
Averaged Reynolds equation for flows between rough surfaces in sliding motion

Journal of Electrocardiology Vol. 29 No. 3 1996
Multiresolution Decomposit ion of the Signal-averaged ECG Using the Mallat
Approach for Prediction of Arrhythmic Events After Myocardial Infarction
G i l b e r t o S i e r r a , P h D , * T h o m a s F e t s c h , M D , * L u t z R e i n h a r d t , M S c , *
A n t o n i M a r t f n e z - R u b i o , M D , * M a r k k u M/ ik i j / i r v i , M D , t
K l a u s B a l k e n h o f f , * M a r t i n B o r g g r e f e , M D , *
a n d G f i n t e r B r e i t h a r d t , M D *
Abstract: The aim of this study was to analyze the ability of the multiresolu- tion decomposition of the signal-averaged electrocardiogram (ECG) to dis- criminate between patients who develop life-threatening ventricular arrhyth- mias after myocardial infarction and those who do not and to compare the predictive values of this approach with those obtained from the analysis of ventricular late potentials in the time domain. Signal-averaged ECGs of 769 prospectively included patients were analyzed. A total of 42 arrhythmic events occurred during the follow-up period. For numerical calculations of wavelet analysis, the total and relative energies of the QRS complex were obtained in seven frequency bands. The combination of the relative energy in the frequency bands 7.8-15.6 Hz and 62.5-125 Hz enhanced statistical perfor- mance as compared with the time-domain parameters (positive predictive accuracy, 11.3 vs 8.2%). Combining wavelet transform and time-domain parameters enhanced the predictive values even more (positive predictive accuracy, 14.3%) compared with applying each method alone. Key words: wavelet transform, signal-averaged ECG, multiresolution decomposition, ven- tricular late potentials.
From the *Department of Cardiology and Angiology, Hospital of the Westfiilische Wilhelms- Universitiit, and Institute for Arteriosclerosis Research, Miinster, Germany, and ~-Helsinki Central Hospital, Helsinki, Finland.
Supported in part by Deutsche Forschungsgemeinschaft (DFG) (grant no~ Br 759/2-2); Bundesministerium ffir Forschung und Technologic (BMFT) (grant no. HKP 314); Deutscher Akademischer Austauschdienst (DAAD); and the
.I~ranz,Loogen,Sfiftung for Cardiological Research. Dr. Gilberto Sierra is a research fellow from the Central Institute of Digital Research, Havana, Cuba, supported by the Deutscher Akademischer Austauschdienst (DAAD).
Reprint requests: Gilberto Sierra, PhD, Centre de Recherche, H6pital du Sacr~-Coeur, 5400 Ouest, Boulevard Gouin, Mon- tr6al, Queb6c, Canada, H4J 1C5.
The use of the s ignal-averaged electrocardiogram (ECG) as one of the noninvas ive methods for risk stratification after acute myocardia l infarction seems wel l - founded according to the results of available studies (1-5). High-resolut ion electrocar- diography using the signal-averaged ECG tech- nique has been developed to detect signals of car- diac electric activation in the microvolt range f rom the body surface (2). Most of the studies in this field have investigated the occurrence of ventr icu- Iar late potentials in the terminal part of the QRS complex (1,3). These signals have been regarded as
223

224 Journal of Electrocardiotogy Vol. 29 No. 3 July 1996
a marker of an arrhythmogenic substrate in which slow conduction may occur as a result of inhomo- geneous electrical transmission and poor cell-to- cell coupling (6).
Several approaches have been applied to detect ventricular late potentials. These techniques, with the exception of beat-to-beat analysis, are primar- ily based on high-gain amplification and averaging of consecutive normal sinus rhythm beats to elimi- nate random noise and to improve the signal-to- noise ratio. Time-domain analysis characterizes the amplitude of the signal in relation to time, whereas frequency-domain analysis measures the power of different spectral components (5). Spectrotemporal mapping represents a three-dimensional display of the power spectrum in relation to time and fre- quency (7). The spectral turbulence analysis intro- duced by Kelen et al. enables the detection of dynamic frequency changes during the entire QRS complex (8). In addition, the fractal dimension has also been used to characterize abnormal ventricu- Iar late potential activity in postinfarction patients (9). However, owing to the increasing interest in noninvasive methods for risk assessment, addi- tional investigations are needed to enhance the sig- nificance of predictive information retrieved from these methods.
The wavelet transform is a recently introduced time-scale representation that has already found applications in a variety of fields, In the field of biosignal processing, wavelet transform has been applied to single evoked potential analysis (10), audiology (11), detection of ventricular late poten- tials (12-14), heart rate variability (I 5), and phono- cardiography (16). The wavelet transform is an alternative to the Fourier transform, particularly for the analysis of nonstationary signals. Among some of the inconveniences of the Fourier trans- form are the lack of temporal information, the assumption that the signal of interest is stationary, and the low-frequency resolution of the analyzing window. The wavelet transform can be considered to belong to the class of time-frequency transforms that includes the Wigner-Ville and Gabor short- time Fourier transforms (15). Advantages to be gained through its use include the ability to localize singularities more accurately in the time domain, near perfect reconstruction from the transform coefficients, and efficient implementation by pyra- midal algorithms (15).
In this study, the ability of the multiresolution decomposition method, using the Mallat algorithm (17), to discriminate between patients who devel- oped serious arrhythmic events after myocardial
infarction and those who did not was assessed. In addition, the predictive values of the results of the wavelet transform when applied to the QRS com- plex of the signal-averaged ECG were compared with the predictive values of the conventional parameters used in the time-domain analysis of ventricular late potentials.
Materials and Methods
Signal-averaged ECGs of 769 prospectively en- rolled patients surviving acute myocardial infarc- tion were recorded 18 _ 9 days after the infarction. These recordings were obtained from the nonin- terventional Post-Infarction Late Potential (PILP) study, of which the main goal was to assess in the first line the prognostic value of ventricular late potentials detected by the signal-averaged ECG. This multicenter study included patients from 17 hospitals, with a mean age of 53 _+ 7 years (range, 22-65 years), of whom 108 (14%) had had a pre- vious myocardial infarction before inclusion in the PILP study.
