
a cross-sectional study on the health status of rubber tappers ...
Upload
khangminh22Category
view
1download
0
Page 1/24
Mobile Health Applications: A Cross-sectional Study ofAwareness, Attitudes, and Practices among MedicalStudents in MalaysiaJulian Valerie John Jembai
Universiti Malaysia SarawakYi Lin, Charlene Wong
Universiti Malaysia SarawakNur Alia Muhammad Amir Bakhtiar
Universiti Malaysia SarawakSiti Nursuraya Md Lazim
Universiti Malaysia SarawakHwei Sung Ling
Universiti Malaysia SarawakPei Xuan Kuan
Digital Health Research and Innovation, Institute for Clinical ResearchPin Fen Chua ( [email protected] )
Universiti Malaysia Sarawak
Research Article
Keywords: Applications, COVID-19, health and �tness, medical education, mobile health
Posted Date: April 15th, 2022
DOI: https://doi.org/10.21203/rs.3.rs-1493720/v1
License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read FullLicense

Page 2/24
AbstractBackground: The popularity of mobile health (mHealth) applications (apps) in health and medical education israpidly growing, especially since the onset of the COVID-19 pandemic. Thus, we aimed to assess awareness,attitudes, practices, and factors associated with mHealth app usage among medical students.
Methods: We conducted a cross-sectional study among medical students at a government university in Sarawak,Malaysia, from February to April 2021. Validated questionnaires were administered to all consenting students. Inaddition to basic demographic information, these questionnaires included questions on awareness of, attitudestoward, and practices with mHealth apps concerned with medical education, health and �tness, and COVID-19management.
Results: Study respondents had favorable attitudes toward mHealth apps [medical education (61.8%), health and�tness (76.3%), and COVID-19 management (82.7%)]. Overall, respondents’ mean attitude scores were four out of�ve for all three app categories. However, respondents showed higher usage of COVID-19 management apps(73.5%) than medical education (35.7%) and �tness (39.0%) apps. Usage of all three app categories wassigni�cantly associated with the respondent’s awareness and attitude. Respondents who were in the top 20% forhousehold income and duration of study were more likely to use medical education apps. A higher percentage ofrespondents in the top 20% household income group used COVID-19 apps compared to those in the other incomegroups. The most common barrier to the use of apps was uncertainty regarding the most suitable apps to choose.
Conclusion: Our study highlighted a discrepancy between awareness of mHealth apps and positive attitudestoward them and their use. Recognition of barriers to the use of mHealth apps by relevant authorities may benecessary to increase the usage of these apps.
BackgroundThe World Health Organization’s Global Observatory de�nes mobile health (mHealth) as a public health practicesupported by mobile devices such as mobile phones, patient monitoring devices, personal digital assistants, andother wireless devices (1). MHealth is used to provide healthcare information to the public, collect health data,monitor patients remotely, access health records, make medical diagnoses, and assist in disease prevention andmanagement (2, 3). MHealth applications are software apps for portable devices such as smartphones or tablets.They are generally grouped into medical education and teaching apps, health and �tness apps for use by patientsand the public, telemedicine and telehealth apps, and others (4).
There are various clinical and teaching apps designed for medical students and health professionals in medicaleducation. These serve to enhance clinical knowledge, aid decision-making, provide telemedicine, and facilitatepatient care (4–6). Drug and clinical reference apps, diagnostic apps, and medical calculators are commonmHealth apps used by healthcare professionals and students. Research has found that health professionals �ndthese apps particularly useful for accessing the latest medical journals during patient care and for patientmanagement (7). Many �nd that these apps save time accessing critical information during clinical practice andprovide access to on-the-job learning (8). Given the valuable functions that they provide, mHealth medicaleducation apps are likely to be adopted widely in every aspect of clinical practice (7).
Health and �tness mHealth apps are used to promote healthy lifestyles, particularly in adolescents and students(9). The common features of �tness apps include step counting, calorie counters, weight loss management, and

Page 3/24
exercise regimes. Use of these apps for home-based exercise is encouraged and expected to rise, especially duringthe COVID-19 pandemic, while movement outside the home is restricted (10, 11). Integrated usage of wearabledevices and mHealth apps increases motivation and practice e�cacy among users seeking healthier lifestyles(12).
The COVID-19 pandemic has led to the development of COVID-19 information and symptom tracking apps. COVID-19 management apps provide users with information on the necessary health measures based on recordedsymptoms (13). COVID-19 apps have also revolutionized public health disease monitoring. One such app usesBluetooth technology to send push noti�cations, alerting those in the vicinity of those with possible COVID-19infection (13). COVID-19 apps also provide the public with information regarding the disease, good hygienepractices, and standard operating procedures (SOPs) (14).
Despite the rise of mHealth app usage, challenges continue to hinder their adoption. Various patterns of mHealthusage have been found in different demographics (15). Socioeconomic factors are a barrier to mHealth adoption(16). Medical students also face challenges to the adoption of these technologies (17). The COVID-19 pandemic isexpected to transform the teaching methods of medical schools through the integration of telemedicine (18).
In tandem with the Fourth Industrial Revolution (4IR), mHealth apps are essential in the rapidly evolving �eld ofdigital healthcare. Despite increasing mobile phone usage in Malaysia, public knowledge regarding mobile phoneutilization for health is lacking. To date, little is known regarding medical students’ awareness, attitudes, andpractices, and the obstacles to their adoption of mHealth during the COVID-19 pandemic. Thus, we aimed toassess mHealth app awareness, attitudes, and practices among medical students at the Universiti MalaysiaSarawak (UNIMAS). This will provide mHealth app providers, medical educators, and health institutions withinsights that allow them to improve mHealth adoption.
Methods
Sample population and designThis cross-sectional study administered a questionnaire to 739 undergraduate medical students from UNIMAS toassess their awareness of, attitudes toward, and practices with mHealth apps. The inclusion criteria for therespondents were year one to year �ve medical students from UNIMAS with access to digital devices. Conveniencesampling was used in this study. The sample size was determined using the open-source calculator Open-SourceEpidemiology Statistics for Public Health (Open Epi) v. 3.01. To attain a con�dence level of 95%, 247 respondentswere required. Allowing for a potential 10% attrition rate, the minimum number of respondents required was 275.Ethical approval was obtained from the Ethics Committee of UNIMAS Faculty of Medicine and Health Sciencesand the Malaysian National Medical Research Register (NMRR) (NMRR-20-2834-57731) and the Medical Researchand Ethics Committee [ref: KKM/NIHSEC/P21-67(4)].
Before we began data collection for the main study, face validity was determined using �ve medical students anda pilot study with 12 medical students was conducted. Questionnaire items on medical, health and �tness, andCOVID-19 mHealth apps were assessed for internal consistency using Cronbach’s alpha (CA). The questionnaireshowed good reliability with a CA of 0.651 for questions on medical apps, 0.777 for questions on health and�tness apps, and 0.907 for questions on COVID-19 apps.
Data collection

