Multiple sclerosis: The importance of early recognition and ...
15
REVIEW m CREDIT ROBERT J. FOX, MD Mellen Center for Multiple Sclerosis Treatment and Research, Department of Neurology, Cleveland Clinic JEFFREY A. COHEN, MD Mellen Center for Multiple Sclerosis Treatment and Research, Department of Neurology, Cleveland Clinic Multiple sclerosis: The importance of early recognition and treatment ABSTRACT Primary practitioners need to know how to expedite the diagnosis and treatment of multiple sclerosis (MS), because treatments that can slow its course appear to be most effective when started early. Several lines of evidence demonstrate that tissue damage occurs very early in the disease, and much of this damage is clinically silent. KEY POINTS After the diagnosis of MS is made and appropriate treatments started, patients require ongoing care. Primary care physicians play an important role in identifying and managing MS symptoms. An effective partnership between the patient's primary care provider and neurologist can help patients remain active by addressing symptoms and complications of MS. In clinical trials, interferon (IFN) beta-1a, IFN beta-1 b, IFN beta-1a(R), and glatiramer acetate reduced the relapse rate by approximately 30%. ECENT STUDIES AND NEW TREATMENTS are changing the approach to multiple sclerosis (MS). The studies have shown that, although clinical manifestations are intermit- tent and often mild early in the disease, patho- logic damage accumulates from the onset. New treatments can slow the progression of neurologic manifestations, but must be started early in the course of the disease. Primary care providers need to be familiar with MS, its complications, and different treat- ments to expedite diagnosis and coordinate treatment. They play a key role in identifying and managing the protean symptoms of MS. • CLINICAL FEATURES OF MS MS is a chronic inflammatory disorder of the central nervous system (CNS—brain, optic nerves, and spinal cord) characterized patho- logically by demyelination and axonal dam- age. In the United States, an estimated 250,000 to 350,000 people have MS. Symptoms Because the lesions in MS are multifocal and can develop in any location within the central nervous system, the possible clinical manifes- tations are diverse ( TABLE 1). Symptoms vary markedly from patient to patient and in indi- vidual patients over time. Motor deficits in MS include weakness, spasticity, and ataxia. Weakness usually is central in character and accompanied by spas- ticity (abnormal increased muscle tone), hyperreflexia, and abnormal cutaneous reflexes (eg, the Babinski sign). These physi- CLEVELAND CLINIC JOURNAL OF MEDICINE VOLUME 68 • NUMBER 2 FEBRUARY 2001 157 on April 21, 2022. For personal use only. All other uses require permission. www.ccjm.org Downloaded from
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Multiple sclerosis: The importance of early recognition and ...

REVIEW
m CREDIT
ROBERT J. FOX, MD Mellen Center for Mult iple Sclerosis Treatment and Research, Department of Neurology, Cleveland Clinic
J E F F R E Y A. COHEN, MD Mellen Center for Mult iple Sclerosis Treatment and Research, Department of Neurology, Cleveland Clinic
Multiple sclerosis: The importance of early recognition and treatment
ABSTRACT Primary practitioners need to know how to expedite the diagnosis and treatment of multiple sclerosis (MS), because treatments that can slow its course appear to be most effective when started early. Several lines of evidence demonstrate that tissue damage occurs very early in the disease, and much of this damage is clinically silent.
KEY POINTS After the diagnosis of MS is made and appropriate treatments started, patients require ongoing care. Primary care physicians play an important role in identifying and managing MS symptoms.
An effective partnership between the patient's primary care provider and neurologist can help patients remain active by addressing symptoms and complications of MS.
In clinical trials, interferon (IFN) beta-1a, IFN beta-1 b, IFN beta-1a(R), and glatiramer acetate reduced the relapse rate by approximately 30%.
E C E N T S T U D I E S A N D N E W T R E A T M E N T S
are changing the approach to multiple sclerosis (MS) . The studies have shown that, although clinical manifestations are intermit-tent and often mild early in the disease, patho-logic damage accumulates from the onset. New treatments can slow the progression of neurologic manifestations, but must be started early in the course of the disease.
Primary care providers need to be familiar with MS, its complications, and different treat-ments to expedite diagnosis and coordinate treatment. They play a key role in identifying and managing the protean symptoms of MS.
• CLINICAL FEATURES OF M S
M S is a chronic inflammatory disorder of the central nervous system (CNS—brain, optic nerves, and spinal cord) characterized patho-logically by demyelination and axonal dam-age. In the United States, an estimated 250,000 to 350,000 people have MS.
S y m p t o m s Because the lesions in MS are multifocal and can develop in any location within the central nervous system, the possible clinical manifes-tations are diverse (TABLE 1 ) . Symptoms vary markedly from patient to patient and in indi-vidual patients over time.
Motor deficits in MS include weakness, spasticity, and ataxia. Weakness usually is central in character and accompanied by spas-ticity (abnormal increased muscle tone), hyperreflexia, and abnormal cutaneous reflexes (eg, the Babinski sign). These physi-
CLEVELAND CLINIC JOURNAL OF MEDICINE V O L U M E 68 • NUMBER 2 FEBRUARY 2 0 0 1 1 5 7
on April 21, 2022. For personal use only. All other uses require permission.www.ccjm.orgDownloaded from

MULTIPLE SCLEROSIS FOX AND COHEN
TABLE 7
T y p i c a l n e u r o l o g i c m a n i f e s t a t i o n s o f M S
MANIFESTATION PERCENT OF PATIENTS WITH MANIFESTATION' AT PRESENTATION DURING THE COURSE
Visua l loss or 49 100 o c u l o m o t o r d y s f u n c t i o n Weakness 43 88 Sensory de f i c i t s 41 87 I n c o o r d i n a t i o n 23 82 Bladder , b o w e l , or 10 63 sexua l d y s f u n c t i o n C o g n i t i v e i m p a i r m e n t 4 39
'To ta l percentages are greater than 1 0 0 % because some pat ients had mul t ip le symptoms
ADAPTED FROM POSER S, WIKSTROM J, BAUER HJ. CLINICAL DATA A N D THE IDENTIFICATION OF SPECIAL FORMS OF MULTIPLE SCLEROSIS IN 1271 CASES STUDIED WITH A STANDARDIZED
DOCUMENTATION SYSTEM. J NEUROL SCI 1979; 4 0 : 1 5 9 - 1 6 8 .
cal findings in a young patient with previous neurologic symptoms may raise the suspicion of MS. Involvement of the cerebellum or its connections leads to appendicular, truncal, gait, bulbar, or ocular ataxia.
Sensory loss can involve any combina-tion of the limbs or trunk and any combina-tion of the senses. Sometimes the pattern of sensory loss can be patchy or can simulate a peripheral nerve or spinal root distribution. Negative sensory symptoms (ie, loss of sensa-tion) often are accompanied by positive sen-sory phenomena (see below). Visual loss in M S reflects the site of involvement of the afferent visual system. Unilateral loss of vision due to optic or retrobulbar neuritis is the most common pattern. Lesions of the efferent visu-al system produce abnormalities of eye move-ments. Diplopia and blurred vision are the most common symptoms.
Urinary symptoms. The most straightfor-ward bladder manifestation is urinary frequen-cy and urgency resulting from detrusor hyper-activity. However, urinary manifestations of MS more commonly include failure of the bladder both to store urine appropriately and to empty completely. Formal urodynamic studies often are necessary to delineate accu-rately the pathophysiology of the urinary dys-function and to distinguish neurogenic mech-
MS patients list fatigue as their most troubling symptom
anisms from structural causes. Similarly, bowel symptoms can include both constipation or urgency and incontinence.
Gait dysfunction caused by MS has spe-cial significance because the resultant disabil-ity has an impact on quality of life and self-image. Potential causes of gait dysfunction include weakness, spasticity, ataxia, vestibular symptoms, sensory loss, and visual distur-bances. Evaluation by a physical therapist can help to sort out the principal cause or causes of gait dysfunction and decide upon compensato-ry strategies.
C o m m o n l y o v e r l o o k e d s y m p t o m s Physicians frequently overlook several com-mon symptoms of MS, including sexual dys-function, cognitive impairment, fatigue, and pain. Because these manifestations can have a significant impact on quality of life, they are important to identify. Each has many possible causes in addition to MS, which need to be considered before attributing these symptoms to MS.