Patients
All consecutive male patients aged 65 years or less who were admitted with the suspicion of myocardial infarction and had survived the acute period were further evaluated for inclusion in the study. The diagnosis of myocardial infarction was based on all three of the following criteria: (1) typi- cal chest pain; (2) typical changes in laboratory tests (creatine kinase; lactate dehydrogenase, serum glutamic-oxaloacetic transaminase) with increases greater than twice normal; and (3) char- acteristic ECG findings. The exclusion criteria used were unwillingness to participate, previous bypass surgery, valvular heart disease, Wolff-Parkin- son-White syndrome, implanted pacemaker, pre- existing left bundle branch block, renal insuffi- ciency requiring permanent dialysis, malignant hypertension, any malignancy detected during the last 5 years, hepatic cirrhosis with esophageal vari- cosis or ascites, and death during the acute phase of myocardial infarction.
Critical Events
The primary objective of the study was to detect the occurrence of death (sudden cardiac death,

Multiresolution Decomposition of Signal-averaged ECG • Sierraet al. 225
nonsudden cardiac death, or noncardiac death) or of symptomatic hemodynamically compromising sustained ventricular tachycardia or ventricular fib- rillation. Sustained ventricular tachycardia was defined as ventricular tachycardia that manifested beat-by-beat uniform surface QRS configurations lasting longer than 30 seconds or that was hemo- dynamically intolerable and needed prior termina- tion. Ventricular fibrillation was defined as com- pletely disorganized sustained cardiac electrical activity that was hemodynamically intolerable and needed defibrillation.
In case of any hospital admission or death, the independent critical event committee of the study gave one of the following final diagnoses: noncar- diac event; arrhythmic event (documented sus- tained ventricular tachycardia or ventricular fibril- lation, aborted sudden death or sudden cardiac death); reinfarction; pulmonary edema; progressive heart failure; and other cardiac causes. All events not considered primary were considered censored. Any arrhythmic event was considered a valid event if it represented the first event and if there was no intermediate reinfarction.
During the 6-54-month follow-up period (median, 23 months), 42 serious arrhythmic events occurred. Sustained monomorphic ventric- ular tachycardia was documented in 16 patients (2.1%), ventricular fibrillation in 9 (1.2%), and sudden cardiac death in 17 (2.2%). Drug therapy and referral for revascularization procedures dur- ing the postinfarction period was at the discretion of the referring physician.
Methods
Signal Averaging. The signal-averaged ECGs were recorded as described by Simson (1) using the original hardware and software. Three bipolar modified Frank leads were recorded. The X elec- trodes were at the right and left midaxillary lines in the fourth intercostal space. The Y electrodes were placed at the superior aspect of the manubrium and the proximal left leg. The anterior Z electrode was at the lead V2 position and the other was at the identical position on the posterior chest. The posi- tive electrodes were left, inferior, and anterior. The signal was amplified with a gain of 1,000, band- width was 0.05-300 Hz, and the sampling rate was 1,000 Hz. The amplified signal was passed through a four-pole 250-Hz low-pass filter and digitized with 12-bit accuracy. Approximately i50 cardiac cycles were averaged, with only beats with devia-
tion less than twice the template standard devia- tion accepted, and stored on disk.
T ime-domain Analysis. Time-domain analysis of the signal-averaged ECGs was performed by using a bidirectional four-pole Butterworth filter at 25-250 Hz. All calculations were performed from the vector magnitude complex, defined as ~x 2 + y2 + z 2, with commerdal software (ART 1200 EPX) (Arrhythmia Research Technology). The mean root-mean-square noise level was 0.9 _+ 1.0 gV for the vector lead. The criteria for abnormality were filtered QRS duration of 120 ms or longer, root-mean-square voltage of the terminal 40 ms of 25 gV or less, and duration of the signal below 40 gV of 38 or longer. Late potentials were considered to be present if two of three criteria were met (4).
Wavelet Transform. In this study, the mul- tiresolutional approach of wavelet analysis was used because it provides a particularly efficient algorithm for calculation of the wavelet transform. The wavelet transform operates on a data vector, transforming it into a numerically different vector of the same length. A wavelet decomposition of a signal amounts to its description in terms of shifted and dilated versions of some basis wavelet func- tions. The shift operation enables signals to be localized in time, while the dilation operation allows the scale of the original signal to be deter- mined. Hence, a signal can be localized in both time and scale dimensions, which gives rise to the term time-scale representation (15). On dilation (stretching in time domain), the wavelet's fre- quency will decrease, allowing analysis at different scales. This dilation results in a decreased ability to localize events in time (although the frequency resolution correspondingly increases) because the wavelet itself becomes less localized (15).
The wavelet transform can be implemented with a specially designed pair of finite impulse response filters called a quadrature mirror filter (QMF) pair. The QMF pairs are distinctive because the frequency responses of the two finite impulse response filters separate the high-frequency and low-trequency components of the input signal (18). Mallat showed that the calculation of the wavelet representation may be accomplished with a pyramidal algorithm based on convolutions with QMFs (17). In our study, the wavelet transform was performed according to Mallat (17) and Chui (19) and the method is restricted to dyadic (binary) analysis. For the calculation of the filter coeffi- cients, the modifications proposed by Allen et al.

226 Journal of Electrocardiology Voi. 29 No. 3 July 1996
were considered (20). The dyadic wavelet analysis is based on the projection of the signal f(x) on the or thonormal basis:
(1) Azjf(x)=2-] ~[ <f(u),%,(u--2-Jn)>(p2J(x--2-Jn)
where n, j e Z, and the basis function (p2J (X) a r e
formed by scaling (by the factor 2J) a given func- tion ~p(x), which is called the scaling function. A2,f(x) can be interpreted as the approximation of the signal that results from low-pass filtering to smooth high-frequency details corresponding to finer resolutions than 2J. Going from A20+l)f(x ) to A2jf(x), the signal information that corresponds exactly to the resolution 2J +1 is suppressed. The dif- ference DxJf(x) between Ax~J+,~f(x) and A>f(x) is called the signal detail at the resolution 2J, and it is computed through the wavelet function ~(x), cor- responding to the scaling function cp(x):
( 2 ) D x i f ( x ) = 2 - J E < f ( u ) , ~ x i ( U - 2 - J n ) > l [ / 2 J ( x - 2 J n ) n = - ~
Here ~2j(x) is formed by scaling (by the factor 2J) the function ~/(x). The discrete approximation (A~j) and the discrete detail (D~j) of f(x) can be estimated by using the inner products at the resolution 2J, as follows:
(3) A~if(n ) = <f(u),%i(u-2dn)>
(4) D~jf(n) = <f(u),~/2i(u-2-Jn)>
The computat ion of Ad2jf(x) and Dd2Jf(x) is carried out by the following recurrence algorithm:
(5) A~jf(n) = • h(2n-k)Adx~j÷,,f(2n-k) k=
+~
d , = -- - ~ - -~(2n-k)Ad0<,f(2n-k) (6) Dzf(nj 5., k = - ~
where h(n) = h(-n), ~(n) = g(-n), h(n) = <(p>,(u), ~p(u-n)>, and g(n) = <~>l(U), q0(u-n)>.
