
Clinical expression of rheumatoid arthritis in Chilean patients
11
Clinical Expression of Rheumatoid Arthritis in Chilean Patients Loreto Massardo, Verbnica Aguirre, M. Eugenia Garcia, Vinicio Cervilla, Sandra Nicovani, Alfonso Gonzdlez, Santiago Rivero, and Sergio Jacobelli In populations such as Northern Europeans in which the HLA-DR4 subtypes Dw14 and Dw4 show strong association with rheumatoid arthritis (RA), these alleles and the double allelic dose of the shared epitope are considered severity markers. The clinical expression of RA varies in different populations, which may be determined by variation in the prevalence of these markers. In the present study we analyzed the expression of RA in 112 consecutive Chilean patients and its relation to the prevalence of genetic factors, prompted by our previous observation that DR4 is weakly associated to RA in this population. Mean age was 50 -+ 14 years; 90% were seropositive and 87% were female, with a disease duration of 10 -+ 8 years. Extra-articular manifestations were found in 383./o of patients, rheumatoid nodules in 27%, vasculitis in 8%, and Sj6gren's syndrome in 29%. Functional capacity (ACR, 1991) I or I1: 82%. 15%of patients stopped working. Hand radiographs scored according to Steinbrocker in 89 patients: I, 21%; II, 15%; III, 43%; IV, 21%. In this series, patients with less formal education seemed to have more benign arthritis. In 97 controls and in 65 (56%) RA patients the presence of DRB1 alleles corresponding to DR1 and DR4 serotypes, to DR4-Dw subtypes, and homozygocity, were determined by ! polymerase chain react=on followed by specific oligonucleotide hybridization. The shared epitope was present in 53% of RA patients and in 30% of controls (P = .0048, odds ratio [OR] = 2.64). A double allelic dose of the epitope was present in 15% of RA patients compared with 4% of controls (P = .026, OR = 4.23). In a subgroup of 31 erosive RA patients we did not find a significant association of disease severity with the shared epitope in a single or double allelic dose. None of the DR4 subtypes that associate with RA in other populations was found significantly more prevalent in our patients. The severity of RA in our study compared with published series was intermediate between British patients with severe RA and Greek patients with milder disease. This may be due to the high prevalence of Dw13"0403 in our population. Copyright © 1995by W.B. Saunders Company INDEX WORDS: Rheumatoid arthritis; immunogenetics; clinical expression; HLA antigens; prognosis. From the Departamento de Immunologia Clinica y Reumatolo- gia, and Departamento de Radiologia, Escuela de Medicina, Pontificia Universidad Cat6lica de Chile, and the Hospital Dr S6tero del Rio, Servicio Metropolitano de Salud Sur Oriente, Santiago, Chile. Loreto Massardo, MD: Assistant Professor of Medicine, Department of Clinical Immunology and Rheumatology; Ver6nica Aguirre, MD: Fellow in Rheumatology; M Eugenia Garcla, MD: Fellow in Rheumatology," Vinicio Cervilla, MD: Associate Professor of Radiology, Department of Radiology, Escuela de Medicina; Sandra Nicovani, BSc: Department of Cellular Biology, Facultad de Ciencias Biol6gicas; Alfonso Gonzfilez, MD, PhD: Associate Professorof Medicine, Depart- ment of Clinical Immunology and Rheumatology; San- tiago Rivero, MD: Associate Professor of Medicine, Depart- ment of Clinical Immunology and Rheumatology; Sergio Jacobelli, MD: Professor of Medicine, Department of Clinical Immunology and Rheumatology, Escuela de Medicina, Pontiff- cia Universidad Cat6lica de Chile. Supported in part by grant 1930596from Fondo Nacional de Ciencia y Tecnologfa. Address reprint requests to: Loreto Massardo, MD, Departa- mento de Immunologla Cldnica y Reumatologia, Escuela de Medicina, Pontificia Universidad CatOlica de Chile, Casilla l14-D, Santiago, CHILE. Copyright © 1995 by W..B. Saunders Company 0049-0172/95/2503-000655.00/0 Seminars in Arthritis and Rheumatism, Vol 25, No 3 (December), 1995: pp 203-213 203
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Clinical expression of rheumatoid arthritis in Chilean patients

Clinical Express ion of Rheumatoid Arthritis in Chilean Patients
Loreto Massardo, Verbnica Aguirre, M. Eugenia Garcia, Vinicio Cervilla, Sandra
Nicovani, Al fonso Gonzdlez, Sant iago Rivero, and Sergio Jacobell i
In populations such as Northern Europeans in which the HLA-DR4 subtypes Dw14 and Dw4 show strong association wi th rheumatoid arthritis (RA), these alleles and the double allelic dose of the shared epitope are considered severity markers. The clinical expression of RA varies in different populations, which may be determined by variation in the prevalence of these markers. In the present study we analyzed the expression of RA in 112 consecutive Chilean patients and its relation to the prevalence of genetic factors, prompted by our previous observation that DR4 is weakly associated to RA in this population. Mean age was 50 -+ 14 years; 90% were seropositive and 87% were female, wi th a disease duration of 10 -+ 8 years. Extra-articular manifestations were found in 383./o of patients, rheumatoid nodules in 27%, vasculitis in 8%, and Sj6gren's syndrome in 29%. Functional capacity (ACR, 1991) I or I1: 82%. 15%of patients stopped working. Hand radiographs scored according to Steinbrocker in 89 patients: I, 21%; II, 15%; III, 43%; IV, 21%. In this series, patients wi th less formal education seemed to have more benign arthritis. In 97 controls and in 65 (56%) RA patients the presence of DRB1 alleles corresponding to DR1 and DR4 serotypes, to DR4-Dw subtypes, and homozygocity, were determined by
! polymerase chain react=on fol lowed by specific oligonucleotide hybridization. The shared epitope was present in 53% of RA patients and in 30% of controls (P = .0048, odds ratio [OR] = 2.64). A double allelic dose of the epitope was present in 15% of RA patients compared wi th 4% of controls (P = .026, OR = 4.23). In a subgroup of 31 erosive RA patients we did not find a significant association of disease severity wi th the shared epitope in a single or double allelic dose. None of the DR4 subtypes that associate wi th RA in other populations was found significantly more prevalent in our patients. The severity of RA in our study compared wi th published series was intermediate between British patients wi th severe RA and Greek patients wi th milder disease. This may be due to the high prevalence of Dw13"0403 in our population. Copyright © 1995 by W.B. Saunders Company
INDEX WORDS: Rheumatoid arthritis; immunogenetics; clinical expression; HLA antigens; prognosis.
From the Departamento de Immunologia Clinica y Reumatolo- gia, and Departamento de Radiologia, Escuela de Medicina, Pontificia Universidad Cat6lica de Chile, and the Hospital Dr S6tero del Rio, Servicio Metropolitano de Salud Sur Oriente, Santiago, Chile.
Loreto Massardo, MD: Assistant Professor of Medicine, Department of Clinical Immunology and Rheumatology; Ver6nica Aguirre, MD: Fellow in Rheumatology; M Eugenia Garcla, MD: Fellow in Rheumatology," Vinicio Cervilla, MD: Associate Professor of Radiology, Department of Radiology, Escuela de Medicina; Sandra Nicovani, BSc: Department of Cellular Biology, Facultad de Ciencias Biol6gicas; Alfonso Gonzfilez, MD, PhD: Associate Professor of Medicine, Depart- ment of Clinical Immunology and Rheumatology; San-
tiago Rivero, MD: Associate Professor of Medicine, Depart- ment of Clinical Immunology and Rheumatology; Sergio Jacobelli, MD: Professor of Medicine, Department of Clinical Immunology and Rheumatology, Escuela de Medicina, Pontiff- cia Universidad Cat6lica de Chile.
