
Progesterone regulation of implantation-related genes: new insights into the role of oestrogen
Upload
independentCategory
view
2download
0
Oestrogen receptor, progesterone receptor, pS2, ERD5, HSP27 and cathepsin D in invasive ductal breast carcinomas
j.HURLIMANN, S.GEBHARD & F.GOMEZ* lnstitut universitaire de pathologie and *Division d’endocrinologie et biochimie clinique, Dipartement de Medecine, kusanne, Switzerland
Date of submission 8 January 199 3 Accepted for publication 9 April 199 3
HURLIMANN J . , GEBHARD S. & GOMEZ F.
(1993) Histopathology 23 , 239-248
Oestrogen receptor, progesterone receptor, pS2, ERD5, HSP2 7 and cathepsin D in invasive ductal breast carcinomas
Hormonal receptors and markers for prognostic evaluation were detected immunohistochemically in 196 infiltrating ductal breast carcinomas. Immunohistochemical detection of progesterone and oestrogen receptor is a method giving results generally concordant with those of the binding assay. However. immunohistochemical detection seems better. It allows the detection of hormonal receptors on small carcinomas, it is not modified by the endogenous hormones, and it has a slightly better correlation with prognosis and with the response to hormone therapy, Immunohisto- chemical detection of progesterone receptor has a prognostic value, sorting a negative subgroup with a poor prognosis from the oestrogen receptor positive tumours. These results can be obtained without quantitative immunohistological methods. ERD5, pS2, HSP27 and cathepsin D are associated with oestrogen receptor positivity. pS2 and HSP27 are interesting markers. They characterize a subgroup of oestrogen receptor negative tumours with a good prognosis. Moreover, pS2 is a marker of response to hormone therapy. EKD5 and cathepsin D do not appear to be of value as markers of prognosis.
Keywords: breast cancer, oestrogen receptor, progesterone receptor. pS2, HSP2 7, EKD 5, cathepsin D
Introduction
Determination of oestrogen receptor (ER 1, progesterone receptor (PR) and several oestrogen regulated proteins in breast carcinomas seems useful for the prediction of prognosis and success of endocrine therapy. However, studies of these markers have not given concordant results. Some of the differences are probably due to the small number of patients and short follow-up periods. However, some of the discordance is due to methodologi- cal problems. Generally, there is a good correlation between biochemical assays of ER and PR on tissue homogenates (binding assays) and their immunohisto- chemical detection on frozen tissues’-’. It has been suggested that the immunohistochemical assessment of ER has an even better prognostic value than biochemical
Address for correspondence: Dr Jean Hurlimann. Institut universitaire de pathologie. Bugnon 25. 101 1 Lausanne. Switzerland.
steroid receptor analysis5. However, the gradation of positivity in immunohistochemistry is variable and its practical utility remains to be established. Several pro- teins, pS2. EKD5, heat shock protein 27 (HSP27) and cathepsin D. have been reported to be synthesized under oestrogen contro19-’2, Their value for the prognosis and response to therapy has been the subject of many studies with contradictory results.
The present study of 196 invasive ductal breast carcinomas was undertaken to establish the value of imrnunohistochemical detection of hormonal receptors and various proteins under oestrogen control. We have compared the immunohistochemical method of ER and PR determination with the biochemical method based on the binding assay. We particularly evaluated the two methods for prognosis of clinical behaviour and response to therapy. The clinical importance of grading the positivity was studied. We also evaluated the prognostic importance of immunohistochemical determination of pS2. HSP27, ERD5 and cathepsin D.
239
240 ].Hurlimunn, SGebhurd and F.Gomez
Materials and methods One hundred and ninety-six patients were studied. All were initially treated by mastectomy and axillary dissec- tion, and entered the study between January 1981 and September 1986. One hundred and fifty-five patients were at stage I or II. 24 at stage 111 and 17 at stage IV. The age range was from 38 to 84 years with an average of 63 years. Clinical data were evaluated on a yearly basis, the last time on 1 April 1992. Seventy patients were followed till death. The observation period was from 66 months to 12 7 months with a median observa- tion of 8 1 months. Fifty-six (29%) patients had died at 5 years and 32 (1 6%) had a recurrence during the 5 years after surgery. No treatment had been given before the tumour was excised.
One hundred and forty-eight patients were treated after surgery: 24 received only hormone treatment, 33 radiotherapy, 15 chemotherapy and 76 a combination of two or three types of treatments. For these patients. the response to each therapy was evaluated, taking into consideration whether adjuvant treatment was given after surgery or only at the time of recurrence or generalized metastasis. Clinical information was obtained from several oncological centres and private physicians. The criteria for therapeutic response were determined following guidelines proposed by Miller and co-workers’ ’.
Invasive ductal carcinomas were selected in order to have an homogeneous group for histological type. The following indices were measured: size of the tumour, number of axillary metastases, and histological grade according to Bloom and Richardson’s and according to an improved modification described by Le Doussal and co-workers’ j.
