Module 8 Young People with Sexually Transmitted Diseases
27
Integration of Adolescent Health and Development Domains into pre-service nursing curriculum 1 Sources: 1. World Health Organization. (2009). World Health Organization: Adolescent Job Aid. World Health Organization. 2. World Health Organization. Orientation Program on Adolescent Health for Health-care Providers. Facilitator Guide - New Modules. World Health Organization. 3. World Health Organization. Orientation Program on Adolescent Health for Health-care Providers. Handout - New Modules. World Health Organization. Prepared for integrating of Adolescent Health and Development Domains into pre-service nursing curriculum at The Hong Kong Polytechnic University, World Health Organization Collaborative Centre for Community Health Services. Supported by WHO, Western Pacific Regional Office Module 8 Young People with Sexually Transmitted Diseases I. Introduction Diseases such as gonorrhoea, syphilis, chancroid, chlamydia and genital herpes are spread by unprotected sex, i.e. sex without a condom. Adolescents are less likely than adults to use a condom because of lack of access or inability to insist on its use. They are therefore at high risk of contracting sexually transmitted infections (STIs) including HIV and AIDS. More than a quarter of a million young people become infected with an STD every day. About 80% of HIV transmission worldwide occurs as a result of unprotected sex. If one partner has a sexually transmitted disease (STD) as well as HIV, the risk of HIV transmission is three to five times greater (WHO, 1998). Adolescents are on the front line of the HIV pandemic. In some African countries, surveys have found one in ten pregnant adolescent girls to be HIV-positive. Worldwide, at least 2.5 million youth were newly infected with HIV during 1997. More than half of all new HIV infections occur in young people. An estimated 10 million adolescents are now living with HIV or are likely to develop AIDS during the next three to 15 years (WHO, 2003). II. Learning objectives Upon completion of this module, learners will be able to: 1. Discuss the global and local prevalence and incidence of STIs, including HIV/AIDS 2. Identify contributing factors and methods of preventing STIs 3. Understand the diagnosis and management of STIs 4. Identify essential features of an STI counselling session and counselling skills using the LEPERS model 5. Identify strategies and health policies related to STIs
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Module 8 Young People with Sexually Transmitted Diseases
Integration of Adolescent Health and Development Domains into pre-service nursing curriculum
1
Sources: 1. World Health Organization. (2009). World Health Organization: Adolescent Job Aid. World Health Organization. 2. World Health Organization. Orientation Program on Adolescent Health for Health-care Providers. Facilitator Guide - New Modules. World Health Organization. 3. World Health Organization. Orientation Program on Adolescent Health for Health-care Providers. Handout - New Modules. World Health Organization.
Prepared for integrating of Adolescent Health and Development Domains into pre-service nursing curriculum at The Hong Kong Polytechnic University, World Health Organization Collaborative Centre for Community Health Services. Supported by WHO, Western Pacific Regional Office
Module 8 Young People with Sexually Transmitted Diseases
I. Introduction Diseases such as gonorrhoea, syphilis, chancroid, chlamydia and genital herpes are spread by unprotected sex, i.e. sex without a condom. Adolescents are less likely than adults to use a condom because of lack of access or inability to insist on its use. They are therefore at high risk of contracting sexually transmitted infections (STIs) including HIV and AIDS. More than a quarter of a million young people become infected with an STD every day. About 80% of HIV transmission worldwide occurs as a result of unprotected sex. If one partner has a sexually transmitted disease (STD) as well as HIV, the risk of HIV transmission is three to five times greater (WHO, 1998). Adolescents are on the front line of the HIV pandemic. In some African countries, surveys have found one in ten pregnant adolescent girls to be HIV-positive. Worldwide, at least 2.5 million youth were newly infected with HIV during 1997. More than half of all new HIV infections occur in young people. An estimated 10 million adolescents are now living with HIV or are likely to develop AIDS during the next three to 15 years (WHO, 2003). II. Learning objectives Upon completion of this module, learners will be able to: 1. Discuss the global and local prevalence and incidence of STIs, including HIV/AIDS 2. Identify contributing factors and methods of preventing STIs 3. Understand the diagnosis and management of STIs 4. Identify essential features of an STI counselling session and counselling skills using the
LEPERS model 5. Identify strategies and health policies related to STIs

