
MOOD DISORDERS IN STROKE PATIENTS: IMPORTANCE OF LOCATION OF LESION
13
Brain (1984), 107, 81-93 MOOD DISORDERS IN STROKE PATIENTS IMPORTANCE OF LOCATION OF LESION by ROBERT G. ROBINSON, 1 - 2 KENNETH L. KUBOS, 1 LYN BOOK STARR, 3 KRISHNA RAO 4 and THOMAS R. PRICE 5 {From the Departments of Psychiatry and Neuroscience, Johns Hopkins University School of Medicine, Baltimore, MD 21205,^ the Departments of Psychiatry, 2 Neurology, 5 Radiology* and Social IVork,-* University of Maryland School of Medicine, Baltimore, MD 21201, USA) SUMMARY In a selected group of right-handed patients with single stroke lesions of either the right (n = 14) or left (n = 22) hemisphere and no predisposing factors for psychiatric disorder, we found that the severity of depression was significantly increased in patients with left anterior lesions as opposed to any other lesion location. In addition, the severity of depression correlated significantly with proximity of the lesion on CT scan to the frontal pole in the left anterior group. The right hemisphere lesion group showed the reverse trend: patients with right posterior lesions were more depressed than patients with right anterior lesions, who were unduly cheerful and apathetic. These findings suggest that intrahemispheric lesion location is in some way related to mood disorder in stroke patients and that there is a graded effect of lesion location on severity of mood change. The neuroanatomy of the biogenic amine-containing pathways in the cerebral cortex might explain this graded effect and provide a neurochemical basis for the mood change. INTRODUCTION During the past several years we have been investigating the occurrence of mood disorders following cerebral ischaemia (Robinson and Szetela, 1981; Robinson and Benson, 1981; Robinson and Price, 1982; Lipsey et al., 1983; Robinson et al., 1983a). We have reported that the frequency and severity of these mood disorders are significantly increased during the period from six months to two years poststroke, and that, in the majority of cases, they last eight to nine months untreated (Robinson and Price, 1982). In addition, we have found that the course and severity of depressive disorders depend on which hemisphere is injured (Robinson and Price, 1982; Robinson et al., 1983a) and, in two studies, one involving left hemisphere injured patients (Robinson and Szetela, 1981) and one involving patients with bilateral brain injury (Lipsey et al., 1983), we reported that the severity of depression was significantly correlated with the proximity of the left hemisphere lesion to the frontal pole as measured on CT scan. Reprint requests and correspondence to Dr Robert G. Robinson, Department of Psychiatry, Adolf Meyer Building 4-119, Johns Hopkins University School of Medicine, Baltimore, MD 21205.
-
Upload
independent -
Category
Documents
-
view
5 -
download
0
Transcript of MOOD DISORDERS IN STROKE PATIENTS: IMPORTANCE OF LOCATION OF LESION

Brain (1984), 107, 81-93
MOOD DISORDERS IN STROKE PATIENTS
IMPORTANCE OF LOCATION OF LESION
by ROBERT G. ROBINSON,1-2 KENNETH L. KUBOS,1
LYN BOOK STARR,3 KRISHNA RAO4 and THOMAS R. PRICE5
{From the Departments of Psychiatry and Neuroscience, Johns Hopkins University School of Medicine,Baltimore, MD 21205,^ the Departments of Psychiatry,2 Neurology,5 Radiology* and Social IVork,-*
University of Maryland School of Medicine, Baltimore, MD 21201, USA)
SUMMARY
In a selected group of right-handed patients with single stroke lesions of either the right (n = 14) or left(n = 22) hemisphere and no predisposing factors for psychiatric disorder, we found that the severity ofdepression was significantly increased in patients with left anterior lesions as opposed to any otherlesion location. In addition, the severity of depression correlated significantly with proximity of thelesion on CT scan to the frontal pole in the left anterior group. The right hemisphere lesion groupshowed the reverse trend: patients with right posterior lesions were more depressed than patients withright anterior lesions, who were unduly cheerful and apathetic. These findings suggest thatintrahemispheric lesion location is in some way related to mood disorder in stroke patients and thatthere is a graded effect of lesion location on severity of mood change. The neuroanatomy of thebiogenic amine-containing pathways in the cerebral cortex might explain this graded effect and providea neurochemical basis for the mood change.
I N T R O D U C T I O N
During the past several years we have been investigating the occurrence of mooddisorders following cerebral ischaemia (Robinson and Szetela, 1981; Robinson andBenson, 1981; Robinson and Price, 1982; Lipsey et al., 1983; Robinson et al.,1983a). We have reported that the frequency and severity of these mood disordersare significantly increased during the period from six months to two yearspoststroke, and that, in the majority of cases, they last eight to nine monthsuntreated (Robinson and Price, 1982). In addition, we have found that the courseand severity of depressive disorders depend on which hemisphere is injured(Robinson and Price, 1982; Robinson et al., 1983a) and, in two studies, oneinvolving left hemisphere injured patients (Robinson and Szetela, 1981) and oneinvolving patients with bilateral brain injury (Lipsey et al., 1983), we reported thatthe severity of depression was significantly correlated with the proximity of the lefthemisphere lesion to the frontal pole as measured on CT scan.
