
Methotrexate therapy for rheumatoid arthritis: clinical practice guidelines based on published...
8
Original article Methotrexate therapy for rheumatoid arthritis: clinical practice guidelines based on published evidence and expert opinion ☆ Stephan Pavy a , Arnaud Constantin b , Thao Pham c , Laure Gossec d , Jean-Francis Maillefert e , Alain Cantagrel b , Bernard Combe f , René-Marc Flipo g , Philippe Goupille h , Xavier Le Loët i , Xavier Mariette j , Xavier Puéchal k , Thierry Schaeverbeke l , Jean Sibilia m , Jacques Tebib n , Daniel Wendling o , Maxime Dougados d, * a Service de rhumatologie A, CHU Cochin, 27, rue du Faubourg-Saint-Jacques, 75014 Paris, France b Service de rhumatologie, CHU Rangueil, Toulouse, France c Service de rhumatologie, CHU de la Conception, Marseille, France d Service de rhumatologie B, CHU Cochin, 27, rue du Faubourg, Saint-Jacques, 75014 Paris, France e Service de rhumatologie, CHU de Dijon, Dijon, France f Service d’immunorhumatologie, CHU Lapeyronie, Montpellier, France g Service de rhumatologie, CHRU Roger-Salengro, Lille, France h Service de rhumatologie, CHU de Trousseau, Tours, France i Service de rhumatologie, CHU de Bois-Guillaume, Rouen, France j Service de rhumatologie, CHU de Bicêtre, Le Kremlin Bicêtre, France k Service de rhumatologie, centre hospitalier, Le Mans, France l Service de rhumatologie, CHU Pellegrin–Tripode, Bordeaux, France m Service de rhumatologie, CHU Hautepierre, Strasbourg, France n Service de rhumatologie, CHU Lyon-Sud, Pierre-Bénite, France o Service de rhumatologie, CHU Jean-Minjoz, Besançon, France Received 5 January 2006; accepted 25 January 2006 Available online 23 March 2006 Abstract Objectives: To develop clinical practice guidelines for the use of methotrexate in rheumatoid arthritis (RA), using the evidence-based ap- proach and expert opinion. Methods: A scientific committee used a Delphi procedure to select five questions, which formed the basis for developing recommendations. Evidence providing answers to the five questions was sought in the Cochrane databases, PubMed, and proceedings of meetings of the French Society for Rheumatology, European League Against Rheumatism, and American College of Rheumatology. Using this evidence, a group of rheumatologists developed and validated the recommendations. For each recommendation, the level of evidence and the extent of agreement among experts were specified. Results: The recommendations were as follows: 1: The starting dosage for methotrexate in patients with RA should not be less than 10 mg/ week and should be determined based on disease severity and patient-related factors; 2: When a patient with RA shows an inadequate response to methotrexate, the dosage should be increased at intervals of 6 weeks, up to 20 mg/week, according to tolerance and patient-related factors; 3: When starting methotrexate treatment in a patient with RA, preference should be given to the oral route. A switch to the intramuscular or subcutaneous route should be considered in patients with poor compliance, inadequate effectiveness, or gastrointestinal side effects; 4: At present, there is no evidence indicating that a change in methotrexate dosage is in order when a TNF antagonist is given concomitantly; 5: The investiga- tions that are mandatory before starting methotrexate therapy in a patient with RA consist of a full blood cell count, serum transaminase levels, serum creatinine with computation of creatinine clearance, and a chest radiograph. In addition, serological tests for the hepatitis viruses B and C http://france.elsevier.com/direct/BONSOI/ Joint Bone Spine 73 (2006) 388–395 ☆ This project was supported by a grant from Abbott France. * Corresponding author. E-mail address: [email protected] (M. Dougados). 1297-319X/$ - see front matter © 2006 Elsevier SAS. All rights reserved. doi:10.1016/j.jbspin.2006.01.007
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Methotrexate therapy for rheumatoid arthritis: clinical practice guidelines based on published...

http://france.elsevier.com/direct/BONSOI/
Joint Bone Spine 73 (2006) 388–395
Original article
☆ This project was supp* Corresponding author.E-mail address: maxim
1297-319X/$ - see front mdoi:10.1016/j.jbspin.2006.
Methotrexate therapy for rheumatoid arthritis:
clinical practice guidelines based on published evidence and expert opinion ☆Stephan Pavy a, Arnaud Constantin b, Thao Pham c, Laure Gossec d, Jean-Francis Maillefert e,Alain Cantagrel b, Bernard Combe f, René-Marc Flipo g, Philippe Goupille h, Xavier Le Loët i,Xavier Mariette j, Xavier Puéchal k, Thierry Schaeverbeke l, Jean Sibilia m, Jacques Tebib n,
Daniel Wendling o, Maxime Dougados d,*
a Service de rhumatologie A, CHU Cochin, 27, rue du Faubourg-Saint-Jacques, 75014 Paris, Franceb Service de rhumatologie, CHU Rangueil, Toulouse, France
c Service de rhumatologie, CHU de la Conception, Marseille, Franced Service de rhumatologie B, CHU Cochin, 27, rue du Faubourg, Saint-Jacques, 75014 Paris, France
e Service de rhumatologie, CHU de Dijon, Dijon, Francef Service d’immunorhumatologie, CHU Lapeyronie, Montpellier, France
g Service de rhumatologie, CHRU Roger-Salengro, Lille, Franceh Service de rhumatologie, CHU de Trousseau, Tours, France
i Service de rhumatologie, CHU de Bois-Guillaume, Rouen, Francej Service de rhumatologie, CHU de Bicêtre, Le Kremlin Bicêtre, France
k Service de rhumatologie, centre hospitalier, Le Mans, Francel Service de rhumatologie, CHU Pellegrin–Tripode, Bordeaux, France
m Service de rhumatologie, CHU Hautepierre, Strasbourg, Francen Service de rhumatologie, CHU Lyon-Sud, Pierre-Bénite, Franceo Service de rhumatologie, CHU Jean-Minjoz, Besançon, France
Received 5 January 2006; accepted 25 January 2006Available online 23 March 2006
Abstract
Objectives: To develop clinical practice guidelines for the use of methotrexate in rheumatoid arthritis (RA), using the evidence-based ap-proach and expert opinion.
Methods: A scientific committee used a Delphi procedure to select five questions, which formed the basis for developing recommendations.Evidence providing answers to the five questions was sought in the Cochrane databases, PubMed, and proceedings of meetings of the FrenchSociety for Rheumatology, European League Against Rheumatism, and American College of Rheumatology. Using this evidence, a group ofrheumatologists developed and validated the recommendations. For each recommendation, the level of evidence and the extent of agreementamong experts were specified.
Results: The recommendations were as follows: 1: The starting dosage for methotrexate in patients with RA should not be less than 10 mg/week and should be determined based on disease severity and patient-related factors; 2: When a patient with RA shows an inadequate response tomethotrexate, the dosage should be increased at intervals of 6 weeks, up to 20 mg/week, according to tolerance and patient-related factors; 3:When starting methotrexate treatment in a patient with RA, preference should be given to the oral route. A switch to the intramuscular orsubcutaneous route should be considered in patients with poor compliance, inadequate effectiveness, or gastrointestinal side effects; 4: At present,there is no evidence indicating that a change in methotrexate dosage is in order when a TNF antagonist is given concomitantly; 5: The investiga-tions that are mandatory before starting methotrexate therapy in a patient with RA consist of a full blood cell count, serum transaminase levels,serum creatinine with computation of creatinine clearance, and a chest radiograph. In addition, serological tests for the hepatitis viruses B and C
orted by a grant from Abbott France.
