches/ MoHSS/
MWACW
2.5.1
Provide training for youth in employable skills (agriculture, computers, and tourism/hospitality) to reduce vulnerability.
MHETEC/MBESC MWACW,NGOs
2.5.1
Establish more recreational facilities for youth. Church/NGOS 2.5.1 Sub-Component 3.1: Capacity development for the expanded treatment, care and support response
3.1
Train Regional Councillors, newly appointed RAC and all RACOC on HIV programme management.
NACOP 3.1.1
Recruit one HBC trainer for each constituency. Run refresher courses on HBC MoHSS 3.1.1 Train more PLWHA as counsellors and in HBC MoHSS 3.1.1 Train health workers on PMTCT/HAART/STIs/TB MoHSS 3.1.1 Train teachers on how to deal with affected children and colleagues MBESC 3.1.2 Sub-Component 3.2 : Treatment, care and support services 3.2 Up-grade laboratory facility in Khorixas and Opuwo to test for HIV and add one in Outjo.
MoHSS/NIP 3.2.1
ARV to roll out in three districts – Outjo, Opuwo, Khorixas MoHSS 3.2.6 Fill HIV/AIDS post in MOHSS MoHSS 3.2.6 ARV drugs (some) to be given at clinics through trained staff. MoHSS 3.2.6 PMTCT and VCT to be implemented in all 3 districts (rapid testing and counselling) – including training of personnel and mobilisation to create demand for services
MoHSS 3.2.3
All TB patients to be consulted regarding testing to know status MoHSS 3.2.5 Counsel STI patients to receive testing and about risk MoHSS 3.2.5 Establish incentives for HBC including training and provision of kits MoHSS 3.2.7 Develop and improve referrals from clinics back to HBC– each district to have a HBC office for this.
MoHSS 3.2.7
Counselling should be provided for those on treatment and those testing positive on positive living (and the family).
3.2.7
Hospitals should have gardens to help with nutritional needs of people on treatment
MoHSS/NGOs/MAWRD
3.2.8
Sub-component 4.1 : Developing the Capacity of Local Responses 4.1 Undertake a survey on number of OVC and affected families - Identify structures already in the community that can be strengthened to care for OVC and nurture and support extended family structures
MWACW 4.1.1

Appendix 2
Medium Plan III for HIV/AIDS 166
Kunene Region’s Commitment Responsible Agency
Ref
Improve coordination mechanisms and monitoring and evaluation. MWACW 4.1.1 Capacity building training for all the stakeholders MoHSS 4.1.1 Sub-Component 4.2 Comprehensive services for OVC and PLWHA 4.2.1 Run programmes on rights of and services for OVC and PLWHA (Maintenance, Disability, Foster grants, fee exemptions)
MBESC/NGOs 4.2.1
RACOC to set up sub-committee on OVC and source funds (including Reg. Dev. Fund). Allocate more resources to these.
RACOC 4.2.1
Ensure the provision of identity documents needed for OVC to access support
MHA 4.2.1
OVC fund has been established in the region. Mobilise resources for this and to establish drop in centres
Regional Council
4.2.1
Sub-Component 4.3: Addressing Poverty 4.3.1 Include a focus in governmental projects on those made vulnerable by HIV/AIDS
All 4.3.1
Promote food security and nutrition MWARD, LFCU, CAA, CAFO,
MoHSS
4.3.1
Produce register of OVC and provide material support to those in need MWACW, CAA, MBESC
4.2.1
Develop and sustain income generating activities identified by local groups – gardens, poultry, tourism
MAWRD 4.3.1
Component 5: Integrated and Coordinated Programme Management 5 Encourage participation at RACOC. Focal people to be given a national and regional calendar of events which they agree to attend.
Focal people/RAC
5.2.1
CACOC to submit annual plans and budget to RAC and RACOC – and report back on funds received. Regional Council to allocated funds to constituencies for HIV/AIDS plans
Regional Councillors
5.2.1
Annual RACOC meeting to look at CACOC annual plans and give feedback
Governor 5.2.1
RAC to attend constituency meetings as planned . RAC 5.2.1 Reg. Dev. Planners should be on RACOC and share recommendations Planner 5.2.1 Strengthen constituency level participation from all sectors – political will needed and in the future transport will be needed.
Regional Councillors
5.2.1
Local Councillors to chair CACOCs one month before RACOC meeting – or a deputised chair- at which activities are assessed and coordinated
Regional Councillor
5.2.1
RACOC activities must have a plan and a budget submitted well in advance and RC should have vote for HIV/AIDS
RAC 5.2.2
Review and up-date sector plans and budgets OPW, Regional Council
5.2.2
Establish proper coordination between line ministries and RACOC RAC 5.2.3 Plans and activities to be clearly set out at national level and shared. NACOP should send info to RAC to be distributed
NACOP/ Ministries/RAC
5.2.3
Establish operating and coordinating procedures between RACOC, CACOC and VDC
RAC/NACOP 5.2.3
Hold community (village level) workshops with different local stakeholders (CBOs, ministry personnel, NGOs etc.)
RAC 5.2.3
Need data base for planning and resource allocation RACOC 5.2.5 Develop M and E tools for RACOC activities RAC 5.3.1 Regional needs assessment to be undertaken Regional
Council 5.4.2

Appendix 2
Medium Plan III for HIV/AIDS 167
Profile:
Ohangwena Region has a population of 228,384 of which 99% live in rural areas. Ohangwena Region has the highest population density at 21.3 persons per square kilometre. Sixty percent of the households are headed by women and a full forty-four percent of the population is under fifteen years of age. Fifty -two percent of the population state that farming is their main source of income and a full twenty percent indicate that pensions are their main source of income. The town of Oshikango is the major gateway to and from Angola. The HIV/AIDS prevalence rate in Ohangwena is 19%, and 18% of the children under fifteen have lost either one or both parents.
Ohangwena Region’s Commitments in MTP III Reference
Ohangwena Region’s Commitment Responsible Agency
Ref
Component 1: Sustained leadership commitment; greater involvement of PLWHA, relevant policies developed and discrimination and stigma reduced.
1
Train all community leaders using trainers, especially those who are living with HIV/AIDS
RACOC, MoHSS 1.1.1
Establish Parish congregation committees Church leaders 1.1.1 Raise awareness of traditional healers and TBAs Traditional
Authorities 1.1.1
Regional Councillors to establish constituency HIV/AIDS Coordinating Committees-11
Regional Councillors
1.1.1
Establish village AIDS Coordinating Committee Traditional Authorities
1.1.1
Provide office accommodation for Support Groups in the constituencies – by 2005
Regional Councillor
1.2.1
Mobilise PLWHA to come out publicly NGOs 1.2.1 Push for legislation to fight HIV/AIDS discrimination – Parliament, Cabinet Governor 1.3.1 Create awareness among minority groups and train peer educators in these groups.(San)
MLRR, RACOC TB Control
1.4.1
Establish regional campaign against discrimination Governors, NACOP,RAC
1.4.1
Component 2: Behaviour change programmes targeting mobile and migrant workers, sex workers and prisoners, young people including OVC and street children, as well as the general population, to reduce new infections
2.
Organise training workshops and refresher courses with latest HIV/AIDS information e.g. ARV, counselling and communication skills etc. for relevant NGOs and community leaders.
NGOs/MoHSS 2.1.1
Strengthen peer educator groups in the region. RACOC/ MoHSS
2.1.1
Arrange workshops on basic info for the region’s special Populations – commercial sex workers, seasonal workers, married couples, the San. And provide IEC materials in the appropriate languages using drama and music when possible.
NGOs/MIB/ MoHSS
2.2.1
School Boards to have a meeting to discuss condom provision – MBESC, NGOS, Councillors
MBESC 2.3.1
Ohangwena Region