Integration of Adolescent Health and Development Domains into pre-service nursing curriculum
2
III. Content Upon completion of this module, learners will be able to: • Discuss the global and local prevalence and incidence of STIs, including HIV/AIDS • Identify contributing factors and methods of preventing STIs • Understand the diagnosis and management of STIs • Identify essential features of an STI counselling session and counselling skills using the
LEPERS model • Identify strategies and health policies related to STIs

Integration of Adolescent Health and Development Domains into pre-service nursing curriculum
3
Objective 1: Discuss the global and local prevalence and incidence of STIs, including HIV/AIDS Activities Activity 8.1: Group discussion Discuss why adolescents are at high risk of contracting STIs, and identify the risk factors and the consequences.
STI infections Note. From Global prevalence and incidence of selected curable sexually transmitted infections: overview and estimate (p.9), by WHO, 2001, Geneva: WHO. Copyright 2001. Chlamydia infections Half of all (48 million) chlamydia infections are reported in South and South East Asian countries. However, the WPRO has previously stated that many prevalence studies in the region were not conducted regularly in most countries, and the data collected may not therefore be reliable. The reported prevalence rates vary greatly and should therefore be interpreted cautiously. The estimated prevalence rates in the adult population in the Western Pacific region were as high as 20% in Papua New Guinea (PNG) and 13% in Pacific Island countries other than Australia, New Zealand and PNG (WPRO, 1999). Note: From Status and Trends of STIs, HIV/AIDS at the end of the Millennium, p.6 by WPRO, 1999. Copyright by the WPRO with permission seeking. *Refer to the WHO Orientation Program on Adolescent Health for Health-care Providers. Facilitator Guide - New Modules. World Health Organization. Module N Young People and HIVs. *Refer to the WHO Orientation Program on Adolescent Health for Health-care Providers. Handout - New Modules. World Health Organization. Module N Young People and HIVs.
Integration of Adolescent Health and Development Domains into pre-service nursing curriculum
4
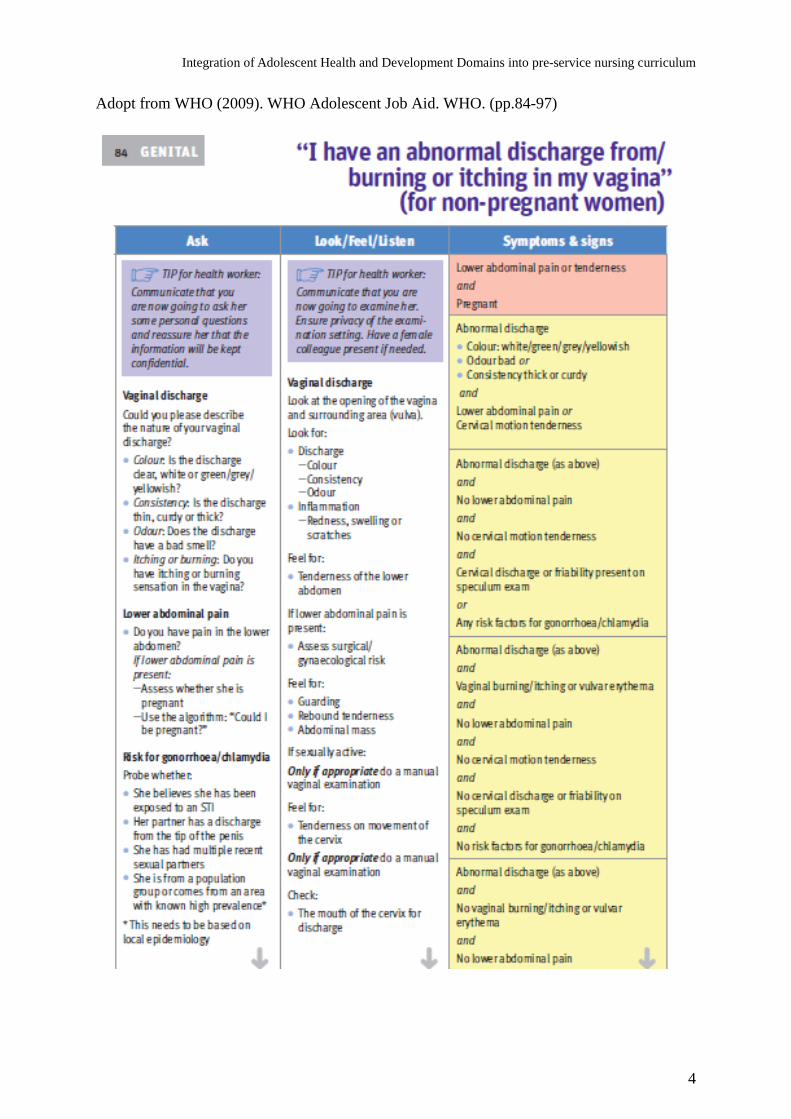
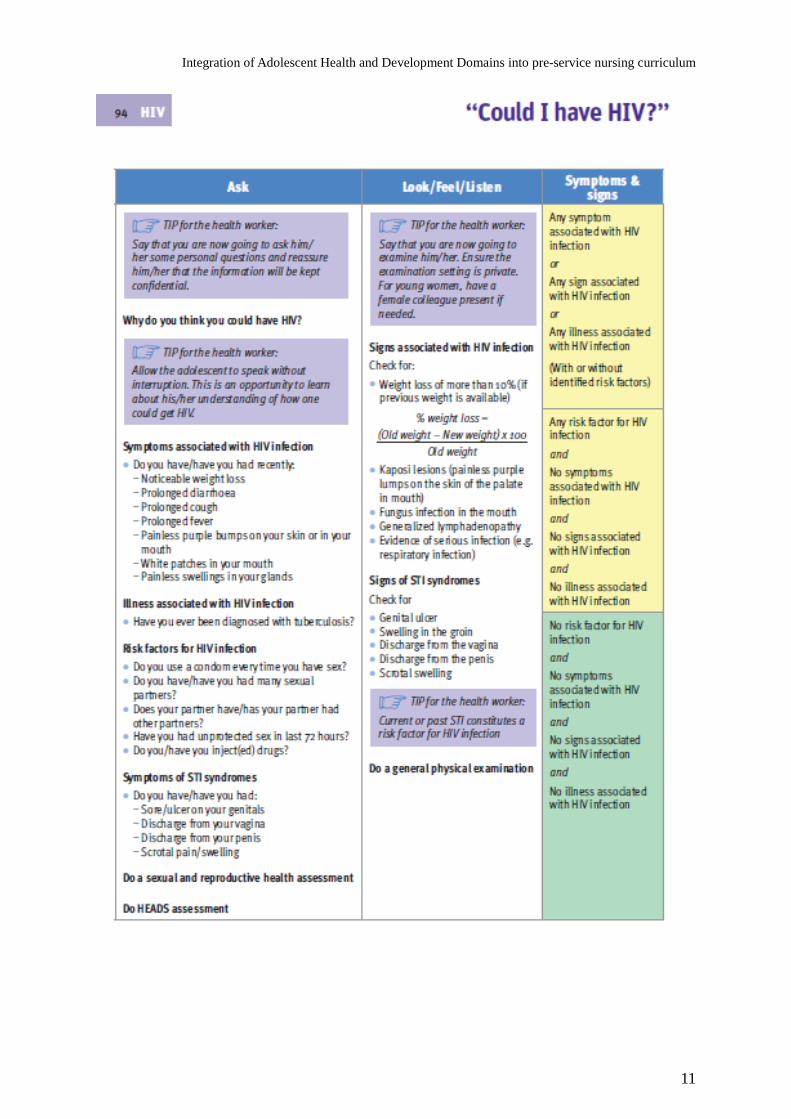
Adopt from WHO (2009). WHO Adolescent Job Aid. WHO. (pp.84-97)