Reprint requests and correspondence to Dr Robert G. Robinson, Department of Psychiatry, Adolf MeyerBuilding 4-119, Johns Hopkins University School of Medicine, Baltimore, MD 21205.

82 ROBERT G. ROBINSON AND OTHERS
Previous investigators have reported that left hemisphere brain injury isassociated with depressive mood while right hemisphere brain injury is associatedwith apathy, cheerfulness, and a tendency to minimize difficulties (Gainotti, 1972;for review, see Pearlson and Robinson, 1982). It has also previously been reportedthat the intrahemispheric location of the lesion is important in determining thepsychopathological manifestations of brain injury (Andersen and Havnik, 1950;Benson, 1973). In general, left frontal injury has been associated with depressivesymptoms while left parietal injury has been associated with unconcern andunawareness (Benson, 1973). In the right hemisphere, Ross and Rush (1981) havedescribed a loss of ability to express emotion with more anterior lesions and a loss ofemotional recognition with more posterior lesions, analogous to the languageorganization in the left hemisphere.
However, the importance of the frontal lobe and the strong relationship betweendistance of the lesion from the frontal pole on CT scan and severity of depressionhave not been reported by other investigators. Our original observations in patientswith left hemisphere injury were undertaken in a group of patients who weremany months past the onset of their illness and in whom there was markedvariability in the duration of their illness (Robinson and Szetela, 1981: Robinsonand Benson, 1981). In addition, we did not exclude any patients in whom there werepremorbid risk factors for psychiatric disorder such as alcoholism, family orpersonal history of psychiatric disorder. Therefore, in the current study, weexamined a selected group of acute stroke patients within a few weeks of their injurywho had identifiable lesions on CT scan and no risk factors for psychiatric disorder.There were two aims of this study. The first was to see if we would replicate ourprevious findings in a better controlled study of patients with left hemisphereinjury, and secondly to see what would be the relationship between lesion locationand psychopathology in patients with right hemisphere lesions.
METHODS
Patient Population
Over a two-year period, we have screened a consecutive series of 184 patients admitted to theUniversity of Maryland Hospital with either a thromboembolic stroke (n = 144) or intracerebralhaemorrhage (n = 40). Of this number, 53 patients could not be interviewed because of a decreasedlevel of consciousness or severe aphasia with comprehension deficits, 7 patients were discharged beforethey could be examined, and 1 patient refused the interview. Of the 123 patients who were examined,we excluded subjects for the present study if they were left handed, or had a previous personal historyof psychiatric treatment, alcohol or drug abuse, family history of psychiatric disorder or if there was aclinical history or CT scan evidence of previous brain injury or the present stroke was not localized onCT scan to one hemisphere. A total of 48 patients survived these exclusion criteria. Of these 48 patients,only patients with lesions which were visualized on CT scan were included. Twenty-two patients metthe criteria and had a positive CT scan with a single left hemisphere lesion (6 had intracerebralhaemorrhage), while 14 met the criteria and had a single right hemisphere infarct (2 had intracerebralhaemorrhage). The fact that in 25 per cent of the patients the lesion was not visualized on CT scan is not

MOOD DISORDER AFTER STROKE 83
unusual since the lesion may have been too small and the tissue changes necessary to produce theneeded density contrasts on CT scan were still evolving during the first few weeks after an infarct (Valk,1980).
Psychiatric and Neurological Examination
The neurological examination and diagnosis were made by the attending neurologist (T.R.P.) inaccord with the examination and diagnostic criteria used by the multicentre NINCDS Pilot StrokeData Bank (Kunitz et ai, 1979).
After obtaining informed consent, patients were given a series of standardized quantifiable measuresof mood, intellectual function and physical impairment which we have previously found to be reliableand valid in stroke patients (Robinson and Szetela, 1981; Robinson and Benson, 1981; Robinson etal.,19836). Examinations were administered in private between 11 a.m. and 2 p.m. in order to minimizeany possible effect of diurnal mood variation. The Hamilton Depression Scale (Hamilton, 1960), a17 item questionnaire measuring psychological and physiological symptoms of depression, was filledout by the interviewer. The Zung Depression Scale (Zung, 1965), a 20 question self-rated depressionquestionnaire was read to each patient, and their responses were scored using the four Zung categories.The modified Present State Examination (PSE) (Wing et al., 1974), a semistructured psychiatricinterview which elicited symptoms related primarily to mood and anxiety, was examiner-scored. Thereliability and validity of this modified version of the PSE has been demonstrated in a previouspublication (Robinson et al., 19836). The Mini-Mental State Examination (Folstein et al., 1975) is an11 item questionnaire which has been found to be reliable and valid in assessing cognitive function instroke patients. Scores may range from 0 to 30, and a score of 23 or below is indicative of significantcognitive impairment. The Johns Hopkins Functioning Inventory (Robinson and Szetela, 1981) is a10 item questionnaire which evaluates the patient's degree of independence in activities of daily livingsuch as walking, dressing and eating. Scores may range from 0 to 27.
