
Double blind controlled phase III multicenter clinical trial with interferon gamma in rheumatoid...
11
Rheumatol Int (1992) 12: 175-185 Rheumalaln I~A~AL W Clinical and Experimental Investigation8 Springer-Verlag 1992 Double blind controlled phase III multicenter clinical trial with interferon gamma in rheumatoid arthritis German Lymphokine Study Group* Received July 1, 1992/Accepted July 2, 1992 Summary. The controlled clinical trial reported here is part of a multicenter clinical and basic research project, sponsored by the German Federal Minister of Science and Technology, directed by a standing commission of * Participants: Organization and documentation P. H. Hofschneider, U. Winter, Max-Planck-Institut fiir Biochemie, Martinsried E.-M. Lemmel, B. Br61z, Staatliches Rheumakrankenhaus Baden- Baden (main investigatol:) W. Gaus, S. Schmid, Universitfit Ulm (clinical documentation) H.-J. Obert, C. Stetter, Bioferon biochemische Substanzen GmbH & Co., Laupheim Hospitals and clinicians I. O. Auer, C. Papst, Medizinische UniversitS.tsklinik, Luitpold- krankenhaus Wfirzburg W. H. Boesken, H. E. Stierle, II. Medizinische Abteilung, Kranken- haus der Barmherzigen Brfider Trier U. Botzenhardt, W. Reemtsen, Rheumatologische Abteilung, Rotes Kreuz-Krankenhaus Bremen D. Brackertz, D. Richter, St. Vincenz-und Elisabeth-Hospital Mainz V. Diehl, A. K. yon Kalle, Medizinische Universit/itsklinik K61n C. G/irtner, S. Herzig, Abteilung Rheumatologie, Krankenhaus Porz/Rhein, K61n J. Goronzy, C. Weyand, Medizinische Poliklinik V Heidelberg J. R. Kalden, F. Strobel, Medizinische Klinik III und Institut ffir klinische Immunologic und Rheumatologie Erlangen E.-M. Lemmel, B. Br61z, Staatliches Rheumakrankenhaus Baden- Baden K. Machalke, Klinik Lippe, Horn-Bad Meinberg H. H. Peter, S. Meske, Abteilung Rheumatologie und klinische Immunologie, Medizinische Universit/itsklinik Freiburg M. Schattenkirchner, K. Krtiger, Rheumaeinheit, Medizinische Poliklinik der Universit/it Mfinchen R. Sprekeler, Diakoniekrankenhaus Rotenburg/Wfimme H. D. Waller, J. G. Saal, Abteilung Inhere Medizin II, Medizinische Klinik Tfibingen H. Warnatz, G. Lemm, Katholisches Krankenhaus Essen-Werden K. Wilms, T. Stolzenburg, Medizinische Poliklinik der Universit/it Wfirzburg Correspondence to: E.-M. Lemmel, Staatliches Rheumakranken- haus, Rotenbachtalstrasse 5, W-7570 Baden-Baden, Federal Re- public of Germany the president of the Max-Planck-Gesellschaft, and co- ordinated by the Max-Planck-Institut ffir Biochemie, Mfinchen. Overall, 249 patients with rheumatoid arthritis (RA) were enrolled by 16 participating hospitals. In addi- tion to NSAID treatment, patients were randomly given either interferon gamma (IFN-7) or placebo. In the IFN-7 group, 107 patients were evaluated and in the control group, 116 patients were evaluated. The response rate after 3 months of treatment, according to joint pain in- dexes, was significantly higher in the IFN-7 group with an error probability of 1%. IFN-7 was able to reduce the quantity of corticosteroids administered. Compared with the control group, the IFN-? group benefited considering all parameters measured. Most important side effects were transient fever and transient influenza-like symp- toms; all other adverse events were comparable in both groups. Key words: Interferon gamma Rheumatoid arthritis - Controlled clinical trial - Multicenter Introduction During the last few years there has been some progress in the development and investigation of natural immuno- regulatory substances that influence rheumatic diseases. Some of these substances are under investigation and clinical testing [1]. Currently, medical treatment for rheumatic patients, especially in the active phases of the disease, is unsatisfactory. Therefore, a therapeutic princi- ple acting directly on the underlying immunologic pro- cesses is urgently required. There is general agreement that inflammation, pain, and destruction occurring in the joint during active rheumatoid arthritis (RA) are caused by a persistent in- crease in the activity of the macrophages and granulo- cytes. This activity results in the release of structure-de- stroying oxygen radicals, increased growth rate of the fibroblasts and the formation of their prostaglandin, Ez,
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Double blind controlled phase III multicenter clinical trial with interferon gamma in rheumatoid...

Rheumatol Int (1992) 12: 175-185 Rheumalaln I~A~AL W Clinical and Experimental Investigation8
�9 Springer-Verlag 1992
Double blind controlled phase III multicenter clinical trial with interferon gamma in rheumatoid arthritis
German Lymphokine Study Group*
Received July 1, 1992/Accepted July 2, 1992
Summary. The controlled clinical trial reported here is part of a multicenter clinical and basic research project, sponsored by the German Federal Minister of Science and Technology, directed by a standing commission of
* Participants:
Organization and documentation
P. H. Hofschneider, U. Winter, Max-Planck-Institut fiir Biochemie, Martinsried E.-M. Lemmel, B. Br61z, Staatliches Rheumakrankenhaus Baden- Baden (main investigatol:) W. Gaus, S. Schmid, Universitfit Ulm (clinical documentation) H.-J. Obert, C. Stetter, Bioferon biochemische Substanzen GmbH & Co., Laupheim
Hospitals and clinicians
I. O. Auer, C. Papst, Medizinische UniversitS.tsklinik, Luitpold- krankenhaus Wfirzburg W. H. Boesken, H. E. Stierle, II. Medizinische Abteilung, Kranken- haus der Barmherzigen Brfider Trier U. Botzenhardt, W. Reemtsen, Rheumatologische Abteilung, Rotes Kreuz-Krankenhaus Bremen D. Brackertz, D. Richter, St. Vincenz- und Elisabeth-Hospital Mainz V. Diehl, A. K. yon Kalle, Medizinische Universit/itsklinik K61n C. G/irtner, S. Herzig, Abteilung Rheumatologie, Krankenhaus Porz/Rhein, K61n J. Goronzy, C. Weyand, Medizinische Poliklinik V Heidelberg J. R. Kalden, F. Strobel, Medizinische Klinik III und Institut ffir klinische Immunologic und Rheumatologie Erlangen E.-M. Lemmel, B. Br61z, Staatliches Rheumakrankenhaus Baden- Baden K. Machalke, Klinik Lippe, Horn-Bad Meinberg H. H. Peter, S. Meske, Abteilung Rheumatologie und klinische Immunologie, Medizinische Universit/itsklinik Freiburg M. Schattenkirchner, K. Krtiger, Rheumaeinheit, Medizinische Poliklinik der Universit/it Mfinchen R. Sprekeler, Diakoniekrankenhaus Rotenburg/Wfimme H. D. Waller, J. G. Saal, Abteilung Inhere Medizin II, Medizinische Klinik Tfibingen H. Warnatz, G. Lemm, Katholisches Krankenhaus Essen-Werden K. Wilms, T. Stolzenburg, Medizinische Poliklinik der Universit/it Wfirzburg Correspondence to: E.-M. Lemmel, Staatliches Rheumakranken- haus, Rotenbachtalstrasse 5, W-7570 Baden-Baden, Federal Re- public of Germany
the president of the Max-Planck-Gesellschaft, and co- ordinated by the Max-Planck-Institut ffir Biochemie, Mfinchen. Overall, 249 patients with rheumatoid arthritis (RA) were enrolled by 16 participating hospitals. In addi- tion to NSAID treatment, patients were randomly given either interferon gamma (IFN-7) or placebo. In the IFN-7 group, 107 patients were evaluated and in the control group, 116 patients were evaluated. The response rate after 3 months of treatment, according to joint pain in- dexes, was significantly higher in the IFN-7 group with an error probability of 1%. IFN-7 was able to reduce the quantity of corticosteroids administered. Compared with the control group, the IFN-? group benefited considering all parameters measured. Most important side effects were transient fever and transient influenza-like symp- toms; all other adverse events were comparable in both groups.
Key words: Interferon gamma Rheumatoid arthritis - Controlled clinical trial - Multicenter
Introduction
During the last few years there has been some progress in the development and investigation of natural immuno- regulatory substances that influence rheumatic diseases. Some of these substances are under investigation and clinical testing [1]. Currently, medical treatment for rheumatic patients, especially in the active phases of the disease, is unsatisfactory. Therefore, a therapeutic princi- ple acting directly on the underlying immunologic pro- cesses is urgently required.
