
Muller cells are living optical fibers in the vertebrate retina

Ms
SNAMa
b
c
d
e
f
g
h
i
h
•••
a
ARAA
KCCMPRC
T
h0
Neuroscience Letters 577 (2014) 95–100
Contents lists available at ScienceDirect
Neuroscience Letters
jo ur nal ho me page: www.elsev ier .com/ locate /neule t
icrovascular network alterations in retina of subjects with cerebralmall vessel disease
aima Hilal a,b,1, Yi-Ting Ongc,d,e,1, Carol Y. Cheungc,d,f, Chuen Seng Tang,arayanaswamy Venketasubramanianh, Wiro J. Niesseni, Henri Vroomani,inur R. Anuard, Merwyn Chewc,d, Christopher Chena,b, Tien Yin Wongc,d,f,ohammad Kamran Ikrama,d,f,∗
Memory, Aging & Cognition Center, National University Health System, Singapore, SingaporeDepartment of Pharmacology, National University of Singapore, Singapore, SingaporeDepartment of Ophthalmology, Yong Loo Lin School of Medicine, National University of Singapore, Singapore, SingaporeSingapore Eye Research Institute, Singapore National Eye Center, Singapore, SingaporeNUS Graduate School for Integrative Sciences and Engineering, National University of Singapore, Singapore, SingaporeOffice of Clinical Sciences, Duke—National University of Singapore Graduate Medical School, Singapore, SingaporeSaw Swee Hock School of Public Health, National University of Singapore, Singapore, SingaporeNeuroscience Clinic, Raffles Hospital, Singapore, SingaporeDepartments of Radiology & Medical Informatics, Erasmus Medical Center, Rotterdam, The Netherlands
i g h l i g h t s
Retinal microvascular network changes were linked previously to stroke and AD.Sparser and more tortuous retinal vascular network was associated with CMB.No significant association was found with lacunar infarcts and WML volume.
r t i c l e i n f o
rticle history:eceived 13 April 2014ccepted 9 June 2014vailable online 14 June 2014
eywords:erebral microbleedserebral small vessel diseaseagnetic resonance imaging
opulation basedetinal microvascular changeshinese
a b s t r a c t
Novel retinal imaging techniques have enabled the assessment of quantitative vascular parameters, whichprovide information on the microvasculature before the appearance of retinopathy signs. Advances inneuroimaging have revealed that cerebral microbleeds (CMB) – besides lacunar infarcts and white matterlesions (WML) – may be a novel marker of cerebral small vessel disease. We examine whether quantitativeretinal vascular parameters are related to cerebral small vessel disease in a Chinese population. Partic-ipants from Epidemiology of Dementia in Singapore Study underwent comprehensive examinations,including 3-Tesla cranial magnetic resonance imaging and retinal-photography. Retinal vascular param-eters (caliber, tortuosity, fractal dimension) were measured from photographs using a semi-automatedcomputer-assisted program. Lacunar infarcts and CMB were visually graded. Total brain and WML volumewere obtained using a validated segmentation tool.
A total of 261subjects were included, of whom 36 had lacunar infarcts, 29 had severe WML, and 83 hadCMB. In age-sex-adjusted models, narrower retinal arteriolar caliber, wider venular caliber and smaller
arteriolar fractal dimension were associated with presence of multiple CMB. In contrast, no associationwas found with lacunar infarcts and WML volume. After multivariate adjustments, associations of venularcaliber, arteriolar fractal dimensions and arteriolar tortuosity with CMB remained statistically significant. In conclusion, subjects with early structural changes in retinal microvasculature were more likely to have CMBs, supporting hypothesis t∗ Corresponding author at: Singapore Eye Research Institute (SERI), The Academia, 20 Cel.: +65 6576 7234.
E-mail address: kamran [email protected] (M.K. Ikram).1 Joint first author.
ttp://dx.doi.org/10.1016/j.neulet.2014.06.024304-3940/© 2014 Elsevier Ireland Ltd. All rights reserved.
hat CMB may be an early manifestation of cerebral small vessel disease.© 2014 Elsevier Ireland Ltd. All rights reserved.
ollege Road, Discovery Tower Level 6, Room 119, 169856 Singapore.

9 ce Let
1
ddhvsbloe[
icnviosrww[
pptsAtiacitM
2
2
p(naot(TpyfgwwbidotTor
external capsules and thalamus) and posterior fossa (brain-
6 S. Hilal et al. / Neuroscien
. Introduction
In addition to Alzheimer’s disease (AD), cerebrovascularisease is an important cause and contributor to cognitiveecline and dementia [1]. Magnetic resonance imaging (MRI)as become increasingly important in unraveling the role ofascular pathology involved in dementia. Improvements in MRcanner hard- and software have made it possible to visualizerain pathology more accurately. Recently, cerebral microb-
eeds (CMB) have been suggested as another manifestationr marker of cerebral small vessel disease, besides mark-rs such as white matter lesions (WML) and lacunar infarcts2].