Integration of Adolescent Health and Development Domains into pre-service nursing curriculum
5

Integration of Adolescent Health and Development Domains into pre-service nursing curriculum
6

Integration of Adolescent Health and Development Domains into pre-service nursing curriculum
7

Integration of Adolescent Health and Development Domains into pre-service nursing curriculum
8

Integration of Adolescent Health and Development Domains into pre-service nursing curriculum
9

Integration of Adolescent Health and Development Domains into pre-service nursing curriculum
10
Integration of Adolescent Health and Development Domains into pre-service nursing curriculum
11

Integration of Adolescent Health and Development Domains into pre-service nursing curriculum
12

Integration of Adolescent Health and Development Domains into pre-service nursing curriculum
13

Integration of Adolescent Health and Development Domains into pre-service nursing curriculum
14
Integration of Adolescent Health and Development Domains into pre-service nursing curriculum
15
Objective 2: Identify contributing factors and methods of preventing STIs Risks associated with adolescence Changing social circumstances have led to changes in sexual behaviour and relationships among young people. These changed circumstances include the following: 1. accelerating urbanization, 2. an earlier start to puberty together with a rise in the mean age of marriage, 3. the rapid spread of mass media communication across cultural boundaries, and Risks factors that are related to STIs: − Curiosity − Self-image − Peer pressure − Stress − Socio-economic status − Sexual education Early unprotected sexuality and use of substances are the leading causes of STIs in adolescence. Adolescence is the transition to adulthood and also a time of learning that necessarily includes risk taking, but the conditions in which these risks are taken will often make the difference between constructive and destructive outcomes. Most significant for reproductive health in adolescents is the phenomenon of unprotected sexual relations among them, whether before or during marriage. This increases the risks associated with sexually transmitted diseases and HIV infection resulting in AIDS. Checklist for identifying STI risk (adapted from WHO, 2003) Answering these questions can help a person recognize if he or she is likely to contract an STI. The answers can also guide the family planning provider: if the client is likely to get an STI, s/he needs a supply of condoms and possibly spermicide, as well as counselling about avoiding STIs, recognizing possible symptoms, and getting treatment if symptoms appear. If the client has any symptoms, s/he also needs diagnosis and treatment or referral Sex workers and their clients face the highest risk of contracting STIs. Among people with lower risk, STI rates are highest among people under age 20 in many countries.

Integration of Adolescent Health and Development Domains into pre-service nursing curriculum
16
The ABCs of preventing STIs (adapted from WHO, 2003) People can avoid STIs by changing their sexual behaviour. They can follow the ABCs - Abstain, Be mutually faithful, and Consistently use condoms Abstain from sex. This is the only guaranteed protection. Be mutually faithful. Always have sex with the same person. This person also must not have sex with anyone else and must not have an STIs IMPORTANT: You usually cannot tell if a person has an STI just by looking at him or her. People with STIs, including HIV, usually do not look sick. Consistently use condoms. Use them every time and use them correctly. To prevent STIs, people at risk should use condoms even if they are using another family planning method. If a woman’s sexual partner will not use condoms, she should try to use a spermicide. However, spermicides may not stop HIV/ AIDS. The diaphragm and cervical cap may also help somewhat in preventing some STIs. *Refer to the WHO Orientation Program on Adolescent Health for Health-care Providers. Facilitator Guide - New Modules. World Health Organization. Module N Young People and HIVs. *Refer to the WHO Orientation Program on Adolescent Health for Health-care Providers. Handout - New Modules. World Health Organization. Module N Young People and HIVs.

