OCRIPLASMIN IN PRACTICE: - Retina Today
16
Sponsored by ThromboGenics, Inc. OCRVMA0297 2/17 OCRIPLASMIN IN PRACTICE: Successful Strategies for Pharmacological Resolution of Symptomatic Vitreomacular Adhesion A summary of the roundtable discussion presented at the 2016 American Society of Retina Specialists Annual Meeting on August 12, 2016, with Peter K. Kaiser, MD, moderator. Advisors: Victor H. Gonzalez, MD; Arshad Khanani, MD, MA; Brian Joondeph, MD, MPS; and Mark H. Nelson, MD, MBA The summary of the discussion provided below is based upon the physicians’ opinions and experiences with ocriplasmin in their practices. The content of this supplement is accurate to the best of the participants’ knowledge at the time of production. This supplement is meant to add to the body of evidence for the use of ocriplasmin in clinical practice. These opinions are not positions held by ThromboGenics. This supplement will only be distributed in the United States. Please refer to the full prescribing information for JETREA®, which can be found at www.Jetrea.com.
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of OCRIPLASMIN IN PRACTICE: - Retina Today

Sponsored by ThromboGenics, Inc. OCRVMA0297 2/17
OCRIPLASMIN IN PRACTICE:Successful Strategies for Pharmacological Resolution of Symptomatic Vitreomacular Adhesion
A summary of the roundtable discussion presented at the 2016 American Society of Retina Specialists Annual Meeting
on August 12, 2016, with Peter K. Kaiser, MD, moderator.
Advisors: Victor H. Gonzalez, MD; Arshad Khanani, MD, MA; Brian Joondeph, MD, MPS; and Mark H. Nelson, MD, MBA
The summary of the discussion provided below is based upon the physicians’ opinions and experiences with ocriplasmin in their practices. The content of this supplement is accurate to the best of the participants’ knowledge at the time of production. This supplement is meant to add to the body of evidence for the use of ocriplasmin in clinical practice. These opinions are not positions held by ThromboGenics. This supplement will only be distributed in the United States.
Please refer to the full prescribing information for JETREA®, which can be found at www.Jetrea.com.

2
ForewordOcriplasmin (ThromboGenics: JETREA®) has now been used as a clinical therapy for more than 5 years for the management of symptomatic vitreomacular adhesion (VMA). During this period, the physicians at this roundtable had the chance to work with this first-in-class drug, not as a replacement for surgery, but instead as a pharmacological treatment for symptomatic VMA. These physicians had the opportunity to observe and refine the treatment practice using ocriplasmin. In this supplement, we bring to you our years of knowledge to help the practitioner understand the clinical perspectives of VMA as a cause of visual disturbances and how to resolve it. I want to thank ThromboGenics for allowing Arshad Khanani, Brian Joondeph, Victor H. Gonzalez, Mark H. Nelson, and myself to have an open discussion to bring our experiences and findings from clinical practice to others considering options on how to best help patients with symptomatic VMA. – Peter K. Kaiser, MD
Faculty Biographies
Peter K. Kaiser, MD, is the Chaney Family Endowed Chair for Ophthalmology Research; a professor of ophthalmology at the Cleveland Clinic Lerner College of Medicine, Cleveland, Ohio; a staff surgeon in the vitreoretinal department at the Cole Eye Institute, Cleveland Clinic, Cleveland, Ohio; and the founding director of the Digital Optical Coherence Tomography Reading Center (DOCTR) at the Cole Eye Institute,
Cleveland Clinic, Cleveland, Ohio. Dr. Kaiser received his medical degree from Harvard Medical School, Boston, Massachusetts and vitreoretinal fellowship at Bascom Palmer Eye Institute, Miami, Florida. Dr. Kaiser has authored more than 200 book chapters, original reports, publications and abstracts. He is an editor of several ophthalmology journals.
Arshad Khanani, MD, MA, is a clinical associate professor at the University of Nevada School of Medicine. He is also a managing partner and the director of clinical research at Sierra Eye Associates in Reno, Nevada. Dr. Khanani graduated magna cum laude in chemistry from Washington University in St. Louis, Missouri, with a bachelor’s and master’s degree. Dr. Khanani obtained his medical degree
from Texas Tech School of Medicine, Lubbock, Texas, and did a fellowship in vitreoretinal diseases at the University of Texas – Southwestern Medical Center, Dallas, Texas. Dr. Khanani has a strong interest in clinical research and has served as a principal investigator for multiple clinical trials. He has been published in numerous ophthalmology journals.
Brian Joondeph, MD, MPS, is a partner of the Colorado Retina Associates and professor of ophthalmology at the Rocky Vista University College of Osteopathic Medicine in Parker, Colorado. He completed fellowships at Retina Bascom Palmer Eye Institute, Miami, Florida, and University of Illinois Eye and Ear Infirmary, Chicago, Illinois. Dr. Joondeph has more than 65 publications and
is a current and past investigator in multiple clinical trials.
Victor H. Gonzalez, MD, is the founder of Valley Retina Institute, McAllen, Texas. Dr. Gonzalez received his medical degree from Harvard Medical School, Boston, Massachusetts, and did a fellowship at the Massachusetts Eye and Ear Infirmary at Harvard Medical School. Dr. Gonzalez authored multiple publications and abstracts. He is an editor of several ophthalmology journals.
Mark H. Nelson, MD, MBA, is an ophthalmologist in Winston-Salem, North Carolina and is affiliated with Novant Health Medical Park Hospital, Winston-Salem, North Carolina. He received his medical degree from Rutgers Robert Wood Johnson Medical School, New Brunswick, New Jersey, and completed his fellowship at Piedmont Hospital, Atlanta, Georgia. He has been in practice for more
than 20 years. Dr. Nelson has authored multiple publications.
Patient Impact of Symptomatic VMAPeter K. Kaiser, MD: How do symptomatic VMA patients typically present in your practice?
Victor H. Gonzalez, MD: Symptomatic VMA presents itself as a nondescript complaint of visual impairment. We have all experienced when patients come in and they are describing some visual disturbance—they are 20/20 and still they are very unhappy with their vision. When I see a patient come in with good vision and dissatisfied with their vision, I begin to seriously consider whether there is something potentially wrong with the surface of the vitreoretinal interface. And quite often, I’m not surprised to find that there is some abnormality caused by traction of the normal vitreous on the retinal surface.
Brian Joondeph, MD, MPS: Our VMA patients can be divided into two groups. One group of patients present with symptoms. Their vision is a little blurry and just not sharp. They are presenting with symptoms of metamorphopsia and will often perceive images to be distorted in size, shape, or inclination. The other group is the patients who are not symptomatic until the referring doctor shows them their OCT [optical coherence tomography]. The patients truly did not know they had a problem until they come in for an annual exam or for another eye problem. Then the doctor shows them a very dramatic OCT and the patients are referred to me for treatment, often quite concerned over the OCT image, but typically not needing intervention based on this being an incidental and asymptomatic finding.

3
Peter K. Kaiser, MD: What are some of the things patients complain about not being able to do in their daily lives? What are some of the complaints you hear?
Arshad Khanani, MD, MA: Most patients who have symptoms recognize that there is an issue with their vision. They have trouble reading, driving, or [with] other disturbances in their daily activities. Their quality of life is deeply affected from the metamorphopsia.
Mark H. Nelson, MD, MBA: Even though these patients are referred for early VMA, most have few visual complaints. I will ask them, “What brought you to the doctor?” They will say that they thought that they needed their glasses changed.” Only when the VMA progresses do they notice vision loss which affects their everyday activities.
Peter K. Kaiser, MD: Describe your protocol to diagnose symptomatic VMA. How do you first examine them? What does the exam consist of? And what are you looking for?
Victor H. Gonzalez, MD: I am quite surprised by how much symptomatic VMA there actually is in my patient population and how often it remains undiagnosed until there is another issue that brings the patient in for an eye exam. A number of my patients are referred for visual disturbances after surgery, and it is important to exclude a complication that arose during the procedure. A majority of the time, the visual disturbances have nothing to do with the surgery.
I start by performing a full eye exam, including an examination of the anterior segment of the eye. Sometimes the patient has dry eye and the visual disturbances disappear when the dry eye is treated. Next, I examine the back of the eye. I check for cystoid macular edema [CME] and other causes of metamorphopsia. I order an OCT to obtain finer detail. The OCT is the best at showing the presence of even a subtle VMT [vitreomacular traction].
Mark H. Nelson, MD, MBA: We have an internet portal where referral doctors send OCTs of patients with VMA. So for the majority of my patients, I know that they have VMA before they come to my office. This process allows for early detection which proves to be a perfect opportunity to use ocriplasmin before macular holes present. When I evaluate a patient with VMA, I specifically look at the anatomy and pathology and see if it correlates to the visual acuity. Alterations to the posterior retina, specifically the ELM [external limiting membrane] or photoreceptor zone usually correlates nicely. If it does not, I look for other reasons for vision loss (ie, macular ischemia, macular degeneration, optic neuropathy, etc.).
Peter K. Kaiser, MD: Any particular scans that you find useful to diagnose VMA on OCT?
Brian Joondeph, MD, MPS: It’s important to observe the scans around the fovea. Something associated with the traction may be seen above or below where the traction is located. We start off with low-volume scanning, and when we start seeing the traction, we repeat it again with a finer scan—higher volume, higher-resolution photos. The higher resolution and multiple images are important if you are going to find a subtle hole. Otherwise, it will be missed on the wider, low-volume scans.
Peter K. Kaiser, MD: The different OCT systems use different acquisition protocols and analysis algorithms. What are your favorite acquisition protocols? Radial line scans versus a macular cube scan? Do you use any advanced visualization features [eg, 3D analysis]?
Victor H. Gonzalez, MD: Not to make the initial diagnosis, but I use the advanced features to determine the best treatment (surgery vs vitreolysis) to resolve symptomatic VMA. Determining the type of treatment requires detailed information about the traction, and to
The Problem of MetamorphopsiaVMA is observed after partial posterior vitreous detachment in which a portion of the posterior vitreous remains attached to the macula.1 Symptomatic VMA occurs when tractional force is excessively exerted on the macula in response to anteroposterior and tangential forces. The pull on the macula may lead to visual distortion and a decrease in visual acuity, and eventually cause functional visual damage. Symptomatic VMA is a painless disease and symptoms may go largely undetected if they occur in the nondominant eye.
One of the most difficult visual challenges faced by patients is metamorphopsia. Patients with metamorphopsia will often perceive images to be distorted in size, shape, or inclination.2 Most patients recognize there is an issue with their vision since metamorphopsia deteriorates reading abilities and facial recognition. They may be upset or unnerved with how poor vision hinders their ability to participate in everyday activities. Recent studies indicate metamorphopsia is a major factor in the deterioration of vision-related quality of life.3 In one study, patients answered the 25-item National Eye Institute Visual Function Questionnaire (VFQ-25) to determine the impact of both metamorphopsia and poor visual acuity on visual quality of life (QoL). The study found a negative correlation between
metamorphopsia and QoL. There was no significant correlation between changes in VFQ-25 composite score and changes in best-corrected visual acuity (BCVA). Thus, patients presenting with symptoms of metamorphopsia may have serious visual problems that can affect QoL.Identifying patients with symptomatic VMA when they present with metamorphopsia is challenging. Problems in visual acuity may not elicit red flags or additional concerns because the change may be small.1 Traditional measures such as visual acuity exams can be complemented with assessment of the patient’s QoL and tests for visual disturbances.4 It may be beneficial for the retina specialist to provide patients with an Amsler Grid and VFQ-25 to monitor for the effects of metamorphopsia. This may prevent further deterioration of vision from symptomatic VMA.5
A specific subset of patients to keep in mind are those with cataracts. Patients with implanted premium lenses account for a higher percentage of symptomatic VMA cases than in previous years. Patients who contemplate and opt for premium lenses expect near-perfect vision.6 The visual distortion associated with symptomatic VMA could hinder patient expectation for pristine vision. Thus, patients undergoing cataract surgery should be tested for symptomatic VMA when visual quality is a concern.

4
Dr. Gonzalez (continued): make that decision, I go straight for a cube. I will do a temporal cube and then a nasal cube. The information obtained from taking the cube in multiple directions gives me a good idea of the dynamics of the vitreous traction. I also use the 3D feature to confirm the morphology of the traction from the macula to the periphery. I use vitreolysis to resolve it; otherwise, I recommend surgery.
To offer my patients pharmacological resolution of symptomatic VMA with ocriplasmin, I need to see a thin traction, meaning a sliver of the vitreous should be attached to the inner retina membrane. A visual analogy can be made with the traction looking like a seagull with evenly expanded wings. The advanced features provide a clearer image of this type of traction and the confidence to provide more accurate guidance on treatment options.
Brian Joondeph, MD, MPS: I also find the 3D view convenient because it can be used as a tool to educate the patient about the disease, show the affected anatomy, and describe treatment to release the traction.
Peter K. Kaiser, MD: Victor [Gonzalez] talked about looking at the dynamics of the traction. What are some of the anatomical features you look for in the OCT images to help you decide how you are going to manage a VMA patient?
Arshad Khanani, MD, MA: Based on the MIVI-TRUST [Microplasmin for Intravitreous Injection-Traction Release without Surgical Treatment] clinical trial data, there are specific anatomical features used to select
appropriate candidates for ocriplasmin treatment. It would appear a candidate targeted for ocriplasmin success to resolve symptomatic VMA would have a focal adhesion [≤1500 μm], smaller FTMH [full-thickness macular hole] [<400 μm], phakic lens status, age younger than 65 years, and the absence of an ERM [epiretinal membrane]. One anecdote to share: when I initially started using the drug, I would still consider patients with a subtle ERM around the fovea as potential candidates. When the MIVI-TRUST subanalysis data was released, I then omitted patients with any signs of ERM, and my success with ocriplasmin increased tremendously. I made similar observations with my patients with phakic eyes—these patients have more success with using ocriplasmin to resolve symptomatic VMA as compared to pseudophakic patients. It is important to watch out for these features for optimal success.
Peter K. Kaiser, MD: Diagnosing an ERM can be difficult even for experienced retina specialists. What are some of the features you look for on an OCT?
Arshad Khanani, MD, MA: I look at all the cuts of the macular cube scan. Any sign of an ERM in the macula is an indication that the patient may not be an optimal candidate for ocriplasmin treatment.
Peter K. Kaiser, MD: I agree that patient selection based on anatomical features is the key to optimal efficacy with ocriplasmin. We have seen in both the MIVI-TRUST and OASIS [Ocriplasmin for Treatment for Symptomatic Vitreomacular Adhesion Including Macular Hole] studies that any presence of an ERM affects
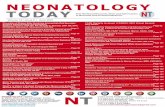
Important Anatomical Features for Diagnosis of Symptomatic VMAWhile changes in visual acuity and metamorphopsia are the presenting symptoms of VMA,1 detection of the traction is the confirmation of symptomatic VMA. Obtaining spectral-domain OCT images to diagnose VMA is standard of care.7 OCT provides detailed information of the vitreomacular anatomy and can accurately identify (1) the size of the adhesion, (2) the size of the macular hole (MH), and (3) the presence of epiretinal membrane (ERM). (Figure 1). The information that the OCT provides may guide decision making with the timing and approach to VMA treatment.
OCT images will present the traction as the vitreous remaining attached above the retinal surface, within a 3-mm (arbitrary)
radius of the fovea.8 VMA can be subclassified as either focal (≤1500 μm) or broad (>1500 μm) based on the diameter of its attachment. The traction can be described as a seagull appearance because of the acute angle between posterior hyaloid and inner retinal surface.
Excessive or chronic vitreomacular traction can result in the development of macular holes.9 A FTMH is a tear in the macula that extends through retinal membrane to the retinal pigment epithelium. A FTMH can be classified as small (<250 μm), medium (250-400 μm), or large (>400 μm).8 Macular hole measurements can be defined on the OCT by taking the maximum width at the base of the retinal pigment epithelium and the minimum width along the hole (largest of the smallest holes).10 All OCT images must be examined to find the largest macular hole and any full-thickness breaks.
Detecting an ERM on the vitreomacular interface is another anatomical feature that is OCT dependent. The ERM will appear as a highly reflective membranous structure at the vitreomacular surface on an OCT image.11,12 More-advanced ERMs can become opaque. ERM assessment is challenging, and several features on the OCT system can assist with more-accurate detection. (See ERM sidebar).6 It is important to detect ERM because it will affect treatment options to release symptomatic VMA tractions.
Figure 1: OCT Images of VMA and Common Anatomical Features
VMA
VMA
+ M
HVM
A + E
RM
(Images courtesy of Arshad Khanani MD, MA)

5
Dr. Kaiser (continued): ocriplasmin success to pharmacologically resolve VMA. While there is no definitive answer at this time, we can hypothesize this: it is derived from the characteristics of the ERM. An ERM is a fibrotic tissue that proliferates and forms sheets of membranes over the surface of the retina. Analysis of the data from the OASIS study confirms that the efficacy of ocriplasmin depends on proper patient selection. About 41.7% of subjects receiving ocriplasmin treatment resolved symptomatic VMA as compared to 6.2% with the sham treatment. However, diagnosing ERM is often difficult. There was variability between investigators’ analysis [of] OCT images when selecting for patients based on the inclusion and exclusion criteria. Some of the investigators allowed patients with ERMs to enter the study. When these patient data were accounted for and reanalyzed with ERMs excluded, the group treated with ocriplasmin experienced a 50.6% pharmacological release rate versus 8% in the sham group. This indicates that a large percentage of patients were enrolled in the study with an ERM, which means that very good retina specialists are still not able to identify an ERM.
Victor H. Gonzalez, MD: That is a good point, and ERM detection is challenging. I do believe many retina specialists can identify an ERM the majority of the time. In my opinion, the detection of ERM was underreported during the OASIS study because we were not looking through the entire cube and examining all the cuts. That is one additional explanation as to why patients that did not meet the inclusion criteria were allowed to enroll in the study.
Peter K. Kaiser, MD: What are some steps we could take to prevent underdiagnosing ERM associated with traction?
Arshad Khanani, MD, MA: An ERM can be missed when most of us are very busy in the clinic. It is easy to look at a printout of one representative OCT on the screen and make a decision. That is why I believe it is crucial that someone should be looking through the entire OCT macular cube. If the physician does not have time to look at the whole cube, the staff may be able to help. It is important for the staff involved with patient care to be trained to look at OCT images for important anatomical features associated with symptomatic VMA. Having good staff training can save you time with each patient if you are not looking at all the OCT scans.
The Case for TreatmentPeter K. Kaiser, MD: When you have a patient who complains about visual disturbances and you have confirmed vitreomacular traction on OCT, what factors do you consider when deciding between treatment and observational management?
Mark H. Nelson, MD, MBA: As I mentioned previously, I look at the correlation of anatomy and visual acuity. The decision to use ocriplasmin also depends on whether it is the first or second eye with VMA/hole formation. If it is the first eye, ocriplasmin is only offered if I see disruption of the posterior retina with corresponding vision loss. If the first eye had a macular hole treated with surgery or ocriplasmin, I am much more likely to treat the second eye sooner. Also patients with VMA who are being treated or who will be needing anti-VEGF [vascular endothelial growth factor] injections will usually be treated with ocriplasmin first. I have seen two patients with VMA undergoing anti-VEGF injections develop full thickness macular holes. If I feel that
a patient is subthreshold for needing ocriplasmin, I will follow them every 4, 8, or 12 weeks depending on the pathology, duration, and visual deficits.
Brian Joondeph, MD, MPS: I use a rule of thumb: about a third get better, a third stay the same, and a third get worse over time. And if it’s worsening and the status changes, then we revisit what treatment options are available. If the symptoms are mild and they have a good quality of life, it is quite reasonable to watch these patients. I have them come back as needed, but like Mark [Nelson], I see them again in 2 to 3 months, and examine for any progression.
Peter K. Kaiser, MD: How often do patients with VMA who are not yet symptomatic actually resolve on their own?
Victor H. Gonzalez, MD: I agree with Brian [Joondeph]. About 30% to 35% of my patients with VMA spontaneously resolve. If they have good visual health in both eyes, I encourage them to monitor their symptoms.
There is one group of patients that I am very concerned about even if they are asymptomatic. This group are the patients that developed a macular hole in one eye and had asymptomatic VMA in the second eye. These patients have a very high risk of progression because one eye [has] already demonstrated worsening pathology. I am very concerned with these patients and advise treatment earlier rather than [waiting] for a worsening pathology to develop. I give them an Amsler Grid to monitor themselves for worsening metamorphopsia. I tend to have a short follow-up scheduled with them, and advise them to come in earlier if they start noticing changes.
Mark H. Nelson, MD, MBA: I see spontaneous resolution often as well. The art of medicine is to know when to and when not to intervene. Again, with a second eye, I am more likely to inject ocriplasmin because the risk to benefit ratio is tilted toward intervention.
Arshad Khanani, MD, MA: I observe a patient if their visual acuity is good and/or if they have mild symptoms that do not affect their daily activities. In my experience, about one-third of my patients with VMA resolve without intervention. Once they become symptomatic, I have an in-depth conversation about ocriplasmin injection versus vitrectomy surgery. Typically, I reserve surgery for patients with larger holes or more severe anatomical features that may respond poorly to ocriplasmin treatment based on MIVI-TRUST data. A number of my patients had ocriplasmin injection in one eye and vitrectomy surgery in the fellow eye. Anecdotally, my patients find the eye treated with ocriplasmin is their better-seeing eye and shows preserved anatomy when imaged on the OCT.
The Ocriplasmin Patient DiscussionPeter K. Kaiser, MD: Arshad [Khanani], you bring up the point of giving your patient the choice between surgery and ocriplasmin treatment. How does this discussion go with the patient? How do you introduce ocriplasmin?
Arshad Khanani, MD, MA: When the patient is ready for a therapeutic option, the discussion goes like this: We have a pharmacological option and a surgical option for your condition. Ocriplasmin is the pharmacological option and it is like chemical surgery. The injection

6
Dr. Khanani (continued): is done in the clinic. If you decide to receive it, you may have flashes and floaters for several days to weeks, and there is a potential for decreased vision from baseline. The success rate for pharmacological resolution with ocriplasmin is based on the OCT parameters. I do not use the same flat success rate for everybody. If they are younger with focal adhesion, or younger with adhesion and a small macular hole, I would give them 50% to 60% success rate based on the subanalysis of the MIVI-TRUST and OASIS trial data. And next, I give the option for surgery and convey the higher success rate. We talk about the positive and negative factors for each option. I do mention that surgery requires one week of facedown positioning if they have a macular hole, and that there is a risk of cataract progression post vitrectomy.
Brian Joondeph, MD, MPS: My discussion with the patient is more general. I discuss the success rates. Moreover, I convey there are safety concerns with injections and with surgery. There is risk of bleeding in the eye, infection, things like that, regardless of which treatment you use. And so I do not go into detail of which risk is higher with which procedure. These are both invasive procedures. And they carry small but finite risks.
Peter K. Kaiser, MD: Victor [Gonzalez], we should also consider the issue of injection technique. How exactly do you perform an ocriplasmin injection on a patient?
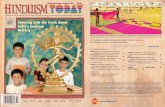
Victor H. Gonzalez, MD: The patient is brought to the injection room, and the staff prepares the patient in the usual manner for an intravitreal injection. I mix the ocriplasmin myself to ensure that no errors occur during handling or dilution. For the injection itself, I use a 30-gauge needle, half an inch long. I aim the tip of the needle toward the macular area, and I proceed to inject in the inferotemporal quadrant, 3.5 mm from the back, using a smooth and continuous motion. The ocriplasmin needs to be delivered directly to the macular area because the effect of the drug is immediate and highly localized. If the macular area is missed, vitreolysis will occur in the wrong location, and the traction will not be released. The targeting of ocriplasmin is different from that of other intravitreal injections, which are usually delivered to the midvitreous (Figure 2).
Arshad Khanani, MD, MA: My procedure is similar. I mix the ocriplasmin right away, and I inject it right away. I insert the tip of the needle all the way toward the macular area.
Peter K. Kaiser, MD: The efficacy rate for ocriplasmin is lower than surgery. How do you discuss the potential resolution rates with your patients?
Victor H. Gonzalez, MD: My discussion about ocriplasmin with the patient includes clinical trial data. I do use the OASIS data in combination with my own experiences. I describe the MIVI-TRUST trial data and describe the reported initial success rate with ocriplasmin at 26%. I explain to patients that this is an active area of research as ocriplasmin is the first of its class. Our knowledge surrounding how to use the drug in VMA has greatly expanded over the past several years. There is an increasing number of clinical trials and real-world data collecting in trials. With this new research data, we were able to get the success rate with ocriplasmin treatment up to almost 45%, 50%; in some subsets, I’ve seen a much higher rate.
Brian Joondeph, MD, MPS: I like to underpromise and overdeliver. The literature and the OASIS clinical trial data describe a roughly 50% success rate. The patients understand the drug may not resolve their VMA and are prepared for surgery. Ocriplasmin does not interfere with the chances for future vitrectomy surgery to release the traction.
Peter K. Kaiser, MD: Do you think there is a general feeling amongst the retina community that the success rate of ocriplasmin is 50%?
Arshad Khanani, MD, MA: Not to my knowledge. When ocriplasmin first became available, the success rate was lower. They may have tried it on 1 or 2 patients, and the drug may not have worked to their expectations. In the beginning, my failure rate was higher because we did not understand the value of certain anatomical features that hindered ocriplasmin success.13 In my personal experience and during my clinical work with the ORBIT trial, we raised ocriplasmin success from 50% to 75%. The key is to select the right patient.
Four Recommendations for Successful ERM DiagnosisPeter K. Kaiser, MD, offered his recommendations to guide the retina specialist to successfully diagnose an ERM when vitreomacular traction is present.
Recommendation #1: Switch OCT imaging from color to grayscale to find an ERM. Grayscale makes subtle details more visible. False or pseudo coloring can make the image look smooth, lose pertinent information, and make it difficult to see the contrast between the ERM and the inner retina.
Recommendation #2: 3D mode may detect early ERM formation on the hyaloid. The traction and details in the area are more exposed as the entire width of the scanned vitreous membrane and retinal surface are visible in the 3D image.
Recommendation #3: Examine all the images in the OCT cube. One image does not span the entire width of the traction. The ERM can be present in other cuts outside the foveal view.
Recommendation #4: Determining ERM status is important to select the correct therapy for a patient with symptomatic VMA. If an ERM is present, it can act like glue holding down that traction. I have examined and reviewed data from many clinical trials, including MIVI-TRUST, OASIS, and ORBIT [Ocriplasmin Research to Better Inform Treatment] showing that the lack of ERM absolutely increases the success rate of the ocriplasmin. There’s no question.