There is general agreement that inflammation, pain, and destruction occurring in the joint during active rheumatoid arthritis (RA) are caused by a persistent in- crease in the activity of the macrophages and granulo- cytes. This activity results in the release of structure-de- stroying oxygen radicals, increased growth rate of the fibroblasts and the formation of their prostaglandin, Ez,

176
and increased activity of the B- and T-lymphocytes with their antibody formation and release of various mediator substances. This immune-mediated inflammation, caus- ing pain and swelling, leads to impairment of movement and function, and ultimately to degradation and destruc- tion of the affected tissue structures. Besides the rheuma- toid factors, the relevant laboratory parameters are those that generally accompany nonspecific inflammation, such as raised erythrocyte sedimentation rate (ESR), anaemia, increased serum copper, decreased serum iron and vari- ous acute-phase proteins.
Interferons (IFN) are a complex group of proteins that occur naturally in the body, the effects of which are large- ly species-specific and show major regulatory effects on many effector cells. Their mode of action is of great inter- est internationally [2-5]. Despite numerous investiga- tions, our knowledge of IFN is still not conclusive, espe- cially regarding their control functions in inflammation and immunologic mechanisms.
Interferon gamma ( IFN- j possesses pronounced im- munomodulating properties. The type of immunomodu- lation, i.e., activation or inhibition, depends mainly on the existing degree of activity: inactive systems are activated, whereas systems that are already activated are inhibited [5, 6].
Synovial fluid mononuclear cells of patients with RA are highly activated and produce spontaneously relative- ly large amounts of interleukin-1 (IL-1). IL-1 is a central mediator of inflammation [7, 8] and is present in the synovial fluid of inflamed rheumatic joints [9-13]. In- active monocytes/macrophages are stimulated by IFN-7 to produce IL-1 [14-16], while in the activated mono- cytes/macrophages, IL-1 production is inhibited by IFN-7 [17 19]. In particular, the self-induced synthesis of IL-1 is reduced [20].
In the rheumatic joint with high inflammatory activity, one would expect a high concentration of the regulating substance IFN-7, but, in fact, only small amounts of IFN-7 are found in the synovial fluid [21-25]. It can, thus, be concluded that small endogenous amounts of IFN-y are insufficient to ensure effective inhibition of the IL-1 synthesis, and, therefore, the inflammatory process con- tinues to develop.
Our knowledge of IFN-y has increased greatly from the results obtained in clinical studies with IFN-y in RA. Overall, 922 patients from phase II studies [26-28], placebo controlled phase III studies [29-32], long-term studies over 12 months [33-36], and a field study [37] are available for assessment of efficacy and safety.
On the basis of these results, IFN-~ was licensed in Germany for the treatment of RA (Polyferon, Dr. Rentschler Arzneimittel GmbH & Co., FRG). IFN-y is a therapeutic agent for patients for whom NSAID therapy is no longer adequate, and where treatment with disease- modifying drugs becomes necessary. Treatment with IFN-~ may stabilize or improve the clinical condition and, thus, reduce the use of corticosteroids. We present the results of mul t icenter trial conducted to confirm the previous findings and to demons t ra te the efficacy of treat- men t in pat ients for whom disease-modifying therapy would be prescribed in addi t ion to NSAIDs.
Materials and methods
Study design. In this multicenter trial, patients were randomly allo- cated to either IFN-7 or placebo in addition to their background antirheumatic treatment for 12 weeks. Treatment was performed in a double-blind manner. At completion of the double-blind phase of the trial, patients were offered the opportunity of receiving IFN-y in an open labeled manner. Approval by an ethics committee was obtained at Wfirzburg University. Informed consent was obtained from all patients. The investigations were performed in accordance with the principles of the Declaration of Helsinki.
Drug administration. Recombinant human IFN-y (rIFN-J, with a a specific activity of greater than 2 x 107 IU/mg protein, was used for the treatment of RA. This interferon is produced by cloning the cDNA of IFN-~ in an expression plasmid [38] and by expression of the gone product in Escherichia coli [39]. The active substance, of which the amino acid sequence has been identified [40], was ob- tained from the crude protein extract of E. coli, purified and made available by Biogen, Cambridge, Mass. (USA) and Bioferon, Laup- helm (FRG).
The preparation used contained 50 gg of the active agent IFN-7, with the following additives: sodium monohydrogen phosphate (an- hydrous), sodium dihydrogen phosphate, and albumin (human). The placebo preparation contained the same additives in identical quantities. Both preparations were presented as lyophilisates in rubber-capped vials of identical appearance. Each vial was labeled with a brief identification of the study and numbered successively. This number identified the hospital and was also the patients' iden- tification number. The coding list was known only to the biometri- cian and the manufacturer of the vials.
Each single dose of 50 gg rIFN-7 or placebo was injected subcu- taneously into the abdominal skin on the morning of every injection day. Patients received seven injections per week for 3 weeks, fol- lowed by three injectons per week every other day for 4 weeks, and finally, two injections per week for 5 weeks.
Additional current medication. Disease modifying drugs were not allowed during the study. Patients having disease modifying drugs before the study were withdrawn from these drugs, e.g., because of ineffectiveness, at least 4 weeks before study entry. Treatment with disease modifying drugs was not initiated during the study. Back- ground antirheumatic medication permitted during the 12 week trial included corticosteroids and nonsteroidal antiinflammatory drugs (NSAIDs). Corticosteroid dosage on entry was allowed to a maximum of 10 mg/day prednisolone equivalents. A decrease in corticosteroid dosage was permitted, an increase in corticosteroid dosage was not permitted and evaluated as a drop-out for ineffica- cy; changes in the corticosteroid dosage had to be documented. NSAIDs and corticosteroids had to be stable for at least 2 weeks before entry into the trial. Additionally, NSAIDs had to be stable for at least the first 3 weeks of the trial, after which time a change in these drugs was permitted but had to be documented.