Since filters g(n) and h(n) are QMFs, the high- pass filter g(n) can be estimated by g(n) = (1)l-n h(1-n). Figure 1 shows the first 30 coefficients of the impulse response of both filters. The algorithm for the computat ion of the discrete approximations by repeating steps 5 and 6 is called the pyramidal transform. It is important to choose a scaling func- tion q0(x) with both good time-localization proper- ties and good low-pass filter characteristics. The scaling function introduced by Mallat, which is based on spline functions of order 3, has these desirable properties because it is characterized by an exponential decay in the time domain and a polynomial decay of w 4 in the frequency domain (17). This function has the additional advantage that the function basis formed by their translations and dilations is or thonormal (21). Additional prop-
Q , 6
"O 0 . 4
• l ~ O . a , z ' l
wml O . Z
e~
0
- 0 . it
0 . 6
0 . 5
~ 0 . 4
0 . 2
,I,¢ O. i
0
- 0 . 3
- 0 . 4
A
1 I I I I '
• 0 1 5 2 O
B
i I t I ; SauNa l e s 5 1 0 1 5 R~O ~
Fig. 1. (A) The impulse response h(n) of the filter corresponding to the scaling function 9(x)- (B) The impulse response g(n) of the filter corresponding to the wavelet function ~(x).
Multiresolution Decomposition of Signal-averaged ECG • Sierra et al. 227
A1 A2 X[n] I 'ow I Low P - - ,
l Filter ~T-"J i Filter ~ : ~ " " '
High Pass ._F,~D 2 Filter
High Pass ~2~ Filter D1
A8 Low Pass
Filter
High Pass Filter
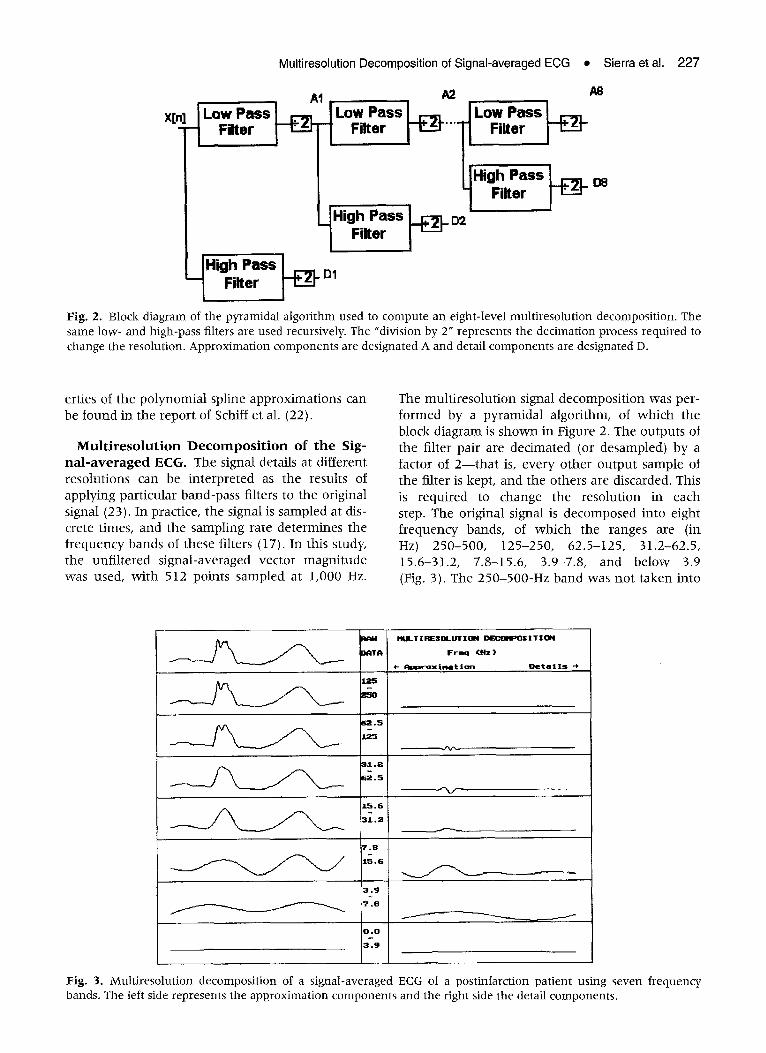
Fig. 2. Block diagram of the pyramidal algorithm used to compute an eight-level multiresolution decomposition. The same low- and high-pass filters are used recursively. The "division by 2" represents the decimation process required to change the resolution. Approximation components are designated A and detail components are designated D.
erties of the polynomial spline approximations can be found in the report of Schiff et al. (22).
M u l t i r e s o l u t i o n D e c o m p o s i t i o n o f t h e Sig- n a l - a v e r a g e d ECG. The signal details at different resolutions can be interpreted as the results of applying particular band-pass filters to the original signal (23). In practice, the signal is sampled at dis- crete times, and the sampling rate determines the f requency bands of these filters (17). In this study, the unfi l tered signal-averaged vector magni tude was used, with 512 points sampled at 1,000 Hz.