Supported in part by grant 1930596 from Fondo Nacional de Ciencia y Tecnologfa.
Address reprint requests to: Loreto Massardo, MD, Departa- mento de Immunologla Cldnica y Reumatologia, Escuela de Medicina, Pontificia Universidad CatOlica de Chile, Casilla l14-D, Santiago, CHILE.
Copyright © 1995 by W..B. Saunders Company 0049-0172/95/2503-000655.00/0
Seminars in Arthritis and Rheumatism, Vol 25, No 3 (December), 1995: pp 203-213 203

204 MASSARDO ET AL
(RA) chronic ] [ ~ HEUMATOID arthritis is a 1 ~ inflammatory disease of unknown etiology that can cause progressive disability. 1-3 Retro- spective analysis has changed the perspectives on some aspects of the disease. Recent studies from Europe and United States have shown that in many patients RA is more severe and resistant to treatment than appreciated hereto- fore. 1-7 Increased mortality also has been docu- mented. 1-14 Long-term prognostic studies have shown that less than 10% of patients have prolonged remission. 1-4,15,16 In most clinic pa- tients functional deterioration is the rule. 1,2,4-7 However, the expression of RA differs across diverse populations, 1,3,~7-23 for reasons un- known, but probably related to genetic or envi- ronmental factors or both.
Studies of HLA class determinants suggest that HLA-DR4 antigens are associated with increased susceptibility to RA and probably play a role in determining disease severity, ls,24-34 While most populations show an association with HLA-DR4, this finding is not univer- sal. 1,3,17,29,35,36 The association between HLA and RA has been further refined and a shared amino acid sequence ("shared epitope") com- mon to the DRB1 chains of all DR specificity associated with RA exists. 29,37 In a recent re- port, Drosos et al is found that there was a striking difference in the clinical expression of RA between Greek and British patients, the Greeks having more benign disease. This could be related to the fact that only 43% of the Greek patients had the shared epitope in con- trast with the 83% of British patients, ls,38
In previous studies we have shown that Chil- ean patients with RA have a weak association with HLA-DR4. 35,36 Because genetic differ- ences could reflect differences in disease expres- sion, we studied the clinical expression of RA in an unselected group of patients attending two large outpatient departments in Santiago.
PATIENTS AND METHODS
This is a prospective descriptive study of a population of 112 patients with RA enrolled from August to September 1992, who spontane- ously consulted at two rheumatology clinics. We examined 49 consecutive adults attending the outpatient rheumatology clinic of the Catholic University Hospital, a private teaching hospital
in downtown Santiago, and 63 patients attend- ing the outpatient rheumatology clinic of the "Hospital Dr. Sdtero del Rio," a national gen- eral hospital of the Southeast Health District that serves a population of nearly 1 million inhabitants of low to middle-low income. Pa- tients had similar opportunities for medical treatment excepting the lesser access to surgery in the Health District hospital. Admission crite- ria was the fulfillment of the American College of Rheumatology (ACR) (formerly the Ameri- can Rheumatism Association) revised criteria for RA. 39 Exclusion criteria were crystal-in- duced arthritis, reactive arthritis, and patients with psoriasis and other connective tissue dis- eases. There were 97 women and 15 men, with an average age of 50 +_ 14 years and an average disease duration of 10 years.
Clinical Expression of RA
Patients were examined according to a writ- ten protocol that included years of formal edu- cation, work status in the year of onset, and in 1992, medical history, ACR criteria, complete clinical evaluation, articular evaluation, and extra-articular manifestations of RA (history of rheumatoid nodules, or pulmonary, cardiac, dermal, ocular, and nervous system involvement and rheumatoid vasculitis: skin vasculitis of nailfold or diagnosed by histomorphology, non- healing ulcers in absence of atherosclerotic disease or venous disease, livedo reticularis, and mononeuritis multiplex). Sj6gren's syndrome (SS) was assessed by a specific questionnaire, and a Schirmer's test was done on all patients. Overt evidence of Felty's syndrome, amyloido- sis, or other major systemic disorders were noted. Rheumatoid factor by latex test was done in 110 patients (normal up to 1/40) and anti- nuclear antibodies by indirect immunofluoeres- cence using HEp-2 cells in 76 patients (positive titer 1/50 or higher). Eleven patients classified as seronegative RA had at least two nega- tive determinations of the latex agglutination test (average was three negative determina- tions), one of which carried out before the use of disease modifying antirheumatic drugs (DMARDs). They fulfilled the criteria for sero- negative RA proposed by Gran and Husby, 4° with the exception of articular erosions.
Clinical data included the ACR criteria for
RA AND THE SHARED EPITOPE IN CHILEAN PATIENTS 205
clinical remission in RA 41 and the number of tender joints as measures of disease activity using the weighted and selective index for actMty of synovitis proposed by Thompson et al. 42 This index includes the simultaneous pres- ence of tenderness and nonbony swelling weighted for joint size. It examines metacarpo- phalangeal and interphalangeal joints of the hand, metatarsophalangeal joints of feet, and large joints (elbow, wrist, knee and ankle [mor- tise]). The presence or absence of extra- articular features, including nodules and vascu- litis, was also recorded. Overall functional status was assessed by the ACR revised criteria for the classification of functional status in RA 43 and by the simplified health assessment questionnaire (HAQ) 44,45 translated into Spanish.
The use of DMARDs (gold salts, D-penicilla- mine, methotrexate, chloroquine, cyclophospha- mid,e, cyclosporine, or azathioprine) and any side effects of medications were recorded. Joint deformities were assessed in hands, elbows, hips, knees, and feet. Use of walking aids, history of previous surgery, and current treat- ment were also recorded.
Hematocrit and erythrocyte sedimentation rate was performed in all the patients. Radio- graphs of hands (PA) from 89 patients were obtained prospectively and read by the same radiologist (V.C.), who was blinded to the clinical findings, using the Steinbrocker sys- tem. 46
In 65 (56%) patients (30 from the University Hospital and 35 from the Health District Hospi- tal) and 97 healthy and unrelated controls (49 from the university hospital and 48 from the Dr S6tero del Rfo Hospital), the presence of DRB1 alleles corresponding to DRI and DR4 sero- types, and to DR4-Dw subtypes (DRB1 04 subtypes Dw4*0401, Dw10*0402, Dw13"0403, Dw14"0404/0408, Dw15"0405) were deter- mined by amplification of HLA class II alleles by polymerase chain reaction followed by spe- cific oligonucleotide hybridization as de- scribed. 38,47,48 The second allele in the DR4 or DR1 patients and controls was subsequently analyzed by using the Quick-Type HLA Class II DRB sequence specific oligonucleotide typing (SSO) (Lifecodes Corp, Stanford, CT) based on the fast HLA-DR typing procedure developed by Zetterquist and Olerup. 49 We did not find
any patient or control with DR10 ('1001) or DR'1402. In addition, six other patients were typed only by the lymphocyte microcytotoxicity test of Terasaki.
Relation between the Clinical Features and Proposed Severity Markers of RA
Any given feature (Appendix) was assessed in patients divided according to age at onset (less than 60 years or 60 years and older), gender, rheumatoid factor, University or Health District Hospital, years of formal education (less than 4 years or 4 years or more), disease duration (divided in 5 groups of less than 2 years, 2 to 6.9, 7 to 11.9, 12 to 16.9, and 17 or more years), with the presence or absence of nodules and/or vasculitis, with HLA-DR4 and with the patients bearing the critical epitope: DRI(DRBI*0101) or the DR4 subtypes Dw4(DRBI*0401), Dw14(DRBl*0404/0408) or Dwl5(DRBI*0405) or patients bearing the double dose of the epitope (DRBI*04/04 or DRBI*04/01). In a subgroup of 31 patients who had erosive hand x-rays, who may be compa- rable to the series of Weyand et al, 33 the prevalence of the shared epitope in relation to the clinical features was assessed.
