
New laboratory markers for the management of rheumatoid arthritis patients
9
Clin Chem Lab Med 2014; 52(12): 1729–1737 Review Daniela P. Foti, Marta Greco, Eleonora Palella and Elio Gulletta* New laboratory markers for the management of rheumatoid arthritis patients Abstract: Rheumatoid arthritis, the most prominent of systemic autoimmune rheumatic diseases, represents an important social health problem. Recent insights into the immunopathogenic mechanism of this complex and multiform illness might open new perspectives for a more appropriate laboratory approach. In this review we focus on the most relevant pathogenetic mechanism; indicat- ing the laboratory biomarkers specifically linked to early diagnosis, prognosis, evolutive aspects of the disease, and therapeutic efficacy. Evidence based on laboratory medi- cine could provide the best outcome for patients. Keywords: evidence-based laboratory medicine (EBLM); immunopathogenesis; laboratory assay; rheumatoid arthritis. DOI 10.1515/cclm-2014-0383 Received April 7, 2014; accepted May 22, 2014; previously published online June 14, 2014 Introduction Rheumatoid arthritis (RA) is the most prominent of sys- temic autoimmune rheumatic diseases that may affect different tissues and organs, although the synovial joints represent the major target. The onset of RA is mainly observed at the end of adolescence or between the 4th and 5th decades of life, while a second peak of incidence is reported between 60 and 70 years. In general, the number of cases increases with age, with a prevalence of 0.5%–1% in industrialized countries, and with rates of 5% in women over 55 years [1]. An early variant of RA is also described in childhood [2]. This disease represents an important social health problem because of its high incidence, invalidat- ing progress and important disabilities. The involvement of the synovial joints, that results in severe dysfunction, leading to limitation of motion, may be accompanied and complicated by several extra-articular manifestations [3–5], such as pleural and pericardial diseases, rheuma- toid nodules, Caplan’s syndrome, bronchiectasis [6, 7]. All these clinical conditions can lead to major reduction in functional and work abilities and health-related quality of life, while the RA-associated increased risk for cardio- vascular disease may reduce life expectancy by 3–18 years [8]. Today, RA is considered a multifactorial disease, in which environmental factors, such as several subsequent viral infections, seem to play a role in the onset and per- sistence of the disease. Smoking is also considered a pre- disposing condition [9]. Genetic factors are, however, also implicated in the susceptibility and the evolution of RA. A genetic association with antigens of the major hysto- compatibility complex (MHC)-II, and in particular human leukocytes antigens (HLA)-DRB1, has been well estab- lished, although non-HLA associated loci have also been linked to the disease [10, 11]. Although the cause of RA is still unknown, autoimmunity plays an important role. It has become increasingly evident that autoantibodies mainly target proteins that undergo citrullination, a post- translational modification frequently occurring during inflammation, apoptosis, and keratinization. Pro-inflam- matory substances released by immune cells are involved in the activation and maintenance of inflammation that causes swelling and subsequent damage of the cartilage and bone inside the joint. It is hypothesized that super- antigens may be also implicated, while self-antigens (col- lagen, proteoglycans, rheumatoid factor and citrullinated proteins) probably play a role in the chronic evolution of the process. At present, there is no universal cure able to ultimately eradicate RA. The therapeutic approach in the management of RA has witnessed revolutionary changes over the last 15 years, thanks to the wider understand- ing of the molecular mechanisms involved in the patho- genesis of the disease. Glucocorticoids, non-steroidal *Corresponding author: Elio Gulletta, MD, Department of Health Sciences, Viale S. Venuta, 88100 Catanzaro, Italy, Phone: +39 0961 3697243, Fax: +39 0961 3697415, E-mail: [email protected] Daniela P. Foti, Marta Greco and Eleonora Palella: Clinical Pathology Unit, Department of Health Sciences, University Magna Graecia, Catanzaro, Italy Unauthenticated Download Date | 6/18/16 7:04 AM
-
Upload
independent -
Category
Documents
-
view
4 -
download
0
Transcript of New laboratory markers for the management of rheumatoid arthritis patients

Clin Chem Lab Med 2014; 52(12): 1729–1737
Review
Daniela P. Foti, Marta Greco, Eleonora Palella and Elio Gulletta*
New laboratory markers for the management of rheumatoid arthritis patients
Abstract: Rheumatoid arthritis, the most prominent of systemic autoimmune rheumatic diseases, represents an important social health problem. Recent insights into the immunopathogenic mechanism of this complex and multiform illness might open new perspectives for a more appropriate laboratory approach. In this review we focus on the most relevant pathogenetic mechanism; indicat-ing the laboratory biomarkers specifically linked to early diagnosis, prognosis, evolutive aspects of the disease, and therapeutic efficacy. Evidence based on laboratory medi-cine could provide the best outcome for patients.
Keywords: evidence-based laboratory medicine (EBLM); immunopathogenesis; laboratory assay; rheumatoid arthritis.