Patient selection criteria. The inclusion criteria were as follows: patients between 18 and 65 years of age, onset of RA between the ages of 16 and 60, confirmed RA according to the diagnostic criteria of the American College of Rheumatology [formerly, the American Rheumatism Association (ARA)] [41, 42], active disease with at least three large or six small joints involved, Westergren erythrocyte sedimentation rate (ESR) of 25 mm/h or greater, and start of ther- apy with disease modifying drugs indicated according to the disease activity or one or more disease modifying drugs administered in the past without satisfactory improvement.
The exclusion criteria were as follows: pregnancy or lactation, any diagnosed malignant disease, overt liver disease, granulocytope- nia (less than 1500 cells/gl), leukocytopenia (less than 2500 cells/gl), insufficient renal function, concomitant infecton of bronchus or urinary tract at study entry, and angina pectoris or recent myocar- dial infarction.
177
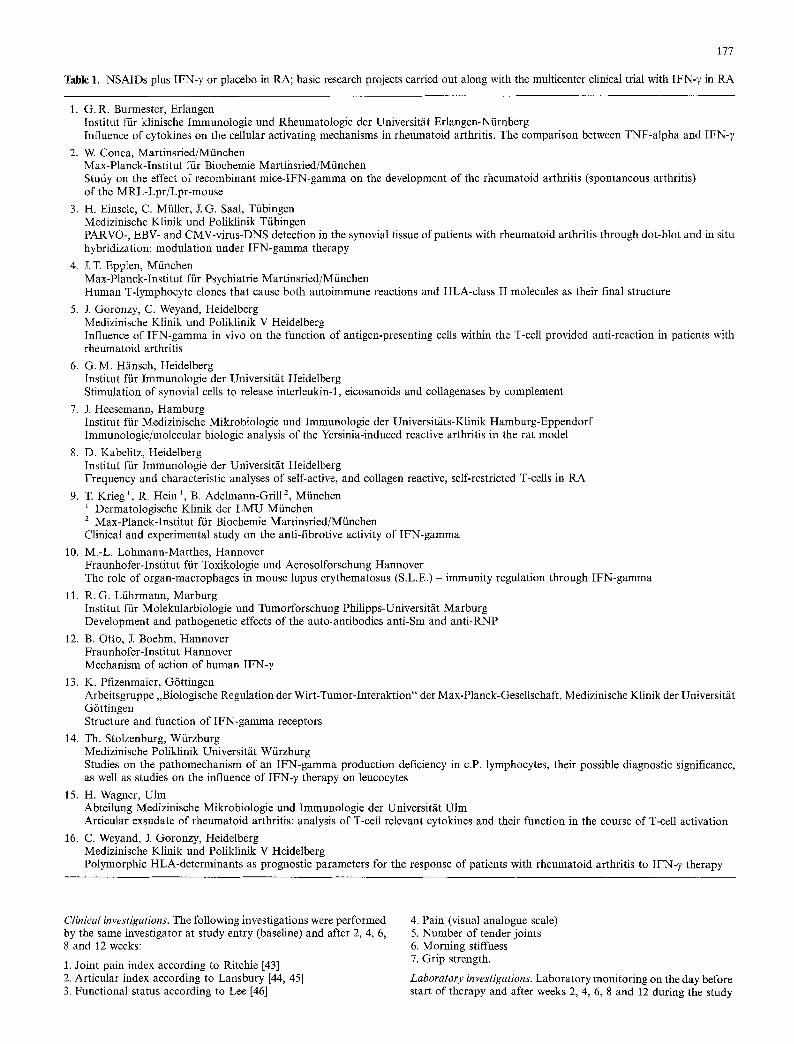
Table 1. NSAIDs plus IFN-y or placebo in RA; basic research projects carried out along with the multicenter clinical trial with IFN-7 in RA
1. G.R. Burmester, Erlangen Institut fiir klinische Immunologie und Rheumatologie der Universitfit Erlangen-Niirnberg Influence of cytokines on the cellular activating mechanisms in rheumatoid arthritis. The comparison between TNF-alpha and IFN- 7
2. W. Conca, Martinsried/Mfinchen Max-Planck-Institut ffir Biochemie Martinsried/Miinchen Study on the effect of recombinant mice-IFN-gamma on the development of the rheumatoid arthritis (spontaneous arthritis) of the MRL-Lpr/Lpr-mouse
3. H. Einsele, C. Miiller, J.G. Saal, Tfibingen Medizinische Klinik und Poliklinik Tiibingen PARVO-, EBV- and CMV-virus-DNS detection in the synovial tissue of patients with rheumatoid arthritis through dot-blot and in situ hybridization: modulation under IFN-gamma therapy
4. J.T. Epplen, Mfinchen Max-Planck-Institut fiir Psychiatrie Martinsried/Miinchen Human T-lymphocyte clones that cause both autoimmune reactions and HLA-class II molecules as their final structure
5. J. Goronzy, C. Weyand, Heidelberg Medizinische Klinik und Poliklinik V Heidelberg Influence of IFN-gamma in vivo on the function of antigen-presenting cells within the T-cell provided anti-reaction in patients with rheumatoid arthritis
6. G.M. Hfinsch, Heidelberg Institut fiir Immunologic der Universitfit Heidelberg Stimulation of synovial cells to release interleukin-1, eicosanoids and collagenases by complement
7. J. Heesemann, Hamburg Institut ffir Medizinische Mikrobiologie und Immunologie der Universit/its-Klinik Hamburg-Eppendorf Immunologic/molecular biologic analysis of the Yersinia-induced reactive arthritis in the rat model
8. D. Kabelitz, Heidelberg Institut ffir Immunologie der Universit/it Heidelberg Frequency and characteristic analyses of self-active, and collagen reactive, self-restricted T-cells in RA
9. T. Krieg 1, R. Hein 1, B. Adelmann-Grill 2, Mfinchen 1 Dermatologische Klinik der LMU Mfinchen 2 Max-Planck-Institut ftir Biochemie Martinsried/Mfinchen Clinical and experimental study on the anti-fibrotive activity of IFN-gamma
10. M.-L. Lohmann-Matthes, Hannover Fraunhofer-Institut ftir Toxikologie und Aerosolforschung Hannover The role of organ-macrophages in mouse lupus erythematosus (S.L.E.) - immunity regulation through IFN-gamma
11. R.G. Lfihrmann, Marburg Institut ffir Molekularbiologie und Tumorforschung Philipps-Universit/it Marburg Development and pathogenetic effects of the auto-antibodies anti-Sm and anti-RNP
12. B. Otto, J. Boehm, Hannover Fraunhofer-Institut Hannover Mechanism of action of human IFN-y
13. K. Pflzenmaier, G6ttingen Arbeitsgruppe ,,Biologische Regulation der Wirt-Tumor-Iuteraktion" der Max-Planck-Gesellschaft, Medizinische Klinik der Universit/it G6ttingen Structure and function of IFN-gamma receptors
14. Th. Stolzenburg, Wiirzburg Medizinische Poliklinik Universit/it W/irzburg Studies on the pathomechanism of an IFN-gamma production deficiency in c.P. lymphocytes, their possible diagnostic significance, as well as studies on the influence of IFN-y therapy on leucocytes
15. H. Wagner, Ulm Abteilung Medizinische Mikrobiologie und Immunologie der Universit/it Ulm Articular exsndate of rheumatoid arthritis: analysis of T-cell relevant cytokines and their function in the course of T-cell activation
16. C. Weyand, J. Goronzy, Heidelberg Medizinische Klinik und Poliklinik V Heidelberg Polymorphic HLA-determinants as prognostic parameters for the response of patients with rheumatoid arthritis to IFN- 7 therapy
Clinical investigations. The following investigations were performed by the same investigator at study entry (baseline) and after 2, 4, 6, 8 and 12 weeks:
1. Joint pain index according to Ritchie [43] 2. Articular index according to Lansbury [44, 45] 3. Functional status according to Lee [46]
4. Pain (visual analogue scale) 5. Number of tender joints 6. Morning stiffness 7. Grip strength.
Laboratory investigations. Laboratory monitoring on the day before start of therapy and after weeks 2, 4, 6, 8 and 12 during the study
178
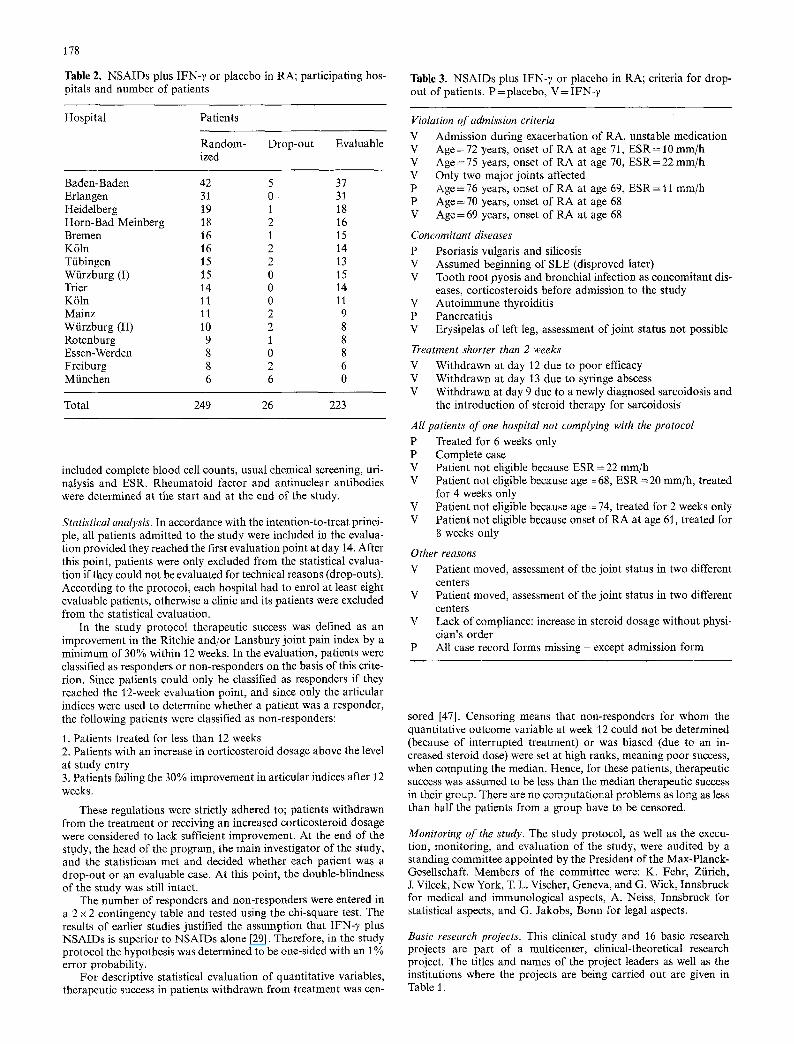
Table 2, NSAIDs plus IFN-7 or placebo in RA; participating hos- pitals and number of patients
Table 3. NSAIDs plus IFN-7 or placebo in RA; criteria for drop- out of patients. P=placebo, V=IFN-y
Hospital Patients
Random- Drop-out Evaluable ized
Baden-Baden 42 5 37 Erlangen 31 0 31 Heidelberg 19 1 18 Horn-Bad Meinberg 18 2 16 Bremen 16 1 15 K61n 16 2 14 Tfibingen 15 2 13 Wiirzburg (I) 15 0 15 Trier 14 0 14 K61n 11 0 11 Mainz 11 2 9 Wfirzburg (II) 10 2 8 Rotenburg 9 1 8 Essen-Werden 8 0 8 Freiburg 8 2 6 Mfinchen 6 6 0
Total 249 26 223
included complete blood cell counts, usual chemical screening, uri- nalysis and ESR. Rheumatoid factor and antinuclear antibodies were determined at the start and at the end of the study.
Stat&tical analysis. In accordance with the intention-to-treat princi- ple, all patients admitted to the study were included in the evalua- tion provided they reached the first evaluation point at day 14. After this point, patients were only excluded from the statistical evalua- tion if they could not be evaluated for technical reasons (drop-outs). According to the protocol, each hospital had to enrol at least eight evaluable patients, otherwise a clinic and its patients were excluded from the statistical evaluation.
In the study protocol therapeutic success was defined as an improvement in the Ritchie and/or Lansbury joint pain index by a minimum of 30% within 12 weeks. In the evaluation, patients were classified as responders or non-responders on the basis of this crite- rion, Since patients could only be classified as responders if they reached the 12-week evaluation point, and since only the articular indices were used to determine whether a patient was a responder, the following patients were classified as non-responders:
1. Patients treated for less than 12 weeks 2. Patients with an increase in corticosteroid dosage above the level at study entry 3. Patients failing the 30% improvement in articular indices after 12 weeks.