[email protected] (M. Dougados).
atter © 2006 Elsevier SAS. All rights reserved.01.007

S. Pavy et al. / Joint Bone Spine 73 (2006) 388–395 389
and a serum albumin assay are recommended. In patients with a history of respiratory disease or current respiratory symptoms, lung function testswith determination of the diffusing capacity for carbon monoxide are recommended; 6: Investigations that are mandatory for monitoring metho-trexate therapy in patients with RA consist of full blood cell counts and serum transaminase and creatinine assays. These tests should be obtainedat least once a month for the first 3 months then every 4–12 weeks; 7: Folate supplementation can be given routinely to patients treated withmethotrexate for RA. In practice, a minimal dosage of 5 mg of folic acid once a week, at a distance from the methotrexate dose, is appropriate; 8:In the event of respiratory symptoms possibly related to methotrexate toxicity, the drug must be stopped and symptom severity evaluated. Shouldevidence of serious disease be found, the patient should be admitted immediately or advice from a pulmonologist should be obtained immedi-ately.
Conclusion: Recommendations about methotrexate therapy for RA were developed. These recommendations should help to improve practiceuniformity and, ultimately, to improve the management of RA.© 2006 Elsevier SAS. All rights reserved.
Keywords: Rheumatoid arthritis; Methotrexate; Recommendations
1. Introduction
Methotrexate is used by most rheumatologists as the first-line disease-modifying antirheumatic drug for patients withrheumatoid arthritis (RA). This choice rests on the good effec-tiveness and safety profile of the drug, its low cost, and theavailability of long-term follow-up data on RA patients givenmethotrexate [1,2]. In addition, recent data indicate that meth-otrexate can produce substantial survival benefits by reducingcardiovascular mortality in patients with RA [3].
However, 20 years after the first randomized controlledtrials (RCTs) demonstrated that methotrexate as monotherapywas effective in decreasing disease activity in RA [4,5],15 years after the first RCTs established its ability to slowthe progression of structural joint damage [6,7], and nearly10 years after the first RCTs of the efficacy and safety of meth-otrexate combined with other conventional disease-modifyingantirheumatic drugs [8,9] or biotherapies [10–12], considerablevariability continues to exist in the modalities of methotrexateuse in RA, most notably regarding starting and maximal do-sages, dosage adjustment, criteria used to monitor patients indaily practice, and the use of folate supplementation.
The objective of this work was to develop clinical practiceguidelines for the use of methotrexate in patients with RA,using evidence from the international literature and expert opi-nion, with the goal of optimizing everyday clinical practice[13].
2. Methods
The procedure for developing the recommendations in-volved several steps, as detailed in the article by Pham et al.[14,15].
2.1. Selection of topics by the scientific committee members
The scientific committee selected three topics: cardiovascu-lar risk and RA [15], use of methotrexate in RA, and nonphar-macological management of patients with recent-onset RA[16]. The use of methotrexate in RA is discussed in this article.
2.2. Selection of questions
Five questions were selected using a Delphi prioritizationprocedure:
1. What dosages and routes of administration should be used:more specifically, what is the optimal starting dose, howand when should the dosage be adjusted, what is the max-imal dosage, and which routes of administration should beused and when?
2. Does the methotrexate dosage deserve special considerationin patients who are also receiving TNFα antagonist therapy?
3. What investigations (including pulmonary investigations)should be performed before starting, and during, low-dosemethotrexate treatment in patients with RA?
4. Should folate supplementation be given routinely (product,dosage, frequency, expected benefit).
5. What is the optimal management strategy when respiratorysymptoms develop in an RA patient taking methotrexate?
2.3. Literature review
We searched the Cochrane databases, PubMed, and the da-tabases of the meetings of the French Society for Rheumatol-ogy (2003 and 2004), European League Against Rheumatism(2003, 2004, and 2005), and American College of Rheumatol-ogy (2003 and 2004). Articles published in French or in Eng-lish before June 2005 were considered. The keywords rheuma-toid arthritis and methotrexate were used in combination withother keywords: dosage, intramuscular, subcutaneous, andparenteral for question 1; adalimumab, etanercept, and inflix-imab for question 2; monitoring, hepatitis B virus, hepatitis Cvirus, hematologic diseases, renal function, respiratory tractdiseases, and pneumonitis for questions 3 and 5; and folic acidand folinic acid for question 4.
Of the 1859 publications retrieved by the literature search,764 were selected based on the titles, and of those 285 basedon the abstracts. The full texts of relevant publications werereviewed. The level of evidence in each publication was deter-mined as recommended by Shekelle et al. [17].
S. Pavy et al. / Joint Bone Spine 73 (2006) 388–395390
The procedure used to select the experts, to present the lit-erature review results to them and to develop and evaluate therecommendations are detailed in the article by Pham et al. [15].