The mult iresolution signal decomposit ion was per- formed by a pyramidal algorithm, of which the block diagram is shown in Figure 2. The outputs of the filter pair are decimated (or desampled) by a factor of 2 - - t h a t is, every other output sample of the filter is kept, and the others are discarded. This is required to change the resolution in each step. The original signal is decomposed into eight f requency bands, of which the ranges are (in Hz) 250-500, i25-250, 62.5-125, 31.2-62.5, 15.6-31.2, 7.8-15.6, 3.9-7.8, and below 3.9 (Fig. 3). The 250-500-Hz band was not taken into
S 2 . 5
3 1 , 2
% 115.6
3 , 9
MULT I RESOLUT I ON DECOHPOg I T I ON
~ T R F r e m ( H = )
~- A l ~ l = v o x l ~ t i o n D e t a i l s -b
7 . 8
L5o6
0 . 0
3 . 9
J
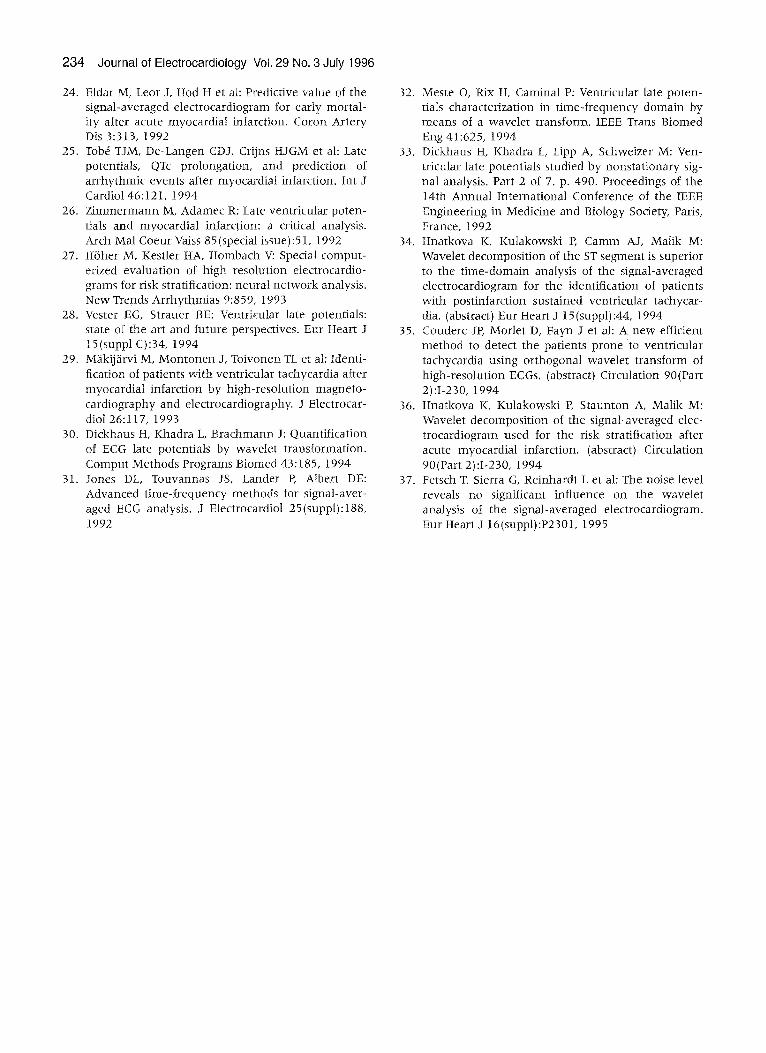
Fig. 3. Multiresolution decomposition of a signal-averaged ECG of a postinfarction patient using seven frequency bands. The left side represents the approximation components and the right side the detail components.

228 Journal of Electrocardiology Vol. 29 No. 3 July 1996
consideration owing to the at tenuat ion produced by the antialias filter of the acquisition system. The total and relative energies of the QRS complex in each f requency band were calculated. The total energy was estimated as the sum of the squares of the detail coefficients. The relative energy was the energy of the detail coefficients in a band with respect to the total energy of the signal. Bertrand et al. showed that the energy of the signal is pre- served by the wavelet t ransform (10).
The algorithm used in this study was writ ten in Turbo Pascal version 7 and executed on an Intel 80486-based IBM-compatible personal computer with a ma th coprocessor included. The algorithm performed the decomposit ion of the signal, its reconstruction, and the calculation of a mean square error of the reconstructed signal with respect to the original. A version of this program permitted analysis of large ECG databases in a batch mode and storage of the results in an ASCII file ready to be imported by the Statistical Package for the Social Sciences (SPSS for Windows, Release 6.0, Chicago, IL) for statistical analyses.
Stat i s t i ca l A n a l y s e s . Univariate analysis of aI1 variables was performed by the M a n n - W h i t n e y U test. Linear dependency between different vari- ables were calculated by means of the bivariate Pearson correlation coefficients. The level of signif- icance (alpha error) was chosen to be .05. The rela- tive cumulative distributions were plotted to deter- mine optimized cutoffs for abnormality, which were used for the calculation of sensitivity, speci- ficity, and total predictive accuracy. Sensitivity was defined as the percentage of patients who in the presence of an event, had an abnormal test result; specificity was defined as the percentage of patients who did not have an event and had a negative test
result. Positive predictive value was defined as the percentage of patients with an abnormal test result and an event among all patients with an abnormal test result; negative predictive value was defined as the percentage of patients with a normal test result and wi thout an event among all patients with a normal test result. Predictive accuracy was defined as the percentage of patients with either a true pos- itive or a true negative test result.
Results
Time-domain Analysis
Table 1 shows the differences in mean values of the t ime-domain parameters be tween the patients who developed serious arrhythmic events after myocardial infarction and those who did not. No significant differences were found in the noise levels. Time-domain analysis showed that 337 patients (44%) presented ventricular late poten- tials. Of the 42 patients who developed arrhythmic events during the follow-up period, 23 (55%) pre- sented late potentials.
Wavelet Transform
The differences in mean values of all wavelet t ransform parameters be tween patients who devel- oped serious arrhythmic events after myocardial infarction and those who did not are also shown in Table 1. The results of univariate analyses of the data for patients with and wi thout arrhythmic events showed significant differences in total energy at 7.8-15.6 Hz (P = .006) and in relative energy at 7.8-15.6 Hz (P = .009), 31.2-62.5 Hz (P = .007), and 62.5-125 Hz (P = .017).
Table 1. Time-domain and Wavelet Transform Parameters That Were Significantly Different Between Patients With and Without Arrhythmic Events
During the Follow-up Period*
Parameters Patients With AEs Patients Without AEs P Values
QRSd (ms) 112 +- 21 105 _+ 17 .009 RMS (gV) 35 _+ 27 46 _+ 32 .007 LAS (ms) 33 _+ 15 29 _+ 13 .04 tE7 (Eu) 141 _+ 124 104+_ 106 .006 rE7 0.095 _+ 0.039 0.081 _+ 0.052 .009 rE31 29_+ 30 (xl0 -3) 49 _+ 61 (×10 -3 ) .007 rE62 3 _+ 3 (xl04) 4_+ 6 (xl04) .017
*Values are mean _+ SD. The nonparametric Mann-Whitney U test was used to calculate P values. QRSd, QRS complex duration; RMS, root mean square of the terminal 40 ms; LAS, duration of the terminat QRS signal below 40 gV; tE7, total energy in the 7.8-15.6-Hz band; rE7, relative energy in the 7.8-15.6-Hz band; rE3l, relative energy in the 31.2-62.5-Hz band; rE62, relative energy in the 62.5-125-Hz band; AE, arrhythmic event; Eu, energy units.

