ENGINEERED BONE BY AUTOLOGOUS OSTEOBLASTS ON POLIMERIC SCAFFOLDS IN MAXILLARY SINUS AUGMENTATION:...
6
Engineered Bone by Autologous Osteoblasts on Polymeric Scaffolds in Maxillary Sinus Augmentation: Histologic Report Carlo Mangano, DDS, MD 1 Adriano Piattelli, DDS, MD 2 Lucia Tettamanti, DDS 1 Francesco Mangano, DDS 3 Alessandro Mangano, DDS 4 Fa ´bio Borges, DDS 5 Giovanna Iezzi, DDS, PhD 6 Susana d’Avila, DDS, MS, PhD 7 Jamil Awad Shibli, DDS, MS, PhD 8 * Several regenerative therapies have been used for maxillary sinus grafting. However, recent advances in modern bone tissue engineering techniques have been evaluated. The aim of this histologic report was to evaluate the bone obtained by a culture of autogenous osteoblasts seeded on polyglycolic-polylactid scaffolds in maxillary sinus augmentation. A 56-year-old partially edentulous male with severe atrophy of the posterior maxilla received 6 polyglycolid- polylactid disks (8 mm diameter 3 2 mm depth, Oral Bone), each carrying 1.5 million autogenous osteoblasts into the depth of the sinus cavity. After 6 months healing, a bone core was harvested and histologically evaluated. The augmented maxillary sinus with engineered bone presented a mean of 28.89% and 71.11% of bone and medullary spaces, respectively. Data from this case report demonstrate that the newly formed bone provided by engineered bone tissue allowed proper initial stability for dental implant placement. However, the role of this new bone in the long-term success of dental implant anchorage needs further investigation. Key Words: maxillary sinus augmentation, engineered bone tissue, human histology, dental implants INTRODUCTION M axillary sinus floor aug- mentation has been used for occlusal rehabilitation with dental implants in the posterior maxilla. 1 Current- ly, several regenerative therapies, including synthetic bone grafts, allogenic and xeno- genic bone matrix, and recombinant growth/ differentiation factors, have been used for maxillary sinus grafting. 1–8 1 Department of Biomaterial Sciences, Insubria Univer- sity, Varese, Italy. 2 Department of Oral Pathology and Oral Medicine, University of Chieti-Pescara, Chieti, Italy. 3 Private practice, Gravedona (COMO), Italy. 4 University of Milan, Milan, Italy. 5 Department of Periodontology, Dental Research Division, Guarulhos University, Guarulhos, SP, Brazil. 6 University of Chieti, Chieti, Italy. 7 Oral Implantology Clinic, Guarulhos University, Guar- ulhos, SP, Brazil. 8 Oral Implantology Clinic, Department of Periodontol- ogy, Dental Research Division, Guarulhos University, Guarulhos, SP, Brazil. * Corresponding author, e-mail: [email protected] DOI: 10.1563/AAID-JOI-D-09-00028 CASE REPORT Journal of Oral Implantology 491
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of ENGINEERED BONE BY AUTOLOGOUS OSTEOBLASTS ON POLIMERIC SCAFFOLDS IN MAXILLARY SINUS AUGMENTATION:...
Engineered Bone by AutologousOsteoblasts on Polymeric Scaffolds inMaxillary Sinus Augmentation:Histologic ReportCarlo Mangano, DDS, MD1
Adriano Piattelli, DDS, MD2
Lucia Tettamanti, DDS1
Francesco Mangano, DDS3
Alessandro Mangano, DDS4
Fabio Borges, DDS5
Giovanna Iezzi, DDS, PhD6
Susana d’Avila, DDS, MS, PhD7
Jamil Awad Shibli, DDS, MS, PhD8*
Several regenerative therapies have been used for maxillary sinus grafting. However, recent
advances in modern bone tissue engineering techniques have been evaluated. The aim of this
histologic report was to evaluate the bone obtained by a culture of autogenous osteoblasts
seeded on polyglycolic-polylactid scaffolds in maxillary sinus augmentation. A 56-year-old
partially edentulous male with severe atrophy of the posterior maxilla received 6 polyglycolid-
polylactid disks (8 mm diameter 3 2 mm depth, Oral Bone), each carrying 1.5 million autogenous
osteoblasts into the depth of the sinus cavity. After 6 months healing, a bone core was harvested
and histologically evaluated. The augmented maxillary sinus with engineered bone presented a
mean of 28.89% and 71.11% of bone and medullary spaces, respectively. Data from this case
report demonstrate that the newly formed bone provided by engineered bone tissue allowed
proper initial stability for dental implant placement. However, the role of this new bone in the
long-term success of dental implant anchorage needs further investigation.