Sexual dysfunction. Although patients and health care professionals often are uncom-fortable raising the issue of sexual dysfunction, it has an important impact on the patient's sense of self-worth and relationships with oth-ers. Erectile dysfunction is common in men, and altered libido and genital sensation are common in both men and women.
Cognitive dysfunction, which is common in MS, most often involves problems with concentration, processing speed, executive function (eg, planning), and visuospatial abil-ities. Formal neuropsychologic testing often is necessary to confirm the presence of cognitive dysfunction and to quantify its severity.
Fatigue. In a survey of patients with MS, fatigue was listed as the most troubling symp-tom. 1 Two types of fatigue are characteristic of MS. First, patients with M S often experience worsening in neurologic function with exer-tion, probably reflecting failure of nerve con-duction in demyelinated.pathways with repeat-ed use or increased body temperature. Second, patients report a chronic lack of energy inde-pendent of exertion. Similar fatigue occurs in a variety of immune and infectious disorders and may result from chronic immune activation and elaboration of immune mediators.
1 5 8 C L E V E L A N D C L I N I C J O U R N A L OF M E D I C I N E V O L U M E 6 8 • N U M B E R 2 F E B R U A R Y 2 0 0 1
on April 21, 2022. For personal use only. All other uses require permission.www.ccjm.orgDownloaded from

T A B L E 2 T A B L E 3 C l a s s i f i c a t i o n o f M S b a s e d on c l i n i c a l c o u r s e
Relapsing-remitting Symptoms and signs develop in the context of clearly defined acute relapses fo l lowed by part ial or complete recovery Clinical manifestations are stable between relapses Secondary progressive After an initial relapsing-remitt ing course, manifestations worsen gradually w i th or w i thou t superimposed acute relapses Primary progressive Manifestations gradually worsen f rom disease onset wi thout relapses
Progressive relapsing Manifestations gradually worsen from disease onset with subsequent superimposed relapses ADAPTED FROM LUBLIN FD, REINGOLD SC. DEFINING THE CLINICAL
COURSE OF MULTIPLE SCLEROSIS: RESULTS OF A N INTERNATIONAL SURVEY. NEUROLOGY 1996; 4 6 : 9 0 7 - 9 1 1 .
Pain. In addition to loss of sensation, patients with MS often complain of positive sensory symptoms, described as uncomfortable tingling, aching, or prickling. These often have a variable distribution and can change over time. At times patients experience frank pain, which may be sharp, lancinating, and paroxys-mal or more chronic burning dysesthesia.
Class i f i ca t ion is b a s e d on d isease course As outlined in TABLE 2 , MS is classified on the basis of the time course over which manifesta-tions develop.2 Since this classification system is empiric and not based on biologic criteria, the pathogenic differences between disease forms remain uncertain. Nonetheless, this classification system provides the framework for an organized approach to diagnosis and long-term management and also allows clini-cal trials to define a more homogeneous pop-ulation for study.
Relapsing-remitting. In approximately 8 5 % of patients, MS initially has a relapsing-remitting course. Symptoms of a relapse typi-cally develop over several days to weeks and then resolve over several weeks to months.
S c h u m a c h e r c r i t e r i a f o r M S
All of the fo l lowing must be present:
Onset of symptoms between ages 20 and 50
Manifestations indicating central nervous system whi te matter disease
Lesions disseminated in t ime and space
Objective abnormalit ies on examinat ion
Manifestations develop as relapses lasting more than 24 hours, spaced 1 month or more apart, or gradual or stepwise progression
Alternative diagnoses el iminated ADAPTED FROM SCHUMACHER GA, BEEBE GW, KIBLER RF, ET AL.
PROBLEMS OF EXPERIMENTAL TRIALS OF THERAPY IN MULTIPLE SCLEROSIS: REPORT BY THE PANEL ON THE EVALUATION OF EXPERI-
MENTAL TRIALS OF THERAPY IN MULTIPLE SCLEROSIS. A N N NY A C A D SCI 1965; 122 :552-568 .
The manifestations can resolve completely, or there may be residual neurologic deficits. Relapses occur on average every 1 to 2 years, although the relapse rate varies markedly both between patients and in individual patients over time.
Secondary progressive. Relapsing-remit-ting MS usually evolves into a secondary pro-gressive course an average of 10 to 15 years after the disease onset.3 When M S lasts 25 years or more, approximately 9 0 % of cases with an initial relapsing-remitting course eventually convert to a secondary progressive course. In secondary progressive MS, preexist-ing neurologic deficits gradually worsen over time. Early in the transition from relapsing-remitting to secondary progressive M S there may be relapses superimposed on gradual worsening, but relapses usually become less evident over time.
Primary progressive. Approximately 15% of patients have gradually worsening manifestations from the onset without clinical relapses: so-called primary progressive MS. Compared with those with relapsing-remit-ting/secondary progressive MS, patients with primary progressive MS typically are older at onset, more often are men, have fewer abnor-malities on magnetic resonance imaging (MRI) of the brain, and respond less readily to diseased-modifying immunotherapies.
Suspect MS in a young adult with relapsing neurologic symptoms
C L E V E L A N D C L I N I C J O U R N A L OF M E D I C I N E V O L U M E 6 8 • N U M B E R 2 F E B R U A R Y 2 0 0 1 1 5 9
on April 21, 2022. For personal use only. All other uses require permission.www.ccjm.orgDownloaded from

MULTIPLE SCLEROSIS FOX AND COHEN
TABLE 7
R e d f l a g s f o r t h e p o t e n t i a l m i s t a k e n d i a g n o s i s o f M S
Onset of symptoms before age 20 or after age 50 Atypical course (eg, gradually progressive from onset w i thou t stabil ization or remissions, or abrupt onset of symptoms) Very prominent family history of a similar disorder Prominent neurologic manifestations unusual for MS (eg, headache) Systemic manifestations (eg, prominent rheumatic symptoms) Unifocal neurologic manifestations even if relapsing Absent features typical of MS (eg, lack of sensory or bladder involvement, or normal MRI), particularly in long-standing or severe disease
Atypical response to t reatment (either lack of any response or an unusually rapid and dramatic response)
Progressive relapsing M S is defined as gradual neurologic worsening from the onset with subsequent superimposed relapses. It is suspected that progressive relapsing MS repre-sents secondary progressive M S in which the initial relapses were unrecognized, forgotten,
Cranial MRI is or clinically silent.
the most useful . . . . . . . . . . . . R„c • D I A G N O S I N G M S
test for MS M S has no pathognomonic clinical, laborato-ry, or imaging finding. Therefore, the diagno-sis ultimately is a clinical decision based on weighing the factors that support the diagno-sis against those that fail to support it or point to the possibility of an alternative diagnosis. The Schumacher criteria^ outline the clinical features typical of MS ( T A B L E 3). Imaging and laboratory studies are used to add support to the diagnosis and rule out other causes of symptoms.
Establishing the diagnosis of M S is straightforward in patients who exhibit classic clinical features and a relapsing-remitting or secondary progressive course. In this situation the likelihood of finding another disorder is small, and testing is unnecessary other than cranial MRI and selected blood work. However, certain "red flags" suggest that a diagnosis other than M S needs to be consid-ered ( T A B L E 4 ) . More extensive testing, guided
by the clinical picture, is warranted in such cases to better confirm the diagnosis of M S and eliminate other disorders.
Cranial MRI is the most useful test in the diagnostic evaluation for MS. It is abnormal in approximately 90% of M S patients, although it may be normal or the findings nonspecific early in the disease course.
MRI of the brain should include long T R images (either fluid-attenuated inversion recovery [FLAIR] or T2-weighted sequences) plus T1-weighted images before and after administration of gadolinium.
Typical findings include multiple ovoid or patchy foci of increased signal on long T R images in the periventricular and subcortical white matter, corpus callosum, brainstem, and cerebellum ( F I G U R E S 1 A N D 2 ) . Often, one or more (but usually not all) of the lesions enhance fol-lowing administration of gadolinium. T h e enhancement results from leakiness of the blood-brain barrier and is thought to indicate lesions with active inflammation. Atrophy of the parenchyma and corpus callosum are well-recognized features of long-standing MS. 5
Spinal MRI should be obtained if cranial MRI is negative, in older patients in whom nonspecific cerebral white lesions sometimes can be found, or if the patient's principal man-ifestations localize to the spinal cord.