Analysis of CT Scan
All CT scans were performed on the same scanner using identical slice thickness, angle toorbital-meatal line and size reduction. Analyses of CT scans were done on 9 consecutive dorsal slices10 mm apart beginning with the first slice that included frontal lobe tissue.
Overall brain size, excluding ventricles, and lesion size were determined in each CT slice by acomputerized area calculation procedure. The area within the lesion was divided by the area within thebrain, excluding the ventricles, giving the lesion size as a percentage of brain volume. Lesion borders oneach slice were determined along the anterior-posterior (AP) axis, and a mean anterior and posteriorborder as a percentage of the maximum AP distance was calculated. The criterion used for establishingwhether a lesion was anterior or posterior was as follows. The lesion was anterior if the anterior borderof the lesion was rostral to 40 per cent of the AP distance and the posterior border was anterior to 60 percent of the AP distance. On the other hand, a lesion was posterior if its anterior border was posterior to40 per cent of the AP distance and the posterior border was caudal to 60 per cent of the AP distance.Thus, we allowed a 20 per cent overlap of anterior and posterior lesions. Lesions that were anterior to40 per cent of the AP distance and posterior to 60 per cent were not used in the data analysis and werecalled both anterior and posterior.
Statistical Analysis
Statistical analysis was done using means and standard deviations, analysis of variance, student'st-tests, and Pearson correlation coefficients. Nonparametric statistics were done using x2 tests withYates modification for small number cells. In order to allow a single depression score to be correlatedwith other variables, an overall depression score (range 0 to 15) was calculated based on the threedepression measures, (i.e. Zung, Hamilton, and PSE) as described in a previous publication (Robinsonand Szetela, 1981). Briefly, the Zung, Hamilton and PSE scores were each translated to a five-point

84 ROBERT G. ROBINSON AND OTHERS
scale, and the scores were summed for each patient. A Zung score of < 40 = 0, 40-49 = 1, 50-59 = 2,etc.; Hamilton < 5 = 0, 6-7 = 1, 8-9 = 2, etc.; PSE < 7 = 0, 8-9 = 1, 10-11 = 2, etc. We havetranslated each depression measure to a five-point scale in order not to 'overweight' one scale, and theycan be summed because of high interscale correlation {see Results) and previously described crossvalidation (Robinson and Szetela, 1981; Robinson el al., 19836).
R E S U L T S
PatientsBackground information revealed no statistically significant differences between
the right and left hemisphere lesion groups (Table 1). There were 10 patients with leftanterior lesions, 8 with left posterior lesions (4 patients could not be classified intoanterior or posterior), 6 with right anterior lesions and 6 with right posterior lesions(2 could not be classified), and there were no statistically significant intergroupdifferences in background demographic data for these four lesion location groups.The patients were predominantly black males in their late fifties or early sixties fromthe middle or lower socioeconomic class. Patients were interviewed generally withinthe first two weeks after the stroke.
Neurological Findings
Except for aphasia, there were no significant differences in the neurologicalsymptoms of the left and right hemisphere stroke groups (Table 2). Between 72 and90 per cent of the patients had a hemiparesis. Between 33 and 67 per cent of bothgroups had a hemisensory loss, and about 20 per cent had a homonymoushemianopia. Aphasia was found only in patients with left hemisphere lesions,although 2 patients with right hemisphere lesions had slurring of speech. Approxi-mately 28 per cent of the left hemisphere damaged patients were aphasic with an
TABLE 1. CHARACTERISTICS OF STUDY POPULATION
Location of stroke lesion
Age (mean ± SD)Sex (% male)Race (% black)Socioeconomic class (Hollingshead cl. 4 or 5)Marital status (% married)No. children (mean ± SD)Origin (% rural)No. siblings (mean ± SD)Tobacco use (% 1 pack per day or greater)Previous medical illness (%) (life threatening)Time since stroke (mean days ± SD)
Left hemisphere(n = 22)57 ± 12
53674090
1.6 ± 1.333
4.5 ± 3.95710
12± 11
Right hemisphere(n = 14)
61 ± 1073634582
2.5 ±2.154
4.8 ± 4.04627
10 ± 7

MOOD DISORDER AFTER STROKE 85
approximately equal distribution of Broca's, Wernicke's, global and anomicaphasias. Comparison of anterior-posterior groups on each side showed 10 of10 patients with left anterior infarct had a hemiparesis while only 3 of 8 patients witha left posterior infarct had this symptom x2 = 4.5, (P < 0.05); 5 of 6 patients withright anterior lesions were hemiparetic while 4 of 6 with right posterior strokes hadthis symptom (n.s.). There were no other statistically significant differences inneurological symptoms between the anterior and posterior groups.
There were 6 of 22 patients with left hemisphere lesions and 2 of 14 with righthemisphere lesions who had intracerebral haemorrhages. Of these 6 with lefthemisphere haemorrhages, 2 had anterior and 3 had posterior lesions (1 was bothanterior and posterior) while in the right hemisphere, none had an anteriorhaemorrhage and one had a posterior haemorrhage (1 was both anterior andposterior). This distribution of infarcts and haemorrhages by location is notsignificantly different than a random distribution (x2 = 2.9, P > 0.25).