Page 4/24
A structured, standardized questionnaire on awareness of, attitudes toward, and practices with mHealth wasadministered to medical students between February 3, 2021, and April 25, 2021. All participants were provided witha subject information sheet and were briefed. After written consent was obtained, the students were given aninternet link to access the self-administered questionnaire.
The questionnaire was developed based on two primary relevant papers (16, 19) and other existing literature (20–24). The questionnaires comprised four sections. Section 1 covered social demographics; section 2 coveredawareness of, attitudes toward, and practices with medical education mHealth apps; section 3 covered awarenessand attitudes; and section 4 covered the use of mHealth �tness and health apps and awareness of, attitudestoward, and practices with COVID-19 mHealth apps.
Sections 2 to 4 assessed students’ attitudes using Likert scale answer formats (scoring from 1 to 5). Each item onthe questionnaire was evaluated for content validity. Face validity was determined via video conference with �vemedical students due to the social distancing requirements of the COVID-19 pandemic.
Measures
Outcome variablesAwareness and use of mHealth apps among the respondents were measured in sections 2 to 4 in a binary fashionas “aware or not aware of mHealth apps” and “use or do not use mHealth apps.” Respondents’ attitudes towardthe three categories of apps were scored in sections 2 to 4 on Likert scales from 1 to 5. The mean (average)attitude score on sections 2 to 4 was determined for each respondent.
Exposure variablesBasic demographic information was gathered. This included age (in years), gender (male or female), ethnicity(Malay, Chinese, Indian, Sarawak Bumiputera/indigenous group, or others), household income [bottom 40 (B40):<RM4849 per month, middle 40 (M40): RM4850–10959 per month, or top 20 (T20): >RM10960 per month], phaseof medical training (clinical or preclinical), ownership of a mobile device (yes or no), and type of device(smartphone, tablet, laptop, or wearable device). Household income classi�cation by the Department of StatisticsMalaysia was used as part of the assessment of the respondent’s family �nancial status (25). We also assessedthe frequency of use for each app (at least once a day, at least once a week, at least once a month, or less thanonce a month). For medical and �tness apps, duration of use was also assessed (less than six months, sixmonths to two years, or more than two years).
Statistical analysisAll demographic data and categorical outcomes were presented as frequencies (n) and percentages (%), exceptthe mean attitude score, which was a continuous variable. Categorical variables were subjected to univariateanalysis using the chi-square test (χ2), and continuous variables were analyzed with an independent t-test.Fischer’s exact test was used when the expected count in a cell was less than 5. P-values of < 0.05 wereconsidered statistically signi�cant. All statistical analyses were performed using SPSS Statistics for Windows, v.24.0 (IBM Corp., Armonk, N.Y., USA) statistical software.
Results