Additional studies. Additional support for the diagnosis of M S can be obtained with the demonstration of intrathecal immuno-globulin production (increased IgG index or oligoclonal bands) on cerebrospinal examina-tion or abnormalities on evoked potentials. In general, these studies are not necessary in patients with clinical and MRI features typical of M S but should be obtained if the clinical and MRI findings fail to adequately support the diagnosis of MS or if atypical features raise the possibility of an alternative diagnosis.
Laboratory tests are necessary to help exclude other disorders that can mimic MS. When a patients clinical and radiologic man-ifestations are typical of relapsing-remitting or secondary progressive MS, only limited labo-ratory studies are necessary: for example an antinuclear antibody ( A N A ) titer and ery-throcyte sedimentation rate to screen for con-nective tissue disorders, serologic tests for syphilis, vitamin B 1 2 level, thyroid-stimulat-
1 6 0 C L E V E L A N D C L I N I C J O U R N A L OF M E D I C I N E V O L U M E 6 8 • N U M B E R 2 F E B R U A R Y 2 0 0 1
on April 21, 2022. For personal use only. All other uses require permission.www.ccjm.orgDownloaded from

ing hormone level to screen for thyroid dis-ease, and a complete blood count. A low-pos-itive A N A titer is common in MS and should not cause confusion. When the clinical pic-ture is atypical, more complete laboratory studies are needed and are directed by the clinical setting.
Should the diagnostic criteria be rede-fined? Current diagnostic criteria do not allow clinicians to diagnose MS at the first clinical manifestation. However, in patients with an isolated inflammatory C N S syndrome consis-tent with an MS relapse, the presence of mul-tiple lesions on brain MRI or evidence of intrathecal immunoglobulin synthesis in cere-brospinal fluid substantially increases the risk of an additional relapse.6'7
Until recently our practice was not to start therapy routinely at this stage. However, two recent studies8'9 reported benefit from initia-tion of disease-modifying therapy with inter-feron (IFN) beta following a single demyeli-nating event. These findings have led to efforts to redefine the diagnostic criteria for MS to allow appropriate initiation of treatment at an early stage.
• PATHOGENESIS OF M S
T h e underlying cause of M S remains unknown. The prevailing hypothesis is that MS results from a cell-mediated autoimmune attack directed against myelin antigens, but emerging evidence suggests that the immunopathogenesis probably is more com-plex.10 T h e genetics of MS involves multiple genes conferring a genetic predisposition and possibly determining disease course and sever-ity.11 A variety of environmental factors have been implicated as potential causes of MS, particularly infectious agents. However, fol-low-up studies have failed to confirm any of these putative causes.
Historically, demyelination has been considered the main pathophysiologic mech-anism producing neurologic manifestations in MS. While inflammatory demyelination and the resultant block of nerve conduction in affected pathways accounts for the reversible neurologic sequelae of acute relapses, several lines of evidence suggest that permanent disability results from axonal
M R I a p p e a r a n c e o f M S : T y p i c a l l e s i o n l o c a t i o n s
FIGURE 1. T 2 - w e i g h t e d m a g n e t i c r e s o n a n c e i m a g e o f a 2 4 - y e a r o l d w o m a n w i t h a 2 - y e a r h i s t o r y o f r e l a p s i n g -r e m i t t i n g MS. T h e r e a r e m u l t i p l e w h i t e - m a t t e r l e s i o n s i n a classic d i s t r i b u t i o n , o v o i d l e s i o n s o r i e n t e d p e r p e n d i c u l a r t o t h e l a t e r a l v e n t r i c l e s ( D a w s o n ' s f i n g e r s , c l o s e d a r r o w h e a d ) , d e e p w h i t e - m a t t e r l e s i o n s ( c l o s e d a r r o w ) , s u b c o r t i c a l l e s i ons i n v o l v i n g U - f i b e r s ( o p e n a r r o w h e a d ) , a n d c o n f l u e n t l e s i o n s a d j a c e n t t o t h e p o s t e r i o r h o r n o f t h e l a t e r a l v e n t r i c l e ( o p e n a r r o w ) . N o n e o f t h e l e s i o n s e n h a n c e d f o l l o w i n g g a d o l i n i u m a d m i n i s t r a t i o n . T h e r e is m o d e r a t e a t r o p h y m a n i f e s t e d as v e n t r i c u l a r e n l a r g e m e n t a n d p r o m i n e n t su lc i . D e s p i t e e a r l y r e l a p s i n g - r e m i t t i n g M S , t h i s p a t i e n t has s e v e r e r a d i o l o g i c a l f i n d i n g s , p l a c i n g h e r a t i n c r e a s e d r isk f o r f u t u r e d i s a b i l i t y .
damage. Two recent autopsy studies1 2 '1 3
demonstrated that extensive axonal damage is a consistent and prominent feature of M S lesions. Cerebral atrophy on MRI is a fre-quent finding in patients with severe long-standing disease, and considerable brain atrophy can be detected in patients with early relapsing-remitting MS and only mild clinical disability.1^15 Clearly, the patho-physiology involves permanent injury, even at an early stage of disease.
C L E V E L A N D C L I N I C J O U F i N A L OF M E D I C I N E V O L U M E 6 8 • N U M B E R 2 F E B R U A R Y 2 0 0 1 1 6 1
on April 21, 2022. For personal use only. All other uses require permission.www.ccjm.orgDownloaded from

MULTIPLE SCLEROSIS FOX AND COHEN
M R I a p p e a r a n c e o f M S : G a d o l i n i u m e n h a n c e m e n t
FIGURE 2. Le f t , T 2 - w e i g h t e d m a g n e t i c r e s o n a n c e i m a g e o f a 2 5 - y e a r - o l d w o m a n w i t h a 5 - y e a r h i s t o r y o f r e l a p s i n g - r e m i t t i n g m u l t i p l e sc le ros is . R i g h t , g a d o l i n i u m -e n h a n c e d T 1 - w e i g h t e d i m a g e o f t h e s a m e p a t i e n t . S o m e o f t h e T 2 l e s i o n s e x h i b i t g a d o l i n i u m e n h a n c e m e n t .
Permanent tissue damage begins to accumulate early in the disease
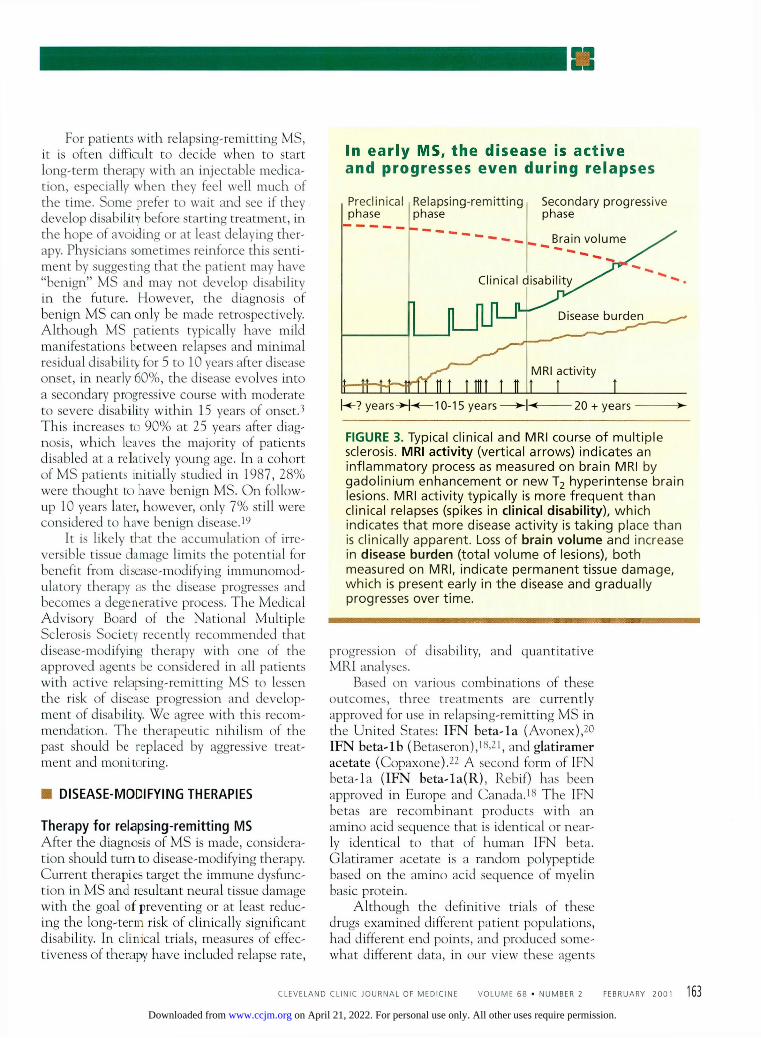
Current concepts of the pathogenesis of MS are summarized in F I G U R E 3 . Approximately 6 0 % to 7 0 % of patients have multiple brain lesions on MRI at the time of the initial clin-ical event,16-17 suggesting that subclinical inflammatory events often predate the clinical presentations. O n average, patients have clin-ical relapses every 1 to 2 years during the relapsing-remitting phase of the disease. Serial MRI studies have shown that MRI-active lesions (defined as new or enlarging T 2 lesions or lesions demonstrating gadolinium enhance-ment) develop up to 10 to 20 times more fre-quently than clinical relapses.
