Multi-modal imaging for assessment of tissue-engineered bone in a critical-sized calvarial defect...
9
Multi-modal imaging for assessment of tissue-engineered bone in a critical-sized calvarial defect mouse model K. A. Wartella 1 , V. Khalilzad-Sharghi 1 , M. L. Kelso 2 , J. L. Kovar 3 , D. L. Kaplan 4 , H. Xu 5 and S. F. Othman 1 * 1 Department of Biological Systems Engineering, University of Nebraska–Lincoln, Lincoln, NE, USA 2 Department of Pharmacy Practice, University of Nebraska Medical Center, Omaha, NE, USA 3 LI-COR Biosciences, Biology Research and Development, Lincoln, NE, USA 4 Department of Biomedical Engineering, Tufts University, Medford, MA, USA 5 School of Engineering and Computer Science, University of the Pacific, Stockton, CA, USA Abstract Tissue-engineered bone (TEB) analysis in vivo relies heavily on tissue histological and end-point eval- uations requiring the sacrifice of animals at specific time points. Due to differences in animal re- sponse to implanted tissues, the conventional analytical methods to evaluate TEB can introduce data inconsistencies. Additionally, the conventional methods increase the number of animals required to provide an acceptable statistical power for hypothesis testing. Alternatively, our non- invasive optical imaging allows for the longitudinal analysis of regenerating tissue, where each ani- mal acts as its own control, thus reducing overall animal numbers. In our 6 month feasibility study, TEB, consisting of a silk protein scaffold with or without differentiated mesenchymal stem cells, was implanted in a critical-sized calvarial defect mouse model. Osteogenesis of the TEB was moni- tored through signal variation, using magnetic resonance imaging (MRI) and near-infrared (NIR) op- tical imaging with IRDye® 800CW BoneTag TM (800CW BT, a bone-specific marker used to label osteogenically differentiated mesenchymal stem cells and mineralization). Histological endpoint measurements and computed tomography (CT) were used to confirm imaging findings. Anatomical MRI revealed decreased signal intensity, indicating mineralization, in the TEB compared to the con- trol (i.e. silk scaffold only) at various growth stages. NIR optical imaging results demonstrated a sig- nal intensity increase of the TEB compared to control. Interpretation of the imaging results were confirmed by histological analysis. Specifically, haematoxylin and eosin staining revealing de novo bone in TEB showed that 80% of the defect was covered by TEB, while only 40% was covered for the control. Taken together, these results demonstrate the potential of multi-modal non-invasive imaging to visualize and quantify TEB for the assessment of regenerative medicine strategies. Copyright © 2015 John Wiley & Sons, Ltd. Received 11 November 2014; Revised 9 April 2015; Accepted 12 June 2015 Keywords tissue-engineered bone (TEB); magnetic resonance imaging (MRI); near-infrared optical imag- ing; calvarial defect model; IRDye 800CW BoneTag 1. Introduction Treatment of bone disease and/or severe bone damage typically involves the use of bone grafts and surgical reconstruction. Still, several difficulties can arise from bone grafts, including morbidity at the donor site, in- fection, immune system reactions and exposure to *Correspondence to: S. F. Othman, Department of Biological Systems Engineering, University of Nebraska–Lincoln (UNL), 249 L. W. Chase Hall, Lincoln, NE 68588-0726, USA. E-mail: [email protected] Copyright © 2015 John Wiley & Sons, Ltd. JOURNAL OF TISSUE ENGINEERING AND REGENERATIVE MEDICINE RESEARCH ARTICLE J Tissue Eng Regen Med (2015) Published online in Wiley Online Library (wileyonlinelibrary.com) DOI: 10.1002/term.2068
Transcript of Multi-modal imaging for assessment of tissue-engineered bone in a critical-sized calvarial defect...
Multi-modal imaging for assessment oftissue-engineered bone in a critical-sizedcalvarial defect mouse modelK. A. Wartella1, V. Khalilzad-Sharghi1, M. L. Kelso2, J. L. Kovar3, D. L. Kaplan4, H. Xu5 andS. F. Othman1*1Department of Biological Systems Engineering, University of Nebraska–Lincoln, Lincoln, NE, USA2Department of Pharmacy Practice, University of Nebraska Medical Center, Omaha, NE, USA3LI-COR Biosciences, Biology Research and Development, Lincoln, NE, USA4Department of Biomedical Engineering, Tufts University, Medford, MA, USA5School of Engineering and Computer Science, University of the Pacific, Stockton, CA, USA
Abstract
Tissue-engineered bone (TEB) analysis in vivo relies heavily on tissue histological and end-point eval-uations requiring the sacrifice of animals at specific time points. Due to differences in animal re-sponse to implanted tissues, the conventional analytical methods to evaluate TEB can introducedata inconsistencies. Additionally, the conventional methods increase the number of animalsrequired to provide an acceptable statistical power for hypothesis testing. Alternatively, our non-invasive optical imaging allows for the longitudinal analysis of regenerating tissue, where each ani-mal acts as its own control, thus reducing overall animal numbers. In our 6 month feasibility study,TEB, consisting of a silk protein scaffold with or without differentiated mesenchymal stem cells,was implanted in a critical-sized calvarial defect mouse model. Osteogenesis of the TEB was moni-tored through signal variation, using magnetic resonance imaging (MRI) and near-infrared (NIR) op-tical imaging with IRDye® 800CW BoneTagTM (800CW BT, a bone-specific marker used to labelosteogenically differentiated mesenchymal stem cells and mineralization). Histological endpointmeasurements and computed tomography (CT) were used to confirm imaging findings. AnatomicalMRI revealed decreased signal intensity, indicating mineralization, in the TEB compared to the con-trol (i.e. silk scaffold only) at various growth stages. NIR optical imaging results demonstrated a sig-nal intensity increase of the TEB compared to control. Interpretation of the imaging results wereconfirmed by histological analysis. Specifically, haematoxylin and eosin staining revealing de novobone in TEB showed that 80% of the defect was covered by TEB, while only 40% was covered for thecontrol. Taken together, these results demonstrate the potential of multi-modal non-invasive imagingto visualize and quantify TEB for the assessment of regenerative medicine strategies. Copyright ©2015 John Wiley & Sons, Ltd.