For statistical analysis, Student's t test, analy- sis of variance, Fisher's exact test, and x-square test with Yate's correction were used where indicated. Spearman correlation was used for HAQ correlation's analysis. Results are ex- pressed as the mean _+ 1 S1-). Odds ratios (OR) with Cornfield 95% confidence limits for OR were calculated. 5°
RESULTS
The Clinical Expression of RA
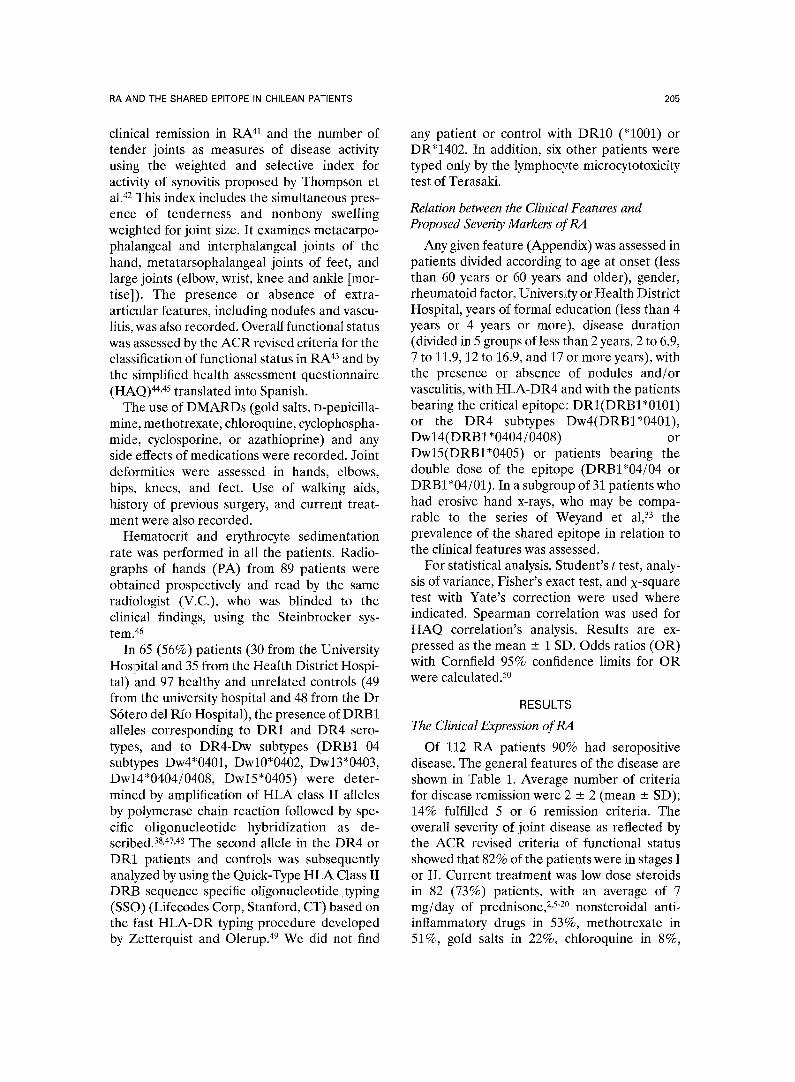
Of 112 RA patients 90% had seropositive disease. The general features of the disease are shown in Table 1. Average number of criteria for disease remission were 2 ___ 2 (mean _ SD); 14% fulfilled 5 or 6 remission criteria. The overall severity of joint disease as reflected by the ACR revised criteria of functional status showed that 82% of the patients were in stages 1 or II. Current treatment was low dose steroids in 82 (73%) patients, with an average of 7 mg/day of prednisoney -2° nonsteroidal anti- inflammatory drugs in 53%, methotrexate in 51%, gold salts in 22%, chloroquine in 8%,
206
Table 1: General Disease Features in 112
Chi lean Patients Wi th Rheumato id Arthri t is
Age (yr); mean _+ SD (range) Age at onset (yr); mean ± SD
(range) Disease duration from onset (yr);
mean ± SD (range) Disease duration from first visit
(yr); mean ± SD (range) Years of formal education;
mean ± SD (range) Number of disease-modifying anti-
rheumatic drugs; mean _+ SD (range)
Number of ACR Criteria for Clinical Remission; mean _+ SD (range)
Health Assessment Questionnaire; mean ± SD (range)
Gender (% female) Seropositive disease (%)
Extra-articular manifestations (%)* Nodules (%) Vasculitis (%) Sj6gren's syndrome (%) Joint deformities (%) Surgery (%)
50 ± 14 (20-80)
39 ± 12 (4-71)
10 ± 8 (0.1-35)
6 ± 6 (0-29)
8 ± 4 (0-17)
3 ± 1 (0-4)
2 ± 2 (0-6)
0.9 ± 0.7 (0-2.7) 87 90 38 27
8 29 73 16
Functional capacity class (%) (ACR 1991 revised criteria) I 47 II 35 III 16 IV 2
Abbreviation: ACR, American College of Rheumatology. *The following were considered in calculating the extra- articular manifestations: rheumatoid nodules, or pulmonary, cardiac, dermal, ocular and nervous system involvement, rheu- matoid vasculitis, and lymphadenopathy.
azathioprine in 3%, and one patient used cyclo- phosphamide and another cyclosporine. Twenty eight (25%) patients had had drug Side effects. Eighty three (73%) patients had joint deformi- ties, 10% used walking-aids, 3% were in a wheel-chair, and 1 patient was bed-ridden. Eigh- teen (16%) patients underwent joint surgery with 24 procedures (the most common were in the foot, followed by the hips, hands, knees, and ankles). Mean HAQ was 0.88 + 0.66. High HAQ values were positively associated with the number of revised criteria for functional status (P < .0001), with a higher index of Thompson (P = .0001) and a greater number of joint defor- mities (P = .002).
Comparisons between the two clinics showed
MASSARDO ET AL
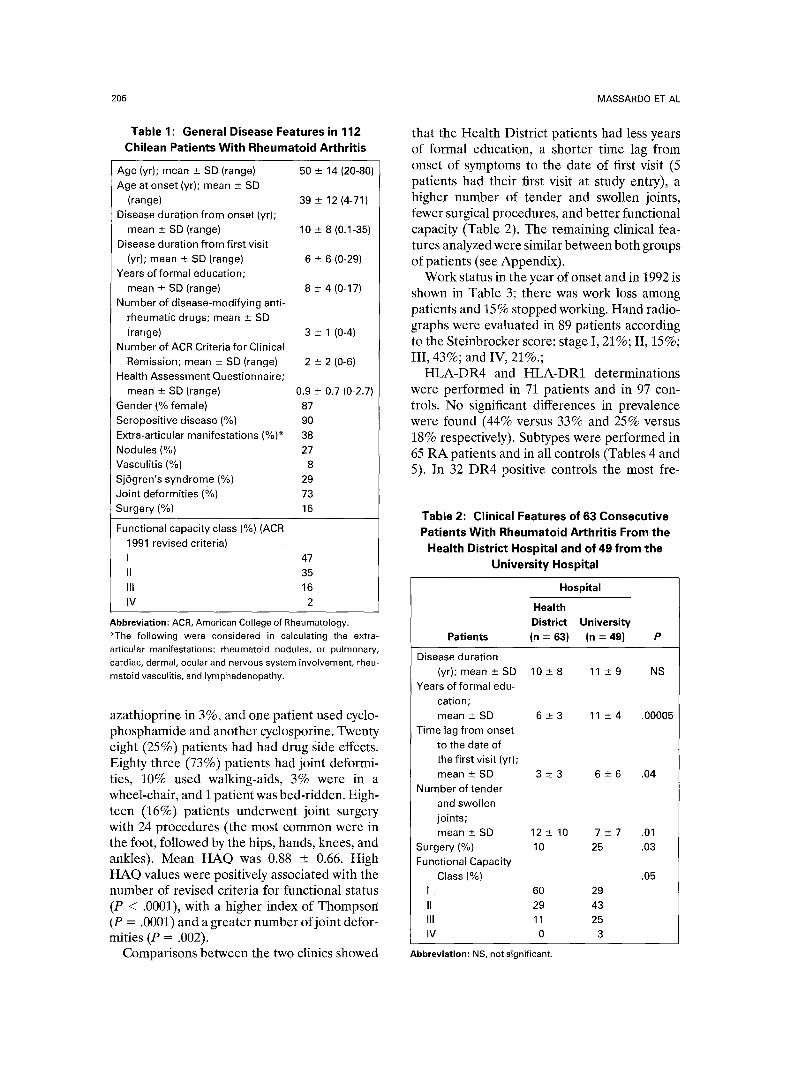
that the Health District patients had less years of formal education, a shorter time lag from onset of symptoms to the date of first visit (5 patients had their first visit at study entry), a higher number of tender and swollen joints, fewer surgical procedures, and better functional capacity (Table 2). The remaining clinical fea- tures analyzed were similar between both groups of patients (see Appendix).