B I N D I N G ASSAY
ER and PR were measured in cytosol preparations obtained from tissue homogenates, using a charcoal assay based on the binding of tritiated oestradiol and a progestogen, as previously describedlh. Tumours containing greater than 10 fmol ER or PR/mg cytosol protein were taken as positive.
IMMUNOHISTOLOGY
For each case, fresh tissues were immediately frozen and kept at - 80°C until immunological processing. We also obtained formalin-fixed paraffin-embedded tissues. The various antigens were immunostained according to the PAP method of Sternberger et a1.” using diaminobenzi- dine as substrate. All steps were performed at room temperature. The sections were f is t incubated for 10 min with normal rabbit serum diluted 1 : 30. All other
incubations in antisera and PAP were of 30 min duration, each separated by washing in Tris-buffered saline (TBS). The antisera and PAP were used at the dilutions mentioned in the antisera paragraph. Finally, all sections were washed in TBS and stained for 10 min in the diamino/H202 substrate (40 mg 3-3’ diaminobeh- zidine in 100 ml TBS containing 35 pI H202). Nuclei were weakly stained with haematoxylin.
Enzymatic digestion was carried out prior to incuba- tion with monoclonal antibody specific for pS2 and polyclonal antibody specific for cathepsin D. Protease VII (Sigma 5255. 1 mg/1.3 ml phosphate-buffered saline) was employed for 10 min at 37°C. Negative controls were obtained by replacing the first step antisera with hybridoma supernatant without specificity for the tis- sues examined.
Antiseru Monoclonal anti-52k procathepsin D ( 1 : 50) was obtained from Transbio, Paris, France. Rabbit antiserum specific for cathepsin D (1 : 400) was produced in our laboratory by immunization with cathepsin D from bovine spleen (Sigma C 3 1 38). Part of the monoclonal antibody to pS2 was kindly provided by Dr P.Chambon, Institut de Chimie biologique. Strasbourg. France and used, diluted 1 : 200, after proteolytic digestion. Another was obtained from CIS Bioindustries, Gif-sur-Yvette. France, and was used, after proteolytic digestion, at 1 : 5 dilution. Prediluted monoclonal antibody to HSP2 7 was obtained from Biogenex Laboratories. San Ramon. CA, USA, Monoclonal antibody to ERD5, diluted 1 : 20. was obtained from Amersham. Buckinghamshire. England. Monoclonal anti-progesterone receptor and anti-oestra- diol receptor were part of ER-ICA and PR-ICA kits and were obtained from Abbott Laboratories, North Chicago, 11,. USA. They were used according to the recommended procedure of the manufacturer.
Normal rabbit serum, rabbit anti-mouse Ig ( 1 : hO), mouse peroxidase-anti-peroxidase complexes (mouse PAP, 1:200) were obtained from Dakopatts A/S, Copenhagen, Denmark.
Methodology Hormonal receptors and cathepsin D detected with monoclonal antibody were analysed on frozen tissues. Cathepsin D detected with polyclonal antiserum, pS2, ERD5 and HSP2 7 were analysed on fixed tissues.
For ER, PR and cathepsin. staining was semi-quantita- tively assessed by estimation of the number and intensity of stained tumour cells as described by Berger and co- workers2. The best conditions for immunostaining on frozen and fixed parafflnembedded tissues were estab- lished on a preliminary study of 20 breast carcinomas. A

Hormottnl receptors in brrnst rvrc*inonms 24 1
Figure 1. Irnrnunohistochemical detection of oestrogen receptor: a most nuclei are positive, b a minority of nuclei are positive.
relationship was established with clinical and histologi- cal parameters and with the therapeutic response.
STATISTICAL METHODS
Statistical analysis was test.
carried out with Fisher's exact
Results Forty-six tumours had diameters less than 2 cm. 72 were between 2 and 2.9 cm and 75 were larger than 3 cm. In three cases, the tumour was not well delimited and the size was not measured. Sixty tumours were of grade 1.82 of grade I1 and 54 of grade 111. Using the modification of Le Doussal et ~ 1 . ' ~ 51 tumours were of grade I. 65 of grade IL34 of grade 111, 38 of grade IV and 8 of grade V. Ninety-one cases had no axillary metastasis, 53 cases had one to three axillary metastases and 4h cases had more than three axillary metastases. Six patients did not have an axillary curettage.
There was a clear relationship between prognosis measured as death at 5 years and the tumour size (P -= 0.00 1) and axillary metastases ( P c 0.001 ). When tumour grade was investigated, the relationship was not as striking and this, irrespective of the grading system employed ( P = O . O 8 ) .
IMMUNOHISTOCHEMICAL DETECTION O F OESTROGEN
RECEPTOR A N D MARKERS
For all the markers, the number and intensity of staining of positive cells were variable. The cases were considered positive if even only rare cells were labelled. For some markers, the number of positive cells was evaluated to see whether a better correlation could be established with usual parameters and prognosis.
