
Sexually Transmitted Infections (STIs) - WHO | World Health ...
60
Moving ahead on elimination of Sexually Transmitted Infections (STIs) in WHO South-East Asia Region - progress and challenges
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Sexually Transmitted Infections (STIs) - WHO | World Health ...

Moving ahead on elimination of
Sexually Transmitted Infections (STIs)in WHO South-East Asia Region - progress and challenges


Moving ahead on elimination of
Sexually Transmitted Infections (STIs) in WHO South-East Asia Region - progress and challenges

Moving ahead on elimination of Sexually Transmitted Infections (STIs) in WHO South-East Asia Region - progress and challengesii
ISBN: 978-92-9022-734-2
© World Health Organization 2019
Some rights reserved. This work is available under the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 IGO licence
(CC BY-NC-SA 3.0 IGO; https://creativecommons.org/licenses/by-nc-sa/3.0/igo).
Under the terms of this licence, you may copy, redistribute and adapt the work for non-commercial purposes, provided the work is appropriately cited, as indicated below. In any use of this work, there should be no suggestion that WHO endorses any specific organization, products or services. The use of the WHO logo is not permitted. If you adapt the work, then you must license your work under the same or equivalent Creative Commons licence. If you create a translation of this work, you should add the following disclaimer along with the suggested citation: “This translation was not created by the World Health Organization (WHO). WHO is not responsible for the content or accuracy of this translation. The original English edition shall be the binding and authentic edition”.
Any mediation relating to disputes arising under the licence shall be conducted in accordance with the mediation rules of the World Intellectual Property Organization.
Suggested citation. Moving ahead on elimination of Sexually Transmitted Infections (STIs) in WHO South-East Asia Region - progress and challenge. New Delhi: World Health Organization, Regional Office for South-East Asia; 2018. Licence: CC BY-NC-SA 3.0 IGO.
Cataloguing-in-Publication (CIP) data. CIP data are available at http://apps.who.int/iris.
Sales, rights and licensing. To purchase WHO publications, see http://apps.who.int/bookorders. To submit requests for commercial use and queries on rights and licensing, see http://www.who.int/about/licensing.
Third-party materials. If you wish to reuse material from this work that is attributed to a third party, such as tables, figures or images, it is your responsibility to determine whether permission is needed for that reuse and to obtain permission from the copyright holder. The risk of claims resulting from infringement of any third-party-owned component in the work rests solely with the user.
General disclaimers. The designations employed and the presentation of the material in this publication do not imply the expression of any opinion what soever on the part of WHO concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted and dashed lines on maps represent approximate border lines for which there may not yet be full agreement.
The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by WHO in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters.
All reasonable precautions have been taken by WHO to verify the information contained in this publication. However, the published material is being distributed without warranty of any kind, either expressed or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall WHO be liable for damages arising from its use.
Printed in India

In the WHO South-East Asia Region the burden of morbidity and mortality from sexually transmitted infections (STIs) is significant, and compromises the sexual and reproductive health of women, as well as newborn and child health. STIs facilitate the sexual transmission of HIV and increase the risk of cervical cancer and have negative financial implications for individuals and health systems.
There are an estimated 357 million new cases annually of four curable STIs – Chlamydia trachomatis, Neisseria gonorrhoeae, syphilis, and Trichomonas vaginalis. An estimated 417 million people are also infected with viral STIs. Approximately 291 million women harbor the human papilloma virus (HPV).
To achieve SDG 3.3, WHO formulated a Global Health Sector Strategy on STIs (2016-21). The strategy aims to end STIs as major public health problem by 2030, envisioning zero new infections, zero STI-related complications and deaths, and zero discrimination. The strategy calls for a 90% reduction of T. pallidum and N. gonorrhoeae incidence and less than 50 cases of congenital syphilis per 100 000 live births.
STIs have caused high morbidity, mortality, disability and adverse pregnancy outcomes in the South-East Asia Region. In the mid-1990s the Region’s Member States accounted for more than a third of new STI infections globally. Large-scale interventions to improve conditions and increase condom use in sex work led to significant STI declines during the late 1990s and early 2000s.Perhaps the greatest overall impact on regional STI epidemiology was achieved during the past 15 years, following substantial progress in India, which accounts for over two thirds of the Region’s population.
The epidemiology of STIs in the Region remains highly heterogeneous. Very low STI incidence and prevalence has been maintained over several decades in Sri Lanka and Thailand, while much higher and variable rates are reported elsewhere. Thailand and Maldives were recently certified as having eliminated mother-to-child transmission of both syphilis and HIV, while Sri Lanka is preparing for validation of the same. Insufficient data on STIs limits epidemiological assessments in most other countries, hindering control efforts.
The current programme response to STIs varies greatly across the Region. For many years Thailand and Sri Lanka have maintained strong commitment and funding. Myanmar has demonstrated early success in a demonstration project of STI control and HIV prevention, achieving 100% targeted condom promotion and the halving of syphilis prevalence. Limited data from Bangladesh show declining syphilis rates, largely due to sex worker mobilization, awareness-raising, condom promotion and the provision of STI services.
This regional report highlights the current situation and response, and the need to urgently take steps to reposition STI control as a public health priority. In doing so, it advocates for resources, staffing and planning independent of HIV programme priorities. There is a need
foreWord
iiiMoving ahead on elimination of Sexually Transmitted Infections (STIs) in WHO South-East Asia Region - progress and challenges

to advocate for and support progress towards STI elimination, including the elimination of mother-to-child transmission (eMTCT), and to prepare elimination cases for infectious syphilis, chancroid and possibly gonorrhoea.
I am certain the report will be of immense benefit to Member States as they strive to reduce STIs, eliminate cervical cancer, achieve SDG 3.3 and with it the goal of ensuring healthy lives and promoting health and well-being for all at all ages.
Poonam Khetrapal Singh
World Health Organization Regional Director
for South-East Asia
Moving ahead on elimination of Sexually Transmitted Infections (STIs) in WHO South-East Asia Region - progress and challengesiv

Moving ahead on elimination of Sexually Transmitted Infections (STIs) in WHO South-East Asia Region - progress and challenges v
Table of ConTenTS
Foreword ......................................................................................................................................... iii
Abbreviations and acronyms ........................................................................................................ vii
Summary ...........................................................................................................................................1
1. Background ...........................................................................................................................5
2. Methods ................................................................................................................................7
3. Findings .................................................................................................................................8
4. Conclusions and recommendations .................................................................................30
References ......................................................................................................................................33
List of resources .............................................................................................................................35
figures
Fig. 1. Literature review: number of STI papers identified from SEA Region .............................9
Fig. 2. WHO global estimates of four curable STIs: proportion from SEA Region ..................10
Fig. 3. Routine STI reporting trends, Sri Lanka ............................................................................16
Fig. 4. Routine STI reporting trends, Thailand ............................................................................18
Fig. 5. Syphilis prevalence trends among pregnant women and KPs in India ..........................20
Fig. 6. Syphilis prevalence trends, Indonesia .............................................................................22
Fig 7. Syphilis prevalence among sex workers in Bangladesh ...................................................23
Fig. 8. STI incidence and syphilis prevalence, Myanmar ............................................................24
Fig. 9. ANC syphilis prevalence, Nepal .......................................................................................25
Fig. 10. Syndromic STI trends, Maldives ......................................................................................27
Fig. 11. Syphilis prevalence among pregnant women, KP and male bridge group, Timor-Leste ....................................................................................................................................28
Fig. 12. Trends of select STI syndromes, Bhutan ........................................................................29

Moving ahead on elimination of Sexually Transmitted Infections (STIs) in WHO South-East Asia Region - progress and challengesvi
Tables
Table 1. Select STI programme components ..............................................................................12
Table 2. Gaps in STI programmes by programmatic area ..........................................................13
Table 3. Various aspects of STI status in Sri Lanka ......................................................................16
Table 4. Various aspects of STI status in Thailand .......................................................................17
Table 5. Various aspects of STI status in India .............................................................................19
Table 6. Various aspects of STI status in Indonesia .....................................................................21
Table 7. Various aspects of STI status in Bangladesh .................................................................22
Table 8. Various aspects of STI status in Myanmar .....................................................................23
Table 9. Various aspects of STI status in Nepal ...........................................................................24
Table 10. Various aspects of STI status in Democratic People’s Republic of Korea .................26
Table 11. Various aspects of STI status in Maldives ....................................................................26
Table 12. Various aspects of STI status in Timor-Leste ...............................................................27
Table 13. Various aspects of STI status in Bhutan .......................................................................28

Moving ahead on elimination of Sexually Transmitted Infections (STIs) in WHO South-East Asia Region - progress and challenges vii
AIDS acquired immune deficiency syndrome
AMR anti-microbial resistance
ANC antenatal clinic
ART antiretroviral therapy
CBO community-based organization
CUP condom use programme
DMSC Durbar Mahila Samanwaya Committee
DSRC designated STI/RTI clinic
eMTCT elimination of mother-to-child transmission
FSW female sex worker
HBV hepatitis B virus
HCV hepatitis C virus
HIV human immunodeficiency virus
HMIS health management information system
HTC HIV testing and counselling
IBBS integrated biological and behavioural surveillance
IDU injecting drug user
KP key population
LGV lymphogranuloma venereum
MoH Ministry of Health
MSM men who have sex with men
MTCT mother-to-child transmission
NAC National AIDS Commission
NACO National AIDS Control Organization
NGO nongovernmental organization
abbrevIaTIonS and aCronymS

Moving ahead on elimination of Sexually Transmitted Infections (STIs) in WHO South-East Asia Region - progress and challengesviii
NSACP National STD/AIDS Control Programme
NSP National Strategic Plan
NSU non-specific urethritis
PPT periodic presumptive treatment
PrEP pre-exposure prophylaxis
RTI reproductive tract infection
SEA South-East Asia
STD sexually transmitted disease
STI sexually transmitted infection
TI targeted intervention
UNAIDS Joint UN Programme on HIV/AIDS
UNICEF United Nations Children’s Fund
WHO World Health Organization

Moving ahead on elimination of Sexually Transmitted Infections (STIs) in WHO South-East Asia Region - progress and challenges 1
This rapid assessment of the sexually transmitted infection (STI) epidemiology and response in the World Health Organization (WHO) South-East Asia (SEA) Region was conducted in April/May 2018.1 Methods included structured interviews with programme managers and WHO focal points, review of the literature and trend analysis of available routine reporting data. The primary focus was on control of common curable STIs – syphilis, gonorrhoea, chlamydia, chancroid and trichomoniasis. Epidemiological interaction and programme overlap with viral STIs, including human immunodeficiency virus (HIV), hepatitis B and C, herpes virus and human papilloma virus, are addressed elsewhere.
Historically, STIs have been among the most serious public health problems in WHO SEA Region, with high associated morbidity, mortality, disability and adverse pregnancy outcomes. WHO estimated that SEA Region countries accounted for more than a third of all new STI infections globally in the mid-1990s.2 The incidence and prevalence of curable STIs, notably ulcerative chancroid and syphilis, were extremely high in urban areas and along well-travelled migrant and trucking networks, and closely linked to rapid early spread of HIV. Where measured, rates of gonococcal, chlamydial and trichomonal infections were often even higher. However, large-scale interventions with package of services, including the promotion of condom use in sex work led to large STI declines and slowing of HIV epidemics during the 1990s and early 2000s, notably in Thailand and parts of India.
Perhaps the greatest overall impact on regional STI epidemiology was achieved during the past 15 years, following marked progress in India, which accounts for over two thirds of the Region’s population. During this period, interventions to reduce HIV/STI transmission among key and bridge populations were scaled up,3 and large STI declines in the most highly affected states were documented. WHO estimates that SEA Region’s share of new STI infections globally was only 11% in 2012, less than a third of what it was in the late 1990s.
Currently, the epidemiology of STIs in the Region remains highly heterogeneous. Very low STI incidence and prevalence have been maintained over several decades in Sri Lanka and Thailand,4 while much higher and variable rates are reported elsewhere. Thailand and Maldives have been certified as having eliminated mother-to-child transmission of both syphilis and HIV, while Sri Lanka is preparing for validation of the same. Yet, insufficient data on STIs limit assessment of the epidemiological situation in most other countries, hindering control efforts.
The current programme response to STIs also varies greatly across the Region. Thailand and Sri Lanka have maintained strong commitment and funding over many years. Elsewhere, the national STI response varies greatly, with many countries struggling to support basic clinical services, maintain stocks of effective STI treatments, conduct outreach to key populations
1 Country data updated in August 2019.2 Estimates of four common, curable STIs: gonorrhoea, chlamydia, syphilis and trichomoniasis.3 Initially supported under Avahan and subsequently transitioned to National AIDS Control Organization (NACO).4 Comparable to Europe (2012 ECDC reported 4.5 syphilis cases per 100 000 population. Thailand reported 3.2 and Sri Lanka
5.4 cases per 100 000).
Summary

Moving ahead on elimination of Sexually Transmitted Infections (STIs) in WHO South-East Asia Region - progress and challenges2
(KPs), maintain basic STI surveillance and monitor antibiotic resistance. Nevertheless, good examples of improving STI control have been described at sub-national levels (notably Kolkata and Mysore in India and Tanjung Pinang in Indonesia), even in large countries where implementation of control efforts has been highly uneven overall. These examples demonstrate the feasibility of improving STI control under a range of conditions. Data from Integrated Biological and Behavioural Surveillance (IBBS) 2014–2015 and special studies from Indonesia demonstrate that STIs have decreased in some areas, particularly among sex workers, following interventions. Myanmar also demonstrated early success in a demonstration project of STI control and HIV prevention with 100% targeted condom promotion. Pilots in four townships demonstrated an increase in condom use among sex workers (from 61% in 2001 to 91% in 2002) and halving of syphilis prevalence. Limited data from Bangladesh show declining syphilis rates, largely due to sex worker mobilization, raising awareness, condom promotion and provision of STI services.
Important gaps and constraints undermining STI control are apparent across the Region. STI control efforts have clearly not been sufficiently scaled up or sustained, and evidence of increasing STI incidence and prevalence is appearing in some areas and among some KPs. As national programmes and donors increasingly promote HIV-specific services like antiretroviral therapy (ART) and recently, pre-exposure prophylaxis (PrEP), often at the expense of broader prevention interventions, there is growing risk of behavioural disinhibition, erosion of condom use and rebounding STI transmission. Yet, STI surveillance is not sufficiently operational and reliable in many countries to detect increasing trends, and weak STI services limit effective responses.
To a large extent, STIs other than HIV have largely fallen off the radar. Echoing this, programme managers described important gaps and constraints related to STI control and surveillance, mainly linked to low perceived priority and insufficient resources.
As attention begins to return to STIs, with global elimination targets proposed for syphilis and gonorrhoea, most countries in the SEA Region will need to strengthen their STI response – including outreach to KPs, service delivery, surveillance and related control efforts. Fortunately, multiple examples of good practice exist in the Region to guide this work. Recommendations for a reinvigorated STI response cover basic areas of surveillance, primary prevention and clinical services.
Key points
epidemiology
• Evidence from multiple sources strongly supports an overall declining trend of curable STIs in the Region over three decades. Shifting patterns are also apparent, with declining proportions of ulcerative and bacterial STIs compared to viral infections.
• Data on syphilis declines are more available and reliable than for other STIs, and useful as markers of sexual transmission trends in general. Triangulation of syphilis surveillance data – from KPs, male STI patients (bridge population), and pregnant women (general population) – can highlight progress and gaps of STI control efforts.

