Microvessel Density in Sinus Augmentation Procedures Using Anorganic Bovine Bone and Autologous...
9
Microvessel Density in Sinus Augmentation Procedures Using Anorganic Bovine Bone and Autologous Bone: 3 Months Results Marco Degidi, MD, DDS,* Luciano Artese, MD,† Corrado Rubini, MD,‡ Vittoria Perrotti, DDS,§ Giovanna Iezzi, DDS, PhD,¶ and Adriano Piattelli, MD, DDS T he maxillary sinus presents a low vascularity and a low oxy- gen tension. 1 Several different materials have been used for sinus augmentation procedures. Autologous bone is considered to be the gold stan- dard. 2–4 Autologous bone carries pro- teins as bone-enhancing substrates, minerals, and vital bone cells 2–4 and shows a fast angiogenic ingrowth of vessels from the surrounding original bone. 5 This latter fact seems to be able to revitalize the graft and its cellular component, which will take part in the local metabolism. 5 The survival of bone grafts is in part determined by the degree and rapidity of revascular- ization. 6 Autologous bone grafts har- vested from the iliac crest present very high success rates with implants loaded and in function. 7 However, the use of iliac grafts increases costs and morbidity, and an 8% incidence of major complications (infection, blood loss, nerve injury) has been reported. 7 The use of intraoral donor sites usually produces less morbidity, but the amount of bone obtained is sometimes not sufficient for bilateral sinus graft- ing. 7 Other bone grafts (i.e., allografts or xenografts) do not carry vital cells and have been shown to be unpredict- able in terms of the amount of osteo- genic promoters that are present. 8,9 Bio-Oss (Geistlich, Wohlhusen, Switzerland) is a deproteinized steril- ized bovine bone with 75% to 80% porosity and a crystal size of approx- imately 10 m in the form of cortical granules. 10 –15 It has been reported that Bio-Oss promotes osteogenesis and has very low resorbability. 16 –21 Bio- Oss has often been used for maxillary sinus floor augmentation proce- dures. 8–14 Bio-Oss has a natural morphologic structure, a chemical com- position identical to that of bone, a large inner surface and porosity comparable to that of bone, a crystalline structure identical to osseous tissue, and purely inorganic composition. 6 Blood vessels are an important component of bone formation and maintenance. 22 Haversian and Volk- mann’s canals represent the vascular- ization of the cortical bone, and through them, nutrients and cytokines reach the osteocytes and the osteo- blasts. 22 This process of vascular in- duction is called angiogenesis and it *Visiting Professor, Dental School, University of Chieti-Pescara, Italy, Private Practice, Bologna, Italy. †Professor of Pathology, University of Chieti-Pescara. ‡Researcher, Department of Pathologic Anatomy and Histopathology, University of Ancona, Italy. §Research Fellow, Dental School, University of Chieti-Pescara. ¶Research Fellow, Dental School, University of Chieti-Pescara. Professor of Oral Pathology and Medicine, Dental School, University of Chieti-Pescara. ISSN 1056-6163/07/01603-317 Implant Dentistry Volume 16 • Number 3 Copyright © 2007 by Lippincott Williams & Wilkins DOI: 10.1097/ID.0b013e3180de4c5f Purpose: This study was an im- munohistochemical evaluation of microvessel density (MVD) in sinus augmentation procedures with au- tologous bone and anorganic bone (Bio-Oss ® ). Materials and Methods: Twenty- four patients (14 men and 10 women – mean age of 48 years with a range from 34 to 53 years) participated in this study. All the patients presented a maxillary partial unilateral edentulism involving the premolar/molar areas, with a residual alveolar ridge height of about 4 to 5 mm. Twelve patients received sinus augmentation proce- dures with 100% autologous bone; 100% Bio-Oss was used in the other 12 patients. Endosseous implants were inserted after a mean period of 3 months. As control, the portions of preexisting subantral bone were used. The mean value of the MVD in control bone was 23.4 / 1.3. The mean value of the MVD in the sinuses aug- mented with autologous bone was 29.0 / 2.4. The mean value of the MVD in the sinuses augmented with Bio-Oss was 23.8 / 2.2. Results: The statistical analysis showed that the differences of the MVD between control bone and si- nuses augmented with Bio-Oss were not statistically significant (P 0.52), while the difference of the MVD be- tween sinuses augmented with autolo- gous bone and those augmented with Bio-Oss was statistically significant (P 0.0008). Conclusions: Autologous bone may act not only as a passive filling material in bone defects but may also release osteogenic growth factors; and particles of autologous bone seem to contain vital osteoprogenitor cells. (Implant Dent 2007;16:317–325) Key Words: anorganic bovine bone, autologous bone, microvessel density, sinus augmentation procedures, xe- nogenic bone IMPLANT DENTISTRY /VOLUME 16, NUMBER 3 2007 317
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Microvessel Density in Sinus Augmentation Procedures Using Anorganic Bovine Bone and Autologous...