One hundred forty-one (72%) cases were positive for ER and 88 (45%) cases for PR, as compared with 146 (75%) and 129 (66%) cases respectively measured with the binding assay. For these two markers the positivity was nuclear (Figure 1).
Ninety-seven (50%) cases were positive for pS2. 94 (48%) were positive for ERD5 and 81 (41%) were positive for HSP2 7. For these three markers the positivity was cytoplasmic (Figure 2).
Two different cells were positive for cathepsin D: the epithelial cells and the histiocytes (Figure 3). The results were similar with monoclonal and polyclonal antibody. The positivity was always cytoplasmic and stronger in histiocytes than in tumour cells. Cathepsin D was also present in normal epithelial cells of the lobular struc- tures. Four main aspects were seen: positivity of histio- cytes only--59 cases: positivity of histiocytes and a minority of tumour cells-28 cases: positivity of histio- cytes and most of tumour cells-94 cases: and positivity of tumour cells only-1 5 cases.
CORRELATION BETWEEN IMMUNOHISTOCHEMICAI.
AND BIOCHEMICAL DETECTION O F STEROID RECEPTORS
Positivity and negativity of ER and PR measured with the biochemical method were defined as previously"'. For ER, detected immunohistochemically, the sensitivity (per cent of positive cases) was 89%, the specificity (per cent negative cases) 78% and the precision (total coincidence) 86%. For PR, detected immunohistochemi- cally, the sensitivity was 68%. the specificity 90% and the precision 72%.
Twenty-seven cases with ER divergence were reviewed. Sixteen cases biochemically positive for ER were immunohistochemically negative: nine had EH zit
11 to 27 fmol/mg protein: seven cases with more than

242 1.Hurlirnann. S.Gebhard and F.Gomez
Figure 2. Immunohistochemical detection of a HSP27 and b pS2.
34 fmol/mg protein were women between 57 and 8 4 years old. Eleven cases biochemically negative for ER were immunohistochemically positive. All cases had a strong desmoplastic reaction in which only rare tumour cells were seen. Fifty-five cases with PR divergence were reviewed. Forty-eight cases biochemically positive for PR were immunohistochemically negative: 2 3 cases had PR at 1 1 to 28 fmol/mg protein, 1 3 cases were women older than 70 years. Twelve cases had no particularity explaining divergence. Seven cases biochemically nega- tive were immunohistochemically positive: all had a strong desmoplastic reaction. Nineteen cases ER - PR + were detected biochemically but only two with immuno- histoc hemistry.
CORRELATION OF HORMONAL RECEPTORS AND MARKERS WITH AGE OF PATIENTS
The results are summarized in Table 1, Oestrogen
receptor wirs detected immunohistochemically in 6 5 to 79% of tumours with no significant difference evident between the age groups. ER was measured biochemi- cally in 86% of tumours from women older than 70 years but only in 68% of tumours from women 40-49 years old (P<0.039) and 66% of tumours from women 50-59 years old (P<O.O10).
PR was detected immunohistochemically in 39 to 56% of the tumours with no significant difference between the age groups. PR was measured biochemi- cally in 52 to 77% of the tumours. In the class of women 59 years old or younger, 75% of the tumours were positive but in women older than 6 0 years, only 58% of the tumours were positive (P=0.008).
pS2. ERDS and cathepsin D showed no variation according to age. HSP27 was present in 44 to 5h'X of the tumours, except for the age group 50-59 years in which only 22% of the turnours were positive ( P = 0.000 3),
klgure 3. lmmunohistochemical detection of cathepsin D. a Positivity of histiocytes only. b Positivity of tumour cells and histiocytes.

50-59 T 3 i t h 4 ) n = 5 8 38(66) 40(70) 43(74) 24(41) 30(52) 13(22) 25(43) ~1 j j ( 9 j )
ER ba. oestrogen receptors measured with binding assay: EK imrn. oestrogen receptors detected immunohistochemically: PR ba. progesterone receptors measured with binding assay: PR imm. progesterone receptors detected immunohistochemically: H. histiocytes: T. tumour cells.
CORRELATION OF MARKERS WITH SIZE OF TUMOUR AND WITH AXILLARY METASTASES
pS2 was present in 61% of small tumours but in only 39%ofthelargesttumours (P=O.O14). Cathepsin D was present in 78% of small tumours and in 61% of the largest (P= 0.040). ERD5 protein was present in 3 7% of small tumours and in 59% of the largest (P=O.O16). There was no difference for HSP27, ER (biochemically and immunohistologically detected) and PR (biochemi- cally measured). For PR detected i nohistologically, only 36% of the largest tumours were 9 ositive compared with 57% of the small ones.
No correlation between markers and axillary meta- stases was established except for PR detected immuno- histochemically and ERD5. PR was present in 53% of tumours without metastases and in 3 3% of the tumours with more than three axillary metastases (P= 0.019). ERD5 was present in 38% of tumours without meta- stases and in 61% of tumours with metastases (P= 0.01).