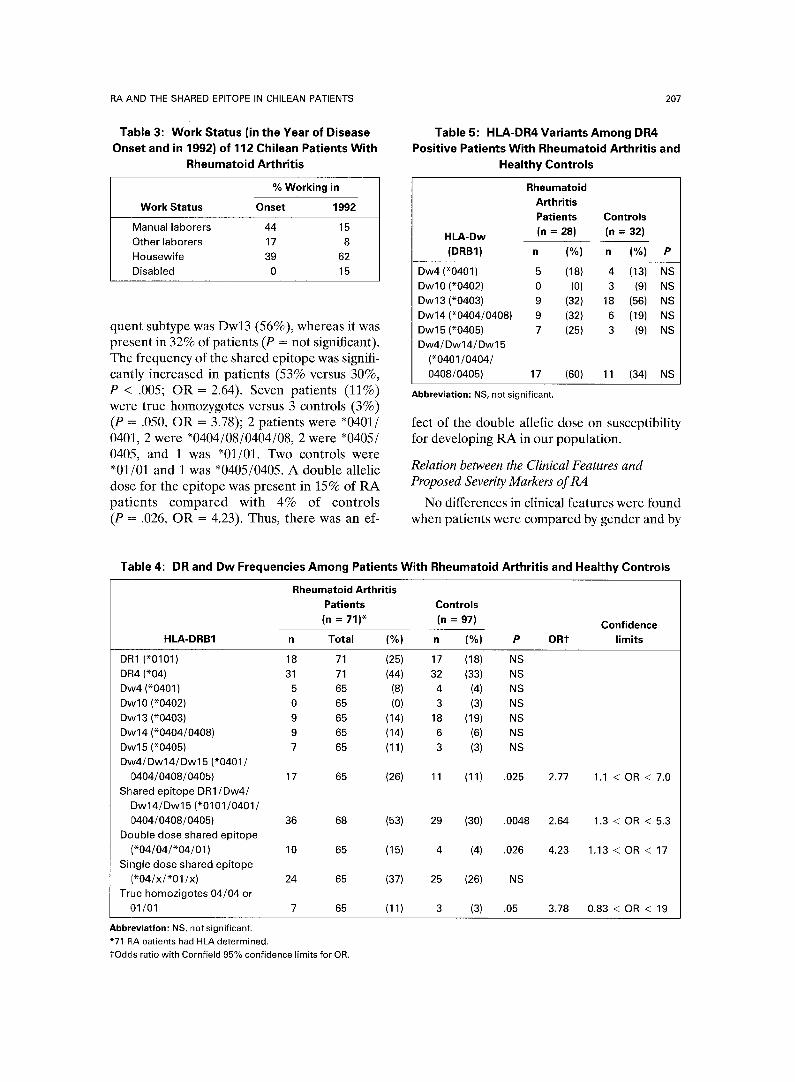
Work status in the year of onset and in 1992 is shown in Table 3; there was work loss among patients and 15% stopped working. Hand radio- graphs were evaluated in 89 patients according to the Steinbrocker score: stage I, 21%; II, 15%; III, 43%; and IV, 21%.;
HLA-DR4 and HLA-DR1 determinations were performed in 71 patients and in 97 con- trols. No significant differences in prevalence were found (44% versus 33% and 25% versus 18% respectively). Subtypes were performed in 65 RA patients and in all controls (Tables 4 and 5). In 32 DR4 positive controls the most fre-
Table 2: Clinical Features of 63 Consecut ive Patients Wi th Rheumato id Arthri t is From the
Health District Hospital and of 49 f rom the Universi ty Hospital
Hospital
Health District University
Patients (n = 63) (n = 49) P
Disease duration (yr); mean ± SD 10 ± 8 11 _+ 9 NS
Years of formal edu- cation; mean ± SD 6 ± 3 11 ± 4 .00005
Time lag from onset to the date of the first visit (yr); m e a n ± S D 3 ± 3 6 -+6 .04
Number of tender and swollen joints; mean ± SD 12 ± 10 7 ± 7 .01
Surgery (%) 10 25 .03 Functional Capacity
Class (%) .05 I , 60 29 II 29 43 Ill 11 25 IV 0 3
Abbreviation: NS, not significant.
RA AND THE SHARED EPITOPE IN CHILEAN PATIENTS
Table 3: Work Status (in the Year of Disease Onset and in 1992) of 112 Chilean Patients Wi th
Rheumatoid Arthrit is
% Working in
Work Status Onset 1992
Manual laborers 44 15 Other laborers 17 8 Housewife 39 62 Disabled 0 15
quent subtype was Dw13 (56%), whereas it was present in 32% of patients (P = not significant). The frequency of the shared epitope was signifi- cantly increased in patients (53% versus 30%, P < .005; OR = 2.64). Seven patients (11%) were true homozygotes versus 3 controls (3%) (P = .050, OR = 3.78); 2 patients were "0401/ 0401, 2 were *0404/08/0404/08, 2 were *0405/ 040:5, and 1 was "01/01. Two controls were "01/01 and 1 was *0405/0405. A double allelic dose for the epitope was present in 15% of RA patients compared with 4% of controls (P = .026, OR -- 4.23). Thus, there was an ef-
2O7
Table 5:HLA-DR4 Variants Among DR4 Positive Patients Wi th Rheumatoid Arthrit is and
Healthy Controls
Rheumatoid Arthritis Patients Controls
HLA-Dw (n = 28) (n = 32)
(DRB1) n (%) n (%) P
Dw4 ('0401) 5 (18) 4 (13) NS D w l 0 (*0402) 0 (0) 3 (9) NS Dw13 (*0403) 9 (32) 18 (56) NS Dw14 (*0404/0408) 9 (32) 6 (19) NS Dw15( '0405) 7 (25) 3 (9) NS Dw4/Dw14/Dw15
( '0401/0404/ 0408/0405) 17 (60) 11 (34) NS
Abbreviation: NS, not significant.
fect of the double allelic dose on susceptibility for developing RA in our population.