Appendix 2
Medium Plan III for HIV/AIDS 168
Ohangwena Region’s Commitment Responsible Agency
Ref
Health education on behavioural change, abstinence and peer education through workshops and in-school and out of school programmes
MFMC, SMA, Red Cross, NAPPA
2.3.2
Create and support more youth clubs
MBESC, Red Cross
2.3.2
Encourage employers to adopt HIV/AIDS policies in the workplace NCCI Branch Ministries
2.4.2
Assess use and needs for condoms, and have regular and consistent provision of male and female condoms at workplaces and schools and public places.
Medical Stores/ RACOC/
2.4.3
Establish VCT throughout region – at all 3 hospitals,1 health centre, Oshikango, Okongo, I mobile –
MoHSS, Lifeline, SMA
2.4.5
STI treatment to be expanded to clinics RMT 2.4.4 Sub-Component 3.1: Capacity development for the expanded treatment, care and support response
3.1
Training on ARV, on referral, on counselling, on communication skills, on monitoring for health workers, labs, pharmacists, HBC, church leaders, traditional leaders, traditional healers, TBAs, LAs, NGOs, private sector, support groups, PLWHA, line ministries –
MoHSS, RACOC, NGOs
3.1.1
Train community health workers and HB C on STIs and OIs
MoHSS CBHC
3.1.1
Ensure that PLWHA and affected vulnerable people receive free health treatment at all facilities – community to be provided with adequate information on this
MoHSS 3.1.2
Sub-Component 3.2: Treatment, care and support services 3.2 Expand PMTCT, and VCT to regional and 3 district hospitals 3.2.3 Re-consider and revise criteria for acceptance into ARV programme to encourage people to come public
MoHSS 3.2.6
Expand HAART (1-2 in the region) to accommodate vast distances and population
RMT 3.2.6
Identify, strengthen and establish HBC groups
MoHSS, Councillors
3.2.7
Sub-component 4.1 : Developing the Capacity of Local Responses 4.1 Identify existing community groups and establish new ones Conduct needs assessment for these groups; mobilise and allocate resources to address these needs - to be specified
MAWRD/ MWACW
4.1.1
Encourage community members to care for OVC and PLWHA Traditional Authorities/ Churches
4.1.1
Sub-Component 4.2: Comprehensive services for OVC and PLWHA 4.2 Financial support for PLWHA – better coverage for all – GRN, Private Sector
MoHSS/Private Sector
4.2.1
Revise and consider qualification for disability grants for PLWHA (AIDS and HIV)
MoHSS 4.2.1
Facilitate allocation of resources to organisations caring for OVC REMU/RACOC 4.2.1 Support and strengthen coordination between RACOC and HBC 4.2.1 Form sub-committee of RACOC to identify and register OVC and PLWHA and facilitate grants to those.
RACOC/REMU 4.2.1
Strengthen local fund raising and resource mobilisation 4.2.1 Sub-Component 4.3: Addressing poverty 4.3 REMU to lobby for national level discussions to look at food and support for PLWHA, and vulnerable families not only during drought
MAWRD/REMU 4.3.1
Identify organisation to develop IGA RDCC 4.3.1 Village EMU to be asked to identify affected families caring for OVC, PLWHA, and HBC
VDC 4.3.1

Appendix 2
Medium Plan III for HIV/AIDS 169
Ohangwena Region’s Commitment Responsible Agency
Ref
Encourage people who are able to work in their fields and establish mini gardens and to plant improved varieties and use improved techniques
MAWRD 4.3.1
Establish how to ensure adequate and fertile land provision and develop irrigation structure and clean drinking water throughout the region
MAWRD 4.3.1
Component 5: Integrated and Coordinated Programme Management 5 RACOC members to be trained (common module) NACOP 5.1.1 Strengthen RACOC by involving regional planner to advise on budget and annual plans
Regional Council
5.2.1
Regional Councillors should chair their CAC; deputy should be health worker; should meet bi-monthly and should develop annual plans.
Regional Councillors
5.2.1
General process of decentralisation needs to be speeded up and the decentralisation of PHC (including HIV/AIDS) needed immediately
MRLGH/ MoHSS
5.2.1
Every ministry, NGO, FBO should appoint a focal person and the focal person should be trained on HIV/AIDS and should be given decision making power for RACOC deliberations. National line ministries to support regional level to facilitate HIV/AIDS work
ALL 5.2.1
Each line ministry, region, NGO to budget for HIV/AIDS All 5.2.2 Establish RACOC sub-committee on resource mobilisation and establish a regional budget for general RACOC activities
Governor/RAC 5.2.2
Transport and office equipment for RAC and transport assistance needed for unemployed RACOC members
Regional Council
5.2.2
Members of RACOC and other stakeholders to be provided with copy of MTP III as soon as possible
NACOP RAC
5.2.3
Improved, clear communication and better flow up and down and more networking in region e.g. more use of media (radio, newspaper)
RAC 5.2.3
Establish monitoring and evaluation committee within RACOC RAC/RACOC should visit all projects in the region to monitor
Governor 5.3.1