Microvessel Density in Sinus AugmentationProcedures Using Anorganic Bovine Boneand Autologous Bone: 3 Months Results
Marco Degidi, MD, DDS,* Luciano Artese, MD,† Corrado Rubini, MD,‡ Vittoria Perrotti, DDS,§Giovanna Iezzi, DDS, PhD,¶ and Adriano Piattelli, MD, DDS�
The maxillary sinus presents alow vascularity and a low oxy-gen tension.1 Several different
materials have been used for sinusaugmentation procedures. Autologousbone is considered to be the gold stan-dard.2–4 Autologous bone carries pro-teins as bone-enhancing substrates,minerals, and vital bone cells2–4 andshows a fast angiogenic ingrowth ofvessels from the surrounding originalbone.5 This latter fact seems to be ableto revitalize the graft and its cellularcomponent, which will take part in thelocal metabolism.5 The survival ofbone grafts is in part determined bythe degree and rapidity of revascular-ization.6 Autologous bone grafts har-vested from the iliac crest present veryhigh success rates with implantsloaded and in function.7 However, theuse of iliac grafts increases costs andmorbidity, and an 8% incidence ofmajor complications (infection, bloodloss, nerve injury) has been reported.7
The use of intraoral donor sites usuallyproduces less morbidity, but theamount of bone obtained is sometimesnot sufficient for bilateral sinus graft-ing.7 Other bone grafts (i.e., allograftsor xenografts) do not carry vital cellsand have been shown to be unpredict-
able in terms of the amount of osteo-genic promoters that are present.8,9
Bio-Oss (Geistlich, Wohlhusen,Switzerland) is a deproteinized steril-ized bovine bone with 75% to 80%porosity and a crystal size of approx-imately 10 �m in the form of corticalgranules.10–15 It has been reported thatBio-Oss promotes osteogenesis andhas very low resorbability.16–21 Bio-Oss has often been used for maxillarysinus floor augmentation proce-dures.8 –14 Bio-Oss has a naturalmorphologic structure, a chemical com-
position identical to that of bone, a largeinner surface and porosity comparableto that of bone, a crystalline structureidentical to osseous tissue, and purelyinorganic composition.6
Blood vessels are an importantcomponent of bone formation andmaintenance.22 Haversian and Volk-mann’s canals represent the vascular-ization of the cortical bone, andthrough them, nutrients and cytokinesreach the osteocytes and the osteo-blasts.22 This process of vascular in-duction is called angiogenesis and it
*Visiting Professor, Dental School, University of Chieti-Pescara,Italy, Private Practice, Bologna, Italy.†Professor of Pathology, University of Chieti-Pescara.‡Researcher, Department of Pathologic Anatomy andHistopathology, University of Ancona, Italy.§Research Fellow, Dental School, University of Chieti-Pescara.¶Research Fellow, Dental School, University of Chieti-Pescara.�Professor of Oral Pathology and Medicine, Dental School,University of Chieti-Pescara.
ISSN 1056-6163/07/01603-317Implant DentistryVolume 16 • Number 3Copyright © 2007 by Lippincott Williams & Wilkins
DOI: 10.1097/ID.0b013e3180de4c5f
Purpose: This study was an im-munohistochemical evaluation ofmicrovessel density (MVD) in sinusaugmentation procedures with au-tologous bone and anorganic bone(Bio-Oss®).
Materials and Methods: Twenty-four patients (14 men and 10 women –mean age of 48 years with a rangefrom 34 to 53 years) participated inthis study. All the patients presented amaxillary partial unilateral edentulisminvolving the premolar/molar areas,with a residual alveolar ridge heightof about 4 to 5 mm. Twelve patientsreceived sinus augmentation proce-dures with 100% autologous bone;100% Bio-Oss was used in the other12 patients. Endosseous implants wereinserted after a mean period of 3months. As control, the portions ofpreexisting subantral bone were used.The mean value of the MVD in controlbone was 23.4 �/� 1.3. The meanvalue of the MVD in the sinuses aug-
mented with autologous bone was 29.0�/� 2.4. The mean value of the MVD inthe sinuses augmented with Bio-Oss was23.8 �/� 2.2.
Results: The statistical analysisshowed that the differences of theMVD between control bone and si-nuses augmented with Bio-Oss werenot statistically significant (P � 0.52),while the difference of the MVD be-tween sinuses augmented with autolo-gous bone and those augmented withBio-Oss was statistically significant(P � 0.0008).
Conclusions: Autologous bonemay act not only as a passive fillingmaterial in bone defects but may alsorelease osteogenic growth factors;and particles of autologous bone seemto contain vital osteoprogenitor cells.(Implant Dent 2007;16:317–325)Key Words: anorganic bovine bone,autologous bone, microvessel density,sinus augmentation procedures, xe-nogenic bone
IMPLANT DENTISTRY / VOLUME 16, NUMBER 3 2007 317

has a relevant role in all regenerationprocedures.22,23 Angiogenesis is im-portant in wound healing, inflamma-tory diseases, and tumors.23 Also thedifferentiation of the bone tissue isaffected by local vascularity. The lowoxygen tension and high metabolic ac-tivity present at injury sites promoteangiogenesis.24 The development of avascular system at injury site is neededfor the delivery of oxygen and nutri-ents and to remove the cellulardebris.22 A complex interplay of molec-ular signals regulates angiogenesis,22
with the involvement of extracellularmatrix remodeling, endothelial cell mi-gration and proliferation, capillary dif-ferentiation, and anastomosis.23 Onemethod used for the evaluation of thepresence of blood vessels in a tissue isthe counting of the microvessel density(MVD).
The aim of this study was to con-duct an immunohistochemical evalua-tion of MVD in bone cores after sinusaugmentation procedures performedwith autogenous bone or anorganicbovine bone (Bio-Oss), and retrievedafter a period of 3 months.
MATERIALS AND METHODS
Twenty-four patients (14 men and10 women – mean age of 48 yearswith a range from 34 to 53 years)participated in this study. All patientsgave their written informed consentand the protocol of the study was ap-proved by the Ethics Committee of theUniversity of Chieti–Pescara. All thepatients presented a maxillary partialunilateral edentulism involving the pre-molar/molar areas, with a residual alve-olar ridge height of about 4 to 5 mm. Allthe patients were nonsmokers; none hadsystemic diseases or maxillary sinus pa-thology. None of the patients had recentextractions in the involved area. All pa-tients had good oral hygiene. At the ini-tial visit the patients received clinicaland occlusal examinations, and periapi-cal and panoramic radiographs; CTscans were performed to evaluate possi-ble intrasinusal pathologies as well asbony walls morphology.