DOI 10.1515/cclm-2014-0383Received April 7, 2014; accepted May 22, 2014; previously published online June 14, 2014
IntroductionRheumatoid arthritis (RA) is the most prominent of sys-temic autoimmune rheumatic diseases that may affect different tissues and organs, although the synovial joints represent the major target. The onset of RA is mainly observed at the end of adolescence or between the 4th and 5th decades of life, while a second peak of incidence is reported between 60 and 70 years. In general, the number of cases increases with age, with a prevalence of 0.5%–1% in industrialized countries, and with rates of 5% in women over 55 years [1]. An early variant of RA is also described in
childhood [2]. This disease represents an important social health problem because of its high incidence, invalidat-ing progress and important disabilities. The involvement of the synovial joints, that results in severe dysfunction, leading to limitation of motion, may be accompanied and complicated by several extra-articular manifestations [3–5], such as pleural and pericardial diseases, rheuma-toid nodules, Caplan’s syndrome, bronchiectasis [6, 7]. All these clinical conditions can lead to major reduction in functional and work abilities and health-related quality of life, while the RA-associated increased risk for cardio-vascular disease may reduce life expectancy by 3–18 years [8]. Today, RA is considered a multifactorial disease, in which environmental factors, such as several subsequent viral infections, seem to play a role in the onset and per-sistence of the disease. Smoking is also considered a pre-disposing condition [9]. Genetic factors are, however, also implicated in the susceptibility and the evolution of RA. A genetic association with antigens of the major hysto-compatibility complex (MHC)-II, and in particular human leukocytes antigens (HLA)-DRB1, has been well estab-lished, although non-HLA associated loci have also been linked to the disease [10, 11]. Although the cause of RA is still unknown, autoimmunity plays an important role. It has become increasingly evident that autoantibodies mainly target proteins that undergo citrullination, a post-translational modification frequently occurring during inflammation, apoptosis, and keratinization. Pro-inflam-matory substances released by immune cells are involved in the activation and maintenance of inflammation that causes swelling and subsequent damage of the cartilage and bone inside the joint. It is hypothesized that super-antigens may be also implicated, while self-antigens (col-lagen, proteoglycans, rheumatoid factor and citrullinated proteins) probably play a role in the chronic evolution of the process. At present, there is no universal cure able to ultimately eradicate RA. The therapeutic approach in the management of RA has witnessed revolutionary changes over the last 15 years, thanks to the wider understand-ing of the molecular mechanisms involved in the patho-genesis of the disease. Glucocorticoids, non-steroidal
*Corresponding author: Elio Gulletta, MD, Department of Health Sciences, Viale S. Venuta, 88100 Catanzaro, Italy, Phone: +39 0961 3697243, Fax: +39 0961 3697415, E-mail: [email protected] P. Foti, Marta Greco and Eleonora Palella: Clinical Pathology Unit, Department of Health Sciences, University Magna Graecia, Catanzaro, Italy
UnauthenticatedDownload Date | 6/18/16 7:04 AM

1730 Foti et al.: Laboratory approach to RA patients
anti-inflammatory drugs, and few disease modifying anti-rheumatic drugs (DMARDs), including methotrexate, sulphasalazine, hydroxychloroquine, and gold have been the only treatment options until two decades ago. Since the discovery of new therapeutic targets, a significant breakthrough has been achieved in rheumatology with the development of biological agents. The first class of biologic agents include tumor necrosis factor (TNF) inhib-itors, followed by many others with different mechanisms of action, such as rituximab, abatacept, and tocilizumab. These agents have changed the fate of patients with RA due to their good efficacy and safety features. Most impor-tantly, the role of B cells in the pathophysiology of RA has been highlighted by depleting peripheral B cells using anti-CD20 agents or inducing apoptosis by the inhibition of B cell receptors and depleting this lymphocyte popula-tion from the germinal center [12]. This novel therapeutic approach can target intracellular B cell signaling and reg-ulatory B cells. Moreover, new cytokine-directed biologi-cal drugs targeting important proinflammatory mediators, such as GM-CSF, interleukin (IL)-1, IL-6 and its receptor, IL-17, IL-20, IL-21, IL-23, have been or will be soon avail-able, hopefully enhancing our therapeutic choices [13]. All recent knowledge on pathogenetic mechanisms has opened a new window upon the efficacious approach of laboratory performances both in the choice of biomarkers, and best practice regarding the patient outcome [14–16].
PathogenesisPresently, a three-step model has been proposed for ACPA-positive RA. In the first step, an environmental risk factor can induce protein citrullination, while the new epitopes may elicit the ACPA production in susceptible individuals, bearing a peculiar haplotype. HLA DRB1 – encoding the most widespread MHC class II HLA-DR β subunit paralog – is the genetic locus most specifically linked to the risk of developing RA in the Caucasian population. Several other genes have been considered as probands for the disease, such as protein tyrosine phosphatase non-receptor type 22 (PTPN22) Arg620→Trp, signal transducer and activa-tor of transcription 4 (STAT4), TNF receptor-associated factors (TRAF)1/C5, all of which are involved in specific protein citrullination induced by environmental factors. The DRB1 allele is responsible for peptide binding specifi-cities and codes for a conserved sequence of amino acids at residues 67–74 of the DR β chain, a region involved in the accommodation of the antigenic peptide and recogni-tion of the T cell receptor [17]. Interestingly, DRB1*0404
or *0401 antigen binding grooves fit better citrullinated, rather than the corresponding arginine-bearing peptides. Genome-wide single nucleotide polymorphism (SNP) analyses of RA patients, compared with healthy con-trols, confirmed the genetic contribution of two of these residues, 71 and 74, and of three other amino acids, all of which are located in the peptide-binding groove, to RA susceptibility [18]. These data classify high-, intermedi-ate-, low-risk and non-susceptibility alleles, depending upon the amino acid sequence between 70 and 74 resi-dues within the groove. Instead, the variant PTPN22 is a gain of function mutation that enhances the ability of its gene product to inhibit T cell activation [19]. PTPN22, in fact, codifies an intracellular tyrosine phosphatase (LyP), which negatively regulates T lymphocyte activity, by modi-fying the intracellular signal of the T cell receptor (TCR). A study on the PTPN22 polymorphism 1858T, anti-cyclic cit-rullinated peptides (CCP) antibodies, rheumatoid factors of all different classes (IgM, IgA, IgG) and shared epitopes genes (HLA-DRB1*0404 or *0401) has established their strong relationship and the high positive predictive value for RA. The presence of PTPN22 1858T polymorphism and anti-CCP antibodies shows 100% specificity for RA [20]. In genetically predisposed individuals, several different environmental factors, depending on the studied popula-tion, can trigger autoimmunity response to citrullinated proteins, impairing tolerance. Among these, smoking and Porphyromonas gingivalis, a self-producing citrullinated protein bacterium involved in periodontitis, are attractive etiological agents playing a role in gene/environment/autoimmunity interactions [21].
In the second step, an inflammatory response can develop into the articular synovial layer, with the recruit-ment of ACPA and the deposition of immunocomplexes. In RA, ACPA are pathogenic, and specific for this disease, and have a strong association with HLA-DRB1 shared epitopes alleles. In rheumatoid synovium, peptidylarginine deimi-nase isoforms peptidylarginine deiminase (PAD)2 and PAD4 are abundant, thereby determining an active local citrullination of proteins, such as fibrin. Citrullinated epitopes appear longer before the clinical symptoms and they are associated with more severe joint erosions and an evolution of clinical course. Citrullination, a modifi-cation of arginine side chains catalyzed by PAD enzymes (deimination) increases the affinity of several peptides for shared epitopes, thus expressing HLA-DR molecules and improving their presentation to T cells. The most well-characterized epitopes are filaggrin, fibrinogen, vimentin, type II collagen, and α-enolase. Cellular survival response can be triggered by misfolded proteins in the endoplas-mic reticulum (ER). ER-stress associated genes are highly
UnauthenticatedDownload Date | 6/18/16 7:04 AM

Foti et al.: Laboratory approach to RA patients 1731
expressed in the rheumatoid synovium and synovial cells. ER chaperone glucose-related protein 78 (GRP78), in vitro, is crucial for the proliferation of synoviocytes and angio-genesis, and strongly contributes to RA pathogenesis [22]. In summary, autoimmunity to citrullinated protein anti-gens has specificity for RA and defines a clinically and genetically distinct form of the disease.