Received 11 November 2014; Revised 9 April 2015; Accepted 12 June 2015
Keywords tissue-engineered bone (TEB); magnetic resonance imaging (MRI); near-infrared optical imag-
ing; calvarial defect model; IRDye 800CW BoneTag
1. Introduction
Treatment of bone disease and/or severe bone damagetypically involves the use of bone grafts and surgicalreconstruction. Still, several difficulties can arise frombone grafts, including morbidity at the donor site, in-fection, immune system reactions and exposure to
*Correspondence to: S. F. Othman, Department of BiologicalSystems Engineering, University of Nebraska–Lincoln (UNL),249 L. W. Chase Hall, Lincoln, NE 68588-0726, USA. E-mail:[email protected]
Copyright © 2015 John Wiley & Sons, Ltd.
JOURNAL OF TISSUE ENGINEERING AND REGENERATIVE MEDICINE RESEARCH ARTICLEJ Tissue Eng Regen Med (2015)Published online in Wiley Online Library (wileyonlinelibrary.com) DOI: 10.1002/term.2068

infectious agents (Baroli, 2009). To overcome difficul-ties associated with bone grafts, researchers have longbeen investigating the potential of tissue-engineered al-ternatives. To engineer bone tissue, a combination ofcells, a biocompatible scaffold and signalling moleculesare used to create bone substitutes (Langer andVacanti, 1993).
Evaluating in vitro data from tissue-engineered bone(TEB) studies allows for the extraction of useful infor-mation, but the experimental conditions cannot be trulyreplicated in the in vivo environment. Hence, animalmodels are critical to assess the biological activation ofosteogenesis, osteoconduction, osteoinduction, masstransport, and biophysical effects during bone regenera-tion (Gomes and Fernandes, 2011; Muschler et al.,2010). Importantly, one widely used model to studybone regeneration is the critical-sized calvarial defectmouse model, for which naturally regenerated bone oc-curs at a rate of < 10% during the lifetime of the ani-mal (Hollinger and Kleinschmidt, 1990). This model isof particular value for studying the development ofTEB in native conditions and the ability of TEB to pro-mote repair of a discontinuous lesion (Gomes andFernandes, 2011). Notably, the defect site has easy sur-gical access, requires no fixation and creates a uniform,easily reproducible, standardized defect (Gomes andFernandes, 2011). Calvarial defect studies are performedusing a broad range of animal models, including mice(Dumas et al., 2009), rats (Cowan et al., 2007), rabbits(Lin et al., 2009) or large animals including dogs(Tanuma et al., 2013), sheep (Xing et al., 2013) or pigs(Wehrhan et al., 2012). Large animal models are ofgreater clinical relevance, given that their skeletal matu-rity more closely resembles that of humans (Muschleret al., 2010).
Currently, most related experiments assess the devel-opment of engineered tissue throughout the course ofthe study at predetermined intervals. Animals aresacrificed for each examination time point in order tocompare changes in longitudinal growth (Studwelland Kotton, 2011). Excised tissues from the sacrificedanimals are subjected to histology, immunohistochemis-try (IHC), real-time polymerase chain reaction (RT–PCR) and micro-computed tomography (mCT) (Meinelet al., 2005; Ye et al., 2011; Zhang et al., 2011). Inorder to reduce the number of animals necessary forstatistical significance and reduce data scattering, anon- and/or less invasive alternative is needed thatdoes not require animal sacrifice.
Imaging modalities, such as ultrasound, computed to-mography (CT), near-infrared (NIR) optical imagingand magnetic resonance imaging (MRI), are non-destructive, permitting serial observations at discretetime points on the same animal. For example, ultrasoundis suitable for early stages of detecting bone regenera-tion, but mature bone cannot be penetrated effectivelywith acoustic waves (Balaban and Hampshire, 2001).CT, on the other hand, provides 3D structural imageswith high spatial resolution and penetration depth and
is clinically translatable for late stages of regenerationthrough assessing the integration and connectivity ofTEB with the host bone tissue. However, CT has limitedsensitivity for pre-mature/immature bone and bone-liketissues. Also, the radiation from CT has been found tosuppress growth and induce breakdown in mouse bone(Klinck et al., 2008; Studwell and Kotton, 2011). Onthe other hand, molecular optical imaging relies on asource of contrast from fluorescence, bioluminescence,absorption or reflectance (Weissleder and Mahmood,2001). Fluorescently-labelled targeted probes that emitsignals in the NIR region (700–900 nm) of the spectrumutilize lower tissue absorption coefficients and result indeeper light penetration compared to imaging at visiblewavelengths. Alternatively, bioluminescence imaging uti-lizes luciferase gene expression systems that emit visiblephotons, based on energy-dependent reactions catalysedby luciferases. For example, Degano et al. (2008) usedbioluminescence to study calvarial bone repair in amouse defect model based on manipulation of the cellsfor gene insertion, verification of gene expression andexpansion of the cells with gene expression. In a previ-ous study of TEB implanted in a subcutaneous mousemodel, NIR dye-labelled targeting agents (IRDye®800CW BoneTagTM; 800CW BT) targeted mineralizedbone or hydroxyapatites and effectively identified bonegrowth (Cowles et al., 2013). Relatedly, MRI provideshigh spatial resolution and detects changes in the watercontent of tissue, thus revealing alterations of the struc-ture and/or functions (Studwell and Kotton, 2011). Al-though each imaging modality provides information onthe tissue-engineering process, no single imaging modal-ity fully characterizes the complex remodelling processof TEB.
This paper presents a feasibility study for the applica-tion of non-invasive multi-modal imaging, MR and opti-cal imaging to assess TEB that is implanted into acritical-sized (5 mm) calvarial defect mouse model.Each mouse served as its own control, with the contra-lateral side of the cranium grafted with a silk proteinimplant without cells. NIR optical imaging with800CW BT and MRI were used to evaluate the implantenvironment for bone regeneration and/or mineraliza-tion in vivo for 6 months. At three time points (i.e. 2,4 and 6 months post-implantation) implants were har-vested and analysed using histology. CT was used to as-sess the regeneration at study completion for onerepresentative mouse.