Multiresolution Decomposition of Signal-averaged ECG • Sierra et al. 229
100
80
60
40
20
[%] I-,-sensitivity -)~specificity --accuracy ]
. . . . . . . . . .
_/ - - - I I I I I
0 5 10 15 20 25
Cutoff (29)
30 35 40 45 50 55 60 65 70 75 80
RMS (pV) Fig. 4. Sensitivity, specificity, and accuracy of the root mean square (RMS) of the terminal 40 ms in tee t ime-domain analysis of ventricular late potentials in postinfarction patients with and without arrhythmic events in the follow-up period. The vertical line shows the opt imum cutoff values (29 gV), sensitivity (55%), specificity (65%), and accuracy (64%).
Receiver Operator Characteristics
To assess t he s ta t is t ica l p e r f o r m a n c e of these resul ts , o p t i m u m cutoff va lue s for sens i t iv i ty a n d
specif ic i ty w e r e ca l cu l a t ed as t he m a x i m u m differ- ences in t he r e l a t ive c u m u l a t i v e d i s t r i bu t i on of
e ach p a r a m e t e r . These cutoff va lues c o r r e s p o n d to t he m a x i m u m s u m of sens i t iv i ty a n d specificity.
The sensi t ivi ty , specificity, a n d to ta l p red ic t ive a c c u r a c y of t h e r o o t - m e a n - s q u a r e p a r a m e t e r is s h o w n in F igure 4 as a n e x a m p l e . The s ta t is t ical resu l t s of b o t h m e t h o d s , as we l l as t he cutoff va lue s ca lcu la ted , a re s h o w n in Table 2. A m o n g the t h r e e t i m e - d o m a i n p a r a m e t e r s of la te p o t e n t i a l analys is , t he QRS d u r a t i o n a n d t h e roo t m e a n squa re in t he t e r m i n a l 40 m s h a d t h e bes t d i s c r i m i n a t i n g va lues . To o b t a i n i n f o r m a t i o n a b o u t t he l i nea r d e p e n d e n c e a m o n g d i f fe ren t var iab les , b iva r i a t e P e a r s o n corre-
l a t ion coeff ic ients w e r e ca l cu l a t ed (Table 3). High co r re l a t ions (.50 < Irl < .96 P < . 0 0 i ) w e r e f o u n d b e t w e e n b o t h t i m e - d o m a i n p a r a m e t e r s (r = - . 56 ) , b e t w e e n the to ta l a n d re la t ive ene rg ie s in t he 7 . 8 - 1 5 . 6 - H z b a n d (r = .77), a n d b e t w e e n the re la- t ive e n e r g y in t he 3 1 . 2 - 6 2 . 5 - H z a n d 6 2 . 5 - 1 2 5 - H z
b a n d s (r = .52). The o t h e r va r i ab le s t ha t w e r e sig- n i f i can t ly c o r r e l a t e d h a d a c o r r e l a t i o n coeff ic ient Irl < .23. A m o n g t i m e - d o m a i n p a r a m e t e r s , t he h igh es t specif ic i ty (65%) , to ta l p r ed i c t i ve accu racy (64%) , a n d pos i t ive p red ic t ive a c c u r a c y (8 .2%) w e r e o b t a i n e d w i t h t he roo t m e a n squa re of t he t e r m i - na l 40 ms.
To e n h a n c e t h e pos i t ive p red i c t i ve va lues o b t a i n e d w i t h t he w a v e l e t t r a n s fo rm , seve ra l com- b i n a t i o n s of t he n o n c o r r e l a t e d p a r a m e t e r s w e r e e v a l u a t e d (Table 4). The bes t resu l t s (11 .3%) was
o b t a i n e d w i t h t he use of t he logical a n d o p e r a t i o n
Table 2. Statistical Analys is Using Time-domain and Mul t i reso lu t ion Decomposi t ion of the Signal-averaged ECG in Postinfarct ion Patients With and Without Arrhythmic Events During the Fo l low-up Period
Parameter and Cutoff Values RMS < 29(~V) QRSd > 99 (ms) tE7 > 69 (Eu) rE7 > 0.07 rE31 < 0.004 rE62 ~< 0.00025
Sensitivity (%) 55 79 74 76 83 69 Specificity (%) 65 41 49 48 40 51 Positive predictive value (%) 8.2 7.2 7.7 7.9 7.4 7.6 Negative predictive value (%) 96 97 97 97 98 97 Total predictive accuracy (%) 64 43 50 50 42 52
RMS, root mean square; QRSd, QRS complex duration; tE7, total energy in the 7.8-15.6-Hz band; rE7, relative energy in the 7.8-15.6-Hz band; rE31, relative energy in the 31.2-62.5-Hz band; rE62, relative energy in the 62.5-125-Hz band; Eu, energy units.

230 Journal of Electrocardiotogy Vot. 29 No. 3 July 1996
Table 3. Correlation Coefficients of Time-domain and Multiresolution Decomposition Parameters Significantly Related to Arrhythmic Events
P a r a m e t e r s R M S Q R S d tE7 rE7 rE31 rE62
RMS t . . . . . QRSd -0 .56* 1 . . . . [E7 0.! t* -0 .07* l - - - - rE7 0.14* -0 .23* 0.77* I - - - - rE31 0 .07~ - - -0 .21 * -0 .2* 1 - - rE62 - - - - - 0 . 1 7 5 - 0 . I 3 " 0.52* 1
*P < . 0 0 1 . ½ P <.05. ~_P < .0 I . RMS, roo t m e a n square ; QRSd, QRS c o m p l e x d u r a t i o n ; tE7, toEal e n e r g y in the 7 . 8 - 1 5 . 6 - H z band ; rE7, r e l a t ive e n e r g y in t he 7 .8 -15 .6 -Hz band ; rE31, r e la t ive e n e r g y in t he 31 .2 -62 .5 -Hz band ; rE62, r e la t ive e n e r g y in t he 6 2 . 5 - 1 2 5 - H z band .