In the final step, the presence of immunocomplexes induces the increasing presence of immunity cells and cytokine production, which can act together to perpetuate, in RA, the chronic inflammation at articular sites. Dysreg-ulated expression of cytokines drives both inflammation and tissue destruction, thereby implicating the evaluation of cytokines pattern for a complete and effective under-standing of patient’s immunoresponse [23]. Recently, the role of IL-36a, which is up-regulated in RA synovium, has been pointed out. This interleukin, expressed by plasma cells, and leading to IL-6 and IL-8 production by synovial fibroblasts, may represent the biological link between autoimmunity and the gradual development of synovi-tis [24]. Hypoxia and Th1 lymphocytes-driven inflamma-tion contribute to the pathogenesis of RA, although Th1 cytokines are not sufficient to induce angiogenesis, even together with hypoxia. Instead, Th2 cytokines induce angiogenic activity in normoxic and hypoxic conditions, suggesting a complex and not yet clarified interaction between hypoxia, angiogenesis and inflammation [25]. The presence of IL-17 in synovial fluid and tissue of RA patients may suggest an important pathogenic role of this cytokine, as supported by several mouse models. IL-17A induces angiogenesis, cell migration and cell invasion, all key processes in the pathogenesis of RA, by stimulating GROα and monocyte chemoattractant protein-1 (MCP-1) expression in RA synovial fibroblasts [26]. Interestingly, MCP-1 and regulated on activation normal T cell expressed and secreted, (RANTES) polymorphisms do not contrib-ute to individual RA susceptibility or severity in the Cau-casian population [27]. Involvement of MCP-1, IL-1β, IL-6, IL-8, TNF-α in RA synovial alterations has been described for many years. In each single patient, the integration of cytokine profiles with autoantibody response may be extremely important for prognosis, for the choice of the most appropriate therapeutic treatment, and the evalu-ation of its efficacy [28]. Moreover, there are more CD4+ CD25high Treg cells present in synovial fluid than in periph-eral blood, where they have shown a functional defect impairing their ability to suppress CD4+ CD25– T cells. This defect can be reversed by anti-TNF-α therapy [29]. Fur-thermore, NK cells seems to play an exclusive role in the pathogenesis of autoimmune disease, and in the case of RA, these specialized cells represent a significant fraction
of the lymphocytes (8%–25%) in the synovial fluid of RA patients and could be detected in the joint early during the disease course [30]. The majority of the NK cells in the synovial fluid of RA patients are CD56bright (approx. 60% of NK cells), a subphenotype also found in the blood of RA patients, but at much lower frequencies (approx. 10% of NK cells). The synovial NK show an elevated expres-sion of CD94/NKG2A and decreased expression of killer immunoglobulin-like receptor (KIR)s and CD16. Due to an upregulated expression of several chemokine recep-tors and adhesion molecules, they may participate in the preferential recruitment into the synovium [31]. The syno-vial CD56bright NK cells express higher levels of activation markers (CD69 and NKp44) and produce more TNF-α and IFN-γ than those from the peripheral blood of the same patients. [32]. Synovial NK cells could induce monocytes to differentiate into DCs, and, as reported, produce IL-22, a cytokine that promotes proliferation of synovial fibro-blasts, thereby representing a target for molecular therapy [33]. Aberrant expression of MHC class I polypeptide-related sequence A in the inflamed synovium may augment CD56bright NK cell activation, resulting in dysregulated production of proinflammatory cytokines rather than in immunoregulation. Taken together, these findings suggest that the enrichment of CD56bright NK cells may contribute to the initiation and/or perpetuation of dysregulated pro-duction of proinflammatory cytokines in the synovium of RA patients [34]. The genetic associations between inflam-matory arthritis and KIR haplotypes support the hypoth-esis that dysregulation of cytokine production by CD56bright NK cells in the synovium and/or decreased cytotoxic-ity by peripheral CD56dim NK cells may contribute to the pathogenesis of RA. Distinct antibody profiles have been associated with subgroups of patients who exhibited high serum levels of TNF-α, IL-1β, IL-6, IL-13, IL-15 and GM-CSF. Significantly increased autoantibody reactivity against citrullinated epitopes was observed in patients within the cytokine “high” subgroup [35, 36]. Increased levels of TNF-α, IL-1α, IL-12p40 and IL-13, and the chemokines eotaxin/chemokine ligand (CCL)11, MCP-1 and interferon-inducible protein 10, were present in early RA as compared with the controls [37]. Between chemokines, only IL8/cysteine x cysteine (CXC)L8 concentrations were higher in patients with psoriatic arthritis and ankylosing spondylitis than in patients with RA [38, 39]. Increased blood levels of pro-inflammatory cytokines are associated with autoantibod-ies targeting citrullinated antigens and surrogate markers of disease activity in patients with early RA [40]. Prot-eomic analysis of serum autoantibodies, cytokines and chemokines enables stratification of patients with RA into molecular subgroups [41] (Table 1).