These regulations were strictly adhered to; patients withdrawn from the treatment or receiving an increased corticosteroid dosage were considered to lack sufficient improvement. At the end of the study, the head of the program, the main investigator of the study, and the statistician met and decided whether each patient was a drop-out or an evaluable case. At this point, the double-blindness of the study was still intact.
The number of responders and non-responders were entered in a 2 x 2 contingency table and tested using the chi-square test. The results of earlier studies justified the assumption that IFN-7 plus NSAIDs is superior to NSAIDs alone [29]. Therefore, in the study protocol the hypothesis was determined to be one-sided with an 1% error probability.
For descriptive statistical evaluation of quantitative variables, therapeutic success in patients withdrawn from treatment was cen-
Violation of admission criteria V Admission during exacerbation of RA, unstable medication V Age = 72 years, onset of RA at age 71, ESR = 10 mm/h V Age = 75 years, onset of RA at age 70, E S R = 22 mm/h V Only two major joints affected P Age= 76 years, onset of RA at age 69, ESR = 11 mm/h P Age = 70 years, onset of RA at age 68 V Age = 69 years, onset of RA at age 68
Concomitant diseases P Psoriasis vulgaris and silicosis V Assumed beginning of SLE (disproved later) V Tooth root pyosis and bronchial infection as concomitant dis-
eases, corticosteroids before admission to the study V Autoimmune thyroiditis P Pancreatitis V Erysipelas of left leg, assessment of joint status not possible
Treatment shorter than 2 weeks V Withdrawn at day 12 due to poor efficacy V Withdrawn at day 13 due to syringe abscess V Withdrawn at day 9 due to a newly diagnosed sarcoidosis and
the introduction of steroid therapy for sarcoidosis
All patients of one hospital not complying with the protocol
P Treated for 6 weeks only P Complete case V Patient not eligible because ESR = 22 mm/h V Patient not eligible because age ~ 68, ESR = 20 ram/h, treated
for 4 weeks only V Patient not eligible because age = 74, treated for 2 weeks only V Patient not eligible because onset of RA at age 61, treated for
8 weeks only
Other reasons V Patient moved, assessment of the joint status in two different
centers V Patient moved, assessment of the joint status in two different
centers V Lack of compliance: increase in steroid dosage without physi-
cian's order P All case record forms missing - except admission form
s0red [47]. Censoring means that non-responders for whom the quantitative outcome variable at week 12 could not be determined (because of interrupted treatment) or was biased (due to an in- creased steroid dose) were set at high ranks, meaning poor success, when computing the median. Hence, for these patients, therapeutic success was assumed to be less than the median therapeutic success in their group. There are no computational problems as long as less than half the patients from a group have to be censored.
Monitoring of the study. The study protocol, as weI1 as the execu- tion, monitoring, and evaluation of the study, were audited by a standing committee appointed by the President of the Max-Planck- Gesellschaft. Members of the committee were: K. Fehr, Ziirich, J. Vilcek, New York, T. L. Vischer, Geneva, and G. Wick, Innsbruck for medical and immunological aspects, A. Neiss, Innsbruck for statistical aspects, and G. Jakobs, Bonn for legal aspects.
Basic research projects. This clinical study and 16 basic research projects are part of a multicenter, clinical-theoretical research project. The titles and names of the project leaders as well as the institutions where the projects are being carried out are given in Table 1.
179
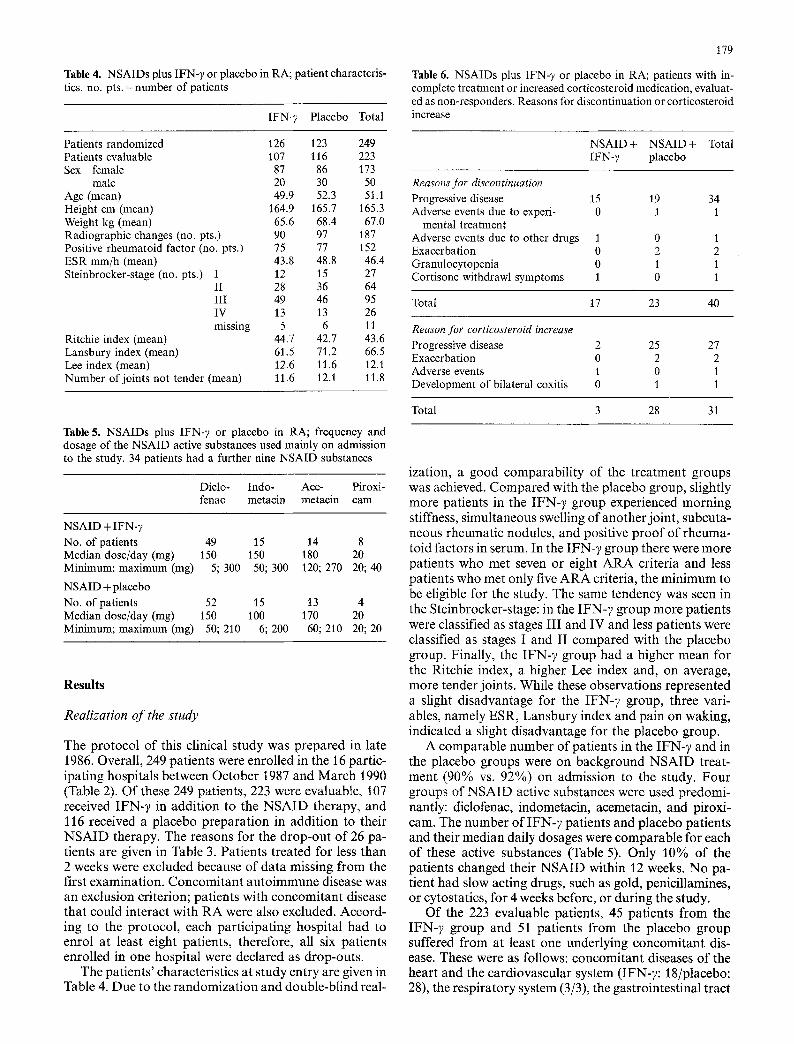
Table 4. NSAIDs plus IFN-7 or placebo in RA; patient characteris- tics. no. pts. = number of patients
IFN-? Placebo Total
Table 6. NSAIDs plus IFN-?) or placebo in RA; patients with in- complete treatment or increased corticosteroid medication, evaluat- ed as non-responders. Reasons for discontinuation or corticosteroid increase
Patients randomized 126 123 249 Patients evaluable 107 116 223 Sex female 87 86 173
male 20 30 50 Age (mean) 49.9 52.3 51.t Height cm (mean) 164.9 165.7 165.3 Weight kg (mean) 65.6 68.4 67.0 Radiographic changes (no. pts.) 90 97 187 Positive rheumatoid factor (no. pts.) 75 77 152 ESR mm/h (mean) 43.8 48.8 46.4 Steinbrocker-stage (no. pts.) I 12 15 27
II 28 36 64 III 49 46 95 IV 13 13 26 missing 5 6 11
Ritchie index (mean) 44.7 42.7 43.6 Lansbury index (mean) 61.5 71.2 66.5 Lee index (mean) 12.6 11.6 12.1 Number of joints not tender (mean) 11.6 12.1 11.8
NSAID+ NSAID+ Total [FN-7 placebo
Reasons for discontinuation Progressive disease 15 19 34 Adverse events due to experi- 0 1 1
mental treatment Adverse events due to other drugs 1 0 1 Exacerbation 0 2 2 Granulocytopenia 0 1 1 Cortisone withdrawl symptoms 1 0 1
Total 17 23 40
Reason for corticosteroid increase Progressive disease 2 25 27 Exacerbation 0 2 2 Adverse events 1 0 1 Development of bilateral coxitis 0 1 1
Total 3 28 31
Table 5. NSAIDs plus IFN-?, or placebo in RA; frequency and dosage of the NSAID active substances used mainly on admission to the study. 34 patients had a further nine NSAID substances
Dido- Indo- Ace- Piroxi- fenac metacin metacin cam
NSAID + IFN-y No. of patients 49 15 14 8 Median dose/day (rag) 150 150 180 20 Minimum; maximum (mg) 5; 300 50; 300 120; 270 20; 40
NSAID + placebo No. of patients 52 15 13 4 Median dose/day (rag) 150 100 170 20 Minimum; maximum (mg) 50; 210 6; 200 60; 210 20; 20
Results
Realization o f the study
The protocol of this clinical study was prepared in late 1986. Overall, 249 patients were enrolled in the 16 partic- ipating hospitals between October 1987 and March 1990 (Table 2). Of these 249 patients, 223 were evaluable, 107 received IFN-~ in addition to the N S A I D therapy, and 116 received a placebo preparat ion in addition to their N S A I D therapy. The reasons for the drop-out of 26 pa- tients are given in Table 3. Patients treated for less than 2 weeks were excluded because of data missing f rom the first examination. Concomitant auto immune disease was an exclusion criterion; patients with concomitant disease that could interact with R A were also excluded. Accord- ing to the protocol, each participating hospital had to enrol at least eight patients, therefore, all six patients enrolled in one hospital were declared as drop-outs.