3. Results and discussion
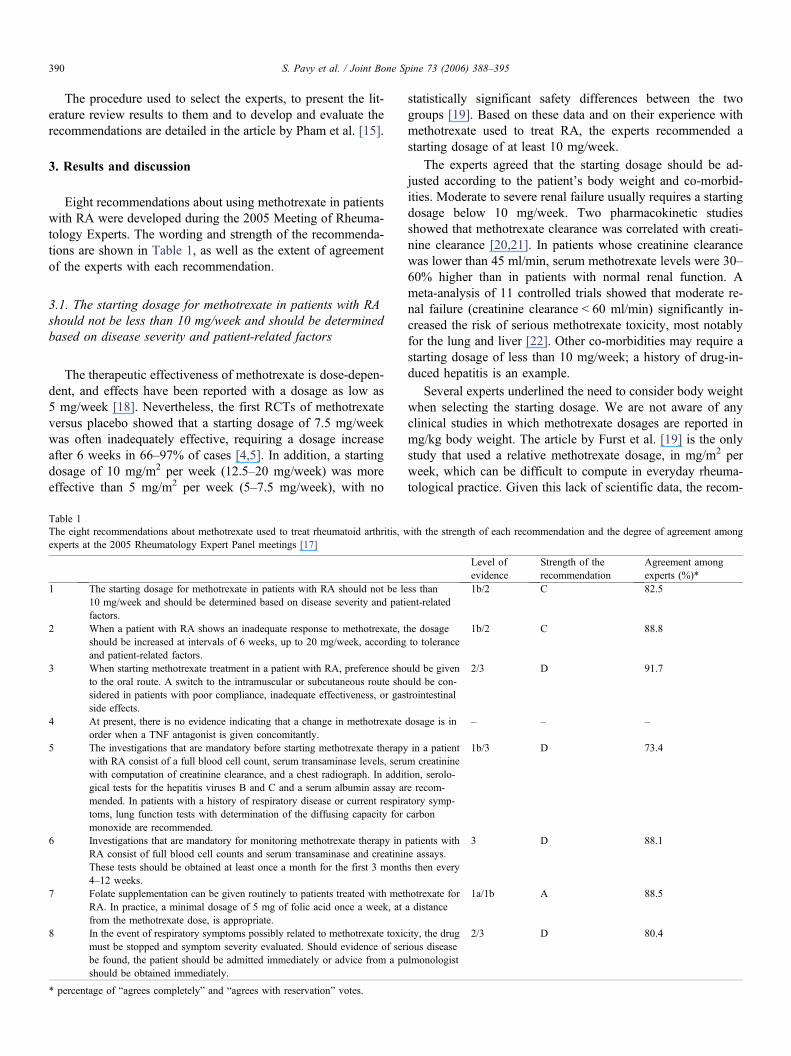
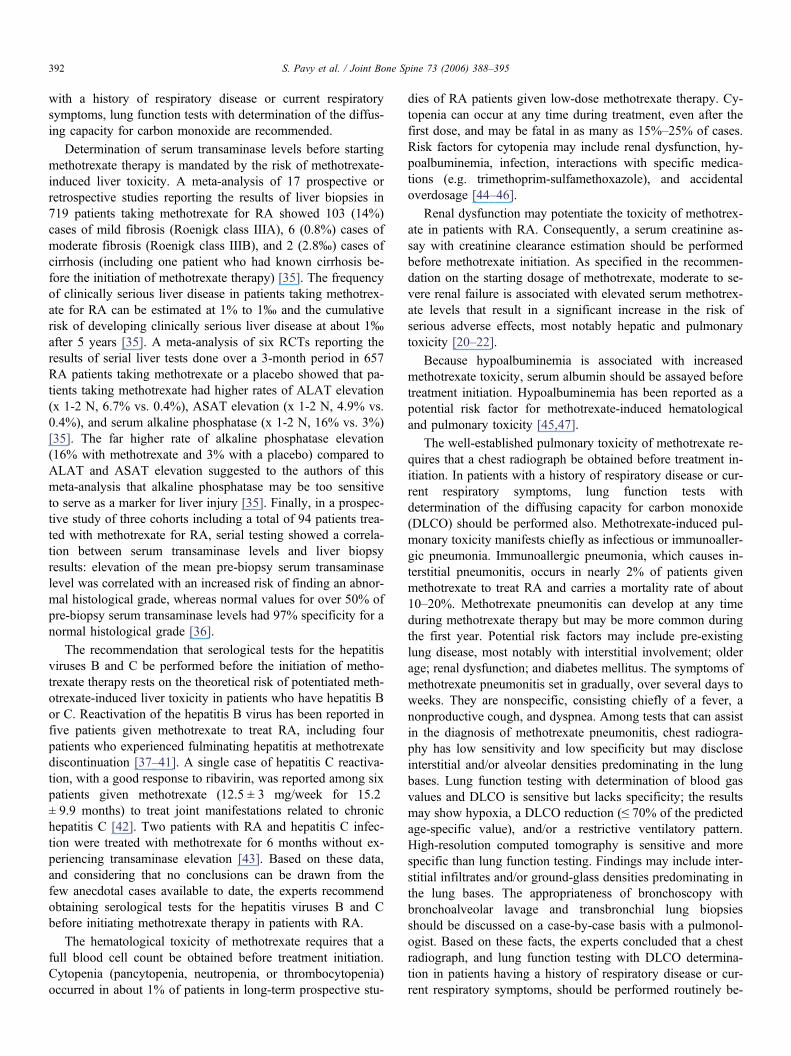
Eight recommendations about using methotrexate in patientswith RA were developed during the 2005 Meeting of Rheuma-tology Experts. The wording and strength of the recommenda-tions are shown in Table 1, as well as the extent of agreementof the experts with each recommendation.
3.1. The starting dosage for methotrexate in patients with RAshould not be less than 10 mg/week and should be determinedbased on disease severity and patient-related factors
The therapeutic effectiveness of methotrexate is dose-depen-dent, and effects have been reported with a dosage as low as5 mg/week [18]. Nevertheless, the first RCTs of methotrexateversus placebo showed that a starting dosage of 7.5 mg/weekwas often inadequately effective, requiring a dosage increaseafter 6 weeks in 66–97% of cases [4,5]. In addition, a startingdosage of 10 mg/m2 per week (12.5–20 mg/week) was moreeffective than 5 mg/m2 per week (5–7.5 mg/week), with no
Table 1The eight recommendations about methotrexate used to treat rheumatoid arthritis, wexperts at the 2005 Rheumatology Expert Panel meetings [17]
1 The starting dosage for methotrexate in patients with RA should not be le10 mg/week and should be determined based on disease severity and patifactors.
2 When a patient with RA shows an inadequate response to methotrexate, tshould be increased at intervals of 6 weeks, up to 20 mg/week, accordingand patient-related factors.
3 When starting methotrexate treatment in a patient with RA, preference shoto the oral route. A switch to the intramuscular or subcutaneous route shosidered in patients with poor compliance, inadequate effectiveness, or gasside effects.
4 At present, there is no evidence indicating that a change in methotrexateorder when a TNF antagonist is given concomitantly.
5 The investigations that are mandatory before starting methotrexate therapywith RA consist of a full blood cell count, serum transaminase levels, seruwith computation of creatinine clearance, and a chest radiograph. In additgical tests for the hepatitis viruses B and C and a serum albumin assay armended. In patients with a history of respiratory disease or current respiratoms, lung function tests with determination of the diffusing capacity formonoxide are recommended.
6 Investigations that are mandatory for monitoring methotrexate therapy inRA consist of full blood cell counts and serum transaminase and creatininThese tests should be obtained at least once a month for the first 3 month4–12 weeks.
7 Folate supplementation can be given routinely to patients treated with metRA. In practice, a minimal dosage of 5 mg of folic acid once a week, atfrom the methotrexate dose, is appropriate.
8 In the event of respiratory symptoms possibly related to methotrexate toxicmust be stopped and symptom severity evaluated. Should evidence of serbe found, the patient should be admitted immediately or advice from a pushould be obtained immediately.
* percentage of “agrees completely” and “agrees with reservation” votes.
statistically significant safety differences between the twogroups [19]. Based on these data and on their experience withmethotrexate used to treat RA, the experts recommended astarting dosage of at least 10 mg/week.
The experts agreed that the starting dosage should be ad-justed according to the patient’s body weight and co-morbid-ities. Moderate to severe renal failure usually requires a startingdosage below 10 mg/week. Two pharmacokinetic studiesshowed that methotrexate clearance was correlated with creati-nine clearance [20,21]. In patients whose creatinine clearancewas lower than 45 ml/min, serum methotrexate levels were 30–60% higher than in patients with normal renal function. Ameta-analysis of 11 controlled trials showed that moderate re-nal failure (creatinine clearance < 60 ml/min) significantly in-creased the risk of serious methotrexate toxicity, most notablyfor the lung and liver [22]. Other co-morbidities may require astarting dosage of less than 10 mg/week; a history of drug-in-duced hepatitis is an example.