UnauthenticatedDownload Date | 6/18/16 7:04 AM
1732 Foti et al.: Laboratory approach to RA patients
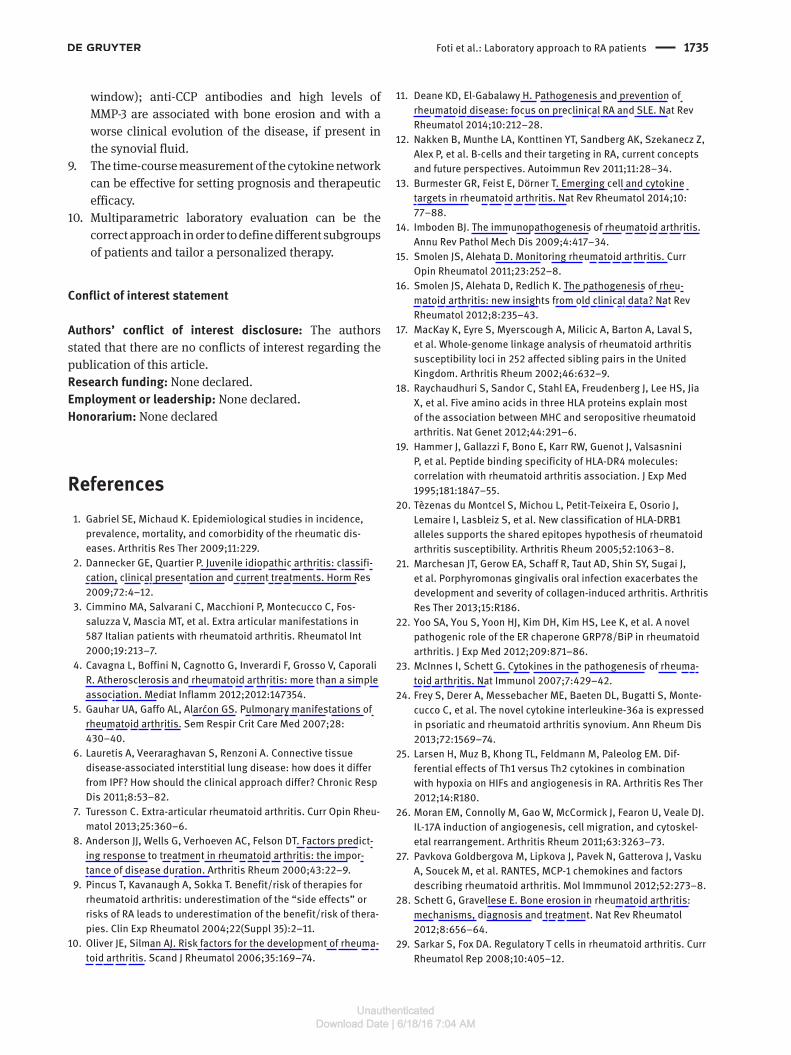
the basis of international guidelines, their assay is still used as corollary procedure for determining a first diag-nosis [42]. Evidence-based laboratory medicine (EBLM) predicts that a laboratory biomarker should have several properties: it should be present in a biosample which is representative of the disease localization; recorded from a patient, and thus specifically linked to his/her disease; and it has to be measured by a standardized and repro-ducible analytical methodology. The ideal biomarker should clearly indicate: health/disease condition; high/low exposure to risk factors; effectiveness/no response to therapy. Thus, each different laboratory biomarker can be used properly in a selected phase of clinical decision (pre-dictivity, diagnosis, prognosis, monitoring therapeutic efficacy or adverse effects), and in all cases, their choice must be related to a real improvement of the patient man-agement [43] (Figure 1).
Common and uncommon laboratory biomarkers of RA are summarized in Table 2.
RF is the prototypic marker of RA for diagnostic and prognostic purposes, since it is associated with joint destruction, even if is not clearly indicated as a mediator of these effects. Moreover, in seropositive RA patients, the levels of RF are not related to bone damage and status of the disease [44]. For several years, evaluation of RF Ig iso-types has been used to enhance the serological diagnosis of RA [45]. More recently, it has been proposed as a useful tool to predict patient response to biological therapy [46]. Several proteolytical enzymes can be involved in the pathogenesis of RA. Between those, metalloprotein-ases represent a family of important factors which cause the destruction of articular tissue. The role that proteo-lytic enzymes play in RA can be summarized as follows: matrix metalloproteinases (MMP 1,2,3,9); cystein protein-ases (cathepsin B,H,L); serin proteinase (elastase, PA, cathepsin G); and aspartic acid proteinase (cathepsin D). MMP-3 can be a very useful marker for the prediction of joint destruction [47]. MMP-3 (stromelisyn-1) is expressed by synovial and articular cells, fibroblasts, chondroblasts,
Table 1 Factors involved in rheumatoid arthritis.
Molecules and receptors PTPN22 TCR/BCR signaling TNFAIP Ubiquitin editing enzyme; TNFR signaling and
NFkB pathway inhibitor TRAF1 TNFR signaling and NF-kB pathway regulator NKp46 Activation of NKTranscription factors REL NF-kB pathway component STAT4 IFN-γ pathway regulatorCytokines and receptors IL-2/IL-21 T cells regulation CTL4 T cells costimulation inhibitor CD40 B/T cells costimulator; production of IgM, TNF-α,
IL-2 TNF-α Proinflammatory; Pro-osteoclastogenesis
(RANKL) IL-6 Proinflammatory; Pro-osteoclastogenesis
(RANKL) IL-1 Moderate pro-inflammatory IL-17 Blocking anti-osteoclastogenetic factors (IL-4,
IFN-γ; IL-12) RANKL Osteoclast differentiation M-CSF Essential for osteoclast differentiation IL-15 Pro-osteoclastogenesis inducing RANKL IL-8 Chemotactic factor IL-22 NK activation IFN-γ Proinflammatory response, NK autocrine functionEnzymes PAD4 Enzymatic peptide citrullinationPolymorphisms VEGF-A Early onset MMP-1; MMP-3 Matrix degradation; hypoxic effect
BiomarkersThe most widely accepted diagnostic criteria for RA suggest that laboratory tests can make an essential contri-bution. Despite the fact that several markers can be meas-ured by widely validated analytical procedures, not all of them allow early diagnosis as they only become positive in the well-established active phase of the disease. On
Figure 1 Evolutive steps in RA.
UnauthenticatedDownload Date | 6/18/16 7:04 AM

Foti et al.: Laboratory approach to RA patients 1733
and osteoclasts. It acts upon extracellular substrates of cartilages, such as fibronectin, collagen IV and V, elastin, proteoglycans, but also together with other MMPs in the disruption of cartilages [48]. It is present in the synovial fluid during the active phase of disease and its levels cor-relate with serum concentrations, independently from patient’s age and severity of the disease. It is produced very early during the course of RA and elevated serum levels can be predictive of articular disruption, within 6–12 months from the event. Together with RF, it can be a laboratory marker of active phlogosis and predictive of invalidant evolution [49]. Polymorphisms in the vascular endothelial factor A (VEGF-A) gene and MMP-1,3 intergenic locus may influence the age of onset of RA [50]. Currently, a more specific immunological profile has been proposed to evaluate each patient at the onset of disease, or their relatives in order to predict the risk of disease. All anti-CCP and RF isotypes analyzed occurred more commonly in unaffected first-degree relatives from multicase families than in the controls, but had different isotype distribution from the patients with RA [51].