Relationship of Anterior-Posterior and Right-Left Lesion Location toPsychopathology
Although about half of all patients with lesions of either the right or lefthemisphere demonstrated symptoms of anxiety and worrying, there were distinctsymptom clusters which were found more frequently in one group than another.Depression and vegetative symptoms (i.e. early morning awakening, decreasedappetite and weight loss or decreased libido) were found in 14 of 22 patients with lefthemisphere injury and in only 2 of 14 patients with right hemisphere injury(x2 = 9.4, P < 0.01). When the intrahemispheric lesion location was taken into
TABLE 2.
WeaknessMildSevere
Sensory deficitMildSevere
Homonymous hemianopiaVisual neglectAphasia
BrocaWernickeGlobalAnomic
NEUROLOGICAL DEFICITS
Lesion
Left hemisphere
Anterior
5/105/10
3/100/101/10
1
1
Posterior
2/81/8
2/82/82/8
211
location
Right hemisphere
Anterior
3/62/6
1/60/61/60/6—
Posterior
0/64/6
1/61/61/62/6—

86 ROBERT G. ROBINSON AND OTHERS
account 7 of 10 patients with left anterior lesions had depression and vegetativesymptoms while 3 of 8 patients with left posterior lesions, 0 of 6 with right anteriorlesions and 1 of 6 with right posterior lesions had these symptoms (x2 = 8.22, df = 3,P < 0.05). On the other hand, patients with right hemisphere lesions were found tohave inappropriate cheerfulness in 6 out of 14 cases (5 of 6 cases were in rightanterior group) while this symptom was found in none of the 22 patients with lefthemisphere injury (x2 = 8.6, P < 0.01).
Analysis of scores from the depression scales were also consistent with the findingof right-left hemisphere group differences as well as anterior posterior groupdifferences. Patients with left anterior hemisphere infarcts had significantly highermean depression scores than patients with left posterior lesions or right anteriorlesions on all three depression scales (Table 3). The right posterior groupdiffered from the left anterior group on the PSE and the overall depressionscore (Table 3).
TABLE 3. INTRAHEMISPHERIC LESION LOCATION RELATED TO DEPRESSION,IMPAIRMENT, SEVERITY, AND SIZE OF LESION
Depression scores (mean ± SD)ZungHamiltonPSEOverall
Cognitive impairmentMini-Mental
Activities of daily livingJHFI
Lesion volume as % of brain volume
Left
Anteriorn = 10
51 ± 1210 ± 618 ± 11
8.4 ± 5.3
19 ± 7
10 ± 64.7 ± 3.5
hemisphere
Posteriorn = 8
36 ±7*4 ±6*5 ±3*
2.6 ± 3.4*
20 ± 6
5 ± 46.3 ±6.1
Right
Anteriorn = 6
35 ±7*5 ±2*5 ±6*
1.5 ±1.2'
27 ±2 +
5 ± 64.1 ±4.9
hemisphere
Posteriorn = 6
42 ± 127 ± 68 ± 6 +
• 5.0 ± 3.5**
23 ± 5
8 ± 55.0 ± 3.4
* Significantly different from left anterior, P < 0.01 +P < 0.05. ** Significantly different from rightanterior, P < 0.02. PSE = Present State.
In contrast to the findings in the left hemisphere, patients with right anteriorlesions had significantly lower mean depression scores on the overall depressionscore than patients with right posterior infarcts (Table 3).
As another way of examining this issue of whether the psychopathologicalsymptoms vary with lesion location, we assessed diagnostic symptom clustersrelated to site of lesion. Using psychiatric Research Diagnostic Criteria (Spitzer etal., 1975), 6 of 10 patients with left anterior infarcts met the criteria for a diagnosis ofmajor depressive disorder with the exception that in some patients, the duration of
MOOD DISORDER AFTER STROKE 87
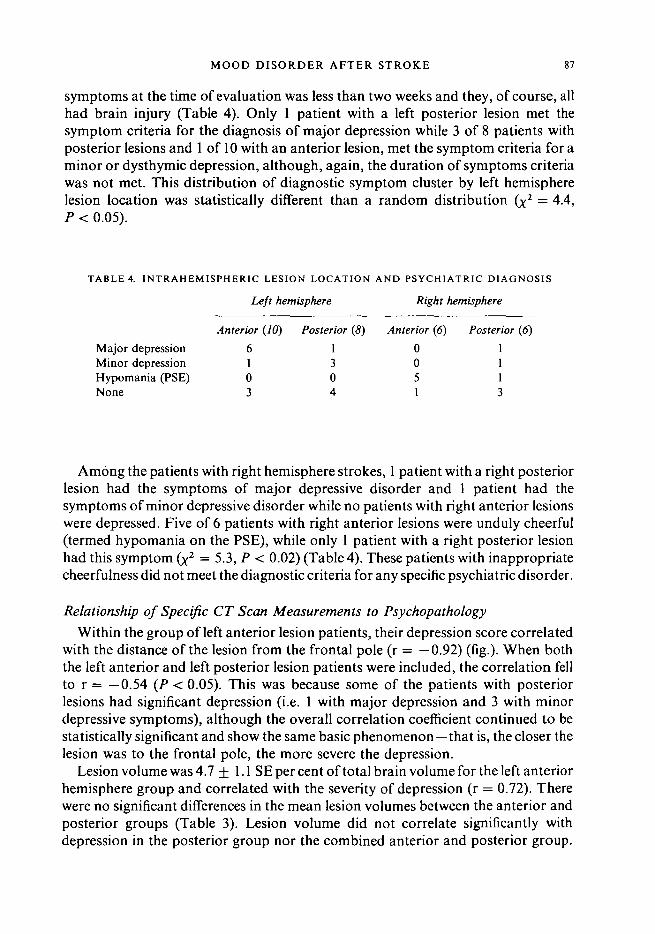
symptoms at the time of evaluation was less than two weeks and they, of course, allhad brain injury (Table 4). Only 1 patient with a left posterior lesion met thesymptom criteria for the diagnosis of major depression while 3 of 8 patients withposterior lesions and 1 of 10 with an anterior lesion, met the symptom criteria for aminor or dysthymic depression, although, again, the duration of symptoms criteriawas not met. This distribution of diagnostic symptom cluster by left hemispherelesion location was statistically different than a random distribution (%2 = 4.4,P < 0.05).