Several experts underlined the need to consider body weightwhen selecting the starting dosage. We are not aware of anyclinical studies in which methotrexate dosages are reported inmg/kg body weight. The article by Furst et al. [19] is the onlystudy that used a relative methotrexate dosage, in mg/m2 perweek, which can be difficult to compute in everyday rheuma-tological practice. Given this lack of scientific data, the recom-
ith the strength of each recommendation and the degree of agreement among
Level ofevidence
Strength of therecommendation
Agreement amongexperts (%)*
ss thanent-related
1b/2 C 82.5
he dosageto tolerance
1b/2 C 88.8
uld be givenuld be con-trointestinal
2/3 D 91.7
dosage is in – – –
in a patientm creatinineion, serolo-e recom-tory symp-carbon
1b/3 D 73.4
patients withe assays.s then every
3 D 88.1
hotrexate fora distance
1a/1b A 88.5
ity, the drugious diseaselmonologist
2/3 D 80.4

S. Pavy et al. / Joint Bone Spine 73 (2006) 388–395 391
mendation states the methotrexate starting dosage as a minimaltotal dosage. However, in overweight patients, a starting do-sage close to the maximum recommended dosage can be used.
The presence of characteristics suggesting particularly severedisease [14] may warrant the use of a starting dosage greaterthan 10 mg/week in order to rapidly induce the maximum treat-ment response, despite the risk of minor side effects [1].
3.2. When a patient with RA shows an inadequate responseto methotrexate, the dosage should be increased at intervalsof 6 weeks, up to 20 mg/week, according to toleranceand patient-related factors
A single RCT investigated the additional efficacy obtainedby increasing the methotrexate dosage above 15 mg/week inpatients with RA [23]. Fifty-four patients with an inadequateresponse to oral methotrexate in a dosage of 15–20 mg/weekwere divided into two groups: the controls received 15 mg/week of methotrexate intramuscularly and the intensive treat-ment group had their intramuscular methotrexate dosage in-creased every 4 weeks as long as the DAS28 was greater than3.2, up to 45 mg/week. At the end of the trial, no significantdifferences were found between the two groups regarding dis-ease activity or the number of patients whose DAS28 was lessthan 3.2. One of the RCTs vs. placebo was started with threemethotrexate dosages, 5, 10, and 20 mg/m2 per week [19].With the highest dosage, which resulted in administration of25–35 mg of methotrexate per week, one third of patients dis-continued methotrexate therapy prematurely because of seriousadverse events, and recruitment to this group was stopped.
The mean relative bioavailability of oral methotrexate com-pared to intramuscular methotrexate varies from 0.64 to 0.85according to the dosage [24,25]. Based on this fact and on theirown experience, the experts decided to recommend 20 mg/week as the maximal dosage. Good tolerance of methotrexatein its current dosage is a prerequisite to a dosage increase.
For the reasons listed in the previous recommendation, in-creasing the methotrexate dosage above 20 mg/week may beappropriate in severely overweight or obese patients. The ex-perts recommended a 6-week interval between dosage incre-ments for inadequate effectiveness. This interval is warrantedby the active nature of the disease. It is consistent with therecommendation about clinical and laboratory test monitoringdeveloped at the 2004 Meeting of Rheumatology Experts [14].
3.3. When starting methotrexate treatment in a patient withRA, preference should be given to the oral route
A switch to the intramuscular or subcutaneous route shouldbe considered in patients with poor compliance, inadequate ef-fectiveness, or gastrointestinal side effects
Bioavailability data for methotrexate in dosages of less than20 mg/week, together with the ease of use and low cost of oralmethotrexate, warrant first-line use of the oral route. Pharma-cokinetic studies have shown that the relative bioavailability of
the oral route compared to the intramuscular route is good withlow dosages but decreases as the methotrexate dosage in-creases. With 7.5 mg/week, the absolute oral bioavailabilityof methotrexate is close to 1 [26]. In a group of patients given10–17.5 mg/week of methotrexate, the mean relative bioavail-ability of the oral route compared to the intramuscular routewas 0.85 (95% CI, 0.77–0.93) [24]. The lower value of 0.64(95% CI, 0.21–0.94) was found with dosages greater than20 mg/week [25]. In these studies, no statistically significantdifferences in bioavailability were detected between the intra-muscular and the subcutaneous routes. The clinical efficacyand/or safety of methotrexate, according to the route of admin-istration has been evaluated only in open-label trials and retro-spective studies. In the above-mentioned study investigatingthe potential benefits of methotrexate dosages greater than15 mg/week [23], 64 patients with inadequate responses to oralmethotrexate in dosages of 15–20 mg/week were given 15 mg/week intramuscularly during the 6 weeks preceding the rando-mization phase. The switch from oral to intramuscular admin-istration resulted in a 0.42 (95% CI, 0.15–0.69) point decreasein the DAS28; this reduced the DAS28 to less than 3.2 in 4(6.25%) patients. A similar open-label prospective studyshowed a significant reduction in the DAS28, by a mean of0.6, in 33 patients switched from oral to intramuscular metho-trexate [27]. Three retrospective studies showed that gastroin-testinal symptoms related to methotrexate administration de-creased after switching from the oral to the parenteral route[28–30].
3.4. At present, there is no evidence indicating that a changein methotrexate dosage is in order when a TNF antagonist isgiven concomitantly
In RCTs of the efficacy and/or safety of methotrexate com-bined with TNF antagonist therapy, the mean methotrexate do-sage ranged from 7.5 to 16 mg with infliximab [10,31], 14.5–18.5 mg with etanercept [11,32], and 17–20 mg with adalimu-mab [12,33]. The influence of the methotrexate dosage on ef-ficacy and safety was not investigated in these studies. In asingle uncontrolled study of 22 RA patients with an inadequateresponse to infliximab (3 mg/kg) and methotrexate in combina-tion, increasing the methotrexate dosage from a mean of 9.9± 3.9 mg/week to a mean of 15 ± 4.3 mg/week improved thetherapeutic response to infliximab in 36.4% of cases (8/22 pa-tients), within 16 weeks. However, this study was not con-trolled, and in seven of the eight patients the improvementwas moderate according to EULAR criteria [34].
3.5. The investigations that are mandatory before startingmethotrexate therapy in a patient with RA consist of a fullblood cell count, serum transaminase levels, serum creatininewith computation of creatinine clearance, and a chestradiograph
In addition, serological tests for the hepatitis viruses B andC and a serum albumin assay are recommended. In patients
S. Pavy et al. / Joint Bone Spine 73 (2006) 388–395392
with a history of respiratory disease or current respiratorysymptoms, lung function tests with determination of the diffus-ing capacity for carbon monoxide are recommended.