Anti-CCP-2 antibodies of both the IgG and IgA iso-types pre-dated the onset of RA by years; also, both IgG and IgA anti-CCP-2 antibodies predicted the development of RA, with the highest predictive value for IgG anti-CCP-2 antibodies; individuals who subsequently developed RA had increased concentrations of several cytokines and chemokines years before the onset of symptoms of joint disease [52].
The immunological profile consists in the definition of haplotype, evaluation of ACPA, and ANA autoantibod-ies (cytoplasmic pattern), measurement of plasma levels of Th1 and Th2 cytokine networks. A seminal paper has
Table 2 Laboratory markers in RA.
Biohumoral Rheumatoid factor (RF) IgM, IgA, IgG hsCRP ESR Metalloproteinases: MMP-3Autoantibodies ANA (cytoplasmic pattern endosomes-lysosomes) ACPA (anti-citrullinated peptides) (vimentin, type II collagen,
α-enolase, fibrinogen) Antibodies antithrombospondin-1 Anti-hnRNP A2/B1 (RA33)Cytokines and molecular markers IL-1β, IL-6, TNF-α, IL-10, IL-17, VEGF, MCP-1Cellular and genetic markers Treg lymphocytes NK, NKT HLA DRB1, PTPN22 Arg620→Trp, STAT4, TRAF1/C5
settled down the importance to identify a complete profile of RA-associated antibodies (AAB) to improve early diag-nosis of the disease and provide prognostic and therag-nostic indications. Anti-CCP antibodies demonstrate the best diagnostic performances for profiling, thus they must be used as first-line screening and identification of subgroups of patients. The use of multiplex assays may facilitate a wider implementation of profiling [53]. More-over, a positive result of the immunoenzymatic evalua-tion of anti-citrullinated peptides (ACPA) against several structural proteins has to be considered the highest specific biomarker for RA. Even if in some patients IgM anti-second generation CCP-2 autoantibodies appear at the initial phase of the disease and seem to persist more frequently, both the IgG and IgA isotypes of anti-CCP-2 antibodies predate the onset of RA by years; the highest positive predictive value is associated with IgG anti-CCP-2 autoantibodies. However, ACPA is not an appropriate marker to monitor the disease [54, 55]. Autoantibodies against citrullinated proteins can be an important factor of osteoclastogenesis. Plasma cells produce ACPA with specificity for citrullinated vimentin, which binds to oste-oclast precursor cells and stimulates the release of TNF, in turn enhancing the differentiation of these cells into mature osteoclasts. During the osteoclast differentiation process, the production of PAD2 enzyme is induced by calcium. The activity of PAD2 leads to the citrullination of vimentin, which is abundantly expressed on the surface of osteoclast-lineage cells [56]. Discrimination between RA and non-RA patients could be performed using CCP antibodies evaluation, especially in RF-negative patients [57]. Evidence to date suggests that the positivity of anti-CCP antibodies may be a predictor of RA onset. This ana-lytical data can have a higher positive predictive value in a population at risk, rather than in a general one, thus the evaluation of haplotype profile can improve the early diagnostic outcome. A multi-biomarker test for the assess-ment of disease activity in RA patients has been performed using CAMERA study. This test may be complementary to the available disease activity laboratory evaluation to improve patient care and outcomes [58]. Four protein bio-markers, whose mass/charge (m/z) values have been well established, were identified as novel biomarkers related to RA, adding great value for laboratory diagnosis of RA [59]. In a recent study, a Multiple Biomarker Disease Activity (MBDA) score algorithm has been tested. It uses the same equation of the Disease Activity Score DAS28-CRP, which takes into account the C-reactive protein (CRP), and bio-markers useful to predict the Swollen Joint Count (SJC28), Tender Joint Count (TJC28), and general health (VAS-GH) as components of the equation (PTJC = predicted TJC;
UnauthenticatedDownload Date | 6/18/16 7:04 AM

1734 Foti et al.: Laboratory approach to RA patients
PSJC = predicted SJC; PVAS-GH = predicted VAS-GH). By using a Venn diagram to predict potential markers, Curtis et al. evaluated and validated this multiple biomarker test to assess RA disease activity with a score, expressed from 1 to 100 [60]. More recently, using a multi-stage approach, the same group tested 130 candidate biomarkers, and ultimately set up an algorithm with 12 protein biomark-ers to obtain an MBDA score for RA patients, with no effects from common comorbidities [61]. A study from a Japanese research group has demonstrated that MMP-3 ELISA method works well in the assessment of MMP-3 serum levels in routinely evaluated RA patients and the test may be important to better characterize the disease outcome in the follow-up [62]. The results of this study suggest that serum MMP-3 can be considered as a predic-tor of joint destruction in RA, treated with a non-biolog-ical disease modifying anti-rheumatic drug. Variations of the MMP-1 and MMP-3 genes affect the serum levels of MMP-1 and -3 and disease activity. MMP-3 is significantly associated with disease activity, inflammatory mediators and cartilage breakdown, making it a potential biomarker of disease severity, but seemingly less useful than CRP and SAA as a biomarker of disease activity in early RA. A conclusive remark is that several closely linked polymor-phisms in the MMP-1-MMP-3 loci have an important role in determining the circulating levels of these MMPs in RA, and that MMP-3 polymorphism is associated with the level of disease activity over time [63].
Recently, using the Quality Assessment of Diagnos-tic Accuracy Studies (QUADAS) tools which is a random-effects method, Zhang et al. were able to summarize sensitivities, specificities, positive and negative likelihood ratio (LR+ and LR–, respectively), and diagnostic odds ratio from 17 studies. They concluded that based upon their high specificity and moderate sensitivity, anti-CCP-2 and anti-CCP-3 played an important role in confirming the diagnosis of RA. Anti-CCP-3 did not have better diagnostic performance than anti-CCP-2, but anti-CCP-2 had evident heterogeneity compared to anti-CCP-3, especially in Amer-ican patients [64].
From pathogenic and clinical evidence, we may suggest a new approach of laboratory medicine to evalu-ate patients in all different evolutive phases of RA. First, the haplotype of the proband should be characterized, and in case of positivity, the relatives must be invited to take the test. This can be useful to predict the risk level of developing the disease. As mentioned before, interna-tionally adopted clinical criteria imply that the laboratory data are important to make the diagnosis. Together with basic laboratory analytical evaluation, in our opinion it is appropriate to measure RF and ACPA. If both tests are
positive, in order to completely and correctly evaluate the patient, a cytokine profile and MMP-3 measurements should be undertaken. The first can be obtained by mul-tiparametric microarray and allows the patient immuno-logical response, the prevalence of Th1 or Th2, cytokine network and the production of Th17 to be evaluated. The latter can be considered the biomarker of disease aggres-siveness and progression. This complete laboratory evalu-ation can produce a correct and personalized therapeutic treatment and prognostic evaluation [65]. In the future, a significant improvement can be obtained by the evalua-tion of genomics and proteomics arrays, in order to char-acterize the individual patient profile at diagnosis and its response to therapeutic treatment.