Key Words: maxillary sinus augmentation, engineered bone tissue, human histology,dental implants
INTRODUCTION
Maxillary sinus floor aug-
mentation has been used
for occlusal rehabilitation
with dental implants in the
posterior maxilla.1 Current-
ly, several regenerative therapies, including
synthetic bone grafts, allogenic and xeno-
genic bone matrix, and recombinant growth/
differentiation factors, have been used for
maxillary sinus grafting.1–8
1 Department of Biomaterial Sciences, Insubria Univer-sity, Varese, Italy.2 Department of Oral Pathology and Oral Medicine,University of Chieti-Pescara, Chieti, Italy.3 Private practice, Gravedona (COMO), Italy.4 University of Milan, Milan, Italy.5 Department of Periodontology, Dental ResearchDivision, Guarulhos University, Guarulhos, SP, Brazil.6 University of Chieti, Chieti, Italy.7 Oral Implantology Clinic, Guarulhos University, Guar-ulhos, SP, Brazil.8 Oral Implantology Clinic, Department of Periodontol-ogy, Dental Research Division, Guarulhos University,Guarulhos, SP, Brazil.* Corresponding author, e-mail: [email protected]: 10.1563/AAID-JOI-D-09-00028
CASE REPORT
Journal of Oral Implantology 491
Modern bone tissue engineering tech-
niques, through their use in combination
with biomaterials and osteogenic cells,
promise to obtain bone regeneration in
difficult contexts, without harvesting autog-
enous bone from other anatomic sites. By
manipulating 3 essential elements—bioma-
terials, growth factors, and osteogenic
cells—bone tissue engineering seeks to
construct the ideal bone graft material,
characterized by the same biological and
structural properties of native bone.9,10
Therefore, the purpose of this case report
was to evaluate the histologic behavior of
the engineered bone tissue, obtained by a
culture of autogenous osteoblasts seeded on
polyglycolic-polylactid scaffolds (Oral Bone,
BioTissue, Friburg, Germany) in maxillary
sinus augmentation.
CASE REPORT
Patient and engineered bone
A 56-year-old partially edentulous male was
referred by his general dentist for implant
therapy for oral rehabilitation with dental
implants. The patient was a healthy non-
smoker with no significant medical history.
After clinical and radiographic examination,
the patient presented missing teeth in the
premolar and molar regions caused by
periodontal disease. The posterior maxilla
presented severe atrophy11 (Figure 1). Max-
illary sinus floor elevation was required to
allow successful implant insertion. The pa-
tient received information on all proposed
treatment, and he provided signed informed
consent before undergoing treatment.
Six weeks before surgery, a specimen (2
3 5 mm) of bone marrow was taken from
the posterior area of the mandible, together
with 100/150 mL of venous blood sample.
The specimen, preserved in a medium
containing antibiotics and antimycotic solu-
tion, was then transferred to BioTissue
Technologies Laboratories to be processed
in a clean room. In the first 28 hours, cells
were enzymatically detached by 0.1% colla-
genase CLSIII (Clostridium histolyticum, Bio-
Chrom, Berlin, Germany) in DMEM/Ham’s F12
(Dulbecco’s substratum modified by Eagle
1:1, Invitrogen GmbH, Karlsruhe, Germany).
After 3 hours, the cellular suspension was
strained and filtered through a 100-mm
mesh, washed 2 times using phosphate-
buffered saline solution (PBS, Invitrogen
GmbH), and seeded as primary culture in
polystyrene culture flasks (Corning, Acton,
Mass). The medium consisted of DMEM/
Ham’s F12 (1:1) with 10% of autologous
patient serum. During the first 2 steps,
penicillin (10 U/mL) and streptomycin
(10 mm/mL) were added prophylactically.