Appendix 2
Medium Plan III for HIV/AIDS 170
Profile:
Omaheke Region has a population of 68,029 (2001 Census) of which seventy-two percent live in rural areas and forty-one percent are under fifteen years of age. Omaheke Region is sparsely populated. Sixty-two percent of children live over five kilometres from a school, and Omaheke has one of the lowest literacy rates in Namibia, 66%. The Trans Kalahari highway runs through Omaheke Region and offers potential for tourisms and economic growth, though it also poses risks for the spread of HIV. Wages and salaries form the main source of household income. The HIV/AIDS prevalence rate for Omaheke is 13%. Ten percent of the children under fifteen have lost one or both parents.
Omaheke Region’s Commitments in MTP III Reference
Omaheke Region’s Commitment Responsible Agency
Ref
Component 1: Enabling environment 1 Motivate leaders to plan and create a conducive environment among the community to improve understanding of HIV/AIDS
RACOC Local
Communities, NGOS, MoHSS
1.1.1
Leaders should be incorporated in various activities/programmes Leaders 1.1.1 Mobilise/solicit funds through local events or approaching donors Leaders 1.1.1 Make accessible relevant HIV/AIDS information and education RACOC 1.2.1 PLWHAs should be encouraged and supported to speak out and participate at national events
Lironga Eparu NANASO
1.2.1
Policies should be clear, well-defined and able to be implemented 1.3 Leaders should be a part of policy formation and implementation Implement intensive sensitisation programmes that must reach people on the ground
ACT MIB ALU
1.4.1
Tailor sensitisation training workshops to different groups and types of leaders
1.4.1
Sensitise people about the multifaceted impact of HIV/AIDS on communities
1.4.1
Sub-Component 2.1: Strengthen capacity to deliver HIV/AIDS prevention programmes
2.1
Train Service providers on conducting needs assessment MoHSS, RACOC OHEP
2.1.1
Train Traditional Healers on Safe Medical Practices Organisation for Traditional
Healers/OHEP
2.1.1
Sub-Component 2.2: Target vulnerable populations 2.2 Design specific Information, Education & Communication materials for specific targeted populations
Prisons, MHETEC MWACW, OHEP
2.2.1
Promote and deliver voluntary counselling and testing services MoHSS, Prisons 2.2.1 Establishment of HIV/AIDS Awareness and Prevention Clubs MHETEC
YHDP/MBESC 2.3.1
Train youth on Behavioural Change and encourage use of condoms CAA MHETEC
2.3.1 2.3.2
Omaheke Region

Appendix 2
Medium Plan III for HIV/AIDS 171
Omaheke Region’s Commitment Responsible Agency
Ref
Ensure HIV/AIDS education is included in all school curricula MBESC 2.3.1 Promote open discussions by parents with children/young people MBESC, parents 2.3.1
2.5.1 Life skills training for In/Out of school youth YHDP
Town Council 2.3.2
Encourage business community to be involved in peer education Private Sector 2.4.2 Promote and ensure the provision of condoms RACOC 2.4.3 Strengthening infection control through training MoHSS 2.4.6 Sub-Component 3.1: Capacity development for the expanded treatment, care and support response
3
Training community members as counsellors for HIV/AIDS infected people and to be recognised by the government for home-based care (HBC)
MoHSS 3.1.1
To train community members to assist in voluntary counselling and testing (VCT)
MoHSS & Community
3.1.1
Train health workers and community members on HIV/AIDS treatment to assist HIV/AIDS infected people with their medication
MoHSS NGOs
3.1.2
Train all health workers so that they are comfortable with HIV/AIDS treatment and care to ensure a continuum of care
MoHSS 3.1.2
Target private and state doctors, ensure that all doctors are trained in pre and post test counselling
MoHSS 3.1.2
Open centres and train people to help improve the taking of medication/treatment whereby a patient sign that he/she received the treatment for his/her own care
MoHSS & Community
3.1.2
Use media and churches to educate communities on HIV/AIDS treatment and care in local languages
Community 3.1.2
Educate community through meetings and workshops on HIV/AIDS treatment and care supervised by community leaders
Community 3.1.2
Sub- Component 3.2: Treatment, care and support services 3.2 Regular distribution of drugs in laboratories and hospitals should be improved
MoHSS 3.2.2
Provide information and education to the general population about HIV/AIDS treatment, care and support programmes.
MoHSS 3.2.2
Increase treatment literacy for people with HIV/AIDS MoHSS 3.2.3 Encourage pregnant women to go for HIV testing and VCT MoHSS &
Community 3.2.3
Education to community on pregnancy and on a healthy lifestyle MoHSS & Community
3.2.3
The encouragement of care at home and the acceptance of the disease
MoHSS 3.2.7
Sub-component 4.1 : Developing the Capacity of Local Responses Good coordination, training, workplace programmes, financial support, education (dissemination of informational material), participatory planning, and M&E
RACOC MoHSS, Ministries,
NGOs, YHDP Private Sector
4.1.1
Psychosocial Support and providing services and financial support for orphans
MoHSS, NGOs & CBOs
4.2
Sub-Component 4.2 Comprehensive services for OVC and PLWHA Needs assessment and registration of those in need of aid MoHSS,
MAWRD, REMU 4.2.1
Training on Income Generating Activities so that they will be able to support themselves
MAWRD, REMU, MLRR, MTI
4.2.1
Outreach programmes to accelerate grants to orphans 4.2.1 More training and support for social workers
4.2.1

Appendix 2
Medium Plan III for HIV/AIDS 172
Omaheke Region’s Commitment Responsible Agency
Ref
Sub-Component 4.3 Addressing poverty Training on income generating activities MWCW,
MAWRD, MLRR 4.3.1
Lobby for food availability and food for work programmes REMU, MoHSS 4.3.1 Advocating municipality for affordable housing RACOC 4.3.1 Implement legislation to eliminate discrimination on housing and insurance policies
4.3.1
Component 5 : Integrated and Coordinated Programme Management 5. Increase membership of RACOCs (e.g. teachers and health workers) RACOC 5.2.1 Give incentives (e.g. snacks/tea) to RACOC members for consistent representation at the meetings
RACOC 5.2.1
Training in proposal writing to seek funding from RACOC. Proposals from lower level to the mother body to solicit funds and mother body will also write proposals for funding
RAC 5.2.2
Raise awareness, develop effective participatory structure at the community level and flow information up to higher levels
RACOC 5.2.3
HIV/AIDS must be mainstreamed in all regional development plans RAC/RDP 5.2.4 Continue Capacity Training in research by skilled people RACOC &
NACOP 5.4.1

Appendix 2
Medium Plan III for HIV/AIDS 173
Profile:
Omusati Region has the second largest population with 228,842 people. The region is overwhelmingly rural with only 1% of the population living in an urban area. 17% of the children under fifteen have lost one or both parents (2001 Census). Sixty two percent of the households are headed by women. Six percent of the population is disabled, with the majority of those being disabled by blindness. Subsistence farming is the main source of income for the people of Omusati, although a full twenty-two percent rely on their pensions as their main source of income. Twenty-three percent of the pregnant women surveyed in 2002 were HIV/AIDS positive in Uutapi.
Omusati Region’s Commitments in MTP III Reference
Commitments Ref. Component 1: Enabling Environment Provide resources and information to enable leaders (political, religious, traditional, NGO) to advocate at village level for example at social functions, funerals and church services on issues of discrimination, isolation of PLWHA, access to treatment, and prevention.
1.1.1
Component 2: Prevention Devise specials programmes for migrant workers returning to Omusati, disabled people, prisoners and those awaiting trial
2.2.1
Devise special programmes for youth 2.3.1 Produce and disseminate IEC in local language. 2.4.1 Organise training for peer educators in all workplaces 2.4.2 Increase condom outlets and appoint community member to ensure provision 2.4.3 Component 3: Treatment, Care and Support Services Sensitise health workers on how to work with volunteers 3.1.1 To expand the provision of VCT throughout the region, starting with Ruacana and Etayi aiming at one per constituency and to train more counsellors
Ensure training and provision of supplies to home-based caregivers through, mapping the existing groups and establishing a HBC network
3.2.4
Train MOHSS staff for the roll out of PMTCT and HAART 3.1.1 Component 4: Impact Mitigation Services Encourage more community participation through training workshops on how to set up projects, raise funds, and monitor.
4.1
Mobilise funds for CACOCs and village organisations especially those caring for the sick and OVC.
4.1
Disseminate information to communities about OVC services through traditional leaders, churches and CACOCs
4.2
Advocate for a streamlined grant application process 4.2 Train community organisations on and provide financial support 4.2 Speed up process of identity documents and birth and death certificates 4.2 Component 5 : Integrated and Coordinated Programme Management Ensure full participation at RACOCs and CACOCs 5.1.1 Provide office assistance to RAC 5.1.1 CACOC apply to RACOC for funds in time for RACOC to submit budget to Regional Council and to MRLGH
5.1.2
OMUSATI REGION