2. Materials and methods
2.1. Tissue-engineered bone (TEB)
Human mesenchymal stem cells (hMSCs) isolated fromfresh adult human bone marrow, obtained commercially(Lonza, Walkersville, MD, USA), were suspended ingrowth medium in a T-75 flask. The medium was
K. A. Wartella et al.
Copyright © 2015 John Wiley & Sons, Ltd. J Tissue Eng Regen Med (2015)DOI: 10.1002/term

composed of Dulbecco’s modified Eagle’s medium(DMEM; Invitrogen, Carlsbad, CA, USA) supplementedwith 10% fetal bovine serum (FBS; Invitrogen) and0.5% antibiotic/antimycotic (Sigma-Aldrich, St Louis,MO, USA) and placed at 37°C and 5% CO2. The me-dium was changed twice weekly and cells were pas-saged up to five times prior to seeding. Aqueousprotein silk sponges with pore size 400–500 mm, diam-eter 5 mm and thickness 2–3 mm were prepared as re-ported previously (Rockwood et al., 2011). The spongeswere next autoclaved, placed in the medium describedabove and conditioned for at least 4 h. Following this,two silk scaffolds were placed in a 24-well plate andseeded with hMSCs at a density of 1 million cells in35 ml medium. Following 2 h of incubation, osteogenicgrowth medium containing DMEM, 10% FBS, 0.5%antibiotic/antimycotic, 100 nM dexamethasone, 10 mMβ-glycerophosphate and 0.05 mm ascorbic acid 2-phosphate (Sigma-Aldrich) was added to the wells.TEB was cultured in osteogenic medium for 2 weeksprior to implantation. On the day of surgery, sterile silkscaffolds and TEB were thinly sliced to < 1 mm, placedin phosphate-buffered saline (PBS) and maintained insterile conditions at 37°C until surgical insertion.
2.2. Mouse critical-sized calvarial defects
All animal procedures were performed using protocolsapproved by the Institutional Animal Care and UseCommittee at the University of Nebraska–Lincoln(UNL). Following UNL guidelines for animal usage, five8 week-old male nude immunodeficient mice (n = 5)(nu/nuJ; Jackson Laboratories, Bar Harbor, ME, USA)were anaesthetized using 2% isoflurane. An iodine so-lution scrub was used to sterilize the surgical areaprior to surgery. A sagittal midline incision was per-formed to reveal the underlying bone, and the perios-teum was removed. A 5 mm stainless steel trephine(Fine Science Tools, Foster City, CA, USA) attached toa drill (Dremel, Racine, WI, USA) was used to gener-ate two contralateral defects/animal, one on each sideof the calvarium (Figure 1) (Meinel et al., 2005). Carewas taken to ensure that the dura remained intact
during drilling and calvarium removal. Forceps wereused to place the silk scaffold and TEB on the leftand right defects, respectively. The incision was closedusing nylon surgical sutures and the animal removedfrom isoflurane exposure. Following surgery, the micewere maintained under aseptic conditions. Sutureswere removed at 1 week post-surgery. Each animalserved as its own control, with the silk scaffold im-plant serving as the control to the TEB implant. Ofthe five animals, one animal was sacrificed and evalu-ated at month 2, another at month 4 and three atmonth 6.
2.3. Near-infrared optical imaging
All mice were anaesthetized with 2% isoflurane inhala-tion for all imaging procedures. The NIR dye-labelledtargeting agent 800CW BT (LI-COR Biosciences,Lincoln, NE, USA) was reconstituted to a dose of 2nM/animal, according to the manufacturer’s instruc-tions; each mouse received a 100 ml intraperitoneal(i.p.) injection. NIR optical images were acquired usingthe Pearl® Impulse Small Animal Imaging System (LI-COR Biosciences). Pre-injection dorsal images (85 mm)of the mice were acquired 24 h post-surgery and at 1month intervals, starting at 1 month post-surgery, andwere continued for 6 months. Each month, followingbaseline imaging, the mice were injected i.p. with800CW BT and imaged 48 h post-injection to allowthe unretained agent to clear. For imaging at months4–6, the implant site was shaved and treated withthe depilatory cream Nair™ (Church and Dwight Co.Inc., Ewing, NJ, USA) to prevent interference from hairgrowth. Prior to month 4, hair growth was minimal.Relative fluorescent units (RFUs) for the silk scaffoldand TEB implants were recorded for each animal byplacing a region of interest (ROI) on the defect areaand analysing it using Pearl Cam Software (LI-CORBiosciences).
2.4. Magnetic resonance imaging
Prior to MRI, mice were anaesthetized and positionedon a custom-designed animal holder (Agilent Inc., PaloAlto, CA, USA). Throughout imaging, the animals weremaintained under anaesthesia (1.2–2% isoflurane), withtheir body temperature and respiration rate closelymonitored and controlled using the Model 1025 Moni-toring and Gating System (SA Instruments, Stony Brook,NY, USA). Both in vivo and ex vivo anatomical images ofthe tissue-engineered constructs were acquired using a9.4 T, 89 mm vertical-bore magnet (Agilent, SantaClara, CA, USA). For the in vivo imaging, images wereacquired using a 4 cm millipede radiofrequency (RF)coil. Micro-imaging triple axis gradients (Agilent, SantaClara, CA, USA) with a maximum strength of 100Gauss/cm and inner diameter of 57 mm were used for
Figure 1. Schematic drawing of mouse calvarial defect for surgi-cal insertion of silk scaffold (left side) and tissue-engineeredbone (right side) implants
Imaging of tissue-engineered bone in a mouse model
Copyright © 2015 John Wiley & Sons, Ltd. J Tissue Eng Regen Med (2015)DOI: 10.1002/term
all experiments. The scanning protocol first obtainedgradient-echo axial slices, using repetition time (TR) =300 ms, echo time (TE) = 2.5 ms, flip angle = 25°,field-of-view (FOV) = 24 cm and slice thickness = 0.3mm, sectioned through the defect site to localize theconstructs. Following localization, the slices wereobliquely aligned orthogonal to the axial slices and tan-gentially to the constructs. The appropriate plane waschosen to acquire a fast-spin-echo sequence (FSEMS)with the following parameters: TR/echo spacing (ESP)= 2000/9.39 ms; echo train length (ETL) = 8; numberof averages = 16; FOV = 23 mm2; matrix size = 1282;slice thickness = 0.2 mm; and imaging time = 8 min 36s. Animals were imaged at 0, 1, 3 and 6 months. Com-parisons were made between the cranial images of thesilk scaffold and the TEB.