Integration of Adolescent Health and Development Domains into pre-service nursing curriculum
17
Objective 3: Understand the diagnosis and management of STIs Table 1: Signs and Symptoms and Treatment of Sexually Transmitted Diseases (STDs) The worldwide incidence of STDs is already high and constantly rising. The ever greater mobility of populations and weakening of traditional customs are increasing the prevalence of people having sexual relations with multiple partners. (Health Systems Development Unit, 2001) Apart from their specific symptoms, STDs also increase the risk of HIV infection. There is considerable evidence that the genital inflammations and lesions caused by STDs increase the risk of sexual transmission of HIV (Health Systems Development Unit, 2001). Signs and symptoms of HIV/AIDS • mouth lesions, small patches of thrush • hairy leukoplakia on the sides of the tongue • lymph nodes swelling • crackling and wheezing sounds in lungs • abdominal pain and diarrhoea Treatment of HIV/AIDS A. Dr. David Ho's cocktail treatment Cocktail treatment, or combination therapy, means the use of multiple anti-viral drugs for treatment, as contrasted with the sole use of one type of drug. Combination therapy is more effective in the sense that it has an inhibiting effects towards HIV, and reduces drug resistance and drug toxicity (Hosein, 2000). B. Vitamins C and E for nuke toxicity Some people who use AZT and other nukes develop muscle weakness. This occurs because AZT appears to damage the power plants or mitochondria (Mt) inside cells. AZT, however, is not the only drug that can damage Mt. In fact, other anti-HIV drugs, particularly other nukes, appear to have the same effect. These drugs can damage Mt in two different ways: • First, the drugs can cause the production of highly active compounds called free radicals.
These compounds damage Mt inside cells in much the same way that rust damages a car. • Second, the drugs appear to interfere with the ability of Mt to extract energy from food.
(Hosein, 2000)

Integration of Adolescent Health and Development Domains into pre-service nursing curriculum
18
Objective 4: Identify essential features of an STI counselling session and counselling skills using the LEPERS model Activities Activity 8.5: Brainstorm What are the essential features of an STI counselling session? “A good counsellor is……” “ A good counselling session takes account of…”
Essential features of an STI counselling session A good counsellor • Is warm • Is trusting • Knows their stuff • Is respectful • Practises confidentiality • Smiles a lot • Is consistent • Treats people fairly • Is supportive • Is friendly • Is sensitive to issues of gender and culture / ethnicity A counselling session takes account of • Time: the value placed on time in the cultural context • Ethics:
Professional ethics Whether using basic counselling skills in a helping way
• The client’s need for confidentiality • The requirement to do the most good and the least harm when there is a dilemma • The requirement to act within the law of the land • Respect for human rights • Location: easy to access
Integration of Adolescent Health and Development Domains into pre-service nursing curriculum
19
The structure of a counselling session • Every session must have a beginning, a middle and an end. • The beginning is where the helper / counsellor introduces himself / herself – who he/she
is and what he/she is there for. • In some sessions it may be appropriate at this point to mention the ethical values of
respect and confidentiality to the client to reassure them. • The middle part of the session is where the helping relationship develops. Here the
counsellor uses basic counselling skills, displays the three core conditions and provides preventative messages.
• The end of the session can be the end of the relationship or the beginning of a long-term relationship. This depends partly on the skills and understanding of the counsellor, but also on the circumstances.
A useful model for problem solving is the LEPERS models (WHO, 2003). LEPERS is: Listening Explaining Providing information Examining Reducing anxiety / providing appropriate reassurance Suggesting strategies An STI counsellor can use the LEPERS model (WHO, 2003) to structure a counselling session. Within the basic structure of counselling, the counsellor uses the relevant skills (active listening, reflection, and paraphrasing and clarification) and displays the three core conditions (empathy, congruence and unconditional positive regard). Introduction and endings An example of an introduction: Hello [or use local greeting] Mary [substitute with local name]. My name is Anne. I work here at the clinic. I will do my best to help. I would like to tell you that whatever you say here today will be held in confidence. Can you tell me what it is that concerns you? • You can change it to suit a standard introduction that all the workers in the clinic use. • You can change it to suit the cultural context you are working in. • The introduction can be peppered with local words or the use of vernacular. An example of an ending: • Mary, can you tell me if you have received the information you wanted when you came
here? • OK! Remember you can always come back and see me again if you have any questions
or need someone to talk to. If you can make an appointment, that will guarantee you will see me again.
• Yes, you can take all the pamphlets, they are free. • Take care, bye, see you again [this depends on what you prefer, and on the wishes of the
person you are helping]