Surgical Protocol
The patients were draped to guar-antee maximum asepsis. The skin wasdisinfected with Betadine and the pa-
tient was asked to rinse with chlo-rhexidine mouthwash 0.2%. Underlocal anesthesia, a crestal incision,slightly toward the palatal aspectthroughout the entire length of theedentulous segment, was performedsupplemented by buccal releasing in-cisions mesially and distally. Fullthickness flaps were elevated to ex-pose the alveolar crest and the lateralwall of the maxillary sinus. Using around bur under cold (4 to 5°C) sterilesaline irrigation, a trap door was madein the lateral sinus wall. The door wasrotated inward and upward with a tophinge to a horizontal position. The si-nus membrane was elevated with cu-rettes of different shapes, until itbecame completely detached from thelateral and inferior walls of the sinus.Half of the sinuses were filled withautologous bone harvested from theiliac crest, and the other half with Bio-Oss mixed with sterile saline solution;both materials were carefully packedin the sinus cavities. A membrane(Biogide, Geistlich, Wolhusen, Swit-zerland) was positioned against thepacked sinus window. The mucoperi-osteal flap was then replaced andsutured with multiple horizontal mat-tress sutures. Amoxicillin (1 g given 2times per day) was prescribed for 1week and analgesics were adminis-tered as required. Sutures were re-moved 2 weeks after surgery. Postsurgical visits were scheduled atmonthly intervals to check the courseof healing. After 3 months, a secondCAT scan was performed; the dimen-sions of the grafts were evaluated and,by means of a surgical template, theimplants were placed. A total of 70implants (50 XiVE and 20 Frialit2,DENTSPLY-Friadent, Mannheim,Germany) were then inserted. From aclinical standpoint, sufficient bonewidth and height was obtained in eachpatient after the sinus augmentationprocedures to allow implant placementin all patients. At the time of implantsurgery, bone cores were harvested us-ing a 3.5 � 10 mm diameter trephineunder a cold (4 to 5°C) sterile salinesolution irrigation. Implants were thenburied and the second stage surgerywas carried out after a healing periodof 6 additional months. Twenty-twobone cores (11 from sinuses aug-mented with autologous bone and 11
from sinuses augmented with Bio-Oss) were retrieved.
These bone cores were pro-cessed for light microscopy andimmunohistochemistry.
Specimen Processing
The decalcification was performedusing the following technique: 37.22 gr.of the natrium salt of the ethylenediami-netetraacetic acid (EDTA) were dis-solved in 1 liter of distilled water, then70 ml of a concentrate of hydrochlorid-ric acid (HCl) were added. After filtra-tion, the specimens were put in thissolution for not more than 2 to 4 hours.The specimens were then put in 70%alcohol solution, dehydrated, and em-bedded in paraffin. All the hematoxylin-eosin stained sections were reviewed,the quality of the slides was checked,and the slides for quantitative evaluationwere selected. Immunostaining forCD34 was performed using the alkalinephosphatase-anti-alkaline phosphatasemethod (APAAP) with a rabbit poly-clonal antibody (Santa Cruz Technol-ogy, Santa Cruz, CA, USA). Sections of4 �m were cut and mounted on poly-L-lysine-coated slides. Paraffin sectionswere dewaxed by xylene, rehydrated,and finally washed in Tris-Buffer (pH7.6) for 10 min. The following stepswere optimized by automatic staining(Dako, TechMate 500, Glostrup, Den-mark). Sections were incubated withprimary antibody solution for CD 34 ata dilution of 1:30.000 for 25 minutes atroom temperature. Slides were rinsed inbuffer (Buffer Kit, Dako, Glostrup,Denmark) and immunoreaction wascompleted with the APAAP kit (Dako,Glostrup, Denmark). The secondary an-tibody was an alkaline phosphatase la-belled monoclonal calf antibody, andthe detection antibody a monoclonalanti-calf mouse antibody. After incuba-tion with a chromogen alkaline phos-phatase substrate (Fast Red, Dako,Glostrp, Denmark), specimens werecounterstained with Mayer’s hematoxy-lin and coverslipped. The antibodyagainst human CD 34-related antigenwas used to highlight the blood mi-crovessels; all the morphologic struc-tures with a lumen surrounded by CD34-positive endothelial cells were con-sidered as blood microvessels. The mi-crovessel count was using an IBAS-ATimage analyzer (Kontron, Munich, Ger-
318 MICROVESSEL DENSITY IN SINUS LIFTING

many); for the evaluation, a 400� mag-nification was used and the individualmicrovessel profiles were circled to pre-vent the duplication or omission of mi-crovessel count. For each case, 10 highpower fields (HPF), corresponding to1.1 square millimeter, were measured.The values were expressed as number ofmicrovessels per square millimeter (mi-crovessel density: MVD). Finally, a sta-tistical analysis was performed, andStudent t test was used to evaluate thepresence of statistically significantdifferences.
RESULTSControl Bone
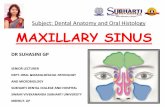
These bone cores showed normalcompact bone with the presence ofregularly scattered vessels of smalland middle dimensions located inHaversian canals and marrow spaces(Fig. 1). Bone trabeculae were present.A few osteoblasts deposing osteoidmatrix were sometimes present.
The mean value of the MVD incontrol bone was 23.4 �/� 1.3.
Autologous Bone
Almost all autologous bone parti-cles were completely lined by newly-formed bone. In some fields rims ofosteoblasts surrounded the newlyformed bone. Compact, mature corti-cal bone was present in some portionsof the bone cores (Fig. 2). The graftedbone had a higher affinity for dyes anda basic fuchsin positive, highly stainedline, similar to the cementing lines,divided the grafted from the newlyformed bone. The grafted autologousbone particles showed very slow re-sorption processes. The mean value ofthe MVD was 29.0 �/� 2.4 (Fig. 3).