Cells were cultured at 37uC with 5% carbon
dioxide (CO2) and 95% humidified air. Every
3 days, 75% of the culture medium was
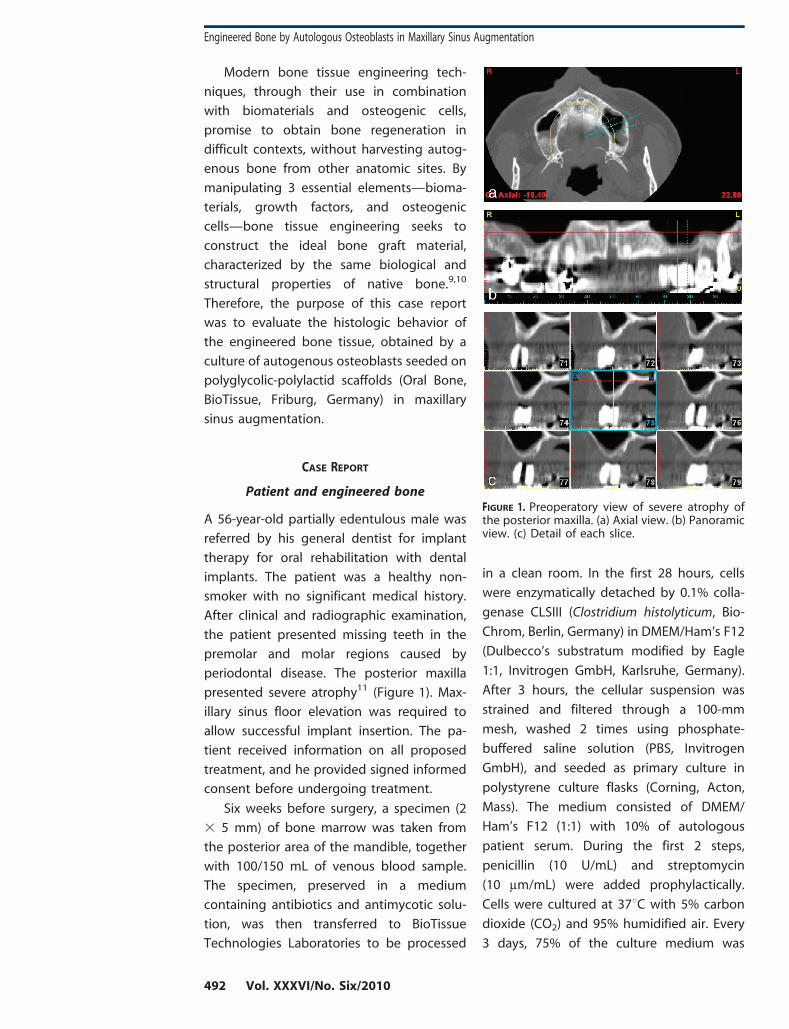
FIGURE 1. Preoperatory view of severe atrophy ofthe posterior maxilla. (a) Axial view. (b) Panoramicview. (c) Detail of each slice.
Engineered Bone by Autologous Osteoblasts in Maxillary Sinus Augmentation
492 Vol. XXXVI/No. Six/2010

replaced. Reaching 70% confluence, cells were
detached from culture flasks with 0.02%
trypsin and 0.02% thylenediaminetet-
raacetic acid, then were subcultivated until
a cell number of 16 to 32 million units was
reached, in 3 to 4 passages. A fraction of
these cells was tested separately for oste-
ogenic reproducibility.12 Cell suspension
was subsequently mixed with fibrinogen
at a ratio of 3:1 (Tissucol Duo S, Baxter,
Vienna, Austria), until a cellular density of
15 million cells/mL (625%) was reached,
and was soaked into biodegradable scaf-
folds (Ethisorb Tamponade, Ethicon, Nor-
densted, Germany), with a volume of
100 mL each. The scaffolds were character-
ized by an unwoven, disk-shaped polygly-
colid-polylactid structure (PLGA) with de-
fined size of 8 mm diameter and 2 mm
height. Scaffold porosity was very high
(.90%). Every single disk was finally capa-
ble of carrying 1.5 million autogenous cells.
The fibrinogen was polymerized by adding
thrombin (diluted 1:10 with PBS). After
polymerization was completed, cell-seeded
constructs were cultured for 1 week in a
specific osteogenic medium (Sigma, Dei-
senhofen, Germany) made of DMEM/Ham’s
F-12 (1:1) enriched with 5% autogenous
serum, ascorbic acid (0.3 mM), dexametha-
sone (1028 mol/L), and beta-glycerophos-
phate (10 mM). After 6 to 9 days of three-
dimensional (3D) culture, cellular vitality
was tested by measurement of cellular
glucose consumption (mg glucose con-
sumption/5 mL of culture medium/48 h).