Integration of Adolescent Health and Development Domains into pre-service nursing curriculum
20
Points for discussion: • For many people, issues of a sexual or reproductive nature can be embarrassing to discuss. To seek assistance is a big step and a person can come with many expectations about the session or the preventative messages that will be provided. Be mindful of this. • Language is an important tool to consider when you are counselling in a helping way. The use of vernacular or slang may assist open communication. Be flexible. • Be mindful of cultural beliefs and expectations and how they influence the thoughts, feelings and behaviour of human beings. Be aware of your own cultural beliefs and expectations. Communication and counselling skills (adapted from WHO, 2003) Counselling • Counselling is a dynamic process. • It involves a contractual agreement between a client and a counsellor who is trained to
practise to an acceptable standard and who is bound by a code of ethics and practice. • Counselling aims to encourage healthy living and requires the client to explore important
personal issues and to identify ways of living with the situation they are in. • Counselling is in no way guidance, advice giving or befriending. Counselling skills • Counselling skills are interpersonal communication skills. • They can be used by anyone—either as a separate set of techniques or as a set of skills
which can be integrated with, or used alongside, an already well established set of professional skills.
• In such a case we may find: – a nurse using counselling skills when he or she listens to a patient or comforts grieving
relatives; or – a manager using counselling skills when an employee tells her that he is thinking of
quitting work to look after his sick child. • Counselling skills contain conditions of empathy, genuineness and the absence of
judgment. • If you are using counselling skills, they will operate within your professional skills and
within other professional ethics.

Integration of Adolescent Health and Development Domains into pre-service nursing curriculum
21
Active listening Active listening is what we pay attention to in the person we are helping. To listen actively we must be aware of and use both verbal and non-verbal signals. Non-verbal signals • Voice quality – soft, hard, confident, timid, strong, weak, etc. • Breathing – deep, shallow, sobbing, relaxed, etc. • Eyes – looking down, looking away, making eye contact, tears, etc. • Facial expression – relaxed, tense, afraid, happy, shocked, etc. • Hand movements – waving about, tapping fingers, etc. • Leg movements – swinging, tapping foot, etc. • Body posture – relaxed, stiff, upright, slumped over, etc. We need to be aware of many things … • We listen with our ears and eyes. • There are cultural reasons why people behave in particular ways. • We need to be aware of the ways people communicate non-verbally. • We also need to be aware of the barriers to communication. • We use non-verbal behaviour to show that we are listening and what we are feeling. • These signals can also be barriers to communication. If we are to help our clients we must … • listen sensitively and accurately to them by being sensitive to their whole person; • be aware of our own emotional blind spots; • be aware of how people express their feelings cross-culturally; and • work to develop our empathic skills. Common counselling errors • Controlling, rather than encouraging, the client’s spontaneous expression of feelings and
needs • Judging, as shown by statements that indicate the client does not meet the counsellor’s
standards • Moralizing, preaching, and patronizing—telling people how they ought to behave or lead
their lives • Labelling, making assumptions about the person rather than trying to find out their
motivations, anxieties and fears • Unwarranted reassuring—trying to induce optimism by making light of the client’s
own version of a problem