Bio-Oss
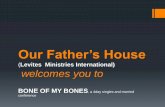
Newly formed mature, compactbone with well-organized osteonslined most of Bio-Oss particles. Insome areas, osteoblasts were seen se-creting osteoid matrix directly on theparticle surfaces. The newly-formedbone was always in close contact withthe particles surface and no gaps werepresent at the bone-particles interface.No inflammatory cell infiltrate waspresent around the particles or at theinterface with bone. Newly formedbone cemented some of the particles.
The Bio-Oss particles presentedmarked staining differences with thehost bone and had a lower affinity forthe dyes. Many small newly formedblood vessels were observed aroundand within the connective tissue insidethe marrow spaces (Figs. 4, 5). Themean value of the MVD was23.8 �/� 2.2.
Statistical Analysis
The statistical analysis showedthat the differences between control
bone and Bio-Oss at 3 months werenot statistically significant (P � 0.52),while the differences between autoge-nous bone and Bio-Oss were statisti-cally significant (P � 0.0008).
DISCUSSION
Autologous bone is the best graftingmaterial due to its nonimmunogenic capa-bilities, low risk of infection, and theosteogenic cell release of growth fac-tors.7,25,26 Its main problem remains itsavailability. For this reason, severaldifferent allografts have been intro-duced in clinical practice. Bio-Oss is axenogeneic bone graft material of bo-vine origin. This material has beendemonstrated to be osteoconductiveand it acts as a scaffold for the forma-tion of new bone.9–15 A hypothesis isthat autologous bone may act not onlyas a passive filling material in bonedefects but also through osteogenicgrowth factors released from theseparticles.7 Moreover, a positive effecton bone formation defects is to beexpected due to the fact that the par-
Fig. 1. Control bone. It is possible to observethe presence of compact bone with the pres-ence of regularly distributed vascular struc-tures of small and middle dimensions locatedin marrow spaces. H & E �200.Fig. 2. Autologous bone. Compact, maturecortical bone was present in some portions ofthe bone cores surrounded by small vessels.H & E �200.Fig. 3. Autologous bone MVD expressionwas higher in small vessels. This expressionpresented a high intensity. CD34 staining�200.
Fig. 4. Bio-Oss at 3 months. Inside the mar-row spaces it was possible to observe thepresence of collagen. The vessels weremainly located in close contact with the bone.H & E �160.Fig. 5. Bio-Oss at 3 months. Inside the mar-row spaces it was possible to observe theCD34� microvessels, located predominantlyin the connective tissue. CD34 staining�160.
IMPLANT DENTISTRY / VOLUME 16, NUMBER 3 2007 319

ticles of autologous bone seem to con-tain vital osteoprogenitor cells.7
Angiogenesis is the process bywhich new blood vessels are formedby sprouting from preexisting ves-sels.27 Osteogenesis in bone regenera-tion has shown to have close links tothe revascularization of the newly-forming tissues, and vessel numberwas found to be positively correlatedwith bone formation rate,28 and atemporal and spatial coupling of an-giogenesis to bone formation and re-sorption has been reported.29 Yao etal28 found that treadmill-running ratsdisplayed bone marrow angiogenesisconcomitant with bone formation in-crease and resorption decrease. Boneformation during distraction osteogen-esis has been reported to be accompa-nied by the induction of factorsassociated with angiogenesis.30 More-over, the highest acceleration of vas-cularization was found to precede thatof new bone formation.31 Regenerat-ing tissues show higher metabolicneeds requiring the presence of acapillary network during the repairprocesses.22 Vessel invasion is an im-portant step in the replacement of thecartilage that leads to bone forma-tion.32 Vessels and osteoblasts arelinked in several ways, such asvasculature-providing preosteopro-genitor cells or microcirculation influ-encing the interstitial temperature.33
Vascular endothelial growth factor(VEGF) is a potent angiogenic mole-cule, and appears to be particularlyimportant in bone formation.34 VEGFregulates recruitment, survival and ac-tivity of endothelial cells, osteoblasts,and osteoclasts.35 In mouse bonesVEGF is expressed before blood ves-sels are detected, and this expressionis tightly associated with osteoblasts.35
During development, VEGF seems tobe essential for blood vessel invasionof hyaline cartilage, growth plate mor-phogenesis and cartilage remodeling.35
Bone morphogenetic protein-2 (BMP-2), an osteoinductive agent, and VEGFare connected through the fact thatBMP stimulates angiogenesis via astimulation of VEGF.36 Furthermore,local delivery of VEGF has been re-ported to increase bone formation inrabbits,35 and the addition of VEGF toa mineralized substrate significantly
increased the production of mineral-ized tissue.37
Aoyama et al38 reported thatVEGF plays a role in the regulation ofangiogenesis at each stage of bone for-mation. In poor vascularity areas theundifferentiated pluripotential cellscan be directed into a chondrogenicand not an osteogenic pathway.24
In a previous study the MVD wasevaluated in alveolar sites augmentedwith autologous bone or Bio-Oss.39 Nosignificant differences were foundwhen comparing the MVD of the sitesregenerated with autologous bone andthose regenerated with Bio-Oss. Theretrieval time was, however, a mean of3 months for the autologous bone sitesand a mean of 6 months for the Bio-Oss sites. It was concluded that thesedata could support the hypothesis of afaster healing for the alveolar sitesaugmented with autologous bone.39
The present study confirms the advan-tages in vascular induction of autolo-gous bone because, we found, after asimilar period of 3 months, an higherand statistically significant differencein the MVD of sinuses grafted withautologous bone than of sinusesgrafted with Bio-Oss. The preferredbone graft material appears to be au-tologous bone as it carries proteins asbone-enhancing substrates, mineralsand vital bone cells, and it has a scaf-fold effect for osteogenic transfer.40–41
Artzi et al41 reported that the rapidhealing of sites augmented with autol-ogous bone is not comparable with theresults obtained with other non-autologous sources. The advantage ofautologous bone as a graft material isthe fast angiogenic ingrowth of vesselsfrom the surrounding host bone.5 Thislatter concept is confirmed by the re-sults of the present study. However,the disadvantages related to the pro-curement of autologous bone and tothe possibility of postoperative com-plications remain.