Moving ahead on elimination of Sexually Transmitted Infections (STIs) in WHO South-East Asia Region - progress and challenges 3
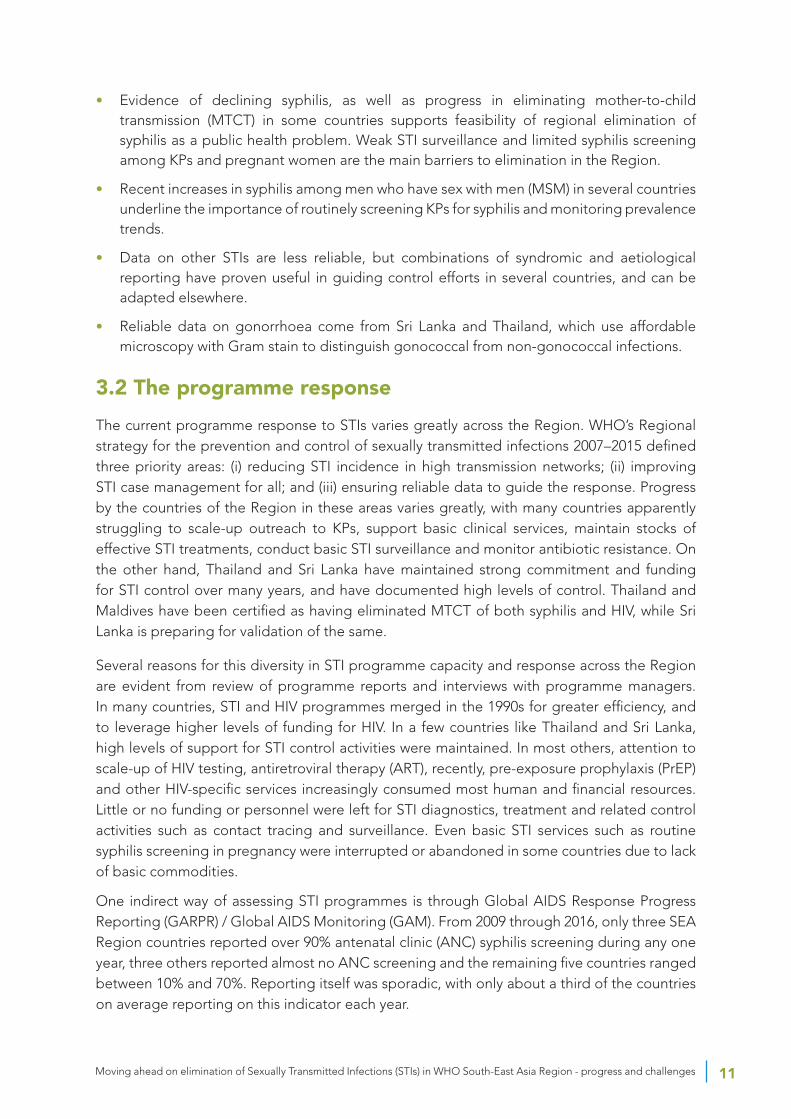
• Evidence of declining syphilis, as well as progress in eliminating mother-to-child transmission (MTCT) in some countries, supports feasibility of regional elimination of syphilis as a public health problem. Weak STI surveillance and limited syphilis screening among KPs and pregnant women are the main barriers to elimination in the Region.
• Recent increases in syphilis among men who have sex with men (MSM) in several countries underlines the importance of routinely screening KPs for syphilis and monitoring prevalence trends.
• Data on other STIs are less reliable, but combinations of syndromic and aetiological reporting have proven useful in guiding control efforts in several countries, and can be adapted elsewhere.
• Reliable data on gonorrhoea come from Sri Lanka and Thailand, which use affordable microscopy with Gram stain to distinguish gonococcal from non-gonococcal infections.
Programme response
• The programme response to STIs varies greatly across the Region, from highly effective to almost non-existent.
• Where STI declines have occurred, evidence strongly supports attribution to programmes that have increased condom use in sex work, while maintaining good clinical services (both targeted and general population) and reliable STI surveillance.
• National experience and sub-national examples highlight multiple effective approaches to reducing STI incidence and prevalence, as well as surveillance and programme monitoring methods.
• STI services for KPs – including quarterly medical checkups, presumptive treatment for asymptomatic infections and regular syphilis screening – have resulted in rapid STI control, including virtual elimination of common STIs in two Indian districts.
Gaps and constraints
• Low perceived priority and programme funding were cited by most countries as the main reasons for declining attention to STI control and surveillance.
• Important gaps in core STI control programme activities were identified in most countries. These have been flagged in this report with recommendations for more in depth assessment and programme strengthening.
Summary of recommendations for strengthening STI control in Sea region
• Urgently take steps to reposition STI control as a public health priority for the Region and advocate for resources, staffing and planning independent of HIV programme priorities (recognizing common ground and potential synergies in STI/HIV control efforts, i.e. offering STI screening/periodic presumptive treatment (PPT) at quarterly PrEP visits).
• Recognize successes in the Region and leverage the considerable experience and expertise available from countries such as Sri Lanka and Thailand and from KP community learning sites like Durbar Mahila Samanwaya Committee (DMSC) and Ashodaya Samithi.

Moving ahead on elimination of Sexually Transmitted Infections (STIs) in WHO South-East Asia Region - progress and challenges4
• Advocate for and support progress towards STI elimination continuing with elimination of mother-to-child transmission (eMTCT) and preparing elimination cases for infectious syphilis, chancroid and possibly gonorrhoea, recognizing that there are strong candidate countries for each of these STI elimination targets in the SEA Region.
• Address the considerable STI data gaps and limitations in most countries, advocating for and supporting basic STI surveillance components including routine reporting (syndromic/aetiological), routine prevalence monitoring (antenatal clinic [ANC] and KP syphilis screening), leveraging regional experience and expertise (mainly from Thailand and Sri Lanka).
• Develop a flexible toolkit of proven interventions for countries at different stages of STI control, including:
¥ appropriate mixed models of aetiological and syndromic management and reporting (as in Thailand and Sri Lanka);
¥ effective community-based models (including microplanning) for high impact STI control with KPs (DMSC, Ashodaya learning sites);
¥ presumptive treatment strategies to rapidly reduce prevalence of curable STIs in sex work, prevent and control STI outbreaks among PrEP users, MSM and other KPs;
¥ rapid response methods to identify and control STI outbreaks (particularly important as countries move towards elimination).
• Country-specific recommendations (see individual assessments) can be considered in several groups with different needs.
¥ Countries with urgent STI control needs (Indonesia, others likely at sub-national level, currently unrecognized due to data gaps)
¥ Countries with significant STI programme limitations to address (India, Bangladesh, Myanmar, Nepal, Democratic People’s Republic of Korea)
¥ Small countries with potential for rapid STI control scale-up (Maldives, Bhutan, Timor-Leste)
¥ Countries with high-level STI control that can prepare elimination cases and assist others (Sri Lanka, Thailand).

Moving ahead on elimination of Sexually Transmitted Infections (STIs) in WHO South-East Asia Region - progress and challenges 5
5 Bangladesh, Bhutan, Democratic People’s Republic of Korea, India, Indonesia, Maldives, Myanmar, Nepal, Sri Lanka, Thailand, Timor-Leste.
6 Estimates of four common, curable STIs: gonorrhoea, chlamydia, syphilis and trichomoniasis.
1. backgroundHistorically, sexually transmitted infections (STIs) have been among the most serious public health problems in the World Health Organization (WHO) South-East Asia (SEA) Region,5 with high associated morbidity, mortality, disability and adverse pregnancy outcomes. Global and regional STI strategies have set ambitious control targets, including 90% reductions of syphilis and gonorrhoea by 2030 (1,2).
According to WHO estimates, SEA Region countries accounted for more than a third of new STI infections6 globally in the mid to late 1990s (3–6). The incidence and prevalence of curable STIs, notably ulcerative chancroid and syphilis, were extremely high and closely linked to rapid early spread of human immunodeficiency virus (HIV) in urban areas and along well-travelled migrant and trucking networks (7). Where measured, rates of gonococcal, chlamydial and trichomonal infections were often even higher. However, large-scale interventions with package of services, including the promotion of condom use in sex work led to large STI declines as well as rapid control of HIV epidemics during the 1990s and early 2000s, notably in Thailand and parts of India.

Moving ahead on elimination of Sexually Transmitted Infections (STIs) in WHO South-East Asia Region - progress and challenges6
7 Initially supported under Avahan and subsequently transitioned to National AIDS Control Organization (NACO).8 Calculated from published estimates after adjusting for population differences in regional groupings.
Progress in India, which accounts for over two thirds of the Region’s population, is likely to have had the greatest overall impact on regional STI epidemiology over the past 15 years. During this period, large scale interventions7 to reduce HIV/STI transmission among key and bridge populations documented large STI declines in several populous and highly affected states. WHO estimates that SEA Region’s share of new STI infections globally was only 11% in 2012, less than a third of what it was in the late 1990s. Although methods used to estimate global STI incidence and prevalence varied over time, such a large change in the regional proportion8 of STI burden calls for more detailed investigation.
The purpose of this report is to assess the current status of STI epidemiology and programmes in the Region.

Moving ahead on elimination of Sexually Transmitted Infections (STIs) in WHO South-East Asia Region - progress and challenges 7
2. methodsThis rapid review of the STI situation in SEA Region was conducted in April–May 2018 (data updated in August 2019) using multiple methods including interviews, review of the literature and analysis of available country data. Interviews using a structured set of questions involved programme managers and WHO country focal points responsible for STI activities. This was followed by inputs from country focal points on the draft report and verification of the data in the report. The responses from an online questionnaire sent to countries by WHO headquarters for the progress on global health sector strategy were also included in the report.

Moving ahead on elimination of Sexually Transmitted Infections (STIs) in WHO South-East Asia Region - progress and challenges8
3. findingsThe main findings of this assessment are grouped under the following categories: (i) epidemiology; (ii) programme response, and (iii) gaps/constraints. Thereafter, country profiles summarize available information on country-level data and experience. Recommendations based on these findings can be found in the report’s conclusion.
3.1 The epidemiology of STIs in the region
WHO global STI estimates are based mainly on review of prevalence studies reported in the published literature (3–6). However, the publication of papers with an STI focus has fluctuated widely over the past decades. Fig. 1 summarizes the number of papers from SEA Region sites mentioning STIs as a main topic since 2000. The number of studies peaked from about 2005 to 2013, a period when donor investment in STI control (including the large Avahan India acquired immune deficiency syndrome [AIDS] Initiative) was highest. Studies with data on STI incidence or prevalence are a subset of the total and follow a similar pattern (6).

Moving ahead on elimination of Sexually Transmitted Infections (STIs) in WHO South-East Asia Region - progress and challenges 9
Fig. 1. Literature review: number of STI papers identified from SEA Region
Total STI Paper for Sear
STI Paper by country
Several limitations are apparent when looking to the literature to estimate STI burden and trends. First, the number and distribution of studies with population-based prevalence data are few and poorly represent regional diversity. In addition, given fluctuations over time, the likelihood of publication bias is high, particularly as sites with donor-supported interventions (and related publications) are likely to have achieved better STI control than those without resources. Most published STI prevalence data come from key populations (KP), bridge groups or clinic-based samples, which are informative for those sub-populations but cannot be directly extrapolated to derive general population estimates.
WHO uses these methods for STI estimation partly due to a lack of reliable routine STI reporting from countries (this is only partially true for SEA Region, as discussed later). Nevertheless, while overall global estimates have changed little over 20 years, the proportion of estimated incident infections from SEA Region has declined sharply, from approximately 36% in 1995 to 11% in 2012 (Fig. 2). Despite limitations of the methods, such a large magnitude of change begs further analysis. An important possibility is that STIs have indeed declined dramatically in SEA Region, more so than in other regions. Evidence for and against this hypothesis is