However, direct in vivo visualization of cerebral small vesselss difficult to achieve. As the retinal and cerebral microvas-ulature share several features [3], the retina may provide aon-invasive “window” into the status of these small cerebralessels. Previous studies have shown that the clinically vis-ble retinopathy signs are associated with an increased riskf stroke and dementia, and subclinical markers of cerebralmall vessel disease [4]. Furthermore, quantitative changes inetinal vessel width, such as narrower arteriolar caliber andider venular caliber, have been shown to be associatedith these subclinical and clinical age-related brain pathologies
5].More recently, a series of novel quantitative retinal vascular
arameters such as fractal dimension and tortuosity have beenroposed to provide information on the cerebral microvascula-ure even before the appearance of retinopathy signs. It has beenhown that both patients with ischemic stroke and those withD have a sparser and more tortuous microvascular network in
he retina [6,7], suggesting that AD and stroke may share sim-lar underlying microvascular pathology. However, data on thessociation between these novel retinal vascular parameters anderebral small vessel disease are largely lacking. Therefore, wenvestigated whether there was a link between these novel quan-itative retinal parameters and cerebral small vessel disease on
RI.
. Materials and methods
.1. Study population
The Epidemiology of Dementia in Singapore (EDIS) study drawsarticipants from the Singapore Epidemiology of Eye DiseaseSEED) Study, which is a population-based study among Chi-ese, Malays and Indians [2]. In the present study we restrictednalysis to the Chinese component of EDIS, as the recruitmentf the other ethnicities is still ongoing. In the first phase ofhe EDIS Study, Chinese participants from SCES aged ≥60 yearsn = 1538) were screened using the 10-point Abbreviated Mentalest (AMT) and a self-report of progressive forgetfulness. Screen-ositives were defined as AMT score ≤6, among those with ≤6ears of formal education, or ≤8 among those with >6 years oformal education; or if the subject or caregiver reported pro-ressive forgetfulness [yes/no]. Screen-positive subjects (n = 612)ere invited to take part in the second phase of this study,hich included an extensive neuropsychological test battery and
rain MRI. Of these 612 participants, 300 agreed to participaten phase II. The details of the study methodology have beenescribed elsewhere [2]. Ethics approval for the EDIS study wasbtained from the SingHealth Institutional Review Board andhe National Healthcare Group Domain-Specific Review Board.he study was conducted in accordance with the Declaration
f Helsinki. Written informed consent was obtained prior toecruitment.ters 577 (2014) 95–100
2.2. Retinal photography
Retinal fundus photographs were taken of each eye with anon-mydriatic digital camera after dilation of pupils with 1% tropi-camide eye drops according to a standardized protocol [6,7]. Retinalimages from all participants were masked and collated for cen-tralized grading at the Reading Centre at Singapore Eye ResearchInstitute. Optic-disc centered images of a randomly selectedeye from each participant were fed through a semi-automatedcomputer-assisted program, Singapore I Vessel Assessment (soft-ware version 3.0), grading to a standardized protocol by trainedgraders. The following retinal vascular parameters were extractedand used for analysis: retinal vascular caliber, fractal dimension,and tortuosity. Details of these parameters and reliability assess-ment have been described elsewhere [6,7].
2.2.1. Retinal vascular caliberThe program calculates retinal arteriolar and venular calibers
as central retinal artery equivalent (CRAE) and central retinal veinequivalent (CRVE), based on the revised Knudtson–Parr–Hubbardformula [6,7].
2.2.2. Retinal vascular fractal dimensionRetinal vascular dimension was evaluated from the skeletonized
vascular network using the box-counting method, and represents a“global” measure that summarizes the whole branching pattern ofthe retinal vascular tree [6,7]. Larger values indicate a more com-plex branching pattern.
2.2.3. Retinal vascular tortuosityRetinal vascular tortuosity was computed as the integral of the
curvature square along the path of the vessel, normalized by thetotal path length; this measure is dimensionless as it represents aratio measure [6,7]. The estimates were summarized as retinal arte-riolar and venular tortuosity separately, representing the averagetortuosity of arterioles and venules, respectively. Retinal vasculartortuosity reflects the extent of curvature in the vessels; a smallertortuosity value indicates a straighter retinal vessel.