CORRELATION OF MARKERS WITH GRADE OF TIJMOUR
Independent of the grading system used, ER, PR. HSP2 7 and cathepsin D were always predominantly expressed in low-grade tumours. with a significant difference between the groups. For ERDS, the difference was significant only with the grading of Bloom and Ri~hardson'~ and for pS2 only with the modified grading of Le Doussal and co-workersI5.
CORRELATION OF OESTROGEN RECEPTOR AND THE OTHER MARKERS
ER positivity (particularly when detected immunohisto-
chemically) was strongly correlated with all the other markers. The results are summarized in Table 2.
CORRELATION OF OESTROGEN RECEPTOR AND
MARKERS WITH PROGNOSIS
Based on death at 5 years as a criterion, hormonal receptors had a prognostic value, especially when they were detected immunohistochemically (Figure 4). With this method, 2 1 % of the ER + PR + cases died at 5 years, compared with 3 5% of the ER + PR - cases (P= 0.056) and 34% of the ER-PR- cases (P=0.067). The same comparison of cases biochemically tested showed 2 5% deaths in the group ER+PR+, 39% in the group ER+PR- (P=0.076), 29% in the group ER-PR- ( P > 0 . 3 ) and 32% in the group ER-PR+ ( b O . 5 ) . No matter how the prognostic value of hormonal receptors changed after 5 years, survival at 6 years was not statistically different in the groups with or without hormonal receptors independent of the method of detec- tion. A few cases were followed during 7 and 8 years and did not allow a statistical analysis. However, no differ- ence could be shown between the cases with or without hormonal receptors.
If the cases were stratified according to the number of metastases (Figure 5) or tumour size, the differences persisted, but they were less significant, particularly in the cases with more than three axillary metastases. There was no correlation between hormonal receptor status and recurrence during the first 5 years.
There was no correlation between pS2, HSPZ 7, ERDS and cathepsin D and survival or tecurrence at 5 years. However, in ER - patients, the subgroup of pS2 + or HSPZ 7 + seemed to have a better prognosis, although the statistical analysis was not significant: there were
244 JHurlimann, S.Gebhard and F.Gomez
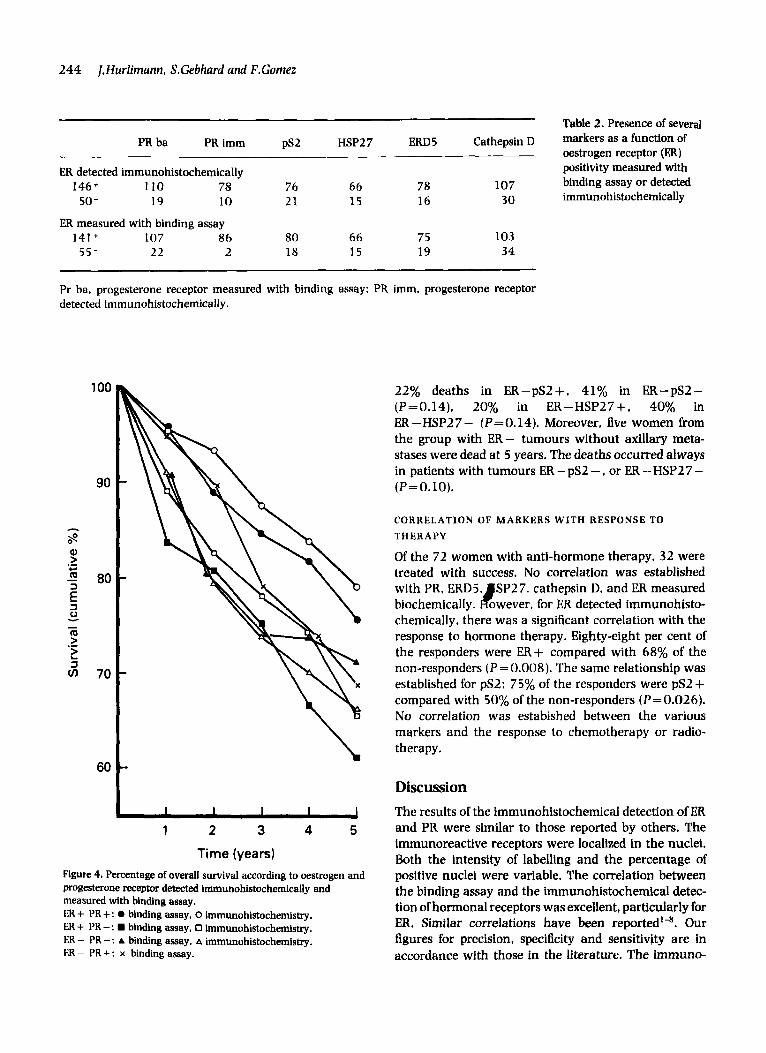
Table 2. Presence of several HSP2 7 m5 Cathepsin D markers as a function of
oestrogen receptor (ER) positivity measured with
107 binding assay or detected 30 immunohistochemically
PR ba PR imm PS2
ER detected immunohistochemically 146+ 110 78 76 66 78
50 - 19 10 21 1 5 16
FR measured with binding assay 141 + 107 86 80 66 75 103
55- 22 2 18 15 19 3 4
Pr ba. progesterone receptor measured with binding assay: PR imm, progesterone receptor detected immunohistochemically.