Thus, although relapsing-remitting M S appears to have clinically active and quiescent periods, inflammatory lesions are developing or evolving almost continuously. Although residual manifestations between relapses often are mild during this stage of disease, there is ongoing tissue damage, manifested as accrual of MRI lesions and progressive brain atro-phy. 14,15,18 Thus, clinical relapses and the pro-gression of disability are a poor reflection of
the ongoing inflammation and resultant tissue damage at early stages of the disease.
A current hypothesis states that overt progression of disability occurs when ongoing irreversible tissue injury exceeds a critical threshold beyond which the nervous system can no longer compensate. This results in the apparent conversion from relapsing-remitting to secondary progressive disease. Ultimately, gadolinium enhancement becomes rare, and patients gradually worsen without acute relapses. It is thought that at this point the dis-ease has become essentially a degenerative process, with neurologic deterioration inde-pendent of ongoing inflammation.
• START THERAPY EARLY
An important implication of this hypothesis is that, to be maximally effective, disease-modi-fying immunomodulatory therapy should be started early in the relapsing-remitting phase and before permanent disability develops ( T A B L E 5 ) .
162 C L E V E L A N D C L I N I C J O U R N A L OF M E D I C I N E V O L U M E 6 8 • N U M B E R 2 F E B R U A R Y 2 0 0 1
on April 21, 2022. For personal use only. All other uses require permission.www.ccjm.orgDownloaded from
For patients with relapsing-remitting MS, it is often difficult to decide when to start long-term therapy with an injectable medica-tion, especially when they feel well much of the time. Some prefer to wait and see if they develop disability before starting treatment, in the hope of avoiding or at least delaying ther-apy. Physicians sometimes reinforce this senti-ment by suggesting that the patient may have "benign" MS and may not develop disability in the future. However, the diagnosis of benign M S can only be made retrospectively. Although MS patients typically have mild manifestations between relapses and minimal residual disability for 5 to 10 years after disease onset, in nearly 60%, the disease evolves into a secondary progressive course with moderate to severe disability within 15 years of onset.3
This increases to 9 0 % at 25 years after diag-nosis, which leaves the majority of patients disabled at a relatively young age. In a cohort of M S patients initially studied in 1987, 2 8 % were thought to have benign MS. On follow-up 10 years later, however, only 7 % still were considered to have benign disease.19
It is likely that the accumulation of irre-versible tissue damage limits the potential for benefit from disease-modifying immunomod-ulatory therapy as the disease progresses and becomes a degenerative process. The Medical Advisory Board of the National Multiple Sclerosis Society recently recommended that disease-modifying therapy with one of the approved agents be considered in all patients with active relapsing-remitting MS to lessen the risk of disease progression and develop-ment of disability. We agree with this recom-mendation. The therapeutic nihilism of the past should be replaced by aggressive treat-ment and monitoring.
• D I S E A S E - M O D I F Y I N G THERAPIES
T h e r a p y fo r r e l a p s i n g - r e m i t t i n g M S After the diagnosis of M S is made, considera-tion should turn to disease-modifying therapy. Current therapies target the immune dysfunc-tion in M S and resultant neural tissue damage with the goal of preventing or at least reduc-ing the long-term risk of clinically significant disability. In clinical trials, measures of effec-tiveness of therapy have included relapse rate,
I n e a r l y M S , t h e d i s e a s e is a c t i v e a n d p r o g r e s s e s e v e n d u r i n g r e l a p s e s
Prec l in ica l R e l a p s i n g - r e m i t t i n g phase
Secondary p r o g r e s s i v e phase
h - ? y e a r s - > - H — 1 0 - 1 5 years 20 + years
FIGURE 3 . T y p i c a l c l i n i c a l a n d M R I c o u r s e o f m u l t i p l e sc le ros is . MRI activity ( v e r t i c a l a r r o w s ) i n d i c a t e s a n i n f l a m m a t o r y p rocess as m e a s u r e d o n b r a i n M R I b y g a d o l i n i u m e n h a n c e m e n t o r n e w T 2 h y p e r i n t e n s e b r a i n l es ions . M R I a c t i v i t y t y p i c a l l y is m o r e f r e q u e n t t h a n c l i n i c a l r e l a p s e s ( sp i kes i n clinical disabil ity), w h i c h i n d i c a t e s t h a t m o r e d i s e a s e a c t i v i t y is t a k i n g p l a c e t h a n is c l i n i c a l l y a p p a r e n t . Loss o f brain v o l u m e a n d i n c r e a s e i n d isease burden ( t o t a l v o l u m e o f l es ions ) , b o t h m e a s u r e d o n M R I , i n d i c a t e p e r m a n e n t t i s s u e d a m a g e , w h i c h is p r e s e n t e a r l y i n t h e d i s e a s e a n d g r a d u a l l y p r o g r e s s e s o v e r t i m e .
progression of disability, and quantitative MRI analyses.
Based on various combinations of these outcomes, three treatments are currently approved for use in relapsing-remitting MS in the United States: IFN beta-la (Avonex),2 0
IFN beta-lb (Betaseron),18 '21 , and glatiramer acetate (Copaxone).2 2 A second form of IFN beta-la ( IFN beta-la(R), Rebif) has been approved in Europe and Canada.18 The IFN betas are recombinant products with an amino acid sequence that is identical or near-ly identical to that of human IFN beta. Glatiramer acetate is a random polypeptide based on the amino acid sequence of myelin basic protein.
Although the definitive trials of these drugs examined different patient populations, had different end points, and produced some-what different data, in our view these agents
C L E V E L A N D C L I N I C J O U F i N A L OF M E D I C I N E V O L U M E 6 8 • N U M B E R 2 F E B R U A R Y 2 0 0 1 1 6 3
on April 21, 2022. For personal use only. All other uses require permission.www.ccjm.orgDownloaded from

MULTIPLE SCLEROSIS FOX A N D COHEN
œ h œ W h y M S s h o u l d b e t r e a t e d e a r l y
Most cases ul t imately evolve into a secondary progressive course w i t h some degree of permanent disabil ity A l though benign MS exists, it is rare The abil ity to predict prognosis in individual patients is l imited Clinical features correlate poorly w i th the ongoing inf lammatory process, w i th resultant progressive irreversible tissue destruction in early, relapsing-remitt ing MS Disease-modifying therapies are available that effectively reduce disease activity and accumulation of disability in relapsing-remit-t ing MS, albeit incompletely; these therapies are preventative, not restorative Extensive experience confirms that, despite troublesome side effects, these agents are safe in general Accumulat ing irreversible pathology, decreasing inf lammation, and evolut ion of MS into a degenerative process l imit the effec-tiveness of disease-modifying therapies late in the disease Emerging evidence suggests increased effectiveness of the avail-able therapies when started early in the disease
appear to have largely comparable clinical efficacy. All four agents reduced the relapse
Benign MS rate by approximately 30%, decreased the ¡S r a r e severity of the relapses, and had beneficial
effects on measures of MS activity and lesion accrual on MRI. As for delay of disability pro-gression, the data were most convincing for IFN beta-la, which produced a 3 7 % reduction in disability progression in a phase 3 trial. It is anticipated that the beneficial effects on relapses, disability progression, and MRI mea-sures of disease activity demonstrated in clini-cal trials lasting for 2 to 3 years will translate into meaningful long-term benefit. However, this prediction is as yet unproven.
Based on the definitive clinical trials and extensive post-marketing experience, all of these agents clearly are safe and effective in relapsing-remitting MS.