7
Victor H. Gonzalez, MD: In all fairness, OCT resolutions have improved. The initial diagnosis for the MIVI-TRUST trials used time-domain OCT. We needed time to transition to spectral-domain OCT, and only then did we have the resolution capabilities to find ERMs and raise the ocriplasmin efficacy rate.
Peter K. Kaiser, MD: How do you describe the potential side effects of ocriplasmin treatment?
Mark H. Nelson, MD, MBA: I separate side effects into those associated with the injection and those specific to the drug. I tell every patient that they will experience an increase in floaters, which indicates that the drug is working effectively. I also tell them that they might experience some mild irritation from the injection, typical of any intravitreal injection. I ask them to contact me if there are any additional concerns, but tell them that mild vision loss and loss of color vision might occur.
Brian Joondeph, MD, MPS: I tell patients their vision may get worse in the short term. They may see flashes, floaters, sparkles, possibly [have] pain in the eye, and there is a chance the adverse events may get worse for a few days post treatment. Patients should contact my office if the pain is severe or if they have severe vision loss. However, more moderate events like flashes, sparkles, or eye pain are perfectly normal. The key is to manage patient expectations about the healing process. I warn my patients about the flashes and sparkles, so they’re not surprised when they occur. I once dealt with a very panicked patient because he was experiencing a ‘light show’, but I explained that this was normal, and it meant that the ocriplasmin is working.
Peter K. Kaiser, MD: Can you describe what happens when ocriplasmin does not resolve the traction?
Victor H. Gonzalez, MD: To me, successful ocriplasmin treatment does not necessarily have to be complete pharmacological resolution of the adhesion. The best outcome is when we can address that nonspecific visual complaint or other visual disturbances that the patient complains of. Quite often, even if the traction is not pharmacologically released, the patient still sees better. More importantly, they verbalize that the disturbance has disappeared or significantly improved.
Arshad Khanani, MD, MA: Most of my patients experience improved symptoms with ocriplasmin even when the adhesion does not resolve. Some have no changes in their symptoms. If their symptoms get worse due to the progression of disease, then I consider vitrectomy.
Peter K. Kaiser, MD: Based on your experience, would you recommend ocriplasmin to your colleagues?
Arshad Khanani, MD, MA: I think ocriplasmin should be one of the tools in our toolbox. The key is proper patient selection and managing patients’ expectations. If you are not offering ocriplasmin to your patient, you may want to consider it in the future as it is a less invasive option that works well in certain patients. I would tell them to look at the current data. The success rate with ocriplasmin in the OASIS trial is 41.7%. This value is even higher when you exclude ERMs—50.6%. I would tell the recent graduates that if they did not try ocriplasmin during their fellowships, they should consider it as an option when they are in practice. I would say, do a little research on your own and ask a colleague who uses it regularly for their advice and experience.
Figure 2: Injection Technique—Comparison of Anti-VEGF Injection and Ocriplasmin Injection14
Adapted from Mastropasqua R, et al., J Ophthalmol. 2016.
(Images courtesy of Mark H. Nelson, MD, MBA)
Patient Case 1: Early and Immediate InterventionMark H. Nelson, MD, MBA: This patient has a small stage 2 macular hole and a VA [visual acuity] of 20/60 (A). This pathology is my preferred indication for ocriplasmin. The decision is easy—the natural history is one of progression therefore treatment has a very good risk-to-benefit ratio. Subsequently, the traction is pharmacologicaly released and the hole is closed. Within one month, the posterior retina aligns perfectly and the vision improved to 20/20 (B).

8
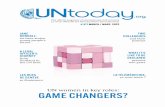
Patient Case 2: Adverse Events Can Be Mild and Are Manageable Post OcriplasminArshad Khanani, MD, MA: A 72-year-old female presented with decreased visual acuity at 20/70 and metamorphopsia in her left eye (A). Her past medical history includes hypertension and cataract surgery in both eyes. After examining the OCT cuts, she was found to have symptomatic VMA and a small macular hole.
The patient was symptomatic and I offered her the choice between ocriplasmin and vitrectomy. She chose to proceed with ocriplasmin. Day 1 post ocriplasmin, the adhesion was not released. Her vision dropped to 20/80, she developed subretinal fluid (SRF), and we detected an ellipsoid zone disruption (B).
She was examined again 2 weeks post-ocriplasmin injection and her VMA released. Her visual acuity improved to 20/40 with the macular hole closed and a decrease in subretinal fluid (C). Only the disruption to the ellipsoid zone persisted. By Month 2, all complications from releasing the VMA subsided, including ellipsoid zone changes. SRF is resolved, and her visual acuity gains persisted at 20/40, and she was quite pleased with her vision (D).
(Images courtesy of Arshad Khanani)
Patient Case 3: Recovery From Severe Decrease in Vision Post-Ocriplasmin InjectionBrian Joondeph, MD, MPS: This was my first experience using ocriplasmin. The patient was a 77-year-old female with a small macular hole in her right [eye] associated with VMA (A). She was phakic and her visual acuity was 20/200. Her fellow left eye had successful surgical treatment of a macular hole several years previously and her visual acuity in that eye was 20/25. Ocriplasmin was recommended as [an] alternative to surgery, postoperative positioning, and expected cataract progression.The day of injection, we reviewed the procedure and the expected postoperative course. On the first post-injection day, she developed pain, redness, and decreased vision-to-hand motions. She was brought in for an exam confirming her visual acuity, and absence of infection or other complications. The VMA was still present (B). At her one-month visit, the vision improved to 20/50 with resolution of VMA and macular hole, but with a small pocket of subretinal fluid (C).At her 9-month visit, her vision was 20/30 with almost complete resolution of subretinal fluid and closed macular hole (D). Subjectively, she felt this eye, treated with ocriplasmin, was her better-seeing eye, compared to her fellow eye treated surgically.This is a good example of transient severe vision loss immediately post-ocriplasmin injection. As this was my first injection, I didn’t know if this was an isolated incident or the normal course of treatment. Fortunately, it is a rare occurrence, and I am confident in my ability to administer ocriplasmin and manage posttreatment expectations and potential adverse events.
(Images courtesy of Brian Joondeph, MD, MPS)
(Images courtesy of Arshad Khanani, MD, MA)
Pre-ocriplasmin VA 20/70
Day 1
Post-ocriplasmin VA 20/80
Month 2
Post-ocriplasmin VA 20/40
Week 2
Post-ocriplasmin VA 20/40
A.
Pre-ocriplasmin VA 20/200 Day 1 Post-ocriplasmin VA: HM
B.
Month 1 Post-ocriplasmin VA 20/50
C.
Month 9 Post-ocriplasmin VA 20/30
D.
D
A
C
B
D