At 6 months post-surgery, one mouse was sacrificed;the head was fixed in 10% buffered formalin and imagedusing the parameters listed above, followed by CT imag-ing (described below). Following the imaging of the fixedhead, the implants were excised, placed in formalin andimaged using a 10 mm RF coil. To increase the signal:noise ratio (SNR), a 10 mm custom-designed RF coil wasused in combination with a magnet. To acquire high-quality images with a short TE, a gradient-echo se-quence was employed to contrast the silk scaffold andTEB. The applied parameters for the gradient-echo se-quence were: TR = 500 ms; TE = 3.19 ms (minimum);flip angle = 25°; number of averages =16; FOV= 21mm2;matrix size = 1282; slice thickness = 0.2 mm; and imagingtime = 4 s 17 min. MRI magnitude images were comparedto calculate the difference in signal intensity for the silkscaffold and TEB.
2.5. Computed tomography
After 6 months of regeneration, the head of one repre-sentative mouse was decapitated and fixed. The entirecranium/head was imaged using CT. Image acquisitionwas accomplished using a FLEX Triumph X-ray com-puted tomography/single photon emission system(CT/SPECT; Gamma Medica Inc., Salem, NH, USA).Data were analysed using software (TriFoil ImagingInc., Northridge, CA, USA) to assess the extent of theregeneration after 6 months, and 1024 CT projectionswith three frames/projection were acquired at 60 kVp
and 210 μA, with a focal spot size of 50 μm. TheseCT/SPECT projections were reconstructed at an opti-mum resolution option using Triumph X-O 4.1 (GammaMedica). The matrix size was 512 μm and the voxelsize was 180 μm. Images were generated using the vi-sualization and analysis software VIVID, which is basedon Amira 4.1 (Visualization Sciences Group, Germany).
2.6. Histology
At 2, 4 and 6 month intervals, an animal was sacrificedand the tissue was excised from each defect site. Sampleswere fixed in 10% buffered formalin and processed forparaffin embedding at the UNL Nebraska Veterinary Diag-nostic Laboratory. Samples were sectioned (5 mm) andstained with haematoxylin and eosin (H&E) or von Kossastain. All slides were examined by a certified pathologistand imaged using a light microscope (AX70, Olympus,Center Valley, PA, USA).
3. Results
3.1. Optical imaging
At 72 h after surgery and 48 h after 800CW BT dye injec-tion, NIR optical imaging revealed probe retention. Thedata were excluded at month 0 because inflammation atthe defect sites biased the optical images. At the 1 month
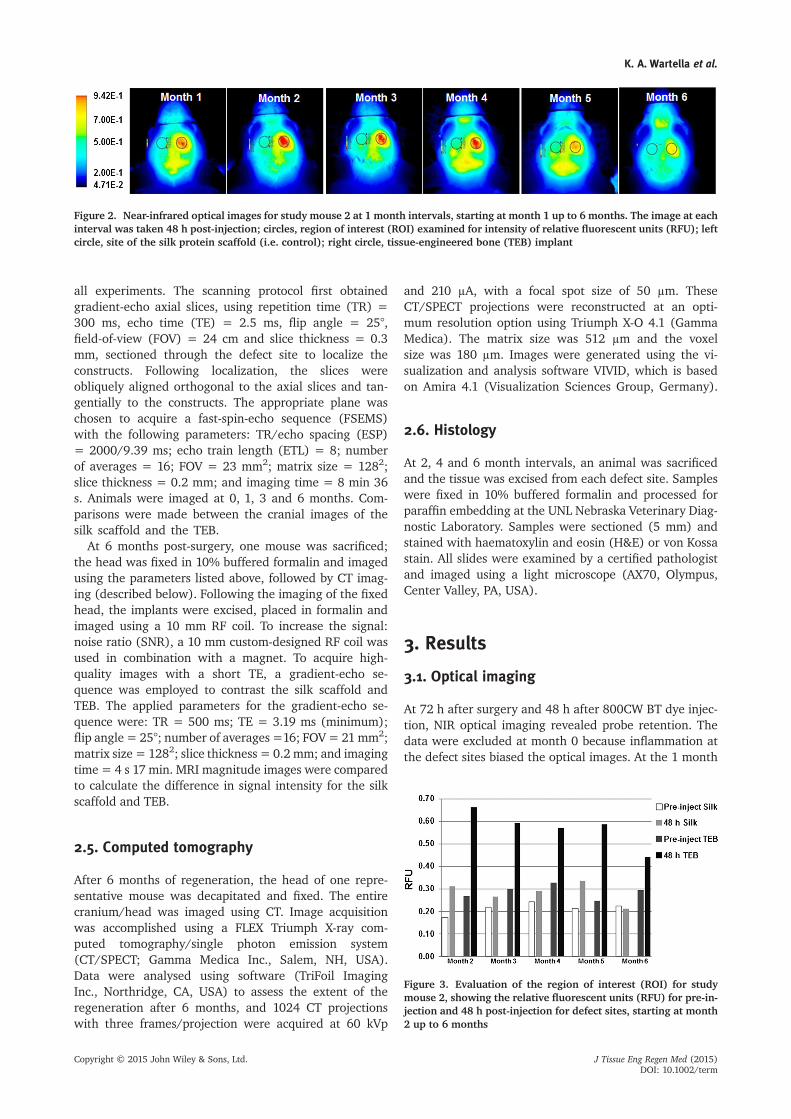
Figure 2. Near-infrared optical images for study mouse 2 at 1 month intervals, starting at month 1 up to 6 months. The image at eachinterval was taken 48 h post-injection; circles, region of interest (ROI) examined for intensity of relative fluorescent units (RFU); leftcircle, site of the silk protein scaffold (i.e. control); right circle, tissue-engineered bone (TEB) implant
Figure 3. Evaluation of the region of interest (ROI) for studymouse 2, showing the relative fluorescent units (RFU) for pre-in-jection and 48 h post-injection for defect sites, starting at month2 up to 6 months