Limitations of therapy. All of the avail-able agents have limitations. All are expen-sive, costing approximately $10,000 per year. All are given by injection one or several times per week, which is inconvenient and unpleas-ant for most patients. And all of these agents have side effects, although serious adverse effects have been extremely rare ( T A B L E 6).
Patients continuing with long-term disease-modifying therapies should receive education about potential side effects and aggressive management of side effects. In general, we rec-ommend that a neurologist familiar with the use of these therapies be consulted when they are initiated.
The most important limitation of the agents available to treat relapsing-remitting MS is their partial effectiveness. A substantial proportion of patients in the active treatment groups in all of the studies continued to have relapses and worsening disability. Emerging evidence of pathological heterogeneity in M S 1 0 suggests that the partial efficacy of these agents for patients as a group may reflect the presence of responders and nonresponders to each agent in the p o p u l a t i o n . 2 3 Ongoing monitoring of patients during treatment is important to detect nonresponders and modi-fy therapy accordingly.
Mitoxantrone (Novantrone) was approved in October 2000 by the U S Food and Drug Administration for "reducing neurologic disability and/or the frequency of clinical relapses in patients with secondary-progressive, progressive-relapsing or worsening relapsing-remitting MS." Mitoxantrone has potent effects on both cellular and humoral immune mechanisms. Typically in MS it is given as an intravenous infusion every 3 months. In clini-cal trials, mitoxantrone treatment led to signif-icant reductions in relapse rates, disability pro-gression, and MRI measures of disease activity and lesion burden in patients with relapsing-remitting and secondary progressive MS.24>25
In general, mitoxantrone has been well toler-ated, the most common adverse effects being nausea, bone marrow suppression, amenorrhea, and infertility. Potential cardiac toxicity is related to total cumulative dose, which limits duration of treatment to about 2 years. Mitoxantrone is also associated with an increased risk of leukemia. Due to its potential toxicity, mitoxantrone should be administered by practitioners familiar with its use.
T r e a t m e n t f o r secondary p r o g r e s s i v e M S Treatment of secondary progressive M S is more problemaric, and, until recently, there were no therapies demonstrated to be of ben-efit.
1 6 4 C L E V E L A N D C L I N I C J O U R N A L OF M E D I C I N E V O L U M E 6 8 • N U M B E R 2 F E B R U A R Y 2 0 0 1
on April 21, 2022. For personal use only. All other uses require permission.www.ccjm.orgDownloaded from

T A B L E 2 TABLE 3
S i d e e f f e c t s o f i m m u n o m o d u l a t i n g t r e a t m e n t s
DRUG AND SIDE EFFECTS' COMMENTS AND TREATMENTS
I FN beta Flulike symptoms
Injection-site reaction
Thyroid dysfunction Depression Headache Menstrual disorders Gastrointestinal symptoms Increased spasticity Alopecia Worsening of psoriasis Leukopenia Increased hepatic transaminases Glat iramer acetate Injection site reaction Systemic post-Injection
reaction (flushing, shortness of breath, palpitations, diaphoresis, anxiety)
M i t o x a n t r o n e Blue sclera, stool, urine Leukopenia, thrombocytopenia Nausea, vomit ing, headache Alopecia
Amenorrhea, inferti l i ty Heart fai lure
Usually decrease over t ime Treatments: acetaminophen, and/or NSAID pretreatment, evening administrat ion Seen w i th IFN beta-1b and IFN beta-1a(R), which are given subcutaneously; rare w i th IFN beta-1a Greatest risk w i th preexisting thyroid dysfunction All are rare
Usually mild Noncardiac, self-l imited, lasts several minutes; reassure patient
Lasts 1 - 2 days after infusion Al though common, usually uncomplicated Mi ld if present Usually only hair th inning Can be irreversible
More common w i th higher doses; mitoxantrone should not be used in those w i th previous heart condit ion
Sexual dysfuntion in MS has important effects on a patient's self-worth
'Listed from most common to least common
A recently published European multicen-ter study26 found IFN beta-lb to be effective in secondary progressive MS. However, European studies of IFN b e t a - l a ( R ) and North American studies of IFN beta-lb found that these agents failed to reduce disability progression, although the drugs did reduce the relapse rate and MRI measures of MS activity.
In another study, mitoxantrone decreased disability progression by 64%, the relapse rate by 69%, and new MRI lesions by 85%, in a group of patients with secondary progressive M S or active relapsing-remitting MS. The cardiac toxicity from mitoxantrone described above limits its use to several years.
Small studies suggested that bimonthly
C L E V E L A N D C L I N I C J O U R N A L OF M E D I C I N E V O L U M E 6 8 • N U M B E R 2 F E B R U A R Y 2 0 0 1 1 6 5
on April 21, 2022. For personal use only. All other uses require permission.www.ccjm.orgDownloaded from

MULTIPLE SCLEROSIS FOX AND COHEN
T A B L E 7
S y m p t o m m a n a g e m e n t i n M S
SYMPTOM AND TREATMENT* COMMENTS
Spasticity
Baclofen 5-20 mg two or three times a day
Tizanidine 4 - 8 mg three or four times a day
Gabapentin 300-900 mg three or four times a day
Diazepam 2-10 mg three times a day
Clonazepam 0.5-5 mg three times a day
Dantrolene 25-100 mg two to four times a day
Neuropathic pain
Gabapentin 300-900 mg three or four times a day
Carbamazepine 200-400 mg three times a day
Phenytoin 300-600 mg daily
Amitriptyline 25-150 mg daily at bedtime
Nortriptyline 25-150 mg daily at bedtime
Fatigue
Amantadine 100 mg twice a day
Modafinil 100-200 mg twice a day
Pemoline 18.75-75 mg daily
Fluoxetine 20-40 mg daily
Depression
Selective serotonin reuptake inhibitors (SSRIs)
Tricyclic antidepressants
Medication should be combined with a regular stretching program
High doses may be helpful but may exacerbate weakness or ataxia
Less tendency to produce weakness compared with baclofen, but more sedating
Useful as adjunct therapy for spasticity when there is concomitant neuropathic pain
Useful for nocturnal spasms
Useful for nocturnal spasms
Least cerebral side effects but produces obligate weakness
Well-tolerated but may require high doses Titrate to avoid sedation
Sedating and may exacerbate ataxia Extended-release form is better tolerated
Sedation and anticholinergic effects may be useful, or may be dose-limiting side effects
Less prominent sedation and anticholinergic effects than amitriptyline
Medication should be combined with a regular exercise program
Need to rule out poor sleep, other medical conditions, and medication side effects
Watch for livedo reticularis
Also improves sleep
Second-line drug
Hepatotoxicity probably rare but must be monitored
Useful when there is concomitant depression
Consider psychotherapy for patients with depression
"Energizing" effect of SSRIs can be helpful wi th fatigue
Useful when there is concomitant pain, detrusor hyperactivity, or sleep disturbance
*Treatments listed in approximate order of usefulness and usual use
1 6 6 C L E V E L A N D C L I N I C J O U R N A L OF M E D I C I N E V O L U M E 6 8 • N U M B E R 2 F E B R U A R Y 2 0 0 1
on April 21, 2022. For personal use only. All other uses require permission.www.ccjm.orgDownloaded from

S Y M P T O M A N D T R E A T M E N T C O M M E N T S
Vertigo
Meclizine 25 mg every 6 hours
Scopolamine patch every 3 days
Ondansetron 8 mg twice a day
Diazepam 2 -10 trig three or four times a day
Ataxic tremor
Ondansetron 8 mg twice a day
Primidone 100-250 mg three or four times a day
Gabapentin 300-900 three or four times a day
Detrusor hyperactivity
Oxybutynin 2.5-5 mg three times a day
Tolterodine 2 mg twice a day
Flaccid bladder
Bethanechol 10-50 mg two to four times a day
Detrusor-sphincter dyssynergia
Terazosin 5 - 1 0 mg daily at bedtime
Constipation
Bulk-forming agents
Lactulose
Bowel urgency
Bulk-forming agents
Impotence
Sildenafil 50 -100 nig as needed
Sedating
Sedating
Medications are rarely effective
Extended-release formulation is useful
Less systemic anticholinergic side effects than oxybutynin but may not be as potent
Patients on anticholinergic therapy need to be monitored for incomplete bladder emptying
Fluid restriction in the evening or low-dose desmopressin acetate may be useful for nocturia, but patients need to avoid restricting fluids during the day
Intermittent catheterization or urinary diversion often are more optimal
Often detrusor-sphincter dyssynergia occurs wi th detrusor hyperactivity; in that setting terazosin or intermittent catheterization can be combined wi th anticholinergic medication
Need to be combined wi th adequate fluid, dietary fiber, and regular exercise
Need to be combined wi th scheduled voiding; biofeedback sometimes is useful
Largely has supplanted other approaches Need to rule out emotional factors, other medical conditions, or medication side effects
C L E V E L A N D C L I N I C J O U F i N A L OF M E D I C I N E V O L U M E 6 8 • N U M B E R 2 F E B R U A R Y 2 0 0 1 1 6 7
on April 21, 2022. For personal use only. All other uses require permission.www.ccjm.orgDownloaded from

MULTIPLE SCLEROSIS FOX AND COHEN
Consider infection in any patient with a relapse
courses of intravenous methylprednisolone,27
low-dose oral methotrexate,28 and glatiramer acetate29 may slow disability progression. Also, several studies reported cyclophosphamide to be of benefit in progressive MS. 3 0 - 3 2 Other studies, however, did not confirm the benefit of cyclophosphamide.33 Owing to its potential toxicity, use of cyclophosphamide mainly has been restricted to patients with rapidly pro-gressive disease.34
Clearly, the later stages of MS are more dif-ficult to treat, and the key to successful treat-ment of MS is to slow the inflammatory process early in the disease. IFN beta and mitox-antrone, used empirically, are appropriate first-line treatments for secondary progressive MS. In selected patients, bimonthly intravenous doses of methylprednisolone, methotrexate, cyclophosphamide, and glatiramer acetate are additional options, although data supporting their utility in secondary progressive MS are less conclusive.
