a cross sectional study of sexually transmitted infections
151
A CROSS SECTIONAL STUDY OF SEXUALLY TRANSMITTED INFECTIONS AMONG HIGH RISK GROUPS ATTENDING SEXUALLY TRANSMITTED INFECTIONS CLINIC IN A TERTIARY CARE HOSPITAL Dissertation Submitted to THE TAMILNADU DR.M.G.R. MEDICAL UNIVERSITY IN PARTIAL FULFILMENT FOR THE AWARD OF THE DEGREE OF DOCTOR OF MEDICINE IN DERMATOLOGY, VENEREOLOGY & LEPROSY Register No.: 201730256 BRANCH XX MAY 2020 DEPARTMENT OF DERMATOLOGY VENEREOLOGY & LEPROSY TIRUNELVELI MEDICAL COLLEGE TIRUNELVELI -11
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of a cross sectional study of sexually transmitted infections
A CROSS SECTIONAL STUDY OF SEXUALLY TRANSMITTED INFECTIONS
AMONG HIGH RISK GROUPS ATTENDING SEXUALLY TRANSMITTED
INFECTIONS CLINIC IN A TERTIARY CARE HOSPITAL
Dissertation Submitted to
THE TAMILNADU DR.M.G.R. MEDICAL UNIVERSITY
IN PARTIAL FULFILMENT FOR THE AWARD OF THE DEGREE OF
DOCTOR OF MEDICINE
IN
DERMATOLOGY, VENEREOLOGY & LEPROSY
Register No.: 201730256
BRANCH XX
MAY 2020
DEPARTMENT OF DERMATOLOGY VENEREOLOGY & LEPROSY
TIRUNELVELI MEDICAL COLLEGE
TIRUNELVELI -11

CERTIFICATE
This is to certify that this dissertation entitled “A CROSS SECTIONAL STUDY OF
SEXUALLY TRANSMITTED INFECTIONS AMONG HIGH RISK GROUPS
ATTENDING SEXUALLY TRANSMITTED INFECTIONS CLINIC IN A TERTIARY
CARE HOSPITAL.” is a bonafide research work done by Dr.VIJAIKUMAR M.G,
Postgraduate student of Department of Dermatology, Venereology and Leprosy,Tirunelveli
Medical College during the academic year 2017 – 2020 for the award of degree of M.D.
Dermatology, Venereology and Leprosy – Branch XX. This work has not previously formed
the basis for the award of any Degree or Diploma.
Guide
Dr.M.Selvakumar M.D. D.D.,Associate Professor,Department of DVL
Head of the Department
Dr.P. Nirmaladevi. M.D.,Professor& HOD,
Department of DVLDepartment of Dermatology, Venereology & Leprosy
Tirunelveli Medical College,Tirunelveli
Dr.S.M.Kannan M.S.Mch.,
The DEAN
Tirunelveli Medical College,
Tirunelveli - 627011

DECLARATION
I solemnly hereby declare that the dissertation entitled “A CROSS SECTIONAL STUDY OF
SEXUALLY TRANSMITTED INFECTIONS AMONG HIGH RISK GROUPS
ATTENDING SEXUALLY TRANSMITTED INFECTIONS CLINIC IN A TERTIARY
CARE HOSPITAL” was done by me at the Department of Dermatology, Venereology &
Leprosy, Tirunelveli Medical College under the guidance and supervision of my Professor.
Dr.M.Selvakumar. The dissertation is submitted for the Degree of Doctor of Medicine in
M.D., Degree Examination, Branch XX in DEPARTMENT OF DERMATOLOGY,
VENEREOLOGY AND LEPROSY.
This is my original work and the dissertation has not formed the basis for the award of
any degree, diploma, associate ship, fellowship or similar other titles. It had not been
submitted to any other university or Institution for the award of any degree or diploma.
Place: Tirunelveli
Date:
Dr.VIJAIKUMAR.M.G.Register No.: 201730256
Post graduate in M.D DVL,Department of DVL,
Tirunelveli Medical College,Tirunelveli-627011

ACKNOWLEDGEMENTLanguage with all elaborations seems to be having limitation especially when it comes
to expression of feelings. It is not possible to convey it in words all the emotions and feelings
one wants to say. It would take pages to acknowledge everyone who, in one way or another
has provided me with assistance, but certain individuals deserve citation for their invaluable
help.
I am grateful to the Dean, Dr.S.M.Kannan MS MCh., Tirunelveli Medical College
and Medical Superintendent, the Tirunelveli Medical College Hospital for allowing me to do
this dissertation and utilize the institutional facilities.
I fall short of words to express my deep sense of gratitude for my esteemed and reverend
teacher, Dr. P.Nirmaladevi MD, my professor & Head of the Department of Dermatology,
Venereology and Leprosy , Tirunelveli Medical College, for her ever-inspiring guidance and
personal supervision. The finest privilege in my professional career has been the opportunity
to work under her inspirational guidance.
I would like to express my sincere and heartfelt thanks to Dr.M. Selvakumar M.D.,
Head of department of Venereology, who has been a guiding light with his constant
encouragement throughout my post-graduation course. I am honoured to have got an
opportunity to be his student during my tenure at this prestigious institute.
I sincerely thank Dr.P.Sivayadevi MD., and Dr.K,Punithavathi MD., Associate
Professors for their valuable suggestions and support throughout the period of this study.
My special thanks to Dr. Seeniammal.S, Assistant Professor for having guided me with
full support throughout the period of this study.
I immensely thank Dr.R.Karthikeyan (late), Dr.A.N.M.Maalik Babu MD, Dr.S.Judith
Joy MD, Dr.P.Kalyanakumar DDVL, Dr.M.Kalaiarasi DDVL, Dr.A.Kamala Nehru DDVL,
my assistant Professors for their constant support and encouragement.

I heartfully thank my seniors Dr.K.Amuthavalli and Dr.P.Sulochana, my colleague
PGs Dr.S.Soundharyaa moorthi, Dr.P.Karthikraja, Dr.M.Aravind Baskar,
Dr.B.Arunkumar, Dr.R.Monisha and friends for their encouragement and support during this
study.
I heartfully thank my family, friends, seniors and junior colleagues for their
involvement for completing this study.
Last but definitely not the least, I would like to thank my patients who cooperated with
me throughout my work. Finally, it is endowment of spiritualism and remembrance of almighty
for all that I achieved. I owe my sincere thanks to all those patients who participated in the
study for their co-operation which made this study possible. Finally, I thank the Almighty for
without Him nothing would have been possible.


CERTIFICATE-II
This is to certify that this dissertation titled “A CROSS SECTIONAL STUDY OF
SEXUALLY TRANSMITTED INFECTIONS AMONG HIGH RISK GROUPS
ATTENDING SEXUALLY TRANSMITTED INFECTIONS CLINIC IN A TERTIARY
CARE HOSPITAL” of the candidate Dr.VIJAIKUMAR M.G with registration number
201730256 for the award of degree of M.D. Dermatology, Venereology and Leprosy. I
personally verified the urkund.com website for the purpose of plagiarism check. I found that
the uploaded file contents from introduction to conclusion page shows 20 percentage of
plagiarism in the dissertation.
Guide & Supervisor sign with seal


CONTENTS
SL.NO. TITLE PAGE NO.
1. INTRODUCTION 1
2. REVIEW OF LITERATURE 3
3. AIMS AND OBJECTIVES 59
4. MATERIALS AND METHODS 60
5. RESULTS 62
6. DISCUSSION 87
7. CONCLUSION 96
8. BIBLIOGRAPHY
9. ANNEXURES
PROFORMA CONSENT FORM
10. MASTER CHART

1
INTRODUCTION
Sexually transmitted infections (STI’s) remains to be a most important
health problem all over India. The prevalence of disease is not even in
community, as behavioural pattern differs among individuals. High risk group
population are more commonly affected with STI’s. Men who have sex with men
(MSM), Commercial Sex Workers (CSW), transgenders (TG), people with
multiple partners, occupation related group like drivers, housekeepers, drug
abusers and migrants are all included under high risk group. It is more and more
felt that these sections of population are especially vulnerable because of their
lack of information, defiance, poor socioeconomic factors, lack of social support,
unprotected measure and other factors.
High-risk sexual behaviour people are those who are having unprotected
sex with partner(s) during sexual intercourse.1 The behavioural risk factors
include age at first intercourse, marital status, frequency of sexual intercourse,
number of lifetime partners, age difference between partners, intravenous drug
abuse, etc. These risk factors augment the increased risk of developing STI’s and
create a great problem at the community level.
High risk sexual practices include oro-anal intercourse, oro-genital
intercourse, ano-genital, dry sex, sex during menstruation, etc.2 Non-usage of
barrier contraceptives are at risk of STI’S including HIV. Safer sex practices like
condom usage is been encouraged by all organizations including NACO for
reducing the STI risk.
2
More than 20 different bacteria, viruses and parasitic infections are
responsible for sexually transmitted infections. Sexual history is very important
for a healthcare provider for proper diagnosis and treatment. He can also advise
on risk reduction by providing prevention counselling. Prevention counselling is
an effective method, if given in an imagined manner to the people's principles,
linguistic, sex, sexual orientation and developmental level. counselling is usually
advised to all sexually active persons who had diagnosed as diseased or who had
STI in the past or who had multiple sex partners. Another major problem that
arose was an increase in adolescent sexual activity in the mid-20th Century. This
led to widespread infection among adolescents and also changed the way for
healthcare policy makers to raise awareness through campaigns.
There is bigger need for detection of STIs, primarily where there is high
concentration of high-risk group, as early diagnosis and treatment can lead to
decrease in complications and reduce the transmission at the community level.
3
REVIEW OF LITERATURE
HISTORY OF STI
Sexually transmitted infections represent a chief public health problem.
STI’s are the cause of acute illness, long term disability, death in men, women
and infants, with tremendous economic consequences at individual and
community level. STIs were previously known as Venereal diseases. Due to the
social stigma of these diseases in the 1970s, the name was changed to Sexually
Transmitted Diseases. Recently, it has been discussed that ‘disease’ is not the
most appropriate term to describe infections, which may remain asymptomatic
for many years or would never develop symptoms. Therefore, the World Health
Organization has suggested instead the use of sexually transmitted infections for
the group of infectious diseases transmitted by sexual activity.3
HUMAN SEXUAL BEHAVIOUR
Human Sexual behavior means broad spectrum of behaviors in which
humans display their sexuality. These behavioral expressions contain biological
elements, cultural influences and sexual arousal (with its physiological changes,
both pronounced and subtle, in the aroused person). It varies from the solitary
(such as autoerotic stimulus and masturbation) to joined sex (genital intercourse,
oral sex, anal sex, non-penetrative sex, etc.) that is involved occasionally.

4
THEORIES OF HUMAN SEXUALITY
Sexual behavior is considered as an inborn energy in the humans: it is even
seen in newborns. Sex drive is altered by various factors like communal, social
and interpersonal factors. Freud ‘s (1905) stages of sex includes the oral stage,
the anal stage, the genital stage, the latency stage and the reawakening of sexual
impulses at puberty.4 Sexuality has a number of different characteristics and
senses depending on variation in person, time, culture, age, and situation.
Sexuality is a part of social collaboration and best explained by opportunity and
reinforcement acting upon a basic biological force. The sexual behavior is
strongly channelized into particular cultural backgrounds. This enforced the
humans to follow traditional sexual behavior patterns which are practiced by
thousands of years ago. Human sexual behavior should be viewed with three
aspects in mind: the biological factors, the learning processes, and finally the
sociocultural environment. The variations in sexual behavior among individuals
is due to various civilizations exists between various groups of individuals in
different places in the world.
CONCEPT OF SEXUAL DEVIANCE
Deviance (psycho-pathology) is the sexual behavior that breaks the
customs and principles of the humanity. The psychopathology is defined as
medical rationalization of the social conditions like homosexuality. Because of
concept of deviance, these individuals will have social stigma, which causes
negative influence in the lives of these deviants (homosexuals).

5
Gagon et al5 proposed a distinction between 3 types of deviance.
1) Normal deviance - The sexual behaviors such as premarital sex, extra
marital sex, masturbation, and oro-genital sex.
2) subcultural deviances - homosexual subcultures
3) individual deviances - exhibitionism or incest
PREVALENCE
About 340 million new cases of the four curable sexually transmitted
infections -gonorrhoea, chlamydia, syphilis, and chancroid are recorded every
year in the world, according to the World Health Organization (WHO).6 National
prevalence of early syphilis cases was 2.1 cases per 1lakh population in the year
2000 and 2001. The rising trend of syphilis has been primarily due to increased
cases among MSM, bisexual and CSW. The increase in syphilis among women
is of associated with an apparent increase in congenital syphilis.7
During 2016–2017, gonorrhoea rate among males increased from 169.7 to
202.5 cases per 100,000 males and the rate among females increased from 120.4
to 141.8 cases per 100,000 females.8 During 2008–2017, the number of reported
cases ranged from 28 in 2009 to six in 2014. Reported cases of chancroid peaked
in 1947 and then declined quickly through 1957, presumably due to the increasing
use of antibiotics like sulphonamides and penicillin. Numerous localized
epidemics, some of which were linked to commercial sex work were identified
during the year 1981–1990.9

6
Prevalence of genital infection with any HPV was 42.5% among adults
aged 18–59 years during 2013–2014. Persistent infection with some HPV
serotypes can cause cervical cancer and recurrent genital warts. HPV serotypes
16 and 18 account for approximately 66% of cervical cancers and approximately
25% of low-grade and 50% of high-grade cervical dysplasia in India.
Genital HSV infection is not a nationally notifiable condition. The overall
percentage of HSV-2 seropositive individuals aged 14–49 years between 1988–
1994 and 2007–2010 remained high-90.7% and 87.4% respectively and most of
them do not report to doctors as it is self-limiting on its own.9
Trichomonas vaginalis is a common sexually transmitted protozoal
infection associated with adverse health consequences such as preterm birth and
symptomatic vaginitis. Prevalence of T. vaginalis in urine specimens obtained
from adults aged 18–59 years was 0.5% among males and 1.8% among females.
MEN WHO HAVE SEX WITH MEN
Bisexual persons may choose persons of both sexes. Homosexual persons
usually choose a sexual partner of the same sex. Homosexual can describe a
person‘s sexual behavior- i.e., a person who predominantly or exclusively has sex
with a person or persons of the same sex 10 and they are termed as - men who
have sex with men‖(MSM). Homosexual can describe a person ‘s sexual identity
– i.e., a person who adopts a sexual life style which is consistent with and self-
defined by same sex desire and same sex behavior can be said to have a
homosexual identity. A man who considers himself homosexual may also have

7
sex with women and men who consider themselves heterosexual may also have
sex with men. Thus, a man who prefers same sex partner may be considered as
homosexual and men who prefers opposite sex partners are referred to as
heterosexual. But if the heterosexual persons have sex with a same sex partner,
they are referred broadly by “MEN WHO HAVE SEX WITH MEN” and
“WOMEN WHO HAVE SEX WITH WOMEN”. Thus, MSM includes both
Homosexuals and Bisexuals.11
HISTORY OF HOMOSEXUALITY:
Homosexual practices played an important role for man in ancient Greece
and other cultures, whereas they have been ritualized and prohibited in various
societies. The term homosexual was first coined by the Hungarian physician
Karoli Maria Kertbeny in 1869 and was later adopted by the influential German
psychiatrist Richard Von Kraft Ebing in his classic Psychopathia Sexualis. It is
often thought that the Greeks were liberal in their attitudes to homosexual and
bisexual behavior. The roman also have accepted homosexuality as a foreseeable
part of man’s sexual life. Julius Caesar was called as the husband of all women
and the wife of all men. Priapus the God of gardens, with a human face was
associated with fertility and thus hostile to homosexual rights.
Kamasutra written by sage vatsayana in 4th to 5th century A.D. contains
an entire topic on homosexuality. In western countries, in 18th century,
homosexual subcultures arose, that allowed people to consider themselves as
being homosexual or Gay such subcultures allowed them to exclusively access
8
male partners. These subcultures allow gay people to live in almost exclusively
gay context with gay doctors, lawyers, accountants, churches and other
businesses catering to them.11
Due to stigmatization and unacceptability of the society, such way of living
was not acceptable as openly as in western countries. In the Asian context, it must
also be noted that unlike many western countries where sexuality and
reproduction are not considered separate issue, the duty of reproduction and issue
of sexual preferences are often entirely separate. Thus, while some persons who
consider themselves as homosexual, they are still likely to get married because of
family compulsions and ethnicities. As a result, the majority of homosexual
people are likely to be married and seek their homosexual contacts secretly
outside the marriage.
Male-to-male sex work is also a significant factor in India cities, where
kothis/hijras, ‘massage boys’, male youth and other males will sell sex to men
because of poverty and unemployment. Without a welfare system, and with
unemployment or low-level incomes, male sex work can be a way out in terms of
supporting the self and family.12
All urban areas have sexualized spaces, such as parks, toilets, railway and
bus stations, specific bazaars, streets, and other public areas where kothis and
hijras would meet potential giryas/panthis, marketing sexual availability through
their feminized social behaviours. Many ‘real men’ also go to these sites, where
they can get caught up “in the heat of moment” and access kothis and hijras there

9
at the time. Such activities play a very important role in the spread of sexually
transmitted infections and HIV/AIDS in this society. Sexual behavioural studies
in India have classified homosexual as anything from 1% of the sexually active
mens to nearly 28% of the occasionally homosexually behavioural males.
In the Indian subcontinent, the most prominent groups are
HIJRAS – transgendered MSM, regarded as a ―third sex. They are often
castrated, dressed as women and are part of a clearly identified social
groups, which is endured by society but sometimes feared as well.
KOTHIS – also called as METIS in Nepal, these are MSM who adopt a
feminine lifestyle but who nevertheless may be married and father of
children.
PANTHIS – also called as Ta in Nepal, these are masculine men who
although live as ordinary males in the community sometimes have insertive
sex with Kothis. They do not have self-identity but are nick-named Panthis
by the Kothis.
DOUBLE DECKERS – mens who were both receptive and insertive
partners.
SEXUAL ROLE BEHAVIOR AMONG MSM
Men change their sexual partners in a number of different contexts and
nowadays increasingly through internet as the world is quickly changing in all its
aspects. They practice variety of sexual practices such as frottage, oro- genital,
oro -anal, penile-anal intercourse, they may likewise use unique techniques of

10
sado-masochism and water sports. Barebacking is the term used for unprotected
anal sex without condom usage and it is practiced by some MSMs who feel
decreased sexual pleasure. These sexual practices are at increased risk of
transmission of HIV and other STIs.13
Homosexuals with anal intercourse can play either the insertive or
receptive role. This produces three role subgroups of men: insertive, receptive
and versatile as opposed to the two role categories of male and female in
heterosexual intercourse. This changes population transmission dynamics, and
the impact depends on the prevalence of each role and the relative transmission
probabilities of insertive and receptive sex.
REASONS FOR HIGH PREVALENCE OF STIS IN MSM
BIOLOGICAL
Semen with higher load of HIV - trauma to anal mucosa
Penis is penetrative organ and transmit semen
Highly receptive columnar epithelial surfaces are involved in Male to
Male sex:
Rectal mucosa, Anorectal squamous-columnar junction, Oropharyngeal
and tonsillar mucosa, Urethral meatal mucosa, Inner surface of prepuce,
SOCIOLOGICAL
Myths and unawareness about male homosexuals-e.g., in countries where
HIV spread is generally heterosexual, many men believe sex with men is
safer.
11
Barrier protection will not prevent reproduction, so condom use is rare.
Illegality discourages open expression of male to male love or sexual
behavior.
Societal stigmatization directly discourages regular open rapport between
two males.
Societal stigmatization thus indirectly encourages multiple casual
partners.
STUDIES OF STI PREVALENCE AND SEXUAL BEHAVIOUR DONE
IN INDIA
A study done in Delhi proposed the percentage of STI among MSM were
33.3%.14 A study at Puducherry showed the prevalence of STI among
MSM as 1.2% with increased prevalence among heterosexuals than
MSM.15
A different sexual behavior survey in Uttar Pradesh reported
approximately 54% of male respondents showed same sex behavior during
their lifetime.16
One study done in rural villages reported that nearly 10 percent of single
men and 3 percent of married men engaged in same sex behavior. 17
Another study conducted at a drop-in center for MSM in Mumbai
disclosed that nearly 23% of MSM were married and that being married
was actually associated with a much higher risk of being HIV positive
(23.8% for married men vs. 9.1% for others).18

12
In 2001 a study from Chennai, analysis of 51 MSM who attended a
community-based survey over a period of three months showed the
following outcomes. Thirteen (26%) MSM were clinically diagnosed to
have one or more STDs. Clinically the following pattern of STDs was
found: Perianal warts - 4 (8%), Genital Herpes - 4 (8%), Perianal herpes -
1 (2%), Secondary syphilis - 1 (2%), Gonococcal urethritis - 1 (2%),
Molluscum contagiosum - 1 (2%), Proctitis - 2 (4%), Scabies - 1 (2%) and
Prostatitis - 1 (2%). Genital dermatoses like Candidal intertrigo - 4 (8%),
Candidal balanoposthitis - 1 (2%), Perianal candidiasis - 1 (2%) and Tinea
cruris were also found. Seven (14%) self-reported as HIV-positive.
COMMERCIAL SEX WORKER
Commercial sex worker or prostitute or call-girl is an individual who
offers sexual service for money or other needs. They are seen in brothels, bars,
parlors and night clubs. They have increased rates of partner adjustment, poor
access to health care, increased duration of contact to infection, and so sexual
contact with CSW is a significant factor for transmitting STI. Sexual intercourse
in exchange for payment is known as prostitution.19 Prostitution is prohibited and
punishable by death in some countries, while completely legal in others.
Due to social stigmatization, prostitutes may also be called as commercial
sex worker’, ‘female sex worker’ or ‘sex trade worker’. Male coordinators of
prostitution are known as pimps. Female coordinators are known as madams.
Places where prostitution take place are called the brothels. These are often

13
located in ‘red light areas’ in big cities like (G.B. road) New Delhi, (Budhwar
peth) Pune, (Sonagachi) Kolkata, (Kamath Pura) Mumbai.
Travelling to lots of poorer nations in search of sexual facilities that is
unavailable or expensive or punishable in one’s own country is sex tourism.
Prostitutes are often defamed in all societies and religion, but their customers are
defamed to a minor extent. Prostitutes have more STIs and abortions, so they can
easily become sterile, but most of them still become pregnant and give birth to
children. An estimated 85% of all prostitutes in Calcutta and Delhi enter the sex
work at an early age.19
HISTORY OF CSW
India has history of prostitution as a profession. In vedic texts prostitutes
were mentioned as ‘loose women’, ‘female vagabonds’ and ‘sadbarani’.
Prostitutes wore red costumes and jewels in vedic times to scare demons as they
live in a wicked zone.
The devadasi system was a ritual in India by 300 AD. In this system,
unmarried girls are dedicated to Hindu temples, where they are used as objects of
sexual pleasure. In the eighteenth century, during the British period there were
many reports of prostitution in large cities. During recent times, prostitution was
not considered as a shameful profession.
Recent data regarding population of brothel-based women is 6000 in
Kolkata. 20 Exact number of sex workers in India would be hard to estimate
because of the secret nature of sex business and their extensive distribution.

14
Present data reveals decreased sexual practices and routine lifestyle of sex
workers has been reduced. The data of these studies revealed that prostitutes had
low standard of living in a depreciated and soiled environment. Pimps, madams
and investors share major portion of their payment. Majority of them are infected
by different STIs irregularly. They usually visit local quacks for seeking health
services who will charge them hugely for treatment, as they may not use
government health facilities due to fear of prejudice.
FACTORS INDUCING WOMEN TO BECOME PROSTITUTES IN
INDIA
When the family and marital life of these CSW fail due to many reasons,
the woman would not be having any confidence on her life. Various reasons of
prostitution are lack of sex education, prior sexual exploitation, bad peer group,
ignorance, acceptance of prostitution, abuse by husband and widowed young
woman.
THEORIES OF PROSTITUTION
1. FUNCTIONALISM: Prostitution is functional for several parties in
society. It provides prostitutes a source of income, and it provides a sexual
alternative for men who lack a sexual partner or are dissatisfied with their
current sexual partner. According to Kingsley Davis, prostitution also
helps keep the divorce rate lower than it would be if prostitution did not
exist.

15
2. CONFLICT THEORY: Prostitution arises from women’s poverty in a
male-controlled society. It also reflects the continuing cultural treatment of
women as sex objects who exist for men’s pleasure
3. SYMBOLIC INTERACTIONISM: Prostitutes and their customers have
various understandings of their behaviour that help them justify why they
engage in this behaviour. Many prostitutes believe they are performing an
important service for their customers, and this belief is perhaps more
common among indoor prostitutes than among street prostitutes. 21
STUDIES COMPARISON
In a study conducted in Chennai, among 248 commercial sex workers,
46.8% were 35 years or more, 59% were educated and 56% were married.
Most of the FSWs (92%) were from different locality. The age at first
sexual intercourse was below 18 years in 48 % of them. In the period of
one month, 30% clients asked for anal sex and 25% of them accepted that
mode of sex too. Consistent condom usage was found in 16%. 27% were
alcoholics and among them, 91% had habit of consumption before sexual
act.22
In a study from Andhra Pradesh, 2005-2006, 3200 female sex workers
were included in the study with following results- 70% were uneducated,
50% were married and 41% of them had sex work as the lone source of
income.23
16
In India, high prevalence states of HIV are Andhra Pradesh, Tamil Nadu,
Karnataka, Maharashtra, Manipur and Nagpur. These states provide 63%
of the total HIV infected persons in whole India.
In a study done in Mexico among 924 FSWs, the prevalence of HIV
infection was 6%, gonococcal infection was 6.4% , chlamydial infection
was 13%, and syphilis was 14.2%.24
According to a ten year study done in Pune, 34% reported regular condom
usage, 52% reported irregular condom usage, 14% had never used condom
among FSW’s. 25
TRANSGENDERS
Transgender have a gender identity or gender appearance that differs from
their own sex. Transgender often called as trans, is also an umbrella term: in
addition to with people whose gender identity is the reverse of their assigned sex
-trans men and trans women. It may include people who are not completely
manly or womanly. Some call transgenders as a third gender. The
word transgender may be defined broadly as cross-dressers. Being transgender is
independent of sexual orientation. Transgender may identify them as
heterosexual, homosexual, bisexual, asexual or may decline to label their sexual
orientation. The opposite of transgender is cisgender, which defines persons
whose gender identity or appearance matches with their assigned sex.
Many transgender experience gender dysphoria, and some search for
medical treatments such as hormone replacement therapy, sex reconstructive
17
surgery, or psychotherapy. Not all transgender desire these modalities and some
cannot undergo these for financial or medical reasons. Many transgender face
discriminations in the workplace and in accessing public accommodations and
healthcare services.
In India, April 2014, the Supreme Court of India declared transgender to
be a 'third gender' in Indian law. Justice KS Radhakrishnan noted in his decision
that, "Seldom, our society appreciates or cares to realize the trauma, agony and
pain which the members of Transgender community suffer, nor appreciates the
innate feelings of the members of the Transgender community, especially of those
whose mind and body disown their biological sex".
They are facing lots of difficulties in the society and have poor quality of
living life as they are not supported with financial support nor from their families.
So, they are forced into high risk sexual practices for money and to survive in the
community. As they are indulged with high risk practices, the chance of STI’s
among them and among the community has increased.
STUDIES RELATED
A 2017 paper used meta-analysis and synthesized national surveys to
estimate that nearly 1 million persons in the United States were transgender. From
2009-2014, 2351 transgenders received an HIV diagnosis in the United States.
84% were transgender women, 15% were transgender men and less than 1% had
another gender identity. Around half of transgenders 43% of transgender women;

18
54% of transgender men who received an HIV diagnosis lived in the South
regions.26
A study conducted in Australia in 43 participants showed 24% of TG and
35% of MSM positive for various STI; chlamydia was detected in 19% of samples
and gonorrhoea in 9% samples. Of the 39 participants tested for syphilis, 3% were
positive and there were no detected cases of HIV.27
A study by Tamilselvan in India, revealed 120 transgenders and they were
all male to females. Almost 46.6% (56) of transgenders belonged to age group
21-30, 25% (30) to 11-20 and 30-40 and 3.4% were >40 years. All of them had
multiple sex partners at certain point of time, of which 25% (31) are now
dedicated to a single partner and 15% (19) were involved in commercial sex. The
safe sexual practice was followed by 68% (84). Among sexual practices, oral
intercourse contributed 97.3% (117), anal 92% (110.4), finger 9% (11), thigh 6%
(7) and vaginal route 24% (28.8). Of 120 patients, 63.3% (76) had infectious
diseases, 42.5% (51) had non-infectious diseases, and 5.9% (7) had both.
RECREATIONAL DRUG USE
Rates of drug usage such as cigarette smoking, alcohol and substance abuse
are higher in MSM when compared to the normal general population. This makes
a potential impression on HIV infected MSMs:
This kind of lifestyle is associated with other high-risk behavior.
Increase risk of atherosclerotic disease and carcinomas which are related
with smoking are compounded by HIV infection.