K. A. Wartella et al.
Copyright © 2015 John Wiley & Sons, Ltd. J Tissue Eng Regen Med (2015)DOI: 10.1002/term
time point, defects were clearly visible in all mice (n = 5),with the TEB displaying higher signal intensity (RFUs)than the control implant. During the entire bone develop-ment period, defects were clearly visible in all mice, withthe TEB implants displaying higher RFUs than the silkscaffold control implants. The strongest signal intensity
occurred at month 2. Figure 2 presents the NIR optical im-ages of a mouse at 1 month intervals, in the range 1–6months. It should be mentioned that pre-injectionbaseline imaging did not occur for month 1, and the datafrom that month could not be used for quantitative butrather for qualitative representation. ROIs (Figure 2,
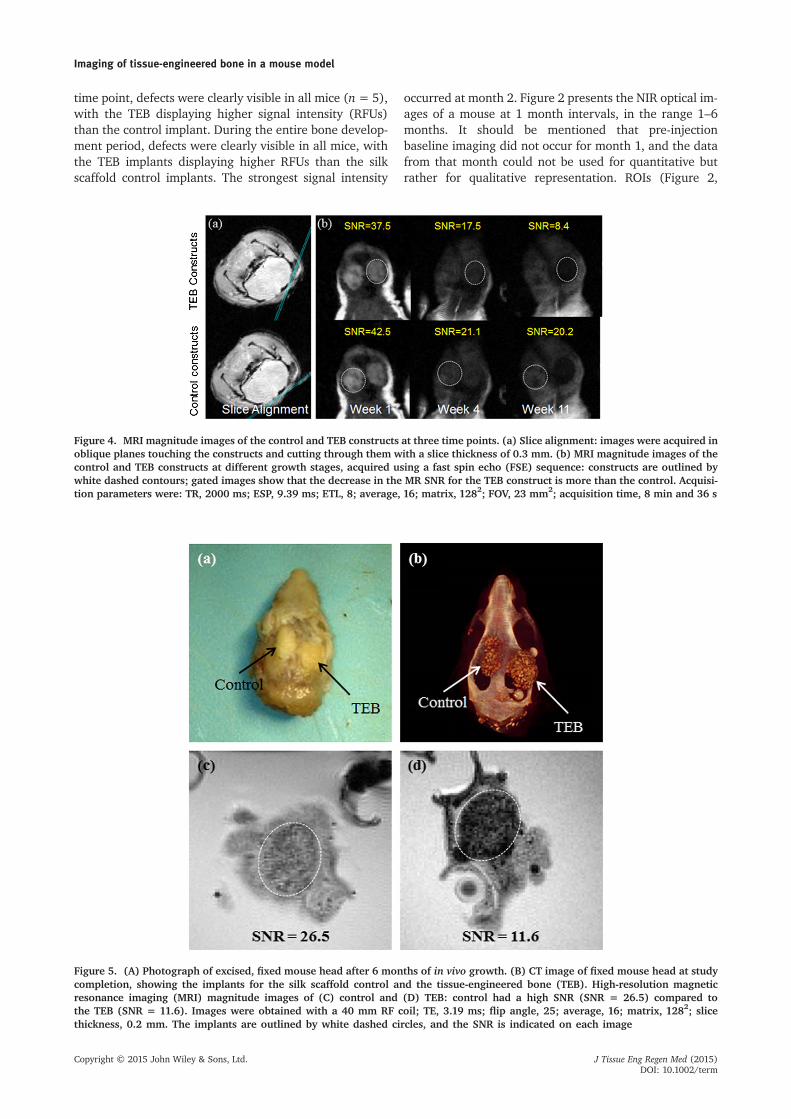
Figure 4. MRI magnitude images of the control and TEB constructs at three time points. (a) Slice alignment: images were acquired inoblique planes touching the constructs and cutting through them with a slice thickness of 0.3 mm. (b) MRI magnitude images of thecontrol and TEB constructs at different growth stages, acquired using a fast spin echo (FSE) sequence: constructs are outlined bywhite dashed contours; gated images show that the decrease in the MR SNR for the TEB construct is more than the control. Acquisi-tion parameters were: TR, 2000 ms; ESP, 9.39 ms; ETL, 8; average, 16; matrix, 1282; FOV, 23 mm2; acquisition time, 8 min and 36 s
Figure 5. (A) Photograph of excised, fixed mouse head after 6 months of in vivo growth. (B) CT image of fixed mouse head at studycompletion, showing the implants for the silk scaffold control and the tissue-engineered bone (TEB). High-resolution magneticresonance imaging (MRI) magnitude images of (C) control and (D) TEB: control had a high SNR (SNR = 26.5) compared tothe TEB (SNR = 11.6). Images were obtained with a 40 mm RF coil; TE, 3.19 ms; flip angle, 25; average, 16; matrix, 1282; slicethickness, 0.2 mm. The implants are outlined by white dashed circles, and the SNR is indicated on each image
Imaging of tissue-engineered bone in a mouse model
Copyright © 2015 John Wiley & Sons, Ltd. J Tissue Eng Regen Med (2015)DOI: 10.1002/term

circles) indicate the ROI for assessing bone growth/mineralization. The control (left side) and the TEB (rightside) were analysed to determine the binding of 800CWBT (Figure 3). At month 2 the data revealed peak fluores-cence for TEB, with RFU = 0.66. There was a constantRFU for months 3–5 (RFU = 0.59, 0.57 and 0.58, respec-tively) and a decline to 0.44 at month 6. Along with peakfluorescence at month 2 of imaging, all mice exhibited ahigher deposition of 800CW BT in the TEB compared tothe control.
3.2. MRI and CT
3.2.1. In vivo imaging
MRI of the control and TEB implants were acquired atthree time points during the study. Figure 4a illustrateshow the slice was aligned for imaging of the defectsites. MRI magnitude images of the control and TEBimplants are shown in Figure 4b, where images fromthe same mouse are shown for different growth stages.With respect to regeneration, both implants exhibited adecrease in SNR. The control SNR was higher com-pared to the TEB; however, the control SNR also de-creased as the study proceeded.
3.2.2. Ex vivo imaging
After 6 months of regeneration, one mouse (out of three)was sacrificed; the head was removed and placed in 10%buffered formalin. Figure 5A shows the control and TEBimplants in the fixed mouse head. Both implants appearintegrated with the native tissue. However, the CT image(Figure 5B) revealed that the control implant covered ap-proximately 40% of the defect site, while the TEB coveredapproximately 80% of the defect site. MRI magnitude im-ages (Figure 5C, D) resulted in a SNR of 11.6 for the TEBand 26.5 for the silk scaffold, indicating greater minerali-zation in the TEB implant. Higher-quality MRI magnitudeimages were acquired by excising the constructs and cap-turing images using the 10 mm RF coil, as shown inFigure 6. The resultant MRI magnitude images illustrateda significant difference (SNR of 11.6 compared to 26.5)between the signal intensity of TEB compared to the con-trol, as shown in Figure 6.