Date: 23-05-2016 Draft: 01 - Op. RI003 EGG
4039
4142
4344
4546
4748
4950
5152
5354
55
Date: 29-06-2016 Draft: 02 - Op. RI003 EGG
Jetrea 2,5 mg/ml USA
05
Date: 07-07-2016 Draft: 03 - Op. RI003 EGGDate: 08-07-2016 Draft: 04 - Op. RI001 EGG
257130 Je01-US-LT-03
Date: 18-07-2016 Draft: 05 - Op. RI003 EGG
HIGHLIGHTS OF PRESCRIBING INFORMATIONThese highlights do not include all the information needed to use JETREA safely and effectively. See full prescribing information for JETREA
JETREA® (ocriplasmin) Intravitreal Injection, 2.5 mg/mLFor intravitreal injectionInitial U.S. Approval: 2012
INDICATIONS AND USAGEJETREA is a proteolytic enzyme indicated for the treatment of symptomatic vitreomacular adhesion. (1)
DOSAGE AND ADMINISTRATION• Must dilute before use. (2.1)• For single use ophthalmic intravitreal injection only. (2.1)• The recommended dose is 0.125 mg (0.1 mL of the diluted solution) administered by intravitreal
injection to the affected eye once as a single dose. (2.2)
DOSAGE FORMS AND STRENGTHSSingle-use glass vial containing JETREA 0.5 mg in 0.2 mL solution for intravitreal injection (2.5 mg/mL). (3)
CONTRAINDICATIONSNone. (4)
WARNINGS AND PRECAUTIONS• Decreases in vision due to progression of the condition with traction may occur requiring surgical
intervention. Patients should be monitored and instructed to report any symptoms without delay. (5.1)• Intravitreal injection procedure associated effects (intraocular inflammation/infection, intraocular
hemorrhage and increased IOP) may occur following an intravitreal injection. Patients should be monitored and instructed to report any symptoms without delay. (5.2)
• Potential for lens subluxation. (5.3)
ADVERSE REACTIONSThe most commonly reported reactions (≥ 5%) in patients treated with JETREA were vitreous floaters, conjunctival hemorrhage, eye pain, photopsia, blurred vision, macular hole, reduced visual acuity, visual impairment, and retinal edema. (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact ThromboGenics Inc. at 1-855-253-7396 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
See 17 for PATIENT COUNSELING INFORMATIONRevised: 03/2016
FULL PRESCRIBING INFORMATION: CONTENTS*
1 INDICATIONS AND USAGE
2 DOSAGE AND ADMINISTRATION2.1 General Dosing Information2.2 Dosing2.3 Preparation for Administration2.4 Administration and Monitoring
3 DOSAGE FORMS AND STRENGTHS
4 CONTRAINDICATIONS
5 WARNINGS AND PRECAUTIONS5.1 Decreased Vision5.2 Intravitreal Injection Procedure Associated Effects5.3 Potential for Lens Subluxation5.4 Retinal Breaks5.5 Dyschromatopsia
6 ADVERSE REACTIONS6.1 Clinical Trials Experience6.2 Immunogenicity6.3 Postmarketing Experience
8 USE IN SPECIFIC POPULATIONS8.1 Pregnancy8.3 Nursing Mothers8.4 Pediatric Use8.5 Geriatric Use
10 OVERDOSAGE
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY12.1 Mechanism of Action12.3 Pharmacokinetics
13 NONCLINICAL TOXICOLOGY13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility13.2 Animal Toxicology and/or Pharmacology
14 CLINICAL STUDIES
16 HOW SUPPLIED/STORAGE AND HANDLING
17 PATIENT COUNSELING INFORMATION
*Sections or subsections omitted from the full prescribing information are not listed.
FULL PRESCRIBING INFORMATION
1 INDICATIONS AND USAGEJETREA® is a proteolytic enzyme indicated for the treatment of symptomatic vitreomacular adhesion.
2 DOSAGE AND ADMINISTRATION
2.1 General Dosing InformationMust be diluted before use. For single-use ophthalmic intravitreal injection only. JETREA must only be administered by a qualified physician.
2.2 DosingThe recommended dose is 0.125 mg (0.1 mL of the diluted solution) administered by intravitreal injection to the affected eye once as a single dose.
2.3 Preparation for AdministrationTo prepare JETREA for intravitreal injection, adhere to the following instructions:1. Remove the vial (2.5 mg/mL corresponding to 0.5 mg ocriplasmin) from the freezer and allow to thaw
at room temperature (within a few minutes).2. Once completely thawed, remove the protective polypropylene flip-off cap from the vial (see Figure 1).
Figure 1:
3. The top of the vial should be disinfected with an alcohol wipe (see Figure 2).
Figure 2:
4. Using aseptic technique, add 0.2 mL of 0.9% w/v Sodium Chloride Injection, USP (sterile, preservative-free) into the JETREA vial (see Figure 3) and gently swirl the vial until the solutions are mixed (see Figure 4).
Figure 3:
Figure 4:
5. Visually inspect the vial for particulate matter. Only a clear, colorless solution without visible particles should be used.
6. Using aseptic technique, withdraw all of the diluted solution using a sterile #19 gauge needle (slightly tilt the vial to ease withdrawal) and discard the needle after withdrawal of the vial contents (see Figure 5). Do not use this needle for the intravitreal injection.
Figure 5:
7. Replace the needle with a sterile #30 gauge needle, carefully expel the air bubbles and excess drug from the syringe and adjust the dose to the 0.1 mL mark on the syringe (corresponding to 0.125 mg ocriplasmin) (see Figure 6).
Figure 6:
8. THE SOLUTION SHOULD BE USED IMMEDIATELY AS IT CONTAINS NO PRESERVATIVES.9. Discard the vial and any unused portion of the diluted solution after single use.
2.4 Administration and MonitoringThe intravitreal injection procedure should be carried out under controlled aseptic conditions, which include the use of sterile gloves, a sterile drape and a sterile eyelid speculum (or equivalent). Adequate anesthesia and a broad spectrum microbiocide should be administered according to standard medical practice. The injection needle should be inserted 3.5 - 4.0 mm posterior to the limbus aiming towards the center of the vitreous cavity, avoiding the horizontal meridian. The injection volume of 0.1 mL is then delivered into the mid-vitreous. Immediately following the intravitreal injection, patients should be monitored for elevation in intraocular pressure. Appropriate monitoring may consist of a check for perfusion of the optic nerve head or tonometry. If required, a sterile paracentesis needle should be available.Following intravitreal injection, patients should be instructed to report any symptoms suggestive of endophthalmitis or retinal detachment (e.g., eye pain, redness of the eye, photophobia, blurred or decreased vision) without delay [see Patient Counseling Information (17)].Each vial should only be used to provide a single injection for the treatment of a single eye. If the contralateral eye requires treatment, a new vial should be used and the sterile field, syringe, gloves, drapes, eyelid speculum, and injection needles should be changed before JETREA is administered to the other eye, however, treatment with JETREA in the other eye is not recommended within 7 days of the initial injection in order to monitor the post-injection course including the potential for decreased vision in the injected eye.Repeated administration of JETREA in the same eye is not recommended [see Nonclinical Toxicology (13.2)].After injection, any unused product must be discarded.No special dosage modification is required for any of the populations that have been studied (e.g. gender, elderly).
3 DOSAGE FORMS AND STRENGTHSSingle-use glass vial containing JETREA 0.5 mg in 0.2 mL solution for intravitreal injection (2.5 mg/mL).
4 CONTRAINDICATIONSNone
5 WARNINGS AND PRECAUTIONS
5.1 Decreased VisionA decrease of ≥ 3 line of best corrected visual acuity (BCVA) was experienced by 5.6% of patients treated with JETREA and 3.2% of patients treated with vehicle in the controlled trials [see Clinical Studies (14)].The majority of these decreases in vision were due to progression of the condition with traction and many required surgical intervention. Patients should be monitored appropriately [see Dosage And Administration (2.4)].
5.2 Intravitreal Injection Procedure Associated EffectsIntravitreal injections are associated with intraocular inflammation / infection, intraocular hemorrhage and increased intraocular pressure (IOP). In the controlled trials, intraocular inflammation occurred in 7.1% of patients injected with JETREA vs. 3.7% of patients injected with vehicle. Most of the post-injection intraocular inflammation events were mild and transient. Intraocular hemorrhage occurred in 2.4% vs. 3.7% of patients injected with JETREA vs. vehicle, respectively. Increased intraocular pressure occurred in 4.1% vs. 5.3% of patients injected with JETREA vs. vehicle, respectively.
5.3 Potential for Lens SubluxationOne case of lens subluxation was reported in a premature infant who received an intravitreal injection of 0.175 mg (1.4 times higher than the recommended dose) [see Use in Specific Populations (8.4)]. Lens subluxation was observed in three animal species (monkey, rabbit, minipig) following a single intravitreal injection that achieved vitreous concentrations of ocriplasmin 1.4 times higher than achieved with the recommended treatment dose. Administration of a second intravitreal dose in monkeys, 28 days apart, produced lens subluxation in 100% of the treated eyes [see Nonclinical Toxicology (13.2)].
5.4 Retinal BreaksIn the controlled trials, the incidence of retinal detachment was 0.9% in the JETREA group and 1.6% in the vehicle group, while the incidence of retinal tear (without detachment) was 1.1% in the JETREA group and 2.7% in the vehicle group. Most of these events occurred during or after vitrectomy in both groups. The incidence of retinal detachment that occurred pre-vitrectomy was 0.4% in the JETREA group and none in the vehicle group, while the incidence of retinal tear (without detachment) that occurred pre-vitrectomy was none in the JETREA group and 0.5% in the vehicle group.
5.5 DyschromatopsiaDyschromatopsia (generally described as yellowish vision) was reported in 2% of all patients injected with JETREA. In approximately half of these dyschromatopsia cases there were also electroretinographic (ERG) changes reported (a- and b-wave amplitude decrease).
6 ADVERSE REACTIONSThe following adverse reactions are described below and elsewhere in the labeling:• Decreased Vision [see Warnings and Precautions (5.1)]• Intravitreal Injection Procedure Associated Effects [see Warnings and Precautions (5.2) and Dosage
And Administration (2.4)]• Potential for Lens Subluxation [see Warnings and Precautions (5.3)]• Retinal Breaks [see Warnings and Precautions (5.4) and Dosage And Administration (2.4)]• Dyschromatopsia [see Warnings and Precautions (5.5)]
6.1 Clinical Trials ExperienceBecause clinical trials are conducted under widely varying conditions, adverse reaction rates in one clinical trial of a drug cannot be directly compared with rates in the clinical trials of the same or another drug and may not reflect the rates observed in practice.Approximately 800 patients have been treated with an intravitreal injection of JETREA. Of these, 465 patients received an intravitreal injection of ocriplasmin 0.125 mg (187 patients received vehicle) in the 2 vehicle-controlled studies (Study 1 and Study 2).The most common adverse reactions (incidence 5% - 20% listed in descending order of frequency) in the vehicle-controlled clinical studies were: vitreous floaters, conjunctival hemorrhage, eye pain, photopsia, blurred vision, macular hole, reduced visual acuity, visual impairment, and retinal edema.Less common adverse reactions observed in the studies at a frequency of < 5% in patients treated with JETREA included macular edema, increased intraocular pressure, anterior chamber cell, photophobia, vitreous detachment, ocular discomfort, iritis, cataract, dry eye, metamorphopsia, pupillary reflex impaired, conjunctival hyperemia, retinal degeneration and visual symptoms perceived in the contralateral eye.Dyschromatopsia was reported in 2% of patients injected with JETREA, with the majority of cases reported from two uncontrolled clinical studies. In approximately half of these dyschromatopsia cases there were also electroretinographic (ERG) changes reported (a- and b-wave amplitude decrease).
6.2 ImmunogenicityAs with all therapeutic proteins, there is potential for immunogenicity. Immunogenicity for this product has not been evaluated.
255919 Je01-US-LT-04 255919 Je01-US-LT-04
Date: 23-05-2016 Draft: 01 - Op. RI003 EGG
4039
4142
4344
4546
4748
4950
5152
5354
55
Date: 29-06-2016 Draft: 02 - Op. RI003 EGG
Jetrea 2,5 mg/ml USA
05
Date: 07-07-2016 Draft: 03 - Op. RI003 EGGDate: 08-07-2016 Draft: 04 - Op. RI001 EGG
257130 Je01-US-LT-03
Date: 18-07-2016 Draft: 05 - Op. RI003 EGG
HIGHLIGHTS OF PRESCRIBING INFORMATIONThese highlights do not include all the information needed to use JETREA safely and effectively. See full prescribing information for JETREA
JETREA® (ocriplasmin) Intravitreal Injection, 2.5 mg/mLFor intravitreal injectionInitial U.S. Approval: 2012
INDICATIONS AND USAGEJETREA is a proteolytic enzyme indicated for the treatment of symptomatic vitreomacular adhesion. (1)
DOSAGE AND ADMINISTRATION• Must dilute before use. (2.1)• For single use ophthalmic intravitreal injection only. (2.1)• The recommended dose is 0.125 mg (0.1 mL of the diluted solution) administered by intravitreal
injection to the affected eye once as a single dose. (2.2)
DOSAGE FORMS AND STRENGTHSSingle-use glass vial containing JETREA 0.5 mg in 0.2 mL solution for intravitreal injection (2.5 mg/mL). (3)
CONTRAINDICATIONSNone. (4)
WARNINGS AND PRECAUTIONS• Decreases in vision due to progression of the condition with traction may occur requiring surgical
intervention. Patients should be monitored and instructed to report any symptoms without delay. (5.1)• Intravitreal injection procedure associated effects (intraocular inflammation/infection, intraocular
hemorrhage and increased IOP) may occur following an intravitreal injection. Patients should be monitored and instructed to report any symptoms without delay. (5.2)
• Potential for lens subluxation. (5.3)
ADVERSE REACTIONSThe most commonly reported reactions (≥ 5%) in patients treated with JETREA were vitreous floaters, conjunctival hemorrhage, eye pain, photopsia, blurred vision, macular hole, reduced visual acuity, visual impairment, and retinal edema. (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact ThromboGenics Inc. at 1-855-253-7396 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
See 17 for PATIENT COUNSELING INFORMATIONRevised: 03/2016
FULL PRESCRIBING INFORMATION: CONTENTS*
1 INDICATIONS AND USAGE
2 DOSAGE AND ADMINISTRATION2.1 General Dosing Information2.2 Dosing2.3 Preparation for Administration2.4 Administration and Monitoring
3 DOSAGE FORMS AND STRENGTHS
4 CONTRAINDICATIONS
5 WARNINGS AND PRECAUTIONS5.1 Decreased Vision5.2 Intravitreal Injection Procedure Associated Effects5.3 Potential for Lens Subluxation5.4 Retinal Breaks5.5 Dyschromatopsia
6 ADVERSE REACTIONS6.1 Clinical Trials Experience6.2 Immunogenicity6.3 Postmarketing Experience
8 USE IN SPECIFIC POPULATIONS8.1 Pregnancy8.3 Nursing Mothers8.4 Pediatric Use8.5 Geriatric Use
10 OVERDOSAGE
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY12.1 Mechanism of Action12.3 Pharmacokinetics
13 NONCLINICAL TOXICOLOGY13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility13.2 Animal Toxicology and/or Pharmacology
14 CLINICAL STUDIES
16 HOW SUPPLIED/STORAGE AND HANDLING
17 PATIENT COUNSELING INFORMATION
*Sections or subsections omitted from the full prescribing information are not listed.
FULL PRESCRIBING INFORMATION
1 INDICATIONS AND USAGEJETREA® is a proteolytic enzyme indicated for the treatment of symptomatic vitreomacular adhesion.
2 DOSAGE AND ADMINISTRATION
2.1 General Dosing InformationMust be diluted before use. For single-use ophthalmic intravitreal injection only. JETREA must only be administered by a qualified physician.
2.2 DosingThe recommended dose is 0.125 mg (0.1 mL of the diluted solution) administered by intravitreal injection to the affected eye once as a single dose.
2.3 Preparation for AdministrationTo prepare JETREA for intravitreal injection, adhere to the following instructions:1. Remove the vial (2.5 mg/mL corresponding to 0.5 mg ocriplasmin) from the freezer and allow to thaw
at room temperature (within a few minutes).2. Once completely thawed, remove the protective polypropylene flip-off cap from the vial (see Figure 1).
Figure 1:
3. The top of the vial should be disinfected with an alcohol wipe (see Figure 2).
Figure 2:
4. Using aseptic technique, add 0.2 mL of 0.9% w/v Sodium Chloride Injection, USP (sterile, preservative-free) into the JETREA vial (see Figure 3) and gently swirl the vial until the solutions are mixed (see Figure 4).
Figure 3:
Figure 4:
5. Visually inspect the vial for particulate matter. Only a clear, colorless solution without visible particles should be used.
6. Using aseptic technique, withdraw all of the diluted solution using a sterile #19 gauge needle (slightly tilt the vial to ease withdrawal) and discard the needle after withdrawal of the vial contents (see Figure 5). Do not use this needle for the intravitreal injection.
Figure 5:
7. Replace the needle with a sterile #30 gauge needle, carefully expel the air bubbles and excess drug from the syringe and adjust the dose to the 0.1 mL mark on the syringe (corresponding to 0.125 mg ocriplasmin) (see Figure 6).
Figure 6:
8. THE SOLUTION SHOULD BE USED IMMEDIATELY AS IT CONTAINS NO PRESERVATIVES.9. Discard the vial and any unused portion of the diluted solution after single use.
2.4 Administration and MonitoringThe intravitreal injection procedure should be carried out under controlled aseptic conditions, which include the use of sterile gloves, a sterile drape and a sterile eyelid speculum (or equivalent). Adequate anesthesia and a broad spectrum microbiocide should be administered according to standard medical practice. The injection needle should be inserted 3.5 - 4.0 mm posterior to the limbus aiming towards the center of the vitreous cavity, avoiding the horizontal meridian. The injection volume of 0.1 mL is then delivered into the mid-vitreous. Immediately following the intravitreal injection, patients should be monitored for elevation in intraocular pressure. Appropriate monitoring may consist of a check for perfusion of the optic nerve head or tonometry. If required, a sterile paracentesis needle should be available.Following intravitreal injection, patients should be instructed to report any symptoms suggestive of endophthalmitis or retinal detachment (e.g., eye pain, redness of the eye, photophobia, blurred or decreased vision) without delay [see Patient Counseling Information (17)].Each vial should only be used to provide a single injection for the treatment of a single eye. If the contralateral eye requires treatment, a new vial should be used and the sterile field, syringe, gloves, drapes, eyelid speculum, and injection needles should be changed before JETREA is administered to the other eye, however, treatment with JETREA in the other eye is not recommended within 7 days of the initial injection in order to monitor the post-injection course including the potential for decreased vision in the injected eye.Repeated administration of JETREA in the same eye is not recommended [see Nonclinical Toxicology (13.2)].After injection, any unused product must be discarded.No special dosage modification is required for any of the populations that have been studied (e.g. gender, elderly).
3 DOSAGE FORMS AND STRENGTHSSingle-use glass vial containing JETREA 0.5 mg in 0.2 mL solution for intravitreal injection (2.5 mg/mL).
4 CONTRAINDICATIONSNone
5 WARNINGS AND PRECAUTIONS
5.1 Decreased VisionA decrease of ≥ 3 line of best corrected visual acuity (BCVA) was experienced by 5.6% of patients treated with JETREA and 3.2% of patients treated with vehicle in the controlled trials [see Clinical Studies (14)].The majority of these decreases in vision were due to progression of the condition with traction and many required surgical intervention. Patients should be monitored appropriately [see Dosage And Administration (2.4)].
5.2 Intravitreal Injection Procedure Associated EffectsIntravitreal injections are associated with intraocular inflammation / infection, intraocular hemorrhage and increased intraocular pressure (IOP). In the controlled trials, intraocular inflammation occurred in 7.1% of patients injected with JETREA vs. 3.7% of patients injected with vehicle. Most of the post-injection intraocular inflammation events were mild and transient. Intraocular hemorrhage occurred in 2.4% vs. 3.7% of patients injected with JETREA vs. vehicle, respectively. Increased intraocular pressure occurred in 4.1% vs. 5.3% of patients injected with JETREA vs. vehicle, respectively.
5.3 Potential for Lens SubluxationOne case of lens subluxation was reported in a premature infant who received an intravitreal injection of 0.175 mg (1.4 times higher than the recommended dose) [see Use in Specific Populations (8.4)]. Lens subluxation was observed in three animal species (monkey, rabbit, minipig) following a single intravitreal injection that achieved vitreous concentrations of ocriplasmin 1.4 times higher than achieved with the recommended treatment dose. Administration of a second intravitreal dose in monkeys, 28 days apart, produced lens subluxation in 100% of the treated eyes [see Nonclinical Toxicology (13.2)].
5.4 Retinal BreaksIn the controlled trials, the incidence of retinal detachment was 0.9% in the JETREA group and 1.6% in the vehicle group, while the incidence of retinal tear (without detachment) was 1.1% in the JETREA group and 2.7% in the vehicle group. Most of these events occurred during or after vitrectomy in both groups. The incidence of retinal detachment that occurred pre-vitrectomy was 0.4% in the JETREA group and none in the vehicle group, while the incidence of retinal tear (without detachment) that occurred pre-vitrectomy was none in the JETREA group and 0.5% in the vehicle group.
5.5 DyschromatopsiaDyschromatopsia (generally described as yellowish vision) was reported in 2% of all patients injected with JETREA. In approximately half of these dyschromatopsia cases there were also electroretinographic (ERG) changes reported (a- and b-wave amplitude decrease).
6 ADVERSE REACTIONSThe following adverse reactions are described below and elsewhere in the labeling:• Decreased Vision [see Warnings and Precautions (5.1)]• Intravitreal Injection Procedure Associated Effects [see Warnings and Precautions (5.2) and Dosage
And Administration (2.4)]• Potential for Lens Subluxation [see Warnings and Precautions (5.3)]• Retinal Breaks [see Warnings and Precautions (5.4) and Dosage And Administration (2.4)]• Dyschromatopsia [see Warnings and Precautions (5.5)]
6.1 Clinical Trials ExperienceBecause clinical trials are conducted under widely varying conditions, adverse reaction rates in one clinical trial of a drug cannot be directly compared with rates in the clinical trials of the same or another drug and may not reflect the rates observed in practice.Approximately 800 patients have been treated with an intravitreal injection of JETREA. Of these, 465 patients received an intravitreal injection of ocriplasmin 0.125 mg (187 patients received vehicle) in the 2 vehicle-controlled studies (Study 1 and Study 2).The most common adverse reactions (incidence 5% - 20% listed in descending order of frequency) in the vehicle-controlled clinical studies were: vitreous floaters, conjunctival hemorrhage, eye pain, photopsia, blurred vision, macular hole, reduced visual acuity, visual impairment, and retinal edema.Less common adverse reactions observed in the studies at a frequency of < 5% in patients treated with JETREA included macular edema, increased intraocular pressure, anterior chamber cell, photophobia, vitreous detachment, ocular discomfort, iritis, cataract, dry eye, metamorphopsia, pupillary reflex impaired, conjunctival hyperemia, retinal degeneration and visual symptoms perceived in the contralateral eye.Dyschromatopsia was reported in 2% of patients injected with JETREA, with the majority of cases reported from two uncontrolled clinical studies. In approximately half of these dyschromatopsia cases there were also electroretinographic (ERG) changes reported (a- and b-wave amplitude decrease).
6.2 ImmunogenicityAs with all therapeutic proteins, there is potential for immunogenicity. Immunogenicity for this product has not been evaluated.
255919 Je01-US-LT-04 255919 Je01-US-LT-04
Date: 23-05-2016 Draft: 01 - Op. RI003 EGG
4039
4142
4344
4546
4748
4950
5152
5354
55
Date: 29-06-2016 Draft: 02 - Op. RI003 EGG
Jetrea 2,5 mg/ml USA
05
Date: 07-07-2016 Draft: 03 - Op. RI003 EGGDate: 08-07-2016 Draft: 04 - Op. RI001 EGG
257130 Je01-US-LT-03
Date: 18-07-2016 Draft: 05 - Op. RI003 EGG
HIGHLIGHTS OF PRESCRIBING INFORMATIONThese highlights do not include all the information needed to use JETREA safely and effectively. See full prescribing information for JETREA
JETREA® (ocriplasmin) Intravitreal Injection, 2.5 mg/mLFor intravitreal injectionInitial U.S. Approval: 2012
INDICATIONS AND USAGEJETREA is a proteolytic enzyme indicated for the treatment of symptomatic vitreomacular adhesion. (1)
DOSAGE AND ADMINISTRATION• Must dilute before use. (2.1)• For single use ophthalmic intravitreal injection only. (2.1)• The recommended dose is 0.125 mg (0.1 mL of the diluted solution) administered by intravitreal
injection to the affected eye once as a single dose. (2.2)
DOSAGE FORMS AND STRENGTHSSingle-use glass vial containing JETREA 0.5 mg in 0.2 mL solution for intravitreal injection (2.5 mg/mL). (3)
CONTRAINDICATIONSNone. (4)
WARNINGS AND PRECAUTIONS• Decreases in vision due to progression of the condition with traction may occur requiring surgical
intervention. Patients should be monitored and instructed to report any symptoms without delay. (5.1)• Intravitreal injection procedure associated effects (intraocular inflammation/infection, intraocular
hemorrhage and increased IOP) may occur following an intravitreal injection. Patients should be monitored and instructed to report any symptoms without delay. (5.2)
• Potential for lens subluxation. (5.3)
ADVERSE REACTIONSThe most commonly reported reactions (≥ 5%) in patients treated with JETREA were vitreous floaters, conjunctival hemorrhage, eye pain, photopsia, blurred vision, macular hole, reduced visual acuity, visual impairment, and retinal edema. (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact ThromboGenics Inc. at 1-855-253-7396 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
See 17 for PATIENT COUNSELING INFORMATIONRevised: 03/2016
FULL PRESCRIBING INFORMATION: CONTENTS*
1 INDICATIONS AND USAGE
2 DOSAGE AND ADMINISTRATION2.1 General Dosing Information2.2 Dosing2.3 Preparation for Administration2.4 Administration and Monitoring
3 DOSAGE FORMS AND STRENGTHS
4 CONTRAINDICATIONS
5 WARNINGS AND PRECAUTIONS5.1 Decreased Vision5.2 Intravitreal Injection Procedure Associated Effects5.3 Potential for Lens Subluxation5.4 Retinal Breaks5.5 Dyschromatopsia
6 ADVERSE REACTIONS6.1 Clinical Trials Experience6.2 Immunogenicity6.3 Postmarketing Experience
8 USE IN SPECIFIC POPULATIONS8.1 Pregnancy8.3 Nursing Mothers8.4 Pediatric Use8.5 Geriatric Use
10 OVERDOSAGE
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY12.1 Mechanism of Action12.3 Pharmacokinetics
13 NONCLINICAL TOXICOLOGY13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility13.2 Animal Toxicology and/or Pharmacology
14 CLINICAL STUDIES
16 HOW SUPPLIED/STORAGE AND HANDLING
17 PATIENT COUNSELING INFORMATION
*Sections or subsections omitted from the full prescribing information are not listed.
FULL PRESCRIBING INFORMATION
1 INDICATIONS AND USAGEJETREA® is a proteolytic enzyme indicated for the treatment of symptomatic vitreomacular adhesion.
2 DOSAGE AND ADMINISTRATION
2.1 General Dosing InformationMust be diluted before use. For single-use ophthalmic intravitreal injection only. JETREA must only be administered by a qualified physician.
2.2 DosingThe recommended dose is 0.125 mg (0.1 mL of the diluted solution) administered by intravitreal injection to the affected eye once as a single dose.
2.3 Preparation for AdministrationTo prepare JETREA for intravitreal injection, adhere to the following instructions:1. Remove the vial (2.5 mg/mL corresponding to 0.5 mg ocriplasmin) from the freezer and allow to thaw
at room temperature (within a few minutes).2. Once completely thawed, remove the protective polypropylene flip-off cap from the vial (see Figure 1).
Figure 1:
3. The top of the vial should be disinfected with an alcohol wipe (see Figure 2).
Figure 2:
4. Using aseptic technique, add 0.2 mL of 0.9% w/v Sodium Chloride Injection, USP (sterile, preservative-free) into the JETREA vial (see Figure 3) and gently swirl the vial until the solutions are mixed (see Figure 4).
Figure 3:
Figure 4:
5. Visually inspect the vial for particulate matter. Only a clear, colorless solution without visible particles should be used.
6. Using aseptic technique, withdraw all of the diluted solution using a sterile #19 gauge needle (slightly tilt the vial to ease withdrawal) and discard the needle after withdrawal of the vial contents (see Figure 5). Do not use this needle for the intravitreal injection.
Figure 5:
7. Replace the needle with a sterile #30 gauge needle, carefully expel the air bubbles and excess drug from the syringe and adjust the dose to the 0.1 mL mark on the syringe (corresponding to 0.125 mg ocriplasmin) (see Figure 6).
Figure 6:
8. THE SOLUTION SHOULD BE USED IMMEDIATELY AS IT CONTAINS NO PRESERVATIVES.9. Discard the vial and any unused portion of the diluted solution after single use.
2.4 Administration and MonitoringThe intravitreal injection procedure should be carried out under controlled aseptic conditions, which include the use of sterile gloves, a sterile drape and a sterile eyelid speculum (or equivalent). Adequate anesthesia and a broad spectrum microbiocide should be administered according to standard medical practice. The injection needle should be inserted 3.5 - 4.0 mm posterior to the limbus aiming towards the center of the vitreous cavity, avoiding the horizontal meridian. The injection volume of 0.1 mL is then delivered into the mid-vitreous. Immediately following the intravitreal injection, patients should be monitored for elevation in intraocular pressure. Appropriate monitoring may consist of a check for perfusion of the optic nerve head or tonometry. If required, a sterile paracentesis needle should be available.Following intravitreal injection, patients should be instructed to report any symptoms suggestive of endophthalmitis or retinal detachment (e.g., eye pain, redness of the eye, photophobia, blurred or decreased vision) without delay [see Patient Counseling Information (17)].Each vial should only be used to provide a single injection for the treatment of a single eye. If the contralateral eye requires treatment, a new vial should be used and the sterile field, syringe, gloves, drapes, eyelid speculum, and injection needles should be changed before JETREA is administered to the other eye, however, treatment with JETREA in the other eye is not recommended within 7 days of the initial injection in order to monitor the post-injection course including the potential for decreased vision in the injected eye.Repeated administration of JETREA in the same eye is not recommended [see Nonclinical Toxicology (13.2)].After injection, any unused product must be discarded.No special dosage modification is required for any of the populations that have been studied (e.g. gender, elderly).
3 DOSAGE FORMS AND STRENGTHSSingle-use glass vial containing JETREA 0.5 mg in 0.2 mL solution for intravitreal injection (2.5 mg/mL).
4 CONTRAINDICATIONSNone
5 WARNINGS AND PRECAUTIONS
5.1 Decreased VisionA decrease of ≥ 3 line of best corrected visual acuity (BCVA) was experienced by 5.6% of patients treated with JETREA and 3.2% of patients treated with vehicle in the controlled trials [see Clinical Studies (14)].The majority of these decreases in vision were due to progression of the condition with traction and many required surgical intervention. Patients should be monitored appropriately [see Dosage And Administration (2.4)].
5.2 Intravitreal Injection Procedure Associated EffectsIntravitreal injections are associated with intraocular inflammation / infection, intraocular hemorrhage and increased intraocular pressure (IOP). In the controlled trials, intraocular inflammation occurred in 7.1% of patients injected with JETREA vs. 3.7% of patients injected with vehicle. Most of the post-injection intraocular inflammation events were mild and transient. Intraocular hemorrhage occurred in 2.4% vs. 3.7% of patients injected with JETREA vs. vehicle, respectively. Increased intraocular pressure occurred in 4.1% vs. 5.3% of patients injected with JETREA vs. vehicle, respectively.
5.3 Potential for Lens SubluxationOne case of lens subluxation was reported in a premature infant who received an intravitreal injection of 0.175 mg (1.4 times higher than the recommended dose) [see Use in Specific Populations (8.4)]. Lens subluxation was observed in three animal species (monkey, rabbit, minipig) following a single intravitreal injection that achieved vitreous concentrations of ocriplasmin 1.4 times higher than achieved with the recommended treatment dose. Administration of a second intravitreal dose in monkeys, 28 days apart, produced lens subluxation in 100% of the treated eyes [see Nonclinical Toxicology (13.2)].
5.4 Retinal BreaksIn the controlled trials, the incidence of retinal detachment was 0.9% in the JETREA group and 1.6% in the vehicle group, while the incidence of retinal tear (without detachment) was 1.1% in the JETREA group and 2.7% in the vehicle group. Most of these events occurred during or after vitrectomy in both groups. The incidence of retinal detachment that occurred pre-vitrectomy was 0.4% in the JETREA group and none in the vehicle group, while the incidence of retinal tear (without detachment) that occurred pre-vitrectomy was none in the JETREA group and 0.5% in the vehicle group.
5.5 DyschromatopsiaDyschromatopsia (generally described as yellowish vision) was reported in 2% of all patients injected with JETREA. In approximately half of these dyschromatopsia cases there were also electroretinographic (ERG) changes reported (a- and b-wave amplitude decrease).
6 ADVERSE REACTIONSThe following adverse reactions are described below and elsewhere in the labeling:• Decreased Vision [see Warnings and Precautions (5.1)]• Intravitreal Injection Procedure Associated Effects [see Warnings and Precautions (5.2) and Dosage
And Administration (2.4)]• Potential for Lens Subluxation [see Warnings and Precautions (5.3)]• Retinal Breaks [see Warnings and Precautions (5.4) and Dosage And Administration (2.4)]• Dyschromatopsia [see Warnings and Precautions (5.5)]
6.1 Clinical Trials ExperienceBecause clinical trials are conducted under widely varying conditions, adverse reaction rates in one clinical trial of a drug cannot be directly compared with rates in the clinical trials of the same or another drug and may not reflect the rates observed in practice.Approximately 800 patients have been treated with an intravitreal injection of JETREA. Of these, 465 patients received an intravitreal injection of ocriplasmin 0.125 mg (187 patients received vehicle) in the 2 vehicle-controlled studies (Study 1 and Study 2).The most common adverse reactions (incidence 5% - 20% listed in descending order of frequency) in the vehicle-controlled clinical studies were: vitreous floaters, conjunctival hemorrhage, eye pain, photopsia, blurred vision, macular hole, reduced visual acuity, visual impairment, and retinal edema.Less common adverse reactions observed in the studies at a frequency of < 5% in patients treated with JETREA included macular edema, increased intraocular pressure, anterior chamber cell, photophobia, vitreous detachment, ocular discomfort, iritis, cataract, dry eye, metamorphopsia, pupillary reflex impaired, conjunctival hyperemia, retinal degeneration and visual symptoms perceived in the contralateral eye.Dyschromatopsia was reported in 2% of patients injected with JETREA, with the majority of cases reported from two uncontrolled clinical studies. In approximately half of these dyschromatopsia cases there were also electroretinographic (ERG) changes reported (a- and b-wave amplitude decrease).
6.2 ImmunogenicityAs with all therapeutic proteins, there is potential for immunogenicity. Immunogenicity for this product has not been evaluated.
255919 Je01-US-LT-04 255919 Je01-US-LT-04