100
90
8
3 80
Q > .- *.,
i 3 0
RI > > 3
I - .- L
70
60
1 2 3 4 5
Time (years) Figure 4. Percentage of overall survival according to oestrogen and progesterone receptor detected immunohistochemically and measured with binding assay. ER + PR + : 0 binding assay, 0 immunohistochemistry. ER + P R - : binding assay, 0 immunohistochemistry. ER - PR-: A binding assay. A immunohistochemistry. ER - PR + : x binding assay.
22% deaths in ER-pSZ+. 41% in ER-pS2- (P=0.14), 20% in ER-HSP27+, 40% in ER-HSP27- (P=0.14). Moreover, five women from the group with ER- tumours without axillary meta- stases were dead at 5 years. The deaths occurred always in patients with tumours ER - pS2 - , or ER - HSP2 7 - (P=O.lO).
CORRELATION OF MARKERS WITH RESPONSE TO THERAPY
Of the 72 women with anti-hormone therapy, 32 were treated with success. No correlation was established with PR, ERD5. SP27. cathepsin D. and ER measured
chemically, there was a significant correlation with the response to hormone therapy. Eighty-eight per cent of the responders were ER+ compared with 68% of the non-responders ( P = 0.008). The same relationship was established for pS2: 75% of the responders were pS2 + compared with 50% of the non-responders (P= 0.026). No correlation was estabished between the various markers and the response to chemotherapy or radio- therapy.
biochemically. B owever, for ER detected immunohisto-
Discussion The results of the immunohistochemical detection of ER and PR were similar to those reported by others. The immunoreactive receptors were localized in the nuclei. Both the intensity of labelling and the percentage of positive nuclei were variable. The correlation between the binding assay and the immunohistochemical detec- tion of hormonal receptors was excellent, particularly for ER. Similar correlations have been reported’-H. Our figures for precision, specificity and sensitivity are in accordance with those in the literature. The immuno-

Hormonal receptors in breast carcinomas 245
C 100
90
80
80
70 Figure 5. Percentage of overall survival according to oestrogen receptor (ER) and progesterone receptor (PR) detected immunohistochemically and measured with binding assay. Influence of axillary 60 metastases. a No axillary metastases, b 1-3 axillary metastases, c More than 3 axillary metastases. For symbols see Figure 4.
11111 1 2 3 4 5
Time (years)
100
90
80
1 s! g 70 .- +- m - z a - 60 L
0
m > 3
- .- v)
50
40
30 - 1 2 3 4 5
Time (years)
histochemical sensitivity for PK was not as good (68%). The discordance between biological and immunohisto- chemical detection of PR has also been stressed by others18. The biochemical assay for PR is not as specific as immunohistochemical detection. PR is probably more labile than ER and its antigenic determinants are masked or destroyed during storage as frozen tissue or during the delay between surgery and tissue processing. The corre- lation between biochemical and immunohistochemical detection of receptors was obtained without semi- quantitative immunohistological method. Our attempt to use a semi-quantitative method did not result in a better correlation with biochemical results or a better evaluation of the patient outcome and we think that, for
- 1 2 3 4 5
practical use, semi-quantitative scoring is not necessary. This has been underscored by Bosman and co-w~rkers'~.
The immunohistochemical detection of hormonal receptors is probably closer to reality than the biochemi- cal measurement. The immunohistochemically EX false negative were tumours from women 65-80 years old with low levels of endogenous oestrogens which could explain the biochemical positivity*". The importance of endogenous oestrogens is also illustrated by the fact that immunohistochemistry detects almost the same percent- age of positive tumours in all age groups but the binding assay detects a higher percentage in elderly women. AN immunohistochemically false positive cases for ER and PR, were turnours with a strong desmoplastic reaction

246 j . Hurlimam. S.Ge6hat-d and F.Gotnez
which explains the negative biochemical test2'. We have never observed cases in which a minority of positive cells could explain the negative binding assay. The PR false negative cases were tumours with a low amount of biochemically detected receptors or tumours from women older than 60 years. In these cases, the very low amount of circulating progesterone could explain the difference between the two methods.