• T R E A T M E N T OF ACUTE RELAPSES
E v a l u a t i o n For patients with known M S experiencing a typical relapse, evaluation should focus on possible precipitating factors, specifically infection. Although the mechanisms remain unclear, infections probably lead to acute M S relapses via immune activation. Fever associ-ated with infections also can exacerbate previ-ous neurologic manifestations in the absence of a true relapse. Increased body temperature decreases the efficiency of nerve transmission in demyelinated pathways, producing a pseu-do-relapse. Therefore, infection needs to be considered in any patient with symptoms of a relapse, particularly if he or she has a fever. If a relapse has atypical symptoms, develops faster or slower than expected, or does not respond to steroid treatment, further laborato-ry and radiologic evaluation should be per-formed as dictated by the clinical picture.
T r e a t m e n t Mild relapses that do not interfere with func-tion do not require treatment. For more severe relapses, corticosteroid therapy accelerates recovery and shortens the relapse duration. However, there is no convincing evidence that
corticosteroid treatment improves the degree of recovery or the long-term course of disease.35-37
A typical regimen is 500 to 1,000 mg of methylprednisolone by daily intravenous infu-sion for 3 to 5 days, followed by a tapering dose of prednisone over several weeks. The optimal dose of intravenous methylprednisolone remains uncertain, as do the duration of treat-ment, whether comparable doses of methyl-prednisolone given orally are equally effective, and the need for an oral taper. Although some practitioners continue to treat relapses with oral prednisone alone, particularly mild relaps-es, the available data suggest that prednisone alone does not effectively shorten relapses.37
Treatment of symptoms and rehabilitation should not be neglected. Several prospective, randomized studies found that intensive inpa-tient rehabilitation for MS improves disability and quality of life, and these benefits can be long-lasting.38~4C The mechanisms behind this improvement remain unclear. Physical thera-py (especially to address gait), occupational therapy, speech therapy, and swallowing ther-apy each can be helpful, and proper referral should be guided by the clinical situation.
• S Y M P T O M M A N A G E M E N T
With increasing emphasis on disease-modify-ing therapy, management of symptoms is sometimes overlooked. However, identifica-tion and treatment of symptoms is an impor-tant aspect of MS management. A variety of symptoms that interfere with daily activities or quality of life can develop at any point in the disease course, either during an acute relapse or more chronically. Many of these potentially troublesome symptoms are amenable to treatment (TABLE 7).
D r u g t r e a t m e n t Patients may have multiple symptoms, and medications used to treat one symptom may exacerbate another. For example, medications used to treat spasticity sometimes produce fatigue. Therefore, it often is necessary to pri-oritize which symptoms are most troublesome.
The clinician must remember that because the manifestations of M S evolve over time, symptom management is an ongoing process, and medications need to be given an adequate
1 6 8 C L E V E L A N D C L I N I C J O U R N A L O F M E D I C I N E V O L U M E 6 8 • N U M B E R 2 F E B R U A R Y 2 0 0 1
on April 21, 2022. For personal use only. All other uses require permission.www.ccjm.orgDownloaded from

trial. Start the dosage at a low level and increase gradually until a therapeutic response is achieved or intolerable side effects occur. If one medication proves ineffective or cannot be tolerated, consider other medications.
A d j u n c t i v e t r e a t m e n t Medications are not the only approach to treating MS symptoms. Adjunct therapies may augment the utility of medications (eg, use of a stretching program to complement medication in the treatment of spasticity; counseling in addition to antidepressant med-ication to treat emotional distress). The assis-tance of other allied health professionals such as social workers and psychologists is critical in addressing issues such as employment, dis-ability, and family stress.
• P R E G N A N C Y A N D REPRODUCTIVE HEALTH
Since M S is more common in women and typ-ically presents in early adulthood, reproduc-tive issues commonly arise. Gynecological care for women with M S does not differ sig-nificantly from routine practice, but there are some special concerns: • Long-term immunosuppressive therapy
may potentially increase the risk of cervi-cal dysplasia and other neoplasms, as well as infections from intrauterine devices.
• Routine examinations are important and should include a breast exam and a Pap smear, especially for women with a history of genital condylomata.
• Urinary tract infections are common in M S patients with impaired bladder func-tion, and frequent antibiotic use can alter the effectiveness of oral contraceptives through the induction of hepatic enzymes. Several excellent reviews concerning
pregnancy and M S have been p u b l i s h e d . 4 l . 4 2
Older studies suggested that pregnancy could precipitate the onset of MS or worsen its course, leading many women with MS to avoid pregnancy. More recent studies showed no convincing evidence that pregnancy caus-es M S or is associated with an increased risk of onset of MS.43 Similarly, there was no sub-stantial deleterious effect of single or multiple pregnancies on the ultimate course of M S or
accumulation of disability. A large prospective study (PRIMS) of 269
pregnancies in 254 women with predominant-ly relapsing-remitting MS provided important information on pregnancy and M S . 4 4 This study confirmed that the relapse rate decreases during pregnancy, but increases during the 3 months after pregnancy. The increased risk of relapse in the postpartum period suggests that disease-modifying therapy should be restarted early after delivery in women with previously active disease. In such cases, breast-feeding needs to be avoided, since these therapies are not recommended while breast-feeding.
MS does not affect fertility or the course of pregnancy. There was no apparent increase in congenital abnormalities or complications of pregnancy, labor, or delivery in the PRIMS study.44 Normally, no special precautions or measures need to be taken during labor or delivery, including with anesthesia. Pregnancy in most patients with MS should not be con-sidered to increase risk, and it is no longer appropriate in most cases to advise women against pregnancy merely because they have MS.
• HEALTH M A I N T E N A N C E IN M S
T h e average life expectancy in MS patients is not substantially different than in the general population. Although a small minority of patients have rapidly progressive disease with premature death, a decreased incidence of traumatic injury balances life expectancy to n e a r - n o r m a l . 4 5 Therefore, standard health maintenance guidelines should be applied to M S patients, including routine mammogra-phy, gynecological exams, colonoscopy, man-agement of chronic conditions such as hyper-tension and diabetes, and immunizations.