The patients ' characteristics at study entry are given in Table 4. Due to the randomizat ion and double-blind real-
ization, a good comparabil i ty of the treatment groups was achieved, Compared with the placebo group, slightly more patients in the IFN-7 group experienced morning stiffness, simultaneous swelling of another joint, subcuta- neous rheumatic nodules, and positive p roof of rheuma- toid factors in serum. In the IFN-7 group there were more patients who met seven or eight A R A criteria and less patients who met only five A R A criteria, the minimum to be eligible for the study. The same tendency was seen in the Steinbrocker-stage: in the IFN-7 group more patients were classified as stages I I I and IV and less patients were classified as stages I and II compared with the placebo group. Finally, the IFN-7 group had a higher mean for the Ritchie index, a higher Lee index and, on average, more tender joints. While these observations represented a slight disadvantage for the IFN-7 group, three vari- ables, namely ESR, Lansbury index and pain on waking, indicated a slight disadvantage for the placebo group.
A comparable number of patients in the IFN-7 and in the placebo groups were on background N S A I D treat- ment (90% vs. 92%) on admission to the study. Four groups of N S A I D active substances were used predomi- nantly: diclofenac, indometacin, acemetacin, and piroxi- cam. The number of IFN-7 patients and placebo patients and their median daily dosages were comparable for each of these active substances (Table 5). Only 10% of the patients changed their N S A I D within 12 weeks. No pa- tient had slow acting drugs, such as gold, penicillamines, or cytostatics, for 4 weeks before, or during the study.
Of the 223 evaluable patients, 45 patients f rom the IFN- 7 group and 51 patients f rom the placebo group suffered f rom at least one underlying concomitant dis- ease. These were as follows: concomitant diseases of the heart and the cardiovascular system (IFN-7: 18/placebo: 28), the respiratory system (3/3), the gastrointestinal tract

180
80- t ' - Q) C~
60-
"~ 40-
E Z
n=107 n--116'--- , I
, I I
. . . . 1 1 . . . .
I . . . .
I
20-
o 0
Week Fig. 1. NSAIDs plus IFN-7 or placebo in RA; censoring of patients because of increased steroid dosage or incomplete treatment with IFN-~, (solid line) and placebo (interrupted line) during the 12-week study period
Table 7. NSAIDs plus IFN-7 or placebo in RA; number of respon- ders and non-responders in the IFN-y and the placebo group after 12 weeks of treatment. Z 2 =5.19, c~=0.011
Responder Non-responder Total
NSAID + IFN-y 53 54 107 NSAID + placebo 40 76 116
Total 93 130 223
Table 8. NSAIDs plus IFN-7 or placebo in RA; classification of responders after 12 weeks of treatment
"Responder" by use of Total
Ritchie Lansbury Ritchie as index index well as Lans- only only bury indices
NSAID + IFN-3, 7 10 36 53 NSAID + placebo 3 8 29 40
Total 10 18 65 93
(9/10), the kidney and urinary tract (4/5), the liver and gallbladder (3/6), the thyroid (7/6), the eyes, ears or nose (4/4), and other diseases ( lUl l ) .
Developments in the number of patients
Patients who received IFN-7 or placebo for less than the total period of the 12-week study, and patients requiring increased corticosteroid dosage were classified as non- responders, but were retained for evaluation. Details on these patients and the criteria for withdrawal are given in Table 6. It was clearly possible to maintain more patients on the combination of background therapy plus IFN-7 than on background therapy plus placebo for the 12 weeks. Overall, 81% of patients on IFN-7 and 56% pa- tients on placebo remained in the study for 12 weeks (Fig. 1).
Results with respect to the main criterion
Improvement in the Ritchie and/or Lansbury joint pain indices by at least 30% after 12 weeks was regarded as the main criterion. In the IFN-7 group, 49.5% of the patients responded to treatment while 34.5% of the patients in the placebo group responded to treatment (Table 7). This result was statistically significant (P=0.011) and, was clearly in favour of the IFN-7 group. Table 8 shows the distribution of responders for the two joint pain indices used. Sixty-eight percent of responders on IFN-,/ and 72.5% of responders on placebo showed a response ac- cording to both the Lansbury and the Ritchie indices. The vast majority of the responders experienced a very distinct response (Table 9). Table 10 shows the number of non-responders in the two study arms. Patients on IFN-7 benefited more in all categories. Fewer patients on IFN-y discontinued their treatment because of insufficient ef- fectiveness, and obviously, fewer patients in the IFN-7 group had to increase their daily steroid dosage. More non-responders in the IFN-7 group (34/107 = 32%) than in the placebo group (25/116 = 22%) were kept on thera- py for the whole duration of the study though not reach-
Table 9. NSAIDs plus IFN-y or placebo in RA; degrees of change of Ritchie and Lansbury indices after 12 weeks treatment in relation to study entry (in %) for all responders (53 IFN-~,, 40 placebo)
[%1
IFN-;:
Lansbury index
- _>70 - 6 0 - 6 9 - 5 0 - 5 9 - 4 0 - 4 9 - 3 0 - 3 9 -0-29-1- _> 1
Placebo
Lansbury index
- > 7 0 - 6 0 - 6 9 - 5 0 - 5 9 - 4 0 - 4 9 - 3 0 - 3 9 - 0 - 2 9 + >1
- >70 - 6 0 - 6 9
.~ - 5 0 - 59 - 4 0 - 4 9 --30-39
~ - - 0 29 ~ + 1 29
+ >30
12 5 2
1
1
3 1 2 1 2 3 2 1 4
2 3 2 t
9 3 1 3 1 1
1 1 1 3 3 2 2 1
2 1 1 1 1 1 1

3 0 ,
2 5 �84
I1)
2 0 �84 x_
o -
"5 to
. i 3
E r
"13
- o t 0 o Q
t r
1 5
2 0 �84
p 2 4 G 12
Week
Fig. 2. NSAIDs plus IFN-? or placebo in RA; cumulated number of patients with an increased or decreased dose of corticosteroids in the IFN-y group (dark columns) or placebo group (light columns); 51 patients in the IFN-7 group and 63 patients in the placebo group received corticosteroids during the course of the 12-week study
Table 10. NSAIDs plus IFN-7 or placebo in RA; classification of non-responders
Non-responder due to Total
Incom- Increased No improve- plete steroids ment in artic- treat- ular index ment after 12 weeks
NSAID + IFN-7 17 3 34 54 NSAID + placebo 23 28 25 76
Total 40 31 59 130
181
ing the 30% improvement demanded for classification as a responder.
Results of the secondary outcome variables
Due to evaluation according to the intention-to-treat principle, it is only possible to give censored medians instead of means for the quantitative parameters em- ployed in comparing the two groups. Excluding the non-responders due to treatment interruption or in- creased steroid dosage would produce biased means and medians.
Table 11 shows the censored medians for the 12 par- ameters determined. All 12 parameters showed a clear advantage for patients treated with IFN-7.
Over the course of the 12-week study period, 51 pa- tients in the IFN-7 group and 63 in the placebo group received corticosteroids. By the end of the study, corti- costeroid dosage had been reduced in 15 and increased in 3 patients on NSAIDs plus IFN-7; the mean dosage re- duction was 2.6 mg, the mean dosage increase was 7.9 mg prednisolone equivalent per patient per day. In contrast, corticosteroid dosage was increased in 28 and reduced in 9 patients on placebo. The mean dosage increase was 5.5 rag, the mean dosage reduction was 3.8 mg pred- nisolone equivalent per patient per day (Fig. 2).