When glucose consumption rates suggest-
ed sufficient viability, constructs were
stored in sterile transport medium and
were transferred to the clinic for the sinus
floor elevation procedure precisely 6 weeks
after biopsy was performed.
Maxillary sinus augmentation
The patient received antibiotics (2 g amox-
icillin) prophylactically 1 hour before surgery.
Local anesthesia (2 mL articaine hydrochlo-
ride 4% with 1/100 000 adrenaline) was
administered. A horizontal crestal incision
and 2 vertical incisions extending beyond
the mucogingival junction were made, and a
full-thickness flap was reflected to expose
the maxillary sinus lateral bone wall. Under
constant irrigation with saline solution, an
osseous window of approximately 1 cm 3
1 cm was demarked and isolated, using a
round diamond-coated bur. The isolated
osseous window was subsequently removed
and conserved in saline solution. The
Schneiderian membrane was exposed and
carefully isolated, using specially designed
elevators, to avoid undesired perforations.
Engineered bone transplants were used for
augmentation in the maxillary sinus. Six
polyglycolid-polylactid disks (8 mm diameter
3 2 mm depth, Oral Bone), each carrying 1.5
million autogenous osteoblasts, were used,
placed, and condensed into the depth of the
sinus cavity. After the sinus augmentation
procedure was completed, the previously
isolated osseous window was repositioned
to close the sinus lateral wall. Sutures were
placed (Supramid, Novaxa Spa, Milan, Italy)
to ensure complete flap closure. Amoxicillin
500 mg capsules was given 3 times daily for
7 days, and ibuprofen 400 mg tablets to be
taken as needed were prescribed for the
patient.
Bone core harvesting
Implant placement surgery was performed
after a 6 month healing period. Bone cores
were harvested through a transcrestal using
a 2.0 3 10 mm diameter trephine bur under
sterile saline solution irrigation. Three im-
plants with sandblasted acid-etched surfaces
(2 implants with 3.75 mm diameter and
13 mm length, and 1 with a 3.75 mm 3
10 mm length) were inserted; primary
stability ranged from 20–40 N/cm. The
second-stage surgery was carried out after
a 5 month healing period.
Mangano et al
Journal of Oral Implantology 493
Specimen processing andhistometric analyses
The biopsies were processed (Precise 1
Automated System, Assing, Rome, Italy) to
obtain thin ground sections as previously
described.13 The specimen was dehydrated in
an ascending series of alcohol rinses and
embedded in glycol methacrylate resin (Tech-
novit 7200 VLC, Kulzer, Wehrheim, Germany).
After polymerization, the specimens was
sectioned lengthwise along the larger axis of
the specimen, using a high-precision dia-
mond disk, to about 150 mm, and were
ground down to about 30 mm. Two slides
obtained from this specimen were stained
with basic fuchsin and toluidine blue. Histo-
morphometry of newly formed bone and
marrow spaces was carried out on the whole
sample at low magnification (325). These
measurements were obtained using a light
microscope (Laborlux S, Leitz, Wetzlar, Ger-
many) connected to a high-resolution video
camera (3CCD, JVC KY-F55B, JVC, Yokohama,
Japan) and interfaced to a monitor and PC
(Intel Pentium III 1200 MMX, Intel, Santa Clara,
Calif). This optical system was linked to a
digitizing pad (Matrix Vision GmbH, Oppen-
weiler, Germany) and a histometry software
package with image capturing capabilities
(Image-Pro Plus 4.5, Media Cybernetics Inc,
Bethesda, Md).