Relation between the Clinical Features and Proposed Severity Markers of RA
No differences in clinical features were found when patients were compared by gender and by
Table 4: DR and Dw Frequencies Among Patients Wi th Rheumatoid Arthritis and Healthy Controls
HLA-DRB1
Rheumatoid Arthritis Patients Controls
(n = 71)* (n = 97) Confidence
n Total (%) n (%} P ORT limits
DR1 ('0101) 18 71 DR4 (*04) 31 71 Dw4 (*0401 ) 5 65 Dw l0 (*0402) 0 65 Dw13 (*0403) 9 65 Dw14 (*0404/0408) 9 65 Dw15 (*0405) 7 65 Dw4/Dw14/Dw15 ('0401 /
0404/0408/0405) 17 65 Shared epi tope DR 1/Dw4/
Dw14/Dw15 ( '0101/0401/ 0404/0408/0405) 36 68
Double dose shared epi tope ( ' 04 /04 / ' 04 /01 ) 10 65
Single dose shared epi tope ( *04 /x / *01 /x ) 24 65
True homozigotes 04/04 or 01/01 7 65
(25) 17 (18) NS (44) 32 (33) NS
(8) 4 (4) NS (0) 3 (3) NS
(14) 18 (19) NS (14) 6 (6) NS (11) 3 (3) NS
(26) 11 (11) .025
(53) 29 (30) .0048
(15) 4 (4) .026
(37) 25 (26) NS
(11) 3 (3) .05
2.77 1.1 < OR < 7.0
2.64 1.3 < OR < 5.3
4.23 1.13 < OR < 17
3.78 0.83 < OR < 19
Abbreviation: NS, not significant. "71 RA patients had HLA determined.
o 1"Odds ratio with Cornfield 95 Yo confidence limits for OR.
208
Table 6:
MASSARDO ET AL
Prevalence of the Shared Epitope in Relation to Clinical Features in 31 Patients With Erosive Hand Radiographs
Shared Epitope
Single Double Nonshared Dose Dose Any Dose Epitope
Patients (n) 9 6 15 16
Age (yr); mean _+ SD 51 -+ 12 57 -+ 12 54 ± 12 53 _+ 14
Age at onset; mean _ SD 40 -+ 12 43 _+ 12 41 ± 12 39 ± 16
Disease duration (yr); mean _+ SD 11 -+ 7 14 -+ 10 13 ± 8 14 ± 8
Total number of drugs; mean -+ SD 2 _+ 1 2 _+ 1 2 ± 1 2 ± 1
Males 0 (0%) 3 (50%) 3 (20%) 2 (13%)
Rheumatoid nodules 3 (33%) 4 (75%) 7 (47%) 5 (31%)
Total extra-articular features 4 (44%) 5 (83%)* 9 (60%) 6 (38%)
Joint surgery 3 (33%) 1 (17%) 4 (25%) 4 (25%)
*Double dose group was compared with the nonshared epitope group P = .07; OR = 8.33; confidence limits: 0.6-246.
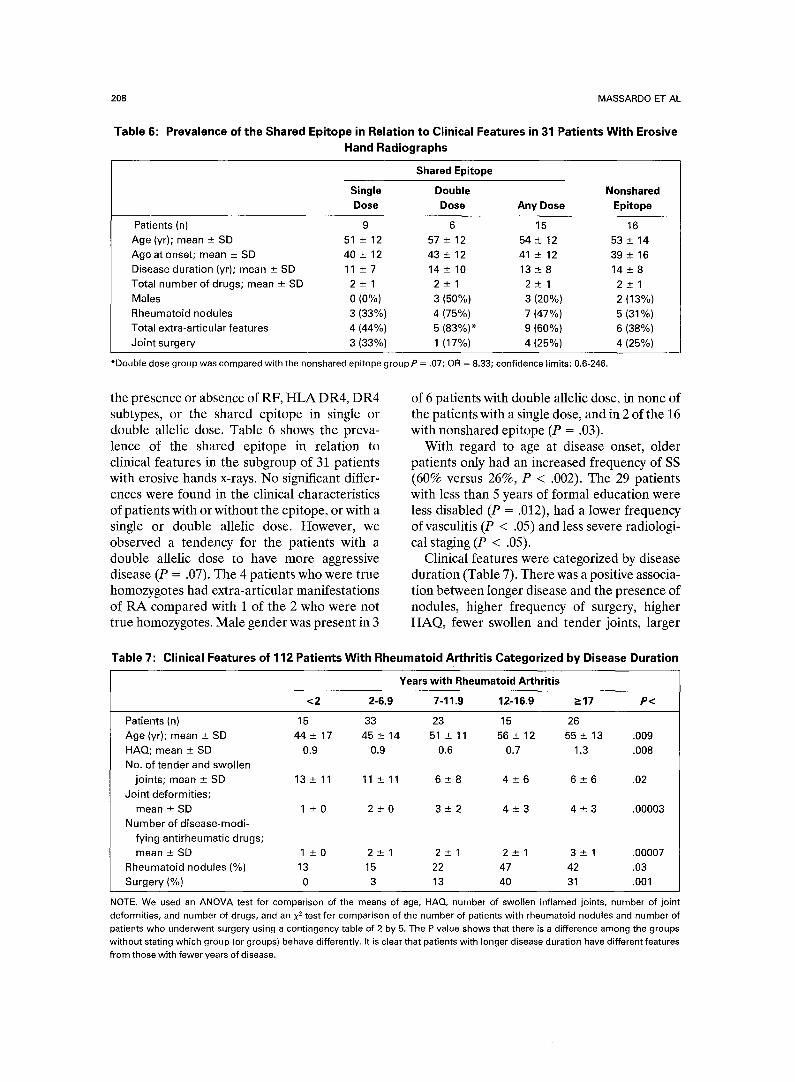
the presence or absence of RF, HLA DR4, DR4 subtypes, or the shared epitope in single or double allelic dose. Table 6 shows the preva- lence of the shared epitope in relation to clinical features in the subgroup of 31 patients with erosive hands x-rays. No significant differ- ences were found in the clinical characteristics of patients with or without the epitope, or with a single or double allelic dose. However, we observed a tendency for the patients with a double allelic dose to have more aggressive disease (P = .07). The 4 patients who were true homozygotes had extra-articular manifestations of RA compared with 1 of the 2 who were not true homozygotes. Male gender was present in 3
of 6 patients with double aIlelic dose, in none of the patients with a single dose, and in 2 of the 16 with nonshared epitope (P = .03).
With regard to age at disease onset, older patients only had an increased frequency of SS (60% versus 26%, P < .002). The 29 patients with less than 5 years of formal education were less disabled (P = .012), had a lower frequency of vasculitis (P < .05) and less severe radiologi- cal staging (P < .05).
Clinical features were categorized by disease duration (Table 7). There was a positive associa- tion between longer disease and the presence of nodules, higher frequency of surgery, higher HAQ, fewer swollen and tender joints, larger
Table 7: Clinical Features of 112 Patients With Rheumatoid Arthritis Categorized by Disease Duration
Years with Rheumatoid Arthritis
<2 2-6.9 7-11.9 12-16.9 ->17 P<
Patients (n) 15 33 23 15 26
Age (yr); mean _+ SD 44_+17 45_+14 51_+11 56_+12 55_+13 .009
HAQ; mean -+ SD 0.9 0.9 0.6 0.7 1.3 .008
No. of tender and swollen
joints; mean _+ SD 13 _+ 11 11 ± 11 6 _+ 8 4 _+ 6 6 + 6 .02
Joint deformities;
mean_+SD 1 _+0 2 -+0 3 -+2 4 -+3 4 -+3 .00003
Number of disease-modi-
fying antirheumatic drugs;
mean _+ SD 1 -+ 0 2 ___ 1 2 -+ 1 2 -+ 1 3 -+ 1 .00007
Rheumatoid nodules (%) 13 15 22 47 42 .03
Surgery (%) 0 3 13 40 31 .001
NOTE. We used an ANOVA test for comparison of the means of age, HAQ, number of swollen inflamed joints, number of joint deformities, and number of drugs, and an x 2 test for comparison of the number of patients with rheumatoid nodules and number of patients who underwent surgery using a contingency table of 2 by 5. The P value shows that there is a difference among the groups without stating which group (or groups) behave differently, it is clear that patients with longer disease duration have different features from those with fewer years of disease.