3.3. Histology
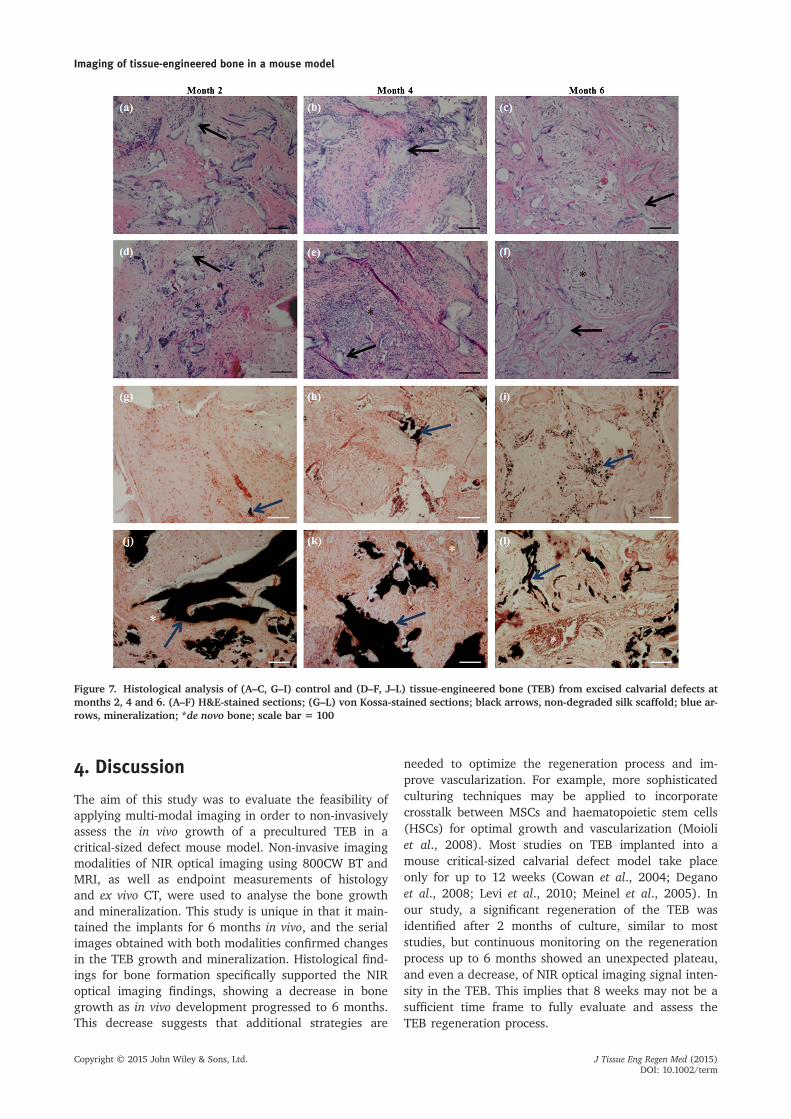
Mice were sacrificed at 2 (n= 1), 4 (n = 1) and 6 (n= 3)months. The calvarial implants were excised and thetissue was processed for histological analysis. H&Estain was used to evaluate the composition and struc-ture of the implants, while von Kossa stain was usedto evaluate mineralization (Figure 7). Observationsusing light microscopy showed that the control implantunderwent some cell migration from the surroundingtissue, but with a large amount of undegraded silk
scaffold visible (Figure 7A). In contrast, the stainedsections of TEB at month 2 (Figure 7D) revealed nu-merous cells and the presence of de novo bone. Withrespect to von Kossa staining at month 2, there wasminor staining in the control (Figure 7G) but an abun-dance of black staining for calcium salts in the TEB(Figure 7J).
The control for the mouse sacrificed at month 4 in-curred an infiltration of cells and was less porous thanat month 2, but had a similar amount of undegradedsilk scaffold (Figure 7B). The month 4 TEB (Figure 7E)demonstrated more new cells than at month 2 and morede novo bone. Similarly, for the control, the von Kossastain at month 4 revealed more calcium salts than themonth 2 sample (Figure 7H) and the TEB appeared sim-ilar in structure to the month 2 sample (Figure 7K).Month 6 staining of the control demonstrated cell infil-tration that appeared similar to the previous samples(Figure 7C). The TEB showed cells and de novo bonebut a decreased amount of both compared to previousmonths (Figure 7F). The von Kossa staining at month6 for the control (Figure 7I) had a similar amount ofcalcium deposition as at month 4. Also, the TEB atmonth 6 exhibited less calcium salts compared to month4 (Figure 6L).
Figure 6. High-resolution MRI magnitude images of the excisedtissue samples upon conclusion of the study after 6 months:white dashed circles outline the (a) control and (b) tissue-engineered bone (TEB). Due to mineralization of the tissue, theTEB produced a lower signal:noise ratio (SNR) compared to thecontrol. For imaging, a 10 mm RF coil was used, with acquisitionparameters for the applied gradient–echo sequence imaging asfollows: TR, 500 ms; TE, 3.19 ms; flip angle, 25; average, 16; ma-trix, 128 × 128; thickness, 0.2 mm; FOV, 17 min and 4 s
K. A. Wartella et al.
Copyright © 2015 John Wiley & Sons, Ltd. J Tissue Eng Regen Med (2015)DOI: 10.1002/term
4. Discussion
The aim of this study was to evaluate the feasibility ofapplying multi-modal imaging in order to non-invasivelyassess the in vivo growth of a precultured TEB in acritical-sized defect mouse model. Non-invasive imagingmodalities of NIR optical imaging using 800CW BT andMRI, as well as endpoint measurements of histologyand ex vivo CT, were used to analyse the bone growthand mineralization. This study is unique in that it main-tained the implants for 6 months in vivo, and the serialimages obtained with both modalities confirmed changesin the TEB growth and mineralization. Histological find-ings for bone formation specifically supported the NIRoptical imaging findings, showing a decrease in bonegrowth as in vivo development progressed to 6 months.This decrease suggests that additional strategies are
needed to optimize the regeneration process and im-prove vascularization. For example, more sophisticatedculturing techniques may be applied to incorporatecrosstalk between MSCs and haematopoietic stem cells(HSCs) for optimal growth and vascularization (Moioliet al., 2008). Most studies on TEB implanted into amouse critical-sized calvarial defect model take placeonly for up to 12 weeks (Cowan et al., 2004; Deganoet al., 2008; Levi et al., 2010; Meinel et al., 2005). Inour study, a significant regeneration of the TEB wasidentified after 2 months of culture, similar to moststudies, but continuous monitoring on the regenerationprocess up to 6 months showed an unexpected plateau,and even a decrease, of NIR optical imaging signal inten-sity in the TEB. This implies that 8 weeks may not be asufficient time frame to fully evaluate and assess theTEB regeneration process.