Moving ahead on elimination of Sexually Transmitted Infections (STIs) in WHO South-East Asia Region - progress and challenges10
examined from national and sub-national data, with special attention to the most populous countries, which have the greatest influence on regional trends.9
Fig. 2. WHO global estimates of four curable STIs: proportion from SEA Region
A large degree of heterogeneity is evident in reviewing SEA Region STI data. From the historic STI declines in Sri Lanka and Thailand to more recent sub-national examples, the feasibility of STI control – approaching elimination in some cases – has been well documented. On the other hand, much poorer STI control persists elsewhere, and the situation remains largely unknown – again due to insufficient data – in several countries. Currently, the epidemiology of STIs in the Region is highly heterogeneous – very low STI incidence10 and prevalence in a few countries, with much higher rates reported by others. Importantly, insufficient data on STIs from much of the Region limits epidemiological assessment and hinders control efforts. Furthermore, the current situation, whether appearing relatively good or bad, is far from static. Evidence of increasing rates of syphilis and other STIs is emerging from a number of Asian countries.
Key points: epidemiology
• Evidence from multiple sources strongly support an overall declining trend of curable STIs in the Region over the past three decades. Shifting patterns are also apparent, with declining proportions of ulcerative and bacterial STIs compared to viral infections.
• Data on syphilis declines are more available and reliable than for other STIs, and can be monitored as markers of sexual transmission trends in general.11
9 Any regional trends in SEA Region are driven strongly by events in India, which accounts for about 68% of the Region’s population.
10 Comparable to Europe (2012 ECDC reported 4.5 syphilis cases per 100 000 population. Thailand reported 3.2 and Sri Lanka 5.4 per 100 000).
11 Triangulation of syphilis surveillance data from KPs, male STI patients (bridge population), and pregnant women (general population) can highlight progress and gaps of STI control efforts.
Moving ahead on elimination of Sexually Transmitted Infections (STIs) in WHO South-East Asia Region - progress and challenges 11
• Evidence of declining syphilis, as well as progress in eliminating mother-to-child transmission (MTCT) in some countries supports feasibility of regional elimination of syphilis as a public health problem. Weak STI surveillance and limited syphilis screening among KPs and pregnant women are the main barriers to elimination in the Region.
• Recent increases in syphilis among men who have sex with men (MSM) in several countries underline the importance of routinely screening KPs for syphilis and monitoring prevalence trends.
• Data on other STIs are less reliable, but combinations of syndromic and aetiological reporting have proven useful in guiding control efforts in several countries, and can be adapted elsewhere.
• Reliable data on gonorrhoea come from Sri Lanka and Thailand, which use affordable microscopy with Gram stain to distinguish gonococcal from non-gonococcal infections.
3.2 The programme response
The current programme response to STIs varies greatly across the Region. WHO’s Regional strategy for the prevention and control of sexually transmitted infections 2007–2015 defined three priority areas: (i) reducing STI incidence in high transmission networks; (ii) improving STI case management for all; and (iii) ensuring reliable data to guide the response. Progress by the countries of the Region in these areas varies greatly, with many countries apparently struggling to scale-up outreach to KPs, support basic clinical services, maintain stocks of effective STI treatments, conduct basic STI surveillance and monitor antibiotic resistance. On the other hand, Thailand and Sri Lanka have maintained strong commitment and funding for STI control over many years, and have documented high levels of control. Thailand and Maldives have been certified as having eliminated MTCT of both syphilis and HIV, while Sri Lanka is preparing for validation of the same.
Several reasons for this diversity in STI programme capacity and response across the Region are evident from review of programme reports and interviews with programme managers. In many countries, STI and HIV programmes merged in the 1990s for greater efficiency, and to leverage higher levels of funding for HIV. In a few countries like Thailand and Sri Lanka, high levels of support for STI control activities were maintained. In most others, attention to scale-up of HIV testing, antiretroviral therapy (ART), recently, pre-exposure prophylaxis (PrEP) and other HIV-specific services increasingly consumed most human and financial resources. Little or no funding or personnel were left for STI diagnostics, treatment and related control activities such as contact tracing and surveillance. Even basic STI services such as routine syphilis screening in pregnancy were interrupted or abandoned in some countries due to lack of basic commodities.
One indirect way of assessing STI programmes is through Global AIDS Response Progress Reporting (GARPR) / Global AIDS Monitoring (GAM). From 2009 through 2016, only three SEA Region countries reported over 90% antenatal clinic (ANC) syphilis screening during any one year, three others reported almost no ANC screening and the remaining five countries ranged between 10% and 70%. Reporting itself was sporadic, with only about a third of the countries on average reporting on this indicator each year.

Moving ahead on elimination of Sexually Transmitted Infections (STIs) in WHO South-East Asia Region - progress and challenges12
Further insight into the functional capacity of national STI control programmes can be gleaned from the Joint United Nations Programme on HIV/AIDS (UNAIDS) narrative progress reports. Sri Lanka presents data on STI programme performance across multiple areas of clinic and community-based interventions in its annual reports; while for most other countries, STI programme activities (excluding HIV) appear to be limited to periodic revision of STI case management guidelines (Table 1).
Table 1. Select STI programme components
STI guidelines (last revision)
reliable STI surveillance (>80% sites reporting)
anC syphilis screening (>90% pregnancies)
STI contact tracing (actively supported)
KP routine STI screening &/or PPT
Bangladesh 2006
Bhutan 2006 Yes
Democratic People’s Republic of Korea
India 2014 Partial Yes Yes
Indonesia 2011
Maldives 2013 Yes Yes Syphilis partially
IDU only (HBV, HCV, syphilis)
Myanmar 2014
Nepal 2014
Sri Lanka 2013 updated, now revising
Yes Yes Yes Yes
Thailand 2016 Yes Yes Yes Yes
Timor-Leste 2014
KP – key populations; PPT – periodic presumptive treatment; IDU – injecting drug user; HBV – hepatitis B virus; HCV – hepatitis C virus; ANC – antenatal clinic
Yet, at sub-national level, several community-based organizations (CBOs) have demonstrated impressive STI control outcomes. These include CBOs working with KPs in Kolkata and Mysore in India and Tanjung Pinang in Indonesia, among others. In fact, most evidence from the Region strongly supports the importance of well-focused interventions with KPs, particularly in sex worker networks, for reducing STI incidence and prevalence across wider populations.
Key points: programme response
• The programme response to STIs varies greatly across the Region, from highly effective to almost non-existent.
• Where STI declines have occurred, evidence strongly supports attribution to programmes that have increased condom use in sex work, while maintaining good clinical services (both targeted and for the general population) and reliable STI surveillance.
• National experience and sub-national examples highlight multiple effective approaches to reducing STI incidence and prevalence, as well as surveillance and programme monitoring methods.

Moving ahead on elimination of Sexually Transmitted Infections (STIs) in WHO South-East Asia Region - progress and challenges 13
• STI services for KPs – including quarterly medical checkups, presumptive treatment for asymptomatic infections and regular syphilis screening – have resulted in rapid STI control, including virtual elimination of common STIs in two Indian districts.
3.3 Gaps and constraints
Multiple gaps in STI control efforts in the Region were identified in the course of this review. Perhaps the most significant is the lack of an identifiable STI control programme in several countries. With the merging of HIV and STI programmes, and increasing focus on HIV-specific activities, attention to a number of key STI prevention and control activities has been diluted or lost. Strategic and operational planning in most countries is dominated by HIV priorities and targets (which are funded). Table 2 summarizes the main gaps and constraints identified during this review.
Table 2. Gaps in STI programmes by programmatic area
Programmatic area Status Gaps/constraintsStrategic planning National strategic plans (NSPs)
for HIV/STI programmes increasingly oriented towards HIV-specific targets; little attention to STI control
STI generally low priority, may include some provision for STI treatment services.
Resources Resource allocation aligned to NSP, including for GFATM and other donors; few resources for STI activities
Lacking separate line items for core STI control activities
Staffing Few or no staff with STI-specific responsibilities in many countries
Often lacking STI programme manager; staff with responsibility for clinical services and surveillance at a minimum
Commodities Condom promotion and distribution for HIV also work for STIs. STI drugs and diagnostics often overlooked
Gaps include reliable supply of STI diagnostics and treatment, logistics and supply management to avoid stockouts
Outreach Outreach to KP and bridge groups works for both HIV and other STIs
Outreach with single focus (i.e. HTC only) misses opportunities for broader STI prevention and risks, alienating KP
Clinical service delivery Variable attention across countries
Variable, often lacking monitoring, supervision, refresher training, etc.
Contact tracing Neglected in most countries Lacking dedicated staff to follow up contacts of index cases
Guidelines development, training and supervision
Many countries in the Region have not updated STI case management guidelines in the past 5 years
Guidelines updates, training and supervision required to maintain effective STI case management
STI surveillance Neglected in most countries Requires dedicated staff to ensure complete, accurate and timely reporting, analyse and disseminate data, etc

Moving ahead on elimination of Sexually Transmitted Infections (STIs) in WHO South-East Asia Region - progress and challenges14
Programmatic area Status Gaps/constraintsAnti-microbial resistance (AMR) monitoring
Neglected in most countries Requires planning, funding and technical assistance for periodic AMR surveys
HTC – HIV testing and counselling
STI control efforts have clearly not been sufficiently scaled up or sustained across the Region, and evidence of increasing STI incidence and prevalence is appearing in some areas and among some populations at high risk. As programmes increasingly promote HIV-specific services like ART and PrEP, there is growing risk of behavioural compensation, including erosion of critical preventive behaviours like condom use, with increasing STI transmission.
Yet, with programme focus on HIV-specific targets, other STIs have largely fallen off the radar. STI surveillance is not even sufficiently operational and reliable in many countries to be able to detect increasing trends.
Key points: gaps and constraints
• Low perceived priority and programme funding were cited by most countries as the main reasons for declining attention to STI control and surveillance.
• Important gaps in core STI control programme activities were identified in most countries. These have been flagged in this report with recommendations for more in depth assessment and programme strengthening.
3.4 Country profiles
A structured question guide was used to assess the STI situation and current response. Responses from the majority of countries indicate that STIs have largely slipped off the radar, and STI control efforts are neglected due in most cases to low perceived priority and insufficient programme resources. Several national and sub-national exceptions are noted here.
The following country profiles focus summarize available information about the epidemiological situation as well as three areas of the response, corresponding to the three objectives of the regional STI strategy – STI services for all, outreach to KPs and STI surveillance.
Moving ahead on elimination of Sexually Transmitted Infections (STIs) in WHO South-East Asia Region - progress and challenges 15
a. Countries with documented high-level control
Sri lankaSTIs have been in decline in Sri Lanka since the mid-1970s due to sustained public health efforts, implemented mainly through district-level STI clinics. All components of STI preventive and curative services are well supported and backed by a simple but reliable surveillance system. The Sri Lanka narrative progress reports to UNAIDS detail how different STI programme components contribute to a comprehensive and highly effective national response to HIV as well as other STIs. Perhaps unique to the Region, the national control programme retained its broad STI focus, incorporating HIV prevention, care and treatment activities within the existing STI programme structures. Moreover, the slow growth of HIV in Sri Lanka has been attributed to the high level of STI control in the country when HIV first appeared.
Sri Lanka has maintained a strong focus on STI surveillance and control since 1952. The national sexually transmitted disease (STD)/AIDS Control Programme (NSACP) of the Ministry of Health has a central STD clinic in Colombo and a well-established network of STD clinics at provincial and district levels. These clinics include both specialist and non-specialist clinicians and public health staff – public health inspectors (PHI) and public health nurses (PHN) – who have both clinic and community outreach responsibilities, including STI contact tracing and outreach visits to sex work venues.
Various aspects of STI status in the country are given in Table 3.

Moving ahead on elimination of Sexually Transmitted Infections (STIs) in WHO South-East Asia Region - progress and challenges16
Table 3. Various aspects of STI status in Sri Lanka
aspects Status notesEpidemiological snapshot
High-level control with low reported incidence of syphilis (4.4 cases per 100000) and gonorrhoea (1.4 cases per 100 000) in 2016
Country is preparing for validation of elimination of MTCT of HIV and Syphilis. The country should be considered a candidate for elimination of STIs as a public health problem (syphilis, chancroid, gonorrhoea)
STI clinical services
Strong network of district-level STD clinics, also supporting peripheral STI services
STI guidelines: last full revision in 2009, minor updates in 2014, currently revising
Outreach/services for KP
Targeted interventions with HIV funding. Also, public heath inspectors/nurses attached to STI clinics do KP outreach
Strengthen programme monitoring of KP coverage, use of services, syphilis prevalence and other STIs, especially among MSM
STI surveillance Strong STI surveillance in place for decades, reliable monitoring of trends, sensitive to outbreaks (early warning system)
Aetiological reporting from district STD clinics, syndromic reports from peripheral levels
Relevant publications
2 STI studies identified
STI clinical services are of high quality and well-organized, with adequate supplies of condoms and essential medicines. STD clinic staff are active in the community and conduct awareness and risk-reduction training for a range of groups, from intermediate to low-risk. Nongovernmental organizations (NGOs) working with sex workers and MSM collaborate with local clinic staff. Pregnant women have been screened for syphilis since 1954, and congenital syphilis has become rare. Over 95% of pregnant women deliver in health-care institutions. STD clinic doctors also conduct professional seminars for doctors in private practice.
Despite progressively improving STI control since the 1980s, outbreaks of gonorrhoea beginning in 2003 and of syphilis in 2012 were detected by surveillance and largely brought back under control.
Routine STI reporting trends are given in Fig. 3.
Fig. 3. Routine STI reporting trends, Sri Lanka

Moving ahead on elimination of Sexually Transmitted Infections (STIs) in WHO South-East Asia Region - progress and challenges 17
ThailandThailand is an excellent example for countries in the Region that are seriously considering STI elimination targets. Building on information from reliable national surveillance, the strategy sets clear disease control targets, aiming to reduce new cases of syphilis from already low levels (from 4.9 cases per 100 000 to less than 3.5), and gonorrhoea (from 10.6 to less than 8 cases per 100 000) by 2021.
New cases of bacterial STIs in Thailand have in fact already decreased by at least 95% since 1989. Measures that contributed to rapid early STI declines include 100% condom use programme (CUP), comprehensive STI management, counselling, promotion of health-seeking behaviour and community participation. Implemented through a network of public health STI clinics, the 100% CUP achieved early success by saturating coverage of sex establishments, where condom use was mandated. While the responsibility for enforcing condom use was on the workplace, the programme provided a range of important services that ensured progressive control of STI/HIV transmission.
Direct services included promotion and distribution of condoms and STI check-ups. STI clinics were expanded and staff conducted regular outreach to sex establishments to promote prevention and STI screening. Importantly, systematic collection of basic data was carried out to inform the programme. This included annual mapping of sex establishments and enumeration of sex workers, behavioural monitoring (focusing on condom use and number of clients) and STI screening. Monitoring activities are largely built into the day-to-day activities of the STI clinics, requiring few special surveys. As sex work changed to more indirect forms (massage, karaoke and bar-based), interventions were adapted to include more outreach and to increase involvement of sex workers.
Various aspects of STI status in the country are given in Table 4.
Table 4. Various aspects of STI status in Thailand
aspects Status notesEpidemiological snapshot
High-level control with low reported incidence of both syphilis (6.2 cases per 100 000) and gonorrhoea (14.6 cases per 100 000)
Plans to validate dual elimination MTCT. The country should be considered a candidate for elimination of STIs as a public health problem (syphilis, chancroid, gonorrhoea)
Validated dual elimination MTCT (syphilis and HIV)
The country should be considered a candidate for elimination of STIs as a public health problem (syphilis, chancroid, gonorrhoea)
STI guidelines: last full revision in 2009, minor updates in 2014, currently revising
STI clinical services
Strong network of STI clinics provide prevention and treatment
STI guidelines as example for other countries interested in aetiological management approaches
Outreach/services for KP
100% CUP and other community-based services to KPs implemented with support of STI clinics
Strengthen programme monitoring of KP coverage, use of services, syphilis prevalence and other STIs, especially among MSM

Moving ahead on elimination of Sexually Transmitted Infections (STIs) in WHO South-East Asia Region - progress and challenges18
aspects Status notesSTI surveillance Strong STI surveillance in place for
decades, reliable monitoring of trends, sensitive to outbreaks (early warning system)
Universal aetiological reporting with case definitions for syphilis, gonorrhoea, NSU, chancroid and LGV
Relevant publications
22 STI studies identified
The initial results in Thailand were dramatic and led to adaptation and replication in other countries. Sex workers were enabled to demand condom use and access STI care, which rapidly slowed transmission. The programme also had a large-scale public heath impact. The incidence rate of reported STI diagnoses (gonorrhoea, non-specific urethritis, syphilis, chancroid and lymphogranuloma venereum [LGV]) decreased from 785 cases/100 000 population in 1986 to 25 cases/100 000 population in 1999. By 2002, an estimated 5.7 million HIV infections had been averted, including averted secondary infections; this not only included sex workers and their clients, but also far larger numbers of people at lower risk. As Thailand’s epidemic began to come under control, implementation of 100% CUP broadened in several ways. Interventions were expanded from establishment-based sex work to others venues; NGOs and CBOs became more involved, especially in non-establishment settings; and clinical services were strengthened. Yet, despite the early success of prevention and treatment programmes, transmission may be increasing among MSM, in particular among young MSM and male sex workers.
STI reporting trends are given in Fig. 4.
Fig. 4. Routine STI reporting trends, Thailand
LGV – lymphogranuloma venereum; NSU – non-specific urethritis