RA AND THE SHARED EPITOPE IN CHILEAN PATIENTS 209
Table 8: Staging of Rheumatoid Arthritis by Hand Radiographs in 89 Chilean Patients
Steinbrocker Staging n (%)
Years With Rheumatoid Arthritis
<2 2-6.9 7-11.9 12-16.9 >-17
I 19 (21) 8 II 13 (15) 2
III 38 (43) 0
IV 19 (21) O
Total 89 10
10 0 1 0
6 3 1 1
9 15 4 10
3 3 3 10
28 21 9 21
P < .ooooool.
number of joint deformities, and greater num- ber of DMARDs. Also a positive association with more severe x-ray staging in the 89 patients examined was noted (Table 8). With hand radiographs and a disease duration longer than 7 years, six still had nonerosive disease at examination. Five of them were seropositive and one was seronegative. These 6 patients had milder disease, no functional disability and used fewer DMARDS.
The 36 (31%) patients who had nodules and/or vasculitis had longer disease duration, an increased frequency of pleuritis and/or peri- carditis, more joint surgery, more joint deformi- ties, and used more DMARDs. One patient had Felty's syndrome.
DISCUSSION
We have previously shown that in our pa- tients, HLA-DR4 has a weak association with RA. 35,36 Because genetic diversity could account, at least in part, for differences in the clinical expression of this disease, we studied the expres- sion of RA in our patients and compared it with reports from other parts of the world.
The general features of our patients were similar to those in white populations. 1,2,19 Dis- ease onset occurred at 39 years, similar to other reports. 2,19 Sex distribution was different, how- ever, with women affected more frequently than men in a ratio of 6-7:1, rather than the 2 or 3:1 ratio shown in rheumatology textbooks. This figure agrees with previous Chilean and Latin Ameri- can 51,52 studies, and is similar to a report from Greece. 17 Disease duration in our patients was 10 years, similar to most series, s,17,s3 Ninety percent of patients had seropositive RA similar to the 85% in a previous Chilean study, s4 83% of Greek pa- tients, 17 and higher than 75% in the United States. 2
Extra-articular manifestations are considered a marker of disease severity; they were present in 42 (38%) patients and intermediate between
66% of British and 20% of Greeks patients (Table 9). 18 The same was seen for the fre- quency of SS. The figures of 8% for vasculitis and 27% for nodules are similar to those re-
Table 9: Clinical Features of Rheumatoid Arthritis in Chilean, British, and Greek Patients
Chilean British Greek Patients Patients Patients
(n = 112)* (n = 107)~ (n = 108)1"
Total extra-ar-
t icular
manifesta-
t ions (%)§ 38 66 20
Rheumatoid
nodules
(%) 27 51 6
Sj6gren's syn-
d rome (%) 29 16 40
Hands radio-
graphs
Stein-
brocker
class (%) n = 89 n = 107 n = 108
i 21 5 37
II 15 34 34
III 43 38 18
IV 21 37 11
Shared epi tope
(%) RA
patients
versus
healthy
controlNI 53 vs 30 83 vs 46 43 vs 16
*Present series. "rReference. TM
§In the British and Greek patients (18) the following were considered in calculating the total extraarticular manifestations: rheumatoid nodules, Raynaud's phenomenon, serositis, skin vasculitis, lymphadenopathy, episcleritis, and livedo reticularis. liThe shared epitope was calculated in 68 Chilean RA patients versus 97 controls, Data for the British population was calcu- lated in 149 RA patients and in lOg controls. 38 Data for the Greek population was calculated in 92 RA patients and in 84 controls. 24

210 MASSARDO ET AL
ported. 2,s5 No amyloidosis was noted in our series as compared with 5% to 10% in Europe or the United States, and 1 patient had Felty's syndrome.
Most patients had joint damage: 73% had joint deformities and 64% were in Steinbrocker radiological stages III or IV in (hand radio- graphs) similar to the British and more destruc- tive than the Greek experience, is Functional capacity, for patients with a similar disease duration, was comparable to other studies. 7 In our patients the HAQ correlated positively with the revised Steinbrocker class, articular joint index, and with the presence of erosions in patients of similar disease duration.
Clinical features of RA analyzed according to disease duration showed that patients with longer disease duration had more severe dis- ease: higher frequency of nodules, more surgi- cal procedures, greater drug use, higher HAQ, higher x-ray stage, and less number of inflamed joints. This finding is similar to published stud- ies. 1,2,4,55,56 As reported previously, the number of tender joints may decline over time, but this does not lead to improved functional status. 1,2,4
In contrast to most published series 1,2,s6,57 we found that none of the 10 patients with less than 2 years of RA and 15 of the 26 between 2 and 6.9 years of RA had erosives in hand radiographs. This data suggests less aggressive disease in our patients compared with other series.
Efforts have been made to correlate progno- sis with clinical indicators, such as age at onset, female gender, polyarticular onset, RF status, low socioeconomic class, or lack of formal education.l-10,13,58,59
Patients whose age at onset was 60 years or older had a shorter disease duration and more SS, with similar extra-articular manifestations, sequelae, functional capacity, HAQ, and x-ray stage compared to patients whose onset was at a younger age. 2 Gender did not influence disease severity. Only 11 patients were seronegative in this series, and they were clinically similar to those who were seropositive.
In our study, two groups of consecutive pa- tients were described, both currently attending rheumatology clinics in two Santiago hospitals, and representing two segments of our popula- tion. Patients from the university hospital tended to be more educated and had more severe disease than those from the health district
hospital. No significant differences were found in HLA-DR4 or shared epitope frequencies between the groups. The difference in time lag from disease onset to first visit (3 _ 3 years for the district hospital and 6-+ 6 years for the university hospital) may be due to the local pattern of referral (Table 2). Patients with less formal education, contrary to what has been reported, had less destructive hand radio- graphs, less vasculitis, and were less dis- abled.5,6,1359,60
At the time of the study, 6% of patients fulfilled the six ACR criteria for remission and 15% met 5 criteria. Felson et al and others have reported that 10% of patients achieve long-term remission. 14,15,16 Seventy-seven percent of pa- tients showed active arthritis on examination with an average of 10 inflamed joints similar to that in British patients and higher than that in Greeks. 18
Work disability occurs in the majority of patients with RA. Job loss or a decrease in hours worked occurs most often in those with severe disease and in those whose jobs require physical labor. 1 There was work loss among our patients and 15% stopped working. Excluding housewives, active work status changed from 58% to 23%; the percentage of housewives increased from 39% to 62% (Table 3). Forty- seven percent of men stopped working. These findings are similar to the findings of Pincus and others. 5,52,61,62 Even patients with less than 2 years of RA stopped working.
The prognosis and severity of RA may be influenced by the presence of genetic and envi- ronmental factors. HLA-DR4 seems to have prognostic value in populations where it is strongly associated with RA. Patients bearing HLA-DR4 have more severe radiographic changes, rheumatoid factor positivity, subcuta- neous nodules, and vasculitis. 3°,31 Felty's syn- drome is associated with Dw4 subtype. 34 Singal et aP 2 have examined extended haplotypes bear- ing DR4 in patients with RA and found that DR4 associated DQw7 were increased in pa- tients with severe disease. In the United States, Britain, and other Northern European coun- tries, RA is most strongly associated with HLA- DRB1 alleles carrying the RA "shared epit- ope", 29'37'38 that is also associated with severity and prognosis. 28 Weyand et aP 3 examined pa- tients who were homozygous for the HLA-DR4

RA AND THE SHARED EPITOPE IN CHILEAN PATIENTS 211
haplotype and found they had more severe disease and more joint surgery.