The prognostic value of immunohistochemical detec- tion of hormonal receptors seems better than the biochemical measurement. We have shown a correla- tion between overall survival at 5 years and ER status only with the immunohistochemical detection. The better prognostic value of immunohistochemistry could be explained by two factors: the method is not under the influence of endogenous oestrogens; the sensitivity of the method gives a better cut off than that established for the biochemical method. However, the importance of the immunohistochemical determination of ER is less strik- ing when the cases are stratified according to tumour size and the number of axillary metastases. Moreover, the prognostic value of hormonal receptors is important only for the first 5 years: we were unable to show a difference in the &year survival rate between the groups with or without hormonal receptors. EK status has also been said to be important for the prediction of the response to hormonal treatmentll. We have shown that immunohistochemically determined, but not biochemi- cally measured, oestrogen receptors correlate with the success of hormonal therapy. We did not show the predictive value of progesterone receptor for response to hormonal therapy. However, a subgroup with a poor prognosis can be sorted out from ER positive tumours based on PR negativity. The positivity of the other markers was cytoplasmic and heterogeneous in distribu- tion and intensity. The percentage of positive tumours for each marker was in accordance with those published for ERD523-24, pS225.2h and HSP2727,28. We confirmed the association of ERD5 with ER2' in contradiction to other^'^*^^. ERD5 was predominantly associated with grade I tumours, but surprisingly, also with tumours with metastases and with the largest tumours. We have no explanation for this exceptional labelling. Like Giri et 01.l~ we were unable to show a relation of this protein with a good response to hormonal treatment. Nor was it possible to demonstrate that this protein was important in the prognosis of breast carcinoma.
We confirmed that pS2 is a protein associated with I:K'i.Lh. This is in accordance with the demonstration of PS2 in vitro under the infuence of oestrogens12. pS2 was also more frequent in small tumours but showed no association with metastases and grade, contrary to the results of Thor et a/.2H and Foekens and co-wor-ers29. In
accordance with Thor et we have not shown the independent predictive value of pS2 for recurrence and for overall survival at 5 years. Other s t u d i e ~ ~ ~ ~ ~ ~ ~ " ' have demonstrated various results for prognosis, depending on the technique used for determination of pS2 and on its cut-off level. However, pS2 seems to have great value in predicting the response to hormonal therapy. It is also a marker of prognosis when the tumours are classified according to ER. In the group of ER- tumours, pS2+ cases have a good prognosis compared with pS2 - cases,
HSP27, described first by Edwards et aLY, has been detected immunohistochemically in breast carcinomas. We have found this protein principally in grade I and FA+ tumours. This is in accordance with studies that have shown an association of this protein with ER in vitrog and in v ~ v o ~ ' . ' ~ . We confirmed that HSP27 did not discriminate between oestrogen responders and non- respondersJ 3. In contradiction to Seymour et a/.34 we did not show a relationship of HSP27 with overall survival or recurrence. However, like pS2. HSP27 sorted out cases with a good prognosis from the ER - group with a bad prognosis.
Cathepsin D in tumour cells was associated with small, EK positive. and grade I tumours. The correlation with EK is not surprising because cathepsin D has been shown to be synthesized under the influence O ~ E R " ' . ~ ~ . ~ ~ . In contradiction to some s tud ie~~ ' -~~) , which have shown that cathepsh D is an important prognostic factor, we have not demonstrated a correlation of cathepsin D and axillary metastases, bone metastases, overall survival or recurrence at 5 years. Similar results have been obtained by Domagala and co-workers" . Moreover, cathepsin D is present in two types of cells. the tumour cells and the histiocytes. It would be necessary to determine the influence of both types of cells. IJntil then, the inter- pretation of cathepsin D levels in tissue extracts is questionable.
Thus, immunohistochemical detection of hormone receptors has several advantages over the biochemical measurement. Immunohistochemistry can be done on small pieces of tissue: it is not modified by endogenous hormones: it detects rare positive cells in desmoplastic tumours and, globally, has a better prognostic value. Moreover, in the future, new monoclonal antibodies will, perhaps, be able to separate ER with different biological properties. For these reasons and in agreement with the conclusion of Tesch et a1.42 we feel that immunohistochemical determination of hormonal receptors should be preferred to the binding assay. Immunohistochemistry is also useful in the dktection of other markers related to ER. pS2 and HSP27 seem promising in sorting out subgroups with a better prognosis and/or a better response to hormone therapy.

Hormonal receptors in breast carcinomas 247
However. imrnunohistochemical detection of cathepsin and ERDS does not appear to be useful.
Acknowhdgements We thank M.M.Bertholet. F.Ahmad, S.Laurini, J.Mai1- lardet and M.Schmidt for their technical assistance, and G.Perriard for manuscript preparation. The help and suggestions of B. Winistorfer during the preparation of the manuscript are also gratefully acknowledged. Dr J.Hurlimann has the financial support of the Ligue Vaudoise contre le cancer, Lausanne.
References I . Charpin C. Martin PM. Ue Victor B et al. Multiparametric study
(SAMBA 200) of estrogen receptor immunocytochemical assay in 400 human breast carcinomas: analysis of estrogen receptor distribution heterogeneity in tissues and correlations with dex- tran-coated charcoal assays and morphological data. Cancer Rcs.
2. Berger U, Wilson P. Thethi S. McClelland RA. Greene GL. Coambes RC. Comparison of an immunocytochemical assay for progest- erone receptor with a biochemical method of measurement and immunocytochemical examination of the relationship between progesterone and estrogen receptors. Citncer Kes. 1 989: 49: 5 1 i h - 51 79.