19
Illicit drug use for-Crack, cocaine, crystal, and methamphetamine lead to
unsafe sexual practices.
Self-injecting the drugs in unsterile manner cause HIV transmission and
hepatitis.
Co-infection with hepatitis causes rapid progression of the disease.
This risky lifestyle will cause poor intake of antiretroviral therapy (ART)
and other medications.
Certain recreational drugs like sildenafil may disturb metabolism of
prescribed drugs.
There is relationship between alcohol and sex among MSM. Alcohol use
serve a unique function in the lives of MSM. Alcohol use among gay and
bisexual men can be a reaction to social marginalization resulting from
their sexual orientation and may be associated with other mental health
issues such as depression, anxiety, and substance use disorders.
Four domains were identified that described the role of substance use in sexual
encounters:
Motivators, Allowers, Rationalizers, Facilitators.
A study of substance uses among HIV-positive MSM found that nearly all
(90%) of the men used drugs to enhance sexual pleasure, and that drug use dulled
negative feelings about living with HIV. A study done in Delhi, 62.4% of IDUs
inject drugs >5 years; whereas in Punjab, it was only 32.4%. The overall HIV
positivity in Delhi and Punjab was 18.3% and 21.2%, respectively. Delhi, the

20
highest HIV positivity is found among the IDUs whose duration of injecting drug
is from 6 months to 1 year (34.5%). In Punjab, the highest positivity is found
among the IDUs who are injecting drugs for more than 5 years (33.5%). In both
the states, the positivity among the IDUs whose frequency of drug use once a
week or less has the maximum positivity; 24.9% in Punjab and 50% in Delhi. 28
OCCUPATIONAL RISK BEHAVIOURS
Occupation is one of the socio-demographic factors, which not only act as
a risk factor for acquiring STI’s but also as a factor of spread of acquired
infection. Major characteristics include:
a high prevalence of unprotected anal intercourse among manual labourers.
increased prevalence of STI’s among truck drivers and housekeepers
a high prevalence of unprotected vaginal intercourse with concurrent alcohol
use and sex with females among hospitality workers
high prevalence of STI’s among salesman and professional industries
people who frequently change their places- migrants
Most individuals are introduced to their sex partners through social
interactions in formal and informal institutional places that work as sex
marketplaces. A study in the United States of America, most individuals meet
long-term buddies through social relations in high school, college or the
workplace, while casual partners are often met through informal sex marketplaces
such as public house and nightclubs. Working in the manual labour and
hospitality industries was related with more sexual risk behaviours than people

21
working in the sales, retail and skilled industries. Those working in manual labour
had higher rate of unprotected anal sex in the past two months than those working
in the hospitality, retail, sales and skilled industries.29 There is a theory that
variance stressors in the work settings by type of occupation lead to sexual risk
behaviours. Conversely, the sexual market structure and social status changes by
sector can be seen as serious factors increasing the possibility of sexual health
liabilities.
A study in India showed that 28% of total STI’s were attributed to unskilled
profession and 50% to job requiring frequent travel. This can be attributed to
widespread unemployment resulting in poverty thereby indulging in various sex
practices and development of various STI’s.30
SEXUALLY TRANSMITTED INFECTIONS AMONG HIGH RISK
GROUPS:
A wide range of microorganisms depend upon human genital tract and
sexual behavior for their survival. More than 20 pathogenic organisms, including
HIV are sexually transmissible and are responsible for high degree of mortality
and morbidity.
It includes,
Syphilis
Gonorrhea
Chancroid
Chlamydia

22
Lymphogranuloma Venereum
Granuloma inguinale
Herpes
Molluscum contagiosum
Warts
Hepatitis B and C
HIV/AIDS
Balanoposthitis
Scabies
Trichomonas vaginalis
Bacterial vaginosis
Vulvovaginal candidiasis 31
Most important concern is the rise of resistance to drugs in these organisms. It
makes the organism more lethal and harder to treat.

23
BACTERIAL INFECTIONS
SYPHILIS
Syphilis caused by the bacteria Treponema pallidum with incubation
period is 9 to 90 days. From a low of fewer than 4 cases of syphilis per one lakh
population in the year 2000, the syphilis incidence has now raised to more than 6
cases per one lakh population.32 Events of active disease occur, followed
by latent periods, where the patient remains infected without signs or symptoms.
Initially syphilis has painless ulcer where the infection entered generally around
the genitals, anus or mouth and may remain unseen. The ulcer is known as a
chancre and this stage is called as primary syphilis. Extensive rash and flu-like
symptoms appear next, which is known as secondary syphilis. If left untreated,
tertiary syphilis develops years later and cause a variety of problems affecting the
brain, eyes, heart and bones.
Syphilis cases are increased among MSM, CSW, persons having multiple
sex partners with unprotected sexual intercourse. Syphilis ulcers are commonly
seen over genitals and anal area but may also be seen on the lips or mouth. Hence,
vaginal, anal or oral sex is the key way of transmitting the infection from one
person to another. Both men and women are equally at risk of syphilis. The
peak incidence rises among the age of 16 and 35 years.

24
PRIMARY SYPHILIS
Approximately 9 to 90 days after the first exposure a skin lesion, called
a chancre, develops at the site of contact. This is classically a single, firm,
painless ulcer with a clean base and sharp borders around 0.5–3.5 cm in size.33 In
the classic form, it evolves from macule to papule and finally to
an ulcer. Occasionally, presents with multiple lesions when coinfected with
HIV. Lesions may be painful in 30% and they may occur at extragenital site (2–
7%). The most common site in women is the cervix (44%),penis in heterosexual
men (99%), anus and rectum in MSM (34%). Lymphadenopathy occurs
frequently (80%) at the site of infection and it occurs 7 to 10 days after chancre
formation. Chancre redux is form of relapsing syphilis in which a chancre appears
at the site of the original infection. It should not be confused with Pseudochancre
redux, in which a tertiary syphilitic gumma develops at the site of the original
chancre. 34
SECONDARY SYPHILIS
Patient is highly infectious during this stage. If chancre left untreated or
treatment was unsuccessful, approximately 3 weeks to 3 months after the 1st
stage, an extensive skin rash develops. Rash may be subtle or appear as reddish-
brown papules or patches. It typically occurs over the trunk and frequently affects
palms and soles not associated with itching. It spontaneously resolves within
weeks to months. Corymbose syphilis describes a central plaque surrounded by
cluster of erythematous papules (resembling a flower). Patchy alopecia over

25
frontal and occipital area. Mucous patches over mouth, throat, genital area,
vagina and anus. Greyish-white moist raised broad based flat topped lesions over
the groin, inner thighs, armpits, perianal region called as condyloma lata.33 Other
symptoms include fever, fatigue, myalgia, headache, joint pains and swollen
lymph glands. Other organs like liver, kidneys, central nervous system and eyes
also affected.
EARLY LATENT (<2 YEARS OF CONTACT)
The patient is infectious at this stage and can transmit the infection to the
partner. Usually there is no signs on clinical examination whereas,
treponemal antibody tests will be positive.
LATE LATENT SYPHILIS (>2 YEARS OF CONTACT)
Patient is non-infectious. Usually there is no signs on clinical examination
whereas, treponemal antibody tests will be positive.
TERTIARY SYPHILIS
Tertiary syphilis may occur roughly 3 to 15 years after the initial infection,
and may be divided into three forms: Gummatous stage
(15%), neurosyphilis (6.5%), and cardiovascular syphilis (10%).35 Tertiary
syphilis patients are not infectious.
Gummatous syphilis or late benign syphilis usually occurs 1 to 45 years
after the primary infection, with an average of 15 years. This stage consists of
chronic gummas, which are soft and vary much in size. They classically affect
the skin, liver, and bone.

26
Neurosyphilis may occur early, being either symptomless or in the form
of meningitis, or late as meningovascular syphilis, general paresis, or tabes
dorsalis, which is associated with poor balance and lightning pains in the lower
limbs. Late neurosyphilis typically occurs 4 to 25 years after initial
infection. There may be Argyll Robertson pupils in which accommodation reflex
is present but light reflex absent.
Cardiovascular syphilis occurs 10–30 years after the primary infection.
The common complication is syphilitic aortitis, associated with aortic
aneurysm development.
A study in India with a total of 124 patients were VDRL reactive, of which
33 (2.25%) were false positive cases and TPHA was reactive in 91 cases (6.22%).
Totally, 91 (6.22%) cases were diagnosed as syphilis. Out of 91 cases, 78
(85.71%) were males and 13 (14.29%) were females. Primary syphilis was
detected in 21 (13.08%), secondary in 38 (41.76%), and latent in 32 (35.16%)
patients. Mixed infection was detected in 7 patients and 8 (8.79%) were HIV
positive. 36
CONGENITAL SYPHILIS
Congenital syphilis can be prevented by treatment before 16 weeks
gestation. The risk to the foetus is high with early untreated maternal syphilis. In
the first few weeks of life it resembles secondary syphilis including vesicle and
bulla, scaly rash, mucous patches and condyloma lata, Snuffles, bone changes,
hepatomegaly and lymphadenopathy are common. Late congenital syphilis

27
affects eyes (interstitial keratitis), ears, joints and CNS. The characteristic signs
include Hutchinson's teeth, typical facial appearance and bowed sabre shins ,
higoumenakis sign, saber shin, or Clutton's joints among others.37
In 2012, an estimated 9,30,000 maternal syphilis infections caused
3,50,000 bad pregnancy outcomes, including 143,000 early fetal
deaths/stillbirths, 62,000 neonatal deaths, 44,000 preterm/low weight births and
102,000 infected infants. Nearly 80% of adverse outcomes occurred among ANC
attendees. From 2008 to 2012 estimates, maternal and congenital syphilis
decreased by 38% (560,000 and 226,000 cases respectively). Despite these
declines, maternal syphilis still causes considerable adverse pregnancy outcomes,
even among women attending ANC. 38
SYPHILIS AND HIV
In the past five years the relation between HIV and syphilis has become
interesting issue for debate and research. As syphilis is an ulcerative sexually
transmitted disease, people with syphilis are at high risk transmitting and
acquiring HIV.39
The clinical presentation of syphilis in HIV patients are
Primary syphilis: bigger, tender multiple ulcers
Secondary syphilis: more genital ulcers with high titres of RPR and
VDRL.
More chance for neurosyphilis.

28
Out of the total 110 patients with syphilis, 27 (24.5%) patients were
seropositive for HIV-1. Of the 27 HIV-positive cases, 18 were diagnosed as
secondary syphilis, 5 were primary, and 4 patients were diagnosed as latent
syphilis. Thirteen patients (48.1%) with HIV co-infection presented with
condyloma lata and two of the HIV-positive patients had persistent generalized
lymphadenopathy.40
TREATMENT GUIDELINES
The diagnosis of syphilis is done by the using dark field microscopy.
Serological non-treponemal tests like VDRL and RPR tests are done. The
commonly used confirmatory test is Treponema Pallidum Hemagglutination Test
(TPHA). Inj. Benzathine Penicillin G single dose given for early syphilis whereas
three doses should be given to late stage of syphilis and persons co-infected with
HIV. Regular follow up is needed at 3, 6, 9, 12, and 24 months post treatment. A
fourfold decline in titre at 6 months after injection is considered as good treatment
response.
GONORRHOEA
Gonorrhoea, colloquially known as the clap, is a sexually transmitted
infection caused by the Neisseria gonorrhoeae, a gram negative
bacteria. Infection may involve the genitals, mouth, and rectum.41 Its incubation
period varies between 1-14 days, with an average 2-5 days. For men in the
community, the prevalence rate varies from 1.7-2.1% and in STI clinics it ranges
from 8.5-25.9%.42

29
Infected Males
Inflammation of the urethra
Creamy or green pus-like discharge from the penis; blood can also be
present
Painful urination
Painful testicles
There are no symptoms at all in 10–15% of men. Rectal symptoms include rectal
pain, pharyngitis that may cause mild to severe difficulty in swallowing may also
occur in MSM with oro-receptive and oro-insertive. Gonococcal infection can be
transmitted by infected fingers to the eyes causing unilateral conjunctivitis with
severe inflammation and a yellowish discharge.
A study by El-Gammel et al, a total of 475 patients over a period of 1 year
attended the study. The subjects were screened for both gonorrhoea and
chlamydia with polymerase chain reaction and Gram's stain using specimens
from the urethral discharge. Out of 475 patients, 125 (26.3%) had gonorrhoea, 47
(9.8%) had chlamydia, and 11 (7.31%) had both diseases. This emphasizes that
co-occurrence of chlamydia and gonorrhoea may be common among males
presenting with urethral discharge.
Infected Females
Often there are no symptoms until the infection has progressed to a more
advanced stage
Creamy or green, pus-like or bloody vaginal discharge

30
Infants
If not treated, gonococcal ophthalmia neonatorum will develop in 28% of
infants born to women with gonorrhoea.
Complications
Ascending infection in the urogenital tract in men, causing painful
inflammation of epididymis and prostate
Urethral scarring in men – possible decreased fertility or bladder-outlet
obstruction
Scarring of the upper reproductive tract in women with PID – possible
infertility, chronic pelvic pain, ectopic pregnancy
Neonatal infection and miscarriage from gonococcal infection in pregnant
women
Systemic involvement such as dermatitis, arthritis, septicaemia,
meningitis, conjunctivitis, pneumonitis, Fitz-Hugh Curtis syndrome,
watercan perineum, perihepatitis.
Treatment guidelines
The gonorrhoea can be diagnosed by gram stain, culture, and PCR.43
The suggested treatment for uncomplicated gonococcal infection is Inj.
Ceftriaxone 250mg I.M stat (or) Azithromycin 2grams stat when
associated with Chlamydial infection .44

31
Antimicrobial susceptibility testing of N. gonorrhoeae isolated in Pune
during the past decade was characterized by high rates of resistance to penicillin
and ciprofloxacin. Cefixime is the first-line drug recommended under syndromic
management of STIs according to the NACO guidelines for treatment of
gonorrhoea. However, emergence of less susceptible strains to ceftriaxone and
cefixime have been reported from WHO regional and reference centre, Delhi
which highlights the importance of routine monitoring antibiotic resistance.
Results of the study support the current recommendations of NACO for use of
third-generation as the first-choice drugs for treatment of gonorrhoea in India.45
NONGONOCOCCAL URETHRITIS (NGU)
Non gonococcal urethritis is an inflammation of the urethra that is not
caused by gonorrhoeal infection.
Symptoms
For men symptoms are discharge from the penis, burning or dysuria,
itching, irritation, increased frequently or tenderness. In women, symptoms are
discharge from vagina, burning or pain during urinating. Abdominal pain or
abnormal vaginal bleeding are indication that the infection has advanced to Pelvic
Inflammatory Disease.
Causes of NGU
Infectious
The most common bacterial cause of NGU is Chlamydia trachomatis, but it can
also be caused by Ureaplasma urealyticum, Haemophilus vaginalis, Mycoplasma

32
genitalium, Mycoplasma hominis, Gardnerella vaginalis, and E.coli. Viruses like
Herpes simplex virus, Adenovirus, Cytomegalovirus .Fungus like Candida
Albicans .Parasite like Trichomonas vaginalis (rare)
Noninfectious
Urethritis can be caused by mechanical injury from a urinary catheter or
a cystoscope or by an irritating chemical like antiseptics or spermicides.
Diagnosis
This can be confirmed by demonstration of polymorphonuclear leucocytes
(PMNL) this can be done by (i) gram stain of urethral discharge should contain
>5 PMNL per high power microscopic fields.46 (ii) positive leucocyte esterase
test on first voided urine. (iii) gram stain of centrifuged sample of first passed
urine should contain >10 PMNL per high power microscopic fields.
Treatment guidelines
Most cases respond to traditional therapy for NGU with
Cap.Doxycycline 100 mg twice a day orally for 7 days or Azithromycin 1 g stat
orally once.
A Thailand study with 237 male urethritis patients were included with GU
and NGU found in 120 (52.9%) and 107 (47.1%) of patients, respectively.
Recurrent urethritis was found in 23.8% of patients and HIV infection was
identified in 11.6%.47

33
CHANCROID
Chancroid is a sexually transmitted infection caused by fastidious gram-
negative bacteria Haemophilus ducreyi. It is characterised by painful ulcers on
the genitals and painful swollen lymph glands. The incubation period ranges from
1 to 14 days. 48
Signs and Symptoms
The ulcer size ranges from 3 to 50 mm. The ulcer is painful, sharply
defined borders with undermined edges. Its base is covered with a grey or
yellowish-grey material and bleeds on manipulation.
dysuria and dyspareunia in females.
Painful swollen lymph nodes occurs in 30 to 60% of patients.
The swollen inguinal lymph nodes and abscesses are often referred to
as buboes.
Common sites
In males , Internal and external surface of prepuce, Coronal sulcus, Frenulum
,Shaft of penis, Preputial orifice, Urethral meatus, Glans penis, Perineum area
In females, Labia majora is most common site. "Kissing ulcers" may develop.
These are ulcers that occur on opposing surfaces of the labia, Labia minora,
Fourchette, Vestibule, Clitoris, Perineal area, Inner thigh.
Clinical variants 49
They are Dwarf chancroid, Giant chancroid, Follicular chancroid, Transient
chancroid, Serpiginous chancroid, Mixed chancroid, Phagedenic chancroid.

34
Diagnosis
Gram stain shows “school of fish appearance”. (ii) culture shows small
non-mucoid yellowish semi opaque colonies appear 2 to 4 days after inoculation.
Studies show that molecular techniques can detect the presence of H. ducreyi
DNA in clinical sample. M-PCR and nested single tube PCR techniques are more
sensitive than standard methods. This can be extremely useful in designing
appropriate syndromic management algorithm for genital ulcer.49
Treatment guidelines
The CDC(2006) guidelines for chancroid is 1 gram of azithromycin stat or
single IM dose (250 mg) of ceftriaxone or erythromycin 500 mg three
times a day orally for 7 days, or oral 500 mg of Ciprofloxacin twice a day
for 3 days.
The buboes should be aspirated, incision and drainage should not be done.
LYMPHOGRANULOMA VENEREUM
Lymphogranuloma venereum (LGV) (also known as Climatic bubo ,
Durand–Nicolas–Favre disease , Lymphogranuloma inguinale and tropical
bubo)50 is a sexually transmitted disease caused by the invasive serovars L1, L2,
L2a, L2b or L3 of Chlamydia trachomatis. incubation period is 3 to 12 days.
Signs and Symptoms 50
The clinical manifestation of LGV depends on the site of entry of the infectious
organism (the sex contact site) and the stage of disease progression.
35
Inoculation at the mucous lining of external sex organs (penis and vagina)
can lead to the inguinal syndrome named after the formation of buboes
or abscesses in the groin. These signs usually appear from 3 days to a
month after exposure.
The rectal syndrome arises if the infection takes place via the rectal
mucosa and is mainly characterized by proctocolitis.51
The pharyngeal syndrome is rare.
Stage 1
Small painless papule appears.
Ulcerates, heals and disappears within a few days and may go unnoticed
Stage 2
Most male patients present during this stage
About 2-6 weeks after the 1st stage painful and swollen inguinal lymph
glands (buboes) develop on one (most common) or both sides of the
groin.in 20% femoral lymph nodes separated by Poupart’s ligament from
enlarged inguinal lymph node producing “GROOVE SIGN OF
GREENBLATT “
Women may present with lower abdominal or back pain (deep pelvic node
involvement).
Other symptoms include malaise, fever, chills, joint and muscular pain and
vomiting.

36
Stage 3
Most female patients present during this stage with fever, pain, itch, pain
on passing stools and urinating, and pus-filled or bloody diarrhoea.
Chronic inflammation may lead to abscesses fistulas, lymphatic
obstruction, rectal strictures and proctocoliltis.
Chronic infection may result in severe scarring causing major deformation
of the genitals.
A Quebec study with 338 cases of LGV, all cases were male, excluding
one transsexual. Most were MSM (99%). 83% reported four sexual partners or
more in the last year, met mostly through the Internet (77%). 83% were HIV-
infected. Recreational drug use was frequent (57%). 52
Treatment guidelines
The diagnosis usually is made serologically (complement fixation) and
Recently a fast Realtime PCR (TaqMan analysis) has been developed to
diagnose LGV.
Treated with Doxycycline 100mg orally bd x 3 weeks or Erythromycin
500mg orally qid x 3 weeks 53
DONOVANOSIS
Granuloma inguinale is a bacterial disease caused by Klebsiella
granulomatis (formerly known as Calymmatobacterium granulomatis)
characterized by genital ulcers. It is also known as granuloma
inguinale, granuloma inguinale tropicum, granuloma venereum, granuloma

37
venereum genitoinguinale, lupoid form of groin ulceration, serpiginous
ulceration of the groin, ulcerating granuloma of the pudendum, and ulcerating
sclerosing granuloma.54
Signs and Symptoms
After contracting the infection, it may take from 1 week to 3 months for any
signs and symptoms to appear. There are several types of lesions that may occur
and symptoms are mild.
The nodular type consists of soft lumps that are typically beefy red in
colour and tend to bleed easily. These are usually painless
despite ulceration.
The hypertrophic or verrucous type consists of large dry warty masses
that resemble genital warts.
The necrotic type presents as dry ulcers that evolve into scarred areas.
A study in Durban, South Africa showed 171 patients with donovanosis in
which Ulcers were present for longer than 28 days in 72 (55.4%) men and 19
(46.3%) women. 95 (55.6%) came from rural areas.55 This shows ulcers are most
common presentation in donovanosis.
Treatment guidelines
The main method of diagnosis is the demonstration of Donovan bodies in
a tissue sample taken by crush preparation or biopsy. Other tests such
as culture, polymerase chain reaction (PCR) or serology are not routinely
available.

38
The recommended regimen is azithromycin 1gram oral/iv once per week,56
alternatively doxycycline 100 mg bd orally or ciprofloxacin 750 mg bd orally
or erythromycin 500 mg orally four times a day or trimethoprim-
sulfamethoxazole one double-strength (160 mg/800 mg) tablet orally twice a day.
BACTERIAL VAGINOSIS
Bacterial vaginosis is a common cause of abnormal vaginal discharge and
malodour in women. Some women have similar findings on vaginal wet
mount and culture but do not have any symptoms. Bacterial vaginosis affects
women of reproductive age. The organisms
like Gardnerella, Bacteroides, Peptostreptococcus and Mobiluncus species
shows over growth.57 These are anaerobic bacteria, that is, they grow in the
absence of oxygen.
Risk factors include vaginal douching, multiple sex partners, antibiotics,
and using an intrauterine device.
According to a study in Nepal, of total 160 cases of vaginal discharge, BV
was seen in 24.4% patients. BV in unmarried women were at higher risk (100%
tested positive) compared to married women (24.2%). Several studies have
documented the occurrence of BV in sexually inactive females or virgins. This
provides support that sexual activity is not a prerequisite for BV. The change in
lifestyle, improper perineal care, food habits, tight clothing, lack of attention
towards menstrual hygiene, and sedentary factor might be the reasons for the
acquisition of BV in unmarried women.58

39
Signs and Symptoms
Common symptoms consist of increased vaginal discharge that usually has
fishy odour. The discharge is white or grey in colour. There may be burning with
urination.59 Occasionally, they are symptomless. The discharge coats the walls of
the vagina, and is generally without irritation, pain, or erythema although
mild itching can sometimes occur.
BV increases the risk of other sexually transmitted infections,
including HIV/AIDS.60 Complications like miscarriage, pre-term delivery, Low
birth weight, Premature rupture of membrane, postpartum endometritis, vaginal
cuff endometritis, Pelvic inflammatory disease and abortions can occur.
BV and HIV
Normally Lactobacilli produce H2O2 which is toxic to HIV, in BV
lactobacilli is reduced. In BV vaginal pH is increased which activates CD4
lymphocytes and become target cells for HIV. BV has also been shown to
increase intravaginal levels of IL-10 which increases susceptibility of
macrophage to HIV.
Treatment guidelines
Clinically BV can be diagnosed using the Amsel criteria 61
Thin, white, homogeneous discharge.
Clue cells on microscopy
pH of vaginal fluid >4.5

40
Release of a fishy odour on adding alkali -10% potassium
hydroxide (KOH) solution.
At least three of the four criteria should be present to confirm the diagnosis.
Gram stain
An alternative is to use a Gram-stained vaginal smear the Nugent criteria.
A score of 0-10 is obtained from combining three other scores. The scores are
as follows:
0–3 is negative for BV
4–6 is intermediate
7+ is indicative of BV.
At least 10–20 high power (1000× oil immersion) fields are counted and an
average determined. Upon examination of 160 nonpregnant women with
symptomatic vaginal discharge, the overall prevalence of BV was 24.4% based
on Nugent’s scoring system.58
Treatment is Metronidazole 400 mg BD orally for 7 days (or)
Metronidazole 2gms single oral dose. Nearly 30% of patients have recurrence of
symptoms within 3 months.62

41
VIRAL INFECTIONS
HERPES GENITALIS
Herpes simplex is one of the commonest genital infections all over the
world. There are two types of herpes simplex virus (HSV); type 1, which is mostly
associated with facial infections and type 2, which is primarily genital, although
there is overlap.
HSV causes lifelong infection with possible reactivation or recurrence.
People often refer only to HSV-2 when discussing genital herpes but both types
can lead to infection in the genital area. Clinically, about 60–70%
of primary genital infections are due to HSV-2 whereas the rest is due to HSV-1.
Primary genital herpes infection
Primary or first genital HSV infections may be mild and unseen, but should
lesions develop, the severity is usually more than in recurrences.
Genital ulceration from herpetic infection is the most common complaint
seen in sexual health clinics. The ulcers are common over the glans,
foreskin and shaft of the penis. They are painful and last for 2 to 3 weeks,
if untreated. The local lymph glands are enlarged and become tender 63.
In women, lesions occur over the external genitalia and mucosae of
the vulva, vagina and cervix. Pain and difficulty in passing urine are
common symptoms.
Some people also have flu-like symptoms like fever, headache and myalgia.
Symptoms tend to be severe in women than in men.