Table 4. Statistical Results of the Combination (LogicaI AND) of Noncorrelated Wavele[ Transform Parameters
P a r a m e t e r s a n d tE7 _> 6 9 ( E u ) A N D tE7 _> 6 9 ( E u ) A N D rE7 _> 0 .07 A N D rE7 ~ 0 .07 A N D Cu to f f V a l u e s rE62 < 0 .00025 rE31 _< 0 .004 rE62 _< 0 .00025 rE31 < 0 .004
Sens i t iv i ty (%) 60 69 60 69 Specif ic i ty (%) 71 62 73 64 Pos i t ive p r ed i c t i ve v a l u e (%) i 0 . 6 9.4 11.3 9.9 Nega t ive p r ed i c t i ve v a l u e (%) 97 97 97 97 Total p r ed i c t i ve a c c u r a c y (%) 71 62 72 64
rE7, to ta i e n e r g y in 7 . 8 -15 .6 -Hz band ; rE7, r e l a t i ve e n e r g y in the 7 .8 -15 .6 -Hz band ; rE31, r e l a t ive e n e r g y in t he 3 l .2 -62 .5 - Hz band ; rE62, r e l a t ive e n e r g y in the 6 2 . 5 - 1 2 5 - H z band; Eu, e n e r g y uni t s .
be tween the energies in the f requency bands 7 .8 - I5 .6 Hz (cutoff > .07) and 62.5-125 Hz (cutoff < .00025). All positive predictive values (> 9.4%) obtained f rom these combinat ions were bet ter than the highest positive predictive value (8.2%) obtained wi th the t ime -doma in parameters . In addition, combinat ions a m o n g the wavele t trans- form paramete rs and the root m e a n square of the terminal 40 ms were performed. The results are shown in Table 5. Several of the positive predictive values are even bet ter than the highest (11.3%) achieved with the wavele t t ransform parameters . The mos t representat ive combina t ion was obtained with the roo t -mean - squa re pa rame te r (cutoff < 29 ,~V) and the relative energy in the 7 .8-15.6-Hz fre-
quency band (cutoff > .07), which together yieided a positive predictive accuracy of 14.3%. Figure 5 shows a compar ison be tween the t ime domain, the wavelet t ransform, and the combinat ion of both methods with respect to these statistical results.
Discussion
Signal-averaged electrocardiography has been shown to identify patients at risk for ventr icular tachycardia and sudden death after acute myocar- dial infarction (1-5,24,25). It represents a promis- ing technique, and the prognostic value of late potentials in the postinfarction period has been
Table 5. Statistical Results of the Combination {Logical AND) of Noncorrelated Wavelet Transform Parameters With the Root Mean Square of the Terminal 40 ms of the Time-domain Method
P a r a m e t e r R M S _< 29 (~V) A N D A N D A N D A N D
rE31 _< 0 . 0 0 4 rE62 <_ 0 .00025 rE7 _> 69 (Eu) rE7 _> 0 .07
Sens i t iv i ty (%) 47 38 38 43 Specif ic i ty (%) 8 i 82 86 85 Pos i t ive p r ed i c t i ve v a l u e {%) I2 .6 10.9 13.6 14.3 Nega t ive p r ed i c t i ve v a l u e (%) 96 96 96 96 Total p r ed i c t i ve a c c u r a c y (%) 79 80 83 83
RMS, roo t m e a n s q u a r e of the t e r m i n a l 40 ms; tE7, to ta l e n e r g y in the 7 .8 -15 .6 -Hz band ; rE7, r e l a t ive e n e r g y in the 7 .8 -15 .6 -Hz band ; rE31, r e l a t ive e n e r g y in the 31 .2-62 .5~Hz band ; rE62, r e l a t ive e n e r g y in t he 6 2 . 5 - 1 2 5 - H z band ; Eu, e n e r g y uni t s .

Multiresolution Decomposition of Signal-averaged ECG • Sierra et al. 231
1 0 0 % -
8 0 % -
60%
40%
20%
0 %
[--ITD EEWT ENBoth
Sensitivity Specificity Pos.pred. Neg.pred. Fig. 5. The most representative results of sensitivity, specificity, and positive and negative predictive values obtained with the parameters of time domain (TD), wavelet transform (WT), and combinations of both methods (Both) for pre- diction of arrhythmic events after acute myocardial infarction. The highest sensitivity (60%) and negative predictive accuracy (97%) for identifying patients with and without arrhythmic events was achieved by the wavelet transform, and the highest specificity (85%) and positive predictive accuracy (14.3%) was achieved by the combination of both methods. All methods had very high negative predictive values (96-97%).
well demonstrated during the last 10 years (26). However, analysis of ventricular late potential in the time domain is limited in terms of its specificity and positive predictive value (27). Its value as a predictor of arrhythmic events and sudden cardiac death is relatively low ( 10-30 %), mainly owing to the low incidence of these events, although it is very reliable in predicting a good outcome, show- ing 95% event-free survival if ventricular late potentials are absent (28). Recently, new tech- niques have been proposed to improve the prog- nostic value of signal-averaged ECG analysis. Some representative examples are the spectral turbu- lence technique (8), high-resolution magnetocar- diography (29), artificial neural networks (27), and the wavelet transform ( 13,14, 30-33).
The wavelet transform of the signal-averaged ECGs from patients with sustained ventricular tachycardia and healthy control subjects was ana- lyzed in the time-frequency plane by Dickhaus et al. (13,30), Meste et al. (32), and Khadra et al. (14). In the study by Dickhaus et al., a quantitative discrimination was performed between patients with ventricular tachycardia (n = 21) and healthy subjects (n = 29), resulting in a sensitivity of 90% and a specifidty of 72% as determined by the
energy under the squared modulus of the time-fre- quency distribution plots of the computed wavelet transforms (13). Morlet et al. applied the wavelet transform to the signal-averaged ECG of the XYZ leads in 20 postinfarction patients with ventricular tachycardia and in 20 patients without ventricular tachycardia, as well as in 10 healthy subjects, using an algorithm based on the coherent detection of the local maxima of the wavelet transform (12). A specificity of 90% and a sensitivity of 85% allowed a distinction between patients with and without ventricular tachycardia. The wavelet transform yielded better results than those obtained from the conventional time-domain approach. Hnatkova et al. applied the wavelet decomposition of the signal- averaged ECG in the ST-segment and the T wave for the identification of patients with sustained ventricular tachycardia after myocardial infarction (34). The population consisted of 53 patients with sustained ventricular tachycardia and 53 patients without arrhythmic events during follow-up evalu- ation. The wavelet decomposition combined with the total QRS duration was significantly superior to the conventional time-domain analysis.