Moving ahead on elimination of Sexually Transmitted Infections (STIs) in WHO South-East Asia Region - progress and challenges 19
b. Countries with partial control or insufficient data
IndiaIndia is the largest country in the Region, accounting for over two thirds of its population. Being geographically large and diverse, it has also shown a large degree of heterogeneity in STI epidemiology and control over the years. Historically, STI transmission, and the early AIDS epidemic, followed migrant pathways to large cities such as Mumbai, Delhi, Kolkata and Chennai. Early control efforts also focused on the large metropolitan areas. From about 2004 onwards, large-scale efforts were made to scale up interventions and services for KPs, first in high-prevalence states (Avahan), then nationwide (National AIDS Control Organization [NACO]). STI prevention, screening and treatment were major programme components. Data from a number of studies provide evidence of significant declines of several common curable STIs during this period, and are supported by more recent programme and survey data.
Various aspects of STI status in the country are given in Table 5.
Table 5. Various aspects of STI status in India
aspects Status notesEpidemiological snapshot
Evidence of declining STI prevalence among key and bridge populations over last 10–15 years from multiple sites and sources
STI declines strongly linked to large-scale interventions (Avahan, NACO)
STI clinical services
Range of services for general population and KPs including syndrome management and presumptive treatment
Increasing attendance/coverage of STI clinics, KP STI services (TI) and ANC syphilis screening have all been documented
Outreach/services for KP
KP interventions for HIV at scale, include range of STI services
Studies/data from multiple sites show large KP STI declines, both population based and among KP using services
STI surveillance Routine STI surveillance with improved reporting (>95% STI clinics, >80% TIs reporting). ANC reporting from two different systems not integrated
Increasing use of STI clinic services. Trend analyses incorporating data from diverse reporting sites could be strengthened
Relevant publications
110 STI studies identified
TI – targeted intervention
STI services and reporting also improved considerably during this period. During the FY 2016–2017, 8.6 million patients were managed for STI/reproductive tract infections (RTIs) following national protocols, which was nearly 95% of the NACO target. STI reporting increased from about 65% in 2008–2009 to 95% of STI clinics (designated STI/RTI clinics [DSRCs]) and 85% of KP targeted intervention (TI) projects in recent years.

Moving ahead on elimination of Sexually Transmitted Infections (STIs) in WHO South-East Asia Region - progress and challenges20
Significant declines in syphilis prevalence were measured between 2005–2006 and 2016–2017 among DSRC attendees, ANC attendees and KPs. HIV Sentinel Surveillance 2014–15 reported 0.14% syphilis prevalence among ANC attendees. However, syphilis prevalence reported from National Health Mission, based on partial ANC testing coverage (17% of 30 million ANC attendees), are significantly higher (1.5%).
Persons with STIs may seek care in the formal health sector comprising the private and public sector-based facilities, in the alternate health sector and in the informal sector. According to IBBS 2014–2015 data, nearly half of female sex workers (FSWs) reported STI/RTI symptoms in the last year, and the majority reported seeking treatment from either NGOs (49%) or government clinics (49%). Similar patterns of treatment seeking was found among MSM (one fifth with STI symptoms).
Syphilis prevalence trends among pregnant women and KPs are given in Fig. 5.
Fig. 5. Syphilis prevalence trends among pregnant women and KPs in India
IndonesiaSTIs are a common public health problem in Indonesia. The STI control programme in Indonesia covers prevention, STI care services and related activities. STI care is available in both the public and private sectors. In the public sector, the syndromic case management approach is used for the management of STIs, and some government-mandated community health clinics (puskemas) provide additional screening services for KPs. Almost no screening of pregnant women for syphilis took place until recently, due to lack of commodities, although this area is now being addressed by the Ministry of Health (MoH).

Moving ahead on elimination of Sexually Transmitted Infections (STIs) in WHO South-East Asia Region - progress and challenges 21
In 2006, an estimated 221 000 women worked in the sex industry serving 4 million clients per year. As early as 1996, the programme began advocating promotion of condoms for all sexual encounters in sex establishments. A 100% condom use policy was adopted as part of the 2003–2007 national strategy. Implementation has been limited and uneven, partly due to health sector decentralization, endorsement by local government and cultural attitudes toward sex work and condoms. Higher condom use and lower STIs have been reported from sites with strong implementation. Several studies report intervention-linked outcomes. Increasing condom use and decreases in gonorrhea, chlamydia and syphilis of up to 80% were reported from two sites following condom promotion/supply, provision of effective STI drugs and periodic presumptive treatment (PPT) for STIs.
Since 2009, national strategies have emphasized prevention of sexual transmission through multi-stakeholder mobilization and support for enabling environments. Interventions aim to empower sex workers to increase condom use and access health services, and are supported by improved condom supply and more comprehensive clinical services. The programme also seeks to increase demand for condom use in sex work among high-risk men through workplace and other programmes, and is addressing MSM and warias (transgenders) with an emphasis on those who sell or buy sex.
Data on STI incidence and prevalence are limited, although routine reporting systems have improved in recent years. Data from IBBS and special studies demonstrate that STIs have decreased in some areas, particularly among sex workers, following interventions. Overall, however, there is no evidence of decreasing trends of syphilis or other STIs among KP or in the general population.
Table 6 gives various aspects of the STI status in the country. Fig. 6 gives the syphilis prevalence trends.
Table 6. Various aspects of STI status in Indonesia
aspects Status notesEpidemiological snapshot
STIs historically high and variable with a few examples of good practice, and many areas with insufficient data
Insufficient and/or unreliable data on STIs limits assessment of current situation and trends
STI clinical services
STI services at puskesmas require training, possibly guidelines review. Very low ANC syphilis screening coverage
ANC syphilis screening targeted for scale-up
Outreach/ services for KP
Under fast-track programme with HIV focus, some STI screening may be done in some areas
Inconsistent response to sex work, KPs with strong services in some areas, brothel closures in others
STI surveillance Partial coverage with SIHA/IMS, no recent analysis of trends
Incomplete reporting is the main challenge
Relevant publications
10 STI studies identified in last 10 years Nearly all papers focus on KP

Moving ahead on elimination of Sexually Transmitted Infections (STIs) in WHO South-East Asia Region - progress and challenges22
Fig. 6. Syphilis prevalence trends, Indonesia
DSW – direct sex worker; ISW – indirect sex worker; MSM – men who have sex with men
note: Waria is an Indonesian word meaning“transgender”.It is derived from a combination of two words – wanita (woman) and pria (man), taking the first syllable from waria and the second syllable from pria.
bangladeshData on STI prevalence and incidence for Bangladesh are limited. Patients with STI, particularly men, usually seek care in the private sector or at health facilities run by NGOs, some medical associations and private medical colleges. The majority of persons with STI are thought to be young persons often following contact with a sex worker. Guidelines for the management of STIs that exist are used mainly in the public sector. STIs are managed by most private medical practitioners according to their own experience.
Various aspects of STI status are given in Table 7.
Table 7. Various aspects of STI status in Bangladesh
aspects Status notesEpidemiological snapshot
Clear declining syphilis trends among sex workers
Few data on other STI
STI clinical services
Provide syndromic management of STI through government and NGO facilities, promote condoms, ensure partner treatment, etc.
Outreach/ services for KP
Sex worker mobilization, raising awareness, condom promotion and provision of STI services
Strengthen programme monitoring of KP coverage, use of services, syphilis prevalence, other STIs
STI surveillance No information
Relevant publications
At least 13 articles with focus on STIs since 2010, covering sex work
UD – urethral discharge; GUD – genital ulcer disease; LAP – lower abdominal pain; OPD – outpatient department

Moving ahead on elimination of Sexually Transmitted Infections (STIs) in WHO South-East Asia Region - progress and challenges 23
Bangladesh acted early to improve HIV/STI prevention among sex workers and clients to mobilize sex workers, raise awareness, promote condom use and provide STI services in brothels and among street-based sex workers. Syphilis prevalence was as high as 57% among the street-based sex workers and 46% at one brothel but has declined greatly since the early 2000s (Fig. 7).
Fig 7. Syphilis prevalence among sex workers in Bangladesh
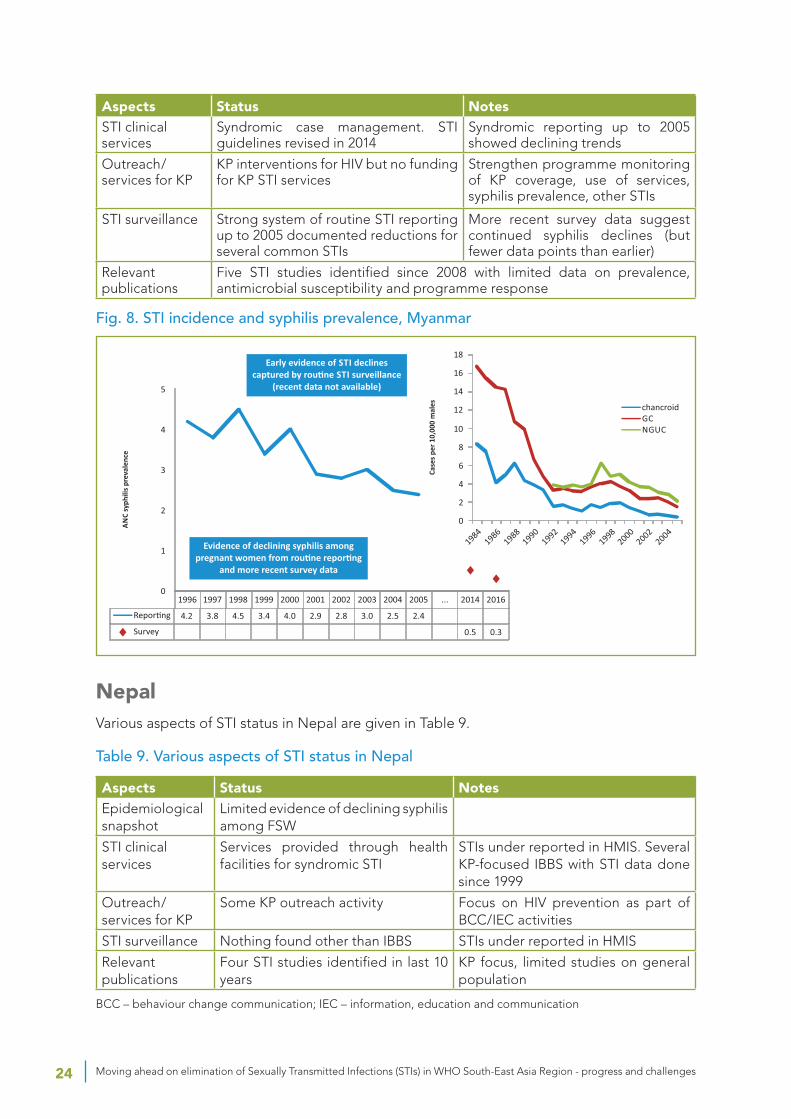
myanmarMyanmar demonstrated early success in a demonstration project of STI control and HIV prevention with 100% targeted condom promotion. Pilots in four townships demonstrated an increase in condom use among sex workers (from 61% in 2001 to 91% in 2002) and halving of syphilis prevalence. By 2006, the programme was reaching almost half the townships in the country, reported condom use had risen to high levels (96% in Mandalay and Yangon) and syphilis trends were declining. By 2019, with HIV prevention services including condom promotion in all 324 townships of the country, reported condom use among sex workers was 81.1% and had risen to 77.1% among MSM (IBBS 2015).
Various aspects of status of STI are given in Table 8. STI incidence and prevention of syphilis are given in Fig. 8.
Table 8. Various aspects of STI status in Myanmar
aspects Status notesEpidemiological snapshot
Declining STI rates and ANC syphilis prevalence up to 2005.Syphilis declines (2014 to 2016):FSW – 6.4% to 5.3%, MSM – 6.0% to 4.4%, ANC – 0.5% to 0.3%
Data on syndromes up to 2005 from routine reporting. Later data from surveys
Moving ahead on elimination of Sexually Transmitted Infections (STIs) in WHO South-East Asia Region - progress and challenges24
aspects Status notesSTI clinical services
Syndromic case management. STI guidelines revised in 2014
Syndromic reporting up to 2005 showed declining trends
Outreach/ services for KP
KP interventions for HIV but no funding for KP STI services
Strengthen programme monitoring of KP coverage, use of services, syphilis prevalence, other STIs
STI surveillance Strong system of routine STI reporting up to 2005 documented reductions for several common STIs
More recent survey data suggest continued syphilis declines (but fewer data points than earlier)
Relevant publications
Five STI studies identified since 2008 with limited data on prevalence, antimicrobial susceptibility and programme response
Fig. 8. STI incidence and syphilis prevalence, Myanmar
nepal Various aspects of STI status in Nepal are given in Table 9.
Table 9. Various aspects of STI status in Nepal
aspects Status notesEpidemiological snapshot
Limited evidence of declining syphilis among FSW
STI clinical services
Services provided through health facilities for syndromic STI
STIs under reported in HMIS. Several KP-focused IBBS with STI data done since 1999
Outreach/ services for KP
Some KP outreach activity Focus on HIV prevention as part of BCC/IEC activities
STI surveillance Nothing found other than IBBS STIs under reported in HMIS
Relevant publications
Four STI studies identified in last 10 years
KP focus, limited studies on general population
BCC – behaviour change communication; IEC – information, education and communication

