
Skin Cleansing without or with Compromise: Soaps and Syndets
Upload
independentCategory
view
0download
0
Middle cerebral artery flow velocity waveforms in normal and small-for-gestational-age fetuses
Giancarlo Marl, MD, and Russell L. Deter, MD
New Haven, Connecticut, and Houston, Texas
The middle cerebral artery flow velocity waveforms were obtained in 16 normal fetuses in a longitudinal
study and in 128 normal fetuses in a cross-sectional study with pulsed Doppler ultrasonography. The
pulsatility index values of the middle cerebral artery were higher at 25 to 30 weeks' gestation than those
observed during the two periods of major cerebral cellular multiplication in the human fetus. In 9 of the 16
fetuses studied longitudinally we compared the pulsatility index values obtained at the end of gestation with those obtained at 1 month after delivery; no significant difference was observed. The pulsatility index
of the middle cerebral artery was also determined in 33 small-for-gestational-age fetuses. A middle
cerebral artery pulsatility index value below our normal range was recorded in 9 of the 33 small-for
gestational-age fetuses (27.3%). These small-for-gestational-age fetuses with abnormal pulsatility index values had a significantly higher incidence of abnormal fetal heart rate and admission into the neonatal
intensive care unit. There were three deaths in the nine small-for-gestational-age fetuses with abnormal pulsatility index values (33.3%) and three deaths in the 24 small-for-gestational-age fetuses with normal pulsatility index values (12.5%). Our data indicate that the pulsatility index of the middle cerebral artery in
the normal human fetus has a parabolic pattern during pregnancy and does not change significantly after
delivery. The results suggest that the small-for-gestational-age fetus with a normal middle cerebral artery pulsatility index is at lower risk than the fetus with abnormal pulsatility index values; moreover,
management of the small-for-gestational-age fetus may be aided by the study of the middle cerebral artery waveforms. (AM J OSSTET GVNECOL 1992;166:1262-70.)
Key words: Middle cerebral artery, small for gestational age, intrauterine growth retardation, pulsatility index, brain-sparing effect
Several studies of fetal cerebral artery blood flow velocity waveforms have been reported in the third trimester of pregnancy in normal, intrauterine growth retarded (IUGR),1. 2 and anemic fetuses.' The studies emphasized a decrease in downstream impedance in the cerebral vasculature of IUGR fetuses attributed to a brain-sparing effect.' Additionally, a reduction in P02
established in the umbilical artery through cordocentesis at the end of gestation' has been associated with the decrease in pulsatility index noted in the cerebral arteries of normal fetuses during this period of gestation.' Normal values for the velocity waveforms of different cerebral arteries have been published by a number of investigators." 2. 5 In many cases the pulsatility index values were derived from cross-sectional Doppler studies, and no longitudinal report on the ce-
From the Departments of Obstetrics and Gynecology, Yale University School of Medicine and Baylor College of Medicine. Received for publication February 11, 1991; revised July 29, 1991; accepted August 8, 1991. Reprint requests: Giancarlo Mari, MD, Yale University School of Medicine, Department of Obstetrics and Gynecology, 123 York St., No. 17-], New Haven, CT 06511. 6/1/33022
1262
rebral blood flow velocity waveforms early in the second trimester of pregnancy (i.e., 15 weeks) has been presented.
Our study presents a serial assessment of the pulsatility index for the middle cerebral artery starting early in the second trimester. Additionally, the pulsatility index of the middle cerebral artery was assessed in 128 normal fetuses in a cross-sectional study. The data obtained in the cross-sectional study have permitted an evaluation of the variability of the pulsatility index within a given population and have provided the basis for the development of normal values of the pulsatility index for the middle cerebral artery in the human fetus. The predicted values derived from the cross-sectional study were compared with the average longitudinal curve. Furthermore, to evaluate the variability of the middle cerebral artery velocity waveforms before delivery and in the first month after delivery, the pulsatility index value of the middle cerebral artery was obtained in nine normal fetuses at the end of gestation and at I month post partum. Finally, middle cerebral artery velocity waveforms of 33 small-for-gestational-age (SGA) fetuses are reported and compared with those obtained in normal fetuses.

Volume 166 Number 4
X Q) ~ c :::7) ... . -... CJ (/) -::;, Q.
< u I:
4
3
2
0 13
Middle cerebral artery velocimetry 1263
18 23 28 33 38 43
Weeks
Fig. 1. Normal range of middle cerebral artery pulsatility index (PI) as a function of gestational age constructed from study of 128 normal fetuses. Lower limit = Predicted pulsatility index -(2 x 0.184 x Predictedpulsatility index); Upperlimit = Predictedpulsatilityindex + (2 x 0.184 x Predicted pulsatility index).