Appendix 2
Medium Plan III for HIV/AIDS 174
Profile:
Oshana Region has a population of 161, 916 (2001 Census) of which 69% live in rural areas. Oshana Region has the second highest population density in the country, concentrated around Oshakati, Ondangwa and Ongwediva. The Oshana Region is a central point for education in the wider area, with a University campus, a teachers’ college and a vocational training centre; however unemployment in Oshana Region is high at 41%. Forty percent of the population is under fifteen, and 54% of the households are headed by women. The HIV/AIDS prevalence rate in Oshana Region is 29% (2002). Oshana Region has the highest number of children under the age of fifteen, 20%, who have lost either one or both parents.
Oshana Region’s Commitments in MTP III Reference
Oshana Region’s Commitment Responsible Agency
Ref
Component 1: Sustained leadership commitment; greater involvement of PLWHA, relevant policies developed and discrimination and stigma reduced
1
Governor’s office to create a platform for all leaders (traditional/church/councillors etc.) to come and discuss their responsibilities and draw up annual plans
Regional Council
1.1.1
Strengthen church activities – setting up congregational HIV/AIDS committees
Church leaders 1.1.1
Traditional leaders to address myths and taboos at monthly meetings Trad. leaders 1.1.1 Community leaders to address social evils of abuse, neglect and social accountability, and to encourage people to go for VCT.
Traditional authorities
1.1.1
PLWHA to serve on main organisations – RACOC and others including line ministries
RAC 1.2.1
Explore how Lironga Eparu can be supported to expand and strengthen its networking and activities. (e.g. visit schools, link with NGOs to share resources, use all forums to address public, radio)
RAC 1.2.1
Relevant legislation to be disseminated –Community Courts/Domestic Violence/ Maintenance Act – in local language
MoJ LAC
1.3.1
Legal measures and policy needed to deal with commercial sex workers (CSW) - registration
MoJ 1.3.1
Evidence of discrimination to be recorded and followed up All leaders 1.4.1 Component 2: Behaviour change programmes targeting mobile and migrant workers, sex workers and prisoners, young people including OVC and street children, as well as the general population, to reduce new infections
2.
Research needed into vulnerable groups especially prisoners, defence, police, unemployed school leavers, sex workers, physically impaired (disabled), abused children, OVC, and OVC headed households, people in informal settlements, road workers and construction workers, truck drivers, taxi drivers, shebeen workers.
Regional Council UNAM MoHSS
2.1.1
Life skills training for teachers MBESC 2.1.1 OVC caregivers to be targeted for communication skills in sexual and reproductive health (addressing taboos)
MWACW 2.1.1
Churches at congregation level to be encouraged to be more open about sexual health and prevention
CCN 2.1.1
Oshana Region

Appendix 2
Medium Plan III for HIV/AIDS 175
Oshana Region’s Commitment Responsible Agency
Ref
Develop and deliver communication skills training for civil servants (nurses etc) and inter-personal communication for others
MoHSS NGOs/UNAM
2.1.1
Establish 10 – 14 year old programme Window of Hope to encourage delay in all schools and other youth venues in the region by 2006
MBESC 2.3.1
Review workplace policies – absenteeism, unpaid leave, sick leave etc. 2.4.2 Every RACOC member should see that condoms are available and accessible in their sector/constituency – e.g. petrol stations
RACOC 2.4.3
Every ministry must develop a workplace programme Ministries 2.4.2 Expand VCT either in every health centre and clinic or mobile clinic – decentralised to rural areas. Disseminate information on VCT
MoHSS 2.4.5
VCTs must refer clients to Support Groups for counselling – for negative clients as well
MoHSS 2.4.5
Employment training for youth, especially heads of households MHETEC 2.5.1 Organise entertainment and youth programmes to provide youth with positive outlets and to disseminate information (leaflets and posters)
MHETEC 2.5.1
Training of youth counsellors and trainers as peer educators MBESC 2.5.1 Sub-Component 3.1: Capacity development for the expanded treatment, care and support response
3.1
Identify and train trainers in NGOs/FBOs and others for PMTCT/VCT MoHSS 3.1.1 Liaise with UNAM to ensure pre-service training (also include lecturers in refreshers)
MoHSS/UNAM 3.1.1
Train and give information to the general public on PMTCT and ARV and STI/TB/Malaria in relation to HIV
MoHSS 3.1.2
Retrain counsellors in PMTCT and HAART MoHSS 3.1.1 Lack of rapid tests and absence of testing centres causing problems – every clinic should have a trained nurse/counsellor
MoHSS 3.1.1
Train health workers need in OI MoHSS 3.1.1 Sub- Component 3.2: Treatment and care services 3.2 Increase social mobilisation on VCT to expand numbers of men and women enrolled in PMTCT
MoHSS 3.2.3
HBC to assist with DOT in TB treatment MoHSS 3.2.5 Enrol as many people as possible in HAART, but people may have no support MoHSS 3.2.6 Study what is causing the bottlenecks in treatment, recommend solutions, and facilitate immediate enrolment and qualifying by expanding hospitals which offer HAART – all district hospitals to become treatment centres
MoHSS 3.2.6
Sensitise public servants to register with Medical Aid in order to get HAART through their medical insurance – train workplaces in this/look at policy
Local Authorities/
Regional Council
3.2.6
HBC volunteers need support through monthly visits coordinated by RAC and SHPA
MoHSS 3.2.7
Strengthen uniform referrals both ways (HBC - hospital – HBC) MoHSS 3.2.7 Sub-component 4.1 : Developing the Capacity of Local Responses 4.1 Strengthen capacity of CBO by giving technical assistance. Help CBOs and HBC groups with financial management (bank accounts etc.)
MAWRD/ MWACW
4.1.1
Train local agencies on behaviour change communication ? 4.1.1 Sub-Component 4.2 Comprehensive services for OVC and PLWHA 4.2 Identify stakeholders in the region to coordinate services to OVC - possibility of HBC caregivers
MWACW
Community leaders to inform communities about the rights and responsibilities of children including problem of neglect
Traditional Authorities
4.2.1
Streamline legal processes for custody – policy change needed MoHSS/ MWACW
4.2.1