The orthogonal wavelet transform of high- resolution ECGs (using dyadic orthogonal Meyer

232 Journal of Electrocardiotogy Vol. 29 No. 3 July 1996
wavelets) was used by Couderc et al. for localiza- tion of micropotentials within the QRS complex (35). They reported an improved detection of patients prone to develop ventricular tachycardias, as compared with the time-domain parameters. Hnatkova et al. reported the use of the wavelet decomposition for risk stratification in 544 sur- vivors of acute myocardial infarction over a follow- up period of 2 years (36). Four parameters were calculated: QRS area, maxima count, surface area, and relative length of the decomposition. In this population, wavelet decomposition of the signal- averaged ECG was a significantly better predictor of postinfarction complications, especially sudden death, than time-domain analysis.
In contrast to most previous reports applying the wavelet transform to signal-averaged ECGs, in this study multiresolution decomposition by the Mallat approach was used to predict postinfarction arrhythmic events. In addition, a population of 769 prospectively enrolled patients was included, which is larger than in any previous report. We expected that the prognostic significance using the complete high-gain QRS complex as a measure of intraventricular conduction abnormalities might be superior to the conventional time-domain approach, which is restricted to the terminal por- tion of the QRS complex. The time-domain para- meters depend strongly on the mean noise level measured in the ST-segment and also on the site of infarction. The prognostic power of time-domain late potentials tends to be lower in anterior than in inferior infarction. This has been attributed to the fact that regional activation takes place earlier in the anterior wall area than in the inferior wall area. Thus, regional slow fractionated activity may be hidden within the QRS complex in anterior myocardial infarction.
On the basis of our results, the most important frequency bands for the discrimination of patients with and without arrhythmic events after myocar- dial infarction are in the frequency bands 7.8-15.6 Hz and 62.5-125 Hz. The results obtained with the relative energy in the 31.2-62.5-Hz band are also considerable. The most important of the time- domain ventricular late potential parameters was the root mean square of the terminal 40 ms. The combination of parameters from the wavelet trans- form and the root-mean-square parameter showed even better predictive values than the wavelet transform alone.
Many studies have found QRS duration to be the most useful parameter for the prediction of arrhythmic events in postinfarction patients, but others have also found the root-mean-square para-
meter to be helpful. These parameters are highly correlated and do not contribute unique informa- tion. These conclusions have been obtained with the criteria commonly used in the detection of ventricular late potentials (eg, QRS duration _> 114 ins at 40 Hz, QRS duration > 120 ms at 25 Hz). In our study, we defined the cutoff value of each parameter as the maximum difference in the rela- tive cumulative distribution. These cutoff values correspond to the maximum sum of sensitivity and specificity. We used the same criteria for the evalu- ation of parameters from different methods, that is, time-domain analysis and the wavelet transform of the vector magnitude. Under these considerations, the root mean square of the terminal 40 ms had higher predictive accuracy than the QRS duration. ~n this study, the total predictive accuracy was strongly correlated with the curve of specificity, owing to the relative low incidence of arrhythmic events in the study group.
The wavelet transform of single-lead ECGs could bring new insights not obtained with the results using the vector magnitude. From a methodologi- cal point of view, special filtering techniques, as in time-domain analysis (eg, bidirectional Butter- worth) are not required; instead, the wavelet algo- rithm can be directly applied to the unfiltered sig- nal-averaged ECG. Although still preliminary, another advantage of the wavelet transform in comparison with analysis of time-domain ventricu- lar late potentials could be lower dependence on the noise level. Fetsch et al. used the Mallat algo- rithm to analyze the signal-averaged ECGs of 31 patients .undergoing cardiac surgery (37). From each patient, two recordings, one before and one during muscle relaxation, were obtained. Neither the total energy nor the relative energy of the wavelet bands was altered significantly. However, in time-domain analyses at 25- and 40-Hz filtering, significant differences in noise level were observed. Because of the limited number of patients included, larger studies have to confirm these findings.
Limitations of Wavelet Transform
Because of the uncertainty principle (19), it is not possible to achieve a simultaneous exact local- ization in the frequency and time domains. Fur- thermore, in dyadic wavelet analysis, the fre- quency resolution is limited by the fact that the filter bandwidth changes by a factor of 2 from one scale of analysis to the next. To obtain a finer fre- quency resolution, it is required to relax the assumption of orthogonality of the wavelet basis

Multiresolution Decomposition of Signal-averaged ECG • Sierra et al. 233
(21). The advantages and disadvantages of other types of wavelet functions for the tasks involved in these analyses remain to be explored.
Limitations of the Study
Potentially lethal arrhythmic events after myocardial infarction occurred only in 42 cases (5.46%). Furthermore, only m en up to 65 years of age with Q wave infarction were included in the study. Therefore, the results of this study should be applied with caution to patients with a non-Q wave myocardial infarction.
Conclusion
The multiresolution decomposit ion of signal- averaged ECGs using the Mallat approach allowed a distinction be tween postinfarction patients with and wi thout arrhythmic events during the follow- up period. The results of the wavelet transform used in this study for prediction of arrhythmic events in postinfarction patients were superior to those achieved with t ime-domain ventricular late potential parameters. Special filtering techniques as used in t ime-domain analysis are not required; instead, the wavelet algorithm can be directly applied to the unfiltered signal-averaged ECG. Combination of wavelet transform and time- domain parameters enhanced predictive values even more.