Date: 23-05-2016 Draft: 01 - Op. RI003 EGG
4039
4142
4344
4546
4748
4950
5152
5354
55
Date: 29-06-2016 Draft: 02 - Op. RI003 EGG
Jetrea 2,5 mg/ml USA
05
Date: 07-07-2016 Draft: 03 - Op. RI003 EGGDate: 08-07-2016 Draft: 04 - Op. RI001 EGG
257130 Je01-US-LT-03
Date: 18-07-2016 Draft: 05 - Op. RI003 EGG
HIGHLIGHTS OF PRESCRIBING INFORMATIONThese highlights do not include all the information needed to use JETREA safely and effectively. See full prescribing information for JETREA
JETREA® (ocriplasmin) Intravitreal Injection, 2.5 mg/mLFor intravitreal injectionInitial U.S. Approval: 2012
INDICATIONS AND USAGEJETREA is a proteolytic enzyme indicated for the treatment of symptomatic vitreomacular adhesion. (1)
DOSAGE AND ADMINISTRATION• Must dilute before use. (2.1)• For single use ophthalmic intravitreal injection only. (2.1)• The recommended dose is 0.125 mg (0.1 mL of the diluted solution) administered by intravitreal
injection to the affected eye once as a single dose. (2.2)
DOSAGE FORMS AND STRENGTHSSingle-use glass vial containing JETREA 0.5 mg in 0.2 mL solution for intravitreal injection (2.5 mg/mL). (3)
CONTRAINDICATIONSNone. (4)
WARNINGS AND PRECAUTIONS• Decreases in vision due to progression of the condition with traction may occur requiring surgical
intervention. Patients should be monitored and instructed to report any symptoms without delay. (5.1)• Intravitreal injection procedure associated effects (intraocular inflammation/infection, intraocular
hemorrhage and increased IOP) may occur following an intravitreal injection. Patients should be monitored and instructed to report any symptoms without delay. (5.2)
• Potential for lens subluxation. (5.3)
ADVERSE REACTIONSThe most commonly reported reactions (≥ 5%) in patients treated with JETREA were vitreous floaters, conjunctival hemorrhage, eye pain, photopsia, blurred vision, macular hole, reduced visual acuity, visual impairment, and retinal edema. (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact ThromboGenics Inc. at 1-855-253-7396 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
See 17 for PATIENT COUNSELING INFORMATIONRevised: 03/2016
FULL PRESCRIBING INFORMATION: CONTENTS*
1 INDICATIONS AND USAGE
2 DOSAGE AND ADMINISTRATION2.1 General Dosing Information2.2 Dosing2.3 Preparation for Administration2.4 Administration and Monitoring
3 DOSAGE FORMS AND STRENGTHS
4 CONTRAINDICATIONS
5 WARNINGS AND PRECAUTIONS5.1 Decreased Vision5.2 Intravitreal Injection Procedure Associated Effects5.3 Potential for Lens Subluxation5.4 Retinal Breaks5.5 Dyschromatopsia
6 ADVERSE REACTIONS6.1 Clinical Trials Experience6.2 Immunogenicity6.3 Postmarketing Experience
8 USE IN SPECIFIC POPULATIONS8.1 Pregnancy8.3 Nursing Mothers8.4 Pediatric Use8.5 Geriatric Use
10 OVERDOSAGE
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY12.1 Mechanism of Action12.3 Pharmacokinetics
13 NONCLINICAL TOXICOLOGY13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility13.2 Animal Toxicology and/or Pharmacology
14 CLINICAL STUDIES
16 HOW SUPPLIED/STORAGE AND HANDLING
17 PATIENT COUNSELING INFORMATION
*Sections or subsections omitted from the full prescribing information are not listed.
FULL PRESCRIBING INFORMATION
1 INDICATIONS AND USAGEJETREA® is a proteolytic enzyme indicated for the treatment of symptomatic vitreomacular adhesion.
2 DOSAGE AND ADMINISTRATION
2.1 General Dosing InformationMust be diluted before use. For single-use ophthalmic intravitreal injection only. JETREA must only be administered by a qualified physician.
2.2 DosingThe recommended dose is 0.125 mg (0.1 mL of the diluted solution) administered by intravitreal injection to the affected eye once as a single dose.
2.3 Preparation for AdministrationTo prepare JETREA for intravitreal injection, adhere to the following instructions:1. Remove the vial (2.5 mg/mL corresponding to 0.5 mg ocriplasmin) from the freezer and allow to thaw
at room temperature (within a few minutes).2. Once completely thawed, remove the protective polypropylene flip-off cap from the vial (see Figure 1).
Figure 1:
3. The top of the vial should be disinfected with an alcohol wipe (see Figure 2).
Figure 2:
4. Using aseptic technique, add 0.2 mL of 0.9% w/v Sodium Chloride Injection, USP (sterile, preservative-free) into the JETREA vial (see Figure 3) and gently swirl the vial until the solutions are mixed (see Figure 4).
Figure 3:
Figure 4:
5. Visually inspect the vial for particulate matter. Only a clear, colorless solution without visible particles should be used.
6. Using aseptic technique, withdraw all of the diluted solution using a sterile #19 gauge needle (slightly tilt the vial to ease withdrawal) and discard the needle after withdrawal of the vial contents (see Figure 5). Do not use this needle for the intravitreal injection.
Figure 5:
7. Replace the needle with a sterile #30 gauge needle, carefully expel the air bubbles and excess drug from the syringe and adjust the dose to the 0.1 mL mark on the syringe (corresponding to 0.125 mg ocriplasmin) (see Figure 6).
Figure 6:
8. THE SOLUTION SHOULD BE USED IMMEDIATELY AS IT CONTAINS NO PRESERVATIVES.9. Discard the vial and any unused portion of the diluted solution after single use.
2.4 Administration and MonitoringThe intravitreal injection procedure should be carried out under controlled aseptic conditions, which include the use of sterile gloves, a sterile drape and a sterile eyelid speculum (or equivalent). Adequate anesthesia and a broad spectrum microbiocide should be administered according to standard medical practice. The injection needle should be inserted 3.5 - 4.0 mm posterior to the limbus aiming towards the center of the vitreous cavity, avoiding the horizontal meridian. The injection volume of 0.1 mL is then delivered into the mid-vitreous. Immediately following the intravitreal injection, patients should be monitored for elevation in intraocular pressure. Appropriate monitoring may consist of a check for perfusion of the optic nerve head or tonometry. If required, a sterile paracentesis needle should be available.Following intravitreal injection, patients should be instructed to report any symptoms suggestive of endophthalmitis or retinal detachment (e.g., eye pain, redness of the eye, photophobia, blurred or decreased vision) without delay [see Patient Counseling Information (17)].Each vial should only be used to provide a single injection for the treatment of a single eye. If the contralateral eye requires treatment, a new vial should be used and the sterile field, syringe, gloves, drapes, eyelid speculum, and injection needles should be changed before JETREA is administered to the other eye, however, treatment with JETREA in the other eye is not recommended within 7 days of the initial injection in order to monitor the post-injection course including the potential for decreased vision in the injected eye.Repeated administration of JETREA in the same eye is not recommended [see Nonclinical Toxicology (13.2)].After injection, any unused product must be discarded.No special dosage modification is required for any of the populations that have been studied (e.g. gender, elderly).
3 DOSAGE FORMS AND STRENGTHSSingle-use glass vial containing JETREA 0.5 mg in 0.2 mL solution for intravitreal injection (2.5 mg/mL).
4 CONTRAINDICATIONSNone
5 WARNINGS AND PRECAUTIONS
5.1 Decreased VisionA decrease of ≥ 3 line of best corrected visual acuity (BCVA) was experienced by 5.6% of patients treated with JETREA and 3.2% of patients treated with vehicle in the controlled trials [see Clinical Studies (14)].The majority of these decreases in vision were due to progression of the condition with traction and many required surgical intervention. Patients should be monitored appropriately [see Dosage And Administration (2.4)].
5.2 Intravitreal Injection Procedure Associated EffectsIntravitreal injections are associated with intraocular inflammation / infection, intraocular hemorrhage and increased intraocular pressure (IOP). In the controlled trials, intraocular inflammation occurred in 7.1% of patients injected with JETREA vs. 3.7% of patients injected with vehicle. Most of the post-injection intraocular inflammation events were mild and transient. Intraocular hemorrhage occurred in 2.4% vs. 3.7% of patients injected with JETREA vs. vehicle, respectively. Increased intraocular pressure occurred in 4.1% vs. 5.3% of patients injected with JETREA vs. vehicle, respectively.
5.3 Potential for Lens SubluxationOne case of lens subluxation was reported in a premature infant who received an intravitreal injection of 0.175 mg (1.4 times higher than the recommended dose) [see Use in Specific Populations (8.4)]. Lens subluxation was observed in three animal species (monkey, rabbit, minipig) following a single intravitreal injection that achieved vitreous concentrations of ocriplasmin 1.4 times higher than achieved with the recommended treatment dose. Administration of a second intravitreal dose in monkeys, 28 days apart, produced lens subluxation in 100% of the treated eyes [see Nonclinical Toxicology (13.2)].
5.4 Retinal BreaksIn the controlled trials, the incidence of retinal detachment was 0.9% in the JETREA group and 1.6% in the vehicle group, while the incidence of retinal tear (without detachment) was 1.1% in the JETREA group and 2.7% in the vehicle group. Most of these events occurred during or after vitrectomy in both groups. The incidence of retinal detachment that occurred pre-vitrectomy was 0.4% in the JETREA group and none in the vehicle group, while the incidence of retinal tear (without detachment) that occurred pre-vitrectomy was none in the JETREA group and 0.5% in the vehicle group.
5.5 DyschromatopsiaDyschromatopsia (generally described as yellowish vision) was reported in 2% of all patients injected with JETREA. In approximately half of these dyschromatopsia cases there were also electroretinographic (ERG) changes reported (a- and b-wave amplitude decrease).
6 ADVERSE REACTIONSThe following adverse reactions are described below and elsewhere in the labeling:• Decreased Vision [see Warnings and Precautions (5.1)]• Intravitreal Injection Procedure Associated Effects [see Warnings and Precautions (5.2) and Dosage
And Administration (2.4)]• Potential for Lens Subluxation [see Warnings and Precautions (5.3)]• Retinal Breaks [see Warnings and Precautions (5.4) and Dosage And Administration (2.4)]• Dyschromatopsia [see Warnings and Precautions (5.5)]
6.1 Clinical Trials ExperienceBecause clinical trials are conducted under widely varying conditions, adverse reaction rates in one clinical trial of a drug cannot be directly compared with rates in the clinical trials of the same or another drug and may not reflect the rates observed in practice.Approximately 800 patients have been treated with an intravitreal injection of JETREA. Of these, 465 patients received an intravitreal injection of ocriplasmin 0.125 mg (187 patients received vehicle) in the 2 vehicle-controlled studies (Study 1 and Study 2).The most common adverse reactions (incidence 5% - 20% listed in descending order of frequency) in the vehicle-controlled clinical studies were: vitreous floaters, conjunctival hemorrhage, eye pain, photopsia, blurred vision, macular hole, reduced visual acuity, visual impairment, and retinal edema.Less common adverse reactions observed in the studies at a frequency of < 5% in patients treated with JETREA included macular edema, increased intraocular pressure, anterior chamber cell, photophobia, vitreous detachment, ocular discomfort, iritis, cataract, dry eye, metamorphopsia, pupillary reflex impaired, conjunctival hyperemia, retinal degeneration and visual symptoms perceived in the contralateral eye.Dyschromatopsia was reported in 2% of patients injected with JETREA, with the majority of cases reported from two uncontrolled clinical studies. In approximately half of these dyschromatopsia cases there were also electroretinographic (ERG) changes reported (a- and b-wave amplitude decrease).
6.2 ImmunogenicityAs with all therapeutic proteins, there is potential for immunogenicity. Immunogenicity for this product has not been evaluated.
255919 Je01-US-LT-04 255919 Je01-US-LT-04
Date: 23-05-2016 Draft: 01 - Op. RI003 EGG
4039
4142
4344
4546
4748
4950
5152
5354
55
Date: 29-06-2016 Draft: 02 - Op. RI003 EGG
Jetrea 2,5 mg/ml USA
05
Date: 07-07-2016 Draft: 03 - Op. RI003 EGGDate: 08-07-2016 Draft: 04 - Op. RI001 EGG
257130 Je01-US-LT-03
Date: 18-07-2016 Draft: 05 - Op. RI003 EGG
HIGHLIGHTS OF PRESCRIBING INFORMATIONThese highlights do not include all the information needed to use JETREA safely and effectively. See full prescribing information for JETREA
JETREA® (ocriplasmin) Intravitreal Injection, 2.5 mg/mLFor intravitreal injectionInitial U.S. Approval: 2012
INDICATIONS AND USAGEJETREA is a proteolytic enzyme indicated for the treatment of symptomatic vitreomacular adhesion. (1)
DOSAGE AND ADMINISTRATION• Must dilute before use. (2.1)• For single use ophthalmic intravitreal injection only. (2.1)• The recommended dose is 0.125 mg (0.1 mL of the diluted solution) administered by intravitreal
injection to the affected eye once as a single dose. (2.2)
DOSAGE FORMS AND STRENGTHSSingle-use glass vial containing JETREA 0.5 mg in 0.2 mL solution for intravitreal injection (2.5 mg/mL). (3)
CONTRAINDICATIONSNone. (4)
WARNINGS AND PRECAUTIONS• Decreases in vision due to progression of the condition with traction may occur requiring surgical
intervention. Patients should be monitored and instructed to report any symptoms without delay. (5.1)• Intravitreal injection procedure associated effects (intraocular inflammation/infection, intraocular
hemorrhage and increased IOP) may occur following an intravitreal injection. Patients should be monitored and instructed to report any symptoms without delay. (5.2)
• Potential for lens subluxation. (5.3)
ADVERSE REACTIONSThe most commonly reported reactions (≥ 5%) in patients treated with JETREA were vitreous floaters, conjunctival hemorrhage, eye pain, photopsia, blurred vision, macular hole, reduced visual acuity, visual impairment, and retinal edema. (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact ThromboGenics Inc. at 1-855-253-7396 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
See 17 for PATIENT COUNSELING INFORMATIONRevised: 03/2016
FULL PRESCRIBING INFORMATION: CONTENTS*
1 INDICATIONS AND USAGE
2 DOSAGE AND ADMINISTRATION2.1 General Dosing Information2.2 Dosing2.3 Preparation for Administration2.4 Administration and Monitoring
3 DOSAGE FORMS AND STRENGTHS
4 CONTRAINDICATIONS
5 WARNINGS AND PRECAUTIONS5.1 Decreased Vision5.2 Intravitreal Injection Procedure Associated Effects5.3 Potential for Lens Subluxation5.4 Retinal Breaks5.5 Dyschromatopsia
6 ADVERSE REACTIONS6.1 Clinical Trials Experience6.2 Immunogenicity6.3 Postmarketing Experience
8 USE IN SPECIFIC POPULATIONS8.1 Pregnancy8.3 Nursing Mothers8.4 Pediatric Use8.5 Geriatric Use
10 OVERDOSAGE
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY12.1 Mechanism of Action12.3 Pharmacokinetics
13 NONCLINICAL TOXICOLOGY13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility13.2 Animal Toxicology and/or Pharmacology
14 CLINICAL STUDIES
16 HOW SUPPLIED/STORAGE AND HANDLING
17 PATIENT COUNSELING INFORMATION
*Sections or subsections omitted from the full prescribing information are not listed.
FULL PRESCRIBING INFORMATION
1 INDICATIONS AND USAGEJETREA® is a proteolytic enzyme indicated for the treatment of symptomatic vitreomacular adhesion.
2 DOSAGE AND ADMINISTRATION
2.1 General Dosing InformationMust be diluted before use. For single-use ophthalmic intravitreal injection only. JETREA must only be administered by a qualified physician.
2.2 DosingThe recommended dose is 0.125 mg (0.1 mL of the diluted solution) administered by intravitreal injection to the affected eye once as a single dose.
2.3 Preparation for AdministrationTo prepare JETREA for intravitreal injection, adhere to the following instructions:1. Remove the vial (2.5 mg/mL corresponding to 0.5 mg ocriplasmin) from the freezer and allow to thaw
at room temperature (within a few minutes).2. Once completely thawed, remove the protective polypropylene flip-off cap from the vial (see Figure 1).
Figure 1:
3. The top of the vial should be disinfected with an alcohol wipe (see Figure 2).
Figure 2:
4. Using aseptic technique, add 0.2 mL of 0.9% w/v Sodium Chloride Injection, USP (sterile, preservative-free) into the JETREA vial (see Figure 3) and gently swirl the vial until the solutions are mixed (see Figure 4).
Figure 3:
Figure 4:
5. Visually inspect the vial for particulate matter. Only a clear, colorless solution without visible particles should be used.
6. Using aseptic technique, withdraw all of the diluted solution using a sterile #19 gauge needle (slightly tilt the vial to ease withdrawal) and discard the needle after withdrawal of the vial contents (see Figure 5). Do not use this needle for the intravitreal injection.
Figure 5:
7. Replace the needle with a sterile #30 gauge needle, carefully expel the air bubbles and excess drug from the syringe and adjust the dose to the 0.1 mL mark on the syringe (corresponding to 0.125 mg ocriplasmin) (see Figure 6).
Figure 6:
8. THE SOLUTION SHOULD BE USED IMMEDIATELY AS IT CONTAINS NO PRESERVATIVES.9. Discard the vial and any unused portion of the diluted solution after single use.
2.4 Administration and MonitoringThe intravitreal injection procedure should be carried out under controlled aseptic conditions, which include the use of sterile gloves, a sterile drape and a sterile eyelid speculum (or equivalent). Adequate anesthesia and a broad spectrum microbiocide should be administered according to standard medical practice. The injection needle should be inserted 3.5 - 4.0 mm posterior to the limbus aiming towards the center of the vitreous cavity, avoiding the horizontal meridian. The injection volume of 0.1 mL is then delivered into the mid-vitreous. Immediately following the intravitreal injection, patients should be monitored for elevation in intraocular pressure. Appropriate monitoring may consist of a check for perfusion of the optic nerve head or tonometry. If required, a sterile paracentesis needle should be available.Following intravitreal injection, patients should be instructed to report any symptoms suggestive of endophthalmitis or retinal detachment (e.g., eye pain, redness of the eye, photophobia, blurred or decreased vision) without delay [see Patient Counseling Information (17)].Each vial should only be used to provide a single injection for the treatment of a single eye. If the contralateral eye requires treatment, a new vial should be used and the sterile field, syringe, gloves, drapes, eyelid speculum, and injection needles should be changed before JETREA is administered to the other eye, however, treatment with JETREA in the other eye is not recommended within 7 days of the initial injection in order to monitor the post-injection course including the potential for decreased vision in the injected eye.Repeated administration of JETREA in the same eye is not recommended [see Nonclinical Toxicology (13.2)].After injection, any unused product must be discarded.No special dosage modification is required for any of the populations that have been studied (e.g. gender, elderly).
3 DOSAGE FORMS AND STRENGTHSSingle-use glass vial containing JETREA 0.5 mg in 0.2 mL solution for intravitreal injection (2.5 mg/mL).
4 CONTRAINDICATIONSNone
5 WARNINGS AND PRECAUTIONS
5.1 Decreased VisionA decrease of ≥ 3 line of best corrected visual acuity (BCVA) was experienced by 5.6% of patients treated with JETREA and 3.2% of patients treated with vehicle in the controlled trials [see Clinical Studies (14)].The majority of these decreases in vision were due to progression of the condition with traction and many required surgical intervention. Patients should be monitored appropriately [see Dosage And Administration (2.4)].
5.2 Intravitreal Injection Procedure Associated EffectsIntravitreal injections are associated with intraocular inflammation / infection, intraocular hemorrhage and increased intraocular pressure (IOP). In the controlled trials, intraocular inflammation occurred in 7.1% of patients injected with JETREA vs. 3.7% of patients injected with vehicle. Most of the post-injection intraocular inflammation events were mild and transient. Intraocular hemorrhage occurred in 2.4% vs. 3.7% of patients injected with JETREA vs. vehicle, respectively. Increased intraocular pressure occurred in 4.1% vs. 5.3% of patients injected with JETREA vs. vehicle, respectively.
5.3 Potential for Lens SubluxationOne case of lens subluxation was reported in a premature infant who received an intravitreal injection of 0.175 mg (1.4 times higher than the recommended dose) [see Use in Specific Populations (8.4)]. Lens subluxation was observed in three animal species (monkey, rabbit, minipig) following a single intravitreal injection that achieved vitreous concentrations of ocriplasmin 1.4 times higher than achieved with the recommended treatment dose. Administration of a second intravitreal dose in monkeys, 28 days apart, produced lens subluxation in 100% of the treated eyes [see Nonclinical Toxicology (13.2)].
5.4 Retinal BreaksIn the controlled trials, the incidence of retinal detachment was 0.9% in the JETREA group and 1.6% in the vehicle group, while the incidence of retinal tear (without detachment) was 1.1% in the JETREA group and 2.7% in the vehicle group. Most of these events occurred during or after vitrectomy in both groups. The incidence of retinal detachment that occurred pre-vitrectomy was 0.4% in the JETREA group and none in the vehicle group, while the incidence of retinal tear (without detachment) that occurred pre-vitrectomy was none in the JETREA group and 0.5% in the vehicle group.
5.5 DyschromatopsiaDyschromatopsia (generally described as yellowish vision) was reported in 2% of all patients injected with JETREA. In approximately half of these dyschromatopsia cases there were also electroretinographic (ERG) changes reported (a- and b-wave amplitude decrease).
6 ADVERSE REACTIONSThe following adverse reactions are described below and elsewhere in the labeling:• Decreased Vision [see Warnings and Precautions (5.1)]• Intravitreal Injection Procedure Associated Effects [see Warnings and Precautions (5.2) and Dosage
And Administration (2.4)]• Potential for Lens Subluxation [see Warnings and Precautions (5.3)]• Retinal Breaks [see Warnings and Precautions (5.4) and Dosage And Administration (2.4)]• Dyschromatopsia [see Warnings and Precautions (5.5)]
6.1 Clinical Trials ExperienceBecause clinical trials are conducted under widely varying conditions, adverse reaction rates in one clinical trial of a drug cannot be directly compared with rates in the clinical trials of the same or another drug and may not reflect the rates observed in practice.Approximately 800 patients have been treated with an intravitreal injection of JETREA. Of these, 465 patients received an intravitreal injection of ocriplasmin 0.125 mg (187 patients received vehicle) in the 2 vehicle-controlled studies (Study 1 and Study 2).The most common adverse reactions (incidence 5% - 20% listed in descending order of frequency) in the vehicle-controlled clinical studies were: vitreous floaters, conjunctival hemorrhage, eye pain, photopsia, blurred vision, macular hole, reduced visual acuity, visual impairment, and retinal edema.Less common adverse reactions observed in the studies at a frequency of < 5% in patients treated with JETREA included macular edema, increased intraocular pressure, anterior chamber cell, photophobia, vitreous detachment, ocular discomfort, iritis, cataract, dry eye, metamorphopsia, pupillary reflex impaired, conjunctival hyperemia, retinal degeneration and visual symptoms perceived in the contralateral eye.Dyschromatopsia was reported in 2% of patients injected with JETREA, with the majority of cases reported from two uncontrolled clinical studies. In approximately half of these dyschromatopsia cases there were also electroretinographic (ERG) changes reported (a- and b-wave amplitude decrease).
6.2 ImmunogenicityAs with all therapeutic proteins, there is potential for immunogenicity. Immunogenicity for this product has not been evaluated.
255919 Je01-US-LT-04 255919 Je01-US-LT-04