Page 5/24
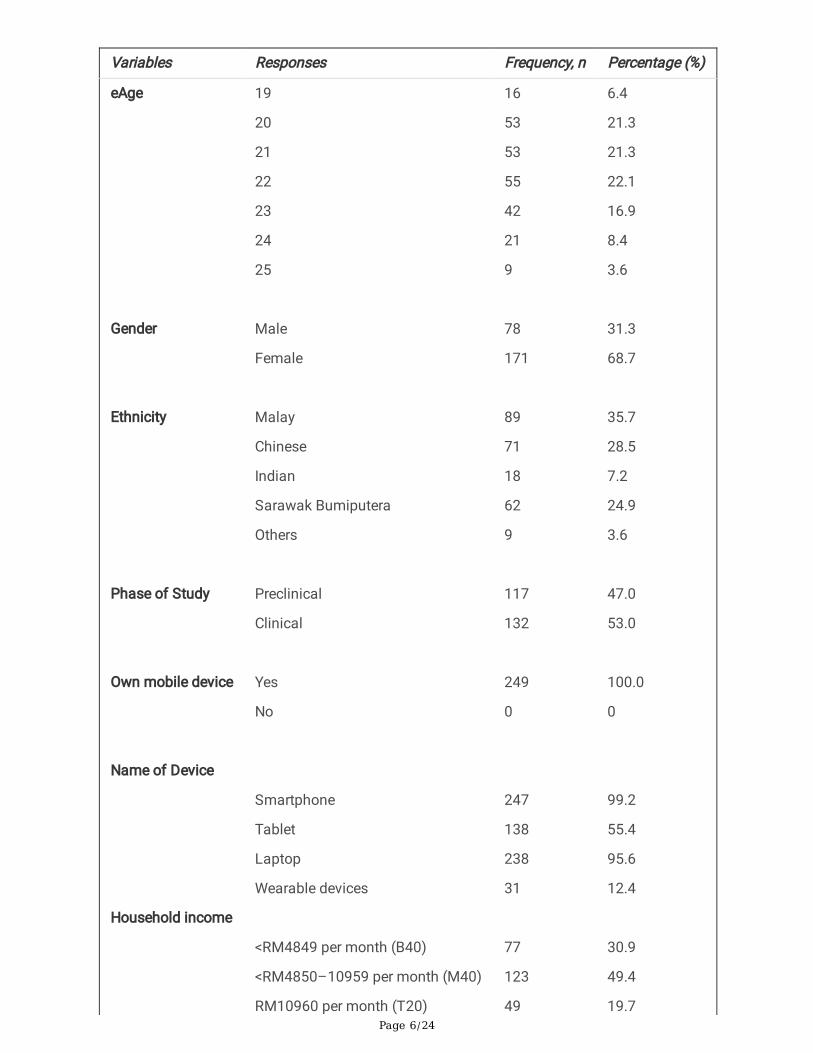
Demographic pro�les of participantsA total of 249 valid questionnaires were returned. The demographic characteristics of the respondents are shownin Table 1. The average age of the respondents was 21 years, and the majority were female (68.7%). Respondentswere undergraduate medical students distributed roughly evenly between the clinical (53%) and preclinical (47%)phases of study. The respondents were ethnically diverse. The majority were in the M40 group (49.4%), denoting afamily income between RM4850 and RM10959. Smartphones (99.2%) and laptops (95.6%) were the most ownedgadgets. Two-thirds of the respondents had > 20 Gb as their monthly telephone company (Telco) data plan.
Table 1: Demographic characteristics of respondents
Page 6/24
Variables Responses Frequency, n Percentage (%)
eAge
Gender
Ethnicity
Phase of Study
Own mobile device
Name of Device
Household income
19
20
21
22
23
24
25
Male
Female
Malay
Chinese
Indian
Sarawak Bumiputera
Others
Preclinical
Clinical
Yes
No
Smartphone
Tablet
Laptop
Wearable devices
<RM4849 per month (B40)
<RM4850–10959 per month (M40)
RM10960 per month (T20)
16
53
53
55
42
21
9
78
171
89
71
18
62
9
117
132
249
0
247
138
238
31
77
123
49
6.4
21.3
21.3
22.1
16.9
8.4
3.6
31.3
68.7
35.7
28.5
7.2
24.9
3.6
47.0
53.0
100.0
0
99.2
55.4
95.6
12.4
30.9
49.4
19.7
Page 7/24
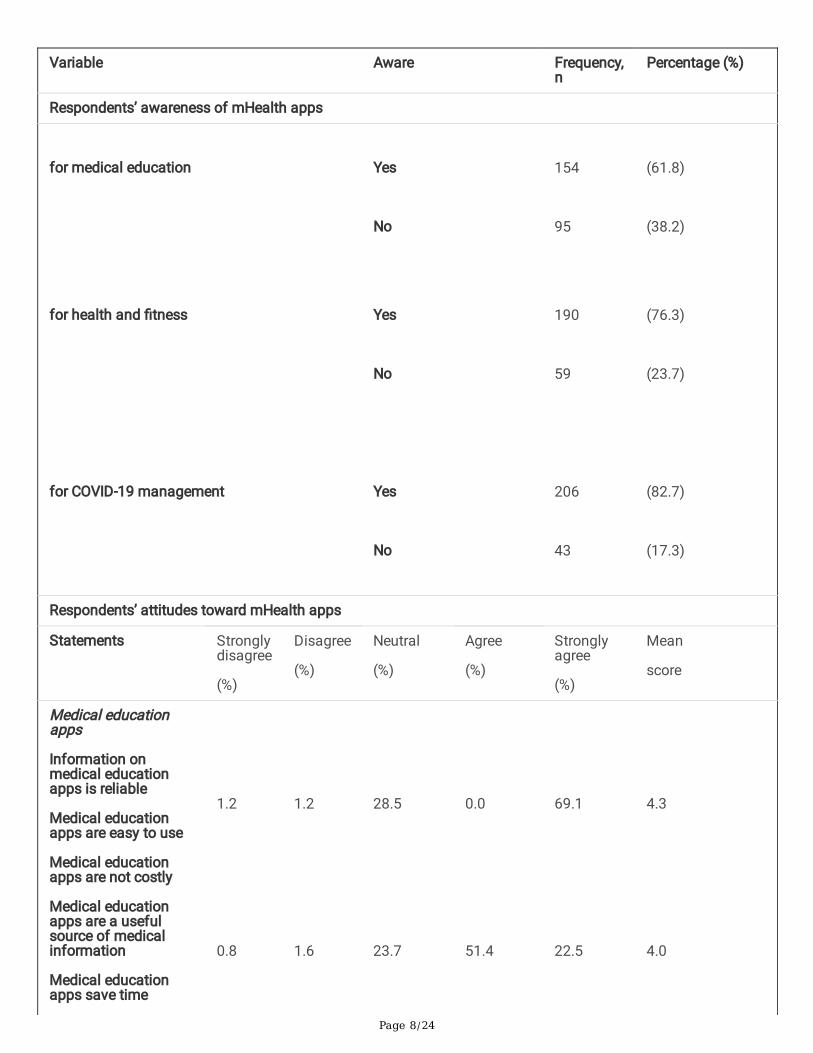
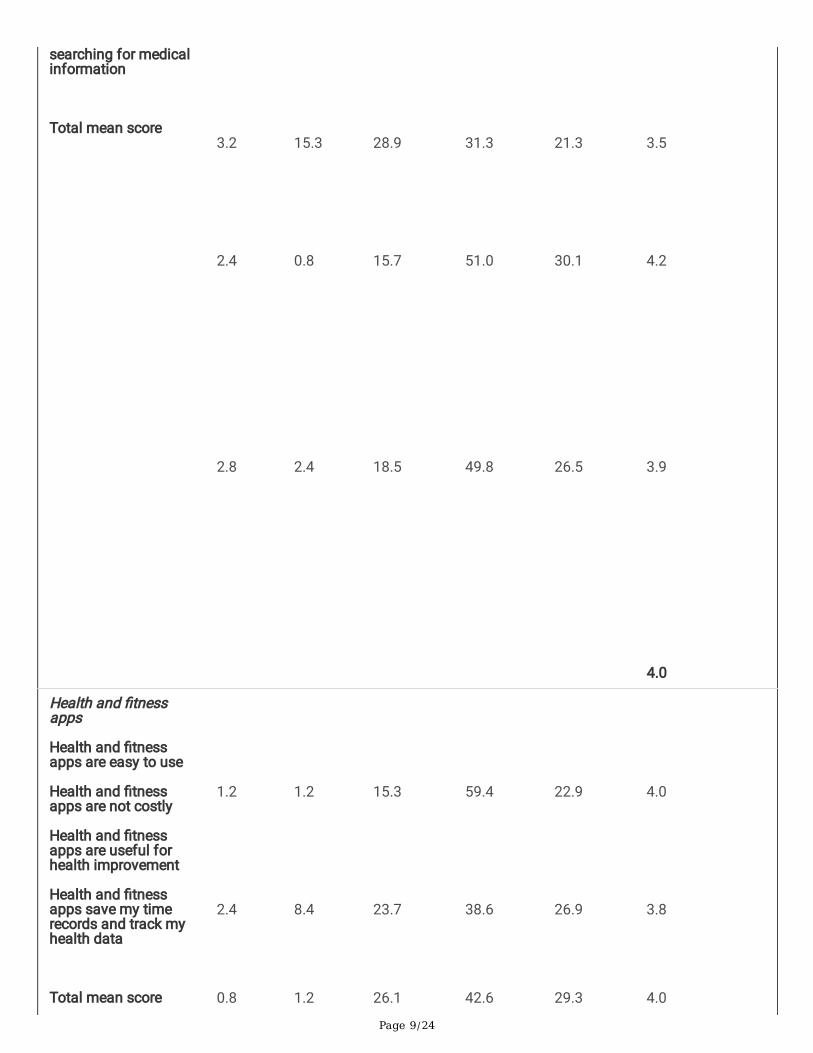
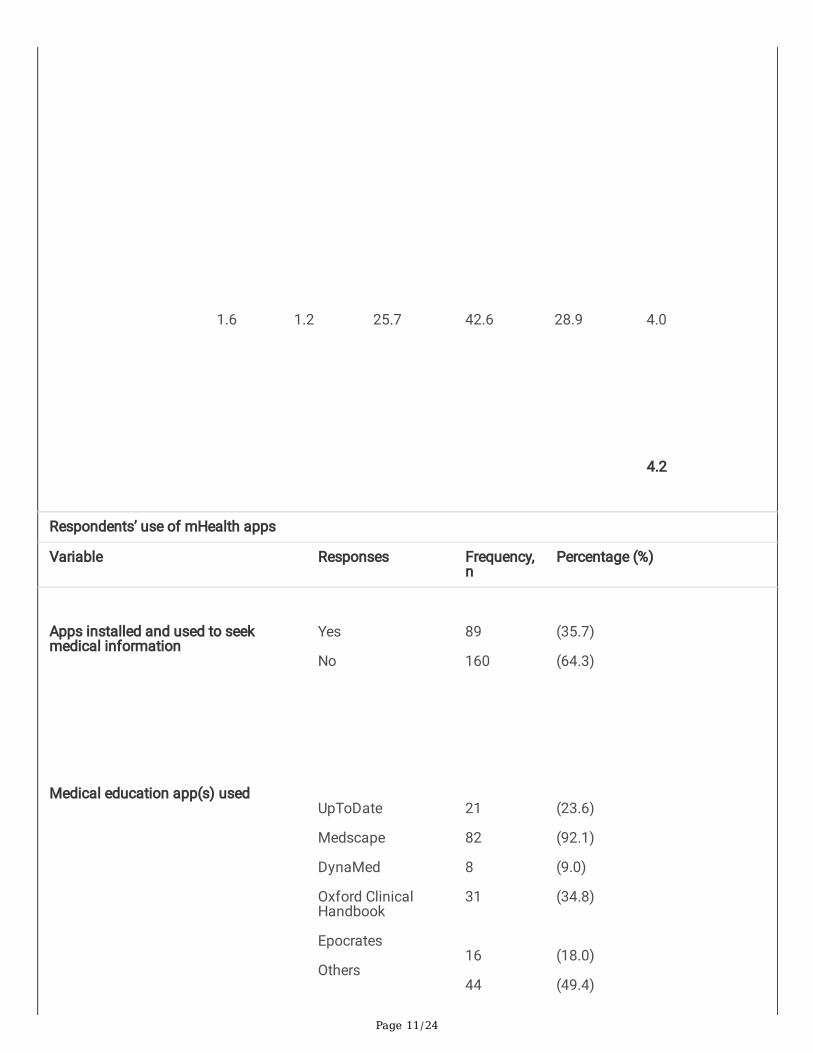
Overall awareness of, attitudes toward, and use of mobile healthapplications among the respondentsAs shown in Table 2, most respondents (82.7%) were aware of the existence and function of COVID-19 apps,followed by personal health and �tness apps (76.3%) and medical education apps (61.8%). The same trend wasseen in positive attitudes (“agree” and “strongly agree”) toward the three types of applications: COVID-19management apps (total mean score: 83), personal health and �tness apps (75.7), and medical education apps(70.6). However, the trend did not persist in respondents’ app usage. Despite the high adoption of COVID-19applications (73.5%), the use of health and �tness (39%) and medical education apps (35.7%) were much lower.My Sejahtera (99.5%), a locally authorized COVID-19 management app; physical activity tracking apps (89.7%);and the medical education app Medscape (92.1%), were the most used applications.
Table 2: Awareness of, attitudes toward, and overall usage of mobile health applications among studyrespondents
Page 8/24
Variable Aware Frequency,n
Percentage (%)
Respondents’ awareness of mHealth apps
for medical education
for health and �tness
for COVID-19 management
Yes
No
Yes
No
Yes
No
154
95
190
59
206
43
(61.8)
(38.2)
(76.3)
(23.7)
(82.7)
(17.3)
Respondents’ attitudes toward mHealth apps
Statements Stronglydisagree
(%)
Disagree
(%)
Neutral
(%)
Agree
(%)
Stronglyagree
(%)
Mean
score
Medical educationapps
Information onmedical educationapps is reliable
Medical educationapps are easy to use
Medical educationapps are not costly
Medical educationapps are a usefulsource of medicalinformation
Medical educationapps save time
1.2
0.8
1.2
1.6
28.5
23.7
0.0
51.4
69.1
22.5
4.3
4.0
Page 9/24
searching for medicalinformation
Total mean score
3.2
2.4
2.8
15.3
0.8
2.4
28.9
15.7
18.5
31.3
51.0
49.8
21.3
30.1
26.5
3.5
4.2
3.9
4.0
Health and �tnessapps
Health and �tnessapps are easy to use
Health and �tnessapps are not costly
Health and �tnessapps are useful forhealth improvement
Health and �tnessapps save my timerecords and track myhealth data
Total mean score
1.2
2.4
0.8
1.2
8.4
1.2
15.3
23.7
26.1
59.4
38.6
42.6
22.9
26.9
29.3
4.0
3.8
4.0