Determination of serum transaminase levels before startingmethotrexate therapy is mandated by the risk of methotrexate-induced liver toxicity. A meta-analysis of 17 prospective orretrospective studies reporting the results of liver biopsies in719 patients taking methotrexate for RA showed 103 (14%)cases of mild fibrosis (Roenigk class IIIA), 6 (0.8%) cases ofmoderate fibrosis (Roenigk class IIIB), and 2 (2.8‰) cases ofcirrhosis (including one patient who had known cirrhosis be-fore the initiation of methotrexate therapy) [35]. The frequencyof clinically serious liver disease in patients taking methotrex-ate for RA can be estimated at 1% to 1‰ and the cumulativerisk of developing clinically serious liver disease at about 1‰after 5 years [35]. A meta-analysis of six RCTs reporting theresults of serial liver tests done over a 3-month period in 657RA patients taking methotrexate or a placebo showed that pa-tients taking methotrexate had higher rates of ALAT elevation(x 1-2 N, 6.7% vs. 0.4%), ASAT elevation (x 1-2 N, 4.9% vs.0.4%), and serum alkaline phosphatase (x 1-2 N, 16% vs. 3%)[35]. The far higher rate of alkaline phosphatase elevation(16% with methotrexate and 3% with a placebo) compared toALAT and ASAT elevation suggested to the authors of thismeta-analysis that alkaline phosphatase may be too sensitiveto serve as a marker for liver injury [35]. Finally, in a prospec-tive study of three cohorts including a total of 94 patients trea-ted with methotrexate for RA, serial testing showed a correla-tion between serum transaminase levels and liver biopsyresults: elevation of the mean pre-biopsy serum transaminaselevel was correlated with an increased risk of finding an abnor-mal histological grade, whereas normal values for over 50% ofpre-biopsy serum transaminase levels had 97% specificity for anormal histological grade [36].
The recommendation that serological tests for the hepatitisviruses B and C be performed before the initiation of metho-trexate therapy rests on the theoretical risk of potentiated meth-otrexate-induced liver toxicity in patients who have hepatitis Bor C. Reactivation of the hepatitis B virus has been reported infive patients given methotrexate to treat RA, including fourpatients who experienced fulminating hepatitis at methotrexatediscontinuation [37–41]. A single case of hepatitis C reactiva-tion, with a good response to ribavirin, was reported among sixpatients given methotrexate (12.5 ± 3 mg/week for 15.2± 9.9 months) to treat joint manifestations related to chronichepatitis C [42]. Two patients with RA and hepatitis C infec-tion were treated with methotrexate for 6 months without ex-periencing transaminase elevation [43]. Based on these data,and considering that no conclusions can be drawn from thefew anecdotal cases available to date, the experts recommendobtaining serological tests for the hepatitis viruses B and Cbefore initiating methotrexate therapy in patients with RA.
The hematological toxicity of methotrexate requires that afull blood cell count be obtained before treatment initiation.Cytopenia (pancytopenia, neutropenia, or thrombocytopenia)occurred in about 1% of patients in long-term prospective stu-
dies of RA patients given low-dose methotrexate therapy. Cy-topenia can occur at any time during treatment, even after thefirst dose, and may be fatal in as many as 15%–25% of cases.Risk factors for cytopenia may include renal dysfunction, hy-poalbuminemia, infection, interactions with specific medica-tions (e.g. trimethoprim-sulfamethoxazole), and accidentaloverdosage [44–46].
Renal dysfunction may potentiate the toxicity of methotrex-ate in patients with RA. Consequently, a serum creatinine as-say with creatinine clearance estimation should be performedbefore methotrexate initiation. As specified in the recommen-dation on the starting dosage of methotrexate, moderate to se-vere renal failure is associated with elevated serum methotrex-ate levels that result in a significant increase in the risk ofserious adverse effects, most notably hepatic and pulmonarytoxicity [20–22].
Because hypoalbuminemia is associated with increasedmethotrexate toxicity, serum albumin should be assayed beforetreatment initiation. Hypoalbuminemia has been reported as apotential risk factor for methotrexate-induced hematologicaland pulmonary toxicity [45,47].
The well-established pulmonary toxicity of methotrexate re-quires that a chest radiograph be obtained before treatment in-itiation. In patients with a history of respiratory disease or cur-rent respiratory symptoms, lung function tests withdetermination of the diffusing capacity for carbon monoxide(DLCO) should be performed also. Methotrexate-induced pul-monary toxicity manifests chiefly as infectious or immunoaller-gic pneumonia. Immunoallergic pneumonia, which causes in-terstitial pneumonitis, occurs in nearly 2% of patients givenmethotrexate to treat RA and carries a mortality rate of about10–20%. Methotrexate pneumonitis can develop at any timeduring methotrexate therapy but may be more common duringthe first year. Potential risk factors may include pre-existinglung disease, most notably with interstitial involvement; olderage; renal dysfunction; and diabetes mellitus. The symptoms ofmethotrexate pneumonitis set in gradually, over several days toweeks. They are nonspecific, consisting chiefly of a fever, anonproductive cough, and dyspnea. Among tests that can assistin the diagnosis of methotrexate pneumonitis, chest radiogra-phy has low sensitivity and low specificity but may discloseinterstitial and/or alveolar densities predominating in the lungbases. Lung function testing with determination of blood gasvalues and DLCO is sensitive but lacks specificity; the resultsmay show hypoxia, a DLCO reduction (≤ 70% of the predictedage-specific value), and/or a restrictive ventilatory pattern.High-resolution computed tomography is sensitive and morespecific than lung function testing. Findings may include inter-stitial infiltrates and/or ground-glass densities predominating inthe lung bases. The appropriateness of bronchoscopy withbronchoalveolar lavage and transbronchial lung biopsiesshould be discussed on a case-by-case basis with a pulmonol-ogist. Based on these facts, the experts concluded that a chestradiograph, and lung function testing with DLCO determina-tion in patients having a history of respiratory disease or cur-rent respiratory symptoms, should be performed routinely be-

S. Pavy et al. / Joint Bone Spine 73 (2006) 388–395 393
fore methotrexate initiation, both to provide baseline data andto ensure identification of potential risk factors for methotrex-ate pneumonitis, such as preexisting interstitial involvement ora low respiratory reserve [47–54].
3.6. Investigations that are mandatory for monitoringmethotrexate therapy in patients with RA consist of full bloodcell counts and serum transaminase and creatinine assays
These tests should be obtained at least once a month for thefirst 3 months then every 4–12 weeks.
Blood cell counts and serum levels of transaminases andcreatinine should be monitored to detect evidence of metho-trexate-induced hepatic and hematological toxicity and to lookfor renal dysfunction, which may potentiate methotrexate toxi-city, as stated regarding recommendation 5. The only evidenceabout the frequency of investigations comes from a meta-ana-lysis of two uncontrolled studies that report the results of liverfunction tests done every 2–6 weeks in RA patients givenmethotrexate for 30 months (N = 45) or 102 months (N = 18)[35]. The optimal frequency of transaminase monitoring was30–60 days [35]. Based on these data, the experts recom-mended a monitoring schedule that is widely used in their clin-ical practice, namely, tests at least once a month during the first3 months and every 4–12 weeks thereafter.
3.7. Folate supplementation can be given routinely to patientstreated with methotrexate for RA
In practice, a minimal dosage of 5 mg of folic acid once aweek, at a distance from the methotrexate dose, is appropriate.