Date: 23-05-2016 Draft: 01 - Op. RI003 EGG
4039
4142
4344
4546
4748
4950
5152
5354
55
Date: 29-06-2016 Draft: 02 - Op. RI003 EGG
Jetrea 2,5 mg/ml USA
05
Date: 07-07-2016 Draft: 03 - Op. RI003 EGGDate: 08-07-2016 Draft: 04 - Op. RI001 EGG
257130 Je01-US-LT-03
Date: 18-07-2016 Draft: 05 - Op. RI003 EGG
HIGHLIGHTS OF PRESCRIBING INFORMATIONThese highlights do not include all the information needed to use JETREA safely and effectively. See full prescribing information for JETREA
JETREA® (ocriplasmin) Intravitreal Injection, 2.5 mg/mLFor intravitreal injectionInitial U.S. Approval: 2012
INDICATIONS AND USAGEJETREA is a proteolytic enzyme indicated for the treatment of symptomatic vitreomacular adhesion. (1)
DOSAGE AND ADMINISTRATION• Must dilute before use. (2.1)• For single use ophthalmic intravitreal injection only. (2.1)• The recommended dose is 0.125 mg (0.1 mL of the diluted solution) administered by intravitreal
injection to the affected eye once as a single dose. (2.2)
DOSAGE FORMS AND STRENGTHSSingle-use glass vial containing JETREA 0.5 mg in 0.2 mL solution for intravitreal injection (2.5 mg/mL). (3)
CONTRAINDICATIONSNone. (4)
WARNINGS AND PRECAUTIONS• Decreases in vision due to progression of the condition with traction may occur requiring surgical
intervention. Patients should be monitored and instructed to report any symptoms without delay. (5.1)• Intravitreal injection procedure associated effects (intraocular inflammation/infection, intraocular
hemorrhage and increased IOP) may occur following an intravitreal injection. Patients should be monitored and instructed to report any symptoms without delay. (5.2)
• Potential for lens subluxation. (5.3)
ADVERSE REACTIONSThe most commonly reported reactions (≥ 5%) in patients treated with JETREA were vitreous floaters, conjunctival hemorrhage, eye pain, photopsia, blurred vision, macular hole, reduced visual acuity, visual impairment, and retinal edema. (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact ThromboGenics Inc. at 1-855-253-7396 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
See 17 for PATIENT COUNSELING INFORMATIONRevised: 03/2016
FULL PRESCRIBING INFORMATION: CONTENTS*
1 INDICATIONS AND USAGE
2 DOSAGE AND ADMINISTRATION2.1 General Dosing Information2.2 Dosing2.3 Preparation for Administration2.4 Administration and Monitoring
3 DOSAGE FORMS AND STRENGTHS
4 CONTRAINDICATIONS
5 WARNINGS AND PRECAUTIONS5.1 Decreased Vision5.2 Intravitreal Injection Procedure Associated Effects5.3 Potential for Lens Subluxation5.4 Retinal Breaks5.5 Dyschromatopsia
6 ADVERSE REACTIONS6.1 Clinical Trials Experience6.2 Immunogenicity6.3 Postmarketing Experience
8 USE IN SPECIFIC POPULATIONS8.1 Pregnancy8.3 Nursing Mothers8.4 Pediatric Use8.5 Geriatric Use
10 OVERDOSAGE
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY12.1 Mechanism of Action12.3 Pharmacokinetics
13 NONCLINICAL TOXICOLOGY13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility13.2 Animal Toxicology and/or Pharmacology
14 CLINICAL STUDIES
16 HOW SUPPLIED/STORAGE AND HANDLING
17 PATIENT COUNSELING INFORMATION
*Sections or subsections omitted from the full prescribing information are not listed.
FULL PRESCRIBING INFORMATION
1 INDICATIONS AND USAGEJETREA® is a proteolytic enzyme indicated for the treatment of symptomatic vitreomacular adhesion.
2 DOSAGE AND ADMINISTRATION
2.1 General Dosing InformationMust be diluted before use. For single-use ophthalmic intravitreal injection only. JETREA must only be administered by a qualified physician.
2.2 DosingThe recommended dose is 0.125 mg (0.1 mL of the diluted solution) administered by intravitreal injection to the affected eye once as a single dose.
2.3 Preparation for AdministrationTo prepare JETREA for intravitreal injection, adhere to the following instructions:1. Remove the vial (2.5 mg/mL corresponding to 0.5 mg ocriplasmin) from the freezer and allow to thaw
at room temperature (within a few minutes).2. Once completely thawed, remove the protective polypropylene flip-off cap from the vial (see Figure 1).
Figure 1:
3. The top of the vial should be disinfected with an alcohol wipe (see Figure 2).
Figure 2:
4. Using aseptic technique, add 0.2 mL of 0.9% w/v Sodium Chloride Injection, USP (sterile, preservative-free) into the JETREA vial (see Figure 3) and gently swirl the vial until the solutions are mixed (see Figure 4).
Figure 3:
Figure 4:
5. Visually inspect the vial for particulate matter. Only a clear, colorless solution without visible particles should be used.
6. Using aseptic technique, withdraw all of the diluted solution using a sterile #19 gauge needle (slightly tilt the vial to ease withdrawal) and discard the needle after withdrawal of the vial contents (see Figure 5). Do not use this needle for the intravitreal injection.
Figure 5:
7. Replace the needle with a sterile #30 gauge needle, carefully expel the air bubbles and excess drug from the syringe and adjust the dose to the 0.1 mL mark on the syringe (corresponding to 0.125 mg ocriplasmin) (see Figure 6).
Figure 6:
8. THE SOLUTION SHOULD BE USED IMMEDIATELY AS IT CONTAINS NO PRESERVATIVES.9. Discard the vial and any unused portion of the diluted solution after single use.
2.4 Administration and MonitoringThe intravitreal injection procedure should be carried out under controlled aseptic conditions, which include the use of sterile gloves, a sterile drape and a sterile eyelid speculum (or equivalent). Adequate anesthesia and a broad spectrum microbiocide should be administered according to standard medical practice. The injection needle should be inserted 3.5 - 4.0 mm posterior to the limbus aiming towards the center of the vitreous cavity, avoiding the horizontal meridian. The injection volume of 0.1 mL is then delivered into the mid-vitreous. Immediately following the intravitreal injection, patients should be monitored for elevation in intraocular pressure. Appropriate monitoring may consist of a check for perfusion of the optic nerve head or tonometry. If required, a sterile paracentesis needle should be available.Following intravitreal injection, patients should be instructed to report any symptoms suggestive of endophthalmitis or retinal detachment (e.g., eye pain, redness of the eye, photophobia, blurred or decreased vision) without delay [see Patient Counseling Information (17)].Each vial should only be used to provide a single injection for the treatment of a single eye. If the contralateral eye requires treatment, a new vial should be used and the sterile field, syringe, gloves, drapes, eyelid speculum, and injection needles should be changed before JETREA is administered to the other eye, however, treatment with JETREA in the other eye is not recommended within 7 days of the initial injection in order to monitor the post-injection course including the potential for decreased vision in the injected eye.Repeated administration of JETREA in the same eye is not recommended [see Nonclinical Toxicology (13.2)].After injection, any unused product must be discarded.No special dosage modification is required for any of the populations that have been studied (e.g. gender, elderly).
3 DOSAGE FORMS AND STRENGTHSSingle-use glass vial containing JETREA 0.5 mg in 0.2 mL solution for intravitreal injection (2.5 mg/mL).
4 CONTRAINDICATIONSNone
5 WARNINGS AND PRECAUTIONS
5.1 Decreased VisionA decrease of ≥ 3 line of best corrected visual acuity (BCVA) was experienced by 5.6% of patients treated with JETREA and 3.2% of patients treated with vehicle in the controlled trials [see Clinical Studies (14)].The majority of these decreases in vision were due to progression of the condition with traction and many required surgical intervention. Patients should be monitored appropriately [see Dosage And Administration (2.4)].
5.2 Intravitreal Injection Procedure Associated EffectsIntravitreal injections are associated with intraocular inflammation / infection, intraocular hemorrhage and increased intraocular pressure (IOP). In the controlled trials, intraocular inflammation occurred in 7.1% of patients injected with JETREA vs. 3.7% of patients injected with vehicle. Most of the post-injection intraocular inflammation events were mild and transient. Intraocular hemorrhage occurred in 2.4% vs. 3.7% of patients injected with JETREA vs. vehicle, respectively. Increased intraocular pressure occurred in 4.1% vs. 5.3% of patients injected with JETREA vs. vehicle, respectively.
5.3 Potential for Lens SubluxationOne case of lens subluxation was reported in a premature infant who received an intravitreal injection of 0.175 mg (1.4 times higher than the recommended dose) [see Use in Specific Populations (8.4)]. Lens subluxation was observed in three animal species (monkey, rabbit, minipig) following a single intravitreal injection that achieved vitreous concentrations of ocriplasmin 1.4 times higher than achieved with the recommended treatment dose. Administration of a second intravitreal dose in monkeys, 28 days apart, produced lens subluxation in 100% of the treated eyes [see Nonclinical Toxicology (13.2)].
5.4 Retinal BreaksIn the controlled trials, the incidence of retinal detachment was 0.9% in the JETREA group and 1.6% in the vehicle group, while the incidence of retinal tear (without detachment) was 1.1% in the JETREA group and 2.7% in the vehicle group. Most of these events occurred during or after vitrectomy in both groups. The incidence of retinal detachment that occurred pre-vitrectomy was 0.4% in the JETREA group and none in the vehicle group, while the incidence of retinal tear (without detachment) that occurred pre-vitrectomy was none in the JETREA group and 0.5% in the vehicle group.
5.5 DyschromatopsiaDyschromatopsia (generally described as yellowish vision) was reported in 2% of all patients injected with JETREA. In approximately half of these dyschromatopsia cases there were also electroretinographic (ERG) changes reported (a- and b-wave amplitude decrease).
6 ADVERSE REACTIONSThe following adverse reactions are described below and elsewhere in the labeling:• Decreased Vision [see Warnings and Precautions (5.1)]• Intravitreal Injection Procedure Associated Effects [see Warnings and Precautions (5.2) and Dosage
And Administration (2.4)]• Potential for Lens Subluxation [see Warnings and Precautions (5.3)]• Retinal Breaks [see Warnings and Precautions (5.4) and Dosage And Administration (2.4)]• Dyschromatopsia [see Warnings and Precautions (5.5)]
6.1 Clinical Trials ExperienceBecause clinical trials are conducted under widely varying conditions, adverse reaction rates in one clinical trial of a drug cannot be directly compared with rates in the clinical trials of the same or another drug and may not reflect the rates observed in practice.Approximately 800 patients have been treated with an intravitreal injection of JETREA. Of these, 465 patients received an intravitreal injection of ocriplasmin 0.125 mg (187 patients received vehicle) in the 2 vehicle-controlled studies (Study 1 and Study 2).The most common adverse reactions (incidence 5% - 20% listed in descending order of frequency) in the vehicle-controlled clinical studies were: vitreous floaters, conjunctival hemorrhage, eye pain, photopsia, blurred vision, macular hole, reduced visual acuity, visual impairment, and retinal edema.Less common adverse reactions observed in the studies at a frequency of < 5% in patients treated with JETREA included macular edema, increased intraocular pressure, anterior chamber cell, photophobia, vitreous detachment, ocular discomfort, iritis, cataract, dry eye, metamorphopsia, pupillary reflex impaired, conjunctival hyperemia, retinal degeneration and visual symptoms perceived in the contralateral eye.Dyschromatopsia was reported in 2% of patients injected with JETREA, with the majority of cases reported from two uncontrolled clinical studies. In approximately half of these dyschromatopsia cases there were also electroretinographic (ERG) changes reported (a- and b-wave amplitude decrease).
6.2 ImmunogenicityAs with all therapeutic proteins, there is potential for immunogenicity. Immunogenicity for this product has not been evaluated.
255919 Je01-US-LT-04 255919 Je01-US-LT-04
Date: 23-05-2016 Draft: 01 - Op. RI003 EGG
4039
4142
4344
4546
4748
4950
5152
5354
55
Date: 29-06-2016 Draft: 02 - Op. RI003 EGG
Jetrea 2,5 mg/ml USA
05
Date: 07-07-2016 Draft: 03 - Op. RI003 EGGDate: 08-07-2016 Draft: 04 - Op. RI001 EGG
257130 Je01-US-LT-03
Date: 18-07-2016 Draft: 05 - Op. RI003 EGG
HIGHLIGHTS OF PRESCRIBING INFORMATIONThese highlights do not include all the information needed to use JETREA safely and effectively. See full prescribing information for JETREA
JETREA® (ocriplasmin) Intravitreal Injection, 2.5 mg/mLFor intravitreal injectionInitial U.S. Approval: 2012
INDICATIONS AND USAGEJETREA is a proteolytic enzyme indicated for the treatment of symptomatic vitreomacular adhesion. (1)
DOSAGE AND ADMINISTRATION• Must dilute before use. (2.1)• For single use ophthalmic intravitreal injection only. (2.1)• The recommended dose is 0.125 mg (0.1 mL of the diluted solution) administered by intravitreal
injection to the affected eye once as a single dose. (2.2)
DOSAGE FORMS AND STRENGTHSSingle-use glass vial containing JETREA 0.5 mg in 0.2 mL solution for intravitreal injection (2.5 mg/mL). (3)
CONTRAINDICATIONSNone. (4)
WARNINGS AND PRECAUTIONS• Decreases in vision due to progression of the condition with traction may occur requiring surgical
intervention. Patients should be monitored and instructed to report any symptoms without delay. (5.1)• Intravitreal injection procedure associated effects (intraocular inflammation/infection, intraocular
hemorrhage and increased IOP) may occur following an intravitreal injection. Patients should be monitored and instructed to report any symptoms without delay. (5.2)
• Potential for lens subluxation. (5.3)
ADVERSE REACTIONSThe most commonly reported reactions (≥ 5%) in patients treated with JETREA were vitreous floaters, conjunctival hemorrhage, eye pain, photopsia, blurred vision, macular hole, reduced visual acuity, visual impairment, and retinal edema. (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact ThromboGenics Inc. at 1-855-253-7396 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
See 17 for PATIENT COUNSELING INFORMATIONRevised: 03/2016
FULL PRESCRIBING INFORMATION: CONTENTS*
1 INDICATIONS AND USAGE
2 DOSAGE AND ADMINISTRATION2.1 General Dosing Information2.2 Dosing2.3 Preparation for Administration2.4 Administration and Monitoring
3 DOSAGE FORMS AND STRENGTHS
4 CONTRAINDICATIONS
5 WARNINGS AND PRECAUTIONS5.1 Decreased Vision5.2 Intravitreal Injection Procedure Associated Effects5.3 Potential for Lens Subluxation5.4 Retinal Breaks5.5 Dyschromatopsia
6 ADVERSE REACTIONS6.1 Clinical Trials Experience6.2 Immunogenicity6.3 Postmarketing Experience
8 USE IN SPECIFIC POPULATIONS8.1 Pregnancy8.3 Nursing Mothers8.4 Pediatric Use8.5 Geriatric Use
10 OVERDOSAGE
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY12.1 Mechanism of Action12.3 Pharmacokinetics
13 NONCLINICAL TOXICOLOGY13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility13.2 Animal Toxicology and/or Pharmacology
14 CLINICAL STUDIES
16 HOW SUPPLIED/STORAGE AND HANDLING
17 PATIENT COUNSELING INFORMATION
*Sections or subsections omitted from the full prescribing information are not listed.
FULL PRESCRIBING INFORMATION
1 INDICATIONS AND USAGEJETREA® is a proteolytic enzyme indicated for the treatment of symptomatic vitreomacular adhesion.
2 DOSAGE AND ADMINISTRATION
2.1 General Dosing InformationMust be diluted before use. For single-use ophthalmic intravitreal injection only. JETREA must only be administered by a qualified physician.
2.2 DosingThe recommended dose is 0.125 mg (0.1 mL of the diluted solution) administered by intravitreal injection to the affected eye once as a single dose.
2.3 Preparation for AdministrationTo prepare JETREA for intravitreal injection, adhere to the following instructions:1. Remove the vial (2.5 mg/mL corresponding to 0.5 mg ocriplasmin) from the freezer and allow to thaw
at room temperature (within a few minutes).2. Once completely thawed, remove the protective polypropylene flip-off cap from the vial (see Figure 1).
Figure 1:
3. The top of the vial should be disinfected with an alcohol wipe (see Figure 2).
Figure 2:
4. Using aseptic technique, add 0.2 mL of 0.9% w/v Sodium Chloride Injection, USP (sterile, preservative-free) into the JETREA vial (see Figure 3) and gently swirl the vial until the solutions are mixed (see Figure 4).
Figure 3:
Figure 4:
5. Visually inspect the vial for particulate matter. Only a clear, colorless solution without visible particles should be used.
6. Using aseptic technique, withdraw all of the diluted solution using a sterile #19 gauge needle (slightly tilt the vial to ease withdrawal) and discard the needle after withdrawal of the vial contents (see Figure 5). Do not use this needle for the intravitreal injection.
Figure 5:
7. Replace the needle with a sterile #30 gauge needle, carefully expel the air bubbles and excess drug from the syringe and adjust the dose to the 0.1 mL mark on the syringe (corresponding to 0.125 mg ocriplasmin) (see Figure 6).
Figure 6:
8. THE SOLUTION SHOULD BE USED IMMEDIATELY AS IT CONTAINS NO PRESERVATIVES.9. Discard the vial and any unused portion of the diluted solution after single use.
2.4 Administration and MonitoringThe intravitreal injection procedure should be carried out under controlled aseptic conditions, which include the use of sterile gloves, a sterile drape and a sterile eyelid speculum (or equivalent). Adequate anesthesia and a broad spectrum microbiocide should be administered according to standard medical practice. The injection needle should be inserted 3.5 - 4.0 mm posterior to the limbus aiming towards the center of the vitreous cavity, avoiding the horizontal meridian. The injection volume of 0.1 mL is then delivered into the mid-vitreous. Immediately following the intravitreal injection, patients should be monitored for elevation in intraocular pressure. Appropriate monitoring may consist of a check for perfusion of the optic nerve head or tonometry. If required, a sterile paracentesis needle should be available.Following intravitreal injection, patients should be instructed to report any symptoms suggestive of endophthalmitis or retinal detachment (e.g., eye pain, redness of the eye, photophobia, blurred or decreased vision) without delay [see Patient Counseling Information (17)].Each vial should only be used to provide a single injection for the treatment of a single eye. If the contralateral eye requires treatment, a new vial should be used and the sterile field, syringe, gloves, drapes, eyelid speculum, and injection needles should be changed before JETREA is administered to the other eye, however, treatment with JETREA in the other eye is not recommended within 7 days of the initial injection in order to monitor the post-injection course including the potential for decreased vision in the injected eye.Repeated administration of JETREA in the same eye is not recommended [see Nonclinical Toxicology (13.2)].After injection, any unused product must be discarded.No special dosage modification is required for any of the populations that have been studied (e.g. gender, elderly).
3 DOSAGE FORMS AND STRENGTHSSingle-use glass vial containing JETREA 0.5 mg in 0.2 mL solution for intravitreal injection (2.5 mg/mL).
4 CONTRAINDICATIONSNone
5 WARNINGS AND PRECAUTIONS
5.1 Decreased VisionA decrease of ≥ 3 line of best corrected visual acuity (BCVA) was experienced by 5.6% of patients treated with JETREA and 3.2% of patients treated with vehicle in the controlled trials [see Clinical Studies (14)].The majority of these decreases in vision were due to progression of the condition with traction and many required surgical intervention. Patients should be monitored appropriately [see Dosage And Administration (2.4)].
5.2 Intravitreal Injection Procedure Associated EffectsIntravitreal injections are associated with intraocular inflammation / infection, intraocular hemorrhage and increased intraocular pressure (IOP). In the controlled trials, intraocular inflammation occurred in 7.1% of patients injected with JETREA vs. 3.7% of patients injected with vehicle. Most of the post-injection intraocular inflammation events were mild and transient. Intraocular hemorrhage occurred in 2.4% vs. 3.7% of patients injected with JETREA vs. vehicle, respectively. Increased intraocular pressure occurred in 4.1% vs. 5.3% of patients injected with JETREA vs. vehicle, respectively.
5.3 Potential for Lens SubluxationOne case of lens subluxation was reported in a premature infant who received an intravitreal injection of 0.175 mg (1.4 times higher than the recommended dose) [see Use in Specific Populations (8.4)]. Lens subluxation was observed in three animal species (monkey, rabbit, minipig) following a single intravitreal injection that achieved vitreous concentrations of ocriplasmin 1.4 times higher than achieved with the recommended treatment dose. Administration of a second intravitreal dose in monkeys, 28 days apart, produced lens subluxation in 100% of the treated eyes [see Nonclinical Toxicology (13.2)].
5.4 Retinal BreaksIn the controlled trials, the incidence of retinal detachment was 0.9% in the JETREA group and 1.6% in the vehicle group, while the incidence of retinal tear (without detachment) was 1.1% in the JETREA group and 2.7% in the vehicle group. Most of these events occurred during or after vitrectomy in both groups. The incidence of retinal detachment that occurred pre-vitrectomy was 0.4% in the JETREA group and none in the vehicle group, while the incidence of retinal tear (without detachment) that occurred pre-vitrectomy was none in the JETREA group and 0.5% in the vehicle group.
5.5 DyschromatopsiaDyschromatopsia (generally described as yellowish vision) was reported in 2% of all patients injected with JETREA. In approximately half of these dyschromatopsia cases there were also electroretinographic (ERG) changes reported (a- and b-wave amplitude decrease).
6 ADVERSE REACTIONSThe following adverse reactions are described below and elsewhere in the labeling:• Decreased Vision [see Warnings and Precautions (5.1)]• Intravitreal Injection Procedure Associated Effects [see Warnings and Precautions (5.2) and Dosage
And Administration (2.4)]• Potential for Lens Subluxation [see Warnings and Precautions (5.3)]• Retinal Breaks [see Warnings and Precautions (5.4) and Dosage And Administration (2.4)]• Dyschromatopsia [see Warnings and Precautions (5.5)]
6.1 Clinical Trials ExperienceBecause clinical trials are conducted under widely varying conditions, adverse reaction rates in one clinical trial of a drug cannot be directly compared with rates in the clinical trials of the same or another drug and may not reflect the rates observed in practice.Approximately 800 patients have been treated with an intravitreal injection of JETREA. Of these, 465 patients received an intravitreal injection of ocriplasmin 0.125 mg (187 patients received vehicle) in the 2 vehicle-controlled studies (Study 1 and Study 2).The most common adverse reactions (incidence 5% - 20% listed in descending order of frequency) in the vehicle-controlled clinical studies were: vitreous floaters, conjunctival hemorrhage, eye pain, photopsia, blurred vision, macular hole, reduced visual acuity, visual impairment, and retinal edema.Less common adverse reactions observed in the studies at a frequency of < 5% in patients treated with JETREA included macular edema, increased intraocular pressure, anterior chamber cell, photophobia, vitreous detachment, ocular discomfort, iritis, cataract, dry eye, metamorphopsia, pupillary reflex impaired, conjunctival hyperemia, retinal degeneration and visual symptoms perceived in the contralateral eye.Dyschromatopsia was reported in 2% of patients injected with JETREA, with the majority of cases reported from two uncontrolled clinical studies. In approximately half of these dyschromatopsia cases there were also electroretinographic (ERG) changes reported (a- and b-wave amplitude decrease).
6.2 ImmunogenicityAs with all therapeutic proteins, there is potential for immunogenicity. Immunogenicity for this product has not been evaluated.
255919 Je01-US-LT-04 255919 Je01-US-LT-04

Date: 23-05-2016 Draft: 01 - Op. RI003 EGG
4039
4142
4344
4546
4748
4950
5152
5354
55
Date: 29-06-2016 Draft: 02 - Op. RI003 EGG
Jetrea 2,5 mg/ml USA
05
Date: 07-07-2016 Draft: 03 - Op. RI003 EGGDate: 08-07-2016 Draft: 04 - Op. RI001 EGG
257130 Je01-US-LT-03
Date: 18-07-2016 Draft: 05 - Op. RI003 EGG
HIGHLIGHTS OF PRESCRIBING INFORMATIONThese highlights do not include all the information needed to use JETREA safely and effectively. See full prescribing information for JETREA
JETREA® (ocriplasmin) Intravitreal Injection, 2.5 mg/mLFor intravitreal injectionInitial U.S. Approval: 2012
INDICATIONS AND USAGEJETREA is a proteolytic enzyme indicated for the treatment of symptomatic vitreomacular adhesion. (1)
DOSAGE AND ADMINISTRATION• Must dilute before use. (2.1)• For single use ophthalmic intravitreal injection only. (2.1)• The recommended dose is 0.125 mg (0.1 mL of the diluted solution) administered by intravitreal
injection to the affected eye once as a single dose. (2.2)
DOSAGE FORMS AND STRENGTHSSingle-use glass vial containing JETREA 0.5 mg in 0.2 mL solution for intravitreal injection (2.5 mg/mL). (3)
CONTRAINDICATIONSNone. (4)
WARNINGS AND PRECAUTIONS• Decreases in vision due to progression of the condition with traction may occur requiring surgical
intervention. Patients should be monitored and instructed to report any symptoms without delay. (5.1)• Intravitreal injection procedure associated effects (intraocular inflammation/infection, intraocular
hemorrhage and increased IOP) may occur following an intravitreal injection. Patients should be monitored and instructed to report any symptoms without delay. (5.2)
• Potential for lens subluxation. (5.3)
ADVERSE REACTIONSThe most commonly reported reactions (≥ 5%) in patients treated with JETREA were vitreous floaters, conjunctival hemorrhage, eye pain, photopsia, blurred vision, macular hole, reduced visual acuity, visual impairment, and retinal edema. (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact ThromboGenics Inc. at 1-855-253-7396 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
See 17 for PATIENT COUNSELING INFORMATIONRevised: 03/2016
FULL PRESCRIBING INFORMATION: CONTENTS*
1 INDICATIONS AND USAGE
2 DOSAGE AND ADMINISTRATION2.1 General Dosing Information2.2 Dosing2.3 Preparation for Administration2.4 Administration and Monitoring
3 DOSAGE FORMS AND STRENGTHS
4 CONTRAINDICATIONS
5 WARNINGS AND PRECAUTIONS5.1 Decreased Vision5.2 Intravitreal Injection Procedure Associated Effects5.3 Potential for Lens Subluxation5.4 Retinal Breaks5.5 Dyschromatopsia
6 ADVERSE REACTIONS6.1 Clinical Trials Experience6.2 Immunogenicity6.3 Postmarketing Experience
8 USE IN SPECIFIC POPULATIONS8.1 Pregnancy8.3 Nursing Mothers8.4 Pediatric Use8.5 Geriatric Use
10 OVERDOSAGE
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY12.1 Mechanism of Action12.3 Pharmacokinetics
13 NONCLINICAL TOXICOLOGY13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility13.2 Animal Toxicology and/or Pharmacology
14 CLINICAL STUDIES
16 HOW SUPPLIED/STORAGE AND HANDLING
17 PATIENT COUNSELING INFORMATION
*Sections or subsections omitted from the full prescribing information are not listed.
FULL PRESCRIBING INFORMATION
1 INDICATIONS AND USAGEJETREA® is a proteolytic enzyme indicated for the treatment of symptomatic vitreomacular adhesion.
2 DOSAGE AND ADMINISTRATION
2.1 General Dosing InformationMust be diluted before use. For single-use ophthalmic intravitreal injection only. JETREA must only be administered by a qualified physician.
2.2 DosingThe recommended dose is 0.125 mg (0.1 mL of the diluted solution) administered by intravitreal injection to the affected eye once as a single dose.
2.3 Preparation for AdministrationTo prepare JETREA for intravitreal injection, adhere to the following instructions:1. Remove the vial (2.5 mg/mL corresponding to 0.5 mg ocriplasmin) from the freezer and allow to thaw
at room temperature (within a few minutes).2. Once completely thawed, remove the protective polypropylene flip-off cap from the vial (see Figure 1).
Figure 1:
3. The top of the vial should be disinfected with an alcohol wipe (see Figure 2).
Figure 2:
4. Using aseptic technique, add 0.2 mL of 0.9% w/v Sodium Chloride Injection, USP (sterile, preservative-free) into the JETREA vial (see Figure 3) and gently swirl the vial until the solutions are mixed (see Figure 4).
Figure 3:
Figure 4:
5. Visually inspect the vial for particulate matter. Only a clear, colorless solution without visible particles should be used.
6. Using aseptic technique, withdraw all of the diluted solution using a sterile #19 gauge needle (slightly tilt the vial to ease withdrawal) and discard the needle after withdrawal of the vial contents (see Figure 5). Do not use this needle for the intravitreal injection.
Figure 5:
7. Replace the needle with a sterile #30 gauge needle, carefully expel the air bubbles and excess drug from the syringe and adjust the dose to the 0.1 mL mark on the syringe (corresponding to 0.125 mg ocriplasmin) (see Figure 6).
Figure 6:
8. THE SOLUTION SHOULD BE USED IMMEDIATELY AS IT CONTAINS NO PRESERVATIVES.9. Discard the vial and any unused portion of the diluted solution after single use.
2.4 Administration and MonitoringThe intravitreal injection procedure should be carried out under controlled aseptic conditions, which include the use of sterile gloves, a sterile drape and a sterile eyelid speculum (or equivalent). Adequate anesthesia and a broad spectrum microbiocide should be administered according to standard medical practice. The injection needle should be inserted 3.5 - 4.0 mm posterior to the limbus aiming towards the center of the vitreous cavity, avoiding the horizontal meridian. The injection volume of 0.1 mL is then delivered into the mid-vitreous. Immediately following the intravitreal injection, patients should be monitored for elevation in intraocular pressure. Appropriate monitoring may consist of a check for perfusion of the optic nerve head or tonometry. If required, a sterile paracentesis needle should be available.Following intravitreal injection, patients should be instructed to report any symptoms suggestive of endophthalmitis or retinal detachment (e.g., eye pain, redness of the eye, photophobia, blurred or decreased vision) without delay [see Patient Counseling Information (17)].Each vial should only be used to provide a single injection for the treatment of a single eye. If the contralateral eye requires treatment, a new vial should be used and the sterile field, syringe, gloves, drapes, eyelid speculum, and injection needles should be changed before JETREA is administered to the other eye, however, treatment with JETREA in the other eye is not recommended within 7 days of the initial injection in order to monitor the post-injection course including the potential for decreased vision in the injected eye.Repeated administration of JETREA in the same eye is not recommended [see Nonclinical Toxicology (13.2)].After injection, any unused product must be discarded.No special dosage modification is required for any of the populations that have been studied (e.g. gender, elderly).
3 DOSAGE FORMS AND STRENGTHSSingle-use glass vial containing JETREA 0.5 mg in 0.2 mL solution for intravitreal injection (2.5 mg/mL).
4 CONTRAINDICATIONSNone
5 WARNINGS AND PRECAUTIONS
5.1 Decreased VisionA decrease of ≥ 3 line of best corrected visual acuity (BCVA) was experienced by 5.6% of patients treated with JETREA and 3.2% of patients treated with vehicle in the controlled trials [see Clinical Studies (14)].The majority of these decreases in vision were due to progression of the condition with traction and many required surgical intervention. Patients should be monitored appropriately [see Dosage And Administration (2.4)].
5.2 Intravitreal Injection Procedure Associated EffectsIntravitreal injections are associated with intraocular inflammation / infection, intraocular hemorrhage and increased intraocular pressure (IOP). In the controlled trials, intraocular inflammation occurred in 7.1% of patients injected with JETREA vs. 3.7% of patients injected with vehicle. Most of the post-injection intraocular inflammation events were mild and transient. Intraocular hemorrhage occurred in 2.4% vs. 3.7% of patients injected with JETREA vs. vehicle, respectively. Increased intraocular pressure occurred in 4.1% vs. 5.3% of patients injected with JETREA vs. vehicle, respectively.
5.3 Potential for Lens SubluxationOne case of lens subluxation was reported in a premature infant who received an intravitreal injection of 0.175 mg (1.4 times higher than the recommended dose) [see Use in Specific Populations (8.4)]. Lens subluxation was observed in three animal species (monkey, rabbit, minipig) following a single intravitreal injection that achieved vitreous concentrations of ocriplasmin 1.4 times higher than achieved with the recommended treatment dose. Administration of a second intravitreal dose in monkeys, 28 days apart, produced lens subluxation in 100% of the treated eyes [see Nonclinical Toxicology (13.2)].
5.4 Retinal BreaksIn the controlled trials, the incidence of retinal detachment was 0.9% in the JETREA group and 1.6% in the vehicle group, while the incidence of retinal tear (without detachment) was 1.1% in the JETREA group and 2.7% in the vehicle group. Most of these events occurred during or after vitrectomy in both groups. The incidence of retinal detachment that occurred pre-vitrectomy was 0.4% in the JETREA group and none in the vehicle group, while the incidence of retinal tear (without detachment) that occurred pre-vitrectomy was none in the JETREA group and 0.5% in the vehicle group.
5.5 DyschromatopsiaDyschromatopsia (generally described as yellowish vision) was reported in 2% of all patients injected with JETREA. In approximately half of these dyschromatopsia cases there were also electroretinographic (ERG) changes reported (a- and b-wave amplitude decrease).
6 ADVERSE REACTIONSThe following adverse reactions are described below and elsewhere in the labeling:• Decreased Vision [see Warnings and Precautions (5.1)]• Intravitreal Injection Procedure Associated Effects [see Warnings and Precautions (5.2) and Dosage
And Administration (2.4)]• Potential for Lens Subluxation [see Warnings and Precautions (5.3)]• Retinal Breaks [see Warnings and Precautions (5.4) and Dosage And Administration (2.4)]• Dyschromatopsia [see Warnings and Precautions (5.5)]
6.1 Clinical Trials ExperienceBecause clinical trials are conducted under widely varying conditions, adverse reaction rates in one clinical trial of a drug cannot be directly compared with rates in the clinical trials of the same or another drug and may not reflect the rates observed in practice.Approximately 800 patients have been treated with an intravitreal injection of JETREA. Of these, 465 patients received an intravitreal injection of ocriplasmin 0.125 mg (187 patients received vehicle) in the 2 vehicle-controlled studies (Study 1 and Study 2).The most common adverse reactions (incidence 5% - 20% listed in descending order of frequency) in the vehicle-controlled clinical studies were: vitreous floaters, conjunctival hemorrhage, eye pain, photopsia, blurred vision, macular hole, reduced visual acuity, visual impairment, and retinal edema.Less common adverse reactions observed in the studies at a frequency of < 5% in patients treated with JETREA included macular edema, increased intraocular pressure, anterior chamber cell, photophobia, vitreous detachment, ocular discomfort, iritis, cataract, dry eye, metamorphopsia, pupillary reflex impaired, conjunctival hyperemia, retinal degeneration and visual symptoms perceived in the contralateral eye.Dyschromatopsia was reported in 2% of patients injected with JETREA, with the majority of cases reported from two uncontrolled clinical studies. In approximately half of these dyschromatopsia cases there were also electroretinographic (ERG) changes reported (a- and b-wave amplitude decrease).
6.2 ImmunogenicityAs with all therapeutic proteins, there is potential for immunogenicity. Immunogenicity for this product has not been evaluated.
255919 Je01-US-LT-04 255919 Je01-US-LT-04