Appendix 2
Medium Plan III for HIV/AIDS 176
Oshana Region’s Commitment Responsible Agency
Ref
Develop/Establish policy regarding inheritance to protect widows and OVC
MoJ 4.2.1
Develop radio campaign on what services are available MIB/NBC 4.2.1 Standardising criteria for identifying PLWHA qualifying for grants (e.g. viral load etc.)
MoHSS 4.4.1
Streamline process registration/identification of OVC and school fee exemption and other services – give responsibility and training to others e.g. trad. leaders etc.
MWACW 4.2.1
Sub-Component 4.3 Addressing poverty 4.3 Vulnerable groups helped to establish gardens and IGA MAWRC 4.3.1 Improved plans for seed dissemination and nutrition training through existing policy in MAWRD – vulnerable families) to be targeted
MAWRD 4.3.1
REMU to expand policies for food distribution to target families affected by HIV/AIDS – qualifying factors for those to benefit from drought relief to be re-considered (e.g. those in settlement areas not only those in rural areas) – national level EMU in OPM to set policy
REMU/EMU 4.3.1
Component 5 : Integrated and Coordinated Programme Management 5 Capacity development and awareness raising for each sector so that it has a dedicated focal person, a policy, counselling services available, resources for HIV/AIDS
RACOC 5.1.1
Strengthen coordination of services through RACOC meetings RAC 5.2.1 Hold quarterly RACOC meetings where members share plan of actions, budgets, progress reports and extra-ordinary meetings when necessary
RAC/ Governor
5.2.1
Develop capacity of constituency HIV/AIDS committees through providing information, making regular support visits from the RAC, identifying and mobilising funds, financial management training.
Regional Councillor/
RAC
5.2.1
CACOCs to be chaired by regional councillors and they should meet every second month in preparation for quarterly RACOC meetings
Regional Councillors
5.2.1
The regional sector focal people to be supported by their department heads.
Ministries 5.2.1
RAC to be supported by a technical team consisting of RAC/SHPA/Regional finance officer/Dev. Planner/an NGO rep. The RAC also to have an administrative assistant in the office.
Regional Council
5.2.1
Development Planner to help with preparation of RACOC annual plans and budgeting and demarcating areas of operations for different implementers
Regional Council
5.2.2
Every ministry must have a budget line item for HIV/AIDS NPC 5.2.2 Improve communication through RACOC newsletter and use public media and public days to share information and learning
RAC 5.2.3
The region would like to see national committees meeting more regularly to bring together national and regional stakeholders
NAEC 5.2.3
Research needed into causes and indications of discrimination IEC/ Advocacy Committee
5.4.3

Appendix 2
Medium Plan III for HIV/AIDS 177
Profile:
The population of Oshikoto Region is 161,007 (2001 census) with 91% of the people living in rural areas. Oshikoto Region is divided into ten constituencies, but has only one proclaimed municipality Tsumeb. Although Oshikoto Region attracts a great number of tourists at Etosha Park, the unemployment rate in Oshikoto Region is the highest in the country at 45%. Forty-three percent of the population is under fifteen, and 50% percent of the households are headed by women. The HIV/AIDS prevalence rate in Onandjokwe was 28% and in Tsumeb, 25%. Sixteen percent of the children under fifteen have lost either one or both parents.
Oshikoto Region’s Commitments in MTP III Reference
Oshikoto Region’s Commitment Responsible Agency
Ref
Component 1: Sustained leadership commitment; greater involvement of PLWHA, relevant policies developed and discrimination and stigma reduced
1
Regular and intensive public meetings to be conducted at all levels – regions, constituency, villages - different leaders to be assigned specific sectors/segments to address - RACOC
Traditional leaders/
RC, churches
1.1.1
Introduce IEC materials, condoms etc. where they are not yet available RACOC 1.1.1 Establish more support groups for PLWHA through traditional authorities and churches.
Communities 1.2.1
Undertake operational research on alcohol, drug abuse, unemployment, poverty (RAC) and disseminate to leaders
MoHSS NGOs
1.1.1
Leaders to address members of the community on stigma and discrimination and to give moral support to PLWHA so everyone is welcomed
Village AIDS committees
1.2.1
Establish educational awareness campaign and involve PLWHA among community members – especially where they do not yet exist.
all leaders/ NGOs/
1.4.1
Component 2: Behaviour change programmes targeting mobile and migrant workers, sex workers and prisoners, young people including OVC and street children, as well as the general population, to reduce new infections
2.
The region plans to target commercial farmers and workers, students, hospitality and transport workers, and those in isolated rural areas with the help of NCCI branches, NNFA, MOHSS, Regional Councillors and Traditional leaders
All 2.2.1
Establish awareness campaigns and social activities in the rural areas CACOC 2.1.1 Village HIV/AIDS committees to develop and distribute their own information in local languages and accessible format.
Traditional leaders
2.1.1
Continue Awareness programmes for prison inmates MPCS/MIB 2.2.1 Encourage children’s programmes and sex education programmes at schools and include awareness of VCT
MBESC/ MHETEC / MIB
2.3.1
MBESC to establish its own counsellor training for HIV/AIDS to supplement MFMC training
MBESC 2.3.1
Provide special information to youth about their own issues MHETEC/MIB/ 2.3.2 Make condoms available in hospitals, clinics, shebeens, schools and other places where youth meet
RACOC members
2.4.3
Introduce accessible VCT in regions, 5 fixed and 1 -2 mobile (test acceptability) – Establish counselling programmes at all VCT centres.
MoHSS/NGOs 2.4.5
Oshikoto Region