The interactions between boneformation and angiogenesis remain tobe fully characterized and, in the fu-ture, more studies will certainly benecessary to evaluate and elucidatethis problem even if the success of anybone graft is primarily related to thedegree of vascularization.41 Evidencepoints to the close relationship be-tween bone vascularization and
osteogenic cells; and a significant re-lationship was found between vesselnumber and bone formation.42
Disclosure
The authors claim to have no finan-cial interest in any company or any ofthe products mentioned in this article.
ACKNOWLEDGMENTS
This work was partially supported bythe National Research Council(C.N.R.), Rome, Italy, by the Ministryof the Education, University, Research(M.I.U.R.), Rome, Italy, and byAROD (Research Association forDentistry and Dermatology), Chieti,Italy.
REFERENCES
1. Butterfield KJ, Bennett J, GronowitzG, et al. Effect of platelet-rich plasma withautogenous bone graft for maxillary sinusaugmentation in a rabbit model. J OralMaxillofac Surg. 2005;63:370-376.
2. Hallman M, Lederlund A, LinsskogS, et al. A clinical histologic study of bovinehydroxyapatite in combination with autog-enous bone and fibrin glue for maxillary si-nus floor augmentation. Results after 8months of healing. Clin Oral Implants Res.2001;12:135-143.
3. Froum SJ, Tarnow DP, Wallace SS, etal. Sinus floor elevation using anorganic bo-vine bone matrix (Osteograf/N) with andwithout autogenous bone: a clinical, histo-logic, radiographic, and histomorphometricanalysis – Part 2 of an ongoing prospectivestudy. Int J Periodontics Restorative Dent.1998;18:529-543.
4. Garg AK. Grafting materials in repairand restoration. In: Lynch SE, Genco RJ,Marz RE. Tissue Engineering. Applicationsin Maxillofacial Surgery and Periodontics.Chicago: Quintessence; 1999:83-101.
5. Schlegel KA, Fichtner G, Schultze-Mosgau, et al. Histological findings in sinusaugmentation with autogenous bone chipsversus a bovine bone substitute. Int J OralMaxillofac Implants. 2003;18:53-58.
6. Merkx MAW, Maltha JC, FreihoferHPM, et al. Incorporation of particulatedbone implants in the facial skeleton. Bio-materials 1999;20:2029-2035.
7. Wada K, Niimi A, Watanabe K, et al.Maxillary sinus floor augmentation inrabbits: a comparative histologic-histomorphometric study betweenrhBMP-2 and autogenous bone. Int J Pe-riodontics Restorative Dent. 2001;21:253-263.
8. Piattelli M, Favero GF, Scarano A, etal. Bone reactions to anorganic bovinebone (Bio-Oss) used in sinus augmenta-
320 MICROVESSEL DENSITY IN SINUS LIFTING

tion procedures - A histologic long-termreport of 20 cases in humans. Int J OralMaxillofac Implants. 1999;14:835-840.
9. Valentini P, Abensur D. Maxillary si-nus floor elevation for implant placementwith demineralized freeze-dried bone andbovine bone (Bio-Oss): a clinical study of20 patients. Int J Periodontics RestorativeDent. 1997;17:233-241.
10. Tadjoedin ES, de Lange GL, Bron-ckers ALJJ, et al. Deproteinized cancellousbovine bone (Bio-Oss) as bone substitutefor sinus floor elevation. A retrospective,histomorphometrical study of five cases.J Clin Periodontol. 2003;30:261-270.
11. Valentini P, Abensur D. Maxillary si-nus floor elevation for implant placementwith demineralized freeze-dried bone andbovine bone (Bio-Oss). Int J PeriodonticsRestorative Dent. 1997;17:233-241.
12. Merkx MAW, Maltha JC, StoelingaPJW. Assessment of the value of anor-ganic bone additives in sinus flooraugmentation: a review of clinical reports.Int J Oral Maxillofac Surg. 2003;32:1-6.
13. Maiorana C, Sommariva L, BrivioP, et al. Maxillary sinus augmentation withanorganic bovine bone (Bio-Oss) and au-tologous platelet-rich plasma: preliminaryclinical and histologic evaluations. Int J Pe-riodontics Restorative Dent. 2003;23:227-235.
14. Haas R, Baron M, Donath K, et al.Porous hydroxyapatite for grafting themaxillary sinus: a comparative histomor-phometric study in sheep. Int J Oral Maxil-lofac Implants. 2002;17:337-346.
15. Artzi Z, Nemcovsky CE, Dayan D.Bovine-HA spongiosa blocks and immedi-ate implant placement in sinus augmenta-tion procedures. Histopathological andhistomorphometric observations on differ-ent histological stainings in 10 consecutivepatients. Clin Oral Implants Res. 2002;13:420-427.
16. Wetzel AC, Stich H, Caffesse RG.Bone apposition onto oral implants in thesinus area filled with different grafting ma-terials. A histologic study in the beagledogs. Clin Oral Implants Res. 1995;6:155-163.
17. Landi L, Pretel RW, Hakimi NM, etal. Maxillary sinus floor elevation using acombination of DFDBA and bovine-derived porous hydroxyapatite: a prelimi-nary histologic and histomorphometricreport. Int J Periodontics Restorative Dent.2000;20:575-583.
18. Rodriguez A, Anastasou GE, LeeH, et al. Maxillary sinus augmentation withdeproteinized bovine bone and plateletrich plasma with simultaneous insertion ofendosseous implants. J Oral Maxillofac Im-plants. 2003;61:157-163.