Adverse events
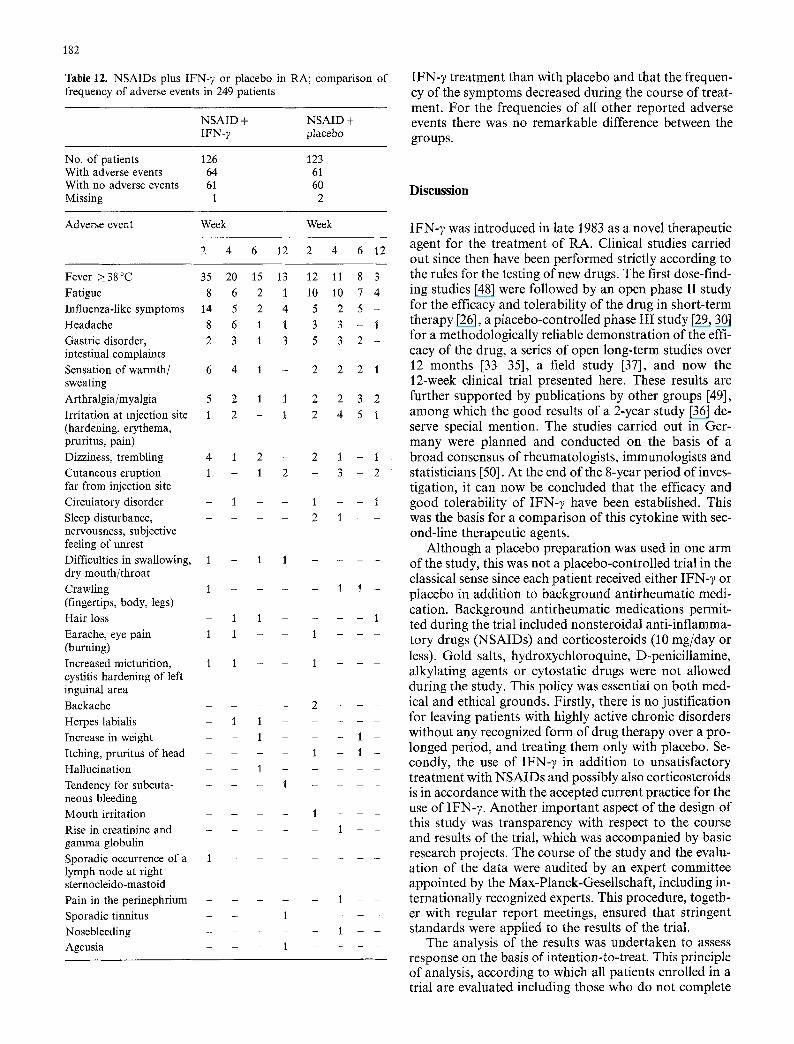
Out of a total of 249 randomized patients, 64 patients in the IFN- 7 group and 61 patients in the placebo group showed at least one adverse event at least once in the 12 weeks of treatment and 2 weeks of further observa- tion. The adverse event most often occurring was in- creased body temperature of or above 38 ~ centigrade. This, and influenza-like symptoms are already well- known side effects of IFN-7. Table 12 shows that fever and influenza-like symptoms occurred more often with
Table 11. NSAIDs plus IFN- 7 or placebo in RA; results of secondary outcome variables (censored medians). Therapeutic success in patients withdrawn from treatment (drop-outs) was censored according to "intention-to-treat" principle [47]. Censoring produces medians with a tendency towards a negative statement. From this reason the medians over 12 weeks were worse than the actual clinical course of the disease
Variable (censored medians) NSAID plus IFN- 7 Timepoint of evaluation (week)
NSAID plus placebo Timepoint of evaluation (week)
0 2 4 6 8 12 0 2 4 6 8 i2
Ritchie index (points) 45 37 35 35 33 37 42 35 42 42 44 56 Lansbury index (points) 58 55 58 58 58 58 68 53 60 60 67 87 Lee index (points) 11 11 11 11 13 14 10 10 9 13 14 17 Grip strength right (kPascal) 20 21 22 20 19 18 22 24 21 18 15 10 Grip strength left (kPascal) 20 19 23 20 20 19 21 21 20 19 16 10 Pain (visual analogue scale) (ram) 50 54 55 55 48 55 50 52 55 56 62 95 Number of tender joints 17 15 15 16 15 16 16 14 16 17 18 22 Morning stiffness (min) 90 60 45 60 60 60 90 60 75 75 110 180 ESR 1 h (mm) 36 40 44 45 48 50 44 46 52 62 68 85 Leukocytes ( x 1000/gl) 8.0 6.7 7.6 8.0 8.2 8.3 7.8 8.0 9.2 9.3 9.7 11.5 Thrombocytes (x 1000/gl) 340 340 350 380 410 420 360 390 425 425 465 530 Hemoglobin (g/dl) 12.3 12.4 12.0 12.0 12.0 11.7 12.3 12.2 11.7 11.4 11.0 10.0
182
Table 12. NSAIDs plus IFN-7 or placebo in RA; comparison of frequency of adverse events in 249 patients
NSAID + NSAID + IFN-7 placebo
No. of patients 126 With adverse events 64 With no adverse events 61 Missing 1
123 61 60
2
I F N - 7 t r ea tmen t than with p lacebo and tha t the f requen- cy o f the s y m p t o m s decreased dur ing the course o f t rea t - ment . F o r the frequencies o f all o ther r e p o r t e d adverse events there was no r e m a r k a b l e difference be tween the groups .
D i s c u s s i o n
Adverse event Week Week
2 4 6 12 2 4 6 12
Fever ~38~ 35 20 15 13 12 11 8 3 Fatigue 8 6 2 1 t0 10 7 4 Influenza-like symptoms 14 5 2 4 5 2 5 - Headache 8 6 1 1 3 3 - 1 Gastric disorder, 2 3 1 3 5 3 2 - intestinal complaints Sensation of warmth/ 6 4 1 - 2 2 2 1 sweating Arthralgia/myalgia 5 2 1 1 2 2 3 2 Irritation at injection site 1 2 - 1 2 4 5 1 (hardening, erythema, pruritus, pain) Dizziness, trembling 4 1 2 - 2 1 - 1 Cutaneous eruption 1 - 1 2 - 3 - 2
far from injection site Circulatory disorder - 1 - - 1 1 Sleep disturbance, - - - - 2 1 nervousness, subjective feeling of unrest Difficulties in swallowing, 1 - 1 1 - dry mouth/throat Crawling 1 . . . . 1 1 - (fingertips, body, legs) Hair loss - 1 1 - - 1 Earache, eye pain l 1 - - 1 (burning) Increased micturition, 1 1 - - 1 cystitis hardening of left inguinal area Backache . . . . 2 Herpes labialis - 1 1 - - Increase in weight - - 1 - - - 1 -
I t c h i n g , pruritus of head . . . . 1 - 1 - Hallucination - - 1 - - Tendency for subcuta . . . . 1 - neous bleeding Mouth irritation - - 1 Rise in creatinine and - - - 1 gamma globulin Sporadic occurrence of a 1 - - lymph node at right sternocleido-mastoid Pain in the perinephrium - - l
Sporadic tinnitus 1 - Nosebleeding - 1 Ageusia 1 -
I F N - y was i n t roduced in late ]983 as a novel the rapeu t i c agent for the t r ea tmen t o f R A . Cl inical s tudies car r ied ou t since then have been p e r f o r m e d str ict ly accord ing to the rules for the test ing o f new drugs. The first dose- f ind- ing studies [48] were fo l lowed by an open phase II s tudy for the efficacy and to le rab i l i ty o f the d rug in shor t - t e rm the r a py [26], a p l acebo -con t ro l l ed phase I I I s tudy [29, 30] for a m e t h o d o l o g i c a l l y re l iable d e m o n s t r a t i o n o f the effi- cacy o f the drug, a series o f open long - t e rm studies over 12 m o n t h s [33-351, a field s tudy [37], and now the 12-week cl inical t r ial p resen ted here. These results are fur ther s u p p o r t e d by pub l i ca t ions by o the r g roups [49], a m o n g which the g o o d results o f a 2 -year s tudy [36] de- serve special men t ion . The studies car r ied out in Ger - m a n y were p l a n n e d and conduc t ed on the basis o f a b r o a d consensus o f rheumato log i s t s , immuno log i s t s and s ta t i s t ic ians [50]. A t the end o f the 8-year pe r iod o f inves- t iga t ion , it can now be conc luded tha t the efficacy and g o o d to le rab i l i ty o f I F N - 7 have been es tabl ished. This was the basis for a c o m p a r i s o n o f this cy tok ine wi th sec- ond- l ine the rapeu t i c agents.
A l t h o u g h a p lacebo p r e p a r a t i o n was used in one a rm o f the s tudy, this was no t a p l acebo -con t ro l l ed tr ial in the classical sense since each pa t i en t received ei ther I F N - 7 or p l acebo in a d d i t i o n to b a c k g r o u n d an t i rheuma t i c medi- cat ion. B a c k g r o u n d an t i rheuma t i c med ica t ions pe rmi t - ted du r ing the tr ial inc luded nons t e ro ida l an t i - i n f l amma- to ry drugs ( N S A I D s ) and cor t i cos te ro ids (10 r ag /day or less). G o l d salts, h y d r o x y c h l o r o q u i n e , D-penic i l l amine , a lky la t ing agents or cy tos ta t ic d rugs were no t a l lowed dur ing the s tudy. This po l icy was essent ia l on bo th med- ical and ethical g rounds . Fi rs t ly , there is no jus t i f ica t ion for leaving pa t ien t s wi th h ighly act ive chronic d i sorders w i thou t any recognized fo rm o f d rug t h e r a p y over a p ro - longed per iod , and t rea t ing them only with p lacebo . Se- condly , the use o f I F N - 7 in a d d i t i o n to unsa t i s f ac to ry t r e a t m e n t wi th N S A I D s and poss ib ly also cor t i cos te ro ids is in acco rdance wi th the accepted cur ren t prac t ice for the use o f IFN-7 . A n o t h e r i m p o r t a n t aspec t o f the design o f this s tudy was t r a n spa re nc y wi th respect to the course and resul ts o f the trial , which was a c c o m p a n i e d by basic research projects . The course o f the s tudy and the evalu- a t ion o f the d a t a were aud i t ed by an exper t commi t t ee a p p o i n t e d by the Max-P lanck -Gese l l s cha f t , inc luding in- t e rna t iona l ly recognized experts . This p rocedure , toge th- er wi th regu la r r e p o r t meet ings, ensured tha t s t r ingent s t anda rds were app l i ed to the results o f the trial .