RESULTS
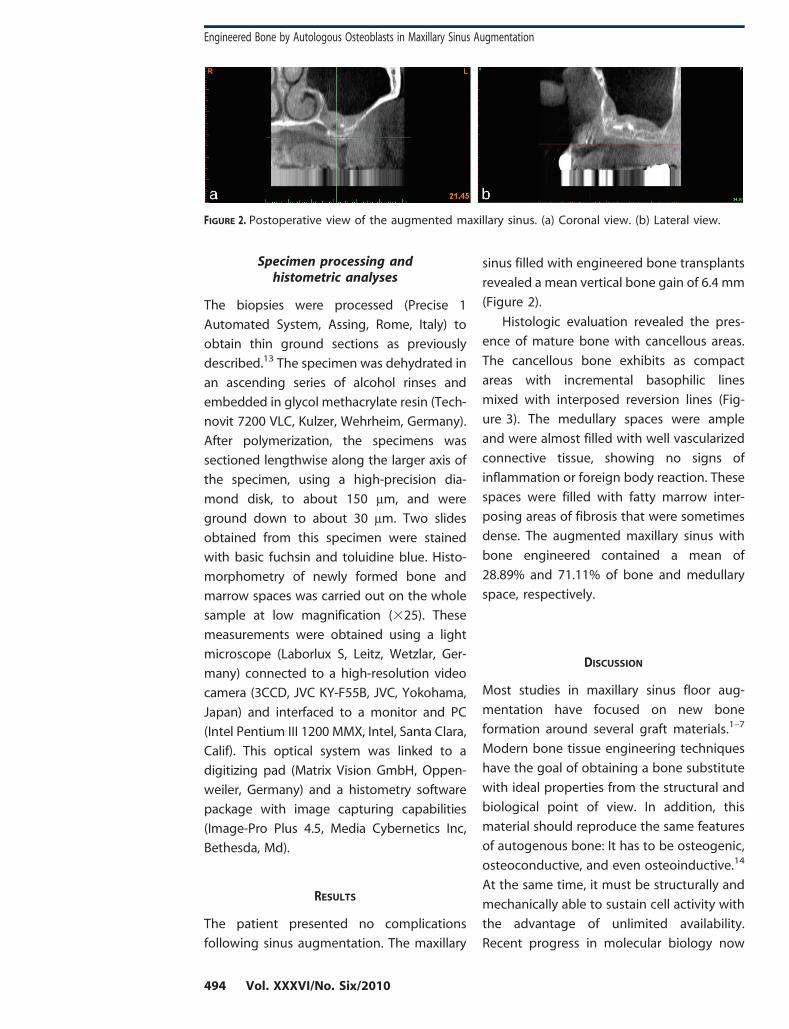
The patient presented no complications
following sinus augmentation. The maxillary
sinus filled with engineered bone transplants
revealed a mean vertical bone gain of 6.4 mm
(Figure 2).
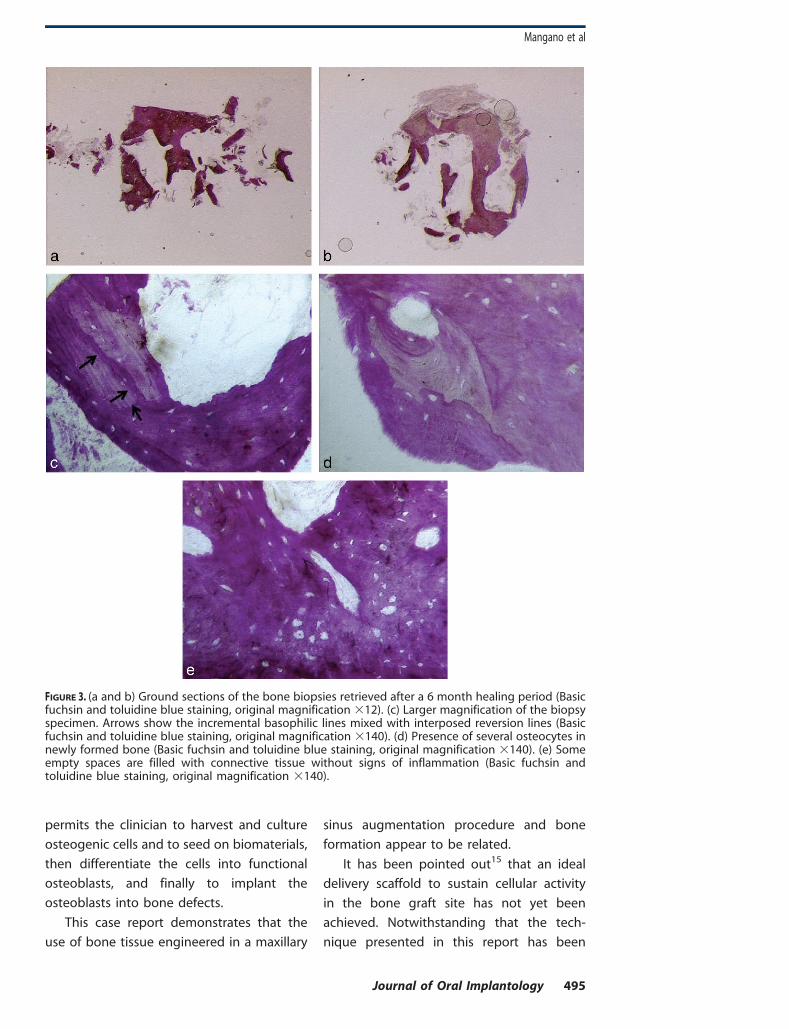
Histologic evaluation revealed the pres-
ence of mature bone with cancellous areas.