Figure 7. Histological analysis of (A–C, G–I) control and (D–F, J–L) tissue-engineered bone (TEB) from excised calvarial defects atmonths 2, 4 and 6. (A–F) H&E-stained sections; (G–L) von Kossa-stained sections; black arrows, non-degraded silk scaffold; blue ar-rows, mineralization; *de novo bone; scale bar = 100
Imaging of tissue-engineered bone in a mouse model
Copyright © 2015 John Wiley & Sons, Ltd. J Tissue Eng Regen Med (2015)DOI: 10.1002/term

For NIR optical imaging, mice were administered aNIR-labelled agent, 800CW BT, which is specific tobone tissue, and imaged at 1 month intervals. Thistechnique is ideal for evaluating mouse calvarial defectsbecause the defect site is only a few millimeters indepth, and thus the light absorption and scattering ofNIR waves are reduced compared to visible wave-lengths, enabling non-invasive analysis of the bone re-modelling and mineralization (Kovar et al., 2007,2011). The 800CW BT used in this study was previouslyevaluated with an assay to compare undifferentiatedhMSCs and osteogenically differentiated hMSCs in amonolayer. In this previous evaluation, the resultsshowed preferential binding and statistical significance,with the signal intensity 4.45–7.75 times higher forthe differentiated cells. Such results were confirmedwith positive calcium staining using von Kossa (Cowleset al., 2013). In our study, all animals at all intervalsdemonstrated a higher RFU signal in the TEB than inthe control; the RFU peaked at month 2. The resultsfrom the NIR optical imaging of calvarial defectsshowed mineralization in the TEB implant, which alsopeaked at month 2; however, the signal intensity fromthe animals sacrificed at month 6 were not consistent.We posit that these findings resulted from the quality ofthe TEB samples. In order to optimize the TEB implant, itmay be necessary to use an improved cultivation systemfor pre-implantation growth, and also to culture the TEBfor more than 2 weeks. For example, Meinel et al. (2005)used a bioreactor to provide dynamic culture conditionsfor tissue-engineered constructs for 5 weeks prior to im-plantation in a mouse calvarial defect model; this strategyresulted in the improved generation of a trabecular-likenetwork in the TEB implant.
To compare the signal intensity of the control and TEBimplants, MRI was used to evaluate the calvarial defectimplants non-invasively at specific time points. Comparedto NIR optical imaging, MRI magnitude images indicateddecreased signal intensity between TEB and control im-plants at each imaging interval. Additionally, the intensitydecreased between the intervals (e.g. at month 0, TEBand control SNRs were greater than at month 3). Previ-ously, MRI was successfully used to monitor in vitrogrowth of TEB, showing a statistically significant decreasein T2 relaxation times from increased deposition of min-erals and extracellular matrix. Additionally, these resultswere supported by histological findings with von Kossastaining, which indicated extensive calcium deposition(Xu et al., 2006). The results reinforce that MRI can beused to assess bone growth in an in vivo mouse calvarialdefect model. Notably, MRI results were in alignmentwith NIR optical images up month 2. However, the MRISNR of the TEB and the control continued to decrease fol-lowing month 2. This SNR decrease can be interpreted asnon-specific calcified tissue development within the TEBand the control. X-ray diffraction has been used to assessthe crystalline nature of the deposited bone tissue inTEB in vitro (Meinel et al., 2005), and should be appliedin future in vivo studies where implants can be extracted
to assess the quality of mineralization. Preliminary CTdata demonstrated that the TEB implant covered a largerarea of the defect compared to the control. However, seg-mentation algorithms are needed to differentiate mineral-ized from non-mineralized tissues (Meinel et al., 2005).
The control and TEB evaluated in a critical-sizedcalvarial defect showed apparent histological differencesbetween the observed animals. For example, the osteo-genic implant showed an abundance of cells, with themost visible at the month 4. The control had some cellularintegration from the surrounding native mouse tissue.The TEB showed de novo bone at all intervals of 2, 4 and6 months. The control exhibited a small amount of denovo bone at month 4, suggesting that host cells inte-grated into the silk and produced developing bone, whichwas also supported by mineralization in the von Kossa re-sults. The von Kossa results from the TEB corroboratedthe findings from the NIR imaging, showing a peak inbone growth at month 2, with a small decrease formonths 3–5 and a greater decrease at month 6.
To improve the results obtained from this feasibilitystudy, it is necessary to verify and enhance the quality ofTEB implanted into the defect model. Use of a spinnerflask or a bioreactor for the pre-implantation culture is ex-pected to increase the quality of the tissue. Additionally,in order to provide an even distribution of hMSCs, im-proved seeding methods could be used for the silk scaffolddimensions, rather than sectioning and implanting it imme-diately prior to surgery. Furthermore, it may be necessary toverify the quality of the TEB prior to surgery. An empty de-fect control with no scaffold could be used to compare withTEB regeneration in future studies. Based on this study, fi-duciary markers are needed to register images acquiredvia different modalities, and more comprehensive TEB evo-lution could be recorded. The same fiduciary markers couldbe used for the imaging modalities to improve replication ofanimal positioning as the animals grow.
In conclusion, this study demonstrates the feasibility ofmulti-modal imaging, using NIR optical imaging and MRI,to non-invasively evaluate TEB growth in critical-sizedcalvarial mouse defect implants. With some modificationsto the current study, as discussed above, these imagingmodalities couid be used to provide improved results forfuture studies and for translating the new methods to clin-ical studies. NIR imaging with 800CW BT can effectivelyvisualize hydroxyapatite (HA), a good biological osteo-genic marker. MRI was effective for anatomical imaging,as well as for visualization of collagen through the identi-fication of different markers, using advanced imagingtechniques such as the magnetization transfer ratio.Finally, CT with proper threshold and segmentationroutines could be used to visualize the integration andconnectivity of TEB with the host bone.