Date: 23-05-2016 Draft: 01 - Op. RI003 EGG
4039
4142
4344
4546
4748
4950
5152
5354
55
Date: 29-06-2016 Draft: 02 - Op. RI003 EGG
Jetrea 2,5 mg/ml USA
05
Date: 07-07-2016 Draft: 03 - Op. RI003 EGGDate: 08-07-2016 Draft: 04 - Op. RI001 EGG
257130 Je01-US-LT-03
Date: 18-07-2016 Draft: 05 - Op. RI003 EGG
HIGHLIGHTS OF PRESCRIBING INFORMATIONThese highlights do not include all the information needed to use JETREA safely and effectively. See full prescribing information for JETREA
JETREA® (ocriplasmin) Intravitreal Injection, 2.5 mg/mLFor intravitreal injectionInitial U.S. Approval: 2012
INDICATIONS AND USAGEJETREA is a proteolytic enzyme indicated for the treatment of symptomatic vitreomacular adhesion. (1)
DOSAGE AND ADMINISTRATION• Must dilute before use. (2.1)• For single use ophthalmic intravitreal injection only. (2.1)• The recommended dose is 0.125 mg (0.1 mL of the diluted solution) administered by intravitreal
injection to the affected eye once as a single dose. (2.2)
DOSAGE FORMS AND STRENGTHSSingle-use glass vial containing JETREA 0.5 mg in 0.2 mL solution for intravitreal injection (2.5 mg/mL). (3)
CONTRAINDICATIONSNone. (4)
WARNINGS AND PRECAUTIONS• Decreases in vision due to progression of the condition with traction may occur requiring surgical
intervention. Patients should be monitored and instructed to report any symptoms without delay. (5.1)• Intravitreal injection procedure associated effects (intraocular inflammation/infection, intraocular
hemorrhage and increased IOP) may occur following an intravitreal injection. Patients should be monitored and instructed to report any symptoms without delay. (5.2)
• Potential for lens subluxation. (5.3)
ADVERSE REACTIONSThe most commonly reported reactions (≥ 5%) in patients treated with JETREA were vitreous floaters, conjunctival hemorrhage, eye pain, photopsia, blurred vision, macular hole, reduced visual acuity, visual impairment, and retinal edema. (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact ThromboGenics Inc. at 1-855-253-7396 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
See 17 for PATIENT COUNSELING INFORMATIONRevised: 03/2016
FULL PRESCRIBING INFORMATION: CONTENTS*
1 INDICATIONS AND USAGE
2 DOSAGE AND ADMINISTRATION2.1 General Dosing Information2.2 Dosing2.3 Preparation for Administration2.4 Administration and Monitoring
3 DOSAGE FORMS AND STRENGTHS
4 CONTRAINDICATIONS
5 WARNINGS AND PRECAUTIONS5.1 Decreased Vision5.2 Intravitreal Injection Procedure Associated Effects5.3 Potential for Lens Subluxation5.4 Retinal Breaks5.5 Dyschromatopsia
6 ADVERSE REACTIONS6.1 Clinical Trials Experience6.2 Immunogenicity6.3 Postmarketing Experience
8 USE IN SPECIFIC POPULATIONS8.1 Pregnancy8.3 Nursing Mothers8.4 Pediatric Use8.5 Geriatric Use
10 OVERDOSAGE
11 DESCRIPTION
12 CLINICAL PHARMACOLOGY12.1 Mechanism of Action12.3 Pharmacokinetics
13 NONCLINICAL TOXICOLOGY13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility13.2 Animal Toxicology and/or Pharmacology
14 CLINICAL STUDIES
16 HOW SUPPLIED/STORAGE AND HANDLING
17 PATIENT COUNSELING INFORMATION
*Sections or subsections omitted from the full prescribing information are not listed.
FULL PRESCRIBING INFORMATION
1 INDICATIONS AND USAGEJETREA® is a proteolytic enzyme indicated for the treatment of symptomatic vitreomacular adhesion.
2 DOSAGE AND ADMINISTRATION
2.1 General Dosing InformationMust be diluted before use. For single-use ophthalmic intravitreal injection only. JETREA must only be administered by a qualified physician.
2.2 DosingThe recommended dose is 0.125 mg (0.1 mL of the diluted solution) administered by intravitreal injection to the affected eye once as a single dose.
2.3 Preparation for AdministrationTo prepare JETREA for intravitreal injection, adhere to the following instructions:1. Remove the vial (2.5 mg/mL corresponding to 0.5 mg ocriplasmin) from the freezer and allow to thaw
at room temperature (within a few minutes).2. Once completely thawed, remove the protective polypropylene flip-off cap from the vial (see Figure 1).
Figure 1:
3. The top of the vial should be disinfected with an alcohol wipe (see Figure 2).
Figure 2:
4. Using aseptic technique, add 0.2 mL of 0.9% w/v Sodium Chloride Injection, USP (sterile, preservative-free) into the JETREA vial (see Figure 3) and gently swirl the vial until the solutions are mixed (see Figure 4).
Figure 3:
Figure 4:
5. Visually inspect the vial for particulate matter. Only a clear, colorless solution without visible particles should be used.
6. Using aseptic technique, withdraw all of the diluted solution using a sterile #19 gauge needle (slightly tilt the vial to ease withdrawal) and discard the needle after withdrawal of the vial contents (see Figure 5). Do not use this needle for the intravitreal injection.
Figure 5:
7. Replace the needle with a sterile #30 gauge needle, carefully expel the air bubbles and excess drug from the syringe and adjust the dose to the 0.1 mL mark on the syringe (corresponding to 0.125 mg ocriplasmin) (see Figure 6).
Figure 6:
8. THE SOLUTION SHOULD BE USED IMMEDIATELY AS IT CONTAINS NO PRESERVATIVES.9. Discard the vial and any unused portion of the diluted solution after single use.
2.4 Administration and MonitoringThe intravitreal injection procedure should be carried out under controlled aseptic conditions, which include the use of sterile gloves, a sterile drape and a sterile eyelid speculum (or equivalent). Adequate anesthesia and a broad spectrum microbiocide should be administered according to standard medical practice. The injection needle should be inserted 3.5 - 4.0 mm posterior to the limbus aiming towards the center of the vitreous cavity, avoiding the horizontal meridian. The injection volume of 0.1 mL is then delivered into the mid-vitreous. Immediately following the intravitreal injection, patients should be monitored for elevation in intraocular pressure. Appropriate monitoring may consist of a check for perfusion of the optic nerve head or tonometry. If required, a sterile paracentesis needle should be available.Following intravitreal injection, patients should be instructed to report any symptoms suggestive of endophthalmitis or retinal detachment (e.g., eye pain, redness of the eye, photophobia, blurred or decreased vision) without delay [see Patient Counseling Information (17)].Each vial should only be used to provide a single injection for the treatment of a single eye. If the contralateral eye requires treatment, a new vial should be used and the sterile field, syringe, gloves, drapes, eyelid speculum, and injection needles should be changed before JETREA is administered to the other eye, however, treatment with JETREA in the other eye is not recommended within 7 days of the initial injection in order to monitor the post-injection course including the potential for decreased vision in the injected eye.Repeated administration of JETREA in the same eye is not recommended [see Nonclinical Toxicology (13.2)].After injection, any unused product must be discarded.No special dosage modification is required for any of the populations that have been studied (e.g. gender, elderly).
3 DOSAGE FORMS AND STRENGTHSSingle-use glass vial containing JETREA 0.5 mg in 0.2 mL solution for intravitreal injection (2.5 mg/mL).
4 CONTRAINDICATIONSNone
5 WARNINGS AND PRECAUTIONS
5.1 Decreased VisionA decrease of ≥ 3 line of best corrected visual acuity (BCVA) was experienced by 5.6% of patients treated with JETREA and 3.2% of patients treated with vehicle in the controlled trials [see Clinical Studies (14)].The majority of these decreases in vision were due to progression of the condition with traction and many required surgical intervention. Patients should be monitored appropriately [see Dosage And Administration (2.4)].
5.2 Intravitreal Injection Procedure Associated EffectsIntravitreal injections are associated with intraocular inflammation / infection, intraocular hemorrhage and increased intraocular pressure (IOP). In the controlled trials, intraocular inflammation occurred in 7.1% of patients injected with JETREA vs. 3.7% of patients injected with vehicle. Most of the post-injection intraocular inflammation events were mild and transient. Intraocular hemorrhage occurred in 2.4% vs. 3.7% of patients injected with JETREA vs. vehicle, respectively. Increased intraocular pressure occurred in 4.1% vs. 5.3% of patients injected with JETREA vs. vehicle, respectively.
5.3 Potential for Lens SubluxationOne case of lens subluxation was reported in a premature infant who received an intravitreal injection of 0.175 mg (1.4 times higher than the recommended dose) [see Use in Specific Populations (8.4)]. Lens subluxation was observed in three animal species (monkey, rabbit, minipig) following a single intravitreal injection that achieved vitreous concentrations of ocriplasmin 1.4 times higher than achieved with the recommended treatment dose. Administration of a second intravitreal dose in monkeys, 28 days apart, produced lens subluxation in 100% of the treated eyes [see Nonclinical Toxicology (13.2)].
5.4 Retinal BreaksIn the controlled trials, the incidence of retinal detachment was 0.9% in the JETREA group and 1.6% in the vehicle group, while the incidence of retinal tear (without detachment) was 1.1% in the JETREA group and 2.7% in the vehicle group. Most of these events occurred during or after vitrectomy in both groups. The incidence of retinal detachment that occurred pre-vitrectomy was 0.4% in the JETREA group and none in the vehicle group, while the incidence of retinal tear (without detachment) that occurred pre-vitrectomy was none in the JETREA group and 0.5% in the vehicle group.
5.5 DyschromatopsiaDyschromatopsia (generally described as yellowish vision) was reported in 2% of all patients injected with JETREA. In approximately half of these dyschromatopsia cases there were also electroretinographic (ERG) changes reported (a- and b-wave amplitude decrease).
6 ADVERSE REACTIONSThe following adverse reactions are described below and elsewhere in the labeling:• Decreased Vision [see Warnings and Precautions (5.1)]• Intravitreal Injection Procedure Associated Effects [see Warnings and Precautions (5.2) and Dosage
And Administration (2.4)]• Potential for Lens Subluxation [see Warnings and Precautions (5.3)]• Retinal Breaks [see Warnings and Precautions (5.4) and Dosage And Administration (2.4)]• Dyschromatopsia [see Warnings and Precautions (5.5)]
6.1 Clinical Trials ExperienceBecause clinical trials are conducted under widely varying conditions, adverse reaction rates in one clinical trial of a drug cannot be directly compared with rates in the clinical trials of the same or another drug and may not reflect the rates observed in practice.Approximately 800 patients have been treated with an intravitreal injection of JETREA. Of these, 465 patients received an intravitreal injection of ocriplasmin 0.125 mg (187 patients received vehicle) in the 2 vehicle-controlled studies (Study 1 and Study 2).The most common adverse reactions (incidence 5% - 20% listed in descending order of frequency) in the vehicle-controlled clinical studies were: vitreous floaters, conjunctival hemorrhage, eye pain, photopsia, blurred vision, macular hole, reduced visual acuity, visual impairment, and retinal edema.Less common adverse reactions observed in the studies at a frequency of < 5% in patients treated with JETREA included macular edema, increased intraocular pressure, anterior chamber cell, photophobia, vitreous detachment, ocular discomfort, iritis, cataract, dry eye, metamorphopsia, pupillary reflex impaired, conjunctival hyperemia, retinal degeneration and visual symptoms perceived in the contralateral eye.Dyschromatopsia was reported in 2% of patients injected with JETREA, with the majority of cases reported from two uncontrolled clinical studies. In approximately half of these dyschromatopsia cases there were also electroretinographic (ERG) changes reported (a- and b-wave amplitude decrease).
6.2 ImmunogenicityAs with all therapeutic proteins, there is potential for immunogenicity. Immunogenicity for this product has not been evaluated.
255919 Je01-US-LT-04 255919 Je01-US-LT-04
Date: 23-05-2016 Draft: 01 - Op. RI003 EGG
4039
4142
4344
4546
4748
4950
5152
5354
55
Date: 29-06-2016 Draft: 02 - Op. RI003 EGG
Jetrea 2,5 mg/ml USA
05
Date: 07-07-2016 Draft: 03 - Op. RI003 EGGDate: 08-07-2016 Draft: 04 - Op. RI001 EGG
257130 Je01-US-LT-03
Date: 18-07-2016 Draft: 05 - Op. RI003 EGG
6.3 Postmarketing ExperienceNight blindness has been identified during post-approval use of JETREA. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
8 USE IN SPECIFIC POPULATIONS
8.1 PregnancyTeratogenic EffectsPregnancy Category C. Animal reproduction studies have not been conducted with ocriplasmin. There are no adequate and well-controlled studies of ocriplasmin in pregnant women. It is not known whether ocriplasmin can cause fetal harm when administered to a pregnant woman or can affect reproduction capacity. The systemic exposure to ocriplasmin is expected to be low after intravitreal injection of a single 0.125 mg dose. Assuming 100% systemic absorption (and a plasma volume of 2700 mL), the estimated plasma concentration is 46 ng/mL. JETREA should be given to a pregnant woman only if clearly needed.
8.3 Nursing MothersIt is not known whether ocriplasmin is excreted in human milk. Because many drugs are excreted in human milk, and because the potential for absorption and harm to infant growth and development exists, caution should be exercised when JETREA is administered to a nursing woman.
8.4 Pediatric UseThe use of JETREA in pediatric patients is not recommended. A single center, randomized, placebo controlled, double masked clinical study to investigate the safety and efficacy of a single intravitreal injection of 0.175 mg ocriplasmin in pediatric subjects as an adjunct to vitrectomy was conducted in 24 eyes of 22 patients. There were no statistical or clinical differences between groups for the induction of total macular PVD, any of the secondary endpoints or adverse events.
8.5 Geriatric UseIn the clinical studies, 384 and 145 patients were ≥ 65 years and of these 192 and 73 patients were ≥ 75 years in the JETREA and vehicle groups respectively. No significant differences in efficacy or safety were seen with increasing age in these studies.
10 OVERDOSAGEThe clinical data on the effects of JETREA overdose are limited. One case of accidental overdose of 0.250 mg ocriplasmin (twice the recommended dose) was reported to be associated with inflammation and a decrease in visual acuity.
11 DESCRIPTIONOcriplasmin is a recombinant truncated form of human plasmin with a molecular weight of 27.2 kDa produced by recombinant DNA technology in a Pichia pastoris expression system. JETREA is a sterile, clear and colorless solution with no preservatives in a single-use glass vial containing 0.5 mg ocriplasmin in 0.2 mL solution for intravitreal injection after dilution. Each vial contains 0.5 mg ocriplasmin (active) and 0.21 mg citric acid, 0.75 mg mannitol, sodium hydroxide (for pH adjustment) and water for injection. The pH of the solution is 3.1.
12 CLINICAL PHARMACOLOGY12.1 Mechanism of ActionOcriplasmin has proteolytic activity against protein components of the vitreous body and the vitreoretinal interface (VRI) (e.g. laminin, fibronectin and collagen), thereby dissolving the protein matrix responsible for the vitreomacular adhesion (VMA).
12.3 PharmacokineticsThe intravitreal pharmacokinetics of ocriplasmin were determined in a clinical study in patients scheduled for vitrectomy where 0.125 mg ocriplasmin (corresponding to an average concentration of 29 mcg ocriplasmin per mL vitreous volume [approximately 4.3 mL/eye]) was administered as a single intravitreal dose at different time points prior to vitrectomy. The mean ocriplasmin activity levels decreased with time from injection to time of sampling as illustrated in Table 1, according to a second-order kinetic process. At 24 hours post-injection the levels in the vitreous were below 3% of the theoretical concentration reached immediately after injection. Because of the small dose administered (0.125 mg), detectable levels of ocriplasmin in systemic circulation are not expected after intravitreal injection.
Table 1: Mean Ocriplasmin Activity Levels in Vitreous Samples after Intravitreal Injection of 0.125 mg Ocriplasmin
Time post-injection (subjects)
5-30min(n=8)
31-60min(n=8)
2-4hours(n=8)
24hr ± 2hr(n=4)
7days ± 1day (n=4)
Mean ± SD Ocriplasmin levels (mcg/mL)
12 ±7.6 8.1 ±5.2 2.6 ±1.6 0.5 ±0.3a < 0.27b
a 2 subjects below lower limit of detection, other 2 subjects at 0.88 and 0.57 mcg/mLb Lower limit of detection
Ocriplasmin enters the endogenous protein catabolism pathway through which it is rapidly inactivated via its interactions with protease inhibitor α2-antiplasmin or α2-macroglobulin.
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of FertilityNo carcinogenicity, mutagenicity or reproductive and developmental toxicity studies were conducted with ocriplasmin.
13.2 Animal Toxicology and/or PharmacologyThe ocular toxicity of ocriplasmin after a single intravitreal dose has been evaluated in rabbits, monkeys and minipigs. Ocriplasmin induced an inflammatory response and transient ERG changes in rabbits and monkeys, which tended to resolve over time. Lens subluxation was observed in the 3 species at ocriplasmin concentrations in the vitreous at or above 41 mcg/mL, a concentration 1.4-fold above the intended clinical concentration in the vitreous of 29 mcg/mL. Intraocular hemorrhage was observed in rabbits and monkeys.A second intravitreal administration of ocriplasmin (28 days apart) in monkeys at doses of 75 mcg/eye (41 mcg/mL vitreous) or 125 mcg/eye (68 mcg/mL vitreous) was associated with lens subluxation in all ocriplasmin treated eyes. Sustained increases in IOP occurred in two animals with lens subluxation. Microscopic findings in the eye included vitreous liquefaction, degeneration/disruption of the hyaloideocapsular ligament (with loss of ciliary zonular fibers), lens degeneration, mononuclear cell infiltration of the vitreous, and vacuolation of the retinal inner nuclear cell layer. These doses are 1.4-fold and 2.3-fold the intended clinical concentration in the vitreous of 29 mcg/mL, respectively.
14 CLINICAL STUDIESThe efficacy and safety of JETREA was demonstrated in two multicenter, randomized, double masked, vehicle-controlled, 6 month studies in patients with symptomatic vitreomacular adhesion (VMA). A total of 652 patients (JETREA 464, vehicle 188) were randomized in these 2 studies. Randomization was 2:1 (JETREA:vehicle) in Study 1 and 3:1 in Study 2.Patients were treated with a single injection of JETREA or vehicle. In both of the studies, the proportion of patients who achieved VMA resolution at Day 28 (i.e., achieved success on the primary endpoint) was significantly higher in the ocriplasmin group compared with the vehicle group through Month 6 (Table 2 and Figure 7).
Table 2: Proportion of Patients with VMA Resolution in the Study Eye (Study 1, Study 2: Full Analysis Set)
Study 1 Study 2
VehicleN=107
JETREAN=219
Difference(95% CI)
VehicleN=81
JETREAN=245
Difference(95% CI)
n (%) n (%) n (%) n (%)
Day 7 8 (7.5) 54 (24.7) 17.2 (9.6, 24.8) 1 (1.2) 36 (14.7) 13.5 (8.4, 18.5)
Day 14 12 (11.2) 57 (26.0) 14.8 (6.5, 23.2) 1 (1.2) 44 (18.0) 16.7 (11.4, 22.1)
Day 28 14 (13.1) 61 (27.9) 14.8 (6.0, 23.5) 5 (6.2) 62 (25.3) 19.1 (11.6, 26.7)
Month 3 16 (15.0) 58 (26.5) 11.5 (2.6, 20.5) 7 (8.6) 62 (25.3) 16.7 (8.5, 24.9)
Month 6 15 (14.0) 60 (27.4) 13.4 (4.5, 22.2) 10 (12.3) 65 (26.5) 14.2 (5.1, 23.2)
Figure 7: Proportion of Patients with VMA Resolution in the Study Eye (Study 1 and Study 2)
Study 1 JETREA
Study 2 JETREA
Study 1 Vehicle
Study 2 Vehicle
Days Post-Injection
At all post-injection days, p≤0.02 in Study 1 and p≤0.01 in Study 2
Total posterior vitreous detachment (PVD) induction in symptomatic vitreomacular adhesion patients was evaluated by B-scan ultrasound. A statistically significantly higher percentage of JETREA treated patients achieved total PVD at Day 28 compared to vehicle treated patients in Study 1 (16% vs. 6%; p=0.014) and in Study 2 (11% vs. 0%; p<0.01).The number of patients with at least 3 lines increase in visual acuity was numerically higher in the ocriplasmin
group compared to vehicle in both trials, however, the number of patients with at least a 3 lines decrease in visual acuity was also higher in the ocriplasmin group in one of the studies (Table 3 and Figure 8).
Table 3: Categorical Change from Baseline in BCVA at Month 6, Irrespective of Vitrectomy (Study 1 and Study 2)
Study 1 Study 2
JETREA Vehicle Difference JETREA Vehicle Difference
N=219 N=107 (95% CI) N=245 N=81 (95% CI)
≥ 3 line Improvement in BCVA
Month 6 28 (12.8%) 9 (8.4%) 4.4 (-2.5, 11.2)
29 (11.8%) 3 (3.8%) 8.1 (2.3, 13.9)
> 3 line Worsening in BCVA
Month 6 16 (7.3%) 2 (1.9%) 5.4 (1.1, 9.7) 10 (4.1%) 4 (5.0%) -0.9 (-6.3, 4.5)
Figure 8: Percentage of Patients with Gain or Loss of ≥ 3 Lines of BCVA at Protocol- Specified Visits
Study 1 JETREA Study 1 Vehicle Study 2 JETREA Study 2 Vehicle
16 HOW SUPPLIED/STORAGE AND HANDLINGEach vial of JETREA contains 0.5 mg ocriplasmin in 0.2 mL citric-buffered solution (2.5 mg/mL). JETREA is supplied in a 2 mL glass vial with a latex free rubber stopper. Vials are for single use only. NDC 24856-001-00StorageStore frozen at or below -4˚F (-20˚C). Protect the vials from light by storing in the original package until time of use.
17 PATIENT COUNSELING INFORMATIONIn the days following JETREA administration, patients are at risk of developing intraocular inflammation/infection. Advise patients to seek immediate care from an ophthalmologist if the eye becomes red, sensitive to light, painful, or develops a change in vision [see Warnings and Precautions (5.2)].Patients may experience temporary visual impairment after receiving an intravitreal injection of JETREA [see Warnings and Precautions (5.1)]. Advise patients to not drive or operate heavy machinery until this visual impairment has resolved. If visual impairment persists or decreases further, advise patients to seek care from an ophthalmologist.
Manufactured for: ThromboGenics, Inc.101 Wood Avenue South, Suite 610 Iselin, NJ 08830
U.S. License Number: 1866©2012, ThromboGenics, Inc. All rights reserved.Revised March 2016Initial U.S. Approval: 2012ThromboGenics U.S. patents: 7,445,775; 7,547,435; 7,914,783 and other pending patents.
255919Je01-US-LT-04
% V
MA
Res
olu
tio
n
Days
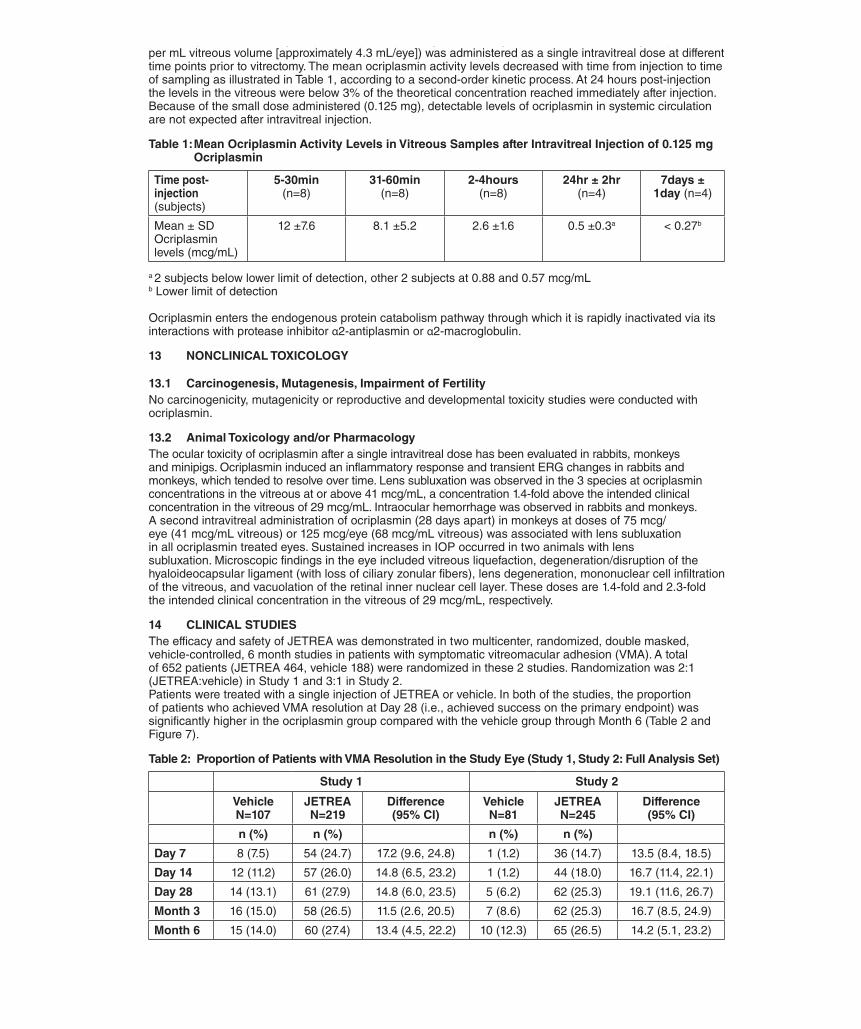
Date: 23-05-2016 Draft: 01 - Op. RI003 EGG
4039
4142
4344
4546
4748
4950
5152
5354
55
Date: 29-06-2016 Draft: 02 - Op. RI003 EGG
Jetrea 2,5 mg/ml USA
05
Date: 07-07-2016 Draft: 03 - Op. RI003 EGGDate: 08-07-2016 Draft: 04 - Op. RI001 EGG
257130 Je01-US-LT-03
Date: 18-07-2016 Draft: 05 - Op. RI003 EGG
6.3 Postmarketing ExperienceNight blindness has been identified during post-approval use of JETREA. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
8 USE IN SPECIFIC POPULATIONS
8.1 PregnancyTeratogenic EffectsPregnancy Category C. Animal reproduction studies have not been conducted with ocriplasmin. There are no adequate and well-controlled studies of ocriplasmin in pregnant women. It is not known whether ocriplasmin can cause fetal harm when administered to a pregnant woman or can affect reproduction capacity. The systemic exposure to ocriplasmin is expected to be low after intravitreal injection of a single 0.125 mg dose. Assuming 100% systemic absorption (and a plasma volume of 2700 mL), the estimated plasma concentration is 46 ng/mL. JETREA should be given to a pregnant woman only if clearly needed.
8.3 Nursing MothersIt is not known whether ocriplasmin is excreted in human milk. Because many drugs are excreted in human milk, and because the potential for absorption and harm to infant growth and development exists, caution should be exercised when JETREA is administered to a nursing woman.
8.4 Pediatric UseThe use of JETREA in pediatric patients is not recommended. A single center, randomized, placebo controlled, double masked clinical study to investigate the safety and efficacy of a single intravitreal injection of 0.175 mg ocriplasmin in pediatric subjects as an adjunct to vitrectomy was conducted in 24 eyes of 22 patients. There were no statistical or clinical differences between groups for the induction of total macular PVD, any of the secondary endpoints or adverse events.
8.5 Geriatric UseIn the clinical studies, 384 and 145 patients were ≥ 65 years and of these 192 and 73 patients were ≥ 75 years in the JETREA and vehicle groups respectively. No significant differences in efficacy or safety were seen with increasing age in these studies.
10 OVERDOSAGEThe clinical data on the effects of JETREA overdose are limited. One case of accidental overdose of 0.250 mg ocriplasmin (twice the recommended dose) was reported to be associated with inflammation and a decrease in visual acuity.
11 DESCRIPTIONOcriplasmin is a recombinant truncated form of human plasmin with a molecular weight of 27.2 kDa produced by recombinant DNA technology in a Pichia pastoris expression system. JETREA is a sterile, clear and colorless solution with no preservatives in a single-use glass vial containing 0.5 mg ocriplasmin in 0.2 mL solution for intravitreal injection after dilution. Each vial contains 0.5 mg ocriplasmin (active) and 0.21 mg citric acid, 0.75 mg mannitol, sodium hydroxide (for pH adjustment) and water for injection. The pH of the solution is 3.1.
12 CLINICAL PHARMACOLOGY12.1 Mechanism of ActionOcriplasmin has proteolytic activity against protein components of the vitreous body and the vitreoretinal interface (VRI) (e.g. laminin, fibronectin and collagen), thereby dissolving the protein matrix responsible for the vitreomacular adhesion (VMA).
12.3 PharmacokineticsThe intravitreal pharmacokinetics of ocriplasmin were determined in a clinical study in patients scheduled for vitrectomy where 0.125 mg ocriplasmin (corresponding to an average concentration of 29 mcg ocriplasmin per mL vitreous volume [approximately 4.3 mL/eye]) was administered as a single intravitreal dose at different time points prior to vitrectomy. The mean ocriplasmin activity levels decreased with time from injection to time of sampling as illustrated in Table 1, according to a second-order kinetic process. At 24 hours post-injection the levels in the vitreous were below 3% of the theoretical concentration reached immediately after injection. Because of the small dose administered (0.125 mg), detectable levels of ocriplasmin in systemic circulation are not expected after intravitreal injection.
Table 1: Mean Ocriplasmin Activity Levels in Vitreous Samples after Intravitreal Injection of 0.125 mg Ocriplasmin
Time post-injection (subjects)
5-30min(n=8)
31-60min(n=8)
2-4hours(n=8)
24hr ± 2hr(n=4)
7days ± 1day (n=4)
Mean ± SD Ocriplasmin levels (mcg/mL)
12 ±7.6 8.1 ±5.2 2.6 ±1.6 0.5 ±0.3a < 0.27b
a 2 subjects below lower limit of detection, other 2 subjects at 0.88 and 0.57 mcg/mLb Lower limit of detection
Ocriplasmin enters the endogenous protein catabolism pathway through which it is rapidly inactivated via its interactions with protease inhibitor α2-antiplasmin or α2-macroglobulin.
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of FertilityNo carcinogenicity, mutagenicity or reproductive and developmental toxicity studies were conducted with ocriplasmin.
13.2 Animal Toxicology and/or PharmacologyThe ocular toxicity of ocriplasmin after a single intravitreal dose has been evaluated in rabbits, monkeys and minipigs. Ocriplasmin induced an inflammatory response and transient ERG changes in rabbits and monkeys, which tended to resolve over time. Lens subluxation was observed in the 3 species at ocriplasmin concentrations in the vitreous at or above 41 mcg/mL, a concentration 1.4-fold above the intended clinical concentration in the vitreous of 29 mcg/mL. Intraocular hemorrhage was observed in rabbits and monkeys.A second intravitreal administration of ocriplasmin (28 days apart) in monkeys at doses of 75 mcg/eye (41 mcg/mL vitreous) or 125 mcg/eye (68 mcg/mL vitreous) was associated with lens subluxation in all ocriplasmin treated eyes. Sustained increases in IOP occurred in two animals with lens subluxation. Microscopic findings in the eye included vitreous liquefaction, degeneration/disruption of the hyaloideocapsular ligament (with loss of ciliary zonular fibers), lens degeneration, mononuclear cell infiltration of the vitreous, and vacuolation of the retinal inner nuclear cell layer. These doses are 1.4-fold and 2.3-fold the intended clinical concentration in the vitreous of 29 mcg/mL, respectively.
14 CLINICAL STUDIESThe efficacy and safety of JETREA was demonstrated in two multicenter, randomized, double masked, vehicle-controlled, 6 month studies in patients with symptomatic vitreomacular adhesion (VMA). A total of 652 patients (JETREA 464, vehicle 188) were randomized in these 2 studies. Randomization was 2:1 (JETREA:vehicle) in Study 1 and 3:1 in Study 2.Patients were treated with a single injection of JETREA or vehicle. In both of the studies, the proportion of patients who achieved VMA resolution at Day 28 (i.e., achieved success on the primary endpoint) was significantly higher in the ocriplasmin group compared with the vehicle group through Month 6 (Table 2 and Figure 7).
Table 2: Proportion of Patients with VMA Resolution in the Study Eye (Study 1, Study 2: Full Analysis Set)
Study 1 Study 2
VehicleN=107
JETREAN=219
Difference(95% CI)
VehicleN=81
JETREAN=245
Difference(95% CI)
n (%) n (%) n (%) n (%)
Day 7 8 (7.5) 54 (24.7) 17.2 (9.6, 24.8) 1 (1.2) 36 (14.7) 13.5 (8.4, 18.5)
Day 14 12 (11.2) 57 (26.0) 14.8 (6.5, 23.2) 1 (1.2) 44 (18.0) 16.7 (11.4, 22.1)
Day 28 14 (13.1) 61 (27.9) 14.8 (6.0, 23.5) 5 (6.2) 62 (25.3) 19.1 (11.6, 26.7)
Month 3 16 (15.0) 58 (26.5) 11.5 (2.6, 20.5) 7 (8.6) 62 (25.3) 16.7 (8.5, 24.9)
Month 6 15 (14.0) 60 (27.4) 13.4 (4.5, 22.2) 10 (12.3) 65 (26.5) 14.2 (5.1, 23.2)
Figure 7: Proportion of Patients with VMA Resolution in the Study Eye (Study 1 and Study 2)
Study 1 JETREA
Study 2 JETREA
Study 1 Vehicle
Study 2 Vehicle
Days Post-Injection
At all post-injection days, p≤0.02 in Study 1 and p≤0.01 in Study 2
Total posterior vitreous detachment (PVD) induction in symptomatic vitreomacular adhesion patients was evaluated by B-scan ultrasound. A statistically significantly higher percentage of JETREA treated patients achieved total PVD at Day 28 compared to vehicle treated patients in Study 1 (16% vs. 6%; p=0.014) and in Study 2 (11% vs. 0%; p<0.01).The number of patients with at least 3 lines increase in visual acuity was numerically higher in the ocriplasmin
group compared to vehicle in both trials, however, the number of patients with at least a 3 lines decrease in visual acuity was also higher in the ocriplasmin group in one of the studies (Table 3 and Figure 8).
Table 3: Categorical Change from Baseline in BCVA at Month 6, Irrespective of Vitrectomy (Study 1 and Study 2)
Study 1 Study 2
JETREA Vehicle Difference JETREA Vehicle Difference
N=219 N=107 (95% CI) N=245 N=81 (95% CI)
≥ 3 line Improvement in BCVA
Month 6 28 (12.8%) 9 (8.4%) 4.4 (-2.5, 11.2)
29 (11.8%) 3 (3.8%) 8.1 (2.3, 13.9)
> 3 line Worsening in BCVA
Month 6 16 (7.3%) 2 (1.9%) 5.4 (1.1, 9.7) 10 (4.1%) 4 (5.0%) -0.9 (-6.3, 4.5)
Figure 8: Percentage of Patients with Gain or Loss of ≥ 3 Lines of BCVA at Protocol- Specified Visits
Study 1 JETREA Study 1 Vehicle Study 2 JETREA Study 2 Vehicle
16 HOW SUPPLIED/STORAGE AND HANDLINGEach vial of JETREA contains 0.5 mg ocriplasmin in 0.2 mL citric-buffered solution (2.5 mg/mL). JETREA is supplied in a 2 mL glass vial with a latex free rubber stopper. Vials are for single use only. NDC 24856-001-00StorageStore frozen at or below -4˚F (-20˚C). Protect the vials from light by storing in the original package until time of use.
17 PATIENT COUNSELING INFORMATIONIn the days following JETREA administration, patients are at risk of developing intraocular inflammation/infection. Advise patients to seek immediate care from an ophthalmologist if the eye becomes red, sensitive to light, painful, or develops a change in vision [see Warnings and Precautions (5.2)].Patients may experience temporary visual impairment after receiving an intravitreal injection of JETREA [see Warnings and Precautions (5.1)]. Advise patients to not drive or operate heavy machinery until this visual impairment has resolved. If visual impairment persists or decreases further, advise patients to seek care from an ophthalmologist.
Manufactured for: ThromboGenics, Inc.101 Wood Avenue South, Suite 610 Iselin, NJ 08830
U.S. License Number: 1866©2012, ThromboGenics, Inc. All rights reserved.Revised March 2016Initial U.S. Approval: 2012ThromboGenics U.S. patents: 7,445,775; 7,547,435; 7,914,783 and other pending patents.
255919Je01-US-LT-04
% V
MA
Res
olu
tio
n
Days