Moving ahead on elimination of Sexually Transmitted Infections (STIs) in WHO South-East Asia Region - progress and challenges 25
In Nepal, interventions with sex workers started slowly from the mid-1990s with education and condom promotion in Kathmandu and a few other towns following description of risks related to sex work. A 2001 survey of 500 Kathmandu Valley sex workers measured 14.3% active syphilis prevalence among street-based sex workers (3.5% among establishment-based). From the mid-1990s, NGOs began peer interventions, opened drop-in centres and provided condoms and STI services to sex workers. Integrated IBBSs for FSWs have been conducted as early as in 1999 in 22 highway districts, and more recently in 2018.
More recent IBBS data (2018) support large HIV prevalence reductions among FSWs (0.7% in 2018, compared to 2.0% recorded in 2003). However, trends of active syphilis prevalence are unstable (0.3% in 2012, 10.3% in 2016 and 1.6 % in 2018 (Fig. 9).
A related IBBS study (2018) conducted on the male labour migrants (MLM) in six eastern districts demonstrated that the most common STI symptoms experienced were genital ulcers or sores (11.6%) and burning sensation (10.2%). Fewer than one third of the surveyed population sought treatment for the symptoms.
Fig. 9. ANC syphilis prevalence, Nepal
democratic People’s republic of KoreaFew data are available on STIs in Democratic People’s Republic of Korea. HIV reportedly does not exist but hepatitis B and C are common enough to justify screening programmes. Blood safety is reportedly ensured by screening but details and data are pending.
Various aspects of STI status are given in Table 10.
Moving ahead on elimination of Sexually Transmitted Infections (STIs) in WHO South-East Asia Region - progress and challenges26
Table 10. Various aspects of STI status in Democratic People’s Republic of Korea
aspects Status notesEpidemiological snapshot Situation largely unknown
STI clinical services Situation largely unknown
Outreach/ services for KP None
STI surveillance Situation largely unknown
Relevant publications No STI studies identified
maldivesThe HIV and STI epidemics in the Maldives are at a very low level. The national strategic plan for HIV/AIDS 2014–2018 prioritizes targeting of prevention services to KPs, and sets coverage targets for sex workers, MSM and IDUs.
Various aspects of STI status are given in Table 11.
Table 11. Various aspects of STI status in Maldives
aspects Status notesEpidemiological snapshot
Low and declining STI rates evident from limited data
While STIs appear to be low, both monitoring and services could be strengthened
STI clinical services
Syndrome management in place with guidelines revised in 2013
Attention to capacity of health-care workers, selective introduction of etiological testing
Outreach/ services for KP
KP interventions mainly for HIV with little attention to STIs
Strengthen programme monitoring of KP coverage, use of services, syphilis prevalence, other STIs
STI surveillance Regular routine reporting (done separately for native and large expat populations)
Monitoring and trend analyses of routine data from all reporting sites could be strengthened
Relevant publications
IBBS 2008
The country does not have a separate programme for STI; STI control is incorporated in the National HIV/AIDS Programme. Syndromic management approach is applied in all health-care facilities except in the regional hospitals and the Indira Gandhi Memorial Hospital where laboratory facilities are available. The country is developing an integrated HIV/STI strategy for 2020–2024 where STI control will be an integral and significant component.
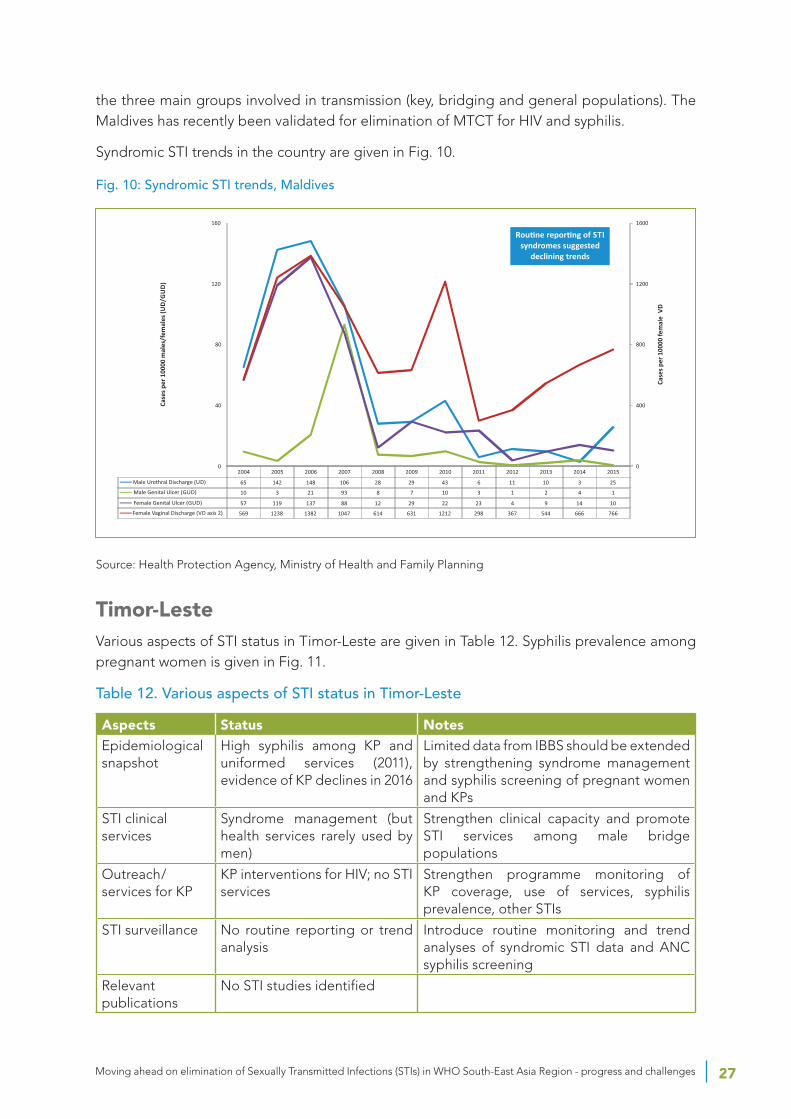
A solid platform for STI surveillance is in place in the Maldives. New STI guidelines were released in 2013, up to date treatment is available, and recent improvements in case reporting permit programme managers to see patterns and trends of major STI syndromes. Initial trend analysis and data triangulation suggest that the common curable STIs may have declined in recent years and be at historically low levels, both for the Maldives and the Region (Fig 10). These patterns and trends need to be investigated further.
Prevalence trends of syphilis and HIV are receiving increased attention. HIV/syphilis screening among pregnant women is strictly monitored and promptly reported and all positive cases are immediately treated. Equivalent prevalence data on KPs is limited to ongoing IBBS. The data from IBBS would provide a more complete picture of sexual transmission trends among
Moving ahead on elimination of Sexually Transmitted Infections (STIs) in WHO South-East Asia Region - progress and challenges 27
the three main groups involved in transmission (key, bridging and general populations). The Maldives has recently been validated for elimination of MTCT for HIV and syphilis.
Syndromic STI trends in the country are given in Fig. 10.
Fig. 10: Syndromic STI trends, Maldives
Source: Health Protection Agency, Ministry of Health and Family Planning
Timor-lesteVarious aspects of STI status in Timor-Leste are given in Table 12. Syphilis prevalence among pregnant women is given in Fig. 11.
Table 12. Various aspects of STI status in Timor-Leste
aspects Status notesEpidemiological snapshot
High syphilis among KP and uniformed services (2011), evidence of KP declines in 2016
Limited data from IBBS should be extended by strengthening syndrome management and syphilis screening of pregnant women and KPs
STI clinical services
Syndrome management (but health services rarely used by men)
Strengthen clinical capacity and promote STI services among male bridge populations
Outreach/ services for KP
KP interventions for HIV; no STI services
Strengthen programme monitoring of KP coverage, use of services, syphilis prevalence, other STIs
STI surveillance No routine reporting or trend analysis
Introduce routine monitoring and trend analyses of syndromic STI data and ANC syphilis screening
Relevant publications
No STI studies identified
Moving ahead on elimination of Sexually Transmitted Infections (STIs) in WHO South-East Asia Region - progress and challenges28
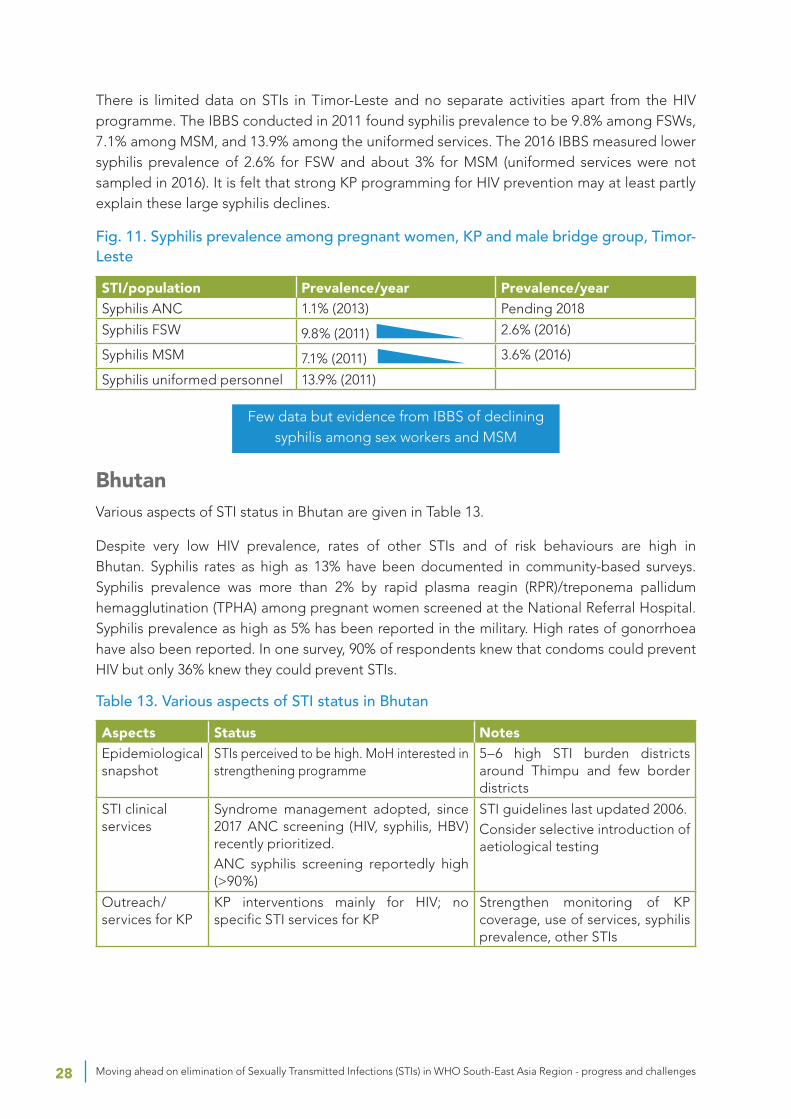
There is limited data on STIs in Timor-Leste and no separate activities apart from the HIV programme. The IBBS conducted in 2011 found syphilis prevalence to be 9.8% among FSWs, 7.1% among MSM, and 13.9% among the uniformed services. The 2016 IBBS measured lower syphilis prevalence of 2.6% for FSW and about 3% for MSM (uniformed services were not sampled in 2016). It is felt that strong KP programming for HIV prevention may at least partly explain these large syphilis declines.
Fig. 11. Syphilis prevalence among pregnant women, KP and male bridge group, Timor-Leste
STI/population Prevalence/year Prevalence/yearSyphilis ANC 1.1% (2013) Pending 2018
Syphilis FSW 9.8% (2011) 2.6% (2016)
Syphilis MSM 7.1% (2011) 3.6% (2016)
Syphilis uniformed personnel 13.9% (2011)
Few data but evidence from IBBS of declining syphilis among sex workers and MSM
bhutanVarious aspects of STI status in Bhutan are given in Table 13.
Despite very low HIV prevalence, rates of other STIs and of risk behaviours are high in Bhutan. Syphilis rates as high as 13% have been documented in community-based surveys. Syphilis prevalence was more than 2% by rapid plasma reagin (RPR)/treponema pallidum hemagglutination (TPHA) among pregnant women screened at the National Referral Hospital. Syphilis prevalence as high as 5% has been reported in the military. High rates of gonorrhoea have also been reported. In one survey, 90% of respondents knew that condoms could prevent HIV but only 36% knew they could prevent STIs.
Table 13. Various aspects of STI status in Bhutan
aspects Status notesEpidemiological snapshot
STIs perceived to be high. MoH interested in strengthening programme
5–6 high STI burden districts around Thimpu and few border districts
STI clinical services
Syndrome management adopted, since 2017 ANC screening (HIV, syphilis, HBV) recently prioritized.ANC syphilis screening reportedly high (>90%)
STI guidelines last updated 2006.Consider selective introduction of aetiological testing
Outreach/ services for KP
KP interventions mainly for HIV; no specific STI services for KP
Strengthen monitoring of KP coverage, use of services, syphilis prevalence, other STIs

Moving ahead on elimination of Sexually Transmitted Infections (STIs) in WHO South-East Asia Region - progress and challenges 29
aspects Status notesSTI surveillance Routine reporting of syndromes since
2010. AMR data from study done 2012–2014
Monitoring and trend analyses of routine data from all reporting sites could be strengthened (including ANC syphilis prevalence trends)
Relevant publications
1 STI study (2013) on knowledge of STIs in two rural districts
There is no private health sector in Bhutan and all persons with STIs seek care at either public sector-based facilities, in the informal sector or by self-medication. STIs continue to be problematic with gonorrhoea being the most common STI. Initiatives that have been implemented to control STIs include outreach, behavioural surveillance, targeted preventive interventions, syndromic management, etc.
The National AIDS and STI Control Programme has made strong initial efforts to strengthen HIV prevention within the broader context of controlling STIs. These efforts have been carried out with active support from several sectors. The primary channels for STI/HIV interventions are health-care facilities, multi-sectoral task forces (MSTFs) and health information and service centres (HISCs). The latter is appropriately targeted to a few districts where risk of STIs and potential for HIV transmission are greatest.
Trends of select STI syndromes in Bhutan are given in Fig. 12.
Fig. 12. Trends of select STI syndromes, Bhutan