ConclusionsThe evaluation of multiple biomarker profiles is funda-mental in order to enrol the patient in a specific target therapy treatment. This is most likely to be effective and safe based on similarities between patient’s disease char-acteristics and the cohort that responds to therapy. In this prospective, analysis of multiple biomarkers, and espe-cially of post-translational biomarkers in RA, can help to stratify the patient’s population in different subsets that exhibit different outcomes and respond to specific thera-peutic treatment.
In summary:1. RA is a complex disease with different clinically
aspects and evolutionary forms.2. HLA-DRB1 shared epitope and PTPN22 (gain-of-
function of Lyp which inhibits T-lymphocytes activation) are two genes strongly associated with the risk of RA.
3. IL-6 and TNF-α play a central role in RA. IL-17 can be measured either in synovial fluid either in compromised tissues.
4. Treg CD4+CD25hi lymphocytes are predominant in synovial fluid, rather than in blood. Their levels can be normalized as effect of anti-TNF therapy.
5. NKp46 cytofluorimetric assay can account for NK activation.
6. Anti-CCP antibodies are specifically present during RA and support distinction between clinically and genetically different forms of RA.
7. All environmental factors which can alter antigenic tolerance against anti-CCP antibodies are not yet defined.
8. Anti-CCP-antibodies are present in serum several years before the early phase of disease (pre-clinical
UnauthenticatedDownload Date | 6/18/16 7:04 AM
Foti et al.: Laboratory approach to RA patients 1735
window); anti-CCP antibodies and high levels of MMP-3 are associated with bone erosion and with a worse clinical evolution of the disease, if present in the synovial fluid.
9. The time-course measurement of the cytokine network can be effective for setting prognosis and therapeutic efficacy.
10. Multiparametric laboratory evaluation can be the correct approach in order to define different subgroups of patients and tailor a personalized therapy.
Conflict of interest statement
Authors’ conflict of interest disclosure: The authors stated that there are no conflicts of interest regarding the publication of this article.Research funding: None declared.Employment or leadership: None declared.Honorarium: None declared
References1. Gabriel SE, Michaud K. Epidemiological studies in incidence,
prevalence, mortality, and comorbidity of the rheumatic dis-eases. Arthritis Res Ther 2009;11:229.
2. Dannecker GE, Quartier P. Juvenile idiopathic arthritis: classifi-cation, clinical presentation and current treatments. Horm Res 2009;72:4–12.
3. Cimmino MA, Salvarani C, Macchioni P, Montecucco C, Fos-saluzza V, Mascia MT, et al. Extra articular manifestations in 587 Italian patients with rheumatoid arthritis. Rheumatol Int 2000;19:213–7.
4. Cavagna L, Boffini N, Cagnotto G, Inverardi F, Grosso V, Caporali R. Atherosclerosis and rheumatoid arthritis: more than a simple association. Mediat Inflamm 2012;2012:147354.
5. Gauhar UA, Gaffo AL, Alarćon GS. Pulmonary manifestations of rheumatoid arthritis. Sem Respir Crit Care Med 2007;28: 430–40.
6. Lauretis A, Veeraraghavan S, Renzoni A. Connective tissue disease-associated interstitial lung disease: how does it differ from IPF? How should the clinical approach differ? Chronic Resp Dis 2011;8:53–82.
7. Turesson C. Extra-articular rheumatoid arthritis. Curr Opin Rheu-matol 2013;25:360–6.
8. Anderson JJ, Wells G, Verhoeven AC, Felson DT. Factors predict-ing response to treatment in rheumatoid arthritis: the impor-tance of disease duration. Arthritis Rheum 2000;43:22–9.
9. Pincus T, Kavanaugh A, Sokka T. Benefit/risk of therapies for rheumatoid arthritis: underestimation of the “side effects” or risks of RA leads to underestimation of the benefit/risk of thera-pies. Clin Exp Rheumatol 2004;22(Suppl 35):2–11.
10. Oliver JE, Silman AJ. Risk factors for the development of rheuma-toid arthritis. Scand J Rheumatol 2006;35:169–74.
11. Deane KD, El-Gabalawy H. Pathogenesis and prevention of rheumatoid disease: focus on preclinical RA and SLE. Nat Rev Rheumatol 2014;10:212–28.
12. Nakken B, Munthe LA, Konttinen YT, Sandberg AK, Szekanecz Z, Alex P, et al. B-cells and their targeting in RA, current concepts and future perspectives. Autoimmun Rev 2011;11:28–34.
13. Burmester GR, Feist E, Dörner T. Emerging cell and cytokine targets in rheumatoid arthritis. Nat Rev Rheumatol 2014;10: 77–88.
14. Imboden BJ. The immunopathogenesis of rheumatoid arthritis. Annu Rev Pathol Mech Dis 2009;4:417–34.
15. Smolen JS, Alehata D. Monitoring rheumatoid arthritis. Curr Opin Rheumatol 2011;23:252–8.
16. Smolen JS, Alehata D, Redlich K. The pathogenesis of rheu-matoid arthritis: new insights from old clinical data? Nat Rev Rheumatol 2012;8:235–43.
17. MacKay K, Eyre S, Myerscough A, Milicic A, Barton A, Laval S, et al. Whole-genome linkage analysis of rheumatoid arthritis susceptibility loci in 252 affected sibling pairs in the United Kingdom. Arthritis Rheum 2002;46:632–9.
18. Raychaudhuri S, Sandor C, Stahl EA, Freudenberg J, Lee HS, Jia X, et al. Five amino acids in three HLA proteins explain most of the association between MHC and seropositive rheumatoid arthritis. Nat Genet 2012;44:291–6.
19. Hammer J, Gallazzi F, Bono E, Karr RW, Guenot J, Valsasnini P, et al. Peptide binding specificity of HLA-DR4 molecules: correlation with rheumatoid arthritis association. J Exp Med 1995;181:1847–55.