2.3. Neuroimaging
MRI was performed on a 3Tesla Siemens Magnetom Trio Timscanner, using a 32-channel head coil, at the Clinical ImagingResearch Centre of the National University of Singapore. Subjectswith claustrophobia, contraindications for MRI, or those who wereunable to tolerate the procedure were excluded. All MRIs weregraded by one radiologist and two clinicians blinded to the neu-ropsychological and clinical data. Any disagreement was broughtto consensus for the final decision [2]. The following MRI markerswere collated for each subject:
(1) Presence of lacune was defined on T2-weighted and Fluid Atten-uated Inversion Recovery (FLAIR) images using the Universityof Edinburgh Neuroimaging stroke scale [2]. The inter- andintrarater reliability as expressed by kappa statistic ranged from0.59 to 0.80.
(2) CMB were graded based on location, size and number onsusceptibility weighted imaging (SWI) sequence using brainobserver microbleed scale [2]. CMB were also categorized intoone of three locations: lobar (cortical gray–white junction,subcortical white matter), deep (basal ganglia, internal and
stem and cerebellum).The inter- and intrarater reliability asexpressed by kappa statistic ranged from 0.78 to 0.89.
ce Letters 577 (2014) 95–100 97
(
2
iwiiw(asSawtdmtt
2
ndtiweTafMadCceaacs
Table 1Baseline characteristics of study participants (n = 261).
Baseline characteristics Mean/N
Age (years) 70 (0.4)Males 122 (46.7)BMI (kg/m2) 24.1 (0.2)Hypertension 196 (75.1)Diabetes 69 (26.4)Hyperlipidemia 154 (59.0)Systolic blood pressure (mmHg) 147.0 (1.2)Diastolic blood pressure (mmHg) 76.7 (0.7)Mean arterial blood pressure (mmHg) 100.2 (0.7)Fasting blood glucose (mmol/l) 5.1 (0.09)Fasting total cholesterol (mmol/l) 4.9 (0.05)Ever smokers 76 (29.1)
S. Hilal et al. / Neuroscien
3) White matter lesions volume, total brain volume, and totalintracranial volume were quantified by automatic segmenta-tion, as described previously [2].
.4. Assessment of other vascular risk factors
Demographic and vascular risk factors including age, sex, smok-ng, hypertension, diabetes, hyperlipidemia, height and weight
ere collected and verified by medical records [2]. Blood testsncluded full blood count, fasting blood glucose and serum lipidsncluding total cholesterol. Systolic and diastolic blood pressures
ere measured using a digital automatic blood pressure monitorOMRON-HEM 7203, Japan) after resting for five minutes. Meanrterial blood pressure was calculated as two-thirds of the dia-tolic blood pressure plus one-third of the systolic blood pressure.ubjects were categorized into non-smokers and smokers (pastnd current smokers). Body mass index (BMI) was defined aseight in kilograms divided by height in meters squared. Hyper-
ension was defined as systolic blood pressure ≥140 mmHg and/oriastolic blood pressure ≥90 mmHg or use of anti-hypertensiveedication. Diabetes was defined as HbA1c ≥6.5%, or receiving
reatment for diabetes. Hyperlipidemia was defined as total choles-erol ≥4.14 mmol/l or use of lipid-lowering medications.