42
Recurrent genital herpes infection 64
After the primary infection, there may be no further clinical manifestations
throughout life. Recurrences are more frequent with type 2 genital herpes than
with type 1.
Recurrences can be triggered by:
Trauma.
Ultraviolet radiation (sun).
Other infections.
Menstruation (flare-ups may occur before period).
Emotional stress.
Recurrent infections differ from primary infections in that the vesicles are
usually smaller in size. They also tend to be of shorter period than the primary
infection, usually 5-7 days.
These produce shallow ulcers, over the glans or shaft of the penis in men
and on the labia, vagina or cervix in women. Recurrences can cause painful
symptoms or the lesions can be unnoticed. Lesions usually heal within 7–10 days
without scarring.
Complications of genital herpes
Urethritis.
Proctitis, rectal pain, watery discharge,
and autonomic nerve dysfunction that may produce difficulty in passing
urine.65

43
Neurogenic pain over leg and thigh pain. This often leads to recurrence.
esophagitis, encephalitis retinitis, thrombocytopenia, mollarets'
meningitis.
Widespread infection.
HSV and HIV
Clinically the lesions are atypical, large often haemorrhagic, deep painful
ulcers with raised margins. Other atypical lesions include hyperkeratotic
verrucous lesions vegetating plaques and a zosteriform appearance.
A study by Chopra et al showed 8 (16%) HIV positive women and 4 (8%)
HIV negative women with genital ulcers among 50 patients. Herpes genitalis was
the cause of genital ulcers in 5 (10%) HIV positive women and 3 (6%) HIV
negative women, trailed by syphilis in 3 (6%) HIV positive women and 1 (2%)
HIV negative women. This shows increased incidence of herpes genitalis among
HIV infected people.(66)
Diagnosis &Treatment guidelines
Tzanck smear, biopsy, blood test for antigen and culture are useful
diagnostic tools. Culture remains the Gold Standard.
Treated with Oral acyclovir 200mg 5 times daily (or) 400mg 3 to 4 times
daily till clinical resolution attained (7-10 days) (or) Famciclovir 500mg twice
daily x 5-10 days (or) valacyclovir 1 g daily x 5-10 day.(67)
A study by Maharajan et al showed 90 clinically diagnosed herpes genitalis
cases, confirmed by Tzanck test and were divided into 3 groups of 30 patients

44
each which were applied topical ZnSO 4 in concentrations of 1%, 2% and 4%
respectively over a period of 3 months. Ten patients of group 1 (1% ZnSO 4)
showed recurrence, 6 patients in group 2 (2% ZnSO 4) and only one patient in
group 3 (4% ZnSO 4) showed recurrence. No serious side effects were
noted. Thus, topical ZnSO 4 has been found to be an effective treatment for
increasing remissions in herpes genitalis. Topical 4% ZnSO 4 has been found to
be most successful out of the three concentrations.68
MOLLUSCOM CONTAGIOSUM
Molluscum contagiosum (MC), also called as water warts or Bateman
disease. Molluscum contagiosum is caused by a poxvirus, the molluscum
contagiosum virus. There are 4 viral subtypes.69
A study was done in Pondicherry for comparing the incidence of genital
MC among children and adults, which showed 14.5% in children and 23% in
adults signifying increased risk of genital MC among sexually active adults.70
Mode of transmission:71
Direct skin-to-skin contact
Sexual transmission in adults.
Indirect contact through shared towels or other items
Auto-inoculation into another site by shaving or scratching.
Signs and Symptoms
Molluscum contagiosum lesions are pearly dome shaped umbilicated waxy
papules with 1–5 mm in diameter.72 Molluscum lesions commonly found on the

45
face, arms, legs in children. Adults classically have MC lesions in the genital
region and this is considered to be a sexually transmitted infection. Because of
this, if children have genital lesions then sexual abuse should be suspected. These
lesions are commonly not painful, but they may be associated with itching or
become irritated. Picking or scratching the lesions may lead to a spread of the
infection, an additional bacterial infection, and scarring. In about 10% of the
cases, eczema develops around the lesions.
Molluscum and HIV
Between 10% to 30% of patients with symptomatic HIV disease have
molluscum contagiosum. MC2 is common in adult men and patients with HIV
infection. The lesions in HIV will be giant(>1cm), multiple (upto 100),
distributed over face, including the eye lids and ears, neck and in intertriginous
areas. In homosexual men the lesions are often seen in ano-genital area. It is
important to differentiate it from keratoacanthoma, cryptococcosis,
histoplasmosis and penicilliosis.
Incidence of MC in HIV infected persons is 5-18%. In patients with CD4
count <200 cells/mm 3, incidence increases to 25-35%. Unusual morphological
variants including giant, tumour like nodular lesions (>1 cm), necrotic lesions,
abscesses, polypoidal or pseudo cystic variants and cutaneous horn have also
been described in HIV seropositive patients.73

46
Treatment guidelines
Molluscum is usually diagnosed by its typical clinical appearance.
Molluscum bodies can often be expressed from the centre of the umblicated
papules. Sometimes, the diagnosis is made by skin biopsy. Histopathology shows
typical intracytoplasmic inclusion bodies.74
There is no single perfect treatment of molluscum contagiosum since we
are currently unable to kill the virus. Physical treatments include needling,
Cryotherapy, Gentle curettage or electrodessication, Laser ablation. Medical
treatments include 10% KOH, Podophyllotoxin cream, salicylic acid ,
Cantharidin solution, cimetidine.75 Imiquimod cream and sinecatechins can be
used but are unproven.
GENITAL WARTS
Anogenital wart is the common superficial skin infection in an anogenital
area that is caused by human papillomavirus (HPV).76 Anogenital warts also
known as condyloma acuminata, genital warts and squamous cell papilloma.
They are generally due to HPV types 6 and 11.
An anogenital wart is a skin coloured papule a few millimetres in diameter.
Warts may join together to form plaques. They may occur in the following sites
like vulva, vagina, corona , prepuce, scrotum, perianal region.77 Warts due to the
same types of HPV can also occur over oral mucosa.
Transmission of warts 78
Sexual contact. This is the most common way among adults.

47
Transmission is likely from visible warts than from subclinical HPV
infection.
Oral sex.
Vertical transmission.
Auto inoculation from one site to another.
Fomites.
HPV and HIV
HIV infected patients have multiple lesions and diffuse involvement of the
anogenital areas. They develop very large genital warts and these become locally
invasive and destructive.79 These tumours are called giant condylomas (or)
BuschkeLowenstein tumours. They do not cause metastasis, but carry a
significant risk of transformation into squamous cell carcinoma. In vitro studies
have revealed that intracellular HIV-1 tat m RNA can transactivate HPV type 16
E6 & E7 an action that is significant in the development of squamous cell
carcinoma. Women with HIV infection appear to be at increased risk for HPV
and related cervical intra epithelial neoplasia.
Treatment guidelines
Genital warts are usually identified clinically. Biopsy is sometimes
necessary to confirm the diagnosis of viral wart or to diagnose an associated
carcinoma.
Treatment for external genital warts includes application of liquid
Nitrogen, Podophyllin 25%, TCA 90%, 5% Imiquimod (or) Podofilox gel 0.5%.80

48
HEPATITIS B & C
Hepatitis B & C is an infectious disease caused by the hepatitis B & C
virus (HBV) that affects the liver.81 It can cause both acute and chronic
infections. Many people have no symptoms during the initial infection. It is 50 to
100 times more infectious than human immunodeficiency virus (HIV). Possible
forms of transmission include sexual contact, blood transfusions and transfusion
with other human blood products, re-use of contaminated needles and syringes,
and vertical transmission from mother to child (MTCT) during childbirth.
Acute viral infection
Symptoms are generally mild and vague, and may include
fatigue, nausea and vomiting, fever, muscle or joint pains, abdominal
pain, decreased appetite and weight loss, jaundice occurs in ~25% of those
infected), dark urine, and clay-coloured stools
Chronic viral infection
Chronic infection after several years may cause cirrhosis or liver cancer.
Liver cirrhosis may lead to portal hypertension, ascites (accumulation of fluid in
the abdomen), easy bruising or bleeding, varices (enlarged veins, especially in
the stomach and oesophagus), jaundice, and a syndrome of cognitive impairment
known as hepatic encephalopathy. Ascites occurs at some stage in more than half
of those who have a chronic infection.

49
Treatment guidelines
HBsAg (Hepatitis B surface antigen) can be present in acute and chronic
HBV infection. Its presence for greater than six months is suggestive of chronic
infections. Anti-HCV indicates prior exposure or infection. PCR for HCV
particles is the most specific test.
Alpha interferon and pegylated interferon slow the replication of the virus
and stimulate immune clearance of the virus. Other effective drugs include
lamivudine, adefovir, entecavir, and telbivudine.
SCABIES
Scabies is an itchy rash caused by a parasitic mite that burrows in the skin.
The human scabies mite's scientific name is Sarcoptes scabiei var. hominis.82
Scabies affects families and communities worldwide. It is most common
in children, young adults and the elderly. Factors leading to the spread of scabies
include Poverty and overcrowding, Institutional care (rest homes, hospitals,
prisons, Refugee camps), immune deficiency or that are immune suppressed, Low
rates of identification and proper treatment of the disease.
Transmission
Scabies is nearly always acquired by skin-to-skin contact with someone else
with scabies.
The contact may be quite brief such as holding hands with an infested
child.
It is sometimes sexually transmitted.

50
Occasionally scabies is acquired via bedding or furnishings.
Signs and Symptoms
The characteristic symptoms of a scabies infection include
intense itching and superficial burrows.83 It is almost diagnostic of the disease. It
involves wrist, inner aspect of arm and forearm, axilla, nipple, umbilicus and
genitals called as “CIRCLE OF HEBRA”.
Scabies and HIV
The clinical features of scabies in the HIV positive patients are often
determined by the degree of immune suppression. As the immunity decreased
(CD4+cells <200/ µL) the more contagious forms of scabies called crusted
scabies (Norwegian (or) hyperkeratotic) become apparent. These patients may
harbour millions of scabies mites. 84
Treatment guidelines
The diagnosis of scabies is made by history and physical findings. Rarely,
lesions can be scraped and mite or mite feces identified by microscopy under oil
immersion.
Treatment is with Permethrin cream 5% applied overnight and
Oral ivermectin 200 mcg/kg is convenient. Rare complications include seizures.
Some experts recommend repeat treatment at 1 week.

51
VULVOVAGINAL CANDIDIASIS
Vulvovaginal candidiasis refers to vaginal and vulval symptoms caused by
a yeast, most commonly Candida albicans.85 It affects 70% of women on at least
one occasion over a lifetime.
Risk factors for VVC are due to increased usage of antibiotics, Oral
contraceptive pills, vaginal douching, IUCDs and tight dresses.
Signs and Symptoms 86
Itching, burning and soreness in the vagina and vulva.
pain when passing urine (dysuria)
Vulval oedema and fissures.
Dense white curdy vaginal discharge
Pustules over inner and outer parts of the vulva, sometimes spreading
widely in the groin to include pubic areas, groin and thighs.
Centres for Disease Control and Prevention had classified VVC:
1. Uncomplicated
Sporadic or infrequent
Mild to moderate VVC
Likely to be candida albicans
Immunocompetent women
2. Complicated 87
Recurrent VVC
Severe VVC

52
Non candida albicans
women with uncontrolled diabetes mellitus or immunosuppression or
pregnant
Treatment guidelines
Diagnosis of VVC depends upon demonstration of pseudo hyphae from
vaginal discharge in 10% KOH mount, culture and PCR. Treatment is by oral
Fluconazole
150mg stat and topical 2% Clotrimazole cream.88
TRICHOMONAS VAGINALIS
Trichomoniasis is an extremely common, sexually
transmitted infection (STI) caused by the protozoan parasite, Trichomonas
vaginalis.89 Females can acquire the disease from infected males or females; but
males usually acquire it only from infected females. The incubation period is
generally between 4 and 28 days. Trichomoniasis is a marker of high-risk sexual
behaviour. Co-infection with other STIs is common, especially Chlamydia
trachomatis and Neisseria gonorrhoeae. It serves as a “TROJAN HORSE”.
Signs and Symptoms
In men it can display symptoms of urethritis. 'Frothy', greenish vaginal
discharge with a 'musty' malodorous smell is characteristic. Only 2% of women
with the infection will have a "strawberry" cervix (colpitis macularis, an
erythematous cervix with pinpoint areas of exudation) or vagina on

53
examination.90 This is due to capillary dilation as a result of the inflammatory
response.
Complications of T. vaginalis in women include: preterm delivery, low
birth weight, and increased mortality as well as predisposing
to HIV infection, AIDS, and cervical cancer. T.vaginalis has also been reported
in the urinary tract, fallopian tubes, and pelvis and can
cause pneumonia, bronchitis, and oral lesions. Condoms are effective at
reducing, but not wholly preventing, transmission. Trichomonas
vaginalis infection in males has been found to cause
asymptomatic urethritis and prostatitis.
Treatment guidelines
Diagnosis is done by demonstration of organism in wet mount of vaginal
discharge, phase contrast microscope, culture, immunological and molecular
methods.
According to CDC 2006 guidelines recommended treatment is
Metronidazole 2 g orally single dose or Metronidazole 500 mg twice orally for 7
days. Sex Partner should be treated and avoid sex till completion of the
treatment.91

54
BALANOPOSTHITIS
Balanitis is inflammation of the glans penis. When the foreskin is also
affected, it is called as balanoposthitis.92
Etiology
Irritation by environmental substances, trauma, and infection such as
bacterial, viral, and fungal. Some of these infections are sexually
transmitted diseases.93
It is less among people who are circumcised as in many cases the prepuce
contributes to the disease. Both not enough cleaning and too much
cleaning can cause complications. Diabetes can make balanoposthitis
more likely, especially if the blood sugar is poorly controlled.
Signs and Symptoms
First signs – small red erosions over glans
Redness of the prepuce.
Erythema of the penis.
Other rashes on the head of the penis
Foul smelling sub preputial discharge
Painful prepuce and penis.
Treatment guidelines
To determine the factors contributing to balanoposthitis, a swab may be
taken for bacterial and yeast culture. Urethral cultures may be necessary and
occasionally, serological tests for syphilis and diabetes. In persistent cases,

55
a skin biopsy is appropriate to determine whether there is an underlying skin
disease or carcinoma.
Treatment modalities consist of Astringent compresses using dilute vinegar
(1% acetic acid ), Burrow's solution (aqueous solution of aluminium acetate)
or potassium permanganate, Topical antifungal medication, Topical antiseptic
or antibiotic, Mild topical steroid. Depending on culture, an oral antifungal
and/or an oral antibiotic may be prescribed. In refractory
cases, circumcision may be necessary to prevent recurrence.
HUMAN IMMUNO DEFICIENCY VIRUS (HIV)
HIV is the etiological agent of AIDS which belongs to the lentivirus
subgroup of family retroviridae. HIV is a RNA virus, a cytopathic virus. 2 major
types are HIV1 and HIV 2. There are three groups of HIV1 group "M" (major),
group "O" (outlier) and group "N. The M group consists of eight subtypes A, B,
C, D, F, G, H and J and as well as four major circulating recombinant forms.
Host factors
The cell surface receptor for HIV-1 is CD4 differentiation antigen. CD4 is
expressed on T helper lymphocytes and less on Dendritic cell, Macrophages and
microglial cells. Another receptor called "galactosyl ceramide" can also serve as
a receptor for HIV in glial and neuroblastoma cell lines. The CC- Chemokine
receptor - 5 (CCR-5) is considered as main coreceptor used by macrophage -
trophic HIV -1 strains. The role of CCR-2 is not well-known.

56
During the early stage, virus propagates mostly in peripheral blood
mononuclear cells. HIV infection usually elicits strong cell mediated immune
response (CD8 + Cytotoxic T-cells) which helps to clear the high viral load but
fail to eradicate HIV infection. During asymptomatic period, virus is active in
lymphoid tissue. In untreated patients after a variable period, CD4 T cell count
falls below a serious level and patient develops highly susceptible to opportunistic
diseases.
The main endogenous factors that control HIV expression are cytokines
and exogenous factors are other microbes with effects on HIV replication.
Coinfections upregulate HIV expression and hasten the progression. The virus
during early, asymptomatic phase are non syncytium inducing variants and during
late stages syncytium inducing variants.
Transmission of HIV
1.Sexual transmission.
In India the epidemic spreads mainly through sexual route. According to
phylogenetic analysis most of Indian HIV-1 strains belong to sub type "C".
Sexual transmission can occur following vaginal and anal intercourse and also
through oral sex.80 Male to female transmission is twice as effective as female
to male transmission.
2.Transmission through pregnancy and breast feeding.
HIV infection to the foetus / new born may occur during Intrauterine,
peripartum and postpartum periods. 50% - 70% of transmission occurs at time of

57
delivery with 30% - 50% in utero. The risk of postpartum infection from breast
feeding is estimated to be approximately 15% - 30%.
3.Blood - borne Transmission.
The connection between the transfusion of blood products and AIDS was
first discovered in 1982. Donor screening and HIV testing of donors can prevent
HIV transmission from blood and blood products. HIV infected injecting drug
users may transmit HIV by syringe (or) needle sharing.
4.Occupational Exposure.
Health care workers are at risk through a percutaneous injury by needles
or other sharp instruments. The risk is found to be approximately 0.3%.
5.Organ and Tissue Donation
HIV transmission can occur following the transplantation of human organs
(or) following bone marrow or bone chip transplantation from infected donors.
6.Household transmission, casual contact and insect factors.
There is considerable epidemiological data available that HIV transmission
not occurs through hugging (or) kissing, sharing clothes or eating and drinking
utensils. There is also no evidence that insects can act as vectors for transmission.
Clinical staging of HIV disease
1.Acute seroconversion syndrome.
It is the complex symptom that is experienced in 80-90% of patients but
not frequently registered. The time of onset is 2-4 weeks from exposure. This
presents as influenza - like illness (or) as infectious mononucleosis like illness.

58
2.Early HIV Disease
Most of the patients are asymptomatic with CD4 cell count greater than
500 cells / mm3 Generalised lymphadenopathy is the common manifestation.
Dermatologic symptoms like seborrheic dermatitis, Eosinophilic folliculitis etc
are common.
3.Intermediate Stage
It Also called as symptomatic HIV infection parallels to category B, CDC
clinical classification with CD4 count between 200-500 cells / mm3 AIDS state
(or) late stage
This stage in characterized by opportunistic infections and malignancies. It
corresponds to CDC category C classification with CD4 cell count 50-200 cells /
mm3.
4.Advanced HIV disease
In this stage CD4 count less than 50 cells / mm3 with infections like
Mycobacterium avium complex, cytomegalovirus retinitis, disseminated fungal
infections, AIDS dementia complex.

59
AIM & OBJECTIVES:
1. To assess and provide clinical and epidemiological data of STIs
among high risk groups attending STI OPD.
2. To study the Age wise distribution of STIs in high risk groups.
3. To study the sexual behaviour pattern and mode of sex among high
risk groups.
4. To study the prevalence of HIV infection in high risk groups.
60
MATERIALS AND METHODS
STUDY DESIGN: Cross sectional observational study
STUDY AREA: Sexually transmitted infections (STI) OPD in Tirunelveli
medical college.
STUDY PERIOD: 18 months (January 2018 – June 2019)
SAMPLE SIZE: The study population included were patients attending our
OPD with history of high-risk sexual behavior. They are registered during the
period from 1st January 2018 to 30th June 2019 in STI OPD in Tirunelveli
medical college. During the study period, a total of 460 patients were registered
and observed.
STUDY SUBJECT: Men who have sex with men, female sex workers and
transgender attending sexually transmitted infections OPD.
INCLUSION CRITERIA:
1. MSM
2. Female sex workers
3. Transgender
4. Multiple sexual partners
5. Drivers, Housekeeping, Migrants.
Methodology
The study patients were questioned regarding their age, occupation, marital
status, presenting complaints, sexual history and their condom use. All the
patients were counselled on STD/ HIV, genital hygiene, sexual practices,

61
regular treatment and follow up. They were given pre and post-test
counselling. All the patients underwent a complete physical examination and
genital examination. All these patients were clinically analysed for the genital
manifestations and supported by laboratory diagnosis. Serological tests for
syphilis including blood RPR, TPHA, HIV, HBsAg and Anti HCV antibodies
were done. In the case of genital ulcers, the following tests were done.
1. Dark field microscopic examination for Treponema pallidum.
2. Gram’s stain for Chancroid and Candida.
3. Tissue smear and Leishman stain for Klebsiella granulomatis.
4. Tzanck test for Multinucleated giant cells.
In the case of genital discharge, the following tests were done.
1. Wet film for Trichomonas vaginalis
2. 10% potassium hydroxide preparation for Candida albicans
3. Gram’s stain to identify Neisseria gonorrhoeae, clue cells and Candida
hyphae.
In addition, the examination of urine, culture of Neisseria gonorrhoea from
specimens of urethral discharge were done. Discharge from ulcers were
subjected to culture and sensitivity if necessary.
Routine baseline laboratory investigations including complete blood count,
urine for albumin, sugar deposits, USG abdomen were done. Liver function test,
Renal function test, Random blood sugar, chest x-ray, ECG, sputum smear for
AFB, blood and urine culture sensitivity were also done if mandatory. Patients
were offered standard treatment according to clinical condition and prophylaxis
for opportunistic infections. Epidose were given to their known contacts.

62
RESULTS
STATISTICS AMONG HIGH RISK GROUPSThese statistics comprises of 460 high risk individuals attended STI OPD
during study period of 18 months (January 2018 – June 2019).
TABLE 1: ANALYSIS OF AGE GROUP AMONG HIGH RISK GROUPS
Age group Frequency Percent10-19 3 0.720-39 295 64.140-64 158 34.3>65 4 0.9
Total 460 100.0
Out of 460 high risk group patients, 295 patients belong to the age group of 20-
39 years followed by 158 patients belongs to 40-64 years of age. Only 3 and 4 patients
were in the age group of 10-19 and >65 years respectively.
0
50
100
150
200
250
300
10-19 20-39 40-64 >65
3
295
158
4
AGE DISTRIBUTION
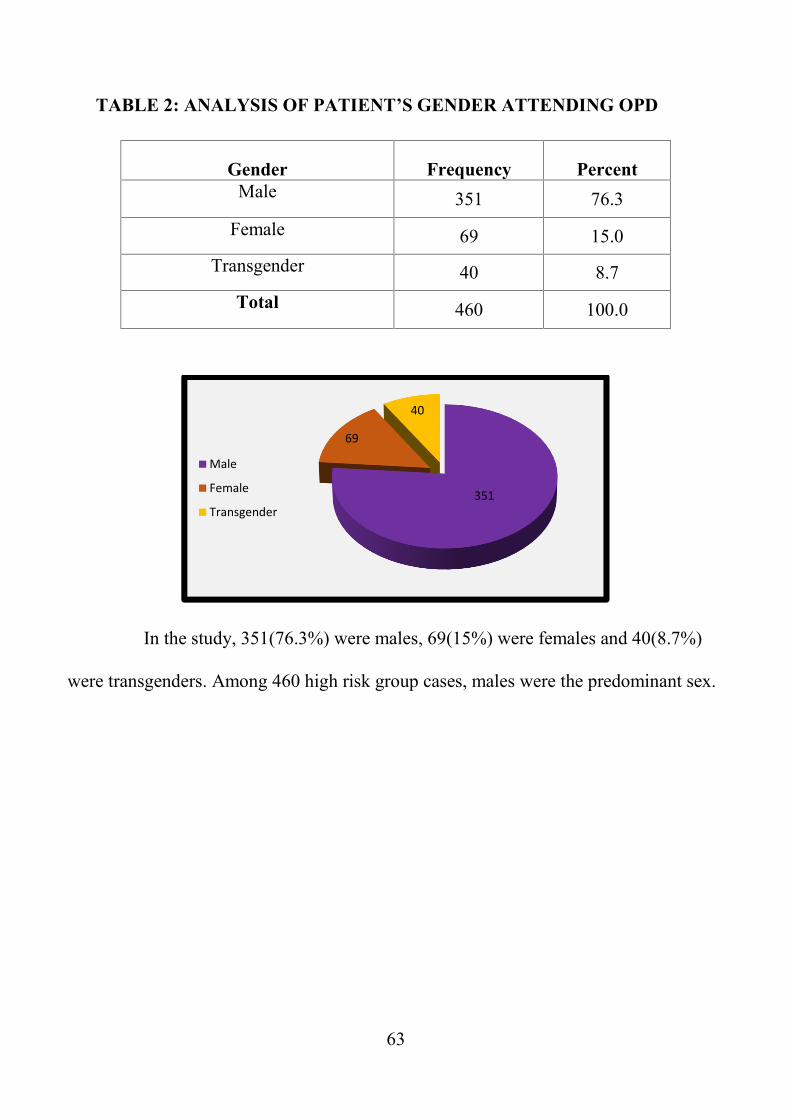
63
TABLE 2: ANALYSIS OF PATIENT’S GENDER ATTENDING OPD
Gender Frequency PercentMale 351 76.3
Female 69 15.0Transgender 40 8.7
Total 460 100.0
In the study, 351(76.3%) were males, 69(15%) were females and 40(8.7%)
were transgenders. Among 460 high risk group cases, males were the predominant sex.
351
69
40
Male
Female
Transgender

64
TABLE 3: LIST OCCUPATION STATUS
Occupation Frequency PercentFEMALE SEX WORKER 28 6.1COOLIE 2 0.4DRIVER 67 14.6HOUSEKEEPING 56 12.2MIGRANTS 33 7.2OTHERS 263 57.2STUDENT 11 2.4Total 460 100.0
In the study, high risk occupational groups were truck drivers (14.6%),
housekeepers (12.2%), migrants (7.2%) and female sex workers (6.1%). 57.2%
of patients had various other occupation which were not considered as high-risk
occupation.
TABLE 4: MARITAL STATUS OF HIGH-RISK GROUPS
Marital Status Frequency PercentMarried 366 79.6
Unmarried 93 20.2Widower 1 0.2
Total 460 100.0
Among 460 patients, 79.6% were married, 20.2% were unmarried and 0.2%
were widower.

65
TABLE 5: ANALYSIS OF SEXUAL BEHAVIOUR PROFILE
Sexual Behaviour Frequency Percent
EMC/PMC 263 57.2
MSM 197 42.8
Total 460 100.0
Regarding sexual behaviour, out of 460 were high risk patients 263(57.2%)
had extra and pre-marital heterosexual contact and 197(43%) were MSM. This
implies heterosexual contact were at increased risk than homosexuals.
57%43%
EMC/PMC
MSM

66
TABLE 6: LIST OF CONTACT PERSON
Status of contact person Frequency PercentKnown male 108 23.5Known female 48 10.4Unknown male 139 30.2Unknown female 165 35.9Total 460 100.0
Regarding status of partner, 66% had recent exposure with unknown
partners and 44% with known partners. This signifies increased risk of
transmission of STI’s among unknown partners.