TABLE 4. INTRAHEMISPHERIC LESION LOCATION AND PSYCHIATRIC DIAGNOSIS
Left hemisphere Right hemisphere
Anterior (10) Posterior (8) Anterior (6) Posterior (6)
Major depression 6 1 0 1Minor depression 1 3 0 1Hypomania (PSE) 0 0 5 1None 3 4 1 3
Among the patients with right hemisphere strokes, 1 patient with a right posteriorlesion had the symptoms of major depressive disorder and 1 patient had thesymptoms of minor depressive disorder while no patients with right anterior lesionswere depressed. Five of 6 patients with right anterior lesions were unduly cheerful(termed hypomania on the PSE), while only 1 patient with a right posterior lesionhad this symptom (x2 = 5.3, P < 0.02) (Table 4). These patients with inappropriatecheerfulness did not meet the diagnostic criteria for any specific psychiatric disorder.
Relationship of Specific CT Scan Measurements to Psychopathology
Within the group of left anterior lesion patients, their depression score correlatedwith the distance of the lesion from the frontal pole (r = —0.92) (fig.). When boththe left anterior and left posterior lesion patients were included, the correlation fellto r = —0.54 (P < 0.05). This was because some of the patients with posteriorlesions had significant depression (i.e. 1 with major depression and 3 with minordepressive symptoms), although the overall correlation coefficient continued to bestatistically significant and show the same basic phenomenon—that is, the closer thelesion was to the frontal pole, the more severe the depression.
Lesion volume was 4.7 ±1.1 SE per cent of total brain volume for the left anteriorhemisphere group and correlated with the severity of depression (r = 0.72). Therewere no significant differences in the mean lesion volumes between the anterior andposterior groups (Table 3). Lesion volume did not correlate significantly withdepression in the posterior group nor the combined anterior and posterior group.

ROBERT G. ROBINSON AND OTHERS
14 -
12
O 4 -
18
20
20 22 24 26 28 30 32 34 36 • Left
24 28 32 36 40 44 48 52 56 • Right
Distance of lesion from frontal pole
FIG. Relationship between overall depression score and distance of the anterior border of the lesion from thefrontal pole for patients with either left anterior hemisphere infarcts or right hemisphere infarcts. The distance fromthe frontal pole is expressed as a percentage of the total anteroposterior distance. The correlation coefficients areindicated on the figure. rlefl, P < 0.001; r r i fh l, P < 0.01.
In the group of patients with right hemisphere strokes, there was a significantcorrelation between the overall depression score and the distance of the lesion fromthe frontal pole for the entire right hemisphere group (r = 0.76) (fig.), that is, thefurther the lesion was from the frontal pole, the more severe the depression. This isexactly the opposite direction of correlation from that found in the left hemispheregroup. Lesion volume was 4.5 ± 1.3 SE per cent of total brain volume. The lesionvolume did not correlate significantly with the depression score in either the anterioror posterior group.
Relationship Between Depression Scores and Physical and Cognitive Impairment
Cognitive impairment as measured by Mini-Mental score, correlated significantlywith the overall depression score in the left hemisphere lesion group (r = —0.43);however, activities of daily living as measured by the Johns Hopkins FunctioningInventory (JHFI) score did not correlate significantly with the overall depressionscore (r = 0.29). In addition, Mini-Mental score, but not JHFI score, correlatedwith lesion volume (r = —0.63, P < 0.01) for the entire left hemisphere lesiongroup. No other correlations between severity of impairment and depression scoresor lesion volume were significant in the left hemisphere injured group.