In Polynesians, RA has a lower prevalence than in most populations and the most frequent DR4 subtype is Dw13, 63 which does not associ- ate with RA. 29,37 In Greeks, RA has a weak association with HLA-DR424,64 and a milder clinical expressionlS; in that study HLA-DR4 was not a severity markerY Thus, the preva- lence and the clinical variability of the disease in different populations may be due to different frequencies of the alleles linked to susceptibility and severity.
The clinical expression of RA in the exam- ined Chilean patients was intermediate in sever- ity between British and Greek patients. 18 In our series, the weak association of RA with DR435,36 may be due to the fact that the most frequent subtype of HLA-DR4 was Dwl3. This could also explain some of the differences observed comparing the extra-articular manifestations with British patients. The shared epitope was found in 53% of RA patients and in 30% of healthy controls (P < .005; OR = 2.64), how- ever, it was not related to disease severity. Severity was not associated with any particular DR4 subtype in our population.
Of the 31 patients with erosive disease who may be comparable to the series of Weyand et al, 33 16 (52%) did not have the shared epitope and 6 of this 16 (38%) had extra-articular features. No significant differences were found in the clinical characteristics of patients with or without the epitope, or with a single or double allelic dose (Table 6). However, a tendency for the patients with double allelic dose to have more aggressive disease was observed (P = .07). With regard to gender, it is difficult to draw a valid conclusion because 87% of patients were female. However, maleness was found mainly in patients with a double allelic dose (P = .03). Because this is a cross sectional study we cannot
comment to the finding of early onset of ero- sions. Although data about joint surgery were obtained, its high cost introduces a strong bias because it was unaffordable for many patients, and it would not be valid to compare surgery among our patients with North American or European series.
In this series, we did not find a significant association of RA severity with the shared epitope in a single or double allelic dose, although a tendency for more severe patients to bear the double dose was observed. We cannot rule out a relationship of HLA with severity; however, we believe its influence is weaker than previously reported in North American or En- glish series. Study of a larger patient population is needed before definite conclusions are drawn.
APPENDIX
The following parameters were studied: age at onset and age at study, gender, years of formal education, work status in the year of onset and in 1992, time lag from onset to the first rheumatology visit, disease duration from onset to date of study, number of ACR criteria for the classification of RA, number of ACR criteria for remission in RA, number of tender and swollen joints of the Thompson Index, functional capacity class, number of joint defor- mities, use of DMARDs, presence of a history of surgery, hand radiographs (Steinbrocker class), presence or absence of antinuclear anti- body, rheumatoid factor, rheumatoid vasculitis, SS, nodules, pleuritis/pericarditis, pulmonary fibrosis, history of eye inflammation, and total number of extra-articular manifestations. The presence of DR4 serotype (71 patients), DR4-Dw subtypes (65 patients), the shared epitope (68 patients), and homozygocity (65 patients) in single or double dose of the epitope were also assessed.
REFERENCES 1. Felson DT: Epidemiology of the Rheumatic diseases,
in McCarty DJ and Koopman WJ (eds): Arthritis and allied conditions (ed 12). A Textbook of Rheumatology. Philadel- phia, PA, Lea & Febiger, 1993, pp 17-47
2. McCarty D J: Clinical picture of Rheumatoid Arthritis, in McCarty DJ and Koopman WJ (eds): Arthritis and allied conditions. A Textbook of Rheumatology (ed 12). Philadel- phia, PA, Lea & Febiger, 1993, pp 781-809
3. Hochberg MC, Spector TD: Epidemiology of rheuma- toid arthritis: update. Epidemiol Rev 12:247-252, 1990
4. Scott DL, Coulton BL, Symmons DPM, et al: Long- term outcome of treating rheumatoid arthritis: results after 20 years. Lancet 16:1108-1111, 1987
5. Pincus T, Callahan LF, Sale WG, et al: Severe func- tional declines, work disability, and increased mortality in seventy-five rheumatoid arthritis patients studied over nine years. Arthritis Rheum 27:864-872, 1984
6. Pincus T, Callahan LF, Vaughn WK: Questionnaire, walking time and button test mortality in rheumatoid arthritis. J Rheumatol 14:240-250, 1987
212 MASSARDO ET AL
7. Sherrer YS, Bloch DA, Mitchell DM, et al: The development of disability in rheumatoid arthritis. Arthritis Rheum 29:494-500, 1986
8. Wolfe F: Clinical, laboratory, and radiographic assess- ments. Curr Opin Rheumatol 5:139-145, 1993
9. Mitchell DM, Spitz PW, Young DY, et al: Survival, prognosis, and causes of death in rheumatoid arthritis. Arthritis Rheum 29:706-714, 1986
10. Vandenbroucke JP, Hazevoet HM, and Cats A: Survival and cause of death in rheumatoid arthritis: a 25-year prospective followup. J Rheumato111:158-161, 1984
11. Reilly PA, Cosh JA, Maddison PJ, et al: Mortality and survival in rheumatoid arthritis: a 25 year prospective study of 100 patients. Ann Rheum Dis 49:363-369, 1990
12. Abruzzo JL: Rheumatoid arthritis and mortality. Arthritis Rheum 25:1020-1023, 1982
13. Pincus T, Callahan LF: Taking mortality in rheuma- toid arthritis seriously--predictive markers, socioeconomic status and comorbidity. J Rheumatol 13:841-845, 1986
14. Kazis LE, Anderson JJ, Meenan RF: Health status as a predictor of mortality in rheumatoid arthritis: A five-year study. J Rheumatol 17:609-613, 1990
15. Pincus T: The paradox of effective therapies but poor long-term outcomes in rheumatoid arthritis. Semin Arthri- tis Rheum 21:2-15, 1992
16. Wolfe F, and Hawley DJ: Remission in rheumatoid arthritis. J Rheumatol 12:245-252, 1985
17. Boki KA, Drosos AA, Tzioufas AG, et al: Examina- tion of HLA-DR4 as a severity marker for rheumatoid arthritis in Greek patients. Ann Rheum Dis 52:517-519, 1993
18. Drosos AA, Lanchbury JS, Panayi GS, Moutsopoulos HM: Rheumatoid arthritis in Greek and British patients. Arthritis Rheum 35:745-748, 1992
19. Spector TD: Rheumatoid arthritis. Epidemiology of Rheumatic Disease. Rheum Dis Clin North Am 16:513-537, 1990
20. Meyers OL, Daynes G, Beighton P: Rheumatoid arthritis in a tribal Xhosa population in the Transkei, Southern Africa. Ann Rheum Dis 36:62-65, 1977
21. Solomon L, Robin G, Valkenburg HA: Rheumatoid arthritis in an urban South African Negro population. Ann Rheum Dis 34:128-135, 1975
22. Beighton P, Solomon L, Valkenburg HA: Rheuma- toid arthritis in a rural South African Negro population. Ann Rheum Dis 34:136-141, 1975
23. Adebajo A, Reid DM: The pattern of rheumatoid arthritis in West Africa and comparison with a cohort of British patients. Q J Med 292:633-640, 1991
24. Boki KA, Panayi GS, Vaughan RW, et al: HLA Class II sequence polymorphisms and susceptibility to rheuma- toid arthritis in Greeks. Arthritis Rheum 35:749-755, 1992