Appendix 2
Medium Plan III for HIV/AIDS 178
Oshikoto Region’s Commitment Responsible Agency
Ref
Strengthen STI syndromic management MoHSS 2.4.4 Establish and encourage youth to join sport clubs, youth clubs, community service groups, and other social activities.
NGOs/Church/MBESC
2.5.1
Sub-Component 3.1: Capacity development for the expanded treatment, care and support response
3.1
Expand training /ARV/OI/STI MoHSS Ensure guidelines on OI are available at all district hospitals and clinics MoHSS 3.1.2 Sub-Component 3.2 : Treatment, care and support services 3.2 Provide PMTCT at every district hospital and provide health education at ante-natal clinics about PMTCT
MoHSS 3.2.3
Ensure clinic cater for OI/TB/STIs MoHSS 3.2.5 Test all family members of TB patients are tested, free of charge MoHSS 3.2.5 Ensure ARV available at all district hospitals by 2007 MoHSS 3.2.6 Provide more HBC kits with re-filling system through all district pharmacists
MoHSS 3.2.7
Sub-component 4.1 : Developing the Capacity of Local Responses 4.1 Use and/or establish village committees to steer and spear awareness campaigns around impact of HIV/AIDS. Donations to be mobilised for these campaigns from donors and private sector.
MAWRD/ MIB
4.1.1
Train focal people of Village HIV Committees at monthly meetings– church leaders, RC, RAC, Village Council
RAC 4.1.1
Give organisations caring for OVC training, especially centres – NGOs/MWACW 4.1.1
Sub-Component 4.2 Comprehensive services for OVC and PLWHA 4.2 MBESC to collaborate with MWACW and MOHSS to see that school fees and other services are exempt from payment from OVC.
MBESC 4.2.1
MWACW to visit the outlying areas with community leaders, councillors, headmen, MOHSS etc. on a regular basis to register OVC.
MWACW 4.2.1
Sub-Component 4.3: Addressing Poverty 4.3 Include food distribution to infected and affected people and OVC in revised drought relief screening and validating procedures
REMU 4.3.1
Train households in IGA and food production for self-reliance and provide land to these groups for gardens, fields, centres. – MWARD – Churches, traditional leaders, MLRR, Division of Community development within MWACW
MAWRD
4.3.1
Component 5: Integrated and Coordinated Programme Management 5 Maintain current structure of RACOC, CACOC and VACOC. These should be chaired by Governor (co-chaired by CMO of MoHSS) and Regional Councillors respectively. They should meet monthly.
RACOC 5.2.1
Create sub-committees of RACOC (advocacy etc.) where necessary RACOC 5.2.1 Establish a technical management team to support the RAC RACOC 5.2.1 Village HIV/AIDS committees to be established and active RAC/RC 5.2.1 Establish regional HIV/AIDS Fund and mobilise local business community and NGOs to contribute
RACOC 5.2.2
Line ministries should have plans of action and budgets for HIV/AIDS that tally and are shared with the RACOC annual plan
All 5.2.2
HIV/AIDS Committees to design local materials on local case studies Reg. Councillor 5.2.3 Establish proper communication and implementation structures between regional and national structures
NACOP/ RAC
5.2.3
Regional Council to endorse the RACOC plan of action and HIV/AIDS should be mainstreamed in all RC activities by better coordination between RC and RAC office
Regional Council
5.2.4

Appendix 2
Medium Plan III for HIV/AIDS 179
Profile:
Otjozondjupa Region has a population of 135,384 (Census 2001) of which 59% live in rural areas. Thirty-eight percent of the population is under fifteen. The region is divided into seven constituencies and has four major towns. Resettlement is occurring on both communal and commercial farming areas. The region has four hospitals, a health centre and sixteen clinics. Although the region has fifty-five schools, the literacy rate is low for Namibia at 67%. The HIV/AIDS prevalence rate for the region is 27.5 % and ten percent of the children under fifteen have lost one or both parents. Factors influencing this relatively high HIV/AIDS prevalence rate are the three army bases in the region and the main transport corridor route linking the north and south of Namibia and neighbouring countries.
Otjozondjupa Region’s Commitments in MTP III Reference
Otjozondjupa Region’s Commitments Ref Component 1: Enabling Environment All leaders actively involved in HIV/AIDS activities 1.1.1 People living with AIDS actively involved at all levels 1.2.1 HIV positive people have become counsellors 1.2.1 Involvement of HIV positive people in treatment literacy programmes 1.2.1 HIV/AIDS support groups established in all constituencies 1.2.1 Increased number of people coming out to live openly and positively with HIV/AIDS 1.2.1 All HIV positive people understand their rights of employment 1.4.1 Housing schemes available for HIV positive people 1.4.2 HIV positive people are able to access insurance cover 1.4.2 Improved family acceptance of HIV positive people 1.4.2 Component 2: Prevention Prevention campaigns to reduce infection levels and stop the further spread of HIV/AIDS among the following special populations: truck drivers, Namibia Defence Force, prisoners, farm workers, mobile workers, refugees, people living with HIV/AIDS (PLWHA), in and out of school youth, widows, and elderly carers.
2.2.1
Targeted prevention messages available to sensitise targets groups on transmission of HIV/AIDS and enhanced behaviour change
2.2.1
Increased distribution points for condoms 2.2.1 Increased number of people using condoms correctly and consistently 2.2.1 People living with HIV/AIDS trained on living positively 2.2.1
Elderly carers of people living with AIDS trained on safe home based care practices 2.2.1 Behaviour change programmes in schools supported and strengthened 2.3.1
Workplace programmes established in each ministry and organisation 2.4.2 Strengthened control of STI, TB HIV/AIDS in the region 2.4.4 Increased number of patients whose partners return for treatment 2.4.4 One Voluntary counselling and testing (VCT) centre functioning at each district hospital with mobile VCT services available for outreach
2.4.5
Reduced alcohol consumption in special groups and among the general population 2.5.1 Cultural aspects that facilitate transmission of HIV e.g. Otjiramwe and wife inheritance identified and interventions in place to address them
2.5.1
Otjozondjupa Region

Appendix 2
Medium Plan III for HIV/AIDS 180
Otjozondjupa Region’s Commitments Ref Component 3: Treatment, Care and Support Services 3.1 Information about treatment care and support available at all levels 3.1.2 Trained trainer of trainers (TOTs) on HIV/AIDS issues in every constituency 3.1.2 PMTCT available for all HIV positive pregnant women in the region 3.2.3 All patients showing signs of immuno suppression to be on prophylactic treatment 3.2.4 Establishment of Direct Observation Treatment Short-course (DOTS) for TB throughout the region
3.2.5
HAART available in all major hospitals in the region 3.2.6 Home based care (HBC) expanded to cover each constituency 3.2.7 Monitoring and evaluation mechanisms in place for HBC services 3.2.7 Improved attitude of health workers towards infected patients 3.2.8 Component 4: Impact mitigation services 4 Increased percentage of orphans and vulnerable children (OVCs) cared for satisfactorily
4.1.2
Continued education for all OVC ensured 4.1.2 Increased awareness and access to disability grants for people living with AIDS 4.4.1 Component 5: Integrated and Coordinated Programme Management 5.1 Constituency AIDS Coordinating Committees functioning in all constituencies 5.2.1 Enhanced regional coordination, accountability and monitoring through an effective Regional AIDS Coordinating Committee
5.2.1