67
TABLE 7: MODE OF SEX AMONG HIGH RISK GROUPS
Mode of Sex
Age groupTotal Percent10-19 20-39 40-64 >65
Count Count Count Count
Vaginal route 1 181 76 0258 56.1
Anoreceptive 2 101 66 4173 37.6
Anoinsertive 2 80 44 4130 28.3
Ororeceptive 2 109 78 4193 42.0
Oroinsertive 2 93 59 4158 34.3
In the study, predominant route of intercourse was vaginal (56.1%)
followed by ororeceptive (42%), anoreceptive (37.6%), oro-insertive (34.3%) and
anoinsertive (28.3%)
1 2 2 2 2
181
101
80
10993
7666
44
78
59
0 4 4 4 40
20
40
60
80
100
120
140
160
180
200
Age group 10-19
Age group 20-39
Age group 40-64
Age group >65

68
TABLE 8: CONDOM USAGE AMONG HIGHRISK GROUPS
Condom use Frequency PercentProtected 32 7.0Unprotected 428 93.0Total 460 100.0
In this study, consistent condom usage is present in 7% of high-risk group.
93% patients had never used condoms. This is the reason for increased STI
transmission among high-risk group people which in turn increase the burden of
STI in the community.
32
428
PROTECTED
UNPROTECTED

69
TABLE 9: STATUS OF CIRCUMCISION & CASTRATION
In the study, 81.3% were uncircumcised and only 0.4% were circumcised.
Among 40 transgenders, 17 (42%) were castrated and remaining 23 (58%) were
not castrated.
2
374
6717
CIRCUMCISED
UNCIRCUMCISED
NONE
CASTRATED
Circumcision Frequency PercentCircumcised 2 0.4
Uncircumcised 374 81.3None 67 14.6
Castrated 17 3.7Total 460 100.0

70
TABLE 10: TOTAL STI’S DIAGNOSED AMONG HIGH RISK GROUPS
Diagnosis Frequency PercentNil 272 59.1STI 188 40.9
Total 460 100.0
Among 460 patients, 188 (40.9%) were diagnosed to have STI and 272
(59.1%) were devoid of STI. All these 272 high risk group cases had routine STI
screening for early diagnosis.
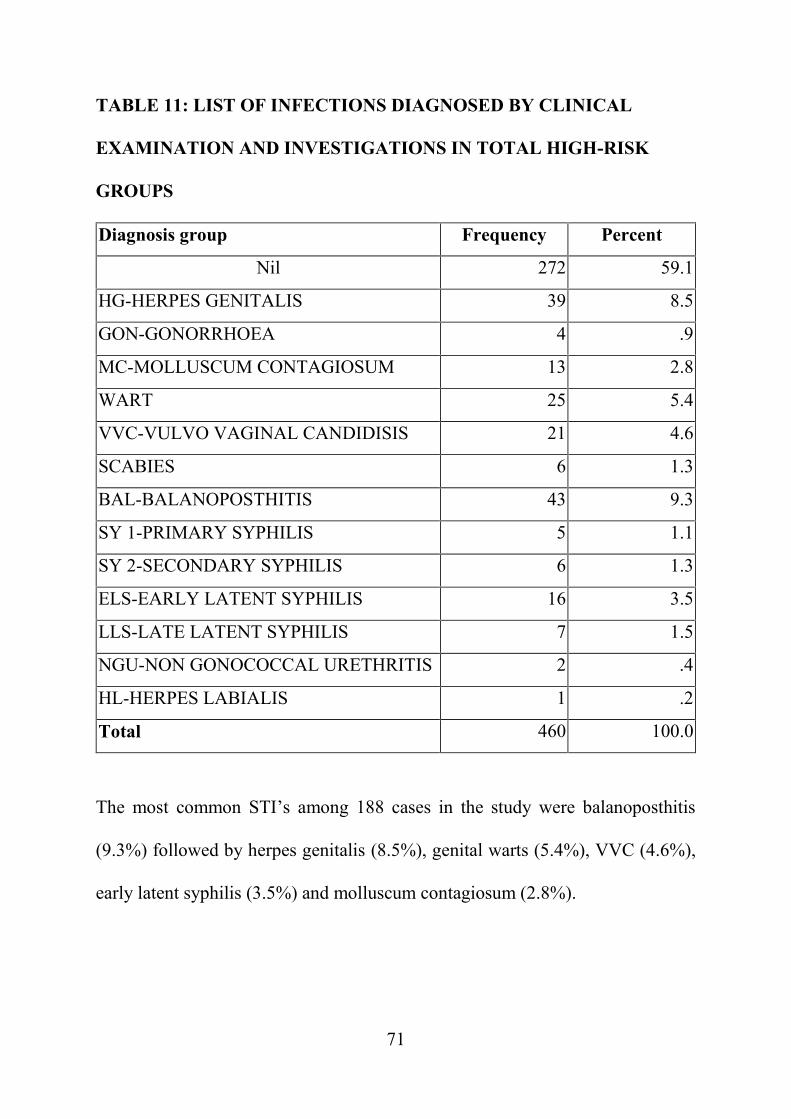
71
TABLE 11: LIST OF INFECTIONS DIAGNOSED BY CLINICAL
EXAMINATION AND INVESTIGATIONS IN TOTAL HIGH-RISK
GROUPS
Diagnosis group Frequency Percent
Nil 272 59.1
HG-HERPES GENITALIS 39 8.5
GON-GONORRHOEA 4 .9
MC-MOLLUSCUM CONTAGIOSUM 13 2.8
WART 25 5.4
VVC-VULVO VAGINAL CANDIDISIS 21 4.6
SCABIES 6 1.3
BAL-BALANOPOSTHITIS 43 9.3
SY 1-PRIMARY SYPHILIS 5 1.1
SY 2-SECONDARY SYPHILIS 6 1.3
ELS-EARLY LATENT SYPHILIS 16 3.5
LLS-LATE LATENT SYPHILIS 7 1.5
NGU-NON GONOCOCCAL URETHRITIS 2 .4
HL-HERPES LABIALIS 1 .2
Total 460 100.0
The most common STI’s among 188 cases in the study were balanoposthitis
(9.3%) followed by herpes genitalis (8.5%), genital warts (5.4%), VVC (4.6%),
early latent syphilis (3.5%) and molluscum contagiosum (2.8%).
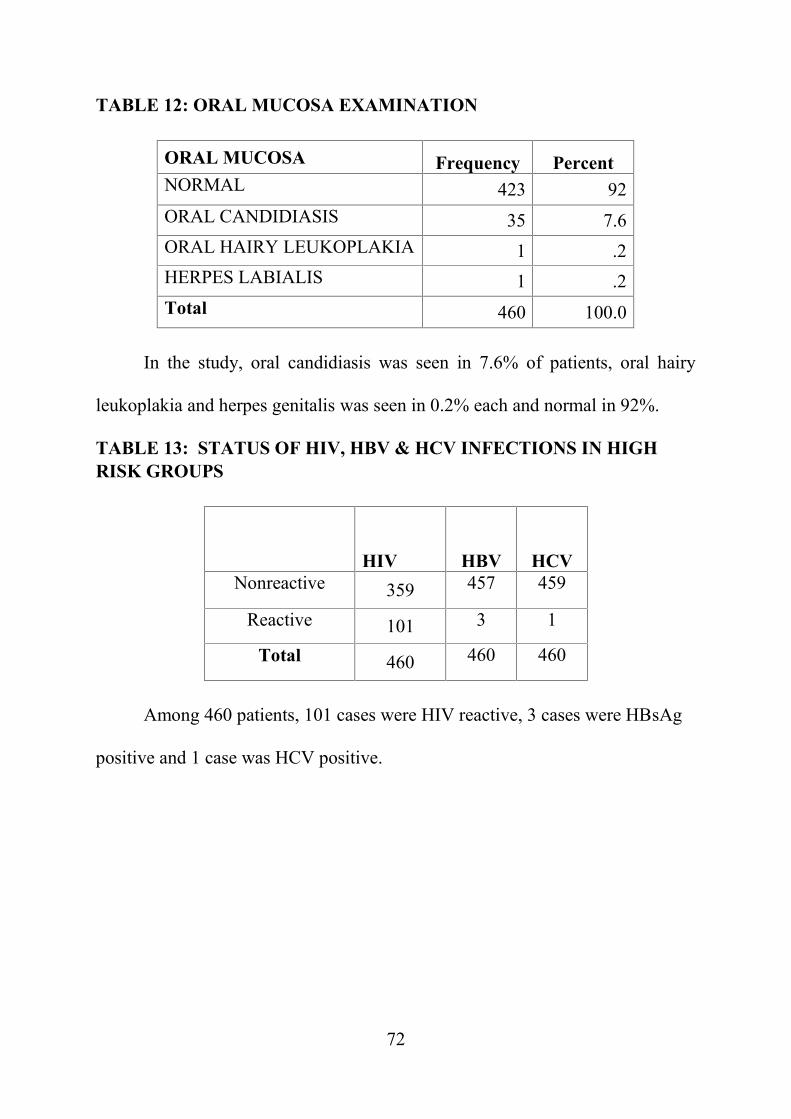
72
TABLE 12: ORAL MUCOSA EXAMINATION
ORAL MUCOSA Frequency PercentNORMAL 423 92ORAL CANDIDIASIS 35 7.6ORAL HAIRY LEUKOPLAKIA 1 .2HERPES LABIALIS 1 .2Total 460 100.0
In the study, oral candidiasis was seen in 7.6% of patients, oral hairy
leukoplakia and herpes genitalis was seen in 0.2% each and normal in 92%.
TABLE 13: STATUS OF HIV, HBV & HCV INFECTIONS IN HIGHRISK GROUPS
HIV HBV HCVNonreactive 359 457 459
Reactive 101 3 1
Total 460 460 460
Among 460 patients, 101 cases were HIV reactive, 3 cases were HBsAg
positive and 1 case was HCV positive.

73
TABLE 14: RPR & TPHA STATUS
POSITIVE NEGATIVE
RPR 34 426
TPHA 34 426
Among 460 high risk group patients, 34 were RPR and TPHA positive
implying 34 cases of syphilis. This indicates increased prevalence of syphilis still
exists in our country.
TABLE 15: STATUS OF DIABETES MELLITUS
frequency Percent
Absent 440 95.7
Present 20 4.3
Total 460 100
Prevalence of diabetes mellitus among 460 high-risk group patients were
20(4.3%) which is of decreased significance. Non-diabetics in the study were
95.7%.

74
STATISTICS AMONG HIGH RISK GROUP WITH STI’SThese statistics comprises of 188 STI cases among 460 high risk
individuals in the study.
TABLE 16: DISTRIBUTION OFAGE GROUP AMONG DISEASED
Age group Frequency Percent20-39 107 56.940-64 80 42.6>65 1 .5Total 188 100.0
Among 188 STI cases in the study, the prevalence of STI’s are more
common between 20-39 years of age (56.9%) followed by 40-64 years of age
(42.6%).
0
20
40
60
80
100
120
20-3940-64
>65
107
80
1
FREQ
UEN
CY
AGE GROUP

75
TABLE 17: ANALYSIS OF GENDER PROFILE
Gender Frequency PercentMale 142 75.5Female 43 22.9Transgender 3 1.6
Total 188 100.0
Among 188 STI cases, 142(75.5%) were males followed by 43(22.9%)
females and 3(1.6%) transgenders.
142
43
3
Male
Female
Transgender

76
TABLE 18: LIST OF OCCUPATION STATUS AMONG STI’S
Occupation Frequency PercentFemale sex worker 26 13.8
Coolie 2 1.1Driver 27 14.4
Housekeeping 24 12.8Migrants 11 5.9Others 88 46.8Student 10 5.3Total 188 100.0
Among 188 STI cases, predominant high-risk group of occupation was
drivers (14.4%), female sex workers (13.8%) and housekeepers (12.8%).
TABLE 19: MARITAL STATUS
Maritalstatus Frequency Percent
Married 140 74.5Unmarried 47 25.0Widower 1 .5
Total 188 100.0
In the group of 188 STI’s, 140 (74.5%) were married, 47(25%) were
unmarried and 1(0.5%) was a widower.

77
TABLE 20: ANALYSIS OF SEXUAL BEHAVIOUR
Sexualbehaviour Frequency PercentEMC/PMC 144 76.6MSM 44 23.4Total 188 100.0
P<0.0001 signifies high association between sexual behaviour and
prevalence of STI’s in the study. Predominant high-risk sexual behavior was seen
in EMC/PMC 144(76.6%) followed by 44(23.4%).
144
44
EMC/PMC
MSM

78
TABLE 21: ANALYSIS OF PERIOD OF LAST CONTACT
Last contact Frequency Percent<2WEEK 38 20.2
2WEEEK TO1MONTH 57 30.3
1MONTH TO 1 YEAR 59 31.4>1YEAR 34 18.1
Total 188 100.0
Diagnosis group Last contactTotal<2 weeks 2 weeks to
1 month1 month to
1 year1year
HG-HERPESGENITALIS
11 14 9 5 39
GON-GONORRHOEA 1 1 2 0 4MC-MOLLUSCUMCONTAGIOSUM
1 5 6 1 13
WART 2 8 12 3 25VVC-VULVO
VAGINALCANDIDISIS
8 8 4 1 21
SCABIES 2 1 2 1 6BAL-
BALANOPOSTHITIS9 13 6 15 43
SY 1-PRIMARYSYPHILIS
2 2 1 0 5
SY 2-SECONDARYSYPHILIS
1 2 3 0 6
ELS-EARLY LATENTSYPHILIS
1 0 13 2 16
LLS-LATE LATENTSYPHILIS
0 1 1 5 7
NGU-NON-GONOCOCCAL
URETHRITIS
0 2 0 0 2
HL-HERPESLABIALIS
0 0 0 1 1
Total 38 57 59 34 188

79
TABLE 22: LIST OF CONTACT PERSON
Contactperson Frequency PercentKnown male 43 22.9Known female 22 11.7Unknown male 43 22.9Unknownfemale 80 42.6
Total 188 100.0
Among 188 cases of STI’s, the prevalence of STI’s were more common
among unknown partners (65.5%) than known partners (34.5%).

80
TABLE 23: ANALYSIS OF MODE OF SEX
Mode ofSex
Age group
TOTAL
PERCENT
PVALU
E
10-19 20-39 40-64 >65Coun
tCoun
tCoun
tCoun
t
Vaginalroute
0 54 33 087 46.3%
0.008
Anoreceptive
0 45 36 182 43.6%
Anoinsertive
0 32 24 157 30.3%
Ororeceptive
0 52 45 198 52.1%
Oroinsertive 0 43 33 177 41.0%
P value for all routes is < 0.05 showing significance between mode of sex
and prevalence of STIs. The increased risk of STI’s was through ororeceptive
and vaginal routes.
0 0 0 0 0
54
45
32
52
43
33 36
24
45
33
0 1 1 1 10
10
20
30
40
50
60
Age group 10-19
Age group 20-39
Age group 40-64
Age group >65

81
TABLE 24: CONDOM USAGE AMONG INFECTED PERSONS
Condom use Frequency PercentProtected
14 7.4
Unprotected174 92.6
Total 188 100.0
In the study of 188 STI cases, p value was >0.05 signifying no association
between condom protection and prevalence of STI’s.
14
174
PROTECTED
UNPROTECTED

82
TABLE 25: STATUS OF CIRCUMCISION / CASTRATION
Circumcision Frequency Percent
Circumcised 2 1.1
Uncircumcised 142 75.5
None 41 21.8Castrated 3 1.6
Total 188 100.0
P value is 0.0001, which shows significance between uncircumcised and
prevalence of STIs which proves increased risk of STI’s among uncircumcised
men.
020406080
100120140160
2
142
41
3

83
TABLE 26: CLINICAL EXAMINATION FINDINGS OF DISEASED
GENITAL ULCER / FISSURE
GENITALULCER/FISSURE Frequency Percent
Painlessindurated ulcer 6 3.2
Painful ulcer 38 20.2Erosions/fissures 43 22.9
Scar 6 3.2None 95 50.5Total 188 100.0
GENITAL DISCHARGE
Genital discharge Frequency PercentUrethral discharge
6 3.2
Curdy white discharge21 11.2
Homogenous paste discharge1 0.5
Sub preputial discharge43 22.9
None 117 62.2Total 188 100.0

84
GENITAL PAPULES
Papules Frequency Percentverrucous papules
26 13.8
Umblicated papules13 6.9
Excoriated papules6 3.2
None 143 76.1Total 188 100.0
LYMPHNODES
Lymph nodes Frequency PercentPresent 51 27.1Absent 137 72.9Total 188 100.0
TABLE 27: STATUS OF HIV, HBV, HCV & DIABETES MELLITUSSTATUS
Frequency PercentHIV 31 16.4
HBsAg 0 0HCV 0 0DM 20 10.6
P value is 0.019 which shows significance between HIV and prevalence
of STI’s. There is no association between HBsAg, HCV and prevalence of
STI’s.

85
TABLE 28: DISTRIBUTION OF STI’S IN HIV POSITIVE GROUP
Diagnosis group FrequencyHG-HERPES GENITALIS 5GON-GONORRHOEA 1MC-MOLLUSCUM CONTAGIOSUM 1WART 8SCABIES 2BAL-BALANOPOSTHITIS 8SY 1-PRIMARY SYPHILIS 1ELS-EARLY LATENT SYPHILIS 2LLS-LATE LATENT SYPHILIS 2NGU-NON-GONOCOCCAL URETHRITIS 1HL-HERPES LABIALIS 1TOTAL 31
Among 31 HIV infected STI cases, the most common diagnosis was genital
warts and balanoposthitis followed by herpes genitalis, syphilis and scabies.
Other STI’s like gonorrhea, molluscum contagiosum, non-gonococcal urethritis
and herpes labialis are seen in one patient each only.

86
TABLE 29: LIST OF INFECTIONS DIAGNOSED BY CLINICALEXAMINATION AND INVESTIGATIONS AMONG DISEASED.Diagnosis group Frequency PercentHG-HERPES GENITALIS 39 20.7GON-GONORRHOEA 4 2.1MC-MOLLUSCUM CONTAGIOSUM 13 7WART 25 13.3VVC-VULVO VAGINAL CANDIDISIS 21 11.2SCABIES 6 3.2BAL-BALANOPOSTHITIS 43 22.9SY 1-PRIMARY SYPHILIS 5 2.7SY 2-SECONDARY SYPHILIS 6 3.2ELS-EARLY LATENT SYPHILIS 16 8.5LLS-LATE LATENT SYPHILIS 7 3.7NGU-NON-GONOCOCCAL URETHRITIS 2 1.1HL-HERPES LABIALIS 1 0.5Total 188 100.0
The most common STI’s among 188 cases in the study were balanoposthitis
(22.9%) followed by herpes genitalis (20.7%), genital warts (13.3%), VVC
(11.2%), early latent syphilis (8.5%) and molluscum contagiosum (7%).
39
4
13
2521
6
43
5 6
16
72 1
05
101520253035404550
TOTA
L CA
SES

87
DISCUSSION
In our study 460 cases were enrolled with high risk behaviour. Among 460
cases, 188 high risk behavior cases were found to have STI’s and remaining 272
cases were not diagnosed with any of the STI and had routine screening for high
risk behaviour. Most of the cases bought by NGOs were MSM and FSW.
In our study comprising 188 patients with STI’s, most common age group
was between 20 – 39 years (56.9%). It is consistent with study done by Arpit C.
Prajapati et al where the most common age group was between 25-35 years.94 As
in this age group , young sexually active people increasingly engage in high risk
sexual behavior like unprotected anal sex, multiple sex partners, MSM and they
use the internet to recruit sex partners which leads on to increased transmission
of STIs. 95
Among 188 STI patients, almost two-third were males (75.5%) whereas
females and transgenders were only 22.9% and 1.6% respectively. This is similar
to the study done in north India by Suvirya et al wherein males were three-fourth
involved.96 This shows men were most commonly indulging in high risk sexual
practices.
In our study out of 188 STI acquired persons, 13.8% were female sex
workers, 14.4% were drivers, 12.8% were housekeeping, migrants were 5.9%,
students were 5.3% and 46.8% belong to non-high-risk occupation groups like
tailors, teachers, clerks, carpenters, homemakers and farmers. This clearly shows

88
that more than half of STI acquired persons belongs to high risk occupation
groups.
In this study among188 STI’s, 140 (74.5%) were married, 47(25%) were
unmarried and 1(0.5%) was a widower. This shows the prevalence of STIs were
more common in married individuals and this leads to risk of STI transmission to
their spouse, thus increasing burden of STI in community. This is similar to the
study done by Kwena et al in Lake Victoria in Kisumu, Kenya where 70% of
individual were married.97
In our study the Predominant high-risk sexual behavior was seen in
EMC/PMC 144(76.6%) followed by MSM 44(23.4%). This is similar to study
done in Malawi where multiple sexual partners(EMC/PMC) are at more risk.98 P
= 0.0001 signifying association within multiple sexual partners and prevalence of
STI.
In our study 50.3% had STI’s when exposed within 1month
duration, 31.4% within 1 month to 1 year and 18.1% when exposed more than 1
year.
Regarding status of partner, 65.5% patients had exposure with unknown
partners and 34.5% had with known partners. This implies the prevalence of STIs
transmission is more in patients who had exposure with unknown partner.
In our study the commonest mode of sex was ororeceptive and vaginal
route. These results were comparable with Kolkata study 99 where penovaginal is

89
the most common mode of sex. P value for all routes is < 0.05 showing
significance between mode of sex and prevalence of STIs.
In our study, the prevalence of STIs are more common in the persons who
did not use condom (92.6%). Our study highlights the fact that barrier usage
should be encouraged strictly in young people, particularly those at high risk of
developing STIs and HIV. Nayyar et al study in 2015 also emphasizes the usage
of condom among high risk sexual behaviour populations.14
Among 188 STI cases 75.5% were uncircumcised followed by 1.1% who
were circumcised. All the transgenders with STI were castrated. P value is
0.0001, which signifies increased risk of STI transmission among uncircumcised
men. The role of circumcision in prevention of HIV/STIs is still debatable. Some
studies have showed that penile foreskin offers a portal of entry for pathogens,
including HIV, as it is more vulnerable to trauma during intercourse, the internal
mucosa of the foreskin has less keratinization and a higher density of target cells
for HIV infection moreover, the microenvironment in uncircumcised foreskin
may be warm, moist offers a suitable site for the pathogens to reproduce. All these
aspects support the role of circumcision in prevention of HIV/STIs. This was
confirmed in Nayyar et al study in 2015 where, the prevalence of STI and HIV
was found to be 14% in circumcised cases and 42.7% in uncircumcised.14
The common clinical finding of genital ulcer in our study was erosions and
fissures 22.9% mostly seen in balanoposthitis followed by painful ulcer 20.2%
90
seen in herpes genitalis. Lymph nodes was present in 27.1% among 188 STI’s in
our study. Various presentation of genital discharge includes urethral discharge
3.2%, curdy white discharge 11.2%, homogenous paste like discharge in 0.5%
and sub preputial discharge in 22.9%. Many cases presented with verrucous
papules 13.8% suggestive of anogenital wart, 6.9% umbilicated papules
suggestive of genital molluscum contagiosum and excoriated papules of scabies
with 3.2%.
The high prevalence of STD's in HIV positives shows the status of
infectivity and predilection cofactors in HIV transmission and acquisition. This
shows the importance of early diagnosis and management of STDs to control HIV
transmission and acquisition.
In our study 31 persons (23 EMC/PMC & 8 MSM) with STI’s were co-
infected with HIV infection. This shows large group of individuals involved in
sexual practices with multiple sexual partners, early age of first sexual exposure
and non-usage of condoms. In our study genital wart (8), balanoposthitis (8),
herpes genitalis (5) were commonly coinfected with HIV. Among 460 total high-
risk population 101 persons were infected with HIV this shows significance (P =
0.019) of HIV infection with high risk groups. So, our study highlights the
importance of strengthening the surveillance, early diagnosis and joint strategies
to control and manage STD's and HIV.
91
Here in our study among 460 patients 35 patients had oral candidiasis and
1 had oral hairy leukoplakia. All these patients are associated with HIV
infections.
In our study we newly diagnosed 20 cases of diabetes mellitus among them
16 patients had balanoposthitis. They were referred to physician and were started
on anti-diabetic drugs.
PATTERNS OF SEXUALLY TRANSMITTED DISEASE IN HIGH RISK
GROUPS
Most of STIs were seen in age group between 20-39 years (56.9%)
followed by 40-60 years of age (42.6%) and majority of them had EMC/PMC
(76.6%) and MSM (23.4%) this shows the most common mode of transmission
in our study India remains heterosexual only i.e. multiple sexual partners
(EMC/PMC). 40.9% of our patients with high risk behaviour had atleast one
significant STI. Among 188 people men (75.5%) were most commonly indulged
in high risk behaviour followed by women (22.9%) and transgenders (1.6%).
SYPHILIS
Total number of high-risk group positive for Syphilis during routine RPR
testing was 34 (18.1%) which was then confirmed with Treponema Pallidum
hemagglutination assay (TPHA). Of the 34 positive patients, 5(14.3%%) were
diagnosed to have primary syphilis, 6 (17.6%) were diagnosed to have secondary
syphilis, 16(47.1%) were early latent syphilis and 7(20.6%) were late latent
syphilis. In patients with primary, secondary and early syphilis one dose inj.

92
Benzathine penicillin 2.4 million units is given and in late syphilis 3 doses of inj.
Benzathine penicillin 2.4 million units is given and advised for follow up. Patients
were asked to bring partner. Among 34 syphilis patients 28 were male and 6 were
female. Among them 19 patients had EMC/PMC whereas 15 had MSM sexual
behaviour and 5(14.8%) patients are co-infected with HIV. This is similar to
study done by sethi et al in north India where more males are infected than
females.100 In study done by Prakash Narayanan 101, the prevalence of syphilis
among MSMs was 6.6% which lesser when compared to our study.
HERPES GENITALIS
It is one of the most common sexually transmitted infection worldwide
including India. In our study 39(20.7%) cases of herpes genitalis were found and
asked to bring partner for screening. Of the 39 patients 30 were male, 8 were
female and 1 transgender. Among them 32 patients had EMC/PMC whereas 7
had MSM sexual behaviour and 5(12.9%) patients are co-infected with HIV. It is
the commonest ulcerative STI diagnosed among HIV positive patients according
to our study. Some cases showed typical morphological features whereas HIV
infected patients showed atypical presentations. They all were treated with red kit
and advised to bring their partners.
GENITAL WART
In our study the prevalence is 26 (13.8%). It is the most common STI
noticed in MSM in our study. out 26, we had 22(85%) penile wart, 4(15%)
perianal wart which were treated with podophyllin toxin. Around 22 males and 4

93
females were affected with 16 (61.5%) EMC/PMC and 10 (38.5%) MSM. Nearly
8 (36.3%) patients were coinfected with HIV which is also highest in our study.
All patients with perianal warts gave history of being anoreceptive. HPV
infection among MSM is highest in those who are coinfected with HIV. The
prevalence of genital wart among MSM in our study was 38.5%, which is of
increased incidence than the study done Garg et al which showed the prevalence
of 26%.102
MOLLUSCUM CONTAGIOSUM
The prevalence of genital molluscum contagiosum has also raised. In
present study 7% (13 cases) were positive for MC. He was treated by doing
needling. Only one case was coinfected with HIV.
URETHRAL DISCHARGE
In our study, 6 (3.2%) patients presented with urethral discharge and
urethritis, among them 4 were due to gonococcal urethritis and 2 were non
gonococcal urethritis (NGU). We encountered a rare complication of gonococcal
infection in MSM – “WATERCAN PERENIUM”. Gonococcal urethritis was
diagnosed by Gram stain and culture and treated with grey kit and episodic
treatment was given for partners. 1 case from each gonococcal and NGU were
HIV positive.