Conflict of interest
Joy Kovar is a scientist at Licor Biosciences.
K. A. Wartella et al.
Copyright © 2015 John Wiley & Sons, Ltd. J Tissue Eng Regen Med (2015)DOI: 10.1002/term

Acknowledgements
We are grateful to Nebraska Stem Cell (Grant No. Stem Cell2013–07) for the support of this study, and the National Institutes
of Health (NIH) Tissue Engineering Resource Center (Grant No.P41 EB002520) for support for the materials used in the study.The authors also thank Ms Melody Montgomery at the Universityof Nebraska Medical Center for help in editing this manuscript.
References
Balaban RS, Hampshire VA. 2001; Challengesin small animal noninvasive imaging. ILARJ 42: 248–262.
Baroli B. 2009; From natural bone grafts totissue engineering therapeutics: brain-storming on pharmaceutical formulativerequirements and challenges. J Pharm Sci98: 1317–1375.
Cowan CM, Aghaloo T, Chou YF et al.2007; MicroCT evaluation of three-dimensional mineralization in responseto BMP-2 doses in vitro and in criticalsized rat calvarial defects. Tissue Eng13: 501–512.
Cowan CM, Shi YY, Aalami OO et al. 2004;Adipose-derived adult stromal cells healcritical-size mouse calvarial defects. NatBiotechnol 22: 560–567.
Cowles EA, Kovar JL, Curtis ET et al. 2013;Near-infrared optical imaging for monitor-ing the regeneration of osteogenic tissue-engineered constructs. Biores Open Access2: 186–191.
Degano IR, Vilalta M, Bago JR et al. 2008;Bioluminescence imaging of calvarial bonerepair using bone marrow and adiposetissue-derived mesenchymal stem cells.Biomaterials 29: 427–437.
Dumas A, Moreau MF, Gherardi RK et al.2009; Bone grafts cultured with bonemarrow stromal cells for the repair ofcritical bone defects: an experimentalstudy in mice. J Biomed Mater Res A 90:1218–1229.
Gomes PS, Fernandes MH. 2011; Rodentmodels in bone-related research: the rele-vance of calvarial defects in the assess-ment of bone regeneration strategies. LabAnim 45: 14–24.
Hollinger JO, Kleinschmidt JC. 1990; Thecritical size defect as an experimental
model to test bone repair materials. JCraniofac Surg 1: 60–68.
Klinck RJ, Campbell GM, Boyd SK 2008; Ra-diation effects on bone architecture inmice and rats resulting from in vivomicro-computed tomography scanning.Med Eng Phys 30: 888–895.
Kovar JL, Simpson MA, Schutz-GeschwenderA et al. 2007; A systematic approach to thedevelopment of fluorescent contrastagents for optical imaging of mouse cancermodels. Anal Biochem 367: 1–12.
Kovar JL, Xu X, Draney D et al. 2011; Near-in-frared-labeled tetracycline derivative is aneffective marker of bone deposition inmice. Anal Biochem 416: 167–173.
Langer R, Vacanti JP 1993; Tissue engineer-ing. Science 260: 920–926.
Levi B, James AW, Nelson ER et al. 2010; Hu-man adipose derived stromal cells healcritical size mouse calvarial defects. PLoSOne 5: e11177.
Lin L, Shen Q, Wei X et al. 2009; Comparisonof osteogenic potentials of BMP4 trans-duced stem cells from autologous bonemarrow and fat tissue in a rabbit modelof calvarial defects. Calcif Tissue Int 85:55–65.
Meinel L, Fajardo R, Hofmann S et al. 2005;Silk implants for the healing of critical sizebone defects. Bone 37: 688–698.
Moioli EK, Clark PA, Chen M et al. 2008;Synergistic actions of hematopoietic andmesenchymal stem/progenitor cells invascularizing bioengineered tissues. PLoSOne 3: e3922.
Muschler GF, Raut VP, Patterson TE et al.2010; The design and use of animalmodels for translational research in bonetissue engineering and regenerative medi-cine. Tissue Eng B Rev 16: 123–145.
Rockwood DN, Preda RC, Yucel T et al.2011; Materials fabrication from Bombyxmori silk fibroin. Nat Protoc 6:1612–1631.
Studwell AJ, Kotton DN. 2011; A shift fromcell cultures to creatures: in vivo imagingof small animals in experimental regenera-tive medicine. Mol Ther 19: 1933–1941.
Tanuma Y, Matsui K, Kawai T et al. 2013;Comparison of bone regeneration betweenoctacalcium phosphate/collagen compos-ite and β-tricalcium phosphate in caninecalvarial defect. Oral Surg Oral Med OralPathol Oral Radiol 115: 9–17.
Wehrhan F, Amann K, Molenberg A et al.2012; PEG matrix enables cell-mediatedlocal BMP-2 gene delivery and increasedbone formation in a porcine critical sizedefect model of craniofacial bone regener-ation. Clin Oral Implants Res 23: 805–813.
Weissleder R, Mahmood U 2001; Molecularimaging. Radiology 219: 316–333.
Z Xing, TO Pedersen, X Wu. 2013; Biologicaleffects of functionalizing copolymer scaf-folds with nanodiamond particles. TissueEng A 19: 1783–1791.
Xu H, Othman SF, Hong L et al. 2006;Magnetic resonance microscopy for mon-itoring osteogenesis in tissue-engineeredconstruct in vitro. Phys Med Biol 51:719–732.
JH Ye, YJ Xu, J Gao. 2011; Critical-sizecalvarial bone defects healing in a mousemodel with silk scaffolds and SATB2-modified iPSCs. Biomaterials 32:5065–5076.
Zhang Y, Fan W, Nothdurft L et al. 2011; Invitro and in vivo evaluation of adenoviruscombined silk fibroin scaffolds for bonemorphogenetic protein-7 gene delivery.Tissue Eng C Methods 17: 789–797.
Imaging of tissue-engineered bone in a mouse model
Copyright © 2015 John Wiley & Sons, Ltd. J Tissue Eng Regen Med (2015)DOI: 10.1002/term