Page 10/24
0.8
1.2
14.9
49.0
34.1
4.1
4.0
COVID-19management apps
COVID-19 appinformation is reliable
Apps are easy to use
Apps are not costly
Apps are useful forpandemic control
Apps save time (e.g.,scan-in to enterpremises, record localhealth risk, and checkthe latest COVID-19information)
User privacy isprotected when usingthe apps
Total mean score
0.8
0.8
0.8
1.2
0.8
1.2
1.2
0.8
1.2
0.8
14.9
12.4
10.8
16.5
9.2
57.4
56.2
44.6
44.6
46.6
25.7
29.3
43.0
36.5
42.6
4.1
4.1
4.3
4.1
4.5
Page 11/24
1.6
1.2
25.7
42.6
28.9
4.0
4.2
Respondents’ use of mHealth apps
Variable Responses Frequency,n
Percentage (%)
Apps installed and used to seekmedical information
Medical education app(s) used
Yes
No
UpToDate
Medscape
DynaMed
Oxford ClinicalHandbook
Epocrates
Others
89
160
21
82
8
31
16
44
(35.7)
(64.3)
(23.6)
(92.1)
(9.0)
(34.8)
(18.0)
(49.4)

Page 12/24
Apps installed and used for healthand �tness purposes
Health and �tness app(s) used
Apps installed and used for COVID-19management
COVID-19 apps used
Yes
No
Physical activity
Food trackers
Fasting apps
Others
Yes
No
My Sejahtera
COVID trace
Qmunity
My Trace
97
152
87
38
18
2
183
66
182
16
33
4
(39.0)
(61.0)
(89.7)
(39.2)
(18.6)
(2.1)
(73.5)
(26.5)
(99.5)
(8.7)
(18.0)
(2.2)
Obstacles to mHealth application use among respondentsAs shown in Table 3, most respondents (up to 73.5%) were uncertain of the most suitable mHealth apps to use.Around one-third of the respondents identi�ed personal budget and data privacy concerns as hindrances to appuse. Of note, uncertainty regarding apps usage (37.5%) and lack of con�dence in the information that they provide(21.3%) were also the barriers to mHealth app use among our respondents.
Table 3: Obstacles to respondent use of mHealth applications