The symptoms of MS overlap those of a variety of medical conditions. Clinicians need to remain vigilant so as not to miss the devel-opment of anemia, thyroid disease, vitamin B j 2 deficiency, or diabetes mellitus in MS patients. Furthermore, MS therapies can pre-dispose td other medical conditions. Steroid use can precipitate or exacerbate hyper-glycemia or hypertension. Corticosteroids and reduced exercise contribute to osteoporosis. Chronic immunosuppression increases the risk
We no longer advise against pregnancy solely on the basis of MS
C L E V E L A N D C L I N I C J O U F i N A L OF M E D I C I N E V O L U M E 6 8 • N U M B E R 2 F E B R U A R Y 2 0 0 1 1 6 9
on April 21, 2022. For personal use only. All other uses require permission.www.ccjm.orgDownloaded from

MULTIPLE SCLEROSIS FOX AND COHEN
of malignancy and infection. Many of the medications used to treat MS can cause drug-induced hepatitis.
In general, immunizations are safe and effective in MS patients.46 Although there is a theoretical concern that activation of the immune system could precipitate a relapse, there is no clear evidence that immunizations are harmful to MS patients. We recommend
B REFERENCES 1. Freal JF, Kraft GH, Coryell JK. Symptomatic fatigue in MS.
Arch Phys Med Rehabil 1984; 65:135-138. 2. Lublin FD, Reingold SC. Defining the clinical course of
multiple sclerosis: Results of an international survey. Neurology 1996; 46:907-911.
3. Weinshenker BG, Bass B, Rice GPA, et al. The natural history of multiple sclerosis: A geographically based study. I. Clinical course and disability. Brain 1989; 112:133-146.
4. Schumacher GA, Beebe GW, Kibler RF, et al. Problems of experimental trials of therapy in multiple sclerosis: Report by the panel on the evaluation of experimental trials of therapy in multiple sclerosis. Ann NY Acad Sci 1965; 122:552-568.
5. Simon J, Holtas S, Schiffer R, et al. Corpus callosum and subcallosal-periventricular lesions in multiple scle-rosis: Detection wi th MR. Radiology 1986; 160:363-367.
6. Optic Neuritis Study Group. The 5-year risk of MS after optic neuritis. Experience of the Optic Neuritis Treatment Trial. Neurology 1997; 49:1404-1413.
7. Cole SR, Beck RW, Moke PS, et al. The predictive value of CSF oligodonal banding for MS 5 years after optic neuritis. Neurology 1998; 51:885-887.
8. Jacobs LD, Beck RW, Simon JH, et al. The effect of initi-ating Interferon beta-la therapy during a first demyelinating event on the development of clinically definite multiple sclerosis. N Engl J Med 2000; 343:898-904.
9. Comi G, Filippi M, Barkhof F, et al. Interferon beta 1a (Rebif) in patients wi th acute neurological syndromes suggestive of multiple sclerosis: A multi-center, ran-domized, double-blind, placebo-controlled study. Neurology 2000; 54 (suppl 3):A85-A86.
10. Lucchinetti CF, Bruck W, Rodriguez M, Lassmann H. Distinct patterns of multiple sclerosis pathology indi-cates heterogeneity in pathogenesis. Brain Pathol 1996; 6:259-274.
11. Haines JL, Terwedow HA, Burgess K, et al. Linkage of the MHC to familial multiple sclerosis suggests genetic heterogeneity. Hum Mol Genet 1998; 7:1229-1234.
12. Ferguson B, Matyszak MK, Esiri MM, Perry VH. Axonal damage in acute multiple sclerosis lesions. Brain 1997; 120:393-399.
13. Trapp BD, Peterson J, Ransohoff RM, et al. Axonal transection in the lesions of multiple sclerosis. N Engl J Med 1998; 338:278-285.
14. Rudick RA, Fisher E, Lee JC, et al. Use of the brain parenchymal fraction to measure whole brain atrophy in relapsing-remitting MS. Neurology 1999; 53:1698-1704.
15. Simon JH, Jacobs LD, Campion MK, et al. A longitudinal study of brain atrophy in relapsing multiple sclerosis. Neurology 1999; 53:139-148.
influenza and pneumococcal vaccinations for disabled patients with respiratory compromise, such as patients who are wheelchair- or bed-restricted. In general, the indications for immunizations in patients with MS are the same as for the general population. •
Acknowledgment. Dr. Fox is supported by a Physician Fellowship Award from the National Multiple Sclerosis Society and a Potiker Fellowship.
16. Beck RW, Arrington J, Murtaugh R, et al. Brain mag-netic resonance imaging in acute optic neuritis. Experience of the Optic Neuritis Study Group. Arch Neurol 1993; 50:841-846.
17. Brex PA, O'Riordan Jl, Miszkiel KA, et al. Multisequence MRI in clinically isolated syndromes and the early development of MS. Neurology 1999; 53:1184-1190.
18. Paty DW, Li DKB, the UBC MS/MRI Study Group, the IFNB Multiple Sclerosis Study Group. Interferon beta-l b is effective in relapsing-remitting multiple sclerosis. II. MRI analysis results of a multicenter, randomized, double-blind, placebo-controlled trial. Neurology 1993; 43:662-667.
19. Hawkins SA, McDonnell GV. Benign multiple sclerosis? Clinical course, long term fol low up, and assessment of prognostic factors. J Neurol Neurosurg Psychiatry 1999; 67:148-152.
20. Jacobs LD, Cookfair DL, Rudick RA, et al. Intramuscular interferon beta-1a for disease progression in relapsing multiple sclerosis. Ann Neurol 1996; 39:285-294.
21. The IFNB Multiple Sclerosis Study Group. Interferon beta-1b is effective in relapsing-remitting multiple sclerosis. I. clinical results of a multicenter, random-ized, double-blind, placebo-controlled trial. Neurology 1993; 43:655-661.
22. Johnson KP, Brooks BR, Cohen JA, et al. Copolymer 1 reduces the relapse rate and improves disability in relapsing-remitting multiple sclerosis: Results of a phase III multicenter, double-blind, placebo-controlled trial. Neurology 1995; 45:1268-1276.
23. Cohen JA, Carter JL, Kinkel RP, Schwid SR. Therapy of relapsing multiple sclerosis. Treatment approaches for nonresponders. J Neuroimmunol 1999; 98:29-36.
24. Härtung H-P, Gonsette R, the MIMS-Study Group. Mitoxantrone in progressive multiple sclerosis (MS): A placebo-controlled, randomized, observer-blind European Phase III multicenter study—Clinical results [abstract]. Mult Scler 1998; 4:325.
25. Krapf H, Morrissey SP, Zenker O, et al. Mitoxantrone in progressive multiple sclerosis (MS): A placebo-con-trolled, randomized, observer-blind European Phase III multicenter study—MRI results [abstract]. Mult Scler 1998; 4:380.
26. European Study Group on Interferon ß-1b in Secondary Progressive MS. Placebo-controlled multi-centre randomized trial of interferon ß-1b in treat-ment of secondary progressive multiple sclerosis. Lancet 1998; 352:1491-1497.
27. Goodkin DE, Kinkel RP, Weinstock-Guttman B, et al. A phase II study of IV methylprednisolone in secondary-progressive multiple sclerosis. Neurology 1998; 51:239-245.
28. Goodkin DE, Rudick RA, Medendorp SV, et al. Low-dose (7.5 mg) oral methotrexate reduces the rate of
1 7 0 C L E V E L A N D C L I N I C J O U R N A L OF M E D I C I N E V O L U M E 6 8 • N U M B E R 2 F E B R U A R Y 2 0 0 1
on April 21, 2022. For personal use only. All other uses require permission.www.ccjm.orgDownloaded from

INSTRUCTIONS FOR AUTHORS
progression in chronic progressive mult iple sclerosis. Ann Neurol 1995, 37:30-41.
29. Bornstein MB, Miller A, Slagle S, et al. A placebo-con-trolled, double-blind, randomized, two-center, pi lot tr ial of Cop 1 in chronic progressive mult iple sclerosis. Neurology 1991; 41:533-539.
30. Hauser SL, Dawson DM, Lehrich JR, et al. Intensive immunosuppression in progressive mult iple sclerosis. A randomized, three-arm study of high-dose intravenous cyclophosphamide, plasma exchange, and ACTH. N Engl J Med 1983; 308:173-180.
31. Weiner HL, IVIackin GA, Orav EJ, et al. Intermittent cyclophosphamide pulse therapy in progressive multiple sclerosis: Final report of the Northeast Cooperative Mult ip le Sclerosis Treatment Group. Neurology 1993; 43:910-918.
32. Goodkin DE, Plencer S, Palmer-Saxerud J, et al. Cyclophosphamide in chronic progressive mult iple scle-rosis. Maintenance vs nonmaintenance therapy. Arch Neurol 1987; 44:823-827.