20. Tèzenas du Montcel S, Michou L, Petit-Teixeira E, Osorio J, Lemaire I, Lasbleiz S, et al. New classification of HLA-DRB1 alleles supports the shared epitopes hypothesis of rheumatoid arthritis susceptibility. Arthritis Rheum 2005;52:1063–8.
21. Marchesan JT, Gerow EA, Schaff R, Taut AD, Shin SY, Sugai J, et al. Porphyromonas gingivalis oral infection exacerbates the development and severity of collagen-induced arthritis. Arthritis Res Ther 2013;15:R186.
22. Yoo SA, You S, Yoon HJ, Kim DH, Kim HS, Lee K, et al. A novel pathogenic role of the ER chaperone GRP78/BiP in rheumatoid arthritis. J Exp Med 2012;209:871–86.
23. McInnes I, Schett G. Cytokines in the pathogenesis of rheuma-toid arthritis. Nat Immunol 2007;7:429–42.
24. Frey S, Derer A, Messebacher ME, Baeten DL, Bugatti S, Monte-cucco C, et al. The novel cytokine interleukine-36a is expressed in psoriatic and rheumatoid arthritis synovium. Ann Rheum Dis 2013;72:1569–74.
25. Larsen H, Muz B, Khong TL, Feldmann M, Paleolog EM. Dif-ferential effects of Th1 versus Th2 cytokines in combination with hypoxia on HIFs and angiogenesis in RA. Arthritis Res Ther 2012;14:R180.
26. Moran EM, Connolly M, Gao W, McCormick J, Fearon U, Veale DJ. IL-17A induction of angiogenesis, cell migration, and cytoskel-etal rearrangement. Arthritis Rheum 2011;63:3263–73.
27. Pavkova Goldbergova M, Lipkova J, Pavek N, Gatterova J, Vasku A, Soucek M, et al. RANTES, MCP-1 chemokines and factors describing rheumatoid arthritis. Mol Immmunol 2012;52:273–8.
28. Schett G, Gravellese E. Bone erosion in rheumatoid arthritis: mechanisms, diagnosis and treatment. Nat Rev Rheumatol 2012;8:656–64.
29. Sarkar S, Fox DA. Regulatory T cells in rheumatoid arthritis. Curr Rheumatol Rep 2008;10:405–12.
UnauthenticatedDownload Date | 6/18/16 7:04 AM

1736 Foti et al.: Laboratory approach to RA patients
30. Fogel LA, Yokoyama WM, French AR. Natural killer cells in human autoimmune disorders. Arthritis Res Ther 2013;15:216–25.
31. Antonelli A, Ferrari SM, Giuggioli D, Ferrannini E, Ferri C, Fallahi P. Chemokine (C-X-C motif) ligand (CXCL)10 in autoimmune diseases. Autoimmun Rev 2014;13:272–80.
32. Huss RS, Huddleston JI, Goodman SB, Butcher EC, Zabel BA. Synovial tissue-infiltrating natural killer cells in osteo-arthritis and periprosthetic inflammation. Arthritis Rheum 2010;62:3799–805.
33. Yang X, Zheng SG. Interleukin-22: a likely target for treatment of autoimmune diseases. Autoimmun Rev 2014;13:615–20.
34. Conigliaro P, Scrivo R, Valesini G, Perricone R. Emerging role for NK cells in the pathogenesis of inflammatory arthropathies. Autoimmun Rev 2011;10:577–81.
35. Hueber W, Tomooka BH, Zhao X, Kidd BA, Drijfhout JW, Fries JF, et al. Proteomic analysis of secreted proteins in early rheuma-toid arthritis: anti-citrulline autoreactivity is associated with up regulation of proinflammatory cytokines. Ann Rheum Dis 2007;66:712–9.
36. Sokolove J, Bromberg R, Deane KD, Lahey LJ, Derber LA, Chandra PE, et al. Autoantibody epitope spreading in the pre-clinical phase predicts progression to rheumatoid arthritis. PLoS One 2012;7:e35296.
37. Hughes-Austin JM, Deane KD, Derber LA, Kolfenbach JR, Zerbe GO, Sokolove J. Multiple cytokines and chemokines are associated with rheumatoid arthritis-related autoimmunity in first-degree relatives without rheumatoid arthritis: studies of the aetiology of rheumatoid arthritis (SERA). Ann Rheum Dis 2013;72:901–7.
38. Proost P, Struyf S, Loos T, Gouwy M, Schutyser E, Conings R, et al. Coexpression and interaction of CXCL10 and CD26 in mesenchymal cells by synergising inflammatory cytokines: CXCL8 and CXCL10 are discriminative markers for autoimmune arthropathies. Arthritis Res Ther 2006;8:R107.
39. Szekanecz Z, Szucs G, Szanto S, Koch AE. Chemokines in rheu-matic diseases. Curr Drug Targets 2006;7:91–102.
40. Noack M, Miossec P. Th17 and regulatory T cell balance in autoimmune and inflammatory diseases. Autoimmun Rev 2014;13:668–77.
41. Li XJ, Xu M, Zhao XQ, Zhao JN, Chen FF, Yu W, et al. Proteomic analysis of synovial fibroblast-like synoviocytes from rheuma-toid arthritis. Clin Exp Rheumatol 2013;31:552–8.
42. Neogi T, Aletaha D. Silman AJ, Naden RL, Felson DT, Aggarwal R, et al. American College of Rheumatology; European League against Rheumatism. The 2010 American College of Rheuma-tology/European League Against Rheumatism classification criteria for rheumatoid arthritis: phase 2 methodological report. Arthritis Rheum 2010;62:2582–91.
43. Lindstrom TM, Robinson WH. Biomarkers for rheumatoid arthri-tis: making it personal. Scand J Clin Lab Invest 2010;70(Suppl 242):79–84.
44. Aletaha D, Alasti F, Smolen JS. Rheumatoid factor determines structural progression of rheumatoid arthritis dependent and independent of disease activity. Ann Rheum Dis 2013;72: 875–80.
45. Kleveland G, Egeland T, Lea T. Quantitation of rheumatoid fac-tors (RF) of IgM, IgA and IgG isotypes by a simple and sensitive ELISA. Discrimination between false and true IgG-RF. Scand J Rheumatol Suppl 1988;75:15–24.
46. Can M, Najip A, Yılmaz N, Inanc N, Yavuz S. Immunoglobulin subtypes predict therapy response to the biologics in patients with rheumatoid arthritis. Rheumatol Int 2013;33:1455–60.