A meta-analysis showed that routine supplementation withfolic acid or folinic acid had no major effects on variables re-flecting the activity of RA [55]. Data from a RCT, however,suggested that folic acid or folinic acid supplementation mightrequire a slight methotrexate dosage increase to maintain effi-cacy [63]. Compared to a placebo, routine folic acid supple-mentation resulted in a 79% decrease in methotrexate-relatedgastrointestinal symptoms (stomatitis, abdominal pain, anorex-ia, nausea, vomiting, diarrhea, and constipation) (odds ratio,0.21; 95% CI, 0.10–0.44; P < 0.0001) [55,58,62]. Comparedto continued folic acid supplementation, stopping supplementa-tion was associated with an increased risk of methotrexate dis-continuation due to gastrointestinal side effects (45% vs. 7%,P = 0.001) [64]. Routine folic acid or folinic acid supplementa-tion decreased the 1-year rate of methotrexate discontinuationbecause of transaminase elevation, compared to a placebo (4%with folic acid and 6% with folinic acid vs. 26% with the pla-cebo, P < 0.001) [63]. Stopping routine folic acid supplementa-tion (compared to continuing supplementation) was associatedwith an increase in the 1-year rate of methotrexate discontinua-tion for neutropenia (< 2000 neutrophils/mm3), although thedifference was not statistically significant, probably becauseof the small number of neutropenia cases [64].
Regarding the overall safety profile of methotrexate, routinefolic acid or folinic acid supplementation decreased the 1-yearrate of methotrexate discontinuation for adverse events (12%with folinic acid, 17% with folic acid, and 38% with the pla-cebo; P < 0.001) [60]. Stopping routine folic acid supplemen-tation increased the 1-year rate of methotrexate discontinuationfor adverse events (46% vs. 21% when supplementation wascontinued, P = 0.02) [64].
The influence of the product used for supplementation (folicacid vs. folinic acid), the dosage, and the dosing schedule(once a day vs. once a week) on the efficacy or safety of meth-otrexate in patients with RA is unclear. Various folate supple-mentation regimens were used in RCTs [55–64]. The results donot suggest major differences between low and high dosages offolic acid (ranges used: 1–5 mg/day and 5–27.5 mg/week) orfolinic acid (ranges used: 1–5 mg/day and 2.5–20 mg/week)[55–64]. Therefore, the experts recommended a simple supple-mentation schedule consistent with existing clinical practice,namely, 5 mg of folic acid or folinic acid once a week, at adistance from the methotrexate dose.
3.8. In the event of respiratory symptoms possibly relatedto methotrexate toxicity, the drug must be stoppedand symptom severity evaluated
Should evidence of serious disease be found, the patientshould be admitted immediately or advice from a pulmonolo-gist should be obtained immediately.
Methotrexate-induced lung toxicity was discussed about therecommendation on investigations required before methotrex-ate initiation in patients with RA. Lower respiratory tract infec-tions and immunoallergic pneumonitis are the main manifesta-tions. These potentially life-threatening complications mayoccur at any time during treatment. The symptoms are nonspe-cific and consist of a fever, a nonproductive cough, and dys-pnea. Respiratory symptoms that develop in an RA patient re-ceiving methotrexate therapy may indicate infection,methotrexate pneumonitis, or another cause of respiratory dis-ease related or unrelated to RA. The first step in differentiatingamong these possibilities is a thorough physical examination.The results are used to choose diagnostic investigations amongthe following: chest radiograph, cytological and microbiologi-cal studies of sputum samples, blood cultures, other direct orindirect tests aimed at detecting infection, lung function testswith determination of blood gas levels and DLCO, high-reso-lution computed tomography, and bronchoscopy with bronch-oalveolar lavage and transbronchial biopsies [47–54]. Giventhe wide diversity of situations encountered in everyday prac-tice, the experts recommended a pragmatic approach involvingmethotrexate discontinuation and a search for evidence of se-vere disease, chiefly hypoxia, dyspnea, and cyanosis. Whensuch evidence is found, the advice of a pulmonologist shouldbe obtained immediately, or the patient should be admitted forimmediate symptomatic treatment and for investigations aimedat identifying the cause of the respiratory symptoms.

[15
[16
[17
[18
[19
[20
[21
[22
[23
[24
[25
[26
[27
[28
[29
[30
[31
[32
[33
S. Pavy et al. / Joint Bone Spine 73 (2006) 388–395394
Acknowledgments
We are grateful to Catherine Mazzacco, Gérard Goldfarb,and Fabrice Michiels at Abbott France for their support; Janinede Palmas and Fabien Moll-François at Margaux Orange fortheir help; and the 75 experts who used their knowledge andtheir experience of rheumatoid arthritis to develop the recom-mendations [15].
References
[1] O’Dell JR. Therapeutic strategies for rheumatoid arthritis. N Engl J Med2004;350:2591–602.
[2] American College of Rheumatology Subcommittee on Rheumatoid Ar-thritis Guidelines. Guidelines for the management of rheumatoid arthritis2002 update. Arthritis Rheum 2002;46:328–46.
[3] Choi HK, Hernán MA, Seeger JD, Robins JM, Wolfe F. Methotrexateand mortality in patients with rheumatoid arthritis: a prospective study.Lancet 2002;359:1173–7.
[4] Williams HJ, Willkens RF, Samuelson Jr. CO, Alarcon GS, GuttadauriaM, Yarboro C, et al. Comparison of low-dose oral pulse methotrexateand placebo in the treatment of rheumatoid arthritis. A controlled clinicaltrial. Arthritis Rheum 1985;28:721–30.
[5] Weinblatt ME, Coblyn JS, Fox DA, Fraser PA, Holdsworth DE,Glass DN, et al. Efficacy of low-dose methotrexate in rheumatoid arthri-tis. N Engl J Med 1985;312:818–22.
[6] Jeurissen MEC, Boerbooms AMT, van de Putte LBA, Doesburg WH,Lemmens AM. Influence of methotrexate and azathioprine on radiologicprogression in rheumatoid arthritis: a randomized, double-blind study.Ann Intern Med 1991;114:999–1004.
[7] Weinblatt ME, Polisson R, Blotner SD. The effects of drug therapy onradiographic progression of rheumatoid arthritis. Results of a 36-weekrandomized trial comparing methotrexate and auranofin. Arthritis Rheum1993;36:613–9.
[8] Boers M, Verhoeven AC, Markusse HM, van de Laar MA, WesthovensR, van Denderen JC, et al. Randomised comparison of combined step-down prednisolone, methotrexate and sulphasalazine with sulphasalazinein early rheumatoid arthritis. Lancet 1997;350:309–18.
[9] Mottonen T, Hannonen P, Leirisalo-Repo M, Nissila M, Kautiainen H,Korpela M, et al. Comparison of combination therapy with single-drugtherapy in early rheumatoid arthritis: a randomised trial. FIN-RACo trialgroup. Lancet 1999;353:1568–73.
[10] Maini R, St Clair EW, Breedveld F, Furst D, Kalden J, Weisman M, et al.Infliximab (chimeric anti-tumour necrosis factor alpha monoclonal anti-body) versus placebo in rheumatoid arthritis patients receiving concomi-tant methotrexate: a randomised phase III trial. ATTRACT Study Group.Lancet 1999;354:1932–9.
[11] Weinblatt ME, Kremer JM, Bankhurst AD, Bulpitt KJ, Fleischmann RM,Fox RI, et al. A trial of etanercept, a recombinant tumor necrosis factorreceptor: Fc fusion protein, in patients with rheumatoid arthritis receivingmethotrexate. N Engl J Med 1999;340:253–9.