Material and methods
This study was done with data from 16 normal fetuses (group 1), 128 normal fetuses in a cross-sectional study (group 2), and 33 SGA fetuses (group 3). Informed consent was obtained from all patients. Twentyfive subjects in our study population participated in other investigations.6 The women in the first two groups were delivered of their fetuses after 37 weeks of gestation; comprehensive pediatric assessment revealed no evidence of growth abnormalities or congenital anomalies. Birth characteristics such as weight, length, head circumference, and abdominal circumference were within the normal ranges for singletons determined by Usher and McLean.' Nine normal fetuses monitored longitudinally were studied 1 month after delivery; two of them were studied four times in the first 6 months after delivery.
Fetal age determination. Fetal age in group 1 was determined from the date of the last menstrual period and confirmed by first-trimester and early secondtrimester ultrasonographic examinations (crown-rump length, biparietal diameter, and femur diaphysis length measurement).8
Gestational age in groups 2 and 3 was determined by both menstrual history and sonographic assessment of fetal biometry from either a scan before 20 weeks' gestation or, if such a scan had not been performed, the first ultrasonographic assessment in this study. Gestational age was based on (I) the date of the last menstrual period when it differed by <2 weeks from the gestational age determined by sonographic parameters or (2) the sonographic assessment if the patient was unsure of the date of her last menstrual period or if
the discrepancy between menstrual and sonographic gestational age was >2 weeks. SGA fetuses were defined on the basis of ultrasonographic measurements of head and abdominal circumferences8 2 or more SD below the mean and confirmed by a low birth weight.'
The data obtained from the Doppler ultrasonographic studies were not used in the clinical management of the patients.
Doppler uItrasonographic examinations. The normal and SGA fetuses were examined when the mothers were in a semirecumbent position. Exposure of the fetal brain to Doppler ultrasonography was kept to a minimum estimated to be around 1 to 5 minutes. Examination of the middle cerebral artery was performed as reported previously.9 A PASS II (General Electric Medical Systems, Milwaukee, Wis.) with pulsed Doppler beam was used in conjunction with a 2.5 MHz real-time imaging device with a 2 mm sample volume. A 0 to 50 Hz pass filter was used . Ultrasonographic energy was 114 m W fe rn" spatial peak temporal average intensity; although it exceeded the 100 mW fcm 2 level recommended by the Food and Drug Administration for fetal Doppler ultrasonography, 10 the intensity was well below the known peak acoustic field emission of 180 m W / cm2
for preenactment ultrasonographic diagnostic devices. In addition, the American Institute of Ultrasound in Medicine recently reported that no independently confirmed significant biologic effects in mammalian tissues have been noted with focused ultrasonographic intensities below 1 W fern'. II
Doppler examinations of the middle cerebral artery in the fetuses of group 1 were carried out at 3- to 4-week intervals from 15 to 18 weeks' gestational age

1264 Mari and Deter April 1992 Am J Obstet Gynecol
Table I. Modeling of individual middle cerebral artery pulsatility index curves obtained in 16 normal fetuses monitored serially during gestation
Patient y= ao + a, (x) +
A Y = -3.203 + 0.416 x B Y = - 1.053 + 0.229 x C Y = - 2.388 + 0.332 x D Y = -2.301 + 0.344 x E y = - 2.496 + 0.336 x F y = - 2.173 + 0.333 x G Y = - 2.339 + 0.328 x H Y = - 2.357 + 0.339 x 1 Y = - 2.380 + 0.339 x J y = -2.397 + 0.341 x K y = - 2.324 + 0.335 x L Y = - 2.368 + 0.333 x M Y = - 2.004 + 0.304 x N Y = -0.881 + 0.240 x 0 y = -2.732 + 0.371 x P Y = 1.324 + 0.259 x
y, Pulsatility index; x, gestational age.
(mean::,: SO: 16.3 ::': 1.5 weeks) to 35 weeks, and at Ito 3-week intervals thereafter until delivery. After 35 weeks we decided to study the middle cerebral artery more frequently because the time of delivery could not be predicted. The middle cerebral artery of nine fetuses in the longitudinal study was studied as seen in utero at 1 month after delivery. In two fetuses the middle cerebral artery was studied at 1, 4, 12, and 24 weeks after delivery.
The gestational age of the fetuses in group 2 at the time of the study ranged between 15 and 41 weeks (29 ::': 7.2 weeks, mean::': SO). In 30 fetuses, two-dimensional directed pulsed Doppler waveforms (Acuson 128; AcusonCo., Mountain View, Calif.) were compared with color-flow Doppler imaging (Acuson 128). Before the middle cerebral artery was interrogated with pulsed Doppler ultrasonography, the color-flow mapping was successively used to confirm that the sample volume had been positioned on the middle cerebral artery and that the angle between the beam and the vessel was <20 degrees.