.5. Statistical analyses
Quantitative retinal vascular measures were used as determi-ants and expressed as per standard deviation (SD) increase orecrease, whereas markers of cerebral small vessel disease wereaken as outcomes. To examine the associations with lacunarnfarcts and CMBs, logistic regression was used. As WML volumes
ere not normally distributed, values were log-transformed. Lin-ar regression was used to model log-transformed WML volumes.hese models were initially adjusted for age and sex, addition-lly for smoking, body mass index, mean arterial blood pressure,asting blood glucose and total cholesterol; and finally for other
RI markers. In order to examine the robustness of any associ-tion with CMB, different categorizations for CMB were used, asescribed previously [2]: (a) multiple (≥2) versus none/single (<2)MB, (b) multiple categories of CMBs (0, 1 or ≥2) and (c) CMBounts using Poisson regression. For the Poisson regression mod-ls, outliers were excluded to satisfy the goodness-of-fit criterion
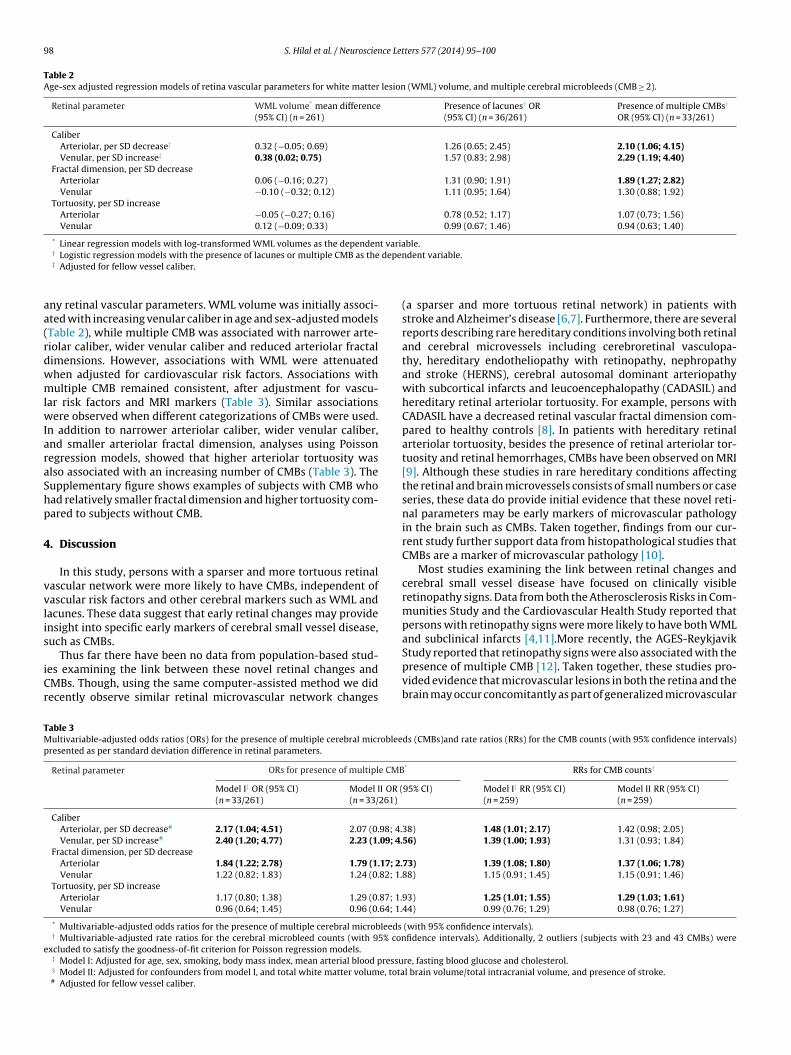
ssessed with the Pearson’s Chi-square statistic. For all the models,ssociation measures were expressed with the corresponding 95%onfidence intervals (CI). All statistical analyses were performed ontandard statistical software (SPSS Version 17, SPSS Inc., USA).Fig. 1. Distribution of cerebral small vessel di
Number between brackets are percentage or standard error of the mean.
3. Results
Out of the 300 subjects who participated in the second phaseof the EDIS Study, 39 subjects were excluded from the analysis:18 had no MRI scans (due to claustrophobia, or contraindications),and 21 subjects did not have gradable retinal photographs. Baselinecharacteristics of the remaining 261 subjects are shown in Table 1.With respect to qualitative MRI markers, 46 subjects (17.6%) hadevidence of ischemic stroke on their MRI scan, of whom 36 (13.8%)had lacunes; while 83 subjects (31.8%) had CMB present, of whom33 (12.6%) had multiple CMB, including 2 subjects who had morethan 20 CMB (23 and 43 CMBs). Among these 33 subjects, 22 hadisolated multiple lobar CMBs, 9 isolated multiple deep or poste-rior fossa CMBs and 2 combination of lobar, deep or posterior fossaCMB. With respect to quantitative MRI markers, mean total brainvolume was 895.6 ml (standard error of the mean [SEM]: 5.4) andmean total intracranial volume 1096 ml (SEM: 6.1). As WML vol-ume showed a skewed distribution, the median WML volume was1.90 ml (interquartile range: 4.48). Fig. 1 shows the prevalence ofthese markers of cerebral small vessel disease stratified accordingto 5-year age categories. All MRI lesions showed a higher prevalencewith increasing age. CMBs were more prevalent in the younger agecategories compared to lacunes, whereas in those aged ≥80 years,the prevalence of CMB and lacunes were comparable. AlthoughWML volume is not directly comparable across age categories withthe other markers, the median WML volume in the youngest cat-egory was relatively small and showed a steep increase at olderage.
Table 2 describes age and sex-adjusted associations of retinalvascular parameters with the different markers of cerebral smallvessel disease. The presence of lacunes was not associated with
sease markers by 5-year age categories.