The cancellous bone exhibits as compact
areas with incremental basophilic lines
mixed with interposed reversion lines (Fig-
ure 3). The medullary spaces were ample
and were almost filled with well vascularized
connective tissue, showing no signs of
inflammation or foreign body reaction. These
spaces were filled with fatty marrow inter-
posing areas of fibrosis that were sometimes
dense. The augmented maxillary sinus with
bone engineered contained a mean of
28.89% and 71.11% of bone and medullary
space, respectively.
DISCUSSION
Most studies in maxillary sinus floor aug-
mentation have focused on new bone
formation around several graft materials.1–7
Modern bone tissue engineering techniques
have the goal of obtaining a bone substitute
with ideal properties from the structural and
biological point of view. In addition, this
material should reproduce the same features
of autogenous bone: It has to be osteogenic,
osteoconductive, and even osteoinductive.14
At the same time, it must be structurally and
mechanically able to sustain cell activity with
the advantage of unlimited availability.
Recent progress in molecular biology now
FIGURE 2. Postoperative view of the augmented maxillary sinus. (a) Coronal view. (b) Lateral view.
Engineered Bone by Autologous Osteoblasts in Maxillary Sinus Augmentation
494 Vol. XXXVI/No. Six/2010
permits the clinician to harvest and culture
osteogenic cells and to seed on biomaterials,
then differentiate the cells into functional
osteoblasts, and finally to implant the
osteoblasts into bone defects.
This case report demonstrates that the
use of bone tissue engineered in a maxillary
sinus augmentation procedure and bone
formation appear to be related.
It has been pointed out15 that an ideal
delivery scaffold to sustain cellular activity
in the bone graft site has not yet been
achieved. Notwithstanding that the tech-
nique presented in this report has been
FIGURE 3. (a and b) Ground sections of the bone biopsies retrieved after a 6 month healing period (Basicfuchsin and toluidine blue staining, original magnification 312). (c) Larger magnification of the biopsyspecimen. Arrows show the incremental basophilic lines mixed with interposed reversion lines (Basicfuchsin and toluidine blue staining, original magnification 3140). (d) Presence of several osteocytes innewly formed bone (Basic fuchsin and toluidine blue staining, original magnification 3140). (e) Someempty spaces are filled with connective tissue without signs of inflammation (Basic fuchsin andtoluidine blue staining, original magnification 3140).
Mangano et al
Journal of Oral Implantology 495
previously described with interesting re-
sults in an earlier study on maxillary sinus
augmentation in humans,16 this strategy for
engineered bone transplant creation may
not ensure sufficient dental implant anchor-
age. Polyglycolid-polylactid (PLGA) synthetic
polymeric scaffolds are characterized by a
rapid resorption rate, which could represent
an unfavorable factor for bone regeneration.
These data have been confirmed in a recent
clinical study17 on maxillary sinus augmenta-
tion in 20 patients. The authors demonstrated
that extended or rapid resorption of the
synthetic polymeric scaffolds could jeopar-
dize bone regeneration, thus making it
impossible to guarantee adequate mechani-
cal stability for osteoblasts delivered to the
graft site. Osteoblasts must adhere to a stable
structure to produce new bone matrix. New
matrix has to subsequently undergo mineral-
ization and maturation processes. To this
issue, fast or extended degradation of the
supporting scaffold determines the inevitable
failure of bone regeneration caused by the
collapse of newly formed bone matrix.