The gestational age of the SGA fetuses (group 2)
ranged from 20 to 37 weeks (31 ± 4.3 weeks, mean ± SO) at the time of the study and from 24 to 42 weeks (33.6 ::': 3.9 weeks, mean ± SO) at the time of delivery.
Data analysis. The Doppler velocity waveforms were recorded on videotape, and a digitized computer system (Digisonics Inc., Houston) calculated the following variables: peak systolic velocity, lowest diastolic velocity, and mean velocity. Three consecutive waveforms were analyzed, and the results were averaged. The pulsatility index (Peak systolic velocity - Lowest diastolic velocity)! Mean velocity)'2 was then calculated. Measurements were obtained only during fetal apnea, which
a2 (x)' p Value R2
-0.008 x' >0.05 66 -0.004 x' >0.05 24 -0.006 x' <0.05 93 -0.007 x' <0.05 80 -0.006 x' <0.05 92 -0.006 x' <0.05 91 -0.006 x' <0.05 93 -0.006 x' <0.05 72 -0.006 x' <0.05 91 -0.006 x' <0.05 83 -0.006 x' <0.05 81 -0.006 x' <0.05 91 -0.006 x' <0.05 88 -0.005 x' >0.05 26 -0.007 x' <0.05 86 -0.005 x' <0.05 88
was defined as the absence of visible changes in the waveform patterns for 2: 15 waveforms.
The intraobserver error (coefficient of variation) for the pulsatility index of the middle cerebral artery was 5.6% as reported previously. 13
Changes in pulsatility index with gestational age for the fetuses of group I were characterized quantitatively by fitting mathematic functions to the experimental data. Regression analysis was used to compare the pulsatility index with gestational age for each fetus. We looked for the optimal polynomial model on the basis of two criteria: (1) coefficients different from zero and (2) maximal coefficient of determination (W). Analysis of variance was used to determine whether the regression accounted for a significant part of the variability in the dependent variable. A p value <0.05 was considered to indicate statistical significance. Assessment of the variability of the pulsatility index of the middle cerebral artery during pregnancy was carried out with the measurements made on the fetuses in group 2. There was only one pulsatility index measurement per fetus in this data set. A second-degree polynomial was fitted to the data with the method of least squares and predicted values calculated at each time point where an actual measurement was made. The differences between actual and predicted pulsatility index values were determined and plotted. Because there appeared to be
an increase in variability with menstrual age, these differences were expressed as a percentage of the predicted values (percent difference). The mean and SD of the percent difference were calculated, and twice the latter was used as the measure of pulsatility index variability at different times in pregnancy (Fig. 1).
A paired Student's t test was used for statistical com-

Volume 166 Number 4
15 Weeks
- 0
18 Weeks - 42
-0
24 Weeks -46
~==:======- - 0
I sec
Middle cerebral artery velocimetry 1265
29 Weeks - 54
- 0
36 Weeks - 104 (J
Q) (/)
........
- 0 E u
39.2 Weeks -91
-0
Fig. 2. Flow velocity waveforms of fetal middle cerebral artery velocity waveforms at different gestational ages.
parison of pulsatility index values in the middle cerebral artery of the fetuses and infants. A probability value of < 0.05 was considered to indicate statistical significance.
The pulsatility index values for the SGA fetuses (group 3) were measured and plotted with our normal range.
In the SGA fetuses we obtained the sensitivity, specificity, positive predictive value, and negative predictive value for the middle cerebral artery pulsatility index, with the test status being above or below our normal reference range for gestational age (predicted value ± 2 SD) and the outcome status being presence or absence of adverse perinatal outcome (defined as admission to the neonatal intensive care unit for> 12 hours or perinatal death).
Results
Initially the patients of group I were 34 normal fetuses. The data of 18 fetuses monitored longitudinally were not included in our analysis because of preterm labor (n = J); first measurement after 18 weeks' gestation , an inadequate number of measurements, or both (n = 13); hypertension (n = 3) ; or multicystic kidney (n = 1). The mothers of group 1 were delivered offetuses between 38 and 42 weeks (39.6 ± l.1 weeks, mean ± SD). A total of 144 examinations were per-
formed . On 16 occasions the middle cerebral artery could not be evaluated on first attempt, because of either fetal position or fetal movement. In these cases the examination was repeated within 1 week. On six occasions the measurement of the middle cerebral artery was not obtained.