References
1. Simson MB: Identification of patients with ventricu- lar tachycardia after myocardial infarction from sig- nals in the terminal QRS complex. Circulation 64:235, 1981
2. Berbari E J, Scherlag B J, Hope RR, Lazzara R: Recording from the body surface of arrhythmogenic ventricular activity during the ST-segment. Am J Cardiol 41:697, 1978
3. Kuchar DL, Thorburn CW, Sammel NL: Prediction of serious arrhythmic events after myocardial infarc- tion: signal-averaged electrocardiogram, Holter monitoring and radionuclide ventriculography. J Am Coll Cardiol 9:531, 1987
4. Breithardt G, Cain ME, E1-Sherif N e t al: Standard for analysis of ventricular late potentials using high- resolution or signal-averaged electrocardiography. Circulation 83:1481, 199I
5. Breithardt G, Wichter T, Fetsch T et ah The signal- averaged ECG: time-domain analysis. Eur Heart J I4 (suppl E):27, 1993
6. Gardner PI, Ursell PC, Fenoglio JT, Wit AL: Electro- physiologic and anatomic basis for fractionated elec- trograms recorded from healed myocardial infarcts. Circulation 72:596, 1985
7. Lander P, Albert DE, Berbari E J: Spectrotemporal analysis of ventricular late potentials. J Electrocar- diol 23:95, 1990
8. Kelen G J, Henkin R, Starr AM et al: Spectral turbu- lence analysis of the signal-averaged electrocardio- gram and its predictive accuracy for inducible sus- tained monomorphic ventricular tachycardia. Am J Cardiol 67:965, 1991
9. Mitchell RH, Escalona O J, Balderson DE, Harron DWG: Detection and characterization of ventricular late potentials using fractals. Proceedings of the World Congress of Medical Physics and Biomedical Engineering, Part 1, 1-660. Rio de Janeiro, Brazil, 1994
10. Bertrand O, Bohorquez J, Pernier J: Time-frequency digital filtering based on an invertible wavelet trans- form: an application to evoked potentials. IEEE Trans Biomed Eng 41:77, 1994
11. Wit HE Van Dijk E Avan P: Wavelet analysis of real ear and synthesized click evoked otoacoustic emis- sions. Heart Res 73:141, 1994
12. Morlet D, Peyrin E Desseigne Pet al: Wavelet analy- sis of high-resolution signal-averaged ECGs in postinfarction patients. J Electrocardiol 26:311, 1993
13. Dickhaus H, Khadra L, Brachmann J: Time-fre- quency analysis of ventricular late potentials. Meth- ods Inf Med 33:187, 1994
14. Khadra L, Dickhaus H, Lipp A: Representations of ECG-late potentials in the time frequency plane. J Med Eng Technol 17:228, 1993
15. Crowe JA, Gibson NM, Woolfson MS, Sonekh MG: Wavelet transform as a potential tool for ECG analy- sis and compression. J Biomed Eng 14:268, 1992
16. Obaidat MS: Phonocardiogram signal analysis: tech- niques and performance comparison. J Med Eng Technol 17:221, i993
17. Mallat SG: A theory for multiresolution signal decomposition: the wavelet representation. IEEE Trans Part Anal Mach IntelI 11:674, 1989
18. Cody MA: The fast wavelet transform. Dr. Dobb's J 4:16, 1992
19. Chui CK: An introduction to wavelets. Academic Press, Boston, 1990
20. Allen RL, Kamangar FA, Stokely EM: Laplacian and orthogonal wavelet pyramid decomposition in coarse-to-fine registration. IEEE Trans Signal Proc 41:3536, 1993
21. Daubechies I: The wavelet transform, time fre- quency localization and signal analysis. IEEE Trans, Info Theory 36:961, 1990
22. Schiff S J, Aldroubi A, Unser M, Sato S: Fast wavelet transformation of EEG. Electroencephalogr Clin Neurophysiol 91:442, 1994
23. Vetterli M: Wavelets and filter banks: theory and design. IEEE Trans Signal Proc 40:2207, 1992
234 Journal of Electrocardiology Voi. 29 No. 3 July 1996
24. Eldar M, Leor J, Hod H et ah Predictive value of the signal-averaged electrocardiogram for early mortal- ity after acute myocardial infarction. Coron Artery Dis 3:313, 1992
25. Tob~ TJM, De-Langen CDJ, Crijns HJGM et ah Late potentials, QTc prolongation, and prediction of arrhythmic events after myocardial infarction. Int J Cardiol 46:121, 1994
26. Zimmermann M, Adamec R: Late ventricular poten- tials and myocardial infarction: a critical analysis. Arch Mal Coeur Vaiss 85(special issue):51, 1992
27. H6her M, Kestler HA, Hombach V: Special comput- erized evaluation of high resolution electrocardio- grams for risk stratification: neural network analysis. New Trends Arrhythmias 9:859, 1993
28. Vester EG, Strauer BE: Ventricular late potentials: state of the art and future perspectives. Eur Heart J 15(suppl C):34, 1994
29. Mfikijfirvi M, Montonen J, Toivonen TL et at: Identi- fication of patients with ventricular tachycardia after myocardial infarction by high-resolution magneto- cardiography and electrocardiography. J Electrocar- diol 26:117, 1993
30. Dickhaus H, Khadra L, Brachmann J: Quantification of ECG late potentials by wavelet transformation. C omput Methods Programs B iomed 43:185, 1994
31. Jones DL, Touvannas JS, Lander E Albert DE: Advanced t ime-frequency methods for signal-aver- aged ECG analysis. J Electrocardiol 25(suppl):188, 1992
32. Meste O, Rix H, Caminal P: Ventricular late poten- tials characterization in t ime-frequency domain by means of a wavelet transform. IEEE Trans Biomed Eng 41:625, 1994
33. Dickhaus H, Khadra L, Lipp A, Schweizer M: Ven- tricular late potentials studied by nonstat ionary sig- nal analysis. Part 2 of 7. p. 490. Proceedings of the 14th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Paris, Erance, 1992
34. Hnatkova K, Kulakowski P, Camm AJ, Malik M: Wavelet decomposition of the ST segment is superior to the t ime-domain analysis of the signal-averaged electrocardiogram for the identification of patients with postinfarction sustained ventricular tachycar- dia. (abstract) Eur Heart J 15 (suppl):44, 1994
35. Couderc JP, Morlet D, Fayn J e t al: A new efficient method to detect the patients prone to ventricular tachycardia using orthogonal wavelet transform of high-resolution ECGs. (abstract) Circulation 90(Part 2):I-230, 1994
36. Hnatkova K, Kulakowski P, Staunton A, Malik M: Wavelet decomposit ion of the signal-averaged elec- trocardiogram used for the risk stratification after acute myocardial infarction. (abstract) Circulation 90(Part 2):I-230, 1994
37. Fetsch T, Sierra G, Reinhardt L e t al: The noise level reveals no significant influence on the wavelet analysis of the signal-averaged electrocardiogram. Eur Heart J 16(suppl):P2301, 1995
Copyright © 2022 FDOKUMEN




