19. Sartori S, Silvestri M, Forni F, et al.Ten-year follow-up in a maxillary sinus aug-mentation using anorganic bovine bone(Bio-Oss). A case report with histomorpho-metric evaluation. Clin Oral Implants Res.2003;14:369-372.
20. Zitzmann NU, Scharer P, MarinelloCP, et al. Alveolar ridge augmentation withBio-Oss: a histologic study in humans. Int JPeriodontics Restorative Dent. 2001;21:289-295.
21. Hammerle CHF, Chiantella GC,Karring T, et al. The effect of deproteinizedbovine bone mineral on bone regenerationaround titanium dental implants. Clin OralImplants Res. 1998;9:151-162.
22. Lakey LA, Akella R, Ranieri JP.Angiogenesis: implications for tissue re-pair. In: Davies JE. Bone Engineering.Toronto: Em Squared Inc; 2000:137-142.
23. Folkman J. Angiogenesis in can-cer, vascular, rheumatoid and other dis-eases. Nature Med. 1995;1:27-31.
24. Carter DR, Loboa Polefka EG,Beaupre GS. Mechanical influences onskeletal regeneration and bone resorption.In: Davies JE. Bone engineering. Toronto:Em Squared Inc; 2000:358-368.
25. Tadjoedin ES, de Lange GL,Lyaruu DM, et al. High concentrations ofbioactive glass material (BiogranR) vs au-togenous bone for sinus floor elevation.Histomorphometrical observations onthree split mouth clinical cases. Clin OralImplants Res. 2002;13:428-436.
26. Silva RV, Camilli JA, Bertran CA, etal. The use of hydroxyapatite and autoge-nous cancellous bone grafts to repair bonedefects in rats. Int J Oral Maxillofac Surg.2005;34:178-184.
27. Johnson RB, Serio FG, Dai X.Vascular endothelial growth factor andprogression of periodontal disease. J Peri-odontol. 1999;70:848-852.
28. Yao Z, Lafage-Proust MH, PlouetJ. Increase of both angiogenesis and bonemass in response to exercise depends onVEGF. J Bone Miner Res. 2004;19:1471-1480.
29. Veillette CJ, von Schroeder HP.Endothelin-1 down-regulates the expres-sion of vascular endothelial growthfactor-A associated with osteoprogenitorproliferation and differentiation. Bone2004;34:288-296.
30. Pacicca DM, Patel N, Lee C, et al.Expression of angiogenic factors duringdistraction osteogenesis. Bone 2003;33:889-898.
31. Rabie AB, Leung FY, Chayanupat-kul A, et al. The correlation between neo-vascularization and bone formation in thecondyle during forward mandibular posi-tioning. Angle Orthod. 2002;72:431-438.
32. Ueno T, Kagawa T, Kanou M, et al.Immunolocalization of vascular endothelialgrowth factor during heterotopic bone for-mation induced from grafted periosteum.Ann Plast Surg. 2004;53:150-154.
33. Winet H. The role of microvascula-ture in normal and perturbed bone healingas revealed by intravital microscopy. Bone1996;19:39S-57S.
34. Huang YC, Kaigler D, Rice KG, etal. Combined angiogenic and osteogenicdelivery enhances bone marrow stromalcell-driven bone regeneration. J BoneMiner Res. 2005;20:848-857.
35. Carano RA, Filvaroff EH. Angiogen-esis and bone repair. Drug Discov Today.2003;8:980-989.
36. Eriksson C, Nygren H, Ohlson K.Implantation of hydrophilic and hydropho-bic titanium discs in rat tibia: cellular reac-tions on the surfaces during the first 3weeks in bone. Biomaterials 2004;25:4759-4766.
37. Murphy WL, Simmons CA, KaiglerD, et al. Bone regeneration via a mineralsubstrate and induced angiogenesis.J Dent Res. 2004;83:204-210.
38. Aoyama J, Tanaka E, Miyauchi M, etal. Immunolocalization of vascular endothe-lial growth factor in rat condylar cartilage dur-ing postnatal development. Histochem CellBiol. 2004;122:35-40.
39. Piattelli A, Degidi M, Di Stefano D,et al. Microvessel density in alveolar ridgeregeneration with autologous and alloplas-tic bone. Implant Dent. 2002;11:370-375.
40. Schliephake H, Dard M, Planck H,et al. Alveolar ridge repair using resorbablemembranes and autogenous bone parti-cles with simultaneous placement ofimplants: an experimental study in dogs.Int J Oral Maxillofac Implants. 2000;15:364-373.
41. Artzi Z, Kozlovsky A, NemcovskyCE, et al. The amount of newly formedbone in sinus grafting procedures dependson tissue depth as well as the type andresidual amount of the grafted material.J Clin Periodontol. 2005;32:193-199.
42. Barou O, Mekraldi S, Vico L, et al.Relationships between trabecular bone re-modeling and bone vascularization: aquantitative study. Bone 2002;30:604-612.