In each of the 30 fetuses studied with pulsed Doppler and color flow mapping the sample volume was found over the middle cerebral artery in the color image after the middle cerebral artery was obtained with pulsed Doppler ultrasonography. The angle was always <20 degrees .
The best model in group I was a second-order polynomial (y = ao + a ,x + a~2) (Table J). Coefficient ao was different from zero in nine cases; coefficient a, was different from zero in 13 cases; and coefficient a2 was different from zero in 14 cases. The middle cerebral artery waveforms manifested a higher diastole at IS to 20 weeks and at the end of gestation (Fig. 2); this was associated with a lower pulsatility index value between 15 and 20 weeks' gestation and, late in the third trimester of pregnancy, a higher value at 25 to 30 weeks' gestation. Fifteen of the 16 individual fetuses showing evidence of a parabolic change in pulsatility index with gestational age were used to specify the average longitudinal curve by determination of the mean coefficient values. The function is given in Table II.
1266 Mari and Deter April 1992 Am J Obslel Gynecol
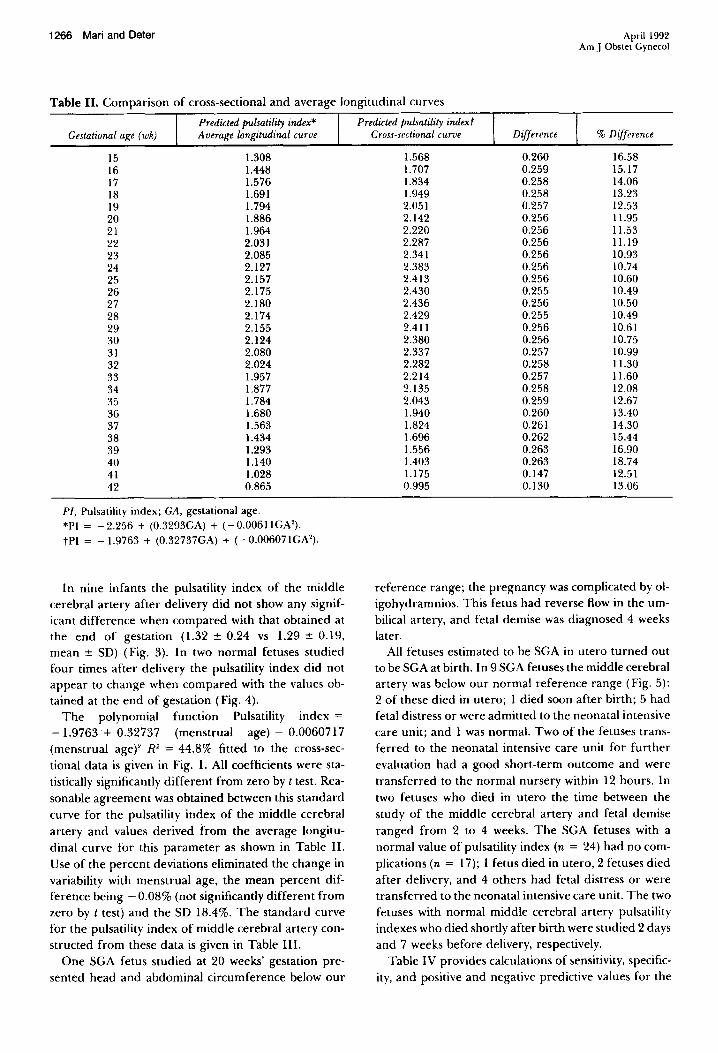
Table II. Comparison of cross-sectional and average longitudinal curves
Predicted pulsatility index* Gestational age (wk) A verage longitudinal curve
IS 1.308 16 1.448 17 1.576 18 1.691 19 1.794 20 1.886 21 1.964 22 2.031 23 2.085 24 2.127 25 2.157 26 2.175 27 2.180 28 2.174 29 2.155 30 2.124 31 2.080 32 2.024 33 1.957 34 1.877 35 1.784 36 1.680 37 1.563 38 1.434 39 1.293 40 1.140 41 1.028 42 0.865
PI, Pulsatility index; GA, gestational age. *PI = -2.256 + (0.3293GA) + (-0.00611GN). tPl = -1.9763 + (0.32737GA) + (-0.00607IGN).
In nine infants the pulsatility index of the middle cerebral artery after delivery did not show any significant difference when compared with that obtained at the end of gestation (1.32:': 0.24 vs 1.29:': 0.19, mean:': SD) (Fig. 3). In two normal fetuses studied four times after delivery the pulsatility index did not appear to change when compared with the values obtained at the end of gestation (Fig. 4).