98 S. Hilal et al. / Neuroscience Letters 577 (2014) 95–100
Table 2Age-sex adjusted regression models of retina vascular parameters for white matter lesion (WML) volume, and multiple cerebral microbleeds (CMB ≥ 2).
Retinal parameter WML volume* mean difference(95% CI) (n = 261)
Presence of lacunes† OR(95% CI) (n = 36/261)
Presence of multiple CMBs†
OR (95% CI) (n = 33/261)
CaliberArteriolar, per SD decrease‡ 0.32 (−0.05; 0.69) 1.26 (0.65; 2.45) 2.10 (1.06; 4.15)Venular, per SD increase‡ 0.38 (0.02; 0.75) 1.57 (0.83; 2.98) 2.29 (1.19; 4.40)
Fractal dimension, per SD decreaseArteriolar 0.06 (−0.16; 0.27) 1.31 (0.90; 1.91) 1.89 (1.27; 2.82)Venular −0.10 (−0.32; 0.12) 1.11 (0.95; 1.64) 1.30 (0.88; 1.92)
Tortuosity, per SD increaseArteriolar −0.05 (−0.27; 0.16) 0.78 (0.52; 1.17) 1.07 (0.73; 1.56)Venular 0.12 (−0.09; 0.33) 0.99 (0.67; 1.46) 0.94 (0.63; 1.40)
* Linear regression models with log-transformed WML volumes as the dependent variable. depen
aa(rdwmlwIaraShp
4
vvlis
iCr
TMp
e
† Logistic regression models with the presence of lacunes or multiple CMB as the‡ Adjusted for fellow vessel caliber.
ny retinal vascular parameters. WML volume was initially associ-ted with increasing venular caliber in age and sex-adjusted modelsTable 2), while multiple CMB was associated with narrower arte-iolar caliber, wider venular caliber and reduced arteriolar fractalimensions. However, associations with WML were attenuatedhen adjusted for cardiovascular risk factors. Associations withultiple CMB remained consistent, after adjustment for vascu-
ar risk factors and MRI markers (Table 3). Similar associationsere observed when different categorizations of CMBs were used.
n addition to narrower arteriolar caliber, wider venular caliber,nd smaller arteriolar fractal dimension, analyses using Poissonegression models, showed that higher arteriolar tortuosity waslso associated with an increasing number of CMBs (Table 3). Theupplementary figure shows examples of subjects with CMB whoad relatively smaller fractal dimension and higher tortuosity com-ared to subjects without CMB.
. Discussion
In this study, persons with a sparser and more tortuous retinalascular network were more likely to have CMBs, independent ofascular risk factors and other cerebral markers such as WML andacunes. These data suggest that early retinal changes may providensight into specific early markers of cerebral small vessel disease,uch as CMBs.
Thus far there have been no data from population-based stud-es examining the link between these novel retinal changes andMBs. Though, using the same computer-assisted method we didecently observe similar retinal microvascular network changes
able 3ultivariable-adjusted odds ratios (ORs) for the presence of multiple cerebral microblee
resented as per standard deviation difference in retinal parameters.
Retinal parameter ORs for presence of multiple CMB
Model I‡ OR (95% CI)(n = 33/261)
Model II OR ((n = 33/261)
CaliberArteriolar, per SD decrease# 2.17 (1.04; 4.51) 2.07 (0.98; 4.Venular, per SD increase# 2.40 (1.20; 4.77) 2.23 (1.09; 4.
Fractal dimension, per SD decreaseArteriolar 1.84 (1.22; 2.78) 1.79 (1.17; 2.Venular 1.22 (0.82; 1.83) 1.24 (0.82; 1.
Tortuosity, per SD increaseArteriolar 1.17 (0.80; 1.38) 1.29 (0.87; 1.Venular 0.96 (0.64; 1.45) 0.96 (0.64; 1.
* Multivariable-adjusted odds ratios for the presence of multiple cerebral microbleeds† Multivariable-adjusted rate ratios for the cerebral microbleed counts (with 95% con
xcluded to satisfy the goodness-of-fit criterion for Poisson regression models.‡ Model I: Adjusted for age, sex, smoking, body mass index, mean arterial blood pressu§ Model II: Adjusted for confounders from model I, and total white matter volume, tota# Adjusted for fellow vessel caliber.
dent variable.