Reprint requests and correspondence to:Prof. Adriano Piattelli, MD, DDSVia F. Sciucchi 6366100 Chieti, ItalyFax: (011) 39-0871-3554076E-mail: [email protected]
IMPLANT DENTISTRY / VOLUME 16, NUMBER 3 2007 321

Abstract Translations
GERMAN / DEUTSCHAUTOR(EN): Marco Degidi, M.D., D.D.S., Luciano Artese,M.D., Corrado Rubini, M.D., Vittoria Perrotti, D.D.S.,Giovanna Iezzi, D.D.S., Ph.D. Adriano Piattelli, M.D.,D.D.S. Schriftverkehr:Prof. Adriano Piattelli, M.D., D.D.S.,Via F. Sciucchi 63, 66100 Chieti (Italien). Fax: 011-39-0871-3554076, eMail: [email protected]ßdichte bei Sinusanreicherungsbehandlungen mit-tels anorganischem Rinderknochengewebe und autologemKnochen: Ergebnisse nach 3monatigem Studienverlauf
ZUSAMMENFASSUNG: Zielsetzung: Die vorliegendeStudie bestand aus einer immunohistochemischen Beurtei-lung der Mikrogefaßdichte (MVD) bei Sinusanreicherungs-behandlungen mittels autologem Knochengewebe undanorganischem Knochen (Bio-Oss®). Materialien undMethoden: Insgesamt 24 Patienten (14 mannliche und 10weibliche im Alter von 34 bis 53 mit einem Durchschnitt-salter von 48 Jahren) nahmen an der Studie teil. Alle Pati-enten litten unter teilweiser, einseitiger Zahnlosigkeit imBereich des Oberkiefers unter Einbeziehung der Pramolarenund Molaren. Dabei belief sich die Hohe des verbleibendenKammes auf 4 bis 5 mm. 12 Behandlungen zur Sinusanhe-bung wurden unter Einsatz von 100% autologemKnochengewebe durchgefuhrt. Die 12 anderen Patientenwurden mit 100% Bio-Oss® behandelt. Knochengewebsinte-grierende Implantate wurden nach durchschnittlich 3Monaten eingepflanzt. Zur Kontrolle wurden Anteile vonbereits bestehendem Knochengewebe im Bereich unter derKieferhohle verwendet. Der durchschnittliche Wert der Mik-rogefaßdichte der Kontrollgruppe lag bei 23,4 �/� 1,3. Furdie mit autologem Knochengewebe durchgefuhrten Behand-lungen der Sinusanhebung lag der Durchschnittswert derMikrogefaßdichte bei 29,0 �/� 2,4. Der durchschnittlicheWert der Mikrogefaßdichte lag fur die Patienten, bei denendie Sinusanhebung unter Zuhilfenahme von Bio-Oss durch-gefuhrt wurde, betrug 23,8 �/� 2,2. Ergebnisse: Die statis-tische Analyse wies aus, dass die Unterschiede in derMikrogefaßdichte zwischen den Kontrollprufknochenteilenund den mit Bio-Oss® zur Sinusanreicherung eingesetztenKnochen statistisch bedeutsam waren (p � 0,0008).Schlussfolgerung: Es wurde die Hypothese aufgestellt,dass autologes Knochengewebe nicht nur passiv als Full-material bei Knochendefekten eingesetzt, sondern sichauch aktiv mit knochenbildenden Wachstumsfaktoren ein-bringen kann. Zusatzlich scheinen die autologen Knochen-partikel auch eigene knochenbildende Zellen zu enthalten.
SCHLUSSELWORTER: Anorganisches Rinderknochengewebe,autologer Knochen, Mikrogefaßdichte, Behandlungen zur Sinu-sanhebung, artfremdes Knochengewebe
SPANISH / ESPAÑOLAUTOR(ES): Marco Degidi, M.D., D.D.S., Luciano Artese,M.D., Corrado Rubini, M.D., Vittoria Perrotti, D.D.S., GiovannaIezzi, D.D.S., Ph.D., Adriano Piattelli, M.D., D.D.S. Correspon-dencia a: Prof. Adriano Piattelli, M.D., D.D.S., Via F. Sciucchi63, 66100 Chieti (Italy). Fax: 011-39-0871-3554076, e-Mail:[email protected] densidad de los microvasos en los procedimientos deaumento del seno usando hueso bovino anorganico y huesoautologo: Resultados a los 3 meses
ABSTRACTO: Proposito: Este estudio fue una evaluacioninmunohistoquımica de la densidad de los microvasos (MVDpor sus siglas en ingles) en los procedimientos de aumentodel seno con hueso autologo y hueso anorganico (Bio-Oss®).Materiales y Metodos: Participaron en este estudio veinticu-atro pacientes (14 hombres y 10 mujeres – media de edad 48con una variacion desde 34 a 55). Todos los pacientes sufrıanun edentulismo unilateral parcial maxilar que incluıan lasareas de los molares y premolares, con una altura residual dela cresta alveolar de aproximadamente 4 a 5 mm. Se realiz-aron doce procedimientos de aumento del seno con huesoautologo en un 100% y en los otros doce pacientes se uso un100% de Bio-Oss®. Los implantes endooseos se colocaronluego de un perıodo medio de 3 meses. Como control, seusaron las partes del hueso subantral preexistentes. El valorde la media de los MVD en el hueso de control fue 23,4 �/�1,3. El valor de la media de los MVD en los senos aumen-tados con hueso autologo fue 29,0 �/� 2,4. El valor de lamedia de los MVD en los senos aumentados con Bio-Oss fue23,8 �/� 2,2. Resultados: El analisis estadıstico demostroque las diferencias de los MVD entre el hueso de control y lossenos aumentados con Bio-Oss® no fueron estadısticamentesignificativas (p � 0,52), mientras que la diferencia de losMVD entre los senos aumentados con hueso autologo yBio-Oss fue estadısticamente significativa (p � 0,0008).Conclusion: La hipotesis es que el hueso autologo puedeservir no solamente como material de relleno pasivo endefectos oseos sino que tambien puede liberar factores decrecimiento osteogenicos; y partıculas de hueso autologoparecen contener celulas vitales osteoprogenitoras.