However, an ideal scaffold for bone regener-
ations is currently under study.17 The Oral
Bone material, with polyglycolid-polylactid
scaffolds, showed efficacy in promoting
cellular activity and bone regeneration as
presented in this case report.
In conclusion, data from this case report
demonstrate that the newly formed bone
provided by bone tissue engineering allowed
proper initial stability for dental implant
placement. However, the role of this new bone
in the long-term success of dental implant
anchorage needs further investigation.
ABBREVIATIONS
CO2: carbon dioxide
3D: 3-dimensional
PBS: phosphate-buffered saline solution
PLGA: polyglycolid-polylactid
REFERENCES
1. Browaeys H, Bouvry P, De Bruyn H. A literaturereview on biomaterials in sinus augmentation proce-dures. Clin Implant Dent Relat Res. 2007;9:166–177.
2. Mangano C, Scarano A, Iezzi G, et al. Maxillarysinus augmentation using an engineered poroushydroxypatite: a clinical, histological and transmissionelectron microscopy study in man. J Oral Implantol.2006;32:122–131.
3. Scarano A, Degidi M, Iezzi G, et al. Maxillary sinusaugmentation with different biomaterials: a compara-tive histologic and histomorphometric study in man.Implant Dent. 2006;15:197–207.
4. Boeck-Neto RJ, Gabrielli M, Lia R, Marcantonio E,Shibli JA, Marcantonio E Jr. Histomorphometrical anal-ysis of bone formed after maxillary sinus floor augmen-tation by grafting with a combination of autogenousbone and demineralized freeze-dried bone allograft orhydroxyapatite. J Periodontol. 2002;73:266–270.
5. Boeck-Neto RJ, Gabrielli MF, Shibli JA, Marcanto-nio E, Lia RC, Marcantonio E Jr. Histomorphometricevaluation of human sinus floor augmentation healingresponses to placement of calcium phosphate orRicinus communis polymer associated with autogenousbone. Clin Implant Dent Relat Res. 2005;7:181–188.
6. Boeck-Neto RJ, Artese L, Piattelli A, et al. VEGF andMVD expression in sinus augmentation with autologousbone and several graft materials. Oral Dis. 2009;15:148–154.
7. Hallman M, Cederlund A, Lindskog S, LundgrenS, Sennerby L. A clinical histologic study of bovinehydroxyapatite in combination with autogenous boneand fibrin glue for maxillary sinus floor augmentation.Clin Oral Implants Res. 2001;12:135–143.
8. Burchardt H. The biology of bone graft repair.Clin Orthop. 1983;174:28–42.
9. Ripamonti U, Duneas N. Tissue engineering ofbone by osteoinductive biomaterials. Mater Res Soc Bull.1996;21:36–39.
10. Young CS, Abukawa H, Asrican R, et al. Tissue-engineered hybrid tooth and bone. Tissue Eng. 2005;11:1599–1610.
11. Cawood JI, Howell RA. A classification of theedentulous jaws. Int J Oral Maxillofac Surg. 1988;17:232–236.
12. Redlich A, Perka C, Schultz O, et al. Boneengineering on the basis of periosteal cells cultured inpolymer fleeces. J Mater Sci Mater Med. 1999;10:767–772.
13. Piattelli A, Scarano A, Quaranta M. High-precision, cost-effective system for producing thinsections of oral tissues containing dental implants.Biomaterials. 1997;18:577–579.
14. Chang SC, Chuang H, Chen YR, et al. Cranialrepair using BMP-2 gene engineered bone marrowstromal cell. J Surg Res. 2004;119:85–91.
15. Meyer U, Wiesmann HP, Berr K, Kubler NR,Handschel J. Cell based bone reconstruction therapies:principles of clinical approaches. Int J Oral MaxillofacImplants. 2006;21:899–906.
16. Schimming R, Schmelzeisen R. Tissue engi-neered bone for maxillary sinus augmentation. J OralMaxillofac Surg. 2004;62:724–729.
17. Zizelmann C, Schoen R, Metzger MC, et al. Boneformation after sinus augmentation with engineeredbone. Clin Oral Impl Res. 2007;18:69–73.
Engineered Bone by Autologous Osteoblasts in Maxillary Sinus Augmentation
496 Vol. XXXVI/No. Six/2010