47. Burrage PS, Mix KS, Brinckerhoff CE. Matrix metalloproteinases: role in arthritis. Front Biosci 2006;11:529–43.
48. Mamehara A, Sugimoto T, Sugiyama D, Morinobu S, Tsuji G, Kawano S, et al. Serum MMP-3 as predictor of joint destruction in RA, treated with non-biological diseases modifying anti-rheu-matic drugs. Kobe J Med Sci 2010;56:E98–107.
49. Houseman M, Potter C, Marshall N, Lakey R, Cawston T, Griffiths I, et al. Baseline serum MMP-3 levels in patients with rheuma-toid arthritis are still independently predictive of radiographic progression in a longitudinal observational cohort at 8 years follow up. Arthritis Res Ther 2012;14:R30.
50. Chen Y, Mattey DL. Age at onset of rheumatoid arthritis: asso-ciation with polymorfisms in the VEGFA gene and an inter-genic locus between MMP 1 and 3 genes. Clin Exp Rheumatol 2012;30:894–8.
51. Ärlestig L, Mullazehi M, Kokkonen H, Rocklöv J, Rönnelid J, Dahlqvist SR. Antibodies against cyclic citrullinated peptides of IgG, IgA and IgM isotype and rheumatoid factor of IgM and IgA isotype are increased in unaffected members of multicase rheumatoid arthritis families from northern Sweden. Ann Rheum Dis 2012;71:825–9.
52. Kokkonen H, Mullazehi M, Berglin E, Hallmans G, Wadell G, Rönnelid J, et al. Antibodies of IgG, IgA and IgM isotypes against cyclic citrullinated peptide precede the development of rheuma-toid arthritis. Arthritis Res Ther 2011;13:R13.
53. Conrad K, Roggenbuck D, Reinhold D, Dörner T. Profiling of rheumatoid arthritis associated autoantibodies. Autoimmun Rev 2010;9:431–5.
54. Jaskowski TD, Hill HR, Russo KL, Lakos G, Szekanecz Z, Teodo-rescu M. Relationship between rheumatoid factor isotypes and IgG anti-cyclic citrullinated peptide antibodies. J Rheumatol 2010;37:1582–8.
55. Szodoray P, Szabo Z, Kapitany A, Gyetvai A, Lakos G, Szanto S, et al. Anti-citrullinated protein/peptide autobodies in asso-ciation with genetic and environmental factors as indicators of disease outcome in rheumatoid arthritis. Autoimmun Rev 2010;9:140–3.
56. Wegner N, Lundberg K, Kinloch A, Fisher B, Malmstrom V, Feld-mann M, et al. Autoimmunity to specific citrullinated proteins gives the first clues to the etiology of rheumatoid arthritis. Immunol Rev 2010;233:34–54.
57. Bizzaro N, Tonutti E, Tozzoli R, Villalta D. Analytical and diag-nostic characteristics of 11 2nd- and 3rd-generation immunoen-zymatic methods for the detection of antibodies to citrullinated proteins. Clin Chem 2007;53:1527–33.
58. Bakker MF, Cavet G, Jacobs JW, Bijlsma JW, Haney DJ, Shen Y, et al. Performance of a multi-biomarker score measuring rheumatoid arthritis disease activity in the CAMERA tight control study. Ann Rheum Dis 2012;71:1692–7.
59. Niu Q, Huang Z, Shi Y, Wang L, Pan X, Hu C. Specific serum pro-tein biomarkers of RA detected by MALDI-TOF-MS combined with magnetic beads. Int Immunol 2010;22:611–8.
60. Curtis JR, van der Helm-van Mil AH, Knevel R, Huizinga TW, Haney DJ, Shen Y, et al. Validation of a novel multi-biomarker test to assess rheumatoid arthritis disease activity. Arthritis Care Res (Hoboken) 2012;64:1794–803.
UnauthenticatedDownload Date | 6/18/16 7:04 AM

Foti et al.: Laboratory approach to RA patients 1737
61. Centola M, Cavet G, Shen Y, Ramanujan S, Knowlton N, Swan KA, et al. Development of a multi-biomarker disease activity test for rheumatoid arthritis. PLoS One 2013;8:e60635.
62. Shinozaki M, Inoue E, Nakajima A, Hara M, Tomatsu T, Kama-tani N, et al. Elevation of serum matrix metalloproteinase-3 as a predictive marker for the long-term disability of rheumatoid arthritis patients in a prospective observational cohort IORRA. Mod Rheumatol 2007;17:403–8.
63. Ally MM, Hodkinson B, Meyer PW, Musenge E, Tikly M, Anderson R. Serum matrix metalloproteinase-3 in comparison with acute
phase proteins as a marker of disease activity and radio-graphic damage in early rheumatoid arthritis. Med Inflamm 2013;2013:183653.
64. Zhang WC, Wu H, Chen WX. Meta-analysis: diagnostic accuracy of anti-cyclic citrullinated peptide 2 antibody and anti-cyclic cit-rullinated peptide 3 antibody in rheumatoid arthritis. Clin Chem Lab Med 2014;16:1–12.
65. Deane KD, Norris JM, Holers VM. Preclinical rheumatoid arthri-tis: identification, evaluation and future directions for investiga-tion. Rheum Dis Clin North Am 2010;36:213–41.
Daniela P. Foti, MD, PhD, Associate professor of Clinical Pathology at University Magna Graecia, Catanzaro, Medical School. Her principal scientific interest is the pathophysiology of Diabetes mel-litus and the best biomedical laboratory performances to evaluate patients affected by chronic degenerative diseases.
Marta Greco, MS Sci., Specialist in Clinical Pathology, Assistant professor of Clinical Pathology at University Magna Graecia, Catan-zaro, Medical School. Her principal scientific interest is dealing with biomedical laboratory evaluation of patients affected by vascular and chronic degenerative diseases.
Eleonora Palella, MD, Post-graduate resident in Clinical Pathology at University Magna Graecia, Catanzaro, Medical School. Her principal scientific interest is dealing with biomedical laboratory evaluation of patients affected by chronic degenerative diseases.
Elio Gulletta, MD, PhD, Full professor and Chair of Clinical Pathology at University Magna Graecia, Catanzaro, Medical School. His princi-pal professional interest is dealing with pathophysiology of chronic inflammatory diseases, and biomedical laboratory performances to increase patient outcomes.
UnauthenticatedDownload Date | 6/18/16 7:04 AM




