Page 13/24
Obstacles to mHealth app use Frequency
n (%)
Medical education apps
Do not know how to assess medical information using mHealth apps
Do not know which app(s) is/are most suitable
Do not trust information provided by the app(s)
Limited budget for app subscription
Health and �tness apps
Do not know which health app(s) is most suitable
Concerns regarding the privacy of personal health data
Limited budget for app subscription
COVID-19 management apps
Do not know how to use the app(s)
Do not know which COVID-19 app(s) is/are most suitable
Do not want to disclose personal information
60 (37.5)
110 (68.8)
34 (21.3)
47 (29.4)
112 (73.7)
40 (26.3)
35 (23.0)
27 (40.9)
37 (56.1)
11 (16.7)
Relationships between respondent demographics and mHealthapp awareness, attitudes, and practicesAs would be expected, the respondents’ awareness of the three categories of mHealth apps signi�cantly affectedtheir usage (Table 4). Higher mHealth apps usage was seen when the respondents were aware of such apps. Ofthe respondents who did not use the apps, 59.1% were not aware of their existence or function.
The mean attitude scores differed signi�cantly between those respondents who used the apps and those who didnot (Table 5). This was true for all three categories of mHealth apps. A higher mean attitude score translated tohigher adoption of apps. COVID-19 apps were used the most (74%) and had the highest mean attitude score(5.45).
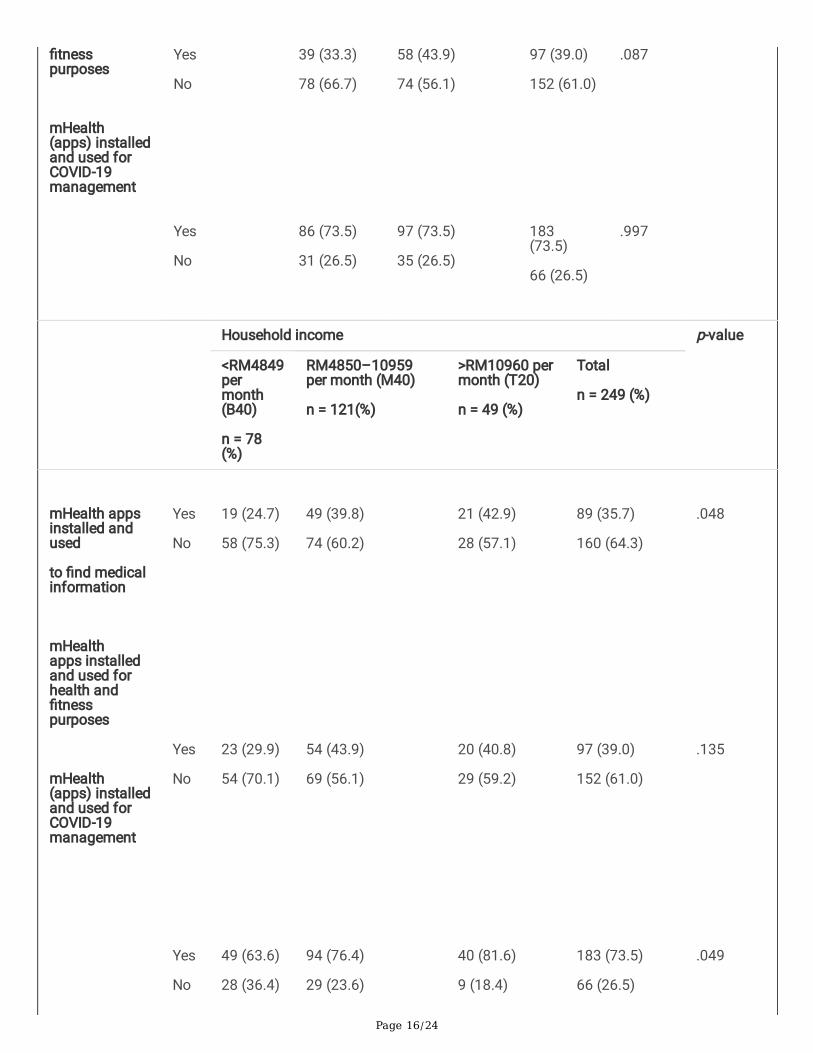
We analyzed the relationships between respondent demographics, including gender, phase of learning, andhousehold income, and the frequency and duration of app usage (see Table 6 and supplementary data). Genderdid not affect app usage. Respondents in the clinical phase of their medical education were more likely to usemedical education applications than those in the preclinical phase (43.2% vs. 27.4%). Respondents with a higherfamily household income, i.e., >RM10960, were more likely to use medical education and COVID-19 mHealth appsthan those with lower household incomes.
Female respondents (20.3%) used medical education apps more frequently (at least once per day) than males(8%). Usage frequency did not differ between those in the clinical and nonclinical phases of study. However, thosein the clinical phase showed a longer duration of medical education app use (more than two years). Although

Page 14/24
respondents with higher household incomes were more likely to use COVID-19 apps, they used them lessfrequently (17.5% at least once a day) than those with poorer �nancial support (81%).
Table 4: MHealth app awareness and use
Respondents’awareness ofapps
Use of medicaleducation apps
p-value Use of healthand �tness apps
p-value Use of COVID-19managementapps
p-value
Yes
n = 89(%)
No
n = 160(%)
Yes
n = 97(%)
No
n = 192(%)
Yes
n = 183(%)
No
n = 66(%)
Aware
Not aware
87(97.8)
2 (2.2)
67(41.9)
93(58.1)
.00 95(97.9)
2(2.1)
95(62.5)
57(37.5)
.00 179(97.8)
4 (1.2)
27(40.9)
39(59.1)
.00
Table 5: Associations between mean scores for attitudes toward mHealth apps and overall app usage
Types of mHealth apps used mHealth app usage n (%) Mean attitude score p-value
Medical education apps Yes
No
89 (36)
160 (34)
4.25
3.64
.00
Health and �tness apps Yes
No
97 (39)
152 (61)
4.18
3.18
.00
COVID-19 management apps Yes
No
183 (74)
66 (26)
4.28
3.75
.00
Table 6: Demographic differences in overall mHealth app use