Appendix 1
Medium Term Plan III for HIV/AIDS 143
1. Overview of international law obligations pertaining to the right to health1
(a) Conventions, treaties and international agreements legally binding on Namibia
The United Nations Charter The International Covenant on Economic, Social and Cultural Rights Convention on the elimination of all forms of racial discrimination Convention on the elimination of all forms of discrimination against women Convention on the rights of the child The African Charter of Human and Peoples’ Rights The Constitution of the World Health Organisation.
(b) Declarations, agreements and other sources of international law that are of a persuasive nature but not legally binding on Namibia
The Universal Declaration of Human Rights Declaration on the Rights of Disabled Persons Declaration on the use of scientific and technological progress in the interests of
peace and for the benefit of mankind Declaration of Alma-Ata on Primary Health Care Cairo, Beijing and Copenhagen Declarations Declaration on the right and responsibility of individuals, groups and organs of
society to promote and protect universally recognised human rights and fundamental freedoms
Millennium Declaration.
2. HIV/AIDS related international commitments made by Namibia2
(a) UN Millennium Declaration and Millennium Development Goals [2000]
Namibia was amongst the 147 heads of State and Government and 189 member states which adopted the Millennium Declaration issued by the United Nations during the Millennium Summit, New York, 6-8 September 2000.
Based on the values of freedom, equality, solidarity, tolerance, respect for nature, and shared responsibility, the Summit identified seven key objectives, of which three are of special relevance for success in the fight against HIV/AIDS in an African context -
Human rights, democracy and good governance, Sustainable development and poverty eradication, and Protecting the vulnerable.
1 This overview is based on a memorandum “Namibia’s international law obligations pertaining to the right to health”, 4 February 2002, compiled by the AIDS Law Unit
2 This section makes no distinction between those commitments which may, or may not be, legally binding or of a persuasive nature but not legally binding
Namibia’s international HIV/AIDS commitments

Appendix 1
Medium Term Plan III for HIV/AIDS 144
As far as HIV/AIDS is concerned, Namibia, along with other member states, resolved –
by the year 2015, to have halted and begun to reverse, the spread of HIV/AIDS [Goal 6: Combat HIV/AIDS, malaria and other major diseases; including Target 7: Have halted by 2015, and begun to reverse, the spread of HIV/AIDS],
to provide special assistance to children orphaned by HIV/AIDS to encourage the pharmaceutical industry to make essential drugs more widely
available and affordable by all who need them in developing countries [United Nations General Assembly Resolution 55/2], and
to give greater opportunities to the private sector, non-governmental organisations and civil society to contribute to the realisation of the above and other Millennium Development Goals and programmes.
The road map for implementation of the Millennium Declaration urged governments of signatory member states to adopt, inter alia, the following strategies towards-
(i) Combating HIV/AIDS
Strengthen health-care systems and addressing factors that affect the provision of HIV-related drugs, including anti-retroviral drugs and their affordability and pricing
Support and encourage the involvement of local communities in making people aware of such diseases
Devote a higher proportion of resources to basic social services in poorer areas since this is crucial for preventing diseases
give greater opportunities to the private sector, non-governmental organisations and civil society to contribute to the realisation of the above and other Millennium Development Goals and programmes.
(ii) Providing assistance to orphans and vulnerable children
Mobilise and strengthen community and family-based actions to support orphaned and vulnerable children;
protect children from violence, abuse, exploitation and discrimination;
provide essential quality social services for children and ensure that orphans and children affected by HIV/AIDS are treated on an equal basis with other children;
Expanding the role of schools as community resource and care centres.
(iii) Making essential drugs more widely available and affordable by all who need them
strengthen health systems for the provision of essential medicines; Increase affordability through differential pricing and the reduction or
elimination of import duties, tariffs and taxes;
Mobilise sustainable financing to support the costs of expanded access to drugs
Namibia is required to monitor its progress towards the achievement of HIV/AIDS-related Millennium Development Goals. [http://www.un.org/millenium/declaration/ares552e.htm visited December 2003; text of United Nations General Assembly Resolution A/56/326; Namibia’s UNGASS country report for January-December 2002].

Appendix 1
Medium Term Plan III for HIV/AIDS 145
(b) The Abuja Declaration and Framework Plan of Action on HIV/AIDS, TB and ORID [2001]
The Abuja Declaration on HIV/AIDS, TB and ORID [Other Related Infectious Diseases], dated 27 April 2001, emerged from the Organisation of African Unity’s African Summit on HIV/AIDS, Tuberculosis, and Other Related Infectious Diseases, held at Abuja, Nigeria, from 24-27 April 2001. During the Summit, African leaders declared AIDS as a State of Emergency in Africa, and the battle against AIDS and related diseases to be their top priority for the first quarter of the 21st century.
After reviewing inter alia, the role played by poverty, poor nutritional conditions, mother to child transmission, the biological vulnerability of women and girls, drug abuse, the vulnerability of youth, by stigmatisation and discrimination, and by insufficient education in the rapid spread of HIV/AIDS, the Declaration committed member African governments inter alia to-
Consolidate a comprehensive, multi-sectoral strategy based on the broadest possible mobilisation of society at all levels, to sensitise the population to the threat of HIV/AIDS and associated opportunistic infections, and to protect those not yet infected through appropriate and effective prevention programmes
Mobilise all human, material and financial resources required to provide care, support and quality treatment to those infected with HIV/AIDS and other related infections
Enact/utilise legislation/trade regulations to ensure the availability of drugs at affordable prices and technologies for treatment, care and prevention of HIV/AIDS
Ensure that the organisational bodies responsible for the strategy are properly convened, and provide a focus for unified national policy-making, programme co-ordination and implementation with respect for equal rights of all
Set a target of allocating at least 15% of the annual budget to the improvement of the health sector.
To assist in attaining the objectives of the Declaration, heads of member states also agreed to a Framework Plan of Action. http//www.aegis.com/news/usis/2001/USO10409.html visited December 2003]
(c) The UNGASS Declaration of Commitment on HIV/AIDS [2001]: “Global crisis – Global Action”
This Declaration, which comprises more than 100 paragraphs, and includes the establishment of the Global AIDS and Health Fund, was adopted during the United Nations General Assembly 26th Special Session on HIV/AIDS held in New York, from 25-27 June 2001.
Broadly, by becoming a signatory to the Declaration, Namibia agreed to the following priorities in the fight against HIV/AIDS-
To ensure that all people, but particularly the youth, know what to do to avoid infection
To stop the transmission of HIV from mother to child To provide treatment to all those infected To intensify the search for a vaccine as well as a cure, and To care for all whose lives have been devastated by AIDS, particularly AIDS orphans.
More particularly, Namibia committed itself inter alia to-
Strong leadership by Government in combating HIV/AIDS, The development and implementation of forthright multi-sectoral national strategies
and financing plans which involve full and active partnerships with civil society, the business community and the private sector
Integrating HIV/AIDS prevention, care, treatment, support and impact-mitigation priorities into mainstream development planning, including poverty alleviation strategies, budget allocations and sectoral development plans
Establishing prevention as the mainstay of the national response