The polynomial function Pulsatility index = -1.9763+ 0.32737 (menstrual age) - 0.0060717 (menstrual agef R2 = 44.8% fitted to the cross-sectional data is given in Fig. I. All coefficients were statistically significantly different from zero by t test. Reasonable agreement was obtained between this standard curve for the pulsatility index of the middle cerebral artery and values derived from the average longitudinal curve for this parameter as shown in Table II. Use of the percent deviations eliminated the change in variability with menstrual age, the mean percent difference being - 0.08% (not significantly different from zero by t test) and the SD 18.4%. The standard curve for the pulsatility index of middle cerebral artery constructed from these data is given in Table III.
One SGA fetus studied at 20 weeks' gestation presented head and abdominal circumference below our
Predicted pulsatility indext Cross-sectional curve Difference % Difference
1.568 0.260 16.58 1.707 0.259 15.17 1.834 0.258 14.06 1.949 0.258 13.23 2.051 0.257 12.53 2.142 0.256 11.95 2.220 0.256 11.53 2.287 0.256 11.19 2.341 0.256 10.93 2.383 0.256 10.74 2.413 0.256 10.60 2.430 0.255 10.49 2.436 0.256 10.50 2.429 0.255 10.49 2.411 0.256 10.61 2.380 0.256 10.75 2.337 0.257 10.99 2.282 0.258 11.30 2.214 0.257 11.60 2.135 0.258 12.08 2.043 0.259 12.67 1.940 0.260 13.40 1.824 0.261 14.30 1.696 0.262 15.44 1.556 0.263 16.90 1.403 0.263 18.74 1.175 0.147 12.51 0.995 0.130 13.06
reference range; the pregnancy was complicated by oligohydramnios. This fetus had reverse flow in the umbilical artery, and fetal demise was diagnosed 4 weeks later.
All fetuses estimated to be SGA in utero turned out to be SGA at birth. In 9 SGA fetuses the middle cerebral artery was below our normal reference range (Fig. 5): 2 of these died in utero; 1 died soon after birth; 5 had fetal distress or were admitted to the neonatal intensive care unit; and 1 was normal. Two of the fetuses transferred to the neonatal intensive care unit for further evaluation had a good short-term outcome and were transferred to the normal nursery within 12 hours. In two fetuses who died in utero the time between the study of the middle cerebral artery and fetal demise ranged from 2 to 4 weeks. The SGA fetuses with a normal value of pulsatility index (n = 24) had no complications (n = 17); I fetus died in utero, 2 fetuses died after delivery, and 4 others had fetal distress or were transferred to the neonatal intensive care unit. The two fetuses with normal middle cerebral artery pulsatility indexes who died shortly after birth were studied 2 days and 7 weeks before delivery, respectively.
Table IV provides calculations of sensitivity, specificity, and positive and negative predictive values for the

Volume 166 Number 4
x OJ "0 ~
Middle cerebral artery velocimetry 1267
I elu s Infanl
Fig. 3. Middle cerebral artery (MCA) pulsatility index values before delivery and at 1 month after delivery in nine normal infants (p > 0.05).
x , 0 OJ "0 ~
:::n +J
• V +J • «l (.I) -~ c.. < 10 U 1:
00
0
• • • • • •
• • • •
-l
WeeKS
• •
10
Fig. 4. Middle cerebral artery (MCA) pulsatility index values in one infant studied from 16 weeks' gestation to 24 weeks after delivery.
middle cerebral artery pulsatility index below the normal range and adverse perinatal outcome.
Table V provides data on the six perinatal deaths. The rate of cesarean sections was 42% in the SGA
fetuses with normal middle cerebral artery pulsatility index and 55% in the SGA fetuses with abnormal middle cerebral artery pulsatility index. Six of the pregnant women of group 2 had hypertension during their pregnancy.
Comment
Wladimiroff et al.I reported that the pulsatility index of the fetal internal carotid artery did not change sig-
nificantly between 26 weeks' gestation and the term of pregnancy. They suggested that IUGR fetuses could undergo a brain-sparing effect, similar to that reported in the animal literature. Successively, Van Den Wijngaard et al. 5 showed that the pulsatility index of the fetal internal carotid artery decreases during gestation. These authors anributed this change to the relatively low oxygen observed by Soothill et aI.' in the umbilical artery at the end of pregnancy.
Vyas et al. 14 studied the middle cerebral artery in normal and hypoxemic fetuses and reported that the end-diastolic velocities were absent in 11 of 42 normal fetuses at 18 to 25 weeks' gestation and in 12 of 50

1268 Mari and Deter
4
X Q)
'0 C
3 :::7) ... ... II:) 2 (/) -::I c.. < u I:
0 13 18
• • •
23
•
•
28
Weeks 33 38
April 1992 Am J Obstet Gynecol
43
Fig. 5. Middle cerebral artery (MeA) pulsatility index of 33 SGA fetuses (squares) plotted on reference range. The large rectangle at 31 weeks' gestation represents 3 pulsatility index values.