Page 15/24
Variable Responses Gender p-value
Male
n (%)
Female
n (%)
Total
n (%)
mHealth appsinstalled andused
to �nd medicalinformation
mHealthapps installedand used forhealth and�tnesspurposes
mHealth(apps) installedand used forCOVID-19management
Yes
No
Yes
No
Yes
No
25 (32.1)
53 (67.9)
30 (38.5)
48 (61.5)
59 (75.6)
19 (24.4)
64 (37.4)
107 (62.6)
67 (39.2)
104 (60.8)
124 (72.5)
47 (27.5)
89 (35.7)
160(64.3)
97 (39.0)
152(61.0)
183(73.5)
66 (26.5)
.412
.914
.604
Phase of study p-value
Preclinical
(year 1–2)
n = 117 (%)
Clinical
(years 3–5)
n = 132 (%)
Total
n = 249(%)
mHealth appsinstalled andused
to �nd medicalinformation
mHealthapps installedand used forhealth and
Yes
No
32 (27.4)
85 (72.6)
57 (43.2)
75 (56.8)
89 (35.7)
160 (64.3)
.009
Page 16/24
�tnesspurposes
mHealth(apps) installedand used forCOVID-19management
Yes
No
Yes
No
39 (33.3)
78 (66.7)
86 (73.5)
31 (26.5)
58 (43.9)
74 (56.1)
97 (73.5)
35 (26.5)
97 (39.0)
152 (61.0)
183(73.5)
66 (26.5)
.087
.997
Household income p-value
<RM4849permonth(B40)
n = 78(%)
RM4850–10959per month (M40)
n = 121(%)
>RM10960 permonth (T20)
n = 49 (%)
Total
n = 249 (%)
mHealth appsinstalled andused
to �nd medicalinformation
mHealthapps installedand used forhealth and�tnesspurposes
mHealth(apps) installedand used forCOVID-19management
Yes
No
Yes
No
Yes
No
19 (24.7)
58 (75.3)
23 (29.9)
54 (70.1)
49 (63.6)
28 (36.4)
49 (39.8)
74 (60.2)
54 (43.9)
69 (56.1)
94 (76.4)
29 (23.6)
21 (42.9)
28 (57.1)
20 (40.8)
29 (59.2)
40 (81.6)
9 (18.4)
89 (35.7)
160 (64.3)
97 (39.0)
152 (61.0)
183 (73.5)
66 (26.5)
.048
.135
.049
Page 17/24
Demographic differences in-app awareness and attitudesOlder respondents (54.5%) and those in the clinical phase of their medical education (60.4%) were more aware ofthe existence of medical education applications (Supplementary Table). However, age and phase of study did notaffect awareness of health and �tness or COVID-19 applications. None of the other demographic featuresmeasured were correlated with the respondents’ attitudes toward the three categories of applications.
DiscussionThe use of mobile health technology is important for medical education (26). The COVID-19 pandemic hascontributed to the growth of mHealth applications, has increased their necessity, and has altered usage patternsamong the medical students (27). This is the �rst cross-sectional study of medical students’ awareness of,attitudes toward, and usage of mobile health applications, including medical education, health and �tness, andCOVID-19 management apps. We also examined obstacles to the use of mHealth apps and investigateddemographic correlations with respondents’ awareness of these apps and their attitude toward their use.
Our respondent demographics were comparable to those of previous studies in terms of student diversity (28).Medical students of different races, �nancial backgrounds, and phase of medical education were included in thestudy. Females were somewhat overrepresented, as has been the case in similar medical school surveys (19, 23,29) Hence, our �ndings are relevant to similar learning centers and multiethnic populations.
In line with previous research, we found that medical students have good awareness of and attitudes towardmHealth apps (16, 28). This may be due to the high rate of mobile device possession due to urbanization and animproved socioeconomic environment in Malaysia (29). The high rate of smartphone ownership was consistentwith the global trend, especially during the COVID-19 pandemic. All of the participants were also equipped withonline access via their mobile devices. Public health awareness is a strong contributor to the adoption of mHealthtechnologies (30), and as has been suggested in previous research, medical students are more likely to be awareof mHealth applications (16). Hence, our students seemed ready to embrace this technology to promote effectivelearning, to promote health and �tness, and to improve their social connectivity (21–23, 31, 32).
The patterns of mHealth app usage among our respondents were noteworthy. The current pandemic is obviouslythe reason for the higher usage rate of COVID-19 management apps compared to �tness apps and medicaleducation apps. Research has shown the importance of a solid national regulatory framework to drive digitalhealth (33). Mobile health apps usage is expected to increase during this outbreak due to the need for self-monitoring, health management, vaccination appointment booking, and contact tracing (11). Although thepandemic could be a potential catalyst for mHealth adoption, another research with a French population foundthat respondents’ distrusted the data protection and e�cacy of these apps during the pandemic, highlighting thedifferent cultural views on this matter (29).
Compared to global mHealth app usage, our study demonstrated infrequent usage of medical education andhealth and �tness apps (5, 19), despite the high mobile device ownership. This may indicate a preference for

Page 18/24
textbooks over medical apps as learning tools. A previous study found that medical students preferred face-to-face lectures and textbook study to medical apps (34). The majority of our respondents indicated that uncertaintyregarding which mHealth apps to choose was an obstacle to their use. By inference, the lack of guidance from themedical curriculum could be an important contributor to low medical education mHealth app usage (35). Our�nding that better �nancial status increased the likelihood of medical education app use indicates that thesubscription costs of mobile applications are also likely to be an obstacle to more widespread use. Increased appuse was observed among students in the clinical phase of their medical education (year three onward in theirmedical program), and these students were also more aware of mHealth apps, consistent with other studies (5).This suggests that earlier exposure to the clinical �eld may aid the integration of mHealth into medical students’learning processes. Our �ndings agreed with an earlier study that device ownership is not a proxy measure of theuse of mHealth technology as this is not the purpose of having the device (16).
Our study demonstrated awareness of health and �tness mHealth apps and favorable attitudes toward them butlow adoption of �tness apps among respondents. A systematic review of studies conducted among the generalpublic revealed a similar phenomenon, illustrating the importance of identifying the obstacles to app usage (36).Although not assessed in this study, poor levels of physical activity among future physicians are common (37).High attrition rates among users of �tness apps may be explained by the lack of entertainment or reward providedby exercise (38). Higher percentage of those who do not use �tness apps among the lower-income group (70.1%)con�rm that cost is an important barrier (39). Among those who used �tness apps, many respondents used themdaily, with the majority installing them during the �rst two years of use. We postulate that decreased access togyms and outdoor exercise resulting from the implementation of the COVID-19 Movement Control Order (MCO)has left our respondents with little alternative but to expand their use of the internet for exercise purposes. As aresult, there has been a drastic increase in mHealth health and �tness app installations worldwide (40).
Although students can afford mobile devices, the cost of apps was still regarded by many as an obstacle to theuse of medical education and �tness apps among our study respondents. A systematic review found cost to beamong the leading factors contributing to low mHealth usage in developing countries (41). Hence, subscription orin-app purchase requirements could be a major hindrance to mHealth app usage.
In contrast to previous research �ndings, there was no gender inequity in mHealth awareness, attitude, or useamong our respondents (29, 42). However, this was a general assessment of app use rather than being focused ona speci�c app. Additionally, respondents of both genders were studying on the same medical program. Thesefactors may explain the homogeneity of our results between genders. Although there was no gender inequity inusage, females were more likely to use the technology frequently when they adopted it. This could be due todifferences in preferred revision and learning methods.
Age and phase of study were signi�cantly associated with the respondents’ awareness of and attitudes towardmedical education apps. This may be due to the greater need for fast access to accurate disease managementinformation when practicing or seeing patients (43). Despite positive attitudes toward mHealth apps, low usagerates of optional mHealth apps were found across the board in our respondents. Previous research has suggestedthat this may be due to the busy schedules of medical students (16, 43). However, those in the clinical phase oftheir training spend most of their learning time in hospitals rather than lecture halls or study rooms. Therefore, theuse of mHealth medical education apps to access medical information has practical value for these students (20).