In the right hemisphere lesion group neither the Mini-Mental score nor the JHFI

MOOD DISORDER AFTER STROKE 89
score correlated significantly with the depression scores. The Mini-Mental score,but not the JHFI score, correlated significantly with the lesion volume (r = —0.42,P < 0.05). The three depression measures were highly significantly correlatedwith each other (Zung-Hamilton, r = 0.80; Zung-PSE, r = 0.82; Hamilton-PSE,r = 0.85).
Relationship Between Aphasia and PsychopathologyAlthough the neurological deficits found in the patients with right and left
cerebral stroke were comparable, aphasia was found, as would be expected, onlyamong patients with left cerebral injury. In order to evaluate whether aphasia wasan important factor in the predominance of depression in left hemisphere strokepatients, we compared left hemisphere lesion patients with and without aphasia onthe various psychopathology scales. There were no significant differences in themean Zung, Hamilton or PSE scores between patients with aphasia and patientswithout aphasia. In a previous publication, we have noted the high frequency ofdepression in patients with nonfluent aphasia (Robinson and Benson, 1981). In thepresent study, aphasia was found in 2 patients with left anterior lesions, 1 of whomhad the symptoms of a major depression and 1 of whom had the symptoms of minordepression. Because there were only 2 patients with aphasia, it was not possible todetermine whether the frequency of depression was higher among these patients ascompared with patients with left anterior brain injury and no aphasia. However, ofthe 7 patients who had the symptoms of major depression, only 2 had aphasia(1 with Broca's and 1 with posterior lesion and global aphasia).
DISCUSSION
We have demonstrated in a selected group of patients with single brain lesions andno predisposing factors for psychiatric disorder that there are important andstatistically significant differences in the distribution, frequency and/or severity ofdepression between patients with anterior or posterior lesions within eachhemisphere. In addition, we have shown that severity of depression correlates withdistance of lesion from the frontal pole across the entire right hemisphere andacross the entire left hemisphere although the correlation is strongest within the leftanterior group.
This finding in the left hemisphere lesion group is a confirmation of our previouslyreported findings in a group of chronic brain-injured patients (Robinson andSzetela, 1981) and in patients with bilateral brain injury (Lipsey et al, 1983). Itshould be noted, however, that the anterior and posterior groups had some overlapin their lesion locations and that the distribution of lesion locations did not cover theentire hemisphere. As shown in the fig. the most anterior lesion was no closer to thefrontal pole than 18 per cent of the A-P distance. Thus, we were evaluating lesionswhich were distributed over about the middle two-thirds of the hemisphere and wereonly 'relatively' more anterior or posterior. Another point which should be made is

90 ROBERT G. ROBINSON AND OTHERS
that in the right hemisphere group we showed a correlation between severity ofdepression and distance of the lesion from the frontal pole. Since the patientswith right hemisphere injury as a group had less severe depression than lefthemisphere lesion patients, the range of scores was lower and the correlation washeavily dependent on two patients with moderate to severe depression. In addition,the interesting finding of inappropriate cheerfulness in patients with right anteriorstrokes could not be correlated with distance of lesion from the frontal pole becausewe were unable to 'grade' inappropriate cheerfulness and could, on the PSE, onlynote its presence or absence. It is possible that severity of this symptom mightcorrelate with proximity of the lesion to the frontal pole as depression did in the lefthemisphere lesion group.
The most obvious implication of this study is that the aetiology of the mooddisorders found in these stroke patients is in some way related to the location oftheir brain injury with left anterior injury being particularly associated withdepression and right anterior injury associated with inappropriate cheerfulness. Themajor question, however, is the nature of this relationship. Does the depressionrepresent a psychological reaction to a particular cognitive or physical impairmentor does it represent the behavioural manifestation of neurophysiological andneurochemical responses to brain injury? We cannot fully answer this question atthe present time and it is possible, for example, that severity of visuospatial deficitsin right posterior lesion patients might correlate strongly with severity of depression.In addition, we have recently reported in our longitudinal study of 103 strokepatients that both severity of cognitive impairment and severity of impairment inactivities of daily living correlate significantly (r values between 0.3 and 0.4) withdepression (Robinson et al., 19836). We are also in the process of a more detailedanalysis of neuropsychological impairment using a much more extensive testbattery to examine the specific kinds of deficits which may correlate with severity ofdepression. Thus, it seems highly likely that severity of impairment plays a role in atleast some poststroke depression, the issue is only whether there is evidence foradditional factors contributing to these mood disorders.
There are several lines of evidence which suggest that neural factors may beinvolved. First, this interesting relationship between the proximity of the lesion tothe frontal pole and severity of depression is a phenomenon which we haverepeatedly demonstrated in several studies (Robinson and Szetela, 1981; Lipsey etal., 1983). This 'graded' effect of lesion location on severity of depression is differentfrom the topographical (Broca, 1861; Wernicke, 1908; Penfield and Boldrey, 1937;Geschwind, 1970) or mass action (Lashley, 1963) relationships between anyneuropsychological function and lesion location. Secondly, the strength of thecorrelation between distance from frontal pole and severity of depression explains50 to 70 per cent of the variance while the relationship to physical or overallcognitive impairment explains 10 to 20 per cent of the variance. Thirdly, thecharacteristic syndrome-like nature of the depression in many of the patients withleft anterior lesions, including both mood and vegetative changes, suggests an

MOOD DISORDER AFTER STROKE 91
'endogenous' aetiology for the depression. Finally, we have yet to find a specificimpairment which occurs in all or most of the severely depressed patients. Forinstance, Broca's aphasia was found in only 1 of the 6 patients with left anteriorlesions and major depressive symptoms. Another patient with an anterior lesion andglobal aphasia did not have major depressive symptoms and 5 of 7 patients withmajor depressive symptoms did not have aphasia.