[12] Weinblatt ME, Keystone EC, Furst DE, Moreland LW, Weisman MH,Birbara CA, et al. Adalimumab, a fully human anti-tumor necrosis factoralpha monoclonal antibody, for the treatment of rheumatoid arthritis inpatients taking concomitant methotrexate: the ARMADA trial. ArthritisRheum 2003;48:35–45.
[13] Dougados M, Betteridge N, Burmester GR, Euller-Ziegler L, GuilleminF, Hirvonen J, et al. EULAR standardised operating procedures for theelaboration, evaluation, dissemination and implementation of recommen-dations endorsed by the EULAR standing committees. Ann Rheum Dis2004;63:1172–6.
[14] Pham T, Gossec L, Fautrel B, Combe B, Flipo RM, Goupille P, et al.Physical examination and laboratory tests in the management of patientswith rheumatoid arthritis: development of recommendations for clinical
practice based on published evidence and expert opinion. Joint BoneSpine 2005;73:222–8.
] Pham T, Gossec L, Constantin A, Pavy S, Bruckert E, Mariette X, et al.Cardiovascular risk and rheumatoid arthritis: clinical practice guidelinesbased on published evidence and expert opinion. Joint Bone Spine 2006;73(2).
] Gossec L, Pavy S, Pham T, Constantin A, Poiraudeau S, Cantagrel A,et al. Nonpharmacological treatments in early rheumatoid arthritis: clini-cal practice guidelines based on published evidence and expert opinion.Joint Bone Spine 2006;73(2).
] Shekelle PG, Woolf SH, Eccles M, Grimshaw J. Clinical guidelines: de-veloping guidelines. BMJ 1999;318:593–6.
] Seideman P. Methotrexate—the relationship between dose and clinicaleffect. Br J Rheumatol 1993;32:751–3.
] Furst DE, Koehnke R, Burmeister LF, Kohler J, Cargill I. Increasingmethotrexate effect with increasing dose in the treatment of resistantrheumatoid arthritis. J Rheumatol 1989;16:313–20.
] Bressolle F, Bologna C, Kinowski JM, Sany J, Combe B. Effects ofmoderate renal insufficiency on pharmacokinetics of methotrexate inrheumatoid arthritis patients. Ann Rheum Dis 1998;57:110–3.
] Ahern M, Booth J, Loxton A, McCarthy P, Meffin P, Kevat S. Metho-trexate kinetics in rheumatoid arthritis: is there an interaction with non-steroidal antiinflammatory drugs? J Rheumatol 1988;15:1356–60.
] Rheumatoid Arthritis Clinical Trial Archive Group. The effect of age andrenal function on the efficacy and toxicity of methotrexate in rheumatoidarthritis. J Rheumatol 1995;22:218–23.
] Lambert CM, Sandhu S, Lochhead A, Hurst NP, McRorie E, Dhillon V.Dose escalation of parenteral methotrexate in active rheumatoid arthritisthat has been unresponsive to conventional doses of methotrexate: a ran-domized, controlled trial. Arthritis Rheum 2004;50:364–71.
] Jundt JW, Browne BA, Fiocco GP, Steele D, Mock D. A comparison oflow dose methotrexate bioavailability: oral solution, oral tablet, subcuta-neous and intramuscular dosing. J Rheumatol 1993;20:1845–9.
] Hoekstra M, Haagsma C, Neef C, Proost J, Knuif A, van de Laar M.Bioavailability of higher dose methotrexate comparing oral and subcuta-neous administration in patients with rheumatoid arthritis. J Rheumatol2004;31:645–8.
] Hamilton RA, Kremer JM. Why intramuscular methotrexate may bemore efficacious than oral dosing in patients with rheumatoid arthritis.Br J Rheumatol 1997;36:86–90.
] Bingham SJ, Buch MH, Lindsay S, Pollard A, White J, Emery P. Parent-eral methotrexate should be given before biological therapy. Rheumatol2003;42:1009–10.
] Moitra RK, Ledingham JM, Hull RG, McCrae FC, Thomas AL, ShabanR, et al. Caveats to the use of parenteral methotrexate in the treatment ofrheumatic disease. Rheumatol 2005;44:256–7.
] Wegrzyn J, Adeleine P, Miossec P. Better efficacy of methotrexate givenby intramuscular injection than orally in patients with rheumatoid arthri-tis. Ann Rheum Dis 2004;63:1232–4.
] Rozin A, Schapira D, Balbir-Gurman A, Braun-Moscovici Y, MarkovitsD, Militianu D, et al. Relapse of rheumatoid arthritis after substitution oforal for parenteral administration of methotrexate. Ann Rheum Dis 2002;61:756–7.
] Maini RN, Breedveld FC, Kalden JR, Smolen JS, Davis D, Macfar-lane JD, et al. Therapeutic efficacy of multiple intravenous infusions ofanti-tumor necrosis factor alpha monoclonal antibody combined withlow-dose weekly methotrexate in rheumatoid arthritis. Arthritis Rheum1998;41:1552–63.
] Keystone EC, Schiff MH, Kremer JM, Kafka S, Lovy M, DeVries T,et al. Once-weekly administration of 50 mg etanercept in patients withactive rheumatoid arthritis: results of a multicenter, randomized, double-blind, placebo-controlled trial. Arthritis Rheum 2004;50:353–63.
] Breedveld FC, Kavanaugh AF, Cohen SB, Pavelka K, van VollenhovenR, Perez JL, et al. Early Treatment of Rheumatoid Arthritis (RA) WithAdalimumab (HUMIRA®) Plus Methotrexate vs. Adalimumab Alone orMethotrexate Alone: The PREMIER Study. 68th Annual Scientific Meet-

[34
[35
[36
[37
[38
[39
[40
[41
[42
[43
[44
[45
[46
[47
[48
[49
[50
[51
[52
[53
[54
[55
[56
[57
[58
[59
[60
[61
[62
[63
[64
S. Pavy et al. / Joint Bone Spine 73 (2006) 388–395 395
ing of the American College of Rheumatology. October 16-21, 2004 inSan Antonio, Texas. Poster Presentation (Presentation Number L5).
] Ornetti P, Solau E, Gaudin P, Sibilia J, Berthelot JM, Puechal X, et al.Increase in methotrexate dose in rheumatoid arthritis patients with an in-adequate response to infliximab. Ann Rheum Dis 2005;64:1379–80.
] Kremer JM, Alarcon GS, Lightfoot Jr. RW, Willkens RF, Furst DE, Wil-liams HJ, et al. Methotrexate for rheumatoid arthritis. Suggested guide-lines for monitoring liver toxicity. American College of Rheumatology.Arthritis Rheum 1994;37:316–28.
] Kremer JM, Furst DE, Weinblatt ME, Blotner SD. Significant changes inserum AST across hepatic histological biopsy grades: prospective analy-sis of 3 cohorts receiving methotrexate therapy for rheumatoid arthritis. JRheumatol 1996;23:459–61.
] Hagiyama H, Kubota T, Komano Y, Kurosaki M, Watanabe M, Miyasa-ka N. Fulminant hepatitis in an asymptomatic chronic carrier of hepatitisB virus mutant after withdrawal of low-dose methotrexate therapy forrheumatoid arthritis. Clin Exp Rheumatol 2004;22:375–6.