Page 19/24
Besides not knowing which app to use and the issue of cost, respondents’ concerns regarding user privacy wereanother signi�cant barrier to using mHealth apps. Although today’s smartphones have security features such aspassword lock, antimalware apps, and data encryption (44), research suggests that there is low utilization of thesesecurity features (45)). Security concerns also include low con�dence in in-app security and data protection (13).We suggest that university administrators and relevant authorities take appropriate action to remove these hurdlesto facilitate increased adoption of mHealth apps among the students.
ConclusionOur study demonstrated high awareness of mHealth apps among medical students, including different categoriesof apps (medical education, health and �tness, and COVID-19 management apps). Although medical students hadpositive attitudes toward mHealth implementation, the practice of mHealth was relatively low. Thus, addressingbarriers to use, such as cost, security concerns, and uncertainty regarding which apps to choose, is essential topromote mHealth app use. The promotion of mHealth app use for educative purposes among medical studentscould facilitate their future implementation in healthcare settings. Recognition by policymakers and regulatorybodies of the barriers to use while taking into account student demographics, interests, and needs would drivemHealth exposure and adoption (41).
Study LimitationsThere were several limitations to this study. First, our respondents were predominantly female, and this may limitthe applicability of our �ndings to both genders. Additionally, the study was a cross-sectional survey ofundergraduate medical students from UNIMAS, so the results may not be fully representative of Malaysianmedical students. Finally, the study was conducted during the COVID-19 pandemic, at which time most medicalstudents were receiving instruction via online distance learning. This interfered with our survey period as thedistribution and return of surveys took longer than it might have face-to-face. It may also have led to moremisinterpretation of survey questions because no face-to-face explanations were possible.
Abbreviations4IR: Fourth Industrial Revolution
3G and 4G: third- and fourth-generation mobile telecommunication
Apps: Applications
B40: Household income < RM4849 per month
CA: Cronbach’s alpha
COVID-19: Coronavirus disease 2019
eHealth: Electronic health
GB: Gigabyte
GPS: Global Positioning System

Page 20/24
GPRS: General Packet Radio Service
IMS: Intercontinental Medical Statistics
IQR: Median
IT: Information technology
KKM: Kementerian Kesihatan Malaysia
M40: Household income of RM4850–10959 per month
MCO: Movement Control Order
mHealth: Mobile health
MREC: Medical Research and Ethics Committee
n: Frequency
NMRR: National Medical Research Register
PLI: Poverty line income
SD: Standard deviation
SOPs: Standard of procedures
SPSS: Statistical Package for the Social Sciences software
T20: Household income > RM10960 per month
UNIMAS: Universiti Malaysia Sarawak
DeclarationsEthics approval and consent to participate
Ethical approval was obtained from the Ethics Committee of UNIMAS Faculty of Medicine and Health Sciences,the Malaysian National Medical Research Register (NMRR) (NMRR-20-2834-57731), and the Medical Research andEthics Committee [ref: KKM/NIHSEC/P21-67(4)]. The investigation conforms with the principles outlined in theDeclaration of Helsinki. All respondents provided written informed consent to participation.
Consent for publication
Not applicable.
Availability of data and materials
The data and materials from this study are available from the corresponding author upon reasonable request.

Page 21/24
Competing interests
The authors declare that they have no competing interests.
Funding
No funding was received for this study. We did not receive any speci�c grant from any funding agencies.
Authors’ contributions
JVJJ contributed to the initial idea, study design, data collection and analysis, manuscript drafting, and �nalpreparation of the paper for publication. YLCW contributed to data collection, data analysis, and the literaturesearch and review. NAMAB and SNML contributed to the design of the instrument for data collection, dataorganization, and formatting of the drafted work. HSL contributed to data collection, data analysis, dataorganization, data interpretation, and drafting of the manuscript. PXK contributed to the initial idea, data analysis,supervision of the project, and editing and critical review of the manuscript. PFC contributed to the initial idea, theliterature search and review, designing the instrument for data collection, supervision of the project, and editingand critical review of the manuscript. All authors read and approved the �nal version of the paper for publication.
Acknowledgments
We would like to express our gratitude to Universiti Malaysia Sarawak for the support to publish this paper. Wewould also like to acknowledge and thank the authors and publishers, Dr. Gajendra Singh, and Dr. Prince Peprahfor their permission and advice on the use of the questionnaires as reference in this study.
References1. Ryu S. Book review: MHealth: New horizons for health through mobile technologies: Based on the �ndings of
the second global survey on eHealth (Global Observatory for EHealth series, volume 3). HealthcareInformatics Research. 2012;18(3):231.
2. Parvin RN, Shahjahan. Knowledge, attitude and practice on eHealth among Doctors Working at selectedprivate hospitals in Dhaka, Bangladesh. Journal of the International Society for Telemedicine and eHealth.2016;4
3. Vaghe� I, Tulu B. The continued use of mobile health apps: Insights from a longitudinal study. JMIR mHealthand uHealth. 2019;7(8):e12983.
4. Boulos MNK, Brewer AC, Karimkhani C, Buller DB, Dellavalle RP. Mobile medical and health apps: State of theart, concerns, regulatory control and certi�cation. Online Journal of Public Health Informatics. 2014;5(3):229.
5. Quant C, Altieri L, Torres J, Craft N. The Self-Perception and Usage of Medical Apps amongst MedicalStudents in the United States: A Cross-Sectional Survey. International Journal of Telemedicine andApplications. 2016;2016:3929741.
�. Mosa ASM, Yoo I, Sheets L. A systematic review of healthcare applications for smartphones. BMC MedicalInformatics and Decision Making. 2012;12:67.
7. Ventola CL. Mobile devices and apps for health care professionals: Uses and bene�ts. P and T.2014;39(5):356–64.