Table III. Middle cerebral artery pulsatility index standard curve (cross-sectional)
Gestational age (wh) Predicted value Upper limitt
15 0.99 1.57 2.14 16 1.08 1. 71 2.33 17 1.16 1.83 2.51 18 1.23 1.95 2.67 19 1.30 2.05 2.81 20 1.35 2.14 2.93 21 1.40 2.22 3.04 22 1.44 2.29 3.13 23 1.48 2.34 3.20 24 1.51 2.38 3.26 25 1.52 2.41 3.30 26 1.54 2.43 3.32 27 1.54 2.44 3.33 28 1.54 2.43 3.32 29 1.52 2.41 3.30 30 1.50 2.38 3.26 31 1.48 2.34 3.20 32 1.44 2.28 3.12 33 1.40 2.21 3.03 34 1.35 2.13 2.92 35 1.29 2.04 2.79 36 1.22 1.94 2.65 37 1.15 1.82 2.49 38 1.07 1.69 2.32 39 0.98 1.56 2.13 40 0.89 1.40 1.92 41 0.78 1.24 1.70 42 0.67 1.06 1.45
PI, Pulsatility index; GA, gestational age. PI = -1.9763 + (0.32737 GA) + ( -0.00611 GN).
*Predicted value - (2 x 0.184 x Predicted value). tPredicted value + (2 x 0.184 x Predicted value).
fetuses at 26 to 33 weeks. They reported that maximum reduction in pulsatility index is reached when the fetal Po. is 2 to 4 SD below normal for gestation. When the oxygen deficit is greater there is a tendency for the
pulsatility index to rise; this presumably reflects the development of brain edema.
Veille and Cohen!5 performed Doppler studies of the middle cerebral artery on 17 fetuses who were SGA at the time of delivery. Results were compared with a group of 25 fetuses who had a normal weight for gestational age at the time of delivery. No difference was found in either the systolic / diastolic ratio!6 or the Pourcelot index!7 of the middle cerebral artery.
It is possible that the physiologic fetal hypoxemia reported by Soothill et al" at the end of gestation could contribute to the low pulsatility index observed in this period of gestation. However, we have observed that the low pulsatility index found in nine normal fetuses late during pregnancy does not change significantly after delivery. Additionally, our study indicates that the pulsatility index of the middle cerebral artery is lowest between 15 and 20 weeks' gestation and at the end of gestation. To postulate another explanation for the low pulsatility index observed in the normal fetus at the end of gestation, the factors that could influence the pulsatility index in the cerebral circulation must be examined. The pulsatility index of the middle cerebral artery is decreased in conditions that suggest a decreased cerebral impedance to blood flow caused by either mechanical factors!S or fetal hypoxemia such as that observed in IUGR fetuses! and in the anemic fetus after intravascular transfusion.' Therefore our results could indicate a decreased cerebral vascular impedance to blood flow during these two periods of gestation.
That reasonable agreement was obtained between the results of the longitudinal and cross-sectional studies in normal fetuses supports the concept that this pattern of change in the pulsatility index of the middle cerebral artery is physiologic. An explanation for lower vascular impedance during early and late pregnancy

Volume 166 Number 4
Table IV. Predictive validity of middle cerebral artery pulsatility index below the normal range for gestational age for adverse perinatal outcome
Test result
Positive (Abnormal) Negative (Normal)
TOTAL
Adverse perinatal outcome*
No. I 6 4
10
%
66.6 16.6
30.3
Disease state
No adverse perinatal outcome
No. I 3
20
23
%
33.3 83.3
69.7
Total
9 24
33
Sensitivity, 60%; specificity, 87%; positive predictive value, 67%; negative predictive value, 83%.
* Admission to neonatal intensive care unit for> 12 hours or perinatal death.
may be found in studies of the development of the human brain. Dobbing and Sands19 studied human fetal brains; they estimated total cell numbers by chemical analysis of deoxyribonucleic acid-phosphorus in the forebrain, cerebellum, and brain stem. These authors calculated the whole brain values as the sum. They assumed that total tissue deoxyribonucleic acid represented total number of cells. They demonstrated that in the human species there are two periods of major cellular multiplication: one at 15 to 20 weeks' gestation and one that commences in the third trimester and probably ends in the second year of postnatal life. We have observed a lower pulsatility index in the middle cerebral artery during these two periods of increased deoxyribonucleic acid synthesis. It can be speculated that during these two periods of major cellular multiplication there is an increased metabolic requirement in the human fetal brain and a lower cerebral vascular impedance to blood flow.