Moving ahead on elimination of Sexually Transmitted Infections (STIs) in WHO South-East Asia Region - progress and challenges30
4. Conclusions and recommendationsEvidence from multiple sources strongly supports an overall declining trend of curable STIs in the Region over the past three decades. Shifting patterns are also apparent, with declining proportions of ulcerative and bacterial STIs compared to viral infections.
Data on syphilis declines are more available and reliable than for other STIs, and useful as markers of sexual transmission trends in general. Triangulation of syphilis surveillance data – from KPs, male STI patients (bridge population) and pregnant women (general population) – can highlight progress and gaps of STI control efforts. Evidence of declining syphilis, as well as progress in eliminating MTCT in some countries, supports the feasibility of regional elimination of syphilis as a public health problem. Weak STI surveillance and limited syphilis screening among KPs and pregnant women are the main barriers to elimination in the Region. Recent increases in syphilis among MSM in several countries underline the importance of routinely screening KPs for syphilis and monitoring prevalence trends.
Data on other STIs are less reliable, but combinations of syndromic and aetiological reporting have proven useful in guiding control efforts in several countries and can be adapted elsewhere. Reliable data on gonorrhoea come from Sri Lanka and Thailand, which use affordable microscopy with Gram stain to distinguish gonococcal from non-gonococcal infections.
Moving ahead on elimination of Sexually Transmitted Infections (STIs) in WHO South-East Asia Region - progress and challenges 31
The programme response to STIs varies greatly across the Region, from highly effective to almost non-existent. Where STI declines have occurred, evidence strongly supports attribution to programmes that have increased condom use in sex work, while maintaining good clinical services (both for targeted and general populations) and reliable STI surveillance. National experience and sub-national examples highlight multiple effective approaches to reducing STI incidence and prevalence, as well as surveillance and programme monitoring methods. STI services for KPs – including quarterly medical checkups, presumptive treatment for asymptomatic infections and regular syphilis screening – have resulted in rapid STI control, including virtual elimination of common STIs in two Indian districts.
A number of important gaps and constraints to STI control were identified in most countries of the Region. These have been flagged in this report with recommendations for more in depth assessment and programme strengthening. Low perceived priority and programme funding were cited by most countries as the main reasons for declining attention to STI control and surveillance.
4.1 Summary of recommendations for strengthening STI control in the Sea region
• Urgently take steps to reposition STI control as a public health priority for the Region and advocate for resources, staffing and planning, independent of HIV programme priorities (recognizing common ground and potential synergies in STI/HIV control efforts, i.e. offering STI screening/PPT at quarterly PrEP visits).
• Recognize successes in the Region and leverage the considerable experience and expertise from countries such as Sri Lanka and Thailand and from KP community learning sites like DMSC and Ashodaya Samithi.
• Advocate for and support progress towards STI elimination, continuing with eMTCT and preparing elimination cases for infectious syphilis, chancroid and possibly gonorrhoea, recognizing that there are strong candidate countries for each of these STI elimination targets in the SEA Region.
• Address the considerable STI data gaps and limitations in most countries, advocating for and supporting basic STI surveillance components including routine reporting (syndromic/aetiological), routine prevalence monitoring (ANC and KP syphilis screening), leveraging regional experience and expertise (mainly from Thailand and Sri Lanka).
• Develop a flexible toolkit of proven interventions for countries at different stages of STI control, including:
¥ appropriate mixed models of aetiological and syndromic management and reporting (as in Thailand and Sri Lanka);
¥ effective community-based models (including microplanning) for high impact STI control with KPs (DMSC, Ashodaya learning sites);
¥ presumptive treatment strategies to rapidly reduce prevalence of curable STIs in sex work, prevent and control STI outbreaks among PrEP users, MSM and other KPs;

Moving ahead on elimination of Sexually Transmitted Infections (STIs) in WHO South-East Asia Region - progress and challenges32
¥ rapid response methods to identify and control STI outbreaks (particularly important as countries move towards elimination).
• Country-specific recommendations (see individual assessments) can be considered in several groups with different needs.
¥ Countries with urgent STI control needs (Indonesia, others likely at sub-national level, currently unrecognized due to data gaps)
¥ Countries with significant STI programme limitations to address (India, Bangladesh, Myanmar, Nepal, Democratic People’s Republic of Korea)
¥ Small countries with potential for rapid STI control scale-up (Maldives, Bhutan, Timor-Leste)
¥ Countries with high-level STI control that can prepare elimination cases and assist others (Sri Lanka, Thailand).

referenCeS

Moving ahead on elimination of Sexually Transmitted Infections (STIs) in WHO South-East Asia Region - progress and challenges34
1. Global health sector strategy on sexually transmitted infections 2016–2021. Doc no. WHA69/2016/REC/1. Geneva: World Health Organization, 2016.
2. Regional strategy for the prevention and control of sexually transmitted infections, 2007–2015. New Delhi: World Health Organization, Regional Office for South-East Asia, 2007.
3. Global prevalence and Incidence of selected curable sexually transmitted infections: overview and estimates. Doc No. WHO/HIV_AIDS/2001.02. Geneva: World Health Organization, 2001.
4. Prevalence and incidence of selected sexually transmitted infections, Chlamydia trachomatis, Neisseria gonorrhoeae, syphilis and Trichomonas vaginalis: methods and results used by WHO to generate 2005 estimates. Geneva: World Health Organization; 2011.
5. Global incidence and prevalence of selected curable sexually transmitted infections - 2008. Geneva: World Health Organization; 2011.
6. Newman L, Rowley J, Vander Hoorn S, Wijesooriya NS, Unemo M, Low N, et al. (2015) Global Estimates of the Prevalence and Incidence of Four Curable Sexually Transmitted Infections in 2012 Based on Systematic Review and Global Reporting. PLoS One. 2015;10(12): e0143304. doi:10.1371/journal. pone.0143304
7. Steen R, Zhao PF, Wi TE, Punchihewa N, Abeyewickreme I, Lo Y-R. Halting and reversing HIV epidemics in Asia by interrupting transmission in sex work: experience and outcomes from ten countries. Expert Review of Anti-infect Ther. 2013;11(10):999–1015.
lIST of reSourCeS

Moving ahead on elimination of Sexually Transmitted Infections (STIs) in WHO South-East Asia Region - progress and challenges36
bangladesh
1. McClair TL, Hossain T, Sultana N, Burnett-Zieman B, Yam EA, Hossain S et al. Paying for Sex by Young Men Who Live on the Streets in Dhaka City: Compounded Sexual Risk in a Vulnerable Migrant Community. J Adolesc Health. 2017;60(2S2):S29–S34.
2. Khanam R, Reza M, Ahmed D, Rahman M, Alam MS, Sultana S et al. Sexually transmitted infections and associated risk factors among street-based and residence-based female sex workers in Dhaka, Bangladesh. Sex Transm Dis. 2017;44(1):21–8.
3. Alam N, Alam A, Fournier P. Medicine sellers for prevention and control of sexually transmitted infections: effect of a quasi-experimental training intervention in Bangladesh. Biomed Res Int. 2015;570340.
4. Kabir H, Saha NC, Gazi R. Female unmarried adolescents’ knowledge on selected reproductive health issues in two low performing areas of Bangladesh: an evaluation study. BMC Public Health. 2015;15:1262.
5. Rahman M, Nakamura K, Seino K, Kizuki M. Intimate partner violence and symptoms of sexually transmitted infections: are the women from low socio-economic strata in Bangladesh at increased risk. Int J Behav Med. 2014;21(2):348–57.
6. Kabir H, Saha NC, Wirtz AL, Gazi R. Treatment-seeking for selected reproductive health problems: behaviours of unmarried female adolescents in two low-performing areas of Bangladesh. Reprod Health. 2014;11:54.
7. McCormick DF, Rahman M, Zadrozny S, Alam A, Ashraf L, Neilsen GA et al. Prevention and control of sexually transmissible infections among hotel-based female sex workers in Dhaka, Bangladesh. Sex Health. 2013;10(6):478–86.
8. Haseen F, Chawdhury FAH, Hossain ME, Huq M, Bhuiyan MU, Imam H et al. Sexually transmitted infections and sexual behaviour among youth clients of hotel-based female sex workers in Dhaka, Bangladesh. Int J STD AIDS. 2012;23(8):553–9.
9. Ahmed A, Reichenbach LJ, Alam N. Symptoms of sexually transmitted infections and care-seeking behaviors of male clients of female sex workers in Bangladesh. Sex Transm Dis. 2012;39(12):979-84.
10. Alam N, Streatfield PK, Shahidullah M, Mitra D, Vermund SH, Kristensen S. Effect of single session counselling on partner referral for sexually transmitted infections management in Bangladesh. Sex Transm Infect. 2011;87(1):46–51.
11. Sarma H, Oliveras E. Improving STI counselling services of non-formal providers in Bangladesh: testing an alternative strategy. Sex Transm Infect. 2011;87(6):47–8.
12. Ahmed MU, Chawdhury FAH, Hossain M, Sultan SZ, Alam M, Salahuddin G et al. Monitoring antimicrobial susceptibility of Neisseria gonorrhoeae isolated from Bangladesh during 1997–2006: emergence and pattern of drug-resistant isolates. J Health Popul Nutr. 2010;28(5):443–9.
13. Alam N, Streatfield PK, Khan SI, Momtaz D, Kristensen S, Vermund SH. Factors associated with partner referral among patients with sexually transmitted infections in Bangladesh. Soc Sci Med. 2010;71(11):1921–6.

Moving ahead on elimination of Sexually Transmitted Infections (STIs) in WHO South-East Asia Region - progress and challenges 37
14. Alam N, Rahman M, Gausia K, Yunus MD, Islam N, Chaudhury P et al. Sexually transmitted infections and risk factors among truck stand workers in Dhaka, Bangladesh. Sex Transm Dis 2007;34(2):99–103.
15. Silverman JG, Decker MR, Kapur NA, Gupta J, Raj A. Violence against wives, sexual risk and sexually transmitted infection among Bangladeshi men. Sex Transm Infect. 2007;83(3):211–5.
16. Ray K, Bala M, Kumari S, Narain JP. Antimicrobial resistance of Neisseria gonorrhoeae in selected World Health Organization Southeast Asia Region countries: an overview. Sex Transm Dis. 2005;32(3):178–84.
17. Nessa K, Waris S-A, Sultan Z, Monira S, Hossain M, Nahar S et al. Epidemiology and etiology of sexually transmitted infection among hotel-based sex workers in Dhaka, Bangladesh. Clin Microbiol. 2004:42(2):618–21.
18. Sabin KM, Rahman M, Hawkes S, Ahsan K, Begum L, Black RE et al. Sexually transmitted infections prevalence rates in slum communities of Dhaka, Bangladesh. Int J STD AIDS. 2003:14(9):614–21.
19. Bogaerts J, Ahmed J, Akhter N, Begum N, Rahman M, Nahar S et al. Sexually transmitted infections among married women in Dhaka, Bangladesh: unexpected high prevalence of herpes simplex type 2 infection. Sex Transm Infect. 2001;77(2):114–9.
20. Rahman M, Alam A, Nessa K, Hossain A, Nahar S, Datta D. Etiology of sexually transmitted infections among street-based female sex workers in Dhaka, Bangladesh. J Clin Microbiol. 2000;38(31):244–6.
21. Hawkes S, Morison L, Foster S, Gausia K, Chakraborty J, Peeling R et al. Reproductive-tract infections in women in low-income, low-prevalence situations: assessment of syndromic management in Matlab, Bangladesh. Lancet. 1999;354(9192):1776–81.
22. Hawkes S. Why include men? Establishing sexual health clinics for men in rural Bangladesh. Health Policy Plan. 1998;13(2):121–30.
India
23. Kulkarni SV, Bala M, Muqeeth SA, Sasikala G, Nirmalkar AP, Thorat R, et al. Antibiotic susceptibility pattern of Neisseria gonorrhoeae strains isolated from five cities in India during 2013-2016. J Med Microbiol. 2018;67:22-8.
24. Arif N, Juyal D, Sebastian S, Khanna N, Dhawan B. Analysis of laboratory testing results for Chlamydia trachomatis infection in an STI clinic in India: Need for extragenital screening. Int J Infect Dis. 2017;57:1-2.
25. Vaz M, Kadyan N, Chalil S, Prasad TLN, Singh AK. Looking for sufficient change: Evaluation of counsellor training for STI syndromic management in India. Eval Program Plann. 2016;58:141-51.
26. Bhattar S, Aggarwal P, Sahani SK, Bhalla P. Co-Infections and Sero-Prevalence of HIV, Syphilis, Hepatitis B and C Infections in Sexually Transmitted Infections Clinic Attendees of Tertiary Care Hospital in North India. J Res Health Sci. 2016;16:162-5.

Moving ahead on elimination of Sexually Transmitted Infections (STIs) in WHO South-East Asia Region - progress and challenges38
27. Prakash R, Manthri S, Tayyaba S, Joy A, Raj SS, Singh D, Agarwal A. Effect of Physical Violence on Sexually Transmitted Infections and Treatment Seeking Behaviour among Female Sex Workers in Thane District, Maharashtra, India. PLoS ONE. 2016;11:e0150347.
28. Lafort Y, Greener R, Roy A, Greener L, Ombidi W, Lessitala F, et al. Where Do Female Sex Workers Seek HIV and Reproductive Health Care and What Motivates These Choices? A Survey in 4 Cities in India, Kenya, Mozambique and South Africa. PLoS ONE. 2016;11:e0160730.
29. Reed E, Erausquin JT, Groves AK, Salazar M, Biradavolu M, Blankenship KM. Client-perpetrated and husband-perpetrated violence among female sex workers in Andhra Pradesh, India: HIV/STI risk across personal and work contexts. Sex Transm Infect. 2016;92:424-9.
30. Lafort Y, Greener R, Roy A, Greener L, Ombidi W, Lessitala F, et al. HIV prevention and care-seeking behaviour among female sex workers in four cities in India, Kenya, Mozambique and South Africa. Trop Med Int Health. 2016;21:1293-303.
31. Erausquin JT, Reed E, Blankenship KM. Change over Time in Police Interactions and HIV Risk Behavior Among Female Sex Workers in Andhra Pradesh, India. AIDS Behav. 2015;19:1108-15.
32. Ramakrishnan L, Ramanathan S, Chakrapani V, Goswami P, Deshpande S, Yadav D, et al. Comparison of Sexual Risk, HIV/STI Prevalence and Intervention Exposure Among Men Who Have Sex with Men and Women (MSMW) and Men Who Have Sex with Men Only (MSMO) in India: Implications for HIV Prevention. AIDS Behav. 2015;19:2255-69.
33. Bharara T, Bhalla P, Rawat D, Garg VK, Sardana K, Chakravarti A. Rising trend of antimicrobial resistance among Neisseria gonorrhoeae isolates and the emergence of N. gonorrhoeae isolate with decreased susceptibility to ceftriaxone. Indian J Med Microbiol. 2015;33:39-42.
34. Abdulkader RS, Kant S, Rai SK, Goswami K, Misra P. Prevalence and determinants of sexually transmitted infections (STIs) among male migrant factory workers in Haryana, North India. Indian J Public Health. 2015;59:30-6.
35. Chen XS, Khaparde S, Prasad TL, Srinivas V, Anyaike C, Ijaodola G, et al. Estimating disease burden of maternal syphilis and associated adverse pregnancy outcomes in India, Nigeria, and Zambia in 2012. Int J Gynaecol Obstet. 2015;130 Suppl 1:S4-9.
36. Beattie TS, Bhattacharjee P, Isac S, Mohan HL, Simic-Lawson M, Ramesh BM, et al. Declines in violence and police arrest among female sex workers in Karnataka state, south India, following a comprehensive HIV prevention programme. J Int AIDS Soc. 2015;18:20079.
37. Sahay S, Deshpande S, Bembalkar S, Kharat M, Parkhe A, Brahme RG, et al. Failure to Use and Sustain Male Condom Usage: Lessons Learned from a Prospective Study among Men Attending STI Clinic in Pune, India. PLoS ONE. 2015;10:e0135071.
38. Hochberg CH, Schneider JA, Dandona R, Lakshmi V, Kumar GA, Sudha T, et al. Population and dyadic-based seroincidence of herpes simplex virus-2 and syphilis in southern India. Sex Transm Infect. 2015;91:375-82.