94
VAGINAL DISCHARGE SYNDROME
During our study period 23 high risk cases presented with vaginal
discharge which include 22 vulvovaginal candidiasis (VVC) and 1 bacterial
vaginosis (BV).
BALANOPOSTHITIS
In our study 43 (22.9%) were diagnosed with balanoposthitis with 35
patients had EMC/PMC and 8 had MSM. HIV coinfection was seen in 8 patients
and comorbidity like diabetes mellitus was found in 16 patients. Mostly these
patients presented with fissures over prepuce and sub preputial discharge. Swab
was taken from the discharge for gram stain, KOH and sent for culture. Mostly
candida albicans was grown in culture.
GENITAL SCABIES
In our study the prevalence was 3.2% (6 cases) all of them were male cases,
who presented with the multiple itchy excoriated papules over penis and scrotum
and treated with 5% permethrin cream overnight application and wash in the
morning and asked to bring the partner for treatment. In a study and 4.4% 102 had
genital scabies.. This may be due unhygienic practices among high risk groups
and poor health seeking behavior. HIV is associated with 2 cases.

95
HEPATITIS B AND C
Infections caused by hepatitis B virus (HBV) and hepatitis C virus (HCV)
show an increasing trend among high risk groups. In our study, among 460
patients 3 were diagnosed with HBV and 1 were diagnosed with HCV
interestingly all four cases had MSM sexual behaviour. In another study done by
Vaux et al 103 also states that MSM sexual behaviour has significant risk factor
for transmission of hepatitis infection.

96
CONCLUSION
High risk groups are the ―bridging population for transmission of STIs and
HIV.
The prevalence of STIs is seen commonly in 2nd to 4th decade of age,
hence they are main target population to be focused in order to prevent
STI/HIV.
Men are most commonly indulged in high risk sexual practice than
female so, they need to be screened regularly.
The population with EMC/PMC sexual behaviour had more STI’s than
MSM and most of them had unprotected intercourse.
Increased prevalence is seen among married high-risk groups with
unknown paid partners.
Increased prevalence of STIs are seen in high risk groups with
unprotected sex.
Most common mode of sex in high risk groups with STI’s was vaginal
route among heterosexual and ororeceptive among MSM.
Most common examination findings among high risk groups was painful
ulcer, fissure, and papules over genitals.
Viral STIs are on the rise when compared to the bacterial infections
among high risk groups. Among viral STIs HIV, Herpes genitalis and
Warts is the commonest, and among bacterial infections, Latent Syphilis
is the common infection and it shows increase in trend of syphilis among

97
high risk groups. Hence consistent screening with RPR and ELISA for
HIV is a must in high risk groups.
Among 101 HIV reactive individual 31 persons were co-infected with
other STIs.
Sex education is essential for high risk groups as earlier the age of sexual
activity.
Discourse the stigma among FSW and TGs to increase the health care
awareness among them.
Partner identification treatment needs to be initiated.
Vaccination for Hepatitis B should be advised.
Counselling for consistent use of condom should be done especially
when contact with unknown partners and during anal sex.
Promoting awareness about HIV-AIDS transmission & its prevention
may alert them to use condom properly during each sexual act.
STIs management in high risk groups requires the expert clinician to be
conversant with risk valuation, the clinical presentation, and current
diagnosis of certain diseases, and to be familiar with new medications.
Successful STI care can be achieved because many infections are easily
identified and treatable with simple single dose therapy.
The current challenges lie in effective risk reduction and enhancing
preventive care in a cost-effective way. Newer diagnostic studies will

98
offer visions into the etiology of several clinical syndromes, but the basis
of care will always rely on listening and talking to patients.
More work is required to govern how to help high risk group minimize
sexual risk, address their mental health concerns, and engage them in
disease free lives.
Regular monitoring of programs and research are necessary for further
success of prevention and control of HIV in this HRG.
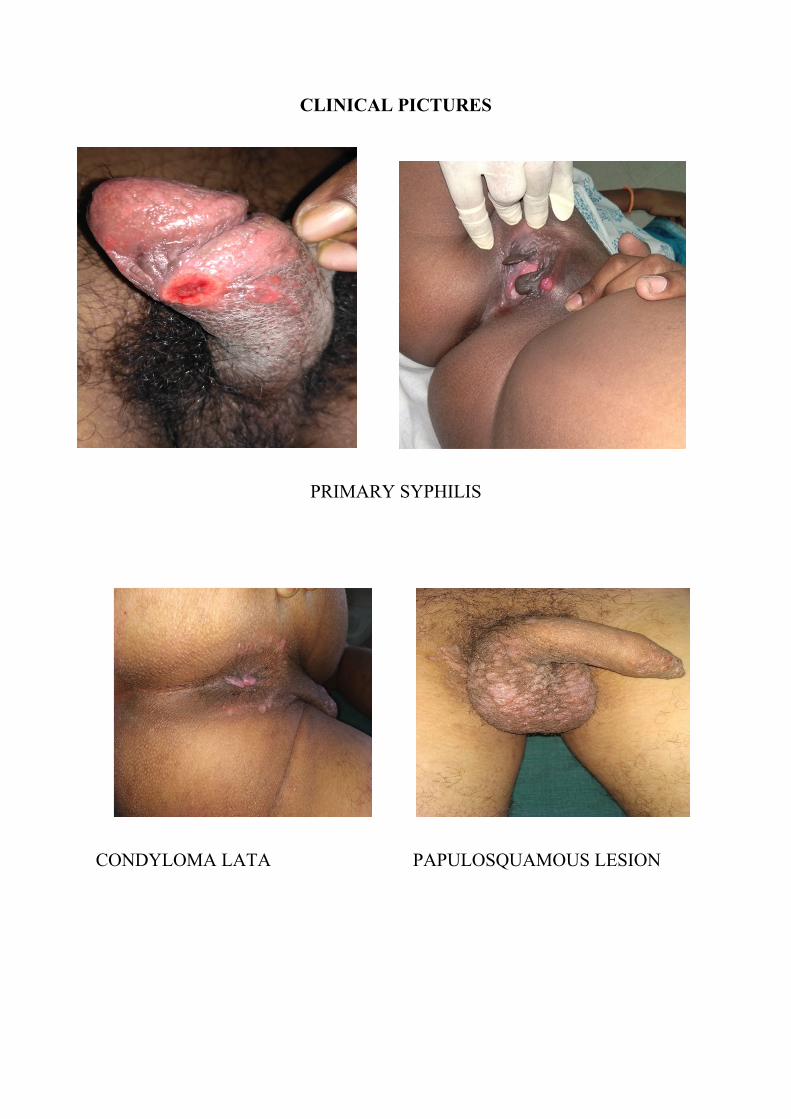
CLINICAL PICTURES
PRIMARY SYPHILIS
CONDYLOMA LATA PAPULOSQUAMOUS LESION

SECONDARY SYPHILIS – ERYTHEMATOUS ANNULAR SCALY PLAQUES
EXTRA GENITAL CHANCRE SY 2- ERYTHEMATOUS PAPULES

GONOCOCCAL URETHRITIS WATERCAN PERENIUM –MULTIPLE FISTULA
GONOCOCCAL CULTURE- SMALL PIN POINT COLONIES

HERPES GENITALIS
HERPES GENITALIS - MULTINUCLEATED GAINT CELLS

MOLLUSCUM CONTAGIOSUM
GENITAL WARTS

BALANOPOSTHITIS
VULVO VAGINAL CANDIDIASIS

GRAM STAIN FOR CANDIDA-GRAM +VE COCCI
PSEUDOHYPHAE & SPORES INKOH
CHROMOGENIC AGAR FOR CANDIDA ALBICANS & NON ALBICANSSPECIES
PINK – CANDIDA KRUSEI
GREEN- CANDIDA ALBICANS

GENITAL SCABIES
RPR - 1:4 DILUTION POSITIVE
TPHA POSITIVITY

REFERENCES
1. Suvirya S, Shukla M, Pathania S, Singhal AK, Agarwal J. Clinico-epidemiological profile and high-risk sexual behavior among clients attendingsexually transmitted infection clinic at a tertiary care hospital in North India.Indian J Sex Transm Dis AIDS. 2018 Jan 1;39(1):38.
2. Vinod K. Sharma. Sexually Transmitted Diseases and HIV / AIDS. 2009.
3. WHO | World Health Organization.4. Freud’s Stages of Psycho-Sexual Development. StudyBix. 2017.
5. Gagnon JH, Simon W, editors. Sexual Deviance. Harper & Row; 1967. 310p.
6. Sexually Transmitted Diseases - Statistics and Epidemiological Profile ofIndia | Medindia.
7. Syphilis - 2017 CDC Sexually Transmitted Diseases Surveillance-Nationalprofile
8. Gonorrhea - 2017 CDC Sexually Transmitted Diseases Surveillance- Nationalprofile
9. Other Sexually Transmitted Diseases - 2017 CDC Sexually TransmittedDiseases Surveillance-National profile
10. Patel VV, Mayer KH, Makadon HJ. Men who have sex with men in India:a diverse population in need of medical attention. Indian J Med Res. 2012Oct;136(4):563–70.
11. Kumar B, Gupta S. Sexually Transmitted Infections. 2nd Revised editionedition. New Dehli: Elsevier India; 2012. 1422 p.
12. Jie W, Ciyong L, Xueqing D, Hui W, Lingyao H (2012) A Syndemic ofPsychosocial Problems Places the MSM (Men Who Have Sex with Men)Population at Greater Risk of HIV Infection. PLoS ONE 7(3): e32312
13. Tamilselvan BP, Mehta N, Shanmugam S, Subramanian K. A study ofbehavioral and disease patterns among transgenders in a tertiary care center.Indian J Sex Transm Dis AIDS. 2018 Jan 1;39(1):18.
14. Nayyar C, Chander R, Gupta P, Sherwal BL. Evaluation of risk factors inpatients attending STI clinic in a tertiary care hospital in North India. IndianJ Sex Transm Dis AIDS. 2015;36(1):48–52.
15. Devi SA, Vetrichevvel TP, Pise GA, Thappa DM. Pattern of sexuallytransmitted infections in a tertiary care centre at Puducherry. Indian JDermatol. 2009 Oct 1;54(4):347.

16. Sexual practices other than peno-vaginal sex: perceptions and practices inan urban community.
17. Verma RK, Collumbien M. Homosexual activity among rural Indian men:implications for HIV interventions. AIDS Lond Engl. 2004 Sep3;18(13):1845–7.
18. Kumta S, Lurie M, Weitzen S, Jerajani H, Gogate A, Row-kavi A, et al.Bisexuality, sexual risk taking, and HIV prevalence among men who have sexwith men accessing voluntary counseling and testing services in Mumbai,India. J Acquir Immune Defic Syndr 1999. 2010 Feb;53(2):227–33.
19. Thappa DM, Singh N, Kaimal S. Prostitution in India and its role in thespread of HIV infection. Indian J Sex Transm Dis AIDS. 2007 Jul 1;28(2):69.
20. Youth partnership project south asia (ypp-sa) (july 2010). "vulnerability ofchildren living in the red light areas of kolkata, india" (PDF). End ChildProstitution and Trafficking. Retrieved 16 December 2018
21. Brewer, D. D., Potterat, J. J., Garrett, S. B., Muth, S. Q., John M. Roberts,J., Kasprzyk, D., et al. (2000). Prostitution and the sex discrepancy in reportednumber of sexual partners. Proceedings of the National Academy of Sciences,97, 12385–12388.
22. Subramanian T, Periannan V, Mehendale S. HIV prevalence and Riskfactors on STIs and AIDS, in Female Sex Workers of Ellapuram PanchayatUnion, Tamil Nadu. 2(3):5.
23. Hemalatha R, Kumar RH, Venkaiah K, Srinivasan K, Brahmam GNV.Prevalence of & knowledge, attitude & practices towards HIV & sexuallytransmitted infections (STIs) among female sex workers (FSWs) in AndhraPradesh. Indian J Med Res. 2011 Oct;134(4):470–5.
24. Patterson TL, Semple SJ, Staines H, Lozada R, Orozovich P, Bucardo J, etal. Prevalence and Correlates of HIV Infection among Female Sex Workersin Two Mexico-U.S. Border Cities. J Infect Dis. 2008 Mar 1;197(5):728–32.
25. Brahme R, Mehta S, Sahay S, Joglekar N, Ghate M, Joshi S, et al.Correlates and trend of HIV prevalence among female sex workers attendingsexually transmitted disease clinics in Pune, India (1993-2002). J AcquirImmune Defic Syndr 1999. 2006 Jan 1;41(1):107–13.
26. Transgender People | Gender | HIV by Group | HIV/AIDS | CDC
27. Veronese V, van Gemert C, Bulu S, Kwarteng T, Bergeri I, Badman S, etal. Sexually transmitted infections among transgender people and men who

have sex with men in Port Vila, Vanuatu. West Pac Surveill Response JWPSAR. 2015 Mar 5;6(1):55–9.
28. Swain P, Das JK, Jha S, Sharnngadharan GK. Determinants of HIVpositivity among injecting drug users in Delhi and Punjab. Indian J SexTransm Dis AIDS. 2017 Jul 1;38(2):121.
29. Muñoz-Laboy M, Severson N, Bannan S. Occupations, social vulnerabilityand HIV/STI risk: The case of bisexual Latino men in the New York Citymetropolitan area. Glob Public Health. 2014;9(10):1167–83.
30. Tiwari R, Shendre M. Role of occupation as a risk factor for sexuallytransmitted disease: A case control study. Indian J Occup Environ Med.2005;9(1):35.
31. Choudhry S, Ramachandran VG, Das S, Bhattacharya SN, Mogha NS.Pattern of sexually transmitted infections and performance of syndromicmanagement against etiological diagnosis in patients attending the sexuallytransmitted infection clinic of a tertiary care hospital. Indian J Sex Transm DisAIDS. 2010 Jul 1;31(2):104.
32. Thomas L. Schwenk, MD reviewing US Preventive Services Task Force(USPSTF). JAMA 2016 Jun 7 Cantor AG et al. JAMA 2016 Jun 7 ClementME and Hicks CB. JAMA 2016 Jun 7
33. Kent ME, Romanelli F. Reexamining Syphilis: An Update onEpidemiology, Clinical Manifestations, and Management. Ann Pharmacother.2008 Feb;42(2):226–36.
34. Eccleston K, Collins L, Higgins SP. Primary syphilis. Int J STD AIDS.2008 Mar;19(3):145–51.
35. Bhatti MT. Optic Neuropathy From Viruses and Spirochetes: IntOphthalmol Clin. 2007;47(4):37–66.
36. Nishal PK, Kapoor A, Jain VK, Dayal S, Aggarwal K. Changing trends inacquired syphilis at a Tertiary Care Center of North India. Indian J SexTransm Dis AIDS. 2015 Jul 1;36(2):149.
37. Woods CR. Congenital Syphilis–Persisting Pestilence: Pediatr Infect DisJ. 2009 Jun;28(6):536–7.
38. Marfatia YS, Pandya I, Jose SK. Congenital syphilis: Marching towardelimination. Indian J Sex Transm Dis AIDS. 2015 Jan 1;36(1):1.
39. French P. Syphilis. BMJ. 2007 Jan 20;334(7585):143–7.

40. Shah BJ, Karia DR, Pawara CL. Syphilis: Is it making resurgence? IndianJ Sex Transm Dis AIDS. 2015 Jul 1;36(2):178.
41. Morgan MK, Decker CF. Gonorrhea. Dis Mon. 2016 Aug;62(8):260–8.
42. Verma R, Sood S, Manjubala, Kapil A, Sharma VK. Diagnostic approachto gonorrhoea: Limitations. Indian J Sex Transm Dis AIDS. 2009 Jan1;30(1):61.
43. Ng L-K, Martin IE. The Laboratory Diagnosis of Neisseria gonorrhoeae.Can J Infect Dis Med Microbiol. 2005;16(1):15–25.
44. Sánchez-Busó L, Golparian D, Corander J, Grad YH, Ohnishi M,Flemming R, et al. The impact of antimicrobials on gonococcal evolution. NatMicrobial. 2019 Jul 29
45. Kulkarni S, Sane S, Mehendale S, Risbud A. Antimicrobial susceptibilityof Neisseria gonorrhoeae in Pune from 1996 to 2007. Indian J Sex Transm DisAIDS. 2011 Jan 1;32(1):58.
46. Swartz SL, Kraus SJ, Herrmann KL, Stargel MD, Brown WJ, Allen SD.Diagnosis and Etiology of Nongonococcal Urethritis. J Infect Dis. 1978 Oct1;138(4):445–54.
47. Leeyaphan C, Jiamton S, Chanyachailert P, Surawan T, Omcharoen V.Treatment outcomes and loss to follow-up rate of male patients withgonococcal and nongonococcal urethritis who attended the sexuallytransmitted disease clinic: An 8-year retrospective study. Indian J Sex TransmDis AIDS. 2017 Jan 1;38(1):37.
48. Trees DL, Morse SA. Chancroid and Haemophilus ducreyi: an update. ClinMicrobiol Rev. 1995 Jul;8(3):357–75.
49. AC I. Chancroid: An update. Indian J Dermatol Venereol Leprol. 2002 Jan1;68(1):5.
50. Ceovic R, Gulin SJ. Lymphogranuloma venereum: diagnostic andtreatment challenges. Infect Drug Resist. 2015 Mar 27;8:39–47.
51. de Vries HJC, Zingoni A, White JA, Ross JDC, Kreuter A. 2013 EuropeanGuideline on the management of proctitis, proctocolitis and enteritis causedby sexually transmissible pathogens. Int J STD AIDS. 2014 Jun;25(7):465–74.
52. Boutin C, Venne S, Fiset M, Fortin C, Murphy D, Severini A, et al.Lymphogranuloma venereum in Quebec: Re-emergence among men whohave sex with men. Can Commun Dis Rep. 2018 Feb 1;44(2):55–61.

53. Kapoor S. Re-emergence of lymphogranuloma venereum. J Eur AcadDermatol Venereol. 2008 Apr;22(4):409–16.
54. O’Farrell N. Donovanosis. Sex Transm Infect. 2002 Dec;78(6):452–7.
55. O’Farrell N. Clinico-epidemiological study of donovanosis in Durban,South Africa. Sex Transm Infect. 1993 Apr 1;69(2):108–11.
56. Granuloma Inguinale (Donovanosis) - 2015 STD Treatment Guidelines
57. Donders GGG, Zodzika J, Rezeberga D. Treatment of bacterial vaginosis:what we have and what we miss. Expert Opin Pharmacother. 2014Apr;15(5):645–57.
58. Ranjit E, Raghubanshi BR, Maskey S, Parajuli P. Prevalence of BacterialVaginosis and Its Association with Risk Factors among Nonpregnant Women:A Hospital Based Study. International Journal of Microbiology. 2018
59. What are the symptoms of bacterial vaginosis? | NICHD - Eunice KennedyShriver National Institute of Child Health and Human Development.
60. Antibiotic treatment for the sexual partners of women with bacterialvaginosis.
61. Amsel R, Totten PA, Spiegel CA, Chen KC, Eschenbach D, Holmes KK.Nonspecific vaginitis. Diagnostic criteria and microbial and epidemiologicassociations. Am J Med. 1983 Jan;74(1):14–22.
62. Oduyebo OO, Anorlu RI, Ogunsola FT. The effects of antimicrobialtherapy on bacterial vaginosis in non-pregnant women. Cochrane DatabaseSyst Rev. 2009 Jul 8;(3):CD006055.
63. STD Facts - Genital Herpes. Centres for Disease Control and Prevention
64. Sauerbrei A. Herpes Genitalis: Diagnosis, Treatment and Prevention.Geburtshilfe Frauenheilkd. 2016 Oct 18;76(12):1310–7.
65. Sakakibara R, Yamanishi T, Uchiyama T, Hattori T. Acute urinaryretention due to benign inflammatory nervous diseases. J Neurol. 2006 Aug1;253(8):1103–10.
66. Chopra D, Sandhu I, Bahl RK, Bhatia R, Goyal A. Prevalence of sexuallytransmitted infections in HIV positive and HIV negative females, in a tertiarycare hospital - An observational study. Indian J Sex Transm Dis AIDS. 2015Jan 1;36(1):59.

67. Patel R, Kennedy OJ, Clarke E, Geretti A, Nilsen A, Lautenschlager S, etal. 2017 European guidelines for the management of genital herpes. Int J STDAIDS. 2017 Dec;28(14):1366–79.
68. Mahajan BB, Dhawan M, Singh R. Herpes genitalis - Topical zinc sulfate:An alternative therapeutic and modality. Indian J Sex Transm Dis AIDS. 2013Jan 1;34(1):32.
69. Molluscum Contagiosum | Poxvirus | Centres for Disease Control andPrevention
70. Laxmisha C, Thappa DM, Jaisankar TJ. Clinical profile of molluscumcontagiosum in children versus adults. Dermatol Online J Aug 24;9(5).
71. Ramdass P, Mullick S, Farber HF. Viral Skin Diseases. Prim Care. 2015Dec;42(4):517–67.
72. Chen X, Anstey AV, Bugert JJ. Molluscum contagiosum virus infection.Lancet Infect Dis. 2013 Oct;13(10):877–88.
73. Poojary SA, Kokane PT. Giant molluscum contagiosum withgranulomatous inflammation and panniculitis: An unusual clinical andhistopathological pattern in an HIV seropositive child. Indian J Sex TransmDis AIDS. 2015 Jan 1;36(1):95.
74. PubMed. In: Wikipedia [Internet]. 2019 [cited 2019 Aug 20]. Availablefrom:https://en.wikipedia.org/w/index.php?title=PubMed&oldid=910486820
75. Scheinfeld N. Cimetidine: A review of the recent developments and reportsin cutaneous medicine. Dermatol Online J:Aug 20;9(2).
76. Genital warts. National Health Survey.UK. 2017
77. Juckett G, Hartman-Adams H. Human papillomavirus: clinicalmanifestations and prevention. Am Fam Physician. 2010 Nov15;82(10):1209–13.
78. Veldhuijzen NJ, Snijders PJ, Reiss P, Meijer CJ, van de Wijgert JH. Factorsaffecting transmission of mucosal human papillomavirus. Lancet Infect Dis.2010 Dec;10(12):862–74.
79. Chopra KF, Tyring SK. The Impact of the Human ImmunodeficiencyVirus on the Human Papillomavirus Epidemic. Arch Dermatol. 1997 May1;133(5):629–33.

80. Lacey CJN, Woodhall SC, Wikstrom A, Ross J. 2012 European guidelinefor the management of anogenital warts. J Eur Acad Dermatol VenereolJEADV. 2013 Mar;27(3):e263-270.
81. WHO | What is hepatitis?. World Health Organisation:2019
82. Prevention C-C for DC and. CDC - Scabies - Epidemiology & Risk Factors
83. Hay RJ. Scabies and pyodermas--diagnosis and treatment. Dermatol Ther.2009 Dec;22(6):466–74.
84. Donabedian H, Khazan U. Norwegian scabies in a patient with AIDS. ClinInfect Dis Off Publ Infect Dis Soc Am. 1992 Jan;14(1):162–4.
85. Ilkit, M; Guzel, AB (August 2011). "The epidemiology, pathogenesis, anddiagnosis of vulvovaginal candidosis: a mycological perspective". CriticalReviews in Microbiology. 37 (3): 250–61
86. Ilkit M, Guzel AB. The epidemiology, pathogenesis, and diagnosis ofvulvovaginal candidosis: a mycological perspective. Crit Rev Microbiol. 2011Aug;37(3):250–61.
87. White DJ, Vanthuyne A. Vulvovaginal candidiasis. Sex Transm Infect.2006 Dec 1;82(suppl 4):iv28–30.
88. Pappas PG, Kauffman CA, Andes DR, Clancy CJ, Marr KA, Ostrosky-Zeichner L, et al. Clinical Practice Guideline for the Management ofCandidiasis: 2016 Update by the Infectious Diseases Society of America. ClinInfect Dis Off Publ Infect Dis Soc Am. 2016 Feb 15;62(4):e1-50.
89. Johnston VJ, Mabey DC. Global epidemiology and control of Trichomonasvaginalis. Curr Opin Infect Dis. 2008 Feb;21(1):56–64.
90. Sonnex C. Colpitis macularis and macular vaginitis unrelated toTrichomonas vaginalis infection. Int J STD AIDS. 1997 Sep;8(9):589–91.
91. Nanda N, Michel RG, Kurdgelashvili G, Wendel KA. Trichomoniasis andits treatment. Expert Rev Anti Infect Ther. 2006 Feb;4(1):125–35.
92. 2013 European guideline for the management of balanoposthitis.
93. Edwards S. Balanitis and balanoposthitis: a review. Genitourin Med. 1996Jun;72(3):155–9.
94. Prajapati AC, Parikh S, Bala DV. Sexual behaviour and practices of menwho have sex with men in Ahmedabad city. Int J Community Med PublicHealth. 2017 Feb 5;2(3):268–74.

95. Sifakis F, Hylton JB, Flynn C, Solomon L, MacKellar DA, Valleroy LA,et al. Prevalence of HIV infection and prior HIV testing among young menwho have sex with men. The Baltimore young men’s survey. AIDS Behav.2010 Aug;14(4):904–12.
96. Suvirya S, Shukla M, Pathania S, Singhal AK, Agarwal J. Clinico-epidemiological profile and high-risk sexual behavior among clients attendingsexually transmitted infection clinic at a tertiary care hospital in North India.Indian J Sex Transm Dis AIDS. 2018 Jan 1;39(1):38.
97. Kwena ZA, Bukusi EA, Ng’ayo MO, Buffardi AL, Nguti R, RichardsonB, et al. Prevalence and risk factors for sexually transmitted infections in ahigh-risk occupational group: the case of fishermen along Lake Victoria inKisumu, Kenya. Int J STD AIDS. 2010 Oct;21(10):708–13.
98. N WC, A S. Associated Risk Factors of STIs and Multiple SexualRelationships among Youths in Malawi. PLoS ONE [Internet]. 2015 Aug 6[cited 2019 Sep 22];10(8). Available from:https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4527764/
99. Pal D, Raut DK, Das A. A study of HIV/STD infections amongstcommercial sex workers in Kolkata. (India) Part-IV laboratory investigationof STD and HIV infections. J Commun Dis. 2004 Mar;36(1):12–6.
100. Sethi S, Mewara A, Hallur V, Prasad A, Sharma K, Raj A. Rising trends ofsyphilis in a tertiary care center in North India. Indian J Sex Transm Dis AIDS.2015 Jul 1;36(2):140.
101. Narayanan. P.An exploration of elevated HIV and STI risk among male sexworkers from India | BMC Public Health.2013 Nov 9;13:1059.
102. Garg T, Chander R, Jain A, Barara M. Sexually transmitted diseases amongmen who have sex with men: A retrospective analysis from Suraksha clinic ina tertiary care hospital. Indian J Sex Transm Dis AIDS. 2012;33(1):16–9.
103. Vaux S, Chevaliez S, Saboni L, Sauvage C, Sommen C, Barin F, et al.Prevalence of hepatitis C infection, screening and associated factors amongmen who have sex with men attending gay venues: a cross-sectional survey(PREVAGAY), France, 2015. BMC Infect Dis. 2019 Apr 11;19(1):315.