Our results are in conflict with those reported by Vyas et al. 14 because we have observed the end-diastolic velocity in the middle cerebral artery velocity waveforms in almost all of the fetuses. This discrepancy may be caused by the use of different high-pass filters: 125 Hz in their study, 0 to 50 Hz in the current study. We think it is important to use a low-frequency high-pass filter when studying the middle cerebral artery because of the possibility of missing the diastolic component of the waveforms, which will affect the pulsatility index.
To date, studies of the fetal cerebral circulation have been directed mainly at recognizing IUGR fetuses. An IUGR fetus can be either a fetus with low growth rate caused by chronic hypoxia at risk for adverse perinatal outcome or a small, normally growing baby. Animal and human experiments have shown that the brainsparing effect is present in conditions of fetal hypox-
Middle cerebral artery velocimetry 1269
Table V. Perinatal deaths
Middle cerebral artery Gestational Time of
Patient pulsatility index age (wk) Diagnosis death
1 0.80 20 IUGR Stillbirth 2 lAO 21 IUGR Neonatal 3 0.92 24 IUGR-PlH Neonatal 4 0.84 25.2 IUGR-LA Stillbirth 5 1.70 26 IUGR Stillbirth 6 1.96 36 IUGR-Hyd Neonatal
PIH, Pregnancy-induced hypertension; LA, lupus anticoagulant; Hyd. hydramnios.
emia. 14. 20 It is reasonable to assume that the brain
sparing effect is present in the fetus with low growth rate and not in the normal small baby. The results of the SGA fetuses reported in this study indicate that in some SGA fetuses there is a pulsatility index value below the normal range, which suggests a brain-sparing effect. The difference between the fetuses with normal versus abnormal middle cerebral arterial pulsatility index may be clinically important. The fetuses with abnormal pulsatility index had a greater incidence of adverse perinatal outcome.
Recently we proposed that the brain-sparing effect is transitory" 1 as reported during prolonged hypoxemia in animal experiments,22 and the overstressed human fetus loses the brain-sparing effect. This hypothesis is further supported by the recent findings of Vyas et al. 14 In our series three SGA fetuses with normal middle cerebral artery pulsatility indexes died, the first in utero and the other two shortly after birth. It is possible that these fetuses had a brain-sparing effect during the pregnancy that was not present when we studied the fetuses.
As our study indicates, the brain-sparing effect can be present early in pregnancy (i.e., 20 weeks). This can be clinically important because of the possibility of early recognition of the fetus at higher risk for adverse perinatal outcome.
In conclusion, our study shows that (1) the pulsatiIity index of the middle cerebral artery of the normal human fetus has a parabolic pattern during pregnancy; (2) a physiologic lower pulsatility index value in the middle cerebral artery of the normal human fetus at 15 to 20 weeks' gestation and late in the third trimester is associated with an increased deoxyribonucleic acid synthesis in the fetal brain; (3) the pulsatility index of the middle cerebral artery after birth in nine normal fetuses did not change significantly from the pulsatility index obtained at the end of gestation; (4) a brainsparing effect can be present early during gestation (i.e., 20 weeks); and (5) an abnormal pulsatility index of the middle cerebral artery in the SGA fetus is associated with worse fetal outcome.

1270 Mari and Deter
I thank Dr. James F. Jekel, Dr. Brian Kirshon, Matthew Massicotte (Yale Medical School Student) and Laura J. Bryson (Baylor Medical School Student) for their help with this article.
REFERENCES
1. Wladimiroff JW, Tonge HM, Stewart PA. Doppler ultrasound assessment of cerebral blood flow in the human fetus. Br J Obstet Gynaecol 1986;93:471-5.
2. WOO JK, Liang ST, Lo RS, Chan FY. Middle cerebral artery Doppler flow velocity waveforms. Obstet Gynecol 1987;70:613-6.
3. Mari G, Moise JK, Deter RL, Carpenter RJ. Flow velocity waveforms of the umbilical and cerebral arteries before and after intravascular transfusion. Obstet Gynecol 1990;75:585-9.
4. Soothill PW, Nicolaides KH, Rodeck CH, Campbell S. Effect of gestational age on fetal and intervillous blood gas and acid-base values in human pregnancy. Fetal Ther 1986; 1: 168-75.
5. Van Den Wijngaard JAGW, Groenenberg IAL, Wladimiroff JW, Hop WCI. Cerebral Doppler ultrasound of the human fetus. Br J Obstet Gynaecol 1989;96:845-9.