The analysis o f the results was u n d e r t a k e n to assess response on the basis o f in ten t ion- to - t rea t . This pr inc ip le o f analysis , accord ing to which all pa t ien ts enro l led in a tr ial are eva lua ted inc luding those who do no t comple t e

the study, has become standard practice especially in on- cological studies. This estabIished principle has only very hesitantly been accepted for clinical research in rheuma- tology, particularly in Germany. In the field of rheuma- tology, use of this principle demands that patients whose treatment has to be stopped due to intolerable side effects must be included in the results, as well as patients deviat- ing from the protocol for therapeutic reasons (e.g., the use of corticosteroids forbidden by the study protocol). In the past, these patients were often declared as drop- outs and the therapeutic success reported by those studies was biased and overestimated due to the exclusion from analysis of patients with poor success. Today, only pa- tients admitted to the study in gross violation of entry criteria and those not evaluable for technical reasons are permitted to be classified as drop-outs and excluded from analysis of the results. In placebo-controlled studies, the decision as to whether a patient is evaluable or not must, of course, be taken in a double-blind manner.
For binary outcome variables, e.g., responder/non-re- sponder, the evaluation procedure based on intention-to- treat presents no problems. Patients withdrawn due to inefficacy or adverse events, and those requiring increases in steroid dosage because of poor therapeutic efficacy, are assigned to the non-responder group and included in the analysis.
This does not pertain to changes in quantitative out- come variables. In patients withdrawn, e.g., after an in- crease in corticosteroids, numerical quantitative results are unavailable or not valid. Methodological approaches for the evaluation of studies with a high drop-out rate have only recently become available [47]. According to this statistical method therapeutic success in patients withdrawn from treatment or requiring increased steroid dosage for descriptive statistical evaluation of quantita- tive outcome variables is censored. Censoring means that therapeutic success in these patients is assumed to be lower than the median therapeutic success in the entire group. The median of the outcome variable can be calcu- lated without any problems if fewer than half the case require censoring. This procedure is the same as that ap- plied to survival times, in which the median survival time can be calculated as soon as half the subjects have died, so that less than half the cases need to be censored.
Censoring, as used in the evaluation of the present study (20 withdrawals in the IFN- 7 group, 51 in the place- bo group), produces medians with a tendency towards a negative statement on a particular parameter as the num- ber of censored patients rises. In contrast to studies in the past with their overestimated therapeutic success rates, the censored median is methodologically stringent and describes in an unbiased manner the therapeutic success achieved for all patients entered in the study. Due to the biased results in the past the results presented in this study are not comparable to results obtained from studies not based upon the intention-to-treat principle. Since the intention-to-treat principle is currently an obligatory re- quirement, e.g., of the American FDA, the results of a large number of earlier clinical studies on the effects of second-line therapeutic agents in RA urgently require reevaluation.
183
The rigid therapeutic guidelines for protocols used in clinical trials place restrictions upon the clinician in- volved. This has less impact for drugs where the dose-re- sponse relationship follows a maximum curve, i.e., where the maximum dose tolerated gives an indication as to the therapeutic dose. On the other hand, immunomodulatory substances such as IFN-7 follow a patient-specific opti- mum curve. In addition, dosage should be reduced in the course of treatment to maintain efficacy [5, 6, 35, 51]. The pre-set dosage regimen of a clinical trial does not permit adequate flexibility for dose adjustments in response to the specific dysregulation of the immune system of indi- vidual patients. These facts must be kept in mind when evaluating our results.
The study discussed here produced four principal re- sults:
1. The response rate to treatment with IFN-y plus NSAIDs was better than that to NSAID treatment alone; the difference was statistically significant. 2. IFN-y permitted reduction in steroid dosage. 3. All parameters of the disease investigated were much better controlled with IFN-y plus NSAIDs than with NSAIDs alone. 4. With the exception of a slight rise in temperature and transient influenza-like symptoms, adverse events with and without IFN-y were equally distributed, implying that IFN-y did not have many side effects.
The therapeutic value of this drug lies in the fact that patients treated with IFN-7 may be maintained at an activity level of the disease where less aggressive therapy is required. On the whole, most patients benefited consid- erably from the treatment though not every single param- eter showed a dramatic improvement. This conclusion also defines the point in time at which interferon ought to enter the patient's treatment plan, namely following pure NSAID therapy and before the introduction of second- line therapeutic agents.
The results of this study require comparison with an- other recently published American placebo-controlled study of IFN-y in RA [52]. The design of the two study protocols was similar. Differences related to two points. In the American study, permitted antirheumatic back- ground treatment included not only NSAIDs and stable corticosteroid doses (10 mg/day or less) but also a stable regimen with hydroxychloroquine, gold salts or D-peni- cillamine. The dosage in the American study was 100 gg IFN-y, 5 days per week for 12 weeks, i.e., the individual doses were higher, and dosage was not progressively scaled down. The results of both studies were compara- ble. The secondary outcome variables showed significant improvement after IFN-y, with the exception of grip strength; with placebo, no significant changes were ob- served after 12 weeks. As expected, in view of the high dosage, side effects were more pronounced in the Ameri- can study but qualitatively were the same as in this German study. There was one important difference be- tween the two studies. Both studies showed a statistically significant improvement in joint indices after 8 weeks, but after 12 weeks this statistically significant improvement was no longer present in the American study. From these

184
observa t ions , we conc luded tha t successful t r ea tmen t can be m a i n t a i n e d by reduc ing the I F N - 7 dosage accord ing to the pa t ien t ' s i nd iv idua l requirements . In the further course of the Amer i can study, dosage was ind iv idua l ly adjus ted . Subsequent ly , the rapeu t i c success was ma in - t a ined for 2 years [36]. Thus, it can be conc luded tha t bo th the s tudy descr ibed here and the Amer i can s tudy of simi- lar design conf i rmed the results of our first con t ro l l ed s tudy [29, 30] as well as those of i n t e rna t iona l s tudies wi thou t p l acebo con t ro l [26, 28].
References
1. Lemmel EM, Bach GL, Bolten W, Brackertz D, Fahmy Z, Mattern H, Stroehmann I, Wittenborg A (1988) Immunmodu- lierende Therapie der chronischen Polyarthritis mit Thymo- pentin. Eine multizentrische placebokontrollierte Studie an 119 Patienten. Dtsch Med Wochenschr 113:172-176
2. Dinarello CA, Mier JW (1987) Lymphokines. N Engl J Med 317:940-945
3. Gastl G, Huber C (1988) The biology of interferon actions. Blut 56:193-199
4. t-Ieremans H, Billiau A (1989) The potential role of interferons and interferon antagonists in inflammatory disease. Drugs 38:957-972
5. Brzoska J, Obert HJ (1990) Immunomodulating effects of inter- ferons: conclusions for therapy. In: Gross G, Jablonska S, Pfister H, Stegner HE (eds) Genital papillomavirus infections: modern diagnosis and treatment. Springer, Berlin Heidelberg New York, pp 379-391
6. Brzoska J, Obert HJ (1987) Interferon gamma: ein janus- k6pfiger Mediator bet Entziindungen. Arzneimittelforschung/ Drug Res 37:1410-1416
7. Dinarello CA (1988) Biology ofinterleukin-l. FASEB J 2:108 115
8. Miller LC, Dinarello CA (1987) Biologic activities of inter- leukin-1 relevant to rheumatic diseases. Pathol Immunopathol Res 6:22 36