PROFORMA
CASE NO:
1. STI NO: OP NO.
2. DATE:
3. AGE:
4. SEX: M / F / TG
5. OCCUPATION:
6.
COMPLAINTS DURATION
GENITAL ULCER
URETHRALDISCHARGEANORECTALDISCHARGEBURNINGMICTURITION
SUBPREPUCIALDISCHARGEGENITAL PAIN
SORE THROAT
BUBO
VESICLES
ORAL ULCERS
LOWERABDOMINAL PAINOTHERCOMPLAINTS

7. MARITAL HISTORY:
1. married /single
LMC- Protected/ unprotected-
8. CONTACT HISTORY:
1. Last contact
2. known/unknown
3. Married/ unmarried
4. Protected /unprotected
5. ororeceptive/ oroinsertive/ anoreceptive/ anoinsertive
9. H/O BLOOD TRANSFUSION:
1O. H/O DRUG ABUSE:
11. ASSOCIATED MEDICAL / SURGICAL CO-MORBIDITIES:
12. GENERAL EXAMINATION:
1. Anaemia / jaundice/ cyanosis/ clubbing/ pedal edema
2. BP
3. Pulse rate
4. Respiratory rate
5. CVS-
6. RS-
7. P/A-
8. CNS-
13. LOCAL EXAMINATION:
1. Circumcised/ uncircumcised
2. Genital ulcers
Site- Size- Border- Induration- Tenderness- Floor-
3. Genital discharge
(i). Urethral/ anorectal-
Mucopurulent- Purulent- Serous-
(ii). Vaginal discharge-
Colour- Quantity- Odour- Nature-
4. lymphadenopathy
1. unilateral/bilateral
2. Tenderness
3. Consistency
4. Matted/ discrete
5. Skin surface
5. Lower abdominal tenderness-
6. Oral mucosa-
7. per rectal examination-
8. Palms and soles-

9. Scalp and hair-
10. nails-
11. Bones and joints-
12. Other cutaneous sites-
13. INVESTIGATIONS (for all patients):
1. RPR-
2. TPHA-
3. ICTC-
4. HBsAg-
5. Anti-HCV-
14. GENITAL ULCER EXAMINATION:
GRAM STAIN- TZANCK SMEAR PUS CULTURE AND SENSITIVITY-
15. GENITAL DISCHARGE EXAMINATION:
GRAM STAIN- KOH MOUNT- WET MOUNT-
16. HISTOPATHOLOGICAL EXAMINATION (If applicable)-
17. PROVISIONAL DIAGNOSIS:

KEY TO MASTER CHART
AGE GROUP
1- 10 to 19 years 2- 20 to 39 years 3- 40 to 64 years 4- >65 years’
SEX
M- Male F- Female TG- Transgender
OCCUPATION
MSW- Male Sex Worker FSW- Female Sex Worker
C- Coolie D- Driver H- Housekeeping M-Migrants
S-Students O-Others
MARITAL STATUS
M- Married UN- Unmarried W-Widow
EMC- Extra Marital Contact
PMC- Pre-Marital Contact
MSM- Men having Sex with Men
LAST CONTACT
1- <2 weeks 2- 2weeks to 1 month 3- 1month to 1 year 4->1 year
CONTACT PERSON
1- known male 2- known female
3- unknown male 4- unknown female
PROTECTED / UNPROTECTED SEX
1- condom used 2- condom not used
MODE OF SEX
1- vaginal route 2- anoreceptive 3- anoinsertive
4- ororeceptive 5-ororeceptive
CIRCUMCISION

1- circumcised 2- un circumcised 3- castrated 4- none
GENITAL ULCER/FISSURE
1-Painless Indurated Ulcer 2-Painful Ulcer with Polycyclic Border
3-Erosions/Fissures 4-Scar 5-None
GENITAL DISCHARGE
1-Urethral Discharge 2-Curdy white Discharge
3-Homogenous Paste Discharge 4-Frothy Greenish Discharge
5-Subpreputial Discharge 6-None
LYMPHNODES
1-Present 2-Absent
PAPULES
1-Verrucous Papules 2-Umblicated Papules
3.Excoriated Papules 4-None
ORAL MUCOSA
OC- Oral Candidiasis OHL- Oral Hairy Leucoplakias
O- Others N-Normal HL- Herpes Labialis
DIABETES MELLITUS
P- Present A- Absent
RPR- Rapid Plasma Reagin test
TPHA- Treponema Pallidum Hemagglutination Test
HIV- Human Immunodeficiency Virus
HBV- Hepatitis B Virus
HCV- Hepatitis C Virus
R- Reactive
NR- Non-Reactive
KOH
1- Pseudo Hyphae with Spores 2- Scabies Mite 3- None

WET MOUNT
1- Motile Organisms 2- Clue Cells 3-None
GRAM STAIN
1- Gram +Ve Cocci 2- Clue Cells 3- Gram -VeDiplococci
4- Gram -Ve Bacilli 5- None
TZANCK SMEAR
1- Multinucleated Giant Cells 2- None
DIAGNOSIS
HG- Herpes Genitalis Gon- Gonorrhoea
MC- Molluscum Contagiosum VVC-Vulvo Vaginal Candidiasis
BAL- Balanoposthitis SY2-Primary Syphilis
SY2- Secondary Syphilis ELS- Early Latent Syphilis
LLS- Late Latent Syphilis NGU- Non-Gonococcal Urethritis
HL- Herpes Labialis.



S.N
O
NA
ME
AG
E
AG
E
SE
X
OC
CU
PA
TIO
N
MA
RIT
AL
ST
AT
US
EM
C/P
MC
/MS
M
LA
ST
CO
NT
AC
T
CO
NT
AC
T P
ER
SO
N
PR
OT
EC
TE
D O
R
UN
PR
OT
EC
TE
D
MO
DE
OF
SE
X
CIR
CU
MC
ISIO
N
GE
NIT
AL
UL
CE
R/F
ISS
UR
E
GE
NIT
AL
DIS
CH
AR
GE
LY
MP
HN
OD
ES
PA
PU
LE
S
OR
AL
MU
CO
SA
DIA
BE
TE
S M
EL
LIT
US
RP
R
TP
HA
ICT
C
HB
sAG
AN
TI
HC
V
KO
H
WE
T M
OU
NT
GR
AM
ST
AIN
TZ
AN
CK
SM
EA
R
DIA
GN
OS
IS
1 ARUMUGAM 45 3 M O M 1 2 2 2 1 1 5 1 1 4 N A NR N NR NR NR 3 3 3 2 GON
2 BHUVAN 21 2 M O M 3 1 3 2 2,3,4,5 2 5 6 2 4 N A R P NR NR NR 3 3 5 2 ELS
3 ANTONY XAVIER 40 3 M O M 3 3 3 2 2,3,4,5, 2 5 6 2 4 N A R P NR NR NR 3 3 5 2 ELS
4 MUTHUKUMAR26 2 M D M 1 3 4 2 1 2 5 1 1 4 N A NR N R NR NR 3 3 3 2 GON
5 MAHARAJA 23 2 M S UN 3 3 3 2 2,3,4,5 2 1 6 1 4 N A R P NR NR NR 3 3 5 2 SY 1
6 POOSAIPANDI 59 3 M H M 1 2 4 2 1 2 5 1 2 4 N A NR N R NR NR 3 3 5 2 NGU
7 SIVA 38 2 M D M 3 1 1 2 2,3,4,5 2 2 6 1 4 N A NR N NR NR NR 3 3 5 1 HG
8 GANAPATHY SUNDARAM32 2 M O UN 3 3 1 2 2,3,45 2 5 6 1 4 N A R P R NR NR 3 3 5 2 ELS
9 HEPSI 39 2 F FSW UN 2 2 1 1 1 3 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
10 ESWARAN 32 2 M H UN 3 1 1 1 4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
11 GANESAN 33 2 M H UN 3 2 1 1 4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
12 MANIKANDAN 28 2 M O UN 3 2 1 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
13 SINDARAPANDI40 3 M D M 3 2 1 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
14 MARIE 38 2 F FSW M 1 3 2 2 1 3 5 2 2 4 N A NR N NR NR NR 1 3 1 2 VVC
15 SURESH 30 2 M D M 3 1 1 2 4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
16 VASANTHAKUMAR26 2 M D UN 2 3 4 2 1 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
17 ARCHANA DEV27 2 M O M 3 2 3 2 2,3,4,5 2 5 6 2 1 N A NR N NR NR NR 3 3 5 2 WART
18 MUTHU 34 2 F FSW M 1 2 3 2 1 3 2 6 1 1 N A NR N NR NR NR 3 3 5 1 HG
19 MARIAPPAN 50 3 M D M 3 4 1 2 4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
20 SENTHUR 23 2 M O UN 3 1 1 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
21 KARTHI 30 2 M D UN 3 2 1 2 2,3 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
22 MUTHAIAH 31 2 M H M 1 2 3 2 1 2 2 6 1 4 N A NR N NR NR NR 3 3 5 1 HG
23 GURUNATHAN60 3 M O M 1 2 2 2 1 2 2 6 1 4 N A NR N NR NR NR 3 3 5 1 HG
24 PONRAM 33 2 M H UM 3 4 3 2 2,3,4,5 2 3 5 2 4 N A NR N NR NR NR 1 3 1 2 BAL
25 MAHALINGAM 46 3 M H M 1 4 4 2 1 2 2 6 1 4 N A NR N NR NR NR 3 3 5 1 HG

S.N
O
NA
ME
AG
E
AG
E
SE
X
OC
CU
PA
TIO
N
MA
RIT
AL
ST
AT
US
EM
C/P
MC
/MS
M
LA
ST
CO
NT
AC
T
CO
NT
AC
T P
ER
SO
N
PR
OT
EC
TE
D O
R
UN
PR
OT
EC
TE
D
MO
DE
OF
SE
X
CIR
CU
MC
ISIO
N
GE
NIT
AL
UL
CE
R/F
ISS
UR
E
GE
NIT
AL
DIS
CH
AR
GE
LY
MP
HN
OD
ES
PA
PU
LE
S
OR
AL
MU
CO
SA
DIA
BE
TE
S M
EL
LIT
US
RP
R
TP
HA
ICT
C
HB
sAG
AN
TI
HC
V
KO
H
WE
T M
OU
NT
GR
AM
ST
AIN
TZ
AN
CK
SM
EA
R
DIA
GN
OS
IS
26 RAJA 30 2 M O UN 3 3 1 2 2,3,4,5 1 5 6 2 1 N A NR N NR NR NR 3 3 5 2 WART
27 BABU 30 2 M O UN 3 3 3 2 2,3,4,5 2 5 6 1 4 N A R P NR NR NR 3 3 5 2 SY 2
28 SUBRAMANI 47 3 M H M 1 2 4 2 1 2 5 6 2 1 N A NR N R NR NR 3 3 5 2 WART
29 JANAKIRAM 37 2 M O M 1 1 4 2 1 2 2 6 1 4 N A NR N NR NR NR 3 3 5 1 HG
30 SURESH 40 3 M O M 1 1 2 2 1 2 2 6 1 4 N A NR N NR NR NR 3 3 5 1 HG
31 JEEVA 34 2 M O M 3 1 1 2 4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
32 VINOTH 29 2 M O UM 3 3 1 2 2,3,4,5 2 5 6 2 4 N A R P NR NR NR 3 3 5 2 ELS
33 MURUGAN 26 2 M D M 1 3 2 2 1 2 4 6 1 4 N A R P NR NR NR 3 3 5 2 ELS
34 FRANCIS 32 2 M O M 1 4 4 2 1 2 2 6 2 4 N A NR N NR NR NR 3 3 5 1 HG
35 MANIKAM 57 3 M D M 1 3 4 2 1 2 3 5 2 4 OC A NR N R NR NR 1 3 1 2 BAL
36 STEFY 28 2 M O M 3 1 3 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
37 DEVDASAN 44 3 M D M 1 4 4 2 1 2 5 6 2 4 OC A NR N R NR NR 3 3 5 2 NIL
38 BALASUBRAMANIAN39 3 M O M 1 3 4 2 1 2 5 6 2 4 OC A NR N R NR NR 3 3 5 2 NIL
39 MUTHAIAH 48 3 M D M 1 4 2 2 1 2 5 6 2 4 N A NR N R NR NR 3 3 5 2 NIL
40 BALAKRISHNAN32 3 M D M 1 4 2 2 1 2 5 6 2 4 N A R P NR NR NR 3 3 5 2 LLS
41 KARTHIKETAN43 3 M O M 3 2 1 2 2,3,4,5 2 3 5 2 4 OC A NR N NR NR NR 1 3 1 2 BAL
42 ATHIMUTHU 49 3 M O M 1 3 4 2 1 2 5 6 2 3 N A NR N NR NR NR 3 3 5 2 SCABIES
43 MAHADEVI 24 2 F FSW UM 2 3 3 2 1 3 5 6 2 4 N A R P NR NR NR 3 3 5 2 ELS
44 RAVI 36 2 M D M 1 3 4 2 1 2 5 6 2 3 N A NR N NR NR NR 3 3 5 2 SCABIES
45 POOVARASAN 21 2 M H UM 3 2 3 2 2,3,4,5 2 2 6 1 4 N A NR N NR NR NR 3 3 5 1 HG
46 AMUTHA 38 2 F O W 1 2 3 2 1 2 2 6 1 4 OC A NR N R NR NR 3 3 5 1 HG
47 SANKARAN 41 3 M H UM 3 3 3 2 2,3,4,5 2 5 6 2 4 N A NR N R NR NR 3 3 5 2 NIL
48 MADASAMY 34 2 M O M 3 3 1 2 4,5 2 5 6 2 4 N A NR N R NR NR 3 3 5 2 NIL
49 SIVASUBRAMANIAN28 2 M O UM 3 2 1 2 2,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
50 PERUMAL 42 3 M O M 1 4 2 2 1 2 5 6 2 4 N A R P R NR NR 3 3 5 2 LLS

S.N
O
NA
ME
AG
E
AG
E
SE
X
OC
CU
PA
TIO
N
MA
RIT
AL
ST
AT
US
EM
C/P
MC
/MS
M
LA
ST
CO
NT
AC
T
CO
NT
AC
T P
ER
SO
N
PR
OT
EC
TE
D O
R
UN
PR
OT
EC
TE
D
MO
DE
OF
SE
X
CIR
CU
MC
ISIO
N
GE
NIT
AL
UL
CE
R/F
ISS
UR
E
GE
NIT
AL
DIS
CH
AR
GE
LY
MP
HN
OD
ES
PA
PU
LE
S
OR
AL
MU
CO
SA
DIA
BE
TE
S M
EL
LIT
US
RP
R
TP
HA
ICT
C
HB
sAG
AN
TI
HC
V
KO
H
WE
T M
OU
NT
GR
AM
ST
AIN
TZ
AN
CK
SM
EA
R
DIA
GN
OS
IS
51 MURALI 28 2 M D M 1 2 2 2 1 3 5 6 2 1 N A NR N NR NR NR 3 3 5 2 WART
52 VANDIMALAYAN28 2 M O M 1 3 4 2 1 2 5 6 2 1 N A NR N NR NR NR 3 3 5 2 WART
53 KARUPUSAMY 58 3 M O M 1 4 2 2 1 2 3 5 2 4 N A NR N R NR NR 1 3 1 2 BAL
54 MAHARAJAN 21 2 M S UM 2 3 2 2 1 2 5 6 2 2 N A NR N NR NR NR 3 3 5 2 MC
55 PARAMESWARAN48 3 M O M 1 4 4 2 1 2 5 6 2 4 OC A NR N R NR NR 3 3 5 2 NIL
56 PAULDURAI 27 2 M O UM 1 4 4 2 1 2 5 6 2 3 N A NR N NR NR NR 3 3 5 2 SCABIES
57 ESAKKIMUTHU27 2 M O UM 1 2 4 2 1 2 5 6 2 2 N A NR N NR NR NR 3 3 5 2 MC
58 LAKSHMANARAJ35 2 M O M 1 1 2 2 1 2 5 6 2 4 OC A NR N R NR NR 3 3 5 2 NIL
59 SUNDARAJAN 35 2 M O M 3 4 2 1 1 2 5 6 2 1 N A NR N NR NR NR 3 3 5 2 WART
60 SUBRAMANIAN37 2 M H M 1 4 4 2 1 2 5 6 2 4 N A NR N R NR NR 3 3 5 2 NIL
61 RANI 33 2 F FSW M 1 3 3 2 1 3 5 3 2 4 N A NR N NR NR NR 3 2 2 2 BV
62 AYYADURAI 45 3 M O M 1 4 4 2 1 2 5 6 2 1 OC A NR N R NR NR 3 3 5 2 WART
63 MUTHUKRISHNAN58 3 M O M 1 3 4 2 1 2 5 6 2 1 N A NR N NR NR NR 3 3 5 2 WART
64 KARUPAIAH 65 3 M O M 1 4 2 2 1 2 2 6 1 4 N A NR N NR NR NR 3 3 5 1 HG
65 VALIAMAL 50 3 F FSW M 1 2 3 2 1 3 5 2 2 4 N A NR N NR NR NR 1 3 1 2 VVC
66 MADASAMHY 32 2 M O M 3 1 2 2 2,3,4,5 2 5 6 2 1 N A NR N R NR NR 3 3 5 2 WART
67 CHANDRAN 31 2 M D M 1 4 4 2 1 2 5 6 2 4 OHL A NR N R NR NR 3 3 5 2 NIL
68 MARIAMMAL 35 2 F FSW M 1 2 3 2 1 2 2 6 1 4 N A NR N NR NR NR 3 3 5 1 HG
69 GANAPATHY 53 3 M D M 1 4 4 2 1 2 3 5 2 4 N P NR N NR NR NR 1 3 1 2 BAL
70 SENTHILKUMAR32 2 M D M 1 4 2 2 1 2 3 5 2 4 N A NR N NR NR NR 1 3 1 2 BAL
71 RAMBA 41 3 TG O UM 3 4 3 2 2,4 4 5 6 2 4 HL P NR N NR NR NR 3 2 5 2 HL
72 SENTHILKUMAR35 2 M O M 3 2 1 1 4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
73 DILIP SARKAR 30 2 M O UM 3 2 1 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
74 THANGAMARIAMMAL36 2 F FSW M 1 3 3 2 1 2 5 6 2 2 N A NR N R NR NR 3 3 5 2 MC
75 KUMAR 39 2 M D M 1 3 4 2 1 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL

S.N
O
NA
ME
AG
E
AG
E
SE
X
OC
CU
PA
TIO
N
MA
RIT
AL
ST
AT
US
EM
C/P
MC
/MS
M
LA
ST
CO
NT
AC
T
CO
NT
AC
T P
ER
SO
N
PR
OT
EC
TE
D O
R
UN
PR
OT
EC
TE
D
MO
DE
OF
SE
X
CIR
CU
MC
ISIO
N
GE
NIT
AL
UL
CE
R/F
ISS
UR
E
GE
NIT
AL
DIS
CH
AR
GE
LY
MP
HN
OD
ES
PA
PU
LE
S
OR
AL
MU
CO
SA
DIA
BE
TE
S M
EL
LIT
US
RP
R
TP
HA
ICT
C
HB
sAG
AN
TI
HC
V
KO
H
WE
T M
OU
NT
GR
AM
ST
AIN
TZ
AN
CK
SM
EA
R
DIA
GN
OS
IS
76 MADASAMY 43 3 M D M 1 3 4 1 1 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
77 VELUSAMY 75 4 M O M 1 4 4 2 1 2 5 6 2 4 OC A NR N R NR NR 3 3 5 2 NIL
78 RAJA 30 2 M H M 1 2 4 2 1 2 3 5 2 4 N A NR N NR NR NR 1 3 1 2 BAL
79 SUNDARAJAN 37 2 M D M 1 4 4 2 1 2 3 5 2 4 N A NR N NR NR NR 1 3 1 2 BAL
80 MUTHALAISAMI24 2 M S UM 1 2 4 2 1 2 5 6 2 1 N A NR N NR NR NR 3 3 5 2 WART
81 ULAGANATHAN63 3 M O M 1 2 2 1 1 2 5 6 2 1 N A NR N NR NR NR 3 3 5 2 WART
82 JEEVA 34 2 M O M 3 3 1 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
83 SARAVANAN 39 2 M O M 1 2 4 2 1 2 3 5 2 4 N A NR N NR NR NR 1 3 1 2 BAL
84 SUNDARAMAHALINGAM36 2 M D M 1 1 4 2 1 2 2 6 1 4 N A NR N NR NR NR 3 3 5 1 HG
85 SUBRAMANIAN40 3 M C M 3 1 1 2 2,3,4,5 2 3 5 2 4 OC A NR N R NR NR 1 3 1 2 BAL
86 SIVA 38 2 M O M 3 1 3 2 2,5 2 2 6 1 4 N A NR N NR NR NR 3 3 5 1 HG
87 RAMAN 45 3 M D M 3 3 1 2 2,3,4,5 2 3 5 2 4 OC A NR N R NR NR 1 3 1 2 BAL
88 MUTHAIAH 44 3 M O M 3 3 1 2 2,3,4,5 2 5 6 2 4 N A NR N R NR NR 3 3 5 2 NIL
89 PARAMESWARI27 2 F FSW M 1 3 3 1 1 3 5 6 2 2 N A NR N NR NR NR 3 3 5 2 MC
90 PONNUSAMI 59 3 M O M 1 4 4 1 1 2 5 6 2 4 N A NR N R NR NR 3 3 5 2 NIL
91 MANIKANDAN 43 3 M D M 1 1 4 2 1 2 2 6 1 4 N A NR N NR NR NR 3 3 5 1 HG
92 PETCHIAMMAL43 3 F FSW M 1 3 1 2 1 3 2 6 1 4 N A NR N R NR NR 3 3 5 1 HG
93 MOHAMED KASI20 2 M M UM 2 3 4 2 1 2 5 6 2 2 N A NR N NR NR NR 3 3 5 2 MC
94 MUTHU 34 3 F FSW M 1 2 3 1 1 3 2 6 1 4 N A NR N NR NR NR 3 3 5 1 HG
95 ESAKKI 55 3 M D M 1 1 4 1 1 2 3 5 2 4 N A NR N NR NR NR 1 3 1 2 BAL
96 KANAMAL 42 3 F FSW M 1 2 3 1 1 3 5 2 2 4 N P NR N NR NR NR 1 3 1 2 VVC
97 RAMAR 45 3 M O M 1 1 4 2 1 2 2 6 1 4 N A NR N NR NR NR 3 3 5 1 HG
98 JOSEPH 25 2 M M UM 2 2 4 2 1 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
99 AVINUSH KUMAR35 2 M C M 1 1 4 2 1 2 3 5 2 4 N P NR N NR NR NR 1 3 1 2 BAL
100 AROKIYASAMY50 3 M O M 1 1 4 2 1 2 3 5 2 4 N P NR N NR NR NR 1 3 1 2 BAL

S.N
O
NA
ME
AG
E
AG
E
SE
X
OC
CU
PA
TIO
N
MA
RIT
AL
ST
AT
US
EM
C/P
MC
/MS
M
LA
ST
CO
NT
AC
T
CO
NT
AC
T P
ER
SO
N
PR
OT
EC
TE
D O
R
UN
PR
OT
EC
TE
D
MO
DE
OF
SE
X
CIR
CU
MC
ISIO
N
GE
NIT
AL
UL
CE
R/F
ISS
UR
E
GE
NIT
AL
DIS
CH
AR
GE
LY
MP
HN
OD
ES
PA
PU
LE
S
OR
AL
MU
CO
SA
DIA
BE
TE
S M
EL
LIT
US
RP
R
TP
HA
ICT
C
HB
sAG
AN
TI
HC
V
KO
H
WE
T M
OU
NT
GR
AM
ST
AIN
TZ
AN
CK
SM
EA
R
DIA
GN
OS
IS
101 ALPHONSE MARY53 3 F O M 1 3 3 2 1 3 5 2 2 4 N P NR N NR NR NR 1 3 1 2 VVC
102 KANNAN 33 2 M D UM 2 4 4 2 1 2 3 5 2 4 N A NR N NR NR NR 1 3 1 2 BAL
103 MARIAPPAN 42 3 M O M 1 2 4 2 1 2 3 5 2 4 N A NR N NR NR NR 1 3 1 2 BAL
104 VIJAIKUMAR 32 2 M O UM 1 2 4 1 1 2 5 1 2 4 N A NR N NR NR NR 3 3 5 2 NGU
105 SUMAN 28 2 M M M 3 3 3 2 2,3,4,5 2 1 6 1 4 N A R P NR NR NR 3 3 5 2 SY 2
106 MARIAPPAN 31 2 M O M 3 4 3 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
107 GANESAN 38 2 M D UM 1 1 4 2 1 2 3 5 2 4 N A NR N NR NR NR 1 3 1 2 BAL
108 KALAISELVSN 31 2 M M UM 2 4 4 2 1 2 2 6 1 4 N A NR N NR NR NR 3 3 5 1 HG
109 PREMKUMAR 27 2 M D UM 2 3 4 1 1 2 3 5 2 4 N A NR N NR NR NR 1 3 1 2 BAL
110 THANGARAJ 58 3 M O M 3 2 1 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
111 MARIAPPAN 28 2 M O UM 3 1 1 2 2,3,4,5 2 5 6 2 1 OC A NR N R NR NR 3 3 5 2 WART
112 INDRA 47 3 F M M 1 1 1 1 1 3 5 2 2 4 N A NR N NR NR NR 1 3 1 2 VVC
113 SUBAIAH 55 3 M O M 1 3 2 2 1 2 2 6 1 4 N A NR N NR NR NR 3 3 5 1 HG
114 MARIAMMAL 35 3 F FSW M 1 2 3 2 1 3 5 2 2 4 N A NR N NR NR NR 1 3 1 2 VVC
115 HARIHARARAJ36 3 M H M 1 3 2 2 1 2 5 6 2 1 N A NR N R NR NR 3 3 5 2 WART
116 CHANDRAN 29 2 F FSW M 1 2 3 1 1 3 5 6 2 1 N A NR N NR NR NR 3 3 5 2 WART
117 LAKSHMIGANTHAN35 2 M D M 1 3 4 2 1 2 2 6 1 4 N A NR N NR NR NR 3 3 5 1 HG
118 SIVANESAN 34 2 M O M 1 3 4 2 1 2 5 6 2 4 N A R P NR NR NR 3 3 5 2 ELS
119 PANDARAPANDIYAN29 2 M M UM 2 2 4 2 1 2 3 5 2 4 N A NR N NR NR NR 1 3 1 2 BAL
120 KARTHI 36 2 M O M 1 2 4 2 1 2 5 6 2 2 N A NR N NR NR NR 3 3 5 2 MC
121 RAMALAKSHMI31 2 F FSW M 1 2 1 2 1 3 5 6 2 2 N A NR N NR NR NR 3 3 5 2 MC
122 SELVI 43 3 F H M 1 2 1 2 1 3 5 6 2 4 N A R P NR NR NR 3 3 5 2 SY 2
123 DHANABAKIYAM32 2 F FSW M 1 1 3 2 1 3 5 2 2 4 N A NR N NR NR NR 1 3 1 2 VVC
124 MOOKAIAH 52 3 M H M 1 4 4 2 1 2 3 5 2 4 N A NR N NR NR NR 1 3 1 2 BAL
125 MARIATHANGAM37 2 F FSW M 1 3 3 2 1 3 5 2 2 4 N A NR N NR NR NR 1 3 1 2 VVC