Page 22/24
�. Altmann V, Gries M. Factors in�uencing the usage intention of mHealth apps: An Empirical Study on theexample of Sweden [Student thesis]. 2017.
9. Dute DJ, Bemelmans WJ, Breda J. Using mobile apps to promote a healthy lifestyle among adolescents andstudents: A review of the theoretical basis and lessons learned. JMIR mHealth and uHealth. 2016;4(2):e39.
10. Mutz M, Müller J, Reimers AK. Use of digital media for home-based sports activities during the COVID-19pandemic: Results from the German SPOVID survey. International Journal of Environmental Research andPublic Health. 2021;18(9):4409.
11. Banskota S, Healy M, Goldberg EM. 15 Smartphone apps for older adults to use while in isolation during theCOVID-19 pandemic. Western Journal of Emergency Medicine. 2020;21(3):514–25.
12. Kinney DA, Nabors LA, Merianos AL, Vidourek RA. College students’ use and perceptions of wearable �tnesstrackers. American Journal of Health Education. 2019;50(5):298–307.
13. Singh H, Couch D, Yap K. Mobile Health Apps That Help With COVID-19 Management: Scoping Review. JMIRNurs. John Leon. 2020;3(1):e20596.
14. Hutchinson A. WhatsApp launches World Health Organization Chatbot to answer COVID-19 queries. 2020.Available from: https://www.socialmediatoday.com/news/whatsapp-launches-world-health-organization-chatbot-to-answer-covid-19-quer/574617/
15. Peng W, Kanthawala S, Yuan S, Hussain SA. A qualitative study of user perceptions of mobile health apps.BMC Public Health. 2016;16(1):1158.
1�. Peprah P, Abalo EM, Agyemang-Duah W, Gyasi RM, Reforce O, Nyonyo J, et al. Knowledge, attitude, and use ofmHealth technology among students in Ghana: A university-based survey. BMC Medical Informatics andDecision Making. 2019;19(1):220.
17. Tudor Car L, Kyaw BM, Nannan Panday RS, van der Kleij R, Chavannes N, Majeed A, Car J. Digital healthtraining programs for medical students: Scoping review. JMIR Medical Education. 2021;7(3):e28275.
1�. Alsou� A, Alsuyihili A, Msherghi A, Elhadi A, Atiyah H, Ashini A, et al. Impact of the COVID-19 pandemic onmedical education: Medical students’ knowledge, attitudes, and practices regarding electronic learning. PLOSONE. 2020;15(11):e0242905.
19. Singh G, Alva S. A survey on usage of mobile health apps among medical undergraduates. CommunityMedicine and Public Health Care. 2019;6(3):1–6.
20. Jebraeily M, Fazlollahi ZZ, Rahimi B. The most common smartphone applications used by medical studentsand barriers of using them. Acta Informatica Medica. 2017;25(4):232.
21. Kayyali R, Peletidi A, Ismail M, Hashim Z, Bandeira P, Bonnah J. Awareness and use of mHealth apps: A studyfrom England. Pharmacy. 2017;5(2).
22. Biruk K, Abetu E. Knowledge and attitude of health professionals toward telemedicine in resource-limitedsettings: A cross-sectional study in North West Ethiopia. Journal of Healthcare Engineering.2018;2018:2389268.
23. Thakre S, Thakre S. Perception of medical students for utility of mobile technology use in medical education.International Journal of Medicine and Public Health. 2015;5(4).
24. Ehteshami A, Hachesu PR, Esfahani MK, Rezazadeh E. Awareness and using of medical students aboutmobile health technology in clinical areas. Acta Informatica Medica. 2013;21(2):109–12.
25. Household Income Estimates and Incidence of Poverty Report, Malaysia, 2020 [press release]. Department ofStatistic Malaysia, 6 August 2021 2020. Available from: https://www.dosm.gov.my/v1/index.php?

Page 23/24
r=column/pdfPrev&id=VTNHRkdiZkFzenBNd1Y1dmg2UUlrZz09
2�. Gaglani SM, Topol EJ. iMedEd: The role of mobile health technologies in medical education. AcademicMedicine. 2014;89(9):1207–9.
27. Katsumata S, Ichikohji T, Nakano S, Yamaguchi S, Ikuine F. Changes in the use of mobile devices during thecrisis: Immediate response to the COVID-19 pandemic. Computers in Human Behavior Reports.2022;5:100168.
2�. Hossain I, Lim ZZ, Ng JJL, Koh WJ, Wong PS. Public attitudes towards mobile health in Singapore: A cross-sectional study. mHealth. 2018;4:41.
29. Khatun F, Heywood AE, Ray PK, Hani� SM, Bhuiya A, Liaw ST. Determinants of readiness to adopt mHealth ina rural community of Bangladesh. International Journal of Medical Informatics. 2015;84(10):847–56.
30. Zhao Y, Ni Q, Zhou R. What factors in�uence the mobile health service adoption? A meta-analysis and themoderating role of age. International Journal of Information Management. 2018;43:342–50.
31. Guma A, Businge PM, Nkamwesiga L, Andogah G. Use of mobile devices by students to support learning inuniversities: A case of Muni University. 2017.
32. David ME, Roberts JA. Smartphone use during the COVID-19 pandemic: Social versus physical distancing.International Journal of Environmental Research and Public Health. 2021;18(3):1034.
33. Jogova M, Shaw J, Jamieson T. The regulatory challenge of mobile health: Lessons for Canada. HealthcarePolicy. 2019;14(3):19–28.
34. Wynter L, Burgess A, Kalman E, Heron JE, Bleasel J. Medical students: What educational resources are theyusing? BMC Medical Education. 2019;19(1):36.
35. Boruff JT, Storie D. Mobile devices in medicine: A survey of how medical students, residents, and faculty usesmartphones and other mobile devices to �nd information. Journal of the Medical Library Association.2014;102(1):22–30.
3�. Szinay D, Jones A, Chadborn T, Brown J, Naughton F. In�uences on the uptake of and engagement with healthand well-being smartphone apps: Systematic review. Journal of Medical Internet Research.2020;22(5):e17572.
37. Rao CR, Darshan B, Das N, Rajan V, Bhogun M, Gupta A. Practice of physical activity among future doctors: Across-sectional analysis. International Journal of Preventive Medicine. 2012;3(5):365.
3�. Huang G, Ren Y. Linking technological functions of �tness mobile apps with continuance usage amongChinese users: Moderating role of exercise self-e�cacy. Computers in Human Behavior. 2020;103:151–60.
39. Canhoto AI, Dibb S. Unpacking the interplay between organisational factors and the economic environment inthe creation of consumer vulnerability. Journal of Marketing Management. 2016;32(3–4):335–56.
40. Ang C. Fitness apps grew by nearly 50% during the �rst half of 2020, study �nds: World Economic Forum.2020 Available from: https://www.weforum.org/agenda/2020/09/�tness-apps-gym-health-downloads/.
41. Kruse C, Betancourt J, Ortiz S, Valdes Luna SM, Bamrah IK, Segovia N. Barriers to the use of mobile health inimproving health outcomes in developing countries: Systematic review. Journal of Medical Internet Research.2019;21(10):e13263.
42. Wesolowski A, Eagle N, Noor AM, Snow RW, Buckee CO. Heterogeneous mobile phone ownership and usagepatterns in Kenya. PLOS ONE. 2012;7(4):e35319.

Page 24/24
43. Chase TJG, Julius A, Chandan JS, Powell E, Hall CS, Phillips BL, et al. Mobile learning in medicine: Anevaluation of attitudes and behaviours of medical students. BMC Medical Education. 2018;18(1):152.
44. Zhou L, Bao J, Watzlaf V, Parmanto B. Barriers to and facilitators of the use of mobile health apps from asecurity perspective: Mixed-methods study. JMIR mHealth and uHealth. 2019;7(4):e11223.
45. Mylonas A, Kastania A, Gritzalis D. Delegate the smartphone user? Security awareness in smartphoneplatforms. Computers and Security. 2013;34:47–66
Supplementary Files
This is a list of supplementary �les associated with this preprint. Click to download.
SupplementaryData.docx
Copyright © 2022 FDOKUMEN




