9. Miyasaka N, Sato K, Goto M, Sasano M, Natsuyama M, Inoue K, Nishioka K (1988) Augmented interleukin-i produc- tion and HLA-DR expression in the synovium of rheumatoid arthritis patients. Possible involvement in joint destruction. Arthritis Rheum 31:480-486
10. Koch B, Baum W, Burmester GR, Rohwer P, Reinke M, Zacher J, Kirchner H, Kalden JR (1989) Prostaglandin-E2-, Inter- leukin-1- und Interferon-Gamma-Produktion mononukle/irer Zellen von Patienten mit entzfindlichen und degenerativen Gelenkerkrankungen. Z Rheumatol 48: 194-199
11. Smith JB, Bocchieri MH, Sherbin-Allen L, Borofsky M, Abruz- zo JL (1989) Occurrence of interleukin-I in human synovial fluid: detection by RIA, bioassay and presence of bioassay-in- hibiting factors. Rheumatol Int 9:53-58
12. Bendtzen K, Petersen J, Halkjrer-Kristensen J, Ingemann- Hansen T (1985) Interleukin-1 like activities in synovial fluids of patients with rheumatoid arthritis and traumatic synovitis. Rheumatol Int 5:79-82
13. Hermann E, Vogt P, Hagmann W, Dunky A, Mfiller W (1988) Synoviaspiegel yon Interleukin-I und C3a bet chronischer Polyarthritis, Psoriasisarthritis und aktivierter Arthrose. Z Rheumatol Int 47:20-25
14. Danis VA, Kulesz A J, Nelson DS, Brooks PM (1990) Cytokine regulation of human monocyte interleukin-1 (IL-1) production in vitro. Enhancement of IL-1 production by interferon (IFN) gamma, tumour necrosis factor-alpha, IL-2 und IL-1, and inhi- bition by IFN-alpha. Clin Exp Immunol 80:435-443
15. Johnson WJ, Breton J, Newman-Tarr T, Connor JR, Meunier PC, Dalton BJ (1990) Interleukin-1 release by rat synovial cells
is dependent on sequential treatment with 7-interferon and lipo- polysaccharide. Arthritis Rheum 33:261-267
16. Harth M, McCain GA, Cousin K (1990) The modulation of interleukin-1 production by interferon gamma, and the in- hibitory effects of gold compounds. Immunopharmacology 20:125-134
17. Brandwein SR (1986) Regulation of interleukin-1 production by mouse peritoneal macrophages. J Biol Chem 261:8624-8632
18. Rowe FM, Edwards J, Cozens PJ (1987) Increased interleukin-1 levels from monocytes of rheumatoid arthritis patients during the early stages of the disease are down regulated in vitro by the addition of interferon-gamma. J Leukocyte Biol 42:600-601
19. Ruschen S, Lemm G, Warnatz H (1989) Spontaneous and LPS-stimutated production of intracellular IL-lfl by synoviai macrophages in rheumatoid arthritis is inhibited by IFN% Clin Exp Immunol 76:246-251
20. Ghezzi P, Dinarello CA (1988) IL-I induces IL-I. III. Specific inhibition of IL-I production by IFN-y. J Immunol 140:4238- 4244
21. Firestein GS, Zvaifler NJ (1987) Peripheral blood and synovial fluid monocyte activation in inflammatory arthritis. II. Low levels of synovial fluid and synovial tissue interferon suggest that 7-interferon is not the primary macrophage activating fac- tor. Arthritis Rheum 30:864-871
22. Ridley M, Panayi G (1988) Comment on the articles by Fire- stein and Zvaifler. Arthritis Rheum 31:1209
23. Buchan G, Barrett K, Fujita T, Taniguchi T, Maini R, Feld- mann M (1988) Detection of activated T cell products in the rheumatoid joint using cDNA probes to Interleukin-2 (IL-2) IL-2 receptor and IFN-~. Clin Exp Immunol 71:395-401
24. Hopkins SJ, Meager A (1988) Cytokines in synovial fluid: II. The presence of tumour necrosis factor and interferon. Clin Exp Immunol 73:88-92
25. Firestein GS, Alvaro-Garcia JM, Maki R (1990) Quantitative analysis of cytokine gene expression in rheumatoid arthritis. J Immunol 144:3347-3353
26. LemmeI EM, Franke M, Gaus W, Hartl PW, Hofschneider PH, Miehlke K, Machalke K, Obert HJ (1987) Results of a phase-II clinical trial on treatment of rheumatoid arthritis with recombi- nant interferon-gamma. Rheumatol Int 7:127-132
27. Zilly A, Obert HJ (1986) Therapie der chronischen Polyarthri- tis. Ergebnisse einer Pilot-Studie mit Lymphokinen. MMW 128:87-89
28. Wolfe F, Cathey MA, Hawley D J, Balser JP, Schindler JD (1986) Clinical trial with r-IFN-gamma in rheumatoid arthritis. In: Pincus SH, Pisetsky DS, Rosenwasser LJ (eds) Biologically based immunomodulators in the therapy of rheumatic diseases. Elsevier, New York, pp 379-395
29. Lemmel EM, Brackertz D, Franke M, Gaus W, Hartl PW, Machalke K, Mielke H, Obert H J, Peter HH, Sieper J, Sprekeler R, Stierle H (1988) Results of a multicenter placebocontrolled double-blind randomized phase III clinical study of treatment of rheumatoid arthritis with recombinant interferon-gamma. Rheumatol Int 8:87-93
30. Lemmel EM, Obert HJ, t-Iofschneider PH (1988) Low-dose gamma interferon treatment of rheumatoid arthritis. Lancet I: 598
31. Cannon GW, Schindler JD, Emkey RD, Denes A, Cohen SA, Wolfe F, Saway A, Jaffer AM, Weaver AL, Cogen L (1987) Double-blind trial of recombinant interferon-gamma versus placebo in rheumatoid arthritis. Arthritis Rheum [Suppl] 30:18
32. Veys EM, Mielants H, Verbruggen G, Grosclaude JP, Luyten F, Meier W, Fiers W, Galazka AR (1987) Recombinant interferon gamma in rheumatoid arthritis. A double-blind study compar- ing Immuneron (recombinant interferon gamma) with placebo. Clin Exp Rheumatol 5 [Suppl 21:53
33. Obert H J, Brzoska JF (1989) Interferon gamma in der Therapie der chronischen Polyarthritis. Die Langzeitbehandlung in der Praxis. Arzneimittelforschung/Drug Res 39:819-822
34. Klein HO (1988) Therapie der rheumatoiden Arthritis mit re- kombinantem Interferon-gamma. Klinischer Verlauf und La-

borparameter w/ihrend einjfihriger Behandlung. Fortschr Med 106:721-725
35. Sprekeler R, Lemmel EM, Obert HJ (1990) Correlation of clinical and serological findings in patients with rheumatoid arthritis treated for one year with interferon-gamma. Z Rheumatol 49:1 - 7
36. Cannon GW, Emkey RD, Denes A, Cohen SA, Saway PA, Wolfe F, Jaffer AM, Weaver AL, Cogen L, GuIinello J, Kennedy SM, Schindler JD (1990) Prospective two-year followup of re- combinant interferon-7 in rheumatoid arthritis. J Rheumato117 [Suppl 3]: 304-310
37. Obert HJ, Brzoska JF (1989) Behandlung der chronischen Poly- arthritis mit Interferon-gamma. Ergebnisse einer Therapie- studie der Phase II bei 476 Patienten. Rheuma 9:286-292
38. Taya Y, Devos R, Tavernier J, Cheroutre H, Engler G, Fiers W (1982) Cloning and structure of the human immune interferon- gamma chromosomal gene. EMBO J 1:953
39. Simons G, Remaut E, Allet B, Devos R, Fiers W (1984) High- level expression of human interferon gamma in Escherichia coli under control of the PL promotor of bacteriophage lambda. Gene 28:55
40. Gray PW, Goeddel DV (1982) Structure of the human immune interferon gene. Nature 298:859-863
41. Ropes M, Bennett GA, Cobb S, Jacox R, Jessar R (1958) 1958 revision of diagnostic criteria for rheumatoid arthritis. Bull Rheum Dis 9:175-176
42. Arnett FC, Edworthy SM, Bloch DA, McShane DJ, Fries JF, Cooper NS, Healey LA, Kaplan SR, Liang MH, Luthra HS, Medsger TA, Mitchell DM, Neustadt DH (1988) The American Rheumatism Association 1987 revised criteria for the classifica- tion of rheumatoid arthritis. Arthritis Rheum 31:315-323
43. Ritchie DM, Boyle JA, McInnes JM, Jasani MK, Dalakos TG, Grieveson P, Buchanan WW (1968) Clinical studies with an
185
articular index for the assessment of joint tenderness in patients with rheumatoid arthritis. Q J Med 37:393-406
44. Lansbury J (1958) Report of a three-year study on the systemic and articular indexes in rheumatoid arthritis. Theoretic and clinical considerations. Arthritis Rheum 1: 505- 522
45. Lansbury J (1967) Methods for evaluating rheumatoid arthritis. In: Hollander JL (ed) Arthritis and allied conditions. Lea and Febiger, Philadelphia, pp 269 291
46. Lee P, Jasani MK, Dick WC, Buchanan WW (1973) Evaluation of a functional index in rheumatoid arthritis. Scand J Rheuma- tol 2:71-77
47. Gaus W (1991) Contributions to robust estimation: trimmed variance and censored median. Presentation at the joint biomet- ric conference of the German and British region, Hamburg, March 19-22, 1991
48. Obert HJ, Hofschneider PH (1985) Interferon bei chronischer Polyarthritis. Positive Wirkung in der klinischen Priifung. Dtsch Med Wochenschr 110:1766 1769
49. Machold KP, Graninger W, Flener R, Smolen JS (1988) Recombinant human gamma-interferon in the treatment of rheumatoid arthritis - a double-blind placebo-controlled cross- over study. Clin Res 36: 534A
50. B6ni A, Hofsehneider PH, Obert HJ (1986) Chronische Poly- arthritis. Erste Ergebnisse mit Interferon-gamma. DIA-GM 7:34-40
51. Obert HJ, Brzoska J (1986) Interferon-gamma in der Therapie der chronischen Polyarthritis. Arzneimittelforschung/Drug Res 36:1557-1560
52. Cannon GW, Pincus SH, Emkey RD, Denes A, Cohen SA, Wolfe F, Saway PA, Jaffer AM, Weaver AL, Cogen L, Schindler JD (1989) Double-blind trial of recombinant y-interferon versus placebo in the treatment of rheumatoid arthritis. Arthritis Rheum 32:964-973




