Date: 23-05-2016 Draft: 01 - Op. RI003 EGG
4039
4142
4344
4546
4748
4950
5152
5354
55
Date: 29-06-2016 Draft: 02 - Op. RI003 EGG
Jetrea 2,5 mg/ml USA
05
Date: 07-07-2016 Draft: 03 - Op. RI003 EGGDate: 08-07-2016 Draft: 04 - Op. RI001 EGG
257130 Je01-US-LT-03
Date: 18-07-2016 Draft: 05 - Op. RI003 EGG
6.3 Postmarketing ExperienceNight blindness has been identified during post-approval use of JETREA. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
8 USE IN SPECIFIC POPULATIONS
8.1 PregnancyTeratogenic EffectsPregnancy Category C. Animal reproduction studies have not been conducted with ocriplasmin. There are no adequate and well-controlled studies of ocriplasmin in pregnant women. It is not known whether ocriplasmin can cause fetal harm when administered to a pregnant woman or can affect reproduction capacity. The systemic exposure to ocriplasmin is expected to be low after intravitreal injection of a single 0.125 mg dose. Assuming 100% systemic absorption (and a plasma volume of 2700 mL), the estimated plasma concentration is 46 ng/mL. JETREA should be given to a pregnant woman only if clearly needed.
8.3 Nursing MothersIt is not known whether ocriplasmin is excreted in human milk. Because many drugs are excreted in human milk, and because the potential for absorption and harm to infant growth and development exists, caution should be exercised when JETREA is administered to a nursing woman.
8.4 Pediatric UseThe use of JETREA in pediatric patients is not recommended. A single center, randomized, placebo controlled, double masked clinical study to investigate the safety and efficacy of a single intravitreal injection of 0.175 mg ocriplasmin in pediatric subjects as an adjunct to vitrectomy was conducted in 24 eyes of 22 patients. There were no statistical or clinical differences between groups for the induction of total macular PVD, any of the secondary endpoints or adverse events.
8.5 Geriatric UseIn the clinical studies, 384 and 145 patients were ≥ 65 years and of these 192 and 73 patients were ≥ 75 years in the JETREA and vehicle groups respectively. No significant differences in efficacy or safety were seen with increasing age in these studies.
10 OVERDOSAGEThe clinical data on the effects of JETREA overdose are limited. One case of accidental overdose of 0.250 mg ocriplasmin (twice the recommended dose) was reported to be associated with inflammation and a decrease in visual acuity.
11 DESCRIPTIONOcriplasmin is a recombinant truncated form of human plasmin with a molecular weight of 27.2 kDa produced by recombinant DNA technology in a Pichia pastoris expression system. JETREA is a sterile, clear and colorless solution with no preservatives in a single-use glass vial containing 0.5 mg ocriplasmin in 0.2 mL solution for intravitreal injection after dilution. Each vial contains 0.5 mg ocriplasmin (active) and 0.21 mg citric acid, 0.75 mg mannitol, sodium hydroxide (for pH adjustment) and water for injection. The pH of the solution is 3.1.
12 CLINICAL PHARMACOLOGY12.1 Mechanism of ActionOcriplasmin has proteolytic activity against protein components of the vitreous body and the vitreoretinal interface (VRI) (e.g. laminin, fibronectin and collagen), thereby dissolving the protein matrix responsible for the vitreomacular adhesion (VMA).
12.3 PharmacokineticsThe intravitreal pharmacokinetics of ocriplasmin were determined in a clinical study in patients scheduled for vitrectomy where 0.125 mg ocriplasmin (corresponding to an average concentration of 29 mcg ocriplasmin per mL vitreous volume [approximately 4.3 mL/eye]) was administered as a single intravitreal dose at different time points prior to vitrectomy. The mean ocriplasmin activity levels decreased with time from injection to time of sampling as illustrated in Table 1, according to a second-order kinetic process. At 24 hours post-injection the levels in the vitreous were below 3% of the theoretical concentration reached immediately after injection. Because of the small dose administered (0.125 mg), detectable levels of ocriplasmin in systemic circulation are not expected after intravitreal injection.
Table 1: Mean Ocriplasmin Activity Levels in Vitreous Samples after Intravitreal Injection of 0.125 mg Ocriplasmin
Time post-injection (subjects)
5-30min(n=8)
31-60min(n=8)
2-4hours(n=8)
24hr ± 2hr(n=4)
7days ± 1day (n=4)
Mean ± SD Ocriplasmin levels (mcg/mL)
12 ±7.6 8.1 ±5.2 2.6 ±1.6 0.5 ±0.3a < 0.27b
a 2 subjects below lower limit of detection, other 2 subjects at 0.88 and 0.57 mcg/mLb Lower limit of detection
Ocriplasmin enters the endogenous protein catabolism pathway through which it is rapidly inactivated via its interactions with protease inhibitor α2-antiplasmin or α2-macroglobulin.
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of FertilityNo carcinogenicity, mutagenicity or reproductive and developmental toxicity studies were conducted with ocriplasmin.
13.2 Animal Toxicology and/or PharmacologyThe ocular toxicity of ocriplasmin after a single intravitreal dose has been evaluated in rabbits, monkeys and minipigs. Ocriplasmin induced an inflammatory response and transient ERG changes in rabbits and monkeys, which tended to resolve over time. Lens subluxation was observed in the 3 species at ocriplasmin concentrations in the vitreous at or above 41 mcg/mL, a concentration 1.4-fold above the intended clinical concentration in the vitreous of 29 mcg/mL. Intraocular hemorrhage was observed in rabbits and monkeys.A second intravitreal administration of ocriplasmin (28 days apart) in monkeys at doses of 75 mcg/eye (41 mcg/mL vitreous) or 125 mcg/eye (68 mcg/mL vitreous) was associated with lens subluxation in all ocriplasmin treated eyes. Sustained increases in IOP occurred in two animals with lens subluxation. Microscopic findings in the eye included vitreous liquefaction, degeneration/disruption of the hyaloideocapsular ligament (with loss of ciliary zonular fibers), lens degeneration, mononuclear cell infiltration of the vitreous, and vacuolation of the retinal inner nuclear cell layer. These doses are 1.4-fold and 2.3-fold the intended clinical concentration in the vitreous of 29 mcg/mL, respectively.
14 CLINICAL STUDIESThe efficacy and safety of JETREA was demonstrated in two multicenter, randomized, double masked, vehicle-controlled, 6 month studies in patients with symptomatic vitreomacular adhesion (VMA). A total of 652 patients (JETREA 464, vehicle 188) were randomized in these 2 studies. Randomization was 2:1 (JETREA:vehicle) in Study 1 and 3:1 in Study 2.Patients were treated with a single injection of JETREA or vehicle. In both of the studies, the proportion of patients who achieved VMA resolution at Day 28 (i.e., achieved success on the primary endpoint) was significantly higher in the ocriplasmin group compared with the vehicle group through Month 6 (Table 2 and Figure 7).
Table 2: Proportion of Patients with VMA Resolution in the Study Eye (Study 1, Study 2: Full Analysis Set)
Study 1 Study 2
VehicleN=107
JETREAN=219
Difference(95% CI)
VehicleN=81
JETREAN=245
Difference(95% CI)
n (%) n (%) n (%) n (%)
Day 7 8 (7.5) 54 (24.7) 17.2 (9.6, 24.8) 1 (1.2) 36 (14.7) 13.5 (8.4, 18.5)
Day 14 12 (11.2) 57 (26.0) 14.8 (6.5, 23.2) 1 (1.2) 44 (18.0) 16.7 (11.4, 22.1)
Day 28 14 (13.1) 61 (27.9) 14.8 (6.0, 23.5) 5 (6.2) 62 (25.3) 19.1 (11.6, 26.7)
Month 3 16 (15.0) 58 (26.5) 11.5 (2.6, 20.5) 7 (8.6) 62 (25.3) 16.7 (8.5, 24.9)
Month 6 15 (14.0) 60 (27.4) 13.4 (4.5, 22.2) 10 (12.3) 65 (26.5) 14.2 (5.1, 23.2)
Figure 7: Proportion of Patients with VMA Resolution in the Study Eye (Study 1 and Study 2)
Study 1 JETREA
Study 2 JETREA
Study 1 Vehicle
Study 2 Vehicle
Days Post-Injection
At all post-injection days, p≤0.02 in Study 1 and p≤0.01 in Study 2
Total posterior vitreous detachment (PVD) induction in symptomatic vitreomacular adhesion patients was evaluated by B-scan ultrasound. A statistically significantly higher percentage of JETREA treated patients achieved total PVD at Day 28 compared to vehicle treated patients in Study 1 (16% vs. 6%; p=0.014) and in Study 2 (11% vs. 0%; p<0.01).The number of patients with at least 3 lines increase in visual acuity was numerically higher in the ocriplasmin
group compared to vehicle in both trials, however, the number of patients with at least a 3 lines decrease in visual acuity was also higher in the ocriplasmin group in one of the studies (Table 3 and Figure 8).
Table 3: Categorical Change from Baseline in BCVA at Month 6, Irrespective of Vitrectomy (Study 1 and Study 2)
Study 1 Study 2
JETREA Vehicle Difference JETREA Vehicle Difference
N=219 N=107 (95% CI) N=245 N=81 (95% CI)
≥ 3 line Improvement in BCVA
Month 6 28 (12.8%) 9 (8.4%) 4.4 (-2.5, 11.2)
29 (11.8%) 3 (3.8%) 8.1 (2.3, 13.9)
> 3 line Worsening in BCVA
Month 6 16 (7.3%) 2 (1.9%) 5.4 (1.1, 9.7) 10 (4.1%) 4 (5.0%) -0.9 (-6.3, 4.5)
Figure 8: Percentage of Patients with Gain or Loss of ≥ 3 Lines of BCVA at Protocol- Specified Visits
Study 1 JETREA Study 1 Vehicle Study 2 JETREA Study 2 Vehicle
16 HOW SUPPLIED/STORAGE AND HANDLINGEach vial of JETREA contains 0.5 mg ocriplasmin in 0.2 mL citric-buffered solution (2.5 mg/mL). JETREA is supplied in a 2 mL glass vial with a latex free rubber stopper. Vials are for single use only. NDC 24856-001-00StorageStore frozen at or below -4˚F (-20˚C). Protect the vials from light by storing in the original package until time of use.
17 PATIENT COUNSELING INFORMATIONIn the days following JETREA administration, patients are at risk of developing intraocular inflammation/infection. Advise patients to seek immediate care from an ophthalmologist if the eye becomes red, sensitive to light, painful, or develops a change in vision [see Warnings and Precautions (5.2)].Patients may experience temporary visual impairment after receiving an intravitreal injection of JETREA [see Warnings and Precautions (5.1)]. Advise patients to not drive or operate heavy machinery until this visual impairment has resolved. If visual impairment persists or decreases further, advise patients to seek care from an ophthalmologist.
Manufactured for: ThromboGenics, Inc.101 Wood Avenue South, Suite 610 Iselin, NJ 08830
U.S. License Number: 1866©2012, ThromboGenics, Inc. All rights reserved.Revised March 2016Initial U.S. Approval: 2012ThromboGenics U.S. patents: 7,445,775; 7,547,435; 7,914,783 and other pending patents.
255919Je01-US-LT-04
% V
MA
Res
olu
tio
n
Days
Date: 23-05-2016 Draft: 01 - Op. RI003 EGG
4039
4142
4344
4546
4748
4950
5152
5354
55
Date: 29-06-2016 Draft: 02 - Op. RI003 EGG
Jetrea 2,5 mg/ml USA
05
Date: 07-07-2016 Draft: 03 - Op. RI003 EGGDate: 08-07-2016 Draft: 04 - Op. RI001 EGG
257130 Je01-US-LT-03
Date: 18-07-2016 Draft: 05 - Op. RI003 EGG
6.3 Postmarketing ExperienceNight blindness has been identified during post-approval use of JETREA. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
8 USE IN SPECIFIC POPULATIONS
8.1 PregnancyTeratogenic EffectsPregnancy Category C. Animal reproduction studies have not been conducted with ocriplasmin. There are no adequate and well-controlled studies of ocriplasmin in pregnant women. It is not known whether ocriplasmin can cause fetal harm when administered to a pregnant woman or can affect reproduction capacity. The systemic exposure to ocriplasmin is expected to be low after intravitreal injection of a single 0.125 mg dose. Assuming 100% systemic absorption (and a plasma volume of 2700 mL), the estimated plasma concentration is 46 ng/mL. JETREA should be given to a pregnant woman only if clearly needed.
8.3 Nursing MothersIt is not known whether ocriplasmin is excreted in human milk. Because many drugs are excreted in human milk, and because the potential for absorption and harm to infant growth and development exists, caution should be exercised when JETREA is administered to a nursing woman.
8.4 Pediatric UseThe use of JETREA in pediatric patients is not recommended. A single center, randomized, placebo controlled, double masked clinical study to investigate the safety and efficacy of a single intravitreal injection of 0.175 mg ocriplasmin in pediatric subjects as an adjunct to vitrectomy was conducted in 24 eyes of 22 patients. There were no statistical or clinical differences between groups for the induction of total macular PVD, any of the secondary endpoints or adverse events.
8.5 Geriatric UseIn the clinical studies, 384 and 145 patients were ≥ 65 years and of these 192 and 73 patients were ≥ 75 years in the JETREA and vehicle groups respectively. No significant differences in efficacy or safety were seen with increasing age in these studies.
10 OVERDOSAGEThe clinical data on the effects of JETREA overdose are limited. One case of accidental overdose of 0.250 mg ocriplasmin (twice the recommended dose) was reported to be associated with inflammation and a decrease in visual acuity.
11 DESCRIPTIONOcriplasmin is a recombinant truncated form of human plasmin with a molecular weight of 27.2 kDa produced by recombinant DNA technology in a Pichia pastoris expression system. JETREA is a sterile, clear and colorless solution with no preservatives in a single-use glass vial containing 0.5 mg ocriplasmin in 0.2 mL solution for intravitreal injection after dilution. Each vial contains 0.5 mg ocriplasmin (active) and 0.21 mg citric acid, 0.75 mg mannitol, sodium hydroxide (for pH adjustment) and water for injection. The pH of the solution is 3.1.
12 CLINICAL PHARMACOLOGY12.1 Mechanism of ActionOcriplasmin has proteolytic activity against protein components of the vitreous body and the vitreoretinal interface (VRI) (e.g. laminin, fibronectin and collagen), thereby dissolving the protein matrix responsible for the vitreomacular adhesion (VMA).
12.3 PharmacokineticsThe intravitreal pharmacokinetics of ocriplasmin were determined in a clinical study in patients scheduled for vitrectomy where 0.125 mg ocriplasmin (corresponding to an average concentration of 29 mcg ocriplasmin per mL vitreous volume [approximately 4.3 mL/eye]) was administered as a single intravitreal dose at different time points prior to vitrectomy. The mean ocriplasmin activity levels decreased with time from injection to time of sampling as illustrated in Table 1, according to a second-order kinetic process. At 24 hours post-injection the levels in the vitreous were below 3% of the theoretical concentration reached immediately after injection. Because of the small dose administered (0.125 mg), detectable levels of ocriplasmin in systemic circulation are not expected after intravitreal injection.
Table 1: Mean Ocriplasmin Activity Levels in Vitreous Samples after Intravitreal Injection of 0.125 mg Ocriplasmin
Time post-injection (subjects)
5-30min(n=8)
31-60min(n=8)
2-4hours(n=8)
24hr ± 2hr(n=4)
7days ± 1day (n=4)
Mean ± SD Ocriplasmin levels (mcg/mL)
12 ±7.6 8.1 ±5.2 2.6 ±1.6 0.5 ±0.3a < 0.27b
a 2 subjects below lower limit of detection, other 2 subjects at 0.88 and 0.57 mcg/mLb Lower limit of detection
Ocriplasmin enters the endogenous protein catabolism pathway through which it is rapidly inactivated via its interactions with protease inhibitor α2-antiplasmin or α2-macroglobulin.
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of FertilityNo carcinogenicity, mutagenicity or reproductive and developmental toxicity studies were conducted with ocriplasmin.
13.2 Animal Toxicology and/or PharmacologyThe ocular toxicity of ocriplasmin after a single intravitreal dose has been evaluated in rabbits, monkeys and minipigs. Ocriplasmin induced an inflammatory response and transient ERG changes in rabbits and monkeys, which tended to resolve over time. Lens subluxation was observed in the 3 species at ocriplasmin concentrations in the vitreous at or above 41 mcg/mL, a concentration 1.4-fold above the intended clinical concentration in the vitreous of 29 mcg/mL. Intraocular hemorrhage was observed in rabbits and monkeys.A second intravitreal administration of ocriplasmin (28 days apart) in monkeys at doses of 75 mcg/eye (41 mcg/mL vitreous) or 125 mcg/eye (68 mcg/mL vitreous) was associated with lens subluxation in all ocriplasmin treated eyes. Sustained increases in IOP occurred in two animals with lens subluxation. Microscopic findings in the eye included vitreous liquefaction, degeneration/disruption of the hyaloideocapsular ligament (with loss of ciliary zonular fibers), lens degeneration, mononuclear cell infiltration of the vitreous, and vacuolation of the retinal inner nuclear cell layer. These doses are 1.4-fold and 2.3-fold the intended clinical concentration in the vitreous of 29 mcg/mL, respectively.
14 CLINICAL STUDIESThe efficacy and safety of JETREA was demonstrated in two multicenter, randomized, double masked, vehicle-controlled, 6 month studies in patients with symptomatic vitreomacular adhesion (VMA). A total of 652 patients (JETREA 464, vehicle 188) were randomized in these 2 studies. Randomization was 2:1 (JETREA:vehicle) in Study 1 and 3:1 in Study 2.Patients were treated with a single injection of JETREA or vehicle. In both of the studies, the proportion of patients who achieved VMA resolution at Day 28 (i.e., achieved success on the primary endpoint) was significantly higher in the ocriplasmin group compared with the vehicle group through Month 6 (Table 2 and Figure 7).
Table 2: Proportion of Patients with VMA Resolution in the Study Eye (Study 1, Study 2: Full Analysis Set)
Study 1 Study 2
VehicleN=107
JETREAN=219
Difference(95% CI)
VehicleN=81
JETREAN=245
Difference(95% CI)
n (%) n (%) n (%) n (%)
Day 7 8 (7.5) 54 (24.7) 17.2 (9.6, 24.8) 1 (1.2) 36 (14.7) 13.5 (8.4, 18.5)
Day 14 12 (11.2) 57 (26.0) 14.8 (6.5, 23.2) 1 (1.2) 44 (18.0) 16.7 (11.4, 22.1)
Day 28 14 (13.1) 61 (27.9) 14.8 (6.0, 23.5) 5 (6.2) 62 (25.3) 19.1 (11.6, 26.7)
Month 3 16 (15.0) 58 (26.5) 11.5 (2.6, 20.5) 7 (8.6) 62 (25.3) 16.7 (8.5, 24.9)
Month 6 15 (14.0) 60 (27.4) 13.4 (4.5, 22.2) 10 (12.3) 65 (26.5) 14.2 (5.1, 23.2)
Figure 7: Proportion of Patients with VMA Resolution in the Study Eye (Study 1 and Study 2)
Study 1 JETREA
Study 2 JETREA
Study 1 Vehicle
Study 2 Vehicle
Days Post-Injection
At all post-injection days, p≤0.02 in Study 1 and p≤0.01 in Study 2
Total posterior vitreous detachment (PVD) induction in symptomatic vitreomacular adhesion patients was evaluated by B-scan ultrasound. A statistically significantly higher percentage of JETREA treated patients achieved total PVD at Day 28 compared to vehicle treated patients in Study 1 (16% vs. 6%; p=0.014) and in Study 2 (11% vs. 0%; p<0.01).The number of patients with at least 3 lines increase in visual acuity was numerically higher in the ocriplasmin
group compared to vehicle in both trials, however, the number of patients with at least a 3 lines decrease in visual acuity was also higher in the ocriplasmin group in one of the studies (Table 3 and Figure 8).
Table 3: Categorical Change from Baseline in BCVA at Month 6, Irrespective of Vitrectomy (Study 1 and Study 2)
Study 1 Study 2
JETREA Vehicle Difference JETREA Vehicle Difference
N=219 N=107 (95% CI) N=245 N=81 (95% CI)
≥ 3 line Improvement in BCVA
Month 6 28 (12.8%) 9 (8.4%) 4.4 (-2.5, 11.2)
29 (11.8%) 3 (3.8%) 8.1 (2.3, 13.9)
> 3 line Worsening in BCVA
Month 6 16 (7.3%) 2 (1.9%) 5.4 (1.1, 9.7) 10 (4.1%) 4 (5.0%) -0.9 (-6.3, 4.5)
Figure 8: Percentage of Patients with Gain or Loss of ≥ 3 Lines of BCVA at Protocol- Specified Visits
Study 1 JETREA Study 1 Vehicle Study 2 JETREA Study 2 Vehicle
16 HOW SUPPLIED/STORAGE AND HANDLINGEach vial of JETREA contains 0.5 mg ocriplasmin in 0.2 mL citric-buffered solution (2.5 mg/mL). JETREA is supplied in a 2 mL glass vial with a latex free rubber stopper. Vials are for single use only. NDC 24856-001-00StorageStore frozen at or below -4˚F (-20˚C). Protect the vials from light by storing in the original package until time of use.
17 PATIENT COUNSELING INFORMATIONIn the days following JETREA administration, patients are at risk of developing intraocular inflammation/infection. Advise patients to seek immediate care from an ophthalmologist if the eye becomes red, sensitive to light, painful, or develops a change in vision [see Warnings and Precautions (5.2)].Patients may experience temporary visual impairment after receiving an intravitreal injection of JETREA [see Warnings and Precautions (5.1)]. Advise patients to not drive or operate heavy machinery until this visual impairment has resolved. If visual impairment persists or decreases further, advise patients to seek care from an ophthalmologist.
Manufactured for: ThromboGenics, Inc.101 Wood Avenue South, Suite 610 Iselin, NJ 08830
U.S. License Number: 1866©2012, ThromboGenics, Inc. All rights reserved.Revised March 2016Initial U.S. Approval: 2012ThromboGenics U.S. patents: 7,445,775; 7,547,435; 7,914,783 and other pending patents.
255919Je01-US-LT-04
% V
MA
Res
olu
tio
n
Days