33. The Canadian Cooperative Mult iple Sclerosis Group. The Canadian cooperative tr ial of cyclophosphamide and plasma exchange in progressive mult iple sclerosis. Lancet 1991; 337:441-446.
34. Weinstock-Guttman B, Kinkel RP, Cohen JA, et al. Treatment of fulminant mult iple sclerosis w i th intra-venous cyclophosphamide. Neurologist 1997; 3:178-185.
35. Mil l igan NM, Newcombe R, Compston DAS. A double-blind controlled trial of high dose methylprednisolone in patients wi th rrult iple sclerosis: 1. clinical effects. J Neurol Neurosurg Psychiatry 1987; 50:511-516.
36. Millar JHD, Vas CJ Noronha MJ, et al. Long-term treat-ment of multiple sclerosis w i th cort icotrophin. Lancet 1967; 2:429-431.
37. Beck RW, deary PA, Anderson MM, et al. A random-ized, controlled t ra i of corticosteroids in the treatment of acute optic neuritis. N Engl J Med 1992; 326:581-588.
38. Freeman JA, Langdon DW, Hobart JC, Thompson AJ. The impact of inpatient rehabil i tat ion on progressive mult iple sclerosis, Neurology 1997; 42:236-244.
39. Freeman JA, Langdon DW, Hobart JC, Thompson AJ. Inpatient rehabilitation in multiple sclerosis: do the benefits carry over into the community? Neurology 1999; 52:50-56.
40. Solari A, Filippini G, Gasco P, et al. Physical rehabilita-t ion has a positive effect on disability in mult iple scle-rosis patients. Neurology 1999; 52:57-62.
41. Damek DM, Shuster EA. Pregnancy and mult iple sclero-sis. Mayo Clin Proc 1997; 72:977-989.
42. Davis RK, Maslow AS. Mult iple sclerosis in pregnancy: a review. Obstet Gynecol Surv 1992; 47:290-296.
43. Leibowitz U, Antonovsky A, Kats R, Aleter M. Does pregnancy increase the risk of mult iple sclerosis? J Neurol Neurosurg Psychiatry 1967; 30:354-357.
44. Confavreux C, Hutchinson M, Hours MM, et al. Rate of pregnancy-related relapse in mult iple sclerosis. N Engl J Med 1998; 339:285-291.
45. Kremenchutzky IVI, Rice GP, Baskerville J, et al. A study of the causes of death in multiple sclerosis. Neurology 2000; 54 (Suppl 3):A350-A351.
46. Miller AE, Morganle LA, Buchwald LY, et al. A multicen-ter, randomized, double-blind, placebo-controlled tr ial of influenza immunization in mult iple sclerosis. Neurology 1997; 48:312-314.
ADDRESS: Robert J. Fox, MD, Mellen Center U-10, The Cleveland Clinic Foundation, 9500 Euclid Avenue, Cleveland, OH 44195; e-mail [email protected].
h e Cleveland Clinic Journal of Medicine p u b l i s h e s c o n c i s e
a r t i c l e s a b o u t n e w d e v e l o p m e n t s o f i m m e d i a t e r e l e v a n c e
d a i l y c l i n i c a l p r a c t i c e o f i n t e r n a l m e d i c i n e a n d c a r d i o l o -
gy. W e e n c o u r a g e a u t h o r s t o d iscuss p o s s i b l e t o p i c s w i t h t h e
E d i t o r , t o p r e v e n t m u l t i p l e s u b m i s s i o n s o n t h e s a m e t o p i c .
S U B M I S S I O N OF M A N U S C R I P T S
Cleveland Clinic Journal of Medicine, N A 3 2 9 5 0 0 E u c l i d A v e n u e ; C l e v e l a n d , O H 4 4 1 9 5 p h o n e ( 2 1 6 ) 4 4 4 - 2 6 6 1 ; f a x ( 2 1 6 ) 4 4 4 - 9 3 8 5 e - m a i l : c c j m @ c c f . o r g
I n c l u d e a c o v e r l e t t e r w i t h full n a m e , address , a n d p h o n e a n d f a x n u m b e r s o f t h e c o r r e s p o n d i n g a u t h o r .
M A N U S C R I P T P R E P A R A T I O N
CLINICAL REVIEW O v e r v i e w o f a d i s c r e t e m e d i c a l p r o b l e m e n c o u n t e r e d in d a i l y p r a c t i c e ; 1 0 t o 15 d o u b l e - s p a c e d pages , i n c l u d i n g a b s t r a c t , r e f e r e n c e s , t a b l e s , a n d l e g e n d s . F o l l o w Uniform Requirements for Manuscripts Submitted to Biomedical Journals (JAMA 1 9 9 7 ; 2 7 7 : 9 2 7 - 9 3 4 ) .
EDITORIAL C o m m e n t a r y o n a c o n t r o v e r s i a l issue; f i v e t o s i x d o u b l e - s p a c e d pages , i n c l u d i n g r e f e r e n c e s , t a b l e s , a n d l e g e n d s .
INTERNAL MEDICINE BOARD REVIEW C l i n i c a l v i g n e t t e s a n d q u e s t i o n s o n t h e d i f f e r e n t i a l d i a g n o s i s a n d t r e a t m e n t o f m e d i c a l c o n d i t i o n s l ike ly t o b e e n c o u n t e r e d o n t h e C e r t i f i c a t i o n E x a m i n a t i o n in M e d i c i n e . U p t o 1 0 p a g e s i n c l u d i n g t a b l e s , l e g e n d s , a n d up t o 1 0 r e f e r e n c e s .
REFERENCES N u m b e r r e f e r e n c e s in t h e o r d e r in w h i c h t h e y a r e c i t e d in t h e t e x t . A b b r e v i a t e p e r i o d i c a l s a c c o r d i n g t o I n d e x M e d i c u s s t y l e . I f a c i t a t i o n h a s s ix o r f e w e r a u t h o r s , list al l a u t h o r s ; i f a c i t a t i o n h a s s e v e n o r m o r e a u t h o r s , list t h e first t h r e e , t h e n " e t a l . " A u t h o r s a r e r e s p o n s i b l e for t h e a c c u r a c y o f r e f e r e n c e s ; a p h o t o s t a t o f t h e first p a g e o f a n y a r t i c l e r e f e r e n c e d s h o u l d b e f u r n i s h e d i f r e q u e s t e d .
FIGURES I n c l u d e t h r e e sets. I f a figure h a s b e e n p u b l i s h e d , p r o v i d e a p e r -m i s s i o n l e t t e r f r o m t h e publ isher , e v e n if it is t h e a u t h o r ' s o w n w o r k . Ident i fy figures by p l a c i n g labe ls o n t h e h a c k . SLibmit c o l o r f igures as 3 5 - m m slides or 5 " x 7 " prints . I n l egends for p h o t o m i -c r o g r a p h s , i n c l u d e t h e type o f s ta in a n d t h e m a g n i f i c a t i o n . A p a t i e n t ' s i d e n t i t y m u s t b e m a s k e d , a n d c o n s e n t t o publ i sh t h e p h o t o g r a p h m u s t a c c o m p a n y t h e m a n u s c r i p t .
PEER R E V I E W
A l l m a n u s c r i p t s are s u b j e c t t o p e e r r e v i e w . A u t h o r s a r e u s u a l l y n o t i f i e d w i t h i n 4 w e e k s a b o u t t h e a c c e p t a b i l i t y o f a m a n u s c r i p t , b u t l o n g e r i n t e r v a l s a r e s o m e t i m e s u n a v o i d a b l e . A l l p a p e r s a c c e p t e d for p u b l i c a t i o n are e d i t e d t o c o n f o r m w i t h t h e Cleveland Clinic Journal of Medicine s ty le . A u t h o r s a r e r e s p o n s i b l e for al l s t a t e m e n t s m a d e in t h e i r w o r k , i n c h i d i n g a n y c h a n g e s m a d e b y t h e c o p y e d i t o r a n d a u t h o r i z e d b y t h e c o r r e -s p o n d i n g a u t h o r .
t o t h e
C L E V E L A N D C L I N I C J O U F i N A L O F M E D I C I N E V O L U M E 6 8 • N U M B E R 2 F E B R U A R Y 2 0 0 1 1 7 1
on April 21, 2022. For personal use only. All other uses require permission.www.ccjm.orgDownloaded from