Moving ahead on elimination of Sexually Transmitted Infections (STIs) in WHO South-East Asia Region - progress and challenges 39
39. Safren SA, Thomas BE, Mayer KH, Biello KB, Mani J, Rajagandhi V, et al. A pilot RCT of an intervention to reduce HIV sexual risk and increase self-acceptance among MSM in Chennai, India. AIDS Behav. 2014;18:1904-12.
40. Ramanathan S, Deshpande S, Gautam A, Pardeshi DB, Ramakrishnan L, Goswami P, et al. Increase in condom use and decline in prevalence of sexually transmitted infections among high-risk men who have sex with men and transgender persons in Maharashtra, India: Avahan, the India AIDS Initiative. BMC Public Health. 2014;14:784.
41. O’Halloran AB, Armstrong G, Medhi GK, Sono CZ, Mahanta J, Kermode M. HIV risks vary according to type of sex work in a cross-sectional survey from Nagaland, India. BMC Womens Health. 2014;14:133.
42. Kokku SB, Mahapatra B, Tucker S, Saggurti N, Prabhakar P. Effect of public-private partnership in treatment of sexually transmitted infections among female sex workers in Andhra Pradesh, India. Indian J Med Res. 2014;139:285-93.
43. Chandrashekar S, Guinness L, Pickles M, Shetty GY, Alary M, Vickerman P, Vassall A. The costs of scaling up HIV prevention for high risk groups: lessons learned from the Avahan Programme in India. PLoS ONE. 2014;9:e106582.
44. Boily MC, Pickles M, Lowndes CM, Ramesh BM, Washington R, Moses S, et al. Positive impact of a large-scale HIV prevention programme among female sex workers and clients in South India. AIDS. 2013;27:1449-60.
45. Charles B, Jeyaseelan L, Edwin Sam A, Kumar Pandian A, Thenmozhi M, Jeyaseelan V. Trends in risk behaviors among female sex workers in south India: priorities for sustaining the reversal of HIV epidemic. AIDS Care. 2013;25:1129-37.
46. Subramanian T, Ramakrishnan L, Aridoss S, Goswami P, Kanguswami B, Shajan M, et al. Increasing condom use and declining STI prevalence in high-risk MSM and TGs: evaluation of a large-scale prevention program in Tamil Nadu, India. BMC Public Health. 2013;13:857.4.
47. Narayanan P, Das A, Morineau G, Prabhakar P, Deshpande GR, Gangakhedkar R, Risbud A. An exploration of elevated HIV and STI risk among male sex workers from India. BMC Public Health. 2013;13:1059.
48. Souverein D, Euser SM, Ramaiah R, Narayana Gowda PR, Shekhar Gowda C, Grootendorst DC, et al. Reduction in STIs in an empowerment intervention programme for female sex workers in Bangalore, India: the Pragati programme. Glob Health Action. 2013;6:22943.
49. Sarna A, Friedland BA, Srikrishnan AK, Katzen LL, Tun W, Abbott SA, et al. Sexually transmitted infections and reproductive health morbidity in a cohort of female sex workers screened for a microbicide feasibility study in Nellore, India. Glob J Health Sci. 2013;5:139-49.
50. Medhi GK, Mahanta J, Hazarika I, Armstrong G, Adhikary R, Mainkar M, Paranjape RS. Syphilis infection among female sex workers in Nagaland, Northeast India: analysing their vulnerability to the infection. Int J STD AIDS. 2013;24:193-7.

Moving ahead on elimination of Sexually Transmitted Infections (STIs) in WHO South-East Asia Region - progress and challenges40
51. Chopra S, Devi P, Devi B. Herpes simplex virus 2 : a boon to develop other sexually transmitted infections. J Indian Med Assoc. 2013;111:236-8.
52. Yadav D, Ramanathan S, Goswami P, Ramakrishnan L, Saggurti N, Sen S, et al. Role of community group exposure in reducing sexually transmitted infection-related risk among female sex workers in India. PLoS ONE. 2013;8:e78361.
53. Das A, Pathni AK, Narayanan P, George B, Morineau G, Saidel T, et al. High rates of reinfection and incidence of bacterial sexually transmitted infections in a cohort of female sex workers from two Indian cities: need for different STI control strategies? Sex Transm Infect. 2013;89:5-10.
54. Ghosh I, Ghosh P, Bharti AC, Mandal R, Biswas J, Basu P. Prevalence of human papillomavirus and co-existent sexually transmitted infections among female sex workers, men having sex with men and injectable drug abusers from eastern India. Asian Pac J Cancer Prev. 2012;13:799-802.
55. Euser SM, Souverein D, Rama Narayana Gowda P, Shekhar Gowda C, Grootendorst D, Ramaiah R, et al. Pragati: an empowerment programme for female sex workers in Bangalore, India. Glob Health Action. 2012;5:1-11.
56. Reed E, Gupta J, Biradavolu M, Blankenship KM. Migration/mobility and risk factors for HIV among female sex workers in Andhra Pradesh, India: implications for HIV prevention. Int J STD AIDS. 2012;23:e7-e13.
57. Sabarwal S, Santhya KG. Treatment-seeking for symptoms of reproductive tract infections among young women in India. Int Perspect Sex Reprod Health. 2012;38:90-8.
58. Sahastrabuddhe S, Gupta A, Stuart E, Godbole S, Ghate M, Sahay S, et al. Sexually transmitted infections and risk behaviors among transgender persons (Hijras) of Pune, India. J Acquir Immune Defic Syndr. 2012;59:72-8.
59. Parimi P, Mishra RM, Tucker S, Saggurti N. Mobilising community collectivisation among female sex workers to promote STI service utilisation from the government healthcare system in Andhra Pradesh, India. J Epidemiol Community Health. 2012;66 Suppl 2:ii62-8.
60. Shrivastava SR, Bobhate PS. Prevalence of HIV and syphilis in patients attending sexually transmitted infections (STI) clinic in an urban slum. J Res Health Sci. 2012;12:7-14.
61. Vidwan NK, Regi A, Steinhoff M, Huppert JS, Staat MA, Dodd C, et al. Low prevalence of Chlamydia trachomatis infection in non-urban pregnant women in Vellore, S. India. PLoS ONE. 2012;7:e34794.
62. Dave SS, Copas A, Richens J, White RG, Kosambiya JK, Desai VK, Stephenson JM. HIV and STI prevalence and determinants among male migrant workers in India. PLoS ONE. 2012;7:e43576.
63. Prabhakar P, Narayanan P, Deshpande GR, Das A, Neilsen G, Mehendale S, Risbud A. Genital ulcer disease in India: etiologies and performance of current syndrome guidelines. Sex Transm Dis. 2012;39:906-10.
64. Raj A, Saggurti N, Cheng DM, Dasgupta A, Bridden C, Pradeshi M, Samet JH. Transactional sex risk and STI among HIV-infected female sex workers and HIV-infected male clients of FSWs in India. AIDS Care. 2011;23:1374-81.

Moving ahead on elimination of Sexually Transmitted Infections (STIs) in WHO South-East Asia Region - progress and challenges 41
65. Rachakulla HK, Kodavalla V, Rajkumar H, Prasad SP, Kallam S, Goswami P, et al. Condom use and prevalence of syphilis and HIV among female sex workers in Andhra Pradesh, India - following a large-scale HIV prevention intervention. BMC Public Health. 2011;11 Suppl 6:S1.
66. Thilakavathi S, Boopathi K, Girish Kumar CP, Santhakumar A, Senthilkumar R, Eswaramurthy C, et al. Assessment of the scale, coverage and outcomes of the Avahan HIV prevention program for female sex workers in Tamil Nadu, India: is there evidence of an effect? BMC Public Health. 2011;11 Suppl 6:S3.
67. Gurung A, Narayanan P, Prabhakar P, Das A, Ranebennur V, Tucker S, et al. Large-scale STI services in Avahan improve utilization and treatment seeking behaviour amongst high-risk groups in India: an analysis of clinical records from six states. BMC Public Health. 2011;11 Suppl 6:S10.
68. Pandey A, Mishra RM, Sahu D, Benara SK, Sengupta U, Paranjape RS, et al. Heading towards the Safer Highways: an assessment of the Avahan prevention programme among long distance truck drivers in India. BMC Public Health. 2011;11 Suppl 6:S15.
69. Hemalatha R, Kumar RH, Venkaiah K, Srinivasan K, Brahmam GN. Prevalence of & knowledge, attitude & practices towards HIV & sexually transmitted infections (STIs) among female sex workers (FSWs) in Andhra Pradesh. Indian J Med Res. 2011;134:470-5.
70. Samanta A, Ghosh S, Mukherjee S. Prevalence and health-seeking behavior of reproductive tract infection/sexually transmitted infections symptomatics: a cross-sectional study of a rural community in the Hooghly district of West Bengal. Indian J Public Health. 2011;55:38-41.
71. Wayal S, Cowan F, Warner P, Copas A, Mabey D, Shahmanesh M. Contraceptive practices, sexual and reproductive health needs of HIV-positive and negative female sex workers in Goa, India. Sex Transm Infect. 2011;87:58-64.
72. Sgaier SK, Mony P, Jayakumar S, McLaughlin C, Arora P, Kumar R, et al. Prevalence and correlates of Herpes Simplex Virus-2 and syphilis infections in the general population in India. Sex Transm Infect. 2011;87:94-100.
73. Arora P, Nagelkerke N, Sgaier SK, Kumar R, Dhingra N, Jha P. HIV, HSV-2 and syphilis among married couples in India: patterns of discordance and concordance. Sex Transm Infect. 2011;87:516-20.
74. Reed E, Gupta J, Biradavolu M, Devireddy V, Blankenship KM. The role of housing in determining HIV risk among female sex workers in Andhra Pradesh, India: considering women’s life contexts. Soc Sci Med. 2011;72:710-6.
75. Gupta K, Vaidehi Y, Majumder N. Spatial mobility, alcohol use, sexual behavior and sexual health among males in India. AIDS Behav. 2010;14 Suppl 1:S18-30.
76. Solomon SS, Srikrishnan AK, Sifakis F, Mehta SH, Vasudevan CK, Balakrishnan P, et al. The emerging HIV epidemic among men who have sex with men in Tamil Nadu, India: geographic diffusion and bisexual concurrency. AIDS Behav. 2010;14:1001-10.

Moving ahead on elimination of Sexually Transmitted Infections (STIs) in WHO South-East Asia Region - progress and challenges42
77. Patel AL, Sachdev D, Nagpal P, Chaudhry U, Sonkar SC, Mendiratta SL, Saluja D. Prevalence of Chlamydia infection among women visiting a gynaecology outpatient department: evaluation of an in-house PCR assay for detection of Chlamydia trachomatis. Ann Clin Microbiol Antimicrob. 2010;9:24.
78. Schneider JA, Lakshmi V, Dandona R, Kumar GA, Sudha T, Dandona L. Population-based seroprevalence of HSV-2 and syphilis in Andhra Pradesh state of India. BMC Infect Dis. 2010;10:59.
79. Beattie TS, Bhattacharjee P, Ramesh BM, Gurnani V, Anthony J, Isac S, et al. Violence against female sex workers in Karnataka state, south India: impact on health, and reductions in violence following an intervention program. BMC Public Health. 2010;10:476.
80. Gutierrez JP, McPherson S, Fakoya A, Matheou A, Bertozzi SM. Community-based prevention leads to an increase in condom use and a reduction in sexually transmitted infections (STIs) among men who have sex with men (MSM) and female sex workers (FSW): the Frontiers Prevention Project (FPP) evaluation results. BMC Public Health. 2010;10:497.
81. Setia MS, Jerajani HR, Brassard P, Boivin JF. Clinical and demographic trends in a sexually transmitted infection clinic in Mumbai (1994-2006): an epidemiologic analysis. Indian J Dermatol Venereol Leprol. 2010;76:387-92.
82. Becker M, Stephen J, Moses S, Washington R, Maclean I, Cheang M, et al. Etiology and determinants of sexually transmitted infections in Karnataka state, south India. Sex Transm Dis. 2010;37:159-64.
83. Ramesh BM, Beattie TS, Shajy I, Washington R, Jagannathan L, Reza-Paul S, et al. Changes in risk behaviours and prevalence of sexually transmitted infections following HIV preventive interventions among female sex workers in five districts in Karnataka state, south India. Sex Transm Infect. 2010;86 Suppl 1:i17-24.
84. Ramakrishnan L, Gautam A, Goswami P, Kallam S, Adhikary R, Mainkar MK, et al. Programme coverage, condom use and STI treatment among FSWs in a large-scale HIV prevention programme: results from cross-sectional surveys in 22 districts in southern India. Sex Transm Infect. 2010;86 Suppl 1:i62-8.
85. Mogasale V, Wi TC, Das A, Kane S, Singh AK, George B, Steen R. Quality assurance and quality improvement using supportive supervision in a large-scale STI intervention with sex workers, men who have sex with men/transgenders and injecting-drug users in India. Sex Transm Infect. 2010;86 Suppl 1:i83-8.
86. Jayanna K, Washington RG, Moses S, Kudur P, Issac S, Balu PS, et al. Assessment of attitudes and practices of providers of services for individuals at high risk of HIV and sexually transmitted infections in Karnataka, south India. Sex Transm Infect. 2010;86:131-5.
87. Mishra S, Naik B, Venugopal B, Kudur P, Washington R, Becker M, et al. Syphilis screening among female sex workers in Bangalore, India: comparison of point-of-care testing and traditional serological approaches. Sex Transm Infect. 2010;86:193-8.
88. Mignone J, Washington R, Ramesh BM, Blanchard JF, Rajaretnam T, Moses S. Discrepancies between the self-reporting of STI preventive care and the actual care provided by male doctors to male patients in Karnataka, India. Sex Transm Infect. 2010;86:391-2.