If some of these poststroke depressions do not represent an understandablereaction to impairment, how then might these findings be explained? The mostobvious explanation is that we have found a 'frontal syndrome' that is different inthe two hemispheres (i.e. left lesions associated with a depressive syndrome, rightlesions associated with inappropriate cheerfulness). Numerous investigators havedescribed a 'frontal syndrome' and recognized the importance of the frontal lobes inaffect (Hecaen and Albert, 1975). However, there is no known neuroanatomy orneurophysiology to account for the importance of the frontal lobe in affect. Ourpresent findings have not only shown a frontal syndrome, but have also shown agraded effect of lesion location on mood from anterior to posterior. These twofindings (i.e. the importance of the frontal lobe in mood disorders and the gradedeffect of lesion location on mood) suggest an intriguing neural hypothesis for theseresults.
Numerous investigators have described the arborizing innervation of thecerebral cortex by noradrenergic neurons in rats (Ungerstedt, 1971; Pickel et al.,1974) and in monkeys (Foote et al., 1981) and Morrison et al. (1979) have recentlydemonstrated that lesions of the anterior cortex disrupt these noradrenergic fibres toa significantly greater extent than do posterior lesions. Our laboratory experimentshave demonstrated that focal cortical lesions in rats produce widespread butasymmetrical depletion of catecholamine concentrations depending upon whichhemisphere is injured (Robinson, 1979; Robinson and Coyle, 1980; Pearlson andRobinson, 1981). Therefore, perhaps the 'lateralized frontal affective syndrome'might be a behavioural manifestation of asymmetrical depletion in the corticalbiogenic amine pathways with more anterior lesions producing greater depletion ofthese amines. Since we were unable to correlate the degree of inappropriatecheerfulness in patients with right hemisphere lesions and proximity of lesion to thefrontal pole, we do not know whether this hypothesis is also applicable to the righthemisphere lesion group. It should be noted, however, that our finding of increaseddepression with more posterior lesions runs counter to what would be expectedon this hypothesis.
Although this suggestion is strictly a hypothesis, there are several strengths toproposing such a hypothesis at this early stage of investigation. First, it is a testablehypothesis which makes certain predictions. For instance, a large lesion shouldinterrupt more pathways than a small lesion in the same location, and therefore leadto greater depression. Our finding of a positive correlation between size of lesion andseverity of depression in the left anterior group is consistent with this prediction. Inaddition, it would be expected that concentrations of biogenic amines which have

92 ROBERT G. ROBINSON AND OTHERS
been implicated in the aetiology of functional depressions (Bunney and Davis, 1965;Schildkraut, 1965) would be decreased in the spinal fluid of patients with depression,and we are currently evaluating this prediction by measuring catecholaminemetabolites in the CSF of depressed stroke patients. This hypothesis also has theadvantage of taking an old observation that there is a distinct 'frontal affect' andgiving it an underlying neuroanatomical substrate.
Regardless of what may be the aetiology of these poststroke mood disorders, thisstudy suggests that there may be an important relationship between both inter- andintrahemisphere lesion location and mood disorder and that depressive disordersare both common (i.e. 13 of 30 patients had clinically significant depression) andfrequently severe. We need to obtain further data on the aetiology of these disordersas well as to investigate effective treatment techniques.
A C K N O W L E D G E M E N T S
The authors would like to thank Paula Bolduc and Curtis Smith for assistance in the preparation ofthe paper. This work was supported in part by NIH Grant Research Scientist Development Award(RGR) MH 00163, NS 15178, NS 18622, NS 9-2302, NS 16332.
R E F E R E N C E S
ANDERSEN A L, HANVIK I J (1950) The psychometric localization of brain lesions: the differential effectof frontal and parietal lesions on MMPI profiles. Journal of Clinical Psychology, 6, 177-180.
BENSON D F (1973) Psychiatric aspects of aphasia. British Journal of Psychiatry, 123, 555-566.BROCA P (1861) New finding of aphasia following a lesion of the posterior part of the second and third
frontal convolutions. Bulletins de la Society Anatomique, 6, 398-407.BUNNEY W E, DAVIS J (1965) Norepinephrine in depressive reactions: a review of supporting evidence.
Archives of General Psychiatry, Chicago, 13, 483-497.FOLSTEIN M F, FOLSTEIN S E, MCHUGH P R (1975) 'Mini-mental state: a practical method for grading
the cognitive state of patients for the clinician. Journal of Psychiatric Research, 12, 189-198.FOOTE S L, MORRISON J H, BLOOM F E, O'CONNER D (1981) Laminar and regional distribution of
norepinephrine fibers in squirrel monkey neocortex as revealed by immunohistochemistry.Society for Neuroscience Abstracts, 7, 792.