Date: 23-05-2016 Draft: 01 - Op. RI003 EGG
4039
4142
4344
4546
4748
4950
5152
5354
55
Date: 29-06-2016 Draft: 02 - Op. RI003 EGG
Jetrea 2,5 mg/ml USA
05
Date: 07-07-2016 Draft: 03 - Op. RI003 EGGDate: 08-07-2016 Draft: 04 - Op. RI001 EGG
257130 Je01-US-LT-03
Date: 18-07-2016 Draft: 05 - Op. RI003 EGG
6.3 Postmarketing ExperienceNight blindness has been identified during post-approval use of JETREA. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
8 USE IN SPECIFIC POPULATIONS
8.1 PregnancyTeratogenic EffectsPregnancy Category C. Animal reproduction studies have not been conducted with ocriplasmin. There are no adequate and well-controlled studies of ocriplasmin in pregnant women. It is not known whether ocriplasmin can cause fetal harm when administered to a pregnant woman or can affect reproduction capacity. The systemic exposure to ocriplasmin is expected to be low after intravitreal injection of a single 0.125 mg dose. Assuming 100% systemic absorption (and a plasma volume of 2700 mL), the estimated plasma concentration is 46 ng/mL. JETREA should be given to a pregnant woman only if clearly needed.
8.3 Nursing MothersIt is not known whether ocriplasmin is excreted in human milk. Because many drugs are excreted in human milk, and because the potential for absorption and harm to infant growth and development exists, caution should be exercised when JETREA is administered to a nursing woman.
8.4 Pediatric UseThe use of JETREA in pediatric patients is not recommended. A single center, randomized, placebo controlled, double masked clinical study to investigate the safety and efficacy of a single intravitreal injection of 0.175 mg ocriplasmin in pediatric subjects as an adjunct to vitrectomy was conducted in 24 eyes of 22 patients. There were no statistical or clinical differences between groups for the induction of total macular PVD, any of the secondary endpoints or adverse events.
8.5 Geriatric UseIn the clinical studies, 384 and 145 patients were ≥ 65 years and of these 192 and 73 patients were ≥ 75 years in the JETREA and vehicle groups respectively. No significant differences in efficacy or safety were seen with increasing age in these studies.
10 OVERDOSAGEThe clinical data on the effects of JETREA overdose are limited. One case of accidental overdose of 0.250 mg ocriplasmin (twice the recommended dose) was reported to be associated with inflammation and a decrease in visual acuity.
11 DESCRIPTIONOcriplasmin is a recombinant truncated form of human plasmin with a molecular weight of 27.2 kDa produced by recombinant DNA technology in a Pichia pastoris expression system. JETREA is a sterile, clear and colorless solution with no preservatives in a single-use glass vial containing 0.5 mg ocriplasmin in 0.2 mL solution for intravitreal injection after dilution. Each vial contains 0.5 mg ocriplasmin (active) and 0.21 mg citric acid, 0.75 mg mannitol, sodium hydroxide (for pH adjustment) and water for injection. The pH of the solution is 3.1.
12 CLINICAL PHARMACOLOGY12.1 Mechanism of ActionOcriplasmin has proteolytic activity against protein components of the vitreous body and the vitreoretinal interface (VRI) (e.g. laminin, fibronectin and collagen), thereby dissolving the protein matrix responsible for the vitreomacular adhesion (VMA).
12.3 PharmacokineticsThe intravitreal pharmacokinetics of ocriplasmin were determined in a clinical study in patients scheduled for vitrectomy where 0.125 mg ocriplasmin (corresponding to an average concentration of 29 mcg ocriplasmin per mL vitreous volume [approximately 4.3 mL/eye]) was administered as a single intravitreal dose at different time points prior to vitrectomy. The mean ocriplasmin activity levels decreased with time from injection to time of sampling as illustrated in Table 1, according to a second-order kinetic process. At 24 hours post-injection the levels in the vitreous were below 3% of the theoretical concentration reached immediately after injection. Because of the small dose administered (0.125 mg), detectable levels of ocriplasmin in systemic circulation are not expected after intravitreal injection.
Table 1: Mean Ocriplasmin Activity Levels in Vitreous Samples after Intravitreal Injection of 0.125 mg Ocriplasmin
Time post-injection (subjects)
5-30min(n=8)
31-60min(n=8)
2-4hours(n=8)
24hr ± 2hr(n=4)
7days ± 1day (n=4)
Mean ± SD Ocriplasmin levels (mcg/mL)
12 ±7.6 8.1 ±5.2 2.6 ±1.6 0.5 ±0.3a < 0.27b
a 2 subjects below lower limit of detection, other 2 subjects at 0.88 and 0.57 mcg/mLb Lower limit of detection
Ocriplasmin enters the endogenous protein catabolism pathway through which it is rapidly inactivated via its interactions with protease inhibitor α2-antiplasmin or α2-macroglobulin.
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, Impairment of FertilityNo carcinogenicity, mutagenicity or reproductive and developmental toxicity studies were conducted with ocriplasmin.
13.2 Animal Toxicology and/or PharmacologyThe ocular toxicity of ocriplasmin after a single intravitreal dose has been evaluated in rabbits, monkeys and minipigs. Ocriplasmin induced an inflammatory response and transient ERG changes in rabbits and monkeys, which tended to resolve over time. Lens subluxation was observed in the 3 species at ocriplasmin concentrations in the vitreous at or above 41 mcg/mL, a concentration 1.4-fold above the intended clinical concentration in the vitreous of 29 mcg/mL. Intraocular hemorrhage was observed in rabbits and monkeys.A second intravitreal administration of ocriplasmin (28 days apart) in monkeys at doses of 75 mcg/eye (41 mcg/mL vitreous) or 125 mcg/eye (68 mcg/mL vitreous) was associated with lens subluxation in all ocriplasmin treated eyes. Sustained increases in IOP occurred in two animals with lens subluxation. Microscopic findings in the eye included vitreous liquefaction, degeneration/disruption of the hyaloideocapsular ligament (with loss of ciliary zonular fibers), lens degeneration, mononuclear cell infiltration of the vitreous, and vacuolation of the retinal inner nuclear cell layer. These doses are 1.4-fold and 2.3-fold the intended clinical concentration in the vitreous of 29 mcg/mL, respectively.
14 CLINICAL STUDIESThe efficacy and safety of JETREA was demonstrated in two multicenter, randomized, double masked, vehicle-controlled, 6 month studies in patients with symptomatic vitreomacular adhesion (VMA). A total of 652 patients (JETREA 464, vehicle 188) were randomized in these 2 studies. Randomization was 2:1 (JETREA:vehicle) in Study 1 and 3:1 in Study 2.Patients were treated with a single injection of JETREA or vehicle. In both of the studies, the proportion of patients who achieved VMA resolution at Day 28 (i.e., achieved success on the primary endpoint) was significantly higher in the ocriplasmin group compared with the vehicle group through Month 6 (Table 2 and Figure 7).
Table 2: Proportion of Patients with VMA Resolution in the Study Eye (Study 1, Study 2: Full Analysis Set)
Study 1 Study 2
VehicleN=107
JETREAN=219
Difference(95% CI)
VehicleN=81
JETREAN=245
Difference(95% CI)
n (%) n (%) n (%) n (%)
Day 7 8 (7.5) 54 (24.7) 17.2 (9.6, 24.8) 1 (1.2) 36 (14.7) 13.5 (8.4, 18.5)
Day 14 12 (11.2) 57 (26.0) 14.8 (6.5, 23.2) 1 (1.2) 44 (18.0) 16.7 (11.4, 22.1)
Day 28 14 (13.1) 61 (27.9) 14.8 (6.0, 23.5) 5 (6.2) 62 (25.3) 19.1 (11.6, 26.7)
Month 3 16 (15.0) 58 (26.5) 11.5 (2.6, 20.5) 7 (8.6) 62 (25.3) 16.7 (8.5, 24.9)
Month 6 15 (14.0) 60 (27.4) 13.4 (4.5, 22.2) 10 (12.3) 65 (26.5) 14.2 (5.1, 23.2)
Figure 7: Proportion of Patients with VMA Resolution in the Study Eye (Study 1 and Study 2)
Study 1 JETREA
Study 2 JETREA
Study 1 Vehicle
Study 2 Vehicle
Days Post-Injection
At all post-injection days, p≤0.02 in Study 1 and p≤0.01 in Study 2
Total posterior vitreous detachment (PVD) induction in symptomatic vitreomacular adhesion patients was evaluated by B-scan ultrasound. A statistically significantly higher percentage of JETREA treated patients achieved total PVD at Day 28 compared to vehicle treated patients in Study 1 (16% vs. 6%; p=0.014) and in Study 2 (11% vs. 0%; p<0.01).The number of patients with at least 3 lines increase in visual acuity was numerically higher in the ocriplasmin
group compared to vehicle in both trials, however, the number of patients with at least a 3 lines decrease in visual acuity was also higher in the ocriplasmin group in one of the studies (Table 3 and Figure 8).
Table 3: Categorical Change from Baseline in BCVA at Month 6, Irrespective of Vitrectomy (Study 1 and Study 2)
Study 1 Study 2
JETREA Vehicle Difference JETREA Vehicle Difference
N=219 N=107 (95% CI) N=245 N=81 (95% CI)
≥ 3 line Improvement in BCVA
Month 6 28 (12.8%) 9 (8.4%) 4.4 (-2.5, 11.2)
29 (11.8%) 3 (3.8%) 8.1 (2.3, 13.9)
> 3 line Worsening in BCVA
Month 6 16 (7.3%) 2 (1.9%) 5.4 (1.1, 9.7) 10 (4.1%) 4 (5.0%) -0.9 (-6.3, 4.5)
Figure 8: Percentage of Patients with Gain or Loss of ≥ 3 Lines of BCVA at Protocol- Specified Visits
Study 1 JETREA Study 1 Vehicle Study 2 JETREA Study 2 Vehicle
16 HOW SUPPLIED/STORAGE AND HANDLINGEach vial of JETREA contains 0.5 mg ocriplasmin in 0.2 mL citric-buffered solution (2.5 mg/mL). JETREA is supplied in a 2 mL glass vial with a latex free rubber stopper. Vials are for single use only. NDC 24856-001-00StorageStore frozen at or below -4˚F (-20˚C). Protect the vials from light by storing in the original package until time of use.
17 PATIENT COUNSELING INFORMATIONIn the days following JETREA administration, patients are at risk of developing intraocular inflammation/infection. Advise patients to seek immediate care from an ophthalmologist if the eye becomes red, sensitive to light, painful, or develops a change in vision [see Warnings and Precautions (5.2)].Patients may experience temporary visual impairment after receiving an intravitreal injection of JETREA [see Warnings and Precautions (5.1)]. Advise patients to not drive or operate heavy machinery until this visual impairment has resolved. If visual impairment persists or decreases further, advise patients to seek care from an ophthalmologist.
Manufactured for: ThromboGenics, Inc.101 Wood Avenue South, Suite 610 Iselin, NJ 08830
U.S. License Number: 1866©2012, ThromboGenics, Inc. All rights reserved.Revised March 2016Initial U.S. Approval: 2012ThromboGenics U.S. patents: 7,445,775; 7,547,435; 7,914,783 and other pending patents.
255919Je01-US-LT-04
% V
MA
Res
olu
tio
n
Days
References: 1. Stalmans P, Benz MS, Gandorfer A, et al. Enzymatic vitreolysis with ocriplasmin for vitreomacular traction and macular holes. N Engl J Med. 2012;367(7):606-615. 2. River Y, Ben Hur T, Steiner I. Reversal of vision metamorphopsia: clinical and anatomical characteristics. Arch Neurol. 1998;55(10):1362-1368. 3. Lina G, Xuemin Q, Qinmei W, Lijun S. Vision-related quality of life, metamorphopsia, and stereopsis after successful surgery for rhegmatogenous retinal detachment. Eye (Lond). 2016;30(1):40-45. 4. Okamoto F, Okamoto Y, Fukuda S, Hiraoka T, Oshika T. Vision-related quality of life and visual function following vitrectomy for proliferative diabetic retinopathy. Am J Ophthalmol. 2008;145(6):1031-1036. 5. Midena E, Vujosevic S. Metamorphopsia: an overlooked visual symptom. Ophthalmic Res. 2015;55(1):26-36. 6. Hyer R. Five pearls for successfully co-managing the premium IOL patient. Optometry Times. 2013. http://optometrytimes.modernmedicine.com/optometrytimes/content/tags/baby-boomers/five-pearls-successfully-co-managing-premium-iol-patient. Accessed January 4, 2017. 7. Stalmans P, Duker JS, Kaiser PK, et al. OCT-based interpretation of the vitreomacular interface and indications for pharmacologic vitreolysis. Retina. 2013; 33(10):2003-2011. 8. Duker JS, Kaiser PK, Binder S, et al. The International Vitreomacular Traction Study Group classification of vitreomacular adhesion, traction, and macular hole. Ophthalmology. 2013;120(12):2611-2619. 9. Johnson MW. Posterior vitreous detachment: evolution and complications of its early stages. Am J Ophthalmol. 2010;149(3):371-382. 10. Moisseiev J, Moroz I, Katz G. Effect of ocriplasmin on the management of macular holes: assessment of the clinical relevance of ocriplasmin. JAMA Ophthalmol. 2014;132(6):709-713. 11. Stevenson W, Prospero Ponce CM, Agarwal DR, Gelman R, Christoforidis JB. Epiretinal membrane: optical coherence tomography-based diagnosis and classification. Clin Ophthalmol. 2016;10:527-534. 12. Koizumi H, Spaide RF, Fisher YL, Freund KB, Klancnik JM, Jr., Yannuzzi LA. Three-dimensional evaluation of vitreomacular traction and epiretinal membrane using spectral-domain optical coherence tomography. Am J Ophthalmol. 2008;145(3):509-517. 13. Khanani A. Improving success with pharmacologic management of symptomatic VMA. Retina Today. 2015;48-50. 14. Mastropasqua R, et al. Comparison of guided and unguided ocriplasmin injection for the treatment of vitreomacular traction: a preliminary study. J Ophthalmol. 2016:6521304.
@2017 ThromboGenics Inc. All rights reserved. ThromboGenics Inc., 101 Wood Avenue South, Suite 610, Iselin NJ 08830-USA. JETREA and the JETREA logo, JETREA CARE and the CARE logo, and THROMBOGENICS and the THROMBOGENICS logo are trademarks or registered trademarks of ThromboGenics, NV.