3. Hanna W. Mobbs B. Comparative evaluation of ER-ICA and enzyme immunoassay for the quantitation of estrogen receptors in breast cancer. Am. /. Clin. Pathol. 1989: 91: 182-186.
4. Kinsel LB. Szabo E. Creene GL. Konrath J. Leight CS. McCarty KS Jr. Immunocytochemical analysis of estrogen receptors as predic- tor of prognosis in breast cancer patients: comparison with quantitative biochemical methods. Canrer Res. 1989: 49: 1051- 1056.
5. Reiner A. Neumeister B. Spona J, Reiner G. Schemper M. Jakess R. Immunocytochemical localization of estrogen and progesterone receptor and prognosis in human primary breast cancer. Cancer Res. 1990: 5 0 7057-7061.
6. Seymour L. Meyer K. Esser J , MacPhail P. Behr A. Berwoda WR. Estimation of PR and ER by immunocytochemistry in breast cancer. Comparison with radioligand binding methods. Am. 1. Clin. Pathol. 1990: 94 (suppl. I): S35-40.
7. Ozzello L, De Rosa C. Habif DV. Creene CL. An immunohisto- chemical evaluation of progesterone receptor in frozen sections, paraffin sections, and cytologic imprints of breast carcinomas. Cancer 1991: 67: 455-462.
8. Masood S, Dee S. Coldstein JD. lmmunocytochemical analysis of progesterone receptors in breast cancer. Am. 1. Clin. Pathol. 199 1:
9. EdwardsDP. Adams DJ. Savage N. McCuire WL. Estrogen induced synthesis of specific proteins in human breast cancer cells. Biochem. Biophys. Res. Cornrn. 1980: 93; 804-8 12.
10. Garcia M. Capony F. Derocq D. Simon D. Pau B. Rochefort H. Characterization of monoclonal antibodies to the estrogen-regu- lated Mr 52000 glycopmtein and their use in MCF-7 cells. Cancer Res. 1985: 45: 709-716.
11 . Coffer AI. Lewis KM, Brockas AJ. King RIB. Monoclonal antibodies
1988: 48: 1578-1 586.
96: 59-63.
against a component related to soluble estrogen receptor. &ncer Res. 1985: 45; 3686-3693.
12. Nun= AM. Jakowlev S, Briand JP et a/. Characterization of the estrogen-induced pS2 protein secreted by the human breast cancer cell line MCF-7. EndocrinologM 1987: 121: 1759-1765.
1 3. Miller AB. Hoogstraten B. Staquet M, Winkler A. Reportingresults of cancer treatment. Cancer 1981: 47: 207-214.
14. Bloom HJG. Richardson WW. Histological grading and prognosis in breast cancer. Br. I. Cancer 1957: 11; 359-377.
1 5. Le Doussal V. Tubiana-Huh M. Friedman S. Hacene K. Spyratos F. Brunet M. Prognostic value of histologic grade nuclear components of Scad-Bloom-Richardson (SBR). An improved score modification based on a multivariate analysis of 1262 invasive ductal breast carcinomas. Cancer 1989: 6 4 19 14-192 1.
16. Vollenweider-Zerargui L. Barrelet L. Wong Y. Lemarchand- Beraud T, Comez F. The predictive value of estrogen and progesterone receptors' concentrations on the clinical behavior of breast cancer in women. Clinical correlation on 547 patients. Cancer 1986: 57: 1171-1180.
1 7. Sternberger LA, Hardy PH Jr, Cuculis J , Meyet HC. The unlabeled antibody enzyme method of immunohistochemistry. Preparation and properties of soluble antigen-antibody complex (horseradish peroxidase-antihorseradish peroxidase) and its use in identitlca- tion of spirochetes. 1. Histodiem. Cytochern. 1970: 18: 3 15-33 3.
18. Helin HI. Helle MJ. Helin ML. Isola JJ. Immunocytochemical detection of estrogen and progesterone receptors in 124 hriman breast cancers. Am. /. Clin. Pathol. 1988: 89: 137-142.
19. Bosman FT, de Ceoij AFPM. Rousch M. Quality control in immunocytochemistry: experiences with the oestrogen receptor assay. I. Clin. Pathol. 1992: 45: 120-124.
20. Wong SY. Carrol EIIS. Ah-See SY. Sewell HF. Detection of estrogen receptor proteins in breast tumors using an improved APA AP immunohistochemical technique. Cancer 1988: 62; 2 171-2 175.
2 1 , I>e Negri F, Campani D. Sarnelli R et al. Comparison of monoclonal immunocytochemical and immunoenzymatic methods for steroid receptor evaluation in breast cancer. Am. 1. Clin. Pathol. 199 1: 96: 53-58.
22. Valavaara R. Tuominen J. Johansson R. Predictive value of tumor estrogen and progesterone receptor levels in postmenopausal women with advanced breast cancer treated with toremifene. Cancer 1990: 66: 2264-2269.