Integration of Adolescent Health and Development Domains into pre-service nursing curriculum
22
HIV-related counselling 4 steps to pre-test counselling care C-confidentiality A-awareness R-reaction E-early testing (WHO, 2003) 5 steps to post-test counselling Give the results simply and clearly. If the result is – ve: • Reinforce strategies to reduce risk of future infection • Discuss the window period and recommend re-testing in three months (WHO, 2003) If the result is + ve: • Address immediate emotional reactions • Discuss personal, family and social implications • Discuss disclosure • Address immediate needs • Make plans for follow-up (WHO, 2003)

Integration of Adolescent Health and Development Domains into pre-service nursing curriculum
23
Objective 5: Examine strategies and health policies related to STIs To address adolescents’ needs, the WHO has developed a regional plan of action that builds on ongoing activities at the country and regional levels, and uses existing interventions as entry points to introduce complementary and/or new interventions. The plan of action is designed to contribute to the development of comprehensive policies, strategies and integrated interventions for adolescent health and development at the country level. Advocacy for the promotion of adolescent health and development Common issues – programmes for adolescent health have concentrated largely on sexual and reproductive health, despite significant morbidity and mortality due to other health problems. Furthermore, programmes have ignored protective factors that help prevent risk taking and promote positive behaviour. More To build the technical capacity to promote adolescent health and development Common issues such as sexually transmitted infections (STIs) – efforts to address adolescent reproductive health and substance abuse issues have resulted in growing technical capacity at the country and regional levels. However, there are limited technical resources for comprehensive promotion and integrated interventions for adolescent health and development. The WHO response, in building technical capacity, aims to bridge that gap. More Development of national policies, strategies and integrated interventions Common issues such as sexually transmitted infections (STIs) – adolescent health and development issues and problems have common roots and are closely connected. They can, therefore, be addressed most effectively by a combination of mutually supportive interventions that promote healthy development. Policies that protect adolescents' rights can facilitate the development and implementation of integrated interventions. Adolescents' participation in developing national policy, strategies and integrated interventions is crucial in meeting their needs. More

Integration of Adolescent Health and Development Domains into pre-service nursing curriculum
24
WHO responses – undertake collaborative work within the WHO and with external partners.
WHO response – develop a five-year regional advocacy and communications strategy and plan of action that aims to encourage countries to develop appropriate policies, strategies and integrated interventions for adolescent health and development. Undertake collaborative work with partners in planning and implementing selected advocacy activities. Support countries in developing (1) the capacity to advocate, and (2) an advocacy and communications strategy and plan of action. Recommendations for action at the country level • Develop an advocacy and communications strategy and plan of action. • Engage adolescents and the community in adolescent health and development
programmes. • Promote positive societal norms and commitment to promoting the healthy
development of adolescents. • Create opportunities and encourage adolescents to engage in healthy modes of
behaviour.
WHO response – support countries in developing a plan of action to build the technical capacity (e.g. advocacy, programming, resource mobilization, etc.) to promote comprehensive adolescent health and development. Strengthen the capacity of existing technical areas (e.g. reproductive health programmes, health-promoting schools) at the country level. Enhance the technical knowledge base by compiling and disseminating information on the latest technical developments and best practice examples in adolescent health and development. Recommendations for action at the country level • Develop and implement a plan of action to build or strengthen technical capacity (e.g.
advocacy, programming, resource mobilization, etc.) to promote comprehensive adolescent health and development.
Recommendations for action at the country level • Develop policies, strategies and integrated interventions with the • participation of key partners, especially adolescents. • Create a supportive environment for implementing adolescent health and development
policies, strategies and interventions. • Identify a multisectoral mechanism for collaboration and coordination at all levels
(national, provincial, community). • Prioritize interventions and identify effective use of resources. • Undertake collaborative work with partners to implement and sustain action.
Integration of Adolescent Health and Development Domains into pre-service nursing curriculum
25
IV. Case Studies Ah Kit is a 27-year-old bachelor working for a large business in China. Since he started working 4 years ago, he has been visiting female sex workers. He has recently agreed, under considerable pressure from his family, to an arranged marriage, at around the same time as he returned a positive VDRL test. This has been successfully treated, but he has also been asked to donate blood as part of his firm’s health awareness programme. Ah Kit is extremely concerned that the blood test following his donation might be positive for HIV, in view of his sexual history. He is also very worried that if he does give blood, the information about his result and his sexual past may somehow get out. He does not know how he would face his parents and fiancée. Group discussion points: 1. What are the issues identified in the case? 2. What can you tell Ah Kit about the issue of confidentiality? 3. Are there any family members or other people/organizations that can be brought in to provide support for Ah Kit? 4. What influences play upon the arrangement of marriages, and how may these be addressed in this situation? 5. What are the prevention implications for Ah Kit?