25. Westedt ML, Breedveld FC, Schreuder GMT, et al: Immunogenetic heterogeneity of rheumatoid arthritis. Ann Rheum Dis 45:534-538, 1986
26. Ollier W, Jaraquemada D, D'Amaro J: HLA antigen associations with extra-articular rheumatoid arthritis. Tis- sue Antigens 24:279-291, 1984
27. De Jongh BM, Van Promunde LKJ, Valkenburg HA, et al: Epidemiological study of HLA and Gm in Rheuma-
toid Arthritis and related symptoms in an open Dutch population. Ann Rheum Dis 43:613-620, 1984
28. Gough A, Faint J, Salmon M, et al: Genetic typing of patients with inflammatory arthritis at presentation can be used to predict outcome. Arthritis Rheum 37:1166-1170, 1994
29. Nepom BS, Nepom GT: Immunogenetics and the Rheumatic Diseases, in Kelley WN, Harris ED, Ruddy S and Sledge CB (eds): Textbook of Rheumatology (ed 4). Philadelphia, PA, Saunders, 1993, pp 89-107
30. Olsen NJ, Callahan LF, Brooks RH, et al: Associa- tions of HLA-DR4 with rheumatoid factor and radio- graphic severity in rheumatoid arthritis. Am J Med 84:257- 264, 1988
31. Alarc6n GS, Koopman WJ, Acton RT: Seronegative rheumatoid arthritis: A distinct immunogenetic disease? Arthritis Rheum 25:502-507, 1982
32. Singal DP, Gren D, Reid B, et al: HLA-D region genes and rheumatoid arthritis (RA): Importance of DR and DQ genes in conferring susceptibility to RA. Ann Rheum Dis 51:23-28, 1992
33. Weyand CM, Hicok KC, Conn DL: The influence of HLA-DRB] genes on disease severity in rheumatoid arthri- tis. Ann Intern Med 117:801-806, 1992
34. Lanchbury JSS, Jaeger EEM, Sansom DM, et al: Strong primary selection for the Dw4 subtype of DR4 accounts for the HLA-DQw7 association with Felty's syn- drome. Human Immunol 32:56-64, 1991
35. Massardo L, Jacobelli S, Rodriguez L, et al: Weak association between HLA-DR4 and rheumatoid arthritis in Chilean patients. Ann Rheum Dis 49:290-292, 1990
36. Gonzfilez A, Nicovani S, Massardo L, et al: Novel genetic markers of rheumatoid arthritis in Chilean patients, by DR serotyping and restriction fragments length polymor- phism analysis. Arthritis Rheum 35:282-289, 1992
37. Gregersen PK, Silver J, Winchester RJ: An approach to understanding the genetics of susceptibility to rheuma- toid arthritis. Arthritis Rheum 30:1205-1213, 1987
38. Wordsworth BP, Lanchbury JS, Sakkas KI, et al: HLA-DR4 subtype frequencies in rheumatoid arthritis indicate that DRB1 is the major susceptibility locus within the HLA class II region. Proc Natl Acad Sci USA 86:10049- 10053, 1989
39. Arnett F, Edworthy SM, Bloch DA, et al: The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum 31:315-324, 1988
40. Gran JT and Husby G: Seronegative rheumatoid arthritis and HLA-DR4: proposal for criteria. J Rheumatol- ogy 14:1079-1082, 1987
41. Pinals RS, Masi AT, Larsen RA, and The Subcommit- tee for Criteria of Remission in Rheumatoid Arthritis of the American Rheumatism Diagnostic and Therapeutic Crite- ria Committee: Preliminary criteria for clinical remission in rheumatoid arthritis. Arthritis Rheum 24:1308-1315, 1981
42. Thompson PW, Silman AJ, Kirwan JR: Articular indices of joint inflammation in rheumatoid arthritis. Arthri- tis Rheum 30:618-623, 1987
43. Hochberg MC, Chang RW, Dwosh I, et al: The American College of Rheumatology 1991 revised criteria

RA AND THE SHARED EPITOPE IN CHILEAN PATIENTS 213
for the classification of global functional status in rheuma- toid arthritis. Arthritis Rheum 35:498-502, 1992
44. Pincus T, Callahan LF, Brooks RH, et al: Self-report questionnaire scores in rheumatoid arthritis compared with traditional physical, radiographic, and laboratory measures. Ann Intern Med 110:259-265, 1989
45. Pincus T, Summey JA, Soraci Jr SA, et al: Assess- ment of patient satisfaction in activities of daily living using a modified Stanford health assessment questionnaire. Arthri- tis RJbeum 26:1346-1352, 1983
46. Steinbrocker O, Traeger CH, Batterman RC: Thera- peutic criteria in rheumatoid arthritis. JAMA 140:659-665, 1949
47. Lanchbury JSS, Hott D, Welsh KI: Sequence analysis of HLA-DR4 beta 1 subtypes additional first domain variability is detected by oligonucleotide hybridization and nucleotide sequencing. Human Immunol 27:136-142, 1990
48. Vaughan RW, Lanchbury JSS, Marsh SGE, et al: The application of oligonucleotide probes to HLA class II typing of the DRB subregion. Tissue Antigens 36:149-155, 1990
49. Zetterquist H, Olerup O. Identification of the HLA DRBl*04,-DRBl*07, and DRBl*09 alleles by PCR ampli- fication and sequence specific primers (PCR-SSP) in 2 hours. Hum Immuno134:64-74, 1992
50. Dean AG, Dean JA, Burton AH, Epi Info, Version 5: A word processing, database, and statistics program for epidemiology on microcomputers. Center for Disease Con- trol, Atlanta, Georgia, USA, 1990
51. Gdmez-Carpio M, Cohen H, Massa F: La dexameta- sona en la Artritis Reumatoidea: Experiencia en 60 casos. Rev Med Chile 88:824-829, 1960
52. Alarc6n GS: Epidemiolofa de las enfermedades reu- matoldgicas en AmErica Latina. Bol Of Sanit Panam 101:309- 326, 1986
53. Wolfe F: 50 years of antirheumatic therapy: the prognosis of rheumatoid arthritis. J Rheumatol 17:24-31, 1990
54. Hurtado R, Losada M, Claure H, and Acchiardo S: Las reacciones de Waaler Rose y del lfitex en la artritis reumatoidea. Rev Med Chile 91:902-907, 1963
55. Bacon PA: Extraarticular features of rheumatoid arthritis, in McCarty DJ, Koopman WJ (eds): Arthritis and allied conditions. A Textbook of Rheumatology (ed 12). Philadelphia, PA, Lea & Febiger, 1993, pp 811-840
56. Fuchs HA, Kaye JJ, Callahan LF: Evidence of signifi- cant radiographic damage in rheumatoid arthritis within the first 2 years of disease. J Rheumatol 16:585-591, 1989
57. Caruso I, Santandrea S, Sarzi Puttini P, et al: Clinical, laboratory and radiographic features in early rheumatoid arthritis. J Rheumatol 17:1263-1267, 1990
58. Van der Heijde DMFM, Van Riel PLCM, Van Rijswijk MH: Influence of prognostic features on the final outcome in rheumatoid arthritis: a review of the literature. Semin Arthritis Rheum 17:284-292, 1988
59. Pincus T: Formal educational level. A marker for the importance of behavioral variables in the pathogenesis, morbidity and mortality of most disease? J Rheumatol 15:1457-1460, 1988
60. Callahan LF, Pincus T: Formal education as a marker of clinical status in rheumatoid arthritis. Arthritis Rheum 31:1346-1357, 1988
61. Reisine ST, Grady KE, Goodenow C, Fifield J: Work disability among women with rheumatoid arthritis. Arthritis Rheum 32:538-543, 1989
62. Yelin E, Meenan R, Nevitt M, Epstein W: Work disability in rheumatoid arthritis: effects of disease, social and work factors. Ann Intern Med 93:551-556, 1980
63. Tan PLJ, Farmiloe S, Roberts M, et al: HLA-DR4 subtypes in New Zealand Polynesians. Predominance of Dwl3 in the healthy population and association of Dwl5 in rheumatoid arthritis. Arthritis Rheum 36:15-19, 1993
64. Papasteriades CA, Kappou ID, Skopouli FN, et al: Lack of HLA-antigen association in Greek rheumatoid arthritis patients. Rheumatol Int 5:201-203, 1985




