Appendix 1
Medium Term Plan III for HIV/AIDS 146
Ensuring that care, support and treatment also form fundamental elements of the response
Reducing vulnerability to HIV/AIDS by realising human rights and fundamental freedoms for all, and particularly, respect for the rights of people living with HIV/AIDS
Giving priority to the vulnerable, and reduce vulnerability by empowering women Providing special assistance to children orphaned and affected by HIV/AIDS Alleviating the social and economic impact of HIV/AIDS Building national research capacity, and accelerate research on the development
of HIV vaccines Integrating HIV/AIDS awareness, prevention, treatment and care elements into
programmes or actions designed to respond to emergency situations Providing substantial and sustained resources to meet the challenge of HIV/AIDS,
and Monitoring and evaluating progress. In this regard, Namibia has submitted its first
country report for the period January to December 2002, and is busy with preparations for improved reporting in 2005 [UNDP/UNAIDS/National Planning Commission/National Aids Executive Committee: Reference documents for the National Initiative to fight HIV/AIDS in Namibia, November 2001; Namibia’s UNGASS country report for January-December 2002].
(d) The New Partnership for Africa’s Development [NEPAD] Statement, October 2001
NEPAD is a “vision and strategic framework for Africa’s renewal” developed in Africa for Africa, and adopted by the Organisation of African Unity at its 37th Summit in July 2001 to act as an integrated strategic socio-economic development framework for Africa.
Although NEPAD’s primary objectives, programme of action, principles make no direct reference to combating HIV/AIDS [http:///www.touchtech.biz/nepad/files/inbrief.html visited December 2003] , member states, including Namibia, are committed to ensuring that all partnerships with NEPAD are linked to the Millennium Development Goals.
While combating HIV/AIDS is not directly mentioned as a sectoral priority either, health [Objective 126] is seen as an integral part of the NEPAD Human Resource Development Initiative, and its first element is to “strengthen programmes for containing communicable diseases, so that they do not fall short of the scale required in order to reduce the burden of disease”.
To achieve the health objectives [paragraph 126], Namibia has inter alia, committed itself to the following actions -
Strengthen participation in processes aimed at procuring affordable drugs Mobilise the resources required to build effective disease interventions and secure
health systems Lead the campaign for increased international financial support for the struggle
against HIV/AIDS and other communicable diseases.
(e) Global Aids and Health Fund
The Global AIDS and Health Fund to fight AIDS, Tuberculosis and Malaria was established in principle by the UNGASS Declaration of Commitment on HIV/AIDS, 2001, to raise international attention to the global health crisis, and to translate that attention into political support and financial commitment. The Fund is intended to reverse the spread of HIV/AIDS, tuberculosis and malaria, and to reduce the consequences of these illnesses.
Namibia’s Country Co-ordination Mechanism for HIV/AIDS, TB and Malaria [NaCCATuM] submitted a proposal to the Global Fund which was conditionally accepted in January 2003, thereby introducing over USD 114,131 million into Namibia over a five-year period. Working with more than 30 partners [NGOs, FBOs, public sector bodies], the proposal seeks to increase overall

Appendix 1
Medium Term Plan III for HIV/AIDS 147
comprehensive care while scaling up interventions in the areas of IEC, Condom distribution, VCT, and OVC. MoHSS plans to roll out the PMTCT+ programme in each of Namibia’s 13 regions within the first year, and all 35 public hospitals by the fifth year. The intention is also to roll out HAART to public hospitals over the next three years. Namibia is required to undertake comprehensive monitoring and evaluation of projects funded through the Global Fund, and provide regular feedback to the Fund [Namibia’s UNGASS country report for January-December 2002, and Annexure 2].
(f) The Maseru Declaration on the fight against HIV/AIDS in the Southern African Development Community [SADC] region, Kingdom of Lesotho, 4 July 2003 and SADC HIV/AIDS Strategic Framework and Programme of Action 2003-2007
The Summit of Heads of State and Governments of SADC on HIV/AIDS was held in Maseru, Lesotho on 4 July 2003, preceded by a meeting of the Ministers of Health, of Finance, and of Gender/Womens Affairs on 3 July, during which the 2003-2007 Strategic framework was drafted.
In the Maseru Declaration, SADC member states including Namibia, inter alia, –
Welcomed and reaffirmed the commitments on HIV/AIDS contained in the 2000 UN Millennium Declaration, the UNGASS declaration, 2001, and the UN General Assembly Declaration on Children
Recognised that the pandemic is best tackled through multi-sectoral interventions, the upholding of human rights and fundamental freedoms and partnerships with stakeholders
Identified several priority areas including access to care, testing and treatment; prevention and social mobilisation; resource mobilisation; a development-oriented approach; and monitoring and evaluation
Affirmed commitment to the SADC HIV/AIDS Strategic Framework and Programme of Action 2003-2007, which aims to reduce the incidence of new infections among the most vulnerable groups in SADC; mitigate the socio-economic impact of HIV/AIDS; review, develop and harmonise policies and legislation relating to HIV prevention, care and support, and treatment within SADC; mobilise and co-ordinate resources for a multi-sectoral response to HIV/AIDS in the region
Established a Regional Fund for the implementation of the 2003-2007 Strategic Framework
Welcomed the US Presidential initiative: Emergency Plan for HIV/AIDS Relief which will provide USD 15 billion within the next five years.
(g) African Union Maputo Declaration on Malaria, HIV/AIDS, Tuberculosis, and other related infectious diseases, Assembly of the African Union, 10-12 July 2003
The Assembly of the African Union devoted a special session to review the current status of HIV/AIDS, TB, Malaria and other related infectious diseases in Africa. Inter alia, the Assembly -
Reaffirmed the commitments on HIV/AIDS contained in the Abuja Declaration, and Committed itself to promote partnerships with the private sector, relevant UN
agencies, pharmaceutical companies and other partners to increase African capacity to produce and distribute affordable generic pharmaceuticals for the management of inter alia, HIV/AIDS and related infectious diseases
Resolved to continue support for the implementation of the Plan of Action for the AU Decade for African Traditional Medicine (2000-2010), especially research on treatment for HIV/AIDS and ORID.

Appendix 1
Medium Term Plan III for HIV/AIDS 148
(h) World Health Organisation Regional Committee for Africa, 53rd session, Brazzaville, Congo, 17-20 June 2003 Resolution AFR/RC53/WP/6 dated 20 June 2003
This resolution by the WHO Regional Committee for Africa pertains to scaling up interventions against HIV/AIDS, Tuberculosis and Malaria in the WHO African Region. The Committee urged member states, of which Namibia is one, inter alia, to-
Develop appropriate policies and legislation to create a supportive environment for scaling up interventions at district and community levels
Allocate increased national resources for activities to fight HIV/AIDS Accelerate the implementation of multi-sectoral responses, clarifying the roles and
contributions of the different sectors and co-ordination structures Improve the quantity and quality of staff involved in management, service delivery
and monitoring and evaluation Promote and fund operational research and research on traditional medicines Engage new and existing partners to participate in programme implementation
and service delivery Decentralise the management of programmes and interventions Incorporate the existing cost-effective intervention packages for HIV/AIDS into the
essential health packages for delivery at all levels Accelerate the implementation of initiatives such as in-country pre-packaging,
distribution to peripheral levels and bulk purchasing arrangement, in order to make drugs, diagnostic tools and other commodities accessible and affordable to the beneficiary groups.