6. Mari G. Arterial blood flow velocity waveforms of the pelvis and lower extremities in normal and IUGR fetuses. AMJ OBSTET GVNECOL 1991;165: 143-51.
7. Usher R, McLean F. Intrauterine growth oflive-born caucasian infants at sea level: standards obtained from measurements in 7 dimensions of infants born between 25 and 44 weeks of gestation. J Pediatr 1969;74:901-10.
8. Deter RL, Hadlock FP, Harrist RB. Evaluation of fetal growth and the detection of intrauterine growth retardation. In: Callen PW, ed. Ultrasonography in obstetrics and gynecology. Phildelphia: WB Saunders, 1983: 113-40.
9. Mari G, Moise KJ, Deter RL, Kirshon B, Carpenter RJ, Huhta JC. Doppler assessment of the pulsatility index in the cerebral circulation of the human fetus. AMJ OBSTET GVNECOL 1989; 160:698-703.
10. Britain RG. Doppler instrumentation. In: Maulik D, McN ellis D, eds. Doppler ultrasound measurement of ma-
April 1992 Am J Obstet Gynecol
ternal-fetal hemodynamics. Ithaca, New York: Perinatology Press, 1987:93-103.
11. American Institute of Ultrasound in Medicine, Bioeffects Committee. Bioeffects considerations for the safety of diagnostic ultrasound. J Ultrasound Med 1988;9S:S1-38.
12. Gosling RG, King DH. Ultrasound angiology. In: Marcus AW, Adamson L, eds. Arteries and veins. New York: Churchill Livingstone, 1975:61-98.
13. Mari G, Moise JK, Deter RL, Kirshon B, Stefos T, Carpenter RJ. Flow velocity waveforms of the vascular system in the anemic fetus before and after intravascular transfusion for severe red blood cell alloimmunization. AM J OBSTETGVNECOL 1990;162:1060-4.
14. Vyas S, Nicolaides KH, Bower S, Campbell S. Middle cerebral artery flow velocity waveforms in fetal hypoxemia. Br J Obstet Gynaecol 1990;97:797-803.
15. Veille JC, Cohen I. Middle cerebral artery blood flow in normal and growth-retarded fetuses. AM J OBSTET GvNECOL 1990;162:391-6.
16. Stuart B, Drumm J, FitzGerald DE, Duignan NM. Fetal blood velocity waveforms in normal pregnancy. Br J Obstet Gynaecol 1980;87:780-5.
17. Pourcelot L. Application c1iniques de I'examen Doppler transcutane: In: Perronneau P, ed. Velocimetrie ultrasonone Doppler. Paris: Seminaire INSERM, 1974:213-40.
18. Mari G, Moise JK, Deter RL, et al. Doppler assessment of the pulsatility index of the middle cerebral artery during constriction of the fetal ductus arteriosus following indomethacin therapy. AM J OBSTET GVNECOL 1989; 161:1528-31.
19. Dobbing J, Sands J. Timing of neuroblast multiplication in developing human brain. Nature 1970;226:639-40.
20. Cohn HE, Sacks EJ, Heymann MA, Rudolph AM. Cardiovascular responses to hypoxemia and acidemia in fetal lambs. AMJ OBSTETGvNECOL 1974;120:817-24.
21. Mari G, Wasserstrum N. Flow velocity waveforms of the fetal circulation preceeding fetal demise in a case oflupus anticoagulant. AMJ OBSTETGVNECOL 1991;164:776-8.
22. Richardson BS, Rurak D, Patrick JE, Homan J, Carmichael L. Cerebral oxidative metabolism during sustained hypoxaemia in fetal sheep. J Dev Physiol 1989; 11 :37-43.
Make researching easier with the Ten-Year Cumulative Index (1978-1 987) to the AMERICAN JOURNAL OF OBSTETRICS AND GYNECOLOGY
The Ten-Year Cumulative Index is a complete guide to more than 30,000 pages of original articles, case reports, letters, and editorials published in the AMERICAN JOURNAL OF OBSTETRICS AND GYNECOLOGY from 1978 through 1987 (volumes 130 to 157). Numbering more than 800 pages, the Cumulative Index includes both a subject and an author index. This hard-cover volume is $64.50 ($69.00 international). Prices include shipping. Payment must accompany all orders and must be in U.S. funds, drawn on a U.S. bank.
Contact Mosby-Year Book, Inc., Subscription Services, 11830 Westline Industrial Drive, St. Louis, MO 63146-3318 USA; phode (314) 453-4394. In the U.S., call toll-free: 1-800-325-4177, ext. 4394. Please allow six weeks for delivery.
Copyright © 2022 FDOKUMEN




