(a sparser and more tortuous retinal network) in patients withstroke and Alzheimer’s disease [6,7]. Furthermore, there are severalreports describing rare hereditary conditions involving both retinaland cerebral microvessels including cerebroretinal vasculopa-thy, hereditary endotheliopathy with retinopathy, nephropathyand stroke (HERNS), cerebral autosomal dominant arteriopathywith subcortical infarcts and leucoencephalopathy (CADASIL) andhereditary retinal arteriolar tortuosity. For example, persons withCADASIL have a decreased retinal vascular fractal dimension com-pared to healthy controls [8]. In patients with hereditary retinalarteriolar tortuosity, besides the presence of retinal arteriolar tor-tuosity and retinal hemorrhages, CMBs have been observed on MRI[9]. Although these studies in rare hereditary conditions affectingthe retinal and brain microvessels consists of small numbers or caseseries, these data do provide initial evidence that these novel reti-nal parameters may be early markers of microvascular pathologyin the brain such as CMBs. Taken together, findings from our cur-rent study further support data from histopathological studies thatCMBs are a marker of microvascular pathology [10].
Most studies examining the link between retinal changes andcerebral small vessel disease have focused on clinically visibleretinopathy signs. Data from both the Atherosclerosis Risks in Com-munities Study and the Cardiovascular Health Study reported thatpersons with retinopathy signs were more likely to have both WMLand subclinical infarcts [4,11].More recently, the AGES-Reykjavik
Study reported that retinopathy signs were also associated with thepresence of multiple CMB [12]. Taken together, these studies pro-vided evidence that microvascular lesions in both the retina and thebrain may occur concomitantly as part of generalized microvasculards (CMBs)and rate ratios (RRs) for the CMB counts (with 95% confidence intervals)
* RRs for CMB counts†
95% CI) Model I‡ RR (95% CI)(n = 259)
Model II RR (95% CI)(n = 259)
38) 1.48 (1.01; 2.17) 1.42 (0.98; 2.05)56) 1.39 (1.00; 1.93) 1.31 (0.93; 1.84)
73) 1.39 (1.08; 1.80) 1.37 (1.06; 1.78)88) 1.15 (0.91; 1.45) 1.15 (0.91; 1.46)
93) 1.25 (1.01; 1.55) 1.29 (1.03; 1.61)44) 0.99 (0.76; 1.29) 0.98 (0.76; 1.27)
(with 95% confidence intervals).fidence intervals). Additionally, 2 outliers (subjects with 23 and 43 CMBs) were
re, fasting blood glucose and cholesterol.l brain volume/total intracranial volume, and presence of stroke.
S. Hilal et al. / Neuroscience Letters 577 (2014) 95–100 99
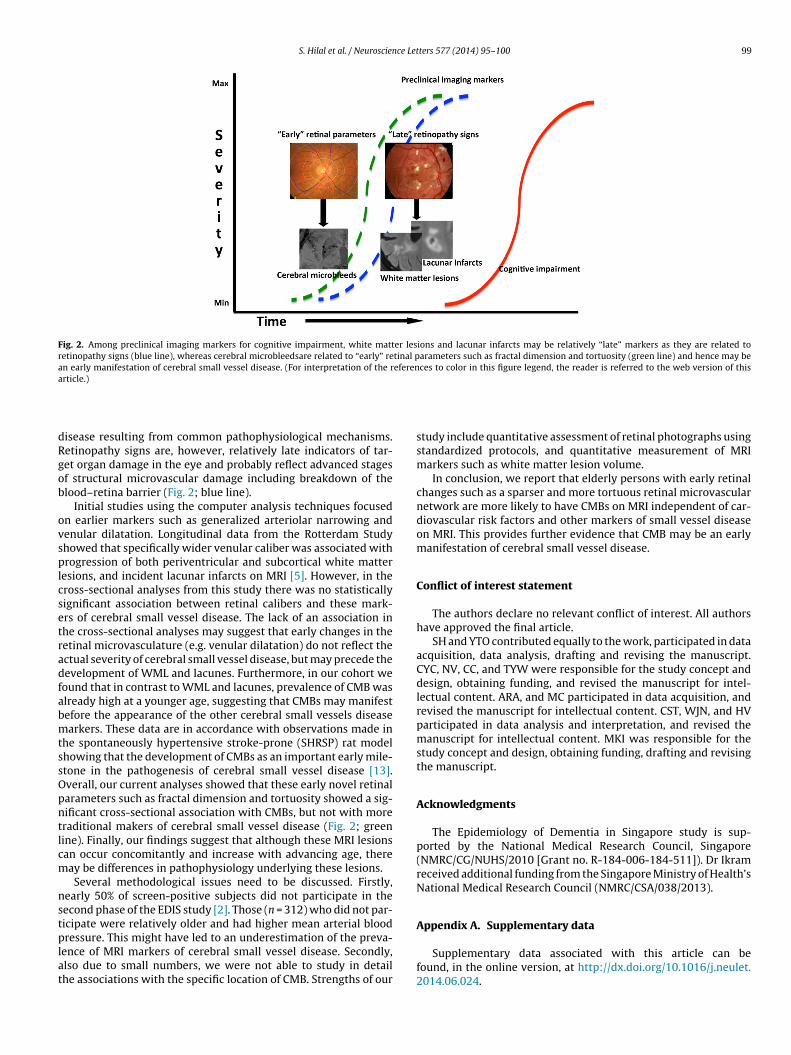
Fig. 2. Among preclinical imaging markers for cognitive impairment, white matter lesions and lacunar infarcts may be relatively “late” markers as they are related toretinopathy signs (blue line), whereas cerebral microbleedsare related to “early” retinal parameters such as fractal dimension and tortuosity (green line) and hence may bean early manifestation of cerebral small vessel disease. (For interpretation of the references to color in this figure legend, the reader is referred to the web version of thisa
dRgob
ovsplcsetradfabmtssOpntlcm
nstplat
Appendix A. Supplementary data
rticle.)