Integration of Adolescent Health and Development Domains into pre-service nursing curriculum
26
V. Summary This module focused on the understanding of risks and consequences related to sexually transmitted infection (STIs) in adolescents. The factors and possible impact on adolescents suffering from STIs were discussed. Prevention is better than cure. Therefore, the possible factors contributing to contracting STIs were identified, which are a key element in the prevention of STIs. The structure of an STI counselling session for adolescents was also addressed. *Refer to the WHO Orientation Program on Adolescent Health for Health-care Providers. Facilitator Guide - New Modules. World Health Organization. Module N Young People and HIVs. *Refer to the WHO Orientation Program on Adolescent Health for Health-care Providers. Handout - New Modules. World Health Organization. Module N Young People and HIVs.
Integration of Adolescent Health and Development Domains into pre-service nursing curriculum
27
VI. References • AIDS epidemic update: December 2002 (http://www.who.int/hiv/facts/epiupdate_en.pdf) • Hockenberry, M., Wilson, D., Winkelstein, M., & Kline, N. (2007). Wong’s nursing care
of infants and children. (8th ed.). St. Louis: Mosby. • Hosein, S.R. (2000). Vitamins C& E for nuke toxicity. CATIE-Research-Treatment
Retrieved March 2000 from http://www.catie.ca/tu.nsf?OpenDatabase&Start=1&Count=100&Expand=30
• McCance, K. L. and Huether, S. E. (2002). Pathophysiology: the biological basis for disease in adults & children (4th ed.). St. Louis: Mosby.
• World Health Organization. (2001). The Second Decade. Improving Adolescent Health and Development. World Health Organization.
• World Health Organization. (2003). STI/HIV Counselling in Pacific Island Countries. Western Pacific Region: WHO.
• World Health Organization. (2009) World Health Organization Adolescent Job Aid. World Health Organization.
• World Health Organization. Orientation Program on Adolescent Health for Health-care Providers. Facilitator Guide - New Modules. World Health Organization.
• World Health Organization. Orientation Program on Adolescent Health for Health-care Providers. Handout - New Modules. World Health Organization.
Resources: • Health Systems Development Unit. (2001). Primary clinical care 3. Sandown: Heinemann
Publisher. • World Health Organization. (1998). Adolescent Health & Development. The second
decade. Western Pacific Region: World Health Organization. • World Health Organization. (1999). Status and trends of STIs, HIV/AIDS at the end of
the millennium (p.6). Western Pacific Region: WHO. • World Health Organization. (2001). Global prevalence and incidence of selected curable
sexually transmitted infections: overview and estimate (p.9). Geneva: WHO. • World Health Organization. (2003). Fact Sheet N 110 March 1996 SEXUALLY
TRANSMITTED DISEASES (STDs). Retrieved April 2000 from http://www.who.int/inf-fs/en/fact110.html
• Guidelines for the management of sexually transmitted infections (http://www.who.int/hiv/hiv_aids_2001_01.pdf)
• Sexually Transmitted Diseases: Treatment Guidelines 2002 • http://www.cdc.gov/std/treatment/TOC2002TG.htm) Recommended websites: • http://www.who.int/health_topics/hiv_infections/en/ • http://www.who.int/health_topics/sexually_transmitted_infections/en • http://www.unaids.org/youngpeople/index.html