Moving ahead on elimination of Sexually Transmitted Infections (STIs) in WHO South-East Asia Region - progress and challenges 43
Indonesia
89. Prabawanti C, Dijkstra A, Riono P, Hartana G. A survey on HIV-related health-seeking behaviors among transgender individuals in Jakarta, based on the theory of planned behavior. BMC Public Health. 2015;15:1138.
90. Prabawanti C, Bollen l, Palupy R, Morineau G, Girault P, Mustikawati DE et al. HIV, sexually transmitted infections, and sexual risk behavior among transgenders in Indonesia. AIDS Behav. 2011;15(3):663–73.
91. Morineau G, Nugrahini N, Riono P, Nurhayati, Girault P, Mustikawati DE et al. Sexual risk taking, STI and HIV prevalence among men who have sex with men in six Indonesian cities. AIDS Behav. 2011;15(5):1033–44.
92. Mawu FO, Davies SC, McKechnie M, Sedyaningsih ER, Widihastuti A, Hillman RJ. Sexually transmissible infections among female sex workers in Manado, Indonesia, using a multiplex polymerase chain reaction-based reverse line blot assay. Sex Health. 2011;8(1):52–60.
93. Silitonga N, Davies SC, Kaldor J, Wignall S, Okoseray M. Prevalence over time and risk factors for sexually transmissible infections among newly-arrived female sex workers in Timika, Indonesia. Sex Health. 2011;8(1):61–4.
94. Bollen LJM, Anartati AS, Morineau G, Sulami S, Prabawanti C, Silfanus FJ et al. Addressing the high prevalence of gonorrhoea and chlamydia among female sex workers in Indonesia: results of an enhanced, comprehensive intervention. Sex Transm Infect. 2010;86(1):61–5.
95. Majid N, Bollen L, Morineau G, Daily SF, Mustikawati DE, Agus N et al. Syphilis among female sex workers in Indonesia: need and opportunity for intervention. Sex Transm Infect. 2010;86(5):377–83.
96. Magnani R, Riono P, Nurhayati, Saputro E, Mustikawati D, Anartati A. Sexual risk behaviours, HIV and other sexually transmitted infections among female sex workers in Indonesia. Sex Transm Infect. 2010;86(50:393–9.
97. Tanudyaya FK, Rahardjo E, Bollen LJM, Madjid N, Daili SF, Priohutomo S et al. Prevalence of sexually transmitted infections and sexual risk behavior among female sex workers in nine provinces in Indonesia, 2005. Southeast Asian J Trop Med Public Health. 2010;41(2):463–¬73.
98. Mustikawati DE, Morineau G, Nurhayati, Irmaningrum Y, Riono P, Priohutomo S et al. Sexual risk taking, sexually transmitted infections and HIV prevalence among four “high-risk” occupational groups of Indonesian men. Sex Transm Infect. 2009;85(5):391–6.
99. Davies SC, Madjid B, Pardohudoyo S, Agung A, Wiraguna GP, Patten JH et al. Prevalence of sexually transmissible infections (STI) among male patients with STI in Denpasar and Makassar, Indonesia: are symptoms of urethritis sufficient to guide syndromic treatment? Sex Health. 2007.4(3):213–5.
100. Davies SC, Taylor JA, Sedyaningsih-Mamahit ER, Gunawan S, Cunningham AL, Mindel A. Prevalence and risk factors for herpes simplex virus type 2 antibodies among low- and high-risk populations in Indonesia. Sex Transm Dis. 2007;34(3):132–8.

Moving ahead on elimination of Sexually Transmitted Infections (STIs) in WHO South-East Asia Region - progress and challenges44
101. Donegan EA, Wirawan DN, Muliawan P, Schachter J, Moncada J, Parekh M et al. Fluoroquinolone-resistant Neisseria gonorrhoeae in Bali, Indonesia: 2004. Sex Transm Dis. 2006;33(10):625–9.
102. Davies SC, Otto B, Partohudoyo S, Chrisnadarmani VAMA, Neilsen GA, Ciaffi L et al. Sexually transmitted infections among female sex workers in Kupang, Indonesia: searching for a screening algorithm to detect cervical gonococcal and chlamydial infections. Sex Transm Dis. 2003:30(9):671–9.
myanmar
103. Hail-Jares K, Choi S, Duo L, Luo Z, Huang ZJ. Occupational and demographic factors associated with drug use among female sex workers at the China-Myanmar border. Drug Alcohol Depend. 2016;161:42–9.
104. Aung WW, Thant M, Wai KT, Aye MM, Ei PW, Myint T et al. Sexually transmitted infections among male highway coach drivers in Myanmar. Southeast Asian J Trop Med Public Health. 2013;44(3):436–47.
105. Khin-Nwe-Oo, Wah-Wah-Aung, Moe-Thida, Khin-Thet-Wai, Hta-Hta-Yi, Win-Win-Mya. Case-control study of ectopic pregnancies in Myanmar: infectious etiological factors. Southeast Asian J Trop Med Public Health. 2011;42(2):347–54.
106. van Wijngaarden JWdL, Brown T, Girault P, Sarkar S, van Griensven F. The epidemiology of human immunodeficiency virus infection, sexually transmitted infections, and associated risk behaviors among men who have sex with men in the Mekong Subregion and China: implications for policy and programming. Sex Transm Dis. 2009;36(5):319–24.
107. Plewes K, Lee T, Kajeechewa l, Thwin MM, Lee SJ, Carrara VI et al. Low seroprevalence of HIV and syphilis in pregnant women in refugee camps on the Thai-Burma border. Int J STD AIDS. 2008;19(12):833–7.
108. Talikowski L, Gillieatt S. Female sex work in Yangon, Myanmar. Sex Health. 2005;2(3):193–202.
nepal
109. Tamang L, Raynes-Greenow C, McGeechan K, Kirsten A, Black I. Knowledge, experience, and utilisation of sexual and reproductive health services amongst Nepalese youth living in the Kathmandu Valley. Sex Reprod Health. 2017;11:25–30.
110. Deuba K, Karki DK, Shrestha R, Aryal UR, Bhatta L, Rai KK. Risk of HIV infection among men having sex with men in Kathmandu Valley, Nepal. Asia Pac J Public Health. 2014:26(2):126–37.
111. Lam Y, Broaddus ET, Surkan PJ. Literacy and healthcare-seeking among women with low educational attainment: analysis of cross-sectional data from the 2011 Nepal Demographic and Health Survey. Int J Equity Health. 2013;12:95.
112. Johnson D, Chamot E, Lhaki P, Broker TR, Steben M, Shrestha S. Prevalence and correlates of cervico-vaginal clinical syndromes among women attending a health camp in Lalitpur district of Nepal. Kathmandu Univ Med J (KUMJ). 2013;11(44):268–73.

Moving ahead on elimination of Sexually Transmitted Infections (STIs) in WHO South-East Asia Region - progress and challenges 45
113. Jaiswal S, Magar BS, Thakali K, Pradhan A, Gurubacharya DL. HIV/AIDS and STI related knowledge, attitude and practice among high school students in Kathmandu valley. Kathmandu Univ Med J (KUMJ). 2005;3(1):69–75.
114. Ray K, Bala M, Kumari S, Narain JP. Antimicrobial resistance of Neisseria gonorrhoeae in selected World Health Organization Southeast Asia Region countries: an overview. Sex Transm Dis. 2005 32 3:178–84.
115. Christian P, Khatry SK, LeClerq SC, Roess AA, Wu L, Yuenger JD et al. Prevalence and risk factors of chlamydia and gonorrhea among rural Nepali women. Sex Transm Infect. 2005;81(3):254–8.
116. Smith-Estelle A, Gruskin S. Vulnerability to HIV/STIs among rural women from migrant communities in Nepal: a health and human rights framework. Reprod Health Matters. 2003;11(22):142–51.
117. Bista KP, Chaudhary P, Slanger TE, Khan MH. The practice of STI treatment among chemists and druggists in Pokhara, Nepal. Sex Transm Infect. 2002;78(3):223.
Thailand
118. Thisyakorn U. Elimination of mother-to-child transmission of HIV: lessons learned from success in Thailand. J Paediatr Int Child Health. 2017;37(2)99–108.
119. Thato R, Daengsaard, E. Determinants of behavior change intention among heterosexual Thai males diagnosed with sexually transmitted diseases. J AIDS Patient Care STDS. 2016;30(11):512–18.
120. Asavapiriyanont S, Chaovarindr U,Kaoien S, Chotigeat U, Kovavisarach E. Prevalence of Sexually Transmitted Infection in Teenage Pregnancy in Rajavithi Hospital, Thailand. J Med Assoc Thai. 2016;99(Suppl 2):S153–60.
121. Marks MA, Gupta S, Liaw K-L, Tadesse A, Kim E, Phongnarisorn C et al. Prevalence and correlates of HPV among women attending family-planning clinics in Thailand. BMC Infect Dis. 2015;15:159.
122. Asavapiriyanont S, Lolekha R, Roongpisuthipong A, Wiratchai A, Kaoiean S, Suksripanich O et al. Sexually transmitted infections among HIV-infected women in Thailand. BMC Public Health. 2013;13:373.
123. Manopaiboon C, Prybylski D, Subhachaturas W, Tanpradech S, Suksripanich O, Siangphoe U et al. Unexpectedly high HIV prevalence among female sex workers in Bangkok, Thailand in a respondent-driven sampling survey. J Int J STD AIDS. 2013;24(1):34–8.
124. Centers for Disease Control and Prevention (CDC). HIV and syphilis infection among men who have sex with men--Bangkok, Thailand, 2005-2011. MMWR Morb Mortal Wkly Rep. 2013;62(25):518–20.
125. Latimore D, Aramrattana A, Sherman SG, Galai N, Srirojn B, Thompson N et al. Sexually transmitted infection risk behaviors in rural Thai adolescents and young adults: support for sex- and age-specific interventions. J Sex Transm Dis. 2013;40(3):216–20.

Moving ahead on elimination of Sexually Transmitted Infections (STIs) in WHO South-East Asia Region - progress and challenges46
126. Sirivongrangson P, Lolekha R, Charoenwatanachokchai A, Siangphoe U, Fox KK, Jirarojwattana N et al. HIV risk behavior among HIV-infected men who have sex with men in Bangkok, Thailand. J AIDS Behav. 2012;16(3):618–25.
127. Choi YP. Heterogeneous and vulnerable: the health risks facing transnational female sex workers. Sociol Health Illn. 2011;33(1):33–49.
128. Rugpao S, Rungruengthanakit K, Werawatanakul Y, Sinchai W, Ruengkris T, Lamlertkittikul S et al. Risk factors and algorithms for chlamydial and gonococcal cervical infections in women attending family planning clinics in Thailand. J Obstet Gynaecol Res. 2010;36(1):147–53.
129. Decker MR, McCauley HL, Phuengsamran D, Janyam S, Seage GR, Silverman JG. Violence victimisation, sexual risk and sexually transmitted infection symptoms among female sex workers in Thailand. J Sex Transm Infect. 2010;86(3):236–40.
130. Nhurod P, Bollen LJM, Smutraprapoot P, Suksripanich O, Siangphoe U, Lolekha R et al. Access to HIV testing for sex workers in Bangkok, Thailand: a high prevalence of HIV among street-based sex workers. J Southeast Asian J Trop Med Public Health. 2010;41(1):153–62.
131. Sutcliffe CG, Aramrattana A, Sherman SG, Sirirojn B, German D, Wongworapat K et al. Incidence of HIV and sexually transmitted infections and risk factors for acquisition among young methamphetamine users in northern Thailand. J Sex Transm Dis. 2009;36(5):284–9.
132. van Wijngaarden JWdL, Brown T, Girault P, Sarkar S, van Griensven F. The epidemiology of human immunodeficiency virus infection, sexually transmitted infections, and associated risk behaviors among men who have sex with men in the Mekong Subregion and China: implications for policy and programming. J Sex Transm Dis. 2009;36(5):319–24.
133. Rugpao S. Women’s reports of condom use in Thai couples under intensive and regular STI/HIV risk reduction counseling. AIDS Behav. 2008;12(3):419–30.
134. Plewes K, Lee T, Kajeechewa L, Thwin MM, Lee SJ, Carrara VI et al. Low seroprevalence of HIV and syphilis in pregnant women in refugee camps on the Thai-Burma border. J Int J STD AIDS. 2008;19(12):833–7.
135. Celentano DD, Sirirojn B, Sutcliffe CG, Quan VM, Thomson N, Keawvichit R et al. Sexually transmitted infections and sexual and substance use correlates among young adults in Chiang Mai, Thailand. J Sex Transm Dis. 2008;35(4):400–5.
136. Turner AN, Morrison CS, Padian NS, Kaufman JS, Behets FM, Salata RA et al. Male circumcision and women’s risk of incident chlamydial, gonococcal, and trichomonal infections. J Sex Transm Dis. 2008;35(7):689–95.
137. Prempree P, Detels R, Ungkasrithongkul M, Meksawasdichai S, Panthong S, Ungpanich V et al. The sources of treatment of sexually transmissible infections in a rural community in central Thailand. J Sex Health. 2007;4(1):17–9.
138. Sirivongrangson P, Bollen LJM, Chaovavanich A, Suksripanich O, Virapat P, Tunthanathip P et al. Screening HIV-infected women for cervical cancer in Thailand: findings from a demonstration project. J Sex Transm Dis. 2007;34(2):104–7.

Moving ahead on elimination of Sexually Transmitted Infections (STIs) in WHO South-East Asia Region - progress and challenges 47
139. Sirivongrangson P, Bollen LJM, Chaovavanich A, Suksripanich O, Jirarojwat N, Virapat P et al. Sexually transmitted infection services as a component of HIV care: findings of a demonstration project among HIV-infected women in Thailand. J Acquir Immune Defic Syndr. 2006;41(5):671–4.
Sri lanka
140. Samarawickrema NA, Tabrizi SN, Young E, Gunawardena P, Garland SM. Prevalence of Trichomonas vaginalis, Chlamydia trachomatis, Neisseria gonorrhoeae and human papillomavirus in a sexual health clinic setting in urban Sri Lanka. Int J STD AIDS. 2015;26(10):733–9. doi: 10.1177/0956462414552813.
141. Jayawardena KA, Silva KT, Jayawardena CK, Samarakoon S. Behavioural risk factors of men associated with transmission of sexually transmitted infections (STIs) in Sri Lanka. WHO South East Asia J Public Health. 2012;1(1):69–75. doi: 10.4103/2224-3151.206916.

noTeS
.............................................................................................................................................................
.............................................................................................................................................................
.............................................................................................................................................................
.............................................................................................................................................................
.............................................................................................................................................................
.............................................................................................................................................................
.............................................................................................................................................................
.............................................................................................................................................................
.............................................................................................................................................................
.............................................................................................................................................................
.............................................................................................................................................................
.............................................................................................................................................................
.............................................................................................................................................................
.............................................................................................................................................................
.............................................................................................................................................................
.............................................................................................................................................................
.............................................................................................................................................................
.............................................................................................................................................................
.............................................................................................................................................................
.............................................................................................................................................................
.............................................................................................................................................................

acknowledgement
The support provided by Dr Richard Steen and Dr T L N Prasad in collection and analysis of STI data from countries for this report is duly acknowledged. We also acknowledge the contribution by WHO country office focal points for STI in getting the required information from national programme

South East Asia RegionWorld Health HouseIndraprastha Estate, Mahatma Gandhi MargNew Delhi 110 002, IndiaPhone: 011 2337 0804
ISBN: 978-92-9022-734-2




