isease resulting from common pathophysiological mechanisms.etinopathy signs are, however, relatively late indicators of tar-et organ damage in the eye and probably reflect advanced stagesf structural microvascular damage including breakdown of thelood–retina barrier (Fig. 2; blue line).
Initial studies using the computer analysis techniques focusedn earlier markers such as generalized arteriolar narrowing andenular dilatation. Longitudinal data from the Rotterdam Studyhowed that specifically wider venular caliber was associated withrogression of both periventricular and subcortical white matter
esions, and incident lacunar infarcts on MRI [5]. However, in theross-sectional analyses from this study there was no statisticallyignificant association between retinal calibers and these mark-rs of cerebral small vessel disease. The lack of an association inhe cross-sectional analyses may suggest that early changes in theetinal microvasculature (e.g. venular dilatation) do not reflect thectual severity of cerebral small vessel disease, but may precede theevelopment of WML and lacunes. Furthermore, in our cohort weound that in contrast to WML and lacunes, prevalence of CMB waslready high at a younger age, suggesting that CMBs may manifestefore the appearance of the other cerebral small vessels diseasearkers. These data are in accordance with observations made in
he spontaneously hypertensive stroke-prone (SHRSP) rat modelhowing that the development of CMBs as an important early mile-tone in the pathogenesis of cerebral small vessel disease [13].verall, our current analyses showed that these early novel retinalarameters such as fractal dimension and tortuosity showed a sig-ificant cross-sectional association with CMBs, but not with moreraditional makers of cerebral small vessel disease (Fig. 2; greenine). Finally, our findings suggest that although these MRI lesionsan occur concomitantly and increase with advancing age, thereay be differences in pathophysiology underlying these lesions.Several methodological issues need to be discussed. Firstly,
early 50% of screen-positive subjects did not participate in theecond phase of the EDIS study [2]. Those (n = 312) who did not par-icipate were relatively older and had higher mean arterial blood
ressure. This might have led to an underestimation of the preva-ence of MRI markers of cerebral small vessel disease. Secondly,lso due to small numbers, we were not able to study in detailhe associations with the specific location of CMB. Strengths of our
study include quantitative assessment of retinal photographs usingstandardized protocols, and quantitative measurement of MRImarkers such as white matter lesion volume.
In conclusion, we report that elderly persons with early retinalchanges such as a sparser and more tortuous retinal microvascularnetwork are more likely to have CMBs on MRI independent of car-diovascular risk factors and other markers of small vessel diseaseon MRI. This provides further evidence that CMB may be an earlymanifestation of cerebral small vessel disease.
Conflict of interest statement
The authors declare no relevant conflict of interest. All authorshave approved the final article.
SH and YTO contributed equally to the work, participated in dataacquisition, data analysis, drafting and revising the manuscript.CYC, NV, CC, and TYW were responsible for the study concept anddesign, obtaining funding, and revised the manuscript for intel-lectual content. ARA, and MC participated in data acquisition, andrevised the manuscript for intellectual content. CST, WJN, and HVparticipated in data analysis and interpretation, and revised themanuscript for intellectual content. MKI was responsible for thestudy concept and design, obtaining funding, drafting and revisingthe manuscript.
Acknowledgments
The Epidemiology of Dementia in Singapore study is sup-ported by the National Medical Research Council, Singapore(NMRC/CG/NUHS/2010 [Grant no. R-184-006-184-511]). Dr Ikramreceived additional funding from the Singapore Ministry of Health’sNational Medical Research Council (NMRC/CSA/038/2013).