] Ostuni P, Botsios C, Punzi L, Sfriso P, Todesco S. Hepatitis B reactiva-tion in a chronic hepatitis B surface antigen carrier with rheumatoid ar-thritis treated with infliximab and low dose methotrexate. Ann RheumDis 2003;62:686–7.
] Ito S, Nakazono K, Murasawa A, Mita Y, Hata K, Saito N, et al. Devel-opment of fulminant hepatitis B (precore variant mutant type) after thediscontinuation of low-dose methotrexate therapy in a rheumatoid arthri-tis patient. Arthritis Rheum 2001;44:339–42.
] Narvaez J, Rodriguez-Moreno J, Martinez-Aguila MD, Clavaguera MT.Severe hepatitis linked to B virus infection after withdrawal of low dosemethotrexate therapy. J Rheumatol 1998;25:2037–8.
] Flowers MA, Heathcote J, Wanless IR, Sherman M, Reynolds WJ, Ca-meron RG, et al. Fulminant hepatitis as a consequence of reactivation ofhepatitis B virus infection after discontinuation of low-dose methotrexatetherapy. Ann Intern Med 1990;112:381–2.
] Nissen MJ, Fontanges E, Allam Y, Zoulim F, Trepo C, Miossec P. Rheu-matological manifestations of hepatitis C: incidence in a rheumatologyand non-rheumatology setting and the effect of methotrexate and interfer-on. Rheumatology 2005;44:1016–20 (2005).
] Mok MY, Ng WL, Yuen MF, Wong RW, Lau CS. Safety of diseasemodifying anti-rheumatic agents in rheumatoid arthritis patients withchronic viral hepatitis. Clin Exp Rheumatol 2000;18:363–8.
] Yazici Y, Sokka T, Kautiainen H, Swearingen C, Kulman I, Pincus T.Long term safety of methotrexate in routine clinical care: discontinuationis unusual and rarely the result of laboratory abnormalities. Ann RheumDis 2005;64:207–11.
] Gutierrez-Urena S, Molina JF, Garcia CO, Cuellar ML, Espinoza LR.Pancytopenia secondary to methotrexate therapy in rheumatoid arthritis.Arthritis Rheum 1996;39:272–6.
] Berthelot JM, Maugars Y, Hamidou M, Chiffoleau A, Barrier J, Grol-leau JY, et al. Pancytopenia and severe cytopenia induced by low-dosemethotrexate. Eight case-reports and a review of one hundred cases fromthe literature (with twenty-four deaths). Rev Rhum Engl Ed 1995;62:477–86.
] Alarcon GS, Kremer JM, Macaluso M, Weinblatt ME, Cannon GW, Pal-mer WR, et al. Risk factors for methotrexate-induced lung injury in pa-tients with rheumatoid arthritis. A multicenter, case-control study. Meth-otrexate-Lung Study Group. Ann Intern Med 1997;127:356–64.
] Saravanan V, Kelly CA. Reducing the risk of methotrexate pneumonitisin rheumatoid arthritis. Rheumatology 2004;43:143–7.
] Hargreaves MR, Mowat AG, Benson MK. Acute pneumonitis associatedwith low dose methotrexate treatment for rheumatoid arthritis: report offive cases and review of published reports. Thorax 1992;47:628–33.
] Ohosone Y, Okano Y, Kameda H, Fujii T, Hama N, Hirakata M, et al.Clinical characteristics of patients with rheumatoid arthritis and metho-trexate induced pneumonitis. J Rheumatol 1997;24:2299–303.
] Golden MR, Katz RS, Balk RA, Golden HE. The relationship of preex-isting lung disease to the development of methotrexate pneumonitis inpatients with rheumatoid arthritis. J Rheumatol 1995;22:1043–7.
] Carson CW, Cannon GW, Egger MJ, Ward JR, Clegg DO. Pulmonarydisease during the treatment of rheumatoid arthritis with low dose pulsemethotrexate. Semin Arthritis Rheum 1987;16:186–95.
] Searles G, McKendry RJ. Methotrexate pneumonitis in rheumatoid ar-thritis: potential risk factors. Four case reports and a review of the litera-ture. J Rheumatol 1987;14:1164–71.
] Kremer JM, Alarcon GS, Weinblatt ME, Kaymakcian MV, Macaluso M,Cannon GW, et al. Clinical, laboratory, radiographic, and histopathologicfeatures of methotrexate-associated lung injury in patients with rheuma-toid arthritis: a multicenter study with literature review. Arthritis Rheum1997;40:1829–37.
] Ortiz Z, Shea B, Suarez Almazor M, Moher D, Wells G, Tugwell P. Fo-lic acid and folinic acid for reducing side effects in patients receivingmethotrexate for rheumatoid arthritis. Cochrane Database Syst Rev2000;2 (CD000951).
] Hanrahan PS, Russell AS. Concurrent use of folinic acid and methotrex-ate in rheumatoid arthritis. J Rheumatol 1988;15:1078–80.
] Buckley LM, Vacek PM, Cooper SM. Administration of folinic acid afterlow dose methotrexate in patients with rheumatoid arthritis. J Rheumatol1990;17:1158–61.
] Morgan SL, Baggott JE, Vaughn WH, Young PK, Austin JV, Krum-dieck CL, et al. The effect of folic acid supplementation on the toxicityof low-dose methotrexate in patients with rheumatoid arthritis. ArthritisRheum 1990;33:9–18.
] Joyce DA, Will RK, Hoffman DM, Laing B, Blackbourn SJ. Exacerba-tion of rheumatoid arthritis in patients treated with methotrexate after ad-ministration of folinic acid. Ann Rheum Dis 1991;50:913–4.
] Shiroky JB, Neville C, Esdaile JM, Choquette D, Zummer M, HazeltineM, et al. Low-dose methotrexate with leucovorin (folinic acid) in themanagement of rheumatoid arthritis. Results of a multicenter rando-mized, double-blind, placebo-controlled trial. Arthritis Rheum 1993;36:795–803.
] Weinblatt ME, Maier AL, Coblyn JS. Low dose leucovorin does not in-terfere with the efficacy of methotrexate in rheumatoid arthritis: an 8-week randomized placebo controlled trial. J Rheumatol 1993;20:950–2.
] Morgan SL, Baggott JE, Vaughn WH, Austin JS, Veitch TA, Lee JY,et al. Supplementation with folic acid during methotrexate therapy forrheumatoid arthritis. A double-blind, placebo-controlled trial. Ann InternMed 1994;121:833–41.
] van Ede AE, Laan RF, Rood MJ, Huizinga TW, van de Laar MA, vanDenderen CJ, et al. Effect of folic or folinic acid supplementation on thetoxicity and efficacy of methotrexate in rheumatoid arthritis: a forty-eightweek, multicenter, randomized, double-blind, placebo-controlled study.Arthritis Rheum 2001;44:1515–24.
] Griffith SM, Fisher J, Clarke S, Montgomery B, Jones PW, Saklatvala J,et al. Do patients with rheumatoid arthritis established on methotrexateand folic acid 5 mg daily need to continue folic acid supplements longterm? Rheumatology 2000;39:1102–9.




