GAINOTTI G (1972) Emotional behavior and hemispheric side of the lesion. Cortex, 8, 41-55.GESCHWIND N (1970) The organization of language and the brain. Science, 170, 940-944.HAMILTON M A (1960) A rating scale for depression. Journal of Neurology, Neurosurgery and
Psychiatry, 23, 56-62.HECAEN H, ALBERT M L (1975) Disorders of mental functioning related to frontal lobe pathology. In:
Psychiatric Aspects of Neurological Disease. Edited by D. F. Benson and D. Blumer. New York:Grune and Stratton, pp. 139-147.
KUNITZ S C, HAUEKOST C L, GROSS C R (1979) Pilot data bank networks for neurological disorders.In: Third Annual Proceedings Symposium of Medical Care, pp. 793-796.
LASHLEY K S (1963) Brain Mechanisms and Intelligence. Chicago: University of Chicago Press.LIPSEY J R, ROBINSON R G, PEARLSON G D, RAO K, PRICE T R (1983) Mood change following
bilateral hemisphere brain injury. British Journal of Psychiatry, 143, 266-273.MORRISON J H, MOLLIVER M E, GRZANNA R (1979) Noradrenergic innervation of cerebral cortex:
widespread effects of local cortical lesions. Science, 205, 313-316.

MOOD DISORDER AFTER STROKE 93
PEARLSON G D, ROBINSON R G (1981) Suction lesions of the frontal cerebral cortex in the rat induceasymmetrical behavioral and catecholaminergic responses. Brain Research, Amsterdam, 218,233-242.
PEARLSON G D, ROBINSON R G (1982) Lateralization of emotional or behavioral responses in intactand hemisphere-damaged humans and rats. In: The Expression of Knowledge. Edited by R. L.Isaacson and N. E. Spear. New York: Plenum Press, pp. 339-390.
PENFTELD W, BOLDREY E (1937) Somatic motor and sensory representation in the cerebral cortex ofman as studied by electrical stimulation. Brain, 60, 389-443.
PICKEL V M, SEGAL M, BLOOM F E (1974) A radioautographic study of the efferent pathways of thenucleus locus coeruleus. Journal of Comparative Neurology, 155, 15-42.
ROBINSON R G (1979) Differential behavioral and biochemical effects of right and left hemisphericcerebral infarction in the rat. Science, 205, 707-710.
ROBINSON R G, BENSON D F (1981) Depression in aphasic patients: frequency, severity andclinical-pathological correlations. Brain and Language, 14, 282-291.
ROBINSON R G, COYLE J T (1980) The differential effect of right versus left hemispheric cerebralinfarction on catecholamines and behavior in the rat. Brain Research, Amsterdam, 188, 63-78.
ROBINSON R G, PRICE T R (1982) Post-stroke depressive disorders: a follow-up study of 103 patients.Stroke, 13, 635-641.
ROBINSON R G, STARR L B, KUBOS K L, PRICE T R (1983a) Post-stroke affective disorders. In:Cerebrovascular Diseases. Edited by M. Reivich and H. I. Hurtig. New York: Raven Press,pp. 137-145.
ROBINSON R G, STARR L B, KUBOS K L, PRICE T R (1983ft) A two year longitudinal study of post-stroke mood disorders: findings during the initial evaluation. Stroke, 14, 736-741.
ROBINSON R G, SZETELA B (1981) Mood change following left hemispheric brain injury. Annals ofNeurology, 9, 447-453.
Ross E D, RUSH A J (1981) Diagnosis and neuroanatomical correlates of depression in brain-damagedpatients. Archives of General Psychiatry, Chicago, 38, 1344-1354.
SCHILDKRAUT J J (1965) The catecholamine hypothesis of affective disorders: a review of supportingevidence. American Journal of Psychiatry, 122, 509-522.
SPITZER R J, ENDICOTT J, ROBINS E (1975) Research Diagnostic Criteria (RDC) for a Group ofFunctional Disorders. New York: Biometrics Research Division, New York Psychiatric Institute.
UNGERSTEDT U (1971) Stereotaxic mapping of monoamine pathways in the rat brain. Ada Physio-logica Scandinavica, Supplement, 367, 1-48.
VALK J (1980) Temporal development of the CT scan image of infarctions. In: Computed Tomographyand Cerebral Infarctions. Edited by J. Valk. New York: Raven Press.
WERNICKE C (1908) The symptom complex of aphasia. In: Modern Clinical Medicine: Diseases of theNervous System. New York: Appleton Press.
WING J K, COOPER E, SORTORIUS N (1974) Measurement and Classification of Psychiatric Symptoms.Cambridge: Cambridge University Press.
ZUNG W W K. (1965) A self-rating depression scale. Archives of General Psychiatry, Chicago, 12,63-70.
(Received March 29, 1983)




