PALABRAS CLAVES: hueso bovino anorganico, hueso au-tologo, densidad de los microvasos, procedimientos de au-mento del seno, hueso xenogenico
PORTUGUESE / PORTUGUÊSAUTOR(ES): Marco Degidi, Medico, Cirurgiao-Dentista,Luciano Artese, Medico, Corrado Rubini, Medico, VittoriaPerrotti, Cirurgia-Dentista, Giovanna Iezzi, Cirurgia-Dentista, Ph.D., Adriano Piattelli, Medico, Cirurgiao-Dentista. Correspondencia para: Prof. Adriano Piattelli,
322 MICROVESSEL DENSITY IN SINUS LIFTING

M.D., D.D.S., Via F. Sciucchi 63, 66100 Chieti (Italy). Fax:011-39-0871-3554076, e-Mail:[email protected] do Microvaso em Procedimentos de Aumento daCavidade Usando Osso Bovino Anorganico e Osso Autol-ogo: Resultados de 3 Meses
RESUMO: Objetivo: Este estudo foi uma avaliacao imuno-histoquımica de densidade do microvaso (MVD) em procedi-mentos de aumento da cavidade com osso autologo e ossoanorganico (Bio-Oss®). Materiais & Metodos: Vinte e quatropacientes (14 homens e 10 mulheres – idade media 48 anoscom um intervalo de 34 a 53) participaram deste estudo.Todos os pacientes apresentaram uma condicao de desden-tado maxilar parcial unilateral envolvendo as areas pre-molares/molares, como uma altura do rebordo alveolarresidual de cerca de 4–5 mm. Doze procedimentos de au-mento da cavidade foram realizados com 100% de ossoautologo, com os outros doze pacientes foi usado 100%Bio-Oss®. Implantes endosseos foram inseridos apos um pe-rıodo medio de 3 meses. Como controle, as porcoes de ossosubantral preexistente foram usadas. O valor medio do MVDem osso de controle foi 23.4 �/� 1.3. O valor medio doMVD nas cavidades aumentadas com osso autologo foi 29.0�/� 2.4. O valor medio do MVD nas cavidades aumentadascom Bio-Oss foi 23.8 �/� 2.2. Resultados: A analise es-tatıstica mostrou que as diferencas do MVD entre osso decontrole e cavidades aumentadas com Bio-Oss® nao foramestatisticamente significativas (p � 0.52), enquanto a dife-renca do MVD entre cavidades aumentadas com osso autol-ogo e Bio-Oss foi estatisticamente significativa (p � 0.0008).Conclusao: A hipotese e que osso autologo pode agir nao socomo material de enchimento passivo em defeitos de osso,mas pode tambem liberar fatores de crescimento osteogenico;e partıculas de osso autologo parecem conter celulas osteo-progenitoras vitais.
PALAVRAS-CHAVE: osso bovino anorganico, osso autol-ogo, densidade do microvaso, procedimentos de aumento dacavidade, osso xenogenico
RUSSIAN /������: Marco Degidi, ������ ������, ���������� ������������ ��, Luciano Artese, ������������,Corrado Rubini, ������ ������, Vittoria Perrotti, ���������� ������������ ��, Giovanna Iezzi, ���������� ������������ ��, ������ ���������, Adriano Piat-telli, ������ ������, ������ ���� ������������ ��.����� ��� ���������� : Prof. Adriano Piattelli, M.D.,D.D.S., Via F. Sciucchi 63, 66100 Chieti (Italy). ����:011-39-0871-3554076, ����� ��������� ���:[email protected]
����� �� 3-��������� ������� ��� ������������������� ��� ����������� ����-������ ����� ���� ����� �������� ������ ����� � �������� �����
��� �! �"#$�%#!: &��: ��� � ����������� �� – �������� ������������������������ �������� ������������ (microvessel density,MVD) ��� ������������ ����-������ � ���� �-��� ������� ����� � ���� ������� ����� (Bio-Oss®). ' ���� � � ������: � �������� �� ����-� �� �� ���� �� � �� ������ � ��� (14 ����� �10 ���� � ���� ��� �� 34 �� 53 ��� , ���������� �� – 48 ���). � ���� � ����� ���� ������������ ������� � ����� ���������� �� ����, � �������� ���������� � �������, ����� ��� ������� ����������� ������� ���� ���� ����� 4–5 ��. ���� ��� � �� ������� ����-������ ���� ��� � �� ������ ����� � �����, ��� ���� ��� � �� � ��� � ���� ��� �������������� Bio-Oss®. !���� ���� ���� � ������ ��� ����� � ������ ����� 3 ���� . ����������� �� ��� �� ����� ������ ��� ����� ������� ������������ � ��� �����. "������ ���� �������� ������������ ��������� ��-��� ���� ���� 23,4 �/� 1,3. "����� � ���� ����-���� ������������ ����� ��������� ����-������ � ���� ���� ������� ����� ���� ����29,0 �/� 2,4. "����� � ���� �������� �������-����� ����� ��������� ����-������ � ���� ����Bio-Oss ���� ���� 23,8 �/� 2,2. ����� ��: # ���� � � �� ����������� ���, � ������ �������� � ������ ��������� ����� � ��� � �������������� ������������ ����� ��������� ����-������ � ���� ���� Bio-Oss � �������� � ��-���� �� �� ����������� ����� ����� (p � 0,52), � ������� � � � �� ����� ��������� ����������������� ��������� ����-������ � ���� ���� ������� ����� � ����� ���� ��� Bio-Oss® ��� �� ���������� � ����� (p � 0,0008). �����:������ ���� ������� , ��� ����� � ����������� �� � ������ � � ������ � �������� ���� � ��� � ������ �������� � �����, � ������ ����������� �� ����� �����, ����� ����,$������, ������ ����� � ������� �����,�������, ������ � ����� � ��� ���������������.
()*!��! $(���: ���� ����� � ����� �����, ����� � �����, �������� ������������,�������� ����-������ , ������ � �����
IMPLANT DENTISTRY / VOLUME 16, NUMBER 3 2007 323

JAPANESE /
CHINESE /
324 MICROVESSEL DENSITY IN SINUS LIFTING

KOREAN /
IMPLANT DENTISTRY / VOLUME 16, NUMBER 3 2007 325