2 3. King RJB. Coffer AI. Gilbert et al. Histochemical studies with a monoclonal antibody raised against a partially purified soluble estradiol receptor preparation from human myometrium. Cancer
24. Ciri DD. Dangefield VJM, Lonsdale R, Rogers K. Immunohistology of oestrogen receptor and D5 antigen in breast cancer: correlation with oestrogen receptor content of adjacent cryostat sections assayed by radioligand binding and enzyme immunoassay. 1. Clin. Pathol. 1987: 40: 734-740.
25. Horne GM. Angus B. Wright C et a/. Relationships between oestrogen receptor. epidermal growth factor receptor. ER-D5 and p24 oestrogen regulated protein in human breast cancer. /. Pathol.
26. Rio MC. Bellocq JP. Gairard B et al. Specific expression of the pS2 gene in subclasses of breast cancers in comparison with expression of the estrogen and progesterone receptors and the oncogene ERBB2. Pror. Natl Arad. Sci. USA 1987: 84; 9243-9247.
27. Schwartz LH. Koerner FC. Edgerton SM et al. pS2 expression and response to hormonal therapy in patients with advanced breast cancer. Cancer Res. 1991: 51: 624-628.
28. Thor AD. Koerner FC. Fdgerton SM. Wood WC. Stracher MA.
R ~ s . 1985: 45: 5728-5733.
1988: 155: 143-150.

248 JHurlimann, S.Gebhard and F.Gomet
Schwa- LH. pS2 expression in primary breast carcinomas: relationship to clinical and histological features and survival. Breast Cancer Res. Treut. 1992: 21; 1 1 1-1 19.
29. Foekens JA. Rio MC. Seguin P et a/. Prediction of relapse and survival in breast cancer patients by pS2 protein status. Cancer Res. 1990: 5 0 3832-3837.
30. Predine J, Spyratos P. Prud'homme JF et a/. Enzyme-linked immunosorbent assay of pS2 in breast cancers, benign tumors and normal breast tissues. Cancer 1992: 69; 2116-2123.
3 1. Adams DJ. McGuire WL. Quantitative enayme-linked immunosor- bent assay for the estrogen-regulated Mr24000 protein in human breast tumors: correlation with estrogen and progesterone recep- tors. Cancer Res. 1985: 45: 2445-2449.
32. Ciocca DR. Stati AO. Amprino de Castro MM. Colocalization of estrogen and progesterone receptors with an estrogen-regulated heat shock protein in parafan sections of human breast and endometrial cancer tissue. Breast Cancer Res. Treat. 1990: 16;
33. Andersen J. Skovbon H. Poulsen HS. Immunocytochemical determination of the oestrogen-regulated protein M 24000 in primary breast cancer and response to endocrine therapy. Eur. 1. Cancer Clin. Oncol. 1989: 25: 641-643.
34. Seymour L. Bezwoda WR. Meyer K. Tumor factors predicting for prognosis in metastatic breast cancer. The presence of P24 predicts for response to treatment and duration of survival. Cancer
243-251.
1990: 66: 2390-2394.
35. Morisset M. Capony F. Rochefort H. Processing and estrogen regulation of the 52-Hodatton protein inside MCF-7 breast cancer cells. Endocrfnologu 1986: 119; 2773-2782.
36. Rochefort H. Capony F. Garcia M et ul. Estrogen-induced lysosomal proteases secreted by breast cancer cells: a role in carcinogenesis? 1. Cell. Biochem. 1987; 35: 17-29.
37. Tandon AK. Clark GM. Chamness GC. Chirgwin JM. McGuire WL. Cathepsin D and prognosis in breast cancer. N. Engl. /. Med. 1 990
38. Namer M, Ramaioli A. Fontana X et a/. Prognostic vdue of total cathepsin D in breast tumors. Breast Cancer Res. Treat. 1991: 1 9 85-93.
39. Thorpe SM, Rochefort H. Garcia Metal. Association between high concentrations of Mr52000 cathepsin D and poor prognosis in primary human breast cancer. Cancer Rrs. 1989: 49: 6008-6014.
40. Henry JA. McCarthy AL. Angus B et al. Prognostic significance of the estrogen-regulated protein. cathepsin D. in breast cancer. An immunohistochemical study. Cancer 1990: 65: 26 5-2 7 1.
41. Domagala W. Striker C. Szadowska A, Dukowicz A. Weber K. Osborn M. Cathepsin D in invasive ductal NOS breast carcinoma as defined by immunohistochemistry. No correlation with sur- vival at 5 years. Am. 1. Patliol. 1992: 141: 1003-1012.
42. Tesch M. Shawwa A. Henderson R. Immunohistochemical deter- mination of estrogen and progesterone receptor status in breast cancer. Am. I . Cliri. Pathol. 199 3: 99: 8- 12.
322: 297-302.
Copyright © 2022 FDOKUMEN




