Supplementary data associated with this article can befound, in the online version, at http://dx.doi.org/10.1016/j.neulet.2014.06.024.
1 ce Let
R
[
[
[
00 S. Hilal et al. / Neuroscien
eferences
[1] L. Pantoni, A. Poggesi, D. Inzitari, Cognitive decline and dementia related tocerebrovascular diseases: some evidence and concepts, Cerebrovasc. Dis. 27(Suppl 1) (2009) 191–196.
[2] S. Hilal, M. Saini, C.S. Tan, J.A. Catindig, W.I. Koay, W.Y. Lee, W.J. Niessen, H.A.Vrooman, T.Y. Wong, C. Chen, M.K. Ikram, N. Venketasubramanian, Cerebralmicrobleeds and cognition in a Chinese population, Alzheimer Dis. Assoc. Dis-ord. 28 (2014) 106–122.
[3] N. Patton, T. Aslam, T. Macgillivray, A. Pattie, I.J. Deary, B. Dhillon, Retinal vas-cular image analysis as a potential screening tool for cerebrovascular disease: arationale based on homology between cerebral and retinal microvasculatures,J. Anat. 206 (2005) 319–348.
[4] M.K. Ikram, C.Y.L. Cheung, T.Y. Wong, C.P.L.H. Chen, Retinal pathology asbiomarker for cognitive impairment and Alzheimer’s disease, J. Neurol. Neuro-surg. Psychiatry 83 (2012) 917–922.
[5] M.K. Ikram, Y.T. Ong, C.Y. Cheung, T.Y. Wong, Retinal vascular caliber mea-surements: clinical significance, current knowledge and future perspectives,Ophthalmologica 229 (2013) 125–136.
[6] Y.T. Ong, D.A. De Silva, C.Y. Cheung, H.M. Chang, C.P. Chen, M.C. Wong, T.Y.Wong, M.K. Ikram, Microvascular structure and network in the retina ofpatients with ischemic stroke, Stroke 44 (2013) 2121–2127.
[7] C.Y. Cheung, Y.-T. Ong, M.K. Ikram, S.Y. Ong, X. Li, S. Hilal, J.-A.S. Catindig, N.Venketasubramanian, P. Yap, D. Seow, C.P. Chen, T.Y. Wong, Microvascular
[
ters 577 (2014) 95–100
network alterations in the retina of patients with Alzheimer’s disease,Alzheimers Dement. 10 (2014) 135–142.
[8] M. Cavallari, T. Falco, M. Frontali, S. Romano, F. Bagnato, F. Orzi, Fractal analysisreveals reduced complexity of retinal vessels in CADASIL, PLoS One 6 (2011)e19150.
[9] K. Vahedi, P. Massin, J.P. Guichard, S. Miocque, M. Polivka, F. Goutières,D. Dress, F. Chapon, M.M. Ruchoux, F. Riant, A. Joutel, A. Gaudric,M.G. Bousser, E. Tournier-Lasserve, Hereditary infantile hemiparesis, reti-nal arteriolar tortuosity, and leukoencephalopathy, Neurology 60 (2003)57–63.
10] A. Charidimou, D.J. Werring, Cerebral microbleeds and cognition in cerebrovas-cular disease: an update, J. Neurol. Sci. 322 (2012) 50–55.
11] W. Longstreth, E.K. Larsen, R. Klein, T.Y. Wong, A.R. Sharrett, D. Lefkowitz, T.A.Manolio, Associations between findings on cranial magnetic resonance imagingand retinal photography in the elderly: the Cardiovascular Health Study, Am.J. Epidemiol. 165 (2007) 78–84.
12] C. Qiu, M.F. Cotch, S. Sigurdsson, P.V. Jonsson, M.K. Jonsdottir, S. Sveinbjrns-dottir, G. Eiriksdottir, R. Klein, T.B. Harris, M.A. van Buchem, V. Gudnason, L.J.Launer, Cerebral microbleeds, retinopathy, and dementia: the AGES-Reykjavik
Study, Neurology 75 (2010) 2221–2228.13] S. Schreiber, C.Z. Bueche, C. Garz, S. Kropf, F. Angenstein, J. Goldschmidt, J.Neumann, H.J. Heinze, M. Goertler, K.G. Reymann, H. Braun, The pathologiccascade of cerebrovascular lesions in SHRSP: is erythrocyte accumulation anearly phase? J. Cereb. Blood Flow Metab. 32 (2012) 278–290.
Copyright © 2022 FDOKUMEN




