S.N
O
NA
ME
AG
E
AG
E
SE
X
OC
CU
PA
TIO
N
MA
RIT
AL
ST
AT
US
EM
C/P
MC
/MS
M
LA
ST
CO
NT
AC
T
CO
NT
AC
T P
ER
SO
N
PR
OT
EC
TE
D O
R
UN
PR
OT
EC
TE
D
MO
DE
OF
SE
X
CIR
CU
MC
ISIO
N
GE
NIT
AL
UL
CE
R/F
ISS
UR
E
GE
NIT
AL
DIS
CH
AR
GE
LY
MP
HN
OD
ES
PA
PU
LE
S
OR
AL
MU
CO
SA
DIA
BE
TE
S M
EL
LIT
US
RP
R
TP
HA
ICT
C
HB
sAG
AN
TI
HC
V
KO
H
WE
T M
OU
NT
GR
AM
ST
AIN
TZ
AN
CK
SM
EA
R
DIA
GN
OS
IS
126 PONMANI 33 2 M O M 3 4 1 1 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
127 ARUNACHALAM56 3 M O M 1 2 4 2 1 2 2 6 1 4 N P NR N NR NR NR 3 3 5 1 HG
128 RAMALAKSHMI29 2 F H M 1 1 1 1 1 3 5 2 2 4 N A NR N NR NR NR 1 3 1 2 VVC
129 ARUMUGANAINAR42 3 M H M 1 4 4 2 1 2 5 6 2 4 N A NR N R NR NR 3 3 5 2 NIL
130 KITTU 51 3 M O M 3 2 3 1 3,4,5 2 3 5 2 4 N P NR N NR NR NR 1 3 1 2 BAL
131 SORNAMMUDI 29 2 M M UM 2 2 4 2 1 2 5 6 2 3 N A NR N R NR NR 3 3 5 2 SCABIES
132 SRINIVASAN 33 2 M H M 1 1 4 2 1 2 3 5 2 4 N A NR N NR NR NR 1 3 1 2 BAL
133 RADHAKRISHNAN55 3 M O M 1 4 4 2 1 2 5 6 2 4 N A R P NR NR NR 3 3 5 2 LLS
134 MANIKANDA PRABHU25 2 M H UM 3 2 1 2 2,3,4,5 2 1 6 1 4 N A R P NR NR NR 3 3 5 2 SY 1
135 KASI 46 3 M D M 1 4 4 2 1 2 5 6 2 4 N A R P NR NR NR 3 3 5 2 LLS
136 RAMACHANDRAN53 3 M O M 1 4 4 2 1 2 3 5 2 4 N P NR N NR NR NR 1 3 1 2 BAL
137 MATHIVANAN 42 3 M H M 1 4 4 2 1 2 3 5 2 4 N A NR N R NR NR 1 3 1 2 BAL
138 KARPAGAM 30 2 F FSW M 1 1 3 2 1 3 5 2 2 4 N A NR N NR NR NR 1 3 1 2 VVC
139 MARIAPPAN 41 3 M M M 1 2 4 2 1 2 3 5 2 4 N A NR N NR NR NR 1 3 1 2 BAL
140 ANDIAPAN 28 2 M D UM 2 2 4 2 1 2 2 6 1 4 N A NR N NR NR NR 3 3 5 1 HG
141 MURUGESWARI37 2 F O M 1 1 3 2 1 3 5 2 2 4 N A NR N NR NR NR 1 3 1 2 VVC
142 PERUMAL 45 3 M D M 3 1 1 2 2,3,4,5 2 2 6 1 4 OC A NR N NR NR NR 3 3 5 1 HG
143 SHANMUGAPANDIAN54 3 M O M 1 3 4 1 1 2 3 5 2 4 N P NR N NR NR NR 1 3 1 2 BAL
144 MARIAMMAL 42 3 F H M 1 3 1 1 1 3 5 6 2 1 N A NR N NR NR NR 3 3 5 2 WART
145 MASOOD 23 2 F O M 1 1 3 2 1 3 2 6 1 4 N A NR N NR NR NR 3 3 5 1 HG
146 MARIA STEPHEN52 3 M O M 1 2 4 2 1 2 5 6 2 4 OC A NR N R NR NR 3 3 5 2 NIL
147 RAMANATHAN54 3 M D M 1 4 2 2 1 2 3 5 2 4 N P NR N NR NR NR 1 3 1 2 BAL
148 THANGAM 43 3 F FSW M 1 1 1 2 1 3 5 2 2 4 N A NR N NR NR NR 1 3 1 2 VVC
149 GOMATHI 45 3 F FSW M 1 1 1 2 1 3 5 2 2 4 N A NR N NR NR NR 1 3 1 2 VVC
150 PALANIVEL 28 2 M O M 1 1 4 2 1 2 3 5 2 4 N A NR N NR NR NR 1 3 1 2 BAL

S.N
O
NA
ME
AG
E
AG
E
SE
X
OC
CU
PA
TIO
N
MA
RIT
AL
ST
AT
US
EM
C/P
MC
/MS
M
LA
ST
CO
NT
AC
T
CO
NT
AC
T P
ER
SO
N
PR
OT
EC
TE
D O
R
UN
PR
OT
EC
TE
D
MO
DE
OF
SE
X
CIR
CU
MC
ISIO
N
GE
NIT
AL
UL
CE
R/F
ISS
UR
E
GE
NIT
AL
DIS
CH
AR
GE
LY
MP
HN
OD
ES
PA
PU
LE
S
OR
AL
MU
CO
SA
DIA
BE
TE
S M
EL
LIT
US
RP
R
TP
HA
ICT
C
HB
sAG
AN
TI
HC
V
KO
H
WE
T M
OU
NT
GR
AM
ST
AIN
TZ
AN
CK
SM
EA
R
DIA
GN
OS
IS
151 DURAIRAJ 41 3 M M M 1 1 4 2 1 2 3 5 2 4 N P NR N NR NR NR 1 3 1 2 BAL
152 KRISHNAN 65 3 M O M 1 1 4 2 1 2 3 5 2 4 N P NR N NR NR NR 1 3 1 2 BAL
153 COLUMBUS 25 2 M O UM 2 2 4 2 1 2 2 6 1 4 N A NR N NR NR NR 3 3 5 1 HG
154 MANI 51 3 M O M 1 2 4 2 1 2 2 6 1 4 N A NR N NR NR NR 3 3 5 1 HG
155 SATHISH 28 2 M D UM 2 3 4 2 1 2 5 6 2 2 N A NR N NR NR NR 3 3 5 2 MC
156 MUTHUKUMAR39 2 M O M 1 3 4 2 1 2 5 6 2 2 N A NR N NR NR NR 3 3 5 2 MC
157 PREETHI 36 2 TG O UM 3 1 1 2 2,3,4,5 4 5 6 2 2 N A NR N NR NR NR 3 3 5 2 MC
158 SIVASHANKAR31 2 M O UM 3 3 3 2 2,3,4,5 2 5 6 2 1 N A NR N NR NR NR 3 3 5 2 WART
159 MARAGATHAM44 3 F FSW M 1 2 3 2 1 3 5 2 2 4 N A NR N NR NR NR 1 3 1 2 VVC
160 KANAGARAJ 51 3 M H M 1 3 4 2 1 2 5 6 2 1 N A NR N R NR NR 3 3 5 2 WART
161 MANI 63 3 M H M 1 3 4 2 1 2 3 5 2 4 OC P NR N R NR NR 1 3 1 2 BAL
162 SORNALAKSHMI27 2 F FSW M 1 2 3 2 1 3 5 2 2 4 N A NR N NR NR NR 1 3 1 2 VVC
163 SAKTHIVEL 29 2 M M M 1 4 4 2 2 2 5 6 2 2 N A NR N NR NR NR 3 3 5 2 MC
164 SIVASAKTHI 29 2 M H UM 2 3 4 2 1 2 5 1 1 4 N A NR N NR NR NR 3 3 3 2 GON
165 ESAKKI 43 3 M O M 3 2 3 2 2,3,4,5 2 3 5 2 4 N P NR N NR NR NR 1 3 1 2 BAL
166 HASSAN 32 2 M M M 3 1 1 2 2,3,4,5 2 5 1 1 4 N A NR N NR NR NR 3 3 3 2 GON
167 SUBRAMANIAN33 2 M O M 1 1 4 2 1 2 1 6 1 4 N A R P NR NR NR 3 3 5 2 SY 1
168 RAMAKRISHNAN47 3 M O M 1 3 4 2 1 2 5 6 2 4 N A R P R NR NR 3 3 5 2 ELS
169 KUMAR 26 2 M H UM 3 1 1 2 2,3,4,5 2 1 6 1 4 N A R P NR NR NR 3 3 5 2 SY 1
170 SURESH 24 2 M O UM 3 1 3 2 2,3,4,5 2 5 6 2 4 N A R P NR NR NR 3 3 5 2 SY 2
171 MURUGAN 43 3 M O M 1 4 4 2 1 2 5 2 2 4 N A NR N NR NR NR 1 3 1 2 VVC
172 PETHCIAMMAL21 2 F S UM 2 2 1 2 1 3 5 2 2 4 N A NR N NR NR NR 1 3 1 2 VVC
173 SHANMUGAM 26 2 M O UM 3 1 3 2 2,3,4,5 2 5 6 2 3 N A NR N R NR NR 3 3 5 2 SCABIES
174 THALAVAI 54 3 M H M 3 2 3 2 2,3,4,5 2 3 5 2 4 N P NR N NR NR NR 1 3 1 2 BAL
175 MANIKANDAN 24 2 M O M 1 4 4 2 1 2 5 6 2 1 OC A NR N R NR NR 3 3 5 2 WART

S.N
O
NA
ME
AG
E
AG
E
SE
X
OC
CU
PA
TIO
N
MA
RIT
AL
ST
AT
US
EM
C/P
MC
/MS
M
LA
ST
CO
NT
AC
T
CO
NT
AC
T P
ER
SO
N
PR
OT
EC
TE
D O
R
UN
PR
OT
EC
TE
D
MO
DE
OF
SE
X
CIR
CU
MC
ISIO
N
GE
NIT
AL
UL
CE
R/F
ISS
UR
E
GE
NIT
AL
DIS
CH
AR
GE
LY
MP
HN
OD
ES
PA
PU
LE
S
OR
AL
MU
CO
SA
DIA
BE
TE
S M
EL
LIT
US
RP
R
TP
HA
ICT
C
HB
sAG
AN
TI
HC
V
KO
H
WE
T M
OU
NT
GR
AM
ST
AIN
TZ
AN
CK
SM
EA
R
DIA
GN
OS
IS
176 MUTHUSELVI 41 3 F FSW M 1 3 3 2 1 3 5 2 2 4 N A NR N NR NR NR 1 3 1 2 VVC
177 RAJA 31 2 M O UM 3 3 1 2 2,3,4,5 2 5 6 2 1 N A NR N NR NR NR 3 3 5 2 WART
178 SUBRAMANIAN47 3 M H M 1 2 4 2 1 2 5 6 2 1 N A NR N R NR NR 3 3 5 2 WART
179 MURUGAN 46 3 M O M 3 4 1 2 2,3 2 5 6 2 4 N A NR N R NR NR 3 3 5 2 NIL
180 RAJAKUMARI 38 2 F FSW M 1 1 1 1 1 3 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
181 KUTRALAM 72 4 M O M 1 4 2 2 1 2 3 5 2 4 N P NR N NR NR NR 1 3 1 2 BAL
182 PAPANASAM 38 2 M O M 1 1 2 2 1 2 5 6 2 3 N A NR N NR NR NR 3 3 5 2 SCABIES
183 KALIRAJ 28 2 M H UM 2 3 4 2 1 2 5 6 2 4 N A R P NR NR NR 3 3 5 2 ELS
184 PRABAKARAN 28 2 M D UM 2 3 4 2 1 2 4 6 1 4 N A R P NR NR NR 3 3 5 2 ELS
185 SUDALAIMUTHU32 2 M O M 3 3 3 2 2,3,4,5 2 4 6 2 4 N A R P NR NR NR 3 3 5 2 ELS
186 ARUL 28 2 M O M 1 3 4 2 1 2 5 6 2 4 N A R P NR NR NR 3 3 5 2 LLS
187 KATHIRAVAN 36 2 M O M 1 4 4 2 1 2 3 5 2 4 O A NR N R NR NR 1 3 1 2 BAL
188 PRIYA 23 2 F S UM 2 3 1 2 1 3 5 6 2 1 N A NR N NR NR NR 3 3 5 2 WART
189 MARIAANTONY39 2 M O M 1 4 4 2 1 2 3 5 2 4 N P NR N NR NR NR 1 3 1 2 BAL
190 CHELLADURAI58 3 M O M 1 4 2 2 1 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
191 PALANIAPPAN 32 2 M H M 1 4 4 2 1 2 3 5 2 4 N A NR N NR NR NR 1 3 1 2 BAL
192 PATTAMMAL 22 2 TG M UM 3 1 1 2 2,3,4,5 4 2 6 1 4 N A NR N NR NR NR 3 3 5 1 HG
193 MAHARAJAN 33 2 M H M 3 4 3 2 2,3,4,5 2 2 6 1 4 N A NR N NR NR NR 3 3 5 1 HG
194 KARUTHAPANDI59 3 M O M 1 3 2 2 1 2 2 6 1 4 N A NR N NR NR NR 3 3 5 1 HG
195 SARAVANAN 41 3 M D M 3 3 3 2 2,3,4,5 2 3 5 2 4 N A NR N NR NR NR 1 3 1 2 BAL
196 MURUGAN 50 3 M O M 1 3 2 2 1 2 2 6 1 4 N A NR N NR NR NR 3 3 5 1 HG
197 VASANTHI 30 2 F FSW M 1 2 1 2 1 3 2 6 1 4 N A NR N NR NR NR 3 3 5 1 HG
198 PARTHIBAN 21 2 M S UM 3 3 1 2 2,3,4,5 2 5 6 2 4 N A R P NR NR NR 3 3 5 2 SY 2
199 ROHINI 22 2 F S UM 2 2 1 2 1 3 5 2 2 4 N A NR N NR NR NR 1 3 1 2 VVC
200 KANNAMMAL 42 3 F FSW M 1 2 1 2 1 3 2 6 1 4 N A NR N NR NR NR 3 3 5 1 HG

S.N
O
NA
ME
AG
E
AG
E
SE
X
OC
CU
PA
TIO
N
MA
RIT
AL
ST
AT
US
EM
C/P
MC
/MS
M
LA
ST
CO
NT
AC
T
CO
NT
AC
T P
ER
SO
N
PR
OT
EC
TE
D O
R
UN
PR
OT
EC
TE
D
MO
DE
OF
SE
X
CIR
CU
MC
ISIO
N
GE
NIT
AL
UL
CE
R/F
ISS
UR
E
GE
NIT
AL
DIS
CH
AR
GE
LY
MP
HN
OD
ES
PA
PU
LE
S
OR
AL
MU
CO
SA
DIA
BE
TE
S M
EL
LIT
US
RP
R
TP
HA
ICT
C
HB
sAG
AN
TI
HC
V
KO
H
WE
T M
OU
NT
GR
AM
ST
AIN
TZ
AN
CK
SM
EA
R
DIA
GN
OS
IS
201 MAHARASI 33 2 F FSW UM 2 2 1 2 1 3 5 6 2 2 N A NR N NR NR NR 3 3 5 2 MC
202 AMALRAJ 40 3 M D M 1 1 4 2 1 2 2 6 1 4 N A NR N NR NR NR 3 3 5 1 HG
203 NAMBIRAJAN 24 2 M O UM 3 3 3 2 2,3,4,5 2 5 6 2 1 N A NR N NR NR NR 3 3 5 2 WART
204 MUTHU 53 3 M O M 1 3 4 2 1 2 2 6 1 4 N A NR N NR NR NR 3 3 5 1 HG
205 ESAKKI 58 3 F O M 1 4 1 2 1 3 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
206 MANONMANI 47 3 F O M 1 4 1 2 1 3 5 6 2 4 N A R P NR NR NR 3 3 5 2 ELS
207 VIJAYALAKSHMI22 2 F S UM 2 3 1 2 1 3 5 6 2 4 N A R P NR NR NR 3 3 5 2 ELS
208 SENTHILKUMAR29 2 M O UM 2 3 1 2 1 2 4 6 2 4 N A R P NR NR NR 3 3 5 2 ELS
209 SUMATHI 45 3 F FSW M 1 2 3 2 1 3 5 6 2 4 N A R P NR NR NR 3 3 5 2 LLS
210 MURUGAN 39 3 M O M 3 2 1 2 2,3,4,5 2 1 6 1 4 N A R P R NR NR 3 3 5 2 SY 1
211 KARUPUSAMY 48 3 M O M 1 3 4 2 1 2 2 6 1 4 N A NR N R NR NR 3 3 5 1 HG
212 THANGAVEL 38 3 M O M 1 2 4 2 1 2 3 5 2 4 N P NR N NR NR NR 1 3 1 2 BAL
213 KAVITHA 28 2 F O M 1 2 1 2 1 3 5 2 2 4 N A NR N NR NR NR 1 3 1 2 VVC
214 SANYASI 39 2 M O M 1 2 4 2 1 2 3 5 2 4 N P NR N NR NR NR 1 3 1 2 BAL
215 RAJINI 36 3 M O M 1 2 4 2 1 2 5 6 2 2 N A NR R NR NR NR 3 3 5 2 MC
216 SUBRAMANI 44 3 M O M 1 2 4 2 1 2 3 5 2 4 N A NR N R NR NR 1 3 1 2 BAL
217 GUNASEELAN 22 2 M S UM 3 3 1 2 2,3,4,5 2 5 6 2 1 N A NR N NR NR NR 3 3 5 2 WART
218 SARANYA 23 2 F S UM 2 2 1 2 1 3 5 6 2 1 N A NR N NR NR NR 3 3 5 2 WART
219 MARIAMMAL 30 2 F O M 1 1 1 2 1 3 5 2 2 4 N A NR N NR NR NR 1 3 1 2 VVC
220 TAMILSELVAN42 3 M O M 3 4 1 2 2,3,4,5 2 4 6 2 4 N A R P NR NR NR 3 3 5 2 ELS
221 SASIKALA 31 2 F O M 1 3 1 2 1 3 4 6 2 4 N A R P NR NR NR 3 3 5 2 ELS
222 NAGAMUTHU 32 2 M O M 3 2 1 2 2,3,4,5 2 5 6 2 4 N A R P NR NR NR 3 3 5 2 SY 2
223 ASWIN RAJ 28 2 M O UM 3 3 1 2 2,3,4,5 2 5 6 2 1 N A NR N NR NR NR 3 3 5 2 WART
224 MANI 50 3 M O M 1 2 4 2 1 2 2 6 1 4 N A NR N R NR NR 3 3 5 1 HG
225 GANESAN 40 3 M O M 3 3 1 2 2,3,4,5 2 2 6 1 4 OC A NR N R NR NR 3 3 5 1 HG
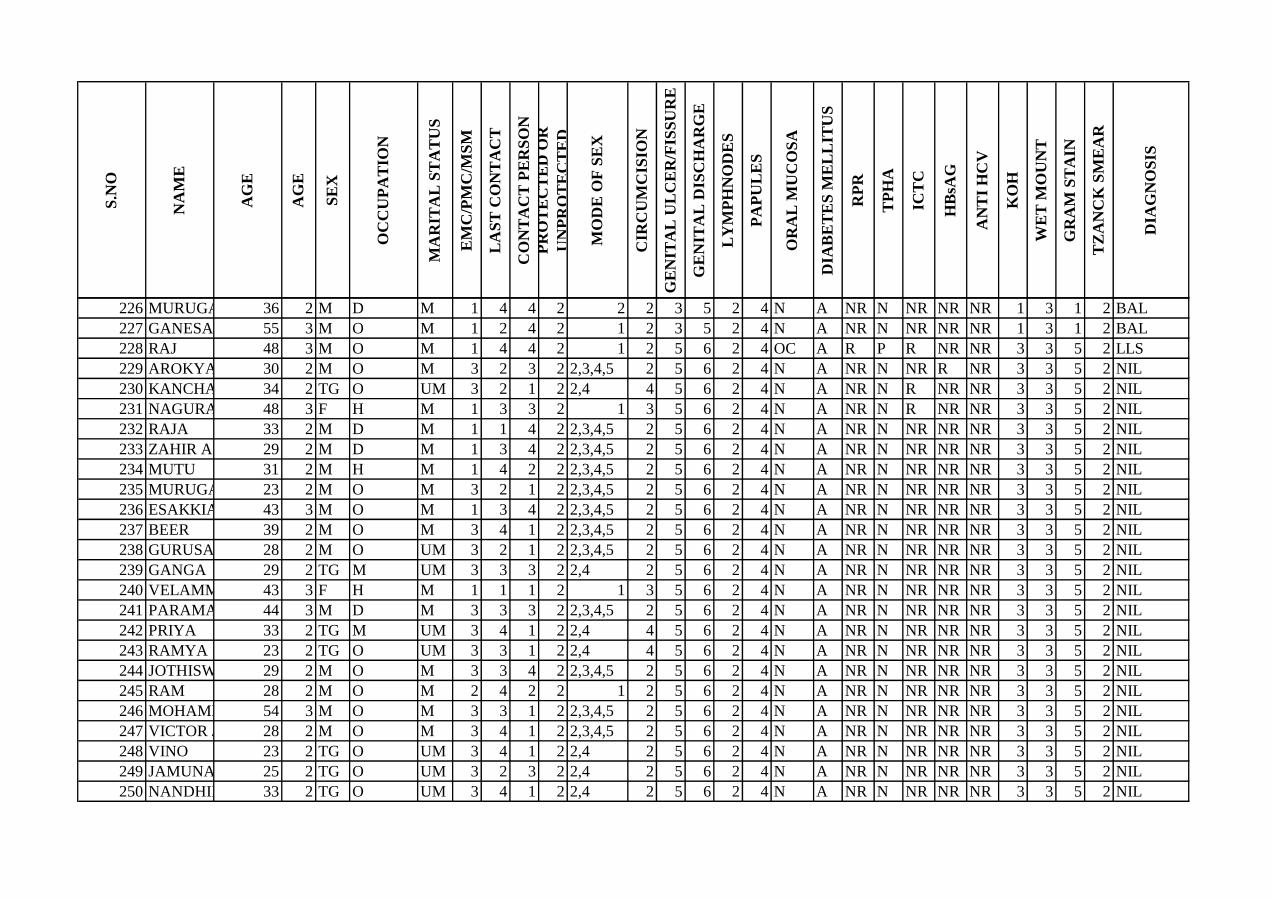
S.N
O
NA
ME
AG
E
AG
E
SE
X
OC
CU
PA
TIO
N
MA
RIT
AL
ST
AT
US
EM
C/P
MC
/MS
M
LA
ST
CO
NT
AC
T
CO
NT
AC
T P
ER
SO
N
PR
OT
EC
TE
D O
R
UN
PR
OT
EC
TE
D
MO
DE
OF
SE
X
CIR
CU
MC
ISIO
N
GE
NIT
AL
UL
CE
R/F
ISS
UR
E
GE
NIT
AL
DIS
CH
AR
GE
LY
MP
HN
OD
ES
PA
PU
LE
S
OR
AL
MU
CO
SA
DIA
BE
TE
S M
EL
LIT
US
RP
R
TP
HA
ICT
C
HB
sAG
AN
TI
HC
V
KO
H
WE
T M
OU
NT
GR
AM
ST
AIN
TZ
AN
CK
SM
EA
R
DIA
GN
OS
IS
226 MURUGAIAH 36 2 M D M 1 4 4 2 2 2 3 5 2 4 N A NR N NR NR NR 1 3 1 2 BAL
227 GANESAN 55 3 M O M 1 2 4 2 1 2 3 5 2 4 N A NR N NR NR NR 1 3 1 2 BAL
228 RAJ 48 3 M O M 1 4 4 2 1 2 5 6 2 4 OC A R P R NR NR 3 3 5 2 LLS
229 AROKYASUDHAN30 2 M O M 3 2 3 2 2,3,4,5 2 5 6 2 4 N A NR N NR R NR 3 3 5 2 NIL
230 KANCHANA 34 2 TG O UM 3 2 1 2 2,4 4 5 6 2 4 N A NR N R NR NR 3 3 5 2 NIL
231 NAGURAMMAL48 3 F H M 1 3 3 2 1 3 5 6 2 4 N A NR N R NR NR 3 3 5 2 NIL
232 RAJA 33 2 M D M 1 1 4 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
233 ZAHIR APPAS 29 2 M D M 1 3 4 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
234 MUTU 31 2 M H M 1 4 2 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
235 MURUGAN 23 2 M O M 3 2 1 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
236 ESAKKIAMMAL43 3 M O M 1 3 4 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
237 BEER 39 2 M O M 3 4 1 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
238 GURUSAMY 28 2 M O UM 3 2 1 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
239 GANGA 29 2 TG M UM 3 3 3 2 2,4 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
240 VELAMMAL 43 3 F H M 1 1 1 2 1 3 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
241 PARAMASIVAM44 3 M D M 3 3 3 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
242 PRIYA 33 2 TG M UM 3 4 1 2 2,4 4 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
243 RAMYA 23 2 TG O UM 3 3 1 2 2,4 4 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
244 JOTHISWARAN29 2 M O M 3 3 4 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
245 RAM 28 2 M O M 2 4 2 2 1 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
246 MOHAMMED ALI54 3 M O M 3 3 1 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
247 VICTOR JEROME28 2 M O M 3 4 1 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
248 VINO 23 2 TG O UM 3 4 1 2 2,4 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
249 JAMUNA 25 2 TG O UM 3 2 3 2 2,4 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
250 NANDHINI 33 2 TG O UM 3 4 1 2 2,4 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL

S.N
O
NA
ME
AG
E
AG
E
SE
X
OC
CU
PA
TIO
N
MA
RIT
AL
ST
AT
US
EM
C/P
MC
/MS
M
LA
ST
CO
NT
AC
T
CO
NT
AC
T P
ER
SO
N
PR
OT
EC
TE
D O
R
UN
PR
OT
EC
TE
D
MO
DE
OF
SE
X
CIR
CU
MC
ISIO
N
GE
NIT
AL
UL
CE
R/F
ISS
UR
E
GE
NIT
AL
DIS
CH
AR
GE
LY
MP
HN
OD
ES
PA
PU
LE
S
OR
AL
MU
CO
SA
DIA
BE
TE
S M
EL
LIT
US
RP
R
TP
HA
ICT
C
HB
sAG
AN
TI
HC
V
KO
H
WE
T M
OU
NT
GR
AM
ST
AIN
TZ
AN
CK
SM
EA
R
DIA
GN
OS
IS
251 HARINI 23 2 TG M UM 3 2 3 2 2,4 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
252 ANJALI 27 2 TG O UM 3 1 1 2 2,4 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
253 SAMBAVI 23 2 TG O M 3 3 3 2 2,4 4 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
254 VITHIYASHREE21 2 TG O UM 3 2 3 2 2,4 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
255 STELLA 29 2 TG O UM 3 3 3 2 2,4 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
256 HASINI 23 2 TG O UM 3 4 1 2 2,4 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
257 SOWMYA 33 2 TG M UM 3 2 1 2 2,4 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
258 RAJA 35 2 M O M 3 1 1 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
259 ALAGESAN 38 2 M O M 1 3 2 2 1 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
260 SWATHI 24 2 TG O M 3 2 3 2 2,3,4,5 4 5 6 2 4 N A NR N R NR NR 3 3 5 2 NIL
261 KATHIRESAN 25 2 M H M 1 4 1 2 1 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
262 RASHEEQ 44 3 M H M 3 4 1 1 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
263 SNEHA 28 2 F O M 1 3 1 2 1 3 5 6 2 4 N A NR N R NR NR 3 3 5 2 NIL
264 NIRMALADEVI 44 3 F O M 1 3 1 2 1 3 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
265 RAJA 27 2 M D M 3 4 3 2 4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
266 ESWARAN 27 2 M O M 3 4 3 2 2,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
267 MUTHURAMALINGAM44 3 M O M 3 2 1 2 3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
268 MARIAPPAN 27 2 M O UM 2 3 2 2 1 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
269 SANKAR GANESH21 2 M O M 3 1 3 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
270 KANNAN 27 2 M O M 3 3 3 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
271 VINOD 25 2 M O UM 2 2 2 2 1 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
272 SAMEER 25 2 M O M 3 3 1 2 2,3 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
273 KANNAM 27 2 M O M 3 4 3 2 4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
274 MURUGAN 54 3 M O M 1 2 4 2 1 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
275 PERIYARAJ 37 2 M D UM 2 3 2 2 1 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL

S.N
O
NA
ME
AG
E
AG
E
SE
X
OC
CU
PA
TIO
N
MA
RIT
AL
ST
AT
US
EM
C/P
MC
/MS
M
LA
ST
CO
NT
AC
T
CO
NT
AC
T P
ER
SO
N
PR
OT
EC
TE
D O
R
UN
PR
OT
EC
TE
D
MO
DE
OF
SE
X
CIR
CU
MC
ISIO
N
GE
NIT
AL
UL
CE
R/F
ISS
UR
E
GE
NIT
AL
DIS
CH
AR
GE
LY
MP
HN
OD
ES
PA
PU
LE
S
OR
AL
MU
CO
SA
DIA
BE
TE
S M
EL
LIT
US
RP
R
TP
HA
ICT
C
HB
sAG
AN
TI
HC
V
KO
H
WE
T M
OU
NT
GR
AM
ST
AIN
TZ
AN
CK
SM
EA
R
DIA
GN
OS
IS
276 NAMBI 34 2 M H UM 2 3 2 2 1 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
277 MARY 37 2 F O M 1 2 4 1 1 3 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
278 INDRA 48 3 F M M 1 3 4 2 1 3 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
279 KRISHNAMOORTHY29 2 M O M 1 4 4 2 1 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
280 SUNDARI 39 2 F O M 1 2 4 2 1 3 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
281 RAJAN 40 3 M O M 3 1 3 2 4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
282 MARY 38 2 F O M 1 3 4 2 1 3 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
283 GANESAN 30 2 M D M 3 4 3 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
284 VEDAMUTHU 63 3 M O M 1 2 4 2 1 2 5 6 2 4 N A NR N R NR NR 3 3 5 2 NIL
285 ALAGENDRAN 23 2 M O UM 2 3 2 2 1 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
286 MALAIRAJAN 50 3 M O M 1 2 4 2 1 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
287 PRABU 22 2 M O M 3 3 3 2 4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
288 MANOHAR 25 2 M O M 3 4 3 2 4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
289 RAMESH 37 2 M O M 3 2 1 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
290 LAKSHMI 33 2 F O M 1 3 4 2 1 3 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
291 MUTHUGANESH26 2 M O M 3 2 1 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
292 TEJASWINI 24 2 TG M M 3 3 3 2 2,4 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
293 SWAPNA 28 2 TG M M 3 2 3 2 2,4 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
294 UMAYAL 29 2 TG M M 3 2 3 2 2,4 4 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
295 ARULPARAI 30 3 M O M 3 3 3 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
296 MANIKANDAN 24 2 M O M 3 4 1 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
297 NISHI 34 2 M O M 3 3 1 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
298 VIGNESH 34 2 M O M 3 4 3 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
299 THANGAM 32 2 F O M 1 2 4 2 1 3 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
300 ISAC 44 3 M O M 1 3 2 2 1 2 5 6 2 4 N A NR N R NR NR 3 3 5 2 NIL

S.N
O
NA
ME
AG
E
AG
E
SE
X
OC
CU
PA
TIO
N
MA
RIT
AL
ST
AT
US
EM
C/P
MC
/MS
M
LA
ST
CO
NT
AC
T
CO
NT
AC
T P
ER
SO
N
PR
OT
EC
TE
D O
R
UN
PR
OT
EC
TE
D
MO
DE
OF
SE
X
CIR
CU
MC
ISIO
N
GE
NIT
AL
UL
CE
R/F
ISS
UR
E
GE
NIT
AL
DIS
CH
AR
GE
LY
MP
HN
OD
ES
PA
PU
LE
S
OR
AL
MU
CO
SA
DIA
BE
TE
S M
EL
LIT
US
RP
R
TP
HA
ICT
C
HB
sAG
AN
TI
HC
V
KO
H
WE
T M
OU
NT
GR
AM
ST
AIN
TZ
AN
CK
SM
EA
R
DIA
GN
OS
IS
301 GANESAN 28 2 M O M 3 1 3 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
302 VINOTH 25 2 M O M 3 2 3 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
303 ELANGOMANI 36 2 M O M 1 3 4 2 1 2 5 6 2 4 OC A NR N R NR NR 3 3 5 2 NIL
304 VELMURUGAN34 2 M O M 3 3 1 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
305 SUNDAR 58 3 M D M 1 4 2 2 1 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
306 SABRUDEEN 48 3 M D M 2 4 2 2 1 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
307 BARATH 24 2 M O M 3 4 3 2 2,3 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
308 MANIKANDAN 38 2 M O M 1 3 4 2 1 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
309 SUNDARRAJ 28 2 M H M 1 2 4 2 1 2 5 6 2 4 N A NR N R NR NR 3 3 5 2 NIL
310 MUTHUPANDI 29 2 M O M 1 3 4 2 1 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
311 SELVASANTHANAM35 2 M O M 1 3 4 2 1 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
312 RAJA 32 2 M O M 1 4 4 2 1 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
313 SANKAR 29 2 M O M 3 3 3 2 4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
314 JOHN PETER 61 3 M H M 3 2 3 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
315 MAHEEB 35 2 M D M 1 4 4 2 1 2 5 6 2 4 N A NR N R NR NR 3 3 5 2 NIL
316 MURUGAN 47 3 M H M 1 2 4 2 1 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
317 SANKARAN 27 2 M O M 3 4 3 2 4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
318 DANIEL 26 2 M O M 3 4 3 2 4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
319 ISMAIL 29 2 M O M 3 4 1 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
320 VIKY 27 2 M O M 3 3 1 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
321 KARTHI 29 2 M D M 3 2 1 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
322 MARIMUTHU 25 2 M O M 3 2 3 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
323 AVUDAIAPPAN29 2 M D M 3 3 3 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
324 SABARIRAJ 40 3 M D M 1 3 4 2 1 2 5 6 2 4 N A NR N R NR NR 3 3 5 2 NIL
325 RAJA 21 2 M D M 3 4 3 2 4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL

S.N
O
NA
ME
AG
E
AG
E
SE
X
OC
CU
PA
TIO
N
MA
RIT
AL
ST
AT
US
EM
C/P
MC
/MS
M
LA
ST
CO
NT
AC
T
CO
NT
AC
T P
ER
SO
N
PR
OT
EC
TE
D O
R
UN
PR
OT
EC
TE
D
MO
DE
OF
SE
X
CIR
CU
MC
ISIO
N
GE
NIT
AL
UL
CE
R/F
ISS
UR
E
GE
NIT
AL
DIS
CH
AR
GE
LY
MP
HN
OD
ES
PA
PU
LE
S
OR
AL
MU
CO
SA
DIA
BE
TE
S M
EL
LIT
US
RP
R
TP
HA
ICT
C
HB
sAG
AN
TI
HC
V
KO
H
WE
T M
OU
NT
GR
AM
ST
AIN
TZ
AN
CK
SM
EA
R
DIA
GN
OS
IS
326 PRAKASH 34 2 M H M 3 4 3 2 3,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
327 KRISHNAN 25 2 M H M 3 2 3 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
328 SENTHILKUMAR26 2 M O M 3 2 3 1 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
329 BALA 23 2 M O M 3 2 3 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
330 GANESAN 39 2 M O M 3 3 3 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
331 GANESAN 29 2 M O M 3 4 3 2 4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
332 RAMKUMAR 26 2 M O M 3 4 3 2 4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
333 AJMAL 22 2 M H M 3 3 3 2 4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
334 MURUGAN 33 2 M D M 1 4 4 2 1 2 5 6 2 4 N A NR N R NR NR 3 3 5 2 NIL
335 KULANTHAIPANDI62 3 M D M 1 3 4 2 1 2 5 6 2 4 N A NR N R NR NR 3 3 5 2 NIL
336 MANMATHARAJ31 2 M H M 1 4 4 2 1 2 5 6 2 4 N A NR N R NR NR 3 3 5 2 NIL
337 AMMU 38 2 M H M 1 3 4 2 1 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
338 DAS 32 2 M O M 3 4 1 2 4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
339 VELMURUGAN39 2 M O M 1 2 4 1 1 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
340 AMMU 36 2 M O M 1 2 4 2 1 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
341 MAHI 27 2 M O M 3 1 1 2 3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
342 RAJA 32 2 M O M 3 3 3 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
343 NARAYANAMOORTHI33 2 M O M 2 4 2 2 1 2 5 6 2 4 N A NR N R NR NR 3 3 5 2 NIL
344 SELVAM 31 2 M O M 3 2 3 2 4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
345 SANTOSH 30 2 M H M 3 3 3 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
346 RAM 24 2 M S UM 3 4 3 2 2,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
347 VICTOR 45 3 M M M 1 3 4 2 1 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
348 KAMARAJ 45 3 M O M 3 4 3 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
349 CHARULATHA 25 2 TG O M 3 2 3 2 2,3,4,5 4 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
350 MUTHAIYAH 47 3 M O M 1 2 4 2 1 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL

S.N
O
NA
ME
AG
E
AG
E
SE
X
OC
CU
PA
TIO
N
MA
RIT
AL
ST
AT
US
EM
C/P
MC
/MS
M
LA
ST
CO
NT
AC
T
CO
NT
AC
T P
ER
SO
N
PR
OT
EC
TE
D O
R
UN
PR
OT
EC
TE
D
MO
DE
OF
SE
X
CIR
CU
MC
ISIO
N
GE
NIT
AL
UL
CE
R/F
ISS
UR
E
GE
NIT
AL
DIS
CH
AR
GE
LY
MP
HN
OD
ES
PA
PU
LE
S
OR
AL
MU
CO
SA
DIA
BE
TE
S M
EL
LIT
US
RP
R
TP
HA
ICT
C
HB
sAG
AN
TI
HC
V
KO
H
WE
T M
OU
NT
GR
AM
ST
AIN
TZ
AN
CK
SM
EA
R
DIA
GN
OS
IS
351 ESAKIRAJA 22 2 M D M 3 3 1 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
352 ROHINI 30 2 TG M M 3 4 3 2 2,4 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
353 BANU 17 1 F O UM 2 2 4 2 1 3 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
354 EDWIN 49 3 M H M 3 3 3 1 2,3,4,5 2 5 6 2 4 N A NR N NR NR R 3 3 5 2 NIL
355 VENKAR 26 2 M O M 3 4 3 2 4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
356 STALIN 38 2 M O M 3 3 3 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
357 GHANARAJ 27 2 M O M 3 2 1 2 2,5 2 5 6 2 4 N A NR N NR R NR 3 3 5 2 NIL
358 VELLADURAI 56 3 M O M 1 4 4 2 1 2 5 6 2 4 N A NR N R NR NR 3 3 5 2 NIL
359 PONNUPANDIYAN55 3 M O M 3 3 3 2 2,3,4,5 2 5 6 2 4 N A NR N R NR NR 3 3 5 2 NIL
360 KUMAR 28 2 M O M 3 2 3 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
361 JEYASRI 31 2 TG M M 3 3 3 2 2,4 4 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
362 SIVASANKARAN23 2 M H M 3 4 1 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
363 SUDHA 37 2 F O M 1 3 4 2 1 3 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
364 NASRUDEEN 32 2 M M M 3 2 3 2 4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
365 THANGARAJ 38 2 M O M 3 2 3 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
366 INDARAAJ 64 3 M O M 1 1 4 2 1 2 5 6 2 4 N A NR N R NR NR 3 3 5 2 NIL
367 OVIYA 30 2 TG M M 3 2 1 2 2,4 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
368 TAMIL 29 2 M O M 1 3 4 2 1 2 5 6 2 4 N A NR N R NR NR 3 3 5 2 NIL
369 MURUGESAN 28 2 M O M 3 4 3 2 2,4,5 2 5 6 2 4 N A NR N NR R NR 3 3 5 2 NIL
370 HAKKINRAJA 31 2 M O M 3 2 3 2 2,3,4,5 2 5 6 2 4 N A NR N R NR NR 3 3 5 2 NIL
371 VIGNESH 25 2 M O M 1 3 4 2 1 2 5 6 2 4 N A NR N R NR NR 3 3 5 2 NIL
372 RAJA 42 3 M O M 3 2 3 2 4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
373 RAJAGOPAL 35 2 M O M 3 3 3 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
374 SARAVANAMUTHU30 2 M O M 3 2 3 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
375 DEIVENDRAN 31 2 M O M 3 3 3 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL

S.N
O
NA
ME
AG
E
AG
E
SE
X
OC
CU
PA
TIO
N
MA
RIT
AL
ST
AT
US
EM
C/P
MC
/MS
M
LA
ST
CO
NT
AC
T
CO
NT
AC
T P
ER
SO
N
PR
OT
EC
TE
D O
R
UN
PR
OT
EC
TE
D
MO
DE
OF
SE
X
CIR
CU
MC
ISIO
N
GE
NIT
AL
UL
CE
R/F
ISS
UR
E
GE
NIT
AL
DIS
CH
AR
GE
LY
MP
HN
OD
ES
PA
PU
LE
S
OR
AL
MU
CO
SA
DIA
BE
TE
S M
EL
LIT
US
RP
R
TP
HA
ICT
C
HB
sAG
AN
TI
HC
V
KO
H
WE
T M
OU
NT
GR
AM
ST
AIN
TZ
AN
CK
SM
EA
R
DIA
GN
OS
IS
376 MUTHUPANDI 23 2 M D M 3 3 3 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
377 NITHYA 34 2 TG M M 3 4 3 1 2,4 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
378 KARTHIKETAN19 1 M O M 3 4 1 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
279 VIJAYASUBBURAJ39 2 M O UM 2 3 2 2 1 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
380 VINOTH 30 2 M O M 1 4 4 2 1 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
381 RAJAMANI 54 3 F O M 1 3 4 2 1 3 5 6 2 4 N A NR N R NR NR 3 3 5 2 NIL
382 PONKALA 35 2 TG M M 3 4 3 2 2,4 4 5 6 2 4 N A NR N R NR NR 3 3 5 2 NIL
383 AIYSHA 30 2 TG O M 3 3 3 2 2,4 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
384 KIRTHIKA 22 2 TG O M 3 2 3 2 2,4 4 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
385 NAKSHTRA 27 2 TG O M 3 3 1 2 2,4 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
386 JINCHANA 19 1 TG M M 3 4 3 2 2,4 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
387 AVANTHIKA 21 2 TG O M 3 3 3 2 2,4 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
388 CHIPPU 36 2 M O M 3 4 3 2 2,4 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
389 MANIARASAN 50 3 M O M 3 2 3 2 2,3,4,5 2 5 6 2 4 N A NR N R NR NR 3 3 5 2 NIL
390 MANIKANDAN 24 2 M O UM 2 3 2 2 1 2 5 6 2 4 N A NR N R NR NR 3 3 5 2 NIL
391 MURUGAN 65 4 M D M 1 4 4 2 1 2 5 6 2 4 N A NR N R NR NR 3 3 5 2 NIL
392 MANIKAM 38 2 M D M 3 2 3 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
393 ARUMUGAM2727 2 M H M 3 4 1 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
394 PATTURAJAN 22 2 M O UM 2 3 2 2 1 2 5 6 2 4 N A NR N R NR NR 3 3 5 2 NIL
395 MANIKANDAN 26 2 M O M 3 2 3 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
396 MAHESHWARI 42 3 F O M 1 4 4 2 1 3 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
397 UIKATTAN 45 3 M O UM 2 2 2 2 1 2 5 6 2 4 OC A NR N R NR NR 3 3 5 2 NIL
398 KARUPPAN 67 4 M O M 1 4 4 2 1 2 5 6 2 4 N A NR N R NR NR 3 3 5 2 NIL
399 ARUN 23 2 M O M 3 3 3 2 2,4 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
400 MAHESHWARI 37 2 F O M 1 3 4 2 1 3 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL

S.N
O
NA
ME
AG
E
AG
E
SE
X
OC
CU
PA
TIO
N
MA
RIT
AL
ST
AT
US
EM
C/P
MC
/MS
M
LA
ST
CO
NT
AC
T
CO
NT
AC
T P
ER
SO
N
PR
OT
EC
TE
D O
R
UN
PR
OT
EC
TE
D
MO
DE
OF
SE
X
CIR
CU
MC
ISIO
N
GE
NIT
AL
UL
CE
R/F
ISS
UR
E
GE
NIT
AL
DIS
CH
AR
GE
LY
MP
HN
OD
ES
PA
PU
LE
S
OR
AL
MU
CO
SA
DIA
BE
TE
S M
EL
LIT
US
RP
R
TP
HA
ICT
C
HB
sAG
AN
TI
HC
V
KO
H
WE
T M
OU
NT
GR
AM
ST
AIN
TZ
AN
CK
SM
EA
R
DIA
GN
OS
IS
401 CHANDRAN 54 3 M O M 1 3 4 2 1 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
402 SANSIYA 38 2 TG M UM 3 4 3 2 2,4 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
403 SUDALAIMUTHU58 3 M O M 1 2 4 2 1 2 5 6 2 4 OC A NR N R NR NR 3 3 5 2 NIL
404 ELAVARASI 27 2 F O M 1 3 4 2 1 3 5 6 2 4 N A NR N R NR NR 3 3 5 2 NIL
405 KUMAR 60 3 M D M 1 2 4 2 1 2 5 6 2 4 OC A NR N R NR NR 3 3 5 2 NIL
406 JEYARAMAN 28 2 M H M 3 3 3 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
407 SUNDAR 30 2 M M M 1 3 2 2 1 2 5 6 2 4 OC A NR N R NR NR 3 3 5 2 NIL
408 MEERAN 44 3 M O M 1 4 4 2 1 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
409 CHANDRALEKAN52 3 M O M 1 2 4 2 1 2 5 6 2 4 OC A NR N R NR NR 3 3 5 2 NIL
410 VIJAYALAKSHMI29 2 TG O UM 3 4 3 2 2,4 4 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
411 THANGADURAI40 3 M O M 1 2 4 2 1 2 5 6 2 4 N A NR N R NR NR 3 3 5 2 NIL
412 VIJAYAN 37 2 M O M 1 4 4 2 1 2 5 6 2 4 N A NR N R NR NR 3 3 5 2 NIL
413 SIVAPNDI 59 3 M O M 1 3 4 2 1 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
414 SANKARAMMAL58 3 F O M 1 1 4 2 1 3 5 6 2 4 N A NR N R NR NR 3 3 5 2 NIL
415 VIJAYASANKARAN34 2 M D M 3 4 3 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
416 NARAYANAN 51 3 M H M 1 3 4 2 1 2 5 6 2 4 OC A NR N R NR NR 3 3 5 2 NIL
417 LAKSHMI 41 3 F D M 1 4 4 2 1 3 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
418 MANIVEL 44 3 M M M 1 2 4 2 1 2 5 6 2 4 OC A NR N R NR NR 3 3 5 2 NIL
419 NAGOORAMMAL40 3 F O M 1 4 4 2 1 3 5 6 2 4 OC A NR N R NR NR 3 3 5 2 NIL
420 SELVAM 47 3 M O M 3 3 3 2 2,3,4,5 2 5 6 2 4 N A NR N R NR NR 3 3 5 2 NIL
421 KANNAN 35 2 M O M 2 2 2 2 1 2 5 6 2 4 OC A NR N R NR NR 3 3 5 2 NIL
422 ANTONY 48 3 M O M 2 1 4 2 1 2 5 6 2 4 OC A NR N R NR NR 3 3 5 2 NIL
423 PERUIYASAMY41 3 M O M 1 2 4 2 1 2 5 6 2 4 OC A NR N R NR NR 3 3 5 2 NIL
424 NARAYANAN 38 2 M O M 1 4 2 2 1 2 5 6 2 4 OC A NR N R NR NR 3 3 5 2 NIL
425 RAJA 26 2 M O M 3 3 3 1 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL

S.N
O
NA
ME
AG
E
AG
E
SE
X
OC
CU
PA
TIO
N
MA
RIT
AL
ST
AT
US
EM
C/P
MC
/MS
M
LA
ST
CO
NT
AC
T
CO
NT
AC
T P
ER
SO
N
PR
OT
EC
TE
D O
R
UN
PR
OT
EC
TE
D
MO
DE
OF
SE
X
CIR
CU
MC
ISIO
N
GE
NIT
AL
UL
CE
R/F
ISS
UR
E
GE
NIT
AL
DIS
CH
AR
GE
LY
MP
HN
OD
ES
PA
PU
LE
S
OR
AL
MU
CO
SA
DIA
BE
TE
S M
EL
LIT
US
RP
R
TP
HA
ICT
C
HB
sAG
AN
TI
HC
V
KO
H
WE
T M
OU
NT
GR
AM
ST
AIN
TZ
AN
CK
SM
EA
R
DIA
GN
OS
IS
426 AMUDHA 35 2 TG M M 3 4 3 2 2,4 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
427 DHANIYA 25 2 TG O UM 3 3 1 2 2,4 4 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
428 VINOSRI 25 2 TG M UM 3 3 1 2 2,4 4 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
429 VINO 26 2 TG O UM 3 3 1 2 2,4 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
430 MAYA 26 2 TG O UM 3 4 1 2 2,4 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
431 MADASAMY 55 3 M O M 1 2 4 2 1 2 5 6 2 4 N A NR N R NR NR 3 3 5 2 NIL
432 ARUMUGAPANDI34 2 M D M 1 3 4 2 1 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
432 KUMAR 40 3 M H M 1 4 4 2 1 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
434 MAHABOOB 47 3 M D M 1 3 4 2 1 2 5 6 2 4 N A NR N R NR NR 3 3 5 2 NIL
435 SAMUEL 20 2 M D UM 3 4 3 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
436 ALI 47 3 M D M 2 3 4 2 1 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
437 DEEPSINGH 64 3 M H M 1 2 4 2 1 2 5 6 2 4 N A NR N R NR NR 3 3 5 2 NIL
438 KUMAR 40 3 M H M 2 4 2 2 1 2 5 6 2 4 N A NR N R NR NR 3 3 5 2 NIL
439 VIJAY VITTAL 25 2 M O M 2 3 2 2 1 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
440 SUNDARRAJ 40 3 M O M 3 2 3 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
441 ESAKIAMMAL 44 3 F O M 1 3 4 2 1 3 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
442 MOTHILAL 32 2 M O M 1 4 4 2 1 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
443 PRIYA 28 2 F H M 1 3 4 2 1 3 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
444 MICHEAL 48 3 M D M 1 4 4 2 1 2 5 6 2 4 OC A NR N R NR NR 3 3 5 2 NIL
445 PERUMAL 34 2 M D M 1 3 3 2 1 2 5 6 2 4 N A NR N R NR NR 3 3 5 2 NIL
446 SABARIRAJ 28 2 M H M 3 2 3 1 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
447 MUTHU 24 2 M O M 3 4 3 2 4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
448 ARUMUGAVADIVU34 2 F O M 1 3 2 2 1 3 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
449 SINDHUKUMAR22 2 M O M 3 2 1 2 2,3,4,5 2 5 6 2 4 OC A NR N R NR NR 3 3 5 2 NIL
450 RAGHU 45 3 M O M 3 3 1 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL

S.N
O
NA
ME
AG
E
AG
E
SE
X
OC
CU
PA
TIO
N
MA
RIT
AL
ST
AT
US
EM
C/P
MC
/MS
M
LA
ST
CO
NT
AC
T
CO
NT
AC
T P
ER
SO
N
PR
OT
EC
TE
D O
R
UN
PR
OT
EC
TE
D
MO
DE
OF
SE
X
CIR
CU
MC
ISIO
N
GE
NIT
AL
UL
CE
R/F
ISS
UR
E
GE
NIT
AL
DIS
CH
AR
GE
LY
MP
HN
OD
ES
PA
PU
LE
S
OR
AL
MU
CO
SA
DIA
BE
TE
S M
EL
LIT
US
RP
R
TP
HA
ICT
C
HB
sAG
AN
TI
HC
V
KO
H
WE
T M
OU
NT
GR
AM
ST
AIN
TZ
AN
CK
SM
EA
R
DIA
GN
OS
IS
451 RAJESHKUMAR41 3 M O M 2 2 2 1 1 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
452 MANIKANDAN 26 2 M H M 3 3 3 2 2,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
453 RAJANDRA PRASAD44 3 M D M 1 4 4 2 1 2 5 6 2 4 OC A NR N R NR NR 3 3 5 2 NIL
454 RAJAIYA 49 3 M D M 1 3 4 2 1 2 5 6 2 4 N A NR N R NR NR 3 3 5 2 NIL
455 SUSAIYAPPAN 42 3 M H M 3 4 3 2 2,3,4,5 2 5 6 2 4 OC A NR N R NR NR 3 3 5 2 NIL
456 VIGNESH 24 2 M O UM 3 3 3 1 2,3,4,5 2 5 6 2 4 N A NR N R NR NR 3 3 5 2 NIL
457 SHEIKMOHAMMED34 2 M O M 3 2 3 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
458 VINOSHRI 24 2 TG O UM 3 4 3 2 2,4 4 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
459 SUNDARI 31 2 F O M 1 3 4 2 1 3 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL
460 RAJA 24 2 M O UM 3 2 3 2 2,3,4,5 2 5 6 2 4 N A NR N NR NR NR 3 3 